User login
Botulinum toxin for men
Men make up an increasing number of dermatology patients seeking cosmetic procedures. According to data from the American Society for Dermatologic Surgery and the American Society of Plastic Surgery, 9%-10% of all cosmetic procedures performed in the United States in 2013 were on men, a 104% increase since 2000. Botulinum toxin is currently the most common minimally invasive cosmetic procedure performed in men. While the overall percentage of men undergoing treatment, compared with women, is relatively small, more than 385,000 botulinum toxin treatments were performed on men last year in the United States, an increase of 310% since 2000.

Studies have shown that men often require more units of onabotulinumtoxinA than women when treating the glabella. In a 2005 study by Alstair and Jean Carruthers, 80 men were randomized to receive 20, 40, 60, or 80 units of onabotulinumtoxinA (Botox or Vistabel). The 40-, 60-, and 80-U doses were consistently more effective than the 20-U dose was in reducing glabellar lines (duration, peak response rate, and improvement from baseline). I find this to be true in my practice. Men may often require 20-60 U in the superficial corrugator and procerus muscles, compared with 20-30 units of onabotulinumtoxinA in the same muscles in women. For the frontalis muscles, I may use 5-20 U in men, compared with 5-10 U of onabotulinumtoxinA in women, but I take care not to inject too inferiorly to avoid a heavy brow or brow ptosis. The orbicularis oculi muscles often require the similar doses of between 6-15 U (most often 12 U/side) depending on degree of muscle contraction and severity of rhytids.

In addition to differences in botulinum toxin dosing between men and women, placement of toxin also may vary. Placement in the superficial corrugator, procerus, frontalis, and orbicularis oculi muscles are often the similar and patient dependent, based on a visual assessment of where their muscles move/contract. The superficial corrugator may insert more laterally in some men, and the brow is often straighter or less arched. The difference in injection site is often at the lateral brow. In women, botulinum toxin is often injected at the lateral brow at the junction where the lateral superior portion of the orbicularis oculi muscle and frontalis meet, in order to help give the brow a "lift." Men, however, often do not want raised or arched brow. Therefore, an injection is often placed about 1 cm above the lateral brow to maintain brow position and avoid overarching, or what some may regard as feminization of the male brow.
The depressor anguli oris and orbicularis oris muscles are injected less frequently in men than in women in my practice because of seemingly decreased rhytid formation in men in these locations. The platysmal muscles may be injected in men, but their average age is older compared with women who receive injections in this location.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
Men make up an increasing number of dermatology patients seeking cosmetic procedures. According to data from the American Society for Dermatologic Surgery and the American Society of Plastic Surgery, 9%-10% of all cosmetic procedures performed in the United States in 2013 were on men, a 104% increase since 2000. Botulinum toxin is currently the most common minimally invasive cosmetic procedure performed in men. While the overall percentage of men undergoing treatment, compared with women, is relatively small, more than 385,000 botulinum toxin treatments were performed on men last year in the United States, an increase of 310% since 2000.
Studies have shown that men often require more units of onabotulinumtoxinA than women when treating the glabella. In a 2005 study by Alstair and Jean Carruthers, 80 men were randomized to receive 20, 40, 60, or 80 units of onabotulinumtoxinA (Botox or Vistabel). The 40-, 60-, and 80-U doses were consistently more effective than the 20-U dose was in reducing glabellar lines (duration, peak response rate, and improvement from baseline). I find this to be true in my practice. Men may often require 20-60 U in the superficial corrugator and procerus muscles, compared with 20-30 units of onabotulinumtoxinA in the same muscles in women. For the frontalis muscles, I may use 5-20 U in men, compared with 5-10 U of onabotulinumtoxinA in women, but I take care not to inject too inferiorly to avoid a heavy brow or brow ptosis. The orbicularis oculi muscles often require the similar doses of between 6-15 U (most often 12 U/side) depending on degree of muscle contraction and severity of rhytids.
In addition to differences in botulinum toxin dosing between men and women, placement of toxin also may vary. Placement in the superficial corrugator, procerus, frontalis, and orbicularis oculi muscles are often the similar and patient dependent, based on a visual assessment of where their muscles move/contract. The superficial corrugator may insert more laterally in some men, and the brow is often straighter or less arched. The difference in injection site is often at the lateral brow. In women, botulinum toxin is often injected at the lateral brow at the junction where the lateral superior portion of the orbicularis oculi muscle and frontalis meet, in order to help give the brow a "lift." Men, however, often do not want raised or arched brow. Therefore, an injection is often placed about 1 cm above the lateral brow to maintain brow position and avoid overarching, or what some may regard as feminization of the male brow.
The depressor anguli oris and orbicularis oris muscles are injected less frequently in men than in women in my practice because of seemingly decreased rhytid formation in men in these locations. The platysmal muscles may be injected in men, but their average age is older compared with women who receive injections in this location.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
Men make up an increasing number of dermatology patients seeking cosmetic procedures. According to data from the American Society for Dermatologic Surgery and the American Society of Plastic Surgery, 9%-10% of all cosmetic procedures performed in the United States in 2013 were on men, a 104% increase since 2000. Botulinum toxin is currently the most common minimally invasive cosmetic procedure performed in men. While the overall percentage of men undergoing treatment, compared with women, is relatively small, more than 385,000 botulinum toxin treatments were performed on men last year in the United States, an increase of 310% since 2000.
Studies have shown that men often require more units of onabotulinumtoxinA than women when treating the glabella. In a 2005 study by Alstair and Jean Carruthers, 80 men were randomized to receive 20, 40, 60, or 80 units of onabotulinumtoxinA (Botox or Vistabel). The 40-, 60-, and 80-U doses were consistently more effective than the 20-U dose was in reducing glabellar lines (duration, peak response rate, and improvement from baseline). I find this to be true in my practice. Men may often require 20-60 U in the superficial corrugator and procerus muscles, compared with 20-30 units of onabotulinumtoxinA in the same muscles in women. For the frontalis muscles, I may use 5-20 U in men, compared with 5-10 U of onabotulinumtoxinA in women, but I take care not to inject too inferiorly to avoid a heavy brow or brow ptosis. The orbicularis oculi muscles often require the similar doses of between 6-15 U (most often 12 U/side) depending on degree of muscle contraction and severity of rhytids.
In addition to differences in botulinum toxin dosing between men and women, placement of toxin also may vary. Placement in the superficial corrugator, procerus, frontalis, and orbicularis oculi muscles are often the similar and patient dependent, based on a visual assessment of where their muscles move/contract. The superficial corrugator may insert more laterally in some men, and the brow is often straighter or less arched. The difference in injection site is often at the lateral brow. In women, botulinum toxin is often injected at the lateral brow at the junction where the lateral superior portion of the orbicularis oculi muscle and frontalis meet, in order to help give the brow a "lift." Men, however, often do not want raised or arched brow. Therefore, an injection is often placed about 1 cm above the lateral brow to maintain brow position and avoid overarching, or what some may regard as feminization of the male brow.
The depressor anguli oris and orbicularis oris muscles are injected less frequently in men than in women in my practice because of seemingly decreased rhytid formation in men in these locations. The platysmal muscles may be injected in men, but their average age is older compared with women who receive injections in this location.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.

FDA looks to make companion diagnostics, lab tests more reliable
Last month, the Food and Drug Administration announced the latest steps it is taking to advance the use of personalized medicine.
First, the agency finalized guidance on the development of companion diagnostics. Second, it signaled its intent to begin oversight of certain laboratory developed tests (LDTs), tests that are designed, manufactured, and used within a single laboratory.
The guidance, initially issued as a draft in July 2011, offers the agency’s thinking on its expectations on the development of companion diagnostics. No substantive changes were made to the final guidance document from its draft version, agency officials said.
"When drug companies develop therapies that will only work on specific subpopulations, it’s important those therapies are approved with a diagnostic test that the FDA knows is accurate and reliable and patients and their physicians can count on," FDA Commissioner Dr. Margaret Hamburg said during a press teleconference.
The agency also revealed its initial thoughts on how it will regulate LDTs in a letter to Congress. The FDA is required to let Congress know 60 days prior to the issuance of draft and final guidance. The forthcoming draft represents a change in how the agency is approaching LDTs.
"The FDA has historically exercised enforcement discretion over LDTs, meaning the agency generally did not enforce applicable regulatory requirements on the tests because they were generally considered lower risk and used on a limited basis within a given institution," Dr. Hamburg said. "Today, they may be marketed and used more broadly and compete with FDA-approved tests without clinical studies to support their use. The deeper concern is about physicians and patients making critical health decisions based on diagnostic tests that have generally not been reviewed by the FDA. Without premarket review by the agency, patients, their health care providers, or the FDA itself cannot be assured those tests are accurate and reliable."
Dr. Hamburg said the agency plans to enforce premarket review requirements for higher-risk LDTs, "including those used to determine medical treatment and that have the same intended use of FDA-approved and FDA-cleared companion diagnostics currently on the market."
The agency’s actions received praise from cancer researchers.
"The recent announcements by the FDA are aimed at providing patients and their physicians with an important level of confidence and certainty with regard to the highly complex molecular and genetic information that these diagnostic tests are determining," American Association for Cancer Research President Dr. Carlos L. Arteaga said in a statement. "As an organization that represents the entire continuum of research, from the laboratory to the clinic, including the clinical researchers and physician-scientists engaged in cancer patient care, the AACR looks forward to continuing to engage with the FDA to ensure that the molecular and genetic diagnostic tests that are being utilized by physicians and patients are based on solidly supported scientific evidence."
Many in the health care community, particularly those in the oncology community, are looking at how best to use personalized medicine as a means of achieving better treatment outcomes and controlling costs of health care.
Last month, the Food and Drug Administration announced the latest steps it is taking to advance the use of personalized medicine.
First, the agency finalized guidance on the development of companion diagnostics. Second, it signaled its intent to begin oversight of certain laboratory developed tests (LDTs), tests that are designed, manufactured, and used within a single laboratory.
The guidance, initially issued as a draft in July 2011, offers the agency’s thinking on its expectations on the development of companion diagnostics. No substantive changes were made to the final guidance document from its draft version, agency officials said.
"When drug companies develop therapies that will only work on specific subpopulations, it’s important those therapies are approved with a diagnostic test that the FDA knows is accurate and reliable and patients and their physicians can count on," FDA Commissioner Dr. Margaret Hamburg said during a press teleconference.
The agency also revealed its initial thoughts on how it will regulate LDTs in a letter to Congress. The FDA is required to let Congress know 60 days prior to the issuance of draft and final guidance. The forthcoming draft represents a change in how the agency is approaching LDTs.
"The FDA has historically exercised enforcement discretion over LDTs, meaning the agency generally did not enforce applicable regulatory requirements on the tests because they were generally considered lower risk and used on a limited basis within a given institution," Dr. Hamburg said. "Today, they may be marketed and used more broadly and compete with FDA-approved tests without clinical studies to support their use. The deeper concern is about physicians and patients making critical health decisions based on diagnostic tests that have generally not been reviewed by the FDA. Without premarket review by the agency, patients, their health care providers, or the FDA itself cannot be assured those tests are accurate and reliable."
Dr. Hamburg said the agency plans to enforce premarket review requirements for higher-risk LDTs, "including those used to determine medical treatment and that have the same intended use of FDA-approved and FDA-cleared companion diagnostics currently on the market."
The agency’s actions received praise from cancer researchers.
"The recent announcements by the FDA are aimed at providing patients and their physicians with an important level of confidence and certainty with regard to the highly complex molecular and genetic information that these diagnostic tests are determining," American Association for Cancer Research President Dr. Carlos L. Arteaga said in a statement. "As an organization that represents the entire continuum of research, from the laboratory to the clinic, including the clinical researchers and physician-scientists engaged in cancer patient care, the AACR looks forward to continuing to engage with the FDA to ensure that the molecular and genetic diagnostic tests that are being utilized by physicians and patients are based on solidly supported scientific evidence."
Many in the health care community, particularly those in the oncology community, are looking at how best to use personalized medicine as a means of achieving better treatment outcomes and controlling costs of health care.
Last month, the Food and Drug Administration announced the latest steps it is taking to advance the use of personalized medicine.
First, the agency finalized guidance on the development of companion diagnostics. Second, it signaled its intent to begin oversight of certain laboratory developed tests (LDTs), tests that are designed, manufactured, and used within a single laboratory.
The guidance, initially issued as a draft in July 2011, offers the agency’s thinking on its expectations on the development of companion diagnostics. No substantive changes were made to the final guidance document from its draft version, agency officials said.
"When drug companies develop therapies that will only work on specific subpopulations, it’s important those therapies are approved with a diagnostic test that the FDA knows is accurate and reliable and patients and their physicians can count on," FDA Commissioner Dr. Margaret Hamburg said during a press teleconference.
The agency also revealed its initial thoughts on how it will regulate LDTs in a letter to Congress. The FDA is required to let Congress know 60 days prior to the issuance of draft and final guidance. The forthcoming draft represents a change in how the agency is approaching LDTs.
"The FDA has historically exercised enforcement discretion over LDTs, meaning the agency generally did not enforce applicable regulatory requirements on the tests because they were generally considered lower risk and used on a limited basis within a given institution," Dr. Hamburg said. "Today, they may be marketed and used more broadly and compete with FDA-approved tests without clinical studies to support their use. The deeper concern is about physicians and patients making critical health decisions based on diagnostic tests that have generally not been reviewed by the FDA. Without premarket review by the agency, patients, their health care providers, or the FDA itself cannot be assured those tests are accurate and reliable."
Dr. Hamburg said the agency plans to enforce premarket review requirements for higher-risk LDTs, "including those used to determine medical treatment and that have the same intended use of FDA-approved and FDA-cleared companion diagnostics currently on the market."
The agency’s actions received praise from cancer researchers.
"The recent announcements by the FDA are aimed at providing patients and their physicians with an important level of confidence and certainty with regard to the highly complex molecular and genetic information that these diagnostic tests are determining," American Association for Cancer Research President Dr. Carlos L. Arteaga said in a statement. "As an organization that represents the entire continuum of research, from the laboratory to the clinic, including the clinical researchers and physician-scientists engaged in cancer patient care, the AACR looks forward to continuing to engage with the FDA to ensure that the molecular and genetic diagnostic tests that are being utilized by physicians and patients are based on solidly supported scientific evidence."
Many in the health care community, particularly those in the oncology community, are looking at how best to use personalized medicine as a means of achieving better treatment outcomes and controlling costs of health care.
Zebrafish research solves mystery of HSC generation

A cure for a range of blood and immune disorders is in sight, according to researchers who say they’ve solved a mystery of hematopoietic stem cell (HSC) generation.
By studying zebrafish embryos, the investigators found that migratory cells from a region known as the endotome are essential for HSC formation.
The team also discovered some of the signals required for HSC generation and identified genes necessary for endotome formation.
The researchers believe these findings, published in Nature, bring us one step closer to creating viable HSCs in the lab.
“HSCs are one of the best therapeutic tools at our disposal because they can make any blood cell in the body,” said study author Peter Currie, PhD, of the Australian Regenerative Medicine Institute at Monash University in Victoria, Australia.
“Potentially, we could use these cells in many more ways than current transplantation strategies to treat serious blood disorders and diseases, but only if we can figure out how they are generated in the first place.”
In an attempt to do just that, Dr Currie and his colleagues studied developing zebrafish. They used high-resolution microscopy to film how HSCs form inside the embryo.
The investigators noted that, in vertebrate embryos, HSCs are initially generated within the dorsal aorta. And previous research showed that signaling relayed from adjacent somites coordinates HSC induction.
Dr Currie and his colleagues found that somite specification of HSCs occurs thanks to an endothelial precursor cell population. These cells arise in a sub-compartment of the zebrafish somite the researchers dubbed “the endotome.”
Endothelial cells from the endotome are specified thanks to activity of the homeobox gene meox1. Specified endotome cells then migrate to and colonize the dorsal aorta, where they induce HSC formation via chemokine signaling that’s activated during endotome formation.
“Endotome cells act like a comfy sofa for pre-HSCs to snuggle into, helping them progress to become fully fledged stem cells,” Dr Currie said. “Not only did we identify some of the cells and signals required for HSC formation, we also pinpointed the genes required for endotome formation in the first place.”
“The really exciting thing about these results is that if we can find the signals present in the endotome cells responsible for embryonic HSC formation, then we can use them in vitro to make different blood cells on demand for all sorts of blood-related disorders.”
For the next phase of this research, Dr Currie and his colleagues are attempting to identify more of the molecular cues that trigger HSC production. ![]()
A cure for a range of blood and immune disorders is in sight, according to researchers who say they’ve solved a mystery of hematopoietic stem cell (HSC) generation.
By studying zebrafish embryos, the investigators found that migratory cells from a region known as the endotome are essential for HSC formation.
The team also discovered some of the signals required for HSC generation and identified genes necessary for endotome formation.
The researchers believe these findings, published in Nature, bring us one step closer to creating viable HSCs in the lab.
“HSCs are one of the best therapeutic tools at our disposal because they can make any blood cell in the body,” said study author Peter Currie, PhD, of the Australian Regenerative Medicine Institute at Monash University in Victoria, Australia.
“Potentially, we could use these cells in many more ways than current transplantation strategies to treat serious blood disorders and diseases, but only if we can figure out how they are generated in the first place.”
In an attempt to do just that, Dr Currie and his colleagues studied developing zebrafish. They used high-resolution microscopy to film how HSCs form inside the embryo.
The investigators noted that, in vertebrate embryos, HSCs are initially generated within the dorsal aorta. And previous research showed that signaling relayed from adjacent somites coordinates HSC induction.
Dr Currie and his colleagues found that somite specification of HSCs occurs thanks to an endothelial precursor cell population. These cells arise in a sub-compartment of the zebrafish somite the researchers dubbed “the endotome.”
Endothelial cells from the endotome are specified thanks to activity of the homeobox gene meox1. Specified endotome cells then migrate to and colonize the dorsal aorta, where they induce HSC formation via chemokine signaling that’s activated during endotome formation.
“Endotome cells act like a comfy sofa for pre-HSCs to snuggle into, helping them progress to become fully fledged stem cells,” Dr Currie said. “Not only did we identify some of the cells and signals required for HSC formation, we also pinpointed the genes required for endotome formation in the first place.”
“The really exciting thing about these results is that if we can find the signals present in the endotome cells responsible for embryonic HSC formation, then we can use them in vitro to make different blood cells on demand for all sorts of blood-related disorders.”
For the next phase of this research, Dr Currie and his colleagues are attempting to identify more of the molecular cues that trigger HSC production. ![]()
A cure for a range of blood and immune disorders is in sight, according to researchers who say they’ve solved a mystery of hematopoietic stem cell (HSC) generation.
By studying zebrafish embryos, the investigators found that migratory cells from a region known as the endotome are essential for HSC formation.
The team also discovered some of the signals required for HSC generation and identified genes necessary for endotome formation.
The researchers believe these findings, published in Nature, bring us one step closer to creating viable HSCs in the lab.
“HSCs are one of the best therapeutic tools at our disposal because they can make any blood cell in the body,” said study author Peter Currie, PhD, of the Australian Regenerative Medicine Institute at Monash University in Victoria, Australia.
“Potentially, we could use these cells in many more ways than current transplantation strategies to treat serious blood disorders and diseases, but only if we can figure out how they are generated in the first place.”
In an attempt to do just that, Dr Currie and his colleagues studied developing zebrafish. They used high-resolution microscopy to film how HSCs form inside the embryo.
The investigators noted that, in vertebrate embryos, HSCs are initially generated within the dorsal aorta. And previous research showed that signaling relayed from adjacent somites coordinates HSC induction.
Dr Currie and his colleagues found that somite specification of HSCs occurs thanks to an endothelial precursor cell population. These cells arise in a sub-compartment of the zebrafish somite the researchers dubbed “the endotome.”
Endothelial cells from the endotome are specified thanks to activity of the homeobox gene meox1. Specified endotome cells then migrate to and colonize the dorsal aorta, where they induce HSC formation via chemokine signaling that’s activated during endotome formation.
“Endotome cells act like a comfy sofa for pre-HSCs to snuggle into, helping them progress to become fully fledged stem cells,” Dr Currie said. “Not only did we identify some of the cells and signals required for HSC formation, we also pinpointed the genes required for endotome formation in the first place.”
“The really exciting thing about these results is that if we can find the signals present in the endotome cells responsible for embryonic HSC formation, then we can use them in vitro to make different blood cells on demand for all sorts of blood-related disorders.”
For the next phase of this research, Dr Currie and his colleagues are attempting to identify more of the molecular cues that trigger HSC production. ![]()
Technique may predict progression in MM

Credit: Graham Colm
Scientists have found that a technique used in Earth science research may be able to help physicians predict the course of multiple myeloma (MM).
The team showed they could use calcium isotope analysis to predict whether MM patients are at risk for developing bone lesions.
The group believes this technique could be used to chart the progression or recurrence of MM and help tailor therapies to better protect patients’ bones.
“At present, there is no good way to track changes in bone balance, except retrospectively using X-ray methods,” said Ariel Anbar, PhD, of Arizona State University in Tempe. “By the time the X-rays show something, the damage has been done.”
“Right now, pain is usually the first indication that cancer is affecting the bones,” added Rafael Fonseca, MD, of the Mayo Clinic in Scottsdale, Arizona. “If we could detect it earlier by an analysis of urine or blood in high-risk patients, it could significantly improve their care.”
To explore this possibility, Drs Fonseca, Anbar, and their colleagues performed calcium isotope analysis using blood samples from MM patients. The team recounted their results in a letter to Leukemia.
As the name suggests, calcium isotope analysis measures calcium isotopes that are naturally present in blood. The technique makes use of a fact well known to Earth scientists but not normally used in biomedicine: different isotopes of a chemical element can react at slightly different rates.
An earlier study testing this technique in healthy subjects showed that when bones form, the lighter isotopes of calcium enter bone a little faster than the heavier isotopes. That difference, called isotope fractionation, is the key to the method.
In healthy, active humans, bone is forming at about the same rate as it resorbs. But if bone loss is occurring, the isotopic composition of blood becomes enriched in the lighter isotopes as bones resorb more quickly than they are formed.
The effect on calcium isotopes is very small, typically less than a 0.02% change in the isotope ratio. But even effects that small can be measured using precise mass spectrometry methods.
Using these methods, the researchers tested peripheral blood samples from 71 adult patients—55 with MM, 9 with smoldering MM, and 7 with monoclonal gammopathy of undetermined significance.
The researchers found an association between how active a patient’s disease was and the change in the isotope ratios. In fact, the isotope ratios predicted disease activity better than, and independent from, standard clinical variables.
Blood samples from patients with active disease had significantly lower mean calcium isotope compositions than samples from patients with non-active disease (mean δ44/42Ca=-0.8 vs -0.67, P=0.025), regardless of diagnosis.
For MM patients specifically, those with active disease had a significantly lower mean δ44/42Ca than patients with non-active disease (-0.79 vs -0.63, P=0.016), which was consistent with resorption of bone containing lighter 42Ca.
Dr Anbar noted that, although calcium isotope analysis has worked in this small set of patients, additional research is needed to verify these initial findings and improve the efficiency of analysis.
“If the method proves to be robust after more careful validation, it could provide earlier detection of bone involvement than presently possible,” he said, “and also provide the possibility to monitor the effectiveness of drugs to combat bone loss.” ![]()
Credit: Graham Colm
Scientists have found that a technique used in Earth science research may be able to help physicians predict the course of multiple myeloma (MM).
The team showed they could use calcium isotope analysis to predict whether MM patients are at risk for developing bone lesions.
The group believes this technique could be used to chart the progression or recurrence of MM and help tailor therapies to better protect patients’ bones.
“At present, there is no good way to track changes in bone balance, except retrospectively using X-ray methods,” said Ariel Anbar, PhD, of Arizona State University in Tempe. “By the time the X-rays show something, the damage has been done.”
“Right now, pain is usually the first indication that cancer is affecting the bones,” added Rafael Fonseca, MD, of the Mayo Clinic in Scottsdale, Arizona. “If we could detect it earlier by an analysis of urine or blood in high-risk patients, it could significantly improve their care.”
To explore this possibility, Drs Fonseca, Anbar, and their colleagues performed calcium isotope analysis using blood samples from MM patients. The team recounted their results in a letter to Leukemia.
As the name suggests, calcium isotope analysis measures calcium isotopes that are naturally present in blood. The technique makes use of a fact well known to Earth scientists but not normally used in biomedicine: different isotopes of a chemical element can react at slightly different rates.
An earlier study testing this technique in healthy subjects showed that when bones form, the lighter isotopes of calcium enter bone a little faster than the heavier isotopes. That difference, called isotope fractionation, is the key to the method.
In healthy, active humans, bone is forming at about the same rate as it resorbs. But if bone loss is occurring, the isotopic composition of blood becomes enriched in the lighter isotopes as bones resorb more quickly than they are formed.
The effect on calcium isotopes is very small, typically less than a 0.02% change in the isotope ratio. But even effects that small can be measured using precise mass spectrometry methods.
Using these methods, the researchers tested peripheral blood samples from 71 adult patients—55 with MM, 9 with smoldering MM, and 7 with monoclonal gammopathy of undetermined significance.
The researchers found an association between how active a patient’s disease was and the change in the isotope ratios. In fact, the isotope ratios predicted disease activity better than, and independent from, standard clinical variables.
Blood samples from patients with active disease had significantly lower mean calcium isotope compositions than samples from patients with non-active disease (mean δ44/42Ca=-0.8 vs -0.67, P=0.025), regardless of diagnosis.
For MM patients specifically, those with active disease had a significantly lower mean δ44/42Ca than patients with non-active disease (-0.79 vs -0.63, P=0.016), which was consistent with resorption of bone containing lighter 42Ca.
Dr Anbar noted that, although calcium isotope analysis has worked in this small set of patients, additional research is needed to verify these initial findings and improve the efficiency of analysis.
“If the method proves to be robust after more careful validation, it could provide earlier detection of bone involvement than presently possible,” he said, “and also provide the possibility to monitor the effectiveness of drugs to combat bone loss.” ![]()
Credit: Graham Colm
Scientists have found that a technique used in Earth science research may be able to help physicians predict the course of multiple myeloma (MM).
The team showed they could use calcium isotope analysis to predict whether MM patients are at risk for developing bone lesions.
The group believes this technique could be used to chart the progression or recurrence of MM and help tailor therapies to better protect patients’ bones.
“At present, there is no good way to track changes in bone balance, except retrospectively using X-ray methods,” said Ariel Anbar, PhD, of Arizona State University in Tempe. “By the time the X-rays show something, the damage has been done.”
“Right now, pain is usually the first indication that cancer is affecting the bones,” added Rafael Fonseca, MD, of the Mayo Clinic in Scottsdale, Arizona. “If we could detect it earlier by an analysis of urine or blood in high-risk patients, it could significantly improve their care.”
To explore this possibility, Drs Fonseca, Anbar, and their colleagues performed calcium isotope analysis using blood samples from MM patients. The team recounted their results in a letter to Leukemia.
As the name suggests, calcium isotope analysis measures calcium isotopes that are naturally present in blood. The technique makes use of a fact well known to Earth scientists but not normally used in biomedicine: different isotopes of a chemical element can react at slightly different rates.
An earlier study testing this technique in healthy subjects showed that when bones form, the lighter isotopes of calcium enter bone a little faster than the heavier isotopes. That difference, called isotope fractionation, is the key to the method.
In healthy, active humans, bone is forming at about the same rate as it resorbs. But if bone loss is occurring, the isotopic composition of blood becomes enriched in the lighter isotopes as bones resorb more quickly than they are formed.
The effect on calcium isotopes is very small, typically less than a 0.02% change in the isotope ratio. But even effects that small can be measured using precise mass spectrometry methods.
Using these methods, the researchers tested peripheral blood samples from 71 adult patients—55 with MM, 9 with smoldering MM, and 7 with monoclonal gammopathy of undetermined significance.
The researchers found an association between how active a patient’s disease was and the change in the isotope ratios. In fact, the isotope ratios predicted disease activity better than, and independent from, standard clinical variables.
Blood samples from patients with active disease had significantly lower mean calcium isotope compositions than samples from patients with non-active disease (mean δ44/42Ca=-0.8 vs -0.67, P=0.025), regardless of diagnosis.
For MM patients specifically, those with active disease had a significantly lower mean δ44/42Ca than patients with non-active disease (-0.79 vs -0.63, P=0.016), which was consistent with resorption of bone containing lighter 42Ca.
Dr Anbar noted that, although calcium isotope analysis has worked in this small set of patients, additional research is needed to verify these initial findings and improve the efficiency of analysis.
“If the method proves to be robust after more careful validation, it could provide earlier detection of bone involvement than presently possible,” he said, “and also provide the possibility to monitor the effectiveness of drugs to combat bone loss.” ![]()
Cancer survivors aren’t living healthy, study shows

Credit: Bill Branson
Childhood cancer survivors are no more likely than their cancer-free peers to adhere to healthy living guidelines, according to a study published in the Journal of Cancer Survivorship.
Survivors were less likely to be smokers and had a lower average body mass index (BMI).
But there were no significant differences between survivors and cancer-free control subjects with regard to overall diet, physical activity, or alcohol consumption.
Chloe Berdan, of Promedica in Toledo, Ohio, and her colleagues uncovered these results by examining data from the Chicago Healthy Living Study.
The team assessed adherence to American Cancer Society Guidelines on Nutrition and Physical Activity via interviews with 431 childhood cancer survivors and 361 control subjects who never had cancer. The survivors, ages 18 to 59, were all diagnosed with a malignant cancer before their 21st birthdays.
There were no significant differences in sex or race between survivors and controls. Survivors were younger than controls (28.4±7.8 vs 29.6± 8.3 years, P=0.04) and had less education (14.0±2.0 vs 14.4±2.0 years, P=0.01).
Overall, there was no significant difference between survivors and control subjects in adhering to the American Cancer Society guidelines.
Survivors and controls also had similar scores for several individual measures, including alcohol consumption, overall physical activity, overall diet, the servings of fruits/vegetables consumed, and the consumption of red/processed meat.
However, survivors were significantly less likely than controls to be smokers—11.4% vs 17.5% (P=0.02). Survivors had, on average, a BMI of about 1.2 kg/m² lower than controls (P=0.01). And survivors consumed significantly less fiber than controls—9.2±3.5 vs 9.7±3.8 kcal (P=0.05).
Only about 1 in 10 survivors (10.2%) met fiber recommendations, 17.7% ate 5 fruits or vegetables per day, and 46.2% met the red/processed meat recommendation of less than 18 oz per week. On average, survivors scored under 50% for the quality of their diets.
Survivors were better at meeting the goal of at least 5 hours of moderate activity per week (60.5%) than to sticking to any of the other guidelines.
About 36% of survivors were within a healthy BMI range, 2.9% were underweight, 28.9% were overweight, and 32.4% were obese.
The 0.7% of survivors who adhered fully to the guidelines tended to be women, non-smokers, and people with a good view of their own health.
“There is still much room for improvement in educating and encouraging survivors to follow healthier diets and lifestyles,” Berdan said. “Adopting such behavior during early adulthood may have a lasting impact on their quality of life and overall survival.” ![]()
Credit: Bill Branson
Childhood cancer survivors are no more likely than their cancer-free peers to adhere to healthy living guidelines, according to a study published in the Journal of Cancer Survivorship.
Survivors were less likely to be smokers and had a lower average body mass index (BMI).
But there were no significant differences between survivors and cancer-free control subjects with regard to overall diet, physical activity, or alcohol consumption.
Chloe Berdan, of Promedica in Toledo, Ohio, and her colleagues uncovered these results by examining data from the Chicago Healthy Living Study.
The team assessed adherence to American Cancer Society Guidelines on Nutrition and Physical Activity via interviews with 431 childhood cancer survivors and 361 control subjects who never had cancer. The survivors, ages 18 to 59, were all diagnosed with a malignant cancer before their 21st birthdays.
There were no significant differences in sex or race between survivors and controls. Survivors were younger than controls (28.4±7.8 vs 29.6± 8.3 years, P=0.04) and had less education (14.0±2.0 vs 14.4±2.0 years, P=0.01).
Overall, there was no significant difference between survivors and control subjects in adhering to the American Cancer Society guidelines.
Survivors and controls also had similar scores for several individual measures, including alcohol consumption, overall physical activity, overall diet, the servings of fruits/vegetables consumed, and the consumption of red/processed meat.
However, survivors were significantly less likely than controls to be smokers—11.4% vs 17.5% (P=0.02). Survivors had, on average, a BMI of about 1.2 kg/m² lower than controls (P=0.01). And survivors consumed significantly less fiber than controls—9.2±3.5 vs 9.7±3.8 kcal (P=0.05).
Only about 1 in 10 survivors (10.2%) met fiber recommendations, 17.7% ate 5 fruits or vegetables per day, and 46.2% met the red/processed meat recommendation of less than 18 oz per week. On average, survivors scored under 50% for the quality of their diets.
Survivors were better at meeting the goal of at least 5 hours of moderate activity per week (60.5%) than to sticking to any of the other guidelines.
About 36% of survivors were within a healthy BMI range, 2.9% were underweight, 28.9% were overweight, and 32.4% were obese.
The 0.7% of survivors who adhered fully to the guidelines tended to be women, non-smokers, and people with a good view of their own health.
“There is still much room for improvement in educating and encouraging survivors to follow healthier diets and lifestyles,” Berdan said. “Adopting such behavior during early adulthood may have a lasting impact on their quality of life and overall survival.” ![]()
Credit: Bill Branson
Childhood cancer survivors are no more likely than their cancer-free peers to adhere to healthy living guidelines, according to a study published in the Journal of Cancer Survivorship.
Survivors were less likely to be smokers and had a lower average body mass index (BMI).
But there were no significant differences between survivors and cancer-free control subjects with regard to overall diet, physical activity, or alcohol consumption.
Chloe Berdan, of Promedica in Toledo, Ohio, and her colleagues uncovered these results by examining data from the Chicago Healthy Living Study.
The team assessed adherence to American Cancer Society Guidelines on Nutrition and Physical Activity via interviews with 431 childhood cancer survivors and 361 control subjects who never had cancer. The survivors, ages 18 to 59, were all diagnosed with a malignant cancer before their 21st birthdays.
There were no significant differences in sex or race between survivors and controls. Survivors were younger than controls (28.4±7.8 vs 29.6± 8.3 years, P=0.04) and had less education (14.0±2.0 vs 14.4±2.0 years, P=0.01).
Overall, there was no significant difference between survivors and control subjects in adhering to the American Cancer Society guidelines.
Survivors and controls also had similar scores for several individual measures, including alcohol consumption, overall physical activity, overall diet, the servings of fruits/vegetables consumed, and the consumption of red/processed meat.
However, survivors were significantly less likely than controls to be smokers—11.4% vs 17.5% (P=0.02). Survivors had, on average, a BMI of about 1.2 kg/m² lower than controls (P=0.01). And survivors consumed significantly less fiber than controls—9.2±3.5 vs 9.7±3.8 kcal (P=0.05).
Only about 1 in 10 survivors (10.2%) met fiber recommendations, 17.7% ate 5 fruits or vegetables per day, and 46.2% met the red/processed meat recommendation of less than 18 oz per week. On average, survivors scored under 50% for the quality of their diets.
Survivors were better at meeting the goal of at least 5 hours of moderate activity per week (60.5%) than to sticking to any of the other guidelines.
About 36% of survivors were within a healthy BMI range, 2.9% were underweight, 28.9% were overweight, and 32.4% were obese.
The 0.7% of survivors who adhered fully to the guidelines tended to be women, non-smokers, and people with a good view of their own health.
“There is still much room for improvement in educating and encouraging survivors to follow healthier diets and lifestyles,” Berdan said. “Adopting such behavior during early adulthood may have a lasting impact on their quality of life and overall survival.” ![]()
A quicker way to manipulate malaria genes

(left) and Jeffrey Wagner
Credit: Bryce Vickmark
The gene-editing technique CRISPR can disrupt a single gene from the malaria parasite Plasmodium falciparum in a matter of weeks, a new study suggests.
Although CRISPR’s success rate ranged from 50% to 100%, the researchers believe the technique shows promise and could greatly speed up gene analysis.
At present, it can take up to a year to determine the function of a single gene in P falciparum, which can hinder efforts to develop drugs and vaccines.
“Even though we’ve sequenced the entire genome of Plasmodium falciparum, half of it still remains functionally uncharacterized,” said Jacquin Niles, MD, PhD, of the Massachusetts Institute of Technology in Cambridge.
“That’s about 2500 genes that, if only we knew what they did, we could think about novel therapeutics, whether it’s drugs or vaccines.”
Dr Niles and his colleagues described their use of CRISPR in P falciparum in Nature Methods.
The team noted that, in P falciparum, gene editing can take up to a year because it relies on homologous recombination, a type of genetic swapping that cells use to repair broken DNA strands and that occurs very rarely in the genome of the malaria parasite.
“You have to rely on this really inefficient process that occurs only if you have spontaneous DNA strand breaks that happen to fall within your region of interest,” Dr Niles said.
More recently, researchers have successfully used zinc finger nucleases to cut out specific genes, but this approach is costly because it requires a new nuclease to be designed for each gene target.
CRISPR exploits a set of bacterial proteins that protect microbes from viral infection. The system includes a DNA-cutting enzyme, Cas9, bound to a short RNA guide strand that is programmed to bind to a specific genome sequence, telling Cas9 where to make its cut. This approach allows scientists to target and delete any gene by simply changing the RNA guide strand sequence.
As soon as researchers proved this system could work in cells other than bacteria, Dr Niles started to think about using it to manipulate P falciparum.
To test this approach, he and his colleagues tried using CRISPR to disrupt 2 genes, kahrp and eba-175, that had previously been knocked out in malaria using traditional approaches.
The kahrp gene produces a protein that causes red blood cells to develop a knobby appearance when infected with malaria. Dr Niles’s team was able to disrupt this gene in 100% of parasites treated with the CRISPR system. The red blood cells infected by parasites remained smooth.
The other gene, eba-175, codes for a protein that binds to red blood cell receptors and helps the malaria parasite enter cells. The researchers were only able to disrupt this gene in 50% to 80% of parasites manipulated with CRISPR.
“We consider this to be a win,” Dr Niles said. “Compared to the efficiency with which P falciparum genetics have been done in the past, even 50% is pretty substantial.”
Now that CRISPR technology has been validated in P falciparum, Dr Niles expects many scientists will adopt it for genetic studies of the parasite. Such efforts could reveal more about how the parasite invades red blood cells and replicates inside cells, which could generate new drug and vaccine targets.
“I think the impact could be quite huge,” he said. “It lowers the barrier to really being more imaginative in terms of how we do experiments and the kinds of questions that we can ask.” ![]()
(left) and Jeffrey Wagner
Credit: Bryce Vickmark
The gene-editing technique CRISPR can disrupt a single gene from the malaria parasite Plasmodium falciparum in a matter of weeks, a new study suggests.
Although CRISPR’s success rate ranged from 50% to 100%, the researchers believe the technique shows promise and could greatly speed up gene analysis.
At present, it can take up to a year to determine the function of a single gene in P falciparum, which can hinder efforts to develop drugs and vaccines.
“Even though we’ve sequenced the entire genome of Plasmodium falciparum, half of it still remains functionally uncharacterized,” said Jacquin Niles, MD, PhD, of the Massachusetts Institute of Technology in Cambridge.
“That’s about 2500 genes that, if only we knew what they did, we could think about novel therapeutics, whether it’s drugs or vaccines.”
Dr Niles and his colleagues described their use of CRISPR in P falciparum in Nature Methods.
The team noted that, in P falciparum, gene editing can take up to a year because it relies on homologous recombination, a type of genetic swapping that cells use to repair broken DNA strands and that occurs very rarely in the genome of the malaria parasite.
“You have to rely on this really inefficient process that occurs only if you have spontaneous DNA strand breaks that happen to fall within your region of interest,” Dr Niles said.
More recently, researchers have successfully used zinc finger nucleases to cut out specific genes, but this approach is costly because it requires a new nuclease to be designed for each gene target.
CRISPR exploits a set of bacterial proteins that protect microbes from viral infection. The system includes a DNA-cutting enzyme, Cas9, bound to a short RNA guide strand that is programmed to bind to a specific genome sequence, telling Cas9 where to make its cut. This approach allows scientists to target and delete any gene by simply changing the RNA guide strand sequence.
As soon as researchers proved this system could work in cells other than bacteria, Dr Niles started to think about using it to manipulate P falciparum.
To test this approach, he and his colleagues tried using CRISPR to disrupt 2 genes, kahrp and eba-175, that had previously been knocked out in malaria using traditional approaches.
The kahrp gene produces a protein that causes red blood cells to develop a knobby appearance when infected with malaria. Dr Niles’s team was able to disrupt this gene in 100% of parasites treated with the CRISPR system. The red blood cells infected by parasites remained smooth.
The other gene, eba-175, codes for a protein that binds to red blood cell receptors and helps the malaria parasite enter cells. The researchers were only able to disrupt this gene in 50% to 80% of parasites manipulated with CRISPR.
“We consider this to be a win,” Dr Niles said. “Compared to the efficiency with which P falciparum genetics have been done in the past, even 50% is pretty substantial.”
Now that CRISPR technology has been validated in P falciparum, Dr Niles expects many scientists will adopt it for genetic studies of the parasite. Such efforts could reveal more about how the parasite invades red blood cells and replicates inside cells, which could generate new drug and vaccine targets.
“I think the impact could be quite huge,” he said. “It lowers the barrier to really being more imaginative in terms of how we do experiments and the kinds of questions that we can ask.” ![]()
(left) and Jeffrey Wagner
Credit: Bryce Vickmark
The gene-editing technique CRISPR can disrupt a single gene from the malaria parasite Plasmodium falciparum in a matter of weeks, a new study suggests.
Although CRISPR’s success rate ranged from 50% to 100%, the researchers believe the technique shows promise and could greatly speed up gene analysis.
At present, it can take up to a year to determine the function of a single gene in P falciparum, which can hinder efforts to develop drugs and vaccines.
“Even though we’ve sequenced the entire genome of Plasmodium falciparum, half of it still remains functionally uncharacterized,” said Jacquin Niles, MD, PhD, of the Massachusetts Institute of Technology in Cambridge.
“That’s about 2500 genes that, if only we knew what they did, we could think about novel therapeutics, whether it’s drugs or vaccines.”
Dr Niles and his colleagues described their use of CRISPR in P falciparum in Nature Methods.
The team noted that, in P falciparum, gene editing can take up to a year because it relies on homologous recombination, a type of genetic swapping that cells use to repair broken DNA strands and that occurs very rarely in the genome of the malaria parasite.
“You have to rely on this really inefficient process that occurs only if you have spontaneous DNA strand breaks that happen to fall within your region of interest,” Dr Niles said.
More recently, researchers have successfully used zinc finger nucleases to cut out specific genes, but this approach is costly because it requires a new nuclease to be designed for each gene target.
CRISPR exploits a set of bacterial proteins that protect microbes from viral infection. The system includes a DNA-cutting enzyme, Cas9, bound to a short RNA guide strand that is programmed to bind to a specific genome sequence, telling Cas9 where to make its cut. This approach allows scientists to target and delete any gene by simply changing the RNA guide strand sequence.
As soon as researchers proved this system could work in cells other than bacteria, Dr Niles started to think about using it to manipulate P falciparum.
To test this approach, he and his colleagues tried using CRISPR to disrupt 2 genes, kahrp and eba-175, that had previously been knocked out in malaria using traditional approaches.
The kahrp gene produces a protein that causes red blood cells to develop a knobby appearance when infected with malaria. Dr Niles’s team was able to disrupt this gene in 100% of parasites treated with the CRISPR system. The red blood cells infected by parasites remained smooth.
The other gene, eba-175, codes for a protein that binds to red blood cell receptors and helps the malaria parasite enter cells. The researchers were only able to disrupt this gene in 50% to 80% of parasites manipulated with CRISPR.
“We consider this to be a win,” Dr Niles said. “Compared to the efficiency with which P falciparum genetics have been done in the past, even 50% is pretty substantial.”
Now that CRISPR technology has been validated in P falciparum, Dr Niles expects many scientists will adopt it for genetic studies of the parasite. Such efforts could reveal more about how the parasite invades red blood cells and replicates inside cells, which could generate new drug and vaccine targets.
“I think the impact could be quite huge,” he said. “It lowers the barrier to really being more imaginative in terms of how we do experiments and the kinds of questions that we can ask.” ![]()
Hospitalists' Use of PPIs
Proton pump inhibitors (PPIs) are commonly used to treat acid‐related disorders but are associated with an increased risk of pneumonia and Clostridium difficile‐associated diarrhea.[1, 2] Initiation of PPIs in hospitalized patients should therefore be limited to specific clinical situations, such as upper gastrointestinal bleeding or stress ulcer prophylaxis in the critically ill.[3] Prior studies suggest significant overuse of PPIs in hospitalized patients exists,[4, 5, 6, 7] but these were published before the widespread implementation of local and national quality improvement efforts targeted at reducing PPI use in medical inpatients (eg, Society of Hospital Medicine's Choosing Wisely list[8]). We aimed to determine the frequency of inappropriate use of PPIs in a contemporary cohort of hospitalized patients in a tertiary care academic medical center.
METHODS
We conducted a retrospective cohort study of 297 patients admitted to a tertiary care center hospitalist service comprised of teaching and nonteaching medical patients who were not critically ill, were admitted between January 1, 2012 and March 31, 2012, and received a PPI during their hospital stay. Three internists used American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy and prior studies to develop criteria to identify appropriate and inappropriate PPI use (Table 1).[4, 5, 6, 7] Appropriate indications included gastrointestinal (GI) bleeding, esophagitis, gastritis, gastroesophageal reflux (GERD), and continuation of home PPI (abrupt discontinuation can trigger reflux symptoms).[9] We extracted the medical records of included patients, applying our prespecified criteria to determine whether use was appropriate. In patients in whom PPI was a continued home medication, we also extracted 2 years of data prior to the index date to determine if the medication was started during a prior hospital admission and, if so, whether this initiation was appropriate. We used descriptive statistics and [2] tests to compare patient characteristics and indications for PPI use.
| Appropriate PPI use | Inappropriate PPI use |
|---|---|
| |
| History of upper GI bleeding | No reason given |
| Endoscopic evidence of peptic ulcer disease | Unspecified GI prophylaxis |
| Esophagitis | Nonspecific abdominal pain |
| Gastritis and duodenitis | Heartburn (nonchronic) |
| Eradication of H pylori | Acute pancreatitis |
| GERD | Anemia |
| Barrett's esophagus | Heparin use for DVT prophylaxis |
| Continued on home PPI | Use of aspirin, NSAID, steroids or Coumadin (as a single agent) |
| Acute esophageal variceal bleeding | |
| NSAID used in patient >65 years‐old | |
| High‐risk groups; combination of 2 or more of aspirin, NSAID, clopidogrel, or Coumadin | |
RESULTS
Of 297 patients, the mean age was 64.4 years (standard deviation 16.3 years), most were white (69%), and 56% were women (Table 2). PPI use was appropriate in 231 (78%, 95% confidence interval: 72.6%‐82.4%) patients. Of these, a majority (172, 75%) of patients received a PPI because it was a continued home medication. Only 40 of the 172 patients had the medication started during a recent hospitalization, and in half of those cases (20) the PPI use was appropriate.
| Demographics | PPI Not Indicated, N=66 | PPI Indicated, N=231 | Total=297 | |||
|---|---|---|---|---|---|---|
| ||||||
| Age, y, mean (SD) | 62.5 | (16.2) | 64.9 | (16.3) | 64.4 | (16.3) |
| Sex, % No. | ||||||
| Female | 51.5% | 34 | 56.7% | 131 | 55.6% | 165 |
| Male | 48.5% | 32 | 43.3% | 100 | 44.4% | 132 |
| Race, % No. | ||||||
| Asian | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Black | 10.6% | 7 | 9.1% | 21 | 9.4% | 28 |
| Hispanic | 18.2% | 12 | 19.5% | 45 | 19.2% | 57 |
| Unknown | 0.0% | 0 | 2.2% | 5 | 1.7% | 5 |
| White | 71.2% | 47 | 68.4% | 158 | 69.0% | 205 |
| Insurance, % No. | ||||||
| Insured | 95.5% | 63 | 87.4% | 202 | 89.2% | 265 |
| Uninsured | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Unknown | 4.5% | 3 | 11.7% | 27 | 10.1% | 30 |
| Service, % No. | ||||||
| Teaching | 25.8% | 17 | 32.9% | 76 | 31.3% | 93 |
| Nonteaching | 74.2% | 49 | 66.7% | 154 | 68.4% | 203 |
| Unknown | 0.0% | 0 | 0.4% | 1 | 0.3% | 1 |
| Chronic disease, % No. | ||||||
| Cardiac disease | 16.7% | 11 | 13.4% | 31 | 14.1% | 42 |
| Pulmonary disease | 16.7% | 11 | 14.7% | 34 | 15.2% | 45 |
| Gastrointestinal disease | 13.6% | 9 | 19.5% | 45 | 18.2% | 54 |
| Hepatic disease | 7.6% | 5 | 3.9% | 9 | 4.7% | 14 |
| Stroke | 1.5% | 1 | 5.2% | 12 | 4.4% | 13 |
| Sepsis | 12.1% | 8 | 13.0% | 30 | 12.8% | 38 |
| Other | 33.3% | 22 | 29.4% | 68 | 30.3% | 90 |
| PPI status, % No. | ||||||
| Continued home PPI | 0.0% | 0 | 74.5% | 172 | 58.1% | 172 |
| Started on PPI in hospital | 100% | 65 | 25.5% | 59 | 41.9% | 124 |
| Discharged on AST, % No. | ||||||
| Yes | 36.4% | 24 | 89.6% | 207 | 22.2% | 231 |
| PPI | 87.5% | 21 | 96.6% | 200 | 95.7% | 221 |
| Brand | 52.4% | 11 | 59.5% | 119 | 58.8% | 130 |
| Generic | 47.6% | 10 | 40.5% | 81 | 41.2% | 91 |
| H2 blocker | 12.5% | 3 | 3.4% | 7 | 4.3% | 10 |
| Brand | 0.0% | 0 | 71.4% | 5 | 50.0% | 5 |
| Generic | 100.0% | 3 | 28.6% | 2 | 50.0% | 5 |
| Medications, % No. | ||||||
| Aspirin | 36.4% | 24 | 43.7% | 101 | 42.1% | 125 |
| NSAID | 10.6% | 4 | 6.5% | 15 | 6.4% | 19 |
| Corticosteroids | 13.6% | 9 | 16.9% | 39 | 16.2% | 48 |
| Warfarin | 0.0% | 5 | 19.0% | 44 | 16.5% | 49 |
| Clopidogrel | 12.1% | 8 | 10.8% | 25 | 11.1% | 33 |
The second most common appropriate diagnosis was GERD (31%), followed by history of GI bleeding (19%) and treatment for esophagitis or gastritis (18%). Among the 66 patients receiving a PPI inappropriately, the majority of patients (56%) had no documented reason for PPI use, and only 11 patients (17%) were receiving PPI for stress ulcer prophylaxis (Figure 1). Five patients (8%) were treated prophylactically because of steroid or anticoagulant use. We observed no differences in age, gender, race, or reason for admission between the patients treated appropriately versus inappropriately.

DISCUSSION
In a contemporary cohort, chronic PPI use prior to admission was the most common reason PPIs were prescribed in the hospital. About 20% of hospitalized patients were started on a PPI for an inappropriate indication, the majority of whom lacked documentation concerning the reason for use. Among patients treated inappropriately, 36% were discharged on acid‐suppressive therapy.
The prior literature has reported a much higher percentages of unnecessary PPI use in hospitalized patients.[4, 5, 6, 7] Gupta et al. found that 70% of patients admitted to an internal medicine service received acid‐suppressive therapy, 73% of whom were treated unnecessarily.[5] Similarly, Nardino et al. found that 65% of acid‐suppressive therapy in hospitalized medical patients was not indicated.[4] If we had excluded patients on home PPIs from our study cohort, we would have found a higher rate of inappropriate use due to a smaller overall patient population. However, we chose to include these patients because they represented the vast majority of hospitalist‐prescribed PPIs. Notably, most of these prior prescriptions were not written during a recent hospital stay, indicating that the majority were initiated by outpatient physicians.
Our study is limited by its small sample size, single‐center design, and inability to determine the indications for outpatient PPI use. Still, it has important implications. Prior work has suggested that focusing efforts on PPI overuse may be premature in the absence of valid risk‐prediction models defining the patient populations that most benefit from PPI therapy.[10] Our work additionally suggests that hospital rates of inappropriate initiation may be relatively low, perhaps because hospitalist culture and practice have been affected by both local and national quality improvement efforts and by evidence dissemination.[8] Quality improvement efforts focused on reducing inpatient PPI use are likely to reveal diminishing returns, as admitting hospitalists are unlikely to abruptly discontinue PPIs prescribed in the outpatient setting.[9] Hospitalists should be encouraged to assess and document the need for PPIs during admission, hospitalization, and discharge processes. However, future efforts to reduce PPI overuse among hospitalized patients should predominately be focused on reducing inappropriate chronic PPI use in the outpatient setting.
Acknowledgements
The authors acknowledge Peter Lindenauer for his comments on an earlier draft of this manuscript.
Disclosures: The study was conducted with funding from the Department of Medicine at Baystate Medical Center. Dr. Lagu is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K01HL114745. Drs. Lagu and Albugeaey had full access to all of the data in the study, and they take responsibility for the integrity of the data and the accuracy of the data analysis. Drs. Lagu, Albugeaey, and Seiler conceived of the study. Drs. Albugeaey and Al Faraj acquired the data. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb analyzed and interpreted the data. Drs. Albugeaey and Lagu drafted the manuscript. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb critically reviewed the manuscript for important intellectual content. Dr. Albugeaey is a recipient of a scholarship from the Ministry of Higher Education, Kingdom of Saudi Arabia. The authors report no conflicts of interest.
- , , , , . Acid‐suppressive medication use and the risk for nosocomial gastrointestinal tract bleeding. Arch Intern Med. 2011;171(11):991–997.
- , , , . Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia. JAMA. 2009;301(20):2120–2128.
- , . Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107(3):345–360; quiz 361.
- , , . Overuse of acid‐suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95(11):3118–3122.
- , , , et al. Overuse of acid suppression therapy in hospitalized patients. South Med J. 2010;103(3):207–211.
- , , , , , . Inappropriate prescribing of proton pump inhibitors in hospitalized patients. J Hosp Med. 2012;7(5):421–425.
- , , , . Inappropriate utilization of intravenous proton pump inhibitors in hospital practice—a prospective study of the extent of the problem and predictive factors. QJM. 2010;103(5):327–335.
- Choosing Wisely, Society of Hospital Medicine, Adult Hospital Medicine. Available at:http://www.choosingwisely.org/doctor‐patient‐lists/society‐of‐hospital‐medicine‐adult‐hospital‐medicine. Accessed April 11, 2014.
- , , , . Safety of the long‐term use of proton pump inhibitors. World J Gastroenterol. 2010;16(19):2323–2330.
- , . Prophylaxis rates for venous thromboembolism and gastrointestinal bleeding in general medical patients: too low or too high? BMJ. 2012;344:e3248.
Proton pump inhibitors (PPIs) are commonly used to treat acid‐related disorders but are associated with an increased risk of pneumonia and Clostridium difficile‐associated diarrhea.[1, 2] Initiation of PPIs in hospitalized patients should therefore be limited to specific clinical situations, such as upper gastrointestinal bleeding or stress ulcer prophylaxis in the critically ill.[3] Prior studies suggest significant overuse of PPIs in hospitalized patients exists,[4, 5, 6, 7] but these were published before the widespread implementation of local and national quality improvement efforts targeted at reducing PPI use in medical inpatients (eg, Society of Hospital Medicine's Choosing Wisely list[8]). We aimed to determine the frequency of inappropriate use of PPIs in a contemporary cohort of hospitalized patients in a tertiary care academic medical center.
METHODS
We conducted a retrospective cohort study of 297 patients admitted to a tertiary care center hospitalist service comprised of teaching and nonteaching medical patients who were not critically ill, were admitted between January 1, 2012 and March 31, 2012, and received a PPI during their hospital stay. Three internists used American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy and prior studies to develop criteria to identify appropriate and inappropriate PPI use (Table 1).[4, 5, 6, 7] Appropriate indications included gastrointestinal (GI) bleeding, esophagitis, gastritis, gastroesophageal reflux (GERD), and continuation of home PPI (abrupt discontinuation can trigger reflux symptoms).[9] We extracted the medical records of included patients, applying our prespecified criteria to determine whether use was appropriate. In patients in whom PPI was a continued home medication, we also extracted 2 years of data prior to the index date to determine if the medication was started during a prior hospital admission and, if so, whether this initiation was appropriate. We used descriptive statistics and [2] tests to compare patient characteristics and indications for PPI use.
| Appropriate PPI use | Inappropriate PPI use |
|---|---|
| |
| History of upper GI bleeding | No reason given |
| Endoscopic evidence of peptic ulcer disease | Unspecified GI prophylaxis |
| Esophagitis | Nonspecific abdominal pain |
| Gastritis and duodenitis | Heartburn (nonchronic) |
| Eradication of H pylori | Acute pancreatitis |
| GERD | Anemia |
| Barrett's esophagus | Heparin use for DVT prophylaxis |
| Continued on home PPI | Use of aspirin, NSAID, steroids or Coumadin (as a single agent) |
| Acute esophageal variceal bleeding | |
| NSAID used in patient >65 years‐old | |
| High‐risk groups; combination of 2 or more of aspirin, NSAID, clopidogrel, or Coumadin | |
RESULTS
Of 297 patients, the mean age was 64.4 years (standard deviation 16.3 years), most were white (69%), and 56% were women (Table 2). PPI use was appropriate in 231 (78%, 95% confidence interval: 72.6%‐82.4%) patients. Of these, a majority (172, 75%) of patients received a PPI because it was a continued home medication. Only 40 of the 172 patients had the medication started during a recent hospitalization, and in half of those cases (20) the PPI use was appropriate.
| Demographics | PPI Not Indicated, N=66 | PPI Indicated, N=231 | Total=297 | |||
|---|---|---|---|---|---|---|
| ||||||
| Age, y, mean (SD) | 62.5 | (16.2) | 64.9 | (16.3) | 64.4 | (16.3) |
| Sex, % No. | ||||||
| Female | 51.5% | 34 | 56.7% | 131 | 55.6% | 165 |
| Male | 48.5% | 32 | 43.3% | 100 | 44.4% | 132 |
| Race, % No. | ||||||
| Asian | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Black | 10.6% | 7 | 9.1% | 21 | 9.4% | 28 |
| Hispanic | 18.2% | 12 | 19.5% | 45 | 19.2% | 57 |
| Unknown | 0.0% | 0 | 2.2% | 5 | 1.7% | 5 |
| White | 71.2% | 47 | 68.4% | 158 | 69.0% | 205 |
| Insurance, % No. | ||||||
| Insured | 95.5% | 63 | 87.4% | 202 | 89.2% | 265 |
| Uninsured | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Unknown | 4.5% | 3 | 11.7% | 27 | 10.1% | 30 |
| Service, % No. | ||||||
| Teaching | 25.8% | 17 | 32.9% | 76 | 31.3% | 93 |
| Nonteaching | 74.2% | 49 | 66.7% | 154 | 68.4% | 203 |
| Unknown | 0.0% | 0 | 0.4% | 1 | 0.3% | 1 |
| Chronic disease, % No. | ||||||
| Cardiac disease | 16.7% | 11 | 13.4% | 31 | 14.1% | 42 |
| Pulmonary disease | 16.7% | 11 | 14.7% | 34 | 15.2% | 45 |
| Gastrointestinal disease | 13.6% | 9 | 19.5% | 45 | 18.2% | 54 |
| Hepatic disease | 7.6% | 5 | 3.9% | 9 | 4.7% | 14 |
| Stroke | 1.5% | 1 | 5.2% | 12 | 4.4% | 13 |
| Sepsis | 12.1% | 8 | 13.0% | 30 | 12.8% | 38 |
| Other | 33.3% | 22 | 29.4% | 68 | 30.3% | 90 |
| PPI status, % No. | ||||||
| Continued home PPI | 0.0% | 0 | 74.5% | 172 | 58.1% | 172 |
| Started on PPI in hospital | 100% | 65 | 25.5% | 59 | 41.9% | 124 |
| Discharged on AST, % No. | ||||||
| Yes | 36.4% | 24 | 89.6% | 207 | 22.2% | 231 |
| PPI | 87.5% | 21 | 96.6% | 200 | 95.7% | 221 |
| Brand | 52.4% | 11 | 59.5% | 119 | 58.8% | 130 |
| Generic | 47.6% | 10 | 40.5% | 81 | 41.2% | 91 |
| H2 blocker | 12.5% | 3 | 3.4% | 7 | 4.3% | 10 |
| Brand | 0.0% | 0 | 71.4% | 5 | 50.0% | 5 |
| Generic | 100.0% | 3 | 28.6% | 2 | 50.0% | 5 |
| Medications, % No. | ||||||
| Aspirin | 36.4% | 24 | 43.7% | 101 | 42.1% | 125 |
| NSAID | 10.6% | 4 | 6.5% | 15 | 6.4% | 19 |
| Corticosteroids | 13.6% | 9 | 16.9% | 39 | 16.2% | 48 |
| Warfarin | 0.0% | 5 | 19.0% | 44 | 16.5% | 49 |
| Clopidogrel | 12.1% | 8 | 10.8% | 25 | 11.1% | 33 |
The second most common appropriate diagnosis was GERD (31%), followed by history of GI bleeding (19%) and treatment for esophagitis or gastritis (18%). Among the 66 patients receiving a PPI inappropriately, the majority of patients (56%) had no documented reason for PPI use, and only 11 patients (17%) were receiving PPI for stress ulcer prophylaxis (Figure 1). Five patients (8%) were treated prophylactically because of steroid or anticoagulant use. We observed no differences in age, gender, race, or reason for admission between the patients treated appropriately versus inappropriately.
DISCUSSION
In a contemporary cohort, chronic PPI use prior to admission was the most common reason PPIs were prescribed in the hospital. About 20% of hospitalized patients were started on a PPI for an inappropriate indication, the majority of whom lacked documentation concerning the reason for use. Among patients treated inappropriately, 36% were discharged on acid‐suppressive therapy.
The prior literature has reported a much higher percentages of unnecessary PPI use in hospitalized patients.[4, 5, 6, 7] Gupta et al. found that 70% of patients admitted to an internal medicine service received acid‐suppressive therapy, 73% of whom were treated unnecessarily.[5] Similarly, Nardino et al. found that 65% of acid‐suppressive therapy in hospitalized medical patients was not indicated.[4] If we had excluded patients on home PPIs from our study cohort, we would have found a higher rate of inappropriate use due to a smaller overall patient population. However, we chose to include these patients because they represented the vast majority of hospitalist‐prescribed PPIs. Notably, most of these prior prescriptions were not written during a recent hospital stay, indicating that the majority were initiated by outpatient physicians.
Our study is limited by its small sample size, single‐center design, and inability to determine the indications for outpatient PPI use. Still, it has important implications. Prior work has suggested that focusing efforts on PPI overuse may be premature in the absence of valid risk‐prediction models defining the patient populations that most benefit from PPI therapy.[10] Our work additionally suggests that hospital rates of inappropriate initiation may be relatively low, perhaps because hospitalist culture and practice have been affected by both local and national quality improvement efforts and by evidence dissemination.[8] Quality improvement efforts focused on reducing inpatient PPI use are likely to reveal diminishing returns, as admitting hospitalists are unlikely to abruptly discontinue PPIs prescribed in the outpatient setting.[9] Hospitalists should be encouraged to assess and document the need for PPIs during admission, hospitalization, and discharge processes. However, future efforts to reduce PPI overuse among hospitalized patients should predominately be focused on reducing inappropriate chronic PPI use in the outpatient setting.
Acknowledgements
The authors acknowledge Peter Lindenauer for his comments on an earlier draft of this manuscript.
Disclosures: The study was conducted with funding from the Department of Medicine at Baystate Medical Center. Dr. Lagu is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K01HL114745. Drs. Lagu and Albugeaey had full access to all of the data in the study, and they take responsibility for the integrity of the data and the accuracy of the data analysis. Drs. Lagu, Albugeaey, and Seiler conceived of the study. Drs. Albugeaey and Al Faraj acquired the data. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb analyzed and interpreted the data. Drs. Albugeaey and Lagu drafted the manuscript. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb critically reviewed the manuscript for important intellectual content. Dr. Albugeaey is a recipient of a scholarship from the Ministry of Higher Education, Kingdom of Saudi Arabia. The authors report no conflicts of interest.
Proton pump inhibitors (PPIs) are commonly used to treat acid‐related disorders but are associated with an increased risk of pneumonia and Clostridium difficile‐associated diarrhea.[1, 2] Initiation of PPIs in hospitalized patients should therefore be limited to specific clinical situations, such as upper gastrointestinal bleeding or stress ulcer prophylaxis in the critically ill.[3] Prior studies suggest significant overuse of PPIs in hospitalized patients exists,[4, 5, 6, 7] but these were published before the widespread implementation of local and national quality improvement efforts targeted at reducing PPI use in medical inpatients (eg, Society of Hospital Medicine's Choosing Wisely list[8]). We aimed to determine the frequency of inappropriate use of PPIs in a contemporary cohort of hospitalized patients in a tertiary care academic medical center.
METHODS
We conducted a retrospective cohort study of 297 patients admitted to a tertiary care center hospitalist service comprised of teaching and nonteaching medical patients who were not critically ill, were admitted between January 1, 2012 and March 31, 2012, and received a PPI during their hospital stay. Three internists used American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy and prior studies to develop criteria to identify appropriate and inappropriate PPI use (Table 1).[4, 5, 6, 7] Appropriate indications included gastrointestinal (GI) bleeding, esophagitis, gastritis, gastroesophageal reflux (GERD), and continuation of home PPI (abrupt discontinuation can trigger reflux symptoms).[9] We extracted the medical records of included patients, applying our prespecified criteria to determine whether use was appropriate. In patients in whom PPI was a continued home medication, we also extracted 2 years of data prior to the index date to determine if the medication was started during a prior hospital admission and, if so, whether this initiation was appropriate. We used descriptive statistics and [2] tests to compare patient characteristics and indications for PPI use.
| Appropriate PPI use | Inappropriate PPI use |
|---|---|
| |
| History of upper GI bleeding | No reason given |
| Endoscopic evidence of peptic ulcer disease | Unspecified GI prophylaxis |
| Esophagitis | Nonspecific abdominal pain |
| Gastritis and duodenitis | Heartburn (nonchronic) |
| Eradication of H pylori | Acute pancreatitis |
| GERD | Anemia |
| Barrett's esophagus | Heparin use for DVT prophylaxis |
| Continued on home PPI | Use of aspirin, NSAID, steroids or Coumadin (as a single agent) |
| Acute esophageal variceal bleeding | |
| NSAID used in patient >65 years‐old | |
| High‐risk groups; combination of 2 or more of aspirin, NSAID, clopidogrel, or Coumadin | |
RESULTS
Of 297 patients, the mean age was 64.4 years (standard deviation 16.3 years), most were white (69%), and 56% were women (Table 2). PPI use was appropriate in 231 (78%, 95% confidence interval: 72.6%‐82.4%) patients. Of these, a majority (172, 75%) of patients received a PPI because it was a continued home medication. Only 40 of the 172 patients had the medication started during a recent hospitalization, and in half of those cases (20) the PPI use was appropriate.
| Demographics | PPI Not Indicated, N=66 | PPI Indicated, N=231 | Total=297 | |||
|---|---|---|---|---|---|---|
| ||||||
| Age, y, mean (SD) | 62.5 | (16.2) | 64.9 | (16.3) | 64.4 | (16.3) |
| Sex, % No. | ||||||
| Female | 51.5% | 34 | 56.7% | 131 | 55.6% | 165 |
| Male | 48.5% | 32 | 43.3% | 100 | 44.4% | 132 |
| Race, % No. | ||||||
| Asian | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Black | 10.6% | 7 | 9.1% | 21 | 9.4% | 28 |
| Hispanic | 18.2% | 12 | 19.5% | 45 | 19.2% | 57 |
| Unknown | 0.0% | 0 | 2.2% | 5 | 1.7% | 5 |
| White | 71.2% | 47 | 68.4% | 158 | 69.0% | 205 |
| Insurance, % No. | ||||||
| Insured | 95.5% | 63 | 87.4% | 202 | 89.2% | 265 |
| Uninsured | 0.0% | 0 | 0.9% | 2 | 0.7% | 2 |
| Unknown | 4.5% | 3 | 11.7% | 27 | 10.1% | 30 |
| Service, % No. | ||||||
| Teaching | 25.8% | 17 | 32.9% | 76 | 31.3% | 93 |
| Nonteaching | 74.2% | 49 | 66.7% | 154 | 68.4% | 203 |
| Unknown | 0.0% | 0 | 0.4% | 1 | 0.3% | 1 |
| Chronic disease, % No. | ||||||
| Cardiac disease | 16.7% | 11 | 13.4% | 31 | 14.1% | 42 |
| Pulmonary disease | 16.7% | 11 | 14.7% | 34 | 15.2% | 45 |
| Gastrointestinal disease | 13.6% | 9 | 19.5% | 45 | 18.2% | 54 |
| Hepatic disease | 7.6% | 5 | 3.9% | 9 | 4.7% | 14 |
| Stroke | 1.5% | 1 | 5.2% | 12 | 4.4% | 13 |
| Sepsis | 12.1% | 8 | 13.0% | 30 | 12.8% | 38 |
| Other | 33.3% | 22 | 29.4% | 68 | 30.3% | 90 |
| PPI status, % No. | ||||||
| Continued home PPI | 0.0% | 0 | 74.5% | 172 | 58.1% | 172 |
| Started on PPI in hospital | 100% | 65 | 25.5% | 59 | 41.9% | 124 |
| Discharged on AST, % No. | ||||||
| Yes | 36.4% | 24 | 89.6% | 207 | 22.2% | 231 |
| PPI | 87.5% | 21 | 96.6% | 200 | 95.7% | 221 |
| Brand | 52.4% | 11 | 59.5% | 119 | 58.8% | 130 |
| Generic | 47.6% | 10 | 40.5% | 81 | 41.2% | 91 |
| H2 blocker | 12.5% | 3 | 3.4% | 7 | 4.3% | 10 |
| Brand | 0.0% | 0 | 71.4% | 5 | 50.0% | 5 |
| Generic | 100.0% | 3 | 28.6% | 2 | 50.0% | 5 |
| Medications, % No. | ||||||
| Aspirin | 36.4% | 24 | 43.7% | 101 | 42.1% | 125 |
| NSAID | 10.6% | 4 | 6.5% | 15 | 6.4% | 19 |
| Corticosteroids | 13.6% | 9 | 16.9% | 39 | 16.2% | 48 |
| Warfarin | 0.0% | 5 | 19.0% | 44 | 16.5% | 49 |
| Clopidogrel | 12.1% | 8 | 10.8% | 25 | 11.1% | 33 |
The second most common appropriate diagnosis was GERD (31%), followed by history of GI bleeding (19%) and treatment for esophagitis or gastritis (18%). Among the 66 patients receiving a PPI inappropriately, the majority of patients (56%) had no documented reason for PPI use, and only 11 patients (17%) were receiving PPI for stress ulcer prophylaxis (Figure 1). Five patients (8%) were treated prophylactically because of steroid or anticoagulant use. We observed no differences in age, gender, race, or reason for admission between the patients treated appropriately versus inappropriately.
DISCUSSION
In a contemporary cohort, chronic PPI use prior to admission was the most common reason PPIs were prescribed in the hospital. About 20% of hospitalized patients were started on a PPI for an inappropriate indication, the majority of whom lacked documentation concerning the reason for use. Among patients treated inappropriately, 36% were discharged on acid‐suppressive therapy.
The prior literature has reported a much higher percentages of unnecessary PPI use in hospitalized patients.[4, 5, 6, 7] Gupta et al. found that 70% of patients admitted to an internal medicine service received acid‐suppressive therapy, 73% of whom were treated unnecessarily.[5] Similarly, Nardino et al. found that 65% of acid‐suppressive therapy in hospitalized medical patients was not indicated.[4] If we had excluded patients on home PPIs from our study cohort, we would have found a higher rate of inappropriate use due to a smaller overall patient population. However, we chose to include these patients because they represented the vast majority of hospitalist‐prescribed PPIs. Notably, most of these prior prescriptions were not written during a recent hospital stay, indicating that the majority were initiated by outpatient physicians.
Our study is limited by its small sample size, single‐center design, and inability to determine the indications for outpatient PPI use. Still, it has important implications. Prior work has suggested that focusing efforts on PPI overuse may be premature in the absence of valid risk‐prediction models defining the patient populations that most benefit from PPI therapy.[10] Our work additionally suggests that hospital rates of inappropriate initiation may be relatively low, perhaps because hospitalist culture and practice have been affected by both local and national quality improvement efforts and by evidence dissemination.[8] Quality improvement efforts focused on reducing inpatient PPI use are likely to reveal diminishing returns, as admitting hospitalists are unlikely to abruptly discontinue PPIs prescribed in the outpatient setting.[9] Hospitalists should be encouraged to assess and document the need for PPIs during admission, hospitalization, and discharge processes. However, future efforts to reduce PPI overuse among hospitalized patients should predominately be focused on reducing inappropriate chronic PPI use in the outpatient setting.
Acknowledgements
The authors acknowledge Peter Lindenauer for his comments on an earlier draft of this manuscript.
Disclosures: The study was conducted with funding from the Department of Medicine at Baystate Medical Center. Dr. Lagu is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K01HL114745. Drs. Lagu and Albugeaey had full access to all of the data in the study, and they take responsibility for the integrity of the data and the accuracy of the data analysis. Drs. Lagu, Albugeaey, and Seiler conceived of the study. Drs. Albugeaey and Al Faraj acquired the data. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb analyzed and interpreted the data. Drs. Albugeaey and Lagu drafted the manuscript. Drs. Lagu, Albugeaey, Al Faraj, Seiler, and Ms. Garb critically reviewed the manuscript for important intellectual content. Dr. Albugeaey is a recipient of a scholarship from the Ministry of Higher Education, Kingdom of Saudi Arabia. The authors report no conflicts of interest.
- , , , , . Acid‐suppressive medication use and the risk for nosocomial gastrointestinal tract bleeding. Arch Intern Med. 2011;171(11):991–997.
- , , , . Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia. JAMA. 2009;301(20):2120–2128.
- , . Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107(3):345–360; quiz 361.
- , , . Overuse of acid‐suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95(11):3118–3122.
- , , , et al. Overuse of acid suppression therapy in hospitalized patients. South Med J. 2010;103(3):207–211.
- , , , , , . Inappropriate prescribing of proton pump inhibitors in hospitalized patients. J Hosp Med. 2012;7(5):421–425.
- , , , . Inappropriate utilization of intravenous proton pump inhibitors in hospital practice—a prospective study of the extent of the problem and predictive factors. QJM. 2010;103(5):327–335.
- Choosing Wisely, Society of Hospital Medicine, Adult Hospital Medicine. Available at:http://www.choosingwisely.org/doctor‐patient‐lists/society‐of‐hospital‐medicine‐adult‐hospital‐medicine. Accessed April 11, 2014.
- , , , . Safety of the long‐term use of proton pump inhibitors. World J Gastroenterol. 2010;16(19):2323–2330.
- , . Prophylaxis rates for venous thromboembolism and gastrointestinal bleeding in general medical patients: too low or too high? BMJ. 2012;344:e3248.
- , , , , . Acid‐suppressive medication use and the risk for nosocomial gastrointestinal tract bleeding. Arch Intern Med. 2011;171(11):991–997.
- , , , . Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia. JAMA. 2009;301(20):2120–2128.
- , . Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107(3):345–360; quiz 361.
- , , . Overuse of acid‐suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95(11):3118–3122.
- , , , et al. Overuse of acid suppression therapy in hospitalized patients. South Med J. 2010;103(3):207–211.
- , , , , , . Inappropriate prescribing of proton pump inhibitors in hospitalized patients. J Hosp Med. 2012;7(5):421–425.
- , , , . Inappropriate utilization of intravenous proton pump inhibitors in hospital practice—a prospective study of the extent of the problem and predictive factors. QJM. 2010;103(5):327–335.
- Choosing Wisely, Society of Hospital Medicine, Adult Hospital Medicine. Available at:http://www.choosingwisely.org/doctor‐patient‐lists/society‐of‐hospital‐medicine‐adult‐hospital‐medicine. Accessed April 11, 2014.
- , , , . Safety of the long‐term use of proton pump inhibitors. World J Gastroenterol. 2010;16(19):2323–2330.
- , . Prophylaxis rates for venous thromboembolism and gastrointestinal bleeding in general medical patients: too low or too high? BMJ. 2012;344:e3248.
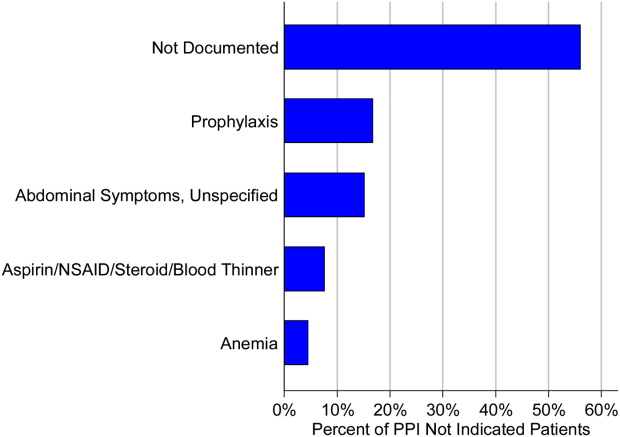
Society of Hospital Medicine (SHM) Calls for Overhaul of Medicare's Observation Status Rules
A hospitalist and SHM Public Policy Committee member is hopeful that SHM's recently released position paper recommending changes to the way the "observation status" designation is used for admitted hospital patients will help improve patient care.
The increasing use of the Centers for Medicare & Medicaid Services' (CMS) patient observation status designation—which grew 88% from 2006 to 2012—has frustrated hospitalists. Under the rule, patients are ineligible for skilled-nursing facility (SNF) care, may not claim insurance coverage for some medications, and may face uncertain cost-sharing and other financial liabilities for their hospitalization.
SHM outlined its concerns about the policy and suggested solutions in the report titled "The Observation Status Problem: Impact and Recommendations for Change."
CMS has attempted to address the issue by creating the "two-midnight rule." The report notes, however, that amid confusion on the application of the "two-midnight rule," Medicare auditing and enforcement have been pushed back several times, most recently to March 31, 2015.
"We still are unclear about what patient vulnerability is under this," says SHM Public Policy Committee member Ann Sheehy, MD, MS, FHM, a hospitalist at the University of Wisconsin School of Medicine and Public Health in Madison, who testified before Congress last May on observation status and other Medicare policies.
"We know that patients can't get SNF coverage when they're under observation," Dr. Sheehy says. "We know that patients are subject to unlimited co-pays when they're under observation, as opposed to when they're hospitalized as inpatients under Medicare Part A, which has a one-time deductible."
The SHM white paper outlines both short- and long-term fixes to the policy. In the near term, SHM recommends:
• Educating providers and patients on the purpose of observation status and raising confidence in when and how it should be applied;
• Changing SNF coverage rules to ensure patients’ eligibility; and
• Reforming the Medicare Recovery Audit Contractor program to improve RAC performance and reduce unintended pressures on admission decisions.
In the long term, the report suggests creating modifiers for diagnosis-related group (DRG) payments to assign to patients needing lower-acuity services, as well as crafting a list of DRGs to assign to patients needing short periods of inpatient care.
"The policy overall is very frustrating," Dr. Sheehy adds. "We hope that any rule change that comes out will address the core problems of observation so that patients can get the care they need with fair and appropriate insurance coverage." TH
Visit our website for more information about patient observation status.
A hospitalist and SHM Public Policy Committee member is hopeful that SHM's recently released position paper recommending changes to the way the "observation status" designation is used for admitted hospital patients will help improve patient care.
The increasing use of the Centers for Medicare & Medicaid Services' (CMS) patient observation status designation—which grew 88% from 2006 to 2012—has frustrated hospitalists. Under the rule, patients are ineligible for skilled-nursing facility (SNF) care, may not claim insurance coverage for some medications, and may face uncertain cost-sharing and other financial liabilities for their hospitalization.
SHM outlined its concerns about the policy and suggested solutions in the report titled "The Observation Status Problem: Impact and Recommendations for Change."
CMS has attempted to address the issue by creating the "two-midnight rule." The report notes, however, that amid confusion on the application of the "two-midnight rule," Medicare auditing and enforcement have been pushed back several times, most recently to March 31, 2015.
"We still are unclear about what patient vulnerability is under this," says SHM Public Policy Committee member Ann Sheehy, MD, MS, FHM, a hospitalist at the University of Wisconsin School of Medicine and Public Health in Madison, who testified before Congress last May on observation status and other Medicare policies.
"We know that patients can't get SNF coverage when they're under observation," Dr. Sheehy says. "We know that patients are subject to unlimited co-pays when they're under observation, as opposed to when they're hospitalized as inpatients under Medicare Part A, which has a one-time deductible."
The SHM white paper outlines both short- and long-term fixes to the policy. In the near term, SHM recommends:
• Educating providers and patients on the purpose of observation status and raising confidence in when and how it should be applied;
• Changing SNF coverage rules to ensure patients’ eligibility; and
• Reforming the Medicare Recovery Audit Contractor program to improve RAC performance and reduce unintended pressures on admission decisions.
In the long term, the report suggests creating modifiers for diagnosis-related group (DRG) payments to assign to patients needing lower-acuity services, as well as crafting a list of DRGs to assign to patients needing short periods of inpatient care.
"The policy overall is very frustrating," Dr. Sheehy adds. "We hope that any rule change that comes out will address the core problems of observation so that patients can get the care they need with fair and appropriate insurance coverage." TH
Visit our website for more information about patient observation status.
A hospitalist and SHM Public Policy Committee member is hopeful that SHM's recently released position paper recommending changes to the way the "observation status" designation is used for admitted hospital patients will help improve patient care.
The increasing use of the Centers for Medicare & Medicaid Services' (CMS) patient observation status designation—which grew 88% from 2006 to 2012—has frustrated hospitalists. Under the rule, patients are ineligible for skilled-nursing facility (SNF) care, may not claim insurance coverage for some medications, and may face uncertain cost-sharing and other financial liabilities for their hospitalization.
SHM outlined its concerns about the policy and suggested solutions in the report titled "The Observation Status Problem: Impact and Recommendations for Change."
CMS has attempted to address the issue by creating the "two-midnight rule." The report notes, however, that amid confusion on the application of the "two-midnight rule," Medicare auditing and enforcement have been pushed back several times, most recently to March 31, 2015.
"We still are unclear about what patient vulnerability is under this," says SHM Public Policy Committee member Ann Sheehy, MD, MS, FHM, a hospitalist at the University of Wisconsin School of Medicine and Public Health in Madison, who testified before Congress last May on observation status and other Medicare policies.
"We know that patients can't get SNF coverage when they're under observation," Dr. Sheehy says. "We know that patients are subject to unlimited co-pays when they're under observation, as opposed to when they're hospitalized as inpatients under Medicare Part A, which has a one-time deductible."
The SHM white paper outlines both short- and long-term fixes to the policy. In the near term, SHM recommends:
• Educating providers and patients on the purpose of observation status and raising confidence in when and how it should be applied;
• Changing SNF coverage rules to ensure patients’ eligibility; and
• Reforming the Medicare Recovery Audit Contractor program to improve RAC performance and reduce unintended pressures on admission decisions.
In the long term, the report suggests creating modifiers for diagnosis-related group (DRG) payments to assign to patients needing lower-acuity services, as well as crafting a list of DRGs to assign to patients needing short periods of inpatient care.
"The policy overall is very frustrating," Dr. Sheehy adds. "We hope that any rule change that comes out will address the core problems of observation so that patients can get the care they need with fair and appropriate insurance coverage." TH
Visit our website for more information about patient observation status.
Patient Safety Experts, Physicians Advocate for Prevention of Medical Errors
In a Senate subcommittee hearing last month, a panel of patient safety experts and physicians raised concerns about the problem of preventable medical errors, which they say can be linked to more than 1,000 patient deaths per day.
For their part, SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, FHM, says hospitalists should demand that their hospitals report better data on patient outcomes.
"When you talk about a patient death, you're talking about the efforts of an entire hospital going into the death or survival of that patient," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York. "If you ask, 'Where did something go wrong?' just looking at the mortality rate doesn't help. What service are you inquiring about? How can you get clean data that’s also useful to the clinician?"
In his testimony before the Subcommittee on Primary Health and Aging, hospitalist Ashish Jha, MD, MPH, referenced a landmark 1999 report from the Institute of Medicine (IOM), "To Err Is Human: Building a Safer Health System," [PDF] which estimated that between 44,000 and 98,000 deaths in the U.S. each year can be attributed to preventable medical errors.
Since the IOM report was published, little has been done to change the systems of care delivery that can lead providers to make errors, said Dr. Jha, an internist at the VA Boston Healthcare System and professor of health policy and management at the Harvard School of Public Health in Boston.
"When a physician orders the wrong medication because two drugs might sound alike, or when a patient develops a central-line infection because a rushed surgeon didn't use proper sterile technique, we now understand that we need to focus on the system that produced the errors," Dr. Jha told Senate subcommittee members.
Both Dr. Jha and panelist Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, said the Centers for Disease Control and Prevention should expand its National Nosocomial Infections Surveillance Program to collect and report data on medical errors.
Several other speakers said hospitals should be mandated to publicly report medical errors.
"Public disclosure is a critical element to preventing these events from happening," said panelist Lisa McGiffert, director of the Consumers Union Safe Patient Project in Austin, Texas. "It informs people about healthcare outcomes and motivates healthcare providers to do more to prevent errors." TH
Visit our website for more information on the impact of medical errors.
In a Senate subcommittee hearing last month, a panel of patient safety experts and physicians raised concerns about the problem of preventable medical errors, which they say can be linked to more than 1,000 patient deaths per day.
For their part, SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, FHM, says hospitalists should demand that their hospitals report better data on patient outcomes.
"When you talk about a patient death, you're talking about the efforts of an entire hospital going into the death or survival of that patient," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York. "If you ask, 'Where did something go wrong?' just looking at the mortality rate doesn't help. What service are you inquiring about? How can you get clean data that’s also useful to the clinician?"
In his testimony before the Subcommittee on Primary Health and Aging, hospitalist Ashish Jha, MD, MPH, referenced a landmark 1999 report from the Institute of Medicine (IOM), "To Err Is Human: Building a Safer Health System," [PDF] which estimated that between 44,000 and 98,000 deaths in the U.S. each year can be attributed to preventable medical errors.
Since the IOM report was published, little has been done to change the systems of care delivery that can lead providers to make errors, said Dr. Jha, an internist at the VA Boston Healthcare System and professor of health policy and management at the Harvard School of Public Health in Boston.
"When a physician orders the wrong medication because two drugs might sound alike, or when a patient develops a central-line infection because a rushed surgeon didn't use proper sterile technique, we now understand that we need to focus on the system that produced the errors," Dr. Jha told Senate subcommittee members.
Both Dr. Jha and panelist Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, said the Centers for Disease Control and Prevention should expand its National Nosocomial Infections Surveillance Program to collect and report data on medical errors.
Several other speakers said hospitals should be mandated to publicly report medical errors.
"Public disclosure is a critical element to preventing these events from happening," said panelist Lisa McGiffert, director of the Consumers Union Safe Patient Project in Austin, Texas. "It informs people about healthcare outcomes and motivates healthcare providers to do more to prevent errors." TH
Visit our website for more information on the impact of medical errors.
In a Senate subcommittee hearing last month, a panel of patient safety experts and physicians raised concerns about the problem of preventable medical errors, which they say can be linked to more than 1,000 patient deaths per day.
For their part, SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, FHM, says hospitalists should demand that their hospitals report better data on patient outcomes.
"When you talk about a patient death, you're talking about the efforts of an entire hospital going into the death or survival of that patient," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York. "If you ask, 'Where did something go wrong?' just looking at the mortality rate doesn't help. What service are you inquiring about? How can you get clean data that’s also useful to the clinician?"
In his testimony before the Subcommittee on Primary Health and Aging, hospitalist Ashish Jha, MD, MPH, referenced a landmark 1999 report from the Institute of Medicine (IOM), "To Err Is Human: Building a Safer Health System," [PDF] which estimated that between 44,000 and 98,000 deaths in the U.S. each year can be attributed to preventable medical errors.
Since the IOM report was published, little has been done to change the systems of care delivery that can lead providers to make errors, said Dr. Jha, an internist at the VA Boston Healthcare System and professor of health policy and management at the Harvard School of Public Health in Boston.
"When a physician orders the wrong medication because two drugs might sound alike, or when a patient develops a central-line infection because a rushed surgeon didn't use proper sterile technique, we now understand that we need to focus on the system that produced the errors," Dr. Jha told Senate subcommittee members.
Both Dr. Jha and panelist Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, said the Centers for Disease Control and Prevention should expand its National Nosocomial Infections Surveillance Program to collect and report data on medical errors.
Several other speakers said hospitals should be mandated to publicly report medical errors.
"Public disclosure is a critical element to preventing these events from happening," said panelist Lisa McGiffert, director of the Consumers Union Safe Patient Project in Austin, Texas. "It informs people about healthcare outcomes and motivates healthcare providers to do more to prevent errors." TH
Visit our website for more information on the impact of medical errors.
Many surgical residents consider quitting during training
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).

Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).
Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).
Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
FROM JAMA Surgery
Major finding: More than half of survey respondents (58%) considered quitting their general surgery residency, an issue more persistent with female respondents.
Data source: Analysis of 288 responses to a survey of general surgery residents in 13 residency programs across different regions (West, Southwest, Midwest, and Northeast) and training centers (university programs, independent programs, or hybrid university-affiliated programs without an onsite university or medical school).
Disclosures: The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
