User login
Official Newspaper of the American College of Surgeons
Stem cell benefits endure 3 years in infants
Infants with congenital heart disease, specifically left heart syndrome, who had cardiac stem-cell therapy after surgery showed improved cardiac and brain function after 3 years when compared with infants who had standard therapy, according to latest results from a clinical trial of progenitor cell infusion in infants.
The prospective, controlled study, published in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150[5]:1198-1208), involved 14 infants with hypoplastic left heart syndrome (HLHS). Dr. Suguru Tarui and colleagues at Okayama University Hospital in Japan infused seven infants with intracoronary cardiosphere-derived cells (CDCs) 1 month after they had two- or three-stage palliative surgery. Seven controls had standard care alone. The trial is known TICAP (Three-year follow-up of the Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single-Ventricle Physiology) (ClinicalTrials.gov ID: NCT01273857).
Infants born with HLHS are known to have poor prognoses. HLHS has been associated with the highest mortality of all congenital heart lesions (Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2015;18[1]:2-6).
The Okayama investigators conducted TICAP in 2011 and demonstrated the feasibility and safety of the intracoronary delivery of CDCs in infants with HLHS after staged procedures. The latest report looks at the secondary outcome of cardiac function through 36 months of follow-up, and is the first clinical trial to report on the mid-term results of cardiac progenitor therapy in congenital heart disease.
“CDC infusion could improve right ventricular function from 3 through 36 months of observation,” Dr. Tarui and colleagues said. “Patients treated by CDCs showed an increase in somatic growth and reduced heart failure status in mid-term follow-up.”
Upon entry into the study, all subjects were of similar age, body weight, and risk profiles. After 36 months, the CDC group showed no complications and significantly improved right ventricular injection fraction compared with controls. As a result, the CDC group had reduced brain natriuretic peptide levels, lower rates of unplanned catheterizations, and higher weight for age. No adverse events occurred in the CDC group, while two patients in the control group had complications (one developed heart failure, another developed enteropathy).
The investigators looked at predictors of cardiac functional efficacy in the CDC group and determined that younger age was associated with greater improvement of right ventricular ejection fraction, as measured on echocardiography. The lower weight-for-age Z score and reduced ejection fraction at the time of infusion may be predictors of cardiac function improvements at 3 years.
“This therapeutic strategy may merit somatic growth enhancement and reduce the incidence of heart failure,” Dr. Tarui and coauthors said.
They noted a number of limitations of their small clinical trial. The study was nonrandomized, and the cardiac interventions were not blinded, among others. “Larger phase II studies focusing on changes in cardiac function, myocardial fibrosis, and quality of life and clinical event rates are warranted to confirm these effects of CDC administration in patients with single ventricular physiology,” they said.
The government of Japan through its ministries of Health, Labor and Welfare, and Education, Culture Sports, Science and Technology provided funding for the study, as did the Research Foundation of Okayama University Hospital. The authors had no disclosures.
The benefits of stem cell treatments for cardiac function beyond the initial follow-up period have “remained an unanswered question,” Dr. Sunjay Kaushal of University of Maryland, Baltimore, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150[5]:1209-11). “The 3-year follow-up data from the TICAP trial, therefore, offers one of the first opportunities to examine the durability of the outcomes found in stem cell-treated patients,” Dr. Kaushal said.
While TICAP provides clues into independent predictors of success with stem cell treatments, the small study population of seven patients makes it difficult to confirm those predictors, he said. “Multivariate analysis of results from future trials with larger sample size will be needed to verify these preliminary findings,” he noted.
Nonetheless, the study adds to the emerging evidence that younger, sicker patients may respond better to stem cell infusion, a concept Dr. Kaushal termed “intriguing.”
“Meanwhile, the TICAP trial and its three-year follow-up should garner enthusiasm for stem cell therapy, and establish the basis for non-ischemic ventricular dysfunction in pediatric patients as an emerging indication for stem cell therapy,” he said.
The benefits of stem cell treatments for cardiac function beyond the initial follow-up period have “remained an unanswered question,” Dr. Sunjay Kaushal of University of Maryland, Baltimore, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150[5]:1209-11). “The 3-year follow-up data from the TICAP trial, therefore, offers one of the first opportunities to examine the durability of the outcomes found in stem cell-treated patients,” Dr. Kaushal said.
While TICAP provides clues into independent predictors of success with stem cell treatments, the small study population of seven patients makes it difficult to confirm those predictors, he said. “Multivariate analysis of results from future trials with larger sample size will be needed to verify these preliminary findings,” he noted.
Nonetheless, the study adds to the emerging evidence that younger, sicker patients may respond better to stem cell infusion, a concept Dr. Kaushal termed “intriguing.”
“Meanwhile, the TICAP trial and its three-year follow-up should garner enthusiasm for stem cell therapy, and establish the basis for non-ischemic ventricular dysfunction in pediatric patients as an emerging indication for stem cell therapy,” he said.
The benefits of stem cell treatments for cardiac function beyond the initial follow-up period have “remained an unanswered question,” Dr. Sunjay Kaushal of University of Maryland, Baltimore, said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150[5]:1209-11). “The 3-year follow-up data from the TICAP trial, therefore, offers one of the first opportunities to examine the durability of the outcomes found in stem cell-treated patients,” Dr. Kaushal said.
While TICAP provides clues into independent predictors of success with stem cell treatments, the small study population of seven patients makes it difficult to confirm those predictors, he said. “Multivariate analysis of results from future trials with larger sample size will be needed to verify these preliminary findings,” he noted.
Nonetheless, the study adds to the emerging evidence that younger, sicker patients may respond better to stem cell infusion, a concept Dr. Kaushal termed “intriguing.”
“Meanwhile, the TICAP trial and its three-year follow-up should garner enthusiasm for stem cell therapy, and establish the basis for non-ischemic ventricular dysfunction in pediatric patients as an emerging indication for stem cell therapy,” he said.
Infants with congenital heart disease, specifically left heart syndrome, who had cardiac stem-cell therapy after surgery showed improved cardiac and brain function after 3 years when compared with infants who had standard therapy, according to latest results from a clinical trial of progenitor cell infusion in infants.
The prospective, controlled study, published in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150[5]:1198-1208), involved 14 infants with hypoplastic left heart syndrome (HLHS). Dr. Suguru Tarui and colleagues at Okayama University Hospital in Japan infused seven infants with intracoronary cardiosphere-derived cells (CDCs) 1 month after they had two- or three-stage palliative surgery. Seven controls had standard care alone. The trial is known TICAP (Three-year follow-up of the Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single-Ventricle Physiology) (ClinicalTrials.gov ID: NCT01273857).
Infants born with HLHS are known to have poor prognoses. HLHS has been associated with the highest mortality of all congenital heart lesions (Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2015;18[1]:2-6).
The Okayama investigators conducted TICAP in 2011 and demonstrated the feasibility and safety of the intracoronary delivery of CDCs in infants with HLHS after staged procedures. The latest report looks at the secondary outcome of cardiac function through 36 months of follow-up, and is the first clinical trial to report on the mid-term results of cardiac progenitor therapy in congenital heart disease.
“CDC infusion could improve right ventricular function from 3 through 36 months of observation,” Dr. Tarui and colleagues said. “Patients treated by CDCs showed an increase in somatic growth and reduced heart failure status in mid-term follow-up.”
Upon entry into the study, all subjects were of similar age, body weight, and risk profiles. After 36 months, the CDC group showed no complications and significantly improved right ventricular injection fraction compared with controls. As a result, the CDC group had reduced brain natriuretic peptide levels, lower rates of unplanned catheterizations, and higher weight for age. No adverse events occurred in the CDC group, while two patients in the control group had complications (one developed heart failure, another developed enteropathy).
The investigators looked at predictors of cardiac functional efficacy in the CDC group and determined that younger age was associated with greater improvement of right ventricular ejection fraction, as measured on echocardiography. The lower weight-for-age Z score and reduced ejection fraction at the time of infusion may be predictors of cardiac function improvements at 3 years.
“This therapeutic strategy may merit somatic growth enhancement and reduce the incidence of heart failure,” Dr. Tarui and coauthors said.
They noted a number of limitations of their small clinical trial. The study was nonrandomized, and the cardiac interventions were not blinded, among others. “Larger phase II studies focusing on changes in cardiac function, myocardial fibrosis, and quality of life and clinical event rates are warranted to confirm these effects of CDC administration in patients with single ventricular physiology,” they said.
The government of Japan through its ministries of Health, Labor and Welfare, and Education, Culture Sports, Science and Technology provided funding for the study, as did the Research Foundation of Okayama University Hospital. The authors had no disclosures.
Infants with congenital heart disease, specifically left heart syndrome, who had cardiac stem-cell therapy after surgery showed improved cardiac and brain function after 3 years when compared with infants who had standard therapy, according to latest results from a clinical trial of progenitor cell infusion in infants.
The prospective, controlled study, published in the November issue of the Journal of Thoracic and Cardiovascular Surgery (2015;150[5]:1198-1208), involved 14 infants with hypoplastic left heart syndrome (HLHS). Dr. Suguru Tarui and colleagues at Okayama University Hospital in Japan infused seven infants with intracoronary cardiosphere-derived cells (CDCs) 1 month after they had two- or three-stage palliative surgery. Seven controls had standard care alone. The trial is known TICAP (Three-year follow-up of the Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single-Ventricle Physiology) (ClinicalTrials.gov ID: NCT01273857).
Infants born with HLHS are known to have poor prognoses. HLHS has been associated with the highest mortality of all congenital heart lesions (Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2015;18[1]:2-6).
The Okayama investigators conducted TICAP in 2011 and demonstrated the feasibility and safety of the intracoronary delivery of CDCs in infants with HLHS after staged procedures. The latest report looks at the secondary outcome of cardiac function through 36 months of follow-up, and is the first clinical trial to report on the mid-term results of cardiac progenitor therapy in congenital heart disease.
“CDC infusion could improve right ventricular function from 3 through 36 months of observation,” Dr. Tarui and colleagues said. “Patients treated by CDCs showed an increase in somatic growth and reduced heart failure status in mid-term follow-up.”
Upon entry into the study, all subjects were of similar age, body weight, and risk profiles. After 36 months, the CDC group showed no complications and significantly improved right ventricular injection fraction compared with controls. As a result, the CDC group had reduced brain natriuretic peptide levels, lower rates of unplanned catheterizations, and higher weight for age. No adverse events occurred in the CDC group, while two patients in the control group had complications (one developed heart failure, another developed enteropathy).
The investigators looked at predictors of cardiac functional efficacy in the CDC group and determined that younger age was associated with greater improvement of right ventricular ejection fraction, as measured on echocardiography. The lower weight-for-age Z score and reduced ejection fraction at the time of infusion may be predictors of cardiac function improvements at 3 years.
“This therapeutic strategy may merit somatic growth enhancement and reduce the incidence of heart failure,” Dr. Tarui and coauthors said.
They noted a number of limitations of their small clinical trial. The study was nonrandomized, and the cardiac interventions were not blinded, among others. “Larger phase II studies focusing on changes in cardiac function, myocardial fibrosis, and quality of life and clinical event rates are warranted to confirm these effects of CDC administration in patients with single ventricular physiology,” they said.
The government of Japan through its ministries of Health, Labor and Welfare, and Education, Culture Sports, Science and Technology provided funding for the study, as did the Research Foundation of Okayama University Hospital. The authors had no disclosures.
FROM JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: This is the first clinical trial to report the midterm safety and efficacy of cardiac progenitor therapy in congenital heart disease.
Major finding: After 36 months, infants who received stem cells for congenital heart failure had better outcomes than did infants who had standard treatment.
Data source: Prospective clinical trial of 14 infants enrolled in the Transcoronary Infusion of Cardiac Progenitor Cells in Hypoplastic Left Heat Syndrome (TICAP) trial, divided evenly between treatment and control groups.
Disclosures: The government of Japan through its ministries of Health, Labor and Welfare, and Education, Culture Sports, Science and Technology provided funding for the study, as did the Research Foundation of Okayama University Hospital. The authors had no disclosures.
Tomotherapy may decrease radiation-induced bowel toxicity in cervical cancer
SAN ANTONIO – Interim results of an ongoing phase III trial show that women who have undergone surgical resection for cervical cancer may be less likely to experience late-onset bowel toxicity if they receive tomotherapy rather than conventionally delivered adjuvant radiotherapy.
In the PARCER trial, grade III or higher radiation-induced bowel toxicity occurred in just 3.2% of women who had adjuvant image-guided intensity-modulated radiation therapy (IG-IMRT) vs. 17.8% of those who received three-dimensional conformal radiation therapy (3D-CRT) at a median of 20 months. The 14.6% absolute difference was statistically significant (P = .02) but this was an exploratory endpoint.

The primary endpoint of late grade II or higher bowel toxicity was not statistically significant, but also showed around a 14% absolute difference between the arms, at 11.4% in the IG-IMRT- and 25% in the 3D-CRT–treated women (P = .13).
Nevertheless, the results are clinically relevant and the trial continues accrual to a target of 240 patients. The stopping rules were not met and there is the potential for the results to become statistically significant with longer follow-up, said Dr. Supriya Chopra of Tata Memorial Centre in Mumbai, India.
Speaking at a press briefing held during the annual meeting of the American Society for Radiation Oncology, she said: “Although this trial was done for cervical cancer, the trial results would impact practice for all endometrial cancer patients as well who would undergo postoperative radiation, and prostate cancer patients.”
“There was a substantial reduction in serious toxicities, something that justifies the added labor intensity and the added resource utilization of the more sophisticated approaches and still adds value to patients because there is a reduction in hospitalization and there is a reduction in the cost of downstream side effects,” said Dr. Brian Kavanagh of the University of Colorado at Denver, Aurora, and president-elect of the ASTRO Board of Directors, in an interview.
Data on 120 patients randomized to date were presented, of whom 58 had received conventional 3D-CRT, and 62 who had undergone IG-IMRT and received 50 Gy of radiation given in 24 fractions over 5 weeks. Patients also received weekly cisplatin (50 mg/m2) and two additional 6 Gy doses of pelvic radiation delivered via brachytherapy. In the IG-IMRT arm, investigators were careful to ensure that very little radiation reached the small bowel. Toxicity was assessed using the Common Toxicity Criteria for Adverse Events version 3.0.
Bowel toxicity can affect a substantial number of women after pelvic irradiation, and it tends to evolve over time, Dr. Chopra said.
“Most of the patients would be continually bothered about having chronic diarrhea or having abdominal bloating sensation which cannot be cured by anything, or just having some lower abdominal pain, which definitely affects their quality of life,” she explained.
The trial thus aimed to see if using the latest radiation technology could help to reduce these side effects.
“These early results are very encouraging but not robust enough to change practice at the moment,” Dr. Chopra said. If the trial is positive, however, she added that IMRT could become the new standard of care.
Final analyses will be undertaken after accrual has been completed and at a median follow-up of 3 years, so potentially by the end of 2018, she said.
SAN ANTONIO – Interim results of an ongoing phase III trial show that women who have undergone surgical resection for cervical cancer may be less likely to experience late-onset bowel toxicity if they receive tomotherapy rather than conventionally delivered adjuvant radiotherapy.
In the PARCER trial, grade III or higher radiation-induced bowel toxicity occurred in just 3.2% of women who had adjuvant image-guided intensity-modulated radiation therapy (IG-IMRT) vs. 17.8% of those who received three-dimensional conformal radiation therapy (3D-CRT) at a median of 20 months. The 14.6% absolute difference was statistically significant (P = .02) but this was an exploratory endpoint.
The primary endpoint of late grade II or higher bowel toxicity was not statistically significant, but also showed around a 14% absolute difference between the arms, at 11.4% in the IG-IMRT- and 25% in the 3D-CRT–treated women (P = .13).
Nevertheless, the results are clinically relevant and the trial continues accrual to a target of 240 patients. The stopping rules were not met and there is the potential for the results to become statistically significant with longer follow-up, said Dr. Supriya Chopra of Tata Memorial Centre in Mumbai, India.
Speaking at a press briefing held during the annual meeting of the American Society for Radiation Oncology, she said: “Although this trial was done for cervical cancer, the trial results would impact practice for all endometrial cancer patients as well who would undergo postoperative radiation, and prostate cancer patients.”
“There was a substantial reduction in serious toxicities, something that justifies the added labor intensity and the added resource utilization of the more sophisticated approaches and still adds value to patients because there is a reduction in hospitalization and there is a reduction in the cost of downstream side effects,” said Dr. Brian Kavanagh of the University of Colorado at Denver, Aurora, and president-elect of the ASTRO Board of Directors, in an interview.
Data on 120 patients randomized to date were presented, of whom 58 had received conventional 3D-CRT, and 62 who had undergone IG-IMRT and received 50 Gy of radiation given in 24 fractions over 5 weeks. Patients also received weekly cisplatin (50 mg/m2) and two additional 6 Gy doses of pelvic radiation delivered via brachytherapy. In the IG-IMRT arm, investigators were careful to ensure that very little radiation reached the small bowel. Toxicity was assessed using the Common Toxicity Criteria for Adverse Events version 3.0.
Bowel toxicity can affect a substantial number of women after pelvic irradiation, and it tends to evolve over time, Dr. Chopra said.
“Most of the patients would be continually bothered about having chronic diarrhea or having abdominal bloating sensation which cannot be cured by anything, or just having some lower abdominal pain, which definitely affects their quality of life,” she explained.
The trial thus aimed to see if using the latest radiation technology could help to reduce these side effects.
“These early results are very encouraging but not robust enough to change practice at the moment,” Dr. Chopra said. If the trial is positive, however, she added that IMRT could become the new standard of care.
Final analyses will be undertaken after accrual has been completed and at a median follow-up of 3 years, so potentially by the end of 2018, she said.
SAN ANTONIO – Interim results of an ongoing phase III trial show that women who have undergone surgical resection for cervical cancer may be less likely to experience late-onset bowel toxicity if they receive tomotherapy rather than conventionally delivered adjuvant radiotherapy.
In the PARCER trial, grade III or higher radiation-induced bowel toxicity occurred in just 3.2% of women who had adjuvant image-guided intensity-modulated radiation therapy (IG-IMRT) vs. 17.8% of those who received three-dimensional conformal radiation therapy (3D-CRT) at a median of 20 months. The 14.6% absolute difference was statistically significant (P = .02) but this was an exploratory endpoint.
The primary endpoint of late grade II or higher bowel toxicity was not statistically significant, but also showed around a 14% absolute difference between the arms, at 11.4% in the IG-IMRT- and 25% in the 3D-CRT–treated women (P = .13).
Nevertheless, the results are clinically relevant and the trial continues accrual to a target of 240 patients. The stopping rules were not met and there is the potential for the results to become statistically significant with longer follow-up, said Dr. Supriya Chopra of Tata Memorial Centre in Mumbai, India.
Speaking at a press briefing held during the annual meeting of the American Society for Radiation Oncology, she said: “Although this trial was done for cervical cancer, the trial results would impact practice for all endometrial cancer patients as well who would undergo postoperative radiation, and prostate cancer patients.”
“There was a substantial reduction in serious toxicities, something that justifies the added labor intensity and the added resource utilization of the more sophisticated approaches and still adds value to patients because there is a reduction in hospitalization and there is a reduction in the cost of downstream side effects,” said Dr. Brian Kavanagh of the University of Colorado at Denver, Aurora, and president-elect of the ASTRO Board of Directors, in an interview.
Data on 120 patients randomized to date were presented, of whom 58 had received conventional 3D-CRT, and 62 who had undergone IG-IMRT and received 50 Gy of radiation given in 24 fractions over 5 weeks. Patients also received weekly cisplatin (50 mg/m2) and two additional 6 Gy doses of pelvic radiation delivered via brachytherapy. In the IG-IMRT arm, investigators were careful to ensure that very little radiation reached the small bowel. Toxicity was assessed using the Common Toxicity Criteria for Adverse Events version 3.0.
Bowel toxicity can affect a substantial number of women after pelvic irradiation, and it tends to evolve over time, Dr. Chopra said.
“Most of the patients would be continually bothered about having chronic diarrhea or having abdominal bloating sensation which cannot be cured by anything, or just having some lower abdominal pain, which definitely affects their quality of life,” she explained.
The trial thus aimed to see if using the latest radiation technology could help to reduce these side effects.
“These early results are very encouraging but not robust enough to change practice at the moment,” Dr. Chopra said. If the trial is positive, however, she added that IMRT could become the new standard of care.
Final analyses will be undertaken after accrual has been completed and at a median follow-up of 3 years, so potentially by the end of 2018, she said.
AT THE ASTRO ANNUAL MEETING

CDC to celebrate best blood clot prevention strategies
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
Endovascular thrombectomy vs tPA: better function, same mortality
Endovascular mechanical thrombectomy yielded better function and revascularization rates but similar mortality and intracranial hemorrhage rates as standard medical therapy using tissue plasminogen activator (tPA) in a meta-analysis of eight high-quality randomized clinical trials comparing the two approaches for acute ischemic stroke.
The results were published online Nov. 3 in JAMA.
This meta-analysis included only large multicenter trials published from 2013 to the present. Previous trials and meta-analyses “had several well-recognized limitations” including inconsistent use of vascular imaging to confirm vessel occlusion before randomization, variable use of tPA in patients who eventually were assigned to endovascular therapy, and reliance on less effective and now outdated mechanical devices, said Dr. Jetan H. Badhiwala of the division of neurosurgery, University of Toronto, and his associates.
The eight trials included 2,423 patients (mean age, 67.4 years); 46.7% were women. A total of 1,313 patients underwent endovascular therapy, defined as the intra-arterial use of a microcatheter or other device for mechanical thrombectomy, with or without the local use of a chemical thrombolytic agent. The remaining 1,110 received standard medical therapy (tPA). The interval between stroke onset and endovascular treatment varied from 5 to 12 hours across these studies, with a mean of 3.8 hours.
Patients who had endovascular thrombectomy showed significantly higher rates of functional independence at 90 days (44.6%) than did those who had tPA (31.8%), for an OR of 1.71 and a number needed to treat of 8. The rate of angiographic revascularization at 24 hours also was markedly higher for endovascular thrombectomy (75.8% vs 34.1%), for an OR of 6.49, the investigators said (JAMA 2015;314:1832-43).
However, there were no significant differences between the two study groups in rates of symptomatic intracranial hemorrhage at 90 days (5.7% vs 5.1%) or all-cause mortality at 90 days (15.8% vs 17.8%), and overall morbidity including in-hospital rates of deep venous thrombosis, MI, and pneumonia also were similar.
No sponsor or source of financial support was reported for this study. Dr. Badhiwala and his associates reported having no relevant financial disclosures.
It is important to note some limitations with this well-conducted meta-analysis. First, functional outcomes showed significant heterogeneity, which the authors attributed to variations in patient-, treatment-, and study-related factors.
Second, the confidence intervals for mortality and intracranial hemorrhage were wide, indicating that more data are necessary to fully inform these outcomes.
Third, five of the eight trials were halted early because of the evident superiority of endovascular thrombectomy, which means they fell substantially short (by up to 74%) of their planned sample sizes. This tends to cause overestimation of treatment effects. Fourth, nearly all these strokes involved carotid territory, nearly all the patients were on the young end of the age spectrum, and very few participants had comorbidities such as AF or diabetes. Such favorable characteristics do not reflect real-world experience with ischemic stroke.
Dr. Joanna M. Wardlaw and Dr. Martin S. Dennis are at the Centre for Clinical Brain Sciences at the University of Edinburgh (Scotland). They reported having no relevant financial disclosures. Dr. Wardlaw and Dr. Dennis made these remarks in an editorial accompanying Dr. Badhiwala’s meta-analysis (JAMA 2015;314:1803-4).
It is important to note some limitations with this well-conducted meta-analysis. First, functional outcomes showed significant heterogeneity, which the authors attributed to variations in patient-, treatment-, and study-related factors.
Second, the confidence intervals for mortality and intracranial hemorrhage were wide, indicating that more data are necessary to fully inform these outcomes.
Third, five of the eight trials were halted early because of the evident superiority of endovascular thrombectomy, which means they fell substantially short (by up to 74%) of their planned sample sizes. This tends to cause overestimation of treatment effects. Fourth, nearly all these strokes involved carotid territory, nearly all the patients were on the young end of the age spectrum, and very few participants had comorbidities such as AF or diabetes. Such favorable characteristics do not reflect real-world experience with ischemic stroke.
Dr. Joanna M. Wardlaw and Dr. Martin S. Dennis are at the Centre for Clinical Brain Sciences at the University of Edinburgh (Scotland). They reported having no relevant financial disclosures. Dr. Wardlaw and Dr. Dennis made these remarks in an editorial accompanying Dr. Badhiwala’s meta-analysis (JAMA 2015;314:1803-4).
It is important to note some limitations with this well-conducted meta-analysis. First, functional outcomes showed significant heterogeneity, which the authors attributed to variations in patient-, treatment-, and study-related factors.
Second, the confidence intervals for mortality and intracranial hemorrhage were wide, indicating that more data are necessary to fully inform these outcomes.
Third, five of the eight trials were halted early because of the evident superiority of endovascular thrombectomy, which means they fell substantially short (by up to 74%) of their planned sample sizes. This tends to cause overestimation of treatment effects. Fourth, nearly all these strokes involved carotid territory, nearly all the patients were on the young end of the age spectrum, and very few participants had comorbidities such as AF or diabetes. Such favorable characteristics do not reflect real-world experience with ischemic stroke.
Dr. Joanna M. Wardlaw and Dr. Martin S. Dennis are at the Centre for Clinical Brain Sciences at the University of Edinburgh (Scotland). They reported having no relevant financial disclosures. Dr. Wardlaw and Dr. Dennis made these remarks in an editorial accompanying Dr. Badhiwala’s meta-analysis (JAMA 2015;314:1803-4).
Endovascular mechanical thrombectomy yielded better function and revascularization rates but similar mortality and intracranial hemorrhage rates as standard medical therapy using tissue plasminogen activator (tPA) in a meta-analysis of eight high-quality randomized clinical trials comparing the two approaches for acute ischemic stroke.
The results were published online Nov. 3 in JAMA.
This meta-analysis included only large multicenter trials published from 2013 to the present. Previous trials and meta-analyses “had several well-recognized limitations” including inconsistent use of vascular imaging to confirm vessel occlusion before randomization, variable use of tPA in patients who eventually were assigned to endovascular therapy, and reliance on less effective and now outdated mechanical devices, said Dr. Jetan H. Badhiwala of the division of neurosurgery, University of Toronto, and his associates.
The eight trials included 2,423 patients (mean age, 67.4 years); 46.7% were women. A total of 1,313 patients underwent endovascular therapy, defined as the intra-arterial use of a microcatheter or other device for mechanical thrombectomy, with or without the local use of a chemical thrombolytic agent. The remaining 1,110 received standard medical therapy (tPA). The interval between stroke onset and endovascular treatment varied from 5 to 12 hours across these studies, with a mean of 3.8 hours.
Patients who had endovascular thrombectomy showed significantly higher rates of functional independence at 90 days (44.6%) than did those who had tPA (31.8%), for an OR of 1.71 and a number needed to treat of 8. The rate of angiographic revascularization at 24 hours also was markedly higher for endovascular thrombectomy (75.8% vs 34.1%), for an OR of 6.49, the investigators said (JAMA 2015;314:1832-43).
However, there were no significant differences between the two study groups in rates of symptomatic intracranial hemorrhage at 90 days (5.7% vs 5.1%) or all-cause mortality at 90 days (15.8% vs 17.8%), and overall morbidity including in-hospital rates of deep venous thrombosis, MI, and pneumonia also were similar.
No sponsor or source of financial support was reported for this study. Dr. Badhiwala and his associates reported having no relevant financial disclosures.
Endovascular mechanical thrombectomy yielded better function and revascularization rates but similar mortality and intracranial hemorrhage rates as standard medical therapy using tissue plasminogen activator (tPA) in a meta-analysis of eight high-quality randomized clinical trials comparing the two approaches for acute ischemic stroke.
The results were published online Nov. 3 in JAMA.
This meta-analysis included only large multicenter trials published from 2013 to the present. Previous trials and meta-analyses “had several well-recognized limitations” including inconsistent use of vascular imaging to confirm vessel occlusion before randomization, variable use of tPA in patients who eventually were assigned to endovascular therapy, and reliance on less effective and now outdated mechanical devices, said Dr. Jetan H. Badhiwala of the division of neurosurgery, University of Toronto, and his associates.
The eight trials included 2,423 patients (mean age, 67.4 years); 46.7% were women. A total of 1,313 patients underwent endovascular therapy, defined as the intra-arterial use of a microcatheter or other device for mechanical thrombectomy, with or without the local use of a chemical thrombolytic agent. The remaining 1,110 received standard medical therapy (tPA). The interval between stroke onset and endovascular treatment varied from 5 to 12 hours across these studies, with a mean of 3.8 hours.
Patients who had endovascular thrombectomy showed significantly higher rates of functional independence at 90 days (44.6%) than did those who had tPA (31.8%), for an OR of 1.71 and a number needed to treat of 8. The rate of angiographic revascularization at 24 hours also was markedly higher for endovascular thrombectomy (75.8% vs 34.1%), for an OR of 6.49, the investigators said (JAMA 2015;314:1832-43).
However, there were no significant differences between the two study groups in rates of symptomatic intracranial hemorrhage at 90 days (5.7% vs 5.1%) or all-cause mortality at 90 days (15.8% vs 17.8%), and overall morbidity including in-hospital rates of deep venous thrombosis, MI, and pneumonia also were similar.
No sponsor or source of financial support was reported for this study. Dr. Badhiwala and his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: Endovascular mechanical thrombectomy yielded better function and angiographic revascularization but similar mortality and rate of intracranial hemorrhage compared with standard medical therapy (tPA) for acute ischemic stroke.
Major finding: Patients who had endovascular thrombectomy showed significantly higher rates of functional independence at 90 days (44.6%) than did those who had tPA (31.8%), for an OR of 1.71 and a number needed to treat of 8.
Data source: A meta-analysis of eight high-quality multicenter randomized clinical trials published during 2013-2015 involving 2,423 adults with acute ischemic stroke.
Disclosures: No sponsor or source of financial support was reported for this study. Dr. Badhiwala and his associates reported having no relevant financial disclosures.
Magnetic sphincter device clicks in real-world GERD patients
CHICAGO – Patients receiving the LINX magnetic sphincter device for gastroesophageal reflux disease (GERD) at a community hospital have outcomes comparable with those achieved at the best academic centers, a study suggests.
“This is a safe and effective operation that, importantly, is very reproducible in the community setting,” Dr. F. Paul “Tripp” Buckley III said at the annual clinical congress of the American College of Surgeons. “Unlike a Nissen [fundoplication] where you have to have 50 [surgeries completed] to be considered an expert and then do over 35 a year to continue to have great outcomes, this is a highly teachable event and can be employed out in the community with little hesitation.”

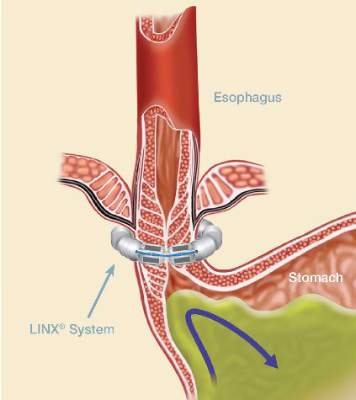
The magnetic sphincter augmentation device (LINX, Torax Medical) was approved in the United States in 2012 for the treatment of GERD and consists of a series of interlinked titanium-encased magnets implanted laparoscopically around the esophagus. The magnets augment a weak lower esophageal sphincter and avoid some of the complications of fundoplication, said Dr. Buckley, who disclosed serving as a proctor and speaker for Torax.
In the 5-year study leading to its approval, 64% of patients achieved the primary outcome of normalization of esophageal acid exposure or at least a 50% reduction in exposure at 1 year after sphincter augmentation and 93% of patients cut their use of proton-pump inhibitors (PPIs) by at least 50%. Six serious adverse events occurred (N Engl J Med. 2013;368:719-27).
Dr. Buckley, of Scott & White Health in Round Rock, Tex., and his associates evaluated their first 102 patients undergoing magnetic sphincter augmentation under general anesthesia at two community hospitals. GERD health-related quality of life (GERD-HRQL) scores were compared before and after surgery and overall results were compared with the clinical trial data. The highest possible total GERD-HRQL score is 75 (worst symptoms) and lowest score 0 (no symptoms).
The community and clinical trial cohorts were similar in age (median, 54 vs. 53 years), sex (both 52% male), median body mass index (both 28 kg/m2), and PPI use (98% vs. 100%), which was a requirement for trial entry.
After patients in the community underwent magnetic sphincter augmentation, PPI use decreased from 98% to 8%, median GERD-HRQL scores declined from 27 to 5, and patient satisfaction with GERD rose from 8% to 84%, which fell short of the satisfaction rate in the clinical trial (84% vs. 94%; P = .05), Dr. Buckley said.

The reduction in PPI use, however, was similar with that reported in the clinical trial, as was the percentage achieving at least 50% improvement in GERD-HRQL scores (86% vs. 92%), and operative times (median 49 vs. 36 minutes), he noted.
Device removal was rare at 1% in the community vs. 6% in the trial (P = .06).
Lower rates of dilation were noted in the community (9% vs. 19%; P = .04), perhaps because of refinements in technique and postoperative management, Dr. Buckley said.
“We know with this device you have to eat normally after implantation so that it will open and close within the scar capsule that’s naturally going to form,” he noted. “You have some patients that scar very tightly and you’ve got other patients that have a little bit of pain with eating and then suddenly they’re back on a liquid diet, which is a death knell for the success of this operation. So you really have to talk with these patients. I tell folks, ‘This is not a fix-it-and-forget-it type of operation.’ You’re going to get to know these patients pretty well, particularly in the early postoperative period.”
Final results recently reported with 5 years of follow-up in the clinical trial showed that 85% of patients were free from daily dependence on PPIs, heartburn was reduced from 89% to 12%, and moderate or severe regurgitation declined from 57% to 1.2%. No migrations or malfunctions occurred (J Laparoendosc Adv Surg Tech A. 2015 Oct;25[10]:787-92).
“One key aspect of this operation, and we think one of the reasons for its success and lack of migrations of the device, is that we keep the phrenoesophogeal ligament intact, so you are never in the mediastinum,” Dr. Buckley said. “For those of us who do a lot of Nissens, you end up blowing through it every time. But here when you keep it intact, you can roll it up on the distal esophagus and you can really reduce the hiatal hernia pretty significantly, even pretty large ones.”
A 3-cm cutoff was used for hiatal hernias in the trial and is recommended for early adoption in the community. A study is planned looking at hernias greater than 3 cm with no upper limit, where the minimal dissection method cannot reduce the hernia and full dissection is required, and the only requirement is that the patient have normal esophageal motility, he said.
Discussant Dr. Douglas Smink from Brigham and Women’s Hospital in Boston, said, “[There is a] lot of interest in this procedure obviously and it’s really nice to see what it’s like outside of the trials and to see your data is very similar.”
He went on to ask whether Dr. Buckley is still recommending fundoplication and, if so, in whom.
The LINX device has supplanted a classic Nissen fundoplication as the first-line operation in patients with good esophageal motility, although the device is not entirely covered by insurance, Dr. Buckley said.
“Basically, I tell patients I think it’s a marginally better operation. It’s not leaps and bounds, but it’s a marginally better operation,” he said, adding that though there has been concern about erosions, their erosion rate is zero and thus far, only seven erosions out of nearly 4,000 devices placed.
CHICAGO – Patients receiving the LINX magnetic sphincter device for gastroesophageal reflux disease (GERD) at a community hospital have outcomes comparable with those achieved at the best academic centers, a study suggests.
“This is a safe and effective operation that, importantly, is very reproducible in the community setting,” Dr. F. Paul “Tripp” Buckley III said at the annual clinical congress of the American College of Surgeons. “Unlike a Nissen [fundoplication] where you have to have 50 [surgeries completed] to be considered an expert and then do over 35 a year to continue to have great outcomes, this is a highly teachable event and can be employed out in the community with little hesitation.”
The magnetic sphincter augmentation device (LINX, Torax Medical) was approved in the United States in 2012 for the treatment of GERD and consists of a series of interlinked titanium-encased magnets implanted laparoscopically around the esophagus. The magnets augment a weak lower esophageal sphincter and avoid some of the complications of fundoplication, said Dr. Buckley, who disclosed serving as a proctor and speaker for Torax.
In the 5-year study leading to its approval, 64% of patients achieved the primary outcome of normalization of esophageal acid exposure or at least a 50% reduction in exposure at 1 year after sphincter augmentation and 93% of patients cut their use of proton-pump inhibitors (PPIs) by at least 50%. Six serious adverse events occurred (N Engl J Med. 2013;368:719-27).
Dr. Buckley, of Scott & White Health in Round Rock, Tex., and his associates evaluated their first 102 patients undergoing magnetic sphincter augmentation under general anesthesia at two community hospitals. GERD health-related quality of life (GERD-HRQL) scores were compared before and after surgery and overall results were compared with the clinical trial data. The highest possible total GERD-HRQL score is 75 (worst symptoms) and lowest score 0 (no symptoms).
The community and clinical trial cohorts were similar in age (median, 54 vs. 53 years), sex (both 52% male), median body mass index (both 28 kg/m2), and PPI use (98% vs. 100%), which was a requirement for trial entry.
After patients in the community underwent magnetic sphincter augmentation, PPI use decreased from 98% to 8%, median GERD-HRQL scores declined from 27 to 5, and patient satisfaction with GERD rose from 8% to 84%, which fell short of the satisfaction rate in the clinical trial (84% vs. 94%; P = .05), Dr. Buckley said.
The reduction in PPI use, however, was similar with that reported in the clinical trial, as was the percentage achieving at least 50% improvement in GERD-HRQL scores (86% vs. 92%), and operative times (median 49 vs. 36 minutes), he noted.
Device removal was rare at 1% in the community vs. 6% in the trial (P = .06).
Lower rates of dilation were noted in the community (9% vs. 19%; P = .04), perhaps because of refinements in technique and postoperative management, Dr. Buckley said.
“We know with this device you have to eat normally after implantation so that it will open and close within the scar capsule that’s naturally going to form,” he noted. “You have some patients that scar very tightly and you’ve got other patients that have a little bit of pain with eating and then suddenly they’re back on a liquid diet, which is a death knell for the success of this operation. So you really have to talk with these patients. I tell folks, ‘This is not a fix-it-and-forget-it type of operation.’ You’re going to get to know these patients pretty well, particularly in the early postoperative period.”
Final results recently reported with 5 years of follow-up in the clinical trial showed that 85% of patients were free from daily dependence on PPIs, heartburn was reduced from 89% to 12%, and moderate or severe regurgitation declined from 57% to 1.2%. No migrations or malfunctions occurred (J Laparoendosc Adv Surg Tech A. 2015 Oct;25[10]:787-92).
“One key aspect of this operation, and we think one of the reasons for its success and lack of migrations of the device, is that we keep the phrenoesophogeal ligament intact, so you are never in the mediastinum,” Dr. Buckley said. “For those of us who do a lot of Nissens, you end up blowing through it every time. But here when you keep it intact, you can roll it up on the distal esophagus and you can really reduce the hiatal hernia pretty significantly, even pretty large ones.”
A 3-cm cutoff was used for hiatal hernias in the trial and is recommended for early adoption in the community. A study is planned looking at hernias greater than 3 cm with no upper limit, where the minimal dissection method cannot reduce the hernia and full dissection is required, and the only requirement is that the patient have normal esophageal motility, he said.
Discussant Dr. Douglas Smink from Brigham and Women’s Hospital in Boston, said, “[There is a] lot of interest in this procedure obviously and it’s really nice to see what it’s like outside of the trials and to see your data is very similar.”
He went on to ask whether Dr. Buckley is still recommending fundoplication and, if so, in whom.
The LINX device has supplanted a classic Nissen fundoplication as the first-line operation in patients with good esophageal motility, although the device is not entirely covered by insurance, Dr. Buckley said.
“Basically, I tell patients I think it’s a marginally better operation. It’s not leaps and bounds, but it’s a marginally better operation,” he said, adding that though there has been concern about erosions, their erosion rate is zero and thus far, only seven erosions out of nearly 4,000 devices placed.
CHICAGO – Patients receiving the LINX magnetic sphincter device for gastroesophageal reflux disease (GERD) at a community hospital have outcomes comparable with those achieved at the best academic centers, a study suggests.
“This is a safe and effective operation that, importantly, is very reproducible in the community setting,” Dr. F. Paul “Tripp” Buckley III said at the annual clinical congress of the American College of Surgeons. “Unlike a Nissen [fundoplication] where you have to have 50 [surgeries completed] to be considered an expert and then do over 35 a year to continue to have great outcomes, this is a highly teachable event and can be employed out in the community with little hesitation.”
The magnetic sphincter augmentation device (LINX, Torax Medical) was approved in the United States in 2012 for the treatment of GERD and consists of a series of interlinked titanium-encased magnets implanted laparoscopically around the esophagus. The magnets augment a weak lower esophageal sphincter and avoid some of the complications of fundoplication, said Dr. Buckley, who disclosed serving as a proctor and speaker for Torax.
In the 5-year study leading to its approval, 64% of patients achieved the primary outcome of normalization of esophageal acid exposure or at least a 50% reduction in exposure at 1 year after sphincter augmentation and 93% of patients cut their use of proton-pump inhibitors (PPIs) by at least 50%. Six serious adverse events occurred (N Engl J Med. 2013;368:719-27).
Dr. Buckley, of Scott & White Health in Round Rock, Tex., and his associates evaluated their first 102 patients undergoing magnetic sphincter augmentation under general anesthesia at two community hospitals. GERD health-related quality of life (GERD-HRQL) scores were compared before and after surgery and overall results were compared with the clinical trial data. The highest possible total GERD-HRQL score is 75 (worst symptoms) and lowest score 0 (no symptoms).
The community and clinical trial cohorts were similar in age (median, 54 vs. 53 years), sex (both 52% male), median body mass index (both 28 kg/m2), and PPI use (98% vs. 100%), which was a requirement for trial entry.
After patients in the community underwent magnetic sphincter augmentation, PPI use decreased from 98% to 8%, median GERD-HRQL scores declined from 27 to 5, and patient satisfaction with GERD rose from 8% to 84%, which fell short of the satisfaction rate in the clinical trial (84% vs. 94%; P = .05), Dr. Buckley said.
The reduction in PPI use, however, was similar with that reported in the clinical trial, as was the percentage achieving at least 50% improvement in GERD-HRQL scores (86% vs. 92%), and operative times (median 49 vs. 36 minutes), he noted.
Device removal was rare at 1% in the community vs. 6% in the trial (P = .06).
Lower rates of dilation were noted in the community (9% vs. 19%; P = .04), perhaps because of refinements in technique and postoperative management, Dr. Buckley said.
“We know with this device you have to eat normally after implantation so that it will open and close within the scar capsule that’s naturally going to form,” he noted. “You have some patients that scar very tightly and you’ve got other patients that have a little bit of pain with eating and then suddenly they’re back on a liquid diet, which is a death knell for the success of this operation. So you really have to talk with these patients. I tell folks, ‘This is not a fix-it-and-forget-it type of operation.’ You’re going to get to know these patients pretty well, particularly in the early postoperative period.”
Final results recently reported with 5 years of follow-up in the clinical trial showed that 85% of patients were free from daily dependence on PPIs, heartburn was reduced from 89% to 12%, and moderate or severe regurgitation declined from 57% to 1.2%. No migrations or malfunctions occurred (J Laparoendosc Adv Surg Tech A. 2015 Oct;25[10]:787-92).
“One key aspect of this operation, and we think one of the reasons for its success and lack of migrations of the device, is that we keep the phrenoesophogeal ligament intact, so you are never in the mediastinum,” Dr. Buckley said. “For those of us who do a lot of Nissens, you end up blowing through it every time. But here when you keep it intact, you can roll it up on the distal esophagus and you can really reduce the hiatal hernia pretty significantly, even pretty large ones.”
A 3-cm cutoff was used for hiatal hernias in the trial and is recommended for early adoption in the community. A study is planned looking at hernias greater than 3 cm with no upper limit, where the minimal dissection method cannot reduce the hernia and full dissection is required, and the only requirement is that the patient have normal esophageal motility, he said.
Discussant Dr. Douglas Smink from Brigham and Women’s Hospital in Boston, said, “[There is a] lot of interest in this procedure obviously and it’s really nice to see what it’s like outside of the trials and to see your data is very similar.”
He went on to ask whether Dr. Buckley is still recommending fundoplication and, if so, in whom.
The LINX device has supplanted a classic Nissen fundoplication as the first-line operation in patients with good esophageal motility, although the device is not entirely covered by insurance, Dr. Buckley said.
“Basically, I tell patients I think it’s a marginally better operation. It’s not leaps and bounds, but it’s a marginally better operation,” he said, adding that though there has been concern about erosions, their erosion rate is zero and thus far, only seven erosions out of nearly 4,000 devices placed.
AT THE ACS CLINICAL CONGRESS
Key clinical point: Magnetic sphincter augmentation in the community setting provides results comparable with those seen in clinical trials.
Major finding: PPI use decreased from 98% to 8% after magnetic sphincter augmentation.
Data source: Prospective study in 102 patients with gastroesophageal reflux disease.
Disclosures: Dr. Buckley reported serving as a proctor and speaker for Torax Medical, which markets the Linx system.
The Role of Liposomal Bupivacaine in Postsurgical Analgesia
A supplement to ACS Surgery News®. This supplement is sponsored by Pacira Pharmaceuticals, Inc.
Wound Infiltration Technique video:
TAP Infiltration Technique video
A supplement to ACS Surgery News®. This supplement is sponsored by Pacira Pharmaceuticals, Inc.
Wound Infiltration Technique video:
TAP Infiltration Technique video
A supplement to ACS Surgery News®. This supplement is sponsored by Pacira Pharmaceuticals, Inc.
Wound Infiltration Technique video:
TAP Infiltration Technique video
CMS finalizes 2016 fee schedule with payment for advance care planning
Officials at the Centers for Medicare & Medicaid Services have issued the final 2016 fee schedule for physicians, making modifications to the Physician Quality Reporting System (PQRS) and loosening requirements for its controversial two-midnight rule.
The fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes changes to payment policies, modifications to misvalued codes, and updates to quality performance metrics under the PQRS, the Medicare Shared Savings Program, and Physician Compare, among others.

As part of the final fee schedule rule, released Oct. 30, CMS is relaxing its two-midnight rule to allow doctors greater flexibility when determining whether hospital stays are subject to the regulation.
For hospital stays for which physicians expect the patient will need less than two midnights of hospital care, an inpatient admission may still be payable under Medicare Part A on a case-by-case basis based on the admitting physician’s judgment, according to the final rule. Additionally, the agency does not plan to send recovery auditors after doctors suspected of violating the two-midnight rule. Instead, CMS plans to use Beneficiary and Family Centered Care Quality Improvement Organizations to conduct initial medical reviews of claims for short-stay inpatient admissions. The claim reviews will focus on educating physicians and hospitals about the policy for inpatient admissions.
Only physicians with questionable practice patterns, such as high rates of claims denial after medical review, will be referred to auditors, according to CMS.
“These changes continue CMS’ long-standing emphasis on the importance of a physician’s medical judgment in meeting the needs of Medicare beneficiaries,” CMS officials stated in a fact sheet.
CMS also finalized two new advance care planning codes that will pay physicians for time spent discussing patient options for advance directives. The first code will cover an initial 30 minutes of the physicians’ time, and the second code will cover additional 30-minute blocks as necessary.
The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015, but CMS delayed the codes’ enactment until collecting public comment.
Modifications to quality programs include a new reporting option under the PQRS that will allow group practices to report quality measure data using a Qualified Clinical Data Registry. In 2016, there will be 281 measures in the PQRS measure set and 18 measures in the Group Practice Reporting Option (GPRO) Web Interface, according to the final rule.
The 2018 payment adjustment will be the last adjustment under the PQRS. Starting in 2019, adjustments to payment for quality reporting and other factors will be made under the Merit-Based Incentive Payment System (MIPS), as required by MACRA.
Changes to the Value-Based Payment Modifier program are also coming in 2016:
• CMS will apply the quality-tiering methodology to all groups and solo practitioners that meet the criteria to avoid the downward adjustment under the PQRS. Groups and solo practitioners would be subject to upward, neutral, or downward adjustments derived under the quality-tiering methodology.
• CMS will continue to set the maximum upward adjustment under the quality-tiering methodology for the CY 2018 value modifier at four times an adjustment factor for groups of physicians with 10 or more eligible professionals, and two times an adjustment factor for groups of physicians with between two and nine eligible professionals and physician solo practitioners.
• CMS will use calendar year 2016 as the performance period for the calendar 2018 value modifier and continue to apply the 2018 value modifier based on participation in the PQRS by groups and solo practitioners.
The fee schedule also includes modifications to the Medicare Shared Savings Program including a new measure on statin therapy for the prevention and treatment of cardiovascular disease in the “preventive health domain” of the Shared Savings Program quality measure set. The final rule also clarifies how PQRS-eligible professionals participating within an Accountable Care Organization can meet reporting requirements.
On Twitter @legal_med
Officials at the Centers for Medicare & Medicaid Services have issued the final 2016 fee schedule for physicians, making modifications to the Physician Quality Reporting System (PQRS) and loosening requirements for its controversial two-midnight rule.
The fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes changes to payment policies, modifications to misvalued codes, and updates to quality performance metrics under the PQRS, the Medicare Shared Savings Program, and Physician Compare, among others.
As part of the final fee schedule rule, released Oct. 30, CMS is relaxing its two-midnight rule to allow doctors greater flexibility when determining whether hospital stays are subject to the regulation.
For hospital stays for which physicians expect the patient will need less than two midnights of hospital care, an inpatient admission may still be payable under Medicare Part A on a case-by-case basis based on the admitting physician’s judgment, according to the final rule. Additionally, the agency does not plan to send recovery auditors after doctors suspected of violating the two-midnight rule. Instead, CMS plans to use Beneficiary and Family Centered Care Quality Improvement Organizations to conduct initial medical reviews of claims for short-stay inpatient admissions. The claim reviews will focus on educating physicians and hospitals about the policy for inpatient admissions.
Only physicians with questionable practice patterns, such as high rates of claims denial after medical review, will be referred to auditors, according to CMS.
“These changes continue CMS’ long-standing emphasis on the importance of a physician’s medical judgment in meeting the needs of Medicare beneficiaries,” CMS officials stated in a fact sheet.
CMS also finalized two new advance care planning codes that will pay physicians for time spent discussing patient options for advance directives. The first code will cover an initial 30 minutes of the physicians’ time, and the second code will cover additional 30-minute blocks as necessary.
The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015, but CMS delayed the codes’ enactment until collecting public comment.
Modifications to quality programs include a new reporting option under the PQRS that will allow group practices to report quality measure data using a Qualified Clinical Data Registry. In 2016, there will be 281 measures in the PQRS measure set and 18 measures in the Group Practice Reporting Option (GPRO) Web Interface, according to the final rule.
The 2018 payment adjustment will be the last adjustment under the PQRS. Starting in 2019, adjustments to payment for quality reporting and other factors will be made under the Merit-Based Incentive Payment System (MIPS), as required by MACRA.
Changes to the Value-Based Payment Modifier program are also coming in 2016:
• CMS will apply the quality-tiering methodology to all groups and solo practitioners that meet the criteria to avoid the downward adjustment under the PQRS. Groups and solo practitioners would be subject to upward, neutral, or downward adjustments derived under the quality-tiering methodology.
• CMS will continue to set the maximum upward adjustment under the quality-tiering methodology for the CY 2018 value modifier at four times an adjustment factor for groups of physicians with 10 or more eligible professionals, and two times an adjustment factor for groups of physicians with between two and nine eligible professionals and physician solo practitioners.
• CMS will use calendar year 2016 as the performance period for the calendar 2018 value modifier and continue to apply the 2018 value modifier based on participation in the PQRS by groups and solo practitioners.
The fee schedule also includes modifications to the Medicare Shared Savings Program including a new measure on statin therapy for the prevention and treatment of cardiovascular disease in the “preventive health domain” of the Shared Savings Program quality measure set. The final rule also clarifies how PQRS-eligible professionals participating within an Accountable Care Organization can meet reporting requirements.
On Twitter @legal_med
Officials at the Centers for Medicare & Medicaid Services have issued the final 2016 fee schedule for physicians, making modifications to the Physician Quality Reporting System (PQRS) and loosening requirements for its controversial two-midnight rule.
The fee schedule – the first since repeal of the Sustainable Growth Rate (SGR) formula and enactment of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – includes changes to payment policies, modifications to misvalued codes, and updates to quality performance metrics under the PQRS, the Medicare Shared Savings Program, and Physician Compare, among others.
As part of the final fee schedule rule, released Oct. 30, CMS is relaxing its two-midnight rule to allow doctors greater flexibility when determining whether hospital stays are subject to the regulation.
For hospital stays for which physicians expect the patient will need less than two midnights of hospital care, an inpatient admission may still be payable under Medicare Part A on a case-by-case basis based on the admitting physician’s judgment, according to the final rule. Additionally, the agency does not plan to send recovery auditors after doctors suspected of violating the two-midnight rule. Instead, CMS plans to use Beneficiary and Family Centered Care Quality Improvement Organizations to conduct initial medical reviews of claims for short-stay inpatient admissions. The claim reviews will focus on educating physicians and hospitals about the policy for inpatient admissions.
Only physicians with questionable practice patterns, such as high rates of claims denial after medical review, will be referred to auditors, according to CMS.
“These changes continue CMS’ long-standing emphasis on the importance of a physician’s medical judgment in meeting the needs of Medicare beneficiaries,” CMS officials stated in a fact sheet.
CMS also finalized two new advance care planning codes that will pay physicians for time spent discussing patient options for advance directives. The first code will cover an initial 30 minutes of the physicians’ time, and the second code will cover additional 30-minute blocks as necessary.
The AMA Current Procedural Terminology (CPT) Editorial Panel and the AMA Relative Value Update Committee (RUC) created the new CPT codes and recommended the associated payments for calendar year 2015, but CMS delayed the codes’ enactment until collecting public comment.
Modifications to quality programs include a new reporting option under the PQRS that will allow group practices to report quality measure data using a Qualified Clinical Data Registry. In 2016, there will be 281 measures in the PQRS measure set and 18 measures in the Group Practice Reporting Option (GPRO) Web Interface, according to the final rule.
The 2018 payment adjustment will be the last adjustment under the PQRS. Starting in 2019, adjustments to payment for quality reporting and other factors will be made under the Merit-Based Incentive Payment System (MIPS), as required by MACRA.
Changes to the Value-Based Payment Modifier program are also coming in 2016:
• CMS will apply the quality-tiering methodology to all groups and solo practitioners that meet the criteria to avoid the downward adjustment under the PQRS. Groups and solo practitioners would be subject to upward, neutral, or downward adjustments derived under the quality-tiering methodology.
• CMS will continue to set the maximum upward adjustment under the quality-tiering methodology for the CY 2018 value modifier at four times an adjustment factor for groups of physicians with 10 or more eligible professionals, and two times an adjustment factor for groups of physicians with between two and nine eligible professionals and physician solo practitioners.
• CMS will use calendar year 2016 as the performance period for the calendar 2018 value modifier and continue to apply the 2018 value modifier based on participation in the PQRS by groups and solo practitioners.
The fee schedule also includes modifications to the Medicare Shared Savings Program including a new measure on statin therapy for the prevention and treatment of cardiovascular disease in the “preventive health domain” of the Shared Savings Program quality measure set. The final rule also clarifies how PQRS-eligible professionals participating within an Accountable Care Organization can meet reporting requirements.
On Twitter @legal_med

Study: High rate of medical errors in postop drug administrations
Medication errors or adverse drug events after surgery occur in as many as one in twenty perioperative medication administrations, according to data published online in the journal Anesthesiology.
A prospective observational study of 277 surgical operations and 3,671 medication administrations found 193 cases (5.3%) involved a medication error or adverse drug event, nearly four-fifths (79.3%) of which were preventable and 68.9% of which were serious (Anesthesiology. 2015 Oct. doi:10.1097/ALN.0000000000000904).

Among the 51 medication errors that led to adverse reactions, nearly half were the result of inappropriate medication doses and 31.4% were due to omitted medications or failure to act, but the most common overall error type was a labeling error.
The medications most commonly associated with errors were propofol, phenylephrine, and fentanyl, and operations greater than 6 hours in duration or with 13 or more medication administrations were associated with a significantly greater risk of errors.
“Examples of technology-based interventions [to minimize perioperative MEs and/or ADEs] include bar code–assisted syringe labeling systems, point-of-care bar code–assisted anesthesia documentation systems, specific drug decision support, and alerts,” wrote the study’s lead author Dr. Karen C. Nanji of Massachusetts General Hospital in Boston, and her coauthors.
The study was supported by the Doctors Company Foundation and the National Institute of General Medical Sciences of the National Institutes of Health. One coauthor – Dr. David Bates – declared financial interests in medical decision support software, as well as funding and positions with a variety of medical technology companies.
Medication errors or adverse drug events after surgery occur in as many as one in twenty perioperative medication administrations, according to data published online in the journal Anesthesiology.
A prospective observational study of 277 surgical operations and 3,671 medication administrations found 193 cases (5.3%) involved a medication error or adverse drug event, nearly four-fifths (79.3%) of which were preventable and 68.9% of which were serious (Anesthesiology. 2015 Oct. doi:10.1097/ALN.0000000000000904).
Among the 51 medication errors that led to adverse reactions, nearly half were the result of inappropriate medication doses and 31.4% were due to omitted medications or failure to act, but the most common overall error type was a labeling error.
The medications most commonly associated with errors were propofol, phenylephrine, and fentanyl, and operations greater than 6 hours in duration or with 13 or more medication administrations were associated with a significantly greater risk of errors.
“Examples of technology-based interventions [to minimize perioperative MEs and/or ADEs] include bar code–assisted syringe labeling systems, point-of-care bar code–assisted anesthesia documentation systems, specific drug decision support, and alerts,” wrote the study’s lead author Dr. Karen C. Nanji of Massachusetts General Hospital in Boston, and her coauthors.
The study was supported by the Doctors Company Foundation and the National Institute of General Medical Sciences of the National Institutes of Health. One coauthor – Dr. David Bates – declared financial interests in medical decision support software, as well as funding and positions with a variety of medical technology companies.
Medication errors or adverse drug events after surgery occur in as many as one in twenty perioperative medication administrations, according to data published online in the journal Anesthesiology.
A prospective observational study of 277 surgical operations and 3,671 medication administrations found 193 cases (5.3%) involved a medication error or adverse drug event, nearly four-fifths (79.3%) of which were preventable and 68.9% of which were serious (Anesthesiology. 2015 Oct. doi:10.1097/ALN.0000000000000904).
Among the 51 medication errors that led to adverse reactions, nearly half were the result of inappropriate medication doses and 31.4% were due to omitted medications or failure to act, but the most common overall error type was a labeling error.
The medications most commonly associated with errors were propofol, phenylephrine, and fentanyl, and operations greater than 6 hours in duration or with 13 or more medication administrations were associated with a significantly greater risk of errors.
“Examples of technology-based interventions [to minimize perioperative MEs and/or ADEs] include bar code–assisted syringe labeling systems, point-of-care bar code–assisted anesthesia documentation systems, specific drug decision support, and alerts,” wrote the study’s lead author Dr. Karen C. Nanji of Massachusetts General Hospital in Boston, and her coauthors.
The study was supported by the Doctors Company Foundation and the National Institute of General Medical Sciences of the National Institutes of Health. One coauthor – Dr. David Bates – declared financial interests in medical decision support software, as well as funding and positions with a variety of medical technology companies.
FROM ANESTHESIOLOGY
Key clinical point: One in twenty perioperative medication administrations may involve a medication error and/or adverse drug event.
Major finding: Nearly four-fifths of perioperative medication errors or adverse events are preventable.
Data source: A prospective observational study of 277 surgical operations and 3,671 medication administrations.
Disclosures: The study was supported by the Doctors Company Foundation and the National Institute of General Medical Sciences of the National Institutes of Health. One coauthor – Dr. David Bates – declared financial interests in medical decision support software, as well as funding and positions with a variety of medical technology companies.

Concurrent mesh herniorrhaphy with bowel surgery doesn’t up morbidity
Concurrent colorectal surgery and mesh herniorrhaphy can be done safely, according to findings from a case-matched study based on American College of Surgeons National Surgical Quality Improvement Program data.
“Our study suggests that mesh repair for [ventral hernia] in the setting of [colorectal surgery] does not worsen 30-day postoperative outcomes,” wrote Dr. Cigdem Benlice and colleagues of the Cleveland Clinic. The study was published in the American Journal of Surgery (2015; 210[4]:766-771]
These two operations are undertaken concurrently in part to save patients from further procedures and anesthesia, but the practice is limited by safety concerns. The complications anticipated include intra-abdominal adhesions, chronic draining sinus, chronic enteric fistula, chronic wound infection, and mesh migration. Any one of these complications could entail further surgical interventions.
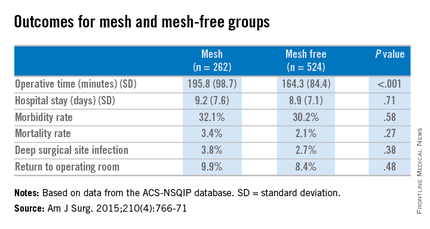
Dr. Benlice and her colleagues used the national, validated, risk-adjusted American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to look at short-term outcomes after concurrent ventral hernia repair (VHR) and colorectal surgery (CS), and the risk factors associated with complications. Data on 2,250 patients having CS and VHR operations simultaneously from 2005 to 2010 were reviewed. Patients having simultaneous VHR with mesh and CS (262) were matched closely with those having both procedures but without mesh (524). The case-matching criteria included diagnosis, type of bowel procedure, and American Society of Anesthesiologists (ASA) class, and follow-up was limited to 30 days.
In a comparison of the mesh and nonmesh groups, morbidity rates were found to be similar (32% vs. 30%, P = .58) as were mortality rates (3.4% vs. 2.1%, P = .27). The rate of deep surgical site infections (3.8% vs. 2.7%, P = .38) were similar between the two groups, and wound disruptions (3.1% vs. 3.1%) rates were the same. The length of hospital stay was also comparable. Mean operating time, however, proved longer in patients who had hernia repair using mesh (196 minutes vs. 164 minutes, P less than .001).
A multivariate analysis showed that open colorectal procedures, III or IV ASA class, smoking, and preoperative open wound or wound infection were significant and independent risk factors (odds ratios, 2.67, 2.51, 2.06, and 2.27, respectively) for surgical site infection.
The limitations of this study reflect some of the limitations of the ACS-NSQIP database. Long-term follow-up, hernia size, type of mesh used, and type of technique used in the operation could not be assessed using the available data. In addition, further analysis of the subgroups of patients with surgical site infections would be needed to examine the impact of mesh (and types of mesh) use on clean-contaminated cases. Researchers noted that at the Cleveland Clinic, type of mesh (biologic vs. nonbiologic) used has been found to have no impact on rates of wound and mesh infection and hernia recurrence, but they were unable to do this kind of analysis with the available data for simultaneous bowel and hernia repair surgery.
The researchers concluded, “the large cohort and strict inclusion, exclusion, and case-matching criteria strengthen the clinical value of this study. When performed simultaneously with CS, VHR with mesh can be performed without increasing perioperative and short-term postoperative morbidity.”
The researchers had no relevant disclosures.
Concurrent colorectal surgery and mesh herniorrhaphy can be done safely, according to findings from a case-matched study based on American College of Surgeons National Surgical Quality Improvement Program data.
“Our study suggests that mesh repair for [ventral hernia] in the setting of [colorectal surgery] does not worsen 30-day postoperative outcomes,” wrote Dr. Cigdem Benlice and colleagues of the Cleveland Clinic. The study was published in the American Journal of Surgery (2015; 210[4]:766-771]
These two operations are undertaken concurrently in part to save patients from further procedures and anesthesia, but the practice is limited by safety concerns. The complications anticipated include intra-abdominal adhesions, chronic draining sinus, chronic enteric fistula, chronic wound infection, and mesh migration. Any one of these complications could entail further surgical interventions.
Dr. Benlice and her colleagues used the national, validated, risk-adjusted American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to look at short-term outcomes after concurrent ventral hernia repair (VHR) and colorectal surgery (CS), and the risk factors associated with complications. Data on 2,250 patients having CS and VHR operations simultaneously from 2005 to 2010 were reviewed. Patients having simultaneous VHR with mesh and CS (262) were matched closely with those having both procedures but without mesh (524). The case-matching criteria included diagnosis, type of bowel procedure, and American Society of Anesthesiologists (ASA) class, and follow-up was limited to 30 days.
In a comparison of the mesh and nonmesh groups, morbidity rates were found to be similar (32% vs. 30%, P = .58) as were mortality rates (3.4% vs. 2.1%, P = .27). The rate of deep surgical site infections (3.8% vs. 2.7%, P = .38) were similar between the two groups, and wound disruptions (3.1% vs. 3.1%) rates were the same. The length of hospital stay was also comparable. Mean operating time, however, proved longer in patients who had hernia repair using mesh (196 minutes vs. 164 minutes, P less than .001).
A multivariate analysis showed that open colorectal procedures, III or IV ASA class, smoking, and preoperative open wound or wound infection were significant and independent risk factors (odds ratios, 2.67, 2.51, 2.06, and 2.27, respectively) for surgical site infection.
The limitations of this study reflect some of the limitations of the ACS-NSQIP database. Long-term follow-up, hernia size, type of mesh used, and type of technique used in the operation could not be assessed using the available data. In addition, further analysis of the subgroups of patients with surgical site infections would be needed to examine the impact of mesh (and types of mesh) use on clean-contaminated cases. Researchers noted that at the Cleveland Clinic, type of mesh (biologic vs. nonbiologic) used has been found to have no impact on rates of wound and mesh infection and hernia recurrence, but they were unable to do this kind of analysis with the available data for simultaneous bowel and hernia repair surgery.
The researchers concluded, “the large cohort and strict inclusion, exclusion, and case-matching criteria strengthen the clinical value of this study. When performed simultaneously with CS, VHR with mesh can be performed without increasing perioperative and short-term postoperative morbidity.”
The researchers had no relevant disclosures.
Concurrent colorectal surgery and mesh herniorrhaphy can be done safely, according to findings from a case-matched study based on American College of Surgeons National Surgical Quality Improvement Program data.
“Our study suggests that mesh repair for [ventral hernia] in the setting of [colorectal surgery] does not worsen 30-day postoperative outcomes,” wrote Dr. Cigdem Benlice and colleagues of the Cleveland Clinic. The study was published in the American Journal of Surgery (2015; 210[4]:766-771]
These two operations are undertaken concurrently in part to save patients from further procedures and anesthesia, but the practice is limited by safety concerns. The complications anticipated include intra-abdominal adhesions, chronic draining sinus, chronic enteric fistula, chronic wound infection, and mesh migration. Any one of these complications could entail further surgical interventions.
Dr. Benlice and her colleagues used the national, validated, risk-adjusted American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to look at short-term outcomes after concurrent ventral hernia repair (VHR) and colorectal surgery (CS), and the risk factors associated with complications. Data on 2,250 patients having CS and VHR operations simultaneously from 2005 to 2010 were reviewed. Patients having simultaneous VHR with mesh and CS (262) were matched closely with those having both procedures but without mesh (524). The case-matching criteria included diagnosis, type of bowel procedure, and American Society of Anesthesiologists (ASA) class, and follow-up was limited to 30 days.
In a comparison of the mesh and nonmesh groups, morbidity rates were found to be similar (32% vs. 30%, P = .58) as were mortality rates (3.4% vs. 2.1%, P = .27). The rate of deep surgical site infections (3.8% vs. 2.7%, P = .38) were similar between the two groups, and wound disruptions (3.1% vs. 3.1%) rates were the same. The length of hospital stay was also comparable. Mean operating time, however, proved longer in patients who had hernia repair using mesh (196 minutes vs. 164 minutes, P less than .001).
A multivariate analysis showed that open colorectal procedures, III or IV ASA class, smoking, and preoperative open wound or wound infection were significant and independent risk factors (odds ratios, 2.67, 2.51, 2.06, and 2.27, respectively) for surgical site infection.
The limitations of this study reflect some of the limitations of the ACS-NSQIP database. Long-term follow-up, hernia size, type of mesh used, and type of technique used in the operation could not be assessed using the available data. In addition, further analysis of the subgroups of patients with surgical site infections would be needed to examine the impact of mesh (and types of mesh) use on clean-contaminated cases. Researchers noted that at the Cleveland Clinic, type of mesh (biologic vs. nonbiologic) used has been found to have no impact on rates of wound and mesh infection and hernia recurrence, but they were unable to do this kind of analysis with the available data for simultaneous bowel and hernia repair surgery.
The researchers concluded, “the large cohort and strict inclusion, exclusion, and case-matching criteria strengthen the clinical value of this study. When performed simultaneously with CS, VHR with mesh can be performed without increasing perioperative and short-term postoperative morbidity.”
The researchers had no relevant disclosures.
FROM THE AMERICAN JOURNAL OF SURGERY
Key clinical point: Simultaneous bowel and hernia surgery with mesh are comparable to a nonmesh operation in terms of postoperative morbidity.
Major finding: In a comparison of the mesh and nonmesh groups, morbidity rates were found to be similar (32% vs. 30%, P = .27) as was the rate of deep surgical site infections (3.8% vs. 2.7%, P = .38).
Data source: ACS-NSQIP data on case-matched patients having concurrent bowel and hernia surgery, with mesh (262) and without mesh (524).
Disclosures: The researchers had no relevant disclosures.
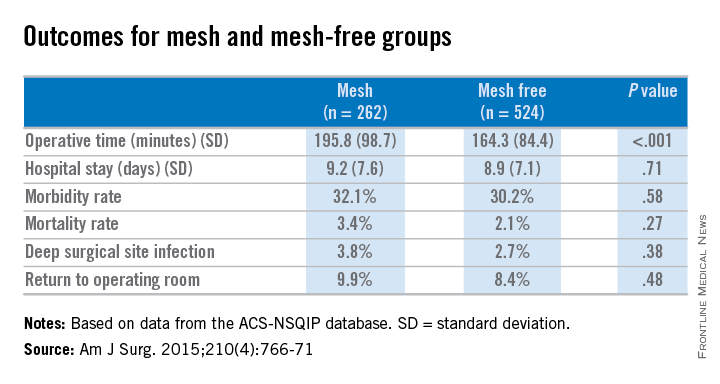
House curbs Medicare premium increase under budget deal
Lawmakers are seeking to limit an increase in Medicare Part B premiums as part of the budget deal negotiated between outgoing House Speaker John Boehner (R-Ohio) and the White House, and approved by the House on Oct. 28.
The House approved the Bipartisan Budget Act by a vote of 266-167. The Senate is expected to act on the deal shortly.

The deal means that some Medicare beneficiaries will avoid seeing their Part B premiums jump from about $105 to $160 per month. Instead, those beneficiaries who are not “held harmless” under Medicare rules – about 30% of Medicare beneficiaries – would see their premiums rise to $120 in 2016. The bulk of Medicare beneficiaries will have stable premiums at about $105 next year.
To pay for the rollback of part of the increase, the budget agreement also calls for those beneficiaries not held harmless under the law to pay an extra $3 per month starting in 2016.
But an analysis of this provision by the National Center for Policy Analysis noted that such adjustments could happen again, as they are tied to the a cost of living adjustment. This is “just another case of Congress kicking the can down the road,” NCPA officials wrote in an Oct. 28 blog post.
The budget deal included only a few other health care–related provisions. The bill would broaden the application of inflation-triggered rebates – the rebates paid by manufacturers when drug price increases outpace inflation – to generic drugs as well as brand name drugs.
Another provision codifies the definition of provider-based off-campus hospital outpatient departments that are not on the main campus and are more than 250 yards away from the main hospital campus. Providers at these off-campus locations would be reimbursed under the ambulatory surgical center prospective payment system or the Medicare physician fee schedule rather than the hospital outpatient prospective payment system.
Finally, the budget bill eliminates a requirement from the Affordable Care Act that mandates that employers with more than 200 workers automatically enroll new full-time employees into a qualifying health plan if it is offered, and automatically reenroll existing employees.
Lawmakers are seeking to limit an increase in Medicare Part B premiums as part of the budget deal negotiated between outgoing House Speaker John Boehner (R-Ohio) and the White House, and approved by the House on Oct. 28.
The House approved the Bipartisan Budget Act by a vote of 266-167. The Senate is expected to act on the deal shortly.
The deal means that some Medicare beneficiaries will avoid seeing their Part B premiums jump from about $105 to $160 per month. Instead, those beneficiaries who are not “held harmless” under Medicare rules – about 30% of Medicare beneficiaries – would see their premiums rise to $120 in 2016. The bulk of Medicare beneficiaries will have stable premiums at about $105 next year.
To pay for the rollback of part of the increase, the budget agreement also calls for those beneficiaries not held harmless under the law to pay an extra $3 per month starting in 2016.
But an analysis of this provision by the National Center for Policy Analysis noted that such adjustments could happen again, as they are tied to the a cost of living adjustment. This is “just another case of Congress kicking the can down the road,” NCPA officials wrote in an Oct. 28 blog post.
The budget deal included only a few other health care–related provisions. The bill would broaden the application of inflation-triggered rebates – the rebates paid by manufacturers when drug price increases outpace inflation – to generic drugs as well as brand name drugs.
Another provision codifies the definition of provider-based off-campus hospital outpatient departments that are not on the main campus and are more than 250 yards away from the main hospital campus. Providers at these off-campus locations would be reimbursed under the ambulatory surgical center prospective payment system or the Medicare physician fee schedule rather than the hospital outpatient prospective payment system.
Finally, the budget bill eliminates a requirement from the Affordable Care Act that mandates that employers with more than 200 workers automatically enroll new full-time employees into a qualifying health plan if it is offered, and automatically reenroll existing employees.
Lawmakers are seeking to limit an increase in Medicare Part B premiums as part of the budget deal negotiated between outgoing House Speaker John Boehner (R-Ohio) and the White House, and approved by the House on Oct. 28.
The House approved the Bipartisan Budget Act by a vote of 266-167. The Senate is expected to act on the deal shortly.
The deal means that some Medicare beneficiaries will avoid seeing their Part B premiums jump from about $105 to $160 per month. Instead, those beneficiaries who are not “held harmless” under Medicare rules – about 30% of Medicare beneficiaries – would see their premiums rise to $120 in 2016. The bulk of Medicare beneficiaries will have stable premiums at about $105 next year.
To pay for the rollback of part of the increase, the budget agreement also calls for those beneficiaries not held harmless under the law to pay an extra $3 per month starting in 2016.
But an analysis of this provision by the National Center for Policy Analysis noted that such adjustments could happen again, as they are tied to the a cost of living adjustment. This is “just another case of Congress kicking the can down the road,” NCPA officials wrote in an Oct. 28 blog post.
The budget deal included only a few other health care–related provisions. The bill would broaden the application of inflation-triggered rebates – the rebates paid by manufacturers when drug price increases outpace inflation – to generic drugs as well as brand name drugs.
Another provision codifies the definition of provider-based off-campus hospital outpatient departments that are not on the main campus and are more than 250 yards away from the main hospital campus. Providers at these off-campus locations would be reimbursed under the ambulatory surgical center prospective payment system or the Medicare physician fee schedule rather than the hospital outpatient prospective payment system.
Finally, the budget bill eliminates a requirement from the Affordable Care Act that mandates that employers with more than 200 workers automatically enroll new full-time employees into a qualifying health plan if it is offered, and automatically reenroll existing employees.
