User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
CVS to discontinue sale of tobacco products
CVS Pharmacy will stop selling cigarettes and other tobacco products by October of this year, the company announced Feb. 5.
CVS President and Chief Executive Officer Larry Merlo said in a statement that the sale of tobacco products is contrary to CVS’s responsibility to help patients manage chronic diseases such as high blood pressure, high cholesterol, and diabetes. "All of these conditions are made worse by smoking," he said. "Tobacco products have no place in a setting where health care is delivered."
In addition to pulling cigarettes from its shelves, CVS also plans to launch a national smoking cessation program in the spring for those trying to quit, Mr. Merlo added.
Dr. Troyen A. Brennan, CVS executive vice president and chief medical officer, and Dr. Steven A. Schroeder, of the Smoking Cessation Leadership Center at the University of California, San Francisco, further explained the decision in a JAMA commentary (JAMA 2014 Feb. 5 [doi:10.1001/jama.2014.686]). "This action may not lead many people to stop smoking; smokers will probably simply go elsewhere to buy cigarettes," they wrote. "But if other retailers follow this lead, tobacco products will become much more difficult to obtain."

U.S. Department of Health and Human Services secretary Kathleen Sebelius praised the effort in a statement, calling the move an "unprecedented step in the retail industry" that would contribute to positive health effects for the next generation.
"Nearly 500,000 Americans die early each year due to smoking, and smoking costs us $289 billion annually," she said, citing the recently released 50th Anniversary Surgeon General Report on smoking and health. "If we fail to reverse course, 5.6 million American children alive today will die prematurely due to smoking."
CVS’s decision also drew support from the American Medical Association. AMA president Dr. Ardis Dee Hoven said in a statement that she applauds the company’s decision to put public health first and recognize the importance of "supporting health and wellness instead of contributing to disease and death caused by tobacco use." Dr. Hoven also said she hoped the change would inspire other pharmacies to follow suit by ending cigarette sales in stores.
Dr. W. Michael Alberts, chief medical officer at Moffitt Cancer Center in Tampa, also voiced approval. "This is a major decision by CVS," he said in an interview. "It may even be a watershed moment akin to the decision to ban smoking on airplanes. Let’s hope such decisions become commonplace in corporate boardrooms."
CVS Pharmacy will stop selling cigarettes and other tobacco products by October of this year, the company announced Feb. 5.
CVS President and Chief Executive Officer Larry Merlo said in a statement that the sale of tobacco products is contrary to CVS’s responsibility to help patients manage chronic diseases such as high blood pressure, high cholesterol, and diabetes. "All of these conditions are made worse by smoking," he said. "Tobacco products have no place in a setting where health care is delivered."
In addition to pulling cigarettes from its shelves, CVS also plans to launch a national smoking cessation program in the spring for those trying to quit, Mr. Merlo added.
Dr. Troyen A. Brennan, CVS executive vice president and chief medical officer, and Dr. Steven A. Schroeder, of the Smoking Cessation Leadership Center at the University of California, San Francisco, further explained the decision in a JAMA commentary (JAMA 2014 Feb. 5 [doi:10.1001/jama.2014.686]). "This action may not lead many people to stop smoking; smokers will probably simply go elsewhere to buy cigarettes," they wrote. "But if other retailers follow this lead, tobacco products will become much more difficult to obtain."
U.S. Department of Health and Human Services secretary Kathleen Sebelius praised the effort in a statement, calling the move an "unprecedented step in the retail industry" that would contribute to positive health effects for the next generation.
"Nearly 500,000 Americans die early each year due to smoking, and smoking costs us $289 billion annually," she said, citing the recently released 50th Anniversary Surgeon General Report on smoking and health. "If we fail to reverse course, 5.6 million American children alive today will die prematurely due to smoking."
CVS’s decision also drew support from the American Medical Association. AMA president Dr. Ardis Dee Hoven said in a statement that she applauds the company’s decision to put public health first and recognize the importance of "supporting health and wellness instead of contributing to disease and death caused by tobacco use." Dr. Hoven also said she hoped the change would inspire other pharmacies to follow suit by ending cigarette sales in stores.
Dr. W. Michael Alberts, chief medical officer at Moffitt Cancer Center in Tampa, also voiced approval. "This is a major decision by CVS," he said in an interview. "It may even be a watershed moment akin to the decision to ban smoking on airplanes. Let’s hope such decisions become commonplace in corporate boardrooms."
CVS Pharmacy will stop selling cigarettes and other tobacco products by October of this year, the company announced Feb. 5.
CVS President and Chief Executive Officer Larry Merlo said in a statement that the sale of tobacco products is contrary to CVS’s responsibility to help patients manage chronic diseases such as high blood pressure, high cholesterol, and diabetes. "All of these conditions are made worse by smoking," he said. "Tobacco products have no place in a setting where health care is delivered."
In addition to pulling cigarettes from its shelves, CVS also plans to launch a national smoking cessation program in the spring for those trying to quit, Mr. Merlo added.
Dr. Troyen A. Brennan, CVS executive vice president and chief medical officer, and Dr. Steven A. Schroeder, of the Smoking Cessation Leadership Center at the University of California, San Francisco, further explained the decision in a JAMA commentary (JAMA 2014 Feb. 5 [doi:10.1001/jama.2014.686]). "This action may not lead many people to stop smoking; smokers will probably simply go elsewhere to buy cigarettes," they wrote. "But if other retailers follow this lead, tobacco products will become much more difficult to obtain."
U.S. Department of Health and Human Services secretary Kathleen Sebelius praised the effort in a statement, calling the move an "unprecedented step in the retail industry" that would contribute to positive health effects for the next generation.
"Nearly 500,000 Americans die early each year due to smoking, and smoking costs us $289 billion annually," she said, citing the recently released 50th Anniversary Surgeon General Report on smoking and health. "If we fail to reverse course, 5.6 million American children alive today will die prematurely due to smoking."
CVS’s decision also drew support from the American Medical Association. AMA president Dr. Ardis Dee Hoven said in a statement that she applauds the company’s decision to put public health first and recognize the importance of "supporting health and wellness instead of contributing to disease and death caused by tobacco use." Dr. Hoven also said she hoped the change would inspire other pharmacies to follow suit by ending cigarette sales in stores.
Dr. W. Michael Alberts, chief medical officer at Moffitt Cancer Center in Tampa, also voiced approval. "This is a major decision by CVS," he said in an interview. "It may even be a watershed moment akin to the decision to ban smoking on airplanes. Let’s hope such decisions become commonplace in corporate boardrooms."

Steroids for Acute COPD—But for How Long?
PRACTICE CHANGER
Prescribe a five-day regimen of glucocorticoid therapy for acute exacerbations of chronic obstructive pulmonary disease (COPD); the shorter course of treatment appears to be as effective as a 14-day regimen.1
Strength of recommendation
B: Based on a single well-designed randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 55-year-old man with COPD presents to the emergency department (ED) with progressive shortness of breath, cough, and sputum production in the past four days. He is diagnosed with a COPD exacerbation, treated with corticosteroids, and admitted to the hospital. His inpatient treatment includes antibiotics, inhaled albuterol and ipratropium, supplemental oxygen, and oral corticosteroids.
How many days should he take oral steroids?
Severe exacerbations of COPD are independently associated with mortality,2 regardless of baseline severity. Guidelines and systematic reviews highlight the importance of using oral glucocorticoids in the management of acute COPD exacerbations, as the drugs have been found to shorten recovery time and length of hospital stay, improve lung function, and reduce the risk for early relapse and treatment failure.3-5 What is not clear is how long the course of oral steroids should be.
What we know (and don’t know) about duration
Data supporting a 14-day course of steroids versus a longer (eight-week) duration come from the Systemic Corticosteroids in COPD Exacerbations trial.6 Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria suggest a 10- to 14-day regimen (30 to 40 mg/d) but acknowledge that there is a lack of data from clinical and observational studies to support this recommendation.3 A recent Cochrane review compared a short course of treatment (three to seven days) with a longer regimen (10 to 15 days) and found that the evidence to support a clinical practice change was inconclusive.5
The study detailed in this PURL—a double-blind RCT comparing five-day with 14-day oral steroid treatment in patients hospitalized for acute COPD exacerbation—had more definitive results.1
Continue reading for the study summary...
STUDY SUMMARY
Shorter and longer regimens produce equal results
Leuppi et al1 used noninferiority methodology to compare a five- and a 14-day course of prednisone 40 mg/d to treat patients with COPD exacerbations. A patient was considered to have an exacerbation if he or she had a change from baseline in two or more of the following: dyspnea, cough, sputum quantity, or purulence.
Participants were patients who presented to the EDs of five Swiss teaching hospitals between March 2006 and February 2011. To be eligible, individuals had to be 40 or older and have at least 20 pack-years of smoking. Exclusion criteria included asthma, mild obstruction (FEV1/FVC > 70%), pneumonia, an estimated survival of less than six months, pregnancy, and lactation.
All the participants (N = 311) received 40 mg methylprednisolone intravenously on day 1, followed by prednisone 40 mg orally on days 2 through 5. The researchers then randomly divided participants into two groups: One group continued to take prednisone 40 mg/d and the other group received a matching placebo for an additional nine days. Participants in both groups also received antibiotics for seven days, twice-daily inhaled steroids, daily tiotropium, and nebulized albuterol, as needed; additional oral glucocorticoids could be administered, as well, at the discretion of the treating physicians.
The primary outcome was the time to the next COPD exacerbation, up to 180 days. Noninferiority between the groups was defined as no more than a 15% absolute increase in exacerbations. The dropout rate was 5.7%, evenly divided between groups. Intention to treat and per-protocol analyses were conducted, and hazard ratios (HRs) were calculated using the Kaplan-Meier method and Cox proportional hazards models.
The time to next COPD exacerbation did not differ between the study groups: 56 days for those on the five-day steroid regimen versus 57 days for those on the
14-day regimen in the intention-to-treat analysis (HR, 0.95). Sensitivity analyses adjusting for baseline characteristics provided similar results, as did the per-protocol analysis.
Secondary outcomes (overall survival; need for mechanical ventilation; need for additional corticosteroids; and clinical performance measures, such as dyspnea score and quality of life) also did not differ between groups. Nor were there differences in hyperglycemia, worsening hypertension, infection, or other adverse effects typically associated with glucocorticoid use. The active treatment group took more than 400 mg more prednisone than the placebo group (mean, 793 mg vs 379 mg, respectively).
WHAT’S NEW?
Now we know: five days is enough
While randomized trials have found that glucocorticoids improve COPD symptoms, the optimal treatment dose and duration were not known. Indeed, current guidelines recommend treatment for more than five days.3 This trial clearly demonstrated that 40-mg prednisone for five days is at least as good as a 14-day treatment course. Furthermore, it is unnecessary to taper the short-course therapy, which simplifies the regimen.
CAVEATS
Will the results apply to those less severely ill?
More than 80% of patients with acute COPD exacerbations can be managed in an outpatient setting.3 However, participants in this trial were hospitalized for a median of 8.5 days, and most had severe or very severe COPD—and thus, were not fully representative of COPD patients typically seen in an outpatient practice. Yet patients with less severe disease should be at least as likely to respond to short-course steroids as those whose COPD is more severe.
It is important to note that participants in this study all received optimal guideline-based therapies during hospitalization, which may be difficult to achieve for some patients treated in an outpatient setting. Finally, treatment adherence observed during the hospitalization period in this trial is unlikely to be replicated in the outpatient setting.
CHALLENGES TO IMPLEMENTATION
Identifying patients who need steroids for a longer duration
For patients with new COPD exacerbations or those successfully treated using short-course therapy in the past, a five-day regimen may be appropriate. For those in whom prior attempts at short-course treatment have failed, however, a 14-day course of treatment may be more advisable. That said, no guidelines are available to help us determine which patients previously treated with a longer regimen will find the shorter course of treatment unsuccessful.
Continue for references...
REFERENCES
1. Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE randomized clinical trial. JAMA. 2013;309:2223-2231.
2. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925-931.
3. Global Initiative for Chronic Obstructive Lung Disease, Inc. The global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease. www.goldcopd.org. Accessed January 9, 2014.
4. Quon BS, Gan WQ, Sin DD. Contemporary management of acute exacerbations of COPD: a systematic review and metaanalysis. Chest. 2008;133:756-766.
5. Walters JA, Wang W, Morley C, et al. Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011; (10):CD006897.
6. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340:1941-1947.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL 1RR 024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(1):29-30, 32.
PRACTICE CHANGER
Prescribe a five-day regimen of glucocorticoid therapy for acute exacerbations of chronic obstructive pulmonary disease (COPD); the shorter course of treatment appears to be as effective as a 14-day regimen.1
Strength of recommendation
B: Based on a single well-designed randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 55-year-old man with COPD presents to the emergency department (ED) with progressive shortness of breath, cough, and sputum production in the past four days. He is diagnosed with a COPD exacerbation, treated with corticosteroids, and admitted to the hospital. His inpatient treatment includes antibiotics, inhaled albuterol and ipratropium, supplemental oxygen, and oral corticosteroids.
How many days should he take oral steroids?
Severe exacerbations of COPD are independently associated with mortality,2 regardless of baseline severity. Guidelines and systematic reviews highlight the importance of using oral glucocorticoids in the management of acute COPD exacerbations, as the drugs have been found to shorten recovery time and length of hospital stay, improve lung function, and reduce the risk for early relapse and treatment failure.3-5 What is not clear is how long the course of oral steroids should be.
What we know (and don’t know) about duration
Data supporting a 14-day course of steroids versus a longer (eight-week) duration come from the Systemic Corticosteroids in COPD Exacerbations trial.6 Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria suggest a 10- to 14-day regimen (30 to 40 mg/d) but acknowledge that there is a lack of data from clinical and observational studies to support this recommendation.3 A recent Cochrane review compared a short course of treatment (three to seven days) with a longer regimen (10 to 15 days) and found that the evidence to support a clinical practice change was inconclusive.5
The study detailed in this PURL—a double-blind RCT comparing five-day with 14-day oral steroid treatment in patients hospitalized for acute COPD exacerbation—had more definitive results.1
Continue reading for the study summary...
STUDY SUMMARY
Shorter and longer regimens produce equal results
Leuppi et al1 used noninferiority methodology to compare a five- and a 14-day course of prednisone 40 mg/d to treat patients with COPD exacerbations. A patient was considered to have an exacerbation if he or she had a change from baseline in two or more of the following: dyspnea, cough, sputum quantity, or purulence.
Participants were patients who presented to the EDs of five Swiss teaching hospitals between March 2006 and February 2011. To be eligible, individuals had to be 40 or older and have at least 20 pack-years of smoking. Exclusion criteria included asthma, mild obstruction (FEV1/FVC > 70%), pneumonia, an estimated survival of less than six months, pregnancy, and lactation.
All the participants (N = 311) received 40 mg methylprednisolone intravenously on day 1, followed by prednisone 40 mg orally on days 2 through 5. The researchers then randomly divided participants into two groups: One group continued to take prednisone 40 mg/d and the other group received a matching placebo for an additional nine days. Participants in both groups also received antibiotics for seven days, twice-daily inhaled steroids, daily tiotropium, and nebulized albuterol, as needed; additional oral glucocorticoids could be administered, as well, at the discretion of the treating physicians.
The primary outcome was the time to the next COPD exacerbation, up to 180 days. Noninferiority between the groups was defined as no more than a 15% absolute increase in exacerbations. The dropout rate was 5.7%, evenly divided between groups. Intention to treat and per-protocol analyses were conducted, and hazard ratios (HRs) were calculated using the Kaplan-Meier method and Cox proportional hazards models.
The time to next COPD exacerbation did not differ between the study groups: 56 days for those on the five-day steroid regimen versus 57 days for those on the
14-day regimen in the intention-to-treat analysis (HR, 0.95). Sensitivity analyses adjusting for baseline characteristics provided similar results, as did the per-protocol analysis.
Secondary outcomes (overall survival; need for mechanical ventilation; need for additional corticosteroids; and clinical performance measures, such as dyspnea score and quality of life) also did not differ between groups. Nor were there differences in hyperglycemia, worsening hypertension, infection, or other adverse effects typically associated with glucocorticoid use. The active treatment group took more than 400 mg more prednisone than the placebo group (mean, 793 mg vs 379 mg, respectively).
WHAT’S NEW?
Now we know: five days is enough
While randomized trials have found that glucocorticoids improve COPD symptoms, the optimal treatment dose and duration were not known. Indeed, current guidelines recommend treatment for more than five days.3 This trial clearly demonstrated that 40-mg prednisone for five days is at least as good as a 14-day treatment course. Furthermore, it is unnecessary to taper the short-course therapy, which simplifies the regimen.
CAVEATS
Will the results apply to those less severely ill?
More than 80% of patients with acute COPD exacerbations can be managed in an outpatient setting.3 However, participants in this trial were hospitalized for a median of 8.5 days, and most had severe or very severe COPD—and thus, were not fully representative of COPD patients typically seen in an outpatient practice. Yet patients with less severe disease should be at least as likely to respond to short-course steroids as those whose COPD is more severe.
It is important to note that participants in this study all received optimal guideline-based therapies during hospitalization, which may be difficult to achieve for some patients treated in an outpatient setting. Finally, treatment adherence observed during the hospitalization period in this trial is unlikely to be replicated in the outpatient setting.
CHALLENGES TO IMPLEMENTATION
Identifying patients who need steroids for a longer duration
For patients with new COPD exacerbations or those successfully treated using short-course therapy in the past, a five-day regimen may be appropriate. For those in whom prior attempts at short-course treatment have failed, however, a 14-day course of treatment may be more advisable. That said, no guidelines are available to help us determine which patients previously treated with a longer regimen will find the shorter course of treatment unsuccessful.
Continue for references...
REFERENCES
1. Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE randomized clinical trial. JAMA. 2013;309:2223-2231.
2. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925-931.
3. Global Initiative for Chronic Obstructive Lung Disease, Inc. The global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease. www.goldcopd.org. Accessed January 9, 2014.
4. Quon BS, Gan WQ, Sin DD. Contemporary management of acute exacerbations of COPD: a systematic review and metaanalysis. Chest. 2008;133:756-766.
5. Walters JA, Wang W, Morley C, et al. Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011; (10):CD006897.
6. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340:1941-1947.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL 1RR 024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(1):29-30, 32.
PRACTICE CHANGER
Prescribe a five-day regimen of glucocorticoid therapy for acute exacerbations of chronic obstructive pulmonary disease (COPD); the shorter course of treatment appears to be as effective as a 14-day regimen.1
Strength of recommendation
B: Based on a single well-designed randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 55-year-old man with COPD presents to the emergency department (ED) with progressive shortness of breath, cough, and sputum production in the past four days. He is diagnosed with a COPD exacerbation, treated with corticosteroids, and admitted to the hospital. His inpatient treatment includes antibiotics, inhaled albuterol and ipratropium, supplemental oxygen, and oral corticosteroids.
How many days should he take oral steroids?
Severe exacerbations of COPD are independently associated with mortality,2 regardless of baseline severity. Guidelines and systematic reviews highlight the importance of using oral glucocorticoids in the management of acute COPD exacerbations, as the drugs have been found to shorten recovery time and length of hospital stay, improve lung function, and reduce the risk for early relapse and treatment failure.3-5 What is not clear is how long the course of oral steroids should be.
What we know (and don’t know) about duration
Data supporting a 14-day course of steroids versus a longer (eight-week) duration come from the Systemic Corticosteroids in COPD Exacerbations trial.6 Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria suggest a 10- to 14-day regimen (30 to 40 mg/d) but acknowledge that there is a lack of data from clinical and observational studies to support this recommendation.3 A recent Cochrane review compared a short course of treatment (three to seven days) with a longer regimen (10 to 15 days) and found that the evidence to support a clinical practice change was inconclusive.5
The study detailed in this PURL—a double-blind RCT comparing five-day with 14-day oral steroid treatment in patients hospitalized for acute COPD exacerbation—had more definitive results.1
Continue reading for the study summary...
STUDY SUMMARY
Shorter and longer regimens produce equal results
Leuppi et al1 used noninferiority methodology to compare a five- and a 14-day course of prednisone 40 mg/d to treat patients with COPD exacerbations. A patient was considered to have an exacerbation if he or she had a change from baseline in two or more of the following: dyspnea, cough, sputum quantity, or purulence.
Participants were patients who presented to the EDs of five Swiss teaching hospitals between March 2006 and February 2011. To be eligible, individuals had to be 40 or older and have at least 20 pack-years of smoking. Exclusion criteria included asthma, mild obstruction (FEV1/FVC > 70%), pneumonia, an estimated survival of less than six months, pregnancy, and lactation.
All the participants (N = 311) received 40 mg methylprednisolone intravenously on day 1, followed by prednisone 40 mg orally on days 2 through 5. The researchers then randomly divided participants into two groups: One group continued to take prednisone 40 mg/d and the other group received a matching placebo for an additional nine days. Participants in both groups also received antibiotics for seven days, twice-daily inhaled steroids, daily tiotropium, and nebulized albuterol, as needed; additional oral glucocorticoids could be administered, as well, at the discretion of the treating physicians.
The primary outcome was the time to the next COPD exacerbation, up to 180 days. Noninferiority between the groups was defined as no more than a 15% absolute increase in exacerbations. The dropout rate was 5.7%, evenly divided between groups. Intention to treat and per-protocol analyses were conducted, and hazard ratios (HRs) were calculated using the Kaplan-Meier method and Cox proportional hazards models.
The time to next COPD exacerbation did not differ between the study groups: 56 days for those on the five-day steroid regimen versus 57 days for those on the
14-day regimen in the intention-to-treat analysis (HR, 0.95). Sensitivity analyses adjusting for baseline characteristics provided similar results, as did the per-protocol analysis.
Secondary outcomes (overall survival; need for mechanical ventilation; need for additional corticosteroids; and clinical performance measures, such as dyspnea score and quality of life) also did not differ between groups. Nor were there differences in hyperglycemia, worsening hypertension, infection, or other adverse effects typically associated with glucocorticoid use. The active treatment group took more than 400 mg more prednisone than the placebo group (mean, 793 mg vs 379 mg, respectively).
WHAT’S NEW?
Now we know: five days is enough
While randomized trials have found that glucocorticoids improve COPD symptoms, the optimal treatment dose and duration were not known. Indeed, current guidelines recommend treatment for more than five days.3 This trial clearly demonstrated that 40-mg prednisone for five days is at least as good as a 14-day treatment course. Furthermore, it is unnecessary to taper the short-course therapy, which simplifies the regimen.
CAVEATS
Will the results apply to those less severely ill?
More than 80% of patients with acute COPD exacerbations can be managed in an outpatient setting.3 However, participants in this trial were hospitalized for a median of 8.5 days, and most had severe or very severe COPD—and thus, were not fully representative of COPD patients typically seen in an outpatient practice. Yet patients with less severe disease should be at least as likely to respond to short-course steroids as those whose COPD is more severe.
It is important to note that participants in this study all received optimal guideline-based therapies during hospitalization, which may be difficult to achieve for some patients treated in an outpatient setting. Finally, treatment adherence observed during the hospitalization period in this trial is unlikely to be replicated in the outpatient setting.
CHALLENGES TO IMPLEMENTATION
Identifying patients who need steroids for a longer duration
For patients with new COPD exacerbations or those successfully treated using short-course therapy in the past, a five-day regimen may be appropriate. For those in whom prior attempts at short-course treatment have failed, however, a 14-day course of treatment may be more advisable. That said, no guidelines are available to help us determine which patients previously treated with a longer regimen will find the shorter course of treatment unsuccessful.
Continue for references...
REFERENCES
1. Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE randomized clinical trial. JAMA. 2013;309:2223-2231.
2. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925-931.
3. Global Initiative for Chronic Obstructive Lung Disease, Inc. The global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease. www.goldcopd.org. Accessed January 9, 2014.
4. Quon BS, Gan WQ, Sin DD. Contemporary management of acute exacerbations of COPD: a systematic review and metaanalysis. Chest. 2008;133:756-766.
5. Walters JA, Wang W, Morley C, et al. Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011; (10):CD006897.
6. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340:1941-1947.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL 1RR 024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(1):29-30, 32.
Woman, 78, With Dyspnea, Dry Cough, and Fatigue
A 78-year-old woman presented to the emergency department (ED) complaining of shortness of breath, a dry nonproductive cough, fatigue, hypoxia, and general malaise lasting for several months and worsening over a two-week period. She denied having fever, chills, hemoptysis, weight loss, headache, rashes, or joint pain. She reported sweats, decrease in appetite, wheezing, cough without sputum production, and slight swelling of the legs. The patient complained of chest pain upon admission, but it resolved quickly.
The patient, a retired widow with five grown children, denied recent surgery or exposure to sick people, had not travelled, and reported no changes in her home environment. She claimed to have no pets but admitted to currently smoking about four cigarettes a day; she had previously smoked, on average, three packs of cigarettes per day for 60 years. She denied using alcohol or drugs, including intravenous agents.
The patient’s medical history was significant for paroxysmal atrial fibrillation. She had also been diagnosed with chronic obstructive pulmonary disease (COPD), transient ischemic attack, patent foramen ovale, hyperlipidemia, seizure disorder, and hypothyroidism. She had no known HIV risk factors and had had no exposure to asbestos or tuberculosis.
The patient’s current medications included amiodarone (200 mg/d) for four years; valproic acid (500 mg/d); aspirin (325 mg/d); levothyroxine (50 g/d); rosuvastatin (10 mg/d); daily warfarin, dosed according to the international normalized ratio (INR); and budesonide/formoterol (160/4.5 mg, one puff bid). She denied having any drug allergies.
Physical examination in the ED revealed a pulse of 63 beats/min; blood pressure, 108/50 mm Hg; and respiratory rate, 16 to 20 breaths/min. The patient’s O2 saturation was 84% on room air; 82% to 84% on 4 L to 6 L of supplemental oxygen; 87% to 92% with a venturi mask; and 95% on biphasic positive airway pressure (BiPAP) device. She was afebrile with hypoxia and able to speak in full sentences. Crackles were detected in the upper lung fields, best heard anteriorly, as well as a few scattered wheezes and rhonchi. Her heart sounds were normal with a regular rhythm; her extremities exhibited trace edema bilaterally. The remainder of the physical exam was normal.
The patient’s laboratory values included a normal white blood cell (WBC) count, elevated lactic acid dehydrogenase (LDH) at 448 IU/L (reference range, 84 to 246 IU/L), and no eosinophils. The erythrocyte sedimentation rate (ESR) was not measured on admission. Blood analysis of her N-terminal pro-brain natriuretic peptide (NT-proBNP) was 4,877 pg/mL; for women older than 75, a level higher than 1,800 pg/mL is abnormal.
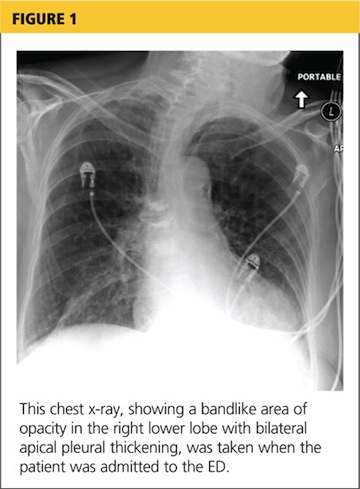
A chest x-ray was performed on admission, showing hyperinflation of the lungs with mild coarsening of the lung markings. A bandlike area of opacity in the right lower lobe with bilateral apical pleural thickening was noted (see Figure 1). Noncontrast CT of the chest revealed diffuse upper lobe ground glass opacities in both lungs, extending into the right middle lobe and lingula as well the superior segments of the lower lobes, with areas of emphysema and septal thickening. Numerous nodules, some of which appeared cavitary, were apparent in the lower lobes.
A two-dimensional echocardiogram demonstrated normal left ventricular size and systolic function, mild tricuspid regurgitation without evidence of pulmonary hypertension, and mild left atrial enlargement.
The patient was admitted to the cardiac unit for evaluation. While there, she received one dose of methylprednisolone (125 mg IV), three doses of ipratropium bromide/albuterol, one dose of ceftriaxone (1 g IV), and one dose of azithromycin (500 mg po). In the absence of significant leg edema and an elevation of jugular venous distention with a normal two-dimensional echocardiogram, heart failure was ruled out. The chest pains reported on initial presentation were ultimately felt to be noncardiac in nature.
After the patient was transferred to the medical floor with an initial diagnosis of exacerbation of her COPD, she was treated with antibiotics, nebulizers, and corticosteroids. She continued to experience episodes of O2 desaturation while on 4 L to 6 L of oxygen via nasal cannula and on a venturi mask. She was then placed on a BiPAP device, set to 12/5, and 50% Fio2 (fraction of inspired oxygen), which improved her oxygenation.
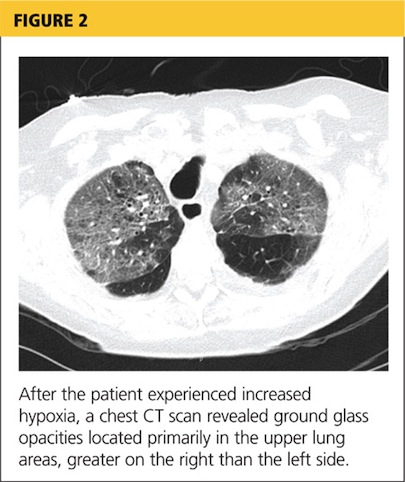
Her hypoxia prompted further radiographic studies. The resulting chest CT scan showed ground glass opacities located primarily in the upper lung areas, greater on the right than on the left side (see Figure 2). The radiologist suggested that the hypoxia was caused by an infection, but because the patient’s presenting symptoms were chronic in nature, drug-induced causes were considered as well. Amiodarone was discontinued.
Cardiology was consulted and agreed that stopping amiodarone was acceptable since the patient was in sinus rhythm at the time. The patient continued to take antibiotics and prednisone. Her symptoms slowly improved during hospitalization, and she required less oxygen. Based on the patient’s presentation, physical exam findings, imaging studies, and laboratory findings, amiodarone-induced pulmonary toxicity (APT) was diagnosed.
She was discharged home on supplemental oxygen at 4 L via cannula, a tapering dosage of prednisone, and metered-dose inhalers for fluticasone/salmeterol and tiotropium bromide. She also had outpatient appointments scheduled, one with the pulmonologist to follow up on her imaging studies and to manage the prednisone taper and the other with the cardiologist to manage her atrial fibrillation.
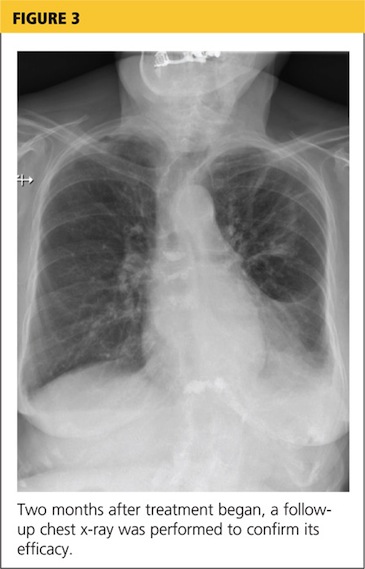
At pulmonology two months later, she had a chest x-ray (see Figure 3) and pulmonary function tests (PFTs). The patient reported feeling progressively better in the past month. Her dyspnea on exertion had improved, and she did not require supplemental oxygen anymore. She stopped smoking cigarettes.
The patient continued to use fluticasone/salmeterol but stopped tiotropium bromide. On physical exam, her O2 saturation was 95% on room air, heart rhythm and rate were regular, and her lungs revealed very minimal crackles at the right base but were otherwise clear.
The plan specified continuing the prednisone taper. The patient was asked to call the office if she had any worsening shortness of breath, cough, and sputum production. She was also encouraged to continue refraining from smoking cigarettes. This patient had done very well, with near complete resolution of symptoms and a clear chest x-ray.
Continue reading for discussion...
DISCUSSION
Amiodarone, a highly effective antiarrhythmic drug, is FDA approved for suppressing ventricular fibrillation and ventricular tachycardia. It is also used off-label as a second- or third-line choice for atrial fibrillation.1
Standard of care requires that, prior to starting amiodarone therapy, patients have a baseline chest x-ray and PFTs with diffusing capacity performed. Thereafter, the patient should be monitored with annual chest x-rays, with one performed promptly if new symptoms develop. Serial PFTs have not offered any benefit for monitoring, but a decrease of more than 15% in total lung capacity or more than 20% in diffusing capacity from baseline is consistent with APT.2
Adverse effects, both cardiac and noncardiac, are common with amiodarone therapy. They include proarrhythmias, bradycardia, and heart block, as well as thyroid and liver dysfunctions; dermatologic conditions such as blue-gray discoloration of the skin and photosensitivity; neurologic effects such as ataxia, paresthesias, and tremor; ocular problems, including corneal microdeposits; gastrointestinal problems such as nausea, anorexia, and constipation; and lung problems such as pulmonary toxicity, pleural effusion, and pleural thickening.3-6 Of these, pulmonary toxicity is the most severe and life threatening.7
APT, also known as amiodarone pneumonitis and amiodarone lung, typically manifests from a few months to a year and a half after treatment is commenced.6 APT can occur even after the drug is discontinued, because amiodarone has a very long elimination half-life of approximately 15 to 45 days and a tendency to concentrate in organs with high blood perfusion and in adipose tissues.8 Patients taking 400 mg/d for two months or longer or 200 mg/d for more than two years are considered at higher risk for APT.9 The severity of disease appears to correlate with the cumulative dose and length of treatment.10
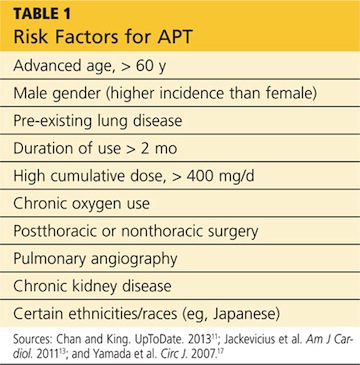
Numerous risk factors for pulmonary toxicity have been reported, including high drug dosage, pre-existing lung disease, patient age, and prior surgery (see Table 1).11 According to an analysis of a database of 237 patients, only age and duration of amiodarone therapy were significant risk factors for APT.9 Its incidence is not precisely known; reported rates range from 1% to 17%.6,12,13
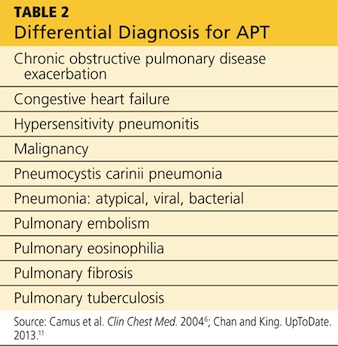
Presentation with such nonspecific symptoms as shortness of breath, nonproductive cough, fatigue, hypoxia, and general malaise is typical for many pulmonary and cardiac illnesses (see Table 2), making APT difficult to diagnose.14 Occasionally, rapid onset with progression to pneumonitis and respiratory failure masquerades as acute respiratory distress syndrome (ARDS).15
Notable, however, is that APT can manifest with nonproductive cough and dyspnea in 50% to 75% of cases. In addition, presenting symptoms will include fever (33% to 50% of cases) with associated malaise, fatigue, chest pain, and weight loss. In patients with APT, the physical exam usually reveals bilateral crackles on inspiration, but diffuse rales may be heard as well.11
Laboratory studies are not very helpful in diagnosing APT. Patients may present with nonspecific elevated WBCs without eosinophilia and an elevated LDH level.11 An elevated ESR may be detected before symptoms of APT manifest and can be present at the time of diagnosis.6
Imaging studies are far more helpful and specific in diagnosing APT. The typical chest x-ray shows bilateral patchy diffuse infiltrates.12 CT of the chest is usually more revealing, demonstrating ground glass opacities in the periphery and subpleural thickening, especially where infiltrates are denser. This thickening may result in pleuritic chest pain.6
The right upper lobe is more often affected in these cases than the left lung.6 Numerous pulmonary nodules in the upper lobes are found rarely and can be confused with lung cancer. These nodules are likely the result of an accumulation of the drug in areas of previous inflammation; a lung mass should prompt the addition of APT in the differential.2,16
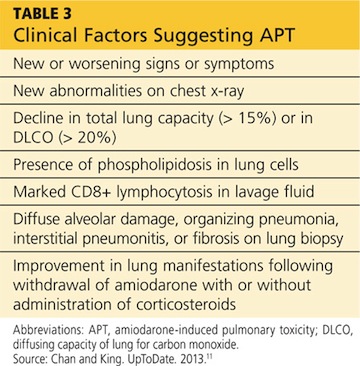
APT is a diagnosis of exclusion, requiring clinical suspicion, drug history, imaging, and consideration of the differential. The presence of three or more clinical factors supports a diagnosis of APT (see Table 3).11
Once APT is recognized, the first action is to have the patient stop taking amiodarone, followed by the administration of corticosteroids (eg, prednisone 40 to 60 mg/d11) for four to 12 months.17 Patients, especially those with underlying lung disease, will typically require temporary oxygen supplementation until hypoxia resolves. Even after the drug has been discontinued, some patients experience worsening symptoms before they see improvement simply because the drug can persist in lung tissue for up to a year following cessation of therapy.6
If APT is diagnosed early, the prognosis is favorable. In one study, a significant number of APT patients stabilized or improved after withdrawal of the drug, regardless of concurrent treatment with corticosteroids.18 Follow-up studies, both imaging and PFT, indicate complete clearing of lung opacities in the majority of patients treated for APT.19 Radiologic improvement may be seen six months after cessation of amiodarone.20 Patients who develop ARDS tend to do poorly and have a mortality rate of approximately 50%.11
Continue reading for the conclusion...
CONCLUSION
Among patients who are taking long-term or high-dose amiodarone, particularly those older than 60, new-onset nonproductive cough and dyspnea signal the need for pulmonary and cardiac work-up. Once the diagnosis of APT is made, treatment is straightforward: Withdraw the amiodarone, and initiate corticosteroid therapy.
REFERENCES
1. Fuster V, Rydén LE, Asinger RW, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation); North American Society of Pacing and Electrophysiology. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. Circulation. 2001; 104(17):2118-2150.
2. Jarand J, Lee A, Leigh R. Amiodaronoma: an unusual form of amiodarone-induced pulmonary toxicity. CMAJ. 2007;176(10):1411-1413.
3. Connolly S. Evidence-based analysis of amiodarone efficacy and safety. Circulation. 1999;100:2025-2034.
4. Amiodarone Trials Meta-Analysis Investigators. Effect of prophylactic amiodarone on mortality after acute myocardial infarction and in congestive heart failure: meta-analysis of individual data from 6500 patients in randomised trials. Lancet. 1997;350(9089):1417-1424.
5. Pollak PT. Clinical organ toxicity of antiarrhythmic compounds: ocular and pulmonary manifestations. Am J Cardiol. 1999;84(9A):37R-45R.
6. Camus P, Martin W, Rosenow E. Amiodarone pulmonary toxicity. Clin Chest Med. 2004;25(1):65-75.
7. Rady MY, Ryan T, Starr NJ. Preoperative therapy with amiodarone and the incidence of acute organ dysfunction after cardiac surgery. Anesth Analg. 1997;85(3):489-497.
8. Canada A, Lesko L, Haffajee C, et al. Amiodarone for tachyarrhythmias: kinetics, and efficacy. Drug Intell Clin Pharm. 1983;17(2):100-104.
9. Ernawati DK, Stafford L, Hughes JD. Amiodarone-induced pulmonary toxicity. Br J Clin Pharmacol. 2008;66(1):82-87.
10. Liu FL, Cohen RD, Downar E, et al. Amiodarone pulmonary toxicity: functional and ultrastructural evaluation. Thorax. 1986;41(2):100-105.
11. Chan E, King TE. Amiodarone pulmonary toxicity. UpToDate. 2013. www.uptodate.com/contents/amiodarone-pulmonary-toxicity. Accessed January 17, 2014.
12. Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43-48.
13. Jackevicius CA, Tom A, Essebag V, et al. Population-level incidence and risk factors for pulmonary toxicity associated with amiodarone. Am J Cardiol. 2011;108:705-710.
14. Jessurun G, Crijns H. Amiodarone pulmonary toxicity [editorial]. BMJ. 1997;314(7081):619-620.
15. Nacca N, Castigliano B, Yuhico L, et al. Severe amiodarone induced pulmonary toxicity. J Thorac Dis. 2012;4(6):667-670.
16. Arnon R, Raz I, Chajek-Shaul T, et al. Amiodarone pulmonary toxicity presenting as a solitary lung mass. Chest. 1988;93(2):425-427.
17. Yamada Y, Shiga T, Matsuda N, et al. Incidence and predictors of pulmonary toxicity in Japanese patients receiving low-dose amiodarone. Circ J. 2007;71(10):1610-1616.
18. Coudert B, Bailly F, Lombard JN, et al. Amiodarone pneumonitis: bronchoalveolar lavage findings in 15 patients and review of the literature. Chest. 1992;102(4):1005-1012.
19. Vernhet H, Bousquet C, Durand G, et al. Reversible amiodarone-induced lung disease: HRCT findings. Eur Radiol. 2001;11(9):1697-1703.
20. Olson LK, Forrest JV, Friedman PJ, et al. Pneumonitis after amiodarone therapy. Radiology. 1984;150(2):327-330.
A 78-year-old woman presented to the emergency department (ED) complaining of shortness of breath, a dry nonproductive cough, fatigue, hypoxia, and general malaise lasting for several months and worsening over a two-week period. She denied having fever, chills, hemoptysis, weight loss, headache, rashes, or joint pain. She reported sweats, decrease in appetite, wheezing, cough without sputum production, and slight swelling of the legs. The patient complained of chest pain upon admission, but it resolved quickly.
The patient, a retired widow with five grown children, denied recent surgery or exposure to sick people, had not travelled, and reported no changes in her home environment. She claimed to have no pets but admitted to currently smoking about four cigarettes a day; she had previously smoked, on average, three packs of cigarettes per day for 60 years. She denied using alcohol or drugs, including intravenous agents.
The patient’s medical history was significant for paroxysmal atrial fibrillation. She had also been diagnosed with chronic obstructive pulmonary disease (COPD), transient ischemic attack, patent foramen ovale, hyperlipidemia, seizure disorder, and hypothyroidism. She had no known HIV risk factors and had had no exposure to asbestos or tuberculosis.
The patient’s current medications included amiodarone (200 mg/d) for four years; valproic acid (500 mg/d); aspirin (325 mg/d); levothyroxine (50 g/d); rosuvastatin (10 mg/d); daily warfarin, dosed according to the international normalized ratio (INR); and budesonide/formoterol (160/4.5 mg, one puff bid). She denied having any drug allergies.
Physical examination in the ED revealed a pulse of 63 beats/min; blood pressure, 108/50 mm Hg; and respiratory rate, 16 to 20 breaths/min. The patient’s O2 saturation was 84% on room air; 82% to 84% on 4 L to 6 L of supplemental oxygen; 87% to 92% with a venturi mask; and 95% on biphasic positive airway pressure (BiPAP) device. She was afebrile with hypoxia and able to speak in full sentences. Crackles were detected in the upper lung fields, best heard anteriorly, as well as a few scattered wheezes and rhonchi. Her heart sounds were normal with a regular rhythm; her extremities exhibited trace edema bilaterally. The remainder of the physical exam was normal.
The patient’s laboratory values included a normal white blood cell (WBC) count, elevated lactic acid dehydrogenase (LDH) at 448 IU/L (reference range, 84 to 246 IU/L), and no eosinophils. The erythrocyte sedimentation rate (ESR) was not measured on admission. Blood analysis of her N-terminal pro-brain natriuretic peptide (NT-proBNP) was 4,877 pg/mL; for women older than 75, a level higher than 1,800 pg/mL is abnormal.
A chest x-ray was performed on admission, showing hyperinflation of the lungs with mild coarsening of the lung markings. A bandlike area of opacity in the right lower lobe with bilateral apical pleural thickening was noted (see Figure 1). Noncontrast CT of the chest revealed diffuse upper lobe ground glass opacities in both lungs, extending into the right middle lobe and lingula as well the superior segments of the lower lobes, with areas of emphysema and septal thickening. Numerous nodules, some of which appeared cavitary, were apparent in the lower lobes.
A two-dimensional echocardiogram demonstrated normal left ventricular size and systolic function, mild tricuspid regurgitation without evidence of pulmonary hypertension, and mild left atrial enlargement.
The patient was admitted to the cardiac unit for evaluation. While there, she received one dose of methylprednisolone (125 mg IV), three doses of ipratropium bromide/albuterol, one dose of ceftriaxone (1 g IV), and one dose of azithromycin (500 mg po). In the absence of significant leg edema and an elevation of jugular venous distention with a normal two-dimensional echocardiogram, heart failure was ruled out. The chest pains reported on initial presentation were ultimately felt to be noncardiac in nature.
After the patient was transferred to the medical floor with an initial diagnosis of exacerbation of her COPD, she was treated with antibiotics, nebulizers, and corticosteroids. She continued to experience episodes of O2 desaturation while on 4 L to 6 L of oxygen via nasal cannula and on a venturi mask. She was then placed on a BiPAP device, set to 12/5, and 50% Fio2 (fraction of inspired oxygen), which improved her oxygenation.
Her hypoxia prompted further radiographic studies. The resulting chest CT scan showed ground glass opacities located primarily in the upper lung areas, greater on the right than on the left side (see Figure 2). The radiologist suggested that the hypoxia was caused by an infection, but because the patient’s presenting symptoms were chronic in nature, drug-induced causes were considered as well. Amiodarone was discontinued.
Cardiology was consulted and agreed that stopping amiodarone was acceptable since the patient was in sinus rhythm at the time. The patient continued to take antibiotics and prednisone. Her symptoms slowly improved during hospitalization, and she required less oxygen. Based on the patient’s presentation, physical exam findings, imaging studies, and laboratory findings, amiodarone-induced pulmonary toxicity (APT) was diagnosed.
She was discharged home on supplemental oxygen at 4 L via cannula, a tapering dosage of prednisone, and metered-dose inhalers for fluticasone/salmeterol and tiotropium bromide. She also had outpatient appointments scheduled, one with the pulmonologist to follow up on her imaging studies and to manage the prednisone taper and the other with the cardiologist to manage her atrial fibrillation.
At pulmonology two months later, she had a chest x-ray (see Figure 3) and pulmonary function tests (PFTs). The patient reported feeling progressively better in the past month. Her dyspnea on exertion had improved, and she did not require supplemental oxygen anymore. She stopped smoking cigarettes.
The patient continued to use fluticasone/salmeterol but stopped tiotropium bromide. On physical exam, her O2 saturation was 95% on room air, heart rhythm and rate were regular, and her lungs revealed very minimal crackles at the right base but were otherwise clear.
The plan specified continuing the prednisone taper. The patient was asked to call the office if she had any worsening shortness of breath, cough, and sputum production. She was also encouraged to continue refraining from smoking cigarettes. This patient had done very well, with near complete resolution of symptoms and a clear chest x-ray.
Continue reading for discussion...
DISCUSSION
Amiodarone, a highly effective antiarrhythmic drug, is FDA approved for suppressing ventricular fibrillation and ventricular tachycardia. It is also used off-label as a second- or third-line choice for atrial fibrillation.1
Standard of care requires that, prior to starting amiodarone therapy, patients have a baseline chest x-ray and PFTs with diffusing capacity performed. Thereafter, the patient should be monitored with annual chest x-rays, with one performed promptly if new symptoms develop. Serial PFTs have not offered any benefit for monitoring, but a decrease of more than 15% in total lung capacity or more than 20% in diffusing capacity from baseline is consistent with APT.2
Adverse effects, both cardiac and noncardiac, are common with amiodarone therapy. They include proarrhythmias, bradycardia, and heart block, as well as thyroid and liver dysfunctions; dermatologic conditions such as blue-gray discoloration of the skin and photosensitivity; neurologic effects such as ataxia, paresthesias, and tremor; ocular problems, including corneal microdeposits; gastrointestinal problems such as nausea, anorexia, and constipation; and lung problems such as pulmonary toxicity, pleural effusion, and pleural thickening.3-6 Of these, pulmonary toxicity is the most severe and life threatening.7
APT, also known as amiodarone pneumonitis and amiodarone lung, typically manifests from a few months to a year and a half after treatment is commenced.6 APT can occur even after the drug is discontinued, because amiodarone has a very long elimination half-life of approximately 15 to 45 days and a tendency to concentrate in organs with high blood perfusion and in adipose tissues.8 Patients taking 400 mg/d for two months or longer or 200 mg/d for more than two years are considered at higher risk for APT.9 The severity of disease appears to correlate with the cumulative dose and length of treatment.10
Numerous risk factors for pulmonary toxicity have been reported, including high drug dosage, pre-existing lung disease, patient age, and prior surgery (see Table 1).11 According to an analysis of a database of 237 patients, only age and duration of amiodarone therapy were significant risk factors for APT.9 Its incidence is not precisely known; reported rates range from 1% to 17%.6,12,13
Presentation with such nonspecific symptoms as shortness of breath, nonproductive cough, fatigue, hypoxia, and general malaise is typical for many pulmonary and cardiac illnesses (see Table 2), making APT difficult to diagnose.14 Occasionally, rapid onset with progression to pneumonitis and respiratory failure masquerades as acute respiratory distress syndrome (ARDS).15
Notable, however, is that APT can manifest with nonproductive cough and dyspnea in 50% to 75% of cases. In addition, presenting symptoms will include fever (33% to 50% of cases) with associated malaise, fatigue, chest pain, and weight loss. In patients with APT, the physical exam usually reveals bilateral crackles on inspiration, but diffuse rales may be heard as well.11
Laboratory studies are not very helpful in diagnosing APT. Patients may present with nonspecific elevated WBCs without eosinophilia and an elevated LDH level.11 An elevated ESR may be detected before symptoms of APT manifest and can be present at the time of diagnosis.6
Imaging studies are far more helpful and specific in diagnosing APT. The typical chest x-ray shows bilateral patchy diffuse infiltrates.12 CT of the chest is usually more revealing, demonstrating ground glass opacities in the periphery and subpleural thickening, especially where infiltrates are denser. This thickening may result in pleuritic chest pain.6
The right upper lobe is more often affected in these cases than the left lung.6 Numerous pulmonary nodules in the upper lobes are found rarely and can be confused with lung cancer. These nodules are likely the result of an accumulation of the drug in areas of previous inflammation; a lung mass should prompt the addition of APT in the differential.2,16
APT is a diagnosis of exclusion, requiring clinical suspicion, drug history, imaging, and consideration of the differential. The presence of three or more clinical factors supports a diagnosis of APT (see Table 3).11
Once APT is recognized, the first action is to have the patient stop taking amiodarone, followed by the administration of corticosteroids (eg, prednisone 40 to 60 mg/d11) for four to 12 months.17 Patients, especially those with underlying lung disease, will typically require temporary oxygen supplementation until hypoxia resolves. Even after the drug has been discontinued, some patients experience worsening symptoms before they see improvement simply because the drug can persist in lung tissue for up to a year following cessation of therapy.6
If APT is diagnosed early, the prognosis is favorable. In one study, a significant number of APT patients stabilized or improved after withdrawal of the drug, regardless of concurrent treatment with corticosteroids.18 Follow-up studies, both imaging and PFT, indicate complete clearing of lung opacities in the majority of patients treated for APT.19 Radiologic improvement may be seen six months after cessation of amiodarone.20 Patients who develop ARDS tend to do poorly and have a mortality rate of approximately 50%.11
Continue reading for the conclusion...
CONCLUSION
Among patients who are taking long-term or high-dose amiodarone, particularly those older than 60, new-onset nonproductive cough and dyspnea signal the need for pulmonary and cardiac work-up. Once the diagnosis of APT is made, treatment is straightforward: Withdraw the amiodarone, and initiate corticosteroid therapy.
REFERENCES
1. Fuster V, Rydén LE, Asinger RW, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation); North American Society of Pacing and Electrophysiology. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. Circulation. 2001; 104(17):2118-2150.
2. Jarand J, Lee A, Leigh R. Amiodaronoma: an unusual form of amiodarone-induced pulmonary toxicity. CMAJ. 2007;176(10):1411-1413.
3. Connolly S. Evidence-based analysis of amiodarone efficacy and safety. Circulation. 1999;100:2025-2034.
4. Amiodarone Trials Meta-Analysis Investigators. Effect of prophylactic amiodarone on mortality after acute myocardial infarction and in congestive heart failure: meta-analysis of individual data from 6500 patients in randomised trials. Lancet. 1997;350(9089):1417-1424.
5. Pollak PT. Clinical organ toxicity of antiarrhythmic compounds: ocular and pulmonary manifestations. Am J Cardiol. 1999;84(9A):37R-45R.
6. Camus P, Martin W, Rosenow E. Amiodarone pulmonary toxicity. Clin Chest Med. 2004;25(1):65-75.
7. Rady MY, Ryan T, Starr NJ. Preoperative therapy with amiodarone and the incidence of acute organ dysfunction after cardiac surgery. Anesth Analg. 1997;85(3):489-497.
8. Canada A, Lesko L, Haffajee C, et al. Amiodarone for tachyarrhythmias: kinetics, and efficacy. Drug Intell Clin Pharm. 1983;17(2):100-104.
9. Ernawati DK, Stafford L, Hughes JD. Amiodarone-induced pulmonary toxicity. Br J Clin Pharmacol. 2008;66(1):82-87.
10. Liu FL, Cohen RD, Downar E, et al. Amiodarone pulmonary toxicity: functional and ultrastructural evaluation. Thorax. 1986;41(2):100-105.
11. Chan E, King TE. Amiodarone pulmonary toxicity. UpToDate. 2013. www.uptodate.com/contents/amiodarone-pulmonary-toxicity. Accessed January 17, 2014.
12. Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43-48.
13. Jackevicius CA, Tom A, Essebag V, et al. Population-level incidence and risk factors for pulmonary toxicity associated with amiodarone. Am J Cardiol. 2011;108:705-710.
14. Jessurun G, Crijns H. Amiodarone pulmonary toxicity [editorial]. BMJ. 1997;314(7081):619-620.
15. Nacca N, Castigliano B, Yuhico L, et al. Severe amiodarone induced pulmonary toxicity. J Thorac Dis. 2012;4(6):667-670.
16. Arnon R, Raz I, Chajek-Shaul T, et al. Amiodarone pulmonary toxicity presenting as a solitary lung mass. Chest. 1988;93(2):425-427.
17. Yamada Y, Shiga T, Matsuda N, et al. Incidence and predictors of pulmonary toxicity in Japanese patients receiving low-dose amiodarone. Circ J. 2007;71(10):1610-1616.
18. Coudert B, Bailly F, Lombard JN, et al. Amiodarone pneumonitis: bronchoalveolar lavage findings in 15 patients and review of the literature. Chest. 1992;102(4):1005-1012.
19. Vernhet H, Bousquet C, Durand G, et al. Reversible amiodarone-induced lung disease: HRCT findings. Eur Radiol. 2001;11(9):1697-1703.
20. Olson LK, Forrest JV, Friedman PJ, et al. Pneumonitis after amiodarone therapy. Radiology. 1984;150(2):327-330.
A 78-year-old woman presented to the emergency department (ED) complaining of shortness of breath, a dry nonproductive cough, fatigue, hypoxia, and general malaise lasting for several months and worsening over a two-week period. She denied having fever, chills, hemoptysis, weight loss, headache, rashes, or joint pain. She reported sweats, decrease in appetite, wheezing, cough without sputum production, and slight swelling of the legs. The patient complained of chest pain upon admission, but it resolved quickly.
The patient, a retired widow with five grown children, denied recent surgery or exposure to sick people, had not travelled, and reported no changes in her home environment. She claimed to have no pets but admitted to currently smoking about four cigarettes a day; she had previously smoked, on average, three packs of cigarettes per day for 60 years. She denied using alcohol or drugs, including intravenous agents.
The patient’s medical history was significant for paroxysmal atrial fibrillation. She had also been diagnosed with chronic obstructive pulmonary disease (COPD), transient ischemic attack, patent foramen ovale, hyperlipidemia, seizure disorder, and hypothyroidism. She had no known HIV risk factors and had had no exposure to asbestos or tuberculosis.
The patient’s current medications included amiodarone (200 mg/d) for four years; valproic acid (500 mg/d); aspirin (325 mg/d); levothyroxine (50 g/d); rosuvastatin (10 mg/d); daily warfarin, dosed according to the international normalized ratio (INR); and budesonide/formoterol (160/4.5 mg, one puff bid). She denied having any drug allergies.
Physical examination in the ED revealed a pulse of 63 beats/min; blood pressure, 108/50 mm Hg; and respiratory rate, 16 to 20 breaths/min. The patient’s O2 saturation was 84% on room air; 82% to 84% on 4 L to 6 L of supplemental oxygen; 87% to 92% with a venturi mask; and 95% on biphasic positive airway pressure (BiPAP) device. She was afebrile with hypoxia and able to speak in full sentences. Crackles were detected in the upper lung fields, best heard anteriorly, as well as a few scattered wheezes and rhonchi. Her heart sounds were normal with a regular rhythm; her extremities exhibited trace edema bilaterally. The remainder of the physical exam was normal.
The patient’s laboratory values included a normal white blood cell (WBC) count, elevated lactic acid dehydrogenase (LDH) at 448 IU/L (reference range, 84 to 246 IU/L), and no eosinophils. The erythrocyte sedimentation rate (ESR) was not measured on admission. Blood analysis of her N-terminal pro-brain natriuretic peptide (NT-proBNP) was 4,877 pg/mL; for women older than 75, a level higher than 1,800 pg/mL is abnormal.
A chest x-ray was performed on admission, showing hyperinflation of the lungs with mild coarsening of the lung markings. A bandlike area of opacity in the right lower lobe with bilateral apical pleural thickening was noted (see Figure 1). Noncontrast CT of the chest revealed diffuse upper lobe ground glass opacities in both lungs, extending into the right middle lobe and lingula as well the superior segments of the lower lobes, with areas of emphysema and septal thickening. Numerous nodules, some of which appeared cavitary, were apparent in the lower lobes.
A two-dimensional echocardiogram demonstrated normal left ventricular size and systolic function, mild tricuspid regurgitation without evidence of pulmonary hypertension, and mild left atrial enlargement.
The patient was admitted to the cardiac unit for evaluation. While there, she received one dose of methylprednisolone (125 mg IV), three doses of ipratropium bromide/albuterol, one dose of ceftriaxone (1 g IV), and one dose of azithromycin (500 mg po). In the absence of significant leg edema and an elevation of jugular venous distention with a normal two-dimensional echocardiogram, heart failure was ruled out. The chest pains reported on initial presentation were ultimately felt to be noncardiac in nature.
After the patient was transferred to the medical floor with an initial diagnosis of exacerbation of her COPD, she was treated with antibiotics, nebulizers, and corticosteroids. She continued to experience episodes of O2 desaturation while on 4 L to 6 L of oxygen via nasal cannula and on a venturi mask. She was then placed on a BiPAP device, set to 12/5, and 50% Fio2 (fraction of inspired oxygen), which improved her oxygenation.
Her hypoxia prompted further radiographic studies. The resulting chest CT scan showed ground glass opacities located primarily in the upper lung areas, greater on the right than on the left side (see Figure 2). The radiologist suggested that the hypoxia was caused by an infection, but because the patient’s presenting symptoms were chronic in nature, drug-induced causes were considered as well. Amiodarone was discontinued.
Cardiology was consulted and agreed that stopping amiodarone was acceptable since the patient was in sinus rhythm at the time. The patient continued to take antibiotics and prednisone. Her symptoms slowly improved during hospitalization, and she required less oxygen. Based on the patient’s presentation, physical exam findings, imaging studies, and laboratory findings, amiodarone-induced pulmonary toxicity (APT) was diagnosed.
She was discharged home on supplemental oxygen at 4 L via cannula, a tapering dosage of prednisone, and metered-dose inhalers for fluticasone/salmeterol and tiotropium bromide. She also had outpatient appointments scheduled, one with the pulmonologist to follow up on her imaging studies and to manage the prednisone taper and the other with the cardiologist to manage her atrial fibrillation.
At pulmonology two months later, she had a chest x-ray (see Figure 3) and pulmonary function tests (PFTs). The patient reported feeling progressively better in the past month. Her dyspnea on exertion had improved, and she did not require supplemental oxygen anymore. She stopped smoking cigarettes.
The patient continued to use fluticasone/salmeterol but stopped tiotropium bromide. On physical exam, her O2 saturation was 95% on room air, heart rhythm and rate were regular, and her lungs revealed very minimal crackles at the right base but were otherwise clear.
The plan specified continuing the prednisone taper. The patient was asked to call the office if she had any worsening shortness of breath, cough, and sputum production. She was also encouraged to continue refraining from smoking cigarettes. This patient had done very well, with near complete resolution of symptoms and a clear chest x-ray.
Continue reading for discussion...
DISCUSSION
Amiodarone, a highly effective antiarrhythmic drug, is FDA approved for suppressing ventricular fibrillation and ventricular tachycardia. It is also used off-label as a second- or third-line choice for atrial fibrillation.1
Standard of care requires that, prior to starting amiodarone therapy, patients have a baseline chest x-ray and PFTs with diffusing capacity performed. Thereafter, the patient should be monitored with annual chest x-rays, with one performed promptly if new symptoms develop. Serial PFTs have not offered any benefit for monitoring, but a decrease of more than 15% in total lung capacity or more than 20% in diffusing capacity from baseline is consistent with APT.2
Adverse effects, both cardiac and noncardiac, are common with amiodarone therapy. They include proarrhythmias, bradycardia, and heart block, as well as thyroid and liver dysfunctions; dermatologic conditions such as blue-gray discoloration of the skin and photosensitivity; neurologic effects such as ataxia, paresthesias, and tremor; ocular problems, including corneal microdeposits; gastrointestinal problems such as nausea, anorexia, and constipation; and lung problems such as pulmonary toxicity, pleural effusion, and pleural thickening.3-6 Of these, pulmonary toxicity is the most severe and life threatening.7
APT, also known as amiodarone pneumonitis and amiodarone lung, typically manifests from a few months to a year and a half after treatment is commenced.6 APT can occur even after the drug is discontinued, because amiodarone has a very long elimination half-life of approximately 15 to 45 days and a tendency to concentrate in organs with high blood perfusion and in adipose tissues.8 Patients taking 400 mg/d for two months or longer or 200 mg/d for more than two years are considered at higher risk for APT.9 The severity of disease appears to correlate with the cumulative dose and length of treatment.10
Numerous risk factors for pulmonary toxicity have been reported, including high drug dosage, pre-existing lung disease, patient age, and prior surgery (see Table 1).11 According to an analysis of a database of 237 patients, only age and duration of amiodarone therapy were significant risk factors for APT.9 Its incidence is not precisely known; reported rates range from 1% to 17%.6,12,13
Presentation with such nonspecific symptoms as shortness of breath, nonproductive cough, fatigue, hypoxia, and general malaise is typical for many pulmonary and cardiac illnesses (see Table 2), making APT difficult to diagnose.14 Occasionally, rapid onset with progression to pneumonitis and respiratory failure masquerades as acute respiratory distress syndrome (ARDS).15
Notable, however, is that APT can manifest with nonproductive cough and dyspnea in 50% to 75% of cases. In addition, presenting symptoms will include fever (33% to 50% of cases) with associated malaise, fatigue, chest pain, and weight loss. In patients with APT, the physical exam usually reveals bilateral crackles on inspiration, but diffuse rales may be heard as well.11
Laboratory studies are not very helpful in diagnosing APT. Patients may present with nonspecific elevated WBCs without eosinophilia and an elevated LDH level.11 An elevated ESR may be detected before symptoms of APT manifest and can be present at the time of diagnosis.6
Imaging studies are far more helpful and specific in diagnosing APT. The typical chest x-ray shows bilateral patchy diffuse infiltrates.12 CT of the chest is usually more revealing, demonstrating ground glass opacities in the periphery and subpleural thickening, especially where infiltrates are denser. This thickening may result in pleuritic chest pain.6
The right upper lobe is more often affected in these cases than the left lung.6 Numerous pulmonary nodules in the upper lobes are found rarely and can be confused with lung cancer. These nodules are likely the result of an accumulation of the drug in areas of previous inflammation; a lung mass should prompt the addition of APT in the differential.2,16
APT is a diagnosis of exclusion, requiring clinical suspicion, drug history, imaging, and consideration of the differential. The presence of three or more clinical factors supports a diagnosis of APT (see Table 3).11
Once APT is recognized, the first action is to have the patient stop taking amiodarone, followed by the administration of corticosteroids (eg, prednisone 40 to 60 mg/d11) for four to 12 months.17 Patients, especially those with underlying lung disease, will typically require temporary oxygen supplementation until hypoxia resolves. Even after the drug has been discontinued, some patients experience worsening symptoms before they see improvement simply because the drug can persist in lung tissue for up to a year following cessation of therapy.6
If APT is diagnosed early, the prognosis is favorable. In one study, a significant number of APT patients stabilized or improved after withdrawal of the drug, regardless of concurrent treatment with corticosteroids.18 Follow-up studies, both imaging and PFT, indicate complete clearing of lung opacities in the majority of patients treated for APT.19 Radiologic improvement may be seen six months after cessation of amiodarone.20 Patients who develop ARDS tend to do poorly and have a mortality rate of approximately 50%.11
Continue reading for the conclusion...
CONCLUSION
Among patients who are taking long-term or high-dose amiodarone, particularly those older than 60, new-onset nonproductive cough and dyspnea signal the need for pulmonary and cardiac work-up. Once the diagnosis of APT is made, treatment is straightforward: Withdraw the amiodarone, and initiate corticosteroid therapy.
REFERENCES
1. Fuster V, Rydén LE, Asinger RW, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation); North American Society of Pacing and Electrophysiology. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. Circulation. 2001; 104(17):2118-2150.
2. Jarand J, Lee A, Leigh R. Amiodaronoma: an unusual form of amiodarone-induced pulmonary toxicity. CMAJ. 2007;176(10):1411-1413.
3. Connolly S. Evidence-based analysis of amiodarone efficacy and safety. Circulation. 1999;100:2025-2034.
4. Amiodarone Trials Meta-Analysis Investigators. Effect of prophylactic amiodarone on mortality after acute myocardial infarction and in congestive heart failure: meta-analysis of individual data from 6500 patients in randomised trials. Lancet. 1997;350(9089):1417-1424.
5. Pollak PT. Clinical organ toxicity of antiarrhythmic compounds: ocular and pulmonary manifestations. Am J Cardiol. 1999;84(9A):37R-45R.
6. Camus P, Martin W, Rosenow E. Amiodarone pulmonary toxicity. Clin Chest Med. 2004;25(1):65-75.
7. Rady MY, Ryan T, Starr NJ. Preoperative therapy with amiodarone and the incidence of acute organ dysfunction after cardiac surgery. Anesth Analg. 1997;85(3):489-497.
8. Canada A, Lesko L, Haffajee C, et al. Amiodarone for tachyarrhythmias: kinetics, and efficacy. Drug Intell Clin Pharm. 1983;17(2):100-104.
9. Ernawati DK, Stafford L, Hughes JD. Amiodarone-induced pulmonary toxicity. Br J Clin Pharmacol. 2008;66(1):82-87.
10. Liu FL, Cohen RD, Downar E, et al. Amiodarone pulmonary toxicity: functional and ultrastructural evaluation. Thorax. 1986;41(2):100-105.
11. Chan E, King TE. Amiodarone pulmonary toxicity. UpToDate. 2013. www.uptodate.com/contents/amiodarone-pulmonary-toxicity. Accessed January 17, 2014.
12. Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43-48.
13. Jackevicius CA, Tom A, Essebag V, et al. Population-level incidence and risk factors for pulmonary toxicity associated with amiodarone. Am J Cardiol. 2011;108:705-710.
14. Jessurun G, Crijns H. Amiodarone pulmonary toxicity [editorial]. BMJ. 1997;314(7081):619-620.
15. Nacca N, Castigliano B, Yuhico L, et al. Severe amiodarone induced pulmonary toxicity. J Thorac Dis. 2012;4(6):667-670.
16. Arnon R, Raz I, Chajek-Shaul T, et al. Amiodarone pulmonary toxicity presenting as a solitary lung mass. Chest. 1988;93(2):425-427.
17. Yamada Y, Shiga T, Matsuda N, et al. Incidence and predictors of pulmonary toxicity in Japanese patients receiving low-dose amiodarone. Circ J. 2007;71(10):1610-1616.
18. Coudert B, Bailly F, Lombard JN, et al. Amiodarone pneumonitis: bronchoalveolar lavage findings in 15 patients and review of the literature. Chest. 1992;102(4):1005-1012.
19. Vernhet H, Bousquet C, Durand G, et al. Reversible amiodarone-induced lung disease: HRCT findings. Eur Radiol. 2001;11(9):1697-1703.
20. Olson LK, Forrest JV, Friedman PJ, et al. Pneumonitis after amiodarone therapy. Radiology. 1984;150(2):327-330.
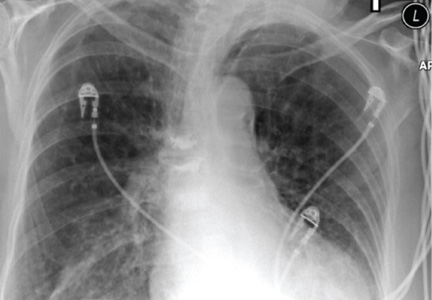
Exam-room posters cut inappropriate antibiotics prescriptions
Exam-room posters declaring a clinician’s commitment to make appropriate antibiotics prescriptions may be a simple, low-cost approach to reducing inappropriate use of antibiotics for acute respiratory infections, according to a report published online Jan. 27 in JAMA Internal Medicine.
Compared with standard practice, the intervention reduced inappropriate prescribing by 20% but had no effect on appropriate prescribing of antibiotics among 11 physicians and three nurse practitioners treating acute respiratory infection at five outpatient primary care clinics. The improvement is comparable to that reported previously for more intensive and expensive interventions, said Daniella Meeker, Ph.D., of RAND Corp., Santa Monica, Calif., and her associates (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14191]).

If these results were extrapolated to the entire United States, the intervention "could eliminate 2.6 million unnecessary antibiotic prescriptions and save $70.4 million annually on drug costs alone," the investigators noted.
"To encourage more judicious use of antibiotics, we designed an intervention that takes advantage of clinicians’ desire to be consistent with their pubic commitments," Dr. Meeker and her colleagues said. "We developed a ... behavioral ‘nudge’ in the form of a public commitment device: a poster-sized letter signed by clinicians and posted in their examination rooms indicating their commitment to reducing inappropriate antibiotic use for acute respiratory infections."
"Public commitment" is a psychological principle that holds that people are much more likely to follow a course of action if they and others have publicly stated that they will do so. It was hoped that an intervention that taps into existing internal motivations would be a more subtle and effective approach than external "reeducation" programs or heavy-handed penalties such as withholding reimbursement for writing too many prescriptions.
Other public commitment approaches have proved successful at increasing participation in recycling programs, getting hotel guests to reuse their towels, increasing donations to organizations serving the disabled, and raising voting rates in elections.
The intervention was a form letter written at the eighth-grade reading level in both English and Spanish and displayed on a poster hung in the exam room. The poster explained why antibiotics were not appropriate for many acute respiratory infections, and it emphasized the clinician’s commitment to follow guidelines for appropriate prescribing. The poster included a photo of the clinician and his or her signature on the letter.
For this study, the posters were used for 12-week periods by clinicians at five Los Angeles community clinics and were used in such a way that an entire 1-year flu cycle was covered. The medical records, including antibiotic prescriptions, were reviewed for all adults seen by the participating clinicians and diagnosed as having an acute respiratory infection for which antibiotics may or may not have been appropriate.
The 14 participating clinicians were randomly assigned to either the intervention (7 using the study condition) or to standard practice (7 control subjects). Eleven of these clinicians were women, and 3 were men. The mean age was 54 years, and the mean duration in practice was 18 years.
A total of 449 patients were included in the intervention group and 505 in the control group. Most (77%) were women, and their mean age was 48 years. Approximately 43% were uninsured.
Diagnoses included acute nasopharyngitis (12 visits), acute laryngitis without obstruction (4 visits), acute laryngopharyngitis (3 visits), acute bronchitis (125 visits), acute upper respiratory tract infections of other sites (10 visits) acute upper respiratory tract infections not otherwise specified (448 visits), bronchitis not specified as acute or chronic (181 visits), nonstreptococcal pharyngitis (161 visits), and influenza with other respiratory manifestations (10 visits).
At baseline, before the intervention was employed, the inappropriate-prescribing rate was 43.5% for clinicians in the intervention group and 42.8% for those in the control group, a nonsignificant difference. During the 12-week intervention period, the inappropriate-prescribing rate dropped to 33.7% for the intervention group but rose to 52.7% for the control group.
That represents a 19.7% reduction for the intervention group, compared with the control group, Dr. Meeker and her associates said.
There was no evidence that the participating clinicians may have undermined the intervention by shifting diagnosis codes away from those that don’t require antibiotics and toward those that might. Diagnostic codes did not change appreciably between baseline and intervention periods in either study group, the researchers said.
Moreover, the rate of appropriate antibiotic prescribing did not change during the intervention period, indicating that clinicians continued to prescribe antibiotics when they were indicated and only stopped prescribing them when they were truly unnecessary.
The intervention, based on a psychological principle, was more effective at curtailing inappropriate prescription of antibiotics than are many others currently in use. Those others typically are based on a model holding that clinicians will change their behavior simply because it makes rational sense to do so, and they use techniques such as education, awareness training, electronic alerts or reminders, and financial incentives, the researchers explained.
"[Our] findings support an alternative model suggesting that clinicians are influenced by interpersonal factors within the context of patient care – in particular, a desire to remain consistent with a prior public commitment," Dr. Meeker and her associates said.
They added that their study was limited because it covered a relatively small geographic area, involved a small number of clinicians, and was of short duration. Moreover, even though the intervention succeeded in reducing inappropriate prescribing significantly, the rate of inappropriate prescribing still remained high among the study participants.
The National Institutes of Health and the National Institute on Aging funded the study. Dr. Meeker and her associates reported no relevant financial conflicts of interest.
Dr. Meeker and her colleagues have developed a novel intervention "based on a sophisticated understanding of how to overcome the psychology that drives behavior linked to inappropriate antibiotic prescription," and it required no complex algorithms, no special technology, no infrastructure, and no enforcement, observed Dr. Brad Spellberg.
"Rather than direct confrontation with the force of education or nagging, they sought a gentler ‘nudging’ approach that worked harmoniously with the underlying psychology of both patient and clinician," he noted.
It remains to be seen whether "this gentle nudge approach" can be generalized to other clinical practices across the country, he added, and whether its effectiveness will be sustained over the long term.
Dr. Spellberg is in the division of general internal medicine at Harbor-UCLA Medical Center and the Los Angeles Biomedical Research Institute in Torrance, Calif. His work is supported by the National Institute of Allergy and Infectious Diseases, and he reported ties to Abbott, Adenium, aRigen, Cardeas, Cempra, GlaxoSmithKline, Meiji, Novan, Pfizer, and Synthetic Biologics. These comments were taken from his invited commentary accompanying Dr. Meeker’s report (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14019]).
Dr. Meeker and her colleagues have developed a novel intervention "based on a sophisticated understanding of how to overcome the psychology that drives behavior linked to inappropriate antibiotic prescription," and it required no complex algorithms, no special technology, no infrastructure, and no enforcement, observed Dr. Brad Spellberg.
"Rather than direct confrontation with the force of education or nagging, they sought a gentler ‘nudging’ approach that worked harmoniously with the underlying psychology of both patient and clinician," he noted.
It remains to be seen whether "this gentle nudge approach" can be generalized to other clinical practices across the country, he added, and whether its effectiveness will be sustained over the long term.
Dr. Spellberg is in the division of general internal medicine at Harbor-UCLA Medical Center and the Los Angeles Biomedical Research Institute in Torrance, Calif. His work is supported by the National Institute of Allergy and Infectious Diseases, and he reported ties to Abbott, Adenium, aRigen, Cardeas, Cempra, GlaxoSmithKline, Meiji, Novan, Pfizer, and Synthetic Biologics. These comments were taken from his invited commentary accompanying Dr. Meeker’s report (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14019]).
Dr. Meeker and her colleagues have developed a novel intervention "based on a sophisticated understanding of how to overcome the psychology that drives behavior linked to inappropriate antibiotic prescription," and it required no complex algorithms, no special technology, no infrastructure, and no enforcement, observed Dr. Brad Spellberg.
"Rather than direct confrontation with the force of education or nagging, they sought a gentler ‘nudging’ approach that worked harmoniously with the underlying psychology of both patient and clinician," he noted.
It remains to be seen whether "this gentle nudge approach" can be generalized to other clinical practices across the country, he added, and whether its effectiveness will be sustained over the long term.
Dr. Spellberg is in the division of general internal medicine at Harbor-UCLA Medical Center and the Los Angeles Biomedical Research Institute in Torrance, Calif. His work is supported by the National Institute of Allergy and Infectious Diseases, and he reported ties to Abbott, Adenium, aRigen, Cardeas, Cempra, GlaxoSmithKline, Meiji, Novan, Pfizer, and Synthetic Biologics. These comments were taken from his invited commentary accompanying Dr. Meeker’s report (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14019]).
Exam-room posters declaring a clinician’s commitment to make appropriate antibiotics prescriptions may be a simple, low-cost approach to reducing inappropriate use of antibiotics for acute respiratory infections, according to a report published online Jan. 27 in JAMA Internal Medicine.
Compared with standard practice, the intervention reduced inappropriate prescribing by 20% but had no effect on appropriate prescribing of antibiotics among 11 physicians and three nurse practitioners treating acute respiratory infection at five outpatient primary care clinics. The improvement is comparable to that reported previously for more intensive and expensive interventions, said Daniella Meeker, Ph.D., of RAND Corp., Santa Monica, Calif., and her associates (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14191]).
If these results were extrapolated to the entire United States, the intervention "could eliminate 2.6 million unnecessary antibiotic prescriptions and save $70.4 million annually on drug costs alone," the investigators noted.
"To encourage more judicious use of antibiotics, we designed an intervention that takes advantage of clinicians’ desire to be consistent with their pubic commitments," Dr. Meeker and her colleagues said. "We developed a ... behavioral ‘nudge’ in the form of a public commitment device: a poster-sized letter signed by clinicians and posted in their examination rooms indicating their commitment to reducing inappropriate antibiotic use for acute respiratory infections."
"Public commitment" is a psychological principle that holds that people are much more likely to follow a course of action if they and others have publicly stated that they will do so. It was hoped that an intervention that taps into existing internal motivations would be a more subtle and effective approach than external "reeducation" programs or heavy-handed penalties such as withholding reimbursement for writing too many prescriptions.
Other public commitment approaches have proved successful at increasing participation in recycling programs, getting hotel guests to reuse their towels, increasing donations to organizations serving the disabled, and raising voting rates in elections.
The intervention was a form letter written at the eighth-grade reading level in both English and Spanish and displayed on a poster hung in the exam room. The poster explained why antibiotics were not appropriate for many acute respiratory infections, and it emphasized the clinician’s commitment to follow guidelines for appropriate prescribing. The poster included a photo of the clinician and his or her signature on the letter.
For this study, the posters were used for 12-week periods by clinicians at five Los Angeles community clinics and were used in such a way that an entire 1-year flu cycle was covered. The medical records, including antibiotic prescriptions, were reviewed for all adults seen by the participating clinicians and diagnosed as having an acute respiratory infection for which antibiotics may or may not have been appropriate.
The 14 participating clinicians were randomly assigned to either the intervention (7 using the study condition) or to standard practice (7 control subjects). Eleven of these clinicians were women, and 3 were men. The mean age was 54 years, and the mean duration in practice was 18 years.
A total of 449 patients were included in the intervention group and 505 in the control group. Most (77%) were women, and their mean age was 48 years. Approximately 43% were uninsured.
Diagnoses included acute nasopharyngitis (12 visits), acute laryngitis without obstruction (4 visits), acute laryngopharyngitis (3 visits), acute bronchitis (125 visits), acute upper respiratory tract infections of other sites (10 visits) acute upper respiratory tract infections not otherwise specified (448 visits), bronchitis not specified as acute or chronic (181 visits), nonstreptococcal pharyngitis (161 visits), and influenza with other respiratory manifestations (10 visits).
At baseline, before the intervention was employed, the inappropriate-prescribing rate was 43.5% for clinicians in the intervention group and 42.8% for those in the control group, a nonsignificant difference. During the 12-week intervention period, the inappropriate-prescribing rate dropped to 33.7% for the intervention group but rose to 52.7% for the control group.
That represents a 19.7% reduction for the intervention group, compared with the control group, Dr. Meeker and her associates said.
There was no evidence that the participating clinicians may have undermined the intervention by shifting diagnosis codes away from those that don’t require antibiotics and toward those that might. Diagnostic codes did not change appreciably between baseline and intervention periods in either study group, the researchers said.
Moreover, the rate of appropriate antibiotic prescribing did not change during the intervention period, indicating that clinicians continued to prescribe antibiotics when they were indicated and only stopped prescribing them when they were truly unnecessary.
The intervention, based on a psychological principle, was more effective at curtailing inappropriate prescription of antibiotics than are many others currently in use. Those others typically are based on a model holding that clinicians will change their behavior simply because it makes rational sense to do so, and they use techniques such as education, awareness training, electronic alerts or reminders, and financial incentives, the researchers explained.
"[Our] findings support an alternative model suggesting that clinicians are influenced by interpersonal factors within the context of patient care – in particular, a desire to remain consistent with a prior public commitment," Dr. Meeker and her associates said.
They added that their study was limited because it covered a relatively small geographic area, involved a small number of clinicians, and was of short duration. Moreover, even though the intervention succeeded in reducing inappropriate prescribing significantly, the rate of inappropriate prescribing still remained high among the study participants.
The National Institutes of Health and the National Institute on Aging funded the study. Dr. Meeker and her associates reported no relevant financial conflicts of interest.
Exam-room posters declaring a clinician’s commitment to make appropriate antibiotics prescriptions may be a simple, low-cost approach to reducing inappropriate use of antibiotics for acute respiratory infections, according to a report published online Jan. 27 in JAMA Internal Medicine.
Compared with standard practice, the intervention reduced inappropriate prescribing by 20% but had no effect on appropriate prescribing of antibiotics among 11 physicians and three nurse practitioners treating acute respiratory infection at five outpatient primary care clinics. The improvement is comparable to that reported previously for more intensive and expensive interventions, said Daniella Meeker, Ph.D., of RAND Corp., Santa Monica, Calif., and her associates (JAMA Intern. Med. 2014 [doi:10.1001/jamainternmed.2013.14191]).
If these results were extrapolated to the entire United States, the intervention "could eliminate 2.6 million unnecessary antibiotic prescriptions and save $70.4 million annually on drug costs alone," the investigators noted.
"To encourage more judicious use of antibiotics, we designed an intervention that takes advantage of clinicians’ desire to be consistent with their pubic commitments," Dr. Meeker and her colleagues said. "We developed a ... behavioral ‘nudge’ in the form of a public commitment device: a poster-sized letter signed by clinicians and posted in their examination rooms indicating their commitment to reducing inappropriate antibiotic use for acute respiratory infections."
"Public commitment" is a psychological principle that holds that people are much more likely to follow a course of action if they and others have publicly stated that they will do so. It was hoped that an intervention that taps into existing internal motivations would be a more subtle and effective approach than external "reeducation" programs or heavy-handed penalties such as withholding reimbursement for writing too many prescriptions.
Other public commitment approaches have proved successful at increasing participation in recycling programs, getting hotel guests to reuse their towels, increasing donations to organizations serving the disabled, and raising voting rates in elections.
The intervention was a form letter written at the eighth-grade reading level in both English and Spanish and displayed on a poster hung in the exam room. The poster explained why antibiotics were not appropriate for many acute respiratory infections, and it emphasized the clinician’s commitment to follow guidelines for appropriate prescribing. The poster included a photo of the clinician and his or her signature on the letter.
For this study, the posters were used for 12-week periods by clinicians at five Los Angeles community clinics and were used in such a way that an entire 1-year flu cycle was covered. The medical records, including antibiotic prescriptions, were reviewed for all adults seen by the participating clinicians and diagnosed as having an acute respiratory infection for which antibiotics may or may not have been appropriate.
The 14 participating clinicians were randomly assigned to either the intervention (7 using the study condition) or to standard practice (7 control subjects). Eleven of these clinicians were women, and 3 were men. The mean age was 54 years, and the mean duration in practice was 18 years.
A total of 449 patients were included in the intervention group and 505 in the control group. Most (77%) were women, and their mean age was 48 years. Approximately 43% were uninsured.
Diagnoses included acute nasopharyngitis (12 visits), acute laryngitis without obstruction (4 visits), acute laryngopharyngitis (3 visits), acute bronchitis (125 visits), acute upper respiratory tract infections of other sites (10 visits) acute upper respiratory tract infections not otherwise specified (448 visits), bronchitis not specified as acute or chronic (181 visits), nonstreptococcal pharyngitis (161 visits), and influenza with other respiratory manifestations (10 visits).
At baseline, before the intervention was employed, the inappropriate-prescribing rate was 43.5% for clinicians in the intervention group and 42.8% for those in the control group, a nonsignificant difference. During the 12-week intervention period, the inappropriate-prescribing rate dropped to 33.7% for the intervention group but rose to 52.7% for the control group.
That represents a 19.7% reduction for the intervention group, compared with the control group, Dr. Meeker and her associates said.
There was no evidence that the participating clinicians may have undermined the intervention by shifting diagnosis codes away from those that don’t require antibiotics and toward those that might. Diagnostic codes did not change appreciably between baseline and intervention periods in either study group, the researchers said.
Moreover, the rate of appropriate antibiotic prescribing did not change during the intervention period, indicating that clinicians continued to prescribe antibiotics when they were indicated and only stopped prescribing them when they were truly unnecessary.
The intervention, based on a psychological principle, was more effective at curtailing inappropriate prescription of antibiotics than are many others currently in use. Those others typically are based on a model holding that clinicians will change their behavior simply because it makes rational sense to do so, and they use techniques such as education, awareness training, electronic alerts or reminders, and financial incentives, the researchers explained.
"[Our] findings support an alternative model suggesting that clinicians are influenced by interpersonal factors within the context of patient care – in particular, a desire to remain consistent with a prior public commitment," Dr. Meeker and her associates said.
They added that their study was limited because it covered a relatively small geographic area, involved a small number of clinicians, and was of short duration. Moreover, even though the intervention succeeded in reducing inappropriate prescribing significantly, the rate of inappropriate prescribing still remained high among the study participants.
The National Institutes of Health and the National Institute on Aging funded the study. Dr. Meeker and her associates reported no relevant financial conflicts of interest.
FROM JAMA INTERNAL MEDICINE
Major finding: During the 12-week intervention period, the inappropriate prescribing rate dropped from 43.5% to 33.7% for the intervention group but rose from 42.8% to 52.7% for the control group, which represents a 19.7% relative reduction with the intervention.
Data source: A randomized clinical trial involving 14 clinicians and 954 of their adult patients who presented with acute respiratory infection during a 1-year period, in which half the clinicians used an intervention to help decrease the inappropriate prescribing of antibiotics.
Disclosures: This study was funded by the National Institutes of Health and the National Institute on Aging. Dr. Meeker and her associates reported no relevant financial conflicts of interest.

Smokers at increased risk after prostate cancer radiation therapy
Patients who undergo external beam radiation therapy for prostate cancer and smoke or have smoked have increased mortality and increased risk of complications, according to Dr. Emily Steinberger and her associates.

Current smoking significantly increased the risk of prostate-specific antigen relapse, distant metastases, and prostate cancer–related death. Current and former smokers were also at a higher risk of external beam radiation therapy–related genitourinary disorders. Smoking did not increase gastrointestinal toxicity, the researchers reported.
Oncologists should encourage patients to participate in smoking-cessation programs before therapy to potentially lower their risk, the researchers recommended.
Read the full article at BJU International (doi:10.1111/bju.12969).
Patients who undergo external beam radiation therapy for prostate cancer and smoke or have smoked have increased mortality and increased risk of complications, according to Dr. Emily Steinberger and her associates.
Current smoking significantly increased the risk of prostate-specific antigen relapse, distant metastases, and prostate cancer–related death. Current and former smokers were also at a higher risk of external beam radiation therapy–related genitourinary disorders. Smoking did not increase gastrointestinal toxicity, the researchers reported.
Oncologists should encourage patients to participate in smoking-cessation programs before therapy to potentially lower their risk, the researchers recommended.
Read the full article at BJU International (doi:10.1111/bju.12969).
Patients who undergo external beam radiation therapy for prostate cancer and smoke or have smoked have increased mortality and increased risk of complications, according to Dr. Emily Steinberger and her associates.
Current smoking significantly increased the risk of prostate-specific antigen relapse, distant metastases, and prostate cancer–related death. Current and former smokers were also at a higher risk of external beam radiation therapy–related genitourinary disorders. Smoking did not increase gastrointestinal toxicity, the researchers reported.
Oncologists should encourage patients to participate in smoking-cessation programs before therapy to potentially lower their risk, the researchers recommended.
Read the full article at BJU International (doi:10.1111/bju.12969).

Zinc for colds
Zinc was recognized as an element in 1509 and as an essential mineral much later. In 1961, zinc deficiency was linked with hypogonadism. Zinc is included in almost all over-the-counter daily vitamins and mineral supplements, typically in the form of zinc oxide, zinc acetate, and zinc gluconate. Zinc is absorbed through the small bowel with an efficiency of 20%-40%. It is the second most important metal in the body after iron and is present in virtually 100% of proteins.
Zinc inhibits viral replication. Because of this, it has been investigated as a way to decrease the duration of symptoms from the common cold. With some evidence suggesting that it works, we know little about the right dose for zinc to exert its magical effects.
In a recently published systematic review, Singh and Das updated a previous Cochrane systematic review and, once again, evaluated the efficacy of zinc in reducing the incidence, severity, and duration of common cold symptoms (Cochrane Database Syst. Rev. 2013;6:CD001364). Studies were included if they were randomized, double-blind, placebo-controlled trials using zinc for at least 5 days for treatment or 5 months for prevention of the common cold.
Sixteen therapeutic trails involving a total of 1,387 people, and two preventive trials with 394 participants were included in the meta-analysis. Zinc came in the form of syrup, lozenges, or tablets. Zinc was associated with statistically significant reductions in the duration but not the severity of symptoms. The mean difference in reduction duration was 1 day (95% confidence interval, –1.72 to –0.34). After 7 days of treatment, significantly fewer subjects had symptoms. Zinc was associated with a reduced incidence of colds, absences from school, and receipt of antibiotics. Bad taste and nausea were significantly higher in patients treated with zinc. The authors suggested that there is a significant reduction in the duration of cold symptoms at a dose of at least 75 mg/day in the lozenge form.
Inhaled zinc can cause permanent anosmia, and so this delivery route was not investigated. Lozenges may be the best bet, since we know the daily dose should be at least 75 mg for treatment. For patients interested in using zinc for prevention, no clear dosage recommendations can be made. Megadose supplementation or high zinc intake has been associated with abdominal pain, diarrhea, nausea, and vomiting. Zinc may interfere with copper absorption, and high zinc intake (greater than 150 mg/day) can lead to copper deficiency and should be avoided.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
Zinc was recognized as an element in 1509 and as an essential mineral much later. In 1961, zinc deficiency was linked with hypogonadism. Zinc is included in almost all over-the-counter daily vitamins and mineral supplements, typically in the form of zinc oxide, zinc acetate, and zinc gluconate. Zinc is absorbed through the small bowel with an efficiency of 20%-40%. It is the second most important metal in the body after iron and is present in virtually 100% of proteins.
Zinc inhibits viral replication. Because of this, it has been investigated as a way to decrease the duration of symptoms from the common cold. With some evidence suggesting that it works, we know little about the right dose for zinc to exert its magical effects.
In a recently published systematic review, Singh and Das updated a previous Cochrane systematic review and, once again, evaluated the efficacy of zinc in reducing the incidence, severity, and duration of common cold symptoms (Cochrane Database Syst. Rev. 2013;6:CD001364). Studies were included if they were randomized, double-blind, placebo-controlled trials using zinc for at least 5 days for treatment or 5 months for prevention of the common cold.
Sixteen therapeutic trails involving a total of 1,387 people, and two preventive trials with 394 participants were included in the meta-analysis. Zinc came in the form of syrup, lozenges, or tablets. Zinc was associated with statistically significant reductions in the duration but not the severity of symptoms. The mean difference in reduction duration was 1 day (95% confidence interval, –1.72 to –0.34). After 7 days of treatment, significantly fewer subjects had symptoms. Zinc was associated with a reduced incidence of colds, absences from school, and receipt of antibiotics. Bad taste and nausea were significantly higher in patients treated with zinc. The authors suggested that there is a significant reduction in the duration of cold symptoms at a dose of at least 75 mg/day in the lozenge form.
Inhaled zinc can cause permanent anosmia, and so this delivery route was not investigated. Lozenges may be the best bet, since we know the daily dose should be at least 75 mg for treatment. For patients interested in using zinc for prevention, no clear dosage recommendations can be made. Megadose supplementation or high zinc intake has been associated with abdominal pain, diarrhea, nausea, and vomiting. Zinc may interfere with copper absorption, and high zinc intake (greater than 150 mg/day) can lead to copper deficiency and should be avoided.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
Zinc was recognized as an element in 1509 and as an essential mineral much later. In 1961, zinc deficiency was linked with hypogonadism. Zinc is included in almost all over-the-counter daily vitamins and mineral supplements, typically in the form of zinc oxide, zinc acetate, and zinc gluconate. Zinc is absorbed through the small bowel with an efficiency of 20%-40%. It is the second most important metal in the body after iron and is present in virtually 100% of proteins.
Zinc inhibits viral replication. Because of this, it has been investigated as a way to decrease the duration of symptoms from the common cold. With some evidence suggesting that it works, we know little about the right dose for zinc to exert its magical effects.
In a recently published systematic review, Singh and Das updated a previous Cochrane systematic review and, once again, evaluated the efficacy of zinc in reducing the incidence, severity, and duration of common cold symptoms (Cochrane Database Syst. Rev. 2013;6:CD001364). Studies were included if they were randomized, double-blind, placebo-controlled trials using zinc for at least 5 days for treatment or 5 months for prevention of the common cold.
Sixteen therapeutic trails involving a total of 1,387 people, and two preventive trials with 394 participants were included in the meta-analysis. Zinc came in the form of syrup, lozenges, or tablets. Zinc was associated with statistically significant reductions in the duration but not the severity of symptoms. The mean difference in reduction duration was 1 day (95% confidence interval, –1.72 to –0.34). After 7 days of treatment, significantly fewer subjects had symptoms. Zinc was associated with a reduced incidence of colds, absences from school, and receipt of antibiotics. Bad taste and nausea were significantly higher in patients treated with zinc. The authors suggested that there is a significant reduction in the duration of cold symptoms at a dose of at least 75 mg/day in the lozenge form.
Inhaled zinc can cause permanent anosmia, and so this delivery route was not investigated. Lozenges may be the best bet, since we know the daily dose should be at least 75 mg for treatment. For patients interested in using zinc for prevention, no clear dosage recommendations can be made. Megadose supplementation or high zinc intake has been associated with abdominal pain, diarrhea, nausea, and vomiting. Zinc may interfere with copper absorption, and high zinc intake (greater than 150 mg/day) can lead to copper deficiency and should be avoided.
Dr. Ebbert is professor of medicine and a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.

Cigarette tax varies considerably among states
New York has the highest cigarette excise tax in the United States and Missouri has the lowest, with a difference of more than $4 in between, the American Lung Association said in a report released Jan. 22.
New York currently adds $4.35 to the price of each pack of cigarettes sold in the state, compared with Missouri’s lowest-in-the-nation rate of 17 cents per pack. Massachusetts has the second-highest tax at $3.51, while Virginia is second lowest at 30 cents. The U.S. average is $1.53 per pack, according to the association’s "State of Tobacco Control 2014" report.
The report noted a general lack of progress among states in smoking cessation and prevention in 2013, with only two states – Massachusetts and Minnesota – passing significant tax increases, "no states approving comprehensive smokefree workplace laws," and two states – Alaska and North Dakota – funding their tobacco prevention programs "at or above levels" recommended by the Centers for Disease Control and Prevention."
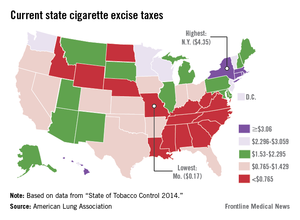
New York has the highest cigarette excise tax in the United States and Missouri has the lowest, with a difference of more than $4 in between, the American Lung Association said in a report released Jan. 22.
New York currently adds $4.35 to the price of each pack of cigarettes sold in the state, compared with Missouri’s lowest-in-the-nation rate of 17 cents per pack. Massachusetts has the second-highest tax at $3.51, while Virginia is second lowest at 30 cents. The U.S. average is $1.53 per pack, according to the association’s "State of Tobacco Control 2014" report.
The report noted a general lack of progress among states in smoking cessation and prevention in 2013, with only two states – Massachusetts and Minnesota – passing significant tax increases, "no states approving comprehensive smokefree workplace laws," and two states – Alaska and North Dakota – funding their tobacco prevention programs "at or above levels" recommended by the Centers for Disease Control and Prevention."
New York has the highest cigarette excise tax in the United States and Missouri has the lowest, with a difference of more than $4 in between, the American Lung Association said in a report released Jan. 22.
New York currently adds $4.35 to the price of each pack of cigarettes sold in the state, compared with Missouri’s lowest-in-the-nation rate of 17 cents per pack. Massachusetts has the second-highest tax at $3.51, while Virginia is second lowest at 30 cents. The U.S. average is $1.53 per pack, according to the association’s "State of Tobacco Control 2014" report.
The report noted a general lack of progress among states in smoking cessation and prevention in 2013, with only two states – Massachusetts and Minnesota – passing significant tax increases, "no states approving comprehensive smokefree workplace laws," and two states – Alaska and North Dakota – funding their tobacco prevention programs "at or above levels" recommended by the Centers for Disease Control and Prevention."
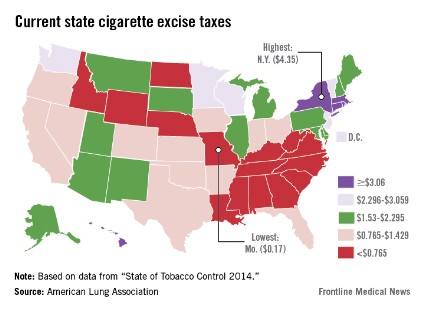
Inpatient safety efforts yield mixed results
Adverse events decreased over the last decade for Medicare inpatients with acute myocardial infarction or heart failure but barely changed for those with pneumonia or conditions requiring surgery, according to an analysis of a Medicare database.
The improvements likely translated to 81,000 fewer adverse events for patients with acute MI (AMI) and heart failure (HF) from 2010 to 2011 alone, according to the study published Jan. 22 in the New England Journal of Medicine.
"Although this suggests that national efforts focused on patient safety have made some inroads, the lack of reductions across the board is disappointing," Yun Wang, Ph.D., of the Harvard School of Public Health, Boston, and his colleagues wrote.
The researchers examined whether hospitalized patients are any better off in light of the current focus on patient safety, including the launch of initiatives such as the American College of Surgeons’ National Surgical Quality Improvement Program and the federal government’s Surgical Infection Prevention Project.
They used three composite outcomes measures: the rate of occurrence for adverse events for which patients were at risk (for instance, only patients receiving warfarin were at risk for warfarin-related events); the proportion of patients with one or more adverse events; and the number of adverse events per 1,000 hospitalizations. They analyzed data on 61,523 patients who were discharged from 4,372 hospitals; the data were extracted from the Medicare Patient Safety Monitoring System database (N. Engl. J. Med. 2014:370;341-51).
The 61,523 patients included 11,399 with AMI, 15,374 with HF, 18,269 with pneumonia, and 16,481 with conditions requiring surgery. Postsurgical patients largely were being treated for joint replacement procedures and other osteoarthritis-related conditions, femur fracture, colon cancer, post-AMI procedures, or other forms of chronic ischemic heart disease.
From 2005-2006 to 2010-2011, AMI and HF patients saw a 1.3 percentage point decline in the rate of adverse events, from 5% to 3.7%. The proportion who had one or more such events decreased from 26% to 19%. The number of adverse events per 1,000 hospitalizations declined from 402 to 262 for AMI patients and from 235 to 167 for HF patients.
Infection-related and drug-related adverse events declined significantly in heart attack and HF patients. There was also a substantial improvement in postprocedure events in HF patients.
Postsurgical patients experienced slight increases in all three outcomes measures, in particular, increases in infection-related and postprocedural events such as venous thromboembolism, and cardiac and catheter-related events. The number of events per 1,000 hospitalizations for pneumonia patients increased insignificantly from 216 to 223. For postsurgical patients, the number of events increased insignificantly from 352/1,000 to 368/1,000.
Patients who had adverse events had significantly longer hospital stays and were at higher risk for death. As the number of adverse events increased, so did the risk of death.
The authors noted that declines in events for AMI and HF patients might be a reflection of the numerous efforts and initiatives to improve care in those two conditions.
But they also found that concerted efforts to improve safety did not necessarily work. There was an increase in pressure ulcers in postsurgical patients, and no decline in ventilator-associated pneumonia in most patients, even though there have been initiatives focused on those conditions.
"Our finding of an increased adverse-event rate among surgical patients indicates a continuing challenge and identifies an important target for patient-safety initiatives," the researchers said.
The study was supported by the Agency for Healthcare Research and Quality as well as academic and federal grants. Dr. Wang was a consultant to and other researchers were employees of the research firm Qualidigm and participated in the analysis. One of the researchers, Dr. Harlan M. Krumholz, disclosed being on a scientific advisory board for UnitedHealthcare and receiving grant money from Medtronic.
On Twitter @aliciaault
Adverse events decreased over the last decade for Medicare inpatients with acute myocardial infarction or heart failure but barely changed for those with pneumonia or conditions requiring surgery, according to an analysis of a Medicare database.
The improvements likely translated to 81,000 fewer adverse events for patients with acute MI (AMI) and heart failure (HF) from 2010 to 2011 alone, according to the study published Jan. 22 in the New England Journal of Medicine.
"Although this suggests that national efforts focused on patient safety have made some inroads, the lack of reductions across the board is disappointing," Yun Wang, Ph.D., of the Harvard School of Public Health, Boston, and his colleagues wrote.
The researchers examined whether hospitalized patients are any better off in light of the current focus on patient safety, including the launch of initiatives such as the American College of Surgeons’ National Surgical Quality Improvement Program and the federal government’s Surgical Infection Prevention Project.
They used three composite outcomes measures: the rate of occurrence for adverse events for which patients were at risk (for instance, only patients receiving warfarin were at risk for warfarin-related events); the proportion of patients with one or more adverse events; and the number of adverse events per 1,000 hospitalizations. They analyzed data on 61,523 patients who were discharged from 4,372 hospitals; the data were extracted from the Medicare Patient Safety Monitoring System database (N. Engl. J. Med. 2014:370;341-51).
The 61,523 patients included 11,399 with AMI, 15,374 with HF, 18,269 with pneumonia, and 16,481 with conditions requiring surgery. Postsurgical patients largely were being treated for joint replacement procedures and other osteoarthritis-related conditions, femur fracture, colon cancer, post-AMI procedures, or other forms of chronic ischemic heart disease.
From 2005-2006 to 2010-2011, AMI and HF patients saw a 1.3 percentage point decline in the rate of adverse events, from 5% to 3.7%. The proportion who had one or more such events decreased from 26% to 19%. The number of adverse events per 1,000 hospitalizations declined from 402 to 262 for AMI patients and from 235 to 167 for HF patients.
Infection-related and drug-related adverse events declined significantly in heart attack and HF patients. There was also a substantial improvement in postprocedure events in HF patients.
Postsurgical patients experienced slight increases in all three outcomes measures, in particular, increases in infection-related and postprocedural events such as venous thromboembolism, and cardiac and catheter-related events. The number of events per 1,000 hospitalizations for pneumonia patients increased insignificantly from 216 to 223. For postsurgical patients, the number of events increased insignificantly from 352/1,000 to 368/1,000.
Patients who had adverse events had significantly longer hospital stays and were at higher risk for death. As the number of adverse events increased, so did the risk of death.
The authors noted that declines in events for AMI and HF patients might be a reflection of the numerous efforts and initiatives to improve care in those two conditions.
But they also found that concerted efforts to improve safety did not necessarily work. There was an increase in pressure ulcers in postsurgical patients, and no decline in ventilator-associated pneumonia in most patients, even though there have been initiatives focused on those conditions.
"Our finding of an increased adverse-event rate among surgical patients indicates a continuing challenge and identifies an important target for patient-safety initiatives," the researchers said.
The study was supported by the Agency for Healthcare Research and Quality as well as academic and federal grants. Dr. Wang was a consultant to and other researchers were employees of the research firm Qualidigm and participated in the analysis. One of the researchers, Dr. Harlan M. Krumholz, disclosed being on a scientific advisory board for UnitedHealthcare and receiving grant money from Medtronic.
On Twitter @aliciaault
Adverse events decreased over the last decade for Medicare inpatients with acute myocardial infarction or heart failure but barely changed for those with pneumonia or conditions requiring surgery, according to an analysis of a Medicare database.
The improvements likely translated to 81,000 fewer adverse events for patients with acute MI (AMI) and heart failure (HF) from 2010 to 2011 alone, according to the study published Jan. 22 in the New England Journal of Medicine.
"Although this suggests that national efforts focused on patient safety have made some inroads, the lack of reductions across the board is disappointing," Yun Wang, Ph.D., of the Harvard School of Public Health, Boston, and his colleagues wrote.
The researchers examined whether hospitalized patients are any better off in light of the current focus on patient safety, including the launch of initiatives such as the American College of Surgeons’ National Surgical Quality Improvement Program and the federal government’s Surgical Infection Prevention Project.
They used three composite outcomes measures: the rate of occurrence for adverse events for which patients were at risk (for instance, only patients receiving warfarin were at risk for warfarin-related events); the proportion of patients with one or more adverse events; and the number of adverse events per 1,000 hospitalizations. They analyzed data on 61,523 patients who were discharged from 4,372 hospitals; the data were extracted from the Medicare Patient Safety Monitoring System database (N. Engl. J. Med. 2014:370;341-51).
The 61,523 patients included 11,399 with AMI, 15,374 with HF, 18,269 with pneumonia, and 16,481 with conditions requiring surgery. Postsurgical patients largely were being treated for joint replacement procedures and other osteoarthritis-related conditions, femur fracture, colon cancer, post-AMI procedures, or other forms of chronic ischemic heart disease.
From 2005-2006 to 2010-2011, AMI and HF patients saw a 1.3 percentage point decline in the rate of adverse events, from 5% to 3.7%. The proportion who had one or more such events decreased from 26% to 19%. The number of adverse events per 1,000 hospitalizations declined from 402 to 262 for AMI patients and from 235 to 167 for HF patients.
Infection-related and drug-related adverse events declined significantly in heart attack and HF patients. There was also a substantial improvement in postprocedure events in HF patients.
Postsurgical patients experienced slight increases in all three outcomes measures, in particular, increases in infection-related and postprocedural events such as venous thromboembolism, and cardiac and catheter-related events. The number of events per 1,000 hospitalizations for pneumonia patients increased insignificantly from 216 to 223. For postsurgical patients, the number of events increased insignificantly from 352/1,000 to 368/1,000.
Patients who had adverse events had significantly longer hospital stays and were at higher risk for death. As the number of adverse events increased, so did the risk of death.
The authors noted that declines in events for AMI and HF patients might be a reflection of the numerous efforts and initiatives to improve care in those two conditions.
But they also found that concerted efforts to improve safety did not necessarily work. There was an increase in pressure ulcers in postsurgical patients, and no decline in ventilator-associated pneumonia in most patients, even though there have been initiatives focused on those conditions.
"Our finding of an increased adverse-event rate among surgical patients indicates a continuing challenge and identifies an important target for patient-safety initiatives," the researchers said.
The study was supported by the Agency for Healthcare Research and Quality as well as academic and federal grants. Dr. Wang was a consultant to and other researchers were employees of the research firm Qualidigm and participated in the analysis. One of the researchers, Dr. Harlan M. Krumholz, disclosed being on a scientific advisory board for UnitedHealthcare and receiving grant money from Medtronic.
On Twitter @aliciaault
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: At least 81,000 adverse events were avoided in a single year in patients hospitalized for acute MI and heart failure.
Data source: A retrospective analysis of data from 61,523 patients in the Medicare Patient Safety Monitoring System.
Disclosures: The study was supported by the Agency for Healthcare Research and Quality as well as academic and federal grants. Dr. Wang was a consultant to and other researchers were employees of the research firm Qualidigm and participated in the analysis. One of the researchers, Dr. Harlan M. Krumholz, disclosed being on a scientific advisory board for UnitedHealthcare and receiving grant money from Medtronic.
Trial immunosuppressive therapy benefits outweigh long-term lymphoma risks in IBD
HOLLYWOOD, FLA. – The benefits of short-term trial immunosuppressive therapy outweigh the risks in inflammatory bowel disease, but certain patient populations require more vigilance than others, Dr. James D. Lewis said at the 2013 Advances in IBD meeting.
"We can probably all agree that thiopurines increase the risk of lymphoma," said Dr. Lewis, of the University of Pennsylvania, Philadelphia, at the conference on inflammatory bowel diseases. "But I’ve gone from ‘probably’ to ‘possibly’ when it comes to using anti-TNF [anti–tumor necrosis factor] therapy. I believe that a short trial of biologics therapy can really inform the risk-benefit balance, moving the conversation from ‘it might make a patient better’ to either it did or it didn’t."
In young males and the elderly, the benefit of combination therapy might not prove worth the risks of the treatment, said Dr. Lewis, "but in the middle ground, I think we have a sweet spot."

Overall, unless ineffective treatment is justifiable for other reasons such as the prevention of antibody formation, it should be discontinued, he said.
Results from the CESAME study, published in 2009, reinforce previously published data, indicating the risk of lymphoma is up to five times higher in IBD patients exposed to thiopurines than in the general population (Lancet 2009;374:1617-25).
"The most important data from CESAME, however, was that patients who discontinued thiopurines had a lymphoma incidence rate that went back to that of the general population," Dr. Lewis said at the meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The link between lymphoma and anti-TNF treatment is harder to establish in IBD patients, because many in this cohort also have been exposed to thiopurines as part of combination therapies, he said.
Combination therapy is possibly associated with a higher risk of lymphoma than thiopurine monotherapy, and it has been shown to lead to a higher incidence rate than biologics monotherapy, said Dr. Lewis.
If you counsel patients that there is a 1 in 2,000 risk of lymphoma per year, he said, but it takes only a quarter of a year to figure out if the drugs are going to work, then the short-term risk is 1.25 per 10,000 that an additional lymphoma would develop because of that 3-month treatment. "And if you stop the treatment, presumably that risk goes away."
The risk-to-benefit ratio would therefore be favorable for most patients who took thiopurines versus those who did not, he said. "The caveat being, the older you get, the more marginal that risk-benefit balance becomes, probably because as you age, your baseline risk for lymphoma is going up."
Regarding the risk of hepatosplenic T-cell lymphoma in patients exposed to immunosuppressive therapy, Dr. Lewis said that when he pooled the risk in person-years from two studies, he "did some back-of-the-envelope calculations and found that in males, the risk might be on the order of 11 in 100,000 person-years of thiopurine exposure."
That means the number needed to harm is about 9,000 patients, which when combined with the possible risk of developing other lymphomas, the number needed to harm is about 6,000 young males for 1 lymphoma death per year, according to Dr. Lewis.
"But I want to caution you that I am almost sure this is an overestimate of the risk, because if this is true, then it means in young males treated with thiopurines who get lymphoma, a third of them would be hepatosplenic lymphomas, and that seems unlikely," he said.
The ultimate magnitude of risk for adding thiopurine therapy for patients, particularly young males, is on par with that of the risk of death from annual use of automobiles, which Dr. Lewis said was approximately 1 in 9,090.
Since "a substantial proportion" of lymphomas associated with immunosuppression are related to the Epstein-Barr virus, according to Dr. Lewis, aside from minimizing unnecessary treatment, which can be hard to define, clinicians might consider discontinuing just thiopurine therapy, or all therapy in the setting of long-term remission. "I’m not endorsing that," he said. "I am saying that is a question for you to consider."
Other considerations include determining the minimum dose of thiopurine or methotrexate necessary to augment the effectiveness of anti-TNF treatment, as well as whether methotrexate is as effective as thiopurines without having an increased lymphoma risk, although only "indirect evidence" currently exists. "It would be nice to see a head-to-head comparison of those," he said.
As for using Epstein-Barr virus serology to help stratify risk, Dr. Lewis said that currently there are no guidelines for it in IBD, and he does not have a set rule to recommend it.
Dr. Lewis disclosed that he consults for AbbVie, Janssen, Prometheus, and Millennium and has received research funding from Centocor and Takeda.
HOLLYWOOD, FLA. – The benefits of short-term trial immunosuppressive therapy outweigh the risks in inflammatory bowel disease, but certain patient populations require more vigilance than others, Dr. James D. Lewis said at the 2013 Advances in IBD meeting.
"We can probably all agree that thiopurines increase the risk of lymphoma," said Dr. Lewis, of the University of Pennsylvania, Philadelphia, at the conference on inflammatory bowel diseases. "But I’ve gone from ‘probably’ to ‘possibly’ when it comes to using anti-TNF [anti–tumor necrosis factor] therapy. I believe that a short trial of biologics therapy can really inform the risk-benefit balance, moving the conversation from ‘it might make a patient better’ to either it did or it didn’t."
In young males and the elderly, the benefit of combination therapy might not prove worth the risks of the treatment, said Dr. Lewis, "but in the middle ground, I think we have a sweet spot."
Overall, unless ineffective treatment is justifiable for other reasons such as the prevention of antibody formation, it should be discontinued, he said.
Results from the CESAME study, published in 2009, reinforce previously published data, indicating the risk of lymphoma is up to five times higher in IBD patients exposed to thiopurines than in the general population (Lancet 2009;374:1617-25).
"The most important data from CESAME, however, was that patients who discontinued thiopurines had a lymphoma incidence rate that went back to that of the general population," Dr. Lewis said at the meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The link between lymphoma and anti-TNF treatment is harder to establish in IBD patients, because many in this cohort also have been exposed to thiopurines as part of combination therapies, he said.
Combination therapy is possibly associated with a higher risk of lymphoma than thiopurine monotherapy, and it has been shown to lead to a higher incidence rate than biologics monotherapy, said Dr. Lewis.
If you counsel patients that there is a 1 in 2,000 risk of lymphoma per year, he said, but it takes only a quarter of a year to figure out if the drugs are going to work, then the short-term risk is 1.25 per 10,000 that an additional lymphoma would develop because of that 3-month treatment. "And if you stop the treatment, presumably that risk goes away."
The risk-to-benefit ratio would therefore be favorable for most patients who took thiopurines versus those who did not, he said. "The caveat being, the older you get, the more marginal that risk-benefit balance becomes, probably because as you age, your baseline risk for lymphoma is going up."
Regarding the risk of hepatosplenic T-cell lymphoma in patients exposed to immunosuppressive therapy, Dr. Lewis said that when he pooled the risk in person-years from two studies, he "did some back-of-the-envelope calculations and found that in males, the risk might be on the order of 11 in 100,000 person-years of thiopurine exposure."
That means the number needed to harm is about 9,000 patients, which when combined with the possible risk of developing other lymphomas, the number needed to harm is about 6,000 young males for 1 lymphoma death per year, according to Dr. Lewis.
"But I want to caution you that I am almost sure this is an overestimate of the risk, because if this is true, then it means in young males treated with thiopurines who get lymphoma, a third of them would be hepatosplenic lymphomas, and that seems unlikely," he said.
The ultimate magnitude of risk for adding thiopurine therapy for patients, particularly young males, is on par with that of the risk of death from annual use of automobiles, which Dr. Lewis said was approximately 1 in 9,090.
Since "a substantial proportion" of lymphomas associated with immunosuppression are related to the Epstein-Barr virus, according to Dr. Lewis, aside from minimizing unnecessary treatment, which can be hard to define, clinicians might consider discontinuing just thiopurine therapy, or all therapy in the setting of long-term remission. "I’m not endorsing that," he said. "I am saying that is a question for you to consider."
Other considerations include determining the minimum dose of thiopurine or methotrexate necessary to augment the effectiveness of anti-TNF treatment, as well as whether methotrexate is as effective as thiopurines without having an increased lymphoma risk, although only "indirect evidence" currently exists. "It would be nice to see a head-to-head comparison of those," he said.
As for using Epstein-Barr virus serology to help stratify risk, Dr. Lewis said that currently there are no guidelines for it in IBD, and he does not have a set rule to recommend it.
Dr. Lewis disclosed that he consults for AbbVie, Janssen, Prometheus, and Millennium and has received research funding from Centocor and Takeda.
HOLLYWOOD, FLA. – The benefits of short-term trial immunosuppressive therapy outweigh the risks in inflammatory bowel disease, but certain patient populations require more vigilance than others, Dr. James D. Lewis said at the 2013 Advances in IBD meeting.
"We can probably all agree that thiopurines increase the risk of lymphoma," said Dr. Lewis, of the University of Pennsylvania, Philadelphia, at the conference on inflammatory bowel diseases. "But I’ve gone from ‘probably’ to ‘possibly’ when it comes to using anti-TNF [anti–tumor necrosis factor] therapy. I believe that a short trial of biologics therapy can really inform the risk-benefit balance, moving the conversation from ‘it might make a patient better’ to either it did or it didn’t."
In young males and the elderly, the benefit of combination therapy might not prove worth the risks of the treatment, said Dr. Lewis, "but in the middle ground, I think we have a sweet spot."
Overall, unless ineffective treatment is justifiable for other reasons such as the prevention of antibody formation, it should be discontinued, he said.
Results from the CESAME study, published in 2009, reinforce previously published data, indicating the risk of lymphoma is up to five times higher in IBD patients exposed to thiopurines than in the general population (Lancet 2009;374:1617-25).
"The most important data from CESAME, however, was that patients who discontinued thiopurines had a lymphoma incidence rate that went back to that of the general population," Dr. Lewis said at the meeting, sponsored by the Crohn’s & Colitis Foundation of America.
The link between lymphoma and anti-TNF treatment is harder to establish in IBD patients, because many in this cohort also have been exposed to thiopurines as part of combination therapies, he said.
Combination therapy is possibly associated with a higher risk of lymphoma than thiopurine monotherapy, and it has been shown to lead to a higher incidence rate than biologics monotherapy, said Dr. Lewis.
If you counsel patients that there is a 1 in 2,000 risk of lymphoma per year, he said, but it takes only a quarter of a year to figure out if the drugs are going to work, then the short-term risk is 1.25 per 10,000 that an additional lymphoma would develop because of that 3-month treatment. "And if you stop the treatment, presumably that risk goes away."
The risk-to-benefit ratio would therefore be favorable for most patients who took thiopurines versus those who did not, he said. "The caveat being, the older you get, the more marginal that risk-benefit balance becomes, probably because as you age, your baseline risk for lymphoma is going up."
Regarding the risk of hepatosplenic T-cell lymphoma in patients exposed to immunosuppressive therapy, Dr. Lewis said that when he pooled the risk in person-years from two studies, he "did some back-of-the-envelope calculations and found that in males, the risk might be on the order of 11 in 100,000 person-years of thiopurine exposure."
That means the number needed to harm is about 9,000 patients, which when combined with the possible risk of developing other lymphomas, the number needed to harm is about 6,000 young males for 1 lymphoma death per year, according to Dr. Lewis.
"But I want to caution you that I am almost sure this is an overestimate of the risk, because if this is true, then it means in young males treated with thiopurines who get lymphoma, a third of them would be hepatosplenic lymphomas, and that seems unlikely," he said.
The ultimate magnitude of risk for adding thiopurine therapy for patients, particularly young males, is on par with that of the risk of death from annual use of automobiles, which Dr. Lewis said was approximately 1 in 9,090.
Since "a substantial proportion" of lymphomas associated with immunosuppression are related to the Epstein-Barr virus, according to Dr. Lewis, aside from minimizing unnecessary treatment, which can be hard to define, clinicians might consider discontinuing just thiopurine therapy, or all therapy in the setting of long-term remission. "I’m not endorsing that," he said. "I am saying that is a question for you to consider."
Other considerations include determining the minimum dose of thiopurine or methotrexate necessary to augment the effectiveness of anti-TNF treatment, as well as whether methotrexate is as effective as thiopurines without having an increased lymphoma risk, although only "indirect evidence" currently exists. "It would be nice to see a head-to-head comparison of those," he said.
As for using Epstein-Barr virus serology to help stratify risk, Dr. Lewis said that currently there are no guidelines for it in IBD, and he does not have a set rule to recommend it.
Dr. Lewis disclosed that he consults for AbbVie, Janssen, Prometheus, and Millennium and has received research funding from Centocor and Takeda.
EXPERT ANALYSIS AT 2013 ADVANCES IN IBD

Imaging, biomarkers, clinical findings guide approach to indeterminate pulmonary nodules
SAN DIEGO – About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We’re encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.

Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it’s important to differentiate – early, accurately, and noninvasively – benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we’re wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It’s not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going – integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.
SAN DIEGO – About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We’re encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.
Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it’s important to differentiate – early, accurately, and noninvasively – benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we’re wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It’s not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going – integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.
SAN DIEGO – About 30% of nodules detected by CT screening fit the criteria for an indeterminate pulmonary nodule. Very few of those nodules represent cancer, and the question is, what do you recommend for those patients in terms of follow-up?
"We’re encountering more and more patients with lung nodules in the clinic, and with the advance of screening, it will become even more of a problem. The numbers are tremendous," Dr. Pierre P. Massion stated at the Joint Conference on the Molecular Origins of Lung Cancer, sponsored by the American Association for Cancer Research and the International Association for the Study of Lung Cancer.
Dr. Massion, the Ingram Professor of Cancer Research at Vanderbilt-Ingram Cancer Center in Nashville, Tenn., said it’s important to differentiate – early, accurately, and noninvasively – benign lesions from cancer. "There is a race for early diagnosis, because surgery is the best chance for cure ... but we also need to decrease the number of thoracotomies performed for benign disease."
Data from eight large trials of lung cancer screening examined the relationship between lesion size and the probability of lung cancer (Chest 2007;132[3 Suppl]:94S-107S). The probability of cancer was 0-1% for lesions less than 5 mm in diameter; 6%-28% for those 5-10 mm, 33%-60% for those 11-20 mm, and 64%-82% for those 21-30 mm.
"The bigger the nodule, the greater the probability of cancer. In fact, however, the number of large nodules is very small," Dr. Massion said. "The indeterminate ones are between 5 and 15 mm in diameter, and these are the ones we struggle with how best to handle." The probability of cancer from indeterminate pulmonary nodules ranges from 6% to 60%, which is a large range.
The shape of the nodule provides additional information, Dr. Massion said. Triangular shape abutting a fissure and central calcification are generally indicators of benign disease and typically do not require follow-up. Alternatively, solid, noncalcified spiculated nodules have a high likelihood of being cancer. Part solid nodules are "very worrisome," he said. "These are most likely to contain malignancy. Nonsolid lesions, also called ground-glass opacities, are troublesome and difficult to assess. They represent about a 20% probability of disease."
The rate of growth of small nodules over time "is probably one of the best imaging markers, [but] for small nodules such as those 5 mm in diameter, the volumetric analysis has a large coefficient of variance," he said.
Prediction models are important to the evaluation of lung nodules, yet even with existing tools "we’re wrong about 30% of the time," he said. The best three prediction models come from studies of patients at the Mayo Clinic (Arch. Intern. Med. 1997;157:849-55) and the Veterans Affairs department (Chest 2007;131:383-88), and from patients enrolled in the PLCO (Prostate, Lung, Colorectal, and Ovarian) Cancer Screening Trial (N. Engl. J. Med. 2013;368:728-36). These prediction models are now recommended for use on nodules greater than 8 mm in diameter in the ACCP 2013 guidelines for evaluation of lung nodules (Chest 2013;143[5 Suppl]:e93S-120S).
"We have no models for never-smokers, which is a huge problem in the community at the moment."
Dr. Massion predicted that serum biomarkers might "come to the rescue" for deciding which patients with indeterminate pulmonary nodules might need to go for a biopsy or resection and which can be carefully watched over time.
In a separate study of 62 lung nodules that integrated clinical, imaging, and protein biomarker findings, clinical information alone resulted in about 50% sensitivity for predicting disease, "which is not great," said Dr. Massion, who was the principal investigator (Cancer Epidemiol. Biomarkers Prev. 2012;21:786-92). The addition of CT imaging increased the area under the curve to about 61%. Adding biomarkers in the blood raised the bar to about 69%.
"It’s not a panacea, but we show a trend toward improvement of classification of these nodules, which is where I think this field is going – integrating information from the clinic, imaging, and the discriminatory power of biomarkers."
Dr. Massion said that he had no relevant financial conflicts to disclose.
EXPERT ANALYSIS AT AN AACR-IASLC JOINT CONFERENCE
