User login
Official Newspaper of the American College of Surgeons
Members in the news
Juan A. Asensio, MD, FACS, FCCM, FRCS, was honored at a formal investiture last November at Saint Patrick’s Cathedral in New York, NY, as a Knight of Malta. Dr. Asensio directs the comprehensive Level I trauma center at CHI Health Creighton University Medical Center, Omaha, NE, where he is a professor of surgery and chief of the division of trauma surgery and surgical critical care. In addition, he is director of the university’s trauma center and trauma program.
The more than 900-year-old Order of Malta is the only remaining active military order from the Crusades. Members assist patients in need, including the young, elderly, handicapped, homeless, and those with terminal illnesses. Through its worldwide relief corps, Malteser International, the order assists refugees and victims of natural disasters, epidemics, and armed conflicts.
Morehouse School of Medicine, Atlanta, GA, in May unveiled a new medical library, named in honor of the late M. Delmar Edwards, MD, FACS, a former trustee of the college; the first African American to practice surgery in Columbus, GA; and a trailblazer for many young surgeons. Dr. Edwards died in Atlanta in 2009 at age 83, but he left a legacy as a surgeon, activist, educator, and philanthropist. Through the former Columbus-Fort Benning Medical Scholarships, one of the largest endowed scholarship funds at the school, now renamed the M. Delmar Edwards, MD, Endowed Scholarship, he helped many medical students complete their education. A native of Arkansas, Dr. Edwards was the third African Americans admitted to the University of Arkansas College of Medicine, Fayetteville.

Stanley J. Kurek, Jr., DO, FACS, professor of surgery, University of South Florida Morsani College of Medicine, and medical director, trauma, acute care surgery and surgical critical care, Lawnwood Regional Medical Center, Ft. Pierce, FL, was recently elected to a one-year term as the 28th president of the Eastern Association for the Surgery of Trauma (EAST). His EAST presidential message is available at www.east.org/news-and-events/news-details/5/message-from-the-east-president.
Barry M. Manuel, MD, FACS, a recipient of the American College of Surgeons (ACS) Distinguished Service Award (DSA) and Past-President of the Massachusetts Chapter of the College, received the Massachusetts Medical Society’s (MMS) 2015 Award for Distinguished Service. The prestigious honor is given annually to an MMS member who has made a lasting contribution to the practice of medicine over a lifetime and made significant contributions to the goals of the MMS.

The award was presented to Dr. Manuel at the MMS annual meeting May 1 in Boston. In 2010, the MMS honored Dr. Manuel with the Lifetime Achievement Award.
Dr. Manuel served as associate dean for continuing medical education, 1980−2014, and professor of surgery, 1982−2014, at the Boston University School of Medicine (BUSM). With his June 30 retirement, he now holds the titles of associate dean emeritus and professor of surgery emeritus. In addition, the Office of Continuing Medical Education at Boston University will be renamed the Barry M. Manuel Office of Continuing Medical Education. Dr. Manuel received the DSA from the ACS in 1993 and in 1997 was the recipient of BUSM’s Distinguished Alumni Award.
Robert W. Panton, MD, FACS, River Forest, IL, was elected vice-speaker of the Illinois State Medical Society (ISMS) during its recent annual meeting. A board-certified specialist in ophthalmologycertified specialist in ophthalmology, Dr. Panton practices at Rush Oak Park Hospital; West Suburban Hospital in Oak Park, IL; and Westlake Hospital and Loyola Gottlieb Memorial Hospital, Melrose Park, IL.

He served as Chicago Medical Society president in 2013–2014. Dr. Panton is also a fellow of the American Academy of Ophthalmology.
.
Juan A. Asensio, MD, FACS, FCCM, FRCS, was honored at a formal investiture last November at Saint Patrick’s Cathedral in New York, NY, as a Knight of Malta. Dr. Asensio directs the comprehensive Level I trauma center at CHI Health Creighton University Medical Center, Omaha, NE, where he is a professor of surgery and chief of the division of trauma surgery and surgical critical care. In addition, he is director of the university’s trauma center and trauma program.
The more than 900-year-old Order of Malta is the only remaining active military order from the Crusades. Members assist patients in need, including the young, elderly, handicapped, homeless, and those with terminal illnesses. Through its worldwide relief corps, Malteser International, the order assists refugees and victims of natural disasters, epidemics, and armed conflicts.
Morehouse School of Medicine, Atlanta, GA, in May unveiled a new medical library, named in honor of the late M. Delmar Edwards, MD, FACS, a former trustee of the college; the first African American to practice surgery in Columbus, GA; and a trailblazer for many young surgeons. Dr. Edwards died in Atlanta in 2009 at age 83, but he left a legacy as a surgeon, activist, educator, and philanthropist. Through the former Columbus-Fort Benning Medical Scholarships, one of the largest endowed scholarship funds at the school, now renamed the M. Delmar Edwards, MD, Endowed Scholarship, he helped many medical students complete their education. A native of Arkansas, Dr. Edwards was the third African Americans admitted to the University of Arkansas College of Medicine, Fayetteville.
Stanley J. Kurek, Jr., DO, FACS, professor of surgery, University of South Florida Morsani College of Medicine, and medical director, trauma, acute care surgery and surgical critical care, Lawnwood Regional Medical Center, Ft. Pierce, FL, was recently elected to a one-year term as the 28th president of the Eastern Association for the Surgery of Trauma (EAST). His EAST presidential message is available at www.east.org/news-and-events/news-details/5/message-from-the-east-president.
Barry M. Manuel, MD, FACS, a recipient of the American College of Surgeons (ACS) Distinguished Service Award (DSA) and Past-President of the Massachusetts Chapter of the College, received the Massachusetts Medical Society’s (MMS) 2015 Award for Distinguished Service. The prestigious honor is given annually to an MMS member who has made a lasting contribution to the practice of medicine over a lifetime and made significant contributions to the goals of the MMS.
The award was presented to Dr. Manuel at the MMS annual meeting May 1 in Boston. In 2010, the MMS honored Dr. Manuel with the Lifetime Achievement Award.
Dr. Manuel served as associate dean for continuing medical education, 1980−2014, and professor of surgery, 1982−2014, at the Boston University School of Medicine (BUSM). With his June 30 retirement, he now holds the titles of associate dean emeritus and professor of surgery emeritus. In addition, the Office of Continuing Medical Education at Boston University will be renamed the Barry M. Manuel Office of Continuing Medical Education. Dr. Manuel received the DSA from the ACS in 1993 and in 1997 was the recipient of BUSM’s Distinguished Alumni Award.
Robert W. Panton, MD, FACS, River Forest, IL, was elected vice-speaker of the Illinois State Medical Society (ISMS) during its recent annual meeting. A board-certified specialist in ophthalmologycertified specialist in ophthalmology, Dr. Panton practices at Rush Oak Park Hospital; West Suburban Hospital in Oak Park, IL; and Westlake Hospital and Loyola Gottlieb Memorial Hospital, Melrose Park, IL.
He served as Chicago Medical Society president in 2013–2014. Dr. Panton is also a fellow of the American Academy of Ophthalmology.
.
Juan A. Asensio, MD, FACS, FCCM, FRCS, was honored at a formal investiture last November at Saint Patrick’s Cathedral in New York, NY, as a Knight of Malta. Dr. Asensio directs the comprehensive Level I trauma center at CHI Health Creighton University Medical Center, Omaha, NE, where he is a professor of surgery and chief of the division of trauma surgery and surgical critical care. In addition, he is director of the university’s trauma center and trauma program.
The more than 900-year-old Order of Malta is the only remaining active military order from the Crusades. Members assist patients in need, including the young, elderly, handicapped, homeless, and those with terminal illnesses. Through its worldwide relief corps, Malteser International, the order assists refugees and victims of natural disasters, epidemics, and armed conflicts.
Morehouse School of Medicine, Atlanta, GA, in May unveiled a new medical library, named in honor of the late M. Delmar Edwards, MD, FACS, a former trustee of the college; the first African American to practice surgery in Columbus, GA; and a trailblazer for many young surgeons. Dr. Edwards died in Atlanta in 2009 at age 83, but he left a legacy as a surgeon, activist, educator, and philanthropist. Through the former Columbus-Fort Benning Medical Scholarships, one of the largest endowed scholarship funds at the school, now renamed the M. Delmar Edwards, MD, Endowed Scholarship, he helped many medical students complete their education. A native of Arkansas, Dr. Edwards was the third African Americans admitted to the University of Arkansas College of Medicine, Fayetteville.
Stanley J. Kurek, Jr., DO, FACS, professor of surgery, University of South Florida Morsani College of Medicine, and medical director, trauma, acute care surgery and surgical critical care, Lawnwood Regional Medical Center, Ft. Pierce, FL, was recently elected to a one-year term as the 28th president of the Eastern Association for the Surgery of Trauma (EAST). His EAST presidential message is available at www.east.org/news-and-events/news-details/5/message-from-the-east-president.
Barry M. Manuel, MD, FACS, a recipient of the American College of Surgeons (ACS) Distinguished Service Award (DSA) and Past-President of the Massachusetts Chapter of the College, received the Massachusetts Medical Society’s (MMS) 2015 Award for Distinguished Service. The prestigious honor is given annually to an MMS member who has made a lasting contribution to the practice of medicine over a lifetime and made significant contributions to the goals of the MMS.
The award was presented to Dr. Manuel at the MMS annual meeting May 1 in Boston. In 2010, the MMS honored Dr. Manuel with the Lifetime Achievement Award.
Dr. Manuel served as associate dean for continuing medical education, 1980−2014, and professor of surgery, 1982−2014, at the Boston University School of Medicine (BUSM). With his June 30 retirement, he now holds the titles of associate dean emeritus and professor of surgery emeritus. In addition, the Office of Continuing Medical Education at Boston University will be renamed the Barry M. Manuel Office of Continuing Medical Education. Dr. Manuel received the DSA from the ACS in 1993 and in 1997 was the recipient of BUSM’s Distinguished Alumni Award.
Robert W. Panton, MD, FACS, River Forest, IL, was elected vice-speaker of the Illinois State Medical Society (ISMS) during its recent annual meeting. A board-certified specialist in ophthalmologycertified specialist in ophthalmology, Dr. Panton practices at Rush Oak Park Hospital; West Suburban Hospital in Oak Park, IL; and Westlake Hospital and Loyola Gottlieb Memorial Hospital, Melrose Park, IL.
He served as Chicago Medical Society president in 2013–2014. Dr. Panton is also a fellow of the American Academy of Ophthalmology.
.
Final days to register for ACS NSQIP National Conference, July 25−28, in Chicago, IL
Space is still available for the 2015 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) Conference, July 25−28, at the Chicago Hilton, IL View the conference agenda at http://goo.gl/TkaKDi.
Attendees at the 10th ACS NSQIP National Conference will enjoy a range of informative workshops, interactive general and breakout sessions on quality improvement, and abundant networking opportunities.
For details regarding registration, contact Registration Services at 312-202-5244, or registration@facs.org. For questions about the conference, contact ACS NSQIP staff at 312-202-5261 or nsqipconference@facs.org
Space is still available for the 2015 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) Conference, July 25−28, at the Chicago Hilton, IL View the conference agenda at http://goo.gl/TkaKDi.
Attendees at the 10th ACS NSQIP National Conference will enjoy a range of informative workshops, interactive general and breakout sessions on quality improvement, and abundant networking opportunities.
For details regarding registration, contact Registration Services at 312-202-5244, or registration@facs.org. For questions about the conference, contact ACS NSQIP staff at 312-202-5261 or nsqipconference@facs.org
Space is still available for the 2015 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®) Conference, July 25−28, at the Chicago Hilton, IL View the conference agenda at http://goo.gl/TkaKDi.
Attendees at the 10th ACS NSQIP National Conference will enjoy a range of informative workshops, interactive general and breakout sessions on quality improvement, and abundant networking opportunities.
For details regarding registration, contact Registration Services at 312-202-5244, or registration@facs.org. For questions about the conference, contact ACS NSQIP staff at 312-202-5261 or nsqipconference@facs.org
View Preliminary Program & Register for AATS International Coronary Congress: State of the Art Surgical Coronary Revascularization
Don’t miss the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
Program, registration & additional information: www.aats.org/CoronaryCongress/
Don’t miss the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
Program, registration & additional information: www.aats.org/CoronaryCongress/
Don’t miss the International Coronary Congress focused on state-of-the-art coronary surgery.
August 21 – 23, 2015
Marriott Marquis, New York
New York City, NY
An international expert faculty will lead this highly practical interdisciplinary program. Topics will include the latest evidence, technologies, tips and tricks for all aspects of coronary revascularization — with a particular emphasis on safely and easily increasing use of arterial grafts.
This two and one-half day program is designed for surgeons, physicians, physician assistants and nurses from around the world. It will include a comprehensive simultaneous curriculum for physician assistants and surgical first assistants.
Surgeons are encouraged to attend with their entire operating team to maximize its unique benefits.
Program Directors
John Puskas
David Taggart
Robert Carlucci
Program Committee Members
Hirokuni Arai
Stephen Fremes
Joseph Sabik
James Tatoulis
Program, registration & additional information: www.aats.org/CoronaryCongress/
WHO recognizes role of surgery and anesthesia in universal health care
At the 68th World Health Assembly on May 22, member states of the World Health Organization (WHO) unanimously passed a historic resolution recognizing emergency and essential surgery and anesthesia as vital components of universal health coverage proposals. View the resolution at http://goo.gl/Un26V7. This resolution is critical in developing safe and cost-effective health care systems in which surgery and anesthesia assume an integral role.
Surgeons treat a range of vital conditions, but recent data published by the Disease Control Priorities Essential Surgery and The Lancet Commission on Global Surgery point to the acute unmet needs of more than 5 billion people worldwide who lack access to basic surgical care. View The Lancet Commission website at http://www.globalsurgery.info/.
The American College of Surgeons (ACS) recognizes that implementation of the WHO resolution will require the collaboration of many stakeholders. The ACS is committed to working with WHO, health ministries around the world, governmental and non-governmental organizations, and other surgical and anesthesia societies for the betterment of surgical care worldwide.
The College also supports the vision established by The Lancet Commission on Global Surgery: Universal Access to Safe, Affordable Surgical and Anaesthesia Care When Needed. The College will continue to promote research on access to safe, affordable, and timely surgery, reporting on the WHO’s and the Lancet Commission’s recommended surgical indicators.
At the 68th World Health Assembly on May 22, member states of the World Health Organization (WHO) unanimously passed a historic resolution recognizing emergency and essential surgery and anesthesia as vital components of universal health coverage proposals. View the resolution at http://goo.gl/Un26V7. This resolution is critical in developing safe and cost-effective health care systems in which surgery and anesthesia assume an integral role.
Surgeons treat a range of vital conditions, but recent data published by the Disease Control Priorities Essential Surgery and The Lancet Commission on Global Surgery point to the acute unmet needs of more than 5 billion people worldwide who lack access to basic surgical care. View The Lancet Commission website at http://www.globalsurgery.info/.
The American College of Surgeons (ACS) recognizes that implementation of the WHO resolution will require the collaboration of many stakeholders. The ACS is committed to working with WHO, health ministries around the world, governmental and non-governmental organizations, and other surgical and anesthesia societies for the betterment of surgical care worldwide.
The College also supports the vision established by The Lancet Commission on Global Surgery: Universal Access to Safe, Affordable Surgical and Anaesthesia Care When Needed. The College will continue to promote research on access to safe, affordable, and timely surgery, reporting on the WHO’s and the Lancet Commission’s recommended surgical indicators.
At the 68th World Health Assembly on May 22, member states of the World Health Organization (WHO) unanimously passed a historic resolution recognizing emergency and essential surgery and anesthesia as vital components of universal health coverage proposals. View the resolution at http://goo.gl/Un26V7. This resolution is critical in developing safe and cost-effective health care systems in which surgery and anesthesia assume an integral role.
Surgeons treat a range of vital conditions, but recent data published by the Disease Control Priorities Essential Surgery and The Lancet Commission on Global Surgery point to the acute unmet needs of more than 5 billion people worldwide who lack access to basic surgical care. View The Lancet Commission website at http://www.globalsurgery.info/.
The American College of Surgeons (ACS) recognizes that implementation of the WHO resolution will require the collaboration of many stakeholders. The ACS is committed to working with WHO, health ministries around the world, governmental and non-governmental organizations, and other surgical and anesthesia societies for the betterment of surgical care worldwide.
The College also supports the vision established by The Lancet Commission on Global Surgery: Universal Access to Safe, Affordable Surgical and Anaesthesia Care When Needed. The College will continue to promote research on access to safe, affordable, and timely surgery, reporting on the WHO’s and the Lancet Commission’s recommended surgical indicators.
2015 Clinical Congress registration is now open
Register now for Clinical Congress 2015, October 4-8, at McCormick Place, Chicago, IL, to take advantage of early-bird pricing. The ACS Clinical Congress remains the premier annual surgical meeting and provides a range of outstanding education and training opportunities for surgeons, surgery residents, medical students, and members of surgical teams.
Earn up to 47.5 Continuing Medical Education (CME) credits while acquiring new skills! A maximum of 28.5 AMA PRA Category 1 Credits™ is available for sessions Monday through Thursday. Physicians should claim only the credit commensurate with the extent of their participation in the activity. A maximum of 19 AMA PRA Category 1 Credits™ can also be earned through completion of Meet-the-Expert Luncheons and weekend Postgraduate courses.
Reasonable hotel rates are also available. Make your hotel reservations and receive special Clinical Congress rates. View more information online at https://www.facs.org/clincon2015.
Register now for Clinical Congress 2015, October 4-8, at McCormick Place, Chicago, IL, to take advantage of early-bird pricing. The ACS Clinical Congress remains the premier annual surgical meeting and provides a range of outstanding education and training opportunities for surgeons, surgery residents, medical students, and members of surgical teams.
Earn up to 47.5 Continuing Medical Education (CME) credits while acquiring new skills! A maximum of 28.5 AMA PRA Category 1 Credits™ is available for sessions Monday through Thursday. Physicians should claim only the credit commensurate with the extent of their participation in the activity. A maximum of 19 AMA PRA Category 1 Credits™ can also be earned through completion of Meet-the-Expert Luncheons and weekend Postgraduate courses.
Reasonable hotel rates are also available. Make your hotel reservations and receive special Clinical Congress rates. View more information online at https://www.facs.org/clincon2015.
Register now for Clinical Congress 2015, October 4-8, at McCormick Place, Chicago, IL, to take advantage of early-bird pricing. The ACS Clinical Congress remains the premier annual surgical meeting and provides a range of outstanding education and training opportunities for surgeons, surgery residents, medical students, and members of surgical teams.
Earn up to 47.5 Continuing Medical Education (CME) credits while acquiring new skills! A maximum of 28.5 AMA PRA Category 1 Credits™ is available for sessions Monday through Thursday. Physicians should claim only the credit commensurate with the extent of their participation in the activity. A maximum of 19 AMA PRA Category 1 Credits™ can also be earned through completion of Meet-the-Expert Luncheons and weekend Postgraduate courses.
Reasonable hotel rates are also available. Make your hotel reservations and receive special Clinical Congress rates. View more information online at https://www.facs.org/clincon2015.
ACS receives accreditation with commendation from ACCME
The Accreditation Council for Continuing Medical Education (ACCME) has awarded the American College of Surgeons (ACS) its highest honor—Accreditation with Commendation. In addition to extending the accreditation term to six years (through November 2020), the ACCME presented the College with a special certificate. The ACS thereby joins an elite group of ACCME-accredited organizations that have achieved this honor. This is the first time the College has received this distinction, which is recognition that the College complies with the ACCME Accreditation Criteria and is a leader and innovator in surgical education.
The Division of Education’s Continuous Professional Development Accreditation Section engaged in a four-year self-study of continuing medical education (CME) activities throughout the College, ACS Chapters, and Joint Providership Program, totaling more than 2,000 activities annually. This extensive accreditation review process included submission of extensive documentation, auditing by the ACCME, interviews with Division of Education leadership, and follow-up reviews by the ACCME Committee and ACCME Board of Directors.
Such an honor is awarded only to those providers that move CME into the arena of improving actual practice, identifying factors that impact patient care, implementing strategies to remove barriers to physician change, and participating within a systems-based framework for quality improvement. The College has taken a leading role in these areas, and the ACCME has recognized this with Accreditation with Commendation. View the ACCME website at http://www.accme.org/.
The Accreditation Council for Continuing Medical Education (ACCME) has awarded the American College of Surgeons (ACS) its highest honor—Accreditation with Commendation. In addition to extending the accreditation term to six years (through November 2020), the ACCME presented the College with a special certificate. The ACS thereby joins an elite group of ACCME-accredited organizations that have achieved this honor. This is the first time the College has received this distinction, which is recognition that the College complies with the ACCME Accreditation Criteria and is a leader and innovator in surgical education.
The Division of Education’s Continuous Professional Development Accreditation Section engaged in a four-year self-study of continuing medical education (CME) activities throughout the College, ACS Chapters, and Joint Providership Program, totaling more than 2,000 activities annually. This extensive accreditation review process included submission of extensive documentation, auditing by the ACCME, interviews with Division of Education leadership, and follow-up reviews by the ACCME Committee and ACCME Board of Directors.
Such an honor is awarded only to those providers that move CME into the arena of improving actual practice, identifying factors that impact patient care, implementing strategies to remove barriers to physician change, and participating within a systems-based framework for quality improvement. The College has taken a leading role in these areas, and the ACCME has recognized this with Accreditation with Commendation. View the ACCME website at http://www.accme.org/.
The Accreditation Council for Continuing Medical Education (ACCME) has awarded the American College of Surgeons (ACS) its highest honor—Accreditation with Commendation. In addition to extending the accreditation term to six years (through November 2020), the ACCME presented the College with a special certificate. The ACS thereby joins an elite group of ACCME-accredited organizations that have achieved this honor. This is the first time the College has received this distinction, which is recognition that the College complies with the ACCME Accreditation Criteria and is a leader and innovator in surgical education.
The Division of Education’s Continuous Professional Development Accreditation Section engaged in a four-year self-study of continuing medical education (CME) activities throughout the College, ACS Chapters, and Joint Providership Program, totaling more than 2,000 activities annually. This extensive accreditation review process included submission of extensive documentation, auditing by the ACCME, interviews with Division of Education leadership, and follow-up reviews by the ACCME Committee and ACCME Board of Directors.
Such an honor is awarded only to those providers that move CME into the arena of improving actual practice, identifying factors that impact patient care, implementing strategies to remove barriers to physician change, and participating within a systems-based framework for quality improvement. The College has taken a leading role in these areas, and the ACCME has recognized this with Accreditation with Commendation. View the ACCME website at http://www.accme.org/.
3 court cases to watch in 2015
Pay close attention to the outcomes of three cases winding their way through the courts this summer, legal experts advise.
On deck are cases that could reshape Stark Law, the Anti-kickback Statute, and the 60-day federal overpayment rule. Decisions on these cases could affect billing practices and practices arrangements, as well as federal reporting obligations. Below is a selection of critical health law cases facing doctors and how they might impact practice.
1. Council for Urological Interests v. Sylvia Burwell et al.
Summary: This case centers on whether the federal Stark Law can prevent physicians from referring patients to hospitals to which the physicians lease equipment, among other things. In 2008, the U.S. Department of Health & Human Services (HHS) issued regulations that effectively prohibit physicians who lease medical equipment to hospitals from referring their Medicare patients to these same hospitals for outpatient care involving that equipment. The regulation prohibits physicians from charging hospitals for the leased equipment on a per-use basis, or a “per-click” basis as it is commonly known. In 2009, the Council for Urological Interests – a nonprofit corporation owned by urologists – sued, claiming the text and legislative history of the Stark Law preclude the HHS from enforcing the per-click ban. The regulation limits the ability of physicians who own joint ventures to refer their patients to receive services under these arrangements, the plaintiffs said. A district court ruled in favor of the HHS, and the Council appealed. A spokeswoman for the U.S. Department of Justice declined to comment for this story.
Case status: In June 2015, the U.S. Court of Appeals for the District of Columbia Circuit ruled that the HHS must reconsider its per-click referral ban. The court suggested that the agency may have misconstrued the legislative history of the Stark Law in order to enact the rule.
Why doctors should care: The ultimate outcome of the case will determine whether or not physicians can engage in per-click leases under Stark Law, said Chicago health law attorney Ericka L. Adler.

“When HHS changed the regulations to no longer allow the per-click arrangement where physicians were self-referring, it caused a lot of deals to be undone,” Ms. Adler said in an interview. “[Certainly], these lease arrangements could, in many cases, be restructured to look more like normal leases and meet the Stark equipment lease exception, but in some cases it created hardships, such as in rural areas.”
Reconsideration of the regulation could mean that the HHS creates more appropriate carve-outs to the rule, Ms. Adler noted.
In the meantime, the appeals court ruling means the per-click ban cannot be enforced while the government reconsiders, which is a positive development for physicians, said Washington health law attorney Thomas L. Mills, who represented the Council for Urological Interests.
“CMS’ permitting per-click leases to non–physician-owned companies while banning them for physician-owned entities made no sense, particularly when the medical procedure is not susceptible to overuse,” Mr. Mills said in an interview. “Perhaps more importantly, the [appeals] decision is a victory for the rule of law. It shows that CMS does not have carte blanche to disadvantage physicians by steering control of the implements of their practices to less important participants in the health care delivery system. ... Physicians should be free to band together to purchase the equipment they believe will provide the most effective treatment for their patients, instead of being forced to rely on the arbitrary procurement decisions of hospitals.”
2. United States v. Continuum Health Partners Inc.
Summary: The federal government contends that three hospitals failed to return overpayments to Medicaid in violation of an Affordable Care Act requirement that they be reported and repaid within 60 days of identification. The government alleges that because of a computer glitch, three hospitals that are operated by Continuum Health Partners Inc., billed both the government and a managed care organization (MCO) for the same services. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum conducted an internal investigation and allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims that Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Continuum argues that the hospitals did not knowingly conceal the overpayments from the government and that the overbillings had not been officially identified. Rather, Continuum argues there is only evidence that administrators discussed potential overpayments. The “mere notice of a potential overpayment does not give rise to an established duty until 60 days after the overpayment is identified,” Continuum said in court documents. Attorneys for the government and for Continuum did not return messages seeking comment.
Case status: The case is before the U.S. District Court for the Southern District of New York.
Why doctors should care: The Continuum case will provide significant guidance to health providers about the ACA 60-day overpayment rule, said Houston health law attorney Micheal E. Clark, who chairs the America Bar Association Health Law Section. As it stands, the federal rule is somewhat unclear, leading to confusion for doctors about their reporting obligations, he said.

“The agency hasn’t really defined what is ‘knowing,’ what is reasonable knowledge of a known overpayment,” Mr. Clark said in an interview. “It’s a gray area. [The ruling] will be very informative about what this is actually going to mean.”
3. Ameritox v. Millennium Laboratories
Summary: Ameritox revolves around whether a laboratory’s giveaway of urine specimen cups to physicians amounted to an illegal kickback. In 2012, lab testing company Ameritox sued Millennium in a Florida district court alleging that Millennium harmed its business by giving the urine cups to doctors in violation of the Stark Law. Physicians used the cups – which have chemically activated strips that contain patient information – to monitor patients’ use of pain medications. Millennium unlawfully obtained physician referrals through free cup agreements, according to Ameritox’s complaint. A federal jury found Millennium had violated the Stark Law as well as the Anti-Kickback Statute by providing the free cups in exchange for referrals and Ameritox was awarded $11 million. Attorneys for both parties did not return messages seeking comment.
Case status: Millennium appealed, and the case is before the 11th U.S. Circuit Court of Appeals. The federal Justice Department has weighed in on the side of Ameritox, arguing that the cup giveaway violated Stark Law and the Anti-Kickback Statute.
Why doctors should care: The Ameritox case makes it clear that doctors should never accept free point-of-care testing cups or similar medical equipment from a lab, said health law attorney Adrienne Dresevic of Southfield, Mich. The case also highlights the broad spectrum of “remuneration,” when it comes to free items or services to doctors, she noted. Under the Anti-Kickback Statute, remuneration refers to the transfer of anything of value, directly or indirectly, overtly or covertly, in cash or in kind.

“The takeaways in Ameritox are applicable to other relationships, such as in the radiology realm,” Ms. Dresevic said in an interview. “Physicians should closely scrutinize any free items or services offered to them to ensure it falls within the exception to what is considered ‘remuneration.’ ”
Exceptions to remuneration could include payments that are a return on an investment interest, such as a dividend or interest income. However, physicians should ensure they are familiar with all exceptions to the law before entering into such agreements, experts advise.
The Ameritox case is important for physicians because more laboratories are approaching doctors with various “arrangements,” and touting that the arrangements are compliant with federal regulations, Ms. Dresevic added. Many doctors are taking the labs’ word for the arrangements’ legality, leading to serious legal risk.
“Physicians need to know how to look beyond what the laboratory representative is presenting to them and make their own determinations, sometimes with the help of health care counsel, regarding the legality of a particular arrangement,” she said.
On Twitter @legal_med
Pay close attention to the outcomes of three cases winding their way through the courts this summer, legal experts advise.
On deck are cases that could reshape Stark Law, the Anti-kickback Statute, and the 60-day federal overpayment rule. Decisions on these cases could affect billing practices and practices arrangements, as well as federal reporting obligations. Below is a selection of critical health law cases facing doctors and how they might impact practice.
1. Council for Urological Interests v. Sylvia Burwell et al.
Summary: This case centers on whether the federal Stark Law can prevent physicians from referring patients to hospitals to which the physicians lease equipment, among other things. In 2008, the U.S. Department of Health & Human Services (HHS) issued regulations that effectively prohibit physicians who lease medical equipment to hospitals from referring their Medicare patients to these same hospitals for outpatient care involving that equipment. The regulation prohibits physicians from charging hospitals for the leased equipment on a per-use basis, or a “per-click” basis as it is commonly known. In 2009, the Council for Urological Interests – a nonprofit corporation owned by urologists – sued, claiming the text and legislative history of the Stark Law preclude the HHS from enforcing the per-click ban. The regulation limits the ability of physicians who own joint ventures to refer their patients to receive services under these arrangements, the plaintiffs said. A district court ruled in favor of the HHS, and the Council appealed. A spokeswoman for the U.S. Department of Justice declined to comment for this story.
Case status: In June 2015, the U.S. Court of Appeals for the District of Columbia Circuit ruled that the HHS must reconsider its per-click referral ban. The court suggested that the agency may have misconstrued the legislative history of the Stark Law in order to enact the rule.
Why doctors should care: The ultimate outcome of the case will determine whether or not physicians can engage in per-click leases under Stark Law, said Chicago health law attorney Ericka L. Adler.
“When HHS changed the regulations to no longer allow the per-click arrangement where physicians were self-referring, it caused a lot of deals to be undone,” Ms. Adler said in an interview. “[Certainly], these lease arrangements could, in many cases, be restructured to look more like normal leases and meet the Stark equipment lease exception, but in some cases it created hardships, such as in rural areas.”
Reconsideration of the regulation could mean that the HHS creates more appropriate carve-outs to the rule, Ms. Adler noted.
In the meantime, the appeals court ruling means the per-click ban cannot be enforced while the government reconsiders, which is a positive development for physicians, said Washington health law attorney Thomas L. Mills, who represented the Council for Urological Interests.
“CMS’ permitting per-click leases to non–physician-owned companies while banning them for physician-owned entities made no sense, particularly when the medical procedure is not susceptible to overuse,” Mr. Mills said in an interview. “Perhaps more importantly, the [appeals] decision is a victory for the rule of law. It shows that CMS does not have carte blanche to disadvantage physicians by steering control of the implements of their practices to less important participants in the health care delivery system. ... Physicians should be free to band together to purchase the equipment they believe will provide the most effective treatment for their patients, instead of being forced to rely on the arbitrary procurement decisions of hospitals.”
2. United States v. Continuum Health Partners Inc.
Summary: The federal government contends that three hospitals failed to return overpayments to Medicaid in violation of an Affordable Care Act requirement that they be reported and repaid within 60 days of identification. The government alleges that because of a computer glitch, three hospitals that are operated by Continuum Health Partners Inc., billed both the government and a managed care organization (MCO) for the same services. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum conducted an internal investigation and allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims that Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Continuum argues that the hospitals did not knowingly conceal the overpayments from the government and that the overbillings had not been officially identified. Rather, Continuum argues there is only evidence that administrators discussed potential overpayments. The “mere notice of a potential overpayment does not give rise to an established duty until 60 days after the overpayment is identified,” Continuum said in court documents. Attorneys for the government and for Continuum did not return messages seeking comment.
Case status: The case is before the U.S. District Court for the Southern District of New York.
Why doctors should care: The Continuum case will provide significant guidance to health providers about the ACA 60-day overpayment rule, said Houston health law attorney Micheal E. Clark, who chairs the America Bar Association Health Law Section. As it stands, the federal rule is somewhat unclear, leading to confusion for doctors about their reporting obligations, he said.
“The agency hasn’t really defined what is ‘knowing,’ what is reasonable knowledge of a known overpayment,” Mr. Clark said in an interview. “It’s a gray area. [The ruling] will be very informative about what this is actually going to mean.”
3. Ameritox v. Millennium Laboratories
Summary: Ameritox revolves around whether a laboratory’s giveaway of urine specimen cups to physicians amounted to an illegal kickback. In 2012, lab testing company Ameritox sued Millennium in a Florida district court alleging that Millennium harmed its business by giving the urine cups to doctors in violation of the Stark Law. Physicians used the cups – which have chemically activated strips that contain patient information – to monitor patients’ use of pain medications. Millennium unlawfully obtained physician referrals through free cup agreements, according to Ameritox’s complaint. A federal jury found Millennium had violated the Stark Law as well as the Anti-Kickback Statute by providing the free cups in exchange for referrals and Ameritox was awarded $11 million. Attorneys for both parties did not return messages seeking comment.
Case status: Millennium appealed, and the case is before the 11th U.S. Circuit Court of Appeals. The federal Justice Department has weighed in on the side of Ameritox, arguing that the cup giveaway violated Stark Law and the Anti-Kickback Statute.
Why doctors should care: The Ameritox case makes it clear that doctors should never accept free point-of-care testing cups or similar medical equipment from a lab, said health law attorney Adrienne Dresevic of Southfield, Mich. The case also highlights the broad spectrum of “remuneration,” when it comes to free items or services to doctors, she noted. Under the Anti-Kickback Statute, remuneration refers to the transfer of anything of value, directly or indirectly, overtly or covertly, in cash or in kind.
“The takeaways in Ameritox are applicable to other relationships, such as in the radiology realm,” Ms. Dresevic said in an interview. “Physicians should closely scrutinize any free items or services offered to them to ensure it falls within the exception to what is considered ‘remuneration.’ ”
Exceptions to remuneration could include payments that are a return on an investment interest, such as a dividend or interest income. However, physicians should ensure they are familiar with all exceptions to the law before entering into such agreements, experts advise.
The Ameritox case is important for physicians because more laboratories are approaching doctors with various “arrangements,” and touting that the arrangements are compliant with federal regulations, Ms. Dresevic added. Many doctors are taking the labs’ word for the arrangements’ legality, leading to serious legal risk.
“Physicians need to know how to look beyond what the laboratory representative is presenting to them and make their own determinations, sometimes with the help of health care counsel, regarding the legality of a particular arrangement,” she said.
On Twitter @legal_med
Pay close attention to the outcomes of three cases winding their way through the courts this summer, legal experts advise.
On deck are cases that could reshape Stark Law, the Anti-kickback Statute, and the 60-day federal overpayment rule. Decisions on these cases could affect billing practices and practices arrangements, as well as federal reporting obligations. Below is a selection of critical health law cases facing doctors and how they might impact practice.
1. Council for Urological Interests v. Sylvia Burwell et al.
Summary: This case centers on whether the federal Stark Law can prevent physicians from referring patients to hospitals to which the physicians lease equipment, among other things. In 2008, the U.S. Department of Health & Human Services (HHS) issued regulations that effectively prohibit physicians who lease medical equipment to hospitals from referring their Medicare patients to these same hospitals for outpatient care involving that equipment. The regulation prohibits physicians from charging hospitals for the leased equipment on a per-use basis, or a “per-click” basis as it is commonly known. In 2009, the Council for Urological Interests – a nonprofit corporation owned by urologists – sued, claiming the text and legislative history of the Stark Law preclude the HHS from enforcing the per-click ban. The regulation limits the ability of physicians who own joint ventures to refer their patients to receive services under these arrangements, the plaintiffs said. A district court ruled in favor of the HHS, and the Council appealed. A spokeswoman for the U.S. Department of Justice declined to comment for this story.
Case status: In June 2015, the U.S. Court of Appeals for the District of Columbia Circuit ruled that the HHS must reconsider its per-click referral ban. The court suggested that the agency may have misconstrued the legislative history of the Stark Law in order to enact the rule.
Why doctors should care: The ultimate outcome of the case will determine whether or not physicians can engage in per-click leases under Stark Law, said Chicago health law attorney Ericka L. Adler.
“When HHS changed the regulations to no longer allow the per-click arrangement where physicians were self-referring, it caused a lot of deals to be undone,” Ms. Adler said in an interview. “[Certainly], these lease arrangements could, in many cases, be restructured to look more like normal leases and meet the Stark equipment lease exception, but in some cases it created hardships, such as in rural areas.”
Reconsideration of the regulation could mean that the HHS creates more appropriate carve-outs to the rule, Ms. Adler noted.
In the meantime, the appeals court ruling means the per-click ban cannot be enforced while the government reconsiders, which is a positive development for physicians, said Washington health law attorney Thomas L. Mills, who represented the Council for Urological Interests.
“CMS’ permitting per-click leases to non–physician-owned companies while banning them for physician-owned entities made no sense, particularly when the medical procedure is not susceptible to overuse,” Mr. Mills said in an interview. “Perhaps more importantly, the [appeals] decision is a victory for the rule of law. It shows that CMS does not have carte blanche to disadvantage physicians by steering control of the implements of their practices to less important participants in the health care delivery system. ... Physicians should be free to band together to purchase the equipment they believe will provide the most effective treatment for their patients, instead of being forced to rely on the arbitrary procurement decisions of hospitals.”
2. United States v. Continuum Health Partners Inc.
Summary: The federal government contends that three hospitals failed to return overpayments to Medicaid in violation of an Affordable Care Act requirement that they be reported and repaid within 60 days of identification. The government alleges that because of a computer glitch, three hospitals that are operated by Continuum Health Partners Inc., billed both the government and a managed care organization (MCO) for the same services. After the New York State Comptroller’s Office alerted Continuum to a possible overbilling, Continuum conducted an internal investigation and allegedly found 900 potentially improper Medicaid claims totaling $1 million, according to court documents. The government claims that Continuum failed to repay the overpayments within 60 days and instead repaid only “small batches” of the affected claims over the next 2 years. Continuum argues that the hospitals did not knowingly conceal the overpayments from the government and that the overbillings had not been officially identified. Rather, Continuum argues there is only evidence that administrators discussed potential overpayments. The “mere notice of a potential overpayment does not give rise to an established duty until 60 days after the overpayment is identified,” Continuum said in court documents. Attorneys for the government and for Continuum did not return messages seeking comment.
Case status: The case is before the U.S. District Court for the Southern District of New York.
Why doctors should care: The Continuum case will provide significant guidance to health providers about the ACA 60-day overpayment rule, said Houston health law attorney Micheal E. Clark, who chairs the America Bar Association Health Law Section. As it stands, the federal rule is somewhat unclear, leading to confusion for doctors about their reporting obligations, he said.
“The agency hasn’t really defined what is ‘knowing,’ what is reasonable knowledge of a known overpayment,” Mr. Clark said in an interview. “It’s a gray area. [The ruling] will be very informative about what this is actually going to mean.”
3. Ameritox v. Millennium Laboratories
Summary: Ameritox revolves around whether a laboratory’s giveaway of urine specimen cups to physicians amounted to an illegal kickback. In 2012, lab testing company Ameritox sued Millennium in a Florida district court alleging that Millennium harmed its business by giving the urine cups to doctors in violation of the Stark Law. Physicians used the cups – which have chemically activated strips that contain patient information – to monitor patients’ use of pain medications. Millennium unlawfully obtained physician referrals through free cup agreements, according to Ameritox’s complaint. A federal jury found Millennium had violated the Stark Law as well as the Anti-Kickback Statute by providing the free cups in exchange for referrals and Ameritox was awarded $11 million. Attorneys for both parties did not return messages seeking comment.
Case status: Millennium appealed, and the case is before the 11th U.S. Circuit Court of Appeals. The federal Justice Department has weighed in on the side of Ameritox, arguing that the cup giveaway violated Stark Law and the Anti-Kickback Statute.
Why doctors should care: The Ameritox case makes it clear that doctors should never accept free point-of-care testing cups or similar medical equipment from a lab, said health law attorney Adrienne Dresevic of Southfield, Mich. The case also highlights the broad spectrum of “remuneration,” when it comes to free items or services to doctors, she noted. Under the Anti-Kickback Statute, remuneration refers to the transfer of anything of value, directly or indirectly, overtly or covertly, in cash or in kind.
“The takeaways in Ameritox are applicable to other relationships, such as in the radiology realm,” Ms. Dresevic said in an interview. “Physicians should closely scrutinize any free items or services offered to them to ensure it falls within the exception to what is considered ‘remuneration.’ ”
Exceptions to remuneration could include payments that are a return on an investment interest, such as a dividend or interest income. However, physicians should ensure they are familiar with all exceptions to the law before entering into such agreements, experts advise.
The Ameritox case is important for physicians because more laboratories are approaching doctors with various “arrangements,” and touting that the arrangements are compliant with federal regulations, Ms. Dresevic added. Many doctors are taking the labs’ word for the arrangements’ legality, leading to serious legal risk.
“Physicians need to know how to look beyond what the laboratory representative is presenting to them and make their own determinations, sometimes with the help of health care counsel, regarding the legality of a particular arrangement,” she said.
On Twitter @legal_med

Bivalirudin in STEMI has low real-world stent thrombosis rate
PARIS – Antithrombotic therapy with bivalirudin for primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction may have been unfairly tarnished as having a high stent thrombosis rate, according to a large, prospective, observational cohort study.
A new analysis from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) showed similarly low stent thrombosis rates within 30 days following primary PCI for STEMI regardless of whether the antithrombotic regimen involved bivalirudin (Angiomax), heparin only, or a glycoprotein IIb/IIIa inhibitor, Dr. Per Grimfjard reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

The SCAAR analysis captured all STEMI patients undergoing primary PCI in Sweden from 2007 through mid-2014. These data reflect real-world interventional practice in Sweden and elsewhere, where bivalirudin is typically administered in a prolonged infusion to protect against early stent thrombosis. In contrast, the randomized trials that linked bivalirudin to high stent thrombosis rates featured protocols in which the drug was stopped immediately after the procedure, noted Dr. Grimfjard, an interventional cardiologist at Uppsala (Sweden) University.
“These are nationwide Swedish numbers, and they are complete. We think the numbers are reassuring in that respect,” he said.
Session chair Dr. Andreas Baumbach said the Swedish data are consistent with his own experience in using bivalirudin in primary PCI for STEMI.
“The headline last year was that bivalirudin has a high stent thrombosis rate. It made the newspapers everywhere. But we never saw that, and we always thought that the difference might be in how we used the drug. There’s a new headline now, that this high stent thrombosis rate is not seen in clinical practice. The practice differs from the randomized trials, and the outcomes differ as well,” observed Dr. Baumbach, professor of interventional cardiology at the University of Bristol (England).
In SCAAR, the 30-day rate of definite, angiographically proven stent thrombosis was 0.84% in 16,860 bivalirudin-treated patients, 0.94% in 3,182 who got heparin only, and 0.83% in 11,216 glycoprotein IIb/IIIa inhibitor recipients. These numeric differences weren’t statistically significant.
All-cause mortality 1 year post-PCI was 9.1% in patients with no stent thrombosis, 16.1% in those who experienced stent thrombosis within 1 day post PCI, and 23.0% in those whose stent thrombosis occurred on days 2-30. Dr. Grimfjard speculated that the explanation for the numerically higher 1-year all-cause mortality rate in patients whose stent thrombosis occurred on days 2-30 as opposed to day 0-1 is probably that they were more likely to have left the hospital when stent thrombosis occurred. That would translate to a longer time to repeat revascularization, hence a larger MI, more heart failure and arrhythmia, and thus a higher long-term risk of death.
Several audience members commented that they weren’t sure what to make of the observational Swedish data because of the looming presence of several potential confounders. For one, clinical practice trends changed considerably during the 7-year time frame of the study, as evidenced by the fact that the use of drug-eluting stents was far more common in bivalirudin-treated patients than in the glycoprotein IIb/IIIa inhibitor group. Also, Swedish cardiologists who put their STEMI patients on bivalirudin were more likely to utilize the more modern radial artery access in performing primary PCI; their practice may have differed from their colleagues’ in other, unrecorded ways as well, it was noted.
Dr. Grimfjard reported having no financial conflicts regarding the study, which was conducted free of commercial support.
PARIS – Antithrombotic therapy with bivalirudin for primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction may have been unfairly tarnished as having a high stent thrombosis rate, according to a large, prospective, observational cohort study.
A new analysis from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) showed similarly low stent thrombosis rates within 30 days following primary PCI for STEMI regardless of whether the antithrombotic regimen involved bivalirudin (Angiomax), heparin only, or a glycoprotein IIb/IIIa inhibitor, Dr. Per Grimfjard reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The SCAAR analysis captured all STEMI patients undergoing primary PCI in Sweden from 2007 through mid-2014. These data reflect real-world interventional practice in Sweden and elsewhere, where bivalirudin is typically administered in a prolonged infusion to protect against early stent thrombosis. In contrast, the randomized trials that linked bivalirudin to high stent thrombosis rates featured protocols in which the drug was stopped immediately after the procedure, noted Dr. Grimfjard, an interventional cardiologist at Uppsala (Sweden) University.
“These are nationwide Swedish numbers, and they are complete. We think the numbers are reassuring in that respect,” he said.
Session chair Dr. Andreas Baumbach said the Swedish data are consistent with his own experience in using bivalirudin in primary PCI for STEMI.
“The headline last year was that bivalirudin has a high stent thrombosis rate. It made the newspapers everywhere. But we never saw that, and we always thought that the difference might be in how we used the drug. There’s a new headline now, that this high stent thrombosis rate is not seen in clinical practice. The practice differs from the randomized trials, and the outcomes differ as well,” observed Dr. Baumbach, professor of interventional cardiology at the University of Bristol (England).
In SCAAR, the 30-day rate of definite, angiographically proven stent thrombosis was 0.84% in 16,860 bivalirudin-treated patients, 0.94% in 3,182 who got heparin only, and 0.83% in 11,216 glycoprotein IIb/IIIa inhibitor recipients. These numeric differences weren’t statistically significant.
All-cause mortality 1 year post-PCI was 9.1% in patients with no stent thrombosis, 16.1% in those who experienced stent thrombosis within 1 day post PCI, and 23.0% in those whose stent thrombosis occurred on days 2-30. Dr. Grimfjard speculated that the explanation for the numerically higher 1-year all-cause mortality rate in patients whose stent thrombosis occurred on days 2-30 as opposed to day 0-1 is probably that they were more likely to have left the hospital when stent thrombosis occurred. That would translate to a longer time to repeat revascularization, hence a larger MI, more heart failure and arrhythmia, and thus a higher long-term risk of death.
Several audience members commented that they weren’t sure what to make of the observational Swedish data because of the looming presence of several potential confounders. For one, clinical practice trends changed considerably during the 7-year time frame of the study, as evidenced by the fact that the use of drug-eluting stents was far more common in bivalirudin-treated patients than in the glycoprotein IIb/IIIa inhibitor group. Also, Swedish cardiologists who put their STEMI patients on bivalirudin were more likely to utilize the more modern radial artery access in performing primary PCI; their practice may have differed from their colleagues’ in other, unrecorded ways as well, it was noted.
Dr. Grimfjard reported having no financial conflicts regarding the study, which was conducted free of commercial support.
PARIS – Antithrombotic therapy with bivalirudin for primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction may have been unfairly tarnished as having a high stent thrombosis rate, according to a large, prospective, observational cohort study.
A new analysis from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) showed similarly low stent thrombosis rates within 30 days following primary PCI for STEMI regardless of whether the antithrombotic regimen involved bivalirudin (Angiomax), heparin only, or a glycoprotein IIb/IIIa inhibitor, Dr. Per Grimfjard reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The SCAAR analysis captured all STEMI patients undergoing primary PCI in Sweden from 2007 through mid-2014. These data reflect real-world interventional practice in Sweden and elsewhere, where bivalirudin is typically administered in a prolonged infusion to protect against early stent thrombosis. In contrast, the randomized trials that linked bivalirudin to high stent thrombosis rates featured protocols in which the drug was stopped immediately after the procedure, noted Dr. Grimfjard, an interventional cardiologist at Uppsala (Sweden) University.
“These are nationwide Swedish numbers, and they are complete. We think the numbers are reassuring in that respect,” he said.
Session chair Dr. Andreas Baumbach said the Swedish data are consistent with his own experience in using bivalirudin in primary PCI for STEMI.
“The headline last year was that bivalirudin has a high stent thrombosis rate. It made the newspapers everywhere. But we never saw that, and we always thought that the difference might be in how we used the drug. There’s a new headline now, that this high stent thrombosis rate is not seen in clinical practice. The practice differs from the randomized trials, and the outcomes differ as well,” observed Dr. Baumbach, professor of interventional cardiology at the University of Bristol (England).
In SCAAR, the 30-day rate of definite, angiographically proven stent thrombosis was 0.84% in 16,860 bivalirudin-treated patients, 0.94% in 3,182 who got heparin only, and 0.83% in 11,216 glycoprotein IIb/IIIa inhibitor recipients. These numeric differences weren’t statistically significant.
All-cause mortality 1 year post-PCI was 9.1% in patients with no stent thrombosis, 16.1% in those who experienced stent thrombosis within 1 day post PCI, and 23.0% in those whose stent thrombosis occurred on days 2-30. Dr. Grimfjard speculated that the explanation for the numerically higher 1-year all-cause mortality rate in patients whose stent thrombosis occurred on days 2-30 as opposed to day 0-1 is probably that they were more likely to have left the hospital when stent thrombosis occurred. That would translate to a longer time to repeat revascularization, hence a larger MI, more heart failure and arrhythmia, and thus a higher long-term risk of death.
Several audience members commented that they weren’t sure what to make of the observational Swedish data because of the looming presence of several potential confounders. For one, clinical practice trends changed considerably during the 7-year time frame of the study, as evidenced by the fact that the use of drug-eluting stents was far more common in bivalirudin-treated patients than in the glycoprotein IIb/IIIa inhibitor group. Also, Swedish cardiologists who put their STEMI patients on bivalirudin were more likely to utilize the more modern radial artery access in performing primary PCI; their practice may have differed from their colleagues’ in other, unrecorded ways as well, it was noted.
Dr. Grimfjard reported having no financial conflicts regarding the study, which was conducted free of commercial support.
AT EUROPCR 2015
Key clinical point: The 30-day incidence of stent thrombosis following primary PCI in a large, real-world STEMI population was reassuringly low regardless of the antithrombotic regimen.
Major finding: The stent thrombosis rate within 30 days after primary PCI for STEMI was 0.84% in patients who received bivalirudin for antithrombotic therapy, 0.94% with heparin only, and 0.83% with a glycoprotein IIb/IIIa inhibitor in this real-world nationwide Swedish registry.
Data source: A prospective observational cohort study which included all patients who underwent primary PCI for STEMI in Sweden during 2007-2014.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was conducted free of commercial support.

Elective colectomy topped medical therapy for advanced ulcerative colitis
For adults with advanced ulcerative colitis (UC) older than 50 years of age, elective colectomy offered a significantly higher survival rate than did medical therapy, according to a retrospective study of 8,371 patients.
Dr. Meenakshi Bewtra of the University of Pennsylvania, Philadelphia, and her coinvestigators matched 830 UC patients seeking elective colectomy for treatment with 7,541 UC patients opting for more traditional medical therapy, all recruited using data from Medicaid and Medicare from 2000 to 2011 (Ann. Intern. Med. July 14, 2015 [doi:10.7326/M14-0960]).
In total, 63 patients who received elective colectomy died, compared with 783 patients in the medical therapy cohort. Mortality rates per cohort were 34 and 54 per 1,000 person-years, respectively. Furthermore, patients were more likely to respond more favorably to elective colectomy than to medical therapy, with an adjusted hazard ratio of 0.67. Additional post hoc analysis revealed higher survival odds with colectomy for patients age 50 years or older (HR, 0.60; P = .032). “These findings warrant discussion with patients when one is weighing the risks and benefits of different medical therapies and total colectomy,” the investigators said.
The authors noted that the study had several limitations, such as potential residual confounding and the possibility of reduced statistical power in subsequent analyses because several databases were used to cull data.
The study was funded by grants from the National Institutes of Health and the Agency for Healthcare Research and Quality. Dr. Bewtra disclosed receiving a grant from NIH and accepting speaking engagements for Imedex and the Crohn’s & Colitis Foundation of America/Robert Michael Educational Institute outside the submitted work.
For adults with advanced ulcerative colitis (UC) older than 50 years of age, elective colectomy offered a significantly higher survival rate than did medical therapy, according to a retrospective study of 8,371 patients.
Dr. Meenakshi Bewtra of the University of Pennsylvania, Philadelphia, and her coinvestigators matched 830 UC patients seeking elective colectomy for treatment with 7,541 UC patients opting for more traditional medical therapy, all recruited using data from Medicaid and Medicare from 2000 to 2011 (Ann. Intern. Med. July 14, 2015 [doi:10.7326/M14-0960]).
In total, 63 patients who received elective colectomy died, compared with 783 patients in the medical therapy cohort. Mortality rates per cohort were 34 and 54 per 1,000 person-years, respectively. Furthermore, patients were more likely to respond more favorably to elective colectomy than to medical therapy, with an adjusted hazard ratio of 0.67. Additional post hoc analysis revealed higher survival odds with colectomy for patients age 50 years or older (HR, 0.60; P = .032). “These findings warrant discussion with patients when one is weighing the risks and benefits of different medical therapies and total colectomy,” the investigators said.
The authors noted that the study had several limitations, such as potential residual confounding and the possibility of reduced statistical power in subsequent analyses because several databases were used to cull data.
The study was funded by grants from the National Institutes of Health and the Agency for Healthcare Research and Quality. Dr. Bewtra disclosed receiving a grant from NIH and accepting speaking engagements for Imedex and the Crohn’s & Colitis Foundation of America/Robert Michael Educational Institute outside the submitted work.
For adults with advanced ulcerative colitis (UC) older than 50 years of age, elective colectomy offered a significantly higher survival rate than did medical therapy, according to a retrospective study of 8,371 patients.
Dr. Meenakshi Bewtra of the University of Pennsylvania, Philadelphia, and her coinvestigators matched 830 UC patients seeking elective colectomy for treatment with 7,541 UC patients opting for more traditional medical therapy, all recruited using data from Medicaid and Medicare from 2000 to 2011 (Ann. Intern. Med. July 14, 2015 [doi:10.7326/M14-0960]).
In total, 63 patients who received elective colectomy died, compared with 783 patients in the medical therapy cohort. Mortality rates per cohort were 34 and 54 per 1,000 person-years, respectively. Furthermore, patients were more likely to respond more favorably to elective colectomy than to medical therapy, with an adjusted hazard ratio of 0.67. Additional post hoc analysis revealed higher survival odds with colectomy for patients age 50 years or older (HR, 0.60; P = .032). “These findings warrant discussion with patients when one is weighing the risks and benefits of different medical therapies and total colectomy,” the investigators said.
The authors noted that the study had several limitations, such as potential residual confounding and the possibility of reduced statistical power in subsequent analyses because several databases were used to cull data.
The study was funded by grants from the National Institutes of Health and the Agency for Healthcare Research and Quality. Dr. Bewtra disclosed receiving a grant from NIH and accepting speaking engagements for Imedex and the Crohn’s & Colitis Foundation of America/Robert Michael Educational Institute outside the submitted work.
FROM THE ANNALS OF INTERNAL MEDICINE
Which specialties are sitting at residents’ popular table?
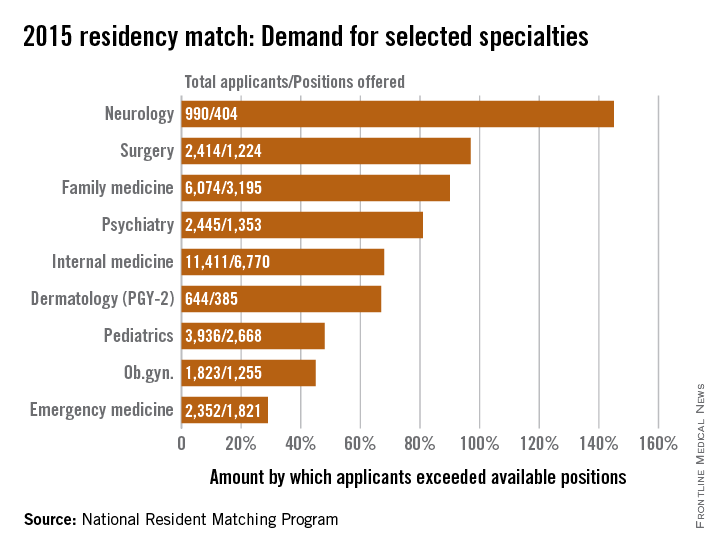
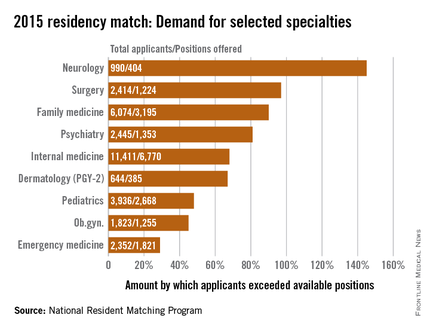
Demand for residency positions exceeded supply for all 47 specialties included in the 2015 residency match, but some specialties were more in demand than others.
Sheer weight of numbers gives the largest specialty, internal medicine, the largest demand – 11,411 total applicants – and the biggest difference between that demand and the number of PGY-1 positions offered: 6,770 slots, leaving 4,641 new doctors to settle for another specialty, according to data from the National Resident Matching Program (NRMP).
There is, however, more than one way to look at Match supply and demand. By doing a little math to take specialty size out of the equation, neurology gets a lot more popular. With 990 residents vying for just 404 positions, the total number of neurology applicants exceeded successful ones by 145%, compared with 68% for internal medicine. Also moving ahead of IM were surgery (97%), family medicine (90%), and psychiatry (81%).
Among the smallest subspecialties – those with less than 100 positions to fill – the demand becomes even more impressive. Radiation oncology had a rate of 600%, while pediatrics-primary put up a rate of 978%. The top of the demand heap, however, is occupied by medicine–preventive medicine, which had 94 applicants for just 7 available slots, according to the NRMP, which means that the number of applicants topped the number accepted by 1,243%.
The total PGY-1 numbers for 2015 look like this: 52,860 applicants filled 27,293 residency positions, so the number of total applicants exceeded those accepted by 94%. Think of it this way: For every residency applicant who matched in 2015, there was nearly one complete applicant who didn’t.
Demand for residency positions exceeded supply for all 47 specialties included in the 2015 residency match, but some specialties were more in demand than others.
Sheer weight of numbers gives the largest specialty, internal medicine, the largest demand – 11,411 total applicants – and the biggest difference between that demand and the number of PGY-1 positions offered: 6,770 slots, leaving 4,641 new doctors to settle for another specialty, according to data from the National Resident Matching Program (NRMP).
There is, however, more than one way to look at Match supply and demand. By doing a little math to take specialty size out of the equation, neurology gets a lot more popular. With 990 residents vying for just 404 positions, the total number of neurology applicants exceeded successful ones by 145%, compared with 68% for internal medicine. Also moving ahead of IM were surgery (97%), family medicine (90%), and psychiatry (81%).
Among the smallest subspecialties – those with less than 100 positions to fill – the demand becomes even more impressive. Radiation oncology had a rate of 600%, while pediatrics-primary put up a rate of 978%. The top of the demand heap, however, is occupied by medicine–preventive medicine, which had 94 applicants for just 7 available slots, according to the NRMP, which means that the number of applicants topped the number accepted by 1,243%.
The total PGY-1 numbers for 2015 look like this: 52,860 applicants filled 27,293 residency positions, so the number of total applicants exceeded those accepted by 94%. Think of it this way: For every residency applicant who matched in 2015, there was nearly one complete applicant who didn’t.
Demand for residency positions exceeded supply for all 47 specialties included in the 2015 residency match, but some specialties were more in demand than others.
Sheer weight of numbers gives the largest specialty, internal medicine, the largest demand – 11,411 total applicants – and the biggest difference between that demand and the number of PGY-1 positions offered: 6,770 slots, leaving 4,641 new doctors to settle for another specialty, according to data from the National Resident Matching Program (NRMP).
There is, however, more than one way to look at Match supply and demand. By doing a little math to take specialty size out of the equation, neurology gets a lot more popular. With 990 residents vying for just 404 positions, the total number of neurology applicants exceeded successful ones by 145%, compared with 68% for internal medicine. Also moving ahead of IM were surgery (97%), family medicine (90%), and psychiatry (81%).
Among the smallest subspecialties – those with less than 100 positions to fill – the demand becomes even more impressive. Radiation oncology had a rate of 600%, while pediatrics-primary put up a rate of 978%. The top of the demand heap, however, is occupied by medicine–preventive medicine, which had 94 applicants for just 7 available slots, according to the NRMP, which means that the number of applicants topped the number accepted by 1,243%.
The total PGY-1 numbers for 2015 look like this: 52,860 applicants filled 27,293 residency positions, so the number of total applicants exceeded those accepted by 94%. Think of it this way: For every residency applicant who matched in 2015, there was nearly one complete applicant who didn’t.