User login
Novel combo boosts response in HER2-negative breast cancer
A novel combination has boosted responses in women with high-risk, HER2-negative breast cancer.
The new combo comprises the immune checkpoint inhibitor durvalumab (Imfinzi, AstraZeneca) and the poly(ADP-ribose) polymerase (PARP) inhibitor olaparib (Lynparza, AstraZeneca).
When this combo was added to standard neoadjuvant chemotherapy, it yielded a significantly higher pathologic complete response (pCR) rate at the time of surgery than was seen with chemotherapy alone.
The superior pCR rate was seen across all HER2-negative breast cancer subtypes, including HER2-negative, estrogen receptor–positive tumors (Mammaprint high risk), and in women with triple-negative breast cancer (TNBC), reported lead investigator Lajos Pusztai, MD, DPhil, from Yale Cancer Center in New Haven, Connecticut.
“These results provide further evidence for the clinical value of immunotherapy in early-stage breast cancer and suggest new avenues for how to exploit these drugs in hormone receptor [HR]–positive breast cancers,” said Pusztai.
He presented the results at the American Association for Cancer Research (AACR) virtual annual meeting, which took place online, owing to the COVID-19 pandemic.
Toxicities, including financial
“The benefits from immunotherapy are clearly emerging in early and metastatic triple-negative breast cancer, likely with PD-L1 expression. However, there’s much more uncertainty in patients with hormone-sensitive tumors whether there is benefit and who will benefit from immunotherapy,” commented Pamela N. Munster, MD, from the University of California, San Francisco, who was the invited discussant.
“The signal of a better pCR rate among patients in the ultra-high Mammaprint group may allow selection of patients with HR-positive disease who may benefit from immunotherapeutic agents and/or PARP inhibitors,” she said.
Munster noted that the approximately 10% higher rate of immune-related adverse events of grade 3 or greater that was seen with the combination appears similar to that seen in other studies, but anemia and fatigue appeared to be less frequent with durvalumab/olaparaib and paclitaxel in comparison with paclitaxel alone.
“In the absence of a clear delineation of the contribution of olaparib, some weight should be given to the financial burden of adding both durvalumab and olaparib to a preoperative regimen,” she said.
The additional cost of durvalumab is approximately $34,000, and adding olaparib boosts that by about $22,000 more, Munster said.
Ongoing platform trial
The new results come from one arm of the ongoing Investigation of Serial Studies to Predict Your Therapeutic Response Through Imaging and Molecular Analysis 2 (I-SPY-2) trial. This is an ongoing platform trial that is exploring the use of new drugs in combination with a standard neoadjuvant therapy backbone for the treatment of high-risk cancers.
In this trial, women with stage II or III breast cancer with tumors 2.5 cm or larger are assessed for one of eight biomarker subtypes according to HER2 status, HR status, and genetic risk factors, as determined on the basis of a 70-gene assay. The patients within each biomarker subtype are randomly assigned to receive standard therapy either with or without an investigational agent.
For each subtrial, a primary endpoint is an improvement in pCR in comparison with the standard of care.
Changes in tumor volume on MRI are used to predict whether patients will achieve a pCR. Those who are considered to have a high Bayesian predictive probability of success are eligible for moving on to phase 3 trials.
The I-SPY-2 trial was described in detail by principal investigator Laura J. Esserman, MD, MBA, from the Helen Diller Comprehensive Cancer Center at the University of California, San Francisco, in a 2017 interview from the annual meeting of the American Society of Clinical Oncology.
As previously reported, the first drugs to “graduate” from the trial were the HER2/HER4 inhibitor neratinib (Nerlynx, Puma Biotechnology) and the investigational PARP inhibitor veliparib (AbbVie).
Study details
The I-SPY-2 results that Pusztai reported at the AACR meeting were based on an analysis of 73 HER2-negative patients, including 21 patients with TNBC and 52 with HR-positive tumors with Mammaprint high-risk features. These patients underwent treatment with durvalumab 1500 mg every 4 weeks for three cycles, olaparib 100 mg twice daily for weeks 1 through 11, and paclitaxel 80 mg/m2 weekly for 12 weeks, followed by AC chemotherapy (doxorubicin and cyclophosphamide) for four cycles.
The 299 patients in the control arm received paclitaxel and chemotherapy only.
In all three biomarker subsets studied, durvalumab and olaparib increased pCR rates compared with controls, as shown in the table.
The probability that the combination was superior to control in each subgroup approached 100%, Pusztai noted.
Adverse events with the combination were consistent with known side effects of the drugs, he commented. Immune-related grade 3 adverse events occurred in 19% of patients in the combination therapy arm, compared with 1.6% in the control arm.
Higher pCR rates were seen in the subset of immune-rich tumors among all cancer subtypes and in both study arms.
“Exploratory analysis suggests several potential predictive markers of durvalumab/olaparib benefit over chemotherapy alone,” Pusztai reported.
These markers included Mammaprint MP2 (ultra high) versus MP1 in HR+/HER2– tumors, and low CD3/CD8 gene signature ratio, high macrophage/Tc-class 2 gene signature ratio, and high proliferation signature, all of which were associated with higher pCR rates in the experimental arm among patients with TNBC.
The trial was supported by the William K. Bowes Jr Foundation, Foundation for the NIH, Give Breast Cancer the Boot, UCSF, the Biomarkers Consortium, IQVIA, the Breast Cancer Research Foundation, Safeway, California Breast Cancer Research Program, Breast Cancer Research–Atwater Trust, and Stand Up to Cancer. Pusztai has received honoraria and consulting fees from AstraZeneca and other companies. Munster has received research and travel support from and has served on the scientific advisory boards of AstraZeneca and other companies.
This article first appeared on Medscape.com.
A novel combination has boosted responses in women with high-risk, HER2-negative breast cancer.
The new combo comprises the immune checkpoint inhibitor durvalumab (Imfinzi, AstraZeneca) and the poly(ADP-ribose) polymerase (PARP) inhibitor olaparib (Lynparza, AstraZeneca).
When this combo was added to standard neoadjuvant chemotherapy, it yielded a significantly higher pathologic complete response (pCR) rate at the time of surgery than was seen with chemotherapy alone.
The superior pCR rate was seen across all HER2-negative breast cancer subtypes, including HER2-negative, estrogen receptor–positive tumors (Mammaprint high risk), and in women with triple-negative breast cancer (TNBC), reported lead investigator Lajos Pusztai, MD, DPhil, from Yale Cancer Center in New Haven, Connecticut.
“These results provide further evidence for the clinical value of immunotherapy in early-stage breast cancer and suggest new avenues for how to exploit these drugs in hormone receptor [HR]–positive breast cancers,” said Pusztai.
He presented the results at the American Association for Cancer Research (AACR) virtual annual meeting, which took place online, owing to the COVID-19 pandemic.
Toxicities, including financial
“The benefits from immunotherapy are clearly emerging in early and metastatic triple-negative breast cancer, likely with PD-L1 expression. However, there’s much more uncertainty in patients with hormone-sensitive tumors whether there is benefit and who will benefit from immunotherapy,” commented Pamela N. Munster, MD, from the University of California, San Francisco, who was the invited discussant.
“The signal of a better pCR rate among patients in the ultra-high Mammaprint group may allow selection of patients with HR-positive disease who may benefit from immunotherapeutic agents and/or PARP inhibitors,” she said.
Munster noted that the approximately 10% higher rate of immune-related adverse events of grade 3 or greater that was seen with the combination appears similar to that seen in other studies, but anemia and fatigue appeared to be less frequent with durvalumab/olaparaib and paclitaxel in comparison with paclitaxel alone.
“In the absence of a clear delineation of the contribution of olaparib, some weight should be given to the financial burden of adding both durvalumab and olaparib to a preoperative regimen,” she said.
The additional cost of durvalumab is approximately $34,000, and adding olaparib boosts that by about $22,000 more, Munster said.
Ongoing platform trial
The new results come from one arm of the ongoing Investigation of Serial Studies to Predict Your Therapeutic Response Through Imaging and Molecular Analysis 2 (I-SPY-2) trial. This is an ongoing platform trial that is exploring the use of new drugs in combination with a standard neoadjuvant therapy backbone for the treatment of high-risk cancers.
In this trial, women with stage II or III breast cancer with tumors 2.5 cm or larger are assessed for one of eight biomarker subtypes according to HER2 status, HR status, and genetic risk factors, as determined on the basis of a 70-gene assay. The patients within each biomarker subtype are randomly assigned to receive standard therapy either with or without an investigational agent.
For each subtrial, a primary endpoint is an improvement in pCR in comparison with the standard of care.
Changes in tumor volume on MRI are used to predict whether patients will achieve a pCR. Those who are considered to have a high Bayesian predictive probability of success are eligible for moving on to phase 3 trials.
The I-SPY-2 trial was described in detail by principal investigator Laura J. Esserman, MD, MBA, from the Helen Diller Comprehensive Cancer Center at the University of California, San Francisco, in a 2017 interview from the annual meeting of the American Society of Clinical Oncology.
As previously reported, the first drugs to “graduate” from the trial were the HER2/HER4 inhibitor neratinib (Nerlynx, Puma Biotechnology) and the investigational PARP inhibitor veliparib (AbbVie).
Study details
The I-SPY-2 results that Pusztai reported at the AACR meeting were based on an analysis of 73 HER2-negative patients, including 21 patients with TNBC and 52 with HR-positive tumors with Mammaprint high-risk features. These patients underwent treatment with durvalumab 1500 mg every 4 weeks for three cycles, olaparib 100 mg twice daily for weeks 1 through 11, and paclitaxel 80 mg/m2 weekly for 12 weeks, followed by AC chemotherapy (doxorubicin and cyclophosphamide) for four cycles.
The 299 patients in the control arm received paclitaxel and chemotherapy only.
In all three biomarker subsets studied, durvalumab and olaparib increased pCR rates compared with controls, as shown in the table.
The probability that the combination was superior to control in each subgroup approached 100%, Pusztai noted.
Adverse events with the combination were consistent with known side effects of the drugs, he commented. Immune-related grade 3 adverse events occurred in 19% of patients in the combination therapy arm, compared with 1.6% in the control arm.
Higher pCR rates were seen in the subset of immune-rich tumors among all cancer subtypes and in both study arms.
“Exploratory analysis suggests several potential predictive markers of durvalumab/olaparib benefit over chemotherapy alone,” Pusztai reported.
These markers included Mammaprint MP2 (ultra high) versus MP1 in HR+/HER2– tumors, and low CD3/CD8 gene signature ratio, high macrophage/Tc-class 2 gene signature ratio, and high proliferation signature, all of which were associated with higher pCR rates in the experimental arm among patients with TNBC.
The trial was supported by the William K. Bowes Jr Foundation, Foundation for the NIH, Give Breast Cancer the Boot, UCSF, the Biomarkers Consortium, IQVIA, the Breast Cancer Research Foundation, Safeway, California Breast Cancer Research Program, Breast Cancer Research–Atwater Trust, and Stand Up to Cancer. Pusztai has received honoraria and consulting fees from AstraZeneca and other companies. Munster has received research and travel support from and has served on the scientific advisory boards of AstraZeneca and other companies.
This article first appeared on Medscape.com.
A novel combination has boosted responses in women with high-risk, HER2-negative breast cancer.
The new combo comprises the immune checkpoint inhibitor durvalumab (Imfinzi, AstraZeneca) and the poly(ADP-ribose) polymerase (PARP) inhibitor olaparib (Lynparza, AstraZeneca).
When this combo was added to standard neoadjuvant chemotherapy, it yielded a significantly higher pathologic complete response (pCR) rate at the time of surgery than was seen with chemotherapy alone.
The superior pCR rate was seen across all HER2-negative breast cancer subtypes, including HER2-negative, estrogen receptor–positive tumors (Mammaprint high risk), and in women with triple-negative breast cancer (TNBC), reported lead investigator Lajos Pusztai, MD, DPhil, from Yale Cancer Center in New Haven, Connecticut.
“These results provide further evidence for the clinical value of immunotherapy in early-stage breast cancer and suggest new avenues for how to exploit these drugs in hormone receptor [HR]–positive breast cancers,” said Pusztai.
He presented the results at the American Association for Cancer Research (AACR) virtual annual meeting, which took place online, owing to the COVID-19 pandemic.
Toxicities, including financial
“The benefits from immunotherapy are clearly emerging in early and metastatic triple-negative breast cancer, likely with PD-L1 expression. However, there’s much more uncertainty in patients with hormone-sensitive tumors whether there is benefit and who will benefit from immunotherapy,” commented Pamela N. Munster, MD, from the University of California, San Francisco, who was the invited discussant.
“The signal of a better pCR rate among patients in the ultra-high Mammaprint group may allow selection of patients with HR-positive disease who may benefit from immunotherapeutic agents and/or PARP inhibitors,” she said.
Munster noted that the approximately 10% higher rate of immune-related adverse events of grade 3 or greater that was seen with the combination appears similar to that seen in other studies, but anemia and fatigue appeared to be less frequent with durvalumab/olaparaib and paclitaxel in comparison with paclitaxel alone.
“In the absence of a clear delineation of the contribution of olaparib, some weight should be given to the financial burden of adding both durvalumab and olaparib to a preoperative regimen,” she said.
The additional cost of durvalumab is approximately $34,000, and adding olaparib boosts that by about $22,000 more, Munster said.
Ongoing platform trial
The new results come from one arm of the ongoing Investigation of Serial Studies to Predict Your Therapeutic Response Through Imaging and Molecular Analysis 2 (I-SPY-2) trial. This is an ongoing platform trial that is exploring the use of new drugs in combination with a standard neoadjuvant therapy backbone for the treatment of high-risk cancers.
In this trial, women with stage II or III breast cancer with tumors 2.5 cm or larger are assessed for one of eight biomarker subtypes according to HER2 status, HR status, and genetic risk factors, as determined on the basis of a 70-gene assay. The patients within each biomarker subtype are randomly assigned to receive standard therapy either with or without an investigational agent.
For each subtrial, a primary endpoint is an improvement in pCR in comparison with the standard of care.
Changes in tumor volume on MRI are used to predict whether patients will achieve a pCR. Those who are considered to have a high Bayesian predictive probability of success are eligible for moving on to phase 3 trials.
The I-SPY-2 trial was described in detail by principal investigator Laura J. Esserman, MD, MBA, from the Helen Diller Comprehensive Cancer Center at the University of California, San Francisco, in a 2017 interview from the annual meeting of the American Society of Clinical Oncology.
As previously reported, the first drugs to “graduate” from the trial were the HER2/HER4 inhibitor neratinib (Nerlynx, Puma Biotechnology) and the investigational PARP inhibitor veliparib (AbbVie).
Study details
The I-SPY-2 results that Pusztai reported at the AACR meeting were based on an analysis of 73 HER2-negative patients, including 21 patients with TNBC and 52 with HR-positive tumors with Mammaprint high-risk features. These patients underwent treatment with durvalumab 1500 mg every 4 weeks for three cycles, olaparib 100 mg twice daily for weeks 1 through 11, and paclitaxel 80 mg/m2 weekly for 12 weeks, followed by AC chemotherapy (doxorubicin and cyclophosphamide) for four cycles.
The 299 patients in the control arm received paclitaxel and chemotherapy only.
In all three biomarker subsets studied, durvalumab and olaparib increased pCR rates compared with controls, as shown in the table.
The probability that the combination was superior to control in each subgroup approached 100%, Pusztai noted.
Adverse events with the combination were consistent with known side effects of the drugs, he commented. Immune-related grade 3 adverse events occurred in 19% of patients in the combination therapy arm, compared with 1.6% in the control arm.
Higher pCR rates were seen in the subset of immune-rich tumors among all cancer subtypes and in both study arms.
“Exploratory analysis suggests several potential predictive markers of durvalumab/olaparib benefit over chemotherapy alone,” Pusztai reported.
These markers included Mammaprint MP2 (ultra high) versus MP1 in HR+/HER2– tumors, and low CD3/CD8 gene signature ratio, high macrophage/Tc-class 2 gene signature ratio, and high proliferation signature, all of which were associated with higher pCR rates in the experimental arm among patients with TNBC.
The trial was supported by the William K. Bowes Jr Foundation, Foundation for the NIH, Give Breast Cancer the Boot, UCSF, the Biomarkers Consortium, IQVIA, the Breast Cancer Research Foundation, Safeway, California Breast Cancer Research Program, Breast Cancer Research–Atwater Trust, and Stand Up to Cancer. Pusztai has received honoraria and consulting fees from AstraZeneca and other companies. Munster has received research and travel support from and has served on the scientific advisory boards of AstraZeneca and other companies.
This article first appeared on Medscape.com.
FROM AACR 2020
Reproductive psychiatry during the COVID-19 pandemic
When last I wrote this column, I was preparing for travel to professional meetings in the spring, planning a presentation for an upcoming grand rounds, and readying to host a scientific advisory board meeting as part of a large scientific project we conduct in Center for Women’s Mental Health. We were also awaiting the relocation of several junior faculty and research staff to Boston this spring and summer as we build our team.

It is now obvious that the COVID-19 pandemic is not a passing squall, but rather a persistent gale that has placed our collective sails in the water. It has not capsized the boat, however, thanks in part to the actions of courageous frontline caregivers and first responders who have mobilized in the wake of this recent public health crisis. From doctors, nurses, and hospital staff to grocery store clerks, home health aides, and neighbors checking in on the elderly – to name just a few – a whole crew of members across society have helped buoy our collective ship. Resilience also is required by all of us who are managing the array of feelings brought about by the day-in, day-out challenges of living life with restricted movement and freedom to engage in pre-COVID-19 activities we took for granted. What seemed like a temporary workaround is now becoming the “new normal” for an unknown amount of time looking forward.
For over 3 decades, my colleagues and I have worked with women who suffer from serious psychiatric disorders and whose treatment has required psychiatric medications such as antidepressants, mood stabilizers, and anxiolytics. The challenge of our work with women who are pregnant or planning pregnancy has been the configuration of the safest ways to navigate treatment on an individual basis for these women across pregnancy and post partum, with continual assessments of how to minimize the risk to fetus from in utero exposure to medications that have been instrumental in the treatment of psychiatric disorders on one hand versus the risks of untreated psychiatric disorder on the other. This work has been the essence of the clinical mission and the cornerstone of the research conducted at the Center for Women’s Mental Health since its inception.
While I have worked shoulder to shoulder with obstetricians for years, my respect for these colleagues during these past weeks has only grown as they have instituted the swiftest protocols to mitigate risk associated with COVID-19 for our pregnant patients, some of whom have tested positive for COVID-19, all in an effort to keep both mother, fetus, and newborn as safe as possible.
For those of us providing mental health services to pregnant women during this time, certain clinical situations have arisen in the context of the COVID-19 pandemic which require particular attention and discussion.
Planned pregnancy and contraception during the COVID-19 pandemic
Half of the pregnancies in this country are unplanned. Now more than ever, it is critical that decisions about moving forward with a plan to conceive be deliberate. These considerations range from the existential to the most concrete. For example, during these last weeks, we have consulted on cases where couples on the cusp of attempts to conceive face concerns about COVID-19, hence making more complicated their timeline with respect to actual plans to get pregnant. These are complicated decisions, particularly for women who may be slightly older and at the reproductive age where delaying pregnancy may have an adverse effect on fertility.
A concrete example of how the pandemic has affected fertility is evident as we encounter situations where women may defer starting a prescription oral contraceptive or lapse in its use because they have had difficulty coordinating visits with health care providers and may fear picking up prescriptions from pharmacies. We also have seen that procedures such as IUD placements have been deferred or canceled, or that some patients decline trips to the hospital or clinic to receive this type of service. These new barriers to access of contraception may require more planning at this time so that decisions about family planning are by design and not default during a time as complicated as the current public health crisis.
Telemedicine: telepsychiatry and obstetrics virtual visits
While wide-scale use of telemedicine platforms was not the standard day-to-day practice in either obstetrics or psychiatry prior to the pandemic, telepsychiatry has come up to speed within a short number of weeks. At our institution, 85% of outpatient visits are being conducted remotely, with in-person visits being reserved for only urgent or emergent visits. Our inpatient psychiatry service remains a setting where psychiatric patients, regardless of their COVID-19 status, can receive necessary care.

The use of telemedicine and specifically telepsychiatry is critical to mitigate the likelihood of exposure to SARS-CoV-2. On our reproductive psychiatry service, it has actually been an opportunity to engage with patients for comprehensive initial consults about reproductive safety of psychiatric medications currently being taken, or for ongoing consultation and direct patient care during follow-up visits during pregnancy to see that patients are sustaining emotional well-being or have changes for treatment implemented if they are not well. An increased frequency of visits allows us more opportunity to capture any signs of early clinical worsening of symptoms that might have been missed previously using the more traditional in-person setting.
Telepsychiatry and “virtual visits” have allowed us to do real-time, nimble modifications of treatment regimens with both pharmacologic and nonpharmacologic interventions to keep women well and to keep them out of the hospital for psychiatric care as often as possible. It also has facilitated a closer collaboration with our colleagues in obstetrics. In a way, the team of providers, including psychiatrists, obstetrical providers, social workers, and therapists can more easily communicate virtually than has sometimes been the case previously, when day-to-day use of telemedicine and virtual team meetings was less common.
Recognition and treatment of anxiety in perinatal patients
Even pregnant women without preexisting anxiety disorders may have heightened anxiety during usual times, and women and their partners cope with this typically in numerous ways including participation in peer-support opportunities, wellness and self-care activities, leveraging support from care providers, and engaging with family. But the previously “typical pregnancy experience” has shifted in the context of COVID-19. Specifically, added concerns of pregnant women about becoming infected, of potential separation from family if they do become ill, or of separation from partners or support systems during labor and delivery (an issue that has been largely resolved in many hospitals), as well as the possibility that a neonate might become ill with exposure to the coronavirus are obviously understandable and real. Such contingencies are unsettling, even for the most settled of our patients. Labor and delivery plans, and plans for outside help from family or others with the baby and older children in the postpartum period, have been upended for many patients.
These are anxious times. The number of nonpharmacologic virtual interventions available to mitigate anxiety are filling email inboxes daily. Curating these options can be a challenge, although several resources are worth noting, such as our department’s page on mental health resources.
During these past weeks, we have seen growing numbers of women for whom the normative anxiety of pregnancy is increasing to the point of causing distress to the level of functional impairment. Many patients for the first time meet criteria for frank anxiety disorders. These patients deserve prompt evaluation by mental health professionals and treatment with evidence-based therapies for anxiety disorders whether nonpharmacologic or pharmacologic so as to mitigate the risk of untreated anxiety on maternal and fetal well-being and also to limit risk for postpartum depression and postpartum anxiety disorders.
Miscarriage and infertility
A 36-year-old patient came to see me in clinic in late January following a miscarriage. She had a history of a previous miscarriage a year before and had an episode of major depression to follow for which she received treatment with an antidepressant and cognitive-behavioral therapy; she also attended a perinatal loss support group. She saw me in early March, anxious to try to conceive but extremely concerned about the risks associated with becoming pregnant at this point in time. Following a lengthy discussion with me and her obstetrician, the patient decided to wait until “the curve flattened” in Boston in terms of new cases of COVID-19, and then start trying to conceive. The case of another patient with a very similar history was presented at our rounds a few weeks ago; she also elected to defer attempts to conceive until life is more settled.
Perhaps one of the most dramatic examples of the impact of COVID-19 on fertility has been for those women with plans to pursue treatment with one of the assisted reproductive technologies. They have been told that professional societies have made recommendations regarding use of assisted reproductive technologies that are not entirely consistent across the country, but where in many places such interventions have been suspended during the COVID-19 pandemic. For many women near the end of their reproductive years, delays in trying to conceive either with or without the aid of fertility treatments may indelibly shape their plans to have children.
Sustaining emotional well-being across pregnancy
Because most psychiatric disorders are chronic in course, it is often the situation where women are treated to wellness for serious psychiatric disorders, with the goal of maintaining wellness across pregnancy and the post partum. One of the most critical takeaway points from 30 years of working with psychiatrically ill pregnant women is the maxim that keeping women well during pregnancy is simply imperative. Maternal psychiatric well-being during pregnancy is a strong predictor of obstetrical and neonatal outcomes, postpartum mental health, and longer-term neurobehavioral outcomes in children. Critically, in the context of the pandemic, keeping women out of psychiatric crises mitigates the necessity of visits to urgent clinical settings such as EDs and psychiatric inpatient units, which can increase the likelihood of exposure to the coronavirus.
Preservation of sleep
Disruption in sleep (duration and quality) can be seen in well over half of women during pregnancy with and without psychiatric disorders, and our experience has been that this has been exacerbated for many women during the COVID-19 crisis. Yet there are very rich data showing that sleep deprivation or sleep dysregulation in women, for example, who suffer from bipolar disorder or major depression can be a strong trigger for psychiatric relapse of underlying illness during pregnancy and the postpartum period.
During a time when normal rhythms of day-to-day life have been shifted – if not frankly disrupted – by swift transitions to remote work, cancellation of school and associated school activities across the country, complaints of insomnia and non-restorative sleep have been exceedingly common. Relevant to all but particularly for pregnant women with histories of psychiatric disorder, attention to sleep hygiene, moderation of caffeine use (if any), and use of any number of biobehavioral interventions to enhance relaxation and modulate stress may be of great value.
Cognitive-behavioral therapy for insomnia (CBT-I) has been demonstrated to be effective in pregnant women. Fortunately, there are user-friendly options on digital platforms that can be used during the pandemic that may play an important role in sustaining emotional well-being for pregnant women who have frank symptoms of insomnia.
Maintenance of ongoing antidepressant treatment during pregnancy among women with histories of mood disorder
Over a decade ago, my colleagues and I wrote about the comparison of outcomes for women with histories of recurrent major depression, demonstrating the value of maintenance treatment with antidepressants, compared with discontinuation of these medications during pregnancy (JAMA. 2006 Feb 1;295[5]:499-507). Recently, I was asked if maintenance antidepressant use in women with histories of recurrent depression was still our clinical recommendation. Over the last decade, we have noted that nearly half of women treated with antidepressants, regardless of illness severity, will discontinue their use of these medications prior to or early on in pregnancy given concerns about potential unknown effects of fetal exposure to medications, even medications for which there are robust data supporting reproductive safety regarding risk of congenital malformations. Routine discontinuation of antidepressants prior to or during pregnancy continues, despite the fact that we showed nearly 70% of those women with past histories of depression on maintenance antidepressant treatment relapsed shortly after discontinuing medication.
While we do not dictate the decisions women make about antidepressant use before, during, or after pregnancy, women with the same severity of illness will frequently make different decisions (a good thing) but we are now having very frank discussions about the particular need during a pandemic to avoid the relapse of serious psychiatric disorders. We typically endorse maintenance medication use with all but a very few number of psychotropic medications for which benefit may not outweigh risk to the fetus. However, for women who have decided nonetheless to discontinue antidepressants or other psychotropics during pregnancy despite the known risk of relapse, we strongly advise that they initiate treatment with evidence-based nonpharmacologic intervention such as CBT or mindfulness-based cognitive therapy (MBCT).
As in other areas of medicine, the pandemic is prompting we professionals in psychiatry, and specifically in perinatal psychiatry, to use all of our tools to keep pregnant and postpartum women well. The availability of digital tools to deliver MBCT and CBT has made the use of such interventions particularly viable at a time of social distancing. That being said, for patients with highly recurrent affective disorder with histories of previous recurrence when they stop their antidepressants, we are more strongly recommending serious consideration of maintenance medication treatment.
Virtual rounds in reproductive psychiatry and women’s mental health
The use of virtual platforms to connect with both patients and colleagues also has provided new opportunities for interaction with the reproductive psychiatry community as a whole. Peer teaching and peer support has been a critical part of our mission, and we decided 1 month ago to establish Virtual Rounds at the Center for Women’s Mental Health. This is a free digital platform, held on a weekly basis with our colleagues from across the country, where we discuss cases that come up in our own clinical rounds and also questions that get put forth by our colleagues in the area of reproductive psychiatry as they manage patients during the pandemic.
Changes in the postpartum experience
The last decade has brought a growing appreciation of postpartum depression and the need to screen and treat postpartum psychiatric disorders, such as postpartum mood and anxiety disorders. Yet in the era of this pandemic, the postpartum experience is itself is changing. Changes in carefully configured plans for the postpartum period – from family coming and going to mobilizing extra support at home and to now having new moms having to manage families and their other children at home – has been an enormous stressor for many women. Plans to have more elderly parents visit during the acute postpartum period, and the increased concerns about people traveling to and from a home where there is a newborn and the need to quarantine, has made the transition to motherhood much more complicated for all postpartum women, let alone for those postpartum women who have histories of psychiatric disorder.
There is a risk of social isolation for postpartum women even under normal circumstances, and this is profoundly more likely during this pandemic. We are actively working with our postpartum patients and optimizing treatment, brainstorming options in terms of using both virtual and real-time support to the extent that it is safe in order to keep women healthy during such a stressful and critical time.
I am heartened by the efforts on the part of organizations such as Postpartum Support International to make available virtually their resources with respect to community-based support and education for women who feel increasingly isolated during the postpartum period, a time where connectedness is so critical.
Summarily, these have been challenging times, but also times of opportunity. The COVID-19 pandemic has prompted us to get even more creative as we configure ways to optimize the emotional well-being of our patients who are planning to get pregnant, who are pregnant, or who are post partum.
The current time, while challenging in so many ways and a time of great pain, loss, and grief for far too many, has also provided an opportunity to work even more collaboratively with our colleagues, coming up with new paradigms of treatments as we weather this historic challenge.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email him at obnews@mdedge.com.
When last I wrote this column, I was preparing for travel to professional meetings in the spring, planning a presentation for an upcoming grand rounds, and readying to host a scientific advisory board meeting as part of a large scientific project we conduct in Center for Women’s Mental Health. We were also awaiting the relocation of several junior faculty and research staff to Boston this spring and summer as we build our team.
It is now obvious that the COVID-19 pandemic is not a passing squall, but rather a persistent gale that has placed our collective sails in the water. It has not capsized the boat, however, thanks in part to the actions of courageous frontline caregivers and first responders who have mobilized in the wake of this recent public health crisis. From doctors, nurses, and hospital staff to grocery store clerks, home health aides, and neighbors checking in on the elderly – to name just a few – a whole crew of members across society have helped buoy our collective ship. Resilience also is required by all of us who are managing the array of feelings brought about by the day-in, day-out challenges of living life with restricted movement and freedom to engage in pre-COVID-19 activities we took for granted. What seemed like a temporary workaround is now becoming the “new normal” for an unknown amount of time looking forward.
For over 3 decades, my colleagues and I have worked with women who suffer from serious psychiatric disorders and whose treatment has required psychiatric medications such as antidepressants, mood stabilizers, and anxiolytics. The challenge of our work with women who are pregnant or planning pregnancy has been the configuration of the safest ways to navigate treatment on an individual basis for these women across pregnancy and post partum, with continual assessments of how to minimize the risk to fetus from in utero exposure to medications that have been instrumental in the treatment of psychiatric disorders on one hand versus the risks of untreated psychiatric disorder on the other. This work has been the essence of the clinical mission and the cornerstone of the research conducted at the Center for Women’s Mental Health since its inception.
While I have worked shoulder to shoulder with obstetricians for years, my respect for these colleagues during these past weeks has only grown as they have instituted the swiftest protocols to mitigate risk associated with COVID-19 for our pregnant patients, some of whom have tested positive for COVID-19, all in an effort to keep both mother, fetus, and newborn as safe as possible.
For those of us providing mental health services to pregnant women during this time, certain clinical situations have arisen in the context of the COVID-19 pandemic which require particular attention and discussion.
Planned pregnancy and contraception during the COVID-19 pandemic
Half of the pregnancies in this country are unplanned. Now more than ever, it is critical that decisions about moving forward with a plan to conceive be deliberate. These considerations range from the existential to the most concrete. For example, during these last weeks, we have consulted on cases where couples on the cusp of attempts to conceive face concerns about COVID-19, hence making more complicated their timeline with respect to actual plans to get pregnant. These are complicated decisions, particularly for women who may be slightly older and at the reproductive age where delaying pregnancy may have an adverse effect on fertility.
A concrete example of how the pandemic has affected fertility is evident as we encounter situations where women may defer starting a prescription oral contraceptive or lapse in its use because they have had difficulty coordinating visits with health care providers and may fear picking up prescriptions from pharmacies. We also have seen that procedures such as IUD placements have been deferred or canceled, or that some patients decline trips to the hospital or clinic to receive this type of service. These new barriers to access of contraception may require more planning at this time so that decisions about family planning are by design and not default during a time as complicated as the current public health crisis.
Telemedicine: telepsychiatry and obstetrics virtual visits
While wide-scale use of telemedicine platforms was not the standard day-to-day practice in either obstetrics or psychiatry prior to the pandemic, telepsychiatry has come up to speed within a short number of weeks. At our institution, 85% of outpatient visits are being conducted remotely, with in-person visits being reserved for only urgent or emergent visits. Our inpatient psychiatry service remains a setting where psychiatric patients, regardless of their COVID-19 status, can receive necessary care.
The use of telemedicine and specifically telepsychiatry is critical to mitigate the likelihood of exposure to SARS-CoV-2. On our reproductive psychiatry service, it has actually been an opportunity to engage with patients for comprehensive initial consults about reproductive safety of psychiatric medications currently being taken, or for ongoing consultation and direct patient care during follow-up visits during pregnancy to see that patients are sustaining emotional well-being or have changes for treatment implemented if they are not well. An increased frequency of visits allows us more opportunity to capture any signs of early clinical worsening of symptoms that might have been missed previously using the more traditional in-person setting.
Telepsychiatry and “virtual visits” have allowed us to do real-time, nimble modifications of treatment regimens with both pharmacologic and nonpharmacologic interventions to keep women well and to keep them out of the hospital for psychiatric care as often as possible. It also has facilitated a closer collaboration with our colleagues in obstetrics. In a way, the team of providers, including psychiatrists, obstetrical providers, social workers, and therapists can more easily communicate virtually than has sometimes been the case previously, when day-to-day use of telemedicine and virtual team meetings was less common.
Recognition and treatment of anxiety in perinatal patients
Even pregnant women without preexisting anxiety disorders may have heightened anxiety during usual times, and women and their partners cope with this typically in numerous ways including participation in peer-support opportunities, wellness and self-care activities, leveraging support from care providers, and engaging with family. But the previously “typical pregnancy experience” has shifted in the context of COVID-19. Specifically, added concerns of pregnant women about becoming infected, of potential separation from family if they do become ill, or of separation from partners or support systems during labor and delivery (an issue that has been largely resolved in many hospitals), as well as the possibility that a neonate might become ill with exposure to the coronavirus are obviously understandable and real. Such contingencies are unsettling, even for the most settled of our patients. Labor and delivery plans, and plans for outside help from family or others with the baby and older children in the postpartum period, have been upended for many patients.
These are anxious times. The number of nonpharmacologic virtual interventions available to mitigate anxiety are filling email inboxes daily. Curating these options can be a challenge, although several resources are worth noting, such as our department’s page on mental health resources.
During these past weeks, we have seen growing numbers of women for whom the normative anxiety of pregnancy is increasing to the point of causing distress to the level of functional impairment. Many patients for the first time meet criteria for frank anxiety disorders. These patients deserve prompt evaluation by mental health professionals and treatment with evidence-based therapies for anxiety disorders whether nonpharmacologic or pharmacologic so as to mitigate the risk of untreated anxiety on maternal and fetal well-being and also to limit risk for postpartum depression and postpartum anxiety disorders.
Miscarriage and infertility
A 36-year-old patient came to see me in clinic in late January following a miscarriage. She had a history of a previous miscarriage a year before and had an episode of major depression to follow for which she received treatment with an antidepressant and cognitive-behavioral therapy; she also attended a perinatal loss support group. She saw me in early March, anxious to try to conceive but extremely concerned about the risks associated with becoming pregnant at this point in time. Following a lengthy discussion with me and her obstetrician, the patient decided to wait until “the curve flattened” in Boston in terms of new cases of COVID-19, and then start trying to conceive. The case of another patient with a very similar history was presented at our rounds a few weeks ago; she also elected to defer attempts to conceive until life is more settled.
Perhaps one of the most dramatic examples of the impact of COVID-19 on fertility has been for those women with plans to pursue treatment with one of the assisted reproductive technologies. They have been told that professional societies have made recommendations regarding use of assisted reproductive technologies that are not entirely consistent across the country, but where in many places such interventions have been suspended during the COVID-19 pandemic. For many women near the end of their reproductive years, delays in trying to conceive either with or without the aid of fertility treatments may indelibly shape their plans to have children.
Sustaining emotional well-being across pregnancy
Because most psychiatric disorders are chronic in course, it is often the situation where women are treated to wellness for serious psychiatric disorders, with the goal of maintaining wellness across pregnancy and the post partum. One of the most critical takeaway points from 30 years of working with psychiatrically ill pregnant women is the maxim that keeping women well during pregnancy is simply imperative. Maternal psychiatric well-being during pregnancy is a strong predictor of obstetrical and neonatal outcomes, postpartum mental health, and longer-term neurobehavioral outcomes in children. Critically, in the context of the pandemic, keeping women out of psychiatric crises mitigates the necessity of visits to urgent clinical settings such as EDs and psychiatric inpatient units, which can increase the likelihood of exposure to the coronavirus.
Preservation of sleep
Disruption in sleep (duration and quality) can be seen in well over half of women during pregnancy with and without psychiatric disorders, and our experience has been that this has been exacerbated for many women during the COVID-19 crisis. Yet there are very rich data showing that sleep deprivation or sleep dysregulation in women, for example, who suffer from bipolar disorder or major depression can be a strong trigger for psychiatric relapse of underlying illness during pregnancy and the postpartum period.
During a time when normal rhythms of day-to-day life have been shifted – if not frankly disrupted – by swift transitions to remote work, cancellation of school and associated school activities across the country, complaints of insomnia and non-restorative sleep have been exceedingly common. Relevant to all but particularly for pregnant women with histories of psychiatric disorder, attention to sleep hygiene, moderation of caffeine use (if any), and use of any number of biobehavioral interventions to enhance relaxation and modulate stress may be of great value.
Cognitive-behavioral therapy for insomnia (CBT-I) has been demonstrated to be effective in pregnant women. Fortunately, there are user-friendly options on digital platforms that can be used during the pandemic that may play an important role in sustaining emotional well-being for pregnant women who have frank symptoms of insomnia.
Maintenance of ongoing antidepressant treatment during pregnancy among women with histories of mood disorder
Over a decade ago, my colleagues and I wrote about the comparison of outcomes for women with histories of recurrent major depression, demonstrating the value of maintenance treatment with antidepressants, compared with discontinuation of these medications during pregnancy (JAMA. 2006 Feb 1;295[5]:499-507). Recently, I was asked if maintenance antidepressant use in women with histories of recurrent depression was still our clinical recommendation. Over the last decade, we have noted that nearly half of women treated with antidepressants, regardless of illness severity, will discontinue their use of these medications prior to or early on in pregnancy given concerns about potential unknown effects of fetal exposure to medications, even medications for which there are robust data supporting reproductive safety regarding risk of congenital malformations. Routine discontinuation of antidepressants prior to or during pregnancy continues, despite the fact that we showed nearly 70% of those women with past histories of depression on maintenance antidepressant treatment relapsed shortly after discontinuing medication.
While we do not dictate the decisions women make about antidepressant use before, during, or after pregnancy, women with the same severity of illness will frequently make different decisions (a good thing) but we are now having very frank discussions about the particular need during a pandemic to avoid the relapse of serious psychiatric disorders. We typically endorse maintenance medication use with all but a very few number of psychotropic medications for which benefit may not outweigh risk to the fetus. However, for women who have decided nonetheless to discontinue antidepressants or other psychotropics during pregnancy despite the known risk of relapse, we strongly advise that they initiate treatment with evidence-based nonpharmacologic intervention such as CBT or mindfulness-based cognitive therapy (MBCT).
As in other areas of medicine, the pandemic is prompting we professionals in psychiatry, and specifically in perinatal psychiatry, to use all of our tools to keep pregnant and postpartum women well. The availability of digital tools to deliver MBCT and CBT has made the use of such interventions particularly viable at a time of social distancing. That being said, for patients with highly recurrent affective disorder with histories of previous recurrence when they stop their antidepressants, we are more strongly recommending serious consideration of maintenance medication treatment.
Virtual rounds in reproductive psychiatry and women’s mental health
The use of virtual platforms to connect with both patients and colleagues also has provided new opportunities for interaction with the reproductive psychiatry community as a whole. Peer teaching and peer support has been a critical part of our mission, and we decided 1 month ago to establish Virtual Rounds at the Center for Women’s Mental Health. This is a free digital platform, held on a weekly basis with our colleagues from across the country, where we discuss cases that come up in our own clinical rounds and also questions that get put forth by our colleagues in the area of reproductive psychiatry as they manage patients during the pandemic.
Changes in the postpartum experience
The last decade has brought a growing appreciation of postpartum depression and the need to screen and treat postpartum psychiatric disorders, such as postpartum mood and anxiety disorders. Yet in the era of this pandemic, the postpartum experience is itself is changing. Changes in carefully configured plans for the postpartum period – from family coming and going to mobilizing extra support at home and to now having new moms having to manage families and their other children at home – has been an enormous stressor for many women. Plans to have more elderly parents visit during the acute postpartum period, and the increased concerns about people traveling to and from a home where there is a newborn and the need to quarantine, has made the transition to motherhood much more complicated for all postpartum women, let alone for those postpartum women who have histories of psychiatric disorder.
There is a risk of social isolation for postpartum women even under normal circumstances, and this is profoundly more likely during this pandemic. We are actively working with our postpartum patients and optimizing treatment, brainstorming options in terms of using both virtual and real-time support to the extent that it is safe in order to keep women healthy during such a stressful and critical time.
I am heartened by the efforts on the part of organizations such as Postpartum Support International to make available virtually their resources with respect to community-based support and education for women who feel increasingly isolated during the postpartum period, a time where connectedness is so critical.
Summarily, these have been challenging times, but also times of opportunity. The COVID-19 pandemic has prompted us to get even more creative as we configure ways to optimize the emotional well-being of our patients who are planning to get pregnant, who are pregnant, or who are post partum.
The current time, while challenging in so many ways and a time of great pain, loss, and grief for far too many, has also provided an opportunity to work even more collaboratively with our colleagues, coming up with new paradigms of treatments as we weather this historic challenge.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email him at obnews@mdedge.com.
When last I wrote this column, I was preparing for travel to professional meetings in the spring, planning a presentation for an upcoming grand rounds, and readying to host a scientific advisory board meeting as part of a large scientific project we conduct in Center for Women’s Mental Health. We were also awaiting the relocation of several junior faculty and research staff to Boston this spring and summer as we build our team.
It is now obvious that the COVID-19 pandemic is not a passing squall, but rather a persistent gale that has placed our collective sails in the water. It has not capsized the boat, however, thanks in part to the actions of courageous frontline caregivers and first responders who have mobilized in the wake of this recent public health crisis. From doctors, nurses, and hospital staff to grocery store clerks, home health aides, and neighbors checking in on the elderly – to name just a few – a whole crew of members across society have helped buoy our collective ship. Resilience also is required by all of us who are managing the array of feelings brought about by the day-in, day-out challenges of living life with restricted movement and freedom to engage in pre-COVID-19 activities we took for granted. What seemed like a temporary workaround is now becoming the “new normal” for an unknown amount of time looking forward.
For over 3 decades, my colleagues and I have worked with women who suffer from serious psychiatric disorders and whose treatment has required psychiatric medications such as antidepressants, mood stabilizers, and anxiolytics. The challenge of our work with women who are pregnant or planning pregnancy has been the configuration of the safest ways to navigate treatment on an individual basis for these women across pregnancy and post partum, with continual assessments of how to minimize the risk to fetus from in utero exposure to medications that have been instrumental in the treatment of psychiatric disorders on one hand versus the risks of untreated psychiatric disorder on the other. This work has been the essence of the clinical mission and the cornerstone of the research conducted at the Center for Women’s Mental Health since its inception.
While I have worked shoulder to shoulder with obstetricians for years, my respect for these colleagues during these past weeks has only grown as they have instituted the swiftest protocols to mitigate risk associated with COVID-19 for our pregnant patients, some of whom have tested positive for COVID-19, all in an effort to keep both mother, fetus, and newborn as safe as possible.
For those of us providing mental health services to pregnant women during this time, certain clinical situations have arisen in the context of the COVID-19 pandemic which require particular attention and discussion.
Planned pregnancy and contraception during the COVID-19 pandemic
Half of the pregnancies in this country are unplanned. Now more than ever, it is critical that decisions about moving forward with a plan to conceive be deliberate. These considerations range from the existential to the most concrete. For example, during these last weeks, we have consulted on cases where couples on the cusp of attempts to conceive face concerns about COVID-19, hence making more complicated their timeline with respect to actual plans to get pregnant. These are complicated decisions, particularly for women who may be slightly older and at the reproductive age where delaying pregnancy may have an adverse effect on fertility.
A concrete example of how the pandemic has affected fertility is evident as we encounter situations where women may defer starting a prescription oral contraceptive or lapse in its use because they have had difficulty coordinating visits with health care providers and may fear picking up prescriptions from pharmacies. We also have seen that procedures such as IUD placements have been deferred or canceled, or that some patients decline trips to the hospital or clinic to receive this type of service. These new barriers to access of contraception may require more planning at this time so that decisions about family planning are by design and not default during a time as complicated as the current public health crisis.
Telemedicine: telepsychiatry and obstetrics virtual visits
While wide-scale use of telemedicine platforms was not the standard day-to-day practice in either obstetrics or psychiatry prior to the pandemic, telepsychiatry has come up to speed within a short number of weeks. At our institution, 85% of outpatient visits are being conducted remotely, with in-person visits being reserved for only urgent or emergent visits. Our inpatient psychiatry service remains a setting where psychiatric patients, regardless of their COVID-19 status, can receive necessary care.
The use of telemedicine and specifically telepsychiatry is critical to mitigate the likelihood of exposure to SARS-CoV-2. On our reproductive psychiatry service, it has actually been an opportunity to engage with patients for comprehensive initial consults about reproductive safety of psychiatric medications currently being taken, or for ongoing consultation and direct patient care during follow-up visits during pregnancy to see that patients are sustaining emotional well-being or have changes for treatment implemented if they are not well. An increased frequency of visits allows us more opportunity to capture any signs of early clinical worsening of symptoms that might have been missed previously using the more traditional in-person setting.
Telepsychiatry and “virtual visits” have allowed us to do real-time, nimble modifications of treatment regimens with both pharmacologic and nonpharmacologic interventions to keep women well and to keep them out of the hospital for psychiatric care as often as possible. It also has facilitated a closer collaboration with our colleagues in obstetrics. In a way, the team of providers, including psychiatrists, obstetrical providers, social workers, and therapists can more easily communicate virtually than has sometimes been the case previously, when day-to-day use of telemedicine and virtual team meetings was less common.
Recognition and treatment of anxiety in perinatal patients
Even pregnant women without preexisting anxiety disorders may have heightened anxiety during usual times, and women and their partners cope with this typically in numerous ways including participation in peer-support opportunities, wellness and self-care activities, leveraging support from care providers, and engaging with family. But the previously “typical pregnancy experience” has shifted in the context of COVID-19. Specifically, added concerns of pregnant women about becoming infected, of potential separation from family if they do become ill, or of separation from partners or support systems during labor and delivery (an issue that has been largely resolved in many hospitals), as well as the possibility that a neonate might become ill with exposure to the coronavirus are obviously understandable and real. Such contingencies are unsettling, even for the most settled of our patients. Labor and delivery plans, and plans for outside help from family or others with the baby and older children in the postpartum period, have been upended for many patients.
These are anxious times. The number of nonpharmacologic virtual interventions available to mitigate anxiety are filling email inboxes daily. Curating these options can be a challenge, although several resources are worth noting, such as our department’s page on mental health resources.
During these past weeks, we have seen growing numbers of women for whom the normative anxiety of pregnancy is increasing to the point of causing distress to the level of functional impairment. Many patients for the first time meet criteria for frank anxiety disorders. These patients deserve prompt evaluation by mental health professionals and treatment with evidence-based therapies for anxiety disorders whether nonpharmacologic or pharmacologic so as to mitigate the risk of untreated anxiety on maternal and fetal well-being and also to limit risk for postpartum depression and postpartum anxiety disorders.
Miscarriage and infertility
A 36-year-old patient came to see me in clinic in late January following a miscarriage. She had a history of a previous miscarriage a year before and had an episode of major depression to follow for which she received treatment with an antidepressant and cognitive-behavioral therapy; she also attended a perinatal loss support group. She saw me in early March, anxious to try to conceive but extremely concerned about the risks associated with becoming pregnant at this point in time. Following a lengthy discussion with me and her obstetrician, the patient decided to wait until “the curve flattened” in Boston in terms of new cases of COVID-19, and then start trying to conceive. The case of another patient with a very similar history was presented at our rounds a few weeks ago; she also elected to defer attempts to conceive until life is more settled.
Perhaps one of the most dramatic examples of the impact of COVID-19 on fertility has been for those women with plans to pursue treatment with one of the assisted reproductive technologies. They have been told that professional societies have made recommendations regarding use of assisted reproductive technologies that are not entirely consistent across the country, but where in many places such interventions have been suspended during the COVID-19 pandemic. For many women near the end of their reproductive years, delays in trying to conceive either with or without the aid of fertility treatments may indelibly shape their plans to have children.
Sustaining emotional well-being across pregnancy
Because most psychiatric disorders are chronic in course, it is often the situation where women are treated to wellness for serious psychiatric disorders, with the goal of maintaining wellness across pregnancy and the post partum. One of the most critical takeaway points from 30 years of working with psychiatrically ill pregnant women is the maxim that keeping women well during pregnancy is simply imperative. Maternal psychiatric well-being during pregnancy is a strong predictor of obstetrical and neonatal outcomes, postpartum mental health, and longer-term neurobehavioral outcomes in children. Critically, in the context of the pandemic, keeping women out of psychiatric crises mitigates the necessity of visits to urgent clinical settings such as EDs and psychiatric inpatient units, which can increase the likelihood of exposure to the coronavirus.
Preservation of sleep
Disruption in sleep (duration and quality) can be seen in well over half of women during pregnancy with and without psychiatric disorders, and our experience has been that this has been exacerbated for many women during the COVID-19 crisis. Yet there are very rich data showing that sleep deprivation or sleep dysregulation in women, for example, who suffer from bipolar disorder or major depression can be a strong trigger for psychiatric relapse of underlying illness during pregnancy and the postpartum period.
During a time when normal rhythms of day-to-day life have been shifted – if not frankly disrupted – by swift transitions to remote work, cancellation of school and associated school activities across the country, complaints of insomnia and non-restorative sleep have been exceedingly common. Relevant to all but particularly for pregnant women with histories of psychiatric disorder, attention to sleep hygiene, moderation of caffeine use (if any), and use of any number of biobehavioral interventions to enhance relaxation and modulate stress may be of great value.
Cognitive-behavioral therapy for insomnia (CBT-I) has been demonstrated to be effective in pregnant women. Fortunately, there are user-friendly options on digital platforms that can be used during the pandemic that may play an important role in sustaining emotional well-being for pregnant women who have frank symptoms of insomnia.
Maintenance of ongoing antidepressant treatment during pregnancy among women with histories of mood disorder
Over a decade ago, my colleagues and I wrote about the comparison of outcomes for women with histories of recurrent major depression, demonstrating the value of maintenance treatment with antidepressants, compared with discontinuation of these medications during pregnancy (JAMA. 2006 Feb 1;295[5]:499-507). Recently, I was asked if maintenance antidepressant use in women with histories of recurrent depression was still our clinical recommendation. Over the last decade, we have noted that nearly half of women treated with antidepressants, regardless of illness severity, will discontinue their use of these medications prior to or early on in pregnancy given concerns about potential unknown effects of fetal exposure to medications, even medications for which there are robust data supporting reproductive safety regarding risk of congenital malformations. Routine discontinuation of antidepressants prior to or during pregnancy continues, despite the fact that we showed nearly 70% of those women with past histories of depression on maintenance antidepressant treatment relapsed shortly after discontinuing medication.
While we do not dictate the decisions women make about antidepressant use before, during, or after pregnancy, women with the same severity of illness will frequently make different decisions (a good thing) but we are now having very frank discussions about the particular need during a pandemic to avoid the relapse of serious psychiatric disorders. We typically endorse maintenance medication use with all but a very few number of psychotropic medications for which benefit may not outweigh risk to the fetus. However, for women who have decided nonetheless to discontinue antidepressants or other psychotropics during pregnancy despite the known risk of relapse, we strongly advise that they initiate treatment with evidence-based nonpharmacologic intervention such as CBT or mindfulness-based cognitive therapy (MBCT).
As in other areas of medicine, the pandemic is prompting we professionals in psychiatry, and specifically in perinatal psychiatry, to use all of our tools to keep pregnant and postpartum women well. The availability of digital tools to deliver MBCT and CBT has made the use of such interventions particularly viable at a time of social distancing. That being said, for patients with highly recurrent affective disorder with histories of previous recurrence when they stop their antidepressants, we are more strongly recommending serious consideration of maintenance medication treatment.
Virtual rounds in reproductive psychiatry and women’s mental health
The use of virtual platforms to connect with both patients and colleagues also has provided new opportunities for interaction with the reproductive psychiatry community as a whole. Peer teaching and peer support has been a critical part of our mission, and we decided 1 month ago to establish Virtual Rounds at the Center for Women’s Mental Health. This is a free digital platform, held on a weekly basis with our colleagues from across the country, where we discuss cases that come up in our own clinical rounds and also questions that get put forth by our colleagues in the area of reproductive psychiatry as they manage patients during the pandemic.
Changes in the postpartum experience
The last decade has brought a growing appreciation of postpartum depression and the need to screen and treat postpartum psychiatric disorders, such as postpartum mood and anxiety disorders. Yet in the era of this pandemic, the postpartum experience is itself is changing. Changes in carefully configured plans for the postpartum period – from family coming and going to mobilizing extra support at home and to now having new moms having to manage families and their other children at home – has been an enormous stressor for many women. Plans to have more elderly parents visit during the acute postpartum period, and the increased concerns about people traveling to and from a home where there is a newborn and the need to quarantine, has made the transition to motherhood much more complicated for all postpartum women, let alone for those postpartum women who have histories of psychiatric disorder.
There is a risk of social isolation for postpartum women even under normal circumstances, and this is profoundly more likely during this pandemic. We are actively working with our postpartum patients and optimizing treatment, brainstorming options in terms of using both virtual and real-time support to the extent that it is safe in order to keep women healthy during such a stressful and critical time.
I am heartened by the efforts on the part of organizations such as Postpartum Support International to make available virtually their resources with respect to community-based support and education for women who feel increasingly isolated during the postpartum period, a time where connectedness is so critical.
Summarily, these have been challenging times, but also times of opportunity. The COVID-19 pandemic has prompted us to get even more creative as we configure ways to optimize the emotional well-being of our patients who are planning to get pregnant, who are pregnant, or who are post partum.
The current time, while challenging in so many ways and a time of great pain, loss, and grief for far too many, has also provided an opportunity to work even more collaboratively with our colleagues, coming up with new paradigms of treatments as we weather this historic challenge.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email him at obnews@mdedge.com.
Contact tracing, isolation have impact, study shows
A far-reaching surveillance initiative was implemented in Shenzhen, China, to isolate and contact trace people suspected of having the COVID-19 coronavirus. This initiative led to faster confirmation of new cases and reduced the window of time during which people were infectious in the community. This potentially reduced the number of new infections that arose from each case, according to a study of patients and contacts over 4 weeks (Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099[20]30287-5).

“The experience of COVID-19 in the city of Shenzhen may demonstrate the huge scale of testing and contact tracing that’s needed to reduce the virus spreading,” said study coauthor Ting Ma, PhD, of Harbin Institute of Technology at Shenzhen.
Dr. Ma acknowledged that some of the measures the program used, such as isolating people outside their homes, may be difficult to impose in other countries, “but we urge governments to consider our findings in the global response to COVID-19.”
The study followed 391 coronavirus cases and 1,286 close contacts identified by the Shenzhen Center for Disease Control and Prevention from Jan. 14 to Feb. 12 this year. The study showed that contact tracing led to confirming new diagnoses within 3.2 days on average vs. 5.5 for symptom-based surveillance, and reduced the time it took to isolate newly infected people by 2 days, from an average of 4.6 to 2.7 days. Eighty-seven people were diagnosed with COVID-19 after they were contact traced and tested. Twenty percent of them had no symptoms, and 29% had no fever. Three deaths occurred in the group during the study period.
The surveillance program was comprehensive and intense. On Jan. 8, the Shenzhen CDC started monitoring travelers from Hubei province, of which Wuhan is the capital, for symptoms of COVID-19. Shenzhen is a city of about 12.5 million people in southeastern China, near Hong Kong, and is about 560 miles south of Wuhan. Over the next 2 weeks, the Shenzhen CDC expanded that surveillance program to all travelers from Hubei regardless of symptoms, along with local hospital patients and people detected by fever screenings at area clinics.
Suspected cases and close contacts underwent nasal-swab testing at 40 different locations in the city. The program identified close contacts through contact tracing, and included anyone who lived in the same dwelling, shared a meal, traveled, or had a social interaction with an index 2 days before symptoms appeared. Casual contacts and some close contacts, such as clinic nurses, who wore masks during the encounters were excluded.
“To achieve similar results, other countries might be able to combine near-universal testing and intensive contact tracing with social distancing and partial lockdowns,” said Dr. Ma. “Although no lockdown measures were introduced in Shenzhen until the end of our study period, Wuhan’s lockdown could have significantly restricted the spread of coronavirus to Shenzhen.”
The researchers noted that children are as susceptible to the virus as are adults, even though their symptoms are not as severe as those of adults. The rate of infection in children 10 and younger was similar to the overall infection rate, 7.4% vs. 6.6%, so the researchers noted that surveillance measures should target them as well.
“This study to me confirms a lot of what we’ve already known,” Aaron E. Glatt, MD, chairman of medicine and an epidemiologist at Mount Sinai South Nassau in Oceanside, N.Y., said in an interview. “It’s an elegant study, but at the same time it sends us a message that we’re at a critical point of time for us to intervene and prevent cases at the very beginning.”
He acknowledged that the Shenzhen effort was intense. “It’s always a resource-intense requirement to do such extensive contact tracing, but that doesn’t mean it shouldn’t be done to the best of your ability to do so,” he said. He was struck by the low relative rate of infection among contacts in the study – around 7%. “There are differences obviously in infection rates in every outbreak,” he said. “Every individual has their own particular infection rate. While we can take ranges and statistical guesses for every individual patient, it could be very high or very low, and that’s most critical to nip it in the bud.”
Lead author Qifang Bi and study coauthors had no financial relationships to disclose.
SOURCE: Bi Q et al. Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099(20)30287-5.
A far-reaching surveillance initiative was implemented in Shenzhen, China, to isolate and contact trace people suspected of having the COVID-19 coronavirus. This initiative led to faster confirmation of new cases and reduced the window of time during which people were infectious in the community. This potentially reduced the number of new infections that arose from each case, according to a study of patients and contacts over 4 weeks (Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099[20]30287-5).
“The experience of COVID-19 in the city of Shenzhen may demonstrate the huge scale of testing and contact tracing that’s needed to reduce the virus spreading,” said study coauthor Ting Ma, PhD, of Harbin Institute of Technology at Shenzhen.
Dr. Ma acknowledged that some of the measures the program used, such as isolating people outside their homes, may be difficult to impose in other countries, “but we urge governments to consider our findings in the global response to COVID-19.”
The study followed 391 coronavirus cases and 1,286 close contacts identified by the Shenzhen Center for Disease Control and Prevention from Jan. 14 to Feb. 12 this year. The study showed that contact tracing led to confirming new diagnoses within 3.2 days on average vs. 5.5 for symptom-based surveillance, and reduced the time it took to isolate newly infected people by 2 days, from an average of 4.6 to 2.7 days. Eighty-seven people were diagnosed with COVID-19 after they were contact traced and tested. Twenty percent of them had no symptoms, and 29% had no fever. Three deaths occurred in the group during the study period.
The surveillance program was comprehensive and intense. On Jan. 8, the Shenzhen CDC started monitoring travelers from Hubei province, of which Wuhan is the capital, for symptoms of COVID-19. Shenzhen is a city of about 12.5 million people in southeastern China, near Hong Kong, and is about 560 miles south of Wuhan. Over the next 2 weeks, the Shenzhen CDC expanded that surveillance program to all travelers from Hubei regardless of symptoms, along with local hospital patients and people detected by fever screenings at area clinics.
Suspected cases and close contacts underwent nasal-swab testing at 40 different locations in the city. The program identified close contacts through contact tracing, and included anyone who lived in the same dwelling, shared a meal, traveled, or had a social interaction with an index 2 days before symptoms appeared. Casual contacts and some close contacts, such as clinic nurses, who wore masks during the encounters were excluded.
“To achieve similar results, other countries might be able to combine near-universal testing and intensive contact tracing with social distancing and partial lockdowns,” said Dr. Ma. “Although no lockdown measures were introduced in Shenzhen until the end of our study period, Wuhan’s lockdown could have significantly restricted the spread of coronavirus to Shenzhen.”
The researchers noted that children are as susceptible to the virus as are adults, even though their symptoms are not as severe as those of adults. The rate of infection in children 10 and younger was similar to the overall infection rate, 7.4% vs. 6.6%, so the researchers noted that surveillance measures should target them as well.
“This study to me confirms a lot of what we’ve already known,” Aaron E. Glatt, MD, chairman of medicine and an epidemiologist at Mount Sinai South Nassau in Oceanside, N.Y., said in an interview. “It’s an elegant study, but at the same time it sends us a message that we’re at a critical point of time for us to intervene and prevent cases at the very beginning.”
He acknowledged that the Shenzhen effort was intense. “It’s always a resource-intense requirement to do such extensive contact tracing, but that doesn’t mean it shouldn’t be done to the best of your ability to do so,” he said. He was struck by the low relative rate of infection among contacts in the study – around 7%. “There are differences obviously in infection rates in every outbreak,” he said. “Every individual has their own particular infection rate. While we can take ranges and statistical guesses for every individual patient, it could be very high or very low, and that’s most critical to nip it in the bud.”
Lead author Qifang Bi and study coauthors had no financial relationships to disclose.
SOURCE: Bi Q et al. Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099(20)30287-5.
A far-reaching surveillance initiative was implemented in Shenzhen, China, to isolate and contact trace people suspected of having the COVID-19 coronavirus. This initiative led to faster confirmation of new cases and reduced the window of time during which people were infectious in the community. This potentially reduced the number of new infections that arose from each case, according to a study of patients and contacts over 4 weeks (Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099[20]30287-5).
“The experience of COVID-19 in the city of Shenzhen may demonstrate the huge scale of testing and contact tracing that’s needed to reduce the virus spreading,” said study coauthor Ting Ma, PhD, of Harbin Institute of Technology at Shenzhen.
Dr. Ma acknowledged that some of the measures the program used, such as isolating people outside their homes, may be difficult to impose in other countries, “but we urge governments to consider our findings in the global response to COVID-19.”
The study followed 391 coronavirus cases and 1,286 close contacts identified by the Shenzhen Center for Disease Control and Prevention from Jan. 14 to Feb. 12 this year. The study showed that contact tracing led to confirming new diagnoses within 3.2 days on average vs. 5.5 for symptom-based surveillance, and reduced the time it took to isolate newly infected people by 2 days, from an average of 4.6 to 2.7 days. Eighty-seven people were diagnosed with COVID-19 after they were contact traced and tested. Twenty percent of them had no symptoms, and 29% had no fever. Three deaths occurred in the group during the study period.
The surveillance program was comprehensive and intense. On Jan. 8, the Shenzhen CDC started monitoring travelers from Hubei province, of which Wuhan is the capital, for symptoms of COVID-19. Shenzhen is a city of about 12.5 million people in southeastern China, near Hong Kong, and is about 560 miles south of Wuhan. Over the next 2 weeks, the Shenzhen CDC expanded that surveillance program to all travelers from Hubei regardless of symptoms, along with local hospital patients and people detected by fever screenings at area clinics.
Suspected cases and close contacts underwent nasal-swab testing at 40 different locations in the city. The program identified close contacts through contact tracing, and included anyone who lived in the same dwelling, shared a meal, traveled, or had a social interaction with an index 2 days before symptoms appeared. Casual contacts and some close contacts, such as clinic nurses, who wore masks during the encounters were excluded.
“To achieve similar results, other countries might be able to combine near-universal testing and intensive contact tracing with social distancing and partial lockdowns,” said Dr. Ma. “Although no lockdown measures were introduced in Shenzhen until the end of our study period, Wuhan’s lockdown could have significantly restricted the spread of coronavirus to Shenzhen.”
The researchers noted that children are as susceptible to the virus as are adults, even though their symptoms are not as severe as those of adults. The rate of infection in children 10 and younger was similar to the overall infection rate, 7.4% vs. 6.6%, so the researchers noted that surveillance measures should target them as well.
“This study to me confirms a lot of what we’ve already known,” Aaron E. Glatt, MD, chairman of medicine and an epidemiologist at Mount Sinai South Nassau in Oceanside, N.Y., said in an interview. “It’s an elegant study, but at the same time it sends us a message that we’re at a critical point of time for us to intervene and prevent cases at the very beginning.”
He acknowledged that the Shenzhen effort was intense. “It’s always a resource-intense requirement to do such extensive contact tracing, but that doesn’t mean it shouldn’t be done to the best of your ability to do so,” he said. He was struck by the low relative rate of infection among contacts in the study – around 7%. “There are differences obviously in infection rates in every outbreak,” he said. “Every individual has their own particular infection rate. While we can take ranges and statistical guesses for every individual patient, it could be very high or very low, and that’s most critical to nip it in the bud.”
Lead author Qifang Bi and study coauthors had no financial relationships to disclose.
SOURCE: Bi Q et al. Lancet Infect Dis. 2020 Apr 27. doi: 10.1016/S1473-3099(20)30287-5.
FROM LANCET INFECTIOUS DISEASE
Acute kidney injury in children hospitalized with diarrheal illness in the U.S.
Clinical question: To determine the incidence and consequences of acute kidney injury among children hospitalized with diarrheal illness in the United States.

Background: Diarrheal illness is the fourth leading cause of death for children younger than 5 years and the fifth leading cause of years of life lost globally. In the United States, diarrheal illness remains a leading cause of hospital admission among young children. Complications of severe diarrheal illness include hypovolemic acute kidney injury (AKI). Hospitalized children who develop AKI experience longer hospital stays and higher mortality. Additionally, children who experience AKI are at increased risk for chronic kidney disease (CKD), hypertension, and proteinuria.
Study design: Retrospective cohort study.
Setting: Kids’ Inpatient Database (KID) from 2009 and 2012. The authors used secondary International Classification of Diseases, Ninth Revision (ICD-9) diagnoses of AKI to identify patients.
Synopsis: The authors reviewed all patients with diarrhea and found that the incidence of AKI in children hospitalized was 0.8%. Those with infectious diarrhea had an incidence of 1% and with noninfectious diarrhea had an incidence of 0.6%. There was a higher incidence of dialysis-requiring AKI in patients with infectious diarrhea. The odds of developing AKI increased with older age in both infectious and noninfectious diarrheal illnesses. As compared with noninfectious diarrheal illness, infectious diarrheal illness was associated with higher odds of AKI (odds ratio, 2.1; 95% confidence interval, 1.7-2.7). Irrespective of diarrhea type, hematologic and rheumatologic conditions, solid organ transplant, CKD, and hypertension were associated with higher odds of developing AKI. AKI in infectious diarrheal illness was also associated with other renal or genitourinary abnormalities, whereas AKI in noninfectious diarrheal illness was associated with diabetes, cardiovascular, and neurologic conditions.
Hospitalizations for diarrheal illness complicated by AKI were associated with higher mortality, prolonged LOS, and higher hospital cost with odds of death increased eightfold with AKI, mean hospital stay was prolonged by 3 days, and costs increased by greater than $9,000 per hospital stay. The development of AKI in hospitalized diarrheal illness was associated with an up to 11-fold increase in the odds of in-hospital mortality for infectious (OR, 10.8; 95% CI, 3.4-34.3) and noninfectious diarrheal illness (OR, 7.0; 95% CI, 3.1-15.7).
The strengths of this study include broad representation of hospitals caring for children across the United States. The study was limited by its use of ICD-9 codes which may misidentify AKI. The authors were unable to determine if identifying AKI could improve outcomes for patients with diarrheal illness.
Bottom line: AKI in diarrhea illnesses is relatively rare. Close attention should be given to AKI in patients with certain serious comorbid illnesses.
Article citation: Bradshaw C, Han J, Chertow GM, Long J, Sutherland SM, Anand S. Acute Kidney Injury in Children Hospitalized With Diarrheal Illness in the United States. Hosp Pediatr. 2019 Dec;9(12):933-941.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, and serves as the pediatrics editor for The Hospitalist.
Clinical question: To determine the incidence and consequences of acute kidney injury among children hospitalized with diarrheal illness in the United States.
Background: Diarrheal illness is the fourth leading cause of death for children younger than 5 years and the fifth leading cause of years of life lost globally. In the United States, diarrheal illness remains a leading cause of hospital admission among young children. Complications of severe diarrheal illness include hypovolemic acute kidney injury (AKI). Hospitalized children who develop AKI experience longer hospital stays and higher mortality. Additionally, children who experience AKI are at increased risk for chronic kidney disease (CKD), hypertension, and proteinuria.
Study design: Retrospective cohort study.
Setting: Kids’ Inpatient Database (KID) from 2009 and 2012. The authors used secondary International Classification of Diseases, Ninth Revision (ICD-9) diagnoses of AKI to identify patients.
Synopsis: The authors reviewed all patients with diarrhea and found that the incidence of AKI in children hospitalized was 0.8%. Those with infectious diarrhea had an incidence of 1% and with noninfectious diarrhea had an incidence of 0.6%. There was a higher incidence of dialysis-requiring AKI in patients with infectious diarrhea. The odds of developing AKI increased with older age in both infectious and noninfectious diarrheal illnesses. As compared with noninfectious diarrheal illness, infectious diarrheal illness was associated with higher odds of AKI (odds ratio, 2.1; 95% confidence interval, 1.7-2.7). Irrespective of diarrhea type, hematologic and rheumatologic conditions, solid organ transplant, CKD, and hypertension were associated with higher odds of developing AKI. AKI in infectious diarrheal illness was also associated with other renal or genitourinary abnormalities, whereas AKI in noninfectious diarrheal illness was associated with diabetes, cardiovascular, and neurologic conditions.
Hospitalizations for diarrheal illness complicated by AKI were associated with higher mortality, prolonged LOS, and higher hospital cost with odds of death increased eightfold with AKI, mean hospital stay was prolonged by 3 days, and costs increased by greater than $9,000 per hospital stay. The development of AKI in hospitalized diarrheal illness was associated with an up to 11-fold increase in the odds of in-hospital mortality for infectious (OR, 10.8; 95% CI, 3.4-34.3) and noninfectious diarrheal illness (OR, 7.0; 95% CI, 3.1-15.7).
The strengths of this study include broad representation of hospitals caring for children across the United States. The study was limited by its use of ICD-9 codes which may misidentify AKI. The authors were unable to determine if identifying AKI could improve outcomes for patients with diarrheal illness.
Bottom line: AKI in diarrhea illnesses is relatively rare. Close attention should be given to AKI in patients with certain serious comorbid illnesses.
Article citation: Bradshaw C, Han J, Chertow GM, Long J, Sutherland SM, Anand S. Acute Kidney Injury in Children Hospitalized With Diarrheal Illness in the United States. Hosp Pediatr. 2019 Dec;9(12):933-941.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, and serves as the pediatrics editor for The Hospitalist.
Clinical question: To determine the incidence and consequences of acute kidney injury among children hospitalized with diarrheal illness in the United States.
Background: Diarrheal illness is the fourth leading cause of death for children younger than 5 years and the fifth leading cause of years of life lost globally. In the United States, diarrheal illness remains a leading cause of hospital admission among young children. Complications of severe diarrheal illness include hypovolemic acute kidney injury (AKI). Hospitalized children who develop AKI experience longer hospital stays and higher mortality. Additionally, children who experience AKI are at increased risk for chronic kidney disease (CKD), hypertension, and proteinuria.
Study design: Retrospective cohort study.
Setting: Kids’ Inpatient Database (KID) from 2009 and 2012. The authors used secondary International Classification of Diseases, Ninth Revision (ICD-9) diagnoses of AKI to identify patients.
Synopsis: The authors reviewed all patients with diarrhea and found that the incidence of AKI in children hospitalized was 0.8%. Those with infectious diarrhea had an incidence of 1% and with noninfectious diarrhea had an incidence of 0.6%. There was a higher incidence of dialysis-requiring AKI in patients with infectious diarrhea. The odds of developing AKI increased with older age in both infectious and noninfectious diarrheal illnesses. As compared with noninfectious diarrheal illness, infectious diarrheal illness was associated with higher odds of AKI (odds ratio, 2.1; 95% confidence interval, 1.7-2.7). Irrespective of diarrhea type, hematologic and rheumatologic conditions, solid organ transplant, CKD, and hypertension were associated with higher odds of developing AKI. AKI in infectious diarrheal illness was also associated with other renal or genitourinary abnormalities, whereas AKI in noninfectious diarrheal illness was associated with diabetes, cardiovascular, and neurologic conditions.
Hospitalizations for diarrheal illness complicated by AKI were associated with higher mortality, prolonged LOS, and higher hospital cost with odds of death increased eightfold with AKI, mean hospital stay was prolonged by 3 days, and costs increased by greater than $9,000 per hospital stay. The development of AKI in hospitalized diarrheal illness was associated with an up to 11-fold increase in the odds of in-hospital mortality for infectious (OR, 10.8; 95% CI, 3.4-34.3) and noninfectious diarrheal illness (OR, 7.0; 95% CI, 3.1-15.7).
The strengths of this study include broad representation of hospitals caring for children across the United States. The study was limited by its use of ICD-9 codes which may misidentify AKI. The authors were unable to determine if identifying AKI could improve outcomes for patients with diarrheal illness.
Bottom line: AKI in diarrhea illnesses is relatively rare. Close attention should be given to AKI in patients with certain serious comorbid illnesses.
Article citation: Bradshaw C, Han J, Chertow GM, Long J, Sutherland SM, Anand S. Acute Kidney Injury in Children Hospitalized With Diarrheal Illness in the United States. Hosp Pediatr. 2019 Dec;9(12):933-941.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, and serves as the pediatrics editor for The Hospitalist.
Supreme Court: Government owes more than $12 billion to health plans
The federal government owes billions of dollars to health insurers under an Affordable Care Act provision intended to help insurers mitigate risk, the U.S. Supreme Court has ruled.

In an 8-to-1 vote announced April 27, justices sided with the plaintiff health plans in Maine Community Health Options v. United States, ruling that the risk corridors statute created a government obligation to pay insurers the full amount originally calculated and that appropriation measures later passed by Congress did not repeal this obligation.
“In establishing the temporary risk corridors program, Congress created a rare money-mandating obligation requiring the federal government to make payments under [Section 1342 of the Affordable Care Act’s] formula,” Associate Justice Sonia Sotomayor wrote in the majority opinion. “Lacking other statutory paths to relief ... petitioners may seek to collect payment through a damages action in the Court of Federal Claims.”
Maine Community Health Options v. United States, which consolidates several lawsuits against the government, centers on the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged by more than $12 billion all together.
The U.S. Department of Justice countered that the government is not required to pay the plans because of measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses.
The U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
The U.S. Supreme Court disagreed. Justices noted that even after Congress enacted the first rider, HHS and the Centers for Medicare & Medicaid Services reiterated that the ACA requires the Secretary to make full payments to issuers and that “HHS [would] record risk corridors payments due as an obligation of the United States government for which full payment is required,” according to the Supreme Court opinion.
“They understood that profitable insurers’ payments to the government would not dispel the Secretary’s obligation to pay unprofitable insurers, even ‘in the event of a shortfall,’ ” Justice Sotomayor wrote in the majority opinion.
Associate Justice Samuel Alito Jr. however, took issue with his fellow justices’ decision. In his dissenting opinion, Justice Alito wrote that under the ruling, billions of taxpayer dollars will be turned over to insurance companies that bet unsuccessfully on the success of the program in question.
“This money will have to be paid even though Congress has pointedly declined to appropriate money for that purpose,” he wrote. “Not only will today’s decision have a massive immediate impact, its potential consequences go much further.”
The high court remanded the consolidated cases to the lower court for further proceedings on details of the disbursement.
The federal government owes billions of dollars to health insurers under an Affordable Care Act provision intended to help insurers mitigate risk, the U.S. Supreme Court has ruled.
In an 8-to-1 vote announced April 27, justices sided with the plaintiff health plans in Maine Community Health Options v. United States, ruling that the risk corridors statute created a government obligation to pay insurers the full amount originally calculated and that appropriation measures later passed by Congress did not repeal this obligation.
“In establishing the temporary risk corridors program, Congress created a rare money-mandating obligation requiring the federal government to make payments under [Section 1342 of the Affordable Care Act’s] formula,” Associate Justice Sonia Sotomayor wrote in the majority opinion. “Lacking other statutory paths to relief ... petitioners may seek to collect payment through a damages action in the Court of Federal Claims.”
Maine Community Health Options v. United States, which consolidates several lawsuits against the government, centers on the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged by more than $12 billion all together.
The U.S. Department of Justice countered that the government is not required to pay the plans because of measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses.
The U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
The U.S. Supreme Court disagreed. Justices noted that even after Congress enacted the first rider, HHS and the Centers for Medicare & Medicaid Services reiterated that the ACA requires the Secretary to make full payments to issuers and that “HHS [would] record risk corridors payments due as an obligation of the United States government for which full payment is required,” according to the Supreme Court opinion.
“They understood that profitable insurers’ payments to the government would not dispel the Secretary’s obligation to pay unprofitable insurers, even ‘in the event of a shortfall,’ ” Justice Sotomayor wrote in the majority opinion.
Associate Justice Samuel Alito Jr. however, took issue with his fellow justices’ decision. In his dissenting opinion, Justice Alito wrote that under the ruling, billions of taxpayer dollars will be turned over to insurance companies that bet unsuccessfully on the success of the program in question.
“This money will have to be paid even though Congress has pointedly declined to appropriate money for that purpose,” he wrote. “Not only will today’s decision have a massive immediate impact, its potential consequences go much further.”
The high court remanded the consolidated cases to the lower court for further proceedings on details of the disbursement.
The federal government owes billions of dollars to health insurers under an Affordable Care Act provision intended to help insurers mitigate risk, the U.S. Supreme Court has ruled.
In an 8-to-1 vote announced April 27, justices sided with the plaintiff health plans in Maine Community Health Options v. United States, ruling that the risk corridors statute created a government obligation to pay insurers the full amount originally calculated and that appropriation measures later passed by Congress did not repeal this obligation.
“In establishing the temporary risk corridors program, Congress created a rare money-mandating obligation requiring the federal government to make payments under [Section 1342 of the Affordable Care Act’s] formula,” Associate Justice Sonia Sotomayor wrote in the majority opinion. “Lacking other statutory paths to relief ... petitioners may seek to collect payment through a damages action in the Court of Federal Claims.”
Maine Community Health Options v. United States, which consolidates several lawsuits against the government, centers on the ACA’s risk corridor program, which required the U.S. Department of Health & Human Services to collect funds from profitable insurers that offered qualified health plans under the exchanges and distribute the funds to insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014, 2015, and 2016, while losses steadily grew, resulting in the HHS paying about 12 cents on the dollar in payments to insurers. More than 150 insurers now allege they were shortchanged by more than $12 billion all together.
The U.S. Department of Justice countered that the government is not required to pay the plans because of measures passed by Congress in 2014 and later years that limited the funding available to compensate insurers for their losses.
The U.S. Court of Appeals for the Federal Circuit decided in favor of the government, ruling that while the ACA required the government to compensate the insurers for their losses, the appropriations measures repealed or suspended that requirement.
The U.S. Supreme Court disagreed. Justices noted that even after Congress enacted the first rider, HHS and the Centers for Medicare & Medicaid Services reiterated that the ACA requires the Secretary to make full payments to issuers and that “HHS [would] record risk corridors payments due as an obligation of the United States government for which full payment is required,” according to the Supreme Court opinion.
“They understood that profitable insurers’ payments to the government would not dispel the Secretary’s obligation to pay unprofitable insurers, even ‘in the event of a shortfall,’ ” Justice Sotomayor wrote in the majority opinion.
Associate Justice Samuel Alito Jr. however, took issue with his fellow justices’ decision. In his dissenting opinion, Justice Alito wrote that under the ruling, billions of taxpayer dollars will be turned over to insurance companies that bet unsuccessfully on the success of the program in question.
“This money will have to be paid even though Congress has pointedly declined to appropriate money for that purpose,” he wrote. “Not only will today’s decision have a massive immediate impact, its potential consequences go much further.”
The high court remanded the consolidated cases to the lower court for further proceedings on details of the disbursement.
REPLENISH: Oral estradiol/progesterone slowed bone turnover as it cut VMS
Menopausal women with an intact uterus treated for a year with a daily, oral, single-pill formulation of estradiol and progesterone for the primary goal of reducing moderate to severe vasomotor symptoms showed evidence of reduced bone turnover in a post hoc, subgroup analysis of 157 women enrolled in the REPLENISH trial.

These findings “provide support for a potential skeletal benefit” when menopausal women with an intact uterus regularly used the tested estradiol plus progesterone formulation to treat moderate to severe vasomotor symptoms (VMS), Risa Kagan, MD, and associates wrote in an abstract released ahead of the study’s scheduled presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. ACOG canceled the meeting, and released abstracts for press coverage.
The reductions reported for three different markers of bone turnover compared with placebo control after 6 and 12 months on treatment with a U.S.-marketed estradiol plus progesterone formulation were ”reassuring and in line with expectations” said Lubna Pal, MBBS, professor of obstetrics, gynecology, and reproductive sciences at Yale University, New Haven, Conn., who was not involved with the study. But the findings fell short of addressing the more clinically relevant issue of whether the tested regimen reduces the rate of bone fractures.

“Only longer-term data can tell us whether this magnitude of effect is sustainable,” which would need to happen to cut fracture incidence, said Dr. Pal, who directs the menopause program at her center. “The reduction in bone-turnover markers is adequate, but magnitude alone doesn’t entirely explain a reduction in fractures.”
The bone-marker findings came from a post hoc analysis of data collected in REPLENISH (Safety and Efficacy Study of the Combination Estradiol and Progesterone to Treat Vasomotor Symptoms in Postmenopausal Women With an Intact Uterus), a phase 3 randomized trial run at 119 U.S. sites that during 2013-2015 enrolled 1,845 menopausal women aged 65 years with an intact uterus and with moderate to severe VMS. The researchers randomized women to alternative daily treatment regimens with a single, oral pill that combined a bioidentical form of 17 beta-estradiol at dosages of 1.0 mg/day, 0.50 mg/day, or 0.25 mg/day, and dosages of bioidentical progesterone at dosages of 100 mg/day or 50 mg/day, or to a placebo control arm; not every possible dosage combination underwent testing.
The original study’s primary safety endpoint was the incidence of endometrial hyperplasia after 12 months on treatment, and the results showed no such events in any dosage arm. The primary efficacy endpoints assessed the frequency and severity of VMS after 4 and 12 weeks on treatment, and the results showed that all four tested formulations of estradiol plus progesterone had similar, statistically significant effects on decreasing VMS frequency, and the four formulations reduced severity in a dose-dependent way (Obstet Gynecol. 2018 Jul;132[1]:161-70). Based in part on results from this pivotal trial, the 1-mg estradiol/100 mg progesterone formulation (Bijuva) received Food and Drug Administration marketing approval in late 2018.
The new analysis of bone-turnover markers focused on a subgroup of women selected from two of the drug-treated arms and control patients who had at least 50 moderate to severe VMS events per week at baseline, were at least 5 years out from their last menstrual period, and had data recorded for three markers of bone turnover at baseline, and after 6 and 12 months on treatment, according to the abstract published in Obstetrics and Gynecology.
The analysis included 56 women treated with 1.0 mg estradiol and 100 mg progesterone daily, 56 who received 0.5 mg estradiol and 100 mg progesterone daily, and 45 women in the placebo arm. It assessed changes from baseline in the on-treatment compared with placebo groups using immunoassays for bone-specific alkaline phosphatase (BSAP), C-terminal telopeptide of type 1 collagen (CTX-1), and N-terminal propeptide of type 1 procollagen (PINP). For this analysis, the researchers combined the two active-treatment arms, and found that all three markers showed statistically significant drops from baseline with treatment, compared with placebo at both 6- and 12-month follow-up. For all three markers, the declines on active treatment grew larger with time, and after 12 months the mean drops from baseline compared with placebo were an 18% relative reduction in BSAP, a 41% relative reduction in CTX-1, and a 29% relative reduction in PINP, reported Dr. Kagan, a gynecologist based in Berkeley, Calif., who is affiliated with the University of California San Francisco.
In addition to not yet providing more clinically meaningful results on bone fracture rates, Dr. Pal cited additional issues that limit interpretation of both these findings and the broader REPLENISH results. First, the new analysis of bone-turnover markers as reported in the abstract does not allow assessment of a possible dose-dependent effect on bone turnover. More importantly, while the full REPLENISH trial provided reassuring data on endometrial protection, it has not yet reported data on the other major safety concern of hormone replacement: the effects of treatment on breast cancer rates. “They need to show no harm” in breast tissue, Dr. Pal said in an interview. In addition, the positive effect reported on markers of bone turnover is not unique to this formulation. Other formulations with estrogen at similar dosages would have similar effects, she said.
Other considerations when using an oral formulation include the reduced risk for prothrombotic effects from estradiol when delivered transdermally instead of orally, although some women have trouble getting insurance coverage for transdermal formulations, Dr. Pal said. Oral estrogen is appropriate only for women without an elevated clotting risk. Daily progesterone treatment also is more problematic than a cyclical dosage regimen, but noncontinuous progesterone results in monthly bleeding, something that some women prefer to avoid. “I’m not convinced that continuous progesterone is a physiologic approach,” said Dr. Pal, a member of the Ob.Gyn. News editorial advisory board. In addition, some women may find the formulation attractive because both the estradiol and progesterone are bioidentical and not synthetic molecules.
In short, the oral estradiol plus progesterone formulation tested in REPLENISH “is another tool” that’s an option for selected menopausal women with a uterus. “The bone findings are in line with expectations and are reassuring. Long-term data are keenly awaited to understand whether the bone marker changes lead to fewer fractures. The impact of the treatment on breast safety will be especially important.” For women who want a bioidentical, oral option and to not have bleeding, the tested formulation can be an effective option providing both symptom benefit and endometrial protection, Dr. Pal said.
REPLENISH was funded by TherapeuticsMD, the company that markets the tested estradiol plus progesterone formulation (Bijuva). Dr. Kagan has been a consultant and adviser to and speaker on behalf of Therapeutics MD, and she has also been a consultant or adviser to or has spoken on behalf of AMAG, Amgen, Astellas, Lupin, Radius, and Warner Chilcott/Allergan, and she has received research funding from Endoceutics. Dr. Pal has been a consultant to Flow Health.
SOURCE: Kagan R et al. Obstet Gynecol. 2020 May;135:62S. doi: 10.1097/01.AOG.0000665076.20231.a8.
Menopausal women with an intact uterus treated for a year with a daily, oral, single-pill formulation of estradiol and progesterone for the primary goal of reducing moderate to severe vasomotor symptoms showed evidence of reduced bone turnover in a post hoc, subgroup analysis of 157 women enrolled in the REPLENISH trial.
These findings “provide support for a potential skeletal benefit” when menopausal women with an intact uterus regularly used the tested estradiol plus progesterone formulation to treat moderate to severe vasomotor symptoms (VMS), Risa Kagan, MD, and associates wrote in an abstract released ahead of the study’s scheduled presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. ACOG canceled the meeting, and released abstracts for press coverage.
The reductions reported for three different markers of bone turnover compared with placebo control after 6 and 12 months on treatment with a U.S.-marketed estradiol plus progesterone formulation were ”reassuring and in line with expectations” said Lubna Pal, MBBS, professor of obstetrics, gynecology, and reproductive sciences at Yale University, New Haven, Conn., who was not involved with the study. But the findings fell short of addressing the more clinically relevant issue of whether the tested regimen reduces the rate of bone fractures.
“Only longer-term data can tell us whether this magnitude of effect is sustainable,” which would need to happen to cut fracture incidence, said Dr. Pal, who directs the menopause program at her center. “The reduction in bone-turnover markers is adequate, but magnitude alone doesn’t entirely explain a reduction in fractures.”
The bone-marker findings came from a post hoc analysis of data collected in REPLENISH (Safety and Efficacy Study of the Combination Estradiol and Progesterone to Treat Vasomotor Symptoms in Postmenopausal Women With an Intact Uterus), a phase 3 randomized trial run at 119 U.S. sites that during 2013-2015 enrolled 1,845 menopausal women aged 65 years with an intact uterus and with moderate to severe VMS. The researchers randomized women to alternative daily treatment regimens with a single, oral pill that combined a bioidentical form of 17 beta-estradiol at dosages of 1.0 mg/day, 0.50 mg/day, or 0.25 mg/day, and dosages of bioidentical progesterone at dosages of 100 mg/day or 50 mg/day, or to a placebo control arm; not every possible dosage combination underwent testing.
The original study’s primary safety endpoint was the incidence of endometrial hyperplasia after 12 months on treatment, and the results showed no such events in any dosage arm. The primary efficacy endpoints assessed the frequency and severity of VMS after 4 and 12 weeks on treatment, and the results showed that all four tested formulations of estradiol plus progesterone had similar, statistically significant effects on decreasing VMS frequency, and the four formulations reduced severity in a dose-dependent way (Obstet Gynecol. 2018 Jul;132[1]:161-70). Based in part on results from this pivotal trial, the 1-mg estradiol/100 mg progesterone formulation (Bijuva) received Food and Drug Administration marketing approval in late 2018.
The new analysis of bone-turnover markers focused on a subgroup of women selected from two of the drug-treated arms and control patients who had at least 50 moderate to severe VMS events per week at baseline, were at least 5 years out from their last menstrual period, and had data recorded for three markers of bone turnover at baseline, and after 6 and 12 months on treatment, according to the abstract published in Obstetrics and Gynecology.
The analysis included 56 women treated with 1.0 mg estradiol and 100 mg progesterone daily, 56 who received 0.5 mg estradiol and 100 mg progesterone daily, and 45 women in the placebo arm. It assessed changes from baseline in the on-treatment compared with placebo groups using immunoassays for bone-specific alkaline phosphatase (BSAP), C-terminal telopeptide of type 1 collagen (CTX-1), and N-terminal propeptide of type 1 procollagen (PINP). For this analysis, the researchers combined the two active-treatment arms, and found that all three markers showed statistically significant drops from baseline with treatment, compared with placebo at both 6- and 12-month follow-up. For all three markers, the declines on active treatment grew larger with time, and after 12 months the mean drops from baseline compared with placebo were an 18% relative reduction in BSAP, a 41% relative reduction in CTX-1, and a 29% relative reduction in PINP, reported Dr. Kagan, a gynecologist based in Berkeley, Calif., who is affiliated with the University of California San Francisco.
In addition to not yet providing more clinically meaningful results on bone fracture rates, Dr. Pal cited additional issues that limit interpretation of both these findings and the broader REPLENISH results. First, the new analysis of bone-turnover markers as reported in the abstract does not allow assessment of a possible dose-dependent effect on bone turnover. More importantly, while the full REPLENISH trial provided reassuring data on endometrial protection, it has not yet reported data on the other major safety concern of hormone replacement: the effects of treatment on breast cancer rates. “They need to show no harm” in breast tissue, Dr. Pal said in an interview. In addition, the positive effect reported on markers of bone turnover is not unique to this formulation. Other formulations with estrogen at similar dosages would have similar effects, she said.
Other considerations when using an oral formulation include the reduced risk for prothrombotic effects from estradiol when delivered transdermally instead of orally, although some women have trouble getting insurance coverage for transdermal formulations, Dr. Pal said. Oral estrogen is appropriate only for women without an elevated clotting risk. Daily progesterone treatment also is more problematic than a cyclical dosage regimen, but noncontinuous progesterone results in monthly bleeding, something that some women prefer to avoid. “I’m not convinced that continuous progesterone is a physiologic approach,” said Dr. Pal, a member of the Ob.Gyn. News editorial advisory board. In addition, some women may find the formulation attractive because both the estradiol and progesterone are bioidentical and not synthetic molecules.
In short, the oral estradiol plus progesterone formulation tested in REPLENISH “is another tool” that’s an option for selected menopausal women with a uterus. “The bone findings are in line with expectations and are reassuring. Long-term data are keenly awaited to understand whether the bone marker changes lead to fewer fractures. The impact of the treatment on breast safety will be especially important.” For women who want a bioidentical, oral option and to not have bleeding, the tested formulation can be an effective option providing both symptom benefit and endometrial protection, Dr. Pal said.
REPLENISH was funded by TherapeuticsMD, the company that markets the tested estradiol plus progesterone formulation (Bijuva). Dr. Kagan has been a consultant and adviser to and speaker on behalf of Therapeutics MD, and she has also been a consultant or adviser to or has spoken on behalf of AMAG, Amgen, Astellas, Lupin, Radius, and Warner Chilcott/Allergan, and she has received research funding from Endoceutics. Dr. Pal has been a consultant to Flow Health.
SOURCE: Kagan R et al. Obstet Gynecol. 2020 May;135:62S. doi: 10.1097/01.AOG.0000665076.20231.a8.
Menopausal women with an intact uterus treated for a year with a daily, oral, single-pill formulation of estradiol and progesterone for the primary goal of reducing moderate to severe vasomotor symptoms showed evidence of reduced bone turnover in a post hoc, subgroup analysis of 157 women enrolled in the REPLENISH trial.
These findings “provide support for a potential skeletal benefit” when menopausal women with an intact uterus regularly used the tested estradiol plus progesterone formulation to treat moderate to severe vasomotor symptoms (VMS), Risa Kagan, MD, and associates wrote in an abstract released ahead of the study’s scheduled presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. ACOG canceled the meeting, and released abstracts for press coverage.
The reductions reported for three different markers of bone turnover compared with placebo control after 6 and 12 months on treatment with a U.S.-marketed estradiol plus progesterone formulation were ”reassuring and in line with expectations” said Lubna Pal, MBBS, professor of obstetrics, gynecology, and reproductive sciences at Yale University, New Haven, Conn., who was not involved with the study. But the findings fell short of addressing the more clinically relevant issue of whether the tested regimen reduces the rate of bone fractures.
“Only longer-term data can tell us whether this magnitude of effect is sustainable,” which would need to happen to cut fracture incidence, said Dr. Pal, who directs the menopause program at her center. “The reduction in bone-turnover markers is adequate, but magnitude alone doesn’t entirely explain a reduction in fractures.”
The bone-marker findings came from a post hoc analysis of data collected in REPLENISH (Safety and Efficacy Study of the Combination Estradiol and Progesterone to Treat Vasomotor Symptoms in Postmenopausal Women With an Intact Uterus), a phase 3 randomized trial run at 119 U.S. sites that during 2013-2015 enrolled 1,845 menopausal women aged 65 years with an intact uterus and with moderate to severe VMS. The researchers randomized women to alternative daily treatment regimens with a single, oral pill that combined a bioidentical form of 17 beta-estradiol at dosages of 1.0 mg/day, 0.50 mg/day, or 0.25 mg/day, and dosages of bioidentical progesterone at dosages of 100 mg/day or 50 mg/day, or to a placebo control arm; not every possible dosage combination underwent testing.
The original study’s primary safety endpoint was the incidence of endometrial hyperplasia after 12 months on treatment, and the results showed no such events in any dosage arm. The primary efficacy endpoints assessed the frequency and severity of VMS after 4 and 12 weeks on treatment, and the results showed that all four tested formulations of estradiol plus progesterone had similar, statistically significant effects on decreasing VMS frequency, and the four formulations reduced severity in a dose-dependent way (Obstet Gynecol. 2018 Jul;132[1]:161-70). Based in part on results from this pivotal trial, the 1-mg estradiol/100 mg progesterone formulation (Bijuva) received Food and Drug Administration marketing approval in late 2018.
The new analysis of bone-turnover markers focused on a subgroup of women selected from two of the drug-treated arms and control patients who had at least 50 moderate to severe VMS events per week at baseline, were at least 5 years out from their last menstrual period, and had data recorded for three markers of bone turnover at baseline, and after 6 and 12 months on treatment, according to the abstract published in Obstetrics and Gynecology.
The analysis included 56 women treated with 1.0 mg estradiol and 100 mg progesterone daily, 56 who received 0.5 mg estradiol and 100 mg progesterone daily, and 45 women in the placebo arm. It assessed changes from baseline in the on-treatment compared with placebo groups using immunoassays for bone-specific alkaline phosphatase (BSAP), C-terminal telopeptide of type 1 collagen (CTX-1), and N-terminal propeptide of type 1 procollagen (PINP). For this analysis, the researchers combined the two active-treatment arms, and found that all three markers showed statistically significant drops from baseline with treatment, compared with placebo at both 6- and 12-month follow-up. For all three markers, the declines on active treatment grew larger with time, and after 12 months the mean drops from baseline compared with placebo were an 18% relative reduction in BSAP, a 41% relative reduction in CTX-1, and a 29% relative reduction in PINP, reported Dr. Kagan, a gynecologist based in Berkeley, Calif., who is affiliated with the University of California San Francisco.
In addition to not yet providing more clinically meaningful results on bone fracture rates, Dr. Pal cited additional issues that limit interpretation of both these findings and the broader REPLENISH results. First, the new analysis of bone-turnover markers as reported in the abstract does not allow assessment of a possible dose-dependent effect on bone turnover. More importantly, while the full REPLENISH trial provided reassuring data on endometrial protection, it has not yet reported data on the other major safety concern of hormone replacement: the effects of treatment on breast cancer rates. “They need to show no harm” in breast tissue, Dr. Pal said in an interview. In addition, the positive effect reported on markers of bone turnover is not unique to this formulation. Other formulations with estrogen at similar dosages would have similar effects, she said.
Other considerations when using an oral formulation include the reduced risk for prothrombotic effects from estradiol when delivered transdermally instead of orally, although some women have trouble getting insurance coverage for transdermal formulations, Dr. Pal said. Oral estrogen is appropriate only for women without an elevated clotting risk. Daily progesterone treatment also is more problematic than a cyclical dosage regimen, but noncontinuous progesterone results in monthly bleeding, something that some women prefer to avoid. “I’m not convinced that continuous progesterone is a physiologic approach,” said Dr. Pal, a member of the Ob.Gyn. News editorial advisory board. In addition, some women may find the formulation attractive because both the estradiol and progesterone are bioidentical and not synthetic molecules.
In short, the oral estradiol plus progesterone formulation tested in REPLENISH “is another tool” that’s an option for selected menopausal women with a uterus. “The bone findings are in line with expectations and are reassuring. Long-term data are keenly awaited to understand whether the bone marker changes lead to fewer fractures. The impact of the treatment on breast safety will be especially important.” For women who want a bioidentical, oral option and to not have bleeding, the tested formulation can be an effective option providing both symptom benefit and endometrial protection, Dr. Pal said.
REPLENISH was funded by TherapeuticsMD, the company that markets the tested estradiol plus progesterone formulation (Bijuva). Dr. Kagan has been a consultant and adviser to and speaker on behalf of Therapeutics MD, and she has also been a consultant or adviser to or has spoken on behalf of AMAG, Amgen, Astellas, Lupin, Radius, and Warner Chilcott/Allergan, and she has received research funding from Endoceutics. Dr. Pal has been a consultant to Flow Health.
SOURCE: Kagan R et al. Obstet Gynecol. 2020 May;135:62S. doi: 10.1097/01.AOG.0000665076.20231.a8.
FROM ACOG 2020
More doctors used digital tools in 2019
The use of digital tools among physicians has markedly risen since 2016, with telehealth visits and remote patient monitoring making the greatest strides in usage, an American Medical Association report shows.
In 2019, 28% of physicians used televisits/virtual visits, up from 14% in 2016, while remote monitoring and management for improved care rose to 22% in 2019, an increase from 13% in 2016, according to the AMA report, released in February 2020. The report, which surveyed 1,359 doctors, includes responses from 672 primary care physicians and 687 specialists.
Remote monitoring for efficiency, meanwhile, grew to 16% in 2019 from 12% in 2016. Remote monitoring for efficiency pertains to smart versions of common clinical devices such as thermometers, blood pressure cuffs, and scales that automatically enter readings in the record. Remote monitoring for improved care refers to mobile applications and devices used for daily measurement of vital signs such as weight, blood pressure, blood glucose.
Adoption of other digital tools by physicians have also grown, including clinical decision support, which climbed to 37% in 2019 from 28% in 2016 and patient engagement tools, which rose to 33% in 2019, up from 26% in 2016. Clinical decision support tools pertain to modules used in conjunction with the electronic health record (EHR), or mobile applications integrated with an EHR that can signify changes in patient data, such as weight gain/loss, or change in blood chemistry. Patient engagement tools, meanwhile, refer to solutions that promote patient wellness and active patient participation in their care.
Tools that encompass use of point of care/workflow enhancement increased to 47% in 2019, from 42% in 2016. This area includes communication and sharing of electronic clinical data to consult with specialists, make referrals and/or transitions of care. Tools that address consumer access to their clinical data, meanwhile, rose to 58% in 2019 from 53% in 2016, the highest adoption rate among the digital health tool categories.
Overall, more physicians see an advantage to digital health solutions than did 3 years ago. More primary care physicians and specialists in 2019 reported a “definite advantage” to digital tools enhancing care of patients than in 2016. Doctors who see no advantage to such tools are trending downward and are concentrated to those age 50 and older, according to the report.
Solo-practice physicians are slowly increasing their use of digital health tools. In 2016, solo physicians reported using an average of 1.5 digital tools, which in 2019 increased to an average of 2.2 digital tools. Small practices with between one and three doctors used an average of 1.4 tools in 2016, which rose to an average of 2.2 tools in 2019, the report found. PCPs used slightly more digital tools, compared with specialists, in both 2016 and 2019.
Female doctors are slightly ahead of their male counterparts when it comes to digital health tools. In 2019, female physicians used an average of 2.6 digital tools, up from 1.9 in 2016. Male doctors used an average of 2.4 tools in 2019, compared with 1.9 tools in 2016.
For the physicians surveyed, the most important factor associated with usage was that digital tools were covered by malpractice insurance, followed by the importance of data privacy/security ensured by the EHR vendor, and that the tools were well integrated with the EHR. Other important factors included that data security was ensured by the practice or hospital, that doctors were reimbursed for their time spent using digital tools, and that the tools were supported by the EHR vendor.
Regarding the top motivator for doctors to use digital tools, 51% of physicians in 2019 said improved efficiency was “very important,” up from 48% in 2016. Other top motivators included that digital tools increased safety, improved diagnostic ability, and addressed physician burnout.
In 2019, the demonstration of safety and efficacy in peer-reviewed publications as it relates to digital tools also grew in importance. Of the physicians surveyed, 36% reported that safety and efficacy demonstrated in peer-reviewed publications was “very important,” an increase from 32% in 2016. Other “very important” factors for physicians are that digital tools used are proven to be as good/superior to traditional care, that they are intuitive/require no special training, that they align with the standard of care, and that their safety and efficacy is validated by the Food and Drug Administration.
“The rise of the digital-native physician will have a profound impact on health care and patient outcomes, and will place digital health technologies under pressure to perform according to higher expectations,” AMA board chair Jesse M. Ehrenfeld, MD, PhD, said in a statement. “The AMA survey provides deep insight into the emerging requirements that physicians expect from digital technologies and sets an industry guidepost for understanding what a growing number of physicians require to adopt new technology.”
The survey was derived from the same physician panel used in 2016, provided by WebMD. For the 2019 survey, the basic 2016 survey was followed in wording and question order, with a few variations to remove some questions no longer relevant. The 2019 sample used careful quotas to ensure a sample composition similar to that of 2016, according to the report.
SOURCE: AMA Digital Health Research: Physicians’ motivations and requirements for adopting digital health – Adoption and attitudinal shifts from 2016 to 2019. American Medical Association. February 2020.
The use of digital tools among physicians has markedly risen since 2016, with telehealth visits and remote patient monitoring making the greatest strides in usage, an American Medical Association report shows.
In 2019, 28% of physicians used televisits/virtual visits, up from 14% in 2016, while remote monitoring and management for improved care rose to 22% in 2019, an increase from 13% in 2016, according to the AMA report, released in February 2020. The report, which surveyed 1,359 doctors, includes responses from 672 primary care physicians and 687 specialists.
Remote monitoring for efficiency, meanwhile, grew to 16% in 2019 from 12% in 2016. Remote monitoring for efficiency pertains to smart versions of common clinical devices such as thermometers, blood pressure cuffs, and scales that automatically enter readings in the record. Remote monitoring for improved care refers to mobile applications and devices used for daily measurement of vital signs such as weight, blood pressure, blood glucose.
Adoption of other digital tools by physicians have also grown, including clinical decision support, which climbed to 37% in 2019 from 28% in 2016 and patient engagement tools, which rose to 33% in 2019, up from 26% in 2016. Clinical decision support tools pertain to modules used in conjunction with the electronic health record (EHR), or mobile applications integrated with an EHR that can signify changes in patient data, such as weight gain/loss, or change in blood chemistry. Patient engagement tools, meanwhile, refer to solutions that promote patient wellness and active patient participation in their care.
Tools that encompass use of point of care/workflow enhancement increased to 47% in 2019, from 42% in 2016. This area includes communication and sharing of electronic clinical data to consult with specialists, make referrals and/or transitions of care. Tools that address consumer access to their clinical data, meanwhile, rose to 58% in 2019 from 53% in 2016, the highest adoption rate among the digital health tool categories.
Overall, more physicians see an advantage to digital health solutions than did 3 years ago. More primary care physicians and specialists in 2019 reported a “definite advantage” to digital tools enhancing care of patients than in 2016. Doctors who see no advantage to such tools are trending downward and are concentrated to those age 50 and older, according to the report.
Solo-practice physicians are slowly increasing their use of digital health tools. In 2016, solo physicians reported using an average of 1.5 digital tools, which in 2019 increased to an average of 2.2 digital tools. Small practices with between one and three doctors used an average of 1.4 tools in 2016, which rose to an average of 2.2 tools in 2019, the report found. PCPs used slightly more digital tools, compared with specialists, in both 2016 and 2019.
Female doctors are slightly ahead of their male counterparts when it comes to digital health tools. In 2019, female physicians used an average of 2.6 digital tools, up from 1.9 in 2016. Male doctors used an average of 2.4 tools in 2019, compared with 1.9 tools in 2016.
For the physicians surveyed, the most important factor associated with usage was that digital tools were covered by malpractice insurance, followed by the importance of data privacy/security ensured by the EHR vendor, and that the tools were well integrated with the EHR. Other important factors included that data security was ensured by the practice or hospital, that doctors were reimbursed for their time spent using digital tools, and that the tools were supported by the EHR vendor.
Regarding the top motivator for doctors to use digital tools, 51% of physicians in 2019 said improved efficiency was “very important,” up from 48% in 2016. Other top motivators included that digital tools increased safety, improved diagnostic ability, and addressed physician burnout.
In 2019, the demonstration of safety and efficacy in peer-reviewed publications as it relates to digital tools also grew in importance. Of the physicians surveyed, 36% reported that safety and efficacy demonstrated in peer-reviewed publications was “very important,” an increase from 32% in 2016. Other “very important” factors for physicians are that digital tools used are proven to be as good/superior to traditional care, that they are intuitive/require no special training, that they align with the standard of care, and that their safety and efficacy is validated by the Food and Drug Administration.
“The rise of the digital-native physician will have a profound impact on health care and patient outcomes, and will place digital health technologies under pressure to perform according to higher expectations,” AMA board chair Jesse M. Ehrenfeld, MD, PhD, said in a statement. “The AMA survey provides deep insight into the emerging requirements that physicians expect from digital technologies and sets an industry guidepost for understanding what a growing number of physicians require to adopt new technology.”
The survey was derived from the same physician panel used in 2016, provided by WebMD. For the 2019 survey, the basic 2016 survey was followed in wording and question order, with a few variations to remove some questions no longer relevant. The 2019 sample used careful quotas to ensure a sample composition similar to that of 2016, according to the report.
SOURCE: AMA Digital Health Research: Physicians’ motivations and requirements for adopting digital health – Adoption and attitudinal shifts from 2016 to 2019. American Medical Association. February 2020.
The use of digital tools among physicians has markedly risen since 2016, with telehealth visits and remote patient monitoring making the greatest strides in usage, an American Medical Association report shows.
In 2019, 28% of physicians used televisits/virtual visits, up from 14% in 2016, while remote monitoring and management for improved care rose to 22% in 2019, an increase from 13% in 2016, according to the AMA report, released in February 2020. The report, which surveyed 1,359 doctors, includes responses from 672 primary care physicians and 687 specialists.
Remote monitoring for efficiency, meanwhile, grew to 16% in 2019 from 12% in 2016. Remote monitoring for efficiency pertains to smart versions of common clinical devices such as thermometers, blood pressure cuffs, and scales that automatically enter readings in the record. Remote monitoring for improved care refers to mobile applications and devices used for daily measurement of vital signs such as weight, blood pressure, blood glucose.
Adoption of other digital tools by physicians have also grown, including clinical decision support, which climbed to 37% in 2019 from 28% in 2016 and patient engagement tools, which rose to 33% in 2019, up from 26% in 2016. Clinical decision support tools pertain to modules used in conjunction with the electronic health record (EHR), or mobile applications integrated with an EHR that can signify changes in patient data, such as weight gain/loss, or change in blood chemistry. Patient engagement tools, meanwhile, refer to solutions that promote patient wellness and active patient participation in their care.
Tools that encompass use of point of care/workflow enhancement increased to 47% in 2019, from 42% in 2016. This area includes communication and sharing of electronic clinical data to consult with specialists, make referrals and/or transitions of care. Tools that address consumer access to their clinical data, meanwhile, rose to 58% in 2019 from 53% in 2016, the highest adoption rate among the digital health tool categories.
Overall, more physicians see an advantage to digital health solutions than did 3 years ago. More primary care physicians and specialists in 2019 reported a “definite advantage” to digital tools enhancing care of patients than in 2016. Doctors who see no advantage to such tools are trending downward and are concentrated to those age 50 and older, according to the report.
Solo-practice physicians are slowly increasing their use of digital health tools. In 2016, solo physicians reported using an average of 1.5 digital tools, which in 2019 increased to an average of 2.2 digital tools. Small practices with between one and three doctors used an average of 1.4 tools in 2016, which rose to an average of 2.2 tools in 2019, the report found. PCPs used slightly more digital tools, compared with specialists, in both 2016 and 2019.
Female doctors are slightly ahead of their male counterparts when it comes to digital health tools. In 2019, female physicians used an average of 2.6 digital tools, up from 1.9 in 2016. Male doctors used an average of 2.4 tools in 2019, compared with 1.9 tools in 2016.
For the physicians surveyed, the most important factor associated with usage was that digital tools were covered by malpractice insurance, followed by the importance of data privacy/security ensured by the EHR vendor, and that the tools were well integrated with the EHR. Other important factors included that data security was ensured by the practice or hospital, that doctors were reimbursed for their time spent using digital tools, and that the tools were supported by the EHR vendor.
Regarding the top motivator for doctors to use digital tools, 51% of physicians in 2019 said improved efficiency was “very important,” up from 48% in 2016. Other top motivators included that digital tools increased safety, improved diagnostic ability, and addressed physician burnout.
In 2019, the demonstration of safety and efficacy in peer-reviewed publications as it relates to digital tools also grew in importance. Of the physicians surveyed, 36% reported that safety and efficacy demonstrated in peer-reviewed publications was “very important,” an increase from 32% in 2016. Other “very important” factors for physicians are that digital tools used are proven to be as good/superior to traditional care, that they are intuitive/require no special training, that they align with the standard of care, and that their safety and efficacy is validated by the Food and Drug Administration.
“The rise of the digital-native physician will have a profound impact on health care and patient outcomes, and will place digital health technologies under pressure to perform according to higher expectations,” AMA board chair Jesse M. Ehrenfeld, MD, PhD, said in a statement. “The AMA survey provides deep insight into the emerging requirements that physicians expect from digital technologies and sets an industry guidepost for understanding what a growing number of physicians require to adopt new technology.”
The survey was derived from the same physician panel used in 2016, provided by WebMD. For the 2019 survey, the basic 2016 survey was followed in wording and question order, with a few variations to remove some questions no longer relevant. The 2019 sample used careful quotas to ensure a sample composition similar to that of 2016, according to the report.
SOURCE: AMA Digital Health Research: Physicians’ motivations and requirements for adopting digital health – Adoption and attitudinal shifts from 2016 to 2019. American Medical Association. February 2020.
Call for Immuno-oncology and Immunotherapy Manuscripts
Federal Practitioner is inviting hematology and oncology health care providers and researchers to contribute to the November 2020 special issue on immuno-oncology. The special issue is produced in cooperation with the Association of VA Hematology/Oncology (AVAHO). The journal is especially interested in new research, case studies, review articles, and patient care program descriptions.
Interested authors can send a brief 2 to 3 sentence abstract to fedprac@mdedge.com by May 29, 2020, or submit a completed article directly into Editorial Manager, a web-based manuscript submission and review system. The updated and complete submission guidelines, including details about the style and format, can be found here:
http://www.mdedge.com/fedprac/
All manuscripts submitted to Federal Practitioner for both special and regular issues will be subject to peer review. Peer reviews are conducted in a double-blind fashion, and the reviewers are asked to comment on the manuscript’s importance, accuracy, relevance, clarity, timeliness, balance, and reference citation. Final decisions on all submitted manuscripts are made by the Editorial Advisory Association Hematology/Oncology special issue advisory board.
Federal Practitioner is inviting hematology and oncology health care providers and researchers to contribute to the November 2020 special issue on immuno-oncology. The special issue is produced in cooperation with the Association of VA Hematology/Oncology (AVAHO). The journal is especially interested in new research, case studies, review articles, and patient care program descriptions.
Interested authors can send a brief 2 to 3 sentence abstract to fedprac@mdedge.com by May 29, 2020, or submit a completed article directly into Editorial Manager, a web-based manuscript submission and review system. The updated and complete submission guidelines, including details about the style and format, can be found here:
http://www.mdedge.com/fedprac/
All manuscripts submitted to Federal Practitioner for both special and regular issues will be subject to peer review. Peer reviews are conducted in a double-blind fashion, and the reviewers are asked to comment on the manuscript’s importance, accuracy, relevance, clarity, timeliness, balance, and reference citation. Final decisions on all submitted manuscripts are made by the Editorial Advisory Association Hematology/Oncology special issue advisory board.
Federal Practitioner is inviting hematology and oncology health care providers and researchers to contribute to the November 2020 special issue on immuno-oncology. The special issue is produced in cooperation with the Association of VA Hematology/Oncology (AVAHO). The journal is especially interested in new research, case studies, review articles, and patient care program descriptions.
Interested authors can send a brief 2 to 3 sentence abstract to fedprac@mdedge.com by May 29, 2020, or submit a completed article directly into Editorial Manager, a web-based manuscript submission and review system. The updated and complete submission guidelines, including details about the style and format, can be found here:
http://www.mdedge.com/fedprac/
All manuscripts submitted to Federal Practitioner for both special and regular issues will be subject to peer review. Peer reviews are conducted in a double-blind fashion, and the reviewers are asked to comment on the manuscript’s importance, accuracy, relevance, clarity, timeliness, balance, and reference citation. Final decisions on all submitted manuscripts are made by the Editorial Advisory Association Hematology/Oncology special issue advisory board.
Tender White Lesions on the Groin
The Diagnosis: Candidal Intertrigo
The biopsy confirmed a diagnosis of severe hyperkeratotic candidal intertrigo with no evidence of Hailey-Hailey disease. Hematoxylin and eosin- stained sections demonstrated irregular acanthosis and variable spongiosis. The stratum corneum was predominantly orthokeratotic with overlying psuedohyphae and yeast fungal elements (Figure 1).
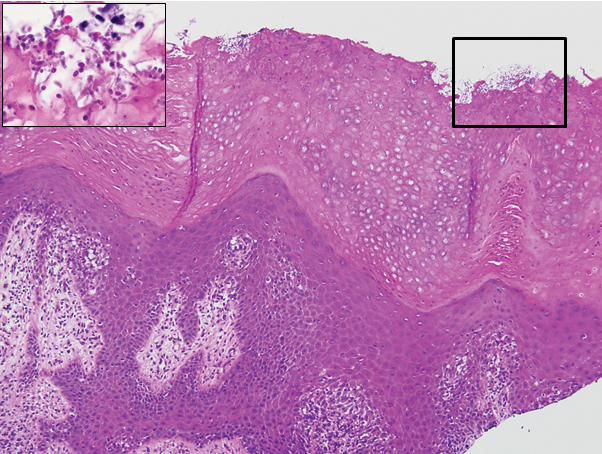
Hyperimmunoglobulinemia E syndrome (HIES), also known as hyper-IgE syndrome or Job syndrome, is a rare immunodeficiency disorder characterized by an eczematous dermatitis-like rash, recurrent skin and lung abscesses, eosinophilia, and elevated serum IgE. Facial asymmetry, prominent forehead, deep-set eyes, broad nose, and roughened facial skin with large pores are characteristic of the sporadic and autosomal-recessive forms. Other common findings include retained primary teeth, hyperextensible joints, and recurrent mucocutaneous candidiasis.1
Although autosomal-dominant and autosomal-recessive inheritance patterns exist, sporadic mutations are the most common cause of HIES.2 Several genes have been implicated depending on the inheritance pattern. The majority of autosomal-dominant cases are associated with inactivating STAT3 (signal transducer and activator of transcription 3) mutations, whereas the majority of autosomal-recessive cases are associated with inactivating DOCK8 (dedicator of cytokinesis 8) mutations.1 Ultimately, all of these mutations lead to an impaired helper T cell (TH17) response, which is crucial for clearing fungal and extracellular bacterial infections.3
Skin eruptions typically are the first manifestation of HIES; they appear within the first week to month of life as papulopustular eruptions on the face and scalp and rapidly generalize to the rest of the body, favoring the shoulders, arms, chest, and buttocks. The pustules then coalesce into crusted plaques that resemble atopic dermatitis, frequently with superimposed Staphylococcus aureus infection. On microscopy, the pustules are folliculocentric and often contain eosinophils, whereas the plaques may contain intraepidermal collections of eosinophils.1
Mucocutaneous candidiasis is seen in approximately 60% of HIES cases and is closely linked to STAT3 inactivating mutations.3 Histologically, there is marked acanthosis with neutrophil exocytosis and abundant yeast and pseudohyphal forms within the stratum corneum (Figure 2).4 Cutaneous candidal infections typically require both oral and topical antifungal agents to clear the infection.3 Most cases of mucocutaneous candidiasis are caused by Candida albicans; however, other known culprits include Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei.5,6 Of note, species identification and antifungal susceptibility studies may be useful in refractory cases, especially with C glabrata, which is known to acquire resistance to azoles, such as fluconazole, with emerging resistance to echinocandins.6

The differential diagnosis of this groin eruption included Hailey-Hailey disease; pemphigus vegetans, Hallopeau type; tinea cruris; and inverse psoriasis. Hailey-Hailey disease can be complicated by a superimposed candidal infection with similar clinical features, and biopsy may be required for definitive diagnosis. Hailey-Hailey disease typically presents with macerated fissured plaques that resemble macerated tissue paper with red fissures (Figure 3). Biopsy confirms full-thickness acantholysis resembling a dilapidated brick wall with minimal dyskeratosis.1 Pemphigus vegetans is a localized variant of pemphigus vulgaris with a predilection for flexural surfaces. The lesions progress to vegetating erosive plaques.4 The Hallopeau type often is studded with pustules and typically remains more localized than the Neumann type. Direct immunofluorescence demonstrates intercellular deposition of IgG and C3, and routine sections characteristically show pseudoepitheliomatous hyperplasia with intraepidermal eosinophilic microabscesses.1,4 Tinea cruris is characterized by erythematous annular lesions with raised scaly borders spreading down the inner thighs.7 The epidermis is variably spongiotic with parakeratosis, and neutrophils often present in a layered stratum corneum with basketweave keratin above a layer of more compact and eosinophilic keratin. Fungal stains, such as periodic acid-Schiff, will highlight the fungal hyphae within the stratum corneum. The inguinal folds are a typical location for inverse psoriasis, which generally appears as thin, sharply demarcated, shiny red plaques with less scale than plaque psoriasis.1 Psoriasiform hyperplasia with a diminished granular layer and tortuous papillary dermal vessels would be expected histologically.1

- James WD, Berger TG, Elston DM. Andrews' Diseases of the Skin. 12th ed. Philadelphia, PA: Elsevier; 2016.
- Schwartz RA, Tarlow MM. Dermatologic manifestations of Job syndrome. Medscape website. https://emedicine.medscape.com/article/1050852-overview. Updated April 22, 2019. Accessed March 28, 2020.
- Minegishi Y, Saito M. Cutaneous manifestations of hyper IgE syndrome. Allergol Int. 2012;61:191-196.
- Patterson JW. Weedon's Skin Pathology. 4th ed. China: Churchill Livingstone Elsevier; 2016.
- Pappas PG, Kauffman CA, Andes DR, et al. Executive summary: clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62:409-417.
- Center for Disease Control and Prevention. Antifungal resistance. https://www.cdc.gov/fungal/antifungal-resistance.html. Updated March 17, 2020. Accessed April 20, 2020.
- Tinea cruris. DermNet NZ website. https://www.dermnetnz.org/topics/tinea-cruris/. Published 2003. Accessed March 28, 2020.
The Diagnosis: Candidal Intertrigo
The biopsy confirmed a diagnosis of severe hyperkeratotic candidal intertrigo with no evidence of Hailey-Hailey disease. Hematoxylin and eosin- stained sections demonstrated irregular acanthosis and variable spongiosis. The stratum corneum was predominantly orthokeratotic with overlying psuedohyphae and yeast fungal elements (Figure 1).
Hyperimmunoglobulinemia E syndrome (HIES), also known as hyper-IgE syndrome or Job syndrome, is a rare immunodeficiency disorder characterized by an eczematous dermatitis-like rash, recurrent skin and lung abscesses, eosinophilia, and elevated serum IgE. Facial asymmetry, prominent forehead, deep-set eyes, broad nose, and roughened facial skin with large pores are characteristic of the sporadic and autosomal-recessive forms. Other common findings include retained primary teeth, hyperextensible joints, and recurrent mucocutaneous candidiasis.1
Although autosomal-dominant and autosomal-recessive inheritance patterns exist, sporadic mutations are the most common cause of HIES.2 Several genes have been implicated depending on the inheritance pattern. The majority of autosomal-dominant cases are associated with inactivating STAT3 (signal transducer and activator of transcription 3) mutations, whereas the majority of autosomal-recessive cases are associated with inactivating DOCK8 (dedicator of cytokinesis 8) mutations.1 Ultimately, all of these mutations lead to an impaired helper T cell (TH17) response, which is crucial for clearing fungal and extracellular bacterial infections.3
Skin eruptions typically are the first manifestation of HIES; they appear within the first week to month of life as papulopustular eruptions on the face and scalp and rapidly generalize to the rest of the body, favoring the shoulders, arms, chest, and buttocks. The pustules then coalesce into crusted plaques that resemble atopic dermatitis, frequently with superimposed Staphylococcus aureus infection. On microscopy, the pustules are folliculocentric and often contain eosinophils, whereas the plaques may contain intraepidermal collections of eosinophils.1
Mucocutaneous candidiasis is seen in approximately 60% of HIES cases and is closely linked to STAT3 inactivating mutations.3 Histologically, there is marked acanthosis with neutrophil exocytosis and abundant yeast and pseudohyphal forms within the stratum corneum (Figure 2).4 Cutaneous candidal infections typically require both oral and topical antifungal agents to clear the infection.3 Most cases of mucocutaneous candidiasis are caused by Candida albicans; however, other known culprits include Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei.5,6 Of note, species identification and antifungal susceptibility studies may be useful in refractory cases, especially with C glabrata, which is known to acquire resistance to azoles, such as fluconazole, with emerging resistance to echinocandins.6
The differential diagnosis of this groin eruption included Hailey-Hailey disease; pemphigus vegetans, Hallopeau type; tinea cruris; and inverse psoriasis. Hailey-Hailey disease can be complicated by a superimposed candidal infection with similar clinical features, and biopsy may be required for definitive diagnosis. Hailey-Hailey disease typically presents with macerated fissured plaques that resemble macerated tissue paper with red fissures (Figure 3). Biopsy confirms full-thickness acantholysis resembling a dilapidated brick wall with minimal dyskeratosis.1 Pemphigus vegetans is a localized variant of pemphigus vulgaris with a predilection for flexural surfaces. The lesions progress to vegetating erosive plaques.4 The Hallopeau type often is studded with pustules and typically remains more localized than the Neumann type. Direct immunofluorescence demonstrates intercellular deposition of IgG and C3, and routine sections characteristically show pseudoepitheliomatous hyperplasia with intraepidermal eosinophilic microabscesses.1,4 Tinea cruris is characterized by erythematous annular lesions with raised scaly borders spreading down the inner thighs.7 The epidermis is variably spongiotic with parakeratosis, and neutrophils often present in a layered stratum corneum with basketweave keratin above a layer of more compact and eosinophilic keratin. Fungal stains, such as periodic acid-Schiff, will highlight the fungal hyphae within the stratum corneum. The inguinal folds are a typical location for inverse psoriasis, which generally appears as thin, sharply demarcated, shiny red plaques with less scale than plaque psoriasis.1 Psoriasiform hyperplasia with a diminished granular layer and tortuous papillary dermal vessels would be expected histologically.1
The Diagnosis: Candidal Intertrigo
The biopsy confirmed a diagnosis of severe hyperkeratotic candidal intertrigo with no evidence of Hailey-Hailey disease. Hematoxylin and eosin- stained sections demonstrated irregular acanthosis and variable spongiosis. The stratum corneum was predominantly orthokeratotic with overlying psuedohyphae and yeast fungal elements (Figure 1).
Hyperimmunoglobulinemia E syndrome (HIES), also known as hyper-IgE syndrome or Job syndrome, is a rare immunodeficiency disorder characterized by an eczematous dermatitis-like rash, recurrent skin and lung abscesses, eosinophilia, and elevated serum IgE. Facial asymmetry, prominent forehead, deep-set eyes, broad nose, and roughened facial skin with large pores are characteristic of the sporadic and autosomal-recessive forms. Other common findings include retained primary teeth, hyperextensible joints, and recurrent mucocutaneous candidiasis.1
Although autosomal-dominant and autosomal-recessive inheritance patterns exist, sporadic mutations are the most common cause of HIES.2 Several genes have been implicated depending on the inheritance pattern. The majority of autosomal-dominant cases are associated with inactivating STAT3 (signal transducer and activator of transcription 3) mutations, whereas the majority of autosomal-recessive cases are associated with inactivating DOCK8 (dedicator of cytokinesis 8) mutations.1 Ultimately, all of these mutations lead to an impaired helper T cell (TH17) response, which is crucial for clearing fungal and extracellular bacterial infections.3
Skin eruptions typically are the first manifestation of HIES; they appear within the first week to month of life as papulopustular eruptions on the face and scalp and rapidly generalize to the rest of the body, favoring the shoulders, arms, chest, and buttocks. The pustules then coalesce into crusted plaques that resemble atopic dermatitis, frequently with superimposed Staphylococcus aureus infection. On microscopy, the pustules are folliculocentric and often contain eosinophils, whereas the plaques may contain intraepidermal collections of eosinophils.1
Mucocutaneous candidiasis is seen in approximately 60% of HIES cases and is closely linked to STAT3 inactivating mutations.3 Histologically, there is marked acanthosis with neutrophil exocytosis and abundant yeast and pseudohyphal forms within the stratum corneum (Figure 2).4 Cutaneous candidal infections typically require both oral and topical antifungal agents to clear the infection.3 Most cases of mucocutaneous candidiasis are caused by Candida albicans; however, other known culprits include Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei.5,6 Of note, species identification and antifungal susceptibility studies may be useful in refractory cases, especially with C glabrata, which is known to acquire resistance to azoles, such as fluconazole, with emerging resistance to echinocandins.6
The differential diagnosis of this groin eruption included Hailey-Hailey disease; pemphigus vegetans, Hallopeau type; tinea cruris; and inverse psoriasis. Hailey-Hailey disease can be complicated by a superimposed candidal infection with similar clinical features, and biopsy may be required for definitive diagnosis. Hailey-Hailey disease typically presents with macerated fissured plaques that resemble macerated tissue paper with red fissures (Figure 3). Biopsy confirms full-thickness acantholysis resembling a dilapidated brick wall with minimal dyskeratosis.1 Pemphigus vegetans is a localized variant of pemphigus vulgaris with a predilection for flexural surfaces. The lesions progress to vegetating erosive plaques.4 The Hallopeau type often is studded with pustules and typically remains more localized than the Neumann type. Direct immunofluorescence demonstrates intercellular deposition of IgG and C3, and routine sections characteristically show pseudoepitheliomatous hyperplasia with intraepidermal eosinophilic microabscesses.1,4 Tinea cruris is characterized by erythematous annular lesions with raised scaly borders spreading down the inner thighs.7 The epidermis is variably spongiotic with parakeratosis, and neutrophils often present in a layered stratum corneum with basketweave keratin above a layer of more compact and eosinophilic keratin. Fungal stains, such as periodic acid-Schiff, will highlight the fungal hyphae within the stratum corneum. The inguinal folds are a typical location for inverse psoriasis, which generally appears as thin, sharply demarcated, shiny red plaques with less scale than plaque psoriasis.1 Psoriasiform hyperplasia with a diminished granular layer and tortuous papillary dermal vessels would be expected histologically.1
- James WD, Berger TG, Elston DM. Andrews' Diseases of the Skin. 12th ed. Philadelphia, PA: Elsevier; 2016.
- Schwartz RA, Tarlow MM. Dermatologic manifestations of Job syndrome. Medscape website. https://emedicine.medscape.com/article/1050852-overview. Updated April 22, 2019. Accessed March 28, 2020.
- Minegishi Y, Saito M. Cutaneous manifestations of hyper IgE syndrome. Allergol Int. 2012;61:191-196.
- Patterson JW. Weedon's Skin Pathology. 4th ed. China: Churchill Livingstone Elsevier; 2016.
- Pappas PG, Kauffman CA, Andes DR, et al. Executive summary: clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62:409-417.
- Center for Disease Control and Prevention. Antifungal resistance. https://www.cdc.gov/fungal/antifungal-resistance.html. Updated March 17, 2020. Accessed April 20, 2020.
- Tinea cruris. DermNet NZ website. https://www.dermnetnz.org/topics/tinea-cruris/. Published 2003. Accessed March 28, 2020.
- James WD, Berger TG, Elston DM. Andrews' Diseases of the Skin. 12th ed. Philadelphia, PA: Elsevier; 2016.
- Schwartz RA, Tarlow MM. Dermatologic manifestations of Job syndrome. Medscape website. https://emedicine.medscape.com/article/1050852-overview. Updated April 22, 2019. Accessed March 28, 2020.
- Minegishi Y, Saito M. Cutaneous manifestations of hyper IgE syndrome. Allergol Int. 2012;61:191-196.
- Patterson JW. Weedon's Skin Pathology. 4th ed. China: Churchill Livingstone Elsevier; 2016.
- Pappas PG, Kauffman CA, Andes DR, et al. Executive summary: clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62:409-417.
- Center for Disease Control and Prevention. Antifungal resistance. https://www.cdc.gov/fungal/antifungal-resistance.html. Updated March 17, 2020. Accessed April 20, 2020.
- Tinea cruris. DermNet NZ website. https://www.dermnetnz.org/topics/tinea-cruris/. Published 2003. Accessed March 28, 2020.

A 28-year-old man with a history of hyperimmunoglobulinemia E syndrome (previously known as Job syndrome), coarse facial features, and multiple skin and soft tissue infections presented to the university dermatology clinic with persistent white, macerated, fissured groin plaques that were present for months. The lesions were tender and pruritic with a burning sensation. Treatment with topical terbinafine and oral fluconazole was attempted without resolution of the eruption. A biopsy of the groin lesion was performed.

Sunless Tanner Caused Persistent Hyperpigmented Patches on the Hands
To the Editor:
The use of sunless tanners has become an alternative for individuals who wish to have tan skin without exposure to UV radiation.1 We present a case of a patient who experienced persistent hyperpigmented patches on the hands months after the use of a sunless tanner containing dihydroxyacetone (DHA), a carbohydrate that reacts with amino acids in the stratum corneum to produce pigments called melanoidins. The hyperpigmentation caused by DHA is due to the Maillard reaction, which is the nonenzymatic glycation of amino groups of proteins by the carbonyl groups of sugar.2 Many sunless tanners contain DHA at varying concentrations. Dermatologists should be aware of the benefits and potential side effects of these alternative products so that they can appropriately counsel patients.
A 20-year-old woman with no history of skin disease presented for evaluation of hyperpigmented patches on the dorsal hands of several months’ duration. Physical examination revealed ill-defined hyperpigmented patches on the dorsal fingers without associated scale or erythema (Figure 1). She had a remote history of Hodgkin lymphoma treated with chemotherapy and was in remission for 5 years prior to the current presentation. Her hematologists referred her to dermatology for evaluation, as they did not believe the patches could be related to her chemotherapy given that she had completed the treatment years before.

A punch biopsy of one of the patches was obtained to elucidate the origin of the hyperpigmentation, which had no obvious triggers according to the patient. Histopathologic examination revealed hyperpigmented parakeratosis and lentiginous hyperplasia along with pigmentation of the stratum corneum (Figures 2A and 2B) with black pigment, which stained positive with Fontana-Masson (Figure 2C).
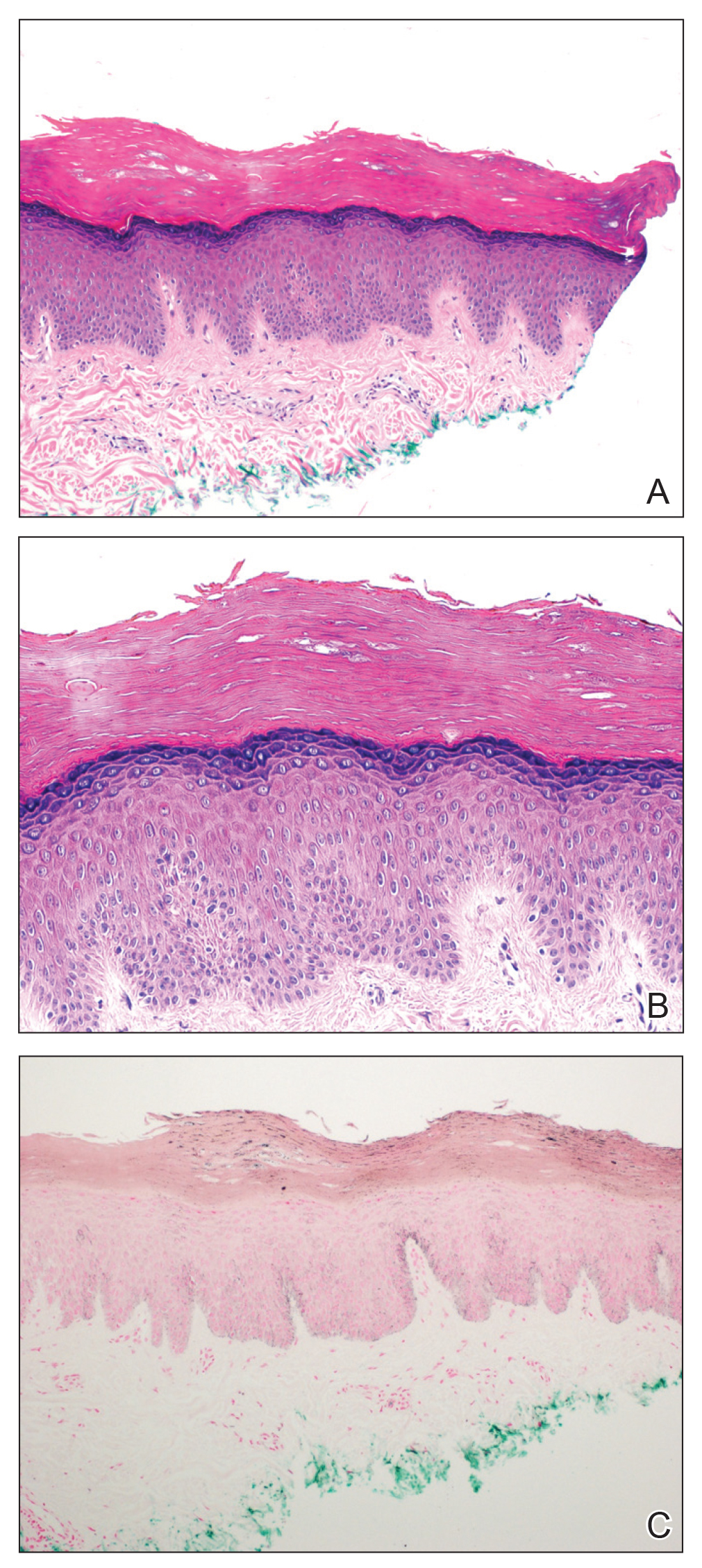
Upon further questioning, it was revealed that our patient had used a sunless tanner 3 months prior to the development of the pigmented patches. She also used urea cream to hasten exfoliation, which resulted in lighter but still apparent hyperpigmentation at follow-up 6 months after the initial presentation.
There has been a rapid growth of the sunless tanning industry in the last several years due to effective public education against UV tanning. Generally, patients apply the sunless tanner and notice an increase in tan within the following 48 hours. Typically, the tan progressively fades with the normal skin exfoliation over the span of weeks. Although most of the DHA binds proteins in the stratum corneum, the US Food and Drug Administration released a report speculating that approximately 11% of the compound reaches the epidermis and dermis.3 There are limited data regarding the effects of the compound should it pass the stratum corneum into the living skin cells.
Products with DHA only confer a sun protection factor of approximately 34; although patients may appear tan, they have no actual decreased risk for sunburn after use. Reports have shown that the use of sunless tanners containing DHA can alter the appearance of melanocytic lesions clinically and has caused pseudochromhidrosis on the palms.3,5,6 A study performed on a human keratinocyte cell line, HaCaT, showed that DHA can induce DNA damage, cell-cycle block, and apoptosis.7 In addition, as described in our case, patients may experience prolonged hyperpigmentation after use.
This case demonstrates the potential for persistent hyperpigmentation months after the use of sunless tanners containing DHA. Asking patients specific questions regarding their history of tanning product use is essential in identifying the pathology. Although a skin biopsy may not be strictly indicated, it may aid diagnosis, especially when the history is unclear. As more dermatologists support the use of sunless tanner, we must be aware of this possible outcome, especially on more cosmetically sensitive areas such as the fingers in this patient. Clinicians should be aware that the US Food and Drug Administration recommends avoiding contact with mucous membranes when applying products containing DHA and also recommends use of a test spot prior to treating the entire body with the product.8 Patients must not only be educated on the benefits of using sunless tanners but on the potential side effects with use of these products as well.
- Garone M, Howard J, Fabrikant J. A review of common tanning methods. J Clin Aesthet Dermatol. 2015;8:43-47.
- Finot PA. Nonenzymatic browning products: physiologic effects and metabolic transit in relation to chemical structure. a review. Diabetes. 1982;31:22-28.
- Yourick JJ, Koenig ML, Yourick DL, et al. Fate of chemicals in skin after dermal application: does the in vitro skin reservoir affect the estimate of systemic absorption? Toxicol Appl Pharmacol. 2004;195:309-320.
- Nguyen B, Kochevar I. Influence of hydration on dihydroxyacetone-induced pigmentation of stratum corneum. J Invest Dermatol. 2003;120:655-661.
- Takita Y, Ichimiya M, Yamaguchi M, et al. A case of pseudochromhidrosis due to dihydroxyacetone. J Dermatol. 2006;33:230-231.
- Yoshida R, Kobayashi S, Amagai M, et al. Brown palm pseudochromhidrosis. Contact Dermatitis. 2002;46:237-238.
- Petersen AB, Wulf HC, Gniadecki R, et al. Dihydroxyacetone, the active browning ingredient in sunless tanning lotions, induces DNA damage, cell-cycle block and apoptosis in cultured HaCaT keratinocytes. Mutat Res. 2004;560:173-186.
- US Food and Drug Administration. Sunless tanners & bronzers. FDA website. http://www.fda.gov/Cosmetics/ProductsIngredients
/Products/ucm134064.htm. Updated March 6, 2018. Accessed April 23, 2020
To the Editor:
The use of sunless tanners has become an alternative for individuals who wish to have tan skin without exposure to UV radiation.1 We present a case of a patient who experienced persistent hyperpigmented patches on the hands months after the use of a sunless tanner containing dihydroxyacetone (DHA), a carbohydrate that reacts with amino acids in the stratum corneum to produce pigments called melanoidins. The hyperpigmentation caused by DHA is due to the Maillard reaction, which is the nonenzymatic glycation of amino groups of proteins by the carbonyl groups of sugar.2 Many sunless tanners contain DHA at varying concentrations. Dermatologists should be aware of the benefits and potential side effects of these alternative products so that they can appropriately counsel patients.
A 20-year-old woman with no history of skin disease presented for evaluation of hyperpigmented patches on the dorsal hands of several months’ duration. Physical examination revealed ill-defined hyperpigmented patches on the dorsal fingers without associated scale or erythema (Figure 1). She had a remote history of Hodgkin lymphoma treated with chemotherapy and was in remission for 5 years prior to the current presentation. Her hematologists referred her to dermatology for evaluation, as they did not believe the patches could be related to her chemotherapy given that she had completed the treatment years before.
A punch biopsy of one of the patches was obtained to elucidate the origin of the hyperpigmentation, which had no obvious triggers according to the patient. Histopathologic examination revealed hyperpigmented parakeratosis and lentiginous hyperplasia along with pigmentation of the stratum corneum (Figures 2A and 2B) with black pigment, which stained positive with Fontana-Masson (Figure 2C).
Upon further questioning, it was revealed that our patient had used a sunless tanner 3 months prior to the development of the pigmented patches. She also used urea cream to hasten exfoliation, which resulted in lighter but still apparent hyperpigmentation at follow-up 6 months after the initial presentation.
There has been a rapid growth of the sunless tanning industry in the last several years due to effective public education against UV tanning. Generally, patients apply the sunless tanner and notice an increase in tan within the following 48 hours. Typically, the tan progressively fades with the normal skin exfoliation over the span of weeks. Although most of the DHA binds proteins in the stratum corneum, the US Food and Drug Administration released a report speculating that approximately 11% of the compound reaches the epidermis and dermis.3 There are limited data regarding the effects of the compound should it pass the stratum corneum into the living skin cells.
Products with DHA only confer a sun protection factor of approximately 34; although patients may appear tan, they have no actual decreased risk for sunburn after use. Reports have shown that the use of sunless tanners containing DHA can alter the appearance of melanocytic lesions clinically and has caused pseudochromhidrosis on the palms.3,5,6 A study performed on a human keratinocyte cell line, HaCaT, showed that DHA can induce DNA damage, cell-cycle block, and apoptosis.7 In addition, as described in our case, patients may experience prolonged hyperpigmentation after use.
This case demonstrates the potential for persistent hyperpigmentation months after the use of sunless tanners containing DHA. Asking patients specific questions regarding their history of tanning product use is essential in identifying the pathology. Although a skin biopsy may not be strictly indicated, it may aid diagnosis, especially when the history is unclear. As more dermatologists support the use of sunless tanner, we must be aware of this possible outcome, especially on more cosmetically sensitive areas such as the fingers in this patient. Clinicians should be aware that the US Food and Drug Administration recommends avoiding contact with mucous membranes when applying products containing DHA and also recommends use of a test spot prior to treating the entire body with the product.8 Patients must not only be educated on the benefits of using sunless tanners but on the potential side effects with use of these products as well.
To the Editor:
The use of sunless tanners has become an alternative for individuals who wish to have tan skin without exposure to UV radiation.1 We present a case of a patient who experienced persistent hyperpigmented patches on the hands months after the use of a sunless tanner containing dihydroxyacetone (DHA), a carbohydrate that reacts with amino acids in the stratum corneum to produce pigments called melanoidins. The hyperpigmentation caused by DHA is due to the Maillard reaction, which is the nonenzymatic glycation of amino groups of proteins by the carbonyl groups of sugar.2 Many sunless tanners contain DHA at varying concentrations. Dermatologists should be aware of the benefits and potential side effects of these alternative products so that they can appropriately counsel patients.
A 20-year-old woman with no history of skin disease presented for evaluation of hyperpigmented patches on the dorsal hands of several months’ duration. Physical examination revealed ill-defined hyperpigmented patches on the dorsal fingers without associated scale or erythema (Figure 1). She had a remote history of Hodgkin lymphoma treated with chemotherapy and was in remission for 5 years prior to the current presentation. Her hematologists referred her to dermatology for evaluation, as they did not believe the patches could be related to her chemotherapy given that she had completed the treatment years before.
A punch biopsy of one of the patches was obtained to elucidate the origin of the hyperpigmentation, which had no obvious triggers according to the patient. Histopathologic examination revealed hyperpigmented parakeratosis and lentiginous hyperplasia along with pigmentation of the stratum corneum (Figures 2A and 2B) with black pigment, which stained positive with Fontana-Masson (Figure 2C).
Upon further questioning, it was revealed that our patient had used a sunless tanner 3 months prior to the development of the pigmented patches. She also used urea cream to hasten exfoliation, which resulted in lighter but still apparent hyperpigmentation at follow-up 6 months after the initial presentation.
There has been a rapid growth of the sunless tanning industry in the last several years due to effective public education against UV tanning. Generally, patients apply the sunless tanner and notice an increase in tan within the following 48 hours. Typically, the tan progressively fades with the normal skin exfoliation over the span of weeks. Although most of the DHA binds proteins in the stratum corneum, the US Food and Drug Administration released a report speculating that approximately 11% of the compound reaches the epidermis and dermis.3 There are limited data regarding the effects of the compound should it pass the stratum corneum into the living skin cells.
Products with DHA only confer a sun protection factor of approximately 34; although patients may appear tan, they have no actual decreased risk for sunburn after use. Reports have shown that the use of sunless tanners containing DHA can alter the appearance of melanocytic lesions clinically and has caused pseudochromhidrosis on the palms.3,5,6 A study performed on a human keratinocyte cell line, HaCaT, showed that DHA can induce DNA damage, cell-cycle block, and apoptosis.7 In addition, as described in our case, patients may experience prolonged hyperpigmentation after use.
This case demonstrates the potential for persistent hyperpigmentation months after the use of sunless tanners containing DHA. Asking patients specific questions regarding their history of tanning product use is essential in identifying the pathology. Although a skin biopsy may not be strictly indicated, it may aid diagnosis, especially when the history is unclear. As more dermatologists support the use of sunless tanner, we must be aware of this possible outcome, especially on more cosmetically sensitive areas such as the fingers in this patient. Clinicians should be aware that the US Food and Drug Administration recommends avoiding contact with mucous membranes when applying products containing DHA and also recommends use of a test spot prior to treating the entire body with the product.8 Patients must not only be educated on the benefits of using sunless tanners but on the potential side effects with use of these products as well.
- Garone M, Howard J, Fabrikant J. A review of common tanning methods. J Clin Aesthet Dermatol. 2015;8:43-47.
- Finot PA. Nonenzymatic browning products: physiologic effects and metabolic transit in relation to chemical structure. a review. Diabetes. 1982;31:22-28.
- Yourick JJ, Koenig ML, Yourick DL, et al. Fate of chemicals in skin after dermal application: does the in vitro skin reservoir affect the estimate of systemic absorption? Toxicol Appl Pharmacol. 2004;195:309-320.
- Nguyen B, Kochevar I. Influence of hydration on dihydroxyacetone-induced pigmentation of stratum corneum. J Invest Dermatol. 2003;120:655-661.
- Takita Y, Ichimiya M, Yamaguchi M, et al. A case of pseudochromhidrosis due to dihydroxyacetone. J Dermatol. 2006;33:230-231.
- Yoshida R, Kobayashi S, Amagai M, et al. Brown palm pseudochromhidrosis. Contact Dermatitis. 2002;46:237-238.
- Petersen AB, Wulf HC, Gniadecki R, et al. Dihydroxyacetone, the active browning ingredient in sunless tanning lotions, induces DNA damage, cell-cycle block and apoptosis in cultured HaCaT keratinocytes. Mutat Res. 2004;560:173-186.
- US Food and Drug Administration. Sunless tanners & bronzers. FDA website. http://www.fda.gov/Cosmetics/ProductsIngredients
/Products/ucm134064.htm. Updated March 6, 2018. Accessed April 23, 2020
- Garone M, Howard J, Fabrikant J. A review of common tanning methods. J Clin Aesthet Dermatol. 2015;8:43-47.
- Finot PA. Nonenzymatic browning products: physiologic effects and metabolic transit in relation to chemical structure. a review. Diabetes. 1982;31:22-28.
- Yourick JJ, Koenig ML, Yourick DL, et al. Fate of chemicals in skin after dermal application: does the in vitro skin reservoir affect the estimate of systemic absorption? Toxicol Appl Pharmacol. 2004;195:309-320.
- Nguyen B, Kochevar I. Influence of hydration on dihydroxyacetone-induced pigmentation of stratum corneum. J Invest Dermatol. 2003;120:655-661.
- Takita Y, Ichimiya M, Yamaguchi M, et al. A case of pseudochromhidrosis due to dihydroxyacetone. J Dermatol. 2006;33:230-231.
- Yoshida R, Kobayashi S, Amagai M, et al. Brown palm pseudochromhidrosis. Contact Dermatitis. 2002;46:237-238.
- Petersen AB, Wulf HC, Gniadecki R, et al. Dihydroxyacetone, the active browning ingredient in sunless tanning lotions, induces DNA damage, cell-cycle block and apoptosis in cultured HaCaT keratinocytes. Mutat Res. 2004;560:173-186.
- US Food and Drug Administration. Sunless tanners & bronzers. FDA website. http://www.fda.gov/Cosmetics/ProductsIngredients
/Products/ucm134064.htm. Updated March 6, 2018. Accessed April 23, 2020
Practice Points
- Patient education on the benefits and risks associated with sunless tanners is critical when using these products.
- Sunless tanners containing dihydroxyacetone potentially can lead to persistent hyperpigmented patches on areas of contact.
- Skin biopsy showing hyperpigmented parakeratosis along with pigmentation of the stratum corneum can aid in diagnosis.
