User login
Official Newspaper of the American College of Surgeons
VIDEO: Immediate breast reconstruction results reassuring in select patients
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
AT THE ACS ANNUAL CONGRESS

Power morcellation risks increase with age
Laparoscopic hysterectomy provides better overall outcomes than either laparoscopic hysterectomy with power morcellation or total abdominal hysterectomy in women with presumed benign gynecologic disease, according to a cohort simulation model.
However, age-related differences in outcomes were apparent in the modeled scenarios, suggesting a need for individualized decision making regarding surgical technique, Dr. Jason D. Wright of Columbia University, New York, and his colleagues reported.
The investigators compared outcomes with the three approaches in a hypothetical cohort of women aged 18-65 years without a preoperative diagnosis of cancer, and found that in women with an underlying malignancy, laparoscopic hysterectomy without power morcellation was the “least costly and most effective modality of hysterectomy” across all scenarios modeled.
When comparing laparoscopic hysterectomy with power morcellation to abdominal hysterectomy, they found that the use of morcellation was associated with 80.83 more intraoperative complications, 199.64 fewer perioperative complications, and 241.80 fewer readmissions per 10,000 women (J Natl Cancer Inst. 2015;109[11]:djv251 doi: 10.1093/jnci/djv251).
Among women younger than age 40 years, laparoscopic hysterectomy with morcellation was associated with 1.57 more cases of disseminated cancer and 0.94 more cancer-associated deaths, but there were 0.97 fewer overall deaths per 10,000 women, compared with abdominal hysterectomy.
The excess cases of disseminated cancer for women who underwent laparoscopy with morcellation increased with age, to 3.75, 12.97, and 47.54 per 10,000 women in those aged 40-49 years, 50-59 years, and 60 years and older, respectively. This translated into excess deaths in all age groups (0.30, 5.07, and 18.14 per 10,000 in those aged 40-49 years, 50-59 years, and 60 years and older, respectively).
Laparoscopic hysterectomy without morcellation was also the least costly approach in all age groups. When compared with abdominal hysterectomy, laparoscopic hysterectomy with morcellation increased life-years among women under age 40 (adding 4.49 years), but decreased life-years in older women (–0.47, –20.64, and –91.19 years per 10,000 women aged 49-50, 50-59, and 60 and older, respectively). But laparoscopic hysterectomy with morcellation became more favorable for those aged 40-49, compared with abdominal hysterectomy, when quality of life was taken into account, with an increase of 11.22 quality-adjusted life-years for that age group.
Although power morcellation, compared with abdominal hysterectomy, was associated with greater quality-adjusted life-years and overall life-years in younger women, the magnitude of benefit was relatively small. And in older women, the risk of electric power morcellation greatly outweighed the benefits, the investigators wrote.
The findings underscore the importance of avoiding unnecessary use of power morcellation, as well as working to detect occult malignancy prior to interventions, they wrote.
The findings are also in accord with a 2014 advisory statement from the Food and Drug Administration warning against the use of electric power morcellators in peri- and postmenopausal women, and demonstrate a need for individualizing surgical technique in all patients and informing patients of the risks of electric power morcellation, the investigators said.
“As women age, the risk of underlying occult malignancy rises, increasing the risks associated with electric power morcellation,” the investigators wrote. “For many women, this risk will outweigh the benefits of minimally invasive surgery, and the procedure should be used with caution.”
The investigators reported having no relevant financial disclosures.
In the wake of reports of dissemination of unrecognized malignancies in patients undergoing laparoscopic hysterectomy with power morcellation of the uterus, the technique has been “virtually discontinued,” despite a lack of analysis of its benefits and potential harms, according to Dr. David G. Mutch.
The work of Wright et al. is a step in the right direction as it begins to assess the real risks of dissemination of malignancy and to determine the benefits and risks to women who might choose to undergo laparoscopy, he wrote in an editorial.
The findings help to more specifically categorize the risk to patients by considering both the risks of dissemination of malignancy and those associated with abdominal hysterectomy.
“More data such as those produced here are needed to better define the real risk so that women give informed consent before undergoing a procedure. Additionally, as other techniques such as morcellation of the uterus in a containment bag become more common, we should obtain data on their safety and efficacy,” he wrote.
Dr. Mutch is with Washington University, St. Louis. He made these remarks in an accompanying editorial (J Natl Cancer Instit. 2005;107[11]:djv283 doi: 10.1093/jnci/djv283).
In the wake of reports of dissemination of unrecognized malignancies in patients undergoing laparoscopic hysterectomy with power morcellation of the uterus, the technique has been “virtually discontinued,” despite a lack of analysis of its benefits and potential harms, according to Dr. David G. Mutch.
The work of Wright et al. is a step in the right direction as it begins to assess the real risks of dissemination of malignancy and to determine the benefits and risks to women who might choose to undergo laparoscopy, he wrote in an editorial.
The findings help to more specifically categorize the risk to patients by considering both the risks of dissemination of malignancy and those associated with abdominal hysterectomy.
“More data such as those produced here are needed to better define the real risk so that women give informed consent before undergoing a procedure. Additionally, as other techniques such as morcellation of the uterus in a containment bag become more common, we should obtain data on their safety and efficacy,” he wrote.
Dr. Mutch is with Washington University, St. Louis. He made these remarks in an accompanying editorial (J Natl Cancer Instit. 2005;107[11]:djv283 doi: 10.1093/jnci/djv283).
In the wake of reports of dissemination of unrecognized malignancies in patients undergoing laparoscopic hysterectomy with power morcellation of the uterus, the technique has been “virtually discontinued,” despite a lack of analysis of its benefits and potential harms, according to Dr. David G. Mutch.
The work of Wright et al. is a step in the right direction as it begins to assess the real risks of dissemination of malignancy and to determine the benefits and risks to women who might choose to undergo laparoscopy, he wrote in an editorial.
The findings help to more specifically categorize the risk to patients by considering both the risks of dissemination of malignancy and those associated with abdominal hysterectomy.
“More data such as those produced here are needed to better define the real risk so that women give informed consent before undergoing a procedure. Additionally, as other techniques such as morcellation of the uterus in a containment bag become more common, we should obtain data on their safety and efficacy,” he wrote.
Dr. Mutch is with Washington University, St. Louis. He made these remarks in an accompanying editorial (J Natl Cancer Instit. 2005;107[11]:djv283 doi: 10.1093/jnci/djv283).
Laparoscopic hysterectomy provides better overall outcomes than either laparoscopic hysterectomy with power morcellation or total abdominal hysterectomy in women with presumed benign gynecologic disease, according to a cohort simulation model.
However, age-related differences in outcomes were apparent in the modeled scenarios, suggesting a need for individualized decision making regarding surgical technique, Dr. Jason D. Wright of Columbia University, New York, and his colleagues reported.
The investigators compared outcomes with the three approaches in a hypothetical cohort of women aged 18-65 years without a preoperative diagnosis of cancer, and found that in women with an underlying malignancy, laparoscopic hysterectomy without power morcellation was the “least costly and most effective modality of hysterectomy” across all scenarios modeled.
When comparing laparoscopic hysterectomy with power morcellation to abdominal hysterectomy, they found that the use of morcellation was associated with 80.83 more intraoperative complications, 199.64 fewer perioperative complications, and 241.80 fewer readmissions per 10,000 women (J Natl Cancer Inst. 2015;109[11]:djv251 doi: 10.1093/jnci/djv251).
Among women younger than age 40 years, laparoscopic hysterectomy with morcellation was associated with 1.57 more cases of disseminated cancer and 0.94 more cancer-associated deaths, but there were 0.97 fewer overall deaths per 10,000 women, compared with abdominal hysterectomy.
The excess cases of disseminated cancer for women who underwent laparoscopy with morcellation increased with age, to 3.75, 12.97, and 47.54 per 10,000 women in those aged 40-49 years, 50-59 years, and 60 years and older, respectively. This translated into excess deaths in all age groups (0.30, 5.07, and 18.14 per 10,000 in those aged 40-49 years, 50-59 years, and 60 years and older, respectively).
Laparoscopic hysterectomy without morcellation was also the least costly approach in all age groups. When compared with abdominal hysterectomy, laparoscopic hysterectomy with morcellation increased life-years among women under age 40 (adding 4.49 years), but decreased life-years in older women (–0.47, –20.64, and –91.19 years per 10,000 women aged 49-50, 50-59, and 60 and older, respectively). But laparoscopic hysterectomy with morcellation became more favorable for those aged 40-49, compared with abdominal hysterectomy, when quality of life was taken into account, with an increase of 11.22 quality-adjusted life-years for that age group.
Although power morcellation, compared with abdominal hysterectomy, was associated with greater quality-adjusted life-years and overall life-years in younger women, the magnitude of benefit was relatively small. And in older women, the risk of electric power morcellation greatly outweighed the benefits, the investigators wrote.
The findings underscore the importance of avoiding unnecessary use of power morcellation, as well as working to detect occult malignancy prior to interventions, they wrote.
The findings are also in accord with a 2014 advisory statement from the Food and Drug Administration warning against the use of electric power morcellators in peri- and postmenopausal women, and demonstrate a need for individualizing surgical technique in all patients and informing patients of the risks of electric power morcellation, the investigators said.
“As women age, the risk of underlying occult malignancy rises, increasing the risks associated with electric power morcellation,” the investigators wrote. “For many women, this risk will outweigh the benefits of minimally invasive surgery, and the procedure should be used with caution.”
The investigators reported having no relevant financial disclosures.
Laparoscopic hysterectomy provides better overall outcomes than either laparoscopic hysterectomy with power morcellation or total abdominal hysterectomy in women with presumed benign gynecologic disease, according to a cohort simulation model.
However, age-related differences in outcomes were apparent in the modeled scenarios, suggesting a need for individualized decision making regarding surgical technique, Dr. Jason D. Wright of Columbia University, New York, and his colleagues reported.
The investigators compared outcomes with the three approaches in a hypothetical cohort of women aged 18-65 years without a preoperative diagnosis of cancer, and found that in women with an underlying malignancy, laparoscopic hysterectomy without power morcellation was the “least costly and most effective modality of hysterectomy” across all scenarios modeled.
When comparing laparoscopic hysterectomy with power morcellation to abdominal hysterectomy, they found that the use of morcellation was associated with 80.83 more intraoperative complications, 199.64 fewer perioperative complications, and 241.80 fewer readmissions per 10,000 women (J Natl Cancer Inst. 2015;109[11]:djv251 doi: 10.1093/jnci/djv251).
Among women younger than age 40 years, laparoscopic hysterectomy with morcellation was associated with 1.57 more cases of disseminated cancer and 0.94 more cancer-associated deaths, but there were 0.97 fewer overall deaths per 10,000 women, compared with abdominal hysterectomy.
The excess cases of disseminated cancer for women who underwent laparoscopy with morcellation increased with age, to 3.75, 12.97, and 47.54 per 10,000 women in those aged 40-49 years, 50-59 years, and 60 years and older, respectively. This translated into excess deaths in all age groups (0.30, 5.07, and 18.14 per 10,000 in those aged 40-49 years, 50-59 years, and 60 years and older, respectively).
Laparoscopic hysterectomy without morcellation was also the least costly approach in all age groups. When compared with abdominal hysterectomy, laparoscopic hysterectomy with morcellation increased life-years among women under age 40 (adding 4.49 years), but decreased life-years in older women (–0.47, –20.64, and –91.19 years per 10,000 women aged 49-50, 50-59, and 60 and older, respectively). But laparoscopic hysterectomy with morcellation became more favorable for those aged 40-49, compared with abdominal hysterectomy, when quality of life was taken into account, with an increase of 11.22 quality-adjusted life-years for that age group.
Although power morcellation, compared with abdominal hysterectomy, was associated with greater quality-adjusted life-years and overall life-years in younger women, the magnitude of benefit was relatively small. And in older women, the risk of electric power morcellation greatly outweighed the benefits, the investigators wrote.
The findings underscore the importance of avoiding unnecessary use of power morcellation, as well as working to detect occult malignancy prior to interventions, they wrote.
The findings are also in accord with a 2014 advisory statement from the Food and Drug Administration warning against the use of electric power morcellators in peri- and postmenopausal women, and demonstrate a need for individualizing surgical technique in all patients and informing patients of the risks of electric power morcellation, the investigators said.
“As women age, the risk of underlying occult malignancy rises, increasing the risks associated with electric power morcellation,” the investigators wrote. “For many women, this risk will outweigh the benefits of minimally invasive surgery, and the procedure should be used with caution.”
The investigators reported having no relevant financial disclosures.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Key clinical point: Laparoscopic hysterectomy without power morcellation was the most effective and least costly method of hysterectomy in women with presumed benign gynecologic disease.
Major finding: The excess deaths associated with laparoscopic hysterectomy with morcellation were 0.30, 5.07, and 18.14 per 10,000 in those aged 40-49 years, 50-59 years, and 60 years and older, respectively, compared with 0.97 fewer deaths in those younger than age 40 years.
Data source: A cohort simulation model involving women aged 18-65 years.
Disclosures: The investigators reported having no relevant financial disclosures.
Small study: Physicians sued for failing to supervise soft-tissue filler procedures
In medical malpractice claims involving soft-tissue fillers, dermatologists and other doctors were frequently named as defendants for allegedly failing to supervise nonphysicians who did the procedures, in a study published in the October issue of the Journal of the American Academy of Dermatology.
In a study of 24 legal and administrative actions, physicians were sued in 13 of the cases, although physician extenders injected the fillers in half of those actions. The results were reported in a research letter (J Am Acad Dermatol. 2015 Oct;73[4]:702-4).

Dr. Navid Ezra, a private practice dermatologist and former resident at Indiana University, Indianapolis, and colleagues analyzed public legal documents from 1995 to 2013 using the national legal research service WestlawNext. They searched three database categories: cases, trial court orders, and administrative guidance and decisions. The categories included opinions by state and federal trial, appellate, and supreme courts, as well as regulatory agencies such as medical boards. A total of 24 legal documents involving soft-tissue fillers were identified – 19 legal cases and 5 disciplinary actions.
Dermatologists and plastic surgeons were sued most often, each accounting for 17% of cases respectively, according to the study. Family practice physicians were named as defendants in 8% of cases. Radiologists, pediatricians, internists, oculoplastic surgeons, and physical medicine/rehabilitation doctors were each named as defendants in 4% of the cases, respectively. Nonphysicians were sued in 25% of cases. Many of the lawsuits named multiple defendants.
The most common injury that resulted in litigation was granuloma formation or other autoimmune reaction. Zyderm was the soft-tissue filler most commonly associated with litigation. However, the authors noted that Zyderm was the first soft-tissue filler approved and temporal bias likely explains the higher number of associated cases.
Of the five disciplinary actions, the majority of doctors were reprimanded for not being present while a nonphysician employee injected patients with soft-tissue fillers. In three of the five reprimands, physicians were functioning as medical directors of medical spas.
The authors concluded that the medico-legal culture is such that physicians are responsible for actions by their physician extenders. They called for further research to evaluate whether the presence of a physician during soft-tissue filler procedures affects the rate of developing complications. They noted that the study’s total number of cases and disciplinary actions underreports the true incidence of legal events related to soft-tissue fillers. The sample size did not include settlements or cases that did not involve an appeal.
On Twitter @legal_med
In medical malpractice claims involving soft-tissue fillers, dermatologists and other doctors were frequently named as defendants for allegedly failing to supervise nonphysicians who did the procedures, in a study published in the October issue of the Journal of the American Academy of Dermatology.
In a study of 24 legal and administrative actions, physicians were sued in 13 of the cases, although physician extenders injected the fillers in half of those actions. The results were reported in a research letter (J Am Acad Dermatol. 2015 Oct;73[4]:702-4).
Dr. Navid Ezra, a private practice dermatologist and former resident at Indiana University, Indianapolis, and colleagues analyzed public legal documents from 1995 to 2013 using the national legal research service WestlawNext. They searched three database categories: cases, trial court orders, and administrative guidance and decisions. The categories included opinions by state and federal trial, appellate, and supreme courts, as well as regulatory agencies such as medical boards. A total of 24 legal documents involving soft-tissue fillers were identified – 19 legal cases and 5 disciplinary actions.
Dermatologists and plastic surgeons were sued most often, each accounting for 17% of cases respectively, according to the study. Family practice physicians were named as defendants in 8% of cases. Radiologists, pediatricians, internists, oculoplastic surgeons, and physical medicine/rehabilitation doctors were each named as defendants in 4% of the cases, respectively. Nonphysicians were sued in 25% of cases. Many of the lawsuits named multiple defendants.
The most common injury that resulted in litigation was granuloma formation or other autoimmune reaction. Zyderm was the soft-tissue filler most commonly associated with litigation. However, the authors noted that Zyderm was the first soft-tissue filler approved and temporal bias likely explains the higher number of associated cases.
Of the five disciplinary actions, the majority of doctors were reprimanded for not being present while a nonphysician employee injected patients with soft-tissue fillers. In three of the five reprimands, physicians were functioning as medical directors of medical spas.
The authors concluded that the medico-legal culture is such that physicians are responsible for actions by their physician extenders. They called for further research to evaluate whether the presence of a physician during soft-tissue filler procedures affects the rate of developing complications. They noted that the study’s total number of cases and disciplinary actions underreports the true incidence of legal events related to soft-tissue fillers. The sample size did not include settlements or cases that did not involve an appeal.
On Twitter @legal_med
In medical malpractice claims involving soft-tissue fillers, dermatologists and other doctors were frequently named as defendants for allegedly failing to supervise nonphysicians who did the procedures, in a study published in the October issue of the Journal of the American Academy of Dermatology.
In a study of 24 legal and administrative actions, physicians were sued in 13 of the cases, although physician extenders injected the fillers in half of those actions. The results were reported in a research letter (J Am Acad Dermatol. 2015 Oct;73[4]:702-4).
Dr. Navid Ezra, a private practice dermatologist and former resident at Indiana University, Indianapolis, and colleagues analyzed public legal documents from 1995 to 2013 using the national legal research service WestlawNext. They searched three database categories: cases, trial court orders, and administrative guidance and decisions. The categories included opinions by state and federal trial, appellate, and supreme courts, as well as regulatory agencies such as medical boards. A total of 24 legal documents involving soft-tissue fillers were identified – 19 legal cases and 5 disciplinary actions.
Dermatologists and plastic surgeons were sued most often, each accounting for 17% of cases respectively, according to the study. Family practice physicians were named as defendants in 8% of cases. Radiologists, pediatricians, internists, oculoplastic surgeons, and physical medicine/rehabilitation doctors were each named as defendants in 4% of the cases, respectively. Nonphysicians were sued in 25% of cases. Many of the lawsuits named multiple defendants.
The most common injury that resulted in litigation was granuloma formation or other autoimmune reaction. Zyderm was the soft-tissue filler most commonly associated with litigation. However, the authors noted that Zyderm was the first soft-tissue filler approved and temporal bias likely explains the higher number of associated cases.
Of the five disciplinary actions, the majority of doctors were reprimanded for not being present while a nonphysician employee injected patients with soft-tissue fillers. In three of the five reprimands, physicians were functioning as medical directors of medical spas.
The authors concluded that the medico-legal culture is such that physicians are responsible for actions by their physician extenders. They called for further research to evaluate whether the presence of a physician during soft-tissue filler procedures affects the rate of developing complications. They noted that the study’s total number of cases and disciplinary actions underreports the true incidence of legal events related to soft-tissue fillers. The sample size did not include settlements or cases that did not involve an appeal.
On Twitter @legal_med
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: A study shows that some medical malpractice claims involving soft-tissue fillers result from procedures performed by nonphysicians, but dermatologists and plastic surgeons are frequently named as defendants for allegedly failing to supervise.
Major finding: In a study of 24 legal and administrative actions, physicians were sued in 13 of the cases, although physician extenders injected the fillers in half of those actions.
Data source: The cases were identified in a search for relevant public legal documents in a national legal database from 1995 to 2013.
Disclosures: The authors had no relevant disclosures; and there was no funding source.

CMS delays Stage 3 meaningful use until 2018, simplifies program
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.

The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.

“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”

She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.
The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.
“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”
She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.
The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.
“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”
She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.

AUDIO: Meaningful use interoperability ‘won’t work without the Internet’
WASHINGTON – The rules for Stage 3 of the meaningful use program have been finalized by the Obama administration, despite questions about physicians’ ability to achieve “interoperability” and pleas from politicians and providers alike to delay its implementation.
Jonathan Bush, cofounder and CEO of athenahealth, said he believes interoperability will be a no-go unless data are seen as common property, and a premium is placed on the seamless transition of medical records by way of the Internet, not faxes.
Speaking about the large sums of money being spent by hospitals to comply with the government’s meaningful use requirements, Mr. Bush said, “they’re going to staff up hundreds of people who aren’t going to be able to run it. It doesn’t connect to anyone.”
In an interview at the annual Washington Ideas Forum sponsored by the Aspen Institute and The Atlantic, Mr. Bush offered his thoughts on how data could be more easily shared.
On Twitter @whitneymcknight
WASHINGTON – The rules for Stage 3 of the meaningful use program have been finalized by the Obama administration, despite questions about physicians’ ability to achieve “interoperability” and pleas from politicians and providers alike to delay its implementation.
Jonathan Bush, cofounder and CEO of athenahealth, said he believes interoperability will be a no-go unless data are seen as common property, and a premium is placed on the seamless transition of medical records by way of the Internet, not faxes.
Speaking about the large sums of money being spent by hospitals to comply with the government’s meaningful use requirements, Mr. Bush said, “they’re going to staff up hundreds of people who aren’t going to be able to run it. It doesn’t connect to anyone.”
In an interview at the annual Washington Ideas Forum sponsored by the Aspen Institute and The Atlantic, Mr. Bush offered his thoughts on how data could be more easily shared.
On Twitter @whitneymcknight
WASHINGTON – The rules for Stage 3 of the meaningful use program have been finalized by the Obama administration, despite questions about physicians’ ability to achieve “interoperability” and pleas from politicians and providers alike to delay its implementation.
Jonathan Bush, cofounder and CEO of athenahealth, said he believes interoperability will be a no-go unless data are seen as common property, and a premium is placed on the seamless transition of medical records by way of the Internet, not faxes.
Speaking about the large sums of money being spent by hospitals to comply with the government’s meaningful use requirements, Mr. Bush said, “they’re going to staff up hundreds of people who aren’t going to be able to run it. It doesn’t connect to anyone.”
In an interview at the annual Washington Ideas Forum sponsored by the Aspen Institute and The Atlantic, Mr. Bush offered his thoughts on how data could be more easily shared.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE WASHINGTON IDEAS FORUM
VIDEO: Take steps now to keep gram-negative resistance at bay
CHICAGO – Gram-negative bacteria are the new frontier of antimicrobial resistance.
Resistant Escherichia coli, Klebsiella, and other organisms are increasingly common in Asia, South America, and southern Europe, but haven’t quite established themselves yet in the United States.
In an interview at the annual clinical congress of the American College of Surgeons, Dr. John Mazuski, a professor of surgery at Washington University in St. Louis, explained what’s known so far, and the steps to take now to keep the organisms in check.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Gram-negative bacteria are the new frontier of antimicrobial resistance.
Resistant Escherichia coli, Klebsiella, and other organisms are increasingly common in Asia, South America, and southern Europe, but haven’t quite established themselves yet in the United States.
In an interview at the annual clinical congress of the American College of Surgeons, Dr. John Mazuski, a professor of surgery at Washington University in St. Louis, explained what’s known so far, and the steps to take now to keep the organisms in check.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Gram-negative bacteria are the new frontier of antimicrobial resistance.
Resistant Escherichia coli, Klebsiella, and other organisms are increasingly common in Asia, South America, and southern Europe, but haven’t quite established themselves yet in the United States.
In an interview at the annual clinical congress of the American College of Surgeons, Dr. John Mazuski, a professor of surgery at Washington University in St. Louis, explained what’s known so far, and the steps to take now to keep the organisms in check.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE ACS CLINICAL CONGRESS

Self-harm emergencies rise 50% after bariatric surgery
The number of self-harm emergencies increases by 50% after bariatric surgery, according to a report published online Oct. 7 in JAMA Surgery.
Mental health problems are common among both morbidly obese adults and patients undergoing bariatric surgery, and a recent meta-analysis of 30 studies found that suicide risk was four times higher among patients undergoing bariatric surgery than in the general population. To examine this association, researchers performed a population-based longitudinal cohort study comparing self-harm behaviors during the 3 years before bariatric surgery with those during the 3 years after bariatric surgery in all 8,815 adults who underwent gastric bypass, intestinal bypass, and sleeve gastrectomy in Ontario during a 5-year period.

This cohort reflects the practice of approximately 200 surgeons. Self-harm behaviors were categorized as medication overdose, alcohol-related, poisoning by toxic chemicals, or physical trauma. Approximately 64% of the study population had a history of anxiety disorders, 7.8% had general mental health disorders, and 0.6% reported alcohol misuse before undergoing bariatric surgery, wrote Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto.
There were 62 self-harm events during the preoperative interval and 96 during the postoperative interval. The mean incidence of self harm was 2.33 events per 1,000 patients during the 3 years before surgery and 3.63 per 1,000 during the 3 years after surgery, for a rate ratio of 1.54. This represents an increase of approximately 50% after bariatric surgery. The postoperative self-harm rate also was three times as high as that in the general Ontario population (1.2 per 1,000 people) during the same period.
Most of these incidents (73%) were medication overdoses. These were considered serious suicide attempts posing significant risk to the patients; they required ambulance transport and hospital admission. Physical trauma such as self-hanging accounted for another 21%. Almost all of the patients with postoperative self-harm behaviors had a known history of mental health problems, chiefly major depression. These findings suggest the need for increased screening and monitoring for excessive drug or alcohol use, as well as activating a reliable support network to mitigate the stress that follows profound changes in diet and lifestyle, Dr. Bhatti and his associates said (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414).
The reason for this rise in self-harm behaviors is not yet known. Some experts contend that changes in alcohol metabolism following bariatric surgery raise the likelihood of intoxication or alcohol-related disinhibition, both of which can escalate impulsivity. Others argue that morbid obesity arises from a food addiction, and after the procedure patients may turn from overeating to alcohol/substance abuse. Most agree that the surgery and the lifestyle changes it requires increase the patient’s stress and anxiety, which can exacerbate preexisting mental health problems. Finally, bariatric surgery itself alters neurohormone levels, which could in turn predispose patients to depression or suicidal behaviors, the investigators said.
This study was limited in that the data didn’t allow the researchers to account for some important surgery-related factors, including patients’ failure to lose a significant amount of weight. In addition, the study focused on self-harm behaviors that led to emergency-department visits; since completed suicides generally don’t include ED visits, some cases of self-harm that ended in death could not be included.
The Canadian Institutes of Health Research, the Canada Research Chair in Medical Decision Sciences, and the Da Souza Chair in Trauma Research funded the study. Dr. Bhatti and his associates reported having no relevant financial disclosures.
Bhatti et al. reported that most self-harm emergencies in this study population occurred in the second and third years following bariatric surgery. But most bariatric surgery programs follow patients only for the first postoperative year, when most weight loss occurs.
This study thus supports the call for longer-term follow-up, especially for patients who have a history of major depressive disorder or self harm. The findings underscore the unique vulnerability of patients undergoing bariatric surgery and force us to closely examine why suicide rates are so much higher in these patients than in the general population.
Amir A. Ghaferi, M.D., and Carol Lindsay-Westphal, Ph.D., are at Ann Arbor (Mich.) Veterans Administration Healthcare System. Dr. Ghaferi is also at the University of Michigan’s Center for Healthcare Outcomes and Policy and department of surgery, and Dr. Lindsay-Westphal is also in the department of psychiatry at the university. Dr. Ghaferi and Dr. Lindsay-Westphal made these remarks in an Invited Commentary accompanying Dr. Bhatti’s report (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3396).
Bhatti et al. reported that most self-harm emergencies in this study population occurred in the second and third years following bariatric surgery. But most bariatric surgery programs follow patients only for the first postoperative year, when most weight loss occurs.
This study thus supports the call for longer-term follow-up, especially for patients who have a history of major depressive disorder or self harm. The findings underscore the unique vulnerability of patients undergoing bariatric surgery and force us to closely examine why suicide rates are so much higher in these patients than in the general population.
Amir A. Ghaferi, M.D., and Carol Lindsay-Westphal, Ph.D., are at Ann Arbor (Mich.) Veterans Administration Healthcare System. Dr. Ghaferi is also at the University of Michigan’s Center for Healthcare Outcomes and Policy and department of surgery, and Dr. Lindsay-Westphal is also in the department of psychiatry at the university. Dr. Ghaferi and Dr. Lindsay-Westphal made these remarks in an Invited Commentary accompanying Dr. Bhatti’s report (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3396).
Bhatti et al. reported that most self-harm emergencies in this study population occurred in the second and third years following bariatric surgery. But most bariatric surgery programs follow patients only for the first postoperative year, when most weight loss occurs.
This study thus supports the call for longer-term follow-up, especially for patients who have a history of major depressive disorder or self harm. The findings underscore the unique vulnerability of patients undergoing bariatric surgery and force us to closely examine why suicide rates are so much higher in these patients than in the general population.
Amir A. Ghaferi, M.D., and Carol Lindsay-Westphal, Ph.D., are at Ann Arbor (Mich.) Veterans Administration Healthcare System. Dr. Ghaferi is also at the University of Michigan’s Center for Healthcare Outcomes and Policy and department of surgery, and Dr. Lindsay-Westphal is also in the department of psychiatry at the university. Dr. Ghaferi and Dr. Lindsay-Westphal made these remarks in an Invited Commentary accompanying Dr. Bhatti’s report (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3396).
The number of self-harm emergencies increases by 50% after bariatric surgery, according to a report published online Oct. 7 in JAMA Surgery.
Mental health problems are common among both morbidly obese adults and patients undergoing bariatric surgery, and a recent meta-analysis of 30 studies found that suicide risk was four times higher among patients undergoing bariatric surgery than in the general population. To examine this association, researchers performed a population-based longitudinal cohort study comparing self-harm behaviors during the 3 years before bariatric surgery with those during the 3 years after bariatric surgery in all 8,815 adults who underwent gastric bypass, intestinal bypass, and sleeve gastrectomy in Ontario during a 5-year period.
This cohort reflects the practice of approximately 200 surgeons. Self-harm behaviors were categorized as medication overdose, alcohol-related, poisoning by toxic chemicals, or physical trauma. Approximately 64% of the study population had a history of anxiety disorders, 7.8% had general mental health disorders, and 0.6% reported alcohol misuse before undergoing bariatric surgery, wrote Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto.
There were 62 self-harm events during the preoperative interval and 96 during the postoperative interval. The mean incidence of self harm was 2.33 events per 1,000 patients during the 3 years before surgery and 3.63 per 1,000 during the 3 years after surgery, for a rate ratio of 1.54. This represents an increase of approximately 50% after bariatric surgery. The postoperative self-harm rate also was three times as high as that in the general Ontario population (1.2 per 1,000 people) during the same period.
Most of these incidents (73%) were medication overdoses. These were considered serious suicide attempts posing significant risk to the patients; they required ambulance transport and hospital admission. Physical trauma such as self-hanging accounted for another 21%. Almost all of the patients with postoperative self-harm behaviors had a known history of mental health problems, chiefly major depression. These findings suggest the need for increased screening and monitoring for excessive drug or alcohol use, as well as activating a reliable support network to mitigate the stress that follows profound changes in diet and lifestyle, Dr. Bhatti and his associates said (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414).
The reason for this rise in self-harm behaviors is not yet known. Some experts contend that changes in alcohol metabolism following bariatric surgery raise the likelihood of intoxication or alcohol-related disinhibition, both of which can escalate impulsivity. Others argue that morbid obesity arises from a food addiction, and after the procedure patients may turn from overeating to alcohol/substance abuse. Most agree that the surgery and the lifestyle changes it requires increase the patient’s stress and anxiety, which can exacerbate preexisting mental health problems. Finally, bariatric surgery itself alters neurohormone levels, which could in turn predispose patients to depression or suicidal behaviors, the investigators said.
This study was limited in that the data didn’t allow the researchers to account for some important surgery-related factors, including patients’ failure to lose a significant amount of weight. In addition, the study focused on self-harm behaviors that led to emergency-department visits; since completed suicides generally don’t include ED visits, some cases of self-harm that ended in death could not be included.
The Canadian Institutes of Health Research, the Canada Research Chair in Medical Decision Sciences, and the Da Souza Chair in Trauma Research funded the study. Dr. Bhatti and his associates reported having no relevant financial disclosures.
The number of self-harm emergencies increases by 50% after bariatric surgery, according to a report published online Oct. 7 in JAMA Surgery.
Mental health problems are common among both morbidly obese adults and patients undergoing bariatric surgery, and a recent meta-analysis of 30 studies found that suicide risk was four times higher among patients undergoing bariatric surgery than in the general population. To examine this association, researchers performed a population-based longitudinal cohort study comparing self-harm behaviors during the 3 years before bariatric surgery with those during the 3 years after bariatric surgery in all 8,815 adults who underwent gastric bypass, intestinal bypass, and sleeve gastrectomy in Ontario during a 5-year period.
This cohort reflects the practice of approximately 200 surgeons. Self-harm behaviors were categorized as medication overdose, alcohol-related, poisoning by toxic chemicals, or physical trauma. Approximately 64% of the study population had a history of anxiety disorders, 7.8% had general mental health disorders, and 0.6% reported alcohol misuse before undergoing bariatric surgery, wrote Junaid A. Bhatti, Ph.D., of the department of evaluative clinical sciences, Sunnybrook Research Institute, Toronto, and the department of surgery, University of Toronto.
There were 62 self-harm events during the preoperative interval and 96 during the postoperative interval. The mean incidence of self harm was 2.33 events per 1,000 patients during the 3 years before surgery and 3.63 per 1,000 during the 3 years after surgery, for a rate ratio of 1.54. This represents an increase of approximately 50% after bariatric surgery. The postoperative self-harm rate also was three times as high as that in the general Ontario population (1.2 per 1,000 people) during the same period.
Most of these incidents (73%) were medication overdoses. These were considered serious suicide attempts posing significant risk to the patients; they required ambulance transport and hospital admission. Physical trauma such as self-hanging accounted for another 21%. Almost all of the patients with postoperative self-harm behaviors had a known history of mental health problems, chiefly major depression. These findings suggest the need for increased screening and monitoring for excessive drug or alcohol use, as well as activating a reliable support network to mitigate the stress that follows profound changes in diet and lifestyle, Dr. Bhatti and his associates said (JAMA Surg. 2015 Oct 7. doi: 10.1001/jamasurg.2015.3414).
The reason for this rise in self-harm behaviors is not yet known. Some experts contend that changes in alcohol metabolism following bariatric surgery raise the likelihood of intoxication or alcohol-related disinhibition, both of which can escalate impulsivity. Others argue that morbid obesity arises from a food addiction, and after the procedure patients may turn from overeating to alcohol/substance abuse. Most agree that the surgery and the lifestyle changes it requires increase the patient’s stress and anxiety, which can exacerbate preexisting mental health problems. Finally, bariatric surgery itself alters neurohormone levels, which could in turn predispose patients to depression or suicidal behaviors, the investigators said.
This study was limited in that the data didn’t allow the researchers to account for some important surgery-related factors, including patients’ failure to lose a significant amount of weight. In addition, the study focused on self-harm behaviors that led to emergency-department visits; since completed suicides generally don’t include ED visits, some cases of self-harm that ended in death could not be included.
The Canadian Institutes of Health Research, the Canada Research Chair in Medical Decision Sciences, and the Da Souza Chair in Trauma Research funded the study. Dr. Bhatti and his associates reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point: The number of self-harm emergencies increased by 50% after bariatric surgery, according to data from a Canadian study.
Major finding: The mean incidence of self harm was 2.33 events per 1,000 patients during the 3 years before surgery and 3.63 per 1,000 during the 3 years after surgery (RR, 1.54).
Data source: A population-based longitudinal cohort study involving all 8,815 adults who had bariatric surgery in Ontario during a 5-year period.
Disclosures: The Canadian Institutes of Health Research, the Canada Research Chair in Medical Decision Sciences, and the Da Souza Chair in Trauma Research funded the study. Dr. Bhatti and his associates reported having no relevant financial disclosures.

BCVI: Screen with CT angiography, confirm with DSA
LAS VEGAS – Management of blunt cerebrovascular injuries using 64-channel computed tomographic angiography screening coupled with digital subtraction angiography for a definitive diagnosis is safe and effective for identifying clinically significant injury and for maintaining a low stroke rate, according to a review of 228 cases.
The computed tomographic angiography (CTA) screening was positive in 189 patients (83%), and digital subtraction angiography (DSA) confirmed injury in 104 (55%) of those. The remaining 39 patients were found to have no injury on DSA, Dr. Charles P. Shahan of the University of Tennessee, Memphis reported at the annual meeting of the American Association for the Surgery of Trauma (AAST).

Stroke related to blunt cerebrovascular injury (BCVI) occurred in five patients (4.8%); three of those patients were symptomatic at the time of presentation, and two became symptomatic while on therapy for a known lesion. None of the patients who had a negative screening CTA, including three with injuries missed on CTA, had a stroke, Dr. Shahan said.
The current study follows a prior study reported at the 2013 AAST annual meeting that suggested that 64-channel multidetector CTA could be the primary screening tool for BCVI. The previously used 32-channel multidetector CTA was found to be inadequate, with a sensitivity of only 52%. Sensitivity increased to 68% with the 64-channel CTA, but the positive predictive value remained remarkably low at 36%, he said.
That study led to a change in the screening algorithm, replacing DSA with CTA for screening, and reserving DSA for definitive BCVI diagnosis following a positive CTA or unexplained neurologic findings, he explained, noting that the rationale was that most injuries missed were low-grade injuries less likely to result in further injury, and that with CTA alone, about two-thirds of patients would be treated unnecessarily because of the false-positive rate.
The purpose of the current study was to evaluate outcomes in the wake of the algorithm change and to assess the potential for missed, clinically significant BCVI.
Study subjects were patients who underwent DSA over an 18-month period after implementation of the algorithm change. Most (64%) were men with a mean age of 43 years and a mean injury severity score of 22 out of 75, indicating moderate or severe injury.
The stroke rate was statistically unchanged in the second study, compared with the first. The findings demonstrate the safety and efficacy of the current management algorithm for BCVI, as well as the value of using DSA to identify false-positive CTA findings. In fact, definitive diagnosis by DSA led to avoidance of potentially harmful anticoagulation in 45% of CTA-positive patients, with no increase in the incidence of strokes resulting from injuries missed by CTA, Dr. Shahan said.
“Considering there were 85 false-positive CTAs, and also considering that our average length of heparin time is approximately 7 days prior to reevaluation, we’ve extrapolated this to nearly 600 heparin infusion days that were avoided by confirmatory DSA testing,” he said, concluding that “CTA with 64-channel multidetector technology with experienced radiology staff in a high-volume center can be safe and effective for BCVI screening.”
He added, however, that false-positive rates with CTA continue to necessitate DSA confirmation to avoid overtreatment.
“We feel that CTA screening with DSA confirmation has allowed us to maintain an acceptably low stroke rate and prevented a tremendous amount of unnecessary anticoagulation in these patients,” he said.
Dr. Clay Cothren Burlew, who was an invited discussant for Dr. Shahan’s paper, applauded Dr. Shahan and his colleagues for “continuing to question the validity of CTA as our primary diagnostic modality for BCVI,” and said the findings made her “stop and think, should we all be doing confirmatory angiography? … Are CTAs actually overcalling 45% of the injuries that we identify?”
Dr. Burlew of the University of Colorado, Denver, questioned whether the high rate of false positives is a result of radiologists who “overcall” questionable findings knowing that a confirmatory angiogram will quickly follow.
“I think this evaluation should be a model for others. Each institution should critically review their individual rates and methods of BCVI diagnosis,” she said, adding that “for centers with a marked increase in the identification of BCVI following institution of CTA as their screening tool, consideration of confirmatory angiography is recommended due to the potential false-positive rate of up to 45%.”
However, confirmatory angiography may not be warranted at centers whose screen yields remain the same with no missed injuries, she said.
“All programs should evaluate their injuries, appropriateness of diagnosis, and impact of subsequent treatment. Only then will we have optimal outcomes,” she concluded.
Dr. Shahan and Dr. Burlew reported having no relevant financial disclosures.
LAS VEGAS – Management of blunt cerebrovascular injuries using 64-channel computed tomographic angiography screening coupled with digital subtraction angiography for a definitive diagnosis is safe and effective for identifying clinically significant injury and for maintaining a low stroke rate, according to a review of 228 cases.
The computed tomographic angiography (CTA) screening was positive in 189 patients (83%), and digital subtraction angiography (DSA) confirmed injury in 104 (55%) of those. The remaining 39 patients were found to have no injury on DSA, Dr. Charles P. Shahan of the University of Tennessee, Memphis reported at the annual meeting of the American Association for the Surgery of Trauma (AAST).
Stroke related to blunt cerebrovascular injury (BCVI) occurred in five patients (4.8%); three of those patients were symptomatic at the time of presentation, and two became symptomatic while on therapy for a known lesion. None of the patients who had a negative screening CTA, including three with injuries missed on CTA, had a stroke, Dr. Shahan said.
The current study follows a prior study reported at the 2013 AAST annual meeting that suggested that 64-channel multidetector CTA could be the primary screening tool for BCVI. The previously used 32-channel multidetector CTA was found to be inadequate, with a sensitivity of only 52%. Sensitivity increased to 68% with the 64-channel CTA, but the positive predictive value remained remarkably low at 36%, he said.
That study led to a change in the screening algorithm, replacing DSA with CTA for screening, and reserving DSA for definitive BCVI diagnosis following a positive CTA or unexplained neurologic findings, he explained, noting that the rationale was that most injuries missed were low-grade injuries less likely to result in further injury, and that with CTA alone, about two-thirds of patients would be treated unnecessarily because of the false-positive rate.
The purpose of the current study was to evaluate outcomes in the wake of the algorithm change and to assess the potential for missed, clinically significant BCVI.
Study subjects were patients who underwent DSA over an 18-month period after implementation of the algorithm change. Most (64%) were men with a mean age of 43 years and a mean injury severity score of 22 out of 75, indicating moderate or severe injury.
The stroke rate was statistically unchanged in the second study, compared with the first. The findings demonstrate the safety and efficacy of the current management algorithm for BCVI, as well as the value of using DSA to identify false-positive CTA findings. In fact, definitive diagnosis by DSA led to avoidance of potentially harmful anticoagulation in 45% of CTA-positive patients, with no increase in the incidence of strokes resulting from injuries missed by CTA, Dr. Shahan said.
“Considering there were 85 false-positive CTAs, and also considering that our average length of heparin time is approximately 7 days prior to reevaluation, we’ve extrapolated this to nearly 600 heparin infusion days that were avoided by confirmatory DSA testing,” he said, concluding that “CTA with 64-channel multidetector technology with experienced radiology staff in a high-volume center can be safe and effective for BCVI screening.”
He added, however, that false-positive rates with CTA continue to necessitate DSA confirmation to avoid overtreatment.
“We feel that CTA screening with DSA confirmation has allowed us to maintain an acceptably low stroke rate and prevented a tremendous amount of unnecessary anticoagulation in these patients,” he said.
Dr. Clay Cothren Burlew, who was an invited discussant for Dr. Shahan’s paper, applauded Dr. Shahan and his colleagues for “continuing to question the validity of CTA as our primary diagnostic modality for BCVI,” and said the findings made her “stop and think, should we all be doing confirmatory angiography? … Are CTAs actually overcalling 45% of the injuries that we identify?”
Dr. Burlew of the University of Colorado, Denver, questioned whether the high rate of false positives is a result of radiologists who “overcall” questionable findings knowing that a confirmatory angiogram will quickly follow.
“I think this evaluation should be a model for others. Each institution should critically review their individual rates and methods of BCVI diagnosis,” she said, adding that “for centers with a marked increase in the identification of BCVI following institution of CTA as their screening tool, consideration of confirmatory angiography is recommended due to the potential false-positive rate of up to 45%.”
However, confirmatory angiography may not be warranted at centers whose screen yields remain the same with no missed injuries, she said.
“All programs should evaluate their injuries, appropriateness of diagnosis, and impact of subsequent treatment. Only then will we have optimal outcomes,” she concluded.
Dr. Shahan and Dr. Burlew reported having no relevant financial disclosures.
LAS VEGAS – Management of blunt cerebrovascular injuries using 64-channel computed tomographic angiography screening coupled with digital subtraction angiography for a definitive diagnosis is safe and effective for identifying clinically significant injury and for maintaining a low stroke rate, according to a review of 228 cases.
The computed tomographic angiography (CTA) screening was positive in 189 patients (83%), and digital subtraction angiography (DSA) confirmed injury in 104 (55%) of those. The remaining 39 patients were found to have no injury on DSA, Dr. Charles P. Shahan of the University of Tennessee, Memphis reported at the annual meeting of the American Association for the Surgery of Trauma (AAST).
Stroke related to blunt cerebrovascular injury (BCVI) occurred in five patients (4.8%); three of those patients were symptomatic at the time of presentation, and two became symptomatic while on therapy for a known lesion. None of the patients who had a negative screening CTA, including three with injuries missed on CTA, had a stroke, Dr. Shahan said.
The current study follows a prior study reported at the 2013 AAST annual meeting that suggested that 64-channel multidetector CTA could be the primary screening tool for BCVI. The previously used 32-channel multidetector CTA was found to be inadequate, with a sensitivity of only 52%. Sensitivity increased to 68% with the 64-channel CTA, but the positive predictive value remained remarkably low at 36%, he said.
That study led to a change in the screening algorithm, replacing DSA with CTA for screening, and reserving DSA for definitive BCVI diagnosis following a positive CTA or unexplained neurologic findings, he explained, noting that the rationale was that most injuries missed were low-grade injuries less likely to result in further injury, and that with CTA alone, about two-thirds of patients would be treated unnecessarily because of the false-positive rate.
The purpose of the current study was to evaluate outcomes in the wake of the algorithm change and to assess the potential for missed, clinically significant BCVI.
Study subjects were patients who underwent DSA over an 18-month period after implementation of the algorithm change. Most (64%) were men with a mean age of 43 years and a mean injury severity score of 22 out of 75, indicating moderate or severe injury.
The stroke rate was statistically unchanged in the second study, compared with the first. The findings demonstrate the safety and efficacy of the current management algorithm for BCVI, as well as the value of using DSA to identify false-positive CTA findings. In fact, definitive diagnosis by DSA led to avoidance of potentially harmful anticoagulation in 45% of CTA-positive patients, with no increase in the incidence of strokes resulting from injuries missed by CTA, Dr. Shahan said.
“Considering there were 85 false-positive CTAs, and also considering that our average length of heparin time is approximately 7 days prior to reevaluation, we’ve extrapolated this to nearly 600 heparin infusion days that were avoided by confirmatory DSA testing,” he said, concluding that “CTA with 64-channel multidetector technology with experienced radiology staff in a high-volume center can be safe and effective for BCVI screening.”
He added, however, that false-positive rates with CTA continue to necessitate DSA confirmation to avoid overtreatment.
“We feel that CTA screening with DSA confirmation has allowed us to maintain an acceptably low stroke rate and prevented a tremendous amount of unnecessary anticoagulation in these patients,” he said.
Dr. Clay Cothren Burlew, who was an invited discussant for Dr. Shahan’s paper, applauded Dr. Shahan and his colleagues for “continuing to question the validity of CTA as our primary diagnostic modality for BCVI,” and said the findings made her “stop and think, should we all be doing confirmatory angiography? … Are CTAs actually overcalling 45% of the injuries that we identify?”
Dr. Burlew of the University of Colorado, Denver, questioned whether the high rate of false positives is a result of radiologists who “overcall” questionable findings knowing that a confirmatory angiogram will quickly follow.
“I think this evaluation should be a model for others. Each institution should critically review their individual rates and methods of BCVI diagnosis,” she said, adding that “for centers with a marked increase in the identification of BCVI following institution of CTA as their screening tool, consideration of confirmatory angiography is recommended due to the potential false-positive rate of up to 45%.”
However, confirmatory angiography may not be warranted at centers whose screen yields remain the same with no missed injuries, she said.
“All programs should evaluate their injuries, appropriateness of diagnosis, and impact of subsequent treatment. Only then will we have optimal outcomes,” she concluded.
Dr. Shahan and Dr. Burlew reported having no relevant financial disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point: Use of 64-channel CT angiography screening coupled with digital subtraction angiography for a definitive diagnosis of blunt cerebrovascular injury is safe and effective for identifying clinically significant injury and for maintaining a low stroke rate.
Major finding: None of the patients who had a negative screening CTA, including three with injuries missed on CTA, had a stroke.
Data source: A review of 228 patients with possible BCVI.
Disclosures: Dr. Shahan and Dr. Burlew reported having no relevant financial disclosures.

Survey: 45% order tests to avoid lawsuits
Almost 45% of physicians say that they have practiced defensive medicine, according to a survey of 1,001 physicians conducted by Physicians Practice, a practice management newspaper and website.
To be exact, 44.6% of respondents said that they had ordered tests or procedures that they “thought were probably not medically necessary just to avoid a potential lawsuit,” Physicians Practice reported in its 2015 Great American Physician Survey.
Almost 44% of the physician respondents said that they had been threatened with a malpractice lawsuit, and nearly 32% reported that they had been the defendant in such a lawsuit, the survey results showed.
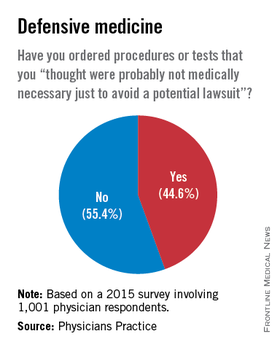
Almost 45% of physicians say that they have practiced defensive medicine, according to a survey of 1,001 physicians conducted by Physicians Practice, a practice management newspaper and website.
To be exact, 44.6% of respondents said that they had ordered tests or procedures that they “thought were probably not medically necessary just to avoid a potential lawsuit,” Physicians Practice reported in its 2015 Great American Physician Survey.
Almost 44% of the physician respondents said that they had been threatened with a malpractice lawsuit, and nearly 32% reported that they had been the defendant in such a lawsuit, the survey results showed.
Almost 45% of physicians say that they have practiced defensive medicine, according to a survey of 1,001 physicians conducted by Physicians Practice, a practice management newspaper and website.
To be exact, 44.6% of respondents said that they had ordered tests or procedures that they “thought were probably not medically necessary just to avoid a potential lawsuit,” Physicians Practice reported in its 2015 Great American Physician Survey.
Almost 44% of the physician respondents said that they had been threatened with a malpractice lawsuit, and nearly 32% reported that they had been the defendant in such a lawsuit, the survey results showed.
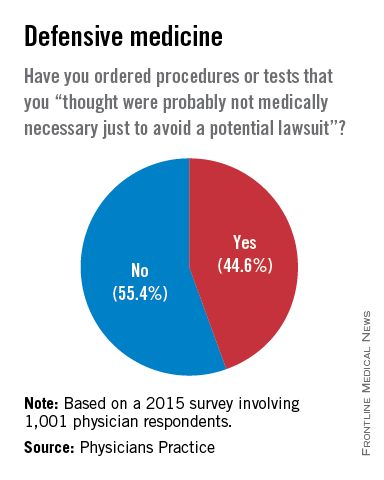
Results mixed in hospital efforts to tackle antimicrobial resistance
SAN DIEGO – Canadian hospitals are making progress in reducing the rates of methicillin-resistant Staphylococcus aureus, but the rates of antimicrobial resistance in Canadian hospitals increased significantly for extended-spectrum beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae, as well as vancomycin-resistant enterococci.
Those are among the key findings from a large national analysis known as CANWARD that were presented at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “What it’s telling us is that some of the things that we’re doing on the antimicrobial resistance side are working,” lead study author George G. Zhanel, Pharm.D., professor of microbiology and infectious diseases at the University of Manitoba, Winnipeg, said in an interview. “But it also tells us that some of these pathogens like [vancomycin-resistant enterococci] and [extended-spectrum beta-lactamase]–producing E. coli continue to go up. So there is some good news and some bad news, but it tells us that it’s not all just doom and gloom. Some progress has been made, but there’s still a long way to go.”
Conducted annually, CANWARD is a national health surveillance study that assesses pathogens causing infections in Canadian hospitals and their patterns of antimicrobial resistance. For the current analysis, Dr. Zhanel and his associates collected 36,607 isolates from patients in tertiary care hospitals in Canada from January 2007 to December 2014. They used Clinical and Laboratory Standards Institute broth microdilution methods to perform antimicrobial susceptibility testing on more than 45 marketed and investigational agents.
Slightly more than half of the patients (55%) were male, and 87% were over age 18. The most common pathogens were E. coli (19.7%), methicillin-susceptible Staphylococcus aureus (MSSA; 16.4%), Pseudomonas aeruginosa (8.7%), S. pneumoniae (6.5%), K. pneumoniae (6.1%), methicillin-resistant S. aureus (MRSA; 4.7%), Enterococcus species (4.0%), and Hemophilus influenzae (4.0%). Susceptibility rates for E. coli were 99.9% for meropenem and tigecycline, 99.7% for ertapenem, 97.7% for piperacillin/tazobactam, 92.5% for ceftriaxone, 90.4% for gentamicin, 77.2% for ciprofloxacin, and 73.0% for trimethoprim and sulfamethoxazole. Susceptibility rates for P. aeruginosa were 94.2% for colistin, 84.3% for piperacillin/tazobactam, 83.3% for ceftazidime, 81.2% for meropenem, 77.6% for gentamicin, and 74.1% for ciprofloxacin. Susceptibility rates for MRSA were 100% for linezolid and telavancin, 99.9% for daptomycin, 99.4% for tigecycline, 99.1% for vancomycin, and 93.3% for trimethoprim and sulfamethoxazole. The rates of resistant organisms between 2007 and 2014 increased significantly for extended-spectrum beta-lactamase–producing E. coli (from 3.4% to 11.6%) and K. pneumoniae (from 1.5% to 6.5%), as well as vancomycin-resistant enterococci (from 1.8% to 7.0%), while rates of MRSA significantly declined (from 26.1% to 20.2%).
“The biggest surprise to me is that the hospital-acquired genotype of MRSA is going down,” Dr. Zhanel commented. “The community-acquired genotype is still going up, but the hospital-acquired [genotype] has plummeted in hospitals.”
He noted that CANWARD data suggest that antimicrobial resistance “is not confined to one part of the hospital. We have resistance happening in medical wards, ICUs, and hospital emergency rooms. We consistently find that resistance is highest in the ICU and by far the lowest in the ER. With clinics we find that it’s a variable scenario.”
The study was supported in part by Abbott, Achaogen, Affinium, Astellas, Astra Zeneca, Bayer, Cerexa/Forest, Cubist, Galderma Laboratories, Merck, Paladin Labs, Pfizer/Wyeth, Sunovion, and the Medicines Co. The researchers reported having no relevant financial disclosures.
SAN DIEGO – Canadian hospitals are making progress in reducing the rates of methicillin-resistant Staphylococcus aureus, but the rates of antimicrobial resistance in Canadian hospitals increased significantly for extended-spectrum beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae, as well as vancomycin-resistant enterococci.
Those are among the key findings from a large national analysis known as CANWARD that were presented at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “What it’s telling us is that some of the things that we’re doing on the antimicrobial resistance side are working,” lead study author George G. Zhanel, Pharm.D., professor of microbiology and infectious diseases at the University of Manitoba, Winnipeg, said in an interview. “But it also tells us that some of these pathogens like [vancomycin-resistant enterococci] and [extended-spectrum beta-lactamase]–producing E. coli continue to go up. So there is some good news and some bad news, but it tells us that it’s not all just doom and gloom. Some progress has been made, but there’s still a long way to go.”
Conducted annually, CANWARD is a national health surveillance study that assesses pathogens causing infections in Canadian hospitals and their patterns of antimicrobial resistance. For the current analysis, Dr. Zhanel and his associates collected 36,607 isolates from patients in tertiary care hospitals in Canada from January 2007 to December 2014. They used Clinical and Laboratory Standards Institute broth microdilution methods to perform antimicrobial susceptibility testing on more than 45 marketed and investigational agents.
Slightly more than half of the patients (55%) were male, and 87% were over age 18. The most common pathogens were E. coli (19.7%), methicillin-susceptible Staphylococcus aureus (MSSA; 16.4%), Pseudomonas aeruginosa (8.7%), S. pneumoniae (6.5%), K. pneumoniae (6.1%), methicillin-resistant S. aureus (MRSA; 4.7%), Enterococcus species (4.0%), and Hemophilus influenzae (4.0%). Susceptibility rates for E. coli were 99.9% for meropenem and tigecycline, 99.7% for ertapenem, 97.7% for piperacillin/tazobactam, 92.5% for ceftriaxone, 90.4% for gentamicin, 77.2% for ciprofloxacin, and 73.0% for trimethoprim and sulfamethoxazole. Susceptibility rates for P. aeruginosa were 94.2% for colistin, 84.3% for piperacillin/tazobactam, 83.3% for ceftazidime, 81.2% for meropenem, 77.6% for gentamicin, and 74.1% for ciprofloxacin. Susceptibility rates for MRSA were 100% for linezolid and telavancin, 99.9% for daptomycin, 99.4% for tigecycline, 99.1% for vancomycin, and 93.3% for trimethoprim and sulfamethoxazole. The rates of resistant organisms between 2007 and 2014 increased significantly for extended-spectrum beta-lactamase–producing E. coli (from 3.4% to 11.6%) and K. pneumoniae (from 1.5% to 6.5%), as well as vancomycin-resistant enterococci (from 1.8% to 7.0%), while rates of MRSA significantly declined (from 26.1% to 20.2%).
“The biggest surprise to me is that the hospital-acquired genotype of MRSA is going down,” Dr. Zhanel commented. “The community-acquired genotype is still going up, but the hospital-acquired [genotype] has plummeted in hospitals.”
He noted that CANWARD data suggest that antimicrobial resistance “is not confined to one part of the hospital. We have resistance happening in medical wards, ICUs, and hospital emergency rooms. We consistently find that resistance is highest in the ICU and by far the lowest in the ER. With clinics we find that it’s a variable scenario.”
The study was supported in part by Abbott, Achaogen, Affinium, Astellas, Astra Zeneca, Bayer, Cerexa/Forest, Cubist, Galderma Laboratories, Merck, Paladin Labs, Pfizer/Wyeth, Sunovion, and the Medicines Co. The researchers reported having no relevant financial disclosures.
SAN DIEGO – Canadian hospitals are making progress in reducing the rates of methicillin-resistant Staphylococcus aureus, but the rates of antimicrobial resistance in Canadian hospitals increased significantly for extended-spectrum beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae, as well as vancomycin-resistant enterococci.
Those are among the key findings from a large national analysis known as CANWARD that were presented at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy. “What it’s telling us is that some of the things that we’re doing on the antimicrobial resistance side are working,” lead study author George G. Zhanel, Pharm.D., professor of microbiology and infectious diseases at the University of Manitoba, Winnipeg, said in an interview. “But it also tells us that some of these pathogens like [vancomycin-resistant enterococci] and [extended-spectrum beta-lactamase]–producing E. coli continue to go up. So there is some good news and some bad news, but it tells us that it’s not all just doom and gloom. Some progress has been made, but there’s still a long way to go.”
Conducted annually, CANWARD is a national health surveillance study that assesses pathogens causing infections in Canadian hospitals and their patterns of antimicrobial resistance. For the current analysis, Dr. Zhanel and his associates collected 36,607 isolates from patients in tertiary care hospitals in Canada from January 2007 to December 2014. They used Clinical and Laboratory Standards Institute broth microdilution methods to perform antimicrobial susceptibility testing on more than 45 marketed and investigational agents.
Slightly more than half of the patients (55%) were male, and 87% were over age 18. The most common pathogens were E. coli (19.7%), methicillin-susceptible Staphylococcus aureus (MSSA; 16.4%), Pseudomonas aeruginosa (8.7%), S. pneumoniae (6.5%), K. pneumoniae (6.1%), methicillin-resistant S. aureus (MRSA; 4.7%), Enterococcus species (4.0%), and Hemophilus influenzae (4.0%). Susceptibility rates for E. coli were 99.9% for meropenem and tigecycline, 99.7% for ertapenem, 97.7% for piperacillin/tazobactam, 92.5% for ceftriaxone, 90.4% for gentamicin, 77.2% for ciprofloxacin, and 73.0% for trimethoprim and sulfamethoxazole. Susceptibility rates for P. aeruginosa were 94.2% for colistin, 84.3% for piperacillin/tazobactam, 83.3% for ceftazidime, 81.2% for meropenem, 77.6% for gentamicin, and 74.1% for ciprofloxacin. Susceptibility rates for MRSA were 100% for linezolid and telavancin, 99.9% for daptomycin, 99.4% for tigecycline, 99.1% for vancomycin, and 93.3% for trimethoprim and sulfamethoxazole. The rates of resistant organisms between 2007 and 2014 increased significantly for extended-spectrum beta-lactamase–producing E. coli (from 3.4% to 11.6%) and K. pneumoniae (from 1.5% to 6.5%), as well as vancomycin-resistant enterococci (from 1.8% to 7.0%), while rates of MRSA significantly declined (from 26.1% to 20.2%).
“The biggest surprise to me is that the hospital-acquired genotype of MRSA is going down,” Dr. Zhanel commented. “The community-acquired genotype is still going up, but the hospital-acquired [genotype] has plummeted in hospitals.”
He noted that CANWARD data suggest that antimicrobial resistance “is not confined to one part of the hospital. We have resistance happening in medical wards, ICUs, and hospital emergency rooms. We consistently find that resistance is highest in the ICU and by far the lowest in the ER. With clinics we find that it’s a variable scenario.”
The study was supported in part by Abbott, Achaogen, Affinium, Astellas, Astra Zeneca, Bayer, Cerexa/Forest, Cubist, Galderma Laboratories, Merck, Paladin Labs, Pfizer/Wyeth, Sunovion, and the Medicines Co. The researchers reported having no relevant financial disclosures.
AT ICAAC 2015
Key clinical point: In Canadian hospitals, the rate of resistant organisms have increased significantly for E. coli and other pathogens but have decreased for MRSA.
Major finding: Rates of resistant organisms between 2007 and 2014 increased significantly for extended-spectrum beta-lactamase–producing E. coli (from 3.4% to 11.6%) and K. pneumoniae (from 1.5% to 6.5%), as well as vancomycin-resistant enterococci (from 1.8% to 7.0%), while rates of MRSA significantly declined (from 26.1% to 20.2%).
Data source: A lab analysis of 36,607 isolates from patients in tertiary care hospitals in Canada from January 2007 to December 2014.
Disclosures: The study was supported in part by Abbott, Achaogen, Affinium, Astellas, Astra Zeneca, Bayer, Cerexa/Forest, Cubist, Galderma Laboratories, Merck, Paladin Labs, Pfizer/Wyeth, Sunovion, and the Medicines Co. The researchers reported having no relevant financial disclosures.