User login
Official Newspaper of the American College of Surgeons
FDA finds long-term clopidogrel does not increase death or cancer risks
Long-term use of the blood-thinning agent clopidogrel did not alter the risk of death in people with heart disease or at risk of developing heart disease, nor did the drug appear to affect cancer risk, according to a statement from the U.S. Food and Drug Administration.
The FDA’s meta-analysis looked at results from 12 trials enrolling a total of 56,799 patients to evaluate the effect of long-term clopidogrel use on all-cause mortality. The incidence of all-cause mortality was 6.7% for the long-term clopidogrel plus aspirin arm and 6.6% for the comparator, resulting in a Mantel Haenszel Risk Difference (MH RD) of 0.04% (95% confidence interval, –0.35%-0.44%).
“The results indicate that long-term (12 months or longer) dual-antiplatelet therapy with clopidogrel and aspirin do not appear to change the overall risk of death, compared with short-term (6 months or less) clopidogrel and aspirin, or aspirin alone,” the agency said in its statement.
The FDA also conducted a meta-analysis looking at nine of these trials (n = 45,374) that had enrolled patients with coronary artery disease or patients at risk of CAD. This also suggested no difference in the risk of all-cause mortality (MH RD –0.07%; 95% CI, –0.43%- 0.29%).
The meta-analysis included results from the Dual-Antiplatelet Therapy Trial (DAPT), whose results included a worrisome safety signal for extended use of clopidogrel (N Engl J Med 2014; 371:2155-66). Patients in the DAPT underwent percutaneous coronary intervention and placement of a drug-eluting stent, after which they received 1 year of clopidogrel or prasugrel plus aspirin. About 1,000 patients were then randomized to 18 additional months of one of the dual-antiplatelet therapies or to aspirin plus placebo. Extended (30-month) use of clopidogrel plus aspirin was associated with a significantly increased risk of death (2.2% for 30 months vs. 1.5% for 12 months), whereas no increased risk was seen for prasugrel plus aspirin. A higher risk of death was mainly due to noncardiovascular causes, including cancer and trauma.
The DAPT did not show an increased risk of cancer-related adverse events related to treatment duration. However, the FDA performed two meta-analyses of other trials, with about 40,000 patients included in each analysis, to determine whether a signal could be found for either cancer-related adverse events or cancer-related death. Neither revealed an increased risk related to long-term clopidogrel use.
Long-term use of the blood-thinning agent clopidogrel did not alter the risk of death in people with heart disease or at risk of developing heart disease, nor did the drug appear to affect cancer risk, according to a statement from the U.S. Food and Drug Administration.
The FDA’s meta-analysis looked at results from 12 trials enrolling a total of 56,799 patients to evaluate the effect of long-term clopidogrel use on all-cause mortality. The incidence of all-cause mortality was 6.7% for the long-term clopidogrel plus aspirin arm and 6.6% for the comparator, resulting in a Mantel Haenszel Risk Difference (MH RD) of 0.04% (95% confidence interval, –0.35%-0.44%).
“The results indicate that long-term (12 months or longer) dual-antiplatelet therapy with clopidogrel and aspirin do not appear to change the overall risk of death, compared with short-term (6 months or less) clopidogrel and aspirin, or aspirin alone,” the agency said in its statement.
The FDA also conducted a meta-analysis looking at nine of these trials (n = 45,374) that had enrolled patients with coronary artery disease or patients at risk of CAD. This also suggested no difference in the risk of all-cause mortality (MH RD –0.07%; 95% CI, –0.43%- 0.29%).
The meta-analysis included results from the Dual-Antiplatelet Therapy Trial (DAPT), whose results included a worrisome safety signal for extended use of clopidogrel (N Engl J Med 2014; 371:2155-66). Patients in the DAPT underwent percutaneous coronary intervention and placement of a drug-eluting stent, after which they received 1 year of clopidogrel or prasugrel plus aspirin. About 1,000 patients were then randomized to 18 additional months of one of the dual-antiplatelet therapies or to aspirin plus placebo. Extended (30-month) use of clopidogrel plus aspirin was associated with a significantly increased risk of death (2.2% for 30 months vs. 1.5% for 12 months), whereas no increased risk was seen for prasugrel plus aspirin. A higher risk of death was mainly due to noncardiovascular causes, including cancer and trauma.
The DAPT did not show an increased risk of cancer-related adverse events related to treatment duration. However, the FDA performed two meta-analyses of other trials, with about 40,000 patients included in each analysis, to determine whether a signal could be found for either cancer-related adverse events or cancer-related death. Neither revealed an increased risk related to long-term clopidogrel use.
Long-term use of the blood-thinning agent clopidogrel did not alter the risk of death in people with heart disease or at risk of developing heart disease, nor did the drug appear to affect cancer risk, according to a statement from the U.S. Food and Drug Administration.
The FDA’s meta-analysis looked at results from 12 trials enrolling a total of 56,799 patients to evaluate the effect of long-term clopidogrel use on all-cause mortality. The incidence of all-cause mortality was 6.7% for the long-term clopidogrel plus aspirin arm and 6.6% for the comparator, resulting in a Mantel Haenszel Risk Difference (MH RD) of 0.04% (95% confidence interval, –0.35%-0.44%).
“The results indicate that long-term (12 months or longer) dual-antiplatelet therapy with clopidogrel and aspirin do not appear to change the overall risk of death, compared with short-term (6 months or less) clopidogrel and aspirin, or aspirin alone,” the agency said in its statement.
The FDA also conducted a meta-analysis looking at nine of these trials (n = 45,374) that had enrolled patients with coronary artery disease or patients at risk of CAD. This also suggested no difference in the risk of all-cause mortality (MH RD –0.07%; 95% CI, –0.43%- 0.29%).
The meta-analysis included results from the Dual-Antiplatelet Therapy Trial (DAPT), whose results included a worrisome safety signal for extended use of clopidogrel (N Engl J Med 2014; 371:2155-66). Patients in the DAPT underwent percutaneous coronary intervention and placement of a drug-eluting stent, after which they received 1 year of clopidogrel or prasugrel plus aspirin. About 1,000 patients were then randomized to 18 additional months of one of the dual-antiplatelet therapies or to aspirin plus placebo. Extended (30-month) use of clopidogrel plus aspirin was associated with a significantly increased risk of death (2.2% for 30 months vs. 1.5% for 12 months), whereas no increased risk was seen for prasugrel plus aspirin. A higher risk of death was mainly due to noncardiovascular causes, including cancer and trauma.
The DAPT did not show an increased risk of cancer-related adverse events related to treatment duration. However, the FDA performed two meta-analyses of other trials, with about 40,000 patients included in each analysis, to determine whether a signal could be found for either cancer-related adverse events or cancer-related death. Neither revealed an increased risk related to long-term clopidogrel use.
Study finds inaccurate reporting of pain by back pain sufferers
SAN DIEGO – Patients with chronic low back pain who report pain scores that do not correlate well with their functional activity level are less satisfied with their pain management treatment, a single-center study found.
“Taking into account that the Affordable Healthcare Act is planning to base physician reimbursements on patient satisfaction with provided treatment, it is imperative to educate patients regarding the necessity to accurately report their pain level using a numeric rating scale. We must also identify other parameters in defining our patients’ chronic pain conditions, such a functionality scales and quality of life questionnaires,” Dr. Nebojsa Nick Knezevic said at the annual meeting of the American Society of Anesthesiologists.

“We rely on many different types of scales for pain, including Likert scales, visual analog scales, and numerical pain rating scales,” said Dr. Knezevic, vice chair for research and education at Advocate Illinois Masonic Medical Center, Chicago. “However, there are many reports talking about the subjectivity of these scales. Interpretation of the pain scores can underestimate or overestimate patient conditions, and they may go on to receive treatments that are not indicated.”
In an effort to assess how numeric pain scores reported by patients with chronic low back pain correlate with their functional activity levels and satisfaction with their pain management, Dr. Knezevic and his associates enrolled 100 patients with radicular low back pain and a mean age of 49 years. Overall, 56% were female, and their average duration of low back pain prior to study enrollment was 14 months.
The investigators asked them to complete pain scores on an 11-point numeric rating scale at rest and during movement, as well as the Oswestry Disability Index (ODI) questionnaire. The researchers evaluated the patients 10 times over a 1-year period at the same time points and asked them to grade their satisfaction with pain management on a scale from 1 to 5, where 1 meant completely dissatisfied, 2 meant dissatisfied, 3 meant somewhat satisfied, 4 meant satisfied, and 5 meant completely satisfied. The investigators multiplied the pain scores by 10 to be on the same 0-100 scale as the ODI and compared the values at each visit. Differences between the ODI and pain scores in the range of –10% to +10% were considered normal, while differences between 11% and 30% were considered mild, differences between 31% and 50% were considered moderate, and differences of more than 50% were considered severe.
Dr. Knezevic reported that pain scores at rest correlated well with ODI in 65% of patients, while mild discrepancies were present in 30% of patients, moderate discrepancies in 4%, and severe discrepancies in 1%. On the other hand, pain scores during movement correlated well with ODI in only 39% of patients, while mild discrepancies were present in 42% of patients, moderate discrepancies in 14%, and severe discrepancies in 5%. More than half of patients (58%) reported pain levels during movement that did not correlate with the level of functional activity indicated by their ODI score. However, inconsistencies between male and female pain score reporting at rest and during movement were equal (P = .606 and P = .928, respectively).
The researchers also found that patients who were taking opioids showed greater discrepancy in reporting pain intensity scores, compared with patients using nonopioid analgesics, as well as those who were not taking medications for their low back pain (P = .038).
“Results of this study showed negative correlation between the degree of discrepancy in pain scores and patient satisfaction with pain management treatment,” Dr. Knezevic concluded.
Dr. Knezevic reported having no financial disclosures.
SAN DIEGO – Patients with chronic low back pain who report pain scores that do not correlate well with their functional activity level are less satisfied with their pain management treatment, a single-center study found.
“Taking into account that the Affordable Healthcare Act is planning to base physician reimbursements on patient satisfaction with provided treatment, it is imperative to educate patients regarding the necessity to accurately report their pain level using a numeric rating scale. We must also identify other parameters in defining our patients’ chronic pain conditions, such a functionality scales and quality of life questionnaires,” Dr. Nebojsa Nick Knezevic said at the annual meeting of the American Society of Anesthesiologists.
“We rely on many different types of scales for pain, including Likert scales, visual analog scales, and numerical pain rating scales,” said Dr. Knezevic, vice chair for research and education at Advocate Illinois Masonic Medical Center, Chicago. “However, there are many reports talking about the subjectivity of these scales. Interpretation of the pain scores can underestimate or overestimate patient conditions, and they may go on to receive treatments that are not indicated.”
In an effort to assess how numeric pain scores reported by patients with chronic low back pain correlate with their functional activity levels and satisfaction with their pain management, Dr. Knezevic and his associates enrolled 100 patients with radicular low back pain and a mean age of 49 years. Overall, 56% were female, and their average duration of low back pain prior to study enrollment was 14 months.
The investigators asked them to complete pain scores on an 11-point numeric rating scale at rest and during movement, as well as the Oswestry Disability Index (ODI) questionnaire. The researchers evaluated the patients 10 times over a 1-year period at the same time points and asked them to grade their satisfaction with pain management on a scale from 1 to 5, where 1 meant completely dissatisfied, 2 meant dissatisfied, 3 meant somewhat satisfied, 4 meant satisfied, and 5 meant completely satisfied. The investigators multiplied the pain scores by 10 to be on the same 0-100 scale as the ODI and compared the values at each visit. Differences between the ODI and pain scores in the range of –10% to +10% were considered normal, while differences between 11% and 30% were considered mild, differences between 31% and 50% were considered moderate, and differences of more than 50% were considered severe.
Dr. Knezevic reported that pain scores at rest correlated well with ODI in 65% of patients, while mild discrepancies were present in 30% of patients, moderate discrepancies in 4%, and severe discrepancies in 1%. On the other hand, pain scores during movement correlated well with ODI in only 39% of patients, while mild discrepancies were present in 42% of patients, moderate discrepancies in 14%, and severe discrepancies in 5%. More than half of patients (58%) reported pain levels during movement that did not correlate with the level of functional activity indicated by their ODI score. However, inconsistencies between male and female pain score reporting at rest and during movement were equal (P = .606 and P = .928, respectively).
The researchers also found that patients who were taking opioids showed greater discrepancy in reporting pain intensity scores, compared with patients using nonopioid analgesics, as well as those who were not taking medications for their low back pain (P = .038).
“Results of this study showed negative correlation between the degree of discrepancy in pain scores and patient satisfaction with pain management treatment,” Dr. Knezevic concluded.
Dr. Knezevic reported having no financial disclosures.
SAN DIEGO – Patients with chronic low back pain who report pain scores that do not correlate well with their functional activity level are less satisfied with their pain management treatment, a single-center study found.
“Taking into account that the Affordable Healthcare Act is planning to base physician reimbursements on patient satisfaction with provided treatment, it is imperative to educate patients regarding the necessity to accurately report their pain level using a numeric rating scale. We must also identify other parameters in defining our patients’ chronic pain conditions, such a functionality scales and quality of life questionnaires,” Dr. Nebojsa Nick Knezevic said at the annual meeting of the American Society of Anesthesiologists.
“We rely on many different types of scales for pain, including Likert scales, visual analog scales, and numerical pain rating scales,” said Dr. Knezevic, vice chair for research and education at Advocate Illinois Masonic Medical Center, Chicago. “However, there are many reports talking about the subjectivity of these scales. Interpretation of the pain scores can underestimate or overestimate patient conditions, and they may go on to receive treatments that are not indicated.”
In an effort to assess how numeric pain scores reported by patients with chronic low back pain correlate with their functional activity levels and satisfaction with their pain management, Dr. Knezevic and his associates enrolled 100 patients with radicular low back pain and a mean age of 49 years. Overall, 56% were female, and their average duration of low back pain prior to study enrollment was 14 months.
The investigators asked them to complete pain scores on an 11-point numeric rating scale at rest and during movement, as well as the Oswestry Disability Index (ODI) questionnaire. The researchers evaluated the patients 10 times over a 1-year period at the same time points and asked them to grade their satisfaction with pain management on a scale from 1 to 5, where 1 meant completely dissatisfied, 2 meant dissatisfied, 3 meant somewhat satisfied, 4 meant satisfied, and 5 meant completely satisfied. The investigators multiplied the pain scores by 10 to be on the same 0-100 scale as the ODI and compared the values at each visit. Differences between the ODI and pain scores in the range of –10% to +10% were considered normal, while differences between 11% and 30% were considered mild, differences between 31% and 50% were considered moderate, and differences of more than 50% were considered severe.
Dr. Knezevic reported that pain scores at rest correlated well with ODI in 65% of patients, while mild discrepancies were present in 30% of patients, moderate discrepancies in 4%, and severe discrepancies in 1%. On the other hand, pain scores during movement correlated well with ODI in only 39% of patients, while mild discrepancies were present in 42% of patients, moderate discrepancies in 14%, and severe discrepancies in 5%. More than half of patients (58%) reported pain levels during movement that did not correlate with the level of functional activity indicated by their ODI score. However, inconsistencies between male and female pain score reporting at rest and during movement were equal (P = .606 and P = .928, respectively).
The researchers also found that patients who were taking opioids showed greater discrepancy in reporting pain intensity scores, compared with patients using nonopioid analgesics, as well as those who were not taking medications for their low back pain (P = .038).
“Results of this study showed negative correlation between the degree of discrepancy in pain scores and patient satisfaction with pain management treatment,” Dr. Knezevic concluded.
Dr. Knezevic reported having no financial disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point: Many patients don’t accurately report their level of back pain when using a numeric rating scale.
Major finding: Pain scores at rest correlated well with the Oswestry Disability Index in 65% of patients, while pain scores during movement correlated well with ODI in only 39% of patients.
Data source: A study of 100 patients with radicular low back pain who completed pain scores on an 11-point numeric rating scale at rest and during movement, as well as the ODI, and were followed for 1 year.
Disclosures: The researchers reported having no financial disclosures.

Small businesses snub Obamacare’s SHOP exchange
After nearly 2 years in operation and millions of dollars spent in development, the small business health insurance exchange created by the Affordable Care Act is struggling to catch on.
Nationally, about 85,000 people, from 11,000 small businesses, have coverage through the online marketplace known as the Small Business Health Options Program, or SHOP, according to the latest federal data released in May. Those totals do not include employers that began coverage in 2014 and have not yet renewed their coverage through HealthCare.gov for 2015.
That’s less than 1% of people with coverage in the U.S. small group insurance market that in 2013 had about 16.7 million people enrolled in health plans, reported Mark Farrah Associates, a market data firm.

The Congressional Budget Office in January estimated 1 million people would enroll for coverage through SHOP in 2015. No one expected the SHOP exchange to have a large enrollment, but industry officials say its early response has been substantially smaller than expected.
“When you look at the cost and look at the take up rate, it certainly raises questions” about whether SHOP has been worthwhile, said Alissa Fox, senior vice president of the Blue Cross Blue Shield Association. “We never thought the business equation made sense.”
Employers with fewer than 50 full-time workers are eligible to buy coverage on SHOP. The federal government even offers businesses an incentive, a tax credit worth up to half of an employer’s share of their workers’ premiums. Among the conditions: The firm must employ fewer than 25 workers and their average salary cannot exceed $50,000. The credit is hardly used in high-cost areas of the country where salaries are higher.
Similar to the health insurance marketplace for individuals, the federal government operates the SHOP exchange in 34 states, and 16 other states plus the District of Columbia run their own small business exchanges. The state exchanges also capture a small share of the small business market, based on more current figures compiled by Kaiser Health News. As of early October, five state-run SHOP exchanges – Idaho, Kentucky, Maryland, Minnesota, and Washington – had sold coverage to fewer than 200 employers. New York and California have the highest enrollments, and together those two states account for about 6,500 employers and nearly 50,000 people.
The Obama administration hoped SHOP would make it easier and cheaper for small employers to offer coverage to employees and for their workers to have a choice of plans.
Unlike the federal- and state-run health insurance exchanges for individuals that limit sign-up to a certain period during the year, the SHOP exchanges allow companies to enroll at any time.
But several factors account for the paltry enrollment in SHOP, say insurance brokers, insurers, and state officials. Brokers say SHOP has fewer health plans and more expensive coverage policies than can be purchased outside the exchange. Several states only have one insurer on their SHOP exchange, including Alabama, Tennessee, North Carolina and Nebraska, according to consulting firm Leavitt Partners.
Many small employers have stuck with plans they purchased outside SHOP because the Obama administration gave them the option to remain with their existing policies until 2017. That enabled employers to stay in plans that don’t meet all the new requirements of the health law, including so-called “essential health benefits.” These additional benefits can drive up the cost of policies, making it harder for the SHOP plans to compete.
Another factor that slowed enrollment in SHOP has been software problems in several states that made it hard for employers and employees to sign up. In addition, the SHOP exchange run by the federal government launched in October 2013 was only available if employers contacted an agent or broker. Its full website was not running until fall 2014.
“With all that stacked up against it, it does not surprise me that the numbers are so low,” said Kevin Lucia, a research professor at Georgetown University Health Policy Institute, who studied the rollout.
Kevin Counihan, the Obama administration’s top insurance exchange official, acknowledges SHOP will only be a “niche product” and most policies will still be sold outside the marketplace. Still, he expects as more employers and insurance brokers learn about SHOP, that its enrollment will grow. Asked in an interview about low enrollment, he said: “It doesn’t really bother me … something like this takes time.”
Mr. Counihan said the key will be to get more brokers interested in selling the SHOP plans.
But many brokers say they don’t see the value of SHOP since it typically offers fewer options than outside the exchanges. “There really is no reason to go to SHOP unless you qualify for the tax credits,” said Ken Stevenson, a Tallahassee, Fla., insurance agent. Four Florida insurers sell on SHOP, fewer than half available in the state. Florida Blue, the state’s largest insurer, said less than 1% of its small group policies are sold on the SHOP.
Other brokers say enrollment on SHOP is more confusing than working directly with carriers. “It’s difficult to get through the website, and it’s a lot easier for employers to pick up the phone and call a broker than spend 4 hours on the SHOP site,” said Alan Schulman, a Bethesda, Md., insurance agent.
The SHOP was set to expand to open for businesses with up to 100 employees in 2016, but Congress and President Obama rescinded that requirement in November.
One company to get the tax credit is Paloma Clothing, a women’s clothing store in Portland, Ore. Co-owner Mike Roach said he signed up for SHOP plan last year on the recommendation of his insurance agent. The credit saved his company about $7,000. That savings, he said, made it affordable for Paloma to keep its share of its employees’ monthly insurance premiums at 85%.
“The tax credit saved us from the terrific, morale-crushing option of decreasing our health insurance coverage for our employees,” he said. Eight of the store’s 15 employees signed up for the SHOP policy sold by Moda Health. Most pay about $45 a month for their share of the premium.
Mr. Roach said he is thankful for the health law. “Wow, finally someone did something to help small businesses deal with the rising cost of providing employees health insurance,” he said. “For so many years … no one did anything but feel sorry for you.”
After nearly 2 years in operation and millions of dollars spent in development, the small business health insurance exchange created by the Affordable Care Act is struggling to catch on.
Nationally, about 85,000 people, from 11,000 small businesses, have coverage through the online marketplace known as the Small Business Health Options Program, or SHOP, according to the latest federal data released in May. Those totals do not include employers that began coverage in 2014 and have not yet renewed their coverage through HealthCare.gov for 2015.
That’s less than 1% of people with coverage in the U.S. small group insurance market that in 2013 had about 16.7 million people enrolled in health plans, reported Mark Farrah Associates, a market data firm.
The Congressional Budget Office in January estimated 1 million people would enroll for coverage through SHOP in 2015. No one expected the SHOP exchange to have a large enrollment, but industry officials say its early response has been substantially smaller than expected.
“When you look at the cost and look at the take up rate, it certainly raises questions” about whether SHOP has been worthwhile, said Alissa Fox, senior vice president of the Blue Cross Blue Shield Association. “We never thought the business equation made sense.”
Employers with fewer than 50 full-time workers are eligible to buy coverage on SHOP. The federal government even offers businesses an incentive, a tax credit worth up to half of an employer’s share of their workers’ premiums. Among the conditions: The firm must employ fewer than 25 workers and their average salary cannot exceed $50,000. The credit is hardly used in high-cost areas of the country where salaries are higher.
Similar to the health insurance marketplace for individuals, the federal government operates the SHOP exchange in 34 states, and 16 other states plus the District of Columbia run their own small business exchanges. The state exchanges also capture a small share of the small business market, based on more current figures compiled by Kaiser Health News. As of early October, five state-run SHOP exchanges – Idaho, Kentucky, Maryland, Minnesota, and Washington – had sold coverage to fewer than 200 employers. New York and California have the highest enrollments, and together those two states account for about 6,500 employers and nearly 50,000 people.
The Obama administration hoped SHOP would make it easier and cheaper for small employers to offer coverage to employees and for their workers to have a choice of plans.
Unlike the federal- and state-run health insurance exchanges for individuals that limit sign-up to a certain period during the year, the SHOP exchanges allow companies to enroll at any time.
But several factors account for the paltry enrollment in SHOP, say insurance brokers, insurers, and state officials. Brokers say SHOP has fewer health plans and more expensive coverage policies than can be purchased outside the exchange. Several states only have one insurer on their SHOP exchange, including Alabama, Tennessee, North Carolina and Nebraska, according to consulting firm Leavitt Partners.
Many small employers have stuck with plans they purchased outside SHOP because the Obama administration gave them the option to remain with their existing policies until 2017. That enabled employers to stay in plans that don’t meet all the new requirements of the health law, including so-called “essential health benefits.” These additional benefits can drive up the cost of policies, making it harder for the SHOP plans to compete.
Another factor that slowed enrollment in SHOP has been software problems in several states that made it hard for employers and employees to sign up. In addition, the SHOP exchange run by the federal government launched in October 2013 was only available if employers contacted an agent or broker. Its full website was not running until fall 2014.
“With all that stacked up against it, it does not surprise me that the numbers are so low,” said Kevin Lucia, a research professor at Georgetown University Health Policy Institute, who studied the rollout.
Kevin Counihan, the Obama administration’s top insurance exchange official, acknowledges SHOP will only be a “niche product” and most policies will still be sold outside the marketplace. Still, he expects as more employers and insurance brokers learn about SHOP, that its enrollment will grow. Asked in an interview about low enrollment, he said: “It doesn’t really bother me … something like this takes time.”
Mr. Counihan said the key will be to get more brokers interested in selling the SHOP plans.
But many brokers say they don’t see the value of SHOP since it typically offers fewer options than outside the exchanges. “There really is no reason to go to SHOP unless you qualify for the tax credits,” said Ken Stevenson, a Tallahassee, Fla., insurance agent. Four Florida insurers sell on SHOP, fewer than half available in the state. Florida Blue, the state’s largest insurer, said less than 1% of its small group policies are sold on the SHOP.
Other brokers say enrollment on SHOP is more confusing than working directly with carriers. “It’s difficult to get through the website, and it’s a lot easier for employers to pick up the phone and call a broker than spend 4 hours on the SHOP site,” said Alan Schulman, a Bethesda, Md., insurance agent.
The SHOP was set to expand to open for businesses with up to 100 employees in 2016, but Congress and President Obama rescinded that requirement in November.
One company to get the tax credit is Paloma Clothing, a women’s clothing store in Portland, Ore. Co-owner Mike Roach said he signed up for SHOP plan last year on the recommendation of his insurance agent. The credit saved his company about $7,000. That savings, he said, made it affordable for Paloma to keep its share of its employees’ monthly insurance premiums at 85%.
“The tax credit saved us from the terrific, morale-crushing option of decreasing our health insurance coverage for our employees,” he said. Eight of the store’s 15 employees signed up for the SHOP policy sold by Moda Health. Most pay about $45 a month for their share of the premium.
Mr. Roach said he is thankful for the health law. “Wow, finally someone did something to help small businesses deal with the rising cost of providing employees health insurance,” he said. “For so many years … no one did anything but feel sorry for you.”
After nearly 2 years in operation and millions of dollars spent in development, the small business health insurance exchange created by the Affordable Care Act is struggling to catch on.
Nationally, about 85,000 people, from 11,000 small businesses, have coverage through the online marketplace known as the Small Business Health Options Program, or SHOP, according to the latest federal data released in May. Those totals do not include employers that began coverage in 2014 and have not yet renewed their coverage through HealthCare.gov for 2015.
That’s less than 1% of people with coverage in the U.S. small group insurance market that in 2013 had about 16.7 million people enrolled in health plans, reported Mark Farrah Associates, a market data firm.
The Congressional Budget Office in January estimated 1 million people would enroll for coverage through SHOP in 2015. No one expected the SHOP exchange to have a large enrollment, but industry officials say its early response has been substantially smaller than expected.
“When you look at the cost and look at the take up rate, it certainly raises questions” about whether SHOP has been worthwhile, said Alissa Fox, senior vice president of the Blue Cross Blue Shield Association. “We never thought the business equation made sense.”
Employers with fewer than 50 full-time workers are eligible to buy coverage on SHOP. The federal government even offers businesses an incentive, a tax credit worth up to half of an employer’s share of their workers’ premiums. Among the conditions: The firm must employ fewer than 25 workers and their average salary cannot exceed $50,000. The credit is hardly used in high-cost areas of the country where salaries are higher.
Similar to the health insurance marketplace for individuals, the federal government operates the SHOP exchange in 34 states, and 16 other states plus the District of Columbia run their own small business exchanges. The state exchanges also capture a small share of the small business market, based on more current figures compiled by Kaiser Health News. As of early October, five state-run SHOP exchanges – Idaho, Kentucky, Maryland, Minnesota, and Washington – had sold coverage to fewer than 200 employers. New York and California have the highest enrollments, and together those two states account for about 6,500 employers and nearly 50,000 people.
The Obama administration hoped SHOP would make it easier and cheaper for small employers to offer coverage to employees and for their workers to have a choice of plans.
Unlike the federal- and state-run health insurance exchanges for individuals that limit sign-up to a certain period during the year, the SHOP exchanges allow companies to enroll at any time.
But several factors account for the paltry enrollment in SHOP, say insurance brokers, insurers, and state officials. Brokers say SHOP has fewer health plans and more expensive coverage policies than can be purchased outside the exchange. Several states only have one insurer on their SHOP exchange, including Alabama, Tennessee, North Carolina and Nebraska, according to consulting firm Leavitt Partners.
Many small employers have stuck with plans they purchased outside SHOP because the Obama administration gave them the option to remain with their existing policies until 2017. That enabled employers to stay in plans that don’t meet all the new requirements of the health law, including so-called “essential health benefits.” These additional benefits can drive up the cost of policies, making it harder for the SHOP plans to compete.
Another factor that slowed enrollment in SHOP has been software problems in several states that made it hard for employers and employees to sign up. In addition, the SHOP exchange run by the federal government launched in October 2013 was only available if employers contacted an agent or broker. Its full website was not running until fall 2014.
“With all that stacked up against it, it does not surprise me that the numbers are so low,” said Kevin Lucia, a research professor at Georgetown University Health Policy Institute, who studied the rollout.
Kevin Counihan, the Obama administration’s top insurance exchange official, acknowledges SHOP will only be a “niche product” and most policies will still be sold outside the marketplace. Still, he expects as more employers and insurance brokers learn about SHOP, that its enrollment will grow. Asked in an interview about low enrollment, he said: “It doesn’t really bother me … something like this takes time.”
Mr. Counihan said the key will be to get more brokers interested in selling the SHOP plans.
But many brokers say they don’t see the value of SHOP since it typically offers fewer options than outside the exchanges. “There really is no reason to go to SHOP unless you qualify for the tax credits,” said Ken Stevenson, a Tallahassee, Fla., insurance agent. Four Florida insurers sell on SHOP, fewer than half available in the state. Florida Blue, the state’s largest insurer, said less than 1% of its small group policies are sold on the SHOP.
Other brokers say enrollment on SHOP is more confusing than working directly with carriers. “It’s difficult to get through the website, and it’s a lot easier for employers to pick up the phone and call a broker than spend 4 hours on the SHOP site,” said Alan Schulman, a Bethesda, Md., insurance agent.
The SHOP was set to expand to open for businesses with up to 100 employees in 2016, but Congress and President Obama rescinded that requirement in November.
One company to get the tax credit is Paloma Clothing, a women’s clothing store in Portland, Ore. Co-owner Mike Roach said he signed up for SHOP plan last year on the recommendation of his insurance agent. The credit saved his company about $7,000. That savings, he said, made it affordable for Paloma to keep its share of its employees’ monthly insurance premiums at 85%.
“The tax credit saved us from the terrific, morale-crushing option of decreasing our health insurance coverage for our employees,” he said. Eight of the store’s 15 employees signed up for the SHOP policy sold by Moda Health. Most pay about $45 a month for their share of the premium.
Mr. Roach said he is thankful for the health law. “Wow, finally someone did something to help small businesses deal with the rising cost of providing employees health insurance,” he said. “For so many years … no one did anything but feel sorry for you.”

AMA expands med schools in education consortium
The American Medical Association has added 20 schools to its Accelerating Change in Medical Education Consortium in an effort to better prepare students for the rapid change in medical practice.
“With medicine and health care delivery in the United States changing in such new and exciting ways, we’ve asked for and are starting to receive a medical education system that keeps pace with this rate of change,” Dr. James Madara, AMA chief operating officer, said during a Nov. 4 press teleconference. “This means trying new content, giving students information they need to know but in the past haven’t been taught, [and] trying new methods,” such as better understanding whether certain content is better shared through lecture or via simulation or electronic channels.

The program launched in 2013 with 11 schools. The new schools added were culled from proposals submitted by 108 of 170 eligible academic institutions.
“We sought proposals that would significantly redesign medical education and these experts reviewed entries with that goal in mind,” said Dr. Susan Skochelak, AMA group vice president for medical education. “The advisory panel evaluated each school’s proposal based on how the project would align with or enhance the 11 founding schools’ work and the projects’ uniqueness and feasibility for implementation at other medical schools.”
Winning programs cover concepts such as care coordination in accountable care organizations, advanced simulation and telemedicine technologies, and addressing the needs of underserved and diverse communities.
The new schools entering the consortium include A. T. Still University School of Osteopathic Medicine, Mesa, Ariz.; Case Western Reserve University, Cleveland; Eastern Virgina Medical School, Norfolk; Emory University, Atlanta; Florida International University, Miami; Harvard Medical School, Boston; Morehouse School of Medicine, Atlanta; Ohio University Heritage College of Osteopathic Medicine, Cleveland campus; Robert Wood Johnson Medical School, New Brunswick, N.J.; City College of New York Sophie Davis School of Biomedical Education, New York; Thomas Jefferson University Sidney Kimmel Medical College, Philadelphia; University of Chicago; University of Connecticut, Farmington; University of Nebraska, Omaha; University of North Carolina at Chapel Hill; University of North Dakota, Grand Forks; University of Texas, Austin; University of Texas Rio Grande Valley School of Medicine, South Texas; University of Utah, Salt Lake City; and University of Washington, Seattle.
“By tripling the number of schools participating in this effort, we know that we will be able to more quickly disseminate the consortium schools’ innovative curriculum models to create the seismic shift that our medical education system needs so that our future physicians can better care for their patients,” Dr. Madara said.
The American Medical Association has added 20 schools to its Accelerating Change in Medical Education Consortium in an effort to better prepare students for the rapid change in medical practice.
“With medicine and health care delivery in the United States changing in such new and exciting ways, we’ve asked for and are starting to receive a medical education system that keeps pace with this rate of change,” Dr. James Madara, AMA chief operating officer, said during a Nov. 4 press teleconference. “This means trying new content, giving students information they need to know but in the past haven’t been taught, [and] trying new methods,” such as better understanding whether certain content is better shared through lecture or via simulation or electronic channels.
The program launched in 2013 with 11 schools. The new schools added were culled from proposals submitted by 108 of 170 eligible academic institutions.
“We sought proposals that would significantly redesign medical education and these experts reviewed entries with that goal in mind,” said Dr. Susan Skochelak, AMA group vice president for medical education. “The advisory panel evaluated each school’s proposal based on how the project would align with or enhance the 11 founding schools’ work and the projects’ uniqueness and feasibility for implementation at other medical schools.”
Winning programs cover concepts such as care coordination in accountable care organizations, advanced simulation and telemedicine technologies, and addressing the needs of underserved and diverse communities.
The new schools entering the consortium include A. T. Still University School of Osteopathic Medicine, Mesa, Ariz.; Case Western Reserve University, Cleveland; Eastern Virgina Medical School, Norfolk; Emory University, Atlanta; Florida International University, Miami; Harvard Medical School, Boston; Morehouse School of Medicine, Atlanta; Ohio University Heritage College of Osteopathic Medicine, Cleveland campus; Robert Wood Johnson Medical School, New Brunswick, N.J.; City College of New York Sophie Davis School of Biomedical Education, New York; Thomas Jefferson University Sidney Kimmel Medical College, Philadelphia; University of Chicago; University of Connecticut, Farmington; University of Nebraska, Omaha; University of North Carolina at Chapel Hill; University of North Dakota, Grand Forks; University of Texas, Austin; University of Texas Rio Grande Valley School of Medicine, South Texas; University of Utah, Salt Lake City; and University of Washington, Seattle.
“By tripling the number of schools participating in this effort, we know that we will be able to more quickly disseminate the consortium schools’ innovative curriculum models to create the seismic shift that our medical education system needs so that our future physicians can better care for their patients,” Dr. Madara said.
The American Medical Association has added 20 schools to its Accelerating Change in Medical Education Consortium in an effort to better prepare students for the rapid change in medical practice.
“With medicine and health care delivery in the United States changing in such new and exciting ways, we’ve asked for and are starting to receive a medical education system that keeps pace with this rate of change,” Dr. James Madara, AMA chief operating officer, said during a Nov. 4 press teleconference. “This means trying new content, giving students information they need to know but in the past haven’t been taught, [and] trying new methods,” such as better understanding whether certain content is better shared through lecture or via simulation or electronic channels.
The program launched in 2013 with 11 schools. The new schools added were culled from proposals submitted by 108 of 170 eligible academic institutions.
“We sought proposals that would significantly redesign medical education and these experts reviewed entries with that goal in mind,” said Dr. Susan Skochelak, AMA group vice president for medical education. “The advisory panel evaluated each school’s proposal based on how the project would align with or enhance the 11 founding schools’ work and the projects’ uniqueness and feasibility for implementation at other medical schools.”
Winning programs cover concepts such as care coordination in accountable care organizations, advanced simulation and telemedicine technologies, and addressing the needs of underserved and diverse communities.
The new schools entering the consortium include A. T. Still University School of Osteopathic Medicine, Mesa, Ariz.; Case Western Reserve University, Cleveland; Eastern Virgina Medical School, Norfolk; Emory University, Atlanta; Florida International University, Miami; Harvard Medical School, Boston; Morehouse School of Medicine, Atlanta; Ohio University Heritage College of Osteopathic Medicine, Cleveland campus; Robert Wood Johnson Medical School, New Brunswick, N.J.; City College of New York Sophie Davis School of Biomedical Education, New York; Thomas Jefferson University Sidney Kimmel Medical College, Philadelphia; University of Chicago; University of Connecticut, Farmington; University of Nebraska, Omaha; University of North Carolina at Chapel Hill; University of North Dakota, Grand Forks; University of Texas, Austin; University of Texas Rio Grande Valley School of Medicine, South Texas; University of Utah, Salt Lake City; and University of Washington, Seattle.
“By tripling the number of schools participating in this effort, we know that we will be able to more quickly disseminate the consortium schools’ innovative curriculum models to create the seismic shift that our medical education system needs so that our future physicians can better care for their patients,” Dr. Madara said.

Adolescent lap band removal rate swells by 5 years
LOS ANGELES – An increasing number of adolescents are undergoing gastric band removal after 2 years post operation, a prospective, longitudinal study shows.
“At 2 years most bands are still in place, with 96% of patients having them. After this point, however, multiple bands are removed each year, demonstrating that 2 years perhaps is only the tip of the iceberg,” Dr. Christine Schad said at Obesity Week.

Indeed, the number of adolescents with bands in place reduced to 87%, 76%, and 53% at years 3, 4, and 5 of follow-up. After 5 years, patients continued to undergo band removal.
Like their adult counterparts, adolescents underwent band removal secondary to weight loss failure, reflux esophagitis, and refractory gastric prolapse, Dr. Schad of Morgan Stanley Children’s Hospital, New York-Presbyterian Columbia University Medical Center, New York, said.
Weight loss seemed to plateau over time among the 79 evaluable adolescents, with less than 39% of patients able to lose more than 50% of their excess body weight over the 5-year study.
“Although gastric banding can be performed safely, 2 years seems inadequate to evaluate efficacy,” she said.
The use of adjustable gastric banding rose rapidly after Food and Drug Administration approval in 2001, thanks to low perioperative morbidity, reversibility, and good early results.
Gastric banding has fallen sharply, however, with recent adult studies showing a high incidence of weight loss failure, weight regain, and device-related complications.
Previous studies have reported on the safety of laparoscopic adjustable gastric banding in adolescents; however, these studies are limited to 3-year follow-up at most, Dr. Schad said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
The investigators enrolled 137 morbidly obese adolescents, aged 14-18 years, who underwent laparoscopic adjustable gastric banding from 2006 to 2011. The current analysis included patients with at least 5 years follow-up and patients who had band removal at any point or who did not survive to study end. There were two deaths. The remaining patients had not reached the 5-year follow-up mark or still had their bands in place.
The 79 evaluable patients had a preoperative weight of 138 kg, body mass index of 49.3 kg/m2, and excess body weight of 47.2%. At the time of surgery, their average age was 16.9 years, 71% were female, 43% Hispanic, 36.7% white, and 16.5% black.
Even though gastric banding is declining, the results are important because there has been little information about adolescents, and in some parts of the country, gastric banding may be the only available option, session comoderator Dr. Robert Carpenter of Scott & White Healthcare in Temple, Tex., said in an interview.
“The other issue is that there are a lot of pediatricians that only want their patients to have nonstapled, nondivided operations,” he said. “If that’s the case, and we now know that perhaps for adolescents there is a 30%, 40%, 50% conversion and/or failure rate, then we are putting these kids at an extreme risk.”
Oftentimes, these adolescents also won’t have an opportunity for another operation.
“Many insurance companies that they’ll transition to away from their parents will actually have a complete exclusion for bariatric surgery or they have a onetime, lifetime operative opportunity,” Dr. Carpenter said. “So, if that’s been burned, it’s burned.”
LOS ANGELES – An increasing number of adolescents are undergoing gastric band removal after 2 years post operation, a prospective, longitudinal study shows.
“At 2 years most bands are still in place, with 96% of patients having them. After this point, however, multiple bands are removed each year, demonstrating that 2 years perhaps is only the tip of the iceberg,” Dr. Christine Schad said at Obesity Week.
Indeed, the number of adolescents with bands in place reduced to 87%, 76%, and 53% at years 3, 4, and 5 of follow-up. After 5 years, patients continued to undergo band removal.
Like their adult counterparts, adolescents underwent band removal secondary to weight loss failure, reflux esophagitis, and refractory gastric prolapse, Dr. Schad of Morgan Stanley Children’s Hospital, New York-Presbyterian Columbia University Medical Center, New York, said.
Weight loss seemed to plateau over time among the 79 evaluable adolescents, with less than 39% of patients able to lose more than 50% of their excess body weight over the 5-year study.
“Although gastric banding can be performed safely, 2 years seems inadequate to evaluate efficacy,” she said.
The use of adjustable gastric banding rose rapidly after Food and Drug Administration approval in 2001, thanks to low perioperative morbidity, reversibility, and good early results.
Gastric banding has fallen sharply, however, with recent adult studies showing a high incidence of weight loss failure, weight regain, and device-related complications.
Previous studies have reported on the safety of laparoscopic adjustable gastric banding in adolescents; however, these studies are limited to 3-year follow-up at most, Dr. Schad said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
The investigators enrolled 137 morbidly obese adolescents, aged 14-18 years, who underwent laparoscopic adjustable gastric banding from 2006 to 2011. The current analysis included patients with at least 5 years follow-up and patients who had band removal at any point or who did not survive to study end. There were two deaths. The remaining patients had not reached the 5-year follow-up mark or still had their bands in place.
The 79 evaluable patients had a preoperative weight of 138 kg, body mass index of 49.3 kg/m2, and excess body weight of 47.2%. At the time of surgery, their average age was 16.9 years, 71% were female, 43% Hispanic, 36.7% white, and 16.5% black.
Even though gastric banding is declining, the results are important because there has been little information about adolescents, and in some parts of the country, gastric banding may be the only available option, session comoderator Dr. Robert Carpenter of Scott & White Healthcare in Temple, Tex., said in an interview.
“The other issue is that there are a lot of pediatricians that only want their patients to have nonstapled, nondivided operations,” he said. “If that’s the case, and we now know that perhaps for adolescents there is a 30%, 40%, 50% conversion and/or failure rate, then we are putting these kids at an extreme risk.”
Oftentimes, these adolescents also won’t have an opportunity for another operation.
“Many insurance companies that they’ll transition to away from their parents will actually have a complete exclusion for bariatric surgery or they have a onetime, lifetime operative opportunity,” Dr. Carpenter said. “So, if that’s been burned, it’s burned.”
LOS ANGELES – An increasing number of adolescents are undergoing gastric band removal after 2 years post operation, a prospective, longitudinal study shows.
“At 2 years most bands are still in place, with 96% of patients having them. After this point, however, multiple bands are removed each year, demonstrating that 2 years perhaps is only the tip of the iceberg,” Dr. Christine Schad said at Obesity Week.
Indeed, the number of adolescents with bands in place reduced to 87%, 76%, and 53% at years 3, 4, and 5 of follow-up. After 5 years, patients continued to undergo band removal.
Like their adult counterparts, adolescents underwent band removal secondary to weight loss failure, reflux esophagitis, and refractory gastric prolapse, Dr. Schad of Morgan Stanley Children’s Hospital, New York-Presbyterian Columbia University Medical Center, New York, said.
Weight loss seemed to plateau over time among the 79 evaluable adolescents, with less than 39% of patients able to lose more than 50% of their excess body weight over the 5-year study.
“Although gastric banding can be performed safely, 2 years seems inadequate to evaluate efficacy,” she said.
The use of adjustable gastric banding rose rapidly after Food and Drug Administration approval in 2001, thanks to low perioperative morbidity, reversibility, and good early results.
Gastric banding has fallen sharply, however, with recent adult studies showing a high incidence of weight loss failure, weight regain, and device-related complications.
Previous studies have reported on the safety of laparoscopic adjustable gastric banding in adolescents; however, these studies are limited to 3-year follow-up at most, Dr. Schad said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
The investigators enrolled 137 morbidly obese adolescents, aged 14-18 years, who underwent laparoscopic adjustable gastric banding from 2006 to 2011. The current analysis included patients with at least 5 years follow-up and patients who had band removal at any point or who did not survive to study end. There were two deaths. The remaining patients had not reached the 5-year follow-up mark or still had their bands in place.
The 79 evaluable patients had a preoperative weight of 138 kg, body mass index of 49.3 kg/m2, and excess body weight of 47.2%. At the time of surgery, their average age was 16.9 years, 71% were female, 43% Hispanic, 36.7% white, and 16.5% black.
Even though gastric banding is declining, the results are important because there has been little information about adolescents, and in some parts of the country, gastric banding may be the only available option, session comoderator Dr. Robert Carpenter of Scott & White Healthcare in Temple, Tex., said in an interview.
“The other issue is that there are a lot of pediatricians that only want their patients to have nonstapled, nondivided operations,” he said. “If that’s the case, and we now know that perhaps for adolescents there is a 30%, 40%, 50% conversion and/or failure rate, then we are putting these kids at an extreme risk.”
Oftentimes, these adolescents also won’t have an opportunity for another operation.
“Many insurance companies that they’ll transition to away from their parents will actually have a complete exclusion for bariatric surgery or they have a onetime, lifetime operative opportunity,” Dr. Carpenter said. “So, if that’s been burned, it’s burned.”
AT OBESITY WEEK 2015
Key clinical point: Adolescents undergo laparoscopic adjustable gastric band removal at increasing numbers after 2 years post operation.
Major finding: The percentage of bands in place was 96% at 2 years, declining to 87%, 76%, and 53% at years 3, 4, and 5.
Data source: Prospective, longitudinal study in 79 adolescents.
Disclosures: Dr. Schad reported having no disclosures.

Conservative management for AR safe at 10 years
Whether to operate on patients with severe aortic regurgitation (AR) before or after symptoms appear has been a point of controversy among cardiothoracic surgeons, but a recent study has found that patients who have early surgery may not fare any better for up to 10 years than those who opt for a more conservative “watchful waiting” course of care.
Investigators from Belgium reported results from an analysis of 160 patients in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1100-08). “In asymptomatic severe AR, delaying surgery until the onset of class I/IIa operative triggers is safe, supporting current guidelines,” said Dr. Christophe de Meester and colleagues at the Catholic University of Louvain and St. Luc University Clinic in Brussels.
The goal of the study was to evaluate long-term outcomes and incidence of cardiac complications in patients with severe AR who did not have any signs and symptoms that called for surgery, and who either had surgery early on or entered conservative management and eventually had an operation when signs and symptoms did appear.
The study found that close follow-up and monitoring of patients with severe AR was a cornerstone of successful conservative management. “We found that survival was similar between the two groups,” Dr. De Meester and coauthors said. “Better survival was nonetheless observed in conservatively managed patients with regular as opposed to no or a looser follow-up.”
The most recent European Society of Cardiology (ESC) guidelines and American Heart Association/American College of Cardiology guidelines state that symptomatic severe AR is a class I indication for surgery regardless of left ventricular (LV) systolic function.
However, Dr. De Meester and colleagues said, the timing of that surgery is not so clear-cut. Earlier studies have shown that surgery could be delayed for patients with minimal symptoms, but more recent evidence has suggested the opposite, according to the study. Two factors favor surgery before symptoms arise – poor aortic valve repair outcomes in patients with symptoms of heart failure and long-standing severe AR, which eventually leads to LV dysfunction.
Yet, the latest ESC guidelines have been “reluctant” to make a strong case for early surgery before symptoms of LV dysfunction appear, and the AHA/ACC guidelines call for surgery only when symptoms of LV dysfunction or LV dilatation develop, Dr. de Meester and his coauthors said.
In the past, the risks of aortic valve replacement were too high to consider early surgery, the study authors said. “However, with the advent of aortic valve repair, operative mortality and long-term outcomes have improved to such an extent that early surgery has become a plausible option for patients.”
But the risk of these patients developing symptoms for surgery was nonetheless low over 10 years, the study found: 7.4% for developing severe LV dilatation; 0.6% for becoming symptomatic; and 0.9% for developing LV dysfunction. Overall, the rate of adverse events in the study population was 9.9% at 10 years.
In the study, 69 patients were initially managed conservatively, 49 of whom were in the watchful waiting group that visited a cardiologist at least annually and another 20 considered an “irregular follow-up subgroup.” Among the watchful waiting group, 31 developed symptoms for surgery (only two declined surgery). Watchful waiting patients had five- and 10-year survival of 100% and 95%, respectively, compared with 90% and 79% among those who had irregular follow-up.
Overall, the conservatively managed group had outcomes better than or equal to the early surgery group. Ten-year cardiovascular survival was 96% in both groups, whereas event-free survival was 92% at 10 years in the conservatively managed group vs. 81% in the early surgery group.
The study was supported by the Belgium National Fund for Scientific Research. The authors had no conflicts to disclose.
The design of the Belgium study “challenges” existing treatment guidelines for asymptomatic chronic aortic insufficiency in two ways, Dr. Leora Balsam and Dr. Abe deAndra Jr., both of the New York University-Langone Medical Center, write in their commentary (J Thorac Cardiovasc Surg. 2015;150:1108-10): first, by making aortic valve repair the preferred surgical treatment in the study and, secondly, by offering surgery to both symptomatic and asymptomatic patients.
“In the era of evidence-based medicine,” Dr. Balsam and Dr. deAndra wrote, “there remains a need for research and innovation even in areas where guidelines exist.”
While many authors have described aortic valve repair as an alternative to aortic valve replacement for chronic severe aortic insufficiency, Dr. Balsam and Dr. deAndra explained that the term aortic valve repair “encompasses a wide array of techniques,” among them valve-sparing aortic root replacement, subcommissural annuloplasty and “myriad” leaf resection, plication, and reconstruction techniques. Because of mounting reports of excellent results with aortic valve repair techniques, growing ranks of cardiothoracic surgeons have advocated for repair as an early intervention for aortic valve problems. But the question remains: “Have we identified the optimal triggers for intervention for aortic insufficiency?” they asked. “The answer is probably no, and that newer technology and diagnostic studies will better discriminate between patients that can benefit from intervention and those that will not.”
Dr. Balsam and Dr. deAndra had no disclosures.
The design of the Belgium study “challenges” existing treatment guidelines for asymptomatic chronic aortic insufficiency in two ways, Dr. Leora Balsam and Dr. Abe deAndra Jr., both of the New York University-Langone Medical Center, write in their commentary (J Thorac Cardiovasc Surg. 2015;150:1108-10): first, by making aortic valve repair the preferred surgical treatment in the study and, secondly, by offering surgery to both symptomatic and asymptomatic patients.
“In the era of evidence-based medicine,” Dr. Balsam and Dr. deAndra wrote, “there remains a need for research and innovation even in areas where guidelines exist.”
While many authors have described aortic valve repair as an alternative to aortic valve replacement for chronic severe aortic insufficiency, Dr. Balsam and Dr. deAndra explained that the term aortic valve repair “encompasses a wide array of techniques,” among them valve-sparing aortic root replacement, subcommissural annuloplasty and “myriad” leaf resection, plication, and reconstruction techniques. Because of mounting reports of excellent results with aortic valve repair techniques, growing ranks of cardiothoracic surgeons have advocated for repair as an early intervention for aortic valve problems. But the question remains: “Have we identified the optimal triggers for intervention for aortic insufficiency?” they asked. “The answer is probably no, and that newer technology and diagnostic studies will better discriminate between patients that can benefit from intervention and those that will not.”
Dr. Balsam and Dr. deAndra had no disclosures.
The design of the Belgium study “challenges” existing treatment guidelines for asymptomatic chronic aortic insufficiency in two ways, Dr. Leora Balsam and Dr. Abe deAndra Jr., both of the New York University-Langone Medical Center, write in their commentary (J Thorac Cardiovasc Surg. 2015;150:1108-10): first, by making aortic valve repair the preferred surgical treatment in the study and, secondly, by offering surgery to both symptomatic and asymptomatic patients.
“In the era of evidence-based medicine,” Dr. Balsam and Dr. deAndra wrote, “there remains a need for research and innovation even in areas where guidelines exist.”
While many authors have described aortic valve repair as an alternative to aortic valve replacement for chronic severe aortic insufficiency, Dr. Balsam and Dr. deAndra explained that the term aortic valve repair “encompasses a wide array of techniques,” among them valve-sparing aortic root replacement, subcommissural annuloplasty and “myriad” leaf resection, plication, and reconstruction techniques. Because of mounting reports of excellent results with aortic valve repair techniques, growing ranks of cardiothoracic surgeons have advocated for repair as an early intervention for aortic valve problems. But the question remains: “Have we identified the optimal triggers for intervention for aortic insufficiency?” they asked. “The answer is probably no, and that newer technology and diagnostic studies will better discriminate between patients that can benefit from intervention and those that will not.”
Dr. Balsam and Dr. deAndra had no disclosures.
Whether to operate on patients with severe aortic regurgitation (AR) before or after symptoms appear has been a point of controversy among cardiothoracic surgeons, but a recent study has found that patients who have early surgery may not fare any better for up to 10 years than those who opt for a more conservative “watchful waiting” course of care.
Investigators from Belgium reported results from an analysis of 160 patients in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1100-08). “In asymptomatic severe AR, delaying surgery until the onset of class I/IIa operative triggers is safe, supporting current guidelines,” said Dr. Christophe de Meester and colleagues at the Catholic University of Louvain and St. Luc University Clinic in Brussels.
The goal of the study was to evaluate long-term outcomes and incidence of cardiac complications in patients with severe AR who did not have any signs and symptoms that called for surgery, and who either had surgery early on or entered conservative management and eventually had an operation when signs and symptoms did appear.
The study found that close follow-up and monitoring of patients with severe AR was a cornerstone of successful conservative management. “We found that survival was similar between the two groups,” Dr. De Meester and coauthors said. “Better survival was nonetheless observed in conservatively managed patients with regular as opposed to no or a looser follow-up.”
The most recent European Society of Cardiology (ESC) guidelines and American Heart Association/American College of Cardiology guidelines state that symptomatic severe AR is a class I indication for surgery regardless of left ventricular (LV) systolic function.
However, Dr. De Meester and colleagues said, the timing of that surgery is not so clear-cut. Earlier studies have shown that surgery could be delayed for patients with minimal symptoms, but more recent evidence has suggested the opposite, according to the study. Two factors favor surgery before symptoms arise – poor aortic valve repair outcomes in patients with symptoms of heart failure and long-standing severe AR, which eventually leads to LV dysfunction.
Yet, the latest ESC guidelines have been “reluctant” to make a strong case for early surgery before symptoms of LV dysfunction appear, and the AHA/ACC guidelines call for surgery only when symptoms of LV dysfunction or LV dilatation develop, Dr. de Meester and his coauthors said.
In the past, the risks of aortic valve replacement were too high to consider early surgery, the study authors said. “However, with the advent of aortic valve repair, operative mortality and long-term outcomes have improved to such an extent that early surgery has become a plausible option for patients.”
But the risk of these patients developing symptoms for surgery was nonetheless low over 10 years, the study found: 7.4% for developing severe LV dilatation; 0.6% for becoming symptomatic; and 0.9% for developing LV dysfunction. Overall, the rate of adverse events in the study population was 9.9% at 10 years.
In the study, 69 patients were initially managed conservatively, 49 of whom were in the watchful waiting group that visited a cardiologist at least annually and another 20 considered an “irregular follow-up subgroup.” Among the watchful waiting group, 31 developed symptoms for surgery (only two declined surgery). Watchful waiting patients had five- and 10-year survival of 100% and 95%, respectively, compared with 90% and 79% among those who had irregular follow-up.
Overall, the conservatively managed group had outcomes better than or equal to the early surgery group. Ten-year cardiovascular survival was 96% in both groups, whereas event-free survival was 92% at 10 years in the conservatively managed group vs. 81% in the early surgery group.
The study was supported by the Belgium National Fund for Scientific Research. The authors had no conflicts to disclose.
Whether to operate on patients with severe aortic regurgitation (AR) before or after symptoms appear has been a point of controversy among cardiothoracic surgeons, but a recent study has found that patients who have early surgery may not fare any better for up to 10 years than those who opt for a more conservative “watchful waiting” course of care.
Investigators from Belgium reported results from an analysis of 160 patients in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1100-08). “In asymptomatic severe AR, delaying surgery until the onset of class I/IIa operative triggers is safe, supporting current guidelines,” said Dr. Christophe de Meester and colleagues at the Catholic University of Louvain and St. Luc University Clinic in Brussels.
The goal of the study was to evaluate long-term outcomes and incidence of cardiac complications in patients with severe AR who did not have any signs and symptoms that called for surgery, and who either had surgery early on or entered conservative management and eventually had an operation when signs and symptoms did appear.
The study found that close follow-up and monitoring of patients with severe AR was a cornerstone of successful conservative management. “We found that survival was similar between the two groups,” Dr. De Meester and coauthors said. “Better survival was nonetheless observed in conservatively managed patients with regular as opposed to no or a looser follow-up.”
The most recent European Society of Cardiology (ESC) guidelines and American Heart Association/American College of Cardiology guidelines state that symptomatic severe AR is a class I indication for surgery regardless of left ventricular (LV) systolic function.
However, Dr. De Meester and colleagues said, the timing of that surgery is not so clear-cut. Earlier studies have shown that surgery could be delayed for patients with minimal symptoms, but more recent evidence has suggested the opposite, according to the study. Two factors favor surgery before symptoms arise – poor aortic valve repair outcomes in patients with symptoms of heart failure and long-standing severe AR, which eventually leads to LV dysfunction.
Yet, the latest ESC guidelines have been “reluctant” to make a strong case for early surgery before symptoms of LV dysfunction appear, and the AHA/ACC guidelines call for surgery only when symptoms of LV dysfunction or LV dilatation develop, Dr. de Meester and his coauthors said.
In the past, the risks of aortic valve replacement were too high to consider early surgery, the study authors said. “However, with the advent of aortic valve repair, operative mortality and long-term outcomes have improved to such an extent that early surgery has become a plausible option for patients.”
But the risk of these patients developing symptoms for surgery was nonetheless low over 10 years, the study found: 7.4% for developing severe LV dilatation; 0.6% for becoming symptomatic; and 0.9% for developing LV dysfunction. Overall, the rate of adverse events in the study population was 9.9% at 10 years.
In the study, 69 patients were initially managed conservatively, 49 of whom were in the watchful waiting group that visited a cardiologist at least annually and another 20 considered an “irregular follow-up subgroup.” Among the watchful waiting group, 31 developed symptoms for surgery (only two declined surgery). Watchful waiting patients had five- and 10-year survival of 100% and 95%, respectively, compared with 90% and 79% among those who had irregular follow-up.
Overall, the conservatively managed group had outcomes better than or equal to the early surgery group. Ten-year cardiovascular survival was 96% in both groups, whereas event-free survival was 92% at 10 years in the conservatively managed group vs. 81% in the early surgery group.
The study was supported by the Belgium National Fund for Scientific Research. The authors had no conflicts to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Delaying surgery until the onset of symptoms of aortic insufficiency is safe, in support of current clinical guidelines.
Major finding: Ten-year cardiovascular survival was equal among conservatively managed and early-surgery groups, but event free survival was 92% at 10 years in the conservatively managed group vs. 81% in the early surgery group.
Data source: Analysis of 160 consecutive asymptomatic patients with severe aortic regurgitation who were assigned to either conservative management or early surgery and followed up for a median of 7.2 years.
Disclosures: The Belgium National Fund of Scientific Research supported the study. The authors had no disclosures.
Robotic surgery progress: Is resistance futile?
Despite the lack of a clear-cut cost-effectiveness case, it appears that the use of robotics in surgery is on its way to becoming the norm.
What may help make that cost-effectiveness case is time, as the hardware becomes cheaper and the technology becomes more widespread.

“I think there are many surgeons who are doing robotic surgery who truly believe that the current of state of the art will bear only a partial resemblance to the state of the art 5-10 years from now,” Dr. Henry Pitt, chief quality officer of the Temple University Health System, Philadelphia, said in an interview. “And part of the persistence by many of the robotic surgeons, while they fully understand that what they are doing is not cost effective now, is that they believe that the next few generations of this technology will become the state of the art and will become cost effective.”
Dr. Pitt, an ACS Fellow, compared the evolution of robotic surgery to that of computers and the application of Moore’s Law, by which the technology advances rapidly while the price eventually comes down.
Spread of robot-assisted surgery
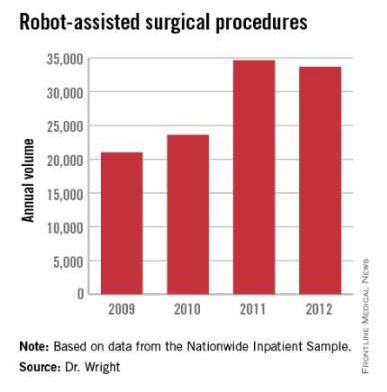
Research by the surgical robot industry and independent investigators shows that use of robotics is on an upward climb. A presentation at the 2015 American College of Surgeons Clinical Congress reveals that, based on retrospective review of the Nationwide Inpatient Sample from 2009-2012 using the ICD-9 code that identifies robot-assisted procedures, there were 113,022 robot-assisted procedures in that period.
In 2009, there were 21,006 procedures, with the volume growing to 33,713 in 2012. Perhaps more telling about the use of robotics is that it is not confined to specialties with a proven track record such as gynecology and urology. The study, led by Dr. G. Paul Wright of Grand Rapids Medical Education Partners and Michigan State University, shows an increase in robotics use in general surgery procedures by 4.5-fold from 2009-2012, with steady increases each year. General surgery accounted for 11.8% of robot-assisted cases in 2012, Dr. Wright and colleagues reported.
Dr. Wright suggested a number of factors contributing to the “surprising” growth of robotics in general surgery.
“I think the growth is stimulated, at least in part, by market forces,” he said in an interview. “For patients who are the consumers of health care, they are often drawn to [surgeons] whom they perceive to be on the cutting edge. Robotic surgery certainly offers that intrigue. With greater access to the technology, if a patient is seeking a robotic surgery that you do not offer as a surgeon, they can likely find that elsewhere, potentially at your competitor. Another driving force is potentially the ease of suturing with the robot which more resembles open surgery while advanced laparoscopic suturing in tight spaces is a more limited skill set among general surgeons.”
Dr. Wright added that “some of the stigma of robotic surgery is dissolving among surgeons as they become more familiar with the technology. I also believe the market forces will help drive down costs in robotics which may help to increase utilization as well.”
Industry touts cost effectiveness
And while Dr. Pitt is looking forward, the industry is energetically promoting the cost effectiveness of robotics today. Intuitive Surgical Inc., manufacturer of the da Vinci surgery robot presented in a recent press briefing data culled from literature found on PubMed showing that robotic surgery, at least with their product, is cost effective now (view the report at http://goo.gl/AfAuT3). But in recent years, the large number of clinical trials comparing robotic vs. laparoscopic surgery for colorectal disease, for example, is equivocal. For many procedures, trials appear to show similar between laparoscopic and robot-assisted approaches, with the main factors in play being length of operation time, hospital stay, and surgical site infection.
According to Intuitive Surgical’s manager of clinical economics, Andrew Yiu, a review of peer-reviewed articles that featured nationwide cohorts of comparisons and included comparisons to both open and laparoscopic procedures outcomes shows improvements across a variety of procedures in terms of hospital stay, lower conversion rates, reduced complications, reduced 30-day readmissions, and improved patient satisfaction, though outcomes were more pronounced in some areas compared with others. Highlighting one procedure in particular – benign hysterectomy – Mr. Yiu noted that rates of minor and major complications associated with robotic vs. laparoscopic surgery were relatively similar but that the conversion rate to open surgery from laparoscopic surgery was 3.9%, compared with 0.9% for da Vinci–assisted surgery.
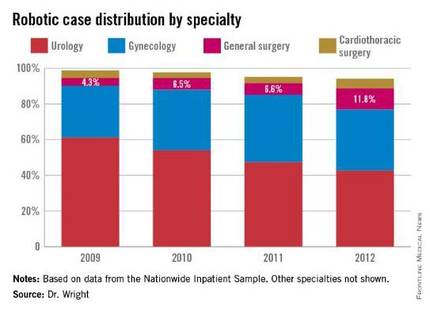
Overall, Intuitive Surgical calculated the potential savings on the episode of care with the da Vinci system at $1,087 vs. laparoscopic procedures and $2,996 over open surgery.
The company is currently promoting its da Vinci IX Surgical System. Cleared by the Food and Drug Administration in April 2014, Intuitive Surgical says that this latest version has broader capabilities than earlier generations and has been optimized for complex, multiquadrant surgeries.
Costs and other trade-offs
In some ways, robot-assisted surgery is following the same path as laparoscopic surgery, observed Dr. Tyler Hughes of the department of general surgery at McPherson (Kan.) Hospital.
“Certainly, we had the issue back in the late ‘80s and early ‘90s of laparoscopy,” Dr. Hughes said in an interview. “Was it cost effective? Because at the time $30,000 or $40,000 for a laparoscopic set-up seemed like a horse-choking amount of money. However, it converted a 5-day in-the-hospital experience to a 4-hour day-surgery experience. The nonclinical benefits to the patient were so enormous that it took the whole place by storm.”
Dr. Hughes, an ACS Fellow, suggested that the leap in savings elsewhere in the episode of care when using laparoscopic surgery over open surgery is not being mirrored in the robotic space and suggested that money should be spent in other areas of need.
“Cost is going to choke the future if we’re not careful. We need nurses. We need infrastructure. We need to be careful to buy things that really make a big difference,” he said.
In a study presented by at the ACS Clinical Congress on a cost-benefit analysis of robotic vs. laparoscopic colectomy, Anastasia Postoev, a fourth-year medical student at Caribbean Medical University in Willemstad, Curacao and her colleagues found little difference in clinical outcomes but higher costs as a result of added time needed to prepare the robot for surgery. The study showed that the potential up-front costs can be $1 to $2 million for the robot in addition to ongoing costs related to training and maintenance. Dr. Hughes said. “It is a terrific marketing tool in the sense that you can certainly attract a lot of people to a hospital with robotic surgery, but whether or not those outcomes are truly different and the cost of those outcomes are justifiable is yet to be determined.”
The ease of use of robotics, however, could end up being a double-edged sword, particularly if there are areas of the country where robotics may not be as pervasive, or in cases when a conversion to open surgery might be required.
“It is a real concern that trainees are being taught robotic surgery for what is not really needed to be robotic in the mainstream,” Dr. Hughes said. “Then they come out with less experience with straight stick laparoscopy and we’ve certainly seen lots of problems in the laparoscopic range for people once they get to the point that they have to convert to open. We really don’t have a large volume of trainee experience in complex open surgery. That’s a big problem. Robotics certainly isn’t going to make that a lot better.”
gtwachtman@frontlinemedcom.com
Despite the lack of a clear-cut cost-effectiveness case, it appears that the use of robotics in surgery is on its way to becoming the norm.
What may help make that cost-effectiveness case is time, as the hardware becomes cheaper and the technology becomes more widespread.
“I think there are many surgeons who are doing robotic surgery who truly believe that the current of state of the art will bear only a partial resemblance to the state of the art 5-10 years from now,” Dr. Henry Pitt, chief quality officer of the Temple University Health System, Philadelphia, said in an interview. “And part of the persistence by many of the robotic surgeons, while they fully understand that what they are doing is not cost effective now, is that they believe that the next few generations of this technology will become the state of the art and will become cost effective.”
Dr. Pitt, an ACS Fellow, compared the evolution of robotic surgery to that of computers and the application of Moore’s Law, by which the technology advances rapidly while the price eventually comes down.
Spread of robot-assisted surgery
Research by the surgical robot industry and independent investigators shows that use of robotics is on an upward climb. A presentation at the 2015 American College of Surgeons Clinical Congress reveals that, based on retrospective review of the Nationwide Inpatient Sample from 2009-2012 using the ICD-9 code that identifies robot-assisted procedures, there were 113,022 robot-assisted procedures in that period.
In 2009, there were 21,006 procedures, with the volume growing to 33,713 in 2012. Perhaps more telling about the use of robotics is that it is not confined to specialties with a proven track record such as gynecology and urology. The study, led by Dr. G. Paul Wright of Grand Rapids Medical Education Partners and Michigan State University, shows an increase in robotics use in general surgery procedures by 4.5-fold from 2009-2012, with steady increases each year. General surgery accounted for 11.8% of robot-assisted cases in 2012, Dr. Wright and colleagues reported.
Dr. Wright suggested a number of factors contributing to the “surprising” growth of robotics in general surgery.
“I think the growth is stimulated, at least in part, by market forces,” he said in an interview. “For patients who are the consumers of health care, they are often drawn to [surgeons] whom they perceive to be on the cutting edge. Robotic surgery certainly offers that intrigue. With greater access to the technology, if a patient is seeking a robotic surgery that you do not offer as a surgeon, they can likely find that elsewhere, potentially at your competitor. Another driving force is potentially the ease of suturing with the robot which more resembles open surgery while advanced laparoscopic suturing in tight spaces is a more limited skill set among general surgeons.”
Dr. Wright added that “some of the stigma of robotic surgery is dissolving among surgeons as they become more familiar with the technology. I also believe the market forces will help drive down costs in robotics which may help to increase utilization as well.”
Industry touts cost effectiveness
And while Dr. Pitt is looking forward, the industry is energetically promoting the cost effectiveness of robotics today. Intuitive Surgical Inc., manufacturer of the da Vinci surgery robot presented in a recent press briefing data culled from literature found on PubMed showing that robotic surgery, at least with their product, is cost effective now (view the report at http://goo.gl/AfAuT3). But in recent years, the large number of clinical trials comparing robotic vs. laparoscopic surgery for colorectal disease, for example, is equivocal. For many procedures, trials appear to show similar between laparoscopic and robot-assisted approaches, with the main factors in play being length of operation time, hospital stay, and surgical site infection.
According to Intuitive Surgical’s manager of clinical economics, Andrew Yiu, a review of peer-reviewed articles that featured nationwide cohorts of comparisons and included comparisons to both open and laparoscopic procedures outcomes shows improvements across a variety of procedures in terms of hospital stay, lower conversion rates, reduced complications, reduced 30-day readmissions, and improved patient satisfaction, though outcomes were more pronounced in some areas compared with others. Highlighting one procedure in particular – benign hysterectomy – Mr. Yiu noted that rates of minor and major complications associated with robotic vs. laparoscopic surgery were relatively similar but that the conversion rate to open surgery from laparoscopic surgery was 3.9%, compared with 0.9% for da Vinci–assisted surgery.
Overall, Intuitive Surgical calculated the potential savings on the episode of care with the da Vinci system at $1,087 vs. laparoscopic procedures and $2,996 over open surgery.
The company is currently promoting its da Vinci IX Surgical System. Cleared by the Food and Drug Administration in April 2014, Intuitive Surgical says that this latest version has broader capabilities than earlier generations and has been optimized for complex, multiquadrant surgeries.
Costs and other trade-offs
In some ways, robot-assisted surgery is following the same path as laparoscopic surgery, observed Dr. Tyler Hughes of the department of general surgery at McPherson (Kan.) Hospital.
“Certainly, we had the issue back in the late ‘80s and early ‘90s of laparoscopy,” Dr. Hughes said in an interview. “Was it cost effective? Because at the time $30,000 or $40,000 for a laparoscopic set-up seemed like a horse-choking amount of money. However, it converted a 5-day in-the-hospital experience to a 4-hour day-surgery experience. The nonclinical benefits to the patient were so enormous that it took the whole place by storm.”
Dr. Hughes, an ACS Fellow, suggested that the leap in savings elsewhere in the episode of care when using laparoscopic surgery over open surgery is not being mirrored in the robotic space and suggested that money should be spent in other areas of need.
“Cost is going to choke the future if we’re not careful. We need nurses. We need infrastructure. We need to be careful to buy things that really make a big difference,” he said.
In a study presented by at the ACS Clinical Congress on a cost-benefit analysis of robotic vs. laparoscopic colectomy, Anastasia Postoev, a fourth-year medical student at Caribbean Medical University in Willemstad, Curacao and her colleagues found little difference in clinical outcomes but higher costs as a result of added time needed to prepare the robot for surgery. The study showed that the potential up-front costs can be $1 to $2 million for the robot in addition to ongoing costs related to training and maintenance. Dr. Hughes said. “It is a terrific marketing tool in the sense that you can certainly attract a lot of people to a hospital with robotic surgery, but whether or not those outcomes are truly different and the cost of those outcomes are justifiable is yet to be determined.”
The ease of use of robotics, however, could end up being a double-edged sword, particularly if there are areas of the country where robotics may not be as pervasive, or in cases when a conversion to open surgery might be required.
“It is a real concern that trainees are being taught robotic surgery for what is not really needed to be robotic in the mainstream,” Dr. Hughes said. “Then they come out with less experience with straight stick laparoscopy and we’ve certainly seen lots of problems in the laparoscopic range for people once they get to the point that they have to convert to open. We really don’t have a large volume of trainee experience in complex open surgery. That’s a big problem. Robotics certainly isn’t going to make that a lot better.”
gtwachtman@frontlinemedcom.com
Despite the lack of a clear-cut cost-effectiveness case, it appears that the use of robotics in surgery is on its way to becoming the norm.
What may help make that cost-effectiveness case is time, as the hardware becomes cheaper and the technology becomes more widespread.
“I think there are many surgeons who are doing robotic surgery who truly believe that the current of state of the art will bear only a partial resemblance to the state of the art 5-10 years from now,” Dr. Henry Pitt, chief quality officer of the Temple University Health System, Philadelphia, said in an interview. “And part of the persistence by many of the robotic surgeons, while they fully understand that what they are doing is not cost effective now, is that they believe that the next few generations of this technology will become the state of the art and will become cost effective.”
Dr. Pitt, an ACS Fellow, compared the evolution of robotic surgery to that of computers and the application of Moore’s Law, by which the technology advances rapidly while the price eventually comes down.
Spread of robot-assisted surgery
Research by the surgical robot industry and independent investigators shows that use of robotics is on an upward climb. A presentation at the 2015 American College of Surgeons Clinical Congress reveals that, based on retrospective review of the Nationwide Inpatient Sample from 2009-2012 using the ICD-9 code that identifies robot-assisted procedures, there were 113,022 robot-assisted procedures in that period.
In 2009, there were 21,006 procedures, with the volume growing to 33,713 in 2012. Perhaps more telling about the use of robotics is that it is not confined to specialties with a proven track record such as gynecology and urology. The study, led by Dr. G. Paul Wright of Grand Rapids Medical Education Partners and Michigan State University, shows an increase in robotics use in general surgery procedures by 4.5-fold from 2009-2012, with steady increases each year. General surgery accounted for 11.8% of robot-assisted cases in 2012, Dr. Wright and colleagues reported.
Dr. Wright suggested a number of factors contributing to the “surprising” growth of robotics in general surgery.
“I think the growth is stimulated, at least in part, by market forces,” he said in an interview. “For patients who are the consumers of health care, they are often drawn to [surgeons] whom they perceive to be on the cutting edge. Robotic surgery certainly offers that intrigue. With greater access to the technology, if a patient is seeking a robotic surgery that you do not offer as a surgeon, they can likely find that elsewhere, potentially at your competitor. Another driving force is potentially the ease of suturing with the robot which more resembles open surgery while advanced laparoscopic suturing in tight spaces is a more limited skill set among general surgeons.”
Dr. Wright added that “some of the stigma of robotic surgery is dissolving among surgeons as they become more familiar with the technology. I also believe the market forces will help drive down costs in robotics which may help to increase utilization as well.”
Industry touts cost effectiveness
And while Dr. Pitt is looking forward, the industry is energetically promoting the cost effectiveness of robotics today. Intuitive Surgical Inc., manufacturer of the da Vinci surgery robot presented in a recent press briefing data culled from literature found on PubMed showing that robotic surgery, at least with their product, is cost effective now (view the report at http://goo.gl/AfAuT3). But in recent years, the large number of clinical trials comparing robotic vs. laparoscopic surgery for colorectal disease, for example, is equivocal. For many procedures, trials appear to show similar between laparoscopic and robot-assisted approaches, with the main factors in play being length of operation time, hospital stay, and surgical site infection.
According to Intuitive Surgical’s manager of clinical economics, Andrew Yiu, a review of peer-reviewed articles that featured nationwide cohorts of comparisons and included comparisons to both open and laparoscopic procedures outcomes shows improvements across a variety of procedures in terms of hospital stay, lower conversion rates, reduced complications, reduced 30-day readmissions, and improved patient satisfaction, though outcomes were more pronounced in some areas compared with others. Highlighting one procedure in particular – benign hysterectomy – Mr. Yiu noted that rates of minor and major complications associated with robotic vs. laparoscopic surgery were relatively similar but that the conversion rate to open surgery from laparoscopic surgery was 3.9%, compared with 0.9% for da Vinci–assisted surgery.
Overall, Intuitive Surgical calculated the potential savings on the episode of care with the da Vinci system at $1,087 vs. laparoscopic procedures and $2,996 over open surgery.
The company is currently promoting its da Vinci IX Surgical System. Cleared by the Food and Drug Administration in April 2014, Intuitive Surgical says that this latest version has broader capabilities than earlier generations and has been optimized for complex, multiquadrant surgeries.
Costs and other trade-offs
In some ways, robot-assisted surgery is following the same path as laparoscopic surgery, observed Dr. Tyler Hughes of the department of general surgery at McPherson (Kan.) Hospital.
“Certainly, we had the issue back in the late ‘80s and early ‘90s of laparoscopy,” Dr. Hughes said in an interview. “Was it cost effective? Because at the time $30,000 or $40,000 for a laparoscopic set-up seemed like a horse-choking amount of money. However, it converted a 5-day in-the-hospital experience to a 4-hour day-surgery experience. The nonclinical benefits to the patient were so enormous that it took the whole place by storm.”
Dr. Hughes, an ACS Fellow, suggested that the leap in savings elsewhere in the episode of care when using laparoscopic surgery over open surgery is not being mirrored in the robotic space and suggested that money should be spent in other areas of need.
“Cost is going to choke the future if we’re not careful. We need nurses. We need infrastructure. We need to be careful to buy things that really make a big difference,” he said.
In a study presented by at the ACS Clinical Congress on a cost-benefit analysis of robotic vs. laparoscopic colectomy, Anastasia Postoev, a fourth-year medical student at Caribbean Medical University in Willemstad, Curacao and her colleagues found little difference in clinical outcomes but higher costs as a result of added time needed to prepare the robot for surgery. The study showed that the potential up-front costs can be $1 to $2 million for the robot in addition to ongoing costs related to training and maintenance. Dr. Hughes said. “It is a terrific marketing tool in the sense that you can certainly attract a lot of people to a hospital with robotic surgery, but whether or not those outcomes are truly different and the cost of those outcomes are justifiable is yet to be determined.”
The ease of use of robotics, however, could end up being a double-edged sword, particularly if there are areas of the country where robotics may not be as pervasive, or in cases when a conversion to open surgery might be required.
“It is a real concern that trainees are being taught robotic surgery for what is not really needed to be robotic in the mainstream,” Dr. Hughes said. “Then they come out with less experience with straight stick laparoscopy and we’ve certainly seen lots of problems in the laparoscopic range for people once they get to the point that they have to convert to open. We really don’t have a large volume of trainee experience in complex open surgery. That’s a big problem. Robotics certainly isn’t going to make that a lot better.”
gtwachtman@frontlinemedcom.com

Does LVAD inhibit cardio protection?
Placement of a left ventricular assist device (LVAD) after a heart attack has been found to suppress certain cellular signaling pathways that protect coronary tissue, but at the same time LVAD placement seemed to help normalize other protective properties in areas of the heart closest to the infarcted region, investigators reported in a recent study.
The findings could have implications in determining the best method for unloading and other medical therapies in the aftermath of a heart attack, Dr. Keshava Rajagopal of the University of Texas, Houston, and associates reported in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1332-41).
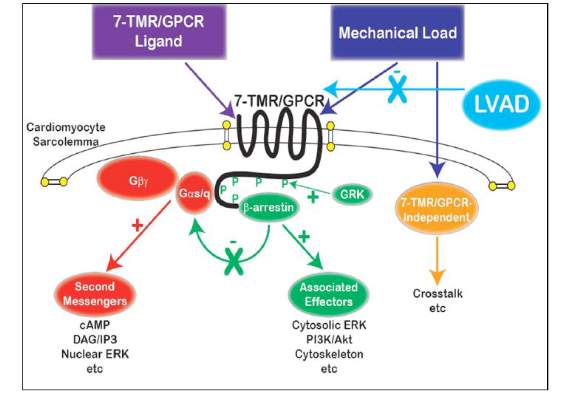
To study the effect of LVAD on cardiac tissue, the investigators induced myocardial infarction in sheep and then placed the animals on LVAD support for 2 weeks. After 10 more weeks of observation, the investigators harvested and analyzed the myocardial specimens. The principal goal of the study was to investigate how heart attack and subsequent short-term mechanical support of the left ventricle can influence signaling controlled by the protein beta-arrestin.
They found that an infarction of myocardial tissue caused activation of the beta-arrestin protein that regulates cellular pathways that can benefit cardiac cells. At the same time, LVAD support inhibited beta-arrestin activation, specifically in regulating pathways of two cardioprotective proteins: Akt, also called protein kinase B (PKB), and, to a lesser extent, ERK-1 and -2.
They also found that MI resulted in regional activation of load-induced signaling of cardiac G protein-coupled receptor (GPCR) via G proteins.
“These studies demonstrate that small platform catheter-based LVAD support exerts suppressive effects on cardioprotective beta-arrestin–mediated signal transduction, while normalizing the signaling networks of G-alpha-q–coupled cardiac GPCRS in the MI-adjacent zone,” Dr. Rajagopal and colleagues said.
They acknowledged that further studies are needed to better understand the roles that specific GPCRs in beta-arrestin–regulated signaling play in left ventricle dysfunction after a heart attack and to help define the optimal timing for LVAD based on signaling and genetic markers along with standard LV functional endpoints.
The authors had no disclosures.
The University of Maryland investigators in this study have joined the ranks of other investigators who have begun to unravel the consequences of mechanical unloading at the cellular level as well as its effect on the heart’s ability to handle calcium after infarction, Dr. William Hiesinger and Dr. Pavan Atluri of the University of Pennsylvania wrote in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1342-3).
“More broadly, these investigations are building the foundation of what will likely be the best platform for an efficacious bridge to recovery: multimodal therapy utilizing the titration of mechanical myocardial unloading,” they said. Dr. Hiesinger and Dr. Atluri commented on the limitations of the University of Maryland study, namely its small sample size and narrow scope. “This is, however, reflective more of the amazing complexity of the biologic and mechanical interactions between the heart and VAD and the need for further investigations of this kind than the quality of the research,” they said.
Understanding the molecular basis and metabolic function cardiac dysfunction after a heart attack is in the “nascent stages,” and even less is known about the effect ventricular loading has on these pathways, Dr. Hiesinger and Dr. Atluri said. “This study offers a concrete platform for both specific treatment and further study,” they wrote.
The University of Maryland investigators in this study have joined the ranks of other investigators who have begun to unravel the consequences of mechanical unloading at the cellular level as well as its effect on the heart’s ability to handle calcium after infarction, Dr. William Hiesinger and Dr. Pavan Atluri of the University of Pennsylvania wrote in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1342-3).
“More broadly, these investigations are building the foundation of what will likely be the best platform for an efficacious bridge to recovery: multimodal therapy utilizing the titration of mechanical myocardial unloading,” they said. Dr. Hiesinger and Dr. Atluri commented on the limitations of the University of Maryland study, namely its small sample size and narrow scope. “This is, however, reflective more of the amazing complexity of the biologic and mechanical interactions between the heart and VAD and the need for further investigations of this kind than the quality of the research,” they said.
Understanding the molecular basis and metabolic function cardiac dysfunction after a heart attack is in the “nascent stages,” and even less is known about the effect ventricular loading has on these pathways, Dr. Hiesinger and Dr. Atluri said. “This study offers a concrete platform for both specific treatment and further study,” they wrote.
The University of Maryland investigators in this study have joined the ranks of other investigators who have begun to unravel the consequences of mechanical unloading at the cellular level as well as its effect on the heart’s ability to handle calcium after infarction, Dr. William Hiesinger and Dr. Pavan Atluri of the University of Pennsylvania wrote in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1342-3).
“More broadly, these investigations are building the foundation of what will likely be the best platform for an efficacious bridge to recovery: multimodal therapy utilizing the titration of mechanical myocardial unloading,” they said. Dr. Hiesinger and Dr. Atluri commented on the limitations of the University of Maryland study, namely its small sample size and narrow scope. “This is, however, reflective more of the amazing complexity of the biologic and mechanical interactions between the heart and VAD and the need for further investigations of this kind than the quality of the research,” they said.
Understanding the molecular basis and metabolic function cardiac dysfunction after a heart attack is in the “nascent stages,” and even less is known about the effect ventricular loading has on these pathways, Dr. Hiesinger and Dr. Atluri said. “This study offers a concrete platform for both specific treatment and further study,” they wrote.
Placement of a left ventricular assist device (LVAD) after a heart attack has been found to suppress certain cellular signaling pathways that protect coronary tissue, but at the same time LVAD placement seemed to help normalize other protective properties in areas of the heart closest to the infarcted region, investigators reported in a recent study.
The findings could have implications in determining the best method for unloading and other medical therapies in the aftermath of a heart attack, Dr. Keshava Rajagopal of the University of Texas, Houston, and associates reported in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1332-41).
To study the effect of LVAD on cardiac tissue, the investigators induced myocardial infarction in sheep and then placed the animals on LVAD support for 2 weeks. After 10 more weeks of observation, the investigators harvested and analyzed the myocardial specimens. The principal goal of the study was to investigate how heart attack and subsequent short-term mechanical support of the left ventricle can influence signaling controlled by the protein beta-arrestin.
They found that an infarction of myocardial tissue caused activation of the beta-arrestin protein that regulates cellular pathways that can benefit cardiac cells. At the same time, LVAD support inhibited beta-arrestin activation, specifically in regulating pathways of two cardioprotective proteins: Akt, also called protein kinase B (PKB), and, to a lesser extent, ERK-1 and -2.
They also found that MI resulted in regional activation of load-induced signaling of cardiac G protein-coupled receptor (GPCR) via G proteins.
“These studies demonstrate that small platform catheter-based LVAD support exerts suppressive effects on cardioprotective beta-arrestin–mediated signal transduction, while normalizing the signaling networks of G-alpha-q–coupled cardiac GPCRS in the MI-adjacent zone,” Dr. Rajagopal and colleagues said.
They acknowledged that further studies are needed to better understand the roles that specific GPCRs in beta-arrestin–regulated signaling play in left ventricle dysfunction after a heart attack and to help define the optimal timing for LVAD based on signaling and genetic markers along with standard LV functional endpoints.
The authors had no disclosures.
Placement of a left ventricular assist device (LVAD) after a heart attack has been found to suppress certain cellular signaling pathways that protect coronary tissue, but at the same time LVAD placement seemed to help normalize other protective properties in areas of the heart closest to the infarcted region, investigators reported in a recent study.
The findings could have implications in determining the best method for unloading and other medical therapies in the aftermath of a heart attack, Dr. Keshava Rajagopal of the University of Texas, Houston, and associates reported in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150:1332-41).
To study the effect of LVAD on cardiac tissue, the investigators induced myocardial infarction in sheep and then placed the animals on LVAD support for 2 weeks. After 10 more weeks of observation, the investigators harvested and analyzed the myocardial specimens. The principal goal of the study was to investigate how heart attack and subsequent short-term mechanical support of the left ventricle can influence signaling controlled by the protein beta-arrestin.
They found that an infarction of myocardial tissue caused activation of the beta-arrestin protein that regulates cellular pathways that can benefit cardiac cells. At the same time, LVAD support inhibited beta-arrestin activation, specifically in regulating pathways of two cardioprotective proteins: Akt, also called protein kinase B (PKB), and, to a lesser extent, ERK-1 and -2.
They also found that MI resulted in regional activation of load-induced signaling of cardiac G protein-coupled receptor (GPCR) via G proteins.
“These studies demonstrate that small platform catheter-based LVAD support exerts suppressive effects on cardioprotective beta-arrestin–mediated signal transduction, while normalizing the signaling networks of G-alpha-q–coupled cardiac GPCRS in the MI-adjacent zone,” Dr. Rajagopal and colleagues said.
They acknowledged that further studies are needed to better understand the roles that specific GPCRs in beta-arrestin–regulated signaling play in left ventricle dysfunction after a heart attack and to help define the optimal timing for LVAD based on signaling and genetic markers along with standard LV functional endpoints.
The authors had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Left ventricular assist device (LVAD) support inhibits pathologic responses to mechanical loading but also can inhibit adaptive responses after myocardial infarction.
Major finding: LVAD support inhibited cardioprotective beta-arrestin–mediated signaling, but net benefits of normalization of load-induced G protein-coupled receptor (GPCR) signaling were observed in the MI-adjacent zone.
Data source: Sheep were induced with myocardial infarction and then placed on LVAD support for 2 weeks and observed for a total of 12 weeks. Then myocardial specimens were harvested and analyzed.
Disclosures: The study authors had no relationships to disclose.
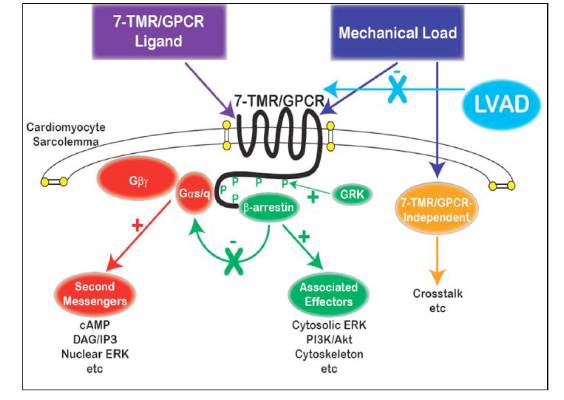
Higher medical spending led to fewer malpractice claims
Greater than average spending was associated with reduced risk of incurring a malpractice claim across all physician specialties in a study of almost 25,000 doctors published Nov. 4 in the BMJ. The finding is consistent with widespread beliefs that higher resource use – sometimes defined as defensive medicine – limits the risk of litigation.
Dr. Anupam B. Jena of Harvard Medical School, Boston, and colleagues compared data from the Florida Agency for Health Care Administration on all acute care hospital discharges from 2000 to 2009 with data from the Florida Office of Insurance Regulation on all closed malpractice claims against Florida physicians during the same period. The data included 24,637 physicians (pediatricians, family physicians, general surgeons, obstetrician-gynecologists, and some subspecialists), more than 18 million hospital admissions, and 4,342 malpractice claims (BMJ 2015;351:h5516. doi: 10.1136/bmj.h5516). They looked at total hospital charges associated with patients treated by a given physician in a given year, averaged across all patients treated by that physician in that year, and adjusted for patient personal and clinical characteristics.

Across all specialties, higher average spending per year was associated with a lower probability of an alleged malpractice incident in the subsequent year. For internists, mean risk-adjusted spending per physician ranged from $19,725 for each hospital admission in the bottom fifth of physician years to $39,379 in the top fifth. The probability for an alleged malpractice claim ranged from 1.5% in the bottom spending fifth to 0.3% in the top spending fifth. Similarly, for ob.gyns., the probability of experiencing an alleged malpractice incident ranged from 1.9% in the bottom fifth of spending to 0.4% in the top fifth. Ob.gyns. on the low end of resource utilization spent a risk-adjusted mean of $8,653, while ob.gyns. on the high end spent $18,162.
Dr. Jena and colleagues also studied more than 1.5 million deliveries performed by 1,625 obstetricians; 15% were cesarean deliveries. In total, 496 malpractice claims were filed against these obstetricians. Ob.gyns. with higher cesarean rates per year were less likely to face a malpractice claim. The probability of being sued ranged from 5.7% in the bottom fifth of cesarean delivery rates to 2.7% in the top fifth.
Authors note that if higher spending is motivated by concerns about malpractice, then the spending would be considered “defensively motivated. However, that spending may not be wasteful if it is associated with fewer errors and therefore lower malpractice claims. More study is needed to compare the costs of additional resource use and the value of reduced errors to learn whether such defensively motivated care is socially wasteful or reflects socially beneficial deterrence.”
The study was supported by the National Institutes of Health.
On Twitter @legal_med
It may be tempting for doctors to view the results of the study by Dr. Jena and colleagues as a means to justify additional tests and procedures to mitigate the risk of a malpractice claim. We would suggest that they should view the study results as a contribution to our understanding of the risk of such claims. We need to better understand defensive medicine, how to define it, how to measure it, and how its practice impacts patients and doctors.
Dr. Tara F. Bishop and Dr. Michael Pesko are with the Department of Health Care Policy and Research at Weill Cornell Medical College in New York. Their comments were taken from an editorial accompanying Dr. Jena’s study (BMJ 2015;351:h5786. doi: 10.1136/bmj.h5786).
It may be tempting for doctors to view the results of the study by Dr. Jena and colleagues as a means to justify additional tests and procedures to mitigate the risk of a malpractice claim. We would suggest that they should view the study results as a contribution to our understanding of the risk of such claims. We need to better understand defensive medicine, how to define it, how to measure it, and how its practice impacts patients and doctors.
Dr. Tara F. Bishop and Dr. Michael Pesko are with the Department of Health Care Policy and Research at Weill Cornell Medical College in New York. Their comments were taken from an editorial accompanying Dr. Jena’s study (BMJ 2015;351:h5786. doi: 10.1136/bmj.h5786).
It may be tempting for doctors to view the results of the study by Dr. Jena and colleagues as a means to justify additional tests and procedures to mitigate the risk of a malpractice claim. We would suggest that they should view the study results as a contribution to our understanding of the risk of such claims. We need to better understand defensive medicine, how to define it, how to measure it, and how its practice impacts patients and doctors.
Dr. Tara F. Bishop and Dr. Michael Pesko are with the Department of Health Care Policy and Research at Weill Cornell Medical College in New York. Their comments were taken from an editorial accompanying Dr. Jena’s study (BMJ 2015;351:h5786. doi: 10.1136/bmj.h5786).
Greater than average spending was associated with reduced risk of incurring a malpractice claim across all physician specialties in a study of almost 25,000 doctors published Nov. 4 in the BMJ. The finding is consistent with widespread beliefs that higher resource use – sometimes defined as defensive medicine – limits the risk of litigation.
Dr. Anupam B. Jena of Harvard Medical School, Boston, and colleagues compared data from the Florida Agency for Health Care Administration on all acute care hospital discharges from 2000 to 2009 with data from the Florida Office of Insurance Regulation on all closed malpractice claims against Florida physicians during the same period. The data included 24,637 physicians (pediatricians, family physicians, general surgeons, obstetrician-gynecologists, and some subspecialists), more than 18 million hospital admissions, and 4,342 malpractice claims (BMJ 2015;351:h5516. doi: 10.1136/bmj.h5516). They looked at total hospital charges associated with patients treated by a given physician in a given year, averaged across all patients treated by that physician in that year, and adjusted for patient personal and clinical characteristics.
Across all specialties, higher average spending per year was associated with a lower probability of an alleged malpractice incident in the subsequent year. For internists, mean risk-adjusted spending per physician ranged from $19,725 for each hospital admission in the bottom fifth of physician years to $39,379 in the top fifth. The probability for an alleged malpractice claim ranged from 1.5% in the bottom spending fifth to 0.3% in the top spending fifth. Similarly, for ob.gyns., the probability of experiencing an alleged malpractice incident ranged from 1.9% in the bottom fifth of spending to 0.4% in the top fifth. Ob.gyns. on the low end of resource utilization spent a risk-adjusted mean of $8,653, while ob.gyns. on the high end spent $18,162.
Dr. Jena and colleagues also studied more than 1.5 million deliveries performed by 1,625 obstetricians; 15% were cesarean deliveries. In total, 496 malpractice claims were filed against these obstetricians. Ob.gyns. with higher cesarean rates per year were less likely to face a malpractice claim. The probability of being sued ranged from 5.7% in the bottom fifth of cesarean delivery rates to 2.7% in the top fifth.
Authors note that if higher spending is motivated by concerns about malpractice, then the spending would be considered “defensively motivated. However, that spending may not be wasteful if it is associated with fewer errors and therefore lower malpractice claims. More study is needed to compare the costs of additional resource use and the value of reduced errors to learn whether such defensively motivated care is socially wasteful or reflects socially beneficial deterrence.”
The study was supported by the National Institutes of Health.
On Twitter @legal_med
Greater than average spending was associated with reduced risk of incurring a malpractice claim across all physician specialties in a study of almost 25,000 doctors published Nov. 4 in the BMJ. The finding is consistent with widespread beliefs that higher resource use – sometimes defined as defensive medicine – limits the risk of litigation.
Dr. Anupam B. Jena of Harvard Medical School, Boston, and colleagues compared data from the Florida Agency for Health Care Administration on all acute care hospital discharges from 2000 to 2009 with data from the Florida Office of Insurance Regulation on all closed malpractice claims against Florida physicians during the same period. The data included 24,637 physicians (pediatricians, family physicians, general surgeons, obstetrician-gynecologists, and some subspecialists), more than 18 million hospital admissions, and 4,342 malpractice claims (BMJ 2015;351:h5516. doi: 10.1136/bmj.h5516). They looked at total hospital charges associated with patients treated by a given physician in a given year, averaged across all patients treated by that physician in that year, and adjusted for patient personal and clinical characteristics.
Across all specialties, higher average spending per year was associated with a lower probability of an alleged malpractice incident in the subsequent year. For internists, mean risk-adjusted spending per physician ranged from $19,725 for each hospital admission in the bottom fifth of physician years to $39,379 in the top fifth. The probability for an alleged malpractice claim ranged from 1.5% in the bottom spending fifth to 0.3% in the top spending fifth. Similarly, for ob.gyns., the probability of experiencing an alleged malpractice incident ranged from 1.9% in the bottom fifth of spending to 0.4% in the top fifth. Ob.gyns. on the low end of resource utilization spent a risk-adjusted mean of $8,653, while ob.gyns. on the high end spent $18,162.
Dr. Jena and colleagues also studied more than 1.5 million deliveries performed by 1,625 obstetricians; 15% were cesarean deliveries. In total, 496 malpractice claims were filed against these obstetricians. Ob.gyns. with higher cesarean rates per year were less likely to face a malpractice claim. The probability of being sued ranged from 5.7% in the bottom fifth of cesarean delivery rates to 2.7% in the top fifth.
Authors note that if higher spending is motivated by concerns about malpractice, then the spending would be considered “defensively motivated. However, that spending may not be wasteful if it is associated with fewer errors and therefore lower malpractice claims. More study is needed to compare the costs of additional resource use and the value of reduced errors to learn whether such defensively motivated care is socially wasteful or reflects socially beneficial deterrence.”
The study was supported by the National Institutes of Health.
On Twitter @legal_med

Hybrid revascularization shows promise, but there are concerns
A hybrid coronary revascularization procedure that combines off-pump left internal mammary artery (LIMA) grafting with percutaneous coronary intervention (PCI) showed good results at 1 year after surgery, but nonetheless showed a rate of adverse events that may raise questions about the procedure.
In a study published in the November issue of the Journal of Thoracic and Cardiovascular Surgery, a team of investigators from Aarhus University Hospital in Denmark reported high rates of graft patency and low rates of death and stroke with the procedure 1 year after a series of 100 operations (J Thorac Cardiovasc Surg. 2015;150:1181-6).
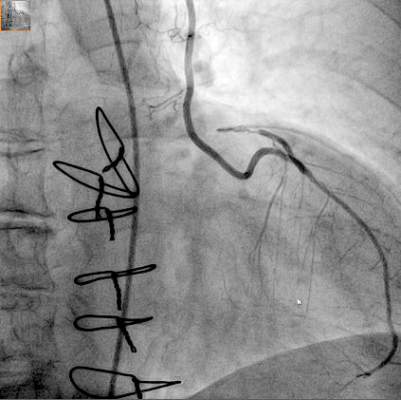
“The high left internal mammary artery graft patency rate and low risk of death and stroke at 1 year seem promising for the long-term outcome of this revascularization strategy,” said Dr. Ivy Susanne Modrau and colleagues.
The single-center study evaluated 1-year clinical and angiographic results of 100 consecutive trial patients with multivessel disease who had the hybrid procedure between October 2010 and February 2012. “The rationale of hybrid coronary revascularization is to achieve the survival benefits of the LIMA to LAD (left anterior descending artery) graft with reduced invasiveness to minimize postprocedural discomfort and morbidity, in particular the risk of stroke,” Dr. Modrau and colleagues said.
The study used the LIMA to LAD graft performed off-pump through a reversed J-hemisternotomy “We chose this technique because of its excellent exposure of the heart, technical ease, low risk of complicating chronic pain, and applicability in virtually all patients,” Dr. Modrau said. Eighty-nine patients had surgery prior to PCI and 11 had PCI prior to surgery.
The primary endpoint was rate of major adverse cardiac or cerebrovascular events (MACCE), the composite of all-cause death, stroke, myocardial infarction, and repeat revascularization by PCI or coronary artery bypass grafting at 1 year. Secondary endpoints included individual components and status of stent and graft patency on angiography.
Overall, 20 patients met the 1-year primary endpoint of MACCE. One patient died, one other had a stroke, and three had heart attacks. Sixteen patients had repeat revascularization procedures, eight performed during the index hospitalization. Graft patency was 98% after 1 year.
Dr. Modrau and coauthors noted the MACCE rate of 20% “was higher than expected,” and certainly higher than results in the SYNTAX study (17.8% in the PCI group and 12.4% in the coronary artery bypass grafting [CABG] group) (Euro. Intervention. 2015;10:e1-e6). One possible reason the Danish investigators cited for higher than expected MACCE rates was that they may be attributed to the learning curve involved with LIMA grafting and the use of early angiography possibly revealing “clinically silent LIMA graft dysfunction due to technical errors.”
The number of repeat revascularizations in the study was more in line with the SYNTAX study: 7% in the Aarhus University study and 6% in the SYNTAX CABG group. However, a meta-analysis of six studies with 1,190 patients reported 1-year repeat revascularization rates of 3.8% after a hybrid procedure and 1.4% after CABG (Am Heart J. 2014;167:585-92).
Ultimately, the safety and efficacy of the hybrid revascularization approach will require long-term follow-up data and head-to-head comparison with conventional CABG and PCI in clinical trials. “Meanwhile, LIMA patency, the cornerstone of surgical revascularization, may be used as a surrogate endpoint for long-term survival after HCR,” Dr. Modrau and coauthors said.
They reported having no disclosures.
Hybrid revascularization procedures are “still not ready for prime time,” Dr. Carlos Mestres of Cleveland Clinic Abu Dhabi, United Arab Emirates, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1028-9).
The study illuminates two key points of concern, Dr. Mestres said: the “unexpectedly high” 20% rate of major adverse cardiac or cerebrovascular events (MACCE); and the in-hospital revascularization rate that was significantly higher than the 1% after CABG that the authors reported in their own institution. That calls into question the reason the investigators would change their own department strategy away from conventional CABG, where they had optimal results, he said.
Dr. Mestres also said the Danish investigators’ conclusion that the study results seemed promising for long-term outcomes of the hybrid procedure “are to be carefully dissected.”
He commended the investigators for collecting angiographic data at 1 year, but said that 1 year of follow-up “is simply not enough” to credibly compare staged procedures with CABG.
Dr. Mestres had no disclosures.
Hybrid revascularization procedures are “still not ready for prime time,” Dr. Carlos Mestres of Cleveland Clinic Abu Dhabi, United Arab Emirates, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1028-9).
The study illuminates two key points of concern, Dr. Mestres said: the “unexpectedly high” 20% rate of major adverse cardiac or cerebrovascular events (MACCE); and the in-hospital revascularization rate that was significantly higher than the 1% after CABG that the authors reported in their own institution. That calls into question the reason the investigators would change their own department strategy away from conventional CABG, where they had optimal results, he said.
Dr. Mestres also said the Danish investigators’ conclusion that the study results seemed promising for long-term outcomes of the hybrid procedure “are to be carefully dissected.”
He commended the investigators for collecting angiographic data at 1 year, but said that 1 year of follow-up “is simply not enough” to credibly compare staged procedures with CABG.
Dr. Mestres had no disclosures.
Hybrid revascularization procedures are “still not ready for prime time,” Dr. Carlos Mestres of Cleveland Clinic Abu Dhabi, United Arab Emirates, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1028-9).
The study illuminates two key points of concern, Dr. Mestres said: the “unexpectedly high” 20% rate of major adverse cardiac or cerebrovascular events (MACCE); and the in-hospital revascularization rate that was significantly higher than the 1% after CABG that the authors reported in their own institution. That calls into question the reason the investigators would change their own department strategy away from conventional CABG, where they had optimal results, he said.
Dr. Mestres also said the Danish investigators’ conclusion that the study results seemed promising for long-term outcomes of the hybrid procedure “are to be carefully dissected.”
He commended the investigators for collecting angiographic data at 1 year, but said that 1 year of follow-up “is simply not enough” to credibly compare staged procedures with CABG.
Dr. Mestres had no disclosures.
A hybrid coronary revascularization procedure that combines off-pump left internal mammary artery (LIMA) grafting with percutaneous coronary intervention (PCI) showed good results at 1 year after surgery, but nonetheless showed a rate of adverse events that may raise questions about the procedure.
In a study published in the November issue of the Journal of Thoracic and Cardiovascular Surgery, a team of investigators from Aarhus University Hospital in Denmark reported high rates of graft patency and low rates of death and stroke with the procedure 1 year after a series of 100 operations (J Thorac Cardiovasc Surg. 2015;150:1181-6).
“The high left internal mammary artery graft patency rate and low risk of death and stroke at 1 year seem promising for the long-term outcome of this revascularization strategy,” said Dr. Ivy Susanne Modrau and colleagues.
The single-center study evaluated 1-year clinical and angiographic results of 100 consecutive trial patients with multivessel disease who had the hybrid procedure between October 2010 and February 2012. “The rationale of hybrid coronary revascularization is to achieve the survival benefits of the LIMA to LAD (left anterior descending artery) graft with reduced invasiveness to minimize postprocedural discomfort and morbidity, in particular the risk of stroke,” Dr. Modrau and colleagues said.
The study used the LIMA to LAD graft performed off-pump through a reversed J-hemisternotomy “We chose this technique because of its excellent exposure of the heart, technical ease, low risk of complicating chronic pain, and applicability in virtually all patients,” Dr. Modrau said. Eighty-nine patients had surgery prior to PCI and 11 had PCI prior to surgery.
The primary endpoint was rate of major adverse cardiac or cerebrovascular events (MACCE), the composite of all-cause death, stroke, myocardial infarction, and repeat revascularization by PCI or coronary artery bypass grafting at 1 year. Secondary endpoints included individual components and status of stent and graft patency on angiography.
Overall, 20 patients met the 1-year primary endpoint of MACCE. One patient died, one other had a stroke, and three had heart attacks. Sixteen patients had repeat revascularization procedures, eight performed during the index hospitalization. Graft patency was 98% after 1 year.
Dr. Modrau and coauthors noted the MACCE rate of 20% “was higher than expected,” and certainly higher than results in the SYNTAX study (17.8% in the PCI group and 12.4% in the coronary artery bypass grafting [CABG] group) (Euro. Intervention. 2015;10:e1-e6). One possible reason the Danish investigators cited for higher than expected MACCE rates was that they may be attributed to the learning curve involved with LIMA grafting and the use of early angiography possibly revealing “clinically silent LIMA graft dysfunction due to technical errors.”
The number of repeat revascularizations in the study was more in line with the SYNTAX study: 7% in the Aarhus University study and 6% in the SYNTAX CABG group. However, a meta-analysis of six studies with 1,190 patients reported 1-year repeat revascularization rates of 3.8% after a hybrid procedure and 1.4% after CABG (Am Heart J. 2014;167:585-92).
Ultimately, the safety and efficacy of the hybrid revascularization approach will require long-term follow-up data and head-to-head comparison with conventional CABG and PCI in clinical trials. “Meanwhile, LIMA patency, the cornerstone of surgical revascularization, may be used as a surrogate endpoint for long-term survival after HCR,” Dr. Modrau and coauthors said.
They reported having no disclosures.
A hybrid coronary revascularization procedure that combines off-pump left internal mammary artery (LIMA) grafting with percutaneous coronary intervention (PCI) showed good results at 1 year after surgery, but nonetheless showed a rate of adverse events that may raise questions about the procedure.
In a study published in the November issue of the Journal of Thoracic and Cardiovascular Surgery, a team of investigators from Aarhus University Hospital in Denmark reported high rates of graft patency and low rates of death and stroke with the procedure 1 year after a series of 100 operations (J Thorac Cardiovasc Surg. 2015;150:1181-6).
“The high left internal mammary artery graft patency rate and low risk of death and stroke at 1 year seem promising for the long-term outcome of this revascularization strategy,” said Dr. Ivy Susanne Modrau and colleagues.
The single-center study evaluated 1-year clinical and angiographic results of 100 consecutive trial patients with multivessel disease who had the hybrid procedure between October 2010 and February 2012. “The rationale of hybrid coronary revascularization is to achieve the survival benefits of the LIMA to LAD (left anterior descending artery) graft with reduced invasiveness to minimize postprocedural discomfort and morbidity, in particular the risk of stroke,” Dr. Modrau and colleagues said.
The study used the LIMA to LAD graft performed off-pump through a reversed J-hemisternotomy “We chose this technique because of its excellent exposure of the heart, technical ease, low risk of complicating chronic pain, and applicability in virtually all patients,” Dr. Modrau said. Eighty-nine patients had surgery prior to PCI and 11 had PCI prior to surgery.
The primary endpoint was rate of major adverse cardiac or cerebrovascular events (MACCE), the composite of all-cause death, stroke, myocardial infarction, and repeat revascularization by PCI or coronary artery bypass grafting at 1 year. Secondary endpoints included individual components and status of stent and graft patency on angiography.
Overall, 20 patients met the 1-year primary endpoint of MACCE. One patient died, one other had a stroke, and three had heart attacks. Sixteen patients had repeat revascularization procedures, eight performed during the index hospitalization. Graft patency was 98% after 1 year.
Dr. Modrau and coauthors noted the MACCE rate of 20% “was higher than expected,” and certainly higher than results in the SYNTAX study (17.8% in the PCI group and 12.4% in the coronary artery bypass grafting [CABG] group) (Euro. Intervention. 2015;10:e1-e6). One possible reason the Danish investigators cited for higher than expected MACCE rates was that they may be attributed to the learning curve involved with LIMA grafting and the use of early angiography possibly revealing “clinically silent LIMA graft dysfunction due to technical errors.”
The number of repeat revascularizations in the study was more in line with the SYNTAX study: 7% in the Aarhus University study and 6% in the SYNTAX CABG group. However, a meta-analysis of six studies with 1,190 patients reported 1-year repeat revascularization rates of 3.8% after a hybrid procedure and 1.4% after CABG (Am Heart J. 2014;167:585-92).
Ultimately, the safety and efficacy of the hybrid revascularization approach will require long-term follow-up data and head-to-head comparison with conventional CABG and PCI in clinical trials. “Meanwhile, LIMA patency, the cornerstone of surgical revascularization, may be used as a surrogate endpoint for long-term survival after HCR,” Dr. Modrau and coauthors said.
They reported having no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:High 1-year left internal mammary artery (LIMA) graft patency and low risk of death and stroke seem promising for long-term outcome after HCR.
Major finding: At 1 year, 98% of patients had patent LIMA grafts but the 20% rate of major adverse cardiac or cerebrovascular events was “higher than expected.”
Data source: Prospective single arm clinical feasibility study including 100 consecutive patients with multivessel disease undergoing staged hybrid coronary revascularization.
Disclosures: The study authors had no disclosures.