User login
Team identifies problems with preclinical research

Poor study design and the tendency to publish positive—but not negative—results threaten the validity of preclinical research, according to an article published in eLife.
“Only a fraction of drugs that show promise in animals end up proving safe and effective in humans,” said study author Jonathan Kimmelman, PhD, of McGill University in Montreal, Quebec, Canada.
“An important reason is because studies in animals are often not well designed and because positive results have a higher chance of being published. They end up skewing what we think we know about the potential of a drug.”
Dr Kimmelman and his colleagues came to this conclusion after evaluating all published animal studies of sunitinib, a drug used to treat advanced kidney cancer, a rare type of stomach cancer, and rare tumors of the neuroendocrine system.
The investigators found evidence to suggest that studies reporting little or no anticancer effect were simply not published, leading anticancer effects of the drug to be overestimated by as much as 45%.
The team noted, however, that these findings do not raise any concerns about the clinical use of sunitinib.
Dr Kimmelman and his colleagues also found that few studies used practices like blinding or randomization. And it was often unclear how many animals had been tested because the sample size was not reported.
The drug was tested against different cancers, and all types tested showed statistically significant anticancer activity, a result that “strains credibility”, according to Dr Kimmelman.
He added that researchers failed to observe the dose-dependent response to the drug that is known to occur in humans.
Finally, the researchers did not test the drug on a range of animal models, focusing instead on juvenile female mice with a compromised immune system. Malignancies tested in a wider range of animal types, such as mice that have spontaneously developed tumors, showed less extreme effect sizes.
“Preclinical research is plagued by poor design and reporting practices, exposing patients to harmful and inactive agents, wasting time in the lab, and driving up the price of drugs,” Dr Kimmelman said.
“Our findings provide compelling reasons for developing and implementing guidelines for the design and reporting of preclinical studies in cancer, similar to those already in use for stroke, epilepsy, and cardiology.” ![]()
Poor study design and the tendency to publish positive—but not negative—results threaten the validity of preclinical research, according to an article published in eLife.
“Only a fraction of drugs that show promise in animals end up proving safe and effective in humans,” said study author Jonathan Kimmelman, PhD, of McGill University in Montreal, Quebec, Canada.
“An important reason is because studies in animals are often not well designed and because positive results have a higher chance of being published. They end up skewing what we think we know about the potential of a drug.”
Dr Kimmelman and his colleagues came to this conclusion after evaluating all published animal studies of sunitinib, a drug used to treat advanced kidney cancer, a rare type of stomach cancer, and rare tumors of the neuroendocrine system.
The investigators found evidence to suggest that studies reporting little or no anticancer effect were simply not published, leading anticancer effects of the drug to be overestimated by as much as 45%.
The team noted, however, that these findings do not raise any concerns about the clinical use of sunitinib.
Dr Kimmelman and his colleagues also found that few studies used practices like blinding or randomization. And it was often unclear how many animals had been tested because the sample size was not reported.
The drug was tested against different cancers, and all types tested showed statistically significant anticancer activity, a result that “strains credibility”, according to Dr Kimmelman.
He added that researchers failed to observe the dose-dependent response to the drug that is known to occur in humans.
Finally, the researchers did not test the drug on a range of animal models, focusing instead on juvenile female mice with a compromised immune system. Malignancies tested in a wider range of animal types, such as mice that have spontaneously developed tumors, showed less extreme effect sizes.
“Preclinical research is plagued by poor design and reporting practices, exposing patients to harmful and inactive agents, wasting time in the lab, and driving up the price of drugs,” Dr Kimmelman said.
“Our findings provide compelling reasons for developing and implementing guidelines for the design and reporting of preclinical studies in cancer, similar to those already in use for stroke, epilepsy, and cardiology.” ![]()
Poor study design and the tendency to publish positive—but not negative—results threaten the validity of preclinical research, according to an article published in eLife.
“Only a fraction of drugs that show promise in animals end up proving safe and effective in humans,” said study author Jonathan Kimmelman, PhD, of McGill University in Montreal, Quebec, Canada.
“An important reason is because studies in animals are often not well designed and because positive results have a higher chance of being published. They end up skewing what we think we know about the potential of a drug.”
Dr Kimmelman and his colleagues came to this conclusion after evaluating all published animal studies of sunitinib, a drug used to treat advanced kidney cancer, a rare type of stomach cancer, and rare tumors of the neuroendocrine system.
The investigators found evidence to suggest that studies reporting little or no anticancer effect were simply not published, leading anticancer effects of the drug to be overestimated by as much as 45%.
The team noted, however, that these findings do not raise any concerns about the clinical use of sunitinib.
Dr Kimmelman and his colleagues also found that few studies used practices like blinding or randomization. And it was often unclear how many animals had been tested because the sample size was not reported.
The drug was tested against different cancers, and all types tested showed statistically significant anticancer activity, a result that “strains credibility”, according to Dr Kimmelman.
He added that researchers failed to observe the dose-dependent response to the drug that is known to occur in humans.
Finally, the researchers did not test the drug on a range of animal models, focusing instead on juvenile female mice with a compromised immune system. Malignancies tested in a wider range of animal types, such as mice that have spontaneously developed tumors, showed less extreme effect sizes.
“Preclinical research is plagued by poor design and reporting practices, exposing patients to harmful and inactive agents, wasting time in the lab, and driving up the price of drugs,” Dr Kimmelman said.
“Our findings provide compelling reasons for developing and implementing guidelines for the design and reporting of preclinical studies in cancer, similar to those already in use for stroke, epilepsy, and cardiology.” ![]()
IDWeek: Rifapentine had best completion rates for health care workers with latent TB
SAN DIEGO – Health care workers with latent tuberculosis infection (LTBI) were significantly more likely to continue a shorter course of weekly rifapentine plus isoniazid (INH) than daily INH monotherapy, researchers reported at an annual scientific meeting on infectious diseases.
“Consideration should be given to no longer routinely recommending INH for the treatment of LTBI among health care workers,” said Dr. Esther Arguello Perez of Memorial Sloan Kettering Cancer Center, New York.

Health care workers face a greater risk of TB infection than the general population, regardless of the income level in the country where they live; patients with undiagnosed laryngeal or pulmonary TB usually pose the greatest risk, especially during procedures that cause coughing, such as sputum induction and bronchoscopy (Int J Tuberc Lung Dis. 2007;11[6]:593-605).
Although occupational TB testing is routine in U.S. health care organizations, more than half of health care workers who start treatment for LTBI historically have failed to finish (Chest. 2010;137[2]:401-9. doi: 10.1378/chest.09-0394). The standard LTBI regimen – 300 mg INH daily for 9 months – has been linked to potentially intolerable adverse effects such as hepatotoxicity, persistent gastrointestinal symptoms, rash, and neuropsychiatric problems (Drug Healthc Patient Saf. 2014;6:145-9. doi: 10.2147/DHPS.S68837).
In a 2011 multicenter trial, investigators reported a significantly higher completion rate for weekly rifapentine plus INH (900 mg each; 82% vs. 69% for daily INH; P < .001). Rates of adverse effects were significantly lower with weekly rifapentine plus INH, although grade 3-4 events and risk of death did not differ between the groups (N Engl J Med. 2011;365:2155-66. doi: 10.1056/NEJMoa1104875). The results of that trial quickly transformed recommendations for LTBI treatment (MMWR. 2011:60(48);1650-53).
Memorial Sloan Kettering implemented weekly rifapentine plus INH for its LTBI personnel in 2011. By 2014, about three-quarters of personnel with LTBI received rifapentine plus INH, while the rest were evenly split between rifampin and INH monotherapy, Dr. Arguello Perez reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
To understand how health care workers’ attitudes and treatment acceptance shifted along with practice, the investigators reviewed records from all health care workers at Memorial Sloan Kettering who were diagnosed with LTBI for 2005-2014. Among 930 patients, only 357 (38%) accepted treatment, although 76% of these individuals finished the regimen they started, she noted. Rifapentine plus INH had the highest completion rate (88%), significantly exceeding rates for a 4-month course of daily rifampin (84%) and for 9 months of INH monotherapy (70%; P < .01 for both differences). In contrast, completion rates for rifampin and INH did not significantly differ, Dr. Arguello Perez said.
Notably, LTBI treatment completion rates among health care workers rose by 26% between 2013, when most prescriptions were for rifampin or INH monotherapy, and 2014, when most were for rifapentine plus INH. “Health care workers might be more likely to accept treatment for LTBI if they know about alternatives to INH,” she concluded.
Dr. Arguello Perez and her associates reported no funding sources and had no financial disclosures.
SAN DIEGO – Health care workers with latent tuberculosis infection (LTBI) were significantly more likely to continue a shorter course of weekly rifapentine plus isoniazid (INH) than daily INH monotherapy, researchers reported at an annual scientific meeting on infectious diseases.
“Consideration should be given to no longer routinely recommending INH for the treatment of LTBI among health care workers,” said Dr. Esther Arguello Perez of Memorial Sloan Kettering Cancer Center, New York.
Health care workers face a greater risk of TB infection than the general population, regardless of the income level in the country where they live; patients with undiagnosed laryngeal or pulmonary TB usually pose the greatest risk, especially during procedures that cause coughing, such as sputum induction and bronchoscopy (Int J Tuberc Lung Dis. 2007;11[6]:593-605).
Although occupational TB testing is routine in U.S. health care organizations, more than half of health care workers who start treatment for LTBI historically have failed to finish (Chest. 2010;137[2]:401-9. doi: 10.1378/chest.09-0394). The standard LTBI regimen – 300 mg INH daily for 9 months – has been linked to potentially intolerable adverse effects such as hepatotoxicity, persistent gastrointestinal symptoms, rash, and neuropsychiatric problems (Drug Healthc Patient Saf. 2014;6:145-9. doi: 10.2147/DHPS.S68837).
In a 2011 multicenter trial, investigators reported a significantly higher completion rate for weekly rifapentine plus INH (900 mg each; 82% vs. 69% for daily INH; P < .001). Rates of adverse effects were significantly lower with weekly rifapentine plus INH, although grade 3-4 events and risk of death did not differ between the groups (N Engl J Med. 2011;365:2155-66. doi: 10.1056/NEJMoa1104875). The results of that trial quickly transformed recommendations for LTBI treatment (MMWR. 2011:60(48);1650-53).
Memorial Sloan Kettering implemented weekly rifapentine plus INH for its LTBI personnel in 2011. By 2014, about three-quarters of personnel with LTBI received rifapentine plus INH, while the rest were evenly split between rifampin and INH monotherapy, Dr. Arguello Perez reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
To understand how health care workers’ attitudes and treatment acceptance shifted along with practice, the investigators reviewed records from all health care workers at Memorial Sloan Kettering who were diagnosed with LTBI for 2005-2014. Among 930 patients, only 357 (38%) accepted treatment, although 76% of these individuals finished the regimen they started, she noted. Rifapentine plus INH had the highest completion rate (88%), significantly exceeding rates for a 4-month course of daily rifampin (84%) and for 9 months of INH monotherapy (70%; P < .01 for both differences). In contrast, completion rates for rifampin and INH did not significantly differ, Dr. Arguello Perez said.
Notably, LTBI treatment completion rates among health care workers rose by 26% between 2013, when most prescriptions were for rifampin or INH monotherapy, and 2014, when most were for rifapentine plus INH. “Health care workers might be more likely to accept treatment for LTBI if they know about alternatives to INH,” she concluded.
Dr. Arguello Perez and her associates reported no funding sources and had no financial disclosures.
SAN DIEGO – Health care workers with latent tuberculosis infection (LTBI) were significantly more likely to continue a shorter course of weekly rifapentine plus isoniazid (INH) than daily INH monotherapy, researchers reported at an annual scientific meeting on infectious diseases.
“Consideration should be given to no longer routinely recommending INH for the treatment of LTBI among health care workers,” said Dr. Esther Arguello Perez of Memorial Sloan Kettering Cancer Center, New York.
Health care workers face a greater risk of TB infection than the general population, regardless of the income level in the country where they live; patients with undiagnosed laryngeal or pulmonary TB usually pose the greatest risk, especially during procedures that cause coughing, such as sputum induction and bronchoscopy (Int J Tuberc Lung Dis. 2007;11[6]:593-605).
Although occupational TB testing is routine in U.S. health care organizations, more than half of health care workers who start treatment for LTBI historically have failed to finish (Chest. 2010;137[2]:401-9. doi: 10.1378/chest.09-0394). The standard LTBI regimen – 300 mg INH daily for 9 months – has been linked to potentially intolerable adverse effects such as hepatotoxicity, persistent gastrointestinal symptoms, rash, and neuropsychiatric problems (Drug Healthc Patient Saf. 2014;6:145-9. doi: 10.2147/DHPS.S68837).
In a 2011 multicenter trial, investigators reported a significantly higher completion rate for weekly rifapentine plus INH (900 mg each; 82% vs. 69% for daily INH; P < .001). Rates of adverse effects were significantly lower with weekly rifapentine plus INH, although grade 3-4 events and risk of death did not differ between the groups (N Engl J Med. 2011;365:2155-66. doi: 10.1056/NEJMoa1104875). The results of that trial quickly transformed recommendations for LTBI treatment (MMWR. 2011:60(48);1650-53).
Memorial Sloan Kettering implemented weekly rifapentine plus INH for its LTBI personnel in 2011. By 2014, about three-quarters of personnel with LTBI received rifapentine plus INH, while the rest were evenly split between rifampin and INH monotherapy, Dr. Arguello Perez reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
To understand how health care workers’ attitudes and treatment acceptance shifted along with practice, the investigators reviewed records from all health care workers at Memorial Sloan Kettering who were diagnosed with LTBI for 2005-2014. Among 930 patients, only 357 (38%) accepted treatment, although 76% of these individuals finished the regimen they started, she noted. Rifapentine plus INH had the highest completion rate (88%), significantly exceeding rates for a 4-month course of daily rifampin (84%) and for 9 months of INH monotherapy (70%; P < .01 for both differences). In contrast, completion rates for rifampin and INH did not significantly differ, Dr. Arguello Perez said.
Notably, LTBI treatment completion rates among health care workers rose by 26% between 2013, when most prescriptions were for rifampin or INH monotherapy, and 2014, when most were for rifapentine plus INH. “Health care workers might be more likely to accept treatment for LTBI if they know about alternatives to INH,” she concluded.
Dr. Arguello Perez and her associates reported no funding sources and had no financial disclosures.
AT IDweek 2015
Key clinical point: Isoniazid monotherapy should not be recommended routinely for health care workers with latent tuberculosis infections.
Major finding: Rates of treatment completion were significantly higher for weekly rifapentine plus isoniazid than for daily isoniazid monotherapy (P < .01).
Data source: Retrospective analysis of all health care workers with LTBI at Memorial Sloan Kettering Cancer Center during 2005-2014.
Disclosures: The researchers reported no funding sources and made no financial disclosures.

Depression, hypertension combo compounds cardiovascular risk
LONDON – The combination of depression and very high systolic blood pressure increased the risk for a major cardiovascular event by 83%, compared with normal blood pressure and no depression, in patients with existing heart disease, diabetes, or stroke.
In a large family practice–based study, the hazard ratio for first hospital admission due to myocardial infarction, stroke or heart failure, or cardiovascular death in patients with high (at least 160 mm Hg) systolic blood pressure who were also depressed was 1.83, a highly significant difference compared with individuals with normal BP and no depression.
The presence of depression also significantly increased the risk for these cardiovascular events by 36% in patients with lower systolic BPs, compared with those with normal BP and no depression.
“Patients with existing heart disease, diabetes, or stroke are more likely to have another heart attack or another stroke or die from heart problems than the general population,” Dr. Bhautesh Jani of the Institute of Health and Wellbeing, University of Glasgow (Scotland), said at the annual congress of the European Society of Cardiology.
“In particular, those who have extremes of blood pressure or those who have depressive symptoms are at higher risk, which has been shown by previous evidence. What is relatively unknown is the combined effect of having extremes of blood pressure and depressive symptoms together, and our study tried to address that problem,” Dr. Jani explained.
The study involved more than 35,500 individuals with existing heart disease, diabetes, or stroke living in Scotland, of whom 3,939 (11%) had at least one major cardiovascular event that needed hospital admission during a 4-year period. Patients had been divided into groups based on their systolic BP, and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) during 2008-2009. A HADS score of more than 7 was considered indicative of depression.
Dr. Jani noted that all the results were adjusted for multiple confounding factors, including age, gender, socioeconomic status, number of comorbid conditions, total cholesterol values, body mass index, and the initiation of antidepressant medication.
“The key implications I would suggest are for secondary prevention and to perhaps focus our resources on monitoring blood pressure and providing treatment in patients with associated depressive symptoms,” Dr. Jani proposed.
Dr. Christi Deaton, professor of clinical nursing research at the University of Cambridge (England), who commented on the study findings, noted that it highlighted the importance of raising awareness among both clinicians and patients of the potential risk associated with a combination of hypertension and depression, particularly among patients with a high level of other risk factors for further cardiovascular events.
“Screening patients for depression is very simple to do and you can start with a couple of questions asking about whether or not the patient felt sad or had low mood, and then go on to use other screening tools,” she observed. “All providers should be screening patients and thinking about the synergy of these two risk factors,” she said.

Other research presented at the ESC Congress by cardiologist Dr. Salim Hayek of Emory University in Atlanta also highlighted the importance of screening for depression, this time in patients with angina. In a study of 5,202 adults enrolled in the university’s biobank between 2004 and 2013 and who underwent left heart catheterization, patients with frequent chest pain were found to have more depressive symptoms than those without angina. Depressive symptoms in this study were assessed using the Patient Health Questionnaire (PHQ-9).
“Chest pain was more frequent in patients with mild depression with and without coronary artery disease, regardless of sex or history of myocardial infarction,” Dr. Hayek said. After multivariate analysis, depression was the most important predictor of frequent chest pain, he added. Other factors independently associated with chest pain frequency were female sex, coronary artery disease severity, history of MI, body mass index, and high blood lipid levels.
“At follow-up, a decrease in depressive symptoms was associated with improvement in chest pain,” Dr. Hayek said, but patients with depression who were revascularized did not show an improvement in chest pain.
The findings suggest that the association between chest pain and depression was independent of the underlying arterial disease and further studies are needed to look at the effect of revascularization and angina relief on depressive symptoms, and conversely if antidepressant medications could help alleviate chest pain.
The study Dr. Jani presented was funded by the Scottish Government. Dr. Jani and Dr. Hayek both reported having no disclosures.
This article was updated February 3, 2016.
LONDON – The combination of depression and very high systolic blood pressure increased the risk for a major cardiovascular event by 83%, compared with normal blood pressure and no depression, in patients with existing heart disease, diabetes, or stroke.
In a large family practice–based study, the hazard ratio for first hospital admission due to myocardial infarction, stroke or heart failure, or cardiovascular death in patients with high (at least 160 mm Hg) systolic blood pressure who were also depressed was 1.83, a highly significant difference compared with individuals with normal BP and no depression.
The presence of depression also significantly increased the risk for these cardiovascular events by 36% in patients with lower systolic BPs, compared with those with normal BP and no depression.
“Patients with existing heart disease, diabetes, or stroke are more likely to have another heart attack or another stroke or die from heart problems than the general population,” Dr. Bhautesh Jani of the Institute of Health and Wellbeing, University of Glasgow (Scotland), said at the annual congress of the European Society of Cardiology.
“In particular, those who have extremes of blood pressure or those who have depressive symptoms are at higher risk, which has been shown by previous evidence. What is relatively unknown is the combined effect of having extremes of blood pressure and depressive symptoms together, and our study tried to address that problem,” Dr. Jani explained.
The study involved more than 35,500 individuals with existing heart disease, diabetes, or stroke living in Scotland, of whom 3,939 (11%) had at least one major cardiovascular event that needed hospital admission during a 4-year period. Patients had been divided into groups based on their systolic BP, and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) during 2008-2009. A HADS score of more than 7 was considered indicative of depression.
Dr. Jani noted that all the results were adjusted for multiple confounding factors, including age, gender, socioeconomic status, number of comorbid conditions, total cholesterol values, body mass index, and the initiation of antidepressant medication.
“The key implications I would suggest are for secondary prevention and to perhaps focus our resources on monitoring blood pressure and providing treatment in patients with associated depressive symptoms,” Dr. Jani proposed.
Dr. Christi Deaton, professor of clinical nursing research at the University of Cambridge (England), who commented on the study findings, noted that it highlighted the importance of raising awareness among both clinicians and patients of the potential risk associated with a combination of hypertension and depression, particularly among patients with a high level of other risk factors for further cardiovascular events.
“Screening patients for depression is very simple to do and you can start with a couple of questions asking about whether or not the patient felt sad or had low mood, and then go on to use other screening tools,” she observed. “All providers should be screening patients and thinking about the synergy of these two risk factors,” she said.
Other research presented at the ESC Congress by cardiologist Dr. Salim Hayek of Emory University in Atlanta also highlighted the importance of screening for depression, this time in patients with angina. In a study of 5,202 adults enrolled in the university’s biobank between 2004 and 2013 and who underwent left heart catheterization, patients with frequent chest pain were found to have more depressive symptoms than those without angina. Depressive symptoms in this study were assessed using the Patient Health Questionnaire (PHQ-9).
“Chest pain was more frequent in patients with mild depression with and without coronary artery disease, regardless of sex or history of myocardial infarction,” Dr. Hayek said. After multivariate analysis, depression was the most important predictor of frequent chest pain, he added. Other factors independently associated with chest pain frequency were female sex, coronary artery disease severity, history of MI, body mass index, and high blood lipid levels.
“At follow-up, a decrease in depressive symptoms was associated with improvement in chest pain,” Dr. Hayek said, but patients with depression who were revascularized did not show an improvement in chest pain.
The findings suggest that the association between chest pain and depression was independent of the underlying arterial disease and further studies are needed to look at the effect of revascularization and angina relief on depressive symptoms, and conversely if antidepressant medications could help alleviate chest pain.
The study Dr. Jani presented was funded by the Scottish Government. Dr. Jani and Dr. Hayek both reported having no disclosures.
This article was updated February 3, 2016.
LONDON – The combination of depression and very high systolic blood pressure increased the risk for a major cardiovascular event by 83%, compared with normal blood pressure and no depression, in patients with existing heart disease, diabetes, or stroke.
In a large family practice–based study, the hazard ratio for first hospital admission due to myocardial infarction, stroke or heart failure, or cardiovascular death in patients with high (at least 160 mm Hg) systolic blood pressure who were also depressed was 1.83, a highly significant difference compared with individuals with normal BP and no depression.
The presence of depression also significantly increased the risk for these cardiovascular events by 36% in patients with lower systolic BPs, compared with those with normal BP and no depression.
“Patients with existing heart disease, diabetes, or stroke are more likely to have another heart attack or another stroke or die from heart problems than the general population,” Dr. Bhautesh Jani of the Institute of Health and Wellbeing, University of Glasgow (Scotland), said at the annual congress of the European Society of Cardiology.
“In particular, those who have extremes of blood pressure or those who have depressive symptoms are at higher risk, which has been shown by previous evidence. What is relatively unknown is the combined effect of having extremes of blood pressure and depressive symptoms together, and our study tried to address that problem,” Dr. Jani explained.
The study involved more than 35,500 individuals with existing heart disease, diabetes, or stroke living in Scotland, of whom 3,939 (11%) had at least one major cardiovascular event that needed hospital admission during a 4-year period. Patients had been divided into groups based on their systolic BP, and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) during 2008-2009. A HADS score of more than 7 was considered indicative of depression.
Dr. Jani noted that all the results were adjusted for multiple confounding factors, including age, gender, socioeconomic status, number of comorbid conditions, total cholesterol values, body mass index, and the initiation of antidepressant medication.
“The key implications I would suggest are for secondary prevention and to perhaps focus our resources on monitoring blood pressure and providing treatment in patients with associated depressive symptoms,” Dr. Jani proposed.
Dr. Christi Deaton, professor of clinical nursing research at the University of Cambridge (England), who commented on the study findings, noted that it highlighted the importance of raising awareness among both clinicians and patients of the potential risk associated with a combination of hypertension and depression, particularly among patients with a high level of other risk factors for further cardiovascular events.
“Screening patients for depression is very simple to do and you can start with a couple of questions asking about whether or not the patient felt sad or had low mood, and then go on to use other screening tools,” she observed. “All providers should be screening patients and thinking about the synergy of these two risk factors,” she said.
Other research presented at the ESC Congress by cardiologist Dr. Salim Hayek of Emory University in Atlanta also highlighted the importance of screening for depression, this time in patients with angina. In a study of 5,202 adults enrolled in the university’s biobank between 2004 and 2013 and who underwent left heart catheterization, patients with frequent chest pain were found to have more depressive symptoms than those without angina. Depressive symptoms in this study were assessed using the Patient Health Questionnaire (PHQ-9).
“Chest pain was more frequent in patients with mild depression with and without coronary artery disease, regardless of sex or history of myocardial infarction,” Dr. Hayek said. After multivariate analysis, depression was the most important predictor of frequent chest pain, he added. Other factors independently associated with chest pain frequency were female sex, coronary artery disease severity, history of MI, body mass index, and high blood lipid levels.
“At follow-up, a decrease in depressive symptoms was associated with improvement in chest pain,” Dr. Hayek said, but patients with depression who were revascularized did not show an improvement in chest pain.
The findings suggest that the association between chest pain and depression was independent of the underlying arterial disease and further studies are needed to look at the effect of revascularization and angina relief on depressive symptoms, and conversely if antidepressant medications could help alleviate chest pain.
The study Dr. Jani presented was funded by the Scottish Government. Dr. Jani and Dr. Hayek both reported having no disclosures.
This article was updated February 3, 2016.
AT THE ESC CONGRESS 2015
Key clinical point: Better monitoring and management of both hypertension and depression could help reduce further cardiovascular morbidity and mortality.
Major finding: The rate of major cardiovascular events was 83% higher in depressed patients with very high (at least 160 mm Hg) systolic BP, compared with individuals with normal pressure and no depression.
Data source: Large family practice study of 35,537 patients with existing coronary heart disease, diabetes, or stroke followed up for 4 years.
Disclosures: The study Dr. Jani presented was funded by the Scottish Government. Dr. Jani had no disclosures.

EADV: Prophylactic photodynamic therapy benefits transplant recipients
COPENHAGEN – Twice-yearly prophylactic photodynamic therapy for primary prevention of actinic keratoses and squamous cell carcinomas is a novel and effective strategy that addresses the problem of accelerated photocarcinogenesis in organ transplant recipients, according to an interim analysis of a multinational, randomized, controlled trial.
“The overall aim is to prevent squamous cell carcinoma development. Photodynamic therapy is well established for secondary prevention of further AKs, and these very early data show that it can also be used for primary prevention in very high-risk patients,” Dr. Katrine Togsverd-Bo said at the annual congress of the European Academy of Dermatology and Venereology.

Accelerated carcinogenesis on sun-exposed skin is a major concern in organ transplant recipients (OTRs). They experience early onset of multiple AKs, with field cancerization and up to a 100-fold increased risk of squamous cell carcinomas (SCCs). Moreover, their SCCs are at substantially greater risk of metastasis than SCCs occurring in the general population, noted Dr. Togsverd-Bo of Bispebjerg Hospital and the University of Copenhagen.
She presented an interim analysis of an ongoing 5-year prospective randomized trial in 50 renal transplant recipients at academic dermatology centers in Copenhagen, Oslo, and Gothenburg, Sweden. All participants had clinically normal-appearing skin at baseline, with no history of AKs or SCCs. They are undergoing twice-yearly, split-side photodynamic therapy (PDT) on the face, forearm, and hand, with the opposite side serving as the untreated control.
To date, 25 patients have completed 3 years of the study. At 3 years of prospective follow-up by blinded evaluators, 50% of patients had AKs on their untreated side, compared with 26% on the prophylactic PDT side. The collective number of AKs on untreated skin was 43, compared with just 8 AKs on PDT-treated skin. Seven patients had AKs only on their untreated side, six had AKs on both sides, and none had any AKs only on their PDT-treated side.
The twice-yearly prophylactic PDT regimen consists of a 3-hour application of 20% methyl aminolevulinate as a photosensitizer followed by applications of a conventional LED light at 37 J/cm2.
Dr. Togsverd-Bo reported having no financial conflicts regarding her study.
COPENHAGEN – Twice-yearly prophylactic photodynamic therapy for primary prevention of actinic keratoses and squamous cell carcinomas is a novel and effective strategy that addresses the problem of accelerated photocarcinogenesis in organ transplant recipients, according to an interim analysis of a multinational, randomized, controlled trial.
“The overall aim is to prevent squamous cell carcinoma development. Photodynamic therapy is well established for secondary prevention of further AKs, and these very early data show that it can also be used for primary prevention in very high-risk patients,” Dr. Katrine Togsverd-Bo said at the annual congress of the European Academy of Dermatology and Venereology.
Accelerated carcinogenesis on sun-exposed skin is a major concern in organ transplant recipients (OTRs). They experience early onset of multiple AKs, with field cancerization and up to a 100-fold increased risk of squamous cell carcinomas (SCCs). Moreover, their SCCs are at substantially greater risk of metastasis than SCCs occurring in the general population, noted Dr. Togsverd-Bo of Bispebjerg Hospital and the University of Copenhagen.
She presented an interim analysis of an ongoing 5-year prospective randomized trial in 50 renal transplant recipients at academic dermatology centers in Copenhagen, Oslo, and Gothenburg, Sweden. All participants had clinically normal-appearing skin at baseline, with no history of AKs or SCCs. They are undergoing twice-yearly, split-side photodynamic therapy (PDT) on the face, forearm, and hand, with the opposite side serving as the untreated control.
To date, 25 patients have completed 3 years of the study. At 3 years of prospective follow-up by blinded evaluators, 50% of patients had AKs on their untreated side, compared with 26% on the prophylactic PDT side. The collective number of AKs on untreated skin was 43, compared with just 8 AKs on PDT-treated skin. Seven patients had AKs only on their untreated side, six had AKs on both sides, and none had any AKs only on their PDT-treated side.
The twice-yearly prophylactic PDT regimen consists of a 3-hour application of 20% methyl aminolevulinate as a photosensitizer followed by applications of a conventional LED light at 37 J/cm2.
Dr. Togsverd-Bo reported having no financial conflicts regarding her study.
COPENHAGEN – Twice-yearly prophylactic photodynamic therapy for primary prevention of actinic keratoses and squamous cell carcinomas is a novel and effective strategy that addresses the problem of accelerated photocarcinogenesis in organ transplant recipients, according to an interim analysis of a multinational, randomized, controlled trial.
“The overall aim is to prevent squamous cell carcinoma development. Photodynamic therapy is well established for secondary prevention of further AKs, and these very early data show that it can also be used for primary prevention in very high-risk patients,” Dr. Katrine Togsverd-Bo said at the annual congress of the European Academy of Dermatology and Venereology.
Accelerated carcinogenesis on sun-exposed skin is a major concern in organ transplant recipients (OTRs). They experience early onset of multiple AKs, with field cancerization and up to a 100-fold increased risk of squamous cell carcinomas (SCCs). Moreover, their SCCs are at substantially greater risk of metastasis than SCCs occurring in the general population, noted Dr. Togsverd-Bo of Bispebjerg Hospital and the University of Copenhagen.
She presented an interim analysis of an ongoing 5-year prospective randomized trial in 50 renal transplant recipients at academic dermatology centers in Copenhagen, Oslo, and Gothenburg, Sweden. All participants had clinically normal-appearing skin at baseline, with no history of AKs or SCCs. They are undergoing twice-yearly, split-side photodynamic therapy (PDT) on the face, forearm, and hand, with the opposite side serving as the untreated control.
To date, 25 patients have completed 3 years of the study. At 3 years of prospective follow-up by blinded evaluators, 50% of patients had AKs on their untreated side, compared with 26% on the prophylactic PDT side. The collective number of AKs on untreated skin was 43, compared with just 8 AKs on PDT-treated skin. Seven patients had AKs only on their untreated side, six had AKs on both sides, and none had any AKs only on their PDT-treated side.
The twice-yearly prophylactic PDT regimen consists of a 3-hour application of 20% methyl aminolevulinate as a photosensitizer followed by applications of a conventional LED light at 37 J/cm2.
Dr. Togsverd-Bo reported having no financial conflicts regarding her study.
AT THE EADV CONGRESS
Key clinical point: Prophylactic photodynamic therapy is a new and effective strategy for primary prevention of actinic keratoses and squamous cell carcinomas in organ transplant recipients.
Major finding: At 3 years of follow-up, 25 renal transplant recipients collectively had 8 actinic keratoses on the side of their face, forearms, and hands treated with twice-yearly prophylactic photodynamic therapy, compared with 43 AKs on the untreated control side.
Data source: This is an interim 3-year analysis from an ongoing 5-year prospective multinational, randomized, controlled trial involving 50 renal transplant recipients.
Disclosures: The presenter reported having no financial conflicts regarding this ongoing study.

NCCN creates tool to aid treatment decisions

patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
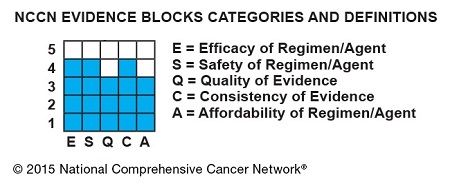
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
Lithium safe, effective for kids with bipolar type I
Lithium appears to be both safe and effective for the management of bipolar I disorder symptoms in pediatric populations, a recently published study from Pediatrics confirms.
Lead author Dr. Robert L. Findling of Johns Hopkins University and his associates conducted a multicenter, randomized, placebo-controlled outpatient trial, gathering data from 153 participants between the ages of 7 and 17 with bipolar I disorder/manic or mixed episodes. Among the participants, 81 were randomized to receive lithium (n = 53) or placebo (n = 28), for up to 8 weeks. Symptoms of bipolar disorder were assessed using the Young Mania Rating Scale (YMRS) score.
Ultimately, the study found that lithium was effective in reducing manic symptoms in nearly one-half (47%) of these participants, with Overall Clinical Global Impression–Improvement scores favoring lithium (n = 25; 47% very much/much improved), compared with placebo (n = 6; 21% very much/much improved) after 8 weeks. The researchers also noted that lithium use was not associated with weight gain, although they observed a statistically significant increase in thyrotropin concentration among the lithium group. Nausea, headache, and vomiting were the most common side effects.
“This study provides evidence to support the efficacy of lithium in the acute treatment of youths with [bipolar I disorder] who are currently in a manic or mixed state. Lithium had an adverse effect profile that was acceptable for most patients,” the authors wrote.
Read the full article in Pediatrics.
Lithium appears to be both safe and effective for the management of bipolar I disorder symptoms in pediatric populations, a recently published study from Pediatrics confirms.
Lead author Dr. Robert L. Findling of Johns Hopkins University and his associates conducted a multicenter, randomized, placebo-controlled outpatient trial, gathering data from 153 participants between the ages of 7 and 17 with bipolar I disorder/manic or mixed episodes. Among the participants, 81 were randomized to receive lithium (n = 53) or placebo (n = 28), for up to 8 weeks. Symptoms of bipolar disorder were assessed using the Young Mania Rating Scale (YMRS) score.
Ultimately, the study found that lithium was effective in reducing manic symptoms in nearly one-half (47%) of these participants, with Overall Clinical Global Impression–Improvement scores favoring lithium (n = 25; 47% very much/much improved), compared with placebo (n = 6; 21% very much/much improved) after 8 weeks. The researchers also noted that lithium use was not associated with weight gain, although they observed a statistically significant increase in thyrotropin concentration among the lithium group. Nausea, headache, and vomiting were the most common side effects.
“This study provides evidence to support the efficacy of lithium in the acute treatment of youths with [bipolar I disorder] who are currently in a manic or mixed state. Lithium had an adverse effect profile that was acceptable for most patients,” the authors wrote.
Read the full article in Pediatrics.
Lithium appears to be both safe and effective for the management of bipolar I disorder symptoms in pediatric populations, a recently published study from Pediatrics confirms.
Lead author Dr. Robert L. Findling of Johns Hopkins University and his associates conducted a multicenter, randomized, placebo-controlled outpatient trial, gathering data from 153 participants between the ages of 7 and 17 with bipolar I disorder/manic or mixed episodes. Among the participants, 81 were randomized to receive lithium (n = 53) or placebo (n = 28), for up to 8 weeks. Symptoms of bipolar disorder were assessed using the Young Mania Rating Scale (YMRS) score.
Ultimately, the study found that lithium was effective in reducing manic symptoms in nearly one-half (47%) of these participants, with Overall Clinical Global Impression–Improvement scores favoring lithium (n = 25; 47% very much/much improved), compared with placebo (n = 6; 21% very much/much improved) after 8 weeks. The researchers also noted that lithium use was not associated with weight gain, although they observed a statistically significant increase in thyrotropin concentration among the lithium group. Nausea, headache, and vomiting were the most common side effects.
“This study provides evidence to support the efficacy of lithium in the acute treatment of youths with [bipolar I disorder] who are currently in a manic or mixed state. Lithium had an adverse effect profile that was acceptable for most patients,” the authors wrote.
Read the full article in Pediatrics.
FROM PEDIATRICS
FDA approves reversal agent for dabigatran

treating a patient
Photo by Tom Watanabe
The US Food and Drug Administration (FDA) has granted accelerated approval for idarucizumab (Praxbind), the first reversal agent for the direct thrombin inhibitor dabigatran (Pradaxa).
Idarucizumab is now approved for use in emergency situations when there is a need to reverse the anticoagulant effect of dabigatran.
The FDA’s accelerated approval program allows the agency to approve drugs for serious conditions that fill an unmet medical need.
Accelerated approval is based on an effect on a surrogate or intermediate clinical endpoint that is reasonably likely to predict a clinical benefit to patients. So the company developing the drug is required to submit additional information after approval to confirm the drug’s clinical benefit.
About dabigatran and idarucizumab
Dabigatran is FDA-approved to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, as well as for the treatment and prevention of deep vein thrombosis and pulmonary embolism.
Idarucizumab is the first reversal agent approved specifically for dabigatran and works by binding to the drug compound to neutralize its effect. Idarucizumab is administered via intravenous injection.
Both idarucizumab and dabigatran are under development by Boehringer Ingelheim.
Idarucizumab has been studied in 3 randomized, double-blind, phase 1 trials of subjects who were not previously taking dabigatran and a phase 3 trial (RE-VERSE AD) of patients who were taking dabigatran and required reversal in an emergency setting.
Phase 1 trials
One phase 1 study (NCT01688830) enrolled 157 healthy male volunteers and consisted of 3 parts. Part 1 included 110 subjects who received placebo or idarucizumab at doses ranging from 20 mg to 8 g.
Idarucizumab (in the absence of dabigatran) was deemed safe and well tolerated. These results were published in Thrombosis and Haemostasis.
Parts 2 and 3 of the study included 47 subjects (part 2, n=35; part 3, n=12), and researchers investigated how well various doses of idarucizumab reversed the anticoagulant effect of dabigatran.
Results from parts 2 and 3 were published in The Lancet. The researchers said idarucizumab (given at 2 g or greater) provided immediate, complete, and sustained reversal of the anticoagulant effect of dabigatran, without producing serious adverse events.
In a second phase 1 study (NCT01955720), researchers evaluated idarucizumab in 46 subjects (males and females). This included healthy volunteers, elderly subjects, and participants with pre-existing mild or moderate kidney impairment.
Idarucizumab immediately and completely reversed dabigatran’s anticoagulant effect in these subjects, and they were able to restart dabigatran within 24 hours of receiving idarucizumab.
In addition, the researchers said there were no clinically relevant adverse events related to idarucizumab, and there were no relevant changes in any of the investigated safety parameters. These results were presented at the 2014 ASH Annual Meeting.
A third phase 1 study (NCT02028780) enrolled 80 healthy Japanese subjects. Researchers assessed the safety, tolerability, and pharmacokinetics of single, increasing doses of idarucizumab, administered both alone and after dabigatran.
Phase 3 trial
In the ongoing phase 3 trial, RE-VERSE AD, researchers are evaluating idarucizumab in emergency settings. The team reported interim results in 90 patients in NEJM and at the 2015 ISTH Congress.
Idarucizumab normalized diluted thrombin time and ecarin clotting time in a majority of patients who had uncontrolled or life-threatening bleeding complications while on dabigatran and in most patients who had to reverse dabigatran’s effects because they required emergency surgery or an invasive procedure.
The researchers said there were no safety concerns related to idarucizumab. However, 23% of patients experienced serious adverse events, 20% died, and several patients had thrombotic or bleeding events after receiving idarucizumab. ![]()
treating a patient
Photo by Tom Watanabe
The US Food and Drug Administration (FDA) has granted accelerated approval for idarucizumab (Praxbind), the first reversal agent for the direct thrombin inhibitor dabigatran (Pradaxa).
Idarucizumab is now approved for use in emergency situations when there is a need to reverse the anticoagulant effect of dabigatran.
The FDA’s accelerated approval program allows the agency to approve drugs for serious conditions that fill an unmet medical need.
Accelerated approval is based on an effect on a surrogate or intermediate clinical endpoint that is reasonably likely to predict a clinical benefit to patients. So the company developing the drug is required to submit additional information after approval to confirm the drug’s clinical benefit.
About dabigatran and idarucizumab
Dabigatran is FDA-approved to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, as well as for the treatment and prevention of deep vein thrombosis and pulmonary embolism.
Idarucizumab is the first reversal agent approved specifically for dabigatran and works by binding to the drug compound to neutralize its effect. Idarucizumab is administered via intravenous injection.
Both idarucizumab and dabigatran are under development by Boehringer Ingelheim.
Idarucizumab has been studied in 3 randomized, double-blind, phase 1 trials of subjects who were not previously taking dabigatran and a phase 3 trial (RE-VERSE AD) of patients who were taking dabigatran and required reversal in an emergency setting.
Phase 1 trials
One phase 1 study (NCT01688830) enrolled 157 healthy male volunteers and consisted of 3 parts. Part 1 included 110 subjects who received placebo or idarucizumab at doses ranging from 20 mg to 8 g.
Idarucizumab (in the absence of dabigatran) was deemed safe and well tolerated. These results were published in Thrombosis and Haemostasis.
Parts 2 and 3 of the study included 47 subjects (part 2, n=35; part 3, n=12), and researchers investigated how well various doses of idarucizumab reversed the anticoagulant effect of dabigatran.
Results from parts 2 and 3 were published in The Lancet. The researchers said idarucizumab (given at 2 g or greater) provided immediate, complete, and sustained reversal of the anticoagulant effect of dabigatran, without producing serious adverse events.
In a second phase 1 study (NCT01955720), researchers evaluated idarucizumab in 46 subjects (males and females). This included healthy volunteers, elderly subjects, and participants with pre-existing mild or moderate kidney impairment.
Idarucizumab immediately and completely reversed dabigatran’s anticoagulant effect in these subjects, and they were able to restart dabigatran within 24 hours of receiving idarucizumab.
In addition, the researchers said there were no clinically relevant adverse events related to idarucizumab, and there were no relevant changes in any of the investigated safety parameters. These results were presented at the 2014 ASH Annual Meeting.
A third phase 1 study (NCT02028780) enrolled 80 healthy Japanese subjects. Researchers assessed the safety, tolerability, and pharmacokinetics of single, increasing doses of idarucizumab, administered both alone and after dabigatran.
Phase 3 trial
In the ongoing phase 3 trial, RE-VERSE AD, researchers are evaluating idarucizumab in emergency settings. The team reported interim results in 90 patients in NEJM and at the 2015 ISTH Congress.
Idarucizumab normalized diluted thrombin time and ecarin clotting time in a majority of patients who had uncontrolled or life-threatening bleeding complications while on dabigatran and in most patients who had to reverse dabigatran’s effects because they required emergency surgery or an invasive procedure.
The researchers said there were no safety concerns related to idarucizumab. However, 23% of patients experienced serious adverse events, 20% died, and several patients had thrombotic or bleeding events after receiving idarucizumab. ![]()
treating a patient
Photo by Tom Watanabe
The US Food and Drug Administration (FDA) has granted accelerated approval for idarucizumab (Praxbind), the first reversal agent for the direct thrombin inhibitor dabigatran (Pradaxa).
Idarucizumab is now approved for use in emergency situations when there is a need to reverse the anticoagulant effect of dabigatran.
The FDA’s accelerated approval program allows the agency to approve drugs for serious conditions that fill an unmet medical need.
Accelerated approval is based on an effect on a surrogate or intermediate clinical endpoint that is reasonably likely to predict a clinical benefit to patients. So the company developing the drug is required to submit additional information after approval to confirm the drug’s clinical benefit.
About dabigatran and idarucizumab
Dabigatran is FDA-approved to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, as well as for the treatment and prevention of deep vein thrombosis and pulmonary embolism.
Idarucizumab is the first reversal agent approved specifically for dabigatran and works by binding to the drug compound to neutralize its effect. Idarucizumab is administered via intravenous injection.
Both idarucizumab and dabigatran are under development by Boehringer Ingelheim.
Idarucizumab has been studied in 3 randomized, double-blind, phase 1 trials of subjects who were not previously taking dabigatran and a phase 3 trial (RE-VERSE AD) of patients who were taking dabigatran and required reversal in an emergency setting.
Phase 1 trials
One phase 1 study (NCT01688830) enrolled 157 healthy male volunteers and consisted of 3 parts. Part 1 included 110 subjects who received placebo or idarucizumab at doses ranging from 20 mg to 8 g.
Idarucizumab (in the absence of dabigatran) was deemed safe and well tolerated. These results were published in Thrombosis and Haemostasis.
Parts 2 and 3 of the study included 47 subjects (part 2, n=35; part 3, n=12), and researchers investigated how well various doses of idarucizumab reversed the anticoagulant effect of dabigatran.
Results from parts 2 and 3 were published in The Lancet. The researchers said idarucizumab (given at 2 g or greater) provided immediate, complete, and sustained reversal of the anticoagulant effect of dabigatran, without producing serious adverse events.
In a second phase 1 study (NCT01955720), researchers evaluated idarucizumab in 46 subjects (males and females). This included healthy volunteers, elderly subjects, and participants with pre-existing mild or moderate kidney impairment.
Idarucizumab immediately and completely reversed dabigatran’s anticoagulant effect in these subjects, and they were able to restart dabigatran within 24 hours of receiving idarucizumab.
In addition, the researchers said there were no clinically relevant adverse events related to idarucizumab, and there were no relevant changes in any of the investigated safety parameters. These results were presented at the 2014 ASH Annual Meeting.
A third phase 1 study (NCT02028780) enrolled 80 healthy Japanese subjects. Researchers assessed the safety, tolerability, and pharmacokinetics of single, increasing doses of idarucizumab, administered both alone and after dabigatran.
Phase 3 trial
In the ongoing phase 3 trial, RE-VERSE AD, researchers are evaluating idarucizumab in emergency settings. The team reported interim results in 90 patients in NEJM and at the 2015 ISTH Congress.
Idarucizumab normalized diluted thrombin time and ecarin clotting time in a majority of patients who had uncontrolled or life-threatening bleeding complications while on dabigatran and in most patients who had to reverse dabigatran’s effects because they required emergency surgery or an invasive procedure.
The researchers said there were no safety concerns related to idarucizumab. However, 23% of patients experienced serious adverse events, 20% died, and several patients had thrombotic or bleeding events after receiving idarucizumab. ![]()
In ALL, early treatment decisions have “irrevocable” implications
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.

Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.
Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.
Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
EXPERT ANALYSIS AT NCCN ANNUAL CONGRESS: HEMATOLOGIC MALIGNANCIES

Idarucizumab approved as first agent to reverse a novel oral anticoagulant
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).

Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).
Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).
Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Endologix announces FDA approval of AFX2 Bifurcated Endograft
The U.S. Food and Drug Administration has approved the AFX2 Bifurcated Endograft System for the treatment of abdominal aortic aneurysms (AAA), the device’s manufacturer, Endologix, announced in a statement.
Endologix also touts the AFX2 as a way to facilitate percutaneous endovascular aneurysm repair (EVAR) by providing low-profile contralateral access through a 7F introducer. The device incorporates Endologix’s ActiveSeal technology, DuraPly expanded polytetrafluoroethylene graft material, and the Vela proximal endograft.
The AFX2 is expected to hit the market in the United States in the first quarter of 2016.
The U.S. Food and Drug Administration has approved the AFX2 Bifurcated Endograft System for the treatment of abdominal aortic aneurysms (AAA), the device’s manufacturer, Endologix, announced in a statement.
Endologix also touts the AFX2 as a way to facilitate percutaneous endovascular aneurysm repair (EVAR) by providing low-profile contralateral access through a 7F introducer. The device incorporates Endologix’s ActiveSeal technology, DuraPly expanded polytetrafluoroethylene graft material, and the Vela proximal endograft.
The AFX2 is expected to hit the market in the United States in the first quarter of 2016.
The U.S. Food and Drug Administration has approved the AFX2 Bifurcated Endograft System for the treatment of abdominal aortic aneurysms (AAA), the device’s manufacturer, Endologix, announced in a statement.
Endologix also touts the AFX2 as a way to facilitate percutaneous endovascular aneurysm repair (EVAR) by providing low-profile contralateral access through a 7F introducer. The device incorporates Endologix’s ActiveSeal technology, DuraPly expanded polytetrafluoroethylene graft material, and the Vela proximal endograft.
The AFX2 is expected to hit the market in the United States in the first quarter of 2016.