User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Solid foods before 17 weeks linked to food allergy
Infants who are introduced to their first solid foods before 17 weeks of age have a higher likelihood of developing food allergies by 2 years, a U.K. team of researchers found.
Additionally, the researchers discovered that infants who receive their first cow’s milk products while still being breastfed were less likely to develop allergies than were those introduced to cow’s milk after breastfeeding had stopped.
The research, led by Kate E.C. Grimshaw, Ph.D., of the University of Southampton, England, and published online Nov. 18 in Pediatrics (2013 [doi:10.1542/peds.2012-3692]), supports current recommendations by the American Academy of Pediatrics that solid food be introduced at between 4 and 6 months*, concurrent with breastfeeding, to prevent allergies (Pediatrics 2008;121:183-91; Pediatrics 2012;129:e827-41).
Dr. Grimshaw and her colleagues’ study identified the 17-week mark as the "crucial time point," with solid food introduced before this time appearing to promote food allergies, while solid food introduced after this time apparently not doing so.
For their research, Dr. Grimshaw and her colleagues used a large prospective cohort study (n = 1,140) to identify mothers of 41 infants diagnosed with food allergies by age 2 years. These infants were matched with 82 controls born on close to the same date. All mothers of infants in the cohort study kept detailed daily food diaries describing their feeding practices through the first year after birth.
Dr. Grimshaw and her colleagues found that solid foods were introduced significantly earlier among the infants with allergies, with 35% of the former receiving their first solids before and including 16 weeks, compared with 14% of control infants (P = .011).
Of the infants who received cow’s milk concurrently with breast milk, the duration of concurrent feeding was longer – 9 weeks – in the control group, compared with 5.5 weeks in the allergy group (P = 0.47), suggesting that the duration of overlap was important and that longer overlap was helpful. However, there was no significant difference between the two groups in terms of the age at when the cow’s milk was introduced into the diet, they said.
Dr. Grimshaw and her colleagues listed as strengths of their study its prospective design that allowed for data collection from birth onward, and before any signs of allergy could become evident; only three infants in the study had evidence of allergy before 24 months. Also, they noted, a thorough diagnostic standard was used to identify allergies.
Although the optimum duration of exclusive breastfeeding has yet to be established, "Health professionals can provide advice that is consistent by encouraging exclusive breastfeeding for as long as possible followed by continued breastfeeding alongside the introduction of complementary foods to maximize the duration of concurrent breastfeeding and solid food introduction," Dr. Grimshaw and her colleagues wrote in their analysis.
The study was funded by the U.K. Food Standards Agency. Dr. Grimshaw declared an advisory relationship with Nutricia, while her coauthor Dr. Graham Roberts disclosed a relationship with Danone Baby Nutrition. Another coauthor on the study, Clare Mills, Ph.D., disclosed associations with Novartis, PepsiCo International, and DBV Technologies.
*Correction, 11/25/13: A previous version of this story misstated the AAP's recommendation for when solid foods should be introduced.
Infants who are introduced to their first solid foods before 17 weeks of age have a higher likelihood of developing food allergies by 2 years, a U.K. team of researchers found.
Additionally, the researchers discovered that infants who receive their first cow’s milk products while still being breastfed were less likely to develop allergies than were those introduced to cow’s milk after breastfeeding had stopped.
The research, led by Kate E.C. Grimshaw, Ph.D., of the University of Southampton, England, and published online Nov. 18 in Pediatrics (2013 [doi:10.1542/peds.2012-3692]), supports current recommendations by the American Academy of Pediatrics that solid food be introduced at between 4 and 6 months*, concurrent with breastfeeding, to prevent allergies (Pediatrics 2008;121:183-91; Pediatrics 2012;129:e827-41).
Dr. Grimshaw and her colleagues’ study identified the 17-week mark as the "crucial time point," with solid food introduced before this time appearing to promote food allergies, while solid food introduced after this time apparently not doing so.
For their research, Dr. Grimshaw and her colleagues used a large prospective cohort study (n = 1,140) to identify mothers of 41 infants diagnosed with food allergies by age 2 years. These infants were matched with 82 controls born on close to the same date. All mothers of infants in the cohort study kept detailed daily food diaries describing their feeding practices through the first year after birth.
Dr. Grimshaw and her colleagues found that solid foods were introduced significantly earlier among the infants with allergies, with 35% of the former receiving their first solids before and including 16 weeks, compared with 14% of control infants (P = .011).
Of the infants who received cow’s milk concurrently with breast milk, the duration of concurrent feeding was longer – 9 weeks – in the control group, compared with 5.5 weeks in the allergy group (P = 0.47), suggesting that the duration of overlap was important and that longer overlap was helpful. However, there was no significant difference between the two groups in terms of the age at when the cow’s milk was introduced into the diet, they said.
Dr. Grimshaw and her colleagues listed as strengths of their study its prospective design that allowed for data collection from birth onward, and before any signs of allergy could become evident; only three infants in the study had evidence of allergy before 24 months. Also, they noted, a thorough diagnostic standard was used to identify allergies.
Although the optimum duration of exclusive breastfeeding has yet to be established, "Health professionals can provide advice that is consistent by encouraging exclusive breastfeeding for as long as possible followed by continued breastfeeding alongside the introduction of complementary foods to maximize the duration of concurrent breastfeeding and solid food introduction," Dr. Grimshaw and her colleagues wrote in their analysis.
The study was funded by the U.K. Food Standards Agency. Dr. Grimshaw declared an advisory relationship with Nutricia, while her coauthor Dr. Graham Roberts disclosed a relationship with Danone Baby Nutrition. Another coauthor on the study, Clare Mills, Ph.D., disclosed associations with Novartis, PepsiCo International, and DBV Technologies.
*Correction, 11/25/13: A previous version of this story misstated the AAP's recommendation for when solid foods should be introduced.
Infants who are introduced to their first solid foods before 17 weeks of age have a higher likelihood of developing food allergies by 2 years, a U.K. team of researchers found.
Additionally, the researchers discovered that infants who receive their first cow’s milk products while still being breastfed were less likely to develop allergies than were those introduced to cow’s milk after breastfeeding had stopped.
The research, led by Kate E.C. Grimshaw, Ph.D., of the University of Southampton, England, and published online Nov. 18 in Pediatrics (2013 [doi:10.1542/peds.2012-3692]), supports current recommendations by the American Academy of Pediatrics that solid food be introduced at between 4 and 6 months*, concurrent with breastfeeding, to prevent allergies (Pediatrics 2008;121:183-91; Pediatrics 2012;129:e827-41).
Dr. Grimshaw and her colleagues’ study identified the 17-week mark as the "crucial time point," with solid food introduced before this time appearing to promote food allergies, while solid food introduced after this time apparently not doing so.
For their research, Dr. Grimshaw and her colleagues used a large prospective cohort study (n = 1,140) to identify mothers of 41 infants diagnosed with food allergies by age 2 years. These infants were matched with 82 controls born on close to the same date. All mothers of infants in the cohort study kept detailed daily food diaries describing their feeding practices through the first year after birth.
Dr. Grimshaw and her colleagues found that solid foods were introduced significantly earlier among the infants with allergies, with 35% of the former receiving their first solids before and including 16 weeks, compared with 14% of control infants (P = .011).
Of the infants who received cow’s milk concurrently with breast milk, the duration of concurrent feeding was longer – 9 weeks – in the control group, compared with 5.5 weeks in the allergy group (P = 0.47), suggesting that the duration of overlap was important and that longer overlap was helpful. However, there was no significant difference between the two groups in terms of the age at when the cow’s milk was introduced into the diet, they said.
Dr. Grimshaw and her colleagues listed as strengths of their study its prospective design that allowed for data collection from birth onward, and before any signs of allergy could become evident; only three infants in the study had evidence of allergy before 24 months. Also, they noted, a thorough diagnostic standard was used to identify allergies.
Although the optimum duration of exclusive breastfeeding has yet to be established, "Health professionals can provide advice that is consistent by encouraging exclusive breastfeeding for as long as possible followed by continued breastfeeding alongside the introduction of complementary foods to maximize the duration of concurrent breastfeeding and solid food introduction," Dr. Grimshaw and her colleagues wrote in their analysis.
The study was funded by the U.K. Food Standards Agency. Dr. Grimshaw declared an advisory relationship with Nutricia, while her coauthor Dr. Graham Roberts disclosed a relationship with Danone Baby Nutrition. Another coauthor on the study, Clare Mills, Ph.D., disclosed associations with Novartis, PepsiCo International, and DBV Technologies.
*Correction, 11/25/13: A previous version of this story misstated the AAP's recommendation for when solid foods should be introduced.
FROM PEDIATRICS
Major finding: Solid foods were introduced significantly earlier among the infants with allergies, with 35% of them receiving their first solids before and including 16 weeks, compared with 14% of control infants (P = .011).
Data source: A study of 41 infants diagnosed with food allergies by age 2 years and 82 age-matched controls.
Disclosures: The study was funded by the U.K. Food Standards Agency. Dr. Grimshaw declared an advisory relationship with Nutricia, while her coauthor Dr. Graham Roberts disclosed a relationship with Danone Baby Nutrition. Another coauthor on the study, Clare Mills, Ph.D., disclosed associations with Novartis, PepsiCo International, and DBV Technologies.
Roflumilast holds up in real world, postapproval studies
CHICAGO – Patients with chronic obstructive pulmonary disease treated with roflumilast had fewer all-cause hospital readmissions and monthly COPD exacerbations than nonusers in two real world database analyses.
Among 1,400 patients, all-cause, 30-day hospital readmissions were 6.9% for those using once-daily oral roflumilast (Daliresp) and 11.1% for nonusers (P = .021).
COPD-related hospital readmissions were also lower with roflumilast, but these findings did not reach statistical significance (6.3% vs. 9.2%; P = .086), Dr. Alpesh N. Amin reported at the annual meeting of the American College of Chest Physicians.
He noted that Medicare recently fined 230 hospitals $227 million for high readmission rates.

"Heart failure, MI, and pneumonia are first on the list, but COPD is right behind that in terms of the penalty issues," said Dr. Amin, chair of the department of medicine and executive director of the hospitalist program at the University of California, Irvine.
Roflumilast, a selective phosphodiesterase-4 inhibitor, was approved in May 2011 to reduce the frequency of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations.
Dr. Amin's retrospective study used data from MarketScan, a large U.S. commercial health insurance claims database, and Medicare supplemental data to evaluate hospitalizations among 15,755 patients discharged for COPD between July 1, 2011, and Dec. 31, 2011. Patients had to have used roflumilast within 14 days after hospitalization or be discharged for COPD without roflumilast use during the entire study period.
After propensity score matching and logistic regression to control for confounding by indication and baseline characteristics, a matched cohort of 350 roflumilast and 1,050 nonroflumilast patients remained.
Conditional logistic regressions showed that roflumilast use is associated with a significantly lower likelihood of all-cause 30-day hospital readmission (odds ratio, 0.59), and a trend toward decreased COPD 30-day readmission (OR, 0.66; P = .089), Dr. Amin said.

All patients in the study were covered by large employer-sponsored private health insurance programs, so generalization of the results to the Medicare and Medicaid populations cannot be assumed, he noted. During the same session, a second database analysis showed that despite being sicker at baseline, adults treated with roflumilast along with other COPD medications had significantly fewer monthly exacerbations than those receiving at least three other COPD maintenance medications.
During the 12-month baseline period, roflumilast patients used significantly more COPD drugs than nonroflumilast patients (mean 3.2 vs. 2.6), were on those drugs significantly longer (mean, 187 days vs. 166 days), and had significantly more baseline ER visits (mean, 0.5 vs. 0.3), and hospitalizations (79% vs. 72%).
The benefit was mainly driven by a reduction in moderate exacerbations, said Dr. Andrew Shorr, a critical care pulmonologist at Washington (D.C.) Hospital Center.
In unadjusted models, rates of combined monthly moderate and severe exacerbations fell 11.1% in the roflumilast group and rose 15.9% among controls, a significant difference.
When looked at separately, the difference was statistically significant for moderate exacerbations (–11.8% vs. +20.7%; P = .001), but not for severe exacerbations requiring hospitalization (–8.8% vs. –5.3%), he said.
After the investigators adjusted for baseline characteristics in a difference-in-difference model, the reduction remained significant for monthly severe/moderate (–0.0160) and moderate exacerbations (–0.0149), but not for severe exacerbations (–0.0012; P = .63).
"We estimated that the magnitude of the effect, after adjusting for baseline imbalances and natural time trends, was about a 23% absolute reduction in monthly exacerbations for the roflumilast group over controls," Dr. Shorr said.
The analysis was based on medical and pharmacy claims in the IMS LifeLink PharMetrics Plus database from May 2010 to December 2012. Data were for 710 COPD patients receiving roflumilast plus other COPD medications and 13,501 patients receiving at least two COPD maintenance medications and prescribed a third maintenance drug during the study index period of May 2011 and September 2012. Patients with asthma or who were corticosteroid dependent were excluded.
Forest Research Institute sponsored the studies. Dr. Amin and Dr. Shorr reported research support and other remuneration from Forest. Some coauthors in each study are Forest employees.
CHICAGO – Patients with chronic obstructive pulmonary disease treated with roflumilast had fewer all-cause hospital readmissions and monthly COPD exacerbations than nonusers in two real world database analyses.
Among 1,400 patients, all-cause, 30-day hospital readmissions were 6.9% for those using once-daily oral roflumilast (Daliresp) and 11.1% for nonusers (P = .021).
COPD-related hospital readmissions were also lower with roflumilast, but these findings did not reach statistical significance (6.3% vs. 9.2%; P = .086), Dr. Alpesh N. Amin reported at the annual meeting of the American College of Chest Physicians.
He noted that Medicare recently fined 230 hospitals $227 million for high readmission rates.
"Heart failure, MI, and pneumonia are first on the list, but COPD is right behind that in terms of the penalty issues," said Dr. Amin, chair of the department of medicine and executive director of the hospitalist program at the University of California, Irvine.
Roflumilast, a selective phosphodiesterase-4 inhibitor, was approved in May 2011 to reduce the frequency of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations.
Dr. Amin's retrospective study used data from MarketScan, a large U.S. commercial health insurance claims database, and Medicare supplemental data to evaluate hospitalizations among 15,755 patients discharged for COPD between July 1, 2011, and Dec. 31, 2011. Patients had to have used roflumilast within 14 days after hospitalization or be discharged for COPD without roflumilast use during the entire study period.
After propensity score matching and logistic regression to control for confounding by indication and baseline characteristics, a matched cohort of 350 roflumilast and 1,050 nonroflumilast patients remained.
Conditional logistic regressions showed that roflumilast use is associated with a significantly lower likelihood of all-cause 30-day hospital readmission (odds ratio, 0.59), and a trend toward decreased COPD 30-day readmission (OR, 0.66; P = .089), Dr. Amin said.
All patients in the study were covered by large employer-sponsored private health insurance programs, so generalization of the results to the Medicare and Medicaid populations cannot be assumed, he noted. During the same session, a second database analysis showed that despite being sicker at baseline, adults treated with roflumilast along with other COPD medications had significantly fewer monthly exacerbations than those receiving at least three other COPD maintenance medications.
During the 12-month baseline period, roflumilast patients used significantly more COPD drugs than nonroflumilast patients (mean 3.2 vs. 2.6), were on those drugs significantly longer (mean, 187 days vs. 166 days), and had significantly more baseline ER visits (mean, 0.5 vs. 0.3), and hospitalizations (79% vs. 72%).
The benefit was mainly driven by a reduction in moderate exacerbations, said Dr. Andrew Shorr, a critical care pulmonologist at Washington (D.C.) Hospital Center.
In unadjusted models, rates of combined monthly moderate and severe exacerbations fell 11.1% in the roflumilast group and rose 15.9% among controls, a significant difference.
When looked at separately, the difference was statistically significant for moderate exacerbations (–11.8% vs. +20.7%; P = .001), but not for severe exacerbations requiring hospitalization (–8.8% vs. –5.3%), he said.
After the investigators adjusted for baseline characteristics in a difference-in-difference model, the reduction remained significant for monthly severe/moderate (–0.0160) and moderate exacerbations (–0.0149), but not for severe exacerbations (–0.0012; P = .63).
"We estimated that the magnitude of the effect, after adjusting for baseline imbalances and natural time trends, was about a 23% absolute reduction in monthly exacerbations for the roflumilast group over controls," Dr. Shorr said.
The analysis was based on medical and pharmacy claims in the IMS LifeLink PharMetrics Plus database from May 2010 to December 2012. Data were for 710 COPD patients receiving roflumilast plus other COPD medications and 13,501 patients receiving at least two COPD maintenance medications and prescribed a third maintenance drug during the study index period of May 2011 and September 2012. Patients with asthma or who were corticosteroid dependent were excluded.
Forest Research Institute sponsored the studies. Dr. Amin and Dr. Shorr reported research support and other remuneration from Forest. Some coauthors in each study are Forest employees.
CHICAGO – Patients with chronic obstructive pulmonary disease treated with roflumilast had fewer all-cause hospital readmissions and monthly COPD exacerbations than nonusers in two real world database analyses.
Among 1,400 patients, all-cause, 30-day hospital readmissions were 6.9% for those using once-daily oral roflumilast (Daliresp) and 11.1% for nonusers (P = .021).
COPD-related hospital readmissions were also lower with roflumilast, but these findings did not reach statistical significance (6.3% vs. 9.2%; P = .086), Dr. Alpesh N. Amin reported at the annual meeting of the American College of Chest Physicians.
He noted that Medicare recently fined 230 hospitals $227 million for high readmission rates.
"Heart failure, MI, and pneumonia are first on the list, but COPD is right behind that in terms of the penalty issues," said Dr. Amin, chair of the department of medicine and executive director of the hospitalist program at the University of California, Irvine.
Roflumilast, a selective phosphodiesterase-4 inhibitor, was approved in May 2011 to reduce the frequency of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations.
Dr. Amin's retrospective study used data from MarketScan, a large U.S. commercial health insurance claims database, and Medicare supplemental data to evaluate hospitalizations among 15,755 patients discharged for COPD between July 1, 2011, and Dec. 31, 2011. Patients had to have used roflumilast within 14 days after hospitalization or be discharged for COPD without roflumilast use during the entire study period.
After propensity score matching and logistic regression to control for confounding by indication and baseline characteristics, a matched cohort of 350 roflumilast and 1,050 nonroflumilast patients remained.
Conditional logistic regressions showed that roflumilast use is associated with a significantly lower likelihood of all-cause 30-day hospital readmission (odds ratio, 0.59), and a trend toward decreased COPD 30-day readmission (OR, 0.66; P = .089), Dr. Amin said.
All patients in the study were covered by large employer-sponsored private health insurance programs, so generalization of the results to the Medicare and Medicaid populations cannot be assumed, he noted. During the same session, a second database analysis showed that despite being sicker at baseline, adults treated with roflumilast along with other COPD medications had significantly fewer monthly exacerbations than those receiving at least three other COPD maintenance medications.
During the 12-month baseline period, roflumilast patients used significantly more COPD drugs than nonroflumilast patients (mean 3.2 vs. 2.6), were on those drugs significantly longer (mean, 187 days vs. 166 days), and had significantly more baseline ER visits (mean, 0.5 vs. 0.3), and hospitalizations (79% vs. 72%).
The benefit was mainly driven by a reduction in moderate exacerbations, said Dr. Andrew Shorr, a critical care pulmonologist at Washington (D.C.) Hospital Center.
In unadjusted models, rates of combined monthly moderate and severe exacerbations fell 11.1% in the roflumilast group and rose 15.9% among controls, a significant difference.
When looked at separately, the difference was statistically significant for moderate exacerbations (–11.8% vs. +20.7%; P = .001), but not for severe exacerbations requiring hospitalization (–8.8% vs. –5.3%), he said.
After the investigators adjusted for baseline characteristics in a difference-in-difference model, the reduction remained significant for monthly severe/moderate (–0.0160) and moderate exacerbations (–0.0149), but not for severe exacerbations (–0.0012; P = .63).
"We estimated that the magnitude of the effect, after adjusting for baseline imbalances and natural time trends, was about a 23% absolute reduction in monthly exacerbations for the roflumilast group over controls," Dr. Shorr said.
The analysis was based on medical and pharmacy claims in the IMS LifeLink PharMetrics Plus database from May 2010 to December 2012. Data were for 710 COPD patients receiving roflumilast plus other COPD medications and 13,501 patients receiving at least two COPD maintenance medications and prescribed a third maintenance drug during the study index period of May 2011 and September 2012. Patients with asthma or who were corticosteroid dependent were excluded.
Forest Research Institute sponsored the studies. Dr. Amin and Dr. Shorr reported research support and other remuneration from Forest. Some coauthors in each study are Forest employees.
AT CHEST 2013
Major finding: 30-day hospital readmissions were 6.9% for those using once-daily oral roflumilast vs. 11.1% for nonusers.
Data source: Two database analyses of COPD patients.
Disclosures: Forest Research Institute sponsored the studies. Dr. Amin and Dr. Shorr reported research support and other remuneration from Forest. Some coauthors in each study are Forest employees.

Biologics inch ahead in asthma treatment
CHICAGO – Targeted biological therapies are working in rheumatoid arthritis, cancer, and irritable bowel disease, leading some experts to question whether their time in asthma has finally arrived.
"We’re still not there yet, but perhaps we can see the light at the end of the tunnel," Dr. Diego J. Maselli said at the annual meeting of the American College of Chest Physicians.
Early successes in animal models of asthma have not translated to humans with asthma, in part because of disparities in immunology, biology, and anatomy, but also because of the heterogeneous nature of the disease.
The benchmark so far for asthma biologics is the anti-immunoglobulin E (anti-IgE) monoclonal antibody omalizumab (Xolair), indicated for moderate to severe persistent asthma that is uncontrolled with inhaled corticosteroids.

Omalizumab gained approval after cutting exacerbations in two trials involving patients with a forced expiratory volume in one second (FEV1) between 40% and 80% predicted, but the drug had no effect on exacerbations in a third trial that did not restrict screening FEV1 and allowed use of long-acting beta2-agonists. In all three studies, exacerbations were not reduced in patients requiring oral steroids as maintenance therapy or those with an FEV1 over 80%.
There is now significant experience with omalizumab, and although there was a concern regarding a slight increase in the incidence of malignancy in the initial studies, large registries have shown no risk for malignant neoplasms or cardiovascular effects, said Dr. Maselli, of the University of Texas Health Science Center, San Antonio.
Promising results with several new agents, however, suggest that phenotypical markers such as IgE, eosinophils, and periostin are necessary to identify patients most likely to benefit from targeted therapy, he noted.
For example, the investigational interleukin 5 (IL-5) antagonist mepolizumab produced mixed initial results, but reduced asthma exacerbations over the course of 50 weeks from a mean of 3.4 to 2 in one study (N. Engl. J. Med. 2009;360:973-84), and by 48% over placebo in a second study when used in highly selected asthma patient populations with confirmed sputum or serum eosinophilia (Lancet 2012;380:651-9).
A recent meta-analysis (PLOS One 2013 March 27 [10.1371/journal.pone.0059872]) of seven mepolizumab studies echoed these findings, but also concluded the drug fails to significantly improve lung function, Dr. Maselli observed.
Provocative results from another biologic suggest that the presence of nasal polyps in eosinophilic asthma may be useful in further selecting patients for IL-5 antagonist therapy. Intravenous treatment with the anti-IL-5 antibody reslizumab (Cinquil) had a greater effect on sputum eosinophilia and asthma exacerbations in poorly controlled asthmatics with nasal polyps (Am. J. Respir. Crit. Care. Med. 2011;184:1125-32).
Serum levels of the matricellular protein periostin are also being used to better target interleukin-13 (IL-13)-directed therapy, Dr. Maselli said. IL-13 induces bronchial epithelial cells to secrete periostin and is thought to play a central role in asthma by promoting mucus secretion and airway remodeling and hyper-reactivity.
Six monthly injections of the experimental anti-IL-13 monoclonal antibody lebrikizumab significantly improved lung function over placebo in asthmatics poorly controlled on inhaled corticosteroids, but produced a more robust increase in FEV1 and a 60% reduction in exacerbations only in the subgroup with high pretreatment periostin levels (N. Engl. J. Med. 2011;365:1088-98). Interestingly, the investigators had hypothesized that high serum IgE plus high peripheral-blood eosinophil counts would serve as a marker for patients with high IL-13 expression.
To further complicate IL-13 blockade, a more recent lebrikizumab study in asthmatic patients not receiving inhaled steroids reported no meaningful differences in FEV1 between various lebrikizumab dose groups and placebo in a periostin subgroup (J. Allergy Clin. Immunol. 2013;132:567-574.e12).
The investigational anti-IL-13 monoclonal antibody tralokinumab also recently failed to meet its primary endpoint of improving Asthma Control Questionnaire scores compared with placebo and modestly improved FEV1 in a phase II study (Eur. Respir. J. 2013;41:330-8).
Finally, strong phase II results are being seen with dupilumab, a monoclonal antibody that inhibits both IL-4 and IL-13 signaling, Dr. Maselli said. Dupilumab cut exacerbations by a dramatic 87%, improved lung function, and decreased biomarkers associated with type 2 helper T-cell-driven inflammation in patients with elevated eosinophil levels and moderate to severe uncontrolled asthma despite use of glucocorticosteroids and long-acting beta-agonists (N. Engl. J. Med. 2013;368:2455-66).
"These agents allow clinicians to target specific asthma phenotypes with the aid of biomarkers such as IgE, eosinophilia, and periostin, and show a glimpse of what the future of ‘personalized medicine’ may offer," he said in an interview. "Ongoing studies will help elucidate which of these newer therapies will prove effective and safe for these difficult-to-treat asthmatics."
Dr. Maselli reported having no financial disclosures.
CHICAGO – Targeted biological therapies are working in rheumatoid arthritis, cancer, and irritable bowel disease, leading some experts to question whether their time in asthma has finally arrived.
"We’re still not there yet, but perhaps we can see the light at the end of the tunnel," Dr. Diego J. Maselli said at the annual meeting of the American College of Chest Physicians.
Early successes in animal models of asthma have not translated to humans with asthma, in part because of disparities in immunology, biology, and anatomy, but also because of the heterogeneous nature of the disease.
The benchmark so far for asthma biologics is the anti-immunoglobulin E (anti-IgE) monoclonal antibody omalizumab (Xolair), indicated for moderate to severe persistent asthma that is uncontrolled with inhaled corticosteroids.
Omalizumab gained approval after cutting exacerbations in two trials involving patients with a forced expiratory volume in one second (FEV1) between 40% and 80% predicted, but the drug had no effect on exacerbations in a third trial that did not restrict screening FEV1 and allowed use of long-acting beta2-agonists. In all three studies, exacerbations were not reduced in patients requiring oral steroids as maintenance therapy or those with an FEV1 over 80%.
There is now significant experience with omalizumab, and although there was a concern regarding a slight increase in the incidence of malignancy in the initial studies, large registries have shown no risk for malignant neoplasms or cardiovascular effects, said Dr. Maselli, of the University of Texas Health Science Center, San Antonio.
Promising results with several new agents, however, suggest that phenotypical markers such as IgE, eosinophils, and periostin are necessary to identify patients most likely to benefit from targeted therapy, he noted.
For example, the investigational interleukin 5 (IL-5) antagonist mepolizumab produced mixed initial results, but reduced asthma exacerbations over the course of 50 weeks from a mean of 3.4 to 2 in one study (N. Engl. J. Med. 2009;360:973-84), and by 48% over placebo in a second study when used in highly selected asthma patient populations with confirmed sputum or serum eosinophilia (Lancet 2012;380:651-9).
A recent meta-analysis (PLOS One 2013 March 27 [10.1371/journal.pone.0059872]) of seven mepolizumab studies echoed these findings, but also concluded the drug fails to significantly improve lung function, Dr. Maselli observed.
Provocative results from another biologic suggest that the presence of nasal polyps in eosinophilic asthma may be useful in further selecting patients for IL-5 antagonist therapy. Intravenous treatment with the anti-IL-5 antibody reslizumab (Cinquil) had a greater effect on sputum eosinophilia and asthma exacerbations in poorly controlled asthmatics with nasal polyps (Am. J. Respir. Crit. Care. Med. 2011;184:1125-32).
Serum levels of the matricellular protein periostin are also being used to better target interleukin-13 (IL-13)-directed therapy, Dr. Maselli said. IL-13 induces bronchial epithelial cells to secrete periostin and is thought to play a central role in asthma by promoting mucus secretion and airway remodeling and hyper-reactivity.
Six monthly injections of the experimental anti-IL-13 monoclonal antibody lebrikizumab significantly improved lung function over placebo in asthmatics poorly controlled on inhaled corticosteroids, but produced a more robust increase in FEV1 and a 60% reduction in exacerbations only in the subgroup with high pretreatment periostin levels (N. Engl. J. Med. 2011;365:1088-98). Interestingly, the investigators had hypothesized that high serum IgE plus high peripheral-blood eosinophil counts would serve as a marker for patients with high IL-13 expression.
To further complicate IL-13 blockade, a more recent lebrikizumab study in asthmatic patients not receiving inhaled steroids reported no meaningful differences in FEV1 between various lebrikizumab dose groups and placebo in a periostin subgroup (J. Allergy Clin. Immunol. 2013;132:567-574.e12).
The investigational anti-IL-13 monoclonal antibody tralokinumab also recently failed to meet its primary endpoint of improving Asthma Control Questionnaire scores compared with placebo and modestly improved FEV1 in a phase II study (Eur. Respir. J. 2013;41:330-8).
Finally, strong phase II results are being seen with dupilumab, a monoclonal antibody that inhibits both IL-4 and IL-13 signaling, Dr. Maselli said. Dupilumab cut exacerbations by a dramatic 87%, improved lung function, and decreased biomarkers associated with type 2 helper T-cell-driven inflammation in patients with elevated eosinophil levels and moderate to severe uncontrolled asthma despite use of glucocorticosteroids and long-acting beta-agonists (N. Engl. J. Med. 2013;368:2455-66).
"These agents allow clinicians to target specific asthma phenotypes with the aid of biomarkers such as IgE, eosinophilia, and periostin, and show a glimpse of what the future of ‘personalized medicine’ may offer," he said in an interview. "Ongoing studies will help elucidate which of these newer therapies will prove effective and safe for these difficult-to-treat asthmatics."
Dr. Maselli reported having no financial disclosures.
CHICAGO – Targeted biological therapies are working in rheumatoid arthritis, cancer, and irritable bowel disease, leading some experts to question whether their time in asthma has finally arrived.
"We’re still not there yet, but perhaps we can see the light at the end of the tunnel," Dr. Diego J. Maselli said at the annual meeting of the American College of Chest Physicians.
Early successes in animal models of asthma have not translated to humans with asthma, in part because of disparities in immunology, biology, and anatomy, but also because of the heterogeneous nature of the disease.
The benchmark so far for asthma biologics is the anti-immunoglobulin E (anti-IgE) monoclonal antibody omalizumab (Xolair), indicated for moderate to severe persistent asthma that is uncontrolled with inhaled corticosteroids.
Omalizumab gained approval after cutting exacerbations in two trials involving patients with a forced expiratory volume in one second (FEV1) between 40% and 80% predicted, but the drug had no effect on exacerbations in a third trial that did not restrict screening FEV1 and allowed use of long-acting beta2-agonists. In all three studies, exacerbations were not reduced in patients requiring oral steroids as maintenance therapy or those with an FEV1 over 80%.
There is now significant experience with omalizumab, and although there was a concern regarding a slight increase in the incidence of malignancy in the initial studies, large registries have shown no risk for malignant neoplasms or cardiovascular effects, said Dr. Maselli, of the University of Texas Health Science Center, San Antonio.
Promising results with several new agents, however, suggest that phenotypical markers such as IgE, eosinophils, and periostin are necessary to identify patients most likely to benefit from targeted therapy, he noted.
For example, the investigational interleukin 5 (IL-5) antagonist mepolizumab produced mixed initial results, but reduced asthma exacerbations over the course of 50 weeks from a mean of 3.4 to 2 in one study (N. Engl. J. Med. 2009;360:973-84), and by 48% over placebo in a second study when used in highly selected asthma patient populations with confirmed sputum or serum eosinophilia (Lancet 2012;380:651-9).
A recent meta-analysis (PLOS One 2013 March 27 [10.1371/journal.pone.0059872]) of seven mepolizumab studies echoed these findings, but also concluded the drug fails to significantly improve lung function, Dr. Maselli observed.
Provocative results from another biologic suggest that the presence of nasal polyps in eosinophilic asthma may be useful in further selecting patients for IL-5 antagonist therapy. Intravenous treatment with the anti-IL-5 antibody reslizumab (Cinquil) had a greater effect on sputum eosinophilia and asthma exacerbations in poorly controlled asthmatics with nasal polyps (Am. J. Respir. Crit. Care. Med. 2011;184:1125-32).
Serum levels of the matricellular protein periostin are also being used to better target interleukin-13 (IL-13)-directed therapy, Dr. Maselli said. IL-13 induces bronchial epithelial cells to secrete periostin and is thought to play a central role in asthma by promoting mucus secretion and airway remodeling and hyper-reactivity.
Six monthly injections of the experimental anti-IL-13 monoclonal antibody lebrikizumab significantly improved lung function over placebo in asthmatics poorly controlled on inhaled corticosteroids, but produced a more robust increase in FEV1 and a 60% reduction in exacerbations only in the subgroup with high pretreatment periostin levels (N. Engl. J. Med. 2011;365:1088-98). Interestingly, the investigators had hypothesized that high serum IgE plus high peripheral-blood eosinophil counts would serve as a marker for patients with high IL-13 expression.
To further complicate IL-13 blockade, a more recent lebrikizumab study in asthmatic patients not receiving inhaled steroids reported no meaningful differences in FEV1 between various lebrikizumab dose groups and placebo in a periostin subgroup (J. Allergy Clin. Immunol. 2013;132:567-574.e12).
The investigational anti-IL-13 monoclonal antibody tralokinumab also recently failed to meet its primary endpoint of improving Asthma Control Questionnaire scores compared with placebo and modestly improved FEV1 in a phase II study (Eur. Respir. J. 2013;41:330-8).
Finally, strong phase II results are being seen with dupilumab, a monoclonal antibody that inhibits both IL-4 and IL-13 signaling, Dr. Maselli said. Dupilumab cut exacerbations by a dramatic 87%, improved lung function, and decreased biomarkers associated with type 2 helper T-cell-driven inflammation in patients with elevated eosinophil levels and moderate to severe uncontrolled asthma despite use of glucocorticosteroids and long-acting beta-agonists (N. Engl. J. Med. 2013;368:2455-66).
"These agents allow clinicians to target specific asthma phenotypes with the aid of biomarkers such as IgE, eosinophilia, and periostin, and show a glimpse of what the future of ‘personalized medicine’ may offer," he said in an interview. "Ongoing studies will help elucidate which of these newer therapies will prove effective and safe for these difficult-to-treat asthmatics."
Dr. Maselli reported having no financial disclosures.
AT CHEST 2013

Clinical phenotypes in COPD lead to better diagnosis, more targeted treatments
CHICAGO – Accurate phenotyping, in the ascendant over the last decade, equates with more effectively targeted treatments for chronic obstructive pulmonary disease, according to a proponent of personalized pulmonary medicine.
"We know that COPD is not the same, but right now we are treating these patients as though one size fits all," Dr. Nicola A. Hanania of the Baylor College of Medicine, Houston, said in a packed session on COPD at the annual meeting of the American College of Chest Physicians.
Because phenotypes describe differences in individuals, they should have relevance to clinically meaningful outcomes. "In COPD, that relates to symptoms, exacerbation, disease progression, response to therapy, and survival," he said.
Potential phenotypes that have been identified according to clinical, physiologic, and radiologic criteria include chronic bronchitis, asthma/COPD overlap, frequent exacerbator, radiologic CT, and persistent systemic inflammation.
Chronic bronchitis
Chronic bronchitis tends to occur more in younger people who smoke. It also is characterized by more wheezing and thicker airway walls. Data presented by Dr. Hanania also showed that this phenotype has more frequent acute exacerbations (Chest 2011;140:1107-8).

In one study, 290 subjects deemed chronically bronchitic – chronic cough and phlegm lasting 3 months of every year for 2 consecutive years – were compared with 771 subjects who were not chronically bronchitic. Investigators found that patients in the first group had more frequent exacerbations per patient: 1.21-1.62 vs. 0.63-1.12 (P < .027). The first group also reported more severe exacerbations: 26.6% vs. 20% (P < .024) (Chest 2011;140:626-33).
Asthma/COPD overlap
"This is a phenotype that deserves more attention. We all have patients where we scratch our head, ‘Is this asthma, or is this COPD?’ " said Dr. Hanania. "We don’t really know because these patients are notoriously excluded from both asthma and COPD studies." He cited estimates suggesting that 13%-20% of COPD patients overlap with asthma (Arch. Bronconeumol. 2012;48:331-7).
Proposed diagnostic criteria for the overlap syndrome phenotype may include two major criteria: marked response to bronchodilators (>15% and >400 mL in forced expiratory volume in 1 second [FEV1]), history of asthma if patient is younger than 40 years, and sputum eosinophilia. Overlap also can be diagnosed by one major criterion and two of the following: response to bronchodilation at least two separate times (>12% and >200 mL in FEV1), history of atopy, and increased total serum IgE. At this time, he said, these criteria are based on expert opinion and on data, "but the clinical implications, once we do the homework, is that these patients deserve to be on antibiotics and corticosteroids early on."
Frequent exacerbator
Defined in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines as two or more exacerbations per year, the frequent exacerbator phenotype was explained in the ECLIPSE study (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints), Dr. Hanania said, which showed that, although exacerbations become more frequent and more severe as COPD progresses, the rate at which they occur appears to reflect an independent susceptibility phenotype (N. Engl. J. Med. 2010; 363:1128-38).
Frequent exacerbators have higher-stage COPD, more severe obstruction, and more hospitalizations, Dr. Hanania noted.
In addition, the ECLIPSE investigators found that, in 2,138 patients, frequent exacerbator types had an odds ratio of 5.72 of having had an exacerbation in the previous year
Although there other risk factors implicating this phenotype, "the most important question to ask the patient is whether they have had an exacerbation in the previous year," he said. Chronic cough is another factor.
The clinical benefit to identifying the frequent exacerbator, according to Dr. Hanania, is that this group has a greater range of comorbidities, including more inflammation, heightened viral susceptibility, and increased cardiovascular risk, among other susceptibilities.
Using CT for phenotyping
Noting that radiologic phenotyping in COPD is more advanced than in asthma at this time, Dr. Hanania said that quantitative and visual assessment of CT radiographs is "promising" and has helped identify COPD subphenotypes such as emphysema because of accurate assessment of lung inflation, wall thickness, and other factors.
Identifying patients with bronchiectasis, pulmonary arterial enlargement, and acute exacerbations in COPD is also possible with CT radiography, making it possible to predict the different outcomes in each situation. "The clinical implication is that these patients tend to have more frequent exacerbation, worse lung function, and infection," he said, noting that nascent research using imaging to determine biomarkers in functional small airways disease also is occurring.
Systemic inflammation
In the ECLIPSE study, 2,164 COPD patients had an odds ratio of 2.23 for being a current smoker and had higher levels of inflammation, as determined using biomarkers such as C-reactive protein, compared with 337 smokers without COPD and 245 nonsmokers. At the 3-year follow-up, this group with persistently higher inflammation also was classified as having significantly higher all-cause mortality than the group with less inflammation (13% vs. 2%); exacerbation rates in this group were also persistently higher (1.5 vs. 0.9) (PLoS ONE 2012;7:e37483).
Therapeutic implications
Coupling these phenotypes with molecular descriptions of mechanisms and their underlying pathologies can lead to accurate, personalized treatment of COPD. "Phenotypes without clear implications for prognosis and treatment are of little clinical use," Dr. Hanania said, noting that longitudinal studies to validate these phenotypes are necessary.
"Research can help identify mechanisms and courses in different phenotypes, including gender differences," he concluded. "Examining therapeutic responses to different phenotypes can lead to future interventions."
Dr. Hanania disclosed several relationships with a variety of pharmaceutical and medical manufacturers, including Genentech, GlaxoSmithKline* and Astra Zeneca.
Beyond GOLD: A tale of two COPD guidelines
Both address severity and comorbidity, but only one COPD guideline takes into account the latest research on phenotyping in chronic obstructive pulmonary disease.
"The GOLD guidelines do not include clinical phenotypes," said Dr. Joan Soriano, a presenter at the meeting. "But the Spanish ones do."
In fact, there is really only one area where the two documents overlap, said Dr. Soriano: how they define COPD, and even that is not the same. "They both mention the fundamental aspect, which is airflow limitation, and also that the mechanism involved is inflammation," he said. The GOLD definition, however, recognizes the importance of comorbidities, which the Spanish guidelines address the role of tobacco and symptomology.
GOLD (Global Initiative for Chronic Obstructive Lung Disease) is an organization of health care professionals from around the world. "I am not a member of GOLD," Dr. Soriano told the packed session.
The Spanish guidelines are issued by SEPAR, the Spanish Society for Pneumology and Thoracic Surgery. Dr. Soriano is the director of epidemiology and clinical research at the International Center of Advanced Respiratory Medicine (CIMERA) in Palma, Spain.
How the two approach diagnosis also differs. The Spanish guidelines begin with the general COPD diagnosis, then move to the characterization and phenotype, then move to the severity of the disease. They are more specific about age (over 35 years), and have lower limit of normal (LLN) values for persons aged over 70 years and less than 50 years. The GOLD guidelines do not address LLN.
To characterize the disease specifically, the Spanish guidelines address the existence of phenotypes, according to Dr. Soriano, beginning with determining the frequency of exacerbation the patient has per year, and then classifying them eventually into four types: mixed, chronic bronchitis, emphysema, and exacerbator. The GOLD guidelines do not mention phenotypes.
When it comes to the multidimensional assessment of COPD, "the GOLD guidelines lump the mild with the severe spirometry. This is very hard for me to understand," he said. Other classification divergence includes that the Spanish guidelines consider the BODE index.
Treatment in the two guidelines begins similarly, but vectors off from there. "Basically, we are looking at the same trials, so the initial treatments should be short-acting bronchodilators," Dr. Soriano said, but because phenotyping allows for more targeted treatment, the Spanish guidelines offer more detailed treatment options.
In a paper coauthored by Dr. Soriano earlier this year, specific treatment per phenotype included phosphodiesterase-4 inhibitors only for those with chronic bronchitis, inhaled corticosteroids for overlap COPD-asthma, and bronchodilators for infrequent exacerbators (Eur. Respir. J. 2013;41:1252-6).
In the end, the guidelines might not follow the same trajectory, but each has value, he said. "Whatever guidelines you choose, don’t go back and forth. Pick one and use them."
Dr. Soriano reported relationships with Novartis Spain, AstraZeneca, Pfizer, and several other pharmaceutical and medical manufacturers.
*CORRECTION, 2/20/2014: An earlier version of this story misstated the name of GlaxoSmithKline.
CHICAGO – Accurate phenotyping, in the ascendant over the last decade, equates with more effectively targeted treatments for chronic obstructive pulmonary disease, according to a proponent of personalized pulmonary medicine.
"We know that COPD is not the same, but right now we are treating these patients as though one size fits all," Dr. Nicola A. Hanania of the Baylor College of Medicine, Houston, said in a packed session on COPD at the annual meeting of the American College of Chest Physicians.
Because phenotypes describe differences in individuals, they should have relevance to clinically meaningful outcomes. "In COPD, that relates to symptoms, exacerbation, disease progression, response to therapy, and survival," he said.
Potential phenotypes that have been identified according to clinical, physiologic, and radiologic criteria include chronic bronchitis, asthma/COPD overlap, frequent exacerbator, radiologic CT, and persistent systemic inflammation.
Chronic bronchitis
Chronic bronchitis tends to occur more in younger people who smoke. It also is characterized by more wheezing and thicker airway walls. Data presented by Dr. Hanania also showed that this phenotype has more frequent acute exacerbations (Chest 2011;140:1107-8).
In one study, 290 subjects deemed chronically bronchitic – chronic cough and phlegm lasting 3 months of every year for 2 consecutive years – were compared with 771 subjects who were not chronically bronchitic. Investigators found that patients in the first group had more frequent exacerbations per patient: 1.21-1.62 vs. 0.63-1.12 (P < .027). The first group also reported more severe exacerbations: 26.6% vs. 20% (P < .024) (Chest 2011;140:626-33).
Asthma/COPD overlap
"This is a phenotype that deserves more attention. We all have patients where we scratch our head, ‘Is this asthma, or is this COPD?’ " said Dr. Hanania. "We don’t really know because these patients are notoriously excluded from both asthma and COPD studies." He cited estimates suggesting that 13%-20% of COPD patients overlap with asthma (Arch. Bronconeumol. 2012;48:331-7).
Proposed diagnostic criteria for the overlap syndrome phenotype may include two major criteria: marked response to bronchodilators (>15% and >400 mL in forced expiratory volume in 1 second [FEV1]), history of asthma if patient is younger than 40 years, and sputum eosinophilia. Overlap also can be diagnosed by one major criterion and two of the following: response to bronchodilation at least two separate times (>12% and >200 mL in FEV1), history of atopy, and increased total serum IgE. At this time, he said, these criteria are based on expert opinion and on data, "but the clinical implications, once we do the homework, is that these patients deserve to be on antibiotics and corticosteroids early on."
Frequent exacerbator
Defined in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines as two or more exacerbations per year, the frequent exacerbator phenotype was explained in the ECLIPSE study (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints), Dr. Hanania said, which showed that, although exacerbations become more frequent and more severe as COPD progresses, the rate at which they occur appears to reflect an independent susceptibility phenotype (N. Engl. J. Med. 2010; 363:1128-38).
Frequent exacerbators have higher-stage COPD, more severe obstruction, and more hospitalizations, Dr. Hanania noted.
In addition, the ECLIPSE investigators found that, in 2,138 patients, frequent exacerbator types had an odds ratio of 5.72 of having had an exacerbation in the previous year
Although there other risk factors implicating this phenotype, "the most important question to ask the patient is whether they have had an exacerbation in the previous year," he said. Chronic cough is another factor.
The clinical benefit to identifying the frequent exacerbator, according to Dr. Hanania, is that this group has a greater range of comorbidities, including more inflammation, heightened viral susceptibility, and increased cardiovascular risk, among other susceptibilities.
Using CT for phenotyping
Noting that radiologic phenotyping in COPD is more advanced than in asthma at this time, Dr. Hanania said that quantitative and visual assessment of CT radiographs is "promising" and has helped identify COPD subphenotypes such as emphysema because of accurate assessment of lung inflation, wall thickness, and other factors.
Identifying patients with bronchiectasis, pulmonary arterial enlargement, and acute exacerbations in COPD is also possible with CT radiography, making it possible to predict the different outcomes in each situation. "The clinical implication is that these patients tend to have more frequent exacerbation, worse lung function, and infection," he said, noting that nascent research using imaging to determine biomarkers in functional small airways disease also is occurring.
Systemic inflammation
In the ECLIPSE study, 2,164 COPD patients had an odds ratio of 2.23 for being a current smoker and had higher levels of inflammation, as determined using biomarkers such as C-reactive protein, compared with 337 smokers without COPD and 245 nonsmokers. At the 3-year follow-up, this group with persistently higher inflammation also was classified as having significantly higher all-cause mortality than the group with less inflammation (13% vs. 2%); exacerbation rates in this group were also persistently higher (1.5 vs. 0.9) (PLoS ONE 2012;7:e37483).
Therapeutic implications
Coupling these phenotypes with molecular descriptions of mechanisms and their underlying pathologies can lead to accurate, personalized treatment of COPD. "Phenotypes without clear implications for prognosis and treatment are of little clinical use," Dr. Hanania said, noting that longitudinal studies to validate these phenotypes are necessary.
"Research can help identify mechanisms and courses in different phenotypes, including gender differences," he concluded. "Examining therapeutic responses to different phenotypes can lead to future interventions."
Dr. Hanania disclosed several relationships with a variety of pharmaceutical and medical manufacturers, including Genentech, GlaxoSmithKline* and Astra Zeneca.
Beyond GOLD: A tale of two COPD guidelines
Both address severity and comorbidity, but only one COPD guideline takes into account the latest research on phenotyping in chronic obstructive pulmonary disease.
"The GOLD guidelines do not include clinical phenotypes," said Dr. Joan Soriano, a presenter at the meeting. "But the Spanish ones do."
In fact, there is really only one area where the two documents overlap, said Dr. Soriano: how they define COPD, and even that is not the same. "They both mention the fundamental aspect, which is airflow limitation, and also that the mechanism involved is inflammation," he said. The GOLD definition, however, recognizes the importance of comorbidities, which the Spanish guidelines address the role of tobacco and symptomology.
GOLD (Global Initiative for Chronic Obstructive Lung Disease) is an organization of health care professionals from around the world. "I am not a member of GOLD," Dr. Soriano told the packed session.
The Spanish guidelines are issued by SEPAR, the Spanish Society for Pneumology and Thoracic Surgery. Dr. Soriano is the director of epidemiology and clinical research at the International Center of Advanced Respiratory Medicine (CIMERA) in Palma, Spain.
How the two approach diagnosis also differs. The Spanish guidelines begin with the general COPD diagnosis, then move to the characterization and phenotype, then move to the severity of the disease. They are more specific about age (over 35 years), and have lower limit of normal (LLN) values for persons aged over 70 years and less than 50 years. The GOLD guidelines do not address LLN.
To characterize the disease specifically, the Spanish guidelines address the existence of phenotypes, according to Dr. Soriano, beginning with determining the frequency of exacerbation the patient has per year, and then classifying them eventually into four types: mixed, chronic bronchitis, emphysema, and exacerbator. The GOLD guidelines do not mention phenotypes.
When it comes to the multidimensional assessment of COPD, "the GOLD guidelines lump the mild with the severe spirometry. This is very hard for me to understand," he said. Other classification divergence includes that the Spanish guidelines consider the BODE index.
Treatment in the two guidelines begins similarly, but vectors off from there. "Basically, we are looking at the same trials, so the initial treatments should be short-acting bronchodilators," Dr. Soriano said, but because phenotyping allows for more targeted treatment, the Spanish guidelines offer more detailed treatment options.
In a paper coauthored by Dr. Soriano earlier this year, specific treatment per phenotype included phosphodiesterase-4 inhibitors only for those with chronic bronchitis, inhaled corticosteroids for overlap COPD-asthma, and bronchodilators for infrequent exacerbators (Eur. Respir. J. 2013;41:1252-6).
In the end, the guidelines might not follow the same trajectory, but each has value, he said. "Whatever guidelines you choose, don’t go back and forth. Pick one and use them."
Dr. Soriano reported relationships with Novartis Spain, AstraZeneca, Pfizer, and several other pharmaceutical and medical manufacturers.
*CORRECTION, 2/20/2014: An earlier version of this story misstated the name of GlaxoSmithKline.
CHICAGO – Accurate phenotyping, in the ascendant over the last decade, equates with more effectively targeted treatments for chronic obstructive pulmonary disease, according to a proponent of personalized pulmonary medicine.
"We know that COPD is not the same, but right now we are treating these patients as though one size fits all," Dr. Nicola A. Hanania of the Baylor College of Medicine, Houston, said in a packed session on COPD at the annual meeting of the American College of Chest Physicians.
Because phenotypes describe differences in individuals, they should have relevance to clinically meaningful outcomes. "In COPD, that relates to symptoms, exacerbation, disease progression, response to therapy, and survival," he said.
Potential phenotypes that have been identified according to clinical, physiologic, and radiologic criteria include chronic bronchitis, asthma/COPD overlap, frequent exacerbator, radiologic CT, and persistent systemic inflammation.
Chronic bronchitis
Chronic bronchitis tends to occur more in younger people who smoke. It also is characterized by more wheezing and thicker airway walls. Data presented by Dr. Hanania also showed that this phenotype has more frequent acute exacerbations (Chest 2011;140:1107-8).
In one study, 290 subjects deemed chronically bronchitic – chronic cough and phlegm lasting 3 months of every year for 2 consecutive years – were compared with 771 subjects who were not chronically bronchitic. Investigators found that patients in the first group had more frequent exacerbations per patient: 1.21-1.62 vs. 0.63-1.12 (P < .027). The first group also reported more severe exacerbations: 26.6% vs. 20% (P < .024) (Chest 2011;140:626-33).
Asthma/COPD overlap
"This is a phenotype that deserves more attention. We all have patients where we scratch our head, ‘Is this asthma, or is this COPD?’ " said Dr. Hanania. "We don’t really know because these patients are notoriously excluded from both asthma and COPD studies." He cited estimates suggesting that 13%-20% of COPD patients overlap with asthma (Arch. Bronconeumol. 2012;48:331-7).
Proposed diagnostic criteria for the overlap syndrome phenotype may include two major criteria: marked response to bronchodilators (>15% and >400 mL in forced expiratory volume in 1 second [FEV1]), history of asthma if patient is younger than 40 years, and sputum eosinophilia. Overlap also can be diagnosed by one major criterion and two of the following: response to bronchodilation at least two separate times (>12% and >200 mL in FEV1), history of atopy, and increased total serum IgE. At this time, he said, these criteria are based on expert opinion and on data, "but the clinical implications, once we do the homework, is that these patients deserve to be on antibiotics and corticosteroids early on."
Frequent exacerbator
Defined in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines as two or more exacerbations per year, the frequent exacerbator phenotype was explained in the ECLIPSE study (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints), Dr. Hanania said, which showed that, although exacerbations become more frequent and more severe as COPD progresses, the rate at which they occur appears to reflect an independent susceptibility phenotype (N. Engl. J. Med. 2010; 363:1128-38).
Frequent exacerbators have higher-stage COPD, more severe obstruction, and more hospitalizations, Dr. Hanania noted.
In addition, the ECLIPSE investigators found that, in 2,138 patients, frequent exacerbator types had an odds ratio of 5.72 of having had an exacerbation in the previous year
Although there other risk factors implicating this phenotype, "the most important question to ask the patient is whether they have had an exacerbation in the previous year," he said. Chronic cough is another factor.
The clinical benefit to identifying the frequent exacerbator, according to Dr. Hanania, is that this group has a greater range of comorbidities, including more inflammation, heightened viral susceptibility, and increased cardiovascular risk, among other susceptibilities.
Using CT for phenotyping
Noting that radiologic phenotyping in COPD is more advanced than in asthma at this time, Dr. Hanania said that quantitative and visual assessment of CT radiographs is "promising" and has helped identify COPD subphenotypes such as emphysema because of accurate assessment of lung inflation, wall thickness, and other factors.
Identifying patients with bronchiectasis, pulmonary arterial enlargement, and acute exacerbations in COPD is also possible with CT radiography, making it possible to predict the different outcomes in each situation. "The clinical implication is that these patients tend to have more frequent exacerbation, worse lung function, and infection," he said, noting that nascent research using imaging to determine biomarkers in functional small airways disease also is occurring.
Systemic inflammation
In the ECLIPSE study, 2,164 COPD patients had an odds ratio of 2.23 for being a current smoker and had higher levels of inflammation, as determined using biomarkers such as C-reactive protein, compared with 337 smokers without COPD and 245 nonsmokers. At the 3-year follow-up, this group with persistently higher inflammation also was classified as having significantly higher all-cause mortality than the group with less inflammation (13% vs. 2%); exacerbation rates in this group were also persistently higher (1.5 vs. 0.9) (PLoS ONE 2012;7:e37483).
Therapeutic implications
Coupling these phenotypes with molecular descriptions of mechanisms and their underlying pathologies can lead to accurate, personalized treatment of COPD. "Phenotypes without clear implications for prognosis and treatment are of little clinical use," Dr. Hanania said, noting that longitudinal studies to validate these phenotypes are necessary.
"Research can help identify mechanisms and courses in different phenotypes, including gender differences," he concluded. "Examining therapeutic responses to different phenotypes can lead to future interventions."
Dr. Hanania disclosed several relationships with a variety of pharmaceutical and medical manufacturers, including Genentech, GlaxoSmithKline* and Astra Zeneca.
Beyond GOLD: A tale of two COPD guidelines
Both address severity and comorbidity, but only one COPD guideline takes into account the latest research on phenotyping in chronic obstructive pulmonary disease.
"The GOLD guidelines do not include clinical phenotypes," said Dr. Joan Soriano, a presenter at the meeting. "But the Spanish ones do."
In fact, there is really only one area where the two documents overlap, said Dr. Soriano: how they define COPD, and even that is not the same. "They both mention the fundamental aspect, which is airflow limitation, and also that the mechanism involved is inflammation," he said. The GOLD definition, however, recognizes the importance of comorbidities, which the Spanish guidelines address the role of tobacco and symptomology.
GOLD (Global Initiative for Chronic Obstructive Lung Disease) is an organization of health care professionals from around the world. "I am not a member of GOLD," Dr. Soriano told the packed session.
The Spanish guidelines are issued by SEPAR, the Spanish Society for Pneumology and Thoracic Surgery. Dr. Soriano is the director of epidemiology and clinical research at the International Center of Advanced Respiratory Medicine (CIMERA) in Palma, Spain.
How the two approach diagnosis also differs. The Spanish guidelines begin with the general COPD diagnosis, then move to the characterization and phenotype, then move to the severity of the disease. They are more specific about age (over 35 years), and have lower limit of normal (LLN) values for persons aged over 70 years and less than 50 years. The GOLD guidelines do not address LLN.
To characterize the disease specifically, the Spanish guidelines address the existence of phenotypes, according to Dr. Soriano, beginning with determining the frequency of exacerbation the patient has per year, and then classifying them eventually into four types: mixed, chronic bronchitis, emphysema, and exacerbator. The GOLD guidelines do not mention phenotypes.
When it comes to the multidimensional assessment of COPD, "the GOLD guidelines lump the mild with the severe spirometry. This is very hard for me to understand," he said. Other classification divergence includes that the Spanish guidelines consider the BODE index.
Treatment in the two guidelines begins similarly, but vectors off from there. "Basically, we are looking at the same trials, so the initial treatments should be short-acting bronchodilators," Dr. Soriano said, but because phenotyping allows for more targeted treatment, the Spanish guidelines offer more detailed treatment options.
In a paper coauthored by Dr. Soriano earlier this year, specific treatment per phenotype included phosphodiesterase-4 inhibitors only for those with chronic bronchitis, inhaled corticosteroids for overlap COPD-asthma, and bronchodilators for infrequent exacerbators (Eur. Respir. J. 2013;41:1252-6).
In the end, the guidelines might not follow the same trajectory, but each has value, he said. "Whatever guidelines you choose, don’t go back and forth. Pick one and use them."
Dr. Soriano reported relationships with Novartis Spain, AstraZeneca, Pfizer, and several other pharmaceutical and medical manufacturers.
*CORRECTION, 2/20/2014: An earlier version of this story misstated the name of GlaxoSmithKline.
EXPERT ANALYSIS FROM CHEST 2013

Off-label use of opioids can provide relief in refractory dyspnea
CHICAGO – Low doses of opioids titrated based on patient ratings of breathing difficulty are effective in managing refractory dyspnea, according to Dr. Donald Mahler.
Because refractory dyspnea is a neuromechanical dissociation, treating more than the pulmonary system can be beneficial, Dr. Mahler said at the annual meeting of the American College of Chest Physicians. "We have targets for the lungs to relieve dyspnea, but we may also have potential targets in the central nervous system that may also provide benefit."
Referring to published data from two randomized controlled studies about the effect of naloxone on blocking opioid signals in patients with COPD who reported breathlessness and perceived "unpleasantness" of dyspnea after exercise, Dr. Mahler said that endogenous opioids modulate the perception of dyspnea; exogenous opioids could therefore do the same (Eur. Respir. J. 2009;33:771-7 and COPD 2011;8:160-6).
Opioid receptors in the limbic system have 100 times greater binding density in the bronchioles and alveolar walls. "That may play a role when thinking about a nebulized approach," said Dr. Mahler of Dartmouth-Hitchcock Medical Center, Lebanon, N.H. The number of side effects, including constipation, was lower with this approach, he added.
Because opioids are known to decrease respiratory drive, there is a "presumable" effect on corollary discharge, which can lead to less perception of breathlessness, according to Dr. Mahler. Narcotics’ dulling effect on the perception of pain and anxiety might also contribute. "Maybe by relieving symptoms, there’s less anxiety as a result," said Dr. Mahler.
He addressed concerns over the "double effect" whereby opioids used to lessen symptoms might actually hasten death in a patient with refractory dyspnea, saying the studies "don’t really support that." Dr. Mahler cited data indicating that higher doses of benzodiazepines used in withdrawal of life-sustaining treatment were not associated with a decreased time from withdrawal of life support to death (CHEST 2004;126:286-93).
As for respiratory depression, Dr. Mahler said he had reviewed 11 studies and found only one report of any change in oxygen saturation after opioid administration.
In deciding whether a patient should be given opioid therapy, Dr. Mahler said physicians should be sure that standard therapies are inadequate and that the risk/benefit ratio favors trial treatment. Establishing treatment goals and confirming that the patient and/or the patient’s family are on board with a trial of opioid treatment is key, he added.
To determine titration, physicians should ask the patients to rate their breathing difficulty. "This is a critical part of the assessment," said Dr. Mahler, noting that the level of breathlessness determines the dose and duration of action.
If dyspnea is episodic, he said, "it doesn’t make sense to administer a long-acting opioid" and so an immediate-release or short-acting form should be considered. If it’s constant, sustained release may be effective, he said.
Dr. Mahler, who said his presentation was related to the off-label use of morphine only, said that the important thing is to "titrate the opioid to achieve the lower effective dose based on the patient’s rating of the dyspnea." Adding an anxiolytic could also be considered, he said. "It’s pretty straightforward that you should discontinue the opioid if there is an unsatisfactory response or if there is an adverse effect."
Dr. Mahler disclosed ties with numerous pharmaceutical manufacturers and other medical organizations, including GlaxoSmithKline, Novartis, and Sunovion.
CHICAGO – Low doses of opioids titrated based on patient ratings of breathing difficulty are effective in managing refractory dyspnea, according to Dr. Donald Mahler.
Because refractory dyspnea is a neuromechanical dissociation, treating more than the pulmonary system can be beneficial, Dr. Mahler said at the annual meeting of the American College of Chest Physicians. "We have targets for the lungs to relieve dyspnea, but we may also have potential targets in the central nervous system that may also provide benefit."
Referring to published data from two randomized controlled studies about the effect of naloxone on blocking opioid signals in patients with COPD who reported breathlessness and perceived "unpleasantness" of dyspnea after exercise, Dr. Mahler said that endogenous opioids modulate the perception of dyspnea; exogenous opioids could therefore do the same (Eur. Respir. J. 2009;33:771-7 and COPD 2011;8:160-6).
Opioid receptors in the limbic system have 100 times greater binding density in the bronchioles and alveolar walls. "That may play a role when thinking about a nebulized approach," said Dr. Mahler of Dartmouth-Hitchcock Medical Center, Lebanon, N.H. The number of side effects, including constipation, was lower with this approach, he added.
Because opioids are known to decrease respiratory drive, there is a "presumable" effect on corollary discharge, which can lead to less perception of breathlessness, according to Dr. Mahler. Narcotics’ dulling effect on the perception of pain and anxiety might also contribute. "Maybe by relieving symptoms, there’s less anxiety as a result," said Dr. Mahler.
He addressed concerns over the "double effect" whereby opioids used to lessen symptoms might actually hasten death in a patient with refractory dyspnea, saying the studies "don’t really support that." Dr. Mahler cited data indicating that higher doses of benzodiazepines used in withdrawal of life-sustaining treatment were not associated with a decreased time from withdrawal of life support to death (CHEST 2004;126:286-93).
As for respiratory depression, Dr. Mahler said he had reviewed 11 studies and found only one report of any change in oxygen saturation after opioid administration.
In deciding whether a patient should be given opioid therapy, Dr. Mahler said physicians should be sure that standard therapies are inadequate and that the risk/benefit ratio favors trial treatment. Establishing treatment goals and confirming that the patient and/or the patient’s family are on board with a trial of opioid treatment is key, he added.
To determine titration, physicians should ask the patients to rate their breathing difficulty. "This is a critical part of the assessment," said Dr. Mahler, noting that the level of breathlessness determines the dose and duration of action.
If dyspnea is episodic, he said, "it doesn’t make sense to administer a long-acting opioid" and so an immediate-release or short-acting form should be considered. If it’s constant, sustained release may be effective, he said.
Dr. Mahler, who said his presentation was related to the off-label use of morphine only, said that the important thing is to "titrate the opioid to achieve the lower effective dose based on the patient’s rating of the dyspnea." Adding an anxiolytic could also be considered, he said. "It’s pretty straightforward that you should discontinue the opioid if there is an unsatisfactory response or if there is an adverse effect."
Dr. Mahler disclosed ties with numerous pharmaceutical manufacturers and other medical organizations, including GlaxoSmithKline, Novartis, and Sunovion.
CHICAGO – Low doses of opioids titrated based on patient ratings of breathing difficulty are effective in managing refractory dyspnea, according to Dr. Donald Mahler.
Because refractory dyspnea is a neuromechanical dissociation, treating more than the pulmonary system can be beneficial, Dr. Mahler said at the annual meeting of the American College of Chest Physicians. "We have targets for the lungs to relieve dyspnea, but we may also have potential targets in the central nervous system that may also provide benefit."
Referring to published data from two randomized controlled studies about the effect of naloxone on blocking opioid signals in patients with COPD who reported breathlessness and perceived "unpleasantness" of dyspnea after exercise, Dr. Mahler said that endogenous opioids modulate the perception of dyspnea; exogenous opioids could therefore do the same (Eur. Respir. J. 2009;33:771-7 and COPD 2011;8:160-6).
Opioid receptors in the limbic system have 100 times greater binding density in the bronchioles and alveolar walls. "That may play a role when thinking about a nebulized approach," said Dr. Mahler of Dartmouth-Hitchcock Medical Center, Lebanon, N.H. The number of side effects, including constipation, was lower with this approach, he added.
Because opioids are known to decrease respiratory drive, there is a "presumable" effect on corollary discharge, which can lead to less perception of breathlessness, according to Dr. Mahler. Narcotics’ dulling effect on the perception of pain and anxiety might also contribute. "Maybe by relieving symptoms, there’s less anxiety as a result," said Dr. Mahler.
He addressed concerns over the "double effect" whereby opioids used to lessen symptoms might actually hasten death in a patient with refractory dyspnea, saying the studies "don’t really support that." Dr. Mahler cited data indicating that higher doses of benzodiazepines used in withdrawal of life-sustaining treatment were not associated with a decreased time from withdrawal of life support to death (CHEST 2004;126:286-93).
As for respiratory depression, Dr. Mahler said he had reviewed 11 studies and found only one report of any change in oxygen saturation after opioid administration.
In deciding whether a patient should be given opioid therapy, Dr. Mahler said physicians should be sure that standard therapies are inadequate and that the risk/benefit ratio favors trial treatment. Establishing treatment goals and confirming that the patient and/or the patient’s family are on board with a trial of opioid treatment is key, he added.
To determine titration, physicians should ask the patients to rate their breathing difficulty. "This is a critical part of the assessment," said Dr. Mahler, noting that the level of breathlessness determines the dose and duration of action.
If dyspnea is episodic, he said, "it doesn’t make sense to administer a long-acting opioid" and so an immediate-release or short-acting form should be considered. If it’s constant, sustained release may be effective, he said.
Dr. Mahler, who said his presentation was related to the off-label use of morphine only, said that the important thing is to "titrate the opioid to achieve the lower effective dose based on the patient’s rating of the dyspnea." Adding an anxiolytic could also be considered, he said. "It’s pretty straightforward that you should discontinue the opioid if there is an unsatisfactory response or if there is an adverse effect."
Dr. Mahler disclosed ties with numerous pharmaceutical manufacturers and other medical organizations, including GlaxoSmithKline, Novartis, and Sunovion.
EXPERT ANALYSIS FROM CHEST 2013
Results vary for pregnancy-related antismoking efforts
Smoking during pregnancy and after delivery decreased moderately but significantly from 2000 to 2010, while the prevalence of smoking before pregnancy dropped only slightly in that time, the Centers for Disease Control and Prevention reported.
The prevalence of smoking during pregnancy went from 13.2% in 2000 to 10.7% in 2010, and the prevalence of smoking after delivery dropped from 18.9% to 15.9%. In comparison, the prevalence of smoking during the 3 months before pregnancy made a nonsignificant drop from 23% in 2000 to 22.5% in 2007, and rose to 23.2% in 2010, according to data from the Pregnancy Risk Assessment Monitoring System (PRAMS).
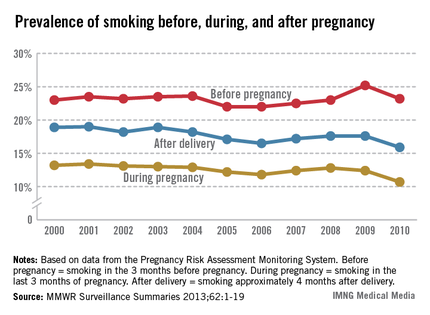
The CDC report noted the Healthy People 2020 goal of reducing the prevalence of prenatal smoking to 1.4% and suggested that, "at the current pace ... it could take another 100 years for the United States to reach this goal" (MMWR Surveillance Summaries 2013;62[SS06]:1-19).
For 2010, the data from 27 PRAMS sites nationwide – 26 states and New York City -– represent approximately 52% of live births.
Smoking during pregnancy and after delivery decreased moderately but significantly from 2000 to 2010, while the prevalence of smoking before pregnancy dropped only slightly in that time, the Centers for Disease Control and Prevention reported.
The prevalence of smoking during pregnancy went from 13.2% in 2000 to 10.7% in 2010, and the prevalence of smoking after delivery dropped from 18.9% to 15.9%. In comparison, the prevalence of smoking during the 3 months before pregnancy made a nonsignificant drop from 23% in 2000 to 22.5% in 2007, and rose to 23.2% in 2010, according to data from the Pregnancy Risk Assessment Monitoring System (PRAMS).
The CDC report noted the Healthy People 2020 goal of reducing the prevalence of prenatal smoking to 1.4% and suggested that, "at the current pace ... it could take another 100 years for the United States to reach this goal" (MMWR Surveillance Summaries 2013;62[SS06]:1-19).
For 2010, the data from 27 PRAMS sites nationwide – 26 states and New York City -– represent approximately 52% of live births.
Smoking during pregnancy and after delivery decreased moderately but significantly from 2000 to 2010, while the prevalence of smoking before pregnancy dropped only slightly in that time, the Centers for Disease Control and Prevention reported.
The prevalence of smoking during pregnancy went from 13.2% in 2000 to 10.7% in 2010, and the prevalence of smoking after delivery dropped from 18.9% to 15.9%. In comparison, the prevalence of smoking during the 3 months before pregnancy made a nonsignificant drop from 23% in 2000 to 22.5% in 2007, and rose to 23.2% in 2010, according to data from the Pregnancy Risk Assessment Monitoring System (PRAMS).
The CDC report noted the Healthy People 2020 goal of reducing the prevalence of prenatal smoking to 1.4% and suggested that, "at the current pace ... it could take another 100 years for the United States to reach this goal" (MMWR Surveillance Summaries 2013;62[SS06]:1-19).
For 2010, the data from 27 PRAMS sites nationwide – 26 states and New York City -– represent approximately 52% of live births.
FROM MMWR
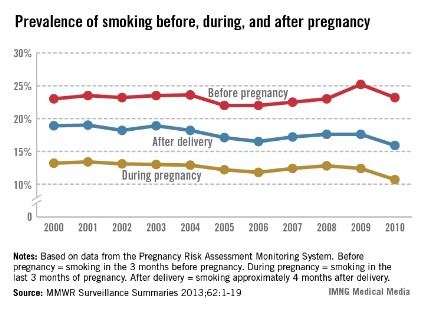
Failure to diagnose
Question: A psychiatrist refers a young woman for possible pneumonia. Her symptoms include episodic dyspnea and hyperventilation. The resident obtained a history of chronic anxiety and depression, for which the patient takes diazepam. There was a history of cigarette smoking and use of oral contraceptives. Physical examination was normal except for obesity, tachycardia, restlessness, and breathlessness. The patient’s cardiovascular and respiratory exams were otherwise normal, and the chest x-ray was read as unremarkable.
The woman was sent home with the tentative diagnosis of anxiety neurosis, but was found dead 24 hours later. Autopsy revealed a massive pulmonary embolus originating from a pelvic vein thrombus.
Which of the following observations is correct?
A. Failure to diagnose is the most common basis for a medical malpractice claim.
B. It is likely that this case will be settled in the decedent’s favor, because all four elements of negligence are satisfied: duty, breach of duty, causation, and damages.
C. The doctor may have been biased, because this was a patient with a psychiatric history.
D. This is an example of framing and anchoring cognitive failure rather than lack of knowledge.
E. All are correct.
Answer: E. This case is modified from an example in the literature on diagnostic errors (N. Engl. J. Med. 2013;368:2445-8). The resident focused his attention on the psychiatric referral diagnoses of pneumonia and anxiety, overlooking the many risk factors for pulmonary embolism that included obesity, cigarette smoking, and the use of oral contraceptives. The case satisfies all four elements for the tort of negligence, and will most likely be decided in the patient’s favor.
It is usually not a lack of knowledge that leads to a diagnostic error, but problems with the clinician’s thought process (cognitive failure). Although physicians well know the pathophysiology of pulmonary embolism, its protean signs and symptoms overlap those of numerous other diseases, and this important diagnosis is frequently missed – in 55% of fatal cases, in one study.
Terms such as "missed diagnosis," "wrong diagnosis," or most commonly "diagnostic error" are used in the medical literature, but the unifying malpractice nomenclature is "failure to diagnose." The term includes the failure to refer to an appropriate specialist if customarily required.
Although reduced physician-patient encounter time is sometimes blamed for missing a diagnosis, this is of course not a legitimate legal defense. There is litigation aplenty over failure-to-diagnose conditions such as myocardial infarction or a dissecting aneurysm (Cardiology 2008;109:263-72). Other examples are pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a recent study in primary care settings (a Veterans Affairs facility and a private clinic), the authors were able to identify diagnostic errors from electronic health record triggers based in part on a patient’s unexpected return visit (JAMA Intern. Med. 2013;173:418-25). Of 190 cases, they identified some 68 unique diagnoses. Commonly presenting with atypical or nonspecific symptoms, these conditions included pneumonia, congestive heart failure, acute renal failure, cancer, and UTIs. Lapses in bedside history taking, physical exam, and test ordering were noted. Significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Diagnostic errors occur more frequently than generally supposed, especially in specialties such as primary care and emergency medicine. They are the most frequent reason for a malpractice claim.
In a review of more than 350,000 closed claims reported to the National Practitioner Data Bank over a 25-year period, researchers from Johns Hopkins University concluded that, "among malpractice claims, diagnostic errors appear to be the most common, most costly, and most dangerous of medical mistakes." They found such errors in 28.6% of all cases, accounting for the highest proportion (35.2%) of total payments.
Diagnostic errors also caused the most severe injuries, especially in hospitalized patients (BMJ Qual. Saf. 2013;22:672-80). It has been reported that roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Diagnostic errors have multifactorial causes, divisible into system-related and cognitive factors (Arch. Intern. Med. 2005;165:1493-9). In a review of 100 internal medicine cases identified through autopsy discrepancies, quality assurance activities, and voluntary reports, the researchers found the absence of fault in only 7% of cases. In the remaining 93 cases, system-related factors were present in 65% and cognitive factors in 74%.
The most common system-related factors were defective, inappropriate, or inefficient policies and procedures, and dysfunctional teamwork and communication. Clinicians know too well that procedural errors can lead to tests that go unordered, results that go unnoticed or misfiled, or a patient who fails to follow up with a referral or return appointment.
One of the most common cognitive problems is faulty synthesis with premature closure, that is, the failure to continue to consider other diagnostic alternatives after forming an initial tentative diagnosis.
Other examples are anchoring bias, where one is locked into an aspect of the case; framing bias, where there is misdirection because of the way the problem was posed; availability bias, where things are judged by what comes readily to mind such as a recent experience; and confirmation bias, where one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary (Acad. Med. 2003;78:775-80).
Errors may be intuitive (automatic) or analytic (controlled). The former, which is the familiar reflexive, blink-of-an-eye diagnosis based on intuition, is the more common error. On the other hand, analytic processes are conscious, deliberate, slower, and generally more reliable, though more resource intensive.
One area deserving of attention: overconfidence and complacency. Critics have pointed out that some physicians are "walking ... in a fog of misplaced optimism" with regard to their confidence, failing to critically examine their assumptions, beliefs, and conclusions (metacognition), and generally underappreciating the likelihood that their diagnoses are wrong (Am. J. Med. 2008;121:S2-S23).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, "Medical Malpractice: Understanding the Law, Managing the Risk" (2006). For additional information, readers may contact the author at siang@hawaii.edu.
Question: A psychiatrist refers a young woman for possible pneumonia. Her symptoms include episodic dyspnea and hyperventilation. The resident obtained a history of chronic anxiety and depression, for which the patient takes diazepam. There was a history of cigarette smoking and use of oral contraceptives. Physical examination was normal except for obesity, tachycardia, restlessness, and breathlessness. The patient’s cardiovascular and respiratory exams were otherwise normal, and the chest x-ray was read as unremarkable.
The woman was sent home with the tentative diagnosis of anxiety neurosis, but was found dead 24 hours later. Autopsy revealed a massive pulmonary embolus originating from a pelvic vein thrombus.
Which of the following observations is correct?
A. Failure to diagnose is the most common basis for a medical malpractice claim.
B. It is likely that this case will be settled in the decedent’s favor, because all four elements of negligence are satisfied: duty, breach of duty, causation, and damages.
C. The doctor may have been biased, because this was a patient with a psychiatric history.
D. This is an example of framing and anchoring cognitive failure rather than lack of knowledge.
E. All are correct.
Answer: E. This case is modified from an example in the literature on diagnostic errors (N. Engl. J. Med. 2013;368:2445-8). The resident focused his attention on the psychiatric referral diagnoses of pneumonia and anxiety, overlooking the many risk factors for pulmonary embolism that included obesity, cigarette smoking, and the use of oral contraceptives. The case satisfies all four elements for the tort of negligence, and will most likely be decided in the patient’s favor.
It is usually not a lack of knowledge that leads to a diagnostic error, but problems with the clinician’s thought process (cognitive failure). Although physicians well know the pathophysiology of pulmonary embolism, its protean signs and symptoms overlap those of numerous other diseases, and this important diagnosis is frequently missed – in 55% of fatal cases, in one study.
Terms such as "missed diagnosis," "wrong diagnosis," or most commonly "diagnostic error" are used in the medical literature, but the unifying malpractice nomenclature is "failure to diagnose." The term includes the failure to refer to an appropriate specialist if customarily required.
Although reduced physician-patient encounter time is sometimes blamed for missing a diagnosis, this is of course not a legitimate legal defense. There is litigation aplenty over failure-to-diagnose conditions such as myocardial infarction or a dissecting aneurysm (Cardiology 2008;109:263-72). Other examples are pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a recent study in primary care settings (a Veterans Affairs facility and a private clinic), the authors were able to identify diagnostic errors from electronic health record triggers based in part on a patient’s unexpected return visit (JAMA Intern. Med. 2013;173:418-25). Of 190 cases, they identified some 68 unique diagnoses. Commonly presenting with atypical or nonspecific symptoms, these conditions included pneumonia, congestive heart failure, acute renal failure, cancer, and UTIs. Lapses in bedside history taking, physical exam, and test ordering were noted. Significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Diagnostic errors occur more frequently than generally supposed, especially in specialties such as primary care and emergency medicine. They are the most frequent reason for a malpractice claim.
In a review of more than 350,000 closed claims reported to the National Practitioner Data Bank over a 25-year period, researchers from Johns Hopkins University concluded that, "among malpractice claims, diagnostic errors appear to be the most common, most costly, and most dangerous of medical mistakes." They found such errors in 28.6% of all cases, accounting for the highest proportion (35.2%) of total payments.
Diagnostic errors also caused the most severe injuries, especially in hospitalized patients (BMJ Qual. Saf. 2013;22:672-80). It has been reported that roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Diagnostic errors have multifactorial causes, divisible into system-related and cognitive factors (Arch. Intern. Med. 2005;165:1493-9). In a review of 100 internal medicine cases identified through autopsy discrepancies, quality assurance activities, and voluntary reports, the researchers found the absence of fault in only 7% of cases. In the remaining 93 cases, system-related factors were present in 65% and cognitive factors in 74%.
The most common system-related factors were defective, inappropriate, or inefficient policies and procedures, and dysfunctional teamwork and communication. Clinicians know too well that procedural errors can lead to tests that go unordered, results that go unnoticed or misfiled, or a patient who fails to follow up with a referral or return appointment.
One of the most common cognitive problems is faulty synthesis with premature closure, that is, the failure to continue to consider other diagnostic alternatives after forming an initial tentative diagnosis.
Other examples are anchoring bias, where one is locked into an aspect of the case; framing bias, where there is misdirection because of the way the problem was posed; availability bias, where things are judged by what comes readily to mind such as a recent experience; and confirmation bias, where one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary (Acad. Med. 2003;78:775-80).
Errors may be intuitive (automatic) or analytic (controlled). The former, which is the familiar reflexive, blink-of-an-eye diagnosis based on intuition, is the more common error. On the other hand, analytic processes are conscious, deliberate, slower, and generally more reliable, though more resource intensive.
One area deserving of attention: overconfidence and complacency. Critics have pointed out that some physicians are "walking ... in a fog of misplaced optimism" with regard to their confidence, failing to critically examine their assumptions, beliefs, and conclusions (metacognition), and generally underappreciating the likelihood that their diagnoses are wrong (Am. J. Med. 2008;121:S2-S23).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, "Medical Malpractice: Understanding the Law, Managing the Risk" (2006). For additional information, readers may contact the author at siang@hawaii.edu.
Question: A psychiatrist refers a young woman for possible pneumonia. Her symptoms include episodic dyspnea and hyperventilation. The resident obtained a history of chronic anxiety and depression, for which the patient takes diazepam. There was a history of cigarette smoking and use of oral contraceptives. Physical examination was normal except for obesity, tachycardia, restlessness, and breathlessness. The patient’s cardiovascular and respiratory exams were otherwise normal, and the chest x-ray was read as unremarkable.
The woman was sent home with the tentative diagnosis of anxiety neurosis, but was found dead 24 hours later. Autopsy revealed a massive pulmonary embolus originating from a pelvic vein thrombus.
Which of the following observations is correct?
A. Failure to diagnose is the most common basis for a medical malpractice claim.
B. It is likely that this case will be settled in the decedent’s favor, because all four elements of negligence are satisfied: duty, breach of duty, causation, and damages.
C. The doctor may have been biased, because this was a patient with a psychiatric history.
D. This is an example of framing and anchoring cognitive failure rather than lack of knowledge.
E. All are correct.
Answer: E. This case is modified from an example in the literature on diagnostic errors (N. Engl. J. Med. 2013;368:2445-8). The resident focused his attention on the psychiatric referral diagnoses of pneumonia and anxiety, overlooking the many risk factors for pulmonary embolism that included obesity, cigarette smoking, and the use of oral contraceptives. The case satisfies all four elements for the tort of negligence, and will most likely be decided in the patient’s favor.
It is usually not a lack of knowledge that leads to a diagnostic error, but problems with the clinician’s thought process (cognitive failure). Although physicians well know the pathophysiology of pulmonary embolism, its protean signs and symptoms overlap those of numerous other diseases, and this important diagnosis is frequently missed – in 55% of fatal cases, in one study.
Terms such as "missed diagnosis," "wrong diagnosis," or most commonly "diagnostic error" are used in the medical literature, but the unifying malpractice nomenclature is "failure to diagnose." The term includes the failure to refer to an appropriate specialist if customarily required.
Although reduced physician-patient encounter time is sometimes blamed for missing a diagnosis, this is of course not a legitimate legal defense. There is litigation aplenty over failure-to-diagnose conditions such as myocardial infarction or a dissecting aneurysm (Cardiology 2008;109:263-72). Other examples are pulmonary embolism, appendicitis, ectopic pregnancy, meningitis, cancers, and fractures.
In a recent study in primary care settings (a Veterans Affairs facility and a private clinic), the authors were able to identify diagnostic errors from electronic health record triggers based in part on a patient’s unexpected return visit (JAMA Intern. Med. 2013;173:418-25). Of 190 cases, they identified some 68 unique diagnoses. Commonly presenting with atypical or nonspecific symptoms, these conditions included pneumonia, congestive heart failure, acute renal failure, cancer, and UTIs. Lapses in bedside history taking, physical exam, and test ordering were noted. Significantly, there was no documentation of an initial differential diagnosis in 80% of misdiagnosed cases.
Diagnostic errors occur more frequently than generally supposed, especially in specialties such as primary care and emergency medicine. They are the most frequent reason for a malpractice claim.
In a review of more than 350,000 closed claims reported to the National Practitioner Data Bank over a 25-year period, researchers from Johns Hopkins University concluded that, "among malpractice claims, diagnostic errors appear to be the most common, most costly, and most dangerous of medical mistakes." They found such errors in 28.6% of all cases, accounting for the highest proportion (35.2%) of total payments.
Diagnostic errors also caused the most severe injuries, especially in hospitalized patients (BMJ Qual. Saf. 2013;22:672-80). It has been reported that roughly 5% of autopsies uncover a diagnostic error that was amenable to appropriate treatment, and some 50,000 annual hospital deaths may be the result of a delayed, incorrect, or overlooked diagnosis.
Diagnostic errors have multifactorial causes, divisible into system-related and cognitive factors (Arch. Intern. Med. 2005;165:1493-9). In a review of 100 internal medicine cases identified through autopsy discrepancies, quality assurance activities, and voluntary reports, the researchers found the absence of fault in only 7% of cases. In the remaining 93 cases, system-related factors were present in 65% and cognitive factors in 74%.
The most common system-related factors were defective, inappropriate, or inefficient policies and procedures, and dysfunctional teamwork and communication. Clinicians know too well that procedural errors can lead to tests that go unordered, results that go unnoticed or misfiled, or a patient who fails to follow up with a referral or return appointment.
One of the most common cognitive problems is faulty synthesis with premature closure, that is, the failure to continue to consider other diagnostic alternatives after forming an initial tentative diagnosis.
Other examples are anchoring bias, where one is locked into an aspect of the case; framing bias, where there is misdirection because of the way the problem was posed; availability bias, where things are judged by what comes readily to mind such as a recent experience; and confirmation bias, where one looks for confirmatory evidence of one’s preferred diagnosis while ignoring evidence to the contrary (Acad. Med. 2003;78:775-80).
Errors may be intuitive (automatic) or analytic (controlled). The former, which is the familiar reflexive, blink-of-an-eye diagnosis based on intuition, is the more common error. On the other hand, analytic processes are conscious, deliberate, slower, and generally more reliable, though more resource intensive.
One area deserving of attention: overconfidence and complacency. Critics have pointed out that some physicians are "walking ... in a fog of misplaced optimism" with regard to their confidence, failing to critically examine their assumptions, beliefs, and conclusions (metacognition), and generally underappreciating the likelihood that their diagnoses are wrong (Am. J. Med. 2008;121:S2-S23).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, "Medical Malpractice: Understanding the Law, Managing the Risk" (2006). For additional information, readers may contact the author at siang@hawaii.edu.
Smartphone technology could enable remote otitis media diagnosis
ORLANDO – A novel smartphone otoscope attachment provides clear, transmittable images of the ear drum or tympanic membrane, and could revolutionize the approach to diagnosing and managing ear infections, according to Dr. Kathryn Rappaport.
In a prospective study involving 63 children who presented to an emergency department between May and December 2012 with upper respiratory tract symptoms, the technology was as effective as a conventional otoscope, and was widely accepted by parents, Dr. Rappaport of Baylor College of Medicine, Houston, reported at the annual meeting of the American Academy of Pediatrics.

After receiving clinical care, each child in the study underwent bilateral otic videoscopy using both the smartphone otoscope (CellScope Oto) and a camera-fitted conventional otoscope. The procedures were performed in random order, said Dr. Rappaport, who was at Emory University in Atlanta when the study was conducted.
Of the children, who had a mean age of 2.9 years, 49 received a clinical diagnosis of acute otitis media by an ED practitioner. Based on independent scoring by four physicians who evaluated 31 CellScope Oto videos and 31 conventional otoscope videos from 26 subjects, there was no difference between the two technologies in either the diagnostic quality of the images or diagnosis confidence ratings.
Diagnosis and treatment decision making were similar with each device. Overall, the physician raters were in fair agreement regarding the clinical ED diagnosis of acute otitis media, while two of the raters had moderate to substantial agreement with the ED diagnosis and two had poor agreement with the ED diagnosis from images obtained via conventional otoscope, Dr. Rappaport said, noting that there was a significant correlation between antimicrobial use and image quality.
This indicated that higher-quality images were more likely to be associated with a definitive diagnosis, she said.
As for parent reactions to the use of the device, most (95%) responded favorably, stating that the CellScope Oto images improved their understanding of their child’s management. Also, 90% said they thought the technology would be easy to use, and they would feel comfortable using it remotely to transmit images to a provider.
The CellScope Oto has the potential to improve diagnosis and management, and to reduce costs associated with acute otitis media in children, Dr. Rappaport said.
The video images can provide a baseline, as well as ongoing documentation of a child’s condition. The video documentation could allow a child to be followed over a period of time – without the need for regular office visits – to help monitor for progression or resolution of middle ear effusion and to guide diagnosis and treatment decision making, she explained.
"Acute otitis media is the most common reason for antimicrobial prescriptions in children. In the future, we would like to study whether the ability to monitor for resolution of a patient’s middle ear effusion using digital imaging with the smartphone otoscope will lead to decreased antimicrobial prescriptions for acute otitis media in children," she said in an interview.
Dr. Rappaport reported having no relevant financial disclosures.
ORLANDO – A novel smartphone otoscope attachment provides clear, transmittable images of the ear drum or tympanic membrane, and could revolutionize the approach to diagnosing and managing ear infections, according to Dr. Kathryn Rappaport.
In a prospective study involving 63 children who presented to an emergency department between May and December 2012 with upper respiratory tract symptoms, the technology was as effective as a conventional otoscope, and was widely accepted by parents, Dr. Rappaport of Baylor College of Medicine, Houston, reported at the annual meeting of the American Academy of Pediatrics.
After receiving clinical care, each child in the study underwent bilateral otic videoscopy using both the smartphone otoscope (CellScope Oto) and a camera-fitted conventional otoscope. The procedures were performed in random order, said Dr. Rappaport, who was at Emory University in Atlanta when the study was conducted.
Of the children, who had a mean age of 2.9 years, 49 received a clinical diagnosis of acute otitis media by an ED practitioner. Based on independent scoring by four physicians who evaluated 31 CellScope Oto videos and 31 conventional otoscope videos from 26 subjects, there was no difference between the two technologies in either the diagnostic quality of the images or diagnosis confidence ratings.
Diagnosis and treatment decision making were similar with each device. Overall, the physician raters were in fair agreement regarding the clinical ED diagnosis of acute otitis media, while two of the raters had moderate to substantial agreement with the ED diagnosis and two had poor agreement with the ED diagnosis from images obtained via conventional otoscope, Dr. Rappaport said, noting that there was a significant correlation between antimicrobial use and image quality.
This indicated that higher-quality images were more likely to be associated with a definitive diagnosis, she said.
As for parent reactions to the use of the device, most (95%) responded favorably, stating that the CellScope Oto images improved their understanding of their child’s management. Also, 90% said they thought the technology would be easy to use, and they would feel comfortable using it remotely to transmit images to a provider.
The CellScope Oto has the potential to improve diagnosis and management, and to reduce costs associated with acute otitis media in children, Dr. Rappaport said.
The video images can provide a baseline, as well as ongoing documentation of a child’s condition. The video documentation could allow a child to be followed over a period of time – without the need for regular office visits – to help monitor for progression or resolution of middle ear effusion and to guide diagnosis and treatment decision making, she explained.
"Acute otitis media is the most common reason for antimicrobial prescriptions in children. In the future, we would like to study whether the ability to monitor for resolution of a patient’s middle ear effusion using digital imaging with the smartphone otoscope will lead to decreased antimicrobial prescriptions for acute otitis media in children," she said in an interview.
Dr. Rappaport reported having no relevant financial disclosures.
ORLANDO – A novel smartphone otoscope attachment provides clear, transmittable images of the ear drum or tympanic membrane, and could revolutionize the approach to diagnosing and managing ear infections, according to Dr. Kathryn Rappaport.
In a prospective study involving 63 children who presented to an emergency department between May and December 2012 with upper respiratory tract symptoms, the technology was as effective as a conventional otoscope, and was widely accepted by parents, Dr. Rappaport of Baylor College of Medicine, Houston, reported at the annual meeting of the American Academy of Pediatrics.
After receiving clinical care, each child in the study underwent bilateral otic videoscopy using both the smartphone otoscope (CellScope Oto) and a camera-fitted conventional otoscope. The procedures were performed in random order, said Dr. Rappaport, who was at Emory University in Atlanta when the study was conducted.
Of the children, who had a mean age of 2.9 years, 49 received a clinical diagnosis of acute otitis media by an ED practitioner. Based on independent scoring by four physicians who evaluated 31 CellScope Oto videos and 31 conventional otoscope videos from 26 subjects, there was no difference between the two technologies in either the diagnostic quality of the images or diagnosis confidence ratings.
Diagnosis and treatment decision making were similar with each device. Overall, the physician raters were in fair agreement regarding the clinical ED diagnosis of acute otitis media, while two of the raters had moderate to substantial agreement with the ED diagnosis and two had poor agreement with the ED diagnosis from images obtained via conventional otoscope, Dr. Rappaport said, noting that there was a significant correlation between antimicrobial use and image quality.
This indicated that higher-quality images were more likely to be associated with a definitive diagnosis, she said.
As for parent reactions to the use of the device, most (95%) responded favorably, stating that the CellScope Oto images improved their understanding of their child’s management. Also, 90% said they thought the technology would be easy to use, and they would feel comfortable using it remotely to transmit images to a provider.
The CellScope Oto has the potential to improve diagnosis and management, and to reduce costs associated with acute otitis media in children, Dr. Rappaport said.
The video images can provide a baseline, as well as ongoing documentation of a child’s condition. The video documentation could allow a child to be followed over a period of time – without the need for regular office visits – to help monitor for progression or resolution of middle ear effusion and to guide diagnosis and treatment decision making, she explained.
"Acute otitis media is the most common reason for antimicrobial prescriptions in children. In the future, we would like to study whether the ability to monitor for resolution of a patient’s middle ear effusion using digital imaging with the smartphone otoscope will lead to decreased antimicrobial prescriptions for acute otitis media in children," she said in an interview.
Dr. Rappaport reported having no relevant financial disclosures.
AT THE AAP NATIONAL CONFERENCE
Major finding: No difference was seen between the smartphone otoscope and a conventional otoscope in either the diagnostic quality of the images or diagnosis confidence ratings.
Data source: A prospective single-site study of 63 children.
Disclosures: Dr. Rappaport reported having no relevant financial disclosures.
Top pulmonary medicine trends at the CHEST 2013 meeting
The buzz at this year's annual meeting of the American College of Chest Physicians included the impact across the field of personalized medicine, disaster preparedness, and accountability in medicine, plus plenty of practical pearls for the community physician.
The buzz at this year's annual meeting of the American College of Chest Physicians included the impact across the field of personalized medicine, disaster preparedness, and accountability in medicine, plus plenty of practical pearls for the community physician.
The buzz at this year's annual meeting of the American College of Chest Physicians included the impact across the field of personalized medicine, disaster preparedness, and accountability in medicine, plus plenty of practical pearls for the community physician.
Early VTE prophylaxis found safe in blunt abdominal injuries
WASHINGTON – Nonoperative prophylaxis for blunt solid abdominal organ trauma was found safe when given 48 hours post injury, according to data presented at the annual clinical congress of the American College of Surgeons.
Because updated guidelines for nonoperative management of solid abdominal organ injuries do not state an optimal time for initiation of prophylaxis, investigators, including presenter Caitlyn Harrison, a third-year medical student at the University of Arizona, Tucson, sought to determine how soon is too soon in this patient population.
Theorizing that there would be no difference in bleeding complications and failure rates associated with early venous thromboembolism (VTE) prevention, the investigators reviewed 7 years of patient data (2005-2011) from a single trauma center to compare the safety of early (less than 48 hours), intermediate (48-72 hours), and late (more than 72 hours) initiation of unfractionated heparin (5,000 units, subcutaneously, every 8 hours) in blunt abdominal injury patients.
Included for review were patients whose abdominal injuries were equal to or greater than 3 on the Abbreviated Injury Scale (AIS). Patients with head injuries that scored 3 or greater on the AIS and those who had been transferred were excluded.
A total of 116 patients were matched according to whether they had received early (n = 58; 67.2% male; mean age, 40 years), intermediate (n = 29; 69% male; mean age, 44.3 years), or late (n = 29; 72.4% male; mean age, 45 years) initiation of VTE prophylaxis.
They also were matched according to organs injured. The investigators found a preponderance of splenic injuries: 41.4% in the early group, 37.9% in the intermediate, and 45.2% in the late group.
The grade of injury and laboratory values including blood pressure and injury severity also were measured.
The researchers found that none of the patients in the intermediate or late groups reached the primary outcome of the need for a post-treatment blood transfusion, although 3.2% of the early group did, Ms. Harrison said.
No patients in any of the three groups required an operative intervention after nonoperative management, although 1.7% of the early group did require embolization, as did 3.4% each of the intermediate and late groups.
Similarly, while thromboembolisms were not found to have occurred in the early group, they did occur in the intermediate and late groups at a rate of 3.4% each. No mortality was recorded as an outcome in any of the three groups, she said, concluding that "early VTE prophylaxis is safe."
Ms. Harrison reported no relevant disclosures.
WASHINGTON – Nonoperative prophylaxis for blunt solid abdominal organ trauma was found safe when given 48 hours post injury, according to data presented at the annual clinical congress of the American College of Surgeons.
Because updated guidelines for nonoperative management of solid abdominal organ injuries do not state an optimal time for initiation of prophylaxis, investigators, including presenter Caitlyn Harrison, a third-year medical student at the University of Arizona, Tucson, sought to determine how soon is too soon in this patient population.
Theorizing that there would be no difference in bleeding complications and failure rates associated with early venous thromboembolism (VTE) prevention, the investigators reviewed 7 years of patient data (2005-2011) from a single trauma center to compare the safety of early (less than 48 hours), intermediate (48-72 hours), and late (more than 72 hours) initiation of unfractionated heparin (5,000 units, subcutaneously, every 8 hours) in blunt abdominal injury patients.
Included for review were patients whose abdominal injuries were equal to or greater than 3 on the Abbreviated Injury Scale (AIS). Patients with head injuries that scored 3 or greater on the AIS and those who had been transferred were excluded.
A total of 116 patients were matched according to whether they had received early (n = 58; 67.2% male; mean age, 40 years), intermediate (n = 29; 69% male; mean age, 44.3 years), or late (n = 29; 72.4% male; mean age, 45 years) initiation of VTE prophylaxis.
They also were matched according to organs injured. The investigators found a preponderance of splenic injuries: 41.4% in the early group, 37.9% in the intermediate, and 45.2% in the late group.
The grade of injury and laboratory values including blood pressure and injury severity also were measured.
The researchers found that none of the patients in the intermediate or late groups reached the primary outcome of the need for a post-treatment blood transfusion, although 3.2% of the early group did, Ms. Harrison said.
No patients in any of the three groups required an operative intervention after nonoperative management, although 1.7% of the early group did require embolization, as did 3.4% each of the intermediate and late groups.
Similarly, while thromboembolisms were not found to have occurred in the early group, they did occur in the intermediate and late groups at a rate of 3.4% each. No mortality was recorded as an outcome in any of the three groups, she said, concluding that "early VTE prophylaxis is safe."
Ms. Harrison reported no relevant disclosures.
WASHINGTON – Nonoperative prophylaxis for blunt solid abdominal organ trauma was found safe when given 48 hours post injury, according to data presented at the annual clinical congress of the American College of Surgeons.
Because updated guidelines for nonoperative management of solid abdominal organ injuries do not state an optimal time for initiation of prophylaxis, investigators, including presenter Caitlyn Harrison, a third-year medical student at the University of Arizona, Tucson, sought to determine how soon is too soon in this patient population.
Theorizing that there would be no difference in bleeding complications and failure rates associated with early venous thromboembolism (VTE) prevention, the investigators reviewed 7 years of patient data (2005-2011) from a single trauma center to compare the safety of early (less than 48 hours), intermediate (48-72 hours), and late (more than 72 hours) initiation of unfractionated heparin (5,000 units, subcutaneously, every 8 hours) in blunt abdominal injury patients.
Included for review were patients whose abdominal injuries were equal to or greater than 3 on the Abbreviated Injury Scale (AIS). Patients with head injuries that scored 3 or greater on the AIS and those who had been transferred were excluded.
A total of 116 patients were matched according to whether they had received early (n = 58; 67.2% male; mean age, 40 years), intermediate (n = 29; 69% male; mean age, 44.3 years), or late (n = 29; 72.4% male; mean age, 45 years) initiation of VTE prophylaxis.
They also were matched according to organs injured. The investigators found a preponderance of splenic injuries: 41.4% in the early group, 37.9% in the intermediate, and 45.2% in the late group.
The grade of injury and laboratory values including blood pressure and injury severity also were measured.
The researchers found that none of the patients in the intermediate or late groups reached the primary outcome of the need for a post-treatment blood transfusion, although 3.2% of the early group did, Ms. Harrison said.
No patients in any of the three groups required an operative intervention after nonoperative management, although 1.7% of the early group did require embolization, as did 3.4% each of the intermediate and late groups.
Similarly, while thromboembolisms were not found to have occurred in the early group, they did occur in the intermediate and late groups at a rate of 3.4% each. No mortality was recorded as an outcome in any of the three groups, she said, concluding that "early VTE prophylaxis is safe."
Ms. Harrison reported no relevant disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: Thromboembolic prophylaxis was found safe in blunt abdominal injury, when administered at either 48, 48-72, or 72 hours post injury.
Data source: Review of 116 blunt solid organ injury patients managed non-operatively at a single trauma center between 2005-2011.
Disclosures: Ms. Harrison reported no relevant disclosures.