User login
When in Doubt, Blame the Drug
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Continue for the outcome >>
OUTCOME
A $5.1 million verdict was returned against the nephrologist.
COMMENT
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.”
“Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture.
Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol). Perhaps the outcome of this case would have been different.
The second physician was a nephrology fellow, who left me with this piece of wisdom: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge.
IN SUM
Before you “missile lock” onto a diagnosis, take a mental step back to consider broad categories of disease. —DML
REFERENCES
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. emedicine.medscape.com/article/229698-overview. Accessed September 16, 2015.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis. J Burn Care Rehabil. 2000;21(3): 199-204.
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Continue for the outcome >>
OUTCOME
A $5.1 million verdict was returned against the nephrologist.
COMMENT
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.”
“Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture.
Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol). Perhaps the outcome of this case would have been different.
The second physician was a nephrology fellow, who left me with this piece of wisdom: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge.
IN SUM
Before you “missile lock” onto a diagnosis, take a mental step back to consider broad categories of disease. —DML
REFERENCES
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. emedicine.medscape.com/article/229698-overview. Accessed September 16, 2015.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis. J Burn Care Rehabil. 2000;21(3): 199-204.
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Continue for the outcome >>
OUTCOME
A $5.1 million verdict was returned against the nephrologist.
COMMENT
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.”
“Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture.
Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol). Perhaps the outcome of this case would have been different.
The second physician was a nephrology fellow, who left me with this piece of wisdom: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge.
IN SUM
Before you “missile lock” onto a diagnosis, take a mental step back to consider broad categories of disease. —DML
REFERENCES
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. emedicine.medscape.com/article/229698-overview. Accessed September 16, 2015.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis. J Burn Care Rehabil. 2000;21(3): 199-204.
Ask, listen, help: Pearls to treat sexual dysfunction in menopause
LAS VEGAS – The first step is to ask. A menopausal woman may be struggling with a female sexual disorder (FSD), but unless her clinician asks, the patient may never volunteer information about her sexual health.
Susan Kellogg Spadt, Ph.D., offered that advice, along with a toolkit of tips, treatments, and pearls for physicians and others caring for the menopausal woman’s sexual health.

Dr. Kellogg Spadt, a certified sexual counselor and professor of obstetrics and gynecology at Drexel University, Philadelphia, addressed FSD in the context of the complicated psychosocial landscape of midlife.
Women at this stage of life may be experiencing life stress as children move out, retirement looms, and aging parents require time and attention. Also, as women age, they are more likely to require medications that can negatively affect sexual health. Body image issues, depression, anxiety, and discrepancy with partner desire levels can all be prevalent in women aged 45-64 years, the group most likely to experience distress from sexual problems, she said at the NAMS 2015 annual meeting.
This is important in the context of a relationship, said Dr. Kellogg Spadt. She pointed out that “when sex is good, it adds a little bit – like icing on the cupcake – to a good relationship.” But when sex is bad or nonexistent, she said, it plays an inordinately negative role, reducing the quality of the relationship by 50%-70% in some studies.
Dr. Kellogg Spadt said a good opening approach should confirm the ubiquity of sexual problems in midlife and normalize concerns. Clinicians can ask: “With menopause, many women have changes in their sexual response. These concerns are very common. Tell me – are you feeling well and complete in your sex life?”

If questioning reveals unsatisfying or nonexistent sex, many problems can be addressed in the office. First, careful questioning and an exam can tease out the extent to which dyspareunia and vaginal dryness may be limiting sexual pleasure. In that case, lubricants, moisturizers, and topical estrogen can be considered.
Office sessions with physical therapists certified in pelvic issues, combined with home use of dilators, can help overcome physical contributors to an uncomfortable sexual experience, she said.
Clinicians can also provide brief office-based counseling using the “PLISSIT” model, which. gives permission for the patient to speak openly about sexual issues; provides limited information to educate the patient about her anatomy and resources available; offers specific suggestions, for example, positioning tips or moisturizer recommendations; and offers intensive therapy, when indicated, such as referring for adjunctive psychotherapy.
Dr. Kellogg Stadt concluded with her top clinical pearls for sexual health in menopausal women:
• Add moisture daily. Using a water-based, bioadhesive lubricant several times a week regardless of sexual frequency can significantly ease comfort and satisfaction with sex and make it easier to have an orgasm.
• Nourish. A Mediterranean diet has been shown to promote sexual function, and regular exercise improves mood and overall health.
• Talk. Partners can use “I” language to talk about sex honestly and in a nonaccusatory way. Clinicians can help provide the vocabulary and communication tips to facilitate this.
• Prioritize pleasure. Intimate time together won’t just happen; even a 20-minute block of time, scheduled weekly, for touching and intimate conversation can clear the way to better sex.
• Think. Reading or watching erotica, being mindful of erotic thoughts as they occur, and focusing on sensation rather than distractions during arousal are all important.
• Stimulate. After menopause, some women need more intense stimulation to reach orgasm, so vibrators can be incorporated into sex play. Women who are uncomfortable with this can use the “doctor’s orders” approach with their partners.
• Try. Just opening up and talking about sex problems shows that a woman is committed to her partner, and taking action shows her level of care and concern for the relationship.
Dr. Kellogg Stadt reported being a consultant or on the advisory board of Neogyn and Nuelle, and on the speakers bureau of Novo Nordisk and Shionogi.
On Twitter @karioakes
LAS VEGAS – The first step is to ask. A menopausal woman may be struggling with a female sexual disorder (FSD), but unless her clinician asks, the patient may never volunteer information about her sexual health.
Susan Kellogg Spadt, Ph.D., offered that advice, along with a toolkit of tips, treatments, and pearls for physicians and others caring for the menopausal woman’s sexual health.
Dr. Kellogg Spadt, a certified sexual counselor and professor of obstetrics and gynecology at Drexel University, Philadelphia, addressed FSD in the context of the complicated psychosocial landscape of midlife.
Women at this stage of life may be experiencing life stress as children move out, retirement looms, and aging parents require time and attention. Also, as women age, they are more likely to require medications that can negatively affect sexual health. Body image issues, depression, anxiety, and discrepancy with partner desire levels can all be prevalent in women aged 45-64 years, the group most likely to experience distress from sexual problems, she said at the NAMS 2015 annual meeting.
This is important in the context of a relationship, said Dr. Kellogg Spadt. She pointed out that “when sex is good, it adds a little bit – like icing on the cupcake – to a good relationship.” But when sex is bad or nonexistent, she said, it plays an inordinately negative role, reducing the quality of the relationship by 50%-70% in some studies.
Dr. Kellogg Spadt said a good opening approach should confirm the ubiquity of sexual problems in midlife and normalize concerns. Clinicians can ask: “With menopause, many women have changes in their sexual response. These concerns are very common. Tell me – are you feeling well and complete in your sex life?”
If questioning reveals unsatisfying or nonexistent sex, many problems can be addressed in the office. First, careful questioning and an exam can tease out the extent to which dyspareunia and vaginal dryness may be limiting sexual pleasure. In that case, lubricants, moisturizers, and topical estrogen can be considered.
Office sessions with physical therapists certified in pelvic issues, combined with home use of dilators, can help overcome physical contributors to an uncomfortable sexual experience, she said.
Clinicians can also provide brief office-based counseling using the “PLISSIT” model, which. gives permission for the patient to speak openly about sexual issues; provides limited information to educate the patient about her anatomy and resources available; offers specific suggestions, for example, positioning tips or moisturizer recommendations; and offers intensive therapy, when indicated, such as referring for adjunctive psychotherapy.
Dr. Kellogg Stadt concluded with her top clinical pearls for sexual health in menopausal women:
• Add moisture daily. Using a water-based, bioadhesive lubricant several times a week regardless of sexual frequency can significantly ease comfort and satisfaction with sex and make it easier to have an orgasm.
• Nourish. A Mediterranean diet has been shown to promote sexual function, and regular exercise improves mood and overall health.
• Talk. Partners can use “I” language to talk about sex honestly and in a nonaccusatory way. Clinicians can help provide the vocabulary and communication tips to facilitate this.
• Prioritize pleasure. Intimate time together won’t just happen; even a 20-minute block of time, scheduled weekly, for touching and intimate conversation can clear the way to better sex.
• Think. Reading or watching erotica, being mindful of erotic thoughts as they occur, and focusing on sensation rather than distractions during arousal are all important.
• Stimulate. After menopause, some women need more intense stimulation to reach orgasm, so vibrators can be incorporated into sex play. Women who are uncomfortable with this can use the “doctor’s orders” approach with their partners.
• Try. Just opening up and talking about sex problems shows that a woman is committed to her partner, and taking action shows her level of care and concern for the relationship.
Dr. Kellogg Stadt reported being a consultant or on the advisory board of Neogyn and Nuelle, and on the speakers bureau of Novo Nordisk and Shionogi.
On Twitter @karioakes
LAS VEGAS – The first step is to ask. A menopausal woman may be struggling with a female sexual disorder (FSD), but unless her clinician asks, the patient may never volunteer information about her sexual health.
Susan Kellogg Spadt, Ph.D., offered that advice, along with a toolkit of tips, treatments, and pearls for physicians and others caring for the menopausal woman’s sexual health.
Dr. Kellogg Spadt, a certified sexual counselor and professor of obstetrics and gynecology at Drexel University, Philadelphia, addressed FSD in the context of the complicated psychosocial landscape of midlife.
Women at this stage of life may be experiencing life stress as children move out, retirement looms, and aging parents require time and attention. Also, as women age, they are more likely to require medications that can negatively affect sexual health. Body image issues, depression, anxiety, and discrepancy with partner desire levels can all be prevalent in women aged 45-64 years, the group most likely to experience distress from sexual problems, she said at the NAMS 2015 annual meeting.
This is important in the context of a relationship, said Dr. Kellogg Spadt. She pointed out that “when sex is good, it adds a little bit – like icing on the cupcake – to a good relationship.” But when sex is bad or nonexistent, she said, it plays an inordinately negative role, reducing the quality of the relationship by 50%-70% in some studies.
Dr. Kellogg Spadt said a good opening approach should confirm the ubiquity of sexual problems in midlife and normalize concerns. Clinicians can ask: “With menopause, many women have changes in their sexual response. These concerns are very common. Tell me – are you feeling well and complete in your sex life?”
If questioning reveals unsatisfying or nonexistent sex, many problems can be addressed in the office. First, careful questioning and an exam can tease out the extent to which dyspareunia and vaginal dryness may be limiting sexual pleasure. In that case, lubricants, moisturizers, and topical estrogen can be considered.
Office sessions with physical therapists certified in pelvic issues, combined with home use of dilators, can help overcome physical contributors to an uncomfortable sexual experience, she said.
Clinicians can also provide brief office-based counseling using the “PLISSIT” model, which. gives permission for the patient to speak openly about sexual issues; provides limited information to educate the patient about her anatomy and resources available; offers specific suggestions, for example, positioning tips or moisturizer recommendations; and offers intensive therapy, when indicated, such as referring for adjunctive psychotherapy.
Dr. Kellogg Stadt concluded with her top clinical pearls for sexual health in menopausal women:
• Add moisture daily. Using a water-based, bioadhesive lubricant several times a week regardless of sexual frequency can significantly ease comfort and satisfaction with sex and make it easier to have an orgasm.
• Nourish. A Mediterranean diet has been shown to promote sexual function, and regular exercise improves mood and overall health.
• Talk. Partners can use “I” language to talk about sex honestly and in a nonaccusatory way. Clinicians can help provide the vocabulary and communication tips to facilitate this.
• Prioritize pleasure. Intimate time together won’t just happen; even a 20-minute block of time, scheduled weekly, for touching and intimate conversation can clear the way to better sex.
• Think. Reading or watching erotica, being mindful of erotic thoughts as they occur, and focusing on sensation rather than distractions during arousal are all important.
• Stimulate. After menopause, some women need more intense stimulation to reach orgasm, so vibrators can be incorporated into sex play. Women who are uncomfortable with this can use the “doctor’s orders” approach with their partners.
• Try. Just opening up and talking about sex problems shows that a woman is committed to her partner, and taking action shows her level of care and concern for the relationship.
Dr. Kellogg Stadt reported being a consultant or on the advisory board of Neogyn and Nuelle, and on the speakers bureau of Novo Nordisk and Shionogi.
On Twitter @karioakes
EXPERT ANALYSIS FROM THE NAMS 2015 ANNUAL MEETING

Colon cancer, colonoscopy, and intestinal issues
Hereditary syndromes in gastroenterology have emerged from being esoteric to being common issues that all of us must deal with, according to Dr. Sapna Syngal of Dana-Farber/Brigham and Women’s Cancer Center, Boston. Screening, surveillance, and treatment of hereditary cancers are all different, compared with sporadic cancer. For colorectal cancers, an excellent resource is http://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf, and there are recent society summaries (Am. J. Gastroenterol. 2015;110:223-62). These recommend a family history of cancer be recorded for all patients, including type of cancer, age at diagnosis, and relationship to patient. Lynch syndrome testing should now be done on all newly diagnosed colorectal cancers by testing of mismatch repair proteins or microsatellite instability. Genetic testing should be done when these are detected and on all family members of affected individuals. Familial adenomatous polyposis testing, including the APC and MUTYH genes, should be done for individuals with more than 10 cumulative adenomas, or a family history of any familial adenomatous condition. Peutz-Jeghers syndrome should be tested for in individuals with perioral/buccal pigmentation or those with two or more hamartomatous polyps. Juvenile polyposis syndrome should be tested for in individuals with five or more juvenile polyps in the colorectum or any juvenile polyps in other parts of the GI tract. Simple clinical questions can help identify those who should be tested (Am. J. Gastroenterol. 2009;104:1508-18).

Modern evidence has refuted several long-held beliefs about diverticulosis and diverticulitis, said Dr. Neil Stollman of the University of California, San Francisco. Evidence now shows that diverticulosis is not associated with a low-fiber diet and that high-fiber diets are associated with higher rates of diverticular complications, although this may be due to confounding. Nonsteroidal anti-inflammatory drugs are associated with increased risk of diverticular bleeding. The risk of diverticulitis is much lower than previously thought. Prior estimates of 10%-25% have now been revised downward to 1%-4%. Nuts and seeds do not cause acute diverticulitis and do not need to be avoided. Diverticulitis is a spectrum of diseases from asymptomatic to symptomatic uncomplicated diverticular disease (SUDD) to acute diverticulitis. Mesalamine may be effective in SUDD and acute diverticulitis but evidence is mixed. Cyclic rifaximin and probiotics may also be helpful in SUDD. Antibiotics, previously thought to be mandatory in acute diverticulitis, have not been clearly beneficial in large randomized trials. Surgery, which was also previously recommended after a second attack of acute diverticulitis, is now considered optional and should be individualized.
Dr. Douglas K. Rex of Indiana University Health, Indianapolis, reviewed key measures of quality in colonoscopy and how to achieve these, even under difficult circumstances. Key measures include adenoma detection rate, which can be improved through careful attention to good technique (looking behind folds, adequate distention, and washing) and recognition of flat and sessile polyps. New technologies include high definition, special endoscope caps that flatten folds, and new wide-angle colonoscopes. Water immersion and CO2 insufflation have also improved quality through easier insertion and less gas distention and pain after the procedure. For removal of large, lateral spreading polyps, the technique of endoscopic mucosal resection has been highly effective. Use of a “bulking agent” for submucosal injection such as hydroxyethyl starch, injectable contrast agent, underwater endoscopic mucosal resection, and avulsion (with cold or hot forceps) of fibrotic/scarred polyps have all been demonstrated to be effective in expert hands.
Dr. Charlene M. Prather of Saint Louis University summarized the increasing prevalence of constipation and reviewed risk factors (decreased activity, low fiber consumption, and use of multiple constipating medications). Constipation can be divided into three types: normal transit, slow transit, and pelvic floor dysfunction (PFD). Physical exam, particularly a high-quality rectal exam, can be very effective with high negative predictive value for PFD. Treatment includes fiber supplementation (most effective for mild/moderate constipation, less helpful in slow transit or PFD), laxatives (best data are for osmotic laxatives and bisacodyl), and newer agents that stimulate chloride secretion. Testing is appropriate for refractory constipation and includes transit time studies, balloon expulsion, and anorectal manometry.
Dr. Brennan Spiegel of the Cedars-Sinai Center for Outcomes Research and Education, Los Angeles, provided a summary of current national efforts to measure, report, and improve quality in gastroenterology. He highlighted several reports of high variability in quality such as adenoma detection, testing in patients with uncomplicated inflammatory bowel disease, and approaches to diagnosis of irritable bowel syndrome. A general approach to achieving quality was outlined, including: 1. standardization, 2. measurement, 3. reporting, 4. incentivizing (getting paid for performance), and 5. improving. U.S. Medicare oversight groups (PQRS) have chosen four general areas of quality (polyp surveillance, gastroesophageal reflux disease, hepatitis C, and IBD) measures. Gastroenterology societies have provided effective tools to measure and report these, including GIQUIC and the AGA Digestive Health Recognition Program.
Dr. Wallace is professor of medicine and director, digestive diseases research program, Mayo Clinic, Jacksonville, Fla. He has received grants from BSCI and Cosmo and has consulted for Olympus and iLumen. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.
Hereditary syndromes in gastroenterology have emerged from being esoteric to being common issues that all of us must deal with, according to Dr. Sapna Syngal of Dana-Farber/Brigham and Women’s Cancer Center, Boston. Screening, surveillance, and treatment of hereditary cancers are all different, compared with sporadic cancer. For colorectal cancers, an excellent resource is http://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf, and there are recent society summaries (Am. J. Gastroenterol. 2015;110:223-62). These recommend a family history of cancer be recorded for all patients, including type of cancer, age at diagnosis, and relationship to patient. Lynch syndrome testing should now be done on all newly diagnosed colorectal cancers by testing of mismatch repair proteins or microsatellite instability. Genetic testing should be done when these are detected and on all family members of affected individuals. Familial adenomatous polyposis testing, including the APC and MUTYH genes, should be done for individuals with more than 10 cumulative adenomas, or a family history of any familial adenomatous condition. Peutz-Jeghers syndrome should be tested for in individuals with perioral/buccal pigmentation or those with two or more hamartomatous polyps. Juvenile polyposis syndrome should be tested for in individuals with five or more juvenile polyps in the colorectum or any juvenile polyps in other parts of the GI tract. Simple clinical questions can help identify those who should be tested (Am. J. Gastroenterol. 2009;104:1508-18).
Modern evidence has refuted several long-held beliefs about diverticulosis and diverticulitis, said Dr. Neil Stollman of the University of California, San Francisco. Evidence now shows that diverticulosis is not associated with a low-fiber diet and that high-fiber diets are associated with higher rates of diverticular complications, although this may be due to confounding. Nonsteroidal anti-inflammatory drugs are associated with increased risk of diverticular bleeding. The risk of diverticulitis is much lower than previously thought. Prior estimates of 10%-25% have now been revised downward to 1%-4%. Nuts and seeds do not cause acute diverticulitis and do not need to be avoided. Diverticulitis is a spectrum of diseases from asymptomatic to symptomatic uncomplicated diverticular disease (SUDD) to acute diverticulitis. Mesalamine may be effective in SUDD and acute diverticulitis but evidence is mixed. Cyclic rifaximin and probiotics may also be helpful in SUDD. Antibiotics, previously thought to be mandatory in acute diverticulitis, have not been clearly beneficial in large randomized trials. Surgery, which was also previously recommended after a second attack of acute diverticulitis, is now considered optional and should be individualized.
Dr. Douglas K. Rex of Indiana University Health, Indianapolis, reviewed key measures of quality in colonoscopy and how to achieve these, even under difficult circumstances. Key measures include adenoma detection rate, which can be improved through careful attention to good technique (looking behind folds, adequate distention, and washing) and recognition of flat and sessile polyps. New technologies include high definition, special endoscope caps that flatten folds, and new wide-angle colonoscopes. Water immersion and CO2 insufflation have also improved quality through easier insertion and less gas distention and pain after the procedure. For removal of large, lateral spreading polyps, the technique of endoscopic mucosal resection has been highly effective. Use of a “bulking agent” for submucosal injection such as hydroxyethyl starch, injectable contrast agent, underwater endoscopic mucosal resection, and avulsion (with cold or hot forceps) of fibrotic/scarred polyps have all been demonstrated to be effective in expert hands.
Dr. Charlene M. Prather of Saint Louis University summarized the increasing prevalence of constipation and reviewed risk factors (decreased activity, low fiber consumption, and use of multiple constipating medications). Constipation can be divided into three types: normal transit, slow transit, and pelvic floor dysfunction (PFD). Physical exam, particularly a high-quality rectal exam, can be very effective with high negative predictive value for PFD. Treatment includes fiber supplementation (most effective for mild/moderate constipation, less helpful in slow transit or PFD), laxatives (best data are for osmotic laxatives and bisacodyl), and newer agents that stimulate chloride secretion. Testing is appropriate for refractory constipation and includes transit time studies, balloon expulsion, and anorectal manometry.
Dr. Brennan Spiegel of the Cedars-Sinai Center for Outcomes Research and Education, Los Angeles, provided a summary of current national efforts to measure, report, and improve quality in gastroenterology. He highlighted several reports of high variability in quality such as adenoma detection, testing in patients with uncomplicated inflammatory bowel disease, and approaches to diagnosis of irritable bowel syndrome. A general approach to achieving quality was outlined, including: 1. standardization, 2. measurement, 3. reporting, 4. incentivizing (getting paid for performance), and 5. improving. U.S. Medicare oversight groups (PQRS) have chosen four general areas of quality (polyp surveillance, gastroesophageal reflux disease, hepatitis C, and IBD) measures. Gastroenterology societies have provided effective tools to measure and report these, including GIQUIC and the AGA Digestive Health Recognition Program.
Dr. Wallace is professor of medicine and director, digestive diseases research program, Mayo Clinic, Jacksonville, Fla. He has received grants from BSCI and Cosmo and has consulted for Olympus and iLumen. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.
Hereditary syndromes in gastroenterology have emerged from being esoteric to being common issues that all of us must deal with, according to Dr. Sapna Syngal of Dana-Farber/Brigham and Women’s Cancer Center, Boston. Screening, surveillance, and treatment of hereditary cancers are all different, compared with sporadic cancer. For colorectal cancers, an excellent resource is http://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf, and there are recent society summaries (Am. J. Gastroenterol. 2015;110:223-62). These recommend a family history of cancer be recorded for all patients, including type of cancer, age at diagnosis, and relationship to patient. Lynch syndrome testing should now be done on all newly diagnosed colorectal cancers by testing of mismatch repair proteins or microsatellite instability. Genetic testing should be done when these are detected and on all family members of affected individuals. Familial adenomatous polyposis testing, including the APC and MUTYH genes, should be done for individuals with more than 10 cumulative adenomas, or a family history of any familial adenomatous condition. Peutz-Jeghers syndrome should be tested for in individuals with perioral/buccal pigmentation or those with two or more hamartomatous polyps. Juvenile polyposis syndrome should be tested for in individuals with five or more juvenile polyps in the colorectum or any juvenile polyps in other parts of the GI tract. Simple clinical questions can help identify those who should be tested (Am. J. Gastroenterol. 2009;104:1508-18).
Modern evidence has refuted several long-held beliefs about diverticulosis and diverticulitis, said Dr. Neil Stollman of the University of California, San Francisco. Evidence now shows that diverticulosis is not associated with a low-fiber diet and that high-fiber diets are associated with higher rates of diverticular complications, although this may be due to confounding. Nonsteroidal anti-inflammatory drugs are associated with increased risk of diverticular bleeding. The risk of diverticulitis is much lower than previously thought. Prior estimates of 10%-25% have now been revised downward to 1%-4%. Nuts and seeds do not cause acute diverticulitis and do not need to be avoided. Diverticulitis is a spectrum of diseases from asymptomatic to symptomatic uncomplicated diverticular disease (SUDD) to acute diverticulitis. Mesalamine may be effective in SUDD and acute diverticulitis but evidence is mixed. Cyclic rifaximin and probiotics may also be helpful in SUDD. Antibiotics, previously thought to be mandatory in acute diverticulitis, have not been clearly beneficial in large randomized trials. Surgery, which was also previously recommended after a second attack of acute diverticulitis, is now considered optional and should be individualized.
Dr. Douglas K. Rex of Indiana University Health, Indianapolis, reviewed key measures of quality in colonoscopy and how to achieve these, even under difficult circumstances. Key measures include adenoma detection rate, which can be improved through careful attention to good technique (looking behind folds, adequate distention, and washing) and recognition of flat and sessile polyps. New technologies include high definition, special endoscope caps that flatten folds, and new wide-angle colonoscopes. Water immersion and CO2 insufflation have also improved quality through easier insertion and less gas distention and pain after the procedure. For removal of large, lateral spreading polyps, the technique of endoscopic mucosal resection has been highly effective. Use of a “bulking agent” for submucosal injection such as hydroxyethyl starch, injectable contrast agent, underwater endoscopic mucosal resection, and avulsion (with cold or hot forceps) of fibrotic/scarred polyps have all been demonstrated to be effective in expert hands.
Dr. Charlene M. Prather of Saint Louis University summarized the increasing prevalence of constipation and reviewed risk factors (decreased activity, low fiber consumption, and use of multiple constipating medications). Constipation can be divided into three types: normal transit, slow transit, and pelvic floor dysfunction (PFD). Physical exam, particularly a high-quality rectal exam, can be very effective with high negative predictive value for PFD. Treatment includes fiber supplementation (most effective for mild/moderate constipation, less helpful in slow transit or PFD), laxatives (best data are for osmotic laxatives and bisacodyl), and newer agents that stimulate chloride secretion. Testing is appropriate for refractory constipation and includes transit time studies, balloon expulsion, and anorectal manometry.
Dr. Brennan Spiegel of the Cedars-Sinai Center for Outcomes Research and Education, Los Angeles, provided a summary of current national efforts to measure, report, and improve quality in gastroenterology. He highlighted several reports of high variability in quality such as adenoma detection, testing in patients with uncomplicated inflammatory bowel disease, and approaches to diagnosis of irritable bowel syndrome. A general approach to achieving quality was outlined, including: 1. standardization, 2. measurement, 3. reporting, 4. incentivizing (getting paid for performance), and 5. improving. U.S. Medicare oversight groups (PQRS) have chosen four general areas of quality (polyp surveillance, gastroesophageal reflux disease, hepatitis C, and IBD) measures. Gastroenterology societies have provided effective tools to measure and report these, including GIQUIC and the AGA Digestive Health Recognition Program.
Dr. Wallace is professor of medicine and director, digestive diseases research program, Mayo Clinic, Jacksonville, Fla. He has received grants from BSCI and Cosmo and has consulted for Olympus and iLumen. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.

Upper GI tract
This year’s session on esophagus/upper GI at the AGA Spring Postgraduate Course was packed with pragmatic, useful information for the evaluation of patients with upper GI disorders. The session began with a talk on the manifestations of extraesophageal reflux disease. The take-home message of this talk was that putative extraesophageal manifestations of gastroesophageal reflux disease rarely respond to high-dose therapy with PPIs (proton-pump inhibitors), in the absence of concurrent esophageal symptoms such as heartburn or regurgitation. In such situations, investigation of other etiologies of patients’ symptoms, including occult postnasal drainage or cough-variant asthma, may be more rewarding than escalating anti-acid therapy.
Dr. John E. Pandolfino, AGAF, of Northwestern University, Chicago, discussed the utilization of high-resolution manometry in the evaluation of dysphagia. A central focus of this discussion was the use of the Chicago classification of motility abnormalities in assessing these patients. In the future, it is likely that the care of these patients will be dictated by the type of abnormality the patient has in this classification scheme. Especially in the setting of achalasia, data are emerging that some subtypes of achalasia are less likely to respond to some therapies. For instance, type 3 achalasia is unlikely to respond to pneumatic balloon dilatation.
Dr. Rhonda Souza of the University of Texas Southwestern Medical Center, Dallas, taught us that a diagnosis of eosinophilic esophagitis requires an 8-week trial of PPI therapy with no resolution of the eosinophilia. Esophageal dilation is generally safe in the setting of a dominant stricture, but it can be delayed prior to medical therapy if the patient is tolerating oral intake well. Although the most commonly used therapies for EoE now involve either swallowed steroids or dietary elimination therapy, several new agents are on the horizon that may give us new treatment options.
Finally, Dr. Amitabh Chak of Case Western Reserve University, Cleveland, reviewed the care of patients with Barrett’s esophagus and low-grade dysplasia. This is an especially difficult group of patients to care for, due in part to the low reproducibility in the diagnosis of low-grade dysplasia, as well as the highly variable reported cancer outcomes in this patient population. Level 1 evidence now exists demonstrating that treatment with radiofrequency ablation decreases the incidence of cancer in patients with low-grade dysplasia, but most patients with this finding will not progress. Therefore, the field would benefit from better risk stratification of these patients.
Dr. Shaheen is professor of medicine and epidemiology and chief of the division of gastroenterology & hepatology, University of North Carolina School of Medicine, Chapel Hill. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.
This year’s session on esophagus/upper GI at the AGA Spring Postgraduate Course was packed with pragmatic, useful information for the evaluation of patients with upper GI disorders. The session began with a talk on the manifestations of extraesophageal reflux disease. The take-home message of this talk was that putative extraesophageal manifestations of gastroesophageal reflux disease rarely respond to high-dose therapy with PPIs (proton-pump inhibitors), in the absence of concurrent esophageal symptoms such as heartburn or regurgitation. In such situations, investigation of other etiologies of patients’ symptoms, including occult postnasal drainage or cough-variant asthma, may be more rewarding than escalating anti-acid therapy.
Dr. John E. Pandolfino, AGAF, of Northwestern University, Chicago, discussed the utilization of high-resolution manometry in the evaluation of dysphagia. A central focus of this discussion was the use of the Chicago classification of motility abnormalities in assessing these patients. In the future, it is likely that the care of these patients will be dictated by the type of abnormality the patient has in this classification scheme. Especially in the setting of achalasia, data are emerging that some subtypes of achalasia are less likely to respond to some therapies. For instance, type 3 achalasia is unlikely to respond to pneumatic balloon dilatation.
Dr. Rhonda Souza of the University of Texas Southwestern Medical Center, Dallas, taught us that a diagnosis of eosinophilic esophagitis requires an 8-week trial of PPI therapy with no resolution of the eosinophilia. Esophageal dilation is generally safe in the setting of a dominant stricture, but it can be delayed prior to medical therapy if the patient is tolerating oral intake well. Although the most commonly used therapies for EoE now involve either swallowed steroids or dietary elimination therapy, several new agents are on the horizon that may give us new treatment options.
Finally, Dr. Amitabh Chak of Case Western Reserve University, Cleveland, reviewed the care of patients with Barrett’s esophagus and low-grade dysplasia. This is an especially difficult group of patients to care for, due in part to the low reproducibility in the diagnosis of low-grade dysplasia, as well as the highly variable reported cancer outcomes in this patient population. Level 1 evidence now exists demonstrating that treatment with radiofrequency ablation decreases the incidence of cancer in patients with low-grade dysplasia, but most patients with this finding will not progress. Therefore, the field would benefit from better risk stratification of these patients.
Dr. Shaheen is professor of medicine and epidemiology and chief of the division of gastroenterology & hepatology, University of North Carolina School of Medicine, Chapel Hill. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.
This year’s session on esophagus/upper GI at the AGA Spring Postgraduate Course was packed with pragmatic, useful information for the evaluation of patients with upper GI disorders. The session began with a talk on the manifestations of extraesophageal reflux disease. The take-home message of this talk was that putative extraesophageal manifestations of gastroesophageal reflux disease rarely respond to high-dose therapy with PPIs (proton-pump inhibitors), in the absence of concurrent esophageal symptoms such as heartburn or regurgitation. In such situations, investigation of other etiologies of patients’ symptoms, including occult postnasal drainage or cough-variant asthma, may be more rewarding than escalating anti-acid therapy.
Dr. John E. Pandolfino, AGAF, of Northwestern University, Chicago, discussed the utilization of high-resolution manometry in the evaluation of dysphagia. A central focus of this discussion was the use of the Chicago classification of motility abnormalities in assessing these patients. In the future, it is likely that the care of these patients will be dictated by the type of abnormality the patient has in this classification scheme. Especially in the setting of achalasia, data are emerging that some subtypes of achalasia are less likely to respond to some therapies. For instance, type 3 achalasia is unlikely to respond to pneumatic balloon dilatation.
Dr. Rhonda Souza of the University of Texas Southwestern Medical Center, Dallas, taught us that a diagnosis of eosinophilic esophagitis requires an 8-week trial of PPI therapy with no resolution of the eosinophilia. Esophageal dilation is generally safe in the setting of a dominant stricture, but it can be delayed prior to medical therapy if the patient is tolerating oral intake well. Although the most commonly used therapies for EoE now involve either swallowed steroids or dietary elimination therapy, several new agents are on the horizon that may give us new treatment options.
Finally, Dr. Amitabh Chak of Case Western Reserve University, Cleveland, reviewed the care of patients with Barrett’s esophagus and low-grade dysplasia. This is an especially difficult group of patients to care for, due in part to the low reproducibility in the diagnosis of low-grade dysplasia, as well as the highly variable reported cancer outcomes in this patient population. Level 1 evidence now exists demonstrating that treatment with radiofrequency ablation decreases the incidence of cancer in patients with low-grade dysplasia, but most patients with this finding will not progress. Therefore, the field would benefit from better risk stratification of these patients.
Dr. Shaheen is professor of medicine and epidemiology and chief of the division of gastroenterology & hepatology, University of North Carolina School of Medicine, Chapel Hill. This is a summary provided by the moderator of one of the spring postgraduate course sessions held at DDW 2015.

EASD: Diabetes doubles death risk from many causes
STOCKHOLM – Having diabetes doubles the risk for death from a multitude of causes and shortens the life span by 5-7 years, judging from evidence from the United Kingdom Prospective Studies Collaboration presented at the annual meeting of the European Association for the Study of Diabetes.
Patients with diabetes were two and a half times more likely than those without it to die from ischemic heart disease (odds ratio, 2.37; 95% confidence interval, 2.23-2.52). They were also more likely to die from ischemic stroke (OR, 2.75; 95% CI, 2.29-3.31) and “a surprising association with” cardiac arrhythmia (OR, 2.47; 95% CI, 1.80-3.38) was found, said the presenting author, Dr. Louisa Gnatiuc of the clinical trial service unit and epidemiological studies unit at Oxford (England) University. She noted, however, that diabetes was more weakly associated with death from nonischemic causes (OR, 1.57; 95% CI, 1.34-1.85).

In addition, diabetic individuals were almost twice as likely as those with no diabetes to die from renal (OR, 1.90; 95% CI, 1.40-2.58) or hepatic (OR, 1.75; 95% CI, 1.36-2.26) causes, and there was a 13% increase in the overall risk for death from cancer (OR, 1.13; 95% CI, 1.06-1.21). The small increased risk for cancer death was largely due to deaths from oral (OR, 1.81; 95% CI, 1.17-2.81), liver (OR, 1.80; 95% CI, 1.26-2.58), and pancreatic (OR, 1.57; 95% CI, 1.21-2.03) cancers, Dr. Gnatiuc observed. Diabetic individuals were also more likely to die from respiratory causes than their nondiabetic counterparts (OR, 1.59; 95% CI, 1.37-1.83).
These data provide further insight into the risk for death from a multitude of causes in patients with diabetes, said Dr. Naveed Sattar, who was not involved in the analysis, in an interview. “While it is pretty much a replication of the Emerging Risk Factor Paper that was published in the New England Journal of Medicine, there is a little bit of new information here, such as the relative risks in women versus men and by age as well,” he observed.
The odds ratio for death from ischemic heart disease was higher among women aged 35-39 years with diabetes versus those with no diabetes than in men aged 35-39 years with diabetes versus no diabetes, at 5.61 (95% CI, 4.08-7.72) and 2.49 (95% CI, 2.16-2.85), respectively. Similar finding were seen at other age ranges, with around a twofold increase in men aged 60-69 years (OR, 2.26; 95% CI, 2.01-2.53) and 70-89 years (OR, 1.89; 95% CI, 1.70-2.11), but a two- to fourfold increase in women aged 60-69 years (OR, 4.15; 95% CI, 3.38-5.10) and 70-79 years (OR, 2.45, 95% CI, 2.11-2.84).
“So it looks like if you develop diabetes younger, your risk for mortality’s higher,” said Dr. Sattar, professor of metabolic medicine at the Institute of Cardiovascular and Medical Sciences, University of Glasgow (Scotland). “That makes sense,” he added, “because if you develop type 2 diabetes at the age of 30, it must be a much more malignant type of diabetes than, say, if you developed diabetes at age 80, and there are other data that now confirm that is the case as well.”
The analysis was based on data from 44 prospective studies that recorded 55,855 deaths in 690,700 adults who had no prior vascular or other chronic diseases at baseline. Men accounted for 60% of the study population, with a mean age of 48 years. During the postpresentation discussion, Dr. Gnatiuc noted that it was difficult to standardize the definition of diabetes used in the study and that all 25,000 cases of diabetes included in the study had been self-reported. It is likely that most cases were type 2. No information on the duration of diabetes was available, but she noted that this should not matter given the prospective nature of the analysis.
During 13 million patient-years of follow up the most common cause of death was ischemic heart disease, accounting for 17,218 deaths, followed by cancer (18,658 deaths). There were 5,466 strokes of which 1,353 were ischemic (OR, 2.75; 95% CI 2.29-3.31), 1,124 hemorrhagic (OR, 1.59; 95% CI 1.26-2.01), 2,563 that were unspecified (OR, 2.30; 95% CI 1.99-2.66), and 626 classed as subarachnoid hemorrhage (OR, 0.62; 95% CI, 0.36-1.08). Vascular causes of death included inflammatory heart disease, sudden death, and atherosclerosis, among others, which were all increased in diabetic versus nondiabetic subjects.
Dr. Gnatiuc noted that the risk for ischemic heart disease increased with increasing age, systolic blood pressure, and total cholesterol in diabetics and in nondiabetics, although it was much higher in those with diabetes than in those without. “Controlling blood pressure, cholesterol, and obesity are particularly important to reduce absolute mortality rates in those with diabetes, she suggested.
The differences between the sexes in terms of ischemic heart disease need further study, she suggested, noting that improved understanding of the sex differences may help better understand and thus reduce the excess mortality seen.
Premature mortality of up to 5 years in men and 7 years in women was observed. “At the age of 70 a man with diabetes would have about 10% less probability to survive up to the age of 90 as compared to their nondiabetic counterparts,” Dr. Gnatiuc said. Women would have about a 30% decrease in survival probability from age 70-90, she added.
STOCKHOLM – Having diabetes doubles the risk for death from a multitude of causes and shortens the life span by 5-7 years, judging from evidence from the United Kingdom Prospective Studies Collaboration presented at the annual meeting of the European Association for the Study of Diabetes.
Patients with diabetes were two and a half times more likely than those without it to die from ischemic heart disease (odds ratio, 2.37; 95% confidence interval, 2.23-2.52). They were also more likely to die from ischemic stroke (OR, 2.75; 95% CI, 2.29-3.31) and “a surprising association with” cardiac arrhythmia (OR, 2.47; 95% CI, 1.80-3.38) was found, said the presenting author, Dr. Louisa Gnatiuc of the clinical trial service unit and epidemiological studies unit at Oxford (England) University. She noted, however, that diabetes was more weakly associated with death from nonischemic causes (OR, 1.57; 95% CI, 1.34-1.85).
In addition, diabetic individuals were almost twice as likely as those with no diabetes to die from renal (OR, 1.90; 95% CI, 1.40-2.58) or hepatic (OR, 1.75; 95% CI, 1.36-2.26) causes, and there was a 13% increase in the overall risk for death from cancer (OR, 1.13; 95% CI, 1.06-1.21). The small increased risk for cancer death was largely due to deaths from oral (OR, 1.81; 95% CI, 1.17-2.81), liver (OR, 1.80; 95% CI, 1.26-2.58), and pancreatic (OR, 1.57; 95% CI, 1.21-2.03) cancers, Dr. Gnatiuc observed. Diabetic individuals were also more likely to die from respiratory causes than their nondiabetic counterparts (OR, 1.59; 95% CI, 1.37-1.83).
These data provide further insight into the risk for death from a multitude of causes in patients with diabetes, said Dr. Naveed Sattar, who was not involved in the analysis, in an interview. “While it is pretty much a replication of the Emerging Risk Factor Paper that was published in the New England Journal of Medicine, there is a little bit of new information here, such as the relative risks in women versus men and by age as well,” he observed.
The odds ratio for death from ischemic heart disease was higher among women aged 35-39 years with diabetes versus those with no diabetes than in men aged 35-39 years with diabetes versus no diabetes, at 5.61 (95% CI, 4.08-7.72) and 2.49 (95% CI, 2.16-2.85), respectively. Similar finding were seen at other age ranges, with around a twofold increase in men aged 60-69 years (OR, 2.26; 95% CI, 2.01-2.53) and 70-89 years (OR, 1.89; 95% CI, 1.70-2.11), but a two- to fourfold increase in women aged 60-69 years (OR, 4.15; 95% CI, 3.38-5.10) and 70-79 years (OR, 2.45, 95% CI, 2.11-2.84).
“So it looks like if you develop diabetes younger, your risk for mortality’s higher,” said Dr. Sattar, professor of metabolic medicine at the Institute of Cardiovascular and Medical Sciences, University of Glasgow (Scotland). “That makes sense,” he added, “because if you develop type 2 diabetes at the age of 30, it must be a much more malignant type of diabetes than, say, if you developed diabetes at age 80, and there are other data that now confirm that is the case as well.”
The analysis was based on data from 44 prospective studies that recorded 55,855 deaths in 690,700 adults who had no prior vascular or other chronic diseases at baseline. Men accounted for 60% of the study population, with a mean age of 48 years. During the postpresentation discussion, Dr. Gnatiuc noted that it was difficult to standardize the definition of diabetes used in the study and that all 25,000 cases of diabetes included in the study had been self-reported. It is likely that most cases were type 2. No information on the duration of diabetes was available, but she noted that this should not matter given the prospective nature of the analysis.
During 13 million patient-years of follow up the most common cause of death was ischemic heart disease, accounting for 17,218 deaths, followed by cancer (18,658 deaths). There were 5,466 strokes of which 1,353 were ischemic (OR, 2.75; 95% CI 2.29-3.31), 1,124 hemorrhagic (OR, 1.59; 95% CI 1.26-2.01), 2,563 that were unspecified (OR, 2.30; 95% CI 1.99-2.66), and 626 classed as subarachnoid hemorrhage (OR, 0.62; 95% CI, 0.36-1.08). Vascular causes of death included inflammatory heart disease, sudden death, and atherosclerosis, among others, which were all increased in diabetic versus nondiabetic subjects.
Dr. Gnatiuc noted that the risk for ischemic heart disease increased with increasing age, systolic blood pressure, and total cholesterol in diabetics and in nondiabetics, although it was much higher in those with diabetes than in those without. “Controlling blood pressure, cholesterol, and obesity are particularly important to reduce absolute mortality rates in those with diabetes, she suggested.
The differences between the sexes in terms of ischemic heart disease need further study, she suggested, noting that improved understanding of the sex differences may help better understand and thus reduce the excess mortality seen.
Premature mortality of up to 5 years in men and 7 years in women was observed. “At the age of 70 a man with diabetes would have about 10% less probability to survive up to the age of 90 as compared to their nondiabetic counterparts,” Dr. Gnatiuc said. Women would have about a 30% decrease in survival probability from age 70-90, she added.
STOCKHOLM – Having diabetes doubles the risk for death from a multitude of causes and shortens the life span by 5-7 years, judging from evidence from the United Kingdom Prospective Studies Collaboration presented at the annual meeting of the European Association for the Study of Diabetes.
Patients with diabetes were two and a half times more likely than those without it to die from ischemic heart disease (odds ratio, 2.37; 95% confidence interval, 2.23-2.52). They were also more likely to die from ischemic stroke (OR, 2.75; 95% CI, 2.29-3.31) and “a surprising association with” cardiac arrhythmia (OR, 2.47; 95% CI, 1.80-3.38) was found, said the presenting author, Dr. Louisa Gnatiuc of the clinical trial service unit and epidemiological studies unit at Oxford (England) University. She noted, however, that diabetes was more weakly associated with death from nonischemic causes (OR, 1.57; 95% CI, 1.34-1.85).
In addition, diabetic individuals were almost twice as likely as those with no diabetes to die from renal (OR, 1.90; 95% CI, 1.40-2.58) or hepatic (OR, 1.75; 95% CI, 1.36-2.26) causes, and there was a 13% increase in the overall risk for death from cancer (OR, 1.13; 95% CI, 1.06-1.21). The small increased risk for cancer death was largely due to deaths from oral (OR, 1.81; 95% CI, 1.17-2.81), liver (OR, 1.80; 95% CI, 1.26-2.58), and pancreatic (OR, 1.57; 95% CI, 1.21-2.03) cancers, Dr. Gnatiuc observed. Diabetic individuals were also more likely to die from respiratory causes than their nondiabetic counterparts (OR, 1.59; 95% CI, 1.37-1.83).
These data provide further insight into the risk for death from a multitude of causes in patients with diabetes, said Dr. Naveed Sattar, who was not involved in the analysis, in an interview. “While it is pretty much a replication of the Emerging Risk Factor Paper that was published in the New England Journal of Medicine, there is a little bit of new information here, such as the relative risks in women versus men and by age as well,” he observed.
The odds ratio for death from ischemic heart disease was higher among women aged 35-39 years with diabetes versus those with no diabetes than in men aged 35-39 years with diabetes versus no diabetes, at 5.61 (95% CI, 4.08-7.72) and 2.49 (95% CI, 2.16-2.85), respectively. Similar finding were seen at other age ranges, with around a twofold increase in men aged 60-69 years (OR, 2.26; 95% CI, 2.01-2.53) and 70-89 years (OR, 1.89; 95% CI, 1.70-2.11), but a two- to fourfold increase in women aged 60-69 years (OR, 4.15; 95% CI, 3.38-5.10) and 70-79 years (OR, 2.45, 95% CI, 2.11-2.84).
“So it looks like if you develop diabetes younger, your risk for mortality’s higher,” said Dr. Sattar, professor of metabolic medicine at the Institute of Cardiovascular and Medical Sciences, University of Glasgow (Scotland). “That makes sense,” he added, “because if you develop type 2 diabetes at the age of 30, it must be a much more malignant type of diabetes than, say, if you developed diabetes at age 80, and there are other data that now confirm that is the case as well.”
The analysis was based on data from 44 prospective studies that recorded 55,855 deaths in 690,700 adults who had no prior vascular or other chronic diseases at baseline. Men accounted for 60% of the study population, with a mean age of 48 years. During the postpresentation discussion, Dr. Gnatiuc noted that it was difficult to standardize the definition of diabetes used in the study and that all 25,000 cases of diabetes included in the study had been self-reported. It is likely that most cases were type 2. No information on the duration of diabetes was available, but she noted that this should not matter given the prospective nature of the analysis.
During 13 million patient-years of follow up the most common cause of death was ischemic heart disease, accounting for 17,218 deaths, followed by cancer (18,658 deaths). There were 5,466 strokes of which 1,353 were ischemic (OR, 2.75; 95% CI 2.29-3.31), 1,124 hemorrhagic (OR, 1.59; 95% CI 1.26-2.01), 2,563 that were unspecified (OR, 2.30; 95% CI 1.99-2.66), and 626 classed as subarachnoid hemorrhage (OR, 0.62; 95% CI, 0.36-1.08). Vascular causes of death included inflammatory heart disease, sudden death, and atherosclerosis, among others, which were all increased in diabetic versus nondiabetic subjects.
Dr. Gnatiuc noted that the risk for ischemic heart disease increased with increasing age, systolic blood pressure, and total cholesterol in diabetics and in nondiabetics, although it was much higher in those with diabetes than in those without. “Controlling blood pressure, cholesterol, and obesity are particularly important to reduce absolute mortality rates in those with diabetes, she suggested.
The differences between the sexes in terms of ischemic heart disease need further study, she suggested, noting that improved understanding of the sex differences may help better understand and thus reduce the excess mortality seen.
Premature mortality of up to 5 years in men and 7 years in women was observed. “At the age of 70 a man with diabetes would have about 10% less probability to survive up to the age of 90 as compared to their nondiabetic counterparts,” Dr. Gnatiuc said. Women would have about a 30% decrease in survival probability from age 70-90, she added.
AT EASD 2015
Key clinical point:Women with diabetes were more likely to die from ischemic heart disease than men with diabetes when compared to those without diabetes.
Major finding: Women with diabetes were more likely to die from ischemic heart disease than men with diabetes when compared to those without diabetes.
Data source: United Kingdom Prospective Studies Collaboration analysis of 44 prospective studies that recorded 55,855 deaths in 690,700 adults who had no prior vascular or other chronic diseases at baseline.
Disclosures: The study was funded by research grants from the British Heart Foundation, UK Medical Research Council, The National Institutes of Health (UK), Cancer Research UK, and the Clinical Trial Service Unit and Epidemiological Studies Unit at Oxford University, UK. Dr. Gnatiuc did not report any personal disclosures.

October 2015 Quiz 2
ANSWER: C
Critique
The first step in managing this patient should not be to stop the tube feedings. Enteral feedings are providing much-needed nutrition to this patient. There is no evidence that either continuous or bolus feedings are superior. Diarrhea has been shown to occur in up to 18% of patients receiving enteral nutrition. Clostridium difficile is the leading cause of health care–associated diarrhea. Antibiotic therapy is the most common risk factor associated with acquisition of C. difficile infection. Internally fed patients are more likely than non–tube fed patients to acquire C. difficile infection and, therefore, it is recommended to check for C. difficile in tube-fed patients, especially when they are receiving antibiotics. The patient has no comorbid conditions that would require elemental formula, such as short bowel syndrome or malabsorption. In addition, it is not clear that elemental formulas are superior to standard formulas in patients with malabsorption or maldigestion. Finally, standard polymeric formulas are lactose free. Other considerations in a patient on enteral feedings with diarrhea include non–C. difficile antibiotic-associated diarrhea, formula composition, sorbitol-containing medication preparations, and side effects of medications as well as hypoalbuminemia.
References
1. Loo V.G., Bourgault A.M., Poirier L., et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. 2011;365:1693-703.
2. Bliss D.Z., Johnson S., Savik K. Acquisition of Clostridium difficile and Clostridium difficile–associated diarrhea in hospitalized patients receiving tube feeding. Ann Intern Med. 1998;129:1012.
3. Macleod J.B., Lefton J., Houghton D., et al. Prospective randomized control trial of intermittent versus continuous gastric feeds for critically ill trauma patients. J Trauma. 2007;63:57.
ANSWER: C
Critique
The first step in managing this patient should not be to stop the tube feedings. Enteral feedings are providing much-needed nutrition to this patient. There is no evidence that either continuous or bolus feedings are superior. Diarrhea has been shown to occur in up to 18% of patients receiving enteral nutrition. Clostridium difficile is the leading cause of health care–associated diarrhea. Antibiotic therapy is the most common risk factor associated with acquisition of C. difficile infection. Internally fed patients are more likely than non–tube fed patients to acquire C. difficile infection and, therefore, it is recommended to check for C. difficile in tube-fed patients, especially when they are receiving antibiotics. The patient has no comorbid conditions that would require elemental formula, such as short bowel syndrome or malabsorption. In addition, it is not clear that elemental formulas are superior to standard formulas in patients with malabsorption or maldigestion. Finally, standard polymeric formulas are lactose free. Other considerations in a patient on enteral feedings with diarrhea include non–C. difficile antibiotic-associated diarrhea, formula composition, sorbitol-containing medication preparations, and side effects of medications as well as hypoalbuminemia.
References
1. Loo V.G., Bourgault A.M., Poirier L., et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. 2011;365:1693-703.
2. Bliss D.Z., Johnson S., Savik K. Acquisition of Clostridium difficile and Clostridium difficile–associated diarrhea in hospitalized patients receiving tube feeding. Ann Intern Med. 1998;129:1012.
3. Macleod J.B., Lefton J., Houghton D., et al. Prospective randomized control trial of intermittent versus continuous gastric feeds for critically ill trauma patients. J Trauma. 2007;63:57.
ANSWER: C
Critique
The first step in managing this patient should not be to stop the tube feedings. Enteral feedings are providing much-needed nutrition to this patient. There is no evidence that either continuous or bolus feedings are superior. Diarrhea has been shown to occur in up to 18% of patients receiving enteral nutrition. Clostridium difficile is the leading cause of health care–associated diarrhea. Antibiotic therapy is the most common risk factor associated with acquisition of C. difficile infection. Internally fed patients are more likely than non–tube fed patients to acquire C. difficile infection and, therefore, it is recommended to check for C. difficile in tube-fed patients, especially when they are receiving antibiotics. The patient has no comorbid conditions that would require elemental formula, such as short bowel syndrome or malabsorption. In addition, it is not clear that elemental formulas are superior to standard formulas in patients with malabsorption or maldigestion. Finally, standard polymeric formulas are lactose free. Other considerations in a patient on enteral feedings with diarrhea include non–C. difficile antibiotic-associated diarrhea, formula composition, sorbitol-containing medication preparations, and side effects of medications as well as hypoalbuminemia.
References
1. Loo V.G., Bourgault A.M., Poirier L., et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. 2011;365:1693-703.
2. Bliss D.Z., Johnson S., Savik K. Acquisition of Clostridium difficile and Clostridium difficile–associated diarrhea in hospitalized patients receiving tube feeding. Ann Intern Med. 1998;129:1012.
3. Macleod J.B., Lefton J., Houghton D., et al. Prospective randomized control trial of intermittent versus continuous gastric feeds for critically ill trauma patients. J Trauma. 2007;63:57.
October 2015 Quiz 1
ANSWER: A
Critique
Extrahepatic biliary atresia accounts for 25%-30% of children with neonatal cholestasis and it is the most commonly identified etiology. Despite the identification and ability to test for many other causes, idiopathic disease still accounts for a similar proportion of infants with cholestasis. Galactosemia, disorders of bile acid biosynthesis, and panhypopituitarism each account for 1% or slightly more of neonatal cholestasis. Autoimmune hepatitis is not a usual consideration in neonates.
Reference
Dellert S., Balistreri W., Neonatal cholestasis. In: Pediatric Gastrointestinal Disease: Pathophysiology, Diagnosis, Management, 3rd ed. Walker A., Durie P., Hamilton R., Walker–Smith J., eds. Hamilton, Ontario: B. C. Decker, 2000;52:880-94.
ANSWER: A
Critique
Extrahepatic biliary atresia accounts for 25%-30% of children with neonatal cholestasis and it is the most commonly identified etiology. Despite the identification and ability to test for many other causes, idiopathic disease still accounts for a similar proportion of infants with cholestasis. Galactosemia, disorders of bile acid biosynthesis, and panhypopituitarism each account for 1% or slightly more of neonatal cholestasis. Autoimmune hepatitis is not a usual consideration in neonates.
Reference
Dellert S., Balistreri W., Neonatal cholestasis. In: Pediatric Gastrointestinal Disease: Pathophysiology, Diagnosis, Management, 3rd ed. Walker A., Durie P., Hamilton R., Walker–Smith J., eds. Hamilton, Ontario: B. C. Decker, 2000;52:880-94.
ANSWER: A
Critique
Extrahepatic biliary atresia accounts for 25%-30% of children with neonatal cholestasis and it is the most commonly identified etiology. Despite the identification and ability to test for many other causes, idiopathic disease still accounts for a similar proportion of infants with cholestasis. Galactosemia, disorders of bile acid biosynthesis, and panhypopituitarism each account for 1% or slightly more of neonatal cholestasis. Autoimmune hepatitis is not a usual consideration in neonates.
Reference
Dellert S., Balistreri W., Neonatal cholestasis. In: Pediatric Gastrointestinal Disease: Pathophysiology, Diagnosis, Management, 3rd ed. Walker A., Durie P., Hamilton R., Walker–Smith J., eds. Hamilton, Ontario: B. C. Decker, 2000;52:880-94.
Does high dietary soy intake affect a woman’s risk of primary or recurrent breast cancer?
No, it doesn’t affect the risk of primary breast cancer, but it does (favorably) affect the risk of cancer recurrence.
Compared with diets low in soy, high dietary intake of soy protein or soy isoflavones isn’t associated with any alteration in the risk of developing primary breast cancer (strength of recommendation [SOR]: B, systematic review of prospective cohort studies). In patients with breast cancer, however, consuming a diet high in soy is associated with a 25% decrease in cancer recurrence and a 15% decrease in mortality (SOR: B, prospective cohort studies).
EVIDENCE SUMMARY
A large systematic review evaluated the relationship between dietary soy intake and risk of a primary breast cancer diagnosis. It included 7 prospective cohort studies, which comprised the best quality evidence available (numerous other reviewed studies were of lower quality). The review found no significant association between dietary soy intake and primary breast cancer (TABLE1-6).
Investigators either surveyed women for intake of soy isoflavones or soy foods or products (tofu, soybeans, lentils, miso) or measured urinary or plasma levels of soy isoflavones. They adjusted for age, alcohol use, smoking status, body mass index, caloric intake, and hormone replacement therapy, then followed subjects for 7 to 23 years, comparing the risk of breast cancer for the lowest and highest levels of soy intake.
Six of the prospective cohort studies found no association between soy intake and breast cancer risk; one study, comprising 4% of the total population, found a lower risk with higher soy intake (effect size=0.44; 95% confidence interval [CI], 0.26-0.73; an effect size of 0.2 is considered small, 0.6 medium, and 1.2 large). The authors didn’t do a meta-analysis of the prospective cohort studies.
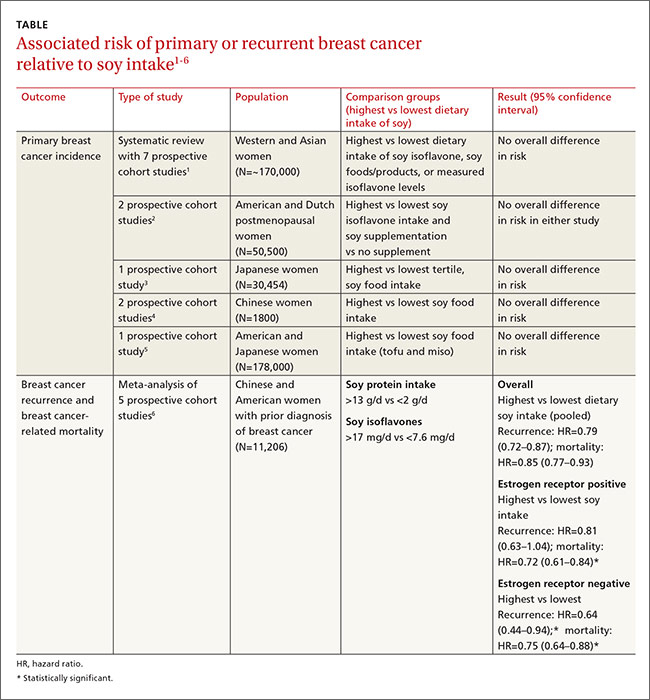
Other cohort studies yield similar findings
Four other large systematic reviews evaluating soy intake and breast cancer risk incorporated a total of 6 individual prospective cohort studies that weren’t included in the previously described review (again, these studies comprised the best quality evidence within the reviews). The 6 studies found no association between soy intake and breast cancer risk.
In 2 of the studies, investigators surveyed postmenopausal women and followed them for 4 to 8 years.2 Investigators in another study adjusted for age, family and gynecologic history, hormone and medication use, exercise, and other factors.3 In 2 other studies, investigators evaluated population subsets that consumed the most vs the fewest servings per week or kilograms per year of soy foods.4 The sixth study compared low with high intake of soy foods and miso.5
Soy intake after breast cancer diagnosis reduces recurrence risk in most studies
Most prospective cohort studies evaluating the association between dietary soy intake after breast cancer diagnosis found an overall 21% decrease in recurrence with high soy intake and a 15% reduction in mortality (TABLE1-6).
Investigators in a meta-analysis of 5 studies that followed women for 4 to 7 years after first breast cancer diagnosis found that higher soy intake was associated with lower mortality but not less recurrence in women who were estrogen receptor positive. Both recurrence and mortality were decreased in estrogen receptor negative women.6
The study also found lower recurrence and mortality in premenopausal women with higher soy intake (recurrence hazard ratio [HR]=0.91; 95% CI, 0.72-1.14; mortality HR=0.78; 95% CI, 0.69-0.88). In postmenopausal women, higher intake was likewise associated with improvement of both outcomes (recurrence HR=0.67; 95% CI, 0.56-0.80; mortality HR=0.81; 95% CI, 0.73-0.91).
An earlier meta-analysis of 4 prospective cohort studies, 2 of which were not included above, also found reduced risk of breast cancer recurrence in groups with high vs low soy isoflavone intake (HR=0.84; 95% CI, 0.70-0.99).7 Women taking tamoxifen showed no difference in mortality or recurrence risk associated with soy intake.
An additional small prospective cohort study (n=256) found similar reductions in recurrence and mortality associated with higher consumption of soy protein.8
1. Chen M, Rao Y, Zheng Y, et al. Association between soy isoflavone intake and breast cancer risk for pre- and post-menopausal women: a meta-analysis of epidemiological studies. PLoS One. 2014;9:e89288.
2. Fritz H, Seely D, Flower G, et al. Soy, red clover, and isoflavones and breast cancer: a systematic review. PLoS One. 2013;8:e81968.
3. Nagata C, Mizoue T, Tanaka K, et al. Soy intake and breast cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn J Clin Oncol. 2014;44:282–295.
4. Liu XO, Huang YB, Gao Y, et al. Association between dietary factors and breast cancer risk among Chinese females: systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15:1291–1298.
5. Qin LQ, Xu JY, Wang PY, et al. Soyfood intake in the prevention of breast cancer risk in women: a meta-analysis of observational epidemiological studies. J Nutr Sci Vitaminol (Tokyo). 2006;52:428–436.
6. Chi F, Wu R, Zeng YC, et al. Post-diagnosis soy food intake and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev. 2013;14:2407–2412.
7. Dong JY, Qin LQ. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: a meta-analysis of prospective studies. Breast Cancer Res Treat. 2011;125:315-323.
8. Kang HB, Zhang YF, Yang JD, et al. Study on soy isoflavone consumption and risk of breast cancer and survival. Asian Pac J Cancer Prev. 2012;13:995–998.
No, it doesn’t affect the risk of primary breast cancer, but it does (favorably) affect the risk of cancer recurrence.
Compared with diets low in soy, high dietary intake of soy protein or soy isoflavones isn’t associated with any alteration in the risk of developing primary breast cancer (strength of recommendation [SOR]: B, systematic review of prospective cohort studies). In patients with breast cancer, however, consuming a diet high in soy is associated with a 25% decrease in cancer recurrence and a 15% decrease in mortality (SOR: B, prospective cohort studies).
EVIDENCE SUMMARY
A large systematic review evaluated the relationship between dietary soy intake and risk of a primary breast cancer diagnosis. It included 7 prospective cohort studies, which comprised the best quality evidence available (numerous other reviewed studies were of lower quality). The review found no significant association between dietary soy intake and primary breast cancer (TABLE1-6).
Investigators either surveyed women for intake of soy isoflavones or soy foods or products (tofu, soybeans, lentils, miso) or measured urinary or plasma levels of soy isoflavones. They adjusted for age, alcohol use, smoking status, body mass index, caloric intake, and hormone replacement therapy, then followed subjects for 7 to 23 years, comparing the risk of breast cancer for the lowest and highest levels of soy intake.
Six of the prospective cohort studies found no association between soy intake and breast cancer risk; one study, comprising 4% of the total population, found a lower risk with higher soy intake (effect size=0.44; 95% confidence interval [CI], 0.26-0.73; an effect size of 0.2 is considered small, 0.6 medium, and 1.2 large). The authors didn’t do a meta-analysis of the prospective cohort studies.
Other cohort studies yield similar findings
Four other large systematic reviews evaluating soy intake and breast cancer risk incorporated a total of 6 individual prospective cohort studies that weren’t included in the previously described review (again, these studies comprised the best quality evidence within the reviews). The 6 studies found no association between soy intake and breast cancer risk.
In 2 of the studies, investigators surveyed postmenopausal women and followed them for 4 to 8 years.2 Investigators in another study adjusted for age, family and gynecologic history, hormone and medication use, exercise, and other factors.3 In 2 other studies, investigators evaluated population subsets that consumed the most vs the fewest servings per week or kilograms per year of soy foods.4 The sixth study compared low with high intake of soy foods and miso.5
Soy intake after breast cancer diagnosis reduces recurrence risk in most studies
Most prospective cohort studies evaluating the association between dietary soy intake after breast cancer diagnosis found an overall 21% decrease in recurrence with high soy intake and a 15% reduction in mortality (TABLE1-6).
Investigators in a meta-analysis of 5 studies that followed women for 4 to 7 years after first breast cancer diagnosis found that higher soy intake was associated with lower mortality but not less recurrence in women who were estrogen receptor positive. Both recurrence and mortality were decreased in estrogen receptor negative women.6
The study also found lower recurrence and mortality in premenopausal women with higher soy intake (recurrence hazard ratio [HR]=0.91; 95% CI, 0.72-1.14; mortality HR=0.78; 95% CI, 0.69-0.88). In postmenopausal women, higher intake was likewise associated with improvement of both outcomes (recurrence HR=0.67; 95% CI, 0.56-0.80; mortality HR=0.81; 95% CI, 0.73-0.91).
An earlier meta-analysis of 4 prospective cohort studies, 2 of which were not included above, also found reduced risk of breast cancer recurrence in groups with high vs low soy isoflavone intake (HR=0.84; 95% CI, 0.70-0.99).7 Women taking tamoxifen showed no difference in mortality or recurrence risk associated with soy intake.
An additional small prospective cohort study (n=256) found similar reductions in recurrence and mortality associated with higher consumption of soy protein.8
No, it doesn’t affect the risk of primary breast cancer, but it does (favorably) affect the risk of cancer recurrence.
Compared with diets low in soy, high dietary intake of soy protein or soy isoflavones isn’t associated with any alteration in the risk of developing primary breast cancer (strength of recommendation [SOR]: B, systematic review of prospective cohort studies). In patients with breast cancer, however, consuming a diet high in soy is associated with a 25% decrease in cancer recurrence and a 15% decrease in mortality (SOR: B, prospective cohort studies).
EVIDENCE SUMMARY
A large systematic review evaluated the relationship between dietary soy intake and risk of a primary breast cancer diagnosis. It included 7 prospective cohort studies, which comprised the best quality evidence available (numerous other reviewed studies were of lower quality). The review found no significant association between dietary soy intake and primary breast cancer (TABLE1-6).
Investigators either surveyed women for intake of soy isoflavones or soy foods or products (tofu, soybeans, lentils, miso) or measured urinary or plasma levels of soy isoflavones. They adjusted for age, alcohol use, smoking status, body mass index, caloric intake, and hormone replacement therapy, then followed subjects for 7 to 23 years, comparing the risk of breast cancer for the lowest and highest levels of soy intake.
Six of the prospective cohort studies found no association between soy intake and breast cancer risk; one study, comprising 4% of the total population, found a lower risk with higher soy intake (effect size=0.44; 95% confidence interval [CI], 0.26-0.73; an effect size of 0.2 is considered small, 0.6 medium, and 1.2 large). The authors didn’t do a meta-analysis of the prospective cohort studies.
Other cohort studies yield similar findings
Four other large systematic reviews evaluating soy intake and breast cancer risk incorporated a total of 6 individual prospective cohort studies that weren’t included in the previously described review (again, these studies comprised the best quality evidence within the reviews). The 6 studies found no association between soy intake and breast cancer risk.
In 2 of the studies, investigators surveyed postmenopausal women and followed them for 4 to 8 years.2 Investigators in another study adjusted for age, family and gynecologic history, hormone and medication use, exercise, and other factors.3 In 2 other studies, investigators evaluated population subsets that consumed the most vs the fewest servings per week or kilograms per year of soy foods.4 The sixth study compared low with high intake of soy foods and miso.5
Soy intake after breast cancer diagnosis reduces recurrence risk in most studies
Most prospective cohort studies evaluating the association between dietary soy intake after breast cancer diagnosis found an overall 21% decrease in recurrence with high soy intake and a 15% reduction in mortality (TABLE1-6).
Investigators in a meta-analysis of 5 studies that followed women for 4 to 7 years after first breast cancer diagnosis found that higher soy intake was associated with lower mortality but not less recurrence in women who were estrogen receptor positive. Both recurrence and mortality were decreased in estrogen receptor negative women.6
The study also found lower recurrence and mortality in premenopausal women with higher soy intake (recurrence hazard ratio [HR]=0.91; 95% CI, 0.72-1.14; mortality HR=0.78; 95% CI, 0.69-0.88). In postmenopausal women, higher intake was likewise associated with improvement of both outcomes (recurrence HR=0.67; 95% CI, 0.56-0.80; mortality HR=0.81; 95% CI, 0.73-0.91).
An earlier meta-analysis of 4 prospective cohort studies, 2 of which were not included above, also found reduced risk of breast cancer recurrence in groups with high vs low soy isoflavone intake (HR=0.84; 95% CI, 0.70-0.99).7 Women taking tamoxifen showed no difference in mortality or recurrence risk associated with soy intake.
An additional small prospective cohort study (n=256) found similar reductions in recurrence and mortality associated with higher consumption of soy protein.8
1. Chen M, Rao Y, Zheng Y, et al. Association between soy isoflavone intake and breast cancer risk for pre- and post-menopausal women: a meta-analysis of epidemiological studies. PLoS One. 2014;9:e89288.
2. Fritz H, Seely D, Flower G, et al. Soy, red clover, and isoflavones and breast cancer: a systematic review. PLoS One. 2013;8:e81968.
3. Nagata C, Mizoue T, Tanaka K, et al. Soy intake and breast cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn J Clin Oncol. 2014;44:282–295.
4. Liu XO, Huang YB, Gao Y, et al. Association between dietary factors and breast cancer risk among Chinese females: systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15:1291–1298.
5. Qin LQ, Xu JY, Wang PY, et al. Soyfood intake in the prevention of breast cancer risk in women: a meta-analysis of observational epidemiological studies. J Nutr Sci Vitaminol (Tokyo). 2006;52:428–436.
6. Chi F, Wu R, Zeng YC, et al. Post-diagnosis soy food intake and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev. 2013;14:2407–2412.
7. Dong JY, Qin LQ. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: a meta-analysis of prospective studies. Breast Cancer Res Treat. 2011;125:315-323.
8. Kang HB, Zhang YF, Yang JD, et al. Study on soy isoflavone consumption and risk of breast cancer and survival. Asian Pac J Cancer Prev. 2012;13:995–998.
1. Chen M, Rao Y, Zheng Y, et al. Association between soy isoflavone intake and breast cancer risk for pre- and post-menopausal women: a meta-analysis of epidemiological studies. PLoS One. 2014;9:e89288.
2. Fritz H, Seely D, Flower G, et al. Soy, red clover, and isoflavones and breast cancer: a systematic review. PLoS One. 2013;8:e81968.
3. Nagata C, Mizoue T, Tanaka K, et al. Soy intake and breast cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn J Clin Oncol. 2014;44:282–295.
4. Liu XO, Huang YB, Gao Y, et al. Association between dietary factors and breast cancer risk among Chinese females: systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15:1291–1298.
5. Qin LQ, Xu JY, Wang PY, et al. Soyfood intake in the prevention of breast cancer risk in women: a meta-analysis of observational epidemiological studies. J Nutr Sci Vitaminol (Tokyo). 2006;52:428–436.
6. Chi F, Wu R, Zeng YC, et al. Post-diagnosis soy food intake and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev. 2013;14:2407–2412.
7. Dong JY, Qin LQ. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: a meta-analysis of prospective studies. Breast Cancer Res Treat. 2011;125:315-323.
8. Kang HB, Zhang YF, Yang JD, et al. Study on soy isoflavone consumption and risk of breast cancer and survival. Asian Pac J Cancer Prev. 2012;13:995–998.
Evidence-based answers from the Family Physicians Inquiries Network

Worsening Migraine in Pregnancy Is Linked to Adverse Outcomes
VALENCIA, SPAIN—Women who present with acute severe migraine during pregnancy are at increased risk for adverse pregnancy outcomes and should be seen in a high-risk pregnancy clinic, according to research presented at the International Headache Congress.
“We should not be seeing these patients in a regular [obstetrician’s or] generalist’s office because oftentimes we need input from neurology, and we need extra surveillance for both the fetus and the mother,” said Tracy B. Grossman, MD, an obstetrics and gynecology resident at Montefiore Medical Center in New York.

Dr. Grossman described a retrospective study of 90 consecutive pregnant patients who presented with acute severe migraine and obtained a neurology consultation at Montefiore Medical Center.
“These patients are different from most migraine patients because most migraine patients actually see improvement of symptoms during pregnancy. So, this is a special group of patients with worsening and refractory migraine,” she said.
Most of the women were in their third trimester. Diagnoses included migraine with aura (11.6%), migraine without aura (59.3%), and both (29.1%). A minority had chronic migraine (12.8%), and 31.4% presented in status migrainosus.
Forty-nine of the 90 patients (54%) experienced one or more adverse pregnancy outcomes. The population’s preterm delivery rate was 28%, which is nearly three times the national average of 11%, as reported by the March of Dimes. The population’s preeclampsia rate was 20.5%, compared with a national rate of 3% to 4%. The low-birth-weight rate of 19.2% was more than double the 8% national average. The rate of cesarean sections was 30.8%.
The study hypothesis was that women with migraine with aura would have higher rates of preeclampsia, preterm delivery, and low birth weight. Although studies of migraine in pregnancy have been few, some investigators have reported these associations. The current study did not find these associations, however, because most of the patients did not have aura, said Dr. Grossman.
“It can’t be purely an aura [or] vascular phenomenon that’s resulting in these adverse outcomes. These high rates of adverse pregnancy outcomes aren’t easily explainable. There’s something going on here that we haven’t teased out yet as to why these migraine patients are special,” she said.
Their risk of adverse pregnancy outcomes was not related to the headache medications that the patients took. Sixty-two patients received a combination of oral and IV therapy with acetaminophen, metoclopramide, and dihydroergotamine. In addition, 30% of patients briefly took barbiturates, and 30% received oxycodone or codeine. Although these drugs raise concerns during pregnancy, the investigators found no associated increase in adverse pregnancy outcomes among women who received them, compared with the women who did not receive those drugs or who did not receive any headache medications.
Dr. Grossman’s own therapeutic preference for patients with severe migraine during pregnancy is a peripheral nerve block with bupivacaine and lidocaine. “It works for the majority of people—we don’t quite know why—and it’s a local therapy that avoids fetal exposure to systemic medications,” she observed.
—Bruce Jancin
VALENCIA, SPAIN—Women who present with acute severe migraine during pregnancy are at increased risk for adverse pregnancy outcomes and should be seen in a high-risk pregnancy clinic, according to research presented at the International Headache Congress.
“We should not be seeing these patients in a regular [obstetrician’s or] generalist’s office because oftentimes we need input from neurology, and we need extra surveillance for both the fetus and the mother,” said Tracy B. Grossman, MD, an obstetrics and gynecology resident at Montefiore Medical Center in New York.
Dr. Grossman described a retrospective study of 90 consecutive pregnant patients who presented with acute severe migraine and obtained a neurology consultation at Montefiore Medical Center.
“These patients are different from most migraine patients because most migraine patients actually see improvement of symptoms during pregnancy. So, this is a special group of patients with worsening and refractory migraine,” she said.
Most of the women were in their third trimester. Diagnoses included migraine with aura (11.6%), migraine without aura (59.3%), and both (29.1%). A minority had chronic migraine (12.8%), and 31.4% presented in status migrainosus.
Forty-nine of the 90 patients (54%) experienced one or more adverse pregnancy outcomes. The population’s preterm delivery rate was 28%, which is nearly three times the national average of 11%, as reported by the March of Dimes. The population’s preeclampsia rate was 20.5%, compared with a national rate of 3% to 4%. The low-birth-weight rate of 19.2% was more than double the 8% national average. The rate of cesarean sections was 30.8%.
The study hypothesis was that women with migraine with aura would have higher rates of preeclampsia, preterm delivery, and low birth weight. Although studies of migraine in pregnancy have been few, some investigators have reported these associations. The current study did not find these associations, however, because most of the patients did not have aura, said Dr. Grossman.
“It can’t be purely an aura [or] vascular phenomenon that’s resulting in these adverse outcomes. These high rates of adverse pregnancy outcomes aren’t easily explainable. There’s something going on here that we haven’t teased out yet as to why these migraine patients are special,” she said.
Their risk of adverse pregnancy outcomes was not related to the headache medications that the patients took. Sixty-two patients received a combination of oral and IV therapy with acetaminophen, metoclopramide, and dihydroergotamine. In addition, 30% of patients briefly took barbiturates, and 30% received oxycodone or codeine. Although these drugs raise concerns during pregnancy, the investigators found no associated increase in adverse pregnancy outcomes among women who received them, compared with the women who did not receive those drugs or who did not receive any headache medications.
Dr. Grossman’s own therapeutic preference for patients with severe migraine during pregnancy is a peripheral nerve block with bupivacaine and lidocaine. “It works for the majority of people—we don’t quite know why—and it’s a local therapy that avoids fetal exposure to systemic medications,” she observed.
—Bruce Jancin
VALENCIA, SPAIN—Women who present with acute severe migraine during pregnancy are at increased risk for adverse pregnancy outcomes and should be seen in a high-risk pregnancy clinic, according to research presented at the International Headache Congress.
“We should not be seeing these patients in a regular [obstetrician’s or] generalist’s office because oftentimes we need input from neurology, and we need extra surveillance for both the fetus and the mother,” said Tracy B. Grossman, MD, an obstetrics and gynecology resident at Montefiore Medical Center in New York.
Dr. Grossman described a retrospective study of 90 consecutive pregnant patients who presented with acute severe migraine and obtained a neurology consultation at Montefiore Medical Center.
“These patients are different from most migraine patients because most migraine patients actually see improvement of symptoms during pregnancy. So, this is a special group of patients with worsening and refractory migraine,” she said.
Most of the women were in their third trimester. Diagnoses included migraine with aura (11.6%), migraine without aura (59.3%), and both (29.1%). A minority had chronic migraine (12.8%), and 31.4% presented in status migrainosus.
Forty-nine of the 90 patients (54%) experienced one or more adverse pregnancy outcomes. The population’s preterm delivery rate was 28%, which is nearly three times the national average of 11%, as reported by the March of Dimes. The population’s preeclampsia rate was 20.5%, compared with a national rate of 3% to 4%. The low-birth-weight rate of 19.2% was more than double the 8% national average. The rate of cesarean sections was 30.8%.
The study hypothesis was that women with migraine with aura would have higher rates of preeclampsia, preterm delivery, and low birth weight. Although studies of migraine in pregnancy have been few, some investigators have reported these associations. The current study did not find these associations, however, because most of the patients did not have aura, said Dr. Grossman.
“It can’t be purely an aura [or] vascular phenomenon that’s resulting in these adverse outcomes. These high rates of adverse pregnancy outcomes aren’t easily explainable. There’s something going on here that we haven’t teased out yet as to why these migraine patients are special,” she said.
Their risk of adverse pregnancy outcomes was not related to the headache medications that the patients took. Sixty-two patients received a combination of oral and IV therapy with acetaminophen, metoclopramide, and dihydroergotamine. In addition, 30% of patients briefly took barbiturates, and 30% received oxycodone or codeine. Although these drugs raise concerns during pregnancy, the investigators found no associated increase in adverse pregnancy outcomes among women who received them, compared with the women who did not receive those drugs or who did not receive any headache medications.
Dr. Grossman’s own therapeutic preference for patients with severe migraine during pregnancy is a peripheral nerve block with bupivacaine and lidocaine. “It works for the majority of people—we don’t quite know why—and it’s a local therapy that avoids fetal exposure to systemic medications,” she observed.
—Bruce Jancin

Scalp Mass Is Painful and Oozes Pus
ANSWER
The correct answer is oral terbinafine or griseofulvin, plus a two-week taper of prednisone (choice “d”); further discussion follows. Most authorities recommend the use of oral steroids with terbinafine (choice “a”) or griseofulvin (choice “b”), to dampen the acute inflammatory reaction to the fungal antigen. Some sources advise the use of itraconazole (choice “c”) but not as a single agent.
DISCUSSION
This case is a classic representation of kerion, a type of tinea capitis. This distinctive presentation results from not only active localized fungal infection with one of the dermatophytes, but also an allergic response to the fungal antigen. (This antigen can also trigger a widespread eczematous rash called an id reaction.) The resulting boggy, tender mass often oozes pus and usually provokes significant localized adenopathy.
A more common type of tinea capitis is uncomplicated dermatophytic infection of the scalp, presenting as mild localized scaling and modest hair loss, with no edema or redness to speak of. Kerion, by contrast, is far more acute and involves an impressive amount of localized redness and edema, along with modest hair loss, purulence, bloody drainage, and marked tenderness. Untreated, kerion can result in permanent scarring alopecia.
Several different dermatophytes have been isolated from kerions, including Trichophyton tonsurans, T violaceum, and various members of the Microsporum family. These zoophilic or geophilic organisms affect children far more than adults. Distinguishing the causative type is significant, because different drugs are required to effectively treat each. This is why a fungal culture is done at the outset.
When the diagnosis is in doubt, a punch biopsy may be necessary, with the sample divided for processing of default H&E stains and for fungal culture. Other information can be obtained by plucking a few hairs from the mass and examining them under 10x power to see if fungal hyphae are confined to the insides of the hair shafts (endothrix) or the outside of the shafts (ectothrix).
This is one situation in which KOH is not helpful for diagnosis: The organisms are too deep to obtain with a superficial scrape.
A number of scalp conditions can mimic a kerion, including lichen planopilaris and folliculitis decalvans. Several years ago, I had a patient who presented with a similar lesion that turned out to be squamous cell carcinoma—which eventually metastasized and led to his death.
TREATMENT
Treatment of more severe types of tinea capitis can be trying, even when the diagnosis is nailed down. The challenge becomes treating the problem long and strong enough to produce a cure.
In this case, I started the patient (who, at age 8, weighed 110 pounds) on a month-long course of terbinafine (250 mg/d) with a two-week taper of prednisone (40 mg). The expectation was that this would rapidly diminish the edema and pain while we waited for the culture results.
If the results showed the expected T tonsurans, treatment would continue as planned. If the cause turned out to be one of the Microsporum species, a switch to griseofulvin, at relatively high doses, would be considered.
ANSWER
The correct answer is oral terbinafine or griseofulvin, plus a two-week taper of prednisone (choice “d”); further discussion follows. Most authorities recommend the use of oral steroids with terbinafine (choice “a”) or griseofulvin (choice “b”), to dampen the acute inflammatory reaction to the fungal antigen. Some sources advise the use of itraconazole (choice “c”) but not as a single agent.
DISCUSSION
This case is a classic representation of kerion, a type of tinea capitis. This distinctive presentation results from not only active localized fungal infection with one of the dermatophytes, but also an allergic response to the fungal antigen. (This antigen can also trigger a widespread eczematous rash called an id reaction.) The resulting boggy, tender mass often oozes pus and usually provokes significant localized adenopathy.
A more common type of tinea capitis is uncomplicated dermatophytic infection of the scalp, presenting as mild localized scaling and modest hair loss, with no edema or redness to speak of. Kerion, by contrast, is far more acute and involves an impressive amount of localized redness and edema, along with modest hair loss, purulence, bloody drainage, and marked tenderness. Untreated, kerion can result in permanent scarring alopecia.
Several different dermatophytes have been isolated from kerions, including Trichophyton tonsurans, T violaceum, and various members of the Microsporum family. These zoophilic or geophilic organisms affect children far more than adults. Distinguishing the causative type is significant, because different drugs are required to effectively treat each. This is why a fungal culture is done at the outset.
When the diagnosis is in doubt, a punch biopsy may be necessary, with the sample divided for processing of default H&E stains and for fungal culture. Other information can be obtained by plucking a few hairs from the mass and examining them under 10x power to see if fungal hyphae are confined to the insides of the hair shafts (endothrix) or the outside of the shafts (ectothrix).
This is one situation in which KOH is not helpful for diagnosis: The organisms are too deep to obtain with a superficial scrape.
A number of scalp conditions can mimic a kerion, including lichen planopilaris and folliculitis decalvans. Several years ago, I had a patient who presented with a similar lesion that turned out to be squamous cell carcinoma—which eventually metastasized and led to his death.
TREATMENT
Treatment of more severe types of tinea capitis can be trying, even when the diagnosis is nailed down. The challenge becomes treating the problem long and strong enough to produce a cure.
In this case, I started the patient (who, at age 8, weighed 110 pounds) on a month-long course of terbinafine (250 mg/d) with a two-week taper of prednisone (40 mg). The expectation was that this would rapidly diminish the edema and pain while we waited for the culture results.
If the results showed the expected T tonsurans, treatment would continue as planned. If the cause turned out to be one of the Microsporum species, a switch to griseofulvin, at relatively high doses, would be considered.
ANSWER
The correct answer is oral terbinafine or griseofulvin, plus a two-week taper of prednisone (choice “d”); further discussion follows. Most authorities recommend the use of oral steroids with terbinafine (choice “a”) or griseofulvin (choice “b”), to dampen the acute inflammatory reaction to the fungal antigen. Some sources advise the use of itraconazole (choice “c”) but not as a single agent.
DISCUSSION
This case is a classic representation of kerion, a type of tinea capitis. This distinctive presentation results from not only active localized fungal infection with one of the dermatophytes, but also an allergic response to the fungal antigen. (This antigen can also trigger a widespread eczematous rash called an id reaction.) The resulting boggy, tender mass often oozes pus and usually provokes significant localized adenopathy.
A more common type of tinea capitis is uncomplicated dermatophytic infection of the scalp, presenting as mild localized scaling and modest hair loss, with no edema or redness to speak of. Kerion, by contrast, is far more acute and involves an impressive amount of localized redness and edema, along with modest hair loss, purulence, bloody drainage, and marked tenderness. Untreated, kerion can result in permanent scarring alopecia.
Several different dermatophytes have been isolated from kerions, including Trichophyton tonsurans, T violaceum, and various members of the Microsporum family. These zoophilic or geophilic organisms affect children far more than adults. Distinguishing the causative type is significant, because different drugs are required to effectively treat each. This is why a fungal culture is done at the outset.
When the diagnosis is in doubt, a punch biopsy may be necessary, with the sample divided for processing of default H&E stains and for fungal culture. Other information can be obtained by plucking a few hairs from the mass and examining them under 10x power to see if fungal hyphae are confined to the insides of the hair shafts (endothrix) or the outside of the shafts (ectothrix).
This is one situation in which KOH is not helpful for diagnosis: The organisms are too deep to obtain with a superficial scrape.
A number of scalp conditions can mimic a kerion, including lichen planopilaris and folliculitis decalvans. Several years ago, I had a patient who presented with a similar lesion that turned out to be squamous cell carcinoma—which eventually metastasized and led to his death.
TREATMENT
Treatment of more severe types of tinea capitis can be trying, even when the diagnosis is nailed down. The challenge becomes treating the problem long and strong enough to produce a cure.
In this case, I started the patient (who, at age 8, weighed 110 pounds) on a month-long course of terbinafine (250 mg/d) with a two-week taper of prednisone (40 mg). The expectation was that this would rapidly diminish the edema and pain while we waited for the culture results.
If the results showed the expected T tonsurans, treatment would continue as planned. If the cause turned out to be one of the Microsporum species, a switch to griseofulvin, at relatively high doses, would be considered.

Four weeks ago, an 8-year-old boy developed a lesion in his scalp that manifested rather quickly and caused pain. Treatment with both topical medications (triple-antibiotic cream and mupirocin cream) and oral antibiotics (cephalexin and trimethoprim/sulfa) has failed to resolve the problem, so his mother brings him to dermatology for evaluation. The patient is afebrile but complains of fatigue. His mother denies any other health problems for the child. There is no history of foreign travel, and the patient’s brother is healthy. The boy is in no acute distress but complains of tenderness on palpation of the lesion. The mass in his left nuchal scalp, which measures 4 cm, is impressively swollen, boggy, wet, and inflamed. Numerous red folliculocentric papules—many oozing pus—are seen on the surface. Located inferiorly to the lesion on the neck is a firm, palpable subcutaneous mass. Examination of the rest of the scalp reveals nothing of note. The clinical presentation and lack of response to oral antibiotics yield a presumptive diagnosis of kerion. A fungal culture is taken, with plans to prescribe appropriate medication.
