User login
Thrombolysis Reduced Survival in Acute PE
DENVER – Adding thrombolytic therapy to standard anticoagulation with heparin did not significantly improve overall survival at 3 months in patients with acute symptomatic pulmonary embolism – and reduced survival rates for some normotensive patients, according to a large international retrospective cohort study.
Thrombolytic therapy as initial treatment did produce a nonsignificant trend toward survival among patients who presented with systolic hypotension, according to a subanalysis of the study data, while significantly worsening survival among normotensive patients.

However, thrombolysis had no significant impact on survival among normotensive patients when researchers accounted for differences in troponin and the presence of right ventricular dysfunction.
"Based on these findings, we cannot recommend thrombolysis in normotensive patients without more data from randomized controlled trials. We need to better determine how to risk stratify these patients," said Dr. David Jimenez of the Ramon y Cajal Hospital and Alcala de Henares University, Madrid.
Current guidelines from the American College of Chest Physicians recommend thrombolytic therapy in addition to anticoagulation for patients with evidence of hemodynamic compromise (grade 1B evidence) and for "selected high-risk patients without hypotension who are judged to have a low risk of bleeding (grade 2B)." The guidelines advise physicians to base that decision on the severity of the pulmonary embolism (PE), the patient’s prognosis, and risk of bleeding (Chest 2008;133:454S-545S).
The current study was done to fill in the evidence gap for those recommendations, explained Dr. Jimenez, who presented the study results at an international meeting of the American Thoracic Society. He and his colleagues from Spain and the United States analyzed data from 15,944 patients with acute pulmonary embolism enrolled in the Spanish registry Registro Informatizado de la Enfermedad Tromboembólica. Thrombolytic therapy had been used in 2.7% (430) of the patients.
In general, those patients were younger, had fewer comorbid conditions, and more signs of clinical severity. In order to overcome that bias, a propensity analysis was conducted in order to match patients for those differences.
Patients were also grouped into those with systolic blood pressure less 100 mm Hg (hypotensive) and those with 100 mm Hg and higher (normotensive).
Comparing 94 propensity score–matched patients with systolic hypotension who received thrombolysis with 94 patients who did not, there was a nonsignificant trend in reduction in all-cause mortality with thrombolytic therapy, with an odds ratio of 0.72.
For two groups of 217 normotensive patients each who received or did not receive thrombolysis, there was a statistically significant increased risk of death for those receiving thrombolysis, with an odds ratio of 2.32. However, when missing troponin and echocardiogram data were added to the analysis, the effect of thrombolysis was no longer significant, with an odds ratio 1.67.
The reasons for the increased risks from thrombolysis for normotensive patients with PE aren’t entirely clear, the investigators said.
However, because the risk of dying from pulmonary embolism is low among normotensive, hemodynamically stable PE patients, those patients’ risk of dying from thrombolysis is therefore elevated by comparison and approaches that of hypotensive patients, Dr. Jimenez speculated. Only half of all patients with pulmonary embolism actually die of the embolism, he noted, while the rest die of other causes such as infections, cancer, and bleeding.
Indeed, there has only been one previous randomized clinical trial showing benefit from thrombolysis in patients with PE, Dr. Jimenez said, and that was in 10 patients with life-threatening PE (J. Thromb. Thrombolysis 1995;2:227-9).
"Thrombolysis is only useful for those who are at high risk for dying from PE," Dr. Jimenez said. "I think we have to test in a randomized, controlled trial whether thrombolysis is helpful in a subgroup of normotensive patients who have high risk due to right ventricular dysfunction and elevated troponin," Dr. Jimenez said.
Such a trial is now underway. The prospective, double-blind, placebo-controlled Pulmonary Embolism Thrombolysis Study (PEITHO) will examine the particular subgroup of normotensive patients with acute PE who have echocardiographic and laboratory evidence of right ventricular dysfunction.
The study investigators want to enroll 1,000 patients at 12 European centers, and they hope to have data by the end of 2012, said Dr. Jimenez, whose hospital is one of the study centers.
Dr. Jimenez stated that he has no financial disclosures.
DENVER – Adding thrombolytic therapy to standard anticoagulation with heparin did not significantly improve overall survival at 3 months in patients with acute symptomatic pulmonary embolism – and reduced survival rates for some normotensive patients, according to a large international retrospective cohort study.
Thrombolytic therapy as initial treatment did produce a nonsignificant trend toward survival among patients who presented with systolic hypotension, according to a subanalysis of the study data, while significantly worsening survival among normotensive patients.
However, thrombolysis had no significant impact on survival among normotensive patients when researchers accounted for differences in troponin and the presence of right ventricular dysfunction.
"Based on these findings, we cannot recommend thrombolysis in normotensive patients without more data from randomized controlled trials. We need to better determine how to risk stratify these patients," said Dr. David Jimenez of the Ramon y Cajal Hospital and Alcala de Henares University, Madrid.
Current guidelines from the American College of Chest Physicians recommend thrombolytic therapy in addition to anticoagulation for patients with evidence of hemodynamic compromise (grade 1B evidence) and for "selected high-risk patients without hypotension who are judged to have a low risk of bleeding (grade 2B)." The guidelines advise physicians to base that decision on the severity of the pulmonary embolism (PE), the patient’s prognosis, and risk of bleeding (Chest 2008;133:454S-545S).
The current study was done to fill in the evidence gap for those recommendations, explained Dr. Jimenez, who presented the study results at an international meeting of the American Thoracic Society. He and his colleagues from Spain and the United States analyzed data from 15,944 patients with acute pulmonary embolism enrolled in the Spanish registry Registro Informatizado de la Enfermedad Tromboembólica. Thrombolytic therapy had been used in 2.7% (430) of the patients.
In general, those patients were younger, had fewer comorbid conditions, and more signs of clinical severity. In order to overcome that bias, a propensity analysis was conducted in order to match patients for those differences.
Patients were also grouped into those with systolic blood pressure less 100 mm Hg (hypotensive) and those with 100 mm Hg and higher (normotensive).
Comparing 94 propensity score–matched patients with systolic hypotension who received thrombolysis with 94 patients who did not, there was a nonsignificant trend in reduction in all-cause mortality with thrombolytic therapy, with an odds ratio of 0.72.
For two groups of 217 normotensive patients each who received or did not receive thrombolysis, there was a statistically significant increased risk of death for those receiving thrombolysis, with an odds ratio of 2.32. However, when missing troponin and echocardiogram data were added to the analysis, the effect of thrombolysis was no longer significant, with an odds ratio 1.67.
The reasons for the increased risks from thrombolysis for normotensive patients with PE aren’t entirely clear, the investigators said.
However, because the risk of dying from pulmonary embolism is low among normotensive, hemodynamically stable PE patients, those patients’ risk of dying from thrombolysis is therefore elevated by comparison and approaches that of hypotensive patients, Dr. Jimenez speculated. Only half of all patients with pulmonary embolism actually die of the embolism, he noted, while the rest die of other causes such as infections, cancer, and bleeding.
Indeed, there has only been one previous randomized clinical trial showing benefit from thrombolysis in patients with PE, Dr. Jimenez said, and that was in 10 patients with life-threatening PE (J. Thromb. Thrombolysis 1995;2:227-9).
"Thrombolysis is only useful for those who are at high risk for dying from PE," Dr. Jimenez said. "I think we have to test in a randomized, controlled trial whether thrombolysis is helpful in a subgroup of normotensive patients who have high risk due to right ventricular dysfunction and elevated troponin," Dr. Jimenez said.
Such a trial is now underway. The prospective, double-blind, placebo-controlled Pulmonary Embolism Thrombolysis Study (PEITHO) will examine the particular subgroup of normotensive patients with acute PE who have echocardiographic and laboratory evidence of right ventricular dysfunction.
The study investigators want to enroll 1,000 patients at 12 European centers, and they hope to have data by the end of 2012, said Dr. Jimenez, whose hospital is one of the study centers.
Dr. Jimenez stated that he has no financial disclosures.
DENVER – Adding thrombolytic therapy to standard anticoagulation with heparin did not significantly improve overall survival at 3 months in patients with acute symptomatic pulmonary embolism – and reduced survival rates for some normotensive patients, according to a large international retrospective cohort study.
Thrombolytic therapy as initial treatment did produce a nonsignificant trend toward survival among patients who presented with systolic hypotension, according to a subanalysis of the study data, while significantly worsening survival among normotensive patients.
However, thrombolysis had no significant impact on survival among normotensive patients when researchers accounted for differences in troponin and the presence of right ventricular dysfunction.
"Based on these findings, we cannot recommend thrombolysis in normotensive patients without more data from randomized controlled trials. We need to better determine how to risk stratify these patients," said Dr. David Jimenez of the Ramon y Cajal Hospital and Alcala de Henares University, Madrid.
Current guidelines from the American College of Chest Physicians recommend thrombolytic therapy in addition to anticoagulation for patients with evidence of hemodynamic compromise (grade 1B evidence) and for "selected high-risk patients without hypotension who are judged to have a low risk of bleeding (grade 2B)." The guidelines advise physicians to base that decision on the severity of the pulmonary embolism (PE), the patient’s prognosis, and risk of bleeding (Chest 2008;133:454S-545S).
The current study was done to fill in the evidence gap for those recommendations, explained Dr. Jimenez, who presented the study results at an international meeting of the American Thoracic Society. He and his colleagues from Spain and the United States analyzed data from 15,944 patients with acute pulmonary embolism enrolled in the Spanish registry Registro Informatizado de la Enfermedad Tromboembólica. Thrombolytic therapy had been used in 2.7% (430) of the patients.
In general, those patients were younger, had fewer comorbid conditions, and more signs of clinical severity. In order to overcome that bias, a propensity analysis was conducted in order to match patients for those differences.
Patients were also grouped into those with systolic blood pressure less 100 mm Hg (hypotensive) and those with 100 mm Hg and higher (normotensive).
Comparing 94 propensity score–matched patients with systolic hypotension who received thrombolysis with 94 patients who did not, there was a nonsignificant trend in reduction in all-cause mortality with thrombolytic therapy, with an odds ratio of 0.72.
For two groups of 217 normotensive patients each who received or did not receive thrombolysis, there was a statistically significant increased risk of death for those receiving thrombolysis, with an odds ratio of 2.32. However, when missing troponin and echocardiogram data were added to the analysis, the effect of thrombolysis was no longer significant, with an odds ratio 1.67.
The reasons for the increased risks from thrombolysis for normotensive patients with PE aren’t entirely clear, the investigators said.
However, because the risk of dying from pulmonary embolism is low among normotensive, hemodynamically stable PE patients, those patients’ risk of dying from thrombolysis is therefore elevated by comparison and approaches that of hypotensive patients, Dr. Jimenez speculated. Only half of all patients with pulmonary embolism actually die of the embolism, he noted, while the rest die of other causes such as infections, cancer, and bleeding.
Indeed, there has only been one previous randomized clinical trial showing benefit from thrombolysis in patients with PE, Dr. Jimenez said, and that was in 10 patients with life-threatening PE (J. Thromb. Thrombolysis 1995;2:227-9).
"Thrombolysis is only useful for those who are at high risk for dying from PE," Dr. Jimenez said. "I think we have to test in a randomized, controlled trial whether thrombolysis is helpful in a subgroup of normotensive patients who have high risk due to right ventricular dysfunction and elevated troponin," Dr. Jimenez said.
Such a trial is now underway. The prospective, double-blind, placebo-controlled Pulmonary Embolism Thrombolysis Study (PEITHO) will examine the particular subgroup of normotensive patients with acute PE who have echocardiographic and laboratory evidence of right ventricular dysfunction.
The study investigators want to enroll 1,000 patients at 12 European centers, and they hope to have data by the end of 2012, said Dr. Jimenez, whose hospital is one of the study centers.
Dr. Jimenez stated that he has no financial disclosures.
FROM AN INTERNATIONAL CONFERENCE OF THE AMERICAN THORACIC SOCIETY
Major Finding: Among 434 normotensive patients with acute symptomatic pulmonary embolism, there was a statistically significant increased risk of death for those receiving thrombolysis, with an odds ratio of 2.32. However, when troponin and right ventricular dysfunction were added to the analysis, the effect of thrombolysis on survival was no longer significant, with an odds ratio 1.67.
Data Source: A retrospective cohort study of data from 15,944 patients with acute pulmonary embolism enrolled in a Spanish registry.
Disclosures: Dr. Jimenez stated that he has no financial disclosures.
Tele-ICU Can Reduce Mortality and Length of Stay
DENVER – An intensive care unit telemedicine intervention was associated with lower hospital and ICU mortality and shorter hospital and ICU lengths of stay in a prospective, unblinded study conducted at one academic medical center over a 2-year period.
The intervention also was associated with significantly higher rates of adherence to critical care best practices and lower rates of complications. More rapid responses to alerts for physiologic instability and off-hours, off-site intensivist care plan reviews were identified as critical care process elements that may have contributed to the lower mortality and shorter lengths of stay associated with the tele-ICU intervention, Dr. Craig M. Lilly reported at an international conference of the American Thoracic Society. The study was simultaneously published online in JAMA (2011;305:E1-9 [doi:10.1001/jama.2011.697]).
Tele-ICU is defined as the provision of care to critically ill patients by health care professionals located remotely. Tele-ICU clinicians use audio, video, and electronic links to assist bedside caregivers in monitoring patients, oversee best practice adherence, and help create and execute care plans, said Dr. Lilly of the University of Massachusetts, Worcester.
Unlike previous studies of the effects of tele-ICU programs, this one focused on changes in the process of care rather than the ICU structure. Prior to the study start, best practices were standardized for the prevention of venous thrombosis, cardiovascular complications, ventilator-associated pneumonia, and stress ulcers. For the primary analysis, a representative sample of preintervention cases was obtained by identifying consecutive hospital discharges from an administrative database for cases managed in each of the seven ICUs (three medical, three surgical, and one mixed cardiovascular). Admission, discharge, and laboratory information was abstracted electronically.
The off-site team included an intensivist and used tele-ICU workstations. The tele-ICU team serially reviewed the care of individual patients, performed real-time audits of best practice adherence, performed workstation-assisted care plan reviews for patients admitted at night, monitored system-generated electronic alerts, audited bedside clinician responses to in-room alarms, and intervened when the responses of bedside clinicians were delayed and patients were deemed physiologically unstable. The off-site team was able to communicate with bedside clinicians or directly manage patients by recording clinician orders for tests, treatments, consultations, and management of life-support devices, Dr. Lilly said.
A total of 6,290 qualifying adult patients were identified from 6,465 electronic admission registrations to any of the seven ICUs, with 1,529 admitted during the preintervention period and 4,761 during the tele-ICU intervention period (the periods were staggered between 2005 and 2007).
Unadjusted ICU mortality was significantly lower in the tele-ICU group, compared with the preintervention group (10.7% vs. 8.6%). When adjusted for acuity, locus of care, physiologic parameters, laboratory values, and time trend, the odds ratio was 0.37. Hospital mortality also was reduced with tele-ICU (13.6% vs. 11.8%). The unadjusted difference was not statistically significant, but hospital mortality was significantly lower with tele-ICU after adjustment for acuity, locus of care, physiological parameters, laboratory values, and time trend, with an odds ratio of 0.40.
Both ICU and hospital mean lengths of stay were significantly lower with tele-ICU. The intervention group had a mean hospital stay of 9.8 days, compared with 13.3 days in the preintervention group. After adjustment for acuity, time trends, physiologic parameters, laboratory values, and locus of care, the hazard ratio was 1.44. For ICU stay, the mean was 4.5 days in the tele-ICU group vs. 6.4 days in the preintervention group. After adjustment for all of the previously listed factors, that hazard ratio was 1.26. Results for medical, surgical, and cardiovascular ICUs were similar, Dr. Lilly said.
To understand how tele-ICU team activities affected care processes and to evaluate the degree to which the association of the intervention with changes in mortality could be attributed to these changes in process, another analysis examined adherence to best practices, incidence of common ICU complications, intensivist involvement for cases admitted during nighttime hours, responses to alerts, and ICU type.
The tele-ICU intervention was associated with significantly better adherence to deep vein thrombosis prevention best practices and cardiovascular protection best practices, as well as lower rates of catheter-related bloodstream infection and ventilator-associated pneumonia. These factors also were associated with significantly lower ICU and hospital mortality. The proportion of the tele-ICU association with lower mortality that could be attributed to adherence to these best practices and complication measures was estimated to be 25% for hospital mortality and 30% for ICU mortality.
"This suggests that there are benefits of a tele-ICU intervention beyond what is provided by daytime bedside intensivist staffing and traditional approaches to quality improvement such as the process changes presented," Dr. Lilly commented.
"These findings suggest that critical care programs that implement processes that increase adherence to best practice, lower rates of complications, shorten response times to alerts and alarms, and support early intensivist case involvement will provide better care at a lower cost. ... Our study suggests that the introduction of a tele-ICU program that collaborates with and supports bedside clinicians is one way to accomplish these aims."
All study authors reported having no conflicts of interest.
Multiple commercial applications of ICU telemedicine now exist, and telemedicine is widely touted as an all-encompassing strategy to improve ICU outcomes. Yet even after 25 years, the optimal role of telemedicine in the ICU remains uncertain. Several previous studies have not demonstrated a benefit. The difference with the telemedicine program in this study is that it was tightly linked to specific quality improvement activities. For this reason, the study by Dr. Lilly and colleagues provides the first convincing evidence that ICU telemedicine can be an effective complement to bedside care in some settings.
The seven ICUs in this study, however, are part of one relatively well-resourced academic medical center that has a strong culture of quality improvement. It is unclear if these results could be replicated in hospitals with fewer resources to devote toward ICU quality. Moreover, all of the telemedicine physicians also worked in the target ICUs, which may have served to increase buy-in among local practitioners. These results may not translate to settings in which the telemedicine unit and hospital unit do not share physicians.
In the right settings and with the right goals, telemedicine can indeed be used to help improve outcomes. Yet, just as with all applications of health information technology, good outcomes should not be assumed. The challenge is to not conclude from this study that ICU telemedicine always is associated with improved quality of care, but instead to continue to explore how telemedicine can be used in clinical settings in which other strategies for quality improvement have not worked. Only then will it be possible to improve the use and avoid the misuse of this complex and evolving technology.
Dr. Jeremy M. Kahn is with the department of critical care medicine and the department of health policy and management at the University of Pittsburgh.
Multiple commercial applications of ICU telemedicine now exist, and telemedicine is widely touted as an all-encompassing strategy to improve ICU outcomes. Yet even after 25 years, the optimal role of telemedicine in the ICU remains uncertain. Several previous studies have not demonstrated a benefit. The difference with the telemedicine program in this study is that it was tightly linked to specific quality improvement activities. For this reason, the study by Dr. Lilly and colleagues provides the first convincing evidence that ICU telemedicine can be an effective complement to bedside care in some settings.
The seven ICUs in this study, however, are part of one relatively well-resourced academic medical center that has a strong culture of quality improvement. It is unclear if these results could be replicated in hospitals with fewer resources to devote toward ICU quality. Moreover, all of the telemedicine physicians also worked in the target ICUs, which may have served to increase buy-in among local practitioners. These results may not translate to settings in which the telemedicine unit and hospital unit do not share physicians.
In the right settings and with the right goals, telemedicine can indeed be used to help improve outcomes. Yet, just as with all applications of health information technology, good outcomes should not be assumed. The challenge is to not conclude from this study that ICU telemedicine always is associated with improved quality of care, but instead to continue to explore how telemedicine can be used in clinical settings in which other strategies for quality improvement have not worked. Only then will it be possible to improve the use and avoid the misuse of this complex and evolving technology.
Dr. Jeremy M. Kahn is with the department of critical care medicine and the department of health policy and management at the University of Pittsburgh.
Multiple commercial applications of ICU telemedicine now exist, and telemedicine is widely touted as an all-encompassing strategy to improve ICU outcomes. Yet even after 25 years, the optimal role of telemedicine in the ICU remains uncertain. Several previous studies have not demonstrated a benefit. The difference with the telemedicine program in this study is that it was tightly linked to specific quality improvement activities. For this reason, the study by Dr. Lilly and colleagues provides the first convincing evidence that ICU telemedicine can be an effective complement to bedside care in some settings.
The seven ICUs in this study, however, are part of one relatively well-resourced academic medical center that has a strong culture of quality improvement. It is unclear if these results could be replicated in hospitals with fewer resources to devote toward ICU quality. Moreover, all of the telemedicine physicians also worked in the target ICUs, which may have served to increase buy-in among local practitioners. These results may not translate to settings in which the telemedicine unit and hospital unit do not share physicians.
In the right settings and with the right goals, telemedicine can indeed be used to help improve outcomes. Yet, just as with all applications of health information technology, good outcomes should not be assumed. The challenge is to not conclude from this study that ICU telemedicine always is associated with improved quality of care, but instead to continue to explore how telemedicine can be used in clinical settings in which other strategies for quality improvement have not worked. Only then will it be possible to improve the use and avoid the misuse of this complex and evolving technology.
Dr. Jeremy M. Kahn is with the department of critical care medicine and the department of health policy and management at the University of Pittsburgh.
DENVER – An intensive care unit telemedicine intervention was associated with lower hospital and ICU mortality and shorter hospital and ICU lengths of stay in a prospective, unblinded study conducted at one academic medical center over a 2-year period.
The intervention also was associated with significantly higher rates of adherence to critical care best practices and lower rates of complications. More rapid responses to alerts for physiologic instability and off-hours, off-site intensivist care plan reviews were identified as critical care process elements that may have contributed to the lower mortality and shorter lengths of stay associated with the tele-ICU intervention, Dr. Craig M. Lilly reported at an international conference of the American Thoracic Society. The study was simultaneously published online in JAMA (2011;305:E1-9 [doi:10.1001/jama.2011.697]).
Tele-ICU is defined as the provision of care to critically ill patients by health care professionals located remotely. Tele-ICU clinicians use audio, video, and electronic links to assist bedside caregivers in monitoring patients, oversee best practice adherence, and help create and execute care plans, said Dr. Lilly of the University of Massachusetts, Worcester.
Unlike previous studies of the effects of tele-ICU programs, this one focused on changes in the process of care rather than the ICU structure. Prior to the study start, best practices were standardized for the prevention of venous thrombosis, cardiovascular complications, ventilator-associated pneumonia, and stress ulcers. For the primary analysis, a representative sample of preintervention cases was obtained by identifying consecutive hospital discharges from an administrative database for cases managed in each of the seven ICUs (three medical, three surgical, and one mixed cardiovascular). Admission, discharge, and laboratory information was abstracted electronically.
The off-site team included an intensivist and used tele-ICU workstations. The tele-ICU team serially reviewed the care of individual patients, performed real-time audits of best practice adherence, performed workstation-assisted care plan reviews for patients admitted at night, monitored system-generated electronic alerts, audited bedside clinician responses to in-room alarms, and intervened when the responses of bedside clinicians were delayed and patients were deemed physiologically unstable. The off-site team was able to communicate with bedside clinicians or directly manage patients by recording clinician orders for tests, treatments, consultations, and management of life-support devices, Dr. Lilly said.
A total of 6,290 qualifying adult patients were identified from 6,465 electronic admission registrations to any of the seven ICUs, with 1,529 admitted during the preintervention period and 4,761 during the tele-ICU intervention period (the periods were staggered between 2005 and 2007).
Unadjusted ICU mortality was significantly lower in the tele-ICU group, compared with the preintervention group (10.7% vs. 8.6%). When adjusted for acuity, locus of care, physiologic parameters, laboratory values, and time trend, the odds ratio was 0.37. Hospital mortality also was reduced with tele-ICU (13.6% vs. 11.8%). The unadjusted difference was not statistically significant, but hospital mortality was significantly lower with tele-ICU after adjustment for acuity, locus of care, physiological parameters, laboratory values, and time trend, with an odds ratio of 0.40.
Both ICU and hospital mean lengths of stay were significantly lower with tele-ICU. The intervention group had a mean hospital stay of 9.8 days, compared with 13.3 days in the preintervention group. After adjustment for acuity, time trends, physiologic parameters, laboratory values, and locus of care, the hazard ratio was 1.44. For ICU stay, the mean was 4.5 days in the tele-ICU group vs. 6.4 days in the preintervention group. After adjustment for all of the previously listed factors, that hazard ratio was 1.26. Results for medical, surgical, and cardiovascular ICUs were similar, Dr. Lilly said.
To understand how tele-ICU team activities affected care processes and to evaluate the degree to which the association of the intervention with changes in mortality could be attributed to these changes in process, another analysis examined adherence to best practices, incidence of common ICU complications, intensivist involvement for cases admitted during nighttime hours, responses to alerts, and ICU type.
The tele-ICU intervention was associated with significantly better adherence to deep vein thrombosis prevention best practices and cardiovascular protection best practices, as well as lower rates of catheter-related bloodstream infection and ventilator-associated pneumonia. These factors also were associated with significantly lower ICU and hospital mortality. The proportion of the tele-ICU association with lower mortality that could be attributed to adherence to these best practices and complication measures was estimated to be 25% for hospital mortality and 30% for ICU mortality.
"This suggests that there are benefits of a tele-ICU intervention beyond what is provided by daytime bedside intensivist staffing and traditional approaches to quality improvement such as the process changes presented," Dr. Lilly commented.
"These findings suggest that critical care programs that implement processes that increase adherence to best practice, lower rates of complications, shorten response times to alerts and alarms, and support early intensivist case involvement will provide better care at a lower cost. ... Our study suggests that the introduction of a tele-ICU program that collaborates with and supports bedside clinicians is one way to accomplish these aims."
All study authors reported having no conflicts of interest.
DENVER – An intensive care unit telemedicine intervention was associated with lower hospital and ICU mortality and shorter hospital and ICU lengths of stay in a prospective, unblinded study conducted at one academic medical center over a 2-year period.
The intervention also was associated with significantly higher rates of adherence to critical care best practices and lower rates of complications. More rapid responses to alerts for physiologic instability and off-hours, off-site intensivist care plan reviews were identified as critical care process elements that may have contributed to the lower mortality and shorter lengths of stay associated with the tele-ICU intervention, Dr. Craig M. Lilly reported at an international conference of the American Thoracic Society. The study was simultaneously published online in JAMA (2011;305:E1-9 [doi:10.1001/jama.2011.697]).
Tele-ICU is defined as the provision of care to critically ill patients by health care professionals located remotely. Tele-ICU clinicians use audio, video, and electronic links to assist bedside caregivers in monitoring patients, oversee best practice adherence, and help create and execute care plans, said Dr. Lilly of the University of Massachusetts, Worcester.
Unlike previous studies of the effects of tele-ICU programs, this one focused on changes in the process of care rather than the ICU structure. Prior to the study start, best practices were standardized for the prevention of venous thrombosis, cardiovascular complications, ventilator-associated pneumonia, and stress ulcers. For the primary analysis, a representative sample of preintervention cases was obtained by identifying consecutive hospital discharges from an administrative database for cases managed in each of the seven ICUs (three medical, three surgical, and one mixed cardiovascular). Admission, discharge, and laboratory information was abstracted electronically.
The off-site team included an intensivist and used tele-ICU workstations. The tele-ICU team serially reviewed the care of individual patients, performed real-time audits of best practice adherence, performed workstation-assisted care plan reviews for patients admitted at night, monitored system-generated electronic alerts, audited bedside clinician responses to in-room alarms, and intervened when the responses of bedside clinicians were delayed and patients were deemed physiologically unstable. The off-site team was able to communicate with bedside clinicians or directly manage patients by recording clinician orders for tests, treatments, consultations, and management of life-support devices, Dr. Lilly said.
A total of 6,290 qualifying adult patients were identified from 6,465 electronic admission registrations to any of the seven ICUs, with 1,529 admitted during the preintervention period and 4,761 during the tele-ICU intervention period (the periods were staggered between 2005 and 2007).
Unadjusted ICU mortality was significantly lower in the tele-ICU group, compared with the preintervention group (10.7% vs. 8.6%). When adjusted for acuity, locus of care, physiologic parameters, laboratory values, and time trend, the odds ratio was 0.37. Hospital mortality also was reduced with tele-ICU (13.6% vs. 11.8%). The unadjusted difference was not statistically significant, but hospital mortality was significantly lower with tele-ICU after adjustment for acuity, locus of care, physiological parameters, laboratory values, and time trend, with an odds ratio of 0.40.
Both ICU and hospital mean lengths of stay were significantly lower with tele-ICU. The intervention group had a mean hospital stay of 9.8 days, compared with 13.3 days in the preintervention group. After adjustment for acuity, time trends, physiologic parameters, laboratory values, and locus of care, the hazard ratio was 1.44. For ICU stay, the mean was 4.5 days in the tele-ICU group vs. 6.4 days in the preintervention group. After adjustment for all of the previously listed factors, that hazard ratio was 1.26. Results for medical, surgical, and cardiovascular ICUs were similar, Dr. Lilly said.
To understand how tele-ICU team activities affected care processes and to evaluate the degree to which the association of the intervention with changes in mortality could be attributed to these changes in process, another analysis examined adherence to best practices, incidence of common ICU complications, intensivist involvement for cases admitted during nighttime hours, responses to alerts, and ICU type.
The tele-ICU intervention was associated with significantly better adherence to deep vein thrombosis prevention best practices and cardiovascular protection best practices, as well as lower rates of catheter-related bloodstream infection and ventilator-associated pneumonia. These factors also were associated with significantly lower ICU and hospital mortality. The proportion of the tele-ICU association with lower mortality that could be attributed to adherence to these best practices and complication measures was estimated to be 25% for hospital mortality and 30% for ICU mortality.
"This suggests that there are benefits of a tele-ICU intervention beyond what is provided by daytime bedside intensivist staffing and traditional approaches to quality improvement such as the process changes presented," Dr. Lilly commented.
"These findings suggest that critical care programs that implement processes that increase adherence to best practice, lower rates of complications, shorten response times to alerts and alarms, and support early intensivist case involvement will provide better care at a lower cost. ... Our study suggests that the introduction of a tele-ICU program that collaborates with and supports bedside clinicians is one way to accomplish these aims."
All study authors reported having no conflicts of interest.
FROM AN INTERNATIONAL CONFERENCE OF THE AMERICAN THORACIC SOCIETY
Major Finding: Unadjusted ICU mortality was significantly lower in the tele-ICU group, compared with the preintervention group (10.7% vs. 8.6%). Hospital mortality also was reduced with tele-ICU (13.6% vs. 11.8%). Both ICU and hospital mean length of stay were significantly shorter with tele-ICU (hospital stay, 9.8 days vs. 13.3 days; ICU stay, 4.5 vs. 6.4 days).
Data Source: Prospective clinical practice study of 6,290 adult patients admitted over 2 years to seven ICUs in an academic medical center.
Disclosures: All study authors reported having no conflicts of interest.
Cryolipolysis Side Effects Mostly Mild and Transient, "Severe Pain" Rare
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system. The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq’s advisory board and have received educational and research support and honoraria from the company.
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system. The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq’s advisory board and have received educational and research support and honoraria from the company.
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system. The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq’s advisory board and have received educational and research support and honoraria from the company.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
Cryolipolysis Side Effects Mostly Mild, "Severe Pain" Rare
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system.
The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq's advisory board and have received educational and research support and honoraria from the company.
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system.
The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq's advisory board and have received educational and research support and honoraria from the company.
GRAPEVINE, TEX. – Risks associated with cryolipolysis for fat reduction are mostly transient and generally mild, according to a recent analysis.
"Severe pain" was reported in approximately 0.05% of all treated patients, said Dr. Nazanin Saedi of the University of California, Irvine.
Reports of severe pain emerged in postmarket surveillance, which traditionally allows for the detection of rare side effects not seen in clinical trials. Of more than 60,000 cryolipolysis treatments between June 2009 and December 2010, there were 23 reports of "severe pain" associated with the Zeltiq system.
The determination that a report was of "severe" pain rather than the known potential discomfort following treatment depended on symptoms. Of the reports, 11 were described as "severe," 8 as "sensitive to touch," 6 as "stabbing," and 6 as "deep/severe burning." (Patients could report more than one symptom). The incidence was calculated based on a denominator of 50,000, giving a rate of 0.00046, or 0.05%.
Zeltiq evaluated the "severe pain" to understand its etiology. The pain does not appear to be associated with the increasing number of larger applicators, because 10 of the 23 of patients reporting "severe pain" underwent treatment with the smaller applicator, Dr. Saedi noted.
Most severe pain involved the abdomen (21 of the 23 patients), arising at a mean of 3.4 days (range, 1-7) following the procedure. The mean time to resolution was 13.9 days (range, 7-28). Just one patient had severe pain lasting for 28 days, while in the majority (16 of the 23), pain had resolved by 2 weeks. Six patients reported that the pain worsened before getting better, peaking at about a week.
Two of the patients had known connective tissue disease, while the etiology was unknown for the rest. Exaggerated panniculitis is one possibility. The pain might also be of focal neuropathic origin, including allodynia, hyperneuralgia, or nerve inflammation arising from cytokine-mediated irritation of nerve fibers during the onset of inflammation following the procedure, said Dr. Saedi. It is likely that there are multiple etiologies.
A variety of therapeutic measures were used to treat the severe pain, but only the topical lidocaine patch was consistently reported as being helpful. Compression garments, lidocaine/tetracaine cream, and Vicodin (hydrocodone bitartrate and acetaminophen) were reported to have some effect, while ibuprofen, Percocet (oxycodone HCl and acetaminophen), Tylenol (acetaminophen) with codeine, ice, and heating pads had little or no effect, Dr. Saedi said.
Hyperpigmentation associated with a first- or second-degree burn of the dermis was another rare adverse event that arose in postmarketing surveillance. A total of four cases were reported, or less than 0.01% of treated patients. Three of the four were deemed to have been a result of operator error. All cases resolved.
Cryolipolysis technology uses controlled cold exposure to reduce subcutaneous fat. Adipocytes are selectively damaged via control and modulation of the cold exposure, while avoiding damage to the overlying epidermis and dermis. The decrease in fat thickness occurs gradually over the subsequent 3 months, and is most pronounced in patients with limited, discrete fatty bulges. The novel technology is among the noninvasive mechanisms for fat reduction that are becoming increasingly popular commercially, she noted.
Since the reports, there have been changes to the user manual as well as revisions in user training, user interface, and procedure monitoring , which make the likelihood of burn injury or subsequent hyperpigmentation more unlikely, even in the event of misuse. In fact, there have been no further reports of burn injury or hyperpigmentation during the last 30,000 procedure cycles, she noted.
"Further postmarket surveillance is needed to identify and better understand rare events," Dr. Saedi concluded.
Dr. Saedi said that she had no relevant financial disclosures. However, her coinvestigators are on Zeltiq's advisory board and have received educational and research support and honoraria from the company.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
AHA Statement Addresses Severe Manifestations of VTE
A scientific statement from the American Heart Association provides guidance for the management of the more severe forms of venous thromboembolism.
The statement focuses on three areas: massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension. “The goal is to provide practical advice to enable the busy clinician to optimize the management of patients with these severe manifestations of [venous thromboembolism],” said the writing committee, cochaired by Dr. Michael R. Jaff and Dr. M. Sean McMurtry (Circulation 2011 Mar. 21 [doi:10.1161/CIR.0b013e318214914f]).« http://www.theheart.org/article/1200965.do»
<[stk -1]>In an interview, Dr. McMurtry noted that because these disease areas have less data to support management strategies than do other areas of cardiovascular medicine, most of the recommendations in the document are class II (“it is reasonable” or “may be considered”) with level of evidence B or C (limited populations evaluated). “The authors hope that this document will inspire more research into these conditions,” said Dr. McMurtry of the University of Alberta, Edmonton.<[etk]>
<[stk -3]>The document begins by defining “massive,” “submassive,” and “low-risk” pulmonary embolism (PE), and provides data for the various techniques used to identify patients at increased risk for adverse short-term outcomes in acute PE. <[etk]>
Beyond initial heparin anticoagulation therapy, the use of fibrinolytic drugs is reasonable for patients with massive acute PE and an acceptable risk of bleeding complications, the statement said. It may also be considered for patients with submassive acute PE judged to have clinical evidence of an adverse prognosis (new hemodynamic instability, worsening respiratory insufficiency, severe right ventricle [RV] dysfunction, or major myocardial necrosis) and a low risk of bleeding.
Fibrinolysis is not recommended for patients with low-risk PE, or submassive PE with minor RV dysfunction, minor myocardial necrosis, and no clinical worsening. Fibrinolysis is also not recommended for undifferentiated cardiac arrest, wrote Dr. McMurtry and Dr. Jaff of Harvard Medical School, and coauthors.
In addition, recommendations are provided for other areas in which data are sparse and optimal management is unclear, including catheter-based therapies. Transcatheter procedures can be performed as an alternative to thrombolysis when there are contraindications or when emergency surgical thrombectomy is unavailable or contraindicated. Catheter interventions can also be performed when thrombolysis has failed to improve hemodynamics in the acute setting.
Hybrid therapy that includes both catheter-based clot fragmentation and local thrombolysis is an emerging strategy, the committee noted.
Adult patients with any confirmed acute PE who have contraindications to anticoagulation or have active bleeding should receive an inferior vena cava (IVC) filter. Further specific guidance is given for the type of filter and for monitoring.
<[stk -1]>Iliofemoral Deep Vein Thrombosis (IVDVT) refers to complete or partial thrombosis of any part of the iliac vein or the common femoral vein, with or without involvement of other lower-extremity veins or the IVC. Under this heading, the document addresses the use of initial coagulant therapy, long-term anticoagulant therapy, compression therapy, IVC filters, and thromboreductive strategies, including systemic, catheter-directed, percutaneous mechanical, and pharmacomechanical thrombolysis. Surgical venous thrombectomy is also discussed as an alternative method of thrombus removal. <[etk]>
«qc'er: pls fact check these next 2 grafs»<[stk -2]>“Reasonable” angiopathy and stenting options for older adolescents and adults include the use of percutaneous transluminal venous angioplasty and stent placement in the iliac vein to treat obstructive lesions after catheter-directed thrombolysis (CDT), pharmacomechanical CDT (PCDT), or surgical venous thrombectomy, and placement of iliac vein stents to reduce postthrombotic symptoms and heal venous ulcers in patients with advanced postthrombotic symptoms and iliac vein obstruction. “For obstructive iliac vein lesions that extend into the common femoral vein, caudal extension of stents into the common femoral vein is reasonable if unavoidable.” Guidelines regarding subsequent therapeutic anticoagulation are also provided. <[etk]>
The authors noted that “the use of percutaneous transluminal venous angioplasty in children may be reasonable, but this practice has not been well studied and may be associated with a greater risk of vasospasm.”
The section on chronic thromboembolic pulmonary hypertension (CTEPH) outlines the classification, risk factors, clinical presentation, diagnosis, and treatment with pulmonary endarterectomy and medical therapies. The condition is a syndrome of dyspnea, fatigue, and exercise intolerance caused by proximal thromboembolic obstruction and distal remodeling of the pulmonary circulation that leads to elevated pulmonary artery pressure and progressive RV failure.
Patients with unexplained dyspnea, exercise intolerance, or clinical evidence of right-sided heart failure, with or without a prior history of symptomatic venous thromboembolism, should be evaluated for CTEPH, and it is reasonable to evaluate patients with an echocardiogram 6 weeks after an acute pulmonary embolism to screen for persistent pulmonary hypertension that may predict the development of CTEPH.
Patients with objectively proven CTEPH should be promptly evaluated for pulmonary endarterectomy, even if symptoms are mild, and receive indefinite therapeutic anticoagulation in the absence of contraindications, they advised.
I have checked the following facts in my story: (Please initial each.)
lf MET drug names and dosages -
lf MET lab test values and their units -
lf MET whether nos. are correct and add up, and whether percentages based on those nos. are correct -
lf MET citation (e.g., JAMA 2008;299:785-92) -
lf MET investigators’ names and affiliations -
lf MET all other proper names (e.g., clinical trials; geographic, company, and test names) –..
lf MET investigators' conflicts of interest and sponsor of study –
Dr. McMurtry reported no relavant disclosures.
********* UNDERSET 1 LINES *********
A scientific statement from the American Heart Association provides guidance for the management of the more severe forms of venous thromboembolism.
The statement focuses on three areas: massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension. “The goal is to provide practical advice to enable the busy clinician to optimize the management of patients with these severe manifestations of [venous thromboembolism],” said the writing committee, cochaired by Dr. Michael R. Jaff and Dr. M. Sean McMurtry (Circulation 2011 Mar. 21 [doi:10.1161/CIR.0b013e318214914f]).« http://www.theheart.org/article/1200965.do»
<[stk -1]>In an interview, Dr. McMurtry noted that because these disease areas have less data to support management strategies than do other areas of cardiovascular medicine, most of the recommendations in the document are class II (“it is reasonable” or “may be considered”) with level of evidence B or C (limited populations evaluated). “The authors hope that this document will inspire more research into these conditions,” said Dr. McMurtry of the University of Alberta, Edmonton.<[etk]>
<[stk -3]>The document begins by defining “massive,” “submassive,” and “low-risk” pulmonary embolism (PE), and provides data for the various techniques used to identify patients at increased risk for adverse short-term outcomes in acute PE. <[etk]>
Beyond initial heparin anticoagulation therapy, the use of fibrinolytic drugs is reasonable for patients with massive acute PE and an acceptable risk of bleeding complications, the statement said. It may also be considered for patients with submassive acute PE judged to have clinical evidence of an adverse prognosis (new hemodynamic instability, worsening respiratory insufficiency, severe right ventricle [RV] dysfunction, or major myocardial necrosis) and a low risk of bleeding.
Fibrinolysis is not recommended for patients with low-risk PE, or submassive PE with minor RV dysfunction, minor myocardial necrosis, and no clinical worsening. Fibrinolysis is also not recommended for undifferentiated cardiac arrest, wrote Dr. McMurtry and Dr. Jaff of Harvard Medical School, and coauthors.
In addition, recommendations are provided for other areas in which data are sparse and optimal management is unclear, including catheter-based therapies. Transcatheter procedures can be performed as an alternative to thrombolysis when there are contraindications or when emergency surgical thrombectomy is unavailable or contraindicated. Catheter interventions can also be performed when thrombolysis has failed to improve hemodynamics in the acute setting.
Hybrid therapy that includes both catheter-based clot fragmentation and local thrombolysis is an emerging strategy, the committee noted.
Adult patients with any confirmed acute PE who have contraindications to anticoagulation or have active bleeding should receive an inferior vena cava (IVC) filter. Further specific guidance is given for the type of filter and for monitoring.
<[stk -1]>Iliofemoral Deep Vein Thrombosis (IVDVT) refers to complete or partial thrombosis of any part of the iliac vein or the common femoral vein, with or without involvement of other lower-extremity veins or the IVC. Under this heading, the document addresses the use of initial coagulant therapy, long-term anticoagulant therapy, compression therapy, IVC filters, and thromboreductive strategies, including systemic, catheter-directed, percutaneous mechanical, and pharmacomechanical thrombolysis. Surgical venous thrombectomy is also discussed as an alternative method of thrombus removal. <[etk]>
«qc'er: pls fact check these next 2 grafs»<[stk -2]>“Reasonable” angiopathy and stenting options for older adolescents and adults include the use of percutaneous transluminal venous angioplasty and stent placement in the iliac vein to treat obstructive lesions after catheter-directed thrombolysis (CDT), pharmacomechanical CDT (PCDT), or surgical venous thrombectomy, and placement of iliac vein stents to reduce postthrombotic symptoms and heal venous ulcers in patients with advanced postthrombotic symptoms and iliac vein obstruction. “For obstructive iliac vein lesions that extend into the common femoral vein, caudal extension of stents into the common femoral vein is reasonable if unavoidable.” Guidelines regarding subsequent therapeutic anticoagulation are also provided. <[etk]>
The authors noted that “the use of percutaneous transluminal venous angioplasty in children may be reasonable, but this practice has not been well studied and may be associated with a greater risk of vasospasm.”
The section on chronic thromboembolic pulmonary hypertension (CTEPH) outlines the classification, risk factors, clinical presentation, diagnosis, and treatment with pulmonary endarterectomy and medical therapies. The condition is a syndrome of dyspnea, fatigue, and exercise intolerance caused by proximal thromboembolic obstruction and distal remodeling of the pulmonary circulation that leads to elevated pulmonary artery pressure and progressive RV failure.
Patients with unexplained dyspnea, exercise intolerance, or clinical evidence of right-sided heart failure, with or without a prior history of symptomatic venous thromboembolism, should be evaluated for CTEPH, and it is reasonable to evaluate patients with an echocardiogram 6 weeks after an acute pulmonary embolism to screen for persistent pulmonary hypertension that may predict the development of CTEPH.
Patients with objectively proven CTEPH should be promptly evaluated for pulmonary endarterectomy, even if symptoms are mild, and receive indefinite therapeutic anticoagulation in the absence of contraindications, they advised.
I have checked the following facts in my story: (Please initial each.)
lf MET drug names and dosages -
lf MET lab test values and their units -
lf MET whether nos. are correct and add up, and whether percentages based on those nos. are correct -
lf MET citation (e.g., JAMA 2008;299:785-92) -
lf MET investigators’ names and affiliations -
lf MET all other proper names (e.g., clinical trials; geographic, company, and test names) –..
lf MET investigators' conflicts of interest and sponsor of study –
Dr. McMurtry reported no relavant disclosures.
********* UNDERSET 1 LINES *********
A scientific statement from the American Heart Association provides guidance for the management of the more severe forms of venous thromboembolism.
The statement focuses on three areas: massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension. “The goal is to provide practical advice to enable the busy clinician to optimize the management of patients with these severe manifestations of [venous thromboembolism],” said the writing committee, cochaired by Dr. Michael R. Jaff and Dr. M. Sean McMurtry (Circulation 2011 Mar. 21 [doi:10.1161/CIR.0b013e318214914f]).« http://www.theheart.org/article/1200965.do»
<[stk -1]>In an interview, Dr. McMurtry noted that because these disease areas have less data to support management strategies than do other areas of cardiovascular medicine, most of the recommendations in the document are class II (“it is reasonable” or “may be considered”) with level of evidence B or C (limited populations evaluated). “The authors hope that this document will inspire more research into these conditions,” said Dr. McMurtry of the University of Alberta, Edmonton.<[etk]>
<[stk -3]>The document begins by defining “massive,” “submassive,” and “low-risk” pulmonary embolism (PE), and provides data for the various techniques used to identify patients at increased risk for adverse short-term outcomes in acute PE. <[etk]>
Beyond initial heparin anticoagulation therapy, the use of fibrinolytic drugs is reasonable for patients with massive acute PE and an acceptable risk of bleeding complications, the statement said. It may also be considered for patients with submassive acute PE judged to have clinical evidence of an adverse prognosis (new hemodynamic instability, worsening respiratory insufficiency, severe right ventricle [RV] dysfunction, or major myocardial necrosis) and a low risk of bleeding.
Fibrinolysis is not recommended for patients with low-risk PE, or submassive PE with minor RV dysfunction, minor myocardial necrosis, and no clinical worsening. Fibrinolysis is also not recommended for undifferentiated cardiac arrest, wrote Dr. McMurtry and Dr. Jaff of Harvard Medical School, and coauthors.
In addition, recommendations are provided for other areas in which data are sparse and optimal management is unclear, including catheter-based therapies. Transcatheter procedures can be performed as an alternative to thrombolysis when there are contraindications or when emergency surgical thrombectomy is unavailable or contraindicated. Catheter interventions can also be performed when thrombolysis has failed to improve hemodynamics in the acute setting.
Hybrid therapy that includes both catheter-based clot fragmentation and local thrombolysis is an emerging strategy, the committee noted.
Adult patients with any confirmed acute PE who have contraindications to anticoagulation or have active bleeding should receive an inferior vena cava (IVC) filter. Further specific guidance is given for the type of filter and for monitoring.
<[stk -1]>Iliofemoral Deep Vein Thrombosis (IVDVT) refers to complete or partial thrombosis of any part of the iliac vein or the common femoral vein, with or without involvement of other lower-extremity veins or the IVC. Under this heading, the document addresses the use of initial coagulant therapy, long-term anticoagulant therapy, compression therapy, IVC filters, and thromboreductive strategies, including systemic, catheter-directed, percutaneous mechanical, and pharmacomechanical thrombolysis. Surgical venous thrombectomy is also discussed as an alternative method of thrombus removal. <[etk]>
«qc'er: pls fact check these next 2 grafs»<[stk -2]>“Reasonable” angiopathy and stenting options for older adolescents and adults include the use of percutaneous transluminal venous angioplasty and stent placement in the iliac vein to treat obstructive lesions after catheter-directed thrombolysis (CDT), pharmacomechanical CDT (PCDT), or surgical venous thrombectomy, and placement of iliac vein stents to reduce postthrombotic symptoms and heal venous ulcers in patients with advanced postthrombotic symptoms and iliac vein obstruction. “For obstructive iliac vein lesions that extend into the common femoral vein, caudal extension of stents into the common femoral vein is reasonable if unavoidable.” Guidelines regarding subsequent therapeutic anticoagulation are also provided. <[etk]>
The authors noted that “the use of percutaneous transluminal venous angioplasty in children may be reasonable, but this practice has not been well studied and may be associated with a greater risk of vasospasm.”
The section on chronic thromboembolic pulmonary hypertension (CTEPH) outlines the classification, risk factors, clinical presentation, diagnosis, and treatment with pulmonary endarterectomy and medical therapies. The condition is a syndrome of dyspnea, fatigue, and exercise intolerance caused by proximal thromboembolic obstruction and distal remodeling of the pulmonary circulation that leads to elevated pulmonary artery pressure and progressive RV failure.
Patients with unexplained dyspnea, exercise intolerance, or clinical evidence of right-sided heart failure, with or without a prior history of symptomatic venous thromboembolism, should be evaluated for CTEPH, and it is reasonable to evaluate patients with an echocardiogram 6 weeks after an acute pulmonary embolism to screen for persistent pulmonary hypertension that may predict the development of CTEPH.
Patients with objectively proven CTEPH should be promptly evaluated for pulmonary endarterectomy, even if symptoms are mild, and receive indefinite therapeutic anticoagulation in the absence of contraindications, they advised.
I have checked the following facts in my story: (Please initial each.)
lf MET drug names and dosages -
lf MET lab test values and their units -
lf MET whether nos. are correct and add up, and whether percentages based on those nos. are correct -
lf MET citation (e.g., JAMA 2008;299:785-92) -
lf MET investigators’ names and affiliations -
lf MET all other proper names (e.g., clinical trials; geographic, company, and test names) –..
lf MET investigators' conflicts of interest and sponsor of study –
Dr. McMurtry reported no relavant disclosures.
********* UNDERSET 1 LINES *********
Studies Highlight Role of Primary Care in HIV-Positive Population
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
FROM THE ARCHIVES OF INTERNAL MEDICINE
Major Finding: HIV Patients in the two studies were found to be at risk for conditions other than HIV, suggesting that because of the success of treatment and the aging of the population, these patients are in need of primary care in addition to infectious disease specialists.
Data Source: Two VA cohort studies and a multisite cluster-randomized controlled trial.
Disclosures: Neither the investigators from the two studies nor the editorialist had any disclosures
Studies Highlight Role of Primary Care in HIV-Positive Population
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
FROM THE ARCHIVES OF INTERNAL MEDICINE
Studies Highlight Role of Primary Care in HIV-Positive Population
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
The overall management of HIV-infected patients need no longer be strictly in the hands of infectious disease experts; primary care physicians have a greater role to play in the management of this patient population, suggest two papers in the April 25 Archives of Internal Medicine.
Conventionally, individuals with HIV infection have been managed by infectious disease specialists. But with the simplification of antiretroviral regimens, the increased ease of viral-load testing, and the subsequent reduction in opportunistic infections and HIV-associated malignancy rates, the management of HIV is far more feasible outside of infectious disease settings, Dr. Mitchell H. Katz said in an accompanying editorial (Arch. Intern. Med. 2011;171:719-20).
Today, the "most common reason for a patient’s condition not being fully suppressed while receiving one of the conventional regimens is nonadherence, a primary care problem if ever there was one," said Dr. Katz of the Los Angeles Department of Health Services.
He added that if "specialty care is less needed than it used to be for HIV-infected patients, it turns out that primary care is more needed. Owing to the advances in HIV treatment, our patients are no longer dying: They are aging!"
In the first paper (an analysis of two cohort studies of veterans), HIV infection was associated with an increased risk for heart failure (HF), independent of conventional risk factors for the heart condition.
Dr. Adeel A. Butt, director of the VA Pittsburgh Healthcare System’s infectious disease/HIV clinic, studied 8,486 patients who did not have prevalent coronary heart disease (CHD), angina, HF, or cancer at baseline. Of those, 2,391 were HIV infected and 6,095 were uninfected. Over a median follow-up of 7.3 years, there were 286 incident HF events and 1,096 deaths. Of the 7,104 patients who did not develop HF or die, 87% completed follow-up (Arch. Intern. Med. 2011:171:737-43).
The median age was 48 years in both groups, and all subjects were male. (Women were excluded because of low numbers.) The age- and race/ethnicity–adjusted rates of incident HF were 7.12 per 1,000 person-years for HIV-infected patients and 4.82 per 1,000 person-years for HIV-uninfected patients. Compared with HIV-uninfected patients, those who were HIV infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, body mass index, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (hazard ratio, 1.81).
Moreover, those with HIV infection who had baseline HIV-1 RNA levels of 500 or more copies/mL had a significantly higher risk of HF than did those who did not have HIV infection (HR, 2.28). However, the HIV-infected patients with HIV-1 RNA levels less than 500 copies/mL did not have an increased risk of HF, Dr. Butt and his associates reported.
Additional analysis excluding patients who developed CHD and/or alcohol abuse or dependence during the follow-up period prior to the HF diagnosis showed that the relationship between HIV and HF persisted, with a hazard ratio of 1.96 for those who developed neither condition, they said.
The exact mechanism by which HIV infection is associated with HF is not well understood. Possible mechanisms include direct effects of the HIV, comorbidities associated with HIV infection, antiretroviral therapy leading to an increased risk of CHD and subsequent HF, nutritional deficiencies, and immunologic damage to the myocardium.
These findings have major clinical implications. "If HF is a major cardiovascular consequence of HIV infection rather than atherosclerotic heart disease, different approaches to manage such consequences are warranted. Cardiovascular risk factor reduction and antiplatelet agents are the mainstay in the management of atherosclerotic heart disease. However, these strategies, plus aggressive blood pressure control and the treatment of the HIV infection, may also be required to prevent development of HF in this population," they concluded.
In the second study, 550 individuals were assigned to a health-promotion intervention that addressed multiple health-related behaviors, and 520 to an HIV/STD risk-reduction intervention. Both interventions consisted of eight weekly, structured, 2-hour sessions delivered by cofacilitators and incorporating brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and risk-reduction knowledge, said Nabila El-Bassel, Ph.D., professor of social work at Columbia University, New York, and her associates.
Those in the health behavior–intervention group were encouraged to exercise throughout the week, including at least 30 minutes of moderate-intensity physical activity on 5 days or at least 20 minutes of vigorous intensity physical activity on 4 days and strength-building activity on at least 2 days. Dietary activities addressed adherence to a diet of five to nine servings of fruits and vegetables daily, including addressing barriers such as cost of fresh produce, taste, and availability (Arch. Intern. Med. 2011;171:728-36).
Sessions also focused on the importance of breast and prostate cancer screening. The health risks of excessive alcohol use, particularly for those infected with hepatitis C, was also covered.
The HIV/STD risk-reduction intervention was structurally similar to the health promotion intervention; however, it focused on the participants as members of couples rather than as individuals.
The mean participant age was 43 years, and the HIV-positive partner was female in 60% of the couples. Attendance at the eight sessions of both interventions was excellent, with a retention rate of 88% at 12 months post intervention, Dr. El-Bassel and her associates reported.
Health promotion–intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. In the health promotion intervention, compared with the HIV/STD intervention, participants consumed fatty foods less frequently (mean difference, –0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
One possible explanation for the lack of an effect of the health promotion intervention on alcohol use is that the HIV/STD intervention also covered the subject, cautioning that alcohol use could be a trigger for unsafe sexual behavior, they noted.
"We are optimistic that the present study offers an approach that may help reduce the disproportionately high morbidity and mortality rates from chronic diseases in African Americans," Dr. El-Bassel and her associates concluded.
Dr. Katz agreed. "Although serodiscordant couples are a highly specialized population, there is no reason to believe that their intervention would not work among other HIV-infected persons. Certainly, this study should encourage others to attempt group health promotion classes because, as I often tell my HIV-infected patients with diabetes, liver disease, or uncontrolled hypertension, ‘It’s not HIV that’s going to kill you.’ "
Neither Dr. Katz nor any of the investigators in either study reported financial disclosures.
FROM THE ARCHIVES OF INTERNAL MEDICINE
Major Finding: In the first study, compared with HIV-uninfected patients, those who were HIV-infected had a significantly increased risk of HF after adjustment for conventional risk factors including race, current smoking, BMI, hypertension, diabetes, and a diagnosis of alcohol abuse or dependence (HR, 1.81). In the second study, health promotion intervention participants were more likely to report consuming five or more servings of fruits and vegetables daily (rate ratio, 1.38) and adhering to physical activity guidelines (RR, 1.39) compared with the HIV/STD intervention participants. Health promotion intervention participants also consumed fatty foods less frequently (mean difference, -0.18), more men received prostate cancer screening (RR, 1.51), and more women received a mammogram (RR, 1.26). Alcohol use did not differ between the intervention groups.
Data Source: Two VA cohort studies and a multisite cluster-randomized controlled trial.
Disclosures: Neither the investigators from the two studies nor the editorialist had any disclosures
Microwave Device Offers Long-Term Treatment for Hyperhidrosis
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
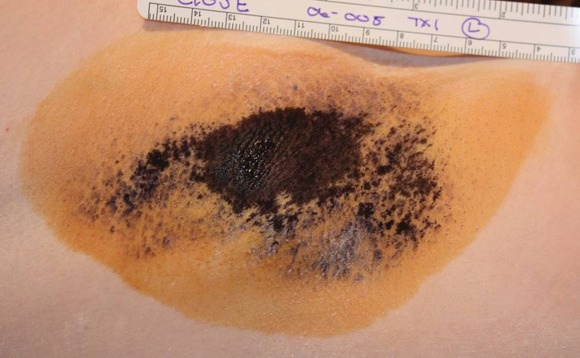
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
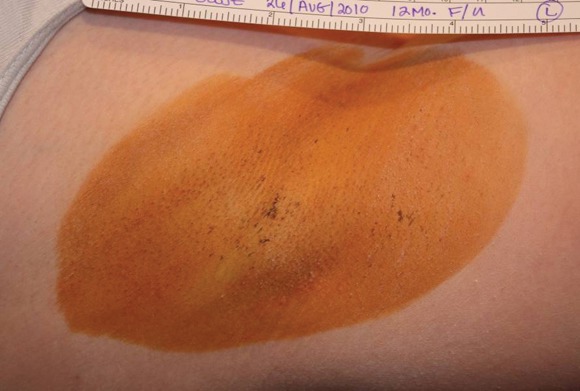
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
Major Finding: First study: Efficacy of treatment in 81 patients as determined by HDSS scores was 89% at 30 days and 67% at 6 months; efficacy of sham treatment in 39 patients was 54% and 44%, respectively. Second study: Of 28 patients seen at 30 days after treatment, all but one had HDSS scores of 1 or 2 (96% efficacy). Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments at 3 months showed that 94% had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Data Source: Two studies of 120 and 31 patients, respectively, with axillary hyperhidrosis
Disclosures: The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
Microwave Device Offers Long-Term Treatment for Hyperhidrosis
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
GRAPEVINE, TEX. – A novel microwave device significantly reduced underarm sweating in two studies involving a total of 151 patients with axillary hyperhidrosis.
The condition affects millions of people, yet current treatments are limited by either duration of effect or efficacy. The microwave device has the potential for a longer-term and possibly even permanent effect via eradication of eccrine sweat glands, Dr. Suzanne L. Kilmer and Dr. Mark Lupin reported in separate presentations at the annual meeting of the American Society for Laser Medicine and Surgery.
Miramar Labs’ miraDry system focuses microwave energy to selectively heat the interface between the skin and underlying fat, where the sweat glands reside. The system comprises a console, handpiece, and disposable tip. The in-office procedure takes approximately 40 minutes. The system was cleared for licensure in the United States by the Food and Drug Administration in January 2011, and will be marketed later this year, according to a company spokesperson.
Dr. Kilmer, of the Laser and Skin Surgery Center of Northern California, Sacramento, presented data on a second-generation version of the device that was FDA approved but never marketed. In a multicenter, sham-controlled study, 120 adults with hyperhidrosis were randomized to miraDry (81) or sham treatment (39) for one to three sessions. The patients had to have a Hyperhidrosis Disease Severity Scale (HDSS) score of 3 or 4 ("my underarm sweating is barely tolerable and frequently/always interferes with my daily activities") at baseline, and gravimetric readings greater than 50 mg at each axilla (in 5 minutes).
Follow-up was 6 months for the sham group and 12 months for the treatment group. Responders were defined as subjects reporting a reduction to an HDSS score of 1 ("My underarm sweating is never noticeable and never interferes with daily activities") or 2 ("My underarm sweating is tolerable but sometimes interferes with daily activities"). The patients had a mean age of 33 years, 58% were female, and 84% were white.
Efficacy for the treatment group was 89% at 30 days, 74% at 3 months, 67% at 6 months, and 69% at the 9- and 12-month visits. In the sham group, efficacy was 54% at 30 days and 44% for the 3- and 6-month visits. At all time points, the differences between the treatment and sham groups were significant, Dr. Kilmer reported.
Treatment-related adverse events were generally mild, and all but one resolved. The most common adverse events in the treatment group were transient patches of altered sensation in the treatment limb, occurring in 8 patients (10%), and axillary pain requiring prescription medication in 5 patients (6%). Most subjects experienced transient post-treatment local sequelae in the axilla such as edema, tenderness, and bruising.
Follow-up of the treated subjects showed stable efficacy through 12 months, she said.
The second study, involving 31 patients, investigated the third-generation, optimized version of the device. As in the earlier study, all patients had to have primary axillary hyperhidrosis with an HDSS score of 3 or 4. The patients also were required to have a gravimetric sweat assessment of at least 50 mg in each axilla (in 5 minutes). None of the patients had surgery for axillary hyperhidrosis or botulinum toxin injections in the axillae in the prior 12 months, said Dr. Lupin of Cosmedica Laser Centre, Victoria, B.C.
The patients had a mean age of 33 years (range 18-65 years), and three-quarters were female. They had a mean BMI of 24.8 kg/m2. Of 28 patients seen at 30 days, all but one (96%) had HDSS scores of 1 or 2. Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments 3 months after treatment showed that 94% of patients had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Nineteen of the 31 initially enrolled patients (61%) experienced at least one treatment-related adverse event, of which most (88%) were rated as mild. The most common were numbness or tingling in an area of the treated limb (12 patients, 39%), and edema in the chest or treatment limb lasting about a week (9 patients, 29%). Most of the patients also experienced acute post-treatment transient effects in the treatment area such as localized edema, tenderness, or erythema. Follow-up of safety is ongoing, Dr. Lupin noted.
"The study is continuing out to 12 months, and at 6 months the preliminary data so far are showing sustained positive improvements in all measures of quality of life, reduction of sweat, and impact on daily living," Dr. Lupin said in an interview. Many patients also reported reduction of axillary hair, and a few patients noted improvement in odor, he said.
Overall, patient satisfaction, as measured by the Dermatology Life Quality Index (DLQI), was 96% at 3 months.
When Dr. Lupin was asked whether miraDry had any disadvantages compared with botulinum toxin type A, he said that there are several short-term advantages to botulinum toxin type A: It is a quicker and easier procedure (about 5-10 minutes) with sweat reduction occurring in just a few days, versus 1 hour for the miraDry procedure, which requires anesthesia and can take a week or longer to produce results. Moreover, botulinum toxin type A is a single treatment and its benefit lasts about 6-8 months, whereas miraDry takes 1-3 sessions for a benefit of at least a year and possibly longer.
Indeed, Dr. Kilmer said in an interview, duration of benefit is an advantage of miraDry over just about every current hyperhidrosis treatment other than sympathectomy, a procedure that is rarely done. So far, the longest miraDry has been studied is 12 months, so "we can’t say for sure, but it didn’t drop off much during that time, so we expect it will last much longer," she said.
Dr. Mathew Avram, director of the Massachusetts General Hospital Dermatology Laser and Cosmetic Center, Boston, said, "This is innovative and interesting technology to address an issue that is very problematic for patients. We need to learn a little more about the duration of these benefits and what if any side effects may be created with repeated treatments over time."
The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
Major Finding: First study: Efficacy of treatment in 81 patients as determined by HDSS scores was 89% at 30 days and 67% at 6 months; efficacy of sham treatment in 39 patients was 54% and 44%, respectively. Second study: Of 28 patients seen at 30 days after treatment, all but one had HDSS scores of 1 or 2 (96% efficacy). Of 25 seen at 3 months, all had HDSS scores of 1 or 2 (100% efficacy). Gravimetric assessments at 3 months showed that 94% had at least a 50% reduction in axillary sweat compared with baseline, with an average sweat reduction of 82%.
Data Source: Two studies of 120 and 31 patients, respectively, with axillary hyperhidrosis
Disclosures: The studies were sponsored by Miramar Labs. Dr. Lupin disclosed that he received a research grant for the study and travel expenses from Miramar, and also received honoraria and travel expenses from Allergan. Dr. Kilmer disclosed that she received research support from Miramar. Dr. Avram is a stockholder in Zeltiq.