User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Palivizumab in preterm infants limits wheezing for 1 year
In otherwise healthy preterm infants, palivizumab injections during the winter months to prevent respiratory syncytial virus also reduced the number of wheezing days by 61% for a full year, according to a report published online May 9 in the New England Journal of Medicine.
"Our study underlines the important role that RSV [respiratory syncytial virus] plays in the pathogenesis of recurrent wheeze. We hypothesize that RSV primarily causes direct pulmonary epithelial damage and local immunologic alterations in the lungs, leading to long-term airway hyperresponsiveness and wheezing," said Dr. Maarten O. Blanken of the division of pediatric immunology and infectious diseases, University Medical Center Utrecht (the Netherlands), and his associates for the Dutch RSV Neonatal Network.

Whether or not RSV plays a causal role in recurrent wheezing has been controversial. Dr. Blanken and his colleagues performed a double-blind randomized trial to further examine the issue.
They enrolled 429 preterm (gestational age, 33-35 weeks) but otherwise healthy infants at 1 university and 15 regional hospitals in the Netherlands during a 2-year period. All the babies were 6 months of age or younger at the start of the RSV season.
The babies were randomly assigned to receive either palivizumab (Synagis, MedImmune) (214 subjects) or placebo (215 subjects) injections during the winter months. Parents recorded airway symptoms, doctor visits, and the use of airway medications until the children reached 1 year of age.
Parents also were instructed to take nasopharyngeal swabs whenever the children developed respiratory symptoms that lasted more than 1 day, to be tested for the presence of RSV RNA.
As expected, the incidence of RSV-related hospitalizations was significantly lower among infants who received palivizumab immunoprophylaxis (0.9%) than among those who received placebo (5.1%). The rate of RSV infection requiring medical attendance but not hospitalization also was significantly lower in the immunoprophylaxis group.
The primary outcome measure of this study was the number of parent-reported days in which the baby wheezed during the first year of life. This was significantly lower in the active-treatment group (1.8% of days) than in the placebo group (4.5% of days), which is a relative reduction of 61%, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1211917]).
In addition, the proportion of babies who developed recurrent wheezing was approximately half as high among those who received palivizumab (11.2%) as among those who received placebo (20.9%). The proportion who were given bronchodilator therapy was similarly lower in the palivizumab group (13%) than in the placebo group (23%).
Notably, the efficacy of immunoprophylaxis was not significantly different between children who had a family history of atopy (54% reduction in wheezing days) and those who did not (72% reduction in wheezing days). Palivizumab’s efficacy was similarly consistent whether the children’s parents had asthma (68% reduction) or did not have asthma (35% reduction).
Children in the RSV-prevention group were less likely than those in the placebo group to have adverse effects requiring hospitalization. There were 32 hospitalizations in 27 children (12.6%) in the palivizumab group, compared with 52 hospitalizations in 47 children (21.9%) in the placebo group, the researchers said.
"In this proof-of-concept study, treatment with a monoclonal antibody for RSV prevention in late preterm infants greatly reduced the number of parent-reported wheezing days during the first year of life, even after the end of therapy and outside the RSV season," Dr. Blanken and his associates said.
"Our results are in line with other studies that acknowledge the relationship between RSV bronchiolitis and recurrent wheeze," they said.
It is unknown whether these results can be generalized to term infants, they added.
This study was supported by an unrestricted grant from Abbott Laboratories and a grant from the Netherlands Organization for Health Research and Development to Dr. Blanken. Dr. Blanken reported conflicts of interest, and his associates reported ties to MedImmune and GlaxoSmithKline.
In otherwise healthy preterm infants, palivizumab injections during the winter months to prevent respiratory syncytial virus also reduced the number of wheezing days by 61% for a full year, according to a report published online May 9 in the New England Journal of Medicine.
"Our study underlines the important role that RSV [respiratory syncytial virus] plays in the pathogenesis of recurrent wheeze. We hypothesize that RSV primarily causes direct pulmonary epithelial damage and local immunologic alterations in the lungs, leading to long-term airway hyperresponsiveness and wheezing," said Dr. Maarten O. Blanken of the division of pediatric immunology and infectious diseases, University Medical Center Utrecht (the Netherlands), and his associates for the Dutch RSV Neonatal Network.
Whether or not RSV plays a causal role in recurrent wheezing has been controversial. Dr. Blanken and his colleagues performed a double-blind randomized trial to further examine the issue.
They enrolled 429 preterm (gestational age, 33-35 weeks) but otherwise healthy infants at 1 university and 15 regional hospitals in the Netherlands during a 2-year period. All the babies were 6 months of age or younger at the start of the RSV season.
The babies were randomly assigned to receive either palivizumab (Synagis, MedImmune) (214 subjects) or placebo (215 subjects) injections during the winter months. Parents recorded airway symptoms, doctor visits, and the use of airway medications until the children reached 1 year of age.
Parents also were instructed to take nasopharyngeal swabs whenever the children developed respiratory symptoms that lasted more than 1 day, to be tested for the presence of RSV RNA.
As expected, the incidence of RSV-related hospitalizations was significantly lower among infants who received palivizumab immunoprophylaxis (0.9%) than among those who received placebo (5.1%). The rate of RSV infection requiring medical attendance but not hospitalization also was significantly lower in the immunoprophylaxis group.
The primary outcome measure of this study was the number of parent-reported days in which the baby wheezed during the first year of life. This was significantly lower in the active-treatment group (1.8% of days) than in the placebo group (4.5% of days), which is a relative reduction of 61%, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1211917]).
In addition, the proportion of babies who developed recurrent wheezing was approximately half as high among those who received palivizumab (11.2%) as among those who received placebo (20.9%). The proportion who were given bronchodilator therapy was similarly lower in the palivizumab group (13%) than in the placebo group (23%).
Notably, the efficacy of immunoprophylaxis was not significantly different between children who had a family history of atopy (54% reduction in wheezing days) and those who did not (72% reduction in wheezing days). Palivizumab’s efficacy was similarly consistent whether the children’s parents had asthma (68% reduction) or did not have asthma (35% reduction).
Children in the RSV-prevention group were less likely than those in the placebo group to have adverse effects requiring hospitalization. There were 32 hospitalizations in 27 children (12.6%) in the palivizumab group, compared with 52 hospitalizations in 47 children (21.9%) in the placebo group, the researchers said.
"In this proof-of-concept study, treatment with a monoclonal antibody for RSV prevention in late preterm infants greatly reduced the number of parent-reported wheezing days during the first year of life, even after the end of therapy and outside the RSV season," Dr. Blanken and his associates said.
"Our results are in line with other studies that acknowledge the relationship between RSV bronchiolitis and recurrent wheeze," they said.
It is unknown whether these results can be generalized to term infants, they added.
This study was supported by an unrestricted grant from Abbott Laboratories and a grant from the Netherlands Organization for Health Research and Development to Dr. Blanken. Dr. Blanken reported conflicts of interest, and his associates reported ties to MedImmune and GlaxoSmithKline.
In otherwise healthy preterm infants, palivizumab injections during the winter months to prevent respiratory syncytial virus also reduced the number of wheezing days by 61% for a full year, according to a report published online May 9 in the New England Journal of Medicine.
"Our study underlines the important role that RSV [respiratory syncytial virus] plays in the pathogenesis of recurrent wheeze. We hypothesize that RSV primarily causes direct pulmonary epithelial damage and local immunologic alterations in the lungs, leading to long-term airway hyperresponsiveness and wheezing," said Dr. Maarten O. Blanken of the division of pediatric immunology and infectious diseases, University Medical Center Utrecht (the Netherlands), and his associates for the Dutch RSV Neonatal Network.
Whether or not RSV plays a causal role in recurrent wheezing has been controversial. Dr. Blanken and his colleagues performed a double-blind randomized trial to further examine the issue.
They enrolled 429 preterm (gestational age, 33-35 weeks) but otherwise healthy infants at 1 university and 15 regional hospitals in the Netherlands during a 2-year period. All the babies were 6 months of age or younger at the start of the RSV season.
The babies were randomly assigned to receive either palivizumab (Synagis, MedImmune) (214 subjects) or placebo (215 subjects) injections during the winter months. Parents recorded airway symptoms, doctor visits, and the use of airway medications until the children reached 1 year of age.
Parents also were instructed to take nasopharyngeal swabs whenever the children developed respiratory symptoms that lasted more than 1 day, to be tested for the presence of RSV RNA.
As expected, the incidence of RSV-related hospitalizations was significantly lower among infants who received palivizumab immunoprophylaxis (0.9%) than among those who received placebo (5.1%). The rate of RSV infection requiring medical attendance but not hospitalization also was significantly lower in the immunoprophylaxis group.
The primary outcome measure of this study was the number of parent-reported days in which the baby wheezed during the first year of life. This was significantly lower in the active-treatment group (1.8% of days) than in the placebo group (4.5% of days), which is a relative reduction of 61%, the investigators said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1211917]).
In addition, the proportion of babies who developed recurrent wheezing was approximately half as high among those who received palivizumab (11.2%) as among those who received placebo (20.9%). The proportion who were given bronchodilator therapy was similarly lower in the palivizumab group (13%) than in the placebo group (23%).
Notably, the efficacy of immunoprophylaxis was not significantly different between children who had a family history of atopy (54% reduction in wheezing days) and those who did not (72% reduction in wheezing days). Palivizumab’s efficacy was similarly consistent whether the children’s parents had asthma (68% reduction) or did not have asthma (35% reduction).
Children in the RSV-prevention group were less likely than those in the placebo group to have adverse effects requiring hospitalization. There were 32 hospitalizations in 27 children (12.6%) in the palivizumab group, compared with 52 hospitalizations in 47 children (21.9%) in the placebo group, the researchers said.
"In this proof-of-concept study, treatment with a monoclonal antibody for RSV prevention in late preterm infants greatly reduced the number of parent-reported wheezing days during the first year of life, even after the end of therapy and outside the RSV season," Dr. Blanken and his associates said.
"Our results are in line with other studies that acknowledge the relationship between RSV bronchiolitis and recurrent wheeze," they said.
It is unknown whether these results can be generalized to term infants, they added.
This study was supported by an unrestricted grant from Abbott Laboratories and a grant from the Netherlands Organization for Health Research and Development to Dr. Blanken. Dr. Blanken reported conflicts of interest, and his associates reported ties to MedImmune and GlaxoSmithKline.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: The number of days in which a healthy preterm baby wheezed during the first year of life was 61% lower with palivizumab (1.8% of days) than with placebo (4.5% of days).
Data source: A randomized proof-of-concept study involving healthy preterm infants who received either RSV prophylaxis with palivizumab (214 infants) or placebo (215 infants) and were followed for 1 year.
Disclosures: This study was supported by an unrestricted grant from Abbott Laboratories and a grant from the Netherlands Organization for Health Research and Development to Dr. Blanken. Dr. Blanken reported no other conflicts of interest, and his associates reported ties to MedImmune and GlaxoSmithKline.
Marijuana habit not linked to lung cancer
WASHINGTON – Regular cannabis smokers are no more likely to develop lung cancer than are people who indulge occasionally.
The finding of no significant increased risk held true whether the smokers imbibed once or twice – or more – each day, and regardless of how many years they had smoked, Dr. Li Rita Zhang reported at the annual meeting of the American Association of Cancer Research.

The study included data from six case-control studies conducted from 1999 to 2012 in the United States, Canada, the United Kingdom, and New Zealand, with a subject pool of 2,159 lung cancer cases and 2,985 controls. All of the studies were part of the International Lung Cancer Consortium (ILCCO), an international group of lung cancer researchers with the aim of sharing comparable data from ongoing and recently completed lung cancer studies from different geographical areas and ethnicities.
Dr. Zhang of the University of California, Los Angeles, performed two analyses. One compared all lung cancer cases and all controls, regardless of concurrent or past tobacco use. Then, to reduce confounding by tobacco, she restricted the analysis to those who had never smoked tobacco. That group comprised 370 cancer cases and 1,358 controls. The models were also adjusted for age, sex, sociodemographic factors, and tobacco pack-years. Habitual use was defined as one joint per day per year.
When compared with cannabis smokers who also used tobacco, habitual pot smokers had no significant increase in cancer risk.
In an analysis of marijuana smokers that excluded tobacco smokers, there were no significant differences in any of the comparisons, including habitual vs. nonhabitual use; number of joints smoked per day; duration of up to 20 years or duration of more than 20 years.
Other literature has shown a link between cannabis smoking and lung cancer, pulmonologist Michael Alberts said in an interview. However, he said, "The conventional wisdom is that cannabis smoking is not as dangerous as cigarette smoking."
The difference in risk is likely related to chemical additives in commercial cigarettes that aren’t present in most methods of inhaling marijuana smoke.
As a general recommendation, smoking anything isn’t good for the respiratory system, said Dr. Alberts, chief medical officer of the Moffitt Cancer Center, Tampa. But for patients using medical marijuana, the benefit could outweigh the risks.
"You can think of it as similar to a CT scan. Radiation isn’t good, but if the scan is something beneficial and the risk is low, you take it. If cannabis is indicated, and if it’s legal, and if there’s literature backing up the indication for use, then you weigh the risk of smoking and the benefit it could bring, and make the decision."
Dr. Zhang declined to comment on the study. In her poster presentation she noted that, "Our results cannot preclude the possibility that cannabis may exhibit an association with lung cancer risk at extremely high dosage over long periods of continued exposure."
Dr. Zhang did not disclosure any financial relationships. Dr. Alberts said he had no disclosures.
WASHINGTON – Regular cannabis smokers are no more likely to develop lung cancer than are people who indulge occasionally.
The finding of no significant increased risk held true whether the smokers imbibed once or twice – or more – each day, and regardless of how many years they had smoked, Dr. Li Rita Zhang reported at the annual meeting of the American Association of Cancer Research.
The study included data from six case-control studies conducted from 1999 to 2012 in the United States, Canada, the United Kingdom, and New Zealand, with a subject pool of 2,159 lung cancer cases and 2,985 controls. All of the studies were part of the International Lung Cancer Consortium (ILCCO), an international group of lung cancer researchers with the aim of sharing comparable data from ongoing and recently completed lung cancer studies from different geographical areas and ethnicities.
Dr. Zhang of the University of California, Los Angeles, performed two analyses. One compared all lung cancer cases and all controls, regardless of concurrent or past tobacco use. Then, to reduce confounding by tobacco, she restricted the analysis to those who had never smoked tobacco. That group comprised 370 cancer cases and 1,358 controls. The models were also adjusted for age, sex, sociodemographic factors, and tobacco pack-years. Habitual use was defined as one joint per day per year.
When compared with cannabis smokers who also used tobacco, habitual pot smokers had no significant increase in cancer risk.
In an analysis of marijuana smokers that excluded tobacco smokers, there were no significant differences in any of the comparisons, including habitual vs. nonhabitual use; number of joints smoked per day; duration of up to 20 years or duration of more than 20 years.
Other literature has shown a link between cannabis smoking and lung cancer, pulmonologist Michael Alberts said in an interview. However, he said, "The conventional wisdom is that cannabis smoking is not as dangerous as cigarette smoking."
The difference in risk is likely related to chemical additives in commercial cigarettes that aren’t present in most methods of inhaling marijuana smoke.
As a general recommendation, smoking anything isn’t good for the respiratory system, said Dr. Alberts, chief medical officer of the Moffitt Cancer Center, Tampa. But for patients using medical marijuana, the benefit could outweigh the risks.
"You can think of it as similar to a CT scan. Radiation isn’t good, but if the scan is something beneficial and the risk is low, you take it. If cannabis is indicated, and if it’s legal, and if there’s literature backing up the indication for use, then you weigh the risk of smoking and the benefit it could bring, and make the decision."
Dr. Zhang declined to comment on the study. In her poster presentation she noted that, "Our results cannot preclude the possibility that cannabis may exhibit an association with lung cancer risk at extremely high dosage over long periods of continued exposure."
Dr. Zhang did not disclosure any financial relationships. Dr. Alberts said he had no disclosures.
WASHINGTON – Regular cannabis smokers are no more likely to develop lung cancer than are people who indulge occasionally.
The finding of no significant increased risk held true whether the smokers imbibed once or twice – or more – each day, and regardless of how many years they had smoked, Dr. Li Rita Zhang reported at the annual meeting of the American Association of Cancer Research.
The study included data from six case-control studies conducted from 1999 to 2012 in the United States, Canada, the United Kingdom, and New Zealand, with a subject pool of 2,159 lung cancer cases and 2,985 controls. All of the studies were part of the International Lung Cancer Consortium (ILCCO), an international group of lung cancer researchers with the aim of sharing comparable data from ongoing and recently completed lung cancer studies from different geographical areas and ethnicities.
Dr. Zhang of the University of California, Los Angeles, performed two analyses. One compared all lung cancer cases and all controls, regardless of concurrent or past tobacco use. Then, to reduce confounding by tobacco, she restricted the analysis to those who had never smoked tobacco. That group comprised 370 cancer cases and 1,358 controls. The models were also adjusted for age, sex, sociodemographic factors, and tobacco pack-years. Habitual use was defined as one joint per day per year.
When compared with cannabis smokers who also used tobacco, habitual pot smokers had no significant increase in cancer risk.
In an analysis of marijuana smokers that excluded tobacco smokers, there were no significant differences in any of the comparisons, including habitual vs. nonhabitual use; number of joints smoked per day; duration of up to 20 years or duration of more than 20 years.
Other literature has shown a link between cannabis smoking and lung cancer, pulmonologist Michael Alberts said in an interview. However, he said, "The conventional wisdom is that cannabis smoking is not as dangerous as cigarette smoking."
The difference in risk is likely related to chemical additives in commercial cigarettes that aren’t present in most methods of inhaling marijuana smoke.
As a general recommendation, smoking anything isn’t good for the respiratory system, said Dr. Alberts, chief medical officer of the Moffitt Cancer Center, Tampa. But for patients using medical marijuana, the benefit could outweigh the risks.
"You can think of it as similar to a CT scan. Radiation isn’t good, but if the scan is something beneficial and the risk is low, you take it. If cannabis is indicated, and if it’s legal, and if there’s literature backing up the indication for use, then you weigh the risk of smoking and the benefit it could bring, and make the decision."
Dr. Zhang declined to comment on the study. In her poster presentation she noted that, "Our results cannot preclude the possibility that cannabis may exhibit an association with lung cancer risk at extremely high dosage over long periods of continued exposure."
Dr. Zhang did not disclosure any financial relationships. Dr. Alberts said he had no disclosures.
AT THE AACR ANNUAL MEETING
Major finding: People who habitually smoked marijuana were no more likely to develop lung cancer than those who didn’t, whether or not they also smoked cigarettes.
Data source: The metaanalysis included 2,159 lung cancer cases and 2,985 controls extracted from six studies.
Disclosures: Neither Dr. Zhang nor Dr. Alberts reported any financial disclosures.

Ambrisentan doesn't help, may worsen pulmonary fibrosis
The endothelin-receptor antagonist ambrisentan not only failed to benefit patients with idiopathic pulmonary fibrosis, it also may have facilitated disease progression in an international phase III clinical trial reported May 7 in Annals of Internal Medicine.
The trial was terminated early when an interim analysis of the data showed that patients treated with ambrisentan were more likely than were control subjects receiving placebo to show progression of idiopathic pulmonary fibrosis (IPF) and to require more hospitalizations for respiratory indications, including acute IPF exacerbations and pneumonia. The findings were the same whether the study subjects had concomitant pulmonary hypertension.

"The observations in this study provide compelling evidence for ambrisentan as an ineffective treatment for patients with IPF and preclude further clinical evaluation of the drug as therapy for the disease. The data provide a basis for explicit guidance to clinicians not to use ambrisentan to treat patients with IPF, regardless of the presence of pulmonary hypertension," said Dr. Ganesh Raghu of the division of pulmonary and critical care medicine, University of Washington Medical Center, Seattle, and his associates.
The researchers undertook this large phase III study because preclinical data suggested that antagonism of endothelin receptors could lessen the severity of pulmonary fibrosis. And in a phase II study involving patients with a variety of interstitial lung diseases, a related endothelin antagonist, bosentan, had improved survival in the subgroup of patients with IPF.
Ambrisentan is a more selective endothelin A-receptor antagonist than bosentan and is currently approved for the treatment of pulmonary arterial hypertension. Dr. Raghu and his colleagues compared it against a matched placebo in 492 IPF patients treated at 136 clinical sites in North America, South America, Europe, Asia, New Zealand, and Australia.
When approximately 75% of the intended total enrollment of 660 patients was reached, an interim safety and efficacy analysis showed that the drug did not improve the primary endpoint, which was a composite of the time to disease progression, death from any cause, hospitalization for respiratory events, or a decrease in lung function. The trial sponsor, Gilead Sciences, terminated the study, and the findings were analyzed on the subjects enrolled up until that point.
The mean interval of exposure to ambrisentan (329 subjects) or placebo (163 subjects) was approximately 35 weeks. At baseline, patients in the active-treatment group and control group were similar regarding demographic traits, pulmonary hemodynamics, lung function, 6-minute walk distance, and quality of life.
Significantly more patients in the ambrisentan group (27.4%) than in the placebo group (17.2%) showed IPF progression. The active-treatment group also had significantly more respiratory hospitalizations (13.4% vs. 5.5%) and deaths (7.9% vs 3.7%) than did the control group, Dr. Raghu and his associates wrote (Ann. Intern. Med. 2013; 158:641-90).
However, there were no significant differences between the two study groups in the secondary endpoints of diffusion capacity for carbon monoxide; forced vital capacity; 6-minute walk distance; scores on the SF-36, which measures quality of life; or scores on the Transitional Dyspnea Index.
These findings were essentially the same when the data were analyzed according to whether or not patients had concomitant pulmonary hypertension at baseline. However, the subset of patients with pulmonary hypertension was small and not adequately powered to demonstrate a significant difference, so this finding should be interpreted with caution, the investigators said.
Regarding adverse events, significantly more patients taking ambrisentan than placebo reported dyspnea, worsening IPF, dizziness, and peripheral edema. Three times as many patients receiving ambrisentan (3%) dropped out of the study because of safety and tolerability issues, compared with those receiving placebo (1%).
This trial was supported by Gilead Sciences, which was involved in all aspects of the study.
The endothelin-receptor antagonist ambrisentan not only failed to benefit patients with idiopathic pulmonary fibrosis, it also may have facilitated disease progression in an international phase III clinical trial reported May 7 in Annals of Internal Medicine.
The trial was terminated early when an interim analysis of the data showed that patients treated with ambrisentan were more likely than were control subjects receiving placebo to show progression of idiopathic pulmonary fibrosis (IPF) and to require more hospitalizations for respiratory indications, including acute IPF exacerbations and pneumonia. The findings were the same whether the study subjects had concomitant pulmonary hypertension.
"The observations in this study provide compelling evidence for ambrisentan as an ineffective treatment for patients with IPF and preclude further clinical evaluation of the drug as therapy for the disease. The data provide a basis for explicit guidance to clinicians not to use ambrisentan to treat patients with IPF, regardless of the presence of pulmonary hypertension," said Dr. Ganesh Raghu of the division of pulmonary and critical care medicine, University of Washington Medical Center, Seattle, and his associates.
The researchers undertook this large phase III study because preclinical data suggested that antagonism of endothelin receptors could lessen the severity of pulmonary fibrosis. And in a phase II study involving patients with a variety of interstitial lung diseases, a related endothelin antagonist, bosentan, had improved survival in the subgroup of patients with IPF.
Ambrisentan is a more selective endothelin A-receptor antagonist than bosentan and is currently approved for the treatment of pulmonary arterial hypertension. Dr. Raghu and his colleagues compared it against a matched placebo in 492 IPF patients treated at 136 clinical sites in North America, South America, Europe, Asia, New Zealand, and Australia.
When approximately 75% of the intended total enrollment of 660 patients was reached, an interim safety and efficacy analysis showed that the drug did not improve the primary endpoint, which was a composite of the time to disease progression, death from any cause, hospitalization for respiratory events, or a decrease in lung function. The trial sponsor, Gilead Sciences, terminated the study, and the findings were analyzed on the subjects enrolled up until that point.
The mean interval of exposure to ambrisentan (329 subjects) or placebo (163 subjects) was approximately 35 weeks. At baseline, patients in the active-treatment group and control group were similar regarding demographic traits, pulmonary hemodynamics, lung function, 6-minute walk distance, and quality of life.
Significantly more patients in the ambrisentan group (27.4%) than in the placebo group (17.2%) showed IPF progression. The active-treatment group also had significantly more respiratory hospitalizations (13.4% vs. 5.5%) and deaths (7.9% vs 3.7%) than did the control group, Dr. Raghu and his associates wrote (Ann. Intern. Med. 2013; 158:641-90).
However, there were no significant differences between the two study groups in the secondary endpoints of diffusion capacity for carbon monoxide; forced vital capacity; 6-minute walk distance; scores on the SF-36, which measures quality of life; or scores on the Transitional Dyspnea Index.
These findings were essentially the same when the data were analyzed according to whether or not patients had concomitant pulmonary hypertension at baseline. However, the subset of patients with pulmonary hypertension was small and not adequately powered to demonstrate a significant difference, so this finding should be interpreted with caution, the investigators said.
Regarding adverse events, significantly more patients taking ambrisentan than placebo reported dyspnea, worsening IPF, dizziness, and peripheral edema. Three times as many patients receiving ambrisentan (3%) dropped out of the study because of safety and tolerability issues, compared with those receiving placebo (1%).
This trial was supported by Gilead Sciences, which was involved in all aspects of the study.
The endothelin-receptor antagonist ambrisentan not only failed to benefit patients with idiopathic pulmonary fibrosis, it also may have facilitated disease progression in an international phase III clinical trial reported May 7 in Annals of Internal Medicine.
The trial was terminated early when an interim analysis of the data showed that patients treated with ambrisentan were more likely than were control subjects receiving placebo to show progression of idiopathic pulmonary fibrosis (IPF) and to require more hospitalizations for respiratory indications, including acute IPF exacerbations and pneumonia. The findings were the same whether the study subjects had concomitant pulmonary hypertension.
"The observations in this study provide compelling evidence for ambrisentan as an ineffective treatment for patients with IPF and preclude further clinical evaluation of the drug as therapy for the disease. The data provide a basis for explicit guidance to clinicians not to use ambrisentan to treat patients with IPF, regardless of the presence of pulmonary hypertension," said Dr. Ganesh Raghu of the division of pulmonary and critical care medicine, University of Washington Medical Center, Seattle, and his associates.
The researchers undertook this large phase III study because preclinical data suggested that antagonism of endothelin receptors could lessen the severity of pulmonary fibrosis. And in a phase II study involving patients with a variety of interstitial lung diseases, a related endothelin antagonist, bosentan, had improved survival in the subgroup of patients with IPF.
Ambrisentan is a more selective endothelin A-receptor antagonist than bosentan and is currently approved for the treatment of pulmonary arterial hypertension. Dr. Raghu and his colleagues compared it against a matched placebo in 492 IPF patients treated at 136 clinical sites in North America, South America, Europe, Asia, New Zealand, and Australia.
When approximately 75% of the intended total enrollment of 660 patients was reached, an interim safety and efficacy analysis showed that the drug did not improve the primary endpoint, which was a composite of the time to disease progression, death from any cause, hospitalization for respiratory events, or a decrease in lung function. The trial sponsor, Gilead Sciences, terminated the study, and the findings were analyzed on the subjects enrolled up until that point.
The mean interval of exposure to ambrisentan (329 subjects) or placebo (163 subjects) was approximately 35 weeks. At baseline, patients in the active-treatment group and control group were similar regarding demographic traits, pulmonary hemodynamics, lung function, 6-minute walk distance, and quality of life.
Significantly more patients in the ambrisentan group (27.4%) than in the placebo group (17.2%) showed IPF progression. The active-treatment group also had significantly more respiratory hospitalizations (13.4% vs. 5.5%) and deaths (7.9% vs 3.7%) than did the control group, Dr. Raghu and his associates wrote (Ann. Intern. Med. 2013; 158:641-90).
However, there were no significant differences between the two study groups in the secondary endpoints of diffusion capacity for carbon monoxide; forced vital capacity; 6-minute walk distance; scores on the SF-36, which measures quality of life; or scores on the Transitional Dyspnea Index.
These findings were essentially the same when the data were analyzed according to whether or not patients had concomitant pulmonary hypertension at baseline. However, the subset of patients with pulmonary hypertension was small and not adequately powered to demonstrate a significant difference, so this finding should be interpreted with caution, the investigators said.
Regarding adverse events, significantly more patients taking ambrisentan than placebo reported dyspnea, worsening IPF, dizziness, and peripheral edema. Three times as many patients receiving ambrisentan (3%) dropped out of the study because of safety and tolerability issues, compared with those receiving placebo (1%).
This trial was supported by Gilead Sciences, which was involved in all aspects of the study.
FROM ANNALS OF INTERNAL MEDICINE
Major Finding: Significantly more patients taking ambrisentan (27.4%) than taking placebo (17.2%) showed IPF progression.
Data Source: A phase III randomized, double-blind clinical trial involving 329 patients with idiopathic pulmonary fibrosis who received ambrisentan and 163 who received a matching placebo for approximately 9 months before the study was terminated.
Disclosures: This trial was supported by ambrisentan-maker Gilead Sciences, which was involved in all aspects of the study.

Eight principles for safe opioid prescribing
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).

And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).
And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).
And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
AT THE AAPM ANNUAL MEETING

Guidelines: SABAs, not LABAs, for exercise-induced bronchoconstriction
Don’t base diagnosis of exercise-induced bronchoconstriction on symptoms alone – but do have patients use inhaled short-acting beta-agonists and do warm-ups before exercise, according to new clinical practice guidelines issued May 1 by the American Thoracic Society.
The guidelines define exercise-induced bronchoconstriction (EIB) as "acute airway narrowing that occurs as a result of exercise."
Considering the high prevalence of EIB, which also affects people without asthma, "evidence-based guidelines for its management are of critical importance," said Dr. Jonathan Parsons, the lead author and chair of the committee that drafted the guidelines, in a statement.

The recommendations "synthesize the latest clinical evidence and will help guide the management of EIB in patients with or without asthma, and in athletes at all levels of competition," added Dr. Parsons, associate professor of internal medicine and associate director of the Ohio State University Asthma Center, Columbus.
The EIB guidelines cover pathogenesis, environmental triggers, diagnosis, treatment, and screening (Am. J. Resp. Crit. Care Med. 2013;187 [doi:10.1164/rccm.201303-0437ST]). Also included is a section on exercise, asthma, and doping – with reminders about which EIB drugs are banned in competitive sports (most beta-agonists) and which are allowed (short-acting inhaled albuterol and inhaled steroids).
Although the guidelines can apply both to adolescents and adults, they cannot be applied reliably to young children, Dr. Parsons noted in an interview.
EIB prevalence among people with asthma is not known, but the estimated prevalence among people who have not been diagnosed with asthma is as high as 20%, according to the ATS. EIB is more prevalent among athletes, affecting 30%-70% of Olympic and elite athletes. Environmental factors likely play a role, such as pollutants emitted from ice surfacing machines in indoor ice rinks, high trichloramine levels in the air of indoor pools, and cold, dry air.
An EIB diagnosis should not be based on symptoms, which are variable, nonspecific, and have poor predictive value. Instead, diagnosis should be made based on changes in lung function provoked by exercise, using serial lung function measurements after a specific exercise or a hyperpnea challenge. Assessing the effects of exercise on forced expiratory volume in 1 second (FEV1) is preferred.
The guidelines grade EIB as mild, moderate, or severe, depending on the percent fall in FEV1 from baseline. They also offer information on alternatives to exercise testing.
The authors rate pharmacologic and nonpharmacologic therapies based on the quality of the supportive evidence. Their first recommendation – administration of an inhaled short-acting beta-agonist (SABA) before exercise – earns a "strong" recommendation based on "high-quality" evidence. Patients typically take SABAs 15 minutes before exercise.
Because of the potential for serious side effects, the authors recommend against daily use of an inhaled long-acting beta-agonist (LABA) for EIB – a strong recommendation based on moderate-quality evidence.
For patients who use an inhaled SABA but continue to have symptoms or need to use the inhaled SABA "daily or more frequently," treatment options before exercise include a daily inhaled corticosteroid (ICS), a daily leukotriene-receptor antagonist, or a mast-cell–stabilizing agent.
"We generally add a daily inhaled ICS or a daily leukotriene-receptor antagonist first, with the choice between these agents made on a case-by-case basis depending upon patient preferences," the guideline authors note. Mast-cell–stabilizing agents and inhaled anticholinergic drugs "play a secondary role," they added. There is also a role for antihistamines in patient with continued symptoms despite treatment, but not for patients without allergies.
Nonpharmacologic measures include interval or combination warm-up exercises before planned exercise, which the guidelines recommend "for all patients" with EIB – a strong recommendation, based on moderate quality evidence. The guidelines cite evidence showing a lower reduction in FEV1 after exercise among people with EIB who engaged in "interval, low-intensity continuous; high-intensity continuous; or combination warm-up" before they exercised.
Another nonpharmacologic recommendation is use of a mask or another device that warms and humidifies the air when patients exercise in a cold climate.
While there is not much evidence supporting dietary modifications, patients interested in this approach can try a low-salt diet, or take fish oil or vitamin C supplements. However, the use of lycopene is not supported, based on the available evidence.
"Our overall recommendations regarding therapy leave a lot of options for the individual patient, which should be discussed with the patient’s physician and tried and evaluated on an ongoing basis," the authors concluded.
The mainstay of treatment "remains maintaining good control of underlying asthma (if present) and preventing or treating symptoms of EIB with SABAs."
The EIB practice guidelines were supported by the ATS and approved by the ATS board of directors. Dr. Parsons’ disclosures include having received lecture fees from AstraZeneca, GlaxoSmithKline, Merck, and Schering Plough. All but one of the other authors disclosed financial relations with a wide range of pharmaceutical companies.
Don’t base diagnosis of exercise-induced bronchoconstriction on symptoms alone – but do have patients use inhaled short-acting beta-agonists and do warm-ups before exercise, according to new clinical practice guidelines issued May 1 by the American Thoracic Society.
The guidelines define exercise-induced bronchoconstriction (EIB) as "acute airway narrowing that occurs as a result of exercise."
Considering the high prevalence of EIB, which also affects people without asthma, "evidence-based guidelines for its management are of critical importance," said Dr. Jonathan Parsons, the lead author and chair of the committee that drafted the guidelines, in a statement.
The recommendations "synthesize the latest clinical evidence and will help guide the management of EIB in patients with or without asthma, and in athletes at all levels of competition," added Dr. Parsons, associate professor of internal medicine and associate director of the Ohio State University Asthma Center, Columbus.
The EIB guidelines cover pathogenesis, environmental triggers, diagnosis, treatment, and screening (Am. J. Resp. Crit. Care Med. 2013;187 [doi:10.1164/rccm.201303-0437ST]). Also included is a section on exercise, asthma, and doping – with reminders about which EIB drugs are banned in competitive sports (most beta-agonists) and which are allowed (short-acting inhaled albuterol and inhaled steroids).
Although the guidelines can apply both to adolescents and adults, they cannot be applied reliably to young children, Dr. Parsons noted in an interview.
EIB prevalence among people with asthma is not known, but the estimated prevalence among people who have not been diagnosed with asthma is as high as 20%, according to the ATS. EIB is more prevalent among athletes, affecting 30%-70% of Olympic and elite athletes. Environmental factors likely play a role, such as pollutants emitted from ice surfacing machines in indoor ice rinks, high trichloramine levels in the air of indoor pools, and cold, dry air.
An EIB diagnosis should not be based on symptoms, which are variable, nonspecific, and have poor predictive value. Instead, diagnosis should be made based on changes in lung function provoked by exercise, using serial lung function measurements after a specific exercise or a hyperpnea challenge. Assessing the effects of exercise on forced expiratory volume in 1 second (FEV1) is preferred.
The guidelines grade EIB as mild, moderate, or severe, depending on the percent fall in FEV1 from baseline. They also offer information on alternatives to exercise testing.
The authors rate pharmacologic and nonpharmacologic therapies based on the quality of the supportive evidence. Their first recommendation – administration of an inhaled short-acting beta-agonist (SABA) before exercise – earns a "strong" recommendation based on "high-quality" evidence. Patients typically take SABAs 15 minutes before exercise.
Because of the potential for serious side effects, the authors recommend against daily use of an inhaled long-acting beta-agonist (LABA) for EIB – a strong recommendation based on moderate-quality evidence.
For patients who use an inhaled SABA but continue to have symptoms or need to use the inhaled SABA "daily or more frequently," treatment options before exercise include a daily inhaled corticosteroid (ICS), a daily leukotriene-receptor antagonist, or a mast-cell–stabilizing agent.
"We generally add a daily inhaled ICS or a daily leukotriene-receptor antagonist first, with the choice between these agents made on a case-by-case basis depending upon patient preferences," the guideline authors note. Mast-cell–stabilizing agents and inhaled anticholinergic drugs "play a secondary role," they added. There is also a role for antihistamines in patient with continued symptoms despite treatment, but not for patients without allergies.
Nonpharmacologic measures include interval or combination warm-up exercises before planned exercise, which the guidelines recommend "for all patients" with EIB – a strong recommendation, based on moderate quality evidence. The guidelines cite evidence showing a lower reduction in FEV1 after exercise among people with EIB who engaged in "interval, low-intensity continuous; high-intensity continuous; or combination warm-up" before they exercised.
Another nonpharmacologic recommendation is use of a mask or another device that warms and humidifies the air when patients exercise in a cold climate.
While there is not much evidence supporting dietary modifications, patients interested in this approach can try a low-salt diet, or take fish oil or vitamin C supplements. However, the use of lycopene is not supported, based on the available evidence.
"Our overall recommendations regarding therapy leave a lot of options for the individual patient, which should be discussed with the patient’s physician and tried and evaluated on an ongoing basis," the authors concluded.
The mainstay of treatment "remains maintaining good control of underlying asthma (if present) and preventing or treating symptoms of EIB with SABAs."
The EIB practice guidelines were supported by the ATS and approved by the ATS board of directors. Dr. Parsons’ disclosures include having received lecture fees from AstraZeneca, GlaxoSmithKline, Merck, and Schering Plough. All but one of the other authors disclosed financial relations with a wide range of pharmaceutical companies.
Don’t base diagnosis of exercise-induced bronchoconstriction on symptoms alone – but do have patients use inhaled short-acting beta-agonists and do warm-ups before exercise, according to new clinical practice guidelines issued May 1 by the American Thoracic Society.
The guidelines define exercise-induced bronchoconstriction (EIB) as "acute airway narrowing that occurs as a result of exercise."
Considering the high prevalence of EIB, which also affects people without asthma, "evidence-based guidelines for its management are of critical importance," said Dr. Jonathan Parsons, the lead author and chair of the committee that drafted the guidelines, in a statement.
The recommendations "synthesize the latest clinical evidence and will help guide the management of EIB in patients with or without asthma, and in athletes at all levels of competition," added Dr. Parsons, associate professor of internal medicine and associate director of the Ohio State University Asthma Center, Columbus.
The EIB guidelines cover pathogenesis, environmental triggers, diagnosis, treatment, and screening (Am. J. Resp. Crit. Care Med. 2013;187 [doi:10.1164/rccm.201303-0437ST]). Also included is a section on exercise, asthma, and doping – with reminders about which EIB drugs are banned in competitive sports (most beta-agonists) and which are allowed (short-acting inhaled albuterol and inhaled steroids).
Although the guidelines can apply both to adolescents and adults, they cannot be applied reliably to young children, Dr. Parsons noted in an interview.
EIB prevalence among people with asthma is not known, but the estimated prevalence among people who have not been diagnosed with asthma is as high as 20%, according to the ATS. EIB is more prevalent among athletes, affecting 30%-70% of Olympic and elite athletes. Environmental factors likely play a role, such as pollutants emitted from ice surfacing machines in indoor ice rinks, high trichloramine levels in the air of indoor pools, and cold, dry air.
An EIB diagnosis should not be based on symptoms, which are variable, nonspecific, and have poor predictive value. Instead, diagnosis should be made based on changes in lung function provoked by exercise, using serial lung function measurements after a specific exercise or a hyperpnea challenge. Assessing the effects of exercise on forced expiratory volume in 1 second (FEV1) is preferred.
The guidelines grade EIB as mild, moderate, or severe, depending on the percent fall in FEV1 from baseline. They also offer information on alternatives to exercise testing.
The authors rate pharmacologic and nonpharmacologic therapies based on the quality of the supportive evidence. Their first recommendation – administration of an inhaled short-acting beta-agonist (SABA) before exercise – earns a "strong" recommendation based on "high-quality" evidence. Patients typically take SABAs 15 minutes before exercise.
Because of the potential for serious side effects, the authors recommend against daily use of an inhaled long-acting beta-agonist (LABA) for EIB – a strong recommendation based on moderate-quality evidence.
For patients who use an inhaled SABA but continue to have symptoms or need to use the inhaled SABA "daily or more frequently," treatment options before exercise include a daily inhaled corticosteroid (ICS), a daily leukotriene-receptor antagonist, or a mast-cell–stabilizing agent.
"We generally add a daily inhaled ICS or a daily leukotriene-receptor antagonist first, with the choice between these agents made on a case-by-case basis depending upon patient preferences," the guideline authors note. Mast-cell–stabilizing agents and inhaled anticholinergic drugs "play a secondary role," they added. There is also a role for antihistamines in patient with continued symptoms despite treatment, but not for patients without allergies.
Nonpharmacologic measures include interval or combination warm-up exercises before planned exercise, which the guidelines recommend "for all patients" with EIB – a strong recommendation, based on moderate quality evidence. The guidelines cite evidence showing a lower reduction in FEV1 after exercise among people with EIB who engaged in "interval, low-intensity continuous; high-intensity continuous; or combination warm-up" before they exercised.
Another nonpharmacologic recommendation is use of a mask or another device that warms and humidifies the air when patients exercise in a cold climate.
While there is not much evidence supporting dietary modifications, patients interested in this approach can try a low-salt diet, or take fish oil or vitamin C supplements. However, the use of lycopene is not supported, based on the available evidence.
"Our overall recommendations regarding therapy leave a lot of options for the individual patient, which should be discussed with the patient’s physician and tried and evaluated on an ongoing basis," the authors concluded.
The mainstay of treatment "remains maintaining good control of underlying asthma (if present) and preventing or treating symptoms of EIB with SABAs."
The EIB practice guidelines were supported by the ATS and approved by the ATS board of directors. Dr. Parsons’ disclosures include having received lecture fees from AstraZeneca, GlaxoSmithKline, Merck, and Schering Plough. All but one of the other authors disclosed financial relations with a wide range of pharmaceutical companies.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE

Infant UTI: Spinal tap for meningitis before ED discharge
LAKE BUENA VISTA, FLA. – Does every baby who presents to the emergency department with a urinary tract infection need a lumbar puncture to rule out meningitis?
Maybe not, Dr. James Callahan said at the Advanced Pediatric Emergency Medicine Assembly. Age, past medical history, and the child’s overall demeanor are the best clues as to whether to proceed with a spinal tap in babies with a confirmed source of infection.
The topic is worth reviewing because childhood meningitis cases are on the decline, said Dr. Callahan of Children’s Hospital of Pennsylvania, Philadelphia.

When a disease begins to fade from a patient population, it also can fade from the collective consciousness of clinicians. "There are residents and fellows in emergency medicine and pediatrics now who have never seen a case of [Haemophilus] influenzae meningitis," he said at the meeting, which was sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics.
That can mean tragedy for patients and families, and disaster for doctors. "Missed meningitis remains the number-one cause of settled lawsuits in pediatric emergency medicine, and carries the highest settlement and indemnity costs," he said.
A number of signs can help rule in the disease, but few can completely rule it out. "Although several clinical features are useful in diagnosing meningitis, no one isolated clinical feature is diagnostic. Nor can any isolated clinical feature completely exclude meningitis as a diagnostic possibility, and it’s not clear what the most accurate combination of clinical features is – or if there even is such a combination," Dr. Callahan explained.
That leaves clinicians with what seems to be the only concrete option – the lumbar puncture. "I personally think an LP is a relatively simple procedure, but there is a lot of parental resistance to it," he noted.
Dr. Callahan examined the question in light of infants’ most common bacterial infection – the urinary tract infection (UTI). Studies from the last 15 years agree that, while the risk of meningitis in conjunction with UTI is very low, it is there.
The largest of these included nearly 2,000 infants with culture-proven UTI. Most (1,609) underwent an LP. Of those patients, 3% had bacterial meningitis. A combination of clinical findings – not clinically ill on exam, no dehydration or acute respiratory distress, no concomitant acute disease or high-risk medical history – ruled out meningitis with a 98% sensitivity and 99.9% negative predictive value (Pediatrics 2010;126:1074-83).
A 2011 study found a 1% rate of meningitis associated with UTI in infants younger than 28 days, but there were no cases at all in the older babies. All of those with meningitis were symptomatic on admission, with fever, irritability, and lethargy (PLoS One 2011;6:e26576).
"Meningitis appears exceedingly rare in children older than 28 days," Dr. Callahan said. "All neonates who present with a culture-proven UTI should have an LP. But those who are older, and who look well, without a negative past history – you might consider not doing one."
Whether or not the child will be admitted to the hospital plays a part in Dr. Callahan’s decision.
"If they have a UTI and they’re getting admitted, but look well and have a negative past medical history, I don’t tap. I really think the data say if they look like they are well, they will not get meningitis."
If, on the other hand, the baby will be going home from the emergency visit, he does the procedure. "And make sure you have someone who’s going to follow that child very closely," he advised.
Dr. Callahan had no financial disclosures.
LAKE BUENA VISTA, FLA. – Does every baby who presents to the emergency department with a urinary tract infection need a lumbar puncture to rule out meningitis?
Maybe not, Dr. James Callahan said at the Advanced Pediatric Emergency Medicine Assembly. Age, past medical history, and the child’s overall demeanor are the best clues as to whether to proceed with a spinal tap in babies with a confirmed source of infection.
The topic is worth reviewing because childhood meningitis cases are on the decline, said Dr. Callahan of Children’s Hospital of Pennsylvania, Philadelphia.
When a disease begins to fade from a patient population, it also can fade from the collective consciousness of clinicians. "There are residents and fellows in emergency medicine and pediatrics now who have never seen a case of [Haemophilus] influenzae meningitis," he said at the meeting, which was sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics.
That can mean tragedy for patients and families, and disaster for doctors. "Missed meningitis remains the number-one cause of settled lawsuits in pediatric emergency medicine, and carries the highest settlement and indemnity costs," he said.
A number of signs can help rule in the disease, but few can completely rule it out. "Although several clinical features are useful in diagnosing meningitis, no one isolated clinical feature is diagnostic. Nor can any isolated clinical feature completely exclude meningitis as a diagnostic possibility, and it’s not clear what the most accurate combination of clinical features is – or if there even is such a combination," Dr. Callahan explained.
That leaves clinicians with what seems to be the only concrete option – the lumbar puncture. "I personally think an LP is a relatively simple procedure, but there is a lot of parental resistance to it," he noted.
Dr. Callahan examined the question in light of infants’ most common bacterial infection – the urinary tract infection (UTI). Studies from the last 15 years agree that, while the risk of meningitis in conjunction with UTI is very low, it is there.
The largest of these included nearly 2,000 infants with culture-proven UTI. Most (1,609) underwent an LP. Of those patients, 3% had bacterial meningitis. A combination of clinical findings – not clinically ill on exam, no dehydration or acute respiratory distress, no concomitant acute disease or high-risk medical history – ruled out meningitis with a 98% sensitivity and 99.9% negative predictive value (Pediatrics 2010;126:1074-83).
A 2011 study found a 1% rate of meningitis associated with UTI in infants younger than 28 days, but there were no cases at all in the older babies. All of those with meningitis were symptomatic on admission, with fever, irritability, and lethargy (PLoS One 2011;6:e26576).
"Meningitis appears exceedingly rare in children older than 28 days," Dr. Callahan said. "All neonates who present with a culture-proven UTI should have an LP. But those who are older, and who look well, without a negative past history – you might consider not doing one."
Whether or not the child will be admitted to the hospital plays a part in Dr. Callahan’s decision.
"If they have a UTI and they’re getting admitted, but look well and have a negative past medical history, I don’t tap. I really think the data say if they look like they are well, they will not get meningitis."
If, on the other hand, the baby will be going home from the emergency visit, he does the procedure. "And make sure you have someone who’s going to follow that child very closely," he advised.
Dr. Callahan had no financial disclosures.
LAKE BUENA VISTA, FLA. – Does every baby who presents to the emergency department with a urinary tract infection need a lumbar puncture to rule out meningitis?
Maybe not, Dr. James Callahan said at the Advanced Pediatric Emergency Medicine Assembly. Age, past medical history, and the child’s overall demeanor are the best clues as to whether to proceed with a spinal tap in babies with a confirmed source of infection.
The topic is worth reviewing because childhood meningitis cases are on the decline, said Dr. Callahan of Children’s Hospital of Pennsylvania, Philadelphia.
When a disease begins to fade from a patient population, it also can fade from the collective consciousness of clinicians. "There are residents and fellows in emergency medicine and pediatrics now who have never seen a case of [Haemophilus] influenzae meningitis," he said at the meeting, which was sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics.
That can mean tragedy for patients and families, and disaster for doctors. "Missed meningitis remains the number-one cause of settled lawsuits in pediatric emergency medicine, and carries the highest settlement and indemnity costs," he said.
A number of signs can help rule in the disease, but few can completely rule it out. "Although several clinical features are useful in diagnosing meningitis, no one isolated clinical feature is diagnostic. Nor can any isolated clinical feature completely exclude meningitis as a diagnostic possibility, and it’s not clear what the most accurate combination of clinical features is – or if there even is such a combination," Dr. Callahan explained.
That leaves clinicians with what seems to be the only concrete option – the lumbar puncture. "I personally think an LP is a relatively simple procedure, but there is a lot of parental resistance to it," he noted.
Dr. Callahan examined the question in light of infants’ most common bacterial infection – the urinary tract infection (UTI). Studies from the last 15 years agree that, while the risk of meningitis in conjunction with UTI is very low, it is there.
The largest of these included nearly 2,000 infants with culture-proven UTI. Most (1,609) underwent an LP. Of those patients, 3% had bacterial meningitis. A combination of clinical findings – not clinically ill on exam, no dehydration or acute respiratory distress, no concomitant acute disease or high-risk medical history – ruled out meningitis with a 98% sensitivity and 99.9% negative predictive value (Pediatrics 2010;126:1074-83).
A 2011 study found a 1% rate of meningitis associated with UTI in infants younger than 28 days, but there were no cases at all in the older babies. All of those with meningitis were symptomatic on admission, with fever, irritability, and lethargy (PLoS One 2011;6:e26576).
"Meningitis appears exceedingly rare in children older than 28 days," Dr. Callahan said. "All neonates who present with a culture-proven UTI should have an LP. But those who are older, and who look well, without a negative past history – you might consider not doing one."
Whether or not the child will be admitted to the hospital plays a part in Dr. Callahan’s decision.
"If they have a UTI and they’re getting admitted, but look well and have a negative past medical history, I don’t tap. I really think the data say if they look like they are well, they will not get meningitis."
If, on the other hand, the baby will be going home from the emergency visit, he does the procedure. "And make sure you have someone who’s going to follow that child very closely," he advised.
Dr. Callahan had no financial disclosures.
EXPERT ANALYSIS FROM THE ADVANCED PEDIATRIC EMERGENCY MEDICINE ASSEMBLY

Older patients report frequent insomnia, sleep treatment use
LOS ANGELES – Most older adults have sleep-related complaints, and most use some form of sleep aid, according to findings from the Successful Aging Evaluation study.
A large number of subjects reported using sleep aids that could have deleterious effects, such as alcohol and over-the-counter remedies.
Of 1,300 subjects included in the Successful Aging Evaluation (SAGE) study, 92.4% had sleep complaints, including waking feeling unrefreshed, early awakening, difficulty falling asleep, and middle of the night awakening. Each of these complaints was reported by between 75% and 79% of subjects, Dr. Nicolas Badre reported in a poster at the annual meeting of the American Association for Geriatric Psychiatry.

More than half (55.5%) of the subjects reported using one or more forms of treatment for sleep disturbance: 8.1% reported using complementary or alternative treatments, 10% reported using alcohol, 14.8% reported using prescription medications, 21.3% reported using over-the-counter remedies, and 39% reported using behavioral techniques, according to Dr. Badre of the University of California, San Diego.
The use of any treatment for sleep was significantly associated with a higher number of doctor visits in the past year, lower Satisfaction With Life Scale scores, a lower average number of hours of sleep per night, depression as measured by the nine-item Patient Health Questionnaire, and reduced physical functioning as measured using the 36-Item Short Form Health Survey.
Clinical depression was associated with a significantly increased odds of any use of treatment for sleep (odds ratio, 2.4), and use of prescription treatment for sleep (OR, 3.3), Dr. Badre noted.
No significant association was seen between the use of any treatment for sleep and cognitive impairment.
The SAGE study was a structured, multicohort population-based study designed to assess successful aging. The survey included a 25-minute phone interview followed by a self-report survey of various domains of functioning. Respondents had a mean age of 77.3 years.
"Results from the SAGE investigation confirm the high prevalence of insomnia and its treatment in older adults," Dr. Badre wrote, noting that decreased activity of the suprachiasmatic nucleus and prescriptions often given to older adults – including stimulants, antihypertensives, respiratory medications, chemotherapy, and decongestants – are among the causes of sleep disturbance in older adults.
The high correlation between the use of any treatment for sleep and depression appears to be a significant risk factor for patients being prescribed medication for sleep, and the high rates of alcohol use and over-the-counter remedies as sleep aids are of concern, he said.
Dr. Badre reported having no relevant financial disclosures.
LOS ANGELES – Most older adults have sleep-related complaints, and most use some form of sleep aid, according to findings from the Successful Aging Evaluation study.
A large number of subjects reported using sleep aids that could have deleterious effects, such as alcohol and over-the-counter remedies.
Of 1,300 subjects included in the Successful Aging Evaluation (SAGE) study, 92.4% had sleep complaints, including waking feeling unrefreshed, early awakening, difficulty falling asleep, and middle of the night awakening. Each of these complaints was reported by between 75% and 79% of subjects, Dr. Nicolas Badre reported in a poster at the annual meeting of the American Association for Geriatric Psychiatry.
More than half (55.5%) of the subjects reported using one or more forms of treatment for sleep disturbance: 8.1% reported using complementary or alternative treatments, 10% reported using alcohol, 14.8% reported using prescription medications, 21.3% reported using over-the-counter remedies, and 39% reported using behavioral techniques, according to Dr. Badre of the University of California, San Diego.
The use of any treatment for sleep was significantly associated with a higher number of doctor visits in the past year, lower Satisfaction With Life Scale scores, a lower average number of hours of sleep per night, depression as measured by the nine-item Patient Health Questionnaire, and reduced physical functioning as measured using the 36-Item Short Form Health Survey.
Clinical depression was associated with a significantly increased odds of any use of treatment for sleep (odds ratio, 2.4), and use of prescription treatment for sleep (OR, 3.3), Dr. Badre noted.
No significant association was seen between the use of any treatment for sleep and cognitive impairment.
The SAGE study was a structured, multicohort population-based study designed to assess successful aging. The survey included a 25-minute phone interview followed by a self-report survey of various domains of functioning. Respondents had a mean age of 77.3 years.
"Results from the SAGE investigation confirm the high prevalence of insomnia and its treatment in older adults," Dr. Badre wrote, noting that decreased activity of the suprachiasmatic nucleus and prescriptions often given to older adults – including stimulants, antihypertensives, respiratory medications, chemotherapy, and decongestants – are among the causes of sleep disturbance in older adults.
The high correlation between the use of any treatment for sleep and depression appears to be a significant risk factor for patients being prescribed medication for sleep, and the high rates of alcohol use and over-the-counter remedies as sleep aids are of concern, he said.
Dr. Badre reported having no relevant financial disclosures.
LOS ANGELES – Most older adults have sleep-related complaints, and most use some form of sleep aid, according to findings from the Successful Aging Evaluation study.
A large number of subjects reported using sleep aids that could have deleterious effects, such as alcohol and over-the-counter remedies.
Of 1,300 subjects included in the Successful Aging Evaluation (SAGE) study, 92.4% had sleep complaints, including waking feeling unrefreshed, early awakening, difficulty falling asleep, and middle of the night awakening. Each of these complaints was reported by between 75% and 79% of subjects, Dr. Nicolas Badre reported in a poster at the annual meeting of the American Association for Geriatric Psychiatry.
More than half (55.5%) of the subjects reported using one or more forms of treatment for sleep disturbance: 8.1% reported using complementary or alternative treatments, 10% reported using alcohol, 14.8% reported using prescription medications, 21.3% reported using over-the-counter remedies, and 39% reported using behavioral techniques, according to Dr. Badre of the University of California, San Diego.
The use of any treatment for sleep was significantly associated with a higher number of doctor visits in the past year, lower Satisfaction With Life Scale scores, a lower average number of hours of sleep per night, depression as measured by the nine-item Patient Health Questionnaire, and reduced physical functioning as measured using the 36-Item Short Form Health Survey.
Clinical depression was associated with a significantly increased odds of any use of treatment for sleep (odds ratio, 2.4), and use of prescription treatment for sleep (OR, 3.3), Dr. Badre noted.
No significant association was seen between the use of any treatment for sleep and cognitive impairment.
The SAGE study was a structured, multicohort population-based study designed to assess successful aging. The survey included a 25-minute phone interview followed by a self-report survey of various domains of functioning. Respondents had a mean age of 77.3 years.
"Results from the SAGE investigation confirm the high prevalence of insomnia and its treatment in older adults," Dr. Badre wrote, noting that decreased activity of the suprachiasmatic nucleus and prescriptions often given to older adults – including stimulants, antihypertensives, respiratory medications, chemotherapy, and decongestants – are among the causes of sleep disturbance in older adults.
The high correlation between the use of any treatment for sleep and depression appears to be a significant risk factor for patients being prescribed medication for sleep, and the high rates of alcohol use and over-the-counter remedies as sleep aids are of concern, he said.
Dr. Badre reported having no relevant financial disclosures.
AT THE AAGP ANNUAL MEETING
Major finding: More than 90% of subjects had sleep complaints; 55.5% reported using a sleep aid, and 10% of these reported using alcohol to sleep.
Data source: A survey of 1,300 older adults.
Disclosures: Dr. Badre reported having no relevant financial disclosures.

FDA panel backs ICS/LABA inhaler for COPD
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel supported the approval of an inhaled powder formulation of fluticasone furoate and vilanterol as a treatment for chronic obstructive pulmonary disease, based on studies of almost 4,000 patients.
At a meeting on April 17, the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted that the results of the studies provided "substantial evidence" to support approval of the fixed-dose combination of 100 mcg of fluticasone furoate (FF) with 25 mcg of vilanterol (VI), administered once a day, for the long-term maintenance treatment of airflow obstruction (in a 9 to 4 vote), and for reducing COPD exacerbations (in an 8 to 5 vote).
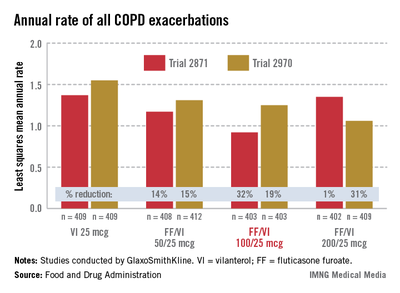
The inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination is formulated in a dry powder, and is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which is developing the product with Theravance.
If the formulation is approved, it would be the first ICS/LABA product that is dosed once a day for COPD, and would be the first such product that would only be available in the combined formulation, since the companies have no plans to pursue approval of the VI component alone. GSK also markets Advair Diskus, the combination of fluticasone propionate and salmeterol, one of the two inhaled ICS/LABA treatments that is FDA approved for the treatment of COPD. The other is the combination of budesonide and formoterol (Symbicort). Both are administered twice a day, and salmeterol and formoterol are both available as separate products for COPD.
The safety and efficacy of three different dosage strengths of FF – 200, 100, and 50 mcg – combined with 25 mcg of VI were evaluated in four pivotal phase III studies of 3,852 mostly Caucasian people (mean age, 62-63 years) with COPD. All patients had a forced expiratory volume in 1 second (FEV1) less than 70% predicted. About half were current smokers.
In two 24-week studies of 2,254 patients evaluating the effect on lung function, the three FF/VI dosage strengths were compared with placebo, FF 100 mcg alone, and VI 25 mcg alone for two primary endpoints: weighted mean FEV1 at 0-4 hours and change from baseline in trough FEV1.
At 24 weeks, there were significant improvements in the weighted mean FEV1 and in trough FEV1 for all three strengths of FF/VI and for VI 25 mcg, compared with placebo. There were also significant improvements in the mean FEV1 (0-4 hours) for all three strengths of FF/VI, compared with FF alone. Improvement in trough FEV1, however, was not significantly better with any of the three doses, when compared with VI 25 mcg alone.
In the two 52-week exacerbation trials of 1,622 patients who had had at least one COPD exacerbation in the previous year, the rate of moderate and severe COPD exacerbations in 1 year was reduced by 21% and 34%, respectively, among those on the FF/VI 100/25 dose over those on VI 25 mcg alone. In one study, the reduction in exacerbations was significant for all three doses, but in the other study, the effect of the proposed 100/25 dose on exacerbations was only numerically, not significantly, improved over the effect of VI 25, the FDA reviewers pointed out. And overall, for the 100/25 dose, the rate of moderate and severe exacerbations was reduced only "by a fraction of an event in 1 year," said Kiya Hamilton, Ph.D., a biostatistician reviewer at the FDA.
Treatment was associated with an increase in local steroid effects, such as oral candidiasis, as expected. In the exacerbation studies, there were more cases of pneumonia and an increase in pneumonia-related deaths with increasing FF doses, and more fractures among those on the FF/VI combination. Bone loss and pneumonia are recognized as adverse effects of ICS in COPD patients, and with one exception, all the deaths were among those on 200/25 mcg dose, which is not going to be marketed, the FDA said.
In a 12 to 1 vote, the panel agreed that the efficacy data provided substantial evidence that the proposed dose provided "a clinically meaningful benefit" for the long-term maintenance treatment of airflow obstruction in COPD. But they were less united on the impact on exacerbations, voting 8 to 5 that the data provided substantial evidence that the reduction in exacerbations seen in the study was clinically meaningful. The panel also voted 10 to 3 that the safety of the 100/25 mcg dose had been adequately demonstrated for the COPD indication.
Panelists supporting approval cited the totality of the database and the utility of having a once a day dose as among the reasons for their votes. Dr. James Stoller, the Jean Wall Bennett Professor of Medicine at the Cleveland Clinic, supported approval and said that the safety profile was acceptable as long as the formulation was not used to treat patients with mild COPD.
Like other panelists who did not support approval, Dr. Paula Carvalho, professor of medicine in the division of pulmonary and critical care medicine, University of Washington, Seattle, said the benefit-risk profile was not adequate. She added that she was more impressed by the effect that treatment with VI 25 mcg alone had on COPD exacerbations than with the combination. Also voting against approval was Peter Peduzzi, Ph.D., professor of public health at the Yale School of Public Health in New Haven, Conn., who said that the impact on trough FEV1 appeared to be driven by the VI component, and like others voting against approval, he cited safety issues.
If approved, GSK plans to market the product as Breo Ellipta. The FDA’s deadline for making a decision on the approval is May 12. The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist might be given a waiver, but not at this meeting.
The product is under review for both COPD and asthma in the European Union and in Japan. It is not under review for asthma in the United States.
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel supported the approval of an inhaled powder formulation of fluticasone furoate and vilanterol as a treatment for chronic obstructive pulmonary disease, based on studies of almost 4,000 patients.
At a meeting on April 17, the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted that the results of the studies provided "substantial evidence" to support approval of the fixed-dose combination of 100 mcg of fluticasone furoate (FF) with 25 mcg of vilanterol (VI), administered once a day, for the long-term maintenance treatment of airflow obstruction (in a 9 to 4 vote), and for reducing COPD exacerbations (in an 8 to 5 vote).
The inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination is formulated in a dry powder, and is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which is developing the product with Theravance.
If the formulation is approved, it would be the first ICS/LABA product that is dosed once a day for COPD, and would be the first such product that would only be available in the combined formulation, since the companies have no plans to pursue approval of the VI component alone. GSK also markets Advair Diskus, the combination of fluticasone propionate and salmeterol, one of the two inhaled ICS/LABA treatments that is FDA approved for the treatment of COPD. The other is the combination of budesonide and formoterol (Symbicort). Both are administered twice a day, and salmeterol and formoterol are both available as separate products for COPD.
The safety and efficacy of three different dosage strengths of FF – 200, 100, and 50 mcg – combined with 25 mcg of VI were evaluated in four pivotal phase III studies of 3,852 mostly Caucasian people (mean age, 62-63 years) with COPD. All patients had a forced expiratory volume in 1 second (FEV1) less than 70% predicted. About half were current smokers.
In two 24-week studies of 2,254 patients evaluating the effect on lung function, the three FF/VI dosage strengths were compared with placebo, FF 100 mcg alone, and VI 25 mcg alone for two primary endpoints: weighted mean FEV1 at 0-4 hours and change from baseline in trough FEV1.
At 24 weeks, there were significant improvements in the weighted mean FEV1 and in trough FEV1 for all three strengths of FF/VI and for VI 25 mcg, compared with placebo. There were also significant improvements in the mean FEV1 (0-4 hours) for all three strengths of FF/VI, compared with FF alone. Improvement in trough FEV1, however, was not significantly better with any of the three doses, when compared with VI 25 mcg alone.
In the two 52-week exacerbation trials of 1,622 patients who had had at least one COPD exacerbation in the previous year, the rate of moderate and severe COPD exacerbations in 1 year was reduced by 21% and 34%, respectively, among those on the FF/VI 100/25 dose over those on VI 25 mcg alone. In one study, the reduction in exacerbations was significant for all three doses, but in the other study, the effect of the proposed 100/25 dose on exacerbations was only numerically, not significantly, improved over the effect of VI 25, the FDA reviewers pointed out. And overall, for the 100/25 dose, the rate of moderate and severe exacerbations was reduced only "by a fraction of an event in 1 year," said Kiya Hamilton, Ph.D., a biostatistician reviewer at the FDA.
Treatment was associated with an increase in local steroid effects, such as oral candidiasis, as expected. In the exacerbation studies, there were more cases of pneumonia and an increase in pneumonia-related deaths with increasing FF doses, and more fractures among those on the FF/VI combination. Bone loss and pneumonia are recognized as adverse effects of ICS in COPD patients, and with one exception, all the deaths were among those on 200/25 mcg dose, which is not going to be marketed, the FDA said.
In a 12 to 1 vote, the panel agreed that the efficacy data provided substantial evidence that the proposed dose provided "a clinically meaningful benefit" for the long-term maintenance treatment of airflow obstruction in COPD. But they were less united on the impact on exacerbations, voting 8 to 5 that the data provided substantial evidence that the reduction in exacerbations seen in the study was clinically meaningful. The panel also voted 10 to 3 that the safety of the 100/25 mcg dose had been adequately demonstrated for the COPD indication.
Panelists supporting approval cited the totality of the database and the utility of having a once a day dose as among the reasons for their votes. Dr. James Stoller, the Jean Wall Bennett Professor of Medicine at the Cleveland Clinic, supported approval and said that the safety profile was acceptable as long as the formulation was not used to treat patients with mild COPD.
Like other panelists who did not support approval, Dr. Paula Carvalho, professor of medicine in the division of pulmonary and critical care medicine, University of Washington, Seattle, said the benefit-risk profile was not adequate. She added that she was more impressed by the effect that treatment with VI 25 mcg alone had on COPD exacerbations than with the combination. Also voting against approval was Peter Peduzzi, Ph.D., professor of public health at the Yale School of Public Health in New Haven, Conn., who said that the impact on trough FEV1 appeared to be driven by the VI component, and like others voting against approval, he cited safety issues.
If approved, GSK plans to market the product as Breo Ellipta. The FDA’s deadline for making a decision on the approval is May 12. The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist might be given a waiver, but not at this meeting.
The product is under review for both COPD and asthma in the European Union and in Japan. It is not under review for asthma in the United States.
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel supported the approval of an inhaled powder formulation of fluticasone furoate and vilanterol as a treatment for chronic obstructive pulmonary disease, based on studies of almost 4,000 patients.
At a meeting on April 17, the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted that the results of the studies provided "substantial evidence" to support approval of the fixed-dose combination of 100 mcg of fluticasone furoate (FF) with 25 mcg of vilanterol (VI), administered once a day, for the long-term maintenance treatment of airflow obstruction (in a 9 to 4 vote), and for reducing COPD exacerbations (in an 8 to 5 vote).
The inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination is formulated in a dry powder, and is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which is developing the product with Theravance.
If the formulation is approved, it would be the first ICS/LABA product that is dosed once a day for COPD, and would be the first such product that would only be available in the combined formulation, since the companies have no plans to pursue approval of the VI component alone. GSK also markets Advair Diskus, the combination of fluticasone propionate and salmeterol, one of the two inhaled ICS/LABA treatments that is FDA approved for the treatment of COPD. The other is the combination of budesonide and formoterol (Symbicort). Both are administered twice a day, and salmeterol and formoterol are both available as separate products for COPD.
The safety and efficacy of three different dosage strengths of FF – 200, 100, and 50 mcg – combined with 25 mcg of VI were evaluated in four pivotal phase III studies of 3,852 mostly Caucasian people (mean age, 62-63 years) with COPD. All patients had a forced expiratory volume in 1 second (FEV1) less than 70% predicted. About half were current smokers.
In two 24-week studies of 2,254 patients evaluating the effect on lung function, the three FF/VI dosage strengths were compared with placebo, FF 100 mcg alone, and VI 25 mcg alone for two primary endpoints: weighted mean FEV1 at 0-4 hours and change from baseline in trough FEV1.
At 24 weeks, there were significant improvements in the weighted mean FEV1 and in trough FEV1 for all three strengths of FF/VI and for VI 25 mcg, compared with placebo. There were also significant improvements in the mean FEV1 (0-4 hours) for all three strengths of FF/VI, compared with FF alone. Improvement in trough FEV1, however, was not significantly better with any of the three doses, when compared with VI 25 mcg alone.
In the two 52-week exacerbation trials of 1,622 patients who had had at least one COPD exacerbation in the previous year, the rate of moderate and severe COPD exacerbations in 1 year was reduced by 21% and 34%, respectively, among those on the FF/VI 100/25 dose over those on VI 25 mcg alone. In one study, the reduction in exacerbations was significant for all three doses, but in the other study, the effect of the proposed 100/25 dose on exacerbations was only numerically, not significantly, improved over the effect of VI 25, the FDA reviewers pointed out. And overall, for the 100/25 dose, the rate of moderate and severe exacerbations was reduced only "by a fraction of an event in 1 year," said Kiya Hamilton, Ph.D., a biostatistician reviewer at the FDA.
Treatment was associated with an increase in local steroid effects, such as oral candidiasis, as expected. In the exacerbation studies, there were more cases of pneumonia and an increase in pneumonia-related deaths with increasing FF doses, and more fractures among those on the FF/VI combination. Bone loss and pneumonia are recognized as adverse effects of ICS in COPD patients, and with one exception, all the deaths were among those on 200/25 mcg dose, which is not going to be marketed, the FDA said.
In a 12 to 1 vote, the panel agreed that the efficacy data provided substantial evidence that the proposed dose provided "a clinically meaningful benefit" for the long-term maintenance treatment of airflow obstruction in COPD. But they were less united on the impact on exacerbations, voting 8 to 5 that the data provided substantial evidence that the reduction in exacerbations seen in the study was clinically meaningful. The panel also voted 10 to 3 that the safety of the 100/25 mcg dose had been adequately demonstrated for the COPD indication.
Panelists supporting approval cited the totality of the database and the utility of having a once a day dose as among the reasons for their votes. Dr. James Stoller, the Jean Wall Bennett Professor of Medicine at the Cleveland Clinic, supported approval and said that the safety profile was acceptable as long as the formulation was not used to treat patients with mild COPD.
Like other panelists who did not support approval, Dr. Paula Carvalho, professor of medicine in the division of pulmonary and critical care medicine, University of Washington, Seattle, said the benefit-risk profile was not adequate. She added that she was more impressed by the effect that treatment with VI 25 mcg alone had on COPD exacerbations than with the combination. Also voting against approval was Peter Peduzzi, Ph.D., professor of public health at the Yale School of Public Health in New Haven, Conn., who said that the impact on trough FEV1 appeared to be driven by the VI component, and like others voting against approval, he cited safety issues.
If approved, GSK plans to market the product as Breo Ellipta. The FDA’s deadline for making a decision on the approval is May 12. The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist might be given a waiver, but not at this meeting.
The product is under review for both COPD and asthma in the European Union and in Japan. It is not under review for asthma in the United States.
AT AN FDA ADVISORY PANEL MEETING
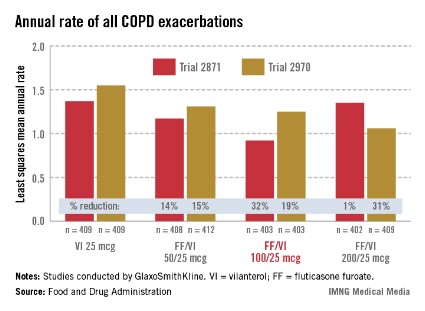
For hypertension, pair CPAP with weight loss
SAN FRANCISCO– A 24-week program combining weight-loss efforts with continuous positive airway pressure produced significantly greater reductions in systolic blood pressure in obese patients with obstructive sleep apnea, compared with either intervention alone, a study of 181 adults found.
In an intent-to-treat analysis, all three groups reduced systolic pressures to a statistically similar extent, compared with baseline – decreases of approximately 8 mm Hg in the combination group and 4 mm Hg with either monotherapy. Among 136 patients who adhered to therapy by completing the trial, however, systolic blood pressure decreased by a mean of 14 mm Hg in the 62 patients randomized to the combination of weight-loss efforts and continuous positive airway pressure (CPAP), a significantly greater decrease than the reductions of approximately 7 mm Hg in 61 patients randomized to weight-loss efforts alone and 3 mm Hg in 58 patients who got CPAP alone.

A 14 mm Hg–drop in systolic blood pressure is an "important reduction" with potentially significant clinical benefits in obese patients with obstructive sleep apnea, Dr. Julio A. Chirinos said at the annual meeting of the American College of Cardiology.
Previous observational studies have shown strong associations in obesity, obstructive sleep apnea, and hypertension but have not been able to assess whether there is any incremental blood pressure benefit to combining treatments for obesity and sleep apnea.
Dr. Chirinos and his associates conducted an ancillary analysis of data from the Cardiovascular Consequences of Obstructive Sleep Apnea trial, which focused primarily on the treatments’ effects on C-reactive protein levels. The study randomized adults with at least moderate obesity and moderate to severe obstructive sleep apnea and C-reactive protein levels greater than 1 mg/L to the three intervention groups. Baseline characteristics were similar among groups. Approximately 41% of patients were hypertensive at baseline.
In the per-protocol analysis of patients who adhered to therapy, the decreases in systolic blood pressure, compared with baseline, were statistically significant in the combination and weight-loss groups but not the CPAP group, reported Dr. Chirinos of the University of Pennsylvania, Philadelphia.
Body weight and body mass index decreased significantly in the weight-loss and combination groups compared with baseline but did not change significantly in the CPAP group. Patients in the weight-loss and combination groups dropped approximately 7 kg in the intent-to-treat analysis and 10-11 kg in the per-protocol analysis. Body mass index decreased by a mean of two to three points in the intent-to-treat analysis and by approximately four points among those who adhered to therapy. No details were provided about the specifics of the weight-loss efforts.
Mean arterial pressure decreased significantly in all three groups, compared with baseline, in both intent-to-treat and per-protocol analyses, but fell significantly more in the combination group, compared with monotherapy, in the per-protocol analysis. Among patients adherent to treatment, mean arterial pressure decreased by more than 10 mm Hg in the combination group, compared with approximately 4 mm Hg–declines with either monotherapy.
Only combination therapy significantly reduced brachial pulse pressure, compared with baseline (by approximately 3 mm Hg), in the intent-to-treat analysis. In the per-protocol analysis, brachial pulse pressure dropped significantly, compared with baseline, in the combination group (a 6 mm Hg decrease) and the weight-loss group (a 4 mm Hg–decrease) but not in the CPAP group.
Brachial pulse pressure decreased significantly with combination therapy in the intent-to-treat analysis but not with either treatment alone. Mean brachial pulse pressure in the per-protocol analysis decreased significantly with combination therapy (a 6 mm Hg–reduction) or weight-loss therapy (a 4 mm Hg–decrease) but increased in the CPAP group.
Carotid-radial pulse pressure amplification measurements did not change significantly from baseline in any group, suggesting that the study’s results were not brought about by missing some changes in central pressure that were not being picked up by brachial measurements, Dr. Chirinos said.
In general, approximately 50% of people with obstructive sleep apnea have hypertension, and around 30% of hypertensive patients have obstructive sleep apnea, he said.
The findings are limited by the study’s strict criteria for patient inclusion or exclusion, its lack of arterial blood pressure monitoring, the use of noninvasive estimates of central pressure measurements, and its duration of only 6 months. The study used carotid tonometry to measure central pulse pressure.
The study excluded patients with blood pressures greater than 160/95 mm Hg, those with predominantly central sleep apnea, patients using supplemental oxygen, and anyone in a high-risk occupation or with a record of dangerous driving. Also excluded were patients with confounders of systemic inflammation, sustained arrhythmia, unstable cardiopulmonary disease, severe restless leg syndrome or chronic pain causing frequent night awakenings, pregnancy, severe depression or other serious medical or psychological conditions that might compromise their safety in the study, and prior CPAP within 8 weeks of the study.
The American Heart Association funded Dr. Chirinos’s analysis. Dr. Chirinos reported having no financial disclosures. Some of his associates reported financial relationships with multiple pharmaceutical companies.
On Twitter @sherryboschert
SAN FRANCISCO– A 24-week program combining weight-loss efforts with continuous positive airway pressure produced significantly greater reductions in systolic blood pressure in obese patients with obstructive sleep apnea, compared with either intervention alone, a study of 181 adults found.
In an intent-to-treat analysis, all three groups reduced systolic pressures to a statistically similar extent, compared with baseline – decreases of approximately 8 mm Hg in the combination group and 4 mm Hg with either monotherapy. Among 136 patients who adhered to therapy by completing the trial, however, systolic blood pressure decreased by a mean of 14 mm Hg in the 62 patients randomized to the combination of weight-loss efforts and continuous positive airway pressure (CPAP), a significantly greater decrease than the reductions of approximately 7 mm Hg in 61 patients randomized to weight-loss efforts alone and 3 mm Hg in 58 patients who got CPAP alone.
A 14 mm Hg–drop in systolic blood pressure is an "important reduction" with potentially significant clinical benefits in obese patients with obstructive sleep apnea, Dr. Julio A. Chirinos said at the annual meeting of the American College of Cardiology.
Previous observational studies have shown strong associations in obesity, obstructive sleep apnea, and hypertension but have not been able to assess whether there is any incremental blood pressure benefit to combining treatments for obesity and sleep apnea.
Dr. Chirinos and his associates conducted an ancillary analysis of data from the Cardiovascular Consequences of Obstructive Sleep Apnea trial, which focused primarily on the treatments’ effects on C-reactive protein levels. The study randomized adults with at least moderate obesity and moderate to severe obstructive sleep apnea and C-reactive protein levels greater than 1 mg/L to the three intervention groups. Baseline characteristics were similar among groups. Approximately 41% of patients were hypertensive at baseline.
In the per-protocol analysis of patients who adhered to therapy, the decreases in systolic blood pressure, compared with baseline, were statistically significant in the combination and weight-loss groups but not the CPAP group, reported Dr. Chirinos of the University of Pennsylvania, Philadelphia.
Body weight and body mass index decreased significantly in the weight-loss and combination groups compared with baseline but did not change significantly in the CPAP group. Patients in the weight-loss and combination groups dropped approximately 7 kg in the intent-to-treat analysis and 10-11 kg in the per-protocol analysis. Body mass index decreased by a mean of two to three points in the intent-to-treat analysis and by approximately four points among those who adhered to therapy. No details were provided about the specifics of the weight-loss efforts.
Mean arterial pressure decreased significantly in all three groups, compared with baseline, in both intent-to-treat and per-protocol analyses, but fell significantly more in the combination group, compared with monotherapy, in the per-protocol analysis. Among patients adherent to treatment, mean arterial pressure decreased by more than 10 mm Hg in the combination group, compared with approximately 4 mm Hg–declines with either monotherapy.
Only combination therapy significantly reduced brachial pulse pressure, compared with baseline (by approximately 3 mm Hg), in the intent-to-treat analysis. In the per-protocol analysis, brachial pulse pressure dropped significantly, compared with baseline, in the combination group (a 6 mm Hg decrease) and the weight-loss group (a 4 mm Hg–decrease) but not in the CPAP group.
Brachial pulse pressure decreased significantly with combination therapy in the intent-to-treat analysis but not with either treatment alone. Mean brachial pulse pressure in the per-protocol analysis decreased significantly with combination therapy (a 6 mm Hg–reduction) or weight-loss therapy (a 4 mm Hg–decrease) but increased in the CPAP group.
Carotid-radial pulse pressure amplification measurements did not change significantly from baseline in any group, suggesting that the study’s results were not brought about by missing some changes in central pressure that were not being picked up by brachial measurements, Dr. Chirinos said.
In general, approximately 50% of people with obstructive sleep apnea have hypertension, and around 30% of hypertensive patients have obstructive sleep apnea, he said.
The findings are limited by the study’s strict criteria for patient inclusion or exclusion, its lack of arterial blood pressure monitoring, the use of noninvasive estimates of central pressure measurements, and its duration of only 6 months. The study used carotid tonometry to measure central pulse pressure.
The study excluded patients with blood pressures greater than 160/95 mm Hg, those with predominantly central sleep apnea, patients using supplemental oxygen, and anyone in a high-risk occupation or with a record of dangerous driving. Also excluded were patients with confounders of systemic inflammation, sustained arrhythmia, unstable cardiopulmonary disease, severe restless leg syndrome or chronic pain causing frequent night awakenings, pregnancy, severe depression or other serious medical or psychological conditions that might compromise their safety in the study, and prior CPAP within 8 weeks of the study.
The American Heart Association funded Dr. Chirinos’s analysis. Dr. Chirinos reported having no financial disclosures. Some of his associates reported financial relationships with multiple pharmaceutical companies.
On Twitter @sherryboschert
SAN FRANCISCO– A 24-week program combining weight-loss efforts with continuous positive airway pressure produced significantly greater reductions in systolic blood pressure in obese patients with obstructive sleep apnea, compared with either intervention alone, a study of 181 adults found.
In an intent-to-treat analysis, all three groups reduced systolic pressures to a statistically similar extent, compared with baseline – decreases of approximately 8 mm Hg in the combination group and 4 mm Hg with either monotherapy. Among 136 patients who adhered to therapy by completing the trial, however, systolic blood pressure decreased by a mean of 14 mm Hg in the 62 patients randomized to the combination of weight-loss efforts and continuous positive airway pressure (CPAP), a significantly greater decrease than the reductions of approximately 7 mm Hg in 61 patients randomized to weight-loss efforts alone and 3 mm Hg in 58 patients who got CPAP alone.
A 14 mm Hg–drop in systolic blood pressure is an "important reduction" with potentially significant clinical benefits in obese patients with obstructive sleep apnea, Dr. Julio A. Chirinos said at the annual meeting of the American College of Cardiology.
Previous observational studies have shown strong associations in obesity, obstructive sleep apnea, and hypertension but have not been able to assess whether there is any incremental blood pressure benefit to combining treatments for obesity and sleep apnea.
Dr. Chirinos and his associates conducted an ancillary analysis of data from the Cardiovascular Consequences of Obstructive Sleep Apnea trial, which focused primarily on the treatments’ effects on C-reactive protein levels. The study randomized adults with at least moderate obesity and moderate to severe obstructive sleep apnea and C-reactive protein levels greater than 1 mg/L to the three intervention groups. Baseline characteristics were similar among groups. Approximately 41% of patients were hypertensive at baseline.
In the per-protocol analysis of patients who adhered to therapy, the decreases in systolic blood pressure, compared with baseline, were statistically significant in the combination and weight-loss groups but not the CPAP group, reported Dr. Chirinos of the University of Pennsylvania, Philadelphia.
Body weight and body mass index decreased significantly in the weight-loss and combination groups compared with baseline but did not change significantly in the CPAP group. Patients in the weight-loss and combination groups dropped approximately 7 kg in the intent-to-treat analysis and 10-11 kg in the per-protocol analysis. Body mass index decreased by a mean of two to three points in the intent-to-treat analysis and by approximately four points among those who adhered to therapy. No details were provided about the specifics of the weight-loss efforts.
Mean arterial pressure decreased significantly in all three groups, compared with baseline, in both intent-to-treat and per-protocol analyses, but fell significantly more in the combination group, compared with monotherapy, in the per-protocol analysis. Among patients adherent to treatment, mean arterial pressure decreased by more than 10 mm Hg in the combination group, compared with approximately 4 mm Hg–declines with either monotherapy.
Only combination therapy significantly reduced brachial pulse pressure, compared with baseline (by approximately 3 mm Hg), in the intent-to-treat analysis. In the per-protocol analysis, brachial pulse pressure dropped significantly, compared with baseline, in the combination group (a 6 mm Hg decrease) and the weight-loss group (a 4 mm Hg–decrease) but not in the CPAP group.
Brachial pulse pressure decreased significantly with combination therapy in the intent-to-treat analysis but not with either treatment alone. Mean brachial pulse pressure in the per-protocol analysis decreased significantly with combination therapy (a 6 mm Hg–reduction) or weight-loss therapy (a 4 mm Hg–decrease) but increased in the CPAP group.
Carotid-radial pulse pressure amplification measurements did not change significantly from baseline in any group, suggesting that the study’s results were not brought about by missing some changes in central pressure that were not being picked up by brachial measurements, Dr. Chirinos said.
In general, approximately 50% of people with obstructive sleep apnea have hypertension, and around 30% of hypertensive patients have obstructive sleep apnea, he said.
The findings are limited by the study’s strict criteria for patient inclusion or exclusion, its lack of arterial blood pressure monitoring, the use of noninvasive estimates of central pressure measurements, and its duration of only 6 months. The study used carotid tonometry to measure central pulse pressure.
The study excluded patients with blood pressures greater than 160/95 mm Hg, those with predominantly central sleep apnea, patients using supplemental oxygen, and anyone in a high-risk occupation or with a record of dangerous driving. Also excluded were patients with confounders of systemic inflammation, sustained arrhythmia, unstable cardiopulmonary disease, severe restless leg syndrome or chronic pain causing frequent night awakenings, pregnancy, severe depression or other serious medical or psychological conditions that might compromise their safety in the study, and prior CPAP within 8 weeks of the study.
The American Heart Association funded Dr. Chirinos’s analysis. Dr. Chirinos reported having no financial disclosures. Some of his associates reported financial relationships with multiple pharmaceutical companies.
On Twitter @sherryboschert
AT ACC 13
Major finding: Mean systolic blood pressure decreased by 14 mm Hg in the combination group at 24 weeks, compared with 7 mm Hg with weight loss alone and 3 mm Hg with CPAP alone in patients who adhered to therapy.
Data source: Secondary analysis of a randomized study of 181 obese adults with obstructive sleep apnea.
Disclosures: The American Heart Association funded Dr. Chirinos’s analysis. Dr. Chirinos reported having no financial disclosures. Some of his associates reported financial relationships with multiple pharmaceutical companies.

Prenatal exposure to air pollution boosts childhood cancer risk
WASHINGTON – Children whose mothers were exposed to air pollution during pregnancy may have a small, but significant, increase in pediatric cancer risk.
A 9-year case-control study found that children who were exposed to the highest levels of traffic-related pollution prenatally and during the first year of life were 19% more likely to develop bilateral retinoblastoma and 17% more likely to develop germ cell tumors than were children who were exposed to the lowest level.

"This is the first study to report upon traffic pollution in relation to retinoblastoma or germ cell tumors, and since both of these are rare, the findings need to be replicated in other studies," Julia E. Heck, Ph.D., said in an interview at the annual meeting of the American Association for Cancer Research.
Dr. Heck, an epidemiologist at the University of California’s Fielding School of Public Health, Los Angeles, used a state air pollution modeling system to detect the patterns in her study. The California Line Source Dispersion Modeling system, version 4 (CALINE4) uses a test fleet of motor vehicles to predict traffic-related carbon monoxide emissions from vehicles in idle, cruise, acceleration, and deceleration.
Her study cohort comprised 3,590 children with cancer who were included in a California cancer registry. All were born between 1998 and 2007 and were aged younger than 6 years. She compared these children to a random selection of 80,224 children drawn form California birth records. The CALINE4 system generated estimates of local traffic exposure based on where the mothers were living during each trimester of pregnancy.
The model imputed emissions from gasoline and diesel vehicles within a 1,500-meter radius of the address. It included data on traffic volume, roadway geometry, vehicle emission rates, and weather patterns, and divided the cohort into quartiles according to exposure. Dr. Heck looked specifically at carbon monoxide measurements in increments of 53 parts per billion.
Each increase in CO emission raised the risk of acute lymphoblastic leukemia by 4%. Each quartile was associated with an overall 14% increased risk of a retinoblastoma, with the risk significantly elevated for bilateral tumors rather than unilateral tumors (a 19% increase). Dr. Heck also saw a 17% increased risk for germ cell tumors for every quartile increase in CO.
Associations with other cancers, including acute myeloid leukemia, non-Hodgkin’s lymphoma, ependymoma, astrocytoma, neuroblastoma, Wilms tumor, hepatoblastoma, and rhabdomyosarcoma, were nonsignificant.
Because Dr. Heck’s study was a retrospective analysis, it cannot prove causation. "The results need to be confirmed in other studies," she said in an interview. "But our findings do support a link between traffic pollution and some childhood cancers."
The field of childhood cancers and air pollution has not been well studied in recent years, Dr. Heck said, although there were a number of such studies in the late 1990s and early 2000s.
One was a British case-control analysis of birth and death records of 12,018 children in the United Kingdom who had been born and died from leukemia and other cancers from 1955 to 1980. The cancer-related deaths were linked to locations of rail and bus stations, ferry terminals, railways, roads, canals, and rivers (J. Epidemiol. Community Health 2005;59:755-60).
"The most striking result is the extraordinary concentration of cancer births within 0.3 km of bus/coach stations (OR = 12.5)," wrote Dr. E.G. Knox, professor emeritus at the University of Birmingham, England. "This was followed by hospitals (OR = 2.6) and heavy transport centers (OR = 1.6)."
Of the individual pollutants examined, both carbon monoxide and 1,3-butadiene more than doubled the risk of cancer.
Because the study encompassed the child’s location at birth, it demonstrated a link to prenatal exposure. "Childhood cancers are strongly determined by prenatal or early postnatal exposures to oil-based combustion gases, especially from engine exhausts," he noted. "The chief carcinogenic agent is probably 1,3-butadiene."
The National Institute for Occupational Safety and Health has recommended that 1,3-butadiene be treated as a potential occupational carcinogen, teratogen, and as a reproduction hazard.
In 2006, Dr. Knox published another study on the same group, in which he attributed about 24% of the cancers to prenatal or early life proximity to areas of high airborne pollutants. "Child cancer initiations are strongly determined by prenatal or early postnatal exposures to engine exhaust gases, probably through maternal inhalation and accumulation of carcinogens over many months," he noted. (J. Epidemiol. Community Health 2006;60:136-41).
Dr. Heck’s study was funded by the National Institutes of Health. She had no financial disclosures.
WASHINGTON – Children whose mothers were exposed to air pollution during pregnancy may have a small, but significant, increase in pediatric cancer risk.
A 9-year case-control study found that children who were exposed to the highest levels of traffic-related pollution prenatally and during the first year of life were 19% more likely to develop bilateral retinoblastoma and 17% more likely to develop germ cell tumors than were children who were exposed to the lowest level.
"This is the first study to report upon traffic pollution in relation to retinoblastoma or germ cell tumors, and since both of these are rare, the findings need to be replicated in other studies," Julia E. Heck, Ph.D., said in an interview at the annual meeting of the American Association for Cancer Research.
Dr. Heck, an epidemiologist at the University of California’s Fielding School of Public Health, Los Angeles, used a state air pollution modeling system to detect the patterns in her study. The California Line Source Dispersion Modeling system, version 4 (CALINE4) uses a test fleet of motor vehicles to predict traffic-related carbon monoxide emissions from vehicles in idle, cruise, acceleration, and deceleration.
Her study cohort comprised 3,590 children with cancer who were included in a California cancer registry. All were born between 1998 and 2007 and were aged younger than 6 years. She compared these children to a random selection of 80,224 children drawn form California birth records. The CALINE4 system generated estimates of local traffic exposure based on where the mothers were living during each trimester of pregnancy.
The model imputed emissions from gasoline and diesel vehicles within a 1,500-meter radius of the address. It included data on traffic volume, roadway geometry, vehicle emission rates, and weather patterns, and divided the cohort into quartiles according to exposure. Dr. Heck looked specifically at carbon monoxide measurements in increments of 53 parts per billion.
Each increase in CO emission raised the risk of acute lymphoblastic leukemia by 4%. Each quartile was associated with an overall 14% increased risk of a retinoblastoma, with the risk significantly elevated for bilateral tumors rather than unilateral tumors (a 19% increase). Dr. Heck also saw a 17% increased risk for germ cell tumors for every quartile increase in CO.
Associations with other cancers, including acute myeloid leukemia, non-Hodgkin’s lymphoma, ependymoma, astrocytoma, neuroblastoma, Wilms tumor, hepatoblastoma, and rhabdomyosarcoma, were nonsignificant.
Because Dr. Heck’s study was a retrospective analysis, it cannot prove causation. "The results need to be confirmed in other studies," she said in an interview. "But our findings do support a link between traffic pollution and some childhood cancers."
The field of childhood cancers and air pollution has not been well studied in recent years, Dr. Heck said, although there were a number of such studies in the late 1990s and early 2000s.
One was a British case-control analysis of birth and death records of 12,018 children in the United Kingdom who had been born and died from leukemia and other cancers from 1955 to 1980. The cancer-related deaths were linked to locations of rail and bus stations, ferry terminals, railways, roads, canals, and rivers (J. Epidemiol. Community Health 2005;59:755-60).
"The most striking result is the extraordinary concentration of cancer births within 0.3 km of bus/coach stations (OR = 12.5)," wrote Dr. E.G. Knox, professor emeritus at the University of Birmingham, England. "This was followed by hospitals (OR = 2.6) and heavy transport centers (OR = 1.6)."
Of the individual pollutants examined, both carbon monoxide and 1,3-butadiene more than doubled the risk of cancer.
Because the study encompassed the child’s location at birth, it demonstrated a link to prenatal exposure. "Childhood cancers are strongly determined by prenatal or early postnatal exposures to oil-based combustion gases, especially from engine exhausts," he noted. "The chief carcinogenic agent is probably 1,3-butadiene."
The National Institute for Occupational Safety and Health has recommended that 1,3-butadiene be treated as a potential occupational carcinogen, teratogen, and as a reproduction hazard.
In 2006, Dr. Knox published another study on the same group, in which he attributed about 24% of the cancers to prenatal or early life proximity to areas of high airborne pollutants. "Child cancer initiations are strongly determined by prenatal or early postnatal exposures to engine exhaust gases, probably through maternal inhalation and accumulation of carcinogens over many months," he noted. (J. Epidemiol. Community Health 2006;60:136-41).
Dr. Heck’s study was funded by the National Institutes of Health. She had no financial disclosures.
WASHINGTON – Children whose mothers were exposed to air pollution during pregnancy may have a small, but significant, increase in pediatric cancer risk.
A 9-year case-control study found that children who were exposed to the highest levels of traffic-related pollution prenatally and during the first year of life were 19% more likely to develop bilateral retinoblastoma and 17% more likely to develop germ cell tumors than were children who were exposed to the lowest level.
"This is the first study to report upon traffic pollution in relation to retinoblastoma or germ cell tumors, and since both of these are rare, the findings need to be replicated in other studies," Julia E. Heck, Ph.D., said in an interview at the annual meeting of the American Association for Cancer Research.
Dr. Heck, an epidemiologist at the University of California’s Fielding School of Public Health, Los Angeles, used a state air pollution modeling system to detect the patterns in her study. The California Line Source Dispersion Modeling system, version 4 (CALINE4) uses a test fleet of motor vehicles to predict traffic-related carbon monoxide emissions from vehicles in idle, cruise, acceleration, and deceleration.
Her study cohort comprised 3,590 children with cancer who were included in a California cancer registry. All were born between 1998 and 2007 and were aged younger than 6 years. She compared these children to a random selection of 80,224 children drawn form California birth records. The CALINE4 system generated estimates of local traffic exposure based on where the mothers were living during each trimester of pregnancy.
The model imputed emissions from gasoline and diesel vehicles within a 1,500-meter radius of the address. It included data on traffic volume, roadway geometry, vehicle emission rates, and weather patterns, and divided the cohort into quartiles according to exposure. Dr. Heck looked specifically at carbon monoxide measurements in increments of 53 parts per billion.
Each increase in CO emission raised the risk of acute lymphoblastic leukemia by 4%. Each quartile was associated with an overall 14% increased risk of a retinoblastoma, with the risk significantly elevated for bilateral tumors rather than unilateral tumors (a 19% increase). Dr. Heck also saw a 17% increased risk for germ cell tumors for every quartile increase in CO.
Associations with other cancers, including acute myeloid leukemia, non-Hodgkin’s lymphoma, ependymoma, astrocytoma, neuroblastoma, Wilms tumor, hepatoblastoma, and rhabdomyosarcoma, were nonsignificant.
Because Dr. Heck’s study was a retrospective analysis, it cannot prove causation. "The results need to be confirmed in other studies," she said in an interview. "But our findings do support a link between traffic pollution and some childhood cancers."
The field of childhood cancers and air pollution has not been well studied in recent years, Dr. Heck said, although there were a number of such studies in the late 1990s and early 2000s.
One was a British case-control analysis of birth and death records of 12,018 children in the United Kingdom who had been born and died from leukemia and other cancers from 1955 to 1980. The cancer-related deaths were linked to locations of rail and bus stations, ferry terminals, railways, roads, canals, and rivers (J. Epidemiol. Community Health 2005;59:755-60).
"The most striking result is the extraordinary concentration of cancer births within 0.3 km of bus/coach stations (OR = 12.5)," wrote Dr. E.G. Knox, professor emeritus at the University of Birmingham, England. "This was followed by hospitals (OR = 2.6) and heavy transport centers (OR = 1.6)."
Of the individual pollutants examined, both carbon monoxide and 1,3-butadiene more than doubled the risk of cancer.
Because the study encompassed the child’s location at birth, it demonstrated a link to prenatal exposure. "Childhood cancers are strongly determined by prenatal or early postnatal exposures to oil-based combustion gases, especially from engine exhausts," he noted. "The chief carcinogenic agent is probably 1,3-butadiene."
The National Institute for Occupational Safety and Health has recommended that 1,3-butadiene be treated as a potential occupational carcinogen, teratogen, and as a reproduction hazard.
In 2006, Dr. Knox published another study on the same group, in which he attributed about 24% of the cancers to prenatal or early life proximity to areas of high airborne pollutants. "Child cancer initiations are strongly determined by prenatal or early postnatal exposures to engine exhaust gases, probably through maternal inhalation and accumulation of carcinogens over many months," he noted. (J. Epidemiol. Community Health 2006;60:136-41).
Dr. Heck’s study was funded by the National Institutes of Health. She had no financial disclosures.
FROM THE AACR ANNUAL MEETING
Major finding: Children exposed prenatally to high levels of motor vehicle exhaust were 19% more likely to develop bilateral retinoblastoma and 17% more likely to develop germ cell tumors than were children with less exposure.
Data source: Case-control analysis of 3,590 children who developed cancer matched to 80,224 controls.
Disclosures: The study was funded by the National Institutes of Health. Dr. Heck had no financial disclosures.
