User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
FDA approves Oralair, first grass-pollen allergy pill
Oralair was approved April 1 by the Food and Drug Administration for the treatment of allergic rhinitis; it is the first sublingual allergen extract approved for use in the United States.
Oralair is indicated to treat allergic rhinitis with or without eye inflammation that is induced by certain grass pollens in people aged 10-65 years. The company had proposed that the treatment be approved for patients aged 5 years and older.
The treatment contains a mixture of freeze-dried extracts from the pollens of five grasses: Kentucky Blue Grass, Orchard, Perennial Rye, Sweet Vernal, and Timothy.

Once-daily Oralair is started 4 months prior to the grass-pollen season and continued throughout the season. The first dose is delivered in the doctor’s office, and the remaining doses can be self-administered at home. Manufacturer Greer Laboratories claims that Oralair may reduce grass allergy symptoms for patients within the first allergy season it is taken.
Treatment with a sublingual tablet would open up the treatment options for the approximately 30 million Americans who suffer from allergic rhinitis every year, said Dr. Linda Cox, immediate past president of the American Academy of Allergy Asthma and Immunology and a practicing allergist in Ft. Lauderdale, Fla.
She said that she sees it as a game changer for the treatment of allergic rhinitis.
"What sublingual immunotherapy offers is home treatment and easier access to care because its safety profile is so good," Dr. Cox said in an interview. "That could potentially open up this treatment for the 90% or so of patients who are not receiving anything and are just treating the symptoms."
She added that Oralair treats the underlying causes of allergic rhinitis, not just the symptoms caused by the disease. "It will bring a group of people who are just suffering through their [allergy] seasons and are getting suboptimal control with various products and give them the potential to just knock out their disease," she added.
Approval of Oralair was based on double-blind, placebo-controlled trials in the United States and Europe that enrolled more than 2,500 adults and children. To assess the treatment’s effectiveness, patients reported their symptoms and additional medications needed to cope with their allergy symptoms. During treatment for one grass-pollen season, patients taking Oralair saw a 16%-30% reduction in symptoms and the need for medications, compared with those who received a placebo.
The trials demonstrated that treatment with Oralair before and during allergy season reduced patients’ allergy symptoms and their need for symptom-relieving medication.
The most common adverse events for Oralair, reported in less than 5% of patients, were oral pruritus, throat irritation, ear pruritus, mouth edema, tongue pruritus, cough, and oropharyngeal pain, Greer Laboratories said in an April 1 statement.
Oralair was first approved in Europe in 2008, and is currently approved in 31 countries.
Oralair was approved April 1 by the Food and Drug Administration for the treatment of allergic rhinitis; it is the first sublingual allergen extract approved for use in the United States.
Oralair is indicated to treat allergic rhinitis with or without eye inflammation that is induced by certain grass pollens in people aged 10-65 years. The company had proposed that the treatment be approved for patients aged 5 years and older.
The treatment contains a mixture of freeze-dried extracts from the pollens of five grasses: Kentucky Blue Grass, Orchard, Perennial Rye, Sweet Vernal, and Timothy.
Once-daily Oralair is started 4 months prior to the grass-pollen season and continued throughout the season. The first dose is delivered in the doctor’s office, and the remaining doses can be self-administered at home. Manufacturer Greer Laboratories claims that Oralair may reduce grass allergy symptoms for patients within the first allergy season it is taken.
Treatment with a sublingual tablet would open up the treatment options for the approximately 30 million Americans who suffer from allergic rhinitis every year, said Dr. Linda Cox, immediate past president of the American Academy of Allergy Asthma and Immunology and a practicing allergist in Ft. Lauderdale, Fla.
She said that she sees it as a game changer for the treatment of allergic rhinitis.
"What sublingual immunotherapy offers is home treatment and easier access to care because its safety profile is so good," Dr. Cox said in an interview. "That could potentially open up this treatment for the 90% or so of patients who are not receiving anything and are just treating the symptoms."
She added that Oralair treats the underlying causes of allergic rhinitis, not just the symptoms caused by the disease. "It will bring a group of people who are just suffering through their [allergy] seasons and are getting suboptimal control with various products and give them the potential to just knock out their disease," she added.
Approval of Oralair was based on double-blind, placebo-controlled trials in the United States and Europe that enrolled more than 2,500 adults and children. To assess the treatment’s effectiveness, patients reported their symptoms and additional medications needed to cope with their allergy symptoms. During treatment for one grass-pollen season, patients taking Oralair saw a 16%-30% reduction in symptoms and the need for medications, compared with those who received a placebo.
The trials demonstrated that treatment with Oralair before and during allergy season reduced patients’ allergy symptoms and their need for symptom-relieving medication.
The most common adverse events for Oralair, reported in less than 5% of patients, were oral pruritus, throat irritation, ear pruritus, mouth edema, tongue pruritus, cough, and oropharyngeal pain, Greer Laboratories said in an April 1 statement.
Oralair was first approved in Europe in 2008, and is currently approved in 31 countries.
Oralair was approved April 1 by the Food and Drug Administration for the treatment of allergic rhinitis; it is the first sublingual allergen extract approved for use in the United States.
Oralair is indicated to treat allergic rhinitis with or without eye inflammation that is induced by certain grass pollens in people aged 10-65 years. The company had proposed that the treatment be approved for patients aged 5 years and older.
The treatment contains a mixture of freeze-dried extracts from the pollens of five grasses: Kentucky Blue Grass, Orchard, Perennial Rye, Sweet Vernal, and Timothy.
Once-daily Oralair is started 4 months prior to the grass-pollen season and continued throughout the season. The first dose is delivered in the doctor’s office, and the remaining doses can be self-administered at home. Manufacturer Greer Laboratories claims that Oralair may reduce grass allergy symptoms for patients within the first allergy season it is taken.
Treatment with a sublingual tablet would open up the treatment options for the approximately 30 million Americans who suffer from allergic rhinitis every year, said Dr. Linda Cox, immediate past president of the American Academy of Allergy Asthma and Immunology and a practicing allergist in Ft. Lauderdale, Fla.
She said that she sees it as a game changer for the treatment of allergic rhinitis.
"What sublingual immunotherapy offers is home treatment and easier access to care because its safety profile is so good," Dr. Cox said in an interview. "That could potentially open up this treatment for the 90% or so of patients who are not receiving anything and are just treating the symptoms."
She added that Oralair treats the underlying causes of allergic rhinitis, not just the symptoms caused by the disease. "It will bring a group of people who are just suffering through their [allergy] seasons and are getting suboptimal control with various products and give them the potential to just knock out their disease," she added.
Approval of Oralair was based on double-blind, placebo-controlled trials in the United States and Europe that enrolled more than 2,500 adults and children. To assess the treatment’s effectiveness, patients reported their symptoms and additional medications needed to cope with their allergy symptoms. During treatment for one grass-pollen season, patients taking Oralair saw a 16%-30% reduction in symptoms and the need for medications, compared with those who received a placebo.
The trials demonstrated that treatment with Oralair before and during allergy season reduced patients’ allergy symptoms and their need for symptom-relieving medication.
The most common adverse events for Oralair, reported in less than 5% of patients, were oral pruritus, throat irritation, ear pruritus, mouth edema, tongue pruritus, cough, and oropharyngeal pain, Greer Laboratories said in an April 1 statement.
Oralair was first approved in Europe in 2008, and is currently approved in 31 countries.

Asthma medication nonadherence mainly unintentional
SAN DIEGO – When patients do not take their asthma medication, it’s usually because they forgot and not because they intentionally made a change in their treatment regimen, a retrospective study of data on 108 adults and 156 children found.
The role of forgetfulness in nonadherence emphasizes the importance of interventions such as text messages, smart inhalers with reminder systems, or Web-based reminder programs to reduce the risk of exacerbations, Dr. Joyce Xiang Wu Lee said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

Dr. Lee, a fellow in allergy and immunology at the Veterans Affairs Greater Los Angeles Medical Center, and her colleagues retrospectively analyzed a subset of data from a previous observational study of the correlation between the Medication Adherence Report ScaleAsthma (MARSA) and other asthma control metrics. They used answers to 10 questions in 283 MARSA surveys completed by the adults (aged 46-77 years) and in 190 MARSA surveys completed by children (aged 4-11 years) during multiple health care visits between June 2010 and May 2011.
The first of the 10 questions asked patients how often they forget to take their asthma medication, and answers were considered indicative of unintentional nonadherence. The other nine questions were used as proxies for intentional nonadherence, including asking how often patients "stop taking it for awhile," "decide to miss a dose," "try to avoid using it," "only use it when I feel breathless," "alter the dose," "use it for a reserve" if other treatments don’t work, "use it before doing something which might make me breathless," "take it less than instructed," or "use it when I need it."
The results suggest that both adult and pediatric patients are more likely to be unintentionally nonadherent to asthma therapy than intentionally adherent, according to statistical analyses using Cronbach’s alpha, nonparametric one-way analysis of variance, and a pairwise comparison using the Bonferroni approach to determine differences between answers to the questions, .
The current analysis excluded patients with chronic obstructive pulmonary disease, other confounding comorbidities, or an inability to perform spirometry or to complete the questionnaire.
Dr. Lee reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – When patients do not take their asthma medication, it’s usually because they forgot and not because they intentionally made a change in their treatment regimen, a retrospective study of data on 108 adults and 156 children found.
The role of forgetfulness in nonadherence emphasizes the importance of interventions such as text messages, smart inhalers with reminder systems, or Web-based reminder programs to reduce the risk of exacerbations, Dr. Joyce Xiang Wu Lee said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Dr. Lee, a fellow in allergy and immunology at the Veterans Affairs Greater Los Angeles Medical Center, and her colleagues retrospectively analyzed a subset of data from a previous observational study of the correlation between the Medication Adherence Report ScaleAsthma (MARSA) and other asthma control metrics. They used answers to 10 questions in 283 MARSA surveys completed by the adults (aged 46-77 years) and in 190 MARSA surveys completed by children (aged 4-11 years) during multiple health care visits between June 2010 and May 2011.
The first of the 10 questions asked patients how often they forget to take their asthma medication, and answers were considered indicative of unintentional nonadherence. The other nine questions were used as proxies for intentional nonadherence, including asking how often patients "stop taking it for awhile," "decide to miss a dose," "try to avoid using it," "only use it when I feel breathless," "alter the dose," "use it for a reserve" if other treatments don’t work, "use it before doing something which might make me breathless," "take it less than instructed," or "use it when I need it."
The results suggest that both adult and pediatric patients are more likely to be unintentionally nonadherent to asthma therapy than intentionally adherent, according to statistical analyses using Cronbach’s alpha, nonparametric one-way analysis of variance, and a pairwise comparison using the Bonferroni approach to determine differences between answers to the questions, .
The current analysis excluded patients with chronic obstructive pulmonary disease, other confounding comorbidities, or an inability to perform spirometry or to complete the questionnaire.
Dr. Lee reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – When patients do not take their asthma medication, it’s usually because they forgot and not because they intentionally made a change in their treatment regimen, a retrospective study of data on 108 adults and 156 children found.
The role of forgetfulness in nonadherence emphasizes the importance of interventions such as text messages, smart inhalers with reminder systems, or Web-based reminder programs to reduce the risk of exacerbations, Dr. Joyce Xiang Wu Lee said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Dr. Lee, a fellow in allergy and immunology at the Veterans Affairs Greater Los Angeles Medical Center, and her colleagues retrospectively analyzed a subset of data from a previous observational study of the correlation between the Medication Adherence Report ScaleAsthma (MARSA) and other asthma control metrics. They used answers to 10 questions in 283 MARSA surveys completed by the adults (aged 46-77 years) and in 190 MARSA surveys completed by children (aged 4-11 years) during multiple health care visits between June 2010 and May 2011.
The first of the 10 questions asked patients how often they forget to take their asthma medication, and answers were considered indicative of unintentional nonadherence. The other nine questions were used as proxies for intentional nonadherence, including asking how often patients "stop taking it for awhile," "decide to miss a dose," "try to avoid using it," "only use it when I feel breathless," "alter the dose," "use it for a reserve" if other treatments don’t work, "use it before doing something which might make me breathless," "take it less than instructed," or "use it when I need it."
The results suggest that both adult and pediatric patients are more likely to be unintentionally nonadherent to asthma therapy than intentionally adherent, according to statistical analyses using Cronbach’s alpha, nonparametric one-way analysis of variance, and a pairwise comparison using the Bonferroni approach to determine differences between answers to the questions, .
The current analysis excluded patients with chronic obstructive pulmonary disease, other confounding comorbidities, or an inability to perform spirometry or to complete the questionnaire.
Dr. Lee reported having no financial disclosures.
On Twitter @sherryboschert
AT 2014 AAAAI ANNUAL MEETING
Major finding: Adults and children were more likely to report unintentional than intentional nonadherence to asthma therapy.
Data source: Retrospective statistical analysis of answers to 10 survey questions completed by 108 adults and 156 children with asthma during multiple health care visits.
Disclosures: Dr. Lee reported having no financial disclosures.

FDA panel backs approval of inhaled insulin for type 1 and 2 diabetes
HYATTSVILLE, MD. – Inhaled insulin will probably become available as a treatment option again, with a Food and Drug Administration advisory panel’s recommendation to approve an orally administered dry powder recombinant insulin formulation for the treatment of both type 1 and type 2 diabetes.
At a meeting on April 1, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee voted 13-1 that the safety and efficacy data for the inhaled insulin, delivered with an inhaler, supported approval for treatment of adults with type 1 diabetes; they voted 14-0 that the data supported approval for treatment of adults with type 2 diabetes. Panelists had unresolved concerns about safety, including the potential for lung cancer and adverse pulmonary effects, acute bronchospasm in people with asthma, and deteriorating pulmonary function over time, which they said should be closely monitored after approval.

Panelists also pointed out that the results of phase III trials indicated that the inhaled insulin product was not as effective as traditional insulin, and that it would not be appropriate for all patients with type 1 and type 2 diabetes. They did note, however, that there was a need for more treatment options and that an inhaled insulin could be useful for certain groups of patients, such as elderly or disabled patients who have physical impairments and have difficulties with injectable insulin and patients who refuse to use needles – and when a dose of insulin is needed to lower blood glucose between meals.
The proposed indication for the Technosphere insulin inhalation system – which provides insulin in cartridges, delivered with the "Gen2" inhaler – is to improve glycemic control in adults with type 1 or type 2 diabetes. The system’s rapid-acting insulin works faster and has a shorter duration of action than regular human insulin or rapid-acting analog insulins, according to the manufacturer, MannKind Corp.
It is administered immediately before or within the first 20 minutes of starting a meal and is used with basal insulin in patients with type 1 diabetes, and it can be used with oral glucose-lowering medications or basal insulin in patients with type 2 diabetes, according to the company, which plans to market the product as Afrezza if approved.
The orally inhaled insulin marketed as Exubera was approved by the FDA in January 2006 for treating adults with type 1 and 2 diabetes, but Pfizer took it off the market in 2007 because of poor sales.

The FDA rejected the approval of the MannKind inhaled insulin twice before because of issues with efficacy and the device, and it asked the company to conduct two new phase III studies with a new inhaler.
In the study of patients with type 1 diabetes, those treated with Afrezza had a mean 0.20–percentage point drop in HbA1c from baseline at 24 weeks, compared with a 0.42–percentage point drop among those on insulin aspart. In the study of patients with type 2 diabetes who were on metformin or at least two other oral diabetes drugs, those treated with Afrezza had a mean 0.84–percentage point drop in HbA1c from baseline, compared with 0.41 at 24 weeks in those on placebo. In trials, the most common adverse events were a dry, transient cough and transient changes in pulmonary function. Lung cancer rates were similar to what would be expected in the general population, according to the company. Hypoglycemia was slightly lower among those on Afrezza in both studies.
There have been four lung cancers in patients treated with Afrezza in clinical trials, including two cases in patients with no smoking history. Since the product delivers a high level of insulin to the lungs, and insulin may activate growth receptors in the lungs, the panel agreed this was a significant issue that should be followed in postmarketing studies. The company has proposed a prospective observational registry of patients to track the incidence of primary lung cancers, as well as other malignancies and serious pulmonary, allergic, and hypoglycemic events that require medical intervention. Labeling would recommend that spirometry be done every 6 months during treatment.
Voting for approval, panel chair Dr. Robert Smith, professor of medicine at Brown University, Providence, R.I., said that inhaled insulin "represents a drug that will serve some patients that are not effectively served by currently available forms of insulin." The data about the potentially serious adverse effects "were not strong enough that I feel it is imperative to resolve those questions" before marketing, he added, but stressed that these safety issues, including the potential for lung cancer and deteriorating lung function, are "very, very important to follow up."
The panelist who voted against approval for type 1diabetes, Dr. David Cooke, clinical director of the division of pediatric endocrinology at Johns Hopkins University, Baltimore, said he was concerned that the risks outweighed the benefits in this group of patients, particularly because of the potential increased risk of cancer. But he said he was more confident about the risk-benefit profile for patients with type 2 diabetes because they would not be exposed to the drug for as long as patients with type 1 diabetes, and that the inhaled insulin may provide some type 2 patients who might otherwise put off taking insulin with a more acceptable and effective option.
The FDA extended the date for completing the review by three months, so the agency can fully review additional information requested from the company, according to a MannKind statement issued April 7.
This article was updated April 7, 2014.
HYATTSVILLE, MD. – Inhaled insulin will probably become available as a treatment option again, with a Food and Drug Administration advisory panel’s recommendation to approve an orally administered dry powder recombinant insulin formulation for the treatment of both type 1 and type 2 diabetes.
At a meeting on April 1, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee voted 13-1 that the safety and efficacy data for the inhaled insulin, delivered with an inhaler, supported approval for treatment of adults with type 1 diabetes; they voted 14-0 that the data supported approval for treatment of adults with type 2 diabetes. Panelists had unresolved concerns about safety, including the potential for lung cancer and adverse pulmonary effects, acute bronchospasm in people with asthma, and deteriorating pulmonary function over time, which they said should be closely monitored after approval.
Panelists also pointed out that the results of phase III trials indicated that the inhaled insulin product was not as effective as traditional insulin, and that it would not be appropriate for all patients with type 1 and type 2 diabetes. They did note, however, that there was a need for more treatment options and that an inhaled insulin could be useful for certain groups of patients, such as elderly or disabled patients who have physical impairments and have difficulties with injectable insulin and patients who refuse to use needles – and when a dose of insulin is needed to lower blood glucose between meals.
The proposed indication for the Technosphere insulin inhalation system – which provides insulin in cartridges, delivered with the "Gen2" inhaler – is to improve glycemic control in adults with type 1 or type 2 diabetes. The system’s rapid-acting insulin works faster and has a shorter duration of action than regular human insulin or rapid-acting analog insulins, according to the manufacturer, MannKind Corp.
It is administered immediately before or within the first 20 minutes of starting a meal and is used with basal insulin in patients with type 1 diabetes, and it can be used with oral glucose-lowering medications or basal insulin in patients with type 2 diabetes, according to the company, which plans to market the product as Afrezza if approved.
The orally inhaled insulin marketed as Exubera was approved by the FDA in January 2006 for treating adults with type 1 and 2 diabetes, but Pfizer took it off the market in 2007 because of poor sales.
The FDA rejected the approval of the MannKind inhaled insulin twice before because of issues with efficacy and the device, and it asked the company to conduct two new phase III studies with a new inhaler.
In the study of patients with type 1 diabetes, those treated with Afrezza had a mean 0.20–percentage point drop in HbA1c from baseline at 24 weeks, compared with a 0.42–percentage point drop among those on insulin aspart. In the study of patients with type 2 diabetes who were on metformin or at least two other oral diabetes drugs, those treated with Afrezza had a mean 0.84–percentage point drop in HbA1c from baseline, compared with 0.41 at 24 weeks in those on placebo. In trials, the most common adverse events were a dry, transient cough and transient changes in pulmonary function. Lung cancer rates were similar to what would be expected in the general population, according to the company. Hypoglycemia was slightly lower among those on Afrezza in both studies.
There have been four lung cancers in patients treated with Afrezza in clinical trials, including two cases in patients with no smoking history. Since the product delivers a high level of insulin to the lungs, and insulin may activate growth receptors in the lungs, the panel agreed this was a significant issue that should be followed in postmarketing studies. The company has proposed a prospective observational registry of patients to track the incidence of primary lung cancers, as well as other malignancies and serious pulmonary, allergic, and hypoglycemic events that require medical intervention. Labeling would recommend that spirometry be done every 6 months during treatment.
Voting for approval, panel chair Dr. Robert Smith, professor of medicine at Brown University, Providence, R.I., said that inhaled insulin "represents a drug that will serve some patients that are not effectively served by currently available forms of insulin." The data about the potentially serious adverse effects "were not strong enough that I feel it is imperative to resolve those questions" before marketing, he added, but stressed that these safety issues, including the potential for lung cancer and deteriorating lung function, are "very, very important to follow up."
The panelist who voted against approval for type 1diabetes, Dr. David Cooke, clinical director of the division of pediatric endocrinology at Johns Hopkins University, Baltimore, said he was concerned that the risks outweighed the benefits in this group of patients, particularly because of the potential increased risk of cancer. But he said he was more confident about the risk-benefit profile for patients with type 2 diabetes because they would not be exposed to the drug for as long as patients with type 1 diabetes, and that the inhaled insulin may provide some type 2 patients who might otherwise put off taking insulin with a more acceptable and effective option.
The FDA extended the date for completing the review by three months, so the agency can fully review additional information requested from the company, according to a MannKind statement issued April 7.
This article was updated April 7, 2014.
HYATTSVILLE, MD. – Inhaled insulin will probably become available as a treatment option again, with a Food and Drug Administration advisory panel’s recommendation to approve an orally administered dry powder recombinant insulin formulation for the treatment of both type 1 and type 2 diabetes.
At a meeting on April 1, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee voted 13-1 that the safety and efficacy data for the inhaled insulin, delivered with an inhaler, supported approval for treatment of adults with type 1 diabetes; they voted 14-0 that the data supported approval for treatment of adults with type 2 diabetes. Panelists had unresolved concerns about safety, including the potential for lung cancer and adverse pulmonary effects, acute bronchospasm in people with asthma, and deteriorating pulmonary function over time, which they said should be closely monitored after approval.
Panelists also pointed out that the results of phase III trials indicated that the inhaled insulin product was not as effective as traditional insulin, and that it would not be appropriate for all patients with type 1 and type 2 diabetes. They did note, however, that there was a need for more treatment options and that an inhaled insulin could be useful for certain groups of patients, such as elderly or disabled patients who have physical impairments and have difficulties with injectable insulin and patients who refuse to use needles – and when a dose of insulin is needed to lower blood glucose between meals.
The proposed indication for the Technosphere insulin inhalation system – which provides insulin in cartridges, delivered with the "Gen2" inhaler – is to improve glycemic control in adults with type 1 or type 2 diabetes. The system’s rapid-acting insulin works faster and has a shorter duration of action than regular human insulin or rapid-acting analog insulins, according to the manufacturer, MannKind Corp.
It is administered immediately before or within the first 20 minutes of starting a meal and is used with basal insulin in patients with type 1 diabetes, and it can be used with oral glucose-lowering medications or basal insulin in patients with type 2 diabetes, according to the company, which plans to market the product as Afrezza if approved.
The orally inhaled insulin marketed as Exubera was approved by the FDA in January 2006 for treating adults with type 1 and 2 diabetes, but Pfizer took it off the market in 2007 because of poor sales.
The FDA rejected the approval of the MannKind inhaled insulin twice before because of issues with efficacy and the device, and it asked the company to conduct two new phase III studies with a new inhaler.
In the study of patients with type 1 diabetes, those treated with Afrezza had a mean 0.20–percentage point drop in HbA1c from baseline at 24 weeks, compared with a 0.42–percentage point drop among those on insulin aspart. In the study of patients with type 2 diabetes who were on metformin or at least two other oral diabetes drugs, those treated with Afrezza had a mean 0.84–percentage point drop in HbA1c from baseline, compared with 0.41 at 24 weeks in those on placebo. In trials, the most common adverse events were a dry, transient cough and transient changes in pulmonary function. Lung cancer rates were similar to what would be expected in the general population, according to the company. Hypoglycemia was slightly lower among those on Afrezza in both studies.
There have been four lung cancers in patients treated with Afrezza in clinical trials, including two cases in patients with no smoking history. Since the product delivers a high level of insulin to the lungs, and insulin may activate growth receptors in the lungs, the panel agreed this was a significant issue that should be followed in postmarketing studies. The company has proposed a prospective observational registry of patients to track the incidence of primary lung cancers, as well as other malignancies and serious pulmonary, allergic, and hypoglycemic events that require medical intervention. Labeling would recommend that spirometry be done every 6 months during treatment.
Voting for approval, panel chair Dr. Robert Smith, professor of medicine at Brown University, Providence, R.I., said that inhaled insulin "represents a drug that will serve some patients that are not effectively served by currently available forms of insulin." The data about the potentially serious adverse effects "were not strong enough that I feel it is imperative to resolve those questions" before marketing, he added, but stressed that these safety issues, including the potential for lung cancer and deteriorating lung function, are "very, very important to follow up."
The panelist who voted against approval for type 1diabetes, Dr. David Cooke, clinical director of the division of pediatric endocrinology at Johns Hopkins University, Baltimore, said he was concerned that the risks outweighed the benefits in this group of patients, particularly because of the potential increased risk of cancer. But he said he was more confident about the risk-benefit profile for patients with type 2 diabetes because they would not be exposed to the drug for as long as patients with type 1 diabetes, and that the inhaled insulin may provide some type 2 patients who might otherwise put off taking insulin with a more acceptable and effective option.
The FDA extended the date for completing the review by three months, so the agency can fully review additional information requested from the company, according to a MannKind statement issued April 7.
This article was updated April 7, 2014.
AT AN FDA ADVISORY PANEL MEETING

It’s Time to Use an Age-based Approach to D-dimer
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
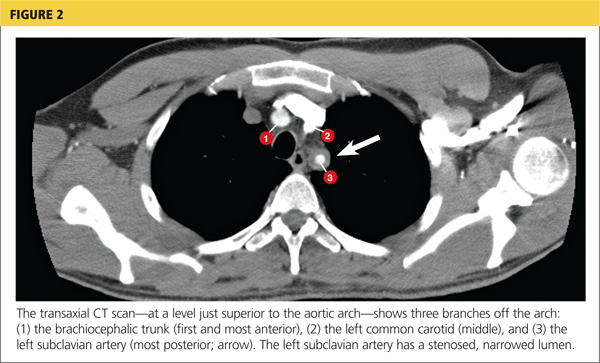
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
Unusual Case of Chest and Left Arm Pain
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
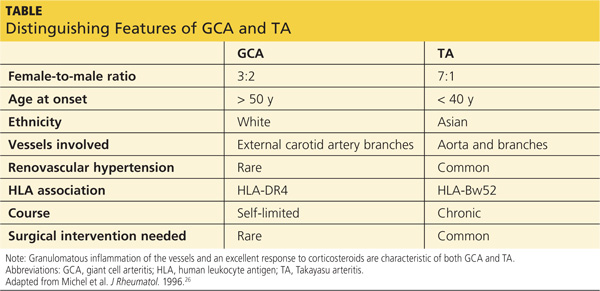
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.
A 37-year-old white man presented to his primary care provider’s office for follow-up after a visit to the emergency department (ED). He had been evaluated at a local ED a week earlier for atypical chest pain and left arm pain. At the ED, blood work was done, along with an ECG, chest x-ray, and chest CT scan, but the results of these evaluations were not available during his initial primary care visit. On discharge from the ED, he was told that his heart was not the cause of his pain and that he should follow up with his primary care provider.
In the office, the patient reported that for the past several months he had been experiencing pain in his left arm when doing heavy or continuous physical labor; he noted that his job as a laborer required vigorous activity. Rest seemed to make his pain go away. He denied pain in the right arm or being awakened by the pain at night. Review of systems was unremarkable, and medical and surgical history was negative.
On physical exam, inspection of his torso and upper and lower extremities did not reveal any apparent abnormalities. Left shoulder and neck exams were normal. Cardiac auscultation was unremarkable, but palpation of the left upper extremity revealed neither a brachial, radial, nor ulnar pulse. Pulses in his right upper extremity were within normal limits. No bruits were appreciated over the carotids or either subclavian artery. Basic Doppler ultrasound over the left upper extremity at the brachial, radial, and ulnar sites showed symmetrical Doppler sounds. The remainder of his exam was unremarkable.
The patient’s ED documents and imaging results were received later in the day, after his office visit. The ECG, blood work results, and chest x-ray were normal. The chest CT results showed no evidence of pulmonary embolism. The radiologist did note mild narrowing at the left subclavian artery secondary to nonspecific surrounding soft tissue, which was noted to possibly represent intramural hemorrhage or atherosclerotic changes. No intimal flap was identified.
Because the diagnosis remained unclear, the patient was asked to bring the disc containing his chest CT images to the office. The radiologist, who was informed about the patient’s history and exam findings by phone, reviewed the CT images and felt there were changes surrounding the three branches off the aortic arch suggestive of inflammation, in addition to the stenosis at the left subclavian artery (see Figure 1 and Figure 2).
Based on the radiologist’s interpretation, additional lab tests were ordered. A complete blood count, comprehensive metabolic panel, prothrombin time/partial thromboplastin time, and lipid panel all yielded results within normal limits. Erythrocyte sedimentation rate (ESR) was 12 mm/h (reference range, 0 to 15 mm/h) and C-reactive protein (CRP) level was 4.9 mg/dL (reference range, 0.1 to 4.9 mg/dL). These laboratory results were essentially unremarkable, and therefore made his diagnosis more elusive.
The patient was referred to a vascular surgeon because of his immediate symptoms. The surgeon performed a thoracic outlet study in which Doppler waveform analysis of the left brachial, radial, and ulnar arteries of the thoracic outlet were analyzed during range-of-motion testing. Results suggested the possibility of thoracic outlet syndrome involving the left upper extremity, with significant baseline arterial insufficiency. A CT angiogram showed critical stenosis of the left subclavian artery and arterial wall thickening. Inflammatory changes were noted as well, and concern for “an inflammatory vasculitis” was described on the CT angiogram. The patient underwent left carotid-to-axillary bypass grafting, after which his left arm pain improved.
Following surgery, the patient returned to the primary care office for evaluation. Although the surgery was successful, the diagnosis was still not clear, requiring additional medical evaluation. The physical exam showed normal pulses in his left upper extremity. Lab tests revealed an elevated ESR of 54 mm/h and a CRP level of 4 mg/dL (reference range, 0.1 to 0.8 mg/dL; a different lab testing site was used, which accounts for the different reference range). In light of the patient’s lab test results, premature arterial vascular disease, and imaging studies suggesting inflammation, Takayasu arteritis (TA) was arrived at as a working diagnosis.
The patient was referred to a rheumatologist, who ordered a repeat ESR and CRP, antineutrophil cytoplasmic antibodies, and a magnetic resonance angiography study of the right brachial artery and major aortic branches to rule out other types of arteritis. Based on the test results, the patient was diagnosed with TA. He was placed on high-dose corticosteroid therapy (prednisone 60 mg/d). Methotrexate 10 mg/wk po was added three months after initiation of the prednisone.
Since being diagnosed with TA, the patient has presented with complaints related to the adverse effects of high-dose corticosteroids (ie, insomnia, weight gain, elevated blood pressure).
Continued on the next page >>
DISCUSSION
The first description of TA is credited to Japanese ophthalmologist Mikito Takayasu, who in 1908 described a wreathlike arteriovenous anastomosis around the optic disc of a 21-year-old woman who had experienced acute vision loss.1-3 Much earlier, in 1761, Italian anatomist Giovanni Battista Morgagni described large-vessel aneurysms and stenosis on a postmortem exam of a 40-year-old woman.2,4 However, TA was not formally labeled a disease until 1975.
TA is a chronic large vessel vasculitis of unknown origin, mainly involving the aorta and its primary branches: the left common carotid, brachiocephalic, and left subclavian arteries. Ongoing inflammation of affected vessels causes fibrotic changes, stenosis, and eventual occlusion and may lead to aneurysm formation.5,6 TA is rare, with an annual incidence in North America of 2.6 cases per million population.6 It occurs most frequently in Asian countries but has been reported in a wide range of ethnic groups.5,7 TA has been characterized as a disease of young women: Between 80% and 97% of patients are women,6,8 and the average age at diagnosis is 25 to 30.8-10
The process of vascular injury in TA begins with inflammation in the vasa vasorum of the aortic vessels. This inflammation, thought to be triggered by an as-yet-unknown antigen, leads to an initial inflammatory cellular infiltration of the aortic media and adventitia; the infiltrate is comprised predominantly of macrophages and T cells.5,9 Inflammatory infiltration causes myointimal proliferation, thickening of the blood vessel wall, and eventual luminal stenosis.5 Cytokines, interleukin 6, interferon , and other chemokines released by infiltrating inflammatory cells within the injured tissue also contribute to the inflammatory response and tissue damage.5,11
Histologically, granulomatous inflammation and giant cells are found in the media.12,13 Destruction of the elastic lamina and the muscular media results in the aneurysmal dilation seen in TA, while dense scarring and continued inflammation of the arterial vasculature results in arterial stenosis.12
Continued on the next page >>
CLINICAL PRESENTATION
Presentation of TA varies widely and can range from asymptomatic disease identified by pulse deficits or impalpable pulses to severe neurologic impairment. The early or prepulseless phase of TA is characterized by inflammatory changes.14 Signs and symptoms are frequently vague and nonspecific, particularly in this early phase, when fatigue, weight loss, and low-grade fever may be seen.12 Headache is another common symptom at the time of disease onset.5
In the later or chronic phase of the disease, individuals will begin to demonstrate signs and symptoms of vascular insufficiency.14 More common physical signs reflect the underlying arterial occlusive disease and include diminished or absent arterial pulses, asymmetrical arm blood pressures, bruits, extremity claudication, and hypertension.5,9,10 Hypertension, generally reflecting renal artery stenosis,10 is present in approximately 40% of cases in the United States and Europe.5,7,15 Neurologic features secondary to hypertension or ischemia affect more than half of patients; in addition to headache, these may include dizziness, syncope, vertigo, transient ischemic attack, and stroke.5
TA can also present with eye, lung, and skin manifestations; however, these features are less common. Although ocular involvement, including amaurosis fugax, has been reported in up to 26% of patients in TA series,5,7,16 permanent loss of vision in North American patients is uncommon.5,7 Pulmonary involvement affecting the large- or medium-sized pulmonary arteries has been reported to occur in approximately 55% of cases5; however, there is uncertainty regarding the prevalence of angiographically demonstrated pulmonary artery involvement, as studies have reported rates ranging from 14.3% to 70%.9,17-20 Pulmonary involvement is often asymptomatic, but features can include dyspnea, cough, and chest pain.5 Skin lesions are seen in up to 28% of cases, most commonly erythema nodosum, erythema induratum, tuberculoidlike eruptions, pyoderma gangrenosum, and cutaneous signs of necrotizing or granulomatous vasculitis.5,21
Continued on the next page >>
DIAGNOSIS
The American College of Rheumatology (ACR) has developed classification criteria for the diagnosis of TA.22 The presence of three or more of the six criteria (age of onset ≤ 40, claudication of the extremities, decreased brachial artery pulse, > 10 mm Hg difference in systolic blood pressure between the arms, bruit over subclavian arteries or aorta, and arteriographic abnormalities) yields a sensitivity of 90.5% and a specificity of 97.8%. Although the ACR classification remains the most widely applied for TA, a limitation of its diagnostic criteria is its failure to distinguish patients with early nonocclusive disease.23
In 1988, the Ishikawa classification criteria were developed, with a modified version subsequently published in 1996.23 Considered superior to the original Ishikawa and ACR criteria based on its application in 106 patients with angiographically proven TA, the modified version has a reported sensitivity and specificity of 92.5% and 95%, respectively.23
With the modified Ishikawa diagnostic criteria, the presence of two major or one major and two or four minor criteria suggests a high probability of TA. The three major criteria consist of lesions of the left mid-subclavian artery and the right mid-subclavian artery and characteristic signs and symptoms of at least 1 mo duration. The 10 minor criteria are high ESR (> 20 mm/h); carotid artery tenderness; hypertension; aortic regurgitation or annuloaortic ectasia; and lesions of pulmonary artery, left mid-common carotid, distal brachiocephalic trunk, descending thoracic aorta, abdominal aorta, and coronary artery.
The diagnosis of TA is based on recognition of clinical findings suggestive of large-vessel vasculitis. Imaging of the arterial tree with CT, MRI, or angiography also demonstrates findings consistent with TA, typically including early-onset vascular wall thickening/enhancement.24 Late imaging studies may reveal arterial stenoses, occlusions, and aneurysms.
Several types of imaging modalities have been used in the diagnosis and management of TA, each with strengths and limitations. Traditional angiography is invasive and requires an arterial puncture. Large doses of radiation are used, exposing the patient to iodinated contrast material, which may be dangerous in patients with poor renal function. However, the primary advantage of traditional angiography is that it allows for interventions such as stent placement and/or angioplasty to be performed.24 Findings on angiography often include long, smooth, tapered stenoses ranging from mild to severe or frank occlusions, as well as collateral vessels or the subclavian steal phenomenon.24
CT imaging is very useful for assessing thickening of the arterial wall. In early TA disease, evaluation of vessel wall thickness may be identified prior to frank stenosis of the artery(s).24 The spectrum of findings on CT angiography includes stenoses; occlusions; aneurysms; and concentric arterial wall thickening affecting the aorta and its branches, the pulmonary arteries, and occasionally the coronary arteries.24
MRI does not require the use of iodinated contrast, nor is there radiation exposure. MRI also has the advantage of evaluating arterial wall thickening, which is often present prior to stenosis (similar to CT imaging).24 Findings of TA on MRI include mural thrombi, signal alterations within and surrounding inflamed vessels, fusiform vascular dilation, thickened aortic valvular cusps, multifocal stenoses, and concentric thickening of the aortic wall.24
Laboratory testing is neither specific nor sensitive. Hoffman and Ahmed studied multiple serologic tests and found that no test reliably distinguishes between patients with active TA and healthy volunteers.25 Increases in the acute phase reactants (ESR and CRP) support the presence of an underlying inflammatory process, and these laboratory tests may be useful in disease monitoring. The ESR and CRP often do not correlate with systemic symptoms or disease progression but are used in conjunction with the clinical exam and serial imaging to gauge treatment success and to monitor disease progression.5,25 Biopsy material typically is not available in the initial diagnosis of TA, but histologic examination at the time of a surgery or procedure is often undertaken to confirm the diagnosis.5
The differential diagnosis of TA includes connective tissue diseases associated with the formation of multiple aneurysms, such as Marfan syndrome and Ehlers-Danlos syndrome.5 However, these diseases do not manifest with large vessel stenosis, the hallmark of TA. Infections known to cause aneurysms of the aorta should also be considered; these include bacterial, fungal, syphilitic, mycotic, and mycobacterial pathogens.5 Blood cultures are used to rule out bacterial agents. Rapid plasma reagin (RPR) and venereal disease research laboratory tests (VDRL) will identify a syphilitic etiology. Fungal cultures or fungal serology will help to rule out a mycotic pathogen.
Autoimmune diseases that can mimic TA include Behçet’s disease, Cogan syndrome, the spondyloarthropathies, and systemic lupus erythematosus. These diseases are not associated with stenosis of large vessels, which differentiates them from TA.5 Giant cell (temporal) arteritis (GCA) may present very similarly to TA, as both diseases affect large arteries.12 The table provides distinguishing features of TA and GCA.26
Continued on the next page >>
TREATMENT
Active phase TA is initially treated with high-dose glucocorticoid therapy (prednisone or methylprednisolone). Typical prednisone doses are 0.5 to 1 mg/kg/d.5 Clinical improvement is seen in almost all patients with glucocorticoid therapy,6,10,23 but relapse is common when prednisone is tapered to less than 20 mg/d.5 The corticosteroid dose is gradually tapered depending on patient response. Common side effects of corticosteroids may include weight gain, elevations in blood glucose, insomnia, increased infection risk, osteoporosis, and slowing of wound healing.
Because nearly half of all patients treated with glucocorticoids alone demonstrate chronic active disease, immunosuppressive therapies are almost always used concomitantly.27 Immune-suppressing drugs that may be used include methotrexate (15 to 25 mg/wk), azathioprine (2 mg/kg/d), and cyclophosphamide (1 to 2 mg/kg/d orally).5,28 Tumor necrosis factor (TNF)–blocking agents used to treat TA include etanercept, infliximab, or adalimumab.28,29 Adverse effects associated with immunosuppressive therapies and TNF-blocking agents include an increased risk for infection(s) and malignancy, bone marrow suppression, and hepatitis B reactivation. Although data are limited on anti-TNF agents, this class of drug has shown promise when used in conjunction with corticosteroids.28
In one open-label study by Hoffman and colleagues, remission rates with methotrexate plus steroids were 81%. Relapse occurred in 44% of study participants when the steroid dose was tapered or decreased to near discontinuation.27 More recently, in an uncontrolled study series involving 15 TA patients from India who were treated with azathioprine plus steroids, remission was achieved following 12 weeks of therapy. Angiographically, there was no progression of arterial disease after one year.30
Surgical and endovascular procedures used to return blood flow in stenotic or occluded vessels include synthetic or autologous vessel bypass, endarterectomy, and percutaneous transluminal angioplasty.5 When aortic insufficiency is present, aortic root replacement or repair is undertaken.5 These procedures are performed by vascular or cardiovascular surgeons and interventional radiologists. Rheumatologists are the medical specialists most involved in the direct care and management of TA patients. Cardiologists are sometimes consulted as well.
Continued on the next page >>
PROGNOSIS
Disability is common in TA. In a National Institutes of Health cohort study, 74% of TA patients reported experiencing functional effects from their disease, and 47% were fully disabled.2,8 In their retrospective review of 107 cases of TA, Lupi-Herrera and colleagues reported a 14% mortality rate.31 Half the deaths in this study were attributed to congestive heart failure (CHF). A cohort study in India that included 88 patients with TA reported cumulative 5- and 10-year survival rates of 91% and 84%, respectively. Of the 10 deaths in this cohort, four were due to CHF.2,32
CONCLUSION
Signs and symptoms of rheumatologic diseases such as TA are often vague, and diagnosis may prove difficult and elusive. Repeat office visits at short intervals may prove to be helpful in making the diagnosis. Referral for radiology and/or rheumatology consultation (face-to-face, if possible) is often necessary.
In cases such as this, completing a personal review of documents and test results done elsewhere, particularly ED/inpatient hospital data, is necessary; relying on the patient’s word that “they told me everything was fine” is insufficient. Clinicians should implement a system that works best for obtaining test results and other documents, follow their instincts, and if the correct diagnosis is not arrived at immediately, keep looking.
References >>
REFERENCES
1. Takayasu M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophthalmol Jpn. 1908;12:554-555.
2. Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: what is the long-term prognosis? Rheum Dis Clin North Am. 2007;33:777-786.
3. Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103-106.
4. Morgagni GB. De sedibus et causis morborum per anatomen indagatis.
(Letter 30).1761. Article 12.
5. Hernandez-Rodriguez J, Maksimowicz-McKinnon K, Hoffman GS. Takayasu’s arteritis. In: Carey WD, ed. Current Clinical Medicine. 2nd ed. Philadelphia: Saunders Elsevier; 2010:1195-1199.
6. Hall S, Barr W, Lie JT, et al. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore). 1985;64:89-99.
7. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Limitations of therapy and a guarded prognosis in an American cohort of Takayasu arteritis patients. Arthritis Rheum. 2007;56:1000-1009.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994:120:919-929.
9. Gornik HL, Creager MA. Aortic diseases: aortitis. Circulation. 2008;117:
3039-3051.
10. Mwipatayi BP, Jeffery PC, Beningfield SJ, et al. Takayasu arteritis: clinical features and management: report of 272 cases. ANZ J Surg. 2005;75:110-117.
11. Noris M. Pathogenesis of Takayasu’s arteritis. J Nephrol. 2001;14:506-513.
12. Hunder GG, Stone JH, Ramirez MP. Clinical features and diagnosis of Takayasu arteritis (2013). www.uptodate.com/contents/clinical-features-and-
diagnosis-of-takayasu-arteritis. Accessed March 24, 2014.
13. Nasu T. Takayasu’s truncoarteritis. Pulseless disease or aortitis syndrome. Acta Pathol Jpn. 1982;32 (suppl 1):117.
14. Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. J Clin Pathol. 2002;55:481-486.
15. Vanoli M, Daina E, Salvarani C, et al. Takayasu’s arteritis: a study of 104 Italian patients. Arthritis Rheum. 2005;53:100-107.
16. Chun YS, Park SJ, Chung H, Lee J. The clinical and ocular manifestations of Takayasu’s arteritis. Retina. 2001;21:132-140.
17. Liu YQ, Jin BL, Ling J. Pulmonary artery involvement in aortoarteritis: an angiographic study. Cardiovasc Intervent Radiol. 1994;17:2-6.
18. Yamada I, Shibuya H, Matsubara O, et al. Pulmonary artery disease in Takayasu’s arteritis: angiographic findings. AJR Am J Roentgenol. 1992;159:
263-269.
19. Sharma S, Kamalakar T, Rajani M, et al. The incidence and patterns of pulmonary artery involvement in Takayasu’s arteritis. Clin Radiol. 1990;42:177-181.
20. He NS, Liu F, Wu EH, et al. Pulmonary artery involvement in aorto-arteritis: an analysis of DSA. Chin Med J (Engl). 1990;103:666-672.
21. Werfel T, Kuipers JG, Zeidler H, et al. Cutaneous manifestations of Takayasu arteritis. Acta Derm Venereol. 1996;76:496-497.
22. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129-1134.
23. Andrews J, Mason JC. Takayasu’s arteritis—recent advances in imaging offer promise. Rheumatology (Oxford). 2007;46:6-15.
24. Gotway MB, Araoz PA, Macedo TA, et al. Imaging findings in Takayasu’s arteritis. AJR Am J Roentgenol. 2005;184:1945-1950.
25. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998;66 (suppl 1):S191-S194.
26. Michel BA, Arend WP, Hunder GG. Clinical differentiation between giant cell (temporal) arteritis and Takayasu’s arteritis. J Rheumatol. 1996;23:106-111.
27. Hoffman GS, Leavitt RY, Kerr GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582.
28. Hunder GG, Stone JH, Ramirez MP. Treatment of Takayasu arteritis (2013). www.uptodate.com/contents/treatment-of-takayasu-arteritis. Accessed March 24, 2014.
29. Schmidt J, Kerman TA, Bacani AK, et al. Tumor necrosis factor inhibitors in patients with Takayasu arteritis: experience from a referral center with long-term followup. Arthritis Care Res (Hoboken). 2012;64:1079-1083.
30. Valsakumar AK, Valappil UC, Jorapur V, et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:1793-1798.
31. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J. 1977;93:94-103.
32. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu’s disease). Circulation. 1989;80:429-437.

VIDEO: Study highlights progress, challenges in nosocomial infections
One in 25 hospitalized patients on any given day has an infection acquired from health care, and as many as 1 in 9 of those will die.
At a press briefing, Dr. Michael Bell discussed new data from a prevalence study conducted by the Centers for Disease Control and Prevention, where he is the deputy director for the division of health care quality promotion. Hospitals, doctors, and patients all have a role to play in decreasing the risks of these infections, he said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
This article was updated 3/28/2014.
One in 25 hospitalized patients on any given day has an infection acquired from health care, and as many as 1 in 9 of those will die.
At a press briefing, Dr. Michael Bell discussed new data from a prevalence study conducted by the Centers for Disease Control and Prevention, where he is the deputy director for the division of health care quality promotion. Hospitals, doctors, and patients all have a role to play in decreasing the risks of these infections, he said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
This article was updated 3/28/2014.
One in 25 hospitalized patients on any given day has an infection acquired from health care, and as many as 1 in 9 of those will die.
At a press briefing, Dr. Michael Bell discussed new data from a prevalence study conducted by the Centers for Disease Control and Prevention, where he is the deputy director for the division of health care quality promotion. Hospitals, doctors, and patients all have a role to play in decreasing the risks of these infections, he said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
This article was updated 3/28/2014.
FROM THE CDC
Smoking bans see 10% declines in preterm births, asthma flares in children
A systematic review and meta-analysis from North America and Europe has found that the introduction of antismoking legislation covering workplaces and public spaces is associated with significant reductions of about 10% in both preterm births and pediatric hospital visits for asthma.
The findings, published online March 27 in the Lancet, also suggest that significant health benefits and associated public-health cost savings from smoking bans may be reaped beginning in the first year after antismoking legislation takes hold (doi:10.1016/S0140-6736[14]60082-9).

For their research, Jasper V. Been, Ph.D., of Maastricht University, the Netherlands, and his colleagues, evaluated 11 studies (5 from North America and 6 from European countries) published during 2008 and 2013. The included studies captured 247,168 million asthma exacerbations and about 2.5 million births. In these study areas, which fell within either local or national bans on smoking in the workplace, public places, and/or restaurants and bars, bans were followed by significant drops in preterm births (–10.4%) and childhood emergency department visits and hospital attendances (–10.1%).
Low birth weight was not seen as significantly changed in Dr. Been and his colleagues’ study (–1.7%; P = .31), but the researchers did see about a 5% decline in children born very small for their gestational age.
For several of the included studies, the drops were immediate. Significant drops in preterm births of 3% or more were seen in the first year following the implementation of some bans, with additional gradual declines occurring in subsequent years. With hospital visits for pediatric asthma, some studies saw drops as high as 20% per year after bans.
In an editorial comment accompanying the study, Dr. Sara Kalkhoran and Stanton A. Glantz, Ph.D., of the University of California, San Francisco, wrote that the findings add to a growing body of evidence that "smoke-free laws bring rapid health benefits and improved lives, whilst, at the same time, reducing medical costs by avoiding emergency department visits and admissions to hospitals."
Dr. Been and his colleagues’ study was funded by the Thrasher Fund, Lung Foundation Netherlands, the International Pediatric Research Fund, Commonwealth Fund, and Maastricht University. None of the study authors or editorial writers declared conflicts of interest.
A systematic review and meta-analysis from North America and Europe has found that the introduction of antismoking legislation covering workplaces and public spaces is associated with significant reductions of about 10% in both preterm births and pediatric hospital visits for asthma.
The findings, published online March 27 in the Lancet, also suggest that significant health benefits and associated public-health cost savings from smoking bans may be reaped beginning in the first year after antismoking legislation takes hold (doi:10.1016/S0140-6736[14]60082-9).
For their research, Jasper V. Been, Ph.D., of Maastricht University, the Netherlands, and his colleagues, evaluated 11 studies (5 from North America and 6 from European countries) published during 2008 and 2013. The included studies captured 247,168 million asthma exacerbations and about 2.5 million births. In these study areas, which fell within either local or national bans on smoking in the workplace, public places, and/or restaurants and bars, bans were followed by significant drops in preterm births (–10.4%) and childhood emergency department visits and hospital attendances (–10.1%).
Low birth weight was not seen as significantly changed in Dr. Been and his colleagues’ study (–1.7%; P = .31), but the researchers did see about a 5% decline in children born very small for their gestational age.
For several of the included studies, the drops were immediate. Significant drops in preterm births of 3% or more were seen in the first year following the implementation of some bans, with additional gradual declines occurring in subsequent years. With hospital visits for pediatric asthma, some studies saw drops as high as 20% per year after bans.
In an editorial comment accompanying the study, Dr. Sara Kalkhoran and Stanton A. Glantz, Ph.D., of the University of California, San Francisco, wrote that the findings add to a growing body of evidence that "smoke-free laws bring rapid health benefits and improved lives, whilst, at the same time, reducing medical costs by avoiding emergency department visits and admissions to hospitals."
Dr. Been and his colleagues’ study was funded by the Thrasher Fund, Lung Foundation Netherlands, the International Pediatric Research Fund, Commonwealth Fund, and Maastricht University. None of the study authors or editorial writers declared conflicts of interest.
A systematic review and meta-analysis from North America and Europe has found that the introduction of antismoking legislation covering workplaces and public spaces is associated with significant reductions of about 10% in both preterm births and pediatric hospital visits for asthma.
The findings, published online March 27 in the Lancet, also suggest that significant health benefits and associated public-health cost savings from smoking bans may be reaped beginning in the first year after antismoking legislation takes hold (doi:10.1016/S0140-6736[14]60082-9).
For their research, Jasper V. Been, Ph.D., of Maastricht University, the Netherlands, and his colleagues, evaluated 11 studies (5 from North America and 6 from European countries) published during 2008 and 2013. The included studies captured 247,168 million asthma exacerbations and about 2.5 million births. In these study areas, which fell within either local or national bans on smoking in the workplace, public places, and/or restaurants and bars, bans were followed by significant drops in preterm births (–10.4%) and childhood emergency department visits and hospital attendances (–10.1%).
Low birth weight was not seen as significantly changed in Dr. Been and his colleagues’ study (–1.7%; P = .31), but the researchers did see about a 5% decline in children born very small for their gestational age.
For several of the included studies, the drops were immediate. Significant drops in preterm births of 3% or more were seen in the first year following the implementation of some bans, with additional gradual declines occurring in subsequent years. With hospital visits for pediatric asthma, some studies saw drops as high as 20% per year after bans.
In an editorial comment accompanying the study, Dr. Sara Kalkhoran and Stanton A. Glantz, Ph.D., of the University of California, San Francisco, wrote that the findings add to a growing body of evidence that "smoke-free laws bring rapid health benefits and improved lives, whilst, at the same time, reducing medical costs by avoiding emergency department visits and admissions to hospitals."
Dr. Been and his colleagues’ study was funded by the Thrasher Fund, Lung Foundation Netherlands, the International Pediatric Research Fund, Commonwealth Fund, and Maastricht University. None of the study authors or editorial writers declared conflicts of interest.
FROM THE LANCET

Sinus surgery: new rigor in research
KEYSTONE, COLO. – Research-minded otolaryngologists have gotten serious about conducting high-quality, patient-centered outcomes studies of endoscopic sinus surgery for chronic rhinosinusitis, which more than 250,000 Americans undergo each year. And the results are eye opening.
Mounting evidence documents that endoscopic sinus surgery (ESS) in properly selected patients with chronic rhinosinusitis (CRS) results in markedly improved quality of life, functional status, and reduced use of medications, compared with medical management, Dr. Todd T. Kingdom said at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
These studies utilize validated measures of patient-centered quality of life and symptoms. They are nothing like the lightweight, less-than-persuasive ESS research published in the 1990s, which reported glowing ‘success’ rates of 80%-97% in single-institution retrospective studies using variable inclusion criteria and often-sketchy definitions of success.

"Those data are not acceptable, but that’s what we had. This was before evidence-based medicine with an emphasis on rigorously designed studies took hold," explained Dr. Kingdom, professor and vice chairman of the department of otolaryngology – head and neck surgery, at the University of Colorado, Denver, and immediate past president of the American Rhinologic Society.
Current research emphasizes the use of modern, validated patient-centered quality of life tools and symptom scores because CRS is a symptom-based diagnosis and it is symptom severity that drives patients to seek treatment. Also, objective measures, such as the Lund-Mackay CT staging system, fail to capture the full experience of disease burden. Nor do objective measures necessarily correlate with patient symptoms, according to the otolaryngologist.
A low point in the field of sinus surgery, in Dr. Kingdom’s view, was the 2006 Cochrane systematic review which concluded ESS "has not been demonstrated to confer additional benefit to that obtained by medical therapy" (Cochrane Database Syst. Rev. 2006:CD004458).
"This review was a disservice," he asserted.
The review was based entirely on three older randomized trials, which not only did not use current treatment paradigms but also did not study the key research question, which Dr. Kingdom believes is this: What’s the comparative effectiveness of ESS vs. continued medical therapy in patients who’ve failed initial medical therapy?
He offered as an example of the contemporary approach to comparative outcomes research in the field of ESS a recent multicenter prospective study led by otolaryngologists at Oregon Health and Science University, Portland. It involved 1 year of prospective follow-up of patients with CRS who had failed initial medical therapy, at which point they elected to undergo ESS or further medical management.
The 65 patients who opted for ESS and the 50 whose chose more medical management were comparable in terms of baseline CRS severity and comorbidities. Both groups showed durable improvement at 12 months, compared with baseline. But ESS was the clear winner, with a mean 71% improvement in the validated Chronic Sinusitis Survey total score, compared with a 46% improvement in the medically managed group. Moreover, during the year of follow-up 17 patients switched over from medical management to ESS and they, too, showed significantly greater improvement than those who remained on medical management (Int. Forum Allergy Rhinol. 2013;3:236-41).
An earlier interim report featuring 6 months of followup showed the surgical group experienced roughly twofold greater improvement, compared with the medical cohort in endpoints including number of days on oral antibiotics or oral corticosteroids and missed days of work or school (Int. Forum Allergy Rhinol. 2011;1:235-41).
Cost-effectiveness studies by various research groups are in the pipeline. The early indication is that the data will show an economic advantage for ESS over medical therapy in patients with recalcitrant disease, according to Dr. Kingdom.
The next research frontier in surgical outcomes in CRS is identification of cellular and molecular markers of disease activity and their genetic underpinnings, which it’s hoped can be used to select the best candidates for ESS, he added.
Dr. Kingdom reported having no financial conflicts of interest.
KEYSTONE, COLO. – Research-minded otolaryngologists have gotten serious about conducting high-quality, patient-centered outcomes studies of endoscopic sinus surgery for chronic rhinosinusitis, which more than 250,000 Americans undergo each year. And the results are eye opening.
Mounting evidence documents that endoscopic sinus surgery (ESS) in properly selected patients with chronic rhinosinusitis (CRS) results in markedly improved quality of life, functional status, and reduced use of medications, compared with medical management, Dr. Todd T. Kingdom said at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
These studies utilize validated measures of patient-centered quality of life and symptoms. They are nothing like the lightweight, less-than-persuasive ESS research published in the 1990s, which reported glowing ‘success’ rates of 80%-97% in single-institution retrospective studies using variable inclusion criteria and often-sketchy definitions of success.
"Those data are not acceptable, but that’s what we had. This was before evidence-based medicine with an emphasis on rigorously designed studies took hold," explained Dr. Kingdom, professor and vice chairman of the department of otolaryngology – head and neck surgery, at the University of Colorado, Denver, and immediate past president of the American Rhinologic Society.
Current research emphasizes the use of modern, validated patient-centered quality of life tools and symptom scores because CRS is a symptom-based diagnosis and it is symptom severity that drives patients to seek treatment. Also, objective measures, such as the Lund-Mackay CT staging system, fail to capture the full experience of disease burden. Nor do objective measures necessarily correlate with patient symptoms, according to the otolaryngologist.
A low point in the field of sinus surgery, in Dr. Kingdom’s view, was the 2006 Cochrane systematic review which concluded ESS "has not been demonstrated to confer additional benefit to that obtained by medical therapy" (Cochrane Database Syst. Rev. 2006:CD004458).
"This review was a disservice," he asserted.
The review was based entirely on three older randomized trials, which not only did not use current treatment paradigms but also did not study the key research question, which Dr. Kingdom believes is this: What’s the comparative effectiveness of ESS vs. continued medical therapy in patients who’ve failed initial medical therapy?
He offered as an example of the contemporary approach to comparative outcomes research in the field of ESS a recent multicenter prospective study led by otolaryngologists at Oregon Health and Science University, Portland. It involved 1 year of prospective follow-up of patients with CRS who had failed initial medical therapy, at which point they elected to undergo ESS or further medical management.
The 65 patients who opted for ESS and the 50 whose chose more medical management were comparable in terms of baseline CRS severity and comorbidities. Both groups showed durable improvement at 12 months, compared with baseline. But ESS was the clear winner, with a mean 71% improvement in the validated Chronic Sinusitis Survey total score, compared with a 46% improvement in the medically managed group. Moreover, during the year of follow-up 17 patients switched over from medical management to ESS and they, too, showed significantly greater improvement than those who remained on medical management (Int. Forum Allergy Rhinol. 2013;3:236-41).
An earlier interim report featuring 6 months of followup showed the surgical group experienced roughly twofold greater improvement, compared with the medical cohort in endpoints including number of days on oral antibiotics or oral corticosteroids and missed days of work or school (Int. Forum Allergy Rhinol. 2011;1:235-41).
Cost-effectiveness studies by various research groups are in the pipeline. The early indication is that the data will show an economic advantage for ESS over medical therapy in patients with recalcitrant disease, according to Dr. Kingdom.
The next research frontier in surgical outcomes in CRS is identification of cellular and molecular markers of disease activity and their genetic underpinnings, which it’s hoped can be used to select the best candidates for ESS, he added.
Dr. Kingdom reported having no financial conflicts of interest.
KEYSTONE, COLO. – Research-minded otolaryngologists have gotten serious about conducting high-quality, patient-centered outcomes studies of endoscopic sinus surgery for chronic rhinosinusitis, which more than 250,000 Americans undergo each year. And the results are eye opening.
Mounting evidence documents that endoscopic sinus surgery (ESS) in properly selected patients with chronic rhinosinusitis (CRS) results in markedly improved quality of life, functional status, and reduced use of medications, compared with medical management, Dr. Todd T. Kingdom said at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
These studies utilize validated measures of patient-centered quality of life and symptoms. They are nothing like the lightweight, less-than-persuasive ESS research published in the 1990s, which reported glowing ‘success’ rates of 80%-97% in single-institution retrospective studies using variable inclusion criteria and often-sketchy definitions of success.
"Those data are not acceptable, but that’s what we had. This was before evidence-based medicine with an emphasis on rigorously designed studies took hold," explained Dr. Kingdom, professor and vice chairman of the department of otolaryngology – head and neck surgery, at the University of Colorado, Denver, and immediate past president of the American Rhinologic Society.
Current research emphasizes the use of modern, validated patient-centered quality of life tools and symptom scores because CRS is a symptom-based diagnosis and it is symptom severity that drives patients to seek treatment. Also, objective measures, such as the Lund-Mackay CT staging system, fail to capture the full experience of disease burden. Nor do objective measures necessarily correlate with patient symptoms, according to the otolaryngologist.
A low point in the field of sinus surgery, in Dr. Kingdom’s view, was the 2006 Cochrane systematic review which concluded ESS "has not been demonstrated to confer additional benefit to that obtained by medical therapy" (Cochrane Database Syst. Rev. 2006:CD004458).
"This review was a disservice," he asserted.
The review was based entirely on three older randomized trials, which not only did not use current treatment paradigms but also did not study the key research question, which Dr. Kingdom believes is this: What’s the comparative effectiveness of ESS vs. continued medical therapy in patients who’ve failed initial medical therapy?
He offered as an example of the contemporary approach to comparative outcomes research in the field of ESS a recent multicenter prospective study led by otolaryngologists at Oregon Health and Science University, Portland. It involved 1 year of prospective follow-up of patients with CRS who had failed initial medical therapy, at which point they elected to undergo ESS or further medical management.
The 65 patients who opted for ESS and the 50 whose chose more medical management were comparable in terms of baseline CRS severity and comorbidities. Both groups showed durable improvement at 12 months, compared with baseline. But ESS was the clear winner, with a mean 71% improvement in the validated Chronic Sinusitis Survey total score, compared with a 46% improvement in the medically managed group. Moreover, during the year of follow-up 17 patients switched over from medical management to ESS and they, too, showed significantly greater improvement than those who remained on medical management (Int. Forum Allergy Rhinol. 2013;3:236-41).
An earlier interim report featuring 6 months of followup showed the surgical group experienced roughly twofold greater improvement, compared with the medical cohort in endpoints including number of days on oral antibiotics or oral corticosteroids and missed days of work or school (Int. Forum Allergy Rhinol. 2011;1:235-41).
Cost-effectiveness studies by various research groups are in the pipeline. The early indication is that the data will show an economic advantage for ESS over medical therapy in patients with recalcitrant disease, according to Dr. Kingdom.
The next research frontier in surgical outcomes in CRS is identification of cellular and molecular markers of disease activity and their genetic underpinnings, which it’s hoped can be used to select the best candidates for ESS, he added.
Dr. Kingdom reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE PULMONARY AND ALLERGY UPDATE

Practice-based asthma navigators trim asthma symptoms, HC utilization
MADRID – Use of practice-based asthma navigators significantly reduced symptoms and emergency room and inpatient visits among inner-city children with moderate to severe asthma in a prospective, case-matched study.
"We’ve seen with our home-visit studies that we’re able to reduce asthma morbidity, but what we hear from the parents all the time is that they feel their communication with providers is lacking, and that they really needed someone to help them navigate the clinical system," Dr. Tyra Bryant-Stephens, founder and director of the Community Asthma Prevention Program at Children’s Hospital of Philadelphia (CHOP), said in an interview.
To overcome this hurdle, CHOP began integrating community health workers as asthma navigators into the clinical team at its inner-city asthma clinics. Key tasks are to teach caregivers about the Asthma Care Plan and proper use of controller medications, facilitate appointment scheduling and set up reminders, contact and share asthma care plans with school nurses, work with social workers to identify appropriate resources for families, and set care coordination goals.

The study enrolled children, aged 2-17 years, on at least two asthma control medications. The participants had been hospitalized or had at least two emergency department (ED) visits in the past year. Their average age was 4.6 years.
After 12 months in the navigator program, preliminary data on 99 children revealed a clear 2- to 3-day reduction over the past 14 days in days using rescue asthma medications (5.28 vs. 3.07; P less than .01), days with symptoms (6.93 to 3.8; P less than .01), and nights with symptoms (6.11 to 3.34; P less than .01), Dr. Bryant-Stephens reported at the world congress of the American College of Chest Physicians.
Compared with baseline, the number of days not taking asthma medications at 12 months was not significantly different (1.48 vs. 1.22) nor was the number of days during which activities had to be slowed (4.41 vs. 3.73).
Enrollment in the navigator program, however, lowered the number of school days missed (16 vs. 2; P less than .05), workdays missed (9.11 vs. 1.13; P less than .01), unscheduled visits to the doctor (2.5 vs. 0.5; P less than .05), ED visits (3.65 vs. 1.31; P less than .01), and hospitalizations (1.73 vs. 0.4; P less than .01).
Although the final analysis comparing participants with matched controls receiving usual care is not yet complete, the data so far show a definite reduction in health care utilization by participants, despite controls being less sick at baseline, Dr. Bryant-Stephens said. This is particularly encouraging because earlier studies at CHOP showed that roughly 50% of asthmatic children never made it back to their primary care physician for follow-up between ED visits.
Making appointments for and keeping follow-up visits were listed by 146 of 157 (93%) caregivers as one of the most important care coordination goals, and were achieved by 80% at 12 months with the assistance of phone calls from the asthma navigator, transportation tokens, and insurance cotransportation, according to the poster presentation.
Success among the other top five caregiver goals was 92% for learning how to properly use asthma medications (126/136 caregivers), 98% for reducing asthma triggers (154/157), 54% for stopping smoking in the house and car (23/42), and 94% for the surprising goal of losing weight in hopes it would reduce asthma symptoms (34/36).
There is no "magic bullet," or single component of the navigator program responsible for the results, but "I think what the navigators have been most effective at is bringing them back to the office. It’s unbelievable compared with the control group," Dr. Bryant-Stephens said at the meeting.
Ultimately, the goal is to make the program self-sufficient, with a pilot program currently underway in which Pennsylvania’s largest Medicaid provider, Keystone First, will pay CHOP to have their clients assigned an asthma navigator when they enroll at an asthma clinic.
Dr. Bryant-Stephens reported funding from the Merck Childhood Asthma Network.
MADRID – Use of practice-based asthma navigators significantly reduced symptoms and emergency room and inpatient visits among inner-city children with moderate to severe asthma in a prospective, case-matched study.
"We’ve seen with our home-visit studies that we’re able to reduce asthma morbidity, but what we hear from the parents all the time is that they feel their communication with providers is lacking, and that they really needed someone to help them navigate the clinical system," Dr. Tyra Bryant-Stephens, founder and director of the Community Asthma Prevention Program at Children’s Hospital of Philadelphia (CHOP), said in an interview.
To overcome this hurdle, CHOP began integrating community health workers as asthma navigators into the clinical team at its inner-city asthma clinics. Key tasks are to teach caregivers about the Asthma Care Plan and proper use of controller medications, facilitate appointment scheduling and set up reminders, contact and share asthma care plans with school nurses, work with social workers to identify appropriate resources for families, and set care coordination goals.
The study enrolled children, aged 2-17 years, on at least two asthma control medications. The participants had been hospitalized or had at least two emergency department (ED) visits in the past year. Their average age was 4.6 years.
After 12 months in the navigator program, preliminary data on 99 children revealed a clear 2- to 3-day reduction over the past 14 days in days using rescue asthma medications (5.28 vs. 3.07; P less than .01), days with symptoms (6.93 to 3.8; P less than .01), and nights with symptoms (6.11 to 3.34; P less than .01), Dr. Bryant-Stephens reported at the world congress of the American College of Chest Physicians.
Compared with baseline, the number of days not taking asthma medications at 12 months was not significantly different (1.48 vs. 1.22) nor was the number of days during which activities had to be slowed (4.41 vs. 3.73).
Enrollment in the navigator program, however, lowered the number of school days missed (16 vs. 2; P less than .05), workdays missed (9.11 vs. 1.13; P less than .01), unscheduled visits to the doctor (2.5 vs. 0.5; P less than .05), ED visits (3.65 vs. 1.31; P less than .01), and hospitalizations (1.73 vs. 0.4; P less than .01).
Although the final analysis comparing participants with matched controls receiving usual care is not yet complete, the data so far show a definite reduction in health care utilization by participants, despite controls being less sick at baseline, Dr. Bryant-Stephens said. This is particularly encouraging because earlier studies at CHOP showed that roughly 50% of asthmatic children never made it back to their primary care physician for follow-up between ED visits.
Making appointments for and keeping follow-up visits were listed by 146 of 157 (93%) caregivers as one of the most important care coordination goals, and were achieved by 80% at 12 months with the assistance of phone calls from the asthma navigator, transportation tokens, and insurance cotransportation, according to the poster presentation.
Success among the other top five caregiver goals was 92% for learning how to properly use asthma medications (126/136 caregivers), 98% for reducing asthma triggers (154/157), 54% for stopping smoking in the house and car (23/42), and 94% for the surprising goal of losing weight in hopes it would reduce asthma symptoms (34/36).
There is no "magic bullet," or single component of the navigator program responsible for the results, but "I think what the navigators have been most effective at is bringing them back to the office. It’s unbelievable compared with the control group," Dr. Bryant-Stephens said at the meeting.
Ultimately, the goal is to make the program self-sufficient, with a pilot program currently underway in which Pennsylvania’s largest Medicaid provider, Keystone First, will pay CHOP to have their clients assigned an asthma navigator when they enroll at an asthma clinic.
Dr. Bryant-Stephens reported funding from the Merck Childhood Asthma Network.
MADRID – Use of practice-based asthma navigators significantly reduced symptoms and emergency room and inpatient visits among inner-city children with moderate to severe asthma in a prospective, case-matched study.
"We’ve seen with our home-visit studies that we’re able to reduce asthma morbidity, but what we hear from the parents all the time is that they feel their communication with providers is lacking, and that they really needed someone to help them navigate the clinical system," Dr. Tyra Bryant-Stephens, founder and director of the Community Asthma Prevention Program at Children’s Hospital of Philadelphia (CHOP), said in an interview.
To overcome this hurdle, CHOP began integrating community health workers as asthma navigators into the clinical team at its inner-city asthma clinics. Key tasks are to teach caregivers about the Asthma Care Plan and proper use of controller medications, facilitate appointment scheduling and set up reminders, contact and share asthma care plans with school nurses, work with social workers to identify appropriate resources for families, and set care coordination goals.
The study enrolled children, aged 2-17 years, on at least two asthma control medications. The participants had been hospitalized or had at least two emergency department (ED) visits in the past year. Their average age was 4.6 years.
After 12 months in the navigator program, preliminary data on 99 children revealed a clear 2- to 3-day reduction over the past 14 days in days using rescue asthma medications (5.28 vs. 3.07; P less than .01), days with symptoms (6.93 to 3.8; P less than .01), and nights with symptoms (6.11 to 3.34; P less than .01), Dr. Bryant-Stephens reported at the world congress of the American College of Chest Physicians.
Compared with baseline, the number of days not taking asthma medications at 12 months was not significantly different (1.48 vs. 1.22) nor was the number of days during which activities had to be slowed (4.41 vs. 3.73).
Enrollment in the navigator program, however, lowered the number of school days missed (16 vs. 2; P less than .05), workdays missed (9.11 vs. 1.13; P less than .01), unscheduled visits to the doctor (2.5 vs. 0.5; P less than .05), ED visits (3.65 vs. 1.31; P less than .01), and hospitalizations (1.73 vs. 0.4; P less than .01).
Although the final analysis comparing participants with matched controls receiving usual care is not yet complete, the data so far show a definite reduction in health care utilization by participants, despite controls being less sick at baseline, Dr. Bryant-Stephens said. This is particularly encouraging because earlier studies at CHOP showed that roughly 50% of asthmatic children never made it back to their primary care physician for follow-up between ED visits.
Making appointments for and keeping follow-up visits were listed by 146 of 157 (93%) caregivers as one of the most important care coordination goals, and were achieved by 80% at 12 months with the assistance of phone calls from the asthma navigator, transportation tokens, and insurance cotransportation, according to the poster presentation.
Success among the other top five caregiver goals was 92% for learning how to properly use asthma medications (126/136 caregivers), 98% for reducing asthma triggers (154/157), 54% for stopping smoking in the house and car (23/42), and 94% for the surprising goal of losing weight in hopes it would reduce asthma symptoms (34/36).
There is no "magic bullet," or single component of the navigator program responsible for the results, but "I think what the navigators have been most effective at is bringing them back to the office. It’s unbelievable compared with the control group," Dr. Bryant-Stephens said at the meeting.
Ultimately, the goal is to make the program self-sufficient, with a pilot program currently underway in which Pennsylvania’s largest Medicaid provider, Keystone First, will pay CHOP to have their clients assigned an asthma navigator when they enroll at an asthma clinic.
Dr. Bryant-Stephens reported funding from the Merck Childhood Asthma Network.
AT CHEST WORLD CONGRESS 2014
Major finding: After 12 months in the asthma navigator program, children had fewer unscheduled visits to the doctor (2.5 vs. 0.5; P less than .05), emergency department visits (3.65 vs. 1.31; P less than .01), and hospitalizations (1.73 vs. 0.4; P less than .01).
Data source: A prospective case-matched study in 99 children with moderate to severe asthma.
Disclosures: Dr. Bryant-Stephens reported funding from the Merck Childhood Asthma Network.

FDA approves omalizumab for chronic idiopathic urticaria
The Food and Drug Administration has approved omalizumab (Xolair) for chronic idiopathic urticaria in people 12 years of age and older who remain symptomatic despite treatment with H1-antihistamine therapy.
Omalizumab was first approved in 2003 for moderate to severe asthma. In 2007, the FDA required the drug to be administered in a doctor’s office only, to monitor for potentially severe anaphylaxis; a boxed warning was added at that time.
According to the drug’s developer, Genentech, omalizumab is the first biologic and the first medicine approved for chronic idiopathic urticaria since nonsedating H1-antihistamines.
The approval was based on the results from two studies, ASTERIA I and ASTERIA II5, which were presented in November 2013 at the annual congress of the European Academy of Dermatology and Venereology.
According to Genentech, about 1.5 million Americans develop chronic idiopathic urticaria at some point, with women twice as likely as men to get the condition.
Chronic idiopathic urticaria "can be a frustrating condition for patients," said Mike Tringale, senior vice president at the Asthma and Allergy Foundation of America in a statement issued by Genentech. "This new use for Xolair gives hope to appropriate patients who can go for months or even years without getting satisfactory itch and hive reduction."
Omalizumab was jointly developed by Genentech and Novartis Pharma, and is copromoted in the United States with Novartis.
aault@frontlinemedcom.com On Twitter @aliciaault
The Food and Drug Administration has approved omalizumab (Xolair) for chronic idiopathic urticaria in people 12 years of age and older who remain symptomatic despite treatment with H1-antihistamine therapy.
Omalizumab was first approved in 2003 for moderate to severe asthma. In 2007, the FDA required the drug to be administered in a doctor’s office only, to monitor for potentially severe anaphylaxis; a boxed warning was added at that time.
According to the drug’s developer, Genentech, omalizumab is the first biologic and the first medicine approved for chronic idiopathic urticaria since nonsedating H1-antihistamines.
The approval was based on the results from two studies, ASTERIA I and ASTERIA II5, which were presented in November 2013 at the annual congress of the European Academy of Dermatology and Venereology.
According to Genentech, about 1.5 million Americans develop chronic idiopathic urticaria at some point, with women twice as likely as men to get the condition.
Chronic idiopathic urticaria "can be a frustrating condition for patients," said Mike Tringale, senior vice president at the Asthma and Allergy Foundation of America in a statement issued by Genentech. "This new use for Xolair gives hope to appropriate patients who can go for months or even years without getting satisfactory itch and hive reduction."
Omalizumab was jointly developed by Genentech and Novartis Pharma, and is copromoted in the United States with Novartis.
aault@frontlinemedcom.com On Twitter @aliciaault
The Food and Drug Administration has approved omalizumab (Xolair) for chronic idiopathic urticaria in people 12 years of age and older who remain symptomatic despite treatment with H1-antihistamine therapy.
Omalizumab was first approved in 2003 for moderate to severe asthma. In 2007, the FDA required the drug to be administered in a doctor’s office only, to monitor for potentially severe anaphylaxis; a boxed warning was added at that time.
According to the drug’s developer, Genentech, omalizumab is the first biologic and the first medicine approved for chronic idiopathic urticaria since nonsedating H1-antihistamines.
The approval was based on the results from two studies, ASTERIA I and ASTERIA II5, which were presented in November 2013 at the annual congress of the European Academy of Dermatology and Venereology.
According to Genentech, about 1.5 million Americans develop chronic idiopathic urticaria at some point, with women twice as likely as men to get the condition.
Chronic idiopathic urticaria "can be a frustrating condition for patients," said Mike Tringale, senior vice president at the Asthma and Allergy Foundation of America in a statement issued by Genentech. "This new use for Xolair gives hope to appropriate patients who can go for months or even years without getting satisfactory itch and hive reduction."
Omalizumab was jointly developed by Genentech and Novartis Pharma, and is copromoted in the United States with Novartis.
aault@frontlinemedcom.com On Twitter @aliciaault