User login
Official Newspaper of the American College of Surgeons
Telehealth boom raises questions about proper practices
For the last few months, family physician Dr. R. Russell Thomas Jr. has split his time between visiting patients at his practice in Eagle Lake, Tex., and treating children who reside more than 300 miles away in Sheffield, Tex. via telemedicine. His virtual tool belt includes an electronic stethoscope that enables Dr. Thomas to hear a patient’s heartbeat in real time and a high-definition camera to view and diagnose skin lesions.
The telehealth services are part of a new initiative at Rice Medical Center, a 25-bed, critical access hospital in rural Eagle Lake – population 3,700. Dr. Thomas has thus far used the technology to treat patients at an at-risk children’s academy and a local primary school. Soon, he and other physicians will also use telemedicine to consult with cardiologists and internists who practice 70 miles away in Houston.

“I look at telemedicine not so much as a practice like cardiology or orthopedics, but more [as] a tool like a percussion hammer or an otoscope,” Dr. Thomas said in an interview. “It’s a tool to practice whatever it is that you do.”
Dr. Thomas is far from alone. Analysts predict vast growth in the telemedicine industry in the coming years. The number of health providers offering telemedicine is expected to rise from 22% in 2014 to 37% in 2015, according to research by Towers Watson. Another report, by BCC Research, shows the global telehospital/clinic and telehome market is expected to reach about $43 billion in 2019, up from $19 billion in 2014.
The explosion of telemedicine is driven by two primary factors, said Dr. Joseph P. McMenamin, a Richmond, Va., attorney who specializes in medical malpractice defense and telemedicine.
“As a society, we are increasingly reliant upon and enamored of electronic methods of communications,” Dr. McMenamin said in an interview. “In one sense, it’s just part of a larger trend. The other, more specific reason, perhaps, is the widespread dissatisfaction with the way our health care system operates today. We are blessed in the United States to have some of the finest physicians in the world. … and then we have this terribly complex, burdensome system for getting people to where they need to be to get care. Telemedicine, by comparison is quick, convenient, and relatively inexpensive.”
Telemedicine is poised to change the way doctors practice. This first of three articles lays out the landscape for how telemedicine is shaping up across the country.
But for doctors, the practice of telemedicine is strewn with challenges. Barriers include reimbursement, licensing, malpractice, and regulation. Topping the barriers is a lack of uniform standards about practices. A key question: What constitutes the responsible use of telemedicine?
States have differing ideas. Some require a physical examination by a physician prior to telemedicine. Some allow that encounter can be conducted via telemedicine, while others mandate the visit is in-person. Alabama, Georgia, and Texas require an in-person follow-up visit after a telemedicine encounter, according to 2015 data from the American Telemedicine Association (ATA). Sixteen states and D.C. have informed consent requirements for telemedicine patients. Still other states have no defined rules for the practice of telemedicine.
To promote consistency and better usage, the Federation of State Medical Boards in 2014 issued a model policy to state medical boards about the recommended practice of telemedicine. The policy maintains that the same standard of care applied to face-to-face encounters be applied to telemedicine encounters, said Lisa A. Robin, chief advocacy officer for the Federation of State Medical Boards (FSMB). At least 29 state boards have telemedicine rules that are consistent with the model policy, Ms. Robin said in an interview.
“As telemedicine continues to evolve, we believe there must be a very strong focus on ensuring patient safety through sound policy making and regulatory practices,” she said.
From practice debate to court dispute
Medical specialty societies are beginning to weigh in on acceptable telehealth practices for doctors. In July, the American Academy of Pediatrics issued guidance advocating that use of telemedicine for episodic care should be done within the context of the medical home and that fragmented telemedicine services should be avoided. Guidance issued by the American Medical Association makes it clears that physicians who prescribe using telemedicine need to first establish a patient-physician relationship. In September, the American College of Physicians (ACP) also issued policy in support of expanded telemedicine use, but cautioned the practice should be between a physician and patient who have an established relationship. The FSMB guidance also states that doctors should establish a relationship with patients before practicing telemedicine.

But how that relationship is created is up for debate. In Texas, disagreement over what creates a physician-patient relationship has led to litigation between national telemedicine company Teladoc and the Texas Medical Board. The case centers on a medical board rule that requires physicians to have a face-to-face visit with patients before treating them through telemedicine. The relationship can be created through telemedicine at an established medical site, but it may not be established through an online questionnaire, e-mail, text, chat, or telephonic evaluation or consultation. Teladoc sued the medical board in April claiming the rule violates federal antitrust laws. Teladoc provides access to medical care via phone or interactive video and treats patients for nonemergency conditions. A judge halted the rule’s enforcement in May.
The company sued to ensure patients have access to the same high-quality telehealth care they’ve received for decades, said Teladoc CEO Jason Gorevic.
“We have employers, health plans, and hospital systems who are coming to us because telehealth is a solution to access-to-care challenges as well as a mechanism to control the cost of care,” Mr. Gorevic said in an interview. “It was our responsibility and quite frankly, our obligation, to take action where there were regulations being adopted that were counter to the interests of patients, payers, and physicians in the state.”
In an April statement, Dr. Michael Arambula, president of the Texas Medical Board (TMB), said the rule represents the best balance of convenience and safety by ensuring quality health care for patients.

“The board recognizes that as technology evolves, so too must regulations governing telemedicine,” Dr. Arambula said in the statement. “However, a telephone medicine scenario that allows a physician to treat an unknown patient without any objective diagnostic data and no ability to follow up with the patient sacrifices the patient’s safety for convenience.”
The Texas Medical Association (TMA) supported the TMB rule. Dr. Thomas, a former TMB member who is active with the TMA, said the rule’s logic is simple.
Without a face-to-face visit, “the doctor has no knowledge of the patient, except for what they tell you in that one encounter,” he said in an interview. “There are no follow-up opportunities, no mechanism for further assessment. It’s episodic care at its worst.”
However, Dr. Reed V. Tuckson, president of the American Telemedicine Association, stresses rules such as the Texas Medical Board’s are unnecessarily intrusive to doctors and diminish the range of possibilities for telemedicine care.
“We do not believe the restrictive covenants that are being applied by far too many state medical boards are appropriate,” Dr. Tuckson said in an interview. “We do not believe they should dictating to physicians, the tools that they should be able to use in partnership with their patients to meet [patients’] individual needs.”
Coming Tuesday, Sept. 29: Who leads the field on paying for telemedicine services?
On Twitter @legal_med
For the last few months, family physician Dr. R. Russell Thomas Jr. has split his time between visiting patients at his practice in Eagle Lake, Tex., and treating children who reside more than 300 miles away in Sheffield, Tex. via telemedicine. His virtual tool belt includes an electronic stethoscope that enables Dr. Thomas to hear a patient’s heartbeat in real time and a high-definition camera to view and diagnose skin lesions.
The telehealth services are part of a new initiative at Rice Medical Center, a 25-bed, critical access hospital in rural Eagle Lake – population 3,700. Dr. Thomas has thus far used the technology to treat patients at an at-risk children’s academy and a local primary school. Soon, he and other physicians will also use telemedicine to consult with cardiologists and internists who practice 70 miles away in Houston.
“I look at telemedicine not so much as a practice like cardiology or orthopedics, but more [as] a tool like a percussion hammer or an otoscope,” Dr. Thomas said in an interview. “It’s a tool to practice whatever it is that you do.”
Dr. Thomas is far from alone. Analysts predict vast growth in the telemedicine industry in the coming years. The number of health providers offering telemedicine is expected to rise from 22% in 2014 to 37% in 2015, according to research by Towers Watson. Another report, by BCC Research, shows the global telehospital/clinic and telehome market is expected to reach about $43 billion in 2019, up from $19 billion in 2014.
The explosion of telemedicine is driven by two primary factors, said Dr. Joseph P. McMenamin, a Richmond, Va., attorney who specializes in medical malpractice defense and telemedicine.
“As a society, we are increasingly reliant upon and enamored of electronic methods of communications,” Dr. McMenamin said in an interview. “In one sense, it’s just part of a larger trend. The other, more specific reason, perhaps, is the widespread dissatisfaction with the way our health care system operates today. We are blessed in the United States to have some of the finest physicians in the world. … and then we have this terribly complex, burdensome system for getting people to where they need to be to get care. Telemedicine, by comparison is quick, convenient, and relatively inexpensive.”
Telemedicine is poised to change the way doctors practice. This first of three articles lays out the landscape for how telemedicine is shaping up across the country.
But for doctors, the practice of telemedicine is strewn with challenges. Barriers include reimbursement, licensing, malpractice, and regulation. Topping the barriers is a lack of uniform standards about practices. A key question: What constitutes the responsible use of telemedicine?
States have differing ideas. Some require a physical examination by a physician prior to telemedicine. Some allow that encounter can be conducted via telemedicine, while others mandate the visit is in-person. Alabama, Georgia, and Texas require an in-person follow-up visit after a telemedicine encounter, according to 2015 data from the American Telemedicine Association (ATA). Sixteen states and D.C. have informed consent requirements for telemedicine patients. Still other states have no defined rules for the practice of telemedicine.
To promote consistency and better usage, the Federation of State Medical Boards in 2014 issued a model policy to state medical boards about the recommended practice of telemedicine. The policy maintains that the same standard of care applied to face-to-face encounters be applied to telemedicine encounters, said Lisa A. Robin, chief advocacy officer for the Federation of State Medical Boards (FSMB). At least 29 state boards have telemedicine rules that are consistent with the model policy, Ms. Robin said in an interview.
“As telemedicine continues to evolve, we believe there must be a very strong focus on ensuring patient safety through sound policy making and regulatory practices,” she said.
From practice debate to court dispute
Medical specialty societies are beginning to weigh in on acceptable telehealth practices for doctors. In July, the American Academy of Pediatrics issued guidance advocating that use of telemedicine for episodic care should be done within the context of the medical home and that fragmented telemedicine services should be avoided. Guidance issued by the American Medical Association makes it clears that physicians who prescribe using telemedicine need to first establish a patient-physician relationship. In September, the American College of Physicians (ACP) also issued policy in support of expanded telemedicine use, but cautioned the practice should be between a physician and patient who have an established relationship. The FSMB guidance also states that doctors should establish a relationship with patients before practicing telemedicine.
But how that relationship is created is up for debate. In Texas, disagreement over what creates a physician-patient relationship has led to litigation between national telemedicine company Teladoc and the Texas Medical Board. The case centers on a medical board rule that requires physicians to have a face-to-face visit with patients before treating them through telemedicine. The relationship can be created through telemedicine at an established medical site, but it may not be established through an online questionnaire, e-mail, text, chat, or telephonic evaluation or consultation. Teladoc sued the medical board in April claiming the rule violates federal antitrust laws. Teladoc provides access to medical care via phone or interactive video and treats patients for nonemergency conditions. A judge halted the rule’s enforcement in May.
The company sued to ensure patients have access to the same high-quality telehealth care they’ve received for decades, said Teladoc CEO Jason Gorevic.
“We have employers, health plans, and hospital systems who are coming to us because telehealth is a solution to access-to-care challenges as well as a mechanism to control the cost of care,” Mr. Gorevic said in an interview. “It was our responsibility and quite frankly, our obligation, to take action where there were regulations being adopted that were counter to the interests of patients, payers, and physicians in the state.”
In an April statement, Dr. Michael Arambula, president of the Texas Medical Board (TMB), said the rule represents the best balance of convenience and safety by ensuring quality health care for patients.
“The board recognizes that as technology evolves, so too must regulations governing telemedicine,” Dr. Arambula said in the statement. “However, a telephone medicine scenario that allows a physician to treat an unknown patient without any objective diagnostic data and no ability to follow up with the patient sacrifices the patient’s safety for convenience.”
The Texas Medical Association (TMA) supported the TMB rule. Dr. Thomas, a former TMB member who is active with the TMA, said the rule’s logic is simple.
Without a face-to-face visit, “the doctor has no knowledge of the patient, except for what they tell you in that one encounter,” he said in an interview. “There are no follow-up opportunities, no mechanism for further assessment. It’s episodic care at its worst.”
However, Dr. Reed V. Tuckson, president of the American Telemedicine Association, stresses rules such as the Texas Medical Board’s are unnecessarily intrusive to doctors and diminish the range of possibilities for telemedicine care.
“We do not believe the restrictive covenants that are being applied by far too many state medical boards are appropriate,” Dr. Tuckson said in an interview. “We do not believe they should dictating to physicians, the tools that they should be able to use in partnership with their patients to meet [patients’] individual needs.”
Coming Tuesday, Sept. 29: Who leads the field on paying for telemedicine services?
On Twitter @legal_med
For the last few months, family physician Dr. R. Russell Thomas Jr. has split his time between visiting patients at his practice in Eagle Lake, Tex., and treating children who reside more than 300 miles away in Sheffield, Tex. via telemedicine. His virtual tool belt includes an electronic stethoscope that enables Dr. Thomas to hear a patient’s heartbeat in real time and a high-definition camera to view and diagnose skin lesions.
The telehealth services are part of a new initiative at Rice Medical Center, a 25-bed, critical access hospital in rural Eagle Lake – population 3,700. Dr. Thomas has thus far used the technology to treat patients at an at-risk children’s academy and a local primary school. Soon, he and other physicians will also use telemedicine to consult with cardiologists and internists who practice 70 miles away in Houston.
“I look at telemedicine not so much as a practice like cardiology or orthopedics, but more [as] a tool like a percussion hammer or an otoscope,” Dr. Thomas said in an interview. “It’s a tool to practice whatever it is that you do.”
Dr. Thomas is far from alone. Analysts predict vast growth in the telemedicine industry in the coming years. The number of health providers offering telemedicine is expected to rise from 22% in 2014 to 37% in 2015, according to research by Towers Watson. Another report, by BCC Research, shows the global telehospital/clinic and telehome market is expected to reach about $43 billion in 2019, up from $19 billion in 2014.
The explosion of telemedicine is driven by two primary factors, said Dr. Joseph P. McMenamin, a Richmond, Va., attorney who specializes in medical malpractice defense and telemedicine.
“As a society, we are increasingly reliant upon and enamored of electronic methods of communications,” Dr. McMenamin said in an interview. “In one sense, it’s just part of a larger trend. The other, more specific reason, perhaps, is the widespread dissatisfaction with the way our health care system operates today. We are blessed in the United States to have some of the finest physicians in the world. … and then we have this terribly complex, burdensome system for getting people to where they need to be to get care. Telemedicine, by comparison is quick, convenient, and relatively inexpensive.”
Telemedicine is poised to change the way doctors practice. This first of three articles lays out the landscape for how telemedicine is shaping up across the country.
But for doctors, the practice of telemedicine is strewn with challenges. Barriers include reimbursement, licensing, malpractice, and regulation. Topping the barriers is a lack of uniform standards about practices. A key question: What constitutes the responsible use of telemedicine?
States have differing ideas. Some require a physical examination by a physician prior to telemedicine. Some allow that encounter can be conducted via telemedicine, while others mandate the visit is in-person. Alabama, Georgia, and Texas require an in-person follow-up visit after a telemedicine encounter, according to 2015 data from the American Telemedicine Association (ATA). Sixteen states and D.C. have informed consent requirements for telemedicine patients. Still other states have no defined rules for the practice of telemedicine.
To promote consistency and better usage, the Federation of State Medical Boards in 2014 issued a model policy to state medical boards about the recommended practice of telemedicine. The policy maintains that the same standard of care applied to face-to-face encounters be applied to telemedicine encounters, said Lisa A. Robin, chief advocacy officer for the Federation of State Medical Boards (FSMB). At least 29 state boards have telemedicine rules that are consistent with the model policy, Ms. Robin said in an interview.
“As telemedicine continues to evolve, we believe there must be a very strong focus on ensuring patient safety through sound policy making and regulatory practices,” she said.
From practice debate to court dispute
Medical specialty societies are beginning to weigh in on acceptable telehealth practices for doctors. In July, the American Academy of Pediatrics issued guidance advocating that use of telemedicine for episodic care should be done within the context of the medical home and that fragmented telemedicine services should be avoided. Guidance issued by the American Medical Association makes it clears that physicians who prescribe using telemedicine need to first establish a patient-physician relationship. In September, the American College of Physicians (ACP) also issued policy in support of expanded telemedicine use, but cautioned the practice should be between a physician and patient who have an established relationship. The FSMB guidance also states that doctors should establish a relationship with patients before practicing telemedicine.
But how that relationship is created is up for debate. In Texas, disagreement over what creates a physician-patient relationship has led to litigation between national telemedicine company Teladoc and the Texas Medical Board. The case centers on a medical board rule that requires physicians to have a face-to-face visit with patients before treating them through telemedicine. The relationship can be created through telemedicine at an established medical site, but it may not be established through an online questionnaire, e-mail, text, chat, or telephonic evaluation or consultation. Teladoc sued the medical board in April claiming the rule violates federal antitrust laws. Teladoc provides access to medical care via phone or interactive video and treats patients for nonemergency conditions. A judge halted the rule’s enforcement in May.
The company sued to ensure patients have access to the same high-quality telehealth care they’ve received for decades, said Teladoc CEO Jason Gorevic.
“We have employers, health plans, and hospital systems who are coming to us because telehealth is a solution to access-to-care challenges as well as a mechanism to control the cost of care,” Mr. Gorevic said in an interview. “It was our responsibility and quite frankly, our obligation, to take action where there were regulations being adopted that were counter to the interests of patients, payers, and physicians in the state.”
In an April statement, Dr. Michael Arambula, president of the Texas Medical Board (TMB), said the rule represents the best balance of convenience and safety by ensuring quality health care for patients.
“The board recognizes that as technology evolves, so too must regulations governing telemedicine,” Dr. Arambula said in the statement. “However, a telephone medicine scenario that allows a physician to treat an unknown patient without any objective diagnostic data and no ability to follow up with the patient sacrifices the patient’s safety for convenience.”
The Texas Medical Association (TMA) supported the TMB rule. Dr. Thomas, a former TMB member who is active with the TMA, said the rule’s logic is simple.
Without a face-to-face visit, “the doctor has no knowledge of the patient, except for what they tell you in that one encounter,” he said in an interview. “There are no follow-up opportunities, no mechanism for further assessment. It’s episodic care at its worst.”
However, Dr. Reed V. Tuckson, president of the American Telemedicine Association, stresses rules such as the Texas Medical Board’s are unnecessarily intrusive to doctors and diminish the range of possibilities for telemedicine care.
“We do not believe the restrictive covenants that are being applied by far too many state medical boards are appropriate,” Dr. Tuckson said in an interview. “We do not believe they should dictating to physicians, the tools that they should be able to use in partnership with their patients to meet [patients’] individual needs.”
Coming Tuesday, Sept. 29: Who leads the field on paying for telemedicine services?
On Twitter @legal_med

Diabetic foot ulcer: Early closure post debridement best
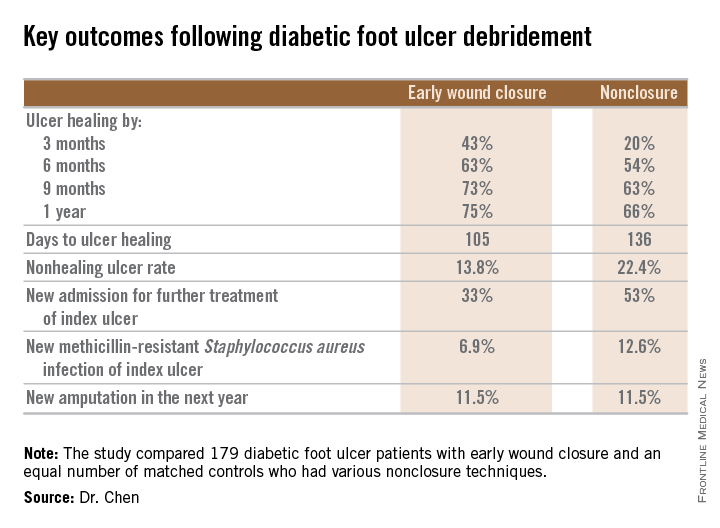
SAN DIEGO – Early wound closure prior to hospital discharge after surgical debridement of infected diabetic foot ulcers yields higher ulcer healing rates and a shorter time to healing, compared with various nonclosure wound management methods, according to a propensity-matched study.
How best to manage the open wound following nonamputative surgery of infected diabetic foot ulcers has been controversial. But early wound closure during the index hospitalization was the clear winner in this comparative study, Dr. Shey-Ying Chen reported at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
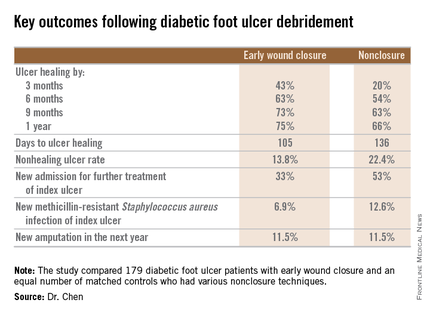
He presented a retrospective comparison between 179 diabetic foot ulcer (DFU) patients with early wound closure after surgical debridement and an equal number of matched controls treated with various nonclosure techniques, including negative pressure wound therapy and the repeated application of moist dressings. The two study groups were matched first on the basis of DFU location – toe, forefoot, midfoot, or rear foot – and then further propensity matched based on demographics, comorbid conditions, the presence of neuropathy, ulcer status by Wagner classification, infection severity, revascularization procedures, and other variables.
During 1 year of follow-up post discharge, ulcer healing occurred in 75% of the early wound closure group, compared with 66% of the nonclosure patients. Readmission for further treatment of the index ulcer occurred in 33% of the early closure group and 52% of the nonclosure group. Other outcomes were also superior in the early wound closure group, noted Dr. Chen of Beth Israel Deaconess Medical Center, Boston.
Two independent predictors of DFU healing during the follow-up period emerged from a Cox regression analysis: early wound closure, with an adjusted odds ratio of 1.63, and acute as opposed to chronic DFU, with an OR of 1.35.
Ulcer healing was significantly less likely in patients with peripheral vascular disease, with an OR of 0.62; neuropathy, with an OR of 0.53; and methicillin-resistant Staphylococcus aureus wound infection, with an OR of 0.59, he continued.
Underscoring the longer-term difficulties faced by patients with DFUs, it’s noteworthy that 11.5% of patients in both study arms underwent new amputations during the year of follow-up. Moreover, a new diagnosis of osteomyelitis was made in 20% of the early wound closure group and 26% of the nonclosure group, a nonsignificant difference.
Dr. Adolf W. Karchmer, Dr. Chen’s senior coinvestigator, said the outcome data are too new to be able to gauge how vascular, orthopedic, and podiatric surgeons will react.
The investigators reported having no financial conflicts with regard to this study, conducted without commercial sponsorship.
SAN DIEGO – Early wound closure prior to hospital discharge after surgical debridement of infected diabetic foot ulcers yields higher ulcer healing rates and a shorter time to healing, compared with various nonclosure wound management methods, according to a propensity-matched study.
How best to manage the open wound following nonamputative surgery of infected diabetic foot ulcers has been controversial. But early wound closure during the index hospitalization was the clear winner in this comparative study, Dr. Shey-Ying Chen reported at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
He presented a retrospective comparison between 179 diabetic foot ulcer (DFU) patients with early wound closure after surgical debridement and an equal number of matched controls treated with various nonclosure techniques, including negative pressure wound therapy and the repeated application of moist dressings. The two study groups were matched first on the basis of DFU location – toe, forefoot, midfoot, or rear foot – and then further propensity matched based on demographics, comorbid conditions, the presence of neuropathy, ulcer status by Wagner classification, infection severity, revascularization procedures, and other variables.
During 1 year of follow-up post discharge, ulcer healing occurred in 75% of the early wound closure group, compared with 66% of the nonclosure patients. Readmission for further treatment of the index ulcer occurred in 33% of the early closure group and 52% of the nonclosure group. Other outcomes were also superior in the early wound closure group, noted Dr. Chen of Beth Israel Deaconess Medical Center, Boston.
Two independent predictors of DFU healing during the follow-up period emerged from a Cox regression analysis: early wound closure, with an adjusted odds ratio of 1.63, and acute as opposed to chronic DFU, with an OR of 1.35.
Ulcer healing was significantly less likely in patients with peripheral vascular disease, with an OR of 0.62; neuropathy, with an OR of 0.53; and methicillin-resistant Staphylococcus aureus wound infection, with an OR of 0.59, he continued.
Underscoring the longer-term difficulties faced by patients with DFUs, it’s noteworthy that 11.5% of patients in both study arms underwent new amputations during the year of follow-up. Moreover, a new diagnosis of osteomyelitis was made in 20% of the early wound closure group and 26% of the nonclosure group, a nonsignificant difference.
Dr. Adolf W. Karchmer, Dr. Chen’s senior coinvestigator, said the outcome data are too new to be able to gauge how vascular, orthopedic, and podiatric surgeons will react.
The investigators reported having no financial conflicts with regard to this study, conducted without commercial sponsorship.
SAN DIEGO – Early wound closure prior to hospital discharge after surgical debridement of infected diabetic foot ulcers yields higher ulcer healing rates and a shorter time to healing, compared with various nonclosure wound management methods, according to a propensity-matched study.
How best to manage the open wound following nonamputative surgery of infected diabetic foot ulcers has been controversial. But early wound closure during the index hospitalization was the clear winner in this comparative study, Dr. Shey-Ying Chen reported at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
He presented a retrospective comparison between 179 diabetic foot ulcer (DFU) patients with early wound closure after surgical debridement and an equal number of matched controls treated with various nonclosure techniques, including negative pressure wound therapy and the repeated application of moist dressings. The two study groups were matched first on the basis of DFU location – toe, forefoot, midfoot, or rear foot – and then further propensity matched based on demographics, comorbid conditions, the presence of neuropathy, ulcer status by Wagner classification, infection severity, revascularization procedures, and other variables.
During 1 year of follow-up post discharge, ulcer healing occurred in 75% of the early wound closure group, compared with 66% of the nonclosure patients. Readmission for further treatment of the index ulcer occurred in 33% of the early closure group and 52% of the nonclosure group. Other outcomes were also superior in the early wound closure group, noted Dr. Chen of Beth Israel Deaconess Medical Center, Boston.
Two independent predictors of DFU healing during the follow-up period emerged from a Cox regression analysis: early wound closure, with an adjusted odds ratio of 1.63, and acute as opposed to chronic DFU, with an OR of 1.35.
Ulcer healing was significantly less likely in patients with peripheral vascular disease, with an OR of 0.62; neuropathy, with an OR of 0.53; and methicillin-resistant Staphylococcus aureus wound infection, with an OR of 0.59, he continued.
Underscoring the longer-term difficulties faced by patients with DFUs, it’s noteworthy that 11.5% of patients in both study arms underwent new amputations during the year of follow-up. Moreover, a new diagnosis of osteomyelitis was made in 20% of the early wound closure group and 26% of the nonclosure group, a nonsignificant difference.
Dr. Adolf W. Karchmer, Dr. Chen’s senior coinvestigator, said the outcome data are too new to be able to gauge how vascular, orthopedic, and podiatric surgeons will react.
The investigators reported having no financial conflicts with regard to this study, conducted without commercial sponsorship.
AT ICAAC 2015
Key clinical point: Diabetic foot ulcers are more likely to heal with early wound closure following surgical debridement than with nonclosure techniques.
Major finding: Healing of diabetic foot ulcers after surgical debridement took an average of 105 days in patients who underwent early wound closure prior to hospital discharge, compared with 136 days in those whose wounds were managed with nonclosure techniques.
Data source: A retrospective, nonrandomized study featuring two propensity score–matched groups, with 179 patients in each, who were followed for 1 year post discharge for surgical debridement of a diabetic foot ulcer.
Disclosures: The presenter reported having no financial conflicts regarding this study, conducted free of commercial support.
Respiratory problems make adenotonsillectomy recovery worse for kids
Respiratory compromise and secondary hemorrhage were the most common early side effects in children who had adenotonsillectomies; children with obstructive sleep apnea (OSA) have nearly five times more respiratory complications after surgery than children without OSA, a multistudy review concluded.

Graziela De Luca Canto, Ph.D., of the Federal University of Santa Catarina, Brazil, and her associates performed a data review by identifying 1,254 different citations found via electronic database searches; after eliminations, only 23 studies were included in the final analysis. Although children with OSA have nearly five times more respiratory complications after adenotonsillectomy than their peers, (odds ratio, 4.90), they are less likely to have postoperative bleeding, compared with children without OSA (OR, 0.41). Among both groups, the most frequent complication was respiratory compromise (9.4%), followed by secondary hemorrhage (2.6%).
Because children with OSA are more likely to require supplemental oxygen, oral or nasal airway insertion, or assisted ventilation in the immediate postoperative period than their peers, the authors suggested that anesthesiologists would be wise to screen patients for snoring, airway dysfunction, and other airway anatomic disorders before performing surgery.
“Children with OSA are clearly at higher anesthetic risk than are patients with normal upper airway function. … Despite the pressure to reduce costs, both surgeons and anesthesiologists should improve screening procedures, perhaps develop alternate surgical approaches, to decrease the risks,” the investigators wrote.
Read the full article in Pediatrics 2015 (doi: 10.1542/peds.2015-1283).
Respiratory compromise and secondary hemorrhage were the most common early side effects in children who had adenotonsillectomies; children with obstructive sleep apnea (OSA) have nearly five times more respiratory complications after surgery than children without OSA, a multistudy review concluded.
Graziela De Luca Canto, Ph.D., of the Federal University of Santa Catarina, Brazil, and her associates performed a data review by identifying 1,254 different citations found via electronic database searches; after eliminations, only 23 studies were included in the final analysis. Although children with OSA have nearly five times more respiratory complications after adenotonsillectomy than their peers, (odds ratio, 4.90), they are less likely to have postoperative bleeding, compared with children without OSA (OR, 0.41). Among both groups, the most frequent complication was respiratory compromise (9.4%), followed by secondary hemorrhage (2.6%).
Because children with OSA are more likely to require supplemental oxygen, oral or nasal airway insertion, or assisted ventilation in the immediate postoperative period than their peers, the authors suggested that anesthesiologists would be wise to screen patients for snoring, airway dysfunction, and other airway anatomic disorders before performing surgery.
“Children with OSA are clearly at higher anesthetic risk than are patients with normal upper airway function. … Despite the pressure to reduce costs, both surgeons and anesthesiologists should improve screening procedures, perhaps develop alternate surgical approaches, to decrease the risks,” the investigators wrote.
Read the full article in Pediatrics 2015 (doi: 10.1542/peds.2015-1283).
Respiratory compromise and secondary hemorrhage were the most common early side effects in children who had adenotonsillectomies; children with obstructive sleep apnea (OSA) have nearly five times more respiratory complications after surgery than children without OSA, a multistudy review concluded.
Graziela De Luca Canto, Ph.D., of the Federal University of Santa Catarina, Brazil, and her associates performed a data review by identifying 1,254 different citations found via electronic database searches; after eliminations, only 23 studies were included in the final analysis. Although children with OSA have nearly five times more respiratory complications after adenotonsillectomy than their peers, (odds ratio, 4.90), they are less likely to have postoperative bleeding, compared with children without OSA (OR, 0.41). Among both groups, the most frequent complication was respiratory compromise (9.4%), followed by secondary hemorrhage (2.6%).
Because children with OSA are more likely to require supplemental oxygen, oral or nasal airway insertion, or assisted ventilation in the immediate postoperative period than their peers, the authors suggested that anesthesiologists would be wise to screen patients for snoring, airway dysfunction, and other airway anatomic disorders before performing surgery.
“Children with OSA are clearly at higher anesthetic risk than are patients with normal upper airway function. … Despite the pressure to reduce costs, both surgeons and anesthesiologists should improve screening procedures, perhaps develop alternate surgical approaches, to decrease the risks,” the investigators wrote.
Read the full article in Pediatrics 2015 (doi: 10.1542/peds.2015-1283).
FROM PEDIATRICS

Readmissions rise with endovascular lower limb procedures
CHICAGO – Endovascular lower-extremity procedures were not associated with lower 30-day readmission rates compared with open surgery in a retrospective review of 7,089 patients.
All-cause, 30-day readmissions were actually higher with an endovascular approach at 12.3% vs. 9.6% for open procedures (Relative risk, 1.28; P = .0003).
Among all patients, an index diagnosis of gangrene was most predictive of readmission (RR, 1.89; P less than .0001), Dr. Todd R. Vogel said at the annual meeting of the Midwestern Vascular Surgical Society.
The data were compiled from 7,089 patients in the Cerner Health Facts database who were admitted for peripheral artery disease and elective lower extremity procedures (3,615 open; 3,474 endo) between September 2008 and March 2014. Their average age was 67.7 years, 44.7% were aged 70 years or older, 60% were men, and 21% were African American.

Older patients and men were significantly more likely to receive endovascular procedures (P less than .0001), said Dr. Vogel, chief of vascular surgery, University of Missouri Health System in Columbia.
Overall, 767 patients (11%) were readmitted (344 open; 423 endo), with gangrene accounting for 21.7% of readmissions.
Other index diagnoses associated with higher 30-day readmissions for all lower extremity procedures were fluid and electrolyte disorders, chronic anemia, lower extremity infection, heart failure, chronic kidney disease, and chronic pulmonary disease.
When stratified by procedure type, the reasons for readmission were very different within the same population of patients based on procedure type, Dr. Vogel said.
Patients who underwent an open procedure were more likely to be readmitted if they had heart failure (RR, 1.78; P less than .0001) or posthemorrhagic anemia (RR, 1.54: P = .006).
Infections – be they lower extremity infection, other infection, postoperative infection, or sepsis – were not predictive of readmission when documented at the index admission for the open cohort.
In contrast, chronic conditions were the major predictors of readmission for patients undergoing endovascular procedures, he said. They included chronic anemia (RR, 1.58; P less than .0001), chronic airway obstruction (RR, 1.36; P = .0095), chronic heart disease (RR, 1.33; P = .0019), chronic kidney disease (RR, 1.37; P = .0013), diabetes (RR, 1.34; P = .0012), and hypertension (RR, 1.27; P = .023).
Fluid and electrolyte disorders (RR, 1.65, P less than .0001) and lower extremity infections (RR, 1.57, P = .0016) were also significant predictors of readmission in the endovascular group.
To ensure there were no disparities between index and readmission diagnoses, a final analysis was performed by procedure type in the 767 readmissions. It confirmed that for the endovascular procedures, chronic problems are bringing patients back to the hospital and not necessarily complications from the procedure, whereas infections, device complications, and hemorrhage are the reasons open surgery patients return, Dr. Vogel said.
“The question is are chronic conditions associated with readmissions the fault of the intervention? As physicians can we hope to curb this in patients who have chronic problems and are then readmitted?” he said.
Some audience members argued that no matter if the patient had a chronic condition or not preoperatively, the responsibility rests with the surgeon because he or she opted to put the patient through an elective endovascular procedure and now they’re returning with chronic heart failure, for example.
Dr. Vogel said this was the first pass at the data and trying to understand what drives readmissions and that it’s possible an endovascular procedure could exacerbate a chronic condition, but that surgeons should take steps to mitigate readmission risk in those with known chronic conditions.
Other attendees questioned how many of the readmissions were planned, hinting that the readmissions may not be directly related to the endovascular technique.
Dr. Vogel said it was difficult using only the ICD-9 codes in the database to determine exactly how many readmissions were planned, but noted that further analyses are intended.
“Reasons for readmission can be exacerbation of chronic patient issues, as seen in the endovascular group, or may be secondary to later complications of the procedure such as wound infections and device complications, as seen after open bypass procedures,” he said in an interview. “Identifying patients with increased risk for readmission after vascular procedures may lead to more effective and higher quality care during the index hospitalization. Our future studies will focus on a more detailed, granular evaluation of these high-risk diagnoses groups through use of the electronic medical record.”
Dr. Vogel reported having no financial disclosures.
On Twitter @pwendl
CHICAGO – Endovascular lower-extremity procedures were not associated with lower 30-day readmission rates compared with open surgery in a retrospective review of 7,089 patients.
All-cause, 30-day readmissions were actually higher with an endovascular approach at 12.3% vs. 9.6% for open procedures (Relative risk, 1.28; P = .0003).
Among all patients, an index diagnosis of gangrene was most predictive of readmission (RR, 1.89; P less than .0001), Dr. Todd R. Vogel said at the annual meeting of the Midwestern Vascular Surgical Society.
The data were compiled from 7,089 patients in the Cerner Health Facts database who were admitted for peripheral artery disease and elective lower extremity procedures (3,615 open; 3,474 endo) between September 2008 and March 2014. Their average age was 67.7 years, 44.7% were aged 70 years or older, 60% were men, and 21% were African American.
Older patients and men were significantly more likely to receive endovascular procedures (P less than .0001), said Dr. Vogel, chief of vascular surgery, University of Missouri Health System in Columbia.
Overall, 767 patients (11%) were readmitted (344 open; 423 endo), with gangrene accounting for 21.7% of readmissions.
Other index diagnoses associated with higher 30-day readmissions for all lower extremity procedures were fluid and electrolyte disorders, chronic anemia, lower extremity infection, heart failure, chronic kidney disease, and chronic pulmonary disease.
When stratified by procedure type, the reasons for readmission were very different within the same population of patients based on procedure type, Dr. Vogel said.
Patients who underwent an open procedure were more likely to be readmitted if they had heart failure (RR, 1.78; P less than .0001) or posthemorrhagic anemia (RR, 1.54: P = .006).
Infections – be they lower extremity infection, other infection, postoperative infection, or sepsis – were not predictive of readmission when documented at the index admission for the open cohort.
In contrast, chronic conditions were the major predictors of readmission for patients undergoing endovascular procedures, he said. They included chronic anemia (RR, 1.58; P less than .0001), chronic airway obstruction (RR, 1.36; P = .0095), chronic heart disease (RR, 1.33; P = .0019), chronic kidney disease (RR, 1.37; P = .0013), diabetes (RR, 1.34; P = .0012), and hypertension (RR, 1.27; P = .023).
Fluid and electrolyte disorders (RR, 1.65, P less than .0001) and lower extremity infections (RR, 1.57, P = .0016) were also significant predictors of readmission in the endovascular group.
To ensure there were no disparities between index and readmission diagnoses, a final analysis was performed by procedure type in the 767 readmissions. It confirmed that for the endovascular procedures, chronic problems are bringing patients back to the hospital and not necessarily complications from the procedure, whereas infections, device complications, and hemorrhage are the reasons open surgery patients return, Dr. Vogel said.
“The question is are chronic conditions associated with readmissions the fault of the intervention? As physicians can we hope to curb this in patients who have chronic problems and are then readmitted?” he said.
Some audience members argued that no matter if the patient had a chronic condition or not preoperatively, the responsibility rests with the surgeon because he or she opted to put the patient through an elective endovascular procedure and now they’re returning with chronic heart failure, for example.
Dr. Vogel said this was the first pass at the data and trying to understand what drives readmissions and that it’s possible an endovascular procedure could exacerbate a chronic condition, but that surgeons should take steps to mitigate readmission risk in those with known chronic conditions.
Other attendees questioned how many of the readmissions were planned, hinting that the readmissions may not be directly related to the endovascular technique.
Dr. Vogel said it was difficult using only the ICD-9 codes in the database to determine exactly how many readmissions were planned, but noted that further analyses are intended.
“Reasons for readmission can be exacerbation of chronic patient issues, as seen in the endovascular group, or may be secondary to later complications of the procedure such as wound infections and device complications, as seen after open bypass procedures,” he said in an interview. “Identifying patients with increased risk for readmission after vascular procedures may lead to more effective and higher quality care during the index hospitalization. Our future studies will focus on a more detailed, granular evaluation of these high-risk diagnoses groups through use of the electronic medical record.”
Dr. Vogel reported having no financial disclosures.
On Twitter @pwendl
CHICAGO – Endovascular lower-extremity procedures were not associated with lower 30-day readmission rates compared with open surgery in a retrospective review of 7,089 patients.
All-cause, 30-day readmissions were actually higher with an endovascular approach at 12.3% vs. 9.6% for open procedures (Relative risk, 1.28; P = .0003).
Among all patients, an index diagnosis of gangrene was most predictive of readmission (RR, 1.89; P less than .0001), Dr. Todd R. Vogel said at the annual meeting of the Midwestern Vascular Surgical Society.
The data were compiled from 7,089 patients in the Cerner Health Facts database who were admitted for peripheral artery disease and elective lower extremity procedures (3,615 open; 3,474 endo) between September 2008 and March 2014. Their average age was 67.7 years, 44.7% were aged 70 years or older, 60% were men, and 21% were African American.
Older patients and men were significantly more likely to receive endovascular procedures (P less than .0001), said Dr. Vogel, chief of vascular surgery, University of Missouri Health System in Columbia.
Overall, 767 patients (11%) were readmitted (344 open; 423 endo), with gangrene accounting for 21.7% of readmissions.
Other index diagnoses associated with higher 30-day readmissions for all lower extremity procedures were fluid and electrolyte disorders, chronic anemia, lower extremity infection, heart failure, chronic kidney disease, and chronic pulmonary disease.
When stratified by procedure type, the reasons for readmission were very different within the same population of patients based on procedure type, Dr. Vogel said.
Patients who underwent an open procedure were more likely to be readmitted if they had heart failure (RR, 1.78; P less than .0001) or posthemorrhagic anemia (RR, 1.54: P = .006).
Infections – be they lower extremity infection, other infection, postoperative infection, or sepsis – were not predictive of readmission when documented at the index admission for the open cohort.
In contrast, chronic conditions were the major predictors of readmission for patients undergoing endovascular procedures, he said. They included chronic anemia (RR, 1.58; P less than .0001), chronic airway obstruction (RR, 1.36; P = .0095), chronic heart disease (RR, 1.33; P = .0019), chronic kidney disease (RR, 1.37; P = .0013), diabetes (RR, 1.34; P = .0012), and hypertension (RR, 1.27; P = .023).
Fluid and electrolyte disorders (RR, 1.65, P less than .0001) and lower extremity infections (RR, 1.57, P = .0016) were also significant predictors of readmission in the endovascular group.
To ensure there were no disparities between index and readmission diagnoses, a final analysis was performed by procedure type in the 767 readmissions. It confirmed that for the endovascular procedures, chronic problems are bringing patients back to the hospital and not necessarily complications from the procedure, whereas infections, device complications, and hemorrhage are the reasons open surgery patients return, Dr. Vogel said.
“The question is are chronic conditions associated with readmissions the fault of the intervention? As physicians can we hope to curb this in patients who have chronic problems and are then readmitted?” he said.
Some audience members argued that no matter if the patient had a chronic condition or not preoperatively, the responsibility rests with the surgeon because he or she opted to put the patient through an elective endovascular procedure and now they’re returning with chronic heart failure, for example.
Dr. Vogel said this was the first pass at the data and trying to understand what drives readmissions and that it’s possible an endovascular procedure could exacerbate a chronic condition, but that surgeons should take steps to mitigate readmission risk in those with known chronic conditions.
Other attendees questioned how many of the readmissions were planned, hinting that the readmissions may not be directly related to the endovascular technique.
Dr. Vogel said it was difficult using only the ICD-9 codes in the database to determine exactly how many readmissions were planned, but noted that further analyses are intended.
“Reasons for readmission can be exacerbation of chronic patient issues, as seen in the endovascular group, or may be secondary to later complications of the procedure such as wound infections and device complications, as seen after open bypass procedures,” he said in an interview. “Identifying patients with increased risk for readmission after vascular procedures may lead to more effective and higher quality care during the index hospitalization. Our future studies will focus on a more detailed, granular evaluation of these high-risk diagnoses groups through use of the electronic medical record.”
Dr. Vogel reported having no financial disclosures.
On Twitter @pwendl
AT MIDWESTERN VASCULAR 2015
Key clinical point: Endovascular procedures were not superior to open surgery in reducing 30-day readmissions in patients undergoing lower extremity procedures.
Major finding: All-cause 30-day readmissions were 12.3% for endovascular and 9.6% for open (P = .0003).
Data source: Retrospective study in 7,089 patients undergoing elective lower extremity procedures.
Disclosures: The research was supported by an award from the Agency for Healthcare Research and Quality. Dr. Vogel reported having no conflicts of interest.

Debunking five myths about minilaparoscopy
NEW YORK – The next big advance in gynecologic minimally invasive surgery could be the wider adoption of minilaparoscopy using newer, frictionless instruments.
Minilaparoscopy is commonly used in cholecystectomy, but is making inroads in gynecology. Minilaparoscopy performed with the newer, smaller instruments is especially well suited for fertility procedures and endometriosis surgery, according to Dr. Gustavo Carvalho, a pioneer in minilaparoscopy. Gynecologists are using minilaparoscopy successfully in hysterectomy as well, but the mini-instruments are not strong enough to survive many hysterectomies, he added.
“Traditional laparoscopy is suited for brutal procedures, such as hysterectomy, but minilap is better for delicate procedures requiring precise, tiny instruments,” Dr. Carvalho said at the meeting.
Despite the promise of utilizing the newer instruments, many surgeons have misconceptions about them.
“This is partly related to instruments used in older procedures called minilap. But after they try it with these newer instruments and learn how to do it, they actually prefer it for many procedures,” Dr. Carvalho, an associate professor of general surgery at Pernambuco University, Recife, Brazil, said in an interview.
Dr. Carvalho debunked the following “myths” about minilaparoscopy:
1. Single-port laparoscopy is cosmetically superior to minilaparoscopy. That’s not the case, Dr. Carvalho said. The few published papers on this subject compared single-port laparoscopy with older, high-friction instruments for minilaparoscopy, he said.
2. Minilaparoscopy should not be performed on obese patients. That’s false, Dr. Carvalho said. “Using newer instruments, we can move around better and see better for delicate operations in obese patients, but surgeons need special training,” he said.
3. Patients don’t want minilaparoscopy. The only published paper looking at patient preference did not offer patients minilaparoscopy with the newer instruments, Dr. Carvalho said. He and his colleagues plans to publish a paper based on research showing that 47% of patients prefer minilaparoscopy, compared with 27% who preferred single-port procedures. “There is a role for single-port procedures,” he added.
4. Minilaparoscopy hurts more than single-port laparoscopy. “No one can prove that minilap hurts less, but it is obvious and intuitive that smaller trocars and instruments cause less pain,” Dr. Carvalho said. “Surgeons want randomized trials, but they won’t be done because this is obvious.”
5. Surgeons lose dexterity and precision with minilaparoscopy. In new research that will be published in the Journal of the Society Laparoendoscopic Surgeons, Dr. Caravalho and his colleagues demonstrate that newer minilaparoscopy instruments are better than larger instruments for delicate tasks. In this study, 22 medical students and 22 surgical residents were given one gross task and three delicate tasks to perform randomly with a 3-mm frictionless trocar, a 3-mm high-friction trocar, and a 5-mm trocar. The larger instruments were significantly better for the gross task, while the smaller instruments were significantly better for the delicate tasks, Dr. Carvalho said. “This study shows the utility of precise, delicate instruments for delicate procedures,” he said.
Dr. Caravalho reported that he is an unpaid consultant for Karl Storz on the development of minilaparoscopic low-friction trocars.
NEW YORK – The next big advance in gynecologic minimally invasive surgery could be the wider adoption of minilaparoscopy using newer, frictionless instruments.
Minilaparoscopy is commonly used in cholecystectomy, but is making inroads in gynecology. Minilaparoscopy performed with the newer, smaller instruments is especially well suited for fertility procedures and endometriosis surgery, according to Dr. Gustavo Carvalho, a pioneer in minilaparoscopy. Gynecologists are using minilaparoscopy successfully in hysterectomy as well, but the mini-instruments are not strong enough to survive many hysterectomies, he added.
“Traditional laparoscopy is suited for brutal procedures, such as hysterectomy, but minilap is better for delicate procedures requiring precise, tiny instruments,” Dr. Carvalho said at the meeting.
Despite the promise of utilizing the newer instruments, many surgeons have misconceptions about them.
“This is partly related to instruments used in older procedures called minilap. But after they try it with these newer instruments and learn how to do it, they actually prefer it for many procedures,” Dr. Carvalho, an associate professor of general surgery at Pernambuco University, Recife, Brazil, said in an interview.
Dr. Carvalho debunked the following “myths” about minilaparoscopy:
1. Single-port laparoscopy is cosmetically superior to minilaparoscopy. That’s not the case, Dr. Carvalho said. The few published papers on this subject compared single-port laparoscopy with older, high-friction instruments for minilaparoscopy, he said.
2. Minilaparoscopy should not be performed on obese patients. That’s false, Dr. Carvalho said. “Using newer instruments, we can move around better and see better for delicate operations in obese patients, but surgeons need special training,” he said.
3. Patients don’t want minilaparoscopy. The only published paper looking at patient preference did not offer patients minilaparoscopy with the newer instruments, Dr. Carvalho said. He and his colleagues plans to publish a paper based on research showing that 47% of patients prefer minilaparoscopy, compared with 27% who preferred single-port procedures. “There is a role for single-port procedures,” he added.
4. Minilaparoscopy hurts more than single-port laparoscopy. “No one can prove that minilap hurts less, but it is obvious and intuitive that smaller trocars and instruments cause less pain,” Dr. Carvalho said. “Surgeons want randomized trials, but they won’t be done because this is obvious.”
5. Surgeons lose dexterity and precision with minilaparoscopy. In new research that will be published in the Journal of the Society Laparoendoscopic Surgeons, Dr. Caravalho and his colleagues demonstrate that newer minilaparoscopy instruments are better than larger instruments for delicate tasks. In this study, 22 medical students and 22 surgical residents were given one gross task and three delicate tasks to perform randomly with a 3-mm frictionless trocar, a 3-mm high-friction trocar, and a 5-mm trocar. The larger instruments were significantly better for the gross task, while the smaller instruments were significantly better for the delicate tasks, Dr. Carvalho said. “This study shows the utility of precise, delicate instruments for delicate procedures,” he said.
Dr. Caravalho reported that he is an unpaid consultant for Karl Storz on the development of minilaparoscopic low-friction trocars.
NEW YORK – The next big advance in gynecologic minimally invasive surgery could be the wider adoption of minilaparoscopy using newer, frictionless instruments.
Minilaparoscopy is commonly used in cholecystectomy, but is making inroads in gynecology. Minilaparoscopy performed with the newer, smaller instruments is especially well suited for fertility procedures and endometriosis surgery, according to Dr. Gustavo Carvalho, a pioneer in minilaparoscopy. Gynecologists are using minilaparoscopy successfully in hysterectomy as well, but the mini-instruments are not strong enough to survive many hysterectomies, he added.
“Traditional laparoscopy is suited for brutal procedures, such as hysterectomy, but minilap is better for delicate procedures requiring precise, tiny instruments,” Dr. Carvalho said at the meeting.
Despite the promise of utilizing the newer instruments, many surgeons have misconceptions about them.
“This is partly related to instruments used in older procedures called minilap. But after they try it with these newer instruments and learn how to do it, they actually prefer it for many procedures,” Dr. Carvalho, an associate professor of general surgery at Pernambuco University, Recife, Brazil, said in an interview.
Dr. Carvalho debunked the following “myths” about minilaparoscopy:
1. Single-port laparoscopy is cosmetically superior to minilaparoscopy. That’s not the case, Dr. Carvalho said. The few published papers on this subject compared single-port laparoscopy with older, high-friction instruments for minilaparoscopy, he said.
2. Minilaparoscopy should not be performed on obese patients. That’s false, Dr. Carvalho said. “Using newer instruments, we can move around better and see better for delicate operations in obese patients, but surgeons need special training,” he said.
3. Patients don’t want minilaparoscopy. The only published paper looking at patient preference did not offer patients minilaparoscopy with the newer instruments, Dr. Carvalho said. He and his colleagues plans to publish a paper based on research showing that 47% of patients prefer minilaparoscopy, compared with 27% who preferred single-port procedures. “There is a role for single-port procedures,” he added.
4. Minilaparoscopy hurts more than single-port laparoscopy. “No one can prove that minilap hurts less, but it is obvious and intuitive that smaller trocars and instruments cause less pain,” Dr. Carvalho said. “Surgeons want randomized trials, but they won’t be done because this is obvious.”
5. Surgeons lose dexterity and precision with minilaparoscopy. In new research that will be published in the Journal of the Society Laparoendoscopic Surgeons, Dr. Caravalho and his colleagues demonstrate that newer minilaparoscopy instruments are better than larger instruments for delicate tasks. In this study, 22 medical students and 22 surgical residents were given one gross task and three delicate tasks to perform randomly with a 3-mm frictionless trocar, a 3-mm high-friction trocar, and a 5-mm trocar. The larger instruments were significantly better for the gross task, while the smaller instruments were significantly better for the delicate tasks, Dr. Carvalho said. “This study shows the utility of precise, delicate instruments for delicate procedures,” he said.
Dr. Caravalho reported that he is an unpaid consultant for Karl Storz on the development of minilaparoscopic low-friction trocars.
EXPERT ANALYSIS FROM MINIMALLY INVASIVE SURGERY WEEK
Smoother orthopedic implants may minimize bacterial adherence
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”

He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”
He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
SAN DIEGO – Rough materials used for orthopedic implants, such as cobalt chromium and titanium, increased bacterial adherence, while smoother materials such as stainless steel did not, results from an image analysis demonstrated.
“In light of these results, it is important to question why we utilize the types of materials we use for various orthopedic procedures,” Dioscaris R. Garcia, Ph.D., said in an interview in advance of the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “There was no one-size-fits-all material to minimize adherence per the findings of this study, but the findings may suggest that having a smoother surface may minimize the ability of bacterial pathogens to adhere to the surface.”
He characterized the topic of bacterial adherence to orthopedic implants as “an issue of great interest due to how little is known about the biological implications of the materials utilized. The most researched of these materials is titanium, which is touted for its biocompatibility. This study aims to provide a base and a glimpse into how the most commonly utilized orthopedic-relevant materials interact with some of the most commonly encountered pathogens.”
For the study, Dr. Garcia, a molecular pharmacologist at Rhode Island Hospital in Providence, Dr. Alan H. Daniels, an orthopedic surgeon at the hospital, and their associates used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens (methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, coagulase-negative Staphylococcus epidermidis, multidrug-resistant Acinetobacter baumannii, Propionibacterium acnes, and vancomycin-resistant Enterococcus faecalis) on five commonly used spinal implant materials (titanium, titanium alloy, stainless steel, cobalt chromium, and polyetherether ketone). The samples were fixed and dehydrated via ethanol dehydration gradient and critical point drying.
The researchers found that some pathogens, such as vancomycin-resistant E. faecalis and multidrug-resistant A. baumannii, were more likely to adhere to more textured materials such as cobalt chromium and titanium, compared with smoother materials such as stainless steel. “Additionally, the findings suggest that the microtopography of these materials may be the driving force behind the adherence of pathogens on the materials themselves,” Dr. Garcia said. Compared with smoother, polished materials, he explained, the rougher materials were more likely to harbor dense proliferation of bacterial pathogens, which could be characterized as biofilms.
“This study has been successful in providing a platform for future studies to build upon and expand to study additional parameters and statistical tools to give further insight into additional driving forces behind adherence and means for improvement of material design,” Dr. Garcia concluded.
Dr. Christopher T. Born, head of the Diane N. Weiss Center for Orthopedic Trauma Research at Rhode Island Hospital, was the study’s principal investigator. The study was supported by Stryker Corp.*
*Correction, 9/19/2015: Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.
AT ICAAC 2015
Key clinical point: Orthopedic implants made from smoother material may minimize bacterial adherence.
Major finding: Some pathogens, such as vancomycin-resistant Enterococcus faecalis and multidrug-resistant Acinetobacter baumannii, were more likely to adhere to more textured materials like cobalt chromium and titanium, compared with smoother materials such as stainless steel.
Data source: A study that used scanning electron microscopy and confocal laser scanning microscopy to evaluate the adherence pattern, density, and propagation of six commonly encountered bacterial pathogens on five commonly used spinal implant materials.
Disclosures: The study was supported by Stryker Corp. Dr. Born is a consultant for Stryker. He also has stock ownership in Biointraface, does consulting for the company, and is a member of its board.*

PROPPR finds resuscitation strategy had no effect on laparotomy outcomes
LAS VEGAS – Choice of damage control resuscitation – plasma-platelet-red blood cell ratio of either 1:1:1 or 1:1:2 – did not affect whether severely injured patients required an emergency laparotomy, nor did it affect time to laparotomy or survival following laparotomy, according to findings from the Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) trial.
“We were unable to detect significant effects of damage control resuscitation on the frequency and time to emergency laparotomy, outcomes, disposition at 30 days, or main endpoint survival,” said Dr. Vicente J. Undurraga Perl of the Oregon Health and Science University, Portland. The lack of a difference between the treatment groups with respect to emergency laparotomy and 30-day survival may be a result of the low overall mortality of 23% and to the study being underpowered to detect a difference between the groups.
The PROPPR trial demonstrated that damage control resuscitation, defined as “a massive transfusion strategy targeting a balanced delivery of plasma-platelet-RBC in a ratio of 1:1:1,” allows earlier achievement of hemostasis in a greater number of severely injured patients than does a 1:1:2 ratio. A corresponding reduction in deaths because of exsanguination was observed in the study subjects, who were enrolled from 12 level-1 trauma centers in North America, where they presented with severe injuries.
Of 680 patients who had severe injuries and were predicted to require massive transfusions, 613 underwent a surgical procedure and 397 underwent a laparotomy. Of the latter, 346 were emergency laparotomies. Of those who received damage control resuscitation using the 1:1:1 ratio, 52% underwent emergency laparotomy (defined as laparotomy within 90 minutes of arrival at a trauma center). Of those who received the 1:1:2 ratio, 50% underwent emergency laparotomy. The difference between the groups was not statistically significant, Dr. Perl reported at the annual meeting of the American Association for the Surgery of Trauma.
The median time to laparotomy was 28 minutes in both groups, and the proportions of patients who survived to 3 hours, 6 hours, 24 hours, and 30 days also were similar in the two groups. For example, 88% and 85% of those in the 1:1:1 and 1:1:2 groups, respectively, survived to 24 hours; 82% and 77%, respectively, survived to 30 days, he said.
There was no overall difference in mortality between the groups (hazard ratio, 0.78), nor was there a difference in survival by study site, he noted.
Dr. Perl reported having no disclosures.
LAS VEGAS – Choice of damage control resuscitation – plasma-platelet-red blood cell ratio of either 1:1:1 or 1:1:2 – did not affect whether severely injured patients required an emergency laparotomy, nor did it affect time to laparotomy or survival following laparotomy, according to findings from the Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) trial.
“We were unable to detect significant effects of damage control resuscitation on the frequency and time to emergency laparotomy, outcomes, disposition at 30 days, or main endpoint survival,” said Dr. Vicente J. Undurraga Perl of the Oregon Health and Science University, Portland. The lack of a difference between the treatment groups with respect to emergency laparotomy and 30-day survival may be a result of the low overall mortality of 23% and to the study being underpowered to detect a difference between the groups.
The PROPPR trial demonstrated that damage control resuscitation, defined as “a massive transfusion strategy targeting a balanced delivery of plasma-platelet-RBC in a ratio of 1:1:1,” allows earlier achievement of hemostasis in a greater number of severely injured patients than does a 1:1:2 ratio. A corresponding reduction in deaths because of exsanguination was observed in the study subjects, who were enrolled from 12 level-1 trauma centers in North America, where they presented with severe injuries.
Of 680 patients who had severe injuries and were predicted to require massive transfusions, 613 underwent a surgical procedure and 397 underwent a laparotomy. Of the latter, 346 were emergency laparotomies. Of those who received damage control resuscitation using the 1:1:1 ratio, 52% underwent emergency laparotomy (defined as laparotomy within 90 minutes of arrival at a trauma center). Of those who received the 1:1:2 ratio, 50% underwent emergency laparotomy. The difference between the groups was not statistically significant, Dr. Perl reported at the annual meeting of the American Association for the Surgery of Trauma.
The median time to laparotomy was 28 minutes in both groups, and the proportions of patients who survived to 3 hours, 6 hours, 24 hours, and 30 days also were similar in the two groups. For example, 88% and 85% of those in the 1:1:1 and 1:1:2 groups, respectively, survived to 24 hours; 82% and 77%, respectively, survived to 30 days, he said.
There was no overall difference in mortality between the groups (hazard ratio, 0.78), nor was there a difference in survival by study site, he noted.
Dr. Perl reported having no disclosures.
LAS VEGAS – Choice of damage control resuscitation – plasma-platelet-red blood cell ratio of either 1:1:1 or 1:1:2 – did not affect whether severely injured patients required an emergency laparotomy, nor did it affect time to laparotomy or survival following laparotomy, according to findings from the Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) trial.
“We were unable to detect significant effects of damage control resuscitation on the frequency and time to emergency laparotomy, outcomes, disposition at 30 days, or main endpoint survival,” said Dr. Vicente J. Undurraga Perl of the Oregon Health and Science University, Portland. The lack of a difference between the treatment groups with respect to emergency laparotomy and 30-day survival may be a result of the low overall mortality of 23% and to the study being underpowered to detect a difference between the groups.
The PROPPR trial demonstrated that damage control resuscitation, defined as “a massive transfusion strategy targeting a balanced delivery of plasma-platelet-RBC in a ratio of 1:1:1,” allows earlier achievement of hemostasis in a greater number of severely injured patients than does a 1:1:2 ratio. A corresponding reduction in deaths because of exsanguination was observed in the study subjects, who were enrolled from 12 level-1 trauma centers in North America, where they presented with severe injuries.
Of 680 patients who had severe injuries and were predicted to require massive transfusions, 613 underwent a surgical procedure and 397 underwent a laparotomy. Of the latter, 346 were emergency laparotomies. Of those who received damage control resuscitation using the 1:1:1 ratio, 52% underwent emergency laparotomy (defined as laparotomy within 90 minutes of arrival at a trauma center). Of those who received the 1:1:2 ratio, 50% underwent emergency laparotomy. The difference between the groups was not statistically significant, Dr. Perl reported at the annual meeting of the American Association for the Surgery of Trauma.
The median time to laparotomy was 28 minutes in both groups, and the proportions of patients who survived to 3 hours, 6 hours, 24 hours, and 30 days also were similar in the two groups. For example, 88% and 85% of those in the 1:1:1 and 1:1:2 groups, respectively, survived to 24 hours; 82% and 77%, respectively, survived to 30 days, he said.
There was no overall difference in mortality between the groups (hazard ratio, 0.78), nor was there a difference in survival by study site, he noted.
Dr. Perl reported having no disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point: Choice of damage control resuscitation – plasma-platelet-red blood cell ratio of either 1:1:1 or 1:1:2 – does not affect whether severely injured patients require an emergency laparotomy, time to laparotomy, or survival following laparotomy.
Major finding: 52% of patients in the 1:1:1-ratio emergency resuscitation group and 50% in the 1:1:2-ratio group underwent emergency laparotomy, and 30-day survival was 82% and 77%, respectively.
Data source: An analysis of data for 680 patients from the PROPPR trial.
Disclosures: Dr. Perl reported having no disclosures.
Uninsured dropped by nearly 9 million between 2013 and 2014
Nearly 9 million Americans gained health insurance between 2013 and 2014, data from the U.S. Census Bureau show.
Results from the U.S. Census Bureau Current Population Survey of 98,000 adults showed that 10.4% of Americans – 33 million people – were uninsured in 2014, down from 13.3% in 2013. The survey is the first to compare data from immediately before the law took full effect and the year it did take full effect.

Although the Affordable Care Act was passed in 2010, it did not reach its full effect until 2014. Citing similar data from a number of other surveys, both public and private, the Commonwealth Fund says the findings provide “further evidence the law is having its intended effect of reducing the number of Americans who lack health insurance.”
The survey also showed that decreases in the uninsured rate tended to be larger in states that expanded Medicaid eligibility. Texas, Florida, and Alaska, where Medicaid eligibility has not been expanded, topped the list of states with the highest uninsured rates at or above 16%. Overall uninsured rates in states that expanded their Medicaid programs ranged from 3.3% in Massachusetts to 15% in Nevada.
U.S. residents most likely to have benefited from the ACA are young adults, older adults with low to moderate incomes, African Americans, and Latinos, all of whom showed at least 3% gains in coverage.
On Twitter @whitneymcknight
Nearly 9 million Americans gained health insurance between 2013 and 2014, data from the U.S. Census Bureau show.
Results from the U.S. Census Bureau Current Population Survey of 98,000 adults showed that 10.4% of Americans – 33 million people – were uninsured in 2014, down from 13.3% in 2013. The survey is the first to compare data from immediately before the law took full effect and the year it did take full effect.
Although the Affordable Care Act was passed in 2010, it did not reach its full effect until 2014. Citing similar data from a number of other surveys, both public and private, the Commonwealth Fund says the findings provide “further evidence the law is having its intended effect of reducing the number of Americans who lack health insurance.”
The survey also showed that decreases in the uninsured rate tended to be larger in states that expanded Medicaid eligibility. Texas, Florida, and Alaska, where Medicaid eligibility has not been expanded, topped the list of states with the highest uninsured rates at or above 16%. Overall uninsured rates in states that expanded their Medicaid programs ranged from 3.3% in Massachusetts to 15% in Nevada.
U.S. residents most likely to have benefited from the ACA are young adults, older adults with low to moderate incomes, African Americans, and Latinos, all of whom showed at least 3% gains in coverage.
On Twitter @whitneymcknight
Nearly 9 million Americans gained health insurance between 2013 and 2014, data from the U.S. Census Bureau show.
Results from the U.S. Census Bureau Current Population Survey of 98,000 adults showed that 10.4% of Americans – 33 million people – were uninsured in 2014, down from 13.3% in 2013. The survey is the first to compare data from immediately before the law took full effect and the year it did take full effect.
Although the Affordable Care Act was passed in 2010, it did not reach its full effect until 2014. Citing similar data from a number of other surveys, both public and private, the Commonwealth Fund says the findings provide “further evidence the law is having its intended effect of reducing the number of Americans who lack health insurance.”
The survey also showed that decreases in the uninsured rate tended to be larger in states that expanded Medicaid eligibility. Texas, Florida, and Alaska, where Medicaid eligibility has not been expanded, topped the list of states with the highest uninsured rates at or above 16%. Overall uninsured rates in states that expanded their Medicaid programs ranged from 3.3% in Massachusetts to 15% in Nevada.
U.S. residents most likely to have benefited from the ACA are young adults, older adults with low to moderate incomes, African Americans, and Latinos, all of whom showed at least 3% gains in coverage.
On Twitter @whitneymcknight

No difference in long-term cost for diabetes treatment with bariatric surgery
There was no difference in long-term health care cost between conventional treatment and bariatric surgery in patients with diabetes, according to a study published in the Lancet online Sept. 17.
Elevated body mass index is associated with an increased risk of diabetes. However, devising effective lifestyle interventions to reduce weight in the severely obese remains a challenge. Data from the Swedish Obese Subjects (SOS) study have demonstrated prevention and remission of type 2 diabetes after bariatric surgery.
Catherine Keating, Ph.D., of the Deakin Health Economics and Baker IDI Heart and Diabetes Institute in Melbourne, and her associates sought to quantify the health care costs during a 15-year period for obese patients treated with bariatric surgery versus conventional treatment.
Data on prescription drug costs were obtained by questionnaires from participants in the SOS study and the Swedish Prescribed Drug Register. The Swedish National Patient Register was used to obtain data on the outpatient and inpatient visits. The participants were followed for up to 15 years.
The original SOS study was a prospective study that compared treatment outcomes and costs in two groups of obese adults: those who underwent bariatric surgery versus a control cohort who received conventional obesity management. The participants ranged from 37 to 60 years old with BMIs of greater than 34 kg/m2 in men and greater than 38 in women. Conventional treatment included behavior modification, lifestyle intervention, or no treatment.
The definition of diabetes was based on a self-report of taking diabetes drugs or a fasting glucose measurement.
After exclusions, 4,030 participants were included; of these, 2,836 were euglycemic, 591 had prediabetes, and 603 were diabetic, the investigators reported (Lancet 2015 Sep 16 [doi: 10.1016/
S2213-8587(15)00290-9]).

Patients in the bariatric surgery groups were on average 6.2 kg heavier (P less than .0001) and 1.5 years younger (P less than .0001) than were the controls. After the 15-year follow-up, weight loss was 16 kg greater in the diabetes subgroup, 18 kg greater in the prediabetes subgroup, and 20 kg greater in the euglycemia subgroup who had bariatric surgery versus conventional treatment (P less than .0001 for all).
After 15 years, the aggregated drug costs were not different between the conventional treatment group and the bariatric surgery group in patients with euglycemia. However, drug costs were lower in the prediabetic participants who had surgery versus conventional treatment (P = .007). Similarly, patients with diabetes who underwent bariatric surgery incurred lower drug costs after 15 years (P less than .0001).
The inpatient hospital costs after 15 years were greater in the surgery group for all glucose levels versus conventional treatment (mean, $51,225 vs. $25,313; P less than .0001).
There were no differences in outpatient costs demonstrated between the glucose subgroups. However, in the diabetes group, there were wide confidence intervals associated with outpatient costs that were thought to be secondary to end-stage renal disease visits.
Finally, the total cost of health care for the euglycemic group was higher in those who underwent surgery versus conventional treatment (P less than .0001). The prediabetic subgroup also incurred a higher total health care cost for surgery versus conventional treatment (P less than .0001). However, there were no differences in total health care cost for patients with diabetes who had surgery versus conventional treatment ($88,572 vs. $79,967, P less than .090).
The total cost was also higher in patients with diabetes for more than 1 year who had surgical intervention versus those who got conventional treatment (P less than .011). However, patients with diabetes for less than 1 year did not show differences in total cost when treated with surgery versus conventional treatments (P less than .476)
“In this study, we show that for obese patients with type 2 diabetes, the upfront costs of bariatric surgery seem to be largely offset by prevention of future health care and drug use,” the authors wrote. In addition, “long-term health care cost results support prioritization of patients with obesity and type 2 diabetes for bariatric surgery.”
This study was supported by a grant from AFA Forsakring. The authors reported multiple disclosures.
Bariatric surgery should be considered, irrespective of body mas index, in patients whose diabetes is not under control, despite the use of medications and lifestyle interventions.
Since the start of the SOS study, bariatric surgery has changed, and present day surgical costs would be lower.
Dr. Ricardo Cohen is affiliated with the Center for Obesity and Diabetes in Sao Paulo, Brazil. These comments were taken from an accompanying editorial (Lancet 2015 Sep 16 [doi: 10.1016/S2213-8587(15)00320-4]). No conflicts of interests were declared.
Bariatric surgery should be considered, irrespective of body mas index, in patients whose diabetes is not under control, despite the use of medications and lifestyle interventions.
Since the start of the SOS study, bariatric surgery has changed, and present day surgical costs would be lower.
Dr. Ricardo Cohen is affiliated with the Center for Obesity and Diabetes in Sao Paulo, Brazil. These comments were taken from an accompanying editorial (Lancet 2015 Sep 16 [doi: 10.1016/S2213-8587(15)00320-4]). No conflicts of interests were declared.
Bariatric surgery should be considered, irrespective of body mas index, in patients whose diabetes is not under control, despite the use of medications and lifestyle interventions.
Since the start of the SOS study, bariatric surgery has changed, and present day surgical costs would be lower.
Dr. Ricardo Cohen is affiliated with the Center for Obesity and Diabetes in Sao Paulo, Brazil. These comments were taken from an accompanying editorial (Lancet 2015 Sep 16 [doi: 10.1016/S2213-8587(15)00320-4]). No conflicts of interests were declared.
There was no difference in long-term health care cost between conventional treatment and bariatric surgery in patients with diabetes, according to a study published in the Lancet online Sept. 17.
Elevated body mass index is associated with an increased risk of diabetes. However, devising effective lifestyle interventions to reduce weight in the severely obese remains a challenge. Data from the Swedish Obese Subjects (SOS) study have demonstrated prevention and remission of type 2 diabetes after bariatric surgery.
Catherine Keating, Ph.D., of the Deakin Health Economics and Baker IDI Heart and Diabetes Institute in Melbourne, and her associates sought to quantify the health care costs during a 15-year period for obese patients treated with bariatric surgery versus conventional treatment.
Data on prescription drug costs were obtained by questionnaires from participants in the SOS study and the Swedish Prescribed Drug Register. The Swedish National Patient Register was used to obtain data on the outpatient and inpatient visits. The participants were followed for up to 15 years.
The original SOS study was a prospective study that compared treatment outcomes and costs in two groups of obese adults: those who underwent bariatric surgery versus a control cohort who received conventional obesity management. The participants ranged from 37 to 60 years old with BMIs of greater than 34 kg/m2 in men and greater than 38 in women. Conventional treatment included behavior modification, lifestyle intervention, or no treatment.
The definition of diabetes was based on a self-report of taking diabetes drugs or a fasting glucose measurement.
After exclusions, 4,030 participants were included; of these, 2,836 were euglycemic, 591 had prediabetes, and 603 were diabetic, the investigators reported (Lancet 2015 Sep 16 [doi: 10.1016/
S2213-8587(15)00290-9]).
Patients in the bariatric surgery groups were on average 6.2 kg heavier (P less than .0001) and 1.5 years younger (P less than .0001) than were the controls. After the 15-year follow-up, weight loss was 16 kg greater in the diabetes subgroup, 18 kg greater in the prediabetes subgroup, and 20 kg greater in the euglycemia subgroup who had bariatric surgery versus conventional treatment (P less than .0001 for all).
After 15 years, the aggregated drug costs were not different between the conventional treatment group and the bariatric surgery group in patients with euglycemia. However, drug costs were lower in the prediabetic participants who had surgery versus conventional treatment (P = .007). Similarly, patients with diabetes who underwent bariatric surgery incurred lower drug costs after 15 years (P less than .0001).
The inpatient hospital costs after 15 years were greater in the surgery group for all glucose levels versus conventional treatment (mean, $51,225 vs. $25,313; P less than .0001).
There were no differences in outpatient costs demonstrated between the glucose subgroups. However, in the diabetes group, there were wide confidence intervals associated with outpatient costs that were thought to be secondary to end-stage renal disease visits.
Finally, the total cost of health care for the euglycemic group was higher in those who underwent surgery versus conventional treatment (P less than .0001). The prediabetic subgroup also incurred a higher total health care cost for surgery versus conventional treatment (P less than .0001). However, there were no differences in total health care cost for patients with diabetes who had surgery versus conventional treatment ($88,572 vs. $79,967, P less than .090).
The total cost was also higher in patients with diabetes for more than 1 year who had surgical intervention versus those who got conventional treatment (P less than .011). However, patients with diabetes for less than 1 year did not show differences in total cost when treated with surgery versus conventional treatments (P less than .476)
“In this study, we show that for obese patients with type 2 diabetes, the upfront costs of bariatric surgery seem to be largely offset by prevention of future health care and drug use,” the authors wrote. In addition, “long-term health care cost results support prioritization of patients with obesity and type 2 diabetes for bariatric surgery.”
This study was supported by a grant from AFA Forsakring. The authors reported multiple disclosures.
There was no difference in long-term health care cost between conventional treatment and bariatric surgery in patients with diabetes, according to a study published in the Lancet online Sept. 17.
Elevated body mass index is associated with an increased risk of diabetes. However, devising effective lifestyle interventions to reduce weight in the severely obese remains a challenge. Data from the Swedish Obese Subjects (SOS) study have demonstrated prevention and remission of type 2 diabetes after bariatric surgery.
Catherine Keating, Ph.D., of the Deakin Health Economics and Baker IDI Heart and Diabetes Institute in Melbourne, and her associates sought to quantify the health care costs during a 15-year period for obese patients treated with bariatric surgery versus conventional treatment.
Data on prescription drug costs were obtained by questionnaires from participants in the SOS study and the Swedish Prescribed Drug Register. The Swedish National Patient Register was used to obtain data on the outpatient and inpatient visits. The participants were followed for up to 15 years.
The original SOS study was a prospective study that compared treatment outcomes and costs in two groups of obese adults: those who underwent bariatric surgery versus a control cohort who received conventional obesity management. The participants ranged from 37 to 60 years old with BMIs of greater than 34 kg/m2 in men and greater than 38 in women. Conventional treatment included behavior modification, lifestyle intervention, or no treatment.
The definition of diabetes was based on a self-report of taking diabetes drugs or a fasting glucose measurement.
After exclusions, 4,030 participants were included; of these, 2,836 were euglycemic, 591 had prediabetes, and 603 were diabetic, the investigators reported (Lancet 2015 Sep 16 [doi: 10.1016/
S2213-8587(15)00290-9]).
Patients in the bariatric surgery groups were on average 6.2 kg heavier (P less than .0001) and 1.5 years younger (P less than .0001) than were the controls. After the 15-year follow-up, weight loss was 16 kg greater in the diabetes subgroup, 18 kg greater in the prediabetes subgroup, and 20 kg greater in the euglycemia subgroup who had bariatric surgery versus conventional treatment (P less than .0001 for all).
After 15 years, the aggregated drug costs were not different between the conventional treatment group and the bariatric surgery group in patients with euglycemia. However, drug costs were lower in the prediabetic participants who had surgery versus conventional treatment (P = .007). Similarly, patients with diabetes who underwent bariatric surgery incurred lower drug costs after 15 years (P less than .0001).
The inpatient hospital costs after 15 years were greater in the surgery group for all glucose levels versus conventional treatment (mean, $51,225 vs. $25,313; P less than .0001).
There were no differences in outpatient costs demonstrated between the glucose subgroups. However, in the diabetes group, there were wide confidence intervals associated with outpatient costs that were thought to be secondary to end-stage renal disease visits.
Finally, the total cost of health care for the euglycemic group was higher in those who underwent surgery versus conventional treatment (P less than .0001). The prediabetic subgroup also incurred a higher total health care cost for surgery versus conventional treatment (P less than .0001). However, there were no differences in total health care cost for patients with diabetes who had surgery versus conventional treatment ($88,572 vs. $79,967, P less than .090).
The total cost was also higher in patients with diabetes for more than 1 year who had surgical intervention versus those who got conventional treatment (P less than .011). However, patients with diabetes for less than 1 year did not show differences in total cost when treated with surgery versus conventional treatments (P less than .476)
“In this study, we show that for obese patients with type 2 diabetes, the upfront costs of bariatric surgery seem to be largely offset by prevention of future health care and drug use,” the authors wrote. In addition, “long-term health care cost results support prioritization of patients with obesity and type 2 diabetes for bariatric surgery.”
This study was supported by a grant from AFA Forsakring. The authors reported multiple disclosures.
THE LANCET
Key clinical point: There was no difference in long-term health care cost between conventional treatment and bariatric surgery in patients with diabetes.
Major finding: There was no difference in total health care cost for patients with diabetes who received surgery versus conventional treatment ($88,572 vs. $79,967, P = .090).
Data source: A 15-year follow-up of Swedish Obese Subjects study participants with additional data obtained on drug costs and inpatient and outpatient visits.
Disclosures: This study was supported by a grant from AFA Forsakring. The authors reported multiple disclosures.

Clinical advances drive lung cancer staging, classification changes
DENVER – The term “precision medicine” can be applied to both clinical care and to pathology, as newly updated staging and classification systems for lung cancer show.
The proposed revised (8th) edition of the TNM staging system for lung cancer gives more weight to tumor size as a prognostic factor, reclassifies some primary tumor (T) descriptors, validates current nodal status (N) descriptors, modifies the definition of some types of metastases (M), and includes additional stages for better prognostic stratification, reported Dr. Ramón Rami-Porta from the Universitari Mútua Terrassa in Barcelona, at a world conference on lung cancer sponsored by the International Association for the Study of Lung Cancer.
Similarly, the updated World Health Organization (WHO) Classification of Lung Tumors, described by Dr. William D. Travis from the Memorial Sloan Kettering Cancer Center in New York, incorporates knowledge gained from immunohistochemistry and molecular testing for common genetic mutations into recommendations for treating the specific clinical circumstances of patients with lung cancer.

WHO’s Next
“The 2015 WHO Classification captures a remarkable decade of advances in every lung cancer specialty, from pathology – including histology, cytology, immunohistochemistry, genetics – to oncology, surgery, radiology, and epidemiology. The rapid expansion of immunohistochemical and molecular tools has had a profound impact on how we were able to reclassify a number of tumors, in addition to how we were able to contribute to improvement of subtyping of lung cancers, particularly non–small cell lung cancer,” Dr. Travis said at a media briefing following his discussion of the new classification at a plenary session.
The changes are expected to improve clinical management of patients with advanced lung cancer by clarifying criteria and terminology for small biopsies and cytology, establishing more accurate histologic subtyping, suggesting strategic management of small tissues, and streamlining the work flow for molecular testing. The classification also emphasizes the need for multidisciplinary cooperation among myriad clinicians, he said.
For surgically resected patients, the classification officially recognizes for the first time subsets of non–small cell lung cancer of adenocarcinoma histology with survival rates of 100% (adenocarcinoma in situ), or nearly 100% (minimally invasive adenocarcinoma).
Among the major changes that will affect the diagnosis of surgically resected patients are the adoption of the 2011 IASLC/ATS/ERS Lung Adenocarcinoma Classification, restriction of a diagnosis of large cell carcinoma to tumors lacking clear differentiation by both immunohistochemistry and morphology, reclassifying of squamous cancers into keratinizing, nonkeratinizing, and basaloid subtypes with elimination of clear cell, small cell, and papillary subtypes. Neuroendocrine subtypes are grouped together, but their classification otherwise remains largely unchanged.
The revised classification is expected to improve prediction of survival and recurrence, predict whether a patient is likely to have a survival benefit with platinum-based chemotherapy, allow radiologic pathologic correlations, and affects TNM staging by emphasizing solid tumor size (vs. whole tumor size), Dr. Travis said.
TNM Changes
The proposed changes to the TNM tumor staging have been submitted for approval to the American Joint Committee on Cancer and the Union for International Cancer Control.
If adopted, they would represent the first significant changes since the 7th edition’s publication in 2009. The changes are based on data on more than 77,000 patients diagnosed with lung cancer from 1999 through 2010.
The proposed changes are not intended, however, to alter clinical practice, and instead “imply a taxonomic refinement rather than new indications of already established treatment protocols,” Dr. Rami-Porta said.

In some cases, the proposed changes would result in an upgrading of the T stage, while others would result in downgrading. For example, tumors that range in size between 1 and 2 cm, designated T1a in the 7th edition, would be T1b in the 8th edition. Similarly, tumors larger than 2 cm and up to 3 cm would be upgraded from T1b to T1c, those larger than 4 up to 5 would go from T2a to T2b, those larger 5 and up to 7 cm would rise from T2b to T3, and those larger than 7 cm would be reclassified from T3 to T4. Tumors invading the diaphragm would also be upgraded from T3 to T4 under the proposed revisions.
In contrast, tumors with limited invasion of the trachea (bronchus less than 2 cm from the carina) would be downgraded from T3 to T2, as would tumors associated with total atelectasis and/or pneumonitis.
The current N descriptors are adequate for predicting prognosis, the investigators determined, prompting the recommendation to retain them in the new edition.
The investigators propose slight changes to the M descriptors of metastases. Although they found no significant differences in survival found among patients with M1a (metastases within the chest cavity) descriptors, when distant metastases outside the chest cavity (M1b) were assessed by to the number of metastases, they found that patients with tumors with one metastasis in one organ had significantly better outcomes than those who had multiple metastases in one or more organs.
The proposed revision would continue to group in the M1a category cases with pleural/pericardial effusions, contralateral/bilateral lung nodules, contralateral/bilateral pleural nodules, or a combination of multiple parameters. However, single metastatic lesions in a single distant organ would be reclassified as M1b, and multiple lesions in a single organ or multiple lesions in multiple organs would be reclassified as M1c.
DENVER – The term “precision medicine” can be applied to both clinical care and to pathology, as newly updated staging and classification systems for lung cancer show.
The proposed revised (8th) edition of the TNM staging system for lung cancer gives more weight to tumor size as a prognostic factor, reclassifies some primary tumor (T) descriptors, validates current nodal status (N) descriptors, modifies the definition of some types of metastases (M), and includes additional stages for better prognostic stratification, reported Dr. Ramón Rami-Porta from the Universitari Mútua Terrassa in Barcelona, at a world conference on lung cancer sponsored by the International Association for the Study of Lung Cancer.
Similarly, the updated World Health Organization (WHO) Classification of Lung Tumors, described by Dr. William D. Travis from the Memorial Sloan Kettering Cancer Center in New York, incorporates knowledge gained from immunohistochemistry and molecular testing for common genetic mutations into recommendations for treating the specific clinical circumstances of patients with lung cancer.
WHO’s Next
“The 2015 WHO Classification captures a remarkable decade of advances in every lung cancer specialty, from pathology – including histology, cytology, immunohistochemistry, genetics – to oncology, surgery, radiology, and epidemiology. The rapid expansion of immunohistochemical and molecular tools has had a profound impact on how we were able to reclassify a number of tumors, in addition to how we were able to contribute to improvement of subtyping of lung cancers, particularly non–small cell lung cancer,” Dr. Travis said at a media briefing following his discussion of the new classification at a plenary session.
The changes are expected to improve clinical management of patients with advanced lung cancer by clarifying criteria and terminology for small biopsies and cytology, establishing more accurate histologic subtyping, suggesting strategic management of small tissues, and streamlining the work flow for molecular testing. The classification also emphasizes the need for multidisciplinary cooperation among myriad clinicians, he said.
For surgically resected patients, the classification officially recognizes for the first time subsets of non–small cell lung cancer of adenocarcinoma histology with survival rates of 100% (adenocarcinoma in situ), or nearly 100% (minimally invasive adenocarcinoma).
Among the major changes that will affect the diagnosis of surgically resected patients are the adoption of the 2011 IASLC/ATS/ERS Lung Adenocarcinoma Classification, restriction of a diagnosis of large cell carcinoma to tumors lacking clear differentiation by both immunohistochemistry and morphology, reclassifying of squamous cancers into keratinizing, nonkeratinizing, and basaloid subtypes with elimination of clear cell, small cell, and papillary subtypes. Neuroendocrine subtypes are grouped together, but their classification otherwise remains largely unchanged.
The revised classification is expected to improve prediction of survival and recurrence, predict whether a patient is likely to have a survival benefit with platinum-based chemotherapy, allow radiologic pathologic correlations, and affects TNM staging by emphasizing solid tumor size (vs. whole tumor size), Dr. Travis said.
TNM Changes
The proposed changes to the TNM tumor staging have been submitted for approval to the American Joint Committee on Cancer and the Union for International Cancer Control.
If adopted, they would represent the first significant changes since the 7th edition’s publication in 2009. The changes are based on data on more than 77,000 patients diagnosed with lung cancer from 1999 through 2010.
The proposed changes are not intended, however, to alter clinical practice, and instead “imply a taxonomic refinement rather than new indications of already established treatment protocols,” Dr. Rami-Porta said.
In some cases, the proposed changes would result in an upgrading of the T stage, while others would result in downgrading. For example, tumors that range in size between 1 and 2 cm, designated T1a in the 7th edition, would be T1b in the 8th edition. Similarly, tumors larger than 2 cm and up to 3 cm would be upgraded from T1b to T1c, those larger than 4 up to 5 would go from T2a to T2b, those larger 5 and up to 7 cm would rise from T2b to T3, and those larger than 7 cm would be reclassified from T3 to T4. Tumors invading the diaphragm would also be upgraded from T3 to T4 under the proposed revisions.
In contrast, tumors with limited invasion of the trachea (bronchus less than 2 cm from the carina) would be downgraded from T3 to T2, as would tumors associated with total atelectasis and/or pneumonitis.
The current N descriptors are adequate for predicting prognosis, the investigators determined, prompting the recommendation to retain them in the new edition.
The investigators propose slight changes to the M descriptors of metastases. Although they found no significant differences in survival found among patients with M1a (metastases within the chest cavity) descriptors, when distant metastases outside the chest cavity (M1b) were assessed by to the number of metastases, they found that patients with tumors with one metastasis in one organ had significantly better outcomes than those who had multiple metastases in one or more organs.
The proposed revision would continue to group in the M1a category cases with pleural/pericardial effusions, contralateral/bilateral lung nodules, contralateral/bilateral pleural nodules, or a combination of multiple parameters. However, single metastatic lesions in a single distant organ would be reclassified as M1b, and multiple lesions in a single organ or multiple lesions in multiple organs would be reclassified as M1c.
DENVER – The term “precision medicine” can be applied to both clinical care and to pathology, as newly updated staging and classification systems for lung cancer show.
The proposed revised (8th) edition of the TNM staging system for lung cancer gives more weight to tumor size as a prognostic factor, reclassifies some primary tumor (T) descriptors, validates current nodal status (N) descriptors, modifies the definition of some types of metastases (M), and includes additional stages for better prognostic stratification, reported Dr. Ramón Rami-Porta from the Universitari Mútua Terrassa in Barcelona, at a world conference on lung cancer sponsored by the International Association for the Study of Lung Cancer.
Similarly, the updated World Health Organization (WHO) Classification of Lung Tumors, described by Dr. William D. Travis from the Memorial Sloan Kettering Cancer Center in New York, incorporates knowledge gained from immunohistochemistry and molecular testing for common genetic mutations into recommendations for treating the specific clinical circumstances of patients with lung cancer.
WHO’s Next
“The 2015 WHO Classification captures a remarkable decade of advances in every lung cancer specialty, from pathology – including histology, cytology, immunohistochemistry, genetics – to oncology, surgery, radiology, and epidemiology. The rapid expansion of immunohistochemical and molecular tools has had a profound impact on how we were able to reclassify a number of tumors, in addition to how we were able to contribute to improvement of subtyping of lung cancers, particularly non–small cell lung cancer,” Dr. Travis said at a media briefing following his discussion of the new classification at a plenary session.
The changes are expected to improve clinical management of patients with advanced lung cancer by clarifying criteria and terminology for small biopsies and cytology, establishing more accurate histologic subtyping, suggesting strategic management of small tissues, and streamlining the work flow for molecular testing. The classification also emphasizes the need for multidisciplinary cooperation among myriad clinicians, he said.
For surgically resected patients, the classification officially recognizes for the first time subsets of non–small cell lung cancer of adenocarcinoma histology with survival rates of 100% (adenocarcinoma in situ), or nearly 100% (minimally invasive adenocarcinoma).
Among the major changes that will affect the diagnosis of surgically resected patients are the adoption of the 2011 IASLC/ATS/ERS Lung Adenocarcinoma Classification, restriction of a diagnosis of large cell carcinoma to tumors lacking clear differentiation by both immunohistochemistry and morphology, reclassifying of squamous cancers into keratinizing, nonkeratinizing, and basaloid subtypes with elimination of clear cell, small cell, and papillary subtypes. Neuroendocrine subtypes are grouped together, but their classification otherwise remains largely unchanged.
The revised classification is expected to improve prediction of survival and recurrence, predict whether a patient is likely to have a survival benefit with platinum-based chemotherapy, allow radiologic pathologic correlations, and affects TNM staging by emphasizing solid tumor size (vs. whole tumor size), Dr. Travis said.
TNM Changes
The proposed changes to the TNM tumor staging have been submitted for approval to the American Joint Committee on Cancer and the Union for International Cancer Control.
If adopted, they would represent the first significant changes since the 7th edition’s publication in 2009. The changes are based on data on more than 77,000 patients diagnosed with lung cancer from 1999 through 2010.
The proposed changes are not intended, however, to alter clinical practice, and instead “imply a taxonomic refinement rather than new indications of already established treatment protocols,” Dr. Rami-Porta said.
In some cases, the proposed changes would result in an upgrading of the T stage, while others would result in downgrading. For example, tumors that range in size between 1 and 2 cm, designated T1a in the 7th edition, would be T1b in the 8th edition. Similarly, tumors larger than 2 cm and up to 3 cm would be upgraded from T1b to T1c, those larger than 4 up to 5 would go from T2a to T2b, those larger 5 and up to 7 cm would rise from T2b to T3, and those larger than 7 cm would be reclassified from T3 to T4. Tumors invading the diaphragm would also be upgraded from T3 to T4 under the proposed revisions.
In contrast, tumors with limited invasion of the trachea (bronchus less than 2 cm from the carina) would be downgraded from T3 to T2, as would tumors associated with total atelectasis and/or pneumonitis.
The current N descriptors are adequate for predicting prognosis, the investigators determined, prompting the recommendation to retain them in the new edition.
The investigators propose slight changes to the M descriptors of metastases. Although they found no significant differences in survival found among patients with M1a (metastases within the chest cavity) descriptors, when distant metastases outside the chest cavity (M1b) were assessed by to the number of metastases, they found that patients with tumors with one metastasis in one organ had significantly better outcomes than those who had multiple metastases in one or more organs.
The proposed revision would continue to group in the M1a category cases with pleural/pericardial effusions, contralateral/bilateral lung nodules, contralateral/bilateral pleural nodules, or a combination of multiple parameters. However, single metastatic lesions in a single distant organ would be reclassified as M1b, and multiple lesions in a single organ or multiple lesions in multiple organs would be reclassified as M1c.
AT THE IASLC WORLD CONFERENCE
Key clinical point: Improved understanding of lung cancer over the last decade has prompted updates to international tumor staging and classification systems.
Major finding: The WHO 2015 Classification of Lung Tumors is expected to aid clinical practice.
Data source: Conference presentation of key changes to the WHO Classification and TNM staging system.
Disclosures: Dr. Travis and Dr. Rami-Porta reported having no disclosures relevant to their presentations.
