User login
Pseudoepitheliomatous Hyperplasia Arising From Purple Tattoo Pigment
To the Editor:
Pseudoepitheliomatous hyperplasia (PEH) is an uncommon type of reactive epidermal proliferation that can occur from a variety of causes, including an underlying infection, inflammation, neoplastic condition, or trauma induced from tattooing.1 Diagnosis can be challenging and requires clinicopathologic correlation, as PEH can mimic malignancy on histopathology.2-4 Histologically, PEH shows irregular hyperplasia of the epidermis and adnexal epithelium, elongation of the rete ridges, and extension of the reactive proliferation into the dermis. Absence of cytologic atypia is key to the diagnosis of PEH, helping to distinguish it from squamous cell carcinoma and keratoacanthoma. Clinically, patients typically present with well-demarcated, erythematous, scaly plaques or nodules in reactive areas, which can be symptomatically pruritic.
A 48-year-old woman presented with scaly and crusted verrucous plaques of 2 months’ duration that were isolated to the areas of purple pigment within a tattoo on the right lower leg. The patient reported pruritus in the affected areas that occurred immediately after obtaining the tattoo, which was her first and only tattoo. She denied any pertinent medical history, including an absence of immunosuppression and autoimmune or chronic inflammatory diseases.
Physical examination revealed scaly and crusted plaques isolated to areas of purple tattoo pigment (Figure 1). Areas of red, green, black, and blue pigmentation within the tattoo were uninvolved. With the initial suspicion of allergic contact dermatitis, two 6-mm punch biopsies were taken from adjacent linear plaques on the right leg for histology and tissue culture. Histopathologic evaluation revealed dermal tattoo pigment with overlying PEH and was negative for signs of infection (Figure 2). Infectious stains such as periodic acid–Schiff, Grocott-Gomori methenamine-silver, and Gram stains were performed and found to be negative. In addition, culture for mycobacteria came back negative. Prurigo was on the differential; however, histopathologic changes were more compatible with a PEH reaction to the tattoo.


Upon diagnosis, the patient was treated with clobetasol ointment 0.05% under occlusion for 1 month without reported improvement. The patient subsequently elected to undergo treatment with intralesional triamcinolone 5 mg/mL to all areas of PEH, except the areas immediately surrounding the healing biopsy sites. Twice-daily application of tacrolimus ointment 0.1% to all affected areas also was initiated. At follow-up 1 month later, she reported symptomatic relief of pruritus with a notable reduction in the thickness of the plaques in all treated areas (Figure 3). A second course of intralesional triamcinolone 5 mg/mL was performed. No additional plaques appeared during the treatment course, and the patient reported high satisfaction with the final result that was achieved.
An increase in the popularity of tattooing has led to more reports of various tattoo skin reactions.4-6 The differential diagnosis is broad for tattoo reactions and includes granulomatous inflammation, sarcoidosis, psoriasis (Köbner phenomenon), allergic contact dermatitis, lichen planus, morphealike reactions, squamous cell carcinoma, and keratoacanthoma,5 which makes clinicopathologic correlation essential for accurate diagnosis. Our case demonstrated the characteristic epithelial hyperplasia in the absence of cytologic atypia. In addition, the presence of mixed dermal inflammation histologically was noted in our patient.

Pseudoepitheliomatous hyperplasia development from a tattoo in areas of both mercury-based and non–mercury-based red pigment is a known association.7-9 Balfour et al10 also reported a case of PEH occurring secondary to manganese-based purple pigment. Because few cases have been reported, the epidemiology for PEH currently is unknown. Treatment of this condition primarily is anecdotal, with prior cases showing success with topical or intralesional steroids.5,7 As with any steroid-based treatment, we recommend less aggressive treatments initially with close follow-up and adaptation as needed to minimize adverse effects such as unwanted atrophy. Some success has been reported with the use of the Q-switched Nd:YAG laser in the setting of a PEH tattoo reaction.5 Similar to other tattoo reactions, surgical removal can be considered with failure of more conservative treatment methods and focal involvement.
We report an unusual case of PEH occurring secondary to purple tattoo pigment. Our report also demonstrates the clinical and symptomatic improvement of PEH that can be achieved through the use of intralesional corticosteroid therapy. Our patient represents a case of PEH reactive to tattooing with purple ink. Further research to elucidate the precise pathogenesis of PEH tattoo reactions would be helpful in identifying high-risk patients and determining the most efficacious treatments.
- Meani RE, Nixon RL, O’Keefe R, et al. Pseudoepitheliomatous hyperplasia secondary to allergic contact dermatitis to Grevillea Robyn Gordon. Australas J Dermatol. 2017;58:E8-E10.
- Chakrabarti S, Chakrabarti P, Agrawal D, et al. Pseudoepitheliomatous hyperplasia: a clinical entity mistaken for squamous cell carcinoma. J Cutan Aesthet Surg. 2014;7:232.
- Kluger N. Issues with keratoacanthoma, pseudoepitheliomatous hyperplasia and squamous cell carcinoma within tattoos: a clinical point of view. J Cutan Pathol. 2009;37:812-813.
- Zayour M, Lazova R. Pseudoepitheliomatous hyperplasia: a review. Am J Dermatopathol. 2011;33:112-126.
- Bassi A, Campolmi P, Cannarozzo G, et al. Tattoo-associated skin reaction: the importance of an early diagnosis and proper treatment [published online July 23, 2014]. Biomed Res Int. 2014;2014:354608.
- Serup J. Diagnostic tools for doctors’ evaluation of tattoo complications. Curr Probl Dermatol. 2017;52:42-57.
- Kazlouskaya V, Junkins-Hopkins JM. Pseudoepitheliomatous hyperplasia in a red pigment tattoo: a separate entity or hypertrophic lichen planus-like reaction? J Clin Aesthet Dermatol. 2015;8:48-52.
- Kluger N, Durand L, Minier-Thoumin C, et al. Pseudoepitheliomatous epidermal hyperplasia in tattoos: report of three cases. Am J Clin Dermatol. 2008;9:337-340.
- Cui W, McGregor DH, Stark SP, et al. Pseudoepitheliomatous hyperplasia—an unusual reaction following tattoo: report of a case and review of the literature. Int J Dermatol. 2007;46:743-745.
- Balfour E, Olhoffer I, Leffell D, et al. Massive pseudoepitheliomatous hyperplasia: an unusual reaction to a tattoo. Am J Dermatopathol. 2003;25:338-340.
To the Editor:
Pseudoepitheliomatous hyperplasia (PEH) is an uncommon type of reactive epidermal proliferation that can occur from a variety of causes, including an underlying infection, inflammation, neoplastic condition, or trauma induced from tattooing.1 Diagnosis can be challenging and requires clinicopathologic correlation, as PEH can mimic malignancy on histopathology.2-4 Histologically, PEH shows irregular hyperplasia of the epidermis and adnexal epithelium, elongation of the rete ridges, and extension of the reactive proliferation into the dermis. Absence of cytologic atypia is key to the diagnosis of PEH, helping to distinguish it from squamous cell carcinoma and keratoacanthoma. Clinically, patients typically present with well-demarcated, erythematous, scaly plaques or nodules in reactive areas, which can be symptomatically pruritic.
A 48-year-old woman presented with scaly and crusted verrucous plaques of 2 months’ duration that were isolated to the areas of purple pigment within a tattoo on the right lower leg. The patient reported pruritus in the affected areas that occurred immediately after obtaining the tattoo, which was her first and only tattoo. She denied any pertinent medical history, including an absence of immunosuppression and autoimmune or chronic inflammatory diseases.
Physical examination revealed scaly and crusted plaques isolated to areas of purple tattoo pigment (Figure 1). Areas of red, green, black, and blue pigmentation within the tattoo were uninvolved. With the initial suspicion of allergic contact dermatitis, two 6-mm punch biopsies were taken from adjacent linear plaques on the right leg for histology and tissue culture. Histopathologic evaluation revealed dermal tattoo pigment with overlying PEH and was negative for signs of infection (Figure 2). Infectious stains such as periodic acid–Schiff, Grocott-Gomori methenamine-silver, and Gram stains were performed and found to be negative. In addition, culture for mycobacteria came back negative. Prurigo was on the differential; however, histopathologic changes were more compatible with a PEH reaction to the tattoo.
Upon diagnosis, the patient was treated with clobetasol ointment 0.05% under occlusion for 1 month without reported improvement. The patient subsequently elected to undergo treatment with intralesional triamcinolone 5 mg/mL to all areas of PEH, except the areas immediately surrounding the healing biopsy sites. Twice-daily application of tacrolimus ointment 0.1% to all affected areas also was initiated. At follow-up 1 month later, she reported symptomatic relief of pruritus with a notable reduction in the thickness of the plaques in all treated areas (Figure 3). A second course of intralesional triamcinolone 5 mg/mL was performed. No additional plaques appeared during the treatment course, and the patient reported high satisfaction with the final result that was achieved.
An increase in the popularity of tattooing has led to more reports of various tattoo skin reactions.4-6 The differential diagnosis is broad for tattoo reactions and includes granulomatous inflammation, sarcoidosis, psoriasis (Köbner phenomenon), allergic contact dermatitis, lichen planus, morphealike reactions, squamous cell carcinoma, and keratoacanthoma,5 which makes clinicopathologic correlation essential for accurate diagnosis. Our case demonstrated the characteristic epithelial hyperplasia in the absence of cytologic atypia. In addition, the presence of mixed dermal inflammation histologically was noted in our patient.
Pseudoepitheliomatous hyperplasia development from a tattoo in areas of both mercury-based and non–mercury-based red pigment is a known association.7-9 Balfour et al10 also reported a case of PEH occurring secondary to manganese-based purple pigment. Because few cases have been reported, the epidemiology for PEH currently is unknown. Treatment of this condition primarily is anecdotal, with prior cases showing success with topical or intralesional steroids.5,7 As with any steroid-based treatment, we recommend less aggressive treatments initially with close follow-up and adaptation as needed to minimize adverse effects such as unwanted atrophy. Some success has been reported with the use of the Q-switched Nd:YAG laser in the setting of a PEH tattoo reaction.5 Similar to other tattoo reactions, surgical removal can be considered with failure of more conservative treatment methods and focal involvement.
We report an unusual case of PEH occurring secondary to purple tattoo pigment. Our report also demonstrates the clinical and symptomatic improvement of PEH that can be achieved through the use of intralesional corticosteroid therapy. Our patient represents a case of PEH reactive to tattooing with purple ink. Further research to elucidate the precise pathogenesis of PEH tattoo reactions would be helpful in identifying high-risk patients and determining the most efficacious treatments.
To the Editor:
Pseudoepitheliomatous hyperplasia (PEH) is an uncommon type of reactive epidermal proliferation that can occur from a variety of causes, including an underlying infection, inflammation, neoplastic condition, or trauma induced from tattooing.1 Diagnosis can be challenging and requires clinicopathologic correlation, as PEH can mimic malignancy on histopathology.2-4 Histologically, PEH shows irregular hyperplasia of the epidermis and adnexal epithelium, elongation of the rete ridges, and extension of the reactive proliferation into the dermis. Absence of cytologic atypia is key to the diagnosis of PEH, helping to distinguish it from squamous cell carcinoma and keratoacanthoma. Clinically, patients typically present with well-demarcated, erythematous, scaly plaques or nodules in reactive areas, which can be symptomatically pruritic.
A 48-year-old woman presented with scaly and crusted verrucous plaques of 2 months’ duration that were isolated to the areas of purple pigment within a tattoo on the right lower leg. The patient reported pruritus in the affected areas that occurred immediately after obtaining the tattoo, which was her first and only tattoo. She denied any pertinent medical history, including an absence of immunosuppression and autoimmune or chronic inflammatory diseases.
Physical examination revealed scaly and crusted plaques isolated to areas of purple tattoo pigment (Figure 1). Areas of red, green, black, and blue pigmentation within the tattoo were uninvolved. With the initial suspicion of allergic contact dermatitis, two 6-mm punch biopsies were taken from adjacent linear plaques on the right leg for histology and tissue culture. Histopathologic evaluation revealed dermal tattoo pigment with overlying PEH and was negative for signs of infection (Figure 2). Infectious stains such as periodic acid–Schiff, Grocott-Gomori methenamine-silver, and Gram stains were performed and found to be negative. In addition, culture for mycobacteria came back negative. Prurigo was on the differential; however, histopathologic changes were more compatible with a PEH reaction to the tattoo.
Upon diagnosis, the patient was treated with clobetasol ointment 0.05% under occlusion for 1 month without reported improvement. The patient subsequently elected to undergo treatment with intralesional triamcinolone 5 mg/mL to all areas of PEH, except the areas immediately surrounding the healing biopsy sites. Twice-daily application of tacrolimus ointment 0.1% to all affected areas also was initiated. At follow-up 1 month later, she reported symptomatic relief of pruritus with a notable reduction in the thickness of the plaques in all treated areas (Figure 3). A second course of intralesional triamcinolone 5 mg/mL was performed. No additional plaques appeared during the treatment course, and the patient reported high satisfaction with the final result that was achieved.
An increase in the popularity of tattooing has led to more reports of various tattoo skin reactions.4-6 The differential diagnosis is broad for tattoo reactions and includes granulomatous inflammation, sarcoidosis, psoriasis (Köbner phenomenon), allergic contact dermatitis, lichen planus, morphealike reactions, squamous cell carcinoma, and keratoacanthoma,5 which makes clinicopathologic correlation essential for accurate diagnosis. Our case demonstrated the characteristic epithelial hyperplasia in the absence of cytologic atypia. In addition, the presence of mixed dermal inflammation histologically was noted in our patient.
Pseudoepitheliomatous hyperplasia development from a tattoo in areas of both mercury-based and non–mercury-based red pigment is a known association.7-9 Balfour et al10 also reported a case of PEH occurring secondary to manganese-based purple pigment. Because few cases have been reported, the epidemiology for PEH currently is unknown. Treatment of this condition primarily is anecdotal, with prior cases showing success with topical or intralesional steroids.5,7 As with any steroid-based treatment, we recommend less aggressive treatments initially with close follow-up and adaptation as needed to minimize adverse effects such as unwanted atrophy. Some success has been reported with the use of the Q-switched Nd:YAG laser in the setting of a PEH tattoo reaction.5 Similar to other tattoo reactions, surgical removal can be considered with failure of more conservative treatment methods and focal involvement.
We report an unusual case of PEH occurring secondary to purple tattoo pigment. Our report also demonstrates the clinical and symptomatic improvement of PEH that can be achieved through the use of intralesional corticosteroid therapy. Our patient represents a case of PEH reactive to tattooing with purple ink. Further research to elucidate the precise pathogenesis of PEH tattoo reactions would be helpful in identifying high-risk patients and determining the most efficacious treatments.
- Meani RE, Nixon RL, O’Keefe R, et al. Pseudoepitheliomatous hyperplasia secondary to allergic contact dermatitis to Grevillea Robyn Gordon. Australas J Dermatol. 2017;58:E8-E10.
- Chakrabarti S, Chakrabarti P, Agrawal D, et al. Pseudoepitheliomatous hyperplasia: a clinical entity mistaken for squamous cell carcinoma. J Cutan Aesthet Surg. 2014;7:232.
- Kluger N. Issues with keratoacanthoma, pseudoepitheliomatous hyperplasia and squamous cell carcinoma within tattoos: a clinical point of view. J Cutan Pathol. 2009;37:812-813.
- Zayour M, Lazova R. Pseudoepitheliomatous hyperplasia: a review. Am J Dermatopathol. 2011;33:112-126.
- Bassi A, Campolmi P, Cannarozzo G, et al. Tattoo-associated skin reaction: the importance of an early diagnosis and proper treatment [published online July 23, 2014]. Biomed Res Int. 2014;2014:354608.
- Serup J. Diagnostic tools for doctors’ evaluation of tattoo complications. Curr Probl Dermatol. 2017;52:42-57.
- Kazlouskaya V, Junkins-Hopkins JM. Pseudoepitheliomatous hyperplasia in a red pigment tattoo: a separate entity or hypertrophic lichen planus-like reaction? J Clin Aesthet Dermatol. 2015;8:48-52.
- Kluger N, Durand L, Minier-Thoumin C, et al. Pseudoepitheliomatous epidermal hyperplasia in tattoos: report of three cases. Am J Clin Dermatol. 2008;9:337-340.
- Cui W, McGregor DH, Stark SP, et al. Pseudoepitheliomatous hyperplasia—an unusual reaction following tattoo: report of a case and review of the literature. Int J Dermatol. 2007;46:743-745.
- Balfour E, Olhoffer I, Leffell D, et al. Massive pseudoepitheliomatous hyperplasia: an unusual reaction to a tattoo. Am J Dermatopathol. 2003;25:338-340.
- Meani RE, Nixon RL, O’Keefe R, et al. Pseudoepitheliomatous hyperplasia secondary to allergic contact dermatitis to Grevillea Robyn Gordon. Australas J Dermatol. 2017;58:E8-E10.
- Chakrabarti S, Chakrabarti P, Agrawal D, et al. Pseudoepitheliomatous hyperplasia: a clinical entity mistaken for squamous cell carcinoma. J Cutan Aesthet Surg. 2014;7:232.
- Kluger N. Issues with keratoacanthoma, pseudoepitheliomatous hyperplasia and squamous cell carcinoma within tattoos: a clinical point of view. J Cutan Pathol. 2009;37:812-813.
- Zayour M, Lazova R. Pseudoepitheliomatous hyperplasia: a review. Am J Dermatopathol. 2011;33:112-126.
- Bassi A, Campolmi P, Cannarozzo G, et al. Tattoo-associated skin reaction: the importance of an early diagnosis and proper treatment [published online July 23, 2014]. Biomed Res Int. 2014;2014:354608.
- Serup J. Diagnostic tools for doctors’ evaluation of tattoo complications. Curr Probl Dermatol. 2017;52:42-57.
- Kazlouskaya V, Junkins-Hopkins JM. Pseudoepitheliomatous hyperplasia in a red pigment tattoo: a separate entity or hypertrophic lichen planus-like reaction? J Clin Aesthet Dermatol. 2015;8:48-52.
- Kluger N, Durand L, Minier-Thoumin C, et al. Pseudoepitheliomatous epidermal hyperplasia in tattoos: report of three cases. Am J Clin Dermatol. 2008;9:337-340.
- Cui W, McGregor DH, Stark SP, et al. Pseudoepitheliomatous hyperplasia—an unusual reaction following tattoo: report of a case and review of the literature. Int J Dermatol. 2007;46:743-745.
- Balfour E, Olhoffer I, Leffell D, et al. Massive pseudoepitheliomatous hyperplasia: an unusual reaction to a tattoo. Am J Dermatopathol. 2003;25:338-340.
Practice Points
- Pseudoepitheliomatous hyperplasia (PEH) is a rare benign condition that can arise in response to multiple underlying triggers such as tattoo pigment.
- Histopathologic evaluation is essential for diagnosis and shows characteristic hyperplasia of the epidermis.
- Clinicians should consider intralesional steroids in the treatment of PEH once atypical mycobacterial and deep fungal infections have been ruled out.

What is the significance of isolated tumor cells in endometrial cancer?
Over the past decade gynecologic oncology surgeons have increasingly adopted the technique of sentinel lymph node (SLN) biopsy to stage endometrial cancer. This is supported by evidence that selective removal of the few lymph nodes which are the first to drain the uterus can accurately detect metastatic disease, sparing the patient a complete lymphadenectomy and its associated risks, such as lymphedema.1 The proposed benefits of SLN biopsy are not just its ability to spare the patient removal of dozens of unnecessary lymph nodes, but also the ability to improve upon the detection of previously unrecognized nodal metastases in locations not routinely sampled by lymphadenectomy and by identifying very-low-volume metastatic disease. This is beneficial only, however, if that previously overlooked low-volume disease is clinically significant.
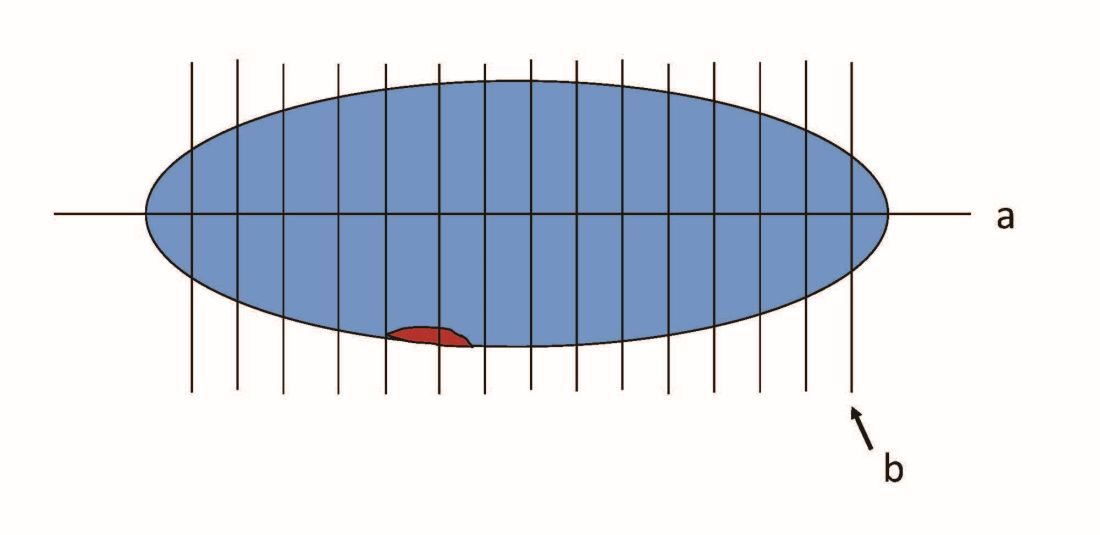
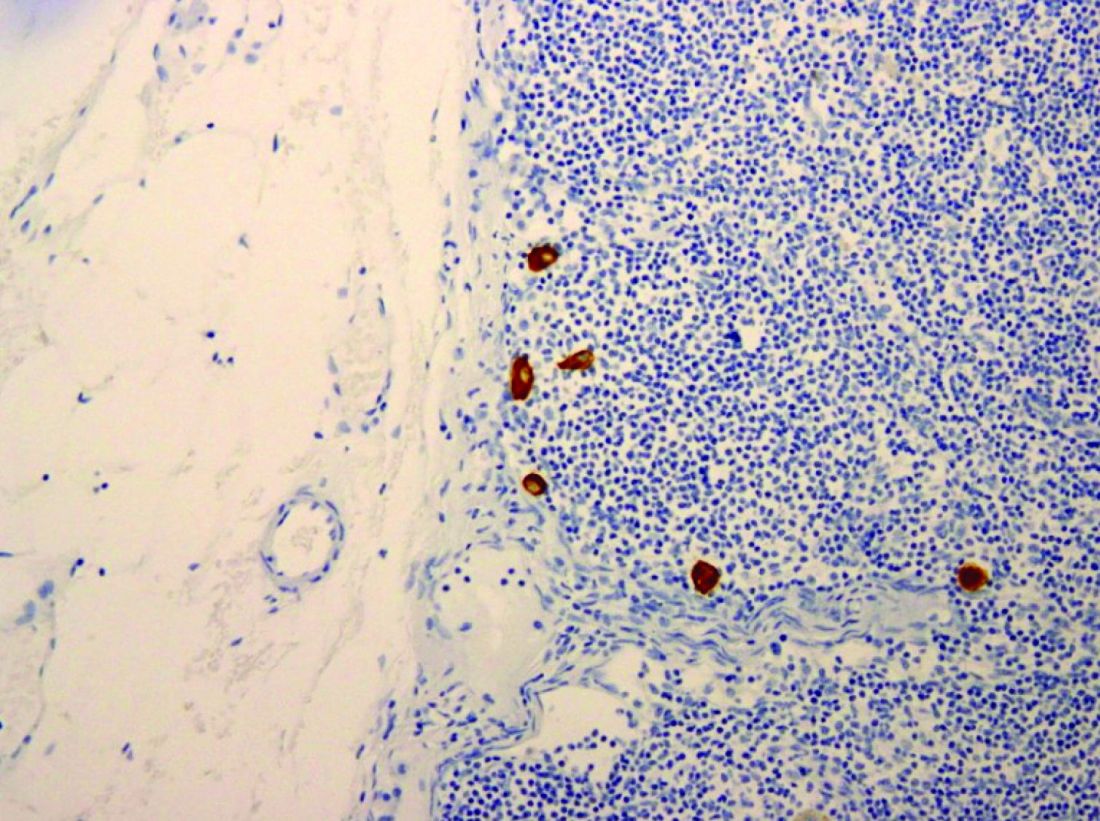
When pathologists evaluate lymph nodes as part of conventional lymphadenectomy, they typically bivalve the lymph node and evaluate with hematoxylin and eosin (H&E) stains. This technique is capable of detecting metastatic lesions greater than 2 mm, but can miss low-volume disease. In contrast, pathologists process SLNs with much finer sectioning (no greater than 2 mm), and, if the node is larger than 4 mm, they will section it perpendicular to the long axis in a bread-loaf fashion. It is not feasible to perform this ultrasectioning on the large numbers of lymph nodes of a complete lymphadenectomy specimen, but when applied to an SLN it allows pathologists to detect much smaller metastatic foci, the so-called “micrometastases” that are between 0.2 and 2 mm in size, and which typically arise in the subcapsular region of the node. The graphic depicts how a traditional longitudinal cut (a) might miss the micrometastasis that could be identified on the finer perpendicular cuts of ultra-sectioning (b). In addition to the ultrasectioning of the node into smaller slices, the pathologist performs additional immunohistochemistry stains for cytokeratin on sentinel nodes which appear negative on preliminary H&E stains. This allows the pathologist to identify even smaller clusters of malignant cells that are less than 0.2 mm, or individual cancer cells, so-called “isolated tumor cells” (ITCs) as shown in the photo. Most SLN series identify that approximately half of their “positive” lymph nodes are low-volume disease (micrometastases and ITCs). ITCs make up the majority of these cases, typically three-quarters.
Clinicians might be reassured by the discovery of low-volume metastatic disease, perceiving that the added attention afforded by the SLN approach helped them to identify metastases that might otherwise have been missed and therefore not treated. This is because node-positive (stage IIIC) disease is not cured by surgery or radiation alone and requires the addition of chemotherapy for survival benefit.2 Alternatively, there is no clear survival benefit derived from treating stage I high/intermediate cancers with chemotherapy, and therefore, the prescription of chemotherapy hinges upon reliable identification of extrauterine disease on pathology.3
It would make sense that if SLNs are more effective in identifying metastatic disease, clinicians who practice SLN biopsy would identify it more of the time. This appears to be the case with a trend towards upstaging in patients who undergo SLN biopsy, compared with those undergoing complete lymphadenectomy.4 It should also follow that if this increased detection of metastatic disease was clinically relevant, we would observe a corresponding improvement in survival outcomes. If not, then the additional identification of low-volume disease may not be value added: imparting toxicity of adjuvant therapy without survival benefit.
Micrometastases (foci sized 0.2-2 mm) are not a new phenomenon to the SLN era. Low-volume lesions were occasionally detected with routine nodal processing and H&E stains. Attention wasn’t paid to nodal volume categorization in pathology reports prior to the SLN era. These were usually reported collectively as stage IIIC disease. It would make sense to continue to approach micrometastases in a manner similar to what we have always done, recognizing that it may represent a continuum of nodal macrometastases. In contrast, ITCs are rarely detected with routine pathologic processing. Perhaps they are less within a continuum of nodal metastases, and more within the continuum of lymphovascular space invasion. We know that ITCs are significantly associated with the cofinding of this uterine phenomenon, which itself is considered a significant risk factor for local recurrence.5
Series have consistently shown the outcomes of women with ITCs to be favorable, compared with those with micrometastases or macrometastases.5,6 However, most retrospective series that evaluated the outcomes of patients with respect to volume of metastatic disease have high rates of treatment of ITCs with chemotherapy, radiotherapy, or both.6 This may mask and confuse whether there is any intrinsically favorable prognostic virtue of ITCs, compared with larger metastatic foci. When ITCs are untreated, it would appear that the rates and patterns of recurrence appear similar to those with negative SLNs, with the caveat that these series all include small numbers.5,7 This would suggest that women with ITCs do not need additional therapy beyond what would be prescribed for their uterine risk factors.

Further supporting the notion that ITCs have more favorable prognosis is that, while SLN biopsy is associated with a higher detection of nodal metastatic disease, it is not necessarily associated with improved survival when compared with complete lymphadenectomy in retrospective series.8 This suggests that finding and treating ITCs may not positively affect outcomes. Or possibly it is a result of inadequate statistical power to show a small benefit should one exist. It is especially difficult to differentiate micrometastases and ITCs with respect to treatment outcomes. Given that ITCs make up the majority of low-volume nodal disease detected through the SLN technique, any potential benefit of increased capture and treatment of the more substantial micrometastases is not likely to be captured. As a result, most series tend to lump patients with micrometastases with those with ITCs in their analysis of patient outcomes. This may be a mistake.
Clearly more research needs to be performed to definitively address the clinical significance of ITCs. While it would be ideal to conduct a prospective trial in which patients with ITCs are randomized to therapy or observation, in reality the scope of such a trial makes it impractical. ITCs are detected in only approximately 5% of all the patients with endometrial cancer, and given that outcomes for this group are, in general, good, it would require enrollment of tens of thousands of patients to establish a statistically satisfactory result. Therefore it is likely that we will need to rely on the results of large retrospective, population-based, observational series to determine if the identification and treatment of ITCs adds value and superior outcomes to patients. In addition, we are making leaps in better understanding the molecular profile of endometrial cancers and how we might incorporate this data with histology and staging results to create treatment algorithms, much like what has been developed for breast cancer. This is likely where the future lies in interpreting the results of staging. In the meantime, it seems reasonable to collect the data regarding volume of metastatic disease including the presence of ITCs, making shared treatment decisions with the patient regarding the addition of adjuvant therapy, recognizing that
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to declare. Email her at obnews@mdedge.com.
References
1. Lancet Oncol. 2017 Mar;18(3):384-92.
2. J Clin Oncol. 2006 Jan 1;24(1):36-44.
3. J Clin Oncol. 2019 Jul 20;37(21):1810-8.
4. Clin Transl Oncol. 2019. doi: 10.1007/s12094-019-02249-x.
5. Gynecol Oncol. 2017 Aug;146(2):240-6.
6. Ann Surg Oncol. 2016 May;23(5):1653-9.
7. Gynecol Oncol. 2019 Jun;153(3):496-9.
8. Gynecol Oncol. 2018 Nov;151(2):235-42.
Over the past decade gynecologic oncology surgeons have increasingly adopted the technique of sentinel lymph node (SLN) biopsy to stage endometrial cancer. This is supported by evidence that selective removal of the few lymph nodes which are the first to drain the uterus can accurately detect metastatic disease, sparing the patient a complete lymphadenectomy and its associated risks, such as lymphedema.1 The proposed benefits of SLN biopsy are not just its ability to spare the patient removal of dozens of unnecessary lymph nodes, but also the ability to improve upon the detection of previously unrecognized nodal metastases in locations not routinely sampled by lymphadenectomy and by identifying very-low-volume metastatic disease. This is beneficial only, however, if that previously overlooked low-volume disease is clinically significant.
When pathologists evaluate lymph nodes as part of conventional lymphadenectomy, they typically bivalve the lymph node and evaluate with hematoxylin and eosin (H&E) stains. This technique is capable of detecting metastatic lesions greater than 2 mm, but can miss low-volume disease. In contrast, pathologists process SLNs with much finer sectioning (no greater than 2 mm), and, if the node is larger than 4 mm, they will section it perpendicular to the long axis in a bread-loaf fashion. It is not feasible to perform this ultrasectioning on the large numbers of lymph nodes of a complete lymphadenectomy specimen, but when applied to an SLN it allows pathologists to detect much smaller metastatic foci, the so-called “micrometastases” that are between 0.2 and 2 mm in size, and which typically arise in the subcapsular region of the node. The graphic depicts how a traditional longitudinal cut (a) might miss the micrometastasis that could be identified on the finer perpendicular cuts of ultra-sectioning (b). In addition to the ultrasectioning of the node into smaller slices, the pathologist performs additional immunohistochemistry stains for cytokeratin on sentinel nodes which appear negative on preliminary H&E stains. This allows the pathologist to identify even smaller clusters of malignant cells that are less than 0.2 mm, or individual cancer cells, so-called “isolated tumor cells” (ITCs) as shown in the photo. Most SLN series identify that approximately half of their “positive” lymph nodes are low-volume disease (micrometastases and ITCs). ITCs make up the majority of these cases, typically three-quarters.
Clinicians might be reassured by the discovery of low-volume metastatic disease, perceiving that the added attention afforded by the SLN approach helped them to identify metastases that might otherwise have been missed and therefore not treated. This is because node-positive (stage IIIC) disease is not cured by surgery or radiation alone and requires the addition of chemotherapy for survival benefit.2 Alternatively, there is no clear survival benefit derived from treating stage I high/intermediate cancers with chemotherapy, and therefore, the prescription of chemotherapy hinges upon reliable identification of extrauterine disease on pathology.3
It would make sense that if SLNs are more effective in identifying metastatic disease, clinicians who practice SLN biopsy would identify it more of the time. This appears to be the case with a trend towards upstaging in patients who undergo SLN biopsy, compared with those undergoing complete lymphadenectomy.4 It should also follow that if this increased detection of metastatic disease was clinically relevant, we would observe a corresponding improvement in survival outcomes. If not, then the additional identification of low-volume disease may not be value added: imparting toxicity of adjuvant therapy without survival benefit.
Micrometastases (foci sized 0.2-2 mm) are not a new phenomenon to the SLN era. Low-volume lesions were occasionally detected with routine nodal processing and H&E stains. Attention wasn’t paid to nodal volume categorization in pathology reports prior to the SLN era. These were usually reported collectively as stage IIIC disease. It would make sense to continue to approach micrometastases in a manner similar to what we have always done, recognizing that it may represent a continuum of nodal macrometastases. In contrast, ITCs are rarely detected with routine pathologic processing. Perhaps they are less within a continuum of nodal metastases, and more within the continuum of lymphovascular space invasion. We know that ITCs are significantly associated with the cofinding of this uterine phenomenon, which itself is considered a significant risk factor for local recurrence.5
Series have consistently shown the outcomes of women with ITCs to be favorable, compared with those with micrometastases or macrometastases.5,6 However, most retrospective series that evaluated the outcomes of patients with respect to volume of metastatic disease have high rates of treatment of ITCs with chemotherapy, radiotherapy, or both.6 This may mask and confuse whether there is any intrinsically favorable prognostic virtue of ITCs, compared with larger metastatic foci. When ITCs are untreated, it would appear that the rates and patterns of recurrence appear similar to those with negative SLNs, with the caveat that these series all include small numbers.5,7 This would suggest that women with ITCs do not need additional therapy beyond what would be prescribed for their uterine risk factors.
Further supporting the notion that ITCs have more favorable prognosis is that, while SLN biopsy is associated with a higher detection of nodal metastatic disease, it is not necessarily associated with improved survival when compared with complete lymphadenectomy in retrospective series.8 This suggests that finding and treating ITCs may not positively affect outcomes. Or possibly it is a result of inadequate statistical power to show a small benefit should one exist. It is especially difficult to differentiate micrometastases and ITCs with respect to treatment outcomes. Given that ITCs make up the majority of low-volume nodal disease detected through the SLN technique, any potential benefit of increased capture and treatment of the more substantial micrometastases is not likely to be captured. As a result, most series tend to lump patients with micrometastases with those with ITCs in their analysis of patient outcomes. This may be a mistake.
Clearly more research needs to be performed to definitively address the clinical significance of ITCs. While it would be ideal to conduct a prospective trial in which patients with ITCs are randomized to therapy or observation, in reality the scope of such a trial makes it impractical. ITCs are detected in only approximately 5% of all the patients with endometrial cancer, and given that outcomes for this group are, in general, good, it would require enrollment of tens of thousands of patients to establish a statistically satisfactory result. Therefore it is likely that we will need to rely on the results of large retrospective, population-based, observational series to determine if the identification and treatment of ITCs adds value and superior outcomes to patients. In addition, we are making leaps in better understanding the molecular profile of endometrial cancers and how we might incorporate this data with histology and staging results to create treatment algorithms, much like what has been developed for breast cancer. This is likely where the future lies in interpreting the results of staging. In the meantime, it seems reasonable to collect the data regarding volume of metastatic disease including the presence of ITCs, making shared treatment decisions with the patient regarding the addition of adjuvant therapy, recognizing that
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to declare. Email her at obnews@mdedge.com.
References
1. Lancet Oncol. 2017 Mar;18(3):384-92.
2. J Clin Oncol. 2006 Jan 1;24(1):36-44.
3. J Clin Oncol. 2019 Jul 20;37(21):1810-8.
4. Clin Transl Oncol. 2019. doi: 10.1007/s12094-019-02249-x.
5. Gynecol Oncol. 2017 Aug;146(2):240-6.
6. Ann Surg Oncol. 2016 May;23(5):1653-9.
7. Gynecol Oncol. 2019 Jun;153(3):496-9.
8. Gynecol Oncol. 2018 Nov;151(2):235-42.
Over the past decade gynecologic oncology surgeons have increasingly adopted the technique of sentinel lymph node (SLN) biopsy to stage endometrial cancer. This is supported by evidence that selective removal of the few lymph nodes which are the first to drain the uterus can accurately detect metastatic disease, sparing the patient a complete lymphadenectomy and its associated risks, such as lymphedema.1 The proposed benefits of SLN biopsy are not just its ability to spare the patient removal of dozens of unnecessary lymph nodes, but also the ability to improve upon the detection of previously unrecognized nodal metastases in locations not routinely sampled by lymphadenectomy and by identifying very-low-volume metastatic disease. This is beneficial only, however, if that previously overlooked low-volume disease is clinically significant.
When pathologists evaluate lymph nodes as part of conventional lymphadenectomy, they typically bivalve the lymph node and evaluate with hematoxylin and eosin (H&E) stains. This technique is capable of detecting metastatic lesions greater than 2 mm, but can miss low-volume disease. In contrast, pathologists process SLNs with much finer sectioning (no greater than 2 mm), and, if the node is larger than 4 mm, they will section it perpendicular to the long axis in a bread-loaf fashion. It is not feasible to perform this ultrasectioning on the large numbers of lymph nodes of a complete lymphadenectomy specimen, but when applied to an SLN it allows pathologists to detect much smaller metastatic foci, the so-called “micrometastases” that are between 0.2 and 2 mm in size, and which typically arise in the subcapsular region of the node. The graphic depicts how a traditional longitudinal cut (a) might miss the micrometastasis that could be identified on the finer perpendicular cuts of ultra-sectioning (b). In addition to the ultrasectioning of the node into smaller slices, the pathologist performs additional immunohistochemistry stains for cytokeratin on sentinel nodes which appear negative on preliminary H&E stains. This allows the pathologist to identify even smaller clusters of malignant cells that are less than 0.2 mm, or individual cancer cells, so-called “isolated tumor cells” (ITCs) as shown in the photo. Most SLN series identify that approximately half of their “positive” lymph nodes are low-volume disease (micrometastases and ITCs). ITCs make up the majority of these cases, typically three-quarters.
Clinicians might be reassured by the discovery of low-volume metastatic disease, perceiving that the added attention afforded by the SLN approach helped them to identify metastases that might otherwise have been missed and therefore not treated. This is because node-positive (stage IIIC) disease is not cured by surgery or radiation alone and requires the addition of chemotherapy for survival benefit.2 Alternatively, there is no clear survival benefit derived from treating stage I high/intermediate cancers with chemotherapy, and therefore, the prescription of chemotherapy hinges upon reliable identification of extrauterine disease on pathology.3
It would make sense that if SLNs are more effective in identifying metastatic disease, clinicians who practice SLN biopsy would identify it more of the time. This appears to be the case with a trend towards upstaging in patients who undergo SLN biopsy, compared with those undergoing complete lymphadenectomy.4 It should also follow that if this increased detection of metastatic disease was clinically relevant, we would observe a corresponding improvement in survival outcomes. If not, then the additional identification of low-volume disease may not be value added: imparting toxicity of adjuvant therapy without survival benefit.
Micrometastases (foci sized 0.2-2 mm) are not a new phenomenon to the SLN era. Low-volume lesions were occasionally detected with routine nodal processing and H&E stains. Attention wasn’t paid to nodal volume categorization in pathology reports prior to the SLN era. These were usually reported collectively as stage IIIC disease. It would make sense to continue to approach micrometastases in a manner similar to what we have always done, recognizing that it may represent a continuum of nodal macrometastases. In contrast, ITCs are rarely detected with routine pathologic processing. Perhaps they are less within a continuum of nodal metastases, and more within the continuum of lymphovascular space invasion. We know that ITCs are significantly associated with the cofinding of this uterine phenomenon, which itself is considered a significant risk factor for local recurrence.5
Series have consistently shown the outcomes of women with ITCs to be favorable, compared with those with micrometastases or macrometastases.5,6 However, most retrospective series that evaluated the outcomes of patients with respect to volume of metastatic disease have high rates of treatment of ITCs with chemotherapy, radiotherapy, or both.6 This may mask and confuse whether there is any intrinsically favorable prognostic virtue of ITCs, compared with larger metastatic foci. When ITCs are untreated, it would appear that the rates and patterns of recurrence appear similar to those with negative SLNs, with the caveat that these series all include small numbers.5,7 This would suggest that women with ITCs do not need additional therapy beyond what would be prescribed for their uterine risk factors.
Further supporting the notion that ITCs have more favorable prognosis is that, while SLN biopsy is associated with a higher detection of nodal metastatic disease, it is not necessarily associated with improved survival when compared with complete lymphadenectomy in retrospective series.8 This suggests that finding and treating ITCs may not positively affect outcomes. Or possibly it is a result of inadequate statistical power to show a small benefit should one exist. It is especially difficult to differentiate micrometastases and ITCs with respect to treatment outcomes. Given that ITCs make up the majority of low-volume nodal disease detected through the SLN technique, any potential benefit of increased capture and treatment of the more substantial micrometastases is not likely to be captured. As a result, most series tend to lump patients with micrometastases with those with ITCs in their analysis of patient outcomes. This may be a mistake.
Clearly more research needs to be performed to definitively address the clinical significance of ITCs. While it would be ideal to conduct a prospective trial in which patients with ITCs are randomized to therapy or observation, in reality the scope of such a trial makes it impractical. ITCs are detected in only approximately 5% of all the patients with endometrial cancer, and given that outcomes for this group are, in general, good, it would require enrollment of tens of thousands of patients to establish a statistically satisfactory result. Therefore it is likely that we will need to rely on the results of large retrospective, population-based, observational series to determine if the identification and treatment of ITCs adds value and superior outcomes to patients. In addition, we are making leaps in better understanding the molecular profile of endometrial cancers and how we might incorporate this data with histology and staging results to create treatment algorithms, much like what has been developed for breast cancer. This is likely where the future lies in interpreting the results of staging. In the meantime, it seems reasonable to collect the data regarding volume of metastatic disease including the presence of ITCs, making shared treatment decisions with the patient regarding the addition of adjuvant therapy, recognizing that
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to declare. Email her at obnews@mdedge.com.
References
1. Lancet Oncol. 2017 Mar;18(3):384-92.
2. J Clin Oncol. 2006 Jan 1;24(1):36-44.
3. J Clin Oncol. 2019 Jul 20;37(21):1810-8.
4. Clin Transl Oncol. 2019. doi: 10.1007/s12094-019-02249-x.
5. Gynecol Oncol. 2017 Aug;146(2):240-6.
6. Ann Surg Oncol. 2016 May;23(5):1653-9.
7. Gynecol Oncol. 2019 Jun;153(3):496-9.
8. Gynecol Oncol. 2018 Nov;151(2):235-42.
SGLT2 inhibitor ertugliflozin shows no CV death or renal benefit
The sodium-glucose transporter 2 (SGLT-2) inhibitor ertugliflozin broke ranks with the other drugs in its class and failed to produce statistically significant drops in the both the combined incidence of cardiovascular (CV) death or heart failure hospitalization, and the rate of adverse renal outcomes, in the mandated CV outcomes trial run for ertugliflozin with more than 8,200 patients with type 2 diabetes and established CV disease.
Merck, one of the companies that markets the drug, announced the topline results in a quarterly financial report released on April 28, 2020.
According to the report, the results from the ertugliflozin cardiovascular outcomes trial “achieved its primary endpoint of noninferiority for major adverse CV events (MACE), compared to placebo in patients with type 2 diabetes mellitus and established atherosclerotic CV disease,” but “the key secondary endpoints of superiority” of ertugliflozin, compared with placebo, “for time to the composite of CV death or hospitalization for heart failure, CV death alone, and the composite of renal death, dialysis/transplant or doubling of serum creatinine from baseline were not met.”
However, the report added that, “while not a prespecified hypothesis for statistical testing, a reduction in hospitalization for heart failure was observed” with ertugliflozin treatment, and the report further said that the drug’s safety profile in the trial “was consistent with that reported in previous studies.” The statement closed by saying that detailed results from the trial are scheduled to be presented on June 16, 2020, at the virtual American Diabetes Association’s 80th Scientific Sessions.
These results came from the VERTIS CV (Evaluation of Ertugliflozin EffIcacy and Safety Cardiovascular Outcomes) trial, which researchers said in 2018 had administered at least one investigational dose to 8,238 randomized patients at centers in any of 34 countries during two enrollment periods in 2013-2015 and 2016-2017 (Am Heart J. 2018 Dec;206:11-23). The tested agent, ertugliflozin (Steglatro) received Food and Drug Administration marketing approval late in 2017 for the indication of improving glycemic control in patients with type 2 diabetes.
The FDA mandated cardiovascular outcomes trials for new glycemic control drugs in guidance the agency issued in 2008 (the FDA released in March 2020 a draft of updated guidance on this topic).
Other FDA-approved agents from the SGLT2 inhibitor class include canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), and all three showed evidence for a statistically significant effect on reducing the incidence of CV disease death and heart failure hospitalizations, as well as renal complications (Can J Diabetes. 2020 Feb;44[1]:61-7). The evidence showing that several SGLT2 drugs have important and consistent effects on endpoints like CV death, heart failure hospitalizations, and renal complications has helped propel this class of agents to the forefront of glycemic control treatments. More recently, one agent from this group, dapagliflozin, also significantly cut the rate of heart failure worsening or CV disease death in patients with heart failure with reduced ejection fraction but without diabetes (N Engl J Med. 2019 Nov 21;381[21]:1995-2008). Based on this evidence, the FDA is currently considering adding a new indication for dapagliflozin that would also label it for use in patients with heart failure with reduced ejection fraction but without diabetes.
The sodium-glucose transporter 2 (SGLT-2) inhibitor ertugliflozin broke ranks with the other drugs in its class and failed to produce statistically significant drops in the both the combined incidence of cardiovascular (CV) death or heart failure hospitalization, and the rate of adverse renal outcomes, in the mandated CV outcomes trial run for ertugliflozin with more than 8,200 patients with type 2 diabetes and established CV disease.
Merck, one of the companies that markets the drug, announced the topline results in a quarterly financial report released on April 28, 2020.
According to the report, the results from the ertugliflozin cardiovascular outcomes trial “achieved its primary endpoint of noninferiority for major adverse CV events (MACE), compared to placebo in patients with type 2 diabetes mellitus and established atherosclerotic CV disease,” but “the key secondary endpoints of superiority” of ertugliflozin, compared with placebo, “for time to the composite of CV death or hospitalization for heart failure, CV death alone, and the composite of renal death, dialysis/transplant or doubling of serum creatinine from baseline were not met.”
However, the report added that, “while not a prespecified hypothesis for statistical testing, a reduction in hospitalization for heart failure was observed” with ertugliflozin treatment, and the report further said that the drug’s safety profile in the trial “was consistent with that reported in previous studies.” The statement closed by saying that detailed results from the trial are scheduled to be presented on June 16, 2020, at the virtual American Diabetes Association’s 80th Scientific Sessions.
These results came from the VERTIS CV (Evaluation of Ertugliflozin EffIcacy and Safety Cardiovascular Outcomes) trial, which researchers said in 2018 had administered at least one investigational dose to 8,238 randomized patients at centers in any of 34 countries during two enrollment periods in 2013-2015 and 2016-2017 (Am Heart J. 2018 Dec;206:11-23). The tested agent, ertugliflozin (Steglatro) received Food and Drug Administration marketing approval late in 2017 for the indication of improving glycemic control in patients with type 2 diabetes.
The FDA mandated cardiovascular outcomes trials for new glycemic control drugs in guidance the agency issued in 2008 (the FDA released in March 2020 a draft of updated guidance on this topic).
Other FDA-approved agents from the SGLT2 inhibitor class include canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), and all three showed evidence for a statistically significant effect on reducing the incidence of CV disease death and heart failure hospitalizations, as well as renal complications (Can J Diabetes. 2020 Feb;44[1]:61-7). The evidence showing that several SGLT2 drugs have important and consistent effects on endpoints like CV death, heart failure hospitalizations, and renal complications has helped propel this class of agents to the forefront of glycemic control treatments. More recently, one agent from this group, dapagliflozin, also significantly cut the rate of heart failure worsening or CV disease death in patients with heart failure with reduced ejection fraction but without diabetes (N Engl J Med. 2019 Nov 21;381[21]:1995-2008). Based on this evidence, the FDA is currently considering adding a new indication for dapagliflozin that would also label it for use in patients with heart failure with reduced ejection fraction but without diabetes.
The sodium-glucose transporter 2 (SGLT-2) inhibitor ertugliflozin broke ranks with the other drugs in its class and failed to produce statistically significant drops in the both the combined incidence of cardiovascular (CV) death or heart failure hospitalization, and the rate of adverse renal outcomes, in the mandated CV outcomes trial run for ertugliflozin with more than 8,200 patients with type 2 diabetes and established CV disease.
Merck, one of the companies that markets the drug, announced the topline results in a quarterly financial report released on April 28, 2020.
According to the report, the results from the ertugliflozin cardiovascular outcomes trial “achieved its primary endpoint of noninferiority for major adverse CV events (MACE), compared to placebo in patients with type 2 diabetes mellitus and established atherosclerotic CV disease,” but “the key secondary endpoints of superiority” of ertugliflozin, compared with placebo, “for time to the composite of CV death or hospitalization for heart failure, CV death alone, and the composite of renal death, dialysis/transplant or doubling of serum creatinine from baseline were not met.”
However, the report added that, “while not a prespecified hypothesis for statistical testing, a reduction in hospitalization for heart failure was observed” with ertugliflozin treatment, and the report further said that the drug’s safety profile in the trial “was consistent with that reported in previous studies.” The statement closed by saying that detailed results from the trial are scheduled to be presented on June 16, 2020, at the virtual American Diabetes Association’s 80th Scientific Sessions.
These results came from the VERTIS CV (Evaluation of Ertugliflozin EffIcacy and Safety Cardiovascular Outcomes) trial, which researchers said in 2018 had administered at least one investigational dose to 8,238 randomized patients at centers in any of 34 countries during two enrollment periods in 2013-2015 and 2016-2017 (Am Heart J. 2018 Dec;206:11-23). The tested agent, ertugliflozin (Steglatro) received Food and Drug Administration marketing approval late in 2017 for the indication of improving glycemic control in patients with type 2 diabetes.
The FDA mandated cardiovascular outcomes trials for new glycemic control drugs in guidance the agency issued in 2008 (the FDA released in March 2020 a draft of updated guidance on this topic).
Other FDA-approved agents from the SGLT2 inhibitor class include canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), and all three showed evidence for a statistically significant effect on reducing the incidence of CV disease death and heart failure hospitalizations, as well as renal complications (Can J Diabetes. 2020 Feb;44[1]:61-7). The evidence showing that several SGLT2 drugs have important and consistent effects on endpoints like CV death, heart failure hospitalizations, and renal complications has helped propel this class of agents to the forefront of glycemic control treatments. More recently, one agent from this group, dapagliflozin, also significantly cut the rate of heart failure worsening or CV disease death in patients with heart failure with reduced ejection fraction but without diabetes (N Engl J Med. 2019 Nov 21;381[21]:1995-2008). Based on this evidence, the FDA is currently considering adding a new indication for dapagliflozin that would also label it for use in patients with heart failure with reduced ejection fraction but without diabetes.
Postapproval data confirm risks with intragastric balloons
The results of two postapproval studies confirm the potential risk of hyperinflation and acute pancreatitis with the Orbera and ReShape liquid-filled intragastric balloon systems used to treat obesity.
The Orbera Intragastric Balloon System is manufactured by Apollo Endosurgery. The ReShape Integrated Dual Balloon System was previously manufactured by ReShape Medical but was acquired by Apollo Endosurgery in December 2018.
In the Orbera postapproval study, 6 of 258 patients (2.3%) experienced balloon hyperinflation, the Food and Drug Administration said today in a letter to health care providers. There were no hyperinflation events detected in the ReShape postapproval study.
Acute pancreatitis was reported in 2 of 159 patients (1.3%) in the ReShape study, with no cases of acute pancreatitis reported in the Orbera study.
No balloon hyperinflation or acute pancreatitis events were reported in the studies the companies submitted to the FDA to gain approval, the agency said.
No deaths were reported in the postapproval studies, though the agency notes that the studies were not powered to detect. However, since Orbera and ReShape were approved in 2015, the FDA has learned of 18 deaths worldwide, including 8 patients in the United States (5 with Orbera and 3 with ReShape).
The FDA issued previous letters to health care providers concerning issues with these devices in June 2018, August 2017, and February 2017.
As of Jan. 1, 2019, Apollo Endosurgery stopped selling the ReShape Balloon. The Orbera balloon remains available.
“The FDA wants to ensure healthcare professionals are aware of the rates of these potential complications observed in the post-approval studies so they can discuss the risks and benefits of weight loss treatments with patients and monitor patients during treatment,” Benjamin Fisher, PhD, director of the Reproductive, Gastro-Renal, Urological, General Hospital Device, and Human Factors Office at the FDA’s Center for Devices and Radiological Health, said in a statement.
“While these devices remain an appropriate treatment option for some patients with obesity, patients should always discuss with their doctors which treatment option is best for them,” said Dr. Fisher.
A version of this article originally appeared on Medscape.com.
The results of two postapproval studies confirm the potential risk of hyperinflation and acute pancreatitis with the Orbera and ReShape liquid-filled intragastric balloon systems used to treat obesity.
The Orbera Intragastric Balloon System is manufactured by Apollo Endosurgery. The ReShape Integrated Dual Balloon System was previously manufactured by ReShape Medical but was acquired by Apollo Endosurgery in December 2018.
In the Orbera postapproval study, 6 of 258 patients (2.3%) experienced balloon hyperinflation, the Food and Drug Administration said today in a letter to health care providers. There were no hyperinflation events detected in the ReShape postapproval study.
Acute pancreatitis was reported in 2 of 159 patients (1.3%) in the ReShape study, with no cases of acute pancreatitis reported in the Orbera study.
No balloon hyperinflation or acute pancreatitis events were reported in the studies the companies submitted to the FDA to gain approval, the agency said.
No deaths were reported in the postapproval studies, though the agency notes that the studies were not powered to detect. However, since Orbera and ReShape were approved in 2015, the FDA has learned of 18 deaths worldwide, including 8 patients in the United States (5 with Orbera and 3 with ReShape).
The FDA issued previous letters to health care providers concerning issues with these devices in June 2018, August 2017, and February 2017.
As of Jan. 1, 2019, Apollo Endosurgery stopped selling the ReShape Balloon. The Orbera balloon remains available.
“The FDA wants to ensure healthcare professionals are aware of the rates of these potential complications observed in the post-approval studies so they can discuss the risks and benefits of weight loss treatments with patients and monitor patients during treatment,” Benjamin Fisher, PhD, director of the Reproductive, Gastro-Renal, Urological, General Hospital Device, and Human Factors Office at the FDA’s Center for Devices and Radiological Health, said in a statement.
“While these devices remain an appropriate treatment option for some patients with obesity, patients should always discuss with their doctors which treatment option is best for them,” said Dr. Fisher.
A version of this article originally appeared on Medscape.com.
The results of two postapproval studies confirm the potential risk of hyperinflation and acute pancreatitis with the Orbera and ReShape liquid-filled intragastric balloon systems used to treat obesity.
The Orbera Intragastric Balloon System is manufactured by Apollo Endosurgery. The ReShape Integrated Dual Balloon System was previously manufactured by ReShape Medical but was acquired by Apollo Endosurgery in December 2018.
In the Orbera postapproval study, 6 of 258 patients (2.3%) experienced balloon hyperinflation, the Food and Drug Administration said today in a letter to health care providers. There were no hyperinflation events detected in the ReShape postapproval study.
Acute pancreatitis was reported in 2 of 159 patients (1.3%) in the ReShape study, with no cases of acute pancreatitis reported in the Orbera study.
No balloon hyperinflation or acute pancreatitis events were reported in the studies the companies submitted to the FDA to gain approval, the agency said.
No deaths were reported in the postapproval studies, though the agency notes that the studies were not powered to detect. However, since Orbera and ReShape were approved in 2015, the FDA has learned of 18 deaths worldwide, including 8 patients in the United States (5 with Orbera and 3 with ReShape).
The FDA issued previous letters to health care providers concerning issues with these devices in June 2018, August 2017, and February 2017.
As of Jan. 1, 2019, Apollo Endosurgery stopped selling the ReShape Balloon. The Orbera balloon remains available.
“The FDA wants to ensure healthcare professionals are aware of the rates of these potential complications observed in the post-approval studies so they can discuss the risks and benefits of weight loss treatments with patients and monitor patients during treatment,” Benjamin Fisher, PhD, director of the Reproductive, Gastro-Renal, Urological, General Hospital Device, and Human Factors Office at the FDA’s Center for Devices and Radiological Health, said in a statement.
“While these devices remain an appropriate treatment option for some patients with obesity, patients should always discuss with their doctors which treatment option is best for them,” said Dr. Fisher.
A version of this article originally appeared on Medscape.com.
A pandemic of pediatric panic
Seventy-three. That is the average number of questions asked daily by preschool-aged children.
Children ask questions to make sense of their world, to learn how things work, to verify their safety, and to interact with others. As a physician, a child and adolescent psychiatrist, and a father to 6-year-old twin daughters, I too am asking more questions these days. Both professionally and personally, these questions are prompted by shifts in routines, uncertainty, and anxiety brought on by the ongoing coronavirus disease 2019 (COVID-19) pandemic. In parallel, I find myself reflecting on my twin daughters’ questions; their questions reverberate with my own, and with the increased anxiety and fears of my patients and their parents.
With this in mind, I’d like to share 2 questions related to pediatric anxiety that may sculpt our clinical work—whether with children, adolescents, or adults—as we provide treatment and comfort to our patients during this pandemic of anxiety.
How do parents affect children’s anxiety?
First, children take cues from their parents. Almost a half century ago, child and adolescent psychiatrist Robert Emde, MD, and others, using elegantly designed experimental settings, documented that a mother’s response strongly influences her young son or daughter’s emotional reaction to a stranger, or to new situations.1 Specifically, very young children were less afraid and interacted more with a stranger and did so more quickly when their mother had a positive (as opposed to neutral or fearful) reaction to the situation.2 Further, in these studies, when the parent’s face was partially covered, very young children became more fearful. Taken together, these findings remind us that children actively seek to read the affective states of those who care for them, and use these reactions to anchor their responses to shifts in routine, such as those brought on by the ongoing COVID-19 pandemic.
Second, in reacting to the pandemic, parents model emotional regulation—an important skill that children and adolescents must develop as they experience intense affect and anxiety. As mental health clinicians, we know that emotional regulation is an essential component of mental health, and problems with it are a hallmark characteristic of several disorders, including anxiety disorders. Further, neuroimaging studies over the past decade have demonstrated that the way in which the medial prefrontal cortex and lower limbic structures (eg, the amygdala) are connected shifts from early childhood through adolescence and into early adulthood.3 It is likely that these shifts in functional connectivity are shaped by the environment as well as intrinsic aspects of the patient’s biology, and that these shifts subtend the developmental expression of anxiety, particularly in times of stress.
How should we talk to children about the pandemic?
Trust is not only the scaffold of our therapeutic relationships, but also a critical component of our conversations with children about the pandemic. Having established a trusting relationship prior to talking with children about their anxiety and about the pandemic, we will do well to remember that there is often more to a question than the actual direct interrogative. From a developmental standpoint, children may repeatedly ask the same question because they are struggling to understand an abstract concept, or are unable to make the same implicit causal link that we—as adults—have made. Also, children may ask the same question multiple times as a way of seeking reassurance. Finally, when a child asks her father “How many people are going to die?” she may actually be asking whether her parents, grandparents, or friends will be safe and healthy. Thus, as we talk with children, we must remember that they may be implicitly asking for more than a number, date, or mechanism. We must think about the motivation for their questions vis a vis their specific fears and past experiences.
For children, adolescents, and adults, the anxiety created by the pandemic constantly shifts, is hard-to-define, and pervades their lives. This ensuing chronic variable stress can worsen both physical and mental health.4 But, it also creates an opportunity for resiliency which—like the coronavirus—can be contagious.5,6 Knowing this, I’d like to ask 4 questions, based on David Brooks’ recent Op-Ed in the New York Times7:
- Can we become “softer and wiser” as a result of the pandemic?
- How can we inoculate our patients against the loneliness and isolation that worsen most psychiatric disorders?
- How can we “see deeper into [our]selves” to provide comfort to our patients, families, and each other as we confront this viral pandemic of anxiety?
- Following “social distancing,” how do we rekindle “social trust”?
1. Emde RN, Gaensbauer TJ, Harmon RJ. Emotional expression in infancy; a biobehavioral study. Psychol Issues. 1976;10(01):1-200.
2. Feinman S, Lewis M. Social referencing at ten months: a second-order effect on infants’ responses to strangers. Child Dev. 1983;54(4):878-887.
3. Gee DG, Gabard-Durnam LJ, Flannery J, et al. Early developmental emergence of human amygdala-prefrontal connectivity after maternal deprivation. Proc Natl Acad Sci U S A. 2013;110(39):15638-15643.
4. Keeshin BR, Cronholm PF, Strawn JR. Physiologic changes associated with violence and abuse exposure: an examination of related medical conditions. Trauma Violence Abuse. 2012;13(1):41-56.
5. Malhi GS, Das P, Bell E, et al. Modelling resilience in adolescence and adversity: a novel framework to inform research and practice. Transl Psychiatry. 2019;9(1):316. doi: 10.1038/s41398-019-0651-y.
6. Rutter M. Annual Research Review: resilience--clinical implications. J Child Psychol Psychiatry. 2013;54(4):474-487.
7. Brooks D. The pandemic of fear and agony. New York Times. April 9, 2020. https://www.nytimes.com/2020/04/09/opinion/covid-anxiety.html. Accessed April 14, 2020.
Seventy-three. That is the average number of questions asked daily by preschool-aged children.
Children ask questions to make sense of their world, to learn how things work, to verify their safety, and to interact with others. As a physician, a child and adolescent psychiatrist, and a father to 6-year-old twin daughters, I too am asking more questions these days. Both professionally and personally, these questions are prompted by shifts in routines, uncertainty, and anxiety brought on by the ongoing coronavirus disease 2019 (COVID-19) pandemic. In parallel, I find myself reflecting on my twin daughters’ questions; their questions reverberate with my own, and with the increased anxiety and fears of my patients and their parents.
With this in mind, I’d like to share 2 questions related to pediatric anxiety that may sculpt our clinical work—whether with children, adolescents, or adults—as we provide treatment and comfort to our patients during this pandemic of anxiety.
How do parents affect children’s anxiety?
First, children take cues from their parents. Almost a half century ago, child and adolescent psychiatrist Robert Emde, MD, and others, using elegantly designed experimental settings, documented that a mother’s response strongly influences her young son or daughter’s emotional reaction to a stranger, or to new situations.1 Specifically, very young children were less afraid and interacted more with a stranger and did so more quickly when their mother had a positive (as opposed to neutral or fearful) reaction to the situation.2 Further, in these studies, when the parent’s face was partially covered, very young children became more fearful. Taken together, these findings remind us that children actively seek to read the affective states of those who care for them, and use these reactions to anchor their responses to shifts in routine, such as those brought on by the ongoing COVID-19 pandemic.
Second, in reacting to the pandemic, parents model emotional regulation—an important skill that children and adolescents must develop as they experience intense affect and anxiety. As mental health clinicians, we know that emotional regulation is an essential component of mental health, and problems with it are a hallmark characteristic of several disorders, including anxiety disorders. Further, neuroimaging studies over the past decade have demonstrated that the way in which the medial prefrontal cortex and lower limbic structures (eg, the amygdala) are connected shifts from early childhood through adolescence and into early adulthood.3 It is likely that these shifts in functional connectivity are shaped by the environment as well as intrinsic aspects of the patient’s biology, and that these shifts subtend the developmental expression of anxiety, particularly in times of stress.
How should we talk to children about the pandemic?
Trust is not only the scaffold of our therapeutic relationships, but also a critical component of our conversations with children about the pandemic. Having established a trusting relationship prior to talking with children about their anxiety and about the pandemic, we will do well to remember that there is often more to a question than the actual direct interrogative. From a developmental standpoint, children may repeatedly ask the same question because they are struggling to understand an abstract concept, or are unable to make the same implicit causal link that we—as adults—have made. Also, children may ask the same question multiple times as a way of seeking reassurance. Finally, when a child asks her father “How many people are going to die?” she may actually be asking whether her parents, grandparents, or friends will be safe and healthy. Thus, as we talk with children, we must remember that they may be implicitly asking for more than a number, date, or mechanism. We must think about the motivation for their questions vis a vis their specific fears and past experiences.
For children, adolescents, and adults, the anxiety created by the pandemic constantly shifts, is hard-to-define, and pervades their lives. This ensuing chronic variable stress can worsen both physical and mental health.4 But, it also creates an opportunity for resiliency which—like the coronavirus—can be contagious.5,6 Knowing this, I’d like to ask 4 questions, based on David Brooks’ recent Op-Ed in the New York Times7:
- Can we become “softer and wiser” as a result of the pandemic?
- How can we inoculate our patients against the loneliness and isolation that worsen most psychiatric disorders?
- How can we “see deeper into [our]selves” to provide comfort to our patients, families, and each other as we confront this viral pandemic of anxiety?
- Following “social distancing,” how do we rekindle “social trust”?
Seventy-three. That is the average number of questions asked daily by preschool-aged children.
Children ask questions to make sense of their world, to learn how things work, to verify their safety, and to interact with others. As a physician, a child and adolescent psychiatrist, and a father to 6-year-old twin daughters, I too am asking more questions these days. Both professionally and personally, these questions are prompted by shifts in routines, uncertainty, and anxiety brought on by the ongoing coronavirus disease 2019 (COVID-19) pandemic. In parallel, I find myself reflecting on my twin daughters’ questions; their questions reverberate with my own, and with the increased anxiety and fears of my patients and their parents.
With this in mind, I’d like to share 2 questions related to pediatric anxiety that may sculpt our clinical work—whether with children, adolescents, or adults—as we provide treatment and comfort to our patients during this pandemic of anxiety.
How do parents affect children’s anxiety?
First, children take cues from their parents. Almost a half century ago, child and adolescent psychiatrist Robert Emde, MD, and others, using elegantly designed experimental settings, documented that a mother’s response strongly influences her young son or daughter’s emotional reaction to a stranger, or to new situations.1 Specifically, very young children were less afraid and interacted more with a stranger and did so more quickly when their mother had a positive (as opposed to neutral or fearful) reaction to the situation.2 Further, in these studies, when the parent’s face was partially covered, very young children became more fearful. Taken together, these findings remind us that children actively seek to read the affective states of those who care for them, and use these reactions to anchor their responses to shifts in routine, such as those brought on by the ongoing COVID-19 pandemic.
Second, in reacting to the pandemic, parents model emotional regulation—an important skill that children and adolescents must develop as they experience intense affect and anxiety. As mental health clinicians, we know that emotional regulation is an essential component of mental health, and problems with it are a hallmark characteristic of several disorders, including anxiety disorders. Further, neuroimaging studies over the past decade have demonstrated that the way in which the medial prefrontal cortex and lower limbic structures (eg, the amygdala) are connected shifts from early childhood through adolescence and into early adulthood.3 It is likely that these shifts in functional connectivity are shaped by the environment as well as intrinsic aspects of the patient’s biology, and that these shifts subtend the developmental expression of anxiety, particularly in times of stress.
How should we talk to children about the pandemic?
Trust is not only the scaffold of our therapeutic relationships, but also a critical component of our conversations with children about the pandemic. Having established a trusting relationship prior to talking with children about their anxiety and about the pandemic, we will do well to remember that there is often more to a question than the actual direct interrogative. From a developmental standpoint, children may repeatedly ask the same question because they are struggling to understand an abstract concept, or are unable to make the same implicit causal link that we—as adults—have made. Also, children may ask the same question multiple times as a way of seeking reassurance. Finally, when a child asks her father “How many people are going to die?” she may actually be asking whether her parents, grandparents, or friends will be safe and healthy. Thus, as we talk with children, we must remember that they may be implicitly asking for more than a number, date, or mechanism. We must think about the motivation for their questions vis a vis their specific fears and past experiences.
For children, adolescents, and adults, the anxiety created by the pandemic constantly shifts, is hard-to-define, and pervades their lives. This ensuing chronic variable stress can worsen both physical and mental health.4 But, it also creates an opportunity for resiliency which—like the coronavirus—can be contagious.5,6 Knowing this, I’d like to ask 4 questions, based on David Brooks’ recent Op-Ed in the New York Times7:
- Can we become “softer and wiser” as a result of the pandemic?
- How can we inoculate our patients against the loneliness and isolation that worsen most psychiatric disorders?
- How can we “see deeper into [our]selves” to provide comfort to our patients, families, and each other as we confront this viral pandemic of anxiety?
- Following “social distancing,” how do we rekindle “social trust”?
1. Emde RN, Gaensbauer TJ, Harmon RJ. Emotional expression in infancy; a biobehavioral study. Psychol Issues. 1976;10(01):1-200.
2. Feinman S, Lewis M. Social referencing at ten months: a second-order effect on infants’ responses to strangers. Child Dev. 1983;54(4):878-887.
3. Gee DG, Gabard-Durnam LJ, Flannery J, et al. Early developmental emergence of human amygdala-prefrontal connectivity after maternal deprivation. Proc Natl Acad Sci U S A. 2013;110(39):15638-15643.
4. Keeshin BR, Cronholm PF, Strawn JR. Physiologic changes associated with violence and abuse exposure: an examination of related medical conditions. Trauma Violence Abuse. 2012;13(1):41-56.
5. Malhi GS, Das P, Bell E, et al. Modelling resilience in adolescence and adversity: a novel framework to inform research and practice. Transl Psychiatry. 2019;9(1):316. doi: 10.1038/s41398-019-0651-y.
6. Rutter M. Annual Research Review: resilience--clinical implications. J Child Psychol Psychiatry. 2013;54(4):474-487.
7. Brooks D. The pandemic of fear and agony. New York Times. April 9, 2020. https://www.nytimes.com/2020/04/09/opinion/covid-anxiety.html. Accessed April 14, 2020.
1. Emde RN, Gaensbauer TJ, Harmon RJ. Emotional expression in infancy; a biobehavioral study. Psychol Issues. 1976;10(01):1-200.
2. Feinman S, Lewis M. Social referencing at ten months: a second-order effect on infants’ responses to strangers. Child Dev. 1983;54(4):878-887.
3. Gee DG, Gabard-Durnam LJ, Flannery J, et al. Early developmental emergence of human amygdala-prefrontal connectivity after maternal deprivation. Proc Natl Acad Sci U S A. 2013;110(39):15638-15643.
4. Keeshin BR, Cronholm PF, Strawn JR. Physiologic changes associated with violence and abuse exposure: an examination of related medical conditions. Trauma Violence Abuse. 2012;13(1):41-56.
5. Malhi GS, Das P, Bell E, et al. Modelling resilience in adolescence and adversity: a novel framework to inform research and practice. Transl Psychiatry. 2019;9(1):316. doi: 10.1038/s41398-019-0651-y.
6. Rutter M. Annual Research Review: resilience--clinical implications. J Child Psychol Psychiatry. 2013;54(4):474-487.
7. Brooks D. The pandemic of fear and agony. New York Times. April 9, 2020. https://www.nytimes.com/2020/04/09/opinion/covid-anxiety.html. Accessed April 14, 2020.

COVID-19 spurs telemedicine, furloughs, retirement
The broad use of telemedicine has been a bright spot in the COVID-19 response, but the pandemic is also creating significant disruption as some physicians are furloughed and others consider practice changes.

A recent survey of physicians conducted by Merritt Hawkins and The Physicians Foundation examined how physicians are being affected by and responding to the pandemic. The findings are based on completed surveys from 842 physicians. About one-third of respondents are primary care physicians, while two-thirds are surgical, medical, and diagnostic specialists and subspecialists.
The survey shines a light on the rapid adoption of telemedicine, with 48% of physicians respondents reporting that they are now treating patients through telemedicine.
“I think that is purely explainable on the situation that COVID has led to with the desire to see patients remotely, still take care of them, and the fact that at the federal level this was recognized and doctors are being compensated for seeing patients remotely,” Gary Price, MD, a plastic surgeon and president of The Physicians Foundation, said in an interview.
“The Foundation does a study of the nation’s physicians every other year and in 2018, when we asked the same question, only 18% of physicians were using some form of telemedicine,” he added.
And Dr. Price said he thinks the shift to telemedicine is here to stay.
“I think that will be a lasting effect of the pandemic,” he said. “More physicians and more patients will be using telemedicine approaches, I think, from here on out. We will see a shift that persists. I think that’s a good thing. Physicians like it. Patients like it. It won’t replace all in-person visits, certainly, but there are a number of health care visits that could be taken care of quite well with a virtual visit and it saves the patients travel time, time away from work, and I think it can make the physicians’ practice more efficient as well.”
The key to sustainability, he said, will be that private insurers and the Centers for Medicare & Medicaid Services continue to pay for it.
“I think we will have had a good demonstration, not only that it can work, but that it does work and that it can be accomplished without any diminishment in the quality of care that’s delivered,” he said.
But the recent survey also identified a number of employment issues that have arisen during the COVID-19 pandemic. Overall, 18% of respondents who were treating COVID-19 patients and 30% of those not treating COVID-19 patients reported that they had been furloughed or experienced a pay cut. Among respondents, just 38.5% reported that they are seeing COVID-19 patients.
“It is unprecedented to my knowledge in the physician employment sphere,” Dr. Price said. “That was the most surprising thing to me. I think you might be able to explain that by the increasing number of physicians who are employees now of larger health systems and the fact that a big portion of those health systems too, in normal times, involves care that right now no one is able to get to or even wants to be seen for because of the risk, of course, of COVID-19.”
The survey also revealed that some respondents had or were planning a change in practice because of COVID-19: 14% said they had or would seek a different practice, 6% reported they had or would find a job without patient care, 7% said they had or would close their practice temporarily, 5% reported that they had or would retire, and 4% said they had or would leave private practice and seek employment at a hospital.
“The survey represents how they are feeling at the time and it doesn’t mean they will necessarily do that, but if even a portion of doctors did that all at once, we would really aggravate an access problem and what we know is a worsening physician shortage in the country,” he said. “So we are very concerned about that.”
Dr. Price also predicted there would be increased consolidation within the health care system as more smaller, independent practices feel the financial stress of the pandemic.
“I hope that I am wrong about that,” he said. “I think smaller practices offer a very cost-effective solution for high-quality care, and their competition in the marketplace for health care is a good and healthy thing.”
The broad use of telemedicine has been a bright spot in the COVID-19 response, but the pandemic is also creating significant disruption as some physicians are furloughed and others consider practice changes.
A recent survey of physicians conducted by Merritt Hawkins and The Physicians Foundation examined how physicians are being affected by and responding to the pandemic. The findings are based on completed surveys from 842 physicians. About one-third of respondents are primary care physicians, while two-thirds are surgical, medical, and diagnostic specialists and subspecialists.
The survey shines a light on the rapid adoption of telemedicine, with 48% of physicians respondents reporting that they are now treating patients through telemedicine.
“I think that is purely explainable on the situation that COVID has led to with the desire to see patients remotely, still take care of them, and the fact that at the federal level this was recognized and doctors are being compensated for seeing patients remotely,” Gary Price, MD, a plastic surgeon and president of The Physicians Foundation, said in an interview.
“The Foundation does a study of the nation’s physicians every other year and in 2018, when we asked the same question, only 18% of physicians were using some form of telemedicine,” he added.
And Dr. Price said he thinks the shift to telemedicine is here to stay.
“I think that will be a lasting effect of the pandemic,” he said. “More physicians and more patients will be using telemedicine approaches, I think, from here on out. We will see a shift that persists. I think that’s a good thing. Physicians like it. Patients like it. It won’t replace all in-person visits, certainly, but there are a number of health care visits that could be taken care of quite well with a virtual visit and it saves the patients travel time, time away from work, and I think it can make the physicians’ practice more efficient as well.”
The key to sustainability, he said, will be that private insurers and the Centers for Medicare & Medicaid Services continue to pay for it.
“I think we will have had a good demonstration, not only that it can work, but that it does work and that it can be accomplished without any diminishment in the quality of care that’s delivered,” he said.
But the recent survey also identified a number of employment issues that have arisen during the COVID-19 pandemic. Overall, 18% of respondents who were treating COVID-19 patients and 30% of those not treating COVID-19 patients reported that they had been furloughed or experienced a pay cut. Among respondents, just 38.5% reported that they are seeing COVID-19 patients.
“It is unprecedented to my knowledge in the physician employment sphere,” Dr. Price said. “That was the most surprising thing to me. I think you might be able to explain that by the increasing number of physicians who are employees now of larger health systems and the fact that a big portion of those health systems too, in normal times, involves care that right now no one is able to get to or even wants to be seen for because of the risk, of course, of COVID-19.”
The survey also revealed that some respondents had or were planning a change in practice because of COVID-19: 14% said they had or would seek a different practice, 6% reported they had or would find a job without patient care, 7% said they had or would close their practice temporarily, 5% reported that they had or would retire, and 4% said they had or would leave private practice and seek employment at a hospital.
“The survey represents how they are feeling at the time and it doesn’t mean they will necessarily do that, but if even a portion of doctors did that all at once, we would really aggravate an access problem and what we know is a worsening physician shortage in the country,” he said. “So we are very concerned about that.”
Dr. Price also predicted there would be increased consolidation within the health care system as more smaller, independent practices feel the financial stress of the pandemic.
“I hope that I am wrong about that,” he said. “I think smaller practices offer a very cost-effective solution for high-quality care, and their competition in the marketplace for health care is a good and healthy thing.”
The broad use of telemedicine has been a bright spot in the COVID-19 response, but the pandemic is also creating significant disruption as some physicians are furloughed and others consider practice changes.
A recent survey of physicians conducted by Merritt Hawkins and The Physicians Foundation examined how physicians are being affected by and responding to the pandemic. The findings are based on completed surveys from 842 physicians. About one-third of respondents are primary care physicians, while two-thirds are surgical, medical, and diagnostic specialists and subspecialists.
The survey shines a light on the rapid adoption of telemedicine, with 48% of physicians respondents reporting that they are now treating patients through telemedicine.
“I think that is purely explainable on the situation that COVID has led to with the desire to see patients remotely, still take care of them, and the fact that at the federal level this was recognized and doctors are being compensated for seeing patients remotely,” Gary Price, MD, a plastic surgeon and president of The Physicians Foundation, said in an interview.
“The Foundation does a study of the nation’s physicians every other year and in 2018, when we asked the same question, only 18% of physicians were using some form of telemedicine,” he added.
And Dr. Price said he thinks the shift to telemedicine is here to stay.
“I think that will be a lasting effect of the pandemic,” he said. “More physicians and more patients will be using telemedicine approaches, I think, from here on out. We will see a shift that persists. I think that’s a good thing. Physicians like it. Patients like it. It won’t replace all in-person visits, certainly, but there are a number of health care visits that could be taken care of quite well with a virtual visit and it saves the patients travel time, time away from work, and I think it can make the physicians’ practice more efficient as well.”
The key to sustainability, he said, will be that private insurers and the Centers for Medicare & Medicaid Services continue to pay for it.
“I think we will have had a good demonstration, not only that it can work, but that it does work and that it can be accomplished without any diminishment in the quality of care that’s delivered,” he said.
But the recent survey also identified a number of employment issues that have arisen during the COVID-19 pandemic. Overall, 18% of respondents who were treating COVID-19 patients and 30% of those not treating COVID-19 patients reported that they had been furloughed or experienced a pay cut. Among respondents, just 38.5% reported that they are seeing COVID-19 patients.
“It is unprecedented to my knowledge in the physician employment sphere,” Dr. Price said. “That was the most surprising thing to me. I think you might be able to explain that by the increasing number of physicians who are employees now of larger health systems and the fact that a big portion of those health systems too, in normal times, involves care that right now no one is able to get to or even wants to be seen for because of the risk, of course, of COVID-19.”
The survey also revealed that some respondents had or were planning a change in practice because of COVID-19: 14% said they had or would seek a different practice, 6% reported they had or would find a job without patient care, 7% said they had or would close their practice temporarily, 5% reported that they had or would retire, and 4% said they had or would leave private practice and seek employment at a hospital.
“The survey represents how they are feeling at the time and it doesn’t mean they will necessarily do that, but if even a portion of doctors did that all at once, we would really aggravate an access problem and what we know is a worsening physician shortage in the country,” he said. “So we are very concerned about that.”
Dr. Price also predicted there would be increased consolidation within the health care system as more smaller, independent practices feel the financial stress of the pandemic.
“I hope that I am wrong about that,” he said. “I think smaller practices offer a very cost-effective solution for high-quality care, and their competition in the marketplace for health care is a good and healthy thing.”
Observation pathway safely reduces acute pancreatitis hospitalization rate
For patients diagnosed with mild acute pancreatitis (AP) in the ED, an observation pathway may significantly reduce hospitalization rate and associated costs without compromising patient safety or quality of care, according to investigators.
Over a 2-year period, the observation pathway at Beth Israel Deaconess Medical Center, Boston, reduced hospitalizations by 31.2%, reported lead author Awais Ahmed, MD, of Harvard Medical School, Boston, and colleagues.
“AP carries a significant burden on the health care system, accounting for the third most common reason for gastrointestinal-related admissions in the United States,” the investigators wrote in the Journal of Clinical Gastroenterology. “As such, streamlining care for AP patients to reduce admissions can reduce the associated financial burden.”
The investigators’ efforts to reduce admissions for patients with AP began in 2016, when they first implemented an observation pathway at Beth Israel. This 6-month pilot study demonstrated proof of concept because it reduced admissions by 22.2% and shortened average length of stay without negatively affecting rates of mortality or readmission.
Based on these encouraging results, the hospital implemented the observation pathway as a standard of care. The present study analyzed 2 years of data from patients diagnosed with AP following the end of the pilot study. The primary outcome was hospitalization rate. Secondary outcomes included health care utilization, 30-day mortality rate, 30-day readmission rate, and median length of stay.
Patients with mild AP entered the observation pathway at the discretion of the supervising clinician, as well as based on absence of exclusion criteria, such as end organ damage, chronic pancreatitis, cholangitis, and other considerations.
Over 2 years, 165 patients were diagnosed with AP in the ED, of whom 118 (71.5%) had mild AP. From this latter group, 54 (45.8%) entered the observation pathway, while 64 (54.2%) were admitted as inpatients, primarily (n = 58) because of exclusion criteria. Within the observation group, 45 out of 54 patients (83.3%) successfully completed the pathway and were discharged. Six of these patients were readmitted within 30 days. Among the 9 patients who did not complete the pathway, 6 failed to meet discharge criteria, resulting in admission, whereas 3 patients left the hospital against medical advice.
Combining data from this 2-year period and the pilot study, the hospitalization rate for mild AP was reduced by 31.2%. In the present study, hospitalization was reduced by 27% for patients with AP of any severity. This figure was steady over a 3-year period, at 25.8%.
Median length of stay for patients with mild AP was significantly shorter in the present study’s observation pathway than in a historical cohort (19.9 vs. 72.0 hours); this remained significant when also including patients from the pilot study (21.2 vs. 72.0 hours). Compared with the historic cohort, patients in the observation had significantly fewer radiographic studies, and more patients were discharged in less than 24 hours. Meanwhile, 30-day readmission and mortality rates remained unchanged.
“In summary, our long-term data of a single center emergency department–based observation management pathway for mild AP demonstrates durability over more than 2 years in maintaining its objective of reducing hospitalization,” the investigators concluded. “This is associated with a [shorter] length of stay, and reduced health care resource utilization, suggesting a possible decrease in financial cost of managing mild AP, without affecting readmission rates or mortality.”
These findings encourage further research, the investigators suggested, while noting that the observation pathway may not be appropriate for all treatment centers.
“The generalizability of the pathway is limited, given its single center location, and tertiary environment,” the investigators wrote. “Smaller hospitals, lacking multidisciplinary support for complications of AP, may find it challenging to implement such a pathway, and thus triage these patients for inpatient admission at their facility or to nearby tertiary centers.”The investigators reported no conflicts of interest.
SOURCE: Ahmed A et al. J Clin Gastroenterol. 2020 Apr 14. doi: 10.1097/MCG.0000000000001354.
Visit the AGA GI Patient Center for information on pancreatitis to share with your patients at https://www.gastro.org/practice-guidance/gi-patient-center/topic/pancreatitis.
For patients diagnosed with mild acute pancreatitis (AP) in the ED, an observation pathway may significantly reduce hospitalization rate and associated costs without compromising patient safety or quality of care, according to investigators.
Over a 2-year period, the observation pathway at Beth Israel Deaconess Medical Center, Boston, reduced hospitalizations by 31.2%, reported lead author Awais Ahmed, MD, of Harvard Medical School, Boston, and colleagues.
“AP carries a significant burden on the health care system, accounting for the third most common reason for gastrointestinal-related admissions in the United States,” the investigators wrote in the Journal of Clinical Gastroenterology. “As such, streamlining care for AP patients to reduce admissions can reduce the associated financial burden.”
The investigators’ efforts to reduce admissions for patients with AP began in 2016, when they first implemented an observation pathway at Beth Israel. This 6-month pilot study demonstrated proof of concept because it reduced admissions by 22.2% and shortened average length of stay without negatively affecting rates of mortality or readmission.
Based on these encouraging results, the hospital implemented the observation pathway as a standard of care. The present study analyzed 2 years of data from patients diagnosed with AP following the end of the pilot study. The primary outcome was hospitalization rate. Secondary outcomes included health care utilization, 30-day mortality rate, 30-day readmission rate, and median length of stay.
Patients with mild AP entered the observation pathway at the discretion of the supervising clinician, as well as based on absence of exclusion criteria, such as end organ damage, chronic pancreatitis, cholangitis, and other considerations.
Over 2 years, 165 patients were diagnosed with AP in the ED, of whom 118 (71.5%) had mild AP. From this latter group, 54 (45.8%) entered the observation pathway, while 64 (54.2%) were admitted as inpatients, primarily (n = 58) because of exclusion criteria. Within the observation group, 45 out of 54 patients (83.3%) successfully completed the pathway and were discharged. Six of these patients were readmitted within 30 days. Among the 9 patients who did not complete the pathway, 6 failed to meet discharge criteria, resulting in admission, whereas 3 patients left the hospital against medical advice.
Combining data from this 2-year period and the pilot study, the hospitalization rate for mild AP was reduced by 31.2%. In the present study, hospitalization was reduced by 27% for patients with AP of any severity. This figure was steady over a 3-year period, at 25.8%.
Median length of stay for patients with mild AP was significantly shorter in the present study’s observation pathway than in a historical cohort (19.9 vs. 72.0 hours); this remained significant when also including patients from the pilot study (21.2 vs. 72.0 hours). Compared with the historic cohort, patients in the observation had significantly fewer radiographic studies, and more patients were discharged in less than 24 hours. Meanwhile, 30-day readmission and mortality rates remained unchanged.
“In summary, our long-term data of a single center emergency department–based observation management pathway for mild AP demonstrates durability over more than 2 years in maintaining its objective of reducing hospitalization,” the investigators concluded. “This is associated with a [shorter] length of stay, and reduced health care resource utilization, suggesting a possible decrease in financial cost of managing mild AP, without affecting readmission rates or mortality.”
These findings encourage further research, the investigators suggested, while noting that the observation pathway may not be appropriate for all treatment centers.
“The generalizability of the pathway is limited, given its single center location, and tertiary environment,” the investigators wrote. “Smaller hospitals, lacking multidisciplinary support for complications of AP, may find it challenging to implement such a pathway, and thus triage these patients for inpatient admission at their facility or to nearby tertiary centers.”The investigators reported no conflicts of interest.
SOURCE: Ahmed A et al. J Clin Gastroenterol. 2020 Apr 14. doi: 10.1097/MCG.0000000000001354.
Visit the AGA GI Patient Center for information on pancreatitis to share with your patients at https://www.gastro.org/practice-guidance/gi-patient-center/topic/pancreatitis.
For patients diagnosed with mild acute pancreatitis (AP) in the ED, an observation pathway may significantly reduce hospitalization rate and associated costs without compromising patient safety or quality of care, according to investigators.
Over a 2-year period, the observation pathway at Beth Israel Deaconess Medical Center, Boston, reduced hospitalizations by 31.2%, reported lead author Awais Ahmed, MD, of Harvard Medical School, Boston, and colleagues.
“AP carries a significant burden on the health care system, accounting for the third most common reason for gastrointestinal-related admissions in the United States,” the investigators wrote in the Journal of Clinical Gastroenterology. “As such, streamlining care for AP patients to reduce admissions can reduce the associated financial burden.”
The investigators’ efforts to reduce admissions for patients with AP began in 2016, when they first implemented an observation pathway at Beth Israel. This 6-month pilot study demonstrated proof of concept because it reduced admissions by 22.2% and shortened average length of stay without negatively affecting rates of mortality or readmission.
Based on these encouraging results, the hospital implemented the observation pathway as a standard of care. The present study analyzed 2 years of data from patients diagnosed with AP following the end of the pilot study. The primary outcome was hospitalization rate. Secondary outcomes included health care utilization, 30-day mortality rate, 30-day readmission rate, and median length of stay.
Patients with mild AP entered the observation pathway at the discretion of the supervising clinician, as well as based on absence of exclusion criteria, such as end organ damage, chronic pancreatitis, cholangitis, and other considerations.
Over 2 years, 165 patients were diagnosed with AP in the ED, of whom 118 (71.5%) had mild AP. From this latter group, 54 (45.8%) entered the observation pathway, while 64 (54.2%) were admitted as inpatients, primarily (n = 58) because of exclusion criteria. Within the observation group, 45 out of 54 patients (83.3%) successfully completed the pathway and were discharged. Six of these patients were readmitted within 30 days. Among the 9 patients who did not complete the pathway, 6 failed to meet discharge criteria, resulting in admission, whereas 3 patients left the hospital against medical advice.
Combining data from this 2-year period and the pilot study, the hospitalization rate for mild AP was reduced by 31.2%. In the present study, hospitalization was reduced by 27% for patients with AP of any severity. This figure was steady over a 3-year period, at 25.8%.
Median length of stay for patients with mild AP was significantly shorter in the present study’s observation pathway than in a historical cohort (19.9 vs. 72.0 hours); this remained significant when also including patients from the pilot study (21.2 vs. 72.0 hours). Compared with the historic cohort, patients in the observation had significantly fewer radiographic studies, and more patients were discharged in less than 24 hours. Meanwhile, 30-day readmission and mortality rates remained unchanged.
“In summary, our long-term data of a single center emergency department–based observation management pathway for mild AP demonstrates durability over more than 2 years in maintaining its objective of reducing hospitalization,” the investigators concluded. “This is associated with a [shorter] length of stay, and reduced health care resource utilization, suggesting a possible decrease in financial cost of managing mild AP, without affecting readmission rates or mortality.”
These findings encourage further research, the investigators suggested, while noting that the observation pathway may not be appropriate for all treatment centers.
“The generalizability of the pathway is limited, given its single center location, and tertiary environment,” the investigators wrote. “Smaller hospitals, lacking multidisciplinary support for complications of AP, may find it challenging to implement such a pathway, and thus triage these patients for inpatient admission at their facility or to nearby tertiary centers.”The investigators reported no conflicts of interest.
SOURCE: Ahmed A et al. J Clin Gastroenterol. 2020 Apr 14. doi: 10.1097/MCG.0000000000001354.
Visit the AGA GI Patient Center for information on pancreatitis to share with your patients at https://www.gastro.org/practice-guidance/gi-patient-center/topic/pancreatitis.
FROM JOURNAL OF CLINICAL GASTROENTEROLOGY
Key clinical point: For patients diagnosed with mild acute pancreatitis in the ED, an observation pathway may significantly reduce hospitalization rate and associated costs without compromising patient safety.
Major finding: An observational approach to mild acute pancreatitis reduced hospitalization rate by 31.2%.
Study details: A prospective trial involving 118 patients with mild acute pancreatitis.
Disclosures: The investigators reported no conflicts of interest.
Source: Ahmed A et al. J Clin Gastroenterol. 2020 Apr 14. doi: 10.1097/MCG.0000000000001354.
Will COVID-19 finally trigger action on health disparities?
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
ESMO gets creative with guidelines for breast cancer care in the COVID-19 era
Like other agencies, the European Society for Medical Oncology has developed guidelines for managing breast cancer patients during the COVID-19 pandemic, recommending when care should be prioritized, delayed, or modified.

ESMO’s breast cancer guidelines expand upon guidelines issued by other groups, addressing a broad spectrum of patient profiles and providing a creative array of treatment options in COVID-19–era clinical practice.
As with ESMO’s other disease-focused COVID-19 guidelines, the breast cancer guidelines are organized by priority levels – high, medium, and low – which are applied to several domains of diagnosis and treatment.
High-priority recommendations apply to patients whose condition is either clinically unstable or whose cancer burden is immediately life-threatening.
Medium-priority recommendations apply to patients for whom delaying care beyond 6 weeks would probably lower the likelihood of a significant benefit from the intervention.
Low-priority recommendations apply to patients for whom services can be delayed for the duration of the COVID-19 pandemic.
Personalized care and high-priority situations
ESMO’s guidelines suggest that multidisciplinary tumor boards should guide decisions about the urgency of care for individual patients, given the complexity of breast cancer biology, the multiplicity of evidence-based treatments, and the possibility of cure or durable high-quality remissions.
The guidelines deliver a clear message that prepandemic discussions about delivering personalized care are even more important now.
ESMO prioritizes investigating high-risk screening mammography results (i.e., BIRADS 5), lumps noted on breast self-examination, clinical evidence of local-regional recurrence, and breast cancer in pregnant women.
Making these scenarios “high priority” will facilitate the best long-term outcomes in time-sensitive scenarios and improve patient satisfaction with care.
Modifications to consider
ESMO provides explicit options for treatment of common breast cancer profiles in which short-term modifications of standard management strategies can safely be considered. Given the generally long natural history of most breast cancer subtypes, these temporary modifications are unlikely to compromise long-term outcomes.
For patients with a new diagnosis of localized breast cancer, the guidelines recommend neoadjuvant chemotherapy, targeted therapy, or hormonal therapy to achieve optimal breast cancer outcomes and safely delay surgery or radiotherapy.
In the metastatic setting, ESMO advises providers to consider:
- Symptom-oriented testing, recognizing the arguable benefit of frequent imaging or serum tumor marker measurement (J Clin Oncol. 2016 Aug 20;34[24]:2820-6).
- Drug holidays, de-escalated maintenance therapy, and protracted schedules of bone-modifying agents.
- Avoiding mTOR and PI3KCA inhibitors as an addition to standard hormonal therapy because of pneumonitis, hyperglycemia, and immunosuppression risks. The guidelines suggest careful thought about adding CDK4/6 inhibitors to standard hormonal therapy because of the added burden of remote safety monitoring with the biologic agents.
ESMO makes suggestions about trimming the duration of adjuvant trastuzumab to 6 months, as in the PERSEPHONE study (Lancet. 2019 Jun 29;393[10191]:2599-612), and modifying the schedule of luteinizing hormone–releasing hormone agonist administration, in an effort to reduce patient exposure to health care personnel (and vice versa).
The guidelines recommend continuing clinical trials if benefits to patients outweigh risks and trials can be modified to enhance patient safety while preserving study endpoint evaluations.
Lower-priority situations
ESMO pointedly assigns a low priority to follow-up of patients who are at high risk of relapse but lack signs or symptoms of relapse.
Like other groups, ESMO recommends that patients with equivocal (i.e., BIRADS 3) screening mammograms should have 6-month follow-up imaging in preference to immediate core needle biopsy of the area(s) of concern.
ESMO uses age to assign priority for postponing adjuvant breast radiation in patients with low- to moderate-risk lesions. However, the guidelines stop surprisingly short of recommending that adjuvant radiation be withheld for older patients with low-risk, stage I, hormonally sensitive, HER2-negative breast cancers who receive endocrine therapy.
Bottom line
The pragmatic adjustments ESMO suggests address the challenges of evaluating and treating breast cancer patients during the COVID-19 pandemic. The guidelines protect each patient’s right to care and safety as well as protecting the safety of caregivers.
The guidelines will likely heighten patients’ satisfaction with care and decrease concern about adequacy of timely evaluation and treatment.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Like other agencies, the European Society for Medical Oncology has developed guidelines for managing breast cancer patients during the COVID-19 pandemic, recommending when care should be prioritized, delayed, or modified.
ESMO’s breast cancer guidelines expand upon guidelines issued by other groups, addressing a broad spectrum of patient profiles and providing a creative array of treatment options in COVID-19–era clinical practice.
As with ESMO’s other disease-focused COVID-19 guidelines, the breast cancer guidelines are organized by priority levels – high, medium, and low – which are applied to several domains of diagnosis and treatment.
High-priority recommendations apply to patients whose condition is either clinically unstable or whose cancer burden is immediately life-threatening.
Medium-priority recommendations apply to patients for whom delaying care beyond 6 weeks would probably lower the likelihood of a significant benefit from the intervention.
Low-priority recommendations apply to patients for whom services can be delayed for the duration of the COVID-19 pandemic.
Personalized care and high-priority situations
ESMO’s guidelines suggest that multidisciplinary tumor boards should guide decisions about the urgency of care for individual patients, given the complexity of breast cancer biology, the multiplicity of evidence-based treatments, and the possibility of cure or durable high-quality remissions.
The guidelines deliver a clear message that prepandemic discussions about delivering personalized care are even more important now.
ESMO prioritizes investigating high-risk screening mammography results (i.e., BIRADS 5), lumps noted on breast self-examination, clinical evidence of local-regional recurrence, and breast cancer in pregnant women.
Making these scenarios “high priority” will facilitate the best long-term outcomes in time-sensitive scenarios and improve patient satisfaction with care.
Modifications to consider
ESMO provides explicit options for treatment of common breast cancer profiles in which short-term modifications of standard management strategies can safely be considered. Given the generally long natural history of most breast cancer subtypes, these temporary modifications are unlikely to compromise long-term outcomes.
For patients with a new diagnosis of localized breast cancer, the guidelines recommend neoadjuvant chemotherapy, targeted therapy, or hormonal therapy to achieve optimal breast cancer outcomes and safely delay surgery or radiotherapy.
In the metastatic setting, ESMO advises providers to consider:
- Symptom-oriented testing, recognizing the arguable benefit of frequent imaging or serum tumor marker measurement (J Clin Oncol. 2016 Aug 20;34[24]:2820-6).
- Drug holidays, de-escalated maintenance therapy, and protracted schedules of bone-modifying agents.
- Avoiding mTOR and PI3KCA inhibitors as an addition to standard hormonal therapy because of pneumonitis, hyperglycemia, and immunosuppression risks. The guidelines suggest careful thought about adding CDK4/6 inhibitors to standard hormonal therapy because of the added burden of remote safety monitoring with the biologic agents.
ESMO makes suggestions about trimming the duration of adjuvant trastuzumab to 6 months, as in the PERSEPHONE study (Lancet. 2019 Jun 29;393[10191]:2599-612), and modifying the schedule of luteinizing hormone–releasing hormone agonist administration, in an effort to reduce patient exposure to health care personnel (and vice versa).
The guidelines recommend continuing clinical trials if benefits to patients outweigh risks and trials can be modified to enhance patient safety while preserving study endpoint evaluations.
Lower-priority situations
ESMO pointedly assigns a low priority to follow-up of patients who are at high risk of relapse but lack signs or symptoms of relapse.
Like other groups, ESMO recommends that patients with equivocal (i.e., BIRADS 3) screening mammograms should have 6-month follow-up imaging in preference to immediate core needle biopsy of the area(s) of concern.
ESMO uses age to assign priority for postponing adjuvant breast radiation in patients with low- to moderate-risk lesions. However, the guidelines stop surprisingly short of recommending that adjuvant radiation be withheld for older patients with low-risk, stage I, hormonally sensitive, HER2-negative breast cancers who receive endocrine therapy.
Bottom line
The pragmatic adjustments ESMO suggests address the challenges of evaluating and treating breast cancer patients during the COVID-19 pandemic. The guidelines protect each patient’s right to care and safety as well as protecting the safety of caregivers.
The guidelines will likely heighten patients’ satisfaction with care and decrease concern about adequacy of timely evaluation and treatment.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Like other agencies, the European Society for Medical Oncology has developed guidelines for managing breast cancer patients during the COVID-19 pandemic, recommending when care should be prioritized, delayed, or modified.
ESMO’s breast cancer guidelines expand upon guidelines issued by other groups, addressing a broad spectrum of patient profiles and providing a creative array of treatment options in COVID-19–era clinical practice.
As with ESMO’s other disease-focused COVID-19 guidelines, the breast cancer guidelines are organized by priority levels – high, medium, and low – which are applied to several domains of diagnosis and treatment.
High-priority recommendations apply to patients whose condition is either clinically unstable or whose cancer burden is immediately life-threatening.
Medium-priority recommendations apply to patients for whom delaying care beyond 6 weeks would probably lower the likelihood of a significant benefit from the intervention.
Low-priority recommendations apply to patients for whom services can be delayed for the duration of the COVID-19 pandemic.
Personalized care and high-priority situations
ESMO’s guidelines suggest that multidisciplinary tumor boards should guide decisions about the urgency of care for individual patients, given the complexity of breast cancer biology, the multiplicity of evidence-based treatments, and the possibility of cure or durable high-quality remissions.
The guidelines deliver a clear message that prepandemic discussions about delivering personalized care are even more important now.
ESMO prioritizes investigating high-risk screening mammography results (i.e., BIRADS 5), lumps noted on breast self-examination, clinical evidence of local-regional recurrence, and breast cancer in pregnant women.
Making these scenarios “high priority” will facilitate the best long-term outcomes in time-sensitive scenarios and improve patient satisfaction with care.
Modifications to consider
ESMO provides explicit options for treatment of common breast cancer profiles in which short-term modifications of standard management strategies can safely be considered. Given the generally long natural history of most breast cancer subtypes, these temporary modifications are unlikely to compromise long-term outcomes.
For patients with a new diagnosis of localized breast cancer, the guidelines recommend neoadjuvant chemotherapy, targeted therapy, or hormonal therapy to achieve optimal breast cancer outcomes and safely delay surgery or radiotherapy.
In the metastatic setting, ESMO advises providers to consider:
- Symptom-oriented testing, recognizing the arguable benefit of frequent imaging or serum tumor marker measurement (J Clin Oncol. 2016 Aug 20;34[24]:2820-6).
- Drug holidays, de-escalated maintenance therapy, and protracted schedules of bone-modifying agents.
- Avoiding mTOR and PI3KCA inhibitors as an addition to standard hormonal therapy because of pneumonitis, hyperglycemia, and immunosuppression risks. The guidelines suggest careful thought about adding CDK4/6 inhibitors to standard hormonal therapy because of the added burden of remote safety monitoring with the biologic agents.
ESMO makes suggestions about trimming the duration of adjuvant trastuzumab to 6 months, as in the PERSEPHONE study (Lancet. 2019 Jun 29;393[10191]:2599-612), and modifying the schedule of luteinizing hormone–releasing hormone agonist administration, in an effort to reduce patient exposure to health care personnel (and vice versa).
The guidelines recommend continuing clinical trials if benefits to patients outweigh risks and trials can be modified to enhance patient safety while preserving study endpoint evaluations.
Lower-priority situations
ESMO pointedly assigns a low priority to follow-up of patients who are at high risk of relapse but lack signs or symptoms of relapse.
Like other groups, ESMO recommends that patients with equivocal (i.e., BIRADS 3) screening mammograms should have 6-month follow-up imaging in preference to immediate core needle biopsy of the area(s) of concern.
ESMO uses age to assign priority for postponing adjuvant breast radiation in patients with low- to moderate-risk lesions. However, the guidelines stop surprisingly short of recommending that adjuvant radiation be withheld for older patients with low-risk, stage I, hormonally sensitive, HER2-negative breast cancers who receive endocrine therapy.
Bottom line
The pragmatic adjustments ESMO suggests address the challenges of evaluating and treating breast cancer patients during the COVID-19 pandemic. The guidelines protect each patient’s right to care and safety as well as protecting the safety of caregivers.
The guidelines will likely heighten patients’ satisfaction with care and decrease concern about adequacy of timely evaluation and treatment.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Adalimumab serum levels and anti-drug antibodies fail to predict responses to other TNFi
Both antiadalimumab (Humira) antibodies and adalimumab serum levels fell short on predicting drug responses in rheumatoid arthritis patients who failed initial adalimumab therapy, based on a retrospective cohort study of 137 adults.
Biologic disease-modifying antirheumatic drugs (bDMARDs), notably adalimumab, are often prescribed for RA, but “approximately 41% of RA patients do not achieve good response after 6 months of treatment with adalimumab,” wrote Evy Ulijn of Sint Maartenskliniek, Nijmegen, the Netherlands, and colleagues. Preliminary studies have suggested that antiadalimumab antibodies (antidrug antibodies, ADA) and adalimumab serum levels (ADL) may predict the response to a second bDMARD in patients who fail initial adalimumab treatment, they said.
In a study published in Annals of the Rheumatic Diseases, the researchers examined data from 137 adult RA patients seen at the clinic during Jan. 2012–Jan. 2018 who failed to respond to adalimumab after at least 3 months of treatment and started another bDMARD. The average age of the patients was 64 years, and approximately 69% were women.
Overall, the presence of ADA was not a significant predictor of a European League Against Rheumatism good response in patients who switched to another TNFi (etanercept, golimumab, infliximab, or certolizumab pegol), with sensitivity of 18% and specificity of 75%. ADA also was not predictive of response to a non-TNFi bDMARD (rituximab, tocilizumab, or abatacept), with sensitivity and specificity of 33% and 70%, respectively.
Similarly, ADL levels in patients who switched to a TNFi or non-TNFi were not significant predictors of treatment response, with sensitivities and specificities of 50% and 52%, respectively, for TNFi and 32% and 69%, respectively, for non-TNFi.
The findings that neither ADA nor ADL showed predictive values contrast with previous studies, the researchers said.
“Not only did the results of this study show no predictive values, in some analyses a prediction is found in the opposite direction of what was expected,” they wrote.
The study findings were limited by several factors, including the random timing of sample collection, retrospective study design, and potential for misclassification of responders or nonresponders, the researchers noted.
However, the results were strengthened by the blinded choice of treatment and outcome assessment, larger sample size than previous studies, and focus on adalimumab in particular, they said.
“While counterintuitive, it is hard to find an explanation for the lack of a positive finding,” they concluded.
More research is needed to confirm the predictive value of ADA and ADL, they said. In the meantime, rheumatologists should base decisions to switch patients to TNFi or non-TNFi treatment after adalimumab failure based on factors including side effects, local protocol, economical aspects, and patient preferences, they said.
The study received no external funding. The researchers had no financial conflicts to disclose.
SOURCE: Ulijn E et al. Ann Rheum Dis. 2020 Apr 21. doi: 10.1136/annrheumdis-2020-216996.
Both antiadalimumab (Humira) antibodies and adalimumab serum levels fell short on predicting drug responses in rheumatoid arthritis patients who failed initial adalimumab therapy, based on a retrospective cohort study of 137 adults.
Biologic disease-modifying antirheumatic drugs (bDMARDs), notably adalimumab, are often prescribed for RA, but “approximately 41% of RA patients do not achieve good response after 6 months of treatment with adalimumab,” wrote Evy Ulijn of Sint Maartenskliniek, Nijmegen, the Netherlands, and colleagues. Preliminary studies have suggested that antiadalimumab antibodies (antidrug antibodies, ADA) and adalimumab serum levels (ADL) may predict the response to a second bDMARD in patients who fail initial adalimumab treatment, they said.
In a study published in Annals of the Rheumatic Diseases, the researchers examined data from 137 adult RA patients seen at the clinic during Jan. 2012–Jan. 2018 who failed to respond to adalimumab after at least 3 months of treatment and started another bDMARD. The average age of the patients was 64 years, and approximately 69% were women.
Overall, the presence of ADA was not a significant predictor of a European League Against Rheumatism good response in patients who switched to another TNFi (etanercept, golimumab, infliximab, or certolizumab pegol), with sensitivity of 18% and specificity of 75%. ADA also was not predictive of response to a non-TNFi bDMARD (rituximab, tocilizumab, or abatacept), with sensitivity and specificity of 33% and 70%, respectively.
Similarly, ADL levels in patients who switched to a TNFi or non-TNFi were not significant predictors of treatment response, with sensitivities and specificities of 50% and 52%, respectively, for TNFi and 32% and 69%, respectively, for non-TNFi.
The findings that neither ADA nor ADL showed predictive values contrast with previous studies, the researchers said.
“Not only did the results of this study show no predictive values, in some analyses a prediction is found in the opposite direction of what was expected,” they wrote.
The study findings were limited by several factors, including the random timing of sample collection, retrospective study design, and potential for misclassification of responders or nonresponders, the researchers noted.
However, the results were strengthened by the blinded choice of treatment and outcome assessment, larger sample size than previous studies, and focus on adalimumab in particular, they said.
“While counterintuitive, it is hard to find an explanation for the lack of a positive finding,” they concluded.
More research is needed to confirm the predictive value of ADA and ADL, they said. In the meantime, rheumatologists should base decisions to switch patients to TNFi or non-TNFi treatment after adalimumab failure based on factors including side effects, local protocol, economical aspects, and patient preferences, they said.
The study received no external funding. The researchers had no financial conflicts to disclose.
SOURCE: Ulijn E et al. Ann Rheum Dis. 2020 Apr 21. doi: 10.1136/annrheumdis-2020-216996.
Both antiadalimumab (Humira) antibodies and adalimumab serum levels fell short on predicting drug responses in rheumatoid arthritis patients who failed initial adalimumab therapy, based on a retrospective cohort study of 137 adults.
Biologic disease-modifying antirheumatic drugs (bDMARDs), notably adalimumab, are often prescribed for RA, but “approximately 41% of RA patients do not achieve good response after 6 months of treatment with adalimumab,” wrote Evy Ulijn of Sint Maartenskliniek, Nijmegen, the Netherlands, and colleagues. Preliminary studies have suggested that antiadalimumab antibodies (antidrug antibodies, ADA) and adalimumab serum levels (ADL) may predict the response to a second bDMARD in patients who fail initial adalimumab treatment, they said.
In a study published in Annals of the Rheumatic Diseases, the researchers examined data from 137 adult RA patients seen at the clinic during Jan. 2012–Jan. 2018 who failed to respond to adalimumab after at least 3 months of treatment and started another bDMARD. The average age of the patients was 64 years, and approximately 69% were women.
Overall, the presence of ADA was not a significant predictor of a European League Against Rheumatism good response in patients who switched to another TNFi (etanercept, golimumab, infliximab, or certolizumab pegol), with sensitivity of 18% and specificity of 75%. ADA also was not predictive of response to a non-TNFi bDMARD (rituximab, tocilizumab, or abatacept), with sensitivity and specificity of 33% and 70%, respectively.
Similarly, ADL levels in patients who switched to a TNFi or non-TNFi were not significant predictors of treatment response, with sensitivities and specificities of 50% and 52%, respectively, for TNFi and 32% and 69%, respectively, for non-TNFi.
The findings that neither ADA nor ADL showed predictive values contrast with previous studies, the researchers said.
“Not only did the results of this study show no predictive values, in some analyses a prediction is found in the opposite direction of what was expected,” they wrote.
The study findings were limited by several factors, including the random timing of sample collection, retrospective study design, and potential for misclassification of responders or nonresponders, the researchers noted.
However, the results were strengthened by the blinded choice of treatment and outcome assessment, larger sample size than previous studies, and focus on adalimumab in particular, they said.
“While counterintuitive, it is hard to find an explanation for the lack of a positive finding,” they concluded.
More research is needed to confirm the predictive value of ADA and ADL, they said. In the meantime, rheumatologists should base decisions to switch patients to TNFi or non-TNFi treatment after adalimumab failure based on factors including side effects, local protocol, economical aspects, and patient preferences, they said.
The study received no external funding. The researchers had no financial conflicts to disclose.
SOURCE: Ulijn E et al. Ann Rheum Dis. 2020 Apr 21. doi: 10.1136/annrheumdis-2020-216996.
FROM ANNALS OF THE RHEUMATIC DISEASES