User login
Official Newspaper of the American College of Surgeons
Poll finds overwhelming support for Medicare coverage of end-of-life talks
The public overwhelmingly supports Medicare’s plan to pay for end-of-life discussions between doctors and patients, despite GOP objections that such chats would lead to rationed care for the elderly and ill, a poll released Sept. 30 finds.
About 8 of every 10 people surveyed by the Kaiser Family Foundation – in a nationally representative sample of 1,202 adults – supported coverage by the government or insurers for planning discussions about the type of care patients preferred in the waning days or weeks of their lives. (KHN is an editorially independent program of the foundation.) These discussions can include whether people would want to be kept alive by artificial means even if they had no chance of regaining consciousness or autonomy and whether they would want their organs to be donated. These preferences can be incorporated into advance directives, or living wills, which are used if someone can no longer communicate.

The Centers for Medicare & Medicaid Services earlier this year proposed paying doctors to have these talks with patients. A final decision is due out soon. The idea had been included in early drafts of the 2010 federal health care law, but former Alaska Gov. Sarah Palin and other opponents of the law labeled the counseling sessions and other provisions “death panels” motivated by desires to save money, and the provision was deleted from the bill.
The notion of helping patients prepare for death has support among many doctors, who sometimes see terminal patients suffer from futile efforts to keep them alive. Last year, the Institute of Medicine issued a report that encouraged end-of-life discussions beginning as early as age 16.
The Kaiser poll found that these talks remain infrequent. Overall, only 17% of those surveyed said they had had such discussions with their doctors or other health care professionals, even though 89% believe doctors should engage in such counseling. A third of respondents said they had talked to doctors about another family member’s wishes for how they would want to be cared for at the end of life.
While none of these proposals calls for the cost of care to weigh on these discussions, the final years of life are indeed expensive for America’s health care system. The Dartmouth Atlas of Health Care has calculated that a third of Medicare spending goes to the care of people with chronic illnesses in their last 2 years of life. That is likely to increase as the population of those older than 65 increases. An analysis by the Kaiser foundation found that Medicare spending per person more than doubled from age 70 to 96, where it peaked at $16,145 per beneficiary in 2011.
The Kaiser poll found less public support for a cost-containment provision that did make it into the health law. The “Cadillac tax” begins in 2018 and will impose a tax on expensive insurance that employers provide to their workers. Sixty percent oppose the plan, which economists have long favored as a way to discourage lavish coverage and make people aware that extensive use of Medicare services is linked to premiums.
The poll also found that 57% of people favor repealing the medical device tax, another piece of the health law that Republicans in Congress are trying to repeal. The tax applies to artificial hips, pacemakers and other devices that doctors implant.
The poll was conducted from Sept. 17 through Sept. 23. The margin of error was +/– 3 percentage points.
Kaiser Health News is a nonprofit national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
The public overwhelmingly supports Medicare’s plan to pay for end-of-life discussions between doctors and patients, despite GOP objections that such chats would lead to rationed care for the elderly and ill, a poll released Sept. 30 finds.
About 8 of every 10 people surveyed by the Kaiser Family Foundation – in a nationally representative sample of 1,202 adults – supported coverage by the government or insurers for planning discussions about the type of care patients preferred in the waning days or weeks of their lives. (KHN is an editorially independent program of the foundation.) These discussions can include whether people would want to be kept alive by artificial means even if they had no chance of regaining consciousness or autonomy and whether they would want their organs to be donated. These preferences can be incorporated into advance directives, or living wills, which are used if someone can no longer communicate.
The Centers for Medicare & Medicaid Services earlier this year proposed paying doctors to have these talks with patients. A final decision is due out soon. The idea had been included in early drafts of the 2010 federal health care law, but former Alaska Gov. Sarah Palin and other opponents of the law labeled the counseling sessions and other provisions “death panels” motivated by desires to save money, and the provision was deleted from the bill.
The notion of helping patients prepare for death has support among many doctors, who sometimes see terminal patients suffer from futile efforts to keep them alive. Last year, the Institute of Medicine issued a report that encouraged end-of-life discussions beginning as early as age 16.
The Kaiser poll found that these talks remain infrequent. Overall, only 17% of those surveyed said they had had such discussions with their doctors or other health care professionals, even though 89% believe doctors should engage in such counseling. A third of respondents said they had talked to doctors about another family member’s wishes for how they would want to be cared for at the end of life.
While none of these proposals calls for the cost of care to weigh on these discussions, the final years of life are indeed expensive for America’s health care system. The Dartmouth Atlas of Health Care has calculated that a third of Medicare spending goes to the care of people with chronic illnesses in their last 2 years of life. That is likely to increase as the population of those older than 65 increases. An analysis by the Kaiser foundation found that Medicare spending per person more than doubled from age 70 to 96, where it peaked at $16,145 per beneficiary in 2011.
The Kaiser poll found less public support for a cost-containment provision that did make it into the health law. The “Cadillac tax” begins in 2018 and will impose a tax on expensive insurance that employers provide to their workers. Sixty percent oppose the plan, which economists have long favored as a way to discourage lavish coverage and make people aware that extensive use of Medicare services is linked to premiums.
The poll also found that 57% of people favor repealing the medical device tax, another piece of the health law that Republicans in Congress are trying to repeal. The tax applies to artificial hips, pacemakers and other devices that doctors implant.
The poll was conducted from Sept. 17 through Sept. 23. The margin of error was +/– 3 percentage points.
Kaiser Health News is a nonprofit national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
The public overwhelmingly supports Medicare’s plan to pay for end-of-life discussions between doctors and patients, despite GOP objections that such chats would lead to rationed care for the elderly and ill, a poll released Sept. 30 finds.
About 8 of every 10 people surveyed by the Kaiser Family Foundation – in a nationally representative sample of 1,202 adults – supported coverage by the government or insurers for planning discussions about the type of care patients preferred in the waning days or weeks of their lives. (KHN is an editorially independent program of the foundation.) These discussions can include whether people would want to be kept alive by artificial means even if they had no chance of regaining consciousness or autonomy and whether they would want their organs to be donated. These preferences can be incorporated into advance directives, or living wills, which are used if someone can no longer communicate.
The Centers for Medicare & Medicaid Services earlier this year proposed paying doctors to have these talks with patients. A final decision is due out soon. The idea had been included in early drafts of the 2010 federal health care law, but former Alaska Gov. Sarah Palin and other opponents of the law labeled the counseling sessions and other provisions “death panels” motivated by desires to save money, and the provision was deleted from the bill.
The notion of helping patients prepare for death has support among many doctors, who sometimes see terminal patients suffer from futile efforts to keep them alive. Last year, the Institute of Medicine issued a report that encouraged end-of-life discussions beginning as early as age 16.
The Kaiser poll found that these talks remain infrequent. Overall, only 17% of those surveyed said they had had such discussions with their doctors or other health care professionals, even though 89% believe doctors should engage in such counseling. A third of respondents said they had talked to doctors about another family member’s wishes for how they would want to be cared for at the end of life.
While none of these proposals calls for the cost of care to weigh on these discussions, the final years of life are indeed expensive for America’s health care system. The Dartmouth Atlas of Health Care has calculated that a third of Medicare spending goes to the care of people with chronic illnesses in their last 2 years of life. That is likely to increase as the population of those older than 65 increases. An analysis by the Kaiser foundation found that Medicare spending per person more than doubled from age 70 to 96, where it peaked at $16,145 per beneficiary in 2011.
The Kaiser poll found less public support for a cost-containment provision that did make it into the health law. The “Cadillac tax” begins in 2018 and will impose a tax on expensive insurance that employers provide to their workers. Sixty percent oppose the plan, which economists have long favored as a way to discourage lavish coverage and make people aware that extensive use of Medicare services is linked to premiums.
The poll also found that 57% of people favor repealing the medical device tax, another piece of the health law that Republicans in Congress are trying to repeal. The tax applies to artificial hips, pacemakers and other devices that doctors implant.
The poll was conducted from Sept. 17 through Sept. 23. The margin of error was +/– 3 percentage points.
Kaiser Health News is a nonprofit national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.

Chlorhexidine gel-pad dressing reduces bloodstream infections
SAN DIEGO – Chlorhexidine-containing intravenous catheter securement dressings significantly reduced the incidence of central venous catheter–related bloodstream infections in neutropenic patients, a multicenter randomized trial showed.
“Central venous catheters impose a risk of catheter-related bloodstream infections, especially when used in neutropenic patients, and the mortality risk has been reported to be up to 36%,” Dr. Lena M. Biehl said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.

One way to prevent catheter-related bloodstream infections is to use chlorhexidine-containing intravenous catheter securement dressings in an effort to decrease skin colonization, said Dr. Biehl of the department of internal medicine at University Hospital of Cologne (Germany). “A few studies have looked at this, but most of them used chlorhexidine-containing sponges. There’s only one study using a more advanced chlorhexidine-containing gel pad, and this study was done in the ICU setting. The gel pad enables you to evaluate the insertion site, so you can see if there are signs of infection without removing the dressing.”
In a multicenter, randomized trial known as the COAT study that was conducted at 10 hematology departments in Germany from February 2012 to September 2014, Dr. Biehl and her associates set out to compare the incidence of central venous catheter–related bloodstream infections in two groups of neutropenic patients: those with chlorhexidine-containing IV catheter-securement dressings that included a gel pad (the chlorhexidine group) and those with conventional IV catheter-securement dressings that lacked a gel pad (the control group). They limited the analysis to patients undergoing intensive chemotherapy with expected neutropenia for at least 5 days and expected central venous catheter use of at least 10 days. The primary endpoint was the incidence of definite catheter-related bloodstream infections within 14 days of central venous catheter placement. The secondary endpoints were overall incidence of definite or probable central venous catheter–related bloodstream infections at 14 days and the overall incidence of definite or probable central venous catheter–related bloodstream infections.
Dr. Biehl presented results from 613 patients. Of these, 307 were in the chlorhexidine group and 306 were in the control group. The median age was 58 years and 59% were male, and the distribution of causative pathogens was similar between the two groups. The incidence of definite catheter-related bloodstream infections at 14 days was 2.6% in the chlorhexidine group, compared with 3.9% in the control group, a difference that did not reach statistical significance (P = .375). However, the overall incidence of definite and probable central venous catheter–related bloodstream infections together at 14 days was 6.5% in the chlorhexidine group, compared with 11.1% in the control group, a difference that reached statistical significance (P = .047). Finally, the overall incidence of definite and probable central venous catheter–related bloodstream infections was 10.4% in the chlorhexidine group, compared with 17% in the control group, a difference that also reached statistical significance (P = .019).
“The chlorhexidine dressings were very well tolerated, and in contrast to previous studies we saw no increase in skin and soft tissue abnormalities or contact dermatitis,” Dr. Biehl said. The researchers also observed no significant difference in mortality between the chlorhexidine and control groups (6.2 % vs. 5.6%, respectively).
The study was supported by a grant from 3M. Dr. Biehl disclosed that she is a member of the speakers bureau for Astellas Pharma and Merck/MSD. She has received travel grants from 3M and Gilead Sciences. Another study investigator, Dr. Maria J. G. T. Vehreschild, disclosed numerous financial ties to industry.
SAN DIEGO – Chlorhexidine-containing intravenous catheter securement dressings significantly reduced the incidence of central venous catheter–related bloodstream infections in neutropenic patients, a multicenter randomized trial showed.
“Central venous catheters impose a risk of catheter-related bloodstream infections, especially when used in neutropenic patients, and the mortality risk has been reported to be up to 36%,” Dr. Lena M. Biehl said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
One way to prevent catheter-related bloodstream infections is to use chlorhexidine-containing intravenous catheter securement dressings in an effort to decrease skin colonization, said Dr. Biehl of the department of internal medicine at University Hospital of Cologne (Germany). “A few studies have looked at this, but most of them used chlorhexidine-containing sponges. There’s only one study using a more advanced chlorhexidine-containing gel pad, and this study was done in the ICU setting. The gel pad enables you to evaluate the insertion site, so you can see if there are signs of infection without removing the dressing.”
In a multicenter, randomized trial known as the COAT study that was conducted at 10 hematology departments in Germany from February 2012 to September 2014, Dr. Biehl and her associates set out to compare the incidence of central venous catheter–related bloodstream infections in two groups of neutropenic patients: those with chlorhexidine-containing IV catheter-securement dressings that included a gel pad (the chlorhexidine group) and those with conventional IV catheter-securement dressings that lacked a gel pad (the control group). They limited the analysis to patients undergoing intensive chemotherapy with expected neutropenia for at least 5 days and expected central venous catheter use of at least 10 days. The primary endpoint was the incidence of definite catheter-related bloodstream infections within 14 days of central venous catheter placement. The secondary endpoints were overall incidence of definite or probable central venous catheter–related bloodstream infections at 14 days and the overall incidence of definite or probable central venous catheter–related bloodstream infections.
Dr. Biehl presented results from 613 patients. Of these, 307 were in the chlorhexidine group and 306 were in the control group. The median age was 58 years and 59% were male, and the distribution of causative pathogens was similar between the two groups. The incidence of definite catheter-related bloodstream infections at 14 days was 2.6% in the chlorhexidine group, compared with 3.9% in the control group, a difference that did not reach statistical significance (P = .375). However, the overall incidence of definite and probable central venous catheter–related bloodstream infections together at 14 days was 6.5% in the chlorhexidine group, compared with 11.1% in the control group, a difference that reached statistical significance (P = .047). Finally, the overall incidence of definite and probable central venous catheter–related bloodstream infections was 10.4% in the chlorhexidine group, compared with 17% in the control group, a difference that also reached statistical significance (P = .019).
“The chlorhexidine dressings were very well tolerated, and in contrast to previous studies we saw no increase in skin and soft tissue abnormalities or contact dermatitis,” Dr. Biehl said. The researchers also observed no significant difference in mortality between the chlorhexidine and control groups (6.2 % vs. 5.6%, respectively).
The study was supported by a grant from 3M. Dr. Biehl disclosed that she is a member of the speakers bureau for Astellas Pharma and Merck/MSD. She has received travel grants from 3M and Gilead Sciences. Another study investigator, Dr. Maria J. G. T. Vehreschild, disclosed numerous financial ties to industry.
SAN DIEGO – Chlorhexidine-containing intravenous catheter securement dressings significantly reduced the incidence of central venous catheter–related bloodstream infections in neutropenic patients, a multicenter randomized trial showed.
“Central venous catheters impose a risk of catheter-related bloodstream infections, especially when used in neutropenic patients, and the mortality risk has been reported to be up to 36%,” Dr. Lena M. Biehl said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
One way to prevent catheter-related bloodstream infections is to use chlorhexidine-containing intravenous catheter securement dressings in an effort to decrease skin colonization, said Dr. Biehl of the department of internal medicine at University Hospital of Cologne (Germany). “A few studies have looked at this, but most of them used chlorhexidine-containing sponges. There’s only one study using a more advanced chlorhexidine-containing gel pad, and this study was done in the ICU setting. The gel pad enables you to evaluate the insertion site, so you can see if there are signs of infection without removing the dressing.”
In a multicenter, randomized trial known as the COAT study that was conducted at 10 hematology departments in Germany from February 2012 to September 2014, Dr. Biehl and her associates set out to compare the incidence of central venous catheter–related bloodstream infections in two groups of neutropenic patients: those with chlorhexidine-containing IV catheter-securement dressings that included a gel pad (the chlorhexidine group) and those with conventional IV catheter-securement dressings that lacked a gel pad (the control group). They limited the analysis to patients undergoing intensive chemotherapy with expected neutropenia for at least 5 days and expected central venous catheter use of at least 10 days. The primary endpoint was the incidence of definite catheter-related bloodstream infections within 14 days of central venous catheter placement. The secondary endpoints were overall incidence of definite or probable central venous catheter–related bloodstream infections at 14 days and the overall incidence of definite or probable central venous catheter–related bloodstream infections.
Dr. Biehl presented results from 613 patients. Of these, 307 were in the chlorhexidine group and 306 were in the control group. The median age was 58 years and 59% were male, and the distribution of causative pathogens was similar between the two groups. The incidence of definite catheter-related bloodstream infections at 14 days was 2.6% in the chlorhexidine group, compared with 3.9% in the control group, a difference that did not reach statistical significance (P = .375). However, the overall incidence of definite and probable central venous catheter–related bloodstream infections together at 14 days was 6.5% in the chlorhexidine group, compared with 11.1% in the control group, a difference that reached statistical significance (P = .047). Finally, the overall incidence of definite and probable central venous catheter–related bloodstream infections was 10.4% in the chlorhexidine group, compared with 17% in the control group, a difference that also reached statistical significance (P = .019).
“The chlorhexidine dressings were very well tolerated, and in contrast to previous studies we saw no increase in skin and soft tissue abnormalities or contact dermatitis,” Dr. Biehl said. The researchers also observed no significant difference in mortality between the chlorhexidine and control groups (6.2 % vs. 5.6%, respectively).
The study was supported by a grant from 3M. Dr. Biehl disclosed that she is a member of the speakers bureau for Astellas Pharma and Merck/MSD. She has received travel grants from 3M and Gilead Sciences. Another study investigator, Dr. Maria J. G. T. Vehreschild, disclosed numerous financial ties to industry.
AT ICAAC 2015
Key clinical point: Using a chlorhexidine-containing securement dressing reduces the incidence of catheter-related bloodstream infections.
Major finding: The overall incidence of definite and probable central venous catheter–related bloodstream infections was 10.4% in the chlorhexidine group, compared with 17% in the control group, a difference that reached statistical significance (P = .019).
Data source: A randomized study of 613 neutropenic patients conducted at 10 hematology departments in Germany.
Disclosures: The study was supported by a grant from 3M. Dr. Biehl disclosed that she is a member of the speakers bureau for Astellas Pharma and Merck/MSD. She has received travel grants from 3M and Gilead Sciences. Another study investigator, Dr. Maria J. G. T. Vehreschild, disclosed numerous financial ties to industry.

Two heads plus four hands equal safe, shorter bilateral mastectomies
SAN FRANCISCO – Two surgeons working in tandem, one on each side of the patient, can significantly reduce the total operative time for bilateral mastectomies without compromising safety or quality of results, according to a study presented at the 2015 ASCO Breast Cancer Symposium.
A review of records on consecutive cases of bilateral mastectomy with tissue expander reconstruction (BMTR) showed that mean overall surgery time (start of incision to closure) was about 23 minutes shorter when two surgeons were working at once, and mean general surgery time (start of incision to end of mastectomy procedure) was 41 minutes shorter with two surgeons vs. a solo operator, reported Dr. Suniti Nimbkar of the department of surgery at Brigham and Women’s Hospital, Boston.
“We did find that there was a significant reduction in time when two surgeons work together, and that reduction is particularly emphasized when you have a patient who is larger, perhaps a heavier patient, and when you have to do more extensive surgery,” she said in an interview at the symposium.
Dual surgeons did take slightly longer to perform the reconstructive surgery portion of the procedure, however.
Effective cosurgery is like a healthy marriage or a successful restaurant kitchen, with partners learning how to anticipate each other’s needs, knowing when to lend a hand, and intuitively grasping when to get out of the way, Dr. Nimbkar suggested.
“As two surgeons work together more and more, they just inevitably grow together in how they operate. I know for example that my direct partner and I operate very similarly, whereas sometimes if I do a cosurgery with a second surgeon that I don’t always operate with we have to work together to understand each other’s approach,” she said.
The investigators scanned the charts of 116 consecutive women who underwent BMTR done by eight breast surgeons at their center, looking for potential differences in operative time and 30-day postoperative complications. In all, 67 of the procedures were cosurgeries, and 49 were done by a single surgeon.
They found that in bivariate analysis, mean general surgery time was 75.8 minutes for the surgical duos, compared with 116.8 minutes for the solo surgeons (P less than .0001). Overall surgery time was also shorter, at 255.2 minutes vs. 278.3 minutes, respectively (P = .005).
Although there were numerically more complications among patients of cosurgeons, there was no statistically significant difference in postoperative complications rates between the twin and singleton surgeons.
A linear regression model showed that factors significantly associated with general surgery time were cosurgeries (P less than .0001), total breast weight (P =.03) and axillary dissection (P = .0003).
The authors noted that although two surgeons cut operative times significantly, the amount of time savings was not proportional to what they expected.
“We also want to know if the plastic surgeons are happy with the results if there are two different surgeons. Do they feel that there is too much of a difference in the way the mastectomy comes out, or is it something they’re fine with? So one of the next steps we’re going to take is to survey the plastic surgeons as to whether they’re comfortable with what we’re doing or if they have ideas about how we can be more uniform,” Dr. Nimbkar said.
SAN FRANCISCO – Two surgeons working in tandem, one on each side of the patient, can significantly reduce the total operative time for bilateral mastectomies without compromising safety or quality of results, according to a study presented at the 2015 ASCO Breast Cancer Symposium.
A review of records on consecutive cases of bilateral mastectomy with tissue expander reconstruction (BMTR) showed that mean overall surgery time (start of incision to closure) was about 23 minutes shorter when two surgeons were working at once, and mean general surgery time (start of incision to end of mastectomy procedure) was 41 minutes shorter with two surgeons vs. a solo operator, reported Dr. Suniti Nimbkar of the department of surgery at Brigham and Women’s Hospital, Boston.
“We did find that there was a significant reduction in time when two surgeons work together, and that reduction is particularly emphasized when you have a patient who is larger, perhaps a heavier patient, and when you have to do more extensive surgery,” she said in an interview at the symposium.
Dual surgeons did take slightly longer to perform the reconstructive surgery portion of the procedure, however.
Effective cosurgery is like a healthy marriage or a successful restaurant kitchen, with partners learning how to anticipate each other’s needs, knowing when to lend a hand, and intuitively grasping when to get out of the way, Dr. Nimbkar suggested.
“As two surgeons work together more and more, they just inevitably grow together in how they operate. I know for example that my direct partner and I operate very similarly, whereas sometimes if I do a cosurgery with a second surgeon that I don’t always operate with we have to work together to understand each other’s approach,” she said.
The investigators scanned the charts of 116 consecutive women who underwent BMTR done by eight breast surgeons at their center, looking for potential differences in operative time and 30-day postoperative complications. In all, 67 of the procedures were cosurgeries, and 49 were done by a single surgeon.
They found that in bivariate analysis, mean general surgery time was 75.8 minutes for the surgical duos, compared with 116.8 minutes for the solo surgeons (P less than .0001). Overall surgery time was also shorter, at 255.2 minutes vs. 278.3 minutes, respectively (P = .005).
Although there were numerically more complications among patients of cosurgeons, there was no statistically significant difference in postoperative complications rates between the twin and singleton surgeons.
A linear regression model showed that factors significantly associated with general surgery time were cosurgeries (P less than .0001), total breast weight (P =.03) and axillary dissection (P = .0003).
The authors noted that although two surgeons cut operative times significantly, the amount of time savings was not proportional to what they expected.
“We also want to know if the plastic surgeons are happy with the results if there are two different surgeons. Do they feel that there is too much of a difference in the way the mastectomy comes out, or is it something they’re fine with? So one of the next steps we’re going to take is to survey the plastic surgeons as to whether they’re comfortable with what we’re doing or if they have ideas about how we can be more uniform,” Dr. Nimbkar said.
SAN FRANCISCO – Two surgeons working in tandem, one on each side of the patient, can significantly reduce the total operative time for bilateral mastectomies without compromising safety or quality of results, according to a study presented at the 2015 ASCO Breast Cancer Symposium.
A review of records on consecutive cases of bilateral mastectomy with tissue expander reconstruction (BMTR) showed that mean overall surgery time (start of incision to closure) was about 23 minutes shorter when two surgeons were working at once, and mean general surgery time (start of incision to end of mastectomy procedure) was 41 minutes shorter with two surgeons vs. a solo operator, reported Dr. Suniti Nimbkar of the department of surgery at Brigham and Women’s Hospital, Boston.
“We did find that there was a significant reduction in time when two surgeons work together, and that reduction is particularly emphasized when you have a patient who is larger, perhaps a heavier patient, and when you have to do more extensive surgery,” she said in an interview at the symposium.
Dual surgeons did take slightly longer to perform the reconstructive surgery portion of the procedure, however.
Effective cosurgery is like a healthy marriage or a successful restaurant kitchen, with partners learning how to anticipate each other’s needs, knowing when to lend a hand, and intuitively grasping when to get out of the way, Dr. Nimbkar suggested.
“As two surgeons work together more and more, they just inevitably grow together in how they operate. I know for example that my direct partner and I operate very similarly, whereas sometimes if I do a cosurgery with a second surgeon that I don’t always operate with we have to work together to understand each other’s approach,” she said.
The investigators scanned the charts of 116 consecutive women who underwent BMTR done by eight breast surgeons at their center, looking for potential differences in operative time and 30-day postoperative complications. In all, 67 of the procedures were cosurgeries, and 49 were done by a single surgeon.
They found that in bivariate analysis, mean general surgery time was 75.8 minutes for the surgical duos, compared with 116.8 minutes for the solo surgeons (P less than .0001). Overall surgery time was also shorter, at 255.2 minutes vs. 278.3 minutes, respectively (P = .005).
Although there were numerically more complications among patients of cosurgeons, there was no statistically significant difference in postoperative complications rates between the twin and singleton surgeons.
A linear regression model showed that factors significantly associated with general surgery time were cosurgeries (P less than .0001), total breast weight (P =.03) and axillary dissection (P = .0003).
The authors noted that although two surgeons cut operative times significantly, the amount of time savings was not proportional to what they expected.
“We also want to know if the plastic surgeons are happy with the results if there are two different surgeons. Do they feel that there is too much of a difference in the way the mastectomy comes out, or is it something they’re fine with? So one of the next steps we’re going to take is to survey the plastic surgeons as to whether they’re comfortable with what we’re doing or if they have ideas about how we can be more uniform,” Dr. Nimbkar said.
AT THE 2015 ASCO BREAST CANCER SYMPOSIUM
Key clinical point:Bilateral mastectomy performed by two surgeons shortens operative time without increasing complications.
Major finding: Mean general surgery time was 75.8 minutes for two surgeons vs. 116.8 minutes for solo surgeons (P less than .0001).
Data source: Retrospective review of records on 116 consecutive patients undergoing bilateral mastectomies.
Disclosures: The study was internally funded. The authors reported no conflicts of interest.
Study reveals higher than expected post-discharge mortality after trauma
LAS VEGAS – A higher-than-expected proportion of trauma-related deaths occur in the months and years after hospital discharge, according to findings from a prospective cohort study.
In 908 trauma patients followed for up to 9.8 years (median, 1.7 years), overall mortality was 27%, and in 509 patients followed for at least 2 years, overall mortality was 38%. Mortality was highest among those who were severely injured (43% at 5 years), Dr. Rachael A. Callcut reported at the annual meeting of the American Association for the Surgery of Trauma.

The median Injury Severity Scale score was 18, but for all ISS groups, survival was significantly worse than predicted actuarial survival for that group – even after exclusion of deaths that occurred within 30 days, she said.
For example, at 5 years, predicted actuarial survival was greater than 95%, but actual survival was about 90% for those with ISS less than 15, about 85% for those with ISS of 15-24, and about 57% for those with ISS greater than 24. This dose-response–like relationship between injury severity and mortality demonstrates that the deaths are not just occurring in “patients who are old and would have died from a heart attack anyway” she explained.
The 30-day mortality in the cohort was 22%, and in-hospital mortality was 22.9%, as eight patients who died after the first 30 days did so in the hospital. Forty-five of the 245 deaths (18%) occurred after 30 days, and 36 of those (80%) occurred after hospital discharge, meaning the out-of-hospital mortality rate was 5.3% overall, and 10% for the most severely injured (hazard ratio, 2.7 for the most severe vs. the least severe injuries).
“I personally found this quite striking given that when a patient leaves the hospital, we feel, to some degree, that we won – only to find out that at least 5% of these patients will go on to subsequently die,” said Dr. Callcut of the University of California San Francisco, adding that “if you look at it slightly differently, which is even more concerning, 37 of the out-of-hospital deaths of the total of 245 deaths, mean that out-of-hospital deaths account for 15% of the total mortality following trauma.”
Further, of the deaths that occurred after 30 days, 53% occurred between 31 days and 1 year after trauma, and trauma was the leading cause of postdischarge death, accounting for 41% of the late deaths, she said.
The patients included in this analysis were all highest level trauma activation patients enrolled in the ongoing study between 2005 and 2012. Comprehensive prospective data were collected, and patients were followed throughout their hospitalization and after discharge. Institutional medical records or death certificates were used to determine timing and cause of death, and survival status was determined based on the last date of care in the institution or by query of the National Death Index for 2013.
These findings provide a rare glimpse of trauma-related outcomes among patients discharged from the hospital. Most prior studies focused on 30-day outcomes, with a few extended out to 90 days, but very few studies have looked at long-term outcomes, Dr. Callcut noted.
“You could say that despite having survived to leave the hospital alive, long-term survival is actually worse than predicted actuarial survival, and this suggests to us that successful hospital discharge does not mean success for your patient,” she concluded.
Dr. Callcut was supported in part by a National Institutes of Health award.
LAS VEGAS – A higher-than-expected proportion of trauma-related deaths occur in the months and years after hospital discharge, according to findings from a prospective cohort study.
In 908 trauma patients followed for up to 9.8 years (median, 1.7 years), overall mortality was 27%, and in 509 patients followed for at least 2 years, overall mortality was 38%. Mortality was highest among those who were severely injured (43% at 5 years), Dr. Rachael A. Callcut reported at the annual meeting of the American Association for the Surgery of Trauma.
The median Injury Severity Scale score was 18, but for all ISS groups, survival was significantly worse than predicted actuarial survival for that group – even after exclusion of deaths that occurred within 30 days, she said.
For example, at 5 years, predicted actuarial survival was greater than 95%, but actual survival was about 90% for those with ISS less than 15, about 85% for those with ISS of 15-24, and about 57% for those with ISS greater than 24. This dose-response–like relationship between injury severity and mortality demonstrates that the deaths are not just occurring in “patients who are old and would have died from a heart attack anyway” she explained.
The 30-day mortality in the cohort was 22%, and in-hospital mortality was 22.9%, as eight patients who died after the first 30 days did so in the hospital. Forty-five of the 245 deaths (18%) occurred after 30 days, and 36 of those (80%) occurred after hospital discharge, meaning the out-of-hospital mortality rate was 5.3% overall, and 10% for the most severely injured (hazard ratio, 2.7 for the most severe vs. the least severe injuries).
“I personally found this quite striking given that when a patient leaves the hospital, we feel, to some degree, that we won – only to find out that at least 5% of these patients will go on to subsequently die,” said Dr. Callcut of the University of California San Francisco, adding that “if you look at it slightly differently, which is even more concerning, 37 of the out-of-hospital deaths of the total of 245 deaths, mean that out-of-hospital deaths account for 15% of the total mortality following trauma.”
Further, of the deaths that occurred after 30 days, 53% occurred between 31 days and 1 year after trauma, and trauma was the leading cause of postdischarge death, accounting for 41% of the late deaths, she said.
The patients included in this analysis were all highest level trauma activation patients enrolled in the ongoing study between 2005 and 2012. Comprehensive prospective data were collected, and patients were followed throughout their hospitalization and after discharge. Institutional medical records or death certificates were used to determine timing and cause of death, and survival status was determined based on the last date of care in the institution or by query of the National Death Index for 2013.
These findings provide a rare glimpse of trauma-related outcomes among patients discharged from the hospital. Most prior studies focused on 30-day outcomes, with a few extended out to 90 days, but very few studies have looked at long-term outcomes, Dr. Callcut noted.
“You could say that despite having survived to leave the hospital alive, long-term survival is actually worse than predicted actuarial survival, and this suggests to us that successful hospital discharge does not mean success for your patient,” she concluded.
Dr. Callcut was supported in part by a National Institutes of Health award.
LAS VEGAS – A higher-than-expected proportion of trauma-related deaths occur in the months and years after hospital discharge, according to findings from a prospective cohort study.
In 908 trauma patients followed for up to 9.8 years (median, 1.7 years), overall mortality was 27%, and in 509 patients followed for at least 2 years, overall mortality was 38%. Mortality was highest among those who were severely injured (43% at 5 years), Dr. Rachael A. Callcut reported at the annual meeting of the American Association for the Surgery of Trauma.
The median Injury Severity Scale score was 18, but for all ISS groups, survival was significantly worse than predicted actuarial survival for that group – even after exclusion of deaths that occurred within 30 days, she said.
For example, at 5 years, predicted actuarial survival was greater than 95%, but actual survival was about 90% for those with ISS less than 15, about 85% for those with ISS of 15-24, and about 57% for those with ISS greater than 24. This dose-response–like relationship between injury severity and mortality demonstrates that the deaths are not just occurring in “patients who are old and would have died from a heart attack anyway” she explained.
The 30-day mortality in the cohort was 22%, and in-hospital mortality was 22.9%, as eight patients who died after the first 30 days did so in the hospital. Forty-five of the 245 deaths (18%) occurred after 30 days, and 36 of those (80%) occurred after hospital discharge, meaning the out-of-hospital mortality rate was 5.3% overall, and 10% for the most severely injured (hazard ratio, 2.7 for the most severe vs. the least severe injuries).
“I personally found this quite striking given that when a patient leaves the hospital, we feel, to some degree, that we won – only to find out that at least 5% of these patients will go on to subsequently die,” said Dr. Callcut of the University of California San Francisco, adding that “if you look at it slightly differently, which is even more concerning, 37 of the out-of-hospital deaths of the total of 245 deaths, mean that out-of-hospital deaths account for 15% of the total mortality following trauma.”
Further, of the deaths that occurred after 30 days, 53% occurred between 31 days and 1 year after trauma, and trauma was the leading cause of postdischarge death, accounting for 41% of the late deaths, she said.
The patients included in this analysis were all highest level trauma activation patients enrolled in the ongoing study between 2005 and 2012. Comprehensive prospective data were collected, and patients were followed throughout their hospitalization and after discharge. Institutional medical records or death certificates were used to determine timing and cause of death, and survival status was determined based on the last date of care in the institution or by query of the National Death Index for 2013.
These findings provide a rare glimpse of trauma-related outcomes among patients discharged from the hospital. Most prior studies focused on 30-day outcomes, with a few extended out to 90 days, but very few studies have looked at long-term outcomes, Dr. Callcut noted.
“You could say that despite having survived to leave the hospital alive, long-term survival is actually worse than predicted actuarial survival, and this suggests to us that successful hospital discharge does not mean success for your patient,” she concluded.
Dr. Callcut was supported in part by a National Institutes of Health award.
AT THE AAST ANNUAL MEETING
Key clinical point: A concerning proportion of trauma-related deaths occur after hospital discharge, according to findings from a prospective cohort study.
Major finding: The out-of-hospital mortality rate was 5.3% overall, and 10% for the most severely injured (hazard ratio, 2.7 for the most vs. least severely injured).
Data source: A prospective cohort study involving 908 patients.
Disclosures: Dr. Callcut was supported in part by a National Institutes of Health award.

HFSA: Next-generation LVAD meets survival goal
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.

Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.

|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.
|
|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.
|
|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.
Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.
Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point: A next-generation left ventricular assist device, HeartMate 3, met its 6-month survival goal to receive CE mark approval in Europe.
Major finding: The advanced heart failure patients who received the HeartMate 3 LVAD had a 92% survival rate after 6 months.
Data source: A prospective series of 50 patients enrolled at 10 centers in six countries.
Disclosures: The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.

Physicians face telemedicine payment challenges
Emergency department personnel at a remote hospital called Dr. James P. Marcin regarding a baby who was just admitted with an upper respiratory infection. Because the patient had cyanotic congenital heart disease, the team was concerned she was too medically complex for their facility, and they were preparing to helicopter her to the pediatric intensive care unit at the University of California, Davis, Children’s Hospital in Sacramento.

But when Dr. Marcin examined the baby via a two-way video, he remembered the child from a previous visit. Although her oxygen levels were low, Dr. Marcin knew they were normal for her condition. Dr. Marcin spoke with the patient’s parents and after learning more about the patient’s symptoms, he was confident the child could remain at the small hospital. She was treated for the upper respiratory infection and later sent home where she improved, said Dr. Marcin, who leads the Pediatric Telemedicine Program at UC Davis.
Despite the positive outcome, Dr. Marcin’s claim was denied by the insurance company, he said.
“Had I not used telemedicine, that child would have been put in a helicopter, flown to our ICU, [and likely incurred] some $20,000 bill,” Dr. Marcin said in an interview. “I saved the insurance company $20,000, and then they ended up denying my 2 hours of critical care time. It’s discouraging.”
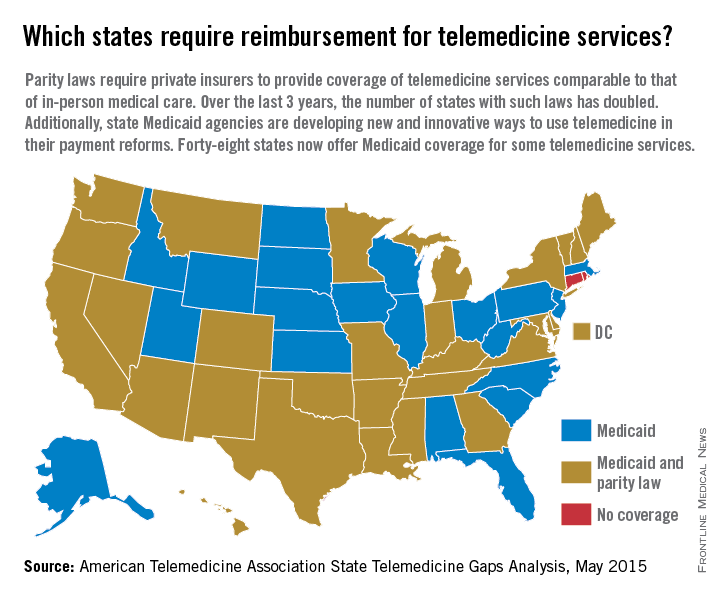
Reimbursement struggles are playing out in medical practices and hospitals across the country. While insurance coverage for telemedicine is growing, experts say payment remains one of the most pressing challenges. So far, 29 states and the District of Columbia have laws that require full parity of coverage and reimbursement for telemedicine services comparable to that of in-person services, according to the American Telemedicine Association (ATA). Medicaid programs in almost all (48) states require some form of compensation for telemedicine, according to a 2015 ATA report.
Payment parity for telemedicine has doubled in the last 2 years, noted Dr. Reed V. Tuckson, ATA president.

“We are seeing, on the side of the private insurance world, really exciting acceptance of telehealth services,” Dr. Tuckson said in an interview. There has been “really great movement forward.”
Enforcement of those parity laws can be spotty, said René Y. Quashie, a Washington health law attorney.
“It’s a mixed bag,” Mr. Quashie said in an interview. “In some states, enforcement is lax so you still have a lot of providers submitting claims that are not being paid or not being paid timely.”
State support equals payment success
In rural Wrightsville, Ga., Dr. Jean R. Sumner regularly gets paid to provide telemedicine. Georgia enacted its parity law in 2006 and has greatly embraced telemedicine capabilities, particularly for its rural populations, said Dr. Sumner, associate dean for rural health at Mercer University in Macon. Part of the success is because of the Georgia Partnership for TeleHealth, a statewide network that focuses on increasing access to care through telemedicine. Its hallmark is the state’s open access network, a web of access points based on existing telemedicine programs that enables secure health information exchange. The goal of the program is for all rural Georgians to access specialty care within 30 miles of their homes.

The state’s strong support of telemedicine contributes to payers taking the modality seriously and doctors getting paid for telemedicine care, Dr. Sumner said in an interview.
“Most insurers pay as long as the visit is equal or superior to an exam done in person,” she said. “It has to be quality care.”
Dr. Sumner also can bill a site fee when telemedicine technology is used at her practice, she said. If a patient visits her practice for a psychiatric consultation while Dr. Sumner is busy, for example, a nurse can connect the patient to a psychiatrist through the office’s telemedicine unit. The site fee is minimal, but it helps cover costs, she said.
In states that do not have parity laws, some larger health plans, such as Anthem and UnitedHealthcare, have proactively covered telemedicine services, said Dr. Peter Antall, president and medical director of American Well’s Online Care Group, a national telehealth service. Smaller health plans on the other hand, are sometimes willing to negotiate with providers and consider adding telemedicine services to a fee schedule, Dr. Antall said in an interview.
“I think we’re moving into a phase where reimbursement is normal or expected in telehealth,” he said. “We’re not quite there yet because there are so many health plans and, within the health plans, there are so many different products and subgroups. It’s still a process that needs to evolve.”
Government payers lag behind
Medicaid policies also vary from state by state. Some state programs cover telemedicine services similar to that of in-person treatment. Others limit coverage by technology or geographic area.
Medicare, by far, ranks the worst in paying physicians for telemedicine, experts said. Of $597 billion in total Medicare payments in 2014, 0.0023% was spent on telemedicine, according to data provided to the Robert J. Waters Center for Telehealth & e-Health Law.
“Unless you’re a patient that presents in a rural community, the Medicare telehealth benefit is not available,” said Mr. Quashie, who is part of the CTeL’s legal resource team. “Medicare is almost a no-go under fee-for-service for telehealth.”
CMS reimburses physicians for telemedicine only when the originating site is in a Health Professional Shortage Area or within a county outside a Metropolitan Statistical Area. The originating site must be a medical facility and not the patient’s home. CMS covers care only on an approved list of medical services.
In its 2016 proposed fee schedule, CMS recommended adding two new codes to its accepted telemedicine services, including codes for prolonged service inpatient care and end-stage renal disease–related services. However, the agency denied a handful of other services requested by the ATA and again, refused to end its patient site limitations.
“We are very concerned about Medicare’s decisions in terms of its ability and willingness to reimburse” telehealth services,” Dr. Tuckson said. “Physicians who are trying to care for our nation’s seniors – so many of whom are presenting real challenges in manging their care in an optimal way – those physicians and patients deserve the opportunity to use [telehealth] tools, and physicians deserve to be reimbursed for the appropriate use of those tools.”
Federal legislation to expand Medicare coverage for telehealth has previously failed. Most recently, Rep. Mike Thompson (D-Calif.) proposed H.R. 2948, the Medicare Telehealth Parity Act of 2015, a bill that would broaden Medicare telemedicine coverage to urban areas and cover more services. The bill has been referred to the House Ways and Means Committee’s Subcommittee on Health.
Coverage of telemedicine by all payers is especially necessary as the health care system shifts to a more value-based care structure, Dr. Marcin said. Telemedicine presents great opportunities for preventing illnesses, keeping patients out of the hospital, and lowering health costs, he said. However, financial incentives to utilize telemedicine in these ways is lacking.
“Even though these technologies have been proven to reduce overall health care costs, they result in lower payments to doctors and hospitals,” Dr. Marcin said. “There’s a malalignment with payments to both hospitals and doctors and what should be the goals of health care, which is to keep patients healthy.”
Coming Tuesday, Oct. 6: Can telemedicine expose you to legal risk?
On Twitter @legal_med
Emergency department personnel at a remote hospital called Dr. James P. Marcin regarding a baby who was just admitted with an upper respiratory infection. Because the patient had cyanotic congenital heart disease, the team was concerned she was too medically complex for their facility, and they were preparing to helicopter her to the pediatric intensive care unit at the University of California, Davis, Children’s Hospital in Sacramento.
But when Dr. Marcin examined the baby via a two-way video, he remembered the child from a previous visit. Although her oxygen levels were low, Dr. Marcin knew they were normal for her condition. Dr. Marcin spoke with the patient’s parents and after learning more about the patient’s symptoms, he was confident the child could remain at the small hospital. She was treated for the upper respiratory infection and later sent home where she improved, said Dr. Marcin, who leads the Pediatric Telemedicine Program at UC Davis.
Despite the positive outcome, Dr. Marcin’s claim was denied by the insurance company, he said.
“Had I not used telemedicine, that child would have been put in a helicopter, flown to our ICU, [and likely incurred] some $20,000 bill,” Dr. Marcin said in an interview. “I saved the insurance company $20,000, and then they ended up denying my 2 hours of critical care time. It’s discouraging.”
Reimbursement struggles are playing out in medical practices and hospitals across the country. While insurance coverage for telemedicine is growing, experts say payment remains one of the most pressing challenges. So far, 29 states and the District of Columbia have laws that require full parity of coverage and reimbursement for telemedicine services comparable to that of in-person services, according to the American Telemedicine Association (ATA). Medicaid programs in almost all (48) states require some form of compensation for telemedicine, according to a 2015 ATA report.
Payment parity for telemedicine has doubled in the last 2 years, noted Dr. Reed V. Tuckson, ATA president.
“We are seeing, on the side of the private insurance world, really exciting acceptance of telehealth services,” Dr. Tuckson said in an interview. There has been “really great movement forward.”
Enforcement of those parity laws can be spotty, said René Y. Quashie, a Washington health law attorney.
“It’s a mixed bag,” Mr. Quashie said in an interview. “In some states, enforcement is lax so you still have a lot of providers submitting claims that are not being paid or not being paid timely.”
State support equals payment success
In rural Wrightsville, Ga., Dr. Jean R. Sumner regularly gets paid to provide telemedicine. Georgia enacted its parity law in 2006 and has greatly embraced telemedicine capabilities, particularly for its rural populations, said Dr. Sumner, associate dean for rural health at Mercer University in Macon. Part of the success is because of the Georgia Partnership for TeleHealth, a statewide network that focuses on increasing access to care through telemedicine. Its hallmark is the state’s open access network, a web of access points based on existing telemedicine programs that enables secure health information exchange. The goal of the program is for all rural Georgians to access specialty care within 30 miles of their homes.
The state’s strong support of telemedicine contributes to payers taking the modality seriously and doctors getting paid for telemedicine care, Dr. Sumner said in an interview.
“Most insurers pay as long as the visit is equal or superior to an exam done in person,” she said. “It has to be quality care.”
Dr. Sumner also can bill a site fee when telemedicine technology is used at her practice, she said. If a patient visits her practice for a psychiatric consultation while Dr. Sumner is busy, for example, a nurse can connect the patient to a psychiatrist through the office’s telemedicine unit. The site fee is minimal, but it helps cover costs, she said.
In states that do not have parity laws, some larger health plans, such as Anthem and UnitedHealthcare, have proactively covered telemedicine services, said Dr. Peter Antall, president and medical director of American Well’s Online Care Group, a national telehealth service. Smaller health plans on the other hand, are sometimes willing to negotiate with providers and consider adding telemedicine services to a fee schedule, Dr. Antall said in an interview.
“I think we’re moving into a phase where reimbursement is normal or expected in telehealth,” he said. “We’re not quite there yet because there are so many health plans and, within the health plans, there are so many different products and subgroups. It’s still a process that needs to evolve.”
Government payers lag behind
Medicaid policies also vary from state by state. Some state programs cover telemedicine services similar to that of in-person treatment. Others limit coverage by technology or geographic area.
Medicare, by far, ranks the worst in paying physicians for telemedicine, experts said. Of $597 billion in total Medicare payments in 2014, 0.0023% was spent on telemedicine, according to data provided to the Robert J. Waters Center for Telehealth & e-Health Law.
“Unless you’re a patient that presents in a rural community, the Medicare telehealth benefit is not available,” said Mr. Quashie, who is part of the CTeL’s legal resource team. “Medicare is almost a no-go under fee-for-service for telehealth.”
CMS reimburses physicians for telemedicine only when the originating site is in a Health Professional Shortage Area or within a county outside a Metropolitan Statistical Area. The originating site must be a medical facility and not the patient’s home. CMS covers care only on an approved list of medical services.
In its 2016 proposed fee schedule, CMS recommended adding two new codes to its accepted telemedicine services, including codes for prolonged service inpatient care and end-stage renal disease–related services. However, the agency denied a handful of other services requested by the ATA and again, refused to end its patient site limitations.
“We are very concerned about Medicare’s decisions in terms of its ability and willingness to reimburse” telehealth services,” Dr. Tuckson said. “Physicians who are trying to care for our nation’s seniors – so many of whom are presenting real challenges in manging their care in an optimal way – those physicians and patients deserve the opportunity to use [telehealth] tools, and physicians deserve to be reimbursed for the appropriate use of those tools.”
Federal legislation to expand Medicare coverage for telehealth has previously failed. Most recently, Rep. Mike Thompson (D-Calif.) proposed H.R. 2948, the Medicare Telehealth Parity Act of 2015, a bill that would broaden Medicare telemedicine coverage to urban areas and cover more services. The bill has been referred to the House Ways and Means Committee’s Subcommittee on Health.
Coverage of telemedicine by all payers is especially necessary as the health care system shifts to a more value-based care structure, Dr. Marcin said. Telemedicine presents great opportunities for preventing illnesses, keeping patients out of the hospital, and lowering health costs, he said. However, financial incentives to utilize telemedicine in these ways is lacking.
“Even though these technologies have been proven to reduce overall health care costs, they result in lower payments to doctors and hospitals,” Dr. Marcin said. “There’s a malalignment with payments to both hospitals and doctors and what should be the goals of health care, which is to keep patients healthy.”
Coming Tuesday, Oct. 6: Can telemedicine expose you to legal risk?
On Twitter @legal_med
Emergency department personnel at a remote hospital called Dr. James P. Marcin regarding a baby who was just admitted with an upper respiratory infection. Because the patient had cyanotic congenital heart disease, the team was concerned she was too medically complex for their facility, and they were preparing to helicopter her to the pediatric intensive care unit at the University of California, Davis, Children’s Hospital in Sacramento.
But when Dr. Marcin examined the baby via a two-way video, he remembered the child from a previous visit. Although her oxygen levels were low, Dr. Marcin knew they were normal for her condition. Dr. Marcin spoke with the patient’s parents and after learning more about the patient’s symptoms, he was confident the child could remain at the small hospital. She was treated for the upper respiratory infection and later sent home where she improved, said Dr. Marcin, who leads the Pediatric Telemedicine Program at UC Davis.
Despite the positive outcome, Dr. Marcin’s claim was denied by the insurance company, he said.
“Had I not used telemedicine, that child would have been put in a helicopter, flown to our ICU, [and likely incurred] some $20,000 bill,” Dr. Marcin said in an interview. “I saved the insurance company $20,000, and then they ended up denying my 2 hours of critical care time. It’s discouraging.”
Reimbursement struggles are playing out in medical practices and hospitals across the country. While insurance coverage for telemedicine is growing, experts say payment remains one of the most pressing challenges. So far, 29 states and the District of Columbia have laws that require full parity of coverage and reimbursement for telemedicine services comparable to that of in-person services, according to the American Telemedicine Association (ATA). Medicaid programs in almost all (48) states require some form of compensation for telemedicine, according to a 2015 ATA report.
Payment parity for telemedicine has doubled in the last 2 years, noted Dr. Reed V. Tuckson, ATA president.
“We are seeing, on the side of the private insurance world, really exciting acceptance of telehealth services,” Dr. Tuckson said in an interview. There has been “really great movement forward.”
Enforcement of those parity laws can be spotty, said René Y. Quashie, a Washington health law attorney.
“It’s a mixed bag,” Mr. Quashie said in an interview. “In some states, enforcement is lax so you still have a lot of providers submitting claims that are not being paid or not being paid timely.”
State support equals payment success
In rural Wrightsville, Ga., Dr. Jean R. Sumner regularly gets paid to provide telemedicine. Georgia enacted its parity law in 2006 and has greatly embraced telemedicine capabilities, particularly for its rural populations, said Dr. Sumner, associate dean for rural health at Mercer University in Macon. Part of the success is because of the Georgia Partnership for TeleHealth, a statewide network that focuses on increasing access to care through telemedicine. Its hallmark is the state’s open access network, a web of access points based on existing telemedicine programs that enables secure health information exchange. The goal of the program is for all rural Georgians to access specialty care within 30 miles of their homes.
The state’s strong support of telemedicine contributes to payers taking the modality seriously and doctors getting paid for telemedicine care, Dr. Sumner said in an interview.
“Most insurers pay as long as the visit is equal or superior to an exam done in person,” she said. “It has to be quality care.”
Dr. Sumner also can bill a site fee when telemedicine technology is used at her practice, she said. If a patient visits her practice for a psychiatric consultation while Dr. Sumner is busy, for example, a nurse can connect the patient to a psychiatrist through the office’s telemedicine unit. The site fee is minimal, but it helps cover costs, she said.
In states that do not have parity laws, some larger health plans, such as Anthem and UnitedHealthcare, have proactively covered telemedicine services, said Dr. Peter Antall, president and medical director of American Well’s Online Care Group, a national telehealth service. Smaller health plans on the other hand, are sometimes willing to negotiate with providers and consider adding telemedicine services to a fee schedule, Dr. Antall said in an interview.
“I think we’re moving into a phase where reimbursement is normal or expected in telehealth,” he said. “We’re not quite there yet because there are so many health plans and, within the health plans, there are so many different products and subgroups. It’s still a process that needs to evolve.”
Government payers lag behind
Medicaid policies also vary from state by state. Some state programs cover telemedicine services similar to that of in-person treatment. Others limit coverage by technology or geographic area.
Medicare, by far, ranks the worst in paying physicians for telemedicine, experts said. Of $597 billion in total Medicare payments in 2014, 0.0023% was spent on telemedicine, according to data provided to the Robert J. Waters Center for Telehealth & e-Health Law.
“Unless you’re a patient that presents in a rural community, the Medicare telehealth benefit is not available,” said Mr. Quashie, who is part of the CTeL’s legal resource team. “Medicare is almost a no-go under fee-for-service for telehealth.”
CMS reimburses physicians for telemedicine only when the originating site is in a Health Professional Shortage Area or within a county outside a Metropolitan Statistical Area. The originating site must be a medical facility and not the patient’s home. CMS covers care only on an approved list of medical services.
In its 2016 proposed fee schedule, CMS recommended adding two new codes to its accepted telemedicine services, including codes for prolonged service inpatient care and end-stage renal disease–related services. However, the agency denied a handful of other services requested by the ATA and again, refused to end its patient site limitations.
“We are very concerned about Medicare’s decisions in terms of its ability and willingness to reimburse” telehealth services,” Dr. Tuckson said. “Physicians who are trying to care for our nation’s seniors – so many of whom are presenting real challenges in manging their care in an optimal way – those physicians and patients deserve the opportunity to use [telehealth] tools, and physicians deserve to be reimbursed for the appropriate use of those tools.”
Federal legislation to expand Medicare coverage for telehealth has previously failed. Most recently, Rep. Mike Thompson (D-Calif.) proposed H.R. 2948, the Medicare Telehealth Parity Act of 2015, a bill that would broaden Medicare telemedicine coverage to urban areas and cover more services. The bill has been referred to the House Ways and Means Committee’s Subcommittee on Health.
Coverage of telemedicine by all payers is especially necessary as the health care system shifts to a more value-based care structure, Dr. Marcin said. Telemedicine presents great opportunities for preventing illnesses, keeping patients out of the hospital, and lowering health costs, he said. However, financial incentives to utilize telemedicine in these ways is lacking.
“Even though these technologies have been proven to reduce overall health care costs, they result in lower payments to doctors and hospitals,” Dr. Marcin said. “There’s a malalignment with payments to both hospitals and doctors and what should be the goals of health care, which is to keep patients healthy.”
Coming Tuesday, Oct. 6: Can telemedicine expose you to legal risk?
On Twitter @legal_med

S. lugdunensis osteoarticular infection often linked to orthopedic devices
SAN DIEGO – Bone and joint infections caused by Staphylococcus lugdunensis are an underestimated hospital-acquired infection often associated with orthopedic devices, according to a multicenter study.
“Consider potential relapse even after 1 year of the end of antibiotic treatment and follow patients with bone and joint infections caused by S. lugdunensis for a minimum 2 years after the end of treatment,” lead study author Dr. Piseth Seng said in an interview at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.

S. lugdunensis is a virulent coagulase-negative staphylococcus which behaves like S. aureus. Prior to the current study, only 47 cases are believed to be published in the medical literature, according to Dr. Seng of the department of internal medicine at Assistance Publique des Hôpitaux de Marseille (France). The purpose of the current study was to report a series of 138 cases of S. lugdunensis osteoarticular infection managed in nine hospital centers and three private clinics in France from January 1995 to December 2014.
The mean age of patients was 61 years, and 68% were male. Of the 138 cases, 113 (82%) were associated with an orthopedic device, including 2 cases of infection after anterior cruciate ligament reconstruction, 66 cases of prosthetic joint infection, and 3 cases of vertebral orthopedic device infection. The majority of orthopedic device infections (88%) occurred more than 1 month after implantation, while the remaining 12% occurred within the first month of implantation.
The researchers identified 30 cases (22%) of bone and joint infection that occurred in the absence of an orthopedic device, including 7 cases of arthritis, 21 cases of osteitis, and 2 cases of vertebral osteomyelitis.
The majority of patients (91%) received a combination of antibiotic and surgical treatment, including amputation (6%), orthopedic prosthesis removal (14%), internal orthopedic device removal (23%), and surgical debridement and retention of the orthopedic device (41%). The proportion of S. lugdunensis strains with reduced susceptibility to antistaphylococcal agents was low. Resistant strains included five to oxacillin, four to fosfomycin, two to fusidic acid, two to co-trimoxazole, one to rifampicin, and one to clindamycin.
To date, relapses have occurred in 19% of the 123 patients in whom researchers have complete follow-up data. The readmission rate among these patients was 76%, and four (3%) died of their infection. “These relapses were not associated with risk factor or comorbidity or polymicrobial infection,” noted Dr. Seng, who characterized the incidence of bone and joint infections caused by S. lugdunensis as being under reported. “S. lugdunensis is known as an organism forming biofilms, but treatment options (surgical debridement or prosthesis removal) did not influence clinical outcomes.”
The mean time to relapse was 305 days and no risk factor or comorbidity was associated with relapse.
Dr. Seng acknowledged that the study was limited by its retrospective design. He and his associates reported having no financial disclosures.
SAN DIEGO – Bone and joint infections caused by Staphylococcus lugdunensis are an underestimated hospital-acquired infection often associated with orthopedic devices, according to a multicenter study.
“Consider potential relapse even after 1 year of the end of antibiotic treatment and follow patients with bone and joint infections caused by S. lugdunensis for a minimum 2 years after the end of treatment,” lead study author Dr. Piseth Seng said in an interview at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
S. lugdunensis is a virulent coagulase-negative staphylococcus which behaves like S. aureus. Prior to the current study, only 47 cases are believed to be published in the medical literature, according to Dr. Seng of the department of internal medicine at Assistance Publique des Hôpitaux de Marseille (France). The purpose of the current study was to report a series of 138 cases of S. lugdunensis osteoarticular infection managed in nine hospital centers and three private clinics in France from January 1995 to December 2014.
The mean age of patients was 61 years, and 68% were male. Of the 138 cases, 113 (82%) were associated with an orthopedic device, including 2 cases of infection after anterior cruciate ligament reconstruction, 66 cases of prosthetic joint infection, and 3 cases of vertebral orthopedic device infection. The majority of orthopedic device infections (88%) occurred more than 1 month after implantation, while the remaining 12% occurred within the first month of implantation.
The researchers identified 30 cases (22%) of bone and joint infection that occurred in the absence of an orthopedic device, including 7 cases of arthritis, 21 cases of osteitis, and 2 cases of vertebral osteomyelitis.
The majority of patients (91%) received a combination of antibiotic and surgical treatment, including amputation (6%), orthopedic prosthesis removal (14%), internal orthopedic device removal (23%), and surgical debridement and retention of the orthopedic device (41%). The proportion of S. lugdunensis strains with reduced susceptibility to antistaphylococcal agents was low. Resistant strains included five to oxacillin, four to fosfomycin, two to fusidic acid, two to co-trimoxazole, one to rifampicin, and one to clindamycin.
To date, relapses have occurred in 19% of the 123 patients in whom researchers have complete follow-up data. The readmission rate among these patients was 76%, and four (3%) died of their infection. “These relapses were not associated with risk factor or comorbidity or polymicrobial infection,” noted Dr. Seng, who characterized the incidence of bone and joint infections caused by S. lugdunensis as being under reported. “S. lugdunensis is known as an organism forming biofilms, but treatment options (surgical debridement or prosthesis removal) did not influence clinical outcomes.”
The mean time to relapse was 305 days and no risk factor or comorbidity was associated with relapse.
Dr. Seng acknowledged that the study was limited by its retrospective design. He and his associates reported having no financial disclosures.
SAN DIEGO – Bone and joint infections caused by Staphylococcus lugdunensis are an underestimated hospital-acquired infection often associated with orthopedic devices, according to a multicenter study.
“Consider potential relapse even after 1 year of the end of antibiotic treatment and follow patients with bone and joint infections caused by S. lugdunensis for a minimum 2 years after the end of treatment,” lead study author Dr. Piseth Seng said in an interview at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
S. lugdunensis is a virulent coagulase-negative staphylococcus which behaves like S. aureus. Prior to the current study, only 47 cases are believed to be published in the medical literature, according to Dr. Seng of the department of internal medicine at Assistance Publique des Hôpitaux de Marseille (France). The purpose of the current study was to report a series of 138 cases of S. lugdunensis osteoarticular infection managed in nine hospital centers and three private clinics in France from January 1995 to December 2014.
The mean age of patients was 61 years, and 68% were male. Of the 138 cases, 113 (82%) were associated with an orthopedic device, including 2 cases of infection after anterior cruciate ligament reconstruction, 66 cases of prosthetic joint infection, and 3 cases of vertebral orthopedic device infection. The majority of orthopedic device infections (88%) occurred more than 1 month after implantation, while the remaining 12% occurred within the first month of implantation.
The researchers identified 30 cases (22%) of bone and joint infection that occurred in the absence of an orthopedic device, including 7 cases of arthritis, 21 cases of osteitis, and 2 cases of vertebral osteomyelitis.
The majority of patients (91%) received a combination of antibiotic and surgical treatment, including amputation (6%), orthopedic prosthesis removal (14%), internal orthopedic device removal (23%), and surgical debridement and retention of the orthopedic device (41%). The proportion of S. lugdunensis strains with reduced susceptibility to antistaphylococcal agents was low. Resistant strains included five to oxacillin, four to fosfomycin, two to fusidic acid, two to co-trimoxazole, one to rifampicin, and one to clindamycin.
To date, relapses have occurred in 19% of the 123 patients in whom researchers have complete follow-up data. The readmission rate among these patients was 76%, and four (3%) died of their infection. “These relapses were not associated with risk factor or comorbidity or polymicrobial infection,” noted Dr. Seng, who characterized the incidence of bone and joint infections caused by S. lugdunensis as being under reported. “S. lugdunensis is known as an organism forming biofilms, but treatment options (surgical debridement or prosthesis removal) did not influence clinical outcomes.”
The mean time to relapse was 305 days and no risk factor or comorbidity was associated with relapse.
Dr. Seng acknowledged that the study was limited by its retrospective design. He and his associates reported having no financial disclosures.
AT ICAAC 2015
Key clinical point: S. lugdunensis infections are often associated with orthopedic devices.
Major finding: Of 138 cases of S. lugdunensis osteoarticular infection, 113 (82%) were associated with an orthopedic device.
Data source: A retrospective study of 138 cases of S. lugdunensis osteoarticular infection managed in nine hospitals and three private clinics in France.
Disclosures: The researchers reported having no financial disclosures.

ASCO: Neoadjuvant chemo does not increase breast cancer surgery complications
SAN FRANCISCO – Breast cancer surgery within 30 days of neoadjuvant chemotherapy appears to be safe, with no significant increase in risk of postoperative complications compared with surgery performed in women who did not receive chemotherapy.
An analysis of data on more than 3,500 patients who underwent surgery for invasive breast cancer after receiving neoadjuvant chemotherapy showed that in an analysis adjusted to better balance patient characteristics, there were no significant differences in postoperative complication rates for patients who received chemotherapy and those who did not, reported Dr. Erin Cordeiro from the Ottawa Hospital in Ontario, Canada, and associates, at a breast cancer symposium sponsored jointly by the American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology.

“I really think this should put to rest the concern that surgeons might have about neoadjuvant chemotherapy particularly because this [study] compressed people within 30 days of the surgery date,” commented Dr. Charles E. Geyer, Jr., from the Virginia Commonwealth University School of Medicine in Richmond. Dr. Geyer was the invited discussant.
The use of neoadjuvant chemotherapy in the treatment of patients with breast cancer continues to increase, growing from 14% in 2006, to 20% in 2011, Dr. Cordeiro said.
But because myelosuppression, particularly neutropenia, is a common side of chemotherapy, surgeons are often concerned that operating too soon after a patient completes a course of chemotherapy could result in increased post-operative complications, she said.
To determine whether neoadjuvant chemotherapy would increase the proportion of overall 30-day postoperative complications among patients undergoing surgery for invasive breast cancer, Dr. Cordeiro drew on the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, which contains validated, risk-adjusted surgical outcomes data from more than 600 hospitals in 49 states, Canada, and Europe.

She identified data on 67,685 patients who underwent surgery for invasive breast cancer from 2005 through 2012. Of this group, 3,624 (5.5%) had received neoadjuvant chemotherapy. Investigators excludedpPatients with high-risk comorbidities and those who underwent other surgery concurrent with breast surgery (e.g., oophorectomy).
In unadjusted analysis, the rate of a composite of overall 30-day post-operative complications, the primary outcome, was 4.9% for patients who had undergone neoadjuvant chemotherapy, compared with 3.7% for patients who did not and this difference was significant (P= .0003). The higher rate among patient who had received chemotherapy recently was largely due to infections, Dr. Cordeiro said.
However, in a multivariate analysis adjusted for propensity score – a measure of the probability of receiving neoeadjuvant chemotherapy by age, diabetes, chronic obstructive pulmonary disease, hypertension, bilateral surgery, and/or year of surgery – the differences between patients who underwent neoadjuvant chemo and those who did not vanished (odds ratio 1.16; 95% confidence interval, 0.98-1.36).
Dr. Cordeiro acknowledged that the study was limited by the use of retrospective data, a lack of knowledge of exactly when chemotherapy was stopped in relation to the surgery data, lack of data on which regimens were used, and no information about prophylatic antibiotics or thromboprophylaxis.
The investigators plan to perform additional subgroup analyses to determine whether there might be differences in complication rates in patients who did or did not receive neoadjuvant chemo by type of breast surgery (breast-conserving vs. mastectomy), type of axillary surgery (sentinel node biopsy vs. axillary lymph node dissection) or among patients who undergo immediate reconstruction.
The study was presented as a poster and in an oral abstract session.
SAN FRANCISCO – Breast cancer surgery within 30 days of neoadjuvant chemotherapy appears to be safe, with no significant increase in risk of postoperative complications compared with surgery performed in women who did not receive chemotherapy.
An analysis of data on more than 3,500 patients who underwent surgery for invasive breast cancer after receiving neoadjuvant chemotherapy showed that in an analysis adjusted to better balance patient characteristics, there were no significant differences in postoperative complication rates for patients who received chemotherapy and those who did not, reported Dr. Erin Cordeiro from the Ottawa Hospital in Ontario, Canada, and associates, at a breast cancer symposium sponsored jointly by the American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology.
“I really think this should put to rest the concern that surgeons might have about neoadjuvant chemotherapy particularly because this [study] compressed people within 30 days of the surgery date,” commented Dr. Charles E. Geyer, Jr., from the Virginia Commonwealth University School of Medicine in Richmond. Dr. Geyer was the invited discussant.
The use of neoadjuvant chemotherapy in the treatment of patients with breast cancer continues to increase, growing from 14% in 2006, to 20% in 2011, Dr. Cordeiro said.
But because myelosuppression, particularly neutropenia, is a common side of chemotherapy, surgeons are often concerned that operating too soon after a patient completes a course of chemotherapy could result in increased post-operative complications, she said.
To determine whether neoadjuvant chemotherapy would increase the proportion of overall 30-day postoperative complications among patients undergoing surgery for invasive breast cancer, Dr. Cordeiro drew on the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, which contains validated, risk-adjusted surgical outcomes data from more than 600 hospitals in 49 states, Canada, and Europe.
She identified data on 67,685 patients who underwent surgery for invasive breast cancer from 2005 through 2012. Of this group, 3,624 (5.5%) had received neoadjuvant chemotherapy. Investigators excludedpPatients with high-risk comorbidities and those who underwent other surgery concurrent with breast surgery (e.g., oophorectomy).
In unadjusted analysis, the rate of a composite of overall 30-day post-operative complications, the primary outcome, was 4.9% for patients who had undergone neoadjuvant chemotherapy, compared with 3.7% for patients who did not and this difference was significant (P= .0003). The higher rate among patient who had received chemotherapy recently was largely due to infections, Dr. Cordeiro said.
However, in a multivariate analysis adjusted for propensity score – a measure of the probability of receiving neoeadjuvant chemotherapy by age, diabetes, chronic obstructive pulmonary disease, hypertension, bilateral surgery, and/or year of surgery – the differences between patients who underwent neoadjuvant chemo and those who did not vanished (odds ratio 1.16; 95% confidence interval, 0.98-1.36).
Dr. Cordeiro acknowledged that the study was limited by the use of retrospective data, a lack of knowledge of exactly when chemotherapy was stopped in relation to the surgery data, lack of data on which regimens were used, and no information about prophylatic antibiotics or thromboprophylaxis.
The investigators plan to perform additional subgroup analyses to determine whether there might be differences in complication rates in patients who did or did not receive neoadjuvant chemo by type of breast surgery (breast-conserving vs. mastectomy), type of axillary surgery (sentinel node biopsy vs. axillary lymph node dissection) or among patients who undergo immediate reconstruction.
The study was presented as a poster and in an oral abstract session.
SAN FRANCISCO – Breast cancer surgery within 30 days of neoadjuvant chemotherapy appears to be safe, with no significant increase in risk of postoperative complications compared with surgery performed in women who did not receive chemotherapy.
An analysis of data on more than 3,500 patients who underwent surgery for invasive breast cancer after receiving neoadjuvant chemotherapy showed that in an analysis adjusted to better balance patient characteristics, there were no significant differences in postoperative complication rates for patients who received chemotherapy and those who did not, reported Dr. Erin Cordeiro from the Ottawa Hospital in Ontario, Canada, and associates, at a breast cancer symposium sponsored jointly by the American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology.
“I really think this should put to rest the concern that surgeons might have about neoadjuvant chemotherapy particularly because this [study] compressed people within 30 days of the surgery date,” commented Dr. Charles E. Geyer, Jr., from the Virginia Commonwealth University School of Medicine in Richmond. Dr. Geyer was the invited discussant.
The use of neoadjuvant chemotherapy in the treatment of patients with breast cancer continues to increase, growing from 14% in 2006, to 20% in 2011, Dr. Cordeiro said.
But because myelosuppression, particularly neutropenia, is a common side of chemotherapy, surgeons are often concerned that operating too soon after a patient completes a course of chemotherapy could result in increased post-operative complications, she said.
To determine whether neoadjuvant chemotherapy would increase the proportion of overall 30-day postoperative complications among patients undergoing surgery for invasive breast cancer, Dr. Cordeiro drew on the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, which contains validated, risk-adjusted surgical outcomes data from more than 600 hospitals in 49 states, Canada, and Europe.
She identified data on 67,685 patients who underwent surgery for invasive breast cancer from 2005 through 2012. Of this group, 3,624 (5.5%) had received neoadjuvant chemotherapy. Investigators excludedpPatients with high-risk comorbidities and those who underwent other surgery concurrent with breast surgery (e.g., oophorectomy).
In unadjusted analysis, the rate of a composite of overall 30-day post-operative complications, the primary outcome, was 4.9% for patients who had undergone neoadjuvant chemotherapy, compared with 3.7% for patients who did not and this difference was significant (P= .0003). The higher rate among patient who had received chemotherapy recently was largely due to infections, Dr. Cordeiro said.
However, in a multivariate analysis adjusted for propensity score – a measure of the probability of receiving neoeadjuvant chemotherapy by age, diabetes, chronic obstructive pulmonary disease, hypertension, bilateral surgery, and/or year of surgery – the differences between patients who underwent neoadjuvant chemo and those who did not vanished (odds ratio 1.16; 95% confidence interval, 0.98-1.36).
Dr. Cordeiro acknowledged that the study was limited by the use of retrospective data, a lack of knowledge of exactly when chemotherapy was stopped in relation to the surgery data, lack of data on which regimens were used, and no information about prophylatic antibiotics or thromboprophylaxis.
The investigators plan to perform additional subgroup analyses to determine whether there might be differences in complication rates in patients who did or did not receive neoadjuvant chemo by type of breast surgery (breast-conserving vs. mastectomy), type of axillary surgery (sentinel node biopsy vs. axillary lymph node dissection) or among patients who undergo immediate reconstruction.
The study was presented as a poster and in an oral abstract session.
AT THE ASCO BREAST CANCER SYMPOSIUM
Key clinical point: Neoadjuvant chemotherapy does not appear to increase the risk for 30-day post-operative complications following surgery for invasive breast cancer.
Major finding: The odds ratio for postoperative complications among patients who underwent chemotherapy was 1.16 but was not statistically significant.
Data source: Retrospective review from a prospective surgical outcomes database on 67,685 patients, 3,624 of whom had neoadjuvant chemotherapy.
Disclosures: Funding for the study was not disclosed. Dr. Cordeiro reported having no conflicts of interest. Dr. Geyer reported a consulting or advisory role with Stennion, research funding from Incyte, and travel expenses from Abbvie, AstraZeneca, and Genetech/Roche.

ICD-10: Feds tout resources available for Oct. 1 switch
Officials from the Centers for Medicare & Medicaid Services sought to assure physicians that the agency is on track for a smooth transition to ICD-10 on Oct. 1.
“We have proven that our claims processing center will be able to accept claims without any problems, and [the claims] will be paid,” Dr. William Rogers, ICD-10 ombudsman at CMS, said in a press conference Sept. 24.

Dr. Patrick H. Conway, CMS principal deputy administrator, added that real-time monitoring of the switch will take place so that the agency can “investigate and address issues as they come in through the ICD-10 coordination center.”
Dr. Rogers and Dr. Conway outlined a number of resources available to assist with the transition:
• General information is available is available at the Road to ICD-10 and www.cms.gov/ICD10.
• Should a problem or concern arise, turn first to your billing vendor or clearinghouse.
• Next, reach out to your Medicare administrative contractor (MAC).
• Questions and concerns can be emailed to the ICD-10 Coordination Center at icd10@cms.hhs.gov.
• If there are still issues, email the ICD-10 ombudsman’s office at icd10_ombudsbman@cms.hhs.gov.Both Dr. Rogers and Dr. Conway downplayed concerns about whether stalled congressional budget negotiations, potentially leading to a government shutdown, would have any impact on the ICD-10 transition. They emphasized that patients will receive the same services on Oct. 1, when ICD-10 officially kicks off, as they did the day before.
Data on claims processing under ICD-10 will be available after one full billing cycle is complete, which should be about 30 days, Dr. Conway said.
On Twitter @whitneymcknight
Officials from the Centers for Medicare & Medicaid Services sought to assure physicians that the agency is on track for a smooth transition to ICD-10 on Oct. 1.
“We have proven that our claims processing center will be able to accept claims without any problems, and [the claims] will be paid,” Dr. William Rogers, ICD-10 ombudsman at CMS, said in a press conference Sept. 24.
Dr. Patrick H. Conway, CMS principal deputy administrator, added that real-time monitoring of the switch will take place so that the agency can “investigate and address issues as they come in through the ICD-10 coordination center.”
Dr. Rogers and Dr. Conway outlined a number of resources available to assist with the transition:
• General information is available is available at the Road to ICD-10 and www.cms.gov/ICD10.
• Should a problem or concern arise, turn first to your billing vendor or clearinghouse.
• Next, reach out to your Medicare administrative contractor (MAC).
• Questions and concerns can be emailed to the ICD-10 Coordination Center at icd10@cms.hhs.gov.
• If there are still issues, email the ICD-10 ombudsman’s office at icd10_ombudsbman@cms.hhs.gov.Both Dr. Rogers and Dr. Conway downplayed concerns about whether stalled congressional budget negotiations, potentially leading to a government shutdown, would have any impact on the ICD-10 transition. They emphasized that patients will receive the same services on Oct. 1, when ICD-10 officially kicks off, as they did the day before.
Data on claims processing under ICD-10 will be available after one full billing cycle is complete, which should be about 30 days, Dr. Conway said.
On Twitter @whitneymcknight
Officials from the Centers for Medicare & Medicaid Services sought to assure physicians that the agency is on track for a smooth transition to ICD-10 on Oct. 1.
“We have proven that our claims processing center will be able to accept claims without any problems, and [the claims] will be paid,” Dr. William Rogers, ICD-10 ombudsman at CMS, said in a press conference Sept. 24.
Dr. Patrick H. Conway, CMS principal deputy administrator, added that real-time monitoring of the switch will take place so that the agency can “investigate and address issues as they come in through the ICD-10 coordination center.”
Dr. Rogers and Dr. Conway outlined a number of resources available to assist with the transition:
• General information is available is available at the Road to ICD-10 and www.cms.gov/ICD10.
• Should a problem or concern arise, turn first to your billing vendor or clearinghouse.
• Next, reach out to your Medicare administrative contractor (MAC).
• Questions and concerns can be emailed to the ICD-10 Coordination Center at icd10@cms.hhs.gov.
• If there are still issues, email the ICD-10 ombudsman’s office at icd10_ombudsbman@cms.hhs.gov.Both Dr. Rogers and Dr. Conway downplayed concerns about whether stalled congressional budget negotiations, potentially leading to a government shutdown, would have any impact on the ICD-10 transition. They emphasized that patients will receive the same services on Oct. 1, when ICD-10 officially kicks off, as they did the day before.
Data on claims processing under ICD-10 will be available after one full billing cycle is complete, which should be about 30 days, Dr. Conway said.
On Twitter @whitneymcknight

Readmissions for C. difficile infections high among elderly
LAS VEGAS – More than one in 10 patients with Clostridium difficile infection at the time of hospital discharge are readmitted for C. difficile infection within 90 days, according to findings from a review of Medicare data from 2009 to 2011.
Of a random sample of nearly 900,000 Part A inpatients and Part D prescription drug claimants during the study period, about 8,500 were hospitalized with a primary or secondary diagnosis of C. difficile infection, and of 7,042 of those who were discharged alive and who were eligible for the study, 945 (13.4%) were readmitted within 90 days, Dr. Charles M. Psoinos reported at the annual meeting of the American Association for the Surgery of Trauma.
Compared with 1,900 patients not readmitted for any reason, those who were readmitted had more baseline comorbidities (average Elixhauser index, 5.9 vs. 4.7), and a significantly shorter length of stay during the index hospitalization (9.2 vs. 11.8 days), and those older than 95 years were twice as likely as those aged 65-70 years to be readmitted, as were those with an emergent vs. nonemergent index hospitalization, said Dr. Psoinos of the University of Massachusetts, Worcester.
Further, the readmission rate was lower in the 39% of patients discharged on oral metronidazole (19%), and in the 12% discharged on oral vancomycin (28%), than among the 38% discharged with no ongoing treatment (48%), while those discharged on both oral metronidazole and vancomycin were at increased risk for readmission (odds ratio, 1.29), he said.
The 90-day all cause mortality rate was nearly doubled in those who were readmitted, compared with those who were not (17.8% vs. 8.9%; OR, 1.77), he said.
Patients who were and were not readmitted did not differ significantly with respect to age (mean of about 80 years) and race distribution, and the outcomes were adjusted for the differences in baseline comorbidities and other confounding factors.
The findings could have important implications for reducing readmissions among Medicare beneficiaries, Dr. Psoinos said.
The incidence of C. difficile infections has increased nearly eightfold in the elderly population over the last several decades, and the elderly now account for more than 70% of hospitalized patients with such infections. Recurrence rates range from 5% to 31% after cessation of therapy, and readmission rates are similar, he explained, noting that treatment recommendations for C. difficile infections are commonly based on symptoms and their severity, with oral metronidazole recommended for mild and moderate disease, vancomycin only for severe disease, and dual therapy for complicated severe disease.
Though limited by the retrospective design of the study, the findings suggest that C. difficile patients discharged from the hospital may benefit from ongoing monotherapy treatment to reduce subclinical infections and induce long-term eradication, and that elderly patients on dual therapy may benefit from continued hospitalization until they are appropriate for discharge on monotherapy.
These strategies could reduce the rate of readmissions, Dr. Psoinos concluded.
Dr. Psoinos reported having no relevant financial conflicts.
LAS VEGAS – More than one in 10 patients with Clostridium difficile infection at the time of hospital discharge are readmitted for C. difficile infection within 90 days, according to findings from a review of Medicare data from 2009 to 2011.
Of a random sample of nearly 900,000 Part A inpatients and Part D prescription drug claimants during the study period, about 8,500 were hospitalized with a primary or secondary diagnosis of C. difficile infection, and of 7,042 of those who were discharged alive and who were eligible for the study, 945 (13.4%) were readmitted within 90 days, Dr. Charles M. Psoinos reported at the annual meeting of the American Association for the Surgery of Trauma.
Compared with 1,900 patients not readmitted for any reason, those who were readmitted had more baseline comorbidities (average Elixhauser index, 5.9 vs. 4.7), and a significantly shorter length of stay during the index hospitalization (9.2 vs. 11.8 days), and those older than 95 years were twice as likely as those aged 65-70 years to be readmitted, as were those with an emergent vs. nonemergent index hospitalization, said Dr. Psoinos of the University of Massachusetts, Worcester.
Further, the readmission rate was lower in the 39% of patients discharged on oral metronidazole (19%), and in the 12% discharged on oral vancomycin (28%), than among the 38% discharged with no ongoing treatment (48%), while those discharged on both oral metronidazole and vancomycin were at increased risk for readmission (odds ratio, 1.29), he said.
The 90-day all cause mortality rate was nearly doubled in those who were readmitted, compared with those who were not (17.8% vs. 8.9%; OR, 1.77), he said.
Patients who were and were not readmitted did not differ significantly with respect to age (mean of about 80 years) and race distribution, and the outcomes were adjusted for the differences in baseline comorbidities and other confounding factors.
The findings could have important implications for reducing readmissions among Medicare beneficiaries, Dr. Psoinos said.
The incidence of C. difficile infections has increased nearly eightfold in the elderly population over the last several decades, and the elderly now account for more than 70% of hospitalized patients with such infections. Recurrence rates range from 5% to 31% after cessation of therapy, and readmission rates are similar, he explained, noting that treatment recommendations for C. difficile infections are commonly based on symptoms and their severity, with oral metronidazole recommended for mild and moderate disease, vancomycin only for severe disease, and dual therapy for complicated severe disease.
Though limited by the retrospective design of the study, the findings suggest that C. difficile patients discharged from the hospital may benefit from ongoing monotherapy treatment to reduce subclinical infections and induce long-term eradication, and that elderly patients on dual therapy may benefit from continued hospitalization until they are appropriate for discharge on monotherapy.
These strategies could reduce the rate of readmissions, Dr. Psoinos concluded.
Dr. Psoinos reported having no relevant financial conflicts.
LAS VEGAS – More than one in 10 patients with Clostridium difficile infection at the time of hospital discharge are readmitted for C. difficile infection within 90 days, according to findings from a review of Medicare data from 2009 to 2011.
Of a random sample of nearly 900,000 Part A inpatients and Part D prescription drug claimants during the study period, about 8,500 were hospitalized with a primary or secondary diagnosis of C. difficile infection, and of 7,042 of those who were discharged alive and who were eligible for the study, 945 (13.4%) were readmitted within 90 days, Dr. Charles M. Psoinos reported at the annual meeting of the American Association for the Surgery of Trauma.
Compared with 1,900 patients not readmitted for any reason, those who were readmitted had more baseline comorbidities (average Elixhauser index, 5.9 vs. 4.7), and a significantly shorter length of stay during the index hospitalization (9.2 vs. 11.8 days), and those older than 95 years were twice as likely as those aged 65-70 years to be readmitted, as were those with an emergent vs. nonemergent index hospitalization, said Dr. Psoinos of the University of Massachusetts, Worcester.
Further, the readmission rate was lower in the 39% of patients discharged on oral metronidazole (19%), and in the 12% discharged on oral vancomycin (28%), than among the 38% discharged with no ongoing treatment (48%), while those discharged on both oral metronidazole and vancomycin were at increased risk for readmission (odds ratio, 1.29), he said.
The 90-day all cause mortality rate was nearly doubled in those who were readmitted, compared with those who were not (17.8% vs. 8.9%; OR, 1.77), he said.
Patients who were and were not readmitted did not differ significantly with respect to age (mean of about 80 years) and race distribution, and the outcomes were adjusted for the differences in baseline comorbidities and other confounding factors.
The findings could have important implications for reducing readmissions among Medicare beneficiaries, Dr. Psoinos said.
The incidence of C. difficile infections has increased nearly eightfold in the elderly population over the last several decades, and the elderly now account for more than 70% of hospitalized patients with such infections. Recurrence rates range from 5% to 31% after cessation of therapy, and readmission rates are similar, he explained, noting that treatment recommendations for C. difficile infections are commonly based on symptoms and their severity, with oral metronidazole recommended for mild and moderate disease, vancomycin only for severe disease, and dual therapy for complicated severe disease.
Though limited by the retrospective design of the study, the findings suggest that C. difficile patients discharged from the hospital may benefit from ongoing monotherapy treatment to reduce subclinical infections and induce long-term eradication, and that elderly patients on dual therapy may benefit from continued hospitalization until they are appropriate for discharge on monotherapy.
These strategies could reduce the rate of readmissions, Dr. Psoinos concluded.
Dr. Psoinos reported having no relevant financial conflicts.
AT THE AAST ANNUAL MEETING
Key clinical point: More than 1 in 10 patients with Clostridium difficile infection at the time of hospital discharge are readmitted for C. difficile infection within 90 days, according to findings from a review of Medicare data from 2009 to 2011.
Major finding: Of 7,042 discharged patients, 945 (13.4%) were readmitted within 90 days.
Data source: A retrospective cohort study of about 900,000 Medicare beneficiaries.
Disclosures: Dr. Psoinos reported having no relevant financial disclosures.