User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Feds abandon fight for graphic cigarette labels
The Food and Drug Administration, facing virulent opposition from the tobacco industry as well as two court decisions that didn’t go its way, has decided to drop its proposals to include graphic, photo-based warning labels on cigarette packs.
Instead, the FDA said it will research new ways to craft warning labels that can reduce tobacco deaths, while still satisfying the courts’ requirements that any regulations not infringe upon tobacco companies’ First Amendment right to free speech. The 2009 Tobacco Control Act requires the FDA to implement new warning labels.
The graphic warning labels, first unveiled in 2011 and intended for placement on all cigarette packages, included disturbing photos such as the corpse of a man who died of tobacco-related causes, disease-riddled lungs, and rotting teeth. Other countries use similar warning labels.
A group of tobacco manufacturers sued the agency to overturn the requirement to use the labels, and two courts – most recently, the U.S. Court of Appeals for the D.C. Circuit – sided with the manufacturers. The Justice Department elected not to appeal the case to the U.S. Supreme Court.
The American Cancer Society Cancer Action Network, the ACS’ advocacy arm, urged the FDA to work quickly to develop new graphic warnings. "The current warning labels have not been changed in 25 years and are widely considered to be ineffective," group president Chris Hansen said in a statement. "Every day that the current warnings remain in place is another day in which ... the health of the nation is compromised."
The Food and Drug Administration, facing virulent opposition from the tobacco industry as well as two court decisions that didn’t go its way, has decided to drop its proposals to include graphic, photo-based warning labels on cigarette packs.
Instead, the FDA said it will research new ways to craft warning labels that can reduce tobacco deaths, while still satisfying the courts’ requirements that any regulations not infringe upon tobacco companies’ First Amendment right to free speech. The 2009 Tobacco Control Act requires the FDA to implement new warning labels.
The graphic warning labels, first unveiled in 2011 and intended for placement on all cigarette packages, included disturbing photos such as the corpse of a man who died of tobacco-related causes, disease-riddled lungs, and rotting teeth. Other countries use similar warning labels.
A group of tobacco manufacturers sued the agency to overturn the requirement to use the labels, and two courts – most recently, the U.S. Court of Appeals for the D.C. Circuit – sided with the manufacturers. The Justice Department elected not to appeal the case to the U.S. Supreme Court.
The American Cancer Society Cancer Action Network, the ACS’ advocacy arm, urged the FDA to work quickly to develop new graphic warnings. "The current warning labels have not been changed in 25 years and are widely considered to be ineffective," group president Chris Hansen said in a statement. "Every day that the current warnings remain in place is another day in which ... the health of the nation is compromised."
The Food and Drug Administration, facing virulent opposition from the tobacco industry as well as two court decisions that didn’t go its way, has decided to drop its proposals to include graphic, photo-based warning labels on cigarette packs.
Instead, the FDA said it will research new ways to craft warning labels that can reduce tobacco deaths, while still satisfying the courts’ requirements that any regulations not infringe upon tobacco companies’ First Amendment right to free speech. The 2009 Tobacco Control Act requires the FDA to implement new warning labels.
The graphic warning labels, first unveiled in 2011 and intended for placement on all cigarette packages, included disturbing photos such as the corpse of a man who died of tobacco-related causes, disease-riddled lungs, and rotting teeth. Other countries use similar warning labels.
A group of tobacco manufacturers sued the agency to overturn the requirement to use the labels, and two courts – most recently, the U.S. Court of Appeals for the D.C. Circuit – sided with the manufacturers. The Justice Department elected not to appeal the case to the U.S. Supreme Court.
The American Cancer Society Cancer Action Network, the ACS’ advocacy arm, urged the FDA to work quickly to develop new graphic warnings. "The current warning labels have not been changed in 25 years and are widely considered to be ineffective," group president Chris Hansen said in a statement. "Every day that the current warnings remain in place is another day in which ... the health of the nation is compromised."
PLCO criteria catch more lung cancers
Modified criteria for screening current or former smokers for lung cancer appeared to be more accurate than currently recommended criteria.
In a post hoc statistical analysis of data on 28,288 people, a version of the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial criteria identified 81 more lung cancers and would have saved an additional 12 lives over a 6-year period, compared with the National Lung Screening Trial (NLST) criteria, Martin C. Tammemägi, Ph.D., and his associates reported.

The modified PLCO criteria were significantly more sensitive than the NLST criteria (83% vs. 71%, respectively) and had a better positive predictive value (4% vs. 3.4%) with no loss of specificity (62% each). Use of the PLCO criteria would have missed 41% fewer cancers, reported Dr. Tammemägi of Brock University, St. Catharines, Ont. (N. Engl. J. Med. 2013;368:728-36).
The American Cancer Society and several other organizations recommend using the NLST criteria, or a version of the criteria, to identify people at high risk of lung cancer who might benefit from screening with low-dose CT imaging. Using the NLST criteria would reduce deaths from lung cancer by 20% (N. Engl. J. Med. 2011;365:395-409). Risk factors include an age between 55 and 74 years, at least a 30 pack-year history of smoking, and no more than 15 years since quitting smoking.
The PLCO criteria added risk factors excluded in the NLST, such as education level (as a proxy for socioeconomic status); body mass index; a family history of lung cancer; chronic obstructive pulmonary disease; chest x-ray within the last 3 years; and not only a history of smoking in pack-years but also the duration of smoking. The PLCO model can be cumbersome to apply because it uses complicated modeling procedures. A spreadsheet for calculating the 6-year risk for lung cancer in a current or former smoker using the PLCO criteria in Dr. Tammemägi’s report can be downloaded here.
The PLCO trial followed patients for a median of 9 years, longer than the median 6-year follow-up in the NLST. The investigators modified the PLCO criteria so that it was directly applicable to patients in the NLST and truncated PLCO follow-up so that they could compare data on 14,144 people in each of the studies. The modified PLCO model was developed and validated using data on 80,375 people in the PLCO trial.
Among people who did not qualify for screening under PLCO criteria, 0.5% developed lung cancer, a significantly smaller proportion than the 0.85% of patients excluded from screening under NLST criteria who then developed lung cancer, Dr. Tammemägi reported. Overall, the modified PLCO criteria identified 12% more of the 678 lung cancers in the total cohort than did NLST criteria. The modified PLCO criteria missed 115 lung cancers; the NLST criteria missed 196.
In the PLCO model, current or former smokers were more likely to develop lung cancer with increasing age; black vs. white race; lower socioeconomic status; lower BMI, self-reported history of chronic obstructive pulmonary disease; family history of lung cancer; current smoking; increasing number of cigarettes smoked per day; duration of smoking; and shorter time since quitting, if no longer smoking.
Prospective studies should evaluate the modified PLCO criteria in different populations and clinical and public health settings, Dr. Tammemägi suggested. Additional risk factors may be added to the model in the future to enhance its predictive accuracy.
Dr. Tammemägi reported having no financial disclosures.
Modified criteria for screening current or former smokers for lung cancer appeared to be more accurate than currently recommended criteria.
In a post hoc statistical analysis of data on 28,288 people, a version of the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial criteria identified 81 more lung cancers and would have saved an additional 12 lives over a 6-year period, compared with the National Lung Screening Trial (NLST) criteria, Martin C. Tammemägi, Ph.D., and his associates reported.
The modified PLCO criteria were significantly more sensitive than the NLST criteria (83% vs. 71%, respectively) and had a better positive predictive value (4% vs. 3.4%) with no loss of specificity (62% each). Use of the PLCO criteria would have missed 41% fewer cancers, reported Dr. Tammemägi of Brock University, St. Catharines, Ont. (N. Engl. J. Med. 2013;368:728-36).
The American Cancer Society and several other organizations recommend using the NLST criteria, or a version of the criteria, to identify people at high risk of lung cancer who might benefit from screening with low-dose CT imaging. Using the NLST criteria would reduce deaths from lung cancer by 20% (N. Engl. J. Med. 2011;365:395-409). Risk factors include an age between 55 and 74 years, at least a 30 pack-year history of smoking, and no more than 15 years since quitting smoking.
The PLCO criteria added risk factors excluded in the NLST, such as education level (as a proxy for socioeconomic status); body mass index; a family history of lung cancer; chronic obstructive pulmonary disease; chest x-ray within the last 3 years; and not only a history of smoking in pack-years but also the duration of smoking. The PLCO model can be cumbersome to apply because it uses complicated modeling procedures. A spreadsheet for calculating the 6-year risk for lung cancer in a current or former smoker using the PLCO criteria in Dr. Tammemägi’s report can be downloaded here.
The PLCO trial followed patients for a median of 9 years, longer than the median 6-year follow-up in the NLST. The investigators modified the PLCO criteria so that it was directly applicable to patients in the NLST and truncated PLCO follow-up so that they could compare data on 14,144 people in each of the studies. The modified PLCO model was developed and validated using data on 80,375 people in the PLCO trial.
Among people who did not qualify for screening under PLCO criteria, 0.5% developed lung cancer, a significantly smaller proportion than the 0.85% of patients excluded from screening under NLST criteria who then developed lung cancer, Dr. Tammemägi reported. Overall, the modified PLCO criteria identified 12% more of the 678 lung cancers in the total cohort than did NLST criteria. The modified PLCO criteria missed 115 lung cancers; the NLST criteria missed 196.
In the PLCO model, current or former smokers were more likely to develop lung cancer with increasing age; black vs. white race; lower socioeconomic status; lower BMI, self-reported history of chronic obstructive pulmonary disease; family history of lung cancer; current smoking; increasing number of cigarettes smoked per day; duration of smoking; and shorter time since quitting, if no longer smoking.
Prospective studies should evaluate the modified PLCO criteria in different populations and clinical and public health settings, Dr. Tammemägi suggested. Additional risk factors may be added to the model in the future to enhance its predictive accuracy.
Dr. Tammemägi reported having no financial disclosures.
Modified criteria for screening current or former smokers for lung cancer appeared to be more accurate than currently recommended criteria.
In a post hoc statistical analysis of data on 28,288 people, a version of the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial criteria identified 81 more lung cancers and would have saved an additional 12 lives over a 6-year period, compared with the National Lung Screening Trial (NLST) criteria, Martin C. Tammemägi, Ph.D., and his associates reported.
The modified PLCO criteria were significantly more sensitive than the NLST criteria (83% vs. 71%, respectively) and had a better positive predictive value (4% vs. 3.4%) with no loss of specificity (62% each). Use of the PLCO criteria would have missed 41% fewer cancers, reported Dr. Tammemägi of Brock University, St. Catharines, Ont. (N. Engl. J. Med. 2013;368:728-36).
The American Cancer Society and several other organizations recommend using the NLST criteria, or a version of the criteria, to identify people at high risk of lung cancer who might benefit from screening with low-dose CT imaging. Using the NLST criteria would reduce deaths from lung cancer by 20% (N. Engl. J. Med. 2011;365:395-409). Risk factors include an age between 55 and 74 years, at least a 30 pack-year history of smoking, and no more than 15 years since quitting smoking.
The PLCO criteria added risk factors excluded in the NLST, such as education level (as a proxy for socioeconomic status); body mass index; a family history of lung cancer; chronic obstructive pulmonary disease; chest x-ray within the last 3 years; and not only a history of smoking in pack-years but also the duration of smoking. The PLCO model can be cumbersome to apply because it uses complicated modeling procedures. A spreadsheet for calculating the 6-year risk for lung cancer in a current or former smoker using the PLCO criteria in Dr. Tammemägi’s report can be downloaded here.
The PLCO trial followed patients for a median of 9 years, longer than the median 6-year follow-up in the NLST. The investigators modified the PLCO criteria so that it was directly applicable to patients in the NLST and truncated PLCO follow-up so that they could compare data on 14,144 people in each of the studies. The modified PLCO model was developed and validated using data on 80,375 people in the PLCO trial.
Among people who did not qualify for screening under PLCO criteria, 0.5% developed lung cancer, a significantly smaller proportion than the 0.85% of patients excluded from screening under NLST criteria who then developed lung cancer, Dr. Tammemägi reported. Overall, the modified PLCO criteria identified 12% more of the 678 lung cancers in the total cohort than did NLST criteria. The modified PLCO criteria missed 115 lung cancers; the NLST criteria missed 196.
In the PLCO model, current or former smokers were more likely to develop lung cancer with increasing age; black vs. white race; lower socioeconomic status; lower BMI, self-reported history of chronic obstructive pulmonary disease; family history of lung cancer; current smoking; increasing number of cigarettes smoked per day; duration of smoking; and shorter time since quitting, if no longer smoking.
Prospective studies should evaluate the modified PLCO criteria in different populations and clinical and public health settings, Dr. Tammemägi suggested. Additional risk factors may be added to the model in the future to enhance its predictive accuracy.
Dr. Tammemägi reported having no financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Using the modified PLCO criteria identified 12% more of the 678 lung cancers in the total cohort than did NLST criteria.
Data Source: Post hoc statistical analyses of data on 28,288 people, 14,144 each from the PLCO trial and the NLST.
Disclosures: Dr. Tammemägi reported having no financial disclosures.

For overweight children, inject epinephrine in lower thigh
SAN ANTONIO – Overweight and obese children in need of epinephrine for anaphylaxis should be injected in the calf or in the lower thigh, rather than upper half of the thigh, to ensure intramuscular administration, according to findings from an ultrasound study of 93 children.
Ultrasound measurement demonstrated that the distance from skin surface to muscle depth was greater than auto-injector needle length at one quarter of the distance down the thigh in 82% of obese children vs. 25% of nonobese children. At three-quarters of the way down the thigh, this was the case in only 17% of obese children and 2% of nonobese children, Dr. Peter Arkwright reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
At a point midway down the calf, the skin surface to muscle depth was less than the length of the auto-injector needle in all of the children, said Dr. Arkwright of the University of Manchester (England).
Intramuscular injection, rather than subcutaneous injection, is imperative for effective delivery of epinephrine, he said, noting that this study was undertaken because of growing concerns that increasing obesity among children could make existing auto-injectors inadequate for providing intramuscular delivery in a significant proportion of patients.
Children included in the study were patients from regional pediatric allergy clinics. All were measured for height, weight, and body mass index, and all underwent ultrasound measurement at set distances down the thigh and leg. Higher weight, BMI, and waist circumference – but not age or gender – were associated with skin surface to muscle depth greater than auto-injector needle length, he noted.
"Based on our study, injecting epinephrine into the lower rather than upper thigh would be advised in overweight or obese children," he said, adding that caregivers of children at risk of anaphylaxis should be advised about the importance of administering epinephrine into the muscle in the most effective way.
For overweight and obese children, this involves injecting into the lower half of the thigh, and for very obese children it involves injecting at the middle of the calf, he said.
Dr. Arkwright reported having no disclosures.
SAN ANTONIO – Overweight and obese children in need of epinephrine for anaphylaxis should be injected in the calf or in the lower thigh, rather than upper half of the thigh, to ensure intramuscular administration, according to findings from an ultrasound study of 93 children.
Ultrasound measurement demonstrated that the distance from skin surface to muscle depth was greater than auto-injector needle length at one quarter of the distance down the thigh in 82% of obese children vs. 25% of nonobese children. At three-quarters of the way down the thigh, this was the case in only 17% of obese children and 2% of nonobese children, Dr. Peter Arkwright reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
At a point midway down the calf, the skin surface to muscle depth was less than the length of the auto-injector needle in all of the children, said Dr. Arkwright of the University of Manchester (England).
Intramuscular injection, rather than subcutaneous injection, is imperative for effective delivery of epinephrine, he said, noting that this study was undertaken because of growing concerns that increasing obesity among children could make existing auto-injectors inadequate for providing intramuscular delivery in a significant proportion of patients.
Children included in the study were patients from regional pediatric allergy clinics. All were measured for height, weight, and body mass index, and all underwent ultrasound measurement at set distances down the thigh and leg. Higher weight, BMI, and waist circumference – but not age or gender – were associated with skin surface to muscle depth greater than auto-injector needle length, he noted.
"Based on our study, injecting epinephrine into the lower rather than upper thigh would be advised in overweight or obese children," he said, adding that caregivers of children at risk of anaphylaxis should be advised about the importance of administering epinephrine into the muscle in the most effective way.
For overweight and obese children, this involves injecting into the lower half of the thigh, and for very obese children it involves injecting at the middle of the calf, he said.
Dr. Arkwright reported having no disclosures.
SAN ANTONIO – Overweight and obese children in need of epinephrine for anaphylaxis should be injected in the calf or in the lower thigh, rather than upper half of the thigh, to ensure intramuscular administration, according to findings from an ultrasound study of 93 children.
Ultrasound measurement demonstrated that the distance from skin surface to muscle depth was greater than auto-injector needle length at one quarter of the distance down the thigh in 82% of obese children vs. 25% of nonobese children. At three-quarters of the way down the thigh, this was the case in only 17% of obese children and 2% of nonobese children, Dr. Peter Arkwright reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
At a point midway down the calf, the skin surface to muscle depth was less than the length of the auto-injector needle in all of the children, said Dr. Arkwright of the University of Manchester (England).
Intramuscular injection, rather than subcutaneous injection, is imperative for effective delivery of epinephrine, he said, noting that this study was undertaken because of growing concerns that increasing obesity among children could make existing auto-injectors inadequate for providing intramuscular delivery in a significant proportion of patients.
Children included in the study were patients from regional pediatric allergy clinics. All were measured for height, weight, and body mass index, and all underwent ultrasound measurement at set distances down the thigh and leg. Higher weight, BMI, and waist circumference – but not age or gender – were associated with skin surface to muscle depth greater than auto-injector needle length, he noted.
"Based on our study, injecting epinephrine into the lower rather than upper thigh would be advised in overweight or obese children," he said, adding that caregivers of children at risk of anaphylaxis should be advised about the importance of administering epinephrine into the muscle in the most effective way.
For overweight and obese children, this involves injecting into the lower half of the thigh, and for very obese children it involves injecting at the middle of the calf, he said.
Dr. Arkwright reported having no disclosures.
AT THE AAAAI ANNUAL MEETING
Major finding: 82% of obese children and 25% of nonobese children had inadequate upper thigh skin surface to muscle depth.
Data source: A prospective study of 93 children.
Disclosures: Dr. Arkwright reported having no disclosures.
NHANES follow-up characterizes asthma/allergy patient mortality
SAN ANTONIO – A diagnosis of asthma, allergic disease, or obstructive or restrictive lung disease among participants in the first National Health and Nutrition Examination Survey conferred a significantly increased long-term risk of all-cause mortality for adults who were aged 40-75 years at baseline but not for those who were aged 25-39 years at baseline, according to findings from the study.
A diagnosis of asthma in the younger group conferred an increased long-term risk of death due to respiratory causes – as did a diagnosis of asthma in the older group, Dr. Jessica R. Savage reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"This association was not likely explained by underlying bronchitis or an increased risk of death due to respiratory infection but was likely due to asthma itself," said Dr. Savage of Brigham and Women’s Hospital, Boston.
"I think the main conclusions are reassuring – no increase in mortality if you are young and have allergies. Some studies show an association between allergy and stroke/heart disease. We were worried that with the rising increase in allergy, there would be also an increase in these other diseases. But we did not see that, fortunately.
"We saw an association with asthma and respiratory death even in the young. Of course, one always needs to remember to be vigilant with asthmatics, but overall for young people the news is good," she said during an interview.
Data were obtained from the National Health and Nutrition Examination Survey (NHANES I), which was conducted from 1971 to 1975 and included 31,937 adults. Of these participants, 14,407 were included in the NHANES I Epidemiologic Follow-Up Study (NHEFS) and were assessed for doctor-diagnosed asthma, allergic rhinitis, food allergy, and urticaria. A subcohort of 6,913 subjects received a more detailed health interview and examination, including prebronchodilator spirometry and percent predicted forced expiratory volume and forced vital capacity. Vital status and cause of death were obtained in 2006.
After adjustment for age, gender, income, education, race, and smoking history, a sensitivity analysis for the association between asthma and mortality demonstrated a significantly increased long-term risk of death in those who were aged 40-75 years at baseline (hazard ratio, 1.22), but not for those aged 25-29 years at baseline (HR, 1.20). The hazard ratios for all-cause mortality in these groups, after exclusion of subjects with bronchitis were not statistically significant (1.16 and 1.52, respectively).
Hazard ratios for the association between asthma and respiratory mortality were significant at 2.03 and 5.87 for the older and younger groups, respectively. The hazard ratios for these groups remained statistically significant at 8.56 and 1.82, respectively, after exclusion of subjects with bronchitis.
This study also demonstrated that older subjects with obstructive lung disease were at significantly increased risk of both all-cause and respiratory mortality and that older subjects with restrictive lung disease were at significantly increased risk of both all-cause and cardiovascular mortality.
Conversely, older adults with urticaria had a reduced risk of cardiovascular mortality.
Cancer-related mortality was slightly, but not significantly, increased in the younger subjects diagnosed with urticaria, and in the older subjects diagnosed with asthma or moderate to severe lung obstruction.
"Asthma and allergic diseases, which typically manifest in childhood, have increased in the United States over the last 3 decades. Asthma and allergy may increase mortality by directly reducing lung function or may be markers of immune dysregulation that could lead to systemic inflammation," Dr. Savage noted, adding that although prior studies have demonstrated associations between allergic sensitization and stroke, hives and cancer, asthma and mortality, and obstructive lung disease and cardiovascular events, the effects of asthma and allergic disease on long-term mortality have been unclear.
"The findings (of this follow-up study) provide some insight regarding the effects of asthma and allergic disease on long-term mortality, Dr. Savage said.
The NHEFS is a joint project of the National Center for Health Statistics and the National Institute on Aging in collaboration with other agencies of the U.S. Public Health Service. Dr. Savage reported having no disclosures.
SAN ANTONIO – A diagnosis of asthma, allergic disease, or obstructive or restrictive lung disease among participants in the first National Health and Nutrition Examination Survey conferred a significantly increased long-term risk of all-cause mortality for adults who were aged 40-75 years at baseline but not for those who were aged 25-39 years at baseline, according to findings from the study.
A diagnosis of asthma in the younger group conferred an increased long-term risk of death due to respiratory causes – as did a diagnosis of asthma in the older group, Dr. Jessica R. Savage reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"This association was not likely explained by underlying bronchitis or an increased risk of death due to respiratory infection but was likely due to asthma itself," said Dr. Savage of Brigham and Women’s Hospital, Boston.
"I think the main conclusions are reassuring – no increase in mortality if you are young and have allergies. Some studies show an association between allergy and stroke/heart disease. We were worried that with the rising increase in allergy, there would be also an increase in these other diseases. But we did not see that, fortunately.
"We saw an association with asthma and respiratory death even in the young. Of course, one always needs to remember to be vigilant with asthmatics, but overall for young people the news is good," she said during an interview.
Data were obtained from the National Health and Nutrition Examination Survey (NHANES I), which was conducted from 1971 to 1975 and included 31,937 adults. Of these participants, 14,407 were included in the NHANES I Epidemiologic Follow-Up Study (NHEFS) and were assessed for doctor-diagnosed asthma, allergic rhinitis, food allergy, and urticaria. A subcohort of 6,913 subjects received a more detailed health interview and examination, including prebronchodilator spirometry and percent predicted forced expiratory volume and forced vital capacity. Vital status and cause of death were obtained in 2006.
After adjustment for age, gender, income, education, race, and smoking history, a sensitivity analysis for the association between asthma and mortality demonstrated a significantly increased long-term risk of death in those who were aged 40-75 years at baseline (hazard ratio, 1.22), but not for those aged 25-29 years at baseline (HR, 1.20). The hazard ratios for all-cause mortality in these groups, after exclusion of subjects with bronchitis were not statistically significant (1.16 and 1.52, respectively).
Hazard ratios for the association between asthma and respiratory mortality were significant at 2.03 and 5.87 for the older and younger groups, respectively. The hazard ratios for these groups remained statistically significant at 8.56 and 1.82, respectively, after exclusion of subjects with bronchitis.
This study also demonstrated that older subjects with obstructive lung disease were at significantly increased risk of both all-cause and respiratory mortality and that older subjects with restrictive lung disease were at significantly increased risk of both all-cause and cardiovascular mortality.
Conversely, older adults with urticaria had a reduced risk of cardiovascular mortality.
Cancer-related mortality was slightly, but not significantly, increased in the younger subjects diagnosed with urticaria, and in the older subjects diagnosed with asthma or moderate to severe lung obstruction.
"Asthma and allergic diseases, which typically manifest in childhood, have increased in the United States over the last 3 decades. Asthma and allergy may increase mortality by directly reducing lung function or may be markers of immune dysregulation that could lead to systemic inflammation," Dr. Savage noted, adding that although prior studies have demonstrated associations between allergic sensitization and stroke, hives and cancer, asthma and mortality, and obstructive lung disease and cardiovascular events, the effects of asthma and allergic disease on long-term mortality have been unclear.
"The findings (of this follow-up study) provide some insight regarding the effects of asthma and allergic disease on long-term mortality, Dr. Savage said.
The NHEFS is a joint project of the National Center for Health Statistics and the National Institute on Aging in collaboration with other agencies of the U.S. Public Health Service. Dr. Savage reported having no disclosures.
SAN ANTONIO – A diagnosis of asthma, allergic disease, or obstructive or restrictive lung disease among participants in the first National Health and Nutrition Examination Survey conferred a significantly increased long-term risk of all-cause mortality for adults who were aged 40-75 years at baseline but not for those who were aged 25-39 years at baseline, according to findings from the study.
A diagnosis of asthma in the younger group conferred an increased long-term risk of death due to respiratory causes – as did a diagnosis of asthma in the older group, Dr. Jessica R. Savage reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"This association was not likely explained by underlying bronchitis or an increased risk of death due to respiratory infection but was likely due to asthma itself," said Dr. Savage of Brigham and Women’s Hospital, Boston.
"I think the main conclusions are reassuring – no increase in mortality if you are young and have allergies. Some studies show an association between allergy and stroke/heart disease. We were worried that with the rising increase in allergy, there would be also an increase in these other diseases. But we did not see that, fortunately.
"We saw an association with asthma and respiratory death even in the young. Of course, one always needs to remember to be vigilant with asthmatics, but overall for young people the news is good," she said during an interview.
Data were obtained from the National Health and Nutrition Examination Survey (NHANES I), which was conducted from 1971 to 1975 and included 31,937 adults. Of these participants, 14,407 were included in the NHANES I Epidemiologic Follow-Up Study (NHEFS) and were assessed for doctor-diagnosed asthma, allergic rhinitis, food allergy, and urticaria. A subcohort of 6,913 subjects received a more detailed health interview and examination, including prebronchodilator spirometry and percent predicted forced expiratory volume and forced vital capacity. Vital status and cause of death were obtained in 2006.
After adjustment for age, gender, income, education, race, and smoking history, a sensitivity analysis for the association between asthma and mortality demonstrated a significantly increased long-term risk of death in those who were aged 40-75 years at baseline (hazard ratio, 1.22), but not for those aged 25-29 years at baseline (HR, 1.20). The hazard ratios for all-cause mortality in these groups, after exclusion of subjects with bronchitis were not statistically significant (1.16 and 1.52, respectively).
Hazard ratios for the association between asthma and respiratory mortality were significant at 2.03 and 5.87 for the older and younger groups, respectively. The hazard ratios for these groups remained statistically significant at 8.56 and 1.82, respectively, after exclusion of subjects with bronchitis.
This study also demonstrated that older subjects with obstructive lung disease were at significantly increased risk of both all-cause and respiratory mortality and that older subjects with restrictive lung disease were at significantly increased risk of both all-cause and cardiovascular mortality.
Conversely, older adults with urticaria had a reduced risk of cardiovascular mortality.
Cancer-related mortality was slightly, but not significantly, increased in the younger subjects diagnosed with urticaria, and in the older subjects diagnosed with asthma or moderate to severe lung obstruction.
"Asthma and allergic diseases, which typically manifest in childhood, have increased in the United States over the last 3 decades. Asthma and allergy may increase mortality by directly reducing lung function or may be markers of immune dysregulation that could lead to systemic inflammation," Dr. Savage noted, adding that although prior studies have demonstrated associations between allergic sensitization and stroke, hives and cancer, asthma and mortality, and obstructive lung disease and cardiovascular events, the effects of asthma and allergic disease on long-term mortality have been unclear.
"The findings (of this follow-up study) provide some insight regarding the effects of asthma and allergic disease on long-term mortality, Dr. Savage said.
The NHEFS is a joint project of the National Center for Health Statistics and the National Institute on Aging in collaboration with other agencies of the U.S. Public Health Service. Dr. Savage reported having no disclosures.
AT THE AAAAI ANNUAL MEETING
Major finding: The long-term risk of death was significantly increased among NHANES 1 subjects with asthma who were aged 40-75 at baseline (hazard ratio, 1.22), but not among those aged 25-29 years at baseline (HR, 1.20).
Data source: Epidemiologic follow-up study (NHEFS) of the longitudinal NHANES 1 study.
Disclosures: The NHEFS is a joint project of the National Center for Health Statistics and the National Institute on Aging in collaboration with other agencies of the Public Health Service. Dr. Savage reported having no disclosures.
Steroids may decrease length of hospital stay for pneumonia
Steroid treatment may not improve mortality in community-acquired pneumonia, but it was associated with significantly shorter hospital stays and an increase in the chance of a clean chest radiograph after treatment.
A meta-analysis of eight studies on the topic showed that steroid treatment reduced the overall length of stay by a little over 1 day. There also was an 87% reduction in the risk of an abnormal chest x-ray at 1 week and an 88% reduction in the risk of delayed shock. These last findings, however, were based on just a few of the analysis’ studies, which were considered only of moderate quality, Dr. Majid Shafiq and colleagues wrote in the March issue of the Journal of Hospital Medicine.

"The data are not strong enough to recommend routine use of steroids among all adults hospitalized with" community-acquired pneumonia (CAP), wrote Dr. Shafiq and his coauthors at the Mayo Clinic in Rochester, Minn. "However, considering that there was no increase in mortality or hospital length of stay with steroid use, it is reasonable to continue steroids if warranted for treatment of underlying comorbid conditions," they noted (J. Hosp. Med. 2013;8:68-75).
The analysis included a total of 1,119 patients, and there were four randomized controlled trials among the studies. In seven studies, the mean patient age ranged from 60 to 80 years. In one study, patients in the experimental arm were a mean of 32 years and those in the control arm were a mean of 41 years. Only one study used a chest x-ray score.
The mean length of stay in the intensive care unit was 13 days for patients taking steroids and 12 for the control patients. The mean hospital length of stay was 10 days for those taking steroids and 14 days for those who did not, said Dr. Shafiq, who is now with Johns Hopkins University, Baltimore, and his associates.
Steroid use did not significantly impact the length of ICU stay or mortality. Four studies showed significantly lower clinical cure rates and a higher number of late failures in patients taking steroids. Two showed no between-group differences in the occurrence of superinfections. Three studies reported that the drugs did not affect gylcemic levels, while four found more frequent hyperglycemia in the steroid group.
"Our study is the first to demonstrate decreased length of hospital stay in this patient population," the investigators wrote. "Importantly, each of the five studies that reported this outcome (including three relatively recent randomized controlled trials) showed the same trend. However, it is not inconceivable that steroid use led to a quicker decline in cytokine levels resulting in an earlier resolution of fever and hence earlier discharge without a faster cure per se."
Dr. Shafiq and his associates reported no financial conflicts.
Steroid treatment may not improve mortality in community-acquired pneumonia, but it was associated with significantly shorter hospital stays and an increase in the chance of a clean chest radiograph after treatment.
A meta-analysis of eight studies on the topic showed that steroid treatment reduced the overall length of stay by a little over 1 day. There also was an 87% reduction in the risk of an abnormal chest x-ray at 1 week and an 88% reduction in the risk of delayed shock. These last findings, however, were based on just a few of the analysis’ studies, which were considered only of moderate quality, Dr. Majid Shafiq and colleagues wrote in the March issue of the Journal of Hospital Medicine.
"The data are not strong enough to recommend routine use of steroids among all adults hospitalized with" community-acquired pneumonia (CAP), wrote Dr. Shafiq and his coauthors at the Mayo Clinic in Rochester, Minn. "However, considering that there was no increase in mortality or hospital length of stay with steroid use, it is reasonable to continue steroids if warranted for treatment of underlying comorbid conditions," they noted (J. Hosp. Med. 2013;8:68-75).
The analysis included a total of 1,119 patients, and there were four randomized controlled trials among the studies. In seven studies, the mean patient age ranged from 60 to 80 years. In one study, patients in the experimental arm were a mean of 32 years and those in the control arm were a mean of 41 years. Only one study used a chest x-ray score.
The mean length of stay in the intensive care unit was 13 days for patients taking steroids and 12 for the control patients. The mean hospital length of stay was 10 days for those taking steroids and 14 days for those who did not, said Dr. Shafiq, who is now with Johns Hopkins University, Baltimore, and his associates.
Steroid use did not significantly impact the length of ICU stay or mortality. Four studies showed significantly lower clinical cure rates and a higher number of late failures in patients taking steroids. Two showed no between-group differences in the occurrence of superinfections. Three studies reported that the drugs did not affect gylcemic levels, while four found more frequent hyperglycemia in the steroid group.
"Our study is the first to demonstrate decreased length of hospital stay in this patient population," the investigators wrote. "Importantly, each of the five studies that reported this outcome (including three relatively recent randomized controlled trials) showed the same trend. However, it is not inconceivable that steroid use led to a quicker decline in cytokine levels resulting in an earlier resolution of fever and hence earlier discharge without a faster cure per se."
Dr. Shafiq and his associates reported no financial conflicts.
Steroid treatment may not improve mortality in community-acquired pneumonia, but it was associated with significantly shorter hospital stays and an increase in the chance of a clean chest radiograph after treatment.
A meta-analysis of eight studies on the topic showed that steroid treatment reduced the overall length of stay by a little over 1 day. There also was an 87% reduction in the risk of an abnormal chest x-ray at 1 week and an 88% reduction in the risk of delayed shock. These last findings, however, were based on just a few of the analysis’ studies, which were considered only of moderate quality, Dr. Majid Shafiq and colleagues wrote in the March issue of the Journal of Hospital Medicine.
"The data are not strong enough to recommend routine use of steroids among all adults hospitalized with" community-acquired pneumonia (CAP), wrote Dr. Shafiq and his coauthors at the Mayo Clinic in Rochester, Minn. "However, considering that there was no increase in mortality or hospital length of stay with steroid use, it is reasonable to continue steroids if warranted for treatment of underlying comorbid conditions," they noted (J. Hosp. Med. 2013;8:68-75).
The analysis included a total of 1,119 patients, and there were four randomized controlled trials among the studies. In seven studies, the mean patient age ranged from 60 to 80 years. In one study, patients in the experimental arm were a mean of 32 years and those in the control arm were a mean of 41 years. Only one study used a chest x-ray score.
The mean length of stay in the intensive care unit was 13 days for patients taking steroids and 12 for the control patients. The mean hospital length of stay was 10 days for those taking steroids and 14 days for those who did not, said Dr. Shafiq, who is now with Johns Hopkins University, Baltimore, and his associates.
Steroid use did not significantly impact the length of ICU stay or mortality. Four studies showed significantly lower clinical cure rates and a higher number of late failures in patients taking steroids. Two showed no between-group differences in the occurrence of superinfections. Three studies reported that the drugs did not affect gylcemic levels, while four found more frequent hyperglycemia in the steroid group.
"Our study is the first to demonstrate decreased length of hospital stay in this patient population," the investigators wrote. "Importantly, each of the five studies that reported this outcome (including three relatively recent randomized controlled trials) showed the same trend. However, it is not inconceivable that steroid use led to a quicker decline in cytokine levels resulting in an earlier resolution of fever and hence earlier discharge without a faster cure per se."
Dr. Shafiq and his associates reported no financial conflicts.
FROM THE JOURNAL OF HOSPITAL MEDICINE
Major Finding: Steroid treatment reduced the overall length of stay by a little more than 1 day in patients with community-acquire pneumonia. The study also showed an 87% reduction in the risk of an abnormal chest x-ray at 1 week and an 88% reduction in the risk of delayed shock, compared with patients who did not take the drugs.
Data Source: Data were drawn from a meta-analysis of eight studies comprising 1,119 patients.
Disclosures: Neither Dr. Shafiq nor his coauthors reported any financial conflicts.
EBSOS implementation improves asthma guideline compliance
SAN ANTONIO – More of the children who present to the pediatric emergency department with asthma exacerbation received recommended care when the staff had instituted a nurse-initiated, evidence-based, standardized order set, according to Dr. Moira E. Breslin.
Specifically, the percentage of patients receiving at least one dose of ipratropium bromide improved from 55.4% before implementation of the order set to 90.9% after implementation. Compliance with the recommendation of the National Asthma Guidelines that patients receive three consecutive nebulized treatments of ipratropium bromide increased from 13.5% to 40.9%, Dr. Breslin of Duke University Medical Center, Durham, N.C., reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The median time to delivery of rescue medication also improved from 21 minutes to 14 minutes for first inhaled bronchodilator administration, and from 41 minutes to 19 minutes for delivery of systemic corticosteroids.
All differences were statistically significant.
The findings are based on a review of charts for 193 patients treated in the pediatric emergency department for status asthmaticus before implementation of the evidence-based standardized order set, or EBSOS, (between Feb. 23, 2009, and Feb. 22, 2012), and for 22 patients treated after implementation (between Feb. 23, 2012, and July 31, 2012).
The EBSOS for the treatment of pediatric asthma used in this study was developed and incorporated into the emergency department electronic ordering system because personnel were not consistently following national asthma treatment guidelines, according to a separate 2010 emergency department records review.
That review showed that 24% of patients admitted for status asthmaticus had not received the recommended ipratropium bromide treatment, and that only 14% of those who did receive ipratropium bromide received the recommended three consecutive doses.
Implementation of the EBSOS involved the use of an algorithm based on a validated Modified Pulmonary Index Score that allowed for triage nurse initiation of the EBSOS. The EBSOS called for continuous pulse oximetry, supplemental oxygen as needed, evaluation by a respiratory therapist, nebulized albuterol administration at 5 mg every 20 minutes for three treatments, administration of nebulized ipratropium bromide at 0.5 mg every 20 minutes for three treatments, and administration of one dose of oral prednisolone at 2 mg/kg up to a maximum of 60 mg.
"Implementation of an EBSOS improved compliance to national asthma guidelines, as evidenced by a higher proportion of pediatric emergency department patients in status asthmaticus receiving ipratropium bromide, as well as shortened time to delivery of inhaled bronchodilators and systemic steroids," Dr. Breslin concluded, noting that future analysis of this review will focus on patient-centered outcomes.
Dr. Breslin reported having no relevant financial disclosures
SAN ANTONIO – More of the children who present to the pediatric emergency department with asthma exacerbation received recommended care when the staff had instituted a nurse-initiated, evidence-based, standardized order set, according to Dr. Moira E. Breslin.
Specifically, the percentage of patients receiving at least one dose of ipratropium bromide improved from 55.4% before implementation of the order set to 90.9% after implementation. Compliance with the recommendation of the National Asthma Guidelines that patients receive three consecutive nebulized treatments of ipratropium bromide increased from 13.5% to 40.9%, Dr. Breslin of Duke University Medical Center, Durham, N.C., reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The median time to delivery of rescue medication also improved from 21 minutes to 14 minutes for first inhaled bronchodilator administration, and from 41 minutes to 19 minutes for delivery of systemic corticosteroids.
All differences were statistically significant.
The findings are based on a review of charts for 193 patients treated in the pediatric emergency department for status asthmaticus before implementation of the evidence-based standardized order set, or EBSOS, (between Feb. 23, 2009, and Feb. 22, 2012), and for 22 patients treated after implementation (between Feb. 23, 2012, and July 31, 2012).
The EBSOS for the treatment of pediatric asthma used in this study was developed and incorporated into the emergency department electronic ordering system because personnel were not consistently following national asthma treatment guidelines, according to a separate 2010 emergency department records review.
That review showed that 24% of patients admitted for status asthmaticus had not received the recommended ipratropium bromide treatment, and that only 14% of those who did receive ipratropium bromide received the recommended three consecutive doses.
Implementation of the EBSOS involved the use of an algorithm based on a validated Modified Pulmonary Index Score that allowed for triage nurse initiation of the EBSOS. The EBSOS called for continuous pulse oximetry, supplemental oxygen as needed, evaluation by a respiratory therapist, nebulized albuterol administration at 5 mg every 20 minutes for three treatments, administration of nebulized ipratropium bromide at 0.5 mg every 20 minutes for three treatments, and administration of one dose of oral prednisolone at 2 mg/kg up to a maximum of 60 mg.
"Implementation of an EBSOS improved compliance to national asthma guidelines, as evidenced by a higher proportion of pediatric emergency department patients in status asthmaticus receiving ipratropium bromide, as well as shortened time to delivery of inhaled bronchodilators and systemic steroids," Dr. Breslin concluded, noting that future analysis of this review will focus on patient-centered outcomes.
Dr. Breslin reported having no relevant financial disclosures
SAN ANTONIO – More of the children who present to the pediatric emergency department with asthma exacerbation received recommended care when the staff had instituted a nurse-initiated, evidence-based, standardized order set, according to Dr. Moira E. Breslin.
Specifically, the percentage of patients receiving at least one dose of ipratropium bromide improved from 55.4% before implementation of the order set to 90.9% after implementation. Compliance with the recommendation of the National Asthma Guidelines that patients receive three consecutive nebulized treatments of ipratropium bromide increased from 13.5% to 40.9%, Dr. Breslin of Duke University Medical Center, Durham, N.C., reported in a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The median time to delivery of rescue medication also improved from 21 minutes to 14 minutes for first inhaled bronchodilator administration, and from 41 minutes to 19 minutes for delivery of systemic corticosteroids.
All differences were statistically significant.
The findings are based on a review of charts for 193 patients treated in the pediatric emergency department for status asthmaticus before implementation of the evidence-based standardized order set, or EBSOS, (between Feb. 23, 2009, and Feb. 22, 2012), and for 22 patients treated after implementation (between Feb. 23, 2012, and July 31, 2012).
The EBSOS for the treatment of pediatric asthma used in this study was developed and incorporated into the emergency department electronic ordering system because personnel were not consistently following national asthma treatment guidelines, according to a separate 2010 emergency department records review.
That review showed that 24% of patients admitted for status asthmaticus had not received the recommended ipratropium bromide treatment, and that only 14% of those who did receive ipratropium bromide received the recommended three consecutive doses.
Implementation of the EBSOS involved the use of an algorithm based on a validated Modified Pulmonary Index Score that allowed for triage nurse initiation of the EBSOS. The EBSOS called for continuous pulse oximetry, supplemental oxygen as needed, evaluation by a respiratory therapist, nebulized albuterol administration at 5 mg every 20 minutes for three treatments, administration of nebulized ipratropium bromide at 0.5 mg every 20 minutes for three treatments, and administration of one dose of oral prednisolone at 2 mg/kg up to a maximum of 60 mg.
"Implementation of an EBSOS improved compliance to national asthma guidelines, as evidenced by a higher proportion of pediatric emergency department patients in status asthmaticus receiving ipratropium bromide, as well as shortened time to delivery of inhaled bronchodilators and systemic steroids," Dr. Breslin concluded, noting that future analysis of this review will focus on patient-centered outcomes.
Dr. Breslin reported having no relevant financial disclosures
AT THE AAAAI ANNUAL MEETING
Major finding: Before order set implementation, 55.4% of patients received at least one dose of ipratropium bromide, compared with 90.9% after EBSOS implementation.
Data source: A pre- and postintervention chart review.
Disclosures: Dr. Breslin reported having no relevant disclosures.
Use of electronic cigarettes on the rise
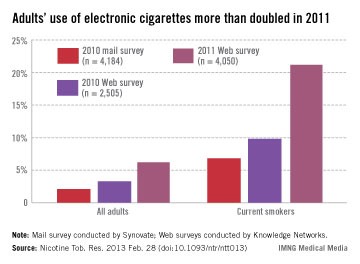
More than twice as many adult smokers used electronic cigarettes in 2011 as in 2010, according to investigators from the Centers for Disease Control and Prevention.
Approximately 21% of current smokers used electronic cigarettes at least once in 2011. The data come from Web-based surveys in 2010 and 2011 and one mail-based survey in 2010. For 2010, smokers’ use of e-cigarettes was 9.8% in the Web survey and 6.8% in the mail survey, said Brian A. King, Ph.D., and his associates at the CDC.
Among all adults, reported use of e-cigarettes was 6.2% in the 2011 survey, compared with 3.3% for the 2010 Web survey and 2.1% for the 2010 mail survey, they reported (Nicotine Tob. Res. 2013 Feb. 28 [doi:10.1093/ntr/ntt013]).
Among former smokers, e-cigarette use was 7.4% in the 2011 survey, 2.5% in the 2010 Web survey, and 0.6% in the 2010 mail survey. There was, however, "no significant difference in ever use of e-cigarettes ... by sex, age, race/ethnicity, education, income, or U.S. region" in any of the surveys, the investigators wrote.
Sample sizes were 4,050 for the 2011 Web survey, 2,505 for the 2010 Web survey, and 4,184 for the 2010 mail survey. Both Web-based surveys were conducted by Knowledge Networks; the mail-based survey was conducted by Synovate. Dr. King and his associates did not declare any financial conflicts of interest.

More than twice as many adult smokers used electronic cigarettes in 2011 as in 2010, according to investigators from the Centers for Disease Control and Prevention.
Approximately 21% of current smokers used electronic cigarettes at least once in 2011. The data come from Web-based surveys in 2010 and 2011 and one mail-based survey in 2010. For 2010, smokers’ use of e-cigarettes was 9.8% in the Web survey and 6.8% in the mail survey, said Brian A. King, Ph.D., and his associates at the CDC.
Among all adults, reported use of e-cigarettes was 6.2% in the 2011 survey, compared with 3.3% for the 2010 Web survey and 2.1% for the 2010 mail survey, they reported (Nicotine Tob. Res. 2013 Feb. 28 [doi:10.1093/ntr/ntt013]).
Among former smokers, e-cigarette use was 7.4% in the 2011 survey, 2.5% in the 2010 Web survey, and 0.6% in the 2010 mail survey. There was, however, "no significant difference in ever use of e-cigarettes ... by sex, age, race/ethnicity, education, income, or U.S. region" in any of the surveys, the investigators wrote.
Sample sizes were 4,050 for the 2011 Web survey, 2,505 for the 2010 Web survey, and 4,184 for the 2010 mail survey. Both Web-based surveys were conducted by Knowledge Networks; the mail-based survey was conducted by Synovate. Dr. King and his associates did not declare any financial conflicts of interest.
More than twice as many adult smokers used electronic cigarettes in 2011 as in 2010, according to investigators from the Centers for Disease Control and Prevention.
Approximately 21% of current smokers used electronic cigarettes at least once in 2011. The data come from Web-based surveys in 2010 and 2011 and one mail-based survey in 2010. For 2010, smokers’ use of e-cigarettes was 9.8% in the Web survey and 6.8% in the mail survey, said Brian A. King, Ph.D., and his associates at the CDC.
Among all adults, reported use of e-cigarettes was 6.2% in the 2011 survey, compared with 3.3% for the 2010 Web survey and 2.1% for the 2010 mail survey, they reported (Nicotine Tob. Res. 2013 Feb. 28 [doi:10.1093/ntr/ntt013]).
Among former smokers, e-cigarette use was 7.4% in the 2011 survey, 2.5% in the 2010 Web survey, and 0.6% in the 2010 mail survey. There was, however, "no significant difference in ever use of e-cigarettes ... by sex, age, race/ethnicity, education, income, or U.S. region" in any of the surveys, the investigators wrote.
Sample sizes were 4,050 for the 2011 Web survey, 2,505 for the 2010 Web survey, and 4,184 for the 2010 mail survey. Both Web-based surveys were conducted by Knowledge Networks; the mail-based survey was conducted by Synovate. Dr. King and his associates did not declare any financial conflicts of interest.
Rivaroxaban ACS indication remains unapproved, manufacturer says
The approval of the oral anticoagulant rivaroxaban for patients with acute coronary syndrome has been delayed for a second time by the Food and Drug Administration, according to the manufacturer, Janssen Pharmaceuticals.
In a March 4 statement, the company announced that the FDA has issued a second Complete Response Letter regarding the application for approval of rivaroxaban, a factor Xa inhibitor marketed as Xarelto, for reducing the risk of cardiovascular events in people with acute coronary syndrome (ACS). The statement says that in response to the FDA’s first Complete Response Letter, issued in June 2012, the company had submitted some of the missing data from the ATLAS ACS 2 TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Aspirin With/Without Thienopyridine Therapy in Subjects With Acute Coronary Syndrome) trial. The data were on 843 (63%) of the people enrolled in the study whose vital status was unknown, which, when included, did not affect the mortality benefit observed in the study, according to the statement.
The phase III ATLAS ACS 2 TIMI 51 results were submitted as part of the application filed in December 2011 for approval of rivaroxaban for reducing the risk of thrombotic cardiovascular events "in patients with ACS [ST-elevation myocardial infarction (STEMI), non–ST-elevation myocardial infarction (NSTEMI), or unstable angina] in combination with aspirin alone or with aspirin plus clopidogrel or ticlopidine," at a 2.5-mg twice-daily dose.
But at a meeting in May 2012, an FDA advisory panel voted 6 to 4, with 1 abstention, against approval of this indication, with those voting no citing a large amount of missing data and safety concerns among the reasons for their votes.
The company statement does not specify the FDA’s reasons for not approving the ACS indication. The FDA issues Complete Response Letters for a drug when there are outstanding issues that need to be resolved before approval, but does not announce when Complete Response Letters are issued. Like the last time, Janssen said that the company is evaluating the FDA’s letter and will continue to work with the FDA to respond to the agency’s questions.
In an interview, Dr. Sanjay Kaul, one of the FDA panelists who voted against approval at the May 2012 panel meeting, said that the company did "a commendable job" of obtaining vital status information in over 60% of those missing this information. However, data are missing in 3.2%, which "is still much higher than that reported in contemporary ACS trials such as TRITON, PLATO, APPRAISE II, or TRACER," he added.

Moreover, although concerns about the missing data dominated the panel deliberations, "it was not the only issue with potential relevance to the approvability of the expanded indication for rivaroxaban," said Dr. Kaul, a professor at the University of California, Los Angeles. Those issues included the lack of a dose response with the 2.5-mg, but not the 5-mg dose, yielding benefit; and "divergent effects" of the two doses on ischemic endpoints (reduction of CV mortality, but not MI, with 2.5 mg and reduction of MI, but not CV mortality, with the 5-mg dose).
Others issues raised at the meeting were the lack of external evidence supporting the role of dual antiplatelet regimen plus novel anticoagulant therapy and the lack of a statistically persuasive treatment benefit, as defined by a robust P value below .001, to allow approval on the basis of one trial, he said.
He said that while he could not speculate as to why the Complete Response Letter was issued, he would not be surprised "if any one or all of these issues played a major role in the FDA’s decision."
Dr. Kaul, who is also attending cardiologist at Cedars-Sinai Medical Center, Los Angeles, disclosed that he owns stock in Johnson & Johnson, of which Janssen is a subsidiary.
First approved in July 2011 for prophylaxis of deep vein thrombosis or pulmonary embolism in patients undergoing hip or knee replacement surgery, rivaroxaban is now approved for six indications, including the treatment of DVT or PE and for reducing the recurrence of DVT and PE after initial treatment.
The approval of the oral anticoagulant rivaroxaban for patients with acute coronary syndrome has been delayed for a second time by the Food and Drug Administration, according to the manufacturer, Janssen Pharmaceuticals.
In a March 4 statement, the company announced that the FDA has issued a second Complete Response Letter regarding the application for approval of rivaroxaban, a factor Xa inhibitor marketed as Xarelto, for reducing the risk of cardiovascular events in people with acute coronary syndrome (ACS). The statement says that in response to the FDA’s first Complete Response Letter, issued in June 2012, the company had submitted some of the missing data from the ATLAS ACS 2 TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Aspirin With/Without Thienopyridine Therapy in Subjects With Acute Coronary Syndrome) trial. The data were on 843 (63%) of the people enrolled in the study whose vital status was unknown, which, when included, did not affect the mortality benefit observed in the study, according to the statement.
The phase III ATLAS ACS 2 TIMI 51 results were submitted as part of the application filed in December 2011 for approval of rivaroxaban for reducing the risk of thrombotic cardiovascular events "in patients with ACS [ST-elevation myocardial infarction (STEMI), non–ST-elevation myocardial infarction (NSTEMI), or unstable angina] in combination with aspirin alone or with aspirin plus clopidogrel or ticlopidine," at a 2.5-mg twice-daily dose.
But at a meeting in May 2012, an FDA advisory panel voted 6 to 4, with 1 abstention, against approval of this indication, with those voting no citing a large amount of missing data and safety concerns among the reasons for their votes.
The company statement does not specify the FDA’s reasons for not approving the ACS indication. The FDA issues Complete Response Letters for a drug when there are outstanding issues that need to be resolved before approval, but does not announce when Complete Response Letters are issued. Like the last time, Janssen said that the company is evaluating the FDA’s letter and will continue to work with the FDA to respond to the agency’s questions.
In an interview, Dr. Sanjay Kaul, one of the FDA panelists who voted against approval at the May 2012 panel meeting, said that the company did "a commendable job" of obtaining vital status information in over 60% of those missing this information. However, data are missing in 3.2%, which "is still much higher than that reported in contemporary ACS trials such as TRITON, PLATO, APPRAISE II, or TRACER," he added.
Moreover, although concerns about the missing data dominated the panel deliberations, "it was not the only issue with potential relevance to the approvability of the expanded indication for rivaroxaban," said Dr. Kaul, a professor at the University of California, Los Angeles. Those issues included the lack of a dose response with the 2.5-mg, but not the 5-mg dose, yielding benefit; and "divergent effects" of the two doses on ischemic endpoints (reduction of CV mortality, but not MI, with 2.5 mg and reduction of MI, but not CV mortality, with the 5-mg dose).
Others issues raised at the meeting were the lack of external evidence supporting the role of dual antiplatelet regimen plus novel anticoagulant therapy and the lack of a statistically persuasive treatment benefit, as defined by a robust P value below .001, to allow approval on the basis of one trial, he said.
He said that while he could not speculate as to why the Complete Response Letter was issued, he would not be surprised "if any one or all of these issues played a major role in the FDA’s decision."
Dr. Kaul, who is also attending cardiologist at Cedars-Sinai Medical Center, Los Angeles, disclosed that he owns stock in Johnson & Johnson, of which Janssen is a subsidiary.
First approved in July 2011 for prophylaxis of deep vein thrombosis or pulmonary embolism in patients undergoing hip or knee replacement surgery, rivaroxaban is now approved for six indications, including the treatment of DVT or PE and for reducing the recurrence of DVT and PE after initial treatment.
The approval of the oral anticoagulant rivaroxaban for patients with acute coronary syndrome has been delayed for a second time by the Food and Drug Administration, according to the manufacturer, Janssen Pharmaceuticals.
In a March 4 statement, the company announced that the FDA has issued a second Complete Response Letter regarding the application for approval of rivaroxaban, a factor Xa inhibitor marketed as Xarelto, for reducing the risk of cardiovascular events in people with acute coronary syndrome (ACS). The statement says that in response to the FDA’s first Complete Response Letter, issued in June 2012, the company had submitted some of the missing data from the ATLAS ACS 2 TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Aspirin With/Without Thienopyridine Therapy in Subjects With Acute Coronary Syndrome) trial. The data were on 843 (63%) of the people enrolled in the study whose vital status was unknown, which, when included, did not affect the mortality benefit observed in the study, according to the statement.
The phase III ATLAS ACS 2 TIMI 51 results were submitted as part of the application filed in December 2011 for approval of rivaroxaban for reducing the risk of thrombotic cardiovascular events "in patients with ACS [ST-elevation myocardial infarction (STEMI), non–ST-elevation myocardial infarction (NSTEMI), or unstable angina] in combination with aspirin alone or with aspirin plus clopidogrel or ticlopidine," at a 2.5-mg twice-daily dose.
But at a meeting in May 2012, an FDA advisory panel voted 6 to 4, with 1 abstention, against approval of this indication, with those voting no citing a large amount of missing data and safety concerns among the reasons for their votes.
The company statement does not specify the FDA’s reasons for not approving the ACS indication. The FDA issues Complete Response Letters for a drug when there are outstanding issues that need to be resolved before approval, but does not announce when Complete Response Letters are issued. Like the last time, Janssen said that the company is evaluating the FDA’s letter and will continue to work with the FDA to respond to the agency’s questions.
In an interview, Dr. Sanjay Kaul, one of the FDA panelists who voted against approval at the May 2012 panel meeting, said that the company did "a commendable job" of obtaining vital status information in over 60% of those missing this information. However, data are missing in 3.2%, which "is still much higher than that reported in contemporary ACS trials such as TRITON, PLATO, APPRAISE II, or TRACER," he added.
Moreover, although concerns about the missing data dominated the panel deliberations, "it was not the only issue with potential relevance to the approvability of the expanded indication for rivaroxaban," said Dr. Kaul, a professor at the University of California, Los Angeles. Those issues included the lack of a dose response with the 2.5-mg, but not the 5-mg dose, yielding benefit; and "divergent effects" of the two doses on ischemic endpoints (reduction of CV mortality, but not MI, with 2.5 mg and reduction of MI, but not CV mortality, with the 5-mg dose).
Others issues raised at the meeting were the lack of external evidence supporting the role of dual antiplatelet regimen plus novel anticoagulant therapy and the lack of a statistically persuasive treatment benefit, as defined by a robust P value below .001, to allow approval on the basis of one trial, he said.
He said that while he could not speculate as to why the Complete Response Letter was issued, he would not be surprised "if any one or all of these issues played a major role in the FDA’s decision."
Dr. Kaul, who is also attending cardiologist at Cedars-Sinai Medical Center, Los Angeles, disclosed that he owns stock in Johnson & Johnson, of which Janssen is a subsidiary.
First approved in July 2011 for prophylaxis of deep vein thrombosis or pulmonary embolism in patients undergoing hip or knee replacement surgery, rivaroxaban is now approved for six indications, including the treatment of DVT or PE and for reducing the recurrence of DVT and PE after initial treatment.

'Contagion' movie built on the One Health message
The chilling final scene of the 2011 movie "Contagion" – which showed the birth of a deadly, worldwide pandemic when a presumably virus-laced morsel of food dropped from the claws of a jungle bat to a piglet that soon graced a Hong Kong restaurant table – won accolades for authenticity and accuracy at the International Meeting on Emerging Diseases and Surveillance in Vienna last month.
In fact, one of the meeting’s speakers, Dr. Mark Smolinski of the Skoll Global Threats Fund, revealed that he was a script consultant for the movie, and that an upfront goal of the film’s producers was to raise public awareness of how emerging infections can occur and the impact they can have.
"It’s an opportunity to use film to bring complicated issues to the general public," said Dr. Smolinski, director of global health for the fund in San Francisco.
A sister company of the Skoll Global Threats Fund is Participant Media, one of the producers of "Contagion." Participant usually releases documentary films, but in this case the "idea was to use a mainstream movie" to educate the public about pandemics and their causes, Dr. Smolinski said. "It emphasized the realities we have today, and a lot of the dialogue we have about One Health," the new paradigm that says animal health and the environment play key roles in determining human health.
"Contagion" began winning fans in the infectious diseases community when it opened 18 months ago. In a blog post, Dr. Larry Madoff, head epidemiologist for the Massachusetts Department of Health, said that in "Contagion," "the science is uncannily true, with rare exceptions. An epidemic like the one described in the film will almost certainly occur, though we can’t predict the details. The notion that an agent like Nipah virus, a pathogen shared by bats, pigs, and humans, and presumably the model for the virus in the movie, will break out of its niche and cause widespread disease is very believable." A not so-unlikely coincidence is that Dr. Madoff also was chairman of the program committee for the meeting last month on new infections where Dr. Smolinski spoke.
"We know that [the movie] has been used a lot for teaching students in various disciplines," Dr. Smolinski added. The movie’s famous last scene depicting the pandemic’s trigger portrays "One Health in one minute," he said.
–Mitchel Zoler
On Twitter @mitchelzoler
The chilling final scene of the 2011 movie "Contagion" – which showed the birth of a deadly, worldwide pandemic when a presumably virus-laced morsel of food dropped from the claws of a jungle bat to a piglet that soon graced a Hong Kong restaurant table – won accolades for authenticity and accuracy at the International Meeting on Emerging Diseases and Surveillance in Vienna last month.
In fact, one of the meeting’s speakers, Dr. Mark Smolinski of the Skoll Global Threats Fund, revealed that he was a script consultant for the movie, and that an upfront goal of the film’s producers was to raise public awareness of how emerging infections can occur and the impact they can have.
"It’s an opportunity to use film to bring complicated issues to the general public," said Dr. Smolinski, director of global health for the fund in San Francisco.
A sister company of the Skoll Global Threats Fund is Participant Media, one of the producers of "Contagion." Participant usually releases documentary films, but in this case the "idea was to use a mainstream movie" to educate the public about pandemics and their causes, Dr. Smolinski said. "It emphasized the realities we have today, and a lot of the dialogue we have about One Health," the new paradigm that says animal health and the environment play key roles in determining human health.
"Contagion" began winning fans in the infectious diseases community when it opened 18 months ago. In a blog post, Dr. Larry Madoff, head epidemiologist for the Massachusetts Department of Health, said that in "Contagion," "the science is uncannily true, with rare exceptions. An epidemic like the one described in the film will almost certainly occur, though we can’t predict the details. The notion that an agent like Nipah virus, a pathogen shared by bats, pigs, and humans, and presumably the model for the virus in the movie, will break out of its niche and cause widespread disease is very believable." A not so-unlikely coincidence is that Dr. Madoff also was chairman of the program committee for the meeting last month on new infections where Dr. Smolinski spoke.
"We know that [the movie] has been used a lot for teaching students in various disciplines," Dr. Smolinski added. The movie’s famous last scene depicting the pandemic’s trigger portrays "One Health in one minute," he said.
–Mitchel Zoler
On Twitter @mitchelzoler
The chilling final scene of the 2011 movie "Contagion" – which showed the birth of a deadly, worldwide pandemic when a presumably virus-laced morsel of food dropped from the claws of a jungle bat to a piglet that soon graced a Hong Kong restaurant table – won accolades for authenticity and accuracy at the International Meeting on Emerging Diseases and Surveillance in Vienna last month.
In fact, one of the meeting’s speakers, Dr. Mark Smolinski of the Skoll Global Threats Fund, revealed that he was a script consultant for the movie, and that an upfront goal of the film’s producers was to raise public awareness of how emerging infections can occur and the impact they can have.
"It’s an opportunity to use film to bring complicated issues to the general public," said Dr. Smolinski, director of global health for the fund in San Francisco.
A sister company of the Skoll Global Threats Fund is Participant Media, one of the producers of "Contagion." Participant usually releases documentary films, but in this case the "idea was to use a mainstream movie" to educate the public about pandemics and their causes, Dr. Smolinski said. "It emphasized the realities we have today, and a lot of the dialogue we have about One Health," the new paradigm that says animal health and the environment play key roles in determining human health.
"Contagion" began winning fans in the infectious diseases community when it opened 18 months ago. In a blog post, Dr. Larry Madoff, head epidemiologist for the Massachusetts Department of Health, said that in "Contagion," "the science is uncannily true, with rare exceptions. An epidemic like the one described in the film will almost certainly occur, though we can’t predict the details. The notion that an agent like Nipah virus, a pathogen shared by bats, pigs, and humans, and presumably the model for the virus in the movie, will break out of its niche and cause widespread disease is very believable." A not so-unlikely coincidence is that Dr. Madoff also was chairman of the program committee for the meeting last month on new infections where Dr. Smolinski spoke.
"We know that [the movie] has been used a lot for teaching students in various disciplines," Dr. Smolinski added. The movie’s famous last scene depicting the pandemic’s trigger portrays "One Health in one minute," he said.
–Mitchel Zoler
On Twitter @mitchelzoler
'Nightmare' CRE infections on the rise, CDC says
Between 2001 and 2011, the percentage of carbapenem-resistant Enterobacteriaceae infections reported by acute-care hospitals in the United States increased nearly fourfold, from 1.2% to 4.2%. More recent data from the first 6 months of 2102 suggest that the percentage of such infections is now slightly higher, at 4.6%.
The findings, which appear in a Vital Signs report released by the Centers for Disease Control and Prevention on March 5, are significant because CRE can kill up to 50% of patients who get bloodstream infections from them.

"It’s not often that our scientists come to me to say that we have a very serious problem and we need to sound an alarm," CDC Director Tom Frieden said during a related telephone press briefing. "But that’s exactly what we’re doing today. This Vital Signs is an early warning about a health care–associated infection that’s happening in hospitals and other inpatient medical facilities. The good news is that we now have an opportunity to prevent its further spread. The sooner we act, the less likely it will get out into the community."
For one component of the report, CDC researchers analyzed data from the National Healthcare Safety Network (NHSN) and its predecessor, the National Nosocomial Infections Surveillance system (NNIS), for the number of Enterobacteriaceae isolates; the percentage reported to be tested against carbapenems; and the percentage reported as carbapenem resistant in 2001 and in 2011. For another component, the researchers evaluated NHSN data for the number and percentage of facilities reporting CRE from a catheter-associated urinary tract infection or central line-associated bloodstream infection between January and June of 2012.
Of the CRE cases reported during the first half of 2012, about 18% occurred in long-term acute care hospitals and about 4% occurred in short-stay hospitals.
Dr. Frieden characterized CRE as a "nightmare bacteria" that poses a triple threat. "First, they’re resistant to all or nearly all antibiotics – even some of our last-resort drugs," he explained. "Second, they have high mortality rates. They kill up to half of people who get serious infections with them. And third, they can spread their resistance to other bacteria such as Escherichia coli and make E. coli resistant to those antibiotics also."
The risk of CRE infection is highest among patients who are receiving complex or long-term medical care, including those in short-stay hospitals or long-term acute care hospitals, or nursing homes. It’s commonly spread by people with unclean hands but "medical devices such as ventilators or catheters [also] increase the risk of life-threatening infection because they allow new bacteria to get deeply into a patient’s body," Dr. Frieden said.
According to the report, health care facilities in Northeastern states report the most cases of CRE, with 42 states reporting having had at least one patient test positive for the infection. In addition, one type of CRE, a resistant form of Klebsiella pneumoniae, demonstrated a nearly sevenfold increase between 2001 and 2011, jumping from 1.6% to 10.4%.
"That’s a very troubling increase," Dr. Frieden said. "In some of those places, these bacteria are now a routine challenge for patients and clinicians."
The good news, he continued, "is that we still have time to stop CRE. Many facilities can act now to prevent CRE from emerging or, if it has emerged, to control it. We need health care leaders, clinicians, and health care departments to act to prevent CRE, so it doesn’t become widespread and spread to the community." He listed six practical ways that health care providers can prevent CRE in their facilities:
• Know if your particular patient has CRE and request immediate alerts from your laboratory every time it identifies any patient with the infection.
• When receiving or transporting patients, make sure to ask or find out if the patient you’re receiving has CRE.
• Protect your patients from CRE by following contact and other precautions whenever you’re treating patients with CRE "so you don’t inadvertently spread their organism to someone else."
• Whenever possible, have specific rooms, equipment, and staff to care for CRE patients. "This reduces the chance that CRE will spread from one patient to others," he said.
• Remove temporary medical devices such as catheters as soon as possible.
• Prescribe antibiotics carefully. "Unfortunately, half of the antibiotics prescribed in this country are either unnecessary or inappropriate," Dr. Frieden said. "Overuse and misuse increases drug-resistant infections. That results in longer inpatient treatment, higher costs, and poorer patient outcomes."
These and other recommendations for hospitals, long-term acute care facilities, nursing homes, and health departments can be found in a CRE prevention toolkit released by the CDC in 2012. "We’re gratified to see that places that have implemented these tools have seen dramatic reductions in their CRE rates," Dr. Frieden said.
Authors of the report acknowledged at least three limitations of the data. First, they wrote, "antimicrobial susceptibility data reported to NNIS and NHSN were generated at individual institutions rather than [at] a central laboratory, and testing methodologies vary between facilities. Second, susceptibility interpretation is based on the recommended break points used when tested. Although carbapenem break points for Enterobacteriaceae were lowered in 2010 and might have influenced the increase in the percentage of isolates that were carbapenem-resistant, most laboratories would not have incorporated those changes by 2011. Finally, in some instances, complete susceptibility test results, particularly for carbapenems, were not reported to NNIS or NHSN, leading to a subset of isolates that were not included in these analyses."
The researchers reported having no relevant financial disclosures.
Between 2001 and 2011, the percentage of carbapenem-resistant Enterobacteriaceae infections reported by acute-care hospitals in the United States increased nearly fourfold, from 1.2% to 4.2%. More recent data from the first 6 months of 2102 suggest that the percentage of such infections is now slightly higher, at 4.6%.
The findings, which appear in a Vital Signs report released by the Centers for Disease Control and Prevention on March 5, are significant because CRE can kill up to 50% of patients who get bloodstream infections from them.
"It’s not often that our scientists come to me to say that we have a very serious problem and we need to sound an alarm," CDC Director Tom Frieden said during a related telephone press briefing. "But that’s exactly what we’re doing today. This Vital Signs is an early warning about a health care–associated infection that’s happening in hospitals and other inpatient medical facilities. The good news is that we now have an opportunity to prevent its further spread. The sooner we act, the less likely it will get out into the community."
For one component of the report, CDC researchers analyzed data from the National Healthcare Safety Network (NHSN) and its predecessor, the National Nosocomial Infections Surveillance system (NNIS), for the number of Enterobacteriaceae isolates; the percentage reported to be tested against carbapenems; and the percentage reported as carbapenem resistant in 2001 and in 2011. For another component, the researchers evaluated NHSN data for the number and percentage of facilities reporting CRE from a catheter-associated urinary tract infection or central line-associated bloodstream infection between January and June of 2012.
Of the CRE cases reported during the first half of 2012, about 18% occurred in long-term acute care hospitals and about 4% occurred in short-stay hospitals.
Dr. Frieden characterized CRE as a "nightmare bacteria" that poses a triple threat. "First, they’re resistant to all or nearly all antibiotics – even some of our last-resort drugs," he explained. "Second, they have high mortality rates. They kill up to half of people who get serious infections with them. And third, they can spread their resistance to other bacteria such as Escherichia coli and make E. coli resistant to those antibiotics also."
The risk of CRE infection is highest among patients who are receiving complex or long-term medical care, including those in short-stay hospitals or long-term acute care hospitals, or nursing homes. It’s commonly spread by people with unclean hands but "medical devices such as ventilators or catheters [also] increase the risk of life-threatening infection because they allow new bacteria to get deeply into a patient’s body," Dr. Frieden said.
According to the report, health care facilities in Northeastern states report the most cases of CRE, with 42 states reporting having had at least one patient test positive for the infection. In addition, one type of CRE, a resistant form of Klebsiella pneumoniae, demonstrated a nearly sevenfold increase between 2001 and 2011, jumping from 1.6% to 10.4%.
"That’s a very troubling increase," Dr. Frieden said. "In some of those places, these bacteria are now a routine challenge for patients and clinicians."
The good news, he continued, "is that we still have time to stop CRE. Many facilities can act now to prevent CRE from emerging or, if it has emerged, to control it. We need health care leaders, clinicians, and health care departments to act to prevent CRE, so it doesn’t become widespread and spread to the community." He listed six practical ways that health care providers can prevent CRE in their facilities:
• Know if your particular patient has CRE and request immediate alerts from your laboratory every time it identifies any patient with the infection.
• When receiving or transporting patients, make sure to ask or find out if the patient you’re receiving has CRE.
• Protect your patients from CRE by following contact and other precautions whenever you’re treating patients with CRE "so you don’t inadvertently spread their organism to someone else."
• Whenever possible, have specific rooms, equipment, and staff to care for CRE patients. "This reduces the chance that CRE will spread from one patient to others," he said.
• Remove temporary medical devices such as catheters as soon as possible.
• Prescribe antibiotics carefully. "Unfortunately, half of the antibiotics prescribed in this country are either unnecessary or inappropriate," Dr. Frieden said. "Overuse and misuse increases drug-resistant infections. That results in longer inpatient treatment, higher costs, and poorer patient outcomes."
These and other recommendations for hospitals, long-term acute care facilities, nursing homes, and health departments can be found in a CRE prevention toolkit released by the CDC in 2012. "We’re gratified to see that places that have implemented these tools have seen dramatic reductions in their CRE rates," Dr. Frieden said.
Authors of the report acknowledged at least three limitations of the data. First, they wrote, "antimicrobial susceptibility data reported to NNIS and NHSN were generated at individual institutions rather than [at] a central laboratory, and testing methodologies vary between facilities. Second, susceptibility interpretation is based on the recommended break points used when tested. Although carbapenem break points for Enterobacteriaceae were lowered in 2010 and might have influenced the increase in the percentage of isolates that were carbapenem-resistant, most laboratories would not have incorporated those changes by 2011. Finally, in some instances, complete susceptibility test results, particularly for carbapenems, were not reported to NNIS or NHSN, leading to a subset of isolates that were not included in these analyses."
The researchers reported having no relevant financial disclosures.
Between 2001 and 2011, the percentage of carbapenem-resistant Enterobacteriaceae infections reported by acute-care hospitals in the United States increased nearly fourfold, from 1.2% to 4.2%. More recent data from the first 6 months of 2102 suggest that the percentage of such infections is now slightly higher, at 4.6%.
The findings, which appear in a Vital Signs report released by the Centers for Disease Control and Prevention on March 5, are significant because CRE can kill up to 50% of patients who get bloodstream infections from them.
"It’s not often that our scientists come to me to say that we have a very serious problem and we need to sound an alarm," CDC Director Tom Frieden said during a related telephone press briefing. "But that’s exactly what we’re doing today. This Vital Signs is an early warning about a health care–associated infection that’s happening in hospitals and other inpatient medical facilities. The good news is that we now have an opportunity to prevent its further spread. The sooner we act, the less likely it will get out into the community."
For one component of the report, CDC researchers analyzed data from the National Healthcare Safety Network (NHSN) and its predecessor, the National Nosocomial Infections Surveillance system (NNIS), for the number of Enterobacteriaceae isolates; the percentage reported to be tested against carbapenems; and the percentage reported as carbapenem resistant in 2001 and in 2011. For another component, the researchers evaluated NHSN data for the number and percentage of facilities reporting CRE from a catheter-associated urinary tract infection or central line-associated bloodstream infection between January and June of 2012.
Of the CRE cases reported during the first half of 2012, about 18% occurred in long-term acute care hospitals and about 4% occurred in short-stay hospitals.
Dr. Frieden characterized CRE as a "nightmare bacteria" that poses a triple threat. "First, they’re resistant to all or nearly all antibiotics – even some of our last-resort drugs," he explained. "Second, they have high mortality rates. They kill up to half of people who get serious infections with them. And third, they can spread their resistance to other bacteria such as Escherichia coli and make E. coli resistant to those antibiotics also."
The risk of CRE infection is highest among patients who are receiving complex or long-term medical care, including those in short-stay hospitals or long-term acute care hospitals, or nursing homes. It’s commonly spread by people with unclean hands but "medical devices such as ventilators or catheters [also] increase the risk of life-threatening infection because they allow new bacteria to get deeply into a patient’s body," Dr. Frieden said.
According to the report, health care facilities in Northeastern states report the most cases of CRE, with 42 states reporting having had at least one patient test positive for the infection. In addition, one type of CRE, a resistant form of Klebsiella pneumoniae, demonstrated a nearly sevenfold increase between 2001 and 2011, jumping from 1.6% to 10.4%.
"That’s a very troubling increase," Dr. Frieden said. "In some of those places, these bacteria are now a routine challenge for patients and clinicians."
The good news, he continued, "is that we still have time to stop CRE. Many facilities can act now to prevent CRE from emerging or, if it has emerged, to control it. We need health care leaders, clinicians, and health care departments to act to prevent CRE, so it doesn’t become widespread and spread to the community." He listed six practical ways that health care providers can prevent CRE in their facilities:
• Know if your particular patient has CRE and request immediate alerts from your laboratory every time it identifies any patient with the infection.
• When receiving or transporting patients, make sure to ask or find out if the patient you’re receiving has CRE.
• Protect your patients from CRE by following contact and other precautions whenever you’re treating patients with CRE "so you don’t inadvertently spread their organism to someone else."
• Whenever possible, have specific rooms, equipment, and staff to care for CRE patients. "This reduces the chance that CRE will spread from one patient to others," he said.
• Remove temporary medical devices such as catheters as soon as possible.
• Prescribe antibiotics carefully. "Unfortunately, half of the antibiotics prescribed in this country are either unnecessary or inappropriate," Dr. Frieden said. "Overuse and misuse increases drug-resistant infections. That results in longer inpatient treatment, higher costs, and poorer patient outcomes."
These and other recommendations for hospitals, long-term acute care facilities, nursing homes, and health departments can be found in a CRE prevention toolkit released by the CDC in 2012. "We’re gratified to see that places that have implemented these tools have seen dramatic reductions in their CRE rates," Dr. Frieden said.
Authors of the report acknowledged at least three limitations of the data. First, they wrote, "antimicrobial susceptibility data reported to NNIS and NHSN were generated at individual institutions rather than [at] a central laboratory, and testing methodologies vary between facilities. Second, susceptibility interpretation is based on the recommended break points used when tested. Although carbapenem break points for Enterobacteriaceae were lowered in 2010 and might have influenced the increase in the percentage of isolates that were carbapenem-resistant, most laboratories would not have incorporated those changes by 2011. Finally, in some instances, complete susceptibility test results, particularly for carbapenems, were not reported to NNIS or NHSN, leading to a subset of isolates that were not included in these analyses."
The researchers reported having no relevant financial disclosures.
FROM CDC VITAL SIGNS
Major Finding: The percentage of carbapenem-resistant Enterobacteriaceae infections reported by acute-care hospitals in the United States increased from 1.2% in 2001 to 4.2% in 2011.
Data Source: CDC analysis of data from the National Healthcare Safety Network (NHSN) and its predecessor, the National Nosocomial Infections Surveillance system (NNIS).
Disclosures: The researchers reported having no relevant financial conflicts.