User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
18% of lung cancers caught by CT screening were indolent
An estimated 18% of the early lung cancers detected by low-dose CT screening in the National Lung Screening Trial were likely indolent and probably represent overdiagnosis, according to a report published online Dec. 9 in JAMA Internal Medicine.
The National Lung Screening Trial (NLST) found "an encouraging" 20% relative reduction in lung cancer–specific mortality among high-risk patients who were screened using low-dose CT, compared with chest radiography. "These findings were met with enthusiasm, but before a widespread public health screening program is implemented, risks of screening also need to be considered," said Dr. Edward F. Patz Jr. of the department of radiology, Duke University Medical Center, Durham, N.C., and his associates in the NLST.
The chief risk in this case is overdiagnosis: identifying an early-stage lesion in an asymptomatic patient that would not progress or affect that patient’s long-term health. It is likely that some of the tumors detected on low-dose CT were just such indolent cancers, and that those patients unnecessarily underwent invasive diagnostic procedures, surgical resection, and multiple follow-up studies.
To estimate how many of the detected cancers in the NLST were indolent – and thus overdiagnosed – Dr. Patz and his colleagues used statistical probability methods to analyze extended follow-up data from the study.
The NLST involved 53,452 men and women aged 55-74 years who were enrolled during 2002-2004 and who had at least a 30-pack-year history of cigarette smoking. The patients were randomly assigned to undergo lung cancer screening using either three annual low-dose CT exams or three annual single-view chest radiographs.
Mean follow-up was approximately 6 years. "At the end of the entire trial, there were 1,089 total lung cancer cases in the low-dose CT arm (649 detected by low-dose CT screening) and 969 cases in the [radiology] arm, for an excess of 120 cases. This gives [an] excess cancer rate of 18.5%," the investigators said (JAMA Intern. Med. 2013 Dec. 9 [doi:10.1001/jamainternmed.2013.12738]).
"The data from this study suggest that ... 18% of persons in the low-dose CT arm with screen-detected lung cancer and 22% of those in the low-dose CT arm with screen-detected NSCLC [non–small cell lung cancer] may be cases of overdiagnosis," Dr. Patz and his associates said. "In other words, if these individuals had not entered the NLST, they would not have received a lung cancer diagnosis or treatment, at least for the next 5 years."
In the future, the study authors noted, "once there are better biomarkers and imaging techniques to predict which individuals with a diagnosis of lung cancer will have more or less aggressive disease, treatment options can be optimized, and a mass screening program can become more valuable."
The National Institutes of Health supported the NSLT. No financial conflicts of interest were reported.
An estimated 18% of the early lung cancers detected by low-dose CT screening in the National Lung Screening Trial were likely indolent and probably represent overdiagnosis, according to a report published online Dec. 9 in JAMA Internal Medicine.
The National Lung Screening Trial (NLST) found "an encouraging" 20% relative reduction in lung cancer–specific mortality among high-risk patients who were screened using low-dose CT, compared with chest radiography. "These findings were met with enthusiasm, but before a widespread public health screening program is implemented, risks of screening also need to be considered," said Dr. Edward F. Patz Jr. of the department of radiology, Duke University Medical Center, Durham, N.C., and his associates in the NLST.
The chief risk in this case is overdiagnosis: identifying an early-stage lesion in an asymptomatic patient that would not progress or affect that patient’s long-term health. It is likely that some of the tumors detected on low-dose CT were just such indolent cancers, and that those patients unnecessarily underwent invasive diagnostic procedures, surgical resection, and multiple follow-up studies.
To estimate how many of the detected cancers in the NLST were indolent – and thus overdiagnosed – Dr. Patz and his colleagues used statistical probability methods to analyze extended follow-up data from the study.
The NLST involved 53,452 men and women aged 55-74 years who were enrolled during 2002-2004 and who had at least a 30-pack-year history of cigarette smoking. The patients were randomly assigned to undergo lung cancer screening using either three annual low-dose CT exams or three annual single-view chest radiographs.
Mean follow-up was approximately 6 years. "At the end of the entire trial, there were 1,089 total lung cancer cases in the low-dose CT arm (649 detected by low-dose CT screening) and 969 cases in the [radiology] arm, for an excess of 120 cases. This gives [an] excess cancer rate of 18.5%," the investigators said (JAMA Intern. Med. 2013 Dec. 9 [doi:10.1001/jamainternmed.2013.12738]).
"The data from this study suggest that ... 18% of persons in the low-dose CT arm with screen-detected lung cancer and 22% of those in the low-dose CT arm with screen-detected NSCLC [non–small cell lung cancer] may be cases of overdiagnosis," Dr. Patz and his associates said. "In other words, if these individuals had not entered the NLST, they would not have received a lung cancer diagnosis or treatment, at least for the next 5 years."
In the future, the study authors noted, "once there are better biomarkers and imaging techniques to predict which individuals with a diagnosis of lung cancer will have more or less aggressive disease, treatment options can be optimized, and a mass screening program can become more valuable."
The National Institutes of Health supported the NSLT. No financial conflicts of interest were reported.
An estimated 18% of the early lung cancers detected by low-dose CT screening in the National Lung Screening Trial were likely indolent and probably represent overdiagnosis, according to a report published online Dec. 9 in JAMA Internal Medicine.
The National Lung Screening Trial (NLST) found "an encouraging" 20% relative reduction in lung cancer–specific mortality among high-risk patients who were screened using low-dose CT, compared with chest radiography. "These findings were met with enthusiasm, but before a widespread public health screening program is implemented, risks of screening also need to be considered," said Dr. Edward F. Patz Jr. of the department of radiology, Duke University Medical Center, Durham, N.C., and his associates in the NLST.
The chief risk in this case is overdiagnosis: identifying an early-stage lesion in an asymptomatic patient that would not progress or affect that patient’s long-term health. It is likely that some of the tumors detected on low-dose CT were just such indolent cancers, and that those patients unnecessarily underwent invasive diagnostic procedures, surgical resection, and multiple follow-up studies.
To estimate how many of the detected cancers in the NLST were indolent – and thus overdiagnosed – Dr. Patz and his colleagues used statistical probability methods to analyze extended follow-up data from the study.
The NLST involved 53,452 men and women aged 55-74 years who were enrolled during 2002-2004 and who had at least a 30-pack-year history of cigarette smoking. The patients were randomly assigned to undergo lung cancer screening using either three annual low-dose CT exams or three annual single-view chest radiographs.
Mean follow-up was approximately 6 years. "At the end of the entire trial, there were 1,089 total lung cancer cases in the low-dose CT arm (649 detected by low-dose CT screening) and 969 cases in the [radiology] arm, for an excess of 120 cases. This gives [an] excess cancer rate of 18.5%," the investigators said (JAMA Intern. Med. 2013 Dec. 9 [doi:10.1001/jamainternmed.2013.12738]).
"The data from this study suggest that ... 18% of persons in the low-dose CT arm with screen-detected lung cancer and 22% of those in the low-dose CT arm with screen-detected NSCLC [non–small cell lung cancer] may be cases of overdiagnosis," Dr. Patz and his associates said. "In other words, if these individuals had not entered the NLST, they would not have received a lung cancer diagnosis or treatment, at least for the next 5 years."
In the future, the study authors noted, "once there are better biomarkers and imaging techniques to predict which individuals with a diagnosis of lung cancer will have more or less aggressive disease, treatment options can be optimized, and a mass screening program can become more valuable."
The National Institutes of Health supported the NSLT. No financial conflicts of interest were reported.
FROM JAMA INTERNAL MEDICINE
Major Finding: An estimated 18% of lung cancers detected by low-dose CT screening in the National Lung Screening Trial were likely indolent and may represent cases of overdiagnosis.
Data Source: A secondary analysis of data from the NLST which involved 53,452 patients aged 55-74 years who were at high risk for lung cancer because of their history of heavy smoking.
Disclosures: The National Institutes of Health supported the NSLT. No financial conflicts of interest were reported.
Smoking cessation agents don’t raise serious CVD risks
The three smoking cessation agents bupropion, varenicline, and nicotine replacement therapy did not raise the risk of serious adverse cardiovascular events in a network meta-analysis of 63 randomized clinical trials reported online Dec. 9 in Circulation.
This finding held true in the main analysis that included 30,508 patients attempting to quit smoking, in a subgroup analysis of the highest-risk patients who had a history of conditions predisposing them to cardiovascular events, and in a sensitivity analysis that broke down cardiovascular events by type and seriousness.

"Given the current findings of low risk of serious CVD events attributed to smoking cessation pharmacotherapies, combined with the well-established CVD and mortality risks of continued smoking, the benefits of use would seem to outweigh the risks," said Edward J. Mills, Ph.D., of the Stanford (Calif.) Prevention Research Center, and his associates.
The investigators performed the meta-analysis because recent reports have raised concerns that these agents may raise cardiovascular risks. They used a statistical technique known as network meta-analysis to examine both direct, head-to-head comparison studies and indirect evidence, "thus increasing the power and interpretability of a comparative analysis."
They included any randomized clinical trial of any of the three pharmacotherapies that were of any duration and that reported on any cardiovascular events. Dr. Mills and his colleagues then considered two separate definitions of cardiovascular events: the first was any such event, including minor occurrences such as palpitations, and the second was only major adverse cardiovascular events as defined by the Food and Drug Administration, which is "considered to be a more stringent definition of important patient outcomes."
A total of 19 of the randomized clinical trials assessed nicotine replacement therapy against placebo, 27 assessed bupropion against placebo, 18 assessed varenicline against placebo, 1 assessed high-dose nicotine replacement therapy against placebo, 1 assessed combination nicotine replacement therapy against a control condition, 2 assessed bupropion against varenicline, 3 assessed bupropion against nicotine replacement therapy, and 1 assessed varenicline against nicotine replacement therapy.
Both a pairwise meta-analysis and the network meta-analysis demonstrated that none of the three pharmacotherapies raised the risk of major adverse cardiovascular events. Bupropion appeared to exert a protective effect against both minor and major events, while varenicline showed no harmful or beneficial effect at all concerning minor or major cardiovascular events.
"Nicotine replacement therapy, the most widely used pharmacotherapy for smoking cessation, was associated with an increase in cardiovascular events that was driven by lower-risk events" such as palpitations and tachycardia, which are "well known and largely benign" effects of nicotine replacement, Dr. Mills and his associates said (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.003961]).
"Concerns about adverse cardiovascular events need to be balanced with the consistent evidence for the benefit of smoking cessation, and patients should be counseled about what adverse events may be associated with smoking cessation therapies, the symptoms associated with the withdrawal period from cigarettes, and symptoms that may be due to existing cardiovascular diseases," the investigators added.
This study was supported by the Canadian Institutes of Health Research, the U.S. National Institutes of Health, and the California Tobacco-Related Disease Research Program. Dr. Mills reported ties to Merck; Pfizer, maker of Chantix (varenicline); Novartis; Takeda; and GlaxoSmithKline, maker of Zyban (bupropion); and his associates reported ties to Pfizer.
Smoking cessation has benefits that extend well beyond cardiovascular disease, both for the individual patient and for the general public, said Dr. Jonathan M. Samet.
Any increased risk for minor cardiovascular events associated with nicotine replacement therapy must be viewed against "the declines in risk for CVD and other diseases that follow successful cessation," he said.
"Even with the assumption of [an excess CVD] risk associated with nicotine replacement therapy, the population-level benefits far exceed the estimated increase."
Dr. Samet is in the department of preventive medicine and the Institute for Global Health at the University of Southern California, Los Angeles. His work is supported by the National Cancer Institute and the FDA Center for Tobacco Products. These remarks were taken from his editorial accompanying Dr. Mills’ report (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.006928]).
Smoking cessation has benefits that extend well beyond cardiovascular disease, both for the individual patient and for the general public, said Dr. Jonathan M. Samet.
Any increased risk for minor cardiovascular events associated with nicotine replacement therapy must be viewed against "the declines in risk for CVD and other diseases that follow successful cessation," he said.
"Even with the assumption of [an excess CVD] risk associated with nicotine replacement therapy, the population-level benefits far exceed the estimated increase."
Dr. Samet is in the department of preventive medicine and the Institute for Global Health at the University of Southern California, Los Angeles. His work is supported by the National Cancer Institute and the FDA Center for Tobacco Products. These remarks were taken from his editorial accompanying Dr. Mills’ report (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.006928]).
Smoking cessation has benefits that extend well beyond cardiovascular disease, both for the individual patient and for the general public, said Dr. Jonathan M. Samet.
Any increased risk for minor cardiovascular events associated with nicotine replacement therapy must be viewed against "the declines in risk for CVD and other diseases that follow successful cessation," he said.
"Even with the assumption of [an excess CVD] risk associated with nicotine replacement therapy, the population-level benefits far exceed the estimated increase."
Dr. Samet is in the department of preventive medicine and the Institute for Global Health at the University of Southern California, Los Angeles. His work is supported by the National Cancer Institute and the FDA Center for Tobacco Products. These remarks were taken from his editorial accompanying Dr. Mills’ report (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.006928]).
The three smoking cessation agents bupropion, varenicline, and nicotine replacement therapy did not raise the risk of serious adverse cardiovascular events in a network meta-analysis of 63 randomized clinical trials reported online Dec. 9 in Circulation.
This finding held true in the main analysis that included 30,508 patients attempting to quit smoking, in a subgroup analysis of the highest-risk patients who had a history of conditions predisposing them to cardiovascular events, and in a sensitivity analysis that broke down cardiovascular events by type and seriousness.
"Given the current findings of low risk of serious CVD events attributed to smoking cessation pharmacotherapies, combined with the well-established CVD and mortality risks of continued smoking, the benefits of use would seem to outweigh the risks," said Edward J. Mills, Ph.D., of the Stanford (Calif.) Prevention Research Center, and his associates.
The investigators performed the meta-analysis because recent reports have raised concerns that these agents may raise cardiovascular risks. They used a statistical technique known as network meta-analysis to examine both direct, head-to-head comparison studies and indirect evidence, "thus increasing the power and interpretability of a comparative analysis."
They included any randomized clinical trial of any of the three pharmacotherapies that were of any duration and that reported on any cardiovascular events. Dr. Mills and his colleagues then considered two separate definitions of cardiovascular events: the first was any such event, including minor occurrences such as palpitations, and the second was only major adverse cardiovascular events as defined by the Food and Drug Administration, which is "considered to be a more stringent definition of important patient outcomes."
A total of 19 of the randomized clinical trials assessed nicotine replacement therapy against placebo, 27 assessed bupropion against placebo, 18 assessed varenicline against placebo, 1 assessed high-dose nicotine replacement therapy against placebo, 1 assessed combination nicotine replacement therapy against a control condition, 2 assessed bupropion against varenicline, 3 assessed bupropion against nicotine replacement therapy, and 1 assessed varenicline against nicotine replacement therapy.
Both a pairwise meta-analysis and the network meta-analysis demonstrated that none of the three pharmacotherapies raised the risk of major adverse cardiovascular events. Bupropion appeared to exert a protective effect against both minor and major events, while varenicline showed no harmful or beneficial effect at all concerning minor or major cardiovascular events.
"Nicotine replacement therapy, the most widely used pharmacotherapy for smoking cessation, was associated with an increase in cardiovascular events that was driven by lower-risk events" such as palpitations and tachycardia, which are "well known and largely benign" effects of nicotine replacement, Dr. Mills and his associates said (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.003961]).
"Concerns about adverse cardiovascular events need to be balanced with the consistent evidence for the benefit of smoking cessation, and patients should be counseled about what adverse events may be associated with smoking cessation therapies, the symptoms associated with the withdrawal period from cigarettes, and symptoms that may be due to existing cardiovascular diseases," the investigators added.
This study was supported by the Canadian Institutes of Health Research, the U.S. National Institutes of Health, and the California Tobacco-Related Disease Research Program. Dr. Mills reported ties to Merck; Pfizer, maker of Chantix (varenicline); Novartis; Takeda; and GlaxoSmithKline, maker of Zyban (bupropion); and his associates reported ties to Pfizer.
The three smoking cessation agents bupropion, varenicline, and nicotine replacement therapy did not raise the risk of serious adverse cardiovascular events in a network meta-analysis of 63 randomized clinical trials reported online Dec. 9 in Circulation.
This finding held true in the main analysis that included 30,508 patients attempting to quit smoking, in a subgroup analysis of the highest-risk patients who had a history of conditions predisposing them to cardiovascular events, and in a sensitivity analysis that broke down cardiovascular events by type and seriousness.
"Given the current findings of low risk of serious CVD events attributed to smoking cessation pharmacotherapies, combined with the well-established CVD and mortality risks of continued smoking, the benefits of use would seem to outweigh the risks," said Edward J. Mills, Ph.D., of the Stanford (Calif.) Prevention Research Center, and his associates.
The investigators performed the meta-analysis because recent reports have raised concerns that these agents may raise cardiovascular risks. They used a statistical technique known as network meta-analysis to examine both direct, head-to-head comparison studies and indirect evidence, "thus increasing the power and interpretability of a comparative analysis."
They included any randomized clinical trial of any of the three pharmacotherapies that were of any duration and that reported on any cardiovascular events. Dr. Mills and his colleagues then considered two separate definitions of cardiovascular events: the first was any such event, including minor occurrences such as palpitations, and the second was only major adverse cardiovascular events as defined by the Food and Drug Administration, which is "considered to be a more stringent definition of important patient outcomes."
A total of 19 of the randomized clinical trials assessed nicotine replacement therapy against placebo, 27 assessed bupropion against placebo, 18 assessed varenicline against placebo, 1 assessed high-dose nicotine replacement therapy against placebo, 1 assessed combination nicotine replacement therapy against a control condition, 2 assessed bupropion against varenicline, 3 assessed bupropion against nicotine replacement therapy, and 1 assessed varenicline against nicotine replacement therapy.
Both a pairwise meta-analysis and the network meta-analysis demonstrated that none of the three pharmacotherapies raised the risk of major adverse cardiovascular events. Bupropion appeared to exert a protective effect against both minor and major events, while varenicline showed no harmful or beneficial effect at all concerning minor or major cardiovascular events.
"Nicotine replacement therapy, the most widely used pharmacotherapy for smoking cessation, was associated with an increase in cardiovascular events that was driven by lower-risk events" such as palpitations and tachycardia, which are "well known and largely benign" effects of nicotine replacement, Dr. Mills and his associates said (Circulation 2013 Dec. 9 [doi:10.1161/circulationaha.113.003961]).
"Concerns about adverse cardiovascular events need to be balanced with the consistent evidence for the benefit of smoking cessation, and patients should be counseled about what adverse events may be associated with smoking cessation therapies, the symptoms associated with the withdrawal period from cigarettes, and symptoms that may be due to existing cardiovascular diseases," the investigators added.
This study was supported by the Canadian Institutes of Health Research, the U.S. National Institutes of Health, and the California Tobacco-Related Disease Research Program. Dr. Mills reported ties to Merck; Pfizer, maker of Chantix (varenicline); Novartis; Takeda; and GlaxoSmithKline, maker of Zyban (bupropion); and his associates reported ties to Pfizer.
FROM CIRCULATION
Major Finding: Bupropion appeared to protect against minor or serious CVD events, varenicline showed no harmful or beneficial effect on minor or serious CVD events, and nicotine replacement therapy showed no effect on serious CVD events but raised the risk of minor events such as palpitations and tachycardia.
Data Source: A network meta-analysis of 63 randomized clinical trials involving 30,508 patients attempting to quit smoking in which cardiovascular events were tracked.
Disclosures: This study was supported by the Canadian Institutes of Health Research, the U.S. National Institutes of Health, and the California Tobacco-Related Disease Research Program. Dr. Mills reported ties to Merck; Pfizer, maker of Chantix (varenicline); Novartis; Takeda; and GlaxoSmithKline, maker of Zyban (bupropion); and his associates reported ties to Pfizer.

Survey identifies need for COPD awareness, discourse
Physicians may miss opportunities to discuss chronic obstructive pulmonary disease with their patients, including former and current smokers with symptoms, according to survey results reported by the National Heart Lung and Blood Institute.
The survey found that the proportion of current smokers who had discussed COPD symptoms with their physicians had increased from 42% in 2009 to 67% in 2013, according to the report. However, during this period, the proportion of former smokers who had talked to their doctors about these symptoms dropped slightly, from 78% in 2009 to 77% in 2013.

Although 74% of current smokers said they had talked to their physicians about their chronic cough, wheezing, or being too short of breath to do normal activities, 26% said no to this question.
Of those who were surveyed who had COPD symptoms and said they had talked to their doctors about having a chronic cough, wheezing, or being too short of breath to do normal activities, only 18% said their doctors told them they might have COPD. Of this group, only 35% said the doctors talked to them about their past or current smoking history.
According to the NHLBI report, the results suggest that awareness of COPD may influence why patients do not talk to their physicians about COPD symptoms: Among those surveyed who were symptomatic and had not talked to their doctors about symptoms, various reasons were mentioned for not doing so, including: "they did not think of it" (cited by 27%), they had the problem for years (20%), "I don’t want another ‘quit smoking’ message" (16%), and the problem "will just go away in time" (16%).
"Regardless of positive developments, the challenge remains that more than 1 in 3 Americans do not know what COPD is or how it affects them – and less than half understand that COPD can be treated," James Kiley, Ph.D., director of the NHLBI Division of Lung Diseases, said in the statement.
http://www.nhlbi.nih.gov/news/press-releases/2013/nih-survey-identifies-barriers-to-effective-patient-provider-dialogue-about-copd.html
The web-based survey is conducted every year by the communications company Porter Novelli, for NHLBI’s "COPD Learn More Breathe Better" campaign. The campaign promotes national awareness about COPD, directed at people with COPD, those at risk of COPD, and health care providers, particularly primary care providers, according to the NHLBI.
The 2013 survey sampled almost 4,500 adults in the United States, with a 66% response rate. Up to half the estimated 24 million people in the United States with COPD have not been diagnosed, and in 2010, COPD replaced stroke as the third leading cause of death in the United States, according to the NHLBI.
Physicians may miss opportunities to discuss chronic obstructive pulmonary disease with their patients, including former and current smokers with symptoms, according to survey results reported by the National Heart Lung and Blood Institute.
The survey found that the proportion of current smokers who had discussed COPD symptoms with their physicians had increased from 42% in 2009 to 67% in 2013, according to the report. However, during this period, the proportion of former smokers who had talked to their doctors about these symptoms dropped slightly, from 78% in 2009 to 77% in 2013.
Although 74% of current smokers said they had talked to their physicians about their chronic cough, wheezing, or being too short of breath to do normal activities, 26% said no to this question.
Of those who were surveyed who had COPD symptoms and said they had talked to their doctors about having a chronic cough, wheezing, or being too short of breath to do normal activities, only 18% said their doctors told them they might have COPD. Of this group, only 35% said the doctors talked to them about their past or current smoking history.
According to the NHLBI report, the results suggest that awareness of COPD may influence why patients do not talk to their physicians about COPD symptoms: Among those surveyed who were symptomatic and had not talked to their doctors about symptoms, various reasons were mentioned for not doing so, including: "they did not think of it" (cited by 27%), they had the problem for years (20%), "I don’t want another ‘quit smoking’ message" (16%), and the problem "will just go away in time" (16%).
"Regardless of positive developments, the challenge remains that more than 1 in 3 Americans do not know what COPD is or how it affects them – and less than half understand that COPD can be treated," James Kiley, Ph.D., director of the NHLBI Division of Lung Diseases, said in the statement.
http://www.nhlbi.nih.gov/news/press-releases/2013/nih-survey-identifies-barriers-to-effective-patient-provider-dialogue-about-copd.html
The web-based survey is conducted every year by the communications company Porter Novelli, for NHLBI’s "COPD Learn More Breathe Better" campaign. The campaign promotes national awareness about COPD, directed at people with COPD, those at risk of COPD, and health care providers, particularly primary care providers, according to the NHLBI.
The 2013 survey sampled almost 4,500 adults in the United States, with a 66% response rate. Up to half the estimated 24 million people in the United States with COPD have not been diagnosed, and in 2010, COPD replaced stroke as the third leading cause of death in the United States, according to the NHLBI.
Physicians may miss opportunities to discuss chronic obstructive pulmonary disease with their patients, including former and current smokers with symptoms, according to survey results reported by the National Heart Lung and Blood Institute.
The survey found that the proportion of current smokers who had discussed COPD symptoms with their physicians had increased from 42% in 2009 to 67% in 2013, according to the report. However, during this period, the proportion of former smokers who had talked to their doctors about these symptoms dropped slightly, from 78% in 2009 to 77% in 2013.
Although 74% of current smokers said they had talked to their physicians about their chronic cough, wheezing, or being too short of breath to do normal activities, 26% said no to this question.
Of those who were surveyed who had COPD symptoms and said they had talked to their doctors about having a chronic cough, wheezing, or being too short of breath to do normal activities, only 18% said their doctors told them they might have COPD. Of this group, only 35% said the doctors talked to them about their past or current smoking history.
According to the NHLBI report, the results suggest that awareness of COPD may influence why patients do not talk to their physicians about COPD symptoms: Among those surveyed who were symptomatic and had not talked to their doctors about symptoms, various reasons were mentioned for not doing so, including: "they did not think of it" (cited by 27%), they had the problem for years (20%), "I don’t want another ‘quit smoking’ message" (16%), and the problem "will just go away in time" (16%).
"Regardless of positive developments, the challenge remains that more than 1 in 3 Americans do not know what COPD is or how it affects them – and less than half understand that COPD can be treated," James Kiley, Ph.D., director of the NHLBI Division of Lung Diseases, said in the statement.
http://www.nhlbi.nih.gov/news/press-releases/2013/nih-survey-identifies-barriers-to-effective-patient-provider-dialogue-about-copd.html
The web-based survey is conducted every year by the communications company Porter Novelli, for NHLBI’s "COPD Learn More Breathe Better" campaign. The campaign promotes national awareness about COPD, directed at people with COPD, those at risk of COPD, and health care providers, particularly primary care providers, according to the NHLBI.
The 2013 survey sampled almost 4,500 adults in the United States, with a 66% response rate. Up to half the estimated 24 million people in the United States with COPD have not been diagnosed, and in 2010, COPD replaced stroke as the third leading cause of death in the United States, according to the NHLBI.

Continued smoking after cancer diagnosis ups mortality risk
Men who continue smoking after a cancer diagnosis have significantly greater risk of death from any cause than did those who quit smoking at the time of diagnosis, according to findings from the prospective population-based Shanghai Cohort Study.
Of 1,632 men from that ongoing study who developed cancer after enrollment and who were eligible for the current analysis, 931 died during 25 years of follow-up, and 747 of those who died were smokers at the time of their cancer diagnosis. Of these smokers, 214 (29%) quit at the time of diagnosis, 197 (26%) smoked persistently after diagnosis, and 336 (45%) smoked intermittently after diagnosis.

After the researchers adjusted for age at diagnosis, education, cumulative number of pack-years of prediagnosis smoking, cancer site, and treatment modalities, the risk of death was 76% greater in those who smoked persistently or intermittently after diagnosis, compared with those who quit at diagnosis, reported Dr. Li Tao of the Cancer Prevention Institute of California, Fremont, and her colleagues.
Median survival was 2.1 years after diagnosis for those who continued smoking, compared with 4.4 years for those who quit, the investigators said.
Using a time-dependent approach, and including all patients with cancer, the overall risk of mortality was 59% greater for smokers vs. nonsmokers after cancer diagnosis.
"When analyzed separately for cancer specific patients, the multivariate-adjusted hazard ratios of death for smoking relative to nonsmoking after cancer diagnosis were 1.92 for patients with lung cancer, 1.76 for patients with stomach cancer, 1.65 for patients with colorectal cancer, and 3.66 for patients with bladder cancer," the investigators wrote.
In a similar analysis that included only current smokers at cancer diagnosis, smoking after cancer diagnosis was associated with a 79% increase risk of death relative to nonsmoking after diagnosis for all patients.
"Among cancer-specific patients, the [hazard ratios] of death for smoking vs. nonsmoking after cancer diagnosis were 2.36 in patients with lung cancer, 1.63 in patients with stomach cancer, 2.31 in patients with colorectal cancer, 2.95 in patients with bladder cancer, 2.27 in patients with prostate cancer, and 1.34 in all other patient with cancer," the investigators said (Cancer Epidemiol. Biomarkers Prev. 2013;22:2404-11).
The Shanghai Cohort Study is investigating the association between lifestyle characteristics and cancer development in more than 18,000 middle-age or older men who were enrolled between Jan.1, 1986, and Sept. 30, 1989. Smoking status is ascertained via annual in-person interviews. Patients in the current analysis had a mean age of 68.8 years and were followed for a mean of 5.3 years after cancer diagnosis. They had a median survival time of 5.4 years after diagnosis.
The findings provide new information about smoking and cancer survival, the investigators said, noting that cancer is the leading cause of death among men in China, and the second leading cause of death among men in the United States.
Tobacco use is the most important recognized cause of cancer-related death, they said, adding that strong evidence demonstrates an association between smoking and cancer risk, and between improved health and smoking cessation.
The impact of smoking after a cancer diagnosis, however, has not been well studied, and existing data are conflicting, they noted.
The findings of the present study, which have important public health implications for cancer survivors, health care providers, and policy makers, underscore the importance of smoking cessation interventions – and the potential benefit of cessation on survival – in patients who are diagnosed with cancer, they said.
Although patients diagnosed with cancer are expected to "show great interest and motivation to quit smoking," many face physical, psychological, and social stress that impedes their ability to do so. Furthermore, only about 50% of smokers diagnosed with cancer in the United States receive formal smoking cessation counseling at diagnosis, during treatment, or during follow-up visits, they noted.
"Therefore, there is noticeable room for the improvement of self-managed or health care provider–assisted smoking cessation in the clinical setting of patients with cancer," they wrote, also noting that the message about inferior survival among those who continue smoking after a cancer diagnosis should be conveyed to patients and their families, and should be included in guidelines and evidence-based clinical practices.
This study has considerable strengths – such as knowledge of baseline smoking status and the prospective design. It also has limitations, including limited treatment data and inclusion of only patients who survived 1 or more years after cancer diagnosis.
Nonetheless, the findings provide strong support for smoking cessation intervention programs that target cancer survivors and should inform future research into the contextual and individual-level factors that may result in inadequate attention to smoking among patients with cancer in the post diagnosis setting, the investigators concluded.
This study was supported by grants from the United States Public Health Service. The costs of publication were defrayed in part by the payment of page charges. The authors reported having no disclosures.
Men who continue smoking after a cancer diagnosis have significantly greater risk of death from any cause than did those who quit smoking at the time of diagnosis, according to findings from the prospective population-based Shanghai Cohort Study.
Of 1,632 men from that ongoing study who developed cancer after enrollment and who were eligible for the current analysis, 931 died during 25 years of follow-up, and 747 of those who died were smokers at the time of their cancer diagnosis. Of these smokers, 214 (29%) quit at the time of diagnosis, 197 (26%) smoked persistently after diagnosis, and 336 (45%) smoked intermittently after diagnosis.
After the researchers adjusted for age at diagnosis, education, cumulative number of pack-years of prediagnosis smoking, cancer site, and treatment modalities, the risk of death was 76% greater in those who smoked persistently or intermittently after diagnosis, compared with those who quit at diagnosis, reported Dr. Li Tao of the Cancer Prevention Institute of California, Fremont, and her colleagues.
Median survival was 2.1 years after diagnosis for those who continued smoking, compared with 4.4 years for those who quit, the investigators said.
Using a time-dependent approach, and including all patients with cancer, the overall risk of mortality was 59% greater for smokers vs. nonsmokers after cancer diagnosis.
"When analyzed separately for cancer specific patients, the multivariate-adjusted hazard ratios of death for smoking relative to nonsmoking after cancer diagnosis were 1.92 for patients with lung cancer, 1.76 for patients with stomach cancer, 1.65 for patients with colorectal cancer, and 3.66 for patients with bladder cancer," the investigators wrote.
In a similar analysis that included only current smokers at cancer diagnosis, smoking after cancer diagnosis was associated with a 79% increase risk of death relative to nonsmoking after diagnosis for all patients.
"Among cancer-specific patients, the [hazard ratios] of death for smoking vs. nonsmoking after cancer diagnosis were 2.36 in patients with lung cancer, 1.63 in patients with stomach cancer, 2.31 in patients with colorectal cancer, 2.95 in patients with bladder cancer, 2.27 in patients with prostate cancer, and 1.34 in all other patient with cancer," the investigators said (Cancer Epidemiol. Biomarkers Prev. 2013;22:2404-11).
The Shanghai Cohort Study is investigating the association between lifestyle characteristics and cancer development in more than 18,000 middle-age or older men who were enrolled between Jan.1, 1986, and Sept. 30, 1989. Smoking status is ascertained via annual in-person interviews. Patients in the current analysis had a mean age of 68.8 years and were followed for a mean of 5.3 years after cancer diagnosis. They had a median survival time of 5.4 years after diagnosis.
The findings provide new information about smoking and cancer survival, the investigators said, noting that cancer is the leading cause of death among men in China, and the second leading cause of death among men in the United States.
Tobacco use is the most important recognized cause of cancer-related death, they said, adding that strong evidence demonstrates an association between smoking and cancer risk, and between improved health and smoking cessation.
The impact of smoking after a cancer diagnosis, however, has not been well studied, and existing data are conflicting, they noted.
The findings of the present study, which have important public health implications for cancer survivors, health care providers, and policy makers, underscore the importance of smoking cessation interventions – and the potential benefit of cessation on survival – in patients who are diagnosed with cancer, they said.
Although patients diagnosed with cancer are expected to "show great interest and motivation to quit smoking," many face physical, psychological, and social stress that impedes their ability to do so. Furthermore, only about 50% of smokers diagnosed with cancer in the United States receive formal smoking cessation counseling at diagnosis, during treatment, or during follow-up visits, they noted.
"Therefore, there is noticeable room for the improvement of self-managed or health care provider–assisted smoking cessation in the clinical setting of patients with cancer," they wrote, also noting that the message about inferior survival among those who continue smoking after a cancer diagnosis should be conveyed to patients and their families, and should be included in guidelines and evidence-based clinical practices.
This study has considerable strengths – such as knowledge of baseline smoking status and the prospective design. It also has limitations, including limited treatment data and inclusion of only patients who survived 1 or more years after cancer diagnosis.
Nonetheless, the findings provide strong support for smoking cessation intervention programs that target cancer survivors and should inform future research into the contextual and individual-level factors that may result in inadequate attention to smoking among patients with cancer in the post diagnosis setting, the investigators concluded.
This study was supported by grants from the United States Public Health Service. The costs of publication were defrayed in part by the payment of page charges. The authors reported having no disclosures.
Men who continue smoking after a cancer diagnosis have significantly greater risk of death from any cause than did those who quit smoking at the time of diagnosis, according to findings from the prospective population-based Shanghai Cohort Study.
Of 1,632 men from that ongoing study who developed cancer after enrollment and who were eligible for the current analysis, 931 died during 25 years of follow-up, and 747 of those who died were smokers at the time of their cancer diagnosis. Of these smokers, 214 (29%) quit at the time of diagnosis, 197 (26%) smoked persistently after diagnosis, and 336 (45%) smoked intermittently after diagnosis.
After the researchers adjusted for age at diagnosis, education, cumulative number of pack-years of prediagnosis smoking, cancer site, and treatment modalities, the risk of death was 76% greater in those who smoked persistently or intermittently after diagnosis, compared with those who quit at diagnosis, reported Dr. Li Tao of the Cancer Prevention Institute of California, Fremont, and her colleagues.
Median survival was 2.1 years after diagnosis for those who continued smoking, compared with 4.4 years for those who quit, the investigators said.
Using a time-dependent approach, and including all patients with cancer, the overall risk of mortality was 59% greater for smokers vs. nonsmokers after cancer diagnosis.
"When analyzed separately for cancer specific patients, the multivariate-adjusted hazard ratios of death for smoking relative to nonsmoking after cancer diagnosis were 1.92 for patients with lung cancer, 1.76 for patients with stomach cancer, 1.65 for patients with colorectal cancer, and 3.66 for patients with bladder cancer," the investigators wrote.
In a similar analysis that included only current smokers at cancer diagnosis, smoking after cancer diagnosis was associated with a 79% increase risk of death relative to nonsmoking after diagnosis for all patients.
"Among cancer-specific patients, the [hazard ratios] of death for smoking vs. nonsmoking after cancer diagnosis were 2.36 in patients with lung cancer, 1.63 in patients with stomach cancer, 2.31 in patients with colorectal cancer, 2.95 in patients with bladder cancer, 2.27 in patients with prostate cancer, and 1.34 in all other patient with cancer," the investigators said (Cancer Epidemiol. Biomarkers Prev. 2013;22:2404-11).
The Shanghai Cohort Study is investigating the association between lifestyle characteristics and cancer development in more than 18,000 middle-age or older men who were enrolled between Jan.1, 1986, and Sept. 30, 1989. Smoking status is ascertained via annual in-person interviews. Patients in the current analysis had a mean age of 68.8 years and were followed for a mean of 5.3 years after cancer diagnosis. They had a median survival time of 5.4 years after diagnosis.
The findings provide new information about smoking and cancer survival, the investigators said, noting that cancer is the leading cause of death among men in China, and the second leading cause of death among men in the United States.
Tobacco use is the most important recognized cause of cancer-related death, they said, adding that strong evidence demonstrates an association between smoking and cancer risk, and between improved health and smoking cessation.
The impact of smoking after a cancer diagnosis, however, has not been well studied, and existing data are conflicting, they noted.
The findings of the present study, which have important public health implications for cancer survivors, health care providers, and policy makers, underscore the importance of smoking cessation interventions – and the potential benefit of cessation on survival – in patients who are diagnosed with cancer, they said.
Although patients diagnosed with cancer are expected to "show great interest and motivation to quit smoking," many face physical, psychological, and social stress that impedes their ability to do so. Furthermore, only about 50% of smokers diagnosed with cancer in the United States receive formal smoking cessation counseling at diagnosis, during treatment, or during follow-up visits, they noted.
"Therefore, there is noticeable room for the improvement of self-managed or health care provider–assisted smoking cessation in the clinical setting of patients with cancer," they wrote, also noting that the message about inferior survival among those who continue smoking after a cancer diagnosis should be conveyed to patients and their families, and should be included in guidelines and evidence-based clinical practices.
This study has considerable strengths – such as knowledge of baseline smoking status and the prospective design. It also has limitations, including limited treatment data and inclusion of only patients who survived 1 or more years after cancer diagnosis.
Nonetheless, the findings provide strong support for smoking cessation intervention programs that target cancer survivors and should inform future research into the contextual and individual-level factors that may result in inadequate attention to smoking among patients with cancer in the post diagnosis setting, the investigators concluded.
This study was supported by grants from the United States Public Health Service. The costs of publication were defrayed in part by the payment of page charges. The authors reported having no disclosures.
FROM CANCER EPIDEMIOLOGY, BIOMARKERS & PREVENTION
Major finding: Among male smokers at the time of cancer diagnosis, the risk of death was 76% greater in those who continued smoking than in those who quit at diagnosis.
Data source: A prospective cohort study involving more than 18,000 men.
Disclosures: This study was supported by grants from the United States Public Health Service. The costs of publication were defrayed in part by the payment of page charges. The authors reported having no disclosures.

Emerging imaging techniques target bronchial thermoplasty
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
CHICAGO – Advanced imaging techniques may play an increasing role in targeting the delivery of bronchial thermoplasty in severe, uncontrolled asthma.
"It’s off-label at this point, but I think this is where we’re going with this therapy," Dr. Mario Castro said at the annual meeting of the American College of Chest Physicians. "Perhaps we can do a better job to target this therapy, just like phenotyping our patients [for novel biologic agents]."
Reconstruction of the airway and parenchyma using diagnostic software during an inspiratory computed tomography (CT) scan allows clinicians to measure all of the lung airways in a systematic way, said Dr. Castro, director of the asthma and airway translational research unit, Washington University School of Medicine, St. Louis.
In the case of a 50-year-old patient with severe persistent asthma, the technique revealed a clearly remodeled airway with a 63% average wall area, but also areas of great heterogeneity in all segmental airways. "What we find is that some airways are remodeled more than others," Dr. Castro said.
The university also now images its patients by combining inhaled hyperpolarized helium gas with magnetic resonance imaging from the apex all the way to the base of the lung. A color algorithm CT mask imposed on the MRI images allows the team to quantify ventilation defects before and after bronchial thermoplasty.
Earlier this year, Dr. Castro’s colleague, Dr. Ajay Sheshadri, reported that patients with severe asthma have a significantly higher baseline ventilation defect percentage (VDP) than healthy subjects (mean 24.4% vs. 3.5%; P = .003). VDP improved by about 7% overall after bronchial thermoplasty (P = .10), with some patients having a marked improvement in VDP, while others did not, Dr. Castro said.
Baseline characteristics were analyzed in an effort to identify responders, and "we were very surprised to find that sputum eosinophilia was the one that trended best in predicting a change in ventilation defect score," he added.
Biopredictors of bronchial thermoplasty response are also being evaluated in a prospective study of patients with severe refractory asthma, led by Dr. Castro, currently recruiting approximately 190 patients at five U.S. sites (NCT01185275).
Dr. Castro’s team is also using xenon gas instead of helium with MRI, because it is more readily available and less expensive. Other groups are using confocal CT to evaluate airways for bronchial thermoplasty, he noted.
Dr. Castro stressed that 13 years of cumulative experience have shown that bronchial thermoplasty is safe and effective, but that careful initial evaluation of candidates remains essential. The American Thoracic Society and European Respiratory Society are expected to release new guidelines early next year for the initial evaluation of all severe asthmatics that recommend six tests, including blood work, spirometry, immunoglobulin E assessment with skin prick tests or an immunoabsorbent assay, and multidetector CT to evaluate for other conditions mimicking asthma.
"With this basic evaluation in our center, we find about one out of every three patients are really not pure asthma; they’re asthma mixed with significant bronchiectasis or no asthma at all, or they have underlying emphysema from prior smoke exposure," said Dr. Castro. "So it is very important that we take a step back with these patients and look."
During a discussion following the presentation, Dr. Castro said he would use bronchial thermoplasty to treat patients with incomplete reversibility of airflow obstruction, but does not advocate repeat treatments because of the potential for additional injury.
"What we do advocate is that we extensively treat all the airways that we can access, and that you treat with continuous therapies," he said. "The average activations in the lower, lower [airway] is around 60, but in some cases I’ve done up to around 140-150 activations, just because they’ve had an extensive bronchial tree that I needed to treat. ... If you have a nonresponder, even 5 years out, I wouldn’t treat because I think smooth muscle is probably not their main problem," he added.
Dr. Castro reported research support, lecturing, and consulting for numerous firms including Boston Scientific, maker of the Alair bronchial thermoplasty system.
AT CHEST 2013
Riociguat benefits persist in pulmonary hypertension
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
CHICAGO – Patients with chronic thromboembolic pulmonary hypertension and pulmonary arterial hypertension maintained benefits with riociguat at 1 year in two long-term extension studies.
Riociguat (Adempas) is the first drug approved for chronic thromboembolic pulmonary hypertension (CTEPH) and the first to show sustained benefits in 6-minute walk distance and functional class in this setting, Dr. Gérald Simonneau said in a late-breaking session at the annual meeting of the American College of Chest Physicians.
The oral soluble guanylate cyclase stimulator was approved in the United States in October 2013 to treat CTEPH and pulmonary arterial hypertension (PAH) based on the phase III CHEST-1 and PATENT-1 studies.
CHEST-1 randomized 261 patients with inoperable CTEPH or persistent pulmonary hypertension after endarterectomy to placebo or riociguat up to 2.5 mg three times daily for 16 weeks.
In all, 237 patients entered CHEST-2, and were either maintained on their optimum riociguat dose, up to 2.5 mg three times daily, or switched to riociguat titrated up to 2.5 mg three times daily. Only 8% of patients required additional PAH drugs at 1 year.
Patients maintained on riociguat gained only 15 m on the 6-minute walk test at 1 year, but added 66 m overall from baseline, said Dr. Simonneau, head of pneumology and intensive care medicine at Hôpital Kremlin Bicêtre, University of Paris-Sud, Le Kremlin-Bicêtre, France.
Patients switching from placebo to riociguat gained 37 m in the walk test at 1 year, but only 45 m from baseline.
WHO functional class improved in about 15% of patients in the riociguat maintenance arm and about 30% of those switched from placebo, he reported.
Freedom from clinical worsening at years 1 and 2 were 88% and 80%, with estimated overall survival rates of 97% and 94%.
During a discussion of the results, Dr. Simonneau observed that the 2-year overall survival rate for CTEPH patients is approximately 92% for patients treated surgically, but only about 70% for those receiving traditional medical therapy.
Adverse events
One fatal pulmonary hemorrhage occurred during CHEST-2, but it was not considered related to the study drug, said Dr. Simonneau, who noted that riociguat's label includes a warning about the risk of pulmonary bleeding events.
Two fatal pulmonary hemorrhages occurred in PATENT-2, and one was related to riociguat, Dr. Lewis Rubin reported during the same session. A third serious pulmonary hemorrhage occurred that was considered related to riociguat, but it resolved.
Hemoptysis was another serious adverse event (SAE) of "interest and concern" in both pulmonary arterial hypertension and CTEPH patients, said Dr. Rubin of the University of California, San Diego. Two patients (1%) had serious hemoptysis in PATENT-1, with seven additional events occurring in the extension phase (2%). All but one case resolved, five were moderate, and no cases were considered related to the study drug, although this could not be entirely excluded.
"The outcome of pulmonary bleeding-related SAEs was, in general, resolved in most cases, and there does not appear to be an association between dose of riociguat used and the occurrence of hemoptysis," said Dr. Rubin. However, "we need some further clarification on the mechanism responsible," he added.
Six serious hemoptysis events occurred in the two CHEST studies (three each), and one patient required bronchial artery embolization. All patients were receiving anticoagulants and none of these events was considered related to the study drug, Dr. Simonneau said.
Overall, 100 (42%) patients in CHEST-2 had a serious AE, and 12 were considered related to riociguat. SAEs were reported in 204 patients (52%) in PATENT-2, with 7% considered study drug related. Syncope was the most common adverse event (2%).
PATENT study
PATENT-1 randomized 443 patients with PAH to placebo or riociguat titrated to 1.5 mg or 2.5 mg three times daily. In all, 98% of patients (434) entered PATENT-2 and received riociguat titrated up to 2.5 mg three times daily. Notably, 54% of patients were on additional PAH medications at 1 year (97% of those pretreated with riociguat and 11% of controls).
Six-minute walk distances increased from a mean of 400 m at the close of PATENT-1 to 417 m in patients initially given the maximum dose of riociguat, for a gain of 17 m; from 406 to 417 m in those initially capped at riociguat 1.5 mg; and from 390 to 426 m in the former placebo group, Dr. Rubin said.
WHO functional class improved by approximately 10% in all three arms.
Freedom from clinical worsening at 1 and 2 years was 88% and 77%, with overall survival estimated at 97% and 93%, he said.
CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies including Bayer.
AT CHEST 2013
Major finding: Patients on continuous riociguat gained an average of 15 m on the 6-minute timed walk test after 1 year in CHEST-2 and 17 m in PATENT-2.
Data source: Prospective extension studies in 237 patients with chronic thromboembolic pulmonary hypertension and 434 patients with pulmonary arterial hypertension.
Disclosures: CHEST-2 and PATENT-2 are supported by Bayer Healthcare, maker of riociguat. Dr. Simonneau and Dr. Lewis reported financial relationships with several drug companies, including Bayer.
LABA/LAMA combo beneficial in moderate, severe COPD
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.

Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.
Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
CHICAGO – A fixed-dose combination of aclidinium bromide and formoterol fumarate improved lung function better than either drug alone without increasing toxicity in patients with moderate to severe chronic obstructive pulmonary disease in the phase III AUGMENT trial.
Aclidinium bromide (Tudorza Pressair) 400 mcg twice daily is a long-acting muscarinic antagonist (LAMA) approved in 2012 for the long-term maintenance treatment of COPD-associated bronchospasm. Formoterol fumarate (Foradil Aerolizer), a long-acting beta2-agonist (LABA), is also used in COPD to control symptoms and prevent wheezing.
Several fixed-dose LABA/LAMA combinations are in development, but none have been approved in COPD.
Combining two agents with different mechanisms of action is often recommended for improved bronchodilation, patient compliance, and cost-effectiveness in patients with COPD, Dr. Anthony D’Urzo said during a late-breaking abstract session at the annual meeting of the American College of Chest Physicians.
AUGMENT investigators (Chest 2013;144[4 MeetingAbstracts]:1025A) evenly randomized 1,692 patients with moderate to severe COPD to one of five twice-daily, metered-dose inhaler treatments: aclidinium 400 mcg plus formoterol 6 mcg or 12 mcg, aclidinium 400 mcg monotherapy, formoterol 12 mcg monotherapy, or placebo. Mean prebronchodilator forced expiratory volume in 1 second (FEV1) was 1.36 mL, and the mean age of the patients was 64 years. About half of the patients were current smokers, an intentional choice to reflect daily clinical practice, he said.
At week 24, the low- and high-dose formoterol combinations significantly increased FEV1 1 hour after morning dosing by 87 mL and 108 mL, respectively, compared with aclidinium alone (both P < .0001), said Dr. D’Urzo, director of the Primary Care Lung Clinic, University of Toronto.
Specifically, peak FEV1 increased by 176 mL with aclidinium alone, 201 mL with formoterol alone, 263 mL with the low-dose combination, and 284 mL with the high-dose combination, and decreased by 37 mL with placebo.
The low- and high-dose formoterol combinations also increased the coprimary endpoint of morning predose (trough) FEV1 at week 24 by 45 mL and 26 mL, respectively, compared with formoterol alone, but the increase was significant only for the higher-dose combination (P = .010), he said.
Specifically, trough FEV1 increased by 102 mL with aclidinium alone, 85 mL with formoterol alone, 111 mL with the low-dose combination, and 130 mL with the high-dose combination, and decreased by 35 mL with placebo.
Session comoderator Dr. Andrew Berman, division director of pulmonary and critical care medicine at Rutgers New Jersey Medical School in Newark, said targeting two different receptors clearly increases the degree of bronchodilation, but he questioned what the combined mechanism of action is and whether there’s perhaps a negative effect when combining two drugs since most clinicians would agree there’s only so much the airways can dilate.
Dr. D’Urzo said the combined mechanism is uncertain, but that there is evidence which suggests that beta2-agonists may augment the bronchial smooth muscle relaxation that is directly induced by muscarinic antagonists via a mechanism that decreases the release of acetylcholine via a modulation of cholinergic neurotransmission.
Adverse events leading to treatment discontinuation were similar across treatment arms, as were serious adverse events reported in 5.7% of patients on the high-dose combination, 5.4% on the low-dose combination, 5% on aclidinium alone, 4.5% on formoterol alone, and 3.6% on placebo. Three deaths occurred in the aclidinium monotherapy arm and one each in the high-dose formoterol combination and formoterol monotherapy arms, but none were thought related to treatment, he said.
Positive results have been reported from a second clinical trial, but codevelopers Forest Laboratories and Almirall announced in August that the New Drug Application submission planned for late 2013 was being delayed in order to resolve concerns raised by the Food and Drug Administration related to "chemistry, manufacturing, and control specifications associated with the combination formula." Forest is preparing a "robust package to address the FDA’s concerns" and is hoping to meet with its officials in early 2014, Forest R&D president Marco Taglietti said during an October earnings conference call.
Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.
AT CHEST 2013
Major finding: Low- and high-dose formoterol combinations increased week-24 peak FEV1 by 87 mL and 108 mL, respectively, over aclidinium alone (P < .0001).
Data source: A prospective study of 1,692 patients with moderate to severe COPD.
Disclosures: Dr. D’Urzo reported having financial ties with several drug firms, including study sponsor Forest Research Institute; two coauthors are Forest employees.

Temperature alone doesn’t rule out flu in the ED
SEATTLE – Lowering the Centers for Disease Control and Prevention’s temperature requirement for influenza-like illness from 100º F to 99º F would likely pick up more cases of true influenza in the emergency department, according to researchers at Rush University Medical Center in Chicago.
At Rush, 203 emergency department (ED) patients tested positive for the virus by polymerase chain reaction (PCR) during the 2012-2013 flu season, but only 135 (67%) were identified as having flu-like illness by the ED’s automated surveillance system, which pulls together provider notes, vital signs, and other information from the electronic records system in real time to identify patients with influenza-like illness (ILI), among other conditions.
On chart review, 29 (43%) of the 68 missed cases met the CDC’s requirements for ILI diagnosis: a temperature of at least 100º F, plus cough and/or sore throat. Most likely, the surveillance system was confused by double-negatives in provider notes or similar problems; Rush investigators are looking into the problem.

However, 39 patients with PCR-confirmed influenza did not meet the CDC’s criteria in the ED; in 15 patients (40%) it was because they had a temperature at or above 99º F, but below the 100º F benchmark.
"If you relabeled the fever criteria to greater than or equal to 99 degrees, you would actually pick up more patients. Your sensitivity would be greater, but we don’t know what would happen to the specificity. We haven’t reprogrammed the surveillance system yet to try it," Dr. Marilyn Hallock, an attending physician in the Rush ED, said a the annual meeting of the American College of Emergency Physicians. It’s something "we might want to explore further," she noted.
In the meantime, "I’m going to think twice before I say patients who come in with that gray-zone temperature between of 99º F and 100 º F don’t have influenza; they might," she said.
The rest of the 39 patients were missed for various reasons. A few arrived in respiratory distress or another condition that precluded an accurate history, while others may not have recalled ILI symptoms or were not asked about them. A number of patients were diagnosed on hospital admission from the ED when more thorough histories were taken, or when they developed the CDC triad after admission.
Dr. Hallock suspects viral PCRs were ordered in the ED for the 39 patients – although they didn’t meet CDC criteria – because it was flu season, and they complained of other flu symptoms such as myalgia and aches. "It was probably just a constellation of symptoms that led physicians to give the test," even though the patients’ ED temperatures were below 100 º F, she said.
In addition to perhaps lowering the ILI requirement to 99 º F, the investigators plan to review ILI symptoms with ED staff and work to improve their documentation, said Dr. Hallock, who indicated that she had no relevant disclosures.
SEATTLE – Lowering the Centers for Disease Control and Prevention’s temperature requirement for influenza-like illness from 100º F to 99º F would likely pick up more cases of true influenza in the emergency department, according to researchers at Rush University Medical Center in Chicago.
At Rush, 203 emergency department (ED) patients tested positive for the virus by polymerase chain reaction (PCR) during the 2012-2013 flu season, but only 135 (67%) were identified as having flu-like illness by the ED’s automated surveillance system, which pulls together provider notes, vital signs, and other information from the electronic records system in real time to identify patients with influenza-like illness (ILI), among other conditions.
On chart review, 29 (43%) of the 68 missed cases met the CDC’s requirements for ILI diagnosis: a temperature of at least 100º F, plus cough and/or sore throat. Most likely, the surveillance system was confused by double-negatives in provider notes or similar problems; Rush investigators are looking into the problem.
However, 39 patients with PCR-confirmed influenza did not meet the CDC’s criteria in the ED; in 15 patients (40%) it was because they had a temperature at or above 99º F, but below the 100º F benchmark.
"If you relabeled the fever criteria to greater than or equal to 99 degrees, you would actually pick up more patients. Your sensitivity would be greater, but we don’t know what would happen to the specificity. We haven’t reprogrammed the surveillance system yet to try it," Dr. Marilyn Hallock, an attending physician in the Rush ED, said a the annual meeting of the American College of Emergency Physicians. It’s something "we might want to explore further," she noted.
In the meantime, "I’m going to think twice before I say patients who come in with that gray-zone temperature between of 99º F and 100 º F don’t have influenza; they might," she said.
The rest of the 39 patients were missed for various reasons. A few arrived in respiratory distress or another condition that precluded an accurate history, while others may not have recalled ILI symptoms or were not asked about them. A number of patients were diagnosed on hospital admission from the ED when more thorough histories were taken, or when they developed the CDC triad after admission.
Dr. Hallock suspects viral PCRs were ordered in the ED for the 39 patients – although they didn’t meet CDC criteria – because it was flu season, and they complained of other flu symptoms such as myalgia and aches. "It was probably just a constellation of symptoms that led physicians to give the test," even though the patients’ ED temperatures were below 100 º F, she said.
In addition to perhaps lowering the ILI requirement to 99 º F, the investigators plan to review ILI symptoms with ED staff and work to improve their documentation, said Dr. Hallock, who indicated that she had no relevant disclosures.
SEATTLE – Lowering the Centers for Disease Control and Prevention’s temperature requirement for influenza-like illness from 100º F to 99º F would likely pick up more cases of true influenza in the emergency department, according to researchers at Rush University Medical Center in Chicago.
At Rush, 203 emergency department (ED) patients tested positive for the virus by polymerase chain reaction (PCR) during the 2012-2013 flu season, but only 135 (67%) were identified as having flu-like illness by the ED’s automated surveillance system, which pulls together provider notes, vital signs, and other information from the electronic records system in real time to identify patients with influenza-like illness (ILI), among other conditions.
On chart review, 29 (43%) of the 68 missed cases met the CDC’s requirements for ILI diagnosis: a temperature of at least 100º F, plus cough and/or sore throat. Most likely, the surveillance system was confused by double-negatives in provider notes or similar problems; Rush investigators are looking into the problem.
However, 39 patients with PCR-confirmed influenza did not meet the CDC’s criteria in the ED; in 15 patients (40%) it was because they had a temperature at or above 99º F, but below the 100º F benchmark.
"If you relabeled the fever criteria to greater than or equal to 99 degrees, you would actually pick up more patients. Your sensitivity would be greater, but we don’t know what would happen to the specificity. We haven’t reprogrammed the surveillance system yet to try it," Dr. Marilyn Hallock, an attending physician in the Rush ED, said a the annual meeting of the American College of Emergency Physicians. It’s something "we might want to explore further," she noted.
In the meantime, "I’m going to think twice before I say patients who come in with that gray-zone temperature between of 99º F and 100 º F don’t have influenza; they might," she said.
The rest of the 39 patients were missed for various reasons. A few arrived in respiratory distress or another condition that precluded an accurate history, while others may not have recalled ILI symptoms or were not asked about them. A number of patients were diagnosed on hospital admission from the ED when more thorough histories were taken, or when they developed the CDC triad after admission.
Dr. Hallock suspects viral PCRs were ordered in the ED for the 39 patients – although they didn’t meet CDC criteria – because it was flu season, and they complained of other flu symptoms such as myalgia and aches. "It was probably just a constellation of symptoms that led physicians to give the test," even though the patients’ ED temperatures were below 100 º F, she said.
In addition to perhaps lowering the ILI requirement to 99 º F, the investigators plan to review ILI symptoms with ED staff and work to improve their documentation, said Dr. Hallock, who indicated that she had no relevant disclosures.
AT THE ACEP SCIENTIFIC ASSEMBLY 2013
Major finding: Thirty-nine of 203 PCR-confirmed influenza patients did not meet CDC influenza-like illness criteria in the ED. Most often, their temperature was below 100º F.
Data Source: Retrospective cross-sectional study.
Disclosures: The presenter has no relevant disclosures.

Radiological guidance does not improve tracheobronchial stent insertion
SYDNEY, AUSTRALIA – Use of radiological guidance for tracheobronchial stent insertion in advanced lung cancer makes no difference to outcomes such as complication rates, length of stay, or survival compared with visually-guided insertion, according to data from 79 patients.
Researchers from Harefield Hospital, London, examined outcomes from patients with advanced primary lung cancer whose airway obstructions were treated with tracheobronchial stenting; 41 were stented under radiological guidance and 38 with direct vision using bronchoscopy.
No cases of stent migration occurred in either group, and there were no significant differences between length of stay and overall survival, Henrietta Wilson, lead investigator, said at a world conference on lung cancer.

However, the use of radiological guidance required more staff and equipment and, by its very nature, led to more radiation exposure than did visually-guided stent insertion, said Ms. Wilson, a thoracic registrar (medical student) at Harefield Hospital.
"I had noticed that with the use of radiological guidance, it seemed to add an amount of time and organization onto the cases that we were doing, with having to get a larger number of people coming to perform the procedure, with the logistics of getting all of the equipment into theater, and that can sometimes also prolong the time of the general anesthetic while getting all of that set up," she said at the conference, which was sponsored by the International Association for the Study of Lung Cancer.
The average length of stay following the procedure was 2.73 days in the radiologically-guided group and 2.26 days in the visually-guided group (P = .93), with 69% of patients discharged on the same day, or the day after. The overall mean survival was 2.6 months, with 20% of patients alive at one year.
"I think probably those who advocate radiological guidance would feel that you get a better position of the stent and so they may have felt that it would get fewer complications from stent migration or malposition of the stent, or people requiring repeat procedures, but that certainly wasn’t something that we found," she said.
Ms. Wilson noted that tracheobronchial stenting was used generally in urgent cases of acute airway obstruction, either as a palliative procedure in itself or to provide short-term relief for patients awaiting further radiotherapy or chemotherapy.
"Acute airway obstruction can be very distressing, so if we’re able to just improve that then it may only be for weeks or a month at most but we find from a quality of life point of view, that’s a real benefit," she said in an interview.
Radiologically-guided stenting required an x-ray C-arm to enable real-time imaging of the stent placement, while in visually-guided placement, the surgeon would use a bronchoscope to assess the position of the tumor, and then use the guide wire to position the stent, Ms. Wilson noted.
Additional research is underway to examine the impact of guidance methods on the duration of the procedure and anesthetic.
Dr. Eleanor Summerhill, FCCP, comments: This small, single- center, retrospective study found no significant differences in rates of stent complications, hospital length of stay, or survival in patients with airway obstruction caused by primary lung cancers stented via direct visualization compared to under radiological guidance.
As the authors note, there are a number of disadvantages to placement under radiologic guidance. These include the need for additional equipment and staffing, as well as more radiation exposure and time under anesthesia.
This study suggests that these measures may not lead to improved outcomes, and will hopefully lead the way to a subsequent multicenter, randomized control trial.
Dr. Summerhill is the director of the Internal Medicine Residency Program at the Memorial Hospital of Rhode Island and Assistant Professor of Medicine
Alpert Medical School of Brown University.
There were no conflicts of interest declared.
SYDNEY, AUSTRALIA – Use of radiological guidance for tracheobronchial stent insertion in advanced lung cancer makes no difference to outcomes such as complication rates, length of stay, or survival compared with visually-guided insertion, according to data from 79 patients.
Researchers from Harefield Hospital, London, examined outcomes from patients with advanced primary lung cancer whose airway obstructions were treated with tracheobronchial stenting; 41 were stented under radiological guidance and 38 with direct vision using bronchoscopy.
No cases of stent migration occurred in either group, and there were no significant differences between length of stay and overall survival, Henrietta Wilson, lead investigator, said at a world conference on lung cancer.
However, the use of radiological guidance required more staff and equipment and, by its very nature, led to more radiation exposure than did visually-guided stent insertion, said Ms. Wilson, a thoracic registrar (medical student) at Harefield Hospital.
"I had noticed that with the use of radiological guidance, it seemed to add an amount of time and organization onto the cases that we were doing, with having to get a larger number of people coming to perform the procedure, with the logistics of getting all of the equipment into theater, and that can sometimes also prolong the time of the general anesthetic while getting all of that set up," she said at the conference, which was sponsored by the International Association for the Study of Lung Cancer.
The average length of stay following the procedure was 2.73 days in the radiologically-guided group and 2.26 days in the visually-guided group (P = .93), with 69% of patients discharged on the same day, or the day after. The overall mean survival was 2.6 months, with 20% of patients alive at one year.
"I think probably those who advocate radiological guidance would feel that you get a better position of the stent and so they may have felt that it would get fewer complications from stent migration or malposition of the stent, or people requiring repeat procedures, but that certainly wasn’t something that we found," she said.
Ms. Wilson noted that tracheobronchial stenting was used generally in urgent cases of acute airway obstruction, either as a palliative procedure in itself or to provide short-term relief for patients awaiting further radiotherapy or chemotherapy.
"Acute airway obstruction can be very distressing, so if we’re able to just improve that then it may only be for weeks or a month at most but we find from a quality of life point of view, that’s a real benefit," she said in an interview.
Radiologically-guided stenting required an x-ray C-arm to enable real-time imaging of the stent placement, while in visually-guided placement, the surgeon would use a bronchoscope to assess the position of the tumor, and then use the guide wire to position the stent, Ms. Wilson noted.
Additional research is underway to examine the impact of guidance methods on the duration of the procedure and anesthetic.
Dr. Eleanor Summerhill, FCCP, comments: This small, single- center, retrospective study found no significant differences in rates of stent complications, hospital length of stay, or survival in patients with airway obstruction caused by primary lung cancers stented via direct visualization compared to under radiological guidance.
As the authors note, there are a number of disadvantages to placement under radiologic guidance. These include the need for additional equipment and staffing, as well as more radiation exposure and time under anesthesia.
This study suggests that these measures may not lead to improved outcomes, and will hopefully lead the way to a subsequent multicenter, randomized control trial.
Dr. Summerhill is the director of the Internal Medicine Residency Program at the Memorial Hospital of Rhode Island and Assistant Professor of Medicine
Alpert Medical School of Brown University.
There were no conflicts of interest declared.
SYDNEY, AUSTRALIA – Use of radiological guidance for tracheobronchial stent insertion in advanced lung cancer makes no difference to outcomes such as complication rates, length of stay, or survival compared with visually-guided insertion, according to data from 79 patients.
Researchers from Harefield Hospital, London, examined outcomes from patients with advanced primary lung cancer whose airway obstructions were treated with tracheobronchial stenting; 41 were stented under radiological guidance and 38 with direct vision using bronchoscopy.
No cases of stent migration occurred in either group, and there were no significant differences between length of stay and overall survival, Henrietta Wilson, lead investigator, said at a world conference on lung cancer.
However, the use of radiological guidance required more staff and equipment and, by its very nature, led to more radiation exposure than did visually-guided stent insertion, said Ms. Wilson, a thoracic registrar (medical student) at Harefield Hospital.
"I had noticed that with the use of radiological guidance, it seemed to add an amount of time and organization onto the cases that we were doing, with having to get a larger number of people coming to perform the procedure, with the logistics of getting all of the equipment into theater, and that can sometimes also prolong the time of the general anesthetic while getting all of that set up," she said at the conference, which was sponsored by the International Association for the Study of Lung Cancer.
The average length of stay following the procedure was 2.73 days in the radiologically-guided group and 2.26 days in the visually-guided group (P = .93), with 69% of patients discharged on the same day, or the day after. The overall mean survival was 2.6 months, with 20% of patients alive at one year.
"I think probably those who advocate radiological guidance would feel that you get a better position of the stent and so they may have felt that it would get fewer complications from stent migration or malposition of the stent, or people requiring repeat procedures, but that certainly wasn’t something that we found," she said.
Ms. Wilson noted that tracheobronchial stenting was used generally in urgent cases of acute airway obstruction, either as a palliative procedure in itself or to provide short-term relief for patients awaiting further radiotherapy or chemotherapy.
"Acute airway obstruction can be very distressing, so if we’re able to just improve that then it may only be for weeks or a month at most but we find from a quality of life point of view, that’s a real benefit," she said in an interview.
Radiologically-guided stenting required an x-ray C-arm to enable real-time imaging of the stent placement, while in visually-guided placement, the surgeon would use a bronchoscope to assess the position of the tumor, and then use the guide wire to position the stent, Ms. Wilson noted.
Additional research is underway to examine the impact of guidance methods on the duration of the procedure and anesthetic.
Dr. Eleanor Summerhill, FCCP, comments: This small, single- center, retrospective study found no significant differences in rates of stent complications, hospital length of stay, or survival in patients with airway obstruction caused by primary lung cancers stented via direct visualization compared to under radiological guidance.
As the authors note, there are a number of disadvantages to placement under radiologic guidance. These include the need for additional equipment and staffing, as well as more radiation exposure and time under anesthesia.
This study suggests that these measures may not lead to improved outcomes, and will hopefully lead the way to a subsequent multicenter, randomized control trial.
Dr. Summerhill is the director of the Internal Medicine Residency Program at the Memorial Hospital of Rhode Island and Assistant Professor of Medicine
Alpert Medical School of Brown University.
There were no conflicts of interest declared.
AT THE IASLC WORLD CONFERENCE
Major finding: The average length of stay following tracheobronchial stent insertion was 2.73 days in the radiologically-guided group and 2.26 days in the visually-guided group (P = .93).
Data source: Retrospective study of 79 patients.
Disclosures: No conflicts of interest declared.

High schoolers smoking more cigars, pipes, e-cigarettes
Overall use of tobacco among high school students decreased from 2011 to 2012, but cigar and pipe smoking went up, as did the use of some nonconventional products, the Centers for Disease Control and Prevention reported.
In 2012, 23.3% of high school students surveyed reported current tobacco use, compared with 24.3% in 2011. Use of cigars, driven largely by a significant increase among non-Hispanic black students, went from 11.6% in 2011 to 12.6% in 2012, and pipe use rose from 4.0% to 4.5%, according to data from the National Youth Tobacco Survey.
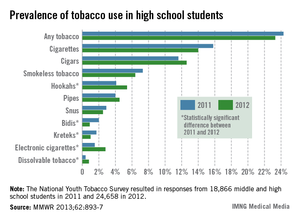
"Youths are known to have higher rates of cigar use than adults, which might be related to the lower price of some cigars (e.g., cigarillos and ‘little cigars’) relative to cigarettes, or the marketing of flavored cigars that might appeal to youths," the report said (MMWR 2013;62;893-7).
Significant increases in use were seen for electronic cigarettes (1.5% in 2011 to 2.8% in 2012) and hookahs (4.1% to 5.4%), but the use of other nonconventional products such as bidis (small brown cigarettes wrapped in a leaf), kreteks (clove cigarettes), and snus declined, the CDC noted.
The 2012 National Youth Tobacco Survey was conducted at 228 schools, with 24,658 middle and high school students responding. The 2011 survey had a sample size of 18,866.
Overall use of tobacco among high school students decreased from 2011 to 2012, but cigar and pipe smoking went up, as did the use of some nonconventional products, the Centers for Disease Control and Prevention reported.
In 2012, 23.3% of high school students surveyed reported current tobacco use, compared with 24.3% in 2011. Use of cigars, driven largely by a significant increase among non-Hispanic black students, went from 11.6% in 2011 to 12.6% in 2012, and pipe use rose from 4.0% to 4.5%, according to data from the National Youth Tobacco Survey.
"Youths are known to have higher rates of cigar use than adults, which might be related to the lower price of some cigars (e.g., cigarillos and ‘little cigars’) relative to cigarettes, or the marketing of flavored cigars that might appeal to youths," the report said (MMWR 2013;62;893-7).
Significant increases in use were seen for electronic cigarettes (1.5% in 2011 to 2.8% in 2012) and hookahs (4.1% to 5.4%), but the use of other nonconventional products such as bidis (small brown cigarettes wrapped in a leaf), kreteks (clove cigarettes), and snus declined, the CDC noted.
The 2012 National Youth Tobacco Survey was conducted at 228 schools, with 24,658 middle and high school students responding. The 2011 survey had a sample size of 18,866.
Overall use of tobacco among high school students decreased from 2011 to 2012, but cigar and pipe smoking went up, as did the use of some nonconventional products, the Centers for Disease Control and Prevention reported.
In 2012, 23.3% of high school students surveyed reported current tobacco use, compared with 24.3% in 2011. Use of cigars, driven largely by a significant increase among non-Hispanic black students, went from 11.6% in 2011 to 12.6% in 2012, and pipe use rose from 4.0% to 4.5%, according to data from the National Youth Tobacco Survey.
"Youths are known to have higher rates of cigar use than adults, which might be related to the lower price of some cigars (e.g., cigarillos and ‘little cigars’) relative to cigarettes, or the marketing of flavored cigars that might appeal to youths," the report said (MMWR 2013;62;893-7).
Significant increases in use were seen for electronic cigarettes (1.5% in 2011 to 2.8% in 2012) and hookahs (4.1% to 5.4%), but the use of other nonconventional products such as bidis (small brown cigarettes wrapped in a leaf), kreteks (clove cigarettes), and snus declined, the CDC noted.
The 2012 National Youth Tobacco Survey was conducted at 228 schools, with 24,658 middle and high school students responding. The 2011 survey had a sample size of 18,866.
FROM MMWR