User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Lung cancer rates highest in West Virginia
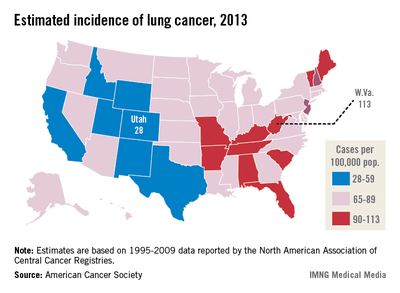
The incidence of lung cancer in the United States for 2013 is expected to be highest in West Virginia and lowest in Utah, according to the American Cancer Society.
The estimated incidence is approximately 113 cases per 100,000 population in West Virginia and 28 cases per 100,000 in Utah. Nationally, it is estimated that there will be approximately 228,190 new cases in 2013, for an incidence of about 73 cases per 100,000 people, according to the ACS data.
The incidence of lung cancer in the United States for 2013 is expected to be highest in West Virginia and lowest in Utah, according to the American Cancer Society.
The estimated incidence is approximately 113 cases per 100,000 population in West Virginia and 28 cases per 100,000 in Utah. Nationally, it is estimated that there will be approximately 228,190 new cases in 2013, for an incidence of about 73 cases per 100,000 people, according to the ACS data.
The incidence of lung cancer in the United States for 2013 is expected to be highest in West Virginia and lowest in Utah, according to the American Cancer Society.
The estimated incidence is approximately 113 cases per 100,000 population in West Virginia and 28 cases per 100,000 in Utah. Nationally, it is estimated that there will be approximately 228,190 new cases in 2013, for an incidence of about 73 cases per 100,000 people, according to the ACS data.
Tailored online feedback may boost asthma control
SAN FRANCISCO – A website designed to give people with asthma tailored feedback about whether they need to see a doctor and what questions to ask when they do may have helped improve asthma control in a randomized, controlled trial in 325 patients.
The study randomized patients to get access to one of two modules in a "patient activation website." The asthma module provided tailored feedback about patients’ asthma control, helped them decide whether they needed to visit a medical provider sooner than already scheduled, and suggested questions for patients to ask their providers. The control group got access to a module that suggested questions they should ask their primary care providers about preventive services such as cancer screening.
Among 325 adults who completed 12 months of follow-up (157 in the intervention group and 168 in the control group), measures of asthma control improved significantly in both groups, with most measures improving significantly more in the intervention group compared with the control group.
Mean scores on the Asthma Control Test (ACT) increased from 17.7 at baseline to 19.9 at 12 months in the intervention group and from 17.9 to 19.1 in the control group, both of which were significant improvements. The greater improvement in the intervention group was statistically significant compared with the control group, Jennifer M. Poger and her associates reported in a poster presentation at the annual meeting of the Society of Behavioral Medicine.
The proportions of patients with controlled asthma (defined as an ACT score of 20 or greater) increased from 50% at baseline to 73% at 12 months in the intervention group and from 53% to 67% in the control group, both of which were statistically significant improvements. The difference between groups, however, did not reach statistical significance, reported Ms. Poger, a researcher at Pennsylvania State University, Hershey, Penn.
The mean number of inhaled asthma medications being used increased by 0.4 in the intervention group between baseline and the 12-month follow-up, compared with 0.2 more medications in the control group, a statistically significant difference between groups.
The results suggest that websites that provide tailored feedback to patients with chronic conditions such as asthma may help them control their diseases, Ms. Poger said.
The investigators’ financial disclosures were not available.
SAN FRANCISCO – A website designed to give people with asthma tailored feedback about whether they need to see a doctor and what questions to ask when they do may have helped improve asthma control in a randomized, controlled trial in 325 patients.
The study randomized patients to get access to one of two modules in a "patient activation website." The asthma module provided tailored feedback about patients’ asthma control, helped them decide whether they needed to visit a medical provider sooner than already scheduled, and suggested questions for patients to ask their providers. The control group got access to a module that suggested questions they should ask their primary care providers about preventive services such as cancer screening.
Among 325 adults who completed 12 months of follow-up (157 in the intervention group and 168 in the control group), measures of asthma control improved significantly in both groups, with most measures improving significantly more in the intervention group compared with the control group.
Mean scores on the Asthma Control Test (ACT) increased from 17.7 at baseline to 19.9 at 12 months in the intervention group and from 17.9 to 19.1 in the control group, both of which were significant improvements. The greater improvement in the intervention group was statistically significant compared with the control group, Jennifer M. Poger and her associates reported in a poster presentation at the annual meeting of the Society of Behavioral Medicine.
The proportions of patients with controlled asthma (defined as an ACT score of 20 or greater) increased from 50% at baseline to 73% at 12 months in the intervention group and from 53% to 67% in the control group, both of which were statistically significant improvements. The difference between groups, however, did not reach statistical significance, reported Ms. Poger, a researcher at Pennsylvania State University, Hershey, Penn.
The mean number of inhaled asthma medications being used increased by 0.4 in the intervention group between baseline and the 12-month follow-up, compared with 0.2 more medications in the control group, a statistically significant difference between groups.
The results suggest that websites that provide tailored feedback to patients with chronic conditions such as asthma may help them control their diseases, Ms. Poger said.
The investigators’ financial disclosures were not available.
SAN FRANCISCO – A website designed to give people with asthma tailored feedback about whether they need to see a doctor and what questions to ask when they do may have helped improve asthma control in a randomized, controlled trial in 325 patients.
The study randomized patients to get access to one of two modules in a "patient activation website." The asthma module provided tailored feedback about patients’ asthma control, helped them decide whether they needed to visit a medical provider sooner than already scheduled, and suggested questions for patients to ask their providers. The control group got access to a module that suggested questions they should ask their primary care providers about preventive services such as cancer screening.
Among 325 adults who completed 12 months of follow-up (157 in the intervention group and 168 in the control group), measures of asthma control improved significantly in both groups, with most measures improving significantly more in the intervention group compared with the control group.
Mean scores on the Asthma Control Test (ACT) increased from 17.7 at baseline to 19.9 at 12 months in the intervention group and from 17.9 to 19.1 in the control group, both of which were significant improvements. The greater improvement in the intervention group was statistically significant compared with the control group, Jennifer M. Poger and her associates reported in a poster presentation at the annual meeting of the Society of Behavioral Medicine.
The proportions of patients with controlled asthma (defined as an ACT score of 20 or greater) increased from 50% at baseline to 73% at 12 months in the intervention group and from 53% to 67% in the control group, both of which were statistically significant improvements. The difference between groups, however, did not reach statistical significance, reported Ms. Poger, a researcher at Pennsylvania State University, Hershey, Penn.
The mean number of inhaled asthma medications being used increased by 0.4 in the intervention group between baseline and the 12-month follow-up, compared with 0.2 more medications in the control group, a statistically significant difference between groups.
The results suggest that websites that provide tailored feedback to patients with chronic conditions such as asthma may help them control their diseases, Ms. Poger said.
The investigators’ financial disclosures were not available.
AT THE ANNUAL MEETING OF THE SOCIETY OF BEHAVIORAL MEDICINE
Immunotherapy for kids' food allergies is taking baby steps
SAN ANTONIO – Oral and sublingual immunotherapy strategies aren’t yet ready for prime time, but they continue to show promise for inducing tolerance in children with food allergies.
Oral immunotherapy
Preliminary findings from a study of low-dose oral immunotherapy (OIT) for peanut allergy, for example, suggest this approach is an effective early-intervention strategy, Dr. Brian Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a randomized, controlled trial involving 49 peanut-sensitized children aged 9-36 months, both low- and high-dose immunotherapy resulted in a significant reduction in both peanut-specific IgE (psIgE) and skin prick test values after a median of 19 treatments, said Dr. Vickery, who is a pediatric allergist and immunologist at the University of North Carolina at Chapel Hill.
The degree of change was similar in those treated with low-dose and high-dose oral immunotherapy. The low dose slope coefficient for psIgE was -2.53 for the low dose group, compared with –1.63 for the high-dose group; and the low dose slope coefficient for the skin prick test was –0.007, compared with –0.009 for the high-dose group, he said.
Of eight subjects who met the criteria for tolerance evaluation as of the time of Dr. Vickery’s presentation, seven had successfully achieved tolerance and now eat peanut ad lib, he noted.
Study subjects were enrolled within 6 months of their index reaction or demonstration of psIgE greater than 5 kUA/L. After randomization to the low- or high-dose treatment group, they underwent serial analysis of immune responses. After at least 1 year of maintenance oral immunotherapy, clinical tolerance was assessed using a double-blinded placebo-controlled oral food challenge based on predefined clinical and immunologic benchmarks.
The findings are preliminary but suggest that early-intervention peanut oral immunotherapy is a feasible strategy. In addition, low-dose oral immunotherapy – using a 10-fold lower dose of peanut protein (the equivalent of about 1 vs. 10 peanuts comprised the maintenance doses in the low- and high-dose groups, respectively) may be sufficiently immunomodulatory in young children with newly diagnosed peanut allergy, Dr. Vickery said during a press briefing at the meeting.
Furthermore, the findings suggest that such an approach is technically possible in that young children can be recruited and treated in this manner, he noted.
Dr. Robert A. Wood, who is chief of the division of allergy and immunology at Hopkins Children’s Center at Johns Hopkins University, Baltimore, and who also presented oral immunotherapy data, noted during the press briefing that the approach used in this study "is sort of seizing on the opportunity that maybe kids early in life, when their allergy is less established, may be more amenable to treatment."
Peanut allergy that manifests in early childhood typically intensifies over 5-10 years, he explained.
The findings, however, are very preliminary.
"In order for us to really understand the impact of these two doses, we will need to assess all of the endpoints in all of the subjects who are currently enrolled, and then unblind the study at the end of it, and do an assessment to really understand whether low or high dose therapy was effective," Dr. Vickery said.
Sublingual immunotherapy
Sublingual immunotherapy (SLIT) is another promising intervention for food allergic children, according to findings from a study presented by Dr. A. Wesley Burks, who is chair of pediatrics at the University of North Carolina at Chapel Hill and physician in chief of N.C. Children’s Hospital, also in Chapel Hill.
Interim data from that study of 44 patients showed that after 36 months of dosing, peanut SLIT–induced clinical tolerance with concurrent changes in skin testing and peanut-specific immunoglobulin levels.
Of 11 patients who completed 36 months of dosing, 6 passed a peanut oral food challenge to 5,000 mg of peanut protein. The remaining five patients ingested a median of 3,750 mg of peanut protein. After SLIT discontinuation for 1 month, five of six passed an identical oral food challenge, suggesting clinical tolerance.
Children in this study were aged 2-11 years. All received open-label peanut SLIT with a daily maintenance dose of 2 mg of peanut protein, Dr. Burks said.
The findings do not say anything about long-term efficacy of SLIT, but they do show that tolerance can be induced, at least in the short term, Dr. Burke said.
Predictors of tolerance induction
Another study presented by Dr. Burke shed some light on factors associated with induction of tolerance, namely basophil hyporesponsiveness and a low peanut IgE:IgG4 ratio.
In that study of 12 patients who received SLIT and 27 who received OIT, 5 (41.7%) and 18 (66.7%), respectively, developed tolerance following immunotherapy. In the SLIT subjects, basophil responses were significantly lower among those who developed tolerance than among those who did not. This was true for each of the 4 log-fold dilutions of peanut antigen used in the assay, Dr. Burks said.
The vast majority of tolerant subjects (91.3%) had a peanut-IgE:IgG4 ratio below 0.92, compared with only 20% of nontolerant subjects.
All subjects underwent double-blind placebo-controlled food challenges to assess desensitization while they were on daily immunotherapy, and those passing the challenge ceased daily therapy and avoided all peanut products for 4 weeks. At 4 weeks, a second food challenge was administered.
The findings suggest that basophil suppression and the balance of antigen-specific IgE and IgG4 may be important in the development of tolerance following peanut immunotherapy, Dr. Burks said.
Long-term immunotherapy outcomes
One missing piece of the immunotherapy puzzle are data on long-term outcomes, as most studies report only 1-2 year outcomes. Another study presented by Dr. Wood, however, takes a step toward filling the gap – with underwhelming results.
The small study looked at long-term outcomes following milk oral immunotherapy in children, and showed that at 4.5 year follow-up, only about 25% of 32 patients were tolerating at least one serving of milk daily and 25% were consuming only trace amounts or were on strict avoidance mainly because of reactions. About 40% of patients were having frequent reactions to milk, 20% had required epinephrine for reactions, and 30% had experienced systemic reactions.
The patients were treated in two studies during 2006 and 2007 with a dose escalation to 500 mg of milk protein over about 8 weeks, followed by 3 months of maintenance dosing. Dietary milk was introduced in amounts ranging from 500 to 4,000 mg daily based on the results of a double-blind placebo-controlled food challenge.
Of note, one subject who passed a 16-g challenge without symptoms went on to become reactive again and now consumes only minimal milk, Dr. Wood said
In fact, one of the surprising things in this study was that some of the more dramatic failures long-term were in children who had achieved success in the initial studies.
These were children who "looked like absolute successes" at the end of the study, because there were tolerating large amounts of milk, he said.
"We really thought – and we hesitate to use the word "cure" – that they were about as close to cured as we could really imagine. And now, 3-5 years later, they are having anaphylactic reactions and are back on strict milk avoidance," he said.
As a result, the excitement following the initial studies has waned somewhat.
"We had a very high degree of optimism. I’m not saying we lost that optimism, but it is certainly tempered a bit by looking at where these kids now stand 3-5 years out," he said, concluding that more research with respect to long-term outcomes of food oral immunotherapy is needed, including investigation of whether longer treatment would improve outcomes, and whether certain factors can predict response and failure.
"The most important message is that this sort of adds another caveat about why we need more research before we can bring this out to our patient population. A message that I think all of us who are doing this research have come to agree upon is that we need long-term follow-up and that letting these kids go at the end of the study is not the end of the story."
Taken together, the findings of these studies underscore a need for more research regarding SLIT vs. OIT, higher vs. lower dosing, and treatment duration, as well as long-term follow-up, the investigators agreed.
"The message is that what we are doing so far is very encouraging, but it’s not the final answer. Where we need to be to bring this out to the general public is several steps beyond where we are now," Dr. Wood said.
The investigators reported having no disclosures.
SAN ANTONIO – Oral and sublingual immunotherapy strategies aren’t yet ready for prime time, but they continue to show promise for inducing tolerance in children with food allergies.
Oral immunotherapy
Preliminary findings from a study of low-dose oral immunotherapy (OIT) for peanut allergy, for example, suggest this approach is an effective early-intervention strategy, Dr. Brian Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a randomized, controlled trial involving 49 peanut-sensitized children aged 9-36 months, both low- and high-dose immunotherapy resulted in a significant reduction in both peanut-specific IgE (psIgE) and skin prick test values after a median of 19 treatments, said Dr. Vickery, who is a pediatric allergist and immunologist at the University of North Carolina at Chapel Hill.
The degree of change was similar in those treated with low-dose and high-dose oral immunotherapy. The low dose slope coefficient for psIgE was -2.53 for the low dose group, compared with –1.63 for the high-dose group; and the low dose slope coefficient for the skin prick test was –0.007, compared with –0.009 for the high-dose group, he said.
Of eight subjects who met the criteria for tolerance evaluation as of the time of Dr. Vickery’s presentation, seven had successfully achieved tolerance and now eat peanut ad lib, he noted.
Study subjects were enrolled within 6 months of their index reaction or demonstration of psIgE greater than 5 kUA/L. After randomization to the low- or high-dose treatment group, they underwent serial analysis of immune responses. After at least 1 year of maintenance oral immunotherapy, clinical tolerance was assessed using a double-blinded placebo-controlled oral food challenge based on predefined clinical and immunologic benchmarks.
The findings are preliminary but suggest that early-intervention peanut oral immunotherapy is a feasible strategy. In addition, low-dose oral immunotherapy – using a 10-fold lower dose of peanut protein (the equivalent of about 1 vs. 10 peanuts comprised the maintenance doses in the low- and high-dose groups, respectively) may be sufficiently immunomodulatory in young children with newly diagnosed peanut allergy, Dr. Vickery said during a press briefing at the meeting.
Furthermore, the findings suggest that such an approach is technically possible in that young children can be recruited and treated in this manner, he noted.
Dr. Robert A. Wood, who is chief of the division of allergy and immunology at Hopkins Children’s Center at Johns Hopkins University, Baltimore, and who also presented oral immunotherapy data, noted during the press briefing that the approach used in this study "is sort of seizing on the opportunity that maybe kids early in life, when their allergy is less established, may be more amenable to treatment."
Peanut allergy that manifests in early childhood typically intensifies over 5-10 years, he explained.
The findings, however, are very preliminary.
"In order for us to really understand the impact of these two doses, we will need to assess all of the endpoints in all of the subjects who are currently enrolled, and then unblind the study at the end of it, and do an assessment to really understand whether low or high dose therapy was effective," Dr. Vickery said.
Sublingual immunotherapy
Sublingual immunotherapy (SLIT) is another promising intervention for food allergic children, according to findings from a study presented by Dr. A. Wesley Burks, who is chair of pediatrics at the University of North Carolina at Chapel Hill and physician in chief of N.C. Children’s Hospital, also in Chapel Hill.
Interim data from that study of 44 patients showed that after 36 months of dosing, peanut SLIT–induced clinical tolerance with concurrent changes in skin testing and peanut-specific immunoglobulin levels.
Of 11 patients who completed 36 months of dosing, 6 passed a peanut oral food challenge to 5,000 mg of peanut protein. The remaining five patients ingested a median of 3,750 mg of peanut protein. After SLIT discontinuation for 1 month, five of six passed an identical oral food challenge, suggesting clinical tolerance.
Children in this study were aged 2-11 years. All received open-label peanut SLIT with a daily maintenance dose of 2 mg of peanut protein, Dr. Burks said.
The findings do not say anything about long-term efficacy of SLIT, but they do show that tolerance can be induced, at least in the short term, Dr. Burke said.
Predictors of tolerance induction
Another study presented by Dr. Burke shed some light on factors associated with induction of tolerance, namely basophil hyporesponsiveness and a low peanut IgE:IgG4 ratio.
In that study of 12 patients who received SLIT and 27 who received OIT, 5 (41.7%) and 18 (66.7%), respectively, developed tolerance following immunotherapy. In the SLIT subjects, basophil responses were significantly lower among those who developed tolerance than among those who did not. This was true for each of the 4 log-fold dilutions of peanut antigen used in the assay, Dr. Burks said.
The vast majority of tolerant subjects (91.3%) had a peanut-IgE:IgG4 ratio below 0.92, compared with only 20% of nontolerant subjects.
All subjects underwent double-blind placebo-controlled food challenges to assess desensitization while they were on daily immunotherapy, and those passing the challenge ceased daily therapy and avoided all peanut products for 4 weeks. At 4 weeks, a second food challenge was administered.
The findings suggest that basophil suppression and the balance of antigen-specific IgE and IgG4 may be important in the development of tolerance following peanut immunotherapy, Dr. Burks said.
Long-term immunotherapy outcomes
One missing piece of the immunotherapy puzzle are data on long-term outcomes, as most studies report only 1-2 year outcomes. Another study presented by Dr. Wood, however, takes a step toward filling the gap – with underwhelming results.
The small study looked at long-term outcomes following milk oral immunotherapy in children, and showed that at 4.5 year follow-up, only about 25% of 32 patients were tolerating at least one serving of milk daily and 25% were consuming only trace amounts or were on strict avoidance mainly because of reactions. About 40% of patients were having frequent reactions to milk, 20% had required epinephrine for reactions, and 30% had experienced systemic reactions.
The patients were treated in two studies during 2006 and 2007 with a dose escalation to 500 mg of milk protein over about 8 weeks, followed by 3 months of maintenance dosing. Dietary milk was introduced in amounts ranging from 500 to 4,000 mg daily based on the results of a double-blind placebo-controlled food challenge.
Of note, one subject who passed a 16-g challenge without symptoms went on to become reactive again and now consumes only minimal milk, Dr. Wood said
In fact, one of the surprising things in this study was that some of the more dramatic failures long-term were in children who had achieved success in the initial studies.
These were children who "looked like absolute successes" at the end of the study, because there were tolerating large amounts of milk, he said.
"We really thought – and we hesitate to use the word "cure" – that they were about as close to cured as we could really imagine. And now, 3-5 years later, they are having anaphylactic reactions and are back on strict milk avoidance," he said.
As a result, the excitement following the initial studies has waned somewhat.
"We had a very high degree of optimism. I’m not saying we lost that optimism, but it is certainly tempered a bit by looking at where these kids now stand 3-5 years out," he said, concluding that more research with respect to long-term outcomes of food oral immunotherapy is needed, including investigation of whether longer treatment would improve outcomes, and whether certain factors can predict response and failure.
"The most important message is that this sort of adds another caveat about why we need more research before we can bring this out to our patient population. A message that I think all of us who are doing this research have come to agree upon is that we need long-term follow-up and that letting these kids go at the end of the study is not the end of the story."
Taken together, the findings of these studies underscore a need for more research regarding SLIT vs. OIT, higher vs. lower dosing, and treatment duration, as well as long-term follow-up, the investigators agreed.
"The message is that what we are doing so far is very encouraging, but it’s not the final answer. Where we need to be to bring this out to the general public is several steps beyond where we are now," Dr. Wood said.
The investigators reported having no disclosures.
SAN ANTONIO – Oral and sublingual immunotherapy strategies aren’t yet ready for prime time, but they continue to show promise for inducing tolerance in children with food allergies.
Oral immunotherapy
Preliminary findings from a study of low-dose oral immunotherapy (OIT) for peanut allergy, for example, suggest this approach is an effective early-intervention strategy, Dr. Brian Vickery reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a randomized, controlled trial involving 49 peanut-sensitized children aged 9-36 months, both low- and high-dose immunotherapy resulted in a significant reduction in both peanut-specific IgE (psIgE) and skin prick test values after a median of 19 treatments, said Dr. Vickery, who is a pediatric allergist and immunologist at the University of North Carolina at Chapel Hill.
The degree of change was similar in those treated with low-dose and high-dose oral immunotherapy. The low dose slope coefficient for psIgE was -2.53 for the low dose group, compared with –1.63 for the high-dose group; and the low dose slope coefficient for the skin prick test was –0.007, compared with –0.009 for the high-dose group, he said.
Of eight subjects who met the criteria for tolerance evaluation as of the time of Dr. Vickery’s presentation, seven had successfully achieved tolerance and now eat peanut ad lib, he noted.
Study subjects were enrolled within 6 months of their index reaction or demonstration of psIgE greater than 5 kUA/L. After randomization to the low- or high-dose treatment group, they underwent serial analysis of immune responses. After at least 1 year of maintenance oral immunotherapy, clinical tolerance was assessed using a double-blinded placebo-controlled oral food challenge based on predefined clinical and immunologic benchmarks.
The findings are preliminary but suggest that early-intervention peanut oral immunotherapy is a feasible strategy. In addition, low-dose oral immunotherapy – using a 10-fold lower dose of peanut protein (the equivalent of about 1 vs. 10 peanuts comprised the maintenance doses in the low- and high-dose groups, respectively) may be sufficiently immunomodulatory in young children with newly diagnosed peanut allergy, Dr. Vickery said during a press briefing at the meeting.
Furthermore, the findings suggest that such an approach is technically possible in that young children can be recruited and treated in this manner, he noted.
Dr. Robert A. Wood, who is chief of the division of allergy and immunology at Hopkins Children’s Center at Johns Hopkins University, Baltimore, and who also presented oral immunotherapy data, noted during the press briefing that the approach used in this study "is sort of seizing on the opportunity that maybe kids early in life, when their allergy is less established, may be more amenable to treatment."
Peanut allergy that manifests in early childhood typically intensifies over 5-10 years, he explained.
The findings, however, are very preliminary.
"In order for us to really understand the impact of these two doses, we will need to assess all of the endpoints in all of the subjects who are currently enrolled, and then unblind the study at the end of it, and do an assessment to really understand whether low or high dose therapy was effective," Dr. Vickery said.
Sublingual immunotherapy
Sublingual immunotherapy (SLIT) is another promising intervention for food allergic children, according to findings from a study presented by Dr. A. Wesley Burks, who is chair of pediatrics at the University of North Carolina at Chapel Hill and physician in chief of N.C. Children’s Hospital, also in Chapel Hill.
Interim data from that study of 44 patients showed that after 36 months of dosing, peanut SLIT–induced clinical tolerance with concurrent changes in skin testing and peanut-specific immunoglobulin levels.
Of 11 patients who completed 36 months of dosing, 6 passed a peanut oral food challenge to 5,000 mg of peanut protein. The remaining five patients ingested a median of 3,750 mg of peanut protein. After SLIT discontinuation for 1 month, five of six passed an identical oral food challenge, suggesting clinical tolerance.
Children in this study were aged 2-11 years. All received open-label peanut SLIT with a daily maintenance dose of 2 mg of peanut protein, Dr. Burks said.
The findings do not say anything about long-term efficacy of SLIT, but they do show that tolerance can be induced, at least in the short term, Dr. Burke said.
Predictors of tolerance induction
Another study presented by Dr. Burke shed some light on factors associated with induction of tolerance, namely basophil hyporesponsiveness and a low peanut IgE:IgG4 ratio.
In that study of 12 patients who received SLIT and 27 who received OIT, 5 (41.7%) and 18 (66.7%), respectively, developed tolerance following immunotherapy. In the SLIT subjects, basophil responses were significantly lower among those who developed tolerance than among those who did not. This was true for each of the 4 log-fold dilutions of peanut antigen used in the assay, Dr. Burks said.
The vast majority of tolerant subjects (91.3%) had a peanut-IgE:IgG4 ratio below 0.92, compared with only 20% of nontolerant subjects.
All subjects underwent double-blind placebo-controlled food challenges to assess desensitization while they were on daily immunotherapy, and those passing the challenge ceased daily therapy and avoided all peanut products for 4 weeks. At 4 weeks, a second food challenge was administered.
The findings suggest that basophil suppression and the balance of antigen-specific IgE and IgG4 may be important in the development of tolerance following peanut immunotherapy, Dr. Burks said.
Long-term immunotherapy outcomes
One missing piece of the immunotherapy puzzle are data on long-term outcomes, as most studies report only 1-2 year outcomes. Another study presented by Dr. Wood, however, takes a step toward filling the gap – with underwhelming results.
The small study looked at long-term outcomes following milk oral immunotherapy in children, and showed that at 4.5 year follow-up, only about 25% of 32 patients were tolerating at least one serving of milk daily and 25% were consuming only trace amounts or were on strict avoidance mainly because of reactions. About 40% of patients were having frequent reactions to milk, 20% had required epinephrine for reactions, and 30% had experienced systemic reactions.
The patients were treated in two studies during 2006 and 2007 with a dose escalation to 500 mg of milk protein over about 8 weeks, followed by 3 months of maintenance dosing. Dietary milk was introduced in amounts ranging from 500 to 4,000 mg daily based on the results of a double-blind placebo-controlled food challenge.
Of note, one subject who passed a 16-g challenge without symptoms went on to become reactive again and now consumes only minimal milk, Dr. Wood said
In fact, one of the surprising things in this study was that some of the more dramatic failures long-term were in children who had achieved success in the initial studies.
These were children who "looked like absolute successes" at the end of the study, because there were tolerating large amounts of milk, he said.
"We really thought – and we hesitate to use the word "cure" – that they were about as close to cured as we could really imagine. And now, 3-5 years later, they are having anaphylactic reactions and are back on strict milk avoidance," he said.
As a result, the excitement following the initial studies has waned somewhat.
"We had a very high degree of optimism. I’m not saying we lost that optimism, but it is certainly tempered a bit by looking at where these kids now stand 3-5 years out," he said, concluding that more research with respect to long-term outcomes of food oral immunotherapy is needed, including investigation of whether longer treatment would improve outcomes, and whether certain factors can predict response and failure.
"The most important message is that this sort of adds another caveat about why we need more research before we can bring this out to our patient population. A message that I think all of us who are doing this research have come to agree upon is that we need long-term follow-up and that letting these kids go at the end of the study is not the end of the story."
Taken together, the findings of these studies underscore a need for more research regarding SLIT vs. OIT, higher vs. lower dosing, and treatment duration, as well as long-term follow-up, the investigators agreed.
"The message is that what we are doing so far is very encouraging, but it’s not the final answer. Where we need to be to bring this out to the general public is several steps beyond where we are now," Dr. Wood said.
The investigators reported having no disclosures.
AT THE AAAAI ANNUAL MEETING
Role of food allergy in eczema downplayed
MAUI, HAWAII – Current thinking on the role of food allergy in pediatric atopic dermatitis suggests a greatly diminished role for allergy testing compared with times past, according to Dr. Joseph F. Fowler Jr.
Guidelines issued by a National Institute of Allergy and Infectious Diseases expert consensus panel – mostly allergists, with little input from dermatologists – concluded that food allergy is actually fairly uncommon in atopics. It affects less than 10% of children under age 2 who have eczema, and a far smaller percentage of older atopic children.

Moreover, the voluminous 58-page report (J. Allergy Clin. Immunol. 2010;126:S1-58) makes the point that allergy testing is time consuming, costly, and not terribly reliable due to high false-positive rates for both scratch testing and RAST (radioallergosorbent tests).
"The bottom line on all this is you probably don’t need to do food allergy testing very often at all in atopics because in those few who did have an allergy to foods, the big three – eggs, milk, and peanuts – accounted for the vast majority of food allergy. So if you’re not sure, what you can do is eliminate those three from the diet, then add them back in one at a time after a few weeks of elimination. That ought to give you a sense of whether there’s really and truly a food allergy operative in that individual," Dr. Fowler said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
"It’s true that occasionally you see allergy to wheat or fish or chocolate or soy or who knows whatever else, but all those other things are very, very uncommon. So while I wouldn’t say you should never do food allergy testing or send a little atopic with recalcitrant eczema for food allergy testing, I think the yield is really going to be relatively low. Doing the elimination trial first is probably the best thing. A good, motivated, observant caregiver is going to be more informative than what the test will tell you," said Dr. Fowler, clinical professor of dermatology at the University of Louisville (Ky.) and codirector of the SDEF seminar.
SDEF and this news organization are owned by the same parent company.
Dr. Fowler is on the speakers bureaus of Galderma, Ranbaxy, and SmartPractice and has received research grants from numerous pharmaceutical companies.
MAUI, HAWAII – Current thinking on the role of food allergy in pediatric atopic dermatitis suggests a greatly diminished role for allergy testing compared with times past, according to Dr. Joseph F. Fowler Jr.
Guidelines issued by a National Institute of Allergy and Infectious Diseases expert consensus panel – mostly allergists, with little input from dermatologists – concluded that food allergy is actually fairly uncommon in atopics. It affects less than 10% of children under age 2 who have eczema, and a far smaller percentage of older atopic children.
Moreover, the voluminous 58-page report (J. Allergy Clin. Immunol. 2010;126:S1-58) makes the point that allergy testing is time consuming, costly, and not terribly reliable due to high false-positive rates for both scratch testing and RAST (radioallergosorbent tests).
"The bottom line on all this is you probably don’t need to do food allergy testing very often at all in atopics because in those few who did have an allergy to foods, the big three – eggs, milk, and peanuts – accounted for the vast majority of food allergy. So if you’re not sure, what you can do is eliminate those three from the diet, then add them back in one at a time after a few weeks of elimination. That ought to give you a sense of whether there’s really and truly a food allergy operative in that individual," Dr. Fowler said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
"It’s true that occasionally you see allergy to wheat or fish or chocolate or soy or who knows whatever else, but all those other things are very, very uncommon. So while I wouldn’t say you should never do food allergy testing or send a little atopic with recalcitrant eczema for food allergy testing, I think the yield is really going to be relatively low. Doing the elimination trial first is probably the best thing. A good, motivated, observant caregiver is going to be more informative than what the test will tell you," said Dr. Fowler, clinical professor of dermatology at the University of Louisville (Ky.) and codirector of the SDEF seminar.
SDEF and this news organization are owned by the same parent company.
Dr. Fowler is on the speakers bureaus of Galderma, Ranbaxy, and SmartPractice and has received research grants from numerous pharmaceutical companies.
MAUI, HAWAII – Current thinking on the role of food allergy in pediatric atopic dermatitis suggests a greatly diminished role for allergy testing compared with times past, according to Dr. Joseph F. Fowler Jr.
Guidelines issued by a National Institute of Allergy and Infectious Diseases expert consensus panel – mostly allergists, with little input from dermatologists – concluded that food allergy is actually fairly uncommon in atopics. It affects less than 10% of children under age 2 who have eczema, and a far smaller percentage of older atopic children.
Moreover, the voluminous 58-page report (J. Allergy Clin. Immunol. 2010;126:S1-58) makes the point that allergy testing is time consuming, costly, and not terribly reliable due to high false-positive rates for both scratch testing and RAST (radioallergosorbent tests).
"The bottom line on all this is you probably don’t need to do food allergy testing very often at all in atopics because in those few who did have an allergy to foods, the big three – eggs, milk, and peanuts – accounted for the vast majority of food allergy. So if you’re not sure, what you can do is eliminate those three from the diet, then add them back in one at a time after a few weeks of elimination. That ought to give you a sense of whether there’s really and truly a food allergy operative in that individual," Dr. Fowler said at the Hawaii Dermatology Seminar sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
"It’s true that occasionally you see allergy to wheat or fish or chocolate or soy or who knows whatever else, but all those other things are very, very uncommon. So while I wouldn’t say you should never do food allergy testing or send a little atopic with recalcitrant eczema for food allergy testing, I think the yield is really going to be relatively low. Doing the elimination trial first is probably the best thing. A good, motivated, observant caregiver is going to be more informative than what the test will tell you," said Dr. Fowler, clinical professor of dermatology at the University of Louisville (Ky.) and codirector of the SDEF seminar.
SDEF and this news organization are owned by the same parent company.
Dr. Fowler is on the speakers bureaus of Galderma, Ranbaxy, and SmartPractice and has received research grants from numerous pharmaceutical companies.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

Data underscore environment's role in allergic disease
SAN ANTONIO – Children living in the United States who were born elsewhere initially have lower rates of allergic disease than do those born in the United States, but the protection against allergic disease is lost after prolonged U.S. residence, according to an analysis of data from the 2007-2008 National Survey of Children’s Health.
Of 91,642 children aged 0-17 years who were included in the study, those born outside of the United States had significantly lower odds of having any allergic disorder, compared with those born in the United States (odds ratio, 0.48). They also had lower odds of all individual allergic disorders studied, including prior or current asthma (OR 0.53), current asthma (OR 0.34), eczema (OR 0.43), hay fever (OR 0.39), and food allergy (OR 0.60), Dr. Jonathan I. Silverberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The association remained significant after adjustment for age, sex, race/ethnicity, household income, residence in metropolitan areas, and history of moving to a new U.S. residence, said Dr. Silverberg of St. Luke’s–Roosevelt Hospital Center, New York.
Also of note, the prevalence rates of allergic disease were lower for all of the diseases studied for children born outside of the United States whose parents were born outside of the United States, compared with those whose parents were born in the United States.
However, after 10 years or more of United States residence, children born outside of the United States had significantly higher odds of developing an allergic disorder, compared with those born outside of the United States who had lived in the country for only 0-2 years (OR 3.04). This was true for eczema (OR 4.93) and hay fever (OR 6.25), but not for asthma or food allergy, Dr. Silverberg said.
The study was undertaken in the wake of prior data showing that certain racial or ethnic groups have lower rates of allergic disease. Dr. Silverberg and his colleagues set out to investigate whether an association existed between birthplace, length of U.S. residence, and various allergic diseases.
The findings suggest that environmental factors promote the development of allergic disease, he concluded.
Dr. Silverberg reported having no relevant financial disclosures.
SAN ANTONIO – Children living in the United States who were born elsewhere initially have lower rates of allergic disease than do those born in the United States, but the protection against allergic disease is lost after prolonged U.S. residence, according to an analysis of data from the 2007-2008 National Survey of Children’s Health.
Of 91,642 children aged 0-17 years who were included in the study, those born outside of the United States had significantly lower odds of having any allergic disorder, compared with those born in the United States (odds ratio, 0.48). They also had lower odds of all individual allergic disorders studied, including prior or current asthma (OR 0.53), current asthma (OR 0.34), eczema (OR 0.43), hay fever (OR 0.39), and food allergy (OR 0.60), Dr. Jonathan I. Silverberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The association remained significant after adjustment for age, sex, race/ethnicity, household income, residence in metropolitan areas, and history of moving to a new U.S. residence, said Dr. Silverberg of St. Luke’s–Roosevelt Hospital Center, New York.
Also of note, the prevalence rates of allergic disease were lower for all of the diseases studied for children born outside of the United States whose parents were born outside of the United States, compared with those whose parents were born in the United States.
However, after 10 years or more of United States residence, children born outside of the United States had significantly higher odds of developing an allergic disorder, compared with those born outside of the United States who had lived in the country for only 0-2 years (OR 3.04). This was true for eczema (OR 4.93) and hay fever (OR 6.25), but not for asthma or food allergy, Dr. Silverberg said.
The study was undertaken in the wake of prior data showing that certain racial or ethnic groups have lower rates of allergic disease. Dr. Silverberg and his colleagues set out to investigate whether an association existed between birthplace, length of U.S. residence, and various allergic diseases.
The findings suggest that environmental factors promote the development of allergic disease, he concluded.
Dr. Silverberg reported having no relevant financial disclosures.
SAN ANTONIO – Children living in the United States who were born elsewhere initially have lower rates of allergic disease than do those born in the United States, but the protection against allergic disease is lost after prolonged U.S. residence, according to an analysis of data from the 2007-2008 National Survey of Children’s Health.
Of 91,642 children aged 0-17 years who were included in the study, those born outside of the United States had significantly lower odds of having any allergic disorder, compared with those born in the United States (odds ratio, 0.48). They also had lower odds of all individual allergic disorders studied, including prior or current asthma (OR 0.53), current asthma (OR 0.34), eczema (OR 0.43), hay fever (OR 0.39), and food allergy (OR 0.60), Dr. Jonathan I. Silverberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The association remained significant after adjustment for age, sex, race/ethnicity, household income, residence in metropolitan areas, and history of moving to a new U.S. residence, said Dr. Silverberg of St. Luke’s–Roosevelt Hospital Center, New York.
Also of note, the prevalence rates of allergic disease were lower for all of the diseases studied for children born outside of the United States whose parents were born outside of the United States, compared with those whose parents were born in the United States.
However, after 10 years or more of United States residence, children born outside of the United States had significantly higher odds of developing an allergic disorder, compared with those born outside of the United States who had lived in the country for only 0-2 years (OR 3.04). This was true for eczema (OR 4.93) and hay fever (OR 6.25), but not for asthma or food allergy, Dr. Silverberg said.
The study was undertaken in the wake of prior data showing that certain racial or ethnic groups have lower rates of allergic disease. Dr. Silverberg and his colleagues set out to investigate whether an association existed between birthplace, length of U.S. residence, and various allergic diseases.
The findings suggest that environmental factors promote the development of allergic disease, he concluded.
Dr. Silverberg reported having no relevant financial disclosures.
AT THE AAAAI ANNUAL MEETING
Major finding: After 10 years or more of United States residence, children born outside of the United States had significantly higher odds of developing an allergic disorder, compared with those born outside of the United States who had lived in the country for only 0-2 years (odds ratio, 3.04).
Data source: An analysis of data from the 2007-2008 National Survey of Children’s Health including 91,642 children aged 0-17 years.
Disclosures: Dr. Silverberg reported having no relevant financial disclosures.
All glucocorticoids linked to increased risk of VTE
Use of all glucocorticoids is associated with a two- to threefold increased risk of venous thromboembolism, depending on the type of glucocorticoid, the route of administration, and other factors, according to a report published online April 1 in JAMA Internal Medicine.
Systemic glucocorticoids, as compared with inhaled ones or glucocorticoids that act on the intestines, were associated with the highest risk of VTE. New use was linked to higher risk than continuing or past use, and the VTE risk increased as the dose of glucocorticoids increased, said Sigrun A. Johannesdottir of the department of clinical epidemiology, Aarhus (the Netherlands) University Hospital, and her associates.
These findings are from a population-based case-control study, which cannot prove a cause-and-effect relationship. Moreover, it is difficult to statistically account for all the confounding effects of patients’ underlying disease – the reason they were taking glucocorticoids in the first place – because such disorders raise the risk of VTE directly or cause immobility that in turn can lead to VTE.
However, the timing of this adverse effect, the strength of the association across all types of glucocorticoids, and the fact that the association persisted after the data were adjusted to account for multiple confounders all "increase our confidence that the results reflect a true biological effect," the investigators said.
"Clinicians should be aware of this association," they noted.
Ms. Johannesdottir and her colleagues used data from several Danish national medical registries to identify all adults who were diagnosed with VTE in Denmark in 2005-2012, all patients who filled prescriptions for glucocorticoids during the study period, and all indications for the drugs as well as all relevant comorbidities. They matched 10 control subjects for age and sex from the general population to each study subject.
A total of 38,765 VTE cases and 387,650 controls were included in this study. The median age was 67 years, and slightly more than half of those studied were women.
All glucocorticoid users were found to be at increased risk for VTE, particularly for pulmonary embolism, compared with nonusers, the researchers said.
Systemic glucocorticoids, including betamethasone, methylprednisolone, prednisolone, prednisone, triamcinolone, and hydrocortisone, raised VTE risk to the highest degree. (No patients filled prescriptions for dexamethasone in this study.)
Inhaled corticosteroids and corticosteroids that act on the intestines also raised VTE risk significantly. Among the systemic glucocorticoids, prednisolone and prednisone raised VTE risk the most.
New use of glucocorticoids was associated with the highest risk of VTE, but current use, continuing use, and former use also raised the risk significantly. Oral formulations were associated with the highest risk of VTE, but injectable formulations also raised the risk significantly, Ms. Johannesdottir and her associates reported (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.122]).
In particular, new use of systemic glucocorticoids was associated with the highest risk for VTE, with an estimated incidence rate ratio of 3.06, compared with nonuse of glucocorticoids.
The risk of VTE also rose with increasing cumulative doses of all glucocorticoids.
In further analyses, elevated risk for VTE persisted across all the subgroups that were examined.
The findings did not change appreciably in a sensitivity analysis that included only subjects who took glucocorticoids for at least 5 years.
"The temporality of the association (i.e., the strongest effect at initiation of therapy and the absence of an effect after discontinuation) is in line with an effect on coagulation," Ms. Johannesdottir and her associates said.
This study was supported by the Clinical Epidemiological Research Foundation at Aarhus University Hospital. No relevant conflicts of interest were reported.
This study provides strong evidence that glucocorticoids are linked to elevated risk of VTE, an association that is difficult to prove because some of the illnesses that are treated with these drugs may themselves cause VTE or may cause immobility that predisposes patients to VTE, said Dr. Mitchell H. Katz.
The findings don’t change the indications for prescribing glucocorticoids, but they "should remind us to always make sure that the potential benefits of treatment outweigh the risks, and to be prepared to diagnose and treat thromboembolism" in patients taking glucocorticoids, he said.
Dr. Mitchell H. Katz is a deputy editor of JAMA Internal Medicine. His remarks were taken from his editorial accompanying Ms. Johannesdottir’s report (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.93]).
This study provides strong evidence that glucocorticoids are linked to elevated risk of VTE, an association that is difficult to prove because some of the illnesses that are treated with these drugs may themselves cause VTE or may cause immobility that predisposes patients to VTE, said Dr. Mitchell H. Katz.
The findings don’t change the indications for prescribing glucocorticoids, but they "should remind us to always make sure that the potential benefits of treatment outweigh the risks, and to be prepared to diagnose and treat thromboembolism" in patients taking glucocorticoids, he said.
Dr. Mitchell H. Katz is a deputy editor of JAMA Internal Medicine. His remarks were taken from his editorial accompanying Ms. Johannesdottir’s report (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.93]).
This study provides strong evidence that glucocorticoids are linked to elevated risk of VTE, an association that is difficult to prove because some of the illnesses that are treated with these drugs may themselves cause VTE or may cause immobility that predisposes patients to VTE, said Dr. Mitchell H. Katz.
The findings don’t change the indications for prescribing glucocorticoids, but they "should remind us to always make sure that the potential benefits of treatment outweigh the risks, and to be prepared to diagnose and treat thromboembolism" in patients taking glucocorticoids, he said.
Dr. Mitchell H. Katz is a deputy editor of JAMA Internal Medicine. His remarks were taken from his editorial accompanying Ms. Johannesdottir’s report (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.93]).
Use of all glucocorticoids is associated with a two- to threefold increased risk of venous thromboembolism, depending on the type of glucocorticoid, the route of administration, and other factors, according to a report published online April 1 in JAMA Internal Medicine.
Systemic glucocorticoids, as compared with inhaled ones or glucocorticoids that act on the intestines, were associated with the highest risk of VTE. New use was linked to higher risk than continuing or past use, and the VTE risk increased as the dose of glucocorticoids increased, said Sigrun A. Johannesdottir of the department of clinical epidemiology, Aarhus (the Netherlands) University Hospital, and her associates.
These findings are from a population-based case-control study, which cannot prove a cause-and-effect relationship. Moreover, it is difficult to statistically account for all the confounding effects of patients’ underlying disease – the reason they were taking glucocorticoids in the first place – because such disorders raise the risk of VTE directly or cause immobility that in turn can lead to VTE.
However, the timing of this adverse effect, the strength of the association across all types of glucocorticoids, and the fact that the association persisted after the data were adjusted to account for multiple confounders all "increase our confidence that the results reflect a true biological effect," the investigators said.
"Clinicians should be aware of this association," they noted.
Ms. Johannesdottir and her colleagues used data from several Danish national medical registries to identify all adults who were diagnosed with VTE in Denmark in 2005-2012, all patients who filled prescriptions for glucocorticoids during the study period, and all indications for the drugs as well as all relevant comorbidities. They matched 10 control subjects for age and sex from the general population to each study subject.
A total of 38,765 VTE cases and 387,650 controls were included in this study. The median age was 67 years, and slightly more than half of those studied were women.
All glucocorticoid users were found to be at increased risk for VTE, particularly for pulmonary embolism, compared with nonusers, the researchers said.
Systemic glucocorticoids, including betamethasone, methylprednisolone, prednisolone, prednisone, triamcinolone, and hydrocortisone, raised VTE risk to the highest degree. (No patients filled prescriptions for dexamethasone in this study.)
Inhaled corticosteroids and corticosteroids that act on the intestines also raised VTE risk significantly. Among the systemic glucocorticoids, prednisolone and prednisone raised VTE risk the most.
New use of glucocorticoids was associated with the highest risk of VTE, but current use, continuing use, and former use also raised the risk significantly. Oral formulations were associated with the highest risk of VTE, but injectable formulations also raised the risk significantly, Ms. Johannesdottir and her associates reported (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.122]).
In particular, new use of systemic glucocorticoids was associated with the highest risk for VTE, with an estimated incidence rate ratio of 3.06, compared with nonuse of glucocorticoids.
The risk of VTE also rose with increasing cumulative doses of all glucocorticoids.
In further analyses, elevated risk for VTE persisted across all the subgroups that were examined.
The findings did not change appreciably in a sensitivity analysis that included only subjects who took glucocorticoids for at least 5 years.
"The temporality of the association (i.e., the strongest effect at initiation of therapy and the absence of an effect after discontinuation) is in line with an effect on coagulation," Ms. Johannesdottir and her associates said.
This study was supported by the Clinical Epidemiological Research Foundation at Aarhus University Hospital. No relevant conflicts of interest were reported.
Use of all glucocorticoids is associated with a two- to threefold increased risk of venous thromboembolism, depending on the type of glucocorticoid, the route of administration, and other factors, according to a report published online April 1 in JAMA Internal Medicine.
Systemic glucocorticoids, as compared with inhaled ones or glucocorticoids that act on the intestines, were associated with the highest risk of VTE. New use was linked to higher risk than continuing or past use, and the VTE risk increased as the dose of glucocorticoids increased, said Sigrun A. Johannesdottir of the department of clinical epidemiology, Aarhus (the Netherlands) University Hospital, and her associates.
These findings are from a population-based case-control study, which cannot prove a cause-and-effect relationship. Moreover, it is difficult to statistically account for all the confounding effects of patients’ underlying disease – the reason they were taking glucocorticoids in the first place – because such disorders raise the risk of VTE directly or cause immobility that in turn can lead to VTE.
However, the timing of this adverse effect, the strength of the association across all types of glucocorticoids, and the fact that the association persisted after the data were adjusted to account for multiple confounders all "increase our confidence that the results reflect a true biological effect," the investigators said.
"Clinicians should be aware of this association," they noted.
Ms. Johannesdottir and her colleagues used data from several Danish national medical registries to identify all adults who were diagnosed with VTE in Denmark in 2005-2012, all patients who filled prescriptions for glucocorticoids during the study period, and all indications for the drugs as well as all relevant comorbidities. They matched 10 control subjects for age and sex from the general population to each study subject.
A total of 38,765 VTE cases and 387,650 controls were included in this study. The median age was 67 years, and slightly more than half of those studied were women.
All glucocorticoid users were found to be at increased risk for VTE, particularly for pulmonary embolism, compared with nonusers, the researchers said.
Systemic glucocorticoids, including betamethasone, methylprednisolone, prednisolone, prednisone, triamcinolone, and hydrocortisone, raised VTE risk to the highest degree. (No patients filled prescriptions for dexamethasone in this study.)
Inhaled corticosteroids and corticosteroids that act on the intestines also raised VTE risk significantly. Among the systemic glucocorticoids, prednisolone and prednisone raised VTE risk the most.
New use of glucocorticoids was associated with the highest risk of VTE, but current use, continuing use, and former use also raised the risk significantly. Oral formulations were associated with the highest risk of VTE, but injectable formulations also raised the risk significantly, Ms. Johannesdottir and her associates reported (JAMA Intern. Med. 2013 April 1 [doi:10.1001/jamainternmed.2013.122]).
In particular, new use of systemic glucocorticoids was associated with the highest risk for VTE, with an estimated incidence rate ratio of 3.06, compared with nonuse of glucocorticoids.
The risk of VTE also rose with increasing cumulative doses of all glucocorticoids.
In further analyses, elevated risk for VTE persisted across all the subgroups that were examined.
The findings did not change appreciably in a sensitivity analysis that included only subjects who took glucocorticoids for at least 5 years.
"The temporality of the association (i.e., the strongest effect at initiation of therapy and the absence of an effect after discontinuation) is in line with an effect on coagulation," Ms. Johannesdottir and her associates said.
This study was supported by the Clinical Epidemiological Research Foundation at Aarhus University Hospital. No relevant conflicts of interest were reported.
FROM JAMA INTERNAL MEDICINE
Major Finding: New use of systemic glucocorticoids was associated with the highest risk for VTE, with an estimated incidence rate ratio of 3.06, compared with nonuse.
Data Source: A national population-based case-control study involving 38,765 Danish adults who developed VTE in a 7-year period and 387,650 controls.
Disclosures: This study was supported by the Clinical Epidemiological Research Foundation at Aarhus University Hospital. No relevant conflicts of interest were reported.
Asthma still uncontrolled? Try these troubleshooting tips

Help patients control their asthma
• Classify and treat asthma based on the patient’s worst symptom, whether or not it is the symptom that occurs most frequently. C
• Treat patients with poorly controlled asthma aggressively to gain quick control, then scale back slowly to the fewest medications and lowest doses needed to maintain control. A
• Reserve long-acting beta-agonists for use as an adjunct to inhaled corticosteroids for adults with poor baseline pulmonary function tests. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Angela D, a 34-year-old patient, has asthma with recurrent exacerbations. She uses a low-dose inhaled corticosteroid (ICS) daily and an albuterol inhaler, as needed, for shortness of breath or wheezing. She also has allergic rhinitis, for which she uses nasal fluticasone. Yet despite this regimen, Ms. D reports she still experiences wheezing, chest tightness, and shortness of breath 3 to 4 times a week and is awak-ened by coughing at least twice a week. In the past 6 months, she has had one emergency department (ED) visit and completed 2 courses of oral steroids.
Ms. D has gained weight since her last visit 3 months ago; her body mass index has gone from 27.5 to 29 kg/m2. And, while she has always been somewhat anxious, Ms. D notes that her anxiety has gotten progressively worse, as well.
About 25 million Americans—approximately one in 12—suffer from asthma1 and, despite improvements in asthma guidelines and treatment in the last 20 years,2 many still struggle with uncontrolled symptoms.3 The consequences can be severe.
Suboptimal control of asthma is associated with a significant decrease in quality of life, a greater likelihood of absence from work or school, and an increased risk for life-threatening events, trips to the ED, hospital admissions, and death.1 A multifaceted approach, including regular assessment, aggressive medication management, and attention to comorbidities, is needed to alleviate the suffering of patients with persistent asthma. This evidence-based review can help you provide such broad-based treatment.
Diagnosis and classification go hand in hand
The cornerstones of asthma management are accurate diagnosis and assessment of disease severity, based on both qualitative and quantitative measures. Start with a patient history, eliciting information about symptoms, triggers, risk factors, and most importantly, how often symptoms occur. Classic high-pitched wheezing sounds during exhalation, a cough that often worsens at night, shortness of breath, and chest tightness should raise suspicion for an asthma diagnosis.2 But frequency (and timing) of symptoms and exacerbations, as well as changes in the patient’s ability to function normally, help to determine whether asthma is classified as mild intermittent, mild persistent, moderate persistent, or severe persistent (TABLE).2
TABLE
Classifying asthma severity2
| Findings | Mild intermittent | Mild persistent | Moderate persistent | Severe persistent |
|---|---|---|---|---|
| Frequency | ≤2/wk | >2/wk, but <1/d | Daily | Continuous |
| Exacerbations | Rare | <2/wk | ≥2/wk | Frequent |
| Activity level | Normal | May decrease with exacerbation | Frequently limited | Significantly limited |
| Nighttime symptoms | ≤2/mo | >2/mo | >1/wk | Frequent |
| FEV1 (or PEF) predicted | >80% | >80% | >60% to <80% | ≤60% |
| PEF variability | <20% | 20%-30% | >30% | >30% |
| FEV1, forced expiratory volume in one second; PEF, peak expiratory flow. | ||||
Because asthma treatment should be based on its classification, an accurate assessment of disease severity is especially important for patients like Ms. D, who have been treated for asthma but continue to have unresolved symptoms. Keep in mind that asthma classification should be based on the worst symptom a patient has, not necessarily the symptom that occurs most frequently. Thus, a patient who has daytime symptoms requiring use of a rescue inhaler 2 to 3 times a week but is awakened at night with shortness of breath 2 times a week would receive a diagnosis of moderate persistent asthma on the basis of the night-time symptoms.
In assessing asthma severity, it is also important to ask specifically about recent events, including ED visits, hospitalizations, and intubations. This information, as well as answers to questions about smoking status, mental health problems, quality of life, and treatment compliance—and whether the patient can afford to purchase the asthma medications you’ve prescribed—can be used to assess the likelihood of poor outcomes.2
Factor in spirometry findings
History and physical examination alone cannot adequately diagnose and classify asthma severity.4,5 Spirometry, a reimbursable office test that can be administered by trained staff members, can be beneficial for any patient older than 5 years for whom a diagnosis of asthma is being considered or disease severity being determined.2 Other objective measures, such as the Mini Asthma Quality of Life questionnaire (http://erj.ersjournals.com/content/14/1/32.full.pdf+html) and peak expiratory flow measurement, may be helpful, as well.2,6
Spirometry measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) and calculates the FEV1/FVC ratio. Reference spirometry values vary according to patient characteristics, such as age, height, sex, and race, as well as the positioning of the patient during the test.7 (A seated position is optimal to reduce the risk of falls as a result of the light-headedness some patients may experience.) The American Thoracic Society provides a set of criteria (available at http://www.gp-training.net/protocol/respiratory/copd/spirometry.htm) that should be considered in interpreting test results.8
The 3 main spirometry patterns you’ll see are:
- Normal (FEV1 >80% predicted; FVC >80% predicted; FEV1/FVC >70%)
- Obstructive (FEV1 <80% predicted; FVC normal or mildly reduced; FEV1/FVC <70%)
- Restrictive (FEV1 normal or mildly reduced; FVC <80% predicted; FEV1/FVC >70%).
Because asthma is a chronic disease with fluctuating symptomatology and severity, spirometry testing should be repeated and results compared on several occasions as a guide to treatment.9 When an obstructive pattern is found, the patient should receive a bronchodilator treatment, then undergo spirometry 15 to 20 minutes later to determine reversibility. A reversible obstructive pattern, defined as an increase in FEV1 by 12% (≥200 mL), is consistent with an asthma diagnosis. If spirometry results are consistently normal but a high clinical suspicion for obstructive disease remains, the patient should be evaluated with a methacholine or histamine challenge test to definitively rule out asthma.10
Rule out asthma mimics. Many medical conditions can mimic symptoms of asthma and result in misdiagnosis or incorrect severity classification and unnecessary treatment. Patients should be evaluated for alternate or coexisting pulmonary conditions, including restrictive lung disease, vocal cord dysfunction, cough-variant asthma, malignancy, and allergies. For a patient whose asthma diagnosis is in doubt or who has a restrictive pattern on spirometry, additional evaluation based on signs and symptoms may require comprehensive pulmonary function testing, chest x-ray, bronchoscopy, laryngoscopy, computed tomography, and/or allergy testing.2
Peak expiratory flow (PEF). While measuring PEF should not replace spirometry or formal pulmonary function testing, it can be helpful for evaluating disease severity and monitoring treatment. Patients should use their own peak flow meters, and results compared with their personal best measurements. An improvement of 60 L/min or >20% after treatment with a bronchodilator is suggestive of asthma.9 There are a number of free or low-cost apps that patients can use to track their PEF measurements and response to treatment, such as Asthma MD, Huff and Puff (for children), and the Peak Flow Calculator.11-13
An evidence-based approach to asthma treatment
The first step in treating newly diagnosed asthma is to advise the patient to avoid known triggers, such as allergens, stressors, and particular odors or activities, to the extent possible, and, most importantly, to avoid exposure to smoke. If the patient smokes—cigarettes, marijuana, hookah, or pipe—stress the importance of quitting and living in a home that is smoke free. The link between asthma exacerbations and cockroaches is also well documented, particularly affecting those in urban areas. Avoidance of cockroaches and their droppings is critical, and may require the use of pest control services.14,15
A general principle of asthma management is to treat it aggressively initially to help the patient achieve quick control, then gradually cut back to the fewest medications and lowest effective doses required to maintain control.2 The National Heart, Lung, and Blood Institute (NHLBI)’s 2007 Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma (FIGURE)2 call for a stepwise approach.
Short-acting beta-agonists (SABAs) and ICS—first-line asthma therapy—have minimal risks or adverse effects. SABAs help reverse acute shortness of breath and wheezing, and ICS can reduce the frequency of exacerbations.2
FIGURE
Stepwise approach to asthma management for patients ≥12 years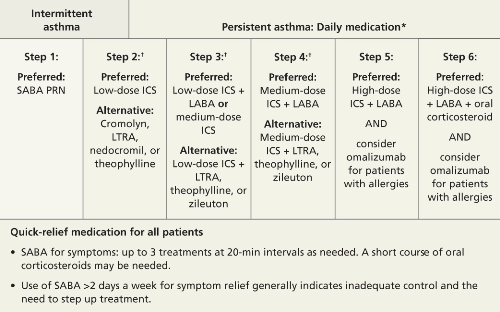
*Consult with an asthma specialist if Step 4 care or higher is required; consider consultation at Step 3.
†Consider subcutaneous allergen immunotherapy for patients with allergic asthma.
ICS, inhaled corticosteroid; LABA, long-acting beta-agonist; LTRA, leukotriene receptor agonist; SABA, short-acting beta-agonist.
Adapted from: National Asthma Education and Prevention Program. J Allergy Clin Immunol. 2007.2
Second-line therapy is less clearcut
There are several options for patients whose symptoms are not well controlled with first-line treatment: (1) Add a long-acting beta-agonist (LABA); (2) add a leukotriene receptor antagonist (LTRA); or (3) increase the ICS dose, the most straightforward approach.
A dose increase avoids both the additional risk of adverse drug reactions and the added cost associated with another medication. But the easiest solution is not necessarily the best. Consider the evidence detailed below, which includes findings from studies published after the NHLBI’s guidelines.
The research on LABAs
LABAs have been widely used as adjunctive therapy for adults with asthma. However, a 2006 study raised safety concerns.16
The Salmeterol Multicenter Asthma Research Trial (SMART) compared the safety of the LABA salmeterol with a placebo added to usual asthma care over a 28-week treatment period. Overall, the primary composite end point—the number of respiratory-related deaths or life-threatening events—was low, and not statistically significant for salmeterol (50 vs 36; relative risk [RR]=1.40; 95% confidence interval [CI], 0.91-2.14).16 However, individual outcomes—respiratory-related deaths, asthma-related deaths, and asthma-related deaths or life-threatening episodes—were significantly more likely in the salmeterol group compared with the placebo group. In subgroup analysis, African American patients were found to be at greatest risk.16
It is hard to draw general conclusions from these data because the study was terminated early and poor outcomes were limited to a particular study year. Nonetheless, many physicians remain wary of LABAs as adjunctive therapy because of these findings and the media publicity they generated.
A 2010 Cochrane review provided additional data on the safety and efficacy of the combination of a LABA and ICS compared with a higher dose of ICS.17 The review, which included 48 randomized controlled trials, found that combination therapy had a lower risk of exacerbations for which oral corticosteroids were required than a higher dose of ICS (RR=0.88; 95% CI, 0.78-0.98; P=.02). The median number needed to treat (NNT) was 73. No significant difference in the risk of overall adverse events (RR=0.99; 95% CI, 0.95-1.03) was found, but there was an increase in the risk of tremor (RR=1.84; 95% CI, 1.20-2.82) and a decrease in risk for oral thrush (RR=0.58; 95% CI, 0.40-0.86) in the combination therapy group.
While the Cochrane review did not show a combination of LABA and ICS to be less safe overall than higher doses of ICS alone, the findings were less favorable for children and patients with higher baseline lung function, in circumstances in which the combination therapy was taken for a longer duration, and when the LABA being studied was formoterol.17
Overall, it is when a LABA is delivered via separate inhaler that adverse outcomes have been reported. Findings have been positive when the LABA is combined with ICS, and this combination is recommended as maintenance therapy for moderate to severe asthma.
Two new studies, published in March 2013, reported successful use of a LABA-ICS combination not only for maintenance via scheduled dosing, but also for early phases of exacerbation via extra dosing—an approach called Single inhaler Maintenance and Reliever Therapy (SMART).18,19 In both studies, SMART resulted in less excessive use of SABAs and less need for oral steroids, fewer hospitalizations for asthma, and fewer cases of progression to a full-blown exacerbation.
The takeaway: LABAs should be reserved for use as an adjunct to ICS in adults with poor baseline pulmonary function tests or severe asthma, and delivered as a combination product with ICS, not as a separate inhaled medication. SMART is a safe and effective means of administering LABA-ICS therapy for some patients at risk for frequent severe exacerbations.
When to consider LTRAs
LTRAs can be valuable medications in asthma management and there are extensive data on their use, particularly in the treatment of children with asthma. A Cochrane review published in 2012, however, supported current guideline recommendations, finding that as monotherapy, ICS are superior to LTRAs.20
When LTRAs as an adjunctive therapy to ICS were compared with ICS monotherapy, researchers found a modest improvement in PEF (weighted mean difference [WMD] =7.7 L/min; 95% CI, 3.6-11.8) in the group receiving combination therapy and a decrease in the need for a SABA as rescue therapy (WMD=1 puff/week; 95% CI, 0.5-2.0).21 There was no significant reduction in the risk of exacerbations requiring systemic steroids (RR=0.64; 95% CI, 0.38-1.07).
LABAs and LTRAs go head to head. A 2010 Cochrane review compared the efficacy and safety of a daily LABA vs a LTRA as add-on therapy for patients whose asthma was not well controlled with ICS monotherapy.22 The LABA/ICS combination was significantly better at reducing the risk of exacerbations requiring systemic corticosteroids than monotherapy with either a LTRA or ICS, reducing the risk from 11% to 9% (RR=0.83; 95% CI, 0.71-0.97). The NNT to prevent one exacerbation over 48 weeks was 38 (95% CI, 22-244).22
The safety of LABAs continues to be a concern, however, as serious adverse events were more common in the LABA group. The number needed to harm (NNH) with LABA therapy vs LTRA over 48 weeks was 78; 95% CI, 33 to infinity.22 (The width of the CI indicates that while harm is possible in as few as 33 patients, it is also possible that an infinite number of patients would need to be treated for one individual to incur harm.) Overall, the evidence suggests that LABAs are superior add-on therapy to ICS for the treatment of uncontrolled asthma compared with LTRAs, but their use nonetheless requires caution and close monitoring in African American and pediatric patients.17
Is there a role for a long-acting anticholinergic inhaler?
Long-acting anticholinergic medication (LAAM)—tiotropium is the only drug in this class on the market, but there are others in clinical trials—is the mainstay of therapy for chronic obstructive pulmonary disease. This drug class was not widely available or studied as an asthma treatment when the NHLBI guidelines were drafted.
A 2010 study of tiotropium challenged the notion that there is no place for LAAMs in asthma therapy. Using a 3-way crossover design, the study compared the addition of tiotropium to ICS with a double dose of ICS or a LABA/ICS combination.23
The results suggest that LAAMs could be useful in treating uncontrolled asthma. Compared with the double dose of ICS, the tiotropium/ICS combination increased PEF by a mean difference of 25.8 L/min (P<.001) and resulted in a statistically significant improvement in the proportion of asthma control days, FEV1, and daily symptom scores.23 As an adjunctive treatment to ICS, tiotropium was not inferior to a LABA.
CASE After a detailed history, physical exam, and diagnostic testing, Ms. D was given a diagnosis of moderate persistent asthma. We recognized the need to step up her treatment. Prior to making any changes in her medication regimen, however, our team, which included a clinical pharmacist, observed her use of inhaled medications and verified that she was using the inhaler properly. We then initiated combination therapy, pairing a LABA and ICS.
Comorbidities complicate asthma management
Asthma management is often complicated by other uncontrolled coexisting medical problems. Common comorbidities that can affect asthma severity include allergic rhinitis, chronic sinusitis, gastroesophageal reflux disease (GERD), obesity, obstructive sleep apnea (OSA), mental health disorders, tobacco use, and hormonal disturbances.2
Allergic rhinitis. Allergic rhinitis has been associated with worse asthma control and a negative impact on quality of life, and the upper airway inflammation associated with it should be treated.24
Antihistamines and nasal steroids are the most effective medical management. Some patients with allergic rhinitis benefit from blood or skin allergy testing for confirmation or to aid in avoidance. Referral to an allergist may be necessary if symptoms are recalcitrant, a food allergy is in question, or the diagnosis is unclear.
GERD. Compared with the general population, patients with asthma have a much higher risk of GERD, although it is not always symptomatic. While results are inconsistent and difficult to predict, treating symptomatic GERD with acid-blocking medications can result in better asthma control for some patients. However, proton pump inhibitors should not be used to treat asthma symptoms in patients with asymptomatic GERD.25,26
Obesity and OSA. Weight loss can significantly improve asthma control, decrease medication use, and improve quality of life.27,28 Obese patients are less likely to respond to treatment with ICS.2 Weight loss also benefits those who suffer from OSA, which may contribute to airway hyperresponsiveness.29
Mental health disorders. Compared with the general population, patients with asthma are more likely to have depression, anxiety, and panic disorders.30 Diagnosis and treatment of these comorbid conditions can lead to better asthma management, increased medication adherence, decreased health care utilization—including fewer ED visits and hospitalizations—and a better quality of life.30
CASE We also addressed our patient’s comorbidities—weight gain, allergic rhinitis, and anxiety. The allergic rhinitis was already well-controlled with a nasal steroid, but we suspected a relationship between Ms. D’s weight gain and increasing anxiety associated with some recent life events. We suggested she see a counselor, and she agreed.
When the patient returned in 12 weeks, she reported that she hardly needed her rescue inhaler anymore and that she was managing her anxiety more effectively. She also told us that she had begun a low-fat dietary regimen, and we confirmed that she had already lost 5 pounds.
CORRESPONDENCE
Stephen A. Wilson, MD, MPH, FAAFP, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; wilsons2@upmc.edu
1. American Academy of Allergy, Asthma, and Immunology. Asthma statistics. Available at: http://www.aaaai.org/about-the-aaaai/newsroom/asthma-statistics.aspx. Accessed March 7, 2012.
2. National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for diagnosis and management of asthma. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
3. Centers for Disease Control and Prevention. National surveillance for asthma—United States, 1980-2004. MMWR Surveill Summ. 2007;56(8):1-54.
4. Stout JW, Visness CM, Enright P, et al. Classification of asthma severity in children. Arch Pediatr Adolesc Med. 2006;160:844-850.
5. Bacharier LB, Strunk RC, Mauger D, et al. Classifying asthma severity in children. Am J Respir Crit Care Med. 2004;170:426-432.
6. Juniper EF, Guyatt GH, Cox FM, et al. Development and validation of the Mini Asthma Quality of Life Questionnaire. Eur Respir J. 1999;14:32-38.
7. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:179-187.
8. Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26:319-338.
9. Bateman ED, Hurd SS, Barnes PJ, et al. Global Strategy for Asthma Management and Prevention. Eur Respir J. 2008;31:143-178.
10. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of COPD. February 2013. Available at: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed March 7, 2013.
11. AsthmaMD. Available at: http://www.asthmamd.org/#resources/iphone_chart.jpg. Accessed March 7, 2013.
12. Indiegogo. Huff & Puff. Available at: http://www.indiegogo.com/projects/the-best-asthma-education-app-in-the-world-period. Accessed March 7, 2013.
13. Vimukti Technologies Pvt Ltd. Peak flow calculator. Available at: http://appworld.blackberry.com/webstore/content/7615. Accessed March 7, 2013,
14. Morgan WJ, Crain EF, Gruchalla RS, et al. Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;35:1068-1080.
15. Phipatanakul W, Matsui E, Portnoy J, et al. Environmental assessment and exposure reduction of rodents: a practice parameter. Ann Allergy Asthma Immunol. 2012;109:375-387.
16. Nelson HS, Weiss ST, Bleeker ER, et al. The Salmeterol Multicenter Asthma Research Trial. Chest. 2006;129:15-26.
17. Ducharme FM, Ni Chroinin M, Greenstone I, et al. Addition of long-acting beta2-agonists to inhaled steroids versus higher dose inhaled steroids in adults and children with persistent asthma. Cochrane Database Syst Rev. 2010;(4):CD005533.-
18. Papi A, Corradi M, Pigeon-Francisco C, et al. Beclometasone-formoterol as maintenance and reliever treatment in patients with asthma. Lancet Respir Med. 2013;1:23-31.
19. Patel M, Pilcher J, Pritchard A, et al. Efficacy and safety of maintenance and reliever combination budesonide-formoterol inhaler in patients with asthma at risk of severe exacerba-tions. Lancet Respir Med. 2013;1:32-42.
20. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.-
21. Ducharme FM. Addition of anti-leukotriene agents to inhaled corticosteroids for chronic asthma. Cochrane Database Syst Rev. 2004;(1):CD003133.-
22. Ducharme FM, Lasserson TJ, Cates CJ. Addition to inhaled corticosteroids of long-acting beta2-agonists versus anti-leukotrienes for chronic asthma. Cochrane Database Syst Rev. 2011;(5):CD003137.-
23. Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010;363:1715-1726.
24. Vandenplas O, Dramaix M, Joos G, et al. The impact of concomitant rhinitis on asthma-related quality of life and asthma control. Allergy. 2010;65:1290-1297.
25. Gibson PG, Henry RL, Coughlan JL. Gastroesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.-
26. The American Lung Association Asthma Clinical Research Centers. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360:1487-1499.
27. Eneli IU, Skybo T, Camargo CA, Jr. Weight loss and asthma. Thorax. 2008;63:671-676.
28. Stenius-Aarniala B, Poussa T, Kvarnstrom J, et al. Immediate and long term effects of weight reduction in obese people with asthma. BMJ. 2000;320:827-832.
29. Sariman N, Levent E, Cubuk R, et al. Bronchial hyperreactivity and airway wall thickening in obstructive sleep apnea patients. Sleep Breath. 2011;15:341-50.
30. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104:22-28.
| Asthma still uncontrolled? Try these troubleshooting tips Jennie Broders, PharmD, BCPS |
Jennie Broders, PharmD, BCPS
UPMC St. Margaret, Pittsburgh, Pa
Krishna Desai, MD
UPMC St. Margaret, Pittsburgh, Pa
Stephen A. Wilson, MD, MPH, FAAFP
UPMC St. Margaret, Pittsburgh, Pa
wilsons2@upmc.edu
The authors reported no potential conflict of interest relevant to this article.
| Asthma still uncontrolled? Try these troubleshooting tips Jennie Broders, PharmD, BCPS |
Jennie Broders, PharmD, BCPS
UPMC St. Margaret, Pittsburgh, Pa
Krishna Desai, MD
UPMC St. Margaret, Pittsburgh, Pa
Stephen A. Wilson, MD, MPH, FAAFP
UPMC St. Margaret, Pittsburgh, Pa
wilsons2@upmc.edu
The authors reported no potential conflict of interest relevant to this article.
| Asthma still uncontrolled? Try these troubleshooting tips Jennie Broders, PharmD, BCPS |
Jennie Broders, PharmD, BCPS
UPMC St. Margaret, Pittsburgh, Pa
Krishna Desai, MD
UPMC St. Margaret, Pittsburgh, Pa
Stephen A. Wilson, MD, MPH, FAAFP
UPMC St. Margaret, Pittsburgh, Pa
wilsons2@upmc.edu
The authors reported no potential conflict of interest relevant to this article.
• Classify and treat asthma based on the patient’s worst symptom, whether or not it is the symptom that occurs most frequently. C
• Treat patients with poorly controlled asthma aggressively to gain quick control, then scale back slowly to the fewest medications and lowest doses needed to maintain control. A
• Reserve long-acting beta-agonists for use as an adjunct to inhaled corticosteroids for adults with poor baseline pulmonary function tests. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Angela D, a 34-year-old patient, has asthma with recurrent exacerbations. She uses a low-dose inhaled corticosteroid (ICS) daily and an albuterol inhaler, as needed, for shortness of breath or wheezing. She also has allergic rhinitis, for which she uses nasal fluticasone. Yet despite this regimen, Ms. D reports she still experiences wheezing, chest tightness, and shortness of breath 3 to 4 times a week and is awak-ened by coughing at least twice a week. In the past 6 months, she has had one emergency department (ED) visit and completed 2 courses of oral steroids.
Ms. D has gained weight since her last visit 3 months ago; her body mass index has gone from 27.5 to 29 kg/m2. And, while she has always been somewhat anxious, Ms. D notes that her anxiety has gotten progressively worse, as well.
About 25 million Americans—approximately one in 12—suffer from asthma1 and, despite improvements in asthma guidelines and treatment in the last 20 years,2 many still struggle with uncontrolled symptoms.3 The consequences can be severe.
Suboptimal control of asthma is associated with a significant decrease in quality of life, a greater likelihood of absence from work or school, and an increased risk for life-threatening events, trips to the ED, hospital admissions, and death.1 A multifaceted approach, including regular assessment, aggressive medication management, and attention to comorbidities, is needed to alleviate the suffering of patients with persistent asthma. This evidence-based review can help you provide such broad-based treatment.
Diagnosis and classification go hand in hand
The cornerstones of asthma management are accurate diagnosis and assessment of disease severity, based on both qualitative and quantitative measures. Start with a patient history, eliciting information about symptoms, triggers, risk factors, and most importantly, how often symptoms occur. Classic high-pitched wheezing sounds during exhalation, a cough that often worsens at night, shortness of breath, and chest tightness should raise suspicion for an asthma diagnosis.2 But frequency (and timing) of symptoms and exacerbations, as well as changes in the patient’s ability to function normally, help to determine whether asthma is classified as mild intermittent, mild persistent, moderate persistent, or severe persistent (TABLE).2
TABLE
Classifying asthma severity2
| Findings | Mild intermittent | Mild persistent | Moderate persistent | Severe persistent |
|---|---|---|---|---|
| Frequency | ≤2/wk | >2/wk, but <1/d | Daily | Continuous |
| Exacerbations | Rare | <2/wk | ≥2/wk | Frequent |
| Activity level | Normal | May decrease with exacerbation | Frequently limited | Significantly limited |
| Nighttime symptoms | ≤2/mo | >2/mo | >1/wk | Frequent |
| FEV1 (or PEF) predicted | >80% | >80% | >60% to <80% | ≤60% |
| PEF variability | <20% | 20%-30% | >30% | >30% |
| FEV1, forced expiratory volume in one second; PEF, peak expiratory flow. | ||||
Because asthma treatment should be based on its classification, an accurate assessment of disease severity is especially important for patients like Ms. D, who have been treated for asthma but continue to have unresolved symptoms. Keep in mind that asthma classification should be based on the worst symptom a patient has, not necessarily the symptom that occurs most frequently. Thus, a patient who has daytime symptoms requiring use of a rescue inhaler 2 to 3 times a week but is awakened at night with shortness of breath 2 times a week would receive a diagnosis of moderate persistent asthma on the basis of the night-time symptoms.
In assessing asthma severity, it is also important to ask specifically about recent events, including ED visits, hospitalizations, and intubations. This information, as well as answers to questions about smoking status, mental health problems, quality of life, and treatment compliance—and whether the patient can afford to purchase the asthma medications you’ve prescribed—can be used to assess the likelihood of poor outcomes.2
Factor in spirometry findings
History and physical examination alone cannot adequately diagnose and classify asthma severity.4,5 Spirometry, a reimbursable office test that can be administered by trained staff members, can be beneficial for any patient older than 5 years for whom a diagnosis of asthma is being considered or disease severity being determined.2 Other objective measures, such as the Mini Asthma Quality of Life questionnaire (http://erj.ersjournals.com/content/14/1/32.full.pdf+html) and peak expiratory flow measurement, may be helpful, as well.2,6
Spirometry measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) and calculates the FEV1/FVC ratio. Reference spirometry values vary according to patient characteristics, such as age, height, sex, and race, as well as the positioning of the patient during the test.7 (A seated position is optimal to reduce the risk of falls as a result of the light-headedness some patients may experience.) The American Thoracic Society provides a set of criteria (available at http://www.gp-training.net/protocol/respiratory/copd/spirometry.htm) that should be considered in interpreting test results.8
The 3 main spirometry patterns you’ll see are:
- Normal (FEV1 >80% predicted; FVC >80% predicted; FEV1/FVC >70%)
- Obstructive (FEV1 <80% predicted; FVC normal or mildly reduced; FEV1/FVC <70%)
- Restrictive (FEV1 normal or mildly reduced; FVC <80% predicted; FEV1/FVC >70%).
Because asthma is a chronic disease with fluctuating symptomatology and severity, spirometry testing should be repeated and results compared on several occasions as a guide to treatment.9 When an obstructive pattern is found, the patient should receive a bronchodilator treatment, then undergo spirometry 15 to 20 minutes later to determine reversibility. A reversible obstructive pattern, defined as an increase in FEV1 by 12% (≥200 mL), is consistent with an asthma diagnosis. If spirometry results are consistently normal but a high clinical suspicion for obstructive disease remains, the patient should be evaluated with a methacholine or histamine challenge test to definitively rule out asthma.10
Rule out asthma mimics. Many medical conditions can mimic symptoms of asthma and result in misdiagnosis or incorrect severity classification and unnecessary treatment. Patients should be evaluated for alternate or coexisting pulmonary conditions, including restrictive lung disease, vocal cord dysfunction, cough-variant asthma, malignancy, and allergies. For a patient whose asthma diagnosis is in doubt or who has a restrictive pattern on spirometry, additional evaluation based on signs and symptoms may require comprehensive pulmonary function testing, chest x-ray, bronchoscopy, laryngoscopy, computed tomography, and/or allergy testing.2
Peak expiratory flow (PEF). While measuring PEF should not replace spirometry or formal pulmonary function testing, it can be helpful for evaluating disease severity and monitoring treatment. Patients should use their own peak flow meters, and results compared with their personal best measurements. An improvement of 60 L/min or >20% after treatment with a bronchodilator is suggestive of asthma.9 There are a number of free or low-cost apps that patients can use to track their PEF measurements and response to treatment, such as Asthma MD, Huff and Puff (for children), and the Peak Flow Calculator.11-13
An evidence-based approach to asthma treatment
The first step in treating newly diagnosed asthma is to advise the patient to avoid known triggers, such as allergens, stressors, and particular odors or activities, to the extent possible, and, most importantly, to avoid exposure to smoke. If the patient smokes—cigarettes, marijuana, hookah, or pipe—stress the importance of quitting and living in a home that is smoke free. The link between asthma exacerbations and cockroaches is also well documented, particularly affecting those in urban areas. Avoidance of cockroaches and their droppings is critical, and may require the use of pest control services.14,15
A general principle of asthma management is to treat it aggressively initially to help the patient achieve quick control, then gradually cut back to the fewest medications and lowest effective doses required to maintain control.2 The National Heart, Lung, and Blood Institute (NHLBI)’s 2007 Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma (FIGURE)2 call for a stepwise approach.
Short-acting beta-agonists (SABAs) and ICS—first-line asthma therapy—have minimal risks or adverse effects. SABAs help reverse acute shortness of breath and wheezing, and ICS can reduce the frequency of exacerbations.2
FIGURE
Stepwise approach to asthma management for patients ≥12 years
*Consult with an asthma specialist if Step 4 care or higher is required; consider consultation at Step 3.
†Consider subcutaneous allergen immunotherapy for patients with allergic asthma.
ICS, inhaled corticosteroid; LABA, long-acting beta-agonist; LTRA, leukotriene receptor agonist; SABA, short-acting beta-agonist.
Adapted from: National Asthma Education and Prevention Program. J Allergy Clin Immunol. 2007.2
Second-line therapy is less clearcut
There are several options for patients whose symptoms are not well controlled with first-line treatment: (1) Add a long-acting beta-agonist (LABA); (2) add a leukotriene receptor antagonist (LTRA); or (3) increase the ICS dose, the most straightforward approach.
A dose increase avoids both the additional risk of adverse drug reactions and the added cost associated with another medication. But the easiest solution is not necessarily the best. Consider the evidence detailed below, which includes findings from studies published after the NHLBI’s guidelines.
The research on LABAs
LABAs have been widely used as adjunctive therapy for adults with asthma. However, a 2006 study raised safety concerns.16
The Salmeterol Multicenter Asthma Research Trial (SMART) compared the safety of the LABA salmeterol with a placebo added to usual asthma care over a 28-week treatment period. Overall, the primary composite end point—the number of respiratory-related deaths or life-threatening events—was low, and not statistically significant for salmeterol (50 vs 36; relative risk [RR]=1.40; 95% confidence interval [CI], 0.91-2.14).16 However, individual outcomes—respiratory-related deaths, asthma-related deaths, and asthma-related deaths or life-threatening episodes—were significantly more likely in the salmeterol group compared with the placebo group. In subgroup analysis, African American patients were found to be at greatest risk.16
It is hard to draw general conclusions from these data because the study was terminated early and poor outcomes were limited to a particular study year. Nonetheless, many physicians remain wary of LABAs as adjunctive therapy because of these findings and the media publicity they generated.
A 2010 Cochrane review provided additional data on the safety and efficacy of the combination of a LABA and ICS compared with a higher dose of ICS.17 The review, which included 48 randomized controlled trials, found that combination therapy had a lower risk of exacerbations for which oral corticosteroids were required than a higher dose of ICS (RR=0.88; 95% CI, 0.78-0.98; P=.02). The median number needed to treat (NNT) was 73. No significant difference in the risk of overall adverse events (RR=0.99; 95% CI, 0.95-1.03) was found, but there was an increase in the risk of tremor (RR=1.84; 95% CI, 1.20-2.82) and a decrease in risk for oral thrush (RR=0.58; 95% CI, 0.40-0.86) in the combination therapy group.
While the Cochrane review did not show a combination of LABA and ICS to be less safe overall than higher doses of ICS alone, the findings were less favorable for children and patients with higher baseline lung function, in circumstances in which the combination therapy was taken for a longer duration, and when the LABA being studied was formoterol.17
Overall, it is when a LABA is delivered via separate inhaler that adverse outcomes have been reported. Findings have been positive when the LABA is combined with ICS, and this combination is recommended as maintenance therapy for moderate to severe asthma.
Two new studies, published in March 2013, reported successful use of a LABA-ICS combination not only for maintenance via scheduled dosing, but also for early phases of exacerbation via extra dosing—an approach called Single inhaler Maintenance and Reliever Therapy (SMART).18,19 In both studies, SMART resulted in less excessive use of SABAs and less need for oral steroids, fewer hospitalizations for asthma, and fewer cases of progression to a full-blown exacerbation.
The takeaway: LABAs should be reserved for use as an adjunct to ICS in adults with poor baseline pulmonary function tests or severe asthma, and delivered as a combination product with ICS, not as a separate inhaled medication. SMART is a safe and effective means of administering LABA-ICS therapy for some patients at risk for frequent severe exacerbations.
When to consider LTRAs
LTRAs can be valuable medications in asthma management and there are extensive data on their use, particularly in the treatment of children with asthma. A Cochrane review published in 2012, however, supported current guideline recommendations, finding that as monotherapy, ICS are superior to LTRAs.20
When LTRAs as an adjunctive therapy to ICS were compared with ICS monotherapy, researchers found a modest improvement in PEF (weighted mean difference [WMD] =7.7 L/min; 95% CI, 3.6-11.8) in the group receiving combination therapy and a decrease in the need for a SABA as rescue therapy (WMD=1 puff/week; 95% CI, 0.5-2.0).21 There was no significant reduction in the risk of exacerbations requiring systemic steroids (RR=0.64; 95% CI, 0.38-1.07).
LABAs and LTRAs go head to head. A 2010 Cochrane review compared the efficacy and safety of a daily LABA vs a LTRA as add-on therapy for patients whose asthma was not well controlled with ICS monotherapy.22 The LABA/ICS combination was significantly better at reducing the risk of exacerbations requiring systemic corticosteroids than monotherapy with either a LTRA or ICS, reducing the risk from 11% to 9% (RR=0.83; 95% CI, 0.71-0.97). The NNT to prevent one exacerbation over 48 weeks was 38 (95% CI, 22-244).22
The safety of LABAs continues to be a concern, however, as serious adverse events were more common in the LABA group. The number needed to harm (NNH) with LABA therapy vs LTRA over 48 weeks was 78; 95% CI, 33 to infinity.22 (The width of the CI indicates that while harm is possible in as few as 33 patients, it is also possible that an infinite number of patients would need to be treated for one individual to incur harm.) Overall, the evidence suggests that LABAs are superior add-on therapy to ICS for the treatment of uncontrolled asthma compared with LTRAs, but their use nonetheless requires caution and close monitoring in African American and pediatric patients.17
Is there a role for a long-acting anticholinergic inhaler?
Long-acting anticholinergic medication (LAAM)—tiotropium is the only drug in this class on the market, but there are others in clinical trials—is the mainstay of therapy for chronic obstructive pulmonary disease. This drug class was not widely available or studied as an asthma treatment when the NHLBI guidelines were drafted.
A 2010 study of tiotropium challenged the notion that there is no place for LAAMs in asthma therapy. Using a 3-way crossover design, the study compared the addition of tiotropium to ICS with a double dose of ICS or a LABA/ICS combination.23
The results suggest that LAAMs could be useful in treating uncontrolled asthma. Compared with the double dose of ICS, the tiotropium/ICS combination increased PEF by a mean difference of 25.8 L/min (P<.001) and resulted in a statistically significant improvement in the proportion of asthma control days, FEV1, and daily symptom scores.23 As an adjunctive treatment to ICS, tiotropium was not inferior to a LABA.
CASE After a detailed history, physical exam, and diagnostic testing, Ms. D was given a diagnosis of moderate persistent asthma. We recognized the need to step up her treatment. Prior to making any changes in her medication regimen, however, our team, which included a clinical pharmacist, observed her use of inhaled medications and verified that she was using the inhaler properly. We then initiated combination therapy, pairing a LABA and ICS.
Comorbidities complicate asthma management
Asthma management is often complicated by other uncontrolled coexisting medical problems. Common comorbidities that can affect asthma severity include allergic rhinitis, chronic sinusitis, gastroesophageal reflux disease (GERD), obesity, obstructive sleep apnea (OSA), mental health disorders, tobacco use, and hormonal disturbances.2
Allergic rhinitis. Allergic rhinitis has been associated with worse asthma control and a negative impact on quality of life, and the upper airway inflammation associated with it should be treated.24
Antihistamines and nasal steroids are the most effective medical management. Some patients with allergic rhinitis benefit from blood or skin allergy testing for confirmation or to aid in avoidance. Referral to an allergist may be necessary if symptoms are recalcitrant, a food allergy is in question, or the diagnosis is unclear.
GERD. Compared with the general population, patients with asthma have a much higher risk of GERD, although it is not always symptomatic. While results are inconsistent and difficult to predict, treating symptomatic GERD with acid-blocking medications can result in better asthma control for some patients. However, proton pump inhibitors should not be used to treat asthma symptoms in patients with asymptomatic GERD.25,26
Obesity and OSA. Weight loss can significantly improve asthma control, decrease medication use, and improve quality of life.27,28 Obese patients are less likely to respond to treatment with ICS.2 Weight loss also benefits those who suffer from OSA, which may contribute to airway hyperresponsiveness.29
Mental health disorders. Compared with the general population, patients with asthma are more likely to have depression, anxiety, and panic disorders.30 Diagnosis and treatment of these comorbid conditions can lead to better asthma management, increased medication adherence, decreased health care utilization—including fewer ED visits and hospitalizations—and a better quality of life.30
CASE We also addressed our patient’s comorbidities—weight gain, allergic rhinitis, and anxiety. The allergic rhinitis was already well-controlled with a nasal steroid, but we suspected a relationship between Ms. D’s weight gain and increasing anxiety associated with some recent life events. We suggested she see a counselor, and she agreed.
When the patient returned in 12 weeks, she reported that she hardly needed her rescue inhaler anymore and that she was managing her anxiety more effectively. She also told us that she had begun a low-fat dietary regimen, and we confirmed that she had already lost 5 pounds.
CORRESPONDENCE
Stephen A. Wilson, MD, MPH, FAAFP, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; wilsons2@upmc.edu
• Classify and treat asthma based on the patient’s worst symptom, whether or not it is the symptom that occurs most frequently. C
• Treat patients with poorly controlled asthma aggressively to gain quick control, then scale back slowly to the fewest medications and lowest doses needed to maintain control. A
• Reserve long-acting beta-agonists for use as an adjunct to inhaled corticosteroids for adults with poor baseline pulmonary function tests. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Angela D, a 34-year-old patient, has asthma with recurrent exacerbations. She uses a low-dose inhaled corticosteroid (ICS) daily and an albuterol inhaler, as needed, for shortness of breath or wheezing. She also has allergic rhinitis, for which she uses nasal fluticasone. Yet despite this regimen, Ms. D reports she still experiences wheezing, chest tightness, and shortness of breath 3 to 4 times a week and is awak-ened by coughing at least twice a week. In the past 6 months, she has had one emergency department (ED) visit and completed 2 courses of oral steroids.
Ms. D has gained weight since her last visit 3 months ago; her body mass index has gone from 27.5 to 29 kg/m2. And, while she has always been somewhat anxious, Ms. D notes that her anxiety has gotten progressively worse, as well.
About 25 million Americans—approximately one in 12—suffer from asthma1 and, despite improvements in asthma guidelines and treatment in the last 20 years,2 many still struggle with uncontrolled symptoms.3 The consequences can be severe.
Suboptimal control of asthma is associated with a significant decrease in quality of life, a greater likelihood of absence from work or school, and an increased risk for life-threatening events, trips to the ED, hospital admissions, and death.1 A multifaceted approach, including regular assessment, aggressive medication management, and attention to comorbidities, is needed to alleviate the suffering of patients with persistent asthma. This evidence-based review can help you provide such broad-based treatment.
Diagnosis and classification go hand in hand
The cornerstones of asthma management are accurate diagnosis and assessment of disease severity, based on both qualitative and quantitative measures. Start with a patient history, eliciting information about symptoms, triggers, risk factors, and most importantly, how often symptoms occur. Classic high-pitched wheezing sounds during exhalation, a cough that often worsens at night, shortness of breath, and chest tightness should raise suspicion for an asthma diagnosis.2 But frequency (and timing) of symptoms and exacerbations, as well as changes in the patient’s ability to function normally, help to determine whether asthma is classified as mild intermittent, mild persistent, moderate persistent, or severe persistent (TABLE).2
TABLE
Classifying asthma severity2
| Findings | Mild intermittent | Mild persistent | Moderate persistent | Severe persistent |
|---|---|---|---|---|
| Frequency | ≤2/wk | >2/wk, but <1/d | Daily | Continuous |
| Exacerbations | Rare | <2/wk | ≥2/wk | Frequent |
| Activity level | Normal | May decrease with exacerbation | Frequently limited | Significantly limited |
| Nighttime symptoms | ≤2/mo | >2/mo | >1/wk | Frequent |
| FEV1 (or PEF) predicted | >80% | >80% | >60% to <80% | ≤60% |
| PEF variability | <20% | 20%-30% | >30% | >30% |
| FEV1, forced expiratory volume in one second; PEF, peak expiratory flow. | ||||
Because asthma treatment should be based on its classification, an accurate assessment of disease severity is especially important for patients like Ms. D, who have been treated for asthma but continue to have unresolved symptoms. Keep in mind that asthma classification should be based on the worst symptom a patient has, not necessarily the symptom that occurs most frequently. Thus, a patient who has daytime symptoms requiring use of a rescue inhaler 2 to 3 times a week but is awakened at night with shortness of breath 2 times a week would receive a diagnosis of moderate persistent asthma on the basis of the night-time symptoms.
In assessing asthma severity, it is also important to ask specifically about recent events, including ED visits, hospitalizations, and intubations. This information, as well as answers to questions about smoking status, mental health problems, quality of life, and treatment compliance—and whether the patient can afford to purchase the asthma medications you’ve prescribed—can be used to assess the likelihood of poor outcomes.2
Factor in spirometry findings
History and physical examination alone cannot adequately diagnose and classify asthma severity.4,5 Spirometry, a reimbursable office test that can be administered by trained staff members, can be beneficial for any patient older than 5 years for whom a diagnosis of asthma is being considered or disease severity being determined.2 Other objective measures, such as the Mini Asthma Quality of Life questionnaire (http://erj.ersjournals.com/content/14/1/32.full.pdf+html) and peak expiratory flow measurement, may be helpful, as well.2,6
Spirometry measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) and calculates the FEV1/FVC ratio. Reference spirometry values vary according to patient characteristics, such as age, height, sex, and race, as well as the positioning of the patient during the test.7 (A seated position is optimal to reduce the risk of falls as a result of the light-headedness some patients may experience.) The American Thoracic Society provides a set of criteria (available at http://www.gp-training.net/protocol/respiratory/copd/spirometry.htm) that should be considered in interpreting test results.8
The 3 main spirometry patterns you’ll see are:
- Normal (FEV1 >80% predicted; FVC >80% predicted; FEV1/FVC >70%)
- Obstructive (FEV1 <80% predicted; FVC normal or mildly reduced; FEV1/FVC <70%)
- Restrictive (FEV1 normal or mildly reduced; FVC <80% predicted; FEV1/FVC >70%).
Because asthma is a chronic disease with fluctuating symptomatology and severity, spirometry testing should be repeated and results compared on several occasions as a guide to treatment.9 When an obstructive pattern is found, the patient should receive a bronchodilator treatment, then undergo spirometry 15 to 20 minutes later to determine reversibility. A reversible obstructive pattern, defined as an increase in FEV1 by 12% (≥200 mL), is consistent with an asthma diagnosis. If spirometry results are consistently normal but a high clinical suspicion for obstructive disease remains, the patient should be evaluated with a methacholine or histamine challenge test to definitively rule out asthma.10
Rule out asthma mimics. Many medical conditions can mimic symptoms of asthma and result in misdiagnosis or incorrect severity classification and unnecessary treatment. Patients should be evaluated for alternate or coexisting pulmonary conditions, including restrictive lung disease, vocal cord dysfunction, cough-variant asthma, malignancy, and allergies. For a patient whose asthma diagnosis is in doubt or who has a restrictive pattern on spirometry, additional evaluation based on signs and symptoms may require comprehensive pulmonary function testing, chest x-ray, bronchoscopy, laryngoscopy, computed tomography, and/or allergy testing.2
Peak expiratory flow (PEF). While measuring PEF should not replace spirometry or formal pulmonary function testing, it can be helpful for evaluating disease severity and monitoring treatment. Patients should use their own peak flow meters, and results compared with their personal best measurements. An improvement of 60 L/min or >20% after treatment with a bronchodilator is suggestive of asthma.9 There are a number of free or low-cost apps that patients can use to track their PEF measurements and response to treatment, such as Asthma MD, Huff and Puff (for children), and the Peak Flow Calculator.11-13
An evidence-based approach to asthma treatment
The first step in treating newly diagnosed asthma is to advise the patient to avoid known triggers, such as allergens, stressors, and particular odors or activities, to the extent possible, and, most importantly, to avoid exposure to smoke. If the patient smokes—cigarettes, marijuana, hookah, or pipe—stress the importance of quitting and living in a home that is smoke free. The link between asthma exacerbations and cockroaches is also well documented, particularly affecting those in urban areas. Avoidance of cockroaches and their droppings is critical, and may require the use of pest control services.14,15
A general principle of asthma management is to treat it aggressively initially to help the patient achieve quick control, then gradually cut back to the fewest medications and lowest effective doses required to maintain control.2 The National Heart, Lung, and Blood Institute (NHLBI)’s 2007 Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma (FIGURE)2 call for a stepwise approach.
Short-acting beta-agonists (SABAs) and ICS—first-line asthma therapy—have minimal risks or adverse effects. SABAs help reverse acute shortness of breath and wheezing, and ICS can reduce the frequency of exacerbations.2
FIGURE
Stepwise approach to asthma management for patients ≥12 years
*Consult with an asthma specialist if Step 4 care or higher is required; consider consultation at Step 3.
†Consider subcutaneous allergen immunotherapy for patients with allergic asthma.
ICS, inhaled corticosteroid; LABA, long-acting beta-agonist; LTRA, leukotriene receptor agonist; SABA, short-acting beta-agonist.
Adapted from: National Asthma Education and Prevention Program. J Allergy Clin Immunol. 2007.2
Second-line therapy is less clearcut
There are several options for patients whose symptoms are not well controlled with first-line treatment: (1) Add a long-acting beta-agonist (LABA); (2) add a leukotriene receptor antagonist (LTRA); or (3) increase the ICS dose, the most straightforward approach.
A dose increase avoids both the additional risk of adverse drug reactions and the added cost associated with another medication. But the easiest solution is not necessarily the best. Consider the evidence detailed below, which includes findings from studies published after the NHLBI’s guidelines.
The research on LABAs
LABAs have been widely used as adjunctive therapy for adults with asthma. However, a 2006 study raised safety concerns.16
The Salmeterol Multicenter Asthma Research Trial (SMART) compared the safety of the LABA salmeterol with a placebo added to usual asthma care over a 28-week treatment period. Overall, the primary composite end point—the number of respiratory-related deaths or life-threatening events—was low, and not statistically significant for salmeterol (50 vs 36; relative risk [RR]=1.40; 95% confidence interval [CI], 0.91-2.14).16 However, individual outcomes—respiratory-related deaths, asthma-related deaths, and asthma-related deaths or life-threatening episodes—were significantly more likely in the salmeterol group compared with the placebo group. In subgroup analysis, African American patients were found to be at greatest risk.16
It is hard to draw general conclusions from these data because the study was terminated early and poor outcomes were limited to a particular study year. Nonetheless, many physicians remain wary of LABAs as adjunctive therapy because of these findings and the media publicity they generated.
A 2010 Cochrane review provided additional data on the safety and efficacy of the combination of a LABA and ICS compared with a higher dose of ICS.17 The review, which included 48 randomized controlled trials, found that combination therapy had a lower risk of exacerbations for which oral corticosteroids were required than a higher dose of ICS (RR=0.88; 95% CI, 0.78-0.98; P=.02). The median number needed to treat (NNT) was 73. No significant difference in the risk of overall adverse events (RR=0.99; 95% CI, 0.95-1.03) was found, but there was an increase in the risk of tremor (RR=1.84; 95% CI, 1.20-2.82) and a decrease in risk for oral thrush (RR=0.58; 95% CI, 0.40-0.86) in the combination therapy group.
While the Cochrane review did not show a combination of LABA and ICS to be less safe overall than higher doses of ICS alone, the findings were less favorable for children and patients with higher baseline lung function, in circumstances in which the combination therapy was taken for a longer duration, and when the LABA being studied was formoterol.17
Overall, it is when a LABA is delivered via separate inhaler that adverse outcomes have been reported. Findings have been positive when the LABA is combined with ICS, and this combination is recommended as maintenance therapy for moderate to severe asthma.
Two new studies, published in March 2013, reported successful use of a LABA-ICS combination not only for maintenance via scheduled dosing, but also for early phases of exacerbation via extra dosing—an approach called Single inhaler Maintenance and Reliever Therapy (SMART).18,19 In both studies, SMART resulted in less excessive use of SABAs and less need for oral steroids, fewer hospitalizations for asthma, and fewer cases of progression to a full-blown exacerbation.
The takeaway: LABAs should be reserved for use as an adjunct to ICS in adults with poor baseline pulmonary function tests or severe asthma, and delivered as a combination product with ICS, not as a separate inhaled medication. SMART is a safe and effective means of administering LABA-ICS therapy for some patients at risk for frequent severe exacerbations.
When to consider LTRAs
LTRAs can be valuable medications in asthma management and there are extensive data on their use, particularly in the treatment of children with asthma. A Cochrane review published in 2012, however, supported current guideline recommendations, finding that as monotherapy, ICS are superior to LTRAs.20
When LTRAs as an adjunctive therapy to ICS were compared with ICS monotherapy, researchers found a modest improvement in PEF (weighted mean difference [WMD] =7.7 L/min; 95% CI, 3.6-11.8) in the group receiving combination therapy and a decrease in the need for a SABA as rescue therapy (WMD=1 puff/week; 95% CI, 0.5-2.0).21 There was no significant reduction in the risk of exacerbations requiring systemic steroids (RR=0.64; 95% CI, 0.38-1.07).
LABAs and LTRAs go head to head. A 2010 Cochrane review compared the efficacy and safety of a daily LABA vs a LTRA as add-on therapy for patients whose asthma was not well controlled with ICS monotherapy.22 The LABA/ICS combination was significantly better at reducing the risk of exacerbations requiring systemic corticosteroids than monotherapy with either a LTRA or ICS, reducing the risk from 11% to 9% (RR=0.83; 95% CI, 0.71-0.97). The NNT to prevent one exacerbation over 48 weeks was 38 (95% CI, 22-244).22
The safety of LABAs continues to be a concern, however, as serious adverse events were more common in the LABA group. The number needed to harm (NNH) with LABA therapy vs LTRA over 48 weeks was 78; 95% CI, 33 to infinity.22 (The width of the CI indicates that while harm is possible in as few as 33 patients, it is also possible that an infinite number of patients would need to be treated for one individual to incur harm.) Overall, the evidence suggests that LABAs are superior add-on therapy to ICS for the treatment of uncontrolled asthma compared with LTRAs, but their use nonetheless requires caution and close monitoring in African American and pediatric patients.17
Is there a role for a long-acting anticholinergic inhaler?
Long-acting anticholinergic medication (LAAM)—tiotropium is the only drug in this class on the market, but there are others in clinical trials—is the mainstay of therapy for chronic obstructive pulmonary disease. This drug class was not widely available or studied as an asthma treatment when the NHLBI guidelines were drafted.
A 2010 study of tiotropium challenged the notion that there is no place for LAAMs in asthma therapy. Using a 3-way crossover design, the study compared the addition of tiotropium to ICS with a double dose of ICS or a LABA/ICS combination.23
The results suggest that LAAMs could be useful in treating uncontrolled asthma. Compared with the double dose of ICS, the tiotropium/ICS combination increased PEF by a mean difference of 25.8 L/min (P<.001) and resulted in a statistically significant improvement in the proportion of asthma control days, FEV1, and daily symptom scores.23 As an adjunctive treatment to ICS, tiotropium was not inferior to a LABA.
CASE After a detailed history, physical exam, and diagnostic testing, Ms. D was given a diagnosis of moderate persistent asthma. We recognized the need to step up her treatment. Prior to making any changes in her medication regimen, however, our team, which included a clinical pharmacist, observed her use of inhaled medications and verified that she was using the inhaler properly. We then initiated combination therapy, pairing a LABA and ICS.
Comorbidities complicate asthma management
Asthma management is often complicated by other uncontrolled coexisting medical problems. Common comorbidities that can affect asthma severity include allergic rhinitis, chronic sinusitis, gastroesophageal reflux disease (GERD), obesity, obstructive sleep apnea (OSA), mental health disorders, tobacco use, and hormonal disturbances.2
Allergic rhinitis. Allergic rhinitis has been associated with worse asthma control and a negative impact on quality of life, and the upper airway inflammation associated with it should be treated.24
Antihistamines and nasal steroids are the most effective medical management. Some patients with allergic rhinitis benefit from blood or skin allergy testing for confirmation or to aid in avoidance. Referral to an allergist may be necessary if symptoms are recalcitrant, a food allergy is in question, or the diagnosis is unclear.
GERD. Compared with the general population, patients with asthma have a much higher risk of GERD, although it is not always symptomatic. While results are inconsistent and difficult to predict, treating symptomatic GERD with acid-blocking medications can result in better asthma control for some patients. However, proton pump inhibitors should not be used to treat asthma symptoms in patients with asymptomatic GERD.25,26
Obesity and OSA. Weight loss can significantly improve asthma control, decrease medication use, and improve quality of life.27,28 Obese patients are less likely to respond to treatment with ICS.2 Weight loss also benefits those who suffer from OSA, which may contribute to airway hyperresponsiveness.29
Mental health disorders. Compared with the general population, patients with asthma are more likely to have depression, anxiety, and panic disorders.30 Diagnosis and treatment of these comorbid conditions can lead to better asthma management, increased medication adherence, decreased health care utilization—including fewer ED visits and hospitalizations—and a better quality of life.30
CASE We also addressed our patient’s comorbidities—weight gain, allergic rhinitis, and anxiety. The allergic rhinitis was already well-controlled with a nasal steroid, but we suspected a relationship between Ms. D’s weight gain and increasing anxiety associated with some recent life events. We suggested she see a counselor, and she agreed.
When the patient returned in 12 weeks, she reported that she hardly needed her rescue inhaler anymore and that she was managing her anxiety more effectively. She also told us that she had begun a low-fat dietary regimen, and we confirmed that she had already lost 5 pounds.
CORRESPONDENCE
Stephen A. Wilson, MD, MPH, FAAFP, UPMC St. Margaret, 815 Freeport Road, Pittsburgh, PA 15215; wilsons2@upmc.edu
1. American Academy of Allergy, Asthma, and Immunology. Asthma statistics. Available at: http://www.aaaai.org/about-the-aaaai/newsroom/asthma-statistics.aspx. Accessed March 7, 2012.
2. National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for diagnosis and management of asthma. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
3. Centers for Disease Control and Prevention. National surveillance for asthma—United States, 1980-2004. MMWR Surveill Summ. 2007;56(8):1-54.
4. Stout JW, Visness CM, Enright P, et al. Classification of asthma severity in children. Arch Pediatr Adolesc Med. 2006;160:844-850.
5. Bacharier LB, Strunk RC, Mauger D, et al. Classifying asthma severity in children. Am J Respir Crit Care Med. 2004;170:426-432.
6. Juniper EF, Guyatt GH, Cox FM, et al. Development and validation of the Mini Asthma Quality of Life Questionnaire. Eur Respir J. 1999;14:32-38.
7. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:179-187.
8. Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26:319-338.
9. Bateman ED, Hurd SS, Barnes PJ, et al. Global Strategy for Asthma Management and Prevention. Eur Respir J. 2008;31:143-178.
10. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of COPD. February 2013. Available at: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed March 7, 2013.
11. AsthmaMD. Available at: http://www.asthmamd.org/#resources/iphone_chart.jpg. Accessed March 7, 2013.
12. Indiegogo. Huff & Puff. Available at: http://www.indiegogo.com/projects/the-best-asthma-education-app-in-the-world-period. Accessed March 7, 2013.
13. Vimukti Technologies Pvt Ltd. Peak flow calculator. Available at: http://appworld.blackberry.com/webstore/content/7615. Accessed March 7, 2013,
14. Morgan WJ, Crain EF, Gruchalla RS, et al. Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;35:1068-1080.
15. Phipatanakul W, Matsui E, Portnoy J, et al. Environmental assessment and exposure reduction of rodents: a practice parameter. Ann Allergy Asthma Immunol. 2012;109:375-387.
16. Nelson HS, Weiss ST, Bleeker ER, et al. The Salmeterol Multicenter Asthma Research Trial. Chest. 2006;129:15-26.
17. Ducharme FM, Ni Chroinin M, Greenstone I, et al. Addition of long-acting beta2-agonists to inhaled steroids versus higher dose inhaled steroids in adults and children with persistent asthma. Cochrane Database Syst Rev. 2010;(4):CD005533.-
18. Papi A, Corradi M, Pigeon-Francisco C, et al. Beclometasone-formoterol as maintenance and reliever treatment in patients with asthma. Lancet Respir Med. 2013;1:23-31.
19. Patel M, Pilcher J, Pritchard A, et al. Efficacy and safety of maintenance and reliever combination budesonide-formoterol inhaler in patients with asthma at risk of severe exacerba-tions. Lancet Respir Med. 2013;1:32-42.
20. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.-
21. Ducharme FM. Addition of anti-leukotriene agents to inhaled corticosteroids for chronic asthma. Cochrane Database Syst Rev. 2004;(1):CD003133.-
22. Ducharme FM, Lasserson TJ, Cates CJ. Addition to inhaled corticosteroids of long-acting beta2-agonists versus anti-leukotrienes for chronic asthma. Cochrane Database Syst Rev. 2011;(5):CD003137.-
23. Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010;363:1715-1726.
24. Vandenplas O, Dramaix M, Joos G, et al. The impact of concomitant rhinitis on asthma-related quality of life and asthma control. Allergy. 2010;65:1290-1297.
25. Gibson PG, Henry RL, Coughlan JL. Gastroesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.-
26. The American Lung Association Asthma Clinical Research Centers. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360:1487-1499.
27. Eneli IU, Skybo T, Camargo CA, Jr. Weight loss and asthma. Thorax. 2008;63:671-676.
28. Stenius-Aarniala B, Poussa T, Kvarnstrom J, et al. Immediate and long term effects of weight reduction in obese people with asthma. BMJ. 2000;320:827-832.
29. Sariman N, Levent E, Cubuk R, et al. Bronchial hyperreactivity and airway wall thickening in obstructive sleep apnea patients. Sleep Breath. 2011;15:341-50.
30. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104:22-28.
1. American Academy of Allergy, Asthma, and Immunology. Asthma statistics. Available at: http://www.aaaai.org/about-the-aaaai/newsroom/asthma-statistics.aspx. Accessed March 7, 2012.
2. National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for diagnosis and management of asthma. J Allergy Clin Immunol. 2007;120(5 suppl):S94-S138.
3. Centers for Disease Control and Prevention. National surveillance for asthma—United States, 1980-2004. MMWR Surveill Summ. 2007;56(8):1-54.
4. Stout JW, Visness CM, Enright P, et al. Classification of asthma severity in children. Arch Pediatr Adolesc Med. 2006;160:844-850.
5. Bacharier LB, Strunk RC, Mauger D, et al. Classifying asthma severity in children. Am J Respir Crit Care Med. 2004;170:426-432.
6. Juniper EF, Guyatt GH, Cox FM, et al. Development and validation of the Mini Asthma Quality of Life Questionnaire. Eur Respir J. 1999;14:32-38.
7. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:179-187.
8. Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26:319-338.
9. Bateman ED, Hurd SS, Barnes PJ, et al. Global Strategy for Asthma Management and Prevention. Eur Respir J. 2008;31:143-178.
10. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of COPD. February 2013. Available at: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed March 7, 2013.
11. AsthmaMD. Available at: http://www.asthmamd.org/#resources/iphone_chart.jpg. Accessed March 7, 2013.
12. Indiegogo. Huff & Puff. Available at: http://www.indiegogo.com/projects/the-best-asthma-education-app-in-the-world-period. Accessed March 7, 2013.
13. Vimukti Technologies Pvt Ltd. Peak flow calculator. Available at: http://appworld.blackberry.com/webstore/content/7615. Accessed March 7, 2013,
14. Morgan WJ, Crain EF, Gruchalla RS, et al. Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;35:1068-1080.
15. Phipatanakul W, Matsui E, Portnoy J, et al. Environmental assessment and exposure reduction of rodents: a practice parameter. Ann Allergy Asthma Immunol. 2012;109:375-387.
16. Nelson HS, Weiss ST, Bleeker ER, et al. The Salmeterol Multicenter Asthma Research Trial. Chest. 2006;129:15-26.
17. Ducharme FM, Ni Chroinin M, Greenstone I, et al. Addition of long-acting beta2-agonists to inhaled steroids versus higher dose inhaled steroids in adults and children with persistent asthma. Cochrane Database Syst Rev. 2010;(4):CD005533.-
18. Papi A, Corradi M, Pigeon-Francisco C, et al. Beclometasone-formoterol as maintenance and reliever treatment in patients with asthma. Lancet Respir Med. 2013;1:23-31.
19. Patel M, Pilcher J, Pritchard A, et al. Efficacy and safety of maintenance and reliever combination budesonide-formoterol inhaler in patients with asthma at risk of severe exacerba-tions. Lancet Respir Med. 2013;1:32-42.
20. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.-
21. Ducharme FM. Addition of anti-leukotriene agents to inhaled corticosteroids for chronic asthma. Cochrane Database Syst Rev. 2004;(1):CD003133.-
22. Ducharme FM, Lasserson TJ, Cates CJ. Addition to inhaled corticosteroids of long-acting beta2-agonists versus anti-leukotrienes for chronic asthma. Cochrane Database Syst Rev. 2011;(5):CD003137.-
23. Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010;363:1715-1726.
24. Vandenplas O, Dramaix M, Joos G, et al. The impact of concomitant rhinitis on asthma-related quality of life and asthma control. Allergy. 2010;65:1290-1297.
25. Gibson PG, Henry RL, Coughlan JL. Gastroesophageal reflux treatment for asthma in adults and children. Cochrane Database Syst Rev. 2003;(2):CD001496.-
26. The American Lung Association Asthma Clinical Research Centers. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360:1487-1499.
27. Eneli IU, Skybo T, Camargo CA, Jr. Weight loss and asthma. Thorax. 2008;63:671-676.
28. Stenius-Aarniala B, Poussa T, Kvarnstrom J, et al. Immediate and long term effects of weight reduction in obese people with asthma. BMJ. 2000;320:827-832.
29. Sariman N, Levent E, Cubuk R, et al. Bronchial hyperreactivity and airway wall thickening in obstructive sleep apnea patients. Sleep Breath. 2011;15:341-50.
30. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104:22-28.
Genetics contribute to smoking habits of adolescents, adults
Genetic risk may contribute to the rapid progression of daily and heavy smoking during adolescence and subsequent problems with nicotine dependence and smoking cessation in adulthood, according to a recent study.
The research may have implications for the development of initiatives that deter smoking in adolescents, reported Daniel W. Belsky, Ph.D., of the University of North Carolina at Chapel Hill and Duke University Medical Center, Durham, N.C., and his associates. The 38-year longitudinal study included 1,037 men and women from the Dunedin Multidisciplinary Health and Development Study of New Zealand. Researchers assessed participants with a multilocus genetic risk score (GRS), originating from three meta-analyses of genome-wide association studies (GWAS) that used the number of cigarettes smoked daily as their phenotype. Dr. Belsky and his team focused their investigation on the single-nucleotide polymorphisms in 15q25.1 and19q13.2 (JAMA Psychiatry 2013 March 27 [doi:10.1001/jamapsychiatry.2013.736]).
Genotyping was possible in 880 Dunedin subjects. In addition to evaluating family history in these individuals, researchers gathered smoking information at eight assessments from the age 11-38 years.
The GRS was not associated with whether or when subjects started smoking. "In fact, daily smokers who did not progress to heavy use were at lower genetic risk than individuals who never smoked," the researchers wrote.
Among 627 ever-smokers in the cohort, those with a higher genetic risk were more likely to rapidly progress to heavy smoking, meaning 20 or more cigarettes daily (hazard ratio, 1.35; 95% confidence interval, 1.14-1.58).
Adolescents with high genetic risk had a greater chance of becoming daily smokers by age 15 (relative risk, 1.24; 95% CI, 1.06-1.45) and progressing to heavy smoking by age 18 (RR, 1.43; 95% CI, 1.10-1.86).
Over the course of the study, subjects with a high genetic risk accumulated more pack-years of smoking. As adults, 27% of ever-smokers became nicotine dependent and those at higher genetic risk had a greater chance of doing so (HR, 1.27; 95% CI, 1.09-1.47). Additionally, of 277 cohort members who smoked daily during their 30s, those with a higher genetic risk were more likely to use smoking to cope with stress.
Further analyses found that smoking cessation was also difficult in adults at high genetic risk. For example, in the cohort of 277 daily smokers, 53% quit smoking a month or longer across 72 months follow-up; however, relapse occurred in 62%. Quitters with a higher genetic risk had a greater chance of relapsing (HR, 1.22; 95% CI, 1.02-1.45).
Only 20% of daily smokers abstained from smoking for a year or more.
Associations detected between the GRS and smoking phenotypes were small, noted the study authors. "Children who our study would classify at high genetic risk are not guaranteed to become addicted if they try smoking, and, even more importantly, children we would classify at low genetic risk are not immune to addiction."
Finally, researchers found that that the GRS score did not correlate with family history. "The GRS contained different information about risk for developmental and mature phenotypes of smoking behavior, compared with family history," reported the study authors.
The authors said that their research "adds a genetic dimension to longstanding arguments" in favor of early cigarette prevention of cigarette consumption, including surtaxes and age restrictions on tobacco purchases.
Funding for this study was provided through grants from various organizations, including the U.S. National Institute on Aging, the U.S. National Institute on Mental Health, and the U.K. Medical Research Council. The Dunedin Multidisciplinary Health and Development Research Unit is supported by the New Zealand Health Research Council.
Genetic risk may contribute to the rapid progression of daily and heavy smoking during adolescence and subsequent problems with nicotine dependence and smoking cessation in adulthood, according to a recent study.
The research may have implications for the development of initiatives that deter smoking in adolescents, reported Daniel W. Belsky, Ph.D., of the University of North Carolina at Chapel Hill and Duke University Medical Center, Durham, N.C., and his associates. The 38-year longitudinal study included 1,037 men and women from the Dunedin Multidisciplinary Health and Development Study of New Zealand. Researchers assessed participants with a multilocus genetic risk score (GRS), originating from three meta-analyses of genome-wide association studies (GWAS) that used the number of cigarettes smoked daily as their phenotype. Dr. Belsky and his team focused their investigation on the single-nucleotide polymorphisms in 15q25.1 and19q13.2 (JAMA Psychiatry 2013 March 27 [doi:10.1001/jamapsychiatry.2013.736]).
Genotyping was possible in 880 Dunedin subjects. In addition to evaluating family history in these individuals, researchers gathered smoking information at eight assessments from the age 11-38 years.
The GRS was not associated with whether or when subjects started smoking. "In fact, daily smokers who did not progress to heavy use were at lower genetic risk than individuals who never smoked," the researchers wrote.
Among 627 ever-smokers in the cohort, those with a higher genetic risk were more likely to rapidly progress to heavy smoking, meaning 20 or more cigarettes daily (hazard ratio, 1.35; 95% confidence interval, 1.14-1.58).
Adolescents with high genetic risk had a greater chance of becoming daily smokers by age 15 (relative risk, 1.24; 95% CI, 1.06-1.45) and progressing to heavy smoking by age 18 (RR, 1.43; 95% CI, 1.10-1.86).
Over the course of the study, subjects with a high genetic risk accumulated more pack-years of smoking. As adults, 27% of ever-smokers became nicotine dependent and those at higher genetic risk had a greater chance of doing so (HR, 1.27; 95% CI, 1.09-1.47). Additionally, of 277 cohort members who smoked daily during their 30s, those with a higher genetic risk were more likely to use smoking to cope with stress.
Further analyses found that smoking cessation was also difficult in adults at high genetic risk. For example, in the cohort of 277 daily smokers, 53% quit smoking a month or longer across 72 months follow-up; however, relapse occurred in 62%. Quitters with a higher genetic risk had a greater chance of relapsing (HR, 1.22; 95% CI, 1.02-1.45).
Only 20% of daily smokers abstained from smoking for a year or more.
Associations detected between the GRS and smoking phenotypes were small, noted the study authors. "Children who our study would classify at high genetic risk are not guaranteed to become addicted if they try smoking, and, even more importantly, children we would classify at low genetic risk are not immune to addiction."
Finally, researchers found that that the GRS score did not correlate with family history. "The GRS contained different information about risk for developmental and mature phenotypes of smoking behavior, compared with family history," reported the study authors.
The authors said that their research "adds a genetic dimension to longstanding arguments" in favor of early cigarette prevention of cigarette consumption, including surtaxes and age restrictions on tobacco purchases.
Funding for this study was provided through grants from various organizations, including the U.S. National Institute on Aging, the U.S. National Institute on Mental Health, and the U.K. Medical Research Council. The Dunedin Multidisciplinary Health and Development Research Unit is supported by the New Zealand Health Research Council.
Genetic risk may contribute to the rapid progression of daily and heavy smoking during adolescence and subsequent problems with nicotine dependence and smoking cessation in adulthood, according to a recent study.
The research may have implications for the development of initiatives that deter smoking in adolescents, reported Daniel W. Belsky, Ph.D., of the University of North Carolina at Chapel Hill and Duke University Medical Center, Durham, N.C., and his associates. The 38-year longitudinal study included 1,037 men and women from the Dunedin Multidisciplinary Health and Development Study of New Zealand. Researchers assessed participants with a multilocus genetic risk score (GRS), originating from three meta-analyses of genome-wide association studies (GWAS) that used the number of cigarettes smoked daily as their phenotype. Dr. Belsky and his team focused their investigation on the single-nucleotide polymorphisms in 15q25.1 and19q13.2 (JAMA Psychiatry 2013 March 27 [doi:10.1001/jamapsychiatry.2013.736]).
Genotyping was possible in 880 Dunedin subjects. In addition to evaluating family history in these individuals, researchers gathered smoking information at eight assessments from the age 11-38 years.
The GRS was not associated with whether or when subjects started smoking. "In fact, daily smokers who did not progress to heavy use were at lower genetic risk than individuals who never smoked," the researchers wrote.
Among 627 ever-smokers in the cohort, those with a higher genetic risk were more likely to rapidly progress to heavy smoking, meaning 20 or more cigarettes daily (hazard ratio, 1.35; 95% confidence interval, 1.14-1.58).
Adolescents with high genetic risk had a greater chance of becoming daily smokers by age 15 (relative risk, 1.24; 95% CI, 1.06-1.45) and progressing to heavy smoking by age 18 (RR, 1.43; 95% CI, 1.10-1.86).
Over the course of the study, subjects with a high genetic risk accumulated more pack-years of smoking. As adults, 27% of ever-smokers became nicotine dependent and those at higher genetic risk had a greater chance of doing so (HR, 1.27; 95% CI, 1.09-1.47). Additionally, of 277 cohort members who smoked daily during their 30s, those with a higher genetic risk were more likely to use smoking to cope with stress.
Further analyses found that smoking cessation was also difficult in adults at high genetic risk. For example, in the cohort of 277 daily smokers, 53% quit smoking a month or longer across 72 months follow-up; however, relapse occurred in 62%. Quitters with a higher genetic risk had a greater chance of relapsing (HR, 1.22; 95% CI, 1.02-1.45).
Only 20% of daily smokers abstained from smoking for a year or more.
Associations detected between the GRS and smoking phenotypes were small, noted the study authors. "Children who our study would classify at high genetic risk are not guaranteed to become addicted if they try smoking, and, even more importantly, children we would classify at low genetic risk are not immune to addiction."
Finally, researchers found that that the GRS score did not correlate with family history. "The GRS contained different information about risk for developmental and mature phenotypes of smoking behavior, compared with family history," reported the study authors.
The authors said that their research "adds a genetic dimension to longstanding arguments" in favor of early cigarette prevention of cigarette consumption, including surtaxes and age restrictions on tobacco purchases.
Funding for this study was provided through grants from various organizations, including the U.S. National Institute on Aging, the U.S. National Institute on Mental Health, and the U.K. Medical Research Council. The Dunedin Multidisciplinary Health and Development Research Unit is supported by the New Zealand Health Research Council.
FROM JAMA PSYCHIATRY
Major finding:Ever-smokers with a higher genetic risk were more likely to rapidly progress to heavy smoking, meaning 20 or more cigarettes daily (hazard ratio 1.35; 95% CI, 1.14-1.58).
Data source: A 38-year, prospective, longitudinal study of a birth cohort consisting of 1,037 subjects.
Disclosures: Funding for this study was provided through grants from various organizations, including the National Institute on Aging, the National Institute on Mental Health, and the U.K. Medical Research Council. The Dunedin Multidisciplinary Health and Development Research Unit is supported by the New Zealand Health Research Council.
Prolonged antibiotic use reduced bronchiectasis exacerbations
Low-dose macrolide antibiotics given for 12 months significantly reduced pulmonary exacerbations in non–cystic fibrosis bronchiectasis, according to findings from two randomized, controlled trials.
However, antibiotic resistance concerns could temper the use of such an approach in clinical practice, the studies’ investigators cautioned.
In BLESS (Bronchiectasis and Low-Dose Erythromycin Study), the annualized mean rate of pulmonary exacerbations per patient per year was 1.29 in patients treated with erythromycin, compared with 1.97 in those given placebo (P = .003) (JAMA 2013;309:1260-7).
In the BAT (Bronchiectasis and Long-Term Azithromycin Treatment) study, the median number of exacerbations after 1 year was 0 in azithromycin-treated patients, compared with 2 in patients given placebo (P less than .001) (JAMA 2013;309:1251-9).
Both studies’ findings are consistent with those of the EMBRACE trial published last year (Lancet 2012;380:660-77), which showed a 500 mg-dose of azithromycin given for 6 months reduced the incidence of pulmonary exacerbations, compared with placebo, in patients who had at least one exacerbation in the past year.
"The BLESS and BAT trials provide robust evidence for a beneficial effect of long-term macrolide maintenance therapy in patients with bronchiectasis," observed Dr. J. Stuart Elborn and Michael Tunney, Ph.D., in an editorial accompanying the articles (JAMA 2013;309:1295-6).
"Given the paucity of evidence for treatments in bronchiectasis, the results of these studies and the recently published EMBRACE trial are welcome, because they provide a good evidence base for an effective therapy for bronchiectasis," added the commentators, both of Queen’s University Belfast, U.K.
Bronchiectasis is characterized by widening of the airways – specifically, the small and medium-size bronchi – mucosal thickening, and bronchial inflammation. Sufferers are usually dogged by a chronic cough and sputum production, impaired lung function, and infection-related exacerbations.
BLESS was a single-center trial conducted in Australia involving 117 outpatients with a history of two or more infective exacerbations in the past year. Patients were treated with twice-daily erythromycin (400 mg) or placebo. The mean ages of antibiotic- and placebo-treated patients were 61.1 years and 63.5 years, respectively.
Treatment with erythromycin resulted in a 43% relative reduction in the mean annualized exacerbation rate. Exacerbations also were significantly decreased in a pre-specified subgroup of patients with Pseudomonas aeruginosa airway infection.
Furthermore, "erythromycin reduced 24-hour sputum production and attenuated lung function," wrote Dr. David Serisier and his colleagues at Mater Adult Hospital in South Brisbane, Australia.
The BAT study was conducted in 14 Dutch hospitals and involved 83 outpatients with a history of three or more lower respiratory tract infections in the past year. Patients were randomized to a daily dose of 250 mg azithromycin or placebo. The mean ages of antibiotic- and placebo-treated patients were 59.9 years and 64.6 years, respectively.
The risk of patients experiencing at least one exacerbation during the trial was significantly lower if they had been treated with the antibiotic rather than being given placebo (46.5% vs. 80%, hazard ratio = 0.29).
"The number of patients needed to treat with azithromycin to maintain clinical stability was 3.0," Dr. Josje Altenburg, Medical Centre Alkmaar, the Netherlands, and associates reported. Azithromycin therapy also was associated with improved lung function, compared with placebo.
One concern with long-term treatment using these antibiotics is the possible development of macrolide resistance. Dr. Altenburg and colleagues reported a macrolide resistance rate of 88% with azithromycin, vs. 26% with placebo. In BLESS, Dr. Serisier and his coauthors observed an increased proportion of macrolide-resistant oropharyngeal streptococci, with a median increase of 27.7%, compared with 0.04% with placebo (P less than .001).
"The bacterial resistance caused by macrolide therapy mandates a cautious application of this therapy in clinical practice," Dr. Serisier and associates acknowledged. They added that the potential for resistance must "curb enthusiasm" for widespread erythromycin use.
"The benefits of long-term macrolide treatment for individual patients with bronchiectasis need to be balanced with increasing concerns regarding the development of resistance to both macrolides and other antibiotics among airway microbiota," Dr. Elborn and Dr. Tunney similarly observed in their accompanying editorial.
"Further long-term studies are required to better determine the relationship between maintenance macrolide treatment, the airway microbiome and resistome, and clinical efficacy in patients with bronchiectasis," they cautioned.
The Mater Adult Respiratory Research Trust Fund funded the BLESS trial. Dr. Serisier reported receiving honoraria, speaker fees, or travel support from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Pharmaxia, and Phebra. The BAT trial was supported by a research grant from the Foreest Medical School, Alkmaar, the Netherlands, and an unrestricted research grant from GlaxoSmithKline. Teva Netherlands provided the azathioprine tablets. Dr. Altenburg, Dr. Elborn, and Dr. Tunney had no disclosures.
Dr. J. Stuart Elborn comments: For years, there has been no specific, evidence-based treatment for non–cystic fibrosis bronchiectasis. Now, with the publication of three trials (BLESS, BAT, and EMBRACE), there is evidence of a benefit with prolonged macrolide antibiotic treatment.
However, the authors of BLESS and the BAT trial both reported high rates of macrolide resistance. This is, of course, a concern with any prolonged antibiotic use.
The researchers are to be commended for addressing the issue of resistance in their studies. They looked for "known pathogens," notably commensal oropharyngeal streptococci in BLESS, and Haemophilus influenzae, Pseudomonas aeruginosa, and Streptococci pneumoniae in the BAT trial. We now know there is a community of bacteria in the sputum of these patients, and resistance in other bacteria may also be an issue.
The studies did not use quantitative cultures to see if a decrease in the total sputum bacterial load or the density of individual species could be linked to the reduced exacerbation frequency, so the mechanism of the improvement is not clear.
Erythromycin and azithromycin have been clearly shown to reduce pulmonary exacerbation rates and improve lung function in these trials. The concern over antibiotic resistance remains. There will be some challenges in extrapolating the results to the wider clinical population and determining which patients could benefit most from long-term macrolide antibiotic treatment; but further evidence of this effective therapy is welcome.
Dr. J. Stuart Elborn is director of the center for infection and immunity, Queen’s University Belfast (U.K.).
Dr. J. Stuart Elborn comments: For years, there has been no specific, evidence-based treatment for non–cystic fibrosis bronchiectasis. Now, with the publication of three trials (BLESS, BAT, and EMBRACE), there is evidence of a benefit with prolonged macrolide antibiotic treatment.
However, the authors of BLESS and the BAT trial both reported high rates of macrolide resistance. This is, of course, a concern with any prolonged antibiotic use.
The researchers are to be commended for addressing the issue of resistance in their studies. They looked for "known pathogens," notably commensal oropharyngeal streptococci in BLESS, and Haemophilus influenzae, Pseudomonas aeruginosa, and Streptococci pneumoniae in the BAT trial. We now know there is a community of bacteria in the sputum of these patients, and resistance in other bacteria may also be an issue.
The studies did not use quantitative cultures to see if a decrease in the total sputum bacterial load or the density of individual species could be linked to the reduced exacerbation frequency, so the mechanism of the improvement is not clear.
Erythromycin and azithromycin have been clearly shown to reduce pulmonary exacerbation rates and improve lung function in these trials. The concern over antibiotic resistance remains. There will be some challenges in extrapolating the results to the wider clinical population and determining which patients could benefit most from long-term macrolide antibiotic treatment; but further evidence of this effective therapy is welcome.
Dr. J. Stuart Elborn is director of the center for infection and immunity, Queen’s University Belfast (U.K.).
Dr. J. Stuart Elborn comments: For years, there has been no specific, evidence-based treatment for non–cystic fibrosis bronchiectasis. Now, with the publication of three trials (BLESS, BAT, and EMBRACE), there is evidence of a benefit with prolonged macrolide antibiotic treatment.
However, the authors of BLESS and the BAT trial both reported high rates of macrolide resistance. This is, of course, a concern with any prolonged antibiotic use.
The researchers are to be commended for addressing the issue of resistance in their studies. They looked for "known pathogens," notably commensal oropharyngeal streptococci in BLESS, and Haemophilus influenzae, Pseudomonas aeruginosa, and Streptococci pneumoniae in the BAT trial. We now know there is a community of bacteria in the sputum of these patients, and resistance in other bacteria may also be an issue.
The studies did not use quantitative cultures to see if a decrease in the total sputum bacterial load or the density of individual species could be linked to the reduced exacerbation frequency, so the mechanism of the improvement is not clear.
Erythromycin and azithromycin have been clearly shown to reduce pulmonary exacerbation rates and improve lung function in these trials. The concern over antibiotic resistance remains. There will be some challenges in extrapolating the results to the wider clinical population and determining which patients could benefit most from long-term macrolide antibiotic treatment; but further evidence of this effective therapy is welcome.
Dr. J. Stuart Elborn is director of the center for infection and immunity, Queen’s University Belfast (U.K.).
Low-dose macrolide antibiotics given for 12 months significantly reduced pulmonary exacerbations in non–cystic fibrosis bronchiectasis, according to findings from two randomized, controlled trials.
However, antibiotic resistance concerns could temper the use of such an approach in clinical practice, the studies’ investigators cautioned.
In BLESS (Bronchiectasis and Low-Dose Erythromycin Study), the annualized mean rate of pulmonary exacerbations per patient per year was 1.29 in patients treated with erythromycin, compared with 1.97 in those given placebo (P = .003) (JAMA 2013;309:1260-7).
In the BAT (Bronchiectasis and Long-Term Azithromycin Treatment) study, the median number of exacerbations after 1 year was 0 in azithromycin-treated patients, compared with 2 in patients given placebo (P less than .001) (JAMA 2013;309:1251-9).
Both studies’ findings are consistent with those of the EMBRACE trial published last year (Lancet 2012;380:660-77), which showed a 500 mg-dose of azithromycin given for 6 months reduced the incidence of pulmonary exacerbations, compared with placebo, in patients who had at least one exacerbation in the past year.
"The BLESS and BAT trials provide robust evidence for a beneficial effect of long-term macrolide maintenance therapy in patients with bronchiectasis," observed Dr. J. Stuart Elborn and Michael Tunney, Ph.D., in an editorial accompanying the articles (JAMA 2013;309:1295-6).
"Given the paucity of evidence for treatments in bronchiectasis, the results of these studies and the recently published EMBRACE trial are welcome, because they provide a good evidence base for an effective therapy for bronchiectasis," added the commentators, both of Queen’s University Belfast, U.K.
Bronchiectasis is characterized by widening of the airways – specifically, the small and medium-size bronchi – mucosal thickening, and bronchial inflammation. Sufferers are usually dogged by a chronic cough and sputum production, impaired lung function, and infection-related exacerbations.
BLESS was a single-center trial conducted in Australia involving 117 outpatients with a history of two or more infective exacerbations in the past year. Patients were treated with twice-daily erythromycin (400 mg) or placebo. The mean ages of antibiotic- and placebo-treated patients were 61.1 years and 63.5 years, respectively.
Treatment with erythromycin resulted in a 43% relative reduction in the mean annualized exacerbation rate. Exacerbations also were significantly decreased in a pre-specified subgroup of patients with Pseudomonas aeruginosa airway infection.
Furthermore, "erythromycin reduced 24-hour sputum production and attenuated lung function," wrote Dr. David Serisier and his colleagues at Mater Adult Hospital in South Brisbane, Australia.
The BAT study was conducted in 14 Dutch hospitals and involved 83 outpatients with a history of three or more lower respiratory tract infections in the past year. Patients were randomized to a daily dose of 250 mg azithromycin or placebo. The mean ages of antibiotic- and placebo-treated patients were 59.9 years and 64.6 years, respectively.
The risk of patients experiencing at least one exacerbation during the trial was significantly lower if they had been treated with the antibiotic rather than being given placebo (46.5% vs. 80%, hazard ratio = 0.29).
"The number of patients needed to treat with azithromycin to maintain clinical stability was 3.0," Dr. Josje Altenburg, Medical Centre Alkmaar, the Netherlands, and associates reported. Azithromycin therapy also was associated with improved lung function, compared with placebo.
One concern with long-term treatment using these antibiotics is the possible development of macrolide resistance. Dr. Altenburg and colleagues reported a macrolide resistance rate of 88% with azithromycin, vs. 26% with placebo. In BLESS, Dr. Serisier and his coauthors observed an increased proportion of macrolide-resistant oropharyngeal streptococci, with a median increase of 27.7%, compared with 0.04% with placebo (P less than .001).
"The bacterial resistance caused by macrolide therapy mandates a cautious application of this therapy in clinical practice," Dr. Serisier and associates acknowledged. They added that the potential for resistance must "curb enthusiasm" for widespread erythromycin use.
"The benefits of long-term macrolide treatment for individual patients with bronchiectasis need to be balanced with increasing concerns regarding the development of resistance to both macrolides and other antibiotics among airway microbiota," Dr. Elborn and Dr. Tunney similarly observed in their accompanying editorial.
"Further long-term studies are required to better determine the relationship between maintenance macrolide treatment, the airway microbiome and resistome, and clinical efficacy in patients with bronchiectasis," they cautioned.
The Mater Adult Respiratory Research Trust Fund funded the BLESS trial. Dr. Serisier reported receiving honoraria, speaker fees, or travel support from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Pharmaxia, and Phebra. The BAT trial was supported by a research grant from the Foreest Medical School, Alkmaar, the Netherlands, and an unrestricted research grant from GlaxoSmithKline. Teva Netherlands provided the azathioprine tablets. Dr. Altenburg, Dr. Elborn, and Dr. Tunney had no disclosures.
Low-dose macrolide antibiotics given for 12 months significantly reduced pulmonary exacerbations in non–cystic fibrosis bronchiectasis, according to findings from two randomized, controlled trials.
However, antibiotic resistance concerns could temper the use of such an approach in clinical practice, the studies’ investigators cautioned.
In BLESS (Bronchiectasis and Low-Dose Erythromycin Study), the annualized mean rate of pulmonary exacerbations per patient per year was 1.29 in patients treated with erythromycin, compared with 1.97 in those given placebo (P = .003) (JAMA 2013;309:1260-7).
In the BAT (Bronchiectasis and Long-Term Azithromycin Treatment) study, the median number of exacerbations after 1 year was 0 in azithromycin-treated patients, compared with 2 in patients given placebo (P less than .001) (JAMA 2013;309:1251-9).
Both studies’ findings are consistent with those of the EMBRACE trial published last year (Lancet 2012;380:660-77), which showed a 500 mg-dose of azithromycin given for 6 months reduced the incidence of pulmonary exacerbations, compared with placebo, in patients who had at least one exacerbation in the past year.
"The BLESS and BAT trials provide robust evidence for a beneficial effect of long-term macrolide maintenance therapy in patients with bronchiectasis," observed Dr. J. Stuart Elborn and Michael Tunney, Ph.D., in an editorial accompanying the articles (JAMA 2013;309:1295-6).
"Given the paucity of evidence for treatments in bronchiectasis, the results of these studies and the recently published EMBRACE trial are welcome, because they provide a good evidence base for an effective therapy for bronchiectasis," added the commentators, both of Queen’s University Belfast, U.K.
Bronchiectasis is characterized by widening of the airways – specifically, the small and medium-size bronchi – mucosal thickening, and bronchial inflammation. Sufferers are usually dogged by a chronic cough and sputum production, impaired lung function, and infection-related exacerbations.
BLESS was a single-center trial conducted in Australia involving 117 outpatients with a history of two or more infective exacerbations in the past year. Patients were treated with twice-daily erythromycin (400 mg) or placebo. The mean ages of antibiotic- and placebo-treated patients were 61.1 years and 63.5 years, respectively.
Treatment with erythromycin resulted in a 43% relative reduction in the mean annualized exacerbation rate. Exacerbations also were significantly decreased in a pre-specified subgroup of patients with Pseudomonas aeruginosa airway infection.
Furthermore, "erythromycin reduced 24-hour sputum production and attenuated lung function," wrote Dr. David Serisier and his colleagues at Mater Adult Hospital in South Brisbane, Australia.
The BAT study was conducted in 14 Dutch hospitals and involved 83 outpatients with a history of three or more lower respiratory tract infections in the past year. Patients were randomized to a daily dose of 250 mg azithromycin or placebo. The mean ages of antibiotic- and placebo-treated patients were 59.9 years and 64.6 years, respectively.
The risk of patients experiencing at least one exacerbation during the trial was significantly lower if they had been treated with the antibiotic rather than being given placebo (46.5% vs. 80%, hazard ratio = 0.29).
"The number of patients needed to treat with azithromycin to maintain clinical stability was 3.0," Dr. Josje Altenburg, Medical Centre Alkmaar, the Netherlands, and associates reported. Azithromycin therapy also was associated with improved lung function, compared with placebo.
One concern with long-term treatment using these antibiotics is the possible development of macrolide resistance. Dr. Altenburg and colleagues reported a macrolide resistance rate of 88% with azithromycin, vs. 26% with placebo. In BLESS, Dr. Serisier and his coauthors observed an increased proportion of macrolide-resistant oropharyngeal streptococci, with a median increase of 27.7%, compared with 0.04% with placebo (P less than .001).
"The bacterial resistance caused by macrolide therapy mandates a cautious application of this therapy in clinical practice," Dr. Serisier and associates acknowledged. They added that the potential for resistance must "curb enthusiasm" for widespread erythromycin use.
"The benefits of long-term macrolide treatment for individual patients with bronchiectasis need to be balanced with increasing concerns regarding the development of resistance to both macrolides and other antibiotics among airway microbiota," Dr. Elborn and Dr. Tunney similarly observed in their accompanying editorial.
"Further long-term studies are required to better determine the relationship between maintenance macrolide treatment, the airway microbiome and resistome, and clinical efficacy in patients with bronchiectasis," they cautioned.
The Mater Adult Respiratory Research Trust Fund funded the BLESS trial. Dr. Serisier reported receiving honoraria, speaker fees, or travel support from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Pharmaxia, and Phebra. The BAT trial was supported by a research grant from the Foreest Medical School, Alkmaar, the Netherlands, and an unrestricted research grant from GlaxoSmithKline. Teva Netherlands provided the azathioprine tablets. Dr. Altenburg, Dr. Elborn, and Dr. Tunney had no disclosures.
FROM JAMA
Major finding: Pulmonary exacerbations occurred less frequently with erythromycin (1.29 vs. 1.97/patient per year, P = .003) or azithromycin (median of 0 vs. 2, P less than .001) than with placebo.
Data source: BLESS and BAT – two randomized, double-blind trials of patients with non–cystic fibrosis bronchiectasis treated with either erythromycin or placebo (n = 117), or azithromycin or placebo (n = 83), for 12 months.
Disclosures: The Mater Adult Respiratory Research Trust Fund funded the BLESS trial. Dr. Serisier reported receiving honoraria, speaker fees, or travel support from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Pharmaxia, and Phebra. The BAT trial was supported by a research grant from the Foreest Medical School, Alkmaar, the Netherlands, and an unrestricted research grant from GlaxoSmithKline. Teva Netherlands provided the azithromycin tablets. Dr. Altenburg, Dr. Elborn, and Dr. Tunney had no disclosures.