User login
Official Newspaper of the American College of Surgeons
IOM report: Teamwork key to reducing medical diagnostic errors
WASHINGTON – Almost every American will experience a medical diagnostic error, but the problem has taken a back seat to other patient safety concerns, an influential panel said in a report out Sept. 22 calling for widespread changes.
Diagnostic errors – defined as inaccurate or delayed diagnoses – account for an estimated 10% of patient deaths, hundreds of thousands of adverse events in hospitals each year, and are a leading cause of paid medical malpractice claims, a blue ribbon panel of the Institute of Medicine (IOM) said in its report.

Such errors can occur with very rare conditions, such as the Liberian man with undetected Ebola who was sent home from a Dallas hospital last September; or more common problems, such as acid reflux being mistaken for a heart attack or a pathology report showing cancer that is never communicated to a patient.
Still, reducing the number won’t be easy, in part because there is no standard, required way to track such errors. Reversing current trends, the report concludes, will require better medical teamwork, training, and computer systems.
“Some people go to their graves with a diagnostic error that is never detected,” said Robert A. Berenson, a research fellow at the Urban Institute in Washington and one of the committee members who wrote the report. “It’s much more difficult to measure than a medication error.”
The report, called “Improving Diagnosis in Health Care,” is the latest in a series launched 15 years ago with “To Err Is Human: Building a Safer Health System,” which fueled the patient-safety movement with its estimate that as many as 98,000 patients die each year because of medical errors. The IOM is part of the private, nonprofit National Academies of Sciences, Engineering and Medicine.
Tuesday’s report has a role for just about everyone in the health system, from computer programmers to clinicians to patients. It recommends better teamwork among health care providers, patients, and families. Citing the dearth of data about diagnostic errors, the report calls for voluntary efforts to report such problems. Dedicated funding is needed for research, the report says, and hospitals and doctors need to develop better ways to identify, reduce, and learn from “near misses.”
Ironically, the report notes that computerized health records, which can help track and coordinate care, can also become a barrier to efficient and correct diagnoses.
The systems, it says, often aren’t compatible from one physician’s office to another or among hospitals, “auto-fill” functions sometimes result in the wrong information being entered, and the sheer volume of inputs and alerts can overwhelm medical staff.
It cites a study of emergency department staff that found clinicians spent more time inputting information into computers than taking care of patients. Another study found that while electronic health record systems provide alerts in response to abnormal diagnostic test results, 70% of medical staff surveyed said they receive more alerts than they can manage.
Making the systems more efficient and allowing patients more timely access to their own medical records to check for and correct errors “could be a game changer,” said Berenson.
Indeed, patients “are going to be critical to the solution,” said Dr. Michael Cohen, another report author and a professor of pathology at the University of Utah, Salt Lake City. “There’s a real opportunity for patients to advocate for themselves and at the same time to challenge the health care providers about the diagnosis being made.”
Helen Haskell, who formed Mothers Against Medical Error after her 15-year-old son died as the result of a medical error, said she was pleased the report focused on better teamwork and communication. She also said patients need better access to their records – particularly hospital records – and said consumers should always ask questions.
“What else can it be? Does this diagnosis match all my symptoms?,” are two of the best questions to ask, said Haskell. “If there is any question, people should get a second opinion.”
Kaiser Health News is a nonprofit national health policy news service that is part of the Henry J. Kaiser Family Foundation.
WASHINGTON – Almost every American will experience a medical diagnostic error, but the problem has taken a back seat to other patient safety concerns, an influential panel said in a report out Sept. 22 calling for widespread changes.
Diagnostic errors – defined as inaccurate or delayed diagnoses – account for an estimated 10% of patient deaths, hundreds of thousands of adverse events in hospitals each year, and are a leading cause of paid medical malpractice claims, a blue ribbon panel of the Institute of Medicine (IOM) said in its report.
Such errors can occur with very rare conditions, such as the Liberian man with undetected Ebola who was sent home from a Dallas hospital last September; or more common problems, such as acid reflux being mistaken for a heart attack or a pathology report showing cancer that is never communicated to a patient.
Still, reducing the number won’t be easy, in part because there is no standard, required way to track such errors. Reversing current trends, the report concludes, will require better medical teamwork, training, and computer systems.
“Some people go to their graves with a diagnostic error that is never detected,” said Robert A. Berenson, a research fellow at the Urban Institute in Washington and one of the committee members who wrote the report. “It’s much more difficult to measure than a medication error.”
The report, called “Improving Diagnosis in Health Care,” is the latest in a series launched 15 years ago with “To Err Is Human: Building a Safer Health System,” which fueled the patient-safety movement with its estimate that as many as 98,000 patients die each year because of medical errors. The IOM is part of the private, nonprofit National Academies of Sciences, Engineering and Medicine.
Tuesday’s report has a role for just about everyone in the health system, from computer programmers to clinicians to patients. It recommends better teamwork among health care providers, patients, and families. Citing the dearth of data about diagnostic errors, the report calls for voluntary efforts to report such problems. Dedicated funding is needed for research, the report says, and hospitals and doctors need to develop better ways to identify, reduce, and learn from “near misses.”
Ironically, the report notes that computerized health records, which can help track and coordinate care, can also become a barrier to efficient and correct diagnoses.
The systems, it says, often aren’t compatible from one physician’s office to another or among hospitals, “auto-fill” functions sometimes result in the wrong information being entered, and the sheer volume of inputs and alerts can overwhelm medical staff.
It cites a study of emergency department staff that found clinicians spent more time inputting information into computers than taking care of patients. Another study found that while electronic health record systems provide alerts in response to abnormal diagnostic test results, 70% of medical staff surveyed said they receive more alerts than they can manage.
Making the systems more efficient and allowing patients more timely access to their own medical records to check for and correct errors “could be a game changer,” said Berenson.
Indeed, patients “are going to be critical to the solution,” said Dr. Michael Cohen, another report author and a professor of pathology at the University of Utah, Salt Lake City. “There’s a real opportunity for patients to advocate for themselves and at the same time to challenge the health care providers about the diagnosis being made.”
Helen Haskell, who formed Mothers Against Medical Error after her 15-year-old son died as the result of a medical error, said she was pleased the report focused on better teamwork and communication. She also said patients need better access to their records – particularly hospital records – and said consumers should always ask questions.
“What else can it be? Does this diagnosis match all my symptoms?,” are two of the best questions to ask, said Haskell. “If there is any question, people should get a second opinion.”
Kaiser Health News is a nonprofit national health policy news service that is part of the Henry J. Kaiser Family Foundation.
WASHINGTON – Almost every American will experience a medical diagnostic error, but the problem has taken a back seat to other patient safety concerns, an influential panel said in a report out Sept. 22 calling for widespread changes.
Diagnostic errors – defined as inaccurate or delayed diagnoses – account for an estimated 10% of patient deaths, hundreds of thousands of adverse events in hospitals each year, and are a leading cause of paid medical malpractice claims, a blue ribbon panel of the Institute of Medicine (IOM) said in its report.
Such errors can occur with very rare conditions, such as the Liberian man with undetected Ebola who was sent home from a Dallas hospital last September; or more common problems, such as acid reflux being mistaken for a heart attack or a pathology report showing cancer that is never communicated to a patient.
Still, reducing the number won’t be easy, in part because there is no standard, required way to track such errors. Reversing current trends, the report concludes, will require better medical teamwork, training, and computer systems.
“Some people go to their graves with a diagnostic error that is never detected,” said Robert A. Berenson, a research fellow at the Urban Institute in Washington and one of the committee members who wrote the report. “It’s much more difficult to measure than a medication error.”
The report, called “Improving Diagnosis in Health Care,” is the latest in a series launched 15 years ago with “To Err Is Human: Building a Safer Health System,” which fueled the patient-safety movement with its estimate that as many as 98,000 patients die each year because of medical errors. The IOM is part of the private, nonprofit National Academies of Sciences, Engineering and Medicine.
Tuesday’s report has a role for just about everyone in the health system, from computer programmers to clinicians to patients. It recommends better teamwork among health care providers, patients, and families. Citing the dearth of data about diagnostic errors, the report calls for voluntary efforts to report such problems. Dedicated funding is needed for research, the report says, and hospitals and doctors need to develop better ways to identify, reduce, and learn from “near misses.”
Ironically, the report notes that computerized health records, which can help track and coordinate care, can also become a barrier to efficient and correct diagnoses.
The systems, it says, often aren’t compatible from one physician’s office to another or among hospitals, “auto-fill” functions sometimes result in the wrong information being entered, and the sheer volume of inputs and alerts can overwhelm medical staff.
It cites a study of emergency department staff that found clinicians spent more time inputting information into computers than taking care of patients. Another study found that while electronic health record systems provide alerts in response to abnormal diagnostic test results, 70% of medical staff surveyed said they receive more alerts than they can manage.
Making the systems more efficient and allowing patients more timely access to their own medical records to check for and correct errors “could be a game changer,” said Berenson.
Indeed, patients “are going to be critical to the solution,” said Dr. Michael Cohen, another report author and a professor of pathology at the University of Utah, Salt Lake City. “There’s a real opportunity for patients to advocate for themselves and at the same time to challenge the health care providers about the diagnosis being made.”
Helen Haskell, who formed Mothers Against Medical Error after her 15-year-old son died as the result of a medical error, said she was pleased the report focused on better teamwork and communication. She also said patients need better access to their records – particularly hospital records – and said consumers should always ask questions.
“What else can it be? Does this diagnosis match all my symptoms?,” are two of the best questions to ask, said Haskell. “If there is any question, people should get a second opinion.”
Kaiser Health News is a nonprofit national health policy news service that is part of the Henry J. Kaiser Family Foundation.

Damage control laparotomy an option for nontrauma secondary peritonitis
LAS VEGAS – Damage control laparotomy is a safe and reliable approach to the surgical management of patients with severe nontrauma secondary peritonitis who require bowel resection, according a review of 182 cases.
For example, the deferred ostomy rate was 16.7% among 72 patients who underwent damage control laparotomy (DCL), which was significantly lower than the primary ostomy rate of 53.6% in 110 patients who underwent a definitive surgical procedure (DSP), Dr. Maria P. Garcia-Garcia reported at the annual meeting of the American Association for the Surgery of Trauma.

Further, the fistula rate was lower among 60 DCL patients who underwent delayed anastomosis, compared with 51 DSP patients who underwent primary anastomosis (26.7% vs. 37.2%), and the mortality rate was lower in the DCL vs. DSP patients (16.7% vs. 24.5%). These differences did not meet statistical significance due to the sample size. Deaths in the DCL group all occurred in those who underwent delayed anastomosis; deaths in the DSP group occurred in 14 ostomy patients and 13 anastomosis patients, said Dr. Garcia-Garcia of Fundacion Valle del Lili, Cali, Colombia.
Disease severity, as measured by APACHE II scores, was similar in the two groups (mean of about 17 for each group). Septic shock was present in 37% at the time of admission. Mean hospital length of stay and mean intensive care unit length of stay did not differ significantly between the groups, nor did the systemic complication rate, or the rates of multiple organ failure and acute respiratory distress syndrome.
Small-bowel perforation occurred in 77 (42.3%), and colon perforation occurred in 105 (57.7%).
The patients included teens and adults aged 16 years or older (mean of 60.3 years) with severe nontrauma secondary peritonitis (NSPT) who were undergoing bowel resection after enteric perforations between 2003 and 2013. The DSP patients underwent either primary anastomosis or primary ostomy, and the DCL patients underwent segmental bowel resection, temporary abdominal closure, and subsequent delayed anastomosis or deferred ostomy.
DCL is a recognized strategy for managing bowel injuries in trauma patients. It was developed in response to the poor outcomes associated with attempting definitive repair, but evidence regarding the role and timing of anastomosis in DCL in NTSP – a condition associated with high morbidity and a 30% in-hospital mortality rate – is lacking, Dr. Garcia-Garcia said, noting that the current findings suggest it is the preferred approach.
“When a definite surgical repair is chosen, there is a 50/50 chance of performing anastomosis or ostomy. However, when a damage control abbreviated laparotomy is performed, there is a high bowel reconstruction success rate of about 80%. Therefore, damage control abbreviated laparotomy is a reliable and safe option in critically ill nontrauma secondary peritonitis patients. At the end of the day it’s your choice: Would you rather leave your patient with an ostomy or tube, or would you give your patient a chance of successful reconstruction without an ostomy?” she said.
Dr. Garcia-Garcia reported having no disclosures.
LAS VEGAS – Damage control laparotomy is a safe and reliable approach to the surgical management of patients with severe nontrauma secondary peritonitis who require bowel resection, according a review of 182 cases.
For example, the deferred ostomy rate was 16.7% among 72 patients who underwent damage control laparotomy (DCL), which was significantly lower than the primary ostomy rate of 53.6% in 110 patients who underwent a definitive surgical procedure (DSP), Dr. Maria P. Garcia-Garcia reported at the annual meeting of the American Association for the Surgery of Trauma.
Further, the fistula rate was lower among 60 DCL patients who underwent delayed anastomosis, compared with 51 DSP patients who underwent primary anastomosis (26.7% vs. 37.2%), and the mortality rate was lower in the DCL vs. DSP patients (16.7% vs. 24.5%). These differences did not meet statistical significance due to the sample size. Deaths in the DCL group all occurred in those who underwent delayed anastomosis; deaths in the DSP group occurred in 14 ostomy patients and 13 anastomosis patients, said Dr. Garcia-Garcia of Fundacion Valle del Lili, Cali, Colombia.
Disease severity, as measured by APACHE II scores, was similar in the two groups (mean of about 17 for each group). Septic shock was present in 37% at the time of admission. Mean hospital length of stay and mean intensive care unit length of stay did not differ significantly between the groups, nor did the systemic complication rate, or the rates of multiple organ failure and acute respiratory distress syndrome.
Small-bowel perforation occurred in 77 (42.3%), and colon perforation occurred in 105 (57.7%).
The patients included teens and adults aged 16 years or older (mean of 60.3 years) with severe nontrauma secondary peritonitis (NSPT) who were undergoing bowel resection after enteric perforations between 2003 and 2013. The DSP patients underwent either primary anastomosis or primary ostomy, and the DCL patients underwent segmental bowel resection, temporary abdominal closure, and subsequent delayed anastomosis or deferred ostomy.
DCL is a recognized strategy for managing bowel injuries in trauma patients. It was developed in response to the poor outcomes associated with attempting definitive repair, but evidence regarding the role and timing of anastomosis in DCL in NTSP – a condition associated with high morbidity and a 30% in-hospital mortality rate – is lacking, Dr. Garcia-Garcia said, noting that the current findings suggest it is the preferred approach.
“When a definite surgical repair is chosen, there is a 50/50 chance of performing anastomosis or ostomy. However, when a damage control abbreviated laparotomy is performed, there is a high bowel reconstruction success rate of about 80%. Therefore, damage control abbreviated laparotomy is a reliable and safe option in critically ill nontrauma secondary peritonitis patients. At the end of the day it’s your choice: Would you rather leave your patient with an ostomy or tube, or would you give your patient a chance of successful reconstruction without an ostomy?” she said.
Dr. Garcia-Garcia reported having no disclosures.
LAS VEGAS – Damage control laparotomy is a safe and reliable approach to the surgical management of patients with severe nontrauma secondary peritonitis who require bowel resection, according a review of 182 cases.
For example, the deferred ostomy rate was 16.7% among 72 patients who underwent damage control laparotomy (DCL), which was significantly lower than the primary ostomy rate of 53.6% in 110 patients who underwent a definitive surgical procedure (DSP), Dr. Maria P. Garcia-Garcia reported at the annual meeting of the American Association for the Surgery of Trauma.
Further, the fistula rate was lower among 60 DCL patients who underwent delayed anastomosis, compared with 51 DSP patients who underwent primary anastomosis (26.7% vs. 37.2%), and the mortality rate was lower in the DCL vs. DSP patients (16.7% vs. 24.5%). These differences did not meet statistical significance due to the sample size. Deaths in the DCL group all occurred in those who underwent delayed anastomosis; deaths in the DSP group occurred in 14 ostomy patients and 13 anastomosis patients, said Dr. Garcia-Garcia of Fundacion Valle del Lili, Cali, Colombia.
Disease severity, as measured by APACHE II scores, was similar in the two groups (mean of about 17 for each group). Septic shock was present in 37% at the time of admission. Mean hospital length of stay and mean intensive care unit length of stay did not differ significantly between the groups, nor did the systemic complication rate, or the rates of multiple organ failure and acute respiratory distress syndrome.
Small-bowel perforation occurred in 77 (42.3%), and colon perforation occurred in 105 (57.7%).
The patients included teens and adults aged 16 years or older (mean of 60.3 years) with severe nontrauma secondary peritonitis (NSPT) who were undergoing bowel resection after enteric perforations between 2003 and 2013. The DSP patients underwent either primary anastomosis or primary ostomy, and the DCL patients underwent segmental bowel resection, temporary abdominal closure, and subsequent delayed anastomosis or deferred ostomy.
DCL is a recognized strategy for managing bowel injuries in trauma patients. It was developed in response to the poor outcomes associated with attempting definitive repair, but evidence regarding the role and timing of anastomosis in DCL in NTSP – a condition associated with high morbidity and a 30% in-hospital mortality rate – is lacking, Dr. Garcia-Garcia said, noting that the current findings suggest it is the preferred approach.
“When a definite surgical repair is chosen, there is a 50/50 chance of performing anastomosis or ostomy. However, when a damage control abbreviated laparotomy is performed, there is a high bowel reconstruction success rate of about 80%. Therefore, damage control abbreviated laparotomy is a reliable and safe option in critically ill nontrauma secondary peritonitis patients. At the end of the day it’s your choice: Would you rather leave your patient with an ostomy or tube, or would you give your patient a chance of successful reconstruction without an ostomy?” she said.
Dr. Garcia-Garcia reported having no disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point: Damage control laparotomy is a safe and reliable approach to the surgical management of patients with severe nontrauma secondary peritonitis who require bowel resection, according a review of 182 cases.
Major finding: The ostomy rate was 16.7% vs. 53.6% with DCL vs. DSP.
Data source: A review of 182 cases.
Disclosures: Dr. Garcia-Garcia reported having no disclosures.

New assay may be a game changer in invasive candidiasis
SAN DIEGO – The T2 magnetic resonance assay for rapid diagnosis or rule-out of invasive candidiasis has the potential to significantly change the management and outcome of this common, deadly, and expensive disease, Dr. Peter G. Pappas asserted at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
This novel diagnostic instrument addresses a longstanding major unmet need in the field of infectious diseases: namely, the necessity for a substantially faster and more accurate test for invasive candidiasis than the decades-old current standard, which is automated blood cultures.

Blood cultures are notoriously insensitive. Indeed, they are negative in roughly 50% of patients with invasive candidiasis, mainly those with deep-seated, noncandidemic invasive candidiasis. And blood cultures are far too slow, taking 2-5 days to finalize results, explained Dr. Pappas, professor of medicine at the University of Alabama, Birmingham. “Management of invasive candidiasis involves time-critical decision making. The earlier we can approach the patient with specific therapy, the better the outcomes. That actually hasn’t been shown prospectively, but it’s a reasonable assumption based upon the available retrospective studies. We would like to be able to initiate effective treatment within 12-24 hours; that’s seldom possible with blood cultures,” he continued.
Dr. Pappas was principal investigator in the direct T2 pivotal clinical trial which led to Food and Drug Administration approval of the T2 magnetic resonance assay, known as the T2Candida platform. In this 1,801-patient multicenter study, the assay provided results in a mean of just over 4 hours with 91.4% sensitivity, 99.4% specificity, and a negative predictive value of 99.2%. In contrast, blood cultures, which were obtained in all participants, required an average of more than 120 hours to provide results (Clin Infect Dis. 2015 Mar 15;60[6]:892-9. doi: 10.1093/cid/ciu959).
At ICAAC 2015, the clinical trial was named one of the top 10 papers of the year in mycology.
Invasive candidiasis is a huge problem that’s seen little in the way of progress over the past 2 decades. Candida infections account for 6% of all hospital-acquired infections in the United States. More than 400,000 cases of invasive candidiasis occur annually worldwide. Attributable mortality rates of up to 49% have been reported. The disease is an important cause of prolonged hospitalization, with episodes adding an average of about $40,000 to the cost of a hospital stay.
The T2Candida test not only enables physicians to get effective antifungal agents started quickly, but a negative result will allow a drastic cutback in the now-routine use of empiric antifungal therapy prescribed during the lengthy wait for blood culture results. This will reduce needless exposure to drug side effects among uninfected patients, discourage the rise of resistant Candida strains, and substantially reduce health care costs.
Extrapolating from this trial’s data, and from other studies, Dr. Pappas said “the sweet spot” for the assay, where it has an impressively high 75%-85% positive predictive value, occurs when it is applied to patients with a pretest probability of invasive candidiasis in the 3%-10% range based upon well-known high-risk factors, including current cancer, neutropenia, organ or stem cell transplantation, having a central venous catheter, or being on steroid therapy.
The new assay bypasses blood cultures entirely, instead employing molecular diagnostics to directly analyze a whole blood sample. It can identify C. albicans and four other clinically relevant Candida species which collectively account for the vast majority of cases of invasive candidiasis. One of the reasons panelists at ICAAC 2015 named the T2Candida pivotal trial to their top-10 list of major papers in mycology is that the T2 magnetic resonance technology is a platform capable of also being applied to the diagnosis of other pathogens whose prompt diagnosis is critical.
Another advantage of the T2Candida platform is that the results are unaffected by antifungal therapy. In contrast, blood cultures become unreliable if a patient has empiric antifungal therapy onboard. In a separate presentation at ICAAC 2015, Dr. Pappas and coworkers presented interim results from an ongoing study that capitalizes on this advantage of the new technology.
To date, the study has enrolled 23 patients with culture-proven candidemia, all of whom underwent daily testing via both blood cultures and T2Candida during their first 7 days on antifungal therapy. Blood cultures remained positive for only two patients on-treatment, whereas T2Candida remained positive for nine patients on all 7 days and also detected one new case of intra-abdominal candidiasis missed by blood cultures.
Thus, the T2Candida platform may be an effective method not only for diagnosis of invasive candidiasis, Dr. Pappas observed, but for monitoring the response to therapy in the form of antifungal agents and/or removal of an offending contaminated catheter.
Dr. Pappas reported receiving research grants from and serving as an advisor to T2 Biosystems, which markets the assay. He has also received research support from Astellas, Gilead, and Merck.
SAN DIEGO – The T2 magnetic resonance assay for rapid diagnosis or rule-out of invasive candidiasis has the potential to significantly change the management and outcome of this common, deadly, and expensive disease, Dr. Peter G. Pappas asserted at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
This novel diagnostic instrument addresses a longstanding major unmet need in the field of infectious diseases: namely, the necessity for a substantially faster and more accurate test for invasive candidiasis than the decades-old current standard, which is automated blood cultures.
Blood cultures are notoriously insensitive. Indeed, they are negative in roughly 50% of patients with invasive candidiasis, mainly those with deep-seated, noncandidemic invasive candidiasis. And blood cultures are far too slow, taking 2-5 days to finalize results, explained Dr. Pappas, professor of medicine at the University of Alabama, Birmingham. “Management of invasive candidiasis involves time-critical decision making. The earlier we can approach the patient with specific therapy, the better the outcomes. That actually hasn’t been shown prospectively, but it’s a reasonable assumption based upon the available retrospective studies. We would like to be able to initiate effective treatment within 12-24 hours; that’s seldom possible with blood cultures,” he continued.
Dr. Pappas was principal investigator in the direct T2 pivotal clinical trial which led to Food and Drug Administration approval of the T2 magnetic resonance assay, known as the T2Candida platform. In this 1,801-patient multicenter study, the assay provided results in a mean of just over 4 hours with 91.4% sensitivity, 99.4% specificity, and a negative predictive value of 99.2%. In contrast, blood cultures, which were obtained in all participants, required an average of more than 120 hours to provide results (Clin Infect Dis. 2015 Mar 15;60[6]:892-9. doi: 10.1093/cid/ciu959).
At ICAAC 2015, the clinical trial was named one of the top 10 papers of the year in mycology.
Invasive candidiasis is a huge problem that’s seen little in the way of progress over the past 2 decades. Candida infections account for 6% of all hospital-acquired infections in the United States. More than 400,000 cases of invasive candidiasis occur annually worldwide. Attributable mortality rates of up to 49% have been reported. The disease is an important cause of prolonged hospitalization, with episodes adding an average of about $40,000 to the cost of a hospital stay.
The T2Candida test not only enables physicians to get effective antifungal agents started quickly, but a negative result will allow a drastic cutback in the now-routine use of empiric antifungal therapy prescribed during the lengthy wait for blood culture results. This will reduce needless exposure to drug side effects among uninfected patients, discourage the rise of resistant Candida strains, and substantially reduce health care costs.
Extrapolating from this trial’s data, and from other studies, Dr. Pappas said “the sweet spot” for the assay, where it has an impressively high 75%-85% positive predictive value, occurs when it is applied to patients with a pretest probability of invasive candidiasis in the 3%-10% range based upon well-known high-risk factors, including current cancer, neutropenia, organ or stem cell transplantation, having a central venous catheter, or being on steroid therapy.
The new assay bypasses blood cultures entirely, instead employing molecular diagnostics to directly analyze a whole blood sample. It can identify C. albicans and four other clinically relevant Candida species which collectively account for the vast majority of cases of invasive candidiasis. One of the reasons panelists at ICAAC 2015 named the T2Candida pivotal trial to their top-10 list of major papers in mycology is that the T2 magnetic resonance technology is a platform capable of also being applied to the diagnosis of other pathogens whose prompt diagnosis is critical.
Another advantage of the T2Candida platform is that the results are unaffected by antifungal therapy. In contrast, blood cultures become unreliable if a patient has empiric antifungal therapy onboard. In a separate presentation at ICAAC 2015, Dr. Pappas and coworkers presented interim results from an ongoing study that capitalizes on this advantage of the new technology.
To date, the study has enrolled 23 patients with culture-proven candidemia, all of whom underwent daily testing via both blood cultures and T2Candida during their first 7 days on antifungal therapy. Blood cultures remained positive for only two patients on-treatment, whereas T2Candida remained positive for nine patients on all 7 days and also detected one new case of intra-abdominal candidiasis missed by blood cultures.
Thus, the T2Candida platform may be an effective method not only for diagnosis of invasive candidiasis, Dr. Pappas observed, but for monitoring the response to therapy in the form of antifungal agents and/or removal of an offending contaminated catheter.
Dr. Pappas reported receiving research grants from and serving as an advisor to T2 Biosystems, which markets the assay. He has also received research support from Astellas, Gilead, and Merck.
SAN DIEGO – The T2 magnetic resonance assay for rapid diagnosis or rule-out of invasive candidiasis has the potential to significantly change the management and outcome of this common, deadly, and expensive disease, Dr. Peter G. Pappas asserted at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
This novel diagnostic instrument addresses a longstanding major unmet need in the field of infectious diseases: namely, the necessity for a substantially faster and more accurate test for invasive candidiasis than the decades-old current standard, which is automated blood cultures.
Blood cultures are notoriously insensitive. Indeed, they are negative in roughly 50% of patients with invasive candidiasis, mainly those with deep-seated, noncandidemic invasive candidiasis. And blood cultures are far too slow, taking 2-5 days to finalize results, explained Dr. Pappas, professor of medicine at the University of Alabama, Birmingham. “Management of invasive candidiasis involves time-critical decision making. The earlier we can approach the patient with specific therapy, the better the outcomes. That actually hasn’t been shown prospectively, but it’s a reasonable assumption based upon the available retrospective studies. We would like to be able to initiate effective treatment within 12-24 hours; that’s seldom possible with blood cultures,” he continued.
Dr. Pappas was principal investigator in the direct T2 pivotal clinical trial which led to Food and Drug Administration approval of the T2 magnetic resonance assay, known as the T2Candida platform. In this 1,801-patient multicenter study, the assay provided results in a mean of just over 4 hours with 91.4% sensitivity, 99.4% specificity, and a negative predictive value of 99.2%. In contrast, blood cultures, which were obtained in all participants, required an average of more than 120 hours to provide results (Clin Infect Dis. 2015 Mar 15;60[6]:892-9. doi: 10.1093/cid/ciu959).
At ICAAC 2015, the clinical trial was named one of the top 10 papers of the year in mycology.
Invasive candidiasis is a huge problem that’s seen little in the way of progress over the past 2 decades. Candida infections account for 6% of all hospital-acquired infections in the United States. More than 400,000 cases of invasive candidiasis occur annually worldwide. Attributable mortality rates of up to 49% have been reported. The disease is an important cause of prolonged hospitalization, with episodes adding an average of about $40,000 to the cost of a hospital stay.
The T2Candida test not only enables physicians to get effective antifungal agents started quickly, but a negative result will allow a drastic cutback in the now-routine use of empiric antifungal therapy prescribed during the lengthy wait for blood culture results. This will reduce needless exposure to drug side effects among uninfected patients, discourage the rise of resistant Candida strains, and substantially reduce health care costs.
Extrapolating from this trial’s data, and from other studies, Dr. Pappas said “the sweet spot” for the assay, where it has an impressively high 75%-85% positive predictive value, occurs when it is applied to patients with a pretest probability of invasive candidiasis in the 3%-10% range based upon well-known high-risk factors, including current cancer, neutropenia, organ or stem cell transplantation, having a central venous catheter, or being on steroid therapy.
The new assay bypasses blood cultures entirely, instead employing molecular diagnostics to directly analyze a whole blood sample. It can identify C. albicans and four other clinically relevant Candida species which collectively account for the vast majority of cases of invasive candidiasis. One of the reasons panelists at ICAAC 2015 named the T2Candida pivotal trial to their top-10 list of major papers in mycology is that the T2 magnetic resonance technology is a platform capable of also being applied to the diagnosis of other pathogens whose prompt diagnosis is critical.
Another advantage of the T2Candida platform is that the results are unaffected by antifungal therapy. In contrast, blood cultures become unreliable if a patient has empiric antifungal therapy onboard. In a separate presentation at ICAAC 2015, Dr. Pappas and coworkers presented interim results from an ongoing study that capitalizes on this advantage of the new technology.
To date, the study has enrolled 23 patients with culture-proven candidemia, all of whom underwent daily testing via both blood cultures and T2Candida during their first 7 days on antifungal therapy. Blood cultures remained positive for only two patients on-treatment, whereas T2Candida remained positive for nine patients on all 7 days and also detected one new case of intra-abdominal candidiasis missed by blood cultures.
Thus, the T2Candida platform may be an effective method not only for diagnosis of invasive candidiasis, Dr. Pappas observed, but for monitoring the response to therapy in the form of antifungal agents and/or removal of an offending contaminated catheter.
Dr. Pappas reported receiving research grants from and serving as an advisor to T2 Biosystems, which markets the assay. He has also received research support from Astellas, Gilead, and Merck.
EXPERT ANALYSIS FROM ICAAC 2015

Hospitalization driving bariatric surgery cost differences
Medicare payments to hospitals for bariatric operations varied by nearly $2,000 per episode of care, mostly because of differences in costs incurred in the initial – or index – hospitalization.
The findings, published online Sept. 16 in JAMA Surgery, offer hospitals a guide to where cost variation is highest (doi:10.1001/jamasurg.2015.2394) for these procedures.
Knowing where costs vary the most is particularly important if hospitals opt to accept bundled Medicare payments for bariatric procedures, which are a proposed addition to 48 other episodes of care that can currently be reimbursed in this way. Under bundled care payment programs, hospitals receive a single payment for all services related to a surgery or other episode of care, thereby accepting more risk when inefficiencies occur.
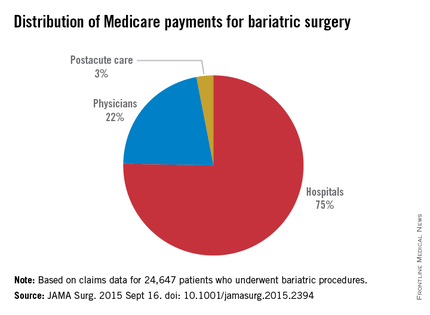
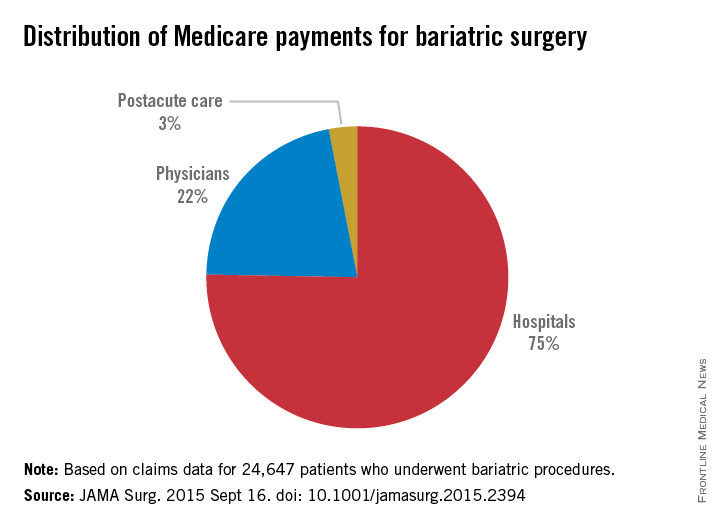
For their research, Dr. Tyler R. Grenda and his colleagues at University of Michigan, Ann Arbor, Center for Healthcare Outcomes and Policy, looked at claims data for 24,647 patients receiving bariatric procedures at 463 hospitals during 2011-2012.
Operations included laparoscopic gastric banding, laparoscopic Roux-en-Y gastric bypass, and open Roux-en-Y gastric bypass, with fewer than 5% of patients receiving other interventions. Mean total payments varied from $11,086 to $13,073 per episode of care, defined as index hospitalization through 30 days postdischarge, for a 16.5% difference between the lowest and highest hospital quartiles.
The index hospitalization was responsible for the largest portion of total payments (75%), seen in the study, followed by physician services (21%) and postacute care services (2.8%).
The large share of costs incurred during the index hospitalization was “likely owing to inpatient complications that drive [diagnosis-related group] up-coding,” the authors wrote, noting that DRG with complications result in higher Medicare payments.
Dr. Grenda and his colleagues concluded that bariatric surgery “appears to have a distinct pattern of hospital cost variation” unlike that seen in other procedures that have been studied to identify drivers of cost differences. “This difference in the pattern of variation emphasizes the importance of understanding cost variation specific to each procedure,” they wrote.
For example, a study that looked at hip fracture repair found that postacute care accounted for a large portion of variation in payments, while less variation was seen for the index hospitalization (Health Serv Res. 2010;45[6, pt 1]:1783-95).
In the current policy environment, in which bundled payments are seen as a way to shift cost accountability to hospitals, “a detailed understanding of variation in the costs for bariatric surgery will be essential for hospitals to identify areas of risk and opportunities for improvement,” the researchers wrote in their analysis.
Dr. Grenda and his colleagues’ research was funded by Agency for Healthcare Research and Quality. One coauthor and the supervisor of the study, Dr. Justin Dimnick, disclosed a financial relationship with ArborMetrix, a health care analytics firm not involved with the study; he is also an editor of JAMA Surgery, which published the study.
Medicare payments to hospitals for bariatric operations varied by nearly $2,000 per episode of care, mostly because of differences in costs incurred in the initial – or index – hospitalization.
The findings, published online Sept. 16 in JAMA Surgery, offer hospitals a guide to where cost variation is highest (doi:10.1001/jamasurg.2015.2394) for these procedures.
Knowing where costs vary the most is particularly important if hospitals opt to accept bundled Medicare payments for bariatric procedures, which are a proposed addition to 48 other episodes of care that can currently be reimbursed in this way. Under bundled care payment programs, hospitals receive a single payment for all services related to a surgery or other episode of care, thereby accepting more risk when inefficiencies occur.
For their research, Dr. Tyler R. Grenda and his colleagues at University of Michigan, Ann Arbor, Center for Healthcare Outcomes and Policy, looked at claims data for 24,647 patients receiving bariatric procedures at 463 hospitals during 2011-2012.
Operations included laparoscopic gastric banding, laparoscopic Roux-en-Y gastric bypass, and open Roux-en-Y gastric bypass, with fewer than 5% of patients receiving other interventions. Mean total payments varied from $11,086 to $13,073 per episode of care, defined as index hospitalization through 30 days postdischarge, for a 16.5% difference between the lowest and highest hospital quartiles.
The index hospitalization was responsible for the largest portion of total payments (75%), seen in the study, followed by physician services (21%) and postacute care services (2.8%).
The large share of costs incurred during the index hospitalization was “likely owing to inpatient complications that drive [diagnosis-related group] up-coding,” the authors wrote, noting that DRG with complications result in higher Medicare payments.
Dr. Grenda and his colleagues concluded that bariatric surgery “appears to have a distinct pattern of hospital cost variation” unlike that seen in other procedures that have been studied to identify drivers of cost differences. “This difference in the pattern of variation emphasizes the importance of understanding cost variation specific to each procedure,” they wrote.
For example, a study that looked at hip fracture repair found that postacute care accounted for a large portion of variation in payments, while less variation was seen for the index hospitalization (Health Serv Res. 2010;45[6, pt 1]:1783-95).
In the current policy environment, in which bundled payments are seen as a way to shift cost accountability to hospitals, “a detailed understanding of variation in the costs for bariatric surgery will be essential for hospitals to identify areas of risk and opportunities for improvement,” the researchers wrote in their analysis.
Dr. Grenda and his colleagues’ research was funded by Agency for Healthcare Research and Quality. One coauthor and the supervisor of the study, Dr. Justin Dimnick, disclosed a financial relationship with ArborMetrix, a health care analytics firm not involved with the study; he is also an editor of JAMA Surgery, which published the study.
Medicare payments to hospitals for bariatric operations varied by nearly $2,000 per episode of care, mostly because of differences in costs incurred in the initial – or index – hospitalization.
The findings, published online Sept. 16 in JAMA Surgery, offer hospitals a guide to where cost variation is highest (doi:10.1001/jamasurg.2015.2394) for these procedures.
Knowing where costs vary the most is particularly important if hospitals opt to accept bundled Medicare payments for bariatric procedures, which are a proposed addition to 48 other episodes of care that can currently be reimbursed in this way. Under bundled care payment programs, hospitals receive a single payment for all services related to a surgery or other episode of care, thereby accepting more risk when inefficiencies occur.
For their research, Dr. Tyler R. Grenda and his colleagues at University of Michigan, Ann Arbor, Center for Healthcare Outcomes and Policy, looked at claims data for 24,647 patients receiving bariatric procedures at 463 hospitals during 2011-2012.
Operations included laparoscopic gastric banding, laparoscopic Roux-en-Y gastric bypass, and open Roux-en-Y gastric bypass, with fewer than 5% of patients receiving other interventions. Mean total payments varied from $11,086 to $13,073 per episode of care, defined as index hospitalization through 30 days postdischarge, for a 16.5% difference between the lowest and highest hospital quartiles.
The index hospitalization was responsible for the largest portion of total payments (75%), seen in the study, followed by physician services (21%) and postacute care services (2.8%).
The large share of costs incurred during the index hospitalization was “likely owing to inpatient complications that drive [diagnosis-related group] up-coding,” the authors wrote, noting that DRG with complications result in higher Medicare payments.
Dr. Grenda and his colleagues concluded that bariatric surgery “appears to have a distinct pattern of hospital cost variation” unlike that seen in other procedures that have been studied to identify drivers of cost differences. “This difference in the pattern of variation emphasizes the importance of understanding cost variation specific to each procedure,” they wrote.
For example, a study that looked at hip fracture repair found that postacute care accounted for a large portion of variation in payments, while less variation was seen for the index hospitalization (Health Serv Res. 2010;45[6, pt 1]:1783-95).
In the current policy environment, in which bundled payments are seen as a way to shift cost accountability to hospitals, “a detailed understanding of variation in the costs for bariatric surgery will be essential for hospitals to identify areas of risk and opportunities for improvement,” the researchers wrote in their analysis.
Dr. Grenda and his colleagues’ research was funded by Agency for Healthcare Research and Quality. One coauthor and the supervisor of the study, Dr. Justin Dimnick, disclosed a financial relationship with ArborMetrix, a health care analytics firm not involved with the study; he is also an editor of JAMA Surgery, which published the study.
FROM JAMA SURGERY
Key clinical point: Initial hospitalization costs account for the lion’s share of cost variation for bariatric operations covered under Medicare.
Major finding: Mean total costs varied from $11,086 to about $13,073 per care episode, a 16.5% difference between the lowest- and highest-quartile hospitals; index hospitalizations accounted for 75% of payments, with less spent on physician fees and aftercare.
Data source: Medicare claims data for nearly 25,000 bariatric procedures performed at U.S. hospitals during 2011-2012.
Disclosures: Study was sponsored by the Agency for Healthcare Research and Quality; one coauthor disclosed financial relationship with a health analytics firm and journal editorship.
Surgical stabilization bests medical management for rib fractures
LAS VEGAS – Surgical stabilization of severe rib fractures leads to better outcomes than does the best medical management in critically ill trauma patients, findings from a 2-year, single-center, clinical trial suggest.
For example, the likelihood of respiratory failure was significantly lower in 35 patients who underwent surgical stabilization of severe rib fractures (SSRF) than among 35 who received optimal medical management (odds ratio, 0.22), and the likelihood of tracheostomy was also significantly lower with SSRF (OR, 0.20). These findings remained significant after controlling for a significantly higher RibScore – a radiographically derived score that predicts pulmonary outcomes in rib fracture patients – in the surgery group (score of 4 vs. 3 on a 0-6 scale), and for a significantly lower incidence of intracranial hemorrhage in the surgery group (5.7% vs. 28.6%), Dr. Fredric Pieracci reported at the annual meeting of the American Association for the Surgery of Trauma.
Further, the average daily spirometry value was 280 mL higher in the operative group, and there were nonsignificant trends toward a decreased likelihood of pneumonia (20.1% vs. 31.5%, respectively), decreased number of ventilator days (6.4 vs. 10.6), decreased ICU length of stay (8.3 vs. 10.4 days), and decreased hospital length of stay (15.2 vs. 25.3 days).
Narcotic requirements were similar in the groups, and no deaths occurred, said Dr. Pieracci, of Denver Health Medical Center.
The study, which was conducted at a level 1 trauma center from 2013 to 2014, enrolled adult patients with various rib fracture patterns, including flail chest, three or more fractures with bicortical displacement, 30% or greater hemithorax volume loss, and either severe pain or respiratory failure despite optimal medical management. Only those who presented within 72 hours of their injury were included.
All eligible patients were managed nonoperatively in the first year of the study, and all were managed operatively in the second year using a standardized technique described recently in the Journal of Trauma and Acute Care Surgery. The nonoperative and operative patient groups were well matched with respect to age, gender, mechanism of injury, preexisting lung pathology, and tobacco use, Dr. Pieracci noted.
“In conclusion, we found that surgical stabilization of severe rib fractures was independently associated with improved pulmonary outcomes, specifically respiratory failure, tracheostomy, duration of mechanical ventilation, and spirometry, and based on this we recommend consideration of surgical stabilization in trauma patients who meet one or more of our inclusion criteria,” he said.
Dr. Pieracci reported serving as a speaker for, and receiving research funding and honorarium from DePuy Synthes.
LAS VEGAS – Surgical stabilization of severe rib fractures leads to better outcomes than does the best medical management in critically ill trauma patients, findings from a 2-year, single-center, clinical trial suggest.
For example, the likelihood of respiratory failure was significantly lower in 35 patients who underwent surgical stabilization of severe rib fractures (SSRF) than among 35 who received optimal medical management (odds ratio, 0.22), and the likelihood of tracheostomy was also significantly lower with SSRF (OR, 0.20). These findings remained significant after controlling for a significantly higher RibScore – a radiographically derived score that predicts pulmonary outcomes in rib fracture patients – in the surgery group (score of 4 vs. 3 on a 0-6 scale), and for a significantly lower incidence of intracranial hemorrhage in the surgery group (5.7% vs. 28.6%), Dr. Fredric Pieracci reported at the annual meeting of the American Association for the Surgery of Trauma.
Further, the average daily spirometry value was 280 mL higher in the operative group, and there were nonsignificant trends toward a decreased likelihood of pneumonia (20.1% vs. 31.5%, respectively), decreased number of ventilator days (6.4 vs. 10.6), decreased ICU length of stay (8.3 vs. 10.4 days), and decreased hospital length of stay (15.2 vs. 25.3 days).
Narcotic requirements were similar in the groups, and no deaths occurred, said Dr. Pieracci, of Denver Health Medical Center.
The study, which was conducted at a level 1 trauma center from 2013 to 2014, enrolled adult patients with various rib fracture patterns, including flail chest, three or more fractures with bicortical displacement, 30% or greater hemithorax volume loss, and either severe pain or respiratory failure despite optimal medical management. Only those who presented within 72 hours of their injury were included.
All eligible patients were managed nonoperatively in the first year of the study, and all were managed operatively in the second year using a standardized technique described recently in the Journal of Trauma and Acute Care Surgery. The nonoperative and operative patient groups were well matched with respect to age, gender, mechanism of injury, preexisting lung pathology, and tobacco use, Dr. Pieracci noted.
“In conclusion, we found that surgical stabilization of severe rib fractures was independently associated with improved pulmonary outcomes, specifically respiratory failure, tracheostomy, duration of mechanical ventilation, and spirometry, and based on this we recommend consideration of surgical stabilization in trauma patients who meet one or more of our inclusion criteria,” he said.
Dr. Pieracci reported serving as a speaker for, and receiving research funding and honorarium from DePuy Synthes.
LAS VEGAS – Surgical stabilization of severe rib fractures leads to better outcomes than does the best medical management in critically ill trauma patients, findings from a 2-year, single-center, clinical trial suggest.
For example, the likelihood of respiratory failure was significantly lower in 35 patients who underwent surgical stabilization of severe rib fractures (SSRF) than among 35 who received optimal medical management (odds ratio, 0.22), and the likelihood of tracheostomy was also significantly lower with SSRF (OR, 0.20). These findings remained significant after controlling for a significantly higher RibScore – a radiographically derived score that predicts pulmonary outcomes in rib fracture patients – in the surgery group (score of 4 vs. 3 on a 0-6 scale), and for a significantly lower incidence of intracranial hemorrhage in the surgery group (5.7% vs. 28.6%), Dr. Fredric Pieracci reported at the annual meeting of the American Association for the Surgery of Trauma.
Further, the average daily spirometry value was 280 mL higher in the operative group, and there were nonsignificant trends toward a decreased likelihood of pneumonia (20.1% vs. 31.5%, respectively), decreased number of ventilator days (6.4 vs. 10.6), decreased ICU length of stay (8.3 vs. 10.4 days), and decreased hospital length of stay (15.2 vs. 25.3 days).
Narcotic requirements were similar in the groups, and no deaths occurred, said Dr. Pieracci, of Denver Health Medical Center.
The study, which was conducted at a level 1 trauma center from 2013 to 2014, enrolled adult patients with various rib fracture patterns, including flail chest, three or more fractures with bicortical displacement, 30% or greater hemithorax volume loss, and either severe pain or respiratory failure despite optimal medical management. Only those who presented within 72 hours of their injury were included.
All eligible patients were managed nonoperatively in the first year of the study, and all were managed operatively in the second year using a standardized technique described recently in the Journal of Trauma and Acute Care Surgery. The nonoperative and operative patient groups were well matched with respect to age, gender, mechanism of injury, preexisting lung pathology, and tobacco use, Dr. Pieracci noted.
“In conclusion, we found that surgical stabilization of severe rib fractures was independently associated with improved pulmonary outcomes, specifically respiratory failure, tracheostomy, duration of mechanical ventilation, and spirometry, and based on this we recommend consideration of surgical stabilization in trauma patients who meet one or more of our inclusion criteria,” he said.
Dr. Pieracci reported serving as a speaker for, and receiving research funding and honorarium from DePuy Synthes.
AT THE AAST ANNUAL MEETING
Key clinical point: Surgical stabilization of severe rib fractures leads to better outcomes than does best medical management in critically ill trauma patients.
Major finding: Surgery patients were significantly less likely than medically managed patients to experience respiratory failure and tracheotomy (OR, 0.22 and 0.20, respectively).
Data source: A prospective, controlled clinical trial involving 70 patients.
Disclosures: Dr. Pieracci reported serving as a speaker for, and receiving research funding and honorarium from DePuy Synthes.
Pioneer ACOs cut out low-value care
In its first year, the Medicare Pioneer accountable care organization (ACO) program resulted in modest reductions in low-value medical services that provide minimal clinical benefit to patients, according to a study published Sept. 21 in JAMA Internal Medicine (doi:10.1001/jamainternmed.2015.4525).
The Pioneer ACO model was associated with a differential reduction of 0.8 in low-value services per 100 beneficiaries or a 1.9% decrease in service quantity, and a 4.5% reduction in spending on low-value services.

Lead author Aaron L. Schwartz, Ph.D., of Harvard Medical School, Boston, and his colleagues compared the use of low-value services by Medicare fee-for-service patients whose providers were in the Pioneer ACO program with use of low-value services by beneficiaries of other health care providers. They examined services from 2009 to 2012 using Medicare claims for a random 20% sample of patients. Comparisons were adjusted for sociodemographic and clinical characteristics and for geography. Low-value services were defined as care providing minimal or no average clinical benefit in specific clinical scenarios.
The greatest reductions in service occurred for the most frequent services, including cancer screening and imaging. Cardiovascular testing and procedures underwent the greatest differential reduction – a 6.3% decrease in low-value services for the Pioneer ACO group. ACOs that were providing more low-value care on average experienced greater reductions.
The study findings are consistent with other conclusions that Pioneer ACO models improve the overall value of health care provided, Dr. Schwartz noted. The findings also demonstrate that patient care preferences may not be major obstacles to reducing low-value service use.
The Medicare Pioneer ACO program aims to improve value and lower cost through incentives and penalties. Participating organizations receive a bonus or a penalty if overall spending for patients is based on meeting a financial benchmark. Performance on 33 quality measures determines the proportion of savings or losses shared by the ACO. In 2012, 32 health care provider organizations volunteered to participate in the Pioneer ACO program. In 2015, there were 19 participating organizations, according to CMS data.
On Twitter @legal_med
The study suggests that some ACOs are capable of slowing health care spending growth without jeopardizing the quality of care.
Participants in the first year of the Medicare Pioneer ACO program precisely targeted reduction of low-value services. All doctors increasingly will be called on to apply similar precision in lowering the cost of delivering valuable services without impairing the quality of care. Individually targeted Medicare payment incentives to improve value will begin for physicians in 2019 via a merit-based incentive payment system. One basis for determining individual physician merit will be prudent use of health care resources.
Although adjusting practice to lower costs is a long stretch from physicians’ traditional role, the well-being of their patients and their communities now depend on it.
Dr. Arnold Milstein of the Standford (Calif.) Clinical Excellence Research Center made these comments in an accompanying editorial (doi:10.1001/jamainternmed.2015.5322). He reported no disclosures.
The study suggests that some ACOs are capable of slowing health care spending growth without jeopardizing the quality of care.
Participants in the first year of the Medicare Pioneer ACO program precisely targeted reduction of low-value services. All doctors increasingly will be called on to apply similar precision in lowering the cost of delivering valuable services without impairing the quality of care. Individually targeted Medicare payment incentives to improve value will begin for physicians in 2019 via a merit-based incentive payment system. One basis for determining individual physician merit will be prudent use of health care resources.
Although adjusting practice to lower costs is a long stretch from physicians’ traditional role, the well-being of their patients and their communities now depend on it.
Dr. Arnold Milstein of the Standford (Calif.) Clinical Excellence Research Center made these comments in an accompanying editorial (doi:10.1001/jamainternmed.2015.5322). He reported no disclosures.
The study suggests that some ACOs are capable of slowing health care spending growth without jeopardizing the quality of care.
Participants in the first year of the Medicare Pioneer ACO program precisely targeted reduction of low-value services. All doctors increasingly will be called on to apply similar precision in lowering the cost of delivering valuable services without impairing the quality of care. Individually targeted Medicare payment incentives to improve value will begin for physicians in 2019 via a merit-based incentive payment system. One basis for determining individual physician merit will be prudent use of health care resources.
Although adjusting practice to lower costs is a long stretch from physicians’ traditional role, the well-being of their patients and their communities now depend on it.
Dr. Arnold Milstein of the Standford (Calif.) Clinical Excellence Research Center made these comments in an accompanying editorial (doi:10.1001/jamainternmed.2015.5322). He reported no disclosures.
In its first year, the Medicare Pioneer accountable care organization (ACO) program resulted in modest reductions in low-value medical services that provide minimal clinical benefit to patients, according to a study published Sept. 21 in JAMA Internal Medicine (doi:10.1001/jamainternmed.2015.4525).
The Pioneer ACO model was associated with a differential reduction of 0.8 in low-value services per 100 beneficiaries or a 1.9% decrease in service quantity, and a 4.5% reduction in spending on low-value services.
Lead author Aaron L. Schwartz, Ph.D., of Harvard Medical School, Boston, and his colleagues compared the use of low-value services by Medicare fee-for-service patients whose providers were in the Pioneer ACO program with use of low-value services by beneficiaries of other health care providers. They examined services from 2009 to 2012 using Medicare claims for a random 20% sample of patients. Comparisons were adjusted for sociodemographic and clinical characteristics and for geography. Low-value services were defined as care providing minimal or no average clinical benefit in specific clinical scenarios.
The greatest reductions in service occurred for the most frequent services, including cancer screening and imaging. Cardiovascular testing and procedures underwent the greatest differential reduction – a 6.3% decrease in low-value services for the Pioneer ACO group. ACOs that were providing more low-value care on average experienced greater reductions.
The study findings are consistent with other conclusions that Pioneer ACO models improve the overall value of health care provided, Dr. Schwartz noted. The findings also demonstrate that patient care preferences may not be major obstacles to reducing low-value service use.
The Medicare Pioneer ACO program aims to improve value and lower cost through incentives and penalties. Participating organizations receive a bonus or a penalty if overall spending for patients is based on meeting a financial benchmark. Performance on 33 quality measures determines the proportion of savings or losses shared by the ACO. In 2012, 32 health care provider organizations volunteered to participate in the Pioneer ACO program. In 2015, there were 19 participating organizations, according to CMS data.
On Twitter @legal_med
In its first year, the Medicare Pioneer accountable care organization (ACO) program resulted in modest reductions in low-value medical services that provide minimal clinical benefit to patients, according to a study published Sept. 21 in JAMA Internal Medicine (doi:10.1001/jamainternmed.2015.4525).
The Pioneer ACO model was associated with a differential reduction of 0.8 in low-value services per 100 beneficiaries or a 1.9% decrease in service quantity, and a 4.5% reduction in spending on low-value services.
Lead author Aaron L. Schwartz, Ph.D., of Harvard Medical School, Boston, and his colleagues compared the use of low-value services by Medicare fee-for-service patients whose providers were in the Pioneer ACO program with use of low-value services by beneficiaries of other health care providers. They examined services from 2009 to 2012 using Medicare claims for a random 20% sample of patients. Comparisons were adjusted for sociodemographic and clinical characteristics and for geography. Low-value services were defined as care providing minimal or no average clinical benefit in specific clinical scenarios.
The greatest reductions in service occurred for the most frequent services, including cancer screening and imaging. Cardiovascular testing and procedures underwent the greatest differential reduction – a 6.3% decrease in low-value services for the Pioneer ACO group. ACOs that were providing more low-value care on average experienced greater reductions.
The study findings are consistent with other conclusions that Pioneer ACO models improve the overall value of health care provided, Dr. Schwartz noted. The findings also demonstrate that patient care preferences may not be major obstacles to reducing low-value service use.
The Medicare Pioneer ACO program aims to improve value and lower cost through incentives and penalties. Participating organizations receive a bonus or a penalty if overall spending for patients is based on meeting a financial benchmark. Performance on 33 quality measures determines the proportion of savings or losses shared by the ACO. In 2012, 32 health care provider organizations volunteered to participate in the Pioneer ACO program. In 2015, there were 19 participating organizations, according to CMS data.
On Twitter @legal_med
FROM JAMA INTERNAL MEDICINE
Key clinical point: The Medicare Pioneer ACO program was associated with modest reductions in low-value services that provide minimal clinical benefit to patients.
Major finding: In its first year, the Medicare Pioneer ACO program was associated with a 0.8 reduction in low-value services per 100 beneficiaries, which was a 1.9% reduction in service quantity and a 4.5% reduction in spending on low-value services.
Data source: Random sample of Medicare claims from the period of 2009-2012.
Disclosures: Dr. Aaron L. Schwartz and Dr. J. Michael McWilliams consult for the Medicare Payment Advisory Commission. Dr. Michael E. Chernew is a partner at VBID Health LLC, which has a contract to develop and market a tool to help insurers and employers quantify spending on low-value services.

Radiation + lumpectomy tied to increased survival in older women with TNBC
Older women with triple-negative breast cancer appear to get an overall survival and disease-specific survival benefit with the addition of radiation to breast-conserving surgery, authors of a retrospective study said.
Among 974 women aged 70 and above with T1-2, N0, M0 triple-negative breast cancer (TNBC; lacking the Her2-neu, estrogen, and progesterone receptors), the addition of radiation to lumpectomy was associated at 23 months’ follow-up with an overall survival (OS) rate of 98.2%, compared with 85.6% for women who received lumpectomy alone (P less than .001). Respective rates of disease-specific survival (DSS) were 99% and 94% (P = .003).
“The use of adjuvant radiation therapy after lumpectomy for elderly women with early-stage TNBC was associated with improved OS and DSS. Noting the potential for selection bias in this study, future prospective study is required to define the management of early-stage triple-negative breast cancer,” wrote Dr. Sean Szjea and colleagues at the University of Texas, Galveston, in a meeting abstract. The study will be presented at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
It’s known that older women with estrogen-receptor positive disease can have good clinical outcomes with lumpectomy and adjuvant therapy alone, but whether adding radiation to breast-conserving surgery in older women with TNBC offers clinical benefit is less certain, the investigators said, prompting them to dive for data into the Surveillance, Epidemiology, and End Results database.
They collected information on 974 women aged 70 or older who underwent lumpectomy for early-stage TNBC with no nodal invasion or metastatic disease from 2010 through 2011. Of this group, 662 (68%) also received radiation therapy.
In addition to determining the OS and DSS rates in the overall population, the investigators conducted multivariate regression modeling controlling for confounding variables, including the use of neoadjuvant chemotherapy, the number of lymph nodes sampled, age, laterality, grade, T stage, the extent of surgery, and the existence of other cancers. They found that the survival benefit for radiation held for both OS (hazard ratio [HR], 0.14; P less than .001) and DSS (HR, 0.14; P = .01).
The authors reported having no relevant financial disclosures.
Older women with triple-negative breast cancer appear to get an overall survival and disease-specific survival benefit with the addition of radiation to breast-conserving surgery, authors of a retrospective study said.
Among 974 women aged 70 and above with T1-2, N0, M0 triple-negative breast cancer (TNBC; lacking the Her2-neu, estrogen, and progesterone receptors), the addition of radiation to lumpectomy was associated at 23 months’ follow-up with an overall survival (OS) rate of 98.2%, compared with 85.6% for women who received lumpectomy alone (P less than .001). Respective rates of disease-specific survival (DSS) were 99% and 94% (P = .003).
“The use of adjuvant radiation therapy after lumpectomy for elderly women with early-stage TNBC was associated with improved OS and DSS. Noting the potential for selection bias in this study, future prospective study is required to define the management of early-stage triple-negative breast cancer,” wrote Dr. Sean Szjea and colleagues at the University of Texas, Galveston, in a meeting abstract. The study will be presented at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
It’s known that older women with estrogen-receptor positive disease can have good clinical outcomes with lumpectomy and adjuvant therapy alone, but whether adding radiation to breast-conserving surgery in older women with TNBC offers clinical benefit is less certain, the investigators said, prompting them to dive for data into the Surveillance, Epidemiology, and End Results database.
They collected information on 974 women aged 70 or older who underwent lumpectomy for early-stage TNBC with no nodal invasion or metastatic disease from 2010 through 2011. Of this group, 662 (68%) also received radiation therapy.
In addition to determining the OS and DSS rates in the overall population, the investigators conducted multivariate regression modeling controlling for confounding variables, including the use of neoadjuvant chemotherapy, the number of lymph nodes sampled, age, laterality, grade, T stage, the extent of surgery, and the existence of other cancers. They found that the survival benefit for radiation held for both OS (hazard ratio [HR], 0.14; P less than .001) and DSS (HR, 0.14; P = .01).
The authors reported having no relevant financial disclosures.
Older women with triple-negative breast cancer appear to get an overall survival and disease-specific survival benefit with the addition of radiation to breast-conserving surgery, authors of a retrospective study said.
Among 974 women aged 70 and above with T1-2, N0, M0 triple-negative breast cancer (TNBC; lacking the Her2-neu, estrogen, and progesterone receptors), the addition of radiation to lumpectomy was associated at 23 months’ follow-up with an overall survival (OS) rate of 98.2%, compared with 85.6% for women who received lumpectomy alone (P less than .001). Respective rates of disease-specific survival (DSS) were 99% and 94% (P = .003).
“The use of adjuvant radiation therapy after lumpectomy for elderly women with early-stage TNBC was associated with improved OS and DSS. Noting the potential for selection bias in this study, future prospective study is required to define the management of early-stage triple-negative breast cancer,” wrote Dr. Sean Szjea and colleagues at the University of Texas, Galveston, in a meeting abstract. The study will be presented at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
It’s known that older women with estrogen-receptor positive disease can have good clinical outcomes with lumpectomy and adjuvant therapy alone, but whether adding radiation to breast-conserving surgery in older women with TNBC offers clinical benefit is less certain, the investigators said, prompting them to dive for data into the Surveillance, Epidemiology, and End Results database.
They collected information on 974 women aged 70 or older who underwent lumpectomy for early-stage TNBC with no nodal invasion or metastatic disease from 2010 through 2011. Of this group, 662 (68%) also received radiation therapy.
In addition to determining the OS and DSS rates in the overall population, the investigators conducted multivariate regression modeling controlling for confounding variables, including the use of neoadjuvant chemotherapy, the number of lymph nodes sampled, age, laterality, grade, T stage, the extent of surgery, and the existence of other cancers. They found that the survival benefit for radiation held for both OS (hazard ratio [HR], 0.14; P less than .001) and DSS (HR, 0.14; P = .01).
The authors reported having no relevant financial disclosures.
FROM THE 2015 ASCO BREAST CANCER SYMPOSIUM
Key clinical point: Radiation added to breast-conserving surgery in women 70 and older with early-stage triple-negative breast cancer was associated with improved survival.
Major finding: Overall survival with radiation and lumpectomy was 98.2%, compared with 85.6% for women who received lumpectomy alone (P less than .001)
Data source: A prospective database review of 974 women aged 70 and older treated from 2010 through 2011.
Disclosures: The authors reported having no relevant financial disclosures.
DCIS recurrences have declined significantly
Recurrence rates of ductal carcinoma in situ (DCIS ) have declined significantly over 3 decades, with the improvements likely because of better screening and pathologic assessment, investigators say.
A retrospective review of 2,996 women who underwent breast-conserving surgery (BCS) for DCIS at Memorial Sloan Kettering Cancer Center in New York from 1978 through 2010 showed that there were 363 recurrences within 5 years of treatment (12%). The 5-year recurrence rate for women treated from 1978 through 1998 was 13.6%, compared with 6.6% for women treated from 1999 through 2010.
The hazard ratio (HR) for more recent treatment was 0.62 (P less than .0001), report Dr. Kimberly J. Van Zee and colleagues at MSKCC in an oral abstract to be presented at the symposium sponsored by the American Society of Clinical Oncology.
The period of treatment remained a significant predictor of lower recurrence after multivariate analysis adjusting for age, family history, radiologic vs. clinical presentation, nuclear grade (nonhigh vs. high), necrosis, number of excisions (two or few vs. three or more), margin status (positive or close margins vs. negative), radiation, and use of endocrine therapy (HR 0.74, P = 0.02).
When the investigators stratified patients by whether they received radiation in addition to BCS, they found that recurrence rates dropped only for those patients who did not receive radiation (HR 0.62, P = 0.003). Among patients who received radiation, recurrence rates did not decline over time (HR 1.13, P = 0.6).

The authors conclude that the lower risk of recurrence over time is only partially explained by changes in clinical practice, such as screening, emphasis on negative surgical margins, and use of adjuvant therapies. The fact that the decline was seen only for women who did not receive radiation suggests that the improvements were not attributable to improvement in radiation therapy techniques. Rather, they may be due to improvements in mammography and in pathologic assessment, the investigators maintain.
“The lower recurrence risk observed for DCIS patients treated in more recent years is important for patient education, especially in view of the widely reported recent increase in use of mastectomy,” they write in the study abstract.
Recurrence rates of ductal carcinoma in situ (DCIS ) have declined significantly over 3 decades, with the improvements likely because of better screening and pathologic assessment, investigators say.
A retrospective review of 2,996 women who underwent breast-conserving surgery (BCS) for DCIS at Memorial Sloan Kettering Cancer Center in New York from 1978 through 2010 showed that there were 363 recurrences within 5 years of treatment (12%). The 5-year recurrence rate for women treated from 1978 through 1998 was 13.6%, compared with 6.6% for women treated from 1999 through 2010.
The hazard ratio (HR) for more recent treatment was 0.62 (P less than .0001), report Dr. Kimberly J. Van Zee and colleagues at MSKCC in an oral abstract to be presented at the symposium sponsored by the American Society of Clinical Oncology.
The period of treatment remained a significant predictor of lower recurrence after multivariate analysis adjusting for age, family history, radiologic vs. clinical presentation, nuclear grade (nonhigh vs. high), necrosis, number of excisions (two or few vs. three or more), margin status (positive or close margins vs. negative), radiation, and use of endocrine therapy (HR 0.74, P = 0.02).
When the investigators stratified patients by whether they received radiation in addition to BCS, they found that recurrence rates dropped only for those patients who did not receive radiation (HR 0.62, P = 0.003). Among patients who received radiation, recurrence rates did not decline over time (HR 1.13, P = 0.6).
The authors conclude that the lower risk of recurrence over time is only partially explained by changes in clinical practice, such as screening, emphasis on negative surgical margins, and use of adjuvant therapies. The fact that the decline was seen only for women who did not receive radiation suggests that the improvements were not attributable to improvement in radiation therapy techniques. Rather, they may be due to improvements in mammography and in pathologic assessment, the investigators maintain.
“The lower recurrence risk observed for DCIS patients treated in more recent years is important for patient education, especially in view of the widely reported recent increase in use of mastectomy,” they write in the study abstract.
Recurrence rates of ductal carcinoma in situ (DCIS ) have declined significantly over 3 decades, with the improvements likely because of better screening and pathologic assessment, investigators say.
A retrospective review of 2,996 women who underwent breast-conserving surgery (BCS) for DCIS at Memorial Sloan Kettering Cancer Center in New York from 1978 through 2010 showed that there were 363 recurrences within 5 years of treatment (12%). The 5-year recurrence rate for women treated from 1978 through 1998 was 13.6%, compared with 6.6% for women treated from 1999 through 2010.
The hazard ratio (HR) for more recent treatment was 0.62 (P less than .0001), report Dr. Kimberly J. Van Zee and colleagues at MSKCC in an oral abstract to be presented at the symposium sponsored by the American Society of Clinical Oncology.
The period of treatment remained a significant predictor of lower recurrence after multivariate analysis adjusting for age, family history, radiologic vs. clinical presentation, nuclear grade (nonhigh vs. high), necrosis, number of excisions (two or few vs. three or more), margin status (positive or close margins vs. negative), radiation, and use of endocrine therapy (HR 0.74, P = 0.02).
When the investigators stratified patients by whether they received radiation in addition to BCS, they found that recurrence rates dropped only for those patients who did not receive radiation (HR 0.62, P = 0.003). Among patients who received radiation, recurrence rates did not decline over time (HR 1.13, P = 0.6).
The authors conclude that the lower risk of recurrence over time is only partially explained by changes in clinical practice, such as screening, emphasis on negative surgical margins, and use of adjuvant therapies. The fact that the decline was seen only for women who did not receive radiation suggests that the improvements were not attributable to improvement in radiation therapy techniques. Rather, they may be due to improvements in mammography and in pathologic assessment, the investigators maintain.
“The lower recurrence risk observed for DCIS patients treated in more recent years is important for patient education, especially in view of the widely reported recent increase in use of mastectomy,” they write in the study abstract.
Key clinical point: Recurrence rates of DCIS in patients treated with breast-conserving surgery declined significantly from 1978 through 2010.
Major finding: The 5-year recurrence rate for women treated from 1978 through 1998 was 13.6%, compared with 6.6% for women treated from 1999 through 2010.
Data source: Retrospective case review of 2,996 women with DCIS treated with breast-conserving surgery with or without radiation.
Disclosures: The funding source was not disclosed. Coauthor Dr. Monica Morrow disclosed receiving honoraria from Genomic Health.
Point/Counterpoint: Does surgery play a role in N2 disease treatment following induction therapy?
POINT: Surgery has its uses for some
BY DR. STEPHEN G. SWISHER
When talking about the role of surgery after induction therapy with persistent N2 disease, one must acknowledge that this is such a heterogeneous disease. You can have single-station N2; resectable, bulky multistation N2; and so on. Then there’s unresectable stage IIIA, but let’s focus mainly on resectable stage IIIA disease.
I can’t tell you how many audiences I’ve faced that absolutely believe the myth that surgery plays no role in Stage IIIA non–small cell lung cancer based on data from stage IIIA disease patients randomized to chemoradiation followed by surgery. The problem with these study results is the high mortality in the pneumonectomy subset. There’s no difference in the overall survival of the two groups, but that doesn’t mean that everyone in that group wouldn’t benefit from surgery.

The curve showed that pneumonectomy did not benefit after chemoradiation in a non–high-volume center. You can see a steep drop in the mortality early on, but it catches up again at the end. If you look at the overall 5-year survival rate, even in the pneumonectomy subset, you’re looking at 22% vs. 24%.
But in the lobectomy set, you see something completely different. You’ve got a doubling of survivors and no mortality early on, and a doubling of 5-year survival from 18% to 36%.
And yet, people continue saying that there’s no role for surgery. Well, I think there is a role for surgery, and there are subsets of N2 for which surgery can be particularly beneficial. We have to move more toward what the medical oncologists do, which is personalize therapy and look at subsets of N2 disease so that we know which patients we can benefit and which ones we can’t.
Moving on to the second myth: Surgery plays no role in N2 residual disease after induction therapy. This myth is based on the results of a couple of prospective studies in the 1980s and ’90s that showed residual N2 disease after chemo- and radiotherapy leads to survival of 16-35 months in most cases. I’d say that those results are true, but it’s not to say there aren’t subsets within these populations that benefited. With preoperative chemo and radiation, it’s basically the same thing – poor prognoses in patients with N2 or N3 disease, so the standard becomes never to operate on these individuals.
A European study prospectively took 30 patients and treated them with induction chemotherapy. They saw a 5-year survival rate of 62% if a patient downgrades to lymph node–negative disease and the positron-emission tomographic (PET) findings were good. But they also saw a subset with a small amount of disease within the lymph nodes at the N2 stage and a poor response on PET; Their 5-year survival rate was around 19%. So I’d argue that PET response and the number of lymph nodes involved are the key criteria, and you shouldn’t routinely deny surgery to these patients.
Our experience at MD Anderson Cancer Center over the last 10 years has been to treat N2 and N3 admissions, with surgery, followed by postoperative radiation of 50 Gy. We’re able to achieve very-low morbidity with this regimen, and no mortality after 30 and 90 days. Just to show the heterogeneity: Single-station, microscopic N2 disease should really be resected.
You just can’t lump together everyone with residual N2 after induction therapy, since PET-CTs and most other diagnostic procedures have high false-negative rates. And like I’ve said, it doesn’t matter because N2 disease is really a subset disease. Microscopic N2 disease behaves in a completely different way than does macroscopic, multiple-level N2 disease. And even more important is how the patient’s primary tumor responds to the chemotherapy or chemoradiation; that will tell you how well they’re going to do even if they have a small amount of residual disease in the lymph nodes.
Dr. Swisher is at the University of Texas MD Anderson Cancer Center in Houston. He disclosed that he is a consultant/advisory board member for GlaxoSmithKline.
COUNTERPOINT: Surgery seems to have little value, adds risk.
BY DR. SCOTT J. SWANSON
Dr. Swisher and I probably agree more than we disagree, but I’m going to start by saying that N2 disease is bad, and most of these populations are heterogeneous. But if you feel that a curve toward the bottom of a graph is good, then you should think twice. Anywhere from a 15%-30% survival rate is not great and shows that we have a long way to go. The overall impression among oncologists in several countries is that it’s not really clear whether surgery adds value. Even in very good centers like MD Anderson where there is minimal risk, surgery inherently still involves some risk.
So then, what do we do with persistent N2 disease? I’d say that most of the time, it should be treated with chemotherapy or chemotherapy and radiation. In some cases, N2 disease can be treated with a creative, mutation-driven immunotherapy approach. Most of the time though, surgery is just not a good idea.

Interestingly, about one-third of lung cancer patients present with stage IIIA disease, so it’s important that we as a medical community sort out these treatment options. I think we’re all in agreement that single-station, microscopic, PET-negative/CT-negative disease is not the same as extranodal or multistation PET-positive disease, so we’ve got to begin to substratify N2 disease.
In an intergroup trial of about 200 patients per arm published in the Lancet, patients went to surgery if they didn’t regress after evaluation. The progression-free survival rate did seem to favor surgery; and, if you look at the lobectomy subset, the results are certainly strong. But again, we’re dealing with curves that are pretty low. The pneumonectomy subset drops off and then starts to catch up, but clearly pneumonectomy was a problem in this multicenter trial. The most important graph to this debate shows subjects that persistently had nodal disease had very poor survival. It’s hard to argue for surgery when results show that only about 24% of them are going to be alive down the road. If oncologists across most of the United States say they believe that surgery isn’t a good idea, we’re not going to use this graph to change their minds; we need to change our way of thinking.
So the conclusion to take away from that presentation is that N0 status at surgery significantly predicts greater 5-year survival. So, conversely, surgery is not helpful for the patient with node-positive disease. Surgical resection should only be considered if lobectomy is the operation in question. Pneumonectomy carries risk, and surgery has no beneficial value, compared with chemotherapy unless the patient has been downstaged.
Our experience at Brigham and Women’s Hospital in Boston is similar to Dr. Swisher’s at MD Anderson. During the first 8 years of our thoracic division, we looked at 103 patients who had surgery after induction therapy for N2 disease. The induction plan in those patients was chemotherapy only for 75, radiation only for 18, and chemoradiation for 10. Almost 40% of patients had pneumonectomies, and the rest had lobectomies.
Mortality was 3.9%, major morbidity was 7%, and about 30% were downstaged. Those 5-year survival rates were about 36%. Persistent nodal disease, either N1 or N2, was seen in about 75%, and most of them were N2; the 5-year survival rate there was about 9% with a median of about 15.9 months. Beauty is in the eye of the beholder, so you may look at that and say that 15.9 months isn’t bad, but there’s still a huge subgroup that’s node positive, so here I’d say that pushing surgery is not the best strategy. We also found in this group that adenocarcinomas were much harder to clear.
We’re on very-safe ground to push surgery in the node-negative group, but you’ve got to be careful in the node-positive group.
Survival is relatively limited in N2 disease in general. Surgery may be of value if you downstage the patient, if you’re doing a lobectomy or if you see squamous cell carcinoma. Going forward, we really ought to focus our attention on identifying responders more reliably and improving downstaging – with different or individualized chemotherapy, or perhaps even immunologic therapy.
For the present, we can talk about radiation dosing. High-dose radiation is clearly a viable option for some patients. In addition, we can improve identification of N2 subgroups. Not all N2 disease is the same, so it should not be treated the same across the board.
Dr. Swanson is at Brigham and Women’s Hospital in Boston. He disclosed that he is a consultant/advisory board member for Covidien and Ethicon Endo-Surgery.
This article grew out of the debate by Dr. Swisher and Dr. Swanson at the annual meeting of the Society of Thoracic Surgeons.
POINT: Surgery has its uses for some
BY DR. STEPHEN G. SWISHER
When talking about the role of surgery after induction therapy with persistent N2 disease, one must acknowledge that this is such a heterogeneous disease. You can have single-station N2; resectable, bulky multistation N2; and so on. Then there’s unresectable stage IIIA, but let’s focus mainly on resectable stage IIIA disease.
I can’t tell you how many audiences I’ve faced that absolutely believe the myth that surgery plays no role in Stage IIIA non–small cell lung cancer based on data from stage IIIA disease patients randomized to chemoradiation followed by surgery. The problem with these study results is the high mortality in the pneumonectomy subset. There’s no difference in the overall survival of the two groups, but that doesn’t mean that everyone in that group wouldn’t benefit from surgery.
The curve showed that pneumonectomy did not benefit after chemoradiation in a non–high-volume center. You can see a steep drop in the mortality early on, but it catches up again at the end. If you look at the overall 5-year survival rate, even in the pneumonectomy subset, you’re looking at 22% vs. 24%.
But in the lobectomy set, you see something completely different. You’ve got a doubling of survivors and no mortality early on, and a doubling of 5-year survival from 18% to 36%.
And yet, people continue saying that there’s no role for surgery. Well, I think there is a role for surgery, and there are subsets of N2 for which surgery can be particularly beneficial. We have to move more toward what the medical oncologists do, which is personalize therapy and look at subsets of N2 disease so that we know which patients we can benefit and which ones we can’t.
Moving on to the second myth: Surgery plays no role in N2 residual disease after induction therapy. This myth is based on the results of a couple of prospective studies in the 1980s and ’90s that showed residual N2 disease after chemo- and radiotherapy leads to survival of 16-35 months in most cases. I’d say that those results are true, but it’s not to say there aren’t subsets within these populations that benefited. With preoperative chemo and radiation, it’s basically the same thing – poor prognoses in patients with N2 or N3 disease, so the standard becomes never to operate on these individuals.
A European study prospectively took 30 patients and treated them with induction chemotherapy. They saw a 5-year survival rate of 62% if a patient downgrades to lymph node–negative disease and the positron-emission tomographic (PET) findings were good. But they also saw a subset with a small amount of disease within the lymph nodes at the N2 stage and a poor response on PET; Their 5-year survival rate was around 19%. So I’d argue that PET response and the number of lymph nodes involved are the key criteria, and you shouldn’t routinely deny surgery to these patients.
Our experience at MD Anderson Cancer Center over the last 10 years has been to treat N2 and N3 admissions, with surgery, followed by postoperative radiation of 50 Gy. We’re able to achieve very-low morbidity with this regimen, and no mortality after 30 and 90 days. Just to show the heterogeneity: Single-station, microscopic N2 disease should really be resected.
You just can’t lump together everyone with residual N2 after induction therapy, since PET-CTs and most other diagnostic procedures have high false-negative rates. And like I’ve said, it doesn’t matter because N2 disease is really a subset disease. Microscopic N2 disease behaves in a completely different way than does macroscopic, multiple-level N2 disease. And even more important is how the patient’s primary tumor responds to the chemotherapy or chemoradiation; that will tell you how well they’re going to do even if they have a small amount of residual disease in the lymph nodes.
Dr. Swisher is at the University of Texas MD Anderson Cancer Center in Houston. He disclosed that he is a consultant/advisory board member for GlaxoSmithKline.
COUNTERPOINT: Surgery seems to have little value, adds risk.
BY DR. SCOTT J. SWANSON
Dr. Swisher and I probably agree more than we disagree, but I’m going to start by saying that N2 disease is bad, and most of these populations are heterogeneous. But if you feel that a curve toward the bottom of a graph is good, then you should think twice. Anywhere from a 15%-30% survival rate is not great and shows that we have a long way to go. The overall impression among oncologists in several countries is that it’s not really clear whether surgery adds value. Even in very good centers like MD Anderson where there is minimal risk, surgery inherently still involves some risk.
So then, what do we do with persistent N2 disease? I’d say that most of the time, it should be treated with chemotherapy or chemotherapy and radiation. In some cases, N2 disease can be treated with a creative, mutation-driven immunotherapy approach. Most of the time though, surgery is just not a good idea.
Interestingly, about one-third of lung cancer patients present with stage IIIA disease, so it’s important that we as a medical community sort out these treatment options. I think we’re all in agreement that single-station, microscopic, PET-negative/CT-negative disease is not the same as extranodal or multistation PET-positive disease, so we’ve got to begin to substratify N2 disease.
In an intergroup trial of about 200 patients per arm published in the Lancet, patients went to surgery if they didn’t regress after evaluation. The progression-free survival rate did seem to favor surgery; and, if you look at the lobectomy subset, the results are certainly strong. But again, we’re dealing with curves that are pretty low. The pneumonectomy subset drops off and then starts to catch up, but clearly pneumonectomy was a problem in this multicenter trial. The most important graph to this debate shows subjects that persistently had nodal disease had very poor survival. It’s hard to argue for surgery when results show that only about 24% of them are going to be alive down the road. If oncologists across most of the United States say they believe that surgery isn’t a good idea, we’re not going to use this graph to change their minds; we need to change our way of thinking.
So the conclusion to take away from that presentation is that N0 status at surgery significantly predicts greater 5-year survival. So, conversely, surgery is not helpful for the patient with node-positive disease. Surgical resection should only be considered if lobectomy is the operation in question. Pneumonectomy carries risk, and surgery has no beneficial value, compared with chemotherapy unless the patient has been downstaged.
Our experience at Brigham and Women’s Hospital in Boston is similar to Dr. Swisher’s at MD Anderson. During the first 8 years of our thoracic division, we looked at 103 patients who had surgery after induction therapy for N2 disease. The induction plan in those patients was chemotherapy only for 75, radiation only for 18, and chemoradiation for 10. Almost 40% of patients had pneumonectomies, and the rest had lobectomies.
Mortality was 3.9%, major morbidity was 7%, and about 30% were downstaged. Those 5-year survival rates were about 36%. Persistent nodal disease, either N1 or N2, was seen in about 75%, and most of them were N2; the 5-year survival rate there was about 9% with a median of about 15.9 months. Beauty is in the eye of the beholder, so you may look at that and say that 15.9 months isn’t bad, but there’s still a huge subgroup that’s node positive, so here I’d say that pushing surgery is not the best strategy. We also found in this group that adenocarcinomas were much harder to clear.
We’re on very-safe ground to push surgery in the node-negative group, but you’ve got to be careful in the node-positive group.
Survival is relatively limited in N2 disease in general. Surgery may be of value if you downstage the patient, if you’re doing a lobectomy or if you see squamous cell carcinoma. Going forward, we really ought to focus our attention on identifying responders more reliably and improving downstaging – with different or individualized chemotherapy, or perhaps even immunologic therapy.
For the present, we can talk about radiation dosing. High-dose radiation is clearly a viable option for some patients. In addition, we can improve identification of N2 subgroups. Not all N2 disease is the same, so it should not be treated the same across the board.
Dr. Swanson is at Brigham and Women’s Hospital in Boston. He disclosed that he is a consultant/advisory board member for Covidien and Ethicon Endo-Surgery.
This article grew out of the debate by Dr. Swisher and Dr. Swanson at the annual meeting of the Society of Thoracic Surgeons.
POINT: Surgery has its uses for some
BY DR. STEPHEN G. SWISHER
When talking about the role of surgery after induction therapy with persistent N2 disease, one must acknowledge that this is such a heterogeneous disease. You can have single-station N2; resectable, bulky multistation N2; and so on. Then there’s unresectable stage IIIA, but let’s focus mainly on resectable stage IIIA disease.
I can’t tell you how many audiences I’ve faced that absolutely believe the myth that surgery plays no role in Stage IIIA non–small cell lung cancer based on data from stage IIIA disease patients randomized to chemoradiation followed by surgery. The problem with these study results is the high mortality in the pneumonectomy subset. There’s no difference in the overall survival of the two groups, but that doesn’t mean that everyone in that group wouldn’t benefit from surgery.
The curve showed that pneumonectomy did not benefit after chemoradiation in a non–high-volume center. You can see a steep drop in the mortality early on, but it catches up again at the end. If you look at the overall 5-year survival rate, even in the pneumonectomy subset, you’re looking at 22% vs. 24%.
But in the lobectomy set, you see something completely different. You’ve got a doubling of survivors and no mortality early on, and a doubling of 5-year survival from 18% to 36%.
And yet, people continue saying that there’s no role for surgery. Well, I think there is a role for surgery, and there are subsets of N2 for which surgery can be particularly beneficial. We have to move more toward what the medical oncologists do, which is personalize therapy and look at subsets of N2 disease so that we know which patients we can benefit and which ones we can’t.
Moving on to the second myth: Surgery plays no role in N2 residual disease after induction therapy. This myth is based on the results of a couple of prospective studies in the 1980s and ’90s that showed residual N2 disease after chemo- and radiotherapy leads to survival of 16-35 months in most cases. I’d say that those results are true, but it’s not to say there aren’t subsets within these populations that benefited. With preoperative chemo and radiation, it’s basically the same thing – poor prognoses in patients with N2 or N3 disease, so the standard becomes never to operate on these individuals.
A European study prospectively took 30 patients and treated them with induction chemotherapy. They saw a 5-year survival rate of 62% if a patient downgrades to lymph node–negative disease and the positron-emission tomographic (PET) findings were good. But they also saw a subset with a small amount of disease within the lymph nodes at the N2 stage and a poor response on PET; Their 5-year survival rate was around 19%. So I’d argue that PET response and the number of lymph nodes involved are the key criteria, and you shouldn’t routinely deny surgery to these patients.
Our experience at MD Anderson Cancer Center over the last 10 years has been to treat N2 and N3 admissions, with surgery, followed by postoperative radiation of 50 Gy. We’re able to achieve very-low morbidity with this regimen, and no mortality after 30 and 90 days. Just to show the heterogeneity: Single-station, microscopic N2 disease should really be resected.
You just can’t lump together everyone with residual N2 after induction therapy, since PET-CTs and most other diagnostic procedures have high false-negative rates. And like I’ve said, it doesn’t matter because N2 disease is really a subset disease. Microscopic N2 disease behaves in a completely different way than does macroscopic, multiple-level N2 disease. And even more important is how the patient’s primary tumor responds to the chemotherapy or chemoradiation; that will tell you how well they’re going to do even if they have a small amount of residual disease in the lymph nodes.
Dr. Swisher is at the University of Texas MD Anderson Cancer Center in Houston. He disclosed that he is a consultant/advisory board member for GlaxoSmithKline.
COUNTERPOINT: Surgery seems to have little value, adds risk.
BY DR. SCOTT J. SWANSON
Dr. Swisher and I probably agree more than we disagree, but I’m going to start by saying that N2 disease is bad, and most of these populations are heterogeneous. But if you feel that a curve toward the bottom of a graph is good, then you should think twice. Anywhere from a 15%-30% survival rate is not great and shows that we have a long way to go. The overall impression among oncologists in several countries is that it’s not really clear whether surgery adds value. Even in very good centers like MD Anderson where there is minimal risk, surgery inherently still involves some risk.
So then, what do we do with persistent N2 disease? I’d say that most of the time, it should be treated with chemotherapy or chemotherapy and radiation. In some cases, N2 disease can be treated with a creative, mutation-driven immunotherapy approach. Most of the time though, surgery is just not a good idea.
Interestingly, about one-third of lung cancer patients present with stage IIIA disease, so it’s important that we as a medical community sort out these treatment options. I think we’re all in agreement that single-station, microscopic, PET-negative/CT-negative disease is not the same as extranodal or multistation PET-positive disease, so we’ve got to begin to substratify N2 disease.
In an intergroup trial of about 200 patients per arm published in the Lancet, patients went to surgery if they didn’t regress after evaluation. The progression-free survival rate did seem to favor surgery; and, if you look at the lobectomy subset, the results are certainly strong. But again, we’re dealing with curves that are pretty low. The pneumonectomy subset drops off and then starts to catch up, but clearly pneumonectomy was a problem in this multicenter trial. The most important graph to this debate shows subjects that persistently had nodal disease had very poor survival. It’s hard to argue for surgery when results show that only about 24% of them are going to be alive down the road. If oncologists across most of the United States say they believe that surgery isn’t a good idea, we’re not going to use this graph to change their minds; we need to change our way of thinking.
So the conclusion to take away from that presentation is that N0 status at surgery significantly predicts greater 5-year survival. So, conversely, surgery is not helpful for the patient with node-positive disease. Surgical resection should only be considered if lobectomy is the operation in question. Pneumonectomy carries risk, and surgery has no beneficial value, compared with chemotherapy unless the patient has been downstaged.
Our experience at Brigham and Women’s Hospital in Boston is similar to Dr. Swisher’s at MD Anderson. During the first 8 years of our thoracic division, we looked at 103 patients who had surgery after induction therapy for N2 disease. The induction plan in those patients was chemotherapy only for 75, radiation only for 18, and chemoradiation for 10. Almost 40% of patients had pneumonectomies, and the rest had lobectomies.
Mortality was 3.9%, major morbidity was 7%, and about 30% were downstaged. Those 5-year survival rates were about 36%. Persistent nodal disease, either N1 or N2, was seen in about 75%, and most of them were N2; the 5-year survival rate there was about 9% with a median of about 15.9 months. Beauty is in the eye of the beholder, so you may look at that and say that 15.9 months isn’t bad, but there’s still a huge subgroup that’s node positive, so here I’d say that pushing surgery is not the best strategy. We also found in this group that adenocarcinomas were much harder to clear.
We’re on very-safe ground to push surgery in the node-negative group, but you’ve got to be careful in the node-positive group.
Survival is relatively limited in N2 disease in general. Surgery may be of value if you downstage the patient, if you’re doing a lobectomy or if you see squamous cell carcinoma. Going forward, we really ought to focus our attention on identifying responders more reliably and improving downstaging – with different or individualized chemotherapy, or perhaps even immunologic therapy.
For the present, we can talk about radiation dosing. High-dose radiation is clearly a viable option for some patients. In addition, we can improve identification of N2 subgroups. Not all N2 disease is the same, so it should not be treated the same across the board.
Dr. Swanson is at Brigham and Women’s Hospital in Boston. He disclosed that he is a consultant/advisory board member for Covidien and Ethicon Endo-Surgery.
This article grew out of the debate by Dr. Swisher and Dr. Swanson at the annual meeting of the Society of Thoracic Surgeons.

No evidence for CLL transmission via blood transfusion
Analysis of data from blood transfusions that took place in Sweden and Denmark over a 30-year period showed no indication that chronic lymphocytic leukemia (CLL) risk is higher among recipients of blood from donors who subsequently developed CLL, according to researchers.
The study compared 7,413 recipients of blood from 796 donors who subsequently developed CLL (exposed group), with 80,431 recipients from 7,477 donors free of CLL (unexposed group). In total, 12 recipients in the exposed group and 107 in the unexposed group were later diagnosed with CLL, for an incidence rate ratio of 0.94 (95% confidence interval, 0.52-1.71). When defining “exposed” as receiving blood less than 10 years before donor CLL diagnosis, the incidence rate ratio was 0.46 (95% CI, 0.12-1.85).
“The analyses provided little evidence that donor MBL [monoclonal B-cell lymphocytosis]/CLL transmission in blood products influences recipient CLL risk,” wrote Dr. Henrik Hjalgrim of the department of epidemiology research at Statens Serum Institut, Copenhagen, and his colleagues (Blood 2015 doi: 10.1182/blood-2015-03-632844).
MBL is fairly common in healthy individuals (estimated at 7.1% in a study of American blood donors aged 45-91 years) and may progress to CLL at various rates depending on the MBL cell count. Results from previous studies investigating the association between transfusion and risk of CLL or small lymphocytic lymphoma have been mixed, they noted.
Using a retrospective approach, Dr. Hjalgrim and his associates first identified donors subsequently diagnosed with CLL, then identified control donors free from CLL who were matched for age, sex, county, number of donations, and blood type.
In case MBL may have progressed in the recipient but not the donor, investigators also examined whether CLL clustered among recipients from an individual donor, regardless of donor CLL status, but found no such clusters.
Limiting the analysis was the lack of donor MBL status, for which postdonation CLL diagnosis substituted. Some recipients in the exposed group may have received blood drawn before the donor developed MBL.
Dr. Hjalgrim and his coauthors reported having no disclosures.
Analysis of data from blood transfusions that took place in Sweden and Denmark over a 30-year period showed no indication that chronic lymphocytic leukemia (CLL) risk is higher among recipients of blood from donors who subsequently developed CLL, according to researchers.
The study compared 7,413 recipients of blood from 796 donors who subsequently developed CLL (exposed group), with 80,431 recipients from 7,477 donors free of CLL (unexposed group). In total, 12 recipients in the exposed group and 107 in the unexposed group were later diagnosed with CLL, for an incidence rate ratio of 0.94 (95% confidence interval, 0.52-1.71). When defining “exposed” as receiving blood less than 10 years before donor CLL diagnosis, the incidence rate ratio was 0.46 (95% CI, 0.12-1.85).
“The analyses provided little evidence that donor MBL [monoclonal B-cell lymphocytosis]/CLL transmission in blood products influences recipient CLL risk,” wrote Dr. Henrik Hjalgrim of the department of epidemiology research at Statens Serum Institut, Copenhagen, and his colleagues (Blood 2015 doi: 10.1182/blood-2015-03-632844).
MBL is fairly common in healthy individuals (estimated at 7.1% in a study of American blood donors aged 45-91 years) and may progress to CLL at various rates depending on the MBL cell count. Results from previous studies investigating the association between transfusion and risk of CLL or small lymphocytic lymphoma have been mixed, they noted.
Using a retrospective approach, Dr. Hjalgrim and his associates first identified donors subsequently diagnosed with CLL, then identified control donors free from CLL who were matched for age, sex, county, number of donations, and blood type.
In case MBL may have progressed in the recipient but not the donor, investigators also examined whether CLL clustered among recipients from an individual donor, regardless of donor CLL status, but found no such clusters.
Limiting the analysis was the lack of donor MBL status, for which postdonation CLL diagnosis substituted. Some recipients in the exposed group may have received blood drawn before the donor developed MBL.
Dr. Hjalgrim and his coauthors reported having no disclosures.
Analysis of data from blood transfusions that took place in Sweden and Denmark over a 30-year period showed no indication that chronic lymphocytic leukemia (CLL) risk is higher among recipients of blood from donors who subsequently developed CLL, according to researchers.
The study compared 7,413 recipients of blood from 796 donors who subsequently developed CLL (exposed group), with 80,431 recipients from 7,477 donors free of CLL (unexposed group). In total, 12 recipients in the exposed group and 107 in the unexposed group were later diagnosed with CLL, for an incidence rate ratio of 0.94 (95% confidence interval, 0.52-1.71). When defining “exposed” as receiving blood less than 10 years before donor CLL diagnosis, the incidence rate ratio was 0.46 (95% CI, 0.12-1.85).
“The analyses provided little evidence that donor MBL [monoclonal B-cell lymphocytosis]/CLL transmission in blood products influences recipient CLL risk,” wrote Dr. Henrik Hjalgrim of the department of epidemiology research at Statens Serum Institut, Copenhagen, and his colleagues (Blood 2015 doi: 10.1182/blood-2015-03-632844).
MBL is fairly common in healthy individuals (estimated at 7.1% in a study of American blood donors aged 45-91 years) and may progress to CLL at various rates depending on the MBL cell count. Results from previous studies investigating the association between transfusion and risk of CLL or small lymphocytic lymphoma have been mixed, they noted.
Using a retrospective approach, Dr. Hjalgrim and his associates first identified donors subsequently diagnosed with CLL, then identified control donors free from CLL who were matched for age, sex, county, number of donations, and blood type.
In case MBL may have progressed in the recipient but not the donor, investigators also examined whether CLL clustered among recipients from an individual donor, regardless of donor CLL status, but found no such clusters.
Limiting the analysis was the lack of donor MBL status, for which postdonation CLL diagnosis substituted. Some recipients in the exposed group may have received blood drawn before the donor developed MBL.
Dr. Hjalgrim and his coauthors reported having no disclosures.
FROM BLOOD
Key clinical point: There is no evidence for higher risk of chronic lymphocytic leukemia (CLL) among recipients of blood products from donors who subsequently were diagnosed with CLL.
Major finding: Among exposed recipients (7,413 who received blood from 796 donors who subsequently developed CLL), 12 were diagnosed with CLL. Among unexposed recipients (80,431 who received blood from 7,477 donors free of CLL), 107 were diagnosed with CLL, for an incidence rate ratio of 0.94 (95% CI, 0.52-1.71).
Data source: The Scandinavian Donations and Transfusions (SCANDAT2) database comprises information, including donor and recipient health outcomes, for more than 20 million blood products handled by blood banks from 1968 to 2010.
Disclosures: Dr. Hjalgrim and his coauthors reported having no disclosures.