User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Tuberculosis rate drops, disparity continues
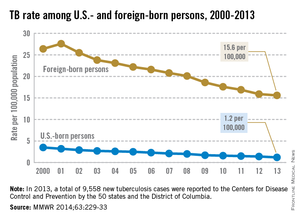
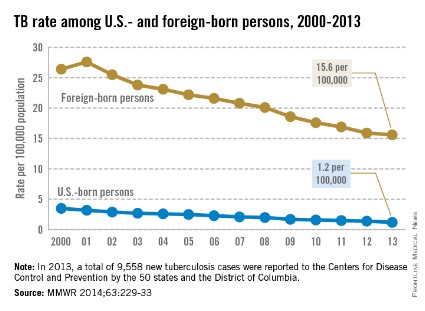
Despite the overall decline in tuberculosis, there continues to be a large disparity in incidence between U.S.-born and foreign-born U.S. residents, the Centers for Disease Control and Prevention reported March 20 in advance of World TB Day, which is on March 24.
In 2013, the TB incidence among foreign-born persons was 15.6 cases per 100,000 population, which was 13 times higher than the rate of 1.2 per 100,000 in U.S.-born persons. The CDC defines a U.S.-born person as anyone born in the United States or in a foreign country but having at least one parent who is a U.S. citizen.
The TB rate declined among both groups from 2012 to 2013, but only by 2.1% among foreign-born persons, compared with 8.4% for U.S.-born persons. Racial/ethnic disparities also continue, with Asians having a TB rate 25.9 times higher and blacks having a rate 6.2 times higher than whites, according to the CDC (MMWR 2014;63:229-33).
In a separate statement, the CDC said that updated recommendations for overseas TB screening of immigrants and refugees have saved the United States an estimated $15 million. Since 2007, people suspected of having TB have been required to undergo a sputum culture instead of a less sensitive microscopic sputum smear test so that their infection could be caught and treated prior to arriving in the United States.
Despite the overall decline in tuberculosis, there continues to be a large disparity in incidence between U.S.-born and foreign-born U.S. residents, the Centers for Disease Control and Prevention reported March 20 in advance of World TB Day, which is on March 24.
In 2013, the TB incidence among foreign-born persons was 15.6 cases per 100,000 population, which was 13 times higher than the rate of 1.2 per 100,000 in U.S.-born persons. The CDC defines a U.S.-born person as anyone born in the United States or in a foreign country but having at least one parent who is a U.S. citizen.
The TB rate declined among both groups from 2012 to 2013, but only by 2.1% among foreign-born persons, compared with 8.4% for U.S.-born persons. Racial/ethnic disparities also continue, with Asians having a TB rate 25.9 times higher and blacks having a rate 6.2 times higher than whites, according to the CDC (MMWR 2014;63:229-33).
In a separate statement, the CDC said that updated recommendations for overseas TB screening of immigrants and refugees have saved the United States an estimated $15 million. Since 2007, people suspected of having TB have been required to undergo a sputum culture instead of a less sensitive microscopic sputum smear test so that their infection could be caught and treated prior to arriving in the United States.
Despite the overall decline in tuberculosis, there continues to be a large disparity in incidence between U.S.-born and foreign-born U.S. residents, the Centers for Disease Control and Prevention reported March 20 in advance of World TB Day, which is on March 24.
In 2013, the TB incidence among foreign-born persons was 15.6 cases per 100,000 population, which was 13 times higher than the rate of 1.2 per 100,000 in U.S.-born persons. The CDC defines a U.S.-born person as anyone born in the United States or in a foreign country but having at least one parent who is a U.S. citizen.
The TB rate declined among both groups from 2012 to 2013, but only by 2.1% among foreign-born persons, compared with 8.4% for U.S.-born persons. Racial/ethnic disparities also continue, with Asians having a TB rate 25.9 times higher and blacks having a rate 6.2 times higher than whites, according to the CDC (MMWR 2014;63:229-33).
In a separate statement, the CDC said that updated recommendations for overseas TB screening of immigrants and refugees have saved the United States an estimated $15 million. Since 2007, people suspected of having TB have been required to undergo a sputum culture instead of a less sensitive microscopic sputum smear test so that their infection could be caught and treated prior to arriving in the United States.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Be wary of asthma’s masqueraders
KEYSTONE, COLO. – The diagnosis of asthma isn’t as simple as it may seem.
Asthma is a clinical syndrome with no specific diagnostic test. So, the response to therapy becomes a key element in finalizing the diagnosis, Dr. Gary R. Cott emphasized at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
"If you have features that make you think of asthma, particularly mild to moderate asthma, and you initiate therapy, you should expect a therapeutic response in 80%-85% of cases. If you don’t get a response, step back and think about whether you made the right diagnosis before you start escalating care," advised Dr. Cott, a pulmonologist and executive vice president of medical and clinical services at National Jewish Health, Denver.
How often do physicians on the front lines get the diagnosis of asthma wrong? The National Jewish experience is illuminating.

In a series of 305 consecutive patients referred to the tertiary center with a preestablished diagnosis of asthma, all of whom were already on treatment for the disease, fully 25% didn’t have asthma at all. A mere 5% were found to have asthma only. A total of 38% had asthma plus an associated contributory respiratory condition, such as allergic rhinitis, rhinosinusitis, or aspirin sensitivity. Another 32% had asthma plus a cardiopulmonary condition that contributed to their symptoms, such as valvular dysfunction, a vascular ring, or pulmonary embolus.
"This experience has been duplicated at other specialty centers. It’s not unique to what we see," according to Dr. Cott.
He defined asthma as a syndrome characterized by increased airway responsiveness to various stimuli, along with variable obstruction of expiratory flow. It’s a physiologic definition. Four elements are essential in establishing the diagnosis: the history, physical exam, spirometry, and response to therapy. A variety of other tests are often helpful in narrowing the differential diagnosis – for example, chest imaging, blood eosinophil measurement, allergy testing, bronchial challenges, diffusing capacity of the lung for carbon monoxide, lung volumes, and elasticity. But they’re not specific for asthma.
"All that wheezes is not asthma. But most is," Dr. Cott observed. "I must say, I’m not very critical of the outside docs who send patients in and say, ‘I think they have asthma,’ and we then say, ‘No, they’ve got something else.’ Asthma is a common disorder. In Colorado, as much as 11% of the population can have asthma. It’s probably the most common thing that will cause an otherwise healthy individual to present with recurring or persistent symptoms.
"I think that sometimes leads us down a path – not always incorrect – of thinking, ‘Let’s try treating for asthma,’ " Dr. Cott noted. "The problem is that when they’re not responding, it’s time to rethink the differential carefully."
The list of disorders involving lower airways obstruction that can mimic asthma is extensive. The top two masqueraders are emphysema and chronic bronchitis. What’s more, asthma, emphysema, and chronic bronchitis aren’t mutually exclusive diseases. A given patient can have any two or even all three.
In contrast to asthma, which is defined physiologically, chronic bronchitis has a historical definition: It’s a condition involving cough with excessive sputum production for at least 3 months per year in at least 2 consecutive years. And emphysema is defined anatomically: permanent enlargement of air spaces distal to the terminal bronchiole with alveolar septae destruction.
It’s important to differentiate these conditions, because their guideline-recommended management strategies differ, as do their prognoses, Dr. Cott continued.
In addition to emphysema and chronic bronchitis, other lower airways disorders that can mimic asthma include infection, sarcoidosis, interstitial lung disease, cystic fibrosis, a tumor or foreign body, and bronchiolitis.
The list of upper airways disorders that can be mistaken for asthma includes vocal cord dysfunction, infection, laryngeal spasm, and laryngeal edema secondary to angioedema. The most useful spirometric clue to upper airways obstruction, in Dr. Cott’s view, is a ratio of the forced expiratory flow at 50% volume to forced inspiratory volume at 50% of 1 or greater.
"That’s virtually always present with upper airway or extrathoracic airways obstruction," he said.
Dr. Cott reported having no conflicts of interest.
KEYSTONE, COLO. – The diagnosis of asthma isn’t as simple as it may seem.
Asthma is a clinical syndrome with no specific diagnostic test. So, the response to therapy becomes a key element in finalizing the diagnosis, Dr. Gary R. Cott emphasized at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
"If you have features that make you think of asthma, particularly mild to moderate asthma, and you initiate therapy, you should expect a therapeutic response in 80%-85% of cases. If you don’t get a response, step back and think about whether you made the right diagnosis before you start escalating care," advised Dr. Cott, a pulmonologist and executive vice president of medical and clinical services at National Jewish Health, Denver.
How often do physicians on the front lines get the diagnosis of asthma wrong? The National Jewish experience is illuminating.
In a series of 305 consecutive patients referred to the tertiary center with a preestablished diagnosis of asthma, all of whom were already on treatment for the disease, fully 25% didn’t have asthma at all. A mere 5% were found to have asthma only. A total of 38% had asthma plus an associated contributory respiratory condition, such as allergic rhinitis, rhinosinusitis, or aspirin sensitivity. Another 32% had asthma plus a cardiopulmonary condition that contributed to their symptoms, such as valvular dysfunction, a vascular ring, or pulmonary embolus.
"This experience has been duplicated at other specialty centers. It’s not unique to what we see," according to Dr. Cott.
He defined asthma as a syndrome characterized by increased airway responsiveness to various stimuli, along with variable obstruction of expiratory flow. It’s a physiologic definition. Four elements are essential in establishing the diagnosis: the history, physical exam, spirometry, and response to therapy. A variety of other tests are often helpful in narrowing the differential diagnosis – for example, chest imaging, blood eosinophil measurement, allergy testing, bronchial challenges, diffusing capacity of the lung for carbon monoxide, lung volumes, and elasticity. But they’re not specific for asthma.
"All that wheezes is not asthma. But most is," Dr. Cott observed. "I must say, I’m not very critical of the outside docs who send patients in and say, ‘I think they have asthma,’ and we then say, ‘No, they’ve got something else.’ Asthma is a common disorder. In Colorado, as much as 11% of the population can have asthma. It’s probably the most common thing that will cause an otherwise healthy individual to present with recurring or persistent symptoms.
"I think that sometimes leads us down a path – not always incorrect – of thinking, ‘Let’s try treating for asthma,’ " Dr. Cott noted. "The problem is that when they’re not responding, it’s time to rethink the differential carefully."
The list of disorders involving lower airways obstruction that can mimic asthma is extensive. The top two masqueraders are emphysema and chronic bronchitis. What’s more, asthma, emphysema, and chronic bronchitis aren’t mutually exclusive diseases. A given patient can have any two or even all three.
In contrast to asthma, which is defined physiologically, chronic bronchitis has a historical definition: It’s a condition involving cough with excessive sputum production for at least 3 months per year in at least 2 consecutive years. And emphysema is defined anatomically: permanent enlargement of air spaces distal to the terminal bronchiole with alveolar septae destruction.
It’s important to differentiate these conditions, because their guideline-recommended management strategies differ, as do their prognoses, Dr. Cott continued.
In addition to emphysema and chronic bronchitis, other lower airways disorders that can mimic asthma include infection, sarcoidosis, interstitial lung disease, cystic fibrosis, a tumor or foreign body, and bronchiolitis.
The list of upper airways disorders that can be mistaken for asthma includes vocal cord dysfunction, infection, laryngeal spasm, and laryngeal edema secondary to angioedema. The most useful spirometric clue to upper airways obstruction, in Dr. Cott’s view, is a ratio of the forced expiratory flow at 50% volume to forced inspiratory volume at 50% of 1 or greater.
"That’s virtually always present with upper airway or extrathoracic airways obstruction," he said.
Dr. Cott reported having no conflicts of interest.
KEYSTONE, COLO. – The diagnosis of asthma isn’t as simple as it may seem.
Asthma is a clinical syndrome with no specific diagnostic test. So, the response to therapy becomes a key element in finalizing the diagnosis, Dr. Gary R. Cott emphasized at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
"If you have features that make you think of asthma, particularly mild to moderate asthma, and you initiate therapy, you should expect a therapeutic response in 80%-85% of cases. If you don’t get a response, step back and think about whether you made the right diagnosis before you start escalating care," advised Dr. Cott, a pulmonologist and executive vice president of medical and clinical services at National Jewish Health, Denver.
How often do physicians on the front lines get the diagnosis of asthma wrong? The National Jewish experience is illuminating.
In a series of 305 consecutive patients referred to the tertiary center with a preestablished diagnosis of asthma, all of whom were already on treatment for the disease, fully 25% didn’t have asthma at all. A mere 5% were found to have asthma only. A total of 38% had asthma plus an associated contributory respiratory condition, such as allergic rhinitis, rhinosinusitis, or aspirin sensitivity. Another 32% had asthma plus a cardiopulmonary condition that contributed to their symptoms, such as valvular dysfunction, a vascular ring, or pulmonary embolus.
"This experience has been duplicated at other specialty centers. It’s not unique to what we see," according to Dr. Cott.
He defined asthma as a syndrome characterized by increased airway responsiveness to various stimuli, along with variable obstruction of expiratory flow. It’s a physiologic definition. Four elements are essential in establishing the diagnosis: the history, physical exam, spirometry, and response to therapy. A variety of other tests are often helpful in narrowing the differential diagnosis – for example, chest imaging, blood eosinophil measurement, allergy testing, bronchial challenges, diffusing capacity of the lung for carbon monoxide, lung volumes, and elasticity. But they’re not specific for asthma.
"All that wheezes is not asthma. But most is," Dr. Cott observed. "I must say, I’m not very critical of the outside docs who send patients in and say, ‘I think they have asthma,’ and we then say, ‘No, they’ve got something else.’ Asthma is a common disorder. In Colorado, as much as 11% of the population can have asthma. It’s probably the most common thing that will cause an otherwise healthy individual to present with recurring or persistent symptoms.
"I think that sometimes leads us down a path – not always incorrect – of thinking, ‘Let’s try treating for asthma,’ " Dr. Cott noted. "The problem is that when they’re not responding, it’s time to rethink the differential carefully."
The list of disorders involving lower airways obstruction that can mimic asthma is extensive. The top two masqueraders are emphysema and chronic bronchitis. What’s more, asthma, emphysema, and chronic bronchitis aren’t mutually exclusive diseases. A given patient can have any two or even all three.
In contrast to asthma, which is defined physiologically, chronic bronchitis has a historical definition: It’s a condition involving cough with excessive sputum production for at least 3 months per year in at least 2 consecutive years. And emphysema is defined anatomically: permanent enlargement of air spaces distal to the terminal bronchiole with alveolar septae destruction.
It’s important to differentiate these conditions, because their guideline-recommended management strategies differ, as do their prognoses, Dr. Cott continued.
In addition to emphysema and chronic bronchitis, other lower airways disorders that can mimic asthma include infection, sarcoidosis, interstitial lung disease, cystic fibrosis, a tumor or foreign body, and bronchiolitis.
The list of upper airways disorders that can be mistaken for asthma includes vocal cord dysfunction, infection, laryngeal spasm, and laryngeal edema secondary to angioedema. The most useful spirometric clue to upper airways obstruction, in Dr. Cott’s view, is a ratio of the forced expiratory flow at 50% volume to forced inspiratory volume at 50% of 1 or greater.
"That’s virtually always present with upper airway or extrathoracic airways obstruction," he said.
Dr. Cott reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE PULMONARY AND ALLERGY UPDATE
Asthma May Increase Risk of Cardiovascular Events
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).
The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).
The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).
The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
AT THE 2014 AAAAI ANNUAL MEETING
Asthma may increase risk of cardiovascular events
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).

The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).
The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Having asthma appears to significantly increase your risk for cardiovascular events, while having allergic rhinitis appears to protect your risk for such events, results from a large cohort study demonstrated.
Studies of mouse models have suggested that Th1 inflammation "is associated with atherosclerosis and plaque development, while the Th2 or general allergic response seems to be protective against atherosclerosis," Dr. Angelina Crans Yoon said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. At the same time, results from human studies regarding the association between allergic rhinitis and cardiovascular events are mixed, said Dr. Crans Yoon, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center.
In an effort to assess the relationship between cardiovascular disease and allergic rhinitis, she and her associates used the Kaiser Permanente Southern California regional database and ICD-9 codes to compare the incidence of cardiovascular and cerebrovascular events and all-cause mortality in a cohort of 109,229 allergic rhinitis patients and 92,775 asthma patients who were seen between Jan. 1, 1995, and Dec. 31, 2012. The cohorts were matched by age, sex, and ethnicity to reference cohorts and followed for a median of 8 years.
Dr. Crans Yoon reported that patients with allergic rhinitis had significantly lower risk for myocardial infarction (hazard ratio, 0.75), cerebrovascular disease (HR, 0.81), and all-cause mortality (HR, 0.51), yet their risk of all cardiovascular events was equal to that of the control cohort (HR, 0.97). At the same time, patients with asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36), yet no significantly higher risk of cerebrovascular disease (HR, 1.03) or all-cause mortality (HR, 1.00).
The findings "led us to think of more questions," Dr. Crans Yoon said. "Why is there this decreased risk of events in patients with allergic rhinitis? What explains the risk of cardiovascular events in patients with asthma? Is atopy related to these differences? We started some secondary analyses looking at medication use. It looks like if you use any medications for allergic rhinitis or asthma, you have a decreased risk of some of these events, except for long-acting beta-agonists, which is consistent with previous reports. We’re also starting to look at specific IgE data on these patients. It looks like positive IgE testing may be associated with a decreased risk of all these events."
She speculated that asthma physiology may explain why patients with asthma had significantly higher risk of cardiovascular disease but not cerebrovascular disease. "The interesting point is that potentially, atopic asthmatics may not have the same increased risk," she said.
Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
AT THE 2014 AAAAI ANNUAL MEETING
Major Finding: Compared with matched controls, patient’s asthma had a significantly higher risk of all cardiovascular disease (HR, 1.36) while patients with allergic rhinitis had a significantly lower risk for myocardial infarction (HR, 0.75).
Data Source: A study of 109,229 patients with allergic rhinitis and 92,775 patients with asthma who were treated at Kaiser Permanente Southern California and followed for a median of 8 years.
Disclosures: Dr. Crans Yoon said that she had no relevant financial conflicts to disclose.
Protocol-based resuscitation fails to beat usual care in early sepsis
Protocol-based resuscitation did not reduce sepsis deaths or morbidity, compared with usual care, in the Protocolized Care for Early Septic Shock study conducted at 31 U.S. academic hospitals.
Among 1,341 evaluable patients, the primary endpoint of 60-day in-hospital mortality was 21% with protocol-based early goal-directed therapy (EGDT), 18.2% with protocol-based standard therapy that did not require the placement of a central venous catheter, administration of inotropes, or blood transfusions, and 18.9% with usual care according to the treating physician’s judgment.
The difference was not statistically significant between the protocol-based interventions and usual care (relative risk, 1.04; P = .83) or between protocol-based EGDT and protocol-based standard therapy (RR, 1.15; P = .31), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published in the New England Journal of Medicine (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1401602]).
The three groups also did not differ significantly with regard to 90-day mortality, incidence of cardiovascular or respiratory failure, length of hospital stay, or discharge disposition.
The results from ProCESS differ from those reported more than a decade ago in the pivotal, single-center Rivers et al. study, in which mortality was significantly reduced for patients with severe sepsis or septic shock treated with 6 hours of EGDT therapy versus standard therapy (N. Engl. J. Med. 2001;345:1368-77).
Though both trials used the same EGDT protocol delivered by a trained, dedicated team at each site, possible reasons for the discordance are that the Rivers study showed nearly perfect adherence to protocol and that its cohort was slightly older, had higher rates of preexisting heart and liver disease, and had a higher initial serum lactate level, noted Dr. Derek Angus, ProCESS principal investigator and chair of critical care medicine at the University of Pittsburgh.
In addition, changes in the management of critically ill patient in the ensuing decade, including use of lower hemoglobin levels as a threshold for transfusion, use of lung-protection strategies, and tighter blood sugar control, "may have helped lower the overall mortality and may have reduced the marginal benefit of alternative resuscitation strategies," he observed.
Dr. Angus received grant support from the National Institutes of General Medical Sciences and nonfinancial support from Edwards Inc. during the trial, grant support to his university from Eisai, and personal fees from Pfizer and MedImmune outside this trial.
"The critical role of the clinician in the early recognition of
sepsis continues to this day to be fundamental to our efforts to improve
the rate of survival," said pulmonologist Dr. Craig M. Lilly of the University of Massachusetts Memorial Medical Center, Boston. (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMe1402564]). He
cautioned, however, on using the findings to come to the "dubious
conclusion that protocols and decision prompts do not have a role in the
treatment of septic shock."
An important contribution of ProCESS
is the evidence it provides on the early recognition of, and antibiotic
treatment for, sepsis in improving survival, Dr. Lilly observed. Shock
was recognized early in most patients (randomization occurred at an
average of 3 hours after ED arrival), 76% received antimicrobial agents
by randomization, and 97% received IV antimicrobials 6 hours after
randomization.
ProCESS also provides "transformative insights
about the treatments for septic shock that bring generalizable benefits"
when septic shock is recognized in the first hours after ED arrival, he
stated. Notably, that use of central hemodynamic and oxygen-saturation
monitoring in the protocol-based EGDT group did not result in better
outcomes than those achieved with clinical assessment of the adequacy of
circulation.
"State legislation and clinical guidelines,
including those endorsed by the National Quality Forum, should be
updated to remove the requirement for central hemodynamic monitoring and
to focus on less costly, lower-risk, and equally effective
alternatives," Dr. Lilly wrote. Dr. Lilly reported no conflicts.
"The critical role of the clinician in the early recognition of
sepsis continues to this day to be fundamental to our efforts to improve
the rate of survival," said pulmonologist Dr. Craig M. Lilly of the University of Massachusetts Memorial Medical Center, Boston. (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMe1402564]). He
cautioned, however, on using the findings to come to the "dubious
conclusion that protocols and decision prompts do not have a role in the
treatment of septic shock."
An important contribution of ProCESS
is the evidence it provides on the early recognition of, and antibiotic
treatment for, sepsis in improving survival, Dr. Lilly observed. Shock
was recognized early in most patients (randomization occurred at an
average of 3 hours after ED arrival), 76% received antimicrobial agents
by randomization, and 97% received IV antimicrobials 6 hours after
randomization.
ProCESS also provides "transformative insights
about the treatments for septic shock that bring generalizable benefits"
when septic shock is recognized in the first hours after ED arrival, he
stated. Notably, that use of central hemodynamic and oxygen-saturation
monitoring in the protocol-based EGDT group did not result in better
outcomes than those achieved with clinical assessment of the adequacy of
circulation.
"State legislation and clinical guidelines,
including those endorsed by the National Quality Forum, should be
updated to remove the requirement for central hemodynamic monitoring and
to focus on less costly, lower-risk, and equally effective
alternatives," Dr. Lilly wrote. Dr. Lilly reported no conflicts.
"The critical role of the clinician in the early recognition of
sepsis continues to this day to be fundamental to our efforts to improve
the rate of survival," said pulmonologist Dr. Craig M. Lilly of the University of Massachusetts Memorial Medical Center, Boston. (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMe1402564]). He
cautioned, however, on using the findings to come to the "dubious
conclusion that protocols and decision prompts do not have a role in the
treatment of septic shock."
An important contribution of ProCESS
is the evidence it provides on the early recognition of, and antibiotic
treatment for, sepsis in improving survival, Dr. Lilly observed. Shock
was recognized early in most patients (randomization occurred at an
average of 3 hours after ED arrival), 76% received antimicrobial agents
by randomization, and 97% received IV antimicrobials 6 hours after
randomization.
ProCESS also provides "transformative insights
about the treatments for septic shock that bring generalizable benefits"
when septic shock is recognized in the first hours after ED arrival, he
stated. Notably, that use of central hemodynamic and oxygen-saturation
monitoring in the protocol-based EGDT group did not result in better
outcomes than those achieved with clinical assessment of the adequacy of
circulation.
"State legislation and clinical guidelines,
including those endorsed by the National Quality Forum, should be
updated to remove the requirement for central hemodynamic monitoring and
to focus on less costly, lower-risk, and equally effective
alternatives," Dr. Lilly wrote. Dr. Lilly reported no conflicts.
Protocol-based resuscitation did not reduce sepsis deaths or morbidity, compared with usual care, in the Protocolized Care for Early Septic Shock study conducted at 31 U.S. academic hospitals.
Among 1,341 evaluable patients, the primary endpoint of 60-day in-hospital mortality was 21% with protocol-based early goal-directed therapy (EGDT), 18.2% with protocol-based standard therapy that did not require the placement of a central venous catheter, administration of inotropes, or blood transfusions, and 18.9% with usual care according to the treating physician’s judgment.
The difference was not statistically significant between the protocol-based interventions and usual care (relative risk, 1.04; P = .83) or between protocol-based EGDT and protocol-based standard therapy (RR, 1.15; P = .31), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published in the New England Journal of Medicine (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1401602]).
The three groups also did not differ significantly with regard to 90-day mortality, incidence of cardiovascular or respiratory failure, length of hospital stay, or discharge disposition.
The results from ProCESS differ from those reported more than a decade ago in the pivotal, single-center Rivers et al. study, in which mortality was significantly reduced for patients with severe sepsis or septic shock treated with 6 hours of EGDT therapy versus standard therapy (N. Engl. J. Med. 2001;345:1368-77).
Though both trials used the same EGDT protocol delivered by a trained, dedicated team at each site, possible reasons for the discordance are that the Rivers study showed nearly perfect adherence to protocol and that its cohort was slightly older, had higher rates of preexisting heart and liver disease, and had a higher initial serum lactate level, noted Dr. Derek Angus, ProCESS principal investigator and chair of critical care medicine at the University of Pittsburgh.
In addition, changes in the management of critically ill patient in the ensuing decade, including use of lower hemoglobin levels as a threshold for transfusion, use of lung-protection strategies, and tighter blood sugar control, "may have helped lower the overall mortality and may have reduced the marginal benefit of alternative resuscitation strategies," he observed.
Dr. Angus received grant support from the National Institutes of General Medical Sciences and nonfinancial support from Edwards Inc. during the trial, grant support to his university from Eisai, and personal fees from Pfizer and MedImmune outside this trial.
Protocol-based resuscitation did not reduce sepsis deaths or morbidity, compared with usual care, in the Protocolized Care for Early Septic Shock study conducted at 31 U.S. academic hospitals.
Among 1,341 evaluable patients, the primary endpoint of 60-day in-hospital mortality was 21% with protocol-based early goal-directed therapy (EGDT), 18.2% with protocol-based standard therapy that did not require the placement of a central venous catheter, administration of inotropes, or blood transfusions, and 18.9% with usual care according to the treating physician’s judgment.
The difference was not statistically significant between the protocol-based interventions and usual care (relative risk, 1.04; P = .83) or between protocol-based EGDT and protocol-based standard therapy (RR, 1.15; P = .31), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published in the New England Journal of Medicine (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1401602]).
The three groups also did not differ significantly with regard to 90-day mortality, incidence of cardiovascular or respiratory failure, length of hospital stay, or discharge disposition.
The results from ProCESS differ from those reported more than a decade ago in the pivotal, single-center Rivers et al. study, in which mortality was significantly reduced for patients with severe sepsis or septic shock treated with 6 hours of EGDT therapy versus standard therapy (N. Engl. J. Med. 2001;345:1368-77).
Though both trials used the same EGDT protocol delivered by a trained, dedicated team at each site, possible reasons for the discordance are that the Rivers study showed nearly perfect adherence to protocol and that its cohort was slightly older, had higher rates of preexisting heart and liver disease, and had a higher initial serum lactate level, noted Dr. Derek Angus, ProCESS principal investigator and chair of critical care medicine at the University of Pittsburgh.
In addition, changes in the management of critically ill patient in the ensuing decade, including use of lower hemoglobin levels as a threshold for transfusion, use of lung-protection strategies, and tighter blood sugar control, "may have helped lower the overall mortality and may have reduced the marginal benefit of alternative resuscitation strategies," he observed.
Dr. Angus received grant support from the National Institutes of General Medical Sciences and nonfinancial support from Edwards Inc. during the trial, grant support to his university from Eisai, and personal fees from Pfizer and MedImmune outside this trial.
FROM ISICEM 2014
Major finding: Sixty-day mortality was 21% with protocol-based EGDT, 18.2% with protocol-based standard therapy, and 18.9% with usual care.
Data source: A prospective study of 1,341 patients with septic shock.
Disclosures: Dr. Angus received grant support from the National Institutes of General Medical Sciences and nonfinancial support from Edwards Inc. during the trial, grant support to his university from Eisai, and personal fees from Pfizer and MedImmune outside this trial.
Recurrent wheeze associated with antibiotic use early in life
SAN DIEGO – Antibiotic use prior to 6 months of age was associated with recurrent wheeze but not with allergic sensitization or other clinical allergic outcomes, results from a large birth cohort study demonstrated.
"In the medical literature, some but not all studies suggest that antibiotic use early in life is related to later childhood asthma and allergic disease," Kyra Jones, M.Ed., said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"It is well known that antibiotics affect the gut microbiome," she added. "What may not be as clear is the impact of the effect and its relationship to allergic outcomes. Since antibiotics affect the gut microbiome, we hypothesized that early antibiotic use would be associated with allergic outcomes."

In an effort to determine whether antibiotic use in the first 6 months of life is associated with allergic sensitization or clinical allergic outcomes at age 2-3 years, Ms. Jones, an epidemiologist in the department of public health sciences at Henry Ford Hospital, Detroit, and her associates obtained data from 1,258 pregnant women who participated in the WHEALS (Wayne County Health, Environment, Allergy, and Asthma Longitudinal Study) prospective birth cohort.
The women, who ranged in age from 21 to 49 years, were recruited between 2003 and 2007 at one of five Henry Ford Health System obstetric clinics in the western Wayne County suburbs or the city of Detroit. They were interviewed at 1, 6, 12, and 24 months following the birth of their child. Next, their children were brought into the clinic at 2-3 years of age and assessed for atopic dermatitis. The researchers analyzed the children’s blood for total IgE and specific IgE to milk, egg, peanut, dog, cat, dust mite, timothy grass, and cockroach and performed skin prick tests for the same allergens.
The primary exposure was defined as the mother reporting that her child had taken one or more of the following antibiotics within the first 6 months of life: cephalosporins, macrolides, penicillin, sulfonamides, and topical antibiotics. Outcomes of interest included total IgE, specific IgE, skin prick test positivity, history of physician diagnosis of atopic dermatitis, and parental report of wheezing at least twice in the first 2-3 years of life – including at least once in the preceding year. The researchers used logistic and linear regression models to assess associations between antibiotic exposure and outcomes.
Ms. Jones reported data from 680 children. More than half (58%) were African American and 51% were male. Slightly more than half (51.2%) had a positive specific IgE, 24.5% had a positive skin prick test, 22.7% had atopic dermatitis, and 15.6% had recurrent wheezing.
At 2 years, most outcomes were similar between children who used antibiotics and those who did not, but 22% of children who took antibiotics had recurrent wheeze, compared with 14% of those who did not, a difference that reached statistical significance (P = 0.03). Multivariate models revealed similar findings (odds ratio of 1.85 for recurrent wheeze in children who received antibiotics vs. those who did not; P = 0.019).
Strengths of the study, Ms. Jones said, include a geographically based, diverse population, while a key limitation was the fact that the children were examined at 2-3 years of age. "This is a little early to diagnose asthma," she noted. "These children have not fully developed their asthmatic and atopic characteristics, so we have to look at them when they’re a little older. Another limitation is the possibility that some of the antibiotics were given for respiratory conditions that were actually early symptoms of asthma."
Ms. Jones said that she had no relevant financial disclosures.
SAN DIEGO – Antibiotic use prior to 6 months of age was associated with recurrent wheeze but not with allergic sensitization or other clinical allergic outcomes, results from a large birth cohort study demonstrated.
"In the medical literature, some but not all studies suggest that antibiotic use early in life is related to later childhood asthma and allergic disease," Kyra Jones, M.Ed., said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"It is well known that antibiotics affect the gut microbiome," she added. "What may not be as clear is the impact of the effect and its relationship to allergic outcomes. Since antibiotics affect the gut microbiome, we hypothesized that early antibiotic use would be associated with allergic outcomes."
In an effort to determine whether antibiotic use in the first 6 months of life is associated with allergic sensitization or clinical allergic outcomes at age 2-3 years, Ms. Jones, an epidemiologist in the department of public health sciences at Henry Ford Hospital, Detroit, and her associates obtained data from 1,258 pregnant women who participated in the WHEALS (Wayne County Health, Environment, Allergy, and Asthma Longitudinal Study) prospective birth cohort.
The women, who ranged in age from 21 to 49 years, were recruited between 2003 and 2007 at one of five Henry Ford Health System obstetric clinics in the western Wayne County suburbs or the city of Detroit. They were interviewed at 1, 6, 12, and 24 months following the birth of their child. Next, their children were brought into the clinic at 2-3 years of age and assessed for atopic dermatitis. The researchers analyzed the children’s blood for total IgE and specific IgE to milk, egg, peanut, dog, cat, dust mite, timothy grass, and cockroach and performed skin prick tests for the same allergens.
The primary exposure was defined as the mother reporting that her child had taken one or more of the following antibiotics within the first 6 months of life: cephalosporins, macrolides, penicillin, sulfonamides, and topical antibiotics. Outcomes of interest included total IgE, specific IgE, skin prick test positivity, history of physician diagnosis of atopic dermatitis, and parental report of wheezing at least twice in the first 2-3 years of life – including at least once in the preceding year. The researchers used logistic and linear regression models to assess associations between antibiotic exposure and outcomes.
Ms. Jones reported data from 680 children. More than half (58%) were African American and 51% were male. Slightly more than half (51.2%) had a positive specific IgE, 24.5% had a positive skin prick test, 22.7% had atopic dermatitis, and 15.6% had recurrent wheezing.
At 2 years, most outcomes were similar between children who used antibiotics and those who did not, but 22% of children who took antibiotics had recurrent wheeze, compared with 14% of those who did not, a difference that reached statistical significance (P = 0.03). Multivariate models revealed similar findings (odds ratio of 1.85 for recurrent wheeze in children who received antibiotics vs. those who did not; P = 0.019).
Strengths of the study, Ms. Jones said, include a geographically based, diverse population, while a key limitation was the fact that the children were examined at 2-3 years of age. "This is a little early to diagnose asthma," she noted. "These children have not fully developed their asthmatic and atopic characteristics, so we have to look at them when they’re a little older. Another limitation is the possibility that some of the antibiotics were given for respiratory conditions that were actually early symptoms of asthma."
Ms. Jones said that she had no relevant financial disclosures.
SAN DIEGO – Antibiotic use prior to 6 months of age was associated with recurrent wheeze but not with allergic sensitization or other clinical allergic outcomes, results from a large birth cohort study demonstrated.
"In the medical literature, some but not all studies suggest that antibiotic use early in life is related to later childhood asthma and allergic disease," Kyra Jones, M.Ed., said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
"It is well known that antibiotics affect the gut microbiome," she added. "What may not be as clear is the impact of the effect and its relationship to allergic outcomes. Since antibiotics affect the gut microbiome, we hypothesized that early antibiotic use would be associated with allergic outcomes."
In an effort to determine whether antibiotic use in the first 6 months of life is associated with allergic sensitization or clinical allergic outcomes at age 2-3 years, Ms. Jones, an epidemiologist in the department of public health sciences at Henry Ford Hospital, Detroit, and her associates obtained data from 1,258 pregnant women who participated in the WHEALS (Wayne County Health, Environment, Allergy, and Asthma Longitudinal Study) prospective birth cohort.
The women, who ranged in age from 21 to 49 years, were recruited between 2003 and 2007 at one of five Henry Ford Health System obstetric clinics in the western Wayne County suburbs or the city of Detroit. They were interviewed at 1, 6, 12, and 24 months following the birth of their child. Next, their children were brought into the clinic at 2-3 years of age and assessed for atopic dermatitis. The researchers analyzed the children’s blood for total IgE and specific IgE to milk, egg, peanut, dog, cat, dust mite, timothy grass, and cockroach and performed skin prick tests for the same allergens.
The primary exposure was defined as the mother reporting that her child had taken one or more of the following antibiotics within the first 6 months of life: cephalosporins, macrolides, penicillin, sulfonamides, and topical antibiotics. Outcomes of interest included total IgE, specific IgE, skin prick test positivity, history of physician diagnosis of atopic dermatitis, and parental report of wheezing at least twice in the first 2-3 years of life – including at least once in the preceding year. The researchers used logistic and linear regression models to assess associations between antibiotic exposure and outcomes.
Ms. Jones reported data from 680 children. More than half (58%) were African American and 51% were male. Slightly more than half (51.2%) had a positive specific IgE, 24.5% had a positive skin prick test, 22.7% had atopic dermatitis, and 15.6% had recurrent wheezing.
At 2 years, most outcomes were similar between children who used antibiotics and those who did not, but 22% of children who took antibiotics had recurrent wheeze, compared with 14% of those who did not, a difference that reached statistical significance (P = 0.03). Multivariate models revealed similar findings (odds ratio of 1.85 for recurrent wheeze in children who received antibiotics vs. those who did not; P = 0.019).
Strengths of the study, Ms. Jones said, include a geographically based, diverse population, while a key limitation was the fact that the children were examined at 2-3 years of age. "This is a little early to diagnose asthma," she noted. "These children have not fully developed their asthmatic and atopic characteristics, so we have to look at them when they’re a little older. Another limitation is the possibility that some of the antibiotics were given for respiratory conditions that were actually early symptoms of asthma."
Ms. Jones said that she had no relevant financial disclosures.
AT 2014 AAAAI ANNUAL MEETING
Major Finding: 22% of children who took antibiotics in the first 6 months of life had recurrent wheeze, compared with 14% of those who did not, a difference that reached statistical significance (P = 0.03).
Data Source: A study of 680 children in the Wayne County, Mich., area that set out to determine whether antibiotic use in the first 6 months of life is associated with allergic sensitization or clinical allergic outcomes at age 2-3 years.
Disclosures: Ms. Jones said that she had no relevant financial disclosures.

New heart valve guideline has more accessible format
The updated practice guideline for managing adults with valvular heart disease has a new, "modular" format to facilitate clinicians’ access to "concise, relevant bytes of information at the point of care, when clinical knowledge is needed most," according to reports published online simultaneously March 3 in Circulation and the Journal of the American College of Cardiology.
The guideline, compiled by a committee of cardiologists, interventionalists, surgeons, and anesthesiologists under the aegis of the American Heart Association and the American College of Cardiology, was last updated in 2008. "Some recommendations from the earlier valvular heart disease guideline have been updated as warranted by new evidence or a better understanding of earlier evidence, whereas others that were inaccurate, irrelevant, or overlapping were deleted or modified," said writing committee cochairs Dr. Rick A. Nishimura of the division of cardiovascular diseases, Mayo Clinic, Rochester, Minn.; and Dr. Catherine M. Otto, director of the University of Washington Medical Center’s Heart Valve Clinic, Seattle.
The narrative text of the guideline is limited, and instead it uses decision pathway diagrams and numerous summary tables of current evidence and recommendations. These include links to relevant references. It is hoped that clinicians can more easily use the new guideline as a quick reference. This format also will enable individual sections to be updated or amended as new evidence comes to light. The PDF of the guideline is available for free.
"This novel approach to evidence-based guideline development will revolutionize the clinical impact of guideline recommendations, ensuring they are always current and allowing seamless integration with electronic medical record systems," Dr. Otto said in a press statement accompanying the reports.
The guideline now includes gradations of disease severity, to help clinicians determine the optimal timing of intervention. Whether or not intervention is indicated depends on five factors: the presence or absence of symptoms, the severity of valvular heart disease, the response of the left and/or right ventricle to the volume or pressure overload caused by the valvular disease, the effect on the pulmonary or systemic circulation, and any change in heart rhythm.
Disease severity ranges from stage A, "at risk," which denotes patients who have risk factors for developing valvular heart disease; through stage B, "progressive," which indicates patients who are asymptomatic but have mildly to moderately severe disease; through stage C, "asymptomatic severe," which includes patients with severe yet still asymptomatic valvular disease in which the left or right ventricle remains compensated or in which the left or right ventricle has decompensated; to stage D, "symptomatic severe," which indicates patients whose severe valvular disease has produced symptoms.
"In patients with stenotic lesions, there is an additional category of ‘very severe’ stenosis based on studies of the natural history showing that prognosis becomes poorer as the severity of stenosis increases," the guideline states.
Information is provided for assessing the various disease states associated with the aortic, mitral, and tricuspid valves, and addresses the issues of valve repair, replacement, and the use of prosthetic valves.
Compared with the previous guideline, the new one suggests surgical intervention at an earlier stage for certain patients. "Due to more knowledge regarding the natural history of untreated patients with severe valvular heart disease and better outcomes from surgery, we’ve lowered the threshold for operation to include more patients with asymptomatic severe disease. Now, select patients with severe asymptomatic aortic stenosis and severe asymptomatic mitral regurgitation can be considered for intervention, depending on certain other factors such as operative mortality and ... the ability to achieve a durable valve repair," Dr. Nishimura said in the press statement.
The new guideline also proposes a new approach to risk assessment, to be applied to all patients for whom intervention is being considered. Previous risk scoring systems were "useful but limited"; the new approach takes into consideration "procedure-specific impediments, major organ system compromise, comorbidities, patient frailty, and the Society of Thoracic Surgeons predicted risk of mortality model."
For the first time, the guideline discusses transcatheter aortic valve replacement and other catheter-based treatments, new technologies that have improved patient care but also have complicated risk assessment. Separate recommendations are now offered regarding the choice and the timing of these interventions.
In addition to the AHA and the ACC, this guideline was developed in collaboration with the American Association for Thoracic Surgery, American Society for Echocardiography, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons.
The complete 2014 Guideline for the Management of Patients With Valvular Heart Disease is available from the American College of Cardiology and the American Heart Association.
Dr. Nishimura and Dr. Otto reported no financial conflicts of interest; their associates on the ACC/AHA Task Force’s writing committee reported ties to Edwards Scientific, Medtronic, and St. Jude Medical.
The updated practice guideline for managing adults with valvular heart disease has a new, "modular" format to facilitate clinicians’ access to "concise, relevant bytes of information at the point of care, when clinical knowledge is needed most," according to reports published online simultaneously March 3 in Circulation and the Journal of the American College of Cardiology.
The guideline, compiled by a committee of cardiologists, interventionalists, surgeons, and anesthesiologists under the aegis of the American Heart Association and the American College of Cardiology, was last updated in 2008. "Some recommendations from the earlier valvular heart disease guideline have been updated as warranted by new evidence or a better understanding of earlier evidence, whereas others that were inaccurate, irrelevant, or overlapping were deleted or modified," said writing committee cochairs Dr. Rick A. Nishimura of the division of cardiovascular diseases, Mayo Clinic, Rochester, Minn.; and Dr. Catherine M. Otto, director of the University of Washington Medical Center’s Heart Valve Clinic, Seattle.
The narrative text of the guideline is limited, and instead it uses decision pathway diagrams and numerous summary tables of current evidence and recommendations. These include links to relevant references. It is hoped that clinicians can more easily use the new guideline as a quick reference. This format also will enable individual sections to be updated or amended as new evidence comes to light. The PDF of the guideline is available for free.
"This novel approach to evidence-based guideline development will revolutionize the clinical impact of guideline recommendations, ensuring they are always current and allowing seamless integration with electronic medical record systems," Dr. Otto said in a press statement accompanying the reports.
The guideline now includes gradations of disease severity, to help clinicians determine the optimal timing of intervention. Whether or not intervention is indicated depends on five factors: the presence or absence of symptoms, the severity of valvular heart disease, the response of the left and/or right ventricle to the volume or pressure overload caused by the valvular disease, the effect on the pulmonary or systemic circulation, and any change in heart rhythm.
Disease severity ranges from stage A, "at risk," which denotes patients who have risk factors for developing valvular heart disease; through stage B, "progressive," which indicates patients who are asymptomatic but have mildly to moderately severe disease; through stage C, "asymptomatic severe," which includes patients with severe yet still asymptomatic valvular disease in which the left or right ventricle remains compensated or in which the left or right ventricle has decompensated; to stage D, "symptomatic severe," which indicates patients whose severe valvular disease has produced symptoms.
"In patients with stenotic lesions, there is an additional category of ‘very severe’ stenosis based on studies of the natural history showing that prognosis becomes poorer as the severity of stenosis increases," the guideline states.
Information is provided for assessing the various disease states associated with the aortic, mitral, and tricuspid valves, and addresses the issues of valve repair, replacement, and the use of prosthetic valves.
Compared with the previous guideline, the new one suggests surgical intervention at an earlier stage for certain patients. "Due to more knowledge regarding the natural history of untreated patients with severe valvular heart disease and better outcomes from surgery, we’ve lowered the threshold for operation to include more patients with asymptomatic severe disease. Now, select patients with severe asymptomatic aortic stenosis and severe asymptomatic mitral regurgitation can be considered for intervention, depending on certain other factors such as operative mortality and ... the ability to achieve a durable valve repair," Dr. Nishimura said in the press statement.
The new guideline also proposes a new approach to risk assessment, to be applied to all patients for whom intervention is being considered. Previous risk scoring systems were "useful but limited"; the new approach takes into consideration "procedure-specific impediments, major organ system compromise, comorbidities, patient frailty, and the Society of Thoracic Surgeons predicted risk of mortality model."
For the first time, the guideline discusses transcatheter aortic valve replacement and other catheter-based treatments, new technologies that have improved patient care but also have complicated risk assessment. Separate recommendations are now offered regarding the choice and the timing of these interventions.
In addition to the AHA and the ACC, this guideline was developed in collaboration with the American Association for Thoracic Surgery, American Society for Echocardiography, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons.
The complete 2014 Guideline for the Management of Patients With Valvular Heart Disease is available from the American College of Cardiology and the American Heart Association.
Dr. Nishimura and Dr. Otto reported no financial conflicts of interest; their associates on the ACC/AHA Task Force’s writing committee reported ties to Edwards Scientific, Medtronic, and St. Jude Medical.
The updated practice guideline for managing adults with valvular heart disease has a new, "modular" format to facilitate clinicians’ access to "concise, relevant bytes of information at the point of care, when clinical knowledge is needed most," according to reports published online simultaneously March 3 in Circulation and the Journal of the American College of Cardiology.
The guideline, compiled by a committee of cardiologists, interventionalists, surgeons, and anesthesiologists under the aegis of the American Heart Association and the American College of Cardiology, was last updated in 2008. "Some recommendations from the earlier valvular heart disease guideline have been updated as warranted by new evidence or a better understanding of earlier evidence, whereas others that were inaccurate, irrelevant, or overlapping were deleted or modified," said writing committee cochairs Dr. Rick A. Nishimura of the division of cardiovascular diseases, Mayo Clinic, Rochester, Minn.; and Dr. Catherine M. Otto, director of the University of Washington Medical Center’s Heart Valve Clinic, Seattle.
The narrative text of the guideline is limited, and instead it uses decision pathway diagrams and numerous summary tables of current evidence and recommendations. These include links to relevant references. It is hoped that clinicians can more easily use the new guideline as a quick reference. This format also will enable individual sections to be updated or amended as new evidence comes to light. The PDF of the guideline is available for free.
"This novel approach to evidence-based guideline development will revolutionize the clinical impact of guideline recommendations, ensuring they are always current and allowing seamless integration with electronic medical record systems," Dr. Otto said in a press statement accompanying the reports.
The guideline now includes gradations of disease severity, to help clinicians determine the optimal timing of intervention. Whether or not intervention is indicated depends on five factors: the presence or absence of symptoms, the severity of valvular heart disease, the response of the left and/or right ventricle to the volume or pressure overload caused by the valvular disease, the effect on the pulmonary or systemic circulation, and any change in heart rhythm.
Disease severity ranges from stage A, "at risk," which denotes patients who have risk factors for developing valvular heart disease; through stage B, "progressive," which indicates patients who are asymptomatic but have mildly to moderately severe disease; through stage C, "asymptomatic severe," which includes patients with severe yet still asymptomatic valvular disease in which the left or right ventricle remains compensated or in which the left or right ventricle has decompensated; to stage D, "symptomatic severe," which indicates patients whose severe valvular disease has produced symptoms.
"In patients with stenotic lesions, there is an additional category of ‘very severe’ stenosis based on studies of the natural history showing that prognosis becomes poorer as the severity of stenosis increases," the guideline states.
Information is provided for assessing the various disease states associated with the aortic, mitral, and tricuspid valves, and addresses the issues of valve repair, replacement, and the use of prosthetic valves.
Compared with the previous guideline, the new one suggests surgical intervention at an earlier stage for certain patients. "Due to more knowledge regarding the natural history of untreated patients with severe valvular heart disease and better outcomes from surgery, we’ve lowered the threshold for operation to include more patients with asymptomatic severe disease. Now, select patients with severe asymptomatic aortic stenosis and severe asymptomatic mitral regurgitation can be considered for intervention, depending on certain other factors such as operative mortality and ... the ability to achieve a durable valve repair," Dr. Nishimura said in the press statement.
The new guideline also proposes a new approach to risk assessment, to be applied to all patients for whom intervention is being considered. Previous risk scoring systems were "useful but limited"; the new approach takes into consideration "procedure-specific impediments, major organ system compromise, comorbidities, patient frailty, and the Society of Thoracic Surgeons predicted risk of mortality model."
For the first time, the guideline discusses transcatheter aortic valve replacement and other catheter-based treatments, new technologies that have improved patient care but also have complicated risk assessment. Separate recommendations are now offered regarding the choice and the timing of these interventions.
In addition to the AHA and the ACC, this guideline was developed in collaboration with the American Association for Thoracic Surgery, American Society for Echocardiography, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons.
The complete 2014 Guideline for the Management of Patients With Valvular Heart Disease is available from the American College of Cardiology and the American Heart Association.
Dr. Nishimura and Dr. Otto reported no financial conflicts of interest; their associates on the ACC/AHA Task Force’s writing committee reported ties to Edwards Scientific, Medtronic, and St. Jude Medical.
FROM CIRCULATION AND THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
VIDEO: Do soy isoflavones improve asthma control?
SAN DIEGO – Greater intake of soy isoflavones has been associated with lower prevalence of asthma in recent studies, but results from the placebo-controlled, federally funded SOYA (Study of Soy Isoflavones in Asthma) trial to assess soy supplements’ impact on asthma control showed that lung function didn’t improve with increased soy isoflavone intake. In a video interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, Dr. Lewis Smith of Northwestern University, Chicago, discusses the study's negative results, and what may have been behind the findings.
SAN DIEGO – Greater intake of soy isoflavones has been associated with lower prevalence of asthma in recent studies, but results from the placebo-controlled, federally funded SOYA (Study of Soy Isoflavones in Asthma) trial to assess soy supplements’ impact on asthma control showed that lung function didn’t improve with increased soy isoflavone intake. In a video interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, Dr. Lewis Smith of Northwestern University, Chicago, discusses the study's negative results, and what may have been behind the findings.
SAN DIEGO – Greater intake of soy isoflavones has been associated with lower prevalence of asthma in recent studies, but results from the placebo-controlled, federally funded SOYA (Study of Soy Isoflavones in Asthma) trial to assess soy supplements’ impact on asthma control showed that lung function didn’t improve with increased soy isoflavone intake. In a video interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, Dr. Lewis Smith of Northwestern University, Chicago, discusses the study's negative results, and what may have been behind the findings.
AT 2014 AAAAI ANNUAL MEETING

Exhaled nitric oxide’s merits in childhood asthma
KEYSTONE, COLO. – Fractional exhaled nitric oxide as a tool for patient care in pediatric asthma has often gotten a bad rap, according to a long-time researcher in the field.
"You’re either an exhaled nitric oxide fan or you’re not, it seems like, in the medical community. Some people expect it to be all things when in fact it’s just one measure. It measures atopic eosinophilic inflammation. We know that asthma is more than one disease, so we need more than one tool. This is a tool that’s useful in a subgroup of asthmatics, but I think the subgroup it’s useful in is big enough that it’s a valuable tool," Dr. Joseph D. Spahn declared at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.

The pediatric allergist published his first study demonstrating the clinical benefits of measuring fractional exhaled nitric oxide (FeNO) well before the technology won Food and Drug Administration approval and became commercially available.
An American Thoracic Society clinical practice guideline addressing the clinical utility of the test was a long time coming. Finally, several years ago, the ATS issued an official guideline declaring "FeNO offers added advantages for patient care" over conventional tests for asthma, such as FEV1 [forced expiratory volume in 1 second] reversibility and provocation tests (Am. J. Respir. Crit. Care Med. 2011;184:602-15).
The guideline describes three major clinical uses for FeNO testing: diagnosing asthma, predicting response to inhaled corticosteroids, and monitoring adherence to this cornerstone therapy.
FeNO’s role in diagnosing asthma
FeNO is significantly elevated in allergic asthma but not in other neutrophilic diseases that can masquerade as asthma, including primary immunodeficiencies, bronchopulmonary dysplasia, alpha-1antitrypsin deficiency, and cystic fibrosis, all of which feature either low or normal FeNO levels.
But it’s important to understand where the test is most likely to prove useful.
"FeNO is the only noninvasive tool we have for assessing airway inflammation. It’s a marker of atopic and Th2-driven inflammation. Many severe adult asthmatics don’t seem to have a Th2-driven disease process. Many little kids with nonatopic asthma and viral-induced wheezing don’t have Th2-driven inflammation. As a result, FeNO is not going to be a great tool in those situations. But for those individuals in which atopy plays a role, it’s a great measure of active airway inflammation," explained Dr. Spahn of the University of Colorado, Denver, and National Jewish Health.
In one representative head-to-head comparative study, a 15% or greater improvement in FEV1 in response to an inhaled corticosteroid – widely considered a gold standard test in support of a diagnosis of asthma – had a 12% sensitivity for the diagnosis, while a reduction of greater than 20 ppb in FeNO had an 88% sensitivity (Am. J. Respir. Crit. Care Med. 2004;169:473-8).
Predicting response to steroid therapy
The ATS guidelines state that symptomatic patients who present initially with a high FeNO – more than 35 ppb in children or 50 ppb in adults – are likely to benefit from a trial of inhaled corticosteroids, and that it’s appropriate to probe for allergen exposure in such patients. The guidelines further recommend that patients with a low baseline FeNO of less than 20 ppb in children or 25 ppb in adults are less likely to have eosinophilic inflammation and are unlikely to benefit from inhaled corticosteroid therapy. Consideration of a therapeutic trial with serial FeNO monitoring is recommended in patients with intermediate levels.
Years ago, Dr. Spahn and his coworkers showed in a double-blind, randomized, crossover study that FeNO values could predict whether children with mild to moderate asthma were more likely to respond to fluticasone (Flonase) or montelukast (Singulair); the higher the initial FeNO, the more likely fluticasone was the more effective option (J. Allergy Clin. Immunol. 2005;115:233-42).
Dr. Spahn also finds FeNO results helpful in combating parental steroid phobia. "Steroid phobia still exists in the pediatric world. I know we as health care providers don’t really worry about inhaled corticosteroids having significant side effects, but parents do," he observed.
He shared a story of a 10-year-old with a severe chronic cough and newly diagnosed asthma.
"This kid was extremely disabled from his cough. If you’re coughing every 30 seconds, it’s not going to be easy for you to function normally in school. But when I mentioned that he needed to be on inhaled corticosteroid therapy, the mom acted like I’d just given her kid a death sentence. So the FeNO was a tool that I used to help convince her that there was inflammation in his airways and the way to treat it was with an inhaled corticosteroid.
"After spending half an hour convincing her of the benefits and safety of inhaled corticosteroids, she agreed. I saw him back 6 weeks later. His cough was pretty much gone, his lung function was completely normalized, and his FeNO had fallen 90%. That’s my record: A 90% reduction is about as good as it gets," Dr. Spahn said.
Assessing steroid adherence
Placing an allergic asthma patient on inhaled corticosteroid therapy should result in at least a 50% reduction in an elevated baseline FeNO. A lesser response, or an increasing FeNO during follow-up visits, is an indicator of an adherence problem.
"I like to tell people who’ve been in practice 20 years or longer that FeNO is to inhaled steroids as the theophylline blood level was to theophylline therapy. Back in the day when we used theophylline, our measure of adherence was checking someone’s theophylline level. If it was low and the patient was poorly controlled, we could blame their poor control on their poor adherence to theophylline. Up until FeNO, we didn’t have that ability with inhaled steroids. We can’t measure inhaled steroid levels due to the fact that they’re so small in the bloodstream," Dr. Spahn explained.
He reported receiving honoraria from GlaxoSmithKline as well as from Aerocrine, which markets an FeNO analyzer.
KEYSTONE, COLO. – Fractional exhaled nitric oxide as a tool for patient care in pediatric asthma has often gotten a bad rap, according to a long-time researcher in the field.
"You’re either an exhaled nitric oxide fan or you’re not, it seems like, in the medical community. Some people expect it to be all things when in fact it’s just one measure. It measures atopic eosinophilic inflammation. We know that asthma is more than one disease, so we need more than one tool. This is a tool that’s useful in a subgroup of asthmatics, but I think the subgroup it’s useful in is big enough that it’s a valuable tool," Dr. Joseph D. Spahn declared at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
The pediatric allergist published his first study demonstrating the clinical benefits of measuring fractional exhaled nitric oxide (FeNO) well before the technology won Food and Drug Administration approval and became commercially available.
An American Thoracic Society clinical practice guideline addressing the clinical utility of the test was a long time coming. Finally, several years ago, the ATS issued an official guideline declaring "FeNO offers added advantages for patient care" over conventional tests for asthma, such as FEV1 [forced expiratory volume in 1 second] reversibility and provocation tests (Am. J. Respir. Crit. Care Med. 2011;184:602-15).
The guideline describes three major clinical uses for FeNO testing: diagnosing asthma, predicting response to inhaled corticosteroids, and monitoring adherence to this cornerstone therapy.
FeNO’s role in diagnosing asthma
FeNO is significantly elevated in allergic asthma but not in other neutrophilic diseases that can masquerade as asthma, including primary immunodeficiencies, bronchopulmonary dysplasia, alpha-1antitrypsin deficiency, and cystic fibrosis, all of which feature either low or normal FeNO levels.
But it’s important to understand where the test is most likely to prove useful.
"FeNO is the only noninvasive tool we have for assessing airway inflammation. It’s a marker of atopic and Th2-driven inflammation. Many severe adult asthmatics don’t seem to have a Th2-driven disease process. Many little kids with nonatopic asthma and viral-induced wheezing don’t have Th2-driven inflammation. As a result, FeNO is not going to be a great tool in those situations. But for those individuals in which atopy plays a role, it’s a great measure of active airway inflammation," explained Dr. Spahn of the University of Colorado, Denver, and National Jewish Health.
In one representative head-to-head comparative study, a 15% or greater improvement in FEV1 in response to an inhaled corticosteroid – widely considered a gold standard test in support of a diagnosis of asthma – had a 12% sensitivity for the diagnosis, while a reduction of greater than 20 ppb in FeNO had an 88% sensitivity (Am. J. Respir. Crit. Care Med. 2004;169:473-8).
Predicting response to steroid therapy
The ATS guidelines state that symptomatic patients who present initially with a high FeNO – more than 35 ppb in children or 50 ppb in adults – are likely to benefit from a trial of inhaled corticosteroids, and that it’s appropriate to probe for allergen exposure in such patients. The guidelines further recommend that patients with a low baseline FeNO of less than 20 ppb in children or 25 ppb in adults are less likely to have eosinophilic inflammation and are unlikely to benefit from inhaled corticosteroid therapy. Consideration of a therapeutic trial with serial FeNO monitoring is recommended in patients with intermediate levels.
Years ago, Dr. Spahn and his coworkers showed in a double-blind, randomized, crossover study that FeNO values could predict whether children with mild to moderate asthma were more likely to respond to fluticasone (Flonase) or montelukast (Singulair); the higher the initial FeNO, the more likely fluticasone was the more effective option (J. Allergy Clin. Immunol. 2005;115:233-42).
Dr. Spahn also finds FeNO results helpful in combating parental steroid phobia. "Steroid phobia still exists in the pediatric world. I know we as health care providers don’t really worry about inhaled corticosteroids having significant side effects, but parents do," he observed.
He shared a story of a 10-year-old with a severe chronic cough and newly diagnosed asthma.
"This kid was extremely disabled from his cough. If you’re coughing every 30 seconds, it’s not going to be easy for you to function normally in school. But when I mentioned that he needed to be on inhaled corticosteroid therapy, the mom acted like I’d just given her kid a death sentence. So the FeNO was a tool that I used to help convince her that there was inflammation in his airways and the way to treat it was with an inhaled corticosteroid.
"After spending half an hour convincing her of the benefits and safety of inhaled corticosteroids, she agreed. I saw him back 6 weeks later. His cough was pretty much gone, his lung function was completely normalized, and his FeNO had fallen 90%. That’s my record: A 90% reduction is about as good as it gets," Dr. Spahn said.
Assessing steroid adherence
Placing an allergic asthma patient on inhaled corticosteroid therapy should result in at least a 50% reduction in an elevated baseline FeNO. A lesser response, or an increasing FeNO during follow-up visits, is an indicator of an adherence problem.
"I like to tell people who’ve been in practice 20 years or longer that FeNO is to inhaled steroids as the theophylline blood level was to theophylline therapy. Back in the day when we used theophylline, our measure of adherence was checking someone’s theophylline level. If it was low and the patient was poorly controlled, we could blame their poor control on their poor adherence to theophylline. Up until FeNO, we didn’t have that ability with inhaled steroids. We can’t measure inhaled steroid levels due to the fact that they’re so small in the bloodstream," Dr. Spahn explained.
He reported receiving honoraria from GlaxoSmithKline as well as from Aerocrine, which markets an FeNO analyzer.
KEYSTONE, COLO. – Fractional exhaled nitric oxide as a tool for patient care in pediatric asthma has often gotten a bad rap, according to a long-time researcher in the field.
"You’re either an exhaled nitric oxide fan or you’re not, it seems like, in the medical community. Some people expect it to be all things when in fact it’s just one measure. It measures atopic eosinophilic inflammation. We know that asthma is more than one disease, so we need more than one tool. This is a tool that’s useful in a subgroup of asthmatics, but I think the subgroup it’s useful in is big enough that it’s a valuable tool," Dr. Joseph D. Spahn declared at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
The pediatric allergist published his first study demonstrating the clinical benefits of measuring fractional exhaled nitric oxide (FeNO) well before the technology won Food and Drug Administration approval and became commercially available.
An American Thoracic Society clinical practice guideline addressing the clinical utility of the test was a long time coming. Finally, several years ago, the ATS issued an official guideline declaring "FeNO offers added advantages for patient care" over conventional tests for asthma, such as FEV1 [forced expiratory volume in 1 second] reversibility and provocation tests (Am. J. Respir. Crit. Care Med. 2011;184:602-15).
The guideline describes three major clinical uses for FeNO testing: diagnosing asthma, predicting response to inhaled corticosteroids, and monitoring adherence to this cornerstone therapy.
FeNO’s role in diagnosing asthma
FeNO is significantly elevated in allergic asthma but not in other neutrophilic diseases that can masquerade as asthma, including primary immunodeficiencies, bronchopulmonary dysplasia, alpha-1antitrypsin deficiency, and cystic fibrosis, all of which feature either low or normal FeNO levels.
But it’s important to understand where the test is most likely to prove useful.
"FeNO is the only noninvasive tool we have for assessing airway inflammation. It’s a marker of atopic and Th2-driven inflammation. Many severe adult asthmatics don’t seem to have a Th2-driven disease process. Many little kids with nonatopic asthma and viral-induced wheezing don’t have Th2-driven inflammation. As a result, FeNO is not going to be a great tool in those situations. But for those individuals in which atopy plays a role, it’s a great measure of active airway inflammation," explained Dr. Spahn of the University of Colorado, Denver, and National Jewish Health.
In one representative head-to-head comparative study, a 15% or greater improvement in FEV1 in response to an inhaled corticosteroid – widely considered a gold standard test in support of a diagnosis of asthma – had a 12% sensitivity for the diagnosis, while a reduction of greater than 20 ppb in FeNO had an 88% sensitivity (Am. J. Respir. Crit. Care Med. 2004;169:473-8).
Predicting response to steroid therapy
The ATS guidelines state that symptomatic patients who present initially with a high FeNO – more than 35 ppb in children or 50 ppb in adults – are likely to benefit from a trial of inhaled corticosteroids, and that it’s appropriate to probe for allergen exposure in such patients. The guidelines further recommend that patients with a low baseline FeNO of less than 20 ppb in children or 25 ppb in adults are less likely to have eosinophilic inflammation and are unlikely to benefit from inhaled corticosteroid therapy. Consideration of a therapeutic trial with serial FeNO monitoring is recommended in patients with intermediate levels.
Years ago, Dr. Spahn and his coworkers showed in a double-blind, randomized, crossover study that FeNO values could predict whether children with mild to moderate asthma were more likely to respond to fluticasone (Flonase) or montelukast (Singulair); the higher the initial FeNO, the more likely fluticasone was the more effective option (J. Allergy Clin. Immunol. 2005;115:233-42).
Dr. Spahn also finds FeNO results helpful in combating parental steroid phobia. "Steroid phobia still exists in the pediatric world. I know we as health care providers don’t really worry about inhaled corticosteroids having significant side effects, but parents do," he observed.
He shared a story of a 10-year-old with a severe chronic cough and newly diagnosed asthma.
"This kid was extremely disabled from his cough. If you’re coughing every 30 seconds, it’s not going to be easy for you to function normally in school. But when I mentioned that he needed to be on inhaled corticosteroid therapy, the mom acted like I’d just given her kid a death sentence. So the FeNO was a tool that I used to help convince her that there was inflammation in his airways and the way to treat it was with an inhaled corticosteroid.
"After spending half an hour convincing her of the benefits and safety of inhaled corticosteroids, she agreed. I saw him back 6 weeks later. His cough was pretty much gone, his lung function was completely normalized, and his FeNO had fallen 90%. That’s my record: A 90% reduction is about as good as it gets," Dr. Spahn said.
Assessing steroid adherence
Placing an allergic asthma patient on inhaled corticosteroid therapy should result in at least a 50% reduction in an elevated baseline FeNO. A lesser response, or an increasing FeNO during follow-up visits, is an indicator of an adherence problem.
"I like to tell people who’ve been in practice 20 years or longer that FeNO is to inhaled steroids as the theophylline blood level was to theophylline therapy. Back in the day when we used theophylline, our measure of adherence was checking someone’s theophylline level. If it was low and the patient was poorly controlled, we could blame their poor control on their poor adherence to theophylline. Up until FeNO, we didn’t have that ability with inhaled steroids. We can’t measure inhaled steroid levels due to the fact that they’re so small in the bloodstream," Dr. Spahn explained.
He reported receiving honoraria from GlaxoSmithKline as well as from Aerocrine, which markets an FeNO analyzer.
EXPERT ANALYSIS FROM THE PULMONARY AND ALLERGY UPDATE

First guidelines on pulmonary hypertension in sickle cell disease released
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
"I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.

|
|
In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Susan Millard, pediatric pulmonologist, Helen DeVos Children’s Hospital, Grand Rapids, Mich.; and CHEST board member.
"I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.
|
|
|
In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Susan Millard, pediatric pulmonologist, Helen DeVos Children’s Hospital, Grand Rapids, Mich.; and CHEST board member.
"I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.
|
|
|
In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Susan Millard, pediatric pulmonologist, Helen DeVos Children’s Hospital, Grand Rapids, Mich.; and CHEST board member.
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
FROM AMERICAN JOURNAL OF RESPIRATORY CRITICAL CARE MEDICINE
