User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Second U.S. case of MERS infection confirmed
The Centers for Disease Control and Prevention has confirmed the second case of Middle East Respiratory Syndrome coronavirus (MERS-CoV) in the United States.
The patient, a health care provider working and residing in Saudi Arabia, first began to experience fever, chills, and a cough on a May 1 flight from Jeddah to Boston. The patient then traveled on two more flights – Boston to Atlanta and Atlanta to Orlando, before being admitted with symptoms to a Florida hospital on May 8.
Lab samples were tested and confirmed in Atlanta on May 11, the CDC announced in a May 12 teleconference.
The Florida patient is isolated and in stable condition, though public health officials continue to identify and reach out to the more than 500 people who may have traveled in close proximity to the infected patient.
The new case does not appear to be linked to the first U.S. case of MERS virus in Indiana, which was confirmed on May 2, officials said.
CDC director Dr. Tom Frieden said in the briefing that the MERS infection behaves similarly to the SARS virus, and that "transmission requires close contact, such as caring for someone infected when sick at home or in the hospital."
Though the health care worker is believed to have worked in a Saudi hospital treating patients with the MERS virus, information is not yet available about whether he or she had direct contact with infected patients.
The MERS virus was first reported in Saudi Arabia in 2012. CDC officials said there has been an international uptake in the number of reported cases since March of this year.
"As of May 12, a total of 538 lab-confirmed cases, including 145 deaths due to MERS, have been reported worldwide," said Dr. Anne Schuchat, director of the CDC’s National Center for Immunization and Respiratory Diseases. A vast majority of cases have occurred in Saudi Arabia, which has reported 450 cases and 118 deaths to date, she added.

Dr. Schuchat noted that despite this second importation of the virus into the United States, risk of infection remains "very low" for the general public, and the virus does not appear to spread easily in community settings. "The clusters of spread are seen most frequently on health care workers caring for MERS patients," she said.
There is no vaccine available to prevent MERS-CoV, but Dr. Schuchat emphasized the importance of practicing basic, everyday precautions such as frequent handwashing, keeping hands away from the face and mouth, staying home when sick, and avoiding contact with sick individuals.
The CDC does not recommend making changes to travel plans at this time, but does urge travelers, particularly those employed in health care settings, to seek immediate medical attention if they experience cough, fever, or respiratory illness within 14 days of travel to the Arabian peninsula.
The Centers for Disease Control and Prevention has confirmed the second case of Middle East Respiratory Syndrome coronavirus (MERS-CoV) in the United States.
The patient, a health care provider working and residing in Saudi Arabia, first began to experience fever, chills, and a cough on a May 1 flight from Jeddah to Boston. The patient then traveled on two more flights – Boston to Atlanta and Atlanta to Orlando, before being admitted with symptoms to a Florida hospital on May 8.
Lab samples were tested and confirmed in Atlanta on May 11, the CDC announced in a May 12 teleconference.
The Florida patient is isolated and in stable condition, though public health officials continue to identify and reach out to the more than 500 people who may have traveled in close proximity to the infected patient.
The new case does not appear to be linked to the first U.S. case of MERS virus in Indiana, which was confirmed on May 2, officials said.
CDC director Dr. Tom Frieden said in the briefing that the MERS infection behaves similarly to the SARS virus, and that "transmission requires close contact, such as caring for someone infected when sick at home or in the hospital."
Though the health care worker is believed to have worked in a Saudi hospital treating patients with the MERS virus, information is not yet available about whether he or she had direct contact with infected patients.
The MERS virus was first reported in Saudi Arabia in 2012. CDC officials said there has been an international uptake in the number of reported cases since March of this year.
"As of May 12, a total of 538 lab-confirmed cases, including 145 deaths due to MERS, have been reported worldwide," said Dr. Anne Schuchat, director of the CDC’s National Center for Immunization and Respiratory Diseases. A vast majority of cases have occurred in Saudi Arabia, which has reported 450 cases and 118 deaths to date, she added.
Dr. Schuchat noted that despite this second importation of the virus into the United States, risk of infection remains "very low" for the general public, and the virus does not appear to spread easily in community settings. "The clusters of spread are seen most frequently on health care workers caring for MERS patients," she said.
There is no vaccine available to prevent MERS-CoV, but Dr. Schuchat emphasized the importance of practicing basic, everyday precautions such as frequent handwashing, keeping hands away from the face and mouth, staying home when sick, and avoiding contact with sick individuals.
The CDC does not recommend making changes to travel plans at this time, but does urge travelers, particularly those employed in health care settings, to seek immediate medical attention if they experience cough, fever, or respiratory illness within 14 days of travel to the Arabian peninsula.
The Centers for Disease Control and Prevention has confirmed the second case of Middle East Respiratory Syndrome coronavirus (MERS-CoV) in the United States.
The patient, a health care provider working and residing in Saudi Arabia, first began to experience fever, chills, and a cough on a May 1 flight from Jeddah to Boston. The patient then traveled on two more flights – Boston to Atlanta and Atlanta to Orlando, before being admitted with symptoms to a Florida hospital on May 8.
Lab samples were tested and confirmed in Atlanta on May 11, the CDC announced in a May 12 teleconference.
The Florida patient is isolated and in stable condition, though public health officials continue to identify and reach out to the more than 500 people who may have traveled in close proximity to the infected patient.
The new case does not appear to be linked to the first U.S. case of MERS virus in Indiana, which was confirmed on May 2, officials said.
CDC director Dr. Tom Frieden said in the briefing that the MERS infection behaves similarly to the SARS virus, and that "transmission requires close contact, such as caring for someone infected when sick at home or in the hospital."
Though the health care worker is believed to have worked in a Saudi hospital treating patients with the MERS virus, information is not yet available about whether he or she had direct contact with infected patients.
The MERS virus was first reported in Saudi Arabia in 2012. CDC officials said there has been an international uptake in the number of reported cases since March of this year.
"As of May 12, a total of 538 lab-confirmed cases, including 145 deaths due to MERS, have been reported worldwide," said Dr. Anne Schuchat, director of the CDC’s National Center for Immunization and Respiratory Diseases. A vast majority of cases have occurred in Saudi Arabia, which has reported 450 cases and 118 deaths to date, she added.
Dr. Schuchat noted that despite this second importation of the virus into the United States, risk of infection remains "very low" for the general public, and the virus does not appear to spread easily in community settings. "The clusters of spread are seen most frequently on health care workers caring for MERS patients," she said.
There is no vaccine available to prevent MERS-CoV, but Dr. Schuchat emphasized the importance of practicing basic, everyday precautions such as frequent handwashing, keeping hands away from the face and mouth, staying home when sick, and avoiding contact with sick individuals.
The CDC does not recommend making changes to travel plans at this time, but does urge travelers, particularly those employed in health care settings, to seek immediate medical attention if they experience cough, fever, or respiratory illness within 14 days of travel to the Arabian peninsula.
FROM A CDC TELECONFERENCE
Steroid-sparing therapy is promising for allergic asthma
KEYSTONE, COLO. – A novel toll-like receptor-9 agonist showed impressive clinical efficacy in persistent allergic asthma in a double-blind, placebo-controlled clinical trial.
"This is really interesting," Dr. Harold S. Nelson commented in highlighting the European study as one of the most promising new developments in immunology during the past year in his talk at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
The toll-like receptor-9 agonist under study is known as QbG10. It consists of a protein shell derived from the Q-beta bacteriophage which is wrapped around a core of DNA oligomer G10 rich in A-type CpG motifs. The protein shell protects the G10 CpG so that when the antigen-presenting cell digests that outer coat, the CpG sits like a Trojan horse inside the T cell or macrophage. The G10 CpG induces interferon-alpha production, which in turn causes degradation of transcription factor GATA-3, explained Dr. Nelson, professor of medicine and of pediatrics at the University of Colorado, Denver, and National Jewish Health.
Allergic asthma is a disease in which allergen-specific Th2 responses figure prominently. QbG10 therapy is designed to nudge the immune system toward a Th1-mediated protective response.
What’s particularly intriguing about this novel immunotherapy, he added, is that the clinical efficacy is achieved without administering any allergen. The results are achieved simply by showing the CpG to asthma patients. CpGs are DNA oligonucleotides containing unmethylated deoxycytidylyl-deoxyguanosine dinucleotides.

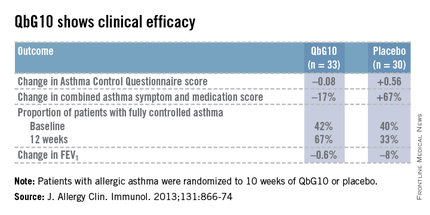
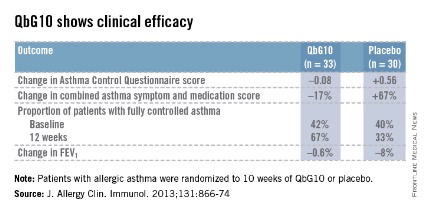
The European proof-of-concept study included 63 patients with allergic asthma being treated with moderate- or high-dose inhaled corticosteroids. They were randomized to receive seven injections of QbG10 or placebo over the course of 10 weeks, during which a controlled steroid withdrawal was carried out. After 4 weeks, the patients’ inhaled steroid dose was cut by 50%. After 8 weeks, the inhaled steroid was discontinued altogether. At evaluation at 12 weeks – 4 weeks after inhaled steroids were halted – two-thirds of QbG10-treated patients had well-controlled asthma as defined by an Asthma Control Questionnaire score of 0.75 or less, compared with one-third of controls. The QbG10 group showed similar advantages on other measures of asthma control, in spite of the steroid taper (see chart).
Local injection site reactions were common in the QbG10 group. The reactions were generally mild to moderate and were most pronounced 1-2 days post injection. The biggest reactions were noted after the third of the seven injections. No systemic reactions occurred (J. Allergy Clin. Immunol. 2013;131:866-74).
Dr. Nelson reported having no financial conflicts of interest regarding this work.
KEYSTONE, COLO. – A novel toll-like receptor-9 agonist showed impressive clinical efficacy in persistent allergic asthma in a double-blind, placebo-controlled clinical trial.
"This is really interesting," Dr. Harold S. Nelson commented in highlighting the European study as one of the most promising new developments in immunology during the past year in his talk at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
The toll-like receptor-9 agonist under study is known as QbG10. It consists of a protein shell derived from the Q-beta bacteriophage which is wrapped around a core of DNA oligomer G10 rich in A-type CpG motifs. The protein shell protects the G10 CpG so that when the antigen-presenting cell digests that outer coat, the CpG sits like a Trojan horse inside the T cell or macrophage. The G10 CpG induces interferon-alpha production, which in turn causes degradation of transcription factor GATA-3, explained Dr. Nelson, professor of medicine and of pediatrics at the University of Colorado, Denver, and National Jewish Health.
Allergic asthma is a disease in which allergen-specific Th2 responses figure prominently. QbG10 therapy is designed to nudge the immune system toward a Th1-mediated protective response.
What’s particularly intriguing about this novel immunotherapy, he added, is that the clinical efficacy is achieved without administering any allergen. The results are achieved simply by showing the CpG to asthma patients. CpGs are DNA oligonucleotides containing unmethylated deoxycytidylyl-deoxyguanosine dinucleotides.
The European proof-of-concept study included 63 patients with allergic asthma being treated with moderate- or high-dose inhaled corticosteroids. They were randomized to receive seven injections of QbG10 or placebo over the course of 10 weeks, during which a controlled steroid withdrawal was carried out. After 4 weeks, the patients’ inhaled steroid dose was cut by 50%. After 8 weeks, the inhaled steroid was discontinued altogether. At evaluation at 12 weeks – 4 weeks after inhaled steroids were halted – two-thirds of QbG10-treated patients had well-controlled asthma as defined by an Asthma Control Questionnaire score of 0.75 or less, compared with one-third of controls. The QbG10 group showed similar advantages on other measures of asthma control, in spite of the steroid taper (see chart).
Local injection site reactions were common in the QbG10 group. The reactions were generally mild to moderate and were most pronounced 1-2 days post injection. The biggest reactions were noted after the third of the seven injections. No systemic reactions occurred (J. Allergy Clin. Immunol. 2013;131:866-74).
Dr. Nelson reported having no financial conflicts of interest regarding this work.
KEYSTONE, COLO. – A novel toll-like receptor-9 agonist showed impressive clinical efficacy in persistent allergic asthma in a double-blind, placebo-controlled clinical trial.
"This is really interesting," Dr. Harold S. Nelson commented in highlighting the European study as one of the most promising new developments in immunology during the past year in his talk at a meeting on allergy and respiratory diseases sponsored by National Jewish Health.
The toll-like receptor-9 agonist under study is known as QbG10. It consists of a protein shell derived from the Q-beta bacteriophage which is wrapped around a core of DNA oligomer G10 rich in A-type CpG motifs. The protein shell protects the G10 CpG so that when the antigen-presenting cell digests that outer coat, the CpG sits like a Trojan horse inside the T cell or macrophage. The G10 CpG induces interferon-alpha production, which in turn causes degradation of transcription factor GATA-3, explained Dr. Nelson, professor of medicine and of pediatrics at the University of Colorado, Denver, and National Jewish Health.
Allergic asthma is a disease in which allergen-specific Th2 responses figure prominently. QbG10 therapy is designed to nudge the immune system toward a Th1-mediated protective response.
What’s particularly intriguing about this novel immunotherapy, he added, is that the clinical efficacy is achieved without administering any allergen. The results are achieved simply by showing the CpG to asthma patients. CpGs are DNA oligonucleotides containing unmethylated deoxycytidylyl-deoxyguanosine dinucleotides.
The European proof-of-concept study included 63 patients with allergic asthma being treated with moderate- or high-dose inhaled corticosteroids. They were randomized to receive seven injections of QbG10 or placebo over the course of 10 weeks, during which a controlled steroid withdrawal was carried out. After 4 weeks, the patients’ inhaled steroid dose was cut by 50%. After 8 weeks, the inhaled steroid was discontinued altogether. At evaluation at 12 weeks – 4 weeks after inhaled steroids were halted – two-thirds of QbG10-treated patients had well-controlled asthma as defined by an Asthma Control Questionnaire score of 0.75 or less, compared with one-third of controls. The QbG10 group showed similar advantages on other measures of asthma control, in spite of the steroid taper (see chart).
Local injection site reactions were common in the QbG10 group. The reactions were generally mild to moderate and were most pronounced 1-2 days post injection. The biggest reactions were noted after the third of the seven injections. No systemic reactions occurred (J. Allergy Clin. Immunol. 2013;131:866-74).
Dr. Nelson reported having no financial conflicts of interest regarding this work.
EXPERT ANALYSIS FROM THE PULMONARY AND ALLERGY UPDATE
Survival gains seen with rituximab and mycophenolate in RA lung disease
LIVERPOOL, ENGLAND – Rituximab and mycophenolate mofetil could offer patients with rheumatoid arthritis and concomitant interstitial lung disease a survival advantage over other therapies, according to findings from a large, retrospective, multicenter study.
Data collated by the British Rheumatoid Interstitial Lung (BRILL) network found all-cause mortality in patients with rheumatoid arthritis (RA) and interstitial lung disease (ILD) treated with rituximab was 8% versus 31% for those treated with anti-tumor necrosis factor (TNF) alpha therapies (P = .03). Death from respiratory causes was also significantly lower in the rituximab-treated patients (4% vs. 15%, P = .04).
All-cause mortality was also significantly lower in patients with RA and ILD treated with mycophenolate mofetil (relative risk, 0.65) when compared with azathioprine (RR, 1.42) or other immunosuppressants, which included cyclophosphamide (RR, 1.65) and tacrolimus (RR, 1.74).
However, these data were retrospective, so prospective therapeutic trials are now needed, said Dr. Clive Kelly of Queen Elizabeth Hospital, Gateshead, England. Dr. Kelly, who was the driving force behind the set up of the BRILL network 2 years ago, stated that plans were already afoot to set up these trials with the intention of recruiting 200 patients with RA and ILD across the United Kingdom.
The aim of future studies would be to compare the use of rituximab versus anti-TNF therapies, with or without methotrexate, and mycophenolate mofetil versus azathioprine, with or without oral steroids, to see if the anticipated survival benefit associated with the newer agents is confirmed. Funding for the trials is yet to be secured, but it is hoped that recruitment can begin next year.
When people think of comorbidity in RA, they tend to think about cardiovascular disease first, Dr. Kelly noted at the British Society for Rheumatology annual conference. He observed that ILD has been associated with RA for well over 50 years and that respiratory disease, largely due to ILD and chronic lung damage, is now a "close second" behind heart disease as a cause of death in patients with RA.
Up to 40% of all cases of ILD are discovered in RA patients postmortem, he said, but with the increased use of high-resolution computed tomography (HRCT) in the 1990s, around a quarter of patients with RA were found to have changes on lung scanning.
Today, the prevalence of clinically significant lung disease is estimated to be around 5% in RA, with a lifetime risk thought to be around 7.7%. Patients with RA who develop ILD are around three times more likely to die than are those who do not, with a reported mean survival around 2.6 years from the diagnosis of lung disease until the advent of these recent studies.
The BRILL network consists of 16 centers located throughout the United Kingdom and was set up to establish a national database of all cases of ILD in RA patients that had been reported by these centers over a 25-year period, beginning in 1988. Patients were included in the database if clinical symptoms, such as shortness of breath or chest crackles, or pulmonary function tests had indicated ILD, and abnormal findings had been confirmed via HRCT.
For the current study, Dr. Kelly and coinvestigators from the BRILL Network looked at a subset of 188 patients with RA and ILD who had been diagnosed between 2000 and 2012. A control group of 188 patients with RA without ILD were included for comparison, matched for age, sex, and duration of RA.
Patients with ILD were more likely than those without to use biologics or immunosuppressants. Of the 188 patients with ILD, 57 were treated with either rituximab or anti-TNF drugs and 83 were treated with immunosuppressants.
The median age at which ILD was identified was 64 years, ranging from 42 to 87 years. The median duration of RA at ILD diagnosis was 9 years and the median duration of ILD was 4 years.
Dr. Kelly reported that RA preceded lung disease in the majority (83%) of cases, while 10% of patients developed ILD before the articular features of their disease became apparent. The onset of RA and ILD was "synchronous" in the remaining 7%.
HRCT results showed that the most common subtype of lung disease was interstitial pneumonia in 65% of cases, which carries the worst overall prognosis, he said. Nonspecific interstitial pneumonia, which is more responsive to early therapy, accounted for 24% of cases. The remaining patients had cryptogenic organizing pneumonia (6%) and or mixed subtypes (5%).
Survival over the 25 years improved, with 67% of RA-ILD patients dying from ILD in 1987-1993, compared with 30% in 2006-2012 (P less than .01). Nevertheless, these data are retrospective, Dr. Kelly observed, and trials are warranted to confirm the effects of specific treatments. He encouraged delegates at the meeting to participate in forthcoming BRILL network studies.
Dr. Kelly had no disclosures.
LIVERPOOL, ENGLAND – Rituximab and mycophenolate mofetil could offer patients with rheumatoid arthritis and concomitant interstitial lung disease a survival advantage over other therapies, according to findings from a large, retrospective, multicenter study.
Data collated by the British Rheumatoid Interstitial Lung (BRILL) network found all-cause mortality in patients with rheumatoid arthritis (RA) and interstitial lung disease (ILD) treated with rituximab was 8% versus 31% for those treated with anti-tumor necrosis factor (TNF) alpha therapies (P = .03). Death from respiratory causes was also significantly lower in the rituximab-treated patients (4% vs. 15%, P = .04).
All-cause mortality was also significantly lower in patients with RA and ILD treated with mycophenolate mofetil (relative risk, 0.65) when compared with azathioprine (RR, 1.42) or other immunosuppressants, which included cyclophosphamide (RR, 1.65) and tacrolimus (RR, 1.74).
However, these data were retrospective, so prospective therapeutic trials are now needed, said Dr. Clive Kelly of Queen Elizabeth Hospital, Gateshead, England. Dr. Kelly, who was the driving force behind the set up of the BRILL network 2 years ago, stated that plans were already afoot to set up these trials with the intention of recruiting 200 patients with RA and ILD across the United Kingdom.
The aim of future studies would be to compare the use of rituximab versus anti-TNF therapies, with or without methotrexate, and mycophenolate mofetil versus azathioprine, with or without oral steroids, to see if the anticipated survival benefit associated with the newer agents is confirmed. Funding for the trials is yet to be secured, but it is hoped that recruitment can begin next year.
When people think of comorbidity in RA, they tend to think about cardiovascular disease first, Dr. Kelly noted at the British Society for Rheumatology annual conference. He observed that ILD has been associated with RA for well over 50 years and that respiratory disease, largely due to ILD and chronic lung damage, is now a "close second" behind heart disease as a cause of death in patients with RA.
Up to 40% of all cases of ILD are discovered in RA patients postmortem, he said, but with the increased use of high-resolution computed tomography (HRCT) in the 1990s, around a quarter of patients with RA were found to have changes on lung scanning.
Today, the prevalence of clinically significant lung disease is estimated to be around 5% in RA, with a lifetime risk thought to be around 7.7%. Patients with RA who develop ILD are around three times more likely to die than are those who do not, with a reported mean survival around 2.6 years from the diagnosis of lung disease until the advent of these recent studies.
The BRILL network consists of 16 centers located throughout the United Kingdom and was set up to establish a national database of all cases of ILD in RA patients that had been reported by these centers over a 25-year period, beginning in 1988. Patients were included in the database if clinical symptoms, such as shortness of breath or chest crackles, or pulmonary function tests had indicated ILD, and abnormal findings had been confirmed via HRCT.
For the current study, Dr. Kelly and coinvestigators from the BRILL Network looked at a subset of 188 patients with RA and ILD who had been diagnosed between 2000 and 2012. A control group of 188 patients with RA without ILD were included for comparison, matched for age, sex, and duration of RA.
Patients with ILD were more likely than those without to use biologics or immunosuppressants. Of the 188 patients with ILD, 57 were treated with either rituximab or anti-TNF drugs and 83 were treated with immunosuppressants.
The median age at which ILD was identified was 64 years, ranging from 42 to 87 years. The median duration of RA at ILD diagnosis was 9 years and the median duration of ILD was 4 years.
Dr. Kelly reported that RA preceded lung disease in the majority (83%) of cases, while 10% of patients developed ILD before the articular features of their disease became apparent. The onset of RA and ILD was "synchronous" in the remaining 7%.
HRCT results showed that the most common subtype of lung disease was interstitial pneumonia in 65% of cases, which carries the worst overall prognosis, he said. Nonspecific interstitial pneumonia, which is more responsive to early therapy, accounted for 24% of cases. The remaining patients had cryptogenic organizing pneumonia (6%) and or mixed subtypes (5%).
Survival over the 25 years improved, with 67% of RA-ILD patients dying from ILD in 1987-1993, compared with 30% in 2006-2012 (P less than .01). Nevertheless, these data are retrospective, Dr. Kelly observed, and trials are warranted to confirm the effects of specific treatments. He encouraged delegates at the meeting to participate in forthcoming BRILL network studies.
Dr. Kelly had no disclosures.
LIVERPOOL, ENGLAND – Rituximab and mycophenolate mofetil could offer patients with rheumatoid arthritis and concomitant interstitial lung disease a survival advantage over other therapies, according to findings from a large, retrospective, multicenter study.
Data collated by the British Rheumatoid Interstitial Lung (BRILL) network found all-cause mortality in patients with rheumatoid arthritis (RA) and interstitial lung disease (ILD) treated with rituximab was 8% versus 31% for those treated with anti-tumor necrosis factor (TNF) alpha therapies (P = .03). Death from respiratory causes was also significantly lower in the rituximab-treated patients (4% vs. 15%, P = .04).
All-cause mortality was also significantly lower in patients with RA and ILD treated with mycophenolate mofetil (relative risk, 0.65) when compared with azathioprine (RR, 1.42) or other immunosuppressants, which included cyclophosphamide (RR, 1.65) and tacrolimus (RR, 1.74).
However, these data were retrospective, so prospective therapeutic trials are now needed, said Dr. Clive Kelly of Queen Elizabeth Hospital, Gateshead, England. Dr. Kelly, who was the driving force behind the set up of the BRILL network 2 years ago, stated that plans were already afoot to set up these trials with the intention of recruiting 200 patients with RA and ILD across the United Kingdom.
The aim of future studies would be to compare the use of rituximab versus anti-TNF therapies, with or without methotrexate, and mycophenolate mofetil versus azathioprine, with or without oral steroids, to see if the anticipated survival benefit associated with the newer agents is confirmed. Funding for the trials is yet to be secured, but it is hoped that recruitment can begin next year.
When people think of comorbidity in RA, they tend to think about cardiovascular disease first, Dr. Kelly noted at the British Society for Rheumatology annual conference. He observed that ILD has been associated with RA for well over 50 years and that respiratory disease, largely due to ILD and chronic lung damage, is now a "close second" behind heart disease as a cause of death in patients with RA.
Up to 40% of all cases of ILD are discovered in RA patients postmortem, he said, but with the increased use of high-resolution computed tomography (HRCT) in the 1990s, around a quarter of patients with RA were found to have changes on lung scanning.
Today, the prevalence of clinically significant lung disease is estimated to be around 5% in RA, with a lifetime risk thought to be around 7.7%. Patients with RA who develop ILD are around three times more likely to die than are those who do not, with a reported mean survival around 2.6 years from the diagnosis of lung disease until the advent of these recent studies.
The BRILL network consists of 16 centers located throughout the United Kingdom and was set up to establish a national database of all cases of ILD in RA patients that had been reported by these centers over a 25-year period, beginning in 1988. Patients were included in the database if clinical symptoms, such as shortness of breath or chest crackles, or pulmonary function tests had indicated ILD, and abnormal findings had been confirmed via HRCT.
For the current study, Dr. Kelly and coinvestigators from the BRILL Network looked at a subset of 188 patients with RA and ILD who had been diagnosed between 2000 and 2012. A control group of 188 patients with RA without ILD were included for comparison, matched for age, sex, and duration of RA.
Patients with ILD were more likely than those without to use biologics or immunosuppressants. Of the 188 patients with ILD, 57 were treated with either rituximab or anti-TNF drugs and 83 were treated with immunosuppressants.
The median age at which ILD was identified was 64 years, ranging from 42 to 87 years. The median duration of RA at ILD diagnosis was 9 years and the median duration of ILD was 4 years.
Dr. Kelly reported that RA preceded lung disease in the majority (83%) of cases, while 10% of patients developed ILD before the articular features of their disease became apparent. The onset of RA and ILD was "synchronous" in the remaining 7%.
HRCT results showed that the most common subtype of lung disease was interstitial pneumonia in 65% of cases, which carries the worst overall prognosis, he said. Nonspecific interstitial pneumonia, which is more responsive to early therapy, accounted for 24% of cases. The remaining patients had cryptogenic organizing pneumonia (6%) and or mixed subtypes (5%).
Survival over the 25 years improved, with 67% of RA-ILD patients dying from ILD in 1987-1993, compared with 30% in 2006-2012 (P less than .01). Nevertheless, these data are retrospective, Dr. Kelly observed, and trials are warranted to confirm the effects of specific treatments. He encouraged delegates at the meeting to participate in forthcoming BRILL network studies.
Dr. Kelly had no disclosures.
AT RHEUMATOLOGY 2014
Key clinical point: Early, retrospective data indicate that in RA-ILD patients, rituximab may improve survival over anti-TNF treatments, while mycophenolate mofetil may reduce mortality when compared with other immunosuppressants.
Major finding: Treatment of RA-ILD with rituximab vs. anti-TNF agents led to all-cause mortality of 8% vs. 31% (P = .03), respectively, and respiratory mortality of 4% vs. 15% (P = .04). The relative risk for death from any cause was 0.65 for mycophenolate treatment, compared with other immunosuppressants.
Data source: Multicenter, retrospective study of 188 patients with rheumatoid arthritis (RA) and interstitial lung disease and 188 with RA and no lung disease as controls.
Disclosures: Dr. Kelly had no conflicts of interest.
Asthma deaths declined modestly during 1999-2010
SAN DIEGO – Between 1999 and 2010, age-adjusted deaths from asthma in the United States declined modestly but significantly, deaths from angioedema increased significantly, and deaths from anaphylaxis remained stable.
Those are key findings from an analysis of Centers for Disease Control and Prevention (CDC) data presented by Dr. Susan J. Kim at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Dr. Kim, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center, and her associate, Jordan C. Brooks, Ph.D., set out to document the number of deaths in the United States in which asthma or allergy played a role between 1990 and 2010, and to determine if there have been secular trends in the incidence of such deaths. The researchers queried the CDC’s online Multiple Cause of Death compressed mortality file for International Classification of Disease (ICD-10) codes relating to asthma, urticaria, angioedema, and anaphylaxis, and proceeded to calculate age-adjusted death rates for 1999-2004 (early period) and 2005-2010 (late period).

During the overall time period, there were 113,778 deaths from asthma of all types, 908 from angioedema, and 2,448 from anaphylaxis. Dr. Kim reported that the total number of deaths from asthma of all types (including status asthmaticus) dropped from 57,935 in the early period to 55,843 in the late period. This represented a significant decline, from a rate of 3.38 per 100,000 persons to 2.95 per 100,000 persons.
Blacks had a significantly higher rate of mortality from asthma than whites (5.85 per 100,000 persons vs. 2.55 per 100,000 persons). "This racial disparity might be attributed to a discrepancy in access to quality medical care and use of medications," Dr. Kim said.
She went on to note that women had a higher rate of mortality from asthma than men (3.61 per 100,000 vs. 2.56 per 100,000). "This is interesting, because when taking all causes of mortality in the United States – cardiovascular disease, malignancy, et cetera – men have a higher mortality rate," she said. "The cause may be due to estrogen and progesterone’s effects on airway contractility and immune function."
The researchers observed a significant increase in total deaths from angioedema, from 0.0157 per 100,000 persons during the early period to 0.0289 per 100,000 persons during the late period. "Perhaps an explanation is that there is a lack of awareness that life-threatening laryngeal attacks and asphyxiation can occur," Dr. Kim hypothesized.
At the same time, no significant trends in anaphylaxis death occurred between the early and late periods. Overall, the death rate from anaphylaxis was 0.0637 per 100,000, or 0.6 per million people. "This mortality rate remained stable between our two time periods," she said. "Previous estimates have ranged from 0.5 and 5.5 per million people."
Dr. Kim acknowledged certain limitations of the study, including the fact that the CDC database used for the analysis is subject to missing data, variability in coding, and miscoding. "There’s also no way for us to know how race was identified," she said. "It also lacked clinical details, including the sequence of events leading to death, and medication reconciliation."
Dr. Kim had no relevant financial conflicts to disclose.
SAN DIEGO – Between 1999 and 2010, age-adjusted deaths from asthma in the United States declined modestly but significantly, deaths from angioedema increased significantly, and deaths from anaphylaxis remained stable.
Those are key findings from an analysis of Centers for Disease Control and Prevention (CDC) data presented by Dr. Susan J. Kim at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Dr. Kim, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center, and her associate, Jordan C. Brooks, Ph.D., set out to document the number of deaths in the United States in which asthma or allergy played a role between 1990 and 2010, and to determine if there have been secular trends in the incidence of such deaths. The researchers queried the CDC’s online Multiple Cause of Death compressed mortality file for International Classification of Disease (ICD-10) codes relating to asthma, urticaria, angioedema, and anaphylaxis, and proceeded to calculate age-adjusted death rates for 1999-2004 (early period) and 2005-2010 (late period).
During the overall time period, there were 113,778 deaths from asthma of all types, 908 from angioedema, and 2,448 from anaphylaxis. Dr. Kim reported that the total number of deaths from asthma of all types (including status asthmaticus) dropped from 57,935 in the early period to 55,843 in the late period. This represented a significant decline, from a rate of 3.38 per 100,000 persons to 2.95 per 100,000 persons.
Blacks had a significantly higher rate of mortality from asthma than whites (5.85 per 100,000 persons vs. 2.55 per 100,000 persons). "This racial disparity might be attributed to a discrepancy in access to quality medical care and use of medications," Dr. Kim said.
She went on to note that women had a higher rate of mortality from asthma than men (3.61 per 100,000 vs. 2.56 per 100,000). "This is interesting, because when taking all causes of mortality in the United States – cardiovascular disease, malignancy, et cetera – men have a higher mortality rate," she said. "The cause may be due to estrogen and progesterone’s effects on airway contractility and immune function."
The researchers observed a significant increase in total deaths from angioedema, from 0.0157 per 100,000 persons during the early period to 0.0289 per 100,000 persons during the late period. "Perhaps an explanation is that there is a lack of awareness that life-threatening laryngeal attacks and asphyxiation can occur," Dr. Kim hypothesized.
At the same time, no significant trends in anaphylaxis death occurred between the early and late periods. Overall, the death rate from anaphylaxis was 0.0637 per 100,000, or 0.6 per million people. "This mortality rate remained stable between our two time periods," she said. "Previous estimates have ranged from 0.5 and 5.5 per million people."
Dr. Kim acknowledged certain limitations of the study, including the fact that the CDC database used for the analysis is subject to missing data, variability in coding, and miscoding. "There’s also no way for us to know how race was identified," she said. "It also lacked clinical details, including the sequence of events leading to death, and medication reconciliation."
Dr. Kim had no relevant financial conflicts to disclose.
SAN DIEGO – Between 1999 and 2010, age-adjusted deaths from asthma in the United States declined modestly but significantly, deaths from angioedema increased significantly, and deaths from anaphylaxis remained stable.
Those are key findings from an analysis of Centers for Disease Control and Prevention (CDC) data presented by Dr. Susan J. Kim at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Dr. Kim, a first-year allergy fellow at Kaiser Permanente Los Angeles Medical Center, and her associate, Jordan C. Brooks, Ph.D., set out to document the number of deaths in the United States in which asthma or allergy played a role between 1990 and 2010, and to determine if there have been secular trends in the incidence of such deaths. The researchers queried the CDC’s online Multiple Cause of Death compressed mortality file for International Classification of Disease (ICD-10) codes relating to asthma, urticaria, angioedema, and anaphylaxis, and proceeded to calculate age-adjusted death rates for 1999-2004 (early period) and 2005-2010 (late period).
During the overall time period, there were 113,778 deaths from asthma of all types, 908 from angioedema, and 2,448 from anaphylaxis. Dr. Kim reported that the total number of deaths from asthma of all types (including status asthmaticus) dropped from 57,935 in the early period to 55,843 in the late period. This represented a significant decline, from a rate of 3.38 per 100,000 persons to 2.95 per 100,000 persons.
Blacks had a significantly higher rate of mortality from asthma than whites (5.85 per 100,000 persons vs. 2.55 per 100,000 persons). "This racial disparity might be attributed to a discrepancy in access to quality medical care and use of medications," Dr. Kim said.
She went on to note that women had a higher rate of mortality from asthma than men (3.61 per 100,000 vs. 2.56 per 100,000). "This is interesting, because when taking all causes of mortality in the United States – cardiovascular disease, malignancy, et cetera – men have a higher mortality rate," she said. "The cause may be due to estrogen and progesterone’s effects on airway contractility and immune function."
The researchers observed a significant increase in total deaths from angioedema, from 0.0157 per 100,000 persons during the early period to 0.0289 per 100,000 persons during the late period. "Perhaps an explanation is that there is a lack of awareness that life-threatening laryngeal attacks and asphyxiation can occur," Dr. Kim hypothesized.
At the same time, no significant trends in anaphylaxis death occurred between the early and late periods. Overall, the death rate from anaphylaxis was 0.0637 per 100,000, or 0.6 per million people. "This mortality rate remained stable between our two time periods," she said. "Previous estimates have ranged from 0.5 and 5.5 per million people."
Dr. Kim acknowledged certain limitations of the study, including the fact that the CDC database used for the analysis is subject to missing data, variability in coding, and miscoding. "There’s also no way for us to know how race was identified," she said. "It also lacked clinical details, including the sequence of events leading to death, and medication reconciliation."
Dr. Kim had no relevant financial conflicts to disclose.
AT THE 2014 AAAAI ANNUAL MEETING
Major Finding: Between 1999 and 2010, mortality from asthma in the United States declined significantly from a rate of 3.38 per 100,000 persons to 2.95 per 100,000 persons, while total deaths from angioedema increased significantly from 0.0157 per 100,000 persons to 0.0289 per 100,000 persons.
Data Source: An analysis of the CDC’s online Multiple Cause of Death compressed mortality file for ICD-10 codes relating to asthma, urticaria, angioedema, and anaphylaxis.
Disclosures: Dr. Kim had no relevant financial conflicts to disclose.

CDC confirms first U.S. case of deadly Middle East Respiratory Syndrome
The Centers for Disease Control and Prevention has confirmed the first case of the deadly Middle East Respiratory Syndrome coronavirus in the United States.
The patient, a health care worker who recently returned from Riyadh, Saudi Arabia, is in stable condition in an Indiana hospital after being admitted with shortness of breath, cough, and fever on April 27.
No other cases have been reported beyond this single case, but investigators are just beginning to reach out to those who came in contact with the patient, said Dr. Anne Schuchat, assistant surgeon general and director of the CDC’s National Center for Immunization and Respiratory Diseases, during a press briefing.
That list could be quite long, as the patient flew on April 24 from Saudi Arabia to London, then on to Chicago, and then traveled by bus to Indiana. The patient is in good condition, and remains in isolation in Community Hospital in Munster, Indiana, according to a statement from the hospital.
Health officials would not release the name of the airline or bus line the patient traveled on.
Indiana state health officials took specimens from the patient, which were then confirmed late today by the CDC.
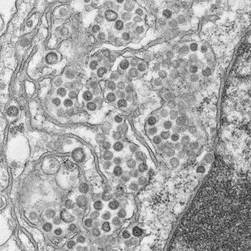
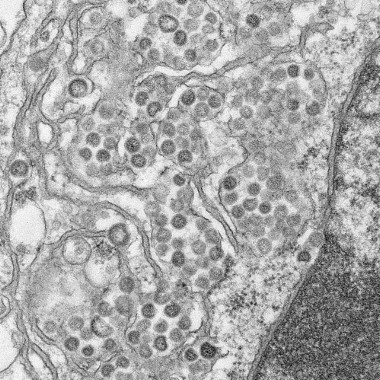
There is no specific treatment for the Middle East Respiratory Syndrome coronavirus (MERS-CoV), which has a case fatality rate of about 30% among symptomatic patients.
Since the virus was first reported in 2012 in Saudi Arabia, 263 cases have been confirmed in 12 countries, with 92 deaths. More than 100 other patients have been confirmed and reported by their ministries of health, but are not included in the World Health Organization tally, Dr. Schuchat said.
The Indiana case represents a "very low risk to the broader general public" because MERS-CoV has not shown the ability to spread easily from person to person in the community setting, she said.
"It is very concerning that the virus has spread in hospitals, and we should not be surprised if additional cases are identified among the health care workers who had close contact with this patient before the patient was isolated and special precautions were implemented," she went on to say.
An outbreak in the spring of 2013 involved 23 confirmed cases at four healthcare facilities, and another surge in cases beginning in March of this year has been identified.
It is unknown whether this represents seasonal variation or mutations in the virus that may make it more easily transmissible. At least one isolate has been sequenced by polymerase chain reaction from a patient in Saudi Arabia, and there were no changes in the virus, Dr. Schuchat said.
"With the SARS virus 10, 11 years ago, we did believe there was a change in the virus that led to more explosive transmission. So we’ll continue to look at that, but we don’t have data right now to confirm that that has happened," she said.
For now, the CDC is not advising people change their travel plans, but is recommending that people who develop a fever, cough, or shortness of breath within 14 days after traveling in or near the Arabian Peninsula see a health care provider, Dr. Schuchat said. Others that should monitor their symptoms include those who have close contact with someone who has these symptoms and travel history.
The CDC is also advising people to use basic respiratory illness precautions such as frequent hand washing, avoiding close contact with people who are sick, and disinfecting frequently touched surfaces.
No specific precautions were given for pediatricians or children, other than to ask for a travel history in patients with respiratory symptoms. The youngest case of MERS-CoV was in a 2 year-old, but the median age is around 51 years, she said.
Dr. Schuchat stressed that guidance may change as this "very fluid" situation evolves. The Indiana Department of Health and the CDC will share additional information on their Web sites and host additional press conferences, as needed, she said.
For more information on Middle East Respiratory Syndrome, go to http://www.cdc.gov/coronavirus/mers/index.html.
The Centers for Disease Control and Prevention has confirmed the first case of the deadly Middle East Respiratory Syndrome coronavirus in the United States.
The patient, a health care worker who recently returned from Riyadh, Saudi Arabia, is in stable condition in an Indiana hospital after being admitted with shortness of breath, cough, and fever on April 27.
No other cases have been reported beyond this single case, but investigators are just beginning to reach out to those who came in contact with the patient, said Dr. Anne Schuchat, assistant surgeon general and director of the CDC’s National Center for Immunization and Respiratory Diseases, during a press briefing.
That list could be quite long, as the patient flew on April 24 from Saudi Arabia to London, then on to Chicago, and then traveled by bus to Indiana. The patient is in good condition, and remains in isolation in Community Hospital in Munster, Indiana, according to a statement from the hospital.
Health officials would not release the name of the airline or bus line the patient traveled on.
Indiana state health officials took specimens from the patient, which were then confirmed late today by the CDC.
There is no specific treatment for the Middle East Respiratory Syndrome coronavirus (MERS-CoV), which has a case fatality rate of about 30% among symptomatic patients.
Since the virus was first reported in 2012 in Saudi Arabia, 263 cases have been confirmed in 12 countries, with 92 deaths. More than 100 other patients have been confirmed and reported by their ministries of health, but are not included in the World Health Organization tally, Dr. Schuchat said.
The Indiana case represents a "very low risk to the broader general public" because MERS-CoV has not shown the ability to spread easily from person to person in the community setting, she said.
"It is very concerning that the virus has spread in hospitals, and we should not be surprised if additional cases are identified among the health care workers who had close contact with this patient before the patient was isolated and special precautions were implemented," she went on to say.
An outbreak in the spring of 2013 involved 23 confirmed cases at four healthcare facilities, and another surge in cases beginning in March of this year has been identified.
It is unknown whether this represents seasonal variation or mutations in the virus that may make it more easily transmissible. At least one isolate has been sequenced by polymerase chain reaction from a patient in Saudi Arabia, and there were no changes in the virus, Dr. Schuchat said.
"With the SARS virus 10, 11 years ago, we did believe there was a change in the virus that led to more explosive transmission. So we’ll continue to look at that, but we don’t have data right now to confirm that that has happened," she said.
For now, the CDC is not advising people change their travel plans, but is recommending that people who develop a fever, cough, or shortness of breath within 14 days after traveling in or near the Arabian Peninsula see a health care provider, Dr. Schuchat said. Others that should monitor their symptoms include those who have close contact with someone who has these symptoms and travel history.
The CDC is also advising people to use basic respiratory illness precautions such as frequent hand washing, avoiding close contact with people who are sick, and disinfecting frequently touched surfaces.
No specific precautions were given for pediatricians or children, other than to ask for a travel history in patients with respiratory symptoms. The youngest case of MERS-CoV was in a 2 year-old, but the median age is around 51 years, she said.
Dr. Schuchat stressed that guidance may change as this "very fluid" situation evolves. The Indiana Department of Health and the CDC will share additional information on their Web sites and host additional press conferences, as needed, she said.
For more information on Middle East Respiratory Syndrome, go to http://www.cdc.gov/coronavirus/mers/index.html.
The Centers for Disease Control and Prevention has confirmed the first case of the deadly Middle East Respiratory Syndrome coronavirus in the United States.
The patient, a health care worker who recently returned from Riyadh, Saudi Arabia, is in stable condition in an Indiana hospital after being admitted with shortness of breath, cough, and fever on April 27.
No other cases have been reported beyond this single case, but investigators are just beginning to reach out to those who came in contact with the patient, said Dr. Anne Schuchat, assistant surgeon general and director of the CDC’s National Center for Immunization and Respiratory Diseases, during a press briefing.
That list could be quite long, as the patient flew on April 24 from Saudi Arabia to London, then on to Chicago, and then traveled by bus to Indiana. The patient is in good condition, and remains in isolation in Community Hospital in Munster, Indiana, according to a statement from the hospital.
Health officials would not release the name of the airline or bus line the patient traveled on.
Indiana state health officials took specimens from the patient, which were then confirmed late today by the CDC.
There is no specific treatment for the Middle East Respiratory Syndrome coronavirus (MERS-CoV), which has a case fatality rate of about 30% among symptomatic patients.
Since the virus was first reported in 2012 in Saudi Arabia, 263 cases have been confirmed in 12 countries, with 92 deaths. More than 100 other patients have been confirmed and reported by their ministries of health, but are not included in the World Health Organization tally, Dr. Schuchat said.
The Indiana case represents a "very low risk to the broader general public" because MERS-CoV has not shown the ability to spread easily from person to person in the community setting, she said.
"It is very concerning that the virus has spread in hospitals, and we should not be surprised if additional cases are identified among the health care workers who had close contact with this patient before the patient was isolated and special precautions were implemented," she went on to say.
An outbreak in the spring of 2013 involved 23 confirmed cases at four healthcare facilities, and another surge in cases beginning in March of this year has been identified.
It is unknown whether this represents seasonal variation or mutations in the virus that may make it more easily transmissible. At least one isolate has been sequenced by polymerase chain reaction from a patient in Saudi Arabia, and there were no changes in the virus, Dr. Schuchat said.
"With the SARS virus 10, 11 years ago, we did believe there was a change in the virus that led to more explosive transmission. So we’ll continue to look at that, but we don’t have data right now to confirm that that has happened," she said.
For now, the CDC is not advising people change their travel plans, but is recommending that people who develop a fever, cough, or shortness of breath within 14 days after traveling in or near the Arabian Peninsula see a health care provider, Dr. Schuchat said. Others that should monitor their symptoms include those who have close contact with someone who has these symptoms and travel history.
The CDC is also advising people to use basic respiratory illness precautions such as frequent hand washing, avoiding close contact with people who are sick, and disinfecting frequently touched surfaces.
No specific precautions were given for pediatricians or children, other than to ask for a travel history in patients with respiratory symptoms. The youngest case of MERS-CoV was in a 2 year-old, but the median age is around 51 years, she said.
Dr. Schuchat stressed that guidance may change as this "very fluid" situation evolves. The Indiana Department of Health and the CDC will share additional information on their Web sites and host additional press conferences, as needed, she said.
For more information on Middle East Respiratory Syndrome, go to http://www.cdc.gov/coronavirus/mers/index.html.
FROM A CDC TELEBRIEFING
CDC: Policy changes could prevent 100,000 deaths a year
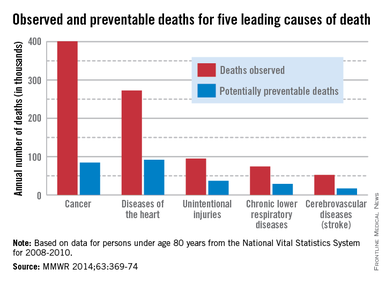
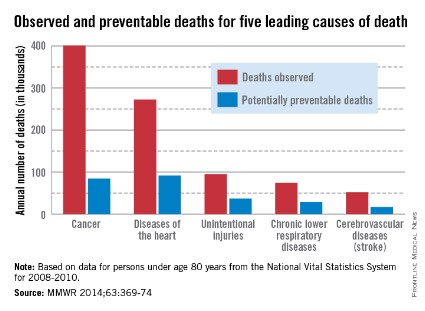
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
FROM MMWR
FDA approves umeclidinium for once-daily COPD maintenance
The Food and Drug Administration has approved umeclidinium as a once-daily, long-term treatment for airflow obstruction for patients with chronic obstructive pulmonary disease, GlaxoSmithKline announced April 30.
Incruse Ellipta (umeclidinium) is a long-acting muscarinic antagonist. It includes 62.5 mcg of umeclidinium delivered with the Ellipta inhaler.
Approximately 27 million people in the United States are affected by COPD, a lung disease that includes chronic bronchitis, emphysema, or both, according to the National Heart, Lung, and Blood Institute.
The phase III clinical trial for umeclidinium included seven clinical trials, which enrolled more than 2,500 COPD patients randomized to umeclidinium or placebo.
The most common adverse events with Incruse Ellipta (and placebo) were nasopharyngitis, 8% (7%); upper respiratory tract infection, 5% (4%); cough, 3% (2%); and arthralgia, 2% (1%). The drug is not recommended during rapidly deteriorating or potentially life-threatening COPD episodes, or as a rescue therapy for acute episodes of bronchospasm.
It is also recommended for the drug to be used with caution in patients with narrow-angle glaucoma and patients with urinary retention, especially prostatic hyperplasia or bladder neck obstruction.
Incruse Ellipta is currently approved in Canada and Europe, and is under review in several other countries. The firm says it plans to launch the drug in the United States in the fourth quarter of 2014.
The Food and Drug Administration has approved umeclidinium as a once-daily, long-term treatment for airflow obstruction for patients with chronic obstructive pulmonary disease, GlaxoSmithKline announced April 30.
Incruse Ellipta (umeclidinium) is a long-acting muscarinic antagonist. It includes 62.5 mcg of umeclidinium delivered with the Ellipta inhaler.
Approximately 27 million people in the United States are affected by COPD, a lung disease that includes chronic bronchitis, emphysema, or both, according to the National Heart, Lung, and Blood Institute.
The phase III clinical trial for umeclidinium included seven clinical trials, which enrolled more than 2,500 COPD patients randomized to umeclidinium or placebo.
The most common adverse events with Incruse Ellipta (and placebo) were nasopharyngitis, 8% (7%); upper respiratory tract infection, 5% (4%); cough, 3% (2%); and arthralgia, 2% (1%). The drug is not recommended during rapidly deteriorating or potentially life-threatening COPD episodes, or as a rescue therapy for acute episodes of bronchospasm.
It is also recommended for the drug to be used with caution in patients with narrow-angle glaucoma and patients with urinary retention, especially prostatic hyperplasia or bladder neck obstruction.
Incruse Ellipta is currently approved in Canada and Europe, and is under review in several other countries. The firm says it plans to launch the drug in the United States in the fourth quarter of 2014.
The Food and Drug Administration has approved umeclidinium as a once-daily, long-term treatment for airflow obstruction for patients with chronic obstructive pulmonary disease, GlaxoSmithKline announced April 30.
Incruse Ellipta (umeclidinium) is a long-acting muscarinic antagonist. It includes 62.5 mcg of umeclidinium delivered with the Ellipta inhaler.
Approximately 27 million people in the United States are affected by COPD, a lung disease that includes chronic bronchitis, emphysema, or both, according to the National Heart, Lung, and Blood Institute.
The phase III clinical trial for umeclidinium included seven clinical trials, which enrolled more than 2,500 COPD patients randomized to umeclidinium or placebo.
The most common adverse events with Incruse Ellipta (and placebo) were nasopharyngitis, 8% (7%); upper respiratory tract infection, 5% (4%); cough, 3% (2%); and arthralgia, 2% (1%). The drug is not recommended during rapidly deteriorating or potentially life-threatening COPD episodes, or as a rescue therapy for acute episodes of bronchospasm.
It is also recommended for the drug to be used with caution in patients with narrow-angle glaucoma and patients with urinary retention, especially prostatic hyperplasia or bladder neck obstruction.
Incruse Ellipta is currently approved in Canada and Europe, and is under review in several other countries. The firm says it plans to launch the drug in the United States in the fourth quarter of 2014.
Nocturnal cortisol levels predicted neurocognitive impairment in sleep apnea
Nocturnal cortisol levels explained up to 16% of changes in learning, memory, and working memory in patients with obstructive sleep apnea, a study showed.
But severity of obstructive sleep apnea (OSA) did not itself predict neurocognitive impairment, said Dr. Kate M. Edwards of the University of Sydney in Lidscombe, Australia, and her associates, who conducted the study at the University of California, San Diego.
"These findings suggest that OSA-related alterations in [hypothalamic-pituitary-adrenal] activity may play a key role in the pathophysiology of neuropsychologic impairments in OSA," the investigators wrote (Sleep Med. 2014;15:27-32).

The researchers enrolled 55 men and women with OSA and measured blood cortisol levels every 2 hours for 24 hours. Participants underwent polysomnography the next night and took a battery of tests to assess seven cognitive domains. The oxygen desaturation index (ODI) was used as an index of OSA severity.
In univariate analyses, the mean apnea-hypopnea index, ODI, and nighttime cortisol levels were significantly associated with global deficit scores and particularly with domains of learning, memory, and working memory, said the investigators. In hierarchical linear regression analyses, nighttime cortisol levels accounted for 9%-16% of variance in the three domains, while ODI (apnea) severity did not predict additional variance, they reported.
"Our data are in line with the literature reporting that chronic exposure to elevated physiologic cortisol levels is associated with a decline in neurocognitive function and hippocampal structure," the investigators said. "The functional effects of cortisol on reduced memory function have been demonstrated by experimental cortisol treatment and stress-induced cortisol level increases."
"The treatment of OSA with CPAP [continuous positive airway pressure] has been reported to show improvements in some aspects of neuropsychologic function, though findings are inconsistent," the investigators wrote.
"It may yield interesting data if future studies address the possibility that CPAP treatment effects on neurocognitive function are mediated by alterations in [hypothalamic-pituitary-adrenal] function, specifically reductions in nighttime cortisol levels."
The work was funded by University of California, San Diego, grants. The authors disclosed no relevant financial conflicts of interest.
Nocturnal cortisol levels explained up to 16% of changes in learning, memory, and working memory in patients with obstructive sleep apnea, a study showed.
But severity of obstructive sleep apnea (OSA) did not itself predict neurocognitive impairment, said Dr. Kate M. Edwards of the University of Sydney in Lidscombe, Australia, and her associates, who conducted the study at the University of California, San Diego.
"These findings suggest that OSA-related alterations in [hypothalamic-pituitary-adrenal] activity may play a key role in the pathophysiology of neuropsychologic impairments in OSA," the investigators wrote (Sleep Med. 2014;15:27-32).
The researchers enrolled 55 men and women with OSA and measured blood cortisol levels every 2 hours for 24 hours. Participants underwent polysomnography the next night and took a battery of tests to assess seven cognitive domains. The oxygen desaturation index (ODI) was used as an index of OSA severity.
In univariate analyses, the mean apnea-hypopnea index, ODI, and nighttime cortisol levels were significantly associated with global deficit scores and particularly with domains of learning, memory, and working memory, said the investigators. In hierarchical linear regression analyses, nighttime cortisol levels accounted for 9%-16% of variance in the three domains, while ODI (apnea) severity did not predict additional variance, they reported.
"Our data are in line with the literature reporting that chronic exposure to elevated physiologic cortisol levels is associated with a decline in neurocognitive function and hippocampal structure," the investigators said. "The functional effects of cortisol on reduced memory function have been demonstrated by experimental cortisol treatment and stress-induced cortisol level increases."
"The treatment of OSA with CPAP [continuous positive airway pressure] has been reported to show improvements in some aspects of neuropsychologic function, though findings are inconsistent," the investigators wrote.
"It may yield interesting data if future studies address the possibility that CPAP treatment effects on neurocognitive function are mediated by alterations in [hypothalamic-pituitary-adrenal] function, specifically reductions in nighttime cortisol levels."
The work was funded by University of California, San Diego, grants. The authors disclosed no relevant financial conflicts of interest.
Nocturnal cortisol levels explained up to 16% of changes in learning, memory, and working memory in patients with obstructive sleep apnea, a study showed.
But severity of obstructive sleep apnea (OSA) did not itself predict neurocognitive impairment, said Dr. Kate M. Edwards of the University of Sydney in Lidscombe, Australia, and her associates, who conducted the study at the University of California, San Diego.
"These findings suggest that OSA-related alterations in [hypothalamic-pituitary-adrenal] activity may play a key role in the pathophysiology of neuropsychologic impairments in OSA," the investigators wrote (Sleep Med. 2014;15:27-32).
The researchers enrolled 55 men and women with OSA and measured blood cortisol levels every 2 hours for 24 hours. Participants underwent polysomnography the next night and took a battery of tests to assess seven cognitive domains. The oxygen desaturation index (ODI) was used as an index of OSA severity.
In univariate analyses, the mean apnea-hypopnea index, ODI, and nighttime cortisol levels were significantly associated with global deficit scores and particularly with domains of learning, memory, and working memory, said the investigators. In hierarchical linear regression analyses, nighttime cortisol levels accounted for 9%-16% of variance in the three domains, while ODI (apnea) severity did not predict additional variance, they reported.
"Our data are in line with the literature reporting that chronic exposure to elevated physiologic cortisol levels is associated with a decline in neurocognitive function and hippocampal structure," the investigators said. "The functional effects of cortisol on reduced memory function have been demonstrated by experimental cortisol treatment and stress-induced cortisol level increases."
"The treatment of OSA with CPAP [continuous positive airway pressure] has been reported to show improvements in some aspects of neuropsychologic function, though findings are inconsistent," the investigators wrote.
"It may yield interesting data if future studies address the possibility that CPAP treatment effects on neurocognitive function are mediated by alterations in [hypothalamic-pituitary-adrenal] function, specifically reductions in nighttime cortisol levels."
The work was funded by University of California, San Diego, grants. The authors disclosed no relevant financial conflicts of interest.
FROM SLEEP MEDICINE
Major finding: Nighttime cortisol levels accounted for 9%-16% of variance in learning, memory, and working memory, and apnea severity did not predict additional variance.
Data source: A cohort study of 55 men and women with obstructive sleep apnea. Tests included blood cortisol measurements, polysomnography, and assessments of seven neurocognitive domains.
Disclosures: The work was funded by University of California, San Diego, grants. The authors disclosed no relevant financial conflicts of interest.

Panel recommends against low-dose CT for lung cancer in Medicare patients
Evidence is insufficient to support lung cancer screening with low-dose computed tomography in the Medicare population, members of the Medicare Evidence Development and Coverage Advisory Committee said at a meeting on April 30.
Specifically, the MEDCAC advisers said that, on average, they had low confidence there is adequate evidence that the benefits outweigh the harms of lung cancer screening with low-dose computed tomography (LDCT) in the Medicare population.

The Centers for Medicare & Medicaid Services accepted two formal requests to initiate a national coverage analysis on lung cancer screening with LDCT, which the U.S. Preventive Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.
"I think it’s almost impossible to extrapolate to the Medicare population the expected results that we would get when I feel it’s our obligation to first do no harm. I didn’t hear that the evidence is there to support benefit beyond harm," said Dr. Curtis Mock, national medical director of UnitedHealthcare Medicare & Retirement.
Most of the MEDCAC advisers said that they were not satisfied by the Medicare-population data in the National Lung Screening Trial (NLST). That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT (N. Engl. J. Med. 2013;368:1980-91). One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
But Medicare-eligible patients – those aged 65-74 years – represented about 25% of patients in the trial, less than the nearly 36% NLST-eligible in the U.S. population.
"I am concerned that we don’t really have a lot of data in the Medicare population, certainly not in the 75-80 [year-old age group], particularly on the harms in the age group that was included in NLST," said Dr. Rita Redberg, MEDCAC chair and professor of medicine at the University of California, San Francisco.
Dr. Redberg also highlighted the additional health complications with Medicare-age patients.
"Surgical mortality increases as one gets older, and the benefits of early detection tend to disappear as you get older because there are more competing causes of death," she said.
The MEDCAC advisers also noted that they were not confident that the harms of lung cancer screening with LDCT (average effective dose of 1.5 mSv) would be minimized if implemented in the Medicare population.
"The harm I worry about will be the intervention of this test on people for which we know nothing about the benefits and harms," said Dr. Allan Fendrick, professor in the department of internal medicine at the University of Michigan, Ann Arbor.
Similarly, Dr. Harry Burke, associate professor at the Uniformed Services University of the Health Sciences in Bethesda, Md., said, "I think the low positive predictive value drives harm. Whether you can balance that harm with the benefit is a very difficult business."
Lastly, the advisors said that they strongly believe there are clinically significant evidence gaps when using LDCT for lung cancer screening in the Medicare population outside a clinical trial.
"The most important gap that I see is based on totality of the data – both from this large NLST trial but also high-quality publications from other trials – to be able to come up with a cohort where we would have much higher confidence that the benefits outweigh the harms than other subgroups," said MEDCAC vice chair Dr. Art Sedrakyan, director of the Patient Centered Comparative Outcomes Research Program at Cornell University, New York.
CMS will take the expert panel’s recommendations into consideration as it develops its national coverage decision for lung cancer screening with LDCT, which it plans to issue by mid-November, followed by a 30-day public comment period.
Evidence is insufficient to support lung cancer screening with low-dose computed tomography in the Medicare population, members of the Medicare Evidence Development and Coverage Advisory Committee said at a meeting on April 30.
Specifically, the MEDCAC advisers said that, on average, they had low confidence there is adequate evidence that the benefits outweigh the harms of lung cancer screening with low-dose computed tomography (LDCT) in the Medicare population.
The Centers for Medicare & Medicaid Services accepted two formal requests to initiate a national coverage analysis on lung cancer screening with LDCT, which the U.S. Preventive Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.
"I think it’s almost impossible to extrapolate to the Medicare population the expected results that we would get when I feel it’s our obligation to first do no harm. I didn’t hear that the evidence is there to support benefit beyond harm," said Dr. Curtis Mock, national medical director of UnitedHealthcare Medicare & Retirement.
Most of the MEDCAC advisers said that they were not satisfied by the Medicare-population data in the National Lung Screening Trial (NLST). That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT (N. Engl. J. Med. 2013;368:1980-91). One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
But Medicare-eligible patients – those aged 65-74 years – represented about 25% of patients in the trial, less than the nearly 36% NLST-eligible in the U.S. population.
"I am concerned that we don’t really have a lot of data in the Medicare population, certainly not in the 75-80 [year-old age group], particularly on the harms in the age group that was included in NLST," said Dr. Rita Redberg, MEDCAC chair and professor of medicine at the University of California, San Francisco.
Dr. Redberg also highlighted the additional health complications with Medicare-age patients.
"Surgical mortality increases as one gets older, and the benefits of early detection tend to disappear as you get older because there are more competing causes of death," she said.
The MEDCAC advisers also noted that they were not confident that the harms of lung cancer screening with LDCT (average effective dose of 1.5 mSv) would be minimized if implemented in the Medicare population.
"The harm I worry about will be the intervention of this test on people for which we know nothing about the benefits and harms," said Dr. Allan Fendrick, professor in the department of internal medicine at the University of Michigan, Ann Arbor.
Similarly, Dr. Harry Burke, associate professor at the Uniformed Services University of the Health Sciences in Bethesda, Md., said, "I think the low positive predictive value drives harm. Whether you can balance that harm with the benefit is a very difficult business."
Lastly, the advisors said that they strongly believe there are clinically significant evidence gaps when using LDCT for lung cancer screening in the Medicare population outside a clinical trial.
"The most important gap that I see is based on totality of the data – both from this large NLST trial but also high-quality publications from other trials – to be able to come up with a cohort where we would have much higher confidence that the benefits outweigh the harms than other subgroups," said MEDCAC vice chair Dr. Art Sedrakyan, director of the Patient Centered Comparative Outcomes Research Program at Cornell University, New York.
CMS will take the expert panel’s recommendations into consideration as it develops its national coverage decision for lung cancer screening with LDCT, which it plans to issue by mid-November, followed by a 30-day public comment period.
Evidence is insufficient to support lung cancer screening with low-dose computed tomography in the Medicare population, members of the Medicare Evidence Development and Coverage Advisory Committee said at a meeting on April 30.
Specifically, the MEDCAC advisers said that, on average, they had low confidence there is adequate evidence that the benefits outweigh the harms of lung cancer screening with low-dose computed tomography (LDCT) in the Medicare population.
The Centers for Medicare & Medicaid Services accepted two formal requests to initiate a national coverage analysis on lung cancer screening with LDCT, which the U.S. Preventive Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.
"I think it’s almost impossible to extrapolate to the Medicare population the expected results that we would get when I feel it’s our obligation to first do no harm. I didn’t hear that the evidence is there to support benefit beyond harm," said Dr. Curtis Mock, national medical director of UnitedHealthcare Medicare & Retirement.
Most of the MEDCAC advisers said that they were not satisfied by the Medicare-population data in the National Lung Screening Trial (NLST). That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT (N. Engl. J. Med. 2013;368:1980-91). One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
But Medicare-eligible patients – those aged 65-74 years – represented about 25% of patients in the trial, less than the nearly 36% NLST-eligible in the U.S. population.
"I am concerned that we don’t really have a lot of data in the Medicare population, certainly not in the 75-80 [year-old age group], particularly on the harms in the age group that was included in NLST," said Dr. Rita Redberg, MEDCAC chair and professor of medicine at the University of California, San Francisco.
Dr. Redberg also highlighted the additional health complications with Medicare-age patients.
"Surgical mortality increases as one gets older, and the benefits of early detection tend to disappear as you get older because there are more competing causes of death," she said.
The MEDCAC advisers also noted that they were not confident that the harms of lung cancer screening with LDCT (average effective dose of 1.5 mSv) would be minimized if implemented in the Medicare population.
"The harm I worry about will be the intervention of this test on people for which we know nothing about the benefits and harms," said Dr. Allan Fendrick, professor in the department of internal medicine at the University of Michigan, Ann Arbor.
Similarly, Dr. Harry Burke, associate professor at the Uniformed Services University of the Health Sciences in Bethesda, Md., said, "I think the low positive predictive value drives harm. Whether you can balance that harm with the benefit is a very difficult business."
Lastly, the advisors said that they strongly believe there are clinically significant evidence gaps when using LDCT for lung cancer screening in the Medicare population outside a clinical trial.
"The most important gap that I see is based on totality of the data – both from this large NLST trial but also high-quality publications from other trials – to be able to come up with a cohort where we would have much higher confidence that the benefits outweigh the harms than other subgroups," said MEDCAC vice chair Dr. Art Sedrakyan, director of the Patient Centered Comparative Outcomes Research Program at Cornell University, New York.
CMS will take the expert panel’s recommendations into consideration as it develops its national coverage decision for lung cancer screening with LDCT, which it plans to issue by mid-November, followed by a 30-day public comment period.
AT A MEDCAC MEETING

Should You Consider Antibiotics for Exacerbations of Mild COPD?
PRACTICE CHANGER
Consider antibiotics for patients with exacerbations of mild to moderate chronic obstructive pulmonary disease (COPD).1
STRENGTH OF RECOMMENDATION
B: Based on a single well-done multicenter randomized controlled trial (RCT) with quality evidence.1
ILLUSTRATIVE CASE
A 45-year-old man with a history of mild COPD seeks treatment for worsening dyspnea and increased (nonpurulent) sputum production. He denies fever or chills. On exam, he has coarse breath sounds and scattered wheezes. Should you add antibiotics to his treatment?
COPD exacerbations—a worsening of symptoms beyond day-to-day variations that leads to a medication change—are part of the disease course and can accelerate lung function decline, decrease quality of life, and, when severe, increase mortality.2 Infections cause an estimated 50% to 70% of COPD exacerbations.2-4
Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend using antibiotics to treat exacerbations in patients with moderate or severe COPD who
• Have increased dyspnea, sputum volume, and sputum purulence;
• Have two of these symptoms if increased sputum purulence is one of them; or
• Require mechanical ventilation.2
According to the GOLD guidelines, the choice of antibiotic should be based on local antibiograms; common options include amoxicillin, amoxicillin/clavulanate, azithromycin, and doxycycline.2 Although the GOLD guidelines cover use of antibiotics for COPD exacerbations, this recommendation is based on analyses of studies that focused on patients with moderate or severe COPD.2 There has been little research on using antibiotics for exacerbations of mild COPD.
STUDY SUMMARY
Using antibiotics often resolves symptoms
Llor et al1 conducted a multicenter, double-blind, placebo-controlled RCT to examine the effectiveness of antibiotic treatment for COPD exacerbations. Participants (ages 40 and older) had mild to moderate COPD, defined as 10 or more pack-years of smoking, an FEV1 greater than 50%, and an FEV1/FVC ratio lower than 0.7. An exacerbation was defined as at least one of the following: increased dyspnea, increased sputum volume, or sputum purulence.
Patients were randomly assigned to receive amoxicillin/clavulanate 500/125 mg or placebo three times a day for eight days. Primary endpoints were clinical cure (resolution of symptoms) and clinical success (resolution or improvement of symptoms) at days 9 to 11, as determined by physician assessment. Secondary measures included cure and clinical success at day 20 and time until next exacerbation. Patients were monitored for one year after the exacerbation.
There were 162 patients in the antibiotic group and 156 in the placebo group; the two groups were demographically similar. In each group, four patients withdrew consent and were removed from analysis. By the 9-to-11-day follow-up visit, 74.1% of patients in the antibiotic group had clinical cure, compared with 59.9% in the placebo group (number needed to treat [NNT] = 7). Clinical success also was significantly greater with antibiotics compared with placebo (90.5% vs 80.9%).
The clinical cure rate at day 20 also was significantly greater in patients on antibiotics compared with placebo (81.6% vs 67.8%; NNT = 7). During the one-year follow-up, 58% of patients in the antibiotic group and 73.2% of those in the placebo group experienced additional exacerbations. Time to next exacerbation was significantly longer in patients taking antibiotics (233 days vs 160 days).
Can CRP level help determine who should receive antibiotics?
Previous studies have identified biomarkers, including C-reactive protein (CRP), that indicate COPD exacerbation but have not linked them to clinical course.5-7 In this study, researchers measured CRP in patients receiving placebo to determine if this biomarker could predict clinical outcomes.
The researchers found that the clinical success rate among patients with a CRP lower than 40 mg/L was 87.6%, while only 34.5% of patients with a CRP greater than 40 mg/L experienced clinical success (sensitivity and specificity for clinical success at this cutoff were 0.655 and 0.876, respectively). This suggests that antibiotics might be appropriate for patients with an exacerbation of mild or moderate COPD who have a CRP greater than 40 mg/L.
There were 35 adverse events: 23 in the antibiotics group and 12 in the placebo group. Two patients in the antibiotics group discontinued treatment as a result. Most adverse events involved mild gastrointestinal problems.
Continued on next page >>
WHAT’S NEW?
Evidence supports antibiotics for mild to moderate COPD
Few placebo-controlled trials have addressed antibiotic use for exacerbations in patients with mild to moderate COPD.2,8,9 This study demonstrated that, compared with placebo, symptom resolution and clinical success is greater with amoxicillin/clavulanate and that antibiotic treatment also may increase time until next exacerbation.
The study also looked at the relationship of CRP and exacerbations in the placebo group. Higher spontaneous clinical cure rates were noted when the CRP was lower than 40 mg/L.
CAVEATS
Effects of concomitant medications are unclear
In both the placebo and antibiotic groups, patients were taking other medications (including short- and long-acting β-agonists, anticholinergics, theophyllines, and oral or inhaled corticosteroids). Roughly the same number of patients in each group took additional medications, but researchers did not conduct a subgroup analysis to see if patients treated with these medications responded differently from those who received antibiotics alone.
GOLD guidelines already suggest antibiotics for exacerbations in patients with moderate COPD.2 In this study, 89% of patients met criteria for moderate COPD and 11% for mild COPD. Though the percentage of patients who had mild COPD was small, we believe the results of this study warrant consideration of antibiotic use in patients with mild disease. Local antibiograms may show increased resistance to amoxicillin/clavulanate; this study did not address the use of other antibiotics.
CHALLENGES TO IMPLEMENTATION
Antibiotic overuse may be a concern
Concerns about antibiotic resistance may make clinicians reluctant to prescribe the drugs for those with mild to moderate COPD.
REFERENCES
1. Llor C, Moragas A, Hernández S, et al. Efficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(8):716-723.
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. January 2014. www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed April 15, 2014.
3. Donaldson GC, Seemungal TA, Bhowmik A, et al. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-852.
4. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
5. Vollenweider DJ, Jarrett H, Steurer-Stey CA, et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257.
6. Bartlett, JG, Sethi S. Management of infection in acute exacerbations of chronic obstructive pulmonary disease. In: Basow DS, ed. UpToDate. www.uptodate.com. Last updated March 27, 2012. Accessed January 2, 2013.
7. Lacoma A, Prat C, Andreo F, et al. Value of procalcitonin, C-reactive protein, and neopterin in exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:157-169.
8. Antonescu-Turcu AL, Tomic R. C-reactive protein and copeptin: prognostic predictors in chronic obstructive pulmonary disease exacerbations. Curr Opin Pulm Med. 2009;15(2):120-125.
9. Thomsen M, Ingebrigtsen TS, Marott JL, et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA. 2013;309(22):2353-2361.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(4):E11-E13.
PRACTICE CHANGER
Consider antibiotics for patients with exacerbations of mild to moderate chronic obstructive pulmonary disease (COPD).1
STRENGTH OF RECOMMENDATION
B: Based on a single well-done multicenter randomized controlled trial (RCT) with quality evidence.1
ILLUSTRATIVE CASE
A 45-year-old man with a history of mild COPD seeks treatment for worsening dyspnea and increased (nonpurulent) sputum production. He denies fever or chills. On exam, he has coarse breath sounds and scattered wheezes. Should you add antibiotics to his treatment?
COPD exacerbations—a worsening of symptoms beyond day-to-day variations that leads to a medication change—are part of the disease course and can accelerate lung function decline, decrease quality of life, and, when severe, increase mortality.2 Infections cause an estimated 50% to 70% of COPD exacerbations.2-4
Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend using antibiotics to treat exacerbations in patients with moderate or severe COPD who
• Have increased dyspnea, sputum volume, and sputum purulence;
• Have two of these symptoms if increased sputum purulence is one of them; or
• Require mechanical ventilation.2
According to the GOLD guidelines, the choice of antibiotic should be based on local antibiograms; common options include amoxicillin, amoxicillin/clavulanate, azithromycin, and doxycycline.2 Although the GOLD guidelines cover use of antibiotics for COPD exacerbations, this recommendation is based on analyses of studies that focused on patients with moderate or severe COPD.2 There has been little research on using antibiotics for exacerbations of mild COPD.
STUDY SUMMARY
Using antibiotics often resolves symptoms
Llor et al1 conducted a multicenter, double-blind, placebo-controlled RCT to examine the effectiveness of antibiotic treatment for COPD exacerbations. Participants (ages 40 and older) had mild to moderate COPD, defined as 10 or more pack-years of smoking, an FEV1 greater than 50%, and an FEV1/FVC ratio lower than 0.7. An exacerbation was defined as at least one of the following: increased dyspnea, increased sputum volume, or sputum purulence.
Patients were randomly assigned to receive amoxicillin/clavulanate 500/125 mg or placebo three times a day for eight days. Primary endpoints were clinical cure (resolution of symptoms) and clinical success (resolution or improvement of symptoms) at days 9 to 11, as determined by physician assessment. Secondary measures included cure and clinical success at day 20 and time until next exacerbation. Patients were monitored for one year after the exacerbation.
There were 162 patients in the antibiotic group and 156 in the placebo group; the two groups were demographically similar. In each group, four patients withdrew consent and were removed from analysis. By the 9-to-11-day follow-up visit, 74.1% of patients in the antibiotic group had clinical cure, compared with 59.9% in the placebo group (number needed to treat [NNT] = 7). Clinical success also was significantly greater with antibiotics compared with placebo (90.5% vs 80.9%).
The clinical cure rate at day 20 also was significantly greater in patients on antibiotics compared with placebo (81.6% vs 67.8%; NNT = 7). During the one-year follow-up, 58% of patients in the antibiotic group and 73.2% of those in the placebo group experienced additional exacerbations. Time to next exacerbation was significantly longer in patients taking antibiotics (233 days vs 160 days).
Can CRP level help determine who should receive antibiotics?
Previous studies have identified biomarkers, including C-reactive protein (CRP), that indicate COPD exacerbation but have not linked them to clinical course.5-7 In this study, researchers measured CRP in patients receiving placebo to determine if this biomarker could predict clinical outcomes.
The researchers found that the clinical success rate among patients with a CRP lower than 40 mg/L was 87.6%, while only 34.5% of patients with a CRP greater than 40 mg/L experienced clinical success (sensitivity and specificity for clinical success at this cutoff were 0.655 and 0.876, respectively). This suggests that antibiotics might be appropriate for patients with an exacerbation of mild or moderate COPD who have a CRP greater than 40 mg/L.
There were 35 adverse events: 23 in the antibiotics group and 12 in the placebo group. Two patients in the antibiotics group discontinued treatment as a result. Most adverse events involved mild gastrointestinal problems.
Continued on next page >>
WHAT’S NEW?
Evidence supports antibiotics for mild to moderate COPD
Few placebo-controlled trials have addressed antibiotic use for exacerbations in patients with mild to moderate COPD.2,8,9 This study demonstrated that, compared with placebo, symptom resolution and clinical success is greater with amoxicillin/clavulanate and that antibiotic treatment also may increase time until next exacerbation.
The study also looked at the relationship of CRP and exacerbations in the placebo group. Higher spontaneous clinical cure rates were noted when the CRP was lower than 40 mg/L.
CAVEATS
Effects of concomitant medications are unclear
In both the placebo and antibiotic groups, patients were taking other medications (including short- and long-acting β-agonists, anticholinergics, theophyllines, and oral or inhaled corticosteroids). Roughly the same number of patients in each group took additional medications, but researchers did not conduct a subgroup analysis to see if patients treated with these medications responded differently from those who received antibiotics alone.
GOLD guidelines already suggest antibiotics for exacerbations in patients with moderate COPD.2 In this study, 89% of patients met criteria for moderate COPD and 11% for mild COPD. Though the percentage of patients who had mild COPD was small, we believe the results of this study warrant consideration of antibiotic use in patients with mild disease. Local antibiograms may show increased resistance to amoxicillin/clavulanate; this study did not address the use of other antibiotics.
CHALLENGES TO IMPLEMENTATION
Antibiotic overuse may be a concern
Concerns about antibiotic resistance may make clinicians reluctant to prescribe the drugs for those with mild to moderate COPD.
REFERENCES
1. Llor C, Moragas A, Hernández S, et al. Efficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(8):716-723.
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. January 2014. www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed April 15, 2014.
3. Donaldson GC, Seemungal TA, Bhowmik A, et al. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-852.
4. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
5. Vollenweider DJ, Jarrett H, Steurer-Stey CA, et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257.
6. Bartlett, JG, Sethi S. Management of infection in acute exacerbations of chronic obstructive pulmonary disease. In: Basow DS, ed. UpToDate. www.uptodate.com. Last updated March 27, 2012. Accessed January 2, 2013.
7. Lacoma A, Prat C, Andreo F, et al. Value of procalcitonin, C-reactive protein, and neopterin in exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:157-169.
8. Antonescu-Turcu AL, Tomic R. C-reactive protein and copeptin: prognostic predictors in chronic obstructive pulmonary disease exacerbations. Curr Opin Pulm Med. 2009;15(2):120-125.
9. Thomsen M, Ingebrigtsen TS, Marott JL, et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA. 2013;309(22):2353-2361.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(4):E11-E13.
PRACTICE CHANGER
Consider antibiotics for patients with exacerbations of mild to moderate chronic obstructive pulmonary disease (COPD).1
STRENGTH OF RECOMMENDATION
B: Based on a single well-done multicenter randomized controlled trial (RCT) with quality evidence.1
ILLUSTRATIVE CASE
A 45-year-old man with a history of mild COPD seeks treatment for worsening dyspnea and increased (nonpurulent) sputum production. He denies fever or chills. On exam, he has coarse breath sounds and scattered wheezes. Should you add antibiotics to his treatment?
COPD exacerbations—a worsening of symptoms beyond day-to-day variations that leads to a medication change—are part of the disease course and can accelerate lung function decline, decrease quality of life, and, when severe, increase mortality.2 Infections cause an estimated 50% to 70% of COPD exacerbations.2-4
Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend using antibiotics to treat exacerbations in patients with moderate or severe COPD who
• Have increased dyspnea, sputum volume, and sputum purulence;
• Have two of these symptoms if increased sputum purulence is one of them; or
• Require mechanical ventilation.2
According to the GOLD guidelines, the choice of antibiotic should be based on local antibiograms; common options include amoxicillin, amoxicillin/clavulanate, azithromycin, and doxycycline.2 Although the GOLD guidelines cover use of antibiotics for COPD exacerbations, this recommendation is based on analyses of studies that focused on patients with moderate or severe COPD.2 There has been little research on using antibiotics for exacerbations of mild COPD.
STUDY SUMMARY
Using antibiotics often resolves symptoms
Llor et al1 conducted a multicenter, double-blind, placebo-controlled RCT to examine the effectiveness of antibiotic treatment for COPD exacerbations. Participants (ages 40 and older) had mild to moderate COPD, defined as 10 or more pack-years of smoking, an FEV1 greater than 50%, and an FEV1/FVC ratio lower than 0.7. An exacerbation was defined as at least one of the following: increased dyspnea, increased sputum volume, or sputum purulence.
Patients were randomly assigned to receive amoxicillin/clavulanate 500/125 mg or placebo three times a day for eight days. Primary endpoints were clinical cure (resolution of symptoms) and clinical success (resolution or improvement of symptoms) at days 9 to 11, as determined by physician assessment. Secondary measures included cure and clinical success at day 20 and time until next exacerbation. Patients were monitored for one year after the exacerbation.
There were 162 patients in the antibiotic group and 156 in the placebo group; the two groups were demographically similar. In each group, four patients withdrew consent and were removed from analysis. By the 9-to-11-day follow-up visit, 74.1% of patients in the antibiotic group had clinical cure, compared with 59.9% in the placebo group (number needed to treat [NNT] = 7). Clinical success also was significantly greater with antibiotics compared with placebo (90.5% vs 80.9%).
The clinical cure rate at day 20 also was significantly greater in patients on antibiotics compared with placebo (81.6% vs 67.8%; NNT = 7). During the one-year follow-up, 58% of patients in the antibiotic group and 73.2% of those in the placebo group experienced additional exacerbations. Time to next exacerbation was significantly longer in patients taking antibiotics (233 days vs 160 days).
Can CRP level help determine who should receive antibiotics?
Previous studies have identified biomarkers, including C-reactive protein (CRP), that indicate COPD exacerbation but have not linked them to clinical course.5-7 In this study, researchers measured CRP in patients receiving placebo to determine if this biomarker could predict clinical outcomes.
The researchers found that the clinical success rate among patients with a CRP lower than 40 mg/L was 87.6%, while only 34.5% of patients with a CRP greater than 40 mg/L experienced clinical success (sensitivity and specificity for clinical success at this cutoff were 0.655 and 0.876, respectively). This suggests that antibiotics might be appropriate for patients with an exacerbation of mild or moderate COPD who have a CRP greater than 40 mg/L.
There were 35 adverse events: 23 in the antibiotics group and 12 in the placebo group. Two patients in the antibiotics group discontinued treatment as a result. Most adverse events involved mild gastrointestinal problems.
Continued on next page >>
WHAT’S NEW?
Evidence supports antibiotics for mild to moderate COPD
Few placebo-controlled trials have addressed antibiotic use for exacerbations in patients with mild to moderate COPD.2,8,9 This study demonstrated that, compared with placebo, symptom resolution and clinical success is greater with amoxicillin/clavulanate and that antibiotic treatment also may increase time until next exacerbation.
The study also looked at the relationship of CRP and exacerbations in the placebo group. Higher spontaneous clinical cure rates were noted when the CRP was lower than 40 mg/L.
CAVEATS
Effects of concomitant medications are unclear
In both the placebo and antibiotic groups, patients were taking other medications (including short- and long-acting β-agonists, anticholinergics, theophyllines, and oral or inhaled corticosteroids). Roughly the same number of patients in each group took additional medications, but researchers did not conduct a subgroup analysis to see if patients treated with these medications responded differently from those who received antibiotics alone.
GOLD guidelines already suggest antibiotics for exacerbations in patients with moderate COPD.2 In this study, 89% of patients met criteria for moderate COPD and 11% for mild COPD. Though the percentage of patients who had mild COPD was small, we believe the results of this study warrant consideration of antibiotic use in patients with mild disease. Local antibiograms may show increased resistance to amoxicillin/clavulanate; this study did not address the use of other antibiotics.
CHALLENGES TO IMPLEMENTATION
Antibiotic overuse may be a concern
Concerns about antibiotic resistance may make clinicians reluctant to prescribe the drugs for those with mild to moderate COPD.
REFERENCES
1. Llor C, Moragas A, Hernández S, et al. Efficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(8):716-723.
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. January 2014. www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html. Accessed April 15, 2014.
3. Donaldson GC, Seemungal TA, Bhowmik A, et al. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-852.
4. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
5. Vollenweider DJ, Jarrett H, Steurer-Stey CA, et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257.
6. Bartlett, JG, Sethi S. Management of infection in acute exacerbations of chronic obstructive pulmonary disease. In: Basow DS, ed. UpToDate. www.uptodate.com. Last updated March 27, 2012. Accessed January 2, 2013.
7. Lacoma A, Prat C, Andreo F, et al. Value of procalcitonin, C-reactive protein, and neopterin in exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:157-169.
8. Antonescu-Turcu AL, Tomic R. C-reactive protein and copeptin: prognostic predictors in chronic obstructive pulmonary disease exacerbations. Curr Opin Pulm Med. 2009;15(2):120-125.
9. Thomsen M, Ingebrigtsen TS, Marott JL, et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA. 2013;309(22):2353-2361.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(4):E11-E13.