User login
Official Newspaper of the American College of Surgeons
Medicare audits: What leads to an exclusion?
WASHINGTON – While the line between an inadvertent billing mistake and intentional coding deception might be blurry, federal investigators are crystal clear about what drives them to exclude health providers from government health programs.
Rejection from Medicaid and Medicare comes down to severity and accountability, said Lisa Re, branch chief of administrative and civil remedies for the Health and Human Services Department Office of Counsel to Inspector General.

“At the end of the day, what we’re looking at is the seriousness of the conduct, cooperation with the compliance program, and whether or not there’s been a sense of financial responsibility – that the program has been made whole from the harm that was done,” Ms. Re said at a meeting sponsored by the American Bar Association.
In 2015, the Office of Inspector General (OIG) excluded 4,112 individuals and entities from participation in federal health care programs, up from 4,017 in 2014, according to a the OIG’s semiannual report to Congress published Nov. 30.
The office expects to recover nearly $3.4 billion in incorrect payments in 2015, down from $4.9 billion last year. The office also reported 925 criminal actions and 682 civil actions in 2015 involving false claims, unjust-enrichment lawsuits, civil settlements, and administrative recoveries.
When it comes to exclusions, investigators rely on the facts and circumstances of each individual case, Ms. Re said. Certain behaviors such as repeated disregard of government inquires and ongoing overbilling can lead to exclusions.
“We’re not trying to punish anyone,” Ms. Re said. “Exclusion is purely remedial. It’s a question of whether or not you have demonstrated sufficient trustworthiness for us to continue doing business with you.”
The OIG considers two types of exclusions – mandatory and permissive. The agency is obligated to exclude a provider if that professional is convicted of program-related crimes, is convicted of patient abuse or neglect, receives a felony health fraud conviction, or is convicted of two mandatory exclusion offenses. The OIG can use its discretion in situations in which a provider receives a misdemeanor conviction related to health fraud, has a license suspended or revoked, fails to disclose required information, fails to take corrective action, or makes false statements to the government, among others. Reinstatement of excluded entities and individuals is not automatic once the exclusion period ends. Those wishing to again participate in a federal health care program must apply for and receive reinstatement permission from the OIG.
Ms. Re stressed that her office is transparent about possible or upcoming exclusions during a payment investigation. If health professionals come under billing scrutiny, she encourages them and their attorneys to contact OIG officials to inquire whether an exclusion is likely or expected.
On Twitter @legal_med
WASHINGTON – While the line between an inadvertent billing mistake and intentional coding deception might be blurry, federal investigators are crystal clear about what drives them to exclude health providers from government health programs.
Rejection from Medicaid and Medicare comes down to severity and accountability, said Lisa Re, branch chief of administrative and civil remedies for the Health and Human Services Department Office of Counsel to Inspector General.
“At the end of the day, what we’re looking at is the seriousness of the conduct, cooperation with the compliance program, and whether or not there’s been a sense of financial responsibility – that the program has been made whole from the harm that was done,” Ms. Re said at a meeting sponsored by the American Bar Association.
In 2015, the Office of Inspector General (OIG) excluded 4,112 individuals and entities from participation in federal health care programs, up from 4,017 in 2014, according to a the OIG’s semiannual report to Congress published Nov. 30.
The office expects to recover nearly $3.4 billion in incorrect payments in 2015, down from $4.9 billion last year. The office also reported 925 criminal actions and 682 civil actions in 2015 involving false claims, unjust-enrichment lawsuits, civil settlements, and administrative recoveries.
When it comes to exclusions, investigators rely on the facts and circumstances of each individual case, Ms. Re said. Certain behaviors such as repeated disregard of government inquires and ongoing overbilling can lead to exclusions.
“We’re not trying to punish anyone,” Ms. Re said. “Exclusion is purely remedial. It’s a question of whether or not you have demonstrated sufficient trustworthiness for us to continue doing business with you.”
The OIG considers two types of exclusions – mandatory and permissive. The agency is obligated to exclude a provider if that professional is convicted of program-related crimes, is convicted of patient abuse or neglect, receives a felony health fraud conviction, or is convicted of two mandatory exclusion offenses. The OIG can use its discretion in situations in which a provider receives a misdemeanor conviction related to health fraud, has a license suspended or revoked, fails to disclose required information, fails to take corrective action, or makes false statements to the government, among others. Reinstatement of excluded entities and individuals is not automatic once the exclusion period ends. Those wishing to again participate in a federal health care program must apply for and receive reinstatement permission from the OIG.
Ms. Re stressed that her office is transparent about possible or upcoming exclusions during a payment investigation. If health professionals come under billing scrutiny, she encourages them and their attorneys to contact OIG officials to inquire whether an exclusion is likely or expected.
On Twitter @legal_med
WASHINGTON – While the line between an inadvertent billing mistake and intentional coding deception might be blurry, federal investigators are crystal clear about what drives them to exclude health providers from government health programs.
Rejection from Medicaid and Medicare comes down to severity and accountability, said Lisa Re, branch chief of administrative and civil remedies for the Health and Human Services Department Office of Counsel to Inspector General.
“At the end of the day, what we’re looking at is the seriousness of the conduct, cooperation with the compliance program, and whether or not there’s been a sense of financial responsibility – that the program has been made whole from the harm that was done,” Ms. Re said at a meeting sponsored by the American Bar Association.
In 2015, the Office of Inspector General (OIG) excluded 4,112 individuals and entities from participation in federal health care programs, up from 4,017 in 2014, according to a the OIG’s semiannual report to Congress published Nov. 30.
The office expects to recover nearly $3.4 billion in incorrect payments in 2015, down from $4.9 billion last year. The office also reported 925 criminal actions and 682 civil actions in 2015 involving false claims, unjust-enrichment lawsuits, civil settlements, and administrative recoveries.
When it comes to exclusions, investigators rely on the facts and circumstances of each individual case, Ms. Re said. Certain behaviors such as repeated disregard of government inquires and ongoing overbilling can lead to exclusions.
“We’re not trying to punish anyone,” Ms. Re said. “Exclusion is purely remedial. It’s a question of whether or not you have demonstrated sufficient trustworthiness for us to continue doing business with you.”
The OIG considers two types of exclusions – mandatory and permissive. The agency is obligated to exclude a provider if that professional is convicted of program-related crimes, is convicted of patient abuse or neglect, receives a felony health fraud conviction, or is convicted of two mandatory exclusion offenses. The OIG can use its discretion in situations in which a provider receives a misdemeanor conviction related to health fraud, has a license suspended or revoked, fails to disclose required information, fails to take corrective action, or makes false statements to the government, among others. Reinstatement of excluded entities and individuals is not automatic once the exclusion period ends. Those wishing to again participate in a federal health care program must apply for and receive reinstatement permission from the OIG.
Ms. Re stressed that her office is transparent about possible or upcoming exclusions during a payment investigation. If health professionals come under billing scrutiny, she encourages them and their attorneys to contact OIG officials to inquire whether an exclusion is likely or expected.
On Twitter @legal_med
AT THE WASHINGTON HEALTH LAW SUMMIT

PROMIS physical function domain outperforms in cervical spine patients
SAN DIEGO – The Neck Disability Index–10 did not perform as well as the Neck Disability Index–5 in assessing patient-reported outcomes in cervical spine patients – and neither was as good as the PROMIS physical function domain delivered by computerized adaptive testing.
Those are the key findings from an analysis of data from more than 500 cervical spine patients treated at University of Utah Health Care in Salt Lake City.

“Previous studies by us and others have shown problems with the NDI [Neck Disability Index] as it is commonly administered” in 10 questions, lead study author Dr. Darrel S. Brodke said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “It has a very poor floor effect, meaning that it does not differentiate between minimally disabled patients, and the scores cannot be appropriately handled with the kinds of statistics that we normally use – though because few of us know this, we still use it as a standard parametric measure.”
In what he said is the first study of its kind, Dr. Brodke, professor of orthopedics at the University of Utah, and his associates set out to compare the psychometric performance of the National Institutes of Health–funded PROMIS (Patient Reported Outcomes Measurement Information System) physical function (PF) domain, administered by computerized adaptive testing, with the standard NDI-10, the NDI-5, and the 36-Item Short Form physical function domain (SF-36 PFD).
In all, 566 patients completed the NDI and PROMIS PF computerized adaptive testing assessments, while 490 also completed the SF-36 PFD.
On average, the NDI-10 took the longest to complete (10 questions in a mean of 183 seconds), followed by the SF-36 PFD (5 questions in a mean of 123 seconds), the NDI-5 (5 questions in a mean of 99 seconds), and the PROMIS PF computerized adaptive testing (between 4 and 12 questions in a mean of 62 seconds).
The psychometric properties of the PROMIS PF computerized adaptive testing were superior to the other outcome measurement tools studied, Dr. Brodke reported. Specifically, the ceiling and floor effects were “excellent” for the PROMIS PF computerized adaptive testing (1.94% and 4.06%, respectively), while the ceiling effects were “fine” for the NDI-10 (4.77%), NDI-5 (7.60%), and SF-36 PFD (11.84%), he said.
However, the floor effects of these three instruments were poor (45.58%, 48.59% and 21.55%, respectively). “The NDI-10 also has the additional challenge of extremely poor raw score to measure correlation,” the researchers noted in their abstract.
“The legacy scale scores significantly predicted the PROMIS PF CAT scores (P less than .0001), with fair correlation for the PF CAT and NDI-10 (0.53) and good correlation of PF CAT and SF-36 PFD (0.62), allowing use of conversion equations to predict scores, which were generated,” the investigators explained.
PROMIS PF computerized adaptive testing “does much better than the NDI or the SF-36 physical function domain at characterizing patients’ physical function, with much better coverage,” Dr. Brodke said. “Not only this, but it is also much faster to fill out, so less burdensome to the patient and the clinic.”
One limitation of the study is that the researchers did not measure the responsiveness aspect of PROMIS performance. “We did not have enough pre- and posttreatment scores to do this measurement yet,” Dr. Brodke said. “The other thing is that minimum clinically important difference [MCID] is not yet worked out for PROMIS in this patient population, though we can infer an MCID as one-half of a standard deviation. More to come in future studies.”
Dr. Brodke reported having no financial disclosures.
SAN DIEGO – The Neck Disability Index–10 did not perform as well as the Neck Disability Index–5 in assessing patient-reported outcomes in cervical spine patients – and neither was as good as the PROMIS physical function domain delivered by computerized adaptive testing.
Those are the key findings from an analysis of data from more than 500 cervical spine patients treated at University of Utah Health Care in Salt Lake City.
“Previous studies by us and others have shown problems with the NDI [Neck Disability Index] as it is commonly administered” in 10 questions, lead study author Dr. Darrel S. Brodke said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “It has a very poor floor effect, meaning that it does not differentiate between minimally disabled patients, and the scores cannot be appropriately handled with the kinds of statistics that we normally use – though because few of us know this, we still use it as a standard parametric measure.”
In what he said is the first study of its kind, Dr. Brodke, professor of orthopedics at the University of Utah, and his associates set out to compare the psychometric performance of the National Institutes of Health–funded PROMIS (Patient Reported Outcomes Measurement Information System) physical function (PF) domain, administered by computerized adaptive testing, with the standard NDI-10, the NDI-5, and the 36-Item Short Form physical function domain (SF-36 PFD).
In all, 566 patients completed the NDI and PROMIS PF computerized adaptive testing assessments, while 490 also completed the SF-36 PFD.
On average, the NDI-10 took the longest to complete (10 questions in a mean of 183 seconds), followed by the SF-36 PFD (5 questions in a mean of 123 seconds), the NDI-5 (5 questions in a mean of 99 seconds), and the PROMIS PF computerized adaptive testing (between 4 and 12 questions in a mean of 62 seconds).
The psychometric properties of the PROMIS PF computerized adaptive testing were superior to the other outcome measurement tools studied, Dr. Brodke reported. Specifically, the ceiling and floor effects were “excellent” for the PROMIS PF computerized adaptive testing (1.94% and 4.06%, respectively), while the ceiling effects were “fine” for the NDI-10 (4.77%), NDI-5 (7.60%), and SF-36 PFD (11.84%), he said.
However, the floor effects of these three instruments were poor (45.58%, 48.59% and 21.55%, respectively). “The NDI-10 also has the additional challenge of extremely poor raw score to measure correlation,” the researchers noted in their abstract.
“The legacy scale scores significantly predicted the PROMIS PF CAT scores (P less than .0001), with fair correlation for the PF CAT and NDI-10 (0.53) and good correlation of PF CAT and SF-36 PFD (0.62), allowing use of conversion equations to predict scores, which were generated,” the investigators explained.
PROMIS PF computerized adaptive testing “does much better than the NDI or the SF-36 physical function domain at characterizing patients’ physical function, with much better coverage,” Dr. Brodke said. “Not only this, but it is also much faster to fill out, so less burdensome to the patient and the clinic.”
One limitation of the study is that the researchers did not measure the responsiveness aspect of PROMIS performance. “We did not have enough pre- and posttreatment scores to do this measurement yet,” Dr. Brodke said. “The other thing is that minimum clinically important difference [MCID] is not yet worked out for PROMIS in this patient population, though we can infer an MCID as one-half of a standard deviation. More to come in future studies.”
Dr. Brodke reported having no financial disclosures.
SAN DIEGO – The Neck Disability Index–10 did not perform as well as the Neck Disability Index–5 in assessing patient-reported outcomes in cervical spine patients – and neither was as good as the PROMIS physical function domain delivered by computerized adaptive testing.
Those are the key findings from an analysis of data from more than 500 cervical spine patients treated at University of Utah Health Care in Salt Lake City.
“Previous studies by us and others have shown problems with the NDI [Neck Disability Index] as it is commonly administered” in 10 questions, lead study author Dr. Darrel S. Brodke said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “It has a very poor floor effect, meaning that it does not differentiate between minimally disabled patients, and the scores cannot be appropriately handled with the kinds of statistics that we normally use – though because few of us know this, we still use it as a standard parametric measure.”
In what he said is the first study of its kind, Dr. Brodke, professor of orthopedics at the University of Utah, and his associates set out to compare the psychometric performance of the National Institutes of Health–funded PROMIS (Patient Reported Outcomes Measurement Information System) physical function (PF) domain, administered by computerized adaptive testing, with the standard NDI-10, the NDI-5, and the 36-Item Short Form physical function domain (SF-36 PFD).
In all, 566 patients completed the NDI and PROMIS PF computerized adaptive testing assessments, while 490 also completed the SF-36 PFD.
On average, the NDI-10 took the longest to complete (10 questions in a mean of 183 seconds), followed by the SF-36 PFD (5 questions in a mean of 123 seconds), the NDI-5 (5 questions in a mean of 99 seconds), and the PROMIS PF computerized adaptive testing (between 4 and 12 questions in a mean of 62 seconds).
The psychometric properties of the PROMIS PF computerized adaptive testing were superior to the other outcome measurement tools studied, Dr. Brodke reported. Specifically, the ceiling and floor effects were “excellent” for the PROMIS PF computerized adaptive testing (1.94% and 4.06%, respectively), while the ceiling effects were “fine” for the NDI-10 (4.77%), NDI-5 (7.60%), and SF-36 PFD (11.84%), he said.
However, the floor effects of these three instruments were poor (45.58%, 48.59% and 21.55%, respectively). “The NDI-10 also has the additional challenge of extremely poor raw score to measure correlation,” the researchers noted in their abstract.
“The legacy scale scores significantly predicted the PROMIS PF CAT scores (P less than .0001), with fair correlation for the PF CAT and NDI-10 (0.53) and good correlation of PF CAT and SF-36 PFD (0.62), allowing use of conversion equations to predict scores, which were generated,” the investigators explained.
PROMIS PF computerized adaptive testing “does much better than the NDI or the SF-36 physical function domain at characterizing patients’ physical function, with much better coverage,” Dr. Brodke said. “Not only this, but it is also much faster to fill out, so less burdensome to the patient and the clinic.”
One limitation of the study is that the researchers did not measure the responsiveness aspect of PROMIS performance. “We did not have enough pre- and posttreatment scores to do this measurement yet,” Dr. Brodke said. “The other thing is that minimum clinically important difference [MCID] is not yet worked out for PROMIS in this patient population, though we can infer an MCID as one-half of a standard deviation. More to come in future studies.”
Dr. Brodke reported having no financial disclosures.
AT CSRS 2015
Key clinical point: In the elective cervical spine surgery population, the PROMIS physical function domain as delivered by computerized adaptive testing outperforms other commonly used tools to measure patient-reported outcomes.
Major finding: The ceiling and floor effects were “excellent” for the PROMIS PF (1.94% and 4.06%, respectively), while the ceiling effects were “fine” for the Neck Disability Index–10 (4.77%), the Neck Disability Index–5 (7.60%), and the 36-Item Short Form physical function domain (11.84%). However, the floor effects of these three instruments were poor (45.58%, 48.59%, and 21.55%, respectively).
Data source: A study of the psychometric performance of the PROMIS physical function domain, administered by computerized adaptive testing, comparing the standard NDI-10, NDI-5, and SF-36 physical function domain.
Disclosures: Dr. Brodke reported having no financial disclosures.

Endobronchial valves improve pulmonary function in emphysema
Endobronchial valves improved pulmonary function, exercise capacity, and quality of life in a prospective randomized controlled trial involving 68 adults with severe emphysema, according to a report published online Dec. 10 in the New England Journal of Medicine.
“The improvements we found were of greater magnitude than those noted with pharmacologic treatment in comparable patients and were similar to improvements with surgical lung-volume reduction, but with significantly less morbidity,” said Karin Klooster of the department of pulmonary diseases, University Medical Center Groningen (the Netherlands) and her associates.
Previous research suggested that bronchoscopic lung-volume reduction using one-way endobronchial valves to block inspiratory but not expiratory air flow would be most effective in patients who had a complete rather than an incomplete fissure between the targeted lobe and the adjacent lobe on high-resolution CT. “A complete fissure on HRCT [high-resolution computed tomography] is a surrogate finding for the absence of interlobar collateral ventilation; if there is collateral ventilation, an occluded lobe can be reinflated through its collaterals,” defeating the purpose of the procedure, the researchers wrote.
During a 3-year period, Ms. Klooster and her associates studied emphysema patients who were older than 35 years (mean age, 58-59) and had a postbronchodilator forced expiratory volume in 1 second (FEV1) less than 60% of predicted volume, a total lung capacity more than 100% of the predicted value, and residual volume more than 150% of predicted volume. On HRCT, all the study participants showed a complete or nearly complete fissure between the targeted lobe and the adjacent lobe. They were randomly assigned to receive endobronchial valves (34 patients) or usual care (34 control subjects) and followed for 6 months. At that time, control subjects were allowed to crossover and receive endobronchial valves as well.
The median procedure time was 18 minutes (range, 6-51 minutes), and the median number of valves placed in each patient was 4 (range, 2-7 valves). The median hospital stay was 1 day (range, 1-13 days).
Compared with the control subjects, patients who received endobronchial valves showed a reduction in target lobar volume of 1,366 mL. This was accompanied by improvements in FEV1 by 191 mL, in forced vital capacity by 442 mL, in residual lung volume, in longer 6-minute walk distance by 106 meters, in scores on the Clinical COPD Questionnaire measuring daily functioning, and in scores on the St. George’s Respiratory Questionnaire measuring quality of life. The results for the control subjects who crossed over to the active-treatment group were very similar, the investigators said (N Engl J Med. 2015 Dec 10;373:2325-35. doi:10.1056/NEJMoa1507807).
However, several adverse effects occurred, and close monitoring of this patient population is crucial. The most common complication was pneumothorax, which developed in 6 of the 34 patients (18%), usually within 1 day of undergoing the procedure. Pneumothorax resolved spontaneously in one patient but required chest-tube drainage in the other five; it resolved in one patient after temporary removal of the valves to promote healing, and in another after permanent removal of all valves.
Other adverse effects, some of which required repeat bronchoscopy, included torsion of the lower-lobe bronchus after upper-lobe treatment (two patients), pneumonia distal to the valves (one patient), increased dyspnea and sputum production (two patients), valve migration (two patients), valve dislocation because of granulation-tissue formation (one patient), and persistent cough (one patient). Despite these setbacks, “the overall outcome of treatment was positive,” Ms. Klooster and her associates said.
All patients who underwent valve removal recovered without any further adverse effects, indicating that this treatment “is fully reversible and doesn’t preclude further therapeutic options,” they added.
The study was supported by the Netherlands Organization for Health Research and Development and the University Medical Center Groningen. Ms. Klooster reported receiving fees, devices, travel support, and grant support from Pulmonx and PneumRx/BTG; her associates reported ties to numerous industry sponsors. Pulmonx commercially supplied the endobronchial valves for the study.
Endobronchial valves improved pulmonary function, exercise capacity, and quality of life in a prospective randomized controlled trial involving 68 adults with severe emphysema, according to a report published online Dec. 10 in the New England Journal of Medicine.
“The improvements we found were of greater magnitude than those noted with pharmacologic treatment in comparable patients and were similar to improvements with surgical lung-volume reduction, but with significantly less morbidity,” said Karin Klooster of the department of pulmonary diseases, University Medical Center Groningen (the Netherlands) and her associates.
Previous research suggested that bronchoscopic lung-volume reduction using one-way endobronchial valves to block inspiratory but not expiratory air flow would be most effective in patients who had a complete rather than an incomplete fissure between the targeted lobe and the adjacent lobe on high-resolution CT. “A complete fissure on HRCT [high-resolution computed tomography] is a surrogate finding for the absence of interlobar collateral ventilation; if there is collateral ventilation, an occluded lobe can be reinflated through its collaterals,” defeating the purpose of the procedure, the researchers wrote.
During a 3-year period, Ms. Klooster and her associates studied emphysema patients who were older than 35 years (mean age, 58-59) and had a postbronchodilator forced expiratory volume in 1 second (FEV1) less than 60% of predicted volume, a total lung capacity more than 100% of the predicted value, and residual volume more than 150% of predicted volume. On HRCT, all the study participants showed a complete or nearly complete fissure between the targeted lobe and the adjacent lobe. They were randomly assigned to receive endobronchial valves (34 patients) or usual care (34 control subjects) and followed for 6 months. At that time, control subjects were allowed to crossover and receive endobronchial valves as well.
The median procedure time was 18 minutes (range, 6-51 minutes), and the median number of valves placed in each patient was 4 (range, 2-7 valves). The median hospital stay was 1 day (range, 1-13 days).
Compared with the control subjects, patients who received endobronchial valves showed a reduction in target lobar volume of 1,366 mL. This was accompanied by improvements in FEV1 by 191 mL, in forced vital capacity by 442 mL, in residual lung volume, in longer 6-minute walk distance by 106 meters, in scores on the Clinical COPD Questionnaire measuring daily functioning, and in scores on the St. George’s Respiratory Questionnaire measuring quality of life. The results for the control subjects who crossed over to the active-treatment group were very similar, the investigators said (N Engl J Med. 2015 Dec 10;373:2325-35. doi:10.1056/NEJMoa1507807).
However, several adverse effects occurred, and close monitoring of this patient population is crucial. The most common complication was pneumothorax, which developed in 6 of the 34 patients (18%), usually within 1 day of undergoing the procedure. Pneumothorax resolved spontaneously in one patient but required chest-tube drainage in the other five; it resolved in one patient after temporary removal of the valves to promote healing, and in another after permanent removal of all valves.
Other adverse effects, some of which required repeat bronchoscopy, included torsion of the lower-lobe bronchus after upper-lobe treatment (two patients), pneumonia distal to the valves (one patient), increased dyspnea and sputum production (two patients), valve migration (two patients), valve dislocation because of granulation-tissue formation (one patient), and persistent cough (one patient). Despite these setbacks, “the overall outcome of treatment was positive,” Ms. Klooster and her associates said.
All patients who underwent valve removal recovered without any further adverse effects, indicating that this treatment “is fully reversible and doesn’t preclude further therapeutic options,” they added.
The study was supported by the Netherlands Organization for Health Research and Development and the University Medical Center Groningen. Ms. Klooster reported receiving fees, devices, travel support, and grant support from Pulmonx and PneumRx/BTG; her associates reported ties to numerous industry sponsors. Pulmonx commercially supplied the endobronchial valves for the study.
Endobronchial valves improved pulmonary function, exercise capacity, and quality of life in a prospective randomized controlled trial involving 68 adults with severe emphysema, according to a report published online Dec. 10 in the New England Journal of Medicine.
“The improvements we found were of greater magnitude than those noted with pharmacologic treatment in comparable patients and were similar to improvements with surgical lung-volume reduction, but with significantly less morbidity,” said Karin Klooster of the department of pulmonary diseases, University Medical Center Groningen (the Netherlands) and her associates.
Previous research suggested that bronchoscopic lung-volume reduction using one-way endobronchial valves to block inspiratory but not expiratory air flow would be most effective in patients who had a complete rather than an incomplete fissure between the targeted lobe and the adjacent lobe on high-resolution CT. “A complete fissure on HRCT [high-resolution computed tomography] is a surrogate finding for the absence of interlobar collateral ventilation; if there is collateral ventilation, an occluded lobe can be reinflated through its collaterals,” defeating the purpose of the procedure, the researchers wrote.
During a 3-year period, Ms. Klooster and her associates studied emphysema patients who were older than 35 years (mean age, 58-59) and had a postbronchodilator forced expiratory volume in 1 second (FEV1) less than 60% of predicted volume, a total lung capacity more than 100% of the predicted value, and residual volume more than 150% of predicted volume. On HRCT, all the study participants showed a complete or nearly complete fissure between the targeted lobe and the adjacent lobe. They were randomly assigned to receive endobronchial valves (34 patients) or usual care (34 control subjects) and followed for 6 months. At that time, control subjects were allowed to crossover and receive endobronchial valves as well.
The median procedure time was 18 minutes (range, 6-51 minutes), and the median number of valves placed in each patient was 4 (range, 2-7 valves). The median hospital stay was 1 day (range, 1-13 days).
Compared with the control subjects, patients who received endobronchial valves showed a reduction in target lobar volume of 1,366 mL. This was accompanied by improvements in FEV1 by 191 mL, in forced vital capacity by 442 mL, in residual lung volume, in longer 6-minute walk distance by 106 meters, in scores on the Clinical COPD Questionnaire measuring daily functioning, and in scores on the St. George’s Respiratory Questionnaire measuring quality of life. The results for the control subjects who crossed over to the active-treatment group were very similar, the investigators said (N Engl J Med. 2015 Dec 10;373:2325-35. doi:10.1056/NEJMoa1507807).
However, several adverse effects occurred, and close monitoring of this patient population is crucial. The most common complication was pneumothorax, which developed in 6 of the 34 patients (18%), usually within 1 day of undergoing the procedure. Pneumothorax resolved spontaneously in one patient but required chest-tube drainage in the other five; it resolved in one patient after temporary removal of the valves to promote healing, and in another after permanent removal of all valves.
Other adverse effects, some of which required repeat bronchoscopy, included torsion of the lower-lobe bronchus after upper-lobe treatment (two patients), pneumonia distal to the valves (one patient), increased dyspnea and sputum production (two patients), valve migration (two patients), valve dislocation because of granulation-tissue formation (one patient), and persistent cough (one patient). Despite these setbacks, “the overall outcome of treatment was positive,” Ms. Klooster and her associates said.
All patients who underwent valve removal recovered without any further adverse effects, indicating that this treatment “is fully reversible and doesn’t preclude further therapeutic options,” they added.
The study was supported by the Netherlands Organization for Health Research and Development and the University Medical Center Groningen. Ms. Klooster reported receiving fees, devices, travel support, and grant support from Pulmonx and PneumRx/BTG; her associates reported ties to numerous industry sponsors. Pulmonx commercially supplied the endobronchial valves for the study.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Endobronchial valves improved pulmonary function, exercise capacity, and QOL in severe emphysema.
Major finding: Patients who received endobronchial valves showed improved FEV1 by 191 mL, forced vital capacity by 442 mL, residual lung volume, 6-minute walk distance by 106 meters, and QOL scores.
Data source: A prospective randomized controlled trial involving 68 patients treated during a 3-year period at a single medical center.
Disclosures: The Netherlands Organization for Health Research and Development and the University Medical Center Groningen funded the study. Ms. Klooster reported receiving fees, devices, travel support, and grant support from Pulmonx and PneumRx/BTG; her associates reported ties to numerous industry sponsors. Pulmonx commercially supplied the endobronchial valves for this study.

Study: TKA patients recover faster with periarticular analgesia injection
Patients more often recovered faster from a total knee arthroplasty (TKA) when they received a periarticular injection of analgesic medication than when they received a femoral nerve block for the same surgery on the opposite knee in a study.
The study included 16 recipients of bilateral primary TKA, who received a femoral nerve block at their first TKA operation and a periarticular injection of an extended-release bupivacaine liposome mixture at the second operation. An average of 2.3 years passed between the two procedures, and the same surgeon performed all surgeries, which occurred between March 2009 and August 2013. Two patients were excluded from the study because of subacute rehabilitation admission delay and a third patient was left out of the study because of respiratory failure, resulting in admission to the ICU.
Following the TKA with a periarticular injection of analgesic medication, the average number of inpatient physical therapy sessions a patient completed was 2.3 (standard deviation: 1.0); the average number of inpatient physical therapy sessions a patient completed after having the TKA with femoral nerve block was 3.5 (SD: 1.3). The average number of hospital days following the TKA with periarticular injection was also a smaller number. The mean number of hospital days following the periarticular injection was 1.5 (SD: 0.6 days). compared with 1.9 days (SD: 0.6 days; P is less than .032) following the femoral nerve block.
“Our data demonstrate that periarticular injection of analgesia allowed patients to complete their inpatient physical therapy sessions and to be discharged sooner, compared with femoral nerve block. This finding suggests that patients who receive periarticular injection of analgesia are able to ambulate independently faster because it does not affect postoperative motor function,” according to Dr. Brandon J. Horn and his colleagues.
Read the full study in the Journal of the American Osteopathic Association (doi: 10.7556/jaoa.2015.146).
Patients more often recovered faster from a total knee arthroplasty (TKA) when they received a periarticular injection of analgesic medication than when they received a femoral nerve block for the same surgery on the opposite knee in a study.
The study included 16 recipients of bilateral primary TKA, who received a femoral nerve block at their first TKA operation and a periarticular injection of an extended-release bupivacaine liposome mixture at the second operation. An average of 2.3 years passed between the two procedures, and the same surgeon performed all surgeries, which occurred between March 2009 and August 2013. Two patients were excluded from the study because of subacute rehabilitation admission delay and a third patient was left out of the study because of respiratory failure, resulting in admission to the ICU.
Following the TKA with a periarticular injection of analgesic medication, the average number of inpatient physical therapy sessions a patient completed was 2.3 (standard deviation: 1.0); the average number of inpatient physical therapy sessions a patient completed after having the TKA with femoral nerve block was 3.5 (SD: 1.3). The average number of hospital days following the TKA with periarticular injection was also a smaller number. The mean number of hospital days following the periarticular injection was 1.5 (SD: 0.6 days). compared with 1.9 days (SD: 0.6 days; P is less than .032) following the femoral nerve block.
“Our data demonstrate that periarticular injection of analgesia allowed patients to complete their inpatient physical therapy sessions and to be discharged sooner, compared with femoral nerve block. This finding suggests that patients who receive periarticular injection of analgesia are able to ambulate independently faster because it does not affect postoperative motor function,” according to Dr. Brandon J. Horn and his colleagues.
Read the full study in the Journal of the American Osteopathic Association (doi: 10.7556/jaoa.2015.146).
Patients more often recovered faster from a total knee arthroplasty (TKA) when they received a periarticular injection of analgesic medication than when they received a femoral nerve block for the same surgery on the opposite knee in a study.
The study included 16 recipients of bilateral primary TKA, who received a femoral nerve block at their first TKA operation and a periarticular injection of an extended-release bupivacaine liposome mixture at the second operation. An average of 2.3 years passed between the two procedures, and the same surgeon performed all surgeries, which occurred between March 2009 and August 2013. Two patients were excluded from the study because of subacute rehabilitation admission delay and a third patient was left out of the study because of respiratory failure, resulting in admission to the ICU.
Following the TKA with a periarticular injection of analgesic medication, the average number of inpatient physical therapy sessions a patient completed was 2.3 (standard deviation: 1.0); the average number of inpatient physical therapy sessions a patient completed after having the TKA with femoral nerve block was 3.5 (SD: 1.3). The average number of hospital days following the TKA with periarticular injection was also a smaller number. The mean number of hospital days following the periarticular injection was 1.5 (SD: 0.6 days). compared with 1.9 days (SD: 0.6 days; P is less than .032) following the femoral nerve block.
“Our data demonstrate that periarticular injection of analgesia allowed patients to complete their inpatient physical therapy sessions and to be discharged sooner, compared with femoral nerve block. This finding suggests that patients who receive periarticular injection of analgesia are able to ambulate independently faster because it does not affect postoperative motor function,” according to Dr. Brandon J. Horn and his colleagues.
Read the full study in the Journal of the American Osteopathic Association (doi: 10.7556/jaoa.2015.146).
FROM THE JOURNAL OF THE AMERICAN OSTEOPATHIC ASSOCIATION
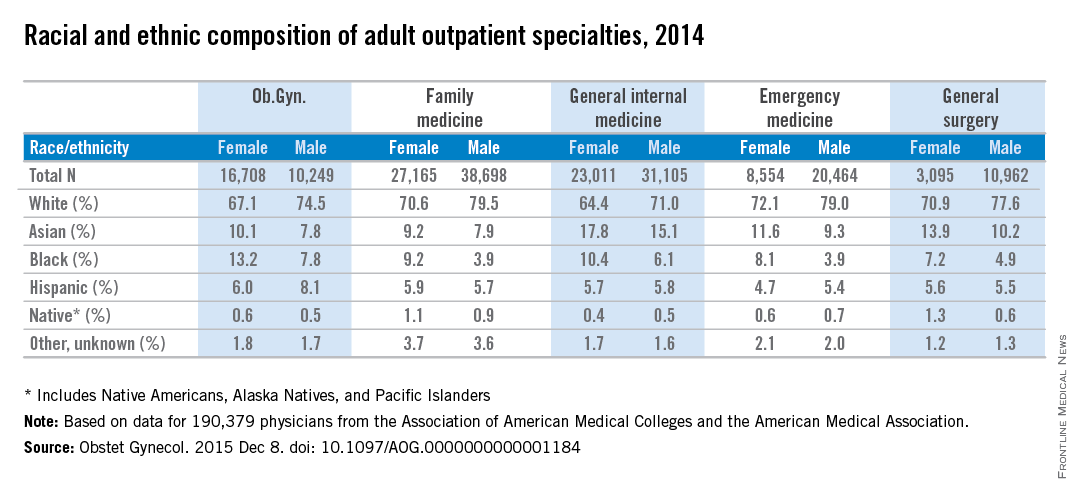
Women physicians outnumber men in ob.gyn., lag in other specialties
Ob.gyn. is the only one of the five largest adult outpatient specialties in which women make up the majority of physicians, according to a new study.
Women made up almost 62% of ob.gyns. in 2014, but none of the other four specialties – family medicine, general internal medicine, emergency medicine, and general surgery – reached 50%, reported Dr. William F. Rayburn of the University of New Mexico, Albuquerque, and his associates.
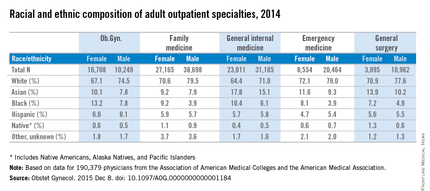
The cross-sectional study of 190,379 physicians also showed that racial and ethnic composition differed between the five specialties, although whites made up the largest racial group in each. Among the minority groups, Asians made up the largest proportion of physicians in the study and were actually overrepresented, compared with the overall U.S. population. Internal medicine had the largest Asian population, followed by general surgery. Asians, along with black physicians, were more likely to be female in each specialty, the investigators said (Obstet Gynecol. 2015 Dec 8. doi: 10.1097/AOG.0000000000001184).
At 18.4%, ob.gyn. had the largest proportion of the underrepresented minorities – blacks, Hispanics, and Natives (Native Americans, Alaska Natives, and Pacific Islanders). Black physicians represented a larger share of ob.gyns. (11.1%) than in any of the other specialties, according to data from the Association of American Medical Colleges and the American Medical Association.
The investigators did not report any conflicts of interest.
Ob.gyn. is the only one of the five largest adult outpatient specialties in which women make up the majority of physicians, according to a new study.
Women made up almost 62% of ob.gyns. in 2014, but none of the other four specialties – family medicine, general internal medicine, emergency medicine, and general surgery – reached 50%, reported Dr. William F. Rayburn of the University of New Mexico, Albuquerque, and his associates.
The cross-sectional study of 190,379 physicians also showed that racial and ethnic composition differed between the five specialties, although whites made up the largest racial group in each. Among the minority groups, Asians made up the largest proportion of physicians in the study and were actually overrepresented, compared with the overall U.S. population. Internal medicine had the largest Asian population, followed by general surgery. Asians, along with black physicians, were more likely to be female in each specialty, the investigators said (Obstet Gynecol. 2015 Dec 8. doi: 10.1097/AOG.0000000000001184).
At 18.4%, ob.gyn. had the largest proportion of the underrepresented minorities – blacks, Hispanics, and Natives (Native Americans, Alaska Natives, and Pacific Islanders). Black physicians represented a larger share of ob.gyns. (11.1%) than in any of the other specialties, according to data from the Association of American Medical Colleges and the American Medical Association.
The investigators did not report any conflicts of interest.
Ob.gyn. is the only one of the five largest adult outpatient specialties in which women make up the majority of physicians, according to a new study.
Women made up almost 62% of ob.gyns. in 2014, but none of the other four specialties – family medicine, general internal medicine, emergency medicine, and general surgery – reached 50%, reported Dr. William F. Rayburn of the University of New Mexico, Albuquerque, and his associates.
The cross-sectional study of 190,379 physicians also showed that racial and ethnic composition differed between the five specialties, although whites made up the largest racial group in each. Among the minority groups, Asians made up the largest proportion of physicians in the study and were actually overrepresented, compared with the overall U.S. population. Internal medicine had the largest Asian population, followed by general surgery. Asians, along with black physicians, were more likely to be female in each specialty, the investigators said (Obstet Gynecol. 2015 Dec 8. doi: 10.1097/AOG.0000000000001184).
At 18.4%, ob.gyn. had the largest proportion of the underrepresented minorities – blacks, Hispanics, and Natives (Native Americans, Alaska Natives, and Pacific Islanders). Black physicians represented a larger share of ob.gyns. (11.1%) than in any of the other specialties, according to data from the Association of American Medical Colleges and the American Medical Association.
The investigators did not report any conflicts of interest.
FROM OBSTETRICS AND GYNECOLOGY
Cigna CEO David Cordani: ACA marketplace is still in ‘version 1.0’
Just days after UnitedHealth Group’s CEO said their move into the new marketplace was a mistake, Cigna CEO David Cordani reaffirmed that his company remains committed for 2016, although the firm is so far losing money on that business.
Cigna has a small share of the health law market with only 230,000 individual customers this year. But that could grow rapidly if a $54 billion purchase bid by insurer Anthem wins federal approval because Anthem is a big player in the individual market. The deal is one of two giant mergers in the works: Aetna is also working to get approval to buy Humana.
If Cigna’s deal is approved, Mr. Cordani is expected to remain with the new company as president and chief operating officer. He sat down with Julie Appleby of Kaiser Health News to discuss the marketplace. This interview has been edited for length.
When looking at the merger, many have asked how can having fewer insurers competing be good for consumers?

When you look at Cigna and Anthem, we are amazingly complementary. Cigna’s strength is for employers … we have unbelievably diverse global set of programs. Anthem is a strong U.S.-based corporation [with] a history and focus really around the individual market and small employers in the states it operates in. We were not historically in the individual market. We’re actually going to create more choice than less. We will be able to take Anthem’s individual infrastructure beyond the 14 states [in which it now operates].
What else?
We’ll take their leading Medicaid program and our leading Medicare program and put them together to design solutions for the dual-eligible population. In terms of employer marketplace, we will be able to bring population health and management programs to their employer programs and help expand the geographic footprint.
UnitedHealth’s CEO last month said the insurer is losing hundreds of millions of dollars on its individual insurance market business and hinted it might pull back from the market in 2017. While Cigna is smaller in that market, did you lose money or make money on Affordable Care Act business in 2014 and 2015?
When the law put in place the exchanges, we took a bit of a different public position than many of our competitors. We saw the exchange marketplace as a potentially attractive long-term viable market. We also said we viewed 2014, 2015, and 2016 as version 1.0 of that market and that it would take those 3 years for the market to shake itself out. We said from day 1 we didn’t expect to make money on it. We didn’t make money on it in 2014 and we aren’t making money on it in 2015.
Two of the reasons United gave for the losses were people moving in and out of the market and higher costs for people who signed up after the official 3-month open enrollment period closed. [There are a number of special exemptions that allow sign-ups during other times of the year.] How could the law be tweaked to lessen those concerns?
Societally, we are just starting to understand how the market is operating. What is the other market with some similarity? Medicare Advantage [the private alternative to traditional Medicare]. It has a one-time limited enrollment period [that is shorter than the ACA] – I think that’s a good thing. Compress the enrollment period, focus it and have a limited number of exceptions.
Secondly, [provide] more flexibility on how [insurers’ provider] networks are designed.
What Medicare Advantage shows us is by offering more choice, and choice is not necessarily different names of insurers, but benefit designs and network configurations, you get the right choice for you … as opposed to socializing things down.
[The market] has to also have a real focus on transparency [for consumers]. It can have more choice aided by transparency [and] network visibility for individuals to understand what they are buying before they sign up.
Only about 40% of the people eligible to enroll have – and they’re mainly concentrated in the income levels with the highest subsidies. What can be done to encourage more people to enroll?
You have to ask the consumer why they’re not enrolling. There’s a perceived affordability challenge. Perception is reality.
If [insurers] are allowed more flexibility in benefit and network configuration, we’re probably going to get solutions that are much more relevant to a part of the population that is not buying.
How would that work? Would you set higher deductibles to get lower premiums?
If you have an individual with a chronic disease, say asthma, you can have a program that is passive: If they want to enroll in a care management plan, they can. Or they can be incented to enroll. Or you can have a plan that is binary: If [you] have that [condition] [you] have to be in that [care management] program. Those are all choices. What we know is if [a patient is] asthmatic and more actively managed, the health outcomes and therefore the affordability can be quite different. This is a case where if you have a chronic illness, you need to be in a management program. We know the quality outcomes will be better and cost outcomes will be more sustainable.
In late December, Cigna will stop paying brokers commissions if they sell gold-level individual plans, which cover more costs than do the less expensive bronze and silver level plans. What is Cigna’s concern with gold products?
Adverse selection. [It’s not that policyholders] are necessarily older or sicker. The whole way the benefits are configured and the way marketplace is working – the performance of those plans – is much less reasonable than all the other plans.
Either there will be more flexibility to configure them in a way to make them sustainable or there won’t be gold plans.
So is Cigna staying in the market?
We’re in for 2016.
How about 2017?
We haven’t made a comment relative to 2017. We view 2014, 2015, and 2016 as version 1.0.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry K. Kaiser Family Foundation.
Just days after UnitedHealth Group’s CEO said their move into the new marketplace was a mistake, Cigna CEO David Cordani reaffirmed that his company remains committed for 2016, although the firm is so far losing money on that business.
Cigna has a small share of the health law market with only 230,000 individual customers this year. But that could grow rapidly if a $54 billion purchase bid by insurer Anthem wins federal approval because Anthem is a big player in the individual market. The deal is one of two giant mergers in the works: Aetna is also working to get approval to buy Humana.
If Cigna’s deal is approved, Mr. Cordani is expected to remain with the new company as president and chief operating officer. He sat down with Julie Appleby of Kaiser Health News to discuss the marketplace. This interview has been edited for length.
When looking at the merger, many have asked how can having fewer insurers competing be good for consumers?
When you look at Cigna and Anthem, we are amazingly complementary. Cigna’s strength is for employers … we have unbelievably diverse global set of programs. Anthem is a strong U.S.-based corporation [with] a history and focus really around the individual market and small employers in the states it operates in. We were not historically in the individual market. We’re actually going to create more choice than less. We will be able to take Anthem’s individual infrastructure beyond the 14 states [in which it now operates].
What else?
We’ll take their leading Medicaid program and our leading Medicare program and put them together to design solutions for the dual-eligible population. In terms of employer marketplace, we will be able to bring population health and management programs to their employer programs and help expand the geographic footprint.
UnitedHealth’s CEO last month said the insurer is losing hundreds of millions of dollars on its individual insurance market business and hinted it might pull back from the market in 2017. While Cigna is smaller in that market, did you lose money or make money on Affordable Care Act business in 2014 and 2015?
When the law put in place the exchanges, we took a bit of a different public position than many of our competitors. We saw the exchange marketplace as a potentially attractive long-term viable market. We also said we viewed 2014, 2015, and 2016 as version 1.0 of that market and that it would take those 3 years for the market to shake itself out. We said from day 1 we didn’t expect to make money on it. We didn’t make money on it in 2014 and we aren’t making money on it in 2015.
Two of the reasons United gave for the losses were people moving in and out of the market and higher costs for people who signed up after the official 3-month open enrollment period closed. [There are a number of special exemptions that allow sign-ups during other times of the year.] How could the law be tweaked to lessen those concerns?
Societally, we are just starting to understand how the market is operating. What is the other market with some similarity? Medicare Advantage [the private alternative to traditional Medicare]. It has a one-time limited enrollment period [that is shorter than the ACA] – I think that’s a good thing. Compress the enrollment period, focus it and have a limited number of exceptions.
Secondly, [provide] more flexibility on how [insurers’ provider] networks are designed.
What Medicare Advantage shows us is by offering more choice, and choice is not necessarily different names of insurers, but benefit designs and network configurations, you get the right choice for you … as opposed to socializing things down.
[The market] has to also have a real focus on transparency [for consumers]. It can have more choice aided by transparency [and] network visibility for individuals to understand what they are buying before they sign up.
Only about 40% of the people eligible to enroll have – and they’re mainly concentrated in the income levels with the highest subsidies. What can be done to encourage more people to enroll?
You have to ask the consumer why they’re not enrolling. There’s a perceived affordability challenge. Perception is reality.
If [insurers] are allowed more flexibility in benefit and network configuration, we’re probably going to get solutions that are much more relevant to a part of the population that is not buying.
How would that work? Would you set higher deductibles to get lower premiums?
If you have an individual with a chronic disease, say asthma, you can have a program that is passive: If they want to enroll in a care management plan, they can. Or they can be incented to enroll. Or you can have a plan that is binary: If [you] have that [condition] [you] have to be in that [care management] program. Those are all choices. What we know is if [a patient is] asthmatic and more actively managed, the health outcomes and therefore the affordability can be quite different. This is a case where if you have a chronic illness, you need to be in a management program. We know the quality outcomes will be better and cost outcomes will be more sustainable.
In late December, Cigna will stop paying brokers commissions if they sell gold-level individual plans, which cover more costs than do the less expensive bronze and silver level plans. What is Cigna’s concern with gold products?
Adverse selection. [It’s not that policyholders] are necessarily older or sicker. The whole way the benefits are configured and the way marketplace is working – the performance of those plans – is much less reasonable than all the other plans.
Either there will be more flexibility to configure them in a way to make them sustainable or there won’t be gold plans.
So is Cigna staying in the market?
We’re in for 2016.
How about 2017?
We haven’t made a comment relative to 2017. We view 2014, 2015, and 2016 as version 1.0.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry K. Kaiser Family Foundation.
Just days after UnitedHealth Group’s CEO said their move into the new marketplace was a mistake, Cigna CEO David Cordani reaffirmed that his company remains committed for 2016, although the firm is so far losing money on that business.
Cigna has a small share of the health law market with only 230,000 individual customers this year. But that could grow rapidly if a $54 billion purchase bid by insurer Anthem wins federal approval because Anthem is a big player in the individual market. The deal is one of two giant mergers in the works: Aetna is also working to get approval to buy Humana.
If Cigna’s deal is approved, Mr. Cordani is expected to remain with the new company as president and chief operating officer. He sat down with Julie Appleby of Kaiser Health News to discuss the marketplace. This interview has been edited for length.
When looking at the merger, many have asked how can having fewer insurers competing be good for consumers?
When you look at Cigna and Anthem, we are amazingly complementary. Cigna’s strength is for employers … we have unbelievably diverse global set of programs. Anthem is a strong U.S.-based corporation [with] a history and focus really around the individual market and small employers in the states it operates in. We were not historically in the individual market. We’re actually going to create more choice than less. We will be able to take Anthem’s individual infrastructure beyond the 14 states [in which it now operates].
What else?
We’ll take their leading Medicaid program and our leading Medicare program and put them together to design solutions for the dual-eligible population. In terms of employer marketplace, we will be able to bring population health and management programs to their employer programs and help expand the geographic footprint.
UnitedHealth’s CEO last month said the insurer is losing hundreds of millions of dollars on its individual insurance market business and hinted it might pull back from the market in 2017. While Cigna is smaller in that market, did you lose money or make money on Affordable Care Act business in 2014 and 2015?
When the law put in place the exchanges, we took a bit of a different public position than many of our competitors. We saw the exchange marketplace as a potentially attractive long-term viable market. We also said we viewed 2014, 2015, and 2016 as version 1.0 of that market and that it would take those 3 years for the market to shake itself out. We said from day 1 we didn’t expect to make money on it. We didn’t make money on it in 2014 and we aren’t making money on it in 2015.
Two of the reasons United gave for the losses were people moving in and out of the market and higher costs for people who signed up after the official 3-month open enrollment period closed. [There are a number of special exemptions that allow sign-ups during other times of the year.] How could the law be tweaked to lessen those concerns?
Societally, we are just starting to understand how the market is operating. What is the other market with some similarity? Medicare Advantage [the private alternative to traditional Medicare]. It has a one-time limited enrollment period [that is shorter than the ACA] – I think that’s a good thing. Compress the enrollment period, focus it and have a limited number of exceptions.
Secondly, [provide] more flexibility on how [insurers’ provider] networks are designed.
What Medicare Advantage shows us is by offering more choice, and choice is not necessarily different names of insurers, but benefit designs and network configurations, you get the right choice for you … as opposed to socializing things down.
[The market] has to also have a real focus on transparency [for consumers]. It can have more choice aided by transparency [and] network visibility for individuals to understand what they are buying before they sign up.
Only about 40% of the people eligible to enroll have – and they’re mainly concentrated in the income levels with the highest subsidies. What can be done to encourage more people to enroll?
You have to ask the consumer why they’re not enrolling. There’s a perceived affordability challenge. Perception is reality.
If [insurers] are allowed more flexibility in benefit and network configuration, we’re probably going to get solutions that are much more relevant to a part of the population that is not buying.
How would that work? Would you set higher deductibles to get lower premiums?
If you have an individual with a chronic disease, say asthma, you can have a program that is passive: If they want to enroll in a care management plan, they can. Or they can be incented to enroll. Or you can have a plan that is binary: If [you] have that [condition] [you] have to be in that [care management] program. Those are all choices. What we know is if [a patient is] asthmatic and more actively managed, the health outcomes and therefore the affordability can be quite different. This is a case where if you have a chronic illness, you need to be in a management program. We know the quality outcomes will be better and cost outcomes will be more sustainable.
In late December, Cigna will stop paying brokers commissions if they sell gold-level individual plans, which cover more costs than do the less expensive bronze and silver level plans. What is Cigna’s concern with gold products?
Adverse selection. [It’s not that policyholders] are necessarily older or sicker. The whole way the benefits are configured and the way marketplace is working – the performance of those plans – is much less reasonable than all the other plans.
Either there will be more flexibility to configure them in a way to make them sustainable or there won’t be gold plans.
So is Cigna staying in the market?
We’re in for 2016.
How about 2017?
We haven’t made a comment relative to 2017. We view 2014, 2015, and 2016 as version 1.0.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry K. Kaiser Family Foundation.

Analysis finds 28.8% prevalence of depression in residents
The estimated prevalence of depression or depressive symptoms was 28.8% among residents and interns worldwide in a meta-analysis of 54 studies of the issue, according to a report published online December 8 in JAMA.
The depression rate ranged from 20.9% to 43.2%, depending on the instrument used to assess symptoms. Eleven studies used the Beck Depression Inventory (BDI), 11 used the Center for Epidemiological Studies Depression Scale (CES-D), 8 used the two-item Primary Care Evaluation of Mental Disorders questionnaire (PRIME-MD), 7 used the nine-item Patient Health Questionnaire (PHQ-9), 4 used the Zung Self-Rating Depression Scale (SDS), 3 used the Harvard Department of Psychiatry/National Depression Screening Day Scale (HANDS), and 11 used other validated methods, said Dr. Douglas A. Mata of the department of pathology, Brigham and Women’s Hospital and Harvard Medical School, Boston, and his associates.
“It is important to note that the vast majority of participants were assessed through self-report inventories that measured depressive symptoms, rather than gold-standard diagnostic clinical interviews for major depressive disorder,” they said.
The meta-analysis included 31 cross-sectional and 23 longitudinal studies published in peer-reviewed journals since 1963 and involving 17,560 residents or interns in North America (35 studies), Asia (9 studies), Europe (5 studies), South America (4 studies), and Africa (1 study). When the results were pooled, the overall prevalence of depression or depressive symptoms was 28.8% (4,969 of 17,560 participants).
In a sensitivity analysis, no individual study affected the overall prevalence estimate by more than 1%. Further analyses showed no significant differences in the prevalence of depression between cross-sectional and longitudinal studies, between U.S. studies and those performed in other countries, between studies of nonsurgical residents only vs. studies of all types of residents, or between studies of interns only vs. studies of upper level residents only. This suggests that the underlying causes of depressive symptoms “are common to the residency experience,” Dr. Mata and his associates said (JAMA. 2015 Dec 8. doi: 10.1001/jama.2015.15845).
The prevalence of depression increased over time. Although this rise was characterized as modest, “it is notable, given efforts by the Accreditation Council for Graduate Medical Education, European Working Time Directive, and others to limit trainee duty hours and improve work conditions. [This] trend may reflect the medical community’s increased awareness of depression or developments external to medical education. Future studies should explore specific factors that may explain this trend,” the investigators said.
The study findings indicate that the long-term health of physicians may be affected, since depression has been linked to a higher risk of future depressive episodes and greater long-term morbidity. Patient care may also be affected, given the established association between physician depression and lower-quality care, they added.

|
Dr. Thomas L. Schwenk |
The meta-analysis by Mata et al. makes it clear that the extent of significant depressive symptomatology, if not overt clinical depression, among physicians-in-training is extraordinarily and unacceptably high. Relieving the burden of depression in these individuals is an issue of professional performance in addition to one of human compassion.
A national conversation about the fundamental structure and function of the graduate medical education system is long overdue, not unlike the discussion that reformed undergraduate medical education after the Flexner Report. The high burden of depressive symptoms among residents and interns has reached a crisis level. It is a marker for deeper and more profound problems in the medical education system, which require equally profound solutions.
Dr. Thomas L. Schwenk is at the University of Nevada, Reno. He reported having no relevant financial disclosures. Dr. Schwenk made these remarks in an editorial accompanying Dr. Mata’s report (JAMA 2015;314:2357-8).
|
|
Dr. Thomas L. Schwenk |
The meta-analysis by Mata et al. makes it clear that the extent of significant depressive symptomatology, if not overt clinical depression, among physicians-in-training is extraordinarily and unacceptably high. Relieving the burden of depression in these individuals is an issue of professional performance in addition to one of human compassion.
A national conversation about the fundamental structure and function of the graduate medical education system is long overdue, not unlike the discussion that reformed undergraduate medical education after the Flexner Report. The high burden of depressive symptoms among residents and interns has reached a crisis level. It is a marker for deeper and more profound problems in the medical education system, which require equally profound solutions.
Dr. Thomas L. Schwenk is at the University of Nevada, Reno. He reported having no relevant financial disclosures. Dr. Schwenk made these remarks in an editorial accompanying Dr. Mata’s report (JAMA 2015;314:2357-8).
|
|
Dr. Thomas L. Schwenk |
The meta-analysis by Mata et al. makes it clear that the extent of significant depressive symptomatology, if not overt clinical depression, among physicians-in-training is extraordinarily and unacceptably high. Relieving the burden of depression in these individuals is an issue of professional performance in addition to one of human compassion.
A national conversation about the fundamental structure and function of the graduate medical education system is long overdue, not unlike the discussion that reformed undergraduate medical education after the Flexner Report. The high burden of depressive symptoms among residents and interns has reached a crisis level. It is a marker for deeper and more profound problems in the medical education system, which require equally profound solutions.
Dr. Thomas L. Schwenk is at the University of Nevada, Reno. He reported having no relevant financial disclosures. Dr. Schwenk made these remarks in an editorial accompanying Dr. Mata’s report (JAMA 2015;314:2357-8).
The estimated prevalence of depression or depressive symptoms was 28.8% among residents and interns worldwide in a meta-analysis of 54 studies of the issue, according to a report published online December 8 in JAMA.
The depression rate ranged from 20.9% to 43.2%, depending on the instrument used to assess symptoms. Eleven studies used the Beck Depression Inventory (BDI), 11 used the Center for Epidemiological Studies Depression Scale (CES-D), 8 used the two-item Primary Care Evaluation of Mental Disorders questionnaire (PRIME-MD), 7 used the nine-item Patient Health Questionnaire (PHQ-9), 4 used the Zung Self-Rating Depression Scale (SDS), 3 used the Harvard Department of Psychiatry/National Depression Screening Day Scale (HANDS), and 11 used other validated methods, said Dr. Douglas A. Mata of the department of pathology, Brigham and Women’s Hospital and Harvard Medical School, Boston, and his associates.
“It is important to note that the vast majority of participants were assessed through self-report inventories that measured depressive symptoms, rather than gold-standard diagnostic clinical interviews for major depressive disorder,” they said.
The meta-analysis included 31 cross-sectional and 23 longitudinal studies published in peer-reviewed journals since 1963 and involving 17,560 residents or interns in North America (35 studies), Asia (9 studies), Europe (5 studies), South America (4 studies), and Africa (1 study). When the results were pooled, the overall prevalence of depression or depressive symptoms was 28.8% (4,969 of 17,560 participants).
In a sensitivity analysis, no individual study affected the overall prevalence estimate by more than 1%. Further analyses showed no significant differences in the prevalence of depression between cross-sectional and longitudinal studies, between U.S. studies and those performed in other countries, between studies of nonsurgical residents only vs. studies of all types of residents, or between studies of interns only vs. studies of upper level residents only. This suggests that the underlying causes of depressive symptoms “are common to the residency experience,” Dr. Mata and his associates said (JAMA. 2015 Dec 8. doi: 10.1001/jama.2015.15845).
The prevalence of depression increased over time. Although this rise was characterized as modest, “it is notable, given efforts by the Accreditation Council for Graduate Medical Education, European Working Time Directive, and others to limit trainee duty hours and improve work conditions. [This] trend may reflect the medical community’s increased awareness of depression or developments external to medical education. Future studies should explore specific factors that may explain this trend,” the investigators said.
The study findings indicate that the long-term health of physicians may be affected, since depression has been linked to a higher risk of future depressive episodes and greater long-term morbidity. Patient care may also be affected, given the established association between physician depression and lower-quality care, they added.
The estimated prevalence of depression or depressive symptoms was 28.8% among residents and interns worldwide in a meta-analysis of 54 studies of the issue, according to a report published online December 8 in JAMA.
The depression rate ranged from 20.9% to 43.2%, depending on the instrument used to assess symptoms. Eleven studies used the Beck Depression Inventory (BDI), 11 used the Center for Epidemiological Studies Depression Scale (CES-D), 8 used the two-item Primary Care Evaluation of Mental Disorders questionnaire (PRIME-MD), 7 used the nine-item Patient Health Questionnaire (PHQ-9), 4 used the Zung Self-Rating Depression Scale (SDS), 3 used the Harvard Department of Psychiatry/National Depression Screening Day Scale (HANDS), and 11 used other validated methods, said Dr. Douglas A. Mata of the department of pathology, Brigham and Women’s Hospital and Harvard Medical School, Boston, and his associates.
“It is important to note that the vast majority of participants were assessed through self-report inventories that measured depressive symptoms, rather than gold-standard diagnostic clinical interviews for major depressive disorder,” they said.
The meta-analysis included 31 cross-sectional and 23 longitudinal studies published in peer-reviewed journals since 1963 and involving 17,560 residents or interns in North America (35 studies), Asia (9 studies), Europe (5 studies), South America (4 studies), and Africa (1 study). When the results were pooled, the overall prevalence of depression or depressive symptoms was 28.8% (4,969 of 17,560 participants).
In a sensitivity analysis, no individual study affected the overall prevalence estimate by more than 1%. Further analyses showed no significant differences in the prevalence of depression between cross-sectional and longitudinal studies, between U.S. studies and those performed in other countries, between studies of nonsurgical residents only vs. studies of all types of residents, or between studies of interns only vs. studies of upper level residents only. This suggests that the underlying causes of depressive symptoms “are common to the residency experience,” Dr. Mata and his associates said (JAMA. 2015 Dec 8. doi: 10.1001/jama.2015.15845).
The prevalence of depression increased over time. Although this rise was characterized as modest, “it is notable, given efforts by the Accreditation Council for Graduate Medical Education, European Working Time Directive, and others to limit trainee duty hours and improve work conditions. [This] trend may reflect the medical community’s increased awareness of depression or developments external to medical education. Future studies should explore specific factors that may explain this trend,” the investigators said.
The study findings indicate that the long-term health of physicians may be affected, since depression has been linked to a higher risk of future depressive episodes and greater long-term morbidity. Patient care may also be affected, given the established association between physician depression and lower-quality care, they added.
FROM JAMA
Key clinical point: The prevalence of depression or depressive symptoms was 28.8% (range, 20.9%-43.2%) among residents in a meta-analysis of 54 studies.
Major finding: The overall prevalence of depression or depressive symptoms was 28.8% (4,969 of 17,560 participants) across all countries, all types of studies, and all types of graduate medical education programs.
Data source: A meta-analysis of 31 cross-sectional and 23 longitudinal studies involving 17,560 residents and interns worldwide.
Disclosures: This study was supported by the U.S. Department of State Fulbright Scholarship program, the National Institutes of Health, and the NIH Medical Scientist Training Program. Dr. Mata and his associates reported having no relevant financial disclosures.

Die not yet cast for lymphazurin and methylene blue dye
CHICAGO – Two commonly used dyes produced mixed results in sentinel lymph node mapping of early stage breast cancer in what was described as the highest-powered study to date.
The average number of sentinel lymph nodes identified per person was significantly higher with 1% methylene blue dye than with 1% lymphazurin (2.89 vs. 2.22; P less than .001).

Although there is extensive support for methylene blue as a safe and efficacious alternative to lymphazurin, this finding on the number of sentinel nodes identified is not replicated in any other study, Dr. Vaishali Patel said at the annual clinical congress of the American College of Surgeons. The study was conducted at the McLaren Flint (Mich.) Medical Center. Dr. Sukamal Saha was principal investigator.
On the other hand, lymphazurin identified significantly more additional lymph nodes than methylene blue (mean 4.48 vs. 2.84; P less than .001).
Nodal positivity was also significantly higher with lymphazurin than methylene blue (14.93% vs. 8.85%; P less than .001), which also has not been reported in other trials.
“We think this does offer a true comparison between the two dyes,” Dr. Patel of Detroit Medical Center Sinai-Grace Hospital said. “The volume of dye and technique were consistent for all 651 patients. … with one surgeon performing the injections and one surgeon performing the procedures.” The 651 consecutive patients were randomly assigned based on agent availability to a preoperative injection of lymphazurin (half intraparenchymal and half subareolar in the upper outer quadrant) or an intraoperative injection of methylene blue over 5 minutes (3 ccs intraparenchymal, 1 cc subareolar, and 1 cc intradermal).
The lymphazurin and methylene blue groups were also similar in number (298 patients vs. 353 patients), age (mean 61.6 years vs. 63.5 years), and T stage (in situ 12% vs. 17.8%; T1 64% vs. 65%; T2 23% vs. 17.5%).
In contrast, three smaller, well-established studies that came to different conclusions used four different surgeons and novel techniques to inject their radiocolloid and supervised residents for lymphatic mapping, she noted.
The radiocolloid lymphazurin first demonstrated superiority over methylene blue in 1990, but alternatives continue to be investigated due to frequent nonavailability and a host of adverse events including blue hives, blue discoloration or tattooing, and anaphylaxis.
Lymphazurin also costs 10-12 times more than methylene blue, which was reflected in the study in an average per patient cost of $815 vs. $75 for methylene blue, Dr. Patel said.
The American Society of Breast Surgeons, however, recommends dual-agent mapping using blue dye and a radioisotope in breast cancer to further improve the success in identifying the sentinel lymph nodes. The improvement is likely because of the dual mechanism at play: radiocolloids become entrapped within the lymph node, whereas certain blue dyes bind to interstitial albumin and are taken up by lymphatics, she explained.
The higher number of sentinel lymph nodes in the methylene blue group may be due to its particle size, which is smaller, weighs less, and diffused faster, Dr. Patel suggested.
The higher number of additional lymph nodes captured with lymphazurin may be because of the higher frequency of nodal dissection in this group than in the methylene blue group (25% vs. 16%).
The finding of greater nodal positivity in the lymphazurin group may be related to mechanism of action or the high percentage of patients with T1 disease enrolled in the study. Still, nodal positivity was higher with lymphazurin than methylene blue regardless of T stage, she said.
The lymphazurin group had higher rates than the methylene blue group of pseudohypoxemia (10% vs. 0%; P less than .0001), but blue hives (1.34% vs. 0%; P = .043) and anaphylaxis (.67% vs. 0%; P = .20) were kept in check. Patients were premedicated and early in the series, the surgeon began excising the area of injected blue skin during the primary surgery, Dr. Patel observed.
Despite being diluted, methylene blue was associated with higher rates of seroma (3.4% vs. 1.7%; P = .005) and skin necrosis (2.55% vs. 9%; P = .005).
Discussant Dr. Alyssa Throckmorton of Baptist Memorial Health Care in Memphis pointed out that more recent data show radiocolloid mapping alone is comparable to dual-agent mapping, suggesting that blue dye may not be needed. That said, there have been national shortages of methylene blue as well as lymphazurin.
“I think in surgeons who are going to use blue dye, with the way drug shortages have become in the last few years, you are going to have to be facile and familiar with both types of dye if you are going to use that as part of your clinical practice,” she said.
CHICAGO – Two commonly used dyes produced mixed results in sentinel lymph node mapping of early stage breast cancer in what was described as the highest-powered study to date.
The average number of sentinel lymph nodes identified per person was significantly higher with 1% methylene blue dye than with 1% lymphazurin (2.89 vs. 2.22; P less than .001).
Although there is extensive support for methylene blue as a safe and efficacious alternative to lymphazurin, this finding on the number of sentinel nodes identified is not replicated in any other study, Dr. Vaishali Patel said at the annual clinical congress of the American College of Surgeons. The study was conducted at the McLaren Flint (Mich.) Medical Center. Dr. Sukamal Saha was principal investigator.
On the other hand, lymphazurin identified significantly more additional lymph nodes than methylene blue (mean 4.48 vs. 2.84; P less than .001).
Nodal positivity was also significantly higher with lymphazurin than methylene blue (14.93% vs. 8.85%; P less than .001), which also has not been reported in other trials.
“We think this does offer a true comparison between the two dyes,” Dr. Patel of Detroit Medical Center Sinai-Grace Hospital said. “The volume of dye and technique were consistent for all 651 patients. … with one surgeon performing the injections and one surgeon performing the procedures.” The 651 consecutive patients were randomly assigned based on agent availability to a preoperative injection of lymphazurin (half intraparenchymal and half subareolar in the upper outer quadrant) or an intraoperative injection of methylene blue over 5 minutes (3 ccs intraparenchymal, 1 cc subareolar, and 1 cc intradermal).
The lymphazurin and methylene blue groups were also similar in number (298 patients vs. 353 patients), age (mean 61.6 years vs. 63.5 years), and T stage (in situ 12% vs. 17.8%; T1 64% vs. 65%; T2 23% vs. 17.5%).
In contrast, three smaller, well-established studies that came to different conclusions used four different surgeons and novel techniques to inject their radiocolloid and supervised residents for lymphatic mapping, she noted.
The radiocolloid lymphazurin first demonstrated superiority over methylene blue in 1990, but alternatives continue to be investigated due to frequent nonavailability and a host of adverse events including blue hives, blue discoloration or tattooing, and anaphylaxis.
Lymphazurin also costs 10-12 times more than methylene blue, which was reflected in the study in an average per patient cost of $815 vs. $75 for methylene blue, Dr. Patel said.
The American Society of Breast Surgeons, however, recommends dual-agent mapping using blue dye and a radioisotope in breast cancer to further improve the success in identifying the sentinel lymph nodes. The improvement is likely because of the dual mechanism at play: radiocolloids become entrapped within the lymph node, whereas certain blue dyes bind to interstitial albumin and are taken up by lymphatics, she explained.
The higher number of sentinel lymph nodes in the methylene blue group may be due to its particle size, which is smaller, weighs less, and diffused faster, Dr. Patel suggested.
The higher number of additional lymph nodes captured with lymphazurin may be because of the higher frequency of nodal dissection in this group than in the methylene blue group (25% vs. 16%).
The finding of greater nodal positivity in the lymphazurin group may be related to mechanism of action or the high percentage of patients with T1 disease enrolled in the study. Still, nodal positivity was higher with lymphazurin than methylene blue regardless of T stage, she said.
The lymphazurin group had higher rates than the methylene blue group of pseudohypoxemia (10% vs. 0%; P less than .0001), but blue hives (1.34% vs. 0%; P = .043) and anaphylaxis (.67% vs. 0%; P = .20) were kept in check. Patients were premedicated and early in the series, the surgeon began excising the area of injected blue skin during the primary surgery, Dr. Patel observed.
Despite being diluted, methylene blue was associated with higher rates of seroma (3.4% vs. 1.7%; P = .005) and skin necrosis (2.55% vs. 9%; P = .005).
Discussant Dr. Alyssa Throckmorton of Baptist Memorial Health Care in Memphis pointed out that more recent data show radiocolloid mapping alone is comparable to dual-agent mapping, suggesting that blue dye may not be needed. That said, there have been national shortages of methylene blue as well as lymphazurin.
“I think in surgeons who are going to use blue dye, with the way drug shortages have become in the last few years, you are going to have to be facile and familiar with both types of dye if you are going to use that as part of your clinical practice,” she said.
CHICAGO – Two commonly used dyes produced mixed results in sentinel lymph node mapping of early stage breast cancer in what was described as the highest-powered study to date.
The average number of sentinel lymph nodes identified per person was significantly higher with 1% methylene blue dye than with 1% lymphazurin (2.89 vs. 2.22; P less than .001).
Although there is extensive support for methylene blue as a safe and efficacious alternative to lymphazurin, this finding on the number of sentinel nodes identified is not replicated in any other study, Dr. Vaishali Patel said at the annual clinical congress of the American College of Surgeons. The study was conducted at the McLaren Flint (Mich.) Medical Center. Dr. Sukamal Saha was principal investigator.
On the other hand, lymphazurin identified significantly more additional lymph nodes than methylene blue (mean 4.48 vs. 2.84; P less than .001).
Nodal positivity was also significantly higher with lymphazurin than methylene blue (14.93% vs. 8.85%; P less than .001), which also has not been reported in other trials.
“We think this does offer a true comparison between the two dyes,” Dr. Patel of Detroit Medical Center Sinai-Grace Hospital said. “The volume of dye and technique were consistent for all 651 patients. … with one surgeon performing the injections and one surgeon performing the procedures.” The 651 consecutive patients were randomly assigned based on agent availability to a preoperative injection of lymphazurin (half intraparenchymal and half subareolar in the upper outer quadrant) or an intraoperative injection of methylene blue over 5 minutes (3 ccs intraparenchymal, 1 cc subareolar, and 1 cc intradermal).
The lymphazurin and methylene blue groups were also similar in number (298 patients vs. 353 patients), age (mean 61.6 years vs. 63.5 years), and T stage (in situ 12% vs. 17.8%; T1 64% vs. 65%; T2 23% vs. 17.5%).
In contrast, three smaller, well-established studies that came to different conclusions used four different surgeons and novel techniques to inject their radiocolloid and supervised residents for lymphatic mapping, she noted.
The radiocolloid lymphazurin first demonstrated superiority over methylene blue in 1990, but alternatives continue to be investigated due to frequent nonavailability and a host of adverse events including blue hives, blue discoloration or tattooing, and anaphylaxis.
Lymphazurin also costs 10-12 times more than methylene blue, which was reflected in the study in an average per patient cost of $815 vs. $75 for methylene blue, Dr. Patel said.
The American Society of Breast Surgeons, however, recommends dual-agent mapping using blue dye and a radioisotope in breast cancer to further improve the success in identifying the sentinel lymph nodes. The improvement is likely because of the dual mechanism at play: radiocolloids become entrapped within the lymph node, whereas certain blue dyes bind to interstitial albumin and are taken up by lymphatics, she explained.
The higher number of sentinel lymph nodes in the methylene blue group may be due to its particle size, which is smaller, weighs less, and diffused faster, Dr. Patel suggested.
The higher number of additional lymph nodes captured with lymphazurin may be because of the higher frequency of nodal dissection in this group than in the methylene blue group (25% vs. 16%).
The finding of greater nodal positivity in the lymphazurin group may be related to mechanism of action or the high percentage of patients with T1 disease enrolled in the study. Still, nodal positivity was higher with lymphazurin than methylene blue regardless of T stage, she said.
The lymphazurin group had higher rates than the methylene blue group of pseudohypoxemia (10% vs. 0%; P less than .0001), but blue hives (1.34% vs. 0%; P = .043) and anaphylaxis (.67% vs. 0%; P = .20) were kept in check. Patients were premedicated and early in the series, the surgeon began excising the area of injected blue skin during the primary surgery, Dr. Patel observed.
Despite being diluted, methylene blue was associated with higher rates of seroma (3.4% vs. 1.7%; P = .005) and skin necrosis (2.55% vs. 9%; P = .005).
Discussant Dr. Alyssa Throckmorton of Baptist Memorial Health Care in Memphis pointed out that more recent data show radiocolloid mapping alone is comparable to dual-agent mapping, suggesting that blue dye may not be needed. That said, there have been national shortages of methylene blue as well as lymphazurin.
“I think in surgeons who are going to use blue dye, with the way drug shortages have become in the last few years, you are going to have to be facile and familiar with both types of dye if you are going to use that as part of your clinical practice,” she said.
AT THE ACS CLINICAL CONGRESS
Key clinical point: Contrary to prior studies, lymph node positivity was higher with lymphazurin than methylene blue in patients with early breast cancer.
Major finding: Nodal positivity was 14.93% with lymphazurin vs. 8.85% with methylene blue (P less than .001).
Data source: Prospective study in 651 patients undergoing lymphatic mapping for breast cancer.
Disclosures: Dr. Patel and Dr. Throckmorton reported having no relevant conflicts.

Postop C. diff infection associated with presurgical antibiotics
A hospital’s rate of postoperative Clostridium difficile infection is related to the number of preoperative antibiotics patients have taken, the complexity of their procedures, and the complexity of the hospital’s surgical program, in addition to known risk factors for the infection, according to a report published online in JAMA Surgery.
Several risk factors for postoperative C. difficile infection have already been identified, including advanced age and comorbidity. To examine known risk factors and identify possible new ones, researchers analyzed information from the Veterans Affairs Surgical Quality Improvement Program’s database, which documents all noncardiac operations at 134 VA medical centers each year.
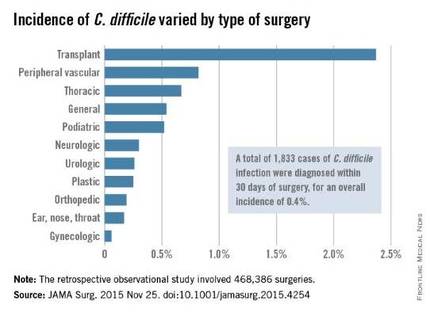
The investigators focused on 468,386 procedures performed during a 4-year period. A total of 1,833 cases of C. difficile infection were diagnosed within 30 days of surgery, for an overall incidence of 0.4% in this predominantly male, elderly population, said Xinli Li, Ph.D., of the Veterans Health Administration, Washington, and associates.
As expected, patients who developed postoperative C. difficile infection were significantly older than those who didn’t (mean age, 67.4 vs. 60.6 years) and were significantly more likely to have comorbidities such as impaired functional status, heart failure, chronic obstructive pulmonary disease, ascites, renal failure, bleeding disorders, wound infection, and recent weight loss.
Unexpectedly, the number of different antibiotics taken during the 60 days preceding surgery also was significantly associated with C. difficile infection. Patients who had taken three or more antibiotics from different classes were nearly six times more likely to develop C. difficile than patients who had taken only one or no antibiotics, the investigators reported (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4263).In addition, patients who underwent more complex surgical procedures were at increased risk of this complication, as were patients at hospitals that frequently handled complex procedures. “These factors reflect the illness of patients, duration of operation, and hospital setting; each is an established risk factor for C. difficile infection,” Dr. Li and associates wrote.
Patients with C. difficile infection had higher rates of postoperative other morbidity (86.0% vs. 7.1%) and 30-day mortality (5.3% vs. 1.0%) and longer postoperative hospital stays (17.9 days vs. 3.6 days).
Contrary to previous studies, this study did not show a temporal increase in C. difficile infection. The overall incidence, as well as the incidences at individual hospitals, remained constant during the entire 4-year study period, the investigators added.
The incidence of C. difficile varied substantially among the 134 VA medical centers, from 0% to 1.35% of all surgical patients. “Surgical administrators and clinical teams may consider the results of this study to target interventions for specific patients undergoing high-risk procedures. Such interventions include selective antibiotic administration, early testing of at-risk patients, hand hygiene with nonalcohol agents, early contact precautions, and specific environmental cleaning protocols,” Dr. Li and associates wrote.
This study was supported by the Veterans Health Administration. Dr. Li and associates reported having no relevant financial disclosures.
The most important finding to highlight in the report by Li et al. is the 12-fold increase in morbidity and 5-fold increase in mortality among patients who developed postoperative C. difficile infection.
The study results underscore the importance of infection control and prevention efforts. They also show how important it is to develop prophylactic strategies, expeditious recognition of C. difficile, adequate supportive care, and improved therapies.
Dr. Paul K. Waltz and Dr. Brian S. Zuckerbraun are at the VA Pittsburgh Healthcare System and the University of Pennsylvania, Pittsburgh. They made these remarks in an invited commentary accompanying Dr. Li’s report (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4254).
The most important finding to highlight in the report by Li et al. is the 12-fold increase in morbidity and 5-fold increase in mortality among patients who developed postoperative C. difficile infection.
The study results underscore the importance of infection control and prevention efforts. They also show how important it is to develop prophylactic strategies, expeditious recognition of C. difficile, adequate supportive care, and improved therapies.
Dr. Paul K. Waltz and Dr. Brian S. Zuckerbraun are at the VA Pittsburgh Healthcare System and the University of Pennsylvania, Pittsburgh. They made these remarks in an invited commentary accompanying Dr. Li’s report (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4254).
The most important finding to highlight in the report by Li et al. is the 12-fold increase in morbidity and 5-fold increase in mortality among patients who developed postoperative C. difficile infection.
The study results underscore the importance of infection control and prevention efforts. They also show how important it is to develop prophylactic strategies, expeditious recognition of C. difficile, adequate supportive care, and improved therapies.
Dr. Paul K. Waltz and Dr. Brian S. Zuckerbraun are at the VA Pittsburgh Healthcare System and the University of Pennsylvania, Pittsburgh. They made these remarks in an invited commentary accompanying Dr. Li’s report (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4254).
A hospital’s rate of postoperative Clostridium difficile infection is related to the number of preoperative antibiotics patients have taken, the complexity of their procedures, and the complexity of the hospital’s surgical program, in addition to known risk factors for the infection, according to a report published online in JAMA Surgery.
Several risk factors for postoperative C. difficile infection have already been identified, including advanced age and comorbidity. To examine known risk factors and identify possible new ones, researchers analyzed information from the Veterans Affairs Surgical Quality Improvement Program’s database, which documents all noncardiac operations at 134 VA medical centers each year.
The investigators focused on 468,386 procedures performed during a 4-year period. A total of 1,833 cases of C. difficile infection were diagnosed within 30 days of surgery, for an overall incidence of 0.4% in this predominantly male, elderly population, said Xinli Li, Ph.D., of the Veterans Health Administration, Washington, and associates.
As expected, patients who developed postoperative C. difficile infection were significantly older than those who didn’t (mean age, 67.4 vs. 60.6 years) and were significantly more likely to have comorbidities such as impaired functional status, heart failure, chronic obstructive pulmonary disease, ascites, renal failure, bleeding disorders, wound infection, and recent weight loss.
Unexpectedly, the number of different antibiotics taken during the 60 days preceding surgery also was significantly associated with C. difficile infection. Patients who had taken three or more antibiotics from different classes were nearly six times more likely to develop C. difficile than patients who had taken only one or no antibiotics, the investigators reported (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4263).In addition, patients who underwent more complex surgical procedures were at increased risk of this complication, as were patients at hospitals that frequently handled complex procedures. “These factors reflect the illness of patients, duration of operation, and hospital setting; each is an established risk factor for C. difficile infection,” Dr. Li and associates wrote.
Patients with C. difficile infection had higher rates of postoperative other morbidity (86.0% vs. 7.1%) and 30-day mortality (5.3% vs. 1.0%) and longer postoperative hospital stays (17.9 days vs. 3.6 days).
Contrary to previous studies, this study did not show a temporal increase in C. difficile infection. The overall incidence, as well as the incidences at individual hospitals, remained constant during the entire 4-year study period, the investigators added.
The incidence of C. difficile varied substantially among the 134 VA medical centers, from 0% to 1.35% of all surgical patients. “Surgical administrators and clinical teams may consider the results of this study to target interventions for specific patients undergoing high-risk procedures. Such interventions include selective antibiotic administration, early testing of at-risk patients, hand hygiene with nonalcohol agents, early contact precautions, and specific environmental cleaning protocols,” Dr. Li and associates wrote.
This study was supported by the Veterans Health Administration. Dr. Li and associates reported having no relevant financial disclosures.
A hospital’s rate of postoperative Clostridium difficile infection is related to the number of preoperative antibiotics patients have taken, the complexity of their procedures, and the complexity of the hospital’s surgical program, in addition to known risk factors for the infection, according to a report published online in JAMA Surgery.
Several risk factors for postoperative C. difficile infection have already been identified, including advanced age and comorbidity. To examine known risk factors and identify possible new ones, researchers analyzed information from the Veterans Affairs Surgical Quality Improvement Program’s database, which documents all noncardiac operations at 134 VA medical centers each year.
The investigators focused on 468,386 procedures performed during a 4-year period. A total of 1,833 cases of C. difficile infection were diagnosed within 30 days of surgery, for an overall incidence of 0.4% in this predominantly male, elderly population, said Xinli Li, Ph.D., of the Veterans Health Administration, Washington, and associates.
As expected, patients who developed postoperative C. difficile infection were significantly older than those who didn’t (mean age, 67.4 vs. 60.6 years) and were significantly more likely to have comorbidities such as impaired functional status, heart failure, chronic obstructive pulmonary disease, ascites, renal failure, bleeding disorders, wound infection, and recent weight loss.
Unexpectedly, the number of different antibiotics taken during the 60 days preceding surgery also was significantly associated with C. difficile infection. Patients who had taken three or more antibiotics from different classes were nearly six times more likely to develop C. difficile than patients who had taken only one or no antibiotics, the investigators reported (JAMA Surg. 2015 Nov 25. doi: 10.1001/jamasurg.2015.4263).In addition, patients who underwent more complex surgical procedures were at increased risk of this complication, as were patients at hospitals that frequently handled complex procedures. “These factors reflect the illness of patients, duration of operation, and hospital setting; each is an established risk factor for C. difficile infection,” Dr. Li and associates wrote.
Patients with C. difficile infection had higher rates of postoperative other morbidity (86.0% vs. 7.1%) and 30-day mortality (5.3% vs. 1.0%) and longer postoperative hospital stays (17.9 days vs. 3.6 days).
Contrary to previous studies, this study did not show a temporal increase in C. difficile infection. The overall incidence, as well as the incidences at individual hospitals, remained constant during the entire 4-year study period, the investigators added.
The incidence of C. difficile varied substantially among the 134 VA medical centers, from 0% to 1.35% of all surgical patients. “Surgical administrators and clinical teams may consider the results of this study to target interventions for specific patients undergoing high-risk procedures. Such interventions include selective antibiotic administration, early testing of at-risk patients, hand hygiene with nonalcohol agents, early contact precautions, and specific environmental cleaning protocols,” Dr. Li and associates wrote.
This study was supported by the Veterans Health Administration. Dr. Li and associates reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point: A hospital’s rate of postoperative C. difficile infection is related to the number of preoperative antibiotics patients took and the complexity of their surgeries.
Major finding: Patients who had taken three or more preoperative antibiotics from different classes were nearly six times more likely to develop C. difficile than patients who had taken only one or no antibiotics.
Data source: A retrospective observational study involving 468,386 surgeries at 134 VA medical centers during a 4-year period.
Disclosures: This study was supported by the Veterans Health Administration. Dr. Li and associates reported having no relevant financial disclosures.
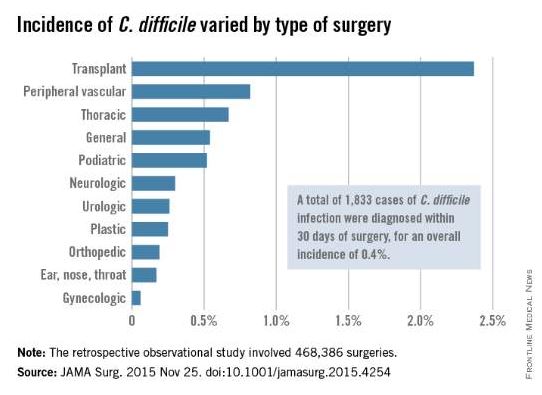
Senate votes to gut ACA, defund Planned Parenthood
WASHINGTON – Several key provisions of the Affordable Care Act would be repealed – and Planned Parenthood would be defunded for a year – under the fiscal year 2016 federal budget reconciliation bill passed Dec. 3 by the Senate.
Building on a budget reconciliation bill (H.R. 3762) passed by the House in October, the legislation would:

• Repeal the individual mandate and the employer mandate to provide health insurance coverage and the associated tax penalties.
• Phase out Medicaid expansion after a 2-year transition period.
• Eliminate federal subsidies to help patients purchase health insurance via the federal health care marketplace.
• Repeal the “Cadillac tax” on high-value health insurance plans.
• Repeal the medical device tax.
• Defund Planned Parenthood for a year and divert some of that funding to community health centers.
The bill passed 52-47, mostly along party lines. Sen. Mark Kirk (R-Ill.) voted with the Democratic minority and Sen. Bernie Sanders (I-Vt.) was absent.*
Senate Majority Leader Mitch McConnell (R-Ky.) hailed the vote. “For years, the American people have been calling on Washington to build a bridge away from Obamacare. For years, Democrats prevented the Senate from passing legislation to do so. But in just a moment, that will change,” he said, calling the vote “a victory for the middle-class families who’ve endured this law’s pain for too long.”
From the Senate floor, Minority Leader Harry Reid (D-Nev.) condemned the action. “Sometimes I wonder what Senate Republicans do when they’re not here in Washington, D.C. Do they talk to their constituents? Do they meet with them? I have a hard time believing my Republican friends are spending much time listening to their constituents’ concerns because it seems that what they are doing runs counter to the needs of their constituents,” Sen. Reid said. “This absurd attempt to repeal the Affordable Care Act through reconciliation is a perfect example.”
The bill now must be considered again by the House since it is not identical to the bill that body passed Oct. 23. Regardless, President Obama is unlikely to sign the bill.
On Twitter @denisefulton
Correction 12/7/15 : An earlier version of this article misstated two senators' votes.
WASHINGTON – Several key provisions of the Affordable Care Act would be repealed – and Planned Parenthood would be defunded for a year – under the fiscal year 2016 federal budget reconciliation bill passed Dec. 3 by the Senate.
Building on a budget reconciliation bill (H.R. 3762) passed by the House in October, the legislation would:
• Repeal the individual mandate and the employer mandate to provide health insurance coverage and the associated tax penalties.
• Phase out Medicaid expansion after a 2-year transition period.
• Eliminate federal subsidies to help patients purchase health insurance via the federal health care marketplace.
• Repeal the “Cadillac tax” on high-value health insurance plans.
• Repeal the medical device tax.
• Defund Planned Parenthood for a year and divert some of that funding to community health centers.
The bill passed 52-47, mostly along party lines. Sen. Mark Kirk (R-Ill.) voted with the Democratic minority and Sen. Bernie Sanders (I-Vt.) was absent.*
Senate Majority Leader Mitch McConnell (R-Ky.) hailed the vote. “For years, the American people have been calling on Washington to build a bridge away from Obamacare. For years, Democrats prevented the Senate from passing legislation to do so. But in just a moment, that will change,” he said, calling the vote “a victory for the middle-class families who’ve endured this law’s pain for too long.”
From the Senate floor, Minority Leader Harry Reid (D-Nev.) condemned the action. “Sometimes I wonder what Senate Republicans do when they’re not here in Washington, D.C. Do they talk to their constituents? Do they meet with them? I have a hard time believing my Republican friends are spending much time listening to their constituents’ concerns because it seems that what they are doing runs counter to the needs of their constituents,” Sen. Reid said. “This absurd attempt to repeal the Affordable Care Act through reconciliation is a perfect example.”
The bill now must be considered again by the House since it is not identical to the bill that body passed Oct. 23. Regardless, President Obama is unlikely to sign the bill.
On Twitter @denisefulton
Correction 12/7/15 : An earlier version of this article misstated two senators' votes.
WASHINGTON – Several key provisions of the Affordable Care Act would be repealed – and Planned Parenthood would be defunded for a year – under the fiscal year 2016 federal budget reconciliation bill passed Dec. 3 by the Senate.
Building on a budget reconciliation bill (H.R. 3762) passed by the House in October, the legislation would:
• Repeal the individual mandate and the employer mandate to provide health insurance coverage and the associated tax penalties.
• Phase out Medicaid expansion after a 2-year transition period.
• Eliminate federal subsidies to help patients purchase health insurance via the federal health care marketplace.
• Repeal the “Cadillac tax” on high-value health insurance plans.
• Repeal the medical device tax.
• Defund Planned Parenthood for a year and divert some of that funding to community health centers.
The bill passed 52-47, mostly along party lines. Sen. Mark Kirk (R-Ill.) voted with the Democratic minority and Sen. Bernie Sanders (I-Vt.) was absent.*
Senate Majority Leader Mitch McConnell (R-Ky.) hailed the vote. “For years, the American people have been calling on Washington to build a bridge away from Obamacare. For years, Democrats prevented the Senate from passing legislation to do so. But in just a moment, that will change,” he said, calling the vote “a victory for the middle-class families who’ve endured this law’s pain for too long.”
From the Senate floor, Minority Leader Harry Reid (D-Nev.) condemned the action. “Sometimes I wonder what Senate Republicans do when they’re not here in Washington, D.C. Do they talk to their constituents? Do they meet with them? I have a hard time believing my Republican friends are spending much time listening to their constituents’ concerns because it seems that what they are doing runs counter to the needs of their constituents,” Sen. Reid said. “This absurd attempt to repeal the Affordable Care Act through reconciliation is a perfect example.”
The bill now must be considered again by the House since it is not identical to the bill that body passed Oct. 23. Regardless, President Obama is unlikely to sign the bill.
On Twitter @denisefulton
Correction 12/7/15 : An earlier version of this article misstated two senators' votes.
