User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Shorter steroid treatment worked for COPD exacerbations
In patients with acute COPD exacerbations, 5-day systemic glucocorticoid therapy was as effective as a conventional 14-day course of the drugs at preventing further exacerbations, according to a report published online May 21 in JAMA.
In a multicenter, randomized clinical trial, the 6-month rate of recurrent COPD exacerbation was 35.9% among patients who received the short course of systemic glucocorticoids, which was noninferior to the 36.8% rate among those who received the usual 2-week course, said Dr. Jörg D. Leuppi of the University Hospital of Basel (Switzerland) and his associates (JAMA 2013 May 21 [doi:10.1001/jama.2013.5023]).
The short-term approach’s main advantage is its significant reduction of patients’ exposure to glucocorticoids, which in turn will likely decrease short-term adverse effects such as hyperglycemia, weight gain, increased blood pressure, and insomnia, the investigators said. The short course also should prevent or delay longer-term steroid toxicities such as diabetes, osteoporosis, bone fractures, adrenal suppression, and ocular complications.
The investigators performed the noninferiority trial, known as the REDUCE (Reduction in the Use of Corticosteroids in Exacerbated COPD) study, because no adequately powered, randomized clinical trial has compared directly the outcomes of these two treatment durations. Despite that, "it has become quite common clinical practice to administer glucocorticoids in COPD exacerbations for shorter periods," the study authors noted.
The REDUCE trial’s results were published online and simultaneously reported at the annual meeting of the American Thoracic Society.
The study included 311 consecutive patients who presented with COPD exacerbations to emergency departments at five Swiss teaching hospitals during a 5-year period. All patients were older than 40 years, were current or past smokers, and had a smoking history of 20 or more pack-years.
All the study subjects received 40 mg of IV methylprednisolone on day 1, followed by 40 mg of oral prednisone on days 2-5. On days 6-14, 155 patients were randomly assigned to continue receiving oral prednisone (conventional therapy) and 156 to receive a matching placebo (short-course therapy). Patients, caregivers, and researchers were blinded to group assignment.
All the patients also received a broad-spectrum antibiotic for 7 days to prevent pneumonia; nebulized short-acting bronchodilators as needed while hospitalized; inhaled glucocorticoids combined with an inhaled beta-agonist twice daily; and inhaled tiotropium once daily. They all also received physiotherapy, supplemental oxygen, and ventilatory support according to accepted guidelines.
Patients who received short-course glucocorticoid therapy had a median cumulative prednisone dose of 200 mg and a mean cumulative dose of 379 mg. In contrast, those who received a longer duration of treatment had a median cumulative prednisone dose of 560 mg and a mean cumulative dose of 793 mg.
After 180 days of follow-up, 56 (35.9%) of patients in the short-course therapy group and 57 (36.8%) in the conventional therapy group reached the primary endpoint of a recurrent COPD exacerbation. The time to recurrence did not differ between the two groups.
In addition, the hazard ratios for experiencing a recurrence were nearly identical between the two study groups in both an intention-to-treat analysis and a per-protocol analysis, "meeting our noninferiority criterion," Dr. Leuppi and his colleagues said.
The findings remained robust in sensitivity analyses that adjusted for variables such as patient age and sex. They also persisted in subgroup analyses that compared patients who had different severities of underlying COPD and different past histories of glucocorticoid use.
Overall survival was not significantly different between patients who received 5 days and those who received 14 days of systemic glucocorticoids. The short-course therapy group also showed no increase in the need for mechanical ventilation during hospitalization.
Measures of forced expiratory volume in 1 second improved significantly in both groups by day 6 and remained stable thereafter, with "almost no differences" between groups. Patients in both groups reported significantly ameliorated dyspnea, as well as similarly improved bronchitis-related quality of life and overall performance.
Regarding short-term adverse effects of exposure to glucocorticoids, rates of new or worsening hypertension and new or worsening hyperglycemia were comparable between the two study groups. "We surmise that the length of hospital stay was insufficient to detect significant differences in blood pressure and blood glucose levels between groups, because these glucocorticoid adverse effects do not develop immediately after initiation of treatment," the researchers said.
There also were no differences in longer-term toxicities such as rates of infection, gastrointestinal bleeding, insomnia, fractures, psychiatric symptoms, or heart failure.
A surprising finding was that patients who received short-term glucocorticoids had a significantly shorter hospital stay (median, 8 days) than did those who received conventional glucocorticoids (median, 9 days). "Because we did not observe significant differences in glucocorticoid-related, short-term adverse effects, we cannot readily explain this observation, which might be a chance finding," Dr. Leuppi and his associates said.
This study was supported by the University Hospital Basel, the Hospital Center of Biel-Bienne, Freiwilligen Akademische Gesellschaft, Fonds für Lehre und Forschung, AstraZeneca, Viollier Laboratory, and Gottfried und Julia Bangerter-Rhyner-Stiftung für Medizinische Forschung. Dr. Leuppi reported ties to these groups and Boehringer-Ingelheim, Chibret, Merck Sharp & Dohme, Novartis, Nycomed, and Pharmaxis, and his associates reported ties to numerous industry sources.
This rigorous, high-quality clinical trial by Leuppi et al. makes it clear that a 5-day regimen of glucocorticoids is sufficient for most COPD exacerbations, and it reduced the cumulative exposure to steroids by 65%, noted Dr. Don D. Sin and Dr. Hye Yun Park.
"This is welcome news for patients with COPD who experience multiple exacerbations annually and are exposed to repeated courses of systemic corticosteroids. These findings will enable clinicians to minimize steroid exposure and reduce the risk of steroid-related toxicity in these patients," they wrote.
Dr. Sin and Dr. Park are at the University of British Columbia James Hogg Research Centre and the Institute for Heart and Lung Health at St. Paul’s Hospital, both in Vancouver. Dr. Park also is in the division of pulmonary and critical care medicine at Samsung Medical Center, Seoul (South Korea). Dr. Park reported no financial conflicts of interest. Dr. Sin reported ties to Merck Frosst, Novartis Canada, AstraZeneca, Grifols, Boehinger Ingelheim, and GlaxoSmithKline. These remarks were taken from their editorial accompanying Dr. Leuppi’s report (JAMA 2013 May 21 [doi:10.1001/jama.2013.5644]).
This rigorous, high-quality clinical trial by Leuppi et al. makes it clear that a 5-day regimen of glucocorticoids is sufficient for most COPD exacerbations, and it reduced the cumulative exposure to steroids by 65%, noted Dr. Don D. Sin and Dr. Hye Yun Park.
"This is welcome news for patients with COPD who experience multiple exacerbations annually and are exposed to repeated courses of systemic corticosteroids. These findings will enable clinicians to minimize steroid exposure and reduce the risk of steroid-related toxicity in these patients," they wrote.
Dr. Sin and Dr. Park are at the University of British Columbia James Hogg Research Centre and the Institute for Heart and Lung Health at St. Paul’s Hospital, both in Vancouver. Dr. Park also is in the division of pulmonary and critical care medicine at Samsung Medical Center, Seoul (South Korea). Dr. Park reported no financial conflicts of interest. Dr. Sin reported ties to Merck Frosst, Novartis Canada, AstraZeneca, Grifols, Boehinger Ingelheim, and GlaxoSmithKline. These remarks were taken from their editorial accompanying Dr. Leuppi’s report (JAMA 2013 May 21 [doi:10.1001/jama.2013.5644]).
This rigorous, high-quality clinical trial by Leuppi et al. makes it clear that a 5-day regimen of glucocorticoids is sufficient for most COPD exacerbations, and it reduced the cumulative exposure to steroids by 65%, noted Dr. Don D. Sin and Dr. Hye Yun Park.
"This is welcome news for patients with COPD who experience multiple exacerbations annually and are exposed to repeated courses of systemic corticosteroids. These findings will enable clinicians to minimize steroid exposure and reduce the risk of steroid-related toxicity in these patients," they wrote.
Dr. Sin and Dr. Park are at the University of British Columbia James Hogg Research Centre and the Institute for Heart and Lung Health at St. Paul’s Hospital, both in Vancouver. Dr. Park also is in the division of pulmonary and critical care medicine at Samsung Medical Center, Seoul (South Korea). Dr. Park reported no financial conflicts of interest. Dr. Sin reported ties to Merck Frosst, Novartis Canada, AstraZeneca, Grifols, Boehinger Ingelheim, and GlaxoSmithKline. These remarks were taken from their editorial accompanying Dr. Leuppi’s report (JAMA 2013 May 21 [doi:10.1001/jama.2013.5644]).
In patients with acute COPD exacerbations, 5-day systemic glucocorticoid therapy was as effective as a conventional 14-day course of the drugs at preventing further exacerbations, according to a report published online May 21 in JAMA.
In a multicenter, randomized clinical trial, the 6-month rate of recurrent COPD exacerbation was 35.9% among patients who received the short course of systemic glucocorticoids, which was noninferior to the 36.8% rate among those who received the usual 2-week course, said Dr. Jörg D. Leuppi of the University Hospital of Basel (Switzerland) and his associates (JAMA 2013 May 21 [doi:10.1001/jama.2013.5023]).
The short-term approach’s main advantage is its significant reduction of patients’ exposure to glucocorticoids, which in turn will likely decrease short-term adverse effects such as hyperglycemia, weight gain, increased blood pressure, and insomnia, the investigators said. The short course also should prevent or delay longer-term steroid toxicities such as diabetes, osteoporosis, bone fractures, adrenal suppression, and ocular complications.
The investigators performed the noninferiority trial, known as the REDUCE (Reduction in the Use of Corticosteroids in Exacerbated COPD) study, because no adequately powered, randomized clinical trial has compared directly the outcomes of these two treatment durations. Despite that, "it has become quite common clinical practice to administer glucocorticoids in COPD exacerbations for shorter periods," the study authors noted.
The REDUCE trial’s results were published online and simultaneously reported at the annual meeting of the American Thoracic Society.
The study included 311 consecutive patients who presented with COPD exacerbations to emergency departments at five Swiss teaching hospitals during a 5-year period. All patients were older than 40 years, were current or past smokers, and had a smoking history of 20 or more pack-years.
All the study subjects received 40 mg of IV methylprednisolone on day 1, followed by 40 mg of oral prednisone on days 2-5. On days 6-14, 155 patients were randomly assigned to continue receiving oral prednisone (conventional therapy) and 156 to receive a matching placebo (short-course therapy). Patients, caregivers, and researchers were blinded to group assignment.
All the patients also received a broad-spectrum antibiotic for 7 days to prevent pneumonia; nebulized short-acting bronchodilators as needed while hospitalized; inhaled glucocorticoids combined with an inhaled beta-agonist twice daily; and inhaled tiotropium once daily. They all also received physiotherapy, supplemental oxygen, and ventilatory support according to accepted guidelines.
Patients who received short-course glucocorticoid therapy had a median cumulative prednisone dose of 200 mg and a mean cumulative dose of 379 mg. In contrast, those who received a longer duration of treatment had a median cumulative prednisone dose of 560 mg and a mean cumulative dose of 793 mg.
After 180 days of follow-up, 56 (35.9%) of patients in the short-course therapy group and 57 (36.8%) in the conventional therapy group reached the primary endpoint of a recurrent COPD exacerbation. The time to recurrence did not differ between the two groups.
In addition, the hazard ratios for experiencing a recurrence were nearly identical between the two study groups in both an intention-to-treat analysis and a per-protocol analysis, "meeting our noninferiority criterion," Dr. Leuppi and his colleagues said.
The findings remained robust in sensitivity analyses that adjusted for variables such as patient age and sex. They also persisted in subgroup analyses that compared patients who had different severities of underlying COPD and different past histories of glucocorticoid use.
Overall survival was not significantly different between patients who received 5 days and those who received 14 days of systemic glucocorticoids. The short-course therapy group also showed no increase in the need for mechanical ventilation during hospitalization.
Measures of forced expiratory volume in 1 second improved significantly in both groups by day 6 and remained stable thereafter, with "almost no differences" between groups. Patients in both groups reported significantly ameliorated dyspnea, as well as similarly improved bronchitis-related quality of life and overall performance.
Regarding short-term adverse effects of exposure to glucocorticoids, rates of new or worsening hypertension and new or worsening hyperglycemia were comparable between the two study groups. "We surmise that the length of hospital stay was insufficient to detect significant differences in blood pressure and blood glucose levels between groups, because these glucocorticoid adverse effects do not develop immediately after initiation of treatment," the researchers said.
There also were no differences in longer-term toxicities such as rates of infection, gastrointestinal bleeding, insomnia, fractures, psychiatric symptoms, or heart failure.
A surprising finding was that patients who received short-term glucocorticoids had a significantly shorter hospital stay (median, 8 days) than did those who received conventional glucocorticoids (median, 9 days). "Because we did not observe significant differences in glucocorticoid-related, short-term adverse effects, we cannot readily explain this observation, which might be a chance finding," Dr. Leuppi and his associates said.
This study was supported by the University Hospital Basel, the Hospital Center of Biel-Bienne, Freiwilligen Akademische Gesellschaft, Fonds für Lehre und Forschung, AstraZeneca, Viollier Laboratory, and Gottfried und Julia Bangerter-Rhyner-Stiftung für Medizinische Forschung. Dr. Leuppi reported ties to these groups and Boehringer-Ingelheim, Chibret, Merck Sharp & Dohme, Novartis, Nycomed, and Pharmaxis, and his associates reported ties to numerous industry sources.
In patients with acute COPD exacerbations, 5-day systemic glucocorticoid therapy was as effective as a conventional 14-day course of the drugs at preventing further exacerbations, according to a report published online May 21 in JAMA.
In a multicenter, randomized clinical trial, the 6-month rate of recurrent COPD exacerbation was 35.9% among patients who received the short course of systemic glucocorticoids, which was noninferior to the 36.8% rate among those who received the usual 2-week course, said Dr. Jörg D. Leuppi of the University Hospital of Basel (Switzerland) and his associates (JAMA 2013 May 21 [doi:10.1001/jama.2013.5023]).
The short-term approach’s main advantage is its significant reduction of patients’ exposure to glucocorticoids, which in turn will likely decrease short-term adverse effects such as hyperglycemia, weight gain, increased blood pressure, and insomnia, the investigators said. The short course also should prevent or delay longer-term steroid toxicities such as diabetes, osteoporosis, bone fractures, adrenal suppression, and ocular complications.
The investigators performed the noninferiority trial, known as the REDUCE (Reduction in the Use of Corticosteroids in Exacerbated COPD) study, because no adequately powered, randomized clinical trial has compared directly the outcomes of these two treatment durations. Despite that, "it has become quite common clinical practice to administer glucocorticoids in COPD exacerbations for shorter periods," the study authors noted.
The REDUCE trial’s results were published online and simultaneously reported at the annual meeting of the American Thoracic Society.
The study included 311 consecutive patients who presented with COPD exacerbations to emergency departments at five Swiss teaching hospitals during a 5-year period. All patients were older than 40 years, were current or past smokers, and had a smoking history of 20 or more pack-years.
All the study subjects received 40 mg of IV methylprednisolone on day 1, followed by 40 mg of oral prednisone on days 2-5. On days 6-14, 155 patients were randomly assigned to continue receiving oral prednisone (conventional therapy) and 156 to receive a matching placebo (short-course therapy). Patients, caregivers, and researchers were blinded to group assignment.
All the patients also received a broad-spectrum antibiotic for 7 days to prevent pneumonia; nebulized short-acting bronchodilators as needed while hospitalized; inhaled glucocorticoids combined with an inhaled beta-agonist twice daily; and inhaled tiotropium once daily. They all also received physiotherapy, supplemental oxygen, and ventilatory support according to accepted guidelines.
Patients who received short-course glucocorticoid therapy had a median cumulative prednisone dose of 200 mg and a mean cumulative dose of 379 mg. In contrast, those who received a longer duration of treatment had a median cumulative prednisone dose of 560 mg and a mean cumulative dose of 793 mg.
After 180 days of follow-up, 56 (35.9%) of patients in the short-course therapy group and 57 (36.8%) in the conventional therapy group reached the primary endpoint of a recurrent COPD exacerbation. The time to recurrence did not differ between the two groups.
In addition, the hazard ratios for experiencing a recurrence were nearly identical between the two study groups in both an intention-to-treat analysis and a per-protocol analysis, "meeting our noninferiority criterion," Dr. Leuppi and his colleagues said.
The findings remained robust in sensitivity analyses that adjusted for variables such as patient age and sex. They also persisted in subgroup analyses that compared patients who had different severities of underlying COPD and different past histories of glucocorticoid use.
Overall survival was not significantly different between patients who received 5 days and those who received 14 days of systemic glucocorticoids. The short-course therapy group also showed no increase in the need for mechanical ventilation during hospitalization.
Measures of forced expiratory volume in 1 second improved significantly in both groups by day 6 and remained stable thereafter, with "almost no differences" between groups. Patients in both groups reported significantly ameliorated dyspnea, as well as similarly improved bronchitis-related quality of life and overall performance.
Regarding short-term adverse effects of exposure to glucocorticoids, rates of new or worsening hypertension and new or worsening hyperglycemia were comparable between the two study groups. "We surmise that the length of hospital stay was insufficient to detect significant differences in blood pressure and blood glucose levels between groups, because these glucocorticoid adverse effects do not develop immediately after initiation of treatment," the researchers said.
There also were no differences in longer-term toxicities such as rates of infection, gastrointestinal bleeding, insomnia, fractures, psychiatric symptoms, or heart failure.
A surprising finding was that patients who received short-term glucocorticoids had a significantly shorter hospital stay (median, 8 days) than did those who received conventional glucocorticoids (median, 9 days). "Because we did not observe significant differences in glucocorticoid-related, short-term adverse effects, we cannot readily explain this observation, which might be a chance finding," Dr. Leuppi and his associates said.
This study was supported by the University Hospital Basel, the Hospital Center of Biel-Bienne, Freiwilligen Akademische Gesellschaft, Fonds für Lehre und Forschung, AstraZeneca, Viollier Laboratory, and Gottfried und Julia Bangerter-Rhyner-Stiftung für Medizinische Forschung. Dr. Leuppi reported ties to these groups and Boehringer-Ingelheim, Chibret, Merck Sharp & Dohme, Novartis, Nycomed, and Pharmaxis, and his associates reported ties to numerous industry sources.
FROM JAMA
Major Finding: After 180 days of follow-up, 56 patients (35.9%) who received short-course glucocorticoids and 57 (36.8%) who received conventional 14-day glucocorticoids reached the primary endpoint of a recurrent COPD exacerbation requiring hospitalization.
Data Source: A blinded, randomized, multicenter clinical trial involving 156 patients with acute COPD exacerbations who received 5 days of glucocorticoid therapy and 155 who received conventional 14-day therapy, all of whom were followed for 6 months.
Disclosures: This study was supported by the University Hospital Basel, the Hospital Center of Biel-Bienne, Freiwilligen Akademische Gesellschaft, Fonds für Lehre und Forschung, AstraZeneca, Viollier Laboratory, and Gottfried und Julia Bangerter-Rhyner-Stiftung für Medizinische Forschung. Dr. Leuppi reported ties to these groups and Boehringer-Ingelheim, Chibret, Merck Sharp & Dohme, Novartis, Nycomed, and Pharmaxis, and his associates reported ties to numerous industry sources.
Gene linked to improved survival in pulmonary fibrosis
A common polymorphism in the promoter of a mucin gene, MUC5B rs35705950, is significantly associated with improved survival in patients who have idiopathic pulmonary fibrosis, according to a report published online May 21 in JAMA.
The 2-year cumulative rate of death was lower among IPF patients who carried one or more copies of this variant than in those who did not in a cohort of 438 patients, and this finding was replicated in a validation cohort of another 148 patients, said Anna L. Peljto, Dr.P.H., of the department of epidemiology, University of Colorado School of Public Health, Denver, and her associates.

Their report was published simultaneously with its presentation at the annual meeting of the American Thoracic Society.
Paradoxically, this same polymorphism was previously reported to be strongly associated with the development of both sporadic IPF and familial interstitial pneumonia, and is considered a risk allele for these disorders.
It is not yet known how the MUC5B rs35705950 polymorphism confers a survival advantage in IPF, but "enhanced mucosal host defense, reduction in infectious complications, a beneficial drug response, and a potential dual role in wound repair should all be considered," the investigators said.
"Regardless of the mechanism, the results suggest that patients with IPF with the MUC5B promoter polymorphism may represent a pathogenically distinct disease entity that incorporates both a significantly higher predisposition to disease and a significantly longer survival," they noted.
Dr. Peljto and her colleagues examined whether carrying this variant affected survival by analyzing data on 438 patients who participated in a 3-year study of interferon treatment for IPF. A total of 37% of study participants were found to carry the MUC5B polymorphism.
The unadjusted 2-year cumulative incidence of death was lower in patients who carried one or more copies of the variant than in those who did not.
The researchers then assessed the polymorphism in a second population: 148 patients treated at the interstitial lung disease clinic at the University of Chicago beginning in the late 2000s and followed for a median of 1.6 years. The frequency of the MUC5B polymorphism was 39%, similar to that in the first cohort.
The unadjusted cumulative incidence of death also was significantly lower in patients who carried the genetic variant in this cohort.
The data from both groups were pooled and adjusted for patient age, sex, smoking history, forced vital capacity at baseline, and diffusing capacity of carbon monoxide at baseline.
"The MUC5B genotype remained a statistically significant predictor of survival," Dr. Peljto and her associates said.
The data were adjusted further to account for study subjects’ plasma concentrations of matrix metalloproteinase-7 (MMP-7); high levels of this substance are associated with poor outcomes in IPF. The association between the MUC5B polymorphism and improved survival remained constant in this analysis.
"This study is, to our knowledge, the first to demonstrate that a genetic variant is associated with survival in IPF," the researchers said (JAMA 2013 May 21 [doi:10.1001/jama.2013.5827]).
However, it would be premature to consider routine clinical genotyping of IPF patients at this time, "given that the addition of MUC5B resulted in relatively small gains in predictive accuracy in patients with established disease."
It may be helpful to combine the predictive value of MUC5B with other genetic and molecular factors to obtain a prognosis in patients who have subclinical or early-stage disease, before lung function has declined notably. "This is especially important because there are currently no IPF pharmalogical therapies approved for use in the United States, and opportunities for early genetic counseling or lung transplantation may be a patient’s only recourse," the investigators said.
This study was supported by the National Heart, Lung, and Blood Institute and the Dorothy P. and Richard P. Simmons Endowed Chair for Pulmonary Research at the University of Pittsburgh. Dr. Peljto reported no relevant financial conflicts; her associates reported numerous ties to industry sources.
A common polymorphism in the promoter of a mucin gene, MUC5B rs35705950, is significantly associated with improved survival in patients who have idiopathic pulmonary fibrosis, according to a report published online May 21 in JAMA.
The 2-year cumulative rate of death was lower among IPF patients who carried one or more copies of this variant than in those who did not in a cohort of 438 patients, and this finding was replicated in a validation cohort of another 148 patients, said Anna L. Peljto, Dr.P.H., of the department of epidemiology, University of Colorado School of Public Health, Denver, and her associates.
Their report was published simultaneously with its presentation at the annual meeting of the American Thoracic Society.
Paradoxically, this same polymorphism was previously reported to be strongly associated with the development of both sporadic IPF and familial interstitial pneumonia, and is considered a risk allele for these disorders.
It is not yet known how the MUC5B rs35705950 polymorphism confers a survival advantage in IPF, but "enhanced mucosal host defense, reduction in infectious complications, a beneficial drug response, and a potential dual role in wound repair should all be considered," the investigators said.
"Regardless of the mechanism, the results suggest that patients with IPF with the MUC5B promoter polymorphism may represent a pathogenically distinct disease entity that incorporates both a significantly higher predisposition to disease and a significantly longer survival," they noted.
Dr. Peljto and her colleagues examined whether carrying this variant affected survival by analyzing data on 438 patients who participated in a 3-year study of interferon treatment for IPF. A total of 37% of study participants were found to carry the MUC5B polymorphism.
The unadjusted 2-year cumulative incidence of death was lower in patients who carried one or more copies of the variant than in those who did not.
The researchers then assessed the polymorphism in a second population: 148 patients treated at the interstitial lung disease clinic at the University of Chicago beginning in the late 2000s and followed for a median of 1.6 years. The frequency of the MUC5B polymorphism was 39%, similar to that in the first cohort.
The unadjusted cumulative incidence of death also was significantly lower in patients who carried the genetic variant in this cohort.
The data from both groups were pooled and adjusted for patient age, sex, smoking history, forced vital capacity at baseline, and diffusing capacity of carbon monoxide at baseline.
"The MUC5B genotype remained a statistically significant predictor of survival," Dr. Peljto and her associates said.
The data were adjusted further to account for study subjects’ plasma concentrations of matrix metalloproteinase-7 (MMP-7); high levels of this substance are associated with poor outcomes in IPF. The association between the MUC5B polymorphism and improved survival remained constant in this analysis.
"This study is, to our knowledge, the first to demonstrate that a genetic variant is associated with survival in IPF," the researchers said (JAMA 2013 May 21 [doi:10.1001/jama.2013.5827]).
However, it would be premature to consider routine clinical genotyping of IPF patients at this time, "given that the addition of MUC5B resulted in relatively small gains in predictive accuracy in patients with established disease."
It may be helpful to combine the predictive value of MUC5B with other genetic and molecular factors to obtain a prognosis in patients who have subclinical or early-stage disease, before lung function has declined notably. "This is especially important because there are currently no IPF pharmalogical therapies approved for use in the United States, and opportunities for early genetic counseling or lung transplantation may be a patient’s only recourse," the investigators said.
This study was supported by the National Heart, Lung, and Blood Institute and the Dorothy P. and Richard P. Simmons Endowed Chair for Pulmonary Research at the University of Pittsburgh. Dr. Peljto reported no relevant financial conflicts; her associates reported numerous ties to industry sources.
A common polymorphism in the promoter of a mucin gene, MUC5B rs35705950, is significantly associated with improved survival in patients who have idiopathic pulmonary fibrosis, according to a report published online May 21 in JAMA.
The 2-year cumulative rate of death was lower among IPF patients who carried one or more copies of this variant than in those who did not in a cohort of 438 patients, and this finding was replicated in a validation cohort of another 148 patients, said Anna L. Peljto, Dr.P.H., of the department of epidemiology, University of Colorado School of Public Health, Denver, and her associates.
Their report was published simultaneously with its presentation at the annual meeting of the American Thoracic Society.
Paradoxically, this same polymorphism was previously reported to be strongly associated with the development of both sporadic IPF and familial interstitial pneumonia, and is considered a risk allele for these disorders.
It is not yet known how the MUC5B rs35705950 polymorphism confers a survival advantage in IPF, but "enhanced mucosal host defense, reduction in infectious complications, a beneficial drug response, and a potential dual role in wound repair should all be considered," the investigators said.
"Regardless of the mechanism, the results suggest that patients with IPF with the MUC5B promoter polymorphism may represent a pathogenically distinct disease entity that incorporates both a significantly higher predisposition to disease and a significantly longer survival," they noted.
Dr. Peljto and her colleagues examined whether carrying this variant affected survival by analyzing data on 438 patients who participated in a 3-year study of interferon treatment for IPF. A total of 37% of study participants were found to carry the MUC5B polymorphism.
The unadjusted 2-year cumulative incidence of death was lower in patients who carried one or more copies of the variant than in those who did not.
The researchers then assessed the polymorphism in a second population: 148 patients treated at the interstitial lung disease clinic at the University of Chicago beginning in the late 2000s and followed for a median of 1.6 years. The frequency of the MUC5B polymorphism was 39%, similar to that in the first cohort.
The unadjusted cumulative incidence of death also was significantly lower in patients who carried the genetic variant in this cohort.
The data from both groups were pooled and adjusted for patient age, sex, smoking history, forced vital capacity at baseline, and diffusing capacity of carbon monoxide at baseline.
"The MUC5B genotype remained a statistically significant predictor of survival," Dr. Peljto and her associates said.
The data were adjusted further to account for study subjects’ plasma concentrations of matrix metalloproteinase-7 (MMP-7); high levels of this substance are associated with poor outcomes in IPF. The association between the MUC5B polymorphism and improved survival remained constant in this analysis.
"This study is, to our knowledge, the first to demonstrate that a genetic variant is associated with survival in IPF," the researchers said (JAMA 2013 May 21 [doi:10.1001/jama.2013.5827]).
However, it would be premature to consider routine clinical genotyping of IPF patients at this time, "given that the addition of MUC5B resulted in relatively small gains in predictive accuracy in patients with established disease."
It may be helpful to combine the predictive value of MUC5B with other genetic and molecular factors to obtain a prognosis in patients who have subclinical or early-stage disease, before lung function has declined notably. "This is especially important because there are currently no IPF pharmalogical therapies approved for use in the United States, and opportunities for early genetic counseling or lung transplantation may be a patient’s only recourse," the investigators said.
This study was supported by the National Heart, Lung, and Blood Institute and the Dorothy P. and Richard P. Simmons Endowed Chair for Pulmonary Research at the University of Pittsburgh. Dr. Peljto reported no relevant financial conflicts; her associates reported numerous ties to industry sources.
FROM JAMA
Major Finding: The 2-year cumulative incidence of death was significantly lower in IPF patients who carried the MUC5B rs35705950 polymorphism than in those who did not.
Data Source: A retrospective cohort study comparing IPF patients who carried a genetic polymorphism with those who did not.
Disclosures: This study was supported by the National Heart, Lung, and Blood Institute and the Dorothy P. and Richard P. Simmons Endowed Chair for Pulmonary Research at the University of Pittsburgh. Dr. Peljto reported no relevant financial disclosures; her associates reported numerous ties to industry sources.

Dupilumab cuts moderate, severe asthma exacerbations
Dupilumab reduced exacerbations of moderate to severe asthma by 87% in adults with poorly controlled disease, and induced rapid and sustained improvements in numerous other measures of asthma severity in an industry-sponsored phase II study published online May 21 in the New England Journal of Medicine.
Dupilumab, a monoclonal antibody that inhibits interleukin-4 and interleukin-13 signaling, "showed substantial efficacy with regard to both objective and patient-reported end points" when it was used concomitantly with inhaled glucocorticoids and long-acting beta-agonists (LABAs), as well as when those background therapies were withdrawn, reported Dr. Sally Wenzel of the University of Pittsburgh and her associates.
"The magnitude and breadth of efficacy that we observed exceed those in other studies of Th2 [type 2 helper T-cell] cytokine inhibition," the researchers noted in the online report, which was presented simultaneously at the annual meeting of the American Thoracic Society.

Dupilumab currently is being assessed for the treatment of several diseases mediated by Th2 pathways. The goal of this phase II trial was to evaluate its safety and efficacy in adults with persistent moderate to severe asthma and elevated eosinophil levels whose symptoms were not well controlled with medium- to high-dose inhaled glucocorticoids plus LABAs (usually fluticasone and salmeterol).
The 104 participants were treated at 28 sites across the United States for 12 weeks, and then followed for another 8 weeks. During the intervention phase of the study, approximately half were randomized to receive once-weekly subcutaneous injections of dupilumab (300 mg) and half to receive matching placebo injections, in addition to the background asthma medications.
At week 4, the study subjects discontinued LABAs, and at weeks 6-9 they tapered off inhaled glucocorticoids. "This approach enabled us to observe the effects of dupilumab when added to background therapy, after LABA discontinuation, during the tapering of inhaled glucocorticoids, and as monotherapy," the researchers said.
The primary endpoint of the study was an asthma exacerbation during the 12-week intervention period. Exacerbations occurred in 3 patients receiving dupilumab (6%), compared with 23 receiving placebo (44%), a highly significant difference.
In addition, the time to an asthma exacerbation was significantly longer with dupilumab than placebo. And forced expiratory volume in 1 second (FEV1) "improved by more than 200 mL when dupilumab, as compared with placebo, was added to inhaled glucocorticoids and LABAs, an increase sustained during their tapering and discontinuation," the researchers noted (N. Engl. J. Med. 2013 May 21 [doi: 10.1056/NEJMoa1304048]).
Several other secondary endpoints also favored dupilumab over placebo, including morning peak expiratory flow values, scores on the Asthma Control Questionnaire (ACQ5), morning and evening asthma symptom scores, and the number of albuterol or levalbuterol inhalations needed per day. These measures improved at the beginning of the intervention in both study groups, then quickly returned to baseline levels in the placebo group while remaining constant in the dupilumab group.
The percentage of patients reporting adverse events was similar between the dupilumab and placebo groups (81% vs. 77%). These events tended to be nonspecific and mild, and included nasopharyngitis, nausea, and headache. One patient developed a progressive papular rash, urticaria, and edema after his ninth injection of dupilumab, which responded to nonurgent treatment of the symptoms and did not recur once the drug was withdrawn.
No serious adverse events were attributed to the study drug, and no patient showed clinically significant changes in vital signs, findings on physical examination, laboratory tests, or ECGs.
"Further studies are needed to confirm these observations and better define the target population, dosing regimen, and long-term efficacy and safety," Dr. Wenzel noted.
However, the study findings support the theory that the Th2 cytokines interleukin-4 and interleukin-13 play a pathogenic role in persistent, moderate-to-severe asthma, she added.
This study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Wenzel reported ties to Sanofi, Regeneron, Amgen, Merck, and other companies. Her associates reported ties to numerous industry sources.
Dupilumab reduced exacerbations of moderate to severe asthma by 87% in adults with poorly controlled disease, and induced rapid and sustained improvements in numerous other measures of asthma severity in an industry-sponsored phase II study published online May 21 in the New England Journal of Medicine.
Dupilumab, a monoclonal antibody that inhibits interleukin-4 and interleukin-13 signaling, "showed substantial efficacy with regard to both objective and patient-reported end points" when it was used concomitantly with inhaled glucocorticoids and long-acting beta-agonists (LABAs), as well as when those background therapies were withdrawn, reported Dr. Sally Wenzel of the University of Pittsburgh and her associates.
"The magnitude and breadth of efficacy that we observed exceed those in other studies of Th2 [type 2 helper T-cell] cytokine inhibition," the researchers noted in the online report, which was presented simultaneously at the annual meeting of the American Thoracic Society.
Dupilumab currently is being assessed for the treatment of several diseases mediated by Th2 pathways. The goal of this phase II trial was to evaluate its safety and efficacy in adults with persistent moderate to severe asthma and elevated eosinophil levels whose symptoms were not well controlled with medium- to high-dose inhaled glucocorticoids plus LABAs (usually fluticasone and salmeterol).
The 104 participants were treated at 28 sites across the United States for 12 weeks, and then followed for another 8 weeks. During the intervention phase of the study, approximately half were randomized to receive once-weekly subcutaneous injections of dupilumab (300 mg) and half to receive matching placebo injections, in addition to the background asthma medications.
At week 4, the study subjects discontinued LABAs, and at weeks 6-9 they tapered off inhaled glucocorticoids. "This approach enabled us to observe the effects of dupilumab when added to background therapy, after LABA discontinuation, during the tapering of inhaled glucocorticoids, and as monotherapy," the researchers said.
The primary endpoint of the study was an asthma exacerbation during the 12-week intervention period. Exacerbations occurred in 3 patients receiving dupilumab (6%), compared with 23 receiving placebo (44%), a highly significant difference.
In addition, the time to an asthma exacerbation was significantly longer with dupilumab than placebo. And forced expiratory volume in 1 second (FEV1) "improved by more than 200 mL when dupilumab, as compared with placebo, was added to inhaled glucocorticoids and LABAs, an increase sustained during their tapering and discontinuation," the researchers noted (N. Engl. J. Med. 2013 May 21 [doi: 10.1056/NEJMoa1304048]).
Several other secondary endpoints also favored dupilumab over placebo, including morning peak expiratory flow values, scores on the Asthma Control Questionnaire (ACQ5), morning and evening asthma symptom scores, and the number of albuterol or levalbuterol inhalations needed per day. These measures improved at the beginning of the intervention in both study groups, then quickly returned to baseline levels in the placebo group while remaining constant in the dupilumab group.
The percentage of patients reporting adverse events was similar between the dupilumab and placebo groups (81% vs. 77%). These events tended to be nonspecific and mild, and included nasopharyngitis, nausea, and headache. One patient developed a progressive papular rash, urticaria, and edema after his ninth injection of dupilumab, which responded to nonurgent treatment of the symptoms and did not recur once the drug was withdrawn.
No serious adverse events were attributed to the study drug, and no patient showed clinically significant changes in vital signs, findings on physical examination, laboratory tests, or ECGs.
"Further studies are needed to confirm these observations and better define the target population, dosing regimen, and long-term efficacy and safety," Dr. Wenzel noted.
However, the study findings support the theory that the Th2 cytokines interleukin-4 and interleukin-13 play a pathogenic role in persistent, moderate-to-severe asthma, she added.
This study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Wenzel reported ties to Sanofi, Regeneron, Amgen, Merck, and other companies. Her associates reported ties to numerous industry sources.
Dupilumab reduced exacerbations of moderate to severe asthma by 87% in adults with poorly controlled disease, and induced rapid and sustained improvements in numerous other measures of asthma severity in an industry-sponsored phase II study published online May 21 in the New England Journal of Medicine.
Dupilumab, a monoclonal antibody that inhibits interleukin-4 and interleukin-13 signaling, "showed substantial efficacy with regard to both objective and patient-reported end points" when it was used concomitantly with inhaled glucocorticoids and long-acting beta-agonists (LABAs), as well as when those background therapies were withdrawn, reported Dr. Sally Wenzel of the University of Pittsburgh and her associates.
"The magnitude and breadth of efficacy that we observed exceed those in other studies of Th2 [type 2 helper T-cell] cytokine inhibition," the researchers noted in the online report, which was presented simultaneously at the annual meeting of the American Thoracic Society.
Dupilumab currently is being assessed for the treatment of several diseases mediated by Th2 pathways. The goal of this phase II trial was to evaluate its safety and efficacy in adults with persistent moderate to severe asthma and elevated eosinophil levels whose symptoms were not well controlled with medium- to high-dose inhaled glucocorticoids plus LABAs (usually fluticasone and salmeterol).
The 104 participants were treated at 28 sites across the United States for 12 weeks, and then followed for another 8 weeks. During the intervention phase of the study, approximately half were randomized to receive once-weekly subcutaneous injections of dupilumab (300 mg) and half to receive matching placebo injections, in addition to the background asthma medications.
At week 4, the study subjects discontinued LABAs, and at weeks 6-9 they tapered off inhaled glucocorticoids. "This approach enabled us to observe the effects of dupilumab when added to background therapy, after LABA discontinuation, during the tapering of inhaled glucocorticoids, and as monotherapy," the researchers said.
The primary endpoint of the study was an asthma exacerbation during the 12-week intervention period. Exacerbations occurred in 3 patients receiving dupilumab (6%), compared with 23 receiving placebo (44%), a highly significant difference.
In addition, the time to an asthma exacerbation was significantly longer with dupilumab than placebo. And forced expiratory volume in 1 second (FEV1) "improved by more than 200 mL when dupilumab, as compared with placebo, was added to inhaled glucocorticoids and LABAs, an increase sustained during their tapering and discontinuation," the researchers noted (N. Engl. J. Med. 2013 May 21 [doi: 10.1056/NEJMoa1304048]).
Several other secondary endpoints also favored dupilumab over placebo, including morning peak expiratory flow values, scores on the Asthma Control Questionnaire (ACQ5), morning and evening asthma symptom scores, and the number of albuterol or levalbuterol inhalations needed per day. These measures improved at the beginning of the intervention in both study groups, then quickly returned to baseline levels in the placebo group while remaining constant in the dupilumab group.
The percentage of patients reporting adverse events was similar between the dupilumab and placebo groups (81% vs. 77%). These events tended to be nonspecific and mild, and included nasopharyngitis, nausea, and headache. One patient developed a progressive papular rash, urticaria, and edema after his ninth injection of dupilumab, which responded to nonurgent treatment of the symptoms and did not recur once the drug was withdrawn.
No serious adverse events were attributed to the study drug, and no patient showed clinically significant changes in vital signs, findings on physical examination, laboratory tests, or ECGs.
"Further studies are needed to confirm these observations and better define the target population, dosing regimen, and long-term efficacy and safety," Dr. Wenzel noted.
However, the study findings support the theory that the Th2 cytokines interleukin-4 and interleukin-13 play a pathogenic role in persistent, moderate-to-severe asthma, she added.
This study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Wenzel reported ties to Sanofi, Regeneron, Amgen, Merck, and other companies. Her associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Dupilumab was associated with an 87% reduction in asthma exacerbation; three patients receiving dupilumab (6%) had an exacerbation during the study, compared with 23 receiving placebo (44%).
Data Source: A randomized, double-blind, phase II clinical trial including 104 adults with persistent moderate to severe asthma.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Wenzel reported ties to Sanofi, Regeneron, Amgen, Merck, and other companies. Her associates reported ties to numerous industry sources.

Vaccine-resistant pertussis strains found in Philadelphia
WASHINGTON – Vaccine-resistant isolates of Bordetella pertussis have appeared in Philadelphia – the first such strains to be seen in the United States.
Of 30 samples analyzed, 18 (60%) showed a variant that conferred resistance to the current vaccine formulation, Dr. Jennifer Vodzak said at the annual meeting of the Pediatric Academic Societies. The strains had developed two different mutations, each of which deleted their expression of pertactin, an outer membrane protein that helps the bacteria adhere to respiratory epithelium. Pertactin is used as an antigen in the acellular pertussis component of the Tdap vaccine.
"It seems that, responding to vaccine pressure, B. pertussis has acquired several adaptations to halt the production of pertactin," said Dr. Vodzak, an infectious disease specialist at St. Christopher’s Hospital for Children, Philadelphia.
For the past decade, pertactin-negative strains have been reported in Japan, France, and Finland. Although the bacteria lack pertactin, French studies have shown that they are just as virulent as the nonmutated strains. The bacteria have simply found a way to cause disease without that particular protein.
Dr. Vodzak and her colleagues first reported their findings in a brief correspondence to the New England Journal Medicine in February. At that time, 11 of 12 isolates cultured from 2011 and 2012 expressed the pertactin variants. Seven expressed stop codons that truncated the protein, and four expressed insertion sequences that disrupted the pertactin coding region. The investigators also noted that these mutations appeared to be unique and not related to those seen in other countries.
Since then, the team has expanded its search, attempting to pinpoint the time these variants first appeared. To do that, they randomly selected 70 samples taken from Philadelphia patients who had culture-proven pertussis from 2007 to 2012. Most (80%) of the samples were from hospitalized patients, the majority of whom (87%) were younger than 1 year. More than half of the patients were younger than 3 months old. So far, 30 of the isolates have been molecularly examined.
After pertussis immunization became widespread in the 1940s, the disease incidence dropped dramatically in the United States. But in the mid-1990s – shortly after the acellular vaccine was introduced in 1991 – a gradual resurgence began. The incidence really picked up in the early 2000s, when annual case reports jumped into the tens of thousands. There were 18,719 cases reported in 2011; in 2012, that number more than doubled, to 41,880 – the highest since 1955.
The rise in cases was temporally related to the initiation of the acellular vaccine, which carries the pertactin antigen. The acellular vaccine also confers a limited immunogenicity. This limited protection and increased surveillance and reporting – not the acellular pertactin-containing vaccine –have caused the rise in cases, according to the Centers for Disease Control and Prevention.
"It does not appear that these strains are the reason the United States has experienced a dramatic increase in the number of reported pertussis cases recently," the agency says on its pertussis pages. "But CDC will continue to closely monitor the situation before drawing any conclusions. There is also no suggestion that these new strains are causing more severe cases of pertussis," or that the mutated strains carry any antibiotic resistance.
The appearance of pertactin-negative strains does seem to parallel the recent jump in cases, but as yet there are no hard data linking these three occurrences, Dr. Vodzak said.
Right now, she added, there’s no way to know if – or when – similar pertactin-negative strains have developed elsewhere in the United States. She and her team are encouraging public health agencies to test their stored samples so a more complete picture can be drawn.
"It will be important to consider the pathogen’s adaptations as we consider both the decreased vaccine effectiveness and vaccine development," she said. "I think the next step is to look at the clinical picture of these variants."
Dr. Vodzak said she had no relevant financial disclosures. Her coauthor, Anne Marie Queenan, Ph.D., is an employee of Janssen Research and Development.
WASHINGTON – Vaccine-resistant isolates of Bordetella pertussis have appeared in Philadelphia – the first such strains to be seen in the United States.
Of 30 samples analyzed, 18 (60%) showed a variant that conferred resistance to the current vaccine formulation, Dr. Jennifer Vodzak said at the annual meeting of the Pediatric Academic Societies. The strains had developed two different mutations, each of which deleted their expression of pertactin, an outer membrane protein that helps the bacteria adhere to respiratory epithelium. Pertactin is used as an antigen in the acellular pertussis component of the Tdap vaccine.
"It seems that, responding to vaccine pressure, B. pertussis has acquired several adaptations to halt the production of pertactin," said Dr. Vodzak, an infectious disease specialist at St. Christopher’s Hospital for Children, Philadelphia.
For the past decade, pertactin-negative strains have been reported in Japan, France, and Finland. Although the bacteria lack pertactin, French studies have shown that they are just as virulent as the nonmutated strains. The bacteria have simply found a way to cause disease without that particular protein.
Dr. Vodzak and her colleagues first reported their findings in a brief correspondence to the New England Journal Medicine in February. At that time, 11 of 12 isolates cultured from 2011 and 2012 expressed the pertactin variants. Seven expressed stop codons that truncated the protein, and four expressed insertion sequences that disrupted the pertactin coding region. The investigators also noted that these mutations appeared to be unique and not related to those seen in other countries.
Since then, the team has expanded its search, attempting to pinpoint the time these variants first appeared. To do that, they randomly selected 70 samples taken from Philadelphia patients who had culture-proven pertussis from 2007 to 2012. Most (80%) of the samples were from hospitalized patients, the majority of whom (87%) were younger than 1 year. More than half of the patients were younger than 3 months old. So far, 30 of the isolates have been molecularly examined.
After pertussis immunization became widespread in the 1940s, the disease incidence dropped dramatically in the United States. But in the mid-1990s – shortly after the acellular vaccine was introduced in 1991 – a gradual resurgence began. The incidence really picked up in the early 2000s, when annual case reports jumped into the tens of thousands. There were 18,719 cases reported in 2011; in 2012, that number more than doubled, to 41,880 – the highest since 1955.
The rise in cases was temporally related to the initiation of the acellular vaccine, which carries the pertactin antigen. The acellular vaccine also confers a limited immunogenicity. This limited protection and increased surveillance and reporting – not the acellular pertactin-containing vaccine –have caused the rise in cases, according to the Centers for Disease Control and Prevention.
"It does not appear that these strains are the reason the United States has experienced a dramatic increase in the number of reported pertussis cases recently," the agency says on its pertussis pages. "But CDC will continue to closely monitor the situation before drawing any conclusions. There is also no suggestion that these new strains are causing more severe cases of pertussis," or that the mutated strains carry any antibiotic resistance.
The appearance of pertactin-negative strains does seem to parallel the recent jump in cases, but as yet there are no hard data linking these three occurrences, Dr. Vodzak said.
Right now, she added, there’s no way to know if – or when – similar pertactin-negative strains have developed elsewhere in the United States. She and her team are encouraging public health agencies to test their stored samples so a more complete picture can be drawn.
"It will be important to consider the pathogen’s adaptations as we consider both the decreased vaccine effectiveness and vaccine development," she said. "I think the next step is to look at the clinical picture of these variants."
Dr. Vodzak said she had no relevant financial disclosures. Her coauthor, Anne Marie Queenan, Ph.D., is an employee of Janssen Research and Development.
WASHINGTON – Vaccine-resistant isolates of Bordetella pertussis have appeared in Philadelphia – the first such strains to be seen in the United States.
Of 30 samples analyzed, 18 (60%) showed a variant that conferred resistance to the current vaccine formulation, Dr. Jennifer Vodzak said at the annual meeting of the Pediatric Academic Societies. The strains had developed two different mutations, each of which deleted their expression of pertactin, an outer membrane protein that helps the bacteria adhere to respiratory epithelium. Pertactin is used as an antigen in the acellular pertussis component of the Tdap vaccine.
"It seems that, responding to vaccine pressure, B. pertussis has acquired several adaptations to halt the production of pertactin," said Dr. Vodzak, an infectious disease specialist at St. Christopher’s Hospital for Children, Philadelphia.
For the past decade, pertactin-negative strains have been reported in Japan, France, and Finland. Although the bacteria lack pertactin, French studies have shown that they are just as virulent as the nonmutated strains. The bacteria have simply found a way to cause disease without that particular protein.
Dr. Vodzak and her colleagues first reported their findings in a brief correspondence to the New England Journal Medicine in February. At that time, 11 of 12 isolates cultured from 2011 and 2012 expressed the pertactin variants. Seven expressed stop codons that truncated the protein, and four expressed insertion sequences that disrupted the pertactin coding region. The investigators also noted that these mutations appeared to be unique and not related to those seen in other countries.
Since then, the team has expanded its search, attempting to pinpoint the time these variants first appeared. To do that, they randomly selected 70 samples taken from Philadelphia patients who had culture-proven pertussis from 2007 to 2012. Most (80%) of the samples were from hospitalized patients, the majority of whom (87%) were younger than 1 year. More than half of the patients were younger than 3 months old. So far, 30 of the isolates have been molecularly examined.
After pertussis immunization became widespread in the 1940s, the disease incidence dropped dramatically in the United States. But in the mid-1990s – shortly after the acellular vaccine was introduced in 1991 – a gradual resurgence began. The incidence really picked up in the early 2000s, when annual case reports jumped into the tens of thousands. There were 18,719 cases reported in 2011; in 2012, that number more than doubled, to 41,880 – the highest since 1955.
The rise in cases was temporally related to the initiation of the acellular vaccine, which carries the pertactin antigen. The acellular vaccine also confers a limited immunogenicity. This limited protection and increased surveillance and reporting – not the acellular pertactin-containing vaccine –have caused the rise in cases, according to the Centers for Disease Control and Prevention.
"It does not appear that these strains are the reason the United States has experienced a dramatic increase in the number of reported pertussis cases recently," the agency says on its pertussis pages. "But CDC will continue to closely monitor the situation before drawing any conclusions. There is also no suggestion that these new strains are causing more severe cases of pertussis," or that the mutated strains carry any antibiotic resistance.
The appearance of pertactin-negative strains does seem to parallel the recent jump in cases, but as yet there are no hard data linking these three occurrences, Dr. Vodzak said.
Right now, she added, there’s no way to know if – or when – similar pertactin-negative strains have developed elsewhere in the United States. She and her team are encouraging public health agencies to test their stored samples so a more complete picture can be drawn.
"It will be important to consider the pathogen’s adaptations as we consider both the decreased vaccine effectiveness and vaccine development," she said. "I think the next step is to look at the clinical picture of these variants."
Dr. Vodzak said she had no relevant financial disclosures. Her coauthor, Anne Marie Queenan, Ph.D., is an employee of Janssen Research and Development.
FROM THE PAS ANNUAL MEETING
Major finding: About 60% of 30 B. pertussis isolates from 2007 to 2012 in Philadelphia showed a mutation that deletes their pertactin expression – making them immune to the pertactin-containing acellular pertussis vaccine.
Data source: An ongoing analysis of 70 isolates taken from Philadelphia residents who had culture-proven pertussis from 2007 to 2012.
Disclosures: Dr. Vodzak said she had no relevant financial disclosures. Her coauthor, Anne Marie Queenan, Ph.D., is an employee of Janssen Research and Development.
WHO, CDC continue monitoring deadly new coronavirus
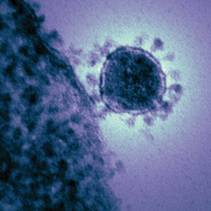
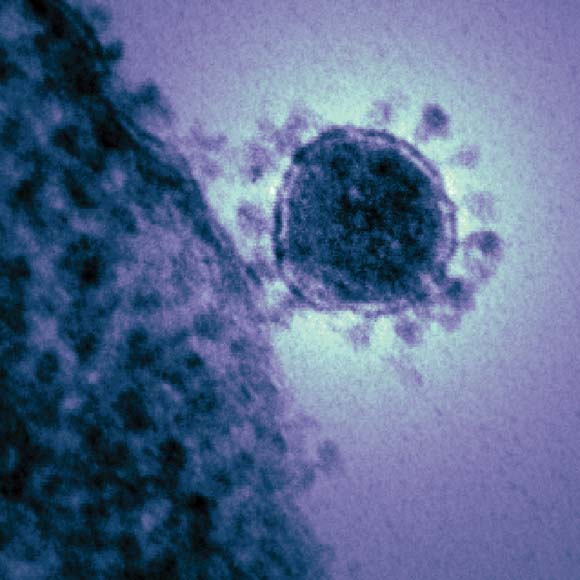
The World Health Organization and the Centers for Disease Control and Prevention are closely following the spread of a new coronavirus that emerged in the Middle East last fall and currently demonstrates a mortality rate of more than 50%.
Widely referred to as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus. By mid May 2013, the new virus had been identified in 38 patients worldwide – in Saudi Arabia, Jordan, France, the United Kingdom, the United Arab Emirates, and Qatar – causing 20 deaths.
"Health care providers are advised to be vigilant among recent travelers returning from areas affected by the virus who develop severe SARI [severe acute respiratory infections]. Specimens from patients’ lower respiratory tracts should be obtained for diagnosis where possible. Clinicians are reminded that NCoV infection should be considered even with atypical signs and symptoms in patients who are significantly immune compromised," WHO said in a written statement May 14.
In a May 13 statement the CDC noted: "So far, there are no reports of anyone in the U.S. getting infected and sick with the novel coronavirus." The CDC added that investigations are underway to determine the source of the novel coronavirus and how it spreads.
The World Health Organization and the Centers for Disease Control and Prevention are closely following the spread of a new coronavirus that emerged in the Middle East last fall and currently demonstrates a mortality rate of more than 50%.
Widely referred to as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus. By mid May 2013, the new virus had been identified in 38 patients worldwide – in Saudi Arabia, Jordan, France, the United Kingdom, the United Arab Emirates, and Qatar – causing 20 deaths.
"Health care providers are advised to be vigilant among recent travelers returning from areas affected by the virus who develop severe SARI [severe acute respiratory infections]. Specimens from patients’ lower respiratory tracts should be obtained for diagnosis where possible. Clinicians are reminded that NCoV infection should be considered even with atypical signs and symptoms in patients who are significantly immune compromised," WHO said in a written statement May 14.
In a May 13 statement the CDC noted: "So far, there are no reports of anyone in the U.S. getting infected and sick with the novel coronavirus." The CDC added that investigations are underway to determine the source of the novel coronavirus and how it spreads.
The World Health Organization and the Centers for Disease Control and Prevention are closely following the spread of a new coronavirus that emerged in the Middle East last fall and currently demonstrates a mortality rate of more than 50%.
Widely referred to as the "novel coronavirus" (NCoV), the new agent is very similar to the severe acute respiratory syndrome (SARS)-associated coronavirus. By mid May 2013, the new virus had been identified in 38 patients worldwide – in Saudi Arabia, Jordan, France, the United Kingdom, the United Arab Emirates, and Qatar – causing 20 deaths.
"Health care providers are advised to be vigilant among recent travelers returning from areas affected by the virus who develop severe SARI [severe acute respiratory infections]. Specimens from patients’ lower respiratory tracts should be obtained for diagnosis where possible. Clinicians are reminded that NCoV infection should be considered even with atypical signs and symptoms in patients who are significantly immune compromised," WHO said in a written statement May 14.
In a May 13 statement the CDC noted: "So far, there are no reports of anyone in the U.S. getting infected and sick with the novel coronavirus." The CDC added that investigations are underway to determine the source of the novel coronavirus and how it spreads.
Lung cancer screening guidelines
Background
Lung cancer is the leading cause of cancer death among men and women in the United States and will account for an estimated 160,000 deaths in 2012. The average 5-year survival for lung cancer is approximately 16%, among the poorest of all cancers. Studies have not shown a significant decrease in lung cancer mortality using chest x-ray (CXR) with and without sputum cytology.
However, the American Cancer Society recently published guidelines for lung cancer screening based on additional data from the National Lung Screening Trial (NLST), which reviewed the utility of low-dose computed tomography (LD-CT) for lung cancer screening.
A survey of 962 primary care physicians in 2006-2007 found that 25% of those surveyed believed that one or more of the national expert groups recommend screening asymptomatic patients for lung cancer. More than 50% of those surveyed had ordered a CXR, and nearly 25% had ordered LD-CT for lung cancer screening of asymptomatic patients in the last 12 months.
Conclusions
NLST randomized patients to annual LD-CT vs. annual CXR over 3 years, with results showing a 20% reduction in cancer death and a 6.7% reduction in death from all causes in the LD-CT arm. Two other randomized, controlled trials using the same endpoints but shorter follow-up were unable to demonstrate this same reduction.
Limitations and harms associated with LD-CT include the psychological stress and anxiety associated with abnormal results, false-positive test results, incidental findings outside of the lung, and morbidity/mortality associated with further diagnostic evaluations in patients with and without lung cancer.
A total of 39% of individuals experienced at least one abnormal CT scan over the 3 years of screening, and most of these patients needed additional imaging to determine the significance of the identified abnormalities. A total of 2.7% of patients ultimately found not have lung cancer underwent invasive procedures for further evaluation, with a complication rate of 0.06%. This is in comparison to the 11.2% complication rate for invasive procedures in patients who were subsequently diagnosed with lung cancer. Radiation exposure was not reported.
A total of 7.5% of participants were found to have incidental findings outside the lung fields on their screening imaging. Currently, there is insufficient evidence to evaluate the potential for overdiagnosis of lung cancer with LD-CT.
The average NLST participant was 62 years old, with approximately a 50-pack-year smoking history. The NLST conclusions suggests LD-CT screening is beneficial in men and women aged 55-74 years who are in reasonably good health, are current smokers or former smokers having quit within the past 15 years, and have a 30 or more pack-year smoking history.
Several studies have shown evidence of higher rates of smoking cessation in patients who have chosen to participate in lung cancer screening programs using LD-CT. A community-based screening program for oral, head, and neck cancer showed some increase in smoking cessation, but other programs targeting lung cancer screening have not replicated this data.
Few insurance programs provide coverage for LD-CT performed for lung cancer screening.
Implementation
The American Cancer Society lung cancer screening guidelines recommend that clinicians initiate a discussion about lung cancer screening with their patients aged 55-74 years who are in reasonably good health, are current smokers or former smokers who quit within the past 15 years, and have a 30 or more pack-year smoking history. Adults who choose to be screened should have annual LD-CT imaging until the age of 74 years.
Adults who choose to undergo lung cancer screening by LD-CT should be referred to an organized screening program. If such a program is not available, then referral should be made to a center that performs a reasonably high volume of CT scans, diagnostics tests, and lung cancer cases. If this is not available, or if the patient is unwilling to travel to a location where this is possible, then screening is not recommended.
Smoking cessation must remain a highest priority for all patients who are currently smoking. LD-CT screening should not be seen as an alternative to smoking cessation.
The American College of Chest Physicians, the American Society of Clinical Oncology, and the American Lung Association also suggest LD-CT screening based on similar NLST criteria.
The National Comprehensive Cancer Network recommends annual LD-CT for persons who meet NSLT entry criteria and for individuals 50 years or older with a smoking history of 20 or more pack-years who have one additional known risk factor for lung cancer.
The American Association for Thoracic Surgery recommends annual lung cancer screening with LD-CT for adults aged 55-79 years with a 30 pack-year history of smoking, annual screening beginning at age 50 years for adults with a 20-pack-year history and an additional calculated cumulative 5-year risk of developing lung cancer of 5% or greater. The 5-year cumulative risk is in conformity with the U.K. Lung Cancer Screening Trial, which uses the Liverpool Lung Project to calculate risk.
The United States Preventative Services Task Force recommendation (most recently updated in 2004) is that the evidence is insufficient to recommend for or against screening asymptomatic persons for lung cancer with LD-CT, CXR, sputum cytology, or a combination of these tests. The USPSTF recommendation has not been revised based on the NLST study. However, the task force is compiling evidence, and a draft of its most current recommendations will be available for public review in 2013.
All decisions regarding lung cancer screening must include an open discussion between physicians and their patients regarding the potential benefits and harms of screening, including false-positive results, the psychological effects of those results, and potential complications related to further diagnostic evaluation. The financial burden to the patient must also be included in this discussion, as initial screening is rarely an insurance-covered benefit.
References
• Wender, R., et al. American Cancer Society lung cancer screening guidelines (CA Cancer J. Clin. 2013;63:106-17).
• Klabude, C., et al. Lung cancer screening practice of primary care physicians: results from a national survey (Ann. Fam. Med. 2012;10:102-10).
• Humphrey, L.L., Teutsch, S., Johnson, M.S. Lung cancer screening with sputum cytologic examination, chest radiography, and computed tomography: an update from the U.S. Preventive Services Task Force (Ann. Intern. Med. 2004;140:740-53).
• Bize, R., Burnand, B., Mueller, Y., Rège-Walther, M., Camain, J.Y., Cornuz, J. Biomedical risk assessment as an aid for smoking cessation (Cochrane Database Syst. Rev. 2012;12:CD004705).
• Ferketich, A.K., Otterson, G.A., King, M., Hall, N., Browning, K.K., Wewers, M.E. A pilot test of a combined tobacco dependence treatment and lung cancer screening program (Lung Cancer 2012;76:211-5).
• van der Aalst, C.M., de Koning, H.J., van den Bergh, K.A., Willemsen, M.C., van Klaveren, R.J. The effectiveness of computer-tailored smoking cessation intervention for participants in lung cancer screening: a randomized control trial (Lung Cancer 2012;76:204-10).
Dr. Vancil is an assistant professor of internal medicine at the University of Arkansas, Little Rock. Dr. Golden is medical director of Arkansas Medicaid and professor of medicine and public health at the University of Arkansas. Dr. Hopkins is director of the division of general internal medicine at the University of Arkansas. E-mail them at imnews@frontlinemedcom.com. They reported having no relevant financial conflicts.
Background
Lung cancer is the leading cause of cancer death among men and women in the United States and will account for an estimated 160,000 deaths in 2012. The average 5-year survival for lung cancer is approximately 16%, among the poorest of all cancers. Studies have not shown a significant decrease in lung cancer mortality using chest x-ray (CXR) with and without sputum cytology.
However, the American Cancer Society recently published guidelines for lung cancer screening based on additional data from the National Lung Screening Trial (NLST), which reviewed the utility of low-dose computed tomography (LD-CT) for lung cancer screening.
A survey of 962 primary care physicians in 2006-2007 found that 25% of those surveyed believed that one or more of the national expert groups recommend screening asymptomatic patients for lung cancer. More than 50% of those surveyed had ordered a CXR, and nearly 25% had ordered LD-CT for lung cancer screening of asymptomatic patients in the last 12 months.
Conclusions
NLST randomized patients to annual LD-CT vs. annual CXR over 3 years, with results showing a 20% reduction in cancer death and a 6.7% reduction in death from all causes in the LD-CT arm. Two other randomized, controlled trials using the same endpoints but shorter follow-up were unable to demonstrate this same reduction.
Limitations and harms associated with LD-CT include the psychological stress and anxiety associated with abnormal results, false-positive test results, incidental findings outside of the lung, and morbidity/mortality associated with further diagnostic evaluations in patients with and without lung cancer.
A total of 39% of individuals experienced at least one abnormal CT scan over the 3 years of screening, and most of these patients needed additional imaging to determine the significance of the identified abnormalities. A total of 2.7% of patients ultimately found not have lung cancer underwent invasive procedures for further evaluation, with a complication rate of 0.06%. This is in comparison to the 11.2% complication rate for invasive procedures in patients who were subsequently diagnosed with lung cancer. Radiation exposure was not reported.
A total of 7.5% of participants were found to have incidental findings outside the lung fields on their screening imaging. Currently, there is insufficient evidence to evaluate the potential for overdiagnosis of lung cancer with LD-CT.
The average NLST participant was 62 years old, with approximately a 50-pack-year smoking history. The NLST conclusions suggests LD-CT screening is beneficial in men and women aged 55-74 years who are in reasonably good health, are current smokers or former smokers having quit within the past 15 years, and have a 30 or more pack-year smoking history.
Several studies have shown evidence of higher rates of smoking cessation in patients who have chosen to participate in lung cancer screening programs using LD-CT. A community-based screening program for oral, head, and neck cancer showed some increase in smoking cessation, but other programs targeting lung cancer screening have not replicated this data.
Few insurance programs provide coverage for LD-CT performed for lung cancer screening.
Implementation
The American Cancer Society lung cancer screening guidelines recommend that clinicians initiate a discussion about lung cancer screening with their patients aged 55-74 years who are in reasonably good health, are current smokers or former smokers who quit within the past 15 years, and have a 30 or more pack-year smoking history. Adults who choose to be screened should have annual LD-CT imaging until the age of 74 years.
Adults who choose to undergo lung cancer screening by LD-CT should be referred to an organized screening program. If such a program is not available, then referral should be made to a center that performs a reasonably high volume of CT scans, diagnostics tests, and lung cancer cases. If this is not available, or if the patient is unwilling to travel to a location where this is possible, then screening is not recommended.
Smoking cessation must remain a highest priority for all patients who are currently smoking. LD-CT screening should not be seen as an alternative to smoking cessation.
The American College of Chest Physicians, the American Society of Clinical Oncology, and the American Lung Association also suggest LD-CT screening based on similar NLST criteria.
The National Comprehensive Cancer Network recommends annual LD-CT for persons who meet NSLT entry criteria and for individuals 50 years or older with a smoking history of 20 or more pack-years who have one additional known risk factor for lung cancer.
The American Association for Thoracic Surgery recommends annual lung cancer screening with LD-CT for adults aged 55-79 years with a 30 pack-year history of smoking, annual screening beginning at age 50 years for adults with a 20-pack-year history and an additional calculated cumulative 5-year risk of developing lung cancer of 5% or greater. The 5-year cumulative risk is in conformity with the U.K. Lung Cancer Screening Trial, which uses the Liverpool Lung Project to calculate risk.
The United States Preventative Services Task Force recommendation (most recently updated in 2004) is that the evidence is insufficient to recommend for or against screening asymptomatic persons for lung cancer with LD-CT, CXR, sputum cytology, or a combination of these tests. The USPSTF recommendation has not been revised based on the NLST study. However, the task force is compiling evidence, and a draft of its most current recommendations will be available for public review in 2013.
All decisions regarding lung cancer screening must include an open discussion between physicians and their patients regarding the potential benefits and harms of screening, including false-positive results, the psychological effects of those results, and potential complications related to further diagnostic evaluation. The financial burden to the patient must also be included in this discussion, as initial screening is rarely an insurance-covered benefit.
References
• Wender, R., et al. American Cancer Society lung cancer screening guidelines (CA Cancer J. Clin. 2013;63:106-17).
• Klabude, C., et al. Lung cancer screening practice of primary care physicians: results from a national survey (Ann. Fam. Med. 2012;10:102-10).
• Humphrey, L.L., Teutsch, S., Johnson, M.S. Lung cancer screening with sputum cytologic examination, chest radiography, and computed tomography: an update from the U.S. Preventive Services Task Force (Ann. Intern. Med. 2004;140:740-53).
• Bize, R., Burnand, B., Mueller, Y., Rège-Walther, M., Camain, J.Y., Cornuz, J. Biomedical risk assessment as an aid for smoking cessation (Cochrane Database Syst. Rev. 2012;12:CD004705).
• Ferketich, A.K., Otterson, G.A., King, M., Hall, N., Browning, K.K., Wewers, M.E. A pilot test of a combined tobacco dependence treatment and lung cancer screening program (Lung Cancer 2012;76:211-5).
• van der Aalst, C.M., de Koning, H.J., van den Bergh, K.A., Willemsen, M.C., van Klaveren, R.J. The effectiveness of computer-tailored smoking cessation intervention for participants in lung cancer screening: a randomized control trial (Lung Cancer 2012;76:204-10).
Dr. Vancil is an assistant professor of internal medicine at the University of Arkansas, Little Rock. Dr. Golden is medical director of Arkansas Medicaid and professor of medicine and public health at the University of Arkansas. Dr. Hopkins is director of the division of general internal medicine at the University of Arkansas. E-mail them at imnews@frontlinemedcom.com. They reported having no relevant financial conflicts.
Background
Lung cancer is the leading cause of cancer death among men and women in the United States and will account for an estimated 160,000 deaths in 2012. The average 5-year survival for lung cancer is approximately 16%, among the poorest of all cancers. Studies have not shown a significant decrease in lung cancer mortality using chest x-ray (CXR) with and without sputum cytology.
However, the American Cancer Society recently published guidelines for lung cancer screening based on additional data from the National Lung Screening Trial (NLST), which reviewed the utility of low-dose computed tomography (LD-CT) for lung cancer screening.
A survey of 962 primary care physicians in 2006-2007 found that 25% of those surveyed believed that one or more of the national expert groups recommend screening asymptomatic patients for lung cancer. More than 50% of those surveyed had ordered a CXR, and nearly 25% had ordered LD-CT for lung cancer screening of asymptomatic patients in the last 12 months.
Conclusions
NLST randomized patients to annual LD-CT vs. annual CXR over 3 years, with results showing a 20% reduction in cancer death and a 6.7% reduction in death from all causes in the LD-CT arm. Two other randomized, controlled trials using the same endpoints but shorter follow-up were unable to demonstrate this same reduction.
Limitations and harms associated with LD-CT include the psychological stress and anxiety associated with abnormal results, false-positive test results, incidental findings outside of the lung, and morbidity/mortality associated with further diagnostic evaluations in patients with and without lung cancer.
A total of 39% of individuals experienced at least one abnormal CT scan over the 3 years of screening, and most of these patients needed additional imaging to determine the significance of the identified abnormalities. A total of 2.7% of patients ultimately found not have lung cancer underwent invasive procedures for further evaluation, with a complication rate of 0.06%. This is in comparison to the 11.2% complication rate for invasive procedures in patients who were subsequently diagnosed with lung cancer. Radiation exposure was not reported.
A total of 7.5% of participants were found to have incidental findings outside the lung fields on their screening imaging. Currently, there is insufficient evidence to evaluate the potential for overdiagnosis of lung cancer with LD-CT.
The average NLST participant was 62 years old, with approximately a 50-pack-year smoking history. The NLST conclusions suggests LD-CT screening is beneficial in men and women aged 55-74 years who are in reasonably good health, are current smokers or former smokers having quit within the past 15 years, and have a 30 or more pack-year smoking history.
Several studies have shown evidence of higher rates of smoking cessation in patients who have chosen to participate in lung cancer screening programs using LD-CT. A community-based screening program for oral, head, and neck cancer showed some increase in smoking cessation, but other programs targeting lung cancer screening have not replicated this data.
Few insurance programs provide coverage for LD-CT performed for lung cancer screening.
Implementation
The American Cancer Society lung cancer screening guidelines recommend that clinicians initiate a discussion about lung cancer screening with their patients aged 55-74 years who are in reasonably good health, are current smokers or former smokers who quit within the past 15 years, and have a 30 or more pack-year smoking history. Adults who choose to be screened should have annual LD-CT imaging until the age of 74 years.
Adults who choose to undergo lung cancer screening by LD-CT should be referred to an organized screening program. If such a program is not available, then referral should be made to a center that performs a reasonably high volume of CT scans, diagnostics tests, and lung cancer cases. If this is not available, or if the patient is unwilling to travel to a location where this is possible, then screening is not recommended.
Smoking cessation must remain a highest priority for all patients who are currently smoking. LD-CT screening should not be seen as an alternative to smoking cessation.
The American College of Chest Physicians, the American Society of Clinical Oncology, and the American Lung Association also suggest LD-CT screening based on similar NLST criteria.
The National Comprehensive Cancer Network recommends annual LD-CT for persons who meet NSLT entry criteria and for individuals 50 years or older with a smoking history of 20 or more pack-years who have one additional known risk factor for lung cancer.
The American Association for Thoracic Surgery recommends annual lung cancer screening with LD-CT for adults aged 55-79 years with a 30 pack-year history of smoking, annual screening beginning at age 50 years for adults with a 20-pack-year history and an additional calculated cumulative 5-year risk of developing lung cancer of 5% or greater. The 5-year cumulative risk is in conformity with the U.K. Lung Cancer Screening Trial, which uses the Liverpool Lung Project to calculate risk.
The United States Preventative Services Task Force recommendation (most recently updated in 2004) is that the evidence is insufficient to recommend for or against screening asymptomatic persons for lung cancer with LD-CT, CXR, sputum cytology, or a combination of these tests. The USPSTF recommendation has not been revised based on the NLST study. However, the task force is compiling evidence, and a draft of its most current recommendations will be available for public review in 2013.
All decisions regarding lung cancer screening must include an open discussion between physicians and their patients regarding the potential benefits and harms of screening, including false-positive results, the psychological effects of those results, and potential complications related to further diagnostic evaluation. The financial burden to the patient must also be included in this discussion, as initial screening is rarely an insurance-covered benefit.
References
• Wender, R., et al. American Cancer Society lung cancer screening guidelines (CA Cancer J. Clin. 2013;63:106-17).
• Klabude, C., et al. Lung cancer screening practice of primary care physicians: results from a national survey (Ann. Fam. Med. 2012;10:102-10).
• Humphrey, L.L., Teutsch, S., Johnson, M.S. Lung cancer screening with sputum cytologic examination, chest radiography, and computed tomography: an update from the U.S. Preventive Services Task Force (Ann. Intern. Med. 2004;140:740-53).
• Bize, R., Burnand, B., Mueller, Y., Rège-Walther, M., Camain, J.Y., Cornuz, J. Biomedical risk assessment as an aid for smoking cessation (Cochrane Database Syst. Rev. 2012;12:CD004705).
• Ferketich, A.K., Otterson, G.A., King, M., Hall, N., Browning, K.K., Wewers, M.E. A pilot test of a combined tobacco dependence treatment and lung cancer screening program (Lung Cancer 2012;76:211-5).
• van der Aalst, C.M., de Koning, H.J., van den Bergh, K.A., Willemsen, M.C., van Klaveren, R.J. The effectiveness of computer-tailored smoking cessation intervention for participants in lung cancer screening: a randomized control trial (Lung Cancer 2012;76:204-10).
Dr. Vancil is an assistant professor of internal medicine at the University of Arkansas, Little Rock. Dr. Golden is medical director of Arkansas Medicaid and professor of medicine and public health at the University of Arkansas. Dr. Hopkins is director of the division of general internal medicine at the University of Arkansas. E-mail them at imnews@frontlinemedcom.com. They reported having no relevant financial conflicts.
Viral testing cut antibiotic use in children with respiratory illness
WASHINGTON – A rapid viral testing panel decreased the odds of inappropriate antibiotic use by 67% in children hospitalized with an acute respiratory illness, allowing about 6% of the children taking them to discontinue them.
Use of such a test could be part of a facility’s overall antibiotic control program, Dr. Russell McCulloh said at the annual meeting of the Pediatric Academic Societies.
"Now we need to talk about when a test like this can be used appropriately," said Dr. McCulloh, an infectious disease specialist at Rhode Island Hospital, Providence. "There is always a strong possibility for a bacterial coinfection in these patients, and that can be very hard to determine because we don’t have a gold standard test for that. Adjunctive diagnostic testing will be necessary if you’re really going to close the loop and implement this as part of an antibiotic stewardship program."
Dr. McCulloh conducted a retrospective chart review of 1,731 children admitted to the hospital for an acute respiratory illness from 2009 to 2011. He then compared the rates of antimicrobial use in children who had the rapid viral panel (809) and those who did not (922). About half of the group (860) had received antibiotics before having the test run, while 255 had received oseltamivir.
Most of the children who had a positive viral panel were prescribed oseltamivir (87%); the drug was used in about 18% of those who had a negative test. A multivariate analysis found that a positive rapid viral panel was the single biggest predictor of getting the antiviral drug, increasing the odds by more than 27 times, Dr. McCulloh said.
Younger age also had a significant association, but the odds ratio was only 1.7. Having a significant past medical history was predictive in an unadjusted analysis, but not in the final model. Abnormal chest x-ray, intensive care unit admission, and abnormal white cell counts had no significant predictive value.
The test also influenced the use of antibiotics, Dr. McCulloh said. Antibiotics were given to 11% of children who had the viral testing, but to 100% of those who did not have it. Antibiotics were used in 51% of those with a positive test, and 67% of those with a negative test. Antibiotics also were discontinued in 6% of children who had a positive viral test.
A multivariate analysis found several factors significantly associated with antibiotic use. A significant past medical history increased the odds by 7%. Stronger predictors included a codiagnosis of acute otitis media (OR 6.0), an abnormal chest x-ray (OR 2.57), and a positive blood culture (OR 3). However, a negative viral panel was associated with a 69% decreased chance of receiving an antibiotic.
The test was a big shaper of physician behavior, Dr. McCulloh said, allowing a more judicious and targeted use of antibiotics while increasing the use of antiviral medication. "Rapid viral panel testing seems to enhance physician decision-making in these patients."
Dr. McCulloh had no financial disclosures.
WASHINGTON – A rapid viral testing panel decreased the odds of inappropriate antibiotic use by 67% in children hospitalized with an acute respiratory illness, allowing about 6% of the children taking them to discontinue them.
Use of such a test could be part of a facility’s overall antibiotic control program, Dr. Russell McCulloh said at the annual meeting of the Pediatric Academic Societies.
"Now we need to talk about when a test like this can be used appropriately," said Dr. McCulloh, an infectious disease specialist at Rhode Island Hospital, Providence. "There is always a strong possibility for a bacterial coinfection in these patients, and that can be very hard to determine because we don’t have a gold standard test for that. Adjunctive diagnostic testing will be necessary if you’re really going to close the loop and implement this as part of an antibiotic stewardship program."
Dr. McCulloh conducted a retrospective chart review of 1,731 children admitted to the hospital for an acute respiratory illness from 2009 to 2011. He then compared the rates of antimicrobial use in children who had the rapid viral panel (809) and those who did not (922). About half of the group (860) had received antibiotics before having the test run, while 255 had received oseltamivir.
Most of the children who had a positive viral panel were prescribed oseltamivir (87%); the drug was used in about 18% of those who had a negative test. A multivariate analysis found that a positive rapid viral panel was the single biggest predictor of getting the antiviral drug, increasing the odds by more than 27 times, Dr. McCulloh said.
Younger age also had a significant association, but the odds ratio was only 1.7. Having a significant past medical history was predictive in an unadjusted analysis, but not in the final model. Abnormal chest x-ray, intensive care unit admission, and abnormal white cell counts had no significant predictive value.
The test also influenced the use of antibiotics, Dr. McCulloh said. Antibiotics were given to 11% of children who had the viral testing, but to 100% of those who did not have it. Antibiotics were used in 51% of those with a positive test, and 67% of those with a negative test. Antibiotics also were discontinued in 6% of children who had a positive viral test.
A multivariate analysis found several factors significantly associated with antibiotic use. A significant past medical history increased the odds by 7%. Stronger predictors included a codiagnosis of acute otitis media (OR 6.0), an abnormal chest x-ray (OR 2.57), and a positive blood culture (OR 3). However, a negative viral panel was associated with a 69% decreased chance of receiving an antibiotic.
The test was a big shaper of physician behavior, Dr. McCulloh said, allowing a more judicious and targeted use of antibiotics while increasing the use of antiviral medication. "Rapid viral panel testing seems to enhance physician decision-making in these patients."
Dr. McCulloh had no financial disclosures.
WASHINGTON – A rapid viral testing panel decreased the odds of inappropriate antibiotic use by 67% in children hospitalized with an acute respiratory illness, allowing about 6% of the children taking them to discontinue them.
Use of such a test could be part of a facility’s overall antibiotic control program, Dr. Russell McCulloh said at the annual meeting of the Pediatric Academic Societies.
"Now we need to talk about when a test like this can be used appropriately," said Dr. McCulloh, an infectious disease specialist at Rhode Island Hospital, Providence. "There is always a strong possibility for a bacterial coinfection in these patients, and that can be very hard to determine because we don’t have a gold standard test for that. Adjunctive diagnostic testing will be necessary if you’re really going to close the loop and implement this as part of an antibiotic stewardship program."
Dr. McCulloh conducted a retrospective chart review of 1,731 children admitted to the hospital for an acute respiratory illness from 2009 to 2011. He then compared the rates of antimicrobial use in children who had the rapid viral panel (809) and those who did not (922). About half of the group (860) had received antibiotics before having the test run, while 255 had received oseltamivir.
Most of the children who had a positive viral panel were prescribed oseltamivir (87%); the drug was used in about 18% of those who had a negative test. A multivariate analysis found that a positive rapid viral panel was the single biggest predictor of getting the antiviral drug, increasing the odds by more than 27 times, Dr. McCulloh said.
Younger age also had a significant association, but the odds ratio was only 1.7. Having a significant past medical history was predictive in an unadjusted analysis, but not in the final model. Abnormal chest x-ray, intensive care unit admission, and abnormal white cell counts had no significant predictive value.
The test also influenced the use of antibiotics, Dr. McCulloh said. Antibiotics were given to 11% of children who had the viral testing, but to 100% of those who did not have it. Antibiotics were used in 51% of those with a positive test, and 67% of those with a negative test. Antibiotics also were discontinued in 6% of children who had a positive viral test.
A multivariate analysis found several factors significantly associated with antibiotic use. A significant past medical history increased the odds by 7%. Stronger predictors included a codiagnosis of acute otitis media (OR 6.0), an abnormal chest x-ray (OR 2.57), and a positive blood culture (OR 3). However, a negative viral panel was associated with a 69% decreased chance of receiving an antibiotic.
The test was a big shaper of physician behavior, Dr. McCulloh said, allowing a more judicious and targeted use of antibiotics while increasing the use of antiviral medication. "Rapid viral panel testing seems to enhance physician decision-making in these patients."
Dr. McCulloh had no financial disclosures.
AT THE PAS ANNUAL MEETING
Major finding: In children hospitalized with an acute respiratory illness, a positive rapid viral panel increased the odds of receiving oseltamivir by more than 27 times, while decreasing the odds of antibiotic use by 69%.
Data source: A retrospective chart review of 1,731 children.
Disclosures: Dr. McCulloh had no financial disclosures.
Preclinical brain amyloid deposition linked to poor sleep
Preclinical beta-amyloid deposition in the brains of cognitively normal volunteers was associated with poor sleep quality but not sleep quantity in a study published in the May issue of JAMA Neurology (formerly Archives of Neurology).
"Our findings support the hypothesis that sleep-wake abnormalities are associated with the presence of amyloid deposition in the preclinical stage of AD [Alzheimer’s disease]," wrote Dr. Yo-El Ju of the Charles F. and Joanne Knight Alzheimer’s Disease Research Center, Washington University, St. Louis, and her associates.
In addition, "our findings may expand the temporal window during which sleep abnormalities are identifiable and potentially modifiable in AD," they noted.

Dr. Ju and her colleagues observed that sleep-wake problems are common in AD, and that early in its course, the disease affects brain regions and pathways important for sleep and wake mechanisms. "Even in mild cognitive impairment, or very mild dementia, there are abnormalities in sleep architecture and electroencephalography measures.
The investigators assessed the sleep of 142 research volunteers aged 45-75 years (mean age, 66 years) using 2 weeks of actigraphy and sleep diary records. They recorded total sleep time, sleep efficiency (sleep time divided by time in bed), and wake time after sleep onset. Some had a parental history of symptomatic AD and were participating in longitudinal studies of healthy aging and dementia. All the study subjects scored 0 on the Clinical Dementia Rating.
Overall, 32 participants (22.5%) had a cerebrospinal fluid level of amyloid beta 42 of less than 500 pg/mL, indicating a strong likelihood of amyloid deposition in the brain.
Study subjects with a strong likelihood of amyloid deposition had significantly worse sleep efficiency (80.4% vs. 83.7%) than did those without amyloid deposition. This association remained significant when the data were adjusted to correct for age, sex, and apolipoprotein E epsilon-4 allele carrier status.
This difference in sleep efficiency also was significant in a subgroup analysis involving only the 100 study subjects who reported that their sleep had not changed during the preceding 5 years.
Wake time after sleep onset also was significantly higher (worse) among subjects with a strong likelihood of amyloid deposition than it was among those without it (63.1 min vs. 54 min).
In contrast, there were no differences between these two study groups in sleep quantity.
The participants with amyloid deposition showed a trend for spending more nonsleeping time in bed, but the trend didn’t reach statistical significance. Similarly, they reported taking more naps per week, but the difference between the groups’ average number of naps didn’t reach statistical significance.
However, "when we looked at the proportion of frequent nappers, defined as those taking naps on 3 or more days per week, this was significantly higher in the group with amyloid deposition, compared with the group without amyloid deposition (31.2% vs. 14.7%)," Dr. Ju and her associates wrote (JAMA Neurol. 2013;70:587-93).
This study could not determine causality. Amyloid deposition could cause sleep-wake disruption through several mechanisms, such as direct interference with neuronal function in areas of the brain that are critical for sleep. But poor sleep could just as well contribute to amyloid deposition, such as by increasing neuronal activity to a pathological degree, which is thought to facilitate deposition. It is likely that both of these processes play a role in a kind of positive feedback loop, the investigators said.
The findings of this study lay important groundwork for future research. "Longitudinal follow-up with ongoing measurement of amyloid and sleep should enable us to begin to tease apart the details of the abnormalities in sleep that begin to occur with the onset of AD pathology, as well as the directionality of the relationship between sleep and amyloid deposition," they noted.
If sleep disruption is found to raise the risk of future AD, "then this provides an even stronger motivation to identify and treat individuals with sleep disorders, such as obstructive sleep apnea," Dr. Ju and her colleagues added.
This study was supported by grants from the U.S. National Institutes of Health, the Ellison Medical Foundation Senior Scholar Award, and the National Center for Research Resources. Dr. Ju reported no financial conflicts of interest, but some of her associates reported ties to UCB, Jazz Pharmaceuticals, and other companies.
Preclinical beta-amyloid deposition in the brains of cognitively normal volunteers was associated with poor sleep quality but not sleep quantity in a study published in the May issue of JAMA Neurology (formerly Archives of Neurology).
"Our findings support the hypothesis that sleep-wake abnormalities are associated with the presence of amyloid deposition in the preclinical stage of AD [Alzheimer’s disease]," wrote Dr. Yo-El Ju of the Charles F. and Joanne Knight Alzheimer’s Disease Research Center, Washington University, St. Louis, and her associates.
In addition, "our findings may expand the temporal window during which sleep abnormalities are identifiable and potentially modifiable in AD," they noted.
Dr. Ju and her colleagues observed that sleep-wake problems are common in AD, and that early in its course, the disease affects brain regions and pathways important for sleep and wake mechanisms. "Even in mild cognitive impairment, or very mild dementia, there are abnormalities in sleep architecture and electroencephalography measures.
The investigators assessed the sleep of 142 research volunteers aged 45-75 years (mean age, 66 years) using 2 weeks of actigraphy and sleep diary records. They recorded total sleep time, sleep efficiency (sleep time divided by time in bed), and wake time after sleep onset. Some had a parental history of symptomatic AD and were participating in longitudinal studies of healthy aging and dementia. All the study subjects scored 0 on the Clinical Dementia Rating.
Overall, 32 participants (22.5%) had a cerebrospinal fluid level of amyloid beta 42 of less than 500 pg/mL, indicating a strong likelihood of amyloid deposition in the brain.
Study subjects with a strong likelihood of amyloid deposition had significantly worse sleep efficiency (80.4% vs. 83.7%) than did those without amyloid deposition. This association remained significant when the data were adjusted to correct for age, sex, and apolipoprotein E epsilon-4 allele carrier status.
This difference in sleep efficiency also was significant in a subgroup analysis involving only the 100 study subjects who reported that their sleep had not changed during the preceding 5 years.
Wake time after sleep onset also was significantly higher (worse) among subjects with a strong likelihood of amyloid deposition than it was among those without it (63.1 min vs. 54 min).
In contrast, there were no differences between these two study groups in sleep quantity.
The participants with amyloid deposition showed a trend for spending more nonsleeping time in bed, but the trend didn’t reach statistical significance. Similarly, they reported taking more naps per week, but the difference between the groups’ average number of naps didn’t reach statistical significance.
However, "when we looked at the proportion of frequent nappers, defined as those taking naps on 3 or more days per week, this was significantly higher in the group with amyloid deposition, compared with the group without amyloid deposition (31.2% vs. 14.7%)," Dr. Ju and her associates wrote (JAMA Neurol. 2013;70:587-93).
This study could not determine causality. Amyloid deposition could cause sleep-wake disruption through several mechanisms, such as direct interference with neuronal function in areas of the brain that are critical for sleep. But poor sleep could just as well contribute to amyloid deposition, such as by increasing neuronal activity to a pathological degree, which is thought to facilitate deposition. It is likely that both of these processes play a role in a kind of positive feedback loop, the investigators said.
The findings of this study lay important groundwork for future research. "Longitudinal follow-up with ongoing measurement of amyloid and sleep should enable us to begin to tease apart the details of the abnormalities in sleep that begin to occur with the onset of AD pathology, as well as the directionality of the relationship between sleep and amyloid deposition," they noted.
If sleep disruption is found to raise the risk of future AD, "then this provides an even stronger motivation to identify and treat individuals with sleep disorders, such as obstructive sleep apnea," Dr. Ju and her colleagues added.
This study was supported by grants from the U.S. National Institutes of Health, the Ellison Medical Foundation Senior Scholar Award, and the National Center for Research Resources. Dr. Ju reported no financial conflicts of interest, but some of her associates reported ties to UCB, Jazz Pharmaceuticals, and other companies.
Preclinical beta-amyloid deposition in the brains of cognitively normal volunteers was associated with poor sleep quality but not sleep quantity in a study published in the May issue of JAMA Neurology (formerly Archives of Neurology).
"Our findings support the hypothesis that sleep-wake abnormalities are associated with the presence of amyloid deposition in the preclinical stage of AD [Alzheimer’s disease]," wrote Dr. Yo-El Ju of the Charles F. and Joanne Knight Alzheimer’s Disease Research Center, Washington University, St. Louis, and her associates.
In addition, "our findings may expand the temporal window during which sleep abnormalities are identifiable and potentially modifiable in AD," they noted.
Dr. Ju and her colleagues observed that sleep-wake problems are common in AD, and that early in its course, the disease affects brain regions and pathways important for sleep and wake mechanisms. "Even in mild cognitive impairment, or very mild dementia, there are abnormalities in sleep architecture and electroencephalography measures.
The investigators assessed the sleep of 142 research volunteers aged 45-75 years (mean age, 66 years) using 2 weeks of actigraphy and sleep diary records. They recorded total sleep time, sleep efficiency (sleep time divided by time in bed), and wake time after sleep onset. Some had a parental history of symptomatic AD and were participating in longitudinal studies of healthy aging and dementia. All the study subjects scored 0 on the Clinical Dementia Rating.
Overall, 32 participants (22.5%) had a cerebrospinal fluid level of amyloid beta 42 of less than 500 pg/mL, indicating a strong likelihood of amyloid deposition in the brain.
Study subjects with a strong likelihood of amyloid deposition had significantly worse sleep efficiency (80.4% vs. 83.7%) than did those without amyloid deposition. This association remained significant when the data were adjusted to correct for age, sex, and apolipoprotein E epsilon-4 allele carrier status.
This difference in sleep efficiency also was significant in a subgroup analysis involving only the 100 study subjects who reported that their sleep had not changed during the preceding 5 years.
Wake time after sleep onset also was significantly higher (worse) among subjects with a strong likelihood of amyloid deposition than it was among those without it (63.1 min vs. 54 min).
In contrast, there were no differences between these two study groups in sleep quantity.
The participants with amyloid deposition showed a trend for spending more nonsleeping time in bed, but the trend didn’t reach statistical significance. Similarly, they reported taking more naps per week, but the difference between the groups’ average number of naps didn’t reach statistical significance.
However, "when we looked at the proportion of frequent nappers, defined as those taking naps on 3 or more days per week, this was significantly higher in the group with amyloid deposition, compared with the group without amyloid deposition (31.2% vs. 14.7%)," Dr. Ju and her associates wrote (JAMA Neurol. 2013;70:587-93).
This study could not determine causality. Amyloid deposition could cause sleep-wake disruption through several mechanisms, such as direct interference with neuronal function in areas of the brain that are critical for sleep. But poor sleep could just as well contribute to amyloid deposition, such as by increasing neuronal activity to a pathological degree, which is thought to facilitate deposition. It is likely that both of these processes play a role in a kind of positive feedback loop, the investigators said.
The findings of this study lay important groundwork for future research. "Longitudinal follow-up with ongoing measurement of amyloid and sleep should enable us to begin to tease apart the details of the abnormalities in sleep that begin to occur with the onset of AD pathology, as well as the directionality of the relationship between sleep and amyloid deposition," they noted.
If sleep disruption is found to raise the risk of future AD, "then this provides an even stronger motivation to identify and treat individuals with sleep disorders, such as obstructive sleep apnea," Dr. Ju and her colleagues added.
This study was supported by grants from the U.S. National Institutes of Health, the Ellison Medical Foundation Senior Scholar Award, and the National Center for Research Resources. Dr. Ju reported no financial conflicts of interest, but some of her associates reported ties to UCB, Jazz Pharmaceuticals, and other companies.
FROM JAMA NEUROLOGY
Major Finding: Study subjects with a strong likelihood of amyloid deposition had significantly worse sleep efficiency (80.4% vs. 83.7%) than did those without amyloid deposition.
Data Source: A cross-sectional study of sleep abnormalities in 32 cognitively normal subjects who had preclinical amyloid deposition in the brain and 110 subjects who did not.
Disclosures: This study was supported by grants from the National Institutes of Health, the Ellison Medical Foundation Senior Scholar Award, and the National Center for Research Resources. Dr. Ju reported no financial conflicts of interest, but some of her associates reported ties to UCB, Jazz Pharmaceuticals, and other companies.

FDA approves once-daily combination drug for COPD
An inhaled powder formulation of the corticosteroid fluticasone furoate and vilanterol, a long-acting beta-2 agonist, has been approved for the long-term, once-daily, maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease, including chronic bronchitis and/or emphysema.
It has also been approved to reduce chronic obstructive pulmonary disease (COPD) exacerbations in patients with a history of exacerbations, according to a statement issued May 10 by the Food and Drug Administration. In studies of 7,700 patients diagnosed with COPD, those treated with the inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination "showed improved lung function and reduced exacerbations compared to placebo," the statement said.
The fixed-dose combination of 100 mcg of fluticasone furoate with 25 mcg of vilanterol is formulated in a dry powder. It is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which developed the product with Theravance. The product will be marketed as Breo Ellipta.
As with other LABAs, the prescribing information for this product includes a boxed warning about the risk of asthma-related deaths, although it is not approved for treating asthma. Nasopharyngitis, oral candidiasis, headache, and upper respiratory tract infections were among the most common side effects reported by patients using the product, according to the FDA.
The approval was announced less than a month after the majority of the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted to support approval of the product for long-term maintenance treatment of airflow obstruction and reducing COPD exacerbations. The panel nearly unanimously agreed that the treatment had "clinically meaningful" benefit as a long-term maintenance treatment for airflow obstruction They voted 8-5 that the data provided "substantial evidence" that reductions in exacerbations were clinically meaningful.
The two inhaled ICS/LABA treatments approved by the FDA for COPD are the combination of fluticasone propionate and salmeterol (Advair Diskus), also marketed by GSK, and the combination of budesonide and formoterol (Symbicort). Both are administered twice a day. Salmeterol and formoterol are both available as separate products to treat COPD. Vilanterol, which is the LABA component of Breo Ellipta, will not be available separately.
The label for Breo Ellipta can be found here.
An inhaled powder formulation of the corticosteroid fluticasone furoate and vilanterol, a long-acting beta-2 agonist, has been approved for the long-term, once-daily, maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease, including chronic bronchitis and/or emphysema.
It has also been approved to reduce chronic obstructive pulmonary disease (COPD) exacerbations in patients with a history of exacerbations, according to a statement issued May 10 by the Food and Drug Administration. In studies of 7,700 patients diagnosed with COPD, those treated with the inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination "showed improved lung function and reduced exacerbations compared to placebo," the statement said.
The fixed-dose combination of 100 mcg of fluticasone furoate with 25 mcg of vilanterol is formulated in a dry powder. It is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which developed the product with Theravance. The product will be marketed as Breo Ellipta.
As with other LABAs, the prescribing information for this product includes a boxed warning about the risk of asthma-related deaths, although it is not approved for treating asthma. Nasopharyngitis, oral candidiasis, headache, and upper respiratory tract infections were among the most common side effects reported by patients using the product, according to the FDA.
The approval was announced less than a month after the majority of the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted to support approval of the product for long-term maintenance treatment of airflow obstruction and reducing COPD exacerbations. The panel nearly unanimously agreed that the treatment had "clinically meaningful" benefit as a long-term maintenance treatment for airflow obstruction They voted 8-5 that the data provided "substantial evidence" that reductions in exacerbations were clinically meaningful.
The two inhaled ICS/LABA treatments approved by the FDA for COPD are the combination of fluticasone propionate and salmeterol (Advair Diskus), also marketed by GSK, and the combination of budesonide and formoterol (Symbicort). Both are administered twice a day. Salmeterol and formoterol are both available as separate products to treat COPD. Vilanterol, which is the LABA component of Breo Ellipta, will not be available separately.
The label for Breo Ellipta can be found here.
An inhaled powder formulation of the corticosteroid fluticasone furoate and vilanterol, a long-acting beta-2 agonist, has been approved for the long-term, once-daily, maintenance treatment of airflow obstruction in patients with chronic obstructive pulmonary disease, including chronic bronchitis and/or emphysema.
It has also been approved to reduce chronic obstructive pulmonary disease (COPD) exacerbations in patients with a history of exacerbations, according to a statement issued May 10 by the Food and Drug Administration. In studies of 7,700 patients diagnosed with COPD, those treated with the inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) combination "showed improved lung function and reduced exacerbations compared to placebo," the statement said.
The fixed-dose combination of 100 mcg of fluticasone furoate with 25 mcg of vilanterol is formulated in a dry powder. It is administered once a day in a new inhaler that provides 30 doses, according to GlaxoSmithKline, which developed the product with Theravance. The product will be marketed as Breo Ellipta.
As with other LABAs, the prescribing information for this product includes a boxed warning about the risk of asthma-related deaths, although it is not approved for treating asthma. Nasopharyngitis, oral candidiasis, headache, and upper respiratory tract infections were among the most common side effects reported by patients using the product, according to the FDA.
The approval was announced less than a month after the majority of the FDA’s Pulmonary-Allergy Drugs Advisory Committee voted to support approval of the product for long-term maintenance treatment of airflow obstruction and reducing COPD exacerbations. The panel nearly unanimously agreed that the treatment had "clinically meaningful" benefit as a long-term maintenance treatment for airflow obstruction They voted 8-5 that the data provided "substantial evidence" that reductions in exacerbations were clinically meaningful.
The two inhaled ICS/LABA treatments approved by the FDA for COPD are the combination of fluticasone propionate and salmeterol (Advair Diskus), also marketed by GSK, and the combination of budesonide and formoterol (Symbicort). Both are administered twice a day. Salmeterol and formoterol are both available as separate products to treat COPD. Vilanterol, which is the LABA component of Breo Ellipta, will not be available separately.
The label for Breo Ellipta can be found here.
AAP guidelines have changed bronchiolitis management
WASHINGTON – The use of radiographs, viral testing, steroids, and bronchodilators for young children with bronchiolitis has declined significantly since the introduction of the American Academy of Pediatrics’ diagnostic and management guidelines.
Before the guidelines were released in 2006 (Pediatrics 2006;118:1774-93), use of all these diagnostic and treatment modalities was on the rise, Dr. Kavita Parikh said at the annual meeting of the Pediatric Academic Societies.

Her retrospective study of more than 130,000 cases demonstrated that the document has had a positive impact on the way bronchiolitis is now managed.
"The AAP practice guideline advocates primarily supportive care," said Dr. Parikh, a pediatric hospitalist at Children’s National Medical Center, Washington. "And as many of us now know, less is more for this illness."
The cases for this study came from a large hospital administration database covering 43 facilities. Dr. Parikh compared diagnostic and treatment resource utilization in three periods: November 2004 to March 2005 (pre-guidelines), November 2007 to March 2008 (early post-guidelines), and November 2011 to March 2012 (late post-guidelines).
The study examined changes in four diagnostic measures (complete blood count [CBC], chest x-rays, respiratory syncytial virus testing, and influenza testing) and three treatment measures (steroids, bronchodilators, and antibiotics).
The study cohort comprised 130,262 children, with a mean age of 4 months. Most (59%) were covered by public insurance.
In the pre-guideline period, CBC was employed in 35% of cases, chest x-ray and RSV testing each in 61%, and influenza testing in 32%. These numbers were essentially unchanged in the early post-guidelines period, but by the late post-guidelines period the recommendations were taking root. All of the measures had decreased significantly: CBC use had gone down by 6%, chest x-rays by about 11%, RSV testing by 20%, and influenza testing by 12%.
Treatment measures changed as well, Dr. Parikh said.
In the pre-guidelines period, steroids were employed in 25% of cases, bronchodilators in 65%, and antibiotics in 34%. Again, the numbers were similar in the early post-guidelines period. By the late post-guidelines period, however, steroid and bronchodilator use had both dropped by 9%. Antibiotic use rose by 3% in the early post-guidelines period but decreased again later for a net change of about 2%. The difference was statistically significant but probably not clinically relevant, Dr. Parikh noted.
"The AAP guidelines have apparently had a positive effect on the way we deal with bronchiolitis, with the greatest impact on chest x-ray, steroid, and bronchodilator use," she said. "We want to continue to look at this and compare local practices to further evaluate implementation by region and hospital type."
Dr. Parikh said that she had no financial disclosures.
WASHINGTON – The use of radiographs, viral testing, steroids, and bronchodilators for young children with bronchiolitis has declined significantly since the introduction of the American Academy of Pediatrics’ diagnostic and management guidelines.
Before the guidelines were released in 2006 (Pediatrics 2006;118:1774-93), use of all these diagnostic and treatment modalities was on the rise, Dr. Kavita Parikh said at the annual meeting of the Pediatric Academic Societies.
Her retrospective study of more than 130,000 cases demonstrated that the document has had a positive impact on the way bronchiolitis is now managed.
"The AAP practice guideline advocates primarily supportive care," said Dr. Parikh, a pediatric hospitalist at Children’s National Medical Center, Washington. "And as many of us now know, less is more for this illness."
The cases for this study came from a large hospital administration database covering 43 facilities. Dr. Parikh compared diagnostic and treatment resource utilization in three periods: November 2004 to March 2005 (pre-guidelines), November 2007 to March 2008 (early post-guidelines), and November 2011 to March 2012 (late post-guidelines).
The study examined changes in four diagnostic measures (complete blood count [CBC], chest x-rays, respiratory syncytial virus testing, and influenza testing) and three treatment measures (steroids, bronchodilators, and antibiotics).
The study cohort comprised 130,262 children, with a mean age of 4 months. Most (59%) were covered by public insurance.
In the pre-guideline period, CBC was employed in 35% of cases, chest x-ray and RSV testing each in 61%, and influenza testing in 32%. These numbers were essentially unchanged in the early post-guidelines period, but by the late post-guidelines period the recommendations were taking root. All of the measures had decreased significantly: CBC use had gone down by 6%, chest x-rays by about 11%, RSV testing by 20%, and influenza testing by 12%.
Treatment measures changed as well, Dr. Parikh said.
In the pre-guidelines period, steroids were employed in 25% of cases, bronchodilators in 65%, and antibiotics in 34%. Again, the numbers were similar in the early post-guidelines period. By the late post-guidelines period, however, steroid and bronchodilator use had both dropped by 9%. Antibiotic use rose by 3% in the early post-guidelines period but decreased again later for a net change of about 2%. The difference was statistically significant but probably not clinically relevant, Dr. Parikh noted.
"The AAP guidelines have apparently had a positive effect on the way we deal with bronchiolitis, with the greatest impact on chest x-ray, steroid, and bronchodilator use," she said. "We want to continue to look at this and compare local practices to further evaluate implementation by region and hospital type."
Dr. Parikh said that she had no financial disclosures.
WASHINGTON – The use of radiographs, viral testing, steroids, and bronchodilators for young children with bronchiolitis has declined significantly since the introduction of the American Academy of Pediatrics’ diagnostic and management guidelines.
Before the guidelines were released in 2006 (Pediatrics 2006;118:1774-93), use of all these diagnostic and treatment modalities was on the rise, Dr. Kavita Parikh said at the annual meeting of the Pediatric Academic Societies.
Her retrospective study of more than 130,000 cases demonstrated that the document has had a positive impact on the way bronchiolitis is now managed.
"The AAP practice guideline advocates primarily supportive care," said Dr. Parikh, a pediatric hospitalist at Children’s National Medical Center, Washington. "And as many of us now know, less is more for this illness."
The cases for this study came from a large hospital administration database covering 43 facilities. Dr. Parikh compared diagnostic and treatment resource utilization in three periods: November 2004 to March 2005 (pre-guidelines), November 2007 to March 2008 (early post-guidelines), and November 2011 to March 2012 (late post-guidelines).
The study examined changes in four diagnostic measures (complete blood count [CBC], chest x-rays, respiratory syncytial virus testing, and influenza testing) and three treatment measures (steroids, bronchodilators, and antibiotics).
The study cohort comprised 130,262 children, with a mean age of 4 months. Most (59%) were covered by public insurance.
In the pre-guideline period, CBC was employed in 35% of cases, chest x-ray and RSV testing each in 61%, and influenza testing in 32%. These numbers were essentially unchanged in the early post-guidelines period, but by the late post-guidelines period the recommendations were taking root. All of the measures had decreased significantly: CBC use had gone down by 6%, chest x-rays by about 11%, RSV testing by 20%, and influenza testing by 12%.
Treatment measures changed as well, Dr. Parikh said.
In the pre-guidelines period, steroids were employed in 25% of cases, bronchodilators in 65%, and antibiotics in 34%. Again, the numbers were similar in the early post-guidelines period. By the late post-guidelines period, however, steroid and bronchodilator use had both dropped by 9%. Antibiotic use rose by 3% in the early post-guidelines period but decreased again later for a net change of about 2%. The difference was statistically significant but probably not clinically relevant, Dr. Parikh noted.
"The AAP guidelines have apparently had a positive effect on the way we deal with bronchiolitis, with the greatest impact on chest x-ray, steroid, and bronchodilator use," she said. "We want to continue to look at this and compare local practices to further evaluate implementation by region and hospital type."
Dr. Parikh said that she had no financial disclosures.
AT THE PAS ANNUAL MEETING
Major finding: Nonrecommended diagnostic and treatment method utilization in bronchiolitis cases decreased by up to 20% within 6 years of the release of disease management guidelines.
Data source: The records review included more than 130,000 cases over an 8-year period.
Disclosures: Dr. Parikh said that she had no financial disclosures.
