User login
Official Newspaper of the American College of Surgeons
AMA: Most physicians still work in small practices
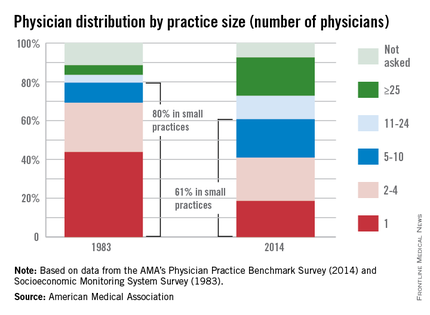
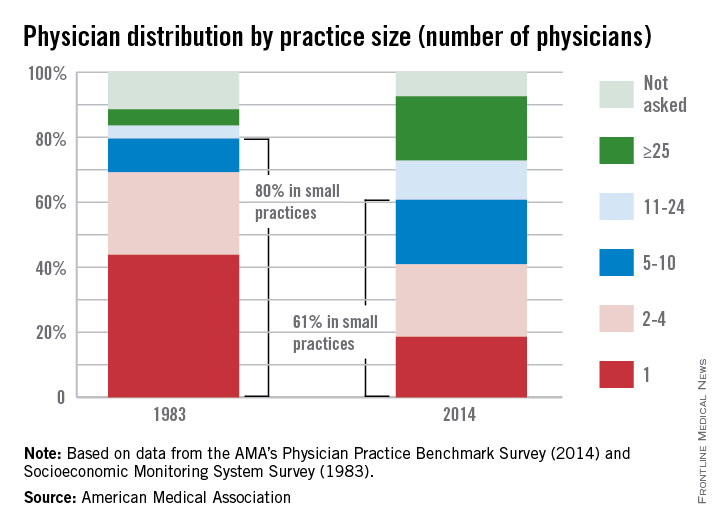
While medical practice arrangements seem to have changed dramatically over the last 30 years, the majority of physicians still work in small practices, the American Medical Association reported.
In a 2014 AMA survey, almost 61% of respondents worked in practices of 10 or fewer physicians. That’s down from the 80% reported by the AMA in 1983, but it still qualifies as majority. Over that same period, the proportion of physicians working in practices of 25 or more increased from 5% to 20%.
These changes in practice size were related to changes in practice ownership, the AMA noted. In 1983, the percentage of physicians who were the owners of their practices was 76%. In 2014, that number was 51%.
Looking at short-term data comparing the 2014 survey with one from 2012, the AMA found that the “share of physicians who worked directly for a hospital or in practices that were at least partially owned by a hospital increased from 29% in 2012 to 32.8% in 2014. Over that 2-year period, the share of physicians who were directly employed by a hospital increased from 5.6% to 7.2%, while the percentage of physicians who were in solo practice decreased from 18.4% to 17.1%, the AMA said.
While medical practice arrangements seem to have changed dramatically over the last 30 years, the majority of physicians still work in small practices, the American Medical Association reported.
In a 2014 AMA survey, almost 61% of respondents worked in practices of 10 or fewer physicians. That’s down from the 80% reported by the AMA in 1983, but it still qualifies as majority. Over that same period, the proportion of physicians working in practices of 25 or more increased from 5% to 20%.
These changes in practice size were related to changes in practice ownership, the AMA noted. In 1983, the percentage of physicians who were the owners of their practices was 76%. In 2014, that number was 51%.
Looking at short-term data comparing the 2014 survey with one from 2012, the AMA found that the “share of physicians who worked directly for a hospital or in practices that were at least partially owned by a hospital increased from 29% in 2012 to 32.8% in 2014. Over that 2-year period, the share of physicians who were directly employed by a hospital increased from 5.6% to 7.2%, while the percentage of physicians who were in solo practice decreased from 18.4% to 17.1%, the AMA said.
While medical practice arrangements seem to have changed dramatically over the last 30 years, the majority of physicians still work in small practices, the American Medical Association reported.
In a 2014 AMA survey, almost 61% of respondents worked in practices of 10 or fewer physicians. That’s down from the 80% reported by the AMA in 1983, but it still qualifies as majority. Over that same period, the proportion of physicians working in practices of 25 or more increased from 5% to 20%.
These changes in practice size were related to changes in practice ownership, the AMA noted. In 1983, the percentage of physicians who were the owners of their practices was 76%. In 2014, that number was 51%.
Looking at short-term data comparing the 2014 survey with one from 2012, the AMA found that the “share of physicians who worked directly for a hospital or in practices that were at least partially owned by a hospital increased from 29% in 2012 to 32.8% in 2014. Over that 2-year period, the share of physicians who were directly employed by a hospital increased from 5.6% to 7.2%, while the percentage of physicians who were in solo practice decreased from 18.4% to 17.1%, the AMA said.
ASCO supports endometrial cancer RT guidelines with some qualifications
The American Society of Clinical Oncology is supporting a guideline on postoperative radiation therapy for endometrial cancer, with some qualifications.
According to the guideline from the American Society for Radiation Oncology, surveillance only is a reasonable course of action in women without residual disease and for women with grade 1 or 2 cancer and less than 50% myometrial invasion (MI). For women with grade 1 or 2 cancer with more than 50% MI and women with grade 3 cancer with less than 50% MI, vaginal brachytherapy is as effective as pelvic radiation is at preventing recurrence and is preferable. Patients with grade 3 cancer above 50% MI will benefit from pelvic radiation therapy.
The ASCO Endorsement Panel gave several qualifications to highlight important points. Qualifications listed include the lack of survival benefit with external beam radiation therapy in early-stage disease, choosing vaginal brachytherapy over external beam radiation therapy in high-intermediate risk disease for locoregional control, chemotherapy in women with high-risk early-stage and advanced disease, the importance of clinical trials, and fertility and quality of life concerns, the panel reported.
Find the full study in the Journal of Clinical Oncology (doi:10.1200/JCO.2015.62.5459)
The American Society of Clinical Oncology is supporting a guideline on postoperative radiation therapy for endometrial cancer, with some qualifications.
According to the guideline from the American Society for Radiation Oncology, surveillance only is a reasonable course of action in women without residual disease and for women with grade 1 or 2 cancer and less than 50% myometrial invasion (MI). For women with grade 1 or 2 cancer with more than 50% MI and women with grade 3 cancer with less than 50% MI, vaginal brachytherapy is as effective as pelvic radiation is at preventing recurrence and is preferable. Patients with grade 3 cancer above 50% MI will benefit from pelvic radiation therapy.
The ASCO Endorsement Panel gave several qualifications to highlight important points. Qualifications listed include the lack of survival benefit with external beam radiation therapy in early-stage disease, choosing vaginal brachytherapy over external beam radiation therapy in high-intermediate risk disease for locoregional control, chemotherapy in women with high-risk early-stage and advanced disease, the importance of clinical trials, and fertility and quality of life concerns, the panel reported.
Find the full study in the Journal of Clinical Oncology (doi:10.1200/JCO.2015.62.5459)
The American Society of Clinical Oncology is supporting a guideline on postoperative radiation therapy for endometrial cancer, with some qualifications.
According to the guideline from the American Society for Radiation Oncology, surveillance only is a reasonable course of action in women without residual disease and for women with grade 1 or 2 cancer and less than 50% myometrial invasion (MI). For women with grade 1 or 2 cancer with more than 50% MI and women with grade 3 cancer with less than 50% MI, vaginal brachytherapy is as effective as pelvic radiation is at preventing recurrence and is preferable. Patients with grade 3 cancer above 50% MI will benefit from pelvic radiation therapy.
The ASCO Endorsement Panel gave several qualifications to highlight important points. Qualifications listed include the lack of survival benefit with external beam radiation therapy in early-stage disease, choosing vaginal brachytherapy over external beam radiation therapy in high-intermediate risk disease for locoregional control, chemotherapy in women with high-risk early-stage and advanced disease, the importance of clinical trials, and fertility and quality of life concerns, the panel reported.
Find the full study in the Journal of Clinical Oncology (doi:10.1200/JCO.2015.62.5459)
CMS pledges flexibility during first year of ICD-10
Physicians will have a year to learn how to properly code under ICD-10 before facing potential penalties or withheld payments, according to a joint announcement from the Centers for Medicare & Medicaid Services and the American Medical Association.
During that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes. However, physicians still will not be able to use ICD-9 codes after Sept. 30, 2015.

“This means that Medicare will not deny payment for these unintentional errors as practices become accustomed to ICD-10 coding,” Dr. Steven Stack, AMA president, wrote in a blog post on the AMA website. “This transition period will give physicians and their practice teams time to get up to speed on the more complicated code set.”
Similarly, physicians will not face penalties under the Physician Quality Reporting System, the value-based modifier, or the meaningful use program based on the specificity of diagnosis codes if the appropriate family of ICD-10 codes are used, according to the AMA. Finally, if a Medicare contractor is unable to process a claim due to coding issues, CMS will authorize an advance payment to the physician.
CMS also plans to create an ICD-10 coordination center and appoint an ombudsman to answer questions about claims submission using ICD-10.
“With easy-to-use tools, a new ICD-10 ombudsman, and added flexibility in our claims audit and quality reporting process, CMS is committed to working with the physician community to work through this transition.” Andy Slavitt, CMS Acting Administrator, said in a statement.
Physicians will have a year to learn how to properly code under ICD-10 before facing potential penalties or withheld payments, according to a joint announcement from the Centers for Medicare & Medicaid Services and the American Medical Association.
During that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes. However, physicians still will not be able to use ICD-9 codes after Sept. 30, 2015.
“This means that Medicare will not deny payment for these unintentional errors as practices become accustomed to ICD-10 coding,” Dr. Steven Stack, AMA president, wrote in a blog post on the AMA website. “This transition period will give physicians and their practice teams time to get up to speed on the more complicated code set.”
Similarly, physicians will not face penalties under the Physician Quality Reporting System, the value-based modifier, or the meaningful use program based on the specificity of diagnosis codes if the appropriate family of ICD-10 codes are used, according to the AMA. Finally, if a Medicare contractor is unable to process a claim due to coding issues, CMS will authorize an advance payment to the physician.
CMS also plans to create an ICD-10 coordination center and appoint an ombudsman to answer questions about claims submission using ICD-10.
“With easy-to-use tools, a new ICD-10 ombudsman, and added flexibility in our claims audit and quality reporting process, CMS is committed to working with the physician community to work through this transition.” Andy Slavitt, CMS Acting Administrator, said in a statement.
Physicians will have a year to learn how to properly code under ICD-10 before facing potential penalties or withheld payments, according to a joint announcement from the Centers for Medicare & Medicaid Services and the American Medical Association.
During that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes. However, physicians still will not be able to use ICD-9 codes after Sept. 30, 2015.
“This means that Medicare will not deny payment for these unintentional errors as practices become accustomed to ICD-10 coding,” Dr. Steven Stack, AMA president, wrote in a blog post on the AMA website. “This transition period will give physicians and their practice teams time to get up to speed on the more complicated code set.”
Similarly, physicians will not face penalties under the Physician Quality Reporting System, the value-based modifier, or the meaningful use program based on the specificity of diagnosis codes if the appropriate family of ICD-10 codes are used, according to the AMA. Finally, if a Medicare contractor is unable to process a claim due to coding issues, CMS will authorize an advance payment to the physician.
CMS also plans to create an ICD-10 coordination center and appoint an ombudsman to answer questions about claims submission using ICD-10.
“With easy-to-use tools, a new ICD-10 ombudsman, and added flexibility in our claims audit and quality reporting process, CMS is committed to working with the physician community to work through this transition.” Andy Slavitt, CMS Acting Administrator, said in a statement.

Survey: Most health care organizations had a recent security breach
More than two-thirds of health care organizations responding to a survey have experienced a significant and recent security event, according to the Health Information and Management Systems Society (HIMSS).
The single largest source of significant security incidents were negligent insiders, defined as well-meaning individuals who unwittingly caused a breach. However, 64% of respondents reported that their organization had been the victim of an attack from an external actor – usually an online scam artist. The results are part of the 2015 HIMSS Cybersecurity Survey, which polled 297 health care leaders and information security officers.

Most of the security incidents resulted in limited disruption of IT systems with limited impact on clinical care, according to the report. The majority of respondents said security incidents were detected within 24 hours of occurrence, “approximately 20% of these security incidents ultimately resulted in loss of patient, financial, or operational data.”
While security breaches may seem like an IT issue, Jennifer Horowitz, senior director of research at HIMSS, said physicians need to be aware of what they can do to help keep their systems secure.
“This is a rapidly changing environment and I think that physicians also need ... to do their part: adhering to the security policies and protocols as their organization,” Ms. Horowitz said in an interivew, highlighting particularly that physicians need to be aware of potential phishing scams sent via email that could comprompise data security.
More than two-thirds of health care organizations responding to a survey have experienced a significant and recent security event, according to the Health Information and Management Systems Society (HIMSS).
The single largest source of significant security incidents were negligent insiders, defined as well-meaning individuals who unwittingly caused a breach. However, 64% of respondents reported that their organization had been the victim of an attack from an external actor – usually an online scam artist. The results are part of the 2015 HIMSS Cybersecurity Survey, which polled 297 health care leaders and information security officers.
Most of the security incidents resulted in limited disruption of IT systems with limited impact on clinical care, according to the report. The majority of respondents said security incidents were detected within 24 hours of occurrence, “approximately 20% of these security incidents ultimately resulted in loss of patient, financial, or operational data.”
While security breaches may seem like an IT issue, Jennifer Horowitz, senior director of research at HIMSS, said physicians need to be aware of what they can do to help keep their systems secure.
“This is a rapidly changing environment and I think that physicians also need ... to do their part: adhering to the security policies and protocols as their organization,” Ms. Horowitz said in an interivew, highlighting particularly that physicians need to be aware of potential phishing scams sent via email that could comprompise data security.
More than two-thirds of health care organizations responding to a survey have experienced a significant and recent security event, according to the Health Information and Management Systems Society (HIMSS).
The single largest source of significant security incidents were negligent insiders, defined as well-meaning individuals who unwittingly caused a breach. However, 64% of respondents reported that their organization had been the victim of an attack from an external actor – usually an online scam artist. The results are part of the 2015 HIMSS Cybersecurity Survey, which polled 297 health care leaders and information security officers.
Most of the security incidents resulted in limited disruption of IT systems with limited impact on clinical care, according to the report. The majority of respondents said security incidents were detected within 24 hours of occurrence, “approximately 20% of these security incidents ultimately resulted in loss of patient, financial, or operational data.”
While security breaches may seem like an IT issue, Jennifer Horowitz, senior director of research at HIMSS, said physicians need to be aware of what they can do to help keep their systems secure.
“This is a rapidly changing environment and I think that physicians also need ... to do their part: adhering to the security policies and protocols as their organization,” Ms. Horowitz said in an interivew, highlighting particularly that physicians need to be aware of potential phishing scams sent via email that could comprompise data security.

DDW: Study finds pancreatic cancer misdiagnosis rate at 31%
WASHINGTON – Initial misdiagnoses were common and were associated with a later disease stage at diagnosis, in a study of 313 patients diagnosed with pancreatic cancer, Dr. Douglas Swords said at the annual Digestive Disease Week.
“By far, the most common misdiagnosis was gallbladder disease,” and there was about a 3-month longer time period, on average, from the first visit to a physician to the actual cancer diagnosis, in patients who were initially misdiagnosed, said Dr. Swords, a surgery resident at the University of Utah, Salt Lake City.

In the series of 313 patients diagnosed with pancreatic cancer, 98 (31.3%) were initially misdiagnosed, with a total of 119 diagnoses other than pancreatic cancer, he said. The most common misdiagnosis was gallbladder disease, which led to a cholecystectomy in 38 cases, followed by gastroesophageal reflux disease in 15 cases, and peptic ulcer disease in 11 cases. Those initially misdiagnosed were an average of about 5 years younger.
Patients with an initial misdiagnosis had significantly greater rates of abdominal pain (about 85% vs. about 60%), weight loss (about 85% vs. about 75%), nausea/vomiting (50% vs. almost 40%), and pancreatitis (almost 30% vs. less than 5%), Dr. Swords said. In addition, patients with an initial misdiagnosis had significantly lower rates of jaundice (about 50% vs. almost 80%). The rates of diarrhea and anorexia were not significantly different between the two groups.
The study also looked at the time intervals from when the patient developed symptoms to the physician visit, from the physician visit to the cancer diagnosis, and from the physician visit to the performance of axial imaging. There was no difference in the time of symptom onset to the first visit with a physician in the two groups (0.5 month among those initially misdiagnosed and 0.7 month among those correctly diagnosed).
However, the time from the physician visit to the cancer diagnosis was 3.5 months among those initially misdiagnosed, vs. less than a month (0.6 month) among those who were correctly diagnosed, a statistically significant difference (P <.001), he said.
In addition, for those patients initially misdiagnosed, it took about 1 month longer from the physician visit to the time a CT scan or other type of axial imaging was ordered (an average of 1.1 months vs. 0.1 month, P <.001).
There was also a statistically significant association between a more advanced stage and initial misdiagnosis. Patients who were initially misdiagnosed had a 1.4-fold greater risk of having stage III or IV disease at the time of the pancreatic cancer diagnosis, Dr. Swords said.
Almost 40% (39) of those who were initially misdiagnosed were diagnosed with stage IV disease when they were correctly diagnosed, compared with 23.7% (51 patients) of those who were correctly diagnosed. The proportion diagnosed with stage III disease was similar, 21.4% among those initially misdiagnosed and 20% of those correctly diagnosed. Almost 51% of those correctly diagnosed were diagnosed with stage II disease, vs. 33.7% of those who were initially misdiagnosed. Of those initially misdiagnosed, 5.1% were diagnosed with stage I disease, compared with 5.6% of those correctly diagnosed.
However, the earlier stage at diagnosis for those with an initial correct diagnosis “did not translate into a survival difference,” Dr. Swords said, noting that there was a trend toward shorter survival among those who were initially misdiagnosed (median overall survival of 9.6 vs. 10.3 months).
Based on these results, Dr. Swords said, “surgeons should consider the diagnosis of pancreatic cancer when a patient referred for cholecystectomy has vague or atypical symptoms.”
He said he had no relevant financial disclosures.
WASHINGTON – Initial misdiagnoses were common and were associated with a later disease stage at diagnosis, in a study of 313 patients diagnosed with pancreatic cancer, Dr. Douglas Swords said at the annual Digestive Disease Week.
“By far, the most common misdiagnosis was gallbladder disease,” and there was about a 3-month longer time period, on average, from the first visit to a physician to the actual cancer diagnosis, in patients who were initially misdiagnosed, said Dr. Swords, a surgery resident at the University of Utah, Salt Lake City.
In the series of 313 patients diagnosed with pancreatic cancer, 98 (31.3%) were initially misdiagnosed, with a total of 119 diagnoses other than pancreatic cancer, he said. The most common misdiagnosis was gallbladder disease, which led to a cholecystectomy in 38 cases, followed by gastroesophageal reflux disease in 15 cases, and peptic ulcer disease in 11 cases. Those initially misdiagnosed were an average of about 5 years younger.
Patients with an initial misdiagnosis had significantly greater rates of abdominal pain (about 85% vs. about 60%), weight loss (about 85% vs. about 75%), nausea/vomiting (50% vs. almost 40%), and pancreatitis (almost 30% vs. less than 5%), Dr. Swords said. In addition, patients with an initial misdiagnosis had significantly lower rates of jaundice (about 50% vs. almost 80%). The rates of diarrhea and anorexia were not significantly different between the two groups.
The study also looked at the time intervals from when the patient developed symptoms to the physician visit, from the physician visit to the cancer diagnosis, and from the physician visit to the performance of axial imaging. There was no difference in the time of symptom onset to the first visit with a physician in the two groups (0.5 month among those initially misdiagnosed and 0.7 month among those correctly diagnosed).
However, the time from the physician visit to the cancer diagnosis was 3.5 months among those initially misdiagnosed, vs. less than a month (0.6 month) among those who were correctly diagnosed, a statistically significant difference (P <.001), he said.
In addition, for those patients initially misdiagnosed, it took about 1 month longer from the physician visit to the time a CT scan or other type of axial imaging was ordered (an average of 1.1 months vs. 0.1 month, P <.001).
There was also a statistically significant association between a more advanced stage and initial misdiagnosis. Patients who were initially misdiagnosed had a 1.4-fold greater risk of having stage III or IV disease at the time of the pancreatic cancer diagnosis, Dr. Swords said.
Almost 40% (39) of those who were initially misdiagnosed were diagnosed with stage IV disease when they were correctly diagnosed, compared with 23.7% (51 patients) of those who were correctly diagnosed. The proportion diagnosed with stage III disease was similar, 21.4% among those initially misdiagnosed and 20% of those correctly diagnosed. Almost 51% of those correctly diagnosed were diagnosed with stage II disease, vs. 33.7% of those who were initially misdiagnosed. Of those initially misdiagnosed, 5.1% were diagnosed with stage I disease, compared with 5.6% of those correctly diagnosed.
However, the earlier stage at diagnosis for those with an initial correct diagnosis “did not translate into a survival difference,” Dr. Swords said, noting that there was a trend toward shorter survival among those who were initially misdiagnosed (median overall survival of 9.6 vs. 10.3 months).
Based on these results, Dr. Swords said, “surgeons should consider the diagnosis of pancreatic cancer when a patient referred for cholecystectomy has vague or atypical symptoms.”
He said he had no relevant financial disclosures.
WASHINGTON – Initial misdiagnoses were common and were associated with a later disease stage at diagnosis, in a study of 313 patients diagnosed with pancreatic cancer, Dr. Douglas Swords said at the annual Digestive Disease Week.
“By far, the most common misdiagnosis was gallbladder disease,” and there was about a 3-month longer time period, on average, from the first visit to a physician to the actual cancer diagnosis, in patients who were initially misdiagnosed, said Dr. Swords, a surgery resident at the University of Utah, Salt Lake City.
In the series of 313 patients diagnosed with pancreatic cancer, 98 (31.3%) were initially misdiagnosed, with a total of 119 diagnoses other than pancreatic cancer, he said. The most common misdiagnosis was gallbladder disease, which led to a cholecystectomy in 38 cases, followed by gastroesophageal reflux disease in 15 cases, and peptic ulcer disease in 11 cases. Those initially misdiagnosed were an average of about 5 years younger.
Patients with an initial misdiagnosis had significantly greater rates of abdominal pain (about 85% vs. about 60%), weight loss (about 85% vs. about 75%), nausea/vomiting (50% vs. almost 40%), and pancreatitis (almost 30% vs. less than 5%), Dr. Swords said. In addition, patients with an initial misdiagnosis had significantly lower rates of jaundice (about 50% vs. almost 80%). The rates of diarrhea and anorexia were not significantly different between the two groups.
The study also looked at the time intervals from when the patient developed symptoms to the physician visit, from the physician visit to the cancer diagnosis, and from the physician visit to the performance of axial imaging. There was no difference in the time of symptom onset to the first visit with a physician in the two groups (0.5 month among those initially misdiagnosed and 0.7 month among those correctly diagnosed).
However, the time from the physician visit to the cancer diagnosis was 3.5 months among those initially misdiagnosed, vs. less than a month (0.6 month) among those who were correctly diagnosed, a statistically significant difference (P <.001), he said.
In addition, for those patients initially misdiagnosed, it took about 1 month longer from the physician visit to the time a CT scan or other type of axial imaging was ordered (an average of 1.1 months vs. 0.1 month, P <.001).
There was also a statistically significant association between a more advanced stage and initial misdiagnosis. Patients who were initially misdiagnosed had a 1.4-fold greater risk of having stage III or IV disease at the time of the pancreatic cancer diagnosis, Dr. Swords said.
Almost 40% (39) of those who were initially misdiagnosed were diagnosed with stage IV disease when they were correctly diagnosed, compared with 23.7% (51 patients) of those who were correctly diagnosed. The proportion diagnosed with stage III disease was similar, 21.4% among those initially misdiagnosed and 20% of those correctly diagnosed. Almost 51% of those correctly diagnosed were diagnosed with stage II disease, vs. 33.7% of those who were initially misdiagnosed. Of those initially misdiagnosed, 5.1% were diagnosed with stage I disease, compared with 5.6% of those correctly diagnosed.
However, the earlier stage at diagnosis for those with an initial correct diagnosis “did not translate into a survival difference,” Dr. Swords said, noting that there was a trend toward shorter survival among those who were initially misdiagnosed (median overall survival of 9.6 vs. 10.3 months).
Based on these results, Dr. Swords said, “surgeons should consider the diagnosis of pancreatic cancer when a patient referred for cholecystectomy has vague or atypical symptoms.”
He said he had no relevant financial disclosures.
AT DDW® 2015
Key clinical point: Pancreatic cancer is often misdiagnosed, and should be considered in patients with vague or atypical symptoms who are referred for a cholecystectomy.
Major finding: About 31% of patients with pancreatic cancer were initially misdiagnosed, most often with a gallbladder disease–related diagnosis.
Data source: A study of 313 patients diagnosed with pancreatic cancer comparing presenting symptoms, the time it took to reach the correct diagnosis, and other features in patients initially misdiagnosed and those who were not misdiagnosed.
Disclosures: Dr. Swords said he had no relevant financial disclosures.
Hospital clinicians commonly work while sick
The vast majority of doctors and other trained medical professionals at a hospital went to work while sick within the past year, even though they realized the risk that decision places on patients, according to a recent study.
In fact, almost 1 in 10 hospital clinicians worked while sick at least five times in the past year, primarily because of staffing concerns or not wanting to let colleagues down, reported Julia Szymczak, Ph.D., and her associates at the Children’s Hospital of Philadelphia (JAMA Pediatr. 2015 July 6 [doi: 10.1001/jamapediatrics.2015.0684]).
“A combination of closed- and open-ended questions illustrated that the decision to work while sick was shaped by systems-level and sociocultural factors that interacted to cause our respondents to work while symptomatic, despite recognizing that this choice may put patients and colleagues at risk,” the authors wrote.

Of 929 surveys sent out, 538 clinicians completed them, which included 280 of 459 physicians (61%) and 256 of 470 advanced-practice clinicians (54.5%). The advanced-practice clinicians included registered nurses, physician assistants, clinical nurse specialists, registered nurse anesthetists, and certified nurse midwives. Of those who responded, 15.7% worked in intensive care, 13.1% in surgery, 12.5% in general pediatrics, and 44.8% in another pediatric subspecialty.
Although 95.3% of respondents believed working while sick put patients at risk, 83.1% reported having done so at least once in the past year. Further, that proportion included 52% of all respondents who reported coming to work sick twice in the past year and 9.3% who worked while ill at least five times in the past year.
Nearly a third of respondents said they would work even if they had diarrhea (30%), while 16% said they would work with a fever, and 55.6% would work with acute respiratory symptoms, including cough, congestion, rhinorrhea, and sore throat.
But doctors were more likely than other professionals to say they would go to work with these symptoms: 38.9% of doctors would work despite diarrhea, compared with 19.9% of advanced-practice clinicians. Doctors and advanced-practice clinicians would also work with acute respiratory symptoms (60% vs. 50.8%, respectively), a fever only (21.8% vs. 9.8%), and fever and chills with body aches (18.6% vs. 10.9%, all P < .03).
Nearly every respondent (98.7%) said they worked despite being sick because they did not want to let their colleagues down, just as almost all of them worried the hospital would not have enough staff (94.9%) or that they would let their patients down (92.5%).
Smaller majorities of respondents also worked because others also work while sick (65%), worried their colleagues would ostracize them (64%) if they didn’t work, were concerned about their patients’ continuity of care (63.8%), had unsupportive leadership (56.2%), or believed they could not be easily replaced (52.6%).
Among the 316 respondents who filled in additional reasons, 64.9% said they had a very hard time finding someone to cover their shift, 61.1% described a strong cultural norm to work unless extremely sick, and 57% expressed uncertainty about what is considered “too sick to work.”
The Centers for Disease Control and Prevention funded the research. The authors reported no disclosures.
For centuries, a guiding principle for health care workers has been primum non nocere, or first do no harm. However, health care workers do exactly that when they work with patients while ill themselves with contagious infections. Even common but untreatable infectious like enterovirus and respiratory syncytial virus can prove deadly to immunocompromised patients.
The propensity to work while ill is influenced by cultural trends. In past years, many ill physicians worked even to the point of receiving intravenous fluids while on the job; working while sick was regarded as a badge of courage. Dr. Szymczak and colleagues identified as an issue the absence of an effective sick relief system that has sufficient flexibility to “staff up” during high rates of health care worker illness. Sick relief systems and policies need to be clear regarding when health care workers should stay away from work, how patient coverage will be ensured, and the availability of and access to paid sick leave.
Determining what constitutes being too sick to work is complicated and lacks a sufficient evidence base. Using a system that bases work restrictions on the presence of key symptoms may add clarity and enable health care workers to recognize when they need to stay home.
Creating a safer and more equitable system of sick leave for health care workers requires a culture change in many institutions to decrease the stigma – internal and external – associated with health care worker illness. Identifying solutions to prioritize patient safety must factor in workforce demands and variability in patient census and emphasize flexibility. Strong administrative and physician leadership and creativity are essential to support appropriate sick leave and ensure adequate staffing. Hospital leadership must ensure that the culture supports a paid sick leave policy that is adequate and nonpunitive.
These comments are selected from an accompanying editorial (JAMA Pediatr. 2015 July 6 [doi:10.1001/jamapediatrics.2015.0994]), written by Dr. Jeffrey R. Starke of the department of pediatrics at Baylor College of Medicine in Houston, and Dr. Mary Anne Jackson of the division of infectious diseases at Children’s Mercy Hospital, University of Missouri–Kansas City. Dr. Starke and Dr. Jackson reported no disclosures.
For centuries, a guiding principle for health care workers has been primum non nocere, or first do no harm. However, health care workers do exactly that when they work with patients while ill themselves with contagious infections. Even common but untreatable infectious like enterovirus and respiratory syncytial virus can prove deadly to immunocompromised patients.
The propensity to work while ill is influenced by cultural trends. In past years, many ill physicians worked even to the point of receiving intravenous fluids while on the job; working while sick was regarded as a badge of courage. Dr. Szymczak and colleagues identified as an issue the absence of an effective sick relief system that has sufficient flexibility to “staff up” during high rates of health care worker illness. Sick relief systems and policies need to be clear regarding when health care workers should stay away from work, how patient coverage will be ensured, and the availability of and access to paid sick leave.
Determining what constitutes being too sick to work is complicated and lacks a sufficient evidence base. Using a system that bases work restrictions on the presence of key symptoms may add clarity and enable health care workers to recognize when they need to stay home.
Creating a safer and more equitable system of sick leave for health care workers requires a culture change in many institutions to decrease the stigma – internal and external – associated with health care worker illness. Identifying solutions to prioritize patient safety must factor in workforce demands and variability in patient census and emphasize flexibility. Strong administrative and physician leadership and creativity are essential to support appropriate sick leave and ensure adequate staffing. Hospital leadership must ensure that the culture supports a paid sick leave policy that is adequate and nonpunitive.
These comments are selected from an accompanying editorial (JAMA Pediatr. 2015 July 6 [doi:10.1001/jamapediatrics.2015.0994]), written by Dr. Jeffrey R. Starke of the department of pediatrics at Baylor College of Medicine in Houston, and Dr. Mary Anne Jackson of the division of infectious diseases at Children’s Mercy Hospital, University of Missouri–Kansas City. Dr. Starke and Dr. Jackson reported no disclosures.
For centuries, a guiding principle for health care workers has been primum non nocere, or first do no harm. However, health care workers do exactly that when they work with patients while ill themselves with contagious infections. Even common but untreatable infectious like enterovirus and respiratory syncytial virus can prove deadly to immunocompromised patients.
The propensity to work while ill is influenced by cultural trends. In past years, many ill physicians worked even to the point of receiving intravenous fluids while on the job; working while sick was regarded as a badge of courage. Dr. Szymczak and colleagues identified as an issue the absence of an effective sick relief system that has sufficient flexibility to “staff up” during high rates of health care worker illness. Sick relief systems and policies need to be clear regarding when health care workers should stay away from work, how patient coverage will be ensured, and the availability of and access to paid sick leave.
Determining what constitutes being too sick to work is complicated and lacks a sufficient evidence base. Using a system that bases work restrictions on the presence of key symptoms may add clarity and enable health care workers to recognize when they need to stay home.
Creating a safer and more equitable system of sick leave for health care workers requires a culture change in many institutions to decrease the stigma – internal and external – associated with health care worker illness. Identifying solutions to prioritize patient safety must factor in workforce demands and variability in patient census and emphasize flexibility. Strong administrative and physician leadership and creativity are essential to support appropriate sick leave and ensure adequate staffing. Hospital leadership must ensure that the culture supports a paid sick leave policy that is adequate and nonpunitive.
These comments are selected from an accompanying editorial (JAMA Pediatr. 2015 July 6 [doi:10.1001/jamapediatrics.2015.0994]), written by Dr. Jeffrey R. Starke of the department of pediatrics at Baylor College of Medicine in Houston, and Dr. Mary Anne Jackson of the division of infectious diseases at Children’s Mercy Hospital, University of Missouri–Kansas City. Dr. Starke and Dr. Jackson reported no disclosures.
The vast majority of doctors and other trained medical professionals at a hospital went to work while sick within the past year, even though they realized the risk that decision places on patients, according to a recent study.
In fact, almost 1 in 10 hospital clinicians worked while sick at least five times in the past year, primarily because of staffing concerns or not wanting to let colleagues down, reported Julia Szymczak, Ph.D., and her associates at the Children’s Hospital of Philadelphia (JAMA Pediatr. 2015 July 6 [doi: 10.1001/jamapediatrics.2015.0684]).
“A combination of closed- and open-ended questions illustrated that the decision to work while sick was shaped by systems-level and sociocultural factors that interacted to cause our respondents to work while symptomatic, despite recognizing that this choice may put patients and colleagues at risk,” the authors wrote.
Of 929 surveys sent out, 538 clinicians completed them, which included 280 of 459 physicians (61%) and 256 of 470 advanced-practice clinicians (54.5%). The advanced-practice clinicians included registered nurses, physician assistants, clinical nurse specialists, registered nurse anesthetists, and certified nurse midwives. Of those who responded, 15.7% worked in intensive care, 13.1% in surgery, 12.5% in general pediatrics, and 44.8% in another pediatric subspecialty.
Although 95.3% of respondents believed working while sick put patients at risk, 83.1% reported having done so at least once in the past year. Further, that proportion included 52% of all respondents who reported coming to work sick twice in the past year and 9.3% who worked while ill at least five times in the past year.
Nearly a third of respondents said they would work even if they had diarrhea (30%), while 16% said they would work with a fever, and 55.6% would work with acute respiratory symptoms, including cough, congestion, rhinorrhea, and sore throat.
But doctors were more likely than other professionals to say they would go to work with these symptoms: 38.9% of doctors would work despite diarrhea, compared with 19.9% of advanced-practice clinicians. Doctors and advanced-practice clinicians would also work with acute respiratory symptoms (60% vs. 50.8%, respectively), a fever only (21.8% vs. 9.8%), and fever and chills with body aches (18.6% vs. 10.9%, all P < .03).
Nearly every respondent (98.7%) said they worked despite being sick because they did not want to let their colleagues down, just as almost all of them worried the hospital would not have enough staff (94.9%) or that they would let their patients down (92.5%).
Smaller majorities of respondents also worked because others also work while sick (65%), worried their colleagues would ostracize them (64%) if they didn’t work, were concerned about their patients’ continuity of care (63.8%), had unsupportive leadership (56.2%), or believed they could not be easily replaced (52.6%).
Among the 316 respondents who filled in additional reasons, 64.9% said they had a very hard time finding someone to cover their shift, 61.1% described a strong cultural norm to work unless extremely sick, and 57% expressed uncertainty about what is considered “too sick to work.”
The Centers for Disease Control and Prevention funded the research. The authors reported no disclosures.
The vast majority of doctors and other trained medical professionals at a hospital went to work while sick within the past year, even though they realized the risk that decision places on patients, according to a recent study.
In fact, almost 1 in 10 hospital clinicians worked while sick at least five times in the past year, primarily because of staffing concerns or not wanting to let colleagues down, reported Julia Szymczak, Ph.D., and her associates at the Children’s Hospital of Philadelphia (JAMA Pediatr. 2015 July 6 [doi: 10.1001/jamapediatrics.2015.0684]).
“A combination of closed- and open-ended questions illustrated that the decision to work while sick was shaped by systems-level and sociocultural factors that interacted to cause our respondents to work while symptomatic, despite recognizing that this choice may put patients and colleagues at risk,” the authors wrote.
Of 929 surveys sent out, 538 clinicians completed them, which included 280 of 459 physicians (61%) and 256 of 470 advanced-practice clinicians (54.5%). The advanced-practice clinicians included registered nurses, physician assistants, clinical nurse specialists, registered nurse anesthetists, and certified nurse midwives. Of those who responded, 15.7% worked in intensive care, 13.1% in surgery, 12.5% in general pediatrics, and 44.8% in another pediatric subspecialty.
Although 95.3% of respondents believed working while sick put patients at risk, 83.1% reported having done so at least once in the past year. Further, that proportion included 52% of all respondents who reported coming to work sick twice in the past year and 9.3% who worked while ill at least five times in the past year.
Nearly a third of respondents said they would work even if they had diarrhea (30%), while 16% said they would work with a fever, and 55.6% would work with acute respiratory symptoms, including cough, congestion, rhinorrhea, and sore throat.
But doctors were more likely than other professionals to say they would go to work with these symptoms: 38.9% of doctors would work despite diarrhea, compared with 19.9% of advanced-practice clinicians. Doctors and advanced-practice clinicians would also work with acute respiratory symptoms (60% vs. 50.8%, respectively), a fever only (21.8% vs. 9.8%), and fever and chills with body aches (18.6% vs. 10.9%, all P < .03).
Nearly every respondent (98.7%) said they worked despite being sick because they did not want to let their colleagues down, just as almost all of them worried the hospital would not have enough staff (94.9%) or that they would let their patients down (92.5%).
Smaller majorities of respondents also worked because others also work while sick (65%), worried their colleagues would ostracize them (64%) if they didn’t work, were concerned about their patients’ continuity of care (63.8%), had unsupportive leadership (56.2%), or believed they could not be easily replaced (52.6%).
Among the 316 respondents who filled in additional reasons, 64.9% said they had a very hard time finding someone to cover their shift, 61.1% described a strong cultural norm to work unless extremely sick, and 57% expressed uncertainty about what is considered “too sick to work.”
The Centers for Disease Control and Prevention funded the research. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: A majority of hospital doctors and other clinicians work while sick.
Major finding: 83.1% of doctors and advanced-practice clinicians worked while ill at least once in the past year; 95.3% recognized the risk to patients and colleagues.
Data source: The findings are based on a cross-sectional, anonymous survey of 280 attending physicians and 256 advanced-practice clinicians at the Children’s Hospital of Philadelphia from January 2014 to March 2014.
Disclosures: The research was funded by the Centers for Disease Control and Prevention. The authors reported no disclosures.

CMS improves Open Payments system, but not enough
Improvements to the Open Payments reporting system are welcome, but don’t go far enough.
That was the message from the American Medical Association upon the July 1 release of another round of data in the financial disclosure system created by the Affordable Care Act.
CMS “has improved our interface for both collecting and reporting this data about compensation and other payments between drug and medical device manufacturers and physicians and teaching hospitals,” Dr. Shantanu Agrawal, CMS deputy administrator and director of the Center for Program Integrity, said in a statement.
“While we appreciate the efforts of the Centers for Medicare & Medicaid Services to verify the data submitted by industry, the complicated and cumbersome process for physicians to register to review their data and seek correction of any inaccuracies continues to hinder their participation in the validation process,” the AMA said in a statement.
Dr. David O. Barbe, a family physician in Mountain Grove, Mo., noted that “the ability to navigate [Open Payments] has substantially improved since the first iteration of this. You can get around the website pretty well. ... You can sort the data. You can search on individuals. You can sort it by large amounts, either by individual physician or by payer.”
However, the approach used still makes it extremely difficult for determining the validity and accuracy of the information that is being presented, said Dr. Barbe, a member of the AMA Board of Trustees.
“I am looking at one physician here who has 511 total transactions,” he said. “There is no way that that physician can legitimately validate or even refute those transactions. I can’t imagine what the record-keeping would be like if he were to attempt to track 511 transactions from industry over the course of the year.”
The complexity of tracking all those data could be the reason so few transactions have been disputed. In 2014, CMS reported data on 10.8 million general payments to physicians and teaching hospitals; 1,732 were transactions disputed. In 2013, data were reported on 4.1 million general payments, with 880 disputed. The value of general payments rose to $2.6 billion ($5.1 million disputed) from $972 million (nearly $2 million disputed).
Open Payments captured payments to 607,000 physicians and to 1,121 teaching hospitals made by 1,444 companies in 2014, up from 470,000 physicians and 1,019 teaching hospitals receiving payments from 1,347 companies in 2013.
But Dr. Barbe said that his primary complaint remains that the information comes without any context and really doesn’t convey any useful information. They’re just data.
“To suppose that because he has a lot of transactions, that means there’s some kind of illicit or nefarious relationship that the physician has with industry, I think is also not necessarily a conclusion one can draw.”
Improvements to the Open Payments reporting system are welcome, but don’t go far enough.
That was the message from the American Medical Association upon the July 1 release of another round of data in the financial disclosure system created by the Affordable Care Act.
CMS “has improved our interface for both collecting and reporting this data about compensation and other payments between drug and medical device manufacturers and physicians and teaching hospitals,” Dr. Shantanu Agrawal, CMS deputy administrator and director of the Center for Program Integrity, said in a statement.
“While we appreciate the efforts of the Centers for Medicare & Medicaid Services to verify the data submitted by industry, the complicated and cumbersome process for physicians to register to review their data and seek correction of any inaccuracies continues to hinder their participation in the validation process,” the AMA said in a statement.
Dr. David O. Barbe, a family physician in Mountain Grove, Mo., noted that “the ability to navigate [Open Payments] has substantially improved since the first iteration of this. You can get around the website pretty well. ... You can sort the data. You can search on individuals. You can sort it by large amounts, either by individual physician or by payer.”
However, the approach used still makes it extremely difficult for determining the validity and accuracy of the information that is being presented, said Dr. Barbe, a member of the AMA Board of Trustees.
“I am looking at one physician here who has 511 total transactions,” he said. “There is no way that that physician can legitimately validate or even refute those transactions. I can’t imagine what the record-keeping would be like if he were to attempt to track 511 transactions from industry over the course of the year.”
The complexity of tracking all those data could be the reason so few transactions have been disputed. In 2014, CMS reported data on 10.8 million general payments to physicians and teaching hospitals; 1,732 were transactions disputed. In 2013, data were reported on 4.1 million general payments, with 880 disputed. The value of general payments rose to $2.6 billion ($5.1 million disputed) from $972 million (nearly $2 million disputed).
Open Payments captured payments to 607,000 physicians and to 1,121 teaching hospitals made by 1,444 companies in 2014, up from 470,000 physicians and 1,019 teaching hospitals receiving payments from 1,347 companies in 2013.
But Dr. Barbe said that his primary complaint remains that the information comes without any context and really doesn’t convey any useful information. They’re just data.
“To suppose that because he has a lot of transactions, that means there’s some kind of illicit or nefarious relationship that the physician has with industry, I think is also not necessarily a conclusion one can draw.”
Improvements to the Open Payments reporting system are welcome, but don’t go far enough.
That was the message from the American Medical Association upon the July 1 release of another round of data in the financial disclosure system created by the Affordable Care Act.
CMS “has improved our interface for both collecting and reporting this data about compensation and other payments between drug and medical device manufacturers and physicians and teaching hospitals,” Dr. Shantanu Agrawal, CMS deputy administrator and director of the Center for Program Integrity, said in a statement.
“While we appreciate the efforts of the Centers for Medicare & Medicaid Services to verify the data submitted by industry, the complicated and cumbersome process for physicians to register to review their data and seek correction of any inaccuracies continues to hinder their participation in the validation process,” the AMA said in a statement.
Dr. David O. Barbe, a family physician in Mountain Grove, Mo., noted that “the ability to navigate [Open Payments] has substantially improved since the first iteration of this. You can get around the website pretty well. ... You can sort the data. You can search on individuals. You can sort it by large amounts, either by individual physician or by payer.”
However, the approach used still makes it extremely difficult for determining the validity and accuracy of the information that is being presented, said Dr. Barbe, a member of the AMA Board of Trustees.
“I am looking at one physician here who has 511 total transactions,” he said. “There is no way that that physician can legitimately validate or even refute those transactions. I can’t imagine what the record-keeping would be like if he were to attempt to track 511 transactions from industry over the course of the year.”
The complexity of tracking all those data could be the reason so few transactions have been disputed. In 2014, CMS reported data on 10.8 million general payments to physicians and teaching hospitals; 1,732 were transactions disputed. In 2013, data were reported on 4.1 million general payments, with 880 disputed. The value of general payments rose to $2.6 billion ($5.1 million disputed) from $972 million (nearly $2 million disputed).
Open Payments captured payments to 607,000 physicians and to 1,121 teaching hospitals made by 1,444 companies in 2014, up from 470,000 physicians and 1,019 teaching hospitals receiving payments from 1,347 companies in 2013.
But Dr. Barbe said that his primary complaint remains that the information comes without any context and really doesn’t convey any useful information. They’re just data.
“To suppose that because he has a lot of transactions, that means there’s some kind of illicit or nefarious relationship that the physician has with industry, I think is also not necessarily a conclusion one can draw.”
DDW: LINX device beneficial, safe for GERD
WASHINGTON – Five-year follow-up data on the magnetic device approved for treating gastroesophageal reflux disease confirm its long-term safety and efficacy, Dr. Robert A. Ganz reported at the annual Digestive Disease Week.
Five years after device implantation, the proportion of patients experiencing moderate to severe regurgitation had dropped to about 1%, from almost 60% at baseline, and two-thirds of patients were not taking any proton pump inhibitors (PPIs), said Dr. Ganz, chief of gastroenterology at Abbott Northwestern Hospital, Minneapolis, and one of the study investigators. These were among the results of the study that evaluated the device, the LINX Reflux Management System. The device was approved by the Food and Drug Administration FDA) in 2012 and is for the treatment of people with GERD as defined by abnormal pH testing, who continue to have chronic GERD symptoms that persist despite maximum medical therapy for the treatment of reflux.
“Magnetic sphincter augmentation should be considered first-line surgical therapy for those with gastroesophageal reflux disease, based on the results of this study,” he said.
The 2-year results of the prospective, multicenter study were the basis of the FDA approval of the device, described by the manufacturer, Torax Medical, as a “small implant [composed] of interlinked titanium beads with magnetic cores,” implanted during standard laparoscopy. The magnetic attraction between the beads augments the existing esophageal sphincter’s barrier function to prevent reflux,” according to the company.
The study enrolled 100 patients with reflux disease with a median age of 53 years, who had experienced typical heartburn for at least 6 months with or without regurgitation and were taking PPIs daily for at least 3 months (median use 5 years). Patients had GERD for a median of 10 years (range: 1-40 years). People who had any type of previous gastric or esophageal surgery, Barrett’s esophagus, a hiatal hernia greater than 3 cm, a body mass index over 35 kg/m2, or grade C or D esophagitis were excluded.
The device was implanted in all patients, who served as their own controls; 85 patients were followed through 5 years (6 were lost to follow-up, the device was explanted in 6 patients, 2 patients did not consent to extended follow-up, and 1 patient died of an unrelated cancer). The median procedure time was 36 minutes with a range of 7-125 minutes); all procedures were successfully completed with no intraoperative complications and all patients were discharged within 24 hours on an unrestricted diet.
The median total Gastroesophageal Reflux Disease–Health-Related Quality of Life (GERD-HRQL) score at baseline was 27 points among those not on PPIs and 11 points on PPIs, dropping to 4 points at 5 years off PPIs. At baseline, 95% of patients expressed dissatisfaction related to reflux, which dropped to 7% at year 5. Moderate to severe heartburn was reported by 89% at baseline, dropping to about 12% at year 5. The proportion of patients experiencing moderate to severe regurgitation dropped from 57% at baseline to about 1% at 5 years, Dr. Ganz said.
At baseline, 100% were taking PPIs every day, compared with 15% at 5 years. (At 5 years, 75% had discontinued PPIs, and about 9% reported PRN use only). Grade A and B esophagitis decreased from 40% at baseline to 16% at 5 years, at which point most cases were grade A, and there were no patients with grade C or D esophagitis, he said. In addition, at 5 years, 100% of patients “reported the ability to belch, and those needing to vomit – about 16% – reported the ability to vomit,” demonstrating that normal physiology was preserved with the device.
At 5 years, there were no device erosions or migrations, or any significant adverse events other than dysphagia, which “was typically mild and not associated with weight loss and tended to resolve over time,” from about 70% in the first few weeks after surgery to 11% at 1 year and 7% at 5 years, Dr. Ganz said.
In seven cases, the device was removed laparoscopically, with no complications and gastric anatomy was preserved for future treatments. All removals were elective. The device was removed in four patients because of dysphagia, which completely resolved in those patients. One patient had the device removed because of vomiting of unknown cause that persisted after removal. Another two patients who “had the device removed for disease management” continued to experience reflux and had “uneventful” Nissen fundoplication,” he said.
“Five years after magnetic augmentation, we have demonstrated objective evidence of reduction in acid exposure and in the majority of patients, normalized pH [and] we demonstrated significant and durable improvement in all group parameters measured, with preservation of fundic anatomy and normal physiology, with the ability to belch and vomit,” Dr. Ganz concluded. The results also show that the “procedure is reproducible, safe and reversible if necessary,” he added, noting that one of the limitations of the study was that subjects served as their own controls. During the discussion period, he was asked about hiatal hernia repairs, an apparent trend to “decay” from years 1 to 5 in some parameters measured, and dysphagia after the procedure.
About 40% of the patients in the study had a hiatal hernia, and about one-third of these patients had a hernia repair. A subgroup analysis of the data is being performed to evaluate the impact of hernia repair, Dr. Ganz said.
PPI use increased from 8% in year 4, to 15% in year 5. The reason for this s difficult to determine but “even though there is a bit of a decay, patients are still quite satisfied at 5 years,” Dr. Ganz remarked, also referring to the marked impact on regurgitation. Many U.S. patients use PPIs for reasons other than reflux, and studies show that many patients are on PPIs after the Nissen procedure in the absence of pathologic pH scores, he pointed out.
Compared with the type of dysphagia patients experience after the Nissen procedure, which is immediate and improves with time, Dr. Ganz said that the dysphagia associated with the device “seemed to peak around 2 weeks and then it slowly improved with time, so this may be more of a scar tissue–associated dysphagia than an edema dysphagia, but … it does improve with time.
Three-year results of the study were published in 2013 (N. Engl. J. Med. 2013;368:719-72), Dr. Ganz was the lead author.
The study was funded by Torax Medical. Dr. Ganz had no disclosures related to the topic of this presentation.
*This story was updated 7/9/2015.
At DDW this year, Dr. Ganz reported on the 5-year follow-up of the original LINX data that was published in the New England Journal of Medicine in 2013 (368:2039-40). The original study enrolled and followed 100 reflux patients for 3 years after implantation of the magnetic sphincter augmentation device, and it appears that the successful outcomes are sustained over the 5-year period. Most notable are the lasting improvement in regurgitation and the dramatic reduction in requirement for maintenance PPI therapy. These findings led the investigators to suggest that this should be considered a first-line surgical therapy for GERD. Overall, this is not an unreasonable statement when one considers the current model wherein antireflux surgery fits in the treatment of GERD. Medical therapy with proton pump inhibitors is extremely safe and effective for a substantial number of patients with GERD and based on this risk/benefit profile should be the first line therapy (Am. J. Gastroenterol. 2013;108:308-28; quiz 329). However, this treatment is not perfect and there are many patients who continue to have persistent symptoms despite PPI therapy (Clin. Gastroenterol. Hepatol. 2012;10:612-9). Although the majority of PPI nonresponders have a functional etiology, there is a distinct population that continue to have refractory reflux-related symptoms, such as regurgitation, that escape the therapeutic target of PPIs. These patients will require an augmentation of the antireflux barrier and the LINX approach appears to be as effective as fundoplication in this regard (J. Am. Coll. Surg. 2015;221:123-8). The question is whether the side effect profile and durability of LINX is better than fundoplication. The answer here is not clear and I would carefully state that LINX and fundoplication can be considered first-line surgical therapies for GERD patients who have documented pathologic acid gastroesophageal reflux and are intolerant to PPIs or not responding to PPIs.
Dr. John E. Pandolfino is professor of medicine and chief of the division of gastroenterology and hepatology at Northwestern University, Chicago. He is a speaker for Astra Zeneca/Takeda and a consultant for EndoGastric Solutions.
At DDW this year, Dr. Ganz reported on the 5-year follow-up of the original LINX data that was published in the New England Journal of Medicine in 2013 (368:2039-40). The original study enrolled and followed 100 reflux patients for 3 years after implantation of the magnetic sphincter augmentation device, and it appears that the successful outcomes are sustained over the 5-year period. Most notable are the lasting improvement in regurgitation and the dramatic reduction in requirement for maintenance PPI therapy. These findings led the investigators to suggest that this should be considered a first-line surgical therapy for GERD. Overall, this is not an unreasonable statement when one considers the current model wherein antireflux surgery fits in the treatment of GERD. Medical therapy with proton pump inhibitors is extremely safe and effective for a substantial number of patients with GERD and based on this risk/benefit profile should be the first line therapy (Am. J. Gastroenterol. 2013;108:308-28; quiz 329). However, this treatment is not perfect and there are many patients who continue to have persistent symptoms despite PPI therapy (Clin. Gastroenterol. Hepatol. 2012;10:612-9). Although the majority of PPI nonresponders have a functional etiology, there is a distinct population that continue to have refractory reflux-related symptoms, such as regurgitation, that escape the therapeutic target of PPIs. These patients will require an augmentation of the antireflux barrier and the LINX approach appears to be as effective as fundoplication in this regard (J. Am. Coll. Surg. 2015;221:123-8). The question is whether the side effect profile and durability of LINX is better than fundoplication. The answer here is not clear and I would carefully state that LINX and fundoplication can be considered first-line surgical therapies for GERD patients who have documented pathologic acid gastroesophageal reflux and are intolerant to PPIs or not responding to PPIs.
Dr. John E. Pandolfino is professor of medicine and chief of the division of gastroenterology and hepatology at Northwestern University, Chicago. He is a speaker for Astra Zeneca/Takeda and a consultant for EndoGastric Solutions.
At DDW this year, Dr. Ganz reported on the 5-year follow-up of the original LINX data that was published in the New England Journal of Medicine in 2013 (368:2039-40). The original study enrolled and followed 100 reflux patients for 3 years after implantation of the magnetic sphincter augmentation device, and it appears that the successful outcomes are sustained over the 5-year period. Most notable are the lasting improvement in regurgitation and the dramatic reduction in requirement for maintenance PPI therapy. These findings led the investigators to suggest that this should be considered a first-line surgical therapy for GERD. Overall, this is not an unreasonable statement when one considers the current model wherein antireflux surgery fits in the treatment of GERD. Medical therapy with proton pump inhibitors is extremely safe and effective for a substantial number of patients with GERD and based on this risk/benefit profile should be the first line therapy (Am. J. Gastroenterol. 2013;108:308-28; quiz 329). However, this treatment is not perfect and there are many patients who continue to have persistent symptoms despite PPI therapy (Clin. Gastroenterol. Hepatol. 2012;10:612-9). Although the majority of PPI nonresponders have a functional etiology, there is a distinct population that continue to have refractory reflux-related symptoms, such as regurgitation, that escape the therapeutic target of PPIs. These patients will require an augmentation of the antireflux barrier and the LINX approach appears to be as effective as fundoplication in this regard (J. Am. Coll. Surg. 2015;221:123-8). The question is whether the side effect profile and durability of LINX is better than fundoplication. The answer here is not clear and I would carefully state that LINX and fundoplication can be considered first-line surgical therapies for GERD patients who have documented pathologic acid gastroesophageal reflux and are intolerant to PPIs or not responding to PPIs.
Dr. John E. Pandolfino is professor of medicine and chief of the division of gastroenterology and hepatology at Northwestern University, Chicago. He is a speaker for Astra Zeneca/Takeda and a consultant for EndoGastric Solutions.
WASHINGTON – Five-year follow-up data on the magnetic device approved for treating gastroesophageal reflux disease confirm its long-term safety and efficacy, Dr. Robert A. Ganz reported at the annual Digestive Disease Week.
Five years after device implantation, the proportion of patients experiencing moderate to severe regurgitation had dropped to about 1%, from almost 60% at baseline, and two-thirds of patients were not taking any proton pump inhibitors (PPIs), said Dr. Ganz, chief of gastroenterology at Abbott Northwestern Hospital, Minneapolis, and one of the study investigators. These were among the results of the study that evaluated the device, the LINX Reflux Management System. The device was approved by the Food and Drug Administration FDA) in 2012 and is for the treatment of people with GERD as defined by abnormal pH testing, who continue to have chronic GERD symptoms that persist despite maximum medical therapy for the treatment of reflux.
“Magnetic sphincter augmentation should be considered first-line surgical therapy for those with gastroesophageal reflux disease, based on the results of this study,” he said.
The 2-year results of the prospective, multicenter study were the basis of the FDA approval of the device, described by the manufacturer, Torax Medical, as a “small implant [composed] of interlinked titanium beads with magnetic cores,” implanted during standard laparoscopy. The magnetic attraction between the beads augments the existing esophageal sphincter’s barrier function to prevent reflux,” according to the company.
The study enrolled 100 patients with reflux disease with a median age of 53 years, who had experienced typical heartburn for at least 6 months with or without regurgitation and were taking PPIs daily for at least 3 months (median use 5 years). Patients had GERD for a median of 10 years (range: 1-40 years). People who had any type of previous gastric or esophageal surgery, Barrett’s esophagus, a hiatal hernia greater than 3 cm, a body mass index over 35 kg/m2, or grade C or D esophagitis were excluded.
The device was implanted in all patients, who served as their own controls; 85 patients were followed through 5 years (6 were lost to follow-up, the device was explanted in 6 patients, 2 patients did not consent to extended follow-up, and 1 patient died of an unrelated cancer). The median procedure time was 36 minutes with a range of 7-125 minutes); all procedures were successfully completed with no intraoperative complications and all patients were discharged within 24 hours on an unrestricted diet.
The median total Gastroesophageal Reflux Disease–Health-Related Quality of Life (GERD-HRQL) score at baseline was 27 points among those not on PPIs and 11 points on PPIs, dropping to 4 points at 5 years off PPIs. At baseline, 95% of patients expressed dissatisfaction related to reflux, which dropped to 7% at year 5. Moderate to severe heartburn was reported by 89% at baseline, dropping to about 12% at year 5. The proportion of patients experiencing moderate to severe regurgitation dropped from 57% at baseline to about 1% at 5 years, Dr. Ganz said.
At baseline, 100% were taking PPIs every day, compared with 15% at 5 years. (At 5 years, 75% had discontinued PPIs, and about 9% reported PRN use only). Grade A and B esophagitis decreased from 40% at baseline to 16% at 5 years, at which point most cases were grade A, and there were no patients with grade C or D esophagitis, he said. In addition, at 5 years, 100% of patients “reported the ability to belch, and those needing to vomit – about 16% – reported the ability to vomit,” demonstrating that normal physiology was preserved with the device.
At 5 years, there were no device erosions or migrations, or any significant adverse events other than dysphagia, which “was typically mild and not associated with weight loss and tended to resolve over time,” from about 70% in the first few weeks after surgery to 11% at 1 year and 7% at 5 years, Dr. Ganz said.
In seven cases, the device was removed laparoscopically, with no complications and gastric anatomy was preserved for future treatments. All removals were elective. The device was removed in four patients because of dysphagia, which completely resolved in those patients. One patient had the device removed because of vomiting of unknown cause that persisted after removal. Another two patients who “had the device removed for disease management” continued to experience reflux and had “uneventful” Nissen fundoplication,” he said.
“Five years after magnetic augmentation, we have demonstrated objective evidence of reduction in acid exposure and in the majority of patients, normalized pH [and] we demonstrated significant and durable improvement in all group parameters measured, with preservation of fundic anatomy and normal physiology, with the ability to belch and vomit,” Dr. Ganz concluded. The results also show that the “procedure is reproducible, safe and reversible if necessary,” he added, noting that one of the limitations of the study was that subjects served as their own controls. During the discussion period, he was asked about hiatal hernia repairs, an apparent trend to “decay” from years 1 to 5 in some parameters measured, and dysphagia after the procedure.
About 40% of the patients in the study had a hiatal hernia, and about one-third of these patients had a hernia repair. A subgroup analysis of the data is being performed to evaluate the impact of hernia repair, Dr. Ganz said.
PPI use increased from 8% in year 4, to 15% in year 5. The reason for this s difficult to determine but “even though there is a bit of a decay, patients are still quite satisfied at 5 years,” Dr. Ganz remarked, also referring to the marked impact on regurgitation. Many U.S. patients use PPIs for reasons other than reflux, and studies show that many patients are on PPIs after the Nissen procedure in the absence of pathologic pH scores, he pointed out.
Compared with the type of dysphagia patients experience after the Nissen procedure, which is immediate and improves with time, Dr. Ganz said that the dysphagia associated with the device “seemed to peak around 2 weeks and then it slowly improved with time, so this may be more of a scar tissue–associated dysphagia than an edema dysphagia, but … it does improve with time.
Three-year results of the study were published in 2013 (N. Engl. J. Med. 2013;368:719-72), Dr. Ganz was the lead author.
The study was funded by Torax Medical. Dr. Ganz had no disclosures related to the topic of this presentation.
*This story was updated 7/9/2015.
WASHINGTON – Five-year follow-up data on the magnetic device approved for treating gastroesophageal reflux disease confirm its long-term safety and efficacy, Dr. Robert A. Ganz reported at the annual Digestive Disease Week.
Five years after device implantation, the proportion of patients experiencing moderate to severe regurgitation had dropped to about 1%, from almost 60% at baseline, and two-thirds of patients were not taking any proton pump inhibitors (PPIs), said Dr. Ganz, chief of gastroenterology at Abbott Northwestern Hospital, Minneapolis, and one of the study investigators. These were among the results of the study that evaluated the device, the LINX Reflux Management System. The device was approved by the Food and Drug Administration FDA) in 2012 and is for the treatment of people with GERD as defined by abnormal pH testing, who continue to have chronic GERD symptoms that persist despite maximum medical therapy for the treatment of reflux.
“Magnetic sphincter augmentation should be considered first-line surgical therapy for those with gastroesophageal reflux disease, based on the results of this study,” he said.
The 2-year results of the prospective, multicenter study were the basis of the FDA approval of the device, described by the manufacturer, Torax Medical, as a “small implant [composed] of interlinked titanium beads with magnetic cores,” implanted during standard laparoscopy. The magnetic attraction between the beads augments the existing esophageal sphincter’s barrier function to prevent reflux,” according to the company.
The study enrolled 100 patients with reflux disease with a median age of 53 years, who had experienced typical heartburn for at least 6 months with or without regurgitation and were taking PPIs daily for at least 3 months (median use 5 years). Patients had GERD for a median of 10 years (range: 1-40 years). People who had any type of previous gastric or esophageal surgery, Barrett’s esophagus, a hiatal hernia greater than 3 cm, a body mass index over 35 kg/m2, or grade C or D esophagitis were excluded.
The device was implanted in all patients, who served as their own controls; 85 patients were followed through 5 years (6 were lost to follow-up, the device was explanted in 6 patients, 2 patients did not consent to extended follow-up, and 1 patient died of an unrelated cancer). The median procedure time was 36 minutes with a range of 7-125 minutes); all procedures were successfully completed with no intraoperative complications and all patients were discharged within 24 hours on an unrestricted diet.
The median total Gastroesophageal Reflux Disease–Health-Related Quality of Life (GERD-HRQL) score at baseline was 27 points among those not on PPIs and 11 points on PPIs, dropping to 4 points at 5 years off PPIs. At baseline, 95% of patients expressed dissatisfaction related to reflux, which dropped to 7% at year 5. Moderate to severe heartburn was reported by 89% at baseline, dropping to about 12% at year 5. The proportion of patients experiencing moderate to severe regurgitation dropped from 57% at baseline to about 1% at 5 years, Dr. Ganz said.
At baseline, 100% were taking PPIs every day, compared with 15% at 5 years. (At 5 years, 75% had discontinued PPIs, and about 9% reported PRN use only). Grade A and B esophagitis decreased from 40% at baseline to 16% at 5 years, at which point most cases were grade A, and there were no patients with grade C or D esophagitis, he said. In addition, at 5 years, 100% of patients “reported the ability to belch, and those needing to vomit – about 16% – reported the ability to vomit,” demonstrating that normal physiology was preserved with the device.
At 5 years, there were no device erosions or migrations, or any significant adverse events other than dysphagia, which “was typically mild and not associated with weight loss and tended to resolve over time,” from about 70% in the first few weeks after surgery to 11% at 1 year and 7% at 5 years, Dr. Ganz said.
In seven cases, the device was removed laparoscopically, with no complications and gastric anatomy was preserved for future treatments. All removals were elective. The device was removed in four patients because of dysphagia, which completely resolved in those patients. One patient had the device removed because of vomiting of unknown cause that persisted after removal. Another two patients who “had the device removed for disease management” continued to experience reflux and had “uneventful” Nissen fundoplication,” he said.
“Five years after magnetic augmentation, we have demonstrated objective evidence of reduction in acid exposure and in the majority of patients, normalized pH [and] we demonstrated significant and durable improvement in all group parameters measured, with preservation of fundic anatomy and normal physiology, with the ability to belch and vomit,” Dr. Ganz concluded. The results also show that the “procedure is reproducible, safe and reversible if necessary,” he added, noting that one of the limitations of the study was that subjects served as their own controls. During the discussion period, he was asked about hiatal hernia repairs, an apparent trend to “decay” from years 1 to 5 in some parameters measured, and dysphagia after the procedure.
About 40% of the patients in the study had a hiatal hernia, and about one-third of these patients had a hernia repair. A subgroup analysis of the data is being performed to evaluate the impact of hernia repair, Dr. Ganz said.
PPI use increased from 8% in year 4, to 15% in year 5. The reason for this s difficult to determine but “even though there is a bit of a decay, patients are still quite satisfied at 5 years,” Dr. Ganz remarked, also referring to the marked impact on regurgitation. Many U.S. patients use PPIs for reasons other than reflux, and studies show that many patients are on PPIs after the Nissen procedure in the absence of pathologic pH scores, he pointed out.
Compared with the type of dysphagia patients experience after the Nissen procedure, which is immediate and improves with time, Dr. Ganz said that the dysphagia associated with the device “seemed to peak around 2 weeks and then it slowly improved with time, so this may be more of a scar tissue–associated dysphagia than an edema dysphagia, but … it does improve with time.
Three-year results of the study were published in 2013 (N. Engl. J. Med. 2013;368:719-72), Dr. Ganz was the lead author.
The study was funded by Torax Medical. Dr. Ganz had no disclosures related to the topic of this presentation.
*This story was updated 7/9/2015.
AT DDW 2015
Key clinical point: A magnetic device designed to augment the lower esophageal sphincter is a surgical option that can be expected to provide long-term control of reflux symptoms in patients with GERD.
Major finding: Improvements 5 years after treatment with the Linx Reflux Management System include a drop from 60% experiencing regurgitation to 1%, and two-third of patients no longer taking PPIs.
Data source: The multicenter, prospective study evaluated the long-term safety and efficacy of the device over 5 years in 100 patients with GERD, who served as their own controls; 85 were included in the 5-year follow-up.
Disclosures: The study was funded by the device manufacturer, Torax Medical. Dr. Ganz had no disclosures related to the topic of this presentation.
Reports of TAVI leaflet thickening downplayed – for now
PARIS – Thought leaders in interventional cardiology have been quick to throw cold water on recent reports of valve leaflet thickening and abnormal leaflet motion being detected in roughly 10% of patients after transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement.
“The take home message for the interventional community is there is no need for clinicians to modify their practice in relation to patient selection, TAVI implantation, or follow-up protocols. Specifically, there is no role for systematic CT or transesophageal echocardiographic follow-up of asymptomatic TAVI patients because they’re not at clinical risk, and these additional procedures carry risk in themselves,” Dr. Bernard Prendergast said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

“Whilst there is room here for speculation and conjecture, I think most of us are confident that some of these findings may represent imaging artifact or reflect the natural history of biological valve leaflets, which has never been examined in such detail in the past,” added Dr. Prendergast, director of the cardiac structural intervention program at Guys and St. Thomas’ Hospital in London and cochair of the special EuroPCR session devoted to the emerging data on valve leaflet abnormalities.
The session featured three separate studies totaling 345 patients who underwent sophisticated, high-resolution 4D CT imaging or transesophageal echocardiography 5 days or more following TAVI or, less frequently, after surgical aortic valve replacement. Roughly 10% of patients showed a spectrum of leaflet abnormalities: thickening, mildly impaired motion, and/or thin films believed to be thrombi.
The leaflet abnormalities weren’t associated with any particular valve. And, as was emphasized by Dr. Prendergast and other speakers, to date these abnormalities haven’t been associated with a single case of stroke, systemic embolism, or valve failure.
Indeed, more than 100,000 TAVI procedures have been performed worldwide, and stroke rates in contemporary randomized trials and large registries are in the 1%-2% range. That’s better than with surgical valve replacement, Dr. Prendergast observed.
“Nowadays we can see much more than we could in the past, when we worked with 2D echocardiography,” observed discussant Dr. Jeroen J. Bax, professor of cardiology and director of noninvasive cardiology imaging at Leiden (the Netherlands) University Medical Center. “We see things that we do not completely understand. We could say that technology has outpaced our clinical understanding. But although we see things, at the moment there is no consequence in terms of hemodynamic performance or clinical outcomes. And this phenomenon of leaflet thickening has been occurring with surgical aortic valve replacement for many, many years and we simply didn’t realize it.”
Dr. Franz-Josef Neumann, who led one of the three studies, reported that 4D CT on day 5 post TAVI revealed leaflet abnormalities, all completely asymptomatic, in 16 of 154 patients. Two-thirds of the study population were on dual antiplatelet therapy at the time, the rest on a single antiplatelet agent. Dual antiplatelet therapy didn’t protect against leaflet thickening or other abnormalities.
All 16 affected patients were placed on an oral vitamin K antagonist with a target international normalized ratio (INR) of 2.5-3.5. To date, 11 of the 16 have undergone follow-up high-resolution CT after a median of 77 days. The leaflet thickening was resolved in all instances, according to Dr. Neumann, medical director of the department of cardiology and angiology at the University of Freiburg (Germany).

Dr. Raj R. Makkar presented a study of 125 patients who underwent high-resolution imaging after TAVI. Importantly, none of those who were on warfarin as part of their post-TAVI regimen developed leaflet abnormalities.
But he cautioned his colleagues against overreacting to the studies he and Dr. Neumann presented by placing all of their TAVI patients on an oral anticoagulant. He noted that the current TAVI population is elderly and laden with many comorbid conditions, placing them at high risk for bleeding complications.
There is at present no standard, guideline-recommended antiplatelet/antithrombotic regimen for before, during, or after TAVI. Working out the optimal protective drug regimen in this population is now a priority in light of the leaflet abnormality findings, but it will take time and require careful study, said Dr. Makkar, associate director of the Cedars Sinai Heart Institute in Los Angeles.
“Everyone is talking about anticoagulation as the imminent solution. But I want to emphasize that it comes with a price in terms of bleeding. These images are beautiful in terms of spatial resolution, but we must resist our temptation while the industry works on designing less thrombogenic valves,” the cardiologist added.
Discussant Dr. Christoph K. Naber confessed he was “stunned” by the images of leaflet abnormalities.
“Although we haven’t seen any clinical consequences, we have to keep in mind that the group of patients is still small. We have very good experience with TAVI; it has saved the lives of many patients. We know it’s a very good therapy. But if we believe we can go further and offer it to younger, lower-risk patients who will have their device for a longer time, then we should take the time and money to understand what is going on here and what consequences it could have. It’s something we should closely watch, especially if we want to extend the indication,” said Dr. Naber, director of the department of cardiology and angiology at the Contilia Cardiovascular Center in Essen, Germany.
He disclosed that he serves as a consultant to Abbott Vascular, Biotronik, Medtronic, and The Medicines Company. Dr. Makkar has received research grants from Edwards Lifesciences, St. Jude Medical, and Boston Scientific. Dr. Prendergast is on the speakers’ bureau for Edwards Lifesciences.
PARIS – Thought leaders in interventional cardiology have been quick to throw cold water on recent reports of valve leaflet thickening and abnormal leaflet motion being detected in roughly 10% of patients after transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement.
“The take home message for the interventional community is there is no need for clinicians to modify their practice in relation to patient selection, TAVI implantation, or follow-up protocols. Specifically, there is no role for systematic CT or transesophageal echocardiographic follow-up of asymptomatic TAVI patients because they’re not at clinical risk, and these additional procedures carry risk in themselves,” Dr. Bernard Prendergast said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Whilst there is room here for speculation and conjecture, I think most of us are confident that some of these findings may represent imaging artifact or reflect the natural history of biological valve leaflets, which has never been examined in such detail in the past,” added Dr. Prendergast, director of the cardiac structural intervention program at Guys and St. Thomas’ Hospital in London and cochair of the special EuroPCR session devoted to the emerging data on valve leaflet abnormalities.
The session featured three separate studies totaling 345 patients who underwent sophisticated, high-resolution 4D CT imaging or transesophageal echocardiography 5 days or more following TAVI or, less frequently, after surgical aortic valve replacement. Roughly 10% of patients showed a spectrum of leaflet abnormalities: thickening, mildly impaired motion, and/or thin films believed to be thrombi.
The leaflet abnormalities weren’t associated with any particular valve. And, as was emphasized by Dr. Prendergast and other speakers, to date these abnormalities haven’t been associated with a single case of stroke, systemic embolism, or valve failure.
Indeed, more than 100,000 TAVI procedures have been performed worldwide, and stroke rates in contemporary randomized trials and large registries are in the 1%-2% range. That’s better than with surgical valve replacement, Dr. Prendergast observed.
“Nowadays we can see much more than we could in the past, when we worked with 2D echocardiography,” observed discussant Dr. Jeroen J. Bax, professor of cardiology and director of noninvasive cardiology imaging at Leiden (the Netherlands) University Medical Center. “We see things that we do not completely understand. We could say that technology has outpaced our clinical understanding. But although we see things, at the moment there is no consequence in terms of hemodynamic performance or clinical outcomes. And this phenomenon of leaflet thickening has been occurring with surgical aortic valve replacement for many, many years and we simply didn’t realize it.”
Dr. Franz-Josef Neumann, who led one of the three studies, reported that 4D CT on day 5 post TAVI revealed leaflet abnormalities, all completely asymptomatic, in 16 of 154 patients. Two-thirds of the study population were on dual antiplatelet therapy at the time, the rest on a single antiplatelet agent. Dual antiplatelet therapy didn’t protect against leaflet thickening or other abnormalities.
All 16 affected patients were placed on an oral vitamin K antagonist with a target international normalized ratio (INR) of 2.5-3.5. To date, 11 of the 16 have undergone follow-up high-resolution CT after a median of 77 days. The leaflet thickening was resolved in all instances, according to Dr. Neumann, medical director of the department of cardiology and angiology at the University of Freiburg (Germany).
Dr. Raj R. Makkar presented a study of 125 patients who underwent high-resolution imaging after TAVI. Importantly, none of those who were on warfarin as part of their post-TAVI regimen developed leaflet abnormalities.
But he cautioned his colleagues against overreacting to the studies he and Dr. Neumann presented by placing all of their TAVI patients on an oral anticoagulant. He noted that the current TAVI population is elderly and laden with many comorbid conditions, placing them at high risk for bleeding complications.
There is at present no standard, guideline-recommended antiplatelet/antithrombotic regimen for before, during, or after TAVI. Working out the optimal protective drug regimen in this population is now a priority in light of the leaflet abnormality findings, but it will take time and require careful study, said Dr. Makkar, associate director of the Cedars Sinai Heart Institute in Los Angeles.
“Everyone is talking about anticoagulation as the imminent solution. But I want to emphasize that it comes with a price in terms of bleeding. These images are beautiful in terms of spatial resolution, but we must resist our temptation while the industry works on designing less thrombogenic valves,” the cardiologist added.
Discussant Dr. Christoph K. Naber confessed he was “stunned” by the images of leaflet abnormalities.
“Although we haven’t seen any clinical consequences, we have to keep in mind that the group of patients is still small. We have very good experience with TAVI; it has saved the lives of many patients. We know it’s a very good therapy. But if we believe we can go further and offer it to younger, lower-risk patients who will have their device for a longer time, then we should take the time and money to understand what is going on here and what consequences it could have. It’s something we should closely watch, especially if we want to extend the indication,” said Dr. Naber, director of the department of cardiology and angiology at the Contilia Cardiovascular Center in Essen, Germany.
He disclosed that he serves as a consultant to Abbott Vascular, Biotronik, Medtronic, and The Medicines Company. Dr. Makkar has received research grants from Edwards Lifesciences, St. Jude Medical, and Boston Scientific. Dr. Prendergast is on the speakers’ bureau for Edwards Lifesciences.
PARIS – Thought leaders in interventional cardiology have been quick to throw cold water on recent reports of valve leaflet thickening and abnormal leaflet motion being detected in roughly 10% of patients after transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement.
“The take home message for the interventional community is there is no need for clinicians to modify their practice in relation to patient selection, TAVI implantation, or follow-up protocols. Specifically, there is no role for systematic CT or transesophageal echocardiographic follow-up of asymptomatic TAVI patients because they’re not at clinical risk, and these additional procedures carry risk in themselves,” Dr. Bernard Prendergast said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Whilst there is room here for speculation and conjecture, I think most of us are confident that some of these findings may represent imaging artifact or reflect the natural history of biological valve leaflets, which has never been examined in such detail in the past,” added Dr. Prendergast, director of the cardiac structural intervention program at Guys and St. Thomas’ Hospital in London and cochair of the special EuroPCR session devoted to the emerging data on valve leaflet abnormalities.
The session featured three separate studies totaling 345 patients who underwent sophisticated, high-resolution 4D CT imaging or transesophageal echocardiography 5 days or more following TAVI or, less frequently, after surgical aortic valve replacement. Roughly 10% of patients showed a spectrum of leaflet abnormalities: thickening, mildly impaired motion, and/or thin films believed to be thrombi.
The leaflet abnormalities weren’t associated with any particular valve. And, as was emphasized by Dr. Prendergast and other speakers, to date these abnormalities haven’t been associated with a single case of stroke, systemic embolism, or valve failure.
Indeed, more than 100,000 TAVI procedures have been performed worldwide, and stroke rates in contemporary randomized trials and large registries are in the 1%-2% range. That’s better than with surgical valve replacement, Dr. Prendergast observed.
“Nowadays we can see much more than we could in the past, when we worked with 2D echocardiography,” observed discussant Dr. Jeroen J. Bax, professor of cardiology and director of noninvasive cardiology imaging at Leiden (the Netherlands) University Medical Center. “We see things that we do not completely understand. We could say that technology has outpaced our clinical understanding. But although we see things, at the moment there is no consequence in terms of hemodynamic performance or clinical outcomes. And this phenomenon of leaflet thickening has been occurring with surgical aortic valve replacement for many, many years and we simply didn’t realize it.”
Dr. Franz-Josef Neumann, who led one of the three studies, reported that 4D CT on day 5 post TAVI revealed leaflet abnormalities, all completely asymptomatic, in 16 of 154 patients. Two-thirds of the study population were on dual antiplatelet therapy at the time, the rest on a single antiplatelet agent. Dual antiplatelet therapy didn’t protect against leaflet thickening or other abnormalities.
All 16 affected patients were placed on an oral vitamin K antagonist with a target international normalized ratio (INR) of 2.5-3.5. To date, 11 of the 16 have undergone follow-up high-resolution CT after a median of 77 days. The leaflet thickening was resolved in all instances, according to Dr. Neumann, medical director of the department of cardiology and angiology at the University of Freiburg (Germany).
Dr. Raj R. Makkar presented a study of 125 patients who underwent high-resolution imaging after TAVI. Importantly, none of those who were on warfarin as part of their post-TAVI regimen developed leaflet abnormalities.
But he cautioned his colleagues against overreacting to the studies he and Dr. Neumann presented by placing all of their TAVI patients on an oral anticoagulant. He noted that the current TAVI population is elderly and laden with many comorbid conditions, placing them at high risk for bleeding complications.
There is at present no standard, guideline-recommended antiplatelet/antithrombotic regimen for before, during, or after TAVI. Working out the optimal protective drug regimen in this population is now a priority in light of the leaflet abnormality findings, but it will take time and require careful study, said Dr. Makkar, associate director of the Cedars Sinai Heart Institute in Los Angeles.
“Everyone is talking about anticoagulation as the imminent solution. But I want to emphasize that it comes with a price in terms of bleeding. These images are beautiful in terms of spatial resolution, but we must resist our temptation while the industry works on designing less thrombogenic valves,” the cardiologist added.
Discussant Dr. Christoph K. Naber confessed he was “stunned” by the images of leaflet abnormalities.
“Although we haven’t seen any clinical consequences, we have to keep in mind that the group of patients is still small. We have very good experience with TAVI; it has saved the lives of many patients. We know it’s a very good therapy. But if we believe we can go further and offer it to younger, lower-risk patients who will have their device for a longer time, then we should take the time and money to understand what is going on here and what consequences it could have. It’s something we should closely watch, especially if we want to extend the indication,” said Dr. Naber, director of the department of cardiology and angiology at the Contilia Cardiovascular Center in Essen, Germany.
He disclosed that he serves as a consultant to Abbott Vascular, Biotronik, Medtronic, and The Medicines Company. Dr. Makkar has received research grants from Edwards Lifesciences, St. Jude Medical, and Boston Scientific. Dr. Prendergast is on the speakers’ bureau for Edwards Lifesciences.
EXPERT ANALYSIS FROM EUROPCR

Cochrane review finds midurethral slings safe, effective
Midurethral sling operations for stress urinary incontinence (SUI) are safe, and – regardless of the routes traversed – are highly effective in the short and mid term, according to a new Cochrane systematic review.
Evidence showing long-term effectiveness is also accruing, but too few of the existing trials have reported outcomes beyond 5 years, Dr. Abigail A. Ford of Bradford (England) Royal Infirmary and her colleagues from the Cochrane Incontinence Group reported.
The findings, based on a review of 81 trials involving a total of 12,113 women, were published July 1 (Cochrane Database Syst. Rev. 2015 [doi:10.1002/14651858.CD006375.pub3]).
Moderate-quality evidence indicates that the transobturator route and retropubic route provide similar rates of subjective and objective cure at up to 1 year (relative risk, 0.98 for both). Low-quality evidence suggests the subjective cure rates are similar with these two approaches at between 1 and 5 years (RR, 0.97), and moderate-quality evidence suggests the subjective cure rates are similar beyond 5 years with the two approaches (RR, 0.95), the investigators said.
Overall, about 80% of women undergoing surgery using either approach experience significant improvement in symptoms at up to 5 years after the surgery; that drops to about 70% after 5 years, based on the few studies that followed patients that long.
Although the overall adverse event rate was low, morbidity rates were higher with the retropubic route. For example, the rate of bladder perforation was 0.6% with the transobturator route vs. 4.5% with the retropubic route. Major vascular/visceral injury, mean operating time, operative blood loss, and hospital length of stay were all lower with the transobturator route. Further, voiding dysfunction was less common with the transobturator route (RR, 0.53).
Groin pain was more common in women in the transobturator vs. retropubic groups (6.4% vs. 1.3%), but suprapubic pain was less common (0.8% vs. 2.9%); both types of pain were of short duration.
The Cochrane investigators also found moderate-quality evidence for the following.
The overall rate of vaginal tape erosion, exposure, or extrusion was low (24 per 1,000 and 21 per 1,000 procedures for the transobturator and retropubic routes, respectively (RR, 1.13).
A retropubic bottom-to-top route was more effective than a top-to-bottom route for subjective cure (RR, 1.10).
Subjective cure rates in the short and mid term were similar when transobturator tape was passed using a medial-to-lateral or lateral-to-medial approach (RR, 1.00 and 1.06, respectively).
Voiding dysfunction was more common with the medial-to-lateral approach (RR, 1.74), but vaginal perforation was less frequent in the medial-to-lateral route (RR, 0.25).
It was unclear, due to very low-quality evidence, whether the lower rates of vaginal epithelial perforation affected vaginal tape erosion, the investigators noted.
The investigators reviewed the literature from 1947 up to June 2014, including only randomized and quasi-randomized controlled trials involving women with stress urinary incontinence, urodynamic stress incontinence, or mixed urinary incontinence, which contribute to up to 80% of cases of urinary incontinence.
They noted that concerns regarding mesh erosion are ongoing, but that the latest white paper and safety communications on meshes released by the Food and Drug Administration in 2011 “relates to ongoing concern with mesh used to treat pelvic organ prolapse and not the small strip of mesh/tape/sling used to treat SUI. In fact, the FDA states that the safety and effectiveness of midurethral slings is well established in clinical trials with 1-year follow-up.”
Overall, the current review highlights the positive impact that midurethral sling operations have on quality of life in women with stress urinary incontinence, but additional reporting of long-term outcomes is needed, the investigators wrote.
“We need to know more about what happens to women in the long term,” Dr. Joseph Ogah, one of the Cochrane investigators and a consultant gynecologist at the University Hospitals of Morecambe Bay NHS Foundation Trust in Cumbria, England, said in a statement. “This review found 35 trials carried out more than 5 years ago: If all the women in these trials were followed up, we would know much more about how long the operations last and, crucially, whether they had developed late but important side effects. Rather than starting any new trials in this area we need to obtain long-term follow-up from the existing trials.”
The review was supported by the National Institute for Health Research in the United Kingdom. Some of the review authors reported industry sponsorship to attend scientific conferences.
Midurethral sling operations for stress urinary incontinence (SUI) are safe, and – regardless of the routes traversed – are highly effective in the short and mid term, according to a new Cochrane systematic review.
Evidence showing long-term effectiveness is also accruing, but too few of the existing trials have reported outcomes beyond 5 years, Dr. Abigail A. Ford of Bradford (England) Royal Infirmary and her colleagues from the Cochrane Incontinence Group reported.
The findings, based on a review of 81 trials involving a total of 12,113 women, were published July 1 (Cochrane Database Syst. Rev. 2015 [doi:10.1002/14651858.CD006375.pub3]).
Moderate-quality evidence indicates that the transobturator route and retropubic route provide similar rates of subjective and objective cure at up to 1 year (relative risk, 0.98 for both). Low-quality evidence suggests the subjective cure rates are similar with these two approaches at between 1 and 5 years (RR, 0.97), and moderate-quality evidence suggests the subjective cure rates are similar beyond 5 years with the two approaches (RR, 0.95), the investigators said.
Overall, about 80% of women undergoing surgery using either approach experience significant improvement in symptoms at up to 5 years after the surgery; that drops to about 70% after 5 years, based on the few studies that followed patients that long.
Although the overall adverse event rate was low, morbidity rates were higher with the retropubic route. For example, the rate of bladder perforation was 0.6% with the transobturator route vs. 4.5% with the retropubic route. Major vascular/visceral injury, mean operating time, operative blood loss, and hospital length of stay were all lower with the transobturator route. Further, voiding dysfunction was less common with the transobturator route (RR, 0.53).
Groin pain was more common in women in the transobturator vs. retropubic groups (6.4% vs. 1.3%), but suprapubic pain was less common (0.8% vs. 2.9%); both types of pain were of short duration.
The Cochrane investigators also found moderate-quality evidence for the following.
The overall rate of vaginal tape erosion, exposure, or extrusion was low (24 per 1,000 and 21 per 1,000 procedures for the transobturator and retropubic routes, respectively (RR, 1.13).
A retropubic bottom-to-top route was more effective than a top-to-bottom route for subjective cure (RR, 1.10).
Subjective cure rates in the short and mid term were similar when transobturator tape was passed using a medial-to-lateral or lateral-to-medial approach (RR, 1.00 and 1.06, respectively).
Voiding dysfunction was more common with the medial-to-lateral approach (RR, 1.74), but vaginal perforation was less frequent in the medial-to-lateral route (RR, 0.25).
It was unclear, due to very low-quality evidence, whether the lower rates of vaginal epithelial perforation affected vaginal tape erosion, the investigators noted.
The investigators reviewed the literature from 1947 up to June 2014, including only randomized and quasi-randomized controlled trials involving women with stress urinary incontinence, urodynamic stress incontinence, or mixed urinary incontinence, which contribute to up to 80% of cases of urinary incontinence.
They noted that concerns regarding mesh erosion are ongoing, but that the latest white paper and safety communications on meshes released by the Food and Drug Administration in 2011 “relates to ongoing concern with mesh used to treat pelvic organ prolapse and not the small strip of mesh/tape/sling used to treat SUI. In fact, the FDA states that the safety and effectiveness of midurethral slings is well established in clinical trials with 1-year follow-up.”
Overall, the current review highlights the positive impact that midurethral sling operations have on quality of life in women with stress urinary incontinence, but additional reporting of long-term outcomes is needed, the investigators wrote.
“We need to know more about what happens to women in the long term,” Dr. Joseph Ogah, one of the Cochrane investigators and a consultant gynecologist at the University Hospitals of Morecambe Bay NHS Foundation Trust in Cumbria, England, said in a statement. “This review found 35 trials carried out more than 5 years ago: If all the women in these trials were followed up, we would know much more about how long the operations last and, crucially, whether they had developed late but important side effects. Rather than starting any new trials in this area we need to obtain long-term follow-up from the existing trials.”
The review was supported by the National Institute for Health Research in the United Kingdom. Some of the review authors reported industry sponsorship to attend scientific conferences.
Midurethral sling operations for stress urinary incontinence (SUI) are safe, and – regardless of the routes traversed – are highly effective in the short and mid term, according to a new Cochrane systematic review.
Evidence showing long-term effectiveness is also accruing, but too few of the existing trials have reported outcomes beyond 5 years, Dr. Abigail A. Ford of Bradford (England) Royal Infirmary and her colleagues from the Cochrane Incontinence Group reported.
The findings, based on a review of 81 trials involving a total of 12,113 women, were published July 1 (Cochrane Database Syst. Rev. 2015 [doi:10.1002/14651858.CD006375.pub3]).
Moderate-quality evidence indicates that the transobturator route and retropubic route provide similar rates of subjective and objective cure at up to 1 year (relative risk, 0.98 for both). Low-quality evidence suggests the subjective cure rates are similar with these two approaches at between 1 and 5 years (RR, 0.97), and moderate-quality evidence suggests the subjective cure rates are similar beyond 5 years with the two approaches (RR, 0.95), the investigators said.
Overall, about 80% of women undergoing surgery using either approach experience significant improvement in symptoms at up to 5 years after the surgery; that drops to about 70% after 5 years, based on the few studies that followed patients that long.
Although the overall adverse event rate was low, morbidity rates were higher with the retropubic route. For example, the rate of bladder perforation was 0.6% with the transobturator route vs. 4.5% with the retropubic route. Major vascular/visceral injury, mean operating time, operative blood loss, and hospital length of stay were all lower with the transobturator route. Further, voiding dysfunction was less common with the transobturator route (RR, 0.53).
Groin pain was more common in women in the transobturator vs. retropubic groups (6.4% vs. 1.3%), but suprapubic pain was less common (0.8% vs. 2.9%); both types of pain were of short duration.
The Cochrane investigators also found moderate-quality evidence for the following.
The overall rate of vaginal tape erosion, exposure, or extrusion was low (24 per 1,000 and 21 per 1,000 procedures for the transobturator and retropubic routes, respectively (RR, 1.13).
A retropubic bottom-to-top route was more effective than a top-to-bottom route for subjective cure (RR, 1.10).
Subjective cure rates in the short and mid term were similar when transobturator tape was passed using a medial-to-lateral or lateral-to-medial approach (RR, 1.00 and 1.06, respectively).
Voiding dysfunction was more common with the medial-to-lateral approach (RR, 1.74), but vaginal perforation was less frequent in the medial-to-lateral route (RR, 0.25).
It was unclear, due to very low-quality evidence, whether the lower rates of vaginal epithelial perforation affected vaginal tape erosion, the investigators noted.
The investigators reviewed the literature from 1947 up to June 2014, including only randomized and quasi-randomized controlled trials involving women with stress urinary incontinence, urodynamic stress incontinence, or mixed urinary incontinence, which contribute to up to 80% of cases of urinary incontinence.
They noted that concerns regarding mesh erosion are ongoing, but that the latest white paper and safety communications on meshes released by the Food and Drug Administration in 2011 “relates to ongoing concern with mesh used to treat pelvic organ prolapse and not the small strip of mesh/tape/sling used to treat SUI. In fact, the FDA states that the safety and effectiveness of midurethral slings is well established in clinical trials with 1-year follow-up.”
Overall, the current review highlights the positive impact that midurethral sling operations have on quality of life in women with stress urinary incontinence, but additional reporting of long-term outcomes is needed, the investigators wrote.
“We need to know more about what happens to women in the long term,” Dr. Joseph Ogah, one of the Cochrane investigators and a consultant gynecologist at the University Hospitals of Morecambe Bay NHS Foundation Trust in Cumbria, England, said in a statement. “This review found 35 trials carried out more than 5 years ago: If all the women in these trials were followed up, we would know much more about how long the operations last and, crucially, whether they had developed late but important side effects. Rather than starting any new trials in this area we need to obtain long-term follow-up from the existing trials.”
The review was supported by the National Institute for Health Research in the United Kingdom. Some of the review authors reported industry sponsorship to attend scientific conferences.
FROM THE COCHRANE DATABASE OF SYSTEMATIC REVIEWS
Key clinical point: Midurethral sling operations for stress urinary incontinence are safe and effective in the short and mid term.
Major finding: About 80% of women continue to experience significant improvement at up to 5 years.
Data source: A systematic review of the literature, including 81 studies involving 12,113 women.
Disclosures: The review was supported by the National Institute for Health Research in the United Kingdom. Some of the review authors reported industry sponsorship to attend scientific conferences.