User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
VIDEO: Hello, this is your inhaler calling
SAN DIEGO – Dr. Bruce Bender of National Jewish Health, Denver, and his colleagues have created an electronic medical records system that reaches out and talks to patients, with the help of speech recognition software. The system notices when kids are due for a new asthma inhaler, and it automatically calls parents to help them order a new one. Over 2 years, it improved asthma inhaler adherence by 25%, without physicians having to lift a finger.
In a video interview, Dr. Bender shared his thoughts about the project at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, and he discussed its potential for conditions beyond asthma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Dr. Bruce Bender of National Jewish Health, Denver, and his colleagues have created an electronic medical records system that reaches out and talks to patients, with the help of speech recognition software. The system notices when kids are due for a new asthma inhaler, and it automatically calls parents to help them order a new one. Over 2 years, it improved asthma inhaler adherence by 25%, without physicians having to lift a finger.
In a video interview, Dr. Bender shared his thoughts about the project at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, and he discussed its potential for conditions beyond asthma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Dr. Bruce Bender of National Jewish Health, Denver, and his colleagues have created an electronic medical records system that reaches out and talks to patients, with the help of speech recognition software. The system notices when kids are due for a new asthma inhaler, and it automatically calls parents to help them order a new one. Over 2 years, it improved asthma inhaler adherence by 25%, without physicians having to lift a finger.
In a video interview, Dr. Bender shared his thoughts about the project at the annual meeting of the American Academy of Allergy, Asthma, and Immunology, and he discussed its potential for conditions beyond asthma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE 2014 AAAAI ANNUAL MEETING
VIDEO: Asthma management app for teens shows promise
SAN DIEGO – A smartphone app designed for children and teenagers with asthma improved medication adherence in a 30-day pilot study of 21 patients. Dr. David Stukus talked with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology about the app’s design and use of evidence-based medicine, how well it worked with adolescents, and a larger prospective trial that’s in the works.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN DIEGO – A smartphone app designed for children and teenagers with asthma improved medication adherence in a 30-day pilot study of 21 patients. Dr. David Stukus talked with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology about the app’s design and use of evidence-based medicine, how well it worked with adolescents, and a larger prospective trial that’s in the works.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN DIEGO – A smartphone app designed for children and teenagers with asthma improved medication adherence in a 30-day pilot study of 21 patients. Dr. David Stukus talked with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology about the app’s design and use of evidence-based medicine, how well it worked with adolescents, and a larger prospective trial that’s in the works.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
AT 2014 AAAAI ANNUAL MEETING
VIDEO: Allergy myths misdirect patients, physicians
SAN DIEGO – Is there really such a thing as a hypoallergenic dog? (Bo Obama, we’re looking at you.) Can blood tests for sale on the Internet identify a child’s allergies? And must parents wait until a child is 1, 2, or 3 years of age to introduce dietary milk, eggs, or nuts?
Dr. David R. Stukus of Nationwide Children’s Hospital in Columbus, Ohio, answers these questions and dispels other allergy-related misperceptions in an interview with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
On Twitter @sherryboschert
SAN DIEGO – Is there really such a thing as a hypoallergenic dog? (Bo Obama, we’re looking at you.) Can blood tests for sale on the Internet identify a child’s allergies? And must parents wait until a child is 1, 2, or 3 years of age to introduce dietary milk, eggs, or nuts?
Dr. David R. Stukus of Nationwide Children’s Hospital in Columbus, Ohio, answers these questions and dispels other allergy-related misperceptions in an interview with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
On Twitter @sherryboschert
SAN DIEGO – Is there really such a thing as a hypoallergenic dog? (Bo Obama, we’re looking at you.) Can blood tests for sale on the Internet identify a child’s allergies? And must parents wait until a child is 1, 2, or 3 years of age to introduce dietary milk, eggs, or nuts?
Dr. David R. Stukus of Nationwide Children’s Hospital in Columbus, Ohio, answers these questions and dispels other allergy-related misperceptions in an interview with us at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
On Twitter @sherryboschert
AT 2014 AAAAI ANNUAL MEETING
Two definitions of Gulf War illness recommended
An Institute of Medicine committee could not reach consensus on a single definition of Gulf War illness and recommended in a new report that clinicians and researchers at least narrow it down to two definitions.
That’s the preferred term – Gulf War illness – for a slew of health problems that occur at a higher rate in the approximately 697,000 U.S. veterans who served in the 1990-1991 Gulf War than in other veterans, the committee said. Gulf War illness is widely used and is more accurate than other terms used over the years for the same problems, including Gulf War syndrome, chronic multisystem illness, unexplained illness, medically unexplained symptoms, and medically unexplained physical symptoms, the report stated.
The Institute of Medicine (IOM) drafted a committee of 16 experts at the request of the Department of Veterans Affairs to try to develop a case definition for what's now called Gulf War illness in order to help standardize diagnosis, inclusion in research studies, and treatments. The committee's 120-page report, "Chronic Multisymptom Illness in Gulf War Veterans: Case Definitions Reexamined," is available on the IOM website.
Unable to find validation for one definition because of methodologic limitations in the studies, the committee recommended using either a broader definition from the Centers for Disease Control and Prevention (CDC) or a more restrictive one from studies of Kansas veterans, depending on the situation. Between the two of them, the definitions capture the most common symptoms of Gulf War illness and provide a framework for more focused research and treatment, the report said.
The committee found 2,033 articles in the literature focused on Gulf War illness symptoms and closely reviewed 718 of them. It found no objective diagnostic criteria but saw cumulative evidence that Gulf War illness is real. Fatigue, pain, and neurocognitive, gastrointestinal, respiratory, and/or dermatologic symptoms were reported with higher frequency in Gulf War veterans than in veterans of the same era who had not been deployed or were deployed elsewhere.
To identify the illness in a Gulf War veteran, the CDC definition requires one or more symptoms in at least two of the following categories: fatigue, pain, or mood and cognition. The Kansas definition requires symptoms in at least three of the following domains: fatigue or sleep, pain, neurologic or cognitive or mood symptoms, gastrointestinal symptoms, respiratory symptoms, and skin symptoms.
The CDC definition identified the illness in 29%-60% of Gulf War veterans, depending on the population studied. The Kansas definition identified the illness in 34% of Kansas veterans of the Gulf War.
The reason the committee couldn’t compile a single case definition is that the studies in the literature do not report on key features of the illness including onset, duration, severity, frequency of symptoms, and exclusionary criteria. The Department of Veterans Affairs should boost efforts to collect these kinds of data, conduct earlier in-depth assessments after deployment when unexpected complaints occur, and track troops’ exposures to vaccinations, drugs, and environmental factors, the report recommends.
The name Gulf War illness won out over Gulf War syndrome because "syndrome" indicates a new group of signs and symptoms, while the types and patterns of symptoms in this illness commonly are seen with other illnesses. The committee rejected "chronic multisymptom illness" because the phrase is not specific to Gulf War veterans.
The committee included experts in clinical medicine, toxicology, psychiatry, neurology, gastroenterology, epidemiology, sociology, psychometrics, biostatistics, occupational medicine, and basic science.
The report does not include potential disclosures of conflicts of interest.
On Twitter @sherryboschert
There has long been debate about whether Gulf War syndrome or Gulf War illness existed. If you remember the time of the Gulf War and shortly afterwards, there were a lot of questions about whether this was "all in their heads." Nobody ever found the sources of the illness. This report says to me that it’s final – that this august institution says, yes, this illness does exist. Whether you use the wider or narrower definition, this is to be taken seriously. That’s very important for physicians to know.
In terms of the two definitions – one narrower to be used for research and one broader to be used clinically – I think this gives people a little bit of latitude, depending on where they fit. The take-home piece is that, since there has been such a smorgasbord of opinions, thoughts, and descriptions, this should help the field by solidifying it further. We do still have two working definitions and we still don’t know a lot such as onset, duration, severity, frequency, and exclusionary criteria. Certainly, more needs to be done, but I think this is a very important step.

|
|
Finally, I think it’s also important that they said "Gulf War illness" rather than "chronic multisymptom illness." Again, I think that lends credibility to the claims of the veterans who have been there. This committee is willing to say, yes, there is something about having been deployed to the first Gulf War at a particular time that helps us understand your medical history. That’s not as far as we’d like to go, but it’s certainly some steps in the right direction.
That was a very short war a long time ago. Now, we’ve had 12 years of a very long war with multiple deployments, yet we haven’t really seen Gulf War illness or its equivalent in this generation of Iraq and Afghanistan veterans. I have expected that at some point we’re going to see these psychosomatic, vague symptoms coming out of this current war. I definitely think there’s time. Traumatic brain injury seems like the cardinal disorder from these wars, but I think we’re going to see some psychosomatic reactions over time.
Dr. Elspeth Cameron Ritchie is an expert on military health issues who retired as a colonel after 28 years in the U.S. Army. These are excerpts of an interview in which she spoke as an individual, not in her current roles as chief clinical officer of the Department of Behavioral Health for the District of Columbia and professor of psychiatry at the Uniformed Services University of the Health Sciences, Bethesda, Md., and at Georgetown University, Washington. She reported having no financial disclosures.
There has long been debate about whether Gulf War syndrome or Gulf War illness existed. If you remember the time of the Gulf War and shortly afterwards, there were a lot of questions about whether this was "all in their heads." Nobody ever found the sources of the illness. This report says to me that it’s final – that this august institution says, yes, this illness does exist. Whether you use the wider or narrower definition, this is to be taken seriously. That’s very important for physicians to know.
In terms of the two definitions – one narrower to be used for research and one broader to be used clinically – I think this gives people a little bit of latitude, depending on where they fit. The take-home piece is that, since there has been such a smorgasbord of opinions, thoughts, and descriptions, this should help the field by solidifying it further. We do still have two working definitions and we still don’t know a lot such as onset, duration, severity, frequency, and exclusionary criteria. Certainly, more needs to be done, but I think this is a very important step.
|
|
|
Finally, I think it’s also important that they said "Gulf War illness" rather than "chronic multisymptom illness." Again, I think that lends credibility to the claims of the veterans who have been there. This committee is willing to say, yes, there is something about having been deployed to the first Gulf War at a particular time that helps us understand your medical history. That’s not as far as we’d like to go, but it’s certainly some steps in the right direction.
That was a very short war a long time ago. Now, we’ve had 12 years of a very long war with multiple deployments, yet we haven’t really seen Gulf War illness or its equivalent in this generation of Iraq and Afghanistan veterans. I have expected that at some point we’re going to see these psychosomatic, vague symptoms coming out of this current war. I definitely think there’s time. Traumatic brain injury seems like the cardinal disorder from these wars, but I think we’re going to see some psychosomatic reactions over time.
Dr. Elspeth Cameron Ritchie is an expert on military health issues who retired as a colonel after 28 years in the U.S. Army. These are excerpts of an interview in which she spoke as an individual, not in her current roles as chief clinical officer of the Department of Behavioral Health for the District of Columbia and professor of psychiatry at the Uniformed Services University of the Health Sciences, Bethesda, Md., and at Georgetown University, Washington. She reported having no financial disclosures.
There has long been debate about whether Gulf War syndrome or Gulf War illness existed. If you remember the time of the Gulf War and shortly afterwards, there were a lot of questions about whether this was "all in their heads." Nobody ever found the sources of the illness. This report says to me that it’s final – that this august institution says, yes, this illness does exist. Whether you use the wider or narrower definition, this is to be taken seriously. That’s very important for physicians to know.
In terms of the two definitions – one narrower to be used for research and one broader to be used clinically – I think this gives people a little bit of latitude, depending on where they fit. The take-home piece is that, since there has been such a smorgasbord of opinions, thoughts, and descriptions, this should help the field by solidifying it further. We do still have two working definitions and we still don’t know a lot such as onset, duration, severity, frequency, and exclusionary criteria. Certainly, more needs to be done, but I think this is a very important step.
|
|
|
Finally, I think it’s also important that they said "Gulf War illness" rather than "chronic multisymptom illness." Again, I think that lends credibility to the claims of the veterans who have been there. This committee is willing to say, yes, there is something about having been deployed to the first Gulf War at a particular time that helps us understand your medical history. That’s not as far as we’d like to go, but it’s certainly some steps in the right direction.
That was a very short war a long time ago. Now, we’ve had 12 years of a very long war with multiple deployments, yet we haven’t really seen Gulf War illness or its equivalent in this generation of Iraq and Afghanistan veterans. I have expected that at some point we’re going to see these psychosomatic, vague symptoms coming out of this current war. I definitely think there’s time. Traumatic brain injury seems like the cardinal disorder from these wars, but I think we’re going to see some psychosomatic reactions over time.
Dr. Elspeth Cameron Ritchie is an expert on military health issues who retired as a colonel after 28 years in the U.S. Army. These are excerpts of an interview in which she spoke as an individual, not in her current roles as chief clinical officer of the Department of Behavioral Health for the District of Columbia and professor of psychiatry at the Uniformed Services University of the Health Sciences, Bethesda, Md., and at Georgetown University, Washington. She reported having no financial disclosures.
An Institute of Medicine committee could not reach consensus on a single definition of Gulf War illness and recommended in a new report that clinicians and researchers at least narrow it down to two definitions.
That’s the preferred term – Gulf War illness – for a slew of health problems that occur at a higher rate in the approximately 697,000 U.S. veterans who served in the 1990-1991 Gulf War than in other veterans, the committee said. Gulf War illness is widely used and is more accurate than other terms used over the years for the same problems, including Gulf War syndrome, chronic multisystem illness, unexplained illness, medically unexplained symptoms, and medically unexplained physical symptoms, the report stated.
The Institute of Medicine (IOM) drafted a committee of 16 experts at the request of the Department of Veterans Affairs to try to develop a case definition for what's now called Gulf War illness in order to help standardize diagnosis, inclusion in research studies, and treatments. The committee's 120-page report, "Chronic Multisymptom Illness in Gulf War Veterans: Case Definitions Reexamined," is available on the IOM website.
Unable to find validation for one definition because of methodologic limitations in the studies, the committee recommended using either a broader definition from the Centers for Disease Control and Prevention (CDC) or a more restrictive one from studies of Kansas veterans, depending on the situation. Between the two of them, the definitions capture the most common symptoms of Gulf War illness and provide a framework for more focused research and treatment, the report said.
The committee found 2,033 articles in the literature focused on Gulf War illness symptoms and closely reviewed 718 of them. It found no objective diagnostic criteria but saw cumulative evidence that Gulf War illness is real. Fatigue, pain, and neurocognitive, gastrointestinal, respiratory, and/or dermatologic symptoms were reported with higher frequency in Gulf War veterans than in veterans of the same era who had not been deployed or were deployed elsewhere.
To identify the illness in a Gulf War veteran, the CDC definition requires one or more symptoms in at least two of the following categories: fatigue, pain, or mood and cognition. The Kansas definition requires symptoms in at least three of the following domains: fatigue or sleep, pain, neurologic or cognitive or mood symptoms, gastrointestinal symptoms, respiratory symptoms, and skin symptoms.
The CDC definition identified the illness in 29%-60% of Gulf War veterans, depending on the population studied. The Kansas definition identified the illness in 34% of Kansas veterans of the Gulf War.
The reason the committee couldn’t compile a single case definition is that the studies in the literature do not report on key features of the illness including onset, duration, severity, frequency of symptoms, and exclusionary criteria. The Department of Veterans Affairs should boost efforts to collect these kinds of data, conduct earlier in-depth assessments after deployment when unexpected complaints occur, and track troops’ exposures to vaccinations, drugs, and environmental factors, the report recommends.
The name Gulf War illness won out over Gulf War syndrome because "syndrome" indicates a new group of signs and symptoms, while the types and patterns of symptoms in this illness commonly are seen with other illnesses. The committee rejected "chronic multisymptom illness" because the phrase is not specific to Gulf War veterans.
The committee included experts in clinical medicine, toxicology, psychiatry, neurology, gastroenterology, epidemiology, sociology, psychometrics, biostatistics, occupational medicine, and basic science.
The report does not include potential disclosures of conflicts of interest.
On Twitter @sherryboschert
An Institute of Medicine committee could not reach consensus on a single definition of Gulf War illness and recommended in a new report that clinicians and researchers at least narrow it down to two definitions.
That’s the preferred term – Gulf War illness – for a slew of health problems that occur at a higher rate in the approximately 697,000 U.S. veterans who served in the 1990-1991 Gulf War than in other veterans, the committee said. Gulf War illness is widely used and is more accurate than other terms used over the years for the same problems, including Gulf War syndrome, chronic multisystem illness, unexplained illness, medically unexplained symptoms, and medically unexplained physical symptoms, the report stated.
The Institute of Medicine (IOM) drafted a committee of 16 experts at the request of the Department of Veterans Affairs to try to develop a case definition for what's now called Gulf War illness in order to help standardize diagnosis, inclusion in research studies, and treatments. The committee's 120-page report, "Chronic Multisymptom Illness in Gulf War Veterans: Case Definitions Reexamined," is available on the IOM website.
Unable to find validation for one definition because of methodologic limitations in the studies, the committee recommended using either a broader definition from the Centers for Disease Control and Prevention (CDC) or a more restrictive one from studies of Kansas veterans, depending on the situation. Between the two of them, the definitions capture the most common symptoms of Gulf War illness and provide a framework for more focused research and treatment, the report said.
The committee found 2,033 articles in the literature focused on Gulf War illness symptoms and closely reviewed 718 of them. It found no objective diagnostic criteria but saw cumulative evidence that Gulf War illness is real. Fatigue, pain, and neurocognitive, gastrointestinal, respiratory, and/or dermatologic symptoms were reported with higher frequency in Gulf War veterans than in veterans of the same era who had not been deployed or were deployed elsewhere.
To identify the illness in a Gulf War veteran, the CDC definition requires one or more symptoms in at least two of the following categories: fatigue, pain, or mood and cognition. The Kansas definition requires symptoms in at least three of the following domains: fatigue or sleep, pain, neurologic or cognitive or mood symptoms, gastrointestinal symptoms, respiratory symptoms, and skin symptoms.
The CDC definition identified the illness in 29%-60% of Gulf War veterans, depending on the population studied. The Kansas definition identified the illness in 34% of Kansas veterans of the Gulf War.
The reason the committee couldn’t compile a single case definition is that the studies in the literature do not report on key features of the illness including onset, duration, severity, frequency of symptoms, and exclusionary criteria. The Department of Veterans Affairs should boost efforts to collect these kinds of data, conduct earlier in-depth assessments after deployment when unexpected complaints occur, and track troops’ exposures to vaccinations, drugs, and environmental factors, the report recommends.
The name Gulf War illness won out over Gulf War syndrome because "syndrome" indicates a new group of signs and symptoms, while the types and patterns of symptoms in this illness commonly are seen with other illnesses. The committee rejected "chronic multisymptom illness" because the phrase is not specific to Gulf War veterans.
The committee included experts in clinical medicine, toxicology, psychiatry, neurology, gastroenterology, epidemiology, sociology, psychometrics, biostatistics, occupational medicine, and basic science.
The report does not include potential disclosures of conflicts of interest.
On Twitter @sherryboschert

FDA issues warning about using doripenem for ventilator-associated pneumonia
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
When used to treat ventilator-associated pneumonia, the antibacterial drug doripenem is linked to a greater risk of mortality and lower clinical cure rates compared with imipenem and cilastatin for injection, according to a drug safety communication issued by the Food and Drug Administration.
Doripenem, an intravenous penem antibacterial drug marketed as Doribax, is not approved to treat any type of pneumonia. A warning about increased mortality in patients with ventilator-associated pneumonia (VAP), for which the use of doripenem is unapproved, has been added to the drug’s label. In a statement posted on March 6, the FDA recommended that health care professionals "consider whether the benefits of Doribax treatment are likely to exceed its potential risks in patients who develop pneumonia while on ventilators."
The safety communication is based on an FDA analysis of a 3-year study comparing 7 days of treatment with doripenem to 10 days of treatment with imipenem and cilastatin in patients with VAP. All-cause mortality over 28 days was 23% among those treated with doripenem, compared with 16.7% among those treated with imipenem and cilastatin. Clinical cure rates also were lower in the doripenem-treated patients in the study, which was stopped prematurely in 2011.
The statement adds that doripenem, approved in 2007, "is still considered safe and effective" for treating adults with complicated intra-abdominal infections and complicated urinary tract infections, including pyelonephritis, which are FDA-approved indications.
In January 2012, the FDA issued a statement about the prematurely terminated study.
The revised doripenem label is available on the FDA website. The label change was made in January. Doripenem is manufactured by Shionogi.
Imipenem and cilastatin for injection is marketed as Primaxin in the United States.
Serious adverse events associated with doripenem should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch/.
Injectable testosterone approved for hypogonadism, with REMS addressing risks
A long-acting intramuscular formulation of testosterone has been approved by the Food and Drug Administration for treating hypogonadism, with a label that includes a boxed warning about the risks of pulmonary oil microembolism and anaphylaxis associated with treatment.
The depot formulation of testosterone undecanoate (TU), in castor oil and benzoyl benzoate, has been approved for treating adult men with primary hypogonadism or hypogonadotropic hypogonadism, congenital or acquired. The indications section includes the statement that it "should only be used in patients who require testosterone replacement therapy and in whom the benefits of the product outweigh the serious risks of pulmonary oil microembolism and anaphylaxis."
The drug will be available, with restrictions, through the Aveed Risk Evaluation and Mitigation Strategy (REMS), according to the manufacturer, Endo Pharmaceuticals, which is marketing the product as Aveed. Under the REMS, prescriber education and certification will be required and distribution of the product will be restricted, according to the company.
The product is available in single-use vials; the recommended dosing is 3 mL (750 mg) at the start of treatment, at 4 weeks, and then at 10-week intervals. After each injection, patients are observed for symptoms of pulmonary oil microembolism (POME) or anaphylaxis for 30 minutes in the physician’s office, clinic, or hospital, the only places where the drug can be administered. Symptoms of serious POME reactions include an urge to cough, dyspnea, throat tightening, chest pain, dizziness, and syncope.
Since Endo filed for approval in 2007, approval of TU has been held up for safety reasons, namely reports of anaphylaxis and POME during or shortly after injections were administered, in clinical and postmarketing studies in countries where the product was approved. At a meeting in April 2013, the FDA’s Advisory Committee for Reproductive Health Drugs and the Drug Safety and Risk Management Advisory Committee split on the safety issue, voting 9-9 on whether they believed the drug had an acceptable safety profile for the proposed use.
Approval was based on the results of a phase III, 84-week, single-arm study of 130 hypogonadal men (mean age, 54 years), which determined that TU was an effective testosterone replacement therapy, based on serum testosterone levels. There was one case of a patient who had mild coughing after the third injection, which was later attributed to POME, according to the prescribing information.
But more cases have been reported after approval in countries outside the United States and in a review of 18 clinical studies; where possible cases of POME were adjudicated, of about 3,500 patients there were 9 cases of POME in 8 patients and 2 cases of anaphylaxis.
The product has been available since 2003 outside the United States, where it is marketed by Bayer Pharma and its subsidiaries.
The company is providing information about the REMS at www.AveedREMS.com and 855-755-0494.
Serious adverse events associated with testosterone undecanoate should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
A long-acting intramuscular formulation of testosterone has been approved by the Food and Drug Administration for treating hypogonadism, with a label that includes a boxed warning about the risks of pulmonary oil microembolism and anaphylaxis associated with treatment.
The depot formulation of testosterone undecanoate (TU), in castor oil and benzoyl benzoate, has been approved for treating adult men with primary hypogonadism or hypogonadotropic hypogonadism, congenital or acquired. The indications section includes the statement that it "should only be used in patients who require testosterone replacement therapy and in whom the benefits of the product outweigh the serious risks of pulmonary oil microembolism and anaphylaxis."
The drug will be available, with restrictions, through the Aveed Risk Evaluation and Mitigation Strategy (REMS), according to the manufacturer, Endo Pharmaceuticals, which is marketing the product as Aveed. Under the REMS, prescriber education and certification will be required and distribution of the product will be restricted, according to the company.
The product is available in single-use vials; the recommended dosing is 3 mL (750 mg) at the start of treatment, at 4 weeks, and then at 10-week intervals. After each injection, patients are observed for symptoms of pulmonary oil microembolism (POME) or anaphylaxis for 30 minutes in the physician’s office, clinic, or hospital, the only places where the drug can be administered. Symptoms of serious POME reactions include an urge to cough, dyspnea, throat tightening, chest pain, dizziness, and syncope.
Since Endo filed for approval in 2007, approval of TU has been held up for safety reasons, namely reports of anaphylaxis and POME during or shortly after injections were administered, in clinical and postmarketing studies in countries where the product was approved. At a meeting in April 2013, the FDA’s Advisory Committee for Reproductive Health Drugs and the Drug Safety and Risk Management Advisory Committee split on the safety issue, voting 9-9 on whether they believed the drug had an acceptable safety profile for the proposed use.
Approval was based on the results of a phase III, 84-week, single-arm study of 130 hypogonadal men (mean age, 54 years), which determined that TU was an effective testosterone replacement therapy, based on serum testosterone levels. There was one case of a patient who had mild coughing after the third injection, which was later attributed to POME, according to the prescribing information.
But more cases have been reported after approval in countries outside the United States and in a review of 18 clinical studies; where possible cases of POME were adjudicated, of about 3,500 patients there were 9 cases of POME in 8 patients and 2 cases of anaphylaxis.
The product has been available since 2003 outside the United States, where it is marketed by Bayer Pharma and its subsidiaries.
The company is providing information about the REMS at www.AveedREMS.com and 855-755-0494.
Serious adverse events associated with testosterone undecanoate should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
A long-acting intramuscular formulation of testosterone has been approved by the Food and Drug Administration for treating hypogonadism, with a label that includes a boxed warning about the risks of pulmonary oil microembolism and anaphylaxis associated with treatment.
The depot formulation of testosterone undecanoate (TU), in castor oil and benzoyl benzoate, has been approved for treating adult men with primary hypogonadism or hypogonadotropic hypogonadism, congenital or acquired. The indications section includes the statement that it "should only be used in patients who require testosterone replacement therapy and in whom the benefits of the product outweigh the serious risks of pulmonary oil microembolism and anaphylaxis."
The drug will be available, with restrictions, through the Aveed Risk Evaluation and Mitigation Strategy (REMS), according to the manufacturer, Endo Pharmaceuticals, which is marketing the product as Aveed. Under the REMS, prescriber education and certification will be required and distribution of the product will be restricted, according to the company.
The product is available in single-use vials; the recommended dosing is 3 mL (750 mg) at the start of treatment, at 4 weeks, and then at 10-week intervals. After each injection, patients are observed for symptoms of pulmonary oil microembolism (POME) or anaphylaxis for 30 minutes in the physician’s office, clinic, or hospital, the only places where the drug can be administered. Symptoms of serious POME reactions include an urge to cough, dyspnea, throat tightening, chest pain, dizziness, and syncope.
Since Endo filed for approval in 2007, approval of TU has been held up for safety reasons, namely reports of anaphylaxis and POME during or shortly after injections were administered, in clinical and postmarketing studies in countries where the product was approved. At a meeting in April 2013, the FDA’s Advisory Committee for Reproductive Health Drugs and the Drug Safety and Risk Management Advisory Committee split on the safety issue, voting 9-9 on whether they believed the drug had an acceptable safety profile for the proposed use.
Approval was based on the results of a phase III, 84-week, single-arm study of 130 hypogonadal men (mean age, 54 years), which determined that TU was an effective testosterone replacement therapy, based on serum testosterone levels. There was one case of a patient who had mild coughing after the third injection, which was later attributed to POME, according to the prescribing information.
But more cases have been reported after approval in countries outside the United States and in a review of 18 clinical studies; where possible cases of POME were adjudicated, of about 3,500 patients there were 9 cases of POME in 8 patients and 2 cases of anaphylaxis.
The product has been available since 2003 outside the United States, where it is marketed by Bayer Pharma and its subsidiaries.
The company is providing information about the REMS at www.AveedREMS.com and 855-755-0494.
Serious adverse events associated with testosterone undecanoate should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
VIDEO: Asthma meds’ safety data reassuring in pregnancy
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ANALYSIS FROM 2014 AAAAI ANNUAL MEETING

CDC sounds alarm on hospital antibiotic use
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
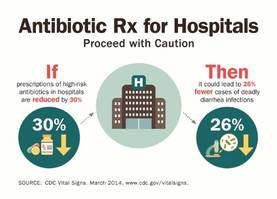
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.

"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.

|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
|
|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
|
|
| Dr. Franklin A. Michota |
Dr. Franklin A. Michota is director of academic affairs, department of hospital medicine, Cleveland Clinic. He reports having no disclosures.
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.
"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.
A scathing new report by the Centers for Disease Control and Prevention found ample room for improvement in inpatient antibiotic prescribing.
Findings include continued overuse of antibiotics in hospitals, errors in prescribing, and the lifesaving potential of efforts to reduce antibiotic use:
• Physicians in some hospitals prescribed three times as many antibiotics as doctors in other hospitals, even though patients were being cared for in similar areas of each hospital.
• Antibiotic prescriptions contained an error in 37% of cases involving treatment for urinary tract infections or use of the common and critical drug, vancomycin (Vancocin).
• Models predicted that a 30% decrease in the use of broad-spectrum antibiotics would lead to a 26% reduction in Clostridium difficile infections, which kill roughly 14,000 hospitalized patients each year.
"Antibiotics are often lifesaving, and we have to protect them before our medicine chests run empty," CDC director Tom Frieden said during a press conference highlighting the report, released in the CDC’s March 4 Morbidity and Mortality Weekly Report (MMWR 2014 March 4;63:1-7).
Dr. Frieden announced that the CDC’s fiscal 2015 budget, part of President Obama’s budget initiative rolled out today, contains a $30 million increase in funds to establish a robust infrastructure in the United States to detect antibiotic threats and protect patients and communities.
The new monies would allow the CDC to extend the "detect and protect" strategy to combat antibiotic resistance outlined last year, help support state and hospital efforts to implement antibiotic stewardship programs, and improve rapid detection of antimicrobial threats and outbreaks.
"One of the things that makes us so focused on antimicrobial resistance is that not only is it a really serious problem, but [also] it’s not too late," Dr. Frieden said.
If funded, he anticipates the CDC and other stakeholders will be able to reverse drug resistance and cut in half the rate of C. difficile and the "nightmare" carbapenem-resistant Enterobacteriaceae infections.
It was noted that robust efforts to improve the use of antibiotics associated with C. difficile in the United Kingdom have resulted in more than a 50% reduction in use of those targeted agents and a roughly 70% reduction in C. difficile infections over the past 6 to 7 years.
The CDC is strongly recommending that every hospital in the United States have an antibiotic stewardship program and is providing a new checklist to help facilities with the task. The checklist contains seven core elements of an effective program: leadership commitment; accountability for outcomes under a single leader; drug expertise under a single pharmacist leader; taking action on at least one prescribing improvement practice; tracking antibiotic prescribing and resistance patterns; reporting regularly to staff about these patterns; and educating staff on antibiotic resistance and improving prescribing practices.
Specific advice was also given to clinicians to order recommended cultures before antibiotics are given and to start drugs promptly; make sure the indication, dose, and expected duration are specified in the patient record; and reassess patients within 48 hours and adjust treatment, if necessary, or stop treatment, if indicated.
Concerns were raised during the briefing over whether voluntary strategies will curb interfacility transmission caused by transfers of patients with multidrug-resistant infections and the failure to report outbreaks between facilities. Dr. John R. Combes, the American Hospital Association’s senior vice president said several groups are working to smooth out these transfers and that the AHA’s "Hospitals in Pursuit of Excellence" program provides best practices to facilitate transfers and foster cooperation with surrounding facilities to prevent infections.
The new CDC report is based on a review of data from all 323 hospitals in the MarketScan Hospital Drug Database and from hospitals in the CDC’s Emerging Infections Program.
Antibiotics were prescribed for 55.7% of patients hospitalized in 2010 in the MarketScan Hospital Drug Database, with 30% receiving at least one dose of broad-spectrum antibiotics.
One or more antibiotics were used to treat active infections in 37% of 11,282 patients treated in 2011 at 183 acute care hospitals evaluated by the Emerging Infections Program. Half of the antibiotics were prescribed for one of three scenarios: lower respiratory tract infections (22.2%), urinary tract infections (14%), and suspected drug-resistant Gram-positive infections such as methicillin-resistant Staphylococcus aureus (17.6%).
The CDC previously called on physicians to address antibiotic resistance in its Antibiotic Threats in the United States, 2013 report and the 2013 Get Smart About Antibiotics Week. The issue also will be tackled in the CDC’s forthcoming Transatlantic Taskforce on Antimicrobial Resistance 2013 report, with additional research expected to focus on contributing factors that led to such wide variances in antibiotic use between hospitals.
Dr. Frieden and Dr. Combes reported having no financial disclosures.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT

Asthma more common in eosinophilic esophagitis than previously thought
SAN DIEGO – Asthma and airway hyperresponsiveness may be underrecognized in children with eosinophilic esophagitis, results from a controlled cross-sectional study demonstrated.
While previous studies have estimated the prevalence of asthma in children with eosinophilic esophagitis (EoE), to range from 24-42%, a recent analysis presented during a late-breaker abstract session at annual meeting of the American Academy of Allergy, Asthma, and Immunology found that up to 70% of children with EoE may suffer from asthma.

"Clinicians treating children with eosinophilic esophagitis should consider asking additional history questions related to asthma symptoms and may also want to consider pulmonary function testing or referral to an asthma specialist for evaluation," lead author Dr. Nadia L. Krupp said in an interview prior to the meeting. "This is the first study to formally evaluate lung function and airway hyperresponsiveness in children with EoE. Prior estimations of asthma have solely come from patient/parent report."
Dr. Krupp, director of the Riley Asthma Care Center in the section of pulmonology, allergy, and critical care medicine at Riley Hospital Children, Indianapolis, and her associates conducted a cross-sectional study of 33 children aged 6-18 years with EoE and 37 healthy controls. The researchers performed methacholine challenge (airway hyperresponsiveness defined as provocative concentration of methacholine less than 8mg/mL), and exhaled nitric oxide. They also analyzed peripheral blood for total IgE, eosinophil count, eotaxin, and serum cytokines.
Baseline spirometry did not significantly differ between EoE subjects and healthy controls. However, airway hyperresponsiveness was present in 33% of children with EoE, compared with only 10.8% of healthy controls (P = .04). In addition, 20% of the 15 EoE subjects with asthma had airway hyperresponsiveness, compared with 44% of the 18 EoE subjects without asthma. Overall, 69.7% of EoE subjects had either asthma or airway hyperresponsiveness.

The researchers found that airway hyperresponsiveness correlated strongly with serum IgE (P less than .0001) and exhaled nitric oxide (P = .0002), while epidermal growth factor (EGF) and fibroblastic growth factor–2 (FGF-2) were elevated in subjects with EoE and asthma, compared to healthy controls and those with EoE but no asthma (P less than .05). In addition, subjects with EoE and asthma who were on asthma controller medications had similar levels of EGF and FGF-2 as healthy controls, while Th2 cytokines and eotaxin did not differ significantly among any groups.
Dr. Krupp said she was surprised "by the fact that airway hyperresponsiveness was more prevalent in those subjects without a history of asthma than those with a known diagnosis, and the fact that Th2-related cytokines were not significantly different between healthy controls and EoE subjects."
She acknowledged certain limitations of the study, including its cross-sectional design and "the fact EoE subjects may have had significant variability in the current activity of their esophageal disease at the time of enrollment."
The study was partially funded by Aerocrine. Dr. Krupp said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Asthma and airway hyperresponsiveness may be underrecognized in children with eosinophilic esophagitis, results from a controlled cross-sectional study demonstrated.
While previous studies have estimated the prevalence of asthma in children with eosinophilic esophagitis (EoE), to range from 24-42%, a recent analysis presented during a late-breaker abstract session at annual meeting of the American Academy of Allergy, Asthma, and Immunology found that up to 70% of children with EoE may suffer from asthma.
"Clinicians treating children with eosinophilic esophagitis should consider asking additional history questions related to asthma symptoms and may also want to consider pulmonary function testing or referral to an asthma specialist for evaluation," lead author Dr. Nadia L. Krupp said in an interview prior to the meeting. "This is the first study to formally evaluate lung function and airway hyperresponsiveness in children with EoE. Prior estimations of asthma have solely come from patient/parent report."
Dr. Krupp, director of the Riley Asthma Care Center in the section of pulmonology, allergy, and critical care medicine at Riley Hospital Children, Indianapolis, and her associates conducted a cross-sectional study of 33 children aged 6-18 years with EoE and 37 healthy controls. The researchers performed methacholine challenge (airway hyperresponsiveness defined as provocative concentration of methacholine less than 8mg/mL), and exhaled nitric oxide. They also analyzed peripheral blood for total IgE, eosinophil count, eotaxin, and serum cytokines.
Baseline spirometry did not significantly differ between EoE subjects and healthy controls. However, airway hyperresponsiveness was present in 33% of children with EoE, compared with only 10.8% of healthy controls (P = .04). In addition, 20% of the 15 EoE subjects with asthma had airway hyperresponsiveness, compared with 44% of the 18 EoE subjects without asthma. Overall, 69.7% of EoE subjects had either asthma or airway hyperresponsiveness.
The researchers found that airway hyperresponsiveness correlated strongly with serum IgE (P less than .0001) and exhaled nitric oxide (P = .0002), while epidermal growth factor (EGF) and fibroblastic growth factor–2 (FGF-2) were elevated in subjects with EoE and asthma, compared to healthy controls and those with EoE but no asthma (P less than .05). In addition, subjects with EoE and asthma who were on asthma controller medications had similar levels of EGF and FGF-2 as healthy controls, while Th2 cytokines and eotaxin did not differ significantly among any groups.
Dr. Krupp said she was surprised "by the fact that airway hyperresponsiveness was more prevalent in those subjects without a history of asthma than those with a known diagnosis, and the fact that Th2-related cytokines were not significantly different between healthy controls and EoE subjects."
She acknowledged certain limitations of the study, including its cross-sectional design and "the fact EoE subjects may have had significant variability in the current activity of their esophageal disease at the time of enrollment."
The study was partially funded by Aerocrine. Dr. Krupp said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Asthma and airway hyperresponsiveness may be underrecognized in children with eosinophilic esophagitis, results from a controlled cross-sectional study demonstrated.
While previous studies have estimated the prevalence of asthma in children with eosinophilic esophagitis (EoE), to range from 24-42%, a recent analysis presented during a late-breaker abstract session at annual meeting of the American Academy of Allergy, Asthma, and Immunology found that up to 70% of children with EoE may suffer from asthma.
"Clinicians treating children with eosinophilic esophagitis should consider asking additional history questions related to asthma symptoms and may also want to consider pulmonary function testing or referral to an asthma specialist for evaluation," lead author Dr. Nadia L. Krupp said in an interview prior to the meeting. "This is the first study to formally evaluate lung function and airway hyperresponsiveness in children with EoE. Prior estimations of asthma have solely come from patient/parent report."
Dr. Krupp, director of the Riley Asthma Care Center in the section of pulmonology, allergy, and critical care medicine at Riley Hospital Children, Indianapolis, and her associates conducted a cross-sectional study of 33 children aged 6-18 years with EoE and 37 healthy controls. The researchers performed methacholine challenge (airway hyperresponsiveness defined as provocative concentration of methacholine less than 8mg/mL), and exhaled nitric oxide. They also analyzed peripheral blood for total IgE, eosinophil count, eotaxin, and serum cytokines.
Baseline spirometry did not significantly differ between EoE subjects and healthy controls. However, airway hyperresponsiveness was present in 33% of children with EoE, compared with only 10.8% of healthy controls (P = .04). In addition, 20% of the 15 EoE subjects with asthma had airway hyperresponsiveness, compared with 44% of the 18 EoE subjects without asthma. Overall, 69.7% of EoE subjects had either asthma or airway hyperresponsiveness.
The researchers found that airway hyperresponsiveness correlated strongly with serum IgE (P less than .0001) and exhaled nitric oxide (P = .0002), while epidermal growth factor (EGF) and fibroblastic growth factor–2 (FGF-2) were elevated in subjects with EoE and asthma, compared to healthy controls and those with EoE but no asthma (P less than .05). In addition, subjects with EoE and asthma who were on asthma controller medications had similar levels of EGF and FGF-2 as healthy controls, while Th2 cytokines and eotaxin did not differ significantly among any groups.
Dr. Krupp said she was surprised "by the fact that airway hyperresponsiveness was more prevalent in those subjects without a history of asthma than those with a known diagnosis, and the fact that Th2-related cytokines were not significantly different between healthy controls and EoE subjects."
She acknowledged certain limitations of the study, including its cross-sectional design and "the fact EoE subjects may have had significant variability in the current activity of their esophageal disease at the time of enrollment."
The study was partially funded by Aerocrine. Dr. Krupp said that she had no relevant financial conflicts to disclose.
AT THE 2014 AAAAI ANNUAL MEETING
Major finding: Airway hyperresponsiveness was present in 33% of children with EoE, compared with only 10.8% of healthy controls (P= .04). In addition, 20% of the 15 EoE subjects with asthma had airway hyperresponsiveness, compared with 44% of the 18 EoE subjects without asthma.
Data source: A cross-sectional study of 33 children aged 6-18 years with EoE and 37 healthy controls.
Disclosures: The study was partially funded by Aerocrine. Dr. Krupp said that she had no relevant financial conflicts to disclose.

Hormone therapy predicted improved lung cancer survival in women
Hormone therapy was associated with improved overall survival in women with non–small-cell lung carcinoma, reported investigators in the March issue of the Journal of Thoracic Oncology.
Long-term hormone use and combinations of estrogen and progesterone predicted the most significant survival benefit, reported Dr. Ann G. Schwartz of the Karmanos Cancer Institute and Wayne State University, both in Detroit, and her associates.
Women with lung cancer usually live longer than do men with the disease. But few prior studies have examined associations between reproductive factors, hormone therapy, and lung cancer outcomes, and results have been inconsistent, investigators said (J. Thorac. Oncol. 2014;9:355-61).
Researchers interviewed 485 women who were diagnosed with non–small-cell lung carcinoma between 2001 and 2005, about their reproductive histories and type, dose, and duration of hormone therapy.
Only hormone therapy predicted overall survival (hazard ratio, 0.69; 95% confidence interval, 0.54-0.89) after accounting for stage at diagnosis, surgery, radiation, education level, cigarette smoke exposure, age, and race, the investigators reported.
Women who received hormone therapy prior to lung cancer diagnosis survived a median of 80 months, compared with 37.5 months for women who did not.
The survival benefit was most significant when hormone therapy lasted 11 years or longer, particularly for combinations of estrogen and progesterone (HR, 0.50; 95% CI, 0.30-0.83). Taking estrogen alone for less than 11 years had no significant effect.
Because patients had to be healthy enough to participate in the survey, results might not apply to all women with non–small-cell lung cancer, Dr. Schwartz and associates noted.
"These findings suggest a complex relationship between exposure to exogenous hormones and lung cancer outcomes," added the researchers. They recommended research to explore the biological reasons for their findings.
This study was supported by the National Institutes of Health. The authors disclosed no relevant financial conflicts of interest.
Hormone therapy was associated with improved overall survival in women with non–small-cell lung carcinoma, reported investigators in the March issue of the Journal of Thoracic Oncology.
Long-term hormone use and combinations of estrogen and progesterone predicted the most significant survival benefit, reported Dr. Ann G. Schwartz of the Karmanos Cancer Institute and Wayne State University, both in Detroit, and her associates.
Women with lung cancer usually live longer than do men with the disease. But few prior studies have examined associations between reproductive factors, hormone therapy, and lung cancer outcomes, and results have been inconsistent, investigators said (J. Thorac. Oncol. 2014;9:355-61).
Researchers interviewed 485 women who were diagnosed with non–small-cell lung carcinoma between 2001 and 2005, about their reproductive histories and type, dose, and duration of hormone therapy.
Only hormone therapy predicted overall survival (hazard ratio, 0.69; 95% confidence interval, 0.54-0.89) after accounting for stage at diagnosis, surgery, radiation, education level, cigarette smoke exposure, age, and race, the investigators reported.
Women who received hormone therapy prior to lung cancer diagnosis survived a median of 80 months, compared with 37.5 months for women who did not.
The survival benefit was most significant when hormone therapy lasted 11 years or longer, particularly for combinations of estrogen and progesterone (HR, 0.50; 95% CI, 0.30-0.83). Taking estrogen alone for less than 11 years had no significant effect.
Because patients had to be healthy enough to participate in the survey, results might not apply to all women with non–small-cell lung cancer, Dr. Schwartz and associates noted.
"These findings suggest a complex relationship between exposure to exogenous hormones and lung cancer outcomes," added the researchers. They recommended research to explore the biological reasons for their findings.
This study was supported by the National Institutes of Health. The authors disclosed no relevant financial conflicts of interest.
Hormone therapy was associated with improved overall survival in women with non–small-cell lung carcinoma, reported investigators in the March issue of the Journal of Thoracic Oncology.
Long-term hormone use and combinations of estrogen and progesterone predicted the most significant survival benefit, reported Dr. Ann G. Schwartz of the Karmanos Cancer Institute and Wayne State University, both in Detroit, and her associates.
Women with lung cancer usually live longer than do men with the disease. But few prior studies have examined associations between reproductive factors, hormone therapy, and lung cancer outcomes, and results have been inconsistent, investigators said (J. Thorac. Oncol. 2014;9:355-61).
Researchers interviewed 485 women who were diagnosed with non–small-cell lung carcinoma between 2001 and 2005, about their reproductive histories and type, dose, and duration of hormone therapy.
Only hormone therapy predicted overall survival (hazard ratio, 0.69; 95% confidence interval, 0.54-0.89) after accounting for stage at diagnosis, surgery, radiation, education level, cigarette smoke exposure, age, and race, the investigators reported.
Women who received hormone therapy prior to lung cancer diagnosis survived a median of 80 months, compared with 37.5 months for women who did not.
The survival benefit was most significant when hormone therapy lasted 11 years or longer, particularly for combinations of estrogen and progesterone (HR, 0.50; 95% CI, 0.30-0.83). Taking estrogen alone for less than 11 years had no significant effect.
Because patients had to be healthy enough to participate in the survey, results might not apply to all women with non–small-cell lung cancer, Dr. Schwartz and associates noted.
"These findings suggest a complex relationship between exposure to exogenous hormones and lung cancer outcomes," added the researchers. They recommended research to explore the biological reasons for their findings.
This study was supported by the National Institutes of Health. The authors disclosed no relevant financial conflicts of interest.
FROM THE JOURNAL OF THORACIC ONCOLOGY
Major Finding: Long-term hormone therapy was associated with significantly improved survival in women with non–small-cell lung cancer (HR, 0.54).
Data Source: A retrospective study of 485 women diagnosed with non–small-cell lung cancer during 2001-2005.
Disclosures: The study was supported by the National Institutes of Health. The authors reported no relevant financial conflicts of interest.