User login
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
SVS Now Accepting Abstracts for VAM 2017
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Best Practices: Protecting Dry Vulnerable Skin with CeraVe® Healing Ointment
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.

- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.

Deprescribing of Proton Pump Inhibitors at the South Texas Veterans Health Care System
Deprescribing of Proton Pump Inhibitors at the South Texas Veterans Health Care System
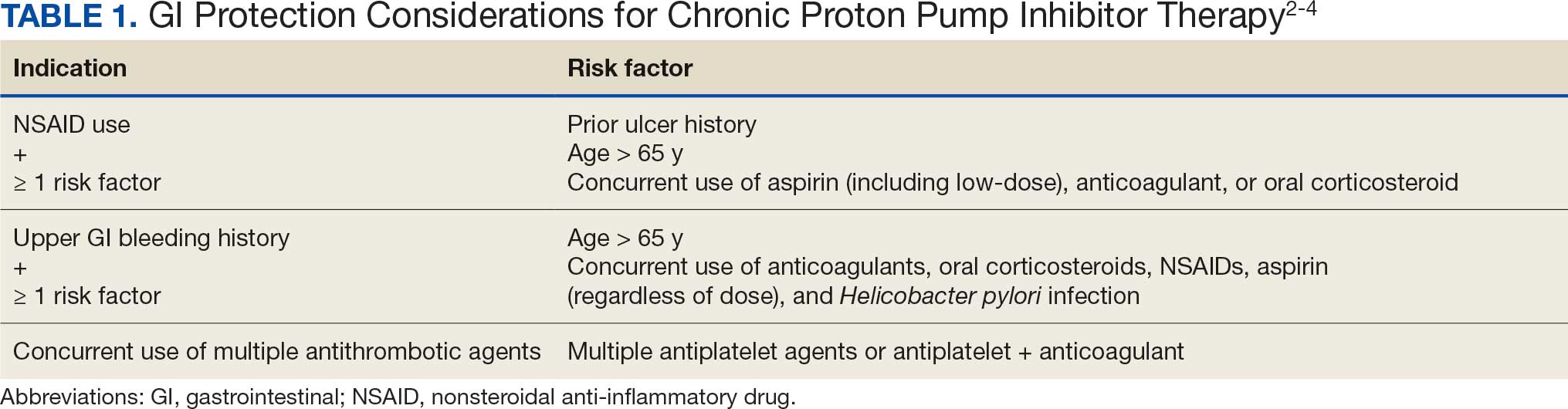
Proton pump inhibitors (PPIs) are widely prescribed medications used to manage various disease states. A systematic review of global trends and practices in PPI use estimated that about 25% of adults use a PPI, accounting for > 28 million users worldwide.1 The duration of PPI therapy varies by indication; however, many patients continue therapy beyond the suggested period. According to the American Gastroenterological Association (AGA) 2022 PPI deprescribing guideline update, regular assessment of PPIs should be performed for ongoing indications, and patients without a definitive indication for chronic PPI use should be considered for safe deprescribing.2 Indications for chronic PPI use include a history of severe erosive esophagitis, esophageal ulcer, peptic stricture, dysphagia, Barrett esophagus, idiopathic pulmonary fibrosis, history of gastrointestinal (GI) bleeding, and GI protection (Table 1).2-4
While PPIs are generally considered safe for short-term use, long-term use has been associated with several adverse effects (AEs) and safety concerns.5 A meta-analysis found a significant risk for Clostridium difficile infections (CDI) in PPI users.6 The effect of PPIs on vitamin B12 deficiency remains controversial; however, there is evidence that vitamin B12 levels may be decreased when gastric acid is suppressed for prolonged periods.7,8 In addition, the use of PPIs may result in decreased absorption of magnesium and calcium. A meta-analysis to examine the association of PPI use and hypomagnesemia found that high-dose PPIs were associated with hypomagnesemia compared with low-dose PPIs.9 Another meta-analysis demonstrated a statistically significant increased risk of hypomagnesemia in patients with PPI use.10 Long-term PPI use has been associated with decreased calcium levels, resulting in osteoporosis and increased risk of bone fractures. Multiple longitudinal observational studies concluded that increased risk for osteoporosis is associated with chronic PPI use.11 Patients who use a PPI long term without a clearly documented indication for chronic PPI therapy may be at risk for unnecessary exposure to PPI-associated AEs.
The US Department of Veterans Affairs (VA) created a dashboard to identify patients with chronic PPI use who may benefit from deprescribing. The Randomized PPI De-Prescribing (RaPPID) Program Dashboard defines chronic PPI use as being prescribed PPI therapy for ≥ 90 days during the 120-day period prior to a scheduled primary care visit. Candidates for deprescribing include those on once-daily PPI with no clear indication for chronic use or with uncomplicated GERD (ie, no erosive esophagitis, stricture, dysphagia, Barrett esophagus), as well as those on a twice-daily PPI for any indication except Zollinger-Ellison syndrome.
The dashboard categorizes deprescribing into 3 methods: (1) discontinuation of once-daily PPIs in the absence of a clear indication or in cases of uncomplicated GERD; (2) dose reduction for patients taking twice-daily PPIs for any non–Zollinger–Ellison indication; and (3) reduce and discontinue, which combines both for patients receiving twice-daily therapy who meet criteria for both strategies. A South Texas Veterans Health Care System (STVHCS) internal medication use evaluation using the VA RaPPID Program Dashboard identified 250 patients on a PPI and concluded that 56.9% of those patients were eligible for PPI deprescribing.12
This quality improvement (QI) project sought to assess PPI use and intervene to improve deprescribing rates at STVHCS. The intervention consisted of an educational in-service presentation delivered to primary care practitioners (PCPs) at a STVHCS patient aligned care team (PACT) collaborative meeting. Follow-up EHR reviews assessed whether PPI therapy was appropriately deprescribed after PCP appointments.
Methods
The primary objective of this QI project was to improve PPI prescribing practices at STVHCS PACT clinics to reduce PPI use in patients with an inappropriate indication by ≥ 10%. Secondary objectives included summarizing the use of vitamin supplementation (ie, cyanocobalamin, magnesium, calcium), reviewing AEs associated with PPI use (ie, CDI, fractures), and evaluating the occurrence of PPI reinitiation, recurrent GERD symptoms, and GI bleeding within 4 weeks of deprescribing.
On November 6, 2024, an in-service presentation was provided to PACT PCPs to educate and encourage the use of the VA RaPPID Program Dashboard, which creates a list of patients with a PCP appointment within 4 weeks of the current date who are eligible for PPI deprescribing. A patient list was generated from the VA RaPPID Program Dashboard on the morning before the in-service presentation. Four weeks following the in-service presentation and after all PCP appointments were conducted, a retrospective EHR review was conducted to assess outcomes. PPI deprescribing was determined collaboratively by the PCP and patient during the appointment, guided by clinical judgment and shared decision-making.
Patients were included if they had a PCP appointment between November 6, 2024, and December 3, 2024 (ie, within 4 weeks of in-service presentation), had an active prescription for an oral PPI from STVHCS and were identified as candidates by the VA RaPPID Program Dashboard for deprescribing as patients with chronic PPI use. Patients were excluded if they had an appropriate indication for chronic use of PPI, canceled or missed their PCP appointment, or failed previous de-escalation attempt (ie, worsening GERD symptoms or developed GI bleed after a deprescribing attempt).
Results
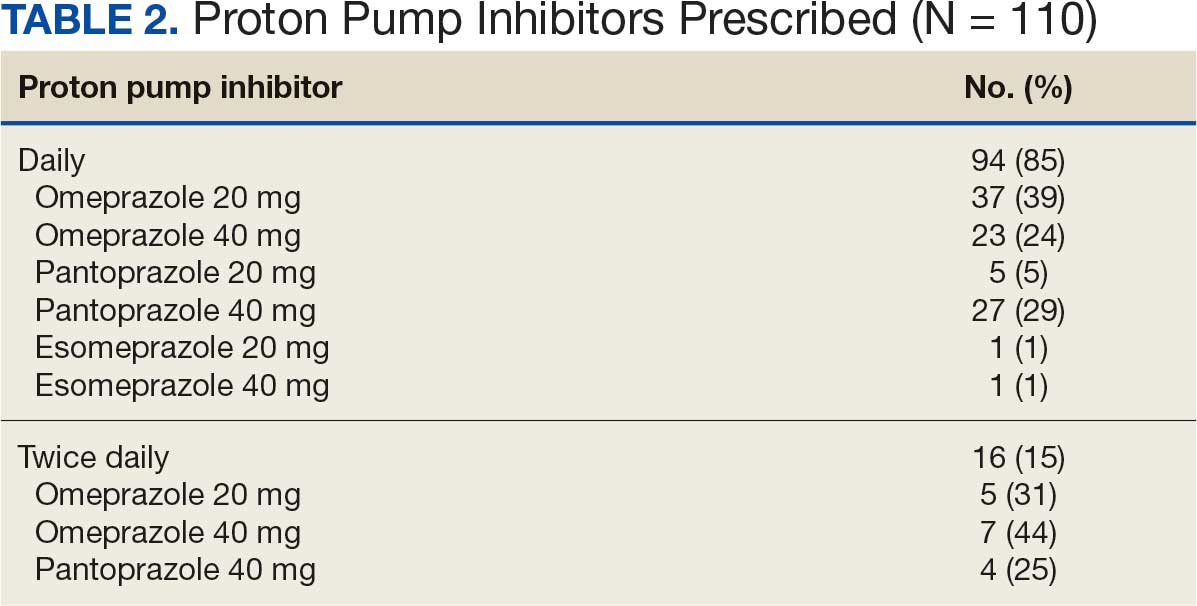
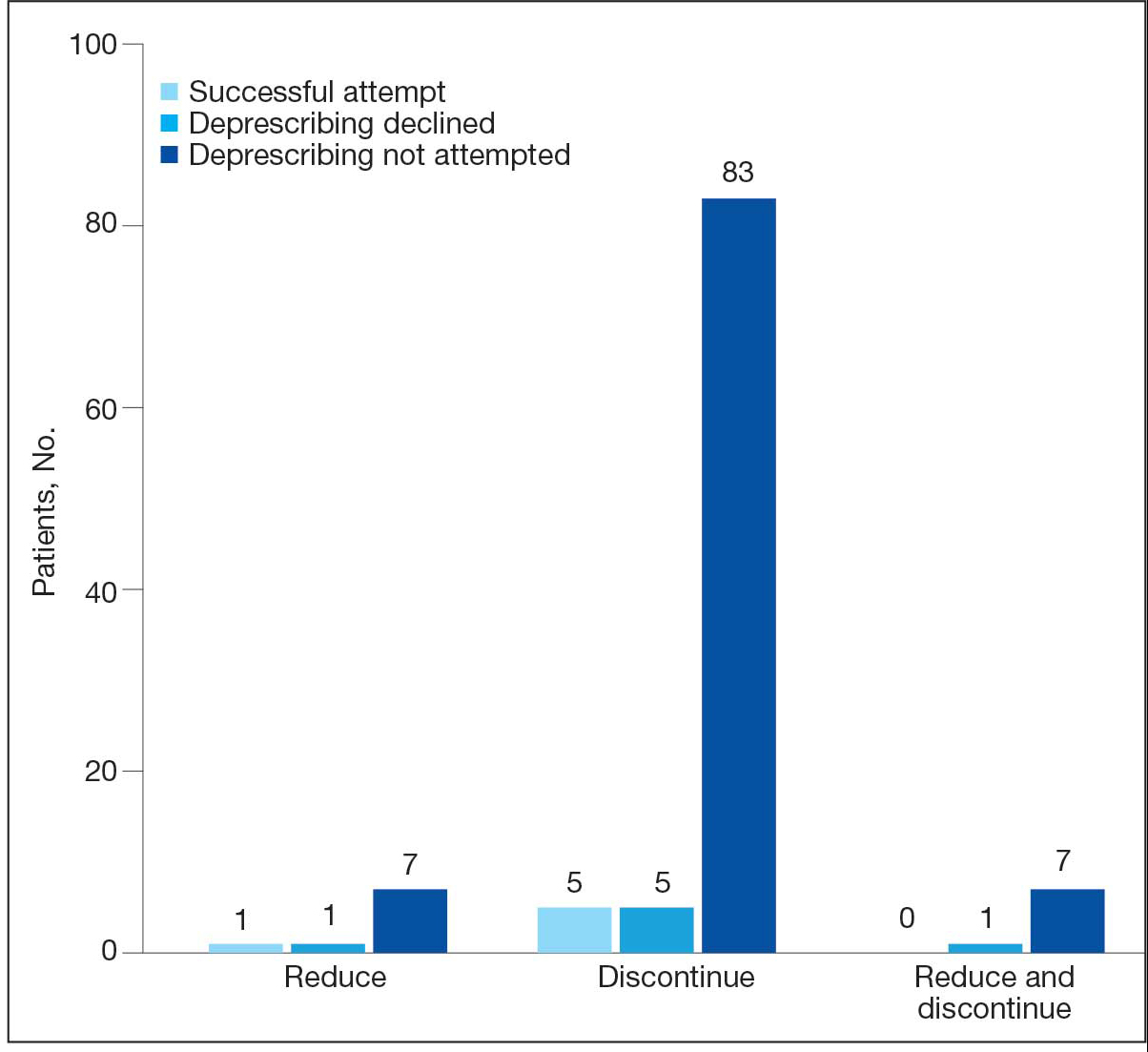
The VA RaPPID Program Dashboard identified 385 patients eligible for PPI deprescribing and 110 patients (29%) met the inclusion criteria and were reviewed. Most patients included were men, with a mean (SD) age of 56 years (13). Ninety-four patients (85%) had a daily PPI prescription with uncomplicated GERD at diagnosis and 16 patients (15%) took PPIs twice daily with uncomplicated GERD (Table 2). Seventy-two patients (65%) took omeprazole, 36 (33%) took pantoprazole, and 2 (2%) took esomeprazole. The dashboard identified 93 patients (85%) as candidates for PPI therapy discontinuation, 9 patients (8%) as candidates for PPI therapy reduction, and 8 patients (7%) as candidates for PPI therapy reduction and discontinuation.
PPIs were deprescribed for 13 of 110 patients (12%). Of the 13 patients offered a trial of PPI deprescribing, 6 (46%) agreed to participate while 7 (54%) declined deprescribing (Figure). The 6 patients who agreed to trial deprescribing were initiated on an individualized tapering regimen.
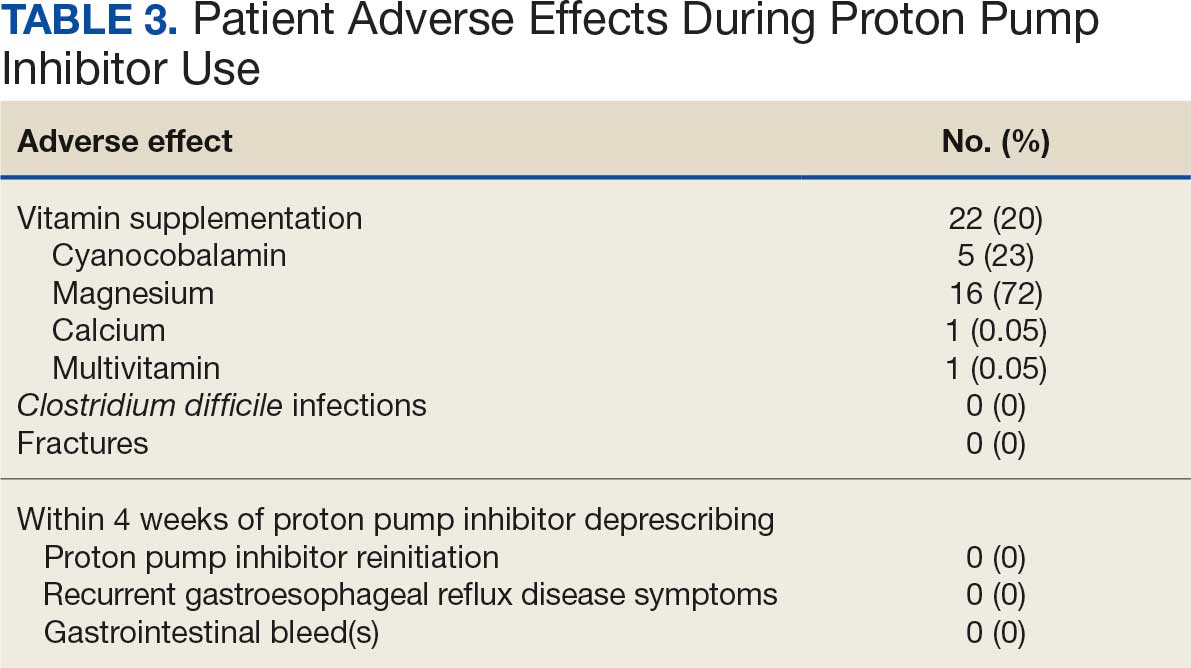
Among all patients, 22 (20%) received vitamin supplementation during PPI therapy. Of those supplemented, 5 (23%) received cyanocobalamin, 16 (73%) received magnesium, 1 (1%) received calcium, and 1 (1%) received a multivitamin. One case of CDI was documented during PPI therapy and no fractures were observed.
The 6 patients who agreed to deprescribe PPIs successfully stopped use and were transitioned to an alternative agent (ie, famotidine) for GERD symptom management. Follow-up EHR review showed no patients reinitiated a PPI, experienced GI bleeding, or had documented recurrence of GERD symptoms within 4 weeks after deprescribing. (Table 3).
Discussion
This STVHCS QI project used the RaPPID Program Dashboard to increase PPI deprescribing rates. A 10% deprescribing goal was established for the single in-service presentation to maintain an attainable, conservative estimate of the expected impact. Six of the 13 patients (46%) successfully deprescribed their PPI, thereby meeting the project’s 10% deprescribing goal. Notably, 1 of the 6 patients was referred to a PACT clinical pharmacist practitioner (CPP) by their PCP for deprescribing and management of GERD symptoms. The patient transitioned from PPI to famotidine and had long-term follow-up care with their assigned PACT CPP, suggesting that greater involvement from PACT CPPs may lead to better adherence to PPI prescribing guidelines.
Our findings align with prior studies that assessed PPI deprescribing. In 2024, Rossi et al examined 66 studies evaluating various PPI deprescribing interventions among patients with mild illness. These included collaborative strategies involving physicians, pharmacists, and other health care professionals; clinical decision-making algorithms; and patient engagement. Rossi et al found that 24% to 67% of patients successfully deprescribed PPI and most patients (51%-88%) did not report any recurring symptoms of heartburn or acid regurgitation after discontinuing PPI therapy.13
In this QI project, famotidine was prescribed as an alternative agent for all 6 patients who successfully discontinued PPI. The AGA guidelines recommend as-needed H2-receptor antagonist use following PPI deprescribing to control symptoms in the short term and prevent immediate resumption of a PPI. Providing an alternative agent for GERD symptoms may encourage patient participation and improve the success of PPI deprescribing initiatives by mitigating concerns over symptom reoccurrence.
Limitations
Secondary outcomes were assessed only within a 4-week period following the PCP visit, and patients may have experienced AEs beyond the 4-week time frame, which may have resulted in their underestimation. It is possible patients may have independently restarted PPI therapy without reporting recurrent symptoms to their PCP, which could further confound the assessment of outcomes. Additionally, while the need for vitamin supplementation and the occurrence of a CDI was observed, it remains unclear whether these events were exclusively caused by PPI use. Potential confounding variables for vitamin supplementation include age and other clinical indications for vitamin supplementation (eg, osteoporosis, migraines, macrocytic anemia, malabsorption syndromes, or concurrent use of other medications associated with vitamin deficiencies). For the patient with CDI, potential confounders include antibiotic use, advanced age, travel history, immunosuppression, or prior GI surgery. These factors limit the ability to draw causal associations to PPI use.
Several factors may explain why deprescribing was only initiated within 12% of eligible patients. First, deprescribing attempts may not have been consistently documented in the PCP visit notes, which may have led to an underestimation of the number of patients who considered deprescribing. Furthermore, time constraints during PCP appointments may have hindered thorough education and documentation. Among patients for whom deprescribing was attempted, about half declined. This hesitancy may have been influenced by their prolonged history of use, perceived medication efficacy, and concern for symptom relapse.
The proposed next step of this QI project would be to involve the PACT CPPs in the PPI deprescribing initiative during patient encounters and assess the impact of their involvement in deprescribing rates, reporting interval outcomes with long-term follow-up. Statistical analysis may also be beneficial to determine whether the observed deprescribing outcomes are statistically significant.
Conclusions
This QI project demonstrated that the use of the VA RaPPID Program Dashboard, in conjunction with targeted clinician education, can positively influence PPI deprescribing. Although a relatively small number of patients considered deprescribing, it was successful in patients who agreed to discontinue PPI therapy. These patients had no recurrence of short-term GERD symptoms or AEs. An H2-receptor antagonist may facilitate successful deprescribing for patients who agree to stop PPI use. The findings of this project highlight the importance of clinician engagement, shared decision-making, and thorough documentation of deprescribing attempts. Further efforts should focus on reinforcing the dashboard, involving PACT CPPs, and evaluating long-term outcomes to enhance the safety and appropriateness of PPI use in the veteran population.
Shanika LGT, Reynolds A, Pattison S, et al. Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol. 2023:1159-1172. doi:10.1007/s00228-023-03534-z
Targownik LE, Fisher DA, Saini SD. AGA clinical practice update on de-prescribing of proton pump inhibitors: expert review. Gastroenterology. 2022:1334-1342. doi:10.1053/j.gastro.2021.12.247
Lanza FL, Chan FKL, Quigley EMM. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. 2009:728-738. doi:10.1038/ajg.2009.115
Abraham NS, Hlatky MA, Antman EM, et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation. 2010:2619-2633. doi:10.1161/CIR.0b013e318202f701
Ament PW, Dicola DB, James ME. Reducing adverse effects of proton pump inhibitors. Am Fam Physician. 2012;86:66-70. Accessed June 18, 2026. https://www.aafp.org/pubs/afp/issues/2012/0701/p66.html
Cao F, Chen CX, Wang M, et al. Updated meta-analysis of controlled observational studies: proton-pump inhibitors and risk of Clostridium difficile infection. J Hosp Infect. 2018:4-13. doi:10.1016/j.jhin.2017.08.017
Losurdo G, Caccavo NLB, Indellicati G, et al. Effect of long-term proton pump inhibitor use on blood vitamins and minerals: a primary care setting study. J Clin Med. 2023:2910. doi:10.3390/jcm12082910
Laine L, Ahnen D, McClain C, et al. Review article: potential gastrointestinal effects of long-term acid suppression with proton pump inhibitors. Aliment Pharmacol Ther. 2000:651-668. doi:10.1046/j.1365-2036.2000.00768.x
Srinutta T, Chewcharat A, Takkavatakarn K, et al. Proton pump inhibitors and hypomagnesemia. Medicine (Baltimore). 2019:e17788. doi:10.1097/MD.0000000000017788
Cheungpasitporn W, Thongprayoon C, Kittanamongkolchai W, et al. Proton pump inhibitors linked to hypomagnesemia: a systematic review and meta-analysis of observational studies. Ren Fail. 2015:1237-1241.doi:10.3109/0886022X.2015.1057800
Thong BKS, Ima-Nirwana S, Chin KY. Proton pump inhibitors and fracture risk: a review of current evidence and mechanisms involved. Int J Environ Res Public Health. 2019:1571. doi:10.3390/ijerph16091571
Errisuriz K. Medication Use Evaluation: Proton Pump Inhibitor De-Prescribing. South Texas Veterans Health Care System; 2024. Unpublished report.
Rossi A, Perrella L, Scotti S, et al. Approaches to deprescribing proton pump inhibitors in clinical practice: a systematic review. J Clin Med. 2024:6283. doi:10.3390/jcm13206283
Proton pump inhibitors (PPIs) are widely prescribed medications used to manage various disease states. A systematic review of global trends and practices in PPI use estimated that about 25% of adults use a PPI, accounting for > 28 million users worldwide.1 The duration of PPI therapy varies by indication; however, many patients continue therapy beyond the suggested period. According to the American Gastroenterological Association (AGA) 2022 PPI deprescribing guideline update, regular assessment of PPIs should be performed for ongoing indications, and patients without a definitive indication for chronic PPI use should be considered for safe deprescribing.2 Indications for chronic PPI use include a history of severe erosive esophagitis, esophageal ulcer, peptic stricture, dysphagia, Barrett esophagus, idiopathic pulmonary fibrosis, history of gastrointestinal (GI) bleeding, and GI protection (Table 1).2-4
While PPIs are generally considered safe for short-term use, long-term use has been associated with several adverse effects (AEs) and safety concerns.5 A meta-analysis found a significant risk for Clostridium difficile infections (CDI) in PPI users.6 The effect of PPIs on vitamin B12 deficiency remains controversial; however, there is evidence that vitamin B12 levels may be decreased when gastric acid is suppressed for prolonged periods.7,8 In addition, the use of PPIs may result in decreased absorption of magnesium and calcium. A meta-analysis to examine the association of PPI use and hypomagnesemia found that high-dose PPIs were associated with hypomagnesemia compared with low-dose PPIs.9 Another meta-analysis demonstrated a statistically significant increased risk of hypomagnesemia in patients with PPI use.10 Long-term PPI use has been associated with decreased calcium levels, resulting in osteoporosis and increased risk of bone fractures. Multiple longitudinal observational studies concluded that increased risk for osteoporosis is associated with chronic PPI use.11 Patients who use a PPI long term without a clearly documented indication for chronic PPI therapy may be at risk for unnecessary exposure to PPI-associated AEs.
The US Department of Veterans Affairs (VA) created a dashboard to identify patients with chronic PPI use who may benefit from deprescribing. The Randomized PPI De-Prescribing (RaPPID) Program Dashboard defines chronic PPI use as being prescribed PPI therapy for ≥ 90 days during the 120-day period prior to a scheduled primary care visit. Candidates for deprescribing include those on once-daily PPI with no clear indication for chronic use or with uncomplicated GERD (ie, no erosive esophagitis, stricture, dysphagia, Barrett esophagus), as well as those on a twice-daily PPI for any indication except Zollinger-Ellison syndrome.
The dashboard categorizes deprescribing into 3 methods: (1) discontinuation of once-daily PPIs in the absence of a clear indication or in cases of uncomplicated GERD; (2) dose reduction for patients taking twice-daily PPIs for any non–Zollinger–Ellison indication; and (3) reduce and discontinue, which combines both for patients receiving twice-daily therapy who meet criteria for both strategies. A South Texas Veterans Health Care System (STVHCS) internal medication use evaluation using the VA RaPPID Program Dashboard identified 250 patients on a PPI and concluded that 56.9% of those patients were eligible for PPI deprescribing.12
This quality improvement (QI) project sought to assess PPI use and intervene to improve deprescribing rates at STVHCS. The intervention consisted of an educational in-service presentation delivered to primary care practitioners (PCPs) at a STVHCS patient aligned care team (PACT) collaborative meeting. Follow-up EHR reviews assessed whether PPI therapy was appropriately deprescribed after PCP appointments.
Methods
The primary objective of this QI project was to improve PPI prescribing practices at STVHCS PACT clinics to reduce PPI use in patients with an inappropriate indication by ≥ 10%. Secondary objectives included summarizing the use of vitamin supplementation (ie, cyanocobalamin, magnesium, calcium), reviewing AEs associated with PPI use (ie, CDI, fractures), and evaluating the occurrence of PPI reinitiation, recurrent GERD symptoms, and GI bleeding within 4 weeks of deprescribing.
On November 6, 2024, an in-service presentation was provided to PACT PCPs to educate and encourage the use of the VA RaPPID Program Dashboard, which creates a list of patients with a PCP appointment within 4 weeks of the current date who are eligible for PPI deprescribing. A patient list was generated from the VA RaPPID Program Dashboard on the morning before the in-service presentation. Four weeks following the in-service presentation and after all PCP appointments were conducted, a retrospective EHR review was conducted to assess outcomes. PPI deprescribing was determined collaboratively by the PCP and patient during the appointment, guided by clinical judgment and shared decision-making.
Patients were included if they had a PCP appointment between November 6, 2024, and December 3, 2024 (ie, within 4 weeks of in-service presentation), had an active prescription for an oral PPI from STVHCS and were identified as candidates by the VA RaPPID Program Dashboard for deprescribing as patients with chronic PPI use. Patients were excluded if they had an appropriate indication for chronic use of PPI, canceled or missed their PCP appointment, or failed previous de-escalation attempt (ie, worsening GERD symptoms or developed GI bleed after a deprescribing attempt).
Results
The VA RaPPID Program Dashboard identified 385 patients eligible for PPI deprescribing and 110 patients (29%) met the inclusion criteria and were reviewed. Most patients included were men, with a mean (SD) age of 56 years (13). Ninety-four patients (85%) had a daily PPI prescription with uncomplicated GERD at diagnosis and 16 patients (15%) took PPIs twice daily with uncomplicated GERD (Table 2). Seventy-two patients (65%) took omeprazole, 36 (33%) took pantoprazole, and 2 (2%) took esomeprazole. The dashboard identified 93 patients (85%) as candidates for PPI therapy discontinuation, 9 patients (8%) as candidates for PPI therapy reduction, and 8 patients (7%) as candidates for PPI therapy reduction and discontinuation.
PPIs were deprescribed for 13 of 110 patients (12%). Of the 13 patients offered a trial of PPI deprescribing, 6 (46%) agreed to participate while 7 (54%) declined deprescribing (Figure). The 6 patients who agreed to trial deprescribing were initiated on an individualized tapering regimen.
Among all patients, 22 (20%) received vitamin supplementation during PPI therapy. Of those supplemented, 5 (23%) received cyanocobalamin, 16 (73%) received magnesium, 1 (1%) received calcium, and 1 (1%) received a multivitamin. One case of CDI was documented during PPI therapy and no fractures were observed.
The 6 patients who agreed to deprescribe PPIs successfully stopped use and were transitioned to an alternative agent (ie, famotidine) for GERD symptom management. Follow-up EHR review showed no patients reinitiated a PPI, experienced GI bleeding, or had documented recurrence of GERD symptoms within 4 weeks after deprescribing. (Table 3).
Discussion
This STVHCS QI project used the RaPPID Program Dashboard to increase PPI deprescribing rates. A 10% deprescribing goal was established for the single in-service presentation to maintain an attainable, conservative estimate of the expected impact. Six of the 13 patients (46%) successfully deprescribed their PPI, thereby meeting the project’s 10% deprescribing goal. Notably, 1 of the 6 patients was referred to a PACT clinical pharmacist practitioner (CPP) by their PCP for deprescribing and management of GERD symptoms. The patient transitioned from PPI to famotidine and had long-term follow-up care with their assigned PACT CPP, suggesting that greater involvement from PACT CPPs may lead to better adherence to PPI prescribing guidelines.
Our findings align with prior studies that assessed PPI deprescribing. In 2024, Rossi et al examined 66 studies evaluating various PPI deprescribing interventions among patients with mild illness. These included collaborative strategies involving physicians, pharmacists, and other health care professionals; clinical decision-making algorithms; and patient engagement. Rossi et al found that 24% to 67% of patients successfully deprescribed PPI and most patients (51%-88%) did not report any recurring symptoms of heartburn or acid regurgitation after discontinuing PPI therapy.13
In this QI project, famotidine was prescribed as an alternative agent for all 6 patients who successfully discontinued PPI. The AGA guidelines recommend as-needed H2-receptor antagonist use following PPI deprescribing to control symptoms in the short term and prevent immediate resumption of a PPI. Providing an alternative agent for GERD symptoms may encourage patient participation and improve the success of PPI deprescribing initiatives by mitigating concerns over symptom reoccurrence.
Limitations
Secondary outcomes were assessed only within a 4-week period following the PCP visit, and patients may have experienced AEs beyond the 4-week time frame, which may have resulted in their underestimation. It is possible patients may have independently restarted PPI therapy without reporting recurrent symptoms to their PCP, which could further confound the assessment of outcomes. Additionally, while the need for vitamin supplementation and the occurrence of a CDI was observed, it remains unclear whether these events were exclusively caused by PPI use. Potential confounding variables for vitamin supplementation include age and other clinical indications for vitamin supplementation (eg, osteoporosis, migraines, macrocytic anemia, malabsorption syndromes, or concurrent use of other medications associated with vitamin deficiencies). For the patient with CDI, potential confounders include antibiotic use, advanced age, travel history, immunosuppression, or prior GI surgery. These factors limit the ability to draw causal associations to PPI use.
Several factors may explain why deprescribing was only initiated within 12% of eligible patients. First, deprescribing attempts may not have been consistently documented in the PCP visit notes, which may have led to an underestimation of the number of patients who considered deprescribing. Furthermore, time constraints during PCP appointments may have hindered thorough education and documentation. Among patients for whom deprescribing was attempted, about half declined. This hesitancy may have been influenced by their prolonged history of use, perceived medication efficacy, and concern for symptom relapse.
The proposed next step of this QI project would be to involve the PACT CPPs in the PPI deprescribing initiative during patient encounters and assess the impact of their involvement in deprescribing rates, reporting interval outcomes with long-term follow-up. Statistical analysis may also be beneficial to determine whether the observed deprescribing outcomes are statistically significant.
Conclusions
This QI project demonstrated that the use of the VA RaPPID Program Dashboard, in conjunction with targeted clinician education, can positively influence PPI deprescribing. Although a relatively small number of patients considered deprescribing, it was successful in patients who agreed to discontinue PPI therapy. These patients had no recurrence of short-term GERD symptoms or AEs. An H2-receptor antagonist may facilitate successful deprescribing for patients who agree to stop PPI use. The findings of this project highlight the importance of clinician engagement, shared decision-making, and thorough documentation of deprescribing attempts. Further efforts should focus on reinforcing the dashboard, involving PACT CPPs, and evaluating long-term outcomes to enhance the safety and appropriateness of PPI use in the veteran population.
Proton pump inhibitors (PPIs) are widely prescribed medications used to manage various disease states. A systematic review of global trends and practices in PPI use estimated that about 25% of adults use a PPI, accounting for > 28 million users worldwide.1 The duration of PPI therapy varies by indication; however, many patients continue therapy beyond the suggested period. According to the American Gastroenterological Association (AGA) 2022 PPI deprescribing guideline update, regular assessment of PPIs should be performed for ongoing indications, and patients without a definitive indication for chronic PPI use should be considered for safe deprescribing.2 Indications for chronic PPI use include a history of severe erosive esophagitis, esophageal ulcer, peptic stricture, dysphagia, Barrett esophagus, idiopathic pulmonary fibrosis, history of gastrointestinal (GI) bleeding, and GI protection (Table 1).2-4
While PPIs are generally considered safe for short-term use, long-term use has been associated with several adverse effects (AEs) and safety concerns.5 A meta-analysis found a significant risk for Clostridium difficile infections (CDI) in PPI users.6 The effect of PPIs on vitamin B12 deficiency remains controversial; however, there is evidence that vitamin B12 levels may be decreased when gastric acid is suppressed for prolonged periods.7,8 In addition, the use of PPIs may result in decreased absorption of magnesium and calcium. A meta-analysis to examine the association of PPI use and hypomagnesemia found that high-dose PPIs were associated with hypomagnesemia compared with low-dose PPIs.9 Another meta-analysis demonstrated a statistically significant increased risk of hypomagnesemia in patients with PPI use.10 Long-term PPI use has been associated with decreased calcium levels, resulting in osteoporosis and increased risk of bone fractures. Multiple longitudinal observational studies concluded that increased risk for osteoporosis is associated with chronic PPI use.11 Patients who use a PPI long term without a clearly documented indication for chronic PPI therapy may be at risk for unnecessary exposure to PPI-associated AEs.
The US Department of Veterans Affairs (VA) created a dashboard to identify patients with chronic PPI use who may benefit from deprescribing. The Randomized PPI De-Prescribing (RaPPID) Program Dashboard defines chronic PPI use as being prescribed PPI therapy for ≥ 90 days during the 120-day period prior to a scheduled primary care visit. Candidates for deprescribing include those on once-daily PPI with no clear indication for chronic use or with uncomplicated GERD (ie, no erosive esophagitis, stricture, dysphagia, Barrett esophagus), as well as those on a twice-daily PPI for any indication except Zollinger-Ellison syndrome.
The dashboard categorizes deprescribing into 3 methods: (1) discontinuation of once-daily PPIs in the absence of a clear indication or in cases of uncomplicated GERD; (2) dose reduction for patients taking twice-daily PPIs for any non–Zollinger–Ellison indication; and (3) reduce and discontinue, which combines both for patients receiving twice-daily therapy who meet criteria for both strategies. A South Texas Veterans Health Care System (STVHCS) internal medication use evaluation using the VA RaPPID Program Dashboard identified 250 patients on a PPI and concluded that 56.9% of those patients were eligible for PPI deprescribing.12
This quality improvement (QI) project sought to assess PPI use and intervene to improve deprescribing rates at STVHCS. The intervention consisted of an educational in-service presentation delivered to primary care practitioners (PCPs) at a STVHCS patient aligned care team (PACT) collaborative meeting. Follow-up EHR reviews assessed whether PPI therapy was appropriately deprescribed after PCP appointments.
Methods
The primary objective of this QI project was to improve PPI prescribing practices at STVHCS PACT clinics to reduce PPI use in patients with an inappropriate indication by ≥ 10%. Secondary objectives included summarizing the use of vitamin supplementation (ie, cyanocobalamin, magnesium, calcium), reviewing AEs associated with PPI use (ie, CDI, fractures), and evaluating the occurrence of PPI reinitiation, recurrent GERD symptoms, and GI bleeding within 4 weeks of deprescribing.
On November 6, 2024, an in-service presentation was provided to PACT PCPs to educate and encourage the use of the VA RaPPID Program Dashboard, which creates a list of patients with a PCP appointment within 4 weeks of the current date who are eligible for PPI deprescribing. A patient list was generated from the VA RaPPID Program Dashboard on the morning before the in-service presentation. Four weeks following the in-service presentation and after all PCP appointments were conducted, a retrospective EHR review was conducted to assess outcomes. PPI deprescribing was determined collaboratively by the PCP and patient during the appointment, guided by clinical judgment and shared decision-making.
Patients were included if they had a PCP appointment between November 6, 2024, and December 3, 2024 (ie, within 4 weeks of in-service presentation), had an active prescription for an oral PPI from STVHCS and were identified as candidates by the VA RaPPID Program Dashboard for deprescribing as patients with chronic PPI use. Patients were excluded if they had an appropriate indication for chronic use of PPI, canceled or missed their PCP appointment, or failed previous de-escalation attempt (ie, worsening GERD symptoms or developed GI bleed after a deprescribing attempt).
Results
The VA RaPPID Program Dashboard identified 385 patients eligible for PPI deprescribing and 110 patients (29%) met the inclusion criteria and were reviewed. Most patients included were men, with a mean (SD) age of 56 years (13). Ninety-four patients (85%) had a daily PPI prescription with uncomplicated GERD at diagnosis and 16 patients (15%) took PPIs twice daily with uncomplicated GERD (Table 2). Seventy-two patients (65%) took omeprazole, 36 (33%) took pantoprazole, and 2 (2%) took esomeprazole. The dashboard identified 93 patients (85%) as candidates for PPI therapy discontinuation, 9 patients (8%) as candidates for PPI therapy reduction, and 8 patients (7%) as candidates for PPI therapy reduction and discontinuation.
PPIs were deprescribed for 13 of 110 patients (12%). Of the 13 patients offered a trial of PPI deprescribing, 6 (46%) agreed to participate while 7 (54%) declined deprescribing (Figure). The 6 patients who agreed to trial deprescribing were initiated on an individualized tapering regimen.
Among all patients, 22 (20%) received vitamin supplementation during PPI therapy. Of those supplemented, 5 (23%) received cyanocobalamin, 16 (73%) received magnesium, 1 (1%) received calcium, and 1 (1%) received a multivitamin. One case of CDI was documented during PPI therapy and no fractures were observed.
The 6 patients who agreed to deprescribe PPIs successfully stopped use and were transitioned to an alternative agent (ie, famotidine) for GERD symptom management. Follow-up EHR review showed no patients reinitiated a PPI, experienced GI bleeding, or had documented recurrence of GERD symptoms within 4 weeks after deprescribing. (Table 3).
Discussion
This STVHCS QI project used the RaPPID Program Dashboard to increase PPI deprescribing rates. A 10% deprescribing goal was established for the single in-service presentation to maintain an attainable, conservative estimate of the expected impact. Six of the 13 patients (46%) successfully deprescribed their PPI, thereby meeting the project’s 10% deprescribing goal. Notably, 1 of the 6 patients was referred to a PACT clinical pharmacist practitioner (CPP) by their PCP for deprescribing and management of GERD symptoms. The patient transitioned from PPI to famotidine and had long-term follow-up care with their assigned PACT CPP, suggesting that greater involvement from PACT CPPs may lead to better adherence to PPI prescribing guidelines.
Our findings align with prior studies that assessed PPI deprescribing. In 2024, Rossi et al examined 66 studies evaluating various PPI deprescribing interventions among patients with mild illness. These included collaborative strategies involving physicians, pharmacists, and other health care professionals; clinical decision-making algorithms; and patient engagement. Rossi et al found that 24% to 67% of patients successfully deprescribed PPI and most patients (51%-88%) did not report any recurring symptoms of heartburn or acid regurgitation after discontinuing PPI therapy.13
In this QI project, famotidine was prescribed as an alternative agent for all 6 patients who successfully discontinued PPI. The AGA guidelines recommend as-needed H2-receptor antagonist use following PPI deprescribing to control symptoms in the short term and prevent immediate resumption of a PPI. Providing an alternative agent for GERD symptoms may encourage patient participation and improve the success of PPI deprescribing initiatives by mitigating concerns over symptom reoccurrence.
Limitations
Secondary outcomes were assessed only within a 4-week period following the PCP visit, and patients may have experienced AEs beyond the 4-week time frame, which may have resulted in their underestimation. It is possible patients may have independently restarted PPI therapy without reporting recurrent symptoms to their PCP, which could further confound the assessment of outcomes. Additionally, while the need for vitamin supplementation and the occurrence of a CDI was observed, it remains unclear whether these events were exclusively caused by PPI use. Potential confounding variables for vitamin supplementation include age and other clinical indications for vitamin supplementation (eg, osteoporosis, migraines, macrocytic anemia, malabsorption syndromes, or concurrent use of other medications associated with vitamin deficiencies). For the patient with CDI, potential confounders include antibiotic use, advanced age, travel history, immunosuppression, or prior GI surgery. These factors limit the ability to draw causal associations to PPI use.
Several factors may explain why deprescribing was only initiated within 12% of eligible patients. First, deprescribing attempts may not have been consistently documented in the PCP visit notes, which may have led to an underestimation of the number of patients who considered deprescribing. Furthermore, time constraints during PCP appointments may have hindered thorough education and documentation. Among patients for whom deprescribing was attempted, about half declined. This hesitancy may have been influenced by their prolonged history of use, perceived medication efficacy, and concern for symptom relapse.
The proposed next step of this QI project would be to involve the PACT CPPs in the PPI deprescribing initiative during patient encounters and assess the impact of their involvement in deprescribing rates, reporting interval outcomes with long-term follow-up. Statistical analysis may also be beneficial to determine whether the observed deprescribing outcomes are statistically significant.
Conclusions
This QI project demonstrated that the use of the VA RaPPID Program Dashboard, in conjunction with targeted clinician education, can positively influence PPI deprescribing. Although a relatively small number of patients considered deprescribing, it was successful in patients who agreed to discontinue PPI therapy. These patients had no recurrence of short-term GERD symptoms or AEs. An H2-receptor antagonist may facilitate successful deprescribing for patients who agree to stop PPI use. The findings of this project highlight the importance of clinician engagement, shared decision-making, and thorough documentation of deprescribing attempts. Further efforts should focus on reinforcing the dashboard, involving PACT CPPs, and evaluating long-term outcomes to enhance the safety and appropriateness of PPI use in the veteran population.
Shanika LGT, Reynolds A, Pattison S, et al. Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol. 2023:1159-1172. doi:10.1007/s00228-023-03534-z
Targownik LE, Fisher DA, Saini SD. AGA clinical practice update on de-prescribing of proton pump inhibitors: expert review. Gastroenterology. 2022:1334-1342. doi:10.1053/j.gastro.2021.12.247
Lanza FL, Chan FKL, Quigley EMM. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. 2009:728-738. doi:10.1038/ajg.2009.115
Abraham NS, Hlatky MA, Antman EM, et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation. 2010:2619-2633. doi:10.1161/CIR.0b013e318202f701
Ament PW, Dicola DB, James ME. Reducing adverse effects of proton pump inhibitors. Am Fam Physician. 2012;86:66-70. Accessed June 18, 2026. https://www.aafp.org/pubs/afp/issues/2012/0701/p66.html
Cao F, Chen CX, Wang M, et al. Updated meta-analysis of controlled observational studies: proton-pump inhibitors and risk of Clostridium difficile infection. J Hosp Infect. 2018:4-13. doi:10.1016/j.jhin.2017.08.017
Losurdo G, Caccavo NLB, Indellicati G, et al. Effect of long-term proton pump inhibitor use on blood vitamins and minerals: a primary care setting study. J Clin Med. 2023:2910. doi:10.3390/jcm12082910
Laine L, Ahnen D, McClain C, et al. Review article: potential gastrointestinal effects of long-term acid suppression with proton pump inhibitors. Aliment Pharmacol Ther. 2000:651-668. doi:10.1046/j.1365-2036.2000.00768.x
Srinutta T, Chewcharat A, Takkavatakarn K, et al. Proton pump inhibitors and hypomagnesemia. Medicine (Baltimore). 2019:e17788. doi:10.1097/MD.0000000000017788
Cheungpasitporn W, Thongprayoon C, Kittanamongkolchai W, et al. Proton pump inhibitors linked to hypomagnesemia: a systematic review and meta-analysis of observational studies. Ren Fail. 2015:1237-1241.doi:10.3109/0886022X.2015.1057800
Thong BKS, Ima-Nirwana S, Chin KY. Proton pump inhibitors and fracture risk: a review of current evidence and mechanisms involved. Int J Environ Res Public Health. 2019:1571. doi:10.3390/ijerph16091571
Errisuriz K. Medication Use Evaluation: Proton Pump Inhibitor De-Prescribing. South Texas Veterans Health Care System; 2024. Unpublished report.
Rossi A, Perrella L, Scotti S, et al. Approaches to deprescribing proton pump inhibitors in clinical practice: a systematic review. J Clin Med. 2024:6283. doi:10.3390/jcm13206283
Shanika LGT, Reynolds A, Pattison S, et al. Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol. 2023:1159-1172. doi:10.1007/s00228-023-03534-z
Targownik LE, Fisher DA, Saini SD. AGA clinical practice update on de-prescribing of proton pump inhibitors: expert review. Gastroenterology. 2022:1334-1342. doi:10.1053/j.gastro.2021.12.247
Lanza FL, Chan FKL, Quigley EMM. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. 2009:728-738. doi:10.1038/ajg.2009.115
Abraham NS, Hlatky MA, Antman EM, et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation. 2010:2619-2633. doi:10.1161/CIR.0b013e318202f701
Ament PW, Dicola DB, James ME. Reducing adverse effects of proton pump inhibitors. Am Fam Physician. 2012;86:66-70. Accessed June 18, 2026. https://www.aafp.org/pubs/afp/issues/2012/0701/p66.html
Cao F, Chen CX, Wang M, et al. Updated meta-analysis of controlled observational studies: proton-pump inhibitors and risk of Clostridium difficile infection. J Hosp Infect. 2018:4-13. doi:10.1016/j.jhin.2017.08.017
Losurdo G, Caccavo NLB, Indellicati G, et al. Effect of long-term proton pump inhibitor use on blood vitamins and minerals: a primary care setting study. J Clin Med. 2023:2910. doi:10.3390/jcm12082910
Laine L, Ahnen D, McClain C, et al. Review article: potential gastrointestinal effects of long-term acid suppression with proton pump inhibitors. Aliment Pharmacol Ther. 2000:651-668. doi:10.1046/j.1365-2036.2000.00768.x
Srinutta T, Chewcharat A, Takkavatakarn K, et al. Proton pump inhibitors and hypomagnesemia. Medicine (Baltimore). 2019:e17788. doi:10.1097/MD.0000000000017788
Cheungpasitporn W, Thongprayoon C, Kittanamongkolchai W, et al. Proton pump inhibitors linked to hypomagnesemia: a systematic review and meta-analysis of observational studies. Ren Fail. 2015:1237-1241.doi:10.3109/0886022X.2015.1057800
Thong BKS, Ima-Nirwana S, Chin KY. Proton pump inhibitors and fracture risk: a review of current evidence and mechanisms involved. Int J Environ Res Public Health. 2019:1571. doi:10.3390/ijerph16091571
Errisuriz K. Medication Use Evaluation: Proton Pump Inhibitor De-Prescribing. South Texas Veterans Health Care System; 2024. Unpublished report.
Rossi A, Perrella L, Scotti S, et al. Approaches to deprescribing proton pump inhibitors in clinical practice: a systematic review. J Clin Med. 2024:6283. doi:10.3390/jcm13206283
Deprescribing of Proton Pump Inhibitors at the South Texas Veterans Health Care System
Deprescribing of Proton Pump Inhibitors at the South Texas Veterans Health Care System

Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.


B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
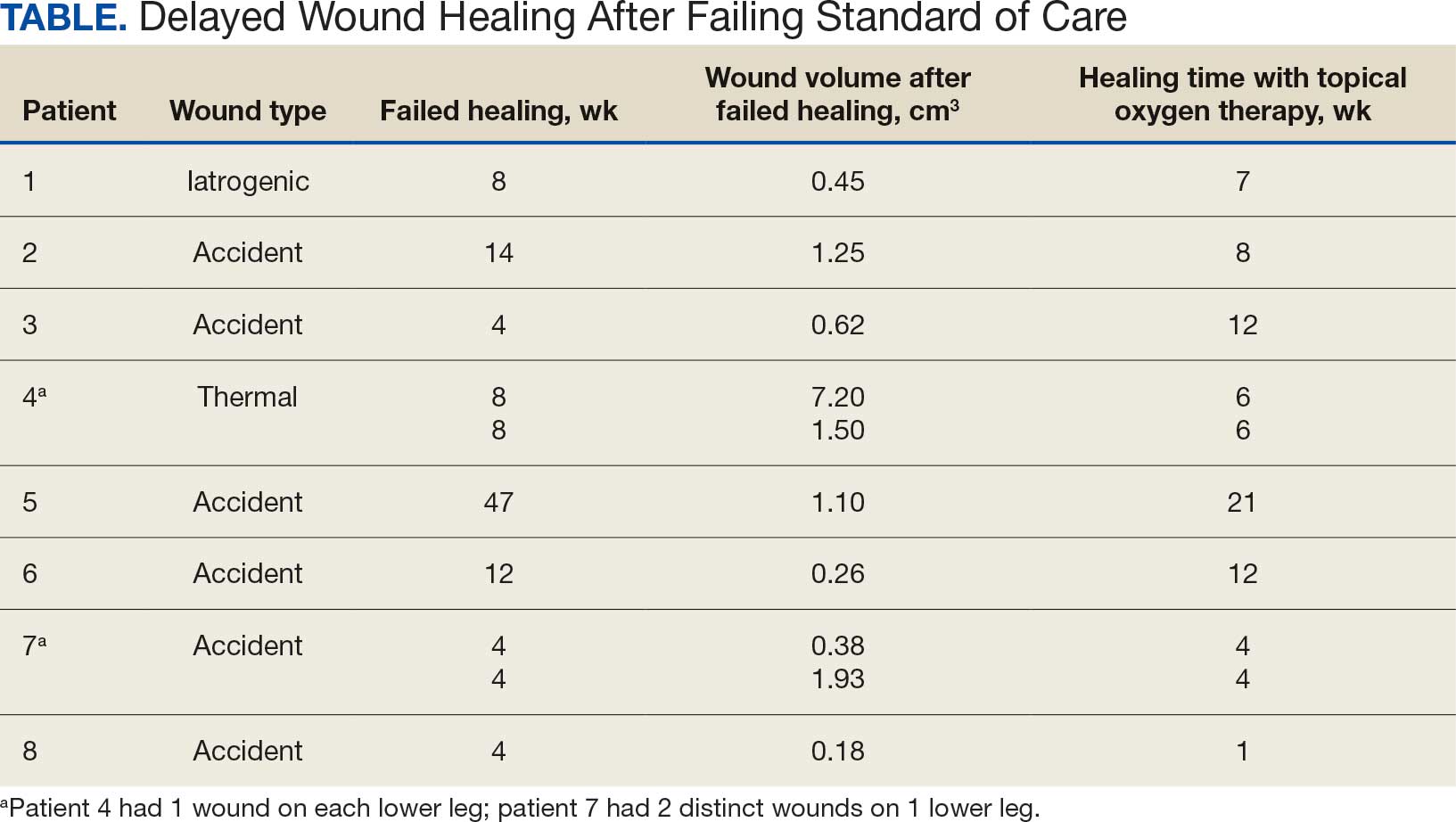
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.
B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.
B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes

Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology

Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
