User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Renal denervation improves glucose metabolism, sleep apnea
MIAMI BEACH – Denervation of the renal arteries improved glucose metabolism and control of drug-resistant hypertension, according to findings from a 2011 pilot study.
"If you thought the impact of renal denervation on hypertension was big, certainly the consideration of renal sympathetic denervation on glucose metabolism raises some real eye-opening opportunities," Dr. Michael R. Jaff said at the International Symposium on Endovascular Therapy 2013.

In 50 patients with drug-resistant hypertension who were enrolled in the pilot study, 37 underwent bilateral renal denervation, and 13 served as controls. Not only did the treated patients experience improvements in blood pressure compared with controls at 3 months (decreases in systolic BP of 32 mm Hg vs. 5 mm Hg, and decreases in diastolic BP of 12 mm Hg vs. 3 mm Hg in treated patients vs. controls, respectively), they also experienced improvements in fasting blood glucose levels.
At 3 months, the treatment group had a 9.4-mg/dL decrease in fasting blood glucose, compared with a 0.9-mg/dL increase in the controls (Circulation 2011;123:1940-6).
"However, I think the most exciting thing is the impact on plasma insulin levels, where there was a real reduction in plasma insulin levels at 1 month and 3 months in patients treated with renal denervation," said Dr. Jaff, who is medical director of the vascular center, the vascular diagnostic laboratory, and the vascular ultrasound core laboratory at Massachusetts General Hospital, Boston.
At 1 month, plasma insulin had decreased by 8.7 mcU/mL in the treated patients, and increased by 6.4 mcU/mL increase in the controls; at 3 months, plasma insulin had decreased by 11.6 mcU/mL in the treated patients, and increased by 0.5 mcU/mL in the controls.
A reduction in the number of patients diagnosed with diabetes and with impaired glucose tolerance was seen at 3 months in the treatment group, while the diabetic cases increased from 23% to 38% and normal glucose tolerance dropped from 31% to 24% in the control group, Dr. Jaff said.
"Admittedly this is a small sample size, but nonetheless, given the basic pathophysiology of this and these early findings, this is a tantalizing impact," he said, adding that if the findings are confirmed, the potential reach of renal denervation is mind-boggling.
"I think the potential is amazing. Could we actually say we could prevent diabetes mellitus in those with resistant hypertension? Could we cure those who already have diabetes? All of this would potentially be on a background of blood pressure control. We’ve all seen these charts that show that the more risk factors you have, it’s almost logarithmic, the impact on atherosclerosis. So being able to manage two major atherosclerotic risk factors with one simple procedure is almost hard to comprehend," he said.
But the "basic pathophysiology" he mentioned offers a plausible path to comprehension of the potential impact of renal sympathetic denervation.
Specifically, sympathetic hyperactivity directly mediates vascular resistance, and increases in vascular resistance shift blood flow from striated muscle to visceral tissues, he said, explaining that visceral tissue is less insulin sensitive than striated muscle.
In one long-term study looking at sympathetic drive in patients with essential hypertension and in normotensive controls, patients with type 2 diabetes had higher sympathetic drive than did controls, and those with hypertension and diabetes had the highest sympathetic drive. The study, which followed patients for 18 years, indicated that sympathetic drive and impaired glucose tolerance were directly related, he said (Metabolism Clin. Exper. 2008;57:1422-7).
"The background on this is that catheter-based denervation has been shown to reduce sympathetic drive as measured by renal norepinephrine spillover at 6 months, with a near 50% reduction in spillover," he said.
The pathophysiology – particularly outflow from the central nervous system and its effect on the clinical symptom of lung congestion – also provides a rationale for multiple other observed and potential "collateral benefits" of renal denervation, such as improvements in obstructive sleep apnea, said Dr. Krishna T. Rocha-Singh, who is director of the Prairie Vascular Institute at St. John’s Hospital, Springfield, Ill.
"Renal sympathetic outflow results in volume reduction and renal blood flow, retention of sodium and volume retention, and can relate to congestion. We can also have an internal reset, if you will, of the chemoreceptors on the brain that can lead to dyspnea and central sleep apnea. And, as [Dr. Jaff] suggested, there can be a reduction in peripheral vascular resistance due to vascular remodeling that improves insulin resistance.
"But more importantly, we have the effect of increased hypertrophy that may induce arrhythmias, oxygen consumption, and promote dyspnea. There’s also a direct connection between that and the brain, again relating to congestion," he said.
Dr. Rocha-Singh said this synergy between two pathophysiological systems – the activation of the sympathetic nervous system and the retention of sodium – relates to vascular resistance and excess volume, and to congestion and the perception of dyspnea.
When a person is in a reclining position, fluid shifts from the legs to the soft tissues. This effect is greater in patients with drug-resistant hypertension than in those with controlled blood pressure, and it occurs irrespective of body mass index and neck circumference, he said.
In a small study of patients who underwent renal denervation, 70% experienced not only blood pressure improvements but also decreases in the severity of sleep apnea as measured using the apnea-hypopnea index at 3 and 6 months’ follow-up, he said.
Additionally, in a small trial involving 27 patients who underwent pulmonary vein isolation or ablation of atrial fibrillation, 69% of those who also underwent renal denervation were free of recurrence of atrial fibrillation at 12 months, compared with only 29% of those who did not undergo renal denervation (J. Am. Coll. Cardiol. 2012;60:1163-70).
These encouraging findings contribute to what Dr. Rocha-Singh called a "tsunami of excitement" surrounding renal denervation. He noted that a quick Internet search identified more than 145 papers that have been published on the topic, and showed that more than 1,700 related provisional patents have been filed.
While, he – like Dr. Jaff – agreed that the enthusiasm must be tempered pending additional procedural and long-term data, he noted that the diversity of the primary and observed collateral benefits of renal denervation is something of a "vuja de" – the opposite of déjà vu.
"We have never experienced anything like this in our professional lives," he said.
Dr. Jaff is a consultant for numerous companies, including Medtronic, the maker of the Symplicity renal denervation device, but he is not compensated by Medtronic. He also has equity in numerous medical device companies, including one – Northwind Medical – that has a renal denervation strategy utilizing a novel mechanism. He is a board member for the nonprofit VIVA Physicians organization. Dr. Rocha-Singh is also a consultant or advisory board member for Medtronic, as well as for CardioSonic.
MIAMI BEACH – Denervation of the renal arteries improved glucose metabolism and control of drug-resistant hypertension, according to findings from a 2011 pilot study.
"If you thought the impact of renal denervation on hypertension was big, certainly the consideration of renal sympathetic denervation on glucose metabolism raises some real eye-opening opportunities," Dr. Michael R. Jaff said at the International Symposium on Endovascular Therapy 2013.
In 50 patients with drug-resistant hypertension who were enrolled in the pilot study, 37 underwent bilateral renal denervation, and 13 served as controls. Not only did the treated patients experience improvements in blood pressure compared with controls at 3 months (decreases in systolic BP of 32 mm Hg vs. 5 mm Hg, and decreases in diastolic BP of 12 mm Hg vs. 3 mm Hg in treated patients vs. controls, respectively), they also experienced improvements in fasting blood glucose levels.
At 3 months, the treatment group had a 9.4-mg/dL decrease in fasting blood glucose, compared with a 0.9-mg/dL increase in the controls (Circulation 2011;123:1940-6).
"However, I think the most exciting thing is the impact on plasma insulin levels, where there was a real reduction in plasma insulin levels at 1 month and 3 months in patients treated with renal denervation," said Dr. Jaff, who is medical director of the vascular center, the vascular diagnostic laboratory, and the vascular ultrasound core laboratory at Massachusetts General Hospital, Boston.
At 1 month, plasma insulin had decreased by 8.7 mcU/mL in the treated patients, and increased by 6.4 mcU/mL increase in the controls; at 3 months, plasma insulin had decreased by 11.6 mcU/mL in the treated patients, and increased by 0.5 mcU/mL in the controls.
A reduction in the number of patients diagnosed with diabetes and with impaired glucose tolerance was seen at 3 months in the treatment group, while the diabetic cases increased from 23% to 38% and normal glucose tolerance dropped from 31% to 24% in the control group, Dr. Jaff said.
"Admittedly this is a small sample size, but nonetheless, given the basic pathophysiology of this and these early findings, this is a tantalizing impact," he said, adding that if the findings are confirmed, the potential reach of renal denervation is mind-boggling.
"I think the potential is amazing. Could we actually say we could prevent diabetes mellitus in those with resistant hypertension? Could we cure those who already have diabetes? All of this would potentially be on a background of blood pressure control. We’ve all seen these charts that show that the more risk factors you have, it’s almost logarithmic, the impact on atherosclerosis. So being able to manage two major atherosclerotic risk factors with one simple procedure is almost hard to comprehend," he said.
But the "basic pathophysiology" he mentioned offers a plausible path to comprehension of the potential impact of renal sympathetic denervation.
Specifically, sympathetic hyperactivity directly mediates vascular resistance, and increases in vascular resistance shift blood flow from striated muscle to visceral tissues, he said, explaining that visceral tissue is less insulin sensitive than striated muscle.
In one long-term study looking at sympathetic drive in patients with essential hypertension and in normotensive controls, patients with type 2 diabetes had higher sympathetic drive than did controls, and those with hypertension and diabetes had the highest sympathetic drive. The study, which followed patients for 18 years, indicated that sympathetic drive and impaired glucose tolerance were directly related, he said (Metabolism Clin. Exper. 2008;57:1422-7).
"The background on this is that catheter-based denervation has been shown to reduce sympathetic drive as measured by renal norepinephrine spillover at 6 months, with a near 50% reduction in spillover," he said.
The pathophysiology – particularly outflow from the central nervous system and its effect on the clinical symptom of lung congestion – also provides a rationale for multiple other observed and potential "collateral benefits" of renal denervation, such as improvements in obstructive sleep apnea, said Dr. Krishna T. Rocha-Singh, who is director of the Prairie Vascular Institute at St. John’s Hospital, Springfield, Ill.
"Renal sympathetic outflow results in volume reduction and renal blood flow, retention of sodium and volume retention, and can relate to congestion. We can also have an internal reset, if you will, of the chemoreceptors on the brain that can lead to dyspnea and central sleep apnea. And, as [Dr. Jaff] suggested, there can be a reduction in peripheral vascular resistance due to vascular remodeling that improves insulin resistance.
"But more importantly, we have the effect of increased hypertrophy that may induce arrhythmias, oxygen consumption, and promote dyspnea. There’s also a direct connection between that and the brain, again relating to congestion," he said.
Dr. Rocha-Singh said this synergy between two pathophysiological systems – the activation of the sympathetic nervous system and the retention of sodium – relates to vascular resistance and excess volume, and to congestion and the perception of dyspnea.
When a person is in a reclining position, fluid shifts from the legs to the soft tissues. This effect is greater in patients with drug-resistant hypertension than in those with controlled blood pressure, and it occurs irrespective of body mass index and neck circumference, he said.
In a small study of patients who underwent renal denervation, 70% experienced not only blood pressure improvements but also decreases in the severity of sleep apnea as measured using the apnea-hypopnea index at 3 and 6 months’ follow-up, he said.
Additionally, in a small trial involving 27 patients who underwent pulmonary vein isolation or ablation of atrial fibrillation, 69% of those who also underwent renal denervation were free of recurrence of atrial fibrillation at 12 months, compared with only 29% of those who did not undergo renal denervation (J. Am. Coll. Cardiol. 2012;60:1163-70).
These encouraging findings contribute to what Dr. Rocha-Singh called a "tsunami of excitement" surrounding renal denervation. He noted that a quick Internet search identified more than 145 papers that have been published on the topic, and showed that more than 1,700 related provisional patents have been filed.
While, he – like Dr. Jaff – agreed that the enthusiasm must be tempered pending additional procedural and long-term data, he noted that the diversity of the primary and observed collateral benefits of renal denervation is something of a "vuja de" – the opposite of déjà vu.
"We have never experienced anything like this in our professional lives," he said.
Dr. Jaff is a consultant for numerous companies, including Medtronic, the maker of the Symplicity renal denervation device, but he is not compensated by Medtronic. He also has equity in numerous medical device companies, including one – Northwind Medical – that has a renal denervation strategy utilizing a novel mechanism. He is a board member for the nonprofit VIVA Physicians organization. Dr. Rocha-Singh is also a consultant or advisory board member for Medtronic, as well as for CardioSonic.
MIAMI BEACH – Denervation of the renal arteries improved glucose metabolism and control of drug-resistant hypertension, according to findings from a 2011 pilot study.
"If you thought the impact of renal denervation on hypertension was big, certainly the consideration of renal sympathetic denervation on glucose metabolism raises some real eye-opening opportunities," Dr. Michael R. Jaff said at the International Symposium on Endovascular Therapy 2013.
In 50 patients with drug-resistant hypertension who were enrolled in the pilot study, 37 underwent bilateral renal denervation, and 13 served as controls. Not only did the treated patients experience improvements in blood pressure compared with controls at 3 months (decreases in systolic BP of 32 mm Hg vs. 5 mm Hg, and decreases in diastolic BP of 12 mm Hg vs. 3 mm Hg in treated patients vs. controls, respectively), they also experienced improvements in fasting blood glucose levels.
At 3 months, the treatment group had a 9.4-mg/dL decrease in fasting blood glucose, compared with a 0.9-mg/dL increase in the controls (Circulation 2011;123:1940-6).
"However, I think the most exciting thing is the impact on plasma insulin levels, where there was a real reduction in plasma insulin levels at 1 month and 3 months in patients treated with renal denervation," said Dr. Jaff, who is medical director of the vascular center, the vascular diagnostic laboratory, and the vascular ultrasound core laboratory at Massachusetts General Hospital, Boston.
At 1 month, plasma insulin had decreased by 8.7 mcU/mL in the treated patients, and increased by 6.4 mcU/mL increase in the controls; at 3 months, plasma insulin had decreased by 11.6 mcU/mL in the treated patients, and increased by 0.5 mcU/mL in the controls.
A reduction in the number of patients diagnosed with diabetes and with impaired glucose tolerance was seen at 3 months in the treatment group, while the diabetic cases increased from 23% to 38% and normal glucose tolerance dropped from 31% to 24% in the control group, Dr. Jaff said.
"Admittedly this is a small sample size, but nonetheless, given the basic pathophysiology of this and these early findings, this is a tantalizing impact," he said, adding that if the findings are confirmed, the potential reach of renal denervation is mind-boggling.
"I think the potential is amazing. Could we actually say we could prevent diabetes mellitus in those with resistant hypertension? Could we cure those who already have diabetes? All of this would potentially be on a background of blood pressure control. We’ve all seen these charts that show that the more risk factors you have, it’s almost logarithmic, the impact on atherosclerosis. So being able to manage two major atherosclerotic risk factors with one simple procedure is almost hard to comprehend," he said.
But the "basic pathophysiology" he mentioned offers a plausible path to comprehension of the potential impact of renal sympathetic denervation.
Specifically, sympathetic hyperactivity directly mediates vascular resistance, and increases in vascular resistance shift blood flow from striated muscle to visceral tissues, he said, explaining that visceral tissue is less insulin sensitive than striated muscle.
In one long-term study looking at sympathetic drive in patients with essential hypertension and in normotensive controls, patients with type 2 diabetes had higher sympathetic drive than did controls, and those with hypertension and diabetes had the highest sympathetic drive. The study, which followed patients for 18 years, indicated that sympathetic drive and impaired glucose tolerance were directly related, he said (Metabolism Clin. Exper. 2008;57:1422-7).
"The background on this is that catheter-based denervation has been shown to reduce sympathetic drive as measured by renal norepinephrine spillover at 6 months, with a near 50% reduction in spillover," he said.
The pathophysiology – particularly outflow from the central nervous system and its effect on the clinical symptom of lung congestion – also provides a rationale for multiple other observed and potential "collateral benefits" of renal denervation, such as improvements in obstructive sleep apnea, said Dr. Krishna T. Rocha-Singh, who is director of the Prairie Vascular Institute at St. John’s Hospital, Springfield, Ill.
"Renal sympathetic outflow results in volume reduction and renal blood flow, retention of sodium and volume retention, and can relate to congestion. We can also have an internal reset, if you will, of the chemoreceptors on the brain that can lead to dyspnea and central sleep apnea. And, as [Dr. Jaff] suggested, there can be a reduction in peripheral vascular resistance due to vascular remodeling that improves insulin resistance.
"But more importantly, we have the effect of increased hypertrophy that may induce arrhythmias, oxygen consumption, and promote dyspnea. There’s also a direct connection between that and the brain, again relating to congestion," he said.
Dr. Rocha-Singh said this synergy between two pathophysiological systems – the activation of the sympathetic nervous system and the retention of sodium – relates to vascular resistance and excess volume, and to congestion and the perception of dyspnea.
When a person is in a reclining position, fluid shifts from the legs to the soft tissues. This effect is greater in patients with drug-resistant hypertension than in those with controlled blood pressure, and it occurs irrespective of body mass index and neck circumference, he said.
In a small study of patients who underwent renal denervation, 70% experienced not only blood pressure improvements but also decreases in the severity of sleep apnea as measured using the apnea-hypopnea index at 3 and 6 months’ follow-up, he said.
Additionally, in a small trial involving 27 patients who underwent pulmonary vein isolation or ablation of atrial fibrillation, 69% of those who also underwent renal denervation were free of recurrence of atrial fibrillation at 12 months, compared with only 29% of those who did not undergo renal denervation (J. Am. Coll. Cardiol. 2012;60:1163-70).
These encouraging findings contribute to what Dr. Rocha-Singh called a "tsunami of excitement" surrounding renal denervation. He noted that a quick Internet search identified more than 145 papers that have been published on the topic, and showed that more than 1,700 related provisional patents have been filed.
While, he – like Dr. Jaff – agreed that the enthusiasm must be tempered pending additional procedural and long-term data, he noted that the diversity of the primary and observed collateral benefits of renal denervation is something of a "vuja de" – the opposite of déjà vu.
"We have never experienced anything like this in our professional lives," he said.
Dr. Jaff is a consultant for numerous companies, including Medtronic, the maker of the Symplicity renal denervation device, but he is not compensated by Medtronic. He also has equity in numerous medical device companies, including one – Northwind Medical – that has a renal denervation strategy utilizing a novel mechanism. He is a board member for the nonprofit VIVA Physicians organization. Dr. Rocha-Singh is also a consultant or advisory board member for Medtronic, as well as for CardioSonic.
EXPERT ANALYSIS FROM ISET 2013

Apixaban, dabigatran found effective, safe for extended post-VTE therapy
Two oral anticoagulants, apixaban and dabigatran, were found to be effective for the extended treatment of venous thromboembolism in three industry-sponsored randomized clinical trials. The results were published online Feb. 21 in the New England Journal of Medicine.
Both medications also reduced the risk of bleeding complications, the investigators said.
In the first trial, two doses of apixaban were compared against placebo in 2,486 patients with venous thromboembolism who had finished 6-12 months of standard anticoagulation therapy and whose physicians were uncertain whether to stop or continue anticoagulation treatment, said Dr. Giancarlo Agnelli and his associates in the Apixaban after the Initial Management of Pulmonary Embolism and DVT with First-Line Therapy–Extended Treatment (AMPLIFY-EXT) study.
Apixaban is an oral factor Xa inhibitor that is administered in fixed doses and doesn’t require laboratory monitoring. The 5-mg (treatment) dose of apixaban has proved effective at preventing stroke in patients with atrial fibrillation, and the 2.5-mg (maintenance) dose has proved effective for thromboprophylaxis after major orthopedic surgery, said Dr. Agnelli of the department of internal and cardiovascular medicine-stroke unit at the University of Perugia (Italy) and his colleagues.
The study subjects were enrolled over a 3-year period at 328 medical centers in 28 countries. They were randomly assigned in double-blind fashion to receive the 2.5-mg dose (840 subjects), the 5-mg dose (813 subjects), or a matching placebo (829 subjects) twice daily for 1 year.
The primary efficacy outcome measure was a composite of symptomatic recurrent VTE or death from any cause. This occurred in 3.8% of the maintenance-dose group and 4.2% of the treatment-dose group, both significantly lower rates than in the placebo group (11.6%). Thus, both doses of apixaban significantly decreased the incidence of recurrent VTE, Dr. Agnelli and his associates said (N. Engl. J. Med. 2013 Feb. 21 [doi10.1056/NEJMoa1207541]).
The primary safety outcome measure was major bleeding, which occurred in 0.2% of the maintenance-dose group and 0.1% of the treatment-dose group, compared with 0.5% of the placebo group. Thus, both doses of apixaban were comparable to placebo in rates of major bleeding.
Clinically relevant nonmajor bleeding occurred in 3.0% of subjects taking 2.5 mg of apixaban and 4.2% of those taking 5 mg of apixaban, which were significantly higher than the 2.3% rate in subjects taking placebo.
The number of patients who would need to be treated with apixaban to prevent a single episode of recurrent VTE was 14. In contrast, the number who would need to be treated to cause an episode of major or clinically relevant nonmajor bleeding was 200, the investigators noted.
"For patients with venous thromboembolism for whom there is uncertainty about the benefits and risks of continued therapy, the results of this study provide a rationale for continuing anticoagulation therapy for an additional 12 months," they said.
"It should be noted, however, that only 15% of the patients in this study were older than 75 years of age, and few had a body weight below 60 kg or moderate or severe renal impairment. Consequently, more data are needed to better determine the benefit-to-risk profile of apixaban with respect to bleeding in such patients," the researchers said.
Further research also is needed to determine the risks and benefits of extending anticoagulation therapy beyond the 12-month mark examined in this study, they added.
In a separate report, Dr. Sam Schulman and his associates in the RE-MEDY and RE-SONATE studies examined the direct thrombin inhibitor dabigatran as a long-term anticoagulation treatment. These trials were extensions of two previous studies of short-term anticoagulation after venous thromboembolism (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMoa1113697]).
In RE-MEDY*, 2,866 VTE patients who had completed at least 3 months of anticoagulation therapy and were considered to be at increased risk for recurrence were randomly assigned to receive either fixed-dose dabigatran twice daily (1,430 subjects) or warfarin (1,426 subjects) for up to 36 months. They were followed at 265 medical centers in 33 countries, said Dr. Schulman of McMaster University Thrombosis and Atherosclerosis Research Institute, Hamilton, Ont., and his colleagues.
The RE-SONATE* trial, in contrast, involved 1,343 VTE patients who had completed at least 3 months of anticoagulation therapy but were not considered to be at increased risk of recurrence, so it was ethical to assess the effect of dabigatran vs. placebo in these patients. The subjects were randomly assigned to receive either fixed-dose dabigatran (681 patients) or a matching placebo (662 patients) and were followed at 147 medical centers in 21 countries.
In both RE-SONATE and RE-MEDY, the primary efficacy outcome measure was recurrent symptomatic VTE or VTE-related death.
In RE-MEDY, this outcome occurred in 1.8% of the dabigatran group and 1.3% of the warfarin group, thus meeting the criteria for noninferiority to warfarin in preventing recurrent or fatal VTE.
In RE-SONATE, this outcome occurred in 0.4% of the dabigatran group, compared with 5.6% of the placebo group, so the drug was significantly more effective than placebo at preventing recurrent or fatal VTE.
Dabigatran was associated with markedly fewer major bleeding events (0.9% vs. 1.8%) and clinically relevant bleeding events (5.6% vs. 10.2%) than was warfarin. However, the drug was associated with more major or clinically relevant bleeding events than was placebo (5.3% vs 1.8%).
In addition, there was a higher rate of acute coronary events with dabigatran (0.9%) than with warfarin (0.2%), although the number of affected patients was small. A recent meta-analysis of seven noninferiority trials also showed a significantly higher risk of MI or acute coronary syndromes with dabigatran than with the comparators. "Whether dabigatran increases the risk of MI is therefore still unclear," Dr. Schulman and his associates said.
AMPLIFY-EXT was funded by Bristol-Myers Squibb (BMS) and Pfizer; Dr. Agnelli reported ties to Bayer, Boehringer Ingelheim (BI), Daiichi Sankyo, BMS, and Sanofi-Aventis, and his associates reported ties to numerous industry sources. RE-MEDY and RE-SONATE were funded by BI; Dr. Schulman and his associates reported ties to numerous industry sources.
UPDATED 2/21: An earlier version of this article transposed the trial names in this instance only. The names were correct in all other instances.
Balancing the risks and benefits of extended anticoagulation is difficult, and deciding whether or when to stop the treatment remains a challenge, said Dr. Jean M. Connors.
Neither apixaban nor dabigatran are approved for short-term or extended treatment of VTE; rivaroxaban is the first of the new anticoagulants to gain such approval. However, the finding that apixaban was as effective in a low dose as it was at the full therapeutic dose, with the same bleeding risk, "may tip the risk-to-benefit ratio in favor of extended treatment for this patient population."
"The crux of using the new oral anticoagulants in clinical practice ... lies in the selection of appropriate patients. Patients in these studies were younger (average age, 56 years), with fewer coexisting diseases and a lower bleeding risk than patients typically seen in practice," and they had no strong indications for continuing anticoagulation, such as cancer or antiphospholipid syndrome.
Patients at the greatest risk of VTE recurrence are the ones who stand to benefit most from extended anticoagulation. Better risk-stratification strategies are needed to identify these patients, she said.
Dr. Connors is in the hematology division, department of medicine, at Brigham and Women’s Hospital, Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Agnelli’s and Dr. Schulman’s reports (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMe1215678]).
Balancing the risks and benefits of extended anticoagulation is difficult, and deciding whether or when to stop the treatment remains a challenge, said Dr. Jean M. Connors.
Neither apixaban nor dabigatran are approved for short-term or extended treatment of VTE; rivaroxaban is the first of the new anticoagulants to gain such approval. However, the finding that apixaban was as effective in a low dose as it was at the full therapeutic dose, with the same bleeding risk, "may tip the risk-to-benefit ratio in favor of extended treatment for this patient population."
"The crux of using the new oral anticoagulants in clinical practice ... lies in the selection of appropriate patients. Patients in these studies were younger (average age, 56 years), with fewer coexisting diseases and a lower bleeding risk than patients typically seen in practice," and they had no strong indications for continuing anticoagulation, such as cancer or antiphospholipid syndrome.
Patients at the greatest risk of VTE recurrence are the ones who stand to benefit most from extended anticoagulation. Better risk-stratification strategies are needed to identify these patients, she said.
Dr. Connors is in the hematology division, department of medicine, at Brigham and Women’s Hospital, Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Agnelli’s and Dr. Schulman’s reports (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMe1215678]).
Balancing the risks and benefits of extended anticoagulation is difficult, and deciding whether or when to stop the treatment remains a challenge, said Dr. Jean M. Connors.
Neither apixaban nor dabigatran are approved for short-term or extended treatment of VTE; rivaroxaban is the first of the new anticoagulants to gain such approval. However, the finding that apixaban was as effective in a low dose as it was at the full therapeutic dose, with the same bleeding risk, "may tip the risk-to-benefit ratio in favor of extended treatment for this patient population."
"The crux of using the new oral anticoagulants in clinical practice ... lies in the selection of appropriate patients. Patients in these studies were younger (average age, 56 years), with fewer coexisting diseases and a lower bleeding risk than patients typically seen in practice," and they had no strong indications for continuing anticoagulation, such as cancer or antiphospholipid syndrome.
Patients at the greatest risk of VTE recurrence are the ones who stand to benefit most from extended anticoagulation. Better risk-stratification strategies are needed to identify these patients, she said.
Dr. Connors is in the hematology division, department of medicine, at Brigham and Women’s Hospital, Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Agnelli’s and Dr. Schulman’s reports (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMe1215678]).
Two oral anticoagulants, apixaban and dabigatran, were found to be effective for the extended treatment of venous thromboembolism in three industry-sponsored randomized clinical trials. The results were published online Feb. 21 in the New England Journal of Medicine.
Both medications also reduced the risk of bleeding complications, the investigators said.
In the first trial, two doses of apixaban were compared against placebo in 2,486 patients with venous thromboembolism who had finished 6-12 months of standard anticoagulation therapy and whose physicians were uncertain whether to stop or continue anticoagulation treatment, said Dr. Giancarlo Agnelli and his associates in the Apixaban after the Initial Management of Pulmonary Embolism and DVT with First-Line Therapy–Extended Treatment (AMPLIFY-EXT) study.
Apixaban is an oral factor Xa inhibitor that is administered in fixed doses and doesn’t require laboratory monitoring. The 5-mg (treatment) dose of apixaban has proved effective at preventing stroke in patients with atrial fibrillation, and the 2.5-mg (maintenance) dose has proved effective for thromboprophylaxis after major orthopedic surgery, said Dr. Agnelli of the department of internal and cardiovascular medicine-stroke unit at the University of Perugia (Italy) and his colleagues.
The study subjects were enrolled over a 3-year period at 328 medical centers in 28 countries. They were randomly assigned in double-blind fashion to receive the 2.5-mg dose (840 subjects), the 5-mg dose (813 subjects), or a matching placebo (829 subjects) twice daily for 1 year.
The primary efficacy outcome measure was a composite of symptomatic recurrent VTE or death from any cause. This occurred in 3.8% of the maintenance-dose group and 4.2% of the treatment-dose group, both significantly lower rates than in the placebo group (11.6%). Thus, both doses of apixaban significantly decreased the incidence of recurrent VTE, Dr. Agnelli and his associates said (N. Engl. J. Med. 2013 Feb. 21 [doi10.1056/NEJMoa1207541]).
The primary safety outcome measure was major bleeding, which occurred in 0.2% of the maintenance-dose group and 0.1% of the treatment-dose group, compared with 0.5% of the placebo group. Thus, both doses of apixaban were comparable to placebo in rates of major bleeding.
Clinically relevant nonmajor bleeding occurred in 3.0% of subjects taking 2.5 mg of apixaban and 4.2% of those taking 5 mg of apixaban, which were significantly higher than the 2.3% rate in subjects taking placebo.
The number of patients who would need to be treated with apixaban to prevent a single episode of recurrent VTE was 14. In contrast, the number who would need to be treated to cause an episode of major or clinically relevant nonmajor bleeding was 200, the investigators noted.
"For patients with venous thromboembolism for whom there is uncertainty about the benefits and risks of continued therapy, the results of this study provide a rationale for continuing anticoagulation therapy for an additional 12 months," they said.
"It should be noted, however, that only 15% of the patients in this study were older than 75 years of age, and few had a body weight below 60 kg or moderate or severe renal impairment. Consequently, more data are needed to better determine the benefit-to-risk profile of apixaban with respect to bleeding in such patients," the researchers said.
Further research also is needed to determine the risks and benefits of extending anticoagulation therapy beyond the 12-month mark examined in this study, they added.
In a separate report, Dr. Sam Schulman and his associates in the RE-MEDY and RE-SONATE studies examined the direct thrombin inhibitor dabigatran as a long-term anticoagulation treatment. These trials were extensions of two previous studies of short-term anticoagulation after venous thromboembolism (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMoa1113697]).
In RE-MEDY*, 2,866 VTE patients who had completed at least 3 months of anticoagulation therapy and were considered to be at increased risk for recurrence were randomly assigned to receive either fixed-dose dabigatran twice daily (1,430 subjects) or warfarin (1,426 subjects) for up to 36 months. They were followed at 265 medical centers in 33 countries, said Dr. Schulman of McMaster University Thrombosis and Atherosclerosis Research Institute, Hamilton, Ont., and his colleagues.
The RE-SONATE* trial, in contrast, involved 1,343 VTE patients who had completed at least 3 months of anticoagulation therapy but were not considered to be at increased risk of recurrence, so it was ethical to assess the effect of dabigatran vs. placebo in these patients. The subjects were randomly assigned to receive either fixed-dose dabigatran (681 patients) or a matching placebo (662 patients) and were followed at 147 medical centers in 21 countries.
In both RE-SONATE and RE-MEDY, the primary efficacy outcome measure was recurrent symptomatic VTE or VTE-related death.
In RE-MEDY, this outcome occurred in 1.8% of the dabigatran group and 1.3% of the warfarin group, thus meeting the criteria for noninferiority to warfarin in preventing recurrent or fatal VTE.
In RE-SONATE, this outcome occurred in 0.4% of the dabigatran group, compared with 5.6% of the placebo group, so the drug was significantly more effective than placebo at preventing recurrent or fatal VTE.
Dabigatran was associated with markedly fewer major bleeding events (0.9% vs. 1.8%) and clinically relevant bleeding events (5.6% vs. 10.2%) than was warfarin. However, the drug was associated with more major or clinically relevant bleeding events than was placebo (5.3% vs 1.8%).
In addition, there was a higher rate of acute coronary events with dabigatran (0.9%) than with warfarin (0.2%), although the number of affected patients was small. A recent meta-analysis of seven noninferiority trials also showed a significantly higher risk of MI or acute coronary syndromes with dabigatran than with the comparators. "Whether dabigatran increases the risk of MI is therefore still unclear," Dr. Schulman and his associates said.
AMPLIFY-EXT was funded by Bristol-Myers Squibb (BMS) and Pfizer; Dr. Agnelli reported ties to Bayer, Boehringer Ingelheim (BI), Daiichi Sankyo, BMS, and Sanofi-Aventis, and his associates reported ties to numerous industry sources. RE-MEDY and RE-SONATE were funded by BI; Dr. Schulman and his associates reported ties to numerous industry sources.
UPDATED 2/21: An earlier version of this article transposed the trial names in this instance only. The names were correct in all other instances.
Two oral anticoagulants, apixaban and dabigatran, were found to be effective for the extended treatment of venous thromboembolism in three industry-sponsored randomized clinical trials. The results were published online Feb. 21 in the New England Journal of Medicine.
Both medications also reduced the risk of bleeding complications, the investigators said.
In the first trial, two doses of apixaban were compared against placebo in 2,486 patients with venous thromboembolism who had finished 6-12 months of standard anticoagulation therapy and whose physicians were uncertain whether to stop or continue anticoagulation treatment, said Dr. Giancarlo Agnelli and his associates in the Apixaban after the Initial Management of Pulmonary Embolism and DVT with First-Line Therapy–Extended Treatment (AMPLIFY-EXT) study.
Apixaban is an oral factor Xa inhibitor that is administered in fixed doses and doesn’t require laboratory monitoring. The 5-mg (treatment) dose of apixaban has proved effective at preventing stroke in patients with atrial fibrillation, and the 2.5-mg (maintenance) dose has proved effective for thromboprophylaxis after major orthopedic surgery, said Dr. Agnelli of the department of internal and cardiovascular medicine-stroke unit at the University of Perugia (Italy) and his colleagues.
The study subjects were enrolled over a 3-year period at 328 medical centers in 28 countries. They were randomly assigned in double-blind fashion to receive the 2.5-mg dose (840 subjects), the 5-mg dose (813 subjects), or a matching placebo (829 subjects) twice daily for 1 year.
The primary efficacy outcome measure was a composite of symptomatic recurrent VTE or death from any cause. This occurred in 3.8% of the maintenance-dose group and 4.2% of the treatment-dose group, both significantly lower rates than in the placebo group (11.6%). Thus, both doses of apixaban significantly decreased the incidence of recurrent VTE, Dr. Agnelli and his associates said (N. Engl. J. Med. 2013 Feb. 21 [doi10.1056/NEJMoa1207541]).
The primary safety outcome measure was major bleeding, which occurred in 0.2% of the maintenance-dose group and 0.1% of the treatment-dose group, compared with 0.5% of the placebo group. Thus, both doses of apixaban were comparable to placebo in rates of major bleeding.
Clinically relevant nonmajor bleeding occurred in 3.0% of subjects taking 2.5 mg of apixaban and 4.2% of those taking 5 mg of apixaban, which were significantly higher than the 2.3% rate in subjects taking placebo.
The number of patients who would need to be treated with apixaban to prevent a single episode of recurrent VTE was 14. In contrast, the number who would need to be treated to cause an episode of major or clinically relevant nonmajor bleeding was 200, the investigators noted.
"For patients with venous thromboembolism for whom there is uncertainty about the benefits and risks of continued therapy, the results of this study provide a rationale for continuing anticoagulation therapy for an additional 12 months," they said.
"It should be noted, however, that only 15% of the patients in this study were older than 75 years of age, and few had a body weight below 60 kg or moderate or severe renal impairment. Consequently, more data are needed to better determine the benefit-to-risk profile of apixaban with respect to bleeding in such patients," the researchers said.
Further research also is needed to determine the risks and benefits of extending anticoagulation therapy beyond the 12-month mark examined in this study, they added.
In a separate report, Dr. Sam Schulman and his associates in the RE-MEDY and RE-SONATE studies examined the direct thrombin inhibitor dabigatran as a long-term anticoagulation treatment. These trials were extensions of two previous studies of short-term anticoagulation after venous thromboembolism (N. Engl. J. Med. 2013 Feb. 21 [doi:10.1056/NEJMoa1113697]).
In RE-MEDY*, 2,866 VTE patients who had completed at least 3 months of anticoagulation therapy and were considered to be at increased risk for recurrence were randomly assigned to receive either fixed-dose dabigatran twice daily (1,430 subjects) or warfarin (1,426 subjects) for up to 36 months. They were followed at 265 medical centers in 33 countries, said Dr. Schulman of McMaster University Thrombosis and Atherosclerosis Research Institute, Hamilton, Ont., and his colleagues.
The RE-SONATE* trial, in contrast, involved 1,343 VTE patients who had completed at least 3 months of anticoagulation therapy but were not considered to be at increased risk of recurrence, so it was ethical to assess the effect of dabigatran vs. placebo in these patients. The subjects were randomly assigned to receive either fixed-dose dabigatran (681 patients) or a matching placebo (662 patients) and were followed at 147 medical centers in 21 countries.
In both RE-SONATE and RE-MEDY, the primary efficacy outcome measure was recurrent symptomatic VTE or VTE-related death.
In RE-MEDY, this outcome occurred in 1.8% of the dabigatran group and 1.3% of the warfarin group, thus meeting the criteria for noninferiority to warfarin in preventing recurrent or fatal VTE.
In RE-SONATE, this outcome occurred in 0.4% of the dabigatran group, compared with 5.6% of the placebo group, so the drug was significantly more effective than placebo at preventing recurrent or fatal VTE.
Dabigatran was associated with markedly fewer major bleeding events (0.9% vs. 1.8%) and clinically relevant bleeding events (5.6% vs. 10.2%) than was warfarin. However, the drug was associated with more major or clinically relevant bleeding events than was placebo (5.3% vs 1.8%).
In addition, there was a higher rate of acute coronary events with dabigatran (0.9%) than with warfarin (0.2%), although the number of affected patients was small. A recent meta-analysis of seven noninferiority trials also showed a significantly higher risk of MI or acute coronary syndromes with dabigatran than with the comparators. "Whether dabigatran increases the risk of MI is therefore still unclear," Dr. Schulman and his associates said.
AMPLIFY-EXT was funded by Bristol-Myers Squibb (BMS) and Pfizer; Dr. Agnelli reported ties to Bayer, Boehringer Ingelheim (BI), Daiichi Sankyo, BMS, and Sanofi-Aventis, and his associates reported ties to numerous industry sources. RE-MEDY and RE-SONATE were funded by BI; Dr. Schulman and his associates reported ties to numerous industry sources.
UPDATED 2/21: An earlier version of this article transposed the trial names in this instance only. The names were correct in all other instances.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Rates of recurrent VTE or death were 3.8% with 2.5 mg apixaban and 4.2% with 5 mg apixaban, vs 11.6% with placebo. Rates of recurrent VTE or VTE-related death were 1.8% with dabigatran vs 1.3% with warfarin and 0.4% with dabigatran vs. 5.6% with placebo.
Data Source: Three double-blind, controlled trials comparing 2.5 mg apixaban (840 subjects) and 5 mg apixiban (813 subjects) with placebo (829 subjects); 150 mg dabigatran (1,430 subjects) with warfarn (1,426 subjects); and 150 mg dabigatran (681 subjects) with placebo (662 subjects).
Disclosures: AMPLIFY-EXT was funded by Bristol-Myers Squibb (BMS) and Pfizer; Dr. Agnelli reported ties to Bayer, Boehringer Ingelheim (BI), Daiichi Sankyo, BMS, and Sanofi-Aventis, and his associates reported ties to numerous industry sources. RE-MEDY and RE-SONATE were funded by BI; Dr. Schulman and his associates reported ties to numerous industry sources.
Bronchiectasis may predict mortality in COPD
Bronchiectasis alone predicted mortality in patients with moderate to severe chronic obstructive pulmonary disease, independent of pulmonary function and other risk factors, a study by Spanish investigators has shown.
That finding means that "bronchiectasis could be a new prognostic factor" for COPD, the study’s authors predicted.
Confirmation of bronchiectasis "would have a major clinical impact," because high-resolution CT can readily diagnose the condition, and effective therapy is available to treat the chronic bronchial inflammation and infection that plague patients, said lead investigator Dr. Miguel Angel Martínez-García of the Polytechnic and University La Fe Hospital in Valencia, Spain, and his colleagues (Am. J. Respir. Crit. Care Med. 2013 Feb. 7 [doi:10.1164/rccm.201208-1518OC]).
Conceivably, those patients could be "subject to different diagnostic and therapeutic approaches and, therefore, define a new phenotype": COPD with bronchiectasis, Dr. Martínez-García said.
Bronchiectasis is already known to be associated with worse exacerbations, more frequent bacterial colonizations, and greater degrees of impairment in COPD patients. But its relationship to mortality – or its utility as a prognostic factor – hasn’t been demonstrated until now, the researchers noted.
The investigators followed 115 patients with moderate to severe COPD and with bronchiectasis and 86 COPD patients without bronchiectasis for a median of 48 months. A total of 43 patients (37%) died in the bronchiectasis group, but only 8 patients (9%) in the nonbronchiectasis group died. COPD exacerbations were the most common cause of death.
COPD patients with bronchiectasis were 2.5 times more likely to die than those without bronchiectasis, after adjustment for factors such as dyspnea, body mass index, the presence of potentially pathogenic respiratory microorganisms, and other potential confounders (hazard ratio, 2.54; 95%CI: 1.16-5.56; P = .02).
Patients with bronchiectasis also presented with "a more severe form of COPD in clinical and functional terms, as well as a greater concentration of parameters of systemic inflammation and a greater presence of" potentially pathogenic microorganisms (PPMs) in their airways, the investigators said.
Bacterial respiratory colonization and subsequent inflammation probably play an important role in dilating the bronchioles and causing bronchiectasis – which leads to more colonization and a vicious cycle. But that cycle might "be broken by the early identification of this subgroup of patients" and the use of oral moxifloxacin or inhaled antibiotics, they said.
A total of 59% (68) of patients with bronchiectasis, but only 20% (17) of those without it, had PPM respiratory isolates, most commonly Haemophilus influenzae, followed by Pseudomonas aeruginosa.
Most of the patients were men and, on average, around 70 years old and overweight. Overall, they had an average smoking history of 60.7 pack-years and had COPD for more than decade. A minority of patients had tuberculosis histories or active pneumonia.
The authors said they had no relevant financial disclosures. Praxis Pharmaceutical funded the study.
COPD, CT, Miguel Angel Martínez-García
Bronchiectasis alone predicted mortality in patients with moderate to severe chronic obstructive pulmonary disease, independent of pulmonary function and other risk factors, a study by Spanish investigators has shown.
That finding means that "bronchiectasis could be a new prognostic factor" for COPD, the study’s authors predicted.
Confirmation of bronchiectasis "would have a major clinical impact," because high-resolution CT can readily diagnose the condition, and effective therapy is available to treat the chronic bronchial inflammation and infection that plague patients, said lead investigator Dr. Miguel Angel Martínez-García of the Polytechnic and University La Fe Hospital in Valencia, Spain, and his colleagues (Am. J. Respir. Crit. Care Med. 2013 Feb. 7 [doi:10.1164/rccm.201208-1518OC]).
Conceivably, those patients could be "subject to different diagnostic and therapeutic approaches and, therefore, define a new phenotype": COPD with bronchiectasis, Dr. Martínez-García said.
Bronchiectasis is already known to be associated with worse exacerbations, more frequent bacterial colonizations, and greater degrees of impairment in COPD patients. But its relationship to mortality – or its utility as a prognostic factor – hasn’t been demonstrated until now, the researchers noted.
The investigators followed 115 patients with moderate to severe COPD and with bronchiectasis and 86 COPD patients without bronchiectasis for a median of 48 months. A total of 43 patients (37%) died in the bronchiectasis group, but only 8 patients (9%) in the nonbronchiectasis group died. COPD exacerbations were the most common cause of death.
COPD patients with bronchiectasis were 2.5 times more likely to die than those without bronchiectasis, after adjustment for factors such as dyspnea, body mass index, the presence of potentially pathogenic respiratory microorganisms, and other potential confounders (hazard ratio, 2.54; 95%CI: 1.16-5.56; P = .02).
Patients with bronchiectasis also presented with "a more severe form of COPD in clinical and functional terms, as well as a greater concentration of parameters of systemic inflammation and a greater presence of" potentially pathogenic microorganisms (PPMs) in their airways, the investigators said.
Bacterial respiratory colonization and subsequent inflammation probably play an important role in dilating the bronchioles and causing bronchiectasis – which leads to more colonization and a vicious cycle. But that cycle might "be broken by the early identification of this subgroup of patients" and the use of oral moxifloxacin or inhaled antibiotics, they said.
A total of 59% (68) of patients with bronchiectasis, but only 20% (17) of those without it, had PPM respiratory isolates, most commonly Haemophilus influenzae, followed by Pseudomonas aeruginosa.
Most of the patients were men and, on average, around 70 years old and overweight. Overall, they had an average smoking history of 60.7 pack-years and had COPD for more than decade. A minority of patients had tuberculosis histories or active pneumonia.
The authors said they had no relevant financial disclosures. Praxis Pharmaceutical funded the study.
Bronchiectasis alone predicted mortality in patients with moderate to severe chronic obstructive pulmonary disease, independent of pulmonary function and other risk factors, a study by Spanish investigators has shown.
That finding means that "bronchiectasis could be a new prognostic factor" for COPD, the study’s authors predicted.
Confirmation of bronchiectasis "would have a major clinical impact," because high-resolution CT can readily diagnose the condition, and effective therapy is available to treat the chronic bronchial inflammation and infection that plague patients, said lead investigator Dr. Miguel Angel Martínez-García of the Polytechnic and University La Fe Hospital in Valencia, Spain, and his colleagues (Am. J. Respir. Crit. Care Med. 2013 Feb. 7 [doi:10.1164/rccm.201208-1518OC]).
Conceivably, those patients could be "subject to different diagnostic and therapeutic approaches and, therefore, define a new phenotype": COPD with bronchiectasis, Dr. Martínez-García said.
Bronchiectasis is already known to be associated with worse exacerbations, more frequent bacterial colonizations, and greater degrees of impairment in COPD patients. But its relationship to mortality – or its utility as a prognostic factor – hasn’t been demonstrated until now, the researchers noted.
The investigators followed 115 patients with moderate to severe COPD and with bronchiectasis and 86 COPD patients without bronchiectasis for a median of 48 months. A total of 43 patients (37%) died in the bronchiectasis group, but only 8 patients (9%) in the nonbronchiectasis group died. COPD exacerbations were the most common cause of death.
COPD patients with bronchiectasis were 2.5 times more likely to die than those without bronchiectasis, after adjustment for factors such as dyspnea, body mass index, the presence of potentially pathogenic respiratory microorganisms, and other potential confounders (hazard ratio, 2.54; 95%CI: 1.16-5.56; P = .02).
Patients with bronchiectasis also presented with "a more severe form of COPD in clinical and functional terms, as well as a greater concentration of parameters of systemic inflammation and a greater presence of" potentially pathogenic microorganisms (PPMs) in their airways, the investigators said.
Bacterial respiratory colonization and subsequent inflammation probably play an important role in dilating the bronchioles and causing bronchiectasis – which leads to more colonization and a vicious cycle. But that cycle might "be broken by the early identification of this subgroup of patients" and the use of oral moxifloxacin or inhaled antibiotics, they said.
A total of 59% (68) of patients with bronchiectasis, but only 20% (17) of those without it, had PPM respiratory isolates, most commonly Haemophilus influenzae, followed by Pseudomonas aeruginosa.
Most of the patients were men and, on average, around 70 years old and overweight. Overall, they had an average smoking history of 60.7 pack-years and had COPD for more than decade. A minority of patients had tuberculosis histories or active pneumonia.
The authors said they had no relevant financial disclosures. Praxis Pharmaceutical funded the study.
COPD, CT, Miguel Angel Martínez-García
COPD, CT, Miguel Angel Martínez-García
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Major Finding: Moderate to severe COPD patients were 2.5 times more likely to die within 2 years if they had bronchiectasis (HR, 2.54; 95% CI: 1.16-5.56; P = .02).
Data Source: A multicenter, prospective observational study in 201 patients.
Disclosures: The investigators said they had no relevant financial disclosures. Praxis Pharmaceutical funded the study.
CDC: Address high smoking rate among mentally ill
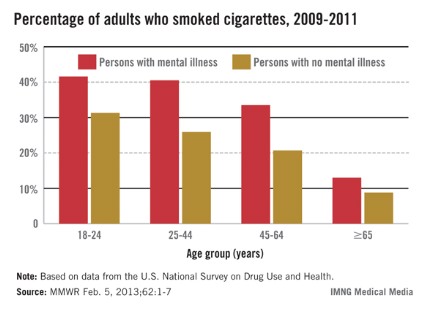
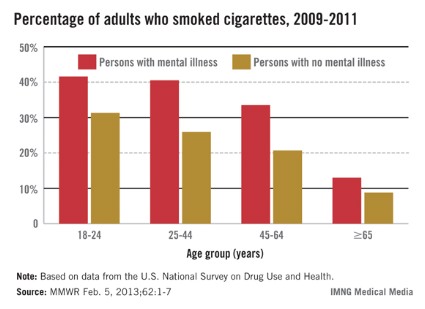
The rate of cigarette smoking among mentally ill adults is 70% higher than among adults without a mental illness and is particularly high in certain groups, including young adults, according to a report released Feb. 5 by the Centers for Disease Control and Prevention and the Substance Abuse and Mental Health Services Administration.
The estimates are based on data from SAMHSA’s 2009-2011 National Survey on Drug Use and Health, which calculated the rates of cigarette smoking among people aged 18 years and older in the United States who reported having "any mental illness," defined as "a diagnosable mental, behavioral, or emotional disorder, excluding developmental and substance use disorders" in the past year.
During this period, 36.1% of adults with a mental illness were current smokers, compared with 21.4% of adults with no mental illness. Those with a mental illness who smoked were heavier smokers, smoking an average of 331 cigarettes a month, compared with 310 a month among adult smokers who do not have a mental illness.
Wide variations were found in the proportion of people with a mental illness who smoked across states, ranging from a low of 18.2% in Utah to almost 50% in West Virginia. In addition to younger adults, the gap in smoking rates was particularly stark among certain populations, including American Indians and Alaska natives (54.7% of those with a mental illness smoked vs. 30.5% of those who did not have a mental illness) and people living below the poverty line (48% vs. 33%). Rates were also higher among people with a mental illness who had lower levels of education (47% among those with less than a high school education and 40.2% of those with a high school education, vs. 19% of college grads).
During a telebriefing held to announce the results, CDC director Dr. Thomas Frieden emphasized that although adults with mental illness smoke more and are less likely to quit, smoking cessation programs work but are underused in this population, and more efforts should be directed toward helping adults with mental illness quit successfully.
"People with mental illness who smoke want to and can quit, and more needs to be done to provide them with the resources and services to help them quit successfully," including making mental health facilities tobacco- and smoke-free, he said at the telebriefing, which was sponsored by the CDC.
The CDC report refers to the activities developed by SAMHSA and the Smoking Cessation Leadership Center to promote smoking cessation efforts in behavioral health care settings. These activities include expansion of the "100 Pioneers for Smoking Cessation Campaign," which provides support for mental health facilities and organizations, according to the CDC press release.
The CDC report is available here. Information on quitting smoking, including a link for health care professionals, is available at www.smokefree.gov.
The rate of cigarette smoking among mentally ill adults is 70% higher than among adults without a mental illness and is particularly high in certain groups, including young adults, according to a report released Feb. 5 by the Centers for Disease Control and Prevention and the Substance Abuse and Mental Health Services Administration.
The estimates are based on data from SAMHSA’s 2009-2011 National Survey on Drug Use and Health, which calculated the rates of cigarette smoking among people aged 18 years and older in the United States who reported having "any mental illness," defined as "a diagnosable mental, behavioral, or emotional disorder, excluding developmental and substance use disorders" in the past year.
During this period, 36.1% of adults with a mental illness were current smokers, compared with 21.4% of adults with no mental illness. Those with a mental illness who smoked were heavier smokers, smoking an average of 331 cigarettes a month, compared with 310 a month among adult smokers who do not have a mental illness.
Wide variations were found in the proportion of people with a mental illness who smoked across states, ranging from a low of 18.2% in Utah to almost 50% in West Virginia. In addition to younger adults, the gap in smoking rates was particularly stark among certain populations, including American Indians and Alaska natives (54.7% of those with a mental illness smoked vs. 30.5% of those who did not have a mental illness) and people living below the poverty line (48% vs. 33%). Rates were also higher among people with a mental illness who had lower levels of education (47% among those with less than a high school education and 40.2% of those with a high school education, vs. 19% of college grads).
During a telebriefing held to announce the results, CDC director Dr. Thomas Frieden emphasized that although adults with mental illness smoke more and are less likely to quit, smoking cessation programs work but are underused in this population, and more efforts should be directed toward helping adults with mental illness quit successfully.
"People with mental illness who smoke want to and can quit, and more needs to be done to provide them with the resources and services to help them quit successfully," including making mental health facilities tobacco- and smoke-free, he said at the telebriefing, which was sponsored by the CDC.
The CDC report refers to the activities developed by SAMHSA and the Smoking Cessation Leadership Center to promote smoking cessation efforts in behavioral health care settings. These activities include expansion of the "100 Pioneers for Smoking Cessation Campaign," which provides support for mental health facilities and organizations, according to the CDC press release.
The CDC report is available here. Information on quitting smoking, including a link for health care professionals, is available at www.smokefree.gov.
The rate of cigarette smoking among mentally ill adults is 70% higher than among adults without a mental illness and is particularly high in certain groups, including young adults, according to a report released Feb. 5 by the Centers for Disease Control and Prevention and the Substance Abuse and Mental Health Services Administration.
The estimates are based on data from SAMHSA’s 2009-2011 National Survey on Drug Use and Health, which calculated the rates of cigarette smoking among people aged 18 years and older in the United States who reported having "any mental illness," defined as "a diagnosable mental, behavioral, or emotional disorder, excluding developmental and substance use disorders" in the past year.
During this period, 36.1% of adults with a mental illness were current smokers, compared with 21.4% of adults with no mental illness. Those with a mental illness who smoked were heavier smokers, smoking an average of 331 cigarettes a month, compared with 310 a month among adult smokers who do not have a mental illness.
Wide variations were found in the proportion of people with a mental illness who smoked across states, ranging from a low of 18.2% in Utah to almost 50% in West Virginia. In addition to younger adults, the gap in smoking rates was particularly stark among certain populations, including American Indians and Alaska natives (54.7% of those with a mental illness smoked vs. 30.5% of those who did not have a mental illness) and people living below the poverty line (48% vs. 33%). Rates were also higher among people with a mental illness who had lower levels of education (47% among those with less than a high school education and 40.2% of those with a high school education, vs. 19% of college grads).
During a telebriefing held to announce the results, CDC director Dr. Thomas Frieden emphasized that although adults with mental illness smoke more and are less likely to quit, smoking cessation programs work but are underused in this population, and more efforts should be directed toward helping adults with mental illness quit successfully.
"People with mental illness who smoke want to and can quit, and more needs to be done to provide them with the resources and services to help them quit successfully," including making mental health facilities tobacco- and smoke-free, he said at the telebriefing, which was sponsored by the CDC.
The CDC report refers to the activities developed by SAMHSA and the Smoking Cessation Leadership Center to promote smoking cessation efforts in behavioral health care settings. These activities include expansion of the "100 Pioneers for Smoking Cessation Campaign," which provides support for mental health facilities and organizations, according to the CDC press release.
The CDC report is available here. Information on quitting smoking, including a link for health care professionals, is available at www.smokefree.gov.
FROM A TELEBRIEFING SPONSORED BY THE CENTERS FOR DISEASE CONTROL AND PREVENTION
Cough aerosols flagged most-infectious TB patients
A new, effective method of assessing tuberculosis infectiousness involves directly measuring aerosols from the coughs of pulmonary TB patients, according to a study published Jan. 10 in the American Journal of Respiratory and Critical Care Medicine.
An analysis of cough aerosols, when available, more accurately predicted transmission than did the traditional method of sputum smear microscopy or culture, reported Dr. Edward C. Jones López of Boston Medical Center and his associates (Am. J. Respir. Crit. Care Med. 2013 Jan. 10 [doi: 10.1164/rccm.201208-1422OC]).
Therefore, the researchers analyzed the number of M. tuberculosis colony forming units (CFUs) in TB patients’ aerosols to see whether the CFU number better predicted new infection in contacts than did an AFB-positive smear. The study group included 96 adult TB patients with sputum AFB-positive culture and their 442 household contacts from May 2009 to January 2011.
The TB patients attended the Mulago Hospital National Tuberculosis and Leprosy Programme in Kampala, Uganda, and lived with at least three household contacts. All had an initial AFB of at least 1+ plus M. tuberculosis culture growth and had received fewer than 6 days of antituberculous treatment or no treatment.
A total of 45% of patients (43) produced culturable M. tuberculosis in aerosols during the two 5-minute coughing periods of sample collection. The 26% of total study group patients who produced high aerosols (at least 10 CFUs) were more likely to transmit an infection to their contacts than the 19% with low aerosols (1-9 CFUs) or the 55% of aerosol-negative cases. Ten was selected as a CFU cut-off, based on an associated increase in tuberculin skin test (TST) conversion risk at this number.
While 69% of the contacts of high aerosol patients were "at-risk" of TST conversion, 25% of contacts of low aerosol patients and 30% of contacts of aerosol negative patients were at risk of TST conversation (P = .009). New infections were diagnosed through a positive tuberculin skin test (TST) or interferon-gamma release assay (IGRA), with retests six weeks later for contacts who tested negative at baseline for both TST and IGRA.
TST conversion risk in low aerosol and aerosol-negative patient contacts was similar (odds ratio, 0.77; 95% confidence interval 0.27-2.17; P = .62). However, the risk in contacts of high-aerosol patients was over five times greater than in contacts of low-aerosol patients (OR, 5.18; 95% CI 1.52-17.61) before adjustment. An adjusted analysis yielded a similar odds ratio (OR, 4.81; 95% CI 1.20-19.23).
Meanwhile, "the same analysis using sputum AFB smear grade to classify exposure groups did not show a clear or consistent risk stratification," the authors wrote. Therefore, high-aerosol TB patients more accurately predicted new TB infections, based on risk of TST conversion.
"In addition to providing a more precise marker of source infectiousness, cough aerosols may help determine the individual risk of M. tuberculosis infection after exposure, which can be variable and is poorly understood," the authors wrote. Yet they acknowledge the limitation that cough aerosols’ predictive value over time is unknown.
They noted three primary implications of their findings, first of which is a "new framework for rational and cost-effective infection control decisions" since the common wisdom that all sputum AFB positive patients are equally infectious is no longer necessarily the case. They also noted that Latent Tuberculosis Infection treatment programs may be improved through more efficient selection of TB contacts with TB exposure.
Finally, the authors suggested that analyzing TB aerosols might offer more accurate classifications of contacts’ inhaled doses of TB, thereby potentially offering an opportunity to better understand how the immune system responds to TB. This information may, in turn, contribute to studies related to TB vaccines, medications and immune responses.
This study was supported by a University of Medicine and Dentistry of New Jersey Foundation award with matching funds from the Division of Infectious Diseases at New Jersey Medical School, funds from the section of infectious diseases at Boston Medical Center and support to Dr. Matthew Fox from the National Institute of Allergy and Infectious Diseases.
A new, effective method of assessing tuberculosis infectiousness involves directly measuring aerosols from the coughs of pulmonary TB patients, according to a study published Jan. 10 in the American Journal of Respiratory and Critical Care Medicine.
An analysis of cough aerosols, when available, more accurately predicted transmission than did the traditional method of sputum smear microscopy or culture, reported Dr. Edward C. Jones López of Boston Medical Center and his associates (Am. J. Respir. Crit. Care Med. 2013 Jan. 10 [doi: 10.1164/rccm.201208-1422OC]).
Therefore, the researchers analyzed the number of M. tuberculosis colony forming units (CFUs) in TB patients’ aerosols to see whether the CFU number better predicted new infection in contacts than did an AFB-positive smear. The study group included 96 adult TB patients with sputum AFB-positive culture and their 442 household contacts from May 2009 to January 2011.
The TB patients attended the Mulago Hospital National Tuberculosis and Leprosy Programme in Kampala, Uganda, and lived with at least three household contacts. All had an initial AFB of at least 1+ plus M. tuberculosis culture growth and had received fewer than 6 days of antituberculous treatment or no treatment.
A total of 45% of patients (43) produced culturable M. tuberculosis in aerosols during the two 5-minute coughing periods of sample collection. The 26% of total study group patients who produced high aerosols (at least 10 CFUs) were more likely to transmit an infection to their contacts than the 19% with low aerosols (1-9 CFUs) or the 55% of aerosol-negative cases. Ten was selected as a CFU cut-off, based on an associated increase in tuberculin skin test (TST) conversion risk at this number.
While 69% of the contacts of high aerosol patients were "at-risk" of TST conversion, 25% of contacts of low aerosol patients and 30% of contacts of aerosol negative patients were at risk of TST conversation (P = .009). New infections were diagnosed through a positive tuberculin skin test (TST) or interferon-gamma release assay (IGRA), with retests six weeks later for contacts who tested negative at baseline for both TST and IGRA.
TST conversion risk in low aerosol and aerosol-negative patient contacts was similar (odds ratio, 0.77; 95% confidence interval 0.27-2.17; P = .62). However, the risk in contacts of high-aerosol patients was over five times greater than in contacts of low-aerosol patients (OR, 5.18; 95% CI 1.52-17.61) before adjustment. An adjusted analysis yielded a similar odds ratio (OR, 4.81; 95% CI 1.20-19.23).
Meanwhile, "the same analysis using sputum AFB smear grade to classify exposure groups did not show a clear or consistent risk stratification," the authors wrote. Therefore, high-aerosol TB patients more accurately predicted new TB infections, based on risk of TST conversion.
"In addition to providing a more precise marker of source infectiousness, cough aerosols may help determine the individual risk of M. tuberculosis infection after exposure, which can be variable and is poorly understood," the authors wrote. Yet they acknowledge the limitation that cough aerosols’ predictive value over time is unknown.
They noted three primary implications of their findings, first of which is a "new framework for rational and cost-effective infection control decisions" since the common wisdom that all sputum AFB positive patients are equally infectious is no longer necessarily the case. They also noted that Latent Tuberculosis Infection treatment programs may be improved through more efficient selection of TB contacts with TB exposure.
Finally, the authors suggested that analyzing TB aerosols might offer more accurate classifications of contacts’ inhaled doses of TB, thereby potentially offering an opportunity to better understand how the immune system responds to TB. This information may, in turn, contribute to studies related to TB vaccines, medications and immune responses.
This study was supported by a University of Medicine and Dentistry of New Jersey Foundation award with matching funds from the Division of Infectious Diseases at New Jersey Medical School, funds from the section of infectious diseases at Boston Medical Center and support to Dr. Matthew Fox from the National Institute of Allergy and Infectious Diseases.
A new, effective method of assessing tuberculosis infectiousness involves directly measuring aerosols from the coughs of pulmonary TB patients, according to a study published Jan. 10 in the American Journal of Respiratory and Critical Care Medicine.
An analysis of cough aerosols, when available, more accurately predicted transmission than did the traditional method of sputum smear microscopy or culture, reported Dr. Edward C. Jones López of Boston Medical Center and his associates (Am. J. Respir. Crit. Care Med. 2013 Jan. 10 [doi: 10.1164/rccm.201208-1422OC]).
Therefore, the researchers analyzed the number of M. tuberculosis colony forming units (CFUs) in TB patients’ aerosols to see whether the CFU number better predicted new infection in contacts than did an AFB-positive smear. The study group included 96 adult TB patients with sputum AFB-positive culture and their 442 household contacts from May 2009 to January 2011.
The TB patients attended the Mulago Hospital National Tuberculosis and Leprosy Programme in Kampala, Uganda, and lived with at least three household contacts. All had an initial AFB of at least 1+ plus M. tuberculosis culture growth and had received fewer than 6 days of antituberculous treatment or no treatment.
A total of 45% of patients (43) produced culturable M. tuberculosis in aerosols during the two 5-minute coughing periods of sample collection. The 26% of total study group patients who produced high aerosols (at least 10 CFUs) were more likely to transmit an infection to their contacts than the 19% with low aerosols (1-9 CFUs) or the 55% of aerosol-negative cases. Ten was selected as a CFU cut-off, based on an associated increase in tuberculin skin test (TST) conversion risk at this number.
While 69% of the contacts of high aerosol patients were "at-risk" of TST conversion, 25% of contacts of low aerosol patients and 30% of contacts of aerosol negative patients were at risk of TST conversation (P = .009). New infections were diagnosed through a positive tuberculin skin test (TST) or interferon-gamma release assay (IGRA), with retests six weeks later for contacts who tested negative at baseline for both TST and IGRA.
TST conversion risk in low aerosol and aerosol-negative patient contacts was similar (odds ratio, 0.77; 95% confidence interval 0.27-2.17; P = .62). However, the risk in contacts of high-aerosol patients was over five times greater than in contacts of low-aerosol patients (OR, 5.18; 95% CI 1.52-17.61) before adjustment. An adjusted analysis yielded a similar odds ratio (OR, 4.81; 95% CI 1.20-19.23).
Meanwhile, "the same analysis using sputum AFB smear grade to classify exposure groups did not show a clear or consistent risk stratification," the authors wrote. Therefore, high-aerosol TB patients more accurately predicted new TB infections, based on risk of TST conversion.
"In addition to providing a more precise marker of source infectiousness, cough aerosols may help determine the individual risk of M. tuberculosis infection after exposure, which can be variable and is poorly understood," the authors wrote. Yet they acknowledge the limitation that cough aerosols’ predictive value over time is unknown.
They noted three primary implications of their findings, first of which is a "new framework for rational and cost-effective infection control decisions" since the common wisdom that all sputum AFB positive patients are equally infectious is no longer necessarily the case. They also noted that Latent Tuberculosis Infection treatment programs may be improved through more efficient selection of TB contacts with TB exposure.
Finally, the authors suggested that analyzing TB aerosols might offer more accurate classifications of contacts’ inhaled doses of TB, thereby potentially offering an opportunity to better understand how the immune system responds to TB. This information may, in turn, contribute to studies related to TB vaccines, medications and immune responses.
This study was supported by a University of Medicine and Dentistry of New Jersey Foundation award with matching funds from the Division of Infectious Diseases at New Jersey Medical School, funds from the section of infectious diseases at Boston Medical Center and support to Dr. Matthew Fox from the National Institute of Allergy and Infectious Diseases.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Major Finding: While 69% of the contacts of the tuberculosis patients who produced cough aerosols with at least 10 M. tuberculosis CFUs were at risk of TST conversion, only 25% of contacts of low-aerosol patients and 30% of the contacts of aerosol-negative patients were at risk of TST conversion. Analysis using sputum of acid-fast bacilli smear grade did not show clear risk stratification.
Data Source: Analysis of 96 sputum AFB-positive TB patients attending Mulago Hospital National Tuberculosis and Leprosy Programme in Kampala, Uganda, from May 2009 to January 2011, plus subsequent new TB infections in their 442 household contacts.
Disclosures: This study was supported by a University of Medicine and Dentistry of New Jersey Foundation, the Division of Infectious Diseases at New Jersey Medical School, Boston Medical Center and the National Institute of Allergy and Infectious Diseases. There were no relevant conflicts of interest.
FDA panel votes against inhaled mannitol for cystic fibrosis
SILVER SPRING, MD. – Uncertainty over safety and efficacy data, particularly in children, moved a Food and Drug Administration advisory panel to unanimously recommend against approval of a dry powder formulation of mannitol for treating cystic fibrosis.
At a Jan. 30 meeting, the Pulmonary-Allergy Drugs Advisory Committee voted 14 to 0 against FDA approval of the product for the management of cystic fibrosis in patients aged 6 years and older, the indication under review. The proposed dose is 400 mg twice a day, administered via a breath-actuated dry powder inhaler over about 5 minutes, using ten 40-mg capsules for the total dose.
Mannitol "hydrates the lung surface, leading to improved airway clearance," according to the Australian manufacturer, Pharmaxis. Dry powder mannitol (DPM) is approved for people aged 6 years and older in Australia and for adults in the European Union.
"I wish I could have voted yes, because I think there is a place for a drug like this, but I think that further studies are necessary," said one of the panelists, Dr. Mary Cataletto, a pediatric pulmonologist and professor of clinical pediatrics at the State University of New York at Stony Brook. Like several other panelists, Dr. Jeffrey Wagener, professor of pediatrics at the University of Colorado, Aurora, said he may have voted in favor of approval if the indication had been limited to adults. "But there was no evidence DPM was effective in children, and "we need more information, more study, in children, particularly long term, looking at exacerbations and other outcomes besides FEV1 [forced expiratory volume in 1 second]," he added.
Pharmaxis presented the results of two phase III studies that enrolled 600 patients aged 6 years and older with cystic fibrosis (mean age about 20-23 years) with a baseline FEV1 of 30% or greater and less than 90% predicted. The trials compared treatment with 400 mg of DPM twice a day to treatment with 50 mg of DPM twice a day (controls). Patients continued other CF treatments, except for hypertonic saline, which, like mannitol, is considered an airway hydrator, and started treatment after passing a mannitol tolerance test.
In one of the studies, conducted outside the United States, the primary endpoint, the average change from baseline in FEV1 over 26 weeks, was significantly greater among those on treatment compared with controls (118 mL vs. 35 mL). But this study had a large amount of missing data because of patients dropping out, an issue raised by the FDA reviewers. In the second study, conducted in the United States, Canada, Argentina, and several European countries, the dropout rate was lower, but improvements in FEV1 from baseline at 26 weeks were only numerically, not significantly, greater among those on treatment compared with controls (107 mL vs. 52 mL).
The safety issue that elicited the most concern among panelists and was the main focus of the safety discussion was the higher rate of hemoptysis associated with treatment, particularly among those under age 18. In the two studies, the rate of hemoptysis (reported as an adverse event, not associated with an exacerbation), was almost 11% in adults on DPM, compared with about 8% of controls. But in those aged 6-17 years, the rate was almost 8% among those on DPM, compared with almost 2% among controls, according to the company, which agreed that hemoptysis in the pediatric age group was a safety signal that needed to be evaluated further.
Other adverse events appeared to be related to tolerability of the treatment, and more patients on DPM stopped treatment because of adverse events (11% vs. 6%), for reasons that included cough and hemoptysis.
FDA reviewers raised statistical issues regarding the data, including the impact missing data had on the primary endpoint in the two studies, particularly in the non-U.S. study, and questioned whether the results provided an accurate estimate of the treatment’s effects.
Several panelists described the efficacy data as "underwhelming," but the panel generally agreed there was some evidence the drug was probably effective in a subset of patients, who have not yet been identified. They also referred to public testimony from several adults with CF who described the benefits of DPM, particularly on their ability to cough up mucus after a treatment, as anecdotal evidence that the drug was effective in some patients.
The FDA usually follows the recommendations of its advisory panels, which are not binding. If approved, Pharmaxis plans to market DPM as Bronchitol. The company markets the Aridol bronchial hyperresponsiveness test that contains 635 mg of inhaled mannitol. A statement released by Pharmaxis after the panel meeting said that the company would continue to work with the FDA to bring the product to the United States.
The FDA’s deadline for making the decision on approval is in March.
FDA panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
SILVER SPRING, MD. – Uncertainty over safety and efficacy data, particularly in children, moved a Food and Drug Administration advisory panel to unanimously recommend against approval of a dry powder formulation of mannitol for treating cystic fibrosis.
At a Jan. 30 meeting, the Pulmonary-Allergy Drugs Advisory Committee voted 14 to 0 against FDA approval of the product for the management of cystic fibrosis in patients aged 6 years and older, the indication under review. The proposed dose is 400 mg twice a day, administered via a breath-actuated dry powder inhaler over about 5 minutes, using ten 40-mg capsules for the total dose.
Mannitol "hydrates the lung surface, leading to improved airway clearance," according to the Australian manufacturer, Pharmaxis. Dry powder mannitol (DPM) is approved for people aged 6 years and older in Australia and for adults in the European Union.
"I wish I could have voted yes, because I think there is a place for a drug like this, but I think that further studies are necessary," said one of the panelists, Dr. Mary Cataletto, a pediatric pulmonologist and professor of clinical pediatrics at the State University of New York at Stony Brook. Like several other panelists, Dr. Jeffrey Wagener, professor of pediatrics at the University of Colorado, Aurora, said he may have voted in favor of approval if the indication had been limited to adults. "But there was no evidence DPM was effective in children, and "we need more information, more study, in children, particularly long term, looking at exacerbations and other outcomes besides FEV1 [forced expiratory volume in 1 second]," he added.
Pharmaxis presented the results of two phase III studies that enrolled 600 patients aged 6 years and older with cystic fibrosis (mean age about 20-23 years) with a baseline FEV1 of 30% or greater and less than 90% predicted. The trials compared treatment with 400 mg of DPM twice a day to treatment with 50 mg of DPM twice a day (controls). Patients continued other CF treatments, except for hypertonic saline, which, like mannitol, is considered an airway hydrator, and started treatment after passing a mannitol tolerance test.
In one of the studies, conducted outside the United States, the primary endpoint, the average change from baseline in FEV1 over 26 weeks, was significantly greater among those on treatment compared with controls (118 mL vs. 35 mL). But this study had a large amount of missing data because of patients dropping out, an issue raised by the FDA reviewers. In the second study, conducted in the United States, Canada, Argentina, and several European countries, the dropout rate was lower, but improvements in FEV1 from baseline at 26 weeks were only numerically, not significantly, greater among those on treatment compared with controls (107 mL vs. 52 mL).
The safety issue that elicited the most concern among panelists and was the main focus of the safety discussion was the higher rate of hemoptysis associated with treatment, particularly among those under age 18. In the two studies, the rate of hemoptysis (reported as an adverse event, not associated with an exacerbation), was almost 11% in adults on DPM, compared with about 8% of controls. But in those aged 6-17 years, the rate was almost 8% among those on DPM, compared with almost 2% among controls, according to the company, which agreed that hemoptysis in the pediatric age group was a safety signal that needed to be evaluated further.
Other adverse events appeared to be related to tolerability of the treatment, and more patients on DPM stopped treatment because of adverse events (11% vs. 6%), for reasons that included cough and hemoptysis.
FDA reviewers raised statistical issues regarding the data, including the impact missing data had on the primary endpoint in the two studies, particularly in the non-U.S. study, and questioned whether the results provided an accurate estimate of the treatment’s effects.
Several panelists described the efficacy data as "underwhelming," but the panel generally agreed there was some evidence the drug was probably effective in a subset of patients, who have not yet been identified. They also referred to public testimony from several adults with CF who described the benefits of DPM, particularly on their ability to cough up mucus after a treatment, as anecdotal evidence that the drug was effective in some patients.
The FDA usually follows the recommendations of its advisory panels, which are not binding. If approved, Pharmaxis plans to market DPM as Bronchitol. The company markets the Aridol bronchial hyperresponsiveness test that contains 635 mg of inhaled mannitol. A statement released by Pharmaxis after the panel meeting said that the company would continue to work with the FDA to bring the product to the United States.
The FDA’s deadline for making the decision on approval is in March.
FDA panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
SILVER SPRING, MD. – Uncertainty over safety and efficacy data, particularly in children, moved a Food and Drug Administration advisory panel to unanimously recommend against approval of a dry powder formulation of mannitol for treating cystic fibrosis.
At a Jan. 30 meeting, the Pulmonary-Allergy Drugs Advisory Committee voted 14 to 0 against FDA approval of the product for the management of cystic fibrosis in patients aged 6 years and older, the indication under review. The proposed dose is 400 mg twice a day, administered via a breath-actuated dry powder inhaler over about 5 minutes, using ten 40-mg capsules for the total dose.
Mannitol "hydrates the lung surface, leading to improved airway clearance," according to the Australian manufacturer, Pharmaxis. Dry powder mannitol (DPM) is approved for people aged 6 years and older in Australia and for adults in the European Union.
"I wish I could have voted yes, because I think there is a place for a drug like this, but I think that further studies are necessary," said one of the panelists, Dr. Mary Cataletto, a pediatric pulmonologist and professor of clinical pediatrics at the State University of New York at Stony Brook. Like several other panelists, Dr. Jeffrey Wagener, professor of pediatrics at the University of Colorado, Aurora, said he may have voted in favor of approval if the indication had been limited to adults. "But there was no evidence DPM was effective in children, and "we need more information, more study, in children, particularly long term, looking at exacerbations and other outcomes besides FEV1 [forced expiratory volume in 1 second]," he added.
Pharmaxis presented the results of two phase III studies that enrolled 600 patients aged 6 years and older with cystic fibrosis (mean age about 20-23 years) with a baseline FEV1 of 30% or greater and less than 90% predicted. The trials compared treatment with 400 mg of DPM twice a day to treatment with 50 mg of DPM twice a day (controls). Patients continued other CF treatments, except for hypertonic saline, which, like mannitol, is considered an airway hydrator, and started treatment after passing a mannitol tolerance test.
In one of the studies, conducted outside the United States, the primary endpoint, the average change from baseline in FEV1 over 26 weeks, was significantly greater among those on treatment compared with controls (118 mL vs. 35 mL). But this study had a large amount of missing data because of patients dropping out, an issue raised by the FDA reviewers. In the second study, conducted in the United States, Canada, Argentina, and several European countries, the dropout rate was lower, but improvements in FEV1 from baseline at 26 weeks were only numerically, not significantly, greater among those on treatment compared with controls (107 mL vs. 52 mL).
The safety issue that elicited the most concern among panelists and was the main focus of the safety discussion was the higher rate of hemoptysis associated with treatment, particularly among those under age 18. In the two studies, the rate of hemoptysis (reported as an adverse event, not associated with an exacerbation), was almost 11% in adults on DPM, compared with about 8% of controls. But in those aged 6-17 years, the rate was almost 8% among those on DPM, compared with almost 2% among controls, according to the company, which agreed that hemoptysis in the pediatric age group was a safety signal that needed to be evaluated further.
Other adverse events appeared to be related to tolerability of the treatment, and more patients on DPM stopped treatment because of adverse events (11% vs. 6%), for reasons that included cough and hemoptysis.
FDA reviewers raised statistical issues regarding the data, including the impact missing data had on the primary endpoint in the two studies, particularly in the non-U.S. study, and questioned whether the results provided an accurate estimate of the treatment’s effects.
Several panelists described the efficacy data as "underwhelming," but the panel generally agreed there was some evidence the drug was probably effective in a subset of patients, who have not yet been identified. They also referred to public testimony from several adults with CF who described the benefits of DPM, particularly on their ability to cough up mucus after a treatment, as anecdotal evidence that the drug was effective in some patients.
The FDA usually follows the recommendations of its advisory panels, which are not binding. If approved, Pharmaxis plans to market DPM as Bronchitol. The company markets the Aridol bronchial hyperresponsiveness test that contains 635 mg of inhaled mannitol. A statement released by Pharmaxis after the panel meeting said that the company would continue to work with the FDA to bring the product to the United States.
The FDA’s deadline for making the decision on approval is in March.
FDA panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
AT A MEETING OF THE FDA'S PULMONARY-ALLERGY DRUGS ADVISORY COMMITTEE
Photo-aging tool dissuades teens from smoking
NEW ORLEANS – Use of photo-aging software helped persuade young people to stop smoking in a small Australian study.
Oksana Burford, a lecturer and doctoral candidate in the School of Pharmacy at Curtin University in Perth, Western Australia, said that she and her colleagues were hoping to find a way to motivate young smokers to quit, as they are generally resistant to most messages. Previous studies have shown, however, that young people do respond to graphic imagery, she said at the annual meeting of the North American Primary Care Research Group.
Ms. Burford decided to test a software program that would show teens and young adults how they would look in their 50s and 60s if they continued to smoke. She used face-aging software – called April – which is marketed by Toronto-based Aprilage Inc.
That company was started in 1998 to help develop the software, which was created for an exhibit at the Ontario Science Center. The Roswell Park Cancer Institute in Buffalo, N.Y., also was very involved in developing the first version of April, and it has been used by many antismoking and substance abuse programs around the world, according to the company.
The photo-aging program is available to clinicians who want to use it in their offices, and individuals also can use the program on the web by visiting http://www.ageme.com/.
Ms. Burford conducted a randomized controlled study at eight pharmacy sites around Western Australia, targeting young smokers. About 1,500 were screened and 213 were deemed eligible for study. In the end, 160 participated – 80 in the control group and 80 in the intervention group. The participants were smokers, aged 18-30, and they had to give informed consent and be available for 6 months of telephone follow-up.
All participants were asked to complete a baseline questionnaire: 56 (70%) in the control group and 48 (60%) in the intervention group completed the form. All received a self-care guide on smoking. For the intervention group, Ms. Burford took a photo of each, downloaded it onto her laptop, and then showed them what they would look like as a smoker or a nonsmoker at age 55. They also were given the photo-aging results to have at home.
Ms. Burford and her colleagues followed up with all subjects by phone at 1, 3, and 6 months.
At 6 months, only 5 of the 80 people in the control group self-reported as nonsmokers. Only 1 of the 5 agreed to a breath test to confirm whether they had actually quit. Just 11 of the 22 in the intervention group who said they had quit agreed to the confirmatory test.
The researchers calculated a Fagerstrom score for all the participants at baseline and at 6 months. Most clinicians use a modified, six-question Fagerstrom quiz, which is a measure of physical dependence on nicotine. The higher the score, the more intense the dependence.
For the control group, 11 moved to a lower category (14%), 68 (85%) had no change, and 1 (1%) moved to a higher category. For the intervention group, 41 (51%) moved to a lower category (this was significant, with a P value of .0001), 39 (49%) had no change, and none moved to a higher group.
The researchers assumed that subjects who did not return follow-up calls continued to smoke, Ms. Burford said. Overall, one in seven smokers quit after viewing their photo-aged selves. Ms. Burford concluded that the software program is an effective motivator in getting young people to quit, but she noted some limitations of the study, including the lack of blinding for participants and researchers and the low number of breath-test verifications in the control group.
Ms. Burford reported no conflicts.
On Twitter @aliciaault
NEW ORLEANS – Use of photo-aging software helped persuade young people to stop smoking in a small Australian study.
Oksana Burford, a lecturer and doctoral candidate in the School of Pharmacy at Curtin University in Perth, Western Australia, said that she and her colleagues were hoping to find a way to motivate young smokers to quit, as they are generally resistant to most messages. Previous studies have shown, however, that young people do respond to graphic imagery, she said at the annual meeting of the North American Primary Care Research Group.
Ms. Burford decided to test a software program that would show teens and young adults how they would look in their 50s and 60s if they continued to smoke. She used face-aging software – called April – which is marketed by Toronto-based Aprilage Inc.
That company was started in 1998 to help develop the software, which was created for an exhibit at the Ontario Science Center. The Roswell Park Cancer Institute in Buffalo, N.Y., also was very involved in developing the first version of April, and it has been used by many antismoking and substance abuse programs around the world, according to the company.
The photo-aging program is available to clinicians who want to use it in their offices, and individuals also can use the program on the web by visiting http://www.ageme.com/.
Ms. Burford conducted a randomized controlled study at eight pharmacy sites around Western Australia, targeting young smokers. About 1,500 were screened and 213 were deemed eligible for study. In the end, 160 participated – 80 in the control group and 80 in the intervention group. The participants were smokers, aged 18-30, and they had to give informed consent and be available for 6 months of telephone follow-up.
All participants were asked to complete a baseline questionnaire: 56 (70%) in the control group and 48 (60%) in the intervention group completed the form. All received a self-care guide on smoking. For the intervention group, Ms. Burford took a photo of each, downloaded it onto her laptop, and then showed them what they would look like as a smoker or a nonsmoker at age 55. They also were given the photo-aging results to have at home.
Ms. Burford and her colleagues followed up with all subjects by phone at 1, 3, and 6 months.
At 6 months, only 5 of the 80 people in the control group self-reported as nonsmokers. Only 1 of the 5 agreed to a breath test to confirm whether they had actually quit. Just 11 of the 22 in the intervention group who said they had quit agreed to the confirmatory test.
The researchers calculated a Fagerstrom score for all the participants at baseline and at 6 months. Most clinicians use a modified, six-question Fagerstrom quiz, which is a measure of physical dependence on nicotine. The higher the score, the more intense the dependence.
For the control group, 11 moved to a lower category (14%), 68 (85%) had no change, and 1 (1%) moved to a higher category. For the intervention group, 41 (51%) moved to a lower category (this was significant, with a P value of .0001), 39 (49%) had no change, and none moved to a higher group.
The researchers assumed that subjects who did not return follow-up calls continued to smoke, Ms. Burford said. Overall, one in seven smokers quit after viewing their photo-aged selves. Ms. Burford concluded that the software program is an effective motivator in getting young people to quit, but she noted some limitations of the study, including the lack of blinding for participants and researchers and the low number of breath-test verifications in the control group.
Ms. Burford reported no conflicts.
On Twitter @aliciaault
NEW ORLEANS – Use of photo-aging software helped persuade young people to stop smoking in a small Australian study.
Oksana Burford, a lecturer and doctoral candidate in the School of Pharmacy at Curtin University in Perth, Western Australia, said that she and her colleagues were hoping to find a way to motivate young smokers to quit, as they are generally resistant to most messages. Previous studies have shown, however, that young people do respond to graphic imagery, she said at the annual meeting of the North American Primary Care Research Group.
Ms. Burford decided to test a software program that would show teens and young adults how they would look in their 50s and 60s if they continued to smoke. She used face-aging software – called April – which is marketed by Toronto-based Aprilage Inc.
That company was started in 1998 to help develop the software, which was created for an exhibit at the Ontario Science Center. The Roswell Park Cancer Institute in Buffalo, N.Y., also was very involved in developing the first version of April, and it has been used by many antismoking and substance abuse programs around the world, according to the company.
The photo-aging program is available to clinicians who want to use it in their offices, and individuals also can use the program on the web by visiting http://www.ageme.com/.
Ms. Burford conducted a randomized controlled study at eight pharmacy sites around Western Australia, targeting young smokers. About 1,500 were screened and 213 were deemed eligible for study. In the end, 160 participated – 80 in the control group and 80 in the intervention group. The participants were smokers, aged 18-30, and they had to give informed consent and be available for 6 months of telephone follow-up.
All participants were asked to complete a baseline questionnaire: 56 (70%) in the control group and 48 (60%) in the intervention group completed the form. All received a self-care guide on smoking. For the intervention group, Ms. Burford took a photo of each, downloaded it onto her laptop, and then showed them what they would look like as a smoker or a nonsmoker at age 55. They also were given the photo-aging results to have at home.
Ms. Burford and her colleagues followed up with all subjects by phone at 1, 3, and 6 months.
At 6 months, only 5 of the 80 people in the control group self-reported as nonsmokers. Only 1 of the 5 agreed to a breath test to confirm whether they had actually quit. Just 11 of the 22 in the intervention group who said they had quit agreed to the confirmatory test.
The researchers calculated a Fagerstrom score for all the participants at baseline and at 6 months. Most clinicians use a modified, six-question Fagerstrom quiz, which is a measure of physical dependence on nicotine. The higher the score, the more intense the dependence.
For the control group, 11 moved to a lower category (14%), 68 (85%) had no change, and 1 (1%) moved to a higher category. For the intervention group, 41 (51%) moved to a lower category (this was significant, with a P value of .0001), 39 (49%) had no change, and none moved to a higher group.
The researchers assumed that subjects who did not return follow-up calls continued to smoke, Ms. Burford said. Overall, one in seven smokers quit after viewing their photo-aged selves. Ms. Burford concluded that the software program is an effective motivator in getting young people to quit, but she noted some limitations of the study, including the lack of blinding for participants and researchers and the low number of breath-test verifications in the control group.
Ms. Burford reported no conflicts.
On Twitter @aliciaault
AT THE ANNUAL MEETING OF THE NORTH AMERICAN PRIMARY CARE RESEARCH GROUP
Major Finding: One in seven young smokers quit 6 months after viewing photo-aged pictures of themselves.
Data Source: A prospective, randomized study of 160 men and women at pharmacy sites in Western Australia.
Disclosures: Ms. Burford reported no conflicts.
Once-daily beta-agonist for COPD earns FDA panel support
SILVER SPRING, MD. – Olodaterol, an inhaled long-acting beta2-adrenergic agonist, is an effective bronchodilator and should be approved for the treatment of chronic obstructive pulmonary disease, based on clinical trials in more than 3,000 patients with moderate to very severe COPD, the majority of a Food and Drug Administration advisory panel agreed at a meeting on Jan. 29.
The FDA’s Pulmonary-Allergy Drugs Advisory Committee voted 15-1, with one abstention, to recommend approval of olodaterol for the long-term, once-daily maintenance bronchodilator treatment of airflow obstruction in patients with COPD including chronic bronchitis and/or emphysema – the indication proposed by the manufacturer, Boehringer Ingelheim. Olodaterol is formulated in an inhalation spray solution, administered once a day via a metered dose inhaler (the Respimat device), at a dose of 5 mcg (two actuations of 2.5 mcg each).
The panelists voting in favor of approval agreed that clinical trial results showed that the drug had a bronchodilator effect comparable to other established bronchodilators, in a real-world setting where patients were on background medications, and at a dosing regimen that was similar to other treatments.
In separate votes on safety and efficacy, the panel also voted 15-1, with 1 abstention, that the data provided "substantial evidence" that the drug was effective; and 15-1, with 1 abstention, that the safety profile was adequate for the proposed indication and was comparable to that of other LABAs. But the panel recommended postmarketing surveillance of safety, including malignancies, and safety in black patients, who made up less than 5% of the enrolled patients in the studies.
In the studies, there were more neoplasms among those treated with olodaterol, but the increase was not statistically significant and did not reach the level of a safety signal, according to the company. But several panelists said that they were struck by the four diagnoses of small-cell lung cancers in patients on the 10-mcg daily dose that was also tested in the studies. While this was not a reason to recommend against approval, they said that malignancies – lung cancers in particular – in treated patients should be closely monitored after approval.
In four pivotal studies presented by the company, treatment with olodaterol (5 mcg or 10 mcg a day) was compared with placebo in 3,104 patients with moderate to very severe COPD (mean age 65 years) who were also on background medications (a muscarinic antagonist in 47%, an anti-inflammatory in 52%, a muscarinic antagonist and an antinflammatory in 29%, and a muscarinic antagonist with an inhaled corticosteroid and a xanthine in 5%).
Compared with placebo, treatment with 5 mcg per day was associated with statistically significant improvements in the two primary endpoints – FEV1 AUC (0-3 hours) and trough FEV1 responses – at 12 weeks in the two studies conducted primarily in the United States, and at 24 weeks in the two studies conducted primarily in Europe. Improvements in lung function with the 5-mcg dose were comparable to the 10-mcg dose, which is not a proposed dose.
Death rates and serious adverse events were similar in patients treated with olodaterol and comparators, and COPD exacerbations were the most common cause of death.
Boehringer Ingelheim has also proposed that the labeling include a claim that treatment with olodaterol increased exercise tolerance, increased respiratory capacity, and reduced lung hyperinflation. If approved by the FDA, this would be the first exercise tolerance claim to be included in labeling of a COPD drug, but based on the comments of the panel, this is unlikely.
In the study, the benefits in exercise tolerance after 6 weeks of treatment were based on effects on exercise tolerance testing performed 2 hours after the morning dose, at the time of the drug’s peak effect, in about 308 patients. It was unclear whether the effects could be maintained if the test had been performed later, which is particularly important because the indication is for maintenance treatment, according to the FDA reviewers.
The panel was not asked to vote on the exercise claim but discussed whether the results were clinically meaningful. Several panelists said that the improvements in exercise tolerance were notable, but since improvements were measured in a laboratory setting 2 hours after patients received the daily dose of olodaterol, it would be useful to evaluate how these improvements affected an individual’s activities of daily living. It would also be useful to provide a measurement later in the day to see if the effects persist throughout a period of time the patient may be active.
If approved, olodaterol will be marketed as Striverdi Respimat. It has already been approved in more than 60 countries.
The LABAs currently approved by the FDA are salmeterol, formoterol, and indacaterol.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
SILVER SPRING, MD. – Olodaterol, an inhaled long-acting beta2-adrenergic agonist, is an effective bronchodilator and should be approved for the treatment of chronic obstructive pulmonary disease, based on clinical trials in more than 3,000 patients with moderate to very severe COPD, the majority of a Food and Drug Administration advisory panel agreed at a meeting on Jan. 29.
The FDA’s Pulmonary-Allergy Drugs Advisory Committee voted 15-1, with one abstention, to recommend approval of olodaterol for the long-term, once-daily maintenance bronchodilator treatment of airflow obstruction in patients with COPD including chronic bronchitis and/or emphysema – the indication proposed by the manufacturer, Boehringer Ingelheim. Olodaterol is formulated in an inhalation spray solution, administered once a day via a metered dose inhaler (the Respimat device), at a dose of 5 mcg (two actuations of 2.5 mcg each).
The panelists voting in favor of approval agreed that clinical trial results showed that the drug had a bronchodilator effect comparable to other established bronchodilators, in a real-world setting where patients were on background medications, and at a dosing regimen that was similar to other treatments.
In separate votes on safety and efficacy, the panel also voted 15-1, with 1 abstention, that the data provided "substantial evidence" that the drug was effective; and 15-1, with 1 abstention, that the safety profile was adequate for the proposed indication and was comparable to that of other LABAs. But the panel recommended postmarketing surveillance of safety, including malignancies, and safety in black patients, who made up less than 5% of the enrolled patients in the studies.
In the studies, there were more neoplasms among those treated with olodaterol, but the increase was not statistically significant and did not reach the level of a safety signal, according to the company. But several panelists said that they were struck by the four diagnoses of small-cell lung cancers in patients on the 10-mcg daily dose that was also tested in the studies. While this was not a reason to recommend against approval, they said that malignancies – lung cancers in particular – in treated patients should be closely monitored after approval.
In four pivotal studies presented by the company, treatment with olodaterol (5 mcg or 10 mcg a day) was compared with placebo in 3,104 patients with moderate to very severe COPD (mean age 65 years) who were also on background medications (a muscarinic antagonist in 47%, an anti-inflammatory in 52%, a muscarinic antagonist and an antinflammatory in 29%, and a muscarinic antagonist with an inhaled corticosteroid and a xanthine in 5%).
Compared with placebo, treatment with 5 mcg per day was associated with statistically significant improvements in the two primary endpoints – FEV1 AUC (0-3 hours) and trough FEV1 responses – at 12 weeks in the two studies conducted primarily in the United States, and at 24 weeks in the two studies conducted primarily in Europe. Improvements in lung function with the 5-mcg dose were comparable to the 10-mcg dose, which is not a proposed dose.
Death rates and serious adverse events were similar in patients treated with olodaterol and comparators, and COPD exacerbations were the most common cause of death.
Boehringer Ingelheim has also proposed that the labeling include a claim that treatment with olodaterol increased exercise tolerance, increased respiratory capacity, and reduced lung hyperinflation. If approved by the FDA, this would be the first exercise tolerance claim to be included in labeling of a COPD drug, but based on the comments of the panel, this is unlikely.
In the study, the benefits in exercise tolerance after 6 weeks of treatment were based on effects on exercise tolerance testing performed 2 hours after the morning dose, at the time of the drug’s peak effect, in about 308 patients. It was unclear whether the effects could be maintained if the test had been performed later, which is particularly important because the indication is for maintenance treatment, according to the FDA reviewers.
The panel was not asked to vote on the exercise claim but discussed whether the results were clinically meaningful. Several panelists said that the improvements in exercise tolerance were notable, but since improvements were measured in a laboratory setting 2 hours after patients received the daily dose of olodaterol, it would be useful to evaluate how these improvements affected an individual’s activities of daily living. It would also be useful to provide a measurement later in the day to see if the effects persist throughout a period of time the patient may be active.
If approved, olodaterol will be marketed as Striverdi Respimat. It has already been approved in more than 60 countries.
The LABAs currently approved by the FDA are salmeterol, formoterol, and indacaterol.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
SILVER SPRING, MD. – Olodaterol, an inhaled long-acting beta2-adrenergic agonist, is an effective bronchodilator and should be approved for the treatment of chronic obstructive pulmonary disease, based on clinical trials in more than 3,000 patients with moderate to very severe COPD, the majority of a Food and Drug Administration advisory panel agreed at a meeting on Jan. 29.
The FDA’s Pulmonary-Allergy Drugs Advisory Committee voted 15-1, with one abstention, to recommend approval of olodaterol for the long-term, once-daily maintenance bronchodilator treatment of airflow obstruction in patients with COPD including chronic bronchitis and/or emphysema – the indication proposed by the manufacturer, Boehringer Ingelheim. Olodaterol is formulated in an inhalation spray solution, administered once a day via a metered dose inhaler (the Respimat device), at a dose of 5 mcg (two actuations of 2.5 mcg each).
The panelists voting in favor of approval agreed that clinical trial results showed that the drug had a bronchodilator effect comparable to other established bronchodilators, in a real-world setting where patients were on background medications, and at a dosing regimen that was similar to other treatments.
In separate votes on safety and efficacy, the panel also voted 15-1, with 1 abstention, that the data provided "substantial evidence" that the drug was effective; and 15-1, with 1 abstention, that the safety profile was adequate for the proposed indication and was comparable to that of other LABAs. But the panel recommended postmarketing surveillance of safety, including malignancies, and safety in black patients, who made up less than 5% of the enrolled patients in the studies.
In the studies, there were more neoplasms among those treated with olodaterol, but the increase was not statistically significant and did not reach the level of a safety signal, according to the company. But several panelists said that they were struck by the four diagnoses of small-cell lung cancers in patients on the 10-mcg daily dose that was also tested in the studies. While this was not a reason to recommend against approval, they said that malignancies – lung cancers in particular – in treated patients should be closely monitored after approval.
In four pivotal studies presented by the company, treatment with olodaterol (5 mcg or 10 mcg a day) was compared with placebo in 3,104 patients with moderate to very severe COPD (mean age 65 years) who were also on background medications (a muscarinic antagonist in 47%, an anti-inflammatory in 52%, a muscarinic antagonist and an antinflammatory in 29%, and a muscarinic antagonist with an inhaled corticosteroid and a xanthine in 5%).
Compared with placebo, treatment with 5 mcg per day was associated with statistically significant improvements in the two primary endpoints – FEV1 AUC (0-3 hours) and trough FEV1 responses – at 12 weeks in the two studies conducted primarily in the United States, and at 24 weeks in the two studies conducted primarily in Europe. Improvements in lung function with the 5-mcg dose were comparable to the 10-mcg dose, which is not a proposed dose.
Death rates and serious adverse events were similar in patients treated with olodaterol and comparators, and COPD exacerbations were the most common cause of death.
Boehringer Ingelheim has also proposed that the labeling include a claim that treatment with olodaterol increased exercise tolerance, increased respiratory capacity, and reduced lung hyperinflation. If approved by the FDA, this would be the first exercise tolerance claim to be included in labeling of a COPD drug, but based on the comments of the panel, this is unlikely.
In the study, the benefits in exercise tolerance after 6 weeks of treatment were based on effects on exercise tolerance testing performed 2 hours after the morning dose, at the time of the drug’s peak effect, in about 308 patients. It was unclear whether the effects could be maintained if the test had been performed later, which is particularly important because the indication is for maintenance treatment, according to the FDA reviewers.
The panel was not asked to vote on the exercise claim but discussed whether the results were clinically meaningful. Several panelists said that the improvements in exercise tolerance were notable, but since improvements were measured in a laboratory setting 2 hours after patients received the daily dose of olodaterol, it would be useful to evaluate how these improvements affected an individual’s activities of daily living. It would also be useful to provide a measurement later in the day to see if the effects persist throughout a period of time the patient may be active.
If approved, olodaterol will be marketed as Striverdi Respimat. It has already been approved in more than 60 countries.
The LABAs currently approved by the FDA are salmeterol, formoterol, and indacaterol.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may be given a waiver, but none were granted at this meeting.
AT A MEETING OF THE FDA'S PULMONARY-ALLERGY DRUGS ADVISORY COMMITTEE
Smoking ups mortality threefold
Both men and women who smoke are three times as likely to die as those who don’t.
Two large population-based studies have come to the same conclusion: Smokers are almost certainly going to die years and years sooner than nonsmokers.

"This analysis showed that a person who had never smoked was about twice as likely as a current smoker to reach 80 years of age," Dr. Prabhat Jha and his associates reported in the Jan. 24 issue of the New England Journal of Medicine (N. Engl. J. Med. 2013:368:341-50). "Among current smokers, survival was shorter by about 11 years for women and by about 12 years for men, as compared with participants who had never smoked."
The report wasn’t all bad news, however. Kicking the habit at any time added years of life, said Dr. Jha of the Center for Global Health Research, Toronto, and his coauthors.
The investigators examined smoking and smoking cessation among 113,752 women and 88,496 men who participated in the U.S. National Health Interview Survey from 1997 to 2004. These data were then correlated to information in the National Death Index up until the end of 2006.
The investigators then calculated the probability of survival in each group from 25 to 79 years of age. The mean follow-up was 7 years, with 10,743 deaths occurring in that age range.
After adjusting for education, alcohol use, and adiposity, men and women who smoked were three times more likely to have died than nonsmokers. The estimated probability of survival to the age of 80 years was 38% among women smokers but 70% for those who had never smoked. For male smokers, the probability of survival to age 80 was 26%, compared with 61% for those who had never smoked.
Both women and men who smoked were significantly more likely than nonsmokers to die in all of the smoking-related conditions examined:
• Lung cancer (hazard ratios of 18 and 15 for women and men, respectively).
• Other cancers (HR, 2 and 2).
• All cancers (HR, 3 and 4).
• Ischemic heart disease (HR, 3.5 and 3).
• Stroke (HR, 3 and 2).
• Other vascular disease (HR, 3 and 2).
• Respiratory disease (HR, 8.5 and 9).
• Other unspecified causes (HR, 2 and 2).
• All medical disorders (HR, 3 and 3).
• Accidents (HR, 4 and 2).
"At 25-79 years of age, about 62% of all deaths among female smokers and 60% of all deaths among male smokers would have been avoided if the rates of death from diseases among smokers had been the same as the rates among those who had never smoked," the authors noted.
Quitting smoking, on the other hand, conferred significant survival benefits, no matter when it occurred. Smokers who quit at age 25-34 years had similar survival to that of never-smokers. "Those who quit smoking gained about 10 years of life, as compared with those who continued to smoke."
Quitting at 35-44 years added 9 years of life, the authors found – not quite as good as those who quit earlier, but still a significant gain. "Smokers who had quit by about 39 years of age still had a 20% excess risk as compared with those who had never smoked. Although this hazard is substantial, it is much smaller than the 200% excess risk among those who continued to smoke."
Smokers who stopped at age 45-54 years gained 6 years of life, and those who quit at age 55-64 years about 4 more years of life. "Even cessation at the age of 45 to 54 years reduced the excess risk of death by about two-thirds," according to Dr. Jha and his coauthors.
While the study concluded that quitting at any age is a good idea, it shouldn’t be construed as a license to smoke longer. "That is not to say, however, that it is safe to smoke until 40 years of age and then stop, for the remaining excess risk of about 20% is substantial; it means that about one in six of these former smokers who dies before the age of 80 years would not have died."
The results are consistent with those of other studies around the world, the investigators said. The implications are staggering, especially for lower-income countries where smoking is more common and quitting less common.
"On the basis of current rates of smoking initiation and cessation, smoking, which killed about 100 million people in the 20th century, will kill about 1 billion in the 21st century."
A second study, also published in the Jan. 24 issue of the New England Journal of Medicine, found, for the first time, that women smokers are dying just as quickly – and from the same conditions – as men who smoke.
"The relative risks of death from lung cancer, chronic obstructive pulmonary disease, ischemic heart disease, any type of stroke, and all causes are now nearly identical for female and male smokers," Dr. Michael Thun and his colleagues wrote (N. Engl. J. Med. 2013:368:351-64). "This finding is new and confirms the prediction that, in relative terms, ‘women who smoke like men die like men.’ "
Dr. Thun, an epidemiologist with the American Cancer Society, and his colleagues drew their three study cohorts from seven national studies and databases. The entire study group comprised 1.32 million women and 899,000 men. Two of the cohorts were considered historical, covering 1959-1988; five were considered contemporary, covering 2000-2010. The participants’ ages by the end of each group’s follow-up period ranged from 50 years to more than 80 years.
For never-smokers, the analysis showed a general overall improvement in mortality between the historical and contemporary cohorts. But smokers did not enjoy this benefit. Between the historical and contemporary cohorts, all-cause mortality was 50% higher in smokers than in nonsmokers.
Again, women were particularly at risk, the investigators noted. "In contrast, there was no temporal decrease in the all-cause death rate among women who were current smokers and there was a 23.6% decrease among men who were current smokers. ... The risk of death from lung cancer among male smokers appears to have stabilized since the 1980s, whereas it continues to increase among female smokers."
Dr. Thun and his associates also found the threefold increase in the risk of death between smokers and never-smokers. Their data determined that at least two-thirds of these deaths were directly associated with smoking, including ischemic heart disease, all other heart disease, stroke, and lung cancer.
A comparison of nonsmokers and smokers within all the time cohorts showed that the highest risks of death for most disorders occurred from 1982 to 1988. Since then, the mortality risks have declined and stabilized but still remain elevated compared with never-smokers. The lung cancer mortality risks were strikingly evident, the authors said: a relative risk of 25 for both men and women.
In contrast to the stabilized rates of other diseases, the mortality risk of chronic obstructive pulmonary disease has continued to increase in smokers. The biggest jump affected smokers older than 55 years and occurred after the 1980s period. The overall COPD mortality risk in the 2000-2010 cohort was more than double that of the 1980s (RR 10 vs. 25.6). The risks were similar for women (RR, 10.3-22.3) and men (RR, 12.5-27.3).
The increase is somewhat of a mystery, the authors said. It can’t be explained by aging, smoking duration, or the improved ability to diagnose COPD. Instead, the finding may be related to changes in the way cigarettes are manufactured.
"For example, the introduction of blended tobacco and genetic selection of tobacco plants lowered the pH of smoke; as a result, inhalation was easier and deeper inhalation was needed for the absorption of protonated nicotine. Other design changes, such as the use of more porous wrapping paper and perforated filters, also diluted the smoke. Deeper inhalation of more dilute smoke increases exposure of the lung parenchyma," they wrote.
Histologic studies have also found a change paralleling these manufacturing differences, the authors noted. The changes "may also have contributed to the shift, beginning in the 1970s, in the histological and topographic features of lung cancers in male smokers, with an increase in the incidence of peripheral adenocarcinomas that largely offset the decrease in squamous-cell and small cell cancers of the central airways. The likely net effect of deeper inhalation on COPD could be wholly detrimental, since COPD results from injury to the lung parenchyma."
Dr. Jha’s study was funded by the Fogarty International Center, the National Institutes of Health, the Canadian Institutes of Health Research, and the Bill and Melinda Gates Foundation. Dr. Thun’s study was funded by the National Institutes of Health and the American Cancer Society. None of the authors of either study had any financial disclosures.
"Everyone knows cigarette smoking is bad for you. Most people in the United States assume that smoking is on its way out. But the grim reality is that smoking still exerts an enormous toll on the health of Americans," Dr. Steven A. Schoeder wrote.
In fact, the striking results of both studies may actually under-report the scope of smoking’s deadly grip on Americans’ health, Dr. Schroeder said in an accompanying editorial (N. Engl. J. Med. 2013:368:389-90).
"Population surveys accurately portray overall trends but omit nuances. Since frequency of smoking was not measured, we don’t know whether less illness occurs among light smokers (an increasing proportion of the smoking population), as compared with heavy smokers. Overall, smoking prevalence in the study by Thun et al. was only 9.5% – half the 2011 prevalence of 19% – because the samples overrepresented people who were better educated. Population groups with high rates of smoking (e.g., incarcerated persons and those with mental illness or substance-abuse disorders) are probably undersampled. Because both articles compared relative risks between smokers and nonsmokers, this omission would not alter the direction of the results. But because smokers in these populations smoke more cigarettes per day, the findings probably underestimate the overall mortality among smokers," he wrote.
Two important messages emerge from these articles, he said.
"First, in terms of health benefits, it is never too late to quit. Clinicians in general, and especially those who care for patients with smoking-related illnesses (e.g., oncologists, cardiologists, pulmonologists, emergency physicians, psychiatrists, and primary care physicians), should do more to stimulate quit attempts. Second, the importance of smoking as a health hazard needs to be elevated."
The public push for more cancer funding in certain diseases is laudable but misses some of the big picture. And smoking runs the risk of social marginalization, which could make it even more invisible to those who set research and policy priorities.
"Because smoking has become a stigmatized behavior concentrated among persons of low social status, it risks becoming invisible to those who set health policies and research priorities. Yet, the need for greater attention to the policies known to reduce the prevalence of smoking remains urgent. As former Australian Health Minister Nicola Roxon has said, ‘We are killing people by not acting,’ " according to Dr. Schroeder.
Dr. Steven Schroeder is director of the Smoking Cessation Leadership Center at the University of California, San Francisco. He had no financial disclosures.
"Everyone knows cigarette smoking is bad for you. Most people in the United States assume that smoking is on its way out. But the grim reality is that smoking still exerts an enormous toll on the health of Americans," Dr. Steven A. Schoeder wrote.
In fact, the striking results of both studies may actually under-report the scope of smoking’s deadly grip on Americans’ health, Dr. Schroeder said in an accompanying editorial (N. Engl. J. Med. 2013:368:389-90).
"Population surveys accurately portray overall trends but omit nuances. Since frequency of smoking was not measured, we don’t know whether less illness occurs among light smokers (an increasing proportion of the smoking population), as compared with heavy smokers. Overall, smoking prevalence in the study by Thun et al. was only 9.5% – half the 2011 prevalence of 19% – because the samples overrepresented people who were better educated. Population groups with high rates of smoking (e.g., incarcerated persons and those with mental illness or substance-abuse disorders) are probably undersampled. Because both articles compared relative risks between smokers and nonsmokers, this omission would not alter the direction of the results. But because smokers in these populations smoke more cigarettes per day, the findings probably underestimate the overall mortality among smokers," he wrote.
Two important messages emerge from these articles, he said.
"First, in terms of health benefits, it is never too late to quit. Clinicians in general, and especially those who care for patients with smoking-related illnesses (e.g., oncologists, cardiologists, pulmonologists, emergency physicians, psychiatrists, and primary care physicians), should do more to stimulate quit attempts. Second, the importance of smoking as a health hazard needs to be elevated."
The public push for more cancer funding in certain diseases is laudable but misses some of the big picture. And smoking runs the risk of social marginalization, which could make it even more invisible to those who set research and policy priorities.
"Because smoking has become a stigmatized behavior concentrated among persons of low social status, it risks becoming invisible to those who set health policies and research priorities. Yet, the need for greater attention to the policies known to reduce the prevalence of smoking remains urgent. As former Australian Health Minister Nicola Roxon has said, ‘We are killing people by not acting,’ " according to Dr. Schroeder.
Dr. Steven Schroeder is director of the Smoking Cessation Leadership Center at the University of California, San Francisco. He had no financial disclosures.
"Everyone knows cigarette smoking is bad for you. Most people in the United States assume that smoking is on its way out. But the grim reality is that smoking still exerts an enormous toll on the health of Americans," Dr. Steven A. Schoeder wrote.
In fact, the striking results of both studies may actually under-report the scope of smoking’s deadly grip on Americans’ health, Dr. Schroeder said in an accompanying editorial (N. Engl. J. Med. 2013:368:389-90).
"Population surveys accurately portray overall trends but omit nuances. Since frequency of smoking was not measured, we don’t know whether less illness occurs among light smokers (an increasing proportion of the smoking population), as compared with heavy smokers. Overall, smoking prevalence in the study by Thun et al. was only 9.5% – half the 2011 prevalence of 19% – because the samples overrepresented people who were better educated. Population groups with high rates of smoking (e.g., incarcerated persons and those with mental illness or substance-abuse disorders) are probably undersampled. Because both articles compared relative risks between smokers and nonsmokers, this omission would not alter the direction of the results. But because smokers in these populations smoke more cigarettes per day, the findings probably underestimate the overall mortality among smokers," he wrote.
Two important messages emerge from these articles, he said.
"First, in terms of health benefits, it is never too late to quit. Clinicians in general, and especially those who care for patients with smoking-related illnesses (e.g., oncologists, cardiologists, pulmonologists, emergency physicians, psychiatrists, and primary care physicians), should do more to stimulate quit attempts. Second, the importance of smoking as a health hazard needs to be elevated."
The public push for more cancer funding in certain diseases is laudable but misses some of the big picture. And smoking runs the risk of social marginalization, which could make it even more invisible to those who set research and policy priorities.
"Because smoking has become a stigmatized behavior concentrated among persons of low social status, it risks becoming invisible to those who set health policies and research priorities. Yet, the need for greater attention to the policies known to reduce the prevalence of smoking remains urgent. As former Australian Health Minister Nicola Roxon has said, ‘We are killing people by not acting,’ " according to Dr. Schroeder.
Dr. Steven Schroeder is director of the Smoking Cessation Leadership Center at the University of California, San Francisco. He had no financial disclosures.
Both men and women who smoke are three times as likely to die as those who don’t.
Two large population-based studies have come to the same conclusion: Smokers are almost certainly going to die years and years sooner than nonsmokers.
"This analysis showed that a person who had never smoked was about twice as likely as a current smoker to reach 80 years of age," Dr. Prabhat Jha and his associates reported in the Jan. 24 issue of the New England Journal of Medicine (N. Engl. J. Med. 2013:368:341-50). "Among current smokers, survival was shorter by about 11 years for women and by about 12 years for men, as compared with participants who had never smoked."
The report wasn’t all bad news, however. Kicking the habit at any time added years of life, said Dr. Jha of the Center for Global Health Research, Toronto, and his coauthors.
The investigators examined smoking and smoking cessation among 113,752 women and 88,496 men who participated in the U.S. National Health Interview Survey from 1997 to 2004. These data were then correlated to information in the National Death Index up until the end of 2006.
The investigators then calculated the probability of survival in each group from 25 to 79 years of age. The mean follow-up was 7 years, with 10,743 deaths occurring in that age range.
After adjusting for education, alcohol use, and adiposity, men and women who smoked were three times more likely to have died than nonsmokers. The estimated probability of survival to the age of 80 years was 38% among women smokers but 70% for those who had never smoked. For male smokers, the probability of survival to age 80 was 26%, compared with 61% for those who had never smoked.
Both women and men who smoked were significantly more likely than nonsmokers to die in all of the smoking-related conditions examined:
• Lung cancer (hazard ratios of 18 and 15 for women and men, respectively).
• Other cancers (HR, 2 and 2).
• All cancers (HR, 3 and 4).
• Ischemic heart disease (HR, 3.5 and 3).
• Stroke (HR, 3 and 2).
• Other vascular disease (HR, 3 and 2).
• Respiratory disease (HR, 8.5 and 9).
• Other unspecified causes (HR, 2 and 2).
• All medical disorders (HR, 3 and 3).
• Accidents (HR, 4 and 2).
"At 25-79 years of age, about 62% of all deaths among female smokers and 60% of all deaths among male smokers would have been avoided if the rates of death from diseases among smokers had been the same as the rates among those who had never smoked," the authors noted.
Quitting smoking, on the other hand, conferred significant survival benefits, no matter when it occurred. Smokers who quit at age 25-34 years had similar survival to that of never-smokers. "Those who quit smoking gained about 10 years of life, as compared with those who continued to smoke."
Quitting at 35-44 years added 9 years of life, the authors found – not quite as good as those who quit earlier, but still a significant gain. "Smokers who had quit by about 39 years of age still had a 20% excess risk as compared with those who had never smoked. Although this hazard is substantial, it is much smaller than the 200% excess risk among those who continued to smoke."
Smokers who stopped at age 45-54 years gained 6 years of life, and those who quit at age 55-64 years about 4 more years of life. "Even cessation at the age of 45 to 54 years reduced the excess risk of death by about two-thirds," according to Dr. Jha and his coauthors.
While the study concluded that quitting at any age is a good idea, it shouldn’t be construed as a license to smoke longer. "That is not to say, however, that it is safe to smoke until 40 years of age and then stop, for the remaining excess risk of about 20% is substantial; it means that about one in six of these former smokers who dies before the age of 80 years would not have died."
The results are consistent with those of other studies around the world, the investigators said. The implications are staggering, especially for lower-income countries where smoking is more common and quitting less common.
"On the basis of current rates of smoking initiation and cessation, smoking, which killed about 100 million people in the 20th century, will kill about 1 billion in the 21st century."
A second study, also published in the Jan. 24 issue of the New England Journal of Medicine, found, for the first time, that women smokers are dying just as quickly – and from the same conditions – as men who smoke.
"The relative risks of death from lung cancer, chronic obstructive pulmonary disease, ischemic heart disease, any type of stroke, and all causes are now nearly identical for female and male smokers," Dr. Michael Thun and his colleagues wrote (N. Engl. J. Med. 2013:368:351-64). "This finding is new and confirms the prediction that, in relative terms, ‘women who smoke like men die like men.’ "
Dr. Thun, an epidemiologist with the American Cancer Society, and his colleagues drew their three study cohorts from seven national studies and databases. The entire study group comprised 1.32 million women and 899,000 men. Two of the cohorts were considered historical, covering 1959-1988; five were considered contemporary, covering 2000-2010. The participants’ ages by the end of each group’s follow-up period ranged from 50 years to more than 80 years.
For never-smokers, the analysis showed a general overall improvement in mortality between the historical and contemporary cohorts. But smokers did not enjoy this benefit. Between the historical and contemporary cohorts, all-cause mortality was 50% higher in smokers than in nonsmokers.
Again, women were particularly at risk, the investigators noted. "In contrast, there was no temporal decrease in the all-cause death rate among women who were current smokers and there was a 23.6% decrease among men who were current smokers. ... The risk of death from lung cancer among male smokers appears to have stabilized since the 1980s, whereas it continues to increase among female smokers."
Dr. Thun and his associates also found the threefold increase in the risk of death between smokers and never-smokers. Their data determined that at least two-thirds of these deaths were directly associated with smoking, including ischemic heart disease, all other heart disease, stroke, and lung cancer.
A comparison of nonsmokers and smokers within all the time cohorts showed that the highest risks of death for most disorders occurred from 1982 to 1988. Since then, the mortality risks have declined and stabilized but still remain elevated compared with never-smokers. The lung cancer mortality risks were strikingly evident, the authors said: a relative risk of 25 for both men and women.
In contrast to the stabilized rates of other diseases, the mortality risk of chronic obstructive pulmonary disease has continued to increase in smokers. The biggest jump affected smokers older than 55 years and occurred after the 1980s period. The overall COPD mortality risk in the 2000-2010 cohort was more than double that of the 1980s (RR 10 vs. 25.6). The risks were similar for women (RR, 10.3-22.3) and men (RR, 12.5-27.3).
The increase is somewhat of a mystery, the authors said. It can’t be explained by aging, smoking duration, or the improved ability to diagnose COPD. Instead, the finding may be related to changes in the way cigarettes are manufactured.
"For example, the introduction of blended tobacco and genetic selection of tobacco plants lowered the pH of smoke; as a result, inhalation was easier and deeper inhalation was needed for the absorption of protonated nicotine. Other design changes, such as the use of more porous wrapping paper and perforated filters, also diluted the smoke. Deeper inhalation of more dilute smoke increases exposure of the lung parenchyma," they wrote.
Histologic studies have also found a change paralleling these manufacturing differences, the authors noted. The changes "may also have contributed to the shift, beginning in the 1970s, in the histological and topographic features of lung cancers in male smokers, with an increase in the incidence of peripheral adenocarcinomas that largely offset the decrease in squamous-cell and small cell cancers of the central airways. The likely net effect of deeper inhalation on COPD could be wholly detrimental, since COPD results from injury to the lung parenchyma."
Dr. Jha’s study was funded by the Fogarty International Center, the National Institutes of Health, the Canadian Institutes of Health Research, and the Bill and Melinda Gates Foundation. Dr. Thun’s study was funded by the National Institutes of Health and the American Cancer Society. None of the authors of either study had any financial disclosures.
Both men and women who smoke are three times as likely to die as those who don’t.
Two large population-based studies have come to the same conclusion: Smokers are almost certainly going to die years and years sooner than nonsmokers.
"This analysis showed that a person who had never smoked was about twice as likely as a current smoker to reach 80 years of age," Dr. Prabhat Jha and his associates reported in the Jan. 24 issue of the New England Journal of Medicine (N. Engl. J. Med. 2013:368:341-50). "Among current smokers, survival was shorter by about 11 years for women and by about 12 years for men, as compared with participants who had never smoked."
The report wasn’t all bad news, however. Kicking the habit at any time added years of life, said Dr. Jha of the Center for Global Health Research, Toronto, and his coauthors.
The investigators examined smoking and smoking cessation among 113,752 women and 88,496 men who participated in the U.S. National Health Interview Survey from 1997 to 2004. These data were then correlated to information in the National Death Index up until the end of 2006.
The investigators then calculated the probability of survival in each group from 25 to 79 years of age. The mean follow-up was 7 years, with 10,743 deaths occurring in that age range.
After adjusting for education, alcohol use, and adiposity, men and women who smoked were three times more likely to have died than nonsmokers. The estimated probability of survival to the age of 80 years was 38% among women smokers but 70% for those who had never smoked. For male smokers, the probability of survival to age 80 was 26%, compared with 61% for those who had never smoked.
Both women and men who smoked were significantly more likely than nonsmokers to die in all of the smoking-related conditions examined:
• Lung cancer (hazard ratios of 18 and 15 for women and men, respectively).
• Other cancers (HR, 2 and 2).
• All cancers (HR, 3 and 4).
• Ischemic heart disease (HR, 3.5 and 3).
• Stroke (HR, 3 and 2).
• Other vascular disease (HR, 3 and 2).
• Respiratory disease (HR, 8.5 and 9).
• Other unspecified causes (HR, 2 and 2).
• All medical disorders (HR, 3 and 3).
• Accidents (HR, 4 and 2).
"At 25-79 years of age, about 62% of all deaths among female smokers and 60% of all deaths among male smokers would have been avoided if the rates of death from diseases among smokers had been the same as the rates among those who had never smoked," the authors noted.
Quitting smoking, on the other hand, conferred significant survival benefits, no matter when it occurred. Smokers who quit at age 25-34 years had similar survival to that of never-smokers. "Those who quit smoking gained about 10 years of life, as compared with those who continued to smoke."
Quitting at 35-44 years added 9 years of life, the authors found – not quite as good as those who quit earlier, but still a significant gain. "Smokers who had quit by about 39 years of age still had a 20% excess risk as compared with those who had never smoked. Although this hazard is substantial, it is much smaller than the 200% excess risk among those who continued to smoke."
Smokers who stopped at age 45-54 years gained 6 years of life, and those who quit at age 55-64 years about 4 more years of life. "Even cessation at the age of 45 to 54 years reduced the excess risk of death by about two-thirds," according to Dr. Jha and his coauthors.
While the study concluded that quitting at any age is a good idea, it shouldn’t be construed as a license to smoke longer. "That is not to say, however, that it is safe to smoke until 40 years of age and then stop, for the remaining excess risk of about 20% is substantial; it means that about one in six of these former smokers who dies before the age of 80 years would not have died."
The results are consistent with those of other studies around the world, the investigators said. The implications are staggering, especially for lower-income countries where smoking is more common and quitting less common.
"On the basis of current rates of smoking initiation and cessation, smoking, which killed about 100 million people in the 20th century, will kill about 1 billion in the 21st century."
A second study, also published in the Jan. 24 issue of the New England Journal of Medicine, found, for the first time, that women smokers are dying just as quickly – and from the same conditions – as men who smoke.
"The relative risks of death from lung cancer, chronic obstructive pulmonary disease, ischemic heart disease, any type of stroke, and all causes are now nearly identical for female and male smokers," Dr. Michael Thun and his colleagues wrote (N. Engl. J. Med. 2013:368:351-64). "This finding is new and confirms the prediction that, in relative terms, ‘women who smoke like men die like men.’ "
Dr. Thun, an epidemiologist with the American Cancer Society, and his colleagues drew their three study cohorts from seven national studies and databases. The entire study group comprised 1.32 million women and 899,000 men. Two of the cohorts were considered historical, covering 1959-1988; five were considered contemporary, covering 2000-2010. The participants’ ages by the end of each group’s follow-up period ranged from 50 years to more than 80 years.
For never-smokers, the analysis showed a general overall improvement in mortality between the historical and contemporary cohorts. But smokers did not enjoy this benefit. Between the historical and contemporary cohorts, all-cause mortality was 50% higher in smokers than in nonsmokers.
Again, women were particularly at risk, the investigators noted. "In contrast, there was no temporal decrease in the all-cause death rate among women who were current smokers and there was a 23.6% decrease among men who were current smokers. ... The risk of death from lung cancer among male smokers appears to have stabilized since the 1980s, whereas it continues to increase among female smokers."
Dr. Thun and his associates also found the threefold increase in the risk of death between smokers and never-smokers. Their data determined that at least two-thirds of these deaths were directly associated with smoking, including ischemic heart disease, all other heart disease, stroke, and lung cancer.
A comparison of nonsmokers and smokers within all the time cohorts showed that the highest risks of death for most disorders occurred from 1982 to 1988. Since then, the mortality risks have declined and stabilized but still remain elevated compared with never-smokers. The lung cancer mortality risks were strikingly evident, the authors said: a relative risk of 25 for both men and women.
In contrast to the stabilized rates of other diseases, the mortality risk of chronic obstructive pulmonary disease has continued to increase in smokers. The biggest jump affected smokers older than 55 years and occurred after the 1980s period. The overall COPD mortality risk in the 2000-2010 cohort was more than double that of the 1980s (RR 10 vs. 25.6). The risks were similar for women (RR, 10.3-22.3) and men (RR, 12.5-27.3).
The increase is somewhat of a mystery, the authors said. It can’t be explained by aging, smoking duration, or the improved ability to diagnose COPD. Instead, the finding may be related to changes in the way cigarettes are manufactured.
"For example, the introduction of blended tobacco and genetic selection of tobacco plants lowered the pH of smoke; as a result, inhalation was easier and deeper inhalation was needed for the absorption of protonated nicotine. Other design changes, such as the use of more porous wrapping paper and perforated filters, also diluted the smoke. Deeper inhalation of more dilute smoke increases exposure of the lung parenchyma," they wrote.
Histologic studies have also found a change paralleling these manufacturing differences, the authors noted. The changes "may also have contributed to the shift, beginning in the 1970s, in the histological and topographic features of lung cancers in male smokers, with an increase in the incidence of peripheral adenocarcinomas that largely offset the decrease in squamous-cell and small cell cancers of the central airways. The likely net effect of deeper inhalation on COPD could be wholly detrimental, since COPD results from injury to the lung parenchyma."
Dr. Jha’s study was funded by the Fogarty International Center, the National Institutes of Health, the Canadian Institutes of Health Research, and the Bill and Melinda Gates Foundation. Dr. Thun’s study was funded by the National Institutes of Health and the American Cancer Society. None of the authors of either study had any financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Smokers are three times more likely to die than nonsmokers, with nearly all of the excess deaths directly attributable to smoking.
Data Source: Two studies comprising nearly 2.5 million people.
Disclosures: The studies were sponsored by the National Institutes of Health, American Cancer Society, Bill and Melinda Gates Foundation, Fogarty International Center, and the Canadian Institutes of Health Research. None of the authors had any financial disclosures.
Pigtail catheters less painful than chest tubes for traumatic pneumothorax
In patients with traumatic pneumothorax, smaller really is better, a study has shown.
The prospective, randomized study found that 14-French pigtail catheters function as well as do traditional, large-bore 28-French chest tubes, and result in significantly less tube-site pain.
The average numerical rating tube-site pain score was 3.2 with the pigtail catheter vs. 7.7 with the chest tube on the day of insertion, 1.9 vs. 6.2 on day 1 (both P values less than .001), and 2.1 vs. 5.5 on day 2 (P = .04).

Chest wall pain was similar between the two groups at all three time points (6.1 vs. 6.0; 5.5 vs. 5.9; and 4.2 vs. 5.9), as was intravenous pain medication use on day 1 (mean 10.3 U vs. 15.4 U) and day 2 (5.0 U vs. 8.6 U). One unit equaled 1 mg morphine, 25 mcg fentanyl, or 0.1 mg hydromorphone HCl (Dilaudid).
It stands to reason that the pigtail catheters are less painful because they’re soft, have a coiled tip, and are inserted with a less-invasive percutaneous technique, whereas traditional, large-bore chest tubes are straight and stiff, and are typically placed via a cutdown technique, Dr. Narong Kulvatunyou said at the annual meeting of the Eastern Association for the Surgery of Trauma.

A recent prospective observational study found no difference in tube-site pain with large (36- to 40-French) versus small (28- to 32-French) chest tubes inserted for chest trauma (J. Trauma Acute Care Surg. 2012;72:422-7), but the analysis still compared two large bores and both used the cutdown technique, he observed.
Based on their early experience in trauma patients, Dr. Kulvatunyou and his colleagues at the University of Arizona, Tucson, reported that 11% of pigtail catheters failed versus 4% of chest tubes (P = .06) (J. Trauma 2011;71:1104-7).
The 2-year review did not assess tube-site pain, prompting the current prospective study involving 40 patients with traumatic pneumothorax evenly randomized to a 14F pigtail catheter placed at the bedside with a modified Seldinger technique or a 28F chest tube placed via a cutdown technique. The tubes were left on suction for 24 hours.
Patients were excluded if they required emergency pigtail or chest tube placement or were unable to respond to the nurse-led pain assessment.
Demographics in the pigtail and chest tube groups were similar in average Injury Severity Score (14.5 vs. 12.2), abbreviated chest injury score (3 vs. 3), blunt trauma injury (85% vs. 80%), rib fractures (both 1.5), and pulmonary contusion (both 25%). Patients’ mean age was 46 years; 80% were male.
Contrary to expectations, tube-site pain was similar whether the pigtail catheter was placed anteriorly between the second and third rib (n = 9) or laterally (n = 11) between the fourth and fifth rib, Dr. Kulvatunyou said.
Failure rate, defined as unresolved or recurrent pneumothorax requiring a second tube, was 5% in the pigtail group and 10% in the chest tube group (P = .55). Secondary endpoints included insertion-related complications (10% for both groups), median number of tube days (2 for both), and median hospital stay (4 days for both).

Invited discussant Dr. David King, a trauma and acute care surgeon at Massachusetts General Hospital, Boston, questioned whether patients were receiving oral pain medications, as this could impact the results, and how the team mitigated a potential Hawthorne effect and observer bias.
"I know you said that the nurses who were getting the pain scores were blinded, but it’s pretty difficult to blind someone to the difference between a garden hose and a straw coming out of their chest wall," he said.
Dr. Kulvatunyou acknowledged that 10 out of 10 patients would prefer a smaller tube if asked, but that patients were asked only whether they would be willing to receive a "different tube that works pretty well," with no mention of tube size. As for the nurses, he said the tubes were typically under dressings and that some nurses may not have noticed the difference – a remark that was not well received based on comments after the session.
Data on oral medications were not collected because they were rarely used in the first 2 days and it was difficult to compare the oral medications, but Dr. Kulvatunyou said the point was well taken.
He noted that pigtail catheters could have a role in other traumatic indications such as hemothorax, hemopneumothorax, and emergency situations, but that additional studies are needed to show that it has equal efficacy to those chest tubes.
"I’m sure everyone puts central lines in pretty quickly, so just imagine if you could do pigtails just as quick as central lines," he said. "It would change everything."
Dr. Kulvatunyou, his coauthors, and Dr. King reported no relevant financial disclosures.
In patients with traumatic pneumothorax, smaller really is better, a study has shown.
The prospective, randomized study found that 14-French pigtail catheters function as well as do traditional, large-bore 28-French chest tubes, and result in significantly less tube-site pain.
The average numerical rating tube-site pain score was 3.2 with the pigtail catheter vs. 7.7 with the chest tube on the day of insertion, 1.9 vs. 6.2 on day 1 (both P values less than .001), and 2.1 vs. 5.5 on day 2 (P = .04).
Chest wall pain was similar between the two groups at all three time points (6.1 vs. 6.0; 5.5 vs. 5.9; and 4.2 vs. 5.9), as was intravenous pain medication use on day 1 (mean 10.3 U vs. 15.4 U) and day 2 (5.0 U vs. 8.6 U). One unit equaled 1 mg morphine, 25 mcg fentanyl, or 0.1 mg hydromorphone HCl (Dilaudid).
It stands to reason that the pigtail catheters are less painful because they’re soft, have a coiled tip, and are inserted with a less-invasive percutaneous technique, whereas traditional, large-bore chest tubes are straight and stiff, and are typically placed via a cutdown technique, Dr. Narong Kulvatunyou said at the annual meeting of the Eastern Association for the Surgery of Trauma.
A recent prospective observational study found no difference in tube-site pain with large (36- to 40-French) versus small (28- to 32-French) chest tubes inserted for chest trauma (J. Trauma Acute Care Surg. 2012;72:422-7), but the analysis still compared two large bores and both used the cutdown technique, he observed.
Based on their early experience in trauma patients, Dr. Kulvatunyou and his colleagues at the University of Arizona, Tucson, reported that 11% of pigtail catheters failed versus 4% of chest tubes (P = .06) (J. Trauma 2011;71:1104-7).
The 2-year review did not assess tube-site pain, prompting the current prospective study involving 40 patients with traumatic pneumothorax evenly randomized to a 14F pigtail catheter placed at the bedside with a modified Seldinger technique or a 28F chest tube placed via a cutdown technique. The tubes were left on suction for 24 hours.
Patients were excluded if they required emergency pigtail or chest tube placement or were unable to respond to the nurse-led pain assessment.
Demographics in the pigtail and chest tube groups were similar in average Injury Severity Score (14.5 vs. 12.2), abbreviated chest injury score (3 vs. 3), blunt trauma injury (85% vs. 80%), rib fractures (both 1.5), and pulmonary contusion (both 25%). Patients’ mean age was 46 years; 80% were male.
Contrary to expectations, tube-site pain was similar whether the pigtail catheter was placed anteriorly between the second and third rib (n = 9) or laterally (n = 11) between the fourth and fifth rib, Dr. Kulvatunyou said.
Failure rate, defined as unresolved or recurrent pneumothorax requiring a second tube, was 5% in the pigtail group and 10% in the chest tube group (P = .55). Secondary endpoints included insertion-related complications (10% for both groups), median number of tube days (2 for both), and median hospital stay (4 days for both).
Invited discussant Dr. David King, a trauma and acute care surgeon at Massachusetts General Hospital, Boston, questioned whether patients were receiving oral pain medications, as this could impact the results, and how the team mitigated a potential Hawthorne effect and observer bias.
"I know you said that the nurses who were getting the pain scores were blinded, but it’s pretty difficult to blind someone to the difference between a garden hose and a straw coming out of their chest wall," he said.
Dr. Kulvatunyou acknowledged that 10 out of 10 patients would prefer a smaller tube if asked, but that patients were asked only whether they would be willing to receive a "different tube that works pretty well," with no mention of tube size. As for the nurses, he said the tubes were typically under dressings and that some nurses may not have noticed the difference – a remark that was not well received based on comments after the session.
Data on oral medications were not collected because they were rarely used in the first 2 days and it was difficult to compare the oral medications, but Dr. Kulvatunyou said the point was well taken.
He noted that pigtail catheters could have a role in other traumatic indications such as hemothorax, hemopneumothorax, and emergency situations, but that additional studies are needed to show that it has equal efficacy to those chest tubes.
"I’m sure everyone puts central lines in pretty quickly, so just imagine if you could do pigtails just as quick as central lines," he said. "It would change everything."
Dr. Kulvatunyou, his coauthors, and Dr. King reported no relevant financial disclosures.
In patients with traumatic pneumothorax, smaller really is better, a study has shown.
The prospective, randomized study found that 14-French pigtail catheters function as well as do traditional, large-bore 28-French chest tubes, and result in significantly less tube-site pain.
The average numerical rating tube-site pain score was 3.2 with the pigtail catheter vs. 7.7 with the chest tube on the day of insertion, 1.9 vs. 6.2 on day 1 (both P values less than .001), and 2.1 vs. 5.5 on day 2 (P = .04).
Chest wall pain was similar between the two groups at all three time points (6.1 vs. 6.0; 5.5 vs. 5.9; and 4.2 vs. 5.9), as was intravenous pain medication use on day 1 (mean 10.3 U vs. 15.4 U) and day 2 (5.0 U vs. 8.6 U). One unit equaled 1 mg morphine, 25 mcg fentanyl, or 0.1 mg hydromorphone HCl (Dilaudid).
It stands to reason that the pigtail catheters are less painful because they’re soft, have a coiled tip, and are inserted with a less-invasive percutaneous technique, whereas traditional, large-bore chest tubes are straight and stiff, and are typically placed via a cutdown technique, Dr. Narong Kulvatunyou said at the annual meeting of the Eastern Association for the Surgery of Trauma.
A recent prospective observational study found no difference in tube-site pain with large (36- to 40-French) versus small (28- to 32-French) chest tubes inserted for chest trauma (J. Trauma Acute Care Surg. 2012;72:422-7), but the analysis still compared two large bores and both used the cutdown technique, he observed.
Based on their early experience in trauma patients, Dr. Kulvatunyou and his colleagues at the University of Arizona, Tucson, reported that 11% of pigtail catheters failed versus 4% of chest tubes (P = .06) (J. Trauma 2011;71:1104-7).
The 2-year review did not assess tube-site pain, prompting the current prospective study involving 40 patients with traumatic pneumothorax evenly randomized to a 14F pigtail catheter placed at the bedside with a modified Seldinger technique or a 28F chest tube placed via a cutdown technique. The tubes were left on suction for 24 hours.
Patients were excluded if they required emergency pigtail or chest tube placement or were unable to respond to the nurse-led pain assessment.
Demographics in the pigtail and chest tube groups were similar in average Injury Severity Score (14.5 vs. 12.2), abbreviated chest injury score (3 vs. 3), blunt trauma injury (85% vs. 80%), rib fractures (both 1.5), and pulmonary contusion (both 25%). Patients’ mean age was 46 years; 80% were male.
Contrary to expectations, tube-site pain was similar whether the pigtail catheter was placed anteriorly between the second and third rib (n = 9) or laterally (n = 11) between the fourth and fifth rib, Dr. Kulvatunyou said.
Failure rate, defined as unresolved or recurrent pneumothorax requiring a second tube, was 5% in the pigtail group and 10% in the chest tube group (P = .55). Secondary endpoints included insertion-related complications (10% for both groups), median number of tube days (2 for both), and median hospital stay (4 days for both).
Invited discussant Dr. David King, a trauma and acute care surgeon at Massachusetts General Hospital, Boston, questioned whether patients were receiving oral pain medications, as this could impact the results, and how the team mitigated a potential Hawthorne effect and observer bias.
"I know you said that the nurses who were getting the pain scores were blinded, but it’s pretty difficult to blind someone to the difference between a garden hose and a straw coming out of their chest wall," he said.
Dr. Kulvatunyou acknowledged that 10 out of 10 patients would prefer a smaller tube if asked, but that patients were asked only whether they would be willing to receive a "different tube that works pretty well," with no mention of tube size. As for the nurses, he said the tubes were typically under dressings and that some nurses may not have noticed the difference – a remark that was not well received based on comments after the session.
Data on oral medications were not collected because they were rarely used in the first 2 days and it was difficult to compare the oral medications, but Dr. Kulvatunyou said the point was well taken.
He noted that pigtail catheters could have a role in other traumatic indications such as hemothorax, hemopneumothorax, and emergency situations, but that additional studies are needed to show that it has equal efficacy to those chest tubes.
"I’m sure everyone puts central lines in pretty quickly, so just imagine if you could do pigtails just as quick as central lines," he said. "It would change everything."
Dr. Kulvatunyou, his coauthors, and Dr. King reported no relevant financial disclosures.
AT THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Major Finding: The average tube-site pain score was 3.2 with the pigtail catheter vs. 7.7 with the chest tube on the day of insertion, 1.9 vs. 6.2 on day 1 (both P values less than .001), and 2.1 vs. 5.5 on day 2 (P = .04).
Data Source: A prospective, randomized trial of 40 patients with traumatic pneumothorax.
Disclosures: Dr. Kulvatunyou, his coauthors, and Dr. King reported no relevant financial disclosures.
