User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Aspirin Sensitivity Signals Asthma Severity
MADRID – Aspirin sensitivity was strongly associated with asthma severity and the presence of chronic rhinosinusitis with nasal polyps in a prospective, multicenter study.
"Aspirin sensitivity may be considered a clinical marker for severe asthma and for the presence of chronic rhinosinusitis with nasal polyps, and a potential marker for united airway disease," Dr. José Antonio Castillo reported at the world congress of the American College of Chest Physicians.
Aspirin-exacerbated respiratory disease is commonly associated with chronic rhinosinusitis (CRS) with nasal polyps, but little information is available on the correlation between aspirin sensitivity and severe asthma.
To evaluate the presence of aspirin sensitivity and CRS with nasal polyps in a cohort of asthmatic patients, pulmonologists and ear, nose, and throat specialists at 23 hospitals in Spain and Latin America recruited 492 patients, aged 18-70 years, attending outpatient clinics with the diagnosis of asthma for at least 1 year. Aspirin sensitivity was assessed by clinical history and/or aspirin challenge, and CRS with nasal polyps was assessed by nasal symptoms, nasal endoscopy, and sinus computed tomography (CT) scan.
Among 473 evaluable patients, 72 (15%) were aspirin sensitive, 14.6% had no nasosinal disease, 12.6% nonallergic rhinitis, 36.8% allergic rhinitis, 16.6% CRS without nasal polyps, and 19.4% CRS with nasal polyps.
*Aspirin-intolerant asthma was strongly related to asthma severity. In all, 3 of the 72 (4.2%) aspirin-intolerant patients were classified as having intermittent asthma (odds ratio, 1); 17 (23.6%) as mild persistent (OR, 4.3); 21 (29.2%) as moderate persistent (OR, 4.3); and 31 (43%) as severe persistent asthma, which was statistically significant (OR, 7.8; P less than .05), reported Dr. Castillo, with the pneumology service at Chiron Dexeus University Hospital, Barcelona.
The presence of CRS with nasal polyps was also significantly associated (38.9%; 28/72 patients) with aspirin sensitivity (OR, 9.05; P less than .001).
Aspirin sensitivity was present in 4.5% of patients with no nasosinal disease, 18.6% of those with nonallergic rhinitis, 9.2% with allergic rhinitis, 17.5% with CRS with no nasal polyps, and 29.8% with CRS and nasal polyps.
Further, patients with aspirin-intolerant asthma showed significantly higher Lund & McKay CT scores than aspirin-tolerant asthmatic patients, according to the poster presentation.
The current results perhaps could be validated by matching aspirin sensitivity with a biomarker of severe asthma, that is, periostin, but are such that they already use aspirin sensitivity as a clinical marker of severe asthma, Dr. Castillo said in an interview.
Patients in the study had a mean age of 45 years and a mean body mass index of 26.9 kg/m2 (range, 16.8-49.8 kg/m2); 70.5% were female, and 9.6% were smokers.
Asthma was intermittent in 85 patients, mild persistent in 122, moderate persistent in 154, and severe persistent in 131, according to Global Initiative for Asthma (GINA) severity criteria.
Dr. Castillo and his coauthors reported no financial disclosures.
*This article was updated 4/7/14
MADRID – Aspirin sensitivity was strongly associated with asthma severity and the presence of chronic rhinosinusitis with nasal polyps in a prospective, multicenter study.
"Aspirin sensitivity may be considered a clinical marker for severe asthma and for the presence of chronic rhinosinusitis with nasal polyps, and a potential marker for united airway disease," Dr. José Antonio Castillo reported at the world congress of the American College of Chest Physicians.
Aspirin-exacerbated respiratory disease is commonly associated with chronic rhinosinusitis (CRS) with nasal polyps, but little information is available on the correlation between aspirin sensitivity and severe asthma.
To evaluate the presence of aspirin sensitivity and CRS with nasal polyps in a cohort of asthmatic patients, pulmonologists and ear, nose, and throat specialists at 23 hospitals in Spain and Latin America recruited 492 patients, aged 18-70 years, attending outpatient clinics with the diagnosis of asthma for at least 1 year. Aspirin sensitivity was assessed by clinical history and/or aspirin challenge, and CRS with nasal polyps was assessed by nasal symptoms, nasal endoscopy, and sinus computed tomography (CT) scan.
Among 473 evaluable patients, 72 (15%) were aspirin sensitive, 14.6% had no nasosinal disease, 12.6% nonallergic rhinitis, 36.8% allergic rhinitis, 16.6% CRS without nasal polyps, and 19.4% CRS with nasal polyps.
*Aspirin-intolerant asthma was strongly related to asthma severity. In all, 3 of the 72 (4.2%) aspirin-intolerant patients were classified as having intermittent asthma (odds ratio, 1); 17 (23.6%) as mild persistent (OR, 4.3); 21 (29.2%) as moderate persistent (OR, 4.3); and 31 (43%) as severe persistent asthma, which was statistically significant (OR, 7.8; P less than .05), reported Dr. Castillo, with the pneumology service at Chiron Dexeus University Hospital, Barcelona.
The presence of CRS with nasal polyps was also significantly associated (38.9%; 28/72 patients) with aspirin sensitivity (OR, 9.05; P less than .001).
Aspirin sensitivity was present in 4.5% of patients with no nasosinal disease, 18.6% of those with nonallergic rhinitis, 9.2% with allergic rhinitis, 17.5% with CRS with no nasal polyps, and 29.8% with CRS and nasal polyps.
Further, patients with aspirin-intolerant asthma showed significantly higher Lund & McKay CT scores than aspirin-tolerant asthmatic patients, according to the poster presentation.
The current results perhaps could be validated by matching aspirin sensitivity with a biomarker of severe asthma, that is, periostin, but are such that they already use aspirin sensitivity as a clinical marker of severe asthma, Dr. Castillo said in an interview.
Patients in the study had a mean age of 45 years and a mean body mass index of 26.9 kg/m2 (range, 16.8-49.8 kg/m2); 70.5% were female, and 9.6% were smokers.
Asthma was intermittent in 85 patients, mild persistent in 122, moderate persistent in 154, and severe persistent in 131, according to Global Initiative for Asthma (GINA) severity criteria.
Dr. Castillo and his coauthors reported no financial disclosures.
*This article was updated 4/7/14
MADRID – Aspirin sensitivity was strongly associated with asthma severity and the presence of chronic rhinosinusitis with nasal polyps in a prospective, multicenter study.
"Aspirin sensitivity may be considered a clinical marker for severe asthma and for the presence of chronic rhinosinusitis with nasal polyps, and a potential marker for united airway disease," Dr. José Antonio Castillo reported at the world congress of the American College of Chest Physicians.
Aspirin-exacerbated respiratory disease is commonly associated with chronic rhinosinusitis (CRS) with nasal polyps, but little information is available on the correlation between aspirin sensitivity and severe asthma.
To evaluate the presence of aspirin sensitivity and CRS with nasal polyps in a cohort of asthmatic patients, pulmonologists and ear, nose, and throat specialists at 23 hospitals in Spain and Latin America recruited 492 patients, aged 18-70 years, attending outpatient clinics with the diagnosis of asthma for at least 1 year. Aspirin sensitivity was assessed by clinical history and/or aspirin challenge, and CRS with nasal polyps was assessed by nasal symptoms, nasal endoscopy, and sinus computed tomography (CT) scan.
Among 473 evaluable patients, 72 (15%) were aspirin sensitive, 14.6% had no nasosinal disease, 12.6% nonallergic rhinitis, 36.8% allergic rhinitis, 16.6% CRS without nasal polyps, and 19.4% CRS with nasal polyps.
*Aspirin-intolerant asthma was strongly related to asthma severity. In all, 3 of the 72 (4.2%) aspirin-intolerant patients were classified as having intermittent asthma (odds ratio, 1); 17 (23.6%) as mild persistent (OR, 4.3); 21 (29.2%) as moderate persistent (OR, 4.3); and 31 (43%) as severe persistent asthma, which was statistically significant (OR, 7.8; P less than .05), reported Dr. Castillo, with the pneumology service at Chiron Dexeus University Hospital, Barcelona.
The presence of CRS with nasal polyps was also significantly associated (38.9%; 28/72 patients) with aspirin sensitivity (OR, 9.05; P less than .001).
Aspirin sensitivity was present in 4.5% of patients with no nasosinal disease, 18.6% of those with nonallergic rhinitis, 9.2% with allergic rhinitis, 17.5% with CRS with no nasal polyps, and 29.8% with CRS and nasal polyps.
Further, patients with aspirin-intolerant asthma showed significantly higher Lund & McKay CT scores than aspirin-tolerant asthmatic patients, according to the poster presentation.
The current results perhaps could be validated by matching aspirin sensitivity with a biomarker of severe asthma, that is, periostin, but are such that they already use aspirin sensitivity as a clinical marker of severe asthma, Dr. Castillo said in an interview.
Patients in the study had a mean age of 45 years and a mean body mass index of 26.9 kg/m2 (range, 16.8-49.8 kg/m2); 70.5% were female, and 9.6% were smokers.
Asthma was intermittent in 85 patients, mild persistent in 122, moderate persistent in 154, and severe persistent in 131, according to Global Initiative for Asthma (GINA) severity criteria.
Dr. Castillo and his coauthors reported no financial disclosures.
*This article was updated 4/7/14
What Are the Benefits and Risks of Inhaled Corticosteroids for COPD?
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
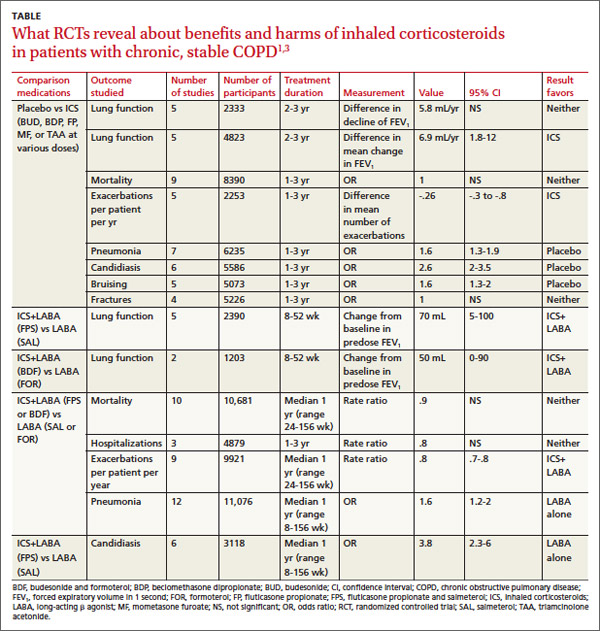
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
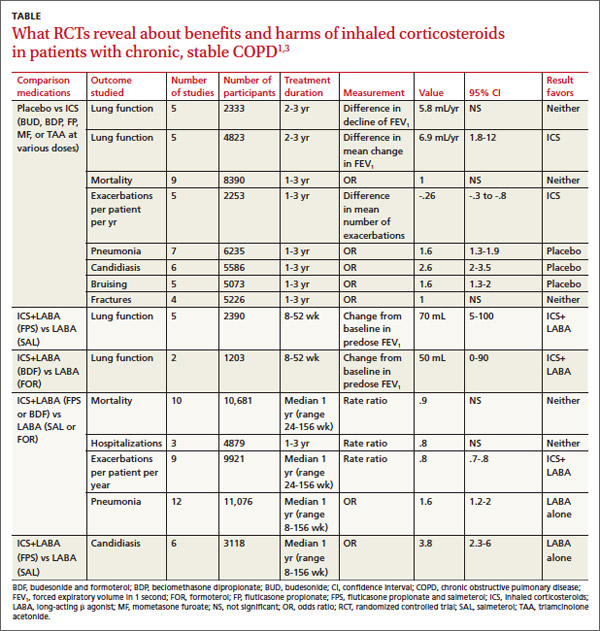
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
Recommendations
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
Recommendations
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
Recommendations
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
What are the benefits and risks of inhaled corticosteroids for COPD?
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
Evidence-based answers from the Family Physicians Inquiries Network
Medicare asks experts to weigh in on low-dose CT lung cancer screening
Should Medicare pay for low-dose computed tomography to screen certain patients for lung cancer? A panel of expert advisers will meet April 30 to review the evidence and make a recommendation.
The Centers for Medicare & Medicaid Services has accepted two formal requests to initiate a national coverage analysis on lung cancer screening with low-dose computed tomography (LDCT), which the U.S. Preventative Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.

CMS is specifically asking its Medicare Evidence Development & Coverage Advisory Committee (MEDCAC) to discuss:
• the evidence that identifies which Medicare patients would benefit the most from the screening.
• screening frequency and duration.
• provider characteristics that optimize benefits and minimize harm.
• criteria to identify a test as positive and the impact of false-positive results.
• follow-up tests or treatments.
The agency also seeks to know how these factors will impact patient education and informed consent in Medicare beneficiaries, including the elderly, younger disabled populations, and patients with end-stage renal disease, and on integrating smoking cessation interventions for current smokers.
In order for CMS to issue a national coverage determination for a preventive service, the following criteria must be met: reasonable and necessary for prevention or early detection of an illness or disability; an A- or B-grade recommendation from USPSTF; and appropriate for Medicare Part A or Medicare Part B beneficiaries.
CMS has asked the panel to vote on whether there is adequate evidence to determine if the benefits of lung cancer screening with LDCT outweigh the harms. The agency will specifically ask if there is adequate evidence to determine if LDCT improves health outcomes: in asymptomatic, high-risk adults over 74 years old; with more than three annual LDCT screens; and if the screening program is implemented outside a clinical study.
The agency is also asking for panel input on the harms of lung cancer screening with LDCT in the Medicare population, specifically harms from the scan itself (an average dose of 1.5 mSv), harms from follow-up evaluation of findings in and outside the lungs, and harms from treatment as a result of positive and false-positive results.
CMS will also ask the panel to identify and discuss any clinically significant evidence gaps regarding the use of LDCT in lung cancer screening outside of a clinical trial.
Last December, the USPSTF recommended annual screening for lung cancer with LDCT in adults aged 55- 80 years who have a 30-pack-year smoking history and currently smoke or have quit in the past 15 years. The recommendation states that screening should be stopped once a person has stopped smoking for 15 years or develops a health problem limiting life expectancy or the ability to have curative lung surgery.
The USPSTF’s recommendations were based largely on a systematic review of several randomized, controlled trials published between 2000 and 2013, including the National Lung Screening Trial. That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT. One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
Under the Affordable Care Act, insurers are required to cover, with no copay requirements, preventative care and screening services that receive a grade A or grade B recommendation from USPSTF.
Should Medicare pay for low-dose computed tomography to screen certain patients for lung cancer? A panel of expert advisers will meet April 30 to review the evidence and make a recommendation.
The Centers for Medicare & Medicaid Services has accepted two formal requests to initiate a national coverage analysis on lung cancer screening with low-dose computed tomography (LDCT), which the U.S. Preventative Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.
CMS is specifically asking its Medicare Evidence Development & Coverage Advisory Committee (MEDCAC) to discuss:
• the evidence that identifies which Medicare patients would benefit the most from the screening.
• screening frequency and duration.
• provider characteristics that optimize benefits and minimize harm.
• criteria to identify a test as positive and the impact of false-positive results.
• follow-up tests or treatments.
The agency also seeks to know how these factors will impact patient education and informed consent in Medicare beneficiaries, including the elderly, younger disabled populations, and patients with end-stage renal disease, and on integrating smoking cessation interventions for current smokers.
In order for CMS to issue a national coverage determination for a preventive service, the following criteria must be met: reasonable and necessary for prevention or early detection of an illness or disability; an A- or B-grade recommendation from USPSTF; and appropriate for Medicare Part A or Medicare Part B beneficiaries.
CMS has asked the panel to vote on whether there is adequate evidence to determine if the benefits of lung cancer screening with LDCT outweigh the harms. The agency will specifically ask if there is adequate evidence to determine if LDCT improves health outcomes: in asymptomatic, high-risk adults over 74 years old; with more than three annual LDCT screens; and if the screening program is implemented outside a clinical study.
The agency is also asking for panel input on the harms of lung cancer screening with LDCT in the Medicare population, specifically harms from the scan itself (an average dose of 1.5 mSv), harms from follow-up evaluation of findings in and outside the lungs, and harms from treatment as a result of positive and false-positive results.
CMS will also ask the panel to identify and discuss any clinically significant evidence gaps regarding the use of LDCT in lung cancer screening outside of a clinical trial.
Last December, the USPSTF recommended annual screening for lung cancer with LDCT in adults aged 55- 80 years who have a 30-pack-year smoking history and currently smoke or have quit in the past 15 years. The recommendation states that screening should be stopped once a person has stopped smoking for 15 years or develops a health problem limiting life expectancy or the ability to have curative lung surgery.
The USPSTF’s recommendations were based largely on a systematic review of several randomized, controlled trials published between 2000 and 2013, including the National Lung Screening Trial. That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT. One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
Under the Affordable Care Act, insurers are required to cover, with no copay requirements, preventative care and screening services that receive a grade A or grade B recommendation from USPSTF.
Should Medicare pay for low-dose computed tomography to screen certain patients for lung cancer? A panel of expert advisers will meet April 30 to review the evidence and make a recommendation.
The Centers for Medicare & Medicaid Services has accepted two formal requests to initiate a national coverage analysis on lung cancer screening with low-dose computed tomography (LDCT), which the U.S. Preventative Services Task Force gave a grade B recommendation for people at high risk for lung cancer based on age and smoking history.
CMS is specifically asking its Medicare Evidence Development & Coverage Advisory Committee (MEDCAC) to discuss:
• the evidence that identifies which Medicare patients would benefit the most from the screening.
• screening frequency and duration.
• provider characteristics that optimize benefits and minimize harm.
• criteria to identify a test as positive and the impact of false-positive results.
• follow-up tests or treatments.
The agency also seeks to know how these factors will impact patient education and informed consent in Medicare beneficiaries, including the elderly, younger disabled populations, and patients with end-stage renal disease, and on integrating smoking cessation interventions for current smokers.
In order for CMS to issue a national coverage determination for a preventive service, the following criteria must be met: reasonable and necessary for prevention or early detection of an illness or disability; an A- or B-grade recommendation from USPSTF; and appropriate for Medicare Part A or Medicare Part B beneficiaries.
CMS has asked the panel to vote on whether there is adequate evidence to determine if the benefits of lung cancer screening with LDCT outweigh the harms. The agency will specifically ask if there is adequate evidence to determine if LDCT improves health outcomes: in asymptomatic, high-risk adults over 74 years old; with more than three annual LDCT screens; and if the screening program is implemented outside a clinical study.
The agency is also asking for panel input on the harms of lung cancer screening with LDCT in the Medicare population, specifically harms from the scan itself (an average dose of 1.5 mSv), harms from follow-up evaluation of findings in and outside the lungs, and harms from treatment as a result of positive and false-positive results.
CMS will also ask the panel to identify and discuss any clinically significant evidence gaps regarding the use of LDCT in lung cancer screening outside of a clinical trial.
Last December, the USPSTF recommended annual screening for lung cancer with LDCT in adults aged 55- 80 years who have a 30-pack-year smoking history and currently smoke or have quit in the past 15 years. The recommendation states that screening should be stopped once a person has stopped smoking for 15 years or develops a health problem limiting life expectancy or the ability to have curative lung surgery.
The USPSTF’s recommendations were based largely on a systematic review of several randomized, controlled trials published between 2000 and 2013, including the National Lung Screening Trial. That study of more than 50,000 asymptomatic adults, aged 55-74 years, showed a 16% reduction in lung cancer mortality and a 6.7% reduction in all-cause mortality when patients were screened using LDCT. One cancer death was averted for every 320 patients screened, and one death from all causes was prevented in every 219 patients screened.
Under the Affordable Care Act, insurers are required to cover, with no copay requirements, preventative care and screening services that receive a grade A or grade B recommendation from USPSTF.

FDA proposes to regulate e-cigarettes, cigars
The Food and Drug Administration’s long-awaited proposal to regulate e-cigarettes, cigars, and other tobacco products as if they were cigarettes does not go far enough to protect the public, and especially children, from the harmful effects of tobacco products, including nicotine addiction, according to its critics.
And, they say, it gives manufacturers too much time to continue selling their products without oversight while the FDA takes an undetermined period of time to consider comments on the proposal and make the rule final.

The 2009 Family Smoking Prevention and Tobacco Control Act gave the FDA authority to extend its regulation of tobacco over all tobacco-derived products. A few years ago, the agency indicated that it would "deem" all tobacco-derived products as similar to cigarettes but had not issued any regulation until now. The new proposal would extend the FDA’s power to regulate e-cigarettes, cigars, pipe tobacco, nicotine gels, water pipe (or hookah) tobacco, and dissolvable tobacco products.
"This proposed rule is the latest step in our efforts to make the next generation tobacco free," said HHS Secretary Kathleen Sebelius, in a statement. The regulation would also allow the FDA to determine whether products like e-cigarettes serve as a gateway to cigarette use, she told reporters.
Mitch Zeller, director of the FDA’s Center for Tobacco Products, said that the agency is "funding massive studies" to get a better handle on the potential benefits and risks of e-cigarettes and the patterns of use. "We have far more questions than answers about who is using e cigarettes and how they are being used," he told reporters, in a briefing.
Under the proposed rule, makers of tobacco products would have to:
• Register with the FDA and report product and ingredient listings.
• Only market new tobacco products after FDA review.
• Only make direct and implied claims of reduced risk if the FDA confirms that scientific evidence supports the claim and that marketing the product will benefit public health as a whole.
• Not distribute free samples.
FDA Commissioner Margaret A. Hamburg said the agency will take comments on the rule for 75 days and then, after analysis, make it final. But she would not give a timetable for when the rule would be made final.
Manufacturers who’ve had products on the market as of February 2007 will be required to submit applications for approval within 24 months of the final rule’s effective date. During that period, they will be allowed to continue to sell their products, subject only to a few regulations that will go into effect immediately. That would include a ban on retail and Internet sales to children under age 18 years; a prohibition on free samples; the requirement that companies register with the FDA; a prohibition on direct or implied claims that the products reduce the risks from tobacco use; and, a prohibition on vending machine sales unless located in facility that never admits youth.
The FDA would not ban Internet sales altogether or prohibit TV ads. The agency would have to issue separate rules on marketing and promotion, said Mr. Zeller.
There’s no proposed ban on flavored tobacco products. That will also require separate rules, once the agency has established jurisdiction over all the products deemed similar, said Mr. Zeller. The agency is also proposing to give so-called "premium" cigars that meet certain criteria a pass on most of the regulation.
Dr. Margaret Foti, CEO of the American Association of Cancer Research said in a statement that FDA regulation of "all tobacco products, including e-cigarettes and cigars," is imperative and that the agency should "prohibit the sale and marketing of these products to children. She added that "the proposed rule is an important step forward in expanding the FDA’s regulation of tobacco and protecting the health of the American people."
The Campaign for Tobacco-Free Kids lauded the FDA for moving forward, but also was disappointed in the decision to not regulate flavorings. The Campaign said in a statement that the flavorings, often found in cigars or e-cigarettes may appeal to youth. It also called the potential premium cigar loophole "deeply disturbing," adding that, "There is no justifiable public health rationale for exempting any category of cigars."
Noting that e-cigarette use is skyrocketing among young Americans, the Campaign said that, "Effective regulation by the FDA and the states is needed to minimize the potential harms of e-cigarettes and ensure any potential health benefits are supported by sound science."
A handful of Democratic senators and a House member who issued a recent report on the apparently concerted effort to market e-cigarettes to teenagers expressed dismay with the FDA proposal. The joint statement said: "Today, after years of waiting for the FDA to act, we are extremely disappointed by its failure to take comprehensive action to prevent e-cigarette companies from continuing to deploy marketing tactics aimed at luring children and teenagers into a candy-flavored nicotine addiction," they said. "As long as e-cigarette companies continue to take pages from Big Tobacco’s old and cynical marketing playbook, our children will remain vulnerable to the grave dangers of nicotine addiction," they added.
The American Cancer Society Cancer Action Network’s chief executive, John R. Seffrin, Ph.D., said that while the FDA’s action was an important step, it was still giving manufacturers a chance to skirt oversight, especially when it came to marketing to children. The companies are using tactics that include "marketing small flavored cigars that look like cigarettes, entering the e-cig market with promotions that could dramatically increase use among children and creating several new types of smokeless products," said Dr. Seffrin, in a statement.
He urged the agency to move quickly. "It should not take several more years for the FDA to be able to specify how it intends to regulate the unfettered marketing of many dangerous tobacco products," he said.
FDA Commissioner Hamburg said that the agency would move quickly. "We are eager to see this process move forward," she said.
On Twitter @aliciaault
The Food and Drug Administration’s long-awaited proposal to regulate e-cigarettes, cigars, and other tobacco products as if they were cigarettes does not go far enough to protect the public, and especially children, from the harmful effects of tobacco products, including nicotine addiction, according to its critics.
And, they say, it gives manufacturers too much time to continue selling their products without oversight while the FDA takes an undetermined period of time to consider comments on the proposal and make the rule final.
The 2009 Family Smoking Prevention and Tobacco Control Act gave the FDA authority to extend its regulation of tobacco over all tobacco-derived products. A few years ago, the agency indicated that it would "deem" all tobacco-derived products as similar to cigarettes but had not issued any regulation until now. The new proposal would extend the FDA’s power to regulate e-cigarettes, cigars, pipe tobacco, nicotine gels, water pipe (or hookah) tobacco, and dissolvable tobacco products.
"This proposed rule is the latest step in our efforts to make the next generation tobacco free," said HHS Secretary Kathleen Sebelius, in a statement. The regulation would also allow the FDA to determine whether products like e-cigarettes serve as a gateway to cigarette use, she told reporters.
Mitch Zeller, director of the FDA’s Center for Tobacco Products, said that the agency is "funding massive studies" to get a better handle on the potential benefits and risks of e-cigarettes and the patterns of use. "We have far more questions than answers about who is using e cigarettes and how they are being used," he told reporters, in a briefing.
Under the proposed rule, makers of tobacco products would have to:
• Register with the FDA and report product and ingredient listings.
• Only market new tobacco products after FDA review.
• Only make direct and implied claims of reduced risk if the FDA confirms that scientific evidence supports the claim and that marketing the product will benefit public health as a whole.
• Not distribute free samples.
FDA Commissioner Margaret A. Hamburg said the agency will take comments on the rule for 75 days and then, after analysis, make it final. But she would not give a timetable for when the rule would be made final.
Manufacturers who’ve had products on the market as of February 2007 will be required to submit applications for approval within 24 months of the final rule’s effective date. During that period, they will be allowed to continue to sell their products, subject only to a few regulations that will go into effect immediately. That would include a ban on retail and Internet sales to children under age 18 years; a prohibition on free samples; the requirement that companies register with the FDA; a prohibition on direct or implied claims that the products reduce the risks from tobacco use; and, a prohibition on vending machine sales unless located in facility that never admits youth.
The FDA would not ban Internet sales altogether or prohibit TV ads. The agency would have to issue separate rules on marketing and promotion, said Mr. Zeller.
There’s no proposed ban on flavored tobacco products. That will also require separate rules, once the agency has established jurisdiction over all the products deemed similar, said Mr. Zeller. The agency is also proposing to give so-called "premium" cigars that meet certain criteria a pass on most of the regulation.
Dr. Margaret Foti, CEO of the American Association of Cancer Research said in a statement that FDA regulation of "all tobacco products, including e-cigarettes and cigars," is imperative and that the agency should "prohibit the sale and marketing of these products to children. She added that "the proposed rule is an important step forward in expanding the FDA’s regulation of tobacco and protecting the health of the American people."
The Campaign for Tobacco-Free Kids lauded the FDA for moving forward, but also was disappointed in the decision to not regulate flavorings. The Campaign said in a statement that the flavorings, often found in cigars or e-cigarettes may appeal to youth. It also called the potential premium cigar loophole "deeply disturbing," adding that, "There is no justifiable public health rationale for exempting any category of cigars."
Noting that e-cigarette use is skyrocketing among young Americans, the Campaign said that, "Effective regulation by the FDA and the states is needed to minimize the potential harms of e-cigarettes and ensure any potential health benefits are supported by sound science."
A handful of Democratic senators and a House member who issued a recent report on the apparently concerted effort to market e-cigarettes to teenagers expressed dismay with the FDA proposal. The joint statement said: "Today, after years of waiting for the FDA to act, we are extremely disappointed by its failure to take comprehensive action to prevent e-cigarette companies from continuing to deploy marketing tactics aimed at luring children and teenagers into a candy-flavored nicotine addiction," they said. "As long as e-cigarette companies continue to take pages from Big Tobacco’s old and cynical marketing playbook, our children will remain vulnerable to the grave dangers of nicotine addiction," they added.
The American Cancer Society Cancer Action Network’s chief executive, John R. Seffrin, Ph.D., said that while the FDA’s action was an important step, it was still giving manufacturers a chance to skirt oversight, especially when it came to marketing to children. The companies are using tactics that include "marketing small flavored cigars that look like cigarettes, entering the e-cig market with promotions that could dramatically increase use among children and creating several new types of smokeless products," said Dr. Seffrin, in a statement.
He urged the agency to move quickly. "It should not take several more years for the FDA to be able to specify how it intends to regulate the unfettered marketing of many dangerous tobacco products," he said.
FDA Commissioner Hamburg said that the agency would move quickly. "We are eager to see this process move forward," she said.
On Twitter @aliciaault
The Food and Drug Administration’s long-awaited proposal to regulate e-cigarettes, cigars, and other tobacco products as if they were cigarettes does not go far enough to protect the public, and especially children, from the harmful effects of tobacco products, including nicotine addiction, according to its critics.
And, they say, it gives manufacturers too much time to continue selling their products without oversight while the FDA takes an undetermined period of time to consider comments on the proposal and make the rule final.
The 2009 Family Smoking Prevention and Tobacco Control Act gave the FDA authority to extend its regulation of tobacco over all tobacco-derived products. A few years ago, the agency indicated that it would "deem" all tobacco-derived products as similar to cigarettes but had not issued any regulation until now. The new proposal would extend the FDA’s power to regulate e-cigarettes, cigars, pipe tobacco, nicotine gels, water pipe (or hookah) tobacco, and dissolvable tobacco products.
"This proposed rule is the latest step in our efforts to make the next generation tobacco free," said HHS Secretary Kathleen Sebelius, in a statement. The regulation would also allow the FDA to determine whether products like e-cigarettes serve as a gateway to cigarette use, she told reporters.
Mitch Zeller, director of the FDA’s Center for Tobacco Products, said that the agency is "funding massive studies" to get a better handle on the potential benefits and risks of e-cigarettes and the patterns of use. "We have far more questions than answers about who is using e cigarettes and how they are being used," he told reporters, in a briefing.
Under the proposed rule, makers of tobacco products would have to:
• Register with the FDA and report product and ingredient listings.
• Only market new tobacco products after FDA review.
• Only make direct and implied claims of reduced risk if the FDA confirms that scientific evidence supports the claim and that marketing the product will benefit public health as a whole.
• Not distribute free samples.
FDA Commissioner Margaret A. Hamburg said the agency will take comments on the rule for 75 days and then, after analysis, make it final. But she would not give a timetable for when the rule would be made final.
Manufacturers who’ve had products on the market as of February 2007 will be required to submit applications for approval within 24 months of the final rule’s effective date. During that period, they will be allowed to continue to sell their products, subject only to a few regulations that will go into effect immediately. That would include a ban on retail and Internet sales to children under age 18 years; a prohibition on free samples; the requirement that companies register with the FDA; a prohibition on direct or implied claims that the products reduce the risks from tobacco use; and, a prohibition on vending machine sales unless located in facility that never admits youth.
The FDA would not ban Internet sales altogether or prohibit TV ads. The agency would have to issue separate rules on marketing and promotion, said Mr. Zeller.
There’s no proposed ban on flavored tobacco products. That will also require separate rules, once the agency has established jurisdiction over all the products deemed similar, said Mr. Zeller. The agency is also proposing to give so-called "premium" cigars that meet certain criteria a pass on most of the regulation.
Dr. Margaret Foti, CEO of the American Association of Cancer Research said in a statement that FDA regulation of "all tobacco products, including e-cigarettes and cigars," is imperative and that the agency should "prohibit the sale and marketing of these products to children. She added that "the proposed rule is an important step forward in expanding the FDA’s regulation of tobacco and protecting the health of the American people."
The Campaign for Tobacco-Free Kids lauded the FDA for moving forward, but also was disappointed in the decision to not regulate flavorings. The Campaign said in a statement that the flavorings, often found in cigars or e-cigarettes may appeal to youth. It also called the potential premium cigar loophole "deeply disturbing," adding that, "There is no justifiable public health rationale for exempting any category of cigars."
Noting that e-cigarette use is skyrocketing among young Americans, the Campaign said that, "Effective regulation by the FDA and the states is needed to minimize the potential harms of e-cigarettes and ensure any potential health benefits are supported by sound science."
A handful of Democratic senators and a House member who issued a recent report on the apparently concerted effort to market e-cigarettes to teenagers expressed dismay with the FDA proposal. The joint statement said: "Today, after years of waiting for the FDA to act, we are extremely disappointed by its failure to take comprehensive action to prevent e-cigarette companies from continuing to deploy marketing tactics aimed at luring children and teenagers into a candy-flavored nicotine addiction," they said. "As long as e-cigarette companies continue to take pages from Big Tobacco’s old and cynical marketing playbook, our children will remain vulnerable to the grave dangers of nicotine addiction," they added.
The American Cancer Society Cancer Action Network’s chief executive, John R. Seffrin, Ph.D., said that while the FDA’s action was an important step, it was still giving manufacturers a chance to skirt oversight, especially when it came to marketing to children. The companies are using tactics that include "marketing small flavored cigars that look like cigarettes, entering the e-cig market with promotions that could dramatically increase use among children and creating several new types of smokeless products," said Dr. Seffrin, in a statement.
He urged the agency to move quickly. "It should not take several more years for the FDA to be able to specify how it intends to regulate the unfettered marketing of many dangerous tobacco products," he said.
FDA Commissioner Hamburg said that the agency would move quickly. "We are eager to see this process move forward," she said.
On Twitter @aliciaault

Benzodiazepines linked to worsened COPD in older adults
Benzodiazepine use is associated with significantly increased risks of adverse respiratory outcomes in older adults with chronic obstructive pulmonary disease, researchers reported online April 17 in the European Respiratory Journal.
New benzodiazepine users were 45% more likely to receive outpatient respiratory medications and 92% more likely to visit the emergency department for respiratory reasons than were non–benzodiazepine users, reported Dr. Nicholas Vozoris of St. Michael’s Hospital and the University of Toronto and his associates.
"These findings are concerning, given that benzodiazepines are known to be frequently used among older adults with COPD and in suboptimal ways," the investigators wrote. "The findings suggest that the potential for adverse respiratory outcomes needs to be considered when administering benzodiazepines to older adults with COPD."
The retrospective population-based cohort study identified 177,355 adults with COPD who were at least 66 years old and lived in Ontario, Canada, during 2003-2010. The researchers used 1:1 propensity score matching without replacement to match 48,915 new benzodiazepine users with the same number of nonusers (Eur. Respir. J. 2014 April 17 [doi: 10.1183/09031936.00008014]).
New users of benzodiazepines were significantly more likely to be prescribed oral corticosteroids or respiratory antibiotics (relative risk, 1.45; 95% confidence interval, 1.36-1.54) and to visit the emergency department for COPD or pneumonia (RR, 1.92; 95% CI, 1.69-2.18).
Furthermore, in the subgroup of patients who had no exacerbation of COPD during the year before baseline, new benzodiazepine users had a significantly greater risk of receiving outpatient respiratory medications (RR, 1.63; 95% CI, 1.44-1.84), visiting an emergency department for COPD or pneumonia (RR, 2.46; 95% CI, 1.90-3.18), being hospitalized for either diagnosis (RR, 1.29; 95% CI, 1.07-1.56), or dying from any cause (RR, 1.19, 95% CI, 1.06-1.34).
The research is consistent with findings from previous smaller, shorter-duration studies, said Dr. Vozoris and his associates. They noted that their definition of COPD had a sensitivity of only 58%, which could limit the generalizability of the findings.
The Canadian Institutes of Health and the Institute for Clinical Evaluative Sciences funded the study. The investigators reported having no conflicts of interest.
Benzodiazepine use is associated with significantly increased risks of adverse respiratory outcomes in older adults with chronic obstructive pulmonary disease, researchers reported online April 17 in the European Respiratory Journal.
New benzodiazepine users were 45% more likely to receive outpatient respiratory medications and 92% more likely to visit the emergency department for respiratory reasons than were non–benzodiazepine users, reported Dr. Nicholas Vozoris of St. Michael’s Hospital and the University of Toronto and his associates.
"These findings are concerning, given that benzodiazepines are known to be frequently used among older adults with COPD and in suboptimal ways," the investigators wrote. "The findings suggest that the potential for adverse respiratory outcomes needs to be considered when administering benzodiazepines to older adults with COPD."
The retrospective population-based cohort study identified 177,355 adults with COPD who were at least 66 years old and lived in Ontario, Canada, during 2003-2010. The researchers used 1:1 propensity score matching without replacement to match 48,915 new benzodiazepine users with the same number of nonusers (Eur. Respir. J. 2014 April 17 [doi: 10.1183/09031936.00008014]).
New users of benzodiazepines were significantly more likely to be prescribed oral corticosteroids or respiratory antibiotics (relative risk, 1.45; 95% confidence interval, 1.36-1.54) and to visit the emergency department for COPD or pneumonia (RR, 1.92; 95% CI, 1.69-2.18).
Furthermore, in the subgroup of patients who had no exacerbation of COPD during the year before baseline, new benzodiazepine users had a significantly greater risk of receiving outpatient respiratory medications (RR, 1.63; 95% CI, 1.44-1.84), visiting an emergency department for COPD or pneumonia (RR, 2.46; 95% CI, 1.90-3.18), being hospitalized for either diagnosis (RR, 1.29; 95% CI, 1.07-1.56), or dying from any cause (RR, 1.19, 95% CI, 1.06-1.34).
The research is consistent with findings from previous smaller, shorter-duration studies, said Dr. Vozoris and his associates. They noted that their definition of COPD had a sensitivity of only 58%, which could limit the generalizability of the findings.
The Canadian Institutes of Health and the Institute for Clinical Evaluative Sciences funded the study. The investigators reported having no conflicts of interest.
Benzodiazepine use is associated with significantly increased risks of adverse respiratory outcomes in older adults with chronic obstructive pulmonary disease, researchers reported online April 17 in the European Respiratory Journal.
New benzodiazepine users were 45% more likely to receive outpatient respiratory medications and 92% more likely to visit the emergency department for respiratory reasons than were non–benzodiazepine users, reported Dr. Nicholas Vozoris of St. Michael’s Hospital and the University of Toronto and his associates.
"These findings are concerning, given that benzodiazepines are known to be frequently used among older adults with COPD and in suboptimal ways," the investigators wrote. "The findings suggest that the potential for adverse respiratory outcomes needs to be considered when administering benzodiazepines to older adults with COPD."
The retrospective population-based cohort study identified 177,355 adults with COPD who were at least 66 years old and lived in Ontario, Canada, during 2003-2010. The researchers used 1:1 propensity score matching without replacement to match 48,915 new benzodiazepine users with the same number of nonusers (Eur. Respir. J. 2014 April 17 [doi: 10.1183/09031936.00008014]).
New users of benzodiazepines were significantly more likely to be prescribed oral corticosteroids or respiratory antibiotics (relative risk, 1.45; 95% confidence interval, 1.36-1.54) and to visit the emergency department for COPD or pneumonia (RR, 1.92; 95% CI, 1.69-2.18).
Furthermore, in the subgroup of patients who had no exacerbation of COPD during the year before baseline, new benzodiazepine users had a significantly greater risk of receiving outpatient respiratory medications (RR, 1.63; 95% CI, 1.44-1.84), visiting an emergency department for COPD or pneumonia (RR, 2.46; 95% CI, 1.90-3.18), being hospitalized for either diagnosis (RR, 1.29; 95% CI, 1.07-1.56), or dying from any cause (RR, 1.19, 95% CI, 1.06-1.34).
The research is consistent with findings from previous smaller, shorter-duration studies, said Dr. Vozoris and his associates. They noted that their definition of COPD had a sensitivity of only 58%, which could limit the generalizability of the findings.
The Canadian Institutes of Health and the Institute for Clinical Evaluative Sciences funded the study. The investigators reported having no conflicts of interest.
FROM THE EUROPEAN RESPIRATORY JOURNAL
Major finding: Compared with nonusers, new users of benzodiazepines were significantly more likely to be prescribed oral corticosteroids or respiratory antibiotics (RR, 1.45; 95% CI, 1.36-1.54) and to visit the emergency department for COPD or pneumonia (RR, 1.92; 95% CI, 1.69-2.18).
Data source: Retrospective population-based cohort study of 177,355 adults with COPD who were aged 66 years or older and lived in Ontario, Canada, during 2003-2010.
Disclosures: The Canadian Institutes of Health and the Institute for Clinical Evaluative Sciences funded the study. The investigators reported having no relevant conflicts of interest.
Air pollution linked to suicide risk
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.

What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.
What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.
What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
AT THE AMERICAN ASSOCIATION OF SUICIDOLOGY ANNUAL MEETING
Major finding: A 20% increase in suicide risk was found when levels of atmospheric nitrogen dioxide are at their highest and a 5% increase when fine particles are at their peak.
Data source: The findings are based on a coupling of air-quality data and the timing of 1,546 suicides from 2000 to 2010.
Disclosures: The lead investigator has no relevant disclosures, and the work received no outside funding.

Obstructive sleep apnea complicates atrial fibrillation
WASHINGTON – About 18% of U.S. patients with atrial fibrillation also have a diagnosis of obstructive sleep apnea, and the confluence of the two appeared linked to increased hospitalizations and further progression of atrial fibrillation, based on a registry of more than 10,000 U.S. atrial fibrillation patients.
In addition, patients who have AF and OSA and who are treated with continuous positive airway pressure (CPAP) have a reduced rate of AF progression, Dr. Jonathan P. Piccini Sr. said at the annual meeting of the American College of Cardiology.
"We probably are not screening for obstructive sleep apnea as aggressively as we should" in AF patients, said Dr. Piccini, an electrophysiologist at Duke University in Durham, N.C. "We know that if obstructive sleep apnea is treated [with CPAP,] the AF burden can be dramatically reduced."

The data Dr. Piccini and his associates analyzed came from the ORBIT-AF (Outcomes Registry for Better Informed Treatment of Atrial Fibrillation), which starting in 2010 enrolled more than 10,000 AF patients from 172 U.S. locations with a variety of practice settings and followed them for more than 2 years. Their medical records showed that at enrollment, 1,841 of the 10,132 enrolled AF patients (18%) had also been diagnosed with OSA. Patients with OSA averaged 69 years old, while those without the disorder averaged 76 years old. Those with OSA had an average body mass index of 34 kg/m2, compared with 28 kg/m2 among those without OSA. Patients with OSA also had higher prevalence rates of dyspnea and fatigue than the enrolled AF patients without OSA.
During 2 years of follow-up, the two subgroups had similar rates of all-cause death, cardiovascular events, major bleeding events, and AF progression, but after multivariate adjustment, patients with OSA had a 12% higher rate of hospitalizations than did patients without OSA, a statistically significant difference.
Further analysis of the 1,624 OSA patients showed that 937 (58%) used CPAP during follow-up as a treatment for OSA. Comparison of the CPAP users and nonusers showed no significant difference in outcomes during follow-up for all-cause death, hospitalizations, cardiovascular events, or major bleeding events, but there was a statistically significant, 34% relative drop in the rate of AF progression among CPAP users compared with nonusers.
The ORBIT-AF registry is sponsored by Johnson & Johnson. Dr. Piccini has received remuneration from Johnson & Johnson, Forest Laboratories, and other companies.
On Twitter @mitchelzoler
WASHINGTON – About 18% of U.S. patients with atrial fibrillation also have a diagnosis of obstructive sleep apnea, and the confluence of the two appeared linked to increased hospitalizations and further progression of atrial fibrillation, based on a registry of more than 10,000 U.S. atrial fibrillation patients.
In addition, patients who have AF and OSA and who are treated with continuous positive airway pressure (CPAP) have a reduced rate of AF progression, Dr. Jonathan P. Piccini Sr. said at the annual meeting of the American College of Cardiology.
"We probably are not screening for obstructive sleep apnea as aggressively as we should" in AF patients, said Dr. Piccini, an electrophysiologist at Duke University in Durham, N.C. "We know that if obstructive sleep apnea is treated [with CPAP,] the AF burden can be dramatically reduced."
The data Dr. Piccini and his associates analyzed came from the ORBIT-AF (Outcomes Registry for Better Informed Treatment of Atrial Fibrillation), which starting in 2010 enrolled more than 10,000 AF patients from 172 U.S. locations with a variety of practice settings and followed them for more than 2 years. Their medical records showed that at enrollment, 1,841 of the 10,132 enrolled AF patients (18%) had also been diagnosed with OSA. Patients with OSA averaged 69 years old, while those without the disorder averaged 76 years old. Those with OSA had an average body mass index of 34 kg/m2, compared with 28 kg/m2 among those without OSA. Patients with OSA also had higher prevalence rates of dyspnea and fatigue than the enrolled AF patients without OSA.
During 2 years of follow-up, the two subgroups had similar rates of all-cause death, cardiovascular events, major bleeding events, and AF progression, but after multivariate adjustment, patients with OSA had a 12% higher rate of hospitalizations than did patients without OSA, a statistically significant difference.
Further analysis of the 1,624 OSA patients showed that 937 (58%) used CPAP during follow-up as a treatment for OSA. Comparison of the CPAP users and nonusers showed no significant difference in outcomes during follow-up for all-cause death, hospitalizations, cardiovascular events, or major bleeding events, but there was a statistically significant, 34% relative drop in the rate of AF progression among CPAP users compared with nonusers.
The ORBIT-AF registry is sponsored by Johnson & Johnson. Dr. Piccini has received remuneration from Johnson & Johnson, Forest Laboratories, and other companies.
On Twitter @mitchelzoler
WASHINGTON – About 18% of U.S. patients with atrial fibrillation also have a diagnosis of obstructive sleep apnea, and the confluence of the two appeared linked to increased hospitalizations and further progression of atrial fibrillation, based on a registry of more than 10,000 U.S. atrial fibrillation patients.
In addition, patients who have AF and OSA and who are treated with continuous positive airway pressure (CPAP) have a reduced rate of AF progression, Dr. Jonathan P. Piccini Sr. said at the annual meeting of the American College of Cardiology.
"We probably are not screening for obstructive sleep apnea as aggressively as we should" in AF patients, said Dr. Piccini, an electrophysiologist at Duke University in Durham, N.C. "We know that if obstructive sleep apnea is treated [with CPAP,] the AF burden can be dramatically reduced."
The data Dr. Piccini and his associates analyzed came from the ORBIT-AF (Outcomes Registry for Better Informed Treatment of Atrial Fibrillation), which starting in 2010 enrolled more than 10,000 AF patients from 172 U.S. locations with a variety of practice settings and followed them for more than 2 years. Their medical records showed that at enrollment, 1,841 of the 10,132 enrolled AF patients (18%) had also been diagnosed with OSA. Patients with OSA averaged 69 years old, while those without the disorder averaged 76 years old. Those with OSA had an average body mass index of 34 kg/m2, compared with 28 kg/m2 among those without OSA. Patients with OSA also had higher prevalence rates of dyspnea and fatigue than the enrolled AF patients without OSA.
During 2 years of follow-up, the two subgroups had similar rates of all-cause death, cardiovascular events, major bleeding events, and AF progression, but after multivariate adjustment, patients with OSA had a 12% higher rate of hospitalizations than did patients without OSA, a statistically significant difference.
Further analysis of the 1,624 OSA patients showed that 937 (58%) used CPAP during follow-up as a treatment for OSA. Comparison of the CPAP users and nonusers showed no significant difference in outcomes during follow-up for all-cause death, hospitalizations, cardiovascular events, or major bleeding events, but there was a statistically significant, 34% relative drop in the rate of AF progression among CPAP users compared with nonusers.
The ORBIT-AF registry is sponsored by Johnson & Johnson. Dr. Piccini has received remuneration from Johnson & Johnson, Forest Laboratories, and other companies.
On Twitter @mitchelzoler
AT ACC 2014
Major finding: Atrial fibrillation patients with sleep apnea had a significant, 12% increased rate of hospitalizations, compared with atrial fibrillation patients without sleep apnea.
Data source: The ORBIT-AF registry, which enrolled 10,132 U.S. patients with atrial fibrillation starting in 2010.
Disclosures: The ORBIT-AF registry is sponsored by Johnson & Johnson. Dr. Piccini has received remuneration from Johnson & Johnson, Forest Laboratories, and other companies.

Better blood pressure, glycemic control in patients with type 2 diabetes on CPAP for apnea
Treatment with continuous positive airway pressure leads to significantly better diabetes and blood pressure control at 5 years among diabetics with obstructive sleep apnea, according to results from a case-control study in 300 patients.
The researchers, led by Julian F. Guest, Ph.D., of Catalyst Health Economics Consultants in Middlesex, England, and King’s College London, examined records from 150 patients with type 2 diabetes and obstructive sleep apnea (OSA) from a national health database who had been treated with continuous positive airway pressure (CPAP) for up to 5 consecutive years, of whom 139 remained on CPAP at year 5, and compared these with 150 controls with both OSA and type 2 diabetes who were not on CPAP.

Dr. Guest and his colleagues sought to discern not only clinical differences between the study groups but also differences in cost effectiveness, and found advantages with CPAP for both. CPAP-treated patients had better-controlled diabetes than did the control patients at 5 years, with hemoglobin A1c of 8.2% in the CPAP group, compared with 12.1% among controls, a significant difference (Diabetes Care 2014 [doi:10.2337/dc13-2539]).
CPAP was also seen increasing patients’ health status significantly, by 0.27 quality-adjusted life years/patient over the 5-year period, while diminishing costs incurred. In both CPAP users and control patients, blood pressure declined over the study period, and patients’ blood pressure in the CPAP-treated group was significantly lower than that of control patients by year 5.
One unexplained finding was that more CPAP-treated than control patients had a diagnosis of cardiac arrhythmias; Dr. Guest and his colleagues suggested that this might be because patients on CPAP may have had more severe OSA at baseline, though this information was not available.
The investigators described their findings as compelling but cautioned that analyses of clinical outcomes "were based on clinicians’ entries into their patients’ records and inevitably subject to a certain amount of imprecision and lack of detail." Moreover, they wrote, the information collected in the database used was done so "for clinical care purposes and not for research."
The study was funded by a grant from ResMed, a maker of CPAP devices, with no other conflicts of interest reported.
Treatment with continuous positive airway pressure leads to significantly better diabetes and blood pressure control at 5 years among diabetics with obstructive sleep apnea, according to results from a case-control study in 300 patients.
The researchers, led by Julian F. Guest, Ph.D., of Catalyst Health Economics Consultants in Middlesex, England, and King’s College London, examined records from 150 patients with type 2 diabetes and obstructive sleep apnea (OSA) from a national health database who had been treated with continuous positive airway pressure (CPAP) for up to 5 consecutive years, of whom 139 remained on CPAP at year 5, and compared these with 150 controls with both OSA and type 2 diabetes who were not on CPAP.
Dr. Guest and his colleagues sought to discern not only clinical differences between the study groups but also differences in cost effectiveness, and found advantages with CPAP for both. CPAP-treated patients had better-controlled diabetes than did the control patients at 5 years, with hemoglobin A1c of 8.2% in the CPAP group, compared with 12.1% among controls, a significant difference (Diabetes Care 2014 [doi:10.2337/dc13-2539]).
CPAP was also seen increasing patients’ health status significantly, by 0.27 quality-adjusted life years/patient over the 5-year period, while diminishing costs incurred. In both CPAP users and control patients, blood pressure declined over the study period, and patients’ blood pressure in the CPAP-treated group was significantly lower than that of control patients by year 5.
One unexplained finding was that more CPAP-treated than control patients had a diagnosis of cardiac arrhythmias; Dr. Guest and his colleagues suggested that this might be because patients on CPAP may have had more severe OSA at baseline, though this information was not available.
The investigators described their findings as compelling but cautioned that analyses of clinical outcomes "were based on clinicians’ entries into their patients’ records and inevitably subject to a certain amount of imprecision and lack of detail." Moreover, they wrote, the information collected in the database used was done so "for clinical care purposes and not for research."
The study was funded by a grant from ResMed, a maker of CPAP devices, with no other conflicts of interest reported.
Treatment with continuous positive airway pressure leads to significantly better diabetes and blood pressure control at 5 years among diabetics with obstructive sleep apnea, according to results from a case-control study in 300 patients.
The researchers, led by Julian F. Guest, Ph.D., of Catalyst Health Economics Consultants in Middlesex, England, and King’s College London, examined records from 150 patients with type 2 diabetes and obstructive sleep apnea (OSA) from a national health database who had been treated with continuous positive airway pressure (CPAP) for up to 5 consecutive years, of whom 139 remained on CPAP at year 5, and compared these with 150 controls with both OSA and type 2 diabetes who were not on CPAP.
Dr. Guest and his colleagues sought to discern not only clinical differences between the study groups but also differences in cost effectiveness, and found advantages with CPAP for both. CPAP-treated patients had better-controlled diabetes than did the control patients at 5 years, with hemoglobin A1c of 8.2% in the CPAP group, compared with 12.1% among controls, a significant difference (Diabetes Care 2014 [doi:10.2337/dc13-2539]).
CPAP was also seen increasing patients’ health status significantly, by 0.27 quality-adjusted life years/patient over the 5-year period, while diminishing costs incurred. In both CPAP users and control patients, blood pressure declined over the study period, and patients’ blood pressure in the CPAP-treated group was significantly lower than that of control patients by year 5.
One unexplained finding was that more CPAP-treated than control patients had a diagnosis of cardiac arrhythmias; Dr. Guest and his colleagues suggested that this might be because patients on CPAP may have had more severe OSA at baseline, though this information was not available.
The investigators described their findings as compelling but cautioned that analyses of clinical outcomes "were based on clinicians’ entries into their patients’ records and inevitably subject to a certain amount of imprecision and lack of detail." Moreover, they wrote, the information collected in the database used was done so "for clinical care purposes and not for research."
The study was funded by a grant from ResMed, a maker of CPAP devices, with no other conflicts of interest reported.
FROM DIABETES CARE
Major finding: OSA patients with T2D patients treated with CPAP had significantly lower HbA1c at 5 years than did those not on CPAP, at 8.2% and 12.1%, respectively.
Data source: A case-control study in 300 patients.
Disclosures: The study was funded by ResMed, a maker of CPAP devices, with no other conflicts of interest reported.

Trivalent flu vaccine effective before age 2 years
The trivalent influenza vaccine was found effective in children younger than 2 years of age in an observational study in Australia, according to a report published online April 21 in Pediatrics.
Data regarding the vaccine’s effectiveness in this age group are limited, so there is ongoing controversy over whether it should be recommended as routine. To assess the effectiveness of the trivalent influenza vaccine, researchers examined rates of immunization and of influenza-like illness treated at the major pediatric teaching hospital in Perth, Western Australia, during a 4-year period. The vaccine was available for free to all children aged 6-59 months in that state during this interval, said Dr. Christopher C. Blyth of the University of Western Australia and the Princess Margaret Hospital for Children, both in Perth, and his associates, on behalf of the WAIVE (Western Australian Influenza Vaccine Effectiveness) Study Team.

A total of 1,903 children were enrolled in the study. The median age was 1.9 years. Culturing of nasopharyngeal swabs showed that 389 (20.4%) had influenza during the study period and another 1,134 (59.6%) had a different respiratory virus; in the remaining children, the cause of the influenza-like illness was nonviral. The most frequently detected noninfluenza viruses were human picornaviruses (673), respiratory syncytial virus A/B (312), human parainfluenza virus types 1 to 4 (193), adenoviruses B through D (157), bocaviruses (126), and coronaviruses OC43/229E (61); 467 children had two or more viruses detected, including 115 children with influenza.
The overall vaccination uptake was low at 24% for the entire study period, and it decreased significantly during the study interval, from 55.1% during 2008-2009 to 9.7% in 2010-2012. This drop-off was due to the temporary suspension of a preschool vaccination program when the FluVax Junior brand it used was linked to a 44-fold rise in febrile convulsions (BMJ Open. 2011 May 30 [10.1136/bmjopen-2010-000016]).
Despite this decrease in use, vaccine efficacy was evident: It was 64.7% overall and 85.8% among children younger than 2 years, the investigators said (Pediatrics 2014;133:e1218-25).
Even among children who did not receive the full schedule of vaccine doses, vaccine efficacy exceeded 81%. "This study provides the strongest evidence to date supporting the effectiveness of the trivalent influenza vaccine in children younger than 2 years of age," Dr. Blyth and his associates said.
This study was funded by the Western Australian Department of Health. The vaccine was provided by Sanofi Pasteur and CSL Biotherapies. Dr. Peter C. Richmond reported past ties to Baxter and GlaxoSmithKline. Dr. Blyth and the remaining associates reported no relevant financial conflicts of interest.
The trivalent influenza vaccine was found effective in children younger than 2 years of age in an observational study in Australia, according to a report published online April 21 in Pediatrics.
Data regarding the vaccine’s effectiveness in this age group are limited, so there is ongoing controversy over whether it should be recommended as routine. To assess the effectiveness of the trivalent influenza vaccine, researchers examined rates of immunization and of influenza-like illness treated at the major pediatric teaching hospital in Perth, Western Australia, during a 4-year period. The vaccine was available for free to all children aged 6-59 months in that state during this interval, said Dr. Christopher C. Blyth of the University of Western Australia and the Princess Margaret Hospital for Children, both in Perth, and his associates, on behalf of the WAIVE (Western Australian Influenza Vaccine Effectiveness) Study Team.
A total of 1,903 children were enrolled in the study. The median age was 1.9 years. Culturing of nasopharyngeal swabs showed that 389 (20.4%) had influenza during the study period and another 1,134 (59.6%) had a different respiratory virus; in the remaining children, the cause of the influenza-like illness was nonviral. The most frequently detected noninfluenza viruses were human picornaviruses (673), respiratory syncytial virus A/B (312), human parainfluenza virus types 1 to 4 (193), adenoviruses B through D (157), bocaviruses (126), and coronaviruses OC43/229E (61); 467 children had two or more viruses detected, including 115 children with influenza.
The overall vaccination uptake was low at 24% for the entire study period, and it decreased significantly during the study interval, from 55.1% during 2008-2009 to 9.7% in 2010-2012. This drop-off was due to the temporary suspension of a preschool vaccination program when the FluVax Junior brand it used was linked to a 44-fold rise in febrile convulsions (BMJ Open. 2011 May 30 [10.1136/bmjopen-2010-000016]).
Despite this decrease in use, vaccine efficacy was evident: It was 64.7% overall and 85.8% among children younger than 2 years, the investigators said (Pediatrics 2014;133:e1218-25).
Even among children who did not receive the full schedule of vaccine doses, vaccine efficacy exceeded 81%. "This study provides the strongest evidence to date supporting the effectiveness of the trivalent influenza vaccine in children younger than 2 years of age," Dr. Blyth and his associates said.
This study was funded by the Western Australian Department of Health. The vaccine was provided by Sanofi Pasteur and CSL Biotherapies. Dr. Peter C. Richmond reported past ties to Baxter and GlaxoSmithKline. Dr. Blyth and the remaining associates reported no relevant financial conflicts of interest.
The trivalent influenza vaccine was found effective in children younger than 2 years of age in an observational study in Australia, according to a report published online April 21 in Pediatrics.
Data regarding the vaccine’s effectiveness in this age group are limited, so there is ongoing controversy over whether it should be recommended as routine. To assess the effectiveness of the trivalent influenza vaccine, researchers examined rates of immunization and of influenza-like illness treated at the major pediatric teaching hospital in Perth, Western Australia, during a 4-year period. The vaccine was available for free to all children aged 6-59 months in that state during this interval, said Dr. Christopher C. Blyth of the University of Western Australia and the Princess Margaret Hospital for Children, both in Perth, and his associates, on behalf of the WAIVE (Western Australian Influenza Vaccine Effectiveness) Study Team.
A total of 1,903 children were enrolled in the study. The median age was 1.9 years. Culturing of nasopharyngeal swabs showed that 389 (20.4%) had influenza during the study period and another 1,134 (59.6%) had a different respiratory virus; in the remaining children, the cause of the influenza-like illness was nonviral. The most frequently detected noninfluenza viruses were human picornaviruses (673), respiratory syncytial virus A/B (312), human parainfluenza virus types 1 to 4 (193), adenoviruses B through D (157), bocaviruses (126), and coronaviruses OC43/229E (61); 467 children had two or more viruses detected, including 115 children with influenza.
The overall vaccination uptake was low at 24% for the entire study period, and it decreased significantly during the study interval, from 55.1% during 2008-2009 to 9.7% in 2010-2012. This drop-off was due to the temporary suspension of a preschool vaccination program when the FluVax Junior brand it used was linked to a 44-fold rise in febrile convulsions (BMJ Open. 2011 May 30 [10.1136/bmjopen-2010-000016]).
Despite this decrease in use, vaccine efficacy was evident: It was 64.7% overall and 85.8% among children younger than 2 years, the investigators said (Pediatrics 2014;133:e1218-25).
Even among children who did not receive the full schedule of vaccine doses, vaccine efficacy exceeded 81%. "This study provides the strongest evidence to date supporting the effectiveness of the trivalent influenza vaccine in children younger than 2 years of age," Dr. Blyth and his associates said.
This study was funded by the Western Australian Department of Health. The vaccine was provided by Sanofi Pasteur and CSL Biotherapies. Dr. Peter C. Richmond reported past ties to Baxter and GlaxoSmithKline. Dr. Blyth and the remaining associates reported no relevant financial conflicts of interest.
FROM PEDIATRICS
Major finding: Vaccine efficacy was 64.7% overall in children under age 5 years, 85.8% among children younger than 2 years, and more than 81% among children who did not receive the full schedule of doses.
Data source: An observational study of 1,903 children aged 6-59 months treated at a single Australian medical center for influenza-like illness during a 4-year period, of whom 24% had received the trivalent influenza vaccine.
Disclosures: This study was funded by the Western Australian Department of Health. The vaccine was provided by Sanofi-Pasteur and CSL Biotherapies. Dr. Peter C. Richmond reported past ties to Baxter and GlaxoSmithKline. Dr. Blyth and the remaining associates reported no relevant financial conflicts of interest.
