User login
Official Newspaper of the American College of Surgeons
From the Washington Office
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.

Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.
Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.
Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.

ACS Clinical Congress: Something for everyone
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.

Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.
Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.
Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.

Mentoring that takes it up a notch
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
More expanded drug indications approved on less rigorous evidence
Hundreds of new – but noninnovative – drugs have been approved in the United States in the last 20 years using expedited review programs designed especially to push forward first-in-class agents for unmet medical needs.
An extensive review of publicly available Food and Drug Administration records also concluded that few of these drugs rely on the more rigorous clinical trials intended to screen out ineffectively or potentially harmful drugs – potentially increasing the availability of poorly investigated agents that may or may not provide much clinical benefit*.

“These data have important implications for patient care,” Dr. Aaron S. Kesselheim and his colleagues wrote (BMJ 2015;351:h4679 doi: 10.1136/bmj.h4679).
“Special regulatory designations allow drugs to be approved at earlier stages based on less rigorous clinical testing; for example, one review showed drugs with orphan designations or granted accelerated approval are also more likely than drugs without these designations to be tested in single-arm studies without placebo or active comparators,” said Dr. Kesselheim of Harvard University and his coinvestigators. “While many physicians and patients trust that FDA-approved products are effective and safe for use, products approved on the basis of more limited data are at greater risk for later changes to their effectiveness or safety profiles.”
A twin study, published in the same issue, found that a lesser class of evidence often supports the approval of supplemental indications. Of 295 supplemental indications approved since 2005, only about one-third were based on trials with active comparators. The rest used nonclinical endpoints like historical controls and biomarkers or imaging data.
Most striking of all, most of the supplemental indications were aimed at pediatric patients, and many extrapolated adult evidence to these young patients, said the authors.
“Although we do not conclude that any of these approvals were mistaken, pediatric patients have unique physiologies and pharmacokinetic characteristics that may require more rigorous trials to confirm both the efficacy and the safety of drugs previously approved only for use in adults.”
Study 1: Expedited review
The authors used the Drugs@FDA database, FDA annual reports, and the Federal Register to identify 774 new agents representing first-in-class agents. Overall, this accounted for a significant increase of 2.6% per year in the number of expedited review and approval programs for each new agent (rate ratio, 1.06) and a 2.4% increase per year in the proportion of agents involved in at least one of these programs. Many approvals were associated with more than one program, and this proportion increased over the study period, from a low of 0.54 in 1987 to a high of 1.72 in 2014.
“Driving this trend was an increase in the proportion of approved, non–first-in-class drugs,” associated with at least one [expedited] program,” the authors noted.
Additionally, not all of the drugs could reasonably be considered as treatments for an urgent, unmet medical need. “For example, bimatoprost (Latisse: Allergan, Dublin) was granted priority review when it was first approved in 2008 for hypotrichosis of the eyelids, a clearly less serious condition.”

While the “breakthrough therapy” pathway was intended for only a handful of drug approvals each year, the FDA received nearly 250 applications in the first 2 years; 68 of these were granted, despite the agency’s prediction than only 2-4 such applications would be approved.
Four of these were for chronic lymphocytic anemia alone – a number the authors suggested might be excessive. “It is doubtful that a single disease condition can be the subject of four true ‘breakthroughs’ in such a short time frame.”
The situation is likely to accelerate, they noted. The 21st Century Cures Act, passed in July by the U.S. House of Representatives, instructs the FDA to develop a new pathway for repurposing approved drugs on the basis of early stage investigators and “high-risk, high-reward research. ... The FDA would also be permitted to approve such indications on the basis of only summaries of data in such circumstances, rather than being required to review the data in detail.”
New antibiotics and antifungals would have particularly lenient evidence requirements, according to the investigators.
However, expedited review is a double-edged sword, the paper noted. An FDA review found that most cancer drugs are later found to be safe and effective in postapproval studies, although such studies are often delayed or – in some cases – never conducted.
The FDA should be granted more authority to punish manufacturers who lag behind these requirements, including having the ability to impose fines and even suspend approval until additional studies are complete, the investigators said.
Study 2: Approval evidence for supplemental indications
The second study concluded that the FDA increasingly approves supplemental indications with less than level I evidence (randomized, controlled trials with placebo or active comparator (BMJ. 2015;351:h4679. doi: 10.1136/bmj.h4679).
Of an examined 295 such approvals since 2005, the largest portion was for oncology (27%). Other indications were infectious disease (15%); cardiovascular disease and prevention (12%); psychiatry (12%); musculoskeletal and rheumatology (10%); neurology (8%); gastroenterology (6%); and other (1%). Orphan drug status accounted for 20% of the approvals.
Only 30% of modified indications were supported by efficacy trials with active comparators. Level I evidence supported half of modified use approvals and 11% of approvals expanding the patient population. Almost all of the expansion approvals were into pediatric populations, and the vast majority (94%) of evidence for those was extrapolated from adult clinical trials.
Uncontrolled trials supported 34% of expanded population approvals, and nine (14%) of these supplemental approvals had no trials with clinical endpoints.
Findings were similar with other approval pathways. Among new indications, 32% had clinical endpoints, as did 30% of modified indications. Only 22% of expanded population indications rested on clinical endpoint data.
“Clinical outcomes were most often used in trials supporting supplemental indication approvals of neurologic (48%) and infectious disease drugs (45%); by contrast, 70% of oncology supplemental indications were supported exclusively by trials using surrogate outcomes.”
Uncontrolled trials supported one-third of expanded population supplements; 14% of these had no clinical trial evidence. Similarly, one-third of orphan drug indications were supported by uncontrolled or historical cohort studies. Significantly fewer orphan than nonorphan approvals were supported by clinical trials (18% vs. 35%).
Again, the situation is likely to accelerate. The Best Pharmaceuticals for Children Act provides up to 6 months of additional market exclusivity for a new approval, “which can be extremely lucrative for the sponsor,” the authors noted. The 21st Century Cures Act will also play into the situation, they said.
“The high degree of heterogeneity of supporting evidence for supplemental indications, in the setting of legislation promoting drug approvals based on decreasing evidentiary standards, underscores the need for a robust system of postapproval drug monitoring for efficacy and safety, timely confirmatory studies, and reexamination of existing legislative incentives to promote the optimal delivery of evidence-based medicine.”
Both studies were supported in part by the Greenwall Faculty Scholars Program in bioethics and the Harvard program in therapeutic science. Dr. Kesselheim and his coinvestigators had no financial disclosures.
On Twitter @alz_gal
*Correction, 9/24/2015: An earlier version of this article misstated the review's findings.
The FDA provides too many expanded drug indications with too little supporting research.
Independent examinations of the agency’s records, including the two studies by Dr. Aaron S. Kesselheim and colleagues, are finding that up to 90% of these approvals provide few or no advantages for patients. The FDA’s flexible criteria and low threshold for approval do not reward more research for breakthroughs but instead reward more research for minor variations that can clear this low threshold.
Patients and doctors have clamored for expedited approval pathways that allow clinical access to new drugs sooner – a process that also generates revenue for drug companies to fund more breakthrough research. But faster approval means taking less time to prove these drugs safe and effective for their new indications. And in an age when prescription drugs are the fourth-leading cause of death in the United States and the third-leading cause in Europe, according to some reports, this doesn’t seem to be a wise move.
Expedited trials – and approvals based on nonclinical data – are incapable of providing patients or doctors with valid information on what new clinical benefits a drug provides.
Patients and doctors must trust the FDA to live up to its claims of providing drugs that work not only for their approved indications, but help more than they harm. But its expedited approval processes only require, in most cases, that the drugs provide “nonzero” levels of effectiveness.
The United States and other countries need an alternative paradigm – one in which research focuses on better medicines for patients rather than for profits, where clinical trials with low risk of bias look for real benefits and faithfully report harms.
Dr. Donald W. Light, an osteopathic physician at Rowan University, Cherry Hill, N.J., and Dr. Joel Lexchin of the School of Health Policy and Management at York University in Toronto made these comments in an accompanying editorial (BMJ 2015;351:h4897). They had no disclosures.
The FDA provides too many expanded drug indications with too little supporting research.
Independent examinations of the agency’s records, including the two studies by Dr. Aaron S. Kesselheim and colleagues, are finding that up to 90% of these approvals provide few or no advantages for patients. The FDA’s flexible criteria and low threshold for approval do not reward more research for breakthroughs but instead reward more research for minor variations that can clear this low threshold.
Patients and doctors have clamored for expedited approval pathways that allow clinical access to new drugs sooner – a process that also generates revenue for drug companies to fund more breakthrough research. But faster approval means taking less time to prove these drugs safe and effective for their new indications. And in an age when prescription drugs are the fourth-leading cause of death in the United States and the third-leading cause in Europe, according to some reports, this doesn’t seem to be a wise move.
Expedited trials – and approvals based on nonclinical data – are incapable of providing patients or doctors with valid information on what new clinical benefits a drug provides.
Patients and doctors must trust the FDA to live up to its claims of providing drugs that work not only for their approved indications, but help more than they harm. But its expedited approval processes only require, in most cases, that the drugs provide “nonzero” levels of effectiveness.
The United States and other countries need an alternative paradigm – one in which research focuses on better medicines for patients rather than for profits, where clinical trials with low risk of bias look for real benefits and faithfully report harms.
Dr. Donald W. Light, an osteopathic physician at Rowan University, Cherry Hill, N.J., and Dr. Joel Lexchin of the School of Health Policy and Management at York University in Toronto made these comments in an accompanying editorial (BMJ 2015;351:h4897). They had no disclosures.
The FDA provides too many expanded drug indications with too little supporting research.
Independent examinations of the agency’s records, including the two studies by Dr. Aaron S. Kesselheim and colleagues, are finding that up to 90% of these approvals provide few or no advantages for patients. The FDA’s flexible criteria and low threshold for approval do not reward more research for breakthroughs but instead reward more research for minor variations that can clear this low threshold.
Patients and doctors have clamored for expedited approval pathways that allow clinical access to new drugs sooner – a process that also generates revenue for drug companies to fund more breakthrough research. But faster approval means taking less time to prove these drugs safe and effective for their new indications. And in an age when prescription drugs are the fourth-leading cause of death in the United States and the third-leading cause in Europe, according to some reports, this doesn’t seem to be a wise move.
Expedited trials – and approvals based on nonclinical data – are incapable of providing patients or doctors with valid information on what new clinical benefits a drug provides.
Patients and doctors must trust the FDA to live up to its claims of providing drugs that work not only for their approved indications, but help more than they harm. But its expedited approval processes only require, in most cases, that the drugs provide “nonzero” levels of effectiveness.
The United States and other countries need an alternative paradigm – one in which research focuses on better medicines for patients rather than for profits, where clinical trials with low risk of bias look for real benefits and faithfully report harms.
Dr. Donald W. Light, an osteopathic physician at Rowan University, Cherry Hill, N.J., and Dr. Joel Lexchin of the School of Health Policy and Management at York University in Toronto made these comments in an accompanying editorial (BMJ 2015;351:h4897). They had no disclosures.
Hundreds of new – but noninnovative – drugs have been approved in the United States in the last 20 years using expedited review programs designed especially to push forward first-in-class agents for unmet medical needs.
An extensive review of publicly available Food and Drug Administration records also concluded that few of these drugs rely on the more rigorous clinical trials intended to screen out ineffectively or potentially harmful drugs – potentially increasing the availability of poorly investigated agents that may or may not provide much clinical benefit*.
“These data have important implications for patient care,” Dr. Aaron S. Kesselheim and his colleagues wrote (BMJ 2015;351:h4679 doi: 10.1136/bmj.h4679).
“Special regulatory designations allow drugs to be approved at earlier stages based on less rigorous clinical testing; for example, one review showed drugs with orphan designations or granted accelerated approval are also more likely than drugs without these designations to be tested in single-arm studies without placebo or active comparators,” said Dr. Kesselheim of Harvard University and his coinvestigators. “While many physicians and patients trust that FDA-approved products are effective and safe for use, products approved on the basis of more limited data are at greater risk for later changes to their effectiveness or safety profiles.”
A twin study, published in the same issue, found that a lesser class of evidence often supports the approval of supplemental indications. Of 295 supplemental indications approved since 2005, only about one-third were based on trials with active comparators. The rest used nonclinical endpoints like historical controls and biomarkers or imaging data.
Most striking of all, most of the supplemental indications were aimed at pediatric patients, and many extrapolated adult evidence to these young patients, said the authors.
“Although we do not conclude that any of these approvals were mistaken, pediatric patients have unique physiologies and pharmacokinetic characteristics that may require more rigorous trials to confirm both the efficacy and the safety of drugs previously approved only for use in adults.”
Study 1: Expedited review
The authors used the Drugs@FDA database, FDA annual reports, and the Federal Register to identify 774 new agents representing first-in-class agents. Overall, this accounted for a significant increase of 2.6% per year in the number of expedited review and approval programs for each new agent (rate ratio, 1.06) and a 2.4% increase per year in the proportion of agents involved in at least one of these programs. Many approvals were associated with more than one program, and this proportion increased over the study period, from a low of 0.54 in 1987 to a high of 1.72 in 2014.
“Driving this trend was an increase in the proportion of approved, non–first-in-class drugs,” associated with at least one [expedited] program,” the authors noted.
Additionally, not all of the drugs could reasonably be considered as treatments for an urgent, unmet medical need. “For example, bimatoprost (Latisse: Allergan, Dublin) was granted priority review when it was first approved in 2008 for hypotrichosis of the eyelids, a clearly less serious condition.”
While the “breakthrough therapy” pathway was intended for only a handful of drug approvals each year, the FDA received nearly 250 applications in the first 2 years; 68 of these were granted, despite the agency’s prediction than only 2-4 such applications would be approved.
Four of these were for chronic lymphocytic anemia alone – a number the authors suggested might be excessive. “It is doubtful that a single disease condition can be the subject of four true ‘breakthroughs’ in such a short time frame.”
The situation is likely to accelerate, they noted. The 21st Century Cures Act, passed in July by the U.S. House of Representatives, instructs the FDA to develop a new pathway for repurposing approved drugs on the basis of early stage investigators and “high-risk, high-reward research. ... The FDA would also be permitted to approve such indications on the basis of only summaries of data in such circumstances, rather than being required to review the data in detail.”
New antibiotics and antifungals would have particularly lenient evidence requirements, according to the investigators.
However, expedited review is a double-edged sword, the paper noted. An FDA review found that most cancer drugs are later found to be safe and effective in postapproval studies, although such studies are often delayed or – in some cases – never conducted.
The FDA should be granted more authority to punish manufacturers who lag behind these requirements, including having the ability to impose fines and even suspend approval until additional studies are complete, the investigators said.
Study 2: Approval evidence for supplemental indications
The second study concluded that the FDA increasingly approves supplemental indications with less than level I evidence (randomized, controlled trials with placebo or active comparator (BMJ. 2015;351:h4679. doi: 10.1136/bmj.h4679).
Of an examined 295 such approvals since 2005, the largest portion was for oncology (27%). Other indications were infectious disease (15%); cardiovascular disease and prevention (12%); psychiatry (12%); musculoskeletal and rheumatology (10%); neurology (8%); gastroenterology (6%); and other (1%). Orphan drug status accounted for 20% of the approvals.
Only 30% of modified indications were supported by efficacy trials with active comparators. Level I evidence supported half of modified use approvals and 11% of approvals expanding the patient population. Almost all of the expansion approvals were into pediatric populations, and the vast majority (94%) of evidence for those was extrapolated from adult clinical trials.
Uncontrolled trials supported 34% of expanded population approvals, and nine (14%) of these supplemental approvals had no trials with clinical endpoints.
Findings were similar with other approval pathways. Among new indications, 32% had clinical endpoints, as did 30% of modified indications. Only 22% of expanded population indications rested on clinical endpoint data.
“Clinical outcomes were most often used in trials supporting supplemental indication approvals of neurologic (48%) and infectious disease drugs (45%); by contrast, 70% of oncology supplemental indications were supported exclusively by trials using surrogate outcomes.”
Uncontrolled trials supported one-third of expanded population supplements; 14% of these had no clinical trial evidence. Similarly, one-third of orphan drug indications were supported by uncontrolled or historical cohort studies. Significantly fewer orphan than nonorphan approvals were supported by clinical trials (18% vs. 35%).
Again, the situation is likely to accelerate. The Best Pharmaceuticals for Children Act provides up to 6 months of additional market exclusivity for a new approval, “which can be extremely lucrative for the sponsor,” the authors noted. The 21st Century Cures Act will also play into the situation, they said.
“The high degree of heterogeneity of supporting evidence for supplemental indications, in the setting of legislation promoting drug approvals based on decreasing evidentiary standards, underscores the need for a robust system of postapproval drug monitoring for efficacy and safety, timely confirmatory studies, and reexamination of existing legislative incentives to promote the optimal delivery of evidence-based medicine.”
Both studies were supported in part by the Greenwall Faculty Scholars Program in bioethics and the Harvard program in therapeutic science. Dr. Kesselheim and his coinvestigators had no financial disclosures.
On Twitter @alz_gal
*Correction, 9/24/2015: An earlier version of this article misstated the review's findings.
Hundreds of new – but noninnovative – drugs have been approved in the United States in the last 20 years using expedited review programs designed especially to push forward first-in-class agents for unmet medical needs.
An extensive review of publicly available Food and Drug Administration records also concluded that few of these drugs rely on the more rigorous clinical trials intended to screen out ineffectively or potentially harmful drugs – potentially increasing the availability of poorly investigated agents that may or may not provide much clinical benefit*.
“These data have important implications for patient care,” Dr. Aaron S. Kesselheim and his colleagues wrote (BMJ 2015;351:h4679 doi: 10.1136/bmj.h4679).
“Special regulatory designations allow drugs to be approved at earlier stages based on less rigorous clinical testing; for example, one review showed drugs with orphan designations or granted accelerated approval are also more likely than drugs without these designations to be tested in single-arm studies without placebo or active comparators,” said Dr. Kesselheim of Harvard University and his coinvestigators. “While many physicians and patients trust that FDA-approved products are effective and safe for use, products approved on the basis of more limited data are at greater risk for later changes to their effectiveness or safety profiles.”
A twin study, published in the same issue, found that a lesser class of evidence often supports the approval of supplemental indications. Of 295 supplemental indications approved since 2005, only about one-third were based on trials with active comparators. The rest used nonclinical endpoints like historical controls and biomarkers or imaging data.
Most striking of all, most of the supplemental indications were aimed at pediatric patients, and many extrapolated adult evidence to these young patients, said the authors.
“Although we do not conclude that any of these approvals were mistaken, pediatric patients have unique physiologies and pharmacokinetic characteristics that may require more rigorous trials to confirm both the efficacy and the safety of drugs previously approved only for use in adults.”
Study 1: Expedited review
The authors used the Drugs@FDA database, FDA annual reports, and the Federal Register to identify 774 new agents representing first-in-class agents. Overall, this accounted for a significant increase of 2.6% per year in the number of expedited review and approval programs for each new agent (rate ratio, 1.06) and a 2.4% increase per year in the proportion of agents involved in at least one of these programs. Many approvals were associated with more than one program, and this proportion increased over the study period, from a low of 0.54 in 1987 to a high of 1.72 in 2014.
“Driving this trend was an increase in the proportion of approved, non–first-in-class drugs,” associated with at least one [expedited] program,” the authors noted.
Additionally, not all of the drugs could reasonably be considered as treatments for an urgent, unmet medical need. “For example, bimatoprost (Latisse: Allergan, Dublin) was granted priority review when it was first approved in 2008 for hypotrichosis of the eyelids, a clearly less serious condition.”
While the “breakthrough therapy” pathway was intended for only a handful of drug approvals each year, the FDA received nearly 250 applications in the first 2 years; 68 of these were granted, despite the agency’s prediction than only 2-4 such applications would be approved.
Four of these were for chronic lymphocytic anemia alone – a number the authors suggested might be excessive. “It is doubtful that a single disease condition can be the subject of four true ‘breakthroughs’ in such a short time frame.”
The situation is likely to accelerate, they noted. The 21st Century Cures Act, passed in July by the U.S. House of Representatives, instructs the FDA to develop a new pathway for repurposing approved drugs on the basis of early stage investigators and “high-risk, high-reward research. ... The FDA would also be permitted to approve such indications on the basis of only summaries of data in such circumstances, rather than being required to review the data in detail.”
New antibiotics and antifungals would have particularly lenient evidence requirements, according to the investigators.
However, expedited review is a double-edged sword, the paper noted. An FDA review found that most cancer drugs are later found to be safe and effective in postapproval studies, although such studies are often delayed or – in some cases – never conducted.
The FDA should be granted more authority to punish manufacturers who lag behind these requirements, including having the ability to impose fines and even suspend approval until additional studies are complete, the investigators said.
Study 2: Approval evidence for supplemental indications
The second study concluded that the FDA increasingly approves supplemental indications with less than level I evidence (randomized, controlled trials with placebo or active comparator (BMJ. 2015;351:h4679. doi: 10.1136/bmj.h4679).
Of an examined 295 such approvals since 2005, the largest portion was for oncology (27%). Other indications were infectious disease (15%); cardiovascular disease and prevention (12%); psychiatry (12%); musculoskeletal and rheumatology (10%); neurology (8%); gastroenterology (6%); and other (1%). Orphan drug status accounted for 20% of the approvals.
Only 30% of modified indications were supported by efficacy trials with active comparators. Level I evidence supported half of modified use approvals and 11% of approvals expanding the patient population. Almost all of the expansion approvals were into pediatric populations, and the vast majority (94%) of evidence for those was extrapolated from adult clinical trials.
Uncontrolled trials supported 34% of expanded population approvals, and nine (14%) of these supplemental approvals had no trials with clinical endpoints.
Findings were similar with other approval pathways. Among new indications, 32% had clinical endpoints, as did 30% of modified indications. Only 22% of expanded population indications rested on clinical endpoint data.
“Clinical outcomes were most often used in trials supporting supplemental indication approvals of neurologic (48%) and infectious disease drugs (45%); by contrast, 70% of oncology supplemental indications were supported exclusively by trials using surrogate outcomes.”
Uncontrolled trials supported one-third of expanded population supplements; 14% of these had no clinical trial evidence. Similarly, one-third of orphan drug indications were supported by uncontrolled or historical cohort studies. Significantly fewer orphan than nonorphan approvals were supported by clinical trials (18% vs. 35%).
Again, the situation is likely to accelerate. The Best Pharmaceuticals for Children Act provides up to 6 months of additional market exclusivity for a new approval, “which can be extremely lucrative for the sponsor,” the authors noted. The 21st Century Cures Act will also play into the situation, they said.
“The high degree of heterogeneity of supporting evidence for supplemental indications, in the setting of legislation promoting drug approvals based on decreasing evidentiary standards, underscores the need for a robust system of postapproval drug monitoring for efficacy and safety, timely confirmatory studies, and reexamination of existing legislative incentives to promote the optimal delivery of evidence-based medicine.”
Both studies were supported in part by the Greenwall Faculty Scholars Program in bioethics and the Harvard program in therapeutic science. Dr. Kesselheim and his coinvestigators had no financial disclosures.
On Twitter @alz_gal
*Correction, 9/24/2015: An earlier version of this article misstated the review's findings.
FROM BMJ

Is Skip N2 metastasis its own category?
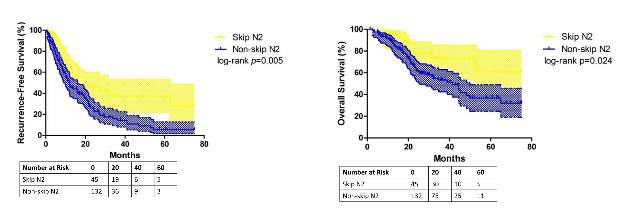
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
Key clinical point: Skip N2 metastases in resectable lung cancer have distinct histological characteristics from non-skip N2 disease.
Major finding: A subset of patients with skip N2 metastasis had higher rates of acinar adenocarcinoma subtype and right-lung disease.
Data source: Retrospective analysis of 177 patients with lung adenocarcinoma and N2 metastasis
Disclosures: The study received funding from the government of China and Shanghai Municipality as well as Shanghai Hospital Development Center. The authors have no relationships to disclose.
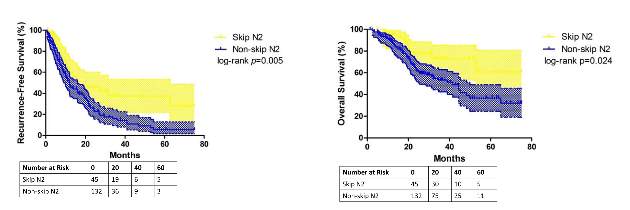
Medicolegal aspects of sleep apnea
Question: A patient who is a commercial truck driver has a long history of snoring and daytime sleepiness. His physical exam was remarkable for obesity, prominent extremities, a large tongue, and a prominent jaw. The treating doctor did not pursue additional work-up or treatment.
One day, the patient fell asleep while driving his truck and hit an oncoming vehicle, resulting in injuries to both patient and the other driver.
In this hypothetical scenario, which of the following statements is best?
A. The doctor may be found negligent for missing the diagnosis of acromegaly and accompanying sleep apnea, and for failing to treat and warn about driving risks.
B. The doctor may be liable to both his patient and the other injured driver.
C. The patient may be terminated from his job as a commercial truck driver, because he poses a danger to himself and the public.
D. Both A and B are correct.
E. All are correct.
Answer: D. Sleep apnea, an underdiagnosed and undertreated disabling condition, places the patient at substantial risk for injuries, chronic hypoxemia, and respiratory arrest. Excessive daytime sleepiness and fatigue may prove hazardous, particularly in those whose undivided attention is a requirement of their jobs, such as with truck drivers.
Diagnosis is established with a formal sleep study (polysomnography), and treatment with a continuous positive airway pressure (CPAP) device is usually effective. In severe or recalcitrant cases, surgical intervention (that is, uvulopalatopharyngoplasty) may be necessary.
In a recent study, Dr. Peter F. Svider of Rutgers New Jersey Medical School, Newark, and his colleagues analyzed 54 litigated sleep apnea cases, of which 33 (61%) were resolved in favor of the defendants (Otolaryngol Head Neck Surg. 2013 Dec;149[6]:947-53). Most of the cases (47) stemmed from patients who underwent surgery with perioperative complications, including death. Inadequate informed consent and monitoring, as well as inappropriate medications, were other findings.
Obstructive sleep apnea is a well-recognized complication of acromegaly with its bony and soft-tissue hypertrophy. The hypothetical situation described above is substantially modified from an actual case in which a 39-year-old man with acromegaly and sleep apnea died from cardiorespiratory arrest (Cornett v. W.O. Moss Regional Hospital, 614 So.2d 189 [La. 1993]). He had presented over the course of several years with repeated complaints of daytime sleepiness and sleeping while driving. Falling asleep in the examination room and abnormal blood gases were giveaway signs. Unfortunately, sleep apnea was left untreated.
Other litigated cases have included anoxic encephalopathy from a lost airway and inappropriate fentanyl dosing during and following aggressive surgery for mild/moderate obstructive sleep apnea, as well as cardiac arrest in a retired sailor during a routine endoscopic procedure. In the latter instance, the plaintiff alleged that there was a failure to take proper precautions in protecting the airway, given that the patient had a known case of obstructive sleep apnea.
What about other liabilities for injuries that are proximately caused by a failure to diagnose and treat?
A doctor is usually liable for negligent care only to his or her own patient, because the duty of care grows out of the doctor-patient relationship and is normally owed to the patient and no one else. However, in very limited circumstances, the duty may extend to other individuals who are family members or even total strangers.
Sleep apnea, by virtue of its sleep disturbances and resulting daytime sleepiness, poses a foreseeable risk of harm. Nonpatient third parties have successfully sued doctors for driving injuries arising out of the failure to diagnose, treat, or warn in a variety of medical conditions.
For example, the Iowa Supreme Court has held that a physician must warn a patient with newly diagnosed seizure disorder about the risks of driving (Freese v. Lemmon, 210 N.W.2d 576 [Iowa 1973]). In that case, a patient with a history of a single seizure injured a woman when he suffered a second seizure while driving.
By analogy, it seems reasonable to assume that the facts given in our hypothetical scenario may give rise to an action against the doctor not only by the patient, but by the injured nonpatient third party as well.
In many jurisdictions, sleep apnea has been accepted as a disability for purposes of the Americans with Disabilities Act (ADA). A disability is defined as a condition evincing substantial interference with a major life activity. Under the ADA, employers are required to make “reasonable accommodation” for disabled employees and cannot simply dismiss them by sole virtue of that disability.
However, qualification for the job must still be shown. One court ruled that a plaintiff with sleep apnea had failed to show that he was a qualified employee even if given his proposed “two-nap-a-day” accommodation (Jackson v. Boise Cascade Corp., 941 F. Supp. 1122 [Ala. 1996]).
Another interesting case involved an anesthesiologist who suffered from sleep apnea and who was snoring and sleeping during surgery. The hospital terminated his contract, and the anesthesiologist filed suit claiming disability discrimination. The 6th U.S. Circuit Court of Appeals affirmed the lower court’s decision in favor of the hospital, finding that the anesthesiologist was fired not because he had a disability, but because he had slept during surgical procedures (Brohm v. JH Properties, 149 F.3d 517 [6th Cir. 1998]).
Distinguishing between discharging someone for unacceptable conduct and discharging someone because of the disability, the court reasoned: “One suffering from chronic sleep deprivation may well be so tired that he cannot stay awake. But such sleep deprivation did not compel Brohm [the anesthesiologist defendant] to administer anesthetics during surgical procedures when he knew he was tired.”
On the other hand, a federal court in 2014 ordered the city of McPherson, Kan., to pay $920,000 in damages to a dismissed police officer suffering from sleep apnea. Although the city cited other factors for the termination, such as insubordination and conduct unbecoming an officer, it had focused on “sleeping on the job” as the basis for the termination. The officer reportedly experienced no further difficulties after he received medical treatment, and the city did not offer the officer an alternative to his graveyard shift or an opportunity to explain his medical condition.
Finally, a discussion of the legal aspects of sleep apnea is incomplete without noting that conducting and billing for sleep studies may occasionally be subject to abuse and/or fraud. The U.S. Department of Health & Human Services Office of Inspector General (OIG) has underscored the high utilization of sleep testing by sleep disorder clinics; in 2010 alone, Medicare reimbursement totaled some $410 million.
The OIG is targeting questionable billing practices under the False Claims Act (31 U.S.C. §§3729-3733) and for self-referrals (Stark Law). Medicare and Medicaid will only reimburse sleep studies that are reasonable and necessary. In addition, there are strict rules such as the mandatory use of properly trained and credentialed sleep technicians, and appropriate level of general physician supervision.
In its most recent prosecution, the federal government is going after the owners of a chain of sleep clinics in the San Francisco Bay area for sleep tests that were conducted in unapproved locations and/or by unlicensed technicians. In addition, the lawsuit alleges a Stark Law violation for self-referrals. The action is being taken in conjunction with a lawsuit filed by a former employee in a whistle-blower action. Under the False Claims Act, whistle-blowers who are private citizens, such as former employees, can file a qui tam action alone or in concert with the government, and they stand to collect a significant (e.g., 25%) portion of any recovery.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: A patient who is a commercial truck driver has a long history of snoring and daytime sleepiness. His physical exam was remarkable for obesity, prominent extremities, a large tongue, and a prominent jaw. The treating doctor did not pursue additional work-up or treatment.
One day, the patient fell asleep while driving his truck and hit an oncoming vehicle, resulting in injuries to both patient and the other driver.
In this hypothetical scenario, which of the following statements is best?
A. The doctor may be found negligent for missing the diagnosis of acromegaly and accompanying sleep apnea, and for failing to treat and warn about driving risks.
B. The doctor may be liable to both his patient and the other injured driver.
C. The patient may be terminated from his job as a commercial truck driver, because he poses a danger to himself and the public.
D. Both A and B are correct.
E. All are correct.
Answer: D. Sleep apnea, an underdiagnosed and undertreated disabling condition, places the patient at substantial risk for injuries, chronic hypoxemia, and respiratory arrest. Excessive daytime sleepiness and fatigue may prove hazardous, particularly in those whose undivided attention is a requirement of their jobs, such as with truck drivers.
Diagnosis is established with a formal sleep study (polysomnography), and treatment with a continuous positive airway pressure (CPAP) device is usually effective. In severe or recalcitrant cases, surgical intervention (that is, uvulopalatopharyngoplasty) may be necessary.
In a recent study, Dr. Peter F. Svider of Rutgers New Jersey Medical School, Newark, and his colleagues analyzed 54 litigated sleep apnea cases, of which 33 (61%) were resolved in favor of the defendants (Otolaryngol Head Neck Surg. 2013 Dec;149[6]:947-53). Most of the cases (47) stemmed from patients who underwent surgery with perioperative complications, including death. Inadequate informed consent and monitoring, as well as inappropriate medications, were other findings.
Obstructive sleep apnea is a well-recognized complication of acromegaly with its bony and soft-tissue hypertrophy. The hypothetical situation described above is substantially modified from an actual case in which a 39-year-old man with acromegaly and sleep apnea died from cardiorespiratory arrest (Cornett v. W.O. Moss Regional Hospital, 614 So.2d 189 [La. 1993]). He had presented over the course of several years with repeated complaints of daytime sleepiness and sleeping while driving. Falling asleep in the examination room and abnormal blood gases were giveaway signs. Unfortunately, sleep apnea was left untreated.
Other litigated cases have included anoxic encephalopathy from a lost airway and inappropriate fentanyl dosing during and following aggressive surgery for mild/moderate obstructive sleep apnea, as well as cardiac arrest in a retired sailor during a routine endoscopic procedure. In the latter instance, the plaintiff alleged that there was a failure to take proper precautions in protecting the airway, given that the patient had a known case of obstructive sleep apnea.
What about other liabilities for injuries that are proximately caused by a failure to diagnose and treat?
A doctor is usually liable for negligent care only to his or her own patient, because the duty of care grows out of the doctor-patient relationship and is normally owed to the patient and no one else. However, in very limited circumstances, the duty may extend to other individuals who are family members or even total strangers.
Sleep apnea, by virtue of its sleep disturbances and resulting daytime sleepiness, poses a foreseeable risk of harm. Nonpatient third parties have successfully sued doctors for driving injuries arising out of the failure to diagnose, treat, or warn in a variety of medical conditions.
For example, the Iowa Supreme Court has held that a physician must warn a patient with newly diagnosed seizure disorder about the risks of driving (Freese v. Lemmon, 210 N.W.2d 576 [Iowa 1973]). In that case, a patient with a history of a single seizure injured a woman when he suffered a second seizure while driving.
By analogy, it seems reasonable to assume that the facts given in our hypothetical scenario may give rise to an action against the doctor not only by the patient, but by the injured nonpatient third party as well.
In many jurisdictions, sleep apnea has been accepted as a disability for purposes of the Americans with Disabilities Act (ADA). A disability is defined as a condition evincing substantial interference with a major life activity. Under the ADA, employers are required to make “reasonable accommodation” for disabled employees and cannot simply dismiss them by sole virtue of that disability.
However, qualification for the job must still be shown. One court ruled that a plaintiff with sleep apnea had failed to show that he was a qualified employee even if given his proposed “two-nap-a-day” accommodation (Jackson v. Boise Cascade Corp., 941 F. Supp. 1122 [Ala. 1996]).
Another interesting case involved an anesthesiologist who suffered from sleep apnea and who was snoring and sleeping during surgery. The hospital terminated his contract, and the anesthesiologist filed suit claiming disability discrimination. The 6th U.S. Circuit Court of Appeals affirmed the lower court’s decision in favor of the hospital, finding that the anesthesiologist was fired not because he had a disability, but because he had slept during surgical procedures (Brohm v. JH Properties, 149 F.3d 517 [6th Cir. 1998]).
Distinguishing between discharging someone for unacceptable conduct and discharging someone because of the disability, the court reasoned: “One suffering from chronic sleep deprivation may well be so tired that he cannot stay awake. But such sleep deprivation did not compel Brohm [the anesthesiologist defendant] to administer anesthetics during surgical procedures when he knew he was tired.”
On the other hand, a federal court in 2014 ordered the city of McPherson, Kan., to pay $920,000 in damages to a dismissed police officer suffering from sleep apnea. Although the city cited other factors for the termination, such as insubordination and conduct unbecoming an officer, it had focused on “sleeping on the job” as the basis for the termination. The officer reportedly experienced no further difficulties after he received medical treatment, and the city did not offer the officer an alternative to his graveyard shift or an opportunity to explain his medical condition.
Finally, a discussion of the legal aspects of sleep apnea is incomplete without noting that conducting and billing for sleep studies may occasionally be subject to abuse and/or fraud. The U.S. Department of Health & Human Services Office of Inspector General (OIG) has underscored the high utilization of sleep testing by sleep disorder clinics; in 2010 alone, Medicare reimbursement totaled some $410 million.
The OIG is targeting questionable billing practices under the False Claims Act (31 U.S.C. §§3729-3733) and for self-referrals (Stark Law). Medicare and Medicaid will only reimburse sleep studies that are reasonable and necessary. In addition, there are strict rules such as the mandatory use of properly trained and credentialed sleep technicians, and appropriate level of general physician supervision.
In its most recent prosecution, the federal government is going after the owners of a chain of sleep clinics in the San Francisco Bay area for sleep tests that were conducted in unapproved locations and/or by unlicensed technicians. In addition, the lawsuit alleges a Stark Law violation for self-referrals. The action is being taken in conjunction with a lawsuit filed by a former employee in a whistle-blower action. Under the False Claims Act, whistle-blowers who are private citizens, such as former employees, can file a qui tam action alone or in concert with the government, and they stand to collect a significant (e.g., 25%) portion of any recovery.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: A patient who is a commercial truck driver has a long history of snoring and daytime sleepiness. His physical exam was remarkable for obesity, prominent extremities, a large tongue, and a prominent jaw. The treating doctor did not pursue additional work-up or treatment.
One day, the patient fell asleep while driving his truck and hit an oncoming vehicle, resulting in injuries to both patient and the other driver.
In this hypothetical scenario, which of the following statements is best?
A. The doctor may be found negligent for missing the diagnosis of acromegaly and accompanying sleep apnea, and for failing to treat and warn about driving risks.
B. The doctor may be liable to both his patient and the other injured driver.
C. The patient may be terminated from his job as a commercial truck driver, because he poses a danger to himself and the public.
D. Both A and B are correct.
E. All are correct.
Answer: D. Sleep apnea, an underdiagnosed and undertreated disabling condition, places the patient at substantial risk for injuries, chronic hypoxemia, and respiratory arrest. Excessive daytime sleepiness and fatigue may prove hazardous, particularly in those whose undivided attention is a requirement of their jobs, such as with truck drivers.
Diagnosis is established with a formal sleep study (polysomnography), and treatment with a continuous positive airway pressure (CPAP) device is usually effective. In severe or recalcitrant cases, surgical intervention (that is, uvulopalatopharyngoplasty) may be necessary.
In a recent study, Dr. Peter F. Svider of Rutgers New Jersey Medical School, Newark, and his colleagues analyzed 54 litigated sleep apnea cases, of which 33 (61%) were resolved in favor of the defendants (Otolaryngol Head Neck Surg. 2013 Dec;149[6]:947-53). Most of the cases (47) stemmed from patients who underwent surgery with perioperative complications, including death. Inadequate informed consent and monitoring, as well as inappropriate medications, were other findings.
Obstructive sleep apnea is a well-recognized complication of acromegaly with its bony and soft-tissue hypertrophy. The hypothetical situation described above is substantially modified from an actual case in which a 39-year-old man with acromegaly and sleep apnea died from cardiorespiratory arrest (Cornett v. W.O. Moss Regional Hospital, 614 So.2d 189 [La. 1993]). He had presented over the course of several years with repeated complaints of daytime sleepiness and sleeping while driving. Falling asleep in the examination room and abnormal blood gases were giveaway signs. Unfortunately, sleep apnea was left untreated.
Other litigated cases have included anoxic encephalopathy from a lost airway and inappropriate fentanyl dosing during and following aggressive surgery for mild/moderate obstructive sleep apnea, as well as cardiac arrest in a retired sailor during a routine endoscopic procedure. In the latter instance, the plaintiff alleged that there was a failure to take proper precautions in protecting the airway, given that the patient had a known case of obstructive sleep apnea.
What about other liabilities for injuries that are proximately caused by a failure to diagnose and treat?
A doctor is usually liable for negligent care only to his or her own patient, because the duty of care grows out of the doctor-patient relationship and is normally owed to the patient and no one else. However, in very limited circumstances, the duty may extend to other individuals who are family members or even total strangers.
Sleep apnea, by virtue of its sleep disturbances and resulting daytime sleepiness, poses a foreseeable risk of harm. Nonpatient third parties have successfully sued doctors for driving injuries arising out of the failure to diagnose, treat, or warn in a variety of medical conditions.
For example, the Iowa Supreme Court has held that a physician must warn a patient with newly diagnosed seizure disorder about the risks of driving (Freese v. Lemmon, 210 N.W.2d 576 [Iowa 1973]). In that case, a patient with a history of a single seizure injured a woman when he suffered a second seizure while driving.
By analogy, it seems reasonable to assume that the facts given in our hypothetical scenario may give rise to an action against the doctor not only by the patient, but by the injured nonpatient third party as well.
In many jurisdictions, sleep apnea has been accepted as a disability for purposes of the Americans with Disabilities Act (ADA). A disability is defined as a condition evincing substantial interference with a major life activity. Under the ADA, employers are required to make “reasonable accommodation” for disabled employees and cannot simply dismiss them by sole virtue of that disability.
However, qualification for the job must still be shown. One court ruled that a plaintiff with sleep apnea had failed to show that he was a qualified employee even if given his proposed “two-nap-a-day” accommodation (Jackson v. Boise Cascade Corp., 941 F. Supp. 1122 [Ala. 1996]).
Another interesting case involved an anesthesiologist who suffered from sleep apnea and who was snoring and sleeping during surgery. The hospital terminated his contract, and the anesthesiologist filed suit claiming disability discrimination. The 6th U.S. Circuit Court of Appeals affirmed the lower court’s decision in favor of the hospital, finding that the anesthesiologist was fired not because he had a disability, but because he had slept during surgical procedures (Brohm v. JH Properties, 149 F.3d 517 [6th Cir. 1998]).
Distinguishing between discharging someone for unacceptable conduct and discharging someone because of the disability, the court reasoned: “One suffering from chronic sleep deprivation may well be so tired that he cannot stay awake. But such sleep deprivation did not compel Brohm [the anesthesiologist defendant] to administer anesthetics during surgical procedures when he knew he was tired.”
On the other hand, a federal court in 2014 ordered the city of McPherson, Kan., to pay $920,000 in damages to a dismissed police officer suffering from sleep apnea. Although the city cited other factors for the termination, such as insubordination and conduct unbecoming an officer, it had focused on “sleeping on the job” as the basis for the termination. The officer reportedly experienced no further difficulties after he received medical treatment, and the city did not offer the officer an alternative to his graveyard shift or an opportunity to explain his medical condition.
Finally, a discussion of the legal aspects of sleep apnea is incomplete without noting that conducting and billing for sleep studies may occasionally be subject to abuse and/or fraud. The U.S. Department of Health & Human Services Office of Inspector General (OIG) has underscored the high utilization of sleep testing by sleep disorder clinics; in 2010 alone, Medicare reimbursement totaled some $410 million.
The OIG is targeting questionable billing practices under the False Claims Act (31 U.S.C. §§3729-3733) and for self-referrals (Stark Law). Medicare and Medicaid will only reimburse sleep studies that are reasonable and necessary. In addition, there are strict rules such as the mandatory use of properly trained and credentialed sleep technicians, and appropriate level of general physician supervision.
In its most recent prosecution, the federal government is going after the owners of a chain of sleep clinics in the San Francisco Bay area for sleep tests that were conducted in unapproved locations and/or by unlicensed technicians. In addition, the lawsuit alleges a Stark Law violation for self-referrals. The action is being taken in conjunction with a lawsuit filed by a former employee in a whistle-blower action. Under the False Claims Act, whistle-blowers who are private citizens, such as former employees, can file a qui tam action alone or in concert with the government, and they stand to collect a significant (e.g., 25%) portion of any recovery.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.

Long-term ceftaroline use associated with neutropenia
SAN DIEGO – The long-term use of ceftaroline is associated with neutropenia, results from a single-center retrospective study showed.
A fifth-generation cephalosporin antibiotic with activity against methicillin-resistant Staphylococcus aureus, ceftaroline is approved for the treatment of community-acquired pneumonia and skin and skin structure infections. It’s also an option for treating orthopedic and endovascular infections when primary therapy fails or is contraindicated, according to one of the study authors, Dr. Hollis R. O’Neal Jr. “There are small case reports of associations between ceftaroline use and neutropenia, and we were noticing that many patients in our clinical practice were developing neutropenia,” Dr. O’Neal, a pulmonologist at Louisiana State University Health Baton Rouge, said in an interview at the Interscience Conference on Antimicrobial Agents and Chemotherapy.
In an effort to determine the incidence, severity, and outcome of neutropenia in patients receiving long-term ceftaroline therapy, Dr. O’Neal and his associates retrospectively evaluated 38 patients who received at least 7 days of ceftaroline initiated at LSU Health Baton Rouge between June 2012 and December 2014. They defined clinically significant neutropenia as having an absolute neutrophil count (ANC) below 2500 cells/mm3 and gathered pertinent data from medical records including comorbidities, chronic medications, and diagnoses.
The median age of the 38 patients was 47 years and their median body mass index was 28 kg/m2. Of the 38 patients, 10 (26%) developed neutropenia. “That was surprising to me,” Dr. O’Neal said. “I thought we would find three or four cases.” Compared with those who were nonneutropenic, those who developed neutropenia tended to be younger (a median of 44 years vs. 51 years), have a lower body mass index (a median of 25 kg/m2 vs. 32 kg/m2), and be more likely to have a longer duration of ceftaroline therapy (a median of 36 days vs. 26 days).
Of the 10 neutropenic patients, 7 had an ANC below 1,500 cells/mm3, and 4 had an ANC below 500 cells/mm3. The median time to first neutropenic day was day 21, with a median nadir of 1,156 cells/mm3. One hospitalization occurred that was believed to be due to neutropenia, but all 30 patients were alive at least 30 days after completing ceftaroline therapy.
“Once the ANC falls below 2,500 cells/mm3, the risk of developing true neutropenia is high,” Dr. O’Neal said. “So what we’re doing is monitoring ANC levels weekly. When they fall below 2,500 we monitor [ANC levels] twice weekly. When they reach 1,500 we stop the drug. So it’s really changed how we monitor the drug’s use.”
The study’s lead author is Dr. Katherine W. Lavie, an infectious diseases fellow at LSU Health Baton Rouge. The researchers reported having no financial disclosures.
SAN DIEGO – The long-term use of ceftaroline is associated with neutropenia, results from a single-center retrospective study showed.
A fifth-generation cephalosporin antibiotic with activity against methicillin-resistant Staphylococcus aureus, ceftaroline is approved for the treatment of community-acquired pneumonia and skin and skin structure infections. It’s also an option for treating orthopedic and endovascular infections when primary therapy fails or is contraindicated, according to one of the study authors, Dr. Hollis R. O’Neal Jr. “There are small case reports of associations between ceftaroline use and neutropenia, and we were noticing that many patients in our clinical practice were developing neutropenia,” Dr. O’Neal, a pulmonologist at Louisiana State University Health Baton Rouge, said in an interview at the Interscience Conference on Antimicrobial Agents and Chemotherapy.
In an effort to determine the incidence, severity, and outcome of neutropenia in patients receiving long-term ceftaroline therapy, Dr. O’Neal and his associates retrospectively evaluated 38 patients who received at least 7 days of ceftaroline initiated at LSU Health Baton Rouge between June 2012 and December 2014. They defined clinically significant neutropenia as having an absolute neutrophil count (ANC) below 2500 cells/mm3 and gathered pertinent data from medical records including comorbidities, chronic medications, and diagnoses.
The median age of the 38 patients was 47 years and their median body mass index was 28 kg/m2. Of the 38 patients, 10 (26%) developed neutropenia. “That was surprising to me,” Dr. O’Neal said. “I thought we would find three or four cases.” Compared with those who were nonneutropenic, those who developed neutropenia tended to be younger (a median of 44 years vs. 51 years), have a lower body mass index (a median of 25 kg/m2 vs. 32 kg/m2), and be more likely to have a longer duration of ceftaroline therapy (a median of 36 days vs. 26 days).
Of the 10 neutropenic patients, 7 had an ANC below 1,500 cells/mm3, and 4 had an ANC below 500 cells/mm3. The median time to first neutropenic day was day 21, with a median nadir of 1,156 cells/mm3. One hospitalization occurred that was believed to be due to neutropenia, but all 30 patients were alive at least 30 days after completing ceftaroline therapy.
“Once the ANC falls below 2,500 cells/mm3, the risk of developing true neutropenia is high,” Dr. O’Neal said. “So what we’re doing is monitoring ANC levels weekly. When they fall below 2,500 we monitor [ANC levels] twice weekly. When they reach 1,500 we stop the drug. So it’s really changed how we monitor the drug’s use.”
The study’s lead author is Dr. Katherine W. Lavie, an infectious diseases fellow at LSU Health Baton Rouge. The researchers reported having no financial disclosures.
SAN DIEGO – The long-term use of ceftaroline is associated with neutropenia, results from a single-center retrospective study showed.
A fifth-generation cephalosporin antibiotic with activity against methicillin-resistant Staphylococcus aureus, ceftaroline is approved for the treatment of community-acquired pneumonia and skin and skin structure infections. It’s also an option for treating orthopedic and endovascular infections when primary therapy fails or is contraindicated, according to one of the study authors, Dr. Hollis R. O’Neal Jr. “There are small case reports of associations between ceftaroline use and neutropenia, and we were noticing that many patients in our clinical practice were developing neutropenia,” Dr. O’Neal, a pulmonologist at Louisiana State University Health Baton Rouge, said in an interview at the Interscience Conference on Antimicrobial Agents and Chemotherapy.
In an effort to determine the incidence, severity, and outcome of neutropenia in patients receiving long-term ceftaroline therapy, Dr. O’Neal and his associates retrospectively evaluated 38 patients who received at least 7 days of ceftaroline initiated at LSU Health Baton Rouge between June 2012 and December 2014. They defined clinically significant neutropenia as having an absolute neutrophil count (ANC) below 2500 cells/mm3 and gathered pertinent data from medical records including comorbidities, chronic medications, and diagnoses.
The median age of the 38 patients was 47 years and their median body mass index was 28 kg/m2. Of the 38 patients, 10 (26%) developed neutropenia. “That was surprising to me,” Dr. O’Neal said. “I thought we would find three or four cases.” Compared with those who were nonneutropenic, those who developed neutropenia tended to be younger (a median of 44 years vs. 51 years), have a lower body mass index (a median of 25 kg/m2 vs. 32 kg/m2), and be more likely to have a longer duration of ceftaroline therapy (a median of 36 days vs. 26 days).
Of the 10 neutropenic patients, 7 had an ANC below 1,500 cells/mm3, and 4 had an ANC below 500 cells/mm3. The median time to first neutropenic day was day 21, with a median nadir of 1,156 cells/mm3. One hospitalization occurred that was believed to be due to neutropenia, but all 30 patients were alive at least 30 days after completing ceftaroline therapy.
“Once the ANC falls below 2,500 cells/mm3, the risk of developing true neutropenia is high,” Dr. O’Neal said. “So what we’re doing is monitoring ANC levels weekly. When they fall below 2,500 we monitor [ANC levels] twice weekly. When they reach 1,500 we stop the drug. So it’s really changed how we monitor the drug’s use.”
The study’s lead author is Dr. Katherine W. Lavie, an infectious diseases fellow at LSU Health Baton Rouge. The researchers reported having no financial disclosures.
AT ICAAC 2015
Key clinical point: Long-term ceftaroline use is associated with neutropenia.
Major finding: Of 38 patients who received at least 7 days of ceftaroline, 10 (26%) developed neutropenia.
Data source: A retrospective cohort study of 38 patients who received long-term ceftaroline therapy between June 2012 and December 2014.
Disclosures: The researchers reported having no financial disclosures.
PsA, PsC do not affect total hip replacement outcomes
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.

The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.
The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
Neither psoriatic arthritis (PsA) nor cutaneous psoriasis (PsC) is an independent predictor of poor postoperative pain or function following a total hip arthroplasty, according to the results of a case-control study by Dr. Lisa A. Mandl and her colleagues.
The study’s participants underwent surgery between May 1, 2007, and Dec. 31, 2010, in a center that performs more than 4,300 THAs annually. All subjects lived for at least 2 years after their operations. The researchers compared pre- and postoperative data from patients in the following three categories: those with PsA, those with PsC without evidence of inflammatory arthritis, and those with osteoarthritis (OA). Patients with OA comprised the control group, which excluded any patient who self-reported a history of PsA, rheumatoid arthritis, lupus erythematosus, or any other systematic rheumatic disease, or who had documentation of skin psoriasis. The researchers acquired postoperative self-report data from 47 PsA patients, 106 PsC patients, and 864 OA patients. Seventeen percent of patients submitted information on their status at 1 year, 69% at 2 years, and 14% at 3-5 years.
The primary outcomes of interest were postoperative pain and function, which were assessed via the Hip Osteoarthritis Outcome Score (HOOS), from which the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was derived.
There were no statistically significant differences in postoperative WOMAC pain or function scores between the three groups of patients (P = .78 and .96, respectively). The mean pain scores were 14.9, 6.1, and 15.8 for patients with PsA, PsC, and OA, respectively. These patients’ mean function scores were 16.3, 19.6, and 18.8 for the PsA, PsC and OA groups, respectively.
Overall levels of satisfaction with the surgery were similar among the three groups (P = .54). Ninety-three percent of the PsA patients, 79% of the PsC patients, and 84% of the OA patients were “very satisfied” with their total hip arthroplasty. Between 1% and 3% of each group reported being “very dissatisfied” with their surgery. The researchers found that extent of skin disease was not associated with worse postoperative pain or function.
“Further work needs to be done to better understand the interplay of disease activity and quality of life on the outcomes of [total hip arthroplasty] in PsA and PsC,” they wrote.
Read the report in Arthritis & Rheumatology (doi: 10.1002/art.39431).
FROM ARTHRITIS & RHEUMATOLOGY

Developing alternatives to unprotected power morcellation
NEW YORK – Power morcellation has been highly controversial since the Food and Drug Administration warned against its use in the majority of women undergoing myomectomy or hysterectomy for fibroid treatment last year. So where does that leave ob.gyns. who perform minimally invasive surgery?
At the annual Minimally Invasive Surgery Week, experts from around the world discussed alternative methods for tumor or organ extraction that are safe and can be used with minimally invasive techniques.
Dr. Antonio Curyof Positivo University in Curitiba, Brazil, highlighted the importance of surgical techniques to prevent port site metastasis.

There are three theories about how these occur: tumor-related, wound-related, and surgical technique–related metastases, he said. Focusing on the surgical technique, he said that contamination is likely the cause.
“Tumor manipulation is the principal factor. Avoid violating the tumor boundary. Avoid gas leakage, as well. I use a single trocar tight to the skin to avoid gas leakage,” Dr. Cury said. “Do not touch the tumor. Use instruments to extract the tumor and avoid rupture.”
Morcellation can be considered cautiously, he said, but use a bag and protect the wound.
“Surgical techniques are related to port site metastasis. Surgical and laparoscopic principles need to be taught. The learning curve is important,” said Dr. Cury, who is on the speakers bureau for and a consultant to Medtronic and Covidien.

In-bag morcellation appears to be the evolving alternative to unprotected power morcellation by minimizing the risk of intraperitoneal tissue dissemination, said Dr. Ceana Nezhat, director of the Nezhat Medical Center in Atlanta.
Tissue extraction transvaginally or via laparoscopic-assisted minilaparotomy is one option. “Using this technique, the patient has the benefit of minimally access surgery without concern about unprotected power morcellation,” said Dr. Nezhat, who reported being a consultant for Karl Storz Endoscopy and a medical adviser to Plasma Surgery, and serving on the advisory board for SurgiQuest.
When performing morcellation with a containment bag, Dr. Jens Rassweiler said it’s important that the bag is stable. “We have to try to get the whole tumor specimen with morcellation. Then we put the pieces together for the pathologist. We have to beware of the risk of tumor spillage,” said Dr. Rassweiler of Klinikum Heilbronn, the academic hospital of the University of Heidelberg, Germany.
The type of extraction bag is important, he said. The bag should be self-opening, have enough working space, and should not be permeable. Several types of extraction bags are available but none is perfect, he told listeners. Newer bags are under development, according to Dr. Rassweiler, who reported having no relevant financial disclosures.
Dr. Nezhat emphasized that surgeons have an important role to play in the public debate on morcellation and its alternatives.
“The power of public opinion has put us where we are. There were reports of injuries, tissue disruption, and dispersion prior to the 2013 public campaign to ban power morcellation. In light of the FDA black box warning, we have to make decisions on how to improve morcellation, with new instrumentation and proper training. We also have to get our patients involved in the decision-making process. It is imperative to educate and inform the patient of the potential risks.”
NEW YORK – Power morcellation has been highly controversial since the Food and Drug Administration warned against its use in the majority of women undergoing myomectomy or hysterectomy for fibroid treatment last year. So where does that leave ob.gyns. who perform minimally invasive surgery?
At the annual Minimally Invasive Surgery Week, experts from around the world discussed alternative methods for tumor or organ extraction that are safe and can be used with minimally invasive techniques.
Dr. Antonio Curyof Positivo University in Curitiba, Brazil, highlighted the importance of surgical techniques to prevent port site metastasis.
There are three theories about how these occur: tumor-related, wound-related, and surgical technique–related metastases, he said. Focusing on the surgical technique, he said that contamination is likely the cause.
“Tumor manipulation is the principal factor. Avoid violating the tumor boundary. Avoid gas leakage, as well. I use a single trocar tight to the skin to avoid gas leakage,” Dr. Cury said. “Do not touch the tumor. Use instruments to extract the tumor and avoid rupture.”
Morcellation can be considered cautiously, he said, but use a bag and protect the wound.
“Surgical techniques are related to port site metastasis. Surgical and laparoscopic principles need to be taught. The learning curve is important,” said Dr. Cury, who is on the speakers bureau for and a consultant to Medtronic and Covidien.
In-bag morcellation appears to be the evolving alternative to unprotected power morcellation by minimizing the risk of intraperitoneal tissue dissemination, said Dr. Ceana Nezhat, director of the Nezhat Medical Center in Atlanta.
Tissue extraction transvaginally or via laparoscopic-assisted minilaparotomy is one option. “Using this technique, the patient has the benefit of minimally access surgery without concern about unprotected power morcellation,” said Dr. Nezhat, who reported being a consultant for Karl Storz Endoscopy and a medical adviser to Plasma Surgery, and serving on the advisory board for SurgiQuest.
When performing morcellation with a containment bag, Dr. Jens Rassweiler said it’s important that the bag is stable. “We have to try to get the whole tumor specimen with morcellation. Then we put the pieces together for the pathologist. We have to beware of the risk of tumor spillage,” said Dr. Rassweiler of Klinikum Heilbronn, the academic hospital of the University of Heidelberg, Germany.
The type of extraction bag is important, he said. The bag should be self-opening, have enough working space, and should not be permeable. Several types of extraction bags are available but none is perfect, he told listeners. Newer bags are under development, according to Dr. Rassweiler, who reported having no relevant financial disclosures.
Dr. Nezhat emphasized that surgeons have an important role to play in the public debate on morcellation and its alternatives.
“The power of public opinion has put us where we are. There were reports of injuries, tissue disruption, and dispersion prior to the 2013 public campaign to ban power morcellation. In light of the FDA black box warning, we have to make decisions on how to improve morcellation, with new instrumentation and proper training. We also have to get our patients involved in the decision-making process. It is imperative to educate and inform the patient of the potential risks.”
NEW YORK – Power morcellation has been highly controversial since the Food and Drug Administration warned against its use in the majority of women undergoing myomectomy or hysterectomy for fibroid treatment last year. So where does that leave ob.gyns. who perform minimally invasive surgery?
At the annual Minimally Invasive Surgery Week, experts from around the world discussed alternative methods for tumor or organ extraction that are safe and can be used with minimally invasive techniques.
Dr. Antonio Curyof Positivo University in Curitiba, Brazil, highlighted the importance of surgical techniques to prevent port site metastasis.
There are three theories about how these occur: tumor-related, wound-related, and surgical technique–related metastases, he said. Focusing on the surgical technique, he said that contamination is likely the cause.
“Tumor manipulation is the principal factor. Avoid violating the tumor boundary. Avoid gas leakage, as well. I use a single trocar tight to the skin to avoid gas leakage,” Dr. Cury said. “Do not touch the tumor. Use instruments to extract the tumor and avoid rupture.”
Morcellation can be considered cautiously, he said, but use a bag and protect the wound.
“Surgical techniques are related to port site metastasis. Surgical and laparoscopic principles need to be taught. The learning curve is important,” said Dr. Cury, who is on the speakers bureau for and a consultant to Medtronic and Covidien.
In-bag morcellation appears to be the evolving alternative to unprotected power morcellation by minimizing the risk of intraperitoneal tissue dissemination, said Dr. Ceana Nezhat, director of the Nezhat Medical Center in Atlanta.
Tissue extraction transvaginally or via laparoscopic-assisted minilaparotomy is one option. “Using this technique, the patient has the benefit of minimally access surgery without concern about unprotected power morcellation,” said Dr. Nezhat, who reported being a consultant for Karl Storz Endoscopy and a medical adviser to Plasma Surgery, and serving on the advisory board for SurgiQuest.
When performing morcellation with a containment bag, Dr. Jens Rassweiler said it’s important that the bag is stable. “We have to try to get the whole tumor specimen with morcellation. Then we put the pieces together for the pathologist. We have to beware of the risk of tumor spillage,” said Dr. Rassweiler of Klinikum Heilbronn, the academic hospital of the University of Heidelberg, Germany.
The type of extraction bag is important, he said. The bag should be self-opening, have enough working space, and should not be permeable. Several types of extraction bags are available but none is perfect, he told listeners. Newer bags are under development, according to Dr. Rassweiler, who reported having no relevant financial disclosures.
Dr. Nezhat emphasized that surgeons have an important role to play in the public debate on morcellation and its alternatives.
“The power of public opinion has put us where we are. There were reports of injuries, tissue disruption, and dispersion prior to the 2013 public campaign to ban power morcellation. In light of the FDA black box warning, we have to make decisions on how to improve morcellation, with new instrumentation and proper training. We also have to get our patients involved in the decision-making process. It is imperative to educate and inform the patient of the potential risks.”
EXPERT ANALYSIS FROM MINIMALLY INVASIVE SURGERY WEEK

IPC maintains first-line status in preventing DVT in most surgical patients
Intermittent pneumatic compression remains the consensus choice as the sole prophylactic agent for deep vein thrombosis in low- or moderate-risk surgical patients, according to a literature analysis published online ahead of print in September in the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Dr. Nirvana Sadaghianloo of the University of Nice (France) Sophia Antipolis and Dr. Alan Dardik of Yale University in New Haven, Conn., used the MEDLINE and Cochrane libraries to find individual studies and meta-analyses published in English since 2011 assessing the efficacy of intermittent pneumatic compression (IPC) in preventing deep vein thrombosis (DVT), which included the American College of Chest Physicians ninth edition guidelines (2012). They stated that, although the overall quality of studies regarding the use of IPC was low, IPC showed efficacy in prevention of DVT for more than 30 years (J Vasc Surg Venous Lymphat Disord. 2015 doi: 10.1016/j.jvsv.2015.07.006).

“IPC represents a good alternative to pharmacologic agents when the risk of thrombosis is moderate or low or when the risk of bleeding is high or may have serious consequences for the patient,” they stated.
However, they also found that most recommendations suggested that, in high-risk patients, IPC plays a role primarily as an additional modality to provide additional benefit in preventing DVT when is used in combination with pharmacologic therapy. They highlighted how the choice of any thromboprophylactic agent required a systematic risk assessment as a critical prerequisite.
Overall, risk stratification was most frequently assessed by the Caprini or Rogers score for most general, abdominal-pelvic, bariatric, vascular, plastic, and gynecologic surgery patients and by the Padua Prediction Score for hospitalized medical patients. In addition, major orthopedic surgery patients and stroke patients with restricted mobility were usually considered high risk, Dr. Sadaghianloo and Dr. Dardik said.
From their assessment of the literature, they determined that “further studies are needed to assess practical clinical questions that remain unanswered, including optimal cuff length and location, sequence and duration of pressure, and whether use of IPC in an outpatient setting can be effective and achieve good compliance.”
The authors reported that they had no conflicts of interest.
Intermittent pneumatic compression remains the consensus choice as the sole prophylactic agent for deep vein thrombosis in low- or moderate-risk surgical patients, according to a literature analysis published online ahead of print in September in the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Dr. Nirvana Sadaghianloo of the University of Nice (France) Sophia Antipolis and Dr. Alan Dardik of Yale University in New Haven, Conn., used the MEDLINE and Cochrane libraries to find individual studies and meta-analyses published in English since 2011 assessing the efficacy of intermittent pneumatic compression (IPC) in preventing deep vein thrombosis (DVT), which included the American College of Chest Physicians ninth edition guidelines (2012). They stated that, although the overall quality of studies regarding the use of IPC was low, IPC showed efficacy in prevention of DVT for more than 30 years (J Vasc Surg Venous Lymphat Disord. 2015 doi: 10.1016/j.jvsv.2015.07.006).
“IPC represents a good alternative to pharmacologic agents when the risk of thrombosis is moderate or low or when the risk of bleeding is high or may have serious consequences for the patient,” they stated.
However, they also found that most recommendations suggested that, in high-risk patients, IPC plays a role primarily as an additional modality to provide additional benefit in preventing DVT when is used in combination with pharmacologic therapy. They highlighted how the choice of any thromboprophylactic agent required a systematic risk assessment as a critical prerequisite.
Overall, risk stratification was most frequently assessed by the Caprini or Rogers score for most general, abdominal-pelvic, bariatric, vascular, plastic, and gynecologic surgery patients and by the Padua Prediction Score for hospitalized medical patients. In addition, major orthopedic surgery patients and stroke patients with restricted mobility were usually considered high risk, Dr. Sadaghianloo and Dr. Dardik said.
From their assessment of the literature, they determined that “further studies are needed to assess practical clinical questions that remain unanswered, including optimal cuff length and location, sequence and duration of pressure, and whether use of IPC in an outpatient setting can be effective and achieve good compliance.”
The authors reported that they had no conflicts of interest.
Intermittent pneumatic compression remains the consensus choice as the sole prophylactic agent for deep vein thrombosis in low- or moderate-risk surgical patients, according to a literature analysis published online ahead of print in September in the Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Dr. Nirvana Sadaghianloo of the University of Nice (France) Sophia Antipolis and Dr. Alan Dardik of Yale University in New Haven, Conn., used the MEDLINE and Cochrane libraries to find individual studies and meta-analyses published in English since 2011 assessing the efficacy of intermittent pneumatic compression (IPC) in preventing deep vein thrombosis (DVT), which included the American College of Chest Physicians ninth edition guidelines (2012). They stated that, although the overall quality of studies regarding the use of IPC was low, IPC showed efficacy in prevention of DVT for more than 30 years (J Vasc Surg Venous Lymphat Disord. 2015 doi: 10.1016/j.jvsv.2015.07.006).
“IPC represents a good alternative to pharmacologic agents when the risk of thrombosis is moderate or low or when the risk of bleeding is high or may have serious consequences for the patient,” they stated.
However, they also found that most recommendations suggested that, in high-risk patients, IPC plays a role primarily as an additional modality to provide additional benefit in preventing DVT when is used in combination with pharmacologic therapy. They highlighted how the choice of any thromboprophylactic agent required a systematic risk assessment as a critical prerequisite.
Overall, risk stratification was most frequently assessed by the Caprini or Rogers score for most general, abdominal-pelvic, bariatric, vascular, plastic, and gynecologic surgery patients and by the Padua Prediction Score for hospitalized medical patients. In addition, major orthopedic surgery patients and stroke patients with restricted mobility were usually considered high risk, Dr. Sadaghianloo and Dr. Dardik said.
From their assessment of the literature, they determined that “further studies are needed to assess practical clinical questions that remain unanswered, including optimal cuff length and location, sequence and duration of pressure, and whether use of IPC in an outpatient setting can be effective and achieve good compliance.”
The authors reported that they had no conflicts of interest.
FROM JOURNAL OF VASCULAR SURGERY: VENOUS AND LYMPHATIC DISORDERS
Key clinical point: IPC is efficacious as the sole prophylactic agent in low- or moderate-risk surgical patients and in patients with high risk of bleeding with drug therapy.
Major finding: In high-risk patients, IPC is an added modality for preventing DVT in combination with pharmacologic prophylaxis.
Data source: Researchers performed an assessment of the literature in English since 2011 in MEDLINE and the Cochrane libraries.
Disclosures: The authors reported that they had no conflicts of interest.
