User login
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
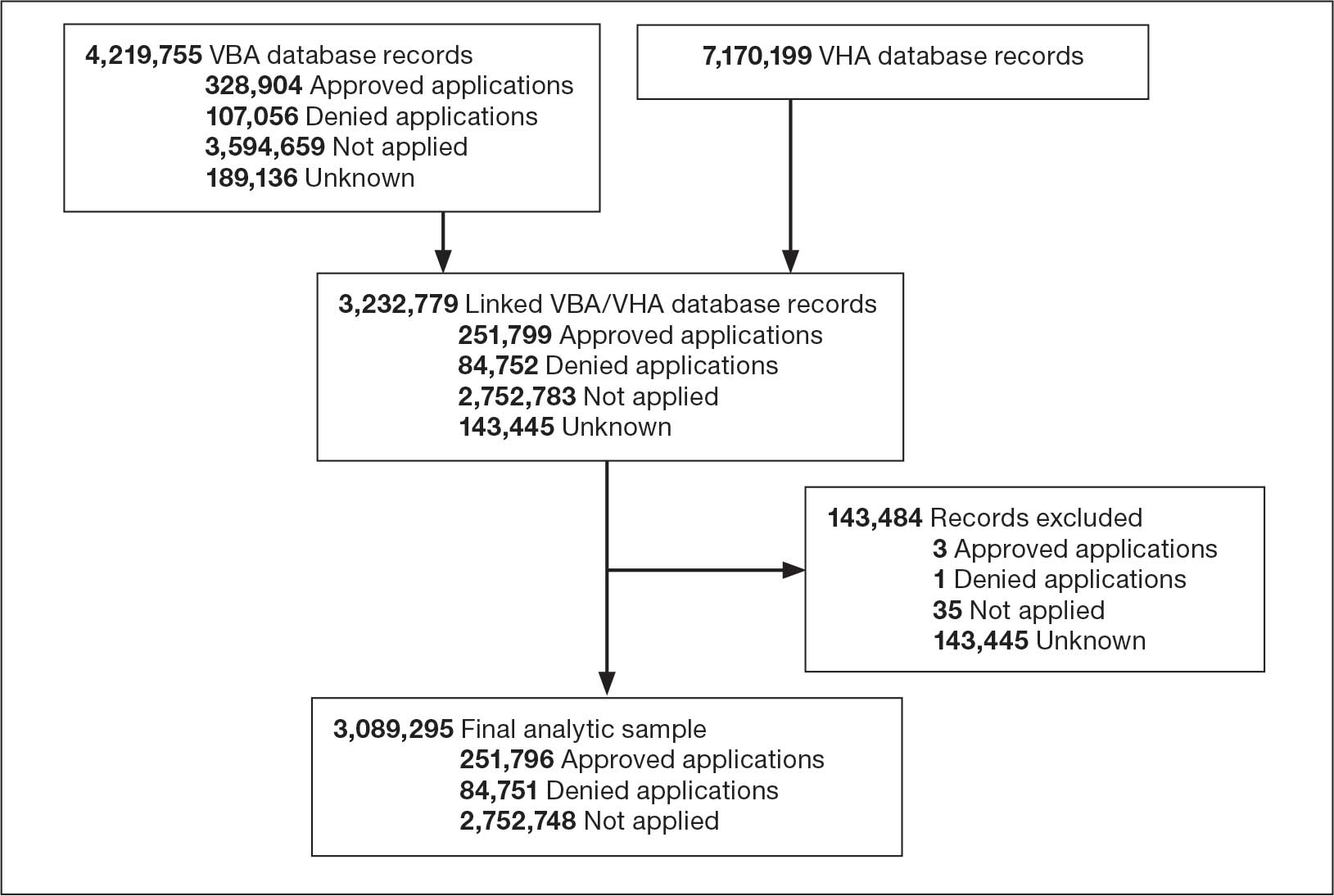
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
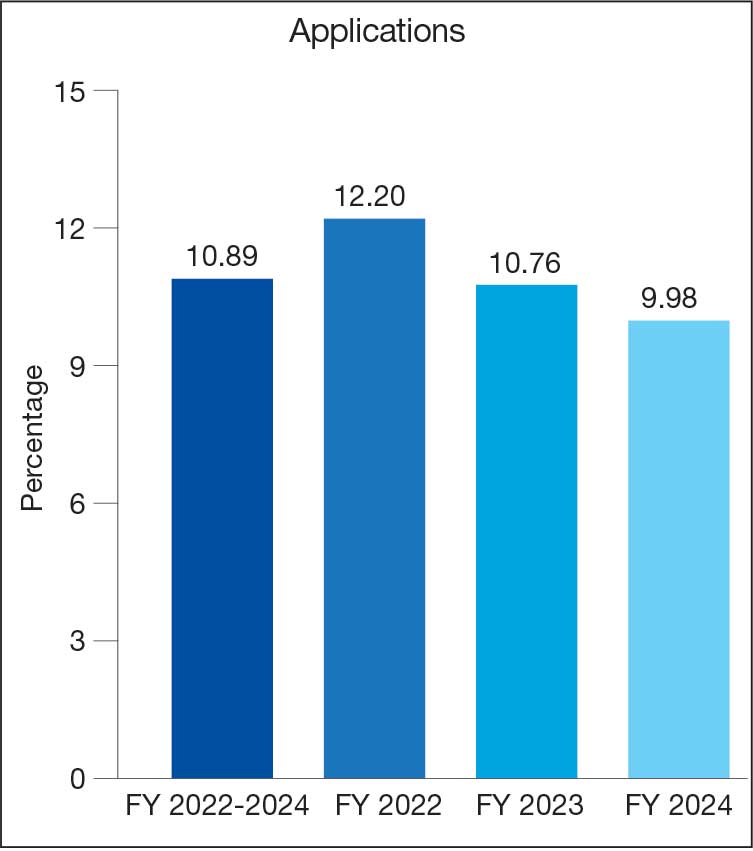
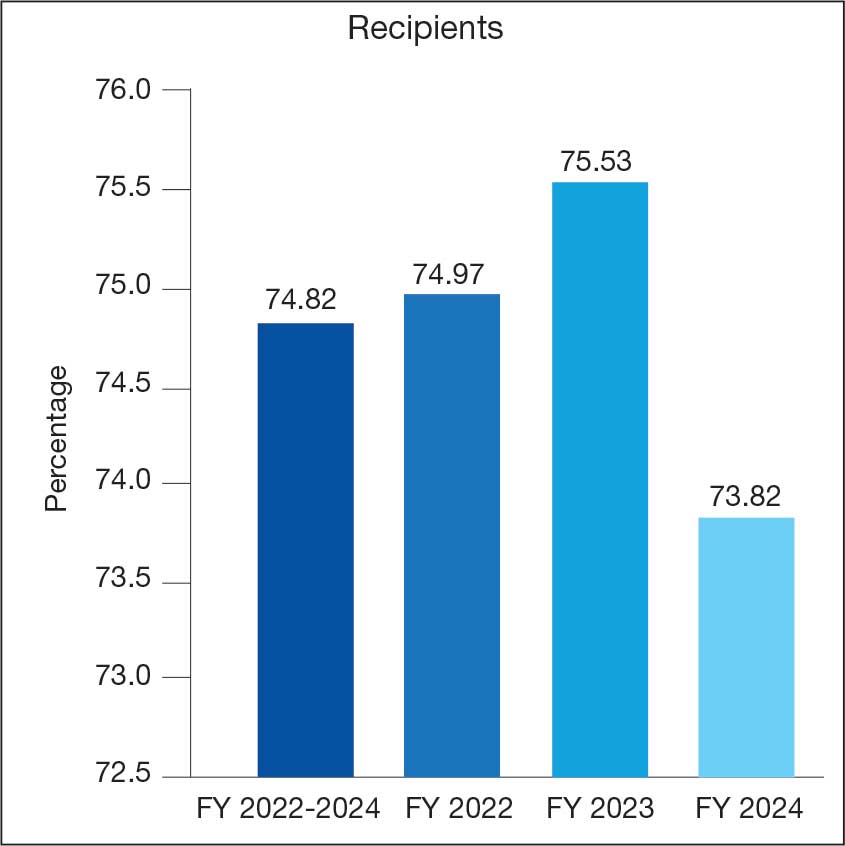
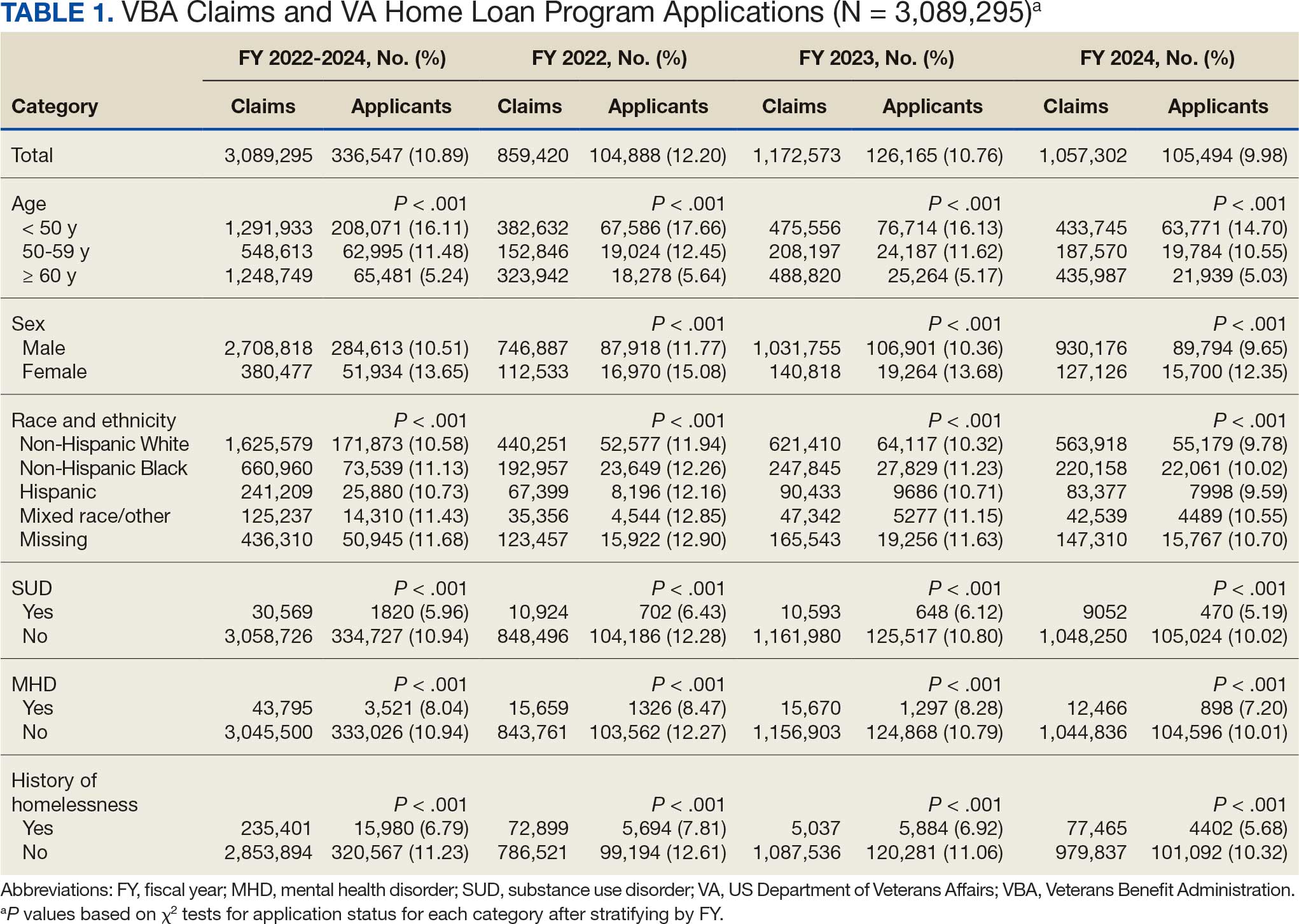
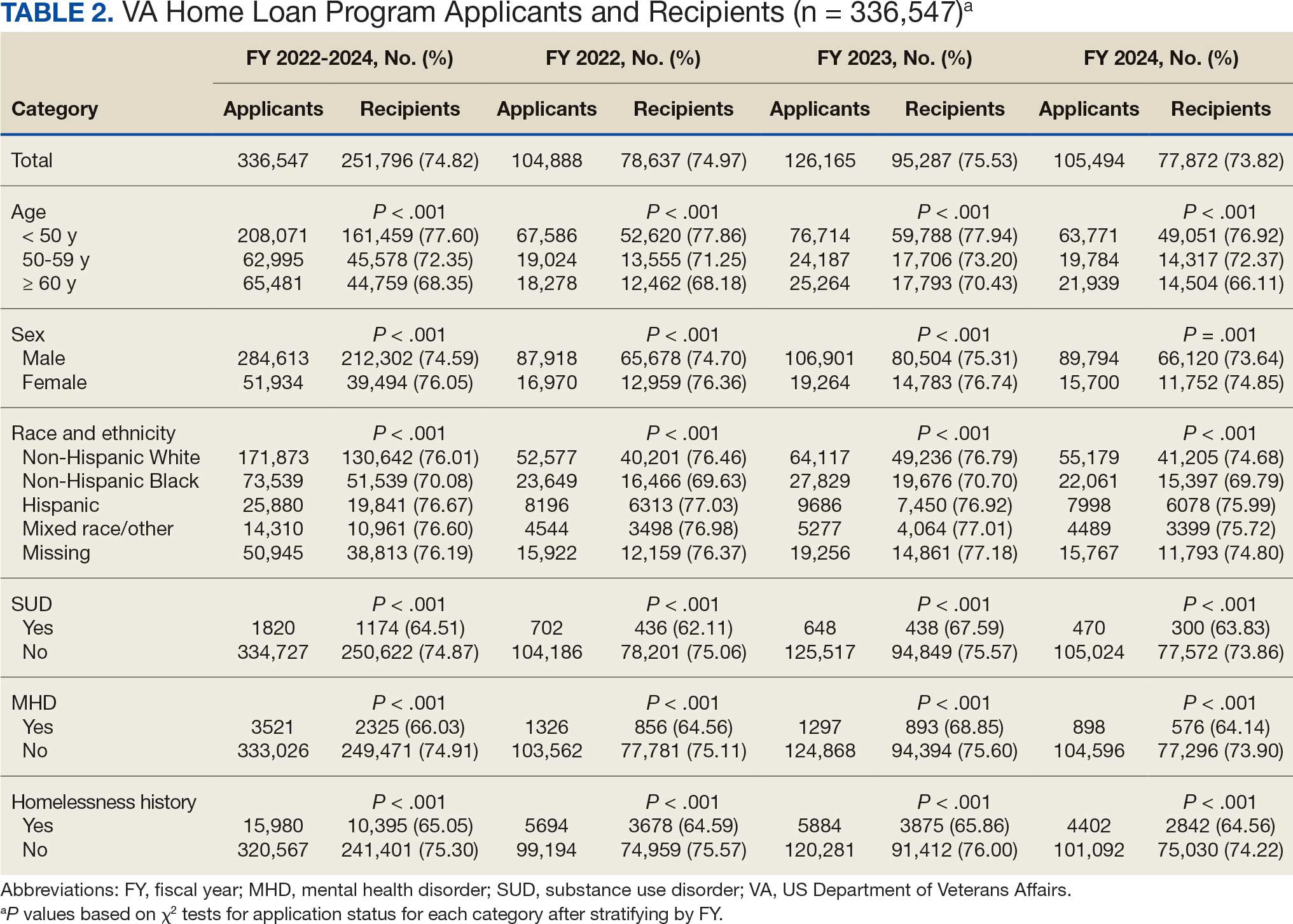
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
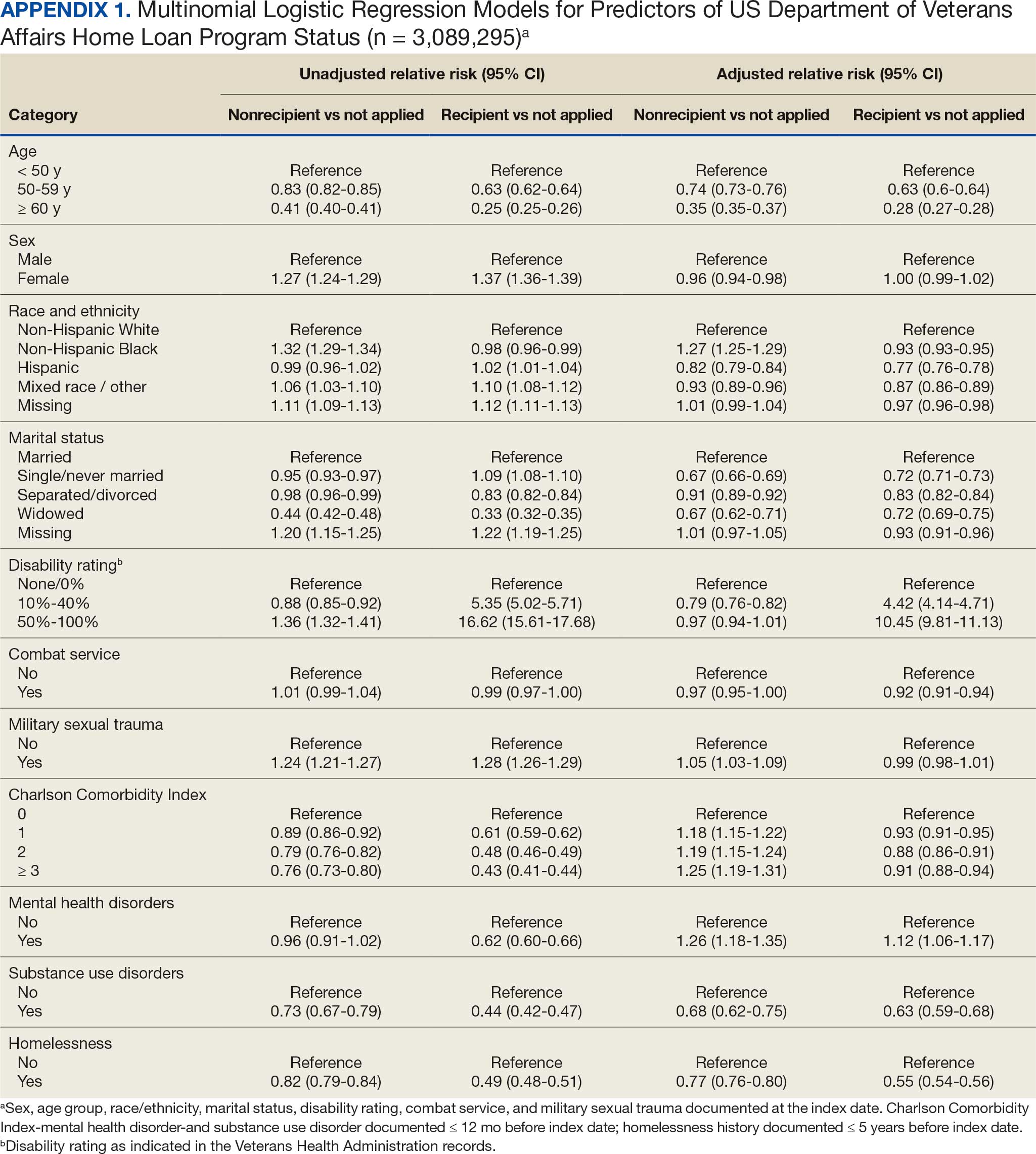
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
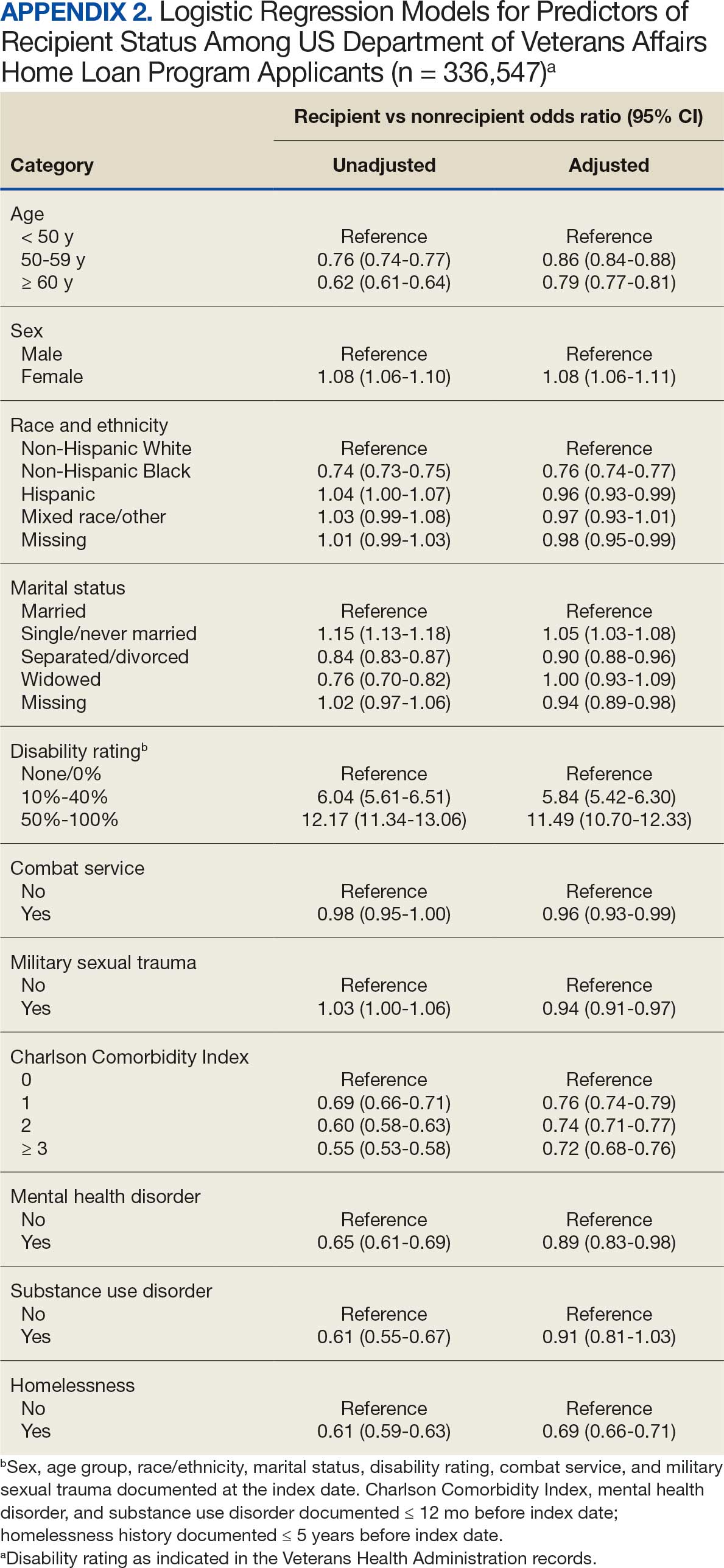
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
The US Department of Veterans Affairs (VA) Home Loan Program, administered by the Veterans Benefits Administration (VBA), is a unique benefit for veterans, active-duty service members, National Guard and Reserve members, and eligible surviving spouses. Established in 1944, the program aims to help these individuals achieve homeownership by leveraging a third-party guarantee, typically from a government agency, to enhance access to credit and improve loan terms for borrowers who may not meet conventional loan qualifications.1 Since its inception, the VA has guaranteed > 28.5 million loans, enabling millions of veterans to buy, build, repair, retain, or adapt homes for personal occupancy.2 The program is designed to support veterans and eligible individuals to become homeowners, recognizing homeownership as a pathway to financial stability and community integration. VA home loans are provided by private lenders (eg, banks, mortgage companies) with a portion guaranteed by the VA, which reduces the risk for lenders and enables them to offer competitive terms, such as no down payment and lower interest rates, making homeownership more accessible to veterans.2
Eligibility criteria for the VA Home Loan Program include military service criteria such as active-duty service members with ≥ 90 continuous days of service; veterans with an honorable discharge meeting minimum service requirements; individuals who served in the National Guard/Reserve for ≥ 90 days of active service or 6 years of service with an honorable discharge; and surviving spouses of veterans who died in service or from a service-connected disability, were designated as missing in action/ prisoner of war, and the spouse is receiving Dependency and Indemnity Compensation. Financial criteria also apply: borrowers must meet lender requirements for credit and income (although VA loans are more flexible than conventional loans) and the home must be for personal occupancy rather than an investment property.3
A June 2025 PubMed literature search did not reveal any prior research on the VA Home Loan Program, although a limited number of studies tackled a wide range of issues related to federal and private home loans.4-12 To our knowledge, there is no prior published examination of the VA Home Loan Program. Understanding VA Home Loan Program usage among Veterans Health Administration (VHA) users can inform the future direction of the program. The VHA operates the largest integrated US health care system, serving > 9 million enrolled veterans annually at 1321 facilities, including 172 medical centers and 1138 outpatient clinics, providing primary and specialized health care, and related medical and social support services for enrolled veterans, including those who are experiencing housing instability or homelessness.13 Specialized VHA programs for homeless veterans include housing, employment, health care, justice, and re-entryrelated services in collaboration with federal and community partners.14 Housing instability has been defined as the state of being at risk of losing housing due to challenges such as difficulties paying rent, overcrowding, frequent relocation, and a substantial proportion of income spent on housing.15,16 Homelessness is a severe manifestation of housing instability that has been defined as the lack of stable, safe, and functioning housing.17,18
Health care and social services, including those that address housing instability and homelessness, are major priorities for the VHA and VBA.19 The VA Home Loan Program may represent an important resource to help veterans achieve long-term housing stability through home ownership. There has been wide public concern about housing affordability and the ability of many Americans, including veterans, to achieve home ownership.20 Homeownership is considered an important part of developing financial assets and achieving financial stability. Lowincome veterans, in particular, may benefit from this program as a national study found that 8.0% of low-income veterans and 13.9% of veterans with a history of homelessness have previously experienced a home foreclosure. 21 A greater understanding of who applies for and receives assistance from the VA Home Loan Program would inform homelessness prevention services and future planning for this program.
We conducted a quality improvement (QI) project on behalf of the VHA Homeless Programs Office and in partnership with the VBA. Our goals were to: (1) describe the annual number of applicants and recipients of the VA Home Loan Program by age group, sex, race/ethnicity, presence of any diagnosed substance use and/or mental health disorder, and history of homelessness; and (2) compare demographic, clinical, and homelessness characteristics among individuals who apply and are granted a loan through this program, individuals who apply and are denied a loan through this program, and individuals who do not apply for a loan through this program.
Methods
This project involved linked VA administrative national databases and was undertaken by the VHA Homeless Programs Office in partnership with the VBA. Specifically, VHA and VBA databases were linked together using veteran identifiers and all data were managed and analyzed on secure VA servers. The project followed VA’s Program Guide 1200.21 for nonresearch activities and institutional review board approval was waived through sponsorship by the VA Homeless Programs Office. The VHA Corporate Data Warehouse (CDW) was accessed to obtain data from the Homeless Operations Management and Evaluation System (HOMES) and other clinical data systems used by VHA clinicians and administrators that capture diagnoses, workload, and other health care data.22,23 HOMES collects intake, progress, and outcome data on homeless veterans within its care system that enables the VA to assess the effectiveness of programs and strategically allocate resources to prevent homelessness.24,25
A list of veterans who filed disability compensation and pension claims was obtained from the VBA Office of Performance Analysis and Integrity, including Social Security number, name, city and state, date of claim submission, grant or increase in benefits, homeless status, VA home loan approval, and homeless aid for dependent children from fiscal year (FY) 2022 through FY 2024. VBA data were linked to VHA CDW electronic health record data from veterans who sought VA health care services and HOMES data on veteran participation in homeless programs who were also experiencing homelessness. VHA data included demographic characteristics (eg, sex, age, race, marital status, combat service) at an index date (earliest visit to the VHA between October 1, 2021, and September 30, 2024); military sexual trauma; clinical characteristics within 12 months prior to the index date (VHA disability rating, substance use disorder [SUD] diagnosis, mental health disorder diagnosis, Charlson Comorbidity Index [CCI] score), and homelessness experience ≤ 5 years prior to the index date.
History of homelessness ≤ 5 years prior to the index date was determined using an operational definition of homelessness based on multiple indicators, including International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code Z59.0; clinic stop codes or HOMES records indicating VA homeless programs clinical encounters; or a positive screen on an annual homelessness screener.16 US Department of Housing and Urban Development-VA Supportive Housing enrollees were excluded because they are considered to no longer be experiencing homelessness, and Veterans Justice Program enrollees were excluded because the program primarily focuses on serving criminal justice-involved veterans. The CCI predicts the risk of death ≤ 1 year by assessing the number and severity of a patient’s coexisting health conditions and is a valuable tool for understanding a patient’s overall health burden, aiding in clinical decision-making and evaluation research studies.26-29 Diagnoses based on ICD-10-CM codes were used to determine SUDs, mental health disorders, and CCI score, using methods that have been described in other publications.30
Population
The VBA cohort of veterans requesting benefits was further restricted to those who met the following eligibility criteria: (1) requested VA benefits FYs 2022 to 2024; (2) sought VHA services ≥ 1 time between FY 2022 and 2024; (3) had matching VBA/VHA records; (4) had no missing data on claim status and/ or demographic, clinical, and homelessness characteristics; and (5) had known home loan status FYs 2022 to 2024. The original VBA dataset consisted of 4,219,755 records and the original VHA dataset consisted of 7,170,199 records (Figure 1). The final linked VBA/VHA dataset after excluding 29 records with missing data on sex, 7 with missing data on age, 6 with missing data on marital status, and an additional 143,444 with unknown VBA claim status, consisted of 3,089,295 records corresponding to 2,260,851 unique veterans. Specifically, 251,796 records corresponded to veterans who had applied and received a loan, 84,751 to veterans who had applied and were nonrecipients of a loan, and 2,752,748 to veterans who did not apply for a loan.
Abbreviations: FY, fiscal year; VBA, Veterans Benefits Administration; VHA, Veterans Health Administration.
Statistical Analysis
All statistical analyses were performed using SAS Enterprise Guide, an application that provides a point-and-click interface for data access, analysis, and management, accommodating both code-based and visual programming. 31 First, we relied on the final analytic sample to calculate the annual proportions of veterans who applied for and/or received a loan through the VA Home Loan Program. We also generated descriptive statistics stratified by age group, sex, race/ethnicity, SUD, mental health disorder, and homelessness, overall and within each FY. Pearson χ2 and Cochran-Armitage trend tests were applied to examine differences in application and receipt of a home loan by baseline characteristics and FY, respectively. Second, we conducted bivariate and multivariable analyses to compare demographic, clinical, and homelessness characteristics between 3 groups of veterans as they pertain to the VA Home Loan Program. Veterans who applied and were nonrecipients of a loan (group 1), veterans who applied and were recipients of a loan (group 2), and veterans who did not apply for a loan (group 3). Similar analyses compared VA Home Loan Program applicants who were recipients of a home loan vs VA Home Loan Program applicants who were nonrecipients of a home loan. Multinomial and binary logistic regression models were constructed to estimate the relative risk ratio (RR) and odds ratio (OR) with 95% CIs for comparisons between these distinct groups on demographic, clinical, and homelessness characteristics. Two-sided statistical tests were evaluated at α = 0.05.
Results
Tables 1 and 2 present the number of VBA applicants, including those who applied for and received benefits through the VA Home Loan Program, by age group, sex, race/ethnicity, as well as histories of SUDs, mental health disorders, and homelessness, overall, and by FY. As shown in Figure 2, 336,547 of 3,089,295 VBA applications (10.9%) pertained to the VA Home Loan Program, with a statistically significant decline in application rates, from 12.2% in FY 2022 to 9.9% in FY 2024 (P < .001 for trend). Among 336,547 veterans who applied for the VA Home Loan Program, 251,796 (74.8%) received a home loan during FYs 2022 to 2024, ranging between 73.8% for FY 2024 and 75.5% for FY 2023 (P < .001 for trend).
Veterans Affairs Home Loan Program, fiscal years (FY) 2022-2024.
Multinomial logistic regression models for demographic, clinical, and homelessness characteristics as predictors of VA Home Loan Program status are provided in Appendix 1. Based on the fully adjusted model, compared with veterans who did not apply to the VA Home Loan Program, those who applied for a home loan were less likely to be aged ≥ 50 years, unmarried, Hispanic ethnicity, mixed race, or other race, diagnosed with a SUD, or history of homelessness. Veterans with higher VA service-connected disability ratings were more frequently recipients of VA home loans, whereas those who self-identified as non-Hispanic Black and those with higher CCI scores were less frequently recipients of VA home loans. Finally, those with mental health disorders were more likely than their counterparts to be applicants (recipients or nonrecipients) of VA home loans.
Binary logistic regression models for demographic, clinical, and homelessness characteristics as predictors of receipt status among applicants to the VA Home Loan Program are provided in Appendix 2. Among applicants, those who were granted a VA home loan were less likely to be aged ≥ 50 years; have a CCI score > 0; have experienced combat service and/or military sexual trauma; be diagnosed with a SUD and/or mental health disorder; or to have a history of homelessness compared with those denied a VA home loan. Applicants granted a VA home loan were also more likely to be female, non-Hispanic White, single or never married, and/or have a VA service-connected disability ratings > 0%.
Discussion
The VA Home Loan Program is a unique benefit and resource for eligible veterans that may be increasingly important in a time of growing concern about the affordability of housing for many Americans. Research on other federally-supported home loan programs as well as private home mortgage programs has been mostly conducted in the economic realm, and studies focused on understanding these programs from a health care system perspective have been sparse.32,33 However, there is a large body of literature documenting the importance of stable, safe, and secure housing on health and well-being.34-37 This study did not focus on evaluating the effects of the VA Home Loan Program, because we wanted to first examine the characteristics of veterans who benefited from the program and how they differed from veterans who did not apply or did apply but had a denied application.
Our findings suggest that several thousands of veterans benefit from the VA Home Loan Program each year. For historical context, the time period examined was one of economic downturn with rising costs of living, including housing, and steady increases in homelessness as reported in the annual point-in-time count of sheltered and unsheltered people experiencing homelessness on a single night as mandated by the US Department of Housing and Urban Development.38-40 The Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded health care and benefits for veterans exposed to burn pits, Agent Orange, and other toxic substances, resulting in more VA disability benefit claims, including large retroactive payments.41-43 Anecdotally, the VBA has noted that the PACT Act helped some homeless veterans with funds and stability to exit homelessness and enroll in the VA Home Loan Program.
Our analysis suggests that beneficiaries of the VA Home Loan Program were frequently aged < 50 years, female, of non-Hispanic White race, and did not have histories of psychiatric disorders or homelessness. Most of these demographic and clinical characteristics were not surprising given the composition of the veteran population, although in-depth analyses are needed to examine sex differences that may have led to more females than males benefiting from the VA Home Loan Program. In addition, it was notable that many younger and non-Hispanic Black veterans had applied. While relatively few veterans with SUDs benefited from the VA Home Loan Program, few had applied. Research is warranted into why veterans with SUDs are less likely to apply for home loans. Quite surprisingly, a sizable proportion of veterans with histories of homelessness reported they had applied to the VA Home Loan Program, although they were less likely than veterans who had not experienced homelessness to be granted a loan.
The examination of differences between veterans who did not apply, were granted, and denied a loan through the VA Home Loan Program revealed several key predictors of application outcomes in multivariable models. Specifically, veterans who applied for home loans were less likely to be aged ≥ 50 years, unmarried, of Hispanic, mixed, or other race/ethnicity, diagnosed with an SUD, or have a history of homelessness. Veterans with higher disability ratings were less frequently denied and more frequently approved, while non-Hispanic Black veterans and those with higher CCI scores were more frequently denied and less frequently approved. VBA applicants with mental health disorders were also more likely to apply for a home loan. Conversely, those granted a home loan were more likely than those denied a home loan to be female, non-Hispanic White, single/unmarried, or to have > 0% VA service-connected disability rating, but less likely to be aged ≥ 50 years, have CCI score > 0, be diagnosed with psychiatric disorders, or have a history of homelessness.
Limitations
This analysis was restricted to a subset of FY 2022 to FY 2024 linked VBA/VHA databases (ie, to veterans who had both VBA and VHA records and met prespecified eligibility criteria). Despite the large number of linked records, a small percentage of these records corresponded to veterans who were applicants or recipients of the VA Home Loan Program. Future studies should expand the time frame to examine variations in application outcomes over time and by background characteristics of veterans enrolled in VHA care who applied for VBA benefits. In addition, we relied on data and ICD-10-CM diagnostic codes from existing electronic health records and claims data to define histories of homelessness, comorbidities, SUDs, and mental health disorders. Given the time-varying nature of these conditions, the temporal sequence of events was difficult to ascertain. Third, it is worth noting that these findings can only be generalized to veterans who applied for VBA benefits and met eligibility criteria, and that these veterans may differ in terms of their demographic and clinical characteristics from those who did not apply for these benefits.
Conclusions
This study analyzed data from 251,796 individuals who applied for and received a VA home loan, 84,751 who were denied a VA home loan, and 2,752,748 veterans who did not apply for a VA home loan from FY 2022 to FY 2024. Accordingly, 11% of applications pertained to the VA Home Loan Program, and 75% of VA Home Loan Program applicants received a home loan. Distinct demographic and clinical characteristics were observed for applicants and recipients of the VA Home Loan Program, which can set the stage for future planning and evaluation of the program. Despite the broad accessibility of veterans to the VA Home Loan Program, there were differences in approval rates among applicants based on sociodemographic and clinical characteristics. Further evaluation, perhaps using qualitative methods, is needed to better understand opportunities and challenges to achieving a VA home loan, especially among underserved veteran populations. Investigation and research can guide future recommendations for any development or corrective actions that can help increase access to veterans who can benefit from the program. Future analyses are also needed to compare veterans enrolled and not enrolled in the VA Home Loan Program on health care-related outcomes.
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
- US Department of Veterans Affairs. Home loans. Accessed April 1, 2026. https://www.benefits.va.gov/homeloans/
- Veterans United Home Loans. VA loans: the complete guide. Accessed April 1, 2026. https://www.veteransunited.com/va-loans/
- US Department of Veterans Affairs. VA-backed veterans home loans. Accessed April 1, 2026. https://www.va.gov/housing-assistance/home-loans/
- Choplin JM, Stark DP. Whispering sweet nothings: a review of verbal behaviors that undermine the effectiveness of government-mandated home-loan disclosures. Cogn Res Princ Implic. 2019;4:6. doi:10.1186/s41235-019-0154-7
- Evans M. Borrowing boon. More explore federal home loan banks backing. Mod Healthc. 2009;39:14.
- Hogarth M. A home loan: how—and how much? Nurs Times. 1973;69:908-909.
- Jacoby SF. Home Owners’ Loan Corporation maps and place-based injury risks: a complex history. Am J Public Health. 2023;113:356-358. doi:10.2105/AJPH.2023.307242
- Merrell C. Finance. Home: a loan. Nurs Times. 1996;92:61-64.
- Namin S, Xu W, Zhou Y, et al. The legacy of the Home Owners’ Loan Corporation and the political ecology of urban trees and air pollution in the United States. Soc Sci Med. 2020;246:112758. doi:10.1016/j.socscimed.2019.112758
- Namin S, Zhou Y, Xu W, et al. Persistence of mortgage lending bias in the United States: 80 years after the Home Owners’ Loan Corporation security maps. J Race Ethn City. 2022;3:70-94. doi:10.1080/26884674.2021.2019568
- Slottow R. The home loan program. J Natl Assoc Hosp Dev. 1990:43-45.
- Wang M, Chen H, Wang L. Locus of control and home mortgage loan behaviour. Int J Psychol. 2008;43:125-129. doi:10.1080/00207590801888760
- US Dept of Veterans Affairs. Veterans Health Administration. About VHA. Updated January 20, 2025. Accessed April 1, 2026. https://www.va.gov/health/aboutvha.asp
- US Dept of Veterans Affairs. VA homeless programs. Updated May 7, 2026. Accessed May 8, 2026. https://department.va.gov/homeless/
- DiTosto JD, Holder K, Soyemi E, et al. Housing instability and adverse perinatal outcomes: a systematic review. Am J Obstet Gynecol MFM. 2021;3:100477. doi:10.1016/j.ajogmf.2021.100477
- Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration medical records. PLoS One. 2022;17:e0279973. doi:10.1371/journal.pone.0279973
- Fowler PJ, Hovmand PS, Marcal KE, et al. Solving homelessness from a complex systems perspective: insights for prevention responses. Annu Rev Public Health. 2019;40: 465-486. doi:10.1146/annurev-publhealth-040617-013553
- US Department of Health and Human Services. Healthy People 2030: housing instability. Accessed April 1, 2026. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
- US Department of Veterans Affairs. VA health care priorities. Accessed April 1, 2026. https://www.va.gov/health/priorities/index.asp
- Tsai J. Federal priorities to address homelessness as a community health problem. Fam Community Health. 2025;48:57-69.
- Tsai J, Hooshyar D. Prevalence of eviction, home foreclosure, and homelessness among low-income US veterans: the National Veteran Homeless and Other Poverty Experiences study. Public Health. 2022;213:181-188. doi:10.1016/j.puhe.2022.10.017
- US Department of Veterans Affairs. Corporate Data Warehouse (CDW). Accessed April 1, 2026. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Price LE, Shea K, Gephart S. The Veterans Affairs Corporate Data Warehouse: uses and implications for nursing research and practice. Nurs Adm Q. 2015;39:311-318. doi:10.1097/NAQ.0000000000000118
- US Department of Veterans Affairs. Homeless Operations Management and Evaluation System (HOMES) User Manual—Phase 1. April 19, 2011. Accessed April 1, 2026. https://www.adldata.org/wp-content/uploads/2016/07/homes.pdf
- Tsai J, Kasprow WJ, Rosenheck RA. Latent homeless risk profiles of a national sample of homeless veterans and their relation to program referral and admission patterns. Am J Public Health. 2013;103:S239-S247. doi:10.2105/AJPH.2013.301322
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted inhospital mortality. J Clin Epidemiol. 2004;57:1288-1294. doi:10.1016/j.jclinepi.2004.03.012
- Beydoun HA, Szymkowiak D, Beydoun MA, et al. Comparing major comorbidity indices as predictors of all-cause mortality in the Veterans Affairs health care system. J Clin Epidemiol. 2025;182:111778. doi:10.1016/j.jclinepi.2025.111778
- Charlson ME, Carrozzino D, Guidi J, et al. Charlson Comorbidity Index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91:8-35. doi:10.1159/000521288
- Glasheen WP, Cordier T, Gumpina R, et al. Charlson Comorbidity Index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12:188-197.
- Beydoun HA, Szymkowiak D, Kinney R, et al. Is the risk of Alzheimer’s disease and related dementias among US veterans influenced by the intersectionality of housing status, HIV/AIDS, hepatitis C, and psychiatric disorders? J Gerontol A Biol Sci Med Sci. 2024;79:glae153. doi:10.1093/gerona/glae153
- SAS Institute. SAS Enterprise Guide. Accessed April 1, 2026. https://www.sas.com/en_us/software/enterprise-guide/features-list.html
- Agarwal S, Amromin G, Chomsisengphet S, et al. Mortgage refinancing, consumer spending, and competition: evidence from the Home Affordable Refinance Program. Rev Econ Stud. 2023;90:499-537.
- Ashcraft A, Bech ML, Frame WS. The Federal Home Loan Bank System: the lender of next-to-last resort? J Money Credit Bank. 2010;42:551-583.
- Gibson M, Petticrew M, Bambra C, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17:175-184. doi:10.1016/j.healthplace.2010.09.011
- Shaw M. Housing and public health. Annu Rev Public Health. 2004; 25:397-418. doi:10.1146/annurev.publhealth.25.101802.123036
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ. 2001;323:187-190. doi:10.1136/bmj.323.7306.187
- Tsai J. Theorizing pathways between eviction filings and increased mortality risk. JAMA. 2024;331:570-571. doi:10.1001/jama.2023.27978
- Bernanke B, Blanchard O. What caused the US pandemicera inflation? Am Econ J Macroecon. 2025;17:1-35.
- Hall SG, Tavlas GS, Wang Y. Drivers and spillover effects of inflation: the United States, the euro area, and the United Kingdom. J Int Money Finance. 2023;131:1-13.
- US Department of Housing and Urban Development. Point-in-Time Count and Housing Inventory Count. Accessed April 1, 2026. https://www.hudexchange.info/programs/hdx/pit-hic/
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act: expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Zychowicz ME. The PACT Act: enhancing health care access for military personnel and veterans. N C Med J. 2023;84:379-380. doi:10.18043/001c.89208
- US Department of Veterans Affairs. The PACT Act and your VA benefits. April 2, 2026. https://www.va.gov/resources/the-pact-act-and-your-va-benefits/
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program
Characteristics of Applicants and Recipients of the Veterans Affairs Home Loan Program

Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
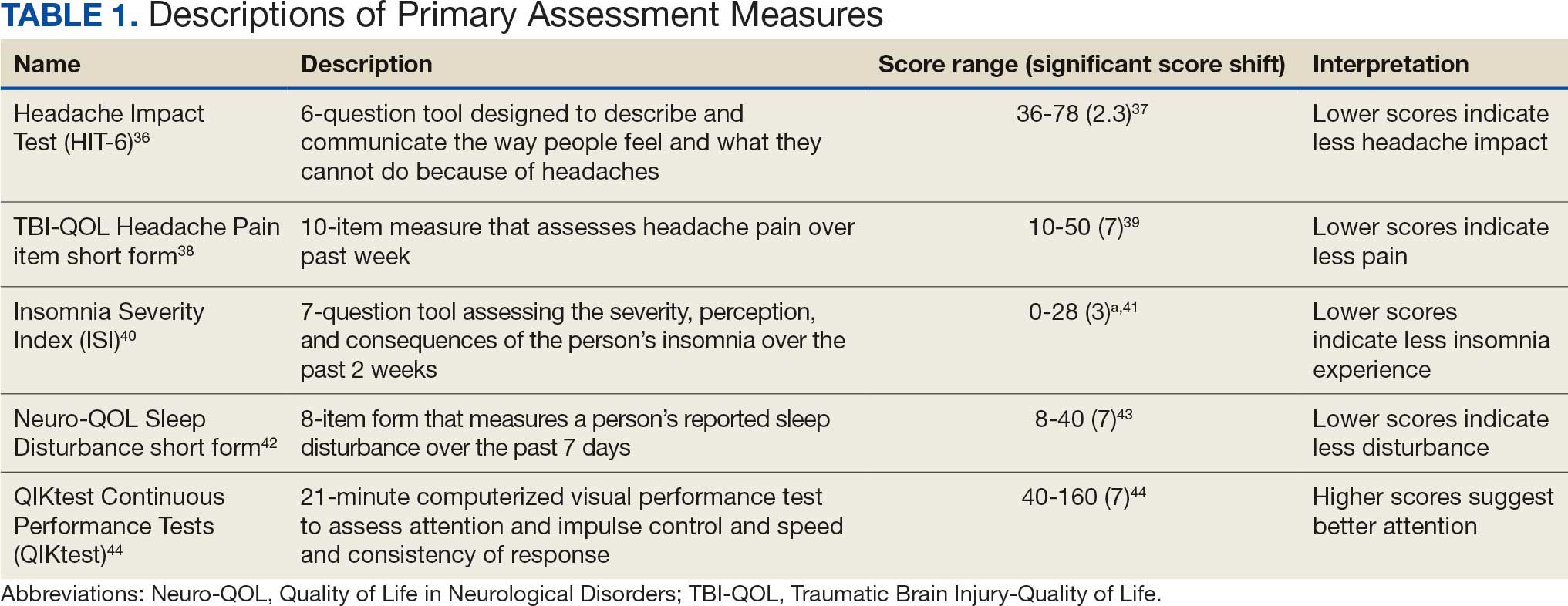
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
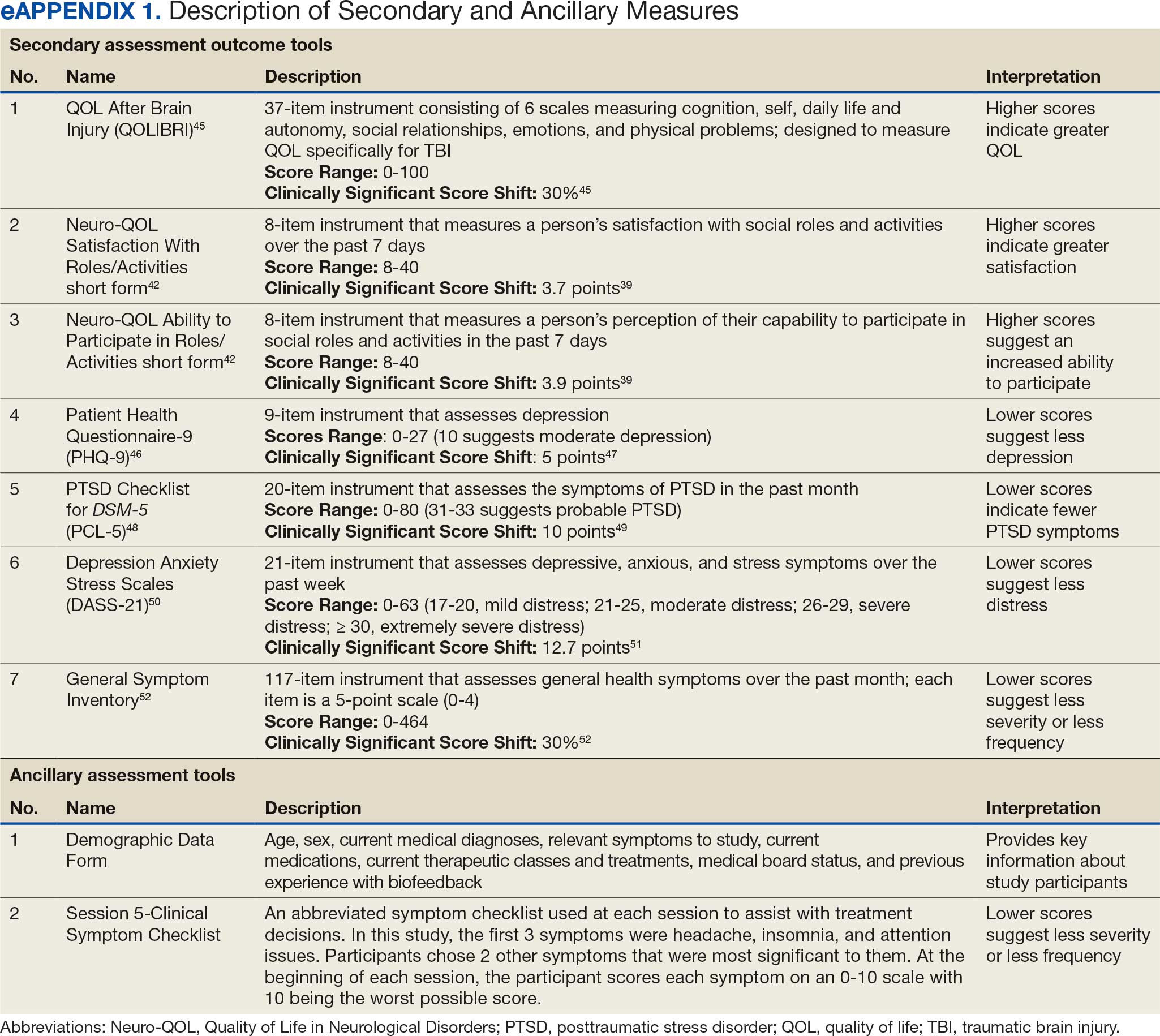
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
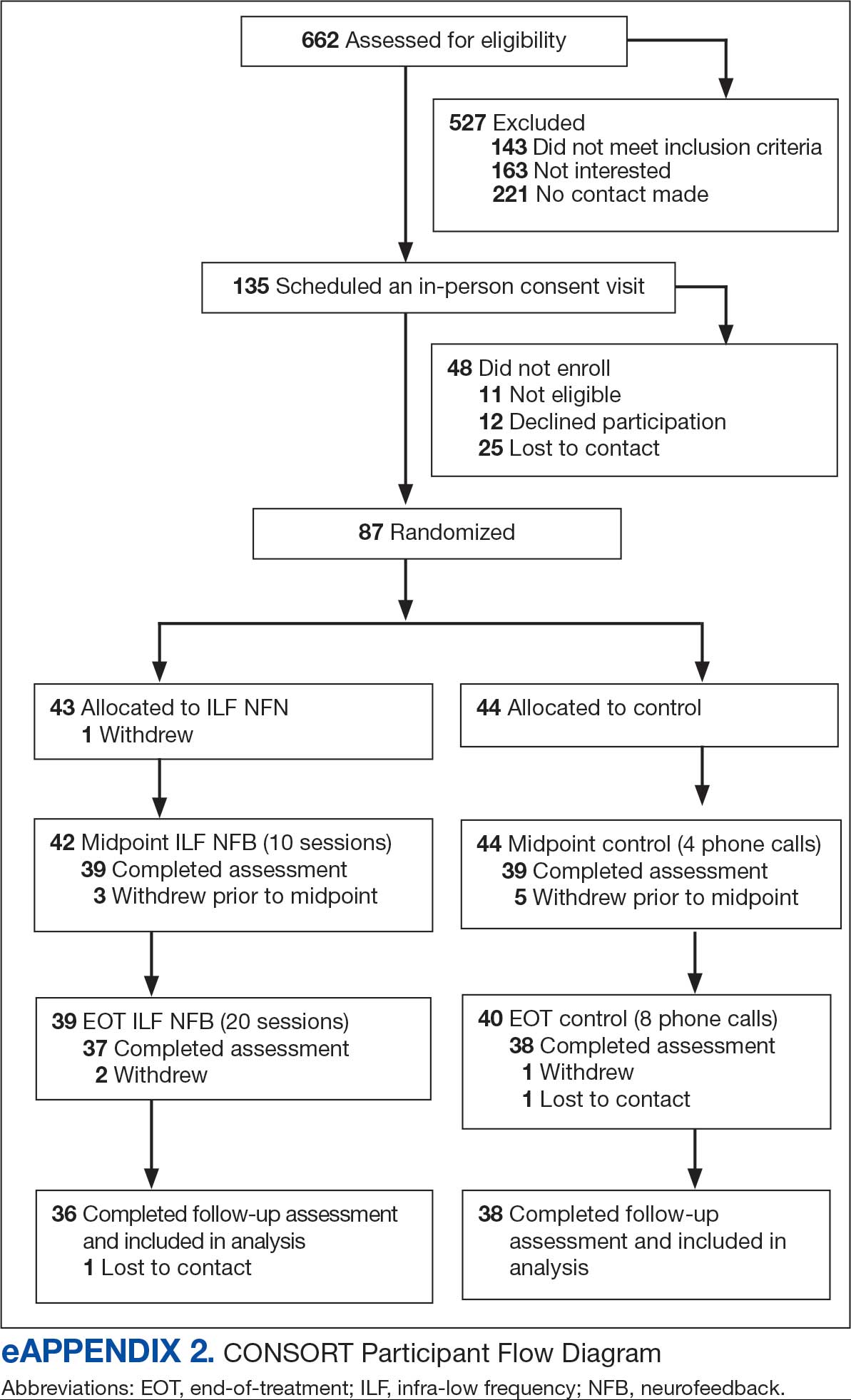
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
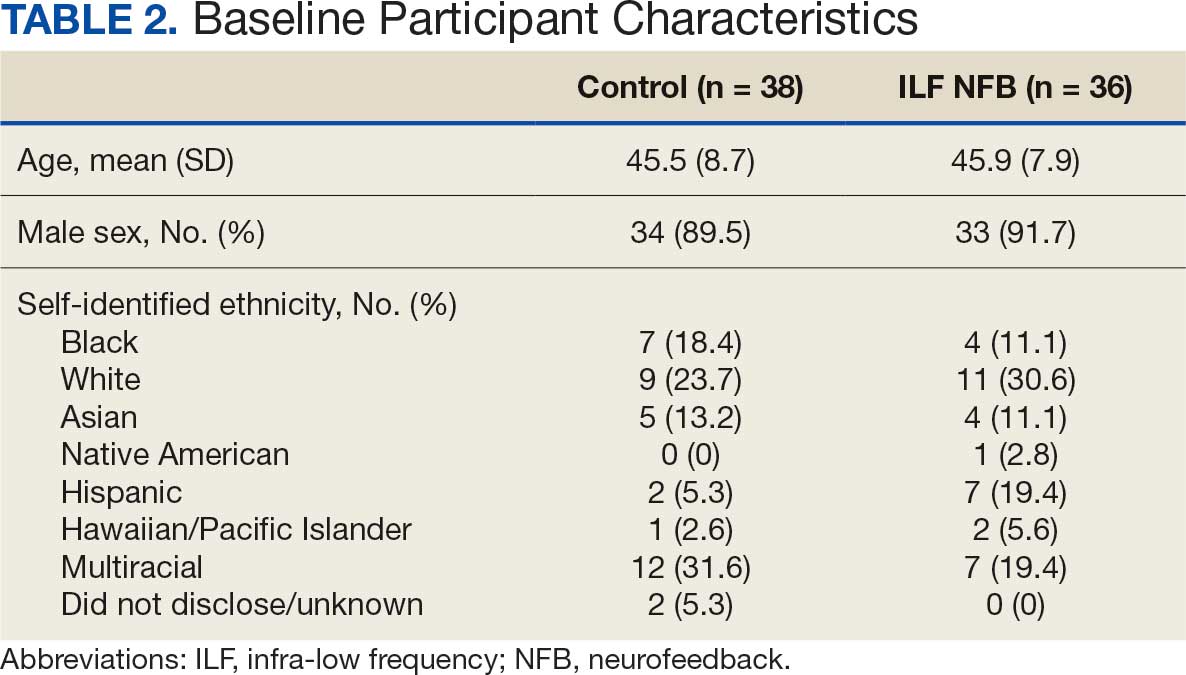
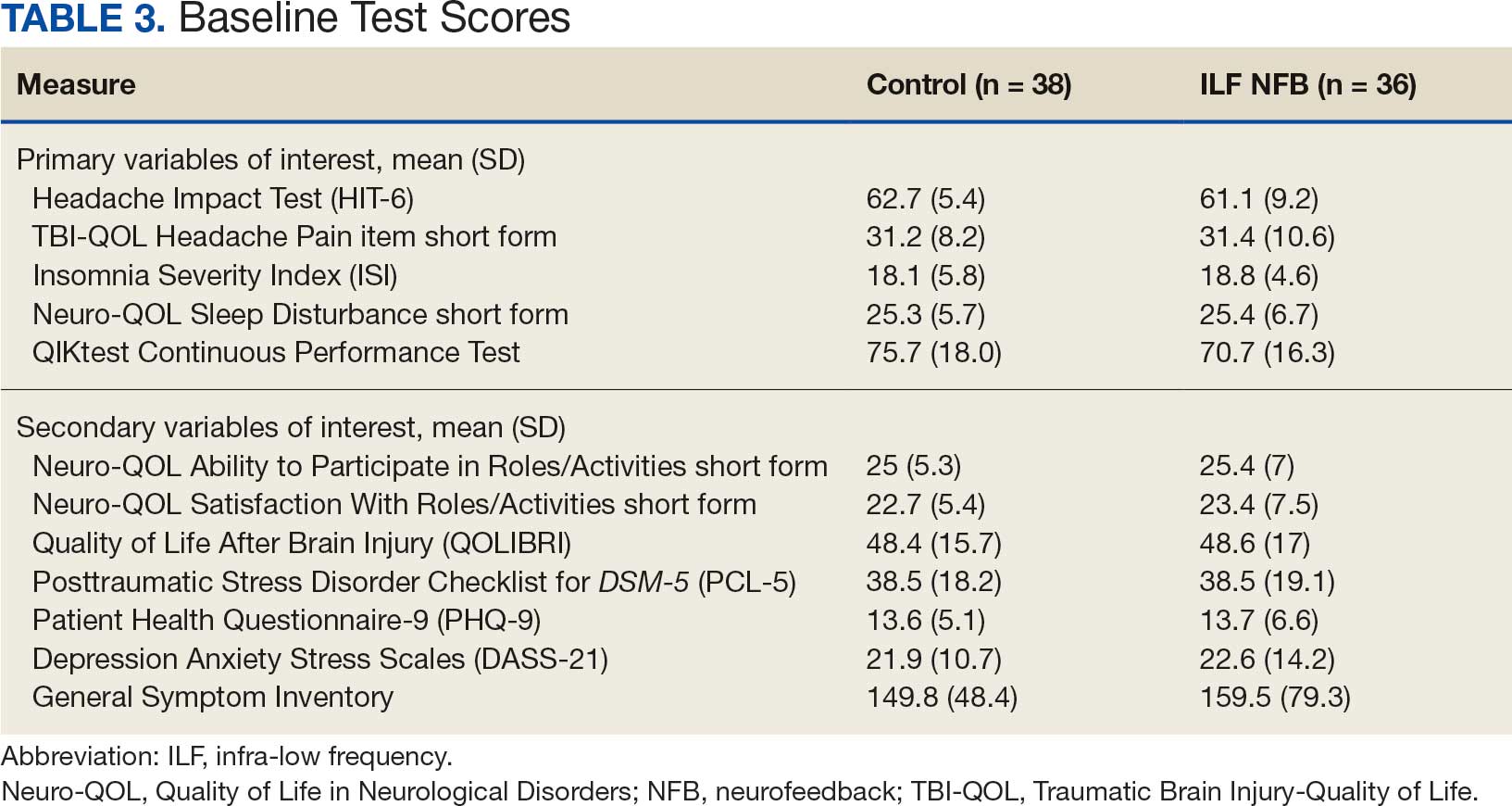
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
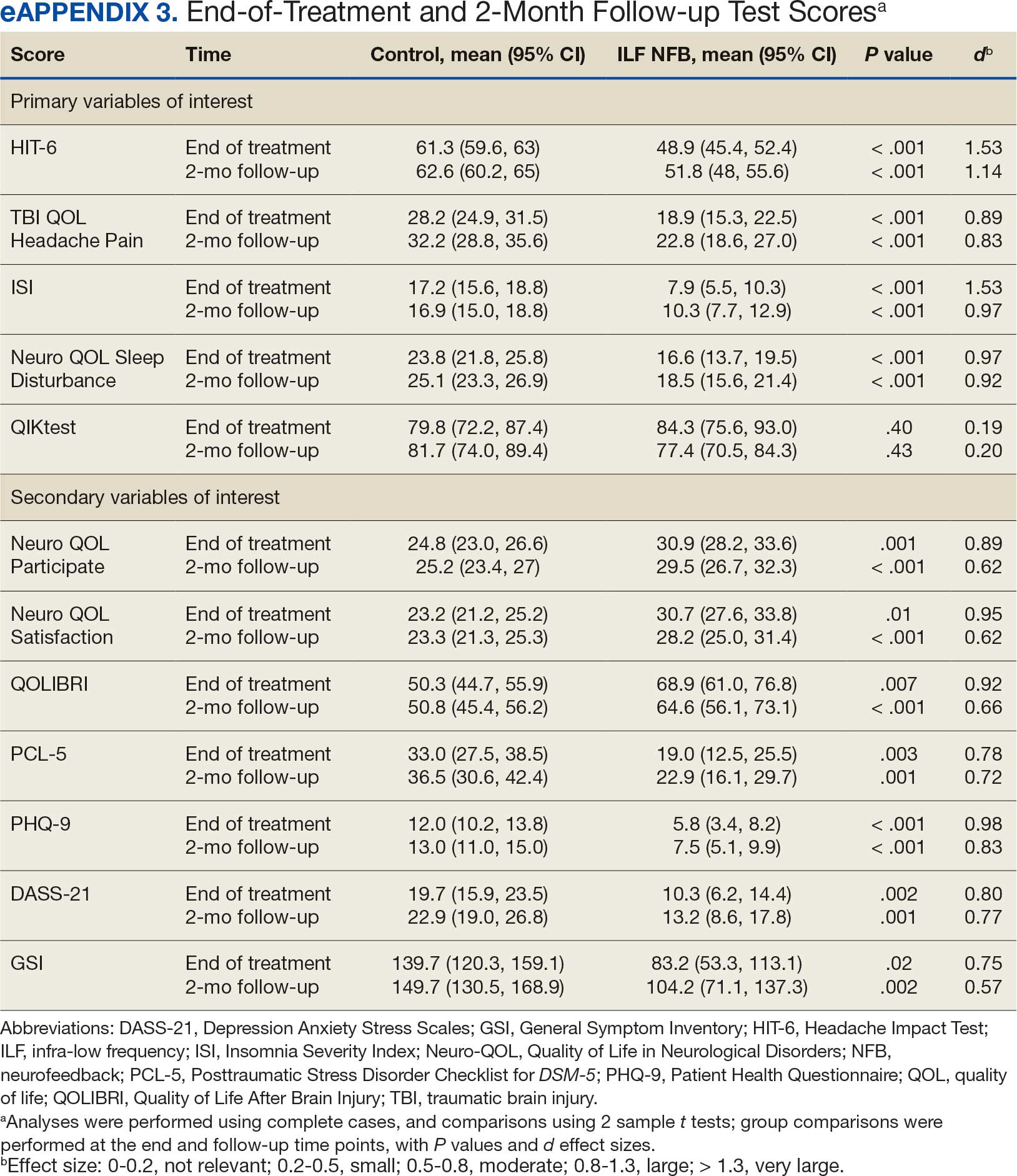
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
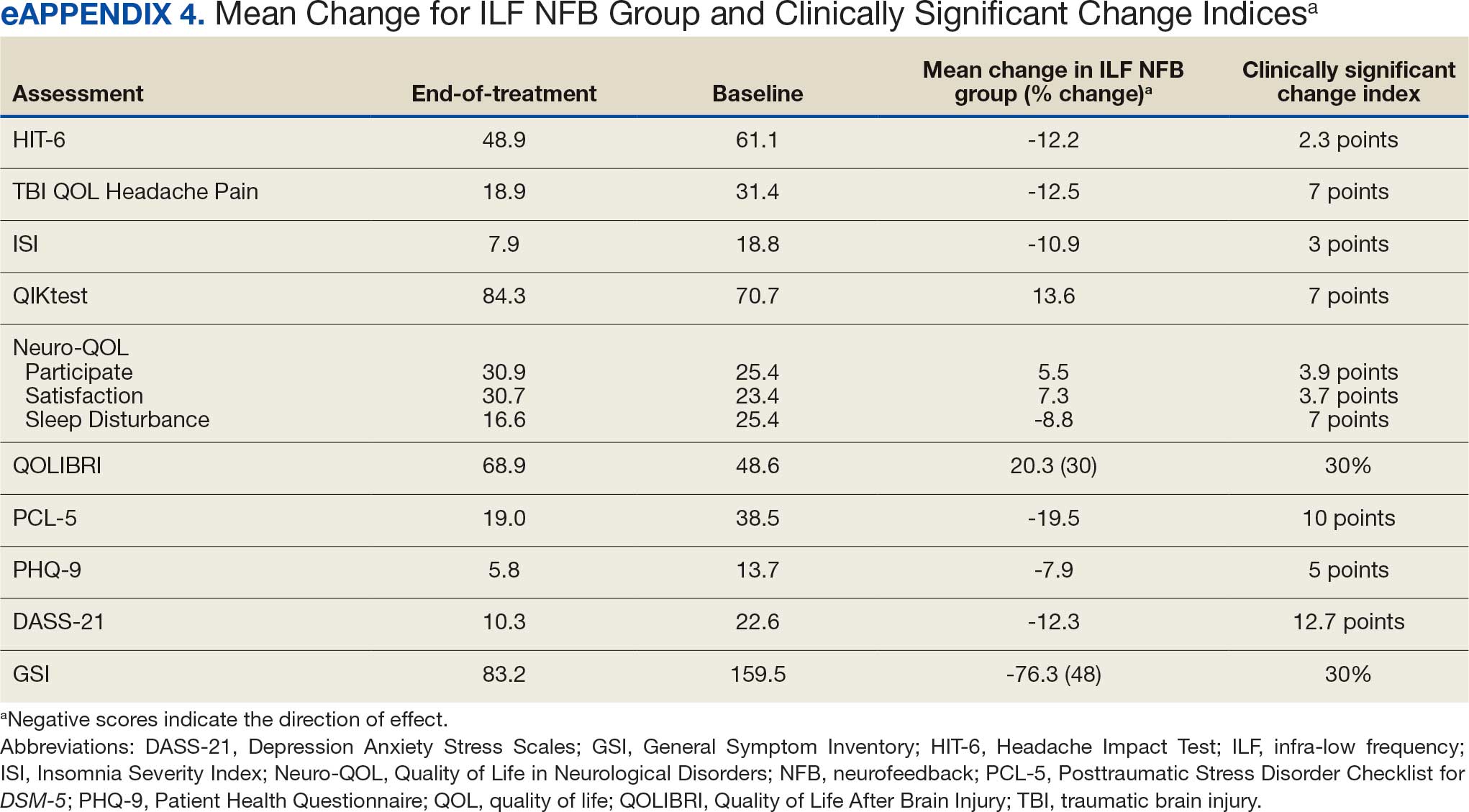
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms

Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
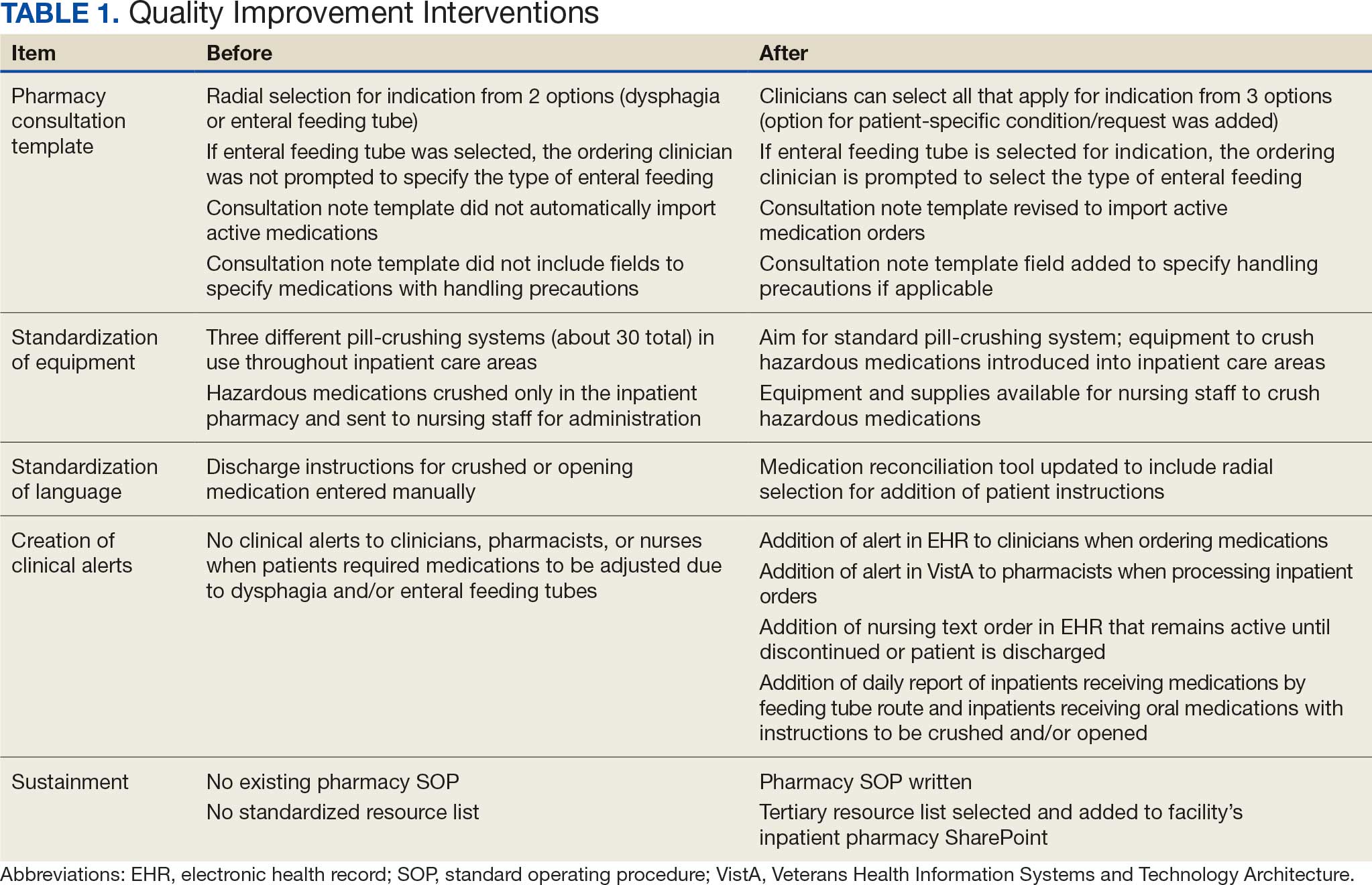
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
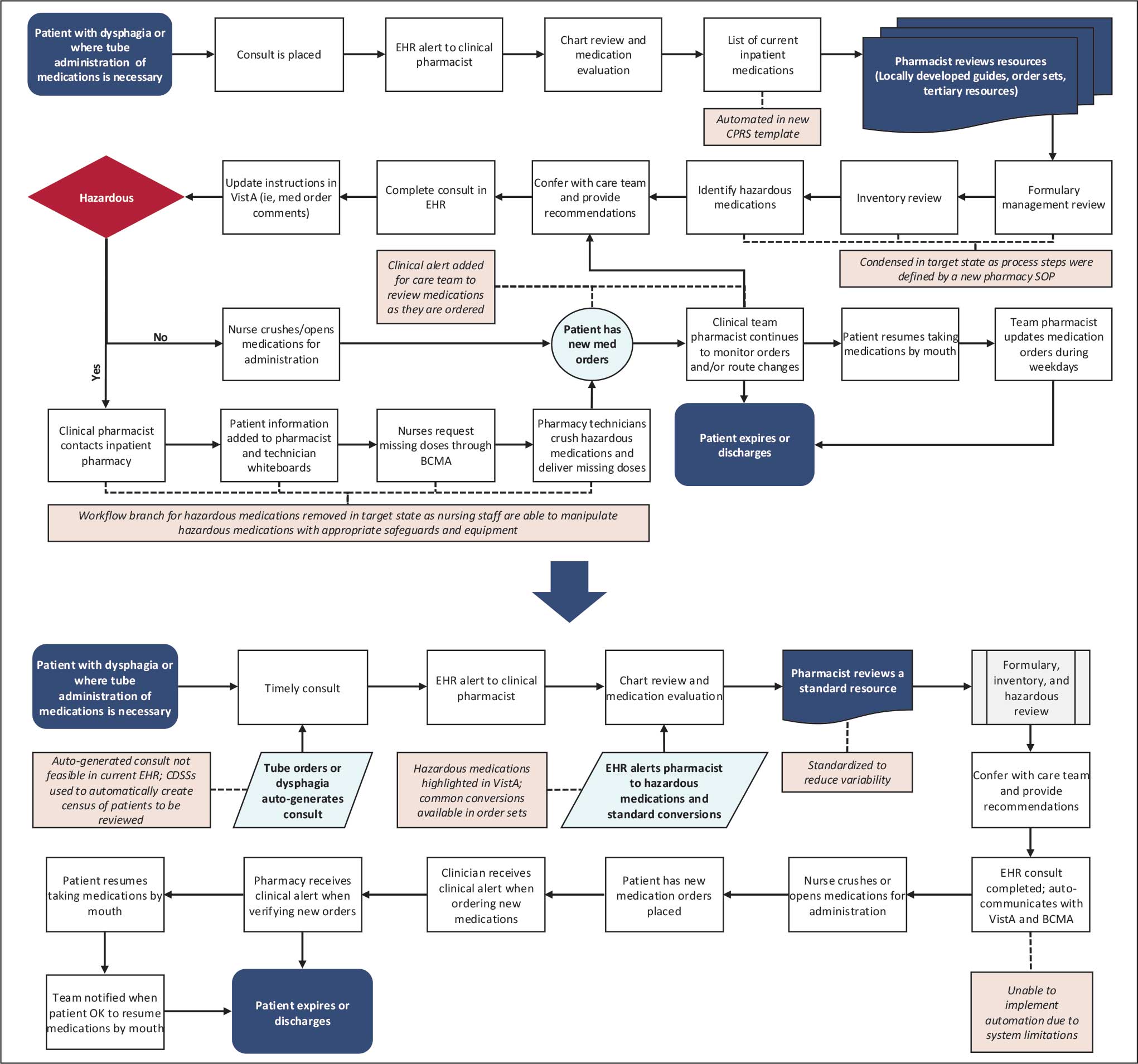
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).

Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes

Frontline Supervisor Perspectives on Enabling High Reliability and Fostering a Just Culture at the VHA
Frontline Supervisor Perspectives on Enabling High Reliability and Fostering a Just Culture at the VHA
The Veterans Health Administration (VHA) is now in the sixth year of its enterprise-wide transformation into a high reliability organization (HRO). This effort began with a 2016 pilot project and is now implemented in 170 VHA medical centers.1-4 This transformation reflects a commitment to implementing standardized and reliable health care practices.
The VHA HRO implementation strategy includes a multifaceted approach to engage leadership through education, training, leader coaching, and change management initiatives.2 Despite the diversity of facilities in terms of cultures, geographies, and complexities, US Department of Veterans Affairs (VA) medical centers (VAMCs) have increasingly embraced standardized HRO practices. These changes are evident in improvements in VHA All Employee Survey scores, which assess 4 key patient safety culture dimensions: risk identification and just culture, error transparency and mitigation, supervisor communication and trust, and team cohesion and engagement.5 Positive trends in these dimensions highlight a cultural shift toward greater reliability, even amid challenges introduced by the COVID-19 pandemic.
However, this progress has encountered some challenges. Leadership turnover, budgetary constraints, and extensive educational demands for implementing and sustaining HRO practices have created obstacles, particularly for frontline health care practitioners.6 Additionally, there are pockets of resistance similar to what the airline industry faced when implementing crew resource management (CRM). Specifically, senior pilots and legacy leaders were reluctant to abandon their high-status, autocratic management styles and embrace CRM, despite its proven benefits for enhancing commercial airline safety.7 Similarly, some VHA staff have expressed resistance to foundational HRO practices, which include safety huddles, safety forums, leader rounding, and visual management systems.6,8
The training requirements for HRO practices range from a 25-minute introductory course (HRO 101) to a 7.5-hour team training session facilitated by the VHA National Center for Patient Safety (NCPS).9 While some supervisors view these requirements as burdensome, others have demonstrated strong enthusiasm for the process.6 Understanding the perspectives of unit and departmental managers regarding factors that enhance or hinder the adoption of HRO practices is critical for continuous improvement.10-12 Research has suggested that fostering psychological safety can create an environment where new ideas are shared openly, helping organizations navigate resistance to change.13-16
A 2024 quality improvement study, drawing on the perceptions of HRO leads, identified key facilitators, including training, coaching, leader approachability, and psychological safety, as well as barriers such as inadequate training and lack of accountability among managers.17 Building on this work, the current study focused on frontline supervisors, who are directly involved in integrating HRO practices into patient care activities. By addressing both barriers and facilitators, this expanded approach aims to provide a more comprehensive understanding of the challenges influencing HRO implementation in day-to-day operations.
Methods
This quality improvement initiative examined facilitators and barriers to establishing just culture and implementing high reliability practices, focusing on frontline supervisors overseeing clinical care teams (eg, emergency department, critical care) or patient-support functions (eg, dietary services). A questionnaire was sent to a randomized sample of VHA facility supervisors.
A qualitative grounded theory approach was employed to provide a deeper understanding of nuanced phenomena that cannot be captured through numerical data alone. This method enables systematic analysis using open, axial, and thematic coding, ensuring that emerging themes achieve saturation.18,19 It is particularly suited for this study, given the limited prior data on frontline supervisors. Additionally, qualitative methods help mitigate biases common in Likert-style scales, where respondents may lean toward agreement, potentially skewing results.20
Inclusion Criteria
Participants were required to have served as a frontline supervisor for ≥ 6 months. Frontline supervisors are assigned responsibility for supporting staff who deliver services to VHA patients, including clinical care, dietary support, and other functions. These staff must complete baseline HRO cultural training as well as NCPS team training and are responsible for supporting quality, safety, and patient experience. Potential participants were identified from a list of frontline supervisors provided by VHA management. A subset was chosen through random sampling across geographically distributed VHA hospital facilities that vary in size and complexity. Invitations to participate in completing the questionnaire were sent via email, explaining the quality improvement initiative’s purpose, and encouraging voluntary participation. Of 2000 frontline supervisors invited to participate in the initiative, 97 completed the questionnaire. Participants represented a mix of VHA sites in terms of geography, size, and complexity.
Procedures
The authors used a qualitative approach and administered a confidential online survey. Demographic data were collected within the survey to understand characteristics of the participant population, including length of time as a frontline supervisor, facility complexity level, and professional background (clinical vs nonclinical). Survey questions were developed to elicit responses to specific areas of interest based on existing literature related to HRO and just culture.
Facilitators were defined as factors that increase the likelihood of establishing or sustaining high reliability practices and/or culture. Barriers were defined as factors that decrease or inhibit the likelihood of establishing or sustaining high reliability practices and/or culture. The questionnaire consisted of open-ended questions asking frontline supervisors to describe HRO practices and just culture at their individual facility and within their role. Participants also were asked to identify facilitators and barriers that helped or hindered their efforts to establish and maintain high reliability practices and just culture. The questionnaire solicited recommendations for additional support, training, resources, or leadership interventions to strengthen high reliability practices and just culture from each participant.
Analysis
Participant characteristics were analyzed using descriptive statistics. Responses to the 7 open-ended questions were coded and analyzed using ATLAS.ti v.24 qualitative data analysis software by an experienced researcher and coauthor. Grounded theory methodology allowed themes to emerge from the data and although the response rate was limited, the themes reached a saturation point.18,19
Ethical Considerations
Institutional review board (IRB) review and approval were not required for this quality improvement initiative. Formal IRB review and approval of a quality improvement initiative are not required by VHA. Participation was confidential and voluntary, and participants could withdraw at any time without consequences. Completion of the survey indicated consent, and facility names and participant identifiers were not used. Unique numbers were assigned to each participant and all responses were kept confidential and nonattributional. Frequency coding was used to identify the facilitators and barriers to high reliability practices implementation and just culture among frontline supervisors until thematic saturation was obtained.
Results
A total of 2000 frontline supervisors were invited to participate, of whom 97 completed the questionnaire (response rate, 4.9%). Participants were first asked to describe just culture and high reliability practices in their own words. The consensus was that a just culture emphasizes a nonpunitive environment where employees can report errors or incidents without fear of retaliation. It encourages accountability at the systems level, focusing on learning from mistakes to improve processes. In response to a question asking respondents to describe HRO practices and just culture in their own words, participants noted that organizations with a just culture promote open communication, allowing staff to discuss safety issues and concerns without fear of personal blame. Additionally, participants agreed that HRO practices were defined as a set of principles and practices aimed at minimizing errors and promoting safety, especially within complex and high-risk environments. Participants responded that key characteristics include a preoccupation with failure, sensitivity to operations, reluctance to simplify, and a commitment to resilience. HRO practices entail proactively identifying and mitigating risks through open communication and collaboration among team members, they added.
Overall, participants were aligned with their view of the role a frontline supervisor plays in supporting just culture and HRO principles at their facility by fostering open communication and psychological safety, encouraging continuous learning and improvement, and promoting team collaboration and shared accountability. Among frontline supervisors, 93 (96%) identified their role as being critical to creating a safe space and reinforcing just culture and HRO principles at their facility, while 4 (4%) failed to identify a single duty.
Identified Themes
Table 1 summarizes 6 key themes identified from participants’ responses, highlighting the most frequently cited facilitators and barriers to implementing and sustaining high reliability practices and a just culture. Table 2 shows the classification of several themes in relation to facility complexity, emphasizing leadership commitment and support as a pivotal facilitator, while listing resistance to change and entrenched attitudes as a prominent barrier.
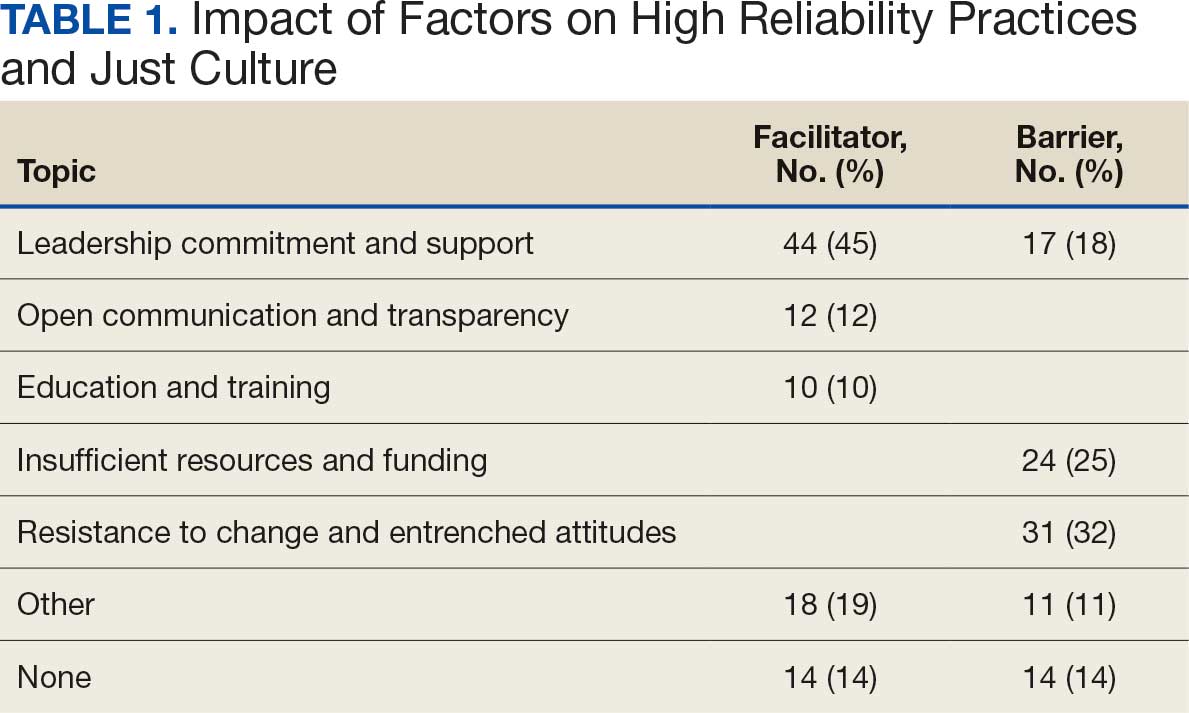
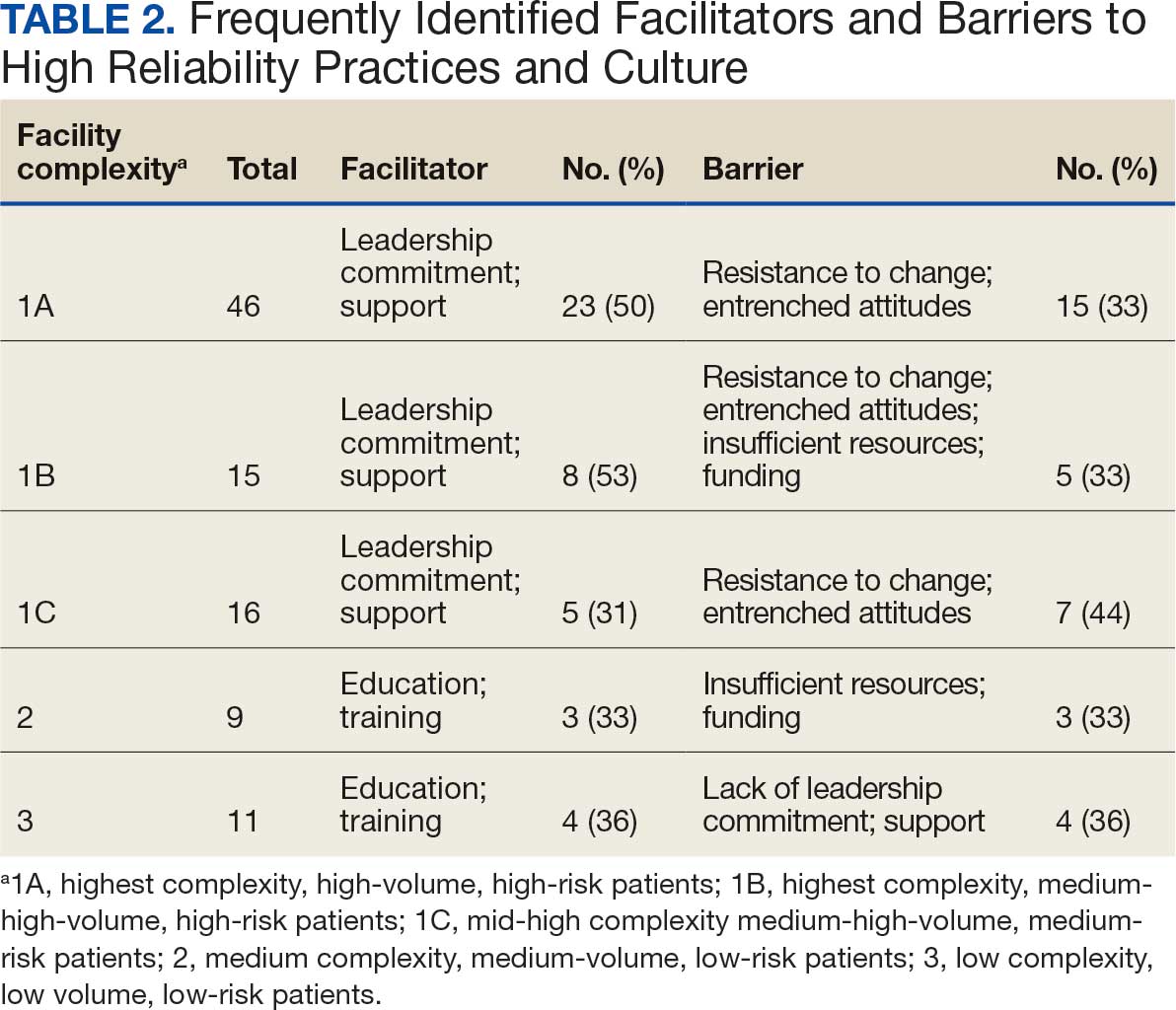
Role of Leadership
Facilitators. Leadership commitment and support were the most frequently identified facilitator, accounting for 44 mentions (45%). This aligns with participants’ descriptions of leadership involvement as crucial, particularly in setting standards and fostering accountability throughout the organization. For example, a frontline supervisor with < 5 years of experience from a nonclinical background at a 1B facility remarked, “Facility leadership are involved, which trickles down to lower-level leads and supervisors, which keeps everyone accountable and holds everyone to the same standards.” Participants frequently identified that leaders setting the standard and communicating expectations as paramount facilitators for strengthening high reliability practices and just culture at their facility.
Barriers. A lack of leadership commitment and support was a significant barrier, cited in 17 responses (18%). Participants described this barrier as a deficiency in follow-through, transparency, and presence, which undermines efforts to sustain just culture and high reliability principles. Notably, the lack of leadership commitment and support stood out as a distinct and recurring theme, underscoring its critical role as an independent challenge to achieving organizational goals. “Many leaders are not yet fully bought in,” a respondent explained. “They take the training and pass it off and go right back to their units and focus on blaming or chastis[ing] people for speaking up.” This theme frequently intersected with mentions of insufficient resources and entrenched attitudes, amplifying other challenges.
Open Communication and Transparency
Facilitators. Open communication and transparency were identified as facilitators in 12 responses (12%). Participants emphasized the importance of mechanisms such as HRO meetings and the sharing of “real” examples of positive outcomes from applying HRO principles. Transparent communication fosters psychological safety, allowing staff to report concerns without fear of reprisal. One participant with < 5 years of experience from a clinical background at a 1A facility encapsulated this theme by saying, “Quarterly ‘fireside chats’ are helpful, [this] creates open dialogue about where the next safety issue may occur, what staff need to do their job safely, while also imparting more of the philosophy of HRO that staff may not be aware of.”
Barriers. While communication serves as a facilitator, participants also highlighted barriers such as siloed communication and fear of reprisal. These reflect challenges in creating open and transparent feedback loops essential to high reliability. For example, a participant concluded, “Leadership does not communicate problem-solving efforts and resolution down the chain, they do not see the problems.” Another participant added, “[HRO principles] are not discussed that much.” While this theme presented as a barrier, it was noted less frequently.
Education and Training
Facilitators. Education and training were noted as facilitators in 10 responses (10%), underscoring their role in establishing high reliability practices. Participants suggested tailored training, simulation-based exercises, and mentorship to enhance practical application. However, they noted the importance of linking training to real change and ensuring leadership enforcement of learned behaviors. This theme is best represented by a participant who concluded, “Trainings have helped, but I think as a supervisor, being involved and interacting with your staff, observing, doing the work they do to help identify potential problems areas, especially when new systems are introduced are key. Being hands-on is the only way to successfully manage your team.”
Barriers. Insufficient resources, including time and staffing constraints, were identified as barriers to education and training, accounting for 24 responses (25%). Participants observed that mandatory training without mentorship or application diminishes its effectiveness.
Insufficient Resources and Funding
Barriers. Resource constraints, including low staffing levels and budget cuts, accounted for 24 responses (25%). Participants reported these limitations prevented staff from attending training and affected the overall implementation of just culture and HRO principles. “Low staffing in supporting services as well as in my own service line have created barriers,” a participant reported. Another participant responded that barriers to HRO were primarily “…financial, as the focus is how to curb costs and bring in more funding rather than taking the time to review and apply the concepts of high reliability.”
Resistance to Change and Entrenched Attitudes
Barriers. Resistance to change was the most frequently identified barrier, with 31 responses (32%). One participant described a persistent “gotcha” culture, where blame and punishment hinder progress toward just culture. This entrenched mindset creates significant obstacles to adopting HRO practices and requires active leadership and supervisor intervention to overcome. This theme is best captured by a respondent who noted that “culture change is difficult, especially among staff with such long tenure. It’s a long game.”
Synthesis and Integration of Findings
The data in Table 1 and Table 2 reinforce the themes identified in the qualitative analysis. Leadership commitment and support are pivotal, both as a facilitator and barrier. Open communication and education and training, while recognized as facilitators, were less frequently mentioned, but still critical. Resistance to change and insufficient resources were the most prominent barriers, indicating where organizational efforts should focus to further foster a culture of high reliability.
By addressing these barriers, particularly resistance to change and resource constraints, and leveraging facilitators like leadership engagement and transparent communication, organizations can enhance their implementation of just culture and high reliability practices. These efforts require deliberate strategies, including effective training, mentorship, and the active presence of leadership.
Discussion
This quality improvement initiative builds on prior research by examining the implementation of HRO practices from the perspective of frontline supervisors. Unlike earlier research focused on HRO leads, this study explores the critical role of supervisors who integrate HRO principles into clinical and administrative operations.17 By analyzing their experiences, this study offers practical insights into facilitating HRO implementation across organizational levels.
The findings highlight broad agreement on the value of just culture and HRO principles in fostering safe, accountable health care environments. Participants described just culture as promoting system—level accountability rather than individual blame, encouraging error reporting and learning for continuous improvement. Similarly, HRO practices—emphasizing a preoccupation with failure, operational sensitivity, and resilience— were seen as vital for patient safety in complex settings.
Frontline supervisors play a pivotal role, with 96% of respondents identifying their influence on fostering open communication, psychological safety, and shared accountability. Key facilitators included leadership commitment, open communication, and mentorship. Active leadership involvement was particularly valued, as it trickles down to reinforce standards across all organizational levels. HRO meetings using real-world examples were seen as instrumental in demonstrating the tangible benefits of these principles, helping embed them into daily practices.
Despite these facilitators, several barriers to implementation were noted. Resistance to change and entrenched attitudes, and a persistent gotcha culture undermined efforts to establish just culture. Resource constraints, including staffing shortages and budget limitations, further hindered the adoption of HRO practices. The lack of consistent leadership engagement, marked by limited visibility, follow-through, and transparency, exacerbated these challenges.
HRO leads are important for promoting education and embedding HRO principles into daily operations. These individuals provide vital support to frontline supervisors, translating HRO concepts into actionable practices. However, organizational challenges such as staff turnover and redirected funding have weakened the infrastructure supporting HRO initiatives. The elimination of HRO lead roles due to budgetary pressures at several facilities reflects a short-term focus on operational demands at the expense of long-term cultural transformation.
Additional barriers included siloed communication, fear of reprisal, bureaucratic obstacles, and outdated technology. These challenges limit progress toward high reliability and diminish the effectiveness of HRO principles.
Participants proposed strategies focused on education, training, and leadership engagement. Simulation-based training tailored to specific roles was identified as an effective tool for preparing staff to apply HRO principles in real-world scenarios. Enhanced communication, such as regular leadership rounding and transparent updates on safety concerns, was also emphasized. Participants stressed the importance of showing staff how their feedback influences organizational decisions to build trust and accountability. Finally, standardizing procedures and protocols across facilities was seen as critical for aligning practices and reducing variability in safety processes.
This study underscores the need for sustained leadership commitment and infrastructure to ensure the long-term success of HRO implementation. Addressing the identified barriers and leveraging the proposed mitigation strategies can foster a culture of safety and reliability across the organization.
Limitations
This quality improvement initiative used qualitative grounded theory methods and sampled a relatively small group of experienced leaders specifically involved in implementing HRO within the VHA. In addition, while saturation of themes was reached, the number of responses represents a small sample of VHA frontline supervisors. As such, the findings may not be fully representative of the perspectives of all unit and departmental leaders across the VHA or other health care systems. A previous qualitative quality improvement initiative focused on the perceptions of HRO leads regarding facilitators and barriers to just culture.17 This quality improvement initiative broadened that focus by examining the perspectives of frontline supervisors in the operational environment, who may not be HRO experts but work to implement HRO principles with the guidance of HRO leads (HRO subject matter experts).
There remains an opportunity to address a critical gap by assessing facilitators and barriers beyond the facility level, incorporating both the Veterans Integrated Service Networks (VISN) and VHA Central Office (VHACO). While qualitative methods, such as those used in this study, provide deep insights and detailed understanding, they are limited in their ability to identify system-wide trends and variations at a more strategic VISN and VHACO level. Addressing this could enhance the broader applicability of HRO principles across the VHA.
Conclusions
Successful implementation of the recommendations reported in this study will require sustained focus and continued commitment from all stakeholders across the VHA. As the VHA enters its seventh year on the HRO journey, the risk of organizational drift remains an ongoing concern. Progress has been made, as evidenced by incremental improvements in All Employee Survey scores and increased reporting of adverse events and near misses, but the challenge will be to maintain focus and continue to build upon progress amid the current climate of budgetary constraints.
This study builds on previous quality improvement efforts and provides valuable insights into the barriers and facilitators that can either hinder or support the VHA’s ongoing pursuit of high reliability. The findings offer a model for understanding the complexities of this journey—one that requires continuous effort and adaptation, as there is no definitive endpoint in the quest for high reliability.
Since completion of this study in 2024, the VHA has entered a period of organizational transition and restructuring. Such transitions are often accompanied by increased operational demands and organizational strain. These include realignments, personnel changes, staffing adjustments, workforce reductions, and continued implementation of a new electronic health record system. In this context, maintaining attention to culture, communication, frontline engagement, and mechanisms that provide visibility into organizational climate is essential to sustain momentum in high-reliability efforts.
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/jhm-D-23-00056
- Sculli GL, Pendley-Louis R, Neily J, et al. A high-reliability organization framework for health care: A multiyear implementation strategy and associated outcomes. J Patient Saf. 2022;18:64-70. doi:10.1097/pts.0000000000000788
- Murray JS, Clifford J, Larson S, Lee JK, Sculli GL. Implementing just culture to improve patient safety. Mil Med. 2023;188:usac115. doi:10.1093/milmed/usac115
- Merchant NB, O’Neal J, Montoya A, Cox GR, Murray JS. Creating a process for the implementation of tiered huddles in a Veterans Affairs Medical Center. Mil Med. 2023;188:901-906. doi:10.1093/milmed/usac073
- Mohr DC, Chen C, Sullivan J, et al. Development and validation of the Veterans Health Administration Patient Safety Culture Survey. J Patient Saf. 2022;18:539-545. doi:10.1097/PTS.0000000000001027
- Leonard C, Gilmartin H, Starr L, Anderson T. Leadership and the high reliability transformation: a qualitative study at Truman VA medical center. J Healthc Risk Manag. 2024;44:17-23. doi:10.1002/jhrm.21580
- Sculli G, Essen K. Soaring to Success: The Path to Developing High-Reliability Teams. HCPro; 2021.
- Gupta JI, Sivils S, Reppert J, Paulot W, Houchens N, Hummel S. Visual management board implementation to enhance high reliability at a large VA health care system. Fed Pract. 2024;41:242-246. doi:10.12788/fp.0507
- Veterans Health Administration. High Reliability Organization Learning Catalog. US Dept of Veterans Affairs; 2024. Internal document.
- Jahn JLS, Black AE. A model of communicative and hierarchical foundations of high reliability organizing in wildland firefighting teams. Manag Commun Q. 2017;31:356-379. doi:10.1177/0893318917691358
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Abrams J. Model the way to navigate difficult topics. The Learning Professional. 2022;43:14-18.
- McCausland T. Creating psychological safety in the workplace. Research-Technology Management. 2023;66:56-58. doi:10.1080/08956308.2023.2164439
- Murray JS, Kelly S, Hanover C. Promoting psychological safety in healthcare organizations. Mil Med. 2022;187:808- 810. doi:10.1093/milmed/usac041
- Sutton RI, Rao H. The friction project: how smart leaders make the right things easier and the wrong things harder. St. Martin’s Press; 2024.
- Clark TR. The 4 stages of psychological safety: defining the path to inclusion and innovation. Berrett-Koehler Publishers, Inc.; 2020.
- Essen K, Villalobos C, Sculli G, Steinbach L. Establishing a just culture: implications for the Veterans Health Administration journey to high reliability. Fed Pract. 2024;41:290- 297. doi:10.12788/fp.0512
- Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 4th ed. SAGE Publications; 2014.
- Patton MQ. Qualitative research & evaluation methods: integrating theory and practice. 4th ed. SAGE Publications, Inc.; 2015.
- Krumpal I. Determinants of social desirability bias in sensitive surveys: a literature review. Qual Quant. 2013;47:2025- 2047. doi:10.1007/s11135-011-9640-9
The Veterans Health Administration (VHA) is now in the sixth year of its enterprise-wide transformation into a high reliability organization (HRO). This effort began with a 2016 pilot project and is now implemented in 170 VHA medical centers.1-4 This transformation reflects a commitment to implementing standardized and reliable health care practices.
The VHA HRO implementation strategy includes a multifaceted approach to engage leadership through education, training, leader coaching, and change management initiatives.2 Despite the diversity of facilities in terms of cultures, geographies, and complexities, US Department of Veterans Affairs (VA) medical centers (VAMCs) have increasingly embraced standardized HRO practices. These changes are evident in improvements in VHA All Employee Survey scores, which assess 4 key patient safety culture dimensions: risk identification and just culture, error transparency and mitigation, supervisor communication and trust, and team cohesion and engagement.5 Positive trends in these dimensions highlight a cultural shift toward greater reliability, even amid challenges introduced by the COVID-19 pandemic.
However, this progress has encountered some challenges. Leadership turnover, budgetary constraints, and extensive educational demands for implementing and sustaining HRO practices have created obstacles, particularly for frontline health care practitioners.6 Additionally, there are pockets of resistance similar to what the airline industry faced when implementing crew resource management (CRM). Specifically, senior pilots and legacy leaders were reluctant to abandon their high-status, autocratic management styles and embrace CRM, despite its proven benefits for enhancing commercial airline safety.7 Similarly, some VHA staff have expressed resistance to foundational HRO practices, which include safety huddles, safety forums, leader rounding, and visual management systems.6,8
The training requirements for HRO practices range from a 25-minute introductory course (HRO 101) to a 7.5-hour team training session facilitated by the VHA National Center for Patient Safety (NCPS).9 While some supervisors view these requirements as burdensome, others have demonstrated strong enthusiasm for the process.6 Understanding the perspectives of unit and departmental managers regarding factors that enhance or hinder the adoption of HRO practices is critical for continuous improvement.10-12 Research has suggested that fostering psychological safety can create an environment where new ideas are shared openly, helping organizations navigate resistance to change.13-16
A 2024 quality improvement study, drawing on the perceptions of HRO leads, identified key facilitators, including training, coaching, leader approachability, and psychological safety, as well as barriers such as inadequate training and lack of accountability among managers.17 Building on this work, the current study focused on frontline supervisors, who are directly involved in integrating HRO practices into patient care activities. By addressing both barriers and facilitators, this expanded approach aims to provide a more comprehensive understanding of the challenges influencing HRO implementation in day-to-day operations.
Methods
This quality improvement initiative examined facilitators and barriers to establishing just culture and implementing high reliability practices, focusing on frontline supervisors overseeing clinical care teams (eg, emergency department, critical care) or patient-support functions (eg, dietary services). A questionnaire was sent to a randomized sample of VHA facility supervisors.
A qualitative grounded theory approach was employed to provide a deeper understanding of nuanced phenomena that cannot be captured through numerical data alone. This method enables systematic analysis using open, axial, and thematic coding, ensuring that emerging themes achieve saturation.18,19 It is particularly suited for this study, given the limited prior data on frontline supervisors. Additionally, qualitative methods help mitigate biases common in Likert-style scales, where respondents may lean toward agreement, potentially skewing results.20
Inclusion Criteria
Participants were required to have served as a frontline supervisor for ≥ 6 months. Frontline supervisors are assigned responsibility for supporting staff who deliver services to VHA patients, including clinical care, dietary support, and other functions. These staff must complete baseline HRO cultural training as well as NCPS team training and are responsible for supporting quality, safety, and patient experience. Potential participants were identified from a list of frontline supervisors provided by VHA management. A subset was chosen through random sampling across geographically distributed VHA hospital facilities that vary in size and complexity. Invitations to participate in completing the questionnaire were sent via email, explaining the quality improvement initiative’s purpose, and encouraging voluntary participation. Of 2000 frontline supervisors invited to participate in the initiative, 97 completed the questionnaire. Participants represented a mix of VHA sites in terms of geography, size, and complexity.
Procedures
The authors used a qualitative approach and administered a confidential online survey. Demographic data were collected within the survey to understand characteristics of the participant population, including length of time as a frontline supervisor, facility complexity level, and professional background (clinical vs nonclinical). Survey questions were developed to elicit responses to specific areas of interest based on existing literature related to HRO and just culture.
Facilitators were defined as factors that increase the likelihood of establishing or sustaining high reliability practices and/or culture. Barriers were defined as factors that decrease or inhibit the likelihood of establishing or sustaining high reliability practices and/or culture. The questionnaire consisted of open-ended questions asking frontline supervisors to describe HRO practices and just culture at their individual facility and within their role. Participants also were asked to identify facilitators and barriers that helped or hindered their efforts to establish and maintain high reliability practices and just culture. The questionnaire solicited recommendations for additional support, training, resources, or leadership interventions to strengthen high reliability practices and just culture from each participant.
Analysis
Participant characteristics were analyzed using descriptive statistics. Responses to the 7 open-ended questions were coded and analyzed using ATLAS.ti v.24 qualitative data analysis software by an experienced researcher and coauthor. Grounded theory methodology allowed themes to emerge from the data and although the response rate was limited, the themes reached a saturation point.18,19
Ethical Considerations
Institutional review board (IRB) review and approval were not required for this quality improvement initiative. Formal IRB review and approval of a quality improvement initiative are not required by VHA. Participation was confidential and voluntary, and participants could withdraw at any time without consequences. Completion of the survey indicated consent, and facility names and participant identifiers were not used. Unique numbers were assigned to each participant and all responses were kept confidential and nonattributional. Frequency coding was used to identify the facilitators and barriers to high reliability practices implementation and just culture among frontline supervisors until thematic saturation was obtained.
Results
A total of 2000 frontline supervisors were invited to participate, of whom 97 completed the questionnaire (response rate, 4.9%). Participants were first asked to describe just culture and high reliability practices in their own words. The consensus was that a just culture emphasizes a nonpunitive environment where employees can report errors or incidents without fear of retaliation. It encourages accountability at the systems level, focusing on learning from mistakes to improve processes. In response to a question asking respondents to describe HRO practices and just culture in their own words, participants noted that organizations with a just culture promote open communication, allowing staff to discuss safety issues and concerns without fear of personal blame. Additionally, participants agreed that HRO practices were defined as a set of principles and practices aimed at minimizing errors and promoting safety, especially within complex and high-risk environments. Participants responded that key characteristics include a preoccupation with failure, sensitivity to operations, reluctance to simplify, and a commitment to resilience. HRO practices entail proactively identifying and mitigating risks through open communication and collaboration among team members, they added.
Overall, participants were aligned with their view of the role a frontline supervisor plays in supporting just culture and HRO principles at their facility by fostering open communication and psychological safety, encouraging continuous learning and improvement, and promoting team collaboration and shared accountability. Among frontline supervisors, 93 (96%) identified their role as being critical to creating a safe space and reinforcing just culture and HRO principles at their facility, while 4 (4%) failed to identify a single duty.
Identified Themes
Table 1 summarizes 6 key themes identified from participants’ responses, highlighting the most frequently cited facilitators and barriers to implementing and sustaining high reliability practices and a just culture. Table 2 shows the classification of several themes in relation to facility complexity, emphasizing leadership commitment and support as a pivotal facilitator, while listing resistance to change and entrenched attitudes as a prominent barrier.
Role of Leadership
Facilitators. Leadership commitment and support were the most frequently identified facilitator, accounting for 44 mentions (45%). This aligns with participants’ descriptions of leadership involvement as crucial, particularly in setting standards and fostering accountability throughout the organization. For example, a frontline supervisor with < 5 years of experience from a nonclinical background at a 1B facility remarked, “Facility leadership are involved, which trickles down to lower-level leads and supervisors, which keeps everyone accountable and holds everyone to the same standards.” Participants frequently identified that leaders setting the standard and communicating expectations as paramount facilitators for strengthening high reliability practices and just culture at their facility.
Barriers. A lack of leadership commitment and support was a significant barrier, cited in 17 responses (18%). Participants described this barrier as a deficiency in follow-through, transparency, and presence, which undermines efforts to sustain just culture and high reliability principles. Notably, the lack of leadership commitment and support stood out as a distinct and recurring theme, underscoring its critical role as an independent challenge to achieving organizational goals. “Many leaders are not yet fully bought in,” a respondent explained. “They take the training and pass it off and go right back to their units and focus on blaming or chastis[ing] people for speaking up.” This theme frequently intersected with mentions of insufficient resources and entrenched attitudes, amplifying other challenges.
Open Communication and Transparency
Facilitators. Open communication and transparency were identified as facilitators in 12 responses (12%). Participants emphasized the importance of mechanisms such as HRO meetings and the sharing of “real” examples of positive outcomes from applying HRO principles. Transparent communication fosters psychological safety, allowing staff to report concerns without fear of reprisal. One participant with < 5 years of experience from a clinical background at a 1A facility encapsulated this theme by saying, “Quarterly ‘fireside chats’ are helpful, [this] creates open dialogue about where the next safety issue may occur, what staff need to do their job safely, while also imparting more of the philosophy of HRO that staff may not be aware of.”
Barriers. While communication serves as a facilitator, participants also highlighted barriers such as siloed communication and fear of reprisal. These reflect challenges in creating open and transparent feedback loops essential to high reliability. For example, a participant concluded, “Leadership does not communicate problem-solving efforts and resolution down the chain, they do not see the problems.” Another participant added, “[HRO principles] are not discussed that much.” While this theme presented as a barrier, it was noted less frequently.
Education and Training
Facilitators. Education and training were noted as facilitators in 10 responses (10%), underscoring their role in establishing high reliability practices. Participants suggested tailored training, simulation-based exercises, and mentorship to enhance practical application. However, they noted the importance of linking training to real change and ensuring leadership enforcement of learned behaviors. This theme is best represented by a participant who concluded, “Trainings have helped, but I think as a supervisor, being involved and interacting with your staff, observing, doing the work they do to help identify potential problems areas, especially when new systems are introduced are key. Being hands-on is the only way to successfully manage your team.”
Barriers. Insufficient resources, including time and staffing constraints, were identified as barriers to education and training, accounting for 24 responses (25%). Participants observed that mandatory training without mentorship or application diminishes its effectiveness.
Insufficient Resources and Funding
Barriers. Resource constraints, including low staffing levels and budget cuts, accounted for 24 responses (25%). Participants reported these limitations prevented staff from attending training and affected the overall implementation of just culture and HRO principles. “Low staffing in supporting services as well as in my own service line have created barriers,” a participant reported. Another participant responded that barriers to HRO were primarily “…financial, as the focus is how to curb costs and bring in more funding rather than taking the time to review and apply the concepts of high reliability.”
Resistance to Change and Entrenched Attitudes
Barriers. Resistance to change was the most frequently identified barrier, with 31 responses (32%). One participant described a persistent “gotcha” culture, where blame and punishment hinder progress toward just culture. This entrenched mindset creates significant obstacles to adopting HRO practices and requires active leadership and supervisor intervention to overcome. This theme is best captured by a respondent who noted that “culture change is difficult, especially among staff with such long tenure. It’s a long game.”
Synthesis and Integration of Findings
The data in Table 1 and Table 2 reinforce the themes identified in the qualitative analysis. Leadership commitment and support are pivotal, both as a facilitator and barrier. Open communication and education and training, while recognized as facilitators, were less frequently mentioned, but still critical. Resistance to change and insufficient resources were the most prominent barriers, indicating where organizational efforts should focus to further foster a culture of high reliability.
By addressing these barriers, particularly resistance to change and resource constraints, and leveraging facilitators like leadership engagement and transparent communication, organizations can enhance their implementation of just culture and high reliability practices. These efforts require deliberate strategies, including effective training, mentorship, and the active presence of leadership.
Discussion
This quality improvement initiative builds on prior research by examining the implementation of HRO practices from the perspective of frontline supervisors. Unlike earlier research focused on HRO leads, this study explores the critical role of supervisors who integrate HRO principles into clinical and administrative operations.17 By analyzing their experiences, this study offers practical insights into facilitating HRO implementation across organizational levels.
The findings highlight broad agreement on the value of just culture and HRO principles in fostering safe, accountable health care environments. Participants described just culture as promoting system—level accountability rather than individual blame, encouraging error reporting and learning for continuous improvement. Similarly, HRO practices—emphasizing a preoccupation with failure, operational sensitivity, and resilience— were seen as vital for patient safety in complex settings.
Frontline supervisors play a pivotal role, with 96% of respondents identifying their influence on fostering open communication, psychological safety, and shared accountability. Key facilitators included leadership commitment, open communication, and mentorship. Active leadership involvement was particularly valued, as it trickles down to reinforce standards across all organizational levels. HRO meetings using real-world examples were seen as instrumental in demonstrating the tangible benefits of these principles, helping embed them into daily practices.
Despite these facilitators, several barriers to implementation were noted. Resistance to change and entrenched attitudes, and a persistent gotcha culture undermined efforts to establish just culture. Resource constraints, including staffing shortages and budget limitations, further hindered the adoption of HRO practices. The lack of consistent leadership engagement, marked by limited visibility, follow-through, and transparency, exacerbated these challenges.
HRO leads are important for promoting education and embedding HRO principles into daily operations. These individuals provide vital support to frontline supervisors, translating HRO concepts into actionable practices. However, organizational challenges such as staff turnover and redirected funding have weakened the infrastructure supporting HRO initiatives. The elimination of HRO lead roles due to budgetary pressures at several facilities reflects a short-term focus on operational demands at the expense of long-term cultural transformation.
Additional barriers included siloed communication, fear of reprisal, bureaucratic obstacles, and outdated technology. These challenges limit progress toward high reliability and diminish the effectiveness of HRO principles.
Participants proposed strategies focused on education, training, and leadership engagement. Simulation-based training tailored to specific roles was identified as an effective tool for preparing staff to apply HRO principles in real-world scenarios. Enhanced communication, such as regular leadership rounding and transparent updates on safety concerns, was also emphasized. Participants stressed the importance of showing staff how their feedback influences organizational decisions to build trust and accountability. Finally, standardizing procedures and protocols across facilities was seen as critical for aligning practices and reducing variability in safety processes.
This study underscores the need for sustained leadership commitment and infrastructure to ensure the long-term success of HRO implementation. Addressing the identified barriers and leveraging the proposed mitigation strategies can foster a culture of safety and reliability across the organization.
Limitations
This quality improvement initiative used qualitative grounded theory methods and sampled a relatively small group of experienced leaders specifically involved in implementing HRO within the VHA. In addition, while saturation of themes was reached, the number of responses represents a small sample of VHA frontline supervisors. As such, the findings may not be fully representative of the perspectives of all unit and departmental leaders across the VHA or other health care systems. A previous qualitative quality improvement initiative focused on the perceptions of HRO leads regarding facilitators and barriers to just culture.17 This quality improvement initiative broadened that focus by examining the perspectives of frontline supervisors in the operational environment, who may not be HRO experts but work to implement HRO principles with the guidance of HRO leads (HRO subject matter experts).
There remains an opportunity to address a critical gap by assessing facilitators and barriers beyond the facility level, incorporating both the Veterans Integrated Service Networks (VISN) and VHA Central Office (VHACO). While qualitative methods, such as those used in this study, provide deep insights and detailed understanding, they are limited in their ability to identify system-wide trends and variations at a more strategic VISN and VHACO level. Addressing this could enhance the broader applicability of HRO principles across the VHA.
Conclusions
Successful implementation of the recommendations reported in this study will require sustained focus and continued commitment from all stakeholders across the VHA. As the VHA enters its seventh year on the HRO journey, the risk of organizational drift remains an ongoing concern. Progress has been made, as evidenced by incremental improvements in All Employee Survey scores and increased reporting of adverse events and near misses, but the challenge will be to maintain focus and continue to build upon progress amid the current climate of budgetary constraints.
This study builds on previous quality improvement efforts and provides valuable insights into the barriers and facilitators that can either hinder or support the VHA’s ongoing pursuit of high reliability. The findings offer a model for understanding the complexities of this journey—one that requires continuous effort and adaptation, as there is no definitive endpoint in the quest for high reliability.
Since completion of this study in 2024, the VHA has entered a period of organizational transition and restructuring. Such transitions are often accompanied by increased operational demands and organizational strain. These include realignments, personnel changes, staffing adjustments, workforce reductions, and continued implementation of a new electronic health record system. In this context, maintaining attention to culture, communication, frontline engagement, and mechanisms that provide visibility into organizational climate is essential to sustain momentum in high-reliability efforts.
The Veterans Health Administration (VHA) is now in the sixth year of its enterprise-wide transformation into a high reliability organization (HRO). This effort began with a 2016 pilot project and is now implemented in 170 VHA medical centers.1-4 This transformation reflects a commitment to implementing standardized and reliable health care practices.
The VHA HRO implementation strategy includes a multifaceted approach to engage leadership through education, training, leader coaching, and change management initiatives.2 Despite the diversity of facilities in terms of cultures, geographies, and complexities, US Department of Veterans Affairs (VA) medical centers (VAMCs) have increasingly embraced standardized HRO practices. These changes are evident in improvements in VHA All Employee Survey scores, which assess 4 key patient safety culture dimensions: risk identification and just culture, error transparency and mitigation, supervisor communication and trust, and team cohesion and engagement.5 Positive trends in these dimensions highlight a cultural shift toward greater reliability, even amid challenges introduced by the COVID-19 pandemic.
However, this progress has encountered some challenges. Leadership turnover, budgetary constraints, and extensive educational demands for implementing and sustaining HRO practices have created obstacles, particularly for frontline health care practitioners.6 Additionally, there are pockets of resistance similar to what the airline industry faced when implementing crew resource management (CRM). Specifically, senior pilots and legacy leaders were reluctant to abandon their high-status, autocratic management styles and embrace CRM, despite its proven benefits for enhancing commercial airline safety.7 Similarly, some VHA staff have expressed resistance to foundational HRO practices, which include safety huddles, safety forums, leader rounding, and visual management systems.6,8
The training requirements for HRO practices range from a 25-minute introductory course (HRO 101) to a 7.5-hour team training session facilitated by the VHA National Center for Patient Safety (NCPS).9 While some supervisors view these requirements as burdensome, others have demonstrated strong enthusiasm for the process.6 Understanding the perspectives of unit and departmental managers regarding factors that enhance or hinder the adoption of HRO practices is critical for continuous improvement.10-12 Research has suggested that fostering psychological safety can create an environment where new ideas are shared openly, helping organizations navigate resistance to change.13-16
A 2024 quality improvement study, drawing on the perceptions of HRO leads, identified key facilitators, including training, coaching, leader approachability, and psychological safety, as well as barriers such as inadequate training and lack of accountability among managers.17 Building on this work, the current study focused on frontline supervisors, who are directly involved in integrating HRO practices into patient care activities. By addressing both barriers and facilitators, this expanded approach aims to provide a more comprehensive understanding of the challenges influencing HRO implementation in day-to-day operations.
Methods
This quality improvement initiative examined facilitators and barriers to establishing just culture and implementing high reliability practices, focusing on frontline supervisors overseeing clinical care teams (eg, emergency department, critical care) or patient-support functions (eg, dietary services). A questionnaire was sent to a randomized sample of VHA facility supervisors.
A qualitative grounded theory approach was employed to provide a deeper understanding of nuanced phenomena that cannot be captured through numerical data alone. This method enables systematic analysis using open, axial, and thematic coding, ensuring that emerging themes achieve saturation.18,19 It is particularly suited for this study, given the limited prior data on frontline supervisors. Additionally, qualitative methods help mitigate biases common in Likert-style scales, where respondents may lean toward agreement, potentially skewing results.20
Inclusion Criteria
Participants were required to have served as a frontline supervisor for ≥ 6 months. Frontline supervisors are assigned responsibility for supporting staff who deliver services to VHA patients, including clinical care, dietary support, and other functions. These staff must complete baseline HRO cultural training as well as NCPS team training and are responsible for supporting quality, safety, and patient experience. Potential participants were identified from a list of frontline supervisors provided by VHA management. A subset was chosen through random sampling across geographically distributed VHA hospital facilities that vary in size and complexity. Invitations to participate in completing the questionnaire were sent via email, explaining the quality improvement initiative’s purpose, and encouraging voluntary participation. Of 2000 frontline supervisors invited to participate in the initiative, 97 completed the questionnaire. Participants represented a mix of VHA sites in terms of geography, size, and complexity.
Procedures
The authors used a qualitative approach and administered a confidential online survey. Demographic data were collected within the survey to understand characteristics of the participant population, including length of time as a frontline supervisor, facility complexity level, and professional background (clinical vs nonclinical). Survey questions were developed to elicit responses to specific areas of interest based on existing literature related to HRO and just culture.
Facilitators were defined as factors that increase the likelihood of establishing or sustaining high reliability practices and/or culture. Barriers were defined as factors that decrease or inhibit the likelihood of establishing or sustaining high reliability practices and/or culture. The questionnaire consisted of open-ended questions asking frontline supervisors to describe HRO practices and just culture at their individual facility and within their role. Participants also were asked to identify facilitators and barriers that helped or hindered their efforts to establish and maintain high reliability practices and just culture. The questionnaire solicited recommendations for additional support, training, resources, or leadership interventions to strengthen high reliability practices and just culture from each participant.
Analysis
Participant characteristics were analyzed using descriptive statistics. Responses to the 7 open-ended questions were coded and analyzed using ATLAS.ti v.24 qualitative data analysis software by an experienced researcher and coauthor. Grounded theory methodology allowed themes to emerge from the data and although the response rate was limited, the themes reached a saturation point.18,19
Ethical Considerations
Institutional review board (IRB) review and approval were not required for this quality improvement initiative. Formal IRB review and approval of a quality improvement initiative are not required by VHA. Participation was confidential and voluntary, and participants could withdraw at any time without consequences. Completion of the survey indicated consent, and facility names and participant identifiers were not used. Unique numbers were assigned to each participant and all responses were kept confidential and nonattributional. Frequency coding was used to identify the facilitators and barriers to high reliability practices implementation and just culture among frontline supervisors until thematic saturation was obtained.
Results
A total of 2000 frontline supervisors were invited to participate, of whom 97 completed the questionnaire (response rate, 4.9%). Participants were first asked to describe just culture and high reliability practices in their own words. The consensus was that a just culture emphasizes a nonpunitive environment where employees can report errors or incidents without fear of retaliation. It encourages accountability at the systems level, focusing on learning from mistakes to improve processes. In response to a question asking respondents to describe HRO practices and just culture in their own words, participants noted that organizations with a just culture promote open communication, allowing staff to discuss safety issues and concerns without fear of personal blame. Additionally, participants agreed that HRO practices were defined as a set of principles and practices aimed at minimizing errors and promoting safety, especially within complex and high-risk environments. Participants responded that key characteristics include a preoccupation with failure, sensitivity to operations, reluctance to simplify, and a commitment to resilience. HRO practices entail proactively identifying and mitigating risks through open communication and collaboration among team members, they added.
Overall, participants were aligned with their view of the role a frontline supervisor plays in supporting just culture and HRO principles at their facility by fostering open communication and psychological safety, encouraging continuous learning and improvement, and promoting team collaboration and shared accountability. Among frontline supervisors, 93 (96%) identified their role as being critical to creating a safe space and reinforcing just culture and HRO principles at their facility, while 4 (4%) failed to identify a single duty.
Identified Themes
Table 1 summarizes 6 key themes identified from participants’ responses, highlighting the most frequently cited facilitators and barriers to implementing and sustaining high reliability practices and a just culture. Table 2 shows the classification of several themes in relation to facility complexity, emphasizing leadership commitment and support as a pivotal facilitator, while listing resistance to change and entrenched attitudes as a prominent barrier.
Role of Leadership
Facilitators. Leadership commitment and support were the most frequently identified facilitator, accounting for 44 mentions (45%). This aligns with participants’ descriptions of leadership involvement as crucial, particularly in setting standards and fostering accountability throughout the organization. For example, a frontline supervisor with < 5 years of experience from a nonclinical background at a 1B facility remarked, “Facility leadership are involved, which trickles down to lower-level leads and supervisors, which keeps everyone accountable and holds everyone to the same standards.” Participants frequently identified that leaders setting the standard and communicating expectations as paramount facilitators for strengthening high reliability practices and just culture at their facility.
Barriers. A lack of leadership commitment and support was a significant barrier, cited in 17 responses (18%). Participants described this barrier as a deficiency in follow-through, transparency, and presence, which undermines efforts to sustain just culture and high reliability principles. Notably, the lack of leadership commitment and support stood out as a distinct and recurring theme, underscoring its critical role as an independent challenge to achieving organizational goals. “Many leaders are not yet fully bought in,” a respondent explained. “They take the training and pass it off and go right back to their units and focus on blaming or chastis[ing] people for speaking up.” This theme frequently intersected with mentions of insufficient resources and entrenched attitudes, amplifying other challenges.
Open Communication and Transparency
Facilitators. Open communication and transparency were identified as facilitators in 12 responses (12%). Participants emphasized the importance of mechanisms such as HRO meetings and the sharing of “real” examples of positive outcomes from applying HRO principles. Transparent communication fosters psychological safety, allowing staff to report concerns without fear of reprisal. One participant with < 5 years of experience from a clinical background at a 1A facility encapsulated this theme by saying, “Quarterly ‘fireside chats’ are helpful, [this] creates open dialogue about where the next safety issue may occur, what staff need to do their job safely, while also imparting more of the philosophy of HRO that staff may not be aware of.”
Barriers. While communication serves as a facilitator, participants also highlighted barriers such as siloed communication and fear of reprisal. These reflect challenges in creating open and transparent feedback loops essential to high reliability. For example, a participant concluded, “Leadership does not communicate problem-solving efforts and resolution down the chain, they do not see the problems.” Another participant added, “[HRO principles] are not discussed that much.” While this theme presented as a barrier, it was noted less frequently.
Education and Training
Facilitators. Education and training were noted as facilitators in 10 responses (10%), underscoring their role in establishing high reliability practices. Participants suggested tailored training, simulation-based exercises, and mentorship to enhance practical application. However, they noted the importance of linking training to real change and ensuring leadership enforcement of learned behaviors. This theme is best represented by a participant who concluded, “Trainings have helped, but I think as a supervisor, being involved and interacting with your staff, observing, doing the work they do to help identify potential problems areas, especially when new systems are introduced are key. Being hands-on is the only way to successfully manage your team.”
Barriers. Insufficient resources, including time and staffing constraints, were identified as barriers to education and training, accounting for 24 responses (25%). Participants observed that mandatory training without mentorship or application diminishes its effectiveness.
Insufficient Resources and Funding
Barriers. Resource constraints, including low staffing levels and budget cuts, accounted for 24 responses (25%). Participants reported these limitations prevented staff from attending training and affected the overall implementation of just culture and HRO principles. “Low staffing in supporting services as well as in my own service line have created barriers,” a participant reported. Another participant responded that barriers to HRO were primarily “…financial, as the focus is how to curb costs and bring in more funding rather than taking the time to review and apply the concepts of high reliability.”
Resistance to Change and Entrenched Attitudes
Barriers. Resistance to change was the most frequently identified barrier, with 31 responses (32%). One participant described a persistent “gotcha” culture, where blame and punishment hinder progress toward just culture. This entrenched mindset creates significant obstacles to adopting HRO practices and requires active leadership and supervisor intervention to overcome. This theme is best captured by a respondent who noted that “culture change is difficult, especially among staff with such long tenure. It’s a long game.”
Synthesis and Integration of Findings
The data in Table 1 and Table 2 reinforce the themes identified in the qualitative analysis. Leadership commitment and support are pivotal, both as a facilitator and barrier. Open communication and education and training, while recognized as facilitators, were less frequently mentioned, but still critical. Resistance to change and insufficient resources were the most prominent barriers, indicating where organizational efforts should focus to further foster a culture of high reliability.
By addressing these barriers, particularly resistance to change and resource constraints, and leveraging facilitators like leadership engagement and transparent communication, organizations can enhance their implementation of just culture and high reliability practices. These efforts require deliberate strategies, including effective training, mentorship, and the active presence of leadership.
Discussion
This quality improvement initiative builds on prior research by examining the implementation of HRO practices from the perspective of frontline supervisors. Unlike earlier research focused on HRO leads, this study explores the critical role of supervisors who integrate HRO principles into clinical and administrative operations.17 By analyzing their experiences, this study offers practical insights into facilitating HRO implementation across organizational levels.
The findings highlight broad agreement on the value of just culture and HRO principles in fostering safe, accountable health care environments. Participants described just culture as promoting system—level accountability rather than individual blame, encouraging error reporting and learning for continuous improvement. Similarly, HRO practices—emphasizing a preoccupation with failure, operational sensitivity, and resilience— were seen as vital for patient safety in complex settings.
Frontline supervisors play a pivotal role, with 96% of respondents identifying their influence on fostering open communication, psychological safety, and shared accountability. Key facilitators included leadership commitment, open communication, and mentorship. Active leadership involvement was particularly valued, as it trickles down to reinforce standards across all organizational levels. HRO meetings using real-world examples were seen as instrumental in demonstrating the tangible benefits of these principles, helping embed them into daily practices.
Despite these facilitators, several barriers to implementation were noted. Resistance to change and entrenched attitudes, and a persistent gotcha culture undermined efforts to establish just culture. Resource constraints, including staffing shortages and budget limitations, further hindered the adoption of HRO practices. The lack of consistent leadership engagement, marked by limited visibility, follow-through, and transparency, exacerbated these challenges.
HRO leads are important for promoting education and embedding HRO principles into daily operations. These individuals provide vital support to frontline supervisors, translating HRO concepts into actionable practices. However, organizational challenges such as staff turnover and redirected funding have weakened the infrastructure supporting HRO initiatives. The elimination of HRO lead roles due to budgetary pressures at several facilities reflects a short-term focus on operational demands at the expense of long-term cultural transformation.
Additional barriers included siloed communication, fear of reprisal, bureaucratic obstacles, and outdated technology. These challenges limit progress toward high reliability and diminish the effectiveness of HRO principles.
Participants proposed strategies focused on education, training, and leadership engagement. Simulation-based training tailored to specific roles was identified as an effective tool for preparing staff to apply HRO principles in real-world scenarios. Enhanced communication, such as regular leadership rounding and transparent updates on safety concerns, was also emphasized. Participants stressed the importance of showing staff how their feedback influences organizational decisions to build trust and accountability. Finally, standardizing procedures and protocols across facilities was seen as critical for aligning practices and reducing variability in safety processes.
This study underscores the need for sustained leadership commitment and infrastructure to ensure the long-term success of HRO implementation. Addressing the identified barriers and leveraging the proposed mitigation strategies can foster a culture of safety and reliability across the organization.
Limitations
This quality improvement initiative used qualitative grounded theory methods and sampled a relatively small group of experienced leaders specifically involved in implementing HRO within the VHA. In addition, while saturation of themes was reached, the number of responses represents a small sample of VHA frontline supervisors. As such, the findings may not be fully representative of the perspectives of all unit and departmental leaders across the VHA or other health care systems. A previous qualitative quality improvement initiative focused on the perceptions of HRO leads regarding facilitators and barriers to just culture.17 This quality improvement initiative broadened that focus by examining the perspectives of frontline supervisors in the operational environment, who may not be HRO experts but work to implement HRO principles with the guidance of HRO leads (HRO subject matter experts).
There remains an opportunity to address a critical gap by assessing facilitators and barriers beyond the facility level, incorporating both the Veterans Integrated Service Networks (VISN) and VHA Central Office (VHACO). While qualitative methods, such as those used in this study, provide deep insights and detailed understanding, they are limited in their ability to identify system-wide trends and variations at a more strategic VISN and VHACO level. Addressing this could enhance the broader applicability of HRO principles across the VHA.
Conclusions
Successful implementation of the recommendations reported in this study will require sustained focus and continued commitment from all stakeholders across the VHA. As the VHA enters its seventh year on the HRO journey, the risk of organizational drift remains an ongoing concern. Progress has been made, as evidenced by incremental improvements in All Employee Survey scores and increased reporting of adverse events and near misses, but the challenge will be to maintain focus and continue to build upon progress amid the current climate of budgetary constraints.
This study builds on previous quality improvement efforts and provides valuable insights into the barriers and facilitators that can either hinder or support the VHA’s ongoing pursuit of high reliability. The findings offer a model for understanding the complexities of this journey—one that requires continuous effort and adaptation, as there is no definitive endpoint in the quest for high reliability.
Since completion of this study in 2024, the VHA has entered a period of organizational transition and restructuring. Such transitions are often accompanied by increased operational demands and organizational strain. These include realignments, personnel changes, staffing adjustments, workforce reductions, and continued implementation of a new electronic health record system. In this context, maintaining attention to culture, communication, frontline engagement, and mechanisms that provide visibility into organizational climate is essential to sustain momentum in high-reliability efforts.
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/jhm-D-23-00056
- Sculli GL, Pendley-Louis R, Neily J, et al. A high-reliability organization framework for health care: A multiyear implementation strategy and associated outcomes. J Patient Saf. 2022;18:64-70. doi:10.1097/pts.0000000000000788
- Murray JS, Clifford J, Larson S, Lee JK, Sculli GL. Implementing just culture to improve patient safety. Mil Med. 2023;188:usac115. doi:10.1093/milmed/usac115
- Merchant NB, O’Neal J, Montoya A, Cox GR, Murray JS. Creating a process for the implementation of tiered huddles in a Veterans Affairs Medical Center. Mil Med. 2023;188:901-906. doi:10.1093/milmed/usac073
- Mohr DC, Chen C, Sullivan J, et al. Development and validation of the Veterans Health Administration Patient Safety Culture Survey. J Patient Saf. 2022;18:539-545. doi:10.1097/PTS.0000000000001027
- Leonard C, Gilmartin H, Starr L, Anderson T. Leadership and the high reliability transformation: a qualitative study at Truman VA medical center. J Healthc Risk Manag. 2024;44:17-23. doi:10.1002/jhrm.21580
- Sculli G, Essen K. Soaring to Success: The Path to Developing High-Reliability Teams. HCPro; 2021.
- Gupta JI, Sivils S, Reppert J, Paulot W, Houchens N, Hummel S. Visual management board implementation to enhance high reliability at a large VA health care system. Fed Pract. 2024;41:242-246. doi:10.12788/fp.0507
- Veterans Health Administration. High Reliability Organization Learning Catalog. US Dept of Veterans Affairs; 2024. Internal document.
- Jahn JLS, Black AE. A model of communicative and hierarchical foundations of high reliability organizing in wildland firefighting teams. Manag Commun Q. 2017;31:356-379. doi:10.1177/0893318917691358
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Abrams J. Model the way to navigate difficult topics. The Learning Professional. 2022;43:14-18.
- McCausland T. Creating psychological safety in the workplace. Research-Technology Management. 2023;66:56-58. doi:10.1080/08956308.2023.2164439
- Murray JS, Kelly S, Hanover C. Promoting psychological safety in healthcare organizations. Mil Med. 2022;187:808- 810. doi:10.1093/milmed/usac041
- Sutton RI, Rao H. The friction project: how smart leaders make the right things easier and the wrong things harder. St. Martin’s Press; 2024.
- Clark TR. The 4 stages of psychological safety: defining the path to inclusion and innovation. Berrett-Koehler Publishers, Inc.; 2020.
- Essen K, Villalobos C, Sculli G, Steinbach L. Establishing a just culture: implications for the Veterans Health Administration journey to high reliability. Fed Pract. 2024;41:290- 297. doi:10.12788/fp.0512
- Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 4th ed. SAGE Publications; 2014.
- Patton MQ. Qualitative research & evaluation methods: integrating theory and practice. 4th ed. SAGE Publications, Inc.; 2015.
- Krumpal I. Determinants of social desirability bias in sensitive surveys: a literature review. Qual Quant. 2013;47:2025- 2047. doi:10.1007/s11135-011-9640-9
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/jhm-D-23-00056
- Sculli GL, Pendley-Louis R, Neily J, et al. A high-reliability organization framework for health care: A multiyear implementation strategy and associated outcomes. J Patient Saf. 2022;18:64-70. doi:10.1097/pts.0000000000000788
- Murray JS, Clifford J, Larson S, Lee JK, Sculli GL. Implementing just culture to improve patient safety. Mil Med. 2023;188:usac115. doi:10.1093/milmed/usac115
- Merchant NB, O’Neal J, Montoya A, Cox GR, Murray JS. Creating a process for the implementation of tiered huddles in a Veterans Affairs Medical Center. Mil Med. 2023;188:901-906. doi:10.1093/milmed/usac073
- Mohr DC, Chen C, Sullivan J, et al. Development and validation of the Veterans Health Administration Patient Safety Culture Survey. J Patient Saf. 2022;18:539-545. doi:10.1097/PTS.0000000000001027
- Leonard C, Gilmartin H, Starr L, Anderson T. Leadership and the high reliability transformation: a qualitative study at Truman VA medical center. J Healthc Risk Manag. 2024;44:17-23. doi:10.1002/jhrm.21580
- Sculli G, Essen K. Soaring to Success: The Path to Developing High-Reliability Teams. HCPro; 2021.
- Gupta JI, Sivils S, Reppert J, Paulot W, Houchens N, Hummel S. Visual management board implementation to enhance high reliability at a large VA health care system. Fed Pract. 2024;41:242-246. doi:10.12788/fp.0507
- Veterans Health Administration. High Reliability Organization Learning Catalog. US Dept of Veterans Affairs; 2024. Internal document.
- Jahn JLS, Black AE. A model of communicative and hierarchical foundations of high reliability organizing in wildland firefighting teams. Manag Commun Q. 2017;31:356-379. doi:10.1177/0893318917691358
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Abrams J. Model the way to navigate difficult topics. The Learning Professional. 2022;43:14-18.
- McCausland T. Creating psychological safety in the workplace. Research-Technology Management. 2023;66:56-58. doi:10.1080/08956308.2023.2164439
- Murray JS, Kelly S, Hanover C. Promoting psychological safety in healthcare organizations. Mil Med. 2022;187:808- 810. doi:10.1093/milmed/usac041
- Sutton RI, Rao H. The friction project: how smart leaders make the right things easier and the wrong things harder. St. Martin’s Press; 2024.
- Clark TR. The 4 stages of psychological safety: defining the path to inclusion and innovation. Berrett-Koehler Publishers, Inc.; 2020.
- Essen K, Villalobos C, Sculli G, Steinbach L. Establishing a just culture: implications for the Veterans Health Administration journey to high reliability. Fed Pract. 2024;41:290- 297. doi:10.12788/fp.0512
- Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 4th ed. SAGE Publications; 2014.
- Patton MQ. Qualitative research & evaluation methods: integrating theory and practice. 4th ed. SAGE Publications, Inc.; 2015.
- Krumpal I. Determinants of social desirability bias in sensitive surveys: a literature review. Qual Quant. 2013;47:2025- 2047. doi:10.1007/s11135-011-9640-9
Frontline Supervisor Perspectives on Enabling High Reliability and Fostering a Just Culture at the VHA
Frontline Supervisor Perspectives on Enabling High Reliability and Fostering a Just Culture at the VHA

Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
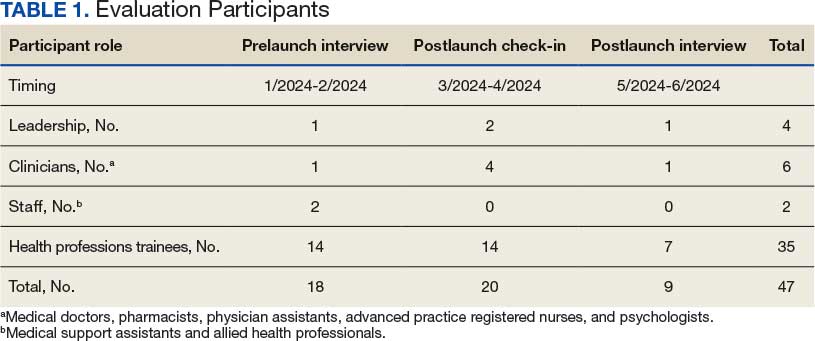
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
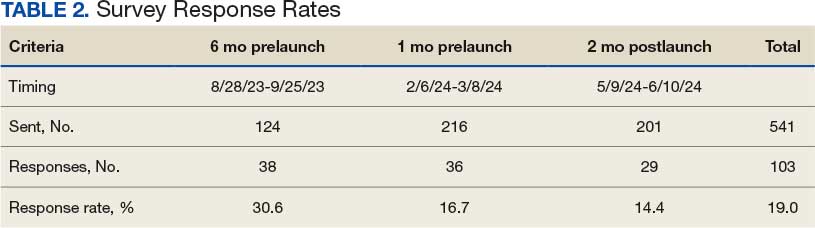
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
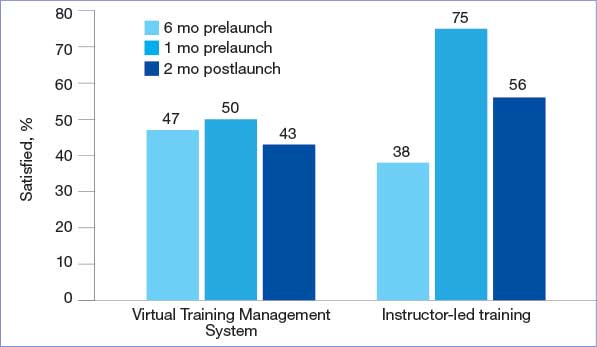
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
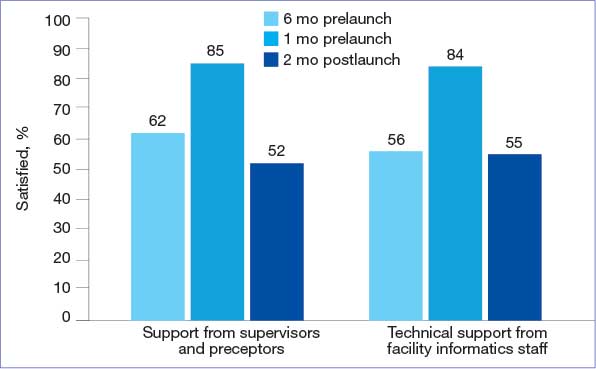
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
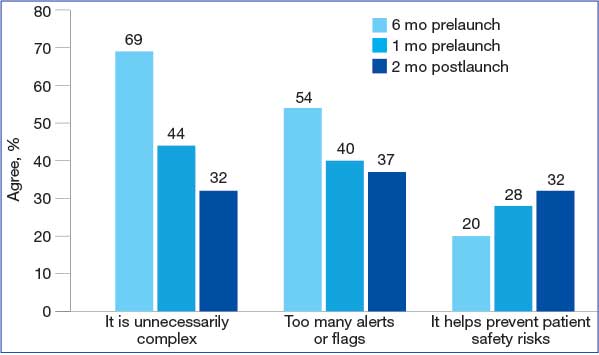
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
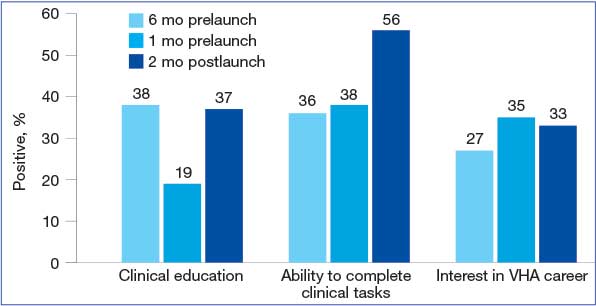
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record

Effectiveness and Safety of Droperidol Use in the VA Greater Los Angeles Healthcare System Emergency Department
Effectiveness and Safety of Droperidol Use in the VA Greater Los Angeles Healthcare System Emergency Department
Droperidol is a butyrophenone antipsychotic approved by the US Food and Drug Administration (FDA) for use in postoperative nausea and vomiting (PONV). Off-label, it has also been utilized for its sedative, anxiolytic, and analgesic properties.1 While its exact mechanism of action remains elusive, it is believed that binding to postsynaptic γ-aminobutyric acid receptors induces anxiolysis and sedation, while dopaminergic activity in the chemoreceptor trigger zone contributes to its antiemetic effects.2 Since the introduction of droperidol in 1967, it has been widely used by emergency physicians, psychiatrists, and anesthesiologists globally.1
Despite its therapeutic efficacy, use of droperidol has been tempered by concerns regarding its cardiovascular safety profile, specifically its potential to prolong the QT interval and precipitate cardiac arrhythmias. In 2001, the FDA placed a boxed warning on droperidol that mandated electrocardiogram (EKG) monitoring before and after treatment. This requirement has led to a widespread decrease in use, and the FDA decision sparked significant controversy among clinicians, with many organizations arguing that the evidence did not support this mandate.1
Further review of the cases cited by the FDA revealed that there were 277 reported cases of droperidol-related adverse events (AEs), but many of these cases were duplicates and occurred outside the US.3 Additionally, the doses of droperidol used in these cases were significantly higher than the typical doses used in the emergency department (ED), ranging from 25 to 250 mg.4 Typical doses for PONV range from 0.625 to 2.5 mg intravenous (IV) or intramuscular (IM). Recommended doses for agitation typically range from 2.5 to 10 mg IV and 5 to 10 mg IM.5
There has been growing interest in reevaluating the risk-benefit profile of droperidol in the ED. Since the original decision by the FDA, multiple publications have challenged the idea that droperidol has significantly higher risks associated with its use. The 2014 review by the Clinical Guidelines Committee of the American Academy of Emergency Medicine did not find evidence that low-dose droperidol (< 2.5 is unsafe for use in the ED.6 A retrospective cohort study from 2020 found no fatalities in 5784 patients. Furthermore, a prospective observational study of 1009 patients at 6 EDs who received high-dose droperidol (≤ 20.0 mg) found no evidence of increased risk for QT prolongation.7 The evidence supports the safety of droperidol for use in prehospital and hospital settings as well as in pediatric, adult, and geriatric populations.8-14 Droperidol was eventually reintroduced in 2019, which led to increased use.
The US Department of Veterans Affairs (VA) formulary has limited options (eg, haloperidol and olanzapine) that have robust evidence supporting their use to treat aggression or psychosis-related agitation. Ziprasidone injections are not on the formulary and require authorization for use, which may delay patient care and pose a safety risk. In 2021, VA Greater Los Angeles Healthcare System (VAGLAHS) received Pharmacy and Therapeutics Committee approval to use droperidol in the ED for agitation or nausea and vomiting. The purpose of this study was to evaluate safety outcomes for patients prescribed droperidol and the need for rescue medications (ie, effectiveness) in the VAGLAHS ED.
Methods
This retrospective chart review analyzed patients administered droperidol in the VAGLAHS ED from February 1, 2021, through April 30, 2023. A list of patients who had droperidol ordered in the VAGLAHS ED was obtained from the Veterans Health Information Systems and Technology Architecture. Charts were reviewed using the Computerized Patient Record System to confirm droperidol administration. Nurse documentation was reviewed to confirm the time, dose, and route of administration. In addition, droperidol dosages were categorized as < 5 mg, 5 to 10 mg, and > 10 mg to review outcomes based on the total amount administered to each patient.
Patients included in the study received droperidol in the ED within the study period, were aged ≥ 18 years, and received droperidol for acute agitation or antiemesis. Patients were excluded if they received droperidol for an indication other than agitation or antiemesis.
The study team reviewed the list of patients and audited the collected data. Reviewers were trained on the study protocols and variables identified. The following data were collected: patient demographics (age, sex, race, height, weight, allergies), Charlson Comorbidity Index (CCI) conditions, cardiac comorbidities, laboratory values at admission, basic metabolic panels, liver function tests, droperidol use (doses, indications, and documentation of safety), concomitant medications ordered with the initial droperidol order, AEs (arrhythmias, extrapyramidal symptoms [EPS], respiratory depression, mortality), medications used within 60 minutes of droperidol administration (rescue medications), other medications used within 24 hours after droperidol administration, and EKG/QTc (corrected QT interval) intervals. The data reviewed and recorded were from the date of the initial patient ED visit.
Outcomes
The primary outcome was all-cause mortality within 24 hours after droperidol administration. This outcome was measured in all patients included in this study. Secondary outcomes included rescue medications needed after droperidol administration, incidence of QT prolongation, incidence of EPS (defined as akathisia, dystonia, parkinsonism, or tardive dyskinesia), and incidence of respiratory depression. Clinically significant QTc was defined as an interval of ≥ 500 ms with incidence of arrhythmias, code blues, or intubations. Baseline risk factors for QTc prolongation were taken into consideration including electrolyte abnormalities, concomitant QT-prolonging medications, CCI score, and cardiac comorbidities. Incidence of EPS was counted if patients received medications such as diphenhydramine or benztropine after droperidol administration in addition to documentation of EPS signs and symptoms. Incidences of EPS findings were reviewed by emergency department physicians to confirm the diagnosis.
Safety was assessed by quantifying mortality rates 24 hours after droperidol administration along with incidence of AEs associated with droperidol use including QT prolongation, EPS, and respiratory depression.
The necessity of rescue medication use was assessed by nursing documentation, additional medications ordered, and/or no additional medications required for agitation within 60 minutes of droperidol administration. Sixty minutes was the chosen timeframe given that the onset of droperidol action is between 3 and 10 minutes and peaks in about 30 minutes. Medications that were considered rescue medications included diphenhydramine < 25 mg, diphenhydramine 25 to 50 mg, lorazepam < 1 mg, lorazepam 1 to 2 mg, diphenhydramine < 25 mg and lorazepam < 1 mg, diphenhydramine < 25 mg and lorazepam 1 to 2 mg, diphenhydramine 25 to 50 mg and lorazepam 1 to 2 mg, and other medications, the names and doses of which were manually documented by investigators.
Statistical Analysis
For all variables in the study, descriptive analysis was used to categorize findings. Microsoft Excel was used to calculate means, frequency counts, percentages, and categorize data.
Results
Between February 1, 2021, and April 16, 2023, 214 patients received droperidol in the VAGLAHS ED, and 207 patients were included in the study. Seven patients did not receive droperidol for the indications included (acute agitation or antiemesis). Most of the study population (89.4%) was male, and the mean age was 51.0 years. The mean CCI was 1.6. In the study, 183 (88.4%) patients received droperidol for agitation and 24 (11.6%) for nausea and vomiting (Table 1).
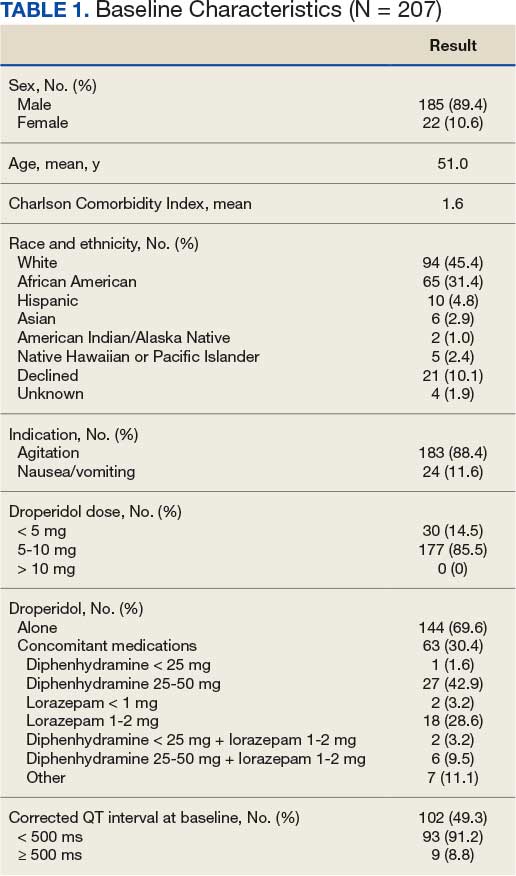
Primary Outcome
No deaths were observed in a 24-hour period after droperidol administration among the 207 patients included in the study. There were also no arrhythmias, code blues, or intubations observed with the administration of droperidol (Table 2).
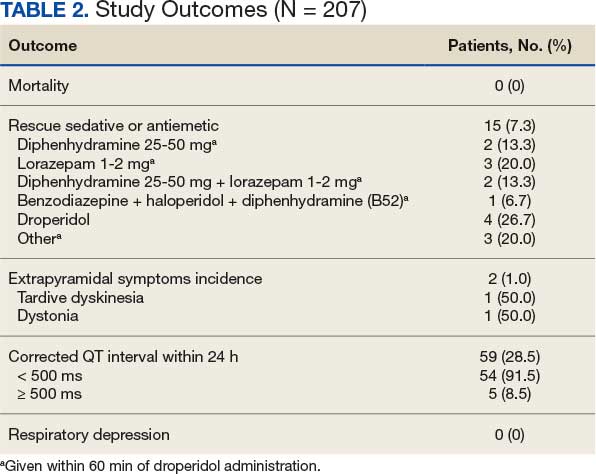
Secondary Outcomes
A total of 144 patients (69.6%) received droperidol alone to resolve agitation or nausea and vomiting. In the remaining population, 63 (30.4%) patients were given medications concomitantly with droperidol.
Fifteen patients (7.2%) required rescue medications that were administered within 60 minutes of droperidol administration. Rescue medications were required for 7 patients (4.9%) who initially received droperidol alone compared with 8 patients (12.7%) who were administered concomitant medications with droperidol (Figure).
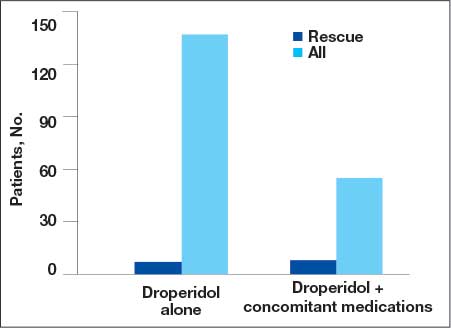
Extrapyramidal Symptoms
EPS occurred in 2 patients (1.0%). There was 1 incidence of tardive dyskinesia (TD) in which the patient received droperidol 2.5 mg IM for emesis. TD was resolved with diphenhydramine 50 mg. A second patient who experienced dystonia received droperidol 10 mg IM for agitation. Dystonia was resolved with benztropine 2 mg. Both patients had a CCI of 0, no cardiac comorbidities, and laboratory test results were within reference ranges. The second patient received olanzapine within 24 hours of droperidol administration; however, it was after the EPS event.
QTc Prolongation
Baseline EKGs (within 6 months prior to ED visit) were available for 102 patients (49.3%). Nine patients (8.8%) had a reported baseline QTc of ≥ 500 ms (Table 3). Of these patients, 6 had a repeat EKG and 5 had a repeat QTc < 500 ms. One patient had a baseline and repeated QTc of 512 ms with essentially no change after droperidol administration. Only 1 patient was on a potentially QTc-prolonging medication at home. None of the patients with baseline QTc > 500 ms experienced arrhythmias after droperidol administration.
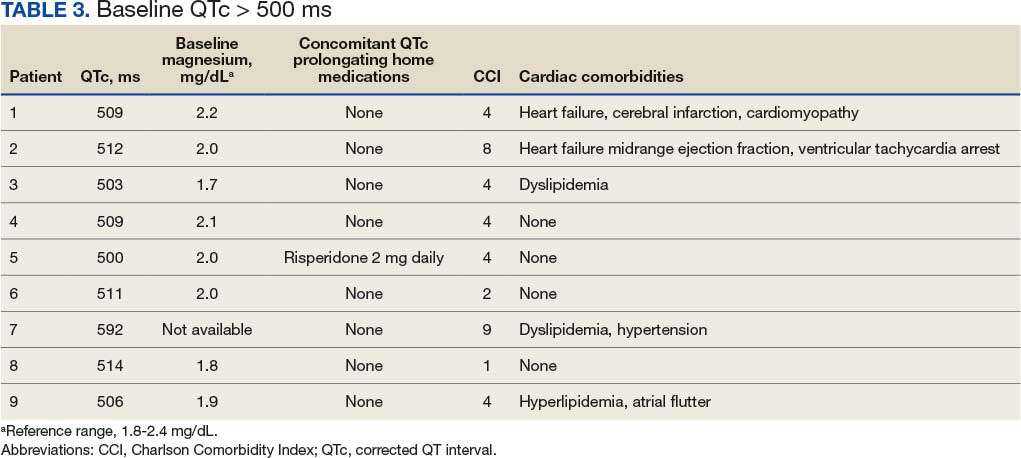
We found that 59 patients (28.5%) had EKGs performed within 24 hours after droperidol administration. Five patients had documented QTc ≥ 500 ms, but no arrhythmias were observed in a 24-hour period. Table 4 describes the additional medications administered after the 60-minute window but within 24 hours after droperidol administration. Quetiapine 300 mg and metoclopramide 5 mg were the only medications documented that can potentially increase QTc. Patient adherence to home medications and the timing of the last dose prior to ED visit were unknown. However, no arrhythmias were noted in these patients with QTc changes. No patients experienced respiratory depression within 24 hours of droperidol administration.
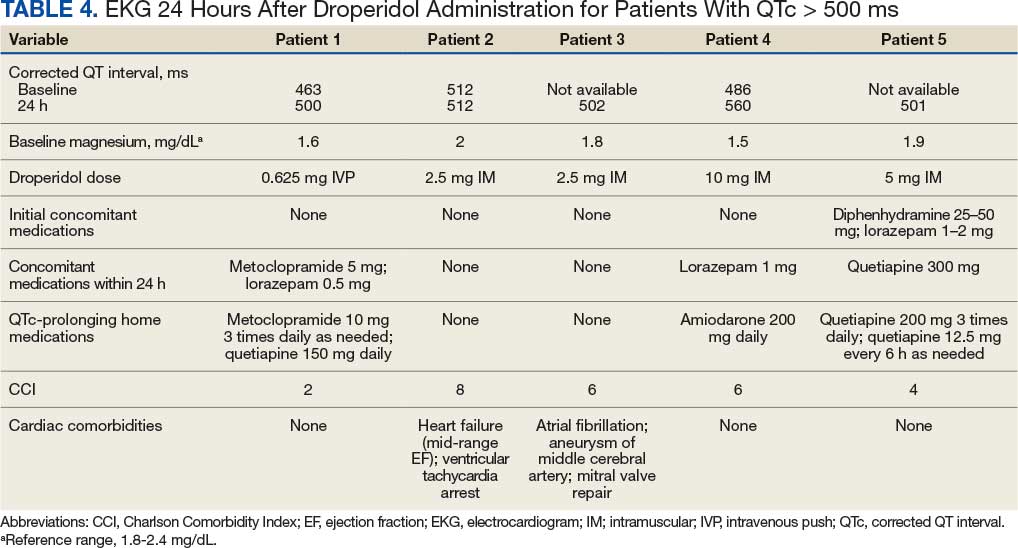
Older Adult Patients
Thirty-eight patients were aged ≥ 65 years with a mean age of 74.2 years. Thirty-four patients (89.5%) received droperidol for agitation and 4 (10.6%) for nausea and vomiting. Only 21 patients had a baseline EKG, and 4 had QTc ≤ 500 ms. At 24 hours, EKGs were performed for 18 patients and 3 had a QTc ≤ 500 ms. No mortality or arrhythmias were reported and there were no incidences of rescue medications, EPS, or respiratory depression.
Discussion
The study included 207 patients who received droperidol for either agitation or nausea/vomiting in the VAGLAHS ED. No mortality occurred within 24 hours of droperidol administration, which is consistent with recent studies.8-14
Furthermore, 59 patients (28.5%) had an EKG performed within 24 hours of droperidol administration; 5 patients had documented QTc ≥ 500 ms. Only 3 of the patients with prolonged QTc had baseline readings for comparison. Only 2 patients had an increase in QTc interval. No arrhythmias were observed; however, the effects of observing QTc prolongation were limited due to the lack of post-EKG readings following droperidol administration. Because of the retrospective nature of the study, neither standardization of EKG at baseline nor 24-hour postadministration were possible. The study found that droperidol was effective with only 15 patients (7.3%) requiring rescue medications. In the patients who were given medications concomitantly with droperidol, it was not possible to conclude whether the patients would have required rescue medications to resolve their agitation or nausea/vomiting. Administration of concomitant medications with droperidol may be attributed to practice patterns associated with haloperidol use, which is frequently administered with concomitant medications such as diphenhydramine and/or a benzodiazepine.
AEs were rare with no documentation of respiratory depression and 2 cases (1.0%) of EPS. Both incidences of EPS resolved with diphenhydramine or benztropine. However, given the reliance on nursing documentation to capture AEs, the number of events may have been underreported.
Limitations
Standardization of dosing was a limiting factor that could affect the need for rescue medications. Another limitation was reliance on nursing reports of resolution of symptoms and comfort with agitated patients. Given the retrospective design and small sample size, this study may not have captured all potential AEs. However, the doses administered within this study population were consistent with what was expected based on other studies.8-14
Conclusions
Droperidol, an antipsychotic, is currently approved for PONV, but is also used off-label for agitation. This study found no fatalities among patients who received droperidol in the ED. The findings suggest that droperidol used for agitation and as an antiemetic, despite its FDA boxed warning, appears to be safe and showed no evidence of mortality, arrhythmias, code blues, or intubations despite the lack of postdose EKG monitoring. Among the 38 patients aged ≥ 65 years, the use of droperidol revealed no increased risks. It should be noted that droperidol appeared safe and few patients required rescue medications within this study population.
- Perkins J, Ho JD, Vilke GM, DeMers G. American Academy of Emergency Medicine Position Statement: Safety of droperidol use in the emergency department. J Emerg Med. 2015;49:91-97. doi:10.1016/j.jemermed.2014.12.024
- Siegel RB, Motov SM, Marcolini EG. Droperidol use in the emergency department: a clinical review. J Emerg Med. 2023;64:289-294. doi:10.1016/j.jemermed.2022.12.012
- Jackson CW, Sheehan AH, Reddan JG. Evidencebased review of the black-box warning for droperidol. Am J Health Syst Pharm. 2007;64:1174-1186. doi:10.2146/ajhp060505
- Habib AS, Gan TJ. Food and Drug Administration black box warning on the perioperative use of droperidol: a review of the cases. Anesth Analg. 2003;96(5):1377-1379. doi:10.1213/01.ane.0000063923.87560.37
- Droperidol. In: Micromedex (electronic version). IBM Watson Health; 2019. Accessed March 2, 2026. https://www .micromedexsolutions.com
- Gaw CM, Cabrera D, Bellolio F, Mattson AE, Lohse CM, Jeffery MM. Effectiveness and safety of droperidol in a United States emergency department. Am J Emerg Med. 2020;38:1310-1314. doi:10.1016/j.ajem.2019.09.007
- Calver L, Page CB, Downes MA, et al. The safety and effectiveness of droperidol for sedation of acute behavioral disturbance in the emergency department. Ann Emerg Med. 2015;66(3):230-238.e1. doi:10.1016/j.annemergmed.2015.03.016
- Ernst R, Wagstaff H, Smith M, et al. Droperidol administration among emergency department patients with abdominal pain, nausea, and vomiting. Am J Emerg Med. 2024;85:44-47. doi:10.1016/j.ajem.2024.07.060
- Szwak K, Sacchetti A. Droperidol use in pediatric emergency department patients. Pediatr Emerg Care. 2010;26:248-250. doi:10.1097/pec.0b013e3181d6d9f2
- Chase PB, Biros MH. A retrospective review of the use and safety of droperidol in a large, high-risk, inner-city emergency department patient population. Acad Emerg Med. 2002;9:1402-1410. doi:10.1111/j.1553-2712.2002.tb01609.x
- Mattson A, Friend K, Brown CS, Cabrera D. Reintegrating droperidol into emergency medicine practice. Am J Health Syst Pharm. 2020;77(22):1838-1845. doi:10.1093/ajhp/zxaa271
- Cole JB, Stang JL, DeVries PA, Martel ML, Miner JR, Driver BE. A prospective study of intramuscular droperidol or olanzapine for acute agitation in the emergency department: a natural experiment owing to drug shortages. Ann Emerg Med. 2021;78(2):274-286. doi:10.1016/j.annemergmed.2021.01.005
- Page CB, Parker LE, Rashford SJ, et al. Prospective study of the safety and effectiveness of droperidol in elderly patients for pre-hospital acute behavioural disturbance. Emerg Med Australas. 2020;32(5):731-736. doi:10.1111/1742-6723.13496
- Page CB, Parker LE, Rashford SJ, et al. A prospective study of the safety and effectiveness of droperidol inchildren for prehospital acute behavioral disturbance. Prehosp Emerg Care. 2018;23:519-526. doi:10.1080/10903127.2018.1542473
Droperidol is a butyrophenone antipsychotic approved by the US Food and Drug Administration (FDA) for use in postoperative nausea and vomiting (PONV). Off-label, it has also been utilized for its sedative, anxiolytic, and analgesic properties.1 While its exact mechanism of action remains elusive, it is believed that binding to postsynaptic γ-aminobutyric acid receptors induces anxiolysis and sedation, while dopaminergic activity in the chemoreceptor trigger zone contributes to its antiemetic effects.2 Since the introduction of droperidol in 1967, it has been widely used by emergency physicians, psychiatrists, and anesthesiologists globally.1
Despite its therapeutic efficacy, use of droperidol has been tempered by concerns regarding its cardiovascular safety profile, specifically its potential to prolong the QT interval and precipitate cardiac arrhythmias. In 2001, the FDA placed a boxed warning on droperidol that mandated electrocardiogram (EKG) monitoring before and after treatment. This requirement has led to a widespread decrease in use, and the FDA decision sparked significant controversy among clinicians, with many organizations arguing that the evidence did not support this mandate.1
Further review of the cases cited by the FDA revealed that there were 277 reported cases of droperidol-related adverse events (AEs), but many of these cases were duplicates and occurred outside the US.3 Additionally, the doses of droperidol used in these cases were significantly higher than the typical doses used in the emergency department (ED), ranging from 25 to 250 mg.4 Typical doses for PONV range from 0.625 to 2.5 mg intravenous (IV) or intramuscular (IM). Recommended doses for agitation typically range from 2.5 to 10 mg IV and 5 to 10 mg IM.5
There has been growing interest in reevaluating the risk-benefit profile of droperidol in the ED. Since the original decision by the FDA, multiple publications have challenged the idea that droperidol has significantly higher risks associated with its use. The 2014 review by the Clinical Guidelines Committee of the American Academy of Emergency Medicine did not find evidence that low-dose droperidol (< 2.5 is unsafe for use in the ED.6 A retrospective cohort study from 2020 found no fatalities in 5784 patients. Furthermore, a prospective observational study of 1009 patients at 6 EDs who received high-dose droperidol (≤ 20.0 mg) found no evidence of increased risk for QT prolongation.7 The evidence supports the safety of droperidol for use in prehospital and hospital settings as well as in pediatric, adult, and geriatric populations.8-14 Droperidol was eventually reintroduced in 2019, which led to increased use.
The US Department of Veterans Affairs (VA) formulary has limited options (eg, haloperidol and olanzapine) that have robust evidence supporting their use to treat aggression or psychosis-related agitation. Ziprasidone injections are not on the formulary and require authorization for use, which may delay patient care and pose a safety risk. In 2021, VA Greater Los Angeles Healthcare System (VAGLAHS) received Pharmacy and Therapeutics Committee approval to use droperidol in the ED for agitation or nausea and vomiting. The purpose of this study was to evaluate safety outcomes for patients prescribed droperidol and the need for rescue medications (ie, effectiveness) in the VAGLAHS ED.
Methods
This retrospective chart review analyzed patients administered droperidol in the VAGLAHS ED from February 1, 2021, through April 30, 2023. A list of patients who had droperidol ordered in the VAGLAHS ED was obtained from the Veterans Health Information Systems and Technology Architecture. Charts were reviewed using the Computerized Patient Record System to confirm droperidol administration. Nurse documentation was reviewed to confirm the time, dose, and route of administration. In addition, droperidol dosages were categorized as < 5 mg, 5 to 10 mg, and > 10 mg to review outcomes based on the total amount administered to each patient.
Patients included in the study received droperidol in the ED within the study period, were aged ≥ 18 years, and received droperidol for acute agitation or antiemesis. Patients were excluded if they received droperidol for an indication other than agitation or antiemesis.
The study team reviewed the list of patients and audited the collected data. Reviewers were trained on the study protocols and variables identified. The following data were collected: patient demographics (age, sex, race, height, weight, allergies), Charlson Comorbidity Index (CCI) conditions, cardiac comorbidities, laboratory values at admission, basic metabolic panels, liver function tests, droperidol use (doses, indications, and documentation of safety), concomitant medications ordered with the initial droperidol order, AEs (arrhythmias, extrapyramidal symptoms [EPS], respiratory depression, mortality), medications used within 60 minutes of droperidol administration (rescue medications), other medications used within 24 hours after droperidol administration, and EKG/QTc (corrected QT interval) intervals. The data reviewed and recorded were from the date of the initial patient ED visit.
Outcomes
The primary outcome was all-cause mortality within 24 hours after droperidol administration. This outcome was measured in all patients included in this study. Secondary outcomes included rescue medications needed after droperidol administration, incidence of QT prolongation, incidence of EPS (defined as akathisia, dystonia, parkinsonism, or tardive dyskinesia), and incidence of respiratory depression. Clinically significant QTc was defined as an interval of ≥ 500 ms with incidence of arrhythmias, code blues, or intubations. Baseline risk factors for QTc prolongation were taken into consideration including electrolyte abnormalities, concomitant QT-prolonging medications, CCI score, and cardiac comorbidities. Incidence of EPS was counted if patients received medications such as diphenhydramine or benztropine after droperidol administration in addition to documentation of EPS signs and symptoms. Incidences of EPS findings were reviewed by emergency department physicians to confirm the diagnosis.
Safety was assessed by quantifying mortality rates 24 hours after droperidol administration along with incidence of AEs associated with droperidol use including QT prolongation, EPS, and respiratory depression.
The necessity of rescue medication use was assessed by nursing documentation, additional medications ordered, and/or no additional medications required for agitation within 60 minutes of droperidol administration. Sixty minutes was the chosen timeframe given that the onset of droperidol action is between 3 and 10 minutes and peaks in about 30 minutes. Medications that were considered rescue medications included diphenhydramine < 25 mg, diphenhydramine 25 to 50 mg, lorazepam < 1 mg, lorazepam 1 to 2 mg, diphenhydramine < 25 mg and lorazepam < 1 mg, diphenhydramine < 25 mg and lorazepam 1 to 2 mg, diphenhydramine 25 to 50 mg and lorazepam 1 to 2 mg, and other medications, the names and doses of which were manually documented by investigators.
Statistical Analysis
For all variables in the study, descriptive analysis was used to categorize findings. Microsoft Excel was used to calculate means, frequency counts, percentages, and categorize data.
Results
Between February 1, 2021, and April 16, 2023, 214 patients received droperidol in the VAGLAHS ED, and 207 patients were included in the study. Seven patients did not receive droperidol for the indications included (acute agitation or antiemesis). Most of the study population (89.4%) was male, and the mean age was 51.0 years. The mean CCI was 1.6. In the study, 183 (88.4%) patients received droperidol for agitation and 24 (11.6%) for nausea and vomiting (Table 1).
Primary Outcome
No deaths were observed in a 24-hour period after droperidol administration among the 207 patients included in the study. There were also no arrhythmias, code blues, or intubations observed with the administration of droperidol (Table 2).
Secondary Outcomes
A total of 144 patients (69.6%) received droperidol alone to resolve agitation or nausea and vomiting. In the remaining population, 63 (30.4%) patients were given medications concomitantly with droperidol.
Fifteen patients (7.2%) required rescue medications that were administered within 60 minutes of droperidol administration. Rescue medications were required for 7 patients (4.9%) who initially received droperidol alone compared with 8 patients (12.7%) who were administered concomitant medications with droperidol (Figure).
Extrapyramidal Symptoms
EPS occurred in 2 patients (1.0%). There was 1 incidence of tardive dyskinesia (TD) in which the patient received droperidol 2.5 mg IM for emesis. TD was resolved with diphenhydramine 50 mg. A second patient who experienced dystonia received droperidol 10 mg IM for agitation. Dystonia was resolved with benztropine 2 mg. Both patients had a CCI of 0, no cardiac comorbidities, and laboratory test results were within reference ranges. The second patient received olanzapine within 24 hours of droperidol administration; however, it was after the EPS event.
QTc Prolongation
Baseline EKGs (within 6 months prior to ED visit) were available for 102 patients (49.3%). Nine patients (8.8%) had a reported baseline QTc of ≥ 500 ms (Table 3). Of these patients, 6 had a repeat EKG and 5 had a repeat QTc < 500 ms. One patient had a baseline and repeated QTc of 512 ms with essentially no change after droperidol administration. Only 1 patient was on a potentially QTc-prolonging medication at home. None of the patients with baseline QTc > 500 ms experienced arrhythmias after droperidol administration.
We found that 59 patients (28.5%) had EKGs performed within 24 hours after droperidol administration. Five patients had documented QTc ≥ 500 ms, but no arrhythmias were observed in a 24-hour period. Table 4 describes the additional medications administered after the 60-minute window but within 24 hours after droperidol administration. Quetiapine 300 mg and metoclopramide 5 mg were the only medications documented that can potentially increase QTc. Patient adherence to home medications and the timing of the last dose prior to ED visit were unknown. However, no arrhythmias were noted in these patients with QTc changes. No patients experienced respiratory depression within 24 hours of droperidol administration.
Older Adult Patients
Thirty-eight patients were aged ≥ 65 years with a mean age of 74.2 years. Thirty-four patients (89.5%) received droperidol for agitation and 4 (10.6%) for nausea and vomiting. Only 21 patients had a baseline EKG, and 4 had QTc ≤ 500 ms. At 24 hours, EKGs were performed for 18 patients and 3 had a QTc ≤ 500 ms. No mortality or arrhythmias were reported and there were no incidences of rescue medications, EPS, or respiratory depression.
Discussion
The study included 207 patients who received droperidol for either agitation or nausea/vomiting in the VAGLAHS ED. No mortality occurred within 24 hours of droperidol administration, which is consistent with recent studies.8-14
Furthermore, 59 patients (28.5%) had an EKG performed within 24 hours of droperidol administration; 5 patients had documented QTc ≥ 500 ms. Only 3 of the patients with prolonged QTc had baseline readings for comparison. Only 2 patients had an increase in QTc interval. No arrhythmias were observed; however, the effects of observing QTc prolongation were limited due to the lack of post-EKG readings following droperidol administration. Because of the retrospective nature of the study, neither standardization of EKG at baseline nor 24-hour postadministration were possible. The study found that droperidol was effective with only 15 patients (7.3%) requiring rescue medications. In the patients who were given medications concomitantly with droperidol, it was not possible to conclude whether the patients would have required rescue medications to resolve their agitation or nausea/vomiting. Administration of concomitant medications with droperidol may be attributed to practice patterns associated with haloperidol use, which is frequently administered with concomitant medications such as diphenhydramine and/or a benzodiazepine.
AEs were rare with no documentation of respiratory depression and 2 cases (1.0%) of EPS. Both incidences of EPS resolved with diphenhydramine or benztropine. However, given the reliance on nursing documentation to capture AEs, the number of events may have been underreported.
Limitations
Standardization of dosing was a limiting factor that could affect the need for rescue medications. Another limitation was reliance on nursing reports of resolution of symptoms and comfort with agitated patients. Given the retrospective design and small sample size, this study may not have captured all potential AEs. However, the doses administered within this study population were consistent with what was expected based on other studies.8-14
Conclusions
Droperidol, an antipsychotic, is currently approved for PONV, but is also used off-label for agitation. This study found no fatalities among patients who received droperidol in the ED. The findings suggest that droperidol used for agitation and as an antiemetic, despite its FDA boxed warning, appears to be safe and showed no evidence of mortality, arrhythmias, code blues, or intubations despite the lack of postdose EKG monitoring. Among the 38 patients aged ≥ 65 years, the use of droperidol revealed no increased risks. It should be noted that droperidol appeared safe and few patients required rescue medications within this study population.
Droperidol is a butyrophenone antipsychotic approved by the US Food and Drug Administration (FDA) for use in postoperative nausea and vomiting (PONV). Off-label, it has also been utilized for its sedative, anxiolytic, and analgesic properties.1 While its exact mechanism of action remains elusive, it is believed that binding to postsynaptic γ-aminobutyric acid receptors induces anxiolysis and sedation, while dopaminergic activity in the chemoreceptor trigger zone contributes to its antiemetic effects.2 Since the introduction of droperidol in 1967, it has been widely used by emergency physicians, psychiatrists, and anesthesiologists globally.1
Despite its therapeutic efficacy, use of droperidol has been tempered by concerns regarding its cardiovascular safety profile, specifically its potential to prolong the QT interval and precipitate cardiac arrhythmias. In 2001, the FDA placed a boxed warning on droperidol that mandated electrocardiogram (EKG) monitoring before and after treatment. This requirement has led to a widespread decrease in use, and the FDA decision sparked significant controversy among clinicians, with many organizations arguing that the evidence did not support this mandate.1
Further review of the cases cited by the FDA revealed that there were 277 reported cases of droperidol-related adverse events (AEs), but many of these cases were duplicates and occurred outside the US.3 Additionally, the doses of droperidol used in these cases were significantly higher than the typical doses used in the emergency department (ED), ranging from 25 to 250 mg.4 Typical doses for PONV range from 0.625 to 2.5 mg intravenous (IV) or intramuscular (IM). Recommended doses for agitation typically range from 2.5 to 10 mg IV and 5 to 10 mg IM.5
There has been growing interest in reevaluating the risk-benefit profile of droperidol in the ED. Since the original decision by the FDA, multiple publications have challenged the idea that droperidol has significantly higher risks associated with its use. The 2014 review by the Clinical Guidelines Committee of the American Academy of Emergency Medicine did not find evidence that low-dose droperidol (< 2.5 is unsafe for use in the ED.6 A retrospective cohort study from 2020 found no fatalities in 5784 patients. Furthermore, a prospective observational study of 1009 patients at 6 EDs who received high-dose droperidol (≤ 20.0 mg) found no evidence of increased risk for QT prolongation.7 The evidence supports the safety of droperidol for use in prehospital and hospital settings as well as in pediatric, adult, and geriatric populations.8-14 Droperidol was eventually reintroduced in 2019, which led to increased use.
The US Department of Veterans Affairs (VA) formulary has limited options (eg, haloperidol and olanzapine) that have robust evidence supporting their use to treat aggression or psychosis-related agitation. Ziprasidone injections are not on the formulary and require authorization for use, which may delay patient care and pose a safety risk. In 2021, VA Greater Los Angeles Healthcare System (VAGLAHS) received Pharmacy and Therapeutics Committee approval to use droperidol in the ED for agitation or nausea and vomiting. The purpose of this study was to evaluate safety outcomes for patients prescribed droperidol and the need for rescue medications (ie, effectiveness) in the VAGLAHS ED.
Methods
This retrospective chart review analyzed patients administered droperidol in the VAGLAHS ED from February 1, 2021, through April 30, 2023. A list of patients who had droperidol ordered in the VAGLAHS ED was obtained from the Veterans Health Information Systems and Technology Architecture. Charts were reviewed using the Computerized Patient Record System to confirm droperidol administration. Nurse documentation was reviewed to confirm the time, dose, and route of administration. In addition, droperidol dosages were categorized as < 5 mg, 5 to 10 mg, and > 10 mg to review outcomes based on the total amount administered to each patient.
Patients included in the study received droperidol in the ED within the study period, were aged ≥ 18 years, and received droperidol for acute agitation or antiemesis. Patients were excluded if they received droperidol for an indication other than agitation or antiemesis.
The study team reviewed the list of patients and audited the collected data. Reviewers were trained on the study protocols and variables identified. The following data were collected: patient demographics (age, sex, race, height, weight, allergies), Charlson Comorbidity Index (CCI) conditions, cardiac comorbidities, laboratory values at admission, basic metabolic panels, liver function tests, droperidol use (doses, indications, and documentation of safety), concomitant medications ordered with the initial droperidol order, AEs (arrhythmias, extrapyramidal symptoms [EPS], respiratory depression, mortality), medications used within 60 minutes of droperidol administration (rescue medications), other medications used within 24 hours after droperidol administration, and EKG/QTc (corrected QT interval) intervals. The data reviewed and recorded were from the date of the initial patient ED visit.
Outcomes
The primary outcome was all-cause mortality within 24 hours after droperidol administration. This outcome was measured in all patients included in this study. Secondary outcomes included rescue medications needed after droperidol administration, incidence of QT prolongation, incidence of EPS (defined as akathisia, dystonia, parkinsonism, or tardive dyskinesia), and incidence of respiratory depression. Clinically significant QTc was defined as an interval of ≥ 500 ms with incidence of arrhythmias, code blues, or intubations. Baseline risk factors for QTc prolongation were taken into consideration including electrolyte abnormalities, concomitant QT-prolonging medications, CCI score, and cardiac comorbidities. Incidence of EPS was counted if patients received medications such as diphenhydramine or benztropine after droperidol administration in addition to documentation of EPS signs and symptoms. Incidences of EPS findings were reviewed by emergency department physicians to confirm the diagnosis.
Safety was assessed by quantifying mortality rates 24 hours after droperidol administration along with incidence of AEs associated with droperidol use including QT prolongation, EPS, and respiratory depression.
The necessity of rescue medication use was assessed by nursing documentation, additional medications ordered, and/or no additional medications required for agitation within 60 minutes of droperidol administration. Sixty minutes was the chosen timeframe given that the onset of droperidol action is between 3 and 10 minutes and peaks in about 30 minutes. Medications that were considered rescue medications included diphenhydramine < 25 mg, diphenhydramine 25 to 50 mg, lorazepam < 1 mg, lorazepam 1 to 2 mg, diphenhydramine < 25 mg and lorazepam < 1 mg, diphenhydramine < 25 mg and lorazepam 1 to 2 mg, diphenhydramine 25 to 50 mg and lorazepam 1 to 2 mg, and other medications, the names and doses of which were manually documented by investigators.
Statistical Analysis
For all variables in the study, descriptive analysis was used to categorize findings. Microsoft Excel was used to calculate means, frequency counts, percentages, and categorize data.
Results
Between February 1, 2021, and April 16, 2023, 214 patients received droperidol in the VAGLAHS ED, and 207 patients were included in the study. Seven patients did not receive droperidol for the indications included (acute agitation or antiemesis). Most of the study population (89.4%) was male, and the mean age was 51.0 years. The mean CCI was 1.6. In the study, 183 (88.4%) patients received droperidol for agitation and 24 (11.6%) for nausea and vomiting (Table 1).
Primary Outcome
No deaths were observed in a 24-hour period after droperidol administration among the 207 patients included in the study. There were also no arrhythmias, code blues, or intubations observed with the administration of droperidol (Table 2).
Secondary Outcomes
A total of 144 patients (69.6%) received droperidol alone to resolve agitation or nausea and vomiting. In the remaining population, 63 (30.4%) patients were given medications concomitantly with droperidol.
Fifteen patients (7.2%) required rescue medications that were administered within 60 minutes of droperidol administration. Rescue medications were required for 7 patients (4.9%) who initially received droperidol alone compared with 8 patients (12.7%) who were administered concomitant medications with droperidol (Figure).
Extrapyramidal Symptoms
EPS occurred in 2 patients (1.0%). There was 1 incidence of tardive dyskinesia (TD) in which the patient received droperidol 2.5 mg IM for emesis. TD was resolved with diphenhydramine 50 mg. A second patient who experienced dystonia received droperidol 10 mg IM for agitation. Dystonia was resolved with benztropine 2 mg. Both patients had a CCI of 0, no cardiac comorbidities, and laboratory test results were within reference ranges. The second patient received olanzapine within 24 hours of droperidol administration; however, it was after the EPS event.
QTc Prolongation
Baseline EKGs (within 6 months prior to ED visit) were available for 102 patients (49.3%). Nine patients (8.8%) had a reported baseline QTc of ≥ 500 ms (Table 3). Of these patients, 6 had a repeat EKG and 5 had a repeat QTc < 500 ms. One patient had a baseline and repeated QTc of 512 ms with essentially no change after droperidol administration. Only 1 patient was on a potentially QTc-prolonging medication at home. None of the patients with baseline QTc > 500 ms experienced arrhythmias after droperidol administration.
We found that 59 patients (28.5%) had EKGs performed within 24 hours after droperidol administration. Five patients had documented QTc ≥ 500 ms, but no arrhythmias were observed in a 24-hour period. Table 4 describes the additional medications administered after the 60-minute window but within 24 hours after droperidol administration. Quetiapine 300 mg and metoclopramide 5 mg were the only medications documented that can potentially increase QTc. Patient adherence to home medications and the timing of the last dose prior to ED visit were unknown. However, no arrhythmias were noted in these patients with QTc changes. No patients experienced respiratory depression within 24 hours of droperidol administration.
Older Adult Patients
Thirty-eight patients were aged ≥ 65 years with a mean age of 74.2 years. Thirty-four patients (89.5%) received droperidol for agitation and 4 (10.6%) for nausea and vomiting. Only 21 patients had a baseline EKG, and 4 had QTc ≤ 500 ms. At 24 hours, EKGs were performed for 18 patients and 3 had a QTc ≤ 500 ms. No mortality or arrhythmias were reported and there were no incidences of rescue medications, EPS, or respiratory depression.
Discussion
The study included 207 patients who received droperidol for either agitation or nausea/vomiting in the VAGLAHS ED. No mortality occurred within 24 hours of droperidol administration, which is consistent with recent studies.8-14
Furthermore, 59 patients (28.5%) had an EKG performed within 24 hours of droperidol administration; 5 patients had documented QTc ≥ 500 ms. Only 3 of the patients with prolonged QTc had baseline readings for comparison. Only 2 patients had an increase in QTc interval. No arrhythmias were observed; however, the effects of observing QTc prolongation were limited due to the lack of post-EKG readings following droperidol administration. Because of the retrospective nature of the study, neither standardization of EKG at baseline nor 24-hour postadministration were possible. The study found that droperidol was effective with only 15 patients (7.3%) requiring rescue medications. In the patients who were given medications concomitantly with droperidol, it was not possible to conclude whether the patients would have required rescue medications to resolve their agitation or nausea/vomiting. Administration of concomitant medications with droperidol may be attributed to practice patterns associated with haloperidol use, which is frequently administered with concomitant medications such as diphenhydramine and/or a benzodiazepine.
AEs were rare with no documentation of respiratory depression and 2 cases (1.0%) of EPS. Both incidences of EPS resolved with diphenhydramine or benztropine. However, given the reliance on nursing documentation to capture AEs, the number of events may have been underreported.
Limitations
Standardization of dosing was a limiting factor that could affect the need for rescue medications. Another limitation was reliance on nursing reports of resolution of symptoms and comfort with agitated patients. Given the retrospective design and small sample size, this study may not have captured all potential AEs. However, the doses administered within this study population were consistent with what was expected based on other studies.8-14
Conclusions
Droperidol, an antipsychotic, is currently approved for PONV, but is also used off-label for agitation. This study found no fatalities among patients who received droperidol in the ED. The findings suggest that droperidol used for agitation and as an antiemetic, despite its FDA boxed warning, appears to be safe and showed no evidence of mortality, arrhythmias, code blues, or intubations despite the lack of postdose EKG monitoring. Among the 38 patients aged ≥ 65 years, the use of droperidol revealed no increased risks. It should be noted that droperidol appeared safe and few patients required rescue medications within this study population.
- Perkins J, Ho JD, Vilke GM, DeMers G. American Academy of Emergency Medicine Position Statement: Safety of droperidol use in the emergency department. J Emerg Med. 2015;49:91-97. doi:10.1016/j.jemermed.2014.12.024
- Siegel RB, Motov SM, Marcolini EG. Droperidol use in the emergency department: a clinical review. J Emerg Med. 2023;64:289-294. doi:10.1016/j.jemermed.2022.12.012
- Jackson CW, Sheehan AH, Reddan JG. Evidencebased review of the black-box warning for droperidol. Am J Health Syst Pharm. 2007;64:1174-1186. doi:10.2146/ajhp060505
- Habib AS, Gan TJ. Food and Drug Administration black box warning on the perioperative use of droperidol: a review of the cases. Anesth Analg. 2003;96(5):1377-1379. doi:10.1213/01.ane.0000063923.87560.37
- Droperidol. In: Micromedex (electronic version). IBM Watson Health; 2019. Accessed March 2, 2026. https://www .micromedexsolutions.com
- Gaw CM, Cabrera D, Bellolio F, Mattson AE, Lohse CM, Jeffery MM. Effectiveness and safety of droperidol in a United States emergency department. Am J Emerg Med. 2020;38:1310-1314. doi:10.1016/j.ajem.2019.09.007
- Calver L, Page CB, Downes MA, et al. The safety and effectiveness of droperidol for sedation of acute behavioral disturbance in the emergency department. Ann Emerg Med. 2015;66(3):230-238.e1. doi:10.1016/j.annemergmed.2015.03.016
- Ernst R, Wagstaff H, Smith M, et al. Droperidol administration among emergency department patients with abdominal pain, nausea, and vomiting. Am J Emerg Med. 2024;85:44-47. doi:10.1016/j.ajem.2024.07.060
- Szwak K, Sacchetti A. Droperidol use in pediatric emergency department patients. Pediatr Emerg Care. 2010;26:248-250. doi:10.1097/pec.0b013e3181d6d9f2
- Chase PB, Biros MH. A retrospective review of the use and safety of droperidol in a large, high-risk, inner-city emergency department patient population. Acad Emerg Med. 2002;9:1402-1410. doi:10.1111/j.1553-2712.2002.tb01609.x
- Mattson A, Friend K, Brown CS, Cabrera D. Reintegrating droperidol into emergency medicine practice. Am J Health Syst Pharm. 2020;77(22):1838-1845. doi:10.1093/ajhp/zxaa271
- Cole JB, Stang JL, DeVries PA, Martel ML, Miner JR, Driver BE. A prospective study of intramuscular droperidol or olanzapine for acute agitation in the emergency department: a natural experiment owing to drug shortages. Ann Emerg Med. 2021;78(2):274-286. doi:10.1016/j.annemergmed.2021.01.005
- Page CB, Parker LE, Rashford SJ, et al. Prospective study of the safety and effectiveness of droperidol in elderly patients for pre-hospital acute behavioural disturbance. Emerg Med Australas. 2020;32(5):731-736. doi:10.1111/1742-6723.13496
- Page CB, Parker LE, Rashford SJ, et al. A prospective study of the safety and effectiveness of droperidol inchildren for prehospital acute behavioral disturbance. Prehosp Emerg Care. 2018;23:519-526. doi:10.1080/10903127.2018.1542473
- Perkins J, Ho JD, Vilke GM, DeMers G. American Academy of Emergency Medicine Position Statement: Safety of droperidol use in the emergency department. J Emerg Med. 2015;49:91-97. doi:10.1016/j.jemermed.2014.12.024
- Siegel RB, Motov SM, Marcolini EG. Droperidol use in the emergency department: a clinical review. J Emerg Med. 2023;64:289-294. doi:10.1016/j.jemermed.2022.12.012
- Jackson CW, Sheehan AH, Reddan JG. Evidencebased review of the black-box warning for droperidol. Am J Health Syst Pharm. 2007;64:1174-1186. doi:10.2146/ajhp060505
- Habib AS, Gan TJ. Food and Drug Administration black box warning on the perioperative use of droperidol: a review of the cases. Anesth Analg. 2003;96(5):1377-1379. doi:10.1213/01.ane.0000063923.87560.37
- Droperidol. In: Micromedex (electronic version). IBM Watson Health; 2019. Accessed March 2, 2026. https://www .micromedexsolutions.com
- Gaw CM, Cabrera D, Bellolio F, Mattson AE, Lohse CM, Jeffery MM. Effectiveness and safety of droperidol in a United States emergency department. Am J Emerg Med. 2020;38:1310-1314. doi:10.1016/j.ajem.2019.09.007
- Calver L, Page CB, Downes MA, et al. The safety and effectiveness of droperidol for sedation of acute behavioral disturbance in the emergency department. Ann Emerg Med. 2015;66(3):230-238.e1. doi:10.1016/j.annemergmed.2015.03.016
- Ernst R, Wagstaff H, Smith M, et al. Droperidol administration among emergency department patients with abdominal pain, nausea, and vomiting. Am J Emerg Med. 2024;85:44-47. doi:10.1016/j.ajem.2024.07.060
- Szwak K, Sacchetti A. Droperidol use in pediatric emergency department patients. Pediatr Emerg Care. 2010;26:248-250. doi:10.1097/pec.0b013e3181d6d9f2
- Chase PB, Biros MH. A retrospective review of the use and safety of droperidol in a large, high-risk, inner-city emergency department patient population. Acad Emerg Med. 2002;9:1402-1410. doi:10.1111/j.1553-2712.2002.tb01609.x
- Mattson A, Friend K, Brown CS, Cabrera D. Reintegrating droperidol into emergency medicine practice. Am J Health Syst Pharm. 2020;77(22):1838-1845. doi:10.1093/ajhp/zxaa271
- Cole JB, Stang JL, DeVries PA, Martel ML, Miner JR, Driver BE. A prospective study of intramuscular droperidol or olanzapine for acute agitation in the emergency department: a natural experiment owing to drug shortages. Ann Emerg Med. 2021;78(2):274-286. doi:10.1016/j.annemergmed.2021.01.005
- Page CB, Parker LE, Rashford SJ, et al. Prospective study of the safety and effectiveness of droperidol in elderly patients for pre-hospital acute behavioural disturbance. Emerg Med Australas. 2020;32(5):731-736. doi:10.1111/1742-6723.13496
- Page CB, Parker LE, Rashford SJ, et al. A prospective study of the safety and effectiveness of droperidol inchildren for prehospital acute behavioral disturbance. Prehosp Emerg Care. 2018;23:519-526. doi:10.1080/10903127.2018.1542473
Effectiveness and Safety of Droperidol Use in the VA Greater Los Angeles Healthcare System Emergency Department
Effectiveness and Safety of Droperidol Use in the VA Greater Los Angeles Healthcare System Emergency Department

Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
