User login
CLL Therapy: Focus on comorbidities, not age
CHICAGO – The majority of patients with chronic lymphocytic leukemia (CLL) are elderly patients over age 65 years, which underscores the need for a careful assessment of fitness for therapy – not necessarily because of age, but because of comorbidity burden, according to Dr. John G. Gribben.

In fact, 68% of CLL patients are over age 65 years (median, 71 years), and 41% are over age 75 years. Perhaps more importantly, 89% of elderly CLL patients have one or more comorbidities, and 46% have at least one major comorbidity, said Dr. Gribben of Barts Cancer Institute, Queen Mary University of London.
Conventional wisdom has long suggested that CLL shortens the life span only in younger patients; older patients were thought to be more likely “to die with CLL rather than of CLL,” he said at the American Society of Hematology Meeting on Hematologic Malignancies.
However, recent findings suggest that CLL shortens the life span of elderly patients as well, he noted.
“I think we probably have been undertreating and underthinking about the impact that CLL can have on these more elderly patients, and I think it does represent an area of unmet need,” he said.
Treatment options in the elderly include FCR (fludarabine, cyclophosphamide, rituximab) in those deemed fit enough to tolerate the regimen, he said, adding, “if you are concerned about neutropenia associated with FCR, there are those who use rituximab-fludarabine [RF], and that’s certainly a good option.”
However, in those with an 11q abnormality, good data show that the addition of the alkylator does add benefit. “I do think that FCR is worthwhile pushing [in those cases],” he said.
Bendamustine-rituximab is also an attractive option, as demonstrated in the CLL10 trial, but it is important to remember that patients in that trial were “fit, healthy patients” based on Clinical Illness Rating Scale (CIRS) scores of less than 6; they were patients who were deemed fit to be randomized to receive FCR.
Chlorambucil-based therapies administered with anti-CD20 monoclonal antibodies are also an option, as are novel agents in those with 17p deletions or a P53 mutation, he said.
When it comes to assessing elderly patients’ fitness for therapy, comorbidities play a more important role than age, he said, explaining that many patients over age 65 are very fit and would do well with therapies such as FCR.
For this reason, comorbidities should be the determining factor in treatment selection, he said.
No standard criteria for assessing fitness exist, but there are a few tools that can help.
Eastern Cooperative Oncology Group performance status and organ function (for example, creatinine clearance) can be helpful and often are used in trial settings, as are criteria for excluding patients from participation, but CIRS, used by the German CLL study group, is a more formal tool for assessing comorbidity.
The German group is not the first to use the tool – CIRS is a widely validated test that provides an objective measurement of fitness for more aggressive chemotherapy regimens – but the group did demonstrate in CLL11 that it could be used to enroll more elderly patients with comorbidities into clinical trials, Dr. Gribben said.
A CIRS score of 6 or lower indicates fitness, whereas increasing scores indicate an increasing lack of fitness, he explained, noting that “like every scoring system there are some issues … somebody could easily have a score higher than 6 with comorbidities that really don’t impact on chemotherapy tolerability.
“But in general terms, this is a good way to be making these sorts of assessments,” he said.
Dr. Gribben has received research funding from the National Institutes of Health, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
CHICAGO – The majority of patients with chronic lymphocytic leukemia (CLL) are elderly patients over age 65 years, which underscores the need for a careful assessment of fitness for therapy – not necessarily because of age, but because of comorbidity burden, according to Dr. John G. Gribben.
In fact, 68% of CLL patients are over age 65 years (median, 71 years), and 41% are over age 75 years. Perhaps more importantly, 89% of elderly CLL patients have one or more comorbidities, and 46% have at least one major comorbidity, said Dr. Gribben of Barts Cancer Institute, Queen Mary University of London.
Conventional wisdom has long suggested that CLL shortens the life span only in younger patients; older patients were thought to be more likely “to die with CLL rather than of CLL,” he said at the American Society of Hematology Meeting on Hematologic Malignancies.
However, recent findings suggest that CLL shortens the life span of elderly patients as well, he noted.
“I think we probably have been undertreating and underthinking about the impact that CLL can have on these more elderly patients, and I think it does represent an area of unmet need,” he said.
Treatment options in the elderly include FCR (fludarabine, cyclophosphamide, rituximab) in those deemed fit enough to tolerate the regimen, he said, adding, “if you are concerned about neutropenia associated with FCR, there are those who use rituximab-fludarabine [RF], and that’s certainly a good option.”
However, in those with an 11q abnormality, good data show that the addition of the alkylator does add benefit. “I do think that FCR is worthwhile pushing [in those cases],” he said.
Bendamustine-rituximab is also an attractive option, as demonstrated in the CLL10 trial, but it is important to remember that patients in that trial were “fit, healthy patients” based on Clinical Illness Rating Scale (CIRS) scores of less than 6; they were patients who were deemed fit to be randomized to receive FCR.
Chlorambucil-based therapies administered with anti-CD20 monoclonal antibodies are also an option, as are novel agents in those with 17p deletions or a P53 mutation, he said.
When it comes to assessing elderly patients’ fitness for therapy, comorbidities play a more important role than age, he said, explaining that many patients over age 65 are very fit and would do well with therapies such as FCR.
For this reason, comorbidities should be the determining factor in treatment selection, he said.
No standard criteria for assessing fitness exist, but there are a few tools that can help.
Eastern Cooperative Oncology Group performance status and organ function (for example, creatinine clearance) can be helpful and often are used in trial settings, as are criteria for excluding patients from participation, but CIRS, used by the German CLL study group, is a more formal tool for assessing comorbidity.
The German group is not the first to use the tool – CIRS is a widely validated test that provides an objective measurement of fitness for more aggressive chemotherapy regimens – but the group did demonstrate in CLL11 that it could be used to enroll more elderly patients with comorbidities into clinical trials, Dr. Gribben said.
A CIRS score of 6 or lower indicates fitness, whereas increasing scores indicate an increasing lack of fitness, he explained, noting that “like every scoring system there are some issues … somebody could easily have a score higher than 6 with comorbidities that really don’t impact on chemotherapy tolerability.
“But in general terms, this is a good way to be making these sorts of assessments,” he said.
Dr. Gribben has received research funding from the National Institutes of Health, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
CHICAGO – The majority of patients with chronic lymphocytic leukemia (CLL) are elderly patients over age 65 years, which underscores the need for a careful assessment of fitness for therapy – not necessarily because of age, but because of comorbidity burden, according to Dr. John G. Gribben.
In fact, 68% of CLL patients are over age 65 years (median, 71 years), and 41% are over age 75 years. Perhaps more importantly, 89% of elderly CLL patients have one or more comorbidities, and 46% have at least one major comorbidity, said Dr. Gribben of Barts Cancer Institute, Queen Mary University of London.
Conventional wisdom has long suggested that CLL shortens the life span only in younger patients; older patients were thought to be more likely “to die with CLL rather than of CLL,” he said at the American Society of Hematology Meeting on Hematologic Malignancies.
However, recent findings suggest that CLL shortens the life span of elderly patients as well, he noted.
“I think we probably have been undertreating and underthinking about the impact that CLL can have on these more elderly patients, and I think it does represent an area of unmet need,” he said.
Treatment options in the elderly include FCR (fludarabine, cyclophosphamide, rituximab) in those deemed fit enough to tolerate the regimen, he said, adding, “if you are concerned about neutropenia associated with FCR, there are those who use rituximab-fludarabine [RF], and that’s certainly a good option.”
However, in those with an 11q abnormality, good data show that the addition of the alkylator does add benefit. “I do think that FCR is worthwhile pushing [in those cases],” he said.
Bendamustine-rituximab is also an attractive option, as demonstrated in the CLL10 trial, but it is important to remember that patients in that trial were “fit, healthy patients” based on Clinical Illness Rating Scale (CIRS) scores of less than 6; they were patients who were deemed fit to be randomized to receive FCR.
Chlorambucil-based therapies administered with anti-CD20 monoclonal antibodies are also an option, as are novel agents in those with 17p deletions or a P53 mutation, he said.
When it comes to assessing elderly patients’ fitness for therapy, comorbidities play a more important role than age, he said, explaining that many patients over age 65 are very fit and would do well with therapies such as FCR.
For this reason, comorbidities should be the determining factor in treatment selection, he said.
No standard criteria for assessing fitness exist, but there are a few tools that can help.
Eastern Cooperative Oncology Group performance status and organ function (for example, creatinine clearance) can be helpful and often are used in trial settings, as are criteria for excluding patients from participation, but CIRS, used by the German CLL study group, is a more formal tool for assessing comorbidity.
The German group is not the first to use the tool – CIRS is a widely validated test that provides an objective measurement of fitness for more aggressive chemotherapy regimens – but the group did demonstrate in CLL11 that it could be used to enroll more elderly patients with comorbidities into clinical trials, Dr. Gribben said.
A CIRS score of 6 or lower indicates fitness, whereas increasing scores indicate an increasing lack of fitness, he explained, noting that “like every scoring system there are some issues … somebody could easily have a score higher than 6 with comorbidities that really don’t impact on chemotherapy tolerability.
“But in general terms, this is a good way to be making these sorts of assessments,” he said.
Dr. Gribben has received research funding from the National Institutes of Health, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
AT MHM 2015

Rash, diarrhea, and eosinophilia
An 83-year-old Iraqi woman was transferred to our inpatient service from the intensive care unit (ICU). She had been admitted to the ICU for respiratory distress and hypotension, where she was treated with stress dose steroids, oseltamivir, vancomycin, piperacillin/tazobactam, and azithromycin. At our inpatient service, she complained of a new pruritic rash on her thighs, abdominal pain, and persistent diarrhea. Her medical history was notable for chronic interstitial lung disease, gastroesophageal reflux disease, and anemia.
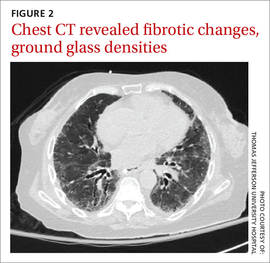
We noted a diffuse maculopapular rash on both of the patient’s inner thighs (FIGURE 1). Laboratory findings revealed leukocytosis and eosinophilia (total white blood cell count of 15,000, with 41% eosinophils). The patient’s eosinophil count—which had improved while she was on steroids in the ICU—had started to rise as steroids were tapered. Blood and cultures from a bronchoscopy were negative. Results from a bronchoalveolar lavage (BAL) were significant for a cell differential of 60% macrophages, 25% neutrophils, 5% lymphocytes, and 10% eosinophils. A stool sample for Clostridium difficile was negative. A computed tomography (CT) scan of the chest revealed bronchiectasis, fibrotic changes, and diffuse ground glass densities (FIGURE 2).
Our patient was a refugee who had arrived in the United States 5 years earlier. Per Centers for Disease Control and Prevention (CDC) guidelines, she had undergone routine stool ova and parasite (O&P) testing upon her arrival in the United States; the results were negative.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Strongyloides stercoralis hyperinfection syndrome
We suspected a parasitic infection because our patient was a refugee with pulmonary, gastrointestinal (GI), and skin complaints, as well as intermittent eosinophilia. Her negative O&P test upon arrival to the United States did not, however, eliminate the possibility of Strongyloides stercoralis, which often goes undetected in routine O&P samples. A serum test for Strongyloides immunoglobulin G (IgG) was positive at 6.39 IV (positive, >2.11 IV). Subsequently, multiple stool samples were tested specifically for the parasite and came back positive, confirming the diagnosis.

Strongyloidiasis is caused by the roundworm S. stercoralis (FIGURE 3), which infects approximately 30 to 100 million people worldwide.1 It is most common in warm, humid climates in subtropical and tropical regions. With increasing trends in migration and travel, strongyloidiasis is now often diagnosed in nonendemic areas.2
The disease is most prevalent in socioeconomically disadvantaged communities and in agricultural settings. Infection in humans occurs when bare skin comes into contact with contaminated soil. The human T-cell lymphotropic virus-1 (HTLV-1) also predisposes individuals to developing strongyloidiasis.1
Infected patients can be asymptomatic or have intermittent symptoms. Patients are likely to complain of a pruritic rash, cough, shortness of breath, abdominal pain, nausea, and/or diarrhea.3,4 The rash, called larva currens, results when the larvae invade the perianal region. The rash typically spreads to the buttocks, groin, and inner thighs.3
Immunosuppressed patients are at a heightened risk. Two serious forms of strongyloidiasis—hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS)—can develop in immunosuppressed individuals. This can occur in patients receiving high-dose corticosteroids.3-5 Immunosuppression can lead to accelerated autoinfection and a large burden of migrating larvae in the body.
HS was suspected in our patient based on her worsening lung disease, recent onset of diarrhea, and rash in the setting of increased eosinophils.
HS is usually limited to the pulmonary, GI, and skin systems, whereas DS can invade numerous other organs. Complications of HS and DS include disseminated bacterial and fungal infections; the mortality rate if either condition is left untreated is close to 90%.3-5
Strongyloidiasis can mimic other infections
The differential diagnosis for S. stercoralis infection includes the following:
Clostridium difficile infection must be excluded in a hospitalized patient with persistent diarrhea. A stool toxin and antigen test is used to make the diagnosis. Patients with C. difficile infection are more likely to have eosinopenia than eosinophilia.6
Schistosomiasis is a helminth infection that can also persist for decades. The signs and symptoms of a chronic infection can be similar to strongyloidiasis. However, patients with schistosomiasis will typically have large organ damage, bloody diarrhea, and/or urinary symptoms. Diagnosis is made from testing multiple stool samples, urine, and serology.6
Adrenal insufficiency occurs with complete or partial loss of endogenous glucocorticoids. There can be resultant eosinophilia, although it is usually not as marked as the eosinophilia observed in our patient. Adrenal insufficiency is diagnosed with an early morning serum cortisol test and a cosyntropin stimulation test.6
A high degree of suspicion in refugees is needed to make the diagnosis
When a patient is from an endemic area, such as Southeast Asia, Latin America, or sub-Saharan Africa7, one’s clinical suspicion should increase. Also, because signs and symptoms of strongyloidiasis are often nonspecific, a high suspicion for the disease is necessary to prompt testing. Eosinophilia may be present, but can be mild, and is not specific for the disease.
Available stool testing is not highly sensitive, and repeated specialized stool examinations are required, with sensitivity reaching close to 100% only after 7 serial samples are examined.3,8 Duodenal aspirate is more sensitive and larvae can also be seen through wet mount of bronchoalveolar lavage fluid. Serologic testing for Strongyloides IgG is available and has high sensitivity. However, specificity can be low because there can be cross-reactivity with other parasites, and the presence of the antibody does not differentiate between past and current infection.3,5,8
Imaging of the lungs is often variable and nonspecific. Findings on a chest x-ray or CT scan of the chest include diffuse alveolar opacities, interstitial infiltrates, pleural effusions, abscess or cavitation, or fibrotic changes.7 However, these findings can also be the result of a bacterial superinfection and not the parasite itself.3,6
Treatment begins with ivermectin
First-line treatment for strongyloidiasis is oral ivermectin, 200 mcg/kg/d.5 Optimal treatment duration is unknown because it is difficult to determine when S. stercoralis has been eradicated due to the low sensitivity of stool samples.4 For a patient with HS or DS, the CDC recommends treatment until stool and/or sputum samples are negative for 2 weeks.5
The CDC recommends that prior to arrival in the United States, all refugees should receive pre-departure treatment for parasites depending on their country of origin. For individuals arriving from the Middle East, the CDC recommends presumptive treatment with ivermectin for Strongyloides and albendazole for infections caused by soil-transmitted helminths.9 However, ivermectin was not routinely administered in the Middle East until January 2014.9,10 As a result of limited pre-departure treatment, US clinicians need to be cognizant of strongyloidiasis and have a high degree of suspicion in patients with nonspecific symptoms, especially when starting treatment with high-dose corticosteroids for other conditions.
We started our patient on a weight-based dose of ivermectin. Piperacillin/tazobactam 3.375 g (IV) every 6 hours was empirically started to cover enteric bacteria in the setting of HS, but was discontinued after blood cultures were negative. An HTLV-1/2 antibody test was negative. A repeat stool O&P test looking specifically for S. stercoralis came back positive on Day 6 of treatment. To determine the course of treatment, repeat O&Ps were done every 72 hours and ivermectin was continued until stool O&Ps were negative for 2 weeks. The total treatment course lasted 22 days.
During the course of treatment, our patient gained weight and her rash, diarrhea, and abdominal pain improved. She was discharged home and followed up with an infectious disease specialist as an outpatient. Three months later, repeat Strongyloides IgG testing was negative.
CORRESPONDENCE
Komal Soin, MD, MPH, Kaiser Permanente Waipio Medical Office, 94-1480 Moaniani Street, Waipahu, HI 96797; komal.soin@gmail.com
1. Centers for Disease Control and Prevention. Parasites - Strongyloides. Epidemiology & risk factors. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/epi.html. Accessed September 4, 2015.
2. Buonfrate D, Angheben A, Gobbi F, et al. Imported strongyloidiasis: epidemiology, presentations, and treatment. Curr Infect Dis Rep. 2012;14:256-262.
3. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040-1047.
4. Buonfrate D, Requena-Mendez A, Angheben A, et al. Severe strongyloidiasis: a systematic review of case reports. BMC Infect Dis. 2013;13:78.
5. Centers for Disease Control and Prevention. Parasites - Strongyloides. Resources for health professionals. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed September 4, 2015.
6. UpToDate. Klion AD, Weller PF. Approach to the patient with unexplained eosinophilia. UpToDate Web site. Available at: http://www.uptodate.com/contents/approach-to-the-patientwith-unexplained-eosinophilia. Accessed August 27, 2015.
7. Mokhlesi B, Shulzhenko O, Garimella PS, et al. Pulmonary strongyloidiasis: the varied clinical presentations. Clin Pulm Med. 2004;11:6-13.
8. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systematic review. PLoS Negl Trop Dis. 2013;7:e2002.
9. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html#me-asia-na-la-caribbean. Accessed April 3, 2014.
10. Centers for Disease Control and Prevention. Treatment options for presumptive parasitic infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/interventions/interventions.html. Accessed April 3, 2014.
An 83-year-old Iraqi woman was transferred to our inpatient service from the intensive care unit (ICU). She had been admitted to the ICU for respiratory distress and hypotension, where she was treated with stress dose steroids, oseltamivir, vancomycin, piperacillin/tazobactam, and azithromycin. At our inpatient service, she complained of a new pruritic rash on her thighs, abdominal pain, and persistent diarrhea. Her medical history was notable for chronic interstitial lung disease, gastroesophageal reflux disease, and anemia.
We noted a diffuse maculopapular rash on both of the patient’s inner thighs (FIGURE 1). Laboratory findings revealed leukocytosis and eosinophilia (total white blood cell count of 15,000, with 41% eosinophils). The patient’s eosinophil count—which had improved while she was on steroids in the ICU—had started to rise as steroids were tapered. Blood and cultures from a bronchoscopy were negative. Results from a bronchoalveolar lavage (BAL) were significant for a cell differential of 60% macrophages, 25% neutrophils, 5% lymphocytes, and 10% eosinophils. A stool sample for Clostridium difficile was negative. A computed tomography (CT) scan of the chest revealed bronchiectasis, fibrotic changes, and diffuse ground glass densities (FIGURE 2).
Our patient was a refugee who had arrived in the United States 5 years earlier. Per Centers for Disease Control and Prevention (CDC) guidelines, she had undergone routine stool ova and parasite (O&P) testing upon her arrival in the United States; the results were negative.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Strongyloides stercoralis hyperinfection syndrome
We suspected a parasitic infection because our patient was a refugee with pulmonary, gastrointestinal (GI), and skin complaints, as well as intermittent eosinophilia. Her negative O&P test upon arrival to the United States did not, however, eliminate the possibility of Strongyloides stercoralis, which often goes undetected in routine O&P samples. A serum test for Strongyloides immunoglobulin G (IgG) was positive at 6.39 IV (positive, >2.11 IV). Subsequently, multiple stool samples were tested specifically for the parasite and came back positive, confirming the diagnosis.
Strongyloidiasis is caused by the roundworm S. stercoralis (FIGURE 3), which infects approximately 30 to 100 million people worldwide.1 It is most common in warm, humid climates in subtropical and tropical regions. With increasing trends in migration and travel, strongyloidiasis is now often diagnosed in nonendemic areas.2
The disease is most prevalent in socioeconomically disadvantaged communities and in agricultural settings. Infection in humans occurs when bare skin comes into contact with contaminated soil. The human T-cell lymphotropic virus-1 (HTLV-1) also predisposes individuals to developing strongyloidiasis.1
Infected patients can be asymptomatic or have intermittent symptoms. Patients are likely to complain of a pruritic rash, cough, shortness of breath, abdominal pain, nausea, and/or diarrhea.3,4 The rash, called larva currens, results when the larvae invade the perianal region. The rash typically spreads to the buttocks, groin, and inner thighs.3
Immunosuppressed patients are at a heightened risk. Two serious forms of strongyloidiasis—hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS)—can develop in immunosuppressed individuals. This can occur in patients receiving high-dose corticosteroids.3-5 Immunosuppression can lead to accelerated autoinfection and a large burden of migrating larvae in the body.
HS was suspected in our patient based on her worsening lung disease, recent onset of diarrhea, and rash in the setting of increased eosinophils.
HS is usually limited to the pulmonary, GI, and skin systems, whereas DS can invade numerous other organs. Complications of HS and DS include disseminated bacterial and fungal infections; the mortality rate if either condition is left untreated is close to 90%.3-5
Strongyloidiasis can mimic other infections
The differential diagnosis for S. stercoralis infection includes the following:
Clostridium difficile infection must be excluded in a hospitalized patient with persistent diarrhea. A stool toxin and antigen test is used to make the diagnosis. Patients with C. difficile infection are more likely to have eosinopenia than eosinophilia.6
Schistosomiasis is a helminth infection that can also persist for decades. The signs and symptoms of a chronic infection can be similar to strongyloidiasis. However, patients with schistosomiasis will typically have large organ damage, bloody diarrhea, and/or urinary symptoms. Diagnosis is made from testing multiple stool samples, urine, and serology.6
Adrenal insufficiency occurs with complete or partial loss of endogenous glucocorticoids. There can be resultant eosinophilia, although it is usually not as marked as the eosinophilia observed in our patient. Adrenal insufficiency is diagnosed with an early morning serum cortisol test and a cosyntropin stimulation test.6
A high degree of suspicion in refugees is needed to make the diagnosis
When a patient is from an endemic area, such as Southeast Asia, Latin America, or sub-Saharan Africa7, one’s clinical suspicion should increase. Also, because signs and symptoms of strongyloidiasis are often nonspecific, a high suspicion for the disease is necessary to prompt testing. Eosinophilia may be present, but can be mild, and is not specific for the disease.
Available stool testing is not highly sensitive, and repeated specialized stool examinations are required, with sensitivity reaching close to 100% only after 7 serial samples are examined.3,8 Duodenal aspirate is more sensitive and larvae can also be seen through wet mount of bronchoalveolar lavage fluid. Serologic testing for Strongyloides IgG is available and has high sensitivity. However, specificity can be low because there can be cross-reactivity with other parasites, and the presence of the antibody does not differentiate between past and current infection.3,5,8
Imaging of the lungs is often variable and nonspecific. Findings on a chest x-ray or CT scan of the chest include diffuse alveolar opacities, interstitial infiltrates, pleural effusions, abscess or cavitation, or fibrotic changes.7 However, these findings can also be the result of a bacterial superinfection and not the parasite itself.3,6
Treatment begins with ivermectin
First-line treatment for strongyloidiasis is oral ivermectin, 200 mcg/kg/d.5 Optimal treatment duration is unknown because it is difficult to determine when S. stercoralis has been eradicated due to the low sensitivity of stool samples.4 For a patient with HS or DS, the CDC recommends treatment until stool and/or sputum samples are negative for 2 weeks.5
The CDC recommends that prior to arrival in the United States, all refugees should receive pre-departure treatment for parasites depending on their country of origin. For individuals arriving from the Middle East, the CDC recommends presumptive treatment with ivermectin for Strongyloides and albendazole for infections caused by soil-transmitted helminths.9 However, ivermectin was not routinely administered in the Middle East until January 2014.9,10 As a result of limited pre-departure treatment, US clinicians need to be cognizant of strongyloidiasis and have a high degree of suspicion in patients with nonspecific symptoms, especially when starting treatment with high-dose corticosteroids for other conditions.
We started our patient on a weight-based dose of ivermectin. Piperacillin/tazobactam 3.375 g (IV) every 6 hours was empirically started to cover enteric bacteria in the setting of HS, but was discontinued after blood cultures were negative. An HTLV-1/2 antibody test was negative. A repeat stool O&P test looking specifically for S. stercoralis came back positive on Day 6 of treatment. To determine the course of treatment, repeat O&Ps were done every 72 hours and ivermectin was continued until stool O&Ps were negative for 2 weeks. The total treatment course lasted 22 days.
During the course of treatment, our patient gained weight and her rash, diarrhea, and abdominal pain improved. She was discharged home and followed up with an infectious disease specialist as an outpatient. Three months later, repeat Strongyloides IgG testing was negative.
CORRESPONDENCE
Komal Soin, MD, MPH, Kaiser Permanente Waipio Medical Office, 94-1480 Moaniani Street, Waipahu, HI 96797; komal.soin@gmail.com
An 83-year-old Iraqi woman was transferred to our inpatient service from the intensive care unit (ICU). She had been admitted to the ICU for respiratory distress and hypotension, where she was treated with stress dose steroids, oseltamivir, vancomycin, piperacillin/tazobactam, and azithromycin. At our inpatient service, she complained of a new pruritic rash on her thighs, abdominal pain, and persistent diarrhea. Her medical history was notable for chronic interstitial lung disease, gastroesophageal reflux disease, and anemia.
We noted a diffuse maculopapular rash on both of the patient’s inner thighs (FIGURE 1). Laboratory findings revealed leukocytosis and eosinophilia (total white blood cell count of 15,000, with 41% eosinophils). The patient’s eosinophil count—which had improved while she was on steroids in the ICU—had started to rise as steroids were tapered. Blood and cultures from a bronchoscopy were negative. Results from a bronchoalveolar lavage (BAL) were significant for a cell differential of 60% macrophages, 25% neutrophils, 5% lymphocytes, and 10% eosinophils. A stool sample for Clostridium difficile was negative. A computed tomography (CT) scan of the chest revealed bronchiectasis, fibrotic changes, and diffuse ground glass densities (FIGURE 2).
Our patient was a refugee who had arrived in the United States 5 years earlier. Per Centers for Disease Control and Prevention (CDC) guidelines, she had undergone routine stool ova and parasite (O&P) testing upon her arrival in the United States; the results were negative.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Strongyloides stercoralis hyperinfection syndrome
We suspected a parasitic infection because our patient was a refugee with pulmonary, gastrointestinal (GI), and skin complaints, as well as intermittent eosinophilia. Her negative O&P test upon arrival to the United States did not, however, eliminate the possibility of Strongyloides stercoralis, which often goes undetected in routine O&P samples. A serum test for Strongyloides immunoglobulin G (IgG) was positive at 6.39 IV (positive, >2.11 IV). Subsequently, multiple stool samples were tested specifically for the parasite and came back positive, confirming the diagnosis.
Strongyloidiasis is caused by the roundworm S. stercoralis (FIGURE 3), which infects approximately 30 to 100 million people worldwide.1 It is most common in warm, humid climates in subtropical and tropical regions. With increasing trends in migration and travel, strongyloidiasis is now often diagnosed in nonendemic areas.2
The disease is most prevalent in socioeconomically disadvantaged communities and in agricultural settings. Infection in humans occurs when bare skin comes into contact with contaminated soil. The human T-cell lymphotropic virus-1 (HTLV-1) also predisposes individuals to developing strongyloidiasis.1
Infected patients can be asymptomatic or have intermittent symptoms. Patients are likely to complain of a pruritic rash, cough, shortness of breath, abdominal pain, nausea, and/or diarrhea.3,4 The rash, called larva currens, results when the larvae invade the perianal region. The rash typically spreads to the buttocks, groin, and inner thighs.3
Immunosuppressed patients are at a heightened risk. Two serious forms of strongyloidiasis—hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS)—can develop in immunosuppressed individuals. This can occur in patients receiving high-dose corticosteroids.3-5 Immunosuppression can lead to accelerated autoinfection and a large burden of migrating larvae in the body.
HS was suspected in our patient based on her worsening lung disease, recent onset of diarrhea, and rash in the setting of increased eosinophils.
HS is usually limited to the pulmonary, GI, and skin systems, whereas DS can invade numerous other organs. Complications of HS and DS include disseminated bacterial and fungal infections; the mortality rate if either condition is left untreated is close to 90%.3-5
Strongyloidiasis can mimic other infections
The differential diagnosis for S. stercoralis infection includes the following:
Clostridium difficile infection must be excluded in a hospitalized patient with persistent diarrhea. A stool toxin and antigen test is used to make the diagnosis. Patients with C. difficile infection are more likely to have eosinopenia than eosinophilia.6
Schistosomiasis is a helminth infection that can also persist for decades. The signs and symptoms of a chronic infection can be similar to strongyloidiasis. However, patients with schistosomiasis will typically have large organ damage, bloody diarrhea, and/or urinary symptoms. Diagnosis is made from testing multiple stool samples, urine, and serology.6
Adrenal insufficiency occurs with complete or partial loss of endogenous glucocorticoids. There can be resultant eosinophilia, although it is usually not as marked as the eosinophilia observed in our patient. Adrenal insufficiency is diagnosed with an early morning serum cortisol test and a cosyntropin stimulation test.6
A high degree of suspicion in refugees is needed to make the diagnosis
When a patient is from an endemic area, such as Southeast Asia, Latin America, or sub-Saharan Africa7, one’s clinical suspicion should increase. Also, because signs and symptoms of strongyloidiasis are often nonspecific, a high suspicion for the disease is necessary to prompt testing. Eosinophilia may be present, but can be mild, and is not specific for the disease.
Available stool testing is not highly sensitive, and repeated specialized stool examinations are required, with sensitivity reaching close to 100% only after 7 serial samples are examined.3,8 Duodenal aspirate is more sensitive and larvae can also be seen through wet mount of bronchoalveolar lavage fluid. Serologic testing for Strongyloides IgG is available and has high sensitivity. However, specificity can be low because there can be cross-reactivity with other parasites, and the presence of the antibody does not differentiate between past and current infection.3,5,8
Imaging of the lungs is often variable and nonspecific. Findings on a chest x-ray or CT scan of the chest include diffuse alveolar opacities, interstitial infiltrates, pleural effusions, abscess or cavitation, or fibrotic changes.7 However, these findings can also be the result of a bacterial superinfection and not the parasite itself.3,6
Treatment begins with ivermectin
First-line treatment for strongyloidiasis is oral ivermectin, 200 mcg/kg/d.5 Optimal treatment duration is unknown because it is difficult to determine when S. stercoralis has been eradicated due to the low sensitivity of stool samples.4 For a patient with HS or DS, the CDC recommends treatment until stool and/or sputum samples are negative for 2 weeks.5
The CDC recommends that prior to arrival in the United States, all refugees should receive pre-departure treatment for parasites depending on their country of origin. For individuals arriving from the Middle East, the CDC recommends presumptive treatment with ivermectin for Strongyloides and albendazole for infections caused by soil-transmitted helminths.9 However, ivermectin was not routinely administered in the Middle East until January 2014.9,10 As a result of limited pre-departure treatment, US clinicians need to be cognizant of strongyloidiasis and have a high degree of suspicion in patients with nonspecific symptoms, especially when starting treatment with high-dose corticosteroids for other conditions.
We started our patient on a weight-based dose of ivermectin. Piperacillin/tazobactam 3.375 g (IV) every 6 hours was empirically started to cover enteric bacteria in the setting of HS, but was discontinued after blood cultures were negative. An HTLV-1/2 antibody test was negative. A repeat stool O&P test looking specifically for S. stercoralis came back positive on Day 6 of treatment. To determine the course of treatment, repeat O&Ps were done every 72 hours and ivermectin was continued until stool O&Ps were negative for 2 weeks. The total treatment course lasted 22 days.
During the course of treatment, our patient gained weight and her rash, diarrhea, and abdominal pain improved. She was discharged home and followed up with an infectious disease specialist as an outpatient. Three months later, repeat Strongyloides IgG testing was negative.
CORRESPONDENCE
Komal Soin, MD, MPH, Kaiser Permanente Waipio Medical Office, 94-1480 Moaniani Street, Waipahu, HI 96797; komal.soin@gmail.com
1. Centers for Disease Control and Prevention. Parasites - Strongyloides. Epidemiology & risk factors. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/epi.html. Accessed September 4, 2015.
2. Buonfrate D, Angheben A, Gobbi F, et al. Imported strongyloidiasis: epidemiology, presentations, and treatment. Curr Infect Dis Rep. 2012;14:256-262.
3. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040-1047.
4. Buonfrate D, Requena-Mendez A, Angheben A, et al. Severe strongyloidiasis: a systematic review of case reports. BMC Infect Dis. 2013;13:78.
5. Centers for Disease Control and Prevention. Parasites - Strongyloides. Resources for health professionals. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed September 4, 2015.
6. UpToDate. Klion AD, Weller PF. Approach to the patient with unexplained eosinophilia. UpToDate Web site. Available at: http://www.uptodate.com/contents/approach-to-the-patientwith-unexplained-eosinophilia. Accessed August 27, 2015.
7. Mokhlesi B, Shulzhenko O, Garimella PS, et al. Pulmonary strongyloidiasis: the varied clinical presentations. Clin Pulm Med. 2004;11:6-13.
8. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systematic review. PLoS Negl Trop Dis. 2013;7:e2002.
9. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html#me-asia-na-la-caribbean. Accessed April 3, 2014.
10. Centers for Disease Control and Prevention. Treatment options for presumptive parasitic infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/interventions/interventions.html. Accessed April 3, 2014.
1. Centers for Disease Control and Prevention. Parasites - Strongyloides. Epidemiology & risk factors. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/epi.html. Accessed September 4, 2015.
2. Buonfrate D, Angheben A, Gobbi F, et al. Imported strongyloidiasis: epidemiology, presentations, and treatment. Curr Infect Dis Rep. 2012;14:256-262.
3. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040-1047.
4. Buonfrate D, Requena-Mendez A, Angheben A, et al. Severe strongyloidiasis: a systematic review of case reports. BMC Infect Dis. 2013;13:78.
5. Centers for Disease Control and Prevention. Parasites - Strongyloides. Resources for health professionals. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed September 4, 2015.
6. UpToDate. Klion AD, Weller PF. Approach to the patient with unexplained eosinophilia. UpToDate Web site. Available at: http://www.uptodate.com/contents/approach-to-the-patientwith-unexplained-eosinophilia. Accessed August 27, 2015.
7. Mokhlesi B, Shulzhenko O, Garimella PS, et al. Pulmonary strongyloidiasis: the varied clinical presentations. Clin Pulm Med. 2004;11:6-13.
8. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systematic review. PLoS Negl Trop Dis. 2013;7:e2002.
9. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html#me-asia-na-la-caribbean. Accessed April 3, 2014.
10. Centers for Disease Control and Prevention. Treatment options for presumptive parasitic infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/interventions/interventions.html. Accessed April 3, 2014.

New and Noteworthy Information—October 2015
Low vitamin D status was associated with accelerated decline in cognitive function in an ethnically diverse older population, according to data published online ahead of print September 14 in JAMA Neurology. Individuals with low vitamin D declined, on average, at a rate two to three times faster than those with adequate vitamin D levels, said the researchers. Serum 25-hydroxyvitamin D was measured at baseline and at five yearly follow-up visits in a longitudinal, multiethnic cohort of 382 patients in an outpatient clinic. Mean age was 75.5. “Independent of race or ethnicity, baseline cognitive abilities, and a host of other risk factors, vitamin D insufficiency was associated with significantly faster declines in both episodic memory and executive function performance,” the researchers reported. “This work, and that of others, suggests that there is enough evidence to recommend that people in their 60s and older discuss taking a daily vitamin D supplement with their physicians.”
Being overweight or obese may be linked to an increased risk of meningioma, according to a meta-analysis published online ahead of print September 16 in Neurology. The meta-analysis looked at available research on BMI, physical activity, and the two most common types of brain tumors—meningioma and glioma. A total of 12 studies on BMI and six on physical activity were analyzed, involving 2,982 meningioma cases and 3,057 glioma cases. Compared with people with a normal weight, overweight people were 21% more likely to develop a meningioma, and obese people were 54% more likely to develop one. “This is an important finding, since there are few known risk factors for meningioma, and the ones we do know about are not things a person can change,” said the investigators. No relationship was found between excess weight and glioma.
Working long hours is linked to an increased risk of stroke and coronary heart disease, compared with working a standard work week, according to research published online ahead of print August 19 in Lancet. Researchers performed a meta-analysis of published studies and unpublished individual-level data examining the effects of longer working hours on cardiovascular disease. Analysis of data from 25 studies involving 603,838 men and women from Europe, the USA, and Australia found a 13% increased risk of incident coronary heart disease in people working 55 or more hours per week, compared with those working a 35- to 40-hour work week. Analysis of data from 17 studies involving 528,908 men and women found a 1.3-times higher risk of stroke in individuals working longer hours per week, compared with those working standard hours. The association remained after controlling for smoking, alcohol consumption, and physical activity, as well as cardiovascular risk factors such as hypertension and high cholesterol.
FDA approved a new indication for Sunovion’s Aptiom (eslicarbazepine acetate): monotherapy for the treatment of partial-onset seizures. Aptiom was approved in 2013 as adjunctive therapy for partial-onset seizures. The new indication approval is based on the results of two phase III trials. Data from the monotherapy trials, in addition to the data generated from the adjunctive trials, confirm that the drug is efficacious and well-tolerated as adjunctive or monotherapy treatment within a daily dose range of 800 to 1,600 mg. The phase III trials evaluated eslicarbazepine acetate (1,600 mg/day or 1,200 mg/day) as monotherapy for partial-onset seizures in patients age 16 or older whose seizures were not well controlled with other antiepileptic drugs (AEDs). Conversion to eslicarbazepine acetate monotherapy was associated with favorable seizure control, compared with historical controls in patients with partial-onset seizures not well controlled by one or two AEDs.
Results of a hospital-based study published online ahead of print August 19 in Neurology offer clinical recommendations regarding acute headache in pregnant women. The investigators conducted a five-year, single-center, retrospective study of consecutive pregnant women presenting to acute care with headache and receiving a neurologic consultation. Their study cohort included 140 women (mean age, 29) who often presented in the third trimester (56.4%). Diagnoses included primary (65%) and secondary (35%) headache disorders. The most common primary headache disorder was migraine (91.2%), and secondary headache disorders were hypertensive disorders. The authors recommend that diagnostic vigilance be heightened in the absence of a headache history and if seizures, hypertension, or fever are present. Attack features may not adequately distinguish primary versus secondary disorders, and low thresholds for neuroimaging and monitoring for preeclampsia are justified, they said.
Short sleepers are four times more likely to catch a cold when exposed to the virus, compared with those who sleep longer, according to a study published in the September issue of Sleep. Researchers recruited 164 volunteers between 2007 and 2011. The recruits underwent two months of health screening, interviews, and questionnaires to establish baselines for stress, temperament, and alcohol and cigarette use. Researchers also measured participants’ normal sleep habits one week prior to sequestering them and administering the cold virus. Subjects who slept less than six hours per night were 4.2 times more likely to catch the cold, compared with those who got more than seven hours of sleep, and those who slept less than five hours were 4.5 times more likely to get sick.
Over the long term, a high dose of a purified form of resveratrol stabilizes a biomarker of Alzheimer’s disease progression, according to clinical trial results published online ahead of print September 11 in Neurology. Resveratrol is a naturally occurring compound found in foods such as red grapes, raspberries, dark chocolate, and some red wines. The randomized, phase II, placebo-controlled, double-blind study enrolled 119 patients with mild to moderate Alzheimer’s disease. The highest dose tested was 1 g orally twice per day. Patients who were treated with increasing doses of resveratrol over 12 months showed little or no change in amyloid-beta40 levels in blood and CSF. Those taking placebo had a decrease in the their levels of amyloid-beta40 over baseline. “We can’t conclude from this study that the effects of resveratrol treatment are beneficial,” said the investigators, but “it does appear that resveratrol was able to penetrate the blood–brain barrier, which is an important observation.”
Survivors of an intracerebral hemorrhage (ICH) who had inadequate blood pressure control during follow-up had a higher risk of ICH recurrence, according to a study in the September 1 issue of JAMA. This association was stronger with worsening severity of hypertension. Investigators studied 1,145 patients with ICH who survived at least 90 days. Median follow-up was 37 months. Blood pressure measurements were obtained at three, six, nine, and 12 months, and every six months thereafter. There were 102 recurrent ICH events among 505 survivors of lobar ICH and 44 recurrent ICH events among 640 survivors of nonlobar ICH. During follow-up, adequate blood pressure control was achieved on at least one measurement by 625 patients (55%) and consistently by 495 patients (43%). The ICH event rate for lobar and nonlobar ICH was higher among patients with inadequate blood pressure control, compared with patients with adequate blood pressure control.
Genetic findings support observational evidence that lower vitamin D levels are associated with increased risk of multiple sclerosis (MS), according to a study published online August 25 in PLOS Medicine. Using Mendelian randomization to reduce the possibility of confounding, the researchers examined whether there was an association between genetically reduced vitamin D levels and susceptibility to MS among participants in the International MS Genetics Consortium Study, which involves 14,498 patients with MS and 24,091 healthy controls. A genetic decrease in the natural-log-transformed vitamin D level by one standard deviation was associated with a twofold increased risk of MS. According to the researchers, “genetically lowered vitamin D levels are strongly associated with increased susceptibility to MS. Whether vitamin D sufficiency can delay or prevent MS onset merits further investigation.”
Diabetes may be linked to the buildup of tangles or tau in the brain, separate from Alzheimer’s disease, according to a study published online ahead of print September 2 in Neurology. The study involved 816 people (average age, 74). Of those, 397 had mild cognitive impairment, 191 had Alzheimer’s disease dementia, and 228 people had no memory or cognitive problems. A total of 124 people had diabetes. The researchers examined the relationship between type 2 diabetes, the loss of brain cells and their connections, levels of beta amyloid, and tau in the spinal fluid of the participants. Those with diabetes had on average 16 pg/mL greater levels of tau in the spinal and brain fluid, irrespective of the diagnosis of dementia. In addition, patients with diabetes had cortical tissue that was an average of 0.03 mm thinner than that of those who did not have diabetes, regardless of their cognitive abilities or dementia status.
Survivors of childhood cancer who have had a stroke have double the risk of a recurrent stroke when compared with noncancer stroke survivors, according to a study published online ahead of print August 26 in Neurology. The main predictors of recurrent stroke were cranial radiation therapy, hypertension, and older age at first stroke. Researchers analyzed retrospective data from the Childhood Cancer Survivor Study, which followed 14,358 survivors of pediatric cancer. Stroke rates were established through surveys and self-report. Of the 271 respondents who reported having a stroke, 70 also reported a second stroke. Overall, the rate of recurrence within the first 10 years after an initial stroke was 21%, which is double the rate in the general population of stroke survivors. The rate was 33% for patients who had received cranial radiation therapy.
—Glenn S. Williams
Low vitamin D status was associated with accelerated decline in cognitive function in an ethnically diverse older population, according to data published online ahead of print September 14 in JAMA Neurology. Individuals with low vitamin D declined, on average, at a rate two to three times faster than those with adequate vitamin D levels, said the researchers. Serum 25-hydroxyvitamin D was measured at baseline and at five yearly follow-up visits in a longitudinal, multiethnic cohort of 382 patients in an outpatient clinic. Mean age was 75.5. “Independent of race or ethnicity, baseline cognitive abilities, and a host of other risk factors, vitamin D insufficiency was associated with significantly faster declines in both episodic memory and executive function performance,” the researchers reported. “This work, and that of others, suggests that there is enough evidence to recommend that people in their 60s and older discuss taking a daily vitamin D supplement with their physicians.”
Being overweight or obese may be linked to an increased risk of meningioma, according to a meta-analysis published online ahead of print September 16 in Neurology. The meta-analysis looked at available research on BMI, physical activity, and the two most common types of brain tumors—meningioma and glioma. A total of 12 studies on BMI and six on physical activity were analyzed, involving 2,982 meningioma cases and 3,057 glioma cases. Compared with people with a normal weight, overweight people were 21% more likely to develop a meningioma, and obese people were 54% more likely to develop one. “This is an important finding, since there are few known risk factors for meningioma, and the ones we do know about are not things a person can change,” said the investigators. No relationship was found between excess weight and glioma.
Working long hours is linked to an increased risk of stroke and coronary heart disease, compared with working a standard work week, according to research published online ahead of print August 19 in Lancet. Researchers performed a meta-analysis of published studies and unpublished individual-level data examining the effects of longer working hours on cardiovascular disease. Analysis of data from 25 studies involving 603,838 men and women from Europe, the USA, and Australia found a 13% increased risk of incident coronary heart disease in people working 55 or more hours per week, compared with those working a 35- to 40-hour work week. Analysis of data from 17 studies involving 528,908 men and women found a 1.3-times higher risk of stroke in individuals working longer hours per week, compared with those working standard hours. The association remained after controlling for smoking, alcohol consumption, and physical activity, as well as cardiovascular risk factors such as hypertension and high cholesterol.
FDA approved a new indication for Sunovion’s Aptiom (eslicarbazepine acetate): monotherapy for the treatment of partial-onset seizures. Aptiom was approved in 2013 as adjunctive therapy for partial-onset seizures. The new indication approval is based on the results of two phase III trials. Data from the monotherapy trials, in addition to the data generated from the adjunctive trials, confirm that the drug is efficacious and well-tolerated as adjunctive or monotherapy treatment within a daily dose range of 800 to 1,600 mg. The phase III trials evaluated eslicarbazepine acetate (1,600 mg/day or 1,200 mg/day) as monotherapy for partial-onset seizures in patients age 16 or older whose seizures were not well controlled with other antiepileptic drugs (AEDs). Conversion to eslicarbazepine acetate monotherapy was associated with favorable seizure control, compared with historical controls in patients with partial-onset seizures not well controlled by one or two AEDs.
Results of a hospital-based study published online ahead of print August 19 in Neurology offer clinical recommendations regarding acute headache in pregnant women. The investigators conducted a five-year, single-center, retrospective study of consecutive pregnant women presenting to acute care with headache and receiving a neurologic consultation. Their study cohort included 140 women (mean age, 29) who often presented in the third trimester (56.4%). Diagnoses included primary (65%) and secondary (35%) headache disorders. The most common primary headache disorder was migraine (91.2%), and secondary headache disorders were hypertensive disorders. The authors recommend that diagnostic vigilance be heightened in the absence of a headache history and if seizures, hypertension, or fever are present. Attack features may not adequately distinguish primary versus secondary disorders, and low thresholds for neuroimaging and monitoring for preeclampsia are justified, they said.
Short sleepers are four times more likely to catch a cold when exposed to the virus, compared with those who sleep longer, according to a study published in the September issue of Sleep. Researchers recruited 164 volunteers between 2007 and 2011. The recruits underwent two months of health screening, interviews, and questionnaires to establish baselines for stress, temperament, and alcohol and cigarette use. Researchers also measured participants’ normal sleep habits one week prior to sequestering them and administering the cold virus. Subjects who slept less than six hours per night were 4.2 times more likely to catch the cold, compared with those who got more than seven hours of sleep, and those who slept less than five hours were 4.5 times more likely to get sick.
Over the long term, a high dose of a purified form of resveratrol stabilizes a biomarker of Alzheimer’s disease progression, according to clinical trial results published online ahead of print September 11 in Neurology. Resveratrol is a naturally occurring compound found in foods such as red grapes, raspberries, dark chocolate, and some red wines. The randomized, phase II, placebo-controlled, double-blind study enrolled 119 patients with mild to moderate Alzheimer’s disease. The highest dose tested was 1 g orally twice per day. Patients who were treated with increasing doses of resveratrol over 12 months showed little or no change in amyloid-beta40 levels in blood and CSF. Those taking placebo had a decrease in the their levels of amyloid-beta40 over baseline. “We can’t conclude from this study that the effects of resveratrol treatment are beneficial,” said the investigators, but “it does appear that resveratrol was able to penetrate the blood–brain barrier, which is an important observation.”
Survivors of an intracerebral hemorrhage (ICH) who had inadequate blood pressure control during follow-up had a higher risk of ICH recurrence, according to a study in the September 1 issue of JAMA. This association was stronger with worsening severity of hypertension. Investigators studied 1,145 patients with ICH who survived at least 90 days. Median follow-up was 37 months. Blood pressure measurements were obtained at three, six, nine, and 12 months, and every six months thereafter. There were 102 recurrent ICH events among 505 survivors of lobar ICH and 44 recurrent ICH events among 640 survivors of nonlobar ICH. During follow-up, adequate blood pressure control was achieved on at least one measurement by 625 patients (55%) and consistently by 495 patients (43%). The ICH event rate for lobar and nonlobar ICH was higher among patients with inadequate blood pressure control, compared with patients with adequate blood pressure control.
Genetic findings support observational evidence that lower vitamin D levels are associated with increased risk of multiple sclerosis (MS), according to a study published online August 25 in PLOS Medicine. Using Mendelian randomization to reduce the possibility of confounding, the researchers examined whether there was an association between genetically reduced vitamin D levels and susceptibility to MS among participants in the International MS Genetics Consortium Study, which involves 14,498 patients with MS and 24,091 healthy controls. A genetic decrease in the natural-log-transformed vitamin D level by one standard deviation was associated with a twofold increased risk of MS. According to the researchers, “genetically lowered vitamin D levels are strongly associated with increased susceptibility to MS. Whether vitamin D sufficiency can delay or prevent MS onset merits further investigation.”
Diabetes may be linked to the buildup of tangles or tau in the brain, separate from Alzheimer’s disease, according to a study published online ahead of print September 2 in Neurology. The study involved 816 people (average age, 74). Of those, 397 had mild cognitive impairment, 191 had Alzheimer’s disease dementia, and 228 people had no memory or cognitive problems. A total of 124 people had diabetes. The researchers examined the relationship between type 2 diabetes, the loss of brain cells and their connections, levels of beta amyloid, and tau in the spinal fluid of the participants. Those with diabetes had on average 16 pg/mL greater levels of tau in the spinal and brain fluid, irrespective of the diagnosis of dementia. In addition, patients with diabetes had cortical tissue that was an average of 0.03 mm thinner than that of those who did not have diabetes, regardless of their cognitive abilities or dementia status.
Survivors of childhood cancer who have had a stroke have double the risk of a recurrent stroke when compared with noncancer stroke survivors, according to a study published online ahead of print August 26 in Neurology. The main predictors of recurrent stroke were cranial radiation therapy, hypertension, and older age at first stroke. Researchers analyzed retrospective data from the Childhood Cancer Survivor Study, which followed 14,358 survivors of pediatric cancer. Stroke rates were established through surveys and self-report. Of the 271 respondents who reported having a stroke, 70 also reported a second stroke. Overall, the rate of recurrence within the first 10 years after an initial stroke was 21%, which is double the rate in the general population of stroke survivors. The rate was 33% for patients who had received cranial radiation therapy.
—Glenn S. Williams
Low vitamin D status was associated with accelerated decline in cognitive function in an ethnically diverse older population, according to data published online ahead of print September 14 in JAMA Neurology. Individuals with low vitamin D declined, on average, at a rate two to three times faster than those with adequate vitamin D levels, said the researchers. Serum 25-hydroxyvitamin D was measured at baseline and at five yearly follow-up visits in a longitudinal, multiethnic cohort of 382 patients in an outpatient clinic. Mean age was 75.5. “Independent of race or ethnicity, baseline cognitive abilities, and a host of other risk factors, vitamin D insufficiency was associated with significantly faster declines in both episodic memory and executive function performance,” the researchers reported. “This work, and that of others, suggests that there is enough evidence to recommend that people in their 60s and older discuss taking a daily vitamin D supplement with their physicians.”
Being overweight or obese may be linked to an increased risk of meningioma, according to a meta-analysis published online ahead of print September 16 in Neurology. The meta-analysis looked at available research on BMI, physical activity, and the two most common types of brain tumors—meningioma and glioma. A total of 12 studies on BMI and six on physical activity were analyzed, involving 2,982 meningioma cases and 3,057 glioma cases. Compared with people with a normal weight, overweight people were 21% more likely to develop a meningioma, and obese people were 54% more likely to develop one. “This is an important finding, since there are few known risk factors for meningioma, and the ones we do know about are not things a person can change,” said the investigators. No relationship was found between excess weight and glioma.
Working long hours is linked to an increased risk of stroke and coronary heart disease, compared with working a standard work week, according to research published online ahead of print August 19 in Lancet. Researchers performed a meta-analysis of published studies and unpublished individual-level data examining the effects of longer working hours on cardiovascular disease. Analysis of data from 25 studies involving 603,838 men and women from Europe, the USA, and Australia found a 13% increased risk of incident coronary heart disease in people working 55 or more hours per week, compared with those working a 35- to 40-hour work week. Analysis of data from 17 studies involving 528,908 men and women found a 1.3-times higher risk of stroke in individuals working longer hours per week, compared with those working standard hours. The association remained after controlling for smoking, alcohol consumption, and physical activity, as well as cardiovascular risk factors such as hypertension and high cholesterol.
FDA approved a new indication for Sunovion’s Aptiom (eslicarbazepine acetate): monotherapy for the treatment of partial-onset seizures. Aptiom was approved in 2013 as adjunctive therapy for partial-onset seizures. The new indication approval is based on the results of two phase III trials. Data from the monotherapy trials, in addition to the data generated from the adjunctive trials, confirm that the drug is efficacious and well-tolerated as adjunctive or monotherapy treatment within a daily dose range of 800 to 1,600 mg. The phase III trials evaluated eslicarbazepine acetate (1,600 mg/day or 1,200 mg/day) as monotherapy for partial-onset seizures in patients age 16 or older whose seizures were not well controlled with other antiepileptic drugs (AEDs). Conversion to eslicarbazepine acetate monotherapy was associated with favorable seizure control, compared with historical controls in patients with partial-onset seizures not well controlled by one or two AEDs.
Results of a hospital-based study published online ahead of print August 19 in Neurology offer clinical recommendations regarding acute headache in pregnant women. The investigators conducted a five-year, single-center, retrospective study of consecutive pregnant women presenting to acute care with headache and receiving a neurologic consultation. Their study cohort included 140 women (mean age, 29) who often presented in the third trimester (56.4%). Diagnoses included primary (65%) and secondary (35%) headache disorders. The most common primary headache disorder was migraine (91.2%), and secondary headache disorders were hypertensive disorders. The authors recommend that diagnostic vigilance be heightened in the absence of a headache history and if seizures, hypertension, or fever are present. Attack features may not adequately distinguish primary versus secondary disorders, and low thresholds for neuroimaging and monitoring for preeclampsia are justified, they said.
Short sleepers are four times more likely to catch a cold when exposed to the virus, compared with those who sleep longer, according to a study published in the September issue of Sleep. Researchers recruited 164 volunteers between 2007 and 2011. The recruits underwent two months of health screening, interviews, and questionnaires to establish baselines for stress, temperament, and alcohol and cigarette use. Researchers also measured participants’ normal sleep habits one week prior to sequestering them and administering the cold virus. Subjects who slept less than six hours per night were 4.2 times more likely to catch the cold, compared with those who got more than seven hours of sleep, and those who slept less than five hours were 4.5 times more likely to get sick.
Over the long term, a high dose of a purified form of resveratrol stabilizes a biomarker of Alzheimer’s disease progression, according to clinical trial results published online ahead of print September 11 in Neurology. Resveratrol is a naturally occurring compound found in foods such as red grapes, raspberries, dark chocolate, and some red wines. The randomized, phase II, placebo-controlled, double-blind study enrolled 119 patients with mild to moderate Alzheimer’s disease. The highest dose tested was 1 g orally twice per day. Patients who were treated with increasing doses of resveratrol over 12 months showed little or no change in amyloid-beta40 levels in blood and CSF. Those taking placebo had a decrease in the their levels of amyloid-beta40 over baseline. “We can’t conclude from this study that the effects of resveratrol treatment are beneficial,” said the investigators, but “it does appear that resveratrol was able to penetrate the blood–brain barrier, which is an important observation.”
Survivors of an intracerebral hemorrhage (ICH) who had inadequate blood pressure control during follow-up had a higher risk of ICH recurrence, according to a study in the September 1 issue of JAMA. This association was stronger with worsening severity of hypertension. Investigators studied 1,145 patients with ICH who survived at least 90 days. Median follow-up was 37 months. Blood pressure measurements were obtained at three, six, nine, and 12 months, and every six months thereafter. There were 102 recurrent ICH events among 505 survivors of lobar ICH and 44 recurrent ICH events among 640 survivors of nonlobar ICH. During follow-up, adequate blood pressure control was achieved on at least one measurement by 625 patients (55%) and consistently by 495 patients (43%). The ICH event rate for lobar and nonlobar ICH was higher among patients with inadequate blood pressure control, compared with patients with adequate blood pressure control.
Genetic findings support observational evidence that lower vitamin D levels are associated with increased risk of multiple sclerosis (MS), according to a study published online August 25 in PLOS Medicine. Using Mendelian randomization to reduce the possibility of confounding, the researchers examined whether there was an association between genetically reduced vitamin D levels and susceptibility to MS among participants in the International MS Genetics Consortium Study, which involves 14,498 patients with MS and 24,091 healthy controls. A genetic decrease in the natural-log-transformed vitamin D level by one standard deviation was associated with a twofold increased risk of MS. According to the researchers, “genetically lowered vitamin D levels are strongly associated with increased susceptibility to MS. Whether vitamin D sufficiency can delay or prevent MS onset merits further investigation.”
Diabetes may be linked to the buildup of tangles or tau in the brain, separate from Alzheimer’s disease, according to a study published online ahead of print September 2 in Neurology. The study involved 816 people (average age, 74). Of those, 397 had mild cognitive impairment, 191 had Alzheimer’s disease dementia, and 228 people had no memory or cognitive problems. A total of 124 people had diabetes. The researchers examined the relationship between type 2 diabetes, the loss of brain cells and their connections, levels of beta amyloid, and tau in the spinal fluid of the participants. Those with diabetes had on average 16 pg/mL greater levels of tau in the spinal and brain fluid, irrespective of the diagnosis of dementia. In addition, patients with diabetes had cortical tissue that was an average of 0.03 mm thinner than that of those who did not have diabetes, regardless of their cognitive abilities or dementia status.
Survivors of childhood cancer who have had a stroke have double the risk of a recurrent stroke when compared with noncancer stroke survivors, according to a study published online ahead of print August 26 in Neurology. The main predictors of recurrent stroke were cranial radiation therapy, hypertension, and older age at first stroke. Researchers analyzed retrospective data from the Childhood Cancer Survivor Study, which followed 14,358 survivors of pediatric cancer. Stroke rates were established through surveys and self-report. Of the 271 respondents who reported having a stroke, 70 also reported a second stroke. Overall, the rate of recurrence within the first 10 years after an initial stroke was 21%, which is double the rate in the general population of stroke survivors. The rate was 33% for patients who had received cranial radiation therapy.
—Glenn S. Williams

What’s Wrong With This Picture?
ANSWER
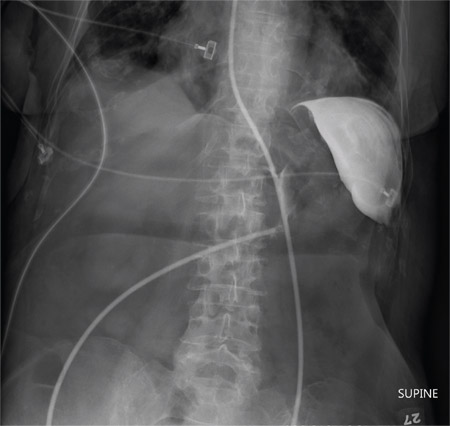
The radiograph shows an enteric tube passing through the gastrointestinal tract. However, it extends low into the left lower quadrant, loops around the right lower quadrant, and then heads up toward the left upper quadrant. Such a course is atypical and concerning for displaced position.
The radiologists concurred, and it was decided to instill some water-soluble contrast and repeat the KUB for further evaluation. That image is shown here. Note that the contrast does not appear to be in the stomach, as no gastric folds are visible. It accumulates in the left upper quadrant, under the diaphragm. Such a finding is concerning for possible gastric perforation.
The tube was promptly withdrawn, and urgent surgical consultation was obtained.
ANSWER
The radiograph shows an enteric tube passing through the gastrointestinal tract. However, it extends low into the left lower quadrant, loops around the right lower quadrant, and then heads up toward the left upper quadrant. Such a course is atypical and concerning for displaced position.
The radiologists concurred, and it was decided to instill some water-soluble contrast and repeat the KUB for further evaluation. That image is shown here. Note that the contrast does not appear to be in the stomach, as no gastric folds are visible. It accumulates in the left upper quadrant, under the diaphragm. Such a finding is concerning for possible gastric perforation.
The tube was promptly withdrawn, and urgent surgical consultation was obtained.
ANSWER
The radiograph shows an enteric tube passing through the gastrointestinal tract. However, it extends low into the left lower quadrant, loops around the right lower quadrant, and then heads up toward the left upper quadrant. Such a course is atypical and concerning for displaced position.
The radiologists concurred, and it was decided to instill some water-soluble contrast and repeat the KUB for further evaluation. That image is shown here. Note that the contrast does not appear to be in the stomach, as no gastric folds are visible. It accumulates in the left upper quadrant, under the diaphragm. Such a finding is concerning for possible gastric perforation.
The tube was promptly withdrawn, and urgent surgical consultation was obtained.

A 90-year-old woman, admitted for altered mental status, just had a nasogastric tube placed to facilitate nutrition and medication delivery. The ICU nurse asks you to review an abdominal radiograph to confirm correct placement, since several attempts by various hospital personnel were required before they felt they had the tube in place. The patient is otherwise currently stable, per the nurse’s report. Her vital signs are stable, and she will arouse to minimal stimulation, although she continues to demonstrate confusion. Portable KUB radiograph is shown. What is your impression?

Tumor Necrosis Factor Inhibitors and Multiple Sclerosis: A Closer Look
With the advent of tumor necrosis factor (TNF) inhibitors, one of the major topics of discussion is the relationship of the drug class with new or worsening multiple sclerosis (MS). Exacerbation of previously quiescent MS and the onset of other demyelinating diseases such as optic neuritis have been reported in patients taking TNF inhibitors. Symptoms included paraesthesia, visual disturbance, and confusion.
Therefore, controversy surrounds the use of TNF-α inhibitors in patients who are more predisposed to developing MS, specifically first-degree relatives of MS patients. The American Academy of Dermatology guidelines for TNF inhibitors state the following: “Because there is an association between anti-TNF therapy and demyelinating diseases (ie, MS), TNF inhibitors should not be used in patients with MS or other demyelinating diseases; first-degree relatives of patients with MS have an increased risk of developing MS, with a sibling relative risk of between 18 and 36, evidence strongly suggests that TNF inhibitors should not be used in first-degree relatives of patients with MS.”
Mansouri et al (J Drugs Dermatol. 2015;14:876-878) presented data suggesting that the number needed to treat is at least an order of magnitude smaller than the number needed to harm across all comparisons of anti–TNF-α agents and first-degree relative relationships. Based on these data, the authors suggest that physicians could weigh the treatment options available and work closely with neurological colleagues when prescribing anti–TNF-α therapy in this patient population, which could be an alternative approach to practicing absolute prohibition of anti–TNF-α agents in patients who have a first-degree relative with MS.
What’s the issue?
This article presents interesting data concerning the risk-benefit of using TNF inhibitors in a potential at-risk population. We are fortunate to have many treatment options available, but in many cases, a TNF inhibitor may be preferable. How will this information affect your use of TNF inhibitors in patients with a first-degree relative with MS?
With the advent of tumor necrosis factor (TNF) inhibitors, one of the major topics of discussion is the relationship of the drug class with new or worsening multiple sclerosis (MS). Exacerbation of previously quiescent MS and the onset of other demyelinating diseases such as optic neuritis have been reported in patients taking TNF inhibitors. Symptoms included paraesthesia, visual disturbance, and confusion.
Therefore, controversy surrounds the use of TNF-α inhibitors in patients who are more predisposed to developing MS, specifically first-degree relatives of MS patients. The American Academy of Dermatology guidelines for TNF inhibitors state the following: “Because there is an association between anti-TNF therapy and demyelinating diseases (ie, MS), TNF inhibitors should not be used in patients with MS or other demyelinating diseases; first-degree relatives of patients with MS have an increased risk of developing MS, with a sibling relative risk of between 18 and 36, evidence strongly suggests that TNF inhibitors should not be used in first-degree relatives of patients with MS.”
Mansouri et al (J Drugs Dermatol. 2015;14:876-878) presented data suggesting that the number needed to treat is at least an order of magnitude smaller than the number needed to harm across all comparisons of anti–TNF-α agents and first-degree relative relationships. Based on these data, the authors suggest that physicians could weigh the treatment options available and work closely with neurological colleagues when prescribing anti–TNF-α therapy in this patient population, which could be an alternative approach to practicing absolute prohibition of anti–TNF-α agents in patients who have a first-degree relative with MS.
What’s the issue?
This article presents interesting data concerning the risk-benefit of using TNF inhibitors in a potential at-risk population. We are fortunate to have many treatment options available, but in many cases, a TNF inhibitor may be preferable. How will this information affect your use of TNF inhibitors in patients with a first-degree relative with MS?
With the advent of tumor necrosis factor (TNF) inhibitors, one of the major topics of discussion is the relationship of the drug class with new or worsening multiple sclerosis (MS). Exacerbation of previously quiescent MS and the onset of other demyelinating diseases such as optic neuritis have been reported in patients taking TNF inhibitors. Symptoms included paraesthesia, visual disturbance, and confusion.
Therefore, controversy surrounds the use of TNF-α inhibitors in patients who are more predisposed to developing MS, specifically first-degree relatives of MS patients. The American Academy of Dermatology guidelines for TNF inhibitors state the following: “Because there is an association between anti-TNF therapy and demyelinating diseases (ie, MS), TNF inhibitors should not be used in patients with MS or other demyelinating diseases; first-degree relatives of patients with MS have an increased risk of developing MS, with a sibling relative risk of between 18 and 36, evidence strongly suggests that TNF inhibitors should not be used in first-degree relatives of patients with MS.”
Mansouri et al (J Drugs Dermatol. 2015;14:876-878) presented data suggesting that the number needed to treat is at least an order of magnitude smaller than the number needed to harm across all comparisons of anti–TNF-α agents and first-degree relative relationships. Based on these data, the authors suggest that physicians could weigh the treatment options available and work closely with neurological colleagues when prescribing anti–TNF-α therapy in this patient population, which could be an alternative approach to practicing absolute prohibition of anti–TNF-α agents in patients who have a first-degree relative with MS.
What’s the issue?
This article presents interesting data concerning the risk-benefit of using TNF inhibitors in a potential at-risk population. We are fortunate to have many treatment options available, but in many cases, a TNF inhibitor may be preferable. How will this information affect your use of TNF inhibitors in patients with a first-degree relative with MS?

Clindamycin–benzoyl peroxide combo effective in moderate and severe acne
A fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% (clindamycin-BP 3.75%) aqueous gel was effective and well tolerated in the treatment of moderate and severe acne vulgaris, reported Dr. Linda Stein Gold of Henry Ford Hospital in Detroit (J Drugs Dermatol. 2015;14[9]:969-74).

A multicenter, double-blind, randomized trial of 498 patients with moderate to severe acne showed that inflammatory and noninflammatory lesions were significantly reduced in patients who received treatment with clindamycin-BP 3.75% topical gel, compared with those in the vehicle group.
In patients with severe acne, 55.1% had a reduction of two grades or more in severity score at 12 weeks. In addition, 30.6% of patients assessed their acne as “clear” or “almost clear,” Dr. Stein Gold wrote. No participants withdrew from the study because of adverse events.
Read the article here.
A fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% (clindamycin-BP 3.75%) aqueous gel was effective and well tolerated in the treatment of moderate and severe acne vulgaris, reported Dr. Linda Stein Gold of Henry Ford Hospital in Detroit (J Drugs Dermatol. 2015;14[9]:969-74).
A multicenter, double-blind, randomized trial of 498 patients with moderate to severe acne showed that inflammatory and noninflammatory lesions were significantly reduced in patients who received treatment with clindamycin-BP 3.75% topical gel, compared with those in the vehicle group.
In patients with severe acne, 55.1% had a reduction of two grades or more in severity score at 12 weeks. In addition, 30.6% of patients assessed their acne as “clear” or “almost clear,” Dr. Stein Gold wrote. No participants withdrew from the study because of adverse events.
Read the article here.
A fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% (clindamycin-BP 3.75%) aqueous gel was effective and well tolerated in the treatment of moderate and severe acne vulgaris, reported Dr. Linda Stein Gold of Henry Ford Hospital in Detroit (J Drugs Dermatol. 2015;14[9]:969-74).
A multicenter, double-blind, randomized trial of 498 patients with moderate to severe acne showed that inflammatory and noninflammatory lesions were significantly reduced in patients who received treatment with clindamycin-BP 3.75% topical gel, compared with those in the vehicle group.
In patients with severe acne, 55.1% had a reduction of two grades or more in severity score at 12 weeks. In addition, 30.6% of patients assessed their acne as “clear” or “almost clear,” Dr. Stein Gold wrote. No participants withdrew from the study because of adverse events.
Read the article here.

Are overweight children likely to become overweight adults?
Yes. Overweight children (body mass index [BMI] ≥85th to <95th percentile) are likely to become overweight or obese adults with a BMI ≥25 (strength of recommendation [SOR]: B, systematic review of high-quality prospective longitudinal studies).
Obese adolescents are significantly more likely to develop severe obesity than normal weight or overweight adolescents (SOR: B, prospective cohort study). (See “Definition of terms” below.)
The trend to overweight and obesity in adulthood is clear
A systematic review of 20 prospective and 5 retrospective trials tracked 179,303 overweight and obese children into adulthood.1 Investigators included studies for evaluation if they were written in English, prospective or retrospective longitudinal in design, described at least one anthropometric measurement, and included odds ratios or risk ratios in the results. The results were not pooled because of heterogeneity among studies.
In high-quality trials, the percentages of overweight or obese children and adolescents who became overweight or obese adults varied: overweight children (76% to 83%), obese children (18% to 60%), overweight adolescents (22% to 58%) and obese adolescents (24% to 90%). Limitations of the review included an inadequate description of the anthropometric measurement protocol, use of self-reported weight and height, and the fact that all studies were conducted in high-income countries.
Obesity in adolescence often progresses to severe obesity later on
A prospective cohort trial followed 8834 nonobese and obese individuals, ages 12 to 21, for 13 years to assess risk of adult obesity.2 Patients were drawn from the National Longitudinal Study of Adolescent Health, which is a representative sample of United States schools from 1994 to 1995 with respect to region, urbanicity, school size, school type, and ethnicity.
Researchers observed a total of 703 incident cases of severe obesity in adulthood, indicating a total incidence rate of 7.9% (95% confidence interval [CI], 7.4%-8.5%). Obese adolescents were significantly more likely to develop severe obesity than nonobese adolescents who were normal weight or overweight (hazard ratio [HR]=16; 95% CI, 12-21).
A significant proportion of obese adolescents became severely obese by their early 30s, with an incidence of 37% in men (95% CI, 31%-44%) and 51% in women (95% CI, 45%-58%). Black women had the highest incidence at 52% (95% CI, 41%-64%). Fewer than 5% of patients (across sex and race) who were normal weight in adolescence became severely obese in adulthood.
Normal weight: Body mass index (BMI) ≥5th to <85th percentile for individuals <20 years old or BMI ≥18.5 to <25 for individuals >20 years.
Overweight: BMI ≥85th to <95th percentile or BMI ≥25 to <30.
Obesity: BMI ≥95th to <120% of 95th percentile or BMI ≥30 to <40.
Severe obesity: BMI ≥120% of 95th percentile; BMI ≥40.
1. Singh AS, Mulder C, Twisk WR, et al. Tracking of childhood overweight into adulthood: a systemic review of the literature. Obes Rev. 2008;9:474-488.
2. The NS, Suchindran C, North KE, et al. Association of adolescent obesity with risk of severe obesity in adulthood. JAMA. 2010;304:2042-2047.
Yes. Overweight children (body mass index [BMI] ≥85th to <95th percentile) are likely to become overweight or obese adults with a BMI ≥25 (strength of recommendation [SOR]: B, systematic review of high-quality prospective longitudinal studies).
Obese adolescents are significantly more likely to develop severe obesity than normal weight or overweight adolescents (SOR: B, prospective cohort study). (See “Definition of terms” below.)
The trend to overweight and obesity in adulthood is clear
A systematic review of 20 prospective and 5 retrospective trials tracked 179,303 overweight and obese children into adulthood.1 Investigators included studies for evaluation if they were written in English, prospective or retrospective longitudinal in design, described at least one anthropometric measurement, and included odds ratios or risk ratios in the results. The results were not pooled because of heterogeneity among studies.
In high-quality trials, the percentages of overweight or obese children and adolescents who became overweight or obese adults varied: overweight children (76% to 83%), obese children (18% to 60%), overweight adolescents (22% to 58%) and obese adolescents (24% to 90%). Limitations of the review included an inadequate description of the anthropometric measurement protocol, use of self-reported weight and height, and the fact that all studies were conducted in high-income countries.
Obesity in adolescence often progresses to severe obesity later on
A prospective cohort trial followed 8834 nonobese and obese individuals, ages 12 to 21, for 13 years to assess risk of adult obesity.2 Patients were drawn from the National Longitudinal Study of Adolescent Health, which is a representative sample of United States schools from 1994 to 1995 with respect to region, urbanicity, school size, school type, and ethnicity.
Researchers observed a total of 703 incident cases of severe obesity in adulthood, indicating a total incidence rate of 7.9% (95% confidence interval [CI], 7.4%-8.5%). Obese adolescents were significantly more likely to develop severe obesity than nonobese adolescents who were normal weight or overweight (hazard ratio [HR]=16; 95% CI, 12-21).
A significant proportion of obese adolescents became severely obese by their early 30s, with an incidence of 37% in men (95% CI, 31%-44%) and 51% in women (95% CI, 45%-58%). Black women had the highest incidence at 52% (95% CI, 41%-64%). Fewer than 5% of patients (across sex and race) who were normal weight in adolescence became severely obese in adulthood.
Normal weight: Body mass index (BMI) ≥5th to <85th percentile for individuals <20 years old or BMI ≥18.5 to <25 for individuals >20 years.
Overweight: BMI ≥85th to <95th percentile or BMI ≥25 to <30.
Obesity: BMI ≥95th to <120% of 95th percentile or BMI ≥30 to <40.
Severe obesity: BMI ≥120% of 95th percentile; BMI ≥40.
Yes. Overweight children (body mass index [BMI] ≥85th to <95th percentile) are likely to become overweight or obese adults with a BMI ≥25 (strength of recommendation [SOR]: B, systematic review of high-quality prospective longitudinal studies).
Obese adolescents are significantly more likely to develop severe obesity than normal weight or overweight adolescents (SOR: B, prospective cohort study). (See “Definition of terms” below.)
The trend to overweight and obesity in adulthood is clear
A systematic review of 20 prospective and 5 retrospective trials tracked 179,303 overweight and obese children into adulthood.1 Investigators included studies for evaluation if they were written in English, prospective or retrospective longitudinal in design, described at least one anthropometric measurement, and included odds ratios or risk ratios in the results. The results were not pooled because of heterogeneity among studies.
In high-quality trials, the percentages of overweight or obese children and adolescents who became overweight or obese adults varied: overweight children (76% to 83%), obese children (18% to 60%), overweight adolescents (22% to 58%) and obese adolescents (24% to 90%). Limitations of the review included an inadequate description of the anthropometric measurement protocol, use of self-reported weight and height, and the fact that all studies were conducted in high-income countries.
Obesity in adolescence often progresses to severe obesity later on
A prospective cohort trial followed 8834 nonobese and obese individuals, ages 12 to 21, for 13 years to assess risk of adult obesity.2 Patients were drawn from the National Longitudinal Study of Adolescent Health, which is a representative sample of United States schools from 1994 to 1995 with respect to region, urbanicity, school size, school type, and ethnicity.
Researchers observed a total of 703 incident cases of severe obesity in adulthood, indicating a total incidence rate of 7.9% (95% confidence interval [CI], 7.4%-8.5%). Obese adolescents were significantly more likely to develop severe obesity than nonobese adolescents who were normal weight or overweight (hazard ratio [HR]=16; 95% CI, 12-21).
A significant proportion of obese adolescents became severely obese by their early 30s, with an incidence of 37% in men (95% CI, 31%-44%) and 51% in women (95% CI, 45%-58%). Black women had the highest incidence at 52% (95% CI, 41%-64%). Fewer than 5% of patients (across sex and race) who were normal weight in adolescence became severely obese in adulthood.
Normal weight: Body mass index (BMI) ≥5th to <85th percentile for individuals <20 years old or BMI ≥18.5 to <25 for individuals >20 years.
Overweight: BMI ≥85th to <95th percentile or BMI ≥25 to <30.
Obesity: BMI ≥95th to <120% of 95th percentile or BMI ≥30 to <40.
Severe obesity: BMI ≥120% of 95th percentile; BMI ≥40.
1. Singh AS, Mulder C, Twisk WR, et al. Tracking of childhood overweight into adulthood: a systemic review of the literature. Obes Rev. 2008;9:474-488.
2. The NS, Suchindran C, North KE, et al. Association of adolescent obesity with risk of severe obesity in adulthood. JAMA. 2010;304:2042-2047.
1. Singh AS, Mulder C, Twisk WR, et al. Tracking of childhood overweight into adulthood: a systemic review of the literature. Obes Rev. 2008;9:474-488.
2. The NS, Suchindran C, North KE, et al. Association of adolescent obesity with risk of severe obesity in adulthood. JAMA. 2010;304:2042-2047.
Evidence-based answers from the Family Physicians Inquiries Network
Office visits should be a “dance,” not a dictate

Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Left subconjunctival hemorrhage • renal dysfunction • international normalized ratio of 4.5 • Dx?
THE CASE
A 71-year-old woman came to our clinic with a left subconjunctival hemorrhage. She had a history of atrial flutter and had received a liver transplant approximately 10 years ago. The patient reported having a procedure 2 weeks before her visit with us to remove a basal cell carcinoma on her lower left eyelid, but had no recent changes in vision or physical damage to the eye.
In the past year, she had been started on dabigatran 150 mg twice daily after developing symptomatic atrial fibrillation. Our patient had also been receiving tacrolimus 3 mg twice daily since her transplant. Other medications she was taking included hydroxychloroquine 200 mg/d for rheumatoid arthritis, propafenone 225 mg twice daily for atrial fibrillation, valsartan 80 mg/d for hypertension, and ranitidine 150 mg/d for reflux.
Venipuncture coagulation tests showed a partial thromboplastin time (PTT) of 75.1 seconds, a prothrombin time (PT) of 46.1 seconds, and an elevated international normalized ratio (INR) of 4.5 (normal range: 0.8-1.2). Point-of-care INR results were not obtained.
A complete blood count (CBC) was unremarkable with the exception of a low platelet count and high red blood cell distribution width (RDW). Our patient’s aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were both within normal limits.
Kidney function tests told another story. The patient’s serum creatinine (SCr) and blood urea nitrogen (BUN) levels were elevated (1.54 mg/dL and 29 mg/dL, respectively) and her creatinine clearance (CrCl; 30.2 mL/min) suggested moderate to severe renal dysfunction.
The patient’s CHADS2 score was calculated as 1, suggesting she had a low-to-moderate risk of stroke.
THE DIAGNOSIS
Our patient had a left subconjunctival hemorrhage and an elevated venipuncture INR. Based on her renal dysfunction, we suspected that her elevated INR was likely due to an excessive dose of dabigatran, as well as an interaction between dabigatran and tacrolimus.
DISCUSSION
Dabigatran is an oral direct thrombin inhibitor approved for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation. An important advantage of dabigatran compared to warfarin is that the fixed-dose regimen does not require routine anticoagulation monitoring. In cases where anticoagulation monitoring is needed, PTT is the preferred method.1
While PT and INR have generally not been shown to accurately reflect the degree of anticoagulation with dabigatran at therapeutic doses, there have been in vitro reports of elevated INRs with supratherapeutic dabigatran levels.2,3 At a typical peak therapeutic dabigatran concentration of approximately 184 ng/mL, the INR generally ranged from 1.1 to 1.7.2 However, at a dabigatran concentration of 1000 ng/mL, the INR was elevated to 4.5,2,3 which is the same venipuncture INR recorded in our patient. While there have been published reports of falsely elevated point-of-care INR results compared to corresponding venipuncture INR results in patients taking dabigatran,4,5 a literature review found only a case of an elevated venipuncture INR in an end-stage renal disease patient receiving hemodialysis.6
In the case noted above, as well as our patient, an accumulation of dabigatran due to the patient’s renal dysfunction likely resulted in high plasma concentrations and therefore an elevated venipuncture INR. The elimination half-life for dabigatran is approximately 14 hours in patients with normal renal function; in a patient with severe renal impairment, the half-life can be up to 28 hours.7 Our patient’s CrCl at the time of presentation was 30.2 mL/min, which indicated moderate to severe renal dysfunction. Based on dabigatran prescribing recommendations, a dose adjustment to 75 mg bid might be appropriate.1 (Our patient was taking 150 mg bid.)
We do not believe our patient’s elevated INR was due to her liver transplant because there were no clinical signs of liver dysfunction. A more likely contributing factor was a drug interaction with tacrolimus. Dabigatran is a moderate affinity P-glycoprotein (P-gp) substrate and tacrolimus is both a P-gp substrate and inhibitor. While an interaction between tacrolimus and dabigatran has not been studied directly, concurrent use of any P-gp inhibitor and dabigatran is contraindicated in patients with severe renal dysfunction (CrCl: 15-30 mL/min).1 For these theoretical interactions, the Drug Interaction Probability Scale (DIPS) has been developed.8 In our patient’s case, the calculated DIPS score of 5 suggests a probable interaction, likely due to P-gp inhibition. The other medications our patient was taking did not have this interaction and were unlikely to contribute to the elevated INR and subconjunctival hemorrhage.
Our patient was instructed to stop taking dabigatran and return in 3 days for additional lab tests. At her follow-up visit, the lab results were PTT, 34.3 seconds; PT, 11.6 seconds; and venipuncture INR, 1.1. Her CBC was unremarkable and unchanged. Shortly after the follow-up visit, our patient was assessed by her cardiologist. Due to her renal dysfunction, risk of bleeding, and relatively low CHADS2 score, the cardiologist decided to discontinue dabigatran and start her on aspirin.
THE TAKEAWAY
Dabigatran may cause elevated INR levels in patients with renal dysfunction and/or those taking other medications that could interact with dabigatran. Concurrent use of any P-gp inhibitor (such as tacrolimus) and dabigatran is contraindicated in patients with severe renal dysfunction. Despite the lack of required routine laboratory monitoring, renal function and drug interactions associated with dabigatran therapy should be monitored closely.
1. Praxada [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
2. van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010;103:1116-1127.
3. Lindahl TL, Baghaei F, Blixter IF, et al; Expert Group on Coagulation of the External Quality Assurance in Laboratory Medicine in Sweden. Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays. Thromb Haemost. 2011;105:371-378.
4. Baruch L, Sherman O. Potential inaccuracy of point-of-care INR in dabigatran-treated patients. Ann Pharmacother. 2011;45:e40.
5. van Ryn J, Baruch L, Clemens A. Interpretation of point-ofcare INR results in patients treated with dabigatran. Am J Med. 2012;125:417-420.
6. Kim J, Yadava M, An IC, et al. Coagulopathy and extremely elevated PT/INR after dabigatran etexilate use in a patient with end-stage renal disease. Case Rep Med. 2013;2013:131395.
7. Stangier J, Rathgen K, Stähle H, et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clin Pharmacokinet. 2010;49:259-268.
8. Horn JR, Hansten PD, Chan LN. Proposal for a new tool to evaluate drug interaction cases. Ann Pharmacother. 2007;41:674-680.
THE CASE
A 71-year-old woman came to our clinic with a left subconjunctival hemorrhage. She had a history of atrial flutter and had received a liver transplant approximately 10 years ago. The patient reported having a procedure 2 weeks before her visit with us to remove a basal cell carcinoma on her lower left eyelid, but had no recent changes in vision or physical damage to the eye.
In the past year, she had been started on dabigatran 150 mg twice daily after developing symptomatic atrial fibrillation. Our patient had also been receiving tacrolimus 3 mg twice daily since her transplant. Other medications she was taking included hydroxychloroquine 200 mg/d for rheumatoid arthritis, propafenone 225 mg twice daily for atrial fibrillation, valsartan 80 mg/d for hypertension, and ranitidine 150 mg/d for reflux.
Venipuncture coagulation tests showed a partial thromboplastin time (PTT) of 75.1 seconds, a prothrombin time (PT) of 46.1 seconds, and an elevated international normalized ratio (INR) of 4.5 (normal range: 0.8-1.2). Point-of-care INR results were not obtained.
A complete blood count (CBC) was unremarkable with the exception of a low platelet count and high red blood cell distribution width (RDW). Our patient’s aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were both within normal limits.
Kidney function tests told another story. The patient’s serum creatinine (SCr) and blood urea nitrogen (BUN) levels were elevated (1.54 mg/dL and 29 mg/dL, respectively) and her creatinine clearance (CrCl; 30.2 mL/min) suggested moderate to severe renal dysfunction.
The patient’s CHADS2 score was calculated as 1, suggesting she had a low-to-moderate risk of stroke.
THE DIAGNOSIS
Our patient had a left subconjunctival hemorrhage and an elevated venipuncture INR. Based on her renal dysfunction, we suspected that her elevated INR was likely due to an excessive dose of dabigatran, as well as an interaction between dabigatran and tacrolimus.
DISCUSSION
Dabigatran is an oral direct thrombin inhibitor approved for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation. An important advantage of dabigatran compared to warfarin is that the fixed-dose regimen does not require routine anticoagulation monitoring. In cases where anticoagulation monitoring is needed, PTT is the preferred method.1
While PT and INR have generally not been shown to accurately reflect the degree of anticoagulation with dabigatran at therapeutic doses, there have been in vitro reports of elevated INRs with supratherapeutic dabigatran levels.2,3 At a typical peak therapeutic dabigatran concentration of approximately 184 ng/mL, the INR generally ranged from 1.1 to 1.7.2 However, at a dabigatran concentration of 1000 ng/mL, the INR was elevated to 4.5,2,3 which is the same venipuncture INR recorded in our patient. While there have been published reports of falsely elevated point-of-care INR results compared to corresponding venipuncture INR results in patients taking dabigatran,4,5 a literature review found only a case of an elevated venipuncture INR in an end-stage renal disease patient receiving hemodialysis.6
In the case noted above, as well as our patient, an accumulation of dabigatran due to the patient’s renal dysfunction likely resulted in high plasma concentrations and therefore an elevated venipuncture INR. The elimination half-life for dabigatran is approximately 14 hours in patients with normal renal function; in a patient with severe renal impairment, the half-life can be up to 28 hours.7 Our patient’s CrCl at the time of presentation was 30.2 mL/min, which indicated moderate to severe renal dysfunction. Based on dabigatran prescribing recommendations, a dose adjustment to 75 mg bid might be appropriate.1 (Our patient was taking 150 mg bid.)
We do not believe our patient’s elevated INR was due to her liver transplant because there were no clinical signs of liver dysfunction. A more likely contributing factor was a drug interaction with tacrolimus. Dabigatran is a moderate affinity P-glycoprotein (P-gp) substrate and tacrolimus is both a P-gp substrate and inhibitor. While an interaction between tacrolimus and dabigatran has not been studied directly, concurrent use of any P-gp inhibitor and dabigatran is contraindicated in patients with severe renal dysfunction (CrCl: 15-30 mL/min).1 For these theoretical interactions, the Drug Interaction Probability Scale (DIPS) has been developed.8 In our patient’s case, the calculated DIPS score of 5 suggests a probable interaction, likely due to P-gp inhibition. The other medications our patient was taking did not have this interaction and were unlikely to contribute to the elevated INR and subconjunctival hemorrhage.
Our patient was instructed to stop taking dabigatran and return in 3 days for additional lab tests. At her follow-up visit, the lab results were PTT, 34.3 seconds; PT, 11.6 seconds; and venipuncture INR, 1.1. Her CBC was unremarkable and unchanged. Shortly after the follow-up visit, our patient was assessed by her cardiologist. Due to her renal dysfunction, risk of bleeding, and relatively low CHADS2 score, the cardiologist decided to discontinue dabigatran and start her on aspirin.
THE TAKEAWAY
Dabigatran may cause elevated INR levels in patients with renal dysfunction and/or those taking other medications that could interact with dabigatran. Concurrent use of any P-gp inhibitor (such as tacrolimus) and dabigatran is contraindicated in patients with severe renal dysfunction. Despite the lack of required routine laboratory monitoring, renal function and drug interactions associated with dabigatran therapy should be monitored closely.
THE CASE
A 71-year-old woman came to our clinic with a left subconjunctival hemorrhage. She had a history of atrial flutter and had received a liver transplant approximately 10 years ago. The patient reported having a procedure 2 weeks before her visit with us to remove a basal cell carcinoma on her lower left eyelid, but had no recent changes in vision or physical damage to the eye.
In the past year, she had been started on dabigatran 150 mg twice daily after developing symptomatic atrial fibrillation. Our patient had also been receiving tacrolimus 3 mg twice daily since her transplant. Other medications she was taking included hydroxychloroquine 200 mg/d for rheumatoid arthritis, propafenone 225 mg twice daily for atrial fibrillation, valsartan 80 mg/d for hypertension, and ranitidine 150 mg/d for reflux.
Venipuncture coagulation tests showed a partial thromboplastin time (PTT) of 75.1 seconds, a prothrombin time (PT) of 46.1 seconds, and an elevated international normalized ratio (INR) of 4.5 (normal range: 0.8-1.2). Point-of-care INR results were not obtained.
A complete blood count (CBC) was unremarkable with the exception of a low platelet count and high red blood cell distribution width (RDW). Our patient’s aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were both within normal limits.
Kidney function tests told another story. The patient’s serum creatinine (SCr) and blood urea nitrogen (BUN) levels were elevated (1.54 mg/dL and 29 mg/dL, respectively) and her creatinine clearance (CrCl; 30.2 mL/min) suggested moderate to severe renal dysfunction.
The patient’s CHADS2 score was calculated as 1, suggesting she had a low-to-moderate risk of stroke.
THE DIAGNOSIS
Our patient had a left subconjunctival hemorrhage and an elevated venipuncture INR. Based on her renal dysfunction, we suspected that her elevated INR was likely due to an excessive dose of dabigatran, as well as an interaction between dabigatran and tacrolimus.
DISCUSSION
Dabigatran is an oral direct thrombin inhibitor approved for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation. An important advantage of dabigatran compared to warfarin is that the fixed-dose regimen does not require routine anticoagulation monitoring. In cases where anticoagulation monitoring is needed, PTT is the preferred method.1
While PT and INR have generally not been shown to accurately reflect the degree of anticoagulation with dabigatran at therapeutic doses, there have been in vitro reports of elevated INRs with supratherapeutic dabigatran levels.2,3 At a typical peak therapeutic dabigatran concentration of approximately 184 ng/mL, the INR generally ranged from 1.1 to 1.7.2 However, at a dabigatran concentration of 1000 ng/mL, the INR was elevated to 4.5,2,3 which is the same venipuncture INR recorded in our patient. While there have been published reports of falsely elevated point-of-care INR results compared to corresponding venipuncture INR results in patients taking dabigatran,4,5 a literature review found only a case of an elevated venipuncture INR in an end-stage renal disease patient receiving hemodialysis.6
In the case noted above, as well as our patient, an accumulation of dabigatran due to the patient’s renal dysfunction likely resulted in high plasma concentrations and therefore an elevated venipuncture INR. The elimination half-life for dabigatran is approximately 14 hours in patients with normal renal function; in a patient with severe renal impairment, the half-life can be up to 28 hours.7 Our patient’s CrCl at the time of presentation was 30.2 mL/min, which indicated moderate to severe renal dysfunction. Based on dabigatran prescribing recommendations, a dose adjustment to 75 mg bid might be appropriate.1 (Our patient was taking 150 mg bid.)
We do not believe our patient’s elevated INR was due to her liver transplant because there were no clinical signs of liver dysfunction. A more likely contributing factor was a drug interaction with tacrolimus. Dabigatran is a moderate affinity P-glycoprotein (P-gp) substrate and tacrolimus is both a P-gp substrate and inhibitor. While an interaction between tacrolimus and dabigatran has not been studied directly, concurrent use of any P-gp inhibitor and dabigatran is contraindicated in patients with severe renal dysfunction (CrCl: 15-30 mL/min).1 For these theoretical interactions, the Drug Interaction Probability Scale (DIPS) has been developed.8 In our patient’s case, the calculated DIPS score of 5 suggests a probable interaction, likely due to P-gp inhibition. The other medications our patient was taking did not have this interaction and were unlikely to contribute to the elevated INR and subconjunctival hemorrhage.
Our patient was instructed to stop taking dabigatran and return in 3 days for additional lab tests. At her follow-up visit, the lab results were PTT, 34.3 seconds; PT, 11.6 seconds; and venipuncture INR, 1.1. Her CBC was unremarkable and unchanged. Shortly after the follow-up visit, our patient was assessed by her cardiologist. Due to her renal dysfunction, risk of bleeding, and relatively low CHADS2 score, the cardiologist decided to discontinue dabigatran and start her on aspirin.
THE TAKEAWAY
Dabigatran may cause elevated INR levels in patients with renal dysfunction and/or those taking other medications that could interact with dabigatran. Concurrent use of any P-gp inhibitor (such as tacrolimus) and dabigatran is contraindicated in patients with severe renal dysfunction. Despite the lack of required routine laboratory monitoring, renal function and drug interactions associated with dabigatran therapy should be monitored closely.
1. Praxada [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
2. van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010;103:1116-1127.
3. Lindahl TL, Baghaei F, Blixter IF, et al; Expert Group on Coagulation of the External Quality Assurance in Laboratory Medicine in Sweden. Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays. Thromb Haemost. 2011;105:371-378.
4. Baruch L, Sherman O. Potential inaccuracy of point-of-care INR in dabigatran-treated patients. Ann Pharmacother. 2011;45:e40.
5. van Ryn J, Baruch L, Clemens A. Interpretation of point-ofcare INR results in patients treated with dabigatran. Am J Med. 2012;125:417-420.
6. Kim J, Yadava M, An IC, et al. Coagulopathy and extremely elevated PT/INR after dabigatran etexilate use in a patient with end-stage renal disease. Case Rep Med. 2013;2013:131395.
7. Stangier J, Rathgen K, Stähle H, et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clin Pharmacokinet. 2010;49:259-268.
8. Horn JR, Hansten PD, Chan LN. Proposal for a new tool to evaluate drug interaction cases. Ann Pharmacother. 2007;41:674-680.
1. Praxada [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
2. van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010;103:1116-1127.
3. Lindahl TL, Baghaei F, Blixter IF, et al; Expert Group on Coagulation of the External Quality Assurance in Laboratory Medicine in Sweden. Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays. Thromb Haemost. 2011;105:371-378.
4. Baruch L, Sherman O. Potential inaccuracy of point-of-care INR in dabigatran-treated patients. Ann Pharmacother. 2011;45:e40.
5. van Ryn J, Baruch L, Clemens A. Interpretation of point-ofcare INR results in patients treated with dabigatran. Am J Med. 2012;125:417-420.
6. Kim J, Yadava M, An IC, et al. Coagulopathy and extremely elevated PT/INR after dabigatran etexilate use in a patient with end-stage renal disease. Case Rep Med. 2013;2013:131395.
7. Stangier J, Rathgen K, Stähle H, et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clin Pharmacokinet. 2010;49:259-268.
8. Horn JR, Hansten PD, Chan LN. Proposal for a new tool to evaluate drug interaction cases. Ann Pharmacother. 2007;41:674-680.

Diagnosing and Managing Depressive Episodes in the DSM-5 Era

