User login
Official Newspaper of the American College of Surgeons
Routine screening sufficient for detecting occult cancer in patients with VTE
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.

Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.
Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.
Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
AT THE 2015 ISTH CONGRESS
Key clinical point: Occult cancers in patients with a first unprovoked VTE are not nearly as common as previously thought, and limited screening for such cancers is appropriate.
Major finding: There were no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%); in overall mortality (1.4% vs. 1.2%), or in cancer-related mortality (1.4% vs. 0.95%).
Data source: A multicenter, open-label, randomized controlled trial of 854 patients with unprovoked VTE.
Disclosures: The trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier reported having no financial disclosures.

SVS: Don’t let TPA delay urgent carotid interventions for mild and moderate strokes
CHICAGO – Urgent carotid interventions were safe after thrombolysis for acute mild to moderate strokes, according to a review of 165 patients at the Ochsner Clinic in New Orleans.
“Our data support the practice of not denying a patient an urgent carotid intervention simply because of TPA [tissue plasminogen activator] administration during the acute stroke period,” said lead investigator Dr. Nicolas Zea, an Ochsner vascular surgeon.
“Urgent carotid endarterectomy [CEA] or coronary artery stenting [CAS] can be safely undertaken in minor to moderate strokes with NIH stroke scale scores less than 10; TPA itself does not appear to be a contraindication, even within 72 hours,” he added.
Urgent carotid interventions are becoming more common after ischemic strokes to prevent recurrences. The approach is most effective within 2 weeks of the index event, but there have been concerns that intracranial hemorrhages (ICH) and other complications might be more likely if patients have had TPA.
Dr. Ochsner and his colleagues conducted their review because, “as vascular surgeons, we are going to encounter a lot more of these patients in the very near future,” Dr. Zea said a meeting hosted by the Society for Vascular Surgery.
From January 2009 to January 2015, 31 patients at Ochsner had carotid interventions – 25 CEA, 6 CAS – a mean of 2.1 days after receiving TPA for transient ischemic attacks (TIA) or ischemic strokes. The patients’ mean National Institutes of Health Stroke Scale (NIHSS) score was 6.6.
Over the same period, 134 patients who had not received TPA had urgent carotid interventions – 110 CEA, 24 CAS – a mean of 2.6 days after TIA or ischemic stroke presentation. Their mean NIHSS score was 6.1.
There were no statistically significant demographic or comorbidity differences between the TPA and no-TPA groups; patients were about 70 years old, on average, and the majority were men. Most had ipsilateral carotid stenosis greater than 70%, or acute occlusions.
The 30-day overall complication rate was 12.9% in the TPA group and 6.7% in the non-TPA group, a nonsignificant difference (P = 0.35).
In the TPA group, there was one (3.2%) ICH, one (3.2%) neck hematoma, and two (6.4%) deaths. In the no-TPA group, there were two (1.5%) ICHs, two (1.5%) neck hematomas, one (0.7%) ischemic stroke, two (1.5%) myocardial infarctions, and two (1.5%) deaths.
In both groups, ICH patients had stroke scores greater than 10. Also, although the rate of death was higher in the TPA group, the deaths “were not necessarily related to thrombolysis,” Dr. Zea noted. One death was from pulmonary embolism, the second from unknown causes. Deaths were due to acute mesenteric ischemia and ICH in the no-TPA group, Dr. Zea said.
There was one (3.2%) hemorrhagic conversion in the TPA group and two (1.5%) in the no-TPA group. Similarly, one (3.2%) TPA patient and two (1.5%) no-TPA patients had complications from access site bleeding. The differences were not statistically significant.
In the TPA group, it didn’t seem to matter if intervention came within 72 hours of administration – as in about half the cases – or afterward, when TPA risks have largely passed. There was one death and one ICH in patients in the earlier group, and one death in the later group, a nonsignificant difference.
There was no outside funding for the study. Dr. Zea had no disclosures. One of the coinvestigators is a consultant for Lutonix.
aotto@frontlinemedcom.com
CHICAGO – Urgent carotid interventions were safe after thrombolysis for acute mild to moderate strokes, according to a review of 165 patients at the Ochsner Clinic in New Orleans.
“Our data support the practice of not denying a patient an urgent carotid intervention simply because of TPA [tissue plasminogen activator] administration during the acute stroke period,” said lead investigator Dr. Nicolas Zea, an Ochsner vascular surgeon.
“Urgent carotid endarterectomy [CEA] or coronary artery stenting [CAS] can be safely undertaken in minor to moderate strokes with NIH stroke scale scores less than 10; TPA itself does not appear to be a contraindication, even within 72 hours,” he added.
Urgent carotid interventions are becoming more common after ischemic strokes to prevent recurrences. The approach is most effective within 2 weeks of the index event, but there have been concerns that intracranial hemorrhages (ICH) and other complications might be more likely if patients have had TPA.
Dr. Ochsner and his colleagues conducted their review because, “as vascular surgeons, we are going to encounter a lot more of these patients in the very near future,” Dr. Zea said a meeting hosted by the Society for Vascular Surgery.
From January 2009 to January 2015, 31 patients at Ochsner had carotid interventions – 25 CEA, 6 CAS – a mean of 2.1 days after receiving TPA for transient ischemic attacks (TIA) or ischemic strokes. The patients’ mean National Institutes of Health Stroke Scale (NIHSS) score was 6.6.
Over the same period, 134 patients who had not received TPA had urgent carotid interventions – 110 CEA, 24 CAS – a mean of 2.6 days after TIA or ischemic stroke presentation. Their mean NIHSS score was 6.1.
There were no statistically significant demographic or comorbidity differences between the TPA and no-TPA groups; patients were about 70 years old, on average, and the majority were men. Most had ipsilateral carotid stenosis greater than 70%, or acute occlusions.
The 30-day overall complication rate was 12.9% in the TPA group and 6.7% in the non-TPA group, a nonsignificant difference (P = 0.35).
In the TPA group, there was one (3.2%) ICH, one (3.2%) neck hematoma, and two (6.4%) deaths. In the no-TPA group, there were two (1.5%) ICHs, two (1.5%) neck hematomas, one (0.7%) ischemic stroke, two (1.5%) myocardial infarctions, and two (1.5%) deaths.
In both groups, ICH patients had stroke scores greater than 10. Also, although the rate of death was higher in the TPA group, the deaths “were not necessarily related to thrombolysis,” Dr. Zea noted. One death was from pulmonary embolism, the second from unknown causes. Deaths were due to acute mesenteric ischemia and ICH in the no-TPA group, Dr. Zea said.
There was one (3.2%) hemorrhagic conversion in the TPA group and two (1.5%) in the no-TPA group. Similarly, one (3.2%) TPA patient and two (1.5%) no-TPA patients had complications from access site bleeding. The differences were not statistically significant.
In the TPA group, it didn’t seem to matter if intervention came within 72 hours of administration – as in about half the cases – or afterward, when TPA risks have largely passed. There was one death and one ICH in patients in the earlier group, and one death in the later group, a nonsignificant difference.
There was no outside funding for the study. Dr. Zea had no disclosures. One of the coinvestigators is a consultant for Lutonix.
aotto@frontlinemedcom.com
CHICAGO – Urgent carotid interventions were safe after thrombolysis for acute mild to moderate strokes, according to a review of 165 patients at the Ochsner Clinic in New Orleans.
“Our data support the practice of not denying a patient an urgent carotid intervention simply because of TPA [tissue plasminogen activator] administration during the acute stroke period,” said lead investigator Dr. Nicolas Zea, an Ochsner vascular surgeon.
“Urgent carotid endarterectomy [CEA] or coronary artery stenting [CAS] can be safely undertaken in minor to moderate strokes with NIH stroke scale scores less than 10; TPA itself does not appear to be a contraindication, even within 72 hours,” he added.
Urgent carotid interventions are becoming more common after ischemic strokes to prevent recurrences. The approach is most effective within 2 weeks of the index event, but there have been concerns that intracranial hemorrhages (ICH) and other complications might be more likely if patients have had TPA.
Dr. Ochsner and his colleagues conducted their review because, “as vascular surgeons, we are going to encounter a lot more of these patients in the very near future,” Dr. Zea said a meeting hosted by the Society for Vascular Surgery.
From January 2009 to January 2015, 31 patients at Ochsner had carotid interventions – 25 CEA, 6 CAS – a mean of 2.1 days after receiving TPA for transient ischemic attacks (TIA) or ischemic strokes. The patients’ mean National Institutes of Health Stroke Scale (NIHSS) score was 6.6.
Over the same period, 134 patients who had not received TPA had urgent carotid interventions – 110 CEA, 24 CAS – a mean of 2.6 days after TIA or ischemic stroke presentation. Their mean NIHSS score was 6.1.
There were no statistically significant demographic or comorbidity differences between the TPA and no-TPA groups; patients were about 70 years old, on average, and the majority were men. Most had ipsilateral carotid stenosis greater than 70%, or acute occlusions.
The 30-day overall complication rate was 12.9% in the TPA group and 6.7% in the non-TPA group, a nonsignificant difference (P = 0.35).
In the TPA group, there was one (3.2%) ICH, one (3.2%) neck hematoma, and two (6.4%) deaths. In the no-TPA group, there were two (1.5%) ICHs, two (1.5%) neck hematomas, one (0.7%) ischemic stroke, two (1.5%) myocardial infarctions, and two (1.5%) deaths.
In both groups, ICH patients had stroke scores greater than 10. Also, although the rate of death was higher in the TPA group, the deaths “were not necessarily related to thrombolysis,” Dr. Zea noted. One death was from pulmonary embolism, the second from unknown causes. Deaths were due to acute mesenteric ischemia and ICH in the no-TPA group, Dr. Zea said.
There was one (3.2%) hemorrhagic conversion in the TPA group and two (1.5%) in the no-TPA group. Similarly, one (3.2%) TPA patient and two (1.5%) no-TPA patients had complications from access site bleeding. The differences were not statistically significant.
In the TPA group, it didn’t seem to matter if intervention came within 72 hours of administration – as in about half the cases – or afterward, when TPA risks have largely passed. There was one death and one ICH in patients in the earlier group, and one death in the later group, a nonsignificant difference.
There was no outside funding for the study. Dr. Zea had no disclosures. One of the coinvestigators is a consultant for Lutonix.
aotto@frontlinemedcom.com
AT THE 2015 VASCULAR ANNUAL MEETING
Key clinical point: Tissue plasminogen activator does not contraindicate urgent carotid endarterectomies or stenting.
Major finding: The 30-day overall complication rate was 12.9% in the TPA group and 6.7% in the no-TPA group, a nonsignificant difference (P = 0.35).
Data source: A retrospective study of 165 patients.
Disclosures: There was no outside funding for the study. Dr. Zea had no disclosures. One of the coinvestigators is a consultant for Lutonix.
Sepsis’ readmission costs dwarf heart attack, heart failure costs
Sepsis-related hospital readmission costs in California adults were more than double those for congestive heart failure (CHF) and more than triple those for acute myocardial infarction (AMI) between 2009 and 2011, a retrospective cohort analysis showed.
The all-cause, 30-day readmission rates among 240,198 sepsis patients, 193,153 CHF patients, and 105,684 AMI patients were 20.4%, 23.6%, and 17.7%, respectively, and the estimated annual costs of those readmissions were $500 million, $229 million, and $142 million, respectively, Dr. Dong W. Chang of Harbor-UCLA Medical Center, Torrance, Calif. and colleagues reported online in Critical Care Medicine (June 30, 2015 [doi:10.1097/CCM.0000000000001159]).
Patient-level factors associated with greater likelihood of 30-day readmission after sepsis included younger age (odds ratio, 1.34 for youngest vs. oldest age categories), black race (odds ratio, 1.29 vs. white race), Native American race (odds ratio, 2.39 vs. white race), and lower income (odds ratio, 1.13 for lowest vs. highest income quartiles). Male gender, residence in metropolitan areas, and greater burden of medical comorbidities were also associated with readmission after sepsis.
Hospital-level factors associated with greater likelihood of readmission included health care delivery to the highest vs. lowest quintile of minorities (odds ratio, 1.28), for-profit status (odds ratio, 1.34), and university vs. nonuniversity hospital setting (odds ratio, 1.35), the investigators found.
The findings, derived from the Healthcare Cost and Utilization Project State Inpatient Database maintained by the Agency for Healthcare Research and Quality, show that sepsis is a leading contributor to excess health care costs related to hospital readmissions.
A better understanding of the causative events leading to sepsis readmissions is needed, the investigators noted, and if studies and policies seeking to reduce hospital readmissions are to be effective, they will need to focus on the problem of sepsis-related readmissions – on a level that is at least comparable to CHF and AMI.
Dr. Chang received research support from the National Institutes of Health.
Sepsis-related hospital readmission costs in California adults were more than double those for congestive heart failure (CHF) and more than triple those for acute myocardial infarction (AMI) between 2009 and 2011, a retrospective cohort analysis showed.
The all-cause, 30-day readmission rates among 240,198 sepsis patients, 193,153 CHF patients, and 105,684 AMI patients were 20.4%, 23.6%, and 17.7%, respectively, and the estimated annual costs of those readmissions were $500 million, $229 million, and $142 million, respectively, Dr. Dong W. Chang of Harbor-UCLA Medical Center, Torrance, Calif. and colleagues reported online in Critical Care Medicine (June 30, 2015 [doi:10.1097/CCM.0000000000001159]).
Patient-level factors associated with greater likelihood of 30-day readmission after sepsis included younger age (odds ratio, 1.34 for youngest vs. oldest age categories), black race (odds ratio, 1.29 vs. white race), Native American race (odds ratio, 2.39 vs. white race), and lower income (odds ratio, 1.13 for lowest vs. highest income quartiles). Male gender, residence in metropolitan areas, and greater burden of medical comorbidities were also associated with readmission after sepsis.
Hospital-level factors associated with greater likelihood of readmission included health care delivery to the highest vs. lowest quintile of minorities (odds ratio, 1.28), for-profit status (odds ratio, 1.34), and university vs. nonuniversity hospital setting (odds ratio, 1.35), the investigators found.
The findings, derived from the Healthcare Cost and Utilization Project State Inpatient Database maintained by the Agency for Healthcare Research and Quality, show that sepsis is a leading contributor to excess health care costs related to hospital readmissions.
A better understanding of the causative events leading to sepsis readmissions is needed, the investigators noted, and if studies and policies seeking to reduce hospital readmissions are to be effective, they will need to focus on the problem of sepsis-related readmissions – on a level that is at least comparable to CHF and AMI.
Dr. Chang received research support from the National Institutes of Health.
Sepsis-related hospital readmission costs in California adults were more than double those for congestive heart failure (CHF) and more than triple those for acute myocardial infarction (AMI) between 2009 and 2011, a retrospective cohort analysis showed.
The all-cause, 30-day readmission rates among 240,198 sepsis patients, 193,153 CHF patients, and 105,684 AMI patients were 20.4%, 23.6%, and 17.7%, respectively, and the estimated annual costs of those readmissions were $500 million, $229 million, and $142 million, respectively, Dr. Dong W. Chang of Harbor-UCLA Medical Center, Torrance, Calif. and colleagues reported online in Critical Care Medicine (June 30, 2015 [doi:10.1097/CCM.0000000000001159]).
Patient-level factors associated with greater likelihood of 30-day readmission after sepsis included younger age (odds ratio, 1.34 for youngest vs. oldest age categories), black race (odds ratio, 1.29 vs. white race), Native American race (odds ratio, 2.39 vs. white race), and lower income (odds ratio, 1.13 for lowest vs. highest income quartiles). Male gender, residence in metropolitan areas, and greater burden of medical comorbidities were also associated with readmission after sepsis.
Hospital-level factors associated with greater likelihood of readmission included health care delivery to the highest vs. lowest quintile of minorities (odds ratio, 1.28), for-profit status (odds ratio, 1.34), and university vs. nonuniversity hospital setting (odds ratio, 1.35), the investigators found.
The findings, derived from the Healthcare Cost and Utilization Project State Inpatient Database maintained by the Agency for Healthcare Research and Quality, show that sepsis is a leading contributor to excess health care costs related to hospital readmissions.
A better understanding of the causative events leading to sepsis readmissions is needed, the investigators noted, and if studies and policies seeking to reduce hospital readmissions are to be effective, they will need to focus on the problem of sepsis-related readmissions – on a level that is at least comparable to CHF and AMI.
Dr. Chang received research support from the National Institutes of Health.
FROM CRITICAL CARE MEDICINE
Key clinical point: Sepsis-related hospital readmission costs in California adults were more than double those for congestive heart failure and more than triple those for acute myocardial infarction between 2009 and 2011.
Major finding: The estimated annual costs of sepsis, CHF, and AMI readmissions were $500 million, $229 million, and $142 million, respectively.
Data source: A retrospective cohort study of more than 539,000 hospitalizations.
Disclosures: Dr. Chang received research support from the National Institutes of Health.
Risk of major bleeding is decreased when AF patients do not receive bridging anticoagulation
TORONTO – Forgoing bridging anticoagulation in patients with atrial fibrillation (AF) is noninferior to perioperative bridging with low-molecular-weight heparin for the prevention of arterial thromboembolism and decreases the risk of major bleeding.
Those results emerged from trial data presented at the International Society on Thrombosis and Haemostasis congress and published simultaneously in the New England Journal of Medicine. Study investigator Dr. Thomas Ortel, chief of the division of hematology at Duke University Medical Center, Durham, N.C., discussed results of the BRIDGE (Effectiveness of Bridging Anticoagulation for Surgery) trial, which evaluated the safety and efficacy of bridging anticoagulant therapy.

Bridging anticoagulation is frequently used in patients taking chronic oral anticoagulant therapy who need their anticoagulation transiently held for an operation or invasive procedure. The need for bridging anticoagulation never has been shown definitively, however, Dr. Ortel said in an interview.
“This is the first prospective, randomized, placebo-controlled, double-blind clinical trial to investigate the role of bridging anticoagulant therapy in patients with AF on chronic anticoagulation with warfarin who need the anticoagulant therapy held for an elective operation or invasive procedure,” he said.
Dr. Ortel and his coauthors evaluated 1,884 patients in the trial, which compared bridging and no bridging in patients with nonvalvular/valvular AF or atrial flutter who required warfarin interruption for elective surgery. The median age was 72.7 years, and 73% of patients were male. A total of 336 patients had a history of stroke or transient ischemic attack.
After stopping warfarin 5 days before the procedure, study participants received dalteparin 100 IU/kg (934 patients) or matching placebo (950 patients) for 3 days before and 5-9 days after the procedure. Dalteparin/placebo was resumed 12-24 hours after minor surgery and 48-72 hours after major surgery.
Warfarin was resumed 24 hours or less after the procedure. Follow-up lasted 30 ± 7 days after the procedure. Primary outcomes were arterial thromboembolism and major bleeding. Secondary outcomes were minor bleeding, death, myocardial infarction, and venous thromboembolism.
Protocol adherence occurred in 81% of patients before the procedure, and in 94.5% of patients post procedure.
The incidence of arterial thromboembolism was 0.4% in the no-bridging group, compared with 0.3% in the bridging group (95% confidence interval, –0.6 to 0.8; P = .01 for noninferiority). The incidence of major bleeding was 1.3% in the no-bridging group and 3.2% in the bridging group (relative risk, 0.41; 95% CI, 0.20-0.78; P = .005 for superiority).
“Current practice guidelines provide weak and inconsistent recommendations concerning the need for bridging anticoagulation,” Dr. Ortel said. “This study provides the highest level of evidence to support a strong recommendation concerning the role of bridging in this patient population.”
It is estimated that approximately one in six warfarin-treated patients with AF will need anticoagulation transiently held for an elective operation or invasive procedure each year, making this a common clinical scenario for providers, Dr. Ortel said. Knowing the findings from the BRIDGE trial will help guide clinicians in making decisions when this situation arises in their patients, he concluded.
“With the introduction of the direct oral anticoagulants, we will now need to develop periprocedural approaches to manage patients on a variety of different agents,” he said. “Warfarin continues to be extensively used in many of these patients, however, and the BRIDGE trial will contribute to improved management for these individuals.”
In response to an audience member’s question about which patients should receive bridging anticoagulation, Dr. Ortel said that “right now, our data would suggest that for AF patients, we don’t need to bridge.”
“I can’t say that, necessarily, for prosthetic heart valves or for venous thromboembolism. I think some of the recommendations that you’ve seen in the guidelines where people try to stratify this by how recently they had thromboembolism or by what type of heart valve they have – those might be the higher-risk patients to consider. But that’s all based on existing guidelines and no prospective data, so I feel comfortable telling you who you don’t need to bridge in, but I’m not going to tell you who you should,” he added.
The BRIDGE Trial was sponsored by the National Heart, Lung, and Blood Institute. Dr. Ortel disclosed grant/research support from Eisai Co. Ltd and Pfizer Inc.
TORONTO – Forgoing bridging anticoagulation in patients with atrial fibrillation (AF) is noninferior to perioperative bridging with low-molecular-weight heparin for the prevention of arterial thromboembolism and decreases the risk of major bleeding.
Those results emerged from trial data presented at the International Society on Thrombosis and Haemostasis congress and published simultaneously in the New England Journal of Medicine. Study investigator Dr. Thomas Ortel, chief of the division of hematology at Duke University Medical Center, Durham, N.C., discussed results of the BRIDGE (Effectiveness of Bridging Anticoagulation for Surgery) trial, which evaluated the safety and efficacy of bridging anticoagulant therapy.
Bridging anticoagulation is frequently used in patients taking chronic oral anticoagulant therapy who need their anticoagulation transiently held for an operation or invasive procedure. The need for bridging anticoagulation never has been shown definitively, however, Dr. Ortel said in an interview.
“This is the first prospective, randomized, placebo-controlled, double-blind clinical trial to investigate the role of bridging anticoagulant therapy in patients with AF on chronic anticoagulation with warfarin who need the anticoagulant therapy held for an elective operation or invasive procedure,” he said.
Dr. Ortel and his coauthors evaluated 1,884 patients in the trial, which compared bridging and no bridging in patients with nonvalvular/valvular AF or atrial flutter who required warfarin interruption for elective surgery. The median age was 72.7 years, and 73% of patients were male. A total of 336 patients had a history of stroke or transient ischemic attack.
After stopping warfarin 5 days before the procedure, study participants received dalteparin 100 IU/kg (934 patients) or matching placebo (950 patients) for 3 days before and 5-9 days after the procedure. Dalteparin/placebo was resumed 12-24 hours after minor surgery and 48-72 hours after major surgery.
Warfarin was resumed 24 hours or less after the procedure. Follow-up lasted 30 ± 7 days after the procedure. Primary outcomes were arterial thromboembolism and major bleeding. Secondary outcomes were minor bleeding, death, myocardial infarction, and venous thromboembolism.
Protocol adherence occurred in 81% of patients before the procedure, and in 94.5% of patients post procedure.
The incidence of arterial thromboembolism was 0.4% in the no-bridging group, compared with 0.3% in the bridging group (95% confidence interval, –0.6 to 0.8; P = .01 for noninferiority). The incidence of major bleeding was 1.3% in the no-bridging group and 3.2% in the bridging group (relative risk, 0.41; 95% CI, 0.20-0.78; P = .005 for superiority).
“Current practice guidelines provide weak and inconsistent recommendations concerning the need for bridging anticoagulation,” Dr. Ortel said. “This study provides the highest level of evidence to support a strong recommendation concerning the role of bridging in this patient population.”
It is estimated that approximately one in six warfarin-treated patients with AF will need anticoagulation transiently held for an elective operation or invasive procedure each year, making this a common clinical scenario for providers, Dr. Ortel said. Knowing the findings from the BRIDGE trial will help guide clinicians in making decisions when this situation arises in their patients, he concluded.
“With the introduction of the direct oral anticoagulants, we will now need to develop periprocedural approaches to manage patients on a variety of different agents,” he said. “Warfarin continues to be extensively used in many of these patients, however, and the BRIDGE trial will contribute to improved management for these individuals.”
In response to an audience member’s question about which patients should receive bridging anticoagulation, Dr. Ortel said that “right now, our data would suggest that for AF patients, we don’t need to bridge.”
“I can’t say that, necessarily, for prosthetic heart valves or for venous thromboembolism. I think some of the recommendations that you’ve seen in the guidelines where people try to stratify this by how recently they had thromboembolism or by what type of heart valve they have – those might be the higher-risk patients to consider. But that’s all based on existing guidelines and no prospective data, so I feel comfortable telling you who you don’t need to bridge in, but I’m not going to tell you who you should,” he added.
The BRIDGE Trial was sponsored by the National Heart, Lung, and Blood Institute. Dr. Ortel disclosed grant/research support from Eisai Co. Ltd and Pfizer Inc.
TORONTO – Forgoing bridging anticoagulation in patients with atrial fibrillation (AF) is noninferior to perioperative bridging with low-molecular-weight heparin for the prevention of arterial thromboembolism and decreases the risk of major bleeding.
Those results emerged from trial data presented at the International Society on Thrombosis and Haemostasis congress and published simultaneously in the New England Journal of Medicine. Study investigator Dr. Thomas Ortel, chief of the division of hematology at Duke University Medical Center, Durham, N.C., discussed results of the BRIDGE (Effectiveness of Bridging Anticoagulation for Surgery) trial, which evaluated the safety and efficacy of bridging anticoagulant therapy.
Bridging anticoagulation is frequently used in patients taking chronic oral anticoagulant therapy who need their anticoagulation transiently held for an operation or invasive procedure. The need for bridging anticoagulation never has been shown definitively, however, Dr. Ortel said in an interview.
“This is the first prospective, randomized, placebo-controlled, double-blind clinical trial to investigate the role of bridging anticoagulant therapy in patients with AF on chronic anticoagulation with warfarin who need the anticoagulant therapy held for an elective operation or invasive procedure,” he said.
Dr. Ortel and his coauthors evaluated 1,884 patients in the trial, which compared bridging and no bridging in patients with nonvalvular/valvular AF or atrial flutter who required warfarin interruption for elective surgery. The median age was 72.7 years, and 73% of patients were male. A total of 336 patients had a history of stroke or transient ischemic attack.
After stopping warfarin 5 days before the procedure, study participants received dalteparin 100 IU/kg (934 patients) or matching placebo (950 patients) for 3 days before and 5-9 days after the procedure. Dalteparin/placebo was resumed 12-24 hours after minor surgery and 48-72 hours after major surgery.
Warfarin was resumed 24 hours or less after the procedure. Follow-up lasted 30 ± 7 days after the procedure. Primary outcomes were arterial thromboembolism and major bleeding. Secondary outcomes were minor bleeding, death, myocardial infarction, and venous thromboembolism.
Protocol adherence occurred in 81% of patients before the procedure, and in 94.5% of patients post procedure.
The incidence of arterial thromboembolism was 0.4% in the no-bridging group, compared with 0.3% in the bridging group (95% confidence interval, –0.6 to 0.8; P = .01 for noninferiority). The incidence of major bleeding was 1.3% in the no-bridging group and 3.2% in the bridging group (relative risk, 0.41; 95% CI, 0.20-0.78; P = .005 for superiority).
“Current practice guidelines provide weak and inconsistent recommendations concerning the need for bridging anticoagulation,” Dr. Ortel said. “This study provides the highest level of evidence to support a strong recommendation concerning the role of bridging in this patient population.”
It is estimated that approximately one in six warfarin-treated patients with AF will need anticoagulation transiently held for an elective operation or invasive procedure each year, making this a common clinical scenario for providers, Dr. Ortel said. Knowing the findings from the BRIDGE trial will help guide clinicians in making decisions when this situation arises in their patients, he concluded.
“With the introduction of the direct oral anticoagulants, we will now need to develop periprocedural approaches to manage patients on a variety of different agents,” he said. “Warfarin continues to be extensively used in many of these patients, however, and the BRIDGE trial will contribute to improved management for these individuals.”
In response to an audience member’s question about which patients should receive bridging anticoagulation, Dr. Ortel said that “right now, our data would suggest that for AF patients, we don’t need to bridge.”
“I can’t say that, necessarily, for prosthetic heart valves or for venous thromboembolism. I think some of the recommendations that you’ve seen in the guidelines where people try to stratify this by how recently they had thromboembolism or by what type of heart valve they have – those might be the higher-risk patients to consider. But that’s all based on existing guidelines and no prospective data, so I feel comfortable telling you who you don’t need to bridge in, but I’m not going to tell you who you should,” he added.
The BRIDGE Trial was sponsored by the National Heart, Lung, and Blood Institute. Dr. Ortel disclosed grant/research support from Eisai Co. Ltd and Pfizer Inc.
FROM 2015 ISTH CONGRESS
Key clinical point: Forgoing bridging anticoagulation in patients with atrial fibrillation is noninferior to perioperative bridging for preventing arterial thromboembolism and decreasing the risk of major bleeding.
Major finding: The incidence of arterial thromboembolism was 0.4% vs. 0.3% in the no-bridging and bridging groups, respectively. The incidence of major bleeding was 1.3% in the no-bridging group and 3.2% in the bridging group.
Data source: A prospective, randomized, placebo-controlled, double-blind trial of 1,884 patients with nonvalvular/valvular AF or atrial flutter who required warfarin interruption for elective surgery.
Disclosures: The BRIDGE Trial was sponsored by the National Heart, Lung, and Blood Institute. Dr. Ortel disclosed grant/research support from Eisai Co. Ltd and Pfizer Inc.

21st Century Cures bill passes House
The House has overwhemingly passed the 21st Century Cures Act, H.R. 6, a broad piece of legislation aimed at streamlining the approval process for medical drugs and devices.
The bill, passed by a 344-77 vote on July 10, also aims to spur innovation in biomedical research and to boost funding to the National Institutes of Health.
Changes made prior to the bill’s introduction to the House floor raised the ire of some legislators and included a reduction in NIH funding and the inclusion of Hyde Amendment language that prohibits the use of federal funds for abortions except in the case of rape, incest, or to save the life of the mother. The bill as it stands is not expected to be picked up in the Senate, which is expected to craft its own legislation.

“I am concerned that the very goal of this legislation set out to achieve, to encourage biomedical innovation and the development of new treatment and cures is undermined somewhat by the reduction in funding for NIH from $10 billion to $8.75 billion,” House Energy and Commerce Committee Ranking Member Frank Pallone, D-N.J., said during the floor debate on July 9.
Despite the concerns over the changes to the bill, support for the bill was overwhelmingly voiced throughout the debate.
“It is time now that we as a nation got serious about curing the major diseases – not treating the diseases, but curing the major diseases – that are affecting this country and affecting us personally,” said House Republican Doctors’ Caucus Chairman Phil Roe, R-Tenn. “I am more passionate about this bill and excited about passing the 21st Century Cures bill than anything I have voted on since I have been in the Congress.”
The House has overwhemingly passed the 21st Century Cures Act, H.R. 6, a broad piece of legislation aimed at streamlining the approval process for medical drugs and devices.
The bill, passed by a 344-77 vote on July 10, also aims to spur innovation in biomedical research and to boost funding to the National Institutes of Health.
Changes made prior to the bill’s introduction to the House floor raised the ire of some legislators and included a reduction in NIH funding and the inclusion of Hyde Amendment language that prohibits the use of federal funds for abortions except in the case of rape, incest, or to save the life of the mother. The bill as it stands is not expected to be picked up in the Senate, which is expected to craft its own legislation.
“I am concerned that the very goal of this legislation set out to achieve, to encourage biomedical innovation and the development of new treatment and cures is undermined somewhat by the reduction in funding for NIH from $10 billion to $8.75 billion,” House Energy and Commerce Committee Ranking Member Frank Pallone, D-N.J., said during the floor debate on July 9.
Despite the concerns over the changes to the bill, support for the bill was overwhelmingly voiced throughout the debate.
“It is time now that we as a nation got serious about curing the major diseases – not treating the diseases, but curing the major diseases – that are affecting this country and affecting us personally,” said House Republican Doctors’ Caucus Chairman Phil Roe, R-Tenn. “I am more passionate about this bill and excited about passing the 21st Century Cures bill than anything I have voted on since I have been in the Congress.”
The House has overwhemingly passed the 21st Century Cures Act, H.R. 6, a broad piece of legislation aimed at streamlining the approval process for medical drugs and devices.
The bill, passed by a 344-77 vote on July 10, also aims to spur innovation in biomedical research and to boost funding to the National Institutes of Health.
Changes made prior to the bill’s introduction to the House floor raised the ire of some legislators and included a reduction in NIH funding and the inclusion of Hyde Amendment language that prohibits the use of federal funds for abortions except in the case of rape, incest, or to save the life of the mother. The bill as it stands is not expected to be picked up in the Senate, which is expected to craft its own legislation.
“I am concerned that the very goal of this legislation set out to achieve, to encourage biomedical innovation and the development of new treatment and cures is undermined somewhat by the reduction in funding for NIH from $10 billion to $8.75 billion,” House Energy and Commerce Committee Ranking Member Frank Pallone, D-N.J., said during the floor debate on July 9.
Despite the concerns over the changes to the bill, support for the bill was overwhelmingly voiced throughout the debate.
“It is time now that we as a nation got serious about curing the major diseases – not treating the diseases, but curing the major diseases – that are affecting this country and affecting us personally,” said House Republican Doctors’ Caucus Chairman Phil Roe, R-Tenn. “I am more passionate about this bill and excited about passing the 21st Century Cures bill than anything I have voted on since I have been in the Congress.”

CMS proposes comprehensive care initiative for hip and knee replacements
The Centers for Medicare & Medicaid Services has proposed a Comprehensive Care for Joint Replacement payment model to improve patient outcomes from hip and knee replacement surgery, the agency announced July 9.
Under the proposed rule, the hospital in which the surgery takes place would be responsible for cost and quality of care from the time of surgery through 90 days after the procedure, or an “episode” of care. Then, based on cost performance and the quality of care delivered, the facility would either receive a financial reward or be required to repay Medicare for a portion of the costs, CMS said in a statement.
“This payment would give hospitals an incentive to work with physicians, home health agencies, and nursing facilities to make sure beneficiaries receive the coordinated care they need with the goal of reducing avoidable hospitalizations and complications,” the agency said.
The new model is an effort to improve the lack of coordinated care that may lead to postsurgery complications and high readmission rates in Medicare beneficiaries who receive these procedures.
“Joint replacements are the most commonly performed Medicare inpatient surgery and their utilization is predicted to continue to grow,” CMS said. “They can require long recoveries that may include extensive rehabilitation or other post-acute care, which provides many opportunities to reward providers that improve patient outcomes.”
Read the proposed rule here: https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-17190.pdf
The Centers for Medicare & Medicaid Services has proposed a Comprehensive Care for Joint Replacement payment model to improve patient outcomes from hip and knee replacement surgery, the agency announced July 9.
Under the proposed rule, the hospital in which the surgery takes place would be responsible for cost and quality of care from the time of surgery through 90 days after the procedure, or an “episode” of care. Then, based on cost performance and the quality of care delivered, the facility would either receive a financial reward or be required to repay Medicare for a portion of the costs, CMS said in a statement.
“This payment would give hospitals an incentive to work with physicians, home health agencies, and nursing facilities to make sure beneficiaries receive the coordinated care they need with the goal of reducing avoidable hospitalizations and complications,” the agency said.
The new model is an effort to improve the lack of coordinated care that may lead to postsurgery complications and high readmission rates in Medicare beneficiaries who receive these procedures.
“Joint replacements are the most commonly performed Medicare inpatient surgery and their utilization is predicted to continue to grow,” CMS said. “They can require long recoveries that may include extensive rehabilitation or other post-acute care, which provides many opportunities to reward providers that improve patient outcomes.”
Read the proposed rule here: https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-17190.pdf
The Centers for Medicare & Medicaid Services has proposed a Comprehensive Care for Joint Replacement payment model to improve patient outcomes from hip and knee replacement surgery, the agency announced July 9.
Under the proposed rule, the hospital in which the surgery takes place would be responsible for cost and quality of care from the time of surgery through 90 days after the procedure, or an “episode” of care. Then, based on cost performance and the quality of care delivered, the facility would either receive a financial reward or be required to repay Medicare for a portion of the costs, CMS said in a statement.
“This payment would give hospitals an incentive to work with physicians, home health agencies, and nursing facilities to make sure beneficiaries receive the coordinated care they need with the goal of reducing avoidable hospitalizations and complications,” the agency said.
The new model is an effort to improve the lack of coordinated care that may lead to postsurgery complications and high readmission rates in Medicare beneficiaries who receive these procedures.
“Joint replacements are the most commonly performed Medicare inpatient surgery and their utilization is predicted to continue to grow,” CMS said. “They can require long recoveries that may include extensive rehabilitation or other post-acute care, which provides many opportunities to reward providers that improve patient outcomes.”
Read the proposed rule here: https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-17190.pdf
Fee schedule update includes advance care planning, PQRS changes
Physicians are praising a new proposal by the Centers for Medicare & Medicaid Services to pay for end-of-life counseling as part of a sweeping draft of updates to its 2016 physician payment schedule.
The proposed fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes modifications to reimbursement policies, changes to misvalued codes, and updates to quality performance metrics for physicians who participate in the Physician Quality Reporting System (PQRS).

As part of the proposal, released on July 8, two new advance care planning codes would be created to pay physicians for time discussing patient options for advance directives. The first code would cover an initial 30 minutes of the doctors’ time, and the second would cover additional 30-minute blocks as necessary.
Dr. Andrew W. Gurman, president-elect of the American Medical Association, said the proposed rule affirms the need to support conversations between doctors and patients about end-of-life wishes before critical medical events occur. The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015.
“This is a patient-centered policy intended to support a careful planning process that is assisted by a physician or other qualified health care professional,” Dr. Gurman said in a statement. “This issue has been mischaracterized in the past and it is time to facilitate patient choices about advance care planning decisions.”
The American College of Physicians (ACP) applauded inclusion of the advance care planning codes, calling it an important step to improve care for Medicare patients with serious illnesses.
“The nation’s physicians believe that conversations among physicians, patients, and loved ones is the standard of care,” ACP President Dr. Wayne J. Riley said in a statement. “The College is pleased that CMS has recognized what the medical community is doing to address the needs and requests made by patients and their loved ones.”
CMS’ proposal also includes updates to the PQRS, the federal program that provides incentive payments to eligible professionals and group practices that report data on quality measures for covered services and/or participate in a qualified clinical data registry (QCDR). The proposal would establish criteria for satisfactory reporting similar to that of previous years, including the general reporting of nine measures covering three National Quality Strategy domains.
Eligible professionals and practices who do not report on PQRS standards in 2016 will see their 2018 Medicare pay cut by 2%. The proposed fee schedule also would eliminate measures that are topped out, duplicative, or are being replaced with more robust measures. If the proposal is finalized, 300 total measures in the PQRS program are slated for 2016.
The proposed fee schedule also would modify the the Medicare Shared Savings Program (MSSP) by:
• Allowing participants to add or delete a measure if it no longer aligns with updated clinical practice or causes patient harm.
• Clarifying how PQRS-eligible professionals participating within an ACO can meet PQRS requirements when their ACO satisfactorily reports quality measures.
• Amending the definition of primary care services to include claims submitted by certain teaching hospitals and excluding those submitted by skilled nursing facilities.
The proposed fee schedule also addresses telemedicine services. CMS says it will pay for telemedicine if the treatment is on the list of approved Medicare telehealth services, and if:
• the service is furnished via an interactive telecommunications system.
• The service is furnished by a physician or authorized practitioner.
• The service is furnished to an eligible telehealth patient.
• The patient receiving the service must be located in a telehealth originating site.
If these conditions are met, Medicare will pay a facility fee to the originating site and make separates payment to the distant site health provider furnishing the service.
CMS is also proposing payment changes for certain specialty services based on codes determined to be misvalued. Specifically, physicians who practice radiation therapy, radiation oncology, and gastroenterology would experience significant decreases to payments for services that they frequently furnish as a result of widespread revisions to the Relative Value Unit (RVU) structure used to establish such codes. Other specialties, such as pathology, would experience significant increases to payments for similar reasons, CMS states. The modifications are a result of an initiative to review misvalued codes and establish new and revised codes.
Meanwhile, CMS is seeking feedback on several components of MACRA, including the definition of clinical practice improvement activities and input on how to define a physician-focused payment model. The agency is also asking for feedback on whether to expand the Comprehensive Primary Care Initiative, a 4-year multipayer pilot that aims to strengthen primary care by offering population-based care management fees and shared savings opportunities to participating health providers.
The proposed rule will be published in the Federal Register on July 15; comments will be accepted through Sept. 8.
On Twitter @legal_med
Physicians are praising a new proposal by the Centers for Medicare & Medicaid Services to pay for end-of-life counseling as part of a sweeping draft of updates to its 2016 physician payment schedule.
The proposed fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes modifications to reimbursement policies, changes to misvalued codes, and updates to quality performance metrics for physicians who participate in the Physician Quality Reporting System (PQRS).
As part of the proposal, released on July 8, two new advance care planning codes would be created to pay physicians for time discussing patient options for advance directives. The first code would cover an initial 30 minutes of the doctors’ time, and the second would cover additional 30-minute blocks as necessary.
Dr. Andrew W. Gurman, president-elect of the American Medical Association, said the proposed rule affirms the need to support conversations between doctors and patients about end-of-life wishes before critical medical events occur. The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015.
“This is a patient-centered policy intended to support a careful planning process that is assisted by a physician or other qualified health care professional,” Dr. Gurman said in a statement. “This issue has been mischaracterized in the past and it is time to facilitate patient choices about advance care planning decisions.”
The American College of Physicians (ACP) applauded inclusion of the advance care planning codes, calling it an important step to improve care for Medicare patients with serious illnesses.
“The nation’s physicians believe that conversations among physicians, patients, and loved ones is the standard of care,” ACP President Dr. Wayne J. Riley said in a statement. “The College is pleased that CMS has recognized what the medical community is doing to address the needs and requests made by patients and their loved ones.”
CMS’ proposal also includes updates to the PQRS, the federal program that provides incentive payments to eligible professionals and group practices that report data on quality measures for covered services and/or participate in a qualified clinical data registry (QCDR). The proposal would establish criteria for satisfactory reporting similar to that of previous years, including the general reporting of nine measures covering three National Quality Strategy domains.
Eligible professionals and practices who do not report on PQRS standards in 2016 will see their 2018 Medicare pay cut by 2%. The proposed fee schedule also would eliminate measures that are topped out, duplicative, or are being replaced with more robust measures. If the proposal is finalized, 300 total measures in the PQRS program are slated for 2016.
The proposed fee schedule also would modify the the Medicare Shared Savings Program (MSSP) by:
• Allowing participants to add or delete a measure if it no longer aligns with updated clinical practice or causes patient harm.
• Clarifying how PQRS-eligible professionals participating within an ACO can meet PQRS requirements when their ACO satisfactorily reports quality measures.
• Amending the definition of primary care services to include claims submitted by certain teaching hospitals and excluding those submitted by skilled nursing facilities.
The proposed fee schedule also addresses telemedicine services. CMS says it will pay for telemedicine if the treatment is on the list of approved Medicare telehealth services, and if:
• the service is furnished via an interactive telecommunications system.
• The service is furnished by a physician or authorized practitioner.
• The service is furnished to an eligible telehealth patient.
• The patient receiving the service must be located in a telehealth originating site.
If these conditions are met, Medicare will pay a facility fee to the originating site and make separates payment to the distant site health provider furnishing the service.
CMS is also proposing payment changes for certain specialty services based on codes determined to be misvalued. Specifically, physicians who practice radiation therapy, radiation oncology, and gastroenterology would experience significant decreases to payments for services that they frequently furnish as a result of widespread revisions to the Relative Value Unit (RVU) structure used to establish such codes. Other specialties, such as pathology, would experience significant increases to payments for similar reasons, CMS states. The modifications are a result of an initiative to review misvalued codes and establish new and revised codes.
Meanwhile, CMS is seeking feedback on several components of MACRA, including the definition of clinical practice improvement activities and input on how to define a physician-focused payment model. The agency is also asking for feedback on whether to expand the Comprehensive Primary Care Initiative, a 4-year multipayer pilot that aims to strengthen primary care by offering population-based care management fees and shared savings opportunities to participating health providers.
The proposed rule will be published in the Federal Register on July 15; comments will be accepted through Sept. 8.
On Twitter @legal_med
Physicians are praising a new proposal by the Centers for Medicare & Medicaid Services to pay for end-of-life counseling as part of a sweeping draft of updates to its 2016 physician payment schedule.
The proposed fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes modifications to reimbursement policies, changes to misvalued codes, and updates to quality performance metrics for physicians who participate in the Physician Quality Reporting System (PQRS).
As part of the proposal, released on July 8, two new advance care planning codes would be created to pay physicians for time discussing patient options for advance directives. The first code would cover an initial 30 minutes of the doctors’ time, and the second would cover additional 30-minute blocks as necessary.
Dr. Andrew W. Gurman, president-elect of the American Medical Association, said the proposed rule affirms the need to support conversations between doctors and patients about end-of-life wishes before critical medical events occur. The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015.
“This is a patient-centered policy intended to support a careful planning process that is assisted by a physician or other qualified health care professional,” Dr. Gurman said in a statement. “This issue has been mischaracterized in the past and it is time to facilitate patient choices about advance care planning decisions.”
The American College of Physicians (ACP) applauded inclusion of the advance care planning codes, calling it an important step to improve care for Medicare patients with serious illnesses.
“The nation’s physicians believe that conversations among physicians, patients, and loved ones is the standard of care,” ACP President Dr. Wayne J. Riley said in a statement. “The College is pleased that CMS has recognized what the medical community is doing to address the needs and requests made by patients and their loved ones.”
CMS’ proposal also includes updates to the PQRS, the federal program that provides incentive payments to eligible professionals and group practices that report data on quality measures for covered services and/or participate in a qualified clinical data registry (QCDR). The proposal would establish criteria for satisfactory reporting similar to that of previous years, including the general reporting of nine measures covering three National Quality Strategy domains.
Eligible professionals and practices who do not report on PQRS standards in 2016 will see their 2018 Medicare pay cut by 2%. The proposed fee schedule also would eliminate measures that are topped out, duplicative, or are being replaced with more robust measures. If the proposal is finalized, 300 total measures in the PQRS program are slated for 2016.
The proposed fee schedule also would modify the the Medicare Shared Savings Program (MSSP) by:
• Allowing participants to add or delete a measure if it no longer aligns with updated clinical practice or causes patient harm.
• Clarifying how PQRS-eligible professionals participating within an ACO can meet PQRS requirements when their ACO satisfactorily reports quality measures.
• Amending the definition of primary care services to include claims submitted by certain teaching hospitals and excluding those submitted by skilled nursing facilities.
The proposed fee schedule also addresses telemedicine services. CMS says it will pay for telemedicine if the treatment is on the list of approved Medicare telehealth services, and if:
• the service is furnished via an interactive telecommunications system.
• The service is furnished by a physician or authorized practitioner.
• The service is furnished to an eligible telehealth patient.
• The patient receiving the service must be located in a telehealth originating site.
If these conditions are met, Medicare will pay a facility fee to the originating site and make separates payment to the distant site health provider furnishing the service.
CMS is also proposing payment changes for certain specialty services based on codes determined to be misvalued. Specifically, physicians who practice radiation therapy, radiation oncology, and gastroenterology would experience significant decreases to payments for services that they frequently furnish as a result of widespread revisions to the Relative Value Unit (RVU) structure used to establish such codes. Other specialties, such as pathology, would experience significant increases to payments for similar reasons, CMS states. The modifications are a result of an initiative to review misvalued codes and establish new and revised codes.
Meanwhile, CMS is seeking feedback on several components of MACRA, including the definition of clinical practice improvement activities and input on how to define a physician-focused payment model. The agency is also asking for feedback on whether to expand the Comprehensive Primary Care Initiative, a 4-year multipayer pilot that aims to strengthen primary care by offering population-based care management fees and shared savings opportunities to participating health providers.
The proposed rule will be published in the Federal Register on July 15; comments will be accepted through Sept. 8.
On Twitter @legal_med

Notice something different about ACS Surgery News?
ACS Surgery News, the official newspaper of the American College of Surgeons, has a new look. The July issue will have a fresh design, new colors, and an increased focus on visual accessibility for readers. The updated format is easier to read and has more graphic elements for quicker access to data. Future issues with the new design will feature opinion columns, updates on critical practice economics issues, and news coverage of cutting-edge surgical technology.

ACS Surgery News readership has surged over the past 2 years. The growing popularity of ACS Surgery News is based on quality content: lively commentary by thought leaders of the surgical profession, timely coverage of surgery meetings, and in-depth features on those issues most important to surgeons.
In addition, the publication website has a fresh look: better layout; easier access to the digital, interactive version of the publication; and more graphic elements.
The next issue of ACS Surgery News mails on July 17. This publication has thrived on commentary, critique, and contributions from readers. Take a look at the new design and let the editorial team know what you think.
ACS Surgery News, the official newspaper of the American College of Surgeons, has a new look. The July issue will have a fresh design, new colors, and an increased focus on visual accessibility for readers. The updated format is easier to read and has more graphic elements for quicker access to data. Future issues with the new design will feature opinion columns, updates on critical practice economics issues, and news coverage of cutting-edge surgical technology.
ACS Surgery News readership has surged over the past 2 years. The growing popularity of ACS Surgery News is based on quality content: lively commentary by thought leaders of the surgical profession, timely coverage of surgery meetings, and in-depth features on those issues most important to surgeons.
In addition, the publication website has a fresh look: better layout; easier access to the digital, interactive version of the publication; and more graphic elements.
The next issue of ACS Surgery News mails on July 17. This publication has thrived on commentary, critique, and contributions from readers. Take a look at the new design and let the editorial team know what you think.
ACS Surgery News, the official newspaper of the American College of Surgeons, has a new look. The July issue will have a fresh design, new colors, and an increased focus on visual accessibility for readers. The updated format is easier to read and has more graphic elements for quicker access to data. Future issues with the new design will feature opinion columns, updates on critical practice economics issues, and news coverage of cutting-edge surgical technology.
ACS Surgery News readership has surged over the past 2 years. The growing popularity of ACS Surgery News is based on quality content: lively commentary by thought leaders of the surgical profession, timely coverage of surgery meetings, and in-depth features on those issues most important to surgeons.
In addition, the publication website has a fresh look: better layout; easier access to the digital, interactive version of the publication; and more graphic elements.
The next issue of ACS Surgery News mails on July 17. This publication has thrived on commentary, critique, and contributions from readers. Take a look at the new design and let the editorial team know what you think.

Where are the really big malpractice awards?
Everything may be bigger in Texas, but New York is the biggest in at least one area: large medical malpractice payments. New York had more than three times as many $1 million–plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank.
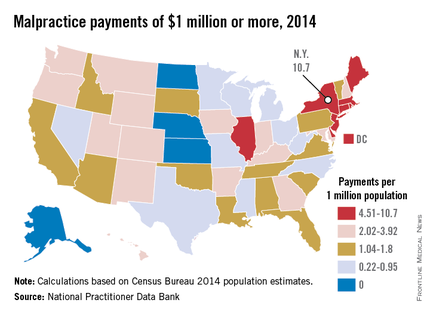
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top five were Massachusetts with 49, followed by California with 43 and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were four states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million–plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22 – just 6 awards from a population of 27 million.
Everything may be bigger in Texas, but New York is the biggest in at least one area: large medical malpractice payments. New York had more than three times as many $1 million–plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank.
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top five were Massachusetts with 49, followed by California with 43 and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were four states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million–plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22 – just 6 awards from a population of 27 million.
Everything may be bigger in Texas, but New York is the biggest in at least one area: large medical malpractice payments. New York had more than three times as many $1 million–plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank.
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top five were Massachusetts with 49, followed by California with 43 and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were four states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million–plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22 – just 6 awards from a population of 27 million.
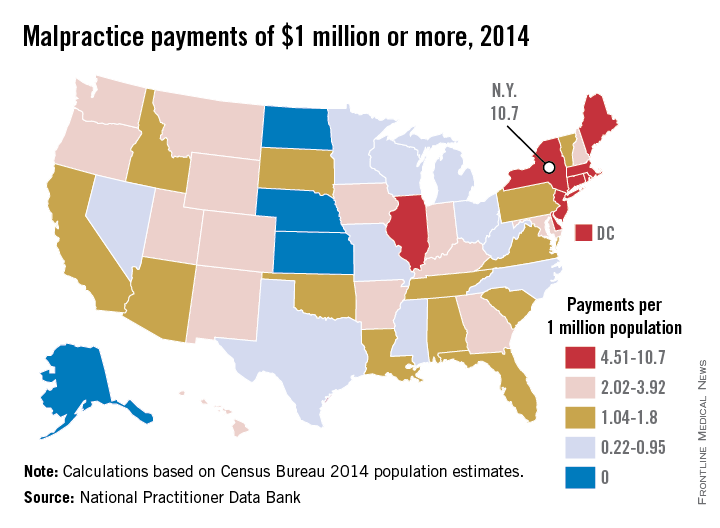
High VTE recurrence risk persists for at least 3 years
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
TORONTO – The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Over a mean of 23 months (median, 30 months), there were 329 VTE recurrences in the study subjects. Cumulative incidence rates were 5.1% at 3 months, and 14.5% at 3 years. The corresponding rates were 8.7% and 24.8% among those with active cancer, 5.2% and 13.0% among those with provoked VTE, and 3.8% and 13.1% among those with unprovoked VTE, Dr. Wei Huang reported at the International Society on Thrombosis and Haemostasis congress.
Independent predictors of recurrence within 3 years after the index event were active cancer with chemotherapy (hazard ratio, 2.59), active cancer without chemotherapy (HR, 1.59), hypercoagulable state (HR, 2.53) superficial thrombophlebitis (HR, 1.62), varicose vein stripping (HR, 1.75), and inferior vena cava (IVC) filter placement (HR, 2.04), said Dr. Huang of the University of Massachusetts, Worcester.
Individuals included in the study were all residents of the Worcester Metropolitan Statistical Area (WMSA) who had a validated diagnosis of acute first-time deep vein thrombosis and/or pulmonary embolism in a hospital or ambulatory care center that provided short-term care for WMSA residents between 1999 and 2009. Medical records and national and local death registry data were reviewed to examine outcomes up to 3 years after the index event.
Subjects were adults with a mean age of 64 years; 44% were men, and 94% where white. Pulmonary embolism with or without deep vein thrombosis occurred in 42%, and 17% of cases were associated with cancer, 43% involved provoked VTE, and 40% involved unprovoked VTE.
Provoked VTE was defined as VTE occurring within 3 months of a prior surgery, pregnancy, trauma, fracture, or hospitalization in patients without presence of active cancer.
Though limited by the lack of information about variations in physician practices across regions, and by the high proportion of white resident in the WMSA, which both raise questions about whether the findings are generalizable to the U.S. population, the identification of these predictors could allow for improved estimation of risk for individual patients, and may aid in the design of new interventional studies, Dr. Huang concluded.
This study was supported by the National Institutes of Health.
AT THE 2015 ISTH CONGRESS
Key clinical point: The risk of recurrence following an initial episode of venous thromboembolism is highest in the first 3 months, but remains high for up to 3 years, according to findings from a population-based study involving 2,989 adults.
Major finding: Active cancer with chemotherapy was the strongest predictor of VTE recurrence (hazard ratio, 2.59).
Data source: Population-based surveillance of 2,989 adults patients.
Disclosures: The National Institutes of Health supported the study.