User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Diagnosis and management of group A streptococcal pharyngitis
Pharyngitis is the major concern for greater than 15 million annual visits to primary care physicians in the United States. Although group A Streptococcus (GAS) is the most common bacterial cause of acute pharyngitis, only 20%-30% of school-age children and only 5%-15% of adults who present to a physician with a sore throat will turn out to have GAS pharyngitis. Treatment of GAS pharyngitis with antibiotics helps to avoid suppurative complications (for example, peritonsillar abscesses, cervical lymphadenitis, etc.), prevent acute rheumatic fever, improve clinical symptoms, decrease contagious transmission to close contacts of the patient, and allow for rapid resumption of normal activities. However, routine empiric treatment of patients with pharyngitis or upper respiratory tract infections with antibiotics has contributed greatly to the worsening of antimicrobial resistance among many common pathogens while failing to provide clinical benefit to patients with pharyngitis that is not caused by GAS. Nationally up to 70% of patients seen in primary care settings for a sore throat are prescribed antibiotics, despite the much lower incidence of GAS pharyngitis. The IDSA guidelines on the diagnosis and management of group A streptococcal pharyngitis provide a comprehensive evidence based statement addressing questions discussed below.
How should the diagnosis of GAS pharyngitis be established?

Diagnosis should be made by throat swab and testing by rapid antigen detection test (RADT) and/or throat culture. Both tonsils, or tonsillar fossae, and posterior pharynx should be swabbed to provide an accurate and adequate sample. RADTs are approximately 95% specific and have a sensitivity of 70%-90%. This means that a positive rapid strep test is most likely a true positive, representing group A pharyngitis. There is no need for confirmatory culture to be performed. A negative rapid strep result, because of its lack of sensitivity, may reflect a false-negative result, meaning that there is a chance that the individual has strep even with a negative test. The likelihood of a false-negative test is highest in those with the greatest likelihood of having GAS: children or people whose clinical picture based on history, symptoms, and signs appear most likely to have strep. In children and adolescents, negative RADTs should have a throat culture performed because of the high incidence of GAS-causing pharyngitis in children, and the likelihood that a negative RADT is inaccurate. Adults with negative RADTs do not warrant additional testing as the incidence of GAS is much lower among adults than children. There is no role for using antistreptococcal antibody titers to help diagnose acute GAS pharyngitis.
Who should undergo testing for GAS pharyngitis?
GAS testing should be performed for individuals with a reasonable likelihood of their pharyngitis being caused by GAS. Testing is not indicated in patients with pharyngitis and symptoms strongly suggestive of viral infection (for example, cough, rhinorrhea, hoarseness, and oral ulcers). In children younger than 3 years old, the incidence of GAS pharyngitis is very low, and testing should be used only in patients who have other risk factors, such as a close household contact with GAS pharyngitis. While GAS causes only 5%-15% of pharyngitis cases in adults, adults with school age children and those who work around children are at an increased risk for GAS pharyngitis. The routine testing of asymptomatic household contacts of patients with GAS pharyngitis is not indicated.
What are the treatment recommendations for patients diagnosed with GAS pharyngitis?
Treatment recommendations for GAS start with narrow spectrum, inexpensive, beta-lactams. Once daily amoxicillin (50 mg/kg [max 1,000 mg]) given for 10 days has been shown to be effective for GAS pharyngitis and is now among the approved regimens. Additional regimens include 10 days of penicillin VK, 250 mg two to three times daily for children; 250 mg four times daily or 500 mg twice daily for adolescents and adults; or 10 days of amoxicillin, 25 mg/kg (max 500 mg) twice daily for adults. Treatment regimens for patients with penicillin allergy include cephalexin 20 mg/kg (max 500 mg) twice daily for 10 days; cefadroxil 30 mg/kg (max 1,000 mg) for 10 days; clindamycin 7 mg/kg per dose (max 300 mg/dose) three times daily for 10 days; or azithromycin 12 mg/kg (max 500 mg) once daily for 5 days; clarithromycin 7.5mg/kg per dose (max 250 mg/dose) twice daily for 10 days. Because of poorer evidence and broader spectrum, the IDSA does not recommended later-generation cephalosporins for the treatment of GAS pharyngitis. Some evidence suggests that because of developing macrolide resistance, 10 days of clarithromycin may be more effective treatment than the shorter 5-day course of azithromycin. Adjunctive therapy with an analgesic/antipyretic to control pain or fever is appropriate, but aspirin should be avoided in children, and corticosteroids are not recommended.
Is the patient with frequent recurrent episodes of apparent GAS pharyngitis likely to be a carrier of pharyngeal GAS?
Clinicians should consider the possibility that some patients with frequent recurrent episodes of GAS pharyngitis may be chronic carriers of GAS and may be experiencing frequent viral infections. Since GAS carriers are unlikely to spread or cause GAS pharyngitis in close contacts, identification of GAS carriers and treatment with the goal of eradication of GAS is not indicated. During winter and spring, as many as 20% of asymptomatic school-age children may be GAS carriers. Tonsillectomy is not recommended solely to reduce GAS pharyngitis episodes.
The bottom line
GAS pharyngitis should be diagnosed with RADTs or throat culture. Treatment options for GAS pharyngitis should start with narrow spectrum beta-lactams, with once-daily amoxicillin now recommended as a treatment option.
Shulman et al. "Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America" (Clin. Infect. Dis. 2012 [doi: 10.1093/cid/cis629]).
Dr. Skolnik is an associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Guthrie is a third-year resident in the hospital’s family medicine program.
Pharyngitis is the major concern for greater than 15 million annual visits to primary care physicians in the United States. Although group A Streptococcus (GAS) is the most common bacterial cause of acute pharyngitis, only 20%-30% of school-age children and only 5%-15% of adults who present to a physician with a sore throat will turn out to have GAS pharyngitis. Treatment of GAS pharyngitis with antibiotics helps to avoid suppurative complications (for example, peritonsillar abscesses, cervical lymphadenitis, etc.), prevent acute rheumatic fever, improve clinical symptoms, decrease contagious transmission to close contacts of the patient, and allow for rapid resumption of normal activities. However, routine empiric treatment of patients with pharyngitis or upper respiratory tract infections with antibiotics has contributed greatly to the worsening of antimicrobial resistance among many common pathogens while failing to provide clinical benefit to patients with pharyngitis that is not caused by GAS. Nationally up to 70% of patients seen in primary care settings for a sore throat are prescribed antibiotics, despite the much lower incidence of GAS pharyngitis. The IDSA guidelines on the diagnosis and management of group A streptococcal pharyngitis provide a comprehensive evidence based statement addressing questions discussed below.
How should the diagnosis of GAS pharyngitis be established?
Diagnosis should be made by throat swab and testing by rapid antigen detection test (RADT) and/or throat culture. Both tonsils, or tonsillar fossae, and posterior pharynx should be swabbed to provide an accurate and adequate sample. RADTs are approximately 95% specific and have a sensitivity of 70%-90%. This means that a positive rapid strep test is most likely a true positive, representing group A pharyngitis. There is no need for confirmatory culture to be performed. A negative rapid strep result, because of its lack of sensitivity, may reflect a false-negative result, meaning that there is a chance that the individual has strep even with a negative test. The likelihood of a false-negative test is highest in those with the greatest likelihood of having GAS: children or people whose clinical picture based on history, symptoms, and signs appear most likely to have strep. In children and adolescents, negative RADTs should have a throat culture performed because of the high incidence of GAS-causing pharyngitis in children, and the likelihood that a negative RADT is inaccurate. Adults with negative RADTs do not warrant additional testing as the incidence of GAS is much lower among adults than children. There is no role for using antistreptococcal antibody titers to help diagnose acute GAS pharyngitis.
Who should undergo testing for GAS pharyngitis?
GAS testing should be performed for individuals with a reasonable likelihood of their pharyngitis being caused by GAS. Testing is not indicated in patients with pharyngitis and symptoms strongly suggestive of viral infection (for example, cough, rhinorrhea, hoarseness, and oral ulcers). In children younger than 3 years old, the incidence of GAS pharyngitis is very low, and testing should be used only in patients who have other risk factors, such as a close household contact with GAS pharyngitis. While GAS causes only 5%-15% of pharyngitis cases in adults, adults with school age children and those who work around children are at an increased risk for GAS pharyngitis. The routine testing of asymptomatic household contacts of patients with GAS pharyngitis is not indicated.
What are the treatment recommendations for patients diagnosed with GAS pharyngitis?
Treatment recommendations for GAS start with narrow spectrum, inexpensive, beta-lactams. Once daily amoxicillin (50 mg/kg [max 1,000 mg]) given for 10 days has been shown to be effective for GAS pharyngitis and is now among the approved regimens. Additional regimens include 10 days of penicillin VK, 250 mg two to three times daily for children; 250 mg four times daily or 500 mg twice daily for adolescents and adults; or 10 days of amoxicillin, 25 mg/kg (max 500 mg) twice daily for adults. Treatment regimens for patients with penicillin allergy include cephalexin 20 mg/kg (max 500 mg) twice daily for 10 days; cefadroxil 30 mg/kg (max 1,000 mg) for 10 days; clindamycin 7 mg/kg per dose (max 300 mg/dose) three times daily for 10 days; or azithromycin 12 mg/kg (max 500 mg) once daily for 5 days; clarithromycin 7.5mg/kg per dose (max 250 mg/dose) twice daily for 10 days. Because of poorer evidence and broader spectrum, the IDSA does not recommended later-generation cephalosporins for the treatment of GAS pharyngitis. Some evidence suggests that because of developing macrolide resistance, 10 days of clarithromycin may be more effective treatment than the shorter 5-day course of azithromycin. Adjunctive therapy with an analgesic/antipyretic to control pain or fever is appropriate, but aspirin should be avoided in children, and corticosteroids are not recommended.
Is the patient with frequent recurrent episodes of apparent GAS pharyngitis likely to be a carrier of pharyngeal GAS?
Clinicians should consider the possibility that some patients with frequent recurrent episodes of GAS pharyngitis may be chronic carriers of GAS and may be experiencing frequent viral infections. Since GAS carriers are unlikely to spread or cause GAS pharyngitis in close contacts, identification of GAS carriers and treatment with the goal of eradication of GAS is not indicated. During winter and spring, as many as 20% of asymptomatic school-age children may be GAS carriers. Tonsillectomy is not recommended solely to reduce GAS pharyngitis episodes.
The bottom line
GAS pharyngitis should be diagnosed with RADTs or throat culture. Treatment options for GAS pharyngitis should start with narrow spectrum beta-lactams, with once-daily amoxicillin now recommended as a treatment option.
Shulman et al. "Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America" (Clin. Infect. Dis. 2012 [doi: 10.1093/cid/cis629]).
Dr. Skolnik is an associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Guthrie is a third-year resident in the hospital’s family medicine program.
Pharyngitis is the major concern for greater than 15 million annual visits to primary care physicians in the United States. Although group A Streptococcus (GAS) is the most common bacterial cause of acute pharyngitis, only 20%-30% of school-age children and only 5%-15% of adults who present to a physician with a sore throat will turn out to have GAS pharyngitis. Treatment of GAS pharyngitis with antibiotics helps to avoid suppurative complications (for example, peritonsillar abscesses, cervical lymphadenitis, etc.), prevent acute rheumatic fever, improve clinical symptoms, decrease contagious transmission to close contacts of the patient, and allow for rapid resumption of normal activities. However, routine empiric treatment of patients with pharyngitis or upper respiratory tract infections with antibiotics has contributed greatly to the worsening of antimicrobial resistance among many common pathogens while failing to provide clinical benefit to patients with pharyngitis that is not caused by GAS. Nationally up to 70% of patients seen in primary care settings for a sore throat are prescribed antibiotics, despite the much lower incidence of GAS pharyngitis. The IDSA guidelines on the diagnosis and management of group A streptococcal pharyngitis provide a comprehensive evidence based statement addressing questions discussed below.
How should the diagnosis of GAS pharyngitis be established?
Diagnosis should be made by throat swab and testing by rapid antigen detection test (RADT) and/or throat culture. Both tonsils, or tonsillar fossae, and posterior pharynx should be swabbed to provide an accurate and adequate sample. RADTs are approximately 95% specific and have a sensitivity of 70%-90%. This means that a positive rapid strep test is most likely a true positive, representing group A pharyngitis. There is no need for confirmatory culture to be performed. A negative rapid strep result, because of its lack of sensitivity, may reflect a false-negative result, meaning that there is a chance that the individual has strep even with a negative test. The likelihood of a false-negative test is highest in those with the greatest likelihood of having GAS: children or people whose clinical picture based on history, symptoms, and signs appear most likely to have strep. In children and adolescents, negative RADTs should have a throat culture performed because of the high incidence of GAS-causing pharyngitis in children, and the likelihood that a negative RADT is inaccurate. Adults with negative RADTs do not warrant additional testing as the incidence of GAS is much lower among adults than children. There is no role for using antistreptococcal antibody titers to help diagnose acute GAS pharyngitis.
Who should undergo testing for GAS pharyngitis?
GAS testing should be performed for individuals with a reasonable likelihood of their pharyngitis being caused by GAS. Testing is not indicated in patients with pharyngitis and symptoms strongly suggestive of viral infection (for example, cough, rhinorrhea, hoarseness, and oral ulcers). In children younger than 3 years old, the incidence of GAS pharyngitis is very low, and testing should be used only in patients who have other risk factors, such as a close household contact with GAS pharyngitis. While GAS causes only 5%-15% of pharyngitis cases in adults, adults with school age children and those who work around children are at an increased risk for GAS pharyngitis. The routine testing of asymptomatic household contacts of patients with GAS pharyngitis is not indicated.
What are the treatment recommendations for patients diagnosed with GAS pharyngitis?
Treatment recommendations for GAS start with narrow spectrum, inexpensive, beta-lactams. Once daily amoxicillin (50 mg/kg [max 1,000 mg]) given for 10 days has been shown to be effective for GAS pharyngitis and is now among the approved regimens. Additional regimens include 10 days of penicillin VK, 250 mg two to three times daily for children; 250 mg four times daily or 500 mg twice daily for adolescents and adults; or 10 days of amoxicillin, 25 mg/kg (max 500 mg) twice daily for adults. Treatment regimens for patients with penicillin allergy include cephalexin 20 mg/kg (max 500 mg) twice daily for 10 days; cefadroxil 30 mg/kg (max 1,000 mg) for 10 days; clindamycin 7 mg/kg per dose (max 300 mg/dose) three times daily for 10 days; or azithromycin 12 mg/kg (max 500 mg) once daily for 5 days; clarithromycin 7.5mg/kg per dose (max 250 mg/dose) twice daily for 10 days. Because of poorer evidence and broader spectrum, the IDSA does not recommended later-generation cephalosporins for the treatment of GAS pharyngitis. Some evidence suggests that because of developing macrolide resistance, 10 days of clarithromycin may be more effective treatment than the shorter 5-day course of azithromycin. Adjunctive therapy with an analgesic/antipyretic to control pain or fever is appropriate, but aspirin should be avoided in children, and corticosteroids are not recommended.
Is the patient with frequent recurrent episodes of apparent GAS pharyngitis likely to be a carrier of pharyngeal GAS?
Clinicians should consider the possibility that some patients with frequent recurrent episodes of GAS pharyngitis may be chronic carriers of GAS and may be experiencing frequent viral infections. Since GAS carriers are unlikely to spread or cause GAS pharyngitis in close contacts, identification of GAS carriers and treatment with the goal of eradication of GAS is not indicated. During winter and spring, as many as 20% of asymptomatic school-age children may be GAS carriers. Tonsillectomy is not recommended solely to reduce GAS pharyngitis episodes.
The bottom line
GAS pharyngitis should be diagnosed with RADTs or throat culture. Treatment options for GAS pharyngitis should start with narrow spectrum beta-lactams, with once-daily amoxicillin now recommended as a treatment option.
Shulman et al. "Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America" (Clin. Infect. Dis. 2012 [doi: 10.1093/cid/cis629]).
Dr. Skolnik is an associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Guthrie is a third-year resident in the hospital’s family medicine program.

Ganetespib trial hints at survival benefit in lung adenocarcinoma
CHICAGO – A novel heat-shock protein inhibitor, ganetespib, showed glimmers of a survival benefit for lung cancer patients in a randomized phase II trial presented at the annual meeting of the American Society of Clinical Oncology.
Tested in combination with docetaxel, the experimental drug appeared to improve overall and progression-free survival, compared with docetaxel alone, as second-line therapy for patients with advanced non–small cell adenocarcinoma of the lung, Dr. Suresh Ramalingam reported.
Neither measure, however, was a primary end point of the study. Heat-shock protein 90 is a chaperone protein that activates other proteins binding to it so that they can perform their normal cellular function. Ganetespib binds to and inhibits Hsp90, causing oncoproteins to become inactivated and to degrade before they have had a chance to unfold into their functional configuration.

In the randomized phase II GALAXY-1 study, median progression-free survival reached 4.5 months among 125 patients assigned to ganetespib and docetaxel, compared with 3.2 months for 127 patients assigned to docetaxel and placebo (hazard ratio, 0.84; P = .038) in an unadjusted analysis.
However, after adjusting for sex, smoking status, lactate dehydrogenase (LDH), performance status, interval since diagnosis, and other common factors, the difference was no longer significant, said Dr. Ramalingam, chief of thoracic oncology and director of medical oncology, at Emory University in Atlanta.
Overall survival, in contrast, was not significantly different in an unadjusted analysis, at a median of 9.8 months for the combination and 7.4 months for docetaxel alone (HR, 0.82), but became significant after adjustment for potential confounders (adjusted HR, 0.73; P = .041).
"This is a first-in-class study showing the potential efficacy of this compound, and I think it presents a potential advance in an area of lung cancer where we haven’t had advances in a long time, and we’re all eagerly awaiting the outcome of the phase III trial," said Dr. Marjorie Zauderer, a medical oncologist and lung cancer specialist at Memorial Sloan-Kettering Cancer Center, New York.
Dr. Zauderer was not involved in the study, but commented on it in a briefing held prior to the presentation of data later in the day.
Overall survival and progression-free survival were secondary end points in the trial. The co-primary end points were progression-free survival in patients with elevated LDH levels or tumors with mutations in KRAS, but these data were not reported. According to Synta Pharmaceuticals, maker of ganetespib, neither KRAS nor epidermal growth factor receptor (EGFR) mutations correlated with an overall survival benefit for the experimental arm of the trial.
When the investigators looked at only those patients who had been diagnosed more than 6 months before being enrolled in the trial (the "6-month population") they found that, in both unadjusted and adjusted analyses, the ganetespib and docetaxel combination was superior to docetaxel and placebo, with median overall survival of 10.7 vs. 6.4 months (unadjusted HR, 0.61; P = .0093; adjusted HR, 0.55; P = .0036), and median progression-free survival of 5.4 vs. 3.4 months (unadjusted HR, 0.61, P = .0041; adjusted HR, 0.62, P = .0075).
About 70% of the patients in the trial were included in the 6-month population. The follow-on GALAXY-2 phase III trial will enroll only those patients who have lived with an adenocarcinoma diagnosis for at least 6 months, the population that derived the greatest benefit in the current study.
The ganetespib and docetaxel combination was generally well tolerated, with manageable mild-to-moderate diarrhea being the most common adverse event.
The study was sponsored by Synta Pharmaceuticals. Dr. Ramalingam said that his institution receives research support from the company but that he had no personal financial disclosures. Dr. Zauderer reported having no conflicts of interest.
CHICAGO – A novel heat-shock protein inhibitor, ganetespib, showed glimmers of a survival benefit for lung cancer patients in a randomized phase II trial presented at the annual meeting of the American Society of Clinical Oncology.
Tested in combination with docetaxel, the experimental drug appeared to improve overall and progression-free survival, compared with docetaxel alone, as second-line therapy for patients with advanced non–small cell adenocarcinoma of the lung, Dr. Suresh Ramalingam reported.
Neither measure, however, was a primary end point of the study. Heat-shock protein 90 is a chaperone protein that activates other proteins binding to it so that they can perform their normal cellular function. Ganetespib binds to and inhibits Hsp90, causing oncoproteins to become inactivated and to degrade before they have had a chance to unfold into their functional configuration.
In the randomized phase II GALAXY-1 study, median progression-free survival reached 4.5 months among 125 patients assigned to ganetespib and docetaxel, compared with 3.2 months for 127 patients assigned to docetaxel and placebo (hazard ratio, 0.84; P = .038) in an unadjusted analysis.
However, after adjusting for sex, smoking status, lactate dehydrogenase (LDH), performance status, interval since diagnosis, and other common factors, the difference was no longer significant, said Dr. Ramalingam, chief of thoracic oncology and director of medical oncology, at Emory University in Atlanta.
Overall survival, in contrast, was not significantly different in an unadjusted analysis, at a median of 9.8 months for the combination and 7.4 months for docetaxel alone (HR, 0.82), but became significant after adjustment for potential confounders (adjusted HR, 0.73; P = .041).
"This is a first-in-class study showing the potential efficacy of this compound, and I think it presents a potential advance in an area of lung cancer where we haven’t had advances in a long time, and we’re all eagerly awaiting the outcome of the phase III trial," said Dr. Marjorie Zauderer, a medical oncologist and lung cancer specialist at Memorial Sloan-Kettering Cancer Center, New York.
Dr. Zauderer was not involved in the study, but commented on it in a briefing held prior to the presentation of data later in the day.
Overall survival and progression-free survival were secondary end points in the trial. The co-primary end points were progression-free survival in patients with elevated LDH levels or tumors with mutations in KRAS, but these data were not reported. According to Synta Pharmaceuticals, maker of ganetespib, neither KRAS nor epidermal growth factor receptor (EGFR) mutations correlated with an overall survival benefit for the experimental arm of the trial.
When the investigators looked at only those patients who had been diagnosed more than 6 months before being enrolled in the trial (the "6-month population") they found that, in both unadjusted and adjusted analyses, the ganetespib and docetaxel combination was superior to docetaxel and placebo, with median overall survival of 10.7 vs. 6.4 months (unadjusted HR, 0.61; P = .0093; adjusted HR, 0.55; P = .0036), and median progression-free survival of 5.4 vs. 3.4 months (unadjusted HR, 0.61, P = .0041; adjusted HR, 0.62, P = .0075).
About 70% of the patients in the trial were included in the 6-month population. The follow-on GALAXY-2 phase III trial will enroll only those patients who have lived with an adenocarcinoma diagnosis for at least 6 months, the population that derived the greatest benefit in the current study.
The ganetespib and docetaxel combination was generally well tolerated, with manageable mild-to-moderate diarrhea being the most common adverse event.
The study was sponsored by Synta Pharmaceuticals. Dr. Ramalingam said that his institution receives research support from the company but that he had no personal financial disclosures. Dr. Zauderer reported having no conflicts of interest.
CHICAGO – A novel heat-shock protein inhibitor, ganetespib, showed glimmers of a survival benefit for lung cancer patients in a randomized phase II trial presented at the annual meeting of the American Society of Clinical Oncology.
Tested in combination with docetaxel, the experimental drug appeared to improve overall and progression-free survival, compared with docetaxel alone, as second-line therapy for patients with advanced non–small cell adenocarcinoma of the lung, Dr. Suresh Ramalingam reported.
Neither measure, however, was a primary end point of the study. Heat-shock protein 90 is a chaperone protein that activates other proteins binding to it so that they can perform their normal cellular function. Ganetespib binds to and inhibits Hsp90, causing oncoproteins to become inactivated and to degrade before they have had a chance to unfold into their functional configuration.
In the randomized phase II GALAXY-1 study, median progression-free survival reached 4.5 months among 125 patients assigned to ganetespib and docetaxel, compared with 3.2 months for 127 patients assigned to docetaxel and placebo (hazard ratio, 0.84; P = .038) in an unadjusted analysis.
However, after adjusting for sex, smoking status, lactate dehydrogenase (LDH), performance status, interval since diagnosis, and other common factors, the difference was no longer significant, said Dr. Ramalingam, chief of thoracic oncology and director of medical oncology, at Emory University in Atlanta.
Overall survival, in contrast, was not significantly different in an unadjusted analysis, at a median of 9.8 months for the combination and 7.4 months for docetaxel alone (HR, 0.82), but became significant after adjustment for potential confounders (adjusted HR, 0.73; P = .041).
"This is a first-in-class study showing the potential efficacy of this compound, and I think it presents a potential advance in an area of lung cancer where we haven’t had advances in a long time, and we’re all eagerly awaiting the outcome of the phase III trial," said Dr. Marjorie Zauderer, a medical oncologist and lung cancer specialist at Memorial Sloan-Kettering Cancer Center, New York.
Dr. Zauderer was not involved in the study, but commented on it in a briefing held prior to the presentation of data later in the day.
Overall survival and progression-free survival were secondary end points in the trial. The co-primary end points were progression-free survival in patients with elevated LDH levels or tumors with mutations in KRAS, but these data were not reported. According to Synta Pharmaceuticals, maker of ganetespib, neither KRAS nor epidermal growth factor receptor (EGFR) mutations correlated with an overall survival benefit for the experimental arm of the trial.
When the investigators looked at only those patients who had been diagnosed more than 6 months before being enrolled in the trial (the "6-month population") they found that, in both unadjusted and adjusted analyses, the ganetespib and docetaxel combination was superior to docetaxel and placebo, with median overall survival of 10.7 vs. 6.4 months (unadjusted HR, 0.61; P = .0093; adjusted HR, 0.55; P = .0036), and median progression-free survival of 5.4 vs. 3.4 months (unadjusted HR, 0.61, P = .0041; adjusted HR, 0.62, P = .0075).
About 70% of the patients in the trial were included in the 6-month population. The follow-on GALAXY-2 phase III trial will enroll only those patients who have lived with an adenocarcinoma diagnosis for at least 6 months, the population that derived the greatest benefit in the current study.
The ganetespib and docetaxel combination was generally well tolerated, with manageable mild-to-moderate diarrhea being the most common adverse event.
The study was sponsored by Synta Pharmaceuticals. Dr. Ramalingam said that his institution receives research support from the company but that he had no personal financial disclosures. Dr. Zauderer reported having no conflicts of interest.
AT THE ASCO ANNUAL MEETING 2013
Major finding: The ganetespib and docetaxel combination was superior to docetaxel and placebo, with median overall survival of 10.7 vs. 6.4 months and median progression-free survival of 5.4 vs. 3.4 months.
Data source: Randomized controlled phase II trial in 252 patients with advanced non–small cell adenocarcinoma of the lung.
Disclosures: The study was sponsored by Synta Pharmaceuticals. Dr. Ramalingam said that his institution receives research support from the company but that he had no personal financial disclosures. Dr. Zauderer reported having no conflicts of interest.
Treating refractory and metastatic lung cancer
CHICAGO – Dr. Roy Herbst of Yale University discusses early results for MPDL3280A, a new PD-L1 antibody for the treatment of non-small cell lung cancer; he also gives his take on other exciting lung cancer data being presented at the annual meeting of the American Society of Clinical Oncology.
CHICAGO – Dr. Roy Herbst of Yale University discusses early results for MPDL3280A, a new PD-L1 antibody for the treatment of non-small cell lung cancer; he also gives his take on other exciting lung cancer data being presented at the annual meeting of the American Society of Clinical Oncology.
CHICAGO – Dr. Roy Herbst of Yale University discusses early results for MPDL3280A, a new PD-L1 antibody for the treatment of non-small cell lung cancer; he also gives his take on other exciting lung cancer data being presented at the annual meeting of the American Society of Clinical Oncology.
AT THE ASCO ANNUAL MEETING 2013

Cough and Back Pain in a Man With COPD
ANSWER
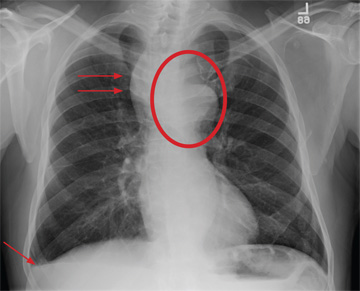
The radiograph shows some evidence of hyperinflated lungs, consistent with COPD. There is a small right effusion evident.
Of note is a superior mediastinal mass, which is causing right-sided and anterior displacement of the intrathoracic trachea. The differential includes possible adenopathy related to a carcinoma or a substernal goiter. Further diagnostic studies and surgical evaluation are warranted.
In this particular case, review of the patient’s imaging history showed he had a chest radiograph two years ago, at which time these findings were present. This favors substernal goiter as the diagnosis. Multinodular goiter was later confirmed with a thyroid ultrasound, and referral to general surgery was made.
ANSWER
The radiograph shows some evidence of hyperinflated lungs, consistent with COPD. There is a small right effusion evident.
Of note is a superior mediastinal mass, which is causing right-sided and anterior displacement of the intrathoracic trachea. The differential includes possible adenopathy related to a carcinoma or a substernal goiter. Further diagnostic studies and surgical evaluation are warranted.
In this particular case, review of the patient’s imaging history showed he had a chest radiograph two years ago, at which time these findings were present. This favors substernal goiter as the diagnosis. Multinodular goiter was later confirmed with a thyroid ultrasound, and referral to general surgery was made.
ANSWER
The radiograph shows some evidence of hyperinflated lungs, consistent with COPD. There is a small right effusion evident.
Of note is a superior mediastinal mass, which is causing right-sided and anterior displacement of the intrathoracic trachea. The differential includes possible adenopathy related to a carcinoma or a substernal goiter. Further diagnostic studies and surgical evaluation are warranted.
In this particular case, review of the patient’s imaging history showed he had a chest radiograph two years ago, at which time these findings were present. This favors substernal goiter as the diagnosis. Multinodular goiter was later confirmed with a thyroid ultrasound, and referral to general surgery was made.

A 60-year-old man presents for evaluation of fever, cough, and back pain. His symptoms have been intermittent but have worsened over the past month or so. He has had no treatment prior to today’s visit. His medical history is significant for hypertension, COPD, and chronic renal insufficiency. He denies any history of tobacco use. On physical exam, you see an older man in no obvious distress. His vital signs are stable. He is afe-brile, with a blood pressure of 150/90 mm Hg, a heart rate of 66 beats/min, and a respiratory rate of 18 breaths/min. His O2 saturation is 98% on room air. His neck is supple, with no evidence of ade-nopathy. Lung sounds are slightly decreased bilaterally, with a few crackles heard. The rest of his physical exam, overall, is normal. You order preliminary lab work as well as a chest radiograph (shown). What is your impression?

Computer prompt boosts flu vaccine rates
WASHINGTON – A pop-up on children’s electronic medical records was enough of a reminder to significantly increase influenza vaccine coverage in four large urban clinics, according to Dr. Melissa S. Stockwell.
"FluAlert" was built into the electronic medical record system and synchronized with the New York City vaccine registry. When it was activated during the winter flu season, children were 9% more likely to be fully vaccinated for influenza than when the reminder system wasn’t engaged, she said at the annual meeting of the Pediatric Academic Societies.

In addition to prompting physicians to vaccinate, the program allowed them to document reasons that the vaccine wasn’t given – a particularly valuable feature, said Dr. Stockwell, a pediatrician who is medical director of the New York–Presbyterian Hospital immunization registry.
"In this world of core measures, documentation of why a child is not vaccinated is becoming increasingly important," she said.
FluAlert was designed based on provider and parent focus groups, and implemented at four urban, community clinics that serve a primarily low-income Hispanic population. When the child’s electronic medical record opens, a FluAlert box appears at the upper-right-hand corner of the screen. The program searches both the provider registry and the larger vaccination registry and displays the vaccination status as having received no vaccine, having received one vaccine, or up to date. It asks, "Do you want to order the flu vaccine today?"
"Our providers wanted the alert to show up early in the visit, when the child’s record is opened, in order to integrate it into conversation with the parent," Dr. Stockwell said. "Doctors can ignore the message, order the vaccine, or document any reason why it wasn’t given. It’s not a forced action."
The alert also offers a look at the child’s overall immunization status, with the opportunity to order those vaccines. A "more info" button offers talking points that can be incorporated into a discussion about the importance of vaccinations.
The program was tested in a randomized study, with each clinic having an on and off period in two flu season phases (October through December and January through February).
When FluAlert was on, it fired for 8,630 visits, identifying the 62% of children who were not up to date on the vaccine. Most of those alerts (77%) came up during well-child and adolescent visits; 16% were acute care visits, 7% were visits specifically for vaccination, and the remaining visits were for Women, Infants, and Children program assessments. Providers acted on the alert 82% of the time: 53% ordered the vaccine. When they did not order the vaccine, providers noted the reason 98% of the time.
Overall, non–up-to-date children who were seen when FluAlert was on were 9% more likely to receive vaccine than children seen during an "off" period.
The program was also associated with significantly more documentation about why a child who needed the flu shot didn’t get it. In total, 625 children left the visit unvaccinated. When FluAlert was on, the reason for not vaccinating was noted for 68%; when it was off, documentation was present for only 41%.
The alert’s relative unobtrusiveness is probably one reason it was embraced as well as it was, Dr. Stockwell added. "What really annoys people is if something pops up and you can’t do anything else until you go through the entire process. So having it sit there as a gentle reminder is more appealing than something that’s always flashing and telling providers what to do."
Dr. Stockwell said she had no relevant financial disclosures
WASHINGTON – A pop-up on children’s electronic medical records was enough of a reminder to significantly increase influenza vaccine coverage in four large urban clinics, according to Dr. Melissa S. Stockwell.
"FluAlert" was built into the electronic medical record system and synchronized with the New York City vaccine registry. When it was activated during the winter flu season, children were 9% more likely to be fully vaccinated for influenza than when the reminder system wasn’t engaged, she said at the annual meeting of the Pediatric Academic Societies.
In addition to prompting physicians to vaccinate, the program allowed them to document reasons that the vaccine wasn’t given – a particularly valuable feature, said Dr. Stockwell, a pediatrician who is medical director of the New York–Presbyterian Hospital immunization registry.
"In this world of core measures, documentation of why a child is not vaccinated is becoming increasingly important," she said.
FluAlert was designed based on provider and parent focus groups, and implemented at four urban, community clinics that serve a primarily low-income Hispanic population. When the child’s electronic medical record opens, a FluAlert box appears at the upper-right-hand corner of the screen. The program searches both the provider registry and the larger vaccination registry and displays the vaccination status as having received no vaccine, having received one vaccine, or up to date. It asks, "Do you want to order the flu vaccine today?"
"Our providers wanted the alert to show up early in the visit, when the child’s record is opened, in order to integrate it into conversation with the parent," Dr. Stockwell said. "Doctors can ignore the message, order the vaccine, or document any reason why it wasn’t given. It’s not a forced action."
The alert also offers a look at the child’s overall immunization status, with the opportunity to order those vaccines. A "more info" button offers talking points that can be incorporated into a discussion about the importance of vaccinations.
The program was tested in a randomized study, with each clinic having an on and off period in two flu season phases (October through December and January through February).
When FluAlert was on, it fired for 8,630 visits, identifying the 62% of children who were not up to date on the vaccine. Most of those alerts (77%) came up during well-child and adolescent visits; 16% were acute care visits, 7% were visits specifically for vaccination, and the remaining visits were for Women, Infants, and Children program assessments. Providers acted on the alert 82% of the time: 53% ordered the vaccine. When they did not order the vaccine, providers noted the reason 98% of the time.
Overall, non–up-to-date children who were seen when FluAlert was on were 9% more likely to receive vaccine than children seen during an "off" period.
The program was also associated with significantly more documentation about why a child who needed the flu shot didn’t get it. In total, 625 children left the visit unvaccinated. When FluAlert was on, the reason for not vaccinating was noted for 68%; when it was off, documentation was present for only 41%.
The alert’s relative unobtrusiveness is probably one reason it was embraced as well as it was, Dr. Stockwell added. "What really annoys people is if something pops up and you can’t do anything else until you go through the entire process. So having it sit there as a gentle reminder is more appealing than something that’s always flashing and telling providers what to do."
Dr. Stockwell said she had no relevant financial disclosures
WASHINGTON – A pop-up on children’s electronic medical records was enough of a reminder to significantly increase influenza vaccine coverage in four large urban clinics, according to Dr. Melissa S. Stockwell.
"FluAlert" was built into the electronic medical record system and synchronized with the New York City vaccine registry. When it was activated during the winter flu season, children were 9% more likely to be fully vaccinated for influenza than when the reminder system wasn’t engaged, she said at the annual meeting of the Pediatric Academic Societies.
In addition to prompting physicians to vaccinate, the program allowed them to document reasons that the vaccine wasn’t given – a particularly valuable feature, said Dr. Stockwell, a pediatrician who is medical director of the New York–Presbyterian Hospital immunization registry.
"In this world of core measures, documentation of why a child is not vaccinated is becoming increasingly important," she said.
FluAlert was designed based on provider and parent focus groups, and implemented at four urban, community clinics that serve a primarily low-income Hispanic population. When the child’s electronic medical record opens, a FluAlert box appears at the upper-right-hand corner of the screen. The program searches both the provider registry and the larger vaccination registry and displays the vaccination status as having received no vaccine, having received one vaccine, or up to date. It asks, "Do you want to order the flu vaccine today?"
"Our providers wanted the alert to show up early in the visit, when the child’s record is opened, in order to integrate it into conversation with the parent," Dr. Stockwell said. "Doctors can ignore the message, order the vaccine, or document any reason why it wasn’t given. It’s not a forced action."
The alert also offers a look at the child’s overall immunization status, with the opportunity to order those vaccines. A "more info" button offers talking points that can be incorporated into a discussion about the importance of vaccinations.
The program was tested in a randomized study, with each clinic having an on and off period in two flu season phases (October through December and January through February).
When FluAlert was on, it fired for 8,630 visits, identifying the 62% of children who were not up to date on the vaccine. Most of those alerts (77%) came up during well-child and adolescent visits; 16% were acute care visits, 7% were visits specifically for vaccination, and the remaining visits were for Women, Infants, and Children program assessments. Providers acted on the alert 82% of the time: 53% ordered the vaccine. When they did not order the vaccine, providers noted the reason 98% of the time.
Overall, non–up-to-date children who were seen when FluAlert was on were 9% more likely to receive vaccine than children seen during an "off" period.
The program was also associated with significantly more documentation about why a child who needed the flu shot didn’t get it. In total, 625 children left the visit unvaccinated. When FluAlert was on, the reason for not vaccinating was noted for 68%; when it was off, documentation was present for only 41%.
The alert’s relative unobtrusiveness is probably one reason it was embraced as well as it was, Dr. Stockwell added. "What really annoys people is if something pops up and you can’t do anything else until you go through the entire process. So having it sit there as a gentle reminder is more appealing than something that’s always flashing and telling providers what to do."
Dr. Stockwell said she had no relevant financial disclosures
AT THE PAS ANNUAL MEETING
Major finding: A pop-up computer reminder resulted in children being 9% more likely to receive flu vaccine than those whose electronic medical record didn’t have the system.
Data source: FluAlert reminder system, piloted in four large urban community clinics.
Disclosures: Dr. Stockwell said he had no relevant financial disclosures.

Familiar respiratory culprits fueled Alabama illnesses
A combination of influenza A, rhinovirus, and bacterial pneumonia – not avian influenza or a novel coronavirus – caused a cluster of serious respiratory illnesses that struck southeastern Alabama, according to state public health officials.
Testing that ruled out avian influenza and novel coronavirus for the cluster of cases, including some that were fatal, is “good news,” said State Health Officer Dr. Donald E. Williamson.
The state's department of health announced its findings in a statement issued May 23.
Earlier in May, seven people with unexplained fever, cough, and shortness of breath had been admitted to the hospital; two cases were fatal. Specimens in six of the seven patients were positive for influenza A, rhinovirus, or a combination of the two; and three patients had bacterial pneumonia, according to the statement. There were no pediatric cases; the ages of the patients ranged from the mid-20s to the 80s, a department spokesperson said.

Enhanced surveillance associated with the cluster of cases was no longer necessary, Dr. Mary McIntyre, assistant state health officer for disease control and prevention, said in the statement. But she encouraged health care providers “to continue routine year-round influenza surveillance activities and submit specimens to the state laboratory for testing.”
Influenza was most likely the main cause of the severe cases, infectious disease specialist Dr. William Schaffner said in an interview. The cluster illustrates that while influenza is a winter infection, it “remains capable of being transmitted and occurring in our population at very low levels” in the summer months, he cautioned.
The investigation of the Alabama cluster “reinforces the need for physicians to be alert constantly, to treat serious disease with respect, get those specimens and, in circumstances like this, at a drop of the hat, notify the public health department,” added Dr. Schaffner, professor and chair of the department of preventive medicine at Vanderbilt University, Nashville, Tenn.
A combination of influenza A, rhinovirus, and bacterial pneumonia – not avian influenza or a novel coronavirus – caused a cluster of serious respiratory illnesses that struck southeastern Alabama, according to state public health officials.
Testing that ruled out avian influenza and novel coronavirus for the cluster of cases, including some that were fatal, is “good news,” said State Health Officer Dr. Donald E. Williamson.
The state's department of health announced its findings in a statement issued May 23.
Earlier in May, seven people with unexplained fever, cough, and shortness of breath had been admitted to the hospital; two cases were fatal. Specimens in six of the seven patients were positive for influenza A, rhinovirus, or a combination of the two; and three patients had bacterial pneumonia, according to the statement. There were no pediatric cases; the ages of the patients ranged from the mid-20s to the 80s, a department spokesperson said.
Enhanced surveillance associated with the cluster of cases was no longer necessary, Dr. Mary McIntyre, assistant state health officer for disease control and prevention, said in the statement. But she encouraged health care providers “to continue routine year-round influenza surveillance activities and submit specimens to the state laboratory for testing.”
Influenza was most likely the main cause of the severe cases, infectious disease specialist Dr. William Schaffner said in an interview. The cluster illustrates that while influenza is a winter infection, it “remains capable of being transmitted and occurring in our population at very low levels” in the summer months, he cautioned.
The investigation of the Alabama cluster “reinforces the need for physicians to be alert constantly, to treat serious disease with respect, get those specimens and, in circumstances like this, at a drop of the hat, notify the public health department,” added Dr. Schaffner, professor and chair of the department of preventive medicine at Vanderbilt University, Nashville, Tenn.
A combination of influenza A, rhinovirus, and bacterial pneumonia – not avian influenza or a novel coronavirus – caused a cluster of serious respiratory illnesses that struck southeastern Alabama, according to state public health officials.
Testing that ruled out avian influenza and novel coronavirus for the cluster of cases, including some that were fatal, is “good news,” said State Health Officer Dr. Donald E. Williamson.
The state's department of health announced its findings in a statement issued May 23.
Earlier in May, seven people with unexplained fever, cough, and shortness of breath had been admitted to the hospital; two cases were fatal. Specimens in six of the seven patients were positive for influenza A, rhinovirus, or a combination of the two; and three patients had bacterial pneumonia, according to the statement. There were no pediatric cases; the ages of the patients ranged from the mid-20s to the 80s, a department spokesperson said.
Enhanced surveillance associated with the cluster of cases was no longer necessary, Dr. Mary McIntyre, assistant state health officer for disease control and prevention, said in the statement. But she encouraged health care providers “to continue routine year-round influenza surveillance activities and submit specimens to the state laboratory for testing.”
Influenza was most likely the main cause of the severe cases, infectious disease specialist Dr. William Schaffner said in an interview. The cluster illustrates that while influenza is a winter infection, it “remains capable of being transmitted and occurring in our population at very low levels” in the summer months, he cautioned.
The investigation of the Alabama cluster “reinforces the need for physicians to be alert constantly, to treat serious disease with respect, get those specimens and, in circumstances like this, at a drop of the hat, notify the public health department,” added Dr. Schaffner, professor and chair of the department of preventive medicine at Vanderbilt University, Nashville, Tenn.

Panel supports lower doses of novel insomnia drug
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel agreed that suvorexant, a drug for insomnia with a novel mechanism of action, was effective in improving the time it took to get to sleep, and for maintenance of sleep in elderly and younger adults. The panel also agreed that its safety profile was acceptable at the lower starting doses.
But at the May 22 meeting, the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee was divided on whether the higher doses recommended for people with inadequate responses on the starting doses were safe, because serious adverse events such as evidence of impaired driving and excessive daytime somnolence were increased at those doses.
The panel was not asked to vote on whether to recommend approval of the drug, which is being reviewed for the treatment of insomnia characterized by difficulties with sleep onset and/or maintenance. If approved, suvorexant, an orexin receptor antagonist, would be the first drug in this class to be approved for insomnia. The FDA usually follows the recommendations of its advisory panels.
The manufacturer, Merck Research Laboratories, studied the drug in almost 3,000 patients, including 1,784 in phase III studies, and has recommended doses of 20 mg (starting dose) up to 40 mg taken at bedtime for adults aged under 65 years, and 15 mg (starting dose) up to 30 mg for people aged 65 and older.
Suvorexant blocks the binding of orexin A and B neuropeptides to orexin receptors, "presumably inhibiting activation of neurons to the arousal system," according to the FDA.
Testing of suvorexant involved three phase III studies – two studies that compared the effects of higher and lower doses against placebo on the onset and maintenance of sleep over 3 months, and a 1-year safety study in a total of 2,809 patients, including 1,784 treated with suvorexant. The drug was effective in improving the onset of and maintenance of sleep, and was sustained for a year, according to the company. In the phase III studies, next-day somnolence was reported by 3% of those on placebo, compared with 7% and 11% of those on low and high doses of suvorexant, respectively. Excessive daytime sleepiness was reported by 0.2% of those on placebo, compared with 0.6% and 1.1%, of those on low and high doses, respectively.
The FDA raised concerns about next-day somnolence, suicidal ideation, impaired driving, and other potentially serious side effects of the drug that appeared to be dose related, and concluded that a dose below 15 mg would be preferable. "Suvorexant is effective but not safe at the higher doses mainly studied," said Dr. Ronald Farkas, clinical team leader in the division of neurology products at the FDA’s Center for Drug Evaluation and Research. The risk-benefit profile may be more favorable at lower doses, since lower doses have similar efficacy, and phase II data suggested that the 10-mg dose may be effective, he told the panel.
In a 16-0 vote with 1 abstention, the panel agreed that based on the clinical trial results, suvorexant was effective for sleep maintenance, and voted 12-4 with 1 abstention, that the drug was effective for improving sleep onset, reflecting less robust effects on this endpoint.
The panel voted 13-3 with 1 abstention that the starting doses were acceptably safe. But they voted 8-7 with 2 abstentions that the safety of the higher doses – 40 mg among those under age 65 and 30 mg among those aged 65 and older – were not acceptable.
"Even though I think the lower doses are probably safe, I have to assume that many patients are going to graduate up to the higher doses," said Dr. Robert Clancy, professor of neurology and pediatrics at the University of Pennsylvania, Philadelphia. Dr. Clancy voted that the safety of the higher doses was not acceptable. He cited the 1.1% rate of excessive daytime sleepiness associated with the higher dose as a particular concern, which he predicted would result in fatalities, although none occurred in trials.
Dr. Ronald Chervin, professor of neurology and director of the sleep disorders center at the University of Michigan, Ann Arbor, was among those who agreed that the higher doses were acceptable. "My gut feeling overall is that we’re not seeing anything different in terms of a dose response on the safety side ... than what we would see for any of the hypnotics that we are currently using," he said.
The company expects the FDA to take action on the drug by mid-year, and if approved, the drug will have to go through the drug scheduling process, the company said in a statement after the meeting.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel agreed that suvorexant, a drug for insomnia with a novel mechanism of action, was effective in improving the time it took to get to sleep, and for maintenance of sleep in elderly and younger adults. The panel also agreed that its safety profile was acceptable at the lower starting doses.
But at the May 22 meeting, the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee was divided on whether the higher doses recommended for people with inadequate responses on the starting doses were safe, because serious adverse events such as evidence of impaired driving and excessive daytime somnolence were increased at those doses.
The panel was not asked to vote on whether to recommend approval of the drug, which is being reviewed for the treatment of insomnia characterized by difficulties with sleep onset and/or maintenance. If approved, suvorexant, an orexin receptor antagonist, would be the first drug in this class to be approved for insomnia. The FDA usually follows the recommendations of its advisory panels.
The manufacturer, Merck Research Laboratories, studied the drug in almost 3,000 patients, including 1,784 in phase III studies, and has recommended doses of 20 mg (starting dose) up to 40 mg taken at bedtime for adults aged under 65 years, and 15 mg (starting dose) up to 30 mg for people aged 65 and older.
Suvorexant blocks the binding of orexin A and B neuropeptides to orexin receptors, "presumably inhibiting activation of neurons to the arousal system," according to the FDA.
Testing of suvorexant involved three phase III studies – two studies that compared the effects of higher and lower doses against placebo on the onset and maintenance of sleep over 3 months, and a 1-year safety study in a total of 2,809 patients, including 1,784 treated with suvorexant. The drug was effective in improving the onset of and maintenance of sleep, and was sustained for a year, according to the company. In the phase III studies, next-day somnolence was reported by 3% of those on placebo, compared with 7% and 11% of those on low and high doses of suvorexant, respectively. Excessive daytime sleepiness was reported by 0.2% of those on placebo, compared with 0.6% and 1.1%, of those on low and high doses, respectively.
The FDA raised concerns about next-day somnolence, suicidal ideation, impaired driving, and other potentially serious side effects of the drug that appeared to be dose related, and concluded that a dose below 15 mg would be preferable. "Suvorexant is effective but not safe at the higher doses mainly studied," said Dr. Ronald Farkas, clinical team leader in the division of neurology products at the FDA’s Center for Drug Evaluation and Research. The risk-benefit profile may be more favorable at lower doses, since lower doses have similar efficacy, and phase II data suggested that the 10-mg dose may be effective, he told the panel.
In a 16-0 vote with 1 abstention, the panel agreed that based on the clinical trial results, suvorexant was effective for sleep maintenance, and voted 12-4 with 1 abstention, that the drug was effective for improving sleep onset, reflecting less robust effects on this endpoint.
The panel voted 13-3 with 1 abstention that the starting doses were acceptably safe. But they voted 8-7 with 2 abstentions that the safety of the higher doses – 40 mg among those under age 65 and 30 mg among those aged 65 and older – were not acceptable.
"Even though I think the lower doses are probably safe, I have to assume that many patients are going to graduate up to the higher doses," said Dr. Robert Clancy, professor of neurology and pediatrics at the University of Pennsylvania, Philadelphia. Dr. Clancy voted that the safety of the higher doses was not acceptable. He cited the 1.1% rate of excessive daytime sleepiness associated with the higher dose as a particular concern, which he predicted would result in fatalities, although none occurred in trials.
Dr. Ronald Chervin, professor of neurology and director of the sleep disorders center at the University of Michigan, Ann Arbor, was among those who agreed that the higher doses were acceptable. "My gut feeling overall is that we’re not seeing anything different in terms of a dose response on the safety side ... than what we would see for any of the hypnotics that we are currently using," he said.
The company expects the FDA to take action on the drug by mid-year, and if approved, the drug will have to go through the drug scheduling process, the company said in a statement after the meeting.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The majority of a Food and Drug Administration advisory panel agreed that suvorexant, a drug for insomnia with a novel mechanism of action, was effective in improving the time it took to get to sleep, and for maintenance of sleep in elderly and younger adults. The panel also agreed that its safety profile was acceptable at the lower starting doses.
But at the May 22 meeting, the FDA’s Peripheral and Central Nervous System Drugs Advisory Committee was divided on whether the higher doses recommended for people with inadequate responses on the starting doses were safe, because serious adverse events such as evidence of impaired driving and excessive daytime somnolence were increased at those doses.
The panel was not asked to vote on whether to recommend approval of the drug, which is being reviewed for the treatment of insomnia characterized by difficulties with sleep onset and/or maintenance. If approved, suvorexant, an orexin receptor antagonist, would be the first drug in this class to be approved for insomnia. The FDA usually follows the recommendations of its advisory panels.
The manufacturer, Merck Research Laboratories, studied the drug in almost 3,000 patients, including 1,784 in phase III studies, and has recommended doses of 20 mg (starting dose) up to 40 mg taken at bedtime for adults aged under 65 years, and 15 mg (starting dose) up to 30 mg for people aged 65 and older.
Suvorexant blocks the binding of orexin A and B neuropeptides to orexin receptors, "presumably inhibiting activation of neurons to the arousal system," according to the FDA.
Testing of suvorexant involved three phase III studies – two studies that compared the effects of higher and lower doses against placebo on the onset and maintenance of sleep over 3 months, and a 1-year safety study in a total of 2,809 patients, including 1,784 treated with suvorexant. The drug was effective in improving the onset of and maintenance of sleep, and was sustained for a year, according to the company. In the phase III studies, next-day somnolence was reported by 3% of those on placebo, compared with 7% and 11% of those on low and high doses of suvorexant, respectively. Excessive daytime sleepiness was reported by 0.2% of those on placebo, compared with 0.6% and 1.1%, of those on low and high doses, respectively.
The FDA raised concerns about next-day somnolence, suicidal ideation, impaired driving, and other potentially serious side effects of the drug that appeared to be dose related, and concluded that a dose below 15 mg would be preferable. "Suvorexant is effective but not safe at the higher doses mainly studied," said Dr. Ronald Farkas, clinical team leader in the division of neurology products at the FDA’s Center for Drug Evaluation and Research. The risk-benefit profile may be more favorable at lower doses, since lower doses have similar efficacy, and phase II data suggested that the 10-mg dose may be effective, he told the panel.
In a 16-0 vote with 1 abstention, the panel agreed that based on the clinical trial results, suvorexant was effective for sleep maintenance, and voted 12-4 with 1 abstention, that the drug was effective for improving sleep onset, reflecting less robust effects on this endpoint.
The panel voted 13-3 with 1 abstention that the starting doses were acceptably safe. But they voted 8-7 with 2 abstentions that the safety of the higher doses – 40 mg among those under age 65 and 30 mg among those aged 65 and older – were not acceptable.
"Even though I think the lower doses are probably safe, I have to assume that many patients are going to graduate up to the higher doses," said Dr. Robert Clancy, professor of neurology and pediatrics at the University of Pennsylvania, Philadelphia. Dr. Clancy voted that the safety of the higher doses was not acceptable. He cited the 1.1% rate of excessive daytime sleepiness associated with the higher dose as a particular concern, which he predicted would result in fatalities, although none occurred in trials.
Dr. Ronald Chervin, professor of neurology and director of the sleep disorders center at the University of Michigan, Ann Arbor, was among those who agreed that the higher doses were acceptable. "My gut feeling overall is that we’re not seeing anything different in terms of a dose response on the safety side ... than what we would see for any of the hypnotics that we are currently using," he said.
The company expects the FDA to take action on the drug by mid-year, and if approved, the drug will have to go through the drug scheduling process, the company said in a statement after the meeting.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
FROM AN FDA ADVISORY PANEL MEETING
CDC urges doctors to help patients quit smoking
WASHINGTON – Doctors need to step up their efforts to counsel patients on smoking cessation.
That was the message from officials at the Centers for Disease Control and Prevention and primary care physicians group at a press briefing May 22.
"Every doctor can help their patients quit, and every doctor should do everything possible to help their patients quit," Dr. Tom Frieden, CDC director, said at a press conference. "Even spending 3-5 minutes on personalized, clear advice will double the likelihood that they will quit for good."
He added that talking about smoking – or about quitting – is still not a part of routine doctor visits.

"That extra moment can make all the difference and help them quit," agreed Surgeon General Regina Benjamin, who also spoke at the briefing.
The CDC estimates that 43 million American adults smoke, and that smoking kills about 440,000 of them each year.
Representatives of the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, and the American Medical Association, joined Dr. Frieden in urging their members and other physicians to do more.
"It’s very important for all of the medical associations to be speaking with one voice," Dr. Charles Cutler, chair of the ACP Board of Regents, said in an interview. "When we’re all saying the same thing, the message for doctors throughout America becomes more resonant."
Advertisements that are part of the CDC’s current "Tips From Former Smokers" campaignwill be tagged with a new line from May 27 through June 2. During that time, ads will say "You can quit. Talk with your doctor for help."
So far, the Tips campaign, which features individuals disfigured from a lifetime of smoking, has generated 200,000 excess calls to the 1-800-QUIT-NOW line managed by the CDC, Dr. Frieden said. The campaign is funded at about $50 million a year with money from the Public Health and Prevention Fund, which was established by the Affordable Care Act.

AAFP president Jeffrey Cain said that physicians are crucial allies for patients who are trying to quit. He noted that the AAFP has several tools to help physicians counsel and care for smokers, including the "Ask and Act Practice Toolkit," and a treating tobacco dependence practice manual. "You have to make it so that tobacco is a vital sign when a patient comes in," said Dr. Cain.
The Tips campaign gives patients a critical way to start conversations about smoking, said Dr. Patrice Harris of the AMA Board of Trustees. "Physicians should talk to every patient who smokes about quitting at every office visit," she said. The AMA’s Healthier Life Steps program helps direct physicians toward resources they can share with patients, she said.
The AAP joined the effort because so many children are exposed to second-hand smoke and because very often, the smoking habit begins in adolescence, said AAP President Thomas K. McInerny. He said that many pediatricians had been remiss in either asking patients or parents about smoking, or encouraging them to quit.
"Pediatricians must intervene during a clinical encounter, yet, unfortunately, many don’t do so," he said.
ACOG president Jeanne A. Conry said that the Tips campaign would help her colleagues improve women’s health and support healthier pregnancies – but only if ob.gyns. make it a part of every visit. "If we are able to discuss tobacco use and well-woman health care with every woman at every time, we will make a difference," she said.
In an editorial published simultaneously in JAMA, Dr. Tim McAfee of the CDC Office on Smoking and Health further underlined and explained the resources available to physicians for smoking cessation counseling (2013;1-2 [doi:10.1001/jama.2013.5975]).

"Physicians have made major strides over the past 2 decades in helping smokers quit, but still fall short of making cessation treatment a routine part of standard care," he wrote. "By making it easier to discuss smoking, the ‘talk with your doctor’ initiative can help bring the nation a step closer to achieving the goal of substantially reducing smoking and smoking-related disease and death."
For smoking cessation counseling information and tools, visit the CDC’s Tips website.
On Twitter @aliciaault
WASHINGTON – Doctors need to step up their efforts to counsel patients on smoking cessation.
That was the message from officials at the Centers for Disease Control and Prevention and primary care physicians group at a press briefing May 22.
"Every doctor can help their patients quit, and every doctor should do everything possible to help their patients quit," Dr. Tom Frieden, CDC director, said at a press conference. "Even spending 3-5 minutes on personalized, clear advice will double the likelihood that they will quit for good."
He added that talking about smoking – or about quitting – is still not a part of routine doctor visits.
"That extra moment can make all the difference and help them quit," agreed Surgeon General Regina Benjamin, who also spoke at the briefing.
The CDC estimates that 43 million American adults smoke, and that smoking kills about 440,000 of them each year.
Representatives of the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, and the American Medical Association, joined Dr. Frieden in urging their members and other physicians to do more.
"It’s very important for all of the medical associations to be speaking with one voice," Dr. Charles Cutler, chair of the ACP Board of Regents, said in an interview. "When we’re all saying the same thing, the message for doctors throughout America becomes more resonant."
Advertisements that are part of the CDC’s current "Tips From Former Smokers" campaignwill be tagged with a new line from May 27 through June 2. During that time, ads will say "You can quit. Talk with your doctor for help."
So far, the Tips campaign, which features individuals disfigured from a lifetime of smoking, has generated 200,000 excess calls to the 1-800-QUIT-NOW line managed by the CDC, Dr. Frieden said. The campaign is funded at about $50 million a year with money from the Public Health and Prevention Fund, which was established by the Affordable Care Act.
AAFP president Jeffrey Cain said that physicians are crucial allies for patients who are trying to quit. He noted that the AAFP has several tools to help physicians counsel and care for smokers, including the "Ask and Act Practice Toolkit," and a treating tobacco dependence practice manual. "You have to make it so that tobacco is a vital sign when a patient comes in," said Dr. Cain.
The Tips campaign gives patients a critical way to start conversations about smoking, said Dr. Patrice Harris of the AMA Board of Trustees. "Physicians should talk to every patient who smokes about quitting at every office visit," she said. The AMA’s Healthier Life Steps program helps direct physicians toward resources they can share with patients, she said.
The AAP joined the effort because so many children are exposed to second-hand smoke and because very often, the smoking habit begins in adolescence, said AAP President Thomas K. McInerny. He said that many pediatricians had been remiss in either asking patients or parents about smoking, or encouraging them to quit.
"Pediatricians must intervene during a clinical encounter, yet, unfortunately, many don’t do so," he said.
ACOG president Jeanne A. Conry said that the Tips campaign would help her colleagues improve women’s health and support healthier pregnancies – but only if ob.gyns. make it a part of every visit. "If we are able to discuss tobacco use and well-woman health care with every woman at every time, we will make a difference," she said.
In an editorial published simultaneously in JAMA, Dr. Tim McAfee of the CDC Office on Smoking and Health further underlined and explained the resources available to physicians for smoking cessation counseling (2013;1-2 [doi:10.1001/jama.2013.5975]).
"Physicians have made major strides over the past 2 decades in helping smokers quit, but still fall short of making cessation treatment a routine part of standard care," he wrote. "By making it easier to discuss smoking, the ‘talk with your doctor’ initiative can help bring the nation a step closer to achieving the goal of substantially reducing smoking and smoking-related disease and death."
For smoking cessation counseling information and tools, visit the CDC’s Tips website.
On Twitter @aliciaault
WASHINGTON – Doctors need to step up their efforts to counsel patients on smoking cessation.
That was the message from officials at the Centers for Disease Control and Prevention and primary care physicians group at a press briefing May 22.
"Every doctor can help their patients quit, and every doctor should do everything possible to help their patients quit," Dr. Tom Frieden, CDC director, said at a press conference. "Even spending 3-5 minutes on personalized, clear advice will double the likelihood that they will quit for good."
He added that talking about smoking – or about quitting – is still not a part of routine doctor visits.
"That extra moment can make all the difference and help them quit," agreed Surgeon General Regina Benjamin, who also spoke at the briefing.
The CDC estimates that 43 million American adults smoke, and that smoking kills about 440,000 of them each year.
Representatives of the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, and the American Medical Association, joined Dr. Frieden in urging their members and other physicians to do more.
"It’s very important for all of the medical associations to be speaking with one voice," Dr. Charles Cutler, chair of the ACP Board of Regents, said in an interview. "When we’re all saying the same thing, the message for doctors throughout America becomes more resonant."
Advertisements that are part of the CDC’s current "Tips From Former Smokers" campaignwill be tagged with a new line from May 27 through June 2. During that time, ads will say "You can quit. Talk with your doctor for help."
So far, the Tips campaign, which features individuals disfigured from a lifetime of smoking, has generated 200,000 excess calls to the 1-800-QUIT-NOW line managed by the CDC, Dr. Frieden said. The campaign is funded at about $50 million a year with money from the Public Health and Prevention Fund, which was established by the Affordable Care Act.
AAFP president Jeffrey Cain said that physicians are crucial allies for patients who are trying to quit. He noted that the AAFP has several tools to help physicians counsel and care for smokers, including the "Ask and Act Practice Toolkit," and a treating tobacco dependence practice manual. "You have to make it so that tobacco is a vital sign when a patient comes in," said Dr. Cain.
The Tips campaign gives patients a critical way to start conversations about smoking, said Dr. Patrice Harris of the AMA Board of Trustees. "Physicians should talk to every patient who smokes about quitting at every office visit," she said. The AMA’s Healthier Life Steps program helps direct physicians toward resources they can share with patients, she said.
The AAP joined the effort because so many children are exposed to second-hand smoke and because very often, the smoking habit begins in adolescence, said AAP President Thomas K. McInerny. He said that many pediatricians had been remiss in either asking patients or parents about smoking, or encouraging them to quit.
"Pediatricians must intervene during a clinical encounter, yet, unfortunately, many don’t do so," he said.
ACOG president Jeanne A. Conry said that the Tips campaign would help her colleagues improve women’s health and support healthier pregnancies – but only if ob.gyns. make it a part of every visit. "If we are able to discuss tobacco use and well-woman health care with every woman at every time, we will make a difference," she said.
In an editorial published simultaneously in JAMA, Dr. Tim McAfee of the CDC Office on Smoking and Health further underlined and explained the resources available to physicians for smoking cessation counseling (2013;1-2 [doi:10.1001/jama.2013.5975]).
"Physicians have made major strides over the past 2 decades in helping smokers quit, but still fall short of making cessation treatment a routine part of standard care," he wrote. "By making it easier to discuss smoking, the ‘talk with your doctor’ initiative can help bring the nation a step closer to achieving the goal of substantially reducing smoking and smoking-related disease and death."
For smoking cessation counseling information and tools, visit the CDC’s Tips website.
On Twitter @aliciaault
FROM A CDC PRESS BRIEFING

Real-world NLST results show CT scans find more early-stage lung cancers
For older Americans who are or used to be heavy smokers, annual CT screening for lung cancer appears to reduce mortality from the disease, according to a report published online in the New England Journal of Medicine.
The results from the initial round of screening in the National Lung Screening Trial show that over a 3-year period, annual low-dose helical CT detected significantly more early-stage lung cancers than conventional chest radiography did, said Dr. Timothy R. Church of the division of environmental health sciences, University of Minnesota School of Public Health, Minneapolis, and his associates in the NLST research group.
In the real-world clinical settings, "a reduction in mortality from lung cancer is achievable at U.S. screening centers that have staff experienced in chest CT," they added.
The findings were published online and simultaneously presented at the annual meeting of the American Thoracic Society.
For this first round of the study, 53,454 asymptomatic men and women aged 55-74 years participated. All had a history of at least 30 pack-years of smoking and were either current smokers or had quit within the preceding 15 years.
The study subjects were treated and followed at 33 sites across the country and were randomly assigned to undergo either low-dose helical CT (26,722 patients) or chest radiography (26,732 patients) to screen for lung cancer every year for 3 years. Eight of these subjects were found to have lung cancer before their first screening could be done and were excluded from the study.
The proportion of study subjects who had positive screening results was markedly higher with low-dose CT scanning (27.3%) than with radiography (9.2%). Lung cancer was diagnosed in 1.1% of the CT group, compared with 0.7% of the radiography group.
In the CT group, 92.5% of the patients who developed lung cancer had a positive screening result (a true-positive result) and 6.2% had a negative screening result (a false-negative result); the remaining subjects missed their scheduled screening visit.
In the radiography group, 71.6% of the patients who developed lung cancer had a true-positive screening result and 25.8% had a false-negative result; the remaining subjects missed their scheduled screening visit.
Thus, the sensitivity and specificity of lung CT were 93.8% and 73.4%, respectively, compared with 73.5% sensitivity and 91.3% specificity for radiography, Dr. Church and his colleagues said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1209120]).
"There were many more bronchioloalveolar carcinomas and adenocarcinomas in the low-dose CT group than in the radiography group (38 vs. 8 and 123 vs. 71, respectively), but the frequencies of other histologic features were similar in the two groups," the investigators said.
The difference between the two groups in the number of detected cancers was almost entirely accounted for by early, stage IA tumors, which were markedly more likely to be identified on CT screening. The rates of detection were fairly comparable between CT and radiography for all the more advanced malignancies.
The study was funded by the National Cancer Institute. No financial conflicts of interest were reported.
For older Americans who are or used to be heavy smokers, annual CT screening for lung cancer appears to reduce mortality from the disease, according to a report published online in the New England Journal of Medicine.
The results from the initial round of screening in the National Lung Screening Trial show that over a 3-year period, annual low-dose helical CT detected significantly more early-stage lung cancers than conventional chest radiography did, said Dr. Timothy R. Church of the division of environmental health sciences, University of Minnesota School of Public Health, Minneapolis, and his associates in the NLST research group.
In the real-world clinical settings, "a reduction in mortality from lung cancer is achievable at U.S. screening centers that have staff experienced in chest CT," they added.
The findings were published online and simultaneously presented at the annual meeting of the American Thoracic Society.
For this first round of the study, 53,454 asymptomatic men and women aged 55-74 years participated. All had a history of at least 30 pack-years of smoking and were either current smokers or had quit within the preceding 15 years.
The study subjects were treated and followed at 33 sites across the country and were randomly assigned to undergo either low-dose helical CT (26,722 patients) or chest radiography (26,732 patients) to screen for lung cancer every year for 3 years. Eight of these subjects were found to have lung cancer before their first screening could be done and were excluded from the study.
The proportion of study subjects who had positive screening results was markedly higher with low-dose CT scanning (27.3%) than with radiography (9.2%). Lung cancer was diagnosed in 1.1% of the CT group, compared with 0.7% of the radiography group.
In the CT group, 92.5% of the patients who developed lung cancer had a positive screening result (a true-positive result) and 6.2% had a negative screening result (a false-negative result); the remaining subjects missed their scheduled screening visit.
In the radiography group, 71.6% of the patients who developed lung cancer had a true-positive screening result and 25.8% had a false-negative result; the remaining subjects missed their scheduled screening visit.
Thus, the sensitivity and specificity of lung CT were 93.8% and 73.4%, respectively, compared with 73.5% sensitivity and 91.3% specificity for radiography, Dr. Church and his colleagues said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1209120]).
"There were many more bronchioloalveolar carcinomas and adenocarcinomas in the low-dose CT group than in the radiography group (38 vs. 8 and 123 vs. 71, respectively), but the frequencies of other histologic features were similar in the two groups," the investigators said.
The difference between the two groups in the number of detected cancers was almost entirely accounted for by early, stage IA tumors, which were markedly more likely to be identified on CT screening. The rates of detection were fairly comparable between CT and radiography for all the more advanced malignancies.
The study was funded by the National Cancer Institute. No financial conflicts of interest were reported.
For older Americans who are or used to be heavy smokers, annual CT screening for lung cancer appears to reduce mortality from the disease, according to a report published online in the New England Journal of Medicine.
The results from the initial round of screening in the National Lung Screening Trial show that over a 3-year period, annual low-dose helical CT detected significantly more early-stage lung cancers than conventional chest radiography did, said Dr. Timothy R. Church of the division of environmental health sciences, University of Minnesota School of Public Health, Minneapolis, and his associates in the NLST research group.
In the real-world clinical settings, "a reduction in mortality from lung cancer is achievable at U.S. screening centers that have staff experienced in chest CT," they added.
The findings were published online and simultaneously presented at the annual meeting of the American Thoracic Society.
For this first round of the study, 53,454 asymptomatic men and women aged 55-74 years participated. All had a history of at least 30 pack-years of smoking and were either current smokers or had quit within the preceding 15 years.
The study subjects were treated and followed at 33 sites across the country and were randomly assigned to undergo either low-dose helical CT (26,722 patients) or chest radiography (26,732 patients) to screen for lung cancer every year for 3 years. Eight of these subjects were found to have lung cancer before their first screening could be done and were excluded from the study.
The proportion of study subjects who had positive screening results was markedly higher with low-dose CT scanning (27.3%) than with radiography (9.2%). Lung cancer was diagnosed in 1.1% of the CT group, compared with 0.7% of the radiography group.
In the CT group, 92.5% of the patients who developed lung cancer had a positive screening result (a true-positive result) and 6.2% had a negative screening result (a false-negative result); the remaining subjects missed their scheduled screening visit.
In the radiography group, 71.6% of the patients who developed lung cancer had a true-positive screening result and 25.8% had a false-negative result; the remaining subjects missed their scheduled screening visit.
Thus, the sensitivity and specificity of lung CT were 93.8% and 73.4%, respectively, compared with 73.5% sensitivity and 91.3% specificity for radiography, Dr. Church and his colleagues said (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1209120]).
"There were many more bronchioloalveolar carcinomas and adenocarcinomas in the low-dose CT group than in the radiography group (38 vs. 8 and 123 vs. 71, respectively), but the frequencies of other histologic features were similar in the two groups," the investigators said.
The difference between the two groups in the number of detected cancers was almost entirely accounted for by early, stage IA tumors, which were markedly more likely to be identified on CT screening. The rates of detection were fairly comparable between CT and radiography for all the more advanced malignancies.
The study was funded by the National Cancer Institute. No financial conflicts of interest were reported.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: The sensitivity and specificity of CT for lung cancer detection were 93.8% and 73.4%, respectively; for radiography, sensitivity was 73.5% and specificity was 91.3%.
Data Source: A descriptive study involving 53,454 asymptomatic current or past smokers randomly assigned to undergo annual lung cancer screening using either low-dose CT or chest radiography and followed for 3 years.
Disclosures: This study was funded by the National Cancer Institute. No financial conflicts of interest were reported.
Early adenotonsillectomy beneficial for obstructive sleep apnea syndrome
Compared with watchful waiting, early adenotonsillectomy did not significantly improve attention or executive function as measured by neuropsychological testing in school-aged children with obstructive sleep apnea syndrome, according to a new report.
The findings were published online May 21 in the New England Journal of Medicine and simultaneously reported at the annual meeting of the American Thoracic Society.
However, early surgery did markedly improve polysomnographic abnormalities, as well as parent- and teacher-reported measures of behavior, executive function, and sleep symptoms, compared with watchful waiting, said Dr. Carole L. Marcus, director of the sleep center at Children’s Hospital of Philadelphia, and her associates.

"We observed no significant difference between the two groups in the change from baseline to follow-up in our primary outcome, the attention and executive-function score of the NEPSY [Developmental NeuroPsychological Assessment]; thus our trial is a negative one. However, other tests showed evidence of changes in behavior," noted Dr. Marcus and her associates in the Childhood Adenotonsillectomy Trial (CHAT).
Previous studies examining cognitive and behavioral outcomes after adenotonsillectomy for obstructive sleep apnea syndrome "have been limited by small samples, lack of randomization or appropriate controls, heterogenous study groups, and sole reliance on parent questionnaires rather than including neuropsychological testing," the investigators said.
In contrast, CHAT involved 453 children aged 5-9 years treated at seven academic sleep centers, who underwent standardized polysomnographic assessments and extensive testing via the Developmental Neuropsychological Assessment (NEPSY); Behavior Rating Inventory of Executive Function (BRIEF); Differential Ability Scales (DAS), which measures general intellectual functioning; Conners’ Rating Scale Revised (CRS-R); Pediatric Sleep Questionnaire sleep-related breathing disorder scale (PSQ-SRBD); Epworth Sleepiness Scale modified for children; Pediatric Quality of Life Inventory (PedsQL); and the Obstructive Sleep Apnea–18 assessment tool that measures disease-specific quality of life.
The children were randomly assigned to undergo adenotonsillectomy within 1 month (226 patients) or to be followed with watchful waiting (227 control subjects), and were formally assessed 7 months later. Demographic and clinical characteristics were well-balanced between the two study groups at baseline, and cognitive and behavioral scores were close to population means. A similar number of children in each group used nasal glucocorticoids or montelukast for allergic rhinitis or asthma.
Approximately half of the children in each group were overweight or obese.
The primary efficacy outcome was change in attention and executive-function score on the NEPSY. These scores improved more in children who underwent adenotonsillectomy than in the controls, but the difference did not reach statistical significance.
However, outcomes were significantly better with surgery than with watchful waiting on measures of obstructive apnea-hypopnea, oxygen desaturation index, hypercapnia, sleep arousal index, and percentage of sleep time in light sleep. This last measure is an indication of improved sleep continuity.
In particular, many more children who underwent early adenotonsillectomy (79%) achieved normalization of the obstructive sleep apnea syndrome, compared with control subjects (46%) (N. Engl. J. Med. 2013 May 21 [doi:10.1056/NEJMoa1215881]).
Adenotonsillectomy also improved outcomes to a significantly greater degree than did watchful waiting on the Conners’ Rating Scale assessing restlessness, impulsiveness, and emotional lability, as well as on all other measures of behavior and quality of life. The effect sizes were in the moderate-to-large range, indicating that the changes were clinically significant.
These benefits were noted in all subgroup analyses, most importantly in both obese and nonobese children. Obese children and children with more severe apnea symptoms showed larger absolute improvements after surgery than did other study subjects.
However, normalization of symptoms was less likely to occur in black children than in those of other races, regardless of treatment assignment. Obstructive sleep apnea has previously been reported to be more severe in black children, as it was in this study population. Black subjects in this study also showed less improvement in parent- and teacher-reported measures after adenotonsillectomy, relative to children of other races.
"The reasons for this racial disparity are unclear. Possible explanations include differences in parents’ expectations, coping mechanisms, or perceptions of their child’s behavior and the presence of risk factors for behavioral problems unrelated to the obstructive sleep apnea syndrome," Dr. Marcus and her associates said.
Regarding adverse effects, the number of serious events was similar between the two study groups. Eight events were related to perioperative complications, but three of these occurred in children assigned to the watchful waiting group who later crossed over to the surgery group.
Overall, the rate of perioperative complications was low, and the only treatment failures in this study occurred in the watchful waiting group. "Thus, this trial supports the overall safety of both early adenotonsillectomy and watchful waiting, but suggests the need for clinical monitoring of children who are being treated conservatively," the researchers said.
They added that it is possible the 7-month follow-up was not long enough to demonstrate "the full response to surgery." It may be that the neurobehavioral sequelae of sleepiness resolve quickly but those related to hypoxemia may stem from neuronal damage and thus take longer to resolve.
This study was limited in that it excluded patients with prolonged oxyhemoglobin desaturation and those taking attention deficit/hyperactivity disorder medications. Therefore "the study results cannot be extrapolated to these vulnerable groups," Dr. Marcus and her colleagues said.
CHAT was supported by the National Institutes of Health. Dr. Marcus reported receiving research equipment from Philips Respironics and Ventus Medical; her associates reported numerous ties to industry sources.
Compared with watchful waiting, early adenotonsillectomy did not significantly improve attention or executive function as measured by neuropsychological testing in school-aged children with obstructive sleep apnea syndrome, according to a new report.
The findings were published online May 21 in the New England Journal of Medicine and simultaneously reported at the annual meeting of the American Thoracic Society.
However, early surgery did markedly improve polysomnographic abnormalities, as well as parent- and teacher-reported measures of behavior, executive function, and sleep symptoms, compared with watchful waiting, said Dr. Carole L. Marcus, director of the sleep center at Children’s Hospital of Philadelphia, and her associates.
"We observed no significant difference between the two groups in the change from baseline to follow-up in our primary outcome, the attention and executive-function score of the NEPSY [Developmental NeuroPsychological Assessment]; thus our trial is a negative one. However, other tests showed evidence of changes in behavior," noted Dr. Marcus and her associates in the Childhood Adenotonsillectomy Trial (CHAT).
Previous studies examining cognitive and behavioral outcomes after adenotonsillectomy for obstructive sleep apnea syndrome "have been limited by small samples, lack of randomization or appropriate controls, heterogenous study groups, and sole reliance on parent questionnaires rather than including neuropsychological testing," the investigators said.
In contrast, CHAT involved 453 children aged 5-9 years treated at seven academic sleep centers, who underwent standardized polysomnographic assessments and extensive testing via the Developmental Neuropsychological Assessment (NEPSY); Behavior Rating Inventory of Executive Function (BRIEF); Differential Ability Scales (DAS), which measures general intellectual functioning; Conners’ Rating Scale Revised (CRS-R); Pediatric Sleep Questionnaire sleep-related breathing disorder scale (PSQ-SRBD); Epworth Sleepiness Scale modified for children; Pediatric Quality of Life Inventory (PedsQL); and the Obstructive Sleep Apnea–18 assessment tool that measures disease-specific quality of life.
The children were randomly assigned to undergo adenotonsillectomy within 1 month (226 patients) or to be followed with watchful waiting (227 control subjects), and were formally assessed 7 months later. Demographic and clinical characteristics were well-balanced between the two study groups at baseline, and cognitive and behavioral scores were close to population means. A similar number of children in each group used nasal glucocorticoids or montelukast for allergic rhinitis or asthma.
Approximately half of the children in each group were overweight or obese.
The primary efficacy outcome was change in attention and executive-function score on the NEPSY. These scores improved more in children who underwent adenotonsillectomy than in the controls, but the difference did not reach statistical significance.
However, outcomes were significantly better with surgery than with watchful waiting on measures of obstructive apnea-hypopnea, oxygen desaturation index, hypercapnia, sleep arousal index, and percentage of sleep time in light sleep. This last measure is an indication of improved sleep continuity.
In particular, many more children who underwent early adenotonsillectomy (79%) achieved normalization of the obstructive sleep apnea syndrome, compared with control subjects (46%) (N. Engl. J. Med. 2013 May 21 [doi:10.1056/NEJMoa1215881]).
Adenotonsillectomy also improved outcomes to a significantly greater degree than did watchful waiting on the Conners’ Rating Scale assessing restlessness, impulsiveness, and emotional lability, as well as on all other measures of behavior and quality of life. The effect sizes were in the moderate-to-large range, indicating that the changes were clinically significant.
These benefits were noted in all subgroup analyses, most importantly in both obese and nonobese children. Obese children and children with more severe apnea symptoms showed larger absolute improvements after surgery than did other study subjects.
However, normalization of symptoms was less likely to occur in black children than in those of other races, regardless of treatment assignment. Obstructive sleep apnea has previously been reported to be more severe in black children, as it was in this study population. Black subjects in this study also showed less improvement in parent- and teacher-reported measures after adenotonsillectomy, relative to children of other races.
"The reasons for this racial disparity are unclear. Possible explanations include differences in parents’ expectations, coping mechanisms, or perceptions of their child’s behavior and the presence of risk factors for behavioral problems unrelated to the obstructive sleep apnea syndrome," Dr. Marcus and her associates said.
Regarding adverse effects, the number of serious events was similar between the two study groups. Eight events were related to perioperative complications, but three of these occurred in children assigned to the watchful waiting group who later crossed over to the surgery group.
Overall, the rate of perioperative complications was low, and the only treatment failures in this study occurred in the watchful waiting group. "Thus, this trial supports the overall safety of both early adenotonsillectomy and watchful waiting, but suggests the need for clinical monitoring of children who are being treated conservatively," the researchers said.
They added that it is possible the 7-month follow-up was not long enough to demonstrate "the full response to surgery." It may be that the neurobehavioral sequelae of sleepiness resolve quickly but those related to hypoxemia may stem from neuronal damage and thus take longer to resolve.
This study was limited in that it excluded patients with prolonged oxyhemoglobin desaturation and those taking attention deficit/hyperactivity disorder medications. Therefore "the study results cannot be extrapolated to these vulnerable groups," Dr. Marcus and her colleagues said.
CHAT was supported by the National Institutes of Health. Dr. Marcus reported receiving research equipment from Philips Respironics and Ventus Medical; her associates reported numerous ties to industry sources.
Compared with watchful waiting, early adenotonsillectomy did not significantly improve attention or executive function as measured by neuropsychological testing in school-aged children with obstructive sleep apnea syndrome, according to a new report.
The findings were published online May 21 in the New England Journal of Medicine and simultaneously reported at the annual meeting of the American Thoracic Society.
However, early surgery did markedly improve polysomnographic abnormalities, as well as parent- and teacher-reported measures of behavior, executive function, and sleep symptoms, compared with watchful waiting, said Dr. Carole L. Marcus, director of the sleep center at Children’s Hospital of Philadelphia, and her associates.
"We observed no significant difference between the two groups in the change from baseline to follow-up in our primary outcome, the attention and executive-function score of the NEPSY [Developmental NeuroPsychological Assessment]; thus our trial is a negative one. However, other tests showed evidence of changes in behavior," noted Dr. Marcus and her associates in the Childhood Adenotonsillectomy Trial (CHAT).
Previous studies examining cognitive and behavioral outcomes after adenotonsillectomy for obstructive sleep apnea syndrome "have been limited by small samples, lack of randomization or appropriate controls, heterogenous study groups, and sole reliance on parent questionnaires rather than including neuropsychological testing," the investigators said.
In contrast, CHAT involved 453 children aged 5-9 years treated at seven academic sleep centers, who underwent standardized polysomnographic assessments and extensive testing via the Developmental Neuropsychological Assessment (NEPSY); Behavior Rating Inventory of Executive Function (BRIEF); Differential Ability Scales (DAS), which measures general intellectual functioning; Conners’ Rating Scale Revised (CRS-R); Pediatric Sleep Questionnaire sleep-related breathing disorder scale (PSQ-SRBD); Epworth Sleepiness Scale modified for children; Pediatric Quality of Life Inventory (PedsQL); and the Obstructive Sleep Apnea–18 assessment tool that measures disease-specific quality of life.
The children were randomly assigned to undergo adenotonsillectomy within 1 month (226 patients) or to be followed with watchful waiting (227 control subjects), and were formally assessed 7 months later. Demographic and clinical characteristics were well-balanced between the two study groups at baseline, and cognitive and behavioral scores were close to population means. A similar number of children in each group used nasal glucocorticoids or montelukast for allergic rhinitis or asthma.
Approximately half of the children in each group were overweight or obese.
The primary efficacy outcome was change in attention and executive-function score on the NEPSY. These scores improved more in children who underwent adenotonsillectomy than in the controls, but the difference did not reach statistical significance.
However, outcomes were significantly better with surgery than with watchful waiting on measures of obstructive apnea-hypopnea, oxygen desaturation index, hypercapnia, sleep arousal index, and percentage of sleep time in light sleep. This last measure is an indication of improved sleep continuity.
In particular, many more children who underwent early adenotonsillectomy (79%) achieved normalization of the obstructive sleep apnea syndrome, compared with control subjects (46%) (N. Engl. J. Med. 2013 May 21 [doi:10.1056/NEJMoa1215881]).
Adenotonsillectomy also improved outcomes to a significantly greater degree than did watchful waiting on the Conners’ Rating Scale assessing restlessness, impulsiveness, and emotional lability, as well as on all other measures of behavior and quality of life. The effect sizes were in the moderate-to-large range, indicating that the changes were clinically significant.
These benefits were noted in all subgroup analyses, most importantly in both obese and nonobese children. Obese children and children with more severe apnea symptoms showed larger absolute improvements after surgery than did other study subjects.
However, normalization of symptoms was less likely to occur in black children than in those of other races, regardless of treatment assignment. Obstructive sleep apnea has previously been reported to be more severe in black children, as it was in this study population. Black subjects in this study also showed less improvement in parent- and teacher-reported measures after adenotonsillectomy, relative to children of other races.
"The reasons for this racial disparity are unclear. Possible explanations include differences in parents’ expectations, coping mechanisms, or perceptions of their child’s behavior and the presence of risk factors for behavioral problems unrelated to the obstructive sleep apnea syndrome," Dr. Marcus and her associates said.
Regarding adverse effects, the number of serious events was similar between the two study groups. Eight events were related to perioperative complications, but three of these occurred in children assigned to the watchful waiting group who later crossed over to the surgery group.
Overall, the rate of perioperative complications was low, and the only treatment failures in this study occurred in the watchful waiting group. "Thus, this trial supports the overall safety of both early adenotonsillectomy and watchful waiting, but suggests the need for clinical monitoring of children who are being treated conservatively," the researchers said.
They added that it is possible the 7-month follow-up was not long enough to demonstrate "the full response to surgery." It may be that the neurobehavioral sequelae of sleepiness resolve quickly but those related to hypoxemia may stem from neuronal damage and thus take longer to resolve.
This study was limited in that it excluded patients with prolonged oxyhemoglobin desaturation and those taking attention deficit/hyperactivity disorder medications. Therefore "the study results cannot be extrapolated to these vulnerable groups," Dr. Marcus and her colleagues said.
CHAT was supported by the National Institutes of Health. Dr. Marcus reported receiving research equipment from Philips Respironics and Ventus Medical; her associates reported numerous ties to industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: Children with obstructive sleep apnea syndrome who underwent adenotonsillectomy did not show greater improvements in attention or executive function than did control subjects, but were markedly more likely to achieve normalization of numerous polysomnographic factors (79% vs. 46%).
Data source: A multicenter randomized clinical trial involving 453 children aged 5-9 years with obstructive sleep apnea syndrome who were assigned to adenotonsillectomy or watchful waiting and followed for 7 months.
Disclosures: CHAT was supported by the National Institutes of Health. Dr. Marcus reported receiving research equipment from Philips Respironics and Ventus Medical; her associates reported numerous ties to industry sources.
