User login
Guidelines back multivessel PCI
New recommendations validate the treatment of partially blocked vessels along with the culprit vessel in patients undergoing a primary percutaneous coronary intervention for ST-elevation myocardial infarction (STEMI).
While 2013 guidelines by the American College of Cardiology and the American Heart Association cautioned against multivessel interventions as nonbeneficial in STEMI, evidence from four recent randomized controlled trials now supports the practice as “reasonable,” the updated guidelines say.
Partially blocked vessels may be treated in hemodynamically stable patients at the time of PCI or as a planned staged procedure.
The guidelines, issued Oct 21 by the ACC/AHA and the Society for Cardiovascular Angiography and Interventions, with collaboration from the American College of Emergency Physicians, have been published online in Journal of the American College of Cardiology (2015 Oct 21;10.1016/jacc.2015.10.005), Circulation, and Catheterization and Cardiovascular Interventions.
The guidelines also downgrade a prior recommendation on routine use of manual aspiration thrombectomy before primary PCI to implant a stent, citing evidence from three randomized trials (INFUSE-AMI, TASTE, and TOTAL) in support of the new class III “no benefit” recommendation. Previously, the organizations had considered this treatment strategy reasonable.
For the advice on primary PCI and multivessel treatment, the guideline authors, led by Dr. Glenn N. Levine of Baylor College of Medicine in Houston, identified four trials (PRAMI, CvLPRIT, DANAMI 3-PRIMULTI, PRAGUE-13) in which multivessel PCI, either staged or at the time of primary PCI, was shown to be nonharmful or beneficial in selected patients with STEMI. In three of these trials, multivessel treatment was shown associated with significant reductions in risk of death and other cardiac events compared to culprit-vessel-only treatment.
Previously, “differing inclusion criteria, study protocols, timing of multivessel PCI, statistical heterogeneity, and variable endpoints” made study results on culprit-only vs. multivessel PCI conflicting, Dr. Levine and colleagues wrote.
While the more recent RCTs have helped clarify a benefit or at least lack of harm, “there are insufficient observational data and no randomized data at this time to inform a recommendation with regard to the optimal timing of nonculprit vessel PCI,” the authors wrote, saying further studies were needed. Clinical data, lesion severity and complexity, and the risk of contrast nephropathy should be considered when determining whether to perform primary or staged multivessel PCI.
Earlier recommendations in 2011 and 2013 favoring aspiration thrombectomy before primary PCI had been based largely on the results of one single-center randomized study enrolling about 1,000 patients (Lancet 2008;371:1915-20).
Since then, much larger trials have shown no significant differences in major cardiac events or death in people who received aspiration thrombectomy prior to primary PCI compared with PCI alone, and a meta-analysis of more than 20,000 patients across 17 trials found no significant reduction in death, reinfarction, or stent thrombosis associated with routine aspiration thrombectomy vs. PCI alone (Circ Cardiovasc Interv. 2015;8:e002258).
The guideline authors clarified that the downgraded recommendation of “no benefit” applies only to routine use of aspiration thrombectomy before primary PCI. Current data remain inadequate to determine a benefit for selective or “bailout” aspiration thrombectomy, which is thrombectomy that, though unplanned, had to be used during the procedure because of an unsatisfactory initial result or a complication.
Several of the ACC/AHA/SCAI guideline authors or reviewers, including both vice chairs of the PCI writing committee, disclosed industry relationships.
New recommendations validate the treatment of partially blocked vessels along with the culprit vessel in patients undergoing a primary percutaneous coronary intervention for ST-elevation myocardial infarction (STEMI).
While 2013 guidelines by the American College of Cardiology and the American Heart Association cautioned against multivessel interventions as nonbeneficial in STEMI, evidence from four recent randomized controlled trials now supports the practice as “reasonable,” the updated guidelines say.
Partially blocked vessels may be treated in hemodynamically stable patients at the time of PCI or as a planned staged procedure.
The guidelines, issued Oct 21 by the ACC/AHA and the Society for Cardiovascular Angiography and Interventions, with collaboration from the American College of Emergency Physicians, have been published online in Journal of the American College of Cardiology (2015 Oct 21;10.1016/jacc.2015.10.005), Circulation, and Catheterization and Cardiovascular Interventions.
The guidelines also downgrade a prior recommendation on routine use of manual aspiration thrombectomy before primary PCI to implant a stent, citing evidence from three randomized trials (INFUSE-AMI, TASTE, and TOTAL) in support of the new class III “no benefit” recommendation. Previously, the organizations had considered this treatment strategy reasonable.
For the advice on primary PCI and multivessel treatment, the guideline authors, led by Dr. Glenn N. Levine of Baylor College of Medicine in Houston, identified four trials (PRAMI, CvLPRIT, DANAMI 3-PRIMULTI, PRAGUE-13) in which multivessel PCI, either staged or at the time of primary PCI, was shown to be nonharmful or beneficial in selected patients with STEMI. In three of these trials, multivessel treatment was shown associated with significant reductions in risk of death and other cardiac events compared to culprit-vessel-only treatment.
Previously, “differing inclusion criteria, study protocols, timing of multivessel PCI, statistical heterogeneity, and variable endpoints” made study results on culprit-only vs. multivessel PCI conflicting, Dr. Levine and colleagues wrote.
While the more recent RCTs have helped clarify a benefit or at least lack of harm, “there are insufficient observational data and no randomized data at this time to inform a recommendation with regard to the optimal timing of nonculprit vessel PCI,” the authors wrote, saying further studies were needed. Clinical data, lesion severity and complexity, and the risk of contrast nephropathy should be considered when determining whether to perform primary or staged multivessel PCI.
Earlier recommendations in 2011 and 2013 favoring aspiration thrombectomy before primary PCI had been based largely on the results of one single-center randomized study enrolling about 1,000 patients (Lancet 2008;371:1915-20).
Since then, much larger trials have shown no significant differences in major cardiac events or death in people who received aspiration thrombectomy prior to primary PCI compared with PCI alone, and a meta-analysis of more than 20,000 patients across 17 trials found no significant reduction in death, reinfarction, or stent thrombosis associated with routine aspiration thrombectomy vs. PCI alone (Circ Cardiovasc Interv. 2015;8:e002258).
The guideline authors clarified that the downgraded recommendation of “no benefit” applies only to routine use of aspiration thrombectomy before primary PCI. Current data remain inadequate to determine a benefit for selective or “bailout” aspiration thrombectomy, which is thrombectomy that, though unplanned, had to be used during the procedure because of an unsatisfactory initial result or a complication.
Several of the ACC/AHA/SCAI guideline authors or reviewers, including both vice chairs of the PCI writing committee, disclosed industry relationships.
New recommendations validate the treatment of partially blocked vessels along with the culprit vessel in patients undergoing a primary percutaneous coronary intervention for ST-elevation myocardial infarction (STEMI).
While 2013 guidelines by the American College of Cardiology and the American Heart Association cautioned against multivessel interventions as nonbeneficial in STEMI, evidence from four recent randomized controlled trials now supports the practice as “reasonable,” the updated guidelines say.
Partially blocked vessels may be treated in hemodynamically stable patients at the time of PCI or as a planned staged procedure.
The guidelines, issued Oct 21 by the ACC/AHA and the Society for Cardiovascular Angiography and Interventions, with collaboration from the American College of Emergency Physicians, have been published online in Journal of the American College of Cardiology (2015 Oct 21;10.1016/jacc.2015.10.005), Circulation, and Catheterization and Cardiovascular Interventions.
The guidelines also downgrade a prior recommendation on routine use of manual aspiration thrombectomy before primary PCI to implant a stent, citing evidence from three randomized trials (INFUSE-AMI, TASTE, and TOTAL) in support of the new class III “no benefit” recommendation. Previously, the organizations had considered this treatment strategy reasonable.
For the advice on primary PCI and multivessel treatment, the guideline authors, led by Dr. Glenn N. Levine of Baylor College of Medicine in Houston, identified four trials (PRAMI, CvLPRIT, DANAMI 3-PRIMULTI, PRAGUE-13) in which multivessel PCI, either staged or at the time of primary PCI, was shown to be nonharmful or beneficial in selected patients with STEMI. In three of these trials, multivessel treatment was shown associated with significant reductions in risk of death and other cardiac events compared to culprit-vessel-only treatment.
Previously, “differing inclusion criteria, study protocols, timing of multivessel PCI, statistical heterogeneity, and variable endpoints” made study results on culprit-only vs. multivessel PCI conflicting, Dr. Levine and colleagues wrote.
While the more recent RCTs have helped clarify a benefit or at least lack of harm, “there are insufficient observational data and no randomized data at this time to inform a recommendation with regard to the optimal timing of nonculprit vessel PCI,” the authors wrote, saying further studies were needed. Clinical data, lesion severity and complexity, and the risk of contrast nephropathy should be considered when determining whether to perform primary or staged multivessel PCI.
Earlier recommendations in 2011 and 2013 favoring aspiration thrombectomy before primary PCI had been based largely on the results of one single-center randomized study enrolling about 1,000 patients (Lancet 2008;371:1915-20).
Since then, much larger trials have shown no significant differences in major cardiac events or death in people who received aspiration thrombectomy prior to primary PCI compared with PCI alone, and a meta-analysis of more than 20,000 patients across 17 trials found no significant reduction in death, reinfarction, or stent thrombosis associated with routine aspiration thrombectomy vs. PCI alone (Circ Cardiovasc Interv. 2015;8:e002258).
The guideline authors clarified that the downgraded recommendation of “no benefit” applies only to routine use of aspiration thrombectomy before primary PCI. Current data remain inadequate to determine a benefit for selective or “bailout” aspiration thrombectomy, which is thrombectomy that, though unplanned, had to be used during the procedure because of an unsatisfactory initial result or a complication.
Several of the ACC/AHA/SCAI guideline authors or reviewers, including both vice chairs of the PCI writing committee, disclosed industry relationships.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
EADV: Best treatments for great saphenous vein reflux
COPENHAGEN – Superior 5-year outcomes for great saphenous vein reflux were achieved with conventional surgery and endovenous laser ablation as compared with ultrasound-guided foam sclerotherapy in a randomized trial, Dr. Simone van der Velden reported at the annual congress of the European Academy of Dermatology and Venereology.
The multicenter study included 224 randomized legs belonging to symptomatic patients with a target great saphenous vein diameter of at least 5 mm. If deemed necessary, patients could undergo one re-treatment at 3 or 12 months after their initial procedure. At 5 years of follow-up, 86% of the treated legs were available for long-term evaluation, noted Dr. van der Velden of Erasmus University Medical Center in Rotterdam, the Netherlands.

The primary endpoint was obliteration or absence of the treated great saphenous vein segment. This was achieved with conventional surgery in 85% of treated cases, in 77% of legs treated with endovenous laser ablation (EVLA), and in 23% with ultrasound-guided foam sclerotherapy (UGFS).
Absence of above-the-knee greater saphenous vein reflux – a secondary endpoint – was achieved in 85% of the conventional surgery group and in 82% of the EVLA group, both of which were significantly better results than the 41% response with UGFS.
Another secondary endpoint was grade II neovascularization. Here again, both conventional surgery and EVLA outperformed UGFS, with rates of 17%, 13%, and 4%, respectively. In contrast, there was no significant difference between the three treatment groups in terms of the presence of refluxing tributaries above or below knee level, she continued.
Scores on the disease-specific Chronic Venous Insufficiency quality of life Questionnaire (CIVIQ) deteriorated over time in the UGFS group, improved in the EVLA-treated patients, and remained stable in the conventional surgery group.
Conventional surgery was performed under general anesthesia and entailed high ligation of the saphenofemoral junction and phlebectomy of tributaries. In contrast, EVLA was done under local tumescent anesthesia using a 940-nm laser. The laser fiber was introduced at knee level, positioned 1-2 cm below the saphenofemoral junction, and delivered an energy of roughly 60 Joules/cm2.
For UGFS, operators utilized a foam comprising 1 mL of sodium tetradecyl sulfate per 3 mL of air. A maximum of 10 mL of foam could be injected per treatment session, depending upon the diameter of the great saphenous vein and length of the refluxing trunk. Phlebectomies in this group were performed only in the event of patient complaints.
Of note, patients in the minimally invasive UGFS group required re-treatment three times more often than did those in the other two study arms.
Dr. van der Velden said she has heard from some UGFS partisans that she and her coinvestigators may have undertreated patients in that study arm because they didn’t routinely perform phlebectomies of the tributaries, and the average amount of foam they injected, about 4.5 mL, was on the low side.
The study was sponsored by Erasmus University. Dr. van der Velden reported having no financial conflicts of interest.
COPENHAGEN – Superior 5-year outcomes for great saphenous vein reflux were achieved with conventional surgery and endovenous laser ablation as compared with ultrasound-guided foam sclerotherapy in a randomized trial, Dr. Simone van der Velden reported at the annual congress of the European Academy of Dermatology and Venereology.
The multicenter study included 224 randomized legs belonging to symptomatic patients with a target great saphenous vein diameter of at least 5 mm. If deemed necessary, patients could undergo one re-treatment at 3 or 12 months after their initial procedure. At 5 years of follow-up, 86% of the treated legs were available for long-term evaluation, noted Dr. van der Velden of Erasmus University Medical Center in Rotterdam, the Netherlands.
The primary endpoint was obliteration or absence of the treated great saphenous vein segment. This was achieved with conventional surgery in 85% of treated cases, in 77% of legs treated with endovenous laser ablation (EVLA), and in 23% with ultrasound-guided foam sclerotherapy (UGFS).
Absence of above-the-knee greater saphenous vein reflux – a secondary endpoint – was achieved in 85% of the conventional surgery group and in 82% of the EVLA group, both of which were significantly better results than the 41% response with UGFS.
Another secondary endpoint was grade II neovascularization. Here again, both conventional surgery and EVLA outperformed UGFS, with rates of 17%, 13%, and 4%, respectively. In contrast, there was no significant difference between the three treatment groups in terms of the presence of refluxing tributaries above or below knee level, she continued.
Scores on the disease-specific Chronic Venous Insufficiency quality of life Questionnaire (CIVIQ) deteriorated over time in the UGFS group, improved in the EVLA-treated patients, and remained stable in the conventional surgery group.
Conventional surgery was performed under general anesthesia and entailed high ligation of the saphenofemoral junction and phlebectomy of tributaries. In contrast, EVLA was done under local tumescent anesthesia using a 940-nm laser. The laser fiber was introduced at knee level, positioned 1-2 cm below the saphenofemoral junction, and delivered an energy of roughly 60 Joules/cm2.
For UGFS, operators utilized a foam comprising 1 mL of sodium tetradecyl sulfate per 3 mL of air. A maximum of 10 mL of foam could be injected per treatment session, depending upon the diameter of the great saphenous vein and length of the refluxing trunk. Phlebectomies in this group were performed only in the event of patient complaints.
Of note, patients in the minimally invasive UGFS group required re-treatment three times more often than did those in the other two study arms.
Dr. van der Velden said she has heard from some UGFS partisans that she and her coinvestigators may have undertreated patients in that study arm because they didn’t routinely perform phlebectomies of the tributaries, and the average amount of foam they injected, about 4.5 mL, was on the low side.
The study was sponsored by Erasmus University. Dr. van der Velden reported having no financial conflicts of interest.
COPENHAGEN – Superior 5-year outcomes for great saphenous vein reflux were achieved with conventional surgery and endovenous laser ablation as compared with ultrasound-guided foam sclerotherapy in a randomized trial, Dr. Simone van der Velden reported at the annual congress of the European Academy of Dermatology and Venereology.
The multicenter study included 224 randomized legs belonging to symptomatic patients with a target great saphenous vein diameter of at least 5 mm. If deemed necessary, patients could undergo one re-treatment at 3 or 12 months after their initial procedure. At 5 years of follow-up, 86% of the treated legs were available for long-term evaluation, noted Dr. van der Velden of Erasmus University Medical Center in Rotterdam, the Netherlands.
The primary endpoint was obliteration or absence of the treated great saphenous vein segment. This was achieved with conventional surgery in 85% of treated cases, in 77% of legs treated with endovenous laser ablation (EVLA), and in 23% with ultrasound-guided foam sclerotherapy (UGFS).
Absence of above-the-knee greater saphenous vein reflux – a secondary endpoint – was achieved in 85% of the conventional surgery group and in 82% of the EVLA group, both of which were significantly better results than the 41% response with UGFS.
Another secondary endpoint was grade II neovascularization. Here again, both conventional surgery and EVLA outperformed UGFS, with rates of 17%, 13%, and 4%, respectively. In contrast, there was no significant difference between the three treatment groups in terms of the presence of refluxing tributaries above or below knee level, she continued.
Scores on the disease-specific Chronic Venous Insufficiency quality of life Questionnaire (CIVIQ) deteriorated over time in the UGFS group, improved in the EVLA-treated patients, and remained stable in the conventional surgery group.
Conventional surgery was performed under general anesthesia and entailed high ligation of the saphenofemoral junction and phlebectomy of tributaries. In contrast, EVLA was done under local tumescent anesthesia using a 940-nm laser. The laser fiber was introduced at knee level, positioned 1-2 cm below the saphenofemoral junction, and delivered an energy of roughly 60 Joules/cm2.
For UGFS, operators utilized a foam comprising 1 mL of sodium tetradecyl sulfate per 3 mL of air. A maximum of 10 mL of foam could be injected per treatment session, depending upon the diameter of the great saphenous vein and length of the refluxing trunk. Phlebectomies in this group were performed only in the event of patient complaints.
Of note, patients in the minimally invasive UGFS group required re-treatment three times more often than did those in the other two study arms.
Dr. van der Velden said she has heard from some UGFS partisans that she and her coinvestigators may have undertreated patients in that study arm because they didn’t routinely perform phlebectomies of the tributaries, and the average amount of foam they injected, about 4.5 mL, was on the low side.
The study was sponsored by Erasmus University. Dr. van der Velden reported having no financial conflicts of interest.
AT THE EADV CONGRESS
Key clinical point: Long-term outcomes for treatment of great saphenous vein reflux were significantly better with conventional surgery or endovenous laser ablation than with ultrasound-guided foam sclerotherapy.
Major finding: Obliteration or absence of the treated great saphenous vein segment was achieved with conventional surgery in 85% of treated cases, with endovenous laser ablation (EVLA) in 77% of legs treated, and with ultrasound-guided foam sclerotherapy (UGFS) in 23%.
Data source: This multicenter clinical trial with 5-year follow-up included 224 legs randomized to one of three popular treatments for great saphenous varicose veins.
Disclosures: The study was sponsored by Erasmus University. The presenter reported having no financial conflicts of interest.

Ibrutinib may prove useful in MM, research shows

showing multiple myeloma
NEW YORK—Results of an open-label, phase 2, dose-escalation study of ibrutinib combined with low-dose dexamethasone suggest the Bruton’s tyrosine kinase (BTK) inhibitor may be useful in treating relapsed or relapsed and refractory patients with multiple myeloma (MM).
In the highest dose cohort, 23% of patients experienced a clinical benefit, which was defined as a minimal response or better by International Myeloma Working Group criteria.
“Ibrutinib is a remarkable agent and, through BTK inhibition, has been a game-changer in CLL [chronic lymphocytic leukemia],” said Paul Richardson, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
Dr Richardson reported results with ibrutinib in MM at Lymphoma & Myeloma 2015.
The rationale for the use of ibrutinib in myeloma is the robust BTK expression in the plasma cells of MM patients as well as its regulation of myeloma “stemness” in the bone marrow.
Ibrutinib plus low-dose dexamethasone has previously demonstrated activity in myeloma at the highest dose tested in a phase 1 trial.
So investigators continued to evaluate ibrutinib in 4 dose cohorts, with and without dexamathesone, and enrolled 92 relapsed/refractory MM patients. Dr Richardson described the results of cohort 4, which met criteria for expansion as of March 2015.
The investigators enrolled 43 patients in cohort 4 to receive 840 mg daily of ibrutinib plus 40 mg of dexamethasone weekly. This dose of ibrutinib is double the dose approved by the US Food and Drug Administration (FDA) for treatment of CLL and Waldenström’s macroglobulinemia.
The patient population was “very typical” for a relapsed/refractory patient population, Dr Richardson noted. The median age was 65 years (range, 43–81), almost two-thirds were male, and they had a median of 4 (range, 2–10) prior therapies.
More than half of patients had an ECOG performance status of 0 or 1, and their median time since diagnosis was 6.5 years.
Nineteen percent had t(11;14), and other chromosomal abnormalities included del 13q14, t(4:14), and del 17p. Twenty-three patients were ISS stage I, 16 were ISS stage II, and 4 were ISS stage III.
Seventy-seven percent of patients had received an autologous stem cell transplant, 95% had prior alkylator treatment, 91% prior lenalidomide, 58% prior thalidomide, and 91% prior bortezomib treatment.
All patients were steroid-refractory. Thirty-five percent were refractory to alkylator treatment, 61% were refractory to lenalidomide, and 49% were refractory to bortezomib.
“And even a number of them had been exposed to pomalidomide and also to carfilzomib,” Dr Richardson said, “recognizing that these are the new and exciting drugs on the block, but, at the same time, a significant number of our patients already received those therapies.”
Five percent of patients achieved a partial response to ibrutinib and low-dose dexamethasone, and 18% achieved a minimal response, for a clinical benefit rate of 23%. Thirty percent had stable disease after 4 or more cycles.
“What was particularly striking,” Dr Richardson said, “was at the top dose, the 840-mg dose, the progression-free survival.”
The median time to disease progression was 5.4 months (range, 0.0–16.4), which the investigators thought was compelling in this large study.
Dr Richardson noted that there were no significant differences in safety observed across all dose cohorts, although 55% of patients experienced a grade 3 or greater treatment-emergent adverse event (AE), while 29% experienced at least 1 serious AE. And 10% of patients experienced peripheral neuropathy (PN), 8 of whom had a prior history of PN.
Treatment-emergent hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included anemia (23%) and thrombocytopenia (21%). Grade 3/4 anemia and thrombocytopenia occurred in 9% of patients in each category.
Treatment-emergent non-hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included diarrhea (63%), fatigue (49%), cough (26%), nausea (23%), and muscle spasms (21%). Two percent of patients had grade 3/4 diarrhea. There were no other grade 3/4 adverse events in the cohort.
Eighty-six percent of patients in cohort 4 discontinued treatment, 60% due to progressive disease, 12% due to an AE, and 2% at the discretion of the investigator. Twelve percent withdrew, were noncompliant, or required concomitant medication that was not permitted by the protocol.
Overall, Dr Richardson said, the safety profile was manageable, similar across the dosing cohorts, and consistent with those seen in CLL and Waldenström’s macroglobulinemia. The 840-mg dose did not increase toxicity and demonstrated activity in this heavily pretreated population.
“The real signal that struck us,” Dr Richardson emphasized, “was the progression-free survival at 5.4 months . . . for a 92-patient, multicenter experience, this is obviously, I think, an encouraging start.”
Investigators continue to explore ibrutinib in 2 ongoing combination studies, one with carfilzomib and dexamethasone (PCYC-1119) and another with pomalidomide and dexamethasone (PCYC-1138). Another trial with lenalidomide and dexamethasone is planned.
Ibrutinib now has 4 FDA-approved indications: patients with CLL who have received at least 1 prior therapy, CLL patients with del 17p, patients with mantle cell lymphoma, and patients with Waldenström’s macroglobulinemia.
Ibrutinib is distributed and marketed as Imbruvica by Pharmacyclics and also marketed by Janssen Biotech, Inc. ![]()
showing multiple myeloma
NEW YORK—Results of an open-label, phase 2, dose-escalation study of ibrutinib combined with low-dose dexamethasone suggest the Bruton’s tyrosine kinase (BTK) inhibitor may be useful in treating relapsed or relapsed and refractory patients with multiple myeloma (MM).
In the highest dose cohort, 23% of patients experienced a clinical benefit, which was defined as a minimal response or better by International Myeloma Working Group criteria.
“Ibrutinib is a remarkable agent and, through BTK inhibition, has been a game-changer in CLL [chronic lymphocytic leukemia],” said Paul Richardson, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
Dr Richardson reported results with ibrutinib in MM at Lymphoma & Myeloma 2015.
The rationale for the use of ibrutinib in myeloma is the robust BTK expression in the plasma cells of MM patients as well as its regulation of myeloma “stemness” in the bone marrow.
Ibrutinib plus low-dose dexamethasone has previously demonstrated activity in myeloma at the highest dose tested in a phase 1 trial.
So investigators continued to evaluate ibrutinib in 4 dose cohorts, with and without dexamathesone, and enrolled 92 relapsed/refractory MM patients. Dr Richardson described the results of cohort 4, which met criteria for expansion as of March 2015.
The investigators enrolled 43 patients in cohort 4 to receive 840 mg daily of ibrutinib plus 40 mg of dexamethasone weekly. This dose of ibrutinib is double the dose approved by the US Food and Drug Administration (FDA) for treatment of CLL and Waldenström’s macroglobulinemia.
The patient population was “very typical” for a relapsed/refractory patient population, Dr Richardson noted. The median age was 65 years (range, 43–81), almost two-thirds were male, and they had a median of 4 (range, 2–10) prior therapies.
More than half of patients had an ECOG performance status of 0 or 1, and their median time since diagnosis was 6.5 years.
Nineteen percent had t(11;14), and other chromosomal abnormalities included del 13q14, t(4:14), and del 17p. Twenty-three patients were ISS stage I, 16 were ISS stage II, and 4 were ISS stage III.
Seventy-seven percent of patients had received an autologous stem cell transplant, 95% had prior alkylator treatment, 91% prior lenalidomide, 58% prior thalidomide, and 91% prior bortezomib treatment.
All patients were steroid-refractory. Thirty-five percent were refractory to alkylator treatment, 61% were refractory to lenalidomide, and 49% were refractory to bortezomib.
“And even a number of them had been exposed to pomalidomide and also to carfilzomib,” Dr Richardson said, “recognizing that these are the new and exciting drugs on the block, but, at the same time, a significant number of our patients already received those therapies.”
Five percent of patients achieved a partial response to ibrutinib and low-dose dexamethasone, and 18% achieved a minimal response, for a clinical benefit rate of 23%. Thirty percent had stable disease after 4 or more cycles.
“What was particularly striking,” Dr Richardson said, “was at the top dose, the 840-mg dose, the progression-free survival.”
The median time to disease progression was 5.4 months (range, 0.0–16.4), which the investigators thought was compelling in this large study.
Dr Richardson noted that there were no significant differences in safety observed across all dose cohorts, although 55% of patients experienced a grade 3 or greater treatment-emergent adverse event (AE), while 29% experienced at least 1 serious AE. And 10% of patients experienced peripheral neuropathy (PN), 8 of whom had a prior history of PN.
Treatment-emergent hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included anemia (23%) and thrombocytopenia (21%). Grade 3/4 anemia and thrombocytopenia occurred in 9% of patients in each category.
Treatment-emergent non-hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included diarrhea (63%), fatigue (49%), cough (26%), nausea (23%), and muscle spasms (21%). Two percent of patients had grade 3/4 diarrhea. There were no other grade 3/4 adverse events in the cohort.
Eighty-six percent of patients in cohort 4 discontinued treatment, 60% due to progressive disease, 12% due to an AE, and 2% at the discretion of the investigator. Twelve percent withdrew, were noncompliant, or required concomitant medication that was not permitted by the protocol.
Overall, Dr Richardson said, the safety profile was manageable, similar across the dosing cohorts, and consistent with those seen in CLL and Waldenström’s macroglobulinemia. The 840-mg dose did not increase toxicity and demonstrated activity in this heavily pretreated population.
“The real signal that struck us,” Dr Richardson emphasized, “was the progression-free survival at 5.4 months . . . for a 92-patient, multicenter experience, this is obviously, I think, an encouraging start.”
Investigators continue to explore ibrutinib in 2 ongoing combination studies, one with carfilzomib and dexamethasone (PCYC-1119) and another with pomalidomide and dexamethasone (PCYC-1138). Another trial with lenalidomide and dexamethasone is planned.
Ibrutinib now has 4 FDA-approved indications: patients with CLL who have received at least 1 prior therapy, CLL patients with del 17p, patients with mantle cell lymphoma, and patients with Waldenström’s macroglobulinemia.
Ibrutinib is distributed and marketed as Imbruvica by Pharmacyclics and also marketed by Janssen Biotech, Inc. ![]()
showing multiple myeloma
NEW YORK—Results of an open-label, phase 2, dose-escalation study of ibrutinib combined with low-dose dexamethasone suggest the Bruton’s tyrosine kinase (BTK) inhibitor may be useful in treating relapsed or relapsed and refractory patients with multiple myeloma (MM).
In the highest dose cohort, 23% of patients experienced a clinical benefit, which was defined as a minimal response or better by International Myeloma Working Group criteria.
“Ibrutinib is a remarkable agent and, through BTK inhibition, has been a game-changer in CLL [chronic lymphocytic leukemia],” said Paul Richardson, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
Dr Richardson reported results with ibrutinib in MM at Lymphoma & Myeloma 2015.
The rationale for the use of ibrutinib in myeloma is the robust BTK expression in the plasma cells of MM patients as well as its regulation of myeloma “stemness” in the bone marrow.
Ibrutinib plus low-dose dexamethasone has previously demonstrated activity in myeloma at the highest dose tested in a phase 1 trial.
So investigators continued to evaluate ibrutinib in 4 dose cohorts, with and without dexamathesone, and enrolled 92 relapsed/refractory MM patients. Dr Richardson described the results of cohort 4, which met criteria for expansion as of March 2015.
The investigators enrolled 43 patients in cohort 4 to receive 840 mg daily of ibrutinib plus 40 mg of dexamethasone weekly. This dose of ibrutinib is double the dose approved by the US Food and Drug Administration (FDA) for treatment of CLL and Waldenström’s macroglobulinemia.
The patient population was “very typical” for a relapsed/refractory patient population, Dr Richardson noted. The median age was 65 years (range, 43–81), almost two-thirds were male, and they had a median of 4 (range, 2–10) prior therapies.
More than half of patients had an ECOG performance status of 0 or 1, and their median time since diagnosis was 6.5 years.
Nineteen percent had t(11;14), and other chromosomal abnormalities included del 13q14, t(4:14), and del 17p. Twenty-three patients were ISS stage I, 16 were ISS stage II, and 4 were ISS stage III.
Seventy-seven percent of patients had received an autologous stem cell transplant, 95% had prior alkylator treatment, 91% prior lenalidomide, 58% prior thalidomide, and 91% prior bortezomib treatment.
All patients were steroid-refractory. Thirty-five percent were refractory to alkylator treatment, 61% were refractory to lenalidomide, and 49% were refractory to bortezomib.
“And even a number of them had been exposed to pomalidomide and also to carfilzomib,” Dr Richardson said, “recognizing that these are the new and exciting drugs on the block, but, at the same time, a significant number of our patients already received those therapies.”
Five percent of patients achieved a partial response to ibrutinib and low-dose dexamethasone, and 18% achieved a minimal response, for a clinical benefit rate of 23%. Thirty percent had stable disease after 4 or more cycles.
“What was particularly striking,” Dr Richardson said, “was at the top dose, the 840-mg dose, the progression-free survival.”
The median time to disease progression was 5.4 months (range, 0.0–16.4), which the investigators thought was compelling in this large study.
Dr Richardson noted that there were no significant differences in safety observed across all dose cohorts, although 55% of patients experienced a grade 3 or greater treatment-emergent adverse event (AE), while 29% experienced at least 1 serious AE. And 10% of patients experienced peripheral neuropathy (PN), 8 of whom had a prior history of PN.
Treatment-emergent hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included anemia (23%) and thrombocytopenia (21%). Grade 3/4 anemia and thrombocytopenia occurred in 9% of patients in each category.
Treatment-emergent non-hematologic AEs of any grade in cohort 4 occurring in more than 20% of patients included diarrhea (63%), fatigue (49%), cough (26%), nausea (23%), and muscle spasms (21%). Two percent of patients had grade 3/4 diarrhea. There were no other grade 3/4 adverse events in the cohort.
Eighty-six percent of patients in cohort 4 discontinued treatment, 60% due to progressive disease, 12% due to an AE, and 2% at the discretion of the investigator. Twelve percent withdrew, were noncompliant, or required concomitant medication that was not permitted by the protocol.
Overall, Dr Richardson said, the safety profile was manageable, similar across the dosing cohorts, and consistent with those seen in CLL and Waldenström’s macroglobulinemia. The 840-mg dose did not increase toxicity and demonstrated activity in this heavily pretreated population.
“The real signal that struck us,” Dr Richardson emphasized, “was the progression-free survival at 5.4 months . . . for a 92-patient, multicenter experience, this is obviously, I think, an encouraging start.”
Investigators continue to explore ibrutinib in 2 ongoing combination studies, one with carfilzomib and dexamethasone (PCYC-1119) and another with pomalidomide and dexamethasone (PCYC-1138). Another trial with lenalidomide and dexamethasone is planned.
Ibrutinib now has 4 FDA-approved indications: patients with CLL who have received at least 1 prior therapy, CLL patients with del 17p, patients with mantle cell lymphoma, and patients with Waldenström’s macroglobulinemia.
Ibrutinib is distributed and marketed as Imbruvica by Pharmacyclics and also marketed by Janssen Biotech, Inc. ![]()
Snake venom helps hydrogels stop bleeding

Hartgerink, PhD, (left)
and Vivek Kumar, PhD
Photo courtesy of
Jeff Fitlow/Rice University
A nanofiber hydrogel infused with snake venom can stop bleeding quickly, even in the presence of anticoagulants, according to researchers.
The hydrogel, SB50, incorporates batroxobin, a venom produced by 2 species of South American pit viper.
SB50 can be injected as a liquid and transforms into a gel that conforms to the site of a wound, keeping it closed and promoting clotting within seconds.
The researchers described this hydrogel in ACS Biomaterials Science and Engineering.
Batroxobin was recognized for its properties as a coagulant in 1936. It has been used to remove excess fibrin proteins from the blood to treat thrombosis and as a topical hemostat. It has also been used as a diagnostic tool to determine blood-clotting time in the presence of heparin.
“From a clinical perspective, that’s far and away the most important issue here,” said study author
Jeffrey Hartgerink, PhD, of Rice University in Houston, Texas.
“There’s a lot of different things that can trigger blood coagulation, but when you’re on heparin, most of them don’t work or they work slowly or poorly. The use of batroxobin allows us to get around this problem because it can immediately start the clotting process, regardless of whether heparin is there or not.”
The batroxobin combined with the researchers’ hydrogels isn’t taken directly from snakes, Dr Hartgerink noted. The substance used for medicine is produced by genetically modified bacteria and then purified, avoiding the risk of other contaminant toxins.
The researchers combined batroxobin with their synthetic, self-assembling nanofibers, which can be loaded into a syringe and injected at the site of a wound, where they reassemble themselves into a gel.
Tests showed the new material stopped a wound from bleeding in as little as 6 seconds, and further prodding of the wound minutes later did not reopen it.
The researchers also tested several other options: the hydrogel without batroxobin, the batroxobin without the hydrogel, a current clinical hemostat known as GelFoam, and an alternative self-assembling hemostat known as Puramatrix. None of these options were as effective, especially in the presence of anticoagulants.
The new work builds upon the researchers’ development of injectable hydrogel scaffolds that help wounds heal and grow natural tissue. The synthetic scaffolds are built from the peptide sequences to mimic natural processes.
“We think SB50 has great potential to stop surgical bleeding, particularly in difficult cases in which the patient is taking heparin or other anticoagulants,” Dr Hartgerink said. “SB50 takes the powerful clotting ability of this snake venom and makes it far more effective by delivering it in an easily localized hydrogel that prevents possible unwanted systemic effects from using batroxobin alone.” ![]()
Hartgerink, PhD, (left)
and Vivek Kumar, PhD
Photo courtesy of
Jeff Fitlow/Rice University
A nanofiber hydrogel infused with snake venom can stop bleeding quickly, even in the presence of anticoagulants, according to researchers.
The hydrogel, SB50, incorporates batroxobin, a venom produced by 2 species of South American pit viper.
SB50 can be injected as a liquid and transforms into a gel that conforms to the site of a wound, keeping it closed and promoting clotting within seconds.
The researchers described this hydrogel in ACS Biomaterials Science and Engineering.
Batroxobin was recognized for its properties as a coagulant in 1936. It has been used to remove excess fibrin proteins from the blood to treat thrombosis and as a topical hemostat. It has also been used as a diagnostic tool to determine blood-clotting time in the presence of heparin.
“From a clinical perspective, that’s far and away the most important issue here,” said study author
Jeffrey Hartgerink, PhD, of Rice University in Houston, Texas.
“There’s a lot of different things that can trigger blood coagulation, but when you’re on heparin, most of them don’t work or they work slowly or poorly. The use of batroxobin allows us to get around this problem because it can immediately start the clotting process, regardless of whether heparin is there or not.”
The batroxobin combined with the researchers’ hydrogels isn’t taken directly from snakes, Dr Hartgerink noted. The substance used for medicine is produced by genetically modified bacteria and then purified, avoiding the risk of other contaminant toxins.
The researchers combined batroxobin with their synthetic, self-assembling nanofibers, which can be loaded into a syringe and injected at the site of a wound, where they reassemble themselves into a gel.
Tests showed the new material stopped a wound from bleeding in as little as 6 seconds, and further prodding of the wound minutes later did not reopen it.
The researchers also tested several other options: the hydrogel without batroxobin, the batroxobin without the hydrogel, a current clinical hemostat known as GelFoam, and an alternative self-assembling hemostat known as Puramatrix. None of these options were as effective, especially in the presence of anticoagulants.
The new work builds upon the researchers’ development of injectable hydrogel scaffolds that help wounds heal and grow natural tissue. The synthetic scaffolds are built from the peptide sequences to mimic natural processes.
“We think SB50 has great potential to stop surgical bleeding, particularly in difficult cases in which the patient is taking heparin or other anticoagulants,” Dr Hartgerink said. “SB50 takes the powerful clotting ability of this snake venom and makes it far more effective by delivering it in an easily localized hydrogel that prevents possible unwanted systemic effects from using batroxobin alone.” ![]()
Hartgerink, PhD, (left)
and Vivek Kumar, PhD
Photo courtesy of
Jeff Fitlow/Rice University
A nanofiber hydrogel infused with snake venom can stop bleeding quickly, even in the presence of anticoagulants, according to researchers.
The hydrogel, SB50, incorporates batroxobin, a venom produced by 2 species of South American pit viper.
SB50 can be injected as a liquid and transforms into a gel that conforms to the site of a wound, keeping it closed and promoting clotting within seconds.
The researchers described this hydrogel in ACS Biomaterials Science and Engineering.
Batroxobin was recognized for its properties as a coagulant in 1936. It has been used to remove excess fibrin proteins from the blood to treat thrombosis and as a topical hemostat. It has also been used as a diagnostic tool to determine blood-clotting time in the presence of heparin.
“From a clinical perspective, that’s far and away the most important issue here,” said study author
Jeffrey Hartgerink, PhD, of Rice University in Houston, Texas.
“There’s a lot of different things that can trigger blood coagulation, but when you’re on heparin, most of them don’t work or they work slowly or poorly. The use of batroxobin allows us to get around this problem because it can immediately start the clotting process, regardless of whether heparin is there or not.”
The batroxobin combined with the researchers’ hydrogels isn’t taken directly from snakes, Dr Hartgerink noted. The substance used for medicine is produced by genetically modified bacteria and then purified, avoiding the risk of other contaminant toxins.
The researchers combined batroxobin with their synthetic, self-assembling nanofibers, which can be loaded into a syringe and injected at the site of a wound, where they reassemble themselves into a gel.
Tests showed the new material stopped a wound from bleeding in as little as 6 seconds, and further prodding of the wound minutes later did not reopen it.
The researchers also tested several other options: the hydrogel without batroxobin, the batroxobin without the hydrogel, a current clinical hemostat known as GelFoam, and an alternative self-assembling hemostat known as Puramatrix. None of these options were as effective, especially in the presence of anticoagulants.
The new work builds upon the researchers’ development of injectable hydrogel scaffolds that help wounds heal and grow natural tissue. The synthetic scaffolds are built from the peptide sequences to mimic natural processes.
“We think SB50 has great potential to stop surgical bleeding, particularly in difficult cases in which the patient is taking heparin or other anticoagulants,” Dr Hartgerink said. “SB50 takes the powerful clotting ability of this snake venom and makes it far more effective by delivering it in an easily localized hydrogel that prevents possible unwanted systemic effects from using batroxobin alone.” ![]()
New test could help fight leukemia

Image courtesy of NIAID
Researchers say they have developed a test that can reveal how the immune system would respond to vaccines for leukemia.
To conduct this test, cancer-specific-proteins are spotted onto a microscope slide.
They are then incubated with a patient blood sample to show whether the immune system can recognize the proteins.
The researchers believe this test could inform immunotherapy trial development and eventually direct the treatment of leukemia.
They described the test in PLOS ONE.
The team explained that cellular arrays using peptide-MHC (pMHC) tetramers allow the simultaneous detection of different antigen-specific T-cell populations that are naturally circulating in leukemia patients and healthy individuals.
The researchers developed a pMHC array to detect CD8+ T-cell populations in leukemia patients that recognize epitopes within viral antigens and leukemia antigens.
Experiments showed this test was at least as sensitive as flow cytometry.
The pMHC array successfully identified more than 40 T-cell populations. It identified T cells that recognized various tumor antigen epitopes in patients with acute myeloid leukemia and acute lymphoblastic leukemia.
“This [test] would allow us to know how good a patients’ immune system is and potentially which proteins their immune system will react to, allowing us to prioritize which proteins we use to develop anticancer vaccines,” said study author Barbara Guinn, PhD, of the University of Southampton in the UK.
“In the future, we may be able to monitor patient immune responses as they are treated in clinical trials, helping us to direct the immune system more efficiently against cancer cells.”
Dr Guinn has spent a large part of her career investigating the differences between cancer cells and normal cells in terms of the proteins they make. She has been able to identify a number of proteins that are overexpressed in tumor cells but not healthy cells.
“Some of these proteins act as biomarkers for patient survival,” she said, “and some of them have helped us understand more about how cancer develops in subgroups of patients with leukemia.” ![]()
Image courtesy of NIAID
Researchers say they have developed a test that can reveal how the immune system would respond to vaccines for leukemia.
To conduct this test, cancer-specific-proteins are spotted onto a microscope slide.
They are then incubated with a patient blood sample to show whether the immune system can recognize the proteins.
The researchers believe this test could inform immunotherapy trial development and eventually direct the treatment of leukemia.
They described the test in PLOS ONE.
The team explained that cellular arrays using peptide-MHC (pMHC) tetramers allow the simultaneous detection of different antigen-specific T-cell populations that are naturally circulating in leukemia patients and healthy individuals.
The researchers developed a pMHC array to detect CD8+ T-cell populations in leukemia patients that recognize epitopes within viral antigens and leukemia antigens.
Experiments showed this test was at least as sensitive as flow cytometry.
The pMHC array successfully identified more than 40 T-cell populations. It identified T cells that recognized various tumor antigen epitopes in patients with acute myeloid leukemia and acute lymphoblastic leukemia.
“This [test] would allow us to know how good a patients’ immune system is and potentially which proteins their immune system will react to, allowing us to prioritize which proteins we use to develop anticancer vaccines,” said study author Barbara Guinn, PhD, of the University of Southampton in the UK.
“In the future, we may be able to monitor patient immune responses as they are treated in clinical trials, helping us to direct the immune system more efficiently against cancer cells.”
Dr Guinn has spent a large part of her career investigating the differences between cancer cells and normal cells in terms of the proteins they make. She has been able to identify a number of proteins that are overexpressed in tumor cells but not healthy cells.
“Some of these proteins act as biomarkers for patient survival,” she said, “and some of them have helped us understand more about how cancer develops in subgroups of patients with leukemia.” ![]()
Image courtesy of NIAID
Researchers say they have developed a test that can reveal how the immune system would respond to vaccines for leukemia.
To conduct this test, cancer-specific-proteins are spotted onto a microscope slide.
They are then incubated with a patient blood sample to show whether the immune system can recognize the proteins.
The researchers believe this test could inform immunotherapy trial development and eventually direct the treatment of leukemia.
They described the test in PLOS ONE.
The team explained that cellular arrays using peptide-MHC (pMHC) tetramers allow the simultaneous detection of different antigen-specific T-cell populations that are naturally circulating in leukemia patients and healthy individuals.
The researchers developed a pMHC array to detect CD8+ T-cell populations in leukemia patients that recognize epitopes within viral antigens and leukemia antigens.
Experiments showed this test was at least as sensitive as flow cytometry.
The pMHC array successfully identified more than 40 T-cell populations. It identified T cells that recognized various tumor antigen epitopes in patients with acute myeloid leukemia and acute lymphoblastic leukemia.
“This [test] would allow us to know how good a patients’ immune system is and potentially which proteins their immune system will react to, allowing us to prioritize which proteins we use to develop anticancer vaccines,” said study author Barbara Guinn, PhD, of the University of Southampton in the UK.
“In the future, we may be able to monitor patient immune responses as they are treated in clinical trials, helping us to direct the immune system more efficiently against cancer cells.”
Dr Guinn has spent a large part of her career investigating the differences between cancer cells and normal cells in terms of the proteins they make. She has been able to identify a number of proteins that are overexpressed in tumor cells but not healthy cells.
“Some of these proteins act as biomarkers for patient survival,” she said, “and some of them have helped us understand more about how cancer develops in subgroups of patients with leukemia.” ![]()
Team aims to inhibit Notch safely

Photo courtesy of the
University of Michigan
A new study suggests a potential way to block one of the most common cancer-causing genes without causing severe side effects.
The Notch gene plays a role in many cancers, and it’s the most common cancer-causing gene in T-cell acute lymphoblastic leukemia (T-ALL).
About 60% of children and adults with T-ALL harbor a Notch mutation.
Unfortunately, drugs that inhibit Notch can cause serious side effects, such as skin cancers.
Now, investigators have discovered a potential new target to inhibit Notch without the toxic effects.
They found that a protein called Zmiz1 sticks to Notch, prompting the gene to turn on its cancer function. But Zmiz1 does not impact normal, healthy Notch functions.
“Notch controls the genes that cause cancer, but it’s also important for normal health,” said Mark Chiang, MD, PhD, of the University of Michigan in Ann Arbor.
“The challenge is to knock out the cancer function of Notch but preserve its normal function. If you unstick Zmiz1 from Notch, the cancer cells die. And Zmiz1 seems to be selective in turning on the cancer functions of Notch.”
Dr Chiang and his colleagues found that mice lived longer when Zmiz1 was deleted. The mice had normal body weight and no severe side effects from Zmiz1 deletion.
The investigators reported these results in Immunity.
“Our goal is to develop a drug to sit right between Notch and Zmiz1 that could break apart the bond,” Dr Chiang said. “We think this would block the Notch cancer pathway without causing toxic side effects, like we see with current Notch inhibitors.”
He noted that a majority of children with T-ALL are cured, but about 20% will relapse. Those children face a grim prognosis.
“We need to develop therapies against Notch to help kids with relapsed cancer and to cure kids with fewer toxicities or long-term effects,” Dr Chiang said. “Our current treatments may often be curative, but there can be a huge price to pay in late effects.”
To further this research, Dr Chiang and his colleagues plan to use X-ray crystallography to create a 3-dimensional image of Notch and Zmiz1 in an effort to understand how they are sticking together. This could help the team to design a drug to separate the proteins. ![]()
Photo courtesy of the
University of Michigan
A new study suggests a potential way to block one of the most common cancer-causing genes without causing severe side effects.
The Notch gene plays a role in many cancers, and it’s the most common cancer-causing gene in T-cell acute lymphoblastic leukemia (T-ALL).
About 60% of children and adults with T-ALL harbor a Notch mutation.
Unfortunately, drugs that inhibit Notch can cause serious side effects, such as skin cancers.
Now, investigators have discovered a potential new target to inhibit Notch without the toxic effects.
They found that a protein called Zmiz1 sticks to Notch, prompting the gene to turn on its cancer function. But Zmiz1 does not impact normal, healthy Notch functions.
“Notch controls the genes that cause cancer, but it’s also important for normal health,” said Mark Chiang, MD, PhD, of the University of Michigan in Ann Arbor.
“The challenge is to knock out the cancer function of Notch but preserve its normal function. If you unstick Zmiz1 from Notch, the cancer cells die. And Zmiz1 seems to be selective in turning on the cancer functions of Notch.”
Dr Chiang and his colleagues found that mice lived longer when Zmiz1 was deleted. The mice had normal body weight and no severe side effects from Zmiz1 deletion.
The investigators reported these results in Immunity.
“Our goal is to develop a drug to sit right between Notch and Zmiz1 that could break apart the bond,” Dr Chiang said. “We think this would block the Notch cancer pathway without causing toxic side effects, like we see with current Notch inhibitors.”
He noted that a majority of children with T-ALL are cured, but about 20% will relapse. Those children face a grim prognosis.
“We need to develop therapies against Notch to help kids with relapsed cancer and to cure kids with fewer toxicities or long-term effects,” Dr Chiang said. “Our current treatments may often be curative, but there can be a huge price to pay in late effects.”
To further this research, Dr Chiang and his colleagues plan to use X-ray crystallography to create a 3-dimensional image of Notch and Zmiz1 in an effort to understand how they are sticking together. This could help the team to design a drug to separate the proteins. ![]()
Photo courtesy of the
University of Michigan
A new study suggests a potential way to block one of the most common cancer-causing genes without causing severe side effects.
The Notch gene plays a role in many cancers, and it’s the most common cancer-causing gene in T-cell acute lymphoblastic leukemia (T-ALL).
About 60% of children and adults with T-ALL harbor a Notch mutation.
Unfortunately, drugs that inhibit Notch can cause serious side effects, such as skin cancers.
Now, investigators have discovered a potential new target to inhibit Notch without the toxic effects.
They found that a protein called Zmiz1 sticks to Notch, prompting the gene to turn on its cancer function. But Zmiz1 does not impact normal, healthy Notch functions.
“Notch controls the genes that cause cancer, but it’s also important for normal health,” said Mark Chiang, MD, PhD, of the University of Michigan in Ann Arbor.
“The challenge is to knock out the cancer function of Notch but preserve its normal function. If you unstick Zmiz1 from Notch, the cancer cells die. And Zmiz1 seems to be selective in turning on the cancer functions of Notch.”
Dr Chiang and his colleagues found that mice lived longer when Zmiz1 was deleted. The mice had normal body weight and no severe side effects from Zmiz1 deletion.
The investigators reported these results in Immunity.
“Our goal is to develop a drug to sit right between Notch and Zmiz1 that could break apart the bond,” Dr Chiang said. “We think this would block the Notch cancer pathway without causing toxic side effects, like we see with current Notch inhibitors.”
He noted that a majority of children with T-ALL are cured, but about 20% will relapse. Those children face a grim prognosis.
“We need to develop therapies against Notch to help kids with relapsed cancer and to cure kids with fewer toxicities or long-term effects,” Dr Chiang said. “Our current treatments may often be curative, but there can be a huge price to pay in late effects.”
To further this research, Dr Chiang and his colleagues plan to use X-ray crystallography to create a 3-dimensional image of Notch and Zmiz1 in an effort to understand how they are sticking together. This could help the team to design a drug to separate the proteins. ![]()
CPR Prior to Defibrillation for VF/VT CPA
Cardiopulmonary arrest (CPA) is a major contributor to overall mortality in both the in‐ and out‐of‐hospital setting.[1, 2, 3] Despite advances in the field of resuscitation science, mortality from CPA remains high.[1, 4] Unlike the out‐of‐hospital environment, inpatient CPA is unique, as trained healthcare providers are the primary responders with a range of expertise available throughout the duration of arrest.
There are inherent opportunities of in‐hospital cardiac arrest that exist, such as the opportunity for near immediate arrest detection, rapid initiation of high‐quality chest compressions, and early defibrillation if indicated. Given the association between improved rates of successful defibrillation and high‐quality chest compressions, the 2005 American Heart Association (AHA) updates changed the recommended guideline ventricular fibrillation/ventricular tachycardia (VF/VT) defibrillation sequence from 3 stacked shocks to a single shock followed by 2 minutes of chest compressions between defibrillation attempts.[5, 6] However, the recommendations were directed primarily at cases of out‐of‐hospital VF/VT CPA, and it currently remains unclear as to whether this strategy offers any advantage to patients who suffer an in‐hospital VF/VT arrest.[7]
Despite the aforementioned findings regarding the benefit of high‐quality chest compressions, there is a paucity of evidence in the medical literature to support whether delivering a period of chest compressions before defibrillation attempt, including initial shock and shock sequence, translate to improved outcomes. With the exception of the statement recommending early defibrillation in case of in‐hospital arrest, there are no formal AHA consensus recommendations.[5, 8, 9] Here we document our experience using the approach of expedited stacked defibrillation shocks in persons experiencing monitored in‐hospital VF/VT arrest.
METHODS
Design
This was a retrospective study of observational data from our in‐hospital resuscitation database. Waiver of informed consent was granted by our institutional investigational review board.
Setting
This study was performed in the University of California San Diego Healthcare System, which includes 2 urban academic hospitals, with a combined total of approximately 500 beds. A designated team is activated in response to code blue requests and includes: code registered nurse (RN), code doctor of medicine (MD), airway MD, respiratory therapist, pharmacist, house nursing supervisor, primary RN, and unit charge RN. Crash carts with defibrillators (ZOLL R and E series; ZOLL Medical Corp., Chelmsford, MA) are located on each inpatient unit. Defibrillator features include real‐time cardiopulmonary resuscitation (CPR) feedback, filtered electrocardiography (ECG), and continuous waveform capnography.
Resuscitation training is provided for all hospital providers as part of the novel Advanced Resuscitation Training (ART) program, which was initiated in 2007.[10] Critical care nurses and physicians receive annual training, whereas noncritical care personnel undergo biennial training. The curriculum is adaptable to institutional treatment algorithms, equipment, and code response. Content is adaptive based on provider type, unit, and opportunities for improvement as revealed by performance improvement data. Resuscitation treatment algorithms are reviewed annually by the Critical Care Committee and Code Blue Subcommittee as part of the ART program, with modifications incorporated into the institutional policies and procedures.
Subjects
All admitted patients with continuous cardiac monitoring who suffered VF/VT arrest between July 2005 and June 2013 were included in this analysis. Patients with active do not attempt resuscitation orders were excluded. Patients were identified from our institutional resuscitation database, into which all in‐hospital cardiopulmonary arrest data are entered. We did not have data on individual patient comorbidity or severity of illness. Overall patient acuity over the course of the study was monitored hospital wide through case‐mix index (CMI). The index is based upon the allocation of hospital resources used to treat a diagnosis‐related group of patients and has previously been used as a surrogate for patient acuity.[11, 12, 13] The code RN who performed the resuscitation is responsible for entering data into a protected performance improvement database. Telecommunications records and the unit log are cross‐referenced to assure complete capture.
Protocols
Specific protocol similarities and differences among the 3 study periods are presented in Table 1.
| Protocol Variable | Stack Shock Period (20052008) | Initial Chest Compression Period (20082011) | Modified Stack Shock Period (20112013) |
|---|---|---|---|
| |||
| Defibrillator type | Medtronic/Physio Control LifePak 12 | Zoll E Series | Zoll E Series |
| Joule increment with defibrillation | 200J‐300J‐360J, manual escalation | 120J‐150J‐200J, manual escalation | 120J‐150J‐200J, automatic escalation |
| Distinction between monitored and unmonitored in‐hospital cardiopulmonary arrest | No | Yes | Yes |
| Chest compressions prior to initial defibrillation | No | Yes | No* |
| Initial defibrillation strategy | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT | 2 minutes of chest compressions prior to initial and in between attempts | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT* |
| Chest compression to ventilation ratio | 15:1 | Continuous chest compressions with ventilation at ratio 10:1 | Continuous chest compressions with ventilation at ratio 10:1 |
| Vasopressors | Epinephrine 1 mg IV/IO every 35 minutes. | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes. |
Stacked Shock Period (20052008)
Historically, our institutional cardiopulmonary arrest protocols advocated early defibrillation with administration of 3 stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT before initiating/resuming chest compressions.
Initial Chest Compression Period (20082011)
In 2008 the protocol was modified to reflect recommendations to perform a 2‐minute period of chest compressions prior to each defibrillation, including the initial attempt.
Modified Stacked Shack Period (20112013)
Finally, in 2011 the protocol was modified again, and defibrillators were configured to allow automatic advancement of defibrillation energy (120J‐150J‐200J). The defibrillation protocol included the following elements.
For an unmonitored arrest, chest compressions and ventilations should be initiated upon recognition of cardiopulmonary arrest. If VF/VT was identified upon placement of defibrillator pads, immediate counter shock was performed and chest compressions resumed immediately for a period of 2 minutes before considering a repeat defibrillation attempt. A dose of epinephrine (1 mg intravenous [IV]/emntraosseous [IO]) or vasopressin (40 units IV/IO) was administered as close to the reinitiation of chest compressions as possible. Defibrillation attempts proceeded with a single shock at a time, each preceded by 2 minutes of chest compressions.
For a monitored arrest, defibrillation attempts were expedited. Chest compressions without ventilations were initiated only until defibrillator pads were placed. Defibrillation attempts were initiated as soon as possible, with at least 3 or more successive shocks administered for persistent VF/VT (stacked shocks). Compressions were performed between shocks if they did not interfere with rhythm analysis. Compressions resumed following the initial series of stacked shocks with persistent CPA, regardless of rhythm, and pressors administered (epinephrine 1 mg IV or vasopressin 40 units IV). Persistent VF/VT received defibrillation attempts every 2 minutes following the initial series of stacked shocks, with compressions performed continuously between attempts. Persistent VF/VT should trigger emergent cardiology consultation for possible emergent percutaneous intervention.
Analysis
The primary outcome measure was defined as survival to hospital discharge at baseline and following each protocol change. 2 was used to compare the 3 time periods, with P < 0.05 defined as statistically significant. Specific group comparisons were made with Bonferroni correction, with P < 0.017 defined as statistically significant. Secondary outcome measures included return of spontaneous circulation (ROSC) and number of shocks required. Demographic and clinical data were also presented for each of the 3 study periods.
RESULTS
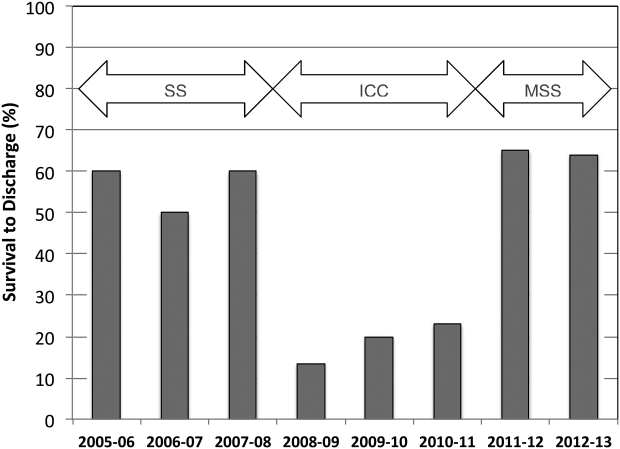
A total of 661 cardiopulmonary arrests of all rhythms were identified during the entire study period. Primary VF/VT arrests was identified in 106 patients (16%). Of these, 102 (96%) were being monitored with continuous ECG at the time of arrest. Demographic and clinical information for the entire study cohort are displayed in Table 2. There were no differences in age, gender, time of arrest, and location of arrest between study periods (all P > 0.05). The incidence of VF/VT arrest did not vary significantly between the study periods (P = 0.16). There were no differences in mean number of defibrillation attempts per arrest; however, there was a significant improvement in the rate of perfusing rhythm after initial set of defibrillation attempts and overall ROSC favoring stacked shocks (all P < 0.05, Table 2). Survival‐to‐hospital discharge for all VF/VT arrest victims decreased, then increased significantly from the stacked shock period to initial chest compression period to modified stacked shock period (58%, 18%, 71%, respectively, P < 0.01, Figure 1). After Bonferroni correction, specific group differences were significant between the stacked shock and initial chest compression groups (P < 0.01) and modified stacked shocks and initial chest compression groups (P < 0.01, Table 2). Finally, the incidence of bystander CPR appeared to be significantly greater in the modified stacked shock period following implementation of our resuscitation program (Table 2). Overall hospital CMI for fiscal years 2005/2006 through 2012/2013 were significantly different (1.47 vs 1.71, P < 0.0001).
| Parameter | Stacked Shocks (n = 31) | Initial Chest Compressions (n = 33) | Modified Stack Shocks (n = 42) |
|---|---|---|---|
| |||
| Age (y) | 54.3 | 64.3 | 59.8 |
| Male gender (%) | 16 (52) | 21 (64) | 21 (50) |
| VF/PVT arrest incidence (per 1,000 admissions) | 0.49 | 0.70 | |
| Arrest 7 am5 pm (%) | 15 (48) | 17 (52) | 21 (50) |
| Non‐ICU location (%) | 13 (42) | 15 (45) | 17 (40) |
| CPR prior to code team arrival (%) | 22 (71)* | 31 (94) | 42 (100) |
| Perfusing rhythm after initial set of defibrillation attempts (%) | 37 | 33 | 70 |
| Mean defibrillation attempts (no.) | 1.3 | 1.8 | 1.5 |
| ROSC (%) | 76 | 56 | 90 |
| Survival‐to‐hospital discharge (%) | 18 (58) | 6 (18) | 30 (71) |
| Case‐mix index (average coefficient by period) | 1.51 | 1.60 | 1.69∥ |
DISCUSSION
The specific focus of this observation was to report on defibrillation strategies that have previously only been reported in an out‐of‐hospital setting. There is no current consensus regarding chest compressions for a predetermined amount of time prior to defibrillation in an inpatient setting. Here we present data suggesting improved outcomes using an approach that expedited defibrillation and included a defibrillation strategy of stacked shocks (stacked shock and modified stack shock, respectively) in monitored inpatient VF/VT arrest.
Early out‐of‐hospital studies initially demonstrated a significant survival benefit for patients who received 1.5 to 3 minutes of chest compressions preceding defibrillation with reported arrest downtimes of 4 to 5 minutes prior to emergency medical services arrival.[14, 15] However, in more recent randomized controlled trials, outcome was not improved when chest compressions were performed prior to defibrillation attempt.[16, 17] Our findings suggest that there is no one size fits all approach to chest compression and defibrillation strategy. Instead, we suggest that factors including whether the arrest occurred while monitored or not aid with decision making and timing of defibrillation.
Our findings favoring expedited defibrillation and stacked shocks in witnessed arrest are consistent with the 3‐phase model of cardiac arrest proposed by Weisfeldt and Becker suggesting that defibrillation success is related to the energy status of the heart.[18] In this model, the first 4 minutes of VF arrest (electrical phase) are characterized by a high‐energy state with higher adenosine triphosphate (ATP)/adenosine monophosphate (AMP) ratios that are associated with increased likelihood for ROSC after defibrillation attempt.[19] Further, VF appears to deplete ATP/AMP ratios after about 4 minutes, at which point the likelihood of defibrillation success is substantially diminished.[18] Between 4 and 10 minutes (circulatory phase), energy stores in the myocardium are severely depleted. However, there is evidence to suggest that high‐quality chest compressions and high chest compression fractionparticularly in conjunction with epinephrinecan replenish ATP stores and increase the likelihood of defibrillation success.[6, 20] Beyond 10 minutes (metabolic phase), survival rates are abysmal, with no therapy yet identified producing clinical utility.
The secondary analyses reveal several interesting trends. We anticipated a higher number of defibrillation attempts during phase II due to a lower likelihood of conversion with a CPR‐first approach. Instead, the number of shocks was similar across all 3 periods. Our findings are consistent with previous reports of a low single or first shock probability of successful defibrillation. However, recent reports document that approximately 80% of patients who ultimately survive to discharge are successfully defibrillated within the first 3 shocks.[21, 22, 23]
It appears that the likelihood of conversion to a perfusing rhythm is higher with expedited, stacked shocks. This underscores the importance of identifying an optimal approach to the treatment of VF/VT, as the initial series of defibrillation attempts may determine outcomes. There also appeared to be an increase in the incidence of VF/VT during the modified stack shock period, although this was not statistically significant. The modified stack shock period correlated temporally with the expansion of our institution's cardiovascular service and the opening of a dedicated inpatient facility, which likely influenced our mixture of inpatients.
These data should be interpreted with consideration of study limitations. Primarily, we did not attempt to determine arrest times prior to initial defibrillation attempts, which is likely an important variable. However, we limited our population studied only to individuals experiencing VF/VT arrest that was witnessed by hospital care staff or occurred while on cardiac monitor. We are confident that these selective criteria resulted in expedited identification and response times well within the electrical phase. We did not evaluate differences or changes in individual patient‐level severity of illness that may have potentially confounded outcome analysis. The effect of individual level in severity of illness and comorbidity are not known. Instead, we used CMI coefficients to explore hospital wide changes in patient acuity during the study period. We noticed an increasing case‐mix coefficient value suggesting higher patient acuity, which would predict increased mortality rather than the decrease noted between the initial chest compression and modified stacked shock periods (Table 2). In addition, we did not integrate CPR process variables, such as depth, rate, recoil, chest compression fraction, and per‐shock pauses, into this analysis. Our previous studies indicated that high‐quality CPR may account for a significant amount of improvement in outcomes following our novel resuscitation program implementation in 2007.[10, 24] Since the program's inception, we have reported continuous improvement in overall in‐hospital mortality that was sustained throughout the duration of the study period despite the significant changes reported in the 3 periods with monitored VF/VT arrest.[10] The use of medications prior to initial defibrillation attempts was not recorded. We have recently reported that during the same period of data collection, there were no significant changes in the use of epinephrine; however, there was a significant increase in the use of vasopressin.[10] It is unclear whether the increased use of vasopressin contributed to the current outcomes. However, given our cohort of witnessed in‐hospital cardiac arrests with an initial shockable rhythm, we anticipate the use of vasopressors as unlikely prior to defibrillation attempt.
Additional important limitations and potential confounding factors in this study were the use of 2 different types of defibrillators, differing escalating energy strategies, and differing defibrillator waveforms. Recent evidence supports biphasic waveforms as more effective than monophasic waveforms.[25, 26, 27] Comparison of defibrillator brand and waveform superiority is out the scope of this study; however, it is interesting to note similar high rates of survival in the stacked shock and modified stack shock phases despite use of different defibrillator brands and waveforms during those respective phases. Regarding escalating energy of defibrillation countershocks, the most recent 2010 AHA guidelines have no position on the superiority of either manual or automatic escalation.[7] However, we noted similar high rates of survival in the stacked shock and modified stack shock periods despite use of differing escalating strategies. Finally, we used survival‐to‐hospital discharge as our main outcome measure rather than neurological status. However, prior studies from our institution suggest that most VF/VT survivors have good neurological outcomes, which are influenced heavily by preadmission functional status.[24]
CONCLUSIONS
Our data suggest that in cases of monitored VF/VT arrest, expeditious defibrillation with use of stacked shocks is associated with a higher rate of ROSC and survival to hospital discharge
Disclosure: Nothing to report.
- , , , et al. Strategies for improving survival after in‐hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–1563.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299:785–792.
- , , , et al. Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146.
- , , , . Predictors of survival from out‐of‐hospital cardiac arrest: a systematic review and meta‐analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81.
- , , , et al. Quality of cardiopulmonary resuscitation during in‐hospital cardiac arrest. JAMA. 2005;293:305–310.
- , , , et al. Chest compression fraction determines survival in patients with out‐of‐hospital ventricular fibrillation. Circulation. 2009;120:1241–1247.
- , , , et al. Part 6: Defibrillation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S325–S337.
- , , , et al. Part 1: executive summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S640—S656.
- , , , et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S729–S767.
- , , , et al. A performance improvement‐based resuscitation programme reduces arrest incidence and increases survival from in‐hospital cardiac arrest. Resuscitation. 2015;92:63–69.
- . The evolution of case‐mix measurement using DRGs: past, present and future. Stud Health Technol Inform. 1994;14:75–83.
- , , , et al. Variability in case‐mix adjusted in‐hospital cardiac arrest rates. Med Care. 2012;50:124–130.
- , , , , . Impact of socioeconomic adjustment on physicians' relative cost of care. Med Care. 2013;51:454–460.
- , , , et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out‐of‐hospital ventricular fibrillation. JAMA. 1999;281:1182–1188.
- , , , et al. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out‐of‐hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289:1389–1395.
- , , , et al. Defibrillation or cardiopulmonary resuscitation first for patients with out‐of‐hospital cardiac arrests found by paramedics to be in ventricular fibrillation? A randomised control trial. Resuscitation. 2008;79:424–431.
- , , , . CPR before defibrillation in out‐of‐hospital cardiac arrest: a randomized trial. Emerg Med Australas. 2005;17:39–45.
- , . Resuscitation after cardiac arrest: a 3‐phase time‐sensitive model. JAMA. 2002;288:3035–3038.
- , , , , . Association of intramyocardial high energy phosphate concentrations with quantitative measures of the ventricular fibrillation electrocardiogram waveform. Resuscitation. 2009;80:946–950.
- , , , et al. Ventricular fibrillation median frequency may not be useful for monitoring during cardiac arrest treated with endothelin‐1 or epinephrine. Anesth Analg. 2004;99:1787–1793, table of contents.
- , , , , . “Probability of successful defibrillation” as a monitor during CPR in out‐of‐hospital cardiac arrested patients. Resuscitation. 2015;48:245–254.
- , , , . Shockable rhythms and defibrillation during in‐hospital pediatric cardiac arrest. Resuscitation. 2014;85:387–391.
- , , , . Beyond the pre‐shock pause: the effect of prehospital defibrillation mode on CPR interruptions and return of spontaneous circulation. Resuscitation. 2013;84:575–579.
- , , . Implementing a “resuscitation bundle” decreases incidence and improves outcomes in inpatient cardiopulmonary arrest. Circulation 2009;120(18 Suppl):S1441.
- , , , et al. Multicenter, randomized, controlled trial of 150‐J biphasic shocks compared with 200‐ to 360‐J monophasic shocks in the resuscitation of out‐of‐hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation. 2000;102:1780–1787.
- , , , , . A prospective, randomised and blinded comparison of first shock success of monophasic and biphasic waveforms in out‐of‐hospital cardiac arrest. Resuscitation. 2003;58:17–24.
- , , , et al. Out‐of‐hospital cardiac arrest rectilinear biphasic to monophasic damped sine defibrillation waveforms with advanced life support intervention trial (ORBIT). Resuscitation. 2005;66:149–157.
Cardiopulmonary arrest (CPA) is a major contributor to overall mortality in both the in‐ and out‐of‐hospital setting.[1, 2, 3] Despite advances in the field of resuscitation science, mortality from CPA remains high.[1, 4] Unlike the out‐of‐hospital environment, inpatient CPA is unique, as trained healthcare providers are the primary responders with a range of expertise available throughout the duration of arrest.
There are inherent opportunities of in‐hospital cardiac arrest that exist, such as the opportunity for near immediate arrest detection, rapid initiation of high‐quality chest compressions, and early defibrillation if indicated. Given the association between improved rates of successful defibrillation and high‐quality chest compressions, the 2005 American Heart Association (AHA) updates changed the recommended guideline ventricular fibrillation/ventricular tachycardia (VF/VT) defibrillation sequence from 3 stacked shocks to a single shock followed by 2 minutes of chest compressions between defibrillation attempts.[5, 6] However, the recommendations were directed primarily at cases of out‐of‐hospital VF/VT CPA, and it currently remains unclear as to whether this strategy offers any advantage to patients who suffer an in‐hospital VF/VT arrest.[7]
Despite the aforementioned findings regarding the benefit of high‐quality chest compressions, there is a paucity of evidence in the medical literature to support whether delivering a period of chest compressions before defibrillation attempt, including initial shock and shock sequence, translate to improved outcomes. With the exception of the statement recommending early defibrillation in case of in‐hospital arrest, there are no formal AHA consensus recommendations.[5, 8, 9] Here we document our experience using the approach of expedited stacked defibrillation shocks in persons experiencing monitored in‐hospital VF/VT arrest.
METHODS
Design
This was a retrospective study of observational data from our in‐hospital resuscitation database. Waiver of informed consent was granted by our institutional investigational review board.
Setting
This study was performed in the University of California San Diego Healthcare System, which includes 2 urban academic hospitals, with a combined total of approximately 500 beds. A designated team is activated in response to code blue requests and includes: code registered nurse (RN), code doctor of medicine (MD), airway MD, respiratory therapist, pharmacist, house nursing supervisor, primary RN, and unit charge RN. Crash carts with defibrillators (ZOLL R and E series; ZOLL Medical Corp., Chelmsford, MA) are located on each inpatient unit. Defibrillator features include real‐time cardiopulmonary resuscitation (CPR) feedback, filtered electrocardiography (ECG), and continuous waveform capnography.
Resuscitation training is provided for all hospital providers as part of the novel Advanced Resuscitation Training (ART) program, which was initiated in 2007.[10] Critical care nurses and physicians receive annual training, whereas noncritical care personnel undergo biennial training. The curriculum is adaptable to institutional treatment algorithms, equipment, and code response. Content is adaptive based on provider type, unit, and opportunities for improvement as revealed by performance improvement data. Resuscitation treatment algorithms are reviewed annually by the Critical Care Committee and Code Blue Subcommittee as part of the ART program, with modifications incorporated into the institutional policies and procedures.
Subjects
All admitted patients with continuous cardiac monitoring who suffered VF/VT arrest between July 2005 and June 2013 were included in this analysis. Patients with active do not attempt resuscitation orders were excluded. Patients were identified from our institutional resuscitation database, into which all in‐hospital cardiopulmonary arrest data are entered. We did not have data on individual patient comorbidity or severity of illness. Overall patient acuity over the course of the study was monitored hospital wide through case‐mix index (CMI). The index is based upon the allocation of hospital resources used to treat a diagnosis‐related group of patients and has previously been used as a surrogate for patient acuity.[11, 12, 13] The code RN who performed the resuscitation is responsible for entering data into a protected performance improvement database. Telecommunications records and the unit log are cross‐referenced to assure complete capture.
Protocols
Specific protocol similarities and differences among the 3 study periods are presented in Table 1.
| Protocol Variable | Stack Shock Period (20052008) | Initial Chest Compression Period (20082011) | Modified Stack Shock Period (20112013) |
|---|---|---|---|
| |||
| Defibrillator type | Medtronic/Physio Control LifePak 12 | Zoll E Series | Zoll E Series |
| Joule increment with defibrillation | 200J‐300J‐360J, manual escalation | 120J‐150J‐200J, manual escalation | 120J‐150J‐200J, automatic escalation |
| Distinction between monitored and unmonitored in‐hospital cardiopulmonary arrest | No | Yes | Yes |
| Chest compressions prior to initial defibrillation | No | Yes | No* |
| Initial defibrillation strategy | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT | 2 minutes of chest compressions prior to initial and in between attempts | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT* |
| Chest compression to ventilation ratio | 15:1 | Continuous chest compressions with ventilation at ratio 10:1 | Continuous chest compressions with ventilation at ratio 10:1 |
| Vasopressors | Epinephrine 1 mg IV/IO every 35 minutes. | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes. |
Stacked Shock Period (20052008)
Historically, our institutional cardiopulmonary arrest protocols advocated early defibrillation with administration of 3 stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT before initiating/resuming chest compressions.
Initial Chest Compression Period (20082011)
In 2008 the protocol was modified to reflect recommendations to perform a 2‐minute period of chest compressions prior to each defibrillation, including the initial attempt.
Modified Stacked Shack Period (20112013)
Finally, in 2011 the protocol was modified again, and defibrillators were configured to allow automatic advancement of defibrillation energy (120J‐150J‐200J). The defibrillation protocol included the following elements.
For an unmonitored arrest, chest compressions and ventilations should be initiated upon recognition of cardiopulmonary arrest. If VF/VT was identified upon placement of defibrillator pads, immediate counter shock was performed and chest compressions resumed immediately for a period of 2 minutes before considering a repeat defibrillation attempt. A dose of epinephrine (1 mg intravenous [IV]/emntraosseous [IO]) or vasopressin (40 units IV/IO) was administered as close to the reinitiation of chest compressions as possible. Defibrillation attempts proceeded with a single shock at a time, each preceded by 2 minutes of chest compressions.
For a monitored arrest, defibrillation attempts were expedited. Chest compressions without ventilations were initiated only until defibrillator pads were placed. Defibrillation attempts were initiated as soon as possible, with at least 3 or more successive shocks administered for persistent VF/VT (stacked shocks). Compressions were performed between shocks if they did not interfere with rhythm analysis. Compressions resumed following the initial series of stacked shocks with persistent CPA, regardless of rhythm, and pressors administered (epinephrine 1 mg IV or vasopressin 40 units IV). Persistent VF/VT received defibrillation attempts every 2 minutes following the initial series of stacked shocks, with compressions performed continuously between attempts. Persistent VF/VT should trigger emergent cardiology consultation for possible emergent percutaneous intervention.
Analysis
The primary outcome measure was defined as survival to hospital discharge at baseline and following each protocol change. 2 was used to compare the 3 time periods, with P < 0.05 defined as statistically significant. Specific group comparisons were made with Bonferroni correction, with P < 0.017 defined as statistically significant. Secondary outcome measures included return of spontaneous circulation (ROSC) and number of shocks required. Demographic and clinical data were also presented for each of the 3 study periods.
RESULTS
A total of 661 cardiopulmonary arrests of all rhythms were identified during the entire study period. Primary VF/VT arrests was identified in 106 patients (16%). Of these, 102 (96%) were being monitored with continuous ECG at the time of arrest. Demographic and clinical information for the entire study cohort are displayed in Table 2. There were no differences in age, gender, time of arrest, and location of arrest between study periods (all P > 0.05). The incidence of VF/VT arrest did not vary significantly between the study periods (P = 0.16). There were no differences in mean number of defibrillation attempts per arrest; however, there was a significant improvement in the rate of perfusing rhythm after initial set of defibrillation attempts and overall ROSC favoring stacked shocks (all P < 0.05, Table 2). Survival‐to‐hospital discharge for all VF/VT arrest victims decreased, then increased significantly from the stacked shock period to initial chest compression period to modified stacked shock period (58%, 18%, 71%, respectively, P < 0.01, Figure 1). After Bonferroni correction, specific group differences were significant between the stacked shock and initial chest compression groups (P < 0.01) and modified stacked shocks and initial chest compression groups (P < 0.01, Table 2). Finally, the incidence of bystander CPR appeared to be significantly greater in the modified stacked shock period following implementation of our resuscitation program (Table 2). Overall hospital CMI for fiscal years 2005/2006 through 2012/2013 were significantly different (1.47 vs 1.71, P < 0.0001).
| Parameter | Stacked Shocks (n = 31) | Initial Chest Compressions (n = 33) | Modified Stack Shocks (n = 42) |
|---|---|---|---|
| |||
| Age (y) | 54.3 | 64.3 | 59.8 |
| Male gender (%) | 16 (52) | 21 (64) | 21 (50) |
| VF/PVT arrest incidence (per 1,000 admissions) | 0.49 | 0.70 | |
| Arrest 7 am5 pm (%) | 15 (48) | 17 (52) | 21 (50) |
| Non‐ICU location (%) | 13 (42) | 15 (45) | 17 (40) |
| CPR prior to code team arrival (%) | 22 (71)* | 31 (94) | 42 (100) |
| Perfusing rhythm after initial set of defibrillation attempts (%) | 37 | 33 | 70 |
| Mean defibrillation attempts (no.) | 1.3 | 1.8 | 1.5 |
| ROSC (%) | 76 | 56 | 90 |
| Survival‐to‐hospital discharge (%) | 18 (58) | 6 (18) | 30 (71) |
| Case‐mix index (average coefficient by period) | 1.51 | 1.60 | 1.69∥ |
DISCUSSION
The specific focus of this observation was to report on defibrillation strategies that have previously only been reported in an out‐of‐hospital setting. There is no current consensus regarding chest compressions for a predetermined amount of time prior to defibrillation in an inpatient setting. Here we present data suggesting improved outcomes using an approach that expedited defibrillation and included a defibrillation strategy of stacked shocks (stacked shock and modified stack shock, respectively) in monitored inpatient VF/VT arrest.
Early out‐of‐hospital studies initially demonstrated a significant survival benefit for patients who received 1.5 to 3 minutes of chest compressions preceding defibrillation with reported arrest downtimes of 4 to 5 minutes prior to emergency medical services arrival.[14, 15] However, in more recent randomized controlled trials, outcome was not improved when chest compressions were performed prior to defibrillation attempt.[16, 17] Our findings suggest that there is no one size fits all approach to chest compression and defibrillation strategy. Instead, we suggest that factors including whether the arrest occurred while monitored or not aid with decision making and timing of defibrillation.
Our findings favoring expedited defibrillation and stacked shocks in witnessed arrest are consistent with the 3‐phase model of cardiac arrest proposed by Weisfeldt and Becker suggesting that defibrillation success is related to the energy status of the heart.[18] In this model, the first 4 minutes of VF arrest (electrical phase) are characterized by a high‐energy state with higher adenosine triphosphate (ATP)/adenosine monophosphate (AMP) ratios that are associated with increased likelihood for ROSC after defibrillation attempt.[19] Further, VF appears to deplete ATP/AMP ratios after about 4 minutes, at which point the likelihood of defibrillation success is substantially diminished.[18] Between 4 and 10 minutes (circulatory phase), energy stores in the myocardium are severely depleted. However, there is evidence to suggest that high‐quality chest compressions and high chest compression fractionparticularly in conjunction with epinephrinecan replenish ATP stores and increase the likelihood of defibrillation success.[6, 20] Beyond 10 minutes (metabolic phase), survival rates are abysmal, with no therapy yet identified producing clinical utility.
The secondary analyses reveal several interesting trends. We anticipated a higher number of defibrillation attempts during phase II due to a lower likelihood of conversion with a CPR‐first approach. Instead, the number of shocks was similar across all 3 periods. Our findings are consistent with previous reports of a low single or first shock probability of successful defibrillation. However, recent reports document that approximately 80% of patients who ultimately survive to discharge are successfully defibrillated within the first 3 shocks.[21, 22, 23]
It appears that the likelihood of conversion to a perfusing rhythm is higher with expedited, stacked shocks. This underscores the importance of identifying an optimal approach to the treatment of VF/VT, as the initial series of defibrillation attempts may determine outcomes. There also appeared to be an increase in the incidence of VF/VT during the modified stack shock period, although this was not statistically significant. The modified stack shock period correlated temporally with the expansion of our institution's cardiovascular service and the opening of a dedicated inpatient facility, which likely influenced our mixture of inpatients.
These data should be interpreted with consideration of study limitations. Primarily, we did not attempt to determine arrest times prior to initial defibrillation attempts, which is likely an important variable. However, we limited our population studied only to individuals experiencing VF/VT arrest that was witnessed by hospital care staff or occurred while on cardiac monitor. We are confident that these selective criteria resulted in expedited identification and response times well within the electrical phase. We did not evaluate differences or changes in individual patient‐level severity of illness that may have potentially confounded outcome analysis. The effect of individual level in severity of illness and comorbidity are not known. Instead, we used CMI coefficients to explore hospital wide changes in patient acuity during the study period. We noticed an increasing case‐mix coefficient value suggesting higher patient acuity, which would predict increased mortality rather than the decrease noted between the initial chest compression and modified stacked shock periods (Table 2). In addition, we did not integrate CPR process variables, such as depth, rate, recoil, chest compression fraction, and per‐shock pauses, into this analysis. Our previous studies indicated that high‐quality CPR may account for a significant amount of improvement in outcomes following our novel resuscitation program implementation in 2007.[10, 24] Since the program's inception, we have reported continuous improvement in overall in‐hospital mortality that was sustained throughout the duration of the study period despite the significant changes reported in the 3 periods with monitored VF/VT arrest.[10] The use of medications prior to initial defibrillation attempts was not recorded. We have recently reported that during the same period of data collection, there were no significant changes in the use of epinephrine; however, there was a significant increase in the use of vasopressin.[10] It is unclear whether the increased use of vasopressin contributed to the current outcomes. However, given our cohort of witnessed in‐hospital cardiac arrests with an initial shockable rhythm, we anticipate the use of vasopressors as unlikely prior to defibrillation attempt.
Additional important limitations and potential confounding factors in this study were the use of 2 different types of defibrillators, differing escalating energy strategies, and differing defibrillator waveforms. Recent evidence supports biphasic waveforms as more effective than monophasic waveforms.[25, 26, 27] Comparison of defibrillator brand and waveform superiority is out the scope of this study; however, it is interesting to note similar high rates of survival in the stacked shock and modified stack shock phases despite use of different defibrillator brands and waveforms during those respective phases. Regarding escalating energy of defibrillation countershocks, the most recent 2010 AHA guidelines have no position on the superiority of either manual or automatic escalation.[7] However, we noted similar high rates of survival in the stacked shock and modified stack shock periods despite use of differing escalating strategies. Finally, we used survival‐to‐hospital discharge as our main outcome measure rather than neurological status. However, prior studies from our institution suggest that most VF/VT survivors have good neurological outcomes, which are influenced heavily by preadmission functional status.[24]
CONCLUSIONS
Our data suggest that in cases of monitored VF/VT arrest, expeditious defibrillation with use of stacked shocks is associated with a higher rate of ROSC and survival to hospital discharge
Disclosure: Nothing to report.
Cardiopulmonary arrest (CPA) is a major contributor to overall mortality in both the in‐ and out‐of‐hospital setting.[1, 2, 3] Despite advances in the field of resuscitation science, mortality from CPA remains high.[1, 4] Unlike the out‐of‐hospital environment, inpatient CPA is unique, as trained healthcare providers are the primary responders with a range of expertise available throughout the duration of arrest.
There are inherent opportunities of in‐hospital cardiac arrest that exist, such as the opportunity for near immediate arrest detection, rapid initiation of high‐quality chest compressions, and early defibrillation if indicated. Given the association between improved rates of successful defibrillation and high‐quality chest compressions, the 2005 American Heart Association (AHA) updates changed the recommended guideline ventricular fibrillation/ventricular tachycardia (VF/VT) defibrillation sequence from 3 stacked shocks to a single shock followed by 2 minutes of chest compressions between defibrillation attempts.[5, 6] However, the recommendations were directed primarily at cases of out‐of‐hospital VF/VT CPA, and it currently remains unclear as to whether this strategy offers any advantage to patients who suffer an in‐hospital VF/VT arrest.[7]
Despite the aforementioned findings regarding the benefit of high‐quality chest compressions, there is a paucity of evidence in the medical literature to support whether delivering a period of chest compressions before defibrillation attempt, including initial shock and shock sequence, translate to improved outcomes. With the exception of the statement recommending early defibrillation in case of in‐hospital arrest, there are no formal AHA consensus recommendations.[5, 8, 9] Here we document our experience using the approach of expedited stacked defibrillation shocks in persons experiencing monitored in‐hospital VF/VT arrest.
METHODS
Design
This was a retrospective study of observational data from our in‐hospital resuscitation database. Waiver of informed consent was granted by our institutional investigational review board.
Setting
This study was performed in the University of California San Diego Healthcare System, which includes 2 urban academic hospitals, with a combined total of approximately 500 beds. A designated team is activated in response to code blue requests and includes: code registered nurse (RN), code doctor of medicine (MD), airway MD, respiratory therapist, pharmacist, house nursing supervisor, primary RN, and unit charge RN. Crash carts with defibrillators (ZOLL R and E series; ZOLL Medical Corp., Chelmsford, MA) are located on each inpatient unit. Defibrillator features include real‐time cardiopulmonary resuscitation (CPR) feedback, filtered electrocardiography (ECG), and continuous waveform capnography.
Resuscitation training is provided for all hospital providers as part of the novel Advanced Resuscitation Training (ART) program, which was initiated in 2007.[10] Critical care nurses and physicians receive annual training, whereas noncritical care personnel undergo biennial training. The curriculum is adaptable to institutional treatment algorithms, equipment, and code response. Content is adaptive based on provider type, unit, and opportunities for improvement as revealed by performance improvement data. Resuscitation treatment algorithms are reviewed annually by the Critical Care Committee and Code Blue Subcommittee as part of the ART program, with modifications incorporated into the institutional policies and procedures.
Subjects
All admitted patients with continuous cardiac monitoring who suffered VF/VT arrest between July 2005 and June 2013 were included in this analysis. Patients with active do not attempt resuscitation orders were excluded. Patients were identified from our institutional resuscitation database, into which all in‐hospital cardiopulmonary arrest data are entered. We did not have data on individual patient comorbidity or severity of illness. Overall patient acuity over the course of the study was monitored hospital wide through case‐mix index (CMI). The index is based upon the allocation of hospital resources used to treat a diagnosis‐related group of patients and has previously been used as a surrogate for patient acuity.[11, 12, 13] The code RN who performed the resuscitation is responsible for entering data into a protected performance improvement database. Telecommunications records and the unit log are cross‐referenced to assure complete capture.
Protocols
Specific protocol similarities and differences among the 3 study periods are presented in Table 1.
| Protocol Variable | Stack Shock Period (20052008) | Initial Chest Compression Period (20082011) | Modified Stack Shock Period (20112013) |
|---|---|---|---|
| |||
| Defibrillator type | Medtronic/Physio Control LifePak 12 | Zoll E Series | Zoll E Series |
| Joule increment with defibrillation | 200J‐300J‐360J, manual escalation | 120J‐150J‐200J, manual escalation | 120J‐150J‐200J, automatic escalation |
| Distinction between monitored and unmonitored in‐hospital cardiopulmonary arrest | No | Yes | Yes |
| Chest compressions prior to initial defibrillation | No | Yes | No* |
| Initial defibrillation strategy | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT | 2 minutes of chest compressions prior to initial and in between attempts | 3 expedited stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT* |
| Chest compression to ventilation ratio | 15:1 | Continuous chest compressions with ventilation at ratio 10:1 | Continuous chest compressions with ventilation at ratio 10:1 |
| Vasopressors | Epinephrine 1 mg IV/IO every 35 minutes. | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes | Epinephrine 1 mg IV/IO or vasopressin 40 units IV/IO every 35 minutes. |
Stacked Shock Period (20052008)
Historically, our institutional cardiopulmonary arrest protocols advocated early defibrillation with administration of 3 stacked shocks with a brief pause between each single defibrillation attempt to confirm sustained VF/VT before initiating/resuming chest compressions.
Initial Chest Compression Period (20082011)
In 2008 the protocol was modified to reflect recommendations to perform a 2‐minute period of chest compressions prior to each defibrillation, including the initial attempt.
Modified Stacked Shack Period (20112013)
Finally, in 2011 the protocol was modified again, and defibrillators were configured to allow automatic advancement of defibrillation energy (120J‐150J‐200J). The defibrillation protocol included the following elements.
For an unmonitored arrest, chest compressions and ventilations should be initiated upon recognition of cardiopulmonary arrest. If VF/VT was identified upon placement of defibrillator pads, immediate counter shock was performed and chest compressions resumed immediately for a period of 2 minutes before considering a repeat defibrillation attempt. A dose of epinephrine (1 mg intravenous [IV]/emntraosseous [IO]) or vasopressin (40 units IV/IO) was administered as close to the reinitiation of chest compressions as possible. Defibrillation attempts proceeded with a single shock at a time, each preceded by 2 minutes of chest compressions.
For a monitored arrest, defibrillation attempts were expedited. Chest compressions without ventilations were initiated only until defibrillator pads were placed. Defibrillation attempts were initiated as soon as possible, with at least 3 or more successive shocks administered for persistent VF/VT (stacked shocks). Compressions were performed between shocks if they did not interfere with rhythm analysis. Compressions resumed following the initial series of stacked shocks with persistent CPA, regardless of rhythm, and pressors administered (epinephrine 1 mg IV or vasopressin 40 units IV). Persistent VF/VT received defibrillation attempts every 2 minutes following the initial series of stacked shocks, with compressions performed continuously between attempts. Persistent VF/VT should trigger emergent cardiology consultation for possible emergent percutaneous intervention.
Analysis
The primary outcome measure was defined as survival to hospital discharge at baseline and following each protocol change. 2 was used to compare the 3 time periods, with P < 0.05 defined as statistically significant. Specific group comparisons were made with Bonferroni correction, with P < 0.017 defined as statistically significant. Secondary outcome measures included return of spontaneous circulation (ROSC) and number of shocks required. Demographic and clinical data were also presented for each of the 3 study periods.
RESULTS
A total of 661 cardiopulmonary arrests of all rhythms were identified during the entire study period. Primary VF/VT arrests was identified in 106 patients (16%). Of these, 102 (96%) were being monitored with continuous ECG at the time of arrest. Demographic and clinical information for the entire study cohort are displayed in Table 2. There were no differences in age, gender, time of arrest, and location of arrest between study periods (all P > 0.05). The incidence of VF/VT arrest did not vary significantly between the study periods (P = 0.16). There were no differences in mean number of defibrillation attempts per arrest; however, there was a significant improvement in the rate of perfusing rhythm after initial set of defibrillation attempts and overall ROSC favoring stacked shocks (all P < 0.05, Table 2). Survival‐to‐hospital discharge for all VF/VT arrest victims decreased, then increased significantly from the stacked shock period to initial chest compression period to modified stacked shock period (58%, 18%, 71%, respectively, P < 0.01, Figure 1). After Bonferroni correction, specific group differences were significant between the stacked shock and initial chest compression groups (P < 0.01) and modified stacked shocks and initial chest compression groups (P < 0.01, Table 2). Finally, the incidence of bystander CPR appeared to be significantly greater in the modified stacked shock period following implementation of our resuscitation program (Table 2). Overall hospital CMI for fiscal years 2005/2006 through 2012/2013 were significantly different (1.47 vs 1.71, P < 0.0001).
| Parameter | Stacked Shocks (n = 31) | Initial Chest Compressions (n = 33) | Modified Stack Shocks (n = 42) |
|---|---|---|---|
| |||
| Age (y) | 54.3 | 64.3 | 59.8 |
| Male gender (%) | 16 (52) | 21 (64) | 21 (50) |
| VF/PVT arrest incidence (per 1,000 admissions) | 0.49 | 0.70 | |
| Arrest 7 am5 pm (%) | 15 (48) | 17 (52) | 21 (50) |
| Non‐ICU location (%) | 13 (42) | 15 (45) | 17 (40) |
| CPR prior to code team arrival (%) | 22 (71)* | 31 (94) | 42 (100) |
| Perfusing rhythm after initial set of defibrillation attempts (%) | 37 | 33 | 70 |
| Mean defibrillation attempts (no.) | 1.3 | 1.8 | 1.5 |
| ROSC (%) | 76 | 56 | 90 |
| Survival‐to‐hospital discharge (%) | 18 (58) | 6 (18) | 30 (71) |
| Case‐mix index (average coefficient by period) | 1.51 | 1.60 | 1.69∥ |
DISCUSSION
The specific focus of this observation was to report on defibrillation strategies that have previously only been reported in an out‐of‐hospital setting. There is no current consensus regarding chest compressions for a predetermined amount of time prior to defibrillation in an inpatient setting. Here we present data suggesting improved outcomes using an approach that expedited defibrillation and included a defibrillation strategy of stacked shocks (stacked shock and modified stack shock, respectively) in monitored inpatient VF/VT arrest.
Early out‐of‐hospital studies initially demonstrated a significant survival benefit for patients who received 1.5 to 3 minutes of chest compressions preceding defibrillation with reported arrest downtimes of 4 to 5 minutes prior to emergency medical services arrival.[14, 15] However, in more recent randomized controlled trials, outcome was not improved when chest compressions were performed prior to defibrillation attempt.[16, 17] Our findings suggest that there is no one size fits all approach to chest compression and defibrillation strategy. Instead, we suggest that factors including whether the arrest occurred while monitored or not aid with decision making and timing of defibrillation.
Our findings favoring expedited defibrillation and stacked shocks in witnessed arrest are consistent with the 3‐phase model of cardiac arrest proposed by Weisfeldt and Becker suggesting that defibrillation success is related to the energy status of the heart.[18] In this model, the first 4 minutes of VF arrest (electrical phase) are characterized by a high‐energy state with higher adenosine triphosphate (ATP)/adenosine monophosphate (AMP) ratios that are associated with increased likelihood for ROSC after defibrillation attempt.[19] Further, VF appears to deplete ATP/AMP ratios after about 4 minutes, at which point the likelihood of defibrillation success is substantially diminished.[18] Between 4 and 10 minutes (circulatory phase), energy stores in the myocardium are severely depleted. However, there is evidence to suggest that high‐quality chest compressions and high chest compression fractionparticularly in conjunction with epinephrinecan replenish ATP stores and increase the likelihood of defibrillation success.[6, 20] Beyond 10 minutes (metabolic phase), survival rates are abysmal, with no therapy yet identified producing clinical utility.
The secondary analyses reveal several interesting trends. We anticipated a higher number of defibrillation attempts during phase II due to a lower likelihood of conversion with a CPR‐first approach. Instead, the number of shocks was similar across all 3 periods. Our findings are consistent with previous reports of a low single or first shock probability of successful defibrillation. However, recent reports document that approximately 80% of patients who ultimately survive to discharge are successfully defibrillated within the first 3 shocks.[21, 22, 23]
It appears that the likelihood of conversion to a perfusing rhythm is higher with expedited, stacked shocks. This underscores the importance of identifying an optimal approach to the treatment of VF/VT, as the initial series of defibrillation attempts may determine outcomes. There also appeared to be an increase in the incidence of VF/VT during the modified stack shock period, although this was not statistically significant. The modified stack shock period correlated temporally with the expansion of our institution's cardiovascular service and the opening of a dedicated inpatient facility, which likely influenced our mixture of inpatients.
These data should be interpreted with consideration of study limitations. Primarily, we did not attempt to determine arrest times prior to initial defibrillation attempts, which is likely an important variable. However, we limited our population studied only to individuals experiencing VF/VT arrest that was witnessed by hospital care staff or occurred while on cardiac monitor. We are confident that these selective criteria resulted in expedited identification and response times well within the electrical phase. We did not evaluate differences or changes in individual patient‐level severity of illness that may have potentially confounded outcome analysis. The effect of individual level in severity of illness and comorbidity are not known. Instead, we used CMI coefficients to explore hospital wide changes in patient acuity during the study period. We noticed an increasing case‐mix coefficient value suggesting higher patient acuity, which would predict increased mortality rather than the decrease noted between the initial chest compression and modified stacked shock periods (Table 2). In addition, we did not integrate CPR process variables, such as depth, rate, recoil, chest compression fraction, and per‐shock pauses, into this analysis. Our previous studies indicated that high‐quality CPR may account for a significant amount of improvement in outcomes following our novel resuscitation program implementation in 2007.[10, 24] Since the program's inception, we have reported continuous improvement in overall in‐hospital mortality that was sustained throughout the duration of the study period despite the significant changes reported in the 3 periods with monitored VF/VT arrest.[10] The use of medications prior to initial defibrillation attempts was not recorded. We have recently reported that during the same period of data collection, there were no significant changes in the use of epinephrine; however, there was a significant increase in the use of vasopressin.[10] It is unclear whether the increased use of vasopressin contributed to the current outcomes. However, given our cohort of witnessed in‐hospital cardiac arrests with an initial shockable rhythm, we anticipate the use of vasopressors as unlikely prior to defibrillation attempt.
Additional important limitations and potential confounding factors in this study were the use of 2 different types of defibrillators, differing escalating energy strategies, and differing defibrillator waveforms. Recent evidence supports biphasic waveforms as more effective than monophasic waveforms.[25, 26, 27] Comparison of defibrillator brand and waveform superiority is out the scope of this study; however, it is interesting to note similar high rates of survival in the stacked shock and modified stack shock phases despite use of different defibrillator brands and waveforms during those respective phases. Regarding escalating energy of defibrillation countershocks, the most recent 2010 AHA guidelines have no position on the superiority of either manual or automatic escalation.[7] However, we noted similar high rates of survival in the stacked shock and modified stack shock periods despite use of differing escalating strategies. Finally, we used survival‐to‐hospital discharge as our main outcome measure rather than neurological status. However, prior studies from our institution suggest that most VF/VT survivors have good neurological outcomes, which are influenced heavily by preadmission functional status.[24]
CONCLUSIONS
Our data suggest that in cases of monitored VF/VT arrest, expeditious defibrillation with use of stacked shocks is associated with a higher rate of ROSC and survival to hospital discharge
Disclosure: Nothing to report.
- , , , et al. Strategies for improving survival after in‐hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–1563.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299:785–792.
- , , , et al. Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146.
- , , , . Predictors of survival from out‐of‐hospital cardiac arrest: a systematic review and meta‐analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81.
- , , , et al. Quality of cardiopulmonary resuscitation during in‐hospital cardiac arrest. JAMA. 2005;293:305–310.
- , , , et al. Chest compression fraction determines survival in patients with out‐of‐hospital ventricular fibrillation. Circulation. 2009;120:1241–1247.
- , , , et al. Part 6: Defibrillation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S325–S337.
- , , , et al. Part 1: executive summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S640—S656.
- , , , et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S729–S767.
- , , , et al. A performance improvement‐based resuscitation programme reduces arrest incidence and increases survival from in‐hospital cardiac arrest. Resuscitation. 2015;92:63–69.
- . The evolution of case‐mix measurement using DRGs: past, present and future. Stud Health Technol Inform. 1994;14:75–83.
- , , , et al. Variability in case‐mix adjusted in‐hospital cardiac arrest rates. Med Care. 2012;50:124–130.
- , , , , . Impact of socioeconomic adjustment on physicians' relative cost of care. Med Care. 2013;51:454–460.
- , , , et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out‐of‐hospital ventricular fibrillation. JAMA. 1999;281:1182–1188.
- , , , et al. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out‐of‐hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289:1389–1395.
- , , , et al. Defibrillation or cardiopulmonary resuscitation first for patients with out‐of‐hospital cardiac arrests found by paramedics to be in ventricular fibrillation? A randomised control trial. Resuscitation. 2008;79:424–431.
- , , , . CPR before defibrillation in out‐of‐hospital cardiac arrest: a randomized trial. Emerg Med Australas. 2005;17:39–45.
- , . Resuscitation after cardiac arrest: a 3‐phase time‐sensitive model. JAMA. 2002;288:3035–3038.
- , , , , . Association of intramyocardial high energy phosphate concentrations with quantitative measures of the ventricular fibrillation electrocardiogram waveform. Resuscitation. 2009;80:946–950.
- , , , et al. Ventricular fibrillation median frequency may not be useful for monitoring during cardiac arrest treated with endothelin‐1 or epinephrine. Anesth Analg. 2004;99:1787–1793, table of contents.
- , , , , . “Probability of successful defibrillation” as a monitor during CPR in out‐of‐hospital cardiac arrested patients. Resuscitation. 2015;48:245–254.
- , , , . Shockable rhythms and defibrillation during in‐hospital pediatric cardiac arrest. Resuscitation. 2014;85:387–391.
- , , , . Beyond the pre‐shock pause: the effect of prehospital defibrillation mode on CPR interruptions and return of spontaneous circulation. Resuscitation. 2013;84:575–579.
- , , . Implementing a “resuscitation bundle” decreases incidence and improves outcomes in inpatient cardiopulmonary arrest. Circulation 2009;120(18 Suppl):S1441.
- , , , et al. Multicenter, randomized, controlled trial of 150‐J biphasic shocks compared with 200‐ to 360‐J monophasic shocks in the resuscitation of out‐of‐hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation. 2000;102:1780–1787.
- , , , , . A prospective, randomised and blinded comparison of first shock success of monophasic and biphasic waveforms in out‐of‐hospital cardiac arrest. Resuscitation. 2003;58:17–24.
- , , , et al. Out‐of‐hospital cardiac arrest rectilinear biphasic to monophasic damped sine defibrillation waveforms with advanced life support intervention trial (ORBIT). Resuscitation. 2005;66:149–157.
- , , , et al. Strategies for improving survival after in‐hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–1563.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299:785–792.
- , , , et al. Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146.
- , , , . Predictors of survival from out‐of‐hospital cardiac arrest: a systematic review and meta‐analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81.
- , , , et al. Quality of cardiopulmonary resuscitation during in‐hospital cardiac arrest. JAMA. 2005;293:305–310.
- , , , et al. Chest compression fraction determines survival in patients with out‐of‐hospital ventricular fibrillation. Circulation. 2009;120:1241–1247.
- , , , et al. Part 6: Defibrillation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S325–S337.
- , , , et al. Part 1: executive summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S640—S656.
- , , , et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S729–S767.
- , , , et al. A performance improvement‐based resuscitation programme reduces arrest incidence and increases survival from in‐hospital cardiac arrest. Resuscitation. 2015;92:63–69.
- . The evolution of case‐mix measurement using DRGs: past, present and future. Stud Health Technol Inform. 1994;14:75–83.
- , , , et al. Variability in case‐mix adjusted in‐hospital cardiac arrest rates. Med Care. 2012;50:124–130.
- , , , , . Impact of socioeconomic adjustment on physicians' relative cost of care. Med Care. 2013;51:454–460.
- , , , et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out‐of‐hospital ventricular fibrillation. JAMA. 1999;281:1182–1188.
- , , , et al. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out‐of‐hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289:1389–1395.
- , , , et al. Defibrillation or cardiopulmonary resuscitation first for patients with out‐of‐hospital cardiac arrests found by paramedics to be in ventricular fibrillation? A randomised control trial. Resuscitation. 2008;79:424–431.
- , , , . CPR before defibrillation in out‐of‐hospital cardiac arrest: a randomized trial. Emerg Med Australas. 2005;17:39–45.
- , . Resuscitation after cardiac arrest: a 3‐phase time‐sensitive model. JAMA. 2002;288:3035–3038.
- , , , , . Association of intramyocardial high energy phosphate concentrations with quantitative measures of the ventricular fibrillation electrocardiogram waveform. Resuscitation. 2009;80:946–950.
- , , , et al. Ventricular fibrillation median frequency may not be useful for monitoring during cardiac arrest treated with endothelin‐1 or epinephrine. Anesth Analg. 2004;99:1787–1793, table of contents.
- , , , , . “Probability of successful defibrillation” as a monitor during CPR in out‐of‐hospital cardiac arrested patients. Resuscitation. 2015;48:245–254.
- , , , . Shockable rhythms and defibrillation during in‐hospital pediatric cardiac arrest. Resuscitation. 2014;85:387–391.
- , , , . Beyond the pre‐shock pause: the effect of prehospital defibrillation mode on CPR interruptions and return of spontaneous circulation. Resuscitation. 2013;84:575–579.
- , , . Implementing a “resuscitation bundle” decreases incidence and improves outcomes in inpatient cardiopulmonary arrest. Circulation 2009;120(18 Suppl):S1441.
- , , , et al. Multicenter, randomized, controlled trial of 150‐J biphasic shocks compared with 200‐ to 360‐J monophasic shocks in the resuscitation of out‐of‐hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation. 2000;102:1780–1787.
- , , , , . A prospective, randomised and blinded comparison of first shock success of monophasic and biphasic waveforms in out‐of‐hospital cardiac arrest. Resuscitation. 2003;58:17–24.
- , , , et al. Out‐of‐hospital cardiac arrest rectilinear biphasic to monophasic damped sine defibrillation waveforms with advanced life support intervention trial (ORBIT). Resuscitation. 2005;66:149–157.
© 2015 Society of Hospital Medicine
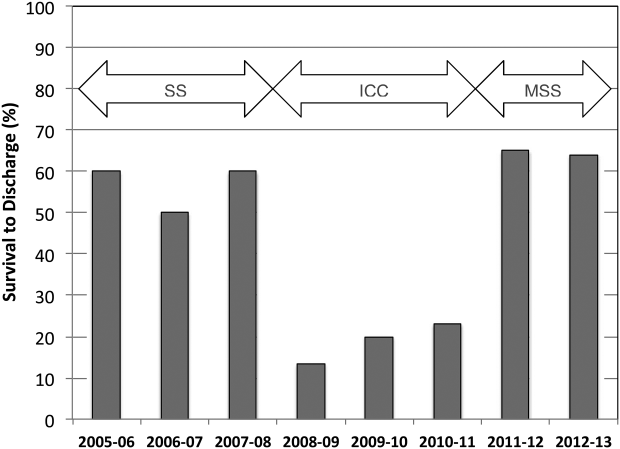
Encouraging Use of the MyFitnessPal App Does Not Lead to Weight Loss in Primary Care Patients
Study Overview
Objective. To evaluate the effectiveness and impact of using MyFitnessPal, a free, popular smartphone application (“app”), for weight loss.
Study design. 2-arm randomized controlled trial.
Setting and participants. Participants were recruited from 2 primary care clinics in the University of California, Los Angeles heath system. The inclusion criteria for the study were ≥ 18 years of age, body mass index (BMI) ≥ 25 kg/m2, an interest in losing weight, and ownership of a smartphone. The exclusion criteria included pregnancy, hemodialysis, life expectancy less than 6 months, lack of interest in weight loss, and current use of a smartphone app for weight loss. Out of 633 individuals assessed, 212 were eligible for the study. Participants were block randomized by BMI 25–30 kg/m2 and BMI > 30 kg/m2 to either usual primary care (n = 107) or usual primary care plus the app (n = 105).
Intervention. MyFitnessPal (MFP) was selected for this study based on previous focus groups with overweight primary care patients. MFP is a calorie-counting app that incorporates evidence-based and theory-based approaches to weight loss. Users can enter their current weight, goal weight, and goal rate of weight loss, which allows the app to generate the user’s daily, individualized calorie goal. MFP users also input daily weight, food intake, and physical activity, which produce certain outputs, including calorie counts, weight trends, and nutritional summaries based on food consumed.
Participants in the intervention arm received help from research assistants in downloading MFP onto their smartphones and received a phone call 1 week after enrollment to assist with any technical issues with the app. Those in the control group were told to choose any preferred activity for weight loss. Both groups received usual care from their primary care provider, with an additional two follow-up visits at 3 and 6 months. At the 3-month follow-up visit, all participants received a nutrition educational handout from www.myplate.gov.
Main outcomes measures. The main outcome measure was weight change at 6 months. Blood pressure, weight, systolic blood pressure (SPB), and 3 self-reported behavioral mediators of weight loss (exercise, diet, and self-efficacy in weight loss) were measured and collected for all participants at baseline and at 3 and 6 months. This study also gathered data from the MyFitnessPal company to measure frequency of app usage. At the 6-month follow-up visit, research assistants asked participants in the intervention arm about their experience using MFP, while those in the control group were asked if they had used MFP in the past 6 months to assess contamination. The authors used a linear mixed effects model (PROC MIXED) in SAS data processing software to investigate the differences in weight change, SBP change, and change in behavioral survey items between the 2 groups while controlling for clinic site. In addition, they performed 2 sensitivity analyses to evaluate the impact of possible informative dropout (income, education, diet experience, treatment group, and baseline value), and the effect of excluding one control group outlier.
Results. The majority of participants were female (73%) with a mean age of 43.4 years (SD = 14.3). The mean BMI was 33.4 kg/m2 (SD = 7.09), and 48% of the participants identified themselves as non-Hispanic white. At the 3-month visit, 26% and 21% of the participants from the intervention and control arms were lost to follow-up. Additionally, at 6 months, 32% and 19% of intervention and control group participants were lost to follow-up.
There was no significant difference in weight change between the two groups at 3 months (control, + 0.54 lb; intervention, –0.06 lb; P = 0.53) or at 6 months (control, +0.6 lb; intervention, –0.07 lb; P = 0.63); between group difference at 3 months was –0.6 lb (95% confidence interval [CI], –2.5 to 1.3 lb; P = 0.53) and at 6 months was –0.67 lb (CI, –3.3 to 2.1 lb; P = 0.63). The sensitivity analysis based on possible missing data also suggested the same outcome with between group difference at 6 months at 0.08 lb (CI, –3.04 to 3.20 lb; P = 0.96). The difference in systolic blood pressure was not significant between the groups.
Participants in the intervention arm used a personal calorie goal more often than those in the control group, with a mean between group difference at 3 months of 1.9 days per week (CI, 1.0 to 2.8; P < 0.001) and a mean between group difference at 6 months of 2.0 days per week (CI, 1.1 to 2.9; P < 0.001). The results also showed that the use of calorie goal feature was significant at 3 months (P < 0.001) and at 6 months (P < 0.001). At the 3-month visit, the authors found that individuals in the intervention group reported decreased self-efficacy in achieving their weight loss goals when compared to their counterparts (–0.85 on a 10-point scale; CI, –1.6 to –0.1; P = 0.026), but self-efficacy was insignificant at the 6-month follow-up. Additionally, the results suggested no difference in self-reported behaviors regarding diet, exercise, and self-efficacy in weight loss between the groups.
The mean number of logins was 61 during the course of the study, and the median total logins was 19. Interestingly, the data showed that there was a rapid decline of logins after enrollment for most participants in the intervention arm. There were 94 users who logged in to the app during the first month and 34 who logged in during the last month of the study. Out of 107 participants from the control group, 14 used MFP during the trial.
Despite a sharp decline in usage, MFP users in the intervention group were satisfied with the app: 79% were somewhat to completely satisfied, 92% would recommend it to a friend, and 80% planned to continue using MFP after the study. The study indicated that there were several aspects that the users liked about MFP including ease of use (100%), feedback on progress (88%), and 48% indicated that it was fun to use. Fewer participants appreciated features such as the reminder feature (42%) and social networking feature (13%). A common theme the authors found in MFP users was increased awareness of food choices, and more caution about food choices. Of those that stopped using MFP, some comments regarding MFP included that it was tedious (84%) and not easy to use (24%).
Conclusion. While most participants were satisfied with MFP, encouraging use of the app did not lead to more weight loss in primary care patients compared to usual care. There was decreased engagement with MFP over time.
Commentary
Despite efforts by the federal government to address the obesity epidemic in the United States, there is still a high prevalence of obesity among children and adults. Approximately 17% of youth and 35% of adults in the United States have a BMI in the obese range (> 30 kg/m2) [1]. In addition to a high association between obesity and chronic diseases such as type 2 diabetes mellitus, hypertension, and hypercholesterolemia[2], the obesity epidemic carries a staggering financial burden. The annual cost of obesity in the U.S. was estimated to be $147 billion in 2008, and the medical costs for each person with obesity was $1429 higher than those with normal weight [3,4]. Therefore, finding cost-effective and easily accessible methods to manage obesity is imperative. The Pew Research Center found that 64% of adults in the U.S. own a smartphone, and 62% of those have used their phone to look up health information[5]. Thus, smartphone applications that deliver weight management information and strategies may be a cost-effective and feasible means to reach a large population.
This study assessed the impact of MyFitnessPal, a free and widely popular mobile application, as an approach to reduce weight among patients in a primary care setting. The authors compared weight change between patients who received usual care from primary care providers (PCPs) and those who used MFP in addition to their usual care. They found no significant difference in weight loss between the two groups at 3 and 6 months during the trial. Despite this negative finding, this study makes important contributions to the e-health literature and highlights important considerations for similar studies.
While the exact reasons for lack of effect are unclear, the lack of effectiveness of such a brief intervention is not surprising. It is important to note that the PCPs did not assist or reinforce the patients to use the MFP app in this study. A systematic review of technology-assisted interventions in primary care suggests that technologies such as smartphone apps could be used as a successful tools for weight loss in the primary care setting, but that there needs to be guidance and feedback from a health care team[6]. Further, the intervention may not have been intense enough to achieve clinically significant weight loss. The U.S. Preventive Service Task Force recommends intensive interventions with at least 12 to 26 visits over 12 months to address obesity[7]. Thus, future studies of this app should include more intensive counseling from the healthcare team to determine if this improves adherence to lifestyle changes.
Strengths of this study include the use of a randomized controlled trial design, double-blinding of both participants and PCPs, and analyses for outlier and missing data. These design considerations increase the validity of the trial outcome. In addition, the authors rigorously assessed the relationship between the exposure and the outcome. The group set a high goal of enrollment to account for potential high rate of attrition (up to 50%). Since there was considerable loss to follow-up at both 3 and 6 months, the authors performed sensitivity analyses to determine if this biased the outcomes. The team assessed crossover contamination at the end of the study by asking participants in the control group if they used MFP during the trial. The authors also conducted a linear regression to examine if baseline self-efficacy was a significant predictor of weight change, controlling for the interaction between self-efficacy and group assignment. Additionally, sensitivity analyses were performed to see if the result from one outlier in the control group who achieved significant weight loss biased the findings.
As one of the first studies to investigate the use of a mobile app for weight loss in the primary care setting, the pragmatic design was impressive. The study showed that introduction to MFP can be done in 5 minutes and that the intervention was highly acceptable to patients. Since research assistants provided minimal guidance to enrolled participants, this study design provided an opportunity to observe the app’s efficacy in the real-world setting for the general public.
Although the authors efficiently designed a valid and pragmatic study, there were several aspects of the study that could be improved. As previously stated by the authors, this study did not explicitly measure the readiness for change, hence it was challenging to accurately and systematically determine the motivation of those in the intervention arm. Additionally, despite the diverse income and race of participants, the majority of the subjects were college-educated. In 2014, only 34% of the U.S. population completed a bachelor’s degree or high, and only 8% completed a master’s or higher degree [8]. This may limit the generalizability of the study, as education level could influence app acceptance and usage behavior.
Applications for Clinical Practice
With a large number of people using smartphones, there are increasing opportunities to use this delivery system to provide weight management information and support strategies for weight loss and lifestyle behavior changes. Previous studies showed that smartphone technology is a promising tool to facilitate weight management[9, 10], but the best practices for implementation of smart phones in the primary setting for weight management are still unknown. Based on this study and previous research done on technology intervention on health, providing the MFP app alone without additional counseling or intervention will not lead to clinically significant weight loss in the majority of patients. Future studies should determine if adding the MFP app is more efficacious when part of a more intensive behavioral intervention. Further studies should also determine whether PCP support in assessing readiness to use health apps and other behavior change technologies increases adherence and weight loss.
—Pich Seekaew, BS, and Melanie Jay MD, MS
1. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
2. Clark JM, Brancati FL. The challenge of obesity-related chronic diseases. J Gen Intern Med 2000;15:828–9.
3. Wang CY, Mcpherson K, Marsh T, et al. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011;378:815–25.
4. Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Affairs 2009;28:822–31.
5. Smith A. U.S. smartphone use in 2015. Pew Research Center Internet Science Tech RSS. 2015.
6. Levine DM, Savarimuthu S, Squires A, et al. Technology-assisted weight loss interventions in primary care: a systematic review. J Gen Intern Med 2014;30:107–17.
7. Moyer VA. Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012;157:373–8.
8. U.S. Department of Education, National Center for Education Statistics. The condition of education 2015 (NCES 2015–144). Educational attainment 2015.
9. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight. J Cardiovasc Nurs 2013; 28:320–9.
10. Hebden L, Cook A, Van Der Ploeg HP, Allman-Farinelli M. Development of smartphone applications for nutrition and physical activity behavior change. JMIR Res Protoc 2012;1:e9.
Study Overview
Objective. To evaluate the effectiveness and impact of using MyFitnessPal, a free, popular smartphone application (“app”), for weight loss.
Study design. 2-arm randomized controlled trial.
Setting and participants. Participants were recruited from 2 primary care clinics in the University of California, Los Angeles heath system. The inclusion criteria for the study were ≥ 18 years of age, body mass index (BMI) ≥ 25 kg/m2, an interest in losing weight, and ownership of a smartphone. The exclusion criteria included pregnancy, hemodialysis, life expectancy less than 6 months, lack of interest in weight loss, and current use of a smartphone app for weight loss. Out of 633 individuals assessed, 212 were eligible for the study. Participants were block randomized by BMI 25–30 kg/m2 and BMI > 30 kg/m2 to either usual primary care (n = 107) or usual primary care plus the app (n = 105).
Intervention. MyFitnessPal (MFP) was selected for this study based on previous focus groups with overweight primary care patients. MFP is a calorie-counting app that incorporates evidence-based and theory-based approaches to weight loss. Users can enter their current weight, goal weight, and goal rate of weight loss, which allows the app to generate the user’s daily, individualized calorie goal. MFP users also input daily weight, food intake, and physical activity, which produce certain outputs, including calorie counts, weight trends, and nutritional summaries based on food consumed.
Participants in the intervention arm received help from research assistants in downloading MFP onto their smartphones and received a phone call 1 week after enrollment to assist with any technical issues with the app. Those in the control group were told to choose any preferred activity for weight loss. Both groups received usual care from their primary care provider, with an additional two follow-up visits at 3 and 6 months. At the 3-month follow-up visit, all participants received a nutrition educational handout from www.myplate.gov.
Main outcomes measures. The main outcome measure was weight change at 6 months. Blood pressure, weight, systolic blood pressure (SPB), and 3 self-reported behavioral mediators of weight loss (exercise, diet, and self-efficacy in weight loss) were measured and collected for all participants at baseline and at 3 and 6 months. This study also gathered data from the MyFitnessPal company to measure frequency of app usage. At the 6-month follow-up visit, research assistants asked participants in the intervention arm about their experience using MFP, while those in the control group were asked if they had used MFP in the past 6 months to assess contamination. The authors used a linear mixed effects model (PROC MIXED) in SAS data processing software to investigate the differences in weight change, SBP change, and change in behavioral survey items between the 2 groups while controlling for clinic site. In addition, they performed 2 sensitivity analyses to evaluate the impact of possible informative dropout (income, education, diet experience, treatment group, and baseline value), and the effect of excluding one control group outlier.
Results. The majority of participants were female (73%) with a mean age of 43.4 years (SD = 14.3). The mean BMI was 33.4 kg/m2 (SD = 7.09), and 48% of the participants identified themselves as non-Hispanic white. At the 3-month visit, 26% and 21% of the participants from the intervention and control arms were lost to follow-up. Additionally, at 6 months, 32% and 19% of intervention and control group participants were lost to follow-up.
There was no significant difference in weight change between the two groups at 3 months (control, + 0.54 lb; intervention, –0.06 lb; P = 0.53) or at 6 months (control, +0.6 lb; intervention, –0.07 lb; P = 0.63); between group difference at 3 months was –0.6 lb (95% confidence interval [CI], –2.5 to 1.3 lb; P = 0.53) and at 6 months was –0.67 lb (CI, –3.3 to 2.1 lb; P = 0.63). The sensitivity analysis based on possible missing data also suggested the same outcome with between group difference at 6 months at 0.08 lb (CI, –3.04 to 3.20 lb; P = 0.96). The difference in systolic blood pressure was not significant between the groups.
Participants in the intervention arm used a personal calorie goal more often than those in the control group, with a mean between group difference at 3 months of 1.9 days per week (CI, 1.0 to 2.8; P < 0.001) and a mean between group difference at 6 months of 2.0 days per week (CI, 1.1 to 2.9; P < 0.001). The results also showed that the use of calorie goal feature was significant at 3 months (P < 0.001) and at 6 months (P < 0.001). At the 3-month visit, the authors found that individuals in the intervention group reported decreased self-efficacy in achieving their weight loss goals when compared to their counterparts (–0.85 on a 10-point scale; CI, –1.6 to –0.1; P = 0.026), but self-efficacy was insignificant at the 6-month follow-up. Additionally, the results suggested no difference in self-reported behaviors regarding diet, exercise, and self-efficacy in weight loss between the groups.
The mean number of logins was 61 during the course of the study, and the median total logins was 19. Interestingly, the data showed that there was a rapid decline of logins after enrollment for most participants in the intervention arm. There were 94 users who logged in to the app during the first month and 34 who logged in during the last month of the study. Out of 107 participants from the control group, 14 used MFP during the trial.
Despite a sharp decline in usage, MFP users in the intervention group were satisfied with the app: 79% were somewhat to completely satisfied, 92% would recommend it to a friend, and 80% planned to continue using MFP after the study. The study indicated that there were several aspects that the users liked about MFP including ease of use (100%), feedback on progress (88%), and 48% indicated that it was fun to use. Fewer participants appreciated features such as the reminder feature (42%) and social networking feature (13%). A common theme the authors found in MFP users was increased awareness of food choices, and more caution about food choices. Of those that stopped using MFP, some comments regarding MFP included that it was tedious (84%) and not easy to use (24%).
Conclusion. While most participants were satisfied with MFP, encouraging use of the app did not lead to more weight loss in primary care patients compared to usual care. There was decreased engagement with MFP over time.
Commentary
Despite efforts by the federal government to address the obesity epidemic in the United States, there is still a high prevalence of obesity among children and adults. Approximately 17% of youth and 35% of adults in the United States have a BMI in the obese range (> 30 kg/m2) [1]. In addition to a high association between obesity and chronic diseases such as type 2 diabetes mellitus, hypertension, and hypercholesterolemia[2], the obesity epidemic carries a staggering financial burden. The annual cost of obesity in the U.S. was estimated to be $147 billion in 2008, and the medical costs for each person with obesity was $1429 higher than those with normal weight [3,4]. Therefore, finding cost-effective and easily accessible methods to manage obesity is imperative. The Pew Research Center found that 64% of adults in the U.S. own a smartphone, and 62% of those have used their phone to look up health information[5]. Thus, smartphone applications that deliver weight management information and strategies may be a cost-effective and feasible means to reach a large population.
This study assessed the impact of MyFitnessPal, a free and widely popular mobile application, as an approach to reduce weight among patients in a primary care setting. The authors compared weight change between patients who received usual care from primary care providers (PCPs) and those who used MFP in addition to their usual care. They found no significant difference in weight loss between the two groups at 3 and 6 months during the trial. Despite this negative finding, this study makes important contributions to the e-health literature and highlights important considerations for similar studies.
While the exact reasons for lack of effect are unclear, the lack of effectiveness of such a brief intervention is not surprising. It is important to note that the PCPs did not assist or reinforce the patients to use the MFP app in this study. A systematic review of technology-assisted interventions in primary care suggests that technologies such as smartphone apps could be used as a successful tools for weight loss in the primary care setting, but that there needs to be guidance and feedback from a health care team[6]. Further, the intervention may not have been intense enough to achieve clinically significant weight loss. The U.S. Preventive Service Task Force recommends intensive interventions with at least 12 to 26 visits over 12 months to address obesity[7]. Thus, future studies of this app should include more intensive counseling from the healthcare team to determine if this improves adherence to lifestyle changes.
Strengths of this study include the use of a randomized controlled trial design, double-blinding of both participants and PCPs, and analyses for outlier and missing data. These design considerations increase the validity of the trial outcome. In addition, the authors rigorously assessed the relationship between the exposure and the outcome. The group set a high goal of enrollment to account for potential high rate of attrition (up to 50%). Since there was considerable loss to follow-up at both 3 and 6 months, the authors performed sensitivity analyses to determine if this biased the outcomes. The team assessed crossover contamination at the end of the study by asking participants in the control group if they used MFP during the trial. The authors also conducted a linear regression to examine if baseline self-efficacy was a significant predictor of weight change, controlling for the interaction between self-efficacy and group assignment. Additionally, sensitivity analyses were performed to see if the result from one outlier in the control group who achieved significant weight loss biased the findings.
As one of the first studies to investigate the use of a mobile app for weight loss in the primary care setting, the pragmatic design was impressive. The study showed that introduction to MFP can be done in 5 minutes and that the intervention was highly acceptable to patients. Since research assistants provided minimal guidance to enrolled participants, this study design provided an opportunity to observe the app’s efficacy in the real-world setting for the general public.
Although the authors efficiently designed a valid and pragmatic study, there were several aspects of the study that could be improved. As previously stated by the authors, this study did not explicitly measure the readiness for change, hence it was challenging to accurately and systematically determine the motivation of those in the intervention arm. Additionally, despite the diverse income and race of participants, the majority of the subjects were college-educated. In 2014, only 34% of the U.S. population completed a bachelor’s degree or high, and only 8% completed a master’s or higher degree [8]. This may limit the generalizability of the study, as education level could influence app acceptance and usage behavior.
Applications for Clinical Practice
With a large number of people using smartphones, there are increasing opportunities to use this delivery system to provide weight management information and support strategies for weight loss and lifestyle behavior changes. Previous studies showed that smartphone technology is a promising tool to facilitate weight management[9, 10], but the best practices for implementation of smart phones in the primary setting for weight management are still unknown. Based on this study and previous research done on technology intervention on health, providing the MFP app alone without additional counseling or intervention will not lead to clinically significant weight loss in the majority of patients. Future studies should determine if adding the MFP app is more efficacious when part of a more intensive behavioral intervention. Further studies should also determine whether PCP support in assessing readiness to use health apps and other behavior change technologies increases adherence and weight loss.
—Pich Seekaew, BS, and Melanie Jay MD, MS
Study Overview
Objective. To evaluate the effectiveness and impact of using MyFitnessPal, a free, popular smartphone application (“app”), for weight loss.
Study design. 2-arm randomized controlled trial.
Setting and participants. Participants were recruited from 2 primary care clinics in the University of California, Los Angeles heath system. The inclusion criteria for the study were ≥ 18 years of age, body mass index (BMI) ≥ 25 kg/m2, an interest in losing weight, and ownership of a smartphone. The exclusion criteria included pregnancy, hemodialysis, life expectancy less than 6 months, lack of interest in weight loss, and current use of a smartphone app for weight loss. Out of 633 individuals assessed, 212 were eligible for the study. Participants were block randomized by BMI 25–30 kg/m2 and BMI > 30 kg/m2 to either usual primary care (n = 107) or usual primary care plus the app (n = 105).
Intervention. MyFitnessPal (MFP) was selected for this study based on previous focus groups with overweight primary care patients. MFP is a calorie-counting app that incorporates evidence-based and theory-based approaches to weight loss. Users can enter their current weight, goal weight, and goal rate of weight loss, which allows the app to generate the user’s daily, individualized calorie goal. MFP users also input daily weight, food intake, and physical activity, which produce certain outputs, including calorie counts, weight trends, and nutritional summaries based on food consumed.
Participants in the intervention arm received help from research assistants in downloading MFP onto their smartphones and received a phone call 1 week after enrollment to assist with any technical issues with the app. Those in the control group were told to choose any preferred activity for weight loss. Both groups received usual care from their primary care provider, with an additional two follow-up visits at 3 and 6 months. At the 3-month follow-up visit, all participants received a nutrition educational handout from www.myplate.gov.
Main outcomes measures. The main outcome measure was weight change at 6 months. Blood pressure, weight, systolic blood pressure (SPB), and 3 self-reported behavioral mediators of weight loss (exercise, diet, and self-efficacy in weight loss) were measured and collected for all participants at baseline and at 3 and 6 months. This study also gathered data from the MyFitnessPal company to measure frequency of app usage. At the 6-month follow-up visit, research assistants asked participants in the intervention arm about their experience using MFP, while those in the control group were asked if they had used MFP in the past 6 months to assess contamination. The authors used a linear mixed effects model (PROC MIXED) in SAS data processing software to investigate the differences in weight change, SBP change, and change in behavioral survey items between the 2 groups while controlling for clinic site. In addition, they performed 2 sensitivity analyses to evaluate the impact of possible informative dropout (income, education, diet experience, treatment group, and baseline value), and the effect of excluding one control group outlier.
Results. The majority of participants were female (73%) with a mean age of 43.4 years (SD = 14.3). The mean BMI was 33.4 kg/m2 (SD = 7.09), and 48% of the participants identified themselves as non-Hispanic white. At the 3-month visit, 26% and 21% of the participants from the intervention and control arms were lost to follow-up. Additionally, at 6 months, 32% and 19% of intervention and control group participants were lost to follow-up.
There was no significant difference in weight change between the two groups at 3 months (control, + 0.54 lb; intervention, –0.06 lb; P = 0.53) or at 6 months (control, +0.6 lb; intervention, –0.07 lb; P = 0.63); between group difference at 3 months was –0.6 lb (95% confidence interval [CI], –2.5 to 1.3 lb; P = 0.53) and at 6 months was –0.67 lb (CI, –3.3 to 2.1 lb; P = 0.63). The sensitivity analysis based on possible missing data also suggested the same outcome with between group difference at 6 months at 0.08 lb (CI, –3.04 to 3.20 lb; P = 0.96). The difference in systolic blood pressure was not significant between the groups.
Participants in the intervention arm used a personal calorie goal more often than those in the control group, with a mean between group difference at 3 months of 1.9 days per week (CI, 1.0 to 2.8; P < 0.001) and a mean between group difference at 6 months of 2.0 days per week (CI, 1.1 to 2.9; P < 0.001). The results also showed that the use of calorie goal feature was significant at 3 months (P < 0.001) and at 6 months (P < 0.001). At the 3-month visit, the authors found that individuals in the intervention group reported decreased self-efficacy in achieving their weight loss goals when compared to their counterparts (–0.85 on a 10-point scale; CI, –1.6 to –0.1; P = 0.026), but self-efficacy was insignificant at the 6-month follow-up. Additionally, the results suggested no difference in self-reported behaviors regarding diet, exercise, and self-efficacy in weight loss between the groups.
The mean number of logins was 61 during the course of the study, and the median total logins was 19. Interestingly, the data showed that there was a rapid decline of logins after enrollment for most participants in the intervention arm. There were 94 users who logged in to the app during the first month and 34 who logged in during the last month of the study. Out of 107 participants from the control group, 14 used MFP during the trial.
Despite a sharp decline in usage, MFP users in the intervention group were satisfied with the app: 79% were somewhat to completely satisfied, 92% would recommend it to a friend, and 80% planned to continue using MFP after the study. The study indicated that there were several aspects that the users liked about MFP including ease of use (100%), feedback on progress (88%), and 48% indicated that it was fun to use. Fewer participants appreciated features such as the reminder feature (42%) and social networking feature (13%). A common theme the authors found in MFP users was increased awareness of food choices, and more caution about food choices. Of those that stopped using MFP, some comments regarding MFP included that it was tedious (84%) and not easy to use (24%).
Conclusion. While most participants were satisfied with MFP, encouraging use of the app did not lead to more weight loss in primary care patients compared to usual care. There was decreased engagement with MFP over time.
Commentary
Despite efforts by the federal government to address the obesity epidemic in the United States, there is still a high prevalence of obesity among children and adults. Approximately 17% of youth and 35% of adults in the United States have a BMI in the obese range (> 30 kg/m2) [1]. In addition to a high association between obesity and chronic diseases such as type 2 diabetes mellitus, hypertension, and hypercholesterolemia[2], the obesity epidemic carries a staggering financial burden. The annual cost of obesity in the U.S. was estimated to be $147 billion in 2008, and the medical costs for each person with obesity was $1429 higher than those with normal weight [3,4]. Therefore, finding cost-effective and easily accessible methods to manage obesity is imperative. The Pew Research Center found that 64% of adults in the U.S. own a smartphone, and 62% of those have used their phone to look up health information[5]. Thus, smartphone applications that deliver weight management information and strategies may be a cost-effective and feasible means to reach a large population.
This study assessed the impact of MyFitnessPal, a free and widely popular mobile application, as an approach to reduce weight among patients in a primary care setting. The authors compared weight change between patients who received usual care from primary care providers (PCPs) and those who used MFP in addition to their usual care. They found no significant difference in weight loss between the two groups at 3 and 6 months during the trial. Despite this negative finding, this study makes important contributions to the e-health literature and highlights important considerations for similar studies.
While the exact reasons for lack of effect are unclear, the lack of effectiveness of such a brief intervention is not surprising. It is important to note that the PCPs did not assist or reinforce the patients to use the MFP app in this study. A systematic review of technology-assisted interventions in primary care suggests that technologies such as smartphone apps could be used as a successful tools for weight loss in the primary care setting, but that there needs to be guidance and feedback from a health care team[6]. Further, the intervention may not have been intense enough to achieve clinically significant weight loss. The U.S. Preventive Service Task Force recommends intensive interventions with at least 12 to 26 visits over 12 months to address obesity[7]. Thus, future studies of this app should include more intensive counseling from the healthcare team to determine if this improves adherence to lifestyle changes.
Strengths of this study include the use of a randomized controlled trial design, double-blinding of both participants and PCPs, and analyses for outlier and missing data. These design considerations increase the validity of the trial outcome. In addition, the authors rigorously assessed the relationship between the exposure and the outcome. The group set a high goal of enrollment to account for potential high rate of attrition (up to 50%). Since there was considerable loss to follow-up at both 3 and 6 months, the authors performed sensitivity analyses to determine if this biased the outcomes. The team assessed crossover contamination at the end of the study by asking participants in the control group if they used MFP during the trial. The authors also conducted a linear regression to examine if baseline self-efficacy was a significant predictor of weight change, controlling for the interaction between self-efficacy and group assignment. Additionally, sensitivity analyses were performed to see if the result from one outlier in the control group who achieved significant weight loss biased the findings.
As one of the first studies to investigate the use of a mobile app for weight loss in the primary care setting, the pragmatic design was impressive. The study showed that introduction to MFP can be done in 5 minutes and that the intervention was highly acceptable to patients. Since research assistants provided minimal guidance to enrolled participants, this study design provided an opportunity to observe the app’s efficacy in the real-world setting for the general public.
Although the authors efficiently designed a valid and pragmatic study, there were several aspects of the study that could be improved. As previously stated by the authors, this study did not explicitly measure the readiness for change, hence it was challenging to accurately and systematically determine the motivation of those in the intervention arm. Additionally, despite the diverse income and race of participants, the majority of the subjects were college-educated. In 2014, only 34% of the U.S. population completed a bachelor’s degree or high, and only 8% completed a master’s or higher degree [8]. This may limit the generalizability of the study, as education level could influence app acceptance and usage behavior.
Applications for Clinical Practice
With a large number of people using smartphones, there are increasing opportunities to use this delivery system to provide weight management information and support strategies for weight loss and lifestyle behavior changes. Previous studies showed that smartphone technology is a promising tool to facilitate weight management[9, 10], but the best practices for implementation of smart phones in the primary setting for weight management are still unknown. Based on this study and previous research done on technology intervention on health, providing the MFP app alone without additional counseling or intervention will not lead to clinically significant weight loss in the majority of patients. Future studies should determine if adding the MFP app is more efficacious when part of a more intensive behavioral intervention. Further studies should also determine whether PCP support in assessing readiness to use health apps and other behavior change technologies increases adherence and weight loss.
—Pich Seekaew, BS, and Melanie Jay MD, MS
1. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
2. Clark JM, Brancati FL. The challenge of obesity-related chronic diseases. J Gen Intern Med 2000;15:828–9.
3. Wang CY, Mcpherson K, Marsh T, et al. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011;378:815–25.
4. Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Affairs 2009;28:822–31.
5. Smith A. U.S. smartphone use in 2015. Pew Research Center Internet Science Tech RSS. 2015.
6. Levine DM, Savarimuthu S, Squires A, et al. Technology-assisted weight loss interventions in primary care: a systematic review. J Gen Intern Med 2014;30:107–17.
7. Moyer VA. Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012;157:373–8.
8. U.S. Department of Education, National Center for Education Statistics. The condition of education 2015 (NCES 2015–144). Educational attainment 2015.
9. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight. J Cardiovasc Nurs 2013; 28:320–9.
10. Hebden L, Cook A, Van Der Ploeg HP, Allman-Farinelli M. Development of smartphone applications for nutrition and physical activity behavior change. JMIR Res Protoc 2012;1:e9.
1. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
2. Clark JM, Brancati FL. The challenge of obesity-related chronic diseases. J Gen Intern Med 2000;15:828–9.
3. Wang CY, Mcpherson K, Marsh T, et al. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011;378:815–25.
4. Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Affairs 2009;28:822–31.
5. Smith A. U.S. smartphone use in 2015. Pew Research Center Internet Science Tech RSS. 2015.
6. Levine DM, Savarimuthu S, Squires A, et al. Technology-assisted weight loss interventions in primary care: a systematic review. J Gen Intern Med 2014;30:107–17.
7. Moyer VA. Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012;157:373–8.
8. U.S. Department of Education, National Center for Education Statistics. The condition of education 2015 (NCES 2015–144). Educational attainment 2015.
9. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight. J Cardiovasc Nurs 2013; 28:320–9.
10. Hebden L, Cook A, Van Der Ploeg HP, Allman-Farinelli M. Development of smartphone applications for nutrition and physical activity behavior change. JMIR Res Protoc 2012;1:e9.
CHA2DS2-VASc Score Modestly Predicts Ischemic Stroke, Thromboembolic Events, and Death in Patients with Heart Failure Without Atrial Fibrillation
Study Overview
Objective. To determine if CHA2DS2-VASc score, a score commonly used to assess risk of cerebrovascular events among adults with atrial fibrillation, predicts ischemic stroke, thromboembolism, and death in a cohort of patients with heart failure with and without atrial fibrillation.
Design. Prospective cohort study.
Setting and participants. Patients in Denmark aged 50 years or older discharged with a primary diagnosis of incident heart failure between 1 Jan 2000 and 31 December 2012. Patients with atrial fibrillation were identified by a hospital diagnosis of atrial fibrillation or atrial flutter from 1994 onwards. The study excluded patients treated with vitamin K antagonist within 6 months prior to heart failure diagnosis and patients with a diagnosis of cancer or chronic obstructive pulmonary disease. The study utilized 3 national Danish registries: the National Patient Registry (which records all hospital admissions and diagnoses using ICD-10), the National Prescription Registry (prescription data), and the Civil Registry System (demographics and vital statistics). The registries were linked and have been well validated.
Main outcome measure. The primary outcome measure was defined as a hospital diagnosis of ischemic stroke or thromboembolic events, transient ischemic attack, systemic embolism, pulmonary embolism or myocardial infarction within 1 year after heart failure diagnosis. A secondary outcome measure was all-cause death at 1 year.
Analysis. Patients were risk stratified using the CHA2DS2-VASc score. Patients were given 1 point for congestive heart failure, hypertension, age 65 to 74 years, diabetes mellitus, vascular disease, and female sex and 2 points for age 75 years or older and previous thromboembolic events. The authors conducted a time-to-event analysis to examine the relationship between CHA2DS2-VASc score and the risk of ischemic stroke, thromboembolic event, and death separately among those with atrial fibrillation and without. Patients were censored if they began anticoagulation therapy during follow-up. The properties of CHA2DS2-VASc score in predicting the risk of outcomes were quantified using C statistics. Multiple sensitivity analyses were conducted to account for patients who had a diagnosis of atrial fibrillation shortly after diagnosis of heart failure, to include patients with chronic obstructive pulmonary disease, and split sample analysis by date of heart failure diagnosis was conducted.
Main results. A total of 42,987 patients with incident heart failure during 2000–2012 were included in the cohort, with 21.9% of these having atrial fibrillation at baseline. The median follow-up period was 1.8 years. For patients with heart failure with or without a diagnosis of atrial fibrillation, the 1-year absolute risk for all outcomes were high and increased with increasing CHA2DS2-VASc score. For ischemic stroke and death, absolute risks were higher among patient with heart failure and atrial fibrillation when compared with patients without atrial fibrillation. At high CHA2DS2-VASc score, the risk of thromboembolism was higher among patients without atrial fibrillation when compared with those with atrial fibrillation. CHA2DS2-VASc score predicted the end point of ischemic stroke at 1 and 5 years modestly with C statistics 0.67 and 0.69 among those without atrial fibrillation and 0.64 and 0.71 among those with atrial fibrillation. The negative predictive value for all events at 1 year was around 90% when using a cutoff score of 1 for patients without atrial fibrillation, but only around 75% at 5 years.
Conclusions. Although the CHA2DS2-VASc score was developed to predict ischemic stroke among patients with atrial fibrillation, it also has modest predictive accuracy when applied to patients with heart failure without atrial fibrillation. Among patients with heart failure with a high CHA2DS2-VASc score, the risks of all adverse outcomes were high regardless of whether concomitant atrial fibrillation was present, and the risk of thromboembolism was higher among those without atrial fibrillation than those with concomitant atrial fibrillation. Because of the modest predictive accuracy, the clinical utility of CHA2DS2-VASc among patients with heart failure needs to be further determined.
Commentary
Clinical prediction rules are increasingly relied upon in clinical setting to drive medical decision making, allowing clinicians to weigh risks and benefits of interventions in a concrete, evidence-based manner [1]. The CHA2DS2-VASc score, endorsed in guidelines for assessing risk of stroke among patients with atrial fibrillation, is widely used in clinical practice [2,3] in helping make decisions about treatment, such as use of anticoagulation. The use of the clinical prediction rule for patients with heart failure but without atrial fibrillation is a novel application of the widely used rule. The rationale is that the CHA2DS2-VASc score includes within it a cluster of stroke risk factors that increases risk of stroke whether atrial fibrillation is present or not and thus perhaps capture stroke risk beyond whether a patient has atrial fibrillation [4]. The authors selected a patient group with high rate of mortality—those with incident heart failure—to evaluate the hypothesis that the CHA2DS2-VASc score could predict stroke outcomes in heart failure patients without atrial fibrillation in a manner similar to that in atrial fibrillation populations, and that at high CHA2DS2-VASc scores, the risk for stroke would be comparable among heart failure patients.
What the authors found is that the scoring algorithm was able to predict stroke occurrence modestly whether or not atrial fibrillation was present, and that stroke risk was high among those at the highest scores regardless of whether patients had atrial fibrillation. These findings underscore the potential use of the scoring algorithm beyond the population with atrial fibrillation, and also highlighted the need for further research in the highest risk group of heart failure patients without atrial fibrillation to determine whether anticoagulation may reduce stroke risk in this population. Minor study limitations included the use of an administrative dataset, in which diagnosis information may be incomplete or erroneous, and the potential limited generalizability of the study, given differences in the makeup of the Danish study population compared with other populations.
Applications for Clinical Practice
The study explores the use of clinical predication rule beyond the condition for which it is developed and found that particularly in high-risk groups, risk scores still predicted adverse events, albeit modestly. For clinicians, it highlights both the utility of the risk scores and the current gap in knowledge about stroke prevention in the highest-risk group of patients without atrial fibrillation. Further studies are needed to determine if anticoagulation therapy applies to this high-risk group for stroke prevention.
—William W. Hung, MD, MPH
1. McGinn TG, Guyatt GH, Wyer PC, et al. Users’ guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence-Based Medicine Working Group. JAMA 2000;284:79–84.
2. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–e76.
3. Camm AJ, Lip GY, De Caterina R, et al; ESC Committee for Practice Guidelines. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Eur Heart J 2012;33:2719–47.
4. Mitchell LB, Southern DA, Galbraith D, et al; APPROACH Investigators. Prediction of stroke or TIA in patients without atrial fibrillation using CHADS2 and CHA2DS2-VASc scores. Heart 2014;100:1524–30.
Study Overview
Objective. To determine if CHA2DS2-VASc score, a score commonly used to assess risk of cerebrovascular events among adults with atrial fibrillation, predicts ischemic stroke, thromboembolism, and death in a cohort of patients with heart failure with and without atrial fibrillation.
Design. Prospective cohort study.
Setting and participants. Patients in Denmark aged 50 years or older discharged with a primary diagnosis of incident heart failure between 1 Jan 2000 and 31 December 2012. Patients with atrial fibrillation were identified by a hospital diagnosis of atrial fibrillation or atrial flutter from 1994 onwards. The study excluded patients treated with vitamin K antagonist within 6 months prior to heart failure diagnosis and patients with a diagnosis of cancer or chronic obstructive pulmonary disease. The study utilized 3 national Danish registries: the National Patient Registry (which records all hospital admissions and diagnoses using ICD-10), the National Prescription Registry (prescription data), and the Civil Registry System (demographics and vital statistics). The registries were linked and have been well validated.
Main outcome measure. The primary outcome measure was defined as a hospital diagnosis of ischemic stroke or thromboembolic events, transient ischemic attack, systemic embolism, pulmonary embolism or myocardial infarction within 1 year after heart failure diagnosis. A secondary outcome measure was all-cause death at 1 year.
Analysis. Patients were risk stratified using the CHA2DS2-VASc score. Patients were given 1 point for congestive heart failure, hypertension, age 65 to 74 years, diabetes mellitus, vascular disease, and female sex and 2 points for age 75 years or older and previous thromboembolic events. The authors conducted a time-to-event analysis to examine the relationship between CHA2DS2-VASc score and the risk of ischemic stroke, thromboembolic event, and death separately among those with atrial fibrillation and without. Patients were censored if they began anticoagulation therapy during follow-up. The properties of CHA2DS2-VASc score in predicting the risk of outcomes were quantified using C statistics. Multiple sensitivity analyses were conducted to account for patients who had a diagnosis of atrial fibrillation shortly after diagnosis of heart failure, to include patients with chronic obstructive pulmonary disease, and split sample analysis by date of heart failure diagnosis was conducted.
Main results. A total of 42,987 patients with incident heart failure during 2000–2012 were included in the cohort, with 21.9% of these having atrial fibrillation at baseline. The median follow-up period was 1.8 years. For patients with heart failure with or without a diagnosis of atrial fibrillation, the 1-year absolute risk for all outcomes were high and increased with increasing CHA2DS2-VASc score. For ischemic stroke and death, absolute risks were higher among patient with heart failure and atrial fibrillation when compared with patients without atrial fibrillation. At high CHA2DS2-VASc score, the risk of thromboembolism was higher among patients without atrial fibrillation when compared with those with atrial fibrillation. CHA2DS2-VASc score predicted the end point of ischemic stroke at 1 and 5 years modestly with C statistics 0.67 and 0.69 among those without atrial fibrillation and 0.64 and 0.71 among those with atrial fibrillation. The negative predictive value for all events at 1 year was around 90% when using a cutoff score of 1 for patients without atrial fibrillation, but only around 75% at 5 years.
Conclusions. Although the CHA2DS2-VASc score was developed to predict ischemic stroke among patients with atrial fibrillation, it also has modest predictive accuracy when applied to patients with heart failure without atrial fibrillation. Among patients with heart failure with a high CHA2DS2-VASc score, the risks of all adverse outcomes were high regardless of whether concomitant atrial fibrillation was present, and the risk of thromboembolism was higher among those without atrial fibrillation than those with concomitant atrial fibrillation. Because of the modest predictive accuracy, the clinical utility of CHA2DS2-VASc among patients with heart failure needs to be further determined.
Commentary
Clinical prediction rules are increasingly relied upon in clinical setting to drive medical decision making, allowing clinicians to weigh risks and benefits of interventions in a concrete, evidence-based manner [1]. The CHA2DS2-VASc score, endorsed in guidelines for assessing risk of stroke among patients with atrial fibrillation, is widely used in clinical practice [2,3] in helping make decisions about treatment, such as use of anticoagulation. The use of the clinical prediction rule for patients with heart failure but without atrial fibrillation is a novel application of the widely used rule. The rationale is that the CHA2DS2-VASc score includes within it a cluster of stroke risk factors that increases risk of stroke whether atrial fibrillation is present or not and thus perhaps capture stroke risk beyond whether a patient has atrial fibrillation [4]. The authors selected a patient group with high rate of mortality—those with incident heart failure—to evaluate the hypothesis that the CHA2DS2-VASc score could predict stroke outcomes in heart failure patients without atrial fibrillation in a manner similar to that in atrial fibrillation populations, and that at high CHA2DS2-VASc scores, the risk for stroke would be comparable among heart failure patients.
What the authors found is that the scoring algorithm was able to predict stroke occurrence modestly whether or not atrial fibrillation was present, and that stroke risk was high among those at the highest scores regardless of whether patients had atrial fibrillation. These findings underscore the potential use of the scoring algorithm beyond the population with atrial fibrillation, and also highlighted the need for further research in the highest risk group of heart failure patients without atrial fibrillation to determine whether anticoagulation may reduce stroke risk in this population. Minor study limitations included the use of an administrative dataset, in which diagnosis information may be incomplete or erroneous, and the potential limited generalizability of the study, given differences in the makeup of the Danish study population compared with other populations.
Applications for Clinical Practice
The study explores the use of clinical predication rule beyond the condition for which it is developed and found that particularly in high-risk groups, risk scores still predicted adverse events, albeit modestly. For clinicians, it highlights both the utility of the risk scores and the current gap in knowledge about stroke prevention in the highest-risk group of patients without atrial fibrillation. Further studies are needed to determine if anticoagulation therapy applies to this high-risk group for stroke prevention.
—William W. Hung, MD, MPH
Study Overview
Objective. To determine if CHA2DS2-VASc score, a score commonly used to assess risk of cerebrovascular events among adults with atrial fibrillation, predicts ischemic stroke, thromboembolism, and death in a cohort of patients with heart failure with and without atrial fibrillation.
Design. Prospective cohort study.
Setting and participants. Patients in Denmark aged 50 years or older discharged with a primary diagnosis of incident heart failure between 1 Jan 2000 and 31 December 2012. Patients with atrial fibrillation were identified by a hospital diagnosis of atrial fibrillation or atrial flutter from 1994 onwards. The study excluded patients treated with vitamin K antagonist within 6 months prior to heart failure diagnosis and patients with a diagnosis of cancer or chronic obstructive pulmonary disease. The study utilized 3 national Danish registries: the National Patient Registry (which records all hospital admissions and diagnoses using ICD-10), the National Prescription Registry (prescription data), and the Civil Registry System (demographics and vital statistics). The registries were linked and have been well validated.
Main outcome measure. The primary outcome measure was defined as a hospital diagnosis of ischemic stroke or thromboembolic events, transient ischemic attack, systemic embolism, pulmonary embolism or myocardial infarction within 1 year after heart failure diagnosis. A secondary outcome measure was all-cause death at 1 year.
Analysis. Patients were risk stratified using the CHA2DS2-VASc score. Patients were given 1 point for congestive heart failure, hypertension, age 65 to 74 years, diabetes mellitus, vascular disease, and female sex and 2 points for age 75 years or older and previous thromboembolic events. The authors conducted a time-to-event analysis to examine the relationship between CHA2DS2-VASc score and the risk of ischemic stroke, thromboembolic event, and death separately among those with atrial fibrillation and without. Patients were censored if they began anticoagulation therapy during follow-up. The properties of CHA2DS2-VASc score in predicting the risk of outcomes were quantified using C statistics. Multiple sensitivity analyses were conducted to account for patients who had a diagnosis of atrial fibrillation shortly after diagnosis of heart failure, to include patients with chronic obstructive pulmonary disease, and split sample analysis by date of heart failure diagnosis was conducted.
Main results. A total of 42,987 patients with incident heart failure during 2000–2012 were included in the cohort, with 21.9% of these having atrial fibrillation at baseline. The median follow-up period was 1.8 years. For patients with heart failure with or without a diagnosis of atrial fibrillation, the 1-year absolute risk for all outcomes were high and increased with increasing CHA2DS2-VASc score. For ischemic stroke and death, absolute risks were higher among patient with heart failure and atrial fibrillation when compared with patients without atrial fibrillation. At high CHA2DS2-VASc score, the risk of thromboembolism was higher among patients without atrial fibrillation when compared with those with atrial fibrillation. CHA2DS2-VASc score predicted the end point of ischemic stroke at 1 and 5 years modestly with C statistics 0.67 and 0.69 among those without atrial fibrillation and 0.64 and 0.71 among those with atrial fibrillation. The negative predictive value for all events at 1 year was around 90% when using a cutoff score of 1 for patients without atrial fibrillation, but only around 75% at 5 years.
Conclusions. Although the CHA2DS2-VASc score was developed to predict ischemic stroke among patients with atrial fibrillation, it also has modest predictive accuracy when applied to patients with heart failure without atrial fibrillation. Among patients with heart failure with a high CHA2DS2-VASc score, the risks of all adverse outcomes were high regardless of whether concomitant atrial fibrillation was present, and the risk of thromboembolism was higher among those without atrial fibrillation than those with concomitant atrial fibrillation. Because of the modest predictive accuracy, the clinical utility of CHA2DS2-VASc among patients with heart failure needs to be further determined.
Commentary
Clinical prediction rules are increasingly relied upon in clinical setting to drive medical decision making, allowing clinicians to weigh risks and benefits of interventions in a concrete, evidence-based manner [1]. The CHA2DS2-VASc score, endorsed in guidelines for assessing risk of stroke among patients with atrial fibrillation, is widely used in clinical practice [2,3] in helping make decisions about treatment, such as use of anticoagulation. The use of the clinical prediction rule for patients with heart failure but without atrial fibrillation is a novel application of the widely used rule. The rationale is that the CHA2DS2-VASc score includes within it a cluster of stroke risk factors that increases risk of stroke whether atrial fibrillation is present or not and thus perhaps capture stroke risk beyond whether a patient has atrial fibrillation [4]. The authors selected a patient group with high rate of mortality—those with incident heart failure—to evaluate the hypothesis that the CHA2DS2-VASc score could predict stroke outcomes in heart failure patients without atrial fibrillation in a manner similar to that in atrial fibrillation populations, and that at high CHA2DS2-VASc scores, the risk for stroke would be comparable among heart failure patients.
What the authors found is that the scoring algorithm was able to predict stroke occurrence modestly whether or not atrial fibrillation was present, and that stroke risk was high among those at the highest scores regardless of whether patients had atrial fibrillation. These findings underscore the potential use of the scoring algorithm beyond the population with atrial fibrillation, and also highlighted the need for further research in the highest risk group of heart failure patients without atrial fibrillation to determine whether anticoagulation may reduce stroke risk in this population. Minor study limitations included the use of an administrative dataset, in which diagnosis information may be incomplete or erroneous, and the potential limited generalizability of the study, given differences in the makeup of the Danish study population compared with other populations.
Applications for Clinical Practice
The study explores the use of clinical predication rule beyond the condition for which it is developed and found that particularly in high-risk groups, risk scores still predicted adverse events, albeit modestly. For clinicians, it highlights both the utility of the risk scores and the current gap in knowledge about stroke prevention in the highest-risk group of patients without atrial fibrillation. Further studies are needed to determine if anticoagulation therapy applies to this high-risk group for stroke prevention.
—William W. Hung, MD, MPH
1. McGinn TG, Guyatt GH, Wyer PC, et al. Users’ guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence-Based Medicine Working Group. JAMA 2000;284:79–84.
2. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–e76.
3. Camm AJ, Lip GY, De Caterina R, et al; ESC Committee for Practice Guidelines. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Eur Heart J 2012;33:2719–47.
4. Mitchell LB, Southern DA, Galbraith D, et al; APPROACH Investigators. Prediction of stroke or TIA in patients without atrial fibrillation using CHADS2 and CHA2DS2-VASc scores. Heart 2014;100:1524–30.
1. McGinn TG, Guyatt GH, Wyer PC, et al. Users’ guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence-Based Medicine Working Group. JAMA 2000;284:79–84.
2. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–e76.
3. Camm AJ, Lip GY, De Caterina R, et al; ESC Committee for Practice Guidelines. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Eur Heart J 2012;33:2719–47.
4. Mitchell LB, Southern DA, Galbraith D, et al; APPROACH Investigators. Prediction of stroke or TIA in patients without atrial fibrillation using CHADS2 and CHA2DS2-VASc scores. Heart 2014;100:1524–30.
A Novel Emergency Department Surge Protocol: Implementation of a Targeted Response Plan
From the Ottawa Hospital, Ottawa, ON Canada.
Abstract
- Objective: Fluctuations in emergency department (ED) visits occur frequently, and traditional global measures of ED crowding do not allow for targeted responses to address root causes. We sought to develop, implement, and evaluate a novel ED surge protocol based on the input-throughput-output (ITO) model of ED flow.
- Methods: This initiative took place at a tertiary care academic teaching hospital. An inter-professional group developed and validated metrics for various levels of surge in relation to the ITO model, measured every 2 hours, which directly linked to specific actions targeting root causes within those components. Main outcome measure was defined as the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively.
- Results: During the 6-month study period, average daily hospital occupancy levels rose above 100% (pre 99.5%, post 101.2%; P = 0.01) and frequency of high surges in the output component increased (pre 7.7%, post 10.8%; P = 0.002). Despite this, frequency of sustained high surges remained stable for input (pre 4.5%, post 0.0%; P = 0.13) and throughput (pre 3.5%, post 2.7%; P = 0.54), while improvement in output reached statistical significance (pre 7.7%, post 2.0%, P = 0.01).
- Conclusions: The ED surge protocol led to effective containment of daily high surges despite significant increase in hospital occupancy levels. This is the first study to describe an ED surge plan capable of identifying within which ITO component surge is happening and linking actions to address specific causes. We believe this protocol can be adapted for any ED.
Emergency department (ED) crowding has been defined as “a situation where the demand for emergency services exceeds the ability to provide care in a reasonable amount of time” [1]. Crowding is an increasingly common occurrence in hospital-based EDs, and overcrowding of EDs has been shown to adversely affect the delivery of emergency care and results in increased patient morbidity and mortality [2,3]. Furthermore, the nature of medical emergencies dictates that rapid daily changes (or surges) in patient volume and acuity occur frequently and unpredictably, contributing to the difficulty of matching resources to demands. Accurate understanding and continuous measurement of where bottlenecks may be occurring within an ED are critical to an effective response to ED surges.
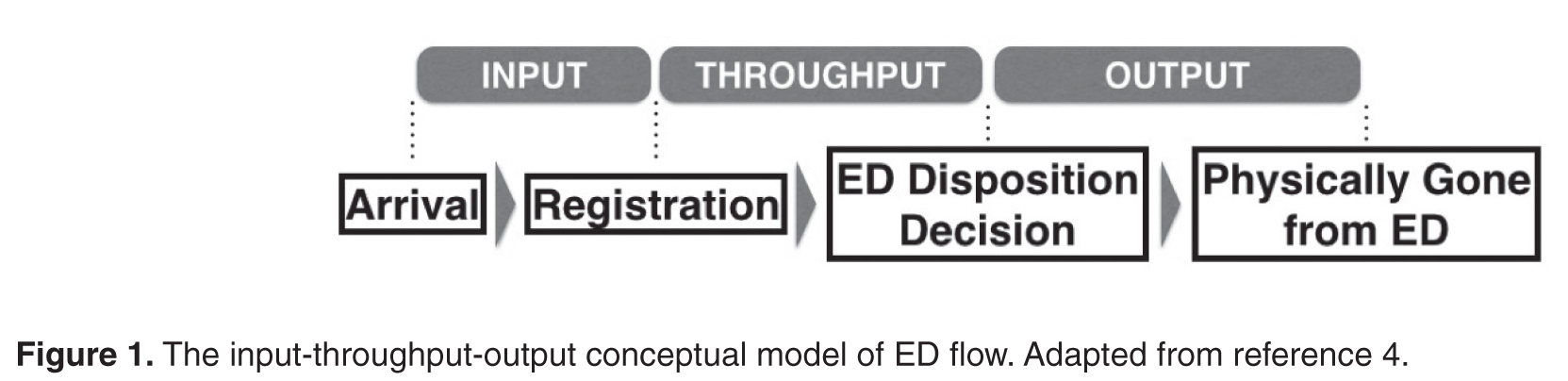
Many of the widely used measurement tools for overcrowding produce one final overall net value on a one-dimensional scale, failing to capture the complexity of the root causes of surges. For example, the National ED Overcrowding Study (NEDOCS) scoring system, validated at various centers and widely used and studied [5–7] utilizes a number of institutional and situational variables to calculate a final NEDOCS score, which translates to “Not Busy,” “Busy,” “Overcrowded,” “Severely Overcrowded,” or “Dangerously Overcrowded” as a global state. Other published scoring systems such as the Emergency Department Work Index (EDWIN), while performing well in comparison to subjective impressions of physicians and nurses, also suffers from computation of a single final score, which makes it difficult to tie to specific actions or solutions [8]. Other surrogate markers quantifying ED crowding have also been used, such as left-without-being-seen rates, ambulance diversions, and total number of boarded patients in the ED; yet they too only measure consequences of crowding and provide little diagnostic information on when and where specific ED surges are actually happening throughout the day [9].
Responding to ED Surges
An effective surge plan should ensure the delivery of safe, effective care in response to various input/throughput/output surges in a coordinated and standardized manner. The ideal ED surge plan should include (1) a prospective continuous tool/method that accurately gauges the surge level (based on objective measures) in various components of the Input-Throughput-Output model of the department, (2) standardized targeted actions that are tied to specific triggers identified within that model to ensure effective solutions, and (3) built-in contingency plans for escalation in the face of sustained/worsening surges. Few studies have been published describing successful implementation of ED surge protocols, with the majority being linked to global ED crowding measures such as the NEDOCS score [10]. As a result, it is difficult to tease out the specific targeted actions that are most effective in dealing with the root causes of a surge.
Local Problem
Prior to the quality improvement initiative we describe below, the Ottawa Hospital ED had no formal process or method of measuring daily surges nor any standardized action plan to respond effectively to those surges. The state of “busy-ness” was often defined by gut feelings of frontline workers, which was quite variable depending on the individuals in charge of departmental patient flow. Often, actions to try and mitigate rising ED surges were triggered too late, resulting in consistent gridlock in the ED that lasted many hours. Several near-misses as well as actual critical incidences had occurred as a result of ineffective management of ED surges, and the authors of this initiative were tasked by senior hospital leadership with designing and implementing a novel solution.
Objectives
We describe our approach to the development, implementation, and evaluation of a novel ED surge protocol at a tertiary care academic hospital based on the principles cited above. Specifically, we sought to:
- define various levels of ED surge and to provide a common language for better communication between all stakeholders
- incorporate the validated Input-Throughput-Output model of ED flow to provide a conceptual framework for measuring surges in real-time and developing targeted action plans
- standardize ED and organizational responses to various ED surges based on identified bottlenecks
- measure and evaluate the effectiveness of the ED surge plan implementation
- continuously modify and improve the ED surge protocol using quality improvement strategies
Methods
Setting
The Ottawa Hospital is an academic tertiary care center with 3 campuses (Civic, General, and Riverside), with the ED providing coverage at 2 physical emergency rooms. The hospital is the regional trauma center as well as referral destination for many subspecialties such as cardiac, vascular and neurosurgical emergencies. This 1163-bed facility handles over 160,000 emergency visits a year, over 1 million ambulatory care visits a year, and roughly 35,000 surgical cases annually. The ED is staffed by 78 staff physicians, approximately 250 registered nurses (RNs), and ~50 emergency medicine residents/trainees.
The EDs are supported by a computerized tracking system that provides real-time metrics. This information is displayed by ED-specific geographical area on electronic whiteboards, which can be accessed on overhead monitors, desktop computers, and personal iPads. Information available to ED physicians and staff at any time includes individual-level data such as location, demographics, Canadian Triage Acuity Score (CTAS), and presenting complaint as well as departmental-level data such as patient volumes, wait times, length of stay (LOS), pending/completed diagnostics, consultation status and final dispositions.
According to the policy and standard operating procedures that govern research at the Ottawa Hospital Research Institute, this work met criteria for quality improvement activities exempt from ethics review.
Intervention
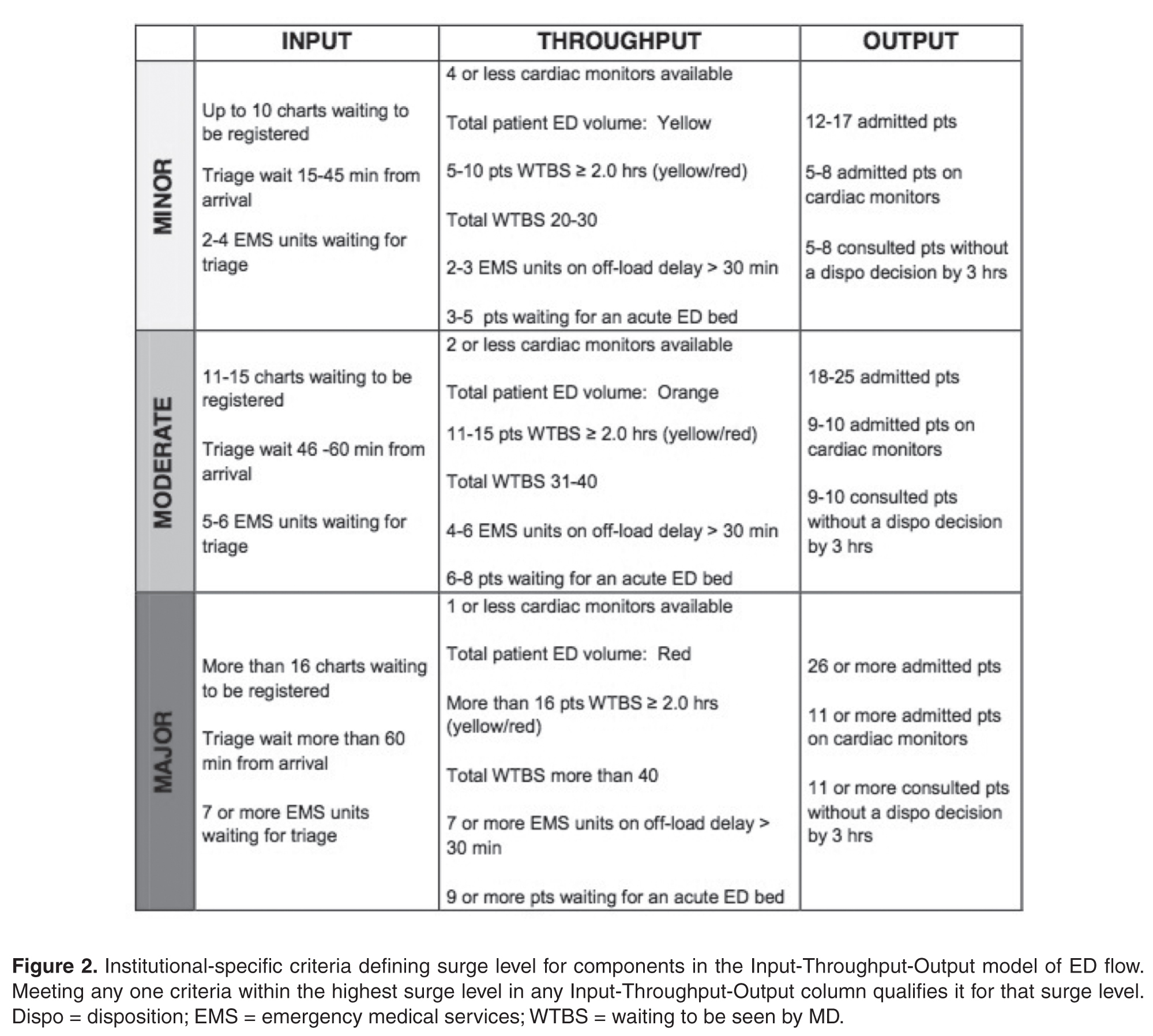
Over a 4-day period care facilitators were polled on an hourly basis to determine what factors were important to the in determining how “busy” they perceived the ED to be. These factors included but were not limited to: total number of patients waiting to be seen; time to physician initial assessment; number of monitored beds available; and number of admitted patients boarded in the ED. Analysis was done to prospectively compare their perception of surge levels to the proposed Surge Plan metrics, and to ensure that the individual criteria for each level was practically meaningful and accurate.
Next, a set of standardized action and response plans were developed and agreed upon that tied specifically to a corresponding component of the different measured ED surge levels (these action plans are detailed in an online Appendix and are also available from the author). The fundamental guiding principles behind the development of each action item was that it should (1) target underlying causes - in a standardized way - specific to the relevant Input-Throughput-Output surge, (2) provide escalating level of effectiveness for each corresponding escalation in the surge level (eg, contacting a staff physician directly for a disposition decision for patents consulted in the ED, if the resident trainees have failed to do so in a timely manner), and (3) coordinate actions by various stakeholders in a planned and organized manner. Practically, the standardized targeted actions span across 5 different roles, which were explicitly listed on action sheets for care facilitators, clinical managers, patient flow managers, evening and night coordinators, and clinical directors.
Stakeholder Engagement
Implementation and Continuous Improvement
Given the complexity of the ED- and hospital-wide nature of the surge protocol, implementation was done over multiple phases and Plan-Do-Study-Act (PDSA) improvement cycles:
Phase I (Apr 2013 - Jun 2013)
The initial proposed ED surge level metrics were measured at a single ED campus. Care facilitators were trained and asked to measure surge levels in the ED every 2 hours. This served as a testing period to gauge the sensitivity and reliability of our proposed surge level metrics, and no actual action items were triggered during this period. Stakeholder meetings were held to determine feasibility of the plan, validate the proposed metrics, and develop “standard work” action plans for each stakeholder group in response to the metrics. This first phase also allowed care facilitators to objectively reflect on ED surge patterns throughout the day, and provided everyone in the ED team a frequent global snapshot of how “busy” the department was at any time. Finally, surge level data during this phase confirmed previous suspicions that the Output component was the biggest driver behind overall ED surge level.
Throughout this phase, the ED clinical manager recorded all the usual actions taken in response to the different level of surges as felt appropriate by the individual care facilitator on duty. The variety of actions and types of escalations were collected and fed back to weekly workgroup meetings to help further refine crafting of standardized action plans for implementation of the surge protocol.
Phase II (June - Aug 2013)
An initial trial of a limited ED surge protocol was rolled out at both ED campuses, with actual action items being triggered in response to specific surge level metrics. The main focus of this PDSA cycle was to collect data on how the care facilitator groups at the 2 campuses utilized the surge protocol, as well as feedback on usability, barriers, and effectiveness. Regular audits were performed to ensure surge measurement and compliance rates. Educational sessions were provided regarding rationale and purpose of the plan so that all team members had a better understanding of ED surges. Frequent meetings with stakeholders to share updates continued throughout Phase II, allowing further engagement as well as fine-tuning of stakeholder action plans based on real-time experiences.
Phase III (Aug 2013 - Dec 2013)
The next phase of implementation expanded beyond the ED and included the hospital’s off-hours and off-service management group. This in effect was the official corporate roll-out of the ED surge protocol including full action plans for all stakeholders, including off-service clinical administrators, inpatient flow managers, and the director of emergency and critical care. Regular audits were performed to ensure compliance of measurement every 2 hours as well as performance of specified action items related to each surge level, with the actual surge level measurement completion rates of 98%.
Data Collection and Analysis
Over the study period April 2013 to December 2013 at the Civic campus and June 2013 to December 2013 at the General campus, ED surge levels were measured every 2 hours by the care facilitators and manually recorded in standardized ED surge protocol booklets. These were subsequently entered into Excel database for tracking and data analysis. Patient volumes and hospital occupancy levels were recorded daily. Perceptions of the primary users of the surge protocol (ie, care facilitators) were obtained via standardized interviews and polls. We present descriptive statistics and statistical process control (SPC) charts. Chi-squared test was performed for comparison of pre- and post-intervention frequencies of outcome measures.
Outcome Measures
The main outcome measure was the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively. High surges were defined as Moderate and Major surges combined. Our expert group consensus was that combinging the Moderate and Major surge categories to represent “high” surge was reasonable since they both require mobilizing resources on a hospital-wide level, and failure to improve despite 6 continuous hours of actively trying to address such high surges would lead to significantly higher risk for quality of care and patient safety issues.
Secondary outcomes include overall frequency of reaching high surge levels at various components of the Input-Throughput-Output ED flow model, hospital occupancy levels, and care facilitators’ perceptions on workload and overall effectiveness of the surge protocol.
Results
ED Flow
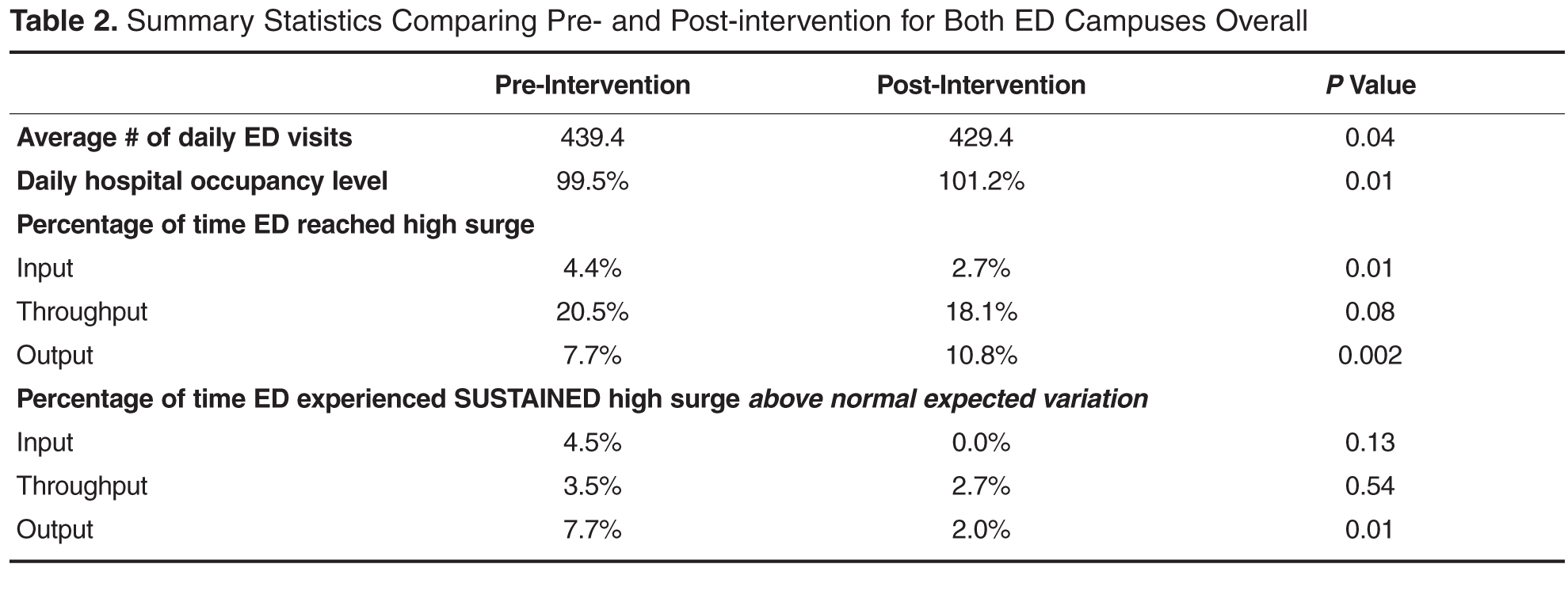
Statistical Process Control Charts
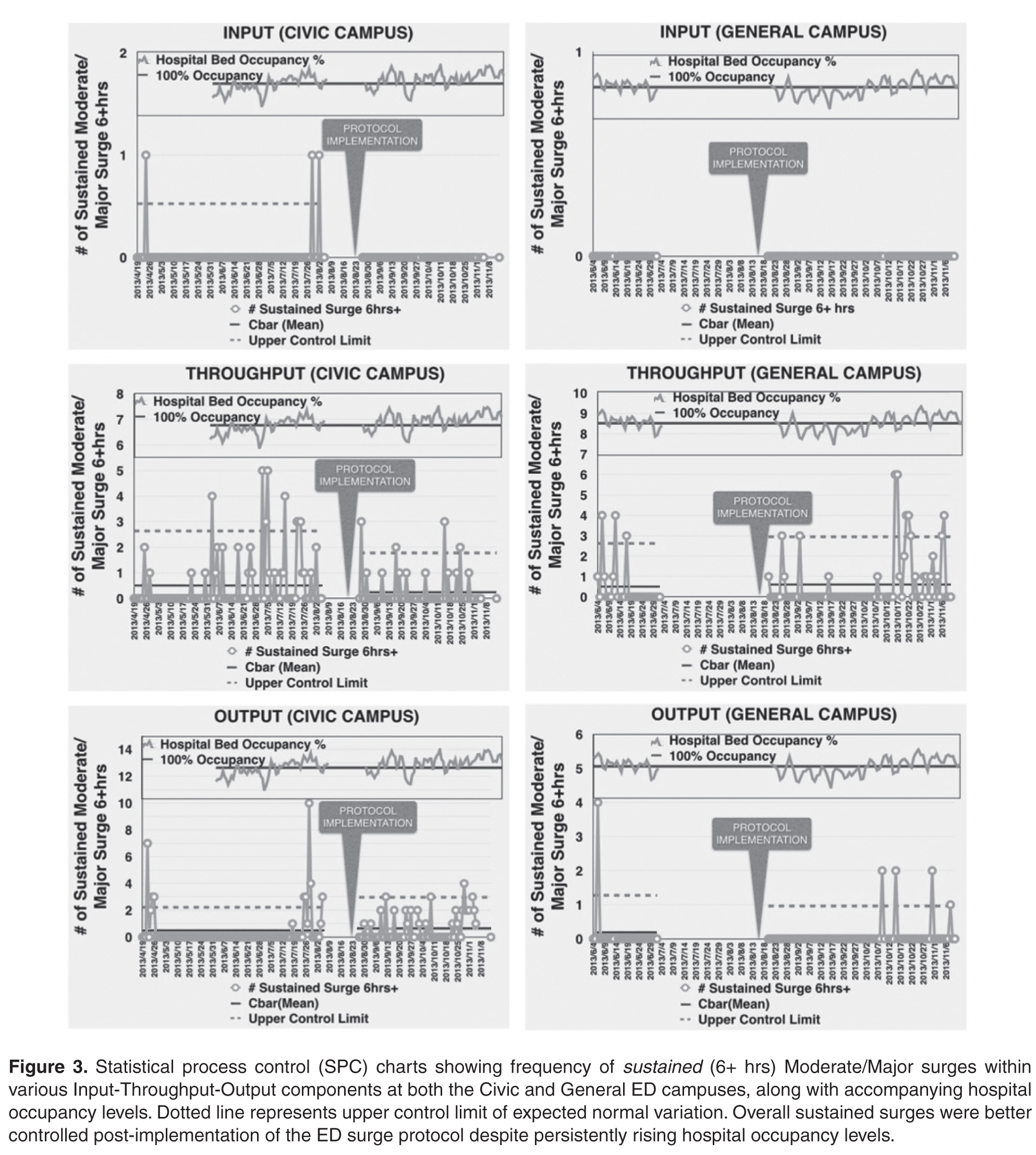
Survey of Care Facilitators
The primary users and drivers of the surge protocol—the care facilitator group—felt strongly that the tool was easy to use and that it made a positive difference. 72% felt that the ED surge protocol has increased their workload but 92% felt that it was good for overall flow of the ED. Specific feedback included having a much more standardized language around communicating (and acting on) surges, and a better overall bird’s-eye view of the department.
Discussion
Despite a call for urgent research on implementing solutions targeting daily ED surges (vs. global ED crowding) over a decade ago at the Academic Emergency Medicine 2006 Consensus Conference [12], little work has been published on distinguishing, measuring, and dealing with ED surges. McCarthy et al proposed the rate of patient arrivals to the ED by time of day as a rudimentary definition of surge, although they provided very little specific guidance on what to do with that information in the setting of responding to spikes in surges [13]. Asplin et al described a number of theoretical models to bridge ED census, daily surges, length of stay and quality of care, however they were never validated in real-life scenarios [14]. A systematic review published in 2009 summarizing articles that described theoretical and practical ED surge responses found a large heterogeneity of different proposed models with little standardization and multiple shortcomings [15].
To our knowledge, this study is the first to report on the actual development, implementation, and evaluation of a daily ED surge protocol that utilizes a widely accepted conceptual model of ED flow. Unlike single global measure of ED crowding, our protocol measures frequent surge levels for various Input-Throughput-Output components of the ED, which are tied directly to standardized specific actions to address underlying root causes. Despite continued rise in hospital occupant levels and budgetary restraints, we found a improvement in the number of times the ED actually hit severe surges with the exception of Output, which is expected since this component of the flow model is intimately tied to hospital occupant levels. When severe surges did happen, we were able to deal with them much more effectively and efficiently, resulting in an overall decrease in sustained surges in the ED including the Output component.
Limitations
Similar to other pragmatic quality improvement projects that rely on manual processes, it was difficult to ensure absolute compliance of surge level measurements throughout the study period. As a result, there were occasional missing surge level data at various times of different days. However, we believe these are relatively nonsignificant occurrences that balanced out over the pre- and post-implementation periods. In addition, we did not have the resources to robustly record and confirm completion of specific action items that were activated in response to various surge levels, although we did confirm verbally with frontline workers regularly that those actions were done. Future Plan-Do-Study-Act cycles will focus on explicit measurement of actual completed action items and further refinement of targeted responses to surge. Finally, while we were able to only collect and present data over a relatively short period of evaluation (and thus potentially susceptible to seasonal variations in ED flow), we believe that our data does support the surge protocol’s effectiveness when compared to the robust trend of hospital occupant levels.
Future Directions
This ED surge protocol can be adapted and modified to fit any ED. The specific criteria defining Minor/Moderate/Major surges can be set up as ratios or percentages relative to total number of monitors, beds, etc., available. The principles of linking actions directly to specific triggers within each Input/Throughput/Output category could be translated to fit any-sized organization. Currently in progress is a longer evaluation period and based upon the results as well as individual feedback, necessary adjustments to our definitions, criteria and action items will be considered as part of ongoing quality improvement. The principles of our surge protocol are not limited to the ED, and we will explore its implementation in other hospital departments as well as methods to link them together in alignment with the hospital’s overall corporate strategy in tackling overcrowding.
Conclusion
In summary, implementation of this novel ED surge protocol led to a more effective response and management of high surges, despite significant increase in overall hospital occupancy rates and associated frequency of surges in the Output component of the ED flow model. Our surge measurement tool is capable of identifying within which area of the ED surges are occurring, and our ED surge protocol links specific actions to address those specific root causes. We believe this will lead not only to more accurate assessments of overall ED crowding but also to more timely and effective departmental and institutional responses.
Corresponding author: Dr. Edmund S.H. Kwok, Dept. of Emergency Medicine, Ottawa Hospital, Civic Campus, 1053 Carling Ave., Ottawa, ON, Canada K1Y 4E9, ekwok@toh.on.ca.
Financial disclosures: None.
1. Bond K. Interventions to reduce overcrowding in emergency departments. [Technology report no 67.4]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.
2. Richardson DB, et al. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 2006;184:213–6.
3. Sprivulis PC, et al. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust 2006; 184:208–12.
4. Asplin BR, Magid DJ, Rhodes KV, et al. A conceptual model of emergency department crowding. Ann Emerg Med 2003; 42:173–80.
5. Affleck A, Parks P, Drummond A, et al. Emergency department overcrowding and access block. CAEP Position Statement. CJEM 2013;15:359–70.
6. Weiss SJ, Derlet R, Arndahl J, et al. Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS). Acad Emerg Med 2004;11:38–50.
7. Weiss SJ, Ernst AA, Nick TG. Comparison of the National Emergency Department Overcrowding Scale and the Emergency Department Work Index for quantifying emergency department crowding. Acad Emerg Med 2006;13:513–8.
8. Jones SS, Allen TL, Welch SJ. An independent evaluation of four quantitative emergency department crowding scales. Acad Emerg Med 2006;13:1204–11
9. Bernstein SL, Verghese V, Leung W, et al. Development and validation of a new index to measure emergency department crowding. Acad Emerg Med 2003;10:938–42
10. General Accounting Office. Hospital emergency departments–crowded conditions vary among hospitals and communities. GAO-03-460. Washington, DC: US General Accounting Office; 2003.
11. Moseley MG, Dickerson CL, Kasey J, et al. Surge: a organizational response to emergency department overcrowding. J Clin Outcomes Manage 2010;17:453–7.
12. Jenkins JL, O’Connor RE, Cone DC. Differentiating large-scale surge versus daily surge. Acad Emerg Med 2006; 13:1169–72.
13. McCarthy ML, Aronsky D, Kelen GD. The measurement of daily surge and its relevance to disaster preparedness. Acad Emerg Med 2006; 13:1138–41.
14. Asplin BR, Flottemesch TJ, Gordon B. Developing models for patient flow and daily surge capacity research. Acad Emerg Med 2006;13:1109–13.
15. Nager AL, Khanna K. Emergency department surge: models and practical implications. J Trauma 2009; 67(2 Suppl):S96–9.
From the Ottawa Hospital, Ottawa, ON Canada.
Abstract
- Objective: Fluctuations in emergency department (ED) visits occur frequently, and traditional global measures of ED crowding do not allow for targeted responses to address root causes. We sought to develop, implement, and evaluate a novel ED surge protocol based on the input-throughput-output (ITO) model of ED flow.
- Methods: This initiative took place at a tertiary care academic teaching hospital. An inter-professional group developed and validated metrics for various levels of surge in relation to the ITO model, measured every 2 hours, which directly linked to specific actions targeting root causes within those components. Main outcome measure was defined as the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively.
- Results: During the 6-month study period, average daily hospital occupancy levels rose above 100% (pre 99.5%, post 101.2%; P = 0.01) and frequency of high surges in the output component increased (pre 7.7%, post 10.8%; P = 0.002). Despite this, frequency of sustained high surges remained stable for input (pre 4.5%, post 0.0%; P = 0.13) and throughput (pre 3.5%, post 2.7%; P = 0.54), while improvement in output reached statistical significance (pre 7.7%, post 2.0%, P = 0.01).
- Conclusions: The ED surge protocol led to effective containment of daily high surges despite significant increase in hospital occupancy levels. This is the first study to describe an ED surge plan capable of identifying within which ITO component surge is happening and linking actions to address specific causes. We believe this protocol can be adapted for any ED.
Emergency department (ED) crowding has been defined as “a situation where the demand for emergency services exceeds the ability to provide care in a reasonable amount of time” [1]. Crowding is an increasingly common occurrence in hospital-based EDs, and overcrowding of EDs has been shown to adversely affect the delivery of emergency care and results in increased patient morbidity and mortality [2,3]. Furthermore, the nature of medical emergencies dictates that rapid daily changes (or surges) in patient volume and acuity occur frequently and unpredictably, contributing to the difficulty of matching resources to demands. Accurate understanding and continuous measurement of where bottlenecks may be occurring within an ED are critical to an effective response to ED surges.
Many of the widely used measurement tools for overcrowding produce one final overall net value on a one-dimensional scale, failing to capture the complexity of the root causes of surges. For example, the National ED Overcrowding Study (NEDOCS) scoring system, validated at various centers and widely used and studied [5–7] utilizes a number of institutional and situational variables to calculate a final NEDOCS score, which translates to “Not Busy,” “Busy,” “Overcrowded,” “Severely Overcrowded,” or “Dangerously Overcrowded” as a global state. Other published scoring systems such as the Emergency Department Work Index (EDWIN), while performing well in comparison to subjective impressions of physicians and nurses, also suffers from computation of a single final score, which makes it difficult to tie to specific actions or solutions [8]. Other surrogate markers quantifying ED crowding have also been used, such as left-without-being-seen rates, ambulance diversions, and total number of boarded patients in the ED; yet they too only measure consequences of crowding and provide little diagnostic information on when and where specific ED surges are actually happening throughout the day [9].
Responding to ED Surges
An effective surge plan should ensure the delivery of safe, effective care in response to various input/throughput/output surges in a coordinated and standardized manner. The ideal ED surge plan should include (1) a prospective continuous tool/method that accurately gauges the surge level (based on objective measures) in various components of the Input-Throughput-Output model of the department, (2) standardized targeted actions that are tied to specific triggers identified within that model to ensure effective solutions, and (3) built-in contingency plans for escalation in the face of sustained/worsening surges. Few studies have been published describing successful implementation of ED surge protocols, with the majority being linked to global ED crowding measures such as the NEDOCS score [10]. As a result, it is difficult to tease out the specific targeted actions that are most effective in dealing with the root causes of a surge.
Local Problem
Prior to the quality improvement initiative we describe below, the Ottawa Hospital ED had no formal process or method of measuring daily surges nor any standardized action plan to respond effectively to those surges. The state of “busy-ness” was often defined by gut feelings of frontline workers, which was quite variable depending on the individuals in charge of departmental patient flow. Often, actions to try and mitigate rising ED surges were triggered too late, resulting in consistent gridlock in the ED that lasted many hours. Several near-misses as well as actual critical incidences had occurred as a result of ineffective management of ED surges, and the authors of this initiative were tasked by senior hospital leadership with designing and implementing a novel solution.
Objectives
We describe our approach to the development, implementation, and evaluation of a novel ED surge protocol at a tertiary care academic hospital based on the principles cited above. Specifically, we sought to:
- define various levels of ED surge and to provide a common language for better communication between all stakeholders
- incorporate the validated Input-Throughput-Output model of ED flow to provide a conceptual framework for measuring surges in real-time and developing targeted action plans
- standardize ED and organizational responses to various ED surges based on identified bottlenecks
- measure and evaluate the effectiveness of the ED surge plan implementation
- continuously modify and improve the ED surge protocol using quality improvement strategies
Methods
Setting
The Ottawa Hospital is an academic tertiary care center with 3 campuses (Civic, General, and Riverside), with the ED providing coverage at 2 physical emergency rooms. The hospital is the regional trauma center as well as referral destination for many subspecialties such as cardiac, vascular and neurosurgical emergencies. This 1163-bed facility handles over 160,000 emergency visits a year, over 1 million ambulatory care visits a year, and roughly 35,000 surgical cases annually. The ED is staffed by 78 staff physicians, approximately 250 registered nurses (RNs), and ~50 emergency medicine residents/trainees.
The EDs are supported by a computerized tracking system that provides real-time metrics. This information is displayed by ED-specific geographical area on electronic whiteboards, which can be accessed on overhead monitors, desktop computers, and personal iPads. Information available to ED physicians and staff at any time includes individual-level data such as location, demographics, Canadian Triage Acuity Score (CTAS), and presenting complaint as well as departmental-level data such as patient volumes, wait times, length of stay (LOS), pending/completed diagnostics, consultation status and final dispositions.
According to the policy and standard operating procedures that govern research at the Ottawa Hospital Research Institute, this work met criteria for quality improvement activities exempt from ethics review.
Intervention
Over a 4-day period care facilitators were polled on an hourly basis to determine what factors were important to the in determining how “busy” they perceived the ED to be. These factors included but were not limited to: total number of patients waiting to be seen; time to physician initial assessment; number of monitored beds available; and number of admitted patients boarded in the ED. Analysis was done to prospectively compare their perception of surge levels to the proposed Surge Plan metrics, and to ensure that the individual criteria for each level was practically meaningful and accurate.
Next, a set of standardized action and response plans were developed and agreed upon that tied specifically to a corresponding component of the different measured ED surge levels (these action plans are detailed in an online Appendix and are also available from the author). The fundamental guiding principles behind the development of each action item was that it should (1) target underlying causes - in a standardized way - specific to the relevant Input-Throughput-Output surge, (2) provide escalating level of effectiveness for each corresponding escalation in the surge level (eg, contacting a staff physician directly for a disposition decision for patents consulted in the ED, if the resident trainees have failed to do so in a timely manner), and (3) coordinate actions by various stakeholders in a planned and organized manner. Practically, the standardized targeted actions span across 5 different roles, which were explicitly listed on action sheets for care facilitators, clinical managers, patient flow managers, evening and night coordinators, and clinical directors.
Stakeholder Engagement
Implementation and Continuous Improvement
Given the complexity of the ED- and hospital-wide nature of the surge protocol, implementation was done over multiple phases and Plan-Do-Study-Act (PDSA) improvement cycles:
Phase I (Apr 2013 - Jun 2013)
The initial proposed ED surge level metrics were measured at a single ED campus. Care facilitators were trained and asked to measure surge levels in the ED every 2 hours. This served as a testing period to gauge the sensitivity and reliability of our proposed surge level metrics, and no actual action items were triggered during this period. Stakeholder meetings were held to determine feasibility of the plan, validate the proposed metrics, and develop “standard work” action plans for each stakeholder group in response to the metrics. This first phase also allowed care facilitators to objectively reflect on ED surge patterns throughout the day, and provided everyone in the ED team a frequent global snapshot of how “busy” the department was at any time. Finally, surge level data during this phase confirmed previous suspicions that the Output component was the biggest driver behind overall ED surge level.
Throughout this phase, the ED clinical manager recorded all the usual actions taken in response to the different level of surges as felt appropriate by the individual care facilitator on duty. The variety of actions and types of escalations were collected and fed back to weekly workgroup meetings to help further refine crafting of standardized action plans for implementation of the surge protocol.
Phase II (June - Aug 2013)
An initial trial of a limited ED surge protocol was rolled out at both ED campuses, with actual action items being triggered in response to specific surge level metrics. The main focus of this PDSA cycle was to collect data on how the care facilitator groups at the 2 campuses utilized the surge protocol, as well as feedback on usability, barriers, and effectiveness. Regular audits were performed to ensure surge measurement and compliance rates. Educational sessions were provided regarding rationale and purpose of the plan so that all team members had a better understanding of ED surges. Frequent meetings with stakeholders to share updates continued throughout Phase II, allowing further engagement as well as fine-tuning of stakeholder action plans based on real-time experiences.
Phase III (Aug 2013 - Dec 2013)
The next phase of implementation expanded beyond the ED and included the hospital’s off-hours and off-service management group. This in effect was the official corporate roll-out of the ED surge protocol including full action plans for all stakeholders, including off-service clinical administrators, inpatient flow managers, and the director of emergency and critical care. Regular audits were performed to ensure compliance of measurement every 2 hours as well as performance of specified action items related to each surge level, with the actual surge level measurement completion rates of 98%.
Data Collection and Analysis
Over the study period April 2013 to December 2013 at the Civic campus and June 2013 to December 2013 at the General campus, ED surge levels were measured every 2 hours by the care facilitators and manually recorded in standardized ED surge protocol booklets. These were subsequently entered into Excel database for tracking and data analysis. Patient volumes and hospital occupancy levels were recorded daily. Perceptions of the primary users of the surge protocol (ie, care facilitators) were obtained via standardized interviews and polls. We present descriptive statistics and statistical process control (SPC) charts. Chi-squared test was performed for comparison of pre- and post-intervention frequencies of outcome measures.
Outcome Measures
The main outcome measure was the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively. High surges were defined as Moderate and Major surges combined. Our expert group consensus was that combinging the Moderate and Major surge categories to represent “high” surge was reasonable since they both require mobilizing resources on a hospital-wide level, and failure to improve despite 6 continuous hours of actively trying to address such high surges would lead to significantly higher risk for quality of care and patient safety issues.
Secondary outcomes include overall frequency of reaching high surge levels at various components of the Input-Throughput-Output ED flow model, hospital occupancy levels, and care facilitators’ perceptions on workload and overall effectiveness of the surge protocol.
Results
ED Flow
Statistical Process Control Charts
Survey of Care Facilitators
The primary users and drivers of the surge protocol—the care facilitator group—felt strongly that the tool was easy to use and that it made a positive difference. 72% felt that the ED surge protocol has increased their workload but 92% felt that it was good for overall flow of the ED. Specific feedback included having a much more standardized language around communicating (and acting on) surges, and a better overall bird’s-eye view of the department.
Discussion
Despite a call for urgent research on implementing solutions targeting daily ED surges (vs. global ED crowding) over a decade ago at the Academic Emergency Medicine 2006 Consensus Conference [12], little work has been published on distinguishing, measuring, and dealing with ED surges. McCarthy et al proposed the rate of patient arrivals to the ED by time of day as a rudimentary definition of surge, although they provided very little specific guidance on what to do with that information in the setting of responding to spikes in surges [13]. Asplin et al described a number of theoretical models to bridge ED census, daily surges, length of stay and quality of care, however they were never validated in real-life scenarios [14]. A systematic review published in 2009 summarizing articles that described theoretical and practical ED surge responses found a large heterogeneity of different proposed models with little standardization and multiple shortcomings [15].
To our knowledge, this study is the first to report on the actual development, implementation, and evaluation of a daily ED surge protocol that utilizes a widely accepted conceptual model of ED flow. Unlike single global measure of ED crowding, our protocol measures frequent surge levels for various Input-Throughput-Output components of the ED, which are tied directly to standardized specific actions to address underlying root causes. Despite continued rise in hospital occupant levels and budgetary restraints, we found a improvement in the number of times the ED actually hit severe surges with the exception of Output, which is expected since this component of the flow model is intimately tied to hospital occupant levels. When severe surges did happen, we were able to deal with them much more effectively and efficiently, resulting in an overall decrease in sustained surges in the ED including the Output component.
Limitations
Similar to other pragmatic quality improvement projects that rely on manual processes, it was difficult to ensure absolute compliance of surge level measurements throughout the study period. As a result, there were occasional missing surge level data at various times of different days. However, we believe these are relatively nonsignificant occurrences that balanced out over the pre- and post-implementation periods. In addition, we did not have the resources to robustly record and confirm completion of specific action items that were activated in response to various surge levels, although we did confirm verbally with frontline workers regularly that those actions were done. Future Plan-Do-Study-Act cycles will focus on explicit measurement of actual completed action items and further refinement of targeted responses to surge. Finally, while we were able to only collect and present data over a relatively short period of evaluation (and thus potentially susceptible to seasonal variations in ED flow), we believe that our data does support the surge protocol’s effectiveness when compared to the robust trend of hospital occupant levels.
Future Directions
This ED surge protocol can be adapted and modified to fit any ED. The specific criteria defining Minor/Moderate/Major surges can be set up as ratios or percentages relative to total number of monitors, beds, etc., available. The principles of linking actions directly to specific triggers within each Input/Throughput/Output category could be translated to fit any-sized organization. Currently in progress is a longer evaluation period and based upon the results as well as individual feedback, necessary adjustments to our definitions, criteria and action items will be considered as part of ongoing quality improvement. The principles of our surge protocol are not limited to the ED, and we will explore its implementation in other hospital departments as well as methods to link them together in alignment with the hospital’s overall corporate strategy in tackling overcrowding.
Conclusion
In summary, implementation of this novel ED surge protocol led to a more effective response and management of high surges, despite significant increase in overall hospital occupancy rates and associated frequency of surges in the Output component of the ED flow model. Our surge measurement tool is capable of identifying within which area of the ED surges are occurring, and our ED surge protocol links specific actions to address those specific root causes. We believe this will lead not only to more accurate assessments of overall ED crowding but also to more timely and effective departmental and institutional responses.
Corresponding author: Dr. Edmund S.H. Kwok, Dept. of Emergency Medicine, Ottawa Hospital, Civic Campus, 1053 Carling Ave., Ottawa, ON, Canada K1Y 4E9, ekwok@toh.on.ca.
Financial disclosures: None.
From the Ottawa Hospital, Ottawa, ON Canada.
Abstract
- Objective: Fluctuations in emergency department (ED) visits occur frequently, and traditional global measures of ED crowding do not allow for targeted responses to address root causes. We sought to develop, implement, and evaluate a novel ED surge protocol based on the input-throughput-output (ITO) model of ED flow.
- Methods: This initiative took place at a tertiary care academic teaching hospital. An inter-professional group developed and validated metrics for various levels of surge in relation to the ITO model, measured every 2 hours, which directly linked to specific actions targeting root causes within those components. Main outcome measure was defined as the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively.
- Results: During the 6-month study period, average daily hospital occupancy levels rose above 100% (pre 99.5%, post 101.2%; P = 0.01) and frequency of high surges in the output component increased (pre 7.7%, post 10.8%; P = 0.002). Despite this, frequency of sustained high surges remained stable for input (pre 4.5%, post 0.0%; P = 0.13) and throughput (pre 3.5%, post 2.7%; P = 0.54), while improvement in output reached statistical significance (pre 7.7%, post 2.0%, P = 0.01).
- Conclusions: The ED surge protocol led to effective containment of daily high surges despite significant increase in hospital occupancy levels. This is the first study to describe an ED surge plan capable of identifying within which ITO component surge is happening and linking actions to address specific causes. We believe this protocol can be adapted for any ED.
Emergency department (ED) crowding has been defined as “a situation where the demand for emergency services exceeds the ability to provide care in a reasonable amount of time” [1]. Crowding is an increasingly common occurrence in hospital-based EDs, and overcrowding of EDs has been shown to adversely affect the delivery of emergency care and results in increased patient morbidity and mortality [2,3]. Furthermore, the nature of medical emergencies dictates that rapid daily changes (or surges) in patient volume and acuity occur frequently and unpredictably, contributing to the difficulty of matching resources to demands. Accurate understanding and continuous measurement of where bottlenecks may be occurring within an ED are critical to an effective response to ED surges.
Many of the widely used measurement tools for overcrowding produce one final overall net value on a one-dimensional scale, failing to capture the complexity of the root causes of surges. For example, the National ED Overcrowding Study (NEDOCS) scoring system, validated at various centers and widely used and studied [5–7] utilizes a number of institutional and situational variables to calculate a final NEDOCS score, which translates to “Not Busy,” “Busy,” “Overcrowded,” “Severely Overcrowded,” or “Dangerously Overcrowded” as a global state. Other published scoring systems such as the Emergency Department Work Index (EDWIN), while performing well in comparison to subjective impressions of physicians and nurses, also suffers from computation of a single final score, which makes it difficult to tie to specific actions or solutions [8]. Other surrogate markers quantifying ED crowding have also been used, such as left-without-being-seen rates, ambulance diversions, and total number of boarded patients in the ED; yet they too only measure consequences of crowding and provide little diagnostic information on when and where specific ED surges are actually happening throughout the day [9].
Responding to ED Surges
An effective surge plan should ensure the delivery of safe, effective care in response to various input/throughput/output surges in a coordinated and standardized manner. The ideal ED surge plan should include (1) a prospective continuous tool/method that accurately gauges the surge level (based on objective measures) in various components of the Input-Throughput-Output model of the department, (2) standardized targeted actions that are tied to specific triggers identified within that model to ensure effective solutions, and (3) built-in contingency plans for escalation in the face of sustained/worsening surges. Few studies have been published describing successful implementation of ED surge protocols, with the majority being linked to global ED crowding measures such as the NEDOCS score [10]. As a result, it is difficult to tease out the specific targeted actions that are most effective in dealing with the root causes of a surge.
Local Problem
Prior to the quality improvement initiative we describe below, the Ottawa Hospital ED had no formal process or method of measuring daily surges nor any standardized action plan to respond effectively to those surges. The state of “busy-ness” was often defined by gut feelings of frontline workers, which was quite variable depending on the individuals in charge of departmental patient flow. Often, actions to try and mitigate rising ED surges were triggered too late, resulting in consistent gridlock in the ED that lasted many hours. Several near-misses as well as actual critical incidences had occurred as a result of ineffective management of ED surges, and the authors of this initiative were tasked by senior hospital leadership with designing and implementing a novel solution.
Objectives
We describe our approach to the development, implementation, and evaluation of a novel ED surge protocol at a tertiary care academic hospital based on the principles cited above. Specifically, we sought to:
- define various levels of ED surge and to provide a common language for better communication between all stakeholders
- incorporate the validated Input-Throughput-Output model of ED flow to provide a conceptual framework for measuring surges in real-time and developing targeted action plans
- standardize ED and organizational responses to various ED surges based on identified bottlenecks
- measure and evaluate the effectiveness of the ED surge plan implementation
- continuously modify and improve the ED surge protocol using quality improvement strategies
Methods
Setting
The Ottawa Hospital is an academic tertiary care center with 3 campuses (Civic, General, and Riverside), with the ED providing coverage at 2 physical emergency rooms. The hospital is the regional trauma center as well as referral destination for many subspecialties such as cardiac, vascular and neurosurgical emergencies. This 1163-bed facility handles over 160,000 emergency visits a year, over 1 million ambulatory care visits a year, and roughly 35,000 surgical cases annually. The ED is staffed by 78 staff physicians, approximately 250 registered nurses (RNs), and ~50 emergency medicine residents/trainees.
The EDs are supported by a computerized tracking system that provides real-time metrics. This information is displayed by ED-specific geographical area on electronic whiteboards, which can be accessed on overhead monitors, desktop computers, and personal iPads. Information available to ED physicians and staff at any time includes individual-level data such as location, demographics, Canadian Triage Acuity Score (CTAS), and presenting complaint as well as departmental-level data such as patient volumes, wait times, length of stay (LOS), pending/completed diagnostics, consultation status and final dispositions.
According to the policy and standard operating procedures that govern research at the Ottawa Hospital Research Institute, this work met criteria for quality improvement activities exempt from ethics review.
Intervention
Over a 4-day period care facilitators were polled on an hourly basis to determine what factors were important to the in determining how “busy” they perceived the ED to be. These factors included but were not limited to: total number of patients waiting to be seen; time to physician initial assessment; number of monitored beds available; and number of admitted patients boarded in the ED. Analysis was done to prospectively compare their perception of surge levels to the proposed Surge Plan metrics, and to ensure that the individual criteria for each level was practically meaningful and accurate.
Next, a set of standardized action and response plans were developed and agreed upon that tied specifically to a corresponding component of the different measured ED surge levels (these action plans are detailed in an online Appendix and are also available from the author). The fundamental guiding principles behind the development of each action item was that it should (1) target underlying causes - in a standardized way - specific to the relevant Input-Throughput-Output surge, (2) provide escalating level of effectiveness for each corresponding escalation in the surge level (eg, contacting a staff physician directly for a disposition decision for patents consulted in the ED, if the resident trainees have failed to do so in a timely manner), and (3) coordinate actions by various stakeholders in a planned and organized manner. Practically, the standardized targeted actions span across 5 different roles, which were explicitly listed on action sheets for care facilitators, clinical managers, patient flow managers, evening and night coordinators, and clinical directors.
Stakeholder Engagement
Implementation and Continuous Improvement
Given the complexity of the ED- and hospital-wide nature of the surge protocol, implementation was done over multiple phases and Plan-Do-Study-Act (PDSA) improvement cycles:
Phase I (Apr 2013 - Jun 2013)
The initial proposed ED surge level metrics were measured at a single ED campus. Care facilitators were trained and asked to measure surge levels in the ED every 2 hours. This served as a testing period to gauge the sensitivity and reliability of our proposed surge level metrics, and no actual action items were triggered during this period. Stakeholder meetings were held to determine feasibility of the plan, validate the proposed metrics, and develop “standard work” action plans for each stakeholder group in response to the metrics. This first phase also allowed care facilitators to objectively reflect on ED surge patterns throughout the day, and provided everyone in the ED team a frequent global snapshot of how “busy” the department was at any time. Finally, surge level data during this phase confirmed previous suspicions that the Output component was the biggest driver behind overall ED surge level.
Throughout this phase, the ED clinical manager recorded all the usual actions taken in response to the different level of surges as felt appropriate by the individual care facilitator on duty. The variety of actions and types of escalations were collected and fed back to weekly workgroup meetings to help further refine crafting of standardized action plans for implementation of the surge protocol.
Phase II (June - Aug 2013)
An initial trial of a limited ED surge protocol was rolled out at both ED campuses, with actual action items being triggered in response to specific surge level metrics. The main focus of this PDSA cycle was to collect data on how the care facilitator groups at the 2 campuses utilized the surge protocol, as well as feedback on usability, barriers, and effectiveness. Regular audits were performed to ensure surge measurement and compliance rates. Educational sessions were provided regarding rationale and purpose of the plan so that all team members had a better understanding of ED surges. Frequent meetings with stakeholders to share updates continued throughout Phase II, allowing further engagement as well as fine-tuning of stakeholder action plans based on real-time experiences.
Phase III (Aug 2013 - Dec 2013)
The next phase of implementation expanded beyond the ED and included the hospital’s off-hours and off-service management group. This in effect was the official corporate roll-out of the ED surge protocol including full action plans for all stakeholders, including off-service clinical administrators, inpatient flow managers, and the director of emergency and critical care. Regular audits were performed to ensure compliance of measurement every 2 hours as well as performance of specified action items related to each surge level, with the actual surge level measurement completion rates of 98%.
Data Collection and Analysis
Over the study period April 2013 to December 2013 at the Civic campus and June 2013 to December 2013 at the General campus, ED surge levels were measured every 2 hours by the care facilitators and manually recorded in standardized ED surge protocol booklets. These were subsequently entered into Excel database for tracking and data analysis. Patient volumes and hospital occupancy levels were recorded daily. Perceptions of the primary users of the surge protocol (ie, care facilitators) were obtained via standardized interviews and polls. We present descriptive statistics and statistical process control (SPC) charts. Chi-squared test was performed for comparison of pre- and post-intervention frequencies of outcome measures.
Outcome Measures
The main outcome measure was the frequency of sustained (≥ 6 hours) high surges, a marker of inability to respond effectively. High surges were defined as Moderate and Major surges combined. Our expert group consensus was that combinging the Moderate and Major surge categories to represent “high” surge was reasonable since they both require mobilizing resources on a hospital-wide level, and failure to improve despite 6 continuous hours of actively trying to address such high surges would lead to significantly higher risk for quality of care and patient safety issues.
Secondary outcomes include overall frequency of reaching high surge levels at various components of the Input-Throughput-Output ED flow model, hospital occupancy levels, and care facilitators’ perceptions on workload and overall effectiveness of the surge protocol.
Results
ED Flow
Statistical Process Control Charts
Survey of Care Facilitators
The primary users and drivers of the surge protocol—the care facilitator group—felt strongly that the tool was easy to use and that it made a positive difference. 72% felt that the ED surge protocol has increased their workload but 92% felt that it was good for overall flow of the ED. Specific feedback included having a much more standardized language around communicating (and acting on) surges, and a better overall bird’s-eye view of the department.
Discussion
Despite a call for urgent research on implementing solutions targeting daily ED surges (vs. global ED crowding) over a decade ago at the Academic Emergency Medicine 2006 Consensus Conference [12], little work has been published on distinguishing, measuring, and dealing with ED surges. McCarthy et al proposed the rate of patient arrivals to the ED by time of day as a rudimentary definition of surge, although they provided very little specific guidance on what to do with that information in the setting of responding to spikes in surges [13]. Asplin et al described a number of theoretical models to bridge ED census, daily surges, length of stay and quality of care, however they were never validated in real-life scenarios [14]. A systematic review published in 2009 summarizing articles that described theoretical and practical ED surge responses found a large heterogeneity of different proposed models with little standardization and multiple shortcomings [15].
To our knowledge, this study is the first to report on the actual development, implementation, and evaluation of a daily ED surge protocol that utilizes a widely accepted conceptual model of ED flow. Unlike single global measure of ED crowding, our protocol measures frequent surge levels for various Input-Throughput-Output components of the ED, which are tied directly to standardized specific actions to address underlying root causes. Despite continued rise in hospital occupant levels and budgetary restraints, we found a improvement in the number of times the ED actually hit severe surges with the exception of Output, which is expected since this component of the flow model is intimately tied to hospital occupant levels. When severe surges did happen, we were able to deal with them much more effectively and efficiently, resulting in an overall decrease in sustained surges in the ED including the Output component.
Limitations
Similar to other pragmatic quality improvement projects that rely on manual processes, it was difficult to ensure absolute compliance of surge level measurements throughout the study period. As a result, there were occasional missing surge level data at various times of different days. However, we believe these are relatively nonsignificant occurrences that balanced out over the pre- and post-implementation periods. In addition, we did not have the resources to robustly record and confirm completion of specific action items that were activated in response to various surge levels, although we did confirm verbally with frontline workers regularly that those actions were done. Future Plan-Do-Study-Act cycles will focus on explicit measurement of actual completed action items and further refinement of targeted responses to surge. Finally, while we were able to only collect and present data over a relatively short period of evaluation (and thus potentially susceptible to seasonal variations in ED flow), we believe that our data does support the surge protocol’s effectiveness when compared to the robust trend of hospital occupant levels.
Future Directions
This ED surge protocol can be adapted and modified to fit any ED. The specific criteria defining Minor/Moderate/Major surges can be set up as ratios or percentages relative to total number of monitors, beds, etc., available. The principles of linking actions directly to specific triggers within each Input/Throughput/Output category could be translated to fit any-sized organization. Currently in progress is a longer evaluation period and based upon the results as well as individual feedback, necessary adjustments to our definitions, criteria and action items will be considered as part of ongoing quality improvement. The principles of our surge protocol are not limited to the ED, and we will explore its implementation in other hospital departments as well as methods to link them together in alignment with the hospital’s overall corporate strategy in tackling overcrowding.
Conclusion
In summary, implementation of this novel ED surge protocol led to a more effective response and management of high surges, despite significant increase in overall hospital occupancy rates and associated frequency of surges in the Output component of the ED flow model. Our surge measurement tool is capable of identifying within which area of the ED surges are occurring, and our ED surge protocol links specific actions to address those specific root causes. We believe this will lead not only to more accurate assessments of overall ED crowding but also to more timely and effective departmental and institutional responses.
Corresponding author: Dr. Edmund S.H. Kwok, Dept. of Emergency Medicine, Ottawa Hospital, Civic Campus, 1053 Carling Ave., Ottawa, ON, Canada K1Y 4E9, ekwok@toh.on.ca.
Financial disclosures: None.
1. Bond K. Interventions to reduce overcrowding in emergency departments. [Technology report no 67.4]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.
2. Richardson DB, et al. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 2006;184:213–6.
3. Sprivulis PC, et al. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust 2006; 184:208–12.
4. Asplin BR, Magid DJ, Rhodes KV, et al. A conceptual model of emergency department crowding. Ann Emerg Med 2003; 42:173–80.
5. Affleck A, Parks P, Drummond A, et al. Emergency department overcrowding and access block. CAEP Position Statement. CJEM 2013;15:359–70.
6. Weiss SJ, Derlet R, Arndahl J, et al. Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS). Acad Emerg Med 2004;11:38–50.
7. Weiss SJ, Ernst AA, Nick TG. Comparison of the National Emergency Department Overcrowding Scale and the Emergency Department Work Index for quantifying emergency department crowding. Acad Emerg Med 2006;13:513–8.
8. Jones SS, Allen TL, Welch SJ. An independent evaluation of four quantitative emergency department crowding scales. Acad Emerg Med 2006;13:1204–11
9. Bernstein SL, Verghese V, Leung W, et al. Development and validation of a new index to measure emergency department crowding. Acad Emerg Med 2003;10:938–42
10. General Accounting Office. Hospital emergency departments–crowded conditions vary among hospitals and communities. GAO-03-460. Washington, DC: US General Accounting Office; 2003.
11. Moseley MG, Dickerson CL, Kasey J, et al. Surge: a organizational response to emergency department overcrowding. J Clin Outcomes Manage 2010;17:453–7.
12. Jenkins JL, O’Connor RE, Cone DC. Differentiating large-scale surge versus daily surge. Acad Emerg Med 2006; 13:1169–72.
13. McCarthy ML, Aronsky D, Kelen GD. The measurement of daily surge and its relevance to disaster preparedness. Acad Emerg Med 2006; 13:1138–41.
14. Asplin BR, Flottemesch TJ, Gordon B. Developing models for patient flow and daily surge capacity research. Acad Emerg Med 2006;13:1109–13.
15. Nager AL, Khanna K. Emergency department surge: models and practical implications. J Trauma 2009; 67(2 Suppl):S96–9.
1. Bond K. Interventions to reduce overcrowding in emergency departments. [Technology report no 67.4]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.
2. Richardson DB, et al. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 2006;184:213–6.
3. Sprivulis PC, et al. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust 2006; 184:208–12.
4. Asplin BR, Magid DJ, Rhodes KV, et al. A conceptual model of emergency department crowding. Ann Emerg Med 2003; 42:173–80.
5. Affleck A, Parks P, Drummond A, et al. Emergency department overcrowding and access block. CAEP Position Statement. CJEM 2013;15:359–70.
6. Weiss SJ, Derlet R, Arndahl J, et al. Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS). Acad Emerg Med 2004;11:38–50.
7. Weiss SJ, Ernst AA, Nick TG. Comparison of the National Emergency Department Overcrowding Scale and the Emergency Department Work Index for quantifying emergency department crowding. Acad Emerg Med 2006;13:513–8.
8. Jones SS, Allen TL, Welch SJ. An independent evaluation of four quantitative emergency department crowding scales. Acad Emerg Med 2006;13:1204–11
9. Bernstein SL, Verghese V, Leung W, et al. Development and validation of a new index to measure emergency department crowding. Acad Emerg Med 2003;10:938–42
10. General Accounting Office. Hospital emergency departments–crowded conditions vary among hospitals and communities. GAO-03-460. Washington, DC: US General Accounting Office; 2003.
11. Moseley MG, Dickerson CL, Kasey J, et al. Surge: a organizational response to emergency department overcrowding. J Clin Outcomes Manage 2010;17:453–7.
12. Jenkins JL, O’Connor RE, Cone DC. Differentiating large-scale surge versus daily surge. Acad Emerg Med 2006; 13:1169–72.
13. McCarthy ML, Aronsky D, Kelen GD. The measurement of daily surge and its relevance to disaster preparedness. Acad Emerg Med 2006; 13:1138–41.
14. Asplin BR, Flottemesch TJ, Gordon B. Developing models for patient flow and daily surge capacity research. Acad Emerg Med 2006;13:1109–13.
15. Nager AL, Khanna K. Emergency department surge: models and practical implications. J Trauma 2009; 67(2 Suppl):S96–9.