User login
California governor signs physician-assisted suicide bill into law
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.

In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.
In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med
California Gov. Jerry Brown (D) has signed into law a controversial measure that allows physicians to help terminally ill patients legally end their lives, making California the fourth state to permit doctor-assisted suicide through its legislature.
Gov. Brown, a former seminary student, approved the End of Life Option Act Oct. 5, after state lawmakers passed the bill Sept. 11.
In a signing message, Gov. Brown said that he had considered all sides of the issue and carefully weighed religious and theological perspectives that shortening a patient’s life is sinful.
“In the end, I was left to reflect on what I would want in the face of my own death,” Gov. Brown said in the message. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Modeled after Oregon’s statute, California’s law requires two doctors to determine that a patient has 6 months or less to live before doctors could prescribe life-ending medication. Patients must have the mental capacity to make medical decisions and would physically have to be able to swallow the drugs.
In addition, patients seeking physician aid in dying must submit two oral requests, a minimum of 15 days apart, and a written request to their physician. The attending physician must receive all three requests directly from the patient and not through a designee. Before prescribing end-of-life drugs, the attending physician must refer the patient to a consulting physician for confirmation of the diagnosis and prognosis and of the patient’s capacity to make the decision.
Oregon, Vermont, and Washington each have laws permitting physician-assisted death. Court rulings in New Mexico and Montana have allowed for the practice, but litigation in those states is ongoing and the decisions have yet to be enforced.
The signing ends nearly a year of passionate debate in California that divided physicians, religious groups, lawmakers, and community members. In May, the California Medical Association (CMA) became the first state medical society to change its stance against physician-assisted suicide to that of being neutral.
“The decision to participate in the End of Life Option Act is a very personal one between a doctor and their patient, which is why CMA has removed policy that outright objects to physicians aiding terminally ill patients in end of life options,” Dr. Luther F. Cobb, CMA president, said in a statement. “We believe it is up to the individual physician and their patient to decide voluntarily whether the End of Life Option Act is something in which they want to engage. Protecting that physician-patient relationship is essential.”
The California law will take effect 90 days after the state legislature adjourns its special session on health care, which may not be until early next year. The earliest likely enactment would be spring 2016.
On Twitter @legal_med

Lavage does not reduce severe complications in perforated diverticulitis
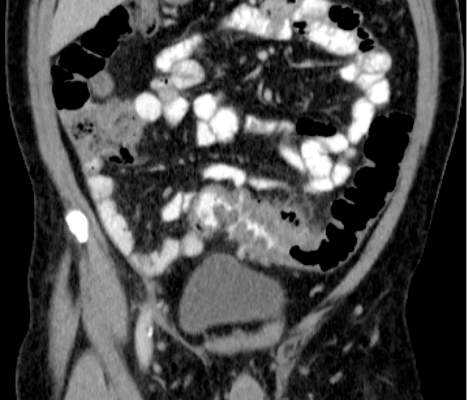
Patients needing emergency surgery for perforated diverticulitis saw no decrease in serious complications when treated with laparoscopic lavage, a minimally invasive procedure, than with primary resection of the colon, according to results from a randomized multicenter trial in Scandinavia.
Likelihood of reoperation also was significantly higher among patients undergoing laparoscopic lavage, and more sigmoid carcinomas were missed.
For their research, published Oct. 6 in JAMA (2015;314:1364-75), a group led by Dr. Johannes Kurt Schultz of the Akershus University Hospital in Lørenskog, Norway, and the University of Oslo sought to eliminate the selection bias that may have contributed to more favorable outcomes associated with laparoscopic lavage in observational studies.
Dr. Schultz and colleagues randomized patients with suspected perforated diverticulitis from 21 centers in Sweden and Norway to laparoscopic peritoneal lavage (n = 101) or colon resection (n = 98), with the choice of open or laparoscopic approach used for resection, as well as the option of colorectal anastomosis, left to the surgeon.
The study did not use laparoscopic Hinchey staging to classify the severity of the perforation prior to treatment assignment as a way of reducing the selection bias that may have occurred in observational studies.
The preoperative randomization resulted in both groups having similar rates of feculent peritonitis and incorrect preoperative diagnoses. Patients assigned to laparoscopic lavage were treated instead with resection if they were found to have fecal peritonitis. Also, patients in both groups whose pathology required additional treatment were treated at surgeon discretion. This left 74 patients randomized to lavage who received it as assigned and 70 patients undergoing resection per assigned protocol. In the intention-to-treat analysis, 31% of patients in the lavage group and 26% of patients in the resection group saw severe postoperative complications within 90 days, a difference of 4.7% that did not reach statistical significance (95% confidence interval, −7.9% to 17%; P = .53). Severe postoperative complications were defined as any complications resulting in a reintervention requiring general anesthesia, a life-threatening organ dysfunction, or death.
Of the patients treated as assigned with lavage, about 20% (n = 15) required reoperation, compared with 6% (n = 4) in the resection arm, a difference of about 14.6% (95% CI, 3.5% to 25.6%; P =.01).
The main reasons for reoperation were secondary peritonitis in the lavage group and wound rupture in the resection group. Intra-abdominal infections were more frequent in the laparoscopic lavage group, Dr. Schultz and colleagues found.
Also in the lavage group, four carcinomas were missed, compared with two in the resection group. “Because of the relatively high rate of missed colon carcinomas in the lavage group, it was essential to perform a colonoscopy after a patient recovered from the perforation,” the researchers wrote in their analysis.
Although patients in the laparoscopic lavage group had significantly shorter operating times, less blood loss, and lower incidence of stoma at 3 months, the researchers concluded that, based on these results, laparoscopic lavage could not be supported in perforated diverticulitis.
Dr. Schultz and colleagues had planned to enroll about half of eligible patients at the study sites. They noted as a limitation of their study that those not enrolled had more severe disease and worse postoperative outcomes, raising the possibility that the results “may not pertain to patients with perforated diverticulitis who are very ill.”
The study was funded by the South-Eastern Norway Regional Health Authority and Akershus University Hospital. None of its authors reported conflicts of interest.
Dr. Schultz and associates detail findings from a randomized, multicenter clinical trial conducted in Scandinavia designed to assess the superiority of laparoscopic lavage plus drainage, compared with laparoscopic or open resection with or without anastomosis for diverticulitis (Hinchey grades I-III) requiring urgent surgery.
The primary outcome was the incidence of severe complications (Clavien-Dindo classification IIIb-V). Of 144 patients, 74 were randomized to receive laparoscopic lavage and 70 to resection. The two groups were similar in characteristics, although significantly fewer of the lavage procedures were performed by a specialty-trained surgeon. Severe complications occurred in 25.7% of patients in the lavage group and 14.3% in the resection group (difference, 11.4%; 95% CI, −1.8 to 24.1), and significantly more patients in the lavage group developed secondary peritonitis (12% vs. 0%) or returned to the operating room (20% vs. 6%). The hospital mortality rates and follow-up quality-of-life scores were comparable between the groups (3% vs. 4% and 0.75 vs. 0.73, respectively). Somewhat worrisome is that four colon cancers were initially missed in patients treated by laparoscopic lavage alone.
Performing laparoscopic lavage is more difficult than merely irrigating the abdomen and placing drains within the pelvis. Surgeons vary in their attitudes related to concomitant adhesiolysis or debridement, and consensus about these procedures is lacking. Furthermore, subjective signs and objective criteria that identify patients at risk for secondary peritonitis or reoperation must be studied, and risk models should be validated to determine which patients are best suited for this less invasive approach. The utility of less intrusive strategies and minimally invasive approaches will undoubtedly expand as technologies evolve, but they must be responsibly incorporated into surgical practice based on evidence rather than subjective reasons.
Dr. Scott A. Strong and Dr. Nathaniel J. Soper are with Northwestern University, Chicago. These comments were taken from an accompanying editorial (JAMA 2015;314[13]:1343-5). They declared no conflicts of interest.
Dr. Schultz and associates detail findings from a randomized, multicenter clinical trial conducted in Scandinavia designed to assess the superiority of laparoscopic lavage plus drainage, compared with laparoscopic or open resection with or without anastomosis for diverticulitis (Hinchey grades I-III) requiring urgent surgery.
The primary outcome was the incidence of severe complications (Clavien-Dindo classification IIIb-V). Of 144 patients, 74 were randomized to receive laparoscopic lavage and 70 to resection. The two groups were similar in characteristics, although significantly fewer of the lavage procedures were performed by a specialty-trained surgeon. Severe complications occurred in 25.7% of patients in the lavage group and 14.3% in the resection group (difference, 11.4%; 95% CI, −1.8 to 24.1), and significantly more patients in the lavage group developed secondary peritonitis (12% vs. 0%) or returned to the operating room (20% vs. 6%). The hospital mortality rates and follow-up quality-of-life scores were comparable between the groups (3% vs. 4% and 0.75 vs. 0.73, respectively). Somewhat worrisome is that four colon cancers were initially missed in patients treated by laparoscopic lavage alone.
Performing laparoscopic lavage is more difficult than merely irrigating the abdomen and placing drains within the pelvis. Surgeons vary in their attitudes related to concomitant adhesiolysis or debridement, and consensus about these procedures is lacking. Furthermore, subjective signs and objective criteria that identify patients at risk for secondary peritonitis or reoperation must be studied, and risk models should be validated to determine which patients are best suited for this less invasive approach. The utility of less intrusive strategies and minimally invasive approaches will undoubtedly expand as technologies evolve, but they must be responsibly incorporated into surgical practice based on evidence rather than subjective reasons.
Dr. Scott A. Strong and Dr. Nathaniel J. Soper are with Northwestern University, Chicago. These comments were taken from an accompanying editorial (JAMA 2015;314[13]:1343-5). They declared no conflicts of interest.
Dr. Schultz and associates detail findings from a randomized, multicenter clinical trial conducted in Scandinavia designed to assess the superiority of laparoscopic lavage plus drainage, compared with laparoscopic or open resection with or without anastomosis for diverticulitis (Hinchey grades I-III) requiring urgent surgery.
The primary outcome was the incidence of severe complications (Clavien-Dindo classification IIIb-V). Of 144 patients, 74 were randomized to receive laparoscopic lavage and 70 to resection. The two groups were similar in characteristics, although significantly fewer of the lavage procedures were performed by a specialty-trained surgeon. Severe complications occurred in 25.7% of patients in the lavage group and 14.3% in the resection group (difference, 11.4%; 95% CI, −1.8 to 24.1), and significantly more patients in the lavage group developed secondary peritonitis (12% vs. 0%) or returned to the operating room (20% vs. 6%). The hospital mortality rates and follow-up quality-of-life scores were comparable between the groups (3% vs. 4% and 0.75 vs. 0.73, respectively). Somewhat worrisome is that four colon cancers were initially missed in patients treated by laparoscopic lavage alone.
Performing laparoscopic lavage is more difficult than merely irrigating the abdomen and placing drains within the pelvis. Surgeons vary in their attitudes related to concomitant adhesiolysis or debridement, and consensus about these procedures is lacking. Furthermore, subjective signs and objective criteria that identify patients at risk for secondary peritonitis or reoperation must be studied, and risk models should be validated to determine which patients are best suited for this less invasive approach. The utility of less intrusive strategies and minimally invasive approaches will undoubtedly expand as technologies evolve, but they must be responsibly incorporated into surgical practice based on evidence rather than subjective reasons.
Dr. Scott A. Strong and Dr. Nathaniel J. Soper are with Northwestern University, Chicago. These comments were taken from an accompanying editorial (JAMA 2015;314[13]:1343-5). They declared no conflicts of interest.
Patients needing emergency surgery for perforated diverticulitis saw no decrease in serious complications when treated with laparoscopic lavage, a minimally invasive procedure, than with primary resection of the colon, according to results from a randomized multicenter trial in Scandinavia.
Likelihood of reoperation also was significantly higher among patients undergoing laparoscopic lavage, and more sigmoid carcinomas were missed.
For their research, published Oct. 6 in JAMA (2015;314:1364-75), a group led by Dr. Johannes Kurt Schultz of the Akershus University Hospital in Lørenskog, Norway, and the University of Oslo sought to eliminate the selection bias that may have contributed to more favorable outcomes associated with laparoscopic lavage in observational studies.
Dr. Schultz and colleagues randomized patients with suspected perforated diverticulitis from 21 centers in Sweden and Norway to laparoscopic peritoneal lavage (n = 101) or colon resection (n = 98), with the choice of open or laparoscopic approach used for resection, as well as the option of colorectal anastomosis, left to the surgeon.
The study did not use laparoscopic Hinchey staging to classify the severity of the perforation prior to treatment assignment as a way of reducing the selection bias that may have occurred in observational studies.
The preoperative randomization resulted in both groups having similar rates of feculent peritonitis and incorrect preoperative diagnoses. Patients assigned to laparoscopic lavage were treated instead with resection if they were found to have fecal peritonitis. Also, patients in both groups whose pathology required additional treatment were treated at surgeon discretion. This left 74 patients randomized to lavage who received it as assigned and 70 patients undergoing resection per assigned protocol. In the intention-to-treat analysis, 31% of patients in the lavage group and 26% of patients in the resection group saw severe postoperative complications within 90 days, a difference of 4.7% that did not reach statistical significance (95% confidence interval, −7.9% to 17%; P = .53). Severe postoperative complications were defined as any complications resulting in a reintervention requiring general anesthesia, a life-threatening organ dysfunction, or death.
Of the patients treated as assigned with lavage, about 20% (n = 15) required reoperation, compared with 6% (n = 4) in the resection arm, a difference of about 14.6% (95% CI, 3.5% to 25.6%; P =.01).
The main reasons for reoperation were secondary peritonitis in the lavage group and wound rupture in the resection group. Intra-abdominal infections were more frequent in the laparoscopic lavage group, Dr. Schultz and colleagues found.
Also in the lavage group, four carcinomas were missed, compared with two in the resection group. “Because of the relatively high rate of missed colon carcinomas in the lavage group, it was essential to perform a colonoscopy after a patient recovered from the perforation,” the researchers wrote in their analysis.
Although patients in the laparoscopic lavage group had significantly shorter operating times, less blood loss, and lower incidence of stoma at 3 months, the researchers concluded that, based on these results, laparoscopic lavage could not be supported in perforated diverticulitis.
Dr. Schultz and colleagues had planned to enroll about half of eligible patients at the study sites. They noted as a limitation of their study that those not enrolled had more severe disease and worse postoperative outcomes, raising the possibility that the results “may not pertain to patients with perforated diverticulitis who are very ill.”
The study was funded by the South-Eastern Norway Regional Health Authority and Akershus University Hospital. None of its authors reported conflicts of interest.
Patients needing emergency surgery for perforated diverticulitis saw no decrease in serious complications when treated with laparoscopic lavage, a minimally invasive procedure, than with primary resection of the colon, according to results from a randomized multicenter trial in Scandinavia.
Likelihood of reoperation also was significantly higher among patients undergoing laparoscopic lavage, and more sigmoid carcinomas were missed.
For their research, published Oct. 6 in JAMA (2015;314:1364-75), a group led by Dr. Johannes Kurt Schultz of the Akershus University Hospital in Lørenskog, Norway, and the University of Oslo sought to eliminate the selection bias that may have contributed to more favorable outcomes associated with laparoscopic lavage in observational studies.
Dr. Schultz and colleagues randomized patients with suspected perforated diverticulitis from 21 centers in Sweden and Norway to laparoscopic peritoneal lavage (n = 101) or colon resection (n = 98), with the choice of open or laparoscopic approach used for resection, as well as the option of colorectal anastomosis, left to the surgeon.
The study did not use laparoscopic Hinchey staging to classify the severity of the perforation prior to treatment assignment as a way of reducing the selection bias that may have occurred in observational studies.
The preoperative randomization resulted in both groups having similar rates of feculent peritonitis and incorrect preoperative diagnoses. Patients assigned to laparoscopic lavage were treated instead with resection if they were found to have fecal peritonitis. Also, patients in both groups whose pathology required additional treatment were treated at surgeon discretion. This left 74 patients randomized to lavage who received it as assigned and 70 patients undergoing resection per assigned protocol. In the intention-to-treat analysis, 31% of patients in the lavage group and 26% of patients in the resection group saw severe postoperative complications within 90 days, a difference of 4.7% that did not reach statistical significance (95% confidence interval, −7.9% to 17%; P = .53). Severe postoperative complications were defined as any complications resulting in a reintervention requiring general anesthesia, a life-threatening organ dysfunction, or death.
Of the patients treated as assigned with lavage, about 20% (n = 15) required reoperation, compared with 6% (n = 4) in the resection arm, a difference of about 14.6% (95% CI, 3.5% to 25.6%; P =.01).
The main reasons for reoperation were secondary peritonitis in the lavage group and wound rupture in the resection group. Intra-abdominal infections were more frequent in the laparoscopic lavage group, Dr. Schultz and colleagues found.
Also in the lavage group, four carcinomas were missed, compared with two in the resection group. “Because of the relatively high rate of missed colon carcinomas in the lavage group, it was essential to perform a colonoscopy after a patient recovered from the perforation,” the researchers wrote in their analysis.
Although patients in the laparoscopic lavage group had significantly shorter operating times, less blood loss, and lower incidence of stoma at 3 months, the researchers concluded that, based on these results, laparoscopic lavage could not be supported in perforated diverticulitis.
Dr. Schultz and colleagues had planned to enroll about half of eligible patients at the study sites. They noted as a limitation of their study that those not enrolled had more severe disease and worse postoperative outcomes, raising the possibility that the results “may not pertain to patients with perforated diverticulitis who are very ill.”
The study was funded by the South-Eastern Norway Regional Health Authority and Akershus University Hospital. None of its authors reported conflicts of interest.
FROM JAMA
Key clinical point: Laparoscopic lavage carries risks of severe postoperative complications similar to colon resection in people presenting with suspected perforated diverticulitis requiring emergency surgery.
Major finding: Mortality and severe complications did not differ significantly at 90 days postoperation between intention-to-treat groups, while reoperation was significantly higher among patients treated with lavage (5.7% for resection vs. 20.3% for lavage, P < .01).
Data source: A multicenter, open-label randomized trial in which patients presenting with likely perforated diverticulitis were randomized to lavage (n = 74) or resection (n = 70).
Disclosures: The study was sponsored by investigator institutions and Norwegian regional government grants. No conflicts of interest were reported.

Radiopeptide therapy sparks unheard of PFS in midgut neuroendocrine tumors
VIENNA – After posting unprecedented results in the phase III NETTER-1 trial, the experimental radiopeptide therapy 177Lu-Dotatate looks poised to become a new treatment option for patients with midgut neuroendocrine tumors that progress on somatostatin analogues.
Median progression-free survival was not reached in patients receiving 177Lu-Dotatate (Lutathera) plus the somatostatin octreotide LAR (Sandostatin), the current standard of care, and was 8.4 months in those given a double dose of octreotide LAR.

This resulted in a hazard ratio of 0.209 (P less than .0001) or almost an 80% reduction in the risk for disease progression or death, Dr. Philippe Ruszniewski of Beaujon Hospital in Clichy, France, said at the European Society for Medical Oncology Congress.
The experimental therapy also was superior to octreotide LAR in terms of objective response rate (19% vs. 3%; P less than .0004). This included one complete response and 18 partial responses to 177Lu-Dotatate vs. 3 partial responses to octreotide LAR alone.
Although few treatment options were up to now available for this rare cancer, “Lu-Dotatate appears as a major advance in these patients,” he said.
Invited discussant Dr. Enrique Grande of Ram<scaps>ó</scaps>n y Cajal University Hospital in Madrid, commented, “This is the most impressive cohort in terms of progression-free survival that we have seen in the neuroendocrine tumors … especially since the comparator arm is a really active one that we are doing in routine practice.”

177Lu-Dotatate belongs to a drug category called peptide receptor radionuclide therapy and is composed of a lutetium radionuclide chelated to a peptide. The 177Lutetium-labeled somatostatin analogue peptide targets somatostatin receptors, which are overexpressed in about 80% of neuroendocrine tumors (NETs).
177Lu-Dotatate has received orphan drug status from the Food and Drug Administration and the European Medicines Agency and in April 2015 also was granted fast-track designation by the FDA.
NETTER-1 enrolled 230 patients with metastatic or locally advanced, inoperable midgut NETs, functioning or not, and evenly randomized them to four doses of 7.4 GBq 177Lu-Dotatate intravenously over 8 weeks plus octreotide LAR 30 mg or to octreotide LAR 60 mg every 28 days given as a deep intragluteal injection. The ileum was the primary tumor site in three-fourths of patients and the liver the site of metastasis in about 83%.
Three-fourths of patients received all four doses of 177Lu-Dotatate and no dose-modifying toxicity was observed in 95% of all 111 treated patients, Dr. Ruszniewski said.
An interim analysis suggested increased overall survival (13 deaths vs. 22 deaths; P less than .018), but the data are immature and need to be confirmed by final analysis, he said.
Treatment-related adverse events of any grade were reported in 86% of patients given 177Lu-Dotatate and 31% on octreotide LAR 60 mg.
Treatment-related serious events occurred in 10 patients in the 177Lu-Dotatate arm vs. 1 in the octreotide arm, with withdrawals because of treatment-related adverse events in 5 vs. 0 patients, respectively.
Serious adverse events related to 177Lu-Dotatate included, but were not limited to, lymphocytopenia in seven patients, thrombocytopenia in three, acute kidney injury in two, and one case each of renal failure and portal hypertension.
When asked in a press briefing whether 177Lu-Dotatate could induce long-term DNA damage after hitting its target, Dr. Ruszniewski said a substudy in 20 unrelated patients will provide pharmacokinetic data on the fate of the radionuclide.
“What we know from phase I and II is that this is probably possible, but rare,” he said. “The two organs that should be carefully watched are the bone marrow and the kidneys.”
To reduce kidney damage, amino acids are infused at the same time as the radionuclide. Myelodysplastic syndrome might occur in 3% to 4% of patients, he added.
The investigators called for additional studies of 177Lu-Dotatate in other types of NETs such as pancreatic and bronchial.
When it was noted that the approved radioactive agent, radium-223 dichloride (Xofigo) also has very good data in pancreatic cancer but is often used behind other drugs because it is a radiopharmaceutical, Dr. Ruszniewski dismissed the suggestion and said NETs are a completely different disease.
Discussant Dr. Grande, however, said that there are logistical considerations surrounding 177-Lu-Dotatate, such as how clinicians would request it, whether it will be widely available, and where it would be delivered.
No special room is needed to treat patients with 177-Lu-Dotatate, but patient urine does have to be controlled, Dr. Ruszniewski noted.
On Twitter @pwendl
VIENNA – After posting unprecedented results in the phase III NETTER-1 trial, the experimental radiopeptide therapy 177Lu-Dotatate looks poised to become a new treatment option for patients with midgut neuroendocrine tumors that progress on somatostatin analogues.
Median progression-free survival was not reached in patients receiving 177Lu-Dotatate (Lutathera) plus the somatostatin octreotide LAR (Sandostatin), the current standard of care, and was 8.4 months in those given a double dose of octreotide LAR.
This resulted in a hazard ratio of 0.209 (P less than .0001) or almost an 80% reduction in the risk for disease progression or death, Dr. Philippe Ruszniewski of Beaujon Hospital in Clichy, France, said at the European Society for Medical Oncology Congress.
The experimental therapy also was superior to octreotide LAR in terms of objective response rate (19% vs. 3%; P less than .0004). This included one complete response and 18 partial responses to 177Lu-Dotatate vs. 3 partial responses to octreotide LAR alone.
Although few treatment options were up to now available for this rare cancer, “Lu-Dotatate appears as a major advance in these patients,” he said.
Invited discussant Dr. Enrique Grande of Ram<scaps>ó</scaps>n y Cajal University Hospital in Madrid, commented, “This is the most impressive cohort in terms of progression-free survival that we have seen in the neuroendocrine tumors … especially since the comparator arm is a really active one that we are doing in routine practice.”
177Lu-Dotatate belongs to a drug category called peptide receptor radionuclide therapy and is composed of a lutetium radionuclide chelated to a peptide. The 177Lutetium-labeled somatostatin analogue peptide targets somatostatin receptors, which are overexpressed in about 80% of neuroendocrine tumors (NETs).
177Lu-Dotatate has received orphan drug status from the Food and Drug Administration and the European Medicines Agency and in April 2015 also was granted fast-track designation by the FDA.
NETTER-1 enrolled 230 patients with metastatic or locally advanced, inoperable midgut NETs, functioning or not, and evenly randomized them to four doses of 7.4 GBq 177Lu-Dotatate intravenously over 8 weeks plus octreotide LAR 30 mg or to octreotide LAR 60 mg every 28 days given as a deep intragluteal injection. The ileum was the primary tumor site in three-fourths of patients and the liver the site of metastasis in about 83%.
Three-fourths of patients received all four doses of 177Lu-Dotatate and no dose-modifying toxicity was observed in 95% of all 111 treated patients, Dr. Ruszniewski said.
An interim analysis suggested increased overall survival (13 deaths vs. 22 deaths; P less than .018), but the data are immature and need to be confirmed by final analysis, he said.
Treatment-related adverse events of any grade were reported in 86% of patients given 177Lu-Dotatate and 31% on octreotide LAR 60 mg.
Treatment-related serious events occurred in 10 patients in the 177Lu-Dotatate arm vs. 1 in the octreotide arm, with withdrawals because of treatment-related adverse events in 5 vs. 0 patients, respectively.
Serious adverse events related to 177Lu-Dotatate included, but were not limited to, lymphocytopenia in seven patients, thrombocytopenia in three, acute kidney injury in two, and one case each of renal failure and portal hypertension.
When asked in a press briefing whether 177Lu-Dotatate could induce long-term DNA damage after hitting its target, Dr. Ruszniewski said a substudy in 20 unrelated patients will provide pharmacokinetic data on the fate of the radionuclide.
“What we know from phase I and II is that this is probably possible, but rare,” he said. “The two organs that should be carefully watched are the bone marrow and the kidneys.”
To reduce kidney damage, amino acids are infused at the same time as the radionuclide. Myelodysplastic syndrome might occur in 3% to 4% of patients, he added.
The investigators called for additional studies of 177Lu-Dotatate in other types of NETs such as pancreatic and bronchial.
When it was noted that the approved radioactive agent, radium-223 dichloride (Xofigo) also has very good data in pancreatic cancer but is often used behind other drugs because it is a radiopharmaceutical, Dr. Ruszniewski dismissed the suggestion and said NETs are a completely different disease.
Discussant Dr. Grande, however, said that there are logistical considerations surrounding 177-Lu-Dotatate, such as how clinicians would request it, whether it will be widely available, and where it would be delivered.
No special room is needed to treat patients with 177-Lu-Dotatate, but patient urine does have to be controlled, Dr. Ruszniewski noted.
On Twitter @pwendl
VIENNA – After posting unprecedented results in the phase III NETTER-1 trial, the experimental radiopeptide therapy 177Lu-Dotatate looks poised to become a new treatment option for patients with midgut neuroendocrine tumors that progress on somatostatin analogues.
Median progression-free survival was not reached in patients receiving 177Lu-Dotatate (Lutathera) plus the somatostatin octreotide LAR (Sandostatin), the current standard of care, and was 8.4 months in those given a double dose of octreotide LAR.
This resulted in a hazard ratio of 0.209 (P less than .0001) or almost an 80% reduction in the risk for disease progression or death, Dr. Philippe Ruszniewski of Beaujon Hospital in Clichy, France, said at the European Society for Medical Oncology Congress.
The experimental therapy also was superior to octreotide LAR in terms of objective response rate (19% vs. 3%; P less than .0004). This included one complete response and 18 partial responses to 177Lu-Dotatate vs. 3 partial responses to octreotide LAR alone.
Although few treatment options were up to now available for this rare cancer, “Lu-Dotatate appears as a major advance in these patients,” he said.
Invited discussant Dr. Enrique Grande of Ram<scaps>ó</scaps>n y Cajal University Hospital in Madrid, commented, “This is the most impressive cohort in terms of progression-free survival that we have seen in the neuroendocrine tumors … especially since the comparator arm is a really active one that we are doing in routine practice.”
177Lu-Dotatate belongs to a drug category called peptide receptor radionuclide therapy and is composed of a lutetium radionuclide chelated to a peptide. The 177Lutetium-labeled somatostatin analogue peptide targets somatostatin receptors, which are overexpressed in about 80% of neuroendocrine tumors (NETs).
177Lu-Dotatate has received orphan drug status from the Food and Drug Administration and the European Medicines Agency and in April 2015 also was granted fast-track designation by the FDA.
NETTER-1 enrolled 230 patients with metastatic or locally advanced, inoperable midgut NETs, functioning or not, and evenly randomized them to four doses of 7.4 GBq 177Lu-Dotatate intravenously over 8 weeks plus octreotide LAR 30 mg or to octreotide LAR 60 mg every 28 days given as a deep intragluteal injection. The ileum was the primary tumor site in three-fourths of patients and the liver the site of metastasis in about 83%.
Three-fourths of patients received all four doses of 177Lu-Dotatate and no dose-modifying toxicity was observed in 95% of all 111 treated patients, Dr. Ruszniewski said.
An interim analysis suggested increased overall survival (13 deaths vs. 22 deaths; P less than .018), but the data are immature and need to be confirmed by final analysis, he said.
Treatment-related adverse events of any grade were reported in 86% of patients given 177Lu-Dotatate and 31% on octreotide LAR 60 mg.
Treatment-related serious events occurred in 10 patients in the 177Lu-Dotatate arm vs. 1 in the octreotide arm, with withdrawals because of treatment-related adverse events in 5 vs. 0 patients, respectively.
Serious adverse events related to 177Lu-Dotatate included, but were not limited to, lymphocytopenia in seven patients, thrombocytopenia in three, acute kidney injury in two, and one case each of renal failure and portal hypertension.
When asked in a press briefing whether 177Lu-Dotatate could induce long-term DNA damage after hitting its target, Dr. Ruszniewski said a substudy in 20 unrelated patients will provide pharmacokinetic data on the fate of the radionuclide.
“What we know from phase I and II is that this is probably possible, but rare,” he said. “The two organs that should be carefully watched are the bone marrow and the kidneys.”
To reduce kidney damage, amino acids are infused at the same time as the radionuclide. Myelodysplastic syndrome might occur in 3% to 4% of patients, he added.
The investigators called for additional studies of 177Lu-Dotatate in other types of NETs such as pancreatic and bronchial.
When it was noted that the approved radioactive agent, radium-223 dichloride (Xofigo) also has very good data in pancreatic cancer but is often used behind other drugs because it is a radiopharmaceutical, Dr. Ruszniewski dismissed the suggestion and said NETs are a completely different disease.
Discussant Dr. Grande, however, said that there are logistical considerations surrounding 177-Lu-Dotatate, such as how clinicians would request it, whether it will be widely available, and where it would be delivered.
No special room is needed to treat patients with 177-Lu-Dotatate, but patient urine does have to be controlled, Dr. Ruszniewski noted.
On Twitter @pwendl
AT EUROPEAN CANCER CONGRESS 2015
Key clinical point: 177Lu-Dotatate plus octreotide LAR was superior to a double-dose of octreotide LAR in terms of progression-free survival and overall response in progressive midgut neuroendocrine tumors.
Major finding: Median progression-free survival was not reached for 177Lu-Dotatate plus octreotide LAR; it was 8.4 months for high-dose octreotide LAR (hazard ratio, 0.2; P less than .001).
Data source: Phase III trial in 230 patients with progressive midgut NETs.
Disclosures: Advanced Accelerator Applications funded the study. Dr. Ruszniewski reported serving as an advisor to AAA and has received honoraria and research funding from AAA, Ipsen, and Novartis.

30-Day Readmission May Be Due to Income or Education
When patients are hospitalized more than once in the same month, it may have more to do with their income or education levels than the quality of care they received, a U.S. study suggests.
Perhaps unsurprisingly, patients 85 and older are more likely to return to the hospital within 30 days of being sent home than people a decade or two younger, according to the analysis of data from Medicare, the U.S. health program for the elderly and disabled.
But patients also have higher odds of returning soon after discharge if they lack a high school diploma, have limited income and assets or have health benefits from Medicaid, the U.S. health program for the poor.
The findings suggest that Medicare penalties for what's known as readmissions under the Affordable Care Act may in some instances mete out punishment for outcomes that are beyond doctors' control, said lead study author Dr. Michael Barnett and senior author Dr. Michael McWilliams, colleagues at Harvard Medical School and Brigham and Women's Hospital in Boston.
"Hospitals are being penalized to a large extent based on the patients they serve," the doctors said by email. "Patients admitted to hospitals with higher readmission rates are sicker and more socially disadvantaged in a variety of ways than patients admitted to hospitals with lower readmission rates."
Under the current penalty system, Medicare deducts 3 percent from inpatient payments to hospitals with higher than expected readmission rates, the researchers report in JAMA Internal Medicine. Expected rates are only adjusted for patients' age, sex and recent diagnoses including the one from their hospital stay.
In 2014, the second year of the program, about 2,600 hospitals were fined a combined $428 million for excessive readmissions, the authors report.
To get a better understanding of how individual patient characteristics might influence repeat hospitalizations, the researchers examined several other variables Medicare doesn't consider in determining expected readmission rates - such as education and income levels, marital status, employment, race and ethnicity, smoking status and drinking habits.
They linked records from a nationwide health and retirement survey of Americans over 50 collected between 2000 and 2010 to data from Medicare claims from 2000 to 2012. The combined analysis assessed more than 8,000 hospital admissions.
The researchers sorted hospitals into quintiles based on readmission rates. They found that at least half of the observed difference in the probability of repeat hospitalizations between hospitals with the highest and lowest readmission rates might be accounted for by patient characteristics not currently considered by Medicare.
When researchers only used Medicare's criteria comparing readmission rates, they found the probability of repeat hospitalization was about 15 percent at facilities with the lowest rates and about 19.5 percent at hospitals with the highest rates.
But when they took another look using more criteria on patients' medical, social and economic characteristics, the gap between hospitals with the lowest and the highest readmission rates narrowed to 16 percent and 18.4 percent, respectively, odds of repeat hospitalization.
One limitation of the study, the authors acknowledge, is the data didn't allow them to calculate how considering individual patient characteristics might impact readmission rates at specific hospitals.
Even so, the findings suggest that the current Medicare penalty system for repeat hospitalizations may put facilities serving poor communities at a distinct financial disadvantage, Dr. Carl van Walraven, a senior scientist at the Ottawa Hospital Research Institute in Canada, noted in an accompanying editorial.
"Differences between hospitals in readmissions may be due to who is treated rather than how they're treated," van Walraven said by email.
When patients are hospitalized more than once in the same month, it may have more to do with their income or education levels than the quality of care they received, a U.S. study suggests.
Perhaps unsurprisingly, patients 85 and older are more likely to return to the hospital within 30 days of being sent home than people a decade or two younger, according to the analysis of data from Medicare, the U.S. health program for the elderly and disabled.
But patients also have higher odds of returning soon after discharge if they lack a high school diploma, have limited income and assets or have health benefits from Medicaid, the U.S. health program for the poor.
The findings suggest that Medicare penalties for what's known as readmissions under the Affordable Care Act may in some instances mete out punishment for outcomes that are beyond doctors' control, said lead study author Dr. Michael Barnett and senior author Dr. Michael McWilliams, colleagues at Harvard Medical School and Brigham and Women's Hospital in Boston.
"Hospitals are being penalized to a large extent based on the patients they serve," the doctors said by email. "Patients admitted to hospitals with higher readmission rates are sicker and more socially disadvantaged in a variety of ways than patients admitted to hospitals with lower readmission rates."
Under the current penalty system, Medicare deducts 3 percent from inpatient payments to hospitals with higher than expected readmission rates, the researchers report in JAMA Internal Medicine. Expected rates are only adjusted for patients' age, sex and recent diagnoses including the one from their hospital stay.
In 2014, the second year of the program, about 2,600 hospitals were fined a combined $428 million for excessive readmissions, the authors report.
To get a better understanding of how individual patient characteristics might influence repeat hospitalizations, the researchers examined several other variables Medicare doesn't consider in determining expected readmission rates - such as education and income levels, marital status, employment, race and ethnicity, smoking status and drinking habits.
They linked records from a nationwide health and retirement survey of Americans over 50 collected between 2000 and 2010 to data from Medicare claims from 2000 to 2012. The combined analysis assessed more than 8,000 hospital admissions.
The researchers sorted hospitals into quintiles based on readmission rates. They found that at least half of the observed difference in the probability of repeat hospitalizations between hospitals with the highest and lowest readmission rates might be accounted for by patient characteristics not currently considered by Medicare.
When researchers only used Medicare's criteria comparing readmission rates, they found the probability of repeat hospitalization was about 15 percent at facilities with the lowest rates and about 19.5 percent at hospitals with the highest rates.
But when they took another look using more criteria on patients' medical, social and economic characteristics, the gap between hospitals with the lowest and the highest readmission rates narrowed to 16 percent and 18.4 percent, respectively, odds of repeat hospitalization.
One limitation of the study, the authors acknowledge, is the data didn't allow them to calculate how considering individual patient characteristics might impact readmission rates at specific hospitals.
Even so, the findings suggest that the current Medicare penalty system for repeat hospitalizations may put facilities serving poor communities at a distinct financial disadvantage, Dr. Carl van Walraven, a senior scientist at the Ottawa Hospital Research Institute in Canada, noted in an accompanying editorial.
"Differences between hospitals in readmissions may be due to who is treated rather than how they're treated," van Walraven said by email.
When patients are hospitalized more than once in the same month, it may have more to do with their income or education levels than the quality of care they received, a U.S. study suggests.
Perhaps unsurprisingly, patients 85 and older are more likely to return to the hospital within 30 days of being sent home than people a decade or two younger, according to the analysis of data from Medicare, the U.S. health program for the elderly and disabled.
But patients also have higher odds of returning soon after discharge if they lack a high school diploma, have limited income and assets or have health benefits from Medicaid, the U.S. health program for the poor.
The findings suggest that Medicare penalties for what's known as readmissions under the Affordable Care Act may in some instances mete out punishment for outcomes that are beyond doctors' control, said lead study author Dr. Michael Barnett and senior author Dr. Michael McWilliams, colleagues at Harvard Medical School and Brigham and Women's Hospital in Boston.
"Hospitals are being penalized to a large extent based on the patients they serve," the doctors said by email. "Patients admitted to hospitals with higher readmission rates are sicker and more socially disadvantaged in a variety of ways than patients admitted to hospitals with lower readmission rates."
Under the current penalty system, Medicare deducts 3 percent from inpatient payments to hospitals with higher than expected readmission rates, the researchers report in JAMA Internal Medicine. Expected rates are only adjusted for patients' age, sex and recent diagnoses including the one from their hospital stay.
In 2014, the second year of the program, about 2,600 hospitals were fined a combined $428 million for excessive readmissions, the authors report.
To get a better understanding of how individual patient characteristics might influence repeat hospitalizations, the researchers examined several other variables Medicare doesn't consider in determining expected readmission rates - such as education and income levels, marital status, employment, race and ethnicity, smoking status and drinking habits.
They linked records from a nationwide health and retirement survey of Americans over 50 collected between 2000 and 2010 to data from Medicare claims from 2000 to 2012. The combined analysis assessed more than 8,000 hospital admissions.
The researchers sorted hospitals into quintiles based on readmission rates. They found that at least half of the observed difference in the probability of repeat hospitalizations between hospitals with the highest and lowest readmission rates might be accounted for by patient characteristics not currently considered by Medicare.
When researchers only used Medicare's criteria comparing readmission rates, they found the probability of repeat hospitalization was about 15 percent at facilities with the lowest rates and about 19.5 percent at hospitals with the highest rates.
But when they took another look using more criteria on patients' medical, social and economic characteristics, the gap between hospitals with the lowest and the highest readmission rates narrowed to 16 percent and 18.4 percent, respectively, odds of repeat hospitalization.
One limitation of the study, the authors acknowledge, is the data didn't allow them to calculate how considering individual patient characteristics might impact readmission rates at specific hospitals.
Even so, the findings suggest that the current Medicare penalty system for repeat hospitalizations may put facilities serving poor communities at a distinct financial disadvantage, Dr. Carl van Walraven, a senior scientist at the Ottawa Hospital Research Institute in Canada, noted in an accompanying editorial.
"Differences between hospitals in readmissions may be due to who is treated rather than how they're treated," van Walraven said by email.
Letter to the Editor: Locum Tenens Helps Avoid Burnout in Hospital Medicine
![]()
So I quit medicine.
I ended up working with a few NGOs (nongovernmental organizations) at the time, becoming the healthcare director of a medium-sized NGO. I learned the enormous amount of red tape that was scattered in that world, and I began missing medicine.
So I unquit medicine.
I decided that the best thing for me was to be my own boss. I didn’t know how to do this. As someone with absolutely no business background, I started reading about different types of work I could do where I was in charge of dictating my hours. Opening up a clinic or starting my own hospitalist group felt like being shackled down in the system again. I talked to my colleagues from residency, and they all seemed underwhelmed with the love of their jobs and overwhelmed by the number of hours that they were working. They still sounded like residents.
After getting a taste of a world outside of medicine, I realized that I had so many hobbies and interests outside of practicing as a hospitalist. I found a love of surfing, I wanted to volunteer and do medical relief work abroad, I wanted to travel the world, and I wanted to study herbal medicine and integrative holistic medicine in great depth—all while being able to keep one foot in the medical system.
That is when I found locum tenens hospitalist-based medicine. Suddenly, I could make my own schedule, decide where and when I would work, and have the flexibility to leave any given hospital if I felt as though I was being pushed into practices that would compromise patient care and safety.
It’s been four years since I began practicing locum tenens hospitalist medicine, and I have never looked back. I have been able to take up surfing more seriously; I’ve traveled around the world and continue to do so—I have been able to travel to Haiti for volunteer work and am traveling to Nepal shortly for medical relief work—and I have been able to dive deeply into integrative holistic medicine. I get to pick and choose how often I work and, most importantly, when I do work, it is an absolute joy. I can happily say I am able to give my patients the care that they deserve without feeling burnt out.
I am a big fan of the way I have decided to practice the art of medicine and can honestly say that I am enjoying my journey.
Geeta Arora, MD, board certified in internal medicine and integrative holistic medicine
![]()
So I quit medicine.
I ended up working with a few NGOs (nongovernmental organizations) at the time, becoming the healthcare director of a medium-sized NGO. I learned the enormous amount of red tape that was scattered in that world, and I began missing medicine.
So I unquit medicine.
I decided that the best thing for me was to be my own boss. I didn’t know how to do this. As someone with absolutely no business background, I started reading about different types of work I could do where I was in charge of dictating my hours. Opening up a clinic or starting my own hospitalist group felt like being shackled down in the system again. I talked to my colleagues from residency, and they all seemed underwhelmed with the love of their jobs and overwhelmed by the number of hours that they were working. They still sounded like residents.
After getting a taste of a world outside of medicine, I realized that I had so many hobbies and interests outside of practicing as a hospitalist. I found a love of surfing, I wanted to volunteer and do medical relief work abroad, I wanted to travel the world, and I wanted to study herbal medicine and integrative holistic medicine in great depth—all while being able to keep one foot in the medical system.
That is when I found locum tenens hospitalist-based medicine. Suddenly, I could make my own schedule, decide where and when I would work, and have the flexibility to leave any given hospital if I felt as though I was being pushed into practices that would compromise patient care and safety.
It’s been four years since I began practicing locum tenens hospitalist medicine, and I have never looked back. I have been able to take up surfing more seriously; I’ve traveled around the world and continue to do so—I have been able to travel to Haiti for volunteer work and am traveling to Nepal shortly for medical relief work—and I have been able to dive deeply into integrative holistic medicine. I get to pick and choose how often I work and, most importantly, when I do work, it is an absolute joy. I can happily say I am able to give my patients the care that they deserve without feeling burnt out.
I am a big fan of the way I have decided to practice the art of medicine and can honestly say that I am enjoying my journey.
Geeta Arora, MD, board certified in internal medicine and integrative holistic medicine
![]()
So I quit medicine.
I ended up working with a few NGOs (nongovernmental organizations) at the time, becoming the healthcare director of a medium-sized NGO. I learned the enormous amount of red tape that was scattered in that world, and I began missing medicine.
So I unquit medicine.
I decided that the best thing for me was to be my own boss. I didn’t know how to do this. As someone with absolutely no business background, I started reading about different types of work I could do where I was in charge of dictating my hours. Opening up a clinic or starting my own hospitalist group felt like being shackled down in the system again. I talked to my colleagues from residency, and they all seemed underwhelmed with the love of their jobs and overwhelmed by the number of hours that they were working. They still sounded like residents.
After getting a taste of a world outside of medicine, I realized that I had so many hobbies and interests outside of practicing as a hospitalist. I found a love of surfing, I wanted to volunteer and do medical relief work abroad, I wanted to travel the world, and I wanted to study herbal medicine and integrative holistic medicine in great depth—all while being able to keep one foot in the medical system.
That is when I found locum tenens hospitalist-based medicine. Suddenly, I could make my own schedule, decide where and when I would work, and have the flexibility to leave any given hospital if I felt as though I was being pushed into practices that would compromise patient care and safety.
It’s been four years since I began practicing locum tenens hospitalist medicine, and I have never looked back. I have been able to take up surfing more seriously; I’ve traveled around the world and continue to do so—I have been able to travel to Haiti for volunteer work and am traveling to Nepal shortly for medical relief work—and I have been able to dive deeply into integrative holistic medicine. I get to pick and choose how often I work and, most importantly, when I do work, it is an absolute joy. I can happily say I am able to give my patients the care that they deserve without feeling burnt out.
I am a big fan of the way I have decided to practice the art of medicine and can honestly say that I am enjoying my journey.
Geeta Arora, MD, board certified in internal medicine and integrative holistic medicine
Society of Hospital Medicine Website Boasts Resources, Guides
SHM’s website offers a wealth of downloadable guides and toolkits, authored by the national experts on topics like:
- End-of-life care;
- Opioid monitoring;
- Antibiotic resistance;
- Post-acute care;
- VTE;
- Pain management; and
- Coronary heart disease (CHD).
SHM’s website offers a wealth of downloadable guides and toolkits, authored by the national experts on topics like:
- End-of-life care;
- Opioid monitoring;
- Antibiotic resistance;
- Post-acute care;
- VTE;
- Pain management; and
- Coronary heart disease (CHD).
SHM’s website offers a wealth of downloadable guides and toolkits, authored by the national experts on topics like:
- End-of-life care;
- Opioid monitoring;
- Antibiotic resistance;
- Post-acute care;
- VTE;
- Pain management; and
- Coronary heart disease (CHD).
How Quality Improvement Programs Improve Hospitals, Communities

And it’s now easier than ever to get started, right from your computer.
Online Webinars
Coaching a Quality Improvement Team: Basics for Being Sure Any QI team and Project Are on the Right Track
Presenter: Jordan Messler, MD, SFHM
Date: October 28, 2015
Time: 1:00 p.m. EDT
Elevating Provider Experience to Improve Patient Experience
Presenter: Mark Rudolph, MD
Date: November 11, 2015
Time: 2:00 p.m. EDT
And it’s now easier than ever to get started, right from your computer.
Online Webinars
Coaching a Quality Improvement Team: Basics for Being Sure Any QI team and Project Are on the Right Track
Presenter: Jordan Messler, MD, SFHM
Date: October 28, 2015
Time: 1:00 p.m. EDT
Elevating Provider Experience to Improve Patient Experience
Presenter: Mark Rudolph, MD
Date: November 11, 2015
Time: 2:00 p.m. EDT
And it’s now easier than ever to get started, right from your computer.
Online Webinars
Coaching a Quality Improvement Team: Basics for Being Sure Any QI team and Project Are on the Right Track
Presenter: Jordan Messler, MD, SFHM
Date: October 28, 2015
Time: 1:00 p.m. EDT
Elevating Provider Experience to Improve Patient Experience
Presenter: Mark Rudolph, MD
Date: November 11, 2015
Time: 2:00 p.m. EDT
Start Planning Now for Hospital Medicine 2016
Hospital Medicine 2016 has been updated to meet the educational needs of hospitalists of all stripes, with new sessions and pre-courses, as well as entirely new tracks on the most cutting-edge topics in the movement.
New tracks planned: post-acute care, health IT for hospitalists, co-management/peri-operative medicine.
Recurring tracks: rapid fire, clinical, young hospitalists, practice management, academic/research, quality, pediatric, potpourri, the doctor-patient relationship.
For an updated list of pre-courses and other sessions, visit Hospital Medicine 2016. Register by Jan. 11, 2016, to save $50.
Hospital Medicine 2016 has been updated to meet the educational needs of hospitalists of all stripes, with new sessions and pre-courses, as well as entirely new tracks on the most cutting-edge topics in the movement.
New tracks planned: post-acute care, health IT for hospitalists, co-management/peri-operative medicine.
Recurring tracks: rapid fire, clinical, young hospitalists, practice management, academic/research, quality, pediatric, potpourri, the doctor-patient relationship.
For an updated list of pre-courses and other sessions, visit Hospital Medicine 2016. Register by Jan. 11, 2016, to save $50.
Hospital Medicine 2016 has been updated to meet the educational needs of hospitalists of all stripes, with new sessions and pre-courses, as well as entirely new tracks on the most cutting-edge topics in the movement.
New tracks planned: post-acute care, health IT for hospitalists, co-management/peri-operative medicine.
Recurring tracks: rapid fire, clinical, young hospitalists, practice management, academic/research, quality, pediatric, potpourri, the doctor-patient relationship.
For an updated list of pre-courses and other sessions, visit Hospital Medicine 2016. Register by Jan. 11, 2016, to save $50.
Society of Hospital Medicine Membership Ambassador Program Ends December 2015
You are one of the best representatives of the hospital medicine movement. You can share your enthusiasm for the specialty and for improving the care of hospitalized patients by telling others about SHM.
And, as an added bonus, you can earn credit toward SHM membership dues.
Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
Active members will be eligible for:
- A $35 credit toward 2016-2017 dues when recruiting one new member;
- A $50 credit toward 2016-2017 dues when recruiting 2-4 new members;
- A $75 credit toward 2016-2017 dues when recruiting 5-9 new members; or
- A $125 credit toward 2016-2017 dues when recruiting 10+ new members.
For every member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to HM16 in San Diego.
Click here for more details.
You are one of the best representatives of the hospital medicine movement. You can share your enthusiasm for the specialty and for improving the care of hospitalized patients by telling others about SHM.
And, as an added bonus, you can earn credit toward SHM membership dues.
Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
Active members will be eligible for:
- A $35 credit toward 2016-2017 dues when recruiting one new member;
- A $50 credit toward 2016-2017 dues when recruiting 2-4 new members;
- A $75 credit toward 2016-2017 dues when recruiting 5-9 new members; or
- A $125 credit toward 2016-2017 dues when recruiting 10+ new members.
For every member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to HM16 in San Diego.
Click here for more details.
You are one of the best representatives of the hospital medicine movement. You can share your enthusiasm for the specialty and for improving the care of hospitalized patients by telling others about SHM.
And, as an added bonus, you can earn credit toward SHM membership dues.
Through the end of the year, all active SHM members can earn 2016-2017 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
Active members will be eligible for:
- A $35 credit toward 2016-2017 dues when recruiting one new member;
- A $50 credit toward 2016-2017 dues when recruiting 2-4 new members;
- A $75 credit toward 2016-2017 dues when recruiting 5-9 new members; or
- A $125 credit toward 2016-2017 dues when recruiting 10+ new members.
For every member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to HM16 in San Diego.
Click here for more details.
Society of Hospital Medicine Awards, Committee, Board Nominations Due October 16

- Nominating yourself or a colleague for one of SHM’s Awards of Excellence, which will be presented at HM16 in San Diego;
- Joining a committee that matches your professional interests or personal passions;
- Applying for SHM’s board of directors; or
- Nominating a colleague for the Master in Hospital Medicine designation, SHM’s most prestigious honor.
For more information, click on the “membership” section of the SHM website.
- Nominating yourself or a colleague for one of SHM’s Awards of Excellence, which will be presented at HM16 in San Diego;
- Joining a committee that matches your professional interests or personal passions;
- Applying for SHM’s board of directors; or
- Nominating a colleague for the Master in Hospital Medicine designation, SHM’s most prestigious honor.
For more information, click on the “membership” section of the SHM website.
- Nominating yourself or a colleague for one of SHM’s Awards of Excellence, which will be presented at HM16 in San Diego;
- Joining a committee that matches your professional interests or personal passions;
- Applying for SHM’s board of directors; or
- Nominating a colleague for the Master in Hospital Medicine designation, SHM’s most prestigious honor.
For more information, click on the “membership” section of the SHM website.