User login
Targeting a protein to improve AML treatment
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
Donor’s lack of sleep may impact HSCT

Sleep-deprived mice make poor donors for hematopoietic stem cell transplants (HSCTs), according to a study published in Nature Communications.
The research showed that a sleep deficit of just 4 hours can reduce—by more than 50%—the ability of HSCs to engraft and reconstitute the blood and bone marrow of an irradiated recipient mouse.
Researchers believe these findings may also apply to humans.
“Considering how little attention we typically pay to sleep in the hospital setting, this finding is troubling,” said study author Asya Rolls, PhD, of Technion–Israel Institute of Technology in Haifa.
“We go to all this trouble to find a matching donor, but this research suggests that, if the donor is not well-rested, it can impact the outcome of the transplantation. However, it’s heartening to think that this is not an insurmountable obstacle. A short period of recovery sleep before transplant can restore the donor’s cells’ ability to function normally.”
Dr Rolls and her colleagues studied mice that had been gently handled for 4 hours to prevent them from sleeping while control mice dozed. The team then collected HSCs from the sleep-deprived and well-rested mice and injected the cells into 12 irradiated mice.
The recipient mice also received an injection of their own HSCs collected prior to radiation so the researchers could quantify the relative abilities of the donated HSCs to engraft successfully.
The team then assessed the prevalence of myeloid cells derived from donated HSCs at 8 weeks and 16 weeks after transplant. At 16 weeks, donor myeloid chimerism was about 26% in HSCT recipients with well-rested donors and about 12% in recipients with sleep-deprived donors (P<0.0001).
Dr Rolls and her colleagues also compared the ability of fluorescently labeled HSCs from sleep-deprived mice and rested mice to home to the bone marrow. After 12 hours, 3.3% percent of HSCs from rested mice were found in the bone marrow, compared to 1.7% of HSCs from sleep-deprived mice (P<0.05).
Further investigation revealed that sleep deprivation downregulates the expression of miR-19b, a negative regulator of the suppressor of cytokine signaling (SOCS) genes, which inhibit HSC migration and homing.
Finally, Dr Rolls and her colleagues found the effects of sleep deprivation on HSCs could be reversed by letting mice catch up on sleep. Even 2 hours of recovery sleep restored the HSCs’ ability to function normally in transplantation tests.
“We still don’t know how sleep deprivation affects us all, not just bone marrow donors,” Dr Rolls said. “The fact that recovery sleep is so helpful only emphasizes how important it is to pay attention to sleep.” ![]()
Sleep-deprived mice make poor donors for hematopoietic stem cell transplants (HSCTs), according to a study published in Nature Communications.
The research showed that a sleep deficit of just 4 hours can reduce—by more than 50%—the ability of HSCs to engraft and reconstitute the blood and bone marrow of an irradiated recipient mouse.
Researchers believe these findings may also apply to humans.
“Considering how little attention we typically pay to sleep in the hospital setting, this finding is troubling,” said study author Asya Rolls, PhD, of Technion–Israel Institute of Technology in Haifa.
“We go to all this trouble to find a matching donor, but this research suggests that, if the donor is not well-rested, it can impact the outcome of the transplantation. However, it’s heartening to think that this is not an insurmountable obstacle. A short period of recovery sleep before transplant can restore the donor’s cells’ ability to function normally.”
Dr Rolls and her colleagues studied mice that had been gently handled for 4 hours to prevent them from sleeping while control mice dozed. The team then collected HSCs from the sleep-deprived and well-rested mice and injected the cells into 12 irradiated mice.
The recipient mice also received an injection of their own HSCs collected prior to radiation so the researchers could quantify the relative abilities of the donated HSCs to engraft successfully.
The team then assessed the prevalence of myeloid cells derived from donated HSCs at 8 weeks and 16 weeks after transplant. At 16 weeks, donor myeloid chimerism was about 26% in HSCT recipients with well-rested donors and about 12% in recipients with sleep-deprived donors (P<0.0001).
Dr Rolls and her colleagues also compared the ability of fluorescently labeled HSCs from sleep-deprived mice and rested mice to home to the bone marrow. After 12 hours, 3.3% percent of HSCs from rested mice were found in the bone marrow, compared to 1.7% of HSCs from sleep-deprived mice (P<0.05).
Further investigation revealed that sleep deprivation downregulates the expression of miR-19b, a negative regulator of the suppressor of cytokine signaling (SOCS) genes, which inhibit HSC migration and homing.
Finally, Dr Rolls and her colleagues found the effects of sleep deprivation on HSCs could be reversed by letting mice catch up on sleep. Even 2 hours of recovery sleep restored the HSCs’ ability to function normally in transplantation tests.
“We still don’t know how sleep deprivation affects us all, not just bone marrow donors,” Dr Rolls said. “The fact that recovery sleep is so helpful only emphasizes how important it is to pay attention to sleep.” ![]()
Sleep-deprived mice make poor donors for hematopoietic stem cell transplants (HSCTs), according to a study published in Nature Communications.
The research showed that a sleep deficit of just 4 hours can reduce—by more than 50%—the ability of HSCs to engraft and reconstitute the blood and bone marrow of an irradiated recipient mouse.
Researchers believe these findings may also apply to humans.
“Considering how little attention we typically pay to sleep in the hospital setting, this finding is troubling,” said study author Asya Rolls, PhD, of Technion–Israel Institute of Technology in Haifa.
“We go to all this trouble to find a matching donor, but this research suggests that, if the donor is not well-rested, it can impact the outcome of the transplantation. However, it’s heartening to think that this is not an insurmountable obstacle. A short period of recovery sleep before transplant can restore the donor’s cells’ ability to function normally.”
Dr Rolls and her colleagues studied mice that had been gently handled for 4 hours to prevent them from sleeping while control mice dozed. The team then collected HSCs from the sleep-deprived and well-rested mice and injected the cells into 12 irradiated mice.
The recipient mice also received an injection of their own HSCs collected prior to radiation so the researchers could quantify the relative abilities of the donated HSCs to engraft successfully.
The team then assessed the prevalence of myeloid cells derived from donated HSCs at 8 weeks and 16 weeks after transplant. At 16 weeks, donor myeloid chimerism was about 26% in HSCT recipients with well-rested donors and about 12% in recipients with sleep-deprived donors (P<0.0001).
Dr Rolls and her colleagues also compared the ability of fluorescently labeled HSCs from sleep-deprived mice and rested mice to home to the bone marrow. After 12 hours, 3.3% percent of HSCs from rested mice were found in the bone marrow, compared to 1.7% of HSCs from sleep-deprived mice (P<0.05).
Further investigation revealed that sleep deprivation downregulates the expression of miR-19b, a negative regulator of the suppressor of cytokine signaling (SOCS) genes, which inhibit HSC migration and homing.
Finally, Dr Rolls and her colleagues found the effects of sleep deprivation on HSCs could be reversed by letting mice catch up on sleep. Even 2 hours of recovery sleep restored the HSCs’ ability to function normally in transplantation tests.
“We still don’t know how sleep deprivation affects us all, not just bone marrow donors,” Dr Rolls said. “The fact that recovery sleep is so helpful only emphasizes how important it is to pay attention to sleep.” ![]()
TCT: Novel drug-coated stent bests bare-metal in patients at high bleeding risk
A novel drug-coated stent halved the need for repeat revascularization and had a superior safety profile, compared with a bare-metal stent, in patients with a high risk of bleeding in the LEADERS FREE trial.
The results could mean that these typically older, sicker patients in whom dual antiplatelet therapy is contraindicated because of hemorrhage risk now have a wider range of revascularization options, said lead investigator Dr. Philip Urban.
“Patients who have a high risk of bleeding during percutaneous coronary intervention (PCI) are often excluded from stent and drug trials but constitute a rapidly growing proportion of PCI candidates, and they suffer high event rates,” said Dr. Urban, director of interventional cardiology at La Tour Hospital in Geneva. As the life expectancy increases, the implications are profound because roughly one-fifth of all PCI patients globally could be candidates for this type of treatment.
The data were presented at the Transcatheter Cardiovascular Therapeutics annual meeting, which was sponsored by the Cardiovascular Research Foundation. The results also were published online (N Engl J Med. 2015 Oct 14. doi: 10.1056/NEJMoa1503943).
“I hope these results will change practice as early as next week in Europe and elsewhere,” he said. The device is currently CE marked in Europe and is available in some parts of Asia. A clinical trial for the device is currently in the preliminary stages in the United States.
The current standard for PCI in patients at high risk for hemorrhage is to use bare-metal, instead of drug-eluting, stents. Although this protocol lowers the potential risk for bleeding and other complications often caused by extended dual antiplatelet therapy (DAPT), it exposes these patients to a higher risk of restenosis.
Rather than use a drug delivery polymer, the Biolimus A9-coated BioFreedom (Biosensors International) is polymer free and uses a stainless steel stent microstructured to hold a proprietary lipophilic drug on its outer surface. The drug is absorbed by the body within a month of placement.
The first of its kind, the double-blinded LEADERS FREE trial randomly assigned 2,466 PCI patients at high risk for bleeding to receive either the test stent or the standard platform Gazelle bare-metal stent. The procedures were performed at nearly 70 participating sites around the world, excluding the United States. More than half of all patients were accessed transradially, which was preferable to transfemoral access, according to Dr. Urban, because of the lower associated bleeding rates.
All patients were given 1 month of antiplatelet therapy after their intervention: about two-thirds of each group received DAPT and one-third received triple antiplatelet therapy. All were then switched to aspirin alone for 1 year.
At 390 days, there was nearly a 50% reduction in the need for repeat revascularization in the 1,221 patients receiving the drug-coated stent (5.1%), compared with 1,221 receiving the bare-metal stent (9.8%), with the difference reaching statistical significance for superiority for this primary efficacy endpoint (P < .001 for superiority).
Patients in the study arm also had a 29% reduction in risk of cardiac death, myocardial infarction, or stent thrombosis, the primary safety endpoint. At 390 days, these events occurred in 9.4% of the drug coated–stent patients, compared with 12.9% of the controls, a statistically significant difference for both noninferiority (P < .0001) and superiority (P = .005).
The study was done in patients typically excluded from such a trial, although, according to Dr. Urban, the PCI procedures performed were no more complex than usual. More than half the patients, three-quarters of whom were men in their mid- to late-70s, also had a range of comorbidities such as diabetes, kidney disease, and atrial fibrillation. Patients taking anticoagulants, those who had experienced a stroke within the past year, those expected to have major surgery within the year, and those who had undergone cancer treatment within the past 3 years also were included.
Bleeding events in the year following did not differ significantly between groups: 18.1% in the study group and 19.1% of controls had BARC 1-5 bleeding; 13.9% in the test arm and 14.7% of controls had BARC 2-5 events; and 7.2% in the study group and 7.3% of controls experienced BARC 3-5 events.
In the past, Dr. Urban had theorized that the trial would help to quantify not only risk for hemorrhage, but also the thrombotic risk in this patient population. In an interview, Dr. Urban said that, while the stent thrombosis rate was nearly identical in both groups in the trial, “the safety advantage of the drug-coated stent was especially apparent in the more thrombotic milieu.”
LEADERS FREE was underwritten by Biosensors International, maker of the BioFreedom stent. Dr. Urban and several of his coinvestigators disclosed relationships with device makers, including Edward Lifesciences, Terumo, Abbott Vascular, and Quest Medical.
On Twitter @whitneymcknight
A novel drug-coated stent halved the need for repeat revascularization and had a superior safety profile, compared with a bare-metal stent, in patients with a high risk of bleeding in the LEADERS FREE trial.
The results could mean that these typically older, sicker patients in whom dual antiplatelet therapy is contraindicated because of hemorrhage risk now have a wider range of revascularization options, said lead investigator Dr. Philip Urban.
“Patients who have a high risk of bleeding during percutaneous coronary intervention (PCI) are often excluded from stent and drug trials but constitute a rapidly growing proportion of PCI candidates, and they suffer high event rates,” said Dr. Urban, director of interventional cardiology at La Tour Hospital in Geneva. As the life expectancy increases, the implications are profound because roughly one-fifth of all PCI patients globally could be candidates for this type of treatment.
The data were presented at the Transcatheter Cardiovascular Therapeutics annual meeting, which was sponsored by the Cardiovascular Research Foundation. The results also were published online (N Engl J Med. 2015 Oct 14. doi: 10.1056/NEJMoa1503943).
“I hope these results will change practice as early as next week in Europe and elsewhere,” he said. The device is currently CE marked in Europe and is available in some parts of Asia. A clinical trial for the device is currently in the preliminary stages in the United States.
The current standard for PCI in patients at high risk for hemorrhage is to use bare-metal, instead of drug-eluting, stents. Although this protocol lowers the potential risk for bleeding and other complications often caused by extended dual antiplatelet therapy (DAPT), it exposes these patients to a higher risk of restenosis.
Rather than use a drug delivery polymer, the Biolimus A9-coated BioFreedom (Biosensors International) is polymer free and uses a stainless steel stent microstructured to hold a proprietary lipophilic drug on its outer surface. The drug is absorbed by the body within a month of placement.
The first of its kind, the double-blinded LEADERS FREE trial randomly assigned 2,466 PCI patients at high risk for bleeding to receive either the test stent or the standard platform Gazelle bare-metal stent. The procedures were performed at nearly 70 participating sites around the world, excluding the United States. More than half of all patients were accessed transradially, which was preferable to transfemoral access, according to Dr. Urban, because of the lower associated bleeding rates.
All patients were given 1 month of antiplatelet therapy after their intervention: about two-thirds of each group received DAPT and one-third received triple antiplatelet therapy. All were then switched to aspirin alone for 1 year.
At 390 days, there was nearly a 50% reduction in the need for repeat revascularization in the 1,221 patients receiving the drug-coated stent (5.1%), compared with 1,221 receiving the bare-metal stent (9.8%), with the difference reaching statistical significance for superiority for this primary efficacy endpoint (P < .001 for superiority).
Patients in the study arm also had a 29% reduction in risk of cardiac death, myocardial infarction, or stent thrombosis, the primary safety endpoint. At 390 days, these events occurred in 9.4% of the drug coated–stent patients, compared with 12.9% of the controls, a statistically significant difference for both noninferiority (P < .0001) and superiority (P = .005).
The study was done in patients typically excluded from such a trial, although, according to Dr. Urban, the PCI procedures performed were no more complex than usual. More than half the patients, three-quarters of whom were men in their mid- to late-70s, also had a range of comorbidities such as diabetes, kidney disease, and atrial fibrillation. Patients taking anticoagulants, those who had experienced a stroke within the past year, those expected to have major surgery within the year, and those who had undergone cancer treatment within the past 3 years also were included.
Bleeding events in the year following did not differ significantly between groups: 18.1% in the study group and 19.1% of controls had BARC 1-5 bleeding; 13.9% in the test arm and 14.7% of controls had BARC 2-5 events; and 7.2% in the study group and 7.3% of controls experienced BARC 3-5 events.
In the past, Dr. Urban had theorized that the trial would help to quantify not only risk for hemorrhage, but also the thrombotic risk in this patient population. In an interview, Dr. Urban said that, while the stent thrombosis rate was nearly identical in both groups in the trial, “the safety advantage of the drug-coated stent was especially apparent in the more thrombotic milieu.”
LEADERS FREE was underwritten by Biosensors International, maker of the BioFreedom stent. Dr. Urban and several of his coinvestigators disclosed relationships with device makers, including Edward Lifesciences, Terumo, Abbott Vascular, and Quest Medical.
On Twitter @whitneymcknight
A novel drug-coated stent halved the need for repeat revascularization and had a superior safety profile, compared with a bare-metal stent, in patients with a high risk of bleeding in the LEADERS FREE trial.
The results could mean that these typically older, sicker patients in whom dual antiplatelet therapy is contraindicated because of hemorrhage risk now have a wider range of revascularization options, said lead investigator Dr. Philip Urban.
“Patients who have a high risk of bleeding during percutaneous coronary intervention (PCI) are often excluded from stent and drug trials but constitute a rapidly growing proportion of PCI candidates, and they suffer high event rates,” said Dr. Urban, director of interventional cardiology at La Tour Hospital in Geneva. As the life expectancy increases, the implications are profound because roughly one-fifth of all PCI patients globally could be candidates for this type of treatment.
The data were presented at the Transcatheter Cardiovascular Therapeutics annual meeting, which was sponsored by the Cardiovascular Research Foundation. The results also were published online (N Engl J Med. 2015 Oct 14. doi: 10.1056/NEJMoa1503943).
“I hope these results will change practice as early as next week in Europe and elsewhere,” he said. The device is currently CE marked in Europe and is available in some parts of Asia. A clinical trial for the device is currently in the preliminary stages in the United States.
The current standard for PCI in patients at high risk for hemorrhage is to use bare-metal, instead of drug-eluting, stents. Although this protocol lowers the potential risk for bleeding and other complications often caused by extended dual antiplatelet therapy (DAPT), it exposes these patients to a higher risk of restenosis.
Rather than use a drug delivery polymer, the Biolimus A9-coated BioFreedom (Biosensors International) is polymer free and uses a stainless steel stent microstructured to hold a proprietary lipophilic drug on its outer surface. The drug is absorbed by the body within a month of placement.
The first of its kind, the double-blinded LEADERS FREE trial randomly assigned 2,466 PCI patients at high risk for bleeding to receive either the test stent or the standard platform Gazelle bare-metal stent. The procedures were performed at nearly 70 participating sites around the world, excluding the United States. More than half of all patients were accessed transradially, which was preferable to transfemoral access, according to Dr. Urban, because of the lower associated bleeding rates.
All patients were given 1 month of antiplatelet therapy after their intervention: about two-thirds of each group received DAPT and one-third received triple antiplatelet therapy. All were then switched to aspirin alone for 1 year.
At 390 days, there was nearly a 50% reduction in the need for repeat revascularization in the 1,221 patients receiving the drug-coated stent (5.1%), compared with 1,221 receiving the bare-metal stent (9.8%), with the difference reaching statistical significance for superiority for this primary efficacy endpoint (P < .001 for superiority).
Patients in the study arm also had a 29% reduction in risk of cardiac death, myocardial infarction, or stent thrombosis, the primary safety endpoint. At 390 days, these events occurred in 9.4% of the drug coated–stent patients, compared with 12.9% of the controls, a statistically significant difference for both noninferiority (P < .0001) and superiority (P = .005).
The study was done in patients typically excluded from such a trial, although, according to Dr. Urban, the PCI procedures performed were no more complex than usual. More than half the patients, three-quarters of whom were men in their mid- to late-70s, also had a range of comorbidities such as diabetes, kidney disease, and atrial fibrillation. Patients taking anticoagulants, those who had experienced a stroke within the past year, those expected to have major surgery within the year, and those who had undergone cancer treatment within the past 3 years also were included.
Bleeding events in the year following did not differ significantly between groups: 18.1% in the study group and 19.1% of controls had BARC 1-5 bleeding; 13.9% in the test arm and 14.7% of controls had BARC 2-5 events; and 7.2% in the study group and 7.3% of controls experienced BARC 3-5 events.
In the past, Dr. Urban had theorized that the trial would help to quantify not only risk for hemorrhage, but also the thrombotic risk in this patient population. In an interview, Dr. Urban said that, while the stent thrombosis rate was nearly identical in both groups in the trial, “the safety advantage of the drug-coated stent was especially apparent in the more thrombotic milieu.”
LEADERS FREE was underwritten by Biosensors International, maker of the BioFreedom stent. Dr. Urban and several of his coinvestigators disclosed relationships with device makers, including Edward Lifesciences, Terumo, Abbott Vascular, and Quest Medical.
On Twitter @whitneymcknight
AT TCT 2015
Key clinical point: Older, sicker acute coronary syndrome patients at higher risk for hemorrhage may now have more PCI options.
Major finding: At 390 days, 5.1% of PCI patients given a drug-coated stent plus 1 month of DAPT required revascularization, compared with 9.8% of the bare metal–stented control group given 1 month of DAPT; 9.4% of those given a drug-coated stent plus 1 month DAPT had adverse events vs. 12.9% of controls.
Data source: LEADERS FREE is a prospective, double-blinded, randomized controlled trial of 2,466 PCI patients at high risk for bleeding.
Disclosures: The study was underwritten by Biosensors International, maker of the BioFreedom stent.
VIDEO: Tranexamic acid didn’t increase postop infections
CHICAGO – Tranexamic acid was not independently associated with any infection within 30 days of injury in U.S. soldiers undergoing trauma surgery, a case-control study showed.
The antifibrinolytic has been used for years to reduce morbidity and the risk of death associated with hemorrhage in the military setting. Tranexamic acid (TXA) made its way into the civilian setting after the 2010 provocative CRASH-2 trial in adult trauma patients.
Because TXA (Cyklokapron, Lysteda) also has anti-inflammatory properties, Dr. Clayton Lewis of Brooke Army Medical Center in San Antonio and his colleagues decided to evaluate the effect of TXA on the development of posttraumatic infections, including time to first infection, in combat casualties.
The findings were presented at the annual clinical congress of the American College of Surgeons, where we caught up with Dr. Lewis for an interview.
Dr. Lewis reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Tranexamic acid was not independently associated with any infection within 30 days of injury in U.S. soldiers undergoing trauma surgery, a case-control study showed.
The antifibrinolytic has been used for years to reduce morbidity and the risk of death associated with hemorrhage in the military setting. Tranexamic acid (TXA) made its way into the civilian setting after the 2010 provocative CRASH-2 trial in adult trauma patients.
Because TXA (Cyklokapron, Lysteda) also has anti-inflammatory properties, Dr. Clayton Lewis of Brooke Army Medical Center in San Antonio and his colleagues decided to evaluate the effect of TXA on the development of posttraumatic infections, including time to first infection, in combat casualties.
The findings were presented at the annual clinical congress of the American College of Surgeons, where we caught up with Dr. Lewis for an interview.
Dr. Lewis reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Tranexamic acid was not independently associated with any infection within 30 days of injury in U.S. soldiers undergoing trauma surgery, a case-control study showed.
The antifibrinolytic has been used for years to reduce morbidity and the risk of death associated with hemorrhage in the military setting. Tranexamic acid (TXA) made its way into the civilian setting after the 2010 provocative CRASH-2 trial in adult trauma patients.
Because TXA (Cyklokapron, Lysteda) also has anti-inflammatory properties, Dr. Clayton Lewis of Brooke Army Medical Center in San Antonio and his colleagues decided to evaluate the effect of TXA on the development of posttraumatic infections, including time to first infection, in combat casualties.
The findings were presented at the annual clinical congress of the American College of Surgeons, where we caught up with Dr. Lewis for an interview.
Dr. Lewis reported having no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ACS CLINICAL CONGRESS
Listen Now: Characteristics of Frequently Hospitalized Patients
The social determinants of health are a root cause of readmissions in the most heavily readmitted patients, according to data analyzed in a recent study published in the Journal of Hospital Medicine. The study's lead author, Marilyn Szekendi, PhD, discusses the research, and Dr. Bradley Flansbaum weighs in on the difficulty of effecting a policy solution for a population without much political voice.
The social determinants of health are a root cause of readmissions in the most heavily readmitted patients, according to data analyzed in a recent study published in the Journal of Hospital Medicine. The study's lead author, Marilyn Szekendi, PhD, discusses the research, and Dr. Bradley Flansbaum weighs in on the difficulty of effecting a policy solution for a population without much political voice.
The social determinants of health are a root cause of readmissions in the most heavily readmitted patients, according to data analyzed in a recent study published in the Journal of Hospital Medicine. The study's lead author, Marilyn Szekendi, PhD, discusses the research, and Dr. Bradley Flansbaum weighs in on the difficulty of effecting a policy solution for a population without much political voice.
CML: Select TKI based on comorbidities, monitor toxicity and adherence
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.

Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
EXPERT ANALYSIS FROM MHM 2015

Solitary Lesion on the Left Ankle
The Diagnosis: Porokeratosis of Mibelli
There are 5 variants of porokeratosis: disseminated superficial actinic porokeratosis (DSAP), linear porokeratosis, porokeratosis of Mibelli, porokeratosis palmaris et plantaris disseminata, and punctate porokeratosis. The most common type is DSAP,1 which is characterized by multiple lesions on the body, particularly in sun-exposed areas. The distinguishing feature of porokeratosis is the cornoid lamella, which is made up of parakeratotic cells extending through the stratum corneum. There also is a thin or absent granular layer beneath it (Figure).2

Patients generally present in the third and fourth decades of life.1 Risk factors for porokeratosis include sun exposure, immunosuppression, and genetics.2-4 Overexpression of the protein p53 in porokeratosis lesions has been demonstrated in studies investigating the genetics of porokeratosis.5,6 A study of Chinese families with DSAP identified 3 different loci associated with DSAP: DSAP1, DSAP2, and DSAP3.2 The progression to cancer has been noted in all types of porokeratosis lesions. Malignancies include squamous cell carcinoma, Bowen disease, and basal cell carcinoma.7,8
Many treatments have been tried for DSAP including cryotherapy, topical 5-fluorouracil, photodynamic therapy, and topical imiquimod with varying success.1 Our patient was treated with cryotherapy but had side effects from treatment including cellulitis and local infections with ulceration before finally healing.
Interestingly, our patient had a single lesion with pathology findings most consistent with DSAP at a later age. Although the pathology suggested DSAP, the size and solitary lesion was more consistent with porokeratosis of Mibelli. Porokeratosis of Mibelli can occur concurrently with DSAP,9 but we have not seen other lesions in this patient. We have educated our patient to be aware of other lesions that may occur in the future. Due to risk for malignant conversion, it is generally viewed as beneficial to treat patients who present with porokeratosis lesions. Our patient’s lesion ultimately cleared and he has not developed new lesions at 1-year follow-up.
Although DSAP generally presents in the third and fourth decades of life and porokeratosis of Mibelli during childhood, it is important to educate both dermatologists and primary care physicians to be aware of the possibility of both diagnoses in the elderly population.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatol Online J. 2012;18:24.
- Murase J, Gilliam AC, et al. Disseminated superficial actinic porokeratosis co-existing with linear and verrucous porokeratosis in an elderly woman: update on the genetics and clinical expression of porokeratosis. J Am Acad Dermatol. 2010;63:886-891.
- Lederman JS, Sober AJ, Lederman GS. Immunosuppression: a cause of porokeratosis? J Am Acad Dermatol. 1985;13:75-79.
- Hernandez MH, Lai CH, Mallory SB. Disseminated porokeratosis associated with chronic renal failure: a new type of disseminated porokeratosis? Arch Dermatol. 2000;136:1568-1569.
- Magee JW, McCalmont TH, LeBoit PE. Overexpression of p53 tumor suppressor protein in porokeratosis. Arch Dermatol. 1994;130:187-190.
- Arranz-Salas I, Sanz-Trelles A, Ojeda DB. p53 alterations in porokeratosis. J Cutan Pathol. 2003;30:455-458.
- Curnow P, Foley P, Baker C. Multiple squamous cell carcinomas complicating linear porokeratosis. Australas J Dermatol. 2003;44:136-139.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Mehta V, Balachandran C. Simultaneous co-occurrence of porokeratosis of Mibelli with disseminated superficial actinic porokeratosis. Indian J Dermatol. 2009;54:390-391.
The Diagnosis: Porokeratosis of Mibelli
There are 5 variants of porokeratosis: disseminated superficial actinic porokeratosis (DSAP), linear porokeratosis, porokeratosis of Mibelli, porokeratosis palmaris et plantaris disseminata, and punctate porokeratosis. The most common type is DSAP,1 which is characterized by multiple lesions on the body, particularly in sun-exposed areas. The distinguishing feature of porokeratosis is the cornoid lamella, which is made up of parakeratotic cells extending through the stratum corneum. There also is a thin or absent granular layer beneath it (Figure).2
Patients generally present in the third and fourth decades of life.1 Risk factors for porokeratosis include sun exposure, immunosuppression, and genetics.2-4 Overexpression of the protein p53 in porokeratosis lesions has been demonstrated in studies investigating the genetics of porokeratosis.5,6 A study of Chinese families with DSAP identified 3 different loci associated with DSAP: DSAP1, DSAP2, and DSAP3.2 The progression to cancer has been noted in all types of porokeratosis lesions. Malignancies include squamous cell carcinoma, Bowen disease, and basal cell carcinoma.7,8
Many treatments have been tried for DSAP including cryotherapy, topical 5-fluorouracil, photodynamic therapy, and topical imiquimod with varying success.1 Our patient was treated with cryotherapy but had side effects from treatment including cellulitis and local infections with ulceration before finally healing.
Interestingly, our patient had a single lesion with pathology findings most consistent with DSAP at a later age. Although the pathology suggested DSAP, the size and solitary lesion was more consistent with porokeratosis of Mibelli. Porokeratosis of Mibelli can occur concurrently with DSAP,9 but we have not seen other lesions in this patient. We have educated our patient to be aware of other lesions that may occur in the future. Due to risk for malignant conversion, it is generally viewed as beneficial to treat patients who present with porokeratosis lesions. Our patient’s lesion ultimately cleared and he has not developed new lesions at 1-year follow-up.
Although DSAP generally presents in the third and fourth decades of life and porokeratosis of Mibelli during childhood, it is important to educate both dermatologists and primary care physicians to be aware of the possibility of both diagnoses in the elderly population.
The Diagnosis: Porokeratosis of Mibelli
There are 5 variants of porokeratosis: disseminated superficial actinic porokeratosis (DSAP), linear porokeratosis, porokeratosis of Mibelli, porokeratosis palmaris et plantaris disseminata, and punctate porokeratosis. The most common type is DSAP,1 which is characterized by multiple lesions on the body, particularly in sun-exposed areas. The distinguishing feature of porokeratosis is the cornoid lamella, which is made up of parakeratotic cells extending through the stratum corneum. There also is a thin or absent granular layer beneath it (Figure).2
Patients generally present in the third and fourth decades of life.1 Risk factors for porokeratosis include sun exposure, immunosuppression, and genetics.2-4 Overexpression of the protein p53 in porokeratosis lesions has been demonstrated in studies investigating the genetics of porokeratosis.5,6 A study of Chinese families with DSAP identified 3 different loci associated with DSAP: DSAP1, DSAP2, and DSAP3.2 The progression to cancer has been noted in all types of porokeratosis lesions. Malignancies include squamous cell carcinoma, Bowen disease, and basal cell carcinoma.7,8
Many treatments have been tried for DSAP including cryotherapy, topical 5-fluorouracil, photodynamic therapy, and topical imiquimod with varying success.1 Our patient was treated with cryotherapy but had side effects from treatment including cellulitis and local infections with ulceration before finally healing.
Interestingly, our patient had a single lesion with pathology findings most consistent with DSAP at a later age. Although the pathology suggested DSAP, the size and solitary lesion was more consistent with porokeratosis of Mibelli. Porokeratosis of Mibelli can occur concurrently with DSAP,9 but we have not seen other lesions in this patient. We have educated our patient to be aware of other lesions that may occur in the future. Due to risk for malignant conversion, it is generally viewed as beneficial to treat patients who present with porokeratosis lesions. Our patient’s lesion ultimately cleared and he has not developed new lesions at 1-year follow-up.
Although DSAP generally presents in the third and fourth decades of life and porokeratosis of Mibelli during childhood, it is important to educate both dermatologists and primary care physicians to be aware of the possibility of both diagnoses in the elderly population.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatol Online J. 2012;18:24.
- Murase J, Gilliam AC, et al. Disseminated superficial actinic porokeratosis co-existing with linear and verrucous porokeratosis in an elderly woman: update on the genetics and clinical expression of porokeratosis. J Am Acad Dermatol. 2010;63:886-891.
- Lederman JS, Sober AJ, Lederman GS. Immunosuppression: a cause of porokeratosis? J Am Acad Dermatol. 1985;13:75-79.
- Hernandez MH, Lai CH, Mallory SB. Disseminated porokeratosis associated with chronic renal failure: a new type of disseminated porokeratosis? Arch Dermatol. 2000;136:1568-1569.
- Magee JW, McCalmont TH, LeBoit PE. Overexpression of p53 tumor suppressor protein in porokeratosis. Arch Dermatol. 1994;130:187-190.
- Arranz-Salas I, Sanz-Trelles A, Ojeda DB. p53 alterations in porokeratosis. J Cutan Pathol. 2003;30:455-458.
- Curnow P, Foley P, Baker C. Multiple squamous cell carcinomas complicating linear porokeratosis. Australas J Dermatol. 2003;44:136-139.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Mehta V, Balachandran C. Simultaneous co-occurrence of porokeratosis of Mibelli with disseminated superficial actinic porokeratosis. Indian J Dermatol. 2009;54:390-391.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatol Online J. 2012;18:24.
- Murase J, Gilliam AC, et al. Disseminated superficial actinic porokeratosis co-existing with linear and verrucous porokeratosis in an elderly woman: update on the genetics and clinical expression of porokeratosis. J Am Acad Dermatol. 2010;63:886-891.
- Lederman JS, Sober AJ, Lederman GS. Immunosuppression: a cause of porokeratosis? J Am Acad Dermatol. 1985;13:75-79.
- Hernandez MH, Lai CH, Mallory SB. Disseminated porokeratosis associated with chronic renal failure: a new type of disseminated porokeratosis? Arch Dermatol. 2000;136:1568-1569.
- Magee JW, McCalmont TH, LeBoit PE. Overexpression of p53 tumor suppressor protein in porokeratosis. Arch Dermatol. 1994;130:187-190.
- Arranz-Salas I, Sanz-Trelles A, Ojeda DB. p53 alterations in porokeratosis. J Cutan Pathol. 2003;30:455-458.
- Curnow P, Foley P, Baker C. Multiple squamous cell carcinomas complicating linear porokeratosis. Australas J Dermatol. 2003;44:136-139.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Mehta V, Balachandran C. Simultaneous co-occurrence of porokeratosis of Mibelli with disseminated superficial actinic porokeratosis. Indian J Dermatol. 2009;54:390-391.

A 69-year-old white man presented with a solitary lesion on the left ankle. His medical history included hypertension and arthritis. He resided in Florida for 11 years but denied tanning and has had sensitive skin throughout his life. He had no other notable skin conditions, except for nummular eczema. He did not have a family history of skin cancer. Physical examination showed the single lesion on the left ankle.

Antibiotics to reduce microbiota may improve treatment of sickle-cell disease
The human body’s microbiota regulates the aging of circulating neutrophils, and aged neutrophils, which are excessively active and adherent, promote tissue injury in inflammatory diseases. These two discoveries appear to point the way toward a simple, effective antibiotic treatment for sickle-cell disease, and may eventually lead to similar therapies for other disorders that induce inflammation-related organ damage, such as septic shock, according to a Research Letter published online Sept. 16 in Nature.
“To our knowledge, this is the first therapy shown to alleviate the chronic tissue damage induced by sickle-cell disease,” said Dachuan Zhang of the Gottesman Institute for Stem Cell and Regenerative Medicine Research and the department of cell biology, Albert Einstein College of Medicine, New York, and his associates. “Our results raise the possibility that manipulation of the microbiome may have sustained implications in disease outcome that should be further studied in clinical trials.”

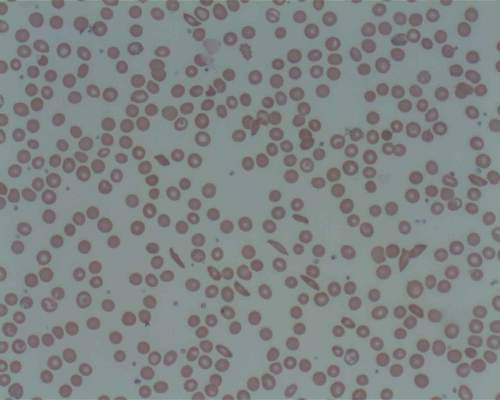
In a series of in vitro and in vivo studies, the researchers demonstrated that aging neutrophils differ from others in that they are overactive and extra-adherent. Adherent neutrophils are already known to precipitate the acute vaso-occlusion that characterizes sickle-cell disease. Aging neutrophils also displayed other traits suggesting that exogenous inflammatory mediators may contribute to their excessive activity and adherence.
Dr. Zhang and his colleagues suspected that molecules in the microbiota – the ecologic community of all microorganisms residing in the body – may be involved, as they are known to cross the intestinal barrier to affect multiple systemic immune-cell populations, and a recent study suggested that the microbiota may regulate neutrophil production and function. To test this hypothesis they treated mice with broad-spectrum antibiotics, which caused dramatic depletion of microbiota volume and composition in the gut. This in turn significantly reduced aged neutrophils in the circulation, which immediately rebounded when the antibiotics were counteracted.
Further mouse studies revealed that neutrophil aging is delayed in a bacterially depleted environment, and that microbiota-derived molecules actually induce neutrophil aging. In a subsequent study of an in vivo model of septic shock, mice that were given antibiotics were protected from neutrophil-mediated damage in the vasculature and showed markedly prolonged survival, compared with untreated mice, the investigators noted (Nature. 2015 Sep 24;525[7570]. doi: 10.1038/nature15367 ).
In an in vivo model of sickle-cell disease, untreated mice with the disease showed markedly increased neutrophil activity and adhesion while affected mice given antibiotics showed marked microbiota depletion; enhanced blood flow; significantly reduced splenomegaly; and marked alleviation of liver necrosis, fibrosis, and inflammation. Survival was significantly improved in the treated mice. Finally, a laboratory-induced replenishment of aging neutrophils in the circulation resulted in acute vaso-occlusive crises and death within 10-30 hours in all affected mice.
“Together, these data suggest that the microbiota regulates aged neutrophil numbers, thereby affecting both acute vaso-occlusive crisis and the ensuing chronic tissue damage in sickle-cell disease,” Dr. Zhang and his associates said.
To assess how their findings applied to human beings, the investigators next studied 23 patients with sickle-cell disease who were not taking antibiotics, 11 patients with sickle-cell disease who were taking penicillin to prevent life-threatening infections, and 9 healthy control subjects. Compared with controls, only the patients who weren’t taking antibiotics showed a dramatic increase in circulating aged neutrophils. This protective effect of antibiotics was consistent across all ages, both genders, and regardless of hydroxyurea intake. Now, a prospective study involving age-matched participants is needed to confirm that antibiotics, by reducing the gut microbiota, decrease aged neutrophils in the circulation and thereby improve vaso-occlusive disease, the researchers said.
The American Heart Association, the National Institutes of Health, and the New York State Stem Cell Science Program funded the study. Dr. Zhang and his associates reported having no relevant disclosures.
The human body’s microbiota regulates the aging of circulating neutrophils, and aged neutrophils, which are excessively active and adherent, promote tissue injury in inflammatory diseases. These two discoveries appear to point the way toward a simple, effective antibiotic treatment for sickle-cell disease, and may eventually lead to similar therapies for other disorders that induce inflammation-related organ damage, such as septic shock, according to a Research Letter published online Sept. 16 in Nature.
“To our knowledge, this is the first therapy shown to alleviate the chronic tissue damage induced by sickle-cell disease,” said Dachuan Zhang of the Gottesman Institute for Stem Cell and Regenerative Medicine Research and the department of cell biology, Albert Einstein College of Medicine, New York, and his associates. “Our results raise the possibility that manipulation of the microbiome may have sustained implications in disease outcome that should be further studied in clinical trials.”
In a series of in vitro and in vivo studies, the researchers demonstrated that aging neutrophils differ from others in that they are overactive and extra-adherent. Adherent neutrophils are already known to precipitate the acute vaso-occlusion that characterizes sickle-cell disease. Aging neutrophils also displayed other traits suggesting that exogenous inflammatory mediators may contribute to their excessive activity and adherence.
Dr. Zhang and his colleagues suspected that molecules in the microbiota – the ecologic community of all microorganisms residing in the body – may be involved, as they are known to cross the intestinal barrier to affect multiple systemic immune-cell populations, and a recent study suggested that the microbiota may regulate neutrophil production and function. To test this hypothesis they treated mice with broad-spectrum antibiotics, which caused dramatic depletion of microbiota volume and composition in the gut. This in turn significantly reduced aged neutrophils in the circulation, which immediately rebounded when the antibiotics were counteracted.
Further mouse studies revealed that neutrophil aging is delayed in a bacterially depleted environment, and that microbiota-derived molecules actually induce neutrophil aging. In a subsequent study of an in vivo model of septic shock, mice that were given antibiotics were protected from neutrophil-mediated damage in the vasculature and showed markedly prolonged survival, compared with untreated mice, the investigators noted (Nature. 2015 Sep 24;525[7570]. doi: 10.1038/nature15367 ).
In an in vivo model of sickle-cell disease, untreated mice with the disease showed markedly increased neutrophil activity and adhesion while affected mice given antibiotics showed marked microbiota depletion; enhanced blood flow; significantly reduced splenomegaly; and marked alleviation of liver necrosis, fibrosis, and inflammation. Survival was significantly improved in the treated mice. Finally, a laboratory-induced replenishment of aging neutrophils in the circulation resulted in acute vaso-occlusive crises and death within 10-30 hours in all affected mice.
“Together, these data suggest that the microbiota regulates aged neutrophil numbers, thereby affecting both acute vaso-occlusive crisis and the ensuing chronic tissue damage in sickle-cell disease,” Dr. Zhang and his associates said.
To assess how their findings applied to human beings, the investigators next studied 23 patients with sickle-cell disease who were not taking antibiotics, 11 patients with sickle-cell disease who were taking penicillin to prevent life-threatening infections, and 9 healthy control subjects. Compared with controls, only the patients who weren’t taking antibiotics showed a dramatic increase in circulating aged neutrophils. This protective effect of antibiotics was consistent across all ages, both genders, and regardless of hydroxyurea intake. Now, a prospective study involving age-matched participants is needed to confirm that antibiotics, by reducing the gut microbiota, decrease aged neutrophils in the circulation and thereby improve vaso-occlusive disease, the researchers said.
The American Heart Association, the National Institutes of Health, and the New York State Stem Cell Science Program funded the study. Dr. Zhang and his associates reported having no relevant disclosures.
The human body’s microbiota regulates the aging of circulating neutrophils, and aged neutrophils, which are excessively active and adherent, promote tissue injury in inflammatory diseases. These two discoveries appear to point the way toward a simple, effective antibiotic treatment for sickle-cell disease, and may eventually lead to similar therapies for other disorders that induce inflammation-related organ damage, such as septic shock, according to a Research Letter published online Sept. 16 in Nature.
“To our knowledge, this is the first therapy shown to alleviate the chronic tissue damage induced by sickle-cell disease,” said Dachuan Zhang of the Gottesman Institute for Stem Cell and Regenerative Medicine Research and the department of cell biology, Albert Einstein College of Medicine, New York, and his associates. “Our results raise the possibility that manipulation of the microbiome may have sustained implications in disease outcome that should be further studied in clinical trials.”
In a series of in vitro and in vivo studies, the researchers demonstrated that aging neutrophils differ from others in that they are overactive and extra-adherent. Adherent neutrophils are already known to precipitate the acute vaso-occlusion that characterizes sickle-cell disease. Aging neutrophils also displayed other traits suggesting that exogenous inflammatory mediators may contribute to their excessive activity and adherence.
Dr. Zhang and his colleagues suspected that molecules in the microbiota – the ecologic community of all microorganisms residing in the body – may be involved, as they are known to cross the intestinal barrier to affect multiple systemic immune-cell populations, and a recent study suggested that the microbiota may regulate neutrophil production and function. To test this hypothesis they treated mice with broad-spectrum antibiotics, which caused dramatic depletion of microbiota volume and composition in the gut. This in turn significantly reduced aged neutrophils in the circulation, which immediately rebounded when the antibiotics were counteracted.
Further mouse studies revealed that neutrophil aging is delayed in a bacterially depleted environment, and that microbiota-derived molecules actually induce neutrophil aging. In a subsequent study of an in vivo model of septic shock, mice that were given antibiotics were protected from neutrophil-mediated damage in the vasculature and showed markedly prolonged survival, compared with untreated mice, the investigators noted (Nature. 2015 Sep 24;525[7570]. doi: 10.1038/nature15367 ).
In an in vivo model of sickle-cell disease, untreated mice with the disease showed markedly increased neutrophil activity and adhesion while affected mice given antibiotics showed marked microbiota depletion; enhanced blood flow; significantly reduced splenomegaly; and marked alleviation of liver necrosis, fibrosis, and inflammation. Survival was significantly improved in the treated mice. Finally, a laboratory-induced replenishment of aging neutrophils in the circulation resulted in acute vaso-occlusive crises and death within 10-30 hours in all affected mice.
“Together, these data suggest that the microbiota regulates aged neutrophil numbers, thereby affecting both acute vaso-occlusive crisis and the ensuing chronic tissue damage in sickle-cell disease,” Dr. Zhang and his associates said.
To assess how their findings applied to human beings, the investigators next studied 23 patients with sickle-cell disease who were not taking antibiotics, 11 patients with sickle-cell disease who were taking penicillin to prevent life-threatening infections, and 9 healthy control subjects. Compared with controls, only the patients who weren’t taking antibiotics showed a dramatic increase in circulating aged neutrophils. This protective effect of antibiotics was consistent across all ages, both genders, and regardless of hydroxyurea intake. Now, a prospective study involving age-matched participants is needed to confirm that antibiotics, by reducing the gut microbiota, decrease aged neutrophils in the circulation and thereby improve vaso-occlusive disease, the researchers said.
The American Heart Association, the National Institutes of Health, and the New York State Stem Cell Science Program funded the study. Dr. Zhang and his associates reported having no relevant disclosures.
FROM NATURE
Key clinical point: The body’s microbiota was found to regulate the aging of circulating neutrophils, a discovery that points the way to easily and markedly improve the chronic tissue damage induced by sickle-cell and perhaps other diseases.
Major finding: In an in vivo mouse model of sickle-cell disease, mice given antibiotics showed marked microbiota depletion; enhanced blood flow; significantly reduced splenomegaly; marked alleviation of liver necrosis, fibrosis, and inflammation; and significantly improved survival.
Data source: A series of in vitro, in vivo, and human studies, the latter involving 23 patients with SCD, 11 with SCD taking prophylactic antibiotics, and 9 healthy control subjects.
Disclosures: The American Heart Association, the National Institutes of Health, and the New York State Stem Cell Science Program funded the study. Dr. Zhang and his associates reported having no relevant disclosures.
The perplexing phantom appointment
How often do you encounter phantom appointments?
What are phantom appointments? They’re patient visits that are nowhere on your schedule.
I’m not talking about someone who shows up on the wrong day or time. That’s at least partially understandable. I’m talking about people who you have no record of but say they have an appointment.
The first impression is to assume they’re scheduled with someone else in the building or another neurologist in my area, but they’ll often pull out a crumpled sheet of paper with my name and address on it, and a time circled.
Where on Earth do these people come from? I have no clue. When asked who made the appointment, it’s always “They made it for me,” or “They told me to be here.” It’s never clear who “they” are. These folks almost never can give you the name of their referring doctor, or who they spoke to. I’m a pretty small office here, just me and my secretary, so there aren’t many people here to talk to.
These aren’t common, maybe a handful per year, but generally unpleasant when they occur. If they happen to show up when I’ve got a gap in the schedule, I’ll try to see them, but the majority end up being turned away. We always offer to make an appointment for them, but most leave, usually angry.
I suspect some were referred for cognitive issues, which partially explains the confusion. Others may be doing it intentionally, hoping that they’ll be seen. (I suspect these are the minority.) Misinterpreted information from other offices likely plays a big part. Perhaps they were given my name and info by another office and told to make an appointment. Somehow, a time for something else got mixed in on the same sheet … and they show up here.
Although they are a minor annoyance on the scale of daily office goings-on, these patients are still a problem. Most are angry and frustrated, as they want to see me. Some are willing to schedule an appointment, but most aren’t. The awkward situation interrupts the routine flow of check-ins and phone calls, and it certainly isn’t something anyone waiting in the lobby wants to overhear. Oftentimes, I have to go up front to handle it, taking me away from a patient. In cases when the patient was referred by another doctor, they might call that office to complain.
It’s a losing situation for all involved. I wish there was some way to prevent them, but their uncertain nature makes it impossible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How often do you encounter phantom appointments?
What are phantom appointments? They’re patient visits that are nowhere on your schedule.
I’m not talking about someone who shows up on the wrong day or time. That’s at least partially understandable. I’m talking about people who you have no record of but say they have an appointment.
The first impression is to assume they’re scheduled with someone else in the building or another neurologist in my area, but they’ll often pull out a crumpled sheet of paper with my name and address on it, and a time circled.
Where on Earth do these people come from? I have no clue. When asked who made the appointment, it’s always “They made it for me,” or “They told me to be here.” It’s never clear who “they” are. These folks almost never can give you the name of their referring doctor, or who they spoke to. I’m a pretty small office here, just me and my secretary, so there aren’t many people here to talk to.
These aren’t common, maybe a handful per year, but generally unpleasant when they occur. If they happen to show up when I’ve got a gap in the schedule, I’ll try to see them, but the majority end up being turned away. We always offer to make an appointment for them, but most leave, usually angry.
I suspect some were referred for cognitive issues, which partially explains the confusion. Others may be doing it intentionally, hoping that they’ll be seen. (I suspect these are the minority.) Misinterpreted information from other offices likely plays a big part. Perhaps they were given my name and info by another office and told to make an appointment. Somehow, a time for something else got mixed in on the same sheet … and they show up here.
Although they are a minor annoyance on the scale of daily office goings-on, these patients are still a problem. Most are angry and frustrated, as they want to see me. Some are willing to schedule an appointment, but most aren’t. The awkward situation interrupts the routine flow of check-ins and phone calls, and it certainly isn’t something anyone waiting in the lobby wants to overhear. Oftentimes, I have to go up front to handle it, taking me away from a patient. In cases when the patient was referred by another doctor, they might call that office to complain.
It’s a losing situation for all involved. I wish there was some way to prevent them, but their uncertain nature makes it impossible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How often do you encounter phantom appointments?
What are phantom appointments? They’re patient visits that are nowhere on your schedule.
I’m not talking about someone who shows up on the wrong day or time. That’s at least partially understandable. I’m talking about people who you have no record of but say they have an appointment.
The first impression is to assume they’re scheduled with someone else in the building or another neurologist in my area, but they’ll often pull out a crumpled sheet of paper with my name and address on it, and a time circled.
Where on Earth do these people come from? I have no clue. When asked who made the appointment, it’s always “They made it for me,” or “They told me to be here.” It’s never clear who “they” are. These folks almost never can give you the name of their referring doctor, or who they spoke to. I’m a pretty small office here, just me and my secretary, so there aren’t many people here to talk to.
These aren’t common, maybe a handful per year, but generally unpleasant when they occur. If they happen to show up when I’ve got a gap in the schedule, I’ll try to see them, but the majority end up being turned away. We always offer to make an appointment for them, but most leave, usually angry.
I suspect some were referred for cognitive issues, which partially explains the confusion. Others may be doing it intentionally, hoping that they’ll be seen. (I suspect these are the minority.) Misinterpreted information from other offices likely plays a big part. Perhaps they were given my name and info by another office and told to make an appointment. Somehow, a time for something else got mixed in on the same sheet … and they show up here.
Although they are a minor annoyance on the scale of daily office goings-on, these patients are still a problem. Most are angry and frustrated, as they want to see me. Some are willing to schedule an appointment, but most aren’t. The awkward situation interrupts the routine flow of check-ins and phone calls, and it certainly isn’t something anyone waiting in the lobby wants to overhear. Oftentimes, I have to go up front to handle it, taking me away from a patient. In cases when the patient was referred by another doctor, they might call that office to complain.
It’s a losing situation for all involved. I wish there was some way to prevent them, but their uncertain nature makes it impossible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Coccidioidomycosis a respiratory threat to construction workers in Southwest
The expansion of the solar energy industry in Coccidioides-endemic areas of the southwestern United States is exposing more workers to the infection, say the authors of a study that found an attack rate of 1.2 cases per 100 workers.
A study among 3,572 workers at two solar power–generating facilities in California identified 44 individuals with the infection between October 2011 and April 2014, 9 of whom were hospitalized, according to a paper published in the Oct. 14 edition of Emerging Infectious Diseases.
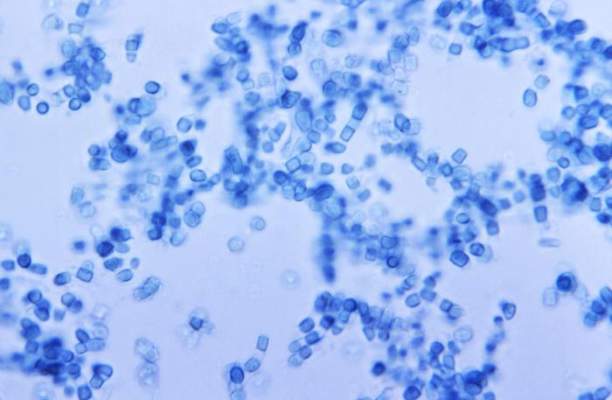
The disease is acquired through inhalation of the soil-dwelling Coccidioides fungus spores and while the majority of the patients said they had received safety training about the risk of coccidioidomycosis, only six of those who regularly performed soil-disruptive work reported regularly using respiratory protection (Emerg Infect Dis. 2015 Oct 14; doi: ).
“Large-scale construction, including solar farm construction, might involve substantial soil disturbance for months, and many employees, particularly from non–Coccidioides-endemic areas, probably lack immunity to Coccidioides,” wrote Jason A. Wilken, Ph.D., of the Centers for Disease Control and Prevention, and his coauthors.
“Medical providers should consider work-related coccidioidomycosis when evaluating construction workers with prolonged febrile respiratory illness, particularly after work in Central or Southern California or in Arizona, and medical providers should follow all statutory requirements for documenting and reporting occupational illness,” Dr. Wilken concluded.
The study was supported by the Centers for Disease Control and Prevention. No conflicts of interest were declared.
The expansion of the solar energy industry in Coccidioides-endemic areas of the southwestern United States is exposing more workers to the infection, say the authors of a study that found an attack rate of 1.2 cases per 100 workers.
A study among 3,572 workers at two solar power–generating facilities in California identified 44 individuals with the infection between October 2011 and April 2014, 9 of whom were hospitalized, according to a paper published in the Oct. 14 edition of Emerging Infectious Diseases.
The disease is acquired through inhalation of the soil-dwelling Coccidioides fungus spores and while the majority of the patients said they had received safety training about the risk of coccidioidomycosis, only six of those who regularly performed soil-disruptive work reported regularly using respiratory protection (Emerg Infect Dis. 2015 Oct 14; doi: ).
“Large-scale construction, including solar farm construction, might involve substantial soil disturbance for months, and many employees, particularly from non–Coccidioides-endemic areas, probably lack immunity to Coccidioides,” wrote Jason A. Wilken, Ph.D., of the Centers for Disease Control and Prevention, and his coauthors.
“Medical providers should consider work-related coccidioidomycosis when evaluating construction workers with prolonged febrile respiratory illness, particularly after work in Central or Southern California or in Arizona, and medical providers should follow all statutory requirements for documenting and reporting occupational illness,” Dr. Wilken concluded.
The study was supported by the Centers for Disease Control and Prevention. No conflicts of interest were declared.
The expansion of the solar energy industry in Coccidioides-endemic areas of the southwestern United States is exposing more workers to the infection, say the authors of a study that found an attack rate of 1.2 cases per 100 workers.
A study among 3,572 workers at two solar power–generating facilities in California identified 44 individuals with the infection between October 2011 and April 2014, 9 of whom were hospitalized, according to a paper published in the Oct. 14 edition of Emerging Infectious Diseases.
The disease is acquired through inhalation of the soil-dwelling Coccidioides fungus spores and while the majority of the patients said they had received safety training about the risk of coccidioidomycosis, only six of those who regularly performed soil-disruptive work reported regularly using respiratory protection (Emerg Infect Dis. 2015 Oct 14; doi: ).
“Large-scale construction, including solar farm construction, might involve substantial soil disturbance for months, and many employees, particularly from non–Coccidioides-endemic areas, probably lack immunity to Coccidioides,” wrote Jason A. Wilken, Ph.D., of the Centers for Disease Control and Prevention, and his coauthors.
“Medical providers should consider work-related coccidioidomycosis when evaluating construction workers with prolonged febrile respiratory illness, particularly after work in Central or Southern California or in Arizona, and medical providers should follow all statutory requirements for documenting and reporting occupational illness,” Dr. Wilken concluded.
The study was supported by the Centers for Disease Control and Prevention. No conflicts of interest were declared.
FROM EMERGING INFECTIOUS DISEASES
Key clinical point:Coccidioidomycosis is a significant risk in workers on solar power–generating facilities in Coccidioides-endemic areas of the Southwestern United States.
Major finding: The attack rate of Coccidioides could be as high 1.2 cases per 100 workers involved in constructing solar power–generating facilities.
Data source: A study among 3,572 workers at two solar power–generating facilities in California.
Disclosures: The study was supported by the Centers for Disease Control and Prevention. No conflicts of interest were declared.