User login
Inflammatory features linked to erosive development in hand OA
Among adults with hand osteoarthritis, ultrasonographic evidence of persistent joint-level inflammation increased the odds of subsequent erosions by as much as 11 times, said authors of a 2-year prospective study.
“These observations implicate a role for inflammation in the pathogenesis of erosive osteoarthritis and might render new therapeutic options that can halt erosive development,” said Dr. Marion C. Kortekaas and her associates at Leiden (the Netherlands) University Medical Center. The findings appeared online in Arthritis & Rheumatology.

The pathogenesis of erosive hand OA remains poorly understood, despite its high clinical burden, the researchers noted. To assess potential risk factors for erosive development, they used standard ultrasonographic methods to examine the interphalangeal joints of 56 consecutive patients who presented to a rheumatology outpatient clinic with hand OA based on American College of Rheumatology criteria. They also scored radiographs for osteophytes or joint-space narrowing with the OARSI method and used the Verbruggen-Veys method to identify and exclude joints that were already eroded (E phase) or remodeled (R phase) at baseline (Arthritis Rheum. 2015 Sep 28. doi: 10.1002/art.39438). At baseline, 18 patients had ultrasonographic evidence of erosions in a total of 51 interphalangeal joints, the investigators said. At the 2.3-year follow-up, a total of 38 interphalangeal joints from 26 patients showed erosive development.
After accounting for age, gender, body mass index, and baseline cartilage and bone abnormalities, all ultrasonographic features of inflammation that were at least grade 1 at baseline and follow-up predicted erosive development. Persistent power Doppler signal was the strongest risk factor, yielding an odds ratio of 11.4 in the adjusted model (95% confidence interval, 2.7-49.1). Other significant risk factors included moderate to severe baseline synovial thickening (OR, 8.8; 95% CI, 2.4-32.3) and power Doppler signal (OR, 7.1; 95% CI, 1.9-26.9).
“The present study confirms that inflammatory US features found at baseline are associated with erosive development on the joint level in hand OA,” the investigators wrote. “These associations are already found after 2 years of follow-up, which is important for future prospective trials.”
The researchers reported having no funding sources or conflicts of interest.
Among adults with hand osteoarthritis, ultrasonographic evidence of persistent joint-level inflammation increased the odds of subsequent erosions by as much as 11 times, said authors of a 2-year prospective study.
“These observations implicate a role for inflammation in the pathogenesis of erosive osteoarthritis and might render new therapeutic options that can halt erosive development,” said Dr. Marion C. Kortekaas and her associates at Leiden (the Netherlands) University Medical Center. The findings appeared online in Arthritis & Rheumatology.
The pathogenesis of erosive hand OA remains poorly understood, despite its high clinical burden, the researchers noted. To assess potential risk factors for erosive development, they used standard ultrasonographic methods to examine the interphalangeal joints of 56 consecutive patients who presented to a rheumatology outpatient clinic with hand OA based on American College of Rheumatology criteria. They also scored radiographs for osteophytes or joint-space narrowing with the OARSI method and used the Verbruggen-Veys method to identify and exclude joints that were already eroded (E phase) or remodeled (R phase) at baseline (Arthritis Rheum. 2015 Sep 28. doi: 10.1002/art.39438). At baseline, 18 patients had ultrasonographic evidence of erosions in a total of 51 interphalangeal joints, the investigators said. At the 2.3-year follow-up, a total of 38 interphalangeal joints from 26 patients showed erosive development.
After accounting for age, gender, body mass index, and baseline cartilage and bone abnormalities, all ultrasonographic features of inflammation that were at least grade 1 at baseline and follow-up predicted erosive development. Persistent power Doppler signal was the strongest risk factor, yielding an odds ratio of 11.4 in the adjusted model (95% confidence interval, 2.7-49.1). Other significant risk factors included moderate to severe baseline synovial thickening (OR, 8.8; 95% CI, 2.4-32.3) and power Doppler signal (OR, 7.1; 95% CI, 1.9-26.9).
“The present study confirms that inflammatory US features found at baseline are associated with erosive development on the joint level in hand OA,” the investigators wrote. “These associations are already found after 2 years of follow-up, which is important for future prospective trials.”
The researchers reported having no funding sources or conflicts of interest.
Among adults with hand osteoarthritis, ultrasonographic evidence of persistent joint-level inflammation increased the odds of subsequent erosions by as much as 11 times, said authors of a 2-year prospective study.
“These observations implicate a role for inflammation in the pathogenesis of erosive osteoarthritis and might render new therapeutic options that can halt erosive development,” said Dr. Marion C. Kortekaas and her associates at Leiden (the Netherlands) University Medical Center. The findings appeared online in Arthritis & Rheumatology.
The pathogenesis of erosive hand OA remains poorly understood, despite its high clinical burden, the researchers noted. To assess potential risk factors for erosive development, they used standard ultrasonographic methods to examine the interphalangeal joints of 56 consecutive patients who presented to a rheumatology outpatient clinic with hand OA based on American College of Rheumatology criteria. They also scored radiographs for osteophytes or joint-space narrowing with the OARSI method and used the Verbruggen-Veys method to identify and exclude joints that were already eroded (E phase) or remodeled (R phase) at baseline (Arthritis Rheum. 2015 Sep 28. doi: 10.1002/art.39438). At baseline, 18 patients had ultrasonographic evidence of erosions in a total of 51 interphalangeal joints, the investigators said. At the 2.3-year follow-up, a total of 38 interphalangeal joints from 26 patients showed erosive development.
After accounting for age, gender, body mass index, and baseline cartilage and bone abnormalities, all ultrasonographic features of inflammation that were at least grade 1 at baseline and follow-up predicted erosive development. Persistent power Doppler signal was the strongest risk factor, yielding an odds ratio of 11.4 in the adjusted model (95% confidence interval, 2.7-49.1). Other significant risk factors included moderate to severe baseline synovial thickening (OR, 8.8; 95% CI, 2.4-32.3) and power Doppler signal (OR, 7.1; 95% CI, 1.9-26.9).
“The present study confirms that inflammatory US features found at baseline are associated with erosive development on the joint level in hand OA,” the investigators wrote. “These associations are already found after 2 years of follow-up, which is important for future prospective trials.”
The researchers reported having no funding sources or conflicts of interest.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Ultrasonographic evidence of inflammation significantly predicted the development of erosions in hand osteoarthritis.
Major finding: All inflammatory ultrasonographic features that were at least grade 1 at baseline and follow-up significantly predicted erosive development.
Data source: Single-center, prospective, ultrasonographic and radiographic study of 56 patients who met ACR criteria for hand OA.
Disclosures: The investigators reported having no funding sources or conflicts of interest.

Word choice affects public perception of drugs

Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Photo courtesy of the FDA
Using the words “breakthrough” and “promising” to describe new drugs affects the public’s perception of the drugs’ effectiveness, according to a study published in JAMA Internal Medicine.
Investigators noted that, in everyday usage, the term “breakthrough” represents a highly significant or definitive advance.
However, the US Food and Drug Administration’s (FDA’s) “breakthrough therapy designation” has a different meaning.
Since the Safety and Innovation Act became law in 2012, the FDA can assign breakthrough designation to a drug that “treats a serious or life-threatening condition” and “may demonstrate a substantial improvement . . . over available therapies” based on preliminary evidence.
And since the creation of the Safety and Innovation Act, all FDA press releases announcing the approval of breakthrough-designated drugs have used the term “breakthrough,” while about half have used the term “promising.”
“Today, patients and their families can easily find FDA press releases on the Internet, or they often hear about them in the news,” said study author Steven Woloshin, MD, of The Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, New Hampshire.
“But the reality is that unless patients fully understand how the FDA is using the term ‘breakthrough,’ they may have unwarranted confidence in the evidence supporting drug claims. So we thought it was important to test how these terms affect the judgement of people without medical training.”
Survey details
The investigators conducted an online survey of 597 Americans. Participants were randomly given 1 of 5 short descriptions of a recently approved drug.
The descriptions were based on an FDA press release for a metastatic lung cancer breakthrough-designated drug that was conditionally approved based on the surrogate outcome of tumor shrinkage.
The first, “facts-only” description described the drug as meeting the criteria for breakthrough designation but did not actually use the term “breakthrough.”
A second and a third description included the facts and added the terms “breakthrough” and “promising,” respectively.
The fourth, “tentative” description included the facts, used the word “breakthrough,” and used the following FDA-required language for professional labeling:
The FDA pointed out that the drug was approved based on tumor shrinkage but that an improvement in survival or disease-related symptoms has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
The fifth, “definitive” description included the same information as the tentative description, but “may be contingent” was changed to “is contingent.”
Participants were then asked to judge the drug’s benefit, harm, and strength of evidence.
Results
The investigators found that adding either “breakthrough” or “promising” in the description significantly increased the percentage of participants who rated the drug as “very” or “completely” effective compared with the facts-only description—23% and 25% vs 11%.
Adding “breakthrough” or “promising” to the description also significantly increased the number of people who reported believing that evidence supporting the drug is “strong” or “extremely strong”—59% and 63% vs 43%.
At the same time, adding either the tentative or definitive explanations significantly reduced the percentage of participants who believed (incorrectly) that the drug had been “proven to save lives”—16% tentative and 10% definitive vs 31% breakthrough.
Finally, when participants were asked which of 2 drugs—one described as “breakthrough,” the other as meeting the breakthrough criteria—they would take for a potentially deadly condition, 92% chose the “breakthrough” drug.
“Our findings clearly indicate that words like ‘breakthrough’ and ‘promising’ increase people’s beliefs in a drug’s effectiveness,” said Lisa Schwartz, MD, of The Dartmouth Institute for Health Policy and Clinical Practice.
“In light of [the findings], press releases with neutral terms and that clearly explain the limited evidence supporting what breakthrough designation and accelerated approval mean might help consumers make more accurate judgements about these drugs.” ![]()
Team identifies therapeutic target for HIT

Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Researchers believe they have identified a therapeutic target for heparin-induced thrombocytopenia (HIT).
The team noted that HIT is caused by antibodies to complexes that form between platelet factor 4 (PF4), which is released from activated platelets, and heparin or cellular glycosaminoglycans.
The researchers elucidated the crystal structure of 3 PF4 complexes and found evidence suggesting that tetramerization of PF4 is targetable.
Zheng Cai, PhD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Nature Communications.
Previously, the researchers identified KKO, a murine monoclonal antibody to PF4/heparin complexes that causes HIT in a murine model. The team said human HIT antibodies compete with KKO for binding to PF4/heparin, and KKO augments the formation of pathogenic immune complexes.
The researchers also identified RTO, an isotype-matched, anti-PF4 antibody that binds to PF4 but does not generate pathogenic complexes.
For the current study, the team described and compared the crystal structures of PF4 in complex with Fabs derived from KKO and RTO to the structure of PF4 in complex with fondaparinux.
The researchers noted that PF4 molecules can exist singly as monomers, doubly as dimers, and as a 4-part complex called a tetramer, which have an “open” end and a “closed” end.
The crystal structure of PF4 in complex with fondaparinux showed that fondaparinux binds to the “closed” end of the PF4 tetramer, which stabilizes the tetramer.
The crystal structure of PF4 in complex with KKO showed that KKO binds to the “open” end of the stabilized tetramer, making contact with 3 of 4 monomers in the tetramer.
The researchers said this helps explain the requirement for heparin as a backbone for the complex. They also said this finding provides new insight into how a normal host protein such as PF4 can be converted into a target of the host immune system, which leads to an autoimmune disorder.
The crystal structure of PF4 in complex with RTO showed that RTO binds to PF4 monomers rather than tetramers. And RTO binds to the monomers in a way that prevents them from combining into tetramers.
Via cell experiments, the researchers confirmed that RTO prevents the formation of antigenic complexes, as well as the activation of platelets by KKO and human HIT antibodies. RTO also prevented clot formation caused by KKO in a mouse model of HIT.
These results suggest that binding of RTO to PF4 monomers prevents the formation of pathogenic complexes that are central to the pathology of HIT. So the researchers believe RTO can provide the basis for new diagnostics and may pave the way for a therapy to stop HIT early in its progression. ![]()
Hematocrit level may predict need for transfusion

Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Photo by Elise Amendola
A young trauma patient’s hematocrit level at hospital admission may predict the need for transfusion, new research suggests.
Results of this retrospective, single-center study indicate that children and adolescents with a hematocrit level of 35% or less at admission are more likely than their peers with higher hematocrit levels to require a transfusion after trauma.
The study was published in the Journal of Trauma and Acute Care Surgery.
“A quick and cost-effective measure, such as admission hematocrit, to identify pediatric patients who are at a high risk for bleeding could provide a critical improvement in optimizing care for children, while reducing costs,” said study author Christopher P. Gayer, MD, PhD, of Children's Hospital Los Angeles (CHLA) in California.
For this research, Dr Gayer and his colleagues examined the medical records of all patients, ages 0 to 17, who presented to the level 1 pediatric trauma center at CHLA between 2005 and 2013.
Of all the patients, 1341 had hematocrit measured at admission. The researchers divided this group into patients who required an intervention—transfusion or operation—for their bleeding (n=93) and those who did not (n=1248).
The mean hematocrit was 38.0 for patients who did not require an intervention and 34.3 for those who did (P<0.01). The mean hematocrit was 26.9 in patients who required a transfusion secondary to bleeding and 36.0 in those who required an operative intervention for nonhemostatic indications (P<0.01).
The researchers then analyzed a subset of patients who had an abdominal CT scan, as these patients had a definitive presence or absence of intra-abdominal injury. There was a significant decrease in admission hematocrit between patients who required a transfusion for an intra-abdominal injury and those who did not—29% and 37%, respectively (P<0.01).
Serial hematocrit values remained significantly lower in the patients who required a transfusion up to 67 hours after admission (P=0.04). The researchers said this suggests that hematocrit is a valuable predictor for requiring a transfusion at least 2 days after an injury, and it may be useful for patients presenting well after their initial injury.
The team then evaluated whether an admission hematocrit cutoff of 35% or less could predict the need for transfusion. For all patients, a cutoff of 35% or less had a sensitivity of 94%, specificity of 77%, positive-predictive value of 5%, and negative predictive value of 99.9%.
In patients who had an abdominal CT, a cutoff hematocrit of 35% or less had a sensitivity of 90%, specificity of 76%, positive predictive value of 21%, and negative predictive value of 99%.
These results led the researchers to conclude that this hematocrit cutoff may be a reliable screening tool.
“Admission hematocrit can be done rapidly in the trauma bay, is relatively inexpensive, causes minimal harm, and can aid in critical decision-making and rapid identification of occult bleeding,” said study author Jamie Golden, MD, of CHLA.
“Our results show that a hematocrit level of less than 35% on admission predicts a greater likelihood for the need of transfusion in pediatric blunt trauma patients.”
The researchers stressed that a doctor's concern in the face of clinical signs of hemorrhagic shock should always take priority over lab data. However, a repeat hematocrit can be quickly and easily performed if clinically indicated.
They added that the results of their study require validation in a prospective, multicenter study. ![]()
Study reveals tumor suppressor in AML

The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said. ![]()
The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said. ![]()
The protein-coding gene hnRNP K acts as a tumor suppressor in acute myeloid leukemia (AML), according to research published in Cancer Cell.
Investigators found that AML patients who carried a partial deletion of chromosome 9 also experienced a significant decrease in hnRNP K expression.
This deletion, 9q21.32, along with the decreased levels of hnRNP K, led to reduced survival and increased tumor formation.
“Our data implicates hnRNP K in the development of blood disorders and suggests it acts as a tumor suppressor,” said Sean Post, PhD, of The University of Texas MD Anderson Cancer Center in Houston.
“Both in vivo and in vitro results indicate that hnRNP K achieves this through regulation of key genetic pathways. Our study found that hnRNP K expression must be maintained for proper cellular regulation and to prevent tumor formation.”
Dr Post and his colleagues examined hnRNP K’s role in tumorigenesis by generating a mouse model harboring an Hnrnpk knockout allele.
They found that Hnrnpk haploinsufficiency resulted in reduced survival, increased tumor formation, genomic instability, and the development of transplantable hematopoietic neoplasms with myeloproliferation.
“Our findings showed that Hnrnpk haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways, which suggests these pathways may be exploited by targeted therapies,” Dr Post said.
Specifically, he and his colleagues found that reduced hnRNP K expression attenuated p21 activation, downregulated C/EBP levels, and activated STAT3 signaling.
The investigators also analyzed samples from AML patients who harbored 9q21.32 and found a significant decrease in hnRNP K expression.
“It was clear that these changes in AML patients with the 9q21.32 deletion resulted in a tumor suppressor gene involved in blood cancer development,” Dr Post said. ![]()
Occupational Contact Dermatitis From Carbapenems
To the Editor:
Contact sensitivity to drugs that are systemically administered can occur among health care workers.1 We report the case of a 28-year-old nurse who developed eczema on the dorsal aspect of the hand (Figure 1A) and the face (Figure 1B) in the workplace. The nurse was working in the hematology department where she usually handled and administered antibiotics such as imipenem, ertapenem, piperacillin, vancomycin, anidulafungin, teicoplanin, and ciprofloxacin. She was moved to a different department where she did not have contact with the suspicious drugs and the dermatitis completely resolved.

One month after the resolution of the eczema she was referred to our allergy department for an allergological evaluation. A dermatologic evaluation was made and a skin biopsy was performed from a lesional area of the left hand. The patient underwent delayed skin test and patch tests with many β-lactam compounds including penicilloyl polylysine, minor determinant mixture, penicillin G, penicillin V, ampicillin, amoxicillin, bacampicillin, piperacillin, mezlocillin and ticarcillin, imipenem-cilastatin, aztreonam, meropenem, ertapenem, and cephalosporins (eg, cephalexin, cefaclor, cefalotin, cefadroxil, cephradine, cefuroxime, ceftriaxone, cefixime, cefoperazone, cefamandole, ceftazidime, cefotaxime). Undiluted solutions of commercial drugs (parenteral drugs when available were used) were used for skin prick test, and if negative, they were tested intradermally as described by Schiavino et al.2 The concentrations used for the skin test and for the patch test are reported in the Table. Histamine (10 mg/mL) and saline were employed as positive and negative controls, respectively. Immediate reactions of at least 3 mm greater in diameter compared to the control for the skin prick test and 5 mm greater for intradermal tests were considered positive. Immediate-type skin tests were read after 20 minutes and also after 48 hours should any delayed reaction occur. An infiltrated erythema with a diameter greater than 5 mm was considered a delayed positive reaction.
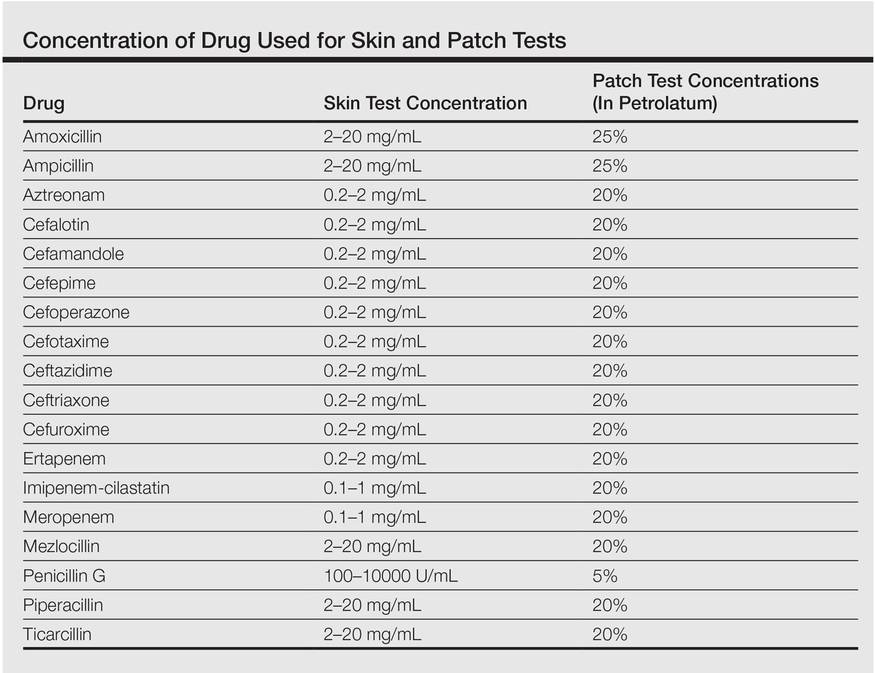
Patch tests were applied to the interscapular region using acrylate adhesive strips with small plates. They were evaluated at 48 and 72 hours. Positivity was assessed according to the indications of the European Network for Drug Allergy.3 Patch tests were carried out using the same drugs as the skin test. All drugs were mixed in petrolatum at 25% wt/wt for ampicillin and amoxicillin, 5% for penicillin G, and 20% for the other drugs as recommended by Schiavino et al.2 We also performed patch tests with ertapenem in 20 healthy controls.
A skin biopsy from lesional skin showed a perivascular infiltrate of the upper dermis with spongiosis of the lesional area similar to eczema. Patch tests and intradermal tests were positive for ertapenem after 48 hours (Figure 2). Imipenem-cilastatin, ampicillin, piperacillin, mezlocillin, and meropenem showed a positive reaction for patch tests. We concluded that the patient had delayed hypersensitivity to carbapenems (ertapenem, imipenem-cilastatin, and meropenem) and semisynthetic penicillins (piperacillin, mezlocillin, and ampicillin).

Drug sensitization in nurses and in health care workers can occur. Natural and semisynthetic penicillin can cause allergic contact dermatitis in health care workers. We report a case of occupational allergy to ertapenem, which is a 1-β-methyl-carbapenem that is administered as a single agent. It is highly active in vitro against bacteria that are generally associated with community-acquired and mixed aerobic and anaerobic infections.4 Occupational contact allergy to other carbapenems such as meropenem also was reported.5 The contact sensitization potential of imipenem has been confirmed in the guinea pig.6 Carbapenems have a bicyclic nucleus composed by a β-lactam ring with an associated 5-membered ring. In our patient, patch tests for ertapenem, imipenem, and meropenem were positive. Although the cross-reactivity between imipenem and penicillin has been demonstrated,2 data on the cross-reactivity between the carbapenems are not strong. Bauer et al7 reported a case of an allergy to imipenem-cilastatin that tolerated treatment with meropenem, but our case showed a complete cross-reactivity between carbapenems. Patch tests for ampicillin, mezlocillin, and piperacillin also were positive; therefore, it can be hypothesized that in our patient, the β-lactam ring was the main epitope recognized by T lymphocytes. Gielen and Goossens1 reported in a study on work-related dermatitis that the most common sensitizers were antibiotics such as penicillins, cephalosporins, and aminoglycosides.
Health care workers should protect their hands with gloves during the preparation of drugs because they have the risk for developing an occupational contact allergy. Detailed allergological and dermatological evaluation is mandatory to confirm or exclude occupational contact allergy.
- Gielen K, Goossens A. Occupational allergic contact dermatitis from drugs in healthcare workers. Contact Dermatitis. 2001;45:273-279.
- Schiavino D, Nucera E, Lombardo C, et al. Cross-reactivity and tolerability of imipenem in patients with delayed-type, cell-mediated hypersensitivity to beta-lactams. Allergy. 2009;64:1644-1648.
- Romano A, Blanca M, Torres MJ, et al. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. 2004;59:1153-1160.
- Teppler H, Gesser RM, Friedland IR, et al. Safety and tolerability of ertapenem. J Antimicrob Chemother. 2004;53(suppl 2):75-81.
- Yesudian PD, King CM. Occupational allergic contact dermatitis from meropenem. Contact Dermatitis. 2001;45:53.
- Nagakura N, Souma S, Shimizu T, et al. Comparison of cross-reactivities of imipenem and other beta-lactam antibiotics by delayed-type hypersensitivity reaction in guinea pigs. Chem Pharm Bull. 1991;39:765-768.
- Bauer SL, Wall GC, Skoglund K, et al. Lack of cross-reactivity to meropenem in a patient with an allergy to imipenem-cilastatin. J Allergy Clin Immunol. 2004;113:173-175.
To the Editor:
Contact sensitivity to drugs that are systemically administered can occur among health care workers.1 We report the case of a 28-year-old nurse who developed eczema on the dorsal aspect of the hand (Figure 1A) and the face (Figure 1B) in the workplace. The nurse was working in the hematology department where she usually handled and administered antibiotics such as imipenem, ertapenem, piperacillin, vancomycin, anidulafungin, teicoplanin, and ciprofloxacin. She was moved to a different department where she did not have contact with the suspicious drugs and the dermatitis completely resolved.
One month after the resolution of the eczema she was referred to our allergy department for an allergological evaluation. A dermatologic evaluation was made and a skin biopsy was performed from a lesional area of the left hand. The patient underwent delayed skin test and patch tests with many β-lactam compounds including penicilloyl polylysine, minor determinant mixture, penicillin G, penicillin V, ampicillin, amoxicillin, bacampicillin, piperacillin, mezlocillin and ticarcillin, imipenem-cilastatin, aztreonam, meropenem, ertapenem, and cephalosporins (eg, cephalexin, cefaclor, cefalotin, cefadroxil, cephradine, cefuroxime, ceftriaxone, cefixime, cefoperazone, cefamandole, ceftazidime, cefotaxime). Undiluted solutions of commercial drugs (parenteral drugs when available were used) were used for skin prick test, and if negative, they were tested intradermally as described by Schiavino et al.2 The concentrations used for the skin test and for the patch test are reported in the Table. Histamine (10 mg/mL) and saline were employed as positive and negative controls, respectively. Immediate reactions of at least 3 mm greater in diameter compared to the control for the skin prick test and 5 mm greater for intradermal tests were considered positive. Immediate-type skin tests were read after 20 minutes and also after 48 hours should any delayed reaction occur. An infiltrated erythema with a diameter greater than 5 mm was considered a delayed positive reaction.
Patch tests were applied to the interscapular region using acrylate adhesive strips with small plates. They were evaluated at 48 and 72 hours. Positivity was assessed according to the indications of the European Network for Drug Allergy.3 Patch tests were carried out using the same drugs as the skin test. All drugs were mixed in petrolatum at 25% wt/wt for ampicillin and amoxicillin, 5% for penicillin G, and 20% for the other drugs as recommended by Schiavino et al.2 We also performed patch tests with ertapenem in 20 healthy controls.
A skin biopsy from lesional skin showed a perivascular infiltrate of the upper dermis with spongiosis of the lesional area similar to eczema. Patch tests and intradermal tests were positive for ertapenem after 48 hours (Figure 2). Imipenem-cilastatin, ampicillin, piperacillin, mezlocillin, and meropenem showed a positive reaction for patch tests. We concluded that the patient had delayed hypersensitivity to carbapenems (ertapenem, imipenem-cilastatin, and meropenem) and semisynthetic penicillins (piperacillin, mezlocillin, and ampicillin).
Drug sensitization in nurses and in health care workers can occur. Natural and semisynthetic penicillin can cause allergic contact dermatitis in health care workers. We report a case of occupational allergy to ertapenem, which is a 1-β-methyl-carbapenem that is administered as a single agent. It is highly active in vitro against bacteria that are generally associated with community-acquired and mixed aerobic and anaerobic infections.4 Occupational contact allergy to other carbapenems such as meropenem also was reported.5 The contact sensitization potential of imipenem has been confirmed in the guinea pig.6 Carbapenems have a bicyclic nucleus composed by a β-lactam ring with an associated 5-membered ring. In our patient, patch tests for ertapenem, imipenem, and meropenem were positive. Although the cross-reactivity between imipenem and penicillin has been demonstrated,2 data on the cross-reactivity between the carbapenems are not strong. Bauer et al7 reported a case of an allergy to imipenem-cilastatin that tolerated treatment with meropenem, but our case showed a complete cross-reactivity between carbapenems. Patch tests for ampicillin, mezlocillin, and piperacillin also were positive; therefore, it can be hypothesized that in our patient, the β-lactam ring was the main epitope recognized by T lymphocytes. Gielen and Goossens1 reported in a study on work-related dermatitis that the most common sensitizers were antibiotics such as penicillins, cephalosporins, and aminoglycosides.
Health care workers should protect their hands with gloves during the preparation of drugs because they have the risk for developing an occupational contact allergy. Detailed allergological and dermatological evaluation is mandatory to confirm or exclude occupational contact allergy.
To the Editor:
Contact sensitivity to drugs that are systemically administered can occur among health care workers.1 We report the case of a 28-year-old nurse who developed eczema on the dorsal aspect of the hand (Figure 1A) and the face (Figure 1B) in the workplace. The nurse was working in the hematology department where she usually handled and administered antibiotics such as imipenem, ertapenem, piperacillin, vancomycin, anidulafungin, teicoplanin, and ciprofloxacin. She was moved to a different department where she did not have contact with the suspicious drugs and the dermatitis completely resolved.
One month after the resolution of the eczema she was referred to our allergy department for an allergological evaluation. A dermatologic evaluation was made and a skin biopsy was performed from a lesional area of the left hand. The patient underwent delayed skin test and patch tests with many β-lactam compounds including penicilloyl polylysine, minor determinant mixture, penicillin G, penicillin V, ampicillin, amoxicillin, bacampicillin, piperacillin, mezlocillin and ticarcillin, imipenem-cilastatin, aztreonam, meropenem, ertapenem, and cephalosporins (eg, cephalexin, cefaclor, cefalotin, cefadroxil, cephradine, cefuroxime, ceftriaxone, cefixime, cefoperazone, cefamandole, ceftazidime, cefotaxime). Undiluted solutions of commercial drugs (parenteral drugs when available were used) were used for skin prick test, and if negative, they were tested intradermally as described by Schiavino et al.2 The concentrations used for the skin test and for the patch test are reported in the Table. Histamine (10 mg/mL) and saline were employed as positive and negative controls, respectively. Immediate reactions of at least 3 mm greater in diameter compared to the control for the skin prick test and 5 mm greater for intradermal tests were considered positive. Immediate-type skin tests were read after 20 minutes and also after 48 hours should any delayed reaction occur. An infiltrated erythema with a diameter greater than 5 mm was considered a delayed positive reaction.
Patch tests were applied to the interscapular region using acrylate adhesive strips with small plates. They were evaluated at 48 and 72 hours. Positivity was assessed according to the indications of the European Network for Drug Allergy.3 Patch tests were carried out using the same drugs as the skin test. All drugs were mixed in petrolatum at 25% wt/wt for ampicillin and amoxicillin, 5% for penicillin G, and 20% for the other drugs as recommended by Schiavino et al.2 We also performed patch tests with ertapenem in 20 healthy controls.
A skin biopsy from lesional skin showed a perivascular infiltrate of the upper dermis with spongiosis of the lesional area similar to eczema. Patch tests and intradermal tests were positive for ertapenem after 48 hours (Figure 2). Imipenem-cilastatin, ampicillin, piperacillin, mezlocillin, and meropenem showed a positive reaction for patch tests. We concluded that the patient had delayed hypersensitivity to carbapenems (ertapenem, imipenem-cilastatin, and meropenem) and semisynthetic penicillins (piperacillin, mezlocillin, and ampicillin).
Drug sensitization in nurses and in health care workers can occur. Natural and semisynthetic penicillin can cause allergic contact dermatitis in health care workers. We report a case of occupational allergy to ertapenem, which is a 1-β-methyl-carbapenem that is administered as a single agent. It is highly active in vitro against bacteria that are generally associated with community-acquired and mixed aerobic and anaerobic infections.4 Occupational contact allergy to other carbapenems such as meropenem also was reported.5 The contact sensitization potential of imipenem has been confirmed in the guinea pig.6 Carbapenems have a bicyclic nucleus composed by a β-lactam ring with an associated 5-membered ring. In our patient, patch tests for ertapenem, imipenem, and meropenem were positive. Although the cross-reactivity between imipenem and penicillin has been demonstrated,2 data on the cross-reactivity between the carbapenems are not strong. Bauer et al7 reported a case of an allergy to imipenem-cilastatin that tolerated treatment with meropenem, but our case showed a complete cross-reactivity between carbapenems. Patch tests for ampicillin, mezlocillin, and piperacillin also were positive; therefore, it can be hypothesized that in our patient, the β-lactam ring was the main epitope recognized by T lymphocytes. Gielen and Goossens1 reported in a study on work-related dermatitis that the most common sensitizers were antibiotics such as penicillins, cephalosporins, and aminoglycosides.
Health care workers should protect their hands with gloves during the preparation of drugs because they have the risk for developing an occupational contact allergy. Detailed allergological and dermatological evaluation is mandatory to confirm or exclude occupational contact allergy.
- Gielen K, Goossens A. Occupational allergic contact dermatitis from drugs in healthcare workers. Contact Dermatitis. 2001;45:273-279.
- Schiavino D, Nucera E, Lombardo C, et al. Cross-reactivity and tolerability of imipenem in patients with delayed-type, cell-mediated hypersensitivity to beta-lactams. Allergy. 2009;64:1644-1648.
- Romano A, Blanca M, Torres MJ, et al. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. 2004;59:1153-1160.
- Teppler H, Gesser RM, Friedland IR, et al. Safety and tolerability of ertapenem. J Antimicrob Chemother. 2004;53(suppl 2):75-81.
- Yesudian PD, King CM. Occupational allergic contact dermatitis from meropenem. Contact Dermatitis. 2001;45:53.
- Nagakura N, Souma S, Shimizu T, et al. Comparison of cross-reactivities of imipenem and other beta-lactam antibiotics by delayed-type hypersensitivity reaction in guinea pigs. Chem Pharm Bull. 1991;39:765-768.
- Bauer SL, Wall GC, Skoglund K, et al. Lack of cross-reactivity to meropenem in a patient with an allergy to imipenem-cilastatin. J Allergy Clin Immunol. 2004;113:173-175.
- Gielen K, Goossens A. Occupational allergic contact dermatitis from drugs in healthcare workers. Contact Dermatitis. 2001;45:273-279.
- Schiavino D, Nucera E, Lombardo C, et al. Cross-reactivity and tolerability of imipenem in patients with delayed-type, cell-mediated hypersensitivity to beta-lactams. Allergy. 2009;64:1644-1648.
- Romano A, Blanca M, Torres MJ, et al. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. 2004;59:1153-1160.
- Teppler H, Gesser RM, Friedland IR, et al. Safety and tolerability of ertapenem. J Antimicrob Chemother. 2004;53(suppl 2):75-81.
- Yesudian PD, King CM. Occupational allergic contact dermatitis from meropenem. Contact Dermatitis. 2001;45:53.
- Nagakura N, Souma S, Shimizu T, et al. Comparison of cross-reactivities of imipenem and other beta-lactam antibiotics by delayed-type hypersensitivity reaction in guinea pigs. Chem Pharm Bull. 1991;39:765-768.
- Bauer SL, Wall GC, Skoglund K, et al. Lack of cross-reactivity to meropenem in a patient with an allergy to imipenem-cilastatin. J Allergy Clin Immunol. 2004;113:173-175.

Joint Commission Resource Educates Patients, Hospitalists about Antibiotics
The Joint Commission has launched a new online resource for patients and hospitalists to help change mindsets and start conversations about proper antibiotic usage.
The SpeakUp: Antibiotics campaign is a package of free materials, including an infographic illustrating which illnesses may require an antibiotic, a list of questions for patients to ask when prescribed an antibiotic, a podcast, and a video reminding patients that antibiotics are not needed for colds or the flu.
“The new SpeakUp campaign provides a variety of resources to help patients and caregivers understand that how they use antibiotics today can affect how well the drugs work for them tomorrow,” says Lisa Waldowski, MS, APRN, CIC, infection control specialist at The Joint Commission.
The primary audience for these materials is the consumer, but hospitalists and healthcare workers are the crucial secondary audience. “This is a partnership; the knowledge needs to go both ways,” Waldowski says. “Sometimes there’s an expectation that when you see a physician, you are somehow shortchanged if you don’t leave with a prescription for an antibiotic.
There’s an education that needs to go on in the mindset of the physician, [in terms of] looking at whether this situation warrants an antibiotic and educating the patient if it does not. It takes time to have that conversation.”
The campaign can also provide a starting point for hospitalists to make changes in the workplace. “The information needs to be digested by everyone individually, but collectively in the organization where you work, this can lead to an antibiotic stewardship program, a coordinated intervention,” she says. She recommends a multidisciplinary approach. “Sometimes successful programs are led by a physician, and they have a strong pharmacy component, working together and supporting one another to use antibiotics appropriately.”
Visit our website for more information on antibiotic overuse.
The Joint Commission has launched a new online resource for patients and hospitalists to help change mindsets and start conversations about proper antibiotic usage.
The SpeakUp: Antibiotics campaign is a package of free materials, including an infographic illustrating which illnesses may require an antibiotic, a list of questions for patients to ask when prescribed an antibiotic, a podcast, and a video reminding patients that antibiotics are not needed for colds or the flu.
“The new SpeakUp campaign provides a variety of resources to help patients and caregivers understand that how they use antibiotics today can affect how well the drugs work for them tomorrow,” says Lisa Waldowski, MS, APRN, CIC, infection control specialist at The Joint Commission.
The primary audience for these materials is the consumer, but hospitalists and healthcare workers are the crucial secondary audience. “This is a partnership; the knowledge needs to go both ways,” Waldowski says. “Sometimes there’s an expectation that when you see a physician, you are somehow shortchanged if you don’t leave with a prescription for an antibiotic.
There’s an education that needs to go on in the mindset of the physician, [in terms of] looking at whether this situation warrants an antibiotic and educating the patient if it does not. It takes time to have that conversation.”
The campaign can also provide a starting point for hospitalists to make changes in the workplace. “The information needs to be digested by everyone individually, but collectively in the organization where you work, this can lead to an antibiotic stewardship program, a coordinated intervention,” she says. She recommends a multidisciplinary approach. “Sometimes successful programs are led by a physician, and they have a strong pharmacy component, working together and supporting one another to use antibiotics appropriately.”
Visit our website for more information on antibiotic overuse.
The Joint Commission has launched a new online resource for patients and hospitalists to help change mindsets and start conversations about proper antibiotic usage.
The SpeakUp: Antibiotics campaign is a package of free materials, including an infographic illustrating which illnesses may require an antibiotic, a list of questions for patients to ask when prescribed an antibiotic, a podcast, and a video reminding patients that antibiotics are not needed for colds or the flu.
“The new SpeakUp campaign provides a variety of resources to help patients and caregivers understand that how they use antibiotics today can affect how well the drugs work for them tomorrow,” says Lisa Waldowski, MS, APRN, CIC, infection control specialist at The Joint Commission.
The primary audience for these materials is the consumer, but hospitalists and healthcare workers are the crucial secondary audience. “This is a partnership; the knowledge needs to go both ways,” Waldowski says. “Sometimes there’s an expectation that when you see a physician, you are somehow shortchanged if you don’t leave with a prescription for an antibiotic.
There’s an education that needs to go on in the mindset of the physician, [in terms of] looking at whether this situation warrants an antibiotic and educating the patient if it does not. It takes time to have that conversation.”
The campaign can also provide a starting point for hospitalists to make changes in the workplace. “The information needs to be digested by everyone individually, but collectively in the organization where you work, this can lead to an antibiotic stewardship program, a coordinated intervention,” she says. She recommends a multidisciplinary approach. “Sometimes successful programs are led by a physician, and they have a strong pharmacy component, working together and supporting one another to use antibiotics appropriately.”
Visit our website for more information on antibiotic overuse.
Medicare Tests New Quality Measure: Readmission Rates for Heart Failure
The Centers for Medicare & Medicaid Services (CMS) has wrapped up a test run of a new measure for readmission of heart failure patients as the federal agency tries to educate hospitals and hospitalists before formally including it as a quality metric in fiscal year 2018.
The trial concludes October 7, 2015, for the new claims-based measurement, excess days in acute care (EDAC) after hospitalization for heart failure. It captures the number of days within the 30-day postdischarge period that a patient spends in acute care following an index admission for heart failure. The measure will be included in CMS’ Hospital Inpatient Quality Reporting Program in fiscal year 2018, but the agency plans to publicly report hospitals’ results on Hospital Compare next year.
CMS hopes the new measure will help educate hospitals and hospitalists about 30-day postdischarge outcomes for patients with heart failure and provide a better understanding of what services are utilized, which could translate to better interventions. CMS spokesperson Alper Ozinal says that hospitalists currently get “little feedback about what happens to their patients after discharge.”
“CMS found substantial variation in utilization across hospitals, which suggests an opportunity for improvement in transitional care practices,” Ozinal says. “CMS anticipates that the measure will support hospital efforts to further optimize quality of care, particularly the quality of transitional care, by providing a more comprehensive picture of postdischarge events.”
The measure’s trial run, which began September 8, 2015, measured Medicare fee-for-service patients age 65 and older who were hospitalized with a principal discharge diagnosis of heart failure. The outcomes are risk-adjusted, taking into account age, sex, and comorbidities.
Once the results are calculated, CMS will post a report on the QualityNet website. Comments are welcome as CMS is expected to discuss whether tweaks are needed in the measure’s methodology.
Visit our website for more information on hospital readmissions.
The Centers for Medicare & Medicaid Services (CMS) has wrapped up a test run of a new measure for readmission of heart failure patients as the federal agency tries to educate hospitals and hospitalists before formally including it as a quality metric in fiscal year 2018.
The trial concludes October 7, 2015, for the new claims-based measurement, excess days in acute care (EDAC) after hospitalization for heart failure. It captures the number of days within the 30-day postdischarge period that a patient spends in acute care following an index admission for heart failure. The measure will be included in CMS’ Hospital Inpatient Quality Reporting Program in fiscal year 2018, but the agency plans to publicly report hospitals’ results on Hospital Compare next year.
CMS hopes the new measure will help educate hospitals and hospitalists about 30-day postdischarge outcomes for patients with heart failure and provide a better understanding of what services are utilized, which could translate to better interventions. CMS spokesperson Alper Ozinal says that hospitalists currently get “little feedback about what happens to their patients after discharge.”
“CMS found substantial variation in utilization across hospitals, which suggests an opportunity for improvement in transitional care practices,” Ozinal says. “CMS anticipates that the measure will support hospital efforts to further optimize quality of care, particularly the quality of transitional care, by providing a more comprehensive picture of postdischarge events.”
The measure’s trial run, which began September 8, 2015, measured Medicare fee-for-service patients age 65 and older who were hospitalized with a principal discharge diagnosis of heart failure. The outcomes are risk-adjusted, taking into account age, sex, and comorbidities.
Once the results are calculated, CMS will post a report on the QualityNet website. Comments are welcome as CMS is expected to discuss whether tweaks are needed in the measure’s methodology.
Visit our website for more information on hospital readmissions.
The Centers for Medicare & Medicaid Services (CMS) has wrapped up a test run of a new measure for readmission of heart failure patients as the federal agency tries to educate hospitals and hospitalists before formally including it as a quality metric in fiscal year 2018.
The trial concludes October 7, 2015, for the new claims-based measurement, excess days in acute care (EDAC) after hospitalization for heart failure. It captures the number of days within the 30-day postdischarge period that a patient spends in acute care following an index admission for heart failure. The measure will be included in CMS’ Hospital Inpatient Quality Reporting Program in fiscal year 2018, but the agency plans to publicly report hospitals’ results on Hospital Compare next year.
CMS hopes the new measure will help educate hospitals and hospitalists about 30-day postdischarge outcomes for patients with heart failure and provide a better understanding of what services are utilized, which could translate to better interventions. CMS spokesperson Alper Ozinal says that hospitalists currently get “little feedback about what happens to their patients after discharge.”
“CMS found substantial variation in utilization across hospitals, which suggests an opportunity for improvement in transitional care practices,” Ozinal says. “CMS anticipates that the measure will support hospital efforts to further optimize quality of care, particularly the quality of transitional care, by providing a more comprehensive picture of postdischarge events.”
The measure’s trial run, which began September 8, 2015, measured Medicare fee-for-service patients age 65 and older who were hospitalized with a principal discharge diagnosis of heart failure. The outcomes are risk-adjusted, taking into account age, sex, and comorbidities.
Once the results are calculated, CMS will post a report on the QualityNet website. Comments are welcome as CMS is expected to discuss whether tweaks are needed in the measure’s methodology.
Visit our website for more information on hospital readmissions.
Billing, Coding Documentation to Support Services, Minimize Risks

The electronic health record (EHR) has many benefits:
- Improved patient care;
- Improved care coordination;
- Improved diagnostics and patient outcomes;
- Increased patient participation; and
- Increased practice efficiencies and cost savings.1
EHRs also introduce risks, however. Heightened concern about EHR misuse and vulnerability elevates the level of scrutiny placed on provider documentation as it relates to billing and coding. Without clear guidelines from the Centers for Medicare and Medicaid Services (CMS) or other payers, the potential for unintentional misapplication exists. Auditor misinterpretation is also possible. Providers should utilize simple defensive documentation principles to support their services and minimize their risks.
Reason for Encounter
Under section 1862 (a)(1)(A) of the Social Security Act, the Medicare Program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).2
A payer can determine if a service is “reasonable and necessary” based on the service indication. The reason for the patient encounter, otherwise known as the chief complaint, must be evident. This can be a symptom, problem, condition, diagnosis, physician-recommended return, or another factor that necessitates the encounter.1 It cannot be inferred and must be clearly stated in the documentation. Without it, a payer may question the medical necessity of the service, especially if it involves hospital-based services in the course of which multiple specialists will see the patient on any given date. Payers are likely to deny services that cannot be easily differentiated (e.g. “no c/o”). Furthermore, payers can deny concurrent care services for the following reasons:3
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate/overlap those of the other provider without any recognizable distinction.
Providers should be specific in identifying the encounter reason, as in the following examples: “Patient seen for shortness of breath” or “Patient with COPD, feeling improved with 3L O2 NC.”
Assessment and Plan
Accurately representing patient complexity for every visit throughout the hospitalization presents its challenges. Although the problem list may not dramatically change day to day, providers must formulate an assessment of the patient’s condition with a corresponding plan of care for each encounter. Documenting problems without a corresponding plan of care does not substantiate physician participation in the management of that problem. Providing a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) minimizes the complexity and effort put forth in the encounter and could result in auditor downgrading upon documentation review.
Developing shortcuts might falsely minimize the provider’s documentation burden. An electronic documentation system might make it possible to copy previous progress notes into the current encounter to save time; however, the previously entered information could include elements that do not require reassessment during a subsequent encounter or contain information about conditions that are being managed concurrently by another specialist (e.g. CKD being managed by the nephrologist). Leaving the copied information unmodified may not accurately reflect the patient’s current condition or the care provided by the hospitalist during the current encounter. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care relevant to that date.
According to the Office of Inspector General (OIG), “inappropriate copy-pasting could facilitate attempts to inflate claims and duplicate or create fraudulent claims.”4
An equally problematic EHR function involves “overdocumentation,” the practice of inserting false or irrelevant documentation to create the appearance of support for billing higher level services.4 EHR technology has the ability to auto-populate fields using templates built into the system or generate extensive documentation on the basis of a single click. The OIG cautions providers to use these features carefully, because they can produce information suggesting the practitioner performed more comprehensive services than were actually rendered.4
An example is the inclusion of the same lab results more than once. Although clinicians include this information as a reference to avoid having to “find it somewhere in the chart” when it is needed—as a basis for comparison, for example—auditors mistake this as an attempt to gain credit for the daily review of the same “old” information. Including only relevant data will mitigate this concern.
Authorship
Dates and signatures are essential to each encounter. Medicare requires services provided/ordered to be authenticated by the author.5 A reviewer must be able to identify each individual who performs, documents, and bills for a service on a given date. Progress notes that fail to identify the service date or service provider will likely result in denial.
Additionally, a service is questioned when two different sets of handwriting appear on a note, yet only one signature is provided. Since the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Notes that contain an illegible signature are equally problematic. If the legibility of the signature prevents the reviewer from correctly identifying the rendering provider, the service may be denied.
CMS has instructed Medicare contractors to request a signed provider attestation before issuing a denial.5 The provider should print his/her name beside the signature or include a separate signature sheet with the requested documentation to assist the reviewer in provider identification. Stamped signatures are not acceptable under any circumstance. Medicare accepts only handwritten or electronic signatures.5
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- HealthIT.gov. Benefits of electronic health records (EHRs). Accessed August 1, 2015.
- Social Security Administration. Exclusions from coverage and Medicare as secondary payer. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15—Covered medical and other health services. Chapter 15, Section 30.E. Concurrent care. Accessed August 1, 2015.
- Department of Health and Human Services. Office of Inspector General. CMS and its contractors have adopted few program integrity practices to address vulnerabilities in EHRs. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Signature guidelines for medical review purposes. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. 1995 documentation guidelines for evaluation and management services. Accessed August 1, 2015.
The electronic health record (EHR) has many benefits:
- Improved patient care;
- Improved care coordination;
- Improved diagnostics and patient outcomes;
- Increased patient participation; and
- Increased practice efficiencies and cost savings.1
EHRs also introduce risks, however. Heightened concern about EHR misuse and vulnerability elevates the level of scrutiny placed on provider documentation as it relates to billing and coding. Without clear guidelines from the Centers for Medicare and Medicaid Services (CMS) or other payers, the potential for unintentional misapplication exists. Auditor misinterpretation is also possible. Providers should utilize simple defensive documentation principles to support their services and minimize their risks.
Reason for Encounter
Under section 1862 (a)(1)(A) of the Social Security Act, the Medicare Program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).2
A payer can determine if a service is “reasonable and necessary” based on the service indication. The reason for the patient encounter, otherwise known as the chief complaint, must be evident. This can be a symptom, problem, condition, diagnosis, physician-recommended return, or another factor that necessitates the encounter.1 It cannot be inferred and must be clearly stated in the documentation. Without it, a payer may question the medical necessity of the service, especially if it involves hospital-based services in the course of which multiple specialists will see the patient on any given date. Payers are likely to deny services that cannot be easily differentiated (e.g. “no c/o”). Furthermore, payers can deny concurrent care services for the following reasons:3
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate/overlap those of the other provider without any recognizable distinction.
Providers should be specific in identifying the encounter reason, as in the following examples: “Patient seen for shortness of breath” or “Patient with COPD, feeling improved with 3L O2 NC.”
Assessment and Plan
Accurately representing patient complexity for every visit throughout the hospitalization presents its challenges. Although the problem list may not dramatically change day to day, providers must formulate an assessment of the patient’s condition with a corresponding plan of care for each encounter. Documenting problems without a corresponding plan of care does not substantiate physician participation in the management of that problem. Providing a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) minimizes the complexity and effort put forth in the encounter and could result in auditor downgrading upon documentation review.
Developing shortcuts might falsely minimize the provider’s documentation burden. An electronic documentation system might make it possible to copy previous progress notes into the current encounter to save time; however, the previously entered information could include elements that do not require reassessment during a subsequent encounter or contain information about conditions that are being managed concurrently by another specialist (e.g. CKD being managed by the nephrologist). Leaving the copied information unmodified may not accurately reflect the patient’s current condition or the care provided by the hospitalist during the current encounter. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care relevant to that date.
According to the Office of Inspector General (OIG), “inappropriate copy-pasting could facilitate attempts to inflate claims and duplicate or create fraudulent claims.”4
An equally problematic EHR function involves “overdocumentation,” the practice of inserting false or irrelevant documentation to create the appearance of support for billing higher level services.4 EHR technology has the ability to auto-populate fields using templates built into the system or generate extensive documentation on the basis of a single click. The OIG cautions providers to use these features carefully, because they can produce information suggesting the practitioner performed more comprehensive services than were actually rendered.4
An example is the inclusion of the same lab results more than once. Although clinicians include this information as a reference to avoid having to “find it somewhere in the chart” when it is needed—as a basis for comparison, for example—auditors mistake this as an attempt to gain credit for the daily review of the same “old” information. Including only relevant data will mitigate this concern.
Authorship
Dates and signatures are essential to each encounter. Medicare requires services provided/ordered to be authenticated by the author.5 A reviewer must be able to identify each individual who performs, documents, and bills for a service on a given date. Progress notes that fail to identify the service date or service provider will likely result in denial.
Additionally, a service is questioned when two different sets of handwriting appear on a note, yet only one signature is provided. Since the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Notes that contain an illegible signature are equally problematic. If the legibility of the signature prevents the reviewer from correctly identifying the rendering provider, the service may be denied.
CMS has instructed Medicare contractors to request a signed provider attestation before issuing a denial.5 The provider should print his/her name beside the signature or include a separate signature sheet with the requested documentation to assist the reviewer in provider identification. Stamped signatures are not acceptable under any circumstance. Medicare accepts only handwritten or electronic signatures.5
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- HealthIT.gov. Benefits of electronic health records (EHRs). Accessed August 1, 2015.
- Social Security Administration. Exclusions from coverage and Medicare as secondary payer. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15—Covered medical and other health services. Chapter 15, Section 30.E. Concurrent care. Accessed August 1, 2015.
- Department of Health and Human Services. Office of Inspector General. CMS and its contractors have adopted few program integrity practices to address vulnerabilities in EHRs. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Signature guidelines for medical review purposes. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. 1995 documentation guidelines for evaluation and management services. Accessed August 1, 2015.
The electronic health record (EHR) has many benefits:
- Improved patient care;
- Improved care coordination;
- Improved diagnostics and patient outcomes;
- Increased patient participation; and
- Increased practice efficiencies and cost savings.1
EHRs also introduce risks, however. Heightened concern about EHR misuse and vulnerability elevates the level of scrutiny placed on provider documentation as it relates to billing and coding. Without clear guidelines from the Centers for Medicare and Medicaid Services (CMS) or other payers, the potential for unintentional misapplication exists. Auditor misinterpretation is also possible. Providers should utilize simple defensive documentation principles to support their services and minimize their risks.
Reason for Encounter
Under section 1862 (a)(1)(A) of the Social Security Act, the Medicare Program may only pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g. colorectal cancer screening).2
A payer can determine if a service is “reasonable and necessary” based on the service indication. The reason for the patient encounter, otherwise known as the chief complaint, must be evident. This can be a symptom, problem, condition, diagnosis, physician-recommended return, or another factor that necessitates the encounter.1 It cannot be inferred and must be clearly stated in the documentation. Without it, a payer may question the medical necessity of the service, especially if it involves hospital-based services in the course of which multiple specialists will see the patient on any given date. Payers are likely to deny services that cannot be easily differentiated (e.g. “no c/o”). Furthermore, payers can deny concurrent care services for the following reasons:3
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate/overlap those of the other provider without any recognizable distinction.
Providers should be specific in identifying the encounter reason, as in the following examples: “Patient seen for shortness of breath” or “Patient with COPD, feeling improved with 3L O2 NC.”
Assessment and Plan
Accurately representing patient complexity for every visit throughout the hospitalization presents its challenges. Although the problem list may not dramatically change day to day, providers must formulate an assessment of the patient’s condition with a corresponding plan of care for each encounter. Documenting problems without a corresponding plan of care does not substantiate physician participation in the management of that problem. Providing a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) minimizes the complexity and effort put forth in the encounter and could result in auditor downgrading upon documentation review.
Developing shortcuts might falsely minimize the provider’s documentation burden. An electronic documentation system might make it possible to copy previous progress notes into the current encounter to save time; however, the previously entered information could include elements that do not require reassessment during a subsequent encounter or contain information about conditions that are being managed concurrently by another specialist (e.g. CKD being managed by the nephrologist). Leaving the copied information unmodified may not accurately reflect the patient’s current condition or the care provided by the hospitalist during the current encounter. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care relevant to that date.
According to the Office of Inspector General (OIG), “inappropriate copy-pasting could facilitate attempts to inflate claims and duplicate or create fraudulent claims.”4
An equally problematic EHR function involves “overdocumentation,” the practice of inserting false or irrelevant documentation to create the appearance of support for billing higher level services.4 EHR technology has the ability to auto-populate fields using templates built into the system or generate extensive documentation on the basis of a single click. The OIG cautions providers to use these features carefully, because they can produce information suggesting the practitioner performed more comprehensive services than were actually rendered.4
An example is the inclusion of the same lab results more than once. Although clinicians include this information as a reference to avoid having to “find it somewhere in the chart” when it is needed—as a basis for comparison, for example—auditors mistake this as an attempt to gain credit for the daily review of the same “old” information. Including only relevant data will mitigate this concern.
Authorship
Dates and signatures are essential to each encounter. Medicare requires services provided/ordered to be authenticated by the author.5 A reviewer must be able to identify each individual who performs, documents, and bills for a service on a given date. Progress notes that fail to identify the service date or service provider will likely result in denial.
Additionally, a service is questioned when two different sets of handwriting appear on a note, yet only one signature is provided. Since the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Notes that contain an illegible signature are equally problematic. If the legibility of the signature prevents the reviewer from correctly identifying the rendering provider, the service may be denied.
CMS has instructed Medicare contractors to request a signed provider attestation before issuing a denial.5 The provider should print his/her name beside the signature or include a separate signature sheet with the requested documentation to assist the reviewer in provider identification. Stamped signatures are not acceptable under any circumstance. Medicare accepts only handwritten or electronic signatures.5
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- HealthIT.gov. Benefits of electronic health records (EHRs). Accessed August 1, 2015.
- Social Security Administration. Exclusions from coverage and Medicare as secondary payer. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15—Covered medical and other health services. Chapter 15, Section 30.E. Concurrent care. Accessed August 1, 2015.
- Department of Health and Human Services. Office of Inspector General. CMS and its contractors have adopted few program integrity practices to address vulnerabilities in EHRs. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. Signature guidelines for medical review purposes. Accessed August 1, 2015.
- Centers for Medicare and Medicaid Services. 1995 documentation guidelines for evaluation and management services. Accessed August 1, 2015.
Do we need lower extremity physiologic studies in the age of duplex scanners?
Lower-Extremity Physiologic Studies Are No Longer Required – Wrong!
Okay Gene, consider an example from the cardiology world.
You walk up a flight of stairs and develop chest pain. Is it angina? If subsequent coronary catheterization reveals a 60% stenosis in your proximal right coronary artery, then you have an anatomic coronary lesion. But is this lesion causing angina? Maybe. If the catheter is pushed across the stenosis and a 12mm Hg resting pressure gradient is identified, the lesion also has hemodynamic significance. But is it causing angina? Possibly.

To clarify things, a functional study is necessary; specifically, you need to stress the heart (using treadmill exercise, biking, infusion of a catecholamine, etc.) and determine the subsequent cardiac response (pain, ECG changes, wall motion abnormalities, sestamibi/thallium uptake, etc.). If stress produces an abnormal cardiac response, does that mean you have angina? Probably.
Yes, it’s so simple a cardiologist can get it. Yet many vascular specialists seem to struggle with the concept that anatomic, hemodynamic, and functional tests provide different types of information about the arterial system. These tests are complimentary; when used properly they combine to yield information that no single test can provide. But the siren song of an image is hard to resist – after all, everyone loves pictures, and Duplex provides nice ones. With imaging, you can scan for aneurysms. You can see what plaque looks like. In some instances you can even perform operations or procedures solely on the basis of Duplex scanning. What more do you need? (Insert my sarcastic sneer here, Gene.)
Duplex even provides basic hemodynamic information about specific lesions (based on blood flow velocity changes across the lesion). However, it’s a mistake to think that hemodynamic changes across a particular lesion tell us much about the overall “hemodynamics” in a limb. Major arteries may be narrowed (or even completely occluded), but if the collateral vessels are good, the resulting hemodynamic compromise may be minimal. Unfortunately, Duplex scanning is relatively poor at identifying and assessing collateral flow. Tests like segmental pressures (and the ankle-brachial index, or ABI) often provide a better assessment of overall arterial status because the adequacy of collateral flow influences (and is reflected in) distal blood pressure measurements. It’s also naive to think that Duplex is the only means for noninvasively obtaining anatomic information about arterial disease; nonimaging tests using segmental pressures, multilevel pulse-volume recordings (PVRs), continuous-wave (CW) Doppler, etc. may not produce pretty pictures, but they can still localize arterial lesions to a particular anatomic level (aortoiliac vs. femoral-popliteal vs. infrapopliteal, etc.).
The combination of hemodynamic and functional testing is typically referred to as “physiologic” testing, but there’s much more to this than just CW Dopplerand pneumatic cuffs. Specific tests using Laser-Doppler to measure skin blood flow or microvascular perfusion pressure make it possible to (physiologically) assess the microcirculation. Transcutaneous Oxygen (TcPO2) measurement is available in many labs; this test provides valuable physiological information about skin viability and healing potential.
Where Duplex scanning meets its biggest challenge is in the area of functional testing. Yes, it’s possible to exercise the legs and identify subsequent flow (velocity) changes across certain lesions or vessels, but any seasoned sonographer knows that these studies are extremely difficult and time consuming. And because they typically can’t assess/account for collateral flow, they are often of questionable value for determining the adverse impact of arterial disease on the patient. In contrast, functional (exercise) studies performed with CW Doppler and air cuffs are simple, inexpensive, reliable, reproducible, and widely applicable.
Bottom line – physiologic studies are an indispensable part of noninvasive arterial testing and will certainly remain so. For any given patient, they are essential for identifying and quantifying the scope and impact of arterial disease. For populations, they are the test of choice for arterial screening. And, from a practical standpoint, they are required for IAC [intersocietal accreditation commission] laboratory accreditation in peripheral arterial testing (as you know, Duplex scanning is optional for arterial accreditation – but physiologic studies are mandatory!)
Finally, the same characteristics that make physiologic tests important for assessing arterial disease are equally – or perhaps even more – relevant for the assessment of venous disease, but the application of this approach remains in its infancy. It’s a good topic for another discussion.
Dr. Rooke is the Krehbiel Professor of Vascular Medicine at the Mayo Clinic, Rochester, Minn. He has no relevant conflicts.
Lower-Extremity Physiologic Studies Are No Longer Required – Yes ... Maybe!
My friend, Thom, makes a strong case for the value of physiologic studies in patients with lower extremity arterial disease – so strong, in fact, that one might wonder if there is any truly cogent “counterpoint” at all. To provide some perspective on this issue, let’s take a look back to see how this field started and consider why someone would even dare make the statement that is being debated here.
When clinical vascular laboratories appeared in the late 1960s, the concept of “nondestructive” or “noninvasive” testing was a novelty that was not widely accepted. The first vascular laboratory tests for the assessment of carotid, peripheral arterial, and venous disease were described as “indirect,” because they relied on detection of the physiologic alterations produced by vascular abnormalities.

These methods included the supraorbital Doppler examination and oculoplethysmography for carotid disease, ankle-brachial indices, segmental pressures, and pulse volume recordings for peripheral arterial disease, and the CW Doppler examination and impedance plethysmography for venous obstruction. In those early days, vascular testing was limited to some vascular surgery practices and physiology laboratories.
While these indirect physiologic tests were helpful for characterizing regional hemodynamics, they did not provide the detailed anatomic information on arterial lesions that vascular surgeons needed to plan treatment. It was not until direct ultrasound imaging of blood vessels became available in the late 1970s and early 1980s that interest in the non-invasive vascular laboratory increased. The “duplex concept” of combining B-mode imaging with Doppler flow detection appeared to overcome the major limitations of the indirect tests by providing two-dimensional images of an arterial lesion along with an assessment of the associated flow patterns – anatomy and hemodynamics – the best of both testing worlds.
The capabilities of duplex ultrasound were so impressive that direct duplex scanning rapidly replaced the indirect or physiologic tests for diagnosis of extracranial carotid disease and lower extremity deep venous thrombosis. But, as Thom points out, peripheral arterial disease is the only testing area in which physiologic studies are still considered as “primary” testing methods according to the IAC Standards and Guidelines for Vascular Testing Accreditation. So the challenge for the modern vascular laboratory is to determine which test to use and how to integrate physiologic testing and duplex scanning in the evaluation of patients with known or suspected peripheral arterial disease.
The clinical role of the vascular laboratory can be divided into the categories of screening, diagnosis, and follow-up. The merits of screening for peripheral arterial disease are beyond the scope of this debate, but screening tests must be safe, inexpensive, and capable of detecting the presence or absence of disease. Clearly, physiologic tests meet these requirements, and in most situations, an ankle-brachial index is all that is needed. Diagnostic testing in patients with signs and symptoms of peripheral arterial disease, including those that may be candidates for intervention, requires the specific anatomic and hemodynamic information that duplex scanning provides, but functional testing (i.e., treadmill exercise) can also be valuable in selected cases. Similarly, follow-up of peripheral arterial interventions usually requires duplex scanning to evaluate the anatomic and hemodynamic features of the treated arterial segment, while follow-up of documented but untreated peripheral arterial disease can often be accomplished primarily by physiologic tests alone.
Are lower-extremity physiologic studies no longer required in the age of modern duplex scanners? Although I am reluctant to admit it, strictly speaking, my friend, Thom, is correct when he responds with an emphatic “Wrong.” There is no reason to completely abandon the physiologic tests that have served us well since before the age of duplex scanning. A simple ankle-brachial index is easy to justify as part of almost any lower extremity arterial evaluation, and exercise treadmill testing is an excellent way to assess the functional status of a patient with peripheral arterial disease. However, vascular laboratories should consider how best to combine the use of physiologic testing and direct duplex imaging for peripheral arterial disease in order to avoid unnecessary or inappropriate testing. For most vascular laboratories, this means that initial screening should be done with physiologic tests, but the primary testing method for diagnosis and follow-up will be duplex scanning, supplemented by selective use of physiologic testing.
Dr. Zierler is professor of surgery at the University of Washington and medical director of the D.E. Strandness Jr. Vascular Laboratory at the University of Washington Medical Center and Harborview Medical Center, Seattle. He has no relevant conflicts.
Lower-Extremity Physiologic Studies Are No Longer Required – Wrong!
Okay Gene, consider an example from the cardiology world.
You walk up a flight of stairs and develop chest pain. Is it angina? If subsequent coronary catheterization reveals a 60% stenosis in your proximal right coronary artery, then you have an anatomic coronary lesion. But is this lesion causing angina? Maybe. If the catheter is pushed across the stenosis and a 12mm Hg resting pressure gradient is identified, the lesion also has hemodynamic significance. But is it causing angina? Possibly.
To clarify things, a functional study is necessary; specifically, you need to stress the heart (using treadmill exercise, biking, infusion of a catecholamine, etc.) and determine the subsequent cardiac response (pain, ECG changes, wall motion abnormalities, sestamibi/thallium uptake, etc.). If stress produces an abnormal cardiac response, does that mean you have angina? Probably.
Yes, it’s so simple a cardiologist can get it. Yet many vascular specialists seem to struggle with the concept that anatomic, hemodynamic, and functional tests provide different types of information about the arterial system. These tests are complimentary; when used properly they combine to yield information that no single test can provide. But the siren song of an image is hard to resist – after all, everyone loves pictures, and Duplex provides nice ones. With imaging, you can scan for aneurysms. You can see what plaque looks like. In some instances you can even perform operations or procedures solely on the basis of Duplex scanning. What more do you need? (Insert my sarcastic sneer here, Gene.)
Duplex even provides basic hemodynamic information about specific lesions (based on blood flow velocity changes across the lesion). However, it’s a mistake to think that hemodynamic changes across a particular lesion tell us much about the overall “hemodynamics” in a limb. Major arteries may be narrowed (or even completely occluded), but if the collateral vessels are good, the resulting hemodynamic compromise may be minimal. Unfortunately, Duplex scanning is relatively poor at identifying and assessing collateral flow. Tests like segmental pressures (and the ankle-brachial index, or ABI) often provide a better assessment of overall arterial status because the adequacy of collateral flow influences (and is reflected in) distal blood pressure measurements. It’s also naive to think that Duplex is the only means for noninvasively obtaining anatomic information about arterial disease; nonimaging tests using segmental pressures, multilevel pulse-volume recordings (PVRs), continuous-wave (CW) Doppler, etc. may not produce pretty pictures, but they can still localize arterial lesions to a particular anatomic level (aortoiliac vs. femoral-popliteal vs. infrapopliteal, etc.).
The combination of hemodynamic and functional testing is typically referred to as “physiologic” testing, but there’s much more to this than just CW Dopplerand pneumatic cuffs. Specific tests using Laser-Doppler to measure skin blood flow or microvascular perfusion pressure make it possible to (physiologically) assess the microcirculation. Transcutaneous Oxygen (TcPO2) measurement is available in many labs; this test provides valuable physiological information about skin viability and healing potential.
Where Duplex scanning meets its biggest challenge is in the area of functional testing. Yes, it’s possible to exercise the legs and identify subsequent flow (velocity) changes across certain lesions or vessels, but any seasoned sonographer knows that these studies are extremely difficult and time consuming. And because they typically can’t assess/account for collateral flow, they are often of questionable value for determining the adverse impact of arterial disease on the patient. In contrast, functional (exercise) studies performed with CW Doppler and air cuffs are simple, inexpensive, reliable, reproducible, and widely applicable.
Bottom line – physiologic studies are an indispensable part of noninvasive arterial testing and will certainly remain so. For any given patient, they are essential for identifying and quantifying the scope and impact of arterial disease. For populations, they are the test of choice for arterial screening. And, from a practical standpoint, they are required for IAC [intersocietal accreditation commission] laboratory accreditation in peripheral arterial testing (as you know, Duplex scanning is optional for arterial accreditation – but physiologic studies are mandatory!)
Finally, the same characteristics that make physiologic tests important for assessing arterial disease are equally – or perhaps even more – relevant for the assessment of venous disease, but the application of this approach remains in its infancy. It’s a good topic for another discussion.
Dr. Rooke is the Krehbiel Professor of Vascular Medicine at the Mayo Clinic, Rochester, Minn. He has no relevant conflicts.
Lower-Extremity Physiologic Studies Are No Longer Required – Yes ... Maybe!
My friend, Thom, makes a strong case for the value of physiologic studies in patients with lower extremity arterial disease – so strong, in fact, that one might wonder if there is any truly cogent “counterpoint” at all. To provide some perspective on this issue, let’s take a look back to see how this field started and consider why someone would even dare make the statement that is being debated here.
When clinical vascular laboratories appeared in the late 1960s, the concept of “nondestructive” or “noninvasive” testing was a novelty that was not widely accepted. The first vascular laboratory tests for the assessment of carotid, peripheral arterial, and venous disease were described as “indirect,” because they relied on detection of the physiologic alterations produced by vascular abnormalities.
These methods included the supraorbital Doppler examination and oculoplethysmography for carotid disease, ankle-brachial indices, segmental pressures, and pulse volume recordings for peripheral arterial disease, and the CW Doppler examination and impedance plethysmography for venous obstruction. In those early days, vascular testing was limited to some vascular surgery practices and physiology laboratories.
While these indirect physiologic tests were helpful for characterizing regional hemodynamics, they did not provide the detailed anatomic information on arterial lesions that vascular surgeons needed to plan treatment. It was not until direct ultrasound imaging of blood vessels became available in the late 1970s and early 1980s that interest in the non-invasive vascular laboratory increased. The “duplex concept” of combining B-mode imaging with Doppler flow detection appeared to overcome the major limitations of the indirect tests by providing two-dimensional images of an arterial lesion along with an assessment of the associated flow patterns – anatomy and hemodynamics – the best of both testing worlds.
The capabilities of duplex ultrasound were so impressive that direct duplex scanning rapidly replaced the indirect or physiologic tests for diagnosis of extracranial carotid disease and lower extremity deep venous thrombosis. But, as Thom points out, peripheral arterial disease is the only testing area in which physiologic studies are still considered as “primary” testing methods according to the IAC Standards and Guidelines for Vascular Testing Accreditation. So the challenge for the modern vascular laboratory is to determine which test to use and how to integrate physiologic testing and duplex scanning in the evaluation of patients with known or suspected peripheral arterial disease.
The clinical role of the vascular laboratory can be divided into the categories of screening, diagnosis, and follow-up. The merits of screening for peripheral arterial disease are beyond the scope of this debate, but screening tests must be safe, inexpensive, and capable of detecting the presence or absence of disease. Clearly, physiologic tests meet these requirements, and in most situations, an ankle-brachial index is all that is needed. Diagnostic testing in patients with signs and symptoms of peripheral arterial disease, including those that may be candidates for intervention, requires the specific anatomic and hemodynamic information that duplex scanning provides, but functional testing (i.e., treadmill exercise) can also be valuable in selected cases. Similarly, follow-up of peripheral arterial interventions usually requires duplex scanning to evaluate the anatomic and hemodynamic features of the treated arterial segment, while follow-up of documented but untreated peripheral arterial disease can often be accomplished primarily by physiologic tests alone.
Are lower-extremity physiologic studies no longer required in the age of modern duplex scanners? Although I am reluctant to admit it, strictly speaking, my friend, Thom, is correct when he responds with an emphatic “Wrong.” There is no reason to completely abandon the physiologic tests that have served us well since before the age of duplex scanning. A simple ankle-brachial index is easy to justify as part of almost any lower extremity arterial evaluation, and exercise treadmill testing is an excellent way to assess the functional status of a patient with peripheral arterial disease. However, vascular laboratories should consider how best to combine the use of physiologic testing and direct duplex imaging for peripheral arterial disease in order to avoid unnecessary or inappropriate testing. For most vascular laboratories, this means that initial screening should be done with physiologic tests, but the primary testing method for diagnosis and follow-up will be duplex scanning, supplemented by selective use of physiologic testing.
Dr. Zierler is professor of surgery at the University of Washington and medical director of the D.E. Strandness Jr. Vascular Laboratory at the University of Washington Medical Center and Harborview Medical Center, Seattle. He has no relevant conflicts.
Lower-Extremity Physiologic Studies Are No Longer Required – Wrong!
Okay Gene, consider an example from the cardiology world.
You walk up a flight of stairs and develop chest pain. Is it angina? If subsequent coronary catheterization reveals a 60% stenosis in your proximal right coronary artery, then you have an anatomic coronary lesion. But is this lesion causing angina? Maybe. If the catheter is pushed across the stenosis and a 12mm Hg resting pressure gradient is identified, the lesion also has hemodynamic significance. But is it causing angina? Possibly.
To clarify things, a functional study is necessary; specifically, you need to stress the heart (using treadmill exercise, biking, infusion of a catecholamine, etc.) and determine the subsequent cardiac response (pain, ECG changes, wall motion abnormalities, sestamibi/thallium uptake, etc.). If stress produces an abnormal cardiac response, does that mean you have angina? Probably.
Yes, it’s so simple a cardiologist can get it. Yet many vascular specialists seem to struggle with the concept that anatomic, hemodynamic, and functional tests provide different types of information about the arterial system. These tests are complimentary; when used properly they combine to yield information that no single test can provide. But the siren song of an image is hard to resist – after all, everyone loves pictures, and Duplex provides nice ones. With imaging, you can scan for aneurysms. You can see what plaque looks like. In some instances you can even perform operations or procedures solely on the basis of Duplex scanning. What more do you need? (Insert my sarcastic sneer here, Gene.)
Duplex even provides basic hemodynamic information about specific lesions (based on blood flow velocity changes across the lesion). However, it’s a mistake to think that hemodynamic changes across a particular lesion tell us much about the overall “hemodynamics” in a limb. Major arteries may be narrowed (or even completely occluded), but if the collateral vessels are good, the resulting hemodynamic compromise may be minimal. Unfortunately, Duplex scanning is relatively poor at identifying and assessing collateral flow. Tests like segmental pressures (and the ankle-brachial index, or ABI) often provide a better assessment of overall arterial status because the adequacy of collateral flow influences (and is reflected in) distal blood pressure measurements. It’s also naive to think that Duplex is the only means for noninvasively obtaining anatomic information about arterial disease; nonimaging tests using segmental pressures, multilevel pulse-volume recordings (PVRs), continuous-wave (CW) Doppler, etc. may not produce pretty pictures, but they can still localize arterial lesions to a particular anatomic level (aortoiliac vs. femoral-popliteal vs. infrapopliteal, etc.).
The combination of hemodynamic and functional testing is typically referred to as “physiologic” testing, but there’s much more to this than just CW Dopplerand pneumatic cuffs. Specific tests using Laser-Doppler to measure skin blood flow or microvascular perfusion pressure make it possible to (physiologically) assess the microcirculation. Transcutaneous Oxygen (TcPO2) measurement is available in many labs; this test provides valuable physiological information about skin viability and healing potential.
Where Duplex scanning meets its biggest challenge is in the area of functional testing. Yes, it’s possible to exercise the legs and identify subsequent flow (velocity) changes across certain lesions or vessels, but any seasoned sonographer knows that these studies are extremely difficult and time consuming. And because they typically can’t assess/account for collateral flow, they are often of questionable value for determining the adverse impact of arterial disease on the patient. In contrast, functional (exercise) studies performed with CW Doppler and air cuffs are simple, inexpensive, reliable, reproducible, and widely applicable.
Bottom line – physiologic studies are an indispensable part of noninvasive arterial testing and will certainly remain so. For any given patient, they are essential for identifying and quantifying the scope and impact of arterial disease. For populations, they are the test of choice for arterial screening. And, from a practical standpoint, they are required for IAC [intersocietal accreditation commission] laboratory accreditation in peripheral arterial testing (as you know, Duplex scanning is optional for arterial accreditation – but physiologic studies are mandatory!)
Finally, the same characteristics that make physiologic tests important for assessing arterial disease are equally – or perhaps even more – relevant for the assessment of venous disease, but the application of this approach remains in its infancy. It’s a good topic for another discussion.
Dr. Rooke is the Krehbiel Professor of Vascular Medicine at the Mayo Clinic, Rochester, Minn. He has no relevant conflicts.
Lower-Extremity Physiologic Studies Are No Longer Required – Yes ... Maybe!
My friend, Thom, makes a strong case for the value of physiologic studies in patients with lower extremity arterial disease – so strong, in fact, that one might wonder if there is any truly cogent “counterpoint” at all. To provide some perspective on this issue, let’s take a look back to see how this field started and consider why someone would even dare make the statement that is being debated here.
When clinical vascular laboratories appeared in the late 1960s, the concept of “nondestructive” or “noninvasive” testing was a novelty that was not widely accepted. The first vascular laboratory tests for the assessment of carotid, peripheral arterial, and venous disease were described as “indirect,” because they relied on detection of the physiologic alterations produced by vascular abnormalities.
These methods included the supraorbital Doppler examination and oculoplethysmography for carotid disease, ankle-brachial indices, segmental pressures, and pulse volume recordings for peripheral arterial disease, and the CW Doppler examination and impedance plethysmography for venous obstruction. In those early days, vascular testing was limited to some vascular surgery practices and physiology laboratories.
While these indirect physiologic tests were helpful for characterizing regional hemodynamics, they did not provide the detailed anatomic information on arterial lesions that vascular surgeons needed to plan treatment. It was not until direct ultrasound imaging of blood vessels became available in the late 1970s and early 1980s that interest in the non-invasive vascular laboratory increased. The “duplex concept” of combining B-mode imaging with Doppler flow detection appeared to overcome the major limitations of the indirect tests by providing two-dimensional images of an arterial lesion along with an assessment of the associated flow patterns – anatomy and hemodynamics – the best of both testing worlds.
The capabilities of duplex ultrasound were so impressive that direct duplex scanning rapidly replaced the indirect or physiologic tests for diagnosis of extracranial carotid disease and lower extremity deep venous thrombosis. But, as Thom points out, peripheral arterial disease is the only testing area in which physiologic studies are still considered as “primary” testing methods according to the IAC Standards and Guidelines for Vascular Testing Accreditation. So the challenge for the modern vascular laboratory is to determine which test to use and how to integrate physiologic testing and duplex scanning in the evaluation of patients with known or suspected peripheral arterial disease.
The clinical role of the vascular laboratory can be divided into the categories of screening, diagnosis, and follow-up. The merits of screening for peripheral arterial disease are beyond the scope of this debate, but screening tests must be safe, inexpensive, and capable of detecting the presence or absence of disease. Clearly, physiologic tests meet these requirements, and in most situations, an ankle-brachial index is all that is needed. Diagnostic testing in patients with signs and symptoms of peripheral arterial disease, including those that may be candidates for intervention, requires the specific anatomic and hemodynamic information that duplex scanning provides, but functional testing (i.e., treadmill exercise) can also be valuable in selected cases. Similarly, follow-up of peripheral arterial interventions usually requires duplex scanning to evaluate the anatomic and hemodynamic features of the treated arterial segment, while follow-up of documented but untreated peripheral arterial disease can often be accomplished primarily by physiologic tests alone.
Are lower-extremity physiologic studies no longer required in the age of modern duplex scanners? Although I am reluctant to admit it, strictly speaking, my friend, Thom, is correct when he responds with an emphatic “Wrong.” There is no reason to completely abandon the physiologic tests that have served us well since before the age of duplex scanning. A simple ankle-brachial index is easy to justify as part of almost any lower extremity arterial evaluation, and exercise treadmill testing is an excellent way to assess the functional status of a patient with peripheral arterial disease. However, vascular laboratories should consider how best to combine the use of physiologic testing and direct duplex imaging for peripheral arterial disease in order to avoid unnecessary or inappropriate testing. For most vascular laboratories, this means that initial screening should be done with physiologic tests, but the primary testing method for diagnosis and follow-up will be duplex scanning, supplemented by selective use of physiologic testing.
Dr. Zierler is professor of surgery at the University of Washington and medical director of the D.E. Strandness Jr. Vascular Laboratory at the University of Washington Medical Center and Harborview Medical Center, Seattle. He has no relevant conflicts.
