User login
Chemo regimen can be ‘highly effective’ against ENKTL

Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
Photo by Larry Young
SAN FRANCISCO—A 3-agent chemotherapy regimen can be “highly effective” in patients with extranodal natural killer/T-cell lymphoma (ENKTL), according to researchers.
In a single-center study, this regimen—pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX)—followed by extensive involved-field radiotherapy (EIFRT) produced high rates of long-term overall survival (OS) and progression-free survival (PFS) in newly diagnosed patients with stage I/II ENKTL.
P-GEMOX also proved effective—though to a much lesser degree—in advanced, relapsed, or refractory ENKTL, and these patients appeared to benefit from autologous stem cell transplant (auto-SCT) as consolidation.
Toxicity associated with P-GEMOX was mild to moderate and tolerable, according to Hui-Qiang Huang, MD, PhD, of State Key Laboratory of Oncology in Southern China, Guangzhou, China.
Dr Huang presented these results at the 8th Annual T-cell Lymphoma Forum.
Newly diagnosed patients
Dr Huang and his colleagues studied 56 patients newly diagnosed with stage I/II, nasal-type ENKTL. Most patients were younger than 60 years of age (80.4%, n=45).
About 79% (n=44) had an ECOG status of 0, and 21.4% (n=12) had a status of 1. About 61% (n=34) had stage I disease, and 39.3% (n=22) had stage II.
All patients received P-GEMOX—gemcitabine at 1000 mg/m2 on days 1 and 8, oxaliplatin at 150 mg/m2 on day 1, and pegaspargase at 2000 U/m2 on day 1. Doses could be adjusted in the event of toxicity.
The regimen was repeated every 3 weeks for a maximum of 4 cycles. Patients then underwent EIFRT—56 Gy in 28 fractions over 4 weeks.
The overall response rate (ORR) after P-GEMOX was 89.3% (50/56). Thirty-five patients achieved a complete response (CR), 15 had a partial response (PR), and 4 had stable disease (SD).
After EIFRT, the ORR increased to 94.6% (53/56). Fifty patients had a CR, 3 had a PR, and 1 had SD.
The median follow-up was 35.2 months (range, 10.6-51.4). Six patients relapsed, and the median time to relapse was 6.2 months.
Five patients died of disease progression. The median time to death was 10.9 months after the completion of EIFRT.
The 4-year OS rate was 90.7±4.0%, and the 4-year PFS rate was 89.1±4.2%.
OS and PFS were superior in patients with stage I disease as compared to stage II (P=0.056 and 0.023, respectively). And OS and PFS were superior in patients who responded to P-GEMOX (P=0.004 and 0.001, respectively).
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (80.3%), thrombocytopenia (55.3%), and hypoproteinemia (75.0%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were granulocytosis (23.2%), thrombocytopenia (19.6%), and hypoproteinemia (10.7%).
Advanced & relapsed/refractory patients
Dr Huang and his colleagues also studied 60 patients with newly diagnosed, stage III/IV ENKTL (25%, n=15), relapsed ENKTL (21.7%, n=19), or refractory disease (43.3%, n=26). Seventy percent of these patients (n=42) had nasal-type ENKTL.
Most patients were younger than 60 years of age (91.7%, n=55). About 73% (n=44) had an ECOG status of 0-1, and 26.7% (n=16) had a status of 2. Fifteen percent of patients (n=9) had stage I disease, 16.7% (n=10) had stage II, 35% (n=21) had stage III, and 33.3% (n=20) had stage IV.
The patients received the same P-GEMOX regimen as the newly diagnosed, stage I/II patients, but they did not receive EIFRT, and responders could undergo auto-SCT.
For the whole cohort, the ORR after P-GEMOX was 70% (42/60). Twenty-one patients had a CR, 21 had a PR, and 9 had SD.
In the newly diagnosed patients, the ORR was 80% (12/15). Four patients had a CR, 8 had a PR, and 2 had SD. In the relapsed/refractory patients, the ORR was 66.7% (30/45). Seventeen patients had a CR, 13 had a PR, and 7 had SD.
The 4-year OS was 43.0±7.3%, and the 4-year PFS was 36.5±6.9%.
There was no significant difference in OS or PFS between the newly diagnosed and relapsed/refractory patients (P=0.653 and 0.825, respectively). However, there was a significant difference in PFS and OS between responders and non-responders (P<0.001 for both).
There was a difference in 3-year OS between patients who went on to auto-SCT and those did not, although it did not reach statistical significance (P=0.08). Eleven patients who achieved a CR went on to auto-SCT.
There were no treatment-related deaths. The most common toxicities (occurring in more than 50% of patients) after P-GEMOX were neutropenia (85%), hypoproteinemia (88.3%), anemia (71.6%), fibrinogen decrease (68.3%), and anorexia (53.3%).
The most common grade 3/4 toxicities (occurring in more than 10% of patients) were neutropenia (31.6%), hypoproteinemia (13.3%), and thrombocytopenia (11.7%).
Dr Huang said this research suggests P-GEMOX can be effective for patients with newly diagnosed or previously treated ENKTL. The next step is to investigate which novel agents could be added to the regimen to improve its efficacy. ![]()
More ob.gyns. find their niche as subspecialists
After 12 years as a private practice ob.gyn., Dr. Brigid McCue was beginning to feel overwhelmed. She loved her work, but keeping up with the kaleidoscope of care components and ever-changing clinical developments was daunting.
“I felt like it was hard to stay really good at all the different aspects of care,” Dr. McCue said. “I was doing fine with obstetrics, and I felt like I was managing my office well, but it’s hard to stay on top of the latest developments, especially in surgical areas. The other thing that was really hard to keep up with was the business aspect of medicine and running a private practice.”
So when an opportunity presented itself, Dr. McCue leaped at the chance to narrow her expertise to obstetrical hospital medicine. She helped establish the ob.gyn. hospitalist program at Beth Israel Deaconess Hospital-Plymouth in Massachusetts, and now serves as chief of ob.gyn. and midwifery for the hospital.

“I love the fact that I now have the time to get really good at [what] I really like, [such as] labor and delivery,” said Dr. McCue, who is president of the Society of OB/GYN Hospitalists. “Since I made this change, I feel like I’m so much more on top of things. I do simulations here on my unit over things like shoulder dystocia. When I was in private practice, I would go to one meeting a year and pray that I never had a shoulder dystocia [case]. Now I really understand the whole process and I take the time to run through that with my midwives and my other nurses and doctors.”
Dr. McCue is one of a growing number of ob.gyns. who have chosen to target their expertise to a single subspecialty or concentrated practice area. Data show subspecialization is on the rise in ob.gyn.
From 1985 to 2015, certificates issued by the American Board of Obstetrics and Gynecology (ABOG) for gynecologic oncology nearly tripled, and certificates issued for reproductive endocrinology and infertility more than doubled, according to data provided by the American Board of Medical Specialties (ABMS). Certificates issued for maternal-fetal medicine rose from 35 in 1985 to 100 in 2015.

Opportunities for ob.gyns. to subspecialize have steadily increased over the last 50 years. The subspecialties of maternal-fetal medicine, gynecologic oncology, and reproductive endocrinology and infertility were first approved for certification by ABOG in 1973. In 1983, ABMS approved a certificate of “added qualification” for ob.gyns. who complete fellowships in critical care. In 1995, ABOG and the American Board of Urology started the subspecialty of female pelvic medicine and reconstructive surgery, which was approved for certification by ABMS in 2011.
ABMS also approved a certificate of “added qualification” for ob.gyns. who complete a fellowship in hospice and palliative medicine in 2008. And fellowships now exist for minimally invasive gynecologic surgery and ob.gyn. hospital medicine.
The reasons that ob.gyns. choose to subspecialize are multifold, said Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill., and one of the medical editors of the Ob.Gyn. News column, Master Class.
“Physicians subspecialize so that they can provide more medical and surgical expertise for a given population,” he said. “Secondly, physicians may be driven to subspecialize for lifestyle reasons. Generalists refer to subspecialists when technical expertise is desired to help with a clinical situation and potentially reduce medical legal risk.”
Ultimately, it’s patients who benefit from the increased care provided by subspecialists, noted Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology, and women’s health at Rutgers, the State University of New Jersey, Newark. Generalist ob.gyns. are tremendously knowledgeable and experienced, he said, but there’s no way for them to know every area, he said. It’s the difference between someone who might be doing a complicated surgery one or twice a year versus someone who is doing that surgery once or twice a week, he added.
“That is ultimately helpful for patients,” Dr. Einstein said. “It’s really about outcomes. This is all better for the patient. That’s the most important thing.”
Not every consequence of subspecialization is positive, however.
“As with everything, subspecialization has both positive and negative effects,” said Dr. Sandra Ann Carson, vice president for education at the American College of Obstetricians and Gynecologists. “The more time one has to focus on a small area, the better that area becomes. However, if all you have is a hammer, everything looks like a nail. The larger population may not need the care that someone with a rare disease may need.”
Dr. Miller refers to this challenge as “losing the forest.” He explains that subspecialists sometimes become so focused on their area of expertise, that they may overlook suitable treatment plans with which they are unfamiliar. An infertility specialist, for example, who neglects to consider a minimally invasive surgical procedure that could allow a patient to become pregnant naturally and instead recommends in vitro fertilization treatment.
“The infertility specialist does not have that particular skill and therefore directs that patient to IVF,” Dr. Miller said. “In the process of subspecializing, we have a tendency to lose the forest and look only at the trees.”
Finding a job is another challenge for the growing number of subspecialists. In many cases, fellowship-trained minimally invasive gynecologic surgeons may have to go back to practicing general gynecology because of a lack of positions, Dr. Miller said.
“We have to be careful that we do not “oversubspecialize” so that we are oversaturating the field,” he said.
In the future, the number of ob.gyn subspecialists will likely continue to grow and become more refined, said Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center in Phoenix.
“I think subspecialists will continue to become more and more developed,” Dr. Chase said. “Perhaps, some areas like family planning or minimally invasive surgery may grow further and become board certified.”
Dr. Carson foresees subspecialization becoming more focused on centralized teaching hospitals, with patients who need special care being sent to these hubs.
“Telemedicine and long-distance communication with a local obstetrician-gynecologist managing the whole patient will allow the best of both worlds,” she said.
Regardless of how subspecialist growth evolves, general ob.gyns. and other primary care physicians will always be needed, said Dr. Mary E. Norton, a maternal-fetal medicine specialist and clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.
“With increasing complexity, experts are needed to interpret advances,” Dr. Norton said. “However, patients also need a ‘medical home’ and primary provider who sees the big picture, and provides ongoing care beyond a single pregnancy or pregnancy complication.”
Why I chose to subspecialize

“I went to medical school with a particular interest in obstetrics. Once there, I was exposed to pediatrics and to high-risk OB, which I found to be fascinating. I particularly enjoyed my exposure to genetics during my pediatrics rotation and cared for a few children with genetic diseases that had a big impact and made a substantial impression on me. I ultimately decided to pursue an ob.gyn. residency and loved the OB part, particularly the prenatal genetics and high-risk OB. I found the balance of maternal and fetal medicine to be an exciting opportunity to care for two patients. I did an elective in prenatal diagnosis during my third year, including a bit of research, and was hooked.”
Dr. Mary E. Norton, a maternal-fetal medicine specialist and a clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.

“In my second year of residency, I became really interested in [gynecology-oncology] because I was fascinated by the surgery and interested in the chemotherapy practice, which is interesting because there’s always new research and new agents and interesting changes in how you treat the various cancers. It’s a very comprehensive, research-based field and that was fascinating to me. It’s a very busy subspecialty with very complex cases on multiple levels. You do these radical surgeries but then you have to be really involved in the choice for which chemotherapy agent to use, what type of radiation to give, and you also get really involved with the families ... Every case is so different and you treat women who are 16 years old, but you also treat women who are 96 years old. You see women from all walks of life with all sorts of different issues. The ability to really get involved with cancer research is a great part of the field.”
Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center, Phoenix.

“I took the opportunity to come to a new program where they were looking for an ob.gyn. hospitalist. That was exciting for me because I got to help establish the program... I feel like we’re a better department because I’m here monitoring labor, but I’m also writing protocols and making sure everyone is up to date. And I still get to do what I love the most, which is birth and babies.”
Dr. Brigid McCue, an ob.gyn. hospitalist and chief of ob.gyn. and midwifery, Beth Israel Deaconess Hospital-Plymouth, Massachusetts.
“I never considered delivering babies for the rest of my life. I was always focused on treating infertile couples. I completed my fellowship in reproductive endocrinology-infertility at the University of Pennsylvania, Philadelphia, at a time when in vitro fertilization was in its infancy and the laparoscope and hysteroscope were virtually diagnostic tools ... As IVF became more successful, I felt it was essential to add this expertise to my armamentarium ... It is truly gratifying to be part of a subspecialty that has advanced so far that the majority of our patients are able to achieve pregnancy via IVF.”

Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill.
“During medical school, I was very interested in the surgical aspects of patient care. When I rotated in gyn-oncology – now knowing that I rotated with some of the best gyn-oncologists who ever practiced – I found myself drawn to the complexity of surgery, acuity of the patients, and the close relationships gyn-oncologists have with their patients. It hit me like a brick that this was the specialty for me. During my residency and fellowship, I was particularly drawn to the multiple modalities we use to treat cancers. I relished the idea that through clinical trials, gyn-oncologists keep pushing the bar to solve the cancer problem. What we do now is different than what we did 5 years ago. It keeps us professionally challenged all the time.”

Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology and women’s health at Rutgers, the State University of New Jersey, Newark.
Throughout 2016, Ob.Gyn. News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @legal_med
After 12 years as a private practice ob.gyn., Dr. Brigid McCue was beginning to feel overwhelmed. She loved her work, but keeping up with the kaleidoscope of care components and ever-changing clinical developments was daunting.
“I felt like it was hard to stay really good at all the different aspects of care,” Dr. McCue said. “I was doing fine with obstetrics, and I felt like I was managing my office well, but it’s hard to stay on top of the latest developments, especially in surgical areas. The other thing that was really hard to keep up with was the business aspect of medicine and running a private practice.”
So when an opportunity presented itself, Dr. McCue leaped at the chance to narrow her expertise to obstetrical hospital medicine. She helped establish the ob.gyn. hospitalist program at Beth Israel Deaconess Hospital-Plymouth in Massachusetts, and now serves as chief of ob.gyn. and midwifery for the hospital.
“I love the fact that I now have the time to get really good at [what] I really like, [such as] labor and delivery,” said Dr. McCue, who is president of the Society of OB/GYN Hospitalists. “Since I made this change, I feel like I’m so much more on top of things. I do simulations here on my unit over things like shoulder dystocia. When I was in private practice, I would go to one meeting a year and pray that I never had a shoulder dystocia [case]. Now I really understand the whole process and I take the time to run through that with my midwives and my other nurses and doctors.”
Dr. McCue is one of a growing number of ob.gyns. who have chosen to target their expertise to a single subspecialty or concentrated practice area. Data show subspecialization is on the rise in ob.gyn.
From 1985 to 2015, certificates issued by the American Board of Obstetrics and Gynecology (ABOG) for gynecologic oncology nearly tripled, and certificates issued for reproductive endocrinology and infertility more than doubled, according to data provided by the American Board of Medical Specialties (ABMS). Certificates issued for maternal-fetal medicine rose from 35 in 1985 to 100 in 2015.
Opportunities for ob.gyns. to subspecialize have steadily increased over the last 50 years. The subspecialties of maternal-fetal medicine, gynecologic oncology, and reproductive endocrinology and infertility were first approved for certification by ABOG in 1973. In 1983, ABMS approved a certificate of “added qualification” for ob.gyns. who complete fellowships in critical care. In 1995, ABOG and the American Board of Urology started the subspecialty of female pelvic medicine and reconstructive surgery, which was approved for certification by ABMS in 2011.
ABMS also approved a certificate of “added qualification” for ob.gyns. who complete a fellowship in hospice and palliative medicine in 2008. And fellowships now exist for minimally invasive gynecologic surgery and ob.gyn. hospital medicine.
The reasons that ob.gyns. choose to subspecialize are multifold, said Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill., and one of the medical editors of the Ob.Gyn. News column, Master Class.
“Physicians subspecialize so that they can provide more medical and surgical expertise for a given population,” he said. “Secondly, physicians may be driven to subspecialize for lifestyle reasons. Generalists refer to subspecialists when technical expertise is desired to help with a clinical situation and potentially reduce medical legal risk.”
Ultimately, it’s patients who benefit from the increased care provided by subspecialists, noted Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology, and women’s health at Rutgers, the State University of New Jersey, Newark. Generalist ob.gyns. are tremendously knowledgeable and experienced, he said, but there’s no way for them to know every area, he said. It’s the difference between someone who might be doing a complicated surgery one or twice a year versus someone who is doing that surgery once or twice a week, he added.
“That is ultimately helpful for patients,” Dr. Einstein said. “It’s really about outcomes. This is all better for the patient. That’s the most important thing.”
Not every consequence of subspecialization is positive, however.
“As with everything, subspecialization has both positive and negative effects,” said Dr. Sandra Ann Carson, vice president for education at the American College of Obstetricians and Gynecologists. “The more time one has to focus on a small area, the better that area becomes. However, if all you have is a hammer, everything looks like a nail. The larger population may not need the care that someone with a rare disease may need.”
Dr. Miller refers to this challenge as “losing the forest.” He explains that subspecialists sometimes become so focused on their area of expertise, that they may overlook suitable treatment plans with which they are unfamiliar. An infertility specialist, for example, who neglects to consider a minimally invasive surgical procedure that could allow a patient to become pregnant naturally and instead recommends in vitro fertilization treatment.
“The infertility specialist does not have that particular skill and therefore directs that patient to IVF,” Dr. Miller said. “In the process of subspecializing, we have a tendency to lose the forest and look only at the trees.”
Finding a job is another challenge for the growing number of subspecialists. In many cases, fellowship-trained minimally invasive gynecologic surgeons may have to go back to practicing general gynecology because of a lack of positions, Dr. Miller said.
“We have to be careful that we do not “oversubspecialize” so that we are oversaturating the field,” he said.
In the future, the number of ob.gyn subspecialists will likely continue to grow and become more refined, said Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center in Phoenix.
“I think subspecialists will continue to become more and more developed,” Dr. Chase said. “Perhaps, some areas like family planning or minimally invasive surgery may grow further and become board certified.”
Dr. Carson foresees subspecialization becoming more focused on centralized teaching hospitals, with patients who need special care being sent to these hubs.
“Telemedicine and long-distance communication with a local obstetrician-gynecologist managing the whole patient will allow the best of both worlds,” she said.
Regardless of how subspecialist growth evolves, general ob.gyns. and other primary care physicians will always be needed, said Dr. Mary E. Norton, a maternal-fetal medicine specialist and clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.
“With increasing complexity, experts are needed to interpret advances,” Dr. Norton said. “However, patients also need a ‘medical home’ and primary provider who sees the big picture, and provides ongoing care beyond a single pregnancy or pregnancy complication.”
Why I chose to subspecialize
“I went to medical school with a particular interest in obstetrics. Once there, I was exposed to pediatrics and to high-risk OB, which I found to be fascinating. I particularly enjoyed my exposure to genetics during my pediatrics rotation and cared for a few children with genetic diseases that had a big impact and made a substantial impression on me. I ultimately decided to pursue an ob.gyn. residency and loved the OB part, particularly the prenatal genetics and high-risk OB. I found the balance of maternal and fetal medicine to be an exciting opportunity to care for two patients. I did an elective in prenatal diagnosis during my third year, including a bit of research, and was hooked.”
Dr. Mary E. Norton, a maternal-fetal medicine specialist and a clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.
“In my second year of residency, I became really interested in [gynecology-oncology] because I was fascinated by the surgery and interested in the chemotherapy practice, which is interesting because there’s always new research and new agents and interesting changes in how you treat the various cancers. It’s a very comprehensive, research-based field and that was fascinating to me. It’s a very busy subspecialty with very complex cases on multiple levels. You do these radical surgeries but then you have to be really involved in the choice for which chemotherapy agent to use, what type of radiation to give, and you also get really involved with the families ... Every case is so different and you treat women who are 16 years old, but you also treat women who are 96 years old. You see women from all walks of life with all sorts of different issues. The ability to really get involved with cancer research is a great part of the field.”
Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center, Phoenix.
“I took the opportunity to come to a new program where they were looking for an ob.gyn. hospitalist. That was exciting for me because I got to help establish the program... I feel like we’re a better department because I’m here monitoring labor, but I’m also writing protocols and making sure everyone is up to date. And I still get to do what I love the most, which is birth and babies.”
Dr. Brigid McCue, an ob.gyn. hospitalist and chief of ob.gyn. and midwifery, Beth Israel Deaconess Hospital-Plymouth, Massachusetts.
“I never considered delivering babies for the rest of my life. I was always focused on treating infertile couples. I completed my fellowship in reproductive endocrinology-infertility at the University of Pennsylvania, Philadelphia, at a time when in vitro fertilization was in its infancy and the laparoscope and hysteroscope were virtually diagnostic tools ... As IVF became more successful, I felt it was essential to add this expertise to my armamentarium ... It is truly gratifying to be part of a subspecialty that has advanced so far that the majority of our patients are able to achieve pregnancy via IVF.”
Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill.
“During medical school, I was very interested in the surgical aspects of patient care. When I rotated in gyn-oncology – now knowing that I rotated with some of the best gyn-oncologists who ever practiced – I found myself drawn to the complexity of surgery, acuity of the patients, and the close relationships gyn-oncologists have with their patients. It hit me like a brick that this was the specialty for me. During my residency and fellowship, I was particularly drawn to the multiple modalities we use to treat cancers. I relished the idea that through clinical trials, gyn-oncologists keep pushing the bar to solve the cancer problem. What we do now is different than what we did 5 years ago. It keeps us professionally challenged all the time.”
Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology and women’s health at Rutgers, the State University of New Jersey, Newark.
Throughout 2016, Ob.Gyn. News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @legal_med
After 12 years as a private practice ob.gyn., Dr. Brigid McCue was beginning to feel overwhelmed. She loved her work, but keeping up with the kaleidoscope of care components and ever-changing clinical developments was daunting.
“I felt like it was hard to stay really good at all the different aspects of care,” Dr. McCue said. “I was doing fine with obstetrics, and I felt like I was managing my office well, but it’s hard to stay on top of the latest developments, especially in surgical areas. The other thing that was really hard to keep up with was the business aspect of medicine and running a private practice.”
So when an opportunity presented itself, Dr. McCue leaped at the chance to narrow her expertise to obstetrical hospital medicine. She helped establish the ob.gyn. hospitalist program at Beth Israel Deaconess Hospital-Plymouth in Massachusetts, and now serves as chief of ob.gyn. and midwifery for the hospital.
“I love the fact that I now have the time to get really good at [what] I really like, [such as] labor and delivery,” said Dr. McCue, who is president of the Society of OB/GYN Hospitalists. “Since I made this change, I feel like I’m so much more on top of things. I do simulations here on my unit over things like shoulder dystocia. When I was in private practice, I would go to one meeting a year and pray that I never had a shoulder dystocia [case]. Now I really understand the whole process and I take the time to run through that with my midwives and my other nurses and doctors.”
Dr. McCue is one of a growing number of ob.gyns. who have chosen to target their expertise to a single subspecialty or concentrated practice area. Data show subspecialization is on the rise in ob.gyn.
From 1985 to 2015, certificates issued by the American Board of Obstetrics and Gynecology (ABOG) for gynecologic oncology nearly tripled, and certificates issued for reproductive endocrinology and infertility more than doubled, according to data provided by the American Board of Medical Specialties (ABMS). Certificates issued for maternal-fetal medicine rose from 35 in 1985 to 100 in 2015.
Opportunities for ob.gyns. to subspecialize have steadily increased over the last 50 years. The subspecialties of maternal-fetal medicine, gynecologic oncology, and reproductive endocrinology and infertility were first approved for certification by ABOG in 1973. In 1983, ABMS approved a certificate of “added qualification” for ob.gyns. who complete fellowships in critical care. In 1995, ABOG and the American Board of Urology started the subspecialty of female pelvic medicine and reconstructive surgery, which was approved for certification by ABMS in 2011.
ABMS also approved a certificate of “added qualification” for ob.gyns. who complete a fellowship in hospice and palliative medicine in 2008. And fellowships now exist for minimally invasive gynecologic surgery and ob.gyn. hospital medicine.
The reasons that ob.gyns. choose to subspecialize are multifold, said Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill., and one of the medical editors of the Ob.Gyn. News column, Master Class.
“Physicians subspecialize so that they can provide more medical and surgical expertise for a given population,” he said. “Secondly, physicians may be driven to subspecialize for lifestyle reasons. Generalists refer to subspecialists when technical expertise is desired to help with a clinical situation and potentially reduce medical legal risk.”
Ultimately, it’s patients who benefit from the increased care provided by subspecialists, noted Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology, and women’s health at Rutgers, the State University of New Jersey, Newark. Generalist ob.gyns. are tremendously knowledgeable and experienced, he said, but there’s no way for them to know every area, he said. It’s the difference between someone who might be doing a complicated surgery one or twice a year versus someone who is doing that surgery once or twice a week, he added.
“That is ultimately helpful for patients,” Dr. Einstein said. “It’s really about outcomes. This is all better for the patient. That’s the most important thing.”
Not every consequence of subspecialization is positive, however.
“As with everything, subspecialization has both positive and negative effects,” said Dr. Sandra Ann Carson, vice president for education at the American College of Obstetricians and Gynecologists. “The more time one has to focus on a small area, the better that area becomes. However, if all you have is a hammer, everything looks like a nail. The larger population may not need the care that someone with a rare disease may need.”
Dr. Miller refers to this challenge as “losing the forest.” He explains that subspecialists sometimes become so focused on their area of expertise, that they may overlook suitable treatment plans with which they are unfamiliar. An infertility specialist, for example, who neglects to consider a minimally invasive surgical procedure that could allow a patient to become pregnant naturally and instead recommends in vitro fertilization treatment.
“The infertility specialist does not have that particular skill and therefore directs that patient to IVF,” Dr. Miller said. “In the process of subspecializing, we have a tendency to lose the forest and look only at the trees.”
Finding a job is another challenge for the growing number of subspecialists. In many cases, fellowship-trained minimally invasive gynecologic surgeons may have to go back to practicing general gynecology because of a lack of positions, Dr. Miller said.
“We have to be careful that we do not “oversubspecialize” so that we are oversaturating the field,” he said.
In the future, the number of ob.gyn subspecialists will likely continue to grow and become more refined, said Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center in Phoenix.
“I think subspecialists will continue to become more and more developed,” Dr. Chase said. “Perhaps, some areas like family planning or minimally invasive surgery may grow further and become board certified.”
Dr. Carson foresees subspecialization becoming more focused on centralized teaching hospitals, with patients who need special care being sent to these hubs.
“Telemedicine and long-distance communication with a local obstetrician-gynecologist managing the whole patient will allow the best of both worlds,” she said.
Regardless of how subspecialist growth evolves, general ob.gyns. and other primary care physicians will always be needed, said Dr. Mary E. Norton, a maternal-fetal medicine specialist and clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.
“With increasing complexity, experts are needed to interpret advances,” Dr. Norton said. “However, patients also need a ‘medical home’ and primary provider who sees the big picture, and provides ongoing care beyond a single pregnancy or pregnancy complication.”
Why I chose to subspecialize
“I went to medical school with a particular interest in obstetrics. Once there, I was exposed to pediatrics and to high-risk OB, which I found to be fascinating. I particularly enjoyed my exposure to genetics during my pediatrics rotation and cared for a few children with genetic diseases that had a big impact and made a substantial impression on me. I ultimately decided to pursue an ob.gyn. residency and loved the OB part, particularly the prenatal genetics and high-risk OB. I found the balance of maternal and fetal medicine to be an exciting opportunity to care for two patients. I did an elective in prenatal diagnosis during my third year, including a bit of research, and was hooked.”
Dr. Mary E. Norton, a maternal-fetal medicine specialist and a clinical geneticist at the Fetal Treatment Center at the University of California, San Francisco.
“In my second year of residency, I became really interested in [gynecology-oncology] because I was fascinated by the surgery and interested in the chemotherapy practice, which is interesting because there’s always new research and new agents and interesting changes in how you treat the various cancers. It’s a very comprehensive, research-based field and that was fascinating to me. It’s a very busy subspecialty with very complex cases on multiple levels. You do these radical surgeries but then you have to be really involved in the choice for which chemotherapy agent to use, what type of radiation to give, and you also get really involved with the families ... Every case is so different and you treat women who are 16 years old, but you also treat women who are 96 years old. You see women from all walks of life with all sorts of different issues. The ability to really get involved with cancer research is a great part of the field.”
Dr. Dana M. Chase, a gynecologic oncologist at the University of Arizona Cancer Center, Phoenix.
“I took the opportunity to come to a new program where they were looking for an ob.gyn. hospitalist. That was exciting for me because I got to help establish the program... I feel like we’re a better department because I’m here monitoring labor, but I’m also writing protocols and making sure everyone is up to date. And I still get to do what I love the most, which is birth and babies.”
Dr. Brigid McCue, an ob.gyn. hospitalist and chief of ob.gyn. and midwifery, Beth Israel Deaconess Hospital-Plymouth, Massachusetts.
“I never considered delivering babies for the rest of my life. I was always focused on treating infertile couples. I completed my fellowship in reproductive endocrinology-infertility at the University of Pennsylvania, Philadelphia, at a time when in vitro fertilization was in its infancy and the laparoscope and hysteroscope were virtually diagnostic tools ... As IVF became more successful, I felt it was essential to add this expertise to my armamentarium ... It is truly gratifying to be part of a subspecialty that has advanced so far that the majority of our patients are able to achieve pregnancy via IVF.”
Dr. Charles E. Miller, a reproductive endocrinologist and minimally invasive gynecologic surgeon in Naperville and Schaumburg, Ill.
“During medical school, I was very interested in the surgical aspects of patient care. When I rotated in gyn-oncology – now knowing that I rotated with some of the best gyn-oncologists who ever practiced – I found myself drawn to the complexity of surgery, acuity of the patients, and the close relationships gyn-oncologists have with their patients. It hit me like a brick that this was the specialty for me. During my residency and fellowship, I was particularly drawn to the multiple modalities we use to treat cancers. I relished the idea that through clinical trials, gyn-oncologists keep pushing the bar to solve the cancer problem. What we do now is different than what we did 5 years ago. It keeps us professionally challenged all the time.”
Dr. Mark H. Einstein, a gynecologic oncologist and chair of obstetrics, gynecology and women’s health at Rutgers, the State University of New Jersey, Newark.
Throughout 2016, Ob.Gyn. News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @legal_med

Method could improve diagnosis of platelet disorders
Courtesy of Dan Cutler
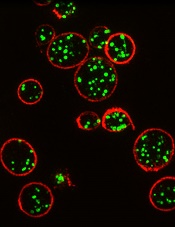
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
Courtesy of Dan Cutler
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
Courtesy of Dan Cutler
A proof-of-concept study suggests structured illumination microscopy (SIM) enables accurate diagnosis of Hermansky-Pudlak syndrome (HPS), an autosomal recessive disorder characterized by platelet dysfunction and prolonged bleeding.
Researchers therefore believe SIM could provide a more accessible and cost-effective method for diagnosing platelet disorders.
They also said SIM provides detailed data that may enable personalized treatments.
The researchers described their results with SIM in the Journal of Thrombosis and Haemostasis.
The team noted that electron microscopy can be used to diagnose HPS and other disorders characterized by platelet dysfunction. But the method is costly, requires fresh samples, gives limited information, and is not widely available.
“We’ve found that SIM has a lot of advantages over whole mount electron microscopy as a diagnosis method,” said study author David Westmoreland, of University College London in the UK.
“Samples don’t need to be analyzed live and can be reanalyzed, and automation means analysis is unbiased and less time-consuming. Given about 75% of patients with a bleeding disorder such as Hermansky-Pudlak syndrome are initially misdiagnosed, and 28% need to see between 4 to 6 specialists before receiving the correct diagnosis, there is a demand for a new method of analysis.”
For this proof-of-concept study, Westmoreland and his colleagues used SIM to image platelet granules in blood samples using a marker protein, CD63.
The imaging technology was custom-built by the team to automatically count the number of granules per platelet, thereby identifying patients with HPS, a rare disorder thought to affect 1 in 500,000 people.
The researchers distinguished the 3 patients with HPS from 7 normal controls with 99% confidence. Automated counting of granules showed that individuals with the disorder had a third as many granules as controls.
“Our limited analysis of this new method is extremely promising, and we hope to take it forward to test for multiple parameters with different markers,” said Dan Cutler, PhD, also of University College London.
“In this way, we could use a single super-resolution image to screen for many different platelet-based blood disorders.” ![]()
Research Shows Inpatient Dermatology Improves Diagnostic Accuracy and Intervention
NEW YORK (Reuters Health) - Inpatient dermatology consultations for skin disorders are associated with improved diagnostic accuracy and faster intervention, researchers have
found.
Information about the impact of hospitalist dermatology consultative services is limited, Dr. Daniela Kroshinsky from Massachusetts General Hospital in Boston and colleagues note in JAMA Dermatology, online January 13.
To learn more, the team conducted a cross-sectional study of data from dermatology consult teams at four academic medical centers in the U.S. Full-time inpatient dermatologists with resident teams performed a total of 1,661 inpatient dermatology consultations within 24 to 48 hours of request over 12 months from 2008 to 2009.
All final diagnoses were based on clinical history, examination findings, and laboratory testing. Each service (primary team) that asked for a dermatology consult provided its presumptive diagnosis at the time of its request.
The most common primary teams were Medicine (47%), followed by Surgery (15%), Intensive Care Units (12%), and Hematology-Oncology (9%). The most commonly undiagnosed or misdiagnosed conditions by the primary teams were cellulitis, leg ulcerations, and viral infections. The majority of primary team preliminary diagnoses included rash/unknown (n=814), followed by cellulitis/abscess (n=115), and drug rash (n=111). The majority of primary diagnoses by dermatologists included drug rash (n=292; 18%), psoriasis/eczema (n=170; 10%), and benign neoplasm (n=168; 10%).
The dermatologists identified additional cutaneous issues in 298 (18%) of consults; diagnosis was confirmed by biopsy in 667 (40%) patients. Overall, dermatology consultation changed the final diagnosis in 71% of consultation requests.
Just under a third of the patients were admitted to the hospitals because of their skin conditions. In the remaining cases, the dermatologic issues were found incidentally or developed during hospitalization.
In 40% of cases, dermatology-specific evaluation and treatment recommendations were carried out in a single visit; 29% required one follow-up evaluation and 16% required two.
"This is the first multicenter national study to define the nature of dermatologic issues presenting to academic medical centers and to demonstrate the impact dermatologists have on improving the correct diagnosis of patients with skin issues,"Dr. Kroshinsky told Reuters Health by email.
Hospitalist dermatology is an important and effective subset of dermatology and hospital medicine, she said.
"Ideally," Dr. Kroshinsky added, "hospitals would have access to a dermatologist in real-time or via teledermatology."
NEW YORK (Reuters Health) - Inpatient dermatology consultations for skin disorders are associated with improved diagnostic accuracy and faster intervention, researchers have
found.
Information about the impact of hospitalist dermatology consultative services is limited, Dr. Daniela Kroshinsky from Massachusetts General Hospital in Boston and colleagues note in JAMA Dermatology, online January 13.
To learn more, the team conducted a cross-sectional study of data from dermatology consult teams at four academic medical centers in the U.S. Full-time inpatient dermatologists with resident teams performed a total of 1,661 inpatient dermatology consultations within 24 to 48 hours of request over 12 months from 2008 to 2009.
All final diagnoses were based on clinical history, examination findings, and laboratory testing. Each service (primary team) that asked for a dermatology consult provided its presumptive diagnosis at the time of its request.
The most common primary teams were Medicine (47%), followed by Surgery (15%), Intensive Care Units (12%), and Hematology-Oncology (9%). The most commonly undiagnosed or misdiagnosed conditions by the primary teams were cellulitis, leg ulcerations, and viral infections. The majority of primary team preliminary diagnoses included rash/unknown (n=814), followed by cellulitis/abscess (n=115), and drug rash (n=111). The majority of primary diagnoses by dermatologists included drug rash (n=292; 18%), psoriasis/eczema (n=170; 10%), and benign neoplasm (n=168; 10%).
The dermatologists identified additional cutaneous issues in 298 (18%) of consults; diagnosis was confirmed by biopsy in 667 (40%) patients. Overall, dermatology consultation changed the final diagnosis in 71% of consultation requests.
Just under a third of the patients were admitted to the hospitals because of their skin conditions. In the remaining cases, the dermatologic issues were found incidentally or developed during hospitalization.
In 40% of cases, dermatology-specific evaluation and treatment recommendations were carried out in a single visit; 29% required one follow-up evaluation and 16% required two.
"This is the first multicenter national study to define the nature of dermatologic issues presenting to academic medical centers and to demonstrate the impact dermatologists have on improving the correct diagnosis of patients with skin issues,"Dr. Kroshinsky told Reuters Health by email.
Hospitalist dermatology is an important and effective subset of dermatology and hospital medicine, she said.
"Ideally," Dr. Kroshinsky added, "hospitals would have access to a dermatologist in real-time or via teledermatology."
NEW YORK (Reuters Health) - Inpatient dermatology consultations for skin disorders are associated with improved diagnostic accuracy and faster intervention, researchers have
found.
Information about the impact of hospitalist dermatology consultative services is limited, Dr. Daniela Kroshinsky from Massachusetts General Hospital in Boston and colleagues note in JAMA Dermatology, online January 13.
To learn more, the team conducted a cross-sectional study of data from dermatology consult teams at four academic medical centers in the U.S. Full-time inpatient dermatologists with resident teams performed a total of 1,661 inpatient dermatology consultations within 24 to 48 hours of request over 12 months from 2008 to 2009.
All final diagnoses were based on clinical history, examination findings, and laboratory testing. Each service (primary team) that asked for a dermatology consult provided its presumptive diagnosis at the time of its request.
The most common primary teams were Medicine (47%), followed by Surgery (15%), Intensive Care Units (12%), and Hematology-Oncology (9%). The most commonly undiagnosed or misdiagnosed conditions by the primary teams were cellulitis, leg ulcerations, and viral infections. The majority of primary team preliminary diagnoses included rash/unknown (n=814), followed by cellulitis/abscess (n=115), and drug rash (n=111). The majority of primary diagnoses by dermatologists included drug rash (n=292; 18%), psoriasis/eczema (n=170; 10%), and benign neoplasm (n=168; 10%).
The dermatologists identified additional cutaneous issues in 298 (18%) of consults; diagnosis was confirmed by biopsy in 667 (40%) patients. Overall, dermatology consultation changed the final diagnosis in 71% of consultation requests.
Just under a third of the patients were admitted to the hospitals because of their skin conditions. In the remaining cases, the dermatologic issues were found incidentally or developed during hospitalization.
In 40% of cases, dermatology-specific evaluation and treatment recommendations were carried out in a single visit; 29% required one follow-up evaluation and 16% required two.
"This is the first multicenter national study to define the nature of dermatologic issues presenting to academic medical centers and to demonstrate the impact dermatologists have on improving the correct diagnosis of patients with skin issues,"Dr. Kroshinsky told Reuters Health by email.
Hospitalist dermatology is an important and effective subset of dermatology and hospital medicine, she said.
"Ideally," Dr. Kroshinsky added, "hospitals would have access to a dermatologist in real-time or via teledermatology."
EBV-CTLs get orphan designation for EBV-PTLD

among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
among uninfected cells (blue)
Image courtesy of
Benjamin Chaigne-Delalande
The US Food and Drug Administration (FDA) has granted orphan designation for cytotoxic T lymphocytes activated against Epstein-Barr virus (EBV-CTLs) to treat EBV post-transplant lymphoproliferative disorder (EBV-PTLD) occurring after solid organ or hematopoietic stem cell transplant.
The FDA grants orphan designation to products intended to treat, diagnose, or prevent disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases, which may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and a 7-year period of marketing exclusivity if the product is approved.
The EBV-CTL product is under development by Atara Biotherapeutics, Inc. It is produced by collecting T cells from third-party donors and exposing the cells to EBV antigens.
The activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient, providing an “off-the-shelf,” allogeneic, cellular therapeutic option for patients.
In the context of EBV-PTLD, Atara’s EBV-CTLs find the cancer cells expressing EBV and kill them. EBV-CTLs are currently being studied in phase 2 trials.
Results of a phase 1/2 study were presented at the APHON 37th Annual Conference and Exhibit and at the 2015 ASCO Annual Meeting.
The FDA previously granted EBV-CTLs breakthrough designation to treat EBV-PTLD. This designation is intended to expedite the development and review of new drugs for serious or life-threatening conditions.
To qualify for breakthrough designation, a drug must show credible evidence of a substantial improvement on a clinically significant endpoint over available therapies, or over placebo if there is no available therapy, or in a study that compares the new treatment plus the standard of care to the standard alone.
The designation confers several benefits, including intensive FDA guidance and eligibility for submission of a rolling biologic license application. ![]()
Gut microbiota linked to severity of malaria

Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Microorganisms in the gut play a role in the severity of malaria, according to a study published in PNAS.
Investigators examined the gut microbiomes of mice and found evidence to suggest that malaria severity is not only a function of the parasite or the host. It is also influenced by the microbes in the infected organism.
And 2 types of bacteria—Bifidobacterium and Lactobacillus—were associated with reduced malaria severity.
“The research provides a potential new avenue to investigate factors that control the severity of malaria,” said study author Steven Wilhelm, PhD, of the University of Tennessee at Knoxville.
“With 1 million people dying [of malaria] each year, many of whom are young children, any approach that may save even a few lives is worth following up on.”
With this study, Dr Wilhelm and his colleagues found that genetically similar mice acquired from different vendors had differences in pathology after malaria infection. There were significant differences in both parasite burden and mortality after infection with multiple Plasmodium species.
The investigators measured gut microbiomes in the mice by sequencing bacteria in the digestive tract and noted significant differences within the different mouse populations.
So the team transferred cecal content from the first set of mice into germ-free mice and found that differences in malaria severity were transferred.
The mice that received transplants from donors that were more resistant to malaria had low parasite burdens. And mice that received transplants from donors that were more susceptible to malaria had high parasite burdens.
The investigators also observed an increased abundance of Bifidobacterium and Lactobacillus bacteria in the mice that exhibited reduced malaria pathology.
So the team took mice that were more susceptible to malaria, treated them with antibiotics, and fed them yogurt containing Bifidobacterium and Lactobacillus. As expected, the severity of malaria in these mice decreased.
“These results demonstrate the possibility of modifying the gut microbiome to prevent severe malaria,” said study author Nathan Schmidt, PhD, of the University of Louisville in Kentucky.
Dr Wilhelm noted that, although the research interventions lessened the severity of malaria in mice, it did not prevent or cure it. And the investigators are a long way from perfecting similar treatments in humans but are working on understanding the mechanism.
“A way to help people who are infected—and especially a simple and cheap way, as much of the infection occurs in the developing world—would be a great service to society,” Dr Wilhelm said. ![]()
Biosimilar infliximab gains FDA Advisory Committee endorsement
A biosimilar agent to Remicade, the brand-name and reference form of infliximab, stayed on track to become the second biosimilar drug to enter the U.S. market when the Arthritis Advisory Committee of the Food and Drug Administration voted overwhelmingly in favor of licensure of the biosimilar at a meeting on Feb. 9.
The vote was 21 in favor and 3 against, with no abstentions.
Because of the way the FDA staff worded the question that the Advisory Committee voted on, the panel not only was in favor of approving biosimilar licensure but also recommended that license for six of the seven diverse indications that Remicade currently has: treatment of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, plaque psoriasis, adult and pediatric Crohn’s disease, and adult ulcerative colitis. The panel did not vote on licensing the biosimilar for treatment of pediatric ulcerative colitis because that specific indication for Remicade remains on patent for a few more years.
The broad range of indications for which the Committee recommended approval was notable because the formulation of biosimilar infliximab under review, manufactured by Celltrion and known in the United States as CT-P13, had been clinically studied only in patients with rheumatoid arthritis or ankylosing spondylitis. The other four recommended indications represented extrapolations, based on the totality of biosimilar evidence presented at the meeting by both Celltrion staffers and consultants as well as analyses presented by FDA staff members.
The overall thrust of the extrapolation issue was that if biosimilarity to Remicade was proven by a range of preclinical and clinical testing, and if safety and efficacy similar to Remicade was shown in trials that enrolled only patients with rheumatoid arthritis or ankylosing spondylitis, then the safety and efficacy previously proven for Remicade for the other indications could be reasonably extrapolated to apply to CT-P13 also, even though CT-P13 was never tested on patients with those conditions. This turned out to often be the key issue that panel members grappled with as they decided whether to vote in favor of the question the FDA asked them to address.
“Many of us are uncomfortable with this new pathway” of extrapolation, said panel member Dr. Beth L. Jonas, a rheumatologist at the University of North Carolina at Chapel Hill.
“I feel we’re taking a risk” with the extrapolations, said Dr. Mary E. Maloney, professor of medicine and chief of dermatology at the University of Massachusetts in Worcester. “We have a responsibility to take a risk to provide biosimilars to patients and to reduce their cost” for needed treatments, she said during the Committee’s discussion of their votes.
“Biosimilar is a new concept, but it’s the future of how we will look at drugs,” explained panel member Dr. Wilma Bergfeld, professor of dermatology at the Cleveland Clinic.
CT-P13 is currently marketed in many other countries worldwide under the brand names Remsima or Inflectra.
The FDA’s staff was clearly behind this application. After summarizing the agency’s internal analysis of the data submitted by Celltrion, Dr. Nikolay Nikolov, clinical team leader for the FDA’s Division of Pulmonary, Allergy and Rheumatology Products, concluded that “the totality of evidence provided by the applicant supports a conclusion that CT-P13 is biosimilar to U.S.-licensed Remicade,” and that “scientific justification for extrapolating the clinical data supports a finding of biosimilarity for all indications for which U.S.-licensed Remicade is licensed.” The FDA’s position makes it seem very likely that the agency will accept the Advisory Committee’s vote and grant CT-P13 license for U.S. marketing in the near future.
CT-P13 also received support during the public comment period of the Committee’s deliberations. At that time, Dr. Gideon P. Smith, a dermatologist at Massachusetts General Hospital in Boston spoke on behalf of the American Academy of Dermatology Association. “Biologics are some of the most important recent developments in treating plaque psoriasis, but cost is an important issue. We hope that biosimilars will decrease the cost of this treatment,” Dr. Smith said. “Infliximab is a complex molecule with a complex production process. We are concerned about the safety and efficacy of treatment. The AADA supports approval based on reducing cost and improving patient access. However, we strongly recommend caution through long-term postmarketing surveillance and using registry data to identify issues of immunogenicity, efficacy, and safety that were not seen in the clinical trials.”
The drug also received support from Dr. Angus B. Worthing, who represented the American College of Rheumatology. “Biosimilars may be the only tool to keep prices of biologics within reason,” said Dr. Worthing, a rheumatologist in Washington. But he also stressed that “extrapolation should be done with caution and not routinely granted.”
CT-P13 has the potential to make a fairly widely used biologic significantly more affordable. In countries where it has come onto the market, it’s been priced at roughly 30% below the prevailing cost of Remicade prior to this competition.
“Infliximab is an extremely important tool in our armamentarium for treatment of both ulcerative colitis and Crohn’s disease,” commented Dr. Stephen B. Hanauer, professor of gastroenterology and hepatology at Northwestern University in Chicago. “Biologic therapies account for an increasing proportion of health care costs for chronic diseases such as inflammatory bowel disease and reducing these costs will be important as increasing numbers of patients are benefiting from long-term biologic therapies. Having reviewed the extensive preclinical and clinical data with CT-P13, I am comfortable with potential substitution or switching as long as physicians are aware of the change and can track any potential reactions to the administered product,” he said in an interview.
“Infliximab is currently used by U.S. rheumatologists to treat certain patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis. It is not the most-widely used tumor necrosis factor inhibitor, which is adalimumab, but it is often used. After FDA approval, biosimilar infliximab is anticipated to be priced lower than Remicade and that would likely increase use of infliximab for rheumatologic conditions,” said Dr. Jonathan Kay, a rheumatologist and professor of medicine at the University of Massachusetts in Worcester. “The clinical experience with CT-P13 in trials and in routine use in other countries show no significant loss of efficacy or any other major problem when changing patients from Remicade to CT-P13. All the data suggest that CT-P13 is highly similar to the reference product. It’s almost akin to comparing one lot of Remicade to another lot of Remicade. I personally would not have a problem initiating a patient on CT-P13 if infliximab was the appropriate drug to use,” Dr. Kay said in an interview.
Dr. Hanauer has been a consultant to Celltrion. Dr. Kay has been a consultant to several drug companies.
On Twitter @mitchelzoler
A biosimilar agent to Remicade, the brand-name and reference form of infliximab, stayed on track to become the second biosimilar drug to enter the U.S. market when the Arthritis Advisory Committee of the Food and Drug Administration voted overwhelmingly in favor of licensure of the biosimilar at a meeting on Feb. 9.
The vote was 21 in favor and 3 against, with no abstentions.
Because of the way the FDA staff worded the question that the Advisory Committee voted on, the panel not only was in favor of approving biosimilar licensure but also recommended that license for six of the seven diverse indications that Remicade currently has: treatment of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, plaque psoriasis, adult and pediatric Crohn’s disease, and adult ulcerative colitis. The panel did not vote on licensing the biosimilar for treatment of pediatric ulcerative colitis because that specific indication for Remicade remains on patent for a few more years.
The broad range of indications for which the Committee recommended approval was notable because the formulation of biosimilar infliximab under review, manufactured by Celltrion and known in the United States as CT-P13, had been clinically studied only in patients with rheumatoid arthritis or ankylosing spondylitis. The other four recommended indications represented extrapolations, based on the totality of biosimilar evidence presented at the meeting by both Celltrion staffers and consultants as well as analyses presented by FDA staff members.
The overall thrust of the extrapolation issue was that if biosimilarity to Remicade was proven by a range of preclinical and clinical testing, and if safety and efficacy similar to Remicade was shown in trials that enrolled only patients with rheumatoid arthritis or ankylosing spondylitis, then the safety and efficacy previously proven for Remicade for the other indications could be reasonably extrapolated to apply to CT-P13 also, even though CT-P13 was never tested on patients with those conditions. This turned out to often be the key issue that panel members grappled with as they decided whether to vote in favor of the question the FDA asked them to address.
“Many of us are uncomfortable with this new pathway” of extrapolation, said panel member Dr. Beth L. Jonas, a rheumatologist at the University of North Carolina at Chapel Hill.
“I feel we’re taking a risk” with the extrapolations, said Dr. Mary E. Maloney, professor of medicine and chief of dermatology at the University of Massachusetts in Worcester. “We have a responsibility to take a risk to provide biosimilars to patients and to reduce their cost” for needed treatments, she said during the Committee’s discussion of their votes.
“Biosimilar is a new concept, but it’s the future of how we will look at drugs,” explained panel member Dr. Wilma Bergfeld, professor of dermatology at the Cleveland Clinic.
CT-P13 is currently marketed in many other countries worldwide under the brand names Remsima or Inflectra.
The FDA’s staff was clearly behind this application. After summarizing the agency’s internal analysis of the data submitted by Celltrion, Dr. Nikolay Nikolov, clinical team leader for the FDA’s Division of Pulmonary, Allergy and Rheumatology Products, concluded that “the totality of evidence provided by the applicant supports a conclusion that CT-P13 is biosimilar to U.S.-licensed Remicade,” and that “scientific justification for extrapolating the clinical data supports a finding of biosimilarity for all indications for which U.S.-licensed Remicade is licensed.” The FDA’s position makes it seem very likely that the agency will accept the Advisory Committee’s vote and grant CT-P13 license for U.S. marketing in the near future.
CT-P13 also received support during the public comment period of the Committee’s deliberations. At that time, Dr. Gideon P. Smith, a dermatologist at Massachusetts General Hospital in Boston spoke on behalf of the American Academy of Dermatology Association. “Biologics are some of the most important recent developments in treating plaque psoriasis, but cost is an important issue. We hope that biosimilars will decrease the cost of this treatment,” Dr. Smith said. “Infliximab is a complex molecule with a complex production process. We are concerned about the safety and efficacy of treatment. The AADA supports approval based on reducing cost and improving patient access. However, we strongly recommend caution through long-term postmarketing surveillance and using registry data to identify issues of immunogenicity, efficacy, and safety that were not seen in the clinical trials.”
The drug also received support from Dr. Angus B. Worthing, who represented the American College of Rheumatology. “Biosimilars may be the only tool to keep prices of biologics within reason,” said Dr. Worthing, a rheumatologist in Washington. But he also stressed that “extrapolation should be done with caution and not routinely granted.”
CT-P13 has the potential to make a fairly widely used biologic significantly more affordable. In countries where it has come onto the market, it’s been priced at roughly 30% below the prevailing cost of Remicade prior to this competition.
“Infliximab is an extremely important tool in our armamentarium for treatment of both ulcerative colitis and Crohn’s disease,” commented Dr. Stephen B. Hanauer, professor of gastroenterology and hepatology at Northwestern University in Chicago. “Biologic therapies account for an increasing proportion of health care costs for chronic diseases such as inflammatory bowel disease and reducing these costs will be important as increasing numbers of patients are benefiting from long-term biologic therapies. Having reviewed the extensive preclinical and clinical data with CT-P13, I am comfortable with potential substitution or switching as long as physicians are aware of the change and can track any potential reactions to the administered product,” he said in an interview.
“Infliximab is currently used by U.S. rheumatologists to treat certain patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis. It is not the most-widely used tumor necrosis factor inhibitor, which is adalimumab, but it is often used. After FDA approval, biosimilar infliximab is anticipated to be priced lower than Remicade and that would likely increase use of infliximab for rheumatologic conditions,” said Dr. Jonathan Kay, a rheumatologist and professor of medicine at the University of Massachusetts in Worcester. “The clinical experience with CT-P13 in trials and in routine use in other countries show no significant loss of efficacy or any other major problem when changing patients from Remicade to CT-P13. All the data suggest that CT-P13 is highly similar to the reference product. It’s almost akin to comparing one lot of Remicade to another lot of Remicade. I personally would not have a problem initiating a patient on CT-P13 if infliximab was the appropriate drug to use,” Dr. Kay said in an interview.
Dr. Hanauer has been a consultant to Celltrion. Dr. Kay has been a consultant to several drug companies.
On Twitter @mitchelzoler
A biosimilar agent to Remicade, the brand-name and reference form of infliximab, stayed on track to become the second biosimilar drug to enter the U.S. market when the Arthritis Advisory Committee of the Food and Drug Administration voted overwhelmingly in favor of licensure of the biosimilar at a meeting on Feb. 9.
The vote was 21 in favor and 3 against, with no abstentions.
Because of the way the FDA staff worded the question that the Advisory Committee voted on, the panel not only was in favor of approving biosimilar licensure but also recommended that license for six of the seven diverse indications that Remicade currently has: treatment of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, plaque psoriasis, adult and pediatric Crohn’s disease, and adult ulcerative colitis. The panel did not vote on licensing the biosimilar for treatment of pediatric ulcerative colitis because that specific indication for Remicade remains on patent for a few more years.
The broad range of indications for which the Committee recommended approval was notable because the formulation of biosimilar infliximab under review, manufactured by Celltrion and known in the United States as CT-P13, had been clinically studied only in patients with rheumatoid arthritis or ankylosing spondylitis. The other four recommended indications represented extrapolations, based on the totality of biosimilar evidence presented at the meeting by both Celltrion staffers and consultants as well as analyses presented by FDA staff members.
The overall thrust of the extrapolation issue was that if biosimilarity to Remicade was proven by a range of preclinical and clinical testing, and if safety and efficacy similar to Remicade was shown in trials that enrolled only patients with rheumatoid arthritis or ankylosing spondylitis, then the safety and efficacy previously proven for Remicade for the other indications could be reasonably extrapolated to apply to CT-P13 also, even though CT-P13 was never tested on patients with those conditions. This turned out to often be the key issue that panel members grappled with as they decided whether to vote in favor of the question the FDA asked them to address.
“Many of us are uncomfortable with this new pathway” of extrapolation, said panel member Dr. Beth L. Jonas, a rheumatologist at the University of North Carolina at Chapel Hill.
“I feel we’re taking a risk” with the extrapolations, said Dr. Mary E. Maloney, professor of medicine and chief of dermatology at the University of Massachusetts in Worcester. “We have a responsibility to take a risk to provide biosimilars to patients and to reduce their cost” for needed treatments, she said during the Committee’s discussion of their votes.
“Biosimilar is a new concept, but it’s the future of how we will look at drugs,” explained panel member Dr. Wilma Bergfeld, professor of dermatology at the Cleveland Clinic.
CT-P13 is currently marketed in many other countries worldwide under the brand names Remsima or Inflectra.
The FDA’s staff was clearly behind this application. After summarizing the agency’s internal analysis of the data submitted by Celltrion, Dr. Nikolay Nikolov, clinical team leader for the FDA’s Division of Pulmonary, Allergy and Rheumatology Products, concluded that “the totality of evidence provided by the applicant supports a conclusion that CT-P13 is biosimilar to U.S.-licensed Remicade,” and that “scientific justification for extrapolating the clinical data supports a finding of biosimilarity for all indications for which U.S.-licensed Remicade is licensed.” The FDA’s position makes it seem very likely that the agency will accept the Advisory Committee’s vote and grant CT-P13 license for U.S. marketing in the near future.
CT-P13 also received support during the public comment period of the Committee’s deliberations. At that time, Dr. Gideon P. Smith, a dermatologist at Massachusetts General Hospital in Boston spoke on behalf of the American Academy of Dermatology Association. “Biologics are some of the most important recent developments in treating plaque psoriasis, but cost is an important issue. We hope that biosimilars will decrease the cost of this treatment,” Dr. Smith said. “Infliximab is a complex molecule with a complex production process. We are concerned about the safety and efficacy of treatment. The AADA supports approval based on reducing cost and improving patient access. However, we strongly recommend caution through long-term postmarketing surveillance and using registry data to identify issues of immunogenicity, efficacy, and safety that were not seen in the clinical trials.”
The drug also received support from Dr. Angus B. Worthing, who represented the American College of Rheumatology. “Biosimilars may be the only tool to keep prices of biologics within reason,” said Dr. Worthing, a rheumatologist in Washington. But he also stressed that “extrapolation should be done with caution and not routinely granted.”
CT-P13 has the potential to make a fairly widely used biologic significantly more affordable. In countries where it has come onto the market, it’s been priced at roughly 30% below the prevailing cost of Remicade prior to this competition.
“Infliximab is an extremely important tool in our armamentarium for treatment of both ulcerative colitis and Crohn’s disease,” commented Dr. Stephen B. Hanauer, professor of gastroenterology and hepatology at Northwestern University in Chicago. “Biologic therapies account for an increasing proportion of health care costs for chronic diseases such as inflammatory bowel disease and reducing these costs will be important as increasing numbers of patients are benefiting from long-term biologic therapies. Having reviewed the extensive preclinical and clinical data with CT-P13, I am comfortable with potential substitution or switching as long as physicians are aware of the change and can track any potential reactions to the administered product,” he said in an interview.
“Infliximab is currently used by U.S. rheumatologists to treat certain patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis. It is not the most-widely used tumor necrosis factor inhibitor, which is adalimumab, but it is often used. After FDA approval, biosimilar infliximab is anticipated to be priced lower than Remicade and that would likely increase use of infliximab for rheumatologic conditions,” said Dr. Jonathan Kay, a rheumatologist and professor of medicine at the University of Massachusetts in Worcester. “The clinical experience with CT-P13 in trials and in routine use in other countries show no significant loss of efficacy or any other major problem when changing patients from Remicade to CT-P13. All the data suggest that CT-P13 is highly similar to the reference product. It’s almost akin to comparing one lot of Remicade to another lot of Remicade. I personally would not have a problem initiating a patient on CT-P13 if infliximab was the appropriate drug to use,” Dr. Kay said in an interview.
Dr. Hanauer has been a consultant to Celltrion. Dr. Kay has been a consultant to several drug companies.
On Twitter @mitchelzoler
A Case of Bloom Syndrome With Uncommon Clinical Manifestations Confirmed on Genetic Testing
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.

After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.
After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.
After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.

When the Doctor Is Not a Doctor

It is now common for patients to arrive in a physician office and never see the physician. Instead, patients are seen by so-called physician extenders. As our population ages, the need for medical care continues to grow beyond the capacity of the 900,000 US physicians that provide required services, particularly in the first level (primary care). The response to the physician shortage has entailed a variety of strategies. There has been a major immigration of foreign physicians, particularly from India; US medical schools have been encouraged to increase enrollment; and new medical schools have been inaugurated. Physicians have been pushed to adopt electronic medical records to permit increased throughput of patients in office practices. These multiple approaches have had an effect, though sometimes the results are undesirable. For example, complicated computer programs often detract from the physician-patient relationship.
One of the early solutions offered to deal with the doctor shortage in primary care was the concept of physician extenders (PEs), also called mid-level practitioners, who are professionals trained to take on a number of the simpler tasks performed by physicians. There are 2 basic classes of PEs: nurse practitioners and physician assistants. Nurse practitioners are originally trained to perform nursing but then undertake a course of study including scientific courses and clinical exposure to various parts of medicine. Physician assistants receive similar training. The duration of training for PEs usually is 18 to 24 months, whereas physicians attend medical school for 4 years. Unlike physicians, mid-level practitioners do not enter physician postgraduate residency training programs, which last many years.
The original concept was that PEs would work side by side with physicians who would supervise the care provided by the PEs. This team concept was designed to free physicians from the more mundane aspects of medical care and allow them to focus on the more challenging diagnostic and therapeutic issues presented by individual patients. In an era in which the burden of documentation has become increasingly onerous, the assistance of paraprofessionals can spare physicians the entry of redundant details in electronic databases that do not contribute to patient welfare.
However, research suggests that the concept of mid-level providers undertaking first-level care side by side with physicians has diverged from the original goal. An article by Coldiron and Ratnarathorn (JAMA Dermatol. 2014;150:1153-1159) studied Medicare billing data. The authors discovered that a variety of activities, many with higher reimbursement than primary care, were billed directly by PEs without apparent physician involvement, including a large number of complex invasive procedures, more than half in dermatology. Their article focused on dermatologic procedures, such as the destruction of skin cancers and advanced surgical repairs, but they listed many other procedures that are typically in the domain of highly trained physicians, including radiologic interpretations such as mammography and joint injections such as spinal injections. The data they presented were substantiated by publications in the medical literature suggesting that mid-level providers at certain hospitals even perform heart catheterizations and gastrointestinal endoscopies.
There have been no apologies for the unsupervised conduct of physician activities by nonphysicians. On the contrary, many PEs claim to be as well trained and proficient as medical doctors. Coldiron and Ratnarathorn argued otherwise. They pointed out that physicians receive an average of 10,000 hours of training compared to 2000 hours for mid-level practitioners, and they raised concerns about misdiagnoses, complications, and unnecessary procedures performed by PEs without supervision. In an editorial, Jalian and Avram (JAMA Dermatol. 2014;150:1149-1151) pointed out that a disproportionate number of cases of lawsuits for laser-induced injuries are related to performance by nonphysicians.
The pressures to allow nonphysicians to practice medicine independently are increasing. There is a shortage of physicians, especially in states such as Massachusetts that have substantial governmental limitation of physician reimbursement. In Massachusetts, regulations encourage mid-level practitioners to practice without physician supervision and even call themselves “doctors.” Furthermore, hospitals have faced residency funding cuts by Medicare and have had regulatory limitation of work hours by medical doctors in residency training. As a result, many institutions have turned to PEs to perform procedures that are typically performed by medical doctors.
Perhaps the greatest pressure favoring use of nonphysicians is financial. Mid-level practitioners receive lower salaries, typically 45% less, than medical doctors. In an era in which lowering costs has supplanted the goal of offering the best medical care possible, the attraction of replacement of a physician by a professional with less training becomes irresistible. It also is of concern that many physicians ignore the requirement to supervise the work of mid-level practitioners to maximize profit. Physicians often hire a mid-level provider rather than finding another physician to partner in their practice. Patients referred to a dermatologist often are seen by a PE and never even see the physician.
The concept of PEs working in a team with physicians remains an excellent approach to remedying the shortage of medical doctors, but we need to return to the original plan. Physician extenders should perform primary care rather than complex and lucrative subspecialties. There must be adequate supervision and definitely participation by physicians in rendering care.
All of the authors in the articles cited argue for greater regulation of unsupervised PEs to prevent performance of procedures where they lack expertise. Although the regulatory approach is sensible, it is more important to ensure that patients choose who gives them their medical care. They should not be obligated to see mid-level practitioners if they want to see a medical doctor. Above all, patients must be informed of the qualifications of those who provide their medical care. They should not be blindsided when they arrive for an appointment with their physician and find themselves shunted to a PE. We must not allow financial considerations to override the integrity of the medical care process.
What do you think is the optimal and safest role for PEs in a dermatology practice?
We want to know your views! Tell us what you think.
It is now common for patients to arrive in a physician office and never see the physician. Instead, patients are seen by so-called physician extenders. As our population ages, the need for medical care continues to grow beyond the capacity of the 900,000 US physicians that provide required services, particularly in the first level (primary care). The response to the physician shortage has entailed a variety of strategies. There has been a major immigration of foreign physicians, particularly from India; US medical schools have been encouraged to increase enrollment; and new medical schools have been inaugurated. Physicians have been pushed to adopt electronic medical records to permit increased throughput of patients in office practices. These multiple approaches have had an effect, though sometimes the results are undesirable. For example, complicated computer programs often detract from the physician-patient relationship.
One of the early solutions offered to deal with the doctor shortage in primary care was the concept of physician extenders (PEs), also called mid-level practitioners, who are professionals trained to take on a number of the simpler tasks performed by physicians. There are 2 basic classes of PEs: nurse practitioners and physician assistants. Nurse practitioners are originally trained to perform nursing but then undertake a course of study including scientific courses and clinical exposure to various parts of medicine. Physician assistants receive similar training. The duration of training for PEs usually is 18 to 24 months, whereas physicians attend medical school for 4 years. Unlike physicians, mid-level practitioners do not enter physician postgraduate residency training programs, which last many years.
The original concept was that PEs would work side by side with physicians who would supervise the care provided by the PEs. This team concept was designed to free physicians from the more mundane aspects of medical care and allow them to focus on the more challenging diagnostic and therapeutic issues presented by individual patients. In an era in which the burden of documentation has become increasingly onerous, the assistance of paraprofessionals can spare physicians the entry of redundant details in electronic databases that do not contribute to patient welfare.
However, research suggests that the concept of mid-level providers undertaking first-level care side by side with physicians has diverged from the original goal. An article by Coldiron and Ratnarathorn (JAMA Dermatol. 2014;150:1153-1159) studied Medicare billing data. The authors discovered that a variety of activities, many with higher reimbursement than primary care, were billed directly by PEs without apparent physician involvement, including a large number of complex invasive procedures, more than half in dermatology. Their article focused on dermatologic procedures, such as the destruction of skin cancers and advanced surgical repairs, but they listed many other procedures that are typically in the domain of highly trained physicians, including radiologic interpretations such as mammography and joint injections such as spinal injections. The data they presented were substantiated by publications in the medical literature suggesting that mid-level providers at certain hospitals even perform heart catheterizations and gastrointestinal endoscopies.
There have been no apologies for the unsupervised conduct of physician activities by nonphysicians. On the contrary, many PEs claim to be as well trained and proficient as medical doctors. Coldiron and Ratnarathorn argued otherwise. They pointed out that physicians receive an average of 10,000 hours of training compared to 2000 hours for mid-level practitioners, and they raised concerns about misdiagnoses, complications, and unnecessary procedures performed by PEs without supervision. In an editorial, Jalian and Avram (JAMA Dermatol. 2014;150:1149-1151) pointed out that a disproportionate number of cases of lawsuits for laser-induced injuries are related to performance by nonphysicians.
The pressures to allow nonphysicians to practice medicine independently are increasing. There is a shortage of physicians, especially in states such as Massachusetts that have substantial governmental limitation of physician reimbursement. In Massachusetts, regulations encourage mid-level practitioners to practice without physician supervision and even call themselves “doctors.” Furthermore, hospitals have faced residency funding cuts by Medicare and have had regulatory limitation of work hours by medical doctors in residency training. As a result, many institutions have turned to PEs to perform procedures that are typically performed by medical doctors.
Perhaps the greatest pressure favoring use of nonphysicians is financial. Mid-level practitioners receive lower salaries, typically 45% less, than medical doctors. In an era in which lowering costs has supplanted the goal of offering the best medical care possible, the attraction of replacement of a physician by a professional with less training becomes irresistible. It also is of concern that many physicians ignore the requirement to supervise the work of mid-level practitioners to maximize profit. Physicians often hire a mid-level provider rather than finding another physician to partner in their practice. Patients referred to a dermatologist often are seen by a PE and never even see the physician.
The concept of PEs working in a team with physicians remains an excellent approach to remedying the shortage of medical doctors, but we need to return to the original plan. Physician extenders should perform primary care rather than complex and lucrative subspecialties. There must be adequate supervision and definitely participation by physicians in rendering care.
All of the authors in the articles cited argue for greater regulation of unsupervised PEs to prevent performance of procedures where they lack expertise. Although the regulatory approach is sensible, it is more important to ensure that patients choose who gives them their medical care. They should not be obligated to see mid-level practitioners if they want to see a medical doctor. Above all, patients must be informed of the qualifications of those who provide their medical care. They should not be blindsided when they arrive for an appointment with their physician and find themselves shunted to a PE. We must not allow financial considerations to override the integrity of the medical care process.
What do you think is the optimal and safest role for PEs in a dermatology practice?
We want to know your views! Tell us what you think.
It is now common for patients to arrive in a physician office and never see the physician. Instead, patients are seen by so-called physician extenders. As our population ages, the need for medical care continues to grow beyond the capacity of the 900,000 US physicians that provide required services, particularly in the first level (primary care). The response to the physician shortage has entailed a variety of strategies. There has been a major immigration of foreign physicians, particularly from India; US medical schools have been encouraged to increase enrollment; and new medical schools have been inaugurated. Physicians have been pushed to adopt electronic medical records to permit increased throughput of patients in office practices. These multiple approaches have had an effect, though sometimes the results are undesirable. For example, complicated computer programs often detract from the physician-patient relationship.
One of the early solutions offered to deal with the doctor shortage in primary care was the concept of physician extenders (PEs), also called mid-level practitioners, who are professionals trained to take on a number of the simpler tasks performed by physicians. There are 2 basic classes of PEs: nurse practitioners and physician assistants. Nurse practitioners are originally trained to perform nursing but then undertake a course of study including scientific courses and clinical exposure to various parts of medicine. Physician assistants receive similar training. The duration of training for PEs usually is 18 to 24 months, whereas physicians attend medical school for 4 years. Unlike physicians, mid-level practitioners do not enter physician postgraduate residency training programs, which last many years.
The original concept was that PEs would work side by side with physicians who would supervise the care provided by the PEs. This team concept was designed to free physicians from the more mundane aspects of medical care and allow them to focus on the more challenging diagnostic and therapeutic issues presented by individual patients. In an era in which the burden of documentation has become increasingly onerous, the assistance of paraprofessionals can spare physicians the entry of redundant details in electronic databases that do not contribute to patient welfare.
However, research suggests that the concept of mid-level providers undertaking first-level care side by side with physicians has diverged from the original goal. An article by Coldiron and Ratnarathorn (JAMA Dermatol. 2014;150:1153-1159) studied Medicare billing data. The authors discovered that a variety of activities, many with higher reimbursement than primary care, were billed directly by PEs without apparent physician involvement, including a large number of complex invasive procedures, more than half in dermatology. Their article focused on dermatologic procedures, such as the destruction of skin cancers and advanced surgical repairs, but they listed many other procedures that are typically in the domain of highly trained physicians, including radiologic interpretations such as mammography and joint injections such as spinal injections. The data they presented were substantiated by publications in the medical literature suggesting that mid-level providers at certain hospitals even perform heart catheterizations and gastrointestinal endoscopies.
There have been no apologies for the unsupervised conduct of physician activities by nonphysicians. On the contrary, many PEs claim to be as well trained and proficient as medical doctors. Coldiron and Ratnarathorn argued otherwise. They pointed out that physicians receive an average of 10,000 hours of training compared to 2000 hours for mid-level practitioners, and they raised concerns about misdiagnoses, complications, and unnecessary procedures performed by PEs without supervision. In an editorial, Jalian and Avram (JAMA Dermatol. 2014;150:1149-1151) pointed out that a disproportionate number of cases of lawsuits for laser-induced injuries are related to performance by nonphysicians.
The pressures to allow nonphysicians to practice medicine independently are increasing. There is a shortage of physicians, especially in states such as Massachusetts that have substantial governmental limitation of physician reimbursement. In Massachusetts, regulations encourage mid-level practitioners to practice without physician supervision and even call themselves “doctors.” Furthermore, hospitals have faced residency funding cuts by Medicare and have had regulatory limitation of work hours by medical doctors in residency training. As a result, many institutions have turned to PEs to perform procedures that are typically performed by medical doctors.
Perhaps the greatest pressure favoring use of nonphysicians is financial. Mid-level practitioners receive lower salaries, typically 45% less, than medical doctors. In an era in which lowering costs has supplanted the goal of offering the best medical care possible, the attraction of replacement of a physician by a professional with less training becomes irresistible. It also is of concern that many physicians ignore the requirement to supervise the work of mid-level practitioners to maximize profit. Physicians often hire a mid-level provider rather than finding another physician to partner in their practice. Patients referred to a dermatologist often are seen by a PE and never even see the physician.
The concept of PEs working in a team with physicians remains an excellent approach to remedying the shortage of medical doctors, but we need to return to the original plan. Physician extenders should perform primary care rather than complex and lucrative subspecialties. There must be adequate supervision and definitely participation by physicians in rendering care.
All of the authors in the articles cited argue for greater regulation of unsupervised PEs to prevent performance of procedures where they lack expertise. Although the regulatory approach is sensible, it is more important to ensure that patients choose who gives them their medical care. They should not be obligated to see mid-level practitioners if they want to see a medical doctor. Above all, patients must be informed of the qualifications of those who provide their medical care. They should not be blindsided when they arrive for an appointment with their physician and find themselves shunted to a PE. We must not allow financial considerations to override the integrity of the medical care process.
What do you think is the optimal and safest role for PEs in a dermatology practice?
We want to know your views! Tell us what you think.

Bringing a baby to the office
I’ve previously written about how my secretary took 8 weeks off for maternity leave. Well, she’s back now, and brought a new staff member with her.
I know several doctors who are horrified that I let her bring the baby to work every day. They tell me it’s unprofessional, a distraction, inconvenient, etc.

Me? I think it’s great.
I have no problem with her being here. If anything, she adds an upbeat vibe to the office. Seeing an adorable newborn up front cheers all comers. She’s quickly become the most popular person here. Nowadays, when I call someone back from the lobby, they jokingly protest and say, but “I’m looking at the baby!” At this point, we’ve even had people coming by just to see her, once word spread there was a baby at my office.
Is it unprofessional? Maybe by someone else’s standards, but not mine. At this stage of life, she’s certainly not in the way. She’s (generally) quiet, sweet, and smiley. Besides, having her here spares my secretary the expense of child care and makes her happy. If keeping your staff happy isn’t part of being professional, I don’t know what is.
Is she a distraction? Perhaps, but not in a bad way. Maybe I take a few seconds here and there to wave at her or help my secretary with something, but nothing that compromises patient care.

Is it inconvenient to have her here? Nope. We have an extra exam room, so it’s easy for my secretary to have a quiet, private place to feed and change her every few hours. If the phones go to voice mail for a few minutes, or I have to keep an ear out for the front door opening, I don’t mind.
She and I both have young families. When we were looking for a new office 3 years ago, one of our requirements was what we called “the sick kid room.” An extra space where, if a kid couldn’t go to school, we wouldn’t be stuck trying to figure out what to do. They’ve always been welcome here, and always will be.
Having kids on site isn’t perfect for every practice. Certainly, a pediatrics office (with a lot more sick kids going in and out) wouldn’t be ideal. But at my place the young lady has brightened things up for all and makes the day more fun.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’ve previously written about how my secretary took 8 weeks off for maternity leave. Well, she’s back now, and brought a new staff member with her.
I know several doctors who are horrified that I let her bring the baby to work every day. They tell me it’s unprofessional, a distraction, inconvenient, etc.
Me? I think it’s great.
I have no problem with her being here. If anything, she adds an upbeat vibe to the office. Seeing an adorable newborn up front cheers all comers. She’s quickly become the most popular person here. Nowadays, when I call someone back from the lobby, they jokingly protest and say, but “I’m looking at the baby!” At this point, we’ve even had people coming by just to see her, once word spread there was a baby at my office.
Is it unprofessional? Maybe by someone else’s standards, but not mine. At this stage of life, she’s certainly not in the way. She’s (generally) quiet, sweet, and smiley. Besides, having her here spares my secretary the expense of child care and makes her happy. If keeping your staff happy isn’t part of being professional, I don’t know what is.
Is she a distraction? Perhaps, but not in a bad way. Maybe I take a few seconds here and there to wave at her or help my secretary with something, but nothing that compromises patient care.
Is it inconvenient to have her here? Nope. We have an extra exam room, so it’s easy for my secretary to have a quiet, private place to feed and change her every few hours. If the phones go to voice mail for a few minutes, or I have to keep an ear out for the front door opening, I don’t mind.
She and I both have young families. When we were looking for a new office 3 years ago, one of our requirements was what we called “the sick kid room.” An extra space where, if a kid couldn’t go to school, we wouldn’t be stuck trying to figure out what to do. They’ve always been welcome here, and always will be.
Having kids on site isn’t perfect for every practice. Certainly, a pediatrics office (with a lot more sick kids going in and out) wouldn’t be ideal. But at my place the young lady has brightened things up for all and makes the day more fun.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’ve previously written about how my secretary took 8 weeks off for maternity leave. Well, she’s back now, and brought a new staff member with her.
I know several doctors who are horrified that I let her bring the baby to work every day. They tell me it’s unprofessional, a distraction, inconvenient, etc.
Me? I think it’s great.
I have no problem with her being here. If anything, she adds an upbeat vibe to the office. Seeing an adorable newborn up front cheers all comers. She’s quickly become the most popular person here. Nowadays, when I call someone back from the lobby, they jokingly protest and say, but “I’m looking at the baby!” At this point, we’ve even had people coming by just to see her, once word spread there was a baby at my office.
Is it unprofessional? Maybe by someone else’s standards, but not mine. At this stage of life, she’s certainly not in the way. She’s (generally) quiet, sweet, and smiley. Besides, having her here spares my secretary the expense of child care and makes her happy. If keeping your staff happy isn’t part of being professional, I don’t know what is.
Is she a distraction? Perhaps, but not in a bad way. Maybe I take a few seconds here and there to wave at her or help my secretary with something, but nothing that compromises patient care.
Is it inconvenient to have her here? Nope. We have an extra exam room, so it’s easy for my secretary to have a quiet, private place to feed and change her every few hours. If the phones go to voice mail for a few minutes, or I have to keep an ear out for the front door opening, I don’t mind.
She and I both have young families. When we were looking for a new office 3 years ago, one of our requirements was what we called “the sick kid room.” An extra space where, if a kid couldn’t go to school, we wouldn’t be stuck trying to figure out what to do. They’ve always been welcome here, and always will be.
Having kids on site isn’t perfect for every practice. Certainly, a pediatrics office (with a lot more sick kids going in and out) wouldn’t be ideal. But at my place the young lady has brightened things up for all and makes the day more fun.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
