User login
EpiPen cost increases far exceed overall medical inflation
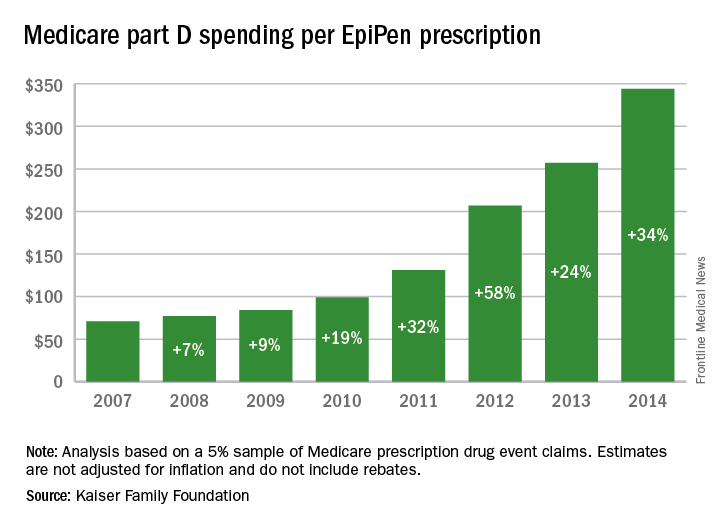
Total Medicare part D spending on EpiPen auto-injectors rose from $7.0 million in 2007 to $87.9 million in 2014 – an increase of 1,151%, according to an analysis released Sept. 20 by the Kaiser Family Foundation.
The number of EpiPen users also increased over that time, however, bringing with it a commensurate 159% rise in the number of prescriptions. Those two trends took the average cost of a single EpiPen prescription from $71 in 2007 to $344 in 2014, the Kaiser analysis showed.
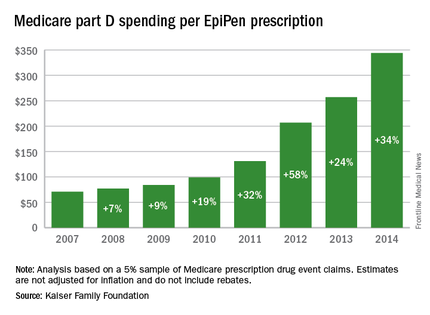
That increase in cost per prescription did not fail to at least double overall medical care price inflation for each year from 2008 to 2014. In 2008, when the two trends were closest together, the EpiPen cost per prescription rose 7.4% from the year before, compared with 3.7% for overall medical spending. In 2014, Medicare part D’s cost for an EpiPen prescription rose 34% from the year before, which was 14 times higher than the 2.4% increase in total medical spending, Kaiser noted.
The analysis was based on a 5% sample of Medicare prescription drug event claims and included beneficiaries who had a least 1 month of part D coverage and one EpiPen prescription during the year. Estimates are not adjusted for inflation and do not include any possible manufacturer discounts, Kaiser said.
Total Medicare part D spending on EpiPen auto-injectors rose from $7.0 million in 2007 to $87.9 million in 2014 – an increase of 1,151%, according to an analysis released Sept. 20 by the Kaiser Family Foundation.
The number of EpiPen users also increased over that time, however, bringing with it a commensurate 159% rise in the number of prescriptions. Those two trends took the average cost of a single EpiPen prescription from $71 in 2007 to $344 in 2014, the Kaiser analysis showed.
That increase in cost per prescription did not fail to at least double overall medical care price inflation for each year from 2008 to 2014. In 2008, when the two trends were closest together, the EpiPen cost per prescription rose 7.4% from the year before, compared with 3.7% for overall medical spending. In 2014, Medicare part D’s cost for an EpiPen prescription rose 34% from the year before, which was 14 times higher than the 2.4% increase in total medical spending, Kaiser noted.
The analysis was based on a 5% sample of Medicare prescription drug event claims and included beneficiaries who had a least 1 month of part D coverage and one EpiPen prescription during the year. Estimates are not adjusted for inflation and do not include any possible manufacturer discounts, Kaiser said.
Total Medicare part D spending on EpiPen auto-injectors rose from $7.0 million in 2007 to $87.9 million in 2014 – an increase of 1,151%, according to an analysis released Sept. 20 by the Kaiser Family Foundation.
The number of EpiPen users also increased over that time, however, bringing with it a commensurate 159% rise in the number of prescriptions. Those two trends took the average cost of a single EpiPen prescription from $71 in 2007 to $344 in 2014, the Kaiser analysis showed.
That increase in cost per prescription did not fail to at least double overall medical care price inflation for each year from 2008 to 2014. In 2008, when the two trends were closest together, the EpiPen cost per prescription rose 7.4% from the year before, compared with 3.7% for overall medical spending. In 2014, Medicare part D’s cost for an EpiPen prescription rose 34% from the year before, which was 14 times higher than the 2.4% increase in total medical spending, Kaiser noted.
The analysis was based on a 5% sample of Medicare prescription drug event claims and included beneficiaries who had a least 1 month of part D coverage and one EpiPen prescription during the year. Estimates are not adjusted for inflation and do not include any possible manufacturer discounts, Kaiser said.
Legislators: Investigate Medicare fraud before paying doctors
Republican leaders in Congress are calling on CMS to impose stricter safeguards against fraudulent Medicare billing by physicians.
The chairmen of the Senate Finance Committee, the House Ways and Means and Energy and Commerce Committees, and the chairmen of key House subcommittees said that the Centers for Medicare & Medicaid Services relies too heavily on the “outdated” pay and chase method and should focus more energy on preventing payment for potential fraudulent claims.
“Improper payments remain an enormous problem for the Medicare program,” the chairmen wrote in a Sept. 12 letter to Acting CMS Administrator Andy Slavitt. “In 2015, the Medicare program had an error rate of 12.1% or $43.3 billion dollars. The billions of dollars lost to Medicare fraud each year underscore the importance of stopping potentially fraudulent payments before they’re made,”

Some health law experts, however, argue that CMS already has a process for in place for pre-identifying inaccurate claims via prepayment audits and reviews. Such efforts can be devastating for physicians who come under scrutiny for unintentional mistakes, said Daniel F. Shay, a Philadelphia health law attorney.
“I can understand why, particularly in an election year, elected officials might send a letter reiterating the need to curb ‘waste, fraud, and abuse,’” Mr. Shay said in an interview. “It’s true that it’s more efficient for the government to investigate a physician’s claim for reimbursement first, and then pay. However, I think we have to take into account the physicians’ perspective, especially physicians in smaller, independent practices.”
The legislators’ letter acknowledges that CMS has taken some proactive steps to prevent health fraud, including creation of the Fraud Prevention System (FPS), which highlights questionable billing patterns and identifies providers who pose high risk to the program. FPS runs analytics on 4.5 million claims daily and has led to more than $820 million in savings, according to CMS. However, legislators said they are still concerned that CMS too often pays claims before investigating whether they’re false. The letter requests that CMS clarify its implementation of the FPS program, including details on fraud investigations and how the agency monitors FPS’s effectiveness.

Houston, Tex.–based health law attorney Michael E. Clark disagrees that CMS is overusing the pay-and-chase method. Quite the contrary, he said.
“The federal government cannot seem to find the right balance on how to address program fraud,” Mr. Clark said in an interview. “While ‘pay and chase’ once was a problem, now the government can effectively destroy health care service providers under a very low threshold without the businesses having a meaningful right to appeal that determination.”
Specifically, CMS can withhold Medicare reimbursement from health providers under an amended 2011 law that permits payments to be suppressed when “credible” allegations of fraud have been made, but are disputed. The term “credible” is a new, lower standard for the administrative action, which was meant to address the pay-and-chase problem, Mr. Clark said. The law defines a “credible allegation of fraud” as an allegation from any source, including but not limited to fraud hotline complaints, data mining of claims, patterns identified through provider audits, civil false claims cases, and law enforcement investigations.
“That standard is easy to meet and agencies have every incentive to claim they’ve got so-called credible allegations of fraud in order to avoid being criticized later on for not preventing the monies from being dissipated,” he said. Because the law precludes health providers from appealing the fraud allegation to a federal court until all administrative remedies have been exhausted, “a health care services provider can quickly be put out of business, even if it turns out that the investigation proves not to be actionable.”
Prepayment reviews of claims can drag on for months, severely impacting a physician’s income, Mr. Shay added. In his experience, the majority of physicians under investigation are not trying to game the system, but rather don’t understand all of the administrative requirements related to filing claims. In some cases, the physicians’ notes are not complete, their bills are too high for services provided, or not enough documentation exists to support medical necessity.
“In the midst of that, you have doctors who are likely well-meaning, who have provided a service to a patient in need, and who are facing real economic hardship without an effective mechanism to challenge or end the prepayment review process,” he said.
Rather than more prepayment investigations, Mr. Shay would like to see CMS focus on physician education.
There needs to be “more emphasis on provider education in terms of compliance with program requirements,” he said. “It shouldn’t require a lawyer getting involved to find out what specifically [CMS] wants them to do. That should be part of the process as a standard.”
On Twitter @legal_med
Republican leaders in Congress are calling on CMS to impose stricter safeguards against fraudulent Medicare billing by physicians.
The chairmen of the Senate Finance Committee, the House Ways and Means and Energy and Commerce Committees, and the chairmen of key House subcommittees said that the Centers for Medicare & Medicaid Services relies too heavily on the “outdated” pay and chase method and should focus more energy on preventing payment for potential fraudulent claims.
“Improper payments remain an enormous problem for the Medicare program,” the chairmen wrote in a Sept. 12 letter to Acting CMS Administrator Andy Slavitt. “In 2015, the Medicare program had an error rate of 12.1% or $43.3 billion dollars. The billions of dollars lost to Medicare fraud each year underscore the importance of stopping potentially fraudulent payments before they’re made,”
Some health law experts, however, argue that CMS already has a process for in place for pre-identifying inaccurate claims via prepayment audits and reviews. Such efforts can be devastating for physicians who come under scrutiny for unintentional mistakes, said Daniel F. Shay, a Philadelphia health law attorney.
“I can understand why, particularly in an election year, elected officials might send a letter reiterating the need to curb ‘waste, fraud, and abuse,’” Mr. Shay said in an interview. “It’s true that it’s more efficient for the government to investigate a physician’s claim for reimbursement first, and then pay. However, I think we have to take into account the physicians’ perspective, especially physicians in smaller, independent practices.”
The legislators’ letter acknowledges that CMS has taken some proactive steps to prevent health fraud, including creation of the Fraud Prevention System (FPS), which highlights questionable billing patterns and identifies providers who pose high risk to the program. FPS runs analytics on 4.5 million claims daily and has led to more than $820 million in savings, according to CMS. However, legislators said they are still concerned that CMS too often pays claims before investigating whether they’re false. The letter requests that CMS clarify its implementation of the FPS program, including details on fraud investigations and how the agency monitors FPS’s effectiveness.
Houston, Tex.–based health law attorney Michael E. Clark disagrees that CMS is overusing the pay-and-chase method. Quite the contrary, he said.
“The federal government cannot seem to find the right balance on how to address program fraud,” Mr. Clark said in an interview. “While ‘pay and chase’ once was a problem, now the government can effectively destroy health care service providers under a very low threshold without the businesses having a meaningful right to appeal that determination.”
Specifically, CMS can withhold Medicare reimbursement from health providers under an amended 2011 law that permits payments to be suppressed when “credible” allegations of fraud have been made, but are disputed. The term “credible” is a new, lower standard for the administrative action, which was meant to address the pay-and-chase problem, Mr. Clark said. The law defines a “credible allegation of fraud” as an allegation from any source, including but not limited to fraud hotline complaints, data mining of claims, patterns identified through provider audits, civil false claims cases, and law enforcement investigations.
“That standard is easy to meet and agencies have every incentive to claim they’ve got so-called credible allegations of fraud in order to avoid being criticized later on for not preventing the monies from being dissipated,” he said. Because the law precludes health providers from appealing the fraud allegation to a federal court until all administrative remedies have been exhausted, “a health care services provider can quickly be put out of business, even if it turns out that the investigation proves not to be actionable.”
Prepayment reviews of claims can drag on for months, severely impacting a physician’s income, Mr. Shay added. In his experience, the majority of physicians under investigation are not trying to game the system, but rather don’t understand all of the administrative requirements related to filing claims. In some cases, the physicians’ notes are not complete, their bills are too high for services provided, or not enough documentation exists to support medical necessity.
“In the midst of that, you have doctors who are likely well-meaning, who have provided a service to a patient in need, and who are facing real economic hardship without an effective mechanism to challenge or end the prepayment review process,” he said.
Rather than more prepayment investigations, Mr. Shay would like to see CMS focus on physician education.
There needs to be “more emphasis on provider education in terms of compliance with program requirements,” he said. “It shouldn’t require a lawyer getting involved to find out what specifically [CMS] wants them to do. That should be part of the process as a standard.”
On Twitter @legal_med
Republican leaders in Congress are calling on CMS to impose stricter safeguards against fraudulent Medicare billing by physicians.
The chairmen of the Senate Finance Committee, the House Ways and Means and Energy and Commerce Committees, and the chairmen of key House subcommittees said that the Centers for Medicare & Medicaid Services relies too heavily on the “outdated” pay and chase method and should focus more energy on preventing payment for potential fraudulent claims.
“Improper payments remain an enormous problem for the Medicare program,” the chairmen wrote in a Sept. 12 letter to Acting CMS Administrator Andy Slavitt. “In 2015, the Medicare program had an error rate of 12.1% or $43.3 billion dollars. The billions of dollars lost to Medicare fraud each year underscore the importance of stopping potentially fraudulent payments before they’re made,”
Some health law experts, however, argue that CMS already has a process for in place for pre-identifying inaccurate claims via prepayment audits and reviews. Such efforts can be devastating for physicians who come under scrutiny for unintentional mistakes, said Daniel F. Shay, a Philadelphia health law attorney.
“I can understand why, particularly in an election year, elected officials might send a letter reiterating the need to curb ‘waste, fraud, and abuse,’” Mr. Shay said in an interview. “It’s true that it’s more efficient for the government to investigate a physician’s claim for reimbursement first, and then pay. However, I think we have to take into account the physicians’ perspective, especially physicians in smaller, independent practices.”
The legislators’ letter acknowledges that CMS has taken some proactive steps to prevent health fraud, including creation of the Fraud Prevention System (FPS), which highlights questionable billing patterns and identifies providers who pose high risk to the program. FPS runs analytics on 4.5 million claims daily and has led to more than $820 million in savings, according to CMS. However, legislators said they are still concerned that CMS too often pays claims before investigating whether they’re false. The letter requests that CMS clarify its implementation of the FPS program, including details on fraud investigations and how the agency monitors FPS’s effectiveness.
Houston, Tex.–based health law attorney Michael E. Clark disagrees that CMS is overusing the pay-and-chase method. Quite the contrary, he said.
“The federal government cannot seem to find the right balance on how to address program fraud,” Mr. Clark said in an interview. “While ‘pay and chase’ once was a problem, now the government can effectively destroy health care service providers under a very low threshold without the businesses having a meaningful right to appeal that determination.”
Specifically, CMS can withhold Medicare reimbursement from health providers under an amended 2011 law that permits payments to be suppressed when “credible” allegations of fraud have been made, but are disputed. The term “credible” is a new, lower standard for the administrative action, which was meant to address the pay-and-chase problem, Mr. Clark said. The law defines a “credible allegation of fraud” as an allegation from any source, including but not limited to fraud hotline complaints, data mining of claims, patterns identified through provider audits, civil false claims cases, and law enforcement investigations.
“That standard is easy to meet and agencies have every incentive to claim they’ve got so-called credible allegations of fraud in order to avoid being criticized later on for not preventing the monies from being dissipated,” he said. Because the law precludes health providers from appealing the fraud allegation to a federal court until all administrative remedies have been exhausted, “a health care services provider can quickly be put out of business, even if it turns out that the investigation proves not to be actionable.”
Prepayment reviews of claims can drag on for months, severely impacting a physician’s income, Mr. Shay added. In his experience, the majority of physicians under investigation are not trying to game the system, but rather don’t understand all of the administrative requirements related to filing claims. In some cases, the physicians’ notes are not complete, their bills are too high for services provided, or not enough documentation exists to support medical necessity.
“In the midst of that, you have doctors who are likely well-meaning, who have provided a service to a patient in need, and who are facing real economic hardship without an effective mechanism to challenge or end the prepayment review process,” he said.
Rather than more prepayment investigations, Mr. Shay would like to see CMS focus on physician education.
There needs to be “more emphasis on provider education in terms of compliance with program requirements,” he said. “It shouldn’t require a lawyer getting involved to find out what specifically [CMS] wants them to do. That should be part of the process as a standard.”
On Twitter @legal_med

Innovation and Cancer Moonshot Highlight AVAHO Conference
The 12th annual Association of VA Hematology/Oncology (AVAHO) Meeting, which begins Friday, September 23 in Dallas, Texas, will present a broad range of topics that focus on innovations in both treatment and patient care. “Innovations are not a one-trick pony,” as William Wachsman, MD, PhD, AVAHO program chair pointed out. “We are broadening how we approach innovations for the entire AVAHO constituency.”
Geoffrey Ling, MD, PhD, director, Defense Advanced Research Projects Agency (DARPA) Biological Technologies Office will be the opening keynote speaker and will offer a peak into the future of the health care technologies being pioneered by the Department of Defense’s advanced research program. Dr. Lin is the office’s founding director and leads a group of scientists working to transform health care, synthetic biology, neuroscience, and other critical biological areas.
In the second keynote address, Deborah Mayer, RN, PhD, AOCN; professor, School of Nursing at the University of North Carolina’s Lineberger Comprehensive Cancer Center will discuss cancer survivorship and how it fits into the cancer moonshot initiative. Dr. Mayer was named to the Moonshot Blue Ribbon Panel earlier this year. Listen to an exclusive interview with Dr. Mayer below.
Click here for more information on the meeting and the complete agenda.
The 12th annual Association of VA Hematology/Oncology (AVAHO) Meeting, which begins Friday, September 23 in Dallas, Texas, will present a broad range of topics that focus on innovations in both treatment and patient care. “Innovations are not a one-trick pony,” as William Wachsman, MD, PhD, AVAHO program chair pointed out. “We are broadening how we approach innovations for the entire AVAHO constituency.”
Geoffrey Ling, MD, PhD, director, Defense Advanced Research Projects Agency (DARPA) Biological Technologies Office will be the opening keynote speaker and will offer a peak into the future of the health care technologies being pioneered by the Department of Defense’s advanced research program. Dr. Lin is the office’s founding director and leads a group of scientists working to transform health care, synthetic biology, neuroscience, and other critical biological areas.
In the second keynote address, Deborah Mayer, RN, PhD, AOCN; professor, School of Nursing at the University of North Carolina’s Lineberger Comprehensive Cancer Center will discuss cancer survivorship and how it fits into the cancer moonshot initiative. Dr. Mayer was named to the Moonshot Blue Ribbon Panel earlier this year. Listen to an exclusive interview with Dr. Mayer below.
Click here for more information on the meeting and the complete agenda.
The 12th annual Association of VA Hematology/Oncology (AVAHO) Meeting, which begins Friday, September 23 in Dallas, Texas, will present a broad range of topics that focus on innovations in both treatment and patient care. “Innovations are not a one-trick pony,” as William Wachsman, MD, PhD, AVAHO program chair pointed out. “We are broadening how we approach innovations for the entire AVAHO constituency.”
Geoffrey Ling, MD, PhD, director, Defense Advanced Research Projects Agency (DARPA) Biological Technologies Office will be the opening keynote speaker and will offer a peak into the future of the health care technologies being pioneered by the Department of Defense’s advanced research program. Dr. Lin is the office’s founding director and leads a group of scientists working to transform health care, synthetic biology, neuroscience, and other critical biological areas.
In the second keynote address, Deborah Mayer, RN, PhD, AOCN; professor, School of Nursing at the University of North Carolina’s Lineberger Comprehensive Cancer Center will discuss cancer survivorship and how it fits into the cancer moonshot initiative. Dr. Mayer was named to the Moonshot Blue Ribbon Panel earlier this year. Listen to an exclusive interview with Dr. Mayer below.
Click here for more information on the meeting and the complete agenda.
President Anita Aggarwal Welcomes Members to the 12th Annual Meeting of AVAHO
I’d like to personally welcome each of you to the 12th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO). It’s an exciting time for AVAHO as we continue to grow and adapt, remaining always receptive, motivated and responsive to our member’s needs.
With more than 630 members nationwide, AVAHO is a membership-driven association. AVAHO members make a difference in the lives of their Veteran patients as an integral part of the health care team. Our current membership includes advanced practice nurses, cancer registrars, medical hematologists and oncologists, pharmacists, physician assistants, registered nurses, radiation oncologists, social workers, surgical oncologists, and other allied health professionals. Our focus on the whole health care team is unique and remains a core aspect of our mission.
The explosion of new technologies for the screening, diagnosis, and treatment of cancer is why we chose the 2016 Annual Meeting theme “Innovation in Hematology and Cancer Care.” By sharing new insights, we can make faster strides against cancer and take better care of our unique Veteran population. Now is the time when we need to adopt new technologies and design studies with new models of providing cancer care to Veterans. Change is inevitable, let’s get out in front and lead.
Data presented at the 2016 Annual Meeting will highlight innovation and technological advances that can improve every aspect of the patient experience—from prevention to diagnosis, treatment, and survivorship.
Based on feedback from last year’s annual meeting and strategic discussions at AVAHO Board meetings, we have embarked on a visionary plan to continue to expand AVAHO’s reach and impact well beyond the annual meeting. We will be sharing with you many of our new initiatives over the next few days. We can only succeed if you are a part of our plan. Please consider how you will be an ACTIVE member!
Sponsor support helps AVAHO advance our mission, broaden our programs, and enhance our member benefits. AVAHO members enjoy the benefits of the sponsored meeting and other activities. As part of its strategic plan, AVAHO plans to broaden our scope and programs, which will necessitate additional funding. Our sponsors, exhibitors and donors are critical to AVAHO’s success. You can help too—don't forget to visit our exhibitors and thank them for supporting our programs. Let us know if you have leads for new sponsors.
Cancer care involves an entire community of caregivers working together on all aspects of the patient’s treatment. The 2016 AVAHO Annual Meeting is a transformative opportunity to learn the latest strategies that can be used in your practice settings.
Thank you for joining me in Dallas where our inspired members have come together to learn, network and advance the mission of AVAHO to provide leadership in delivering quality comprehensive care to Veterans with cancer.
I’d like to personally welcome each of you to the 12th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO). It’s an exciting time for AVAHO as we continue to grow and adapt, remaining always receptive, motivated and responsive to our member’s needs.
With more than 630 members nationwide, AVAHO is a membership-driven association. AVAHO members make a difference in the lives of their Veteran patients as an integral part of the health care team. Our current membership includes advanced practice nurses, cancer registrars, medical hematologists and oncologists, pharmacists, physician assistants, registered nurses, radiation oncologists, social workers, surgical oncologists, and other allied health professionals. Our focus on the whole health care team is unique and remains a core aspect of our mission.
The explosion of new technologies for the screening, diagnosis, and treatment of cancer is why we chose the 2016 Annual Meeting theme “Innovation in Hematology and Cancer Care.” By sharing new insights, we can make faster strides against cancer and take better care of our unique Veteran population. Now is the time when we need to adopt new technologies and design studies with new models of providing cancer care to Veterans. Change is inevitable, let’s get out in front and lead.
Data presented at the 2016 Annual Meeting will highlight innovation and technological advances that can improve every aspect of the patient experience—from prevention to diagnosis, treatment, and survivorship.
Based on feedback from last year’s annual meeting and strategic discussions at AVAHO Board meetings, we have embarked on a visionary plan to continue to expand AVAHO’s reach and impact well beyond the annual meeting. We will be sharing with you many of our new initiatives over the next few days. We can only succeed if you are a part of our plan. Please consider how you will be an ACTIVE member!
Sponsor support helps AVAHO advance our mission, broaden our programs, and enhance our member benefits. AVAHO members enjoy the benefits of the sponsored meeting and other activities. As part of its strategic plan, AVAHO plans to broaden our scope and programs, which will necessitate additional funding. Our sponsors, exhibitors and donors are critical to AVAHO’s success. You can help too—don't forget to visit our exhibitors and thank them for supporting our programs. Let us know if you have leads for new sponsors.
Cancer care involves an entire community of caregivers working together on all aspects of the patient’s treatment. The 2016 AVAHO Annual Meeting is a transformative opportunity to learn the latest strategies that can be used in your practice settings.
Thank you for joining me in Dallas where our inspired members have come together to learn, network and advance the mission of AVAHO to provide leadership in delivering quality comprehensive care to Veterans with cancer.
I’d like to personally welcome each of you to the 12th Annual Meeting of the Association of VA Hematology/Oncology (AVAHO). It’s an exciting time for AVAHO as we continue to grow and adapt, remaining always receptive, motivated and responsive to our member’s needs.
With more than 630 members nationwide, AVAHO is a membership-driven association. AVAHO members make a difference in the lives of their Veteran patients as an integral part of the health care team. Our current membership includes advanced practice nurses, cancer registrars, medical hematologists and oncologists, pharmacists, physician assistants, registered nurses, radiation oncologists, social workers, surgical oncologists, and other allied health professionals. Our focus on the whole health care team is unique and remains a core aspect of our mission.
The explosion of new technologies for the screening, diagnosis, and treatment of cancer is why we chose the 2016 Annual Meeting theme “Innovation in Hematology and Cancer Care.” By sharing new insights, we can make faster strides against cancer and take better care of our unique Veteran population. Now is the time when we need to adopt new technologies and design studies with new models of providing cancer care to Veterans. Change is inevitable, let’s get out in front and lead.
Data presented at the 2016 Annual Meeting will highlight innovation and technological advances that can improve every aspect of the patient experience—from prevention to diagnosis, treatment, and survivorship.
Based on feedback from last year’s annual meeting and strategic discussions at AVAHO Board meetings, we have embarked on a visionary plan to continue to expand AVAHO’s reach and impact well beyond the annual meeting. We will be sharing with you many of our new initiatives over the next few days. We can only succeed if you are a part of our plan. Please consider how you will be an ACTIVE member!
Sponsor support helps AVAHO advance our mission, broaden our programs, and enhance our member benefits. AVAHO members enjoy the benefits of the sponsored meeting and other activities. As part of its strategic plan, AVAHO plans to broaden our scope and programs, which will necessitate additional funding. Our sponsors, exhibitors and donors are critical to AVAHO’s success. You can help too—don't forget to visit our exhibitors and thank them for supporting our programs. Let us know if you have leads for new sponsors.
Cancer care involves an entire community of caregivers working together on all aspects of the patient’s treatment. The 2016 AVAHO Annual Meeting is a transformative opportunity to learn the latest strategies that can be used in your practice settings.
Thank you for joining me in Dallas where our inspired members have come together to learn, network and advance the mission of AVAHO to provide leadership in delivering quality comprehensive care to Veterans with cancer.
3 Ways to Enjoy Dallas
From Friday September 23 through Sunday September 25, the 12th Annual Association of VA Hematology and Oncology Meeting will be held in Dallas, Texas. Not sure what to do outside the meeting? Depending on the type of traveler you are, here is a short list of activities to help you decide.
1. Spend Less, Do More
Just because you’re on a trip doesn’t mean you have to burn a hole in your wallet to enjoy it! If you’re looking to absorb some culture, the Dallas Museum of Art has exhibits and collections from 18th century Rome to modern Texas. If you explore the Dallas Farmers Market, you’ll easily find yourself enthralled by local and specialty produce and cooking demonstrations. But if you can’t resist shopping, pay a visit to the Neiman Marcus flagship store, built in 1914. There are multiple other activities to participate in and around the city for little-to-no cost. Find a list of 50 free things you can do in Dallas here: https://www.tourtexas.com/destinations/50-free-things-to-do-in-Dallas.
2. Eat Away
To get to know a place, you have to immerse yourself in the food. Dallas has no shortage of flavors you can experience. Rich with cultural influences from all over the globe, the variety of cuisines in this city will not disappoint you. In Dallas, traditional Tex-Mex enchiladas, Deep South chicken-fried steak, authentic Vietnamese Pho, and so much more are within reach. Those are just some of the must-have foods to try in Dallas during your trip. Thrillist.com has the entire list of them at https://www.thrillist.com/eat/dallas/the-50-best-things-to-eat-in-dallas.
3. Be One With Nature
Being at peace with nature can be a great break from the busy buzz of the meeting. If enjoying the great outdoors is more your speed, Dallas Park & Recreation offers various features and amenities, such as White Rock Lake, which has 1,015 acres to enjoy. If you’re interested in learning about wildlife and botanical collections, the Texas Discovery Gardens has everything you’re looking for. With 125 miles of trail and 23,242 acres of developed and underdeveloped parkland, there is always someplace in Dallas for you to unwind. For more information on Dallas Park & Recreation, visit http://dallasparks.org.
For additional ways to enjoy Dallas, visit http://www.visitdallas.com.
See you at the 2016 AVAHO Meeting!
From Friday September 23 through Sunday September 25, the 12th Annual Association of VA Hematology and Oncology Meeting will be held in Dallas, Texas. Not sure what to do outside the meeting? Depending on the type of traveler you are, here is a short list of activities to help you decide.
1. Spend Less, Do More
Just because you’re on a trip doesn’t mean you have to burn a hole in your wallet to enjoy it! If you’re looking to absorb some culture, the Dallas Museum of Art has exhibits and collections from 18th century Rome to modern Texas. If you explore the Dallas Farmers Market, you’ll easily find yourself enthralled by local and specialty produce and cooking demonstrations. But if you can’t resist shopping, pay a visit to the Neiman Marcus flagship store, built in 1914. There are multiple other activities to participate in and around the city for little-to-no cost. Find a list of 50 free things you can do in Dallas here: https://www.tourtexas.com/destinations/50-free-things-to-do-in-Dallas.
2. Eat Away
To get to know a place, you have to immerse yourself in the food. Dallas has no shortage of flavors you can experience. Rich with cultural influences from all over the globe, the variety of cuisines in this city will not disappoint you. In Dallas, traditional Tex-Mex enchiladas, Deep South chicken-fried steak, authentic Vietnamese Pho, and so much more are within reach. Those are just some of the must-have foods to try in Dallas during your trip. Thrillist.com has the entire list of them at https://www.thrillist.com/eat/dallas/the-50-best-things-to-eat-in-dallas.
3. Be One With Nature
Being at peace with nature can be a great break from the busy buzz of the meeting. If enjoying the great outdoors is more your speed, Dallas Park & Recreation offers various features and amenities, such as White Rock Lake, which has 1,015 acres to enjoy. If you’re interested in learning about wildlife and botanical collections, the Texas Discovery Gardens has everything you’re looking for. With 125 miles of trail and 23,242 acres of developed and underdeveloped parkland, there is always someplace in Dallas for you to unwind. For more information on Dallas Park & Recreation, visit http://dallasparks.org.
For additional ways to enjoy Dallas, visit http://www.visitdallas.com.
See you at the 2016 AVAHO Meeting!
From Friday September 23 through Sunday September 25, the 12th Annual Association of VA Hematology and Oncology Meeting will be held in Dallas, Texas. Not sure what to do outside the meeting? Depending on the type of traveler you are, here is a short list of activities to help you decide.
1. Spend Less, Do More
Just because you’re on a trip doesn’t mean you have to burn a hole in your wallet to enjoy it! If you’re looking to absorb some culture, the Dallas Museum of Art has exhibits and collections from 18th century Rome to modern Texas. If you explore the Dallas Farmers Market, you’ll easily find yourself enthralled by local and specialty produce and cooking demonstrations. But if you can’t resist shopping, pay a visit to the Neiman Marcus flagship store, built in 1914. There are multiple other activities to participate in and around the city for little-to-no cost. Find a list of 50 free things you can do in Dallas here: https://www.tourtexas.com/destinations/50-free-things-to-do-in-Dallas.
2. Eat Away
To get to know a place, you have to immerse yourself in the food. Dallas has no shortage of flavors you can experience. Rich with cultural influences from all over the globe, the variety of cuisines in this city will not disappoint you. In Dallas, traditional Tex-Mex enchiladas, Deep South chicken-fried steak, authentic Vietnamese Pho, and so much more are within reach. Those are just some of the must-have foods to try in Dallas during your trip. Thrillist.com has the entire list of them at https://www.thrillist.com/eat/dallas/the-50-best-things-to-eat-in-dallas.
3. Be One With Nature
Being at peace with nature can be a great break from the busy buzz of the meeting. If enjoying the great outdoors is more your speed, Dallas Park & Recreation offers various features and amenities, such as White Rock Lake, which has 1,015 acres to enjoy. If you’re interested in learning about wildlife and botanical collections, the Texas Discovery Gardens has everything you’re looking for. With 125 miles of trail and 23,242 acres of developed and underdeveloped parkland, there is always someplace in Dallas for you to unwind. For more information on Dallas Park & Recreation, visit http://dallasparks.org.
For additional ways to enjoy Dallas, visit http://www.visitdallas.com.
See you at the 2016 AVAHO Meeting!
New Center Focuses on Environmental Health Disparities
Nearly half of the Native American population in the US lives in western states where there are an estimated 161,000 abandoned hardrock mines—including > 4,000 abandoned uranium mines. Because of their reliance on natural resources, these tribal communities have direct and frequent contact with metal mixtures through inhalation, drinking water, and eating food. Those exposures are exacerbated by disparities in infrastructure and unique social determinants of health from poverty in rural and isolated locations.
Related: Reducing Health Disparities With Performance Management
That’s the rationale behind the $1.5 million award to the University of New Mexico Health Sciences Center in Albuquerque to establish a Center for Native American Health Equity Research.effort by the Environmental Protection Agency ( EPA) and National Institutes of Health (NIH). The center will tackle those pervasive environmental health disparities with primary biomedical and environmental research and Native American-focused community engagement, says NIH.
The partners in the center are 3 University research programs and the Navajo, Sioux and Crow nations, with plans to expand to a fourth tribal region later. Together they will address research priorities such as examining the distribution of contaminants, cultural practices, and genetic origins of the 3 core tribes to provide a basis for “sorting out the health effects” of metal mixtures in tribal communities.
Related: Unraveling the Causes of Breast Cancer Disparities
The program also will build the research capacity, understanding of data, and interpretation and use of biomedical results across those communities, as well as developing a framework that characterizes the unique exposure pathways, EPA says. Ultimately, the hope is that the research will help define health from a perspective that not only reflects tribal perceptions, but is useful in informing regulatory decision making.
Nearly half of the Native American population in the US lives in western states where there are an estimated 161,000 abandoned hardrock mines—including > 4,000 abandoned uranium mines. Because of their reliance on natural resources, these tribal communities have direct and frequent contact with metal mixtures through inhalation, drinking water, and eating food. Those exposures are exacerbated by disparities in infrastructure and unique social determinants of health from poverty in rural and isolated locations.
Related: Reducing Health Disparities With Performance Management
That’s the rationale behind the $1.5 million award to the University of New Mexico Health Sciences Center in Albuquerque to establish a Center for Native American Health Equity Research.effort by the Environmental Protection Agency ( EPA) and National Institutes of Health (NIH). The center will tackle those pervasive environmental health disparities with primary biomedical and environmental research and Native American-focused community engagement, says NIH.
The partners in the center are 3 University research programs and the Navajo, Sioux and Crow nations, with plans to expand to a fourth tribal region later. Together they will address research priorities such as examining the distribution of contaminants, cultural practices, and genetic origins of the 3 core tribes to provide a basis for “sorting out the health effects” of metal mixtures in tribal communities.
Related: Unraveling the Causes of Breast Cancer Disparities
The program also will build the research capacity, understanding of data, and interpretation and use of biomedical results across those communities, as well as developing a framework that characterizes the unique exposure pathways, EPA says. Ultimately, the hope is that the research will help define health from a perspective that not only reflects tribal perceptions, but is useful in informing regulatory decision making.
Nearly half of the Native American population in the US lives in western states where there are an estimated 161,000 abandoned hardrock mines—including > 4,000 abandoned uranium mines. Because of their reliance on natural resources, these tribal communities have direct and frequent contact with metal mixtures through inhalation, drinking water, and eating food. Those exposures are exacerbated by disparities in infrastructure and unique social determinants of health from poverty in rural and isolated locations.
Related: Reducing Health Disparities With Performance Management
That’s the rationale behind the $1.5 million award to the University of New Mexico Health Sciences Center in Albuquerque to establish a Center for Native American Health Equity Research.effort by the Environmental Protection Agency ( EPA) and National Institutes of Health (NIH). The center will tackle those pervasive environmental health disparities with primary biomedical and environmental research and Native American-focused community engagement, says NIH.
The partners in the center are 3 University research programs and the Navajo, Sioux and Crow nations, with plans to expand to a fourth tribal region later. Together they will address research priorities such as examining the distribution of contaminants, cultural practices, and genetic origins of the 3 core tribes to provide a basis for “sorting out the health effects” of metal mixtures in tribal communities.
Related: Unraveling the Causes of Breast Cancer Disparities
The program also will build the research capacity, understanding of data, and interpretation and use of biomedical results across those communities, as well as developing a framework that characterizes the unique exposure pathways, EPA says. Ultimately, the hope is that the research will help define health from a perspective that not only reflects tribal perceptions, but is useful in informing regulatory decision making.
EMA says plasma/urine-derived meds are safe from Zika

Photo by Cristina Granados
Patients who take plasma-derived or urine-derived medicines do not have to worry about these products being contaminated with Zika virus, according to the European Medicines Agency (EMA).
The agency said assessments have confirmed that manufacturing processes for these medicines—which include coagulation factors, immunoglobulins, and urokinase products—successfully inactivate or remove the Zika virus.
These medicines are produced from body fluids that might be sourced in parts of the world where the Zika virus is prevalent. So regulators in the European Union (EU) sought reassurance that there is no risk of the virus contaminating the final product and thus affecting the patients taking these medicines.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) investigated the potential risk with plasma-derived medicinal products.
And the Co-ordination Group for Mutual Recognition and Decentralised Procedures—Human (CMDh) has coordinated the assessment by EU member states on the potential risk with urine-derived medicinal products.
The CHMP concluded at its meeting last week that the manufacturing processes used for plasma-derived products—including, for example, the solvent/detergent method to inactivate viruses, pasteurization, and virus filtration—inactivate or remove the Zika virus from the finished product.
The CHMP therefore concluded that no additional safety measures, such as the testing or exclusion of certain plasma donors, were necessary.
The CMDh, following an assessment of data, concluded that the manufacturing processes for urine-derived products contain complementary steps with inactivation/removal capacity for enveloped viruses, which are considered sufficient for eliminating Zika virus.
Additional safety measures, such as screening urine donors/donations or deferring donors returning from Zika-affected areas, are not considered necessary.
The findings from these assessments are available in a report from the CHMP’s Biologics Working Party.
The Biologics Working Party recommendation on plasma-derived products is in line with the guidance published in July 2016 by the European Centre for Disease Prevention and Control. ![]()
Photo by Cristina Granados
Patients who take plasma-derived or urine-derived medicines do not have to worry about these products being contaminated with Zika virus, according to the European Medicines Agency (EMA).
The agency said assessments have confirmed that manufacturing processes for these medicines—which include coagulation factors, immunoglobulins, and urokinase products—successfully inactivate or remove the Zika virus.
These medicines are produced from body fluids that might be sourced in parts of the world where the Zika virus is prevalent. So regulators in the European Union (EU) sought reassurance that there is no risk of the virus contaminating the final product and thus affecting the patients taking these medicines.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) investigated the potential risk with plasma-derived medicinal products.
And the Co-ordination Group for Mutual Recognition and Decentralised Procedures—Human (CMDh) has coordinated the assessment by EU member states on the potential risk with urine-derived medicinal products.
The CHMP concluded at its meeting last week that the manufacturing processes used for plasma-derived products—including, for example, the solvent/detergent method to inactivate viruses, pasteurization, and virus filtration—inactivate or remove the Zika virus from the finished product.
The CHMP therefore concluded that no additional safety measures, such as the testing or exclusion of certain plasma donors, were necessary.
The CMDh, following an assessment of data, concluded that the manufacturing processes for urine-derived products contain complementary steps with inactivation/removal capacity for enveloped viruses, which are considered sufficient for eliminating Zika virus.
Additional safety measures, such as screening urine donors/donations or deferring donors returning from Zika-affected areas, are not considered necessary.
The findings from these assessments are available in a report from the CHMP’s Biologics Working Party.
The Biologics Working Party recommendation on plasma-derived products is in line with the guidance published in July 2016 by the European Centre for Disease Prevention and Control. ![]()
Photo by Cristina Granados
Patients who take plasma-derived or urine-derived medicines do not have to worry about these products being contaminated with Zika virus, according to the European Medicines Agency (EMA).
The agency said assessments have confirmed that manufacturing processes for these medicines—which include coagulation factors, immunoglobulins, and urokinase products—successfully inactivate or remove the Zika virus.
These medicines are produced from body fluids that might be sourced in parts of the world where the Zika virus is prevalent. So regulators in the European Union (EU) sought reassurance that there is no risk of the virus contaminating the final product and thus affecting the patients taking these medicines.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) investigated the potential risk with plasma-derived medicinal products.
And the Co-ordination Group for Mutual Recognition and Decentralised Procedures—Human (CMDh) has coordinated the assessment by EU member states on the potential risk with urine-derived medicinal products.
The CHMP concluded at its meeting last week that the manufacturing processes used for plasma-derived products—including, for example, the solvent/detergent method to inactivate viruses, pasteurization, and virus filtration—inactivate or remove the Zika virus from the finished product.
The CHMP therefore concluded that no additional safety measures, such as the testing or exclusion of certain plasma donors, were necessary.
The CMDh, following an assessment of data, concluded that the manufacturing processes for urine-derived products contain complementary steps with inactivation/removal capacity for enveloped viruses, which are considered sufficient for eliminating Zika virus.
Additional safety measures, such as screening urine donors/donations or deferring donors returning from Zika-affected areas, are not considered necessary.
The findings from these assessments are available in a report from the CHMP’s Biologics Working Party.
The Biologics Working Party recommendation on plasma-derived products is in line with the guidance published in July 2016 by the European Centre for Disease Prevention and Control. ![]()
Gene therapy accepted into PRIME program
![]()
Photo by Chad McNeeley
An investigational gene therapy known as LentiGlobin BB305 has been accepted into the European Medicines Agency’s (EMA’s) Priority Medicines (PRIME) program as a treatment for patients with transfusion-dependent beta-thalassemia (TDT).
LentiGlobin BB305 is created by inserting a functional human beta-globin gene into a patient’s hematopoietic stem cells ex vivo. The cells are then returned to the patient via transplant.
The goal of the EMA’s PRIME program is to accelerate the development of therapies that target unmet medical needs. The program provides enhanced EMA support and increased interaction to developers, in order to optimize development plans and speed regulatory evaluations to potentially bring these therapies to patients more quickly.
To be accepted for PRIME, a therapy must demonstrate potential to benefit patients with unmet medical need through early clinical or nonclinical data.
Bluebird bio, the company developing LentiGlobin BB305, is also participating in the EMA’s Adaptive Pathways pilot program.
Like PRIME, the Adaptive Pathways program aims to expedite patient access to therapies with the potential to treat serious conditions with unmet need. It uses the existing European Union (EU) regulatory framework for medicines, including conditional approval.
“PRIME designation will allow bluebird bio to further improve our communication with European regulators as we continue to refine our evidence generation plan in the context of adaptive biomedical innovation,” said David Davidson, MD, chief medical officer of bluebird bio.
“Overall, we believe this will enable us to accelerate development of LentiGlobin drug product for patients with transfusion-dependent beta-thalassemia, a life-shortening disease with significant unmet medical need.”
“Earlier this year, we completed enrollment in the Northstar (HGB-204) global clinical study of LentiGlobin drug product in patients with TDT, which, along with the supporting HGB-205 study, will form the basis of our eventual application for conditional approval in the EU under the Adaptive Pathways pilot program.” ![]()
![]()
Photo by Chad McNeeley
An investigational gene therapy known as LentiGlobin BB305 has been accepted into the European Medicines Agency’s (EMA’s) Priority Medicines (PRIME) program as a treatment for patients with transfusion-dependent beta-thalassemia (TDT).
LentiGlobin BB305 is created by inserting a functional human beta-globin gene into a patient’s hematopoietic stem cells ex vivo. The cells are then returned to the patient via transplant.
The goal of the EMA’s PRIME program is to accelerate the development of therapies that target unmet medical needs. The program provides enhanced EMA support and increased interaction to developers, in order to optimize development plans and speed regulatory evaluations to potentially bring these therapies to patients more quickly.
To be accepted for PRIME, a therapy must demonstrate potential to benefit patients with unmet medical need through early clinical or nonclinical data.
Bluebird bio, the company developing LentiGlobin BB305, is also participating in the EMA’s Adaptive Pathways pilot program.
Like PRIME, the Adaptive Pathways program aims to expedite patient access to therapies with the potential to treat serious conditions with unmet need. It uses the existing European Union (EU) regulatory framework for medicines, including conditional approval.
“PRIME designation will allow bluebird bio to further improve our communication with European regulators as we continue to refine our evidence generation plan in the context of adaptive biomedical innovation,” said David Davidson, MD, chief medical officer of bluebird bio.
“Overall, we believe this will enable us to accelerate development of LentiGlobin drug product for patients with transfusion-dependent beta-thalassemia, a life-shortening disease with significant unmet medical need.”
“Earlier this year, we completed enrollment in the Northstar (HGB-204) global clinical study of LentiGlobin drug product in patients with TDT, which, along with the supporting HGB-205 study, will form the basis of our eventual application for conditional approval in the EU under the Adaptive Pathways pilot program.” ![]()
![]()
Photo by Chad McNeeley
An investigational gene therapy known as LentiGlobin BB305 has been accepted into the European Medicines Agency’s (EMA’s) Priority Medicines (PRIME) program as a treatment for patients with transfusion-dependent beta-thalassemia (TDT).
LentiGlobin BB305 is created by inserting a functional human beta-globin gene into a patient’s hematopoietic stem cells ex vivo. The cells are then returned to the patient via transplant.
The goal of the EMA’s PRIME program is to accelerate the development of therapies that target unmet medical needs. The program provides enhanced EMA support and increased interaction to developers, in order to optimize development plans and speed regulatory evaluations to potentially bring these therapies to patients more quickly.
To be accepted for PRIME, a therapy must demonstrate potential to benefit patients with unmet medical need through early clinical or nonclinical data.
Bluebird bio, the company developing LentiGlobin BB305, is also participating in the EMA’s Adaptive Pathways pilot program.
Like PRIME, the Adaptive Pathways program aims to expedite patient access to therapies with the potential to treat serious conditions with unmet need. It uses the existing European Union (EU) regulatory framework for medicines, including conditional approval.
“PRIME designation will allow bluebird bio to further improve our communication with European regulators as we continue to refine our evidence generation plan in the context of adaptive biomedical innovation,” said David Davidson, MD, chief medical officer of bluebird bio.
“Overall, we believe this will enable us to accelerate development of LentiGlobin drug product for patients with transfusion-dependent beta-thalassemia, a life-shortening disease with significant unmet medical need.”
“Earlier this year, we completed enrollment in the Northstar (HGB-204) global clinical study of LentiGlobin drug product in patients with TDT, which, along with the supporting HGB-205 study, will form the basis of our eventual application for conditional approval in the EU under the Adaptive Pathways pilot program.” ![]()
Compound could treat resistant malaria

of the P falciparum parasite
Image by Mae Melvin/CDC
A novel compound could be effective against malaria infections that are resistant to currently available antimalarial drugs, according to researchers.
In a phase 2 study, the compound, KAF156, proved active against Plasmodium vivax and Plasmodium falciparum malaria.
KAF156 was able to clear both blood and liver stages of malaria parasites, including artemisinin-resistant parasites.
Most of the patients in this study had at least 1 adverse event (AE). However, most were grade 1, and there were no grade 4 or serious AEs.
Results from this study were published in NEJM. The trial was funded, in part, by Novartis, the company developing KAF156.
KAF156 is the first compound from a novel class of drugs called imidazolopiperazines. The drugs’ mechanism of action is still being characterized, but it may be related to a previously uncharacterized gene—Plasmodium falciparum cyclic amine resistance locus (Pfcarl).
From March to August 2013, researchers conducted a phase 2 trial of KAF156 at 5 centers in Thailand and Vietnam.
Twenty-one of the patients in this study had acute, uncomplicated malaria—11 with P vivax and 10 with P falciparum malaria. They received multiple doses of KAF156—400 mg once daily for 3 days.
Twenty-two of the patients studied had uncomplicated, P falciparum malaria and received a single dose of KAF156 at 800 mg.
All patients were assessed for fever and parasite clearance as well as AEs. Patients in the single-dose cohort were also followed for 28 days to assess the cure rate.
Two patients were excluded from the efficacy analysis. One was a P vivax patient receiving the 400 mg dose who turned out to have a mixed infection. And the other was a P falciparum patient who vomited repeatedly after receiving 800 mg of KAF156 (after 3 attempts at dosing).
Efficacy
In the multiple-dose cohorts, the median time to fever clearance after receiving KAF156 was 14 hours (range, 4 to 30) in patients with P vivax malaria and 6 hours (range, 4 to 24) in patients with P falciparum malaria. In the single-dose cohort, the median time to fever clearance was 4 hours (range, 4 to 66).
In the multiple-dose cohorts, the median time to parasite clearance was 24 hours (range, 16 to 36) in patients with P vivax and 45 hours (range, 36 to 66) in patients with P falciparum.
In the single-dose cohort, the median time to parasite clearance was 49 hours (range, 16 to 68). One of these patients had parasite clearance at 66 hours but an asymptomatic recurrence at 84 hours. In all of the other patients, parasitemia cleared.
During follow-up of the single-dose cohort, 1 patient had reinfection, and 7 had recrudescent infections.
Safety
Most patients had at least 1 AE, although none were serious. Seventy-two percent of patients had grade 1 AEs, 35% had grade 2 AEs, and 14% had grade 3 AEs.
Sixty percent of AEs were considered related to treatment. In the multiple-dose cohorts, 14 of the 31 AEs (45%) reported in 7 patients (1 with P vivax and 6 with P falciparum malaria) were considered drug-related. All 22 P falciparum patients in the single-dose cohort had at least 1 AE that was considered drug-related.
The most common AEs were sinus bradycardia, thrombocytopenia, hypokalemia, anemia, and hyperbilirubinemia.
Two patients experienced vomiting of grade 2 or higher. One of these patients discontinued treatment because of repeated vomiting after the 800 mg dose (mentioned above). ![]()
of the P falciparum parasite
Image by Mae Melvin/CDC
A novel compound could be effective against malaria infections that are resistant to currently available antimalarial drugs, according to researchers.
In a phase 2 study, the compound, KAF156, proved active against Plasmodium vivax and Plasmodium falciparum malaria.
KAF156 was able to clear both blood and liver stages of malaria parasites, including artemisinin-resistant parasites.
Most of the patients in this study had at least 1 adverse event (AE). However, most were grade 1, and there were no grade 4 or serious AEs.
Results from this study were published in NEJM. The trial was funded, in part, by Novartis, the company developing KAF156.
KAF156 is the first compound from a novel class of drugs called imidazolopiperazines. The drugs’ mechanism of action is still being characterized, but it may be related to a previously uncharacterized gene—Plasmodium falciparum cyclic amine resistance locus (Pfcarl).
From March to August 2013, researchers conducted a phase 2 trial of KAF156 at 5 centers in Thailand and Vietnam.
Twenty-one of the patients in this study had acute, uncomplicated malaria—11 with P vivax and 10 with P falciparum malaria. They received multiple doses of KAF156—400 mg once daily for 3 days.
Twenty-two of the patients studied had uncomplicated, P falciparum malaria and received a single dose of KAF156 at 800 mg.
All patients were assessed for fever and parasite clearance as well as AEs. Patients in the single-dose cohort were also followed for 28 days to assess the cure rate.
Two patients were excluded from the efficacy analysis. One was a P vivax patient receiving the 400 mg dose who turned out to have a mixed infection. And the other was a P falciparum patient who vomited repeatedly after receiving 800 mg of KAF156 (after 3 attempts at dosing).
Efficacy
In the multiple-dose cohorts, the median time to fever clearance after receiving KAF156 was 14 hours (range, 4 to 30) in patients with P vivax malaria and 6 hours (range, 4 to 24) in patients with P falciparum malaria. In the single-dose cohort, the median time to fever clearance was 4 hours (range, 4 to 66).
In the multiple-dose cohorts, the median time to parasite clearance was 24 hours (range, 16 to 36) in patients with P vivax and 45 hours (range, 36 to 66) in patients with P falciparum.
In the single-dose cohort, the median time to parasite clearance was 49 hours (range, 16 to 68). One of these patients had parasite clearance at 66 hours but an asymptomatic recurrence at 84 hours. In all of the other patients, parasitemia cleared.
During follow-up of the single-dose cohort, 1 patient had reinfection, and 7 had recrudescent infections.
Safety
Most patients had at least 1 AE, although none were serious. Seventy-two percent of patients had grade 1 AEs, 35% had grade 2 AEs, and 14% had grade 3 AEs.
Sixty percent of AEs were considered related to treatment. In the multiple-dose cohorts, 14 of the 31 AEs (45%) reported in 7 patients (1 with P vivax and 6 with P falciparum malaria) were considered drug-related. All 22 P falciparum patients in the single-dose cohort had at least 1 AE that was considered drug-related.
The most common AEs were sinus bradycardia, thrombocytopenia, hypokalemia, anemia, and hyperbilirubinemia.
Two patients experienced vomiting of grade 2 or higher. One of these patients discontinued treatment because of repeated vomiting after the 800 mg dose (mentioned above). ![]()
of the P falciparum parasite
Image by Mae Melvin/CDC
A novel compound could be effective against malaria infections that are resistant to currently available antimalarial drugs, according to researchers.
In a phase 2 study, the compound, KAF156, proved active against Plasmodium vivax and Plasmodium falciparum malaria.
KAF156 was able to clear both blood and liver stages of malaria parasites, including artemisinin-resistant parasites.
Most of the patients in this study had at least 1 adverse event (AE). However, most were grade 1, and there were no grade 4 or serious AEs.
Results from this study were published in NEJM. The trial was funded, in part, by Novartis, the company developing KAF156.
KAF156 is the first compound from a novel class of drugs called imidazolopiperazines. The drugs’ mechanism of action is still being characterized, but it may be related to a previously uncharacterized gene—Plasmodium falciparum cyclic amine resistance locus (Pfcarl).
From March to August 2013, researchers conducted a phase 2 trial of KAF156 at 5 centers in Thailand and Vietnam.
Twenty-one of the patients in this study had acute, uncomplicated malaria—11 with P vivax and 10 with P falciparum malaria. They received multiple doses of KAF156—400 mg once daily for 3 days.
Twenty-two of the patients studied had uncomplicated, P falciparum malaria and received a single dose of KAF156 at 800 mg.
All patients were assessed for fever and parasite clearance as well as AEs. Patients in the single-dose cohort were also followed for 28 days to assess the cure rate.
Two patients were excluded from the efficacy analysis. One was a P vivax patient receiving the 400 mg dose who turned out to have a mixed infection. And the other was a P falciparum patient who vomited repeatedly after receiving 800 mg of KAF156 (after 3 attempts at dosing).
Efficacy
In the multiple-dose cohorts, the median time to fever clearance after receiving KAF156 was 14 hours (range, 4 to 30) in patients with P vivax malaria and 6 hours (range, 4 to 24) in patients with P falciparum malaria. In the single-dose cohort, the median time to fever clearance was 4 hours (range, 4 to 66).
In the multiple-dose cohorts, the median time to parasite clearance was 24 hours (range, 16 to 36) in patients with P vivax and 45 hours (range, 36 to 66) in patients with P falciparum.
In the single-dose cohort, the median time to parasite clearance was 49 hours (range, 16 to 68). One of these patients had parasite clearance at 66 hours but an asymptomatic recurrence at 84 hours. In all of the other patients, parasitemia cleared.
During follow-up of the single-dose cohort, 1 patient had reinfection, and 7 had recrudescent infections.
Safety
Most patients had at least 1 AE, although none were serious. Seventy-two percent of patients had grade 1 AEs, 35% had grade 2 AEs, and 14% had grade 3 AEs.
Sixty percent of AEs were considered related to treatment. In the multiple-dose cohorts, 14 of the 31 AEs (45%) reported in 7 patients (1 with P vivax and 6 with P falciparum malaria) were considered drug-related. All 22 P falciparum patients in the single-dose cohort had at least 1 AE that was considered drug-related.
The most common AEs were sinus bradycardia, thrombocytopenia, hypokalemia, anemia, and hyperbilirubinemia.
Two patients experienced vomiting of grade 2 or higher. One of these patients discontinued treatment because of repeated vomiting after the 800 mg dose (mentioned above). ![]()
Of Cell Phones & Skin Damage
A 54-year-old man is seen for evaluation of various skin problems, none of which he believes to be serious. His concern primarily stems from his job of 30 years, which keeps him outdoors most days with minimal protection from the sun.
In addition to the generally weathered skin on his sun-exposed arms and face, his wife has noticed redness around his neck and chest that is slowly worsening with time.
He denies any discomfort with the changes in his neck skin. He has a history of diabetes and smoking.
EXAMINATION
There is well-defined redness around his neck, especially in the front, that spills down onto his chest. Strangely, instead of matching the scoop neckline of the t-shirts he always wears, the chest redness is asymmetrical. It veers off to the patient’s left, sparing the midline chest. The erythema is partially blanchable with digital pressure but totally macular with no increased warmth.
What is the diagnosis?
DISCUSSION
This patient’s condition is poikiloderma of Civatte (PC), an increase in surface vasculature etched into the skin by chronic overexposure to the sun. PC usually follows a very predictable pattern, mirroring the patient’s usual attire. This made the asymmetry in this patient’s case striking and puzzling. Speculation included uneven sunscreen application or use of clothing such as overalls, which tend to shift during wearing, but the cause remained a mystery—that is, until the patient got dressed.
After putting his shirt back on, he placed his large, heavy cell phone in the left pocket, effectively pulling his shirt down and to the left. This exposed more skin on that side, covering up the right side of the chest. He confirmed that he carried the cell phone in his shirt pocket constantly during his waking hours, at home and on the job.
This conundrum needed to be solved in order to rule out other possible conditions. There’s no rule that prevents a person from having two adjacent diagnoses at the same time, such as PC and Bowen disease (a superficial form of squamous cell carcinoma). In this case, the patient’s skin changes were all consistent with one diagnosis.
TAKE-HOME LEARNING POINTS
• Poikiloderma of Civatte (PC) is the term given to a particular pattern of chronic overexposure to UV rays, typically affecting the neck and upper chest.
• PC is often caused by occupational sun exposure.
• Unless treated with a laser, PC changes are permanent but harmless. They do, however, identify the patient as being at risk for sun-caused skin cancer.
• Atypical presentations of what appear to be common problems may need a bit of investigation to rule out other items in the differential.
A 54-year-old man is seen for evaluation of various skin problems, none of which he believes to be serious. His concern primarily stems from his job of 30 years, which keeps him outdoors most days with minimal protection from the sun.
In addition to the generally weathered skin on his sun-exposed arms and face, his wife has noticed redness around his neck and chest that is slowly worsening with time.
He denies any discomfort with the changes in his neck skin. He has a history of diabetes and smoking.
EXAMINATION
There is well-defined redness around his neck, especially in the front, that spills down onto his chest. Strangely, instead of matching the scoop neckline of the t-shirts he always wears, the chest redness is asymmetrical. It veers off to the patient’s left, sparing the midline chest. The erythema is partially blanchable with digital pressure but totally macular with no increased warmth.
What is the diagnosis?
DISCUSSION
This patient’s condition is poikiloderma of Civatte (PC), an increase in surface vasculature etched into the skin by chronic overexposure to the sun. PC usually follows a very predictable pattern, mirroring the patient’s usual attire. This made the asymmetry in this patient’s case striking and puzzling. Speculation included uneven sunscreen application or use of clothing such as overalls, which tend to shift during wearing, but the cause remained a mystery—that is, until the patient got dressed.
After putting his shirt back on, he placed his large, heavy cell phone in the left pocket, effectively pulling his shirt down and to the left. This exposed more skin on that side, covering up the right side of the chest. He confirmed that he carried the cell phone in his shirt pocket constantly during his waking hours, at home and on the job.
This conundrum needed to be solved in order to rule out other possible conditions. There’s no rule that prevents a person from having two adjacent diagnoses at the same time, such as PC and Bowen disease (a superficial form of squamous cell carcinoma). In this case, the patient’s skin changes were all consistent with one diagnosis.
TAKE-HOME LEARNING POINTS
• Poikiloderma of Civatte (PC) is the term given to a particular pattern of chronic overexposure to UV rays, typically affecting the neck and upper chest.
• PC is often caused by occupational sun exposure.
• Unless treated with a laser, PC changes are permanent but harmless. They do, however, identify the patient as being at risk for sun-caused skin cancer.
• Atypical presentations of what appear to be common problems may need a bit of investigation to rule out other items in the differential.
A 54-year-old man is seen for evaluation of various skin problems, none of which he believes to be serious. His concern primarily stems from his job of 30 years, which keeps him outdoors most days with minimal protection from the sun.
In addition to the generally weathered skin on his sun-exposed arms and face, his wife has noticed redness around his neck and chest that is slowly worsening with time.
He denies any discomfort with the changes in his neck skin. He has a history of diabetes and smoking.
EXAMINATION
There is well-defined redness around his neck, especially in the front, that spills down onto his chest. Strangely, instead of matching the scoop neckline of the t-shirts he always wears, the chest redness is asymmetrical. It veers off to the patient’s left, sparing the midline chest. The erythema is partially blanchable with digital pressure but totally macular with no increased warmth.
What is the diagnosis?
DISCUSSION
This patient’s condition is poikiloderma of Civatte (PC), an increase in surface vasculature etched into the skin by chronic overexposure to the sun. PC usually follows a very predictable pattern, mirroring the patient’s usual attire. This made the asymmetry in this patient’s case striking and puzzling. Speculation included uneven sunscreen application or use of clothing such as overalls, which tend to shift during wearing, but the cause remained a mystery—that is, until the patient got dressed.
After putting his shirt back on, he placed his large, heavy cell phone in the left pocket, effectively pulling his shirt down and to the left. This exposed more skin on that side, covering up the right side of the chest. He confirmed that he carried the cell phone in his shirt pocket constantly during his waking hours, at home and on the job.
This conundrum needed to be solved in order to rule out other possible conditions. There’s no rule that prevents a person from having two adjacent diagnoses at the same time, such as PC and Bowen disease (a superficial form of squamous cell carcinoma). In this case, the patient’s skin changes were all consistent with one diagnosis.
TAKE-HOME LEARNING POINTS
• Poikiloderma of Civatte (PC) is the term given to a particular pattern of chronic overexposure to UV rays, typically affecting the neck and upper chest.
• PC is often caused by occupational sun exposure.
• Unless treated with a laser, PC changes are permanent but harmless. They do, however, identify the patient as being at risk for sun-caused skin cancer.
• Atypical presentations of what appear to be common problems may need a bit of investigation to rule out other items in the differential.
