User login
Official Newspaper of the American College of Surgeons
ASA: Pediatric clinicians over-dispensing opioids, study finds
SAN DIEGO – Pediatric clinicians are dispensing more medicine than needed to treat pain and may be contributing to the epidemic of nonmedical use of prescription opioids, results from a prospective cohort study suggest.
“On the one hand, we have an ethical and more responsibility to treat pain,” Dr. Myron Yaster said in an interview at the annual meeting of the American Society of Anesthesiologists. “I think we’re doing a pretty good job of that. But there’s also a societal issue in what happens to medicines that are left over. That leftover medicine is the most important element in drug addiction. What this study showed is that in the pediatric population, about 60% of what is prescribed is left over.”

As part of a larger ongoing project, Dr. Yaster, professor of pediatric anesthesiology, critical care medicine, and pain management at Johns Hopkins University Hospital, Baltimore, Md., and his associates recruited 433 English-speaking inpatients who were given opioids on discharge from the university’s pediatric hospital. All prescriptions were analyzed by the investigators following discharge for drug, formulation, and amount dispensed. Parents of the patients were interviewed within 2 days of discharge and again up to 2 weeks after discharge to determine if the prescription was filled, to determine pain control on a 4-point Likert scale, how long opioids were used, the amount of medication left at completion of therapy, if patients were given instructions about how to dispose of leftover drug, and if the remaining medications were discarded.
Of the 433 parents, 292 (67%) completed both sets of interviews. The average age of patients was 11 years and their average weight was 44 kg. The majority of patients (89%) were prescribed oxycodone, a liquid formulation 44% of the time. A minority (5%) did not fill their prescriptions, 25% misidentified or did not know the name of their prescription opioid, and patients took opioids for an average of 5 days. “We need to know more about what the prescribers are thinking when they prescribe,” Dr. Yaster said. “Do they actually believe that [patients are] going to take the medicine for 10 days?”
Nearly half of the time (47%), parents rated pain control as “excellent,” followed by “good” (34%), “fair” (10%), or poor (0%). The remaining 9% gave no response. At 2 weeks, an average of 36 opioid tablets and an average of 67 mL of opioid liquid medication remained unused. Overall, patients used only 42% of their prescribed amount.
The researchers also found that 82% of parents were not provided instructions as to what to do with leftover medicine, and only 6% actually did dispose of it. “That means that all that leftover medicine is in people’s medicine cabinets,” Dr. Yaster said. “The study also found that almost half of patients had a teenage sibling. That’s the target population of drug abuse.”
Dr. Yaster reported having no financial disclosures. One of the study authors was Aaron Hsu, a medical student at Johns Hopkins.
SAN DIEGO – Pediatric clinicians are dispensing more medicine than needed to treat pain and may be contributing to the epidemic of nonmedical use of prescription opioids, results from a prospective cohort study suggest.
“On the one hand, we have an ethical and more responsibility to treat pain,” Dr. Myron Yaster said in an interview at the annual meeting of the American Society of Anesthesiologists. “I think we’re doing a pretty good job of that. But there’s also a societal issue in what happens to medicines that are left over. That leftover medicine is the most important element in drug addiction. What this study showed is that in the pediatric population, about 60% of what is prescribed is left over.”
As part of a larger ongoing project, Dr. Yaster, professor of pediatric anesthesiology, critical care medicine, and pain management at Johns Hopkins University Hospital, Baltimore, Md., and his associates recruited 433 English-speaking inpatients who were given opioids on discharge from the university’s pediatric hospital. All prescriptions were analyzed by the investigators following discharge for drug, formulation, and amount dispensed. Parents of the patients were interviewed within 2 days of discharge and again up to 2 weeks after discharge to determine if the prescription was filled, to determine pain control on a 4-point Likert scale, how long opioids were used, the amount of medication left at completion of therapy, if patients were given instructions about how to dispose of leftover drug, and if the remaining medications were discarded.
Of the 433 parents, 292 (67%) completed both sets of interviews. The average age of patients was 11 years and their average weight was 44 kg. The majority of patients (89%) were prescribed oxycodone, a liquid formulation 44% of the time. A minority (5%) did not fill their prescriptions, 25% misidentified or did not know the name of their prescription opioid, and patients took opioids for an average of 5 days. “We need to know more about what the prescribers are thinking when they prescribe,” Dr. Yaster said. “Do they actually believe that [patients are] going to take the medicine for 10 days?”
Nearly half of the time (47%), parents rated pain control as “excellent,” followed by “good” (34%), “fair” (10%), or poor (0%). The remaining 9% gave no response. At 2 weeks, an average of 36 opioid tablets and an average of 67 mL of opioid liquid medication remained unused. Overall, patients used only 42% of their prescribed amount.
The researchers also found that 82% of parents were not provided instructions as to what to do with leftover medicine, and only 6% actually did dispose of it. “That means that all that leftover medicine is in people’s medicine cabinets,” Dr. Yaster said. “The study also found that almost half of patients had a teenage sibling. That’s the target population of drug abuse.”
Dr. Yaster reported having no financial disclosures. One of the study authors was Aaron Hsu, a medical student at Johns Hopkins.
SAN DIEGO – Pediatric clinicians are dispensing more medicine than needed to treat pain and may be contributing to the epidemic of nonmedical use of prescription opioids, results from a prospective cohort study suggest.
“On the one hand, we have an ethical and more responsibility to treat pain,” Dr. Myron Yaster said in an interview at the annual meeting of the American Society of Anesthesiologists. “I think we’re doing a pretty good job of that. But there’s also a societal issue in what happens to medicines that are left over. That leftover medicine is the most important element in drug addiction. What this study showed is that in the pediatric population, about 60% of what is prescribed is left over.”
As part of a larger ongoing project, Dr. Yaster, professor of pediatric anesthesiology, critical care medicine, and pain management at Johns Hopkins University Hospital, Baltimore, Md., and his associates recruited 433 English-speaking inpatients who were given opioids on discharge from the university’s pediatric hospital. All prescriptions were analyzed by the investigators following discharge for drug, formulation, and amount dispensed. Parents of the patients were interviewed within 2 days of discharge and again up to 2 weeks after discharge to determine if the prescription was filled, to determine pain control on a 4-point Likert scale, how long opioids were used, the amount of medication left at completion of therapy, if patients were given instructions about how to dispose of leftover drug, and if the remaining medications were discarded.
Of the 433 parents, 292 (67%) completed both sets of interviews. The average age of patients was 11 years and their average weight was 44 kg. The majority of patients (89%) were prescribed oxycodone, a liquid formulation 44% of the time. A minority (5%) did not fill their prescriptions, 25% misidentified or did not know the name of their prescription opioid, and patients took opioids for an average of 5 days. “We need to know more about what the prescribers are thinking when they prescribe,” Dr. Yaster said. “Do they actually believe that [patients are] going to take the medicine for 10 days?”
Nearly half of the time (47%), parents rated pain control as “excellent,” followed by “good” (34%), “fair” (10%), or poor (0%). The remaining 9% gave no response. At 2 weeks, an average of 36 opioid tablets and an average of 67 mL of opioid liquid medication remained unused. Overall, patients used only 42% of their prescribed amount.
The researchers also found that 82% of parents were not provided instructions as to what to do with leftover medicine, and only 6% actually did dispose of it. “That means that all that leftover medicine is in people’s medicine cabinets,” Dr. Yaster said. “The study also found that almost half of patients had a teenage sibling. That’s the target population of drug abuse.”
Dr. Yaster reported having no financial disclosures. One of the study authors was Aaron Hsu, a medical student at Johns Hopkins.
AT THE ASA ANNUAL MEETING
Key clinical point: Clinicians dispense more opioids than needed to treat pediatric pain.
Major finding: The majority of patients (89%) were prescribed oxycodone, and overall they used only 42% of the opioids they were prescribed.
Data source: A prospective study based on responses from 292 parents of children who were discharged from a university pediatric hospital with an opioid prescription.
Disclosures: Dr. Yaster reported having no financial disclosures.

Experts call for international cooperation on human gene editing
Human gene editing is no longer the stuff of science fiction, and the powerful new technologies that make it possible raise important scientific, ethical, and societal questions.
The organizing committee for a 3-day International Summit On Gene Editing that convened experts from around the world to discuss the issues associated with human gene-editing research, has called upon the international community to work together to establish norms for acceptable uses of human gene editing.

In a statement issued Dec. 3 at the close of the summit, the committee asked the summit cohosts – the U.S. National Academy of Sciences and U.S. National Academy of Medicine, the Royal Society (United Kingdom), and the Chinese Academy of Sciences – to take the lead in creating an ongoing international forum on gene editing and to work on formulating recommendations and guidelines.
“While each nation ultimately has the authority to regulate activities under its jurisdiction, the human genome is shared among all nations,” the committee wrote. “The international community should strive to establish norms concerning acceptable uses of human germline editing and to harmonize regulations, in order to discourage unacceptable activities while advancing human health and welfare.”
The committee also concluded that:
• Intensive basic and preclinical research is needed, with a specific research focus on technologies for editing genetic sequences in human cells, potential benefits and risks of proposed clinical uses for gene editing, and understanding of the biology of human embryos and germline cells. Any early human embryo or germline cells that undergo gene editing should not be used to establish a pregnancy, the committee wrote.
• Improved understanding of the risks of somatic cell editing – such as inaccurate editing – is needed, as is understanding of the potential benefits of each proposed genetic modification. Such uses of gene editing, which are intended to affect only the individual who receives them, can be “appropriately and rigorously evaluated within existing and evolving regulatory frameworks for gene therapy,” they noted.
• Germline editing poses particularly important issues, such as the challenges with predicting harmful effects of genetic changes, including interactions with other genetic variants and with the environment. Moral and ethical considerations, such as the possibility of permanent genetic enhancements that could exacerbate social inequalities or be used coercively, must also be considered. The committee said that “it would be irresponsible to proceed with any clinical use of germline editing” unless and until the safety and efficacy issues have been resolved, and there is broad consensus about the appropriateness of a proposed application.
“At present these criteria have not been met for any proposed clinical use,” the committee wrote, adding that safety issues have not been adequately explored, and the cases of most compelling benefit are limited.
As the science advances and social views evolve, the clinical use of germline editing should be regularly revisited, they wrote.
The presidents of each of the organizations that hosted the summit welcomed the call for ongoing global discussion on issues related to human gene editing.
In a written response they said that they “stand ready to establish a continuing forum for assessment of the many scientific, medical, and ethical questions surrounding the pursuit of human gene-editing applications,” and will coordinate with other academies around the world and other international scientific and medical institutions in that endeavor.
“This is an important moment in human history and we have a responsibility to provide all sections of society with an informed basis for making decisions about this technology, especially for uses that would affect generations to come,” they wrote.
Human gene editing is no longer the stuff of science fiction, and the powerful new technologies that make it possible raise important scientific, ethical, and societal questions.
The organizing committee for a 3-day International Summit On Gene Editing that convened experts from around the world to discuss the issues associated with human gene-editing research, has called upon the international community to work together to establish norms for acceptable uses of human gene editing.
In a statement issued Dec. 3 at the close of the summit, the committee asked the summit cohosts – the U.S. National Academy of Sciences and U.S. National Academy of Medicine, the Royal Society (United Kingdom), and the Chinese Academy of Sciences – to take the lead in creating an ongoing international forum on gene editing and to work on formulating recommendations and guidelines.
“While each nation ultimately has the authority to regulate activities under its jurisdiction, the human genome is shared among all nations,” the committee wrote. “The international community should strive to establish norms concerning acceptable uses of human germline editing and to harmonize regulations, in order to discourage unacceptable activities while advancing human health and welfare.”
The committee also concluded that:
• Intensive basic and preclinical research is needed, with a specific research focus on technologies for editing genetic sequences in human cells, potential benefits and risks of proposed clinical uses for gene editing, and understanding of the biology of human embryos and germline cells. Any early human embryo or germline cells that undergo gene editing should not be used to establish a pregnancy, the committee wrote.
• Improved understanding of the risks of somatic cell editing – such as inaccurate editing – is needed, as is understanding of the potential benefits of each proposed genetic modification. Such uses of gene editing, which are intended to affect only the individual who receives them, can be “appropriately and rigorously evaluated within existing and evolving regulatory frameworks for gene therapy,” they noted.
• Germline editing poses particularly important issues, such as the challenges with predicting harmful effects of genetic changes, including interactions with other genetic variants and with the environment. Moral and ethical considerations, such as the possibility of permanent genetic enhancements that could exacerbate social inequalities or be used coercively, must also be considered. The committee said that “it would be irresponsible to proceed with any clinical use of germline editing” unless and until the safety and efficacy issues have been resolved, and there is broad consensus about the appropriateness of a proposed application.
“At present these criteria have not been met for any proposed clinical use,” the committee wrote, adding that safety issues have not been adequately explored, and the cases of most compelling benefit are limited.
As the science advances and social views evolve, the clinical use of germline editing should be regularly revisited, they wrote.
The presidents of each of the organizations that hosted the summit welcomed the call for ongoing global discussion on issues related to human gene editing.
In a written response they said that they “stand ready to establish a continuing forum for assessment of the many scientific, medical, and ethical questions surrounding the pursuit of human gene-editing applications,” and will coordinate with other academies around the world and other international scientific and medical institutions in that endeavor.
“This is an important moment in human history and we have a responsibility to provide all sections of society with an informed basis for making decisions about this technology, especially for uses that would affect generations to come,” they wrote.
Human gene editing is no longer the stuff of science fiction, and the powerful new technologies that make it possible raise important scientific, ethical, and societal questions.
The organizing committee for a 3-day International Summit On Gene Editing that convened experts from around the world to discuss the issues associated with human gene-editing research, has called upon the international community to work together to establish norms for acceptable uses of human gene editing.
In a statement issued Dec. 3 at the close of the summit, the committee asked the summit cohosts – the U.S. National Academy of Sciences and U.S. National Academy of Medicine, the Royal Society (United Kingdom), and the Chinese Academy of Sciences – to take the lead in creating an ongoing international forum on gene editing and to work on formulating recommendations and guidelines.
“While each nation ultimately has the authority to regulate activities under its jurisdiction, the human genome is shared among all nations,” the committee wrote. “The international community should strive to establish norms concerning acceptable uses of human germline editing and to harmonize regulations, in order to discourage unacceptable activities while advancing human health and welfare.”
The committee also concluded that:
• Intensive basic and preclinical research is needed, with a specific research focus on technologies for editing genetic sequences in human cells, potential benefits and risks of proposed clinical uses for gene editing, and understanding of the biology of human embryos and germline cells. Any early human embryo or germline cells that undergo gene editing should not be used to establish a pregnancy, the committee wrote.
• Improved understanding of the risks of somatic cell editing – such as inaccurate editing – is needed, as is understanding of the potential benefits of each proposed genetic modification. Such uses of gene editing, which are intended to affect only the individual who receives them, can be “appropriately and rigorously evaluated within existing and evolving regulatory frameworks for gene therapy,” they noted.
• Germline editing poses particularly important issues, such as the challenges with predicting harmful effects of genetic changes, including interactions with other genetic variants and with the environment. Moral and ethical considerations, such as the possibility of permanent genetic enhancements that could exacerbate social inequalities or be used coercively, must also be considered. The committee said that “it would be irresponsible to proceed with any clinical use of germline editing” unless and until the safety and efficacy issues have been resolved, and there is broad consensus about the appropriateness of a proposed application.
“At present these criteria have not been met for any proposed clinical use,” the committee wrote, adding that safety issues have not been adequately explored, and the cases of most compelling benefit are limited.
As the science advances and social views evolve, the clinical use of germline editing should be regularly revisited, they wrote.
The presidents of each of the organizations that hosted the summit welcomed the call for ongoing global discussion on issues related to human gene editing.
In a written response they said that they “stand ready to establish a continuing forum for assessment of the many scientific, medical, and ethical questions surrounding the pursuit of human gene-editing applications,” and will coordinate with other academies around the world and other international scientific and medical institutions in that endeavor.
“This is an important moment in human history and we have a responsibility to provide all sections of society with an informed basis for making decisions about this technology, especially for uses that would affect generations to come,” they wrote.
FROM THE INTERNATIONAL SUMMIT ON HUMAN GENE EDITING

Joint Commission names top-performing hospitals
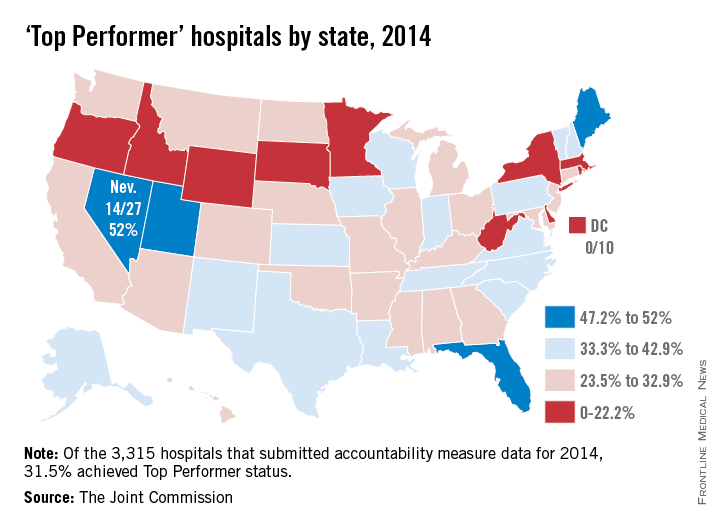
Approximately 31% of U.S. hospitals accredited by the Joint Commission earned “Top Performer” status for 2014, the commission said in its annual report for 2015.
Of the 3,315 hospitals that submitted clinical performance data to the Joint Commission for 2014, 1,043 (31.5%) were recognized as Top Performers. Both numbers were down from 2013, when there were 1,224 (36.9%) top-performing hospitals.

The top-performing state was Nevada, which had 14 of 27 hospitals (52%) recognized by the commission. California and Texas tied for the most recognized hospitals at 95 each, but higher total numbers of hospitals gave those states much lower top-performer rates: 31.3% for California and 37.5% for Texas. Florida, with 47.2% of its hospitals recognized, was the only state with 100 or more hospitals to have a top-performer rate of more than 40%, according to the Joint Commission data.
At the other end of the scale, none of the District of Columbia’s 10 submitting hospitals earned Top Performer status. The state with the lowest rate was Wyoming, where just 1 of 11 hospitals (9.1%) was recognized by the commission. At 18.6%, New York was the only one of the nine states with more than 100 submitting hospitals to have a top-performer rate below 20%, the report noted.
Scores for individual hospitals were derived from 12 sets of accountability measures, which include heart attack care, surgical care, children’s asthma care, and stroke care. Top Performers must “achieve cumulative performance of 95% or above across all reported accountability measures; achieve performance of 95% or above on each and every reported accountability measure with at least 30 denominator cases; and have at least one core measure set with a composite rate of 95% or above and, within that measure set, achieve a performance rate of 95% or above on all applicable individual accountability measures.”
The Top Performer program is going on hiatus for 2016 “due to the evolving national performance measure environment – particularly within the Centers for Medicare & Medicaid Services,” Joint Commission president and chief executive officer Dr. Mark R. Chassin said. “I am confident that hospitals will continue to improve, and that in 2017, we will return with a refreshed program that will better fit the evolving national measure environment.”
Approximately 31% of U.S. hospitals accredited by the Joint Commission earned “Top Performer” status for 2014, the commission said in its annual report for 2015.
Of the 3,315 hospitals that submitted clinical performance data to the Joint Commission for 2014, 1,043 (31.5%) were recognized as Top Performers. Both numbers were down from 2013, when there were 1,224 (36.9%) top-performing hospitals.
The top-performing state was Nevada, which had 14 of 27 hospitals (52%) recognized by the commission. California and Texas tied for the most recognized hospitals at 95 each, but higher total numbers of hospitals gave those states much lower top-performer rates: 31.3% for California and 37.5% for Texas. Florida, with 47.2% of its hospitals recognized, was the only state with 100 or more hospitals to have a top-performer rate of more than 40%, according to the Joint Commission data.
At the other end of the scale, none of the District of Columbia’s 10 submitting hospitals earned Top Performer status. The state with the lowest rate was Wyoming, where just 1 of 11 hospitals (9.1%) was recognized by the commission. At 18.6%, New York was the only one of the nine states with more than 100 submitting hospitals to have a top-performer rate below 20%, the report noted.
Scores for individual hospitals were derived from 12 sets of accountability measures, which include heart attack care, surgical care, children’s asthma care, and stroke care. Top Performers must “achieve cumulative performance of 95% or above across all reported accountability measures; achieve performance of 95% or above on each and every reported accountability measure with at least 30 denominator cases; and have at least one core measure set with a composite rate of 95% or above and, within that measure set, achieve a performance rate of 95% or above on all applicable individual accountability measures.”
The Top Performer program is going on hiatus for 2016 “due to the evolving national performance measure environment – particularly within the Centers for Medicare & Medicaid Services,” Joint Commission president and chief executive officer Dr. Mark R. Chassin said. “I am confident that hospitals will continue to improve, and that in 2017, we will return with a refreshed program that will better fit the evolving national measure environment.”
Approximately 31% of U.S. hospitals accredited by the Joint Commission earned “Top Performer” status for 2014, the commission said in its annual report for 2015.
Of the 3,315 hospitals that submitted clinical performance data to the Joint Commission for 2014, 1,043 (31.5%) were recognized as Top Performers. Both numbers were down from 2013, when there were 1,224 (36.9%) top-performing hospitals.
The top-performing state was Nevada, which had 14 of 27 hospitals (52%) recognized by the commission. California and Texas tied for the most recognized hospitals at 95 each, but higher total numbers of hospitals gave those states much lower top-performer rates: 31.3% for California and 37.5% for Texas. Florida, with 47.2% of its hospitals recognized, was the only state with 100 or more hospitals to have a top-performer rate of more than 40%, according to the Joint Commission data.
At the other end of the scale, none of the District of Columbia’s 10 submitting hospitals earned Top Performer status. The state with the lowest rate was Wyoming, where just 1 of 11 hospitals (9.1%) was recognized by the commission. At 18.6%, New York was the only one of the nine states with more than 100 submitting hospitals to have a top-performer rate below 20%, the report noted.
Scores for individual hospitals were derived from 12 sets of accountability measures, which include heart attack care, surgical care, children’s asthma care, and stroke care. Top Performers must “achieve cumulative performance of 95% or above across all reported accountability measures; achieve performance of 95% or above on each and every reported accountability measure with at least 30 denominator cases; and have at least one core measure set with a composite rate of 95% or above and, within that measure set, achieve a performance rate of 95% or above on all applicable individual accountability measures.”
The Top Performer program is going on hiatus for 2016 “due to the evolving national performance measure environment – particularly within the Centers for Medicare & Medicaid Services,” Joint Commission president and chief executive officer Dr. Mark R. Chassin said. “I am confident that hospitals will continue to improve, and that in 2017, we will return with a refreshed program that will better fit the evolving national measure environment.”
Intrauterine palpator plus 3-D ultrasound boost metroplasty success
LAS VEGAS – The combination of three-dimensional ultrasound and a graduated intrauterine palpator significantly increased the rate of complete metroplasties in a group of women with unexplained infertility or repeat miscarriage.
The instrument, which is marked in millimeters, allows the surgeon to more accurately gauge how much of a uterine septum is removed during the procedure, as well as approximate the shape of what is left. Combined with transvaginal ultrasound visualization, the technique makes a complete, but not overly aggressive, resection more likely, Dr. Attilio Di Spiezio Sardo said at the meeting sponsored by the AAGL.

“One of man’s dilemmas in everyday life is knowing when to stop,” said Dr. Sardo of the University of Naples “Federico II,” Italy. “The same applies to hysteroscopic metroplasties. We still don’t know where to end the incision in order to avoid complications, significant bleeding, or perforation, and in order to avoid abnormal anatomical results.”
The new data he presented builds on his 2009 work, which used 3-D transvaginal ultrasound as the basis for a new subclassification system for uterine anomalies to be used during in-office hysteroscopy.
The aim of the current study was to assess whether the addition of a 5 French graduated intrauterine palpator could improve the accuracy of hysteroscopic metroplasty, compared with that obtained without the instrument. Anatomic results were assessed by 3-D transvaginal ultrasound and second-look hysteroscopy and classified as complete (residual septum less than 5 mm), suboptimal (residual septum 5 mm-10 mm), or incomplete (residual septum greater than 10 mm).
All procedures were performed with the same initial technique under conscious sedation with a 5 mm hysteroscope and miniaturized 5 French instruments. First, the surgeon used a bipolar electrode to remove three-quarters of the septum. Blunt scissors were then used to refine the septal base.
In the intervention group, however, the intrauterine palpator was used to measure the portion of the remaining septum. The metroplasty was stopped when the intrauterine palpator showed that the resected septum corresponded to the presurgical ultrasonographic measures, and had a fundal notch of 1 cm. In the control group, the procedure was stopped when the tubal ostia were clearly visible on the same line and/or hemorrhage from small myometrial vessels of the fundus occurred.
The mean procedural time was similar in the palpator and control groups (12.6 minutes vs. 11.7 minutes). There was one postsurgical intrauterine adhesion in each group.
There were significantly more complete resections in the palpator group than the control group (71% vs. 41%), although the number of suboptimal resections was similar (28% vs. 20%). There were 12 incomplete resections, all of which were in the control group. There was no correlation between septal length and the completeness of resection, Dr. Sardo added.
The combination of 3-D transvaginal ultrasound and a graduated palpator to physically explore the intrauterine space should help improve outcomes in what can be a frustrating procedure, he said.
“I used to think my metroplasties were perfect, and then I reviewed the videos and ultrasounds and sometimes saw that part of the septum was still there,” Dr. Sardo said. “After endometrial ablation, I think hysteroscopic metroplasty is one of the most frustrating problems” for a gynecologic surgeon.
Dr. Sardo reported having no financial disclosures.
LAS VEGAS – The combination of three-dimensional ultrasound and a graduated intrauterine palpator significantly increased the rate of complete metroplasties in a group of women with unexplained infertility or repeat miscarriage.
The instrument, which is marked in millimeters, allows the surgeon to more accurately gauge how much of a uterine septum is removed during the procedure, as well as approximate the shape of what is left. Combined with transvaginal ultrasound visualization, the technique makes a complete, but not overly aggressive, resection more likely, Dr. Attilio Di Spiezio Sardo said at the meeting sponsored by the AAGL.
“One of man’s dilemmas in everyday life is knowing when to stop,” said Dr. Sardo of the University of Naples “Federico II,” Italy. “The same applies to hysteroscopic metroplasties. We still don’t know where to end the incision in order to avoid complications, significant bleeding, or perforation, and in order to avoid abnormal anatomical results.”
The new data he presented builds on his 2009 work, which used 3-D transvaginal ultrasound as the basis for a new subclassification system for uterine anomalies to be used during in-office hysteroscopy.
The aim of the current study was to assess whether the addition of a 5 French graduated intrauterine palpator could improve the accuracy of hysteroscopic metroplasty, compared with that obtained without the instrument. Anatomic results were assessed by 3-D transvaginal ultrasound and second-look hysteroscopy and classified as complete (residual septum less than 5 mm), suboptimal (residual septum 5 mm-10 mm), or incomplete (residual septum greater than 10 mm).
All procedures were performed with the same initial technique under conscious sedation with a 5 mm hysteroscope and miniaturized 5 French instruments. First, the surgeon used a bipolar electrode to remove three-quarters of the septum. Blunt scissors were then used to refine the septal base.
In the intervention group, however, the intrauterine palpator was used to measure the portion of the remaining septum. The metroplasty was stopped when the intrauterine palpator showed that the resected septum corresponded to the presurgical ultrasonographic measures, and had a fundal notch of 1 cm. In the control group, the procedure was stopped when the tubal ostia were clearly visible on the same line and/or hemorrhage from small myometrial vessels of the fundus occurred.
The mean procedural time was similar in the palpator and control groups (12.6 minutes vs. 11.7 minutes). There was one postsurgical intrauterine adhesion in each group.
There were significantly more complete resections in the palpator group than the control group (71% vs. 41%), although the number of suboptimal resections was similar (28% vs. 20%). There were 12 incomplete resections, all of which were in the control group. There was no correlation between septal length and the completeness of resection, Dr. Sardo added.
The combination of 3-D transvaginal ultrasound and a graduated palpator to physically explore the intrauterine space should help improve outcomes in what can be a frustrating procedure, he said.
“I used to think my metroplasties were perfect, and then I reviewed the videos and ultrasounds and sometimes saw that part of the septum was still there,” Dr. Sardo said. “After endometrial ablation, I think hysteroscopic metroplasty is one of the most frustrating problems” for a gynecologic surgeon.
Dr. Sardo reported having no financial disclosures.
LAS VEGAS – The combination of three-dimensional ultrasound and a graduated intrauterine palpator significantly increased the rate of complete metroplasties in a group of women with unexplained infertility or repeat miscarriage.
The instrument, which is marked in millimeters, allows the surgeon to more accurately gauge how much of a uterine septum is removed during the procedure, as well as approximate the shape of what is left. Combined with transvaginal ultrasound visualization, the technique makes a complete, but not overly aggressive, resection more likely, Dr. Attilio Di Spiezio Sardo said at the meeting sponsored by the AAGL.
“One of man’s dilemmas in everyday life is knowing when to stop,” said Dr. Sardo of the University of Naples “Federico II,” Italy. “The same applies to hysteroscopic metroplasties. We still don’t know where to end the incision in order to avoid complications, significant bleeding, or perforation, and in order to avoid abnormal anatomical results.”
The new data he presented builds on his 2009 work, which used 3-D transvaginal ultrasound as the basis for a new subclassification system for uterine anomalies to be used during in-office hysteroscopy.
The aim of the current study was to assess whether the addition of a 5 French graduated intrauterine palpator could improve the accuracy of hysteroscopic metroplasty, compared with that obtained without the instrument. Anatomic results were assessed by 3-D transvaginal ultrasound and second-look hysteroscopy and classified as complete (residual septum less than 5 mm), suboptimal (residual septum 5 mm-10 mm), or incomplete (residual septum greater than 10 mm).
All procedures were performed with the same initial technique under conscious sedation with a 5 mm hysteroscope and miniaturized 5 French instruments. First, the surgeon used a bipolar electrode to remove three-quarters of the septum. Blunt scissors were then used to refine the septal base.
In the intervention group, however, the intrauterine palpator was used to measure the portion of the remaining septum. The metroplasty was stopped when the intrauterine palpator showed that the resected septum corresponded to the presurgical ultrasonographic measures, and had a fundal notch of 1 cm. In the control group, the procedure was stopped when the tubal ostia were clearly visible on the same line and/or hemorrhage from small myometrial vessels of the fundus occurred.
The mean procedural time was similar in the palpator and control groups (12.6 minutes vs. 11.7 minutes). There was one postsurgical intrauterine adhesion in each group.
There were significantly more complete resections in the palpator group than the control group (71% vs. 41%), although the number of suboptimal resections was similar (28% vs. 20%). There were 12 incomplete resections, all of which were in the control group. There was no correlation between septal length and the completeness of resection, Dr. Sardo added.
The combination of 3-D transvaginal ultrasound and a graduated palpator to physically explore the intrauterine space should help improve outcomes in what can be a frustrating procedure, he said.
“I used to think my metroplasties were perfect, and then I reviewed the videos and ultrasounds and sometimes saw that part of the septum was still there,” Dr. Sardo said. “After endometrial ablation, I think hysteroscopic metroplasty is one of the most frustrating problems” for a gynecologic surgeon.
Dr. Sardo reported having no financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Key clinical point: Using a novel, graduated palpator along with transvaginal ultrasound increased the likelihood of a successful metroplasty.
Major finding: A successful procedure occurred in 71% of the intervention group and 41% of the control group.
Data source: A randomized study of 90 women.
Disclosures: Dr. Sardo reported having no financial disclosures.

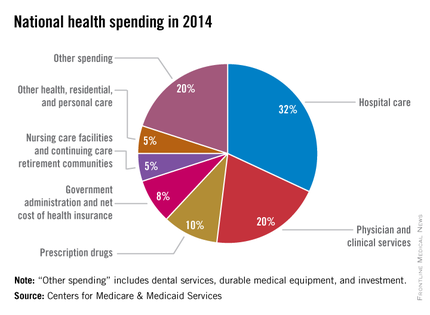
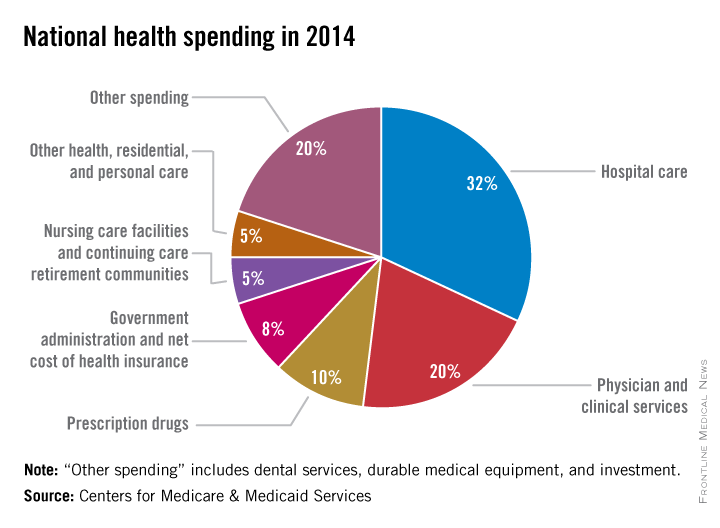
Health spending growth soars after years of low growth
Five years of low growth in national health spending expenditures reversed substantially in 2014, driven by new Affordable Care Act coverage mandates and higher prescription drug spending, largely for new hepatitis C treatments.
U.S. health spending climbed to $3 trillion and grew by 5.3%, as compared with 2013 when growth was 2.9%. Per capita spending in 2014 was up 4.5% to $9,523 from $9,115 in 2013, according to Centers for Medicare & Medicaid Services Office of the Actuary (Health Affairs. 2015 Dec 2 doi: 10.1377/hlthaff.2015.1194).
Anne B. Martin, an economist with actuary’s office, said the 2014 numbers reversed several years of historically low spending growth that tracked with the sluggish economy. She attributed the uptick in growth to the ACA’s access mandates as well as prescription drug purchases, namely those for HCV, which added $11.3 billion in new spending.
“We can’t necessarily say that the [low-growth] cycle has been broken, but this 2014 phenomenon is driven primarily by the ACA expansion and the one-time impact of bringing the new hepatitis C drug into the 2014 mix,” Ms. Martin said.
Between 2013 and 2014, 8.7 million additional patients were enrolled in public and private health insurance, bringing the total insured share of the population from 86% to 88.8%, the highest coverage rate since 1987, according to Ms. Martin and her colleagues.
The growth rate for private health insurance spending went from 1.6% in 2013 to 4.4% in 2014. The $991 billion spent reflected the addition of 2.2 million newly insured patients, and higher rates of spending on medications, clinical services, and inpatient care, compared with 2013.
Federal government spending grew the fastest in 2014 at 11.7%, an 8.2% faster growth rate than in 2013.
In 2014, 28% of all health care purchases were made by the federal government, up from 26% in 2013.
Medicaid-specific spending totaled $495.8 billion, an 11% growth rate in 2014, up from 5.9% in 2013, reflecting the addition of 7.7 million Medicaid enrollees, various increases in prescription drug rebates, and updated provider fees.
Medicare spending jumped to 5.5%, up from 3.0% in 2013, largely due to prescription drugs, although Micah Hartman, a statistician in the Office of the Actuary, said that the per-enrollee spending rate was 2.4% in 2014, up from –0.2% in 2013, which was due to physician and clinical services, higher administrative costs, as well as the net cost of insurance, including fees and administrative costs.
Mr. Hartman singled out Medicare Advantage as a key contributor, noting that the 9.7% increase in growth for that program was from ACA-stipulated fees.
Overall, pharmaceutical spending was $297.7 billion in 2014, according to the report, attributable to novel HCV drugs, other new treatments, fewer-than-normal patent expirations and, in some cases, a doubling of the costs for certain brand-name drugs. The overall 2014 pharmaceutical expenditure growth rate was 12.2%, compared with 2.4% in 2013, the largest differential since 2002.
Physician and clinical services in 2014 went from a growth rate of 2.5% to 4.6%, with total spending at $603.7 billion. Hospital spending last year was $971.8 billion, with a spending growth rate of 4.1%, compared with 3.5% in 2013.
On Twitter @whitneymcknight
Five years of low growth in national health spending expenditures reversed substantially in 2014, driven by new Affordable Care Act coverage mandates and higher prescription drug spending, largely for new hepatitis C treatments.
U.S. health spending climbed to $3 trillion and grew by 5.3%, as compared with 2013 when growth was 2.9%. Per capita spending in 2014 was up 4.5% to $9,523 from $9,115 in 2013, according to Centers for Medicare & Medicaid Services Office of the Actuary (Health Affairs. 2015 Dec 2 doi: 10.1377/hlthaff.2015.1194).
Anne B. Martin, an economist with actuary’s office, said the 2014 numbers reversed several years of historically low spending growth that tracked with the sluggish economy. She attributed the uptick in growth to the ACA’s access mandates as well as prescription drug purchases, namely those for HCV, which added $11.3 billion in new spending.
“We can’t necessarily say that the [low-growth] cycle has been broken, but this 2014 phenomenon is driven primarily by the ACA expansion and the one-time impact of bringing the new hepatitis C drug into the 2014 mix,” Ms. Martin said.
Between 2013 and 2014, 8.7 million additional patients were enrolled in public and private health insurance, bringing the total insured share of the population from 86% to 88.8%, the highest coverage rate since 1987, according to Ms. Martin and her colleagues.
The growth rate for private health insurance spending went from 1.6% in 2013 to 4.4% in 2014. The $991 billion spent reflected the addition of 2.2 million newly insured patients, and higher rates of spending on medications, clinical services, and inpatient care, compared with 2013.
Federal government spending grew the fastest in 2014 at 11.7%, an 8.2% faster growth rate than in 2013.
In 2014, 28% of all health care purchases were made by the federal government, up from 26% in 2013.
Medicaid-specific spending totaled $495.8 billion, an 11% growth rate in 2014, up from 5.9% in 2013, reflecting the addition of 7.7 million Medicaid enrollees, various increases in prescription drug rebates, and updated provider fees.
Medicare spending jumped to 5.5%, up from 3.0% in 2013, largely due to prescription drugs, although Micah Hartman, a statistician in the Office of the Actuary, said that the per-enrollee spending rate was 2.4% in 2014, up from –0.2% in 2013, which was due to physician and clinical services, higher administrative costs, as well as the net cost of insurance, including fees and administrative costs.
Mr. Hartman singled out Medicare Advantage as a key contributor, noting that the 9.7% increase in growth for that program was from ACA-stipulated fees.
Overall, pharmaceutical spending was $297.7 billion in 2014, according to the report, attributable to novel HCV drugs, other new treatments, fewer-than-normal patent expirations and, in some cases, a doubling of the costs for certain brand-name drugs. The overall 2014 pharmaceutical expenditure growth rate was 12.2%, compared with 2.4% in 2013, the largest differential since 2002.
Physician and clinical services in 2014 went from a growth rate of 2.5% to 4.6%, with total spending at $603.7 billion. Hospital spending last year was $971.8 billion, with a spending growth rate of 4.1%, compared with 3.5% in 2013.
On Twitter @whitneymcknight
Five years of low growth in national health spending expenditures reversed substantially in 2014, driven by new Affordable Care Act coverage mandates and higher prescription drug spending, largely for new hepatitis C treatments.
U.S. health spending climbed to $3 trillion and grew by 5.3%, as compared with 2013 when growth was 2.9%. Per capita spending in 2014 was up 4.5% to $9,523 from $9,115 in 2013, according to Centers for Medicare & Medicaid Services Office of the Actuary (Health Affairs. 2015 Dec 2 doi: 10.1377/hlthaff.2015.1194).
Anne B. Martin, an economist with actuary’s office, said the 2014 numbers reversed several years of historically low spending growth that tracked with the sluggish economy. She attributed the uptick in growth to the ACA’s access mandates as well as prescription drug purchases, namely those for HCV, which added $11.3 billion in new spending.
“We can’t necessarily say that the [low-growth] cycle has been broken, but this 2014 phenomenon is driven primarily by the ACA expansion and the one-time impact of bringing the new hepatitis C drug into the 2014 mix,” Ms. Martin said.
Between 2013 and 2014, 8.7 million additional patients were enrolled in public and private health insurance, bringing the total insured share of the population from 86% to 88.8%, the highest coverage rate since 1987, according to Ms. Martin and her colleagues.
The growth rate for private health insurance spending went from 1.6% in 2013 to 4.4% in 2014. The $991 billion spent reflected the addition of 2.2 million newly insured patients, and higher rates of spending on medications, clinical services, and inpatient care, compared with 2013.
Federal government spending grew the fastest in 2014 at 11.7%, an 8.2% faster growth rate than in 2013.
In 2014, 28% of all health care purchases were made by the federal government, up from 26% in 2013.
Medicaid-specific spending totaled $495.8 billion, an 11% growth rate in 2014, up from 5.9% in 2013, reflecting the addition of 7.7 million Medicaid enrollees, various increases in prescription drug rebates, and updated provider fees.
Medicare spending jumped to 5.5%, up from 3.0% in 2013, largely due to prescription drugs, although Micah Hartman, a statistician in the Office of the Actuary, said that the per-enrollee spending rate was 2.4% in 2014, up from –0.2% in 2013, which was due to physician and clinical services, higher administrative costs, as well as the net cost of insurance, including fees and administrative costs.
Mr. Hartman singled out Medicare Advantage as a key contributor, noting that the 9.7% increase in growth for that program was from ACA-stipulated fees.
Overall, pharmaceutical spending was $297.7 billion in 2014, according to the report, attributable to novel HCV drugs, other new treatments, fewer-than-normal patent expirations and, in some cases, a doubling of the costs for certain brand-name drugs. The overall 2014 pharmaceutical expenditure growth rate was 12.2%, compared with 2.4% in 2013, the largest differential since 2002.
Physician and clinical services in 2014 went from a growth rate of 2.5% to 4.6%, with total spending at $603.7 billion. Hospital spending last year was $971.8 billion, with a spending growth rate of 4.1%, compared with 3.5% in 2013.
On Twitter @whitneymcknight
FROM THE JOURNAL HEALTH AFFAIRS
Readmission after esophagectomy raises mortality
About one in five patients who have surgery to remove part or all of the esophagus return to the hospital for complications within 30 days, and when they do their chance of death increases fivefold, compared with those who don’t return to the hospital, investigators at the University of Virginia Health System reported in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1254-60).
“Early recognition of life-threatening readmission diagnoses is essential in order to provide optimal care,” said lead author Dr. Yinin Hu and colleagues. Esophageal cancer is the fastest-growing cancer in the United States, so the study investigators set out to closely examine the reasons for readmissions and death after surgery.
The study identified 1,688 patients in the Surveillance, Epidemiology, and End Results (SEER)-Medicare database aged 66 or older who had surgery for esophageal cancer from 2000 to 2009. The overall 30-day mortality was 6.9%, and the 90-day mortality was 13.9%.
After excluding in-hospital deaths, the investigators’ readmission analysis included 1,543 patients. In this group, overall 90-day mortality following discharge was 6.4%, and the readmission rate within 30 days of discharge was 20.7%
The 90-day mortality for patients who were readmitted was more than four times that for those who were not readmitted, 16.3% vs. 3.8%; their in-hospital mortality was 8.8%. About one-third of readmissions were to facilities different from where patients had the index esophagectomy, and those patients were about seven times more likely to be transferred after readmission than patients admitted to the same facility, 15% vs. 1.9%. Risk-adjusted mortality did not vary significantly across providers.
The most frequent reasons for readmission were pneumonia (11.8%), malnutrition/dehydration (8.1%), pleural effusion (97.5%), and aspiration pneumonitis (6.8%). “Notably, more than one in five patients readmitted with a pulmonary diagnosis subsequently died within 90 days of the operation,” Dr. Hu and coauthors said, indicating that readmissions for pulmonary complications carried the worst prognosis.
This is the first study to demonstrate the gravity of pulmonary readmissions within 30 days of discharge, Dr. Hu and coauthors said. “Patients with nonspecific dyspneic symptoms or small pleural effusions should receive aggressive care upon readmission, as more than 20% will not survive the next few months,” Dr. Hu and coauthors said. “These results reinforce the notion that a fairly benign readmitting diagnosis is often an indicator of a much more severe root process.”
Among nonpulmonary reasons for readmission, dehydration and malnutrition carried the highest risk for death. “While there are many interventions that can promote postoperative nutrition, a readmission due to poor dietary tolerance often indicates other complications such as infection, stenosis, or anastomotic leak,” Dr. Hu and coauthors said. They suggested a thorough root-cause analysis should be part of every readmission.
The study also analyzed the hospital length of stay (LOS) as a predictor for readmission. The median LOS was 13 days, but the most common LOS was 9 days. “In general, the probability of readmission increases with increasing postoperative LOS,” Dr. Hu and colleagues said.
The authors reported no disclosures. Dr. Yinin Hu received funding from the National Institutes of Health and coauthor Dr. Benjamin Kozower received funding from the Agency for Healthcare Research and Quality.
The findings of this study may indicate that patients who stay in the hospital longer have underlying issues that did not surface during their admission for the operation, Dr. Anthony W. Kim of Yale University, New Haven, Conn., said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1030-1). “Therefore, rather than employing a prevention of a failure-to-rescue strategy during a readmission, it may be worthwhile to enact a prevention-of-readmission strategy triggered by a longer than typical [length of stay],” Dr. Kim said. He suggested the root-cause analysis should begin in the hospital on the day after the patient exceeds the median length of stay.

|
Dr. Anthony W. Kim |
But citing the law of unintended consequences, Dr. Kim warns against using readmission as a quality metric as well a instrument to dictate reimbursement. “The law of unintended consequences dictates that when a readmission is taken out of context, using this measure raises the potential conflict of interest between doing what is right for the patient and achieving a specific milestone that may not be in the best interest of an individual patient,” he said. “Discharging a patient early perhaps to the exclusion of adequately addressing inpatient issues for the purposes of achieving a target [length of stay] is perhaps the prime example of these conflicting interests.”
Because of the difficult recovery course after esophagectomy, some readmissions are “necessary, beneficial and, unequivocally, the right decision,” Dr. Kim said. “Ironically, one of the unintended consequences of this article may be that it exposes the fact that until a better system of recording and scrutinizing readmissions exists, governing organizations should exercise considerable caution when assessing a surgeon, hospital, or system and their readmissions,” he said.
To paraphrase the sociologist Robert K. Merton, who devised the law of unintended consequences, the existing state of knowledge limits one’s ability to anticipate the consequences of action. The authors of this study “have added immensely to a body of knowledge that is still growing and deserves ongoing study if policy is to be based upon it,” Dr. Kim said.
Dr. Kim had no disclosures.
The findings of this study may indicate that patients who stay in the hospital longer have underlying issues that did not surface during their admission for the operation, Dr. Anthony W. Kim of Yale University, New Haven, Conn., said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1030-1). “Therefore, rather than employing a prevention of a failure-to-rescue strategy during a readmission, it may be worthwhile to enact a prevention-of-readmission strategy triggered by a longer than typical [length of stay],” Dr. Kim said. He suggested the root-cause analysis should begin in the hospital on the day after the patient exceeds the median length of stay.
|
|
Dr. Anthony W. Kim |
But citing the law of unintended consequences, Dr. Kim warns against using readmission as a quality metric as well a instrument to dictate reimbursement. “The law of unintended consequences dictates that when a readmission is taken out of context, using this measure raises the potential conflict of interest between doing what is right for the patient and achieving a specific milestone that may not be in the best interest of an individual patient,” he said. “Discharging a patient early perhaps to the exclusion of adequately addressing inpatient issues for the purposes of achieving a target [length of stay] is perhaps the prime example of these conflicting interests.”
Because of the difficult recovery course after esophagectomy, some readmissions are “necessary, beneficial and, unequivocally, the right decision,” Dr. Kim said. “Ironically, one of the unintended consequences of this article may be that it exposes the fact that until a better system of recording and scrutinizing readmissions exists, governing organizations should exercise considerable caution when assessing a surgeon, hospital, or system and their readmissions,” he said.
To paraphrase the sociologist Robert K. Merton, who devised the law of unintended consequences, the existing state of knowledge limits one’s ability to anticipate the consequences of action. The authors of this study “have added immensely to a body of knowledge that is still growing and deserves ongoing study if policy is to be based upon it,” Dr. Kim said.
Dr. Kim had no disclosures.
The findings of this study may indicate that patients who stay in the hospital longer have underlying issues that did not surface during their admission for the operation, Dr. Anthony W. Kim of Yale University, New Haven, Conn., said in his invited commentary (J Thorac Cardiovasc Surg. 2015;150:1030-1). “Therefore, rather than employing a prevention of a failure-to-rescue strategy during a readmission, it may be worthwhile to enact a prevention-of-readmission strategy triggered by a longer than typical [length of stay],” Dr. Kim said. He suggested the root-cause analysis should begin in the hospital on the day after the patient exceeds the median length of stay.
|
|
Dr. Anthony W. Kim |
But citing the law of unintended consequences, Dr. Kim warns against using readmission as a quality metric as well a instrument to dictate reimbursement. “The law of unintended consequences dictates that when a readmission is taken out of context, using this measure raises the potential conflict of interest between doing what is right for the patient and achieving a specific milestone that may not be in the best interest of an individual patient,” he said. “Discharging a patient early perhaps to the exclusion of adequately addressing inpatient issues for the purposes of achieving a target [length of stay] is perhaps the prime example of these conflicting interests.”
Because of the difficult recovery course after esophagectomy, some readmissions are “necessary, beneficial and, unequivocally, the right decision,” Dr. Kim said. “Ironically, one of the unintended consequences of this article may be that it exposes the fact that until a better system of recording and scrutinizing readmissions exists, governing organizations should exercise considerable caution when assessing a surgeon, hospital, or system and their readmissions,” he said.
To paraphrase the sociologist Robert K. Merton, who devised the law of unintended consequences, the existing state of knowledge limits one’s ability to anticipate the consequences of action. The authors of this study “have added immensely to a body of knowledge that is still growing and deserves ongoing study if policy is to be based upon it,” Dr. Kim said.
Dr. Kim had no disclosures.
About one in five patients who have surgery to remove part or all of the esophagus return to the hospital for complications within 30 days, and when they do their chance of death increases fivefold, compared with those who don’t return to the hospital, investigators at the University of Virginia Health System reported in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1254-60).
“Early recognition of life-threatening readmission diagnoses is essential in order to provide optimal care,” said lead author Dr. Yinin Hu and colleagues. Esophageal cancer is the fastest-growing cancer in the United States, so the study investigators set out to closely examine the reasons for readmissions and death after surgery.
The study identified 1,688 patients in the Surveillance, Epidemiology, and End Results (SEER)-Medicare database aged 66 or older who had surgery for esophageal cancer from 2000 to 2009. The overall 30-day mortality was 6.9%, and the 90-day mortality was 13.9%.
After excluding in-hospital deaths, the investigators’ readmission analysis included 1,543 patients. In this group, overall 90-day mortality following discharge was 6.4%, and the readmission rate within 30 days of discharge was 20.7%
The 90-day mortality for patients who were readmitted was more than four times that for those who were not readmitted, 16.3% vs. 3.8%; their in-hospital mortality was 8.8%. About one-third of readmissions were to facilities different from where patients had the index esophagectomy, and those patients were about seven times more likely to be transferred after readmission than patients admitted to the same facility, 15% vs. 1.9%. Risk-adjusted mortality did not vary significantly across providers.
The most frequent reasons for readmission were pneumonia (11.8%), malnutrition/dehydration (8.1%), pleural effusion (97.5%), and aspiration pneumonitis (6.8%). “Notably, more than one in five patients readmitted with a pulmonary diagnosis subsequently died within 90 days of the operation,” Dr. Hu and coauthors said, indicating that readmissions for pulmonary complications carried the worst prognosis.
This is the first study to demonstrate the gravity of pulmonary readmissions within 30 days of discharge, Dr. Hu and coauthors said. “Patients with nonspecific dyspneic symptoms or small pleural effusions should receive aggressive care upon readmission, as more than 20% will not survive the next few months,” Dr. Hu and coauthors said. “These results reinforce the notion that a fairly benign readmitting diagnosis is often an indicator of a much more severe root process.”
Among nonpulmonary reasons for readmission, dehydration and malnutrition carried the highest risk for death. “While there are many interventions that can promote postoperative nutrition, a readmission due to poor dietary tolerance often indicates other complications such as infection, stenosis, or anastomotic leak,” Dr. Hu and coauthors said. They suggested a thorough root-cause analysis should be part of every readmission.
The study also analyzed the hospital length of stay (LOS) as a predictor for readmission. The median LOS was 13 days, but the most common LOS was 9 days. “In general, the probability of readmission increases with increasing postoperative LOS,” Dr. Hu and colleagues said.
The authors reported no disclosures. Dr. Yinin Hu received funding from the National Institutes of Health and coauthor Dr. Benjamin Kozower received funding from the Agency for Healthcare Research and Quality.
About one in five patients who have surgery to remove part or all of the esophagus return to the hospital for complications within 30 days, and when they do their chance of death increases fivefold, compared with those who don’t return to the hospital, investigators at the University of Virginia Health System reported in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1254-60).
“Early recognition of life-threatening readmission diagnoses is essential in order to provide optimal care,” said lead author Dr. Yinin Hu and colleagues. Esophageal cancer is the fastest-growing cancer in the United States, so the study investigators set out to closely examine the reasons for readmissions and death after surgery.
The study identified 1,688 patients in the Surveillance, Epidemiology, and End Results (SEER)-Medicare database aged 66 or older who had surgery for esophageal cancer from 2000 to 2009. The overall 30-day mortality was 6.9%, and the 90-day mortality was 13.9%.
After excluding in-hospital deaths, the investigators’ readmission analysis included 1,543 patients. In this group, overall 90-day mortality following discharge was 6.4%, and the readmission rate within 30 days of discharge was 20.7%
The 90-day mortality for patients who were readmitted was more than four times that for those who were not readmitted, 16.3% vs. 3.8%; their in-hospital mortality was 8.8%. About one-third of readmissions were to facilities different from where patients had the index esophagectomy, and those patients were about seven times more likely to be transferred after readmission than patients admitted to the same facility, 15% vs. 1.9%. Risk-adjusted mortality did not vary significantly across providers.
The most frequent reasons for readmission were pneumonia (11.8%), malnutrition/dehydration (8.1%), pleural effusion (97.5%), and aspiration pneumonitis (6.8%). “Notably, more than one in five patients readmitted with a pulmonary diagnosis subsequently died within 90 days of the operation,” Dr. Hu and coauthors said, indicating that readmissions for pulmonary complications carried the worst prognosis.
This is the first study to demonstrate the gravity of pulmonary readmissions within 30 days of discharge, Dr. Hu and coauthors said. “Patients with nonspecific dyspneic symptoms or small pleural effusions should receive aggressive care upon readmission, as more than 20% will not survive the next few months,” Dr. Hu and coauthors said. “These results reinforce the notion that a fairly benign readmitting diagnosis is often an indicator of a much more severe root process.”
Among nonpulmonary reasons for readmission, dehydration and malnutrition carried the highest risk for death. “While there are many interventions that can promote postoperative nutrition, a readmission due to poor dietary tolerance often indicates other complications such as infection, stenosis, or anastomotic leak,” Dr. Hu and coauthors said. They suggested a thorough root-cause analysis should be part of every readmission.
The study also analyzed the hospital length of stay (LOS) as a predictor for readmission. The median LOS was 13 days, but the most common LOS was 9 days. “In general, the probability of readmission increases with increasing postoperative LOS,” Dr. Hu and colleagues said.
The authors reported no disclosures. Dr. Yinin Hu received funding from the National Institutes of Health and coauthor Dr. Benjamin Kozower received funding from the Agency for Healthcare Research and Quality.
Key clinical point: Patients readmitted after esophagectomy are at a greater than fourfold higher risk of death than patients who do not need readmission.
Major finding: The 90-day mortality for patients who were readmitted was greater than four times that for those who were not readmitted, 16.3% vs. 3.8%.
Data source: Analysis of 1,688 patients in the SEER-Medicare database aged 66 or older who had surgery for esophageal cancer from 2000 to 2009.
Disclosures: The authors had no disclosures. Lead author Dr. Yinin Hu received funding from the National Institutes of Health and coauthor Dr. Benjamin Kozower received funding from the Agency for Healthcare Research and Quality.

Does position matter in ViV implantation?
With transcatheter valve-in-valve implantation emerging as a novel treatment for high-risk patients whose existing bioprostheses have deteriorated, a team of investigators at University Heart Center in Hamburg, Germany, has found that the procedure can be done successfully in four different anatomic positions with a variety of bioprostheses.
The findings from the single-center study were published in the December issue of the Journal of Thoracic and Cardiovascular Surgery. (J Thorac Cardiovasc Surg. 2015;150:1557-67). They retrospectively analyzed results of 75 patients who had transcatheter valve-in-valve (ViV) replacement at their institution from 2008 to 2014.
“ViV can be performed in all anatomic positions with acceptable hemodynamic and clinical outcome in high-risk patients,” wrote Dr. Lenard Conradi and coauthors. “Increasing importance of ViV can be anticipated considering growing use of surgical bioprostheses.”
Replacement of biological valves is becoming more common. For surgical aortic valve replacement (SAVR), biological procedures have largely replaced mechanical valve implantation, comprising 87% of all such procedures by 2014, according to data from the German Society for Thoracic and Cardiovascular Surgery (Thorac Cardiovasc Surg. 2014;62:380-92). “Therefore, increasing caseload of patients with deteriorated bioprostheses can be expected,” wrote Dr. Conradi and coauthors.
The four anatomic positions in which the investigators performed the procedures and their share of cases are: aortic (54 patients/72%), mitral (17/22.7%), and tricuspid and pulmonary positions (2/2.7% each). The average interval between the index procedure and ViV was 9 years, with a deviation of nearly 5 years among all procedures. Dr. Conradi and coinvestigators said their study focused on technical aspects of ViV procedures from each position to provide guidance for surgeons.
Overall, the study authors performed ViV successfully in 97.3% of patients, with two patients requiring sequential transcatheter heart valve implantation for initial malpositioning. Thirty-day mortality was 8%, which “ranged lower” than expected when compared to standard preoperative risk stratification, they wrote. Mortality was at 5.6% in the aortic group and 17.6% in the mitral group.
That none of the currently available surgical bioprostheses or transcatheter heart valves (THV) were designed for later ViV procedures in deteriorated bioprostheses – although the CoreValve and Sapein THV have approvals for the indication – “may explain some of the apparent shortcomings of ViV therapy,” the researchers wrote.
The most significant challenge of ViV therapy is dealing with elevated residual gradients, which positioning can influence, according to the study findings. “This is not so much an issue for mitral, tricuspid, or pulmonary positions since surgical bioprostheses implanted in these positions are usually of sufficient size to accommodate the THV,” the researchers noted. “However, in the aortic position, more severe spatial restrictions may apply.”
They cited other reports that described a reverse relationship between size of the bioprosthetic and resulting transvalvular gradient after ViV (JACC Cardiovasc Interv. 2011;4:1218-27; JAMA 2014;312:162-70).
To reduce gradients, the investigators used post-ballooning after aortic ViV with a self-expandable THV in 16 cases, succeeding in 12. “Likely, further THV expansion with active compression of soft leaflet and/or pannus tissue and tighter apposition of THV against the frames of surgical bioprostheses contributed to this desired effect,” wrote the researchers. Patient-prosthesis mismatch probably explained the four cases in which gradients could not be further reduced, they noted.
They issued one “word of caution” regarding aortic ViV in small-sized surgical bioprostheses: “Elevated postprocedural gradients have to be expected and must be weighed against expected benefits and against risk of repeat open heart surgery.”
The six transcatheter heart valves the investigators used were Edwards Sapien (XT)/Sapien3 (52%, 39/75); Medtronic CoreValve/CoreValveEvolut (34.7%, 26); St. Jude Portico and Boston Scientific Lotus (4%, three each); and JenaValve and Medtronic Engager (2.7%, two each). The study also looked at different access routes: transapical in 53.3% (40), transfemoral (transarterial or transvenous) in 42.7% (32), transaortic in 2.7% (2), and transjugular in 1.3% (1).
Dr. Conradi and coauthors Dr. Moritz Seiffert, Dr. Ulrich Schaefer, and Dr. Hendrik Treede disclosed ties with Edwards Lifesciences, JenaValve Technology, Medtronic, Symetis, and St. Jude Medical. Four other coauthors reported no disclosures.
As the population ages and younger patients choose bioprosthetic valves to avoid lifelong warfarin, surgeons are going to face more situations where they will have to decide whether to perform surgical or transcatheter reoperative valve surgery, Dr. Jessica Forcillo of Emory University, Atlanta, and coauthors wrote in an invited commentary (J Thorac Cardiovasc Surg. 2015;150:1568-9).
They called the 8% 30-day mortality rate in the Hamburg study “high” even though the average age of the study population was a “relatively young” 74 years. The Hamburg authors may have learned more had they evaluated fewer prostheses. “With a small number of patients and at the beginning of an experience, focusing on one or two available prostheses may have resulted in more accurate and reliable results,” noted Dr. Forcillo and her colleagues. That 53% of the procedures were done via the transapical approach may also explain the mortality rate, they said.
The overall 30-day mortality rate along with a 17.6% mortality in the mitral ViV group are causes for “some caution against overzealous performance of this procedure and continued monitoring of outcomes in other series,” wrote Dr. Forcillo and her colleagues.
But ViV implantation is a “transformative” technology, they said. “For the elderly, high-risk patients with [structural valve degeneration], transcatheter options may provide improved short-term outcomes,” they added. “The valve community eagerly awaits larger series with adjudicated outcomes of the transcatheter valve-in-valve procedure.”
Dr. Forcillo and coauthor Lillian Tsai had no disclosures. Dr. Vinod Thourani disclosed ties with St. Jude Medical, Edwards Lifesciences, Boston Scientific, Abbott Medical, Medtronic, Directflow, and Sorin Medical.
As the population ages and younger patients choose bioprosthetic valves to avoid lifelong warfarin, surgeons are going to face more situations where they will have to decide whether to perform surgical or transcatheter reoperative valve surgery, Dr. Jessica Forcillo of Emory University, Atlanta, and coauthors wrote in an invited commentary (J Thorac Cardiovasc Surg. 2015;150:1568-9).
They called the 8% 30-day mortality rate in the Hamburg study “high” even though the average age of the study population was a “relatively young” 74 years. The Hamburg authors may have learned more had they evaluated fewer prostheses. “With a small number of patients and at the beginning of an experience, focusing on one or two available prostheses may have resulted in more accurate and reliable results,” noted Dr. Forcillo and her colleagues. That 53% of the procedures were done via the transapical approach may also explain the mortality rate, they said.
The overall 30-day mortality rate along with a 17.6% mortality in the mitral ViV group are causes for “some caution against overzealous performance of this procedure and continued monitoring of outcomes in other series,” wrote Dr. Forcillo and her colleagues.
But ViV implantation is a “transformative” technology, they said. “For the elderly, high-risk patients with [structural valve degeneration], transcatheter options may provide improved short-term outcomes,” they added. “The valve community eagerly awaits larger series with adjudicated outcomes of the transcatheter valve-in-valve procedure.”
Dr. Forcillo and coauthor Lillian Tsai had no disclosures. Dr. Vinod Thourani disclosed ties with St. Jude Medical, Edwards Lifesciences, Boston Scientific, Abbott Medical, Medtronic, Directflow, and Sorin Medical.
As the population ages and younger patients choose bioprosthetic valves to avoid lifelong warfarin, surgeons are going to face more situations where they will have to decide whether to perform surgical or transcatheter reoperative valve surgery, Dr. Jessica Forcillo of Emory University, Atlanta, and coauthors wrote in an invited commentary (J Thorac Cardiovasc Surg. 2015;150:1568-9).
They called the 8% 30-day mortality rate in the Hamburg study “high” even though the average age of the study population was a “relatively young” 74 years. The Hamburg authors may have learned more had they evaluated fewer prostheses. “With a small number of patients and at the beginning of an experience, focusing on one or two available prostheses may have resulted in more accurate and reliable results,” noted Dr. Forcillo and her colleagues. That 53% of the procedures were done via the transapical approach may also explain the mortality rate, they said.
The overall 30-day mortality rate along with a 17.6% mortality in the mitral ViV group are causes for “some caution against overzealous performance of this procedure and continued monitoring of outcomes in other series,” wrote Dr. Forcillo and her colleagues.
But ViV implantation is a “transformative” technology, they said. “For the elderly, high-risk patients with [structural valve degeneration], transcatheter options may provide improved short-term outcomes,” they added. “The valve community eagerly awaits larger series with adjudicated outcomes of the transcatheter valve-in-valve procedure.”
Dr. Forcillo and coauthor Lillian Tsai had no disclosures. Dr. Vinod Thourani disclosed ties with St. Jude Medical, Edwards Lifesciences, Boston Scientific, Abbott Medical, Medtronic, Directflow, and Sorin Medical.
With transcatheter valve-in-valve implantation emerging as a novel treatment for high-risk patients whose existing bioprostheses have deteriorated, a team of investigators at University Heart Center in Hamburg, Germany, has found that the procedure can be done successfully in four different anatomic positions with a variety of bioprostheses.
The findings from the single-center study were published in the December issue of the Journal of Thoracic and Cardiovascular Surgery. (J Thorac Cardiovasc Surg. 2015;150:1557-67). They retrospectively analyzed results of 75 patients who had transcatheter valve-in-valve (ViV) replacement at their institution from 2008 to 2014.
“ViV can be performed in all anatomic positions with acceptable hemodynamic and clinical outcome in high-risk patients,” wrote Dr. Lenard Conradi and coauthors. “Increasing importance of ViV can be anticipated considering growing use of surgical bioprostheses.”
Replacement of biological valves is becoming more common. For surgical aortic valve replacement (SAVR), biological procedures have largely replaced mechanical valve implantation, comprising 87% of all such procedures by 2014, according to data from the German Society for Thoracic and Cardiovascular Surgery (Thorac Cardiovasc Surg. 2014;62:380-92). “Therefore, increasing caseload of patients with deteriorated bioprostheses can be expected,” wrote Dr. Conradi and coauthors.
The four anatomic positions in which the investigators performed the procedures and their share of cases are: aortic (54 patients/72%), mitral (17/22.7%), and tricuspid and pulmonary positions (2/2.7% each). The average interval between the index procedure and ViV was 9 years, with a deviation of nearly 5 years among all procedures. Dr. Conradi and coinvestigators said their study focused on technical aspects of ViV procedures from each position to provide guidance for surgeons.
Overall, the study authors performed ViV successfully in 97.3% of patients, with two patients requiring sequential transcatheter heart valve implantation for initial malpositioning. Thirty-day mortality was 8%, which “ranged lower” than expected when compared to standard preoperative risk stratification, they wrote. Mortality was at 5.6% in the aortic group and 17.6% in the mitral group.
That none of the currently available surgical bioprostheses or transcatheter heart valves (THV) were designed for later ViV procedures in deteriorated bioprostheses – although the CoreValve and Sapein THV have approvals for the indication – “may explain some of the apparent shortcomings of ViV therapy,” the researchers wrote.
The most significant challenge of ViV therapy is dealing with elevated residual gradients, which positioning can influence, according to the study findings. “This is not so much an issue for mitral, tricuspid, or pulmonary positions since surgical bioprostheses implanted in these positions are usually of sufficient size to accommodate the THV,” the researchers noted. “However, in the aortic position, more severe spatial restrictions may apply.”
They cited other reports that described a reverse relationship between size of the bioprosthetic and resulting transvalvular gradient after ViV (JACC Cardiovasc Interv. 2011;4:1218-27; JAMA 2014;312:162-70).
To reduce gradients, the investigators used post-ballooning after aortic ViV with a self-expandable THV in 16 cases, succeeding in 12. “Likely, further THV expansion with active compression of soft leaflet and/or pannus tissue and tighter apposition of THV against the frames of surgical bioprostheses contributed to this desired effect,” wrote the researchers. Patient-prosthesis mismatch probably explained the four cases in which gradients could not be further reduced, they noted.
They issued one “word of caution” regarding aortic ViV in small-sized surgical bioprostheses: “Elevated postprocedural gradients have to be expected and must be weighed against expected benefits and against risk of repeat open heart surgery.”
The six transcatheter heart valves the investigators used were Edwards Sapien (XT)/Sapien3 (52%, 39/75); Medtronic CoreValve/CoreValveEvolut (34.7%, 26); St. Jude Portico and Boston Scientific Lotus (4%, three each); and JenaValve and Medtronic Engager (2.7%, two each). The study also looked at different access routes: transapical in 53.3% (40), transfemoral (transarterial or transvenous) in 42.7% (32), transaortic in 2.7% (2), and transjugular in 1.3% (1).
Dr. Conradi and coauthors Dr. Moritz Seiffert, Dr. Ulrich Schaefer, and Dr. Hendrik Treede disclosed ties with Edwards Lifesciences, JenaValve Technology, Medtronic, Symetis, and St. Jude Medical. Four other coauthors reported no disclosures.
With transcatheter valve-in-valve implantation emerging as a novel treatment for high-risk patients whose existing bioprostheses have deteriorated, a team of investigators at University Heart Center in Hamburg, Germany, has found that the procedure can be done successfully in four different anatomic positions with a variety of bioprostheses.
The findings from the single-center study were published in the December issue of the Journal of Thoracic and Cardiovascular Surgery. (J Thorac Cardiovasc Surg. 2015;150:1557-67). They retrospectively analyzed results of 75 patients who had transcatheter valve-in-valve (ViV) replacement at their institution from 2008 to 2014.
“ViV can be performed in all anatomic positions with acceptable hemodynamic and clinical outcome in high-risk patients,” wrote Dr. Lenard Conradi and coauthors. “Increasing importance of ViV can be anticipated considering growing use of surgical bioprostheses.”
Replacement of biological valves is becoming more common. For surgical aortic valve replacement (SAVR), biological procedures have largely replaced mechanical valve implantation, comprising 87% of all such procedures by 2014, according to data from the German Society for Thoracic and Cardiovascular Surgery (Thorac Cardiovasc Surg. 2014;62:380-92). “Therefore, increasing caseload of patients with deteriorated bioprostheses can be expected,” wrote Dr. Conradi and coauthors.
The four anatomic positions in which the investigators performed the procedures and their share of cases are: aortic (54 patients/72%), mitral (17/22.7%), and tricuspid and pulmonary positions (2/2.7% each). The average interval between the index procedure and ViV was 9 years, with a deviation of nearly 5 years among all procedures. Dr. Conradi and coinvestigators said their study focused on technical aspects of ViV procedures from each position to provide guidance for surgeons.
Overall, the study authors performed ViV successfully in 97.3% of patients, with two patients requiring sequential transcatheter heart valve implantation for initial malpositioning. Thirty-day mortality was 8%, which “ranged lower” than expected when compared to standard preoperative risk stratification, they wrote. Mortality was at 5.6% in the aortic group and 17.6% in the mitral group.
That none of the currently available surgical bioprostheses or transcatheter heart valves (THV) were designed for later ViV procedures in deteriorated bioprostheses – although the CoreValve and Sapein THV have approvals for the indication – “may explain some of the apparent shortcomings of ViV therapy,” the researchers wrote.
The most significant challenge of ViV therapy is dealing with elevated residual gradients, which positioning can influence, according to the study findings. “This is not so much an issue for mitral, tricuspid, or pulmonary positions since surgical bioprostheses implanted in these positions are usually of sufficient size to accommodate the THV,” the researchers noted. “However, in the aortic position, more severe spatial restrictions may apply.”
They cited other reports that described a reverse relationship between size of the bioprosthetic and resulting transvalvular gradient after ViV (JACC Cardiovasc Interv. 2011;4:1218-27; JAMA 2014;312:162-70).
To reduce gradients, the investigators used post-ballooning after aortic ViV with a self-expandable THV in 16 cases, succeeding in 12. “Likely, further THV expansion with active compression of soft leaflet and/or pannus tissue and tighter apposition of THV against the frames of surgical bioprostheses contributed to this desired effect,” wrote the researchers. Patient-prosthesis mismatch probably explained the four cases in which gradients could not be further reduced, they noted.
They issued one “word of caution” regarding aortic ViV in small-sized surgical bioprostheses: “Elevated postprocedural gradients have to be expected and must be weighed against expected benefits and against risk of repeat open heart surgery.”
The six transcatheter heart valves the investigators used were Edwards Sapien (XT)/Sapien3 (52%, 39/75); Medtronic CoreValve/CoreValveEvolut (34.7%, 26); St. Jude Portico and Boston Scientific Lotus (4%, three each); and JenaValve and Medtronic Engager (2.7%, two each). The study also looked at different access routes: transapical in 53.3% (40), transfemoral (transarterial or transvenous) in 42.7% (32), transaortic in 2.7% (2), and transjugular in 1.3% (1).
Dr. Conradi and coauthors Dr. Moritz Seiffert, Dr. Ulrich Schaefer, and Dr. Hendrik Treede disclosed ties with Edwards Lifesciences, JenaValve Technology, Medtronic, Symetis, and St. Jude Medical. Four other coauthors reported no disclosures.
Key clinical point: Transcatheter valve-in-valve (ViV) implantation is a relatively safe treatment for patients with a deteriorated bioprostheses.
Major finding: A ViV implantation when performed in four different positions with six different transcatheter heart valves had a 30-day mortality of 8%.
Data source: Retrospective analysis of 75 consecutive patients receiving ViV procedures from 2008 to 2014 at a single institution.
Disclosures: Dr. Conradi and coauthors Dr. Moritz Seiffert, Dr. Ulrich Schaefer, and Dr. Hendrik Treede disclosed relationships with Edwards Lifesciences, JenaValve Technology, Medtronic, Symetis, and St. Jude Medical. Four other coauthors reported no disclosures.
Surgical ablation endures at 5 years
The Cox-Maze IV procedure (CMPIV) has become the standard for surgical ablation for atrial fibrillation (AF), yet little information has been available on how late outcomes compare with catheter-based ablation. A recent analysis of 576 procedures found that after 5 years, most people who had the procedure remained free of atrial tachyarrhythmias and anticoagulation.
The study, by investigators from Washington University, Barnes-Jewish Hospital in St. Louis, was published in the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1168-78). The researchers first presented the study in April at the American Association for Thoracic Surgery meeting in Seattle.
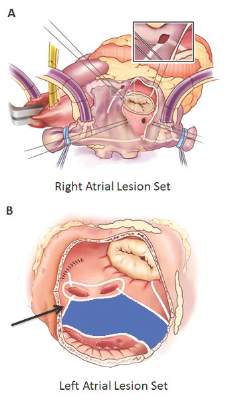
“The results of the CMPIV remain superior to those reported for catheter ablation and other forms of surgical AF ablation, especially for patients with persistent or long-standing AF,” wrote Dr. Matthew C. Henn and his colleagues.
They set out to evaluate late outcomes after CMPIV using current consensus definitions of treatment failure, noting that such outcomes had yet to be reported. They followed 576 patients with atrial fibrillation who had a CMPIV from 2002 to 2014 and compared long-term freedom from atrial fibrillation on and off antiarrhythmic drugs (AADs) across various subgroups. They included the left-sided CMPIV lesion in the analysis because, they said, it had success rates similar to those of biatrial CMPIV.
The Cox-Maze procedure was first introduced by Dr. James Cox in 1987 and updated from the original “cut-and-sew” technique in 2002 to combine bipolar radiofrequency and cryothermal ablation lines in place of most surgical incisions. This iteration was called the Cox-Maze IV procedure. In 2005, CMPIV was modified to include a superior connecting lesion, which formed a “box lesion” by completely isolating the entire posterior left atrium. The study included 512 people who underwent the “box lesion” set procedure.
“The modifications of the CMPIV have allowed it to be performed through a right minithoracotomy (RMT) approach, which has further reduced major morbidity, mortality, and hospital stay compared to those who underwent sternotomy while enjoying equivalent outcomes with regards to freedom from AF,” wrote Dr. Henn and his coauthors.
In the entire cohort, the overall freedom from atrial tachyarrhythmias (ATAs) and anticoagulation were 92% at 1 year, 88% at 2 years, 87% at 3 years, 81% at 4 years, and 73% at 5 years. Overall freedom from ATAs off antiarrhythmic drugs for the entire cohort ranged from 81% at 1 year to 61% at 5 years, and freedom from anticoagulation ranged from 65% at 1 year to 55% at 5 years.
“Freedoms from ATAs on or off AADs were significantly higher in those who underwent box lesion sets when compared to those who did not at 5 years,” noted Dr. Henn and his coauthors. Among the box lesion set group, 78% of those on AADs remained free of ATAs vs. 45% in the non–box lesion set group, and for those off AADs, 66% had no ATAs at 5 years while 33% of the non–box lesion set group did.
Of the overall study population, 41% had paroxysmal AF and 58% had nonparoxysmal AF. Among the latter group, 20% had persistent and 80% had long-standing persistent AF. The nonparoxysmal AF group had a longer duration of preoperative AF, larger left atria and more failed catheter ablations, Dr. Henn and coauthors reported. But, the study showed no differences in freedom from atrial fibrillation on or off AADs at 5 years between patients with paroxysmal AF or persistent/long-standing persistent AF, or between those who underwent stand-alone procedure and those who received a concomitant Cox-Maze procedure. Among those who had a concomitant procedure, 50% had a concomitant mitral valve procedure and 23% had coronary artery bypass grafting.
“The CMPIV results in our series were better than what has been achieved with catheter ablation,” the researchers wrote. They cited studies that showed arrhythmia-free survival after a single ablation procedure ranging from 17% to 29% and “equally poor results.” (Circ Arrhythm Electrophysiol. 2015;8:18-24; J Am Coll Cardiol. 2011;57:160-166; J Am Heart Assoc. 2013;2:e004549.)
“The CMPIV remains the most successful surgical treatment for AF, even in patients with non-paroxysmal AF and regardless of the complexity of the concomitant procedures,” Dr. Henn and his coauthors concluded.
Inconsistencies in this study of the Cox-Maze IV procedure include differing types of atrial fibrillation, heterogeneous concomitant operations, multiple lesion sets and energy sources and inconsistent postablation monitoring, all of which make direct comparisons of surgical ablation strategies or even catheter ablation difficult, Dr. Robert Hawkins and Dr. Gorav Ailawadi of the University of Virginia noted in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1179-80). “Moreover, without controls or selection criteria, it is difficult to account for selection bias,” they wrote.
Yet, this study has “some important findings” despite its shortcomings, namely the “respectable” rates of atrial tachyarrhythmias off antiarrhythmic drugs. These results are superior to other clinical trials, “in part due to the expertise at Washington University,” noted Dr. Hawkins and Dr. Ailawadi.
Adding patients who had the box lesion set approach also improved 5-year outcomes in the study substantially, and left atrium (LA) ablation alone has good results in patients with paroxysmal AF, left atria less than 5.0 cm, and no right atrial enlargement. “Yet, a direct comparison between biatrial and LA lesion sets cannot be made due to the above listed limitations,” they wrote.
The study makes a case for surgical ablation when the preoperative duration of AF is less than 5-10 years and left atrium size is not a problem, and the lesion-set requires further investigation, they said. “Finally, this study highlights the continued need for rigorous monitoring and comparisons of homogeneous patient populations to make stronger conclusions.”
Dr. Ailawadi disclosed relationships with Abbot Vascular, Mitralign, Edwards Lifesciences and St. Jude Medical. Dr. Hawkins had no relationships to disclose.
Inconsistencies in this study of the Cox-Maze IV procedure include differing types of atrial fibrillation, heterogeneous concomitant operations, multiple lesion sets and energy sources and inconsistent postablation monitoring, all of which make direct comparisons of surgical ablation strategies or even catheter ablation difficult, Dr. Robert Hawkins and Dr. Gorav Ailawadi of the University of Virginia noted in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1179-80). “Moreover, without controls or selection criteria, it is difficult to account for selection bias,” they wrote.
Yet, this study has “some important findings” despite its shortcomings, namely the “respectable” rates of atrial tachyarrhythmias off antiarrhythmic drugs. These results are superior to other clinical trials, “in part due to the expertise at Washington University,” noted Dr. Hawkins and Dr. Ailawadi.
Adding patients who had the box lesion set approach also improved 5-year outcomes in the study substantially, and left atrium (LA) ablation alone has good results in patients with paroxysmal AF, left atria less than 5.0 cm, and no right atrial enlargement. “Yet, a direct comparison between biatrial and LA lesion sets cannot be made due to the above listed limitations,” they wrote.
The study makes a case for surgical ablation when the preoperative duration of AF is less than 5-10 years and left atrium size is not a problem, and the lesion-set requires further investigation, they said. “Finally, this study highlights the continued need for rigorous monitoring and comparisons of homogeneous patient populations to make stronger conclusions.”
Dr. Ailawadi disclosed relationships with Abbot Vascular, Mitralign, Edwards Lifesciences and St. Jude Medical. Dr. Hawkins had no relationships to disclose.
Inconsistencies in this study of the Cox-Maze IV procedure include differing types of atrial fibrillation, heterogeneous concomitant operations, multiple lesion sets and energy sources and inconsistent postablation monitoring, all of which make direct comparisons of surgical ablation strategies or even catheter ablation difficult, Dr. Robert Hawkins and Dr. Gorav Ailawadi of the University of Virginia noted in their invited commentary (J Thorac Cardiovasc Surg. 2015;150:1179-80). “Moreover, without controls or selection criteria, it is difficult to account for selection bias,” they wrote.
Yet, this study has “some important findings” despite its shortcomings, namely the “respectable” rates of atrial tachyarrhythmias off antiarrhythmic drugs. These results are superior to other clinical trials, “in part due to the expertise at Washington University,” noted Dr. Hawkins and Dr. Ailawadi.
Adding patients who had the box lesion set approach also improved 5-year outcomes in the study substantially, and left atrium (LA) ablation alone has good results in patients with paroxysmal AF, left atria less than 5.0 cm, and no right atrial enlargement. “Yet, a direct comparison between biatrial and LA lesion sets cannot be made due to the above listed limitations,” they wrote.
The study makes a case for surgical ablation when the preoperative duration of AF is less than 5-10 years and left atrium size is not a problem, and the lesion-set requires further investigation, they said. “Finally, this study highlights the continued need for rigorous monitoring and comparisons of homogeneous patient populations to make stronger conclusions.”
Dr. Ailawadi disclosed relationships with Abbot Vascular, Mitralign, Edwards Lifesciences and St. Jude Medical. Dr. Hawkins had no relationships to disclose.
The Cox-Maze IV procedure (CMPIV) has become the standard for surgical ablation for atrial fibrillation (AF), yet little information has been available on how late outcomes compare with catheter-based ablation. A recent analysis of 576 procedures found that after 5 years, most people who had the procedure remained free of atrial tachyarrhythmias and anticoagulation.
The study, by investigators from Washington University, Barnes-Jewish Hospital in St. Louis, was published in the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1168-78). The researchers first presented the study in April at the American Association for Thoracic Surgery meeting in Seattle.
“The results of the CMPIV remain superior to those reported for catheter ablation and other forms of surgical AF ablation, especially for patients with persistent or long-standing AF,” wrote Dr. Matthew C. Henn and his colleagues.
They set out to evaluate late outcomes after CMPIV using current consensus definitions of treatment failure, noting that such outcomes had yet to be reported. They followed 576 patients with atrial fibrillation who had a CMPIV from 2002 to 2014 and compared long-term freedom from atrial fibrillation on and off antiarrhythmic drugs (AADs) across various subgroups. They included the left-sided CMPIV lesion in the analysis because, they said, it had success rates similar to those of biatrial CMPIV.
The Cox-Maze procedure was first introduced by Dr. James Cox in 1987 and updated from the original “cut-and-sew” technique in 2002 to combine bipolar radiofrequency and cryothermal ablation lines in place of most surgical incisions. This iteration was called the Cox-Maze IV procedure. In 2005, CMPIV was modified to include a superior connecting lesion, which formed a “box lesion” by completely isolating the entire posterior left atrium. The study included 512 people who underwent the “box lesion” set procedure.
“The modifications of the CMPIV have allowed it to be performed through a right minithoracotomy (RMT) approach, which has further reduced major morbidity, mortality, and hospital stay compared to those who underwent sternotomy while enjoying equivalent outcomes with regards to freedom from AF,” wrote Dr. Henn and his coauthors.
In the entire cohort, the overall freedom from atrial tachyarrhythmias (ATAs) and anticoagulation were 92% at 1 year, 88% at 2 years, 87% at 3 years, 81% at 4 years, and 73% at 5 years. Overall freedom from ATAs off antiarrhythmic drugs for the entire cohort ranged from 81% at 1 year to 61% at 5 years, and freedom from anticoagulation ranged from 65% at 1 year to 55% at 5 years.
“Freedoms from ATAs on or off AADs were significantly higher in those who underwent box lesion sets when compared to those who did not at 5 years,” noted Dr. Henn and his coauthors. Among the box lesion set group, 78% of those on AADs remained free of ATAs vs. 45% in the non–box lesion set group, and for those off AADs, 66% had no ATAs at 5 years while 33% of the non–box lesion set group did.
Of the overall study population, 41% had paroxysmal AF and 58% had nonparoxysmal AF. Among the latter group, 20% had persistent and 80% had long-standing persistent AF. The nonparoxysmal AF group had a longer duration of preoperative AF, larger left atria and more failed catheter ablations, Dr. Henn and coauthors reported. But, the study showed no differences in freedom from atrial fibrillation on or off AADs at 5 years between patients with paroxysmal AF or persistent/long-standing persistent AF, or between those who underwent stand-alone procedure and those who received a concomitant Cox-Maze procedure. Among those who had a concomitant procedure, 50% had a concomitant mitral valve procedure and 23% had coronary artery bypass grafting.
“The CMPIV results in our series were better than what has been achieved with catheter ablation,” the researchers wrote. They cited studies that showed arrhythmia-free survival after a single ablation procedure ranging from 17% to 29% and “equally poor results.” (Circ Arrhythm Electrophysiol. 2015;8:18-24; J Am Coll Cardiol. 2011;57:160-166; J Am Heart Assoc. 2013;2:e004549.)
“The CMPIV remains the most successful surgical treatment for AF, even in patients with non-paroxysmal AF and regardless of the complexity of the concomitant procedures,” Dr. Henn and his coauthors concluded.
The Cox-Maze IV procedure (CMPIV) has become the standard for surgical ablation for atrial fibrillation (AF), yet little information has been available on how late outcomes compare with catheter-based ablation. A recent analysis of 576 procedures found that after 5 years, most people who had the procedure remained free of atrial tachyarrhythmias and anticoagulation.
The study, by investigators from Washington University, Barnes-Jewish Hospital in St. Louis, was published in the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1168-78). The researchers first presented the study in April at the American Association for Thoracic Surgery meeting in Seattle.
“The results of the CMPIV remain superior to those reported for catheter ablation and other forms of surgical AF ablation, especially for patients with persistent or long-standing AF,” wrote Dr. Matthew C. Henn and his colleagues.
They set out to evaluate late outcomes after CMPIV using current consensus definitions of treatment failure, noting that such outcomes had yet to be reported. They followed 576 patients with atrial fibrillation who had a CMPIV from 2002 to 2014 and compared long-term freedom from atrial fibrillation on and off antiarrhythmic drugs (AADs) across various subgroups. They included the left-sided CMPIV lesion in the analysis because, they said, it had success rates similar to those of biatrial CMPIV.
The Cox-Maze procedure was first introduced by Dr. James Cox in 1987 and updated from the original “cut-and-sew” technique in 2002 to combine bipolar radiofrequency and cryothermal ablation lines in place of most surgical incisions. This iteration was called the Cox-Maze IV procedure. In 2005, CMPIV was modified to include a superior connecting lesion, which formed a “box lesion” by completely isolating the entire posterior left atrium. The study included 512 people who underwent the “box lesion” set procedure.
“The modifications of the CMPIV have allowed it to be performed through a right minithoracotomy (RMT) approach, which has further reduced major morbidity, mortality, and hospital stay compared to those who underwent sternotomy while enjoying equivalent outcomes with regards to freedom from AF,” wrote Dr. Henn and his coauthors.
In the entire cohort, the overall freedom from atrial tachyarrhythmias (ATAs) and anticoagulation were 92% at 1 year, 88% at 2 years, 87% at 3 years, 81% at 4 years, and 73% at 5 years. Overall freedom from ATAs off antiarrhythmic drugs for the entire cohort ranged from 81% at 1 year to 61% at 5 years, and freedom from anticoagulation ranged from 65% at 1 year to 55% at 5 years.
“Freedoms from ATAs on or off AADs were significantly higher in those who underwent box lesion sets when compared to those who did not at 5 years,” noted Dr. Henn and his coauthors. Among the box lesion set group, 78% of those on AADs remained free of ATAs vs. 45% in the non–box lesion set group, and for those off AADs, 66% had no ATAs at 5 years while 33% of the non–box lesion set group did.
Of the overall study population, 41% had paroxysmal AF and 58% had nonparoxysmal AF. Among the latter group, 20% had persistent and 80% had long-standing persistent AF. The nonparoxysmal AF group had a longer duration of preoperative AF, larger left atria and more failed catheter ablations, Dr. Henn and coauthors reported. But, the study showed no differences in freedom from atrial fibrillation on or off AADs at 5 years between patients with paroxysmal AF or persistent/long-standing persistent AF, or between those who underwent stand-alone procedure and those who received a concomitant Cox-Maze procedure. Among those who had a concomitant procedure, 50% had a concomitant mitral valve procedure and 23% had coronary artery bypass grafting.
“The CMPIV results in our series were better than what has been achieved with catheter ablation,” the researchers wrote. They cited studies that showed arrhythmia-free survival after a single ablation procedure ranging from 17% to 29% and “equally poor results.” (Circ Arrhythm Electrophysiol. 2015;8:18-24; J Am Coll Cardiol. 2011;57:160-166; J Am Heart Assoc. 2013;2:e004549.)
“The CMPIV remains the most successful surgical treatment for AF, even in patients with non-paroxysmal AF and regardless of the complexity of the concomitant procedures,” Dr. Henn and his coauthors concluded.
Key clinical point: Outcomes with the Cox-Maze IV procedure for surgical ablation are superior to catheter ablation and other forms of surgical ablation for atrial fibrillation for up to 5 years duration.
Major finding: Seventy-three percent of the study population was free from atrial tachyarrhythmias and 55% were free from anticoagulation at 5 years.
Data source: Prospective analysis of 576 consecutive patients with atrial fibrillation who had Cox-Maze IV procedure or a left-sized Cox-Maze IV procedure from 2002 to 2014 at a single institution
Disclosures: The National Institutes of Health provided grants for the study. Coauthor Dr. Ralph J. Damiano Jr. disclosed research grants and educational funding from AtriCure and Edwards LifeSciences. The other authors had no disclosures.
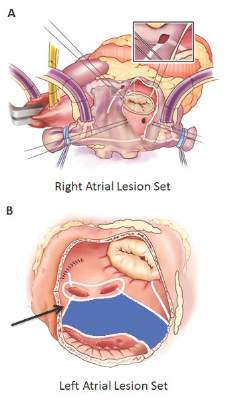
Roux-en-Y improves NASH in obese patients
SAN FRANCISCO – Bariatric surgery is an effective treatment for nonalcoholic steatohepatitis (NASH) in obese patients, a Markov model suggests.
Patients with all classes of obesity, including, mild, moderate, and severe, with all stages of fibrosis, experienced gains in life years following laparoscopic Roux-en-Y gastric bypass, compared with standard management and intensive lifestyle changes, based on the model, Dr. Kathleen Corey reported at the annual meeting of the American Association for the Study of Liver Diseases.

Surgery also increased quality-adjusted life years (QALY) in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis, said Dr Corey of Massachusetts General Hospital, Boston.
The number of F3 patients needed to treat to prevent one liver-related death was favorable across all body mass indexes for those with stage F3 fibrosis. The number needed to treat to prevent one case of cirrhosis in these patients was six to seven, and to prevent one liver-related death was eight to 11, she said.
A cost-effectiveness analysis, with a willingness-to-pay threshold of less than $100,000, also showed that surgery was cost effective for all fibrosis stages for those with severe and moderate obesity.
“The [incremental cost-effectiveness ratio] for BMI of 35-39.9 [kg/m2] was $34,000, for those with a BMI of 40 or greater it was $26,000, and we found that with overweight patients with F3 fibrosis, the ratio was also favorable at $59,000,” she said.
More than 78 million American adults suffer from obesity, and the prevalence of obesity is rising nationwide, she said, adding that obesity results in annual medical costs exceeding $147 billion. Treatment options for obesity are limited, and weight regain after weight loss is frequent, Dr. Corey noted.
“However, bariatric surgery has been shown to be a very effective treatment for obesity. Surgery has been shown to significantly reduce mortality in patients, and reduces progression of many comorbidities, including diabetes,” she said.
Guidelines suggest that bariatric surgery is appropriate for patients with a body mass index of 40 or greater and for those with a BMI of 35 or greater if obesity-related comorbidities such as diabetes or obstructive sleep apnea are present, and data suggest that surgery is also of benefit in those with BMI below 35 with diabetes.
The question remains, though, whether nonalcoholic fatty liver disease (NAFLD) – the most common cause of liver disease in the United States – is an indication in itself for bariatric surgery.
NAFLD is strongly associated with obesity, and its progressive form – NASH – can lead to cirrhosis, hepatocellular carcinoma, and the need for liver transplantation.
“However, there are no FDA-approved therapies for NASH and no randomized controlled trials have been conducted to evaluate the role of bariatric surgery in NASH ... and appropriate BMI cutoffs in those with NASH have not been established,” Dr. Corey said.
Several nonrandomized prospective trials have, however, evaluated bariatric surgery in NASH patients with BMIs of 35 or greater with comorbidities, and in patients with BMIs of 40 or greater, and these have shown that NASH resolution can occur in up to 85% of patients at 1-5 years with fibrosis reduction seen in nearly a third, she said, adding that the risk-benefit ratio for surgery is unknown, as is the value of surgery in NASH patients with BMIs less than 35.
The current study looked at three treatment strategies, including standard management with lifestyle counseling; intensive lifestyle intervention based on a diabetes prevention program with lifestyle, nutrition, and exercise counseling; and bariatric Roux-en-Y gastric bypass in a hypothetical simulated cohort of 45-year-olds with NASH, F0-F3 fibrosis, and varying BMI values.
The findings, though limited by a lack of data on the impact of surgery on patients with a BMI of less than 35, and by evaluation of only one type of surgery, showed that bariatric surgery increased incremental life years at all weight and fibrosis stages vs. standard management and intensive lifestyle intervention, and that surgery increased QALY in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis.
“We found that surgery was cost effective for F3 fibrosis in those with moderate and severe obesity and those with overweight. Randomized trials, though, are needed to assess the management of weight loss surgery for NASH before this can be recommended, certainly in patients with a BMI of less than 35,” she concluded.
Dr. Corey reported serving on an advisory committee or review panel for Gilead, and serving in a speaking or teaching role for Synageva.
SAN FRANCISCO – Bariatric surgery is an effective treatment for nonalcoholic steatohepatitis (NASH) in obese patients, a Markov model suggests.
Patients with all classes of obesity, including, mild, moderate, and severe, with all stages of fibrosis, experienced gains in life years following laparoscopic Roux-en-Y gastric bypass, compared with standard management and intensive lifestyle changes, based on the model, Dr. Kathleen Corey reported at the annual meeting of the American Association for the Study of Liver Diseases.
Surgery also increased quality-adjusted life years (QALY) in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis, said Dr Corey of Massachusetts General Hospital, Boston.
The number of F3 patients needed to treat to prevent one liver-related death was favorable across all body mass indexes for those with stage F3 fibrosis. The number needed to treat to prevent one case of cirrhosis in these patients was six to seven, and to prevent one liver-related death was eight to 11, she said.
A cost-effectiveness analysis, with a willingness-to-pay threshold of less than $100,000, also showed that surgery was cost effective for all fibrosis stages for those with severe and moderate obesity.
“The [incremental cost-effectiveness ratio] for BMI of 35-39.9 [kg/m2] was $34,000, for those with a BMI of 40 or greater it was $26,000, and we found that with overweight patients with F3 fibrosis, the ratio was also favorable at $59,000,” she said.
More than 78 million American adults suffer from obesity, and the prevalence of obesity is rising nationwide, she said, adding that obesity results in annual medical costs exceeding $147 billion. Treatment options for obesity are limited, and weight regain after weight loss is frequent, Dr. Corey noted.
“However, bariatric surgery has been shown to be a very effective treatment for obesity. Surgery has been shown to significantly reduce mortality in patients, and reduces progression of many comorbidities, including diabetes,” she said.
Guidelines suggest that bariatric surgery is appropriate for patients with a body mass index of 40 or greater and for those with a BMI of 35 or greater if obesity-related comorbidities such as diabetes or obstructive sleep apnea are present, and data suggest that surgery is also of benefit in those with BMI below 35 with diabetes.
The question remains, though, whether nonalcoholic fatty liver disease (NAFLD) – the most common cause of liver disease in the United States – is an indication in itself for bariatric surgery.
NAFLD is strongly associated with obesity, and its progressive form – NASH – can lead to cirrhosis, hepatocellular carcinoma, and the need for liver transplantation.
“However, there are no FDA-approved therapies for NASH and no randomized controlled trials have been conducted to evaluate the role of bariatric surgery in NASH ... and appropriate BMI cutoffs in those with NASH have not been established,” Dr. Corey said.
Several nonrandomized prospective trials have, however, evaluated bariatric surgery in NASH patients with BMIs of 35 or greater with comorbidities, and in patients with BMIs of 40 or greater, and these have shown that NASH resolution can occur in up to 85% of patients at 1-5 years with fibrosis reduction seen in nearly a third, she said, adding that the risk-benefit ratio for surgery is unknown, as is the value of surgery in NASH patients with BMIs less than 35.
The current study looked at three treatment strategies, including standard management with lifestyle counseling; intensive lifestyle intervention based on a diabetes prevention program with lifestyle, nutrition, and exercise counseling; and bariatric Roux-en-Y gastric bypass in a hypothetical simulated cohort of 45-year-olds with NASH, F0-F3 fibrosis, and varying BMI values.
The findings, though limited by a lack of data on the impact of surgery on patients with a BMI of less than 35, and by evaluation of only one type of surgery, showed that bariatric surgery increased incremental life years at all weight and fibrosis stages vs. standard management and intensive lifestyle intervention, and that surgery increased QALY in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis.
“We found that surgery was cost effective for F3 fibrosis in those with moderate and severe obesity and those with overweight. Randomized trials, though, are needed to assess the management of weight loss surgery for NASH before this can be recommended, certainly in patients with a BMI of less than 35,” she concluded.
Dr. Corey reported serving on an advisory committee or review panel for Gilead, and serving in a speaking or teaching role for Synageva.
SAN FRANCISCO – Bariatric surgery is an effective treatment for nonalcoholic steatohepatitis (NASH) in obese patients, a Markov model suggests.
Patients with all classes of obesity, including, mild, moderate, and severe, with all stages of fibrosis, experienced gains in life years following laparoscopic Roux-en-Y gastric bypass, compared with standard management and intensive lifestyle changes, based on the model, Dr. Kathleen Corey reported at the annual meeting of the American Association for the Study of Liver Diseases.
Surgery also increased quality-adjusted life years (QALY) in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis, said Dr Corey of Massachusetts General Hospital, Boston.
The number of F3 patients needed to treat to prevent one liver-related death was favorable across all body mass indexes for those with stage F3 fibrosis. The number needed to treat to prevent one case of cirrhosis in these patients was six to seven, and to prevent one liver-related death was eight to 11, she said.
A cost-effectiveness analysis, with a willingness-to-pay threshold of less than $100,000, also showed that surgery was cost effective for all fibrosis stages for those with severe and moderate obesity.
“The [incremental cost-effectiveness ratio] for BMI of 35-39.9 [kg/m2] was $34,000, for those with a BMI of 40 or greater it was $26,000, and we found that with overweight patients with F3 fibrosis, the ratio was also favorable at $59,000,” she said.
More than 78 million American adults suffer from obesity, and the prevalence of obesity is rising nationwide, she said, adding that obesity results in annual medical costs exceeding $147 billion. Treatment options for obesity are limited, and weight regain after weight loss is frequent, Dr. Corey noted.
“However, bariatric surgery has been shown to be a very effective treatment for obesity. Surgery has been shown to significantly reduce mortality in patients, and reduces progression of many comorbidities, including diabetes,” she said.
Guidelines suggest that bariatric surgery is appropriate for patients with a body mass index of 40 or greater and for those with a BMI of 35 or greater if obesity-related comorbidities such as diabetes or obstructive sleep apnea are present, and data suggest that surgery is also of benefit in those with BMI below 35 with diabetes.
The question remains, though, whether nonalcoholic fatty liver disease (NAFLD) – the most common cause of liver disease in the United States – is an indication in itself for bariatric surgery.
NAFLD is strongly associated with obesity, and its progressive form – NASH – can lead to cirrhosis, hepatocellular carcinoma, and the need for liver transplantation.
“However, there are no FDA-approved therapies for NASH and no randomized controlled trials have been conducted to evaluate the role of bariatric surgery in NASH ... and appropriate BMI cutoffs in those with NASH have not been established,” Dr. Corey said.
Several nonrandomized prospective trials have, however, evaluated bariatric surgery in NASH patients with BMIs of 35 or greater with comorbidities, and in patients with BMIs of 40 or greater, and these have shown that NASH resolution can occur in up to 85% of patients at 1-5 years with fibrosis reduction seen in nearly a third, she said, adding that the risk-benefit ratio for surgery is unknown, as is the value of surgery in NASH patients with BMIs less than 35.
The current study looked at three treatment strategies, including standard management with lifestyle counseling; intensive lifestyle intervention based on a diabetes prevention program with lifestyle, nutrition, and exercise counseling; and bariatric Roux-en-Y gastric bypass in a hypothetical simulated cohort of 45-year-olds with NASH, F0-F3 fibrosis, and varying BMI values.
The findings, though limited by a lack of data on the impact of surgery on patients with a BMI of less than 35, and by evaluation of only one type of surgery, showed that bariatric surgery increased incremental life years at all weight and fibrosis stages vs. standard management and intensive lifestyle intervention, and that surgery increased QALY in those with moderate and severe obesity with all fibrosis stages, those with mild obesity and F2-F3 fibrosis, and in overweight patients with F3 fibrosis.
“We found that surgery was cost effective for F3 fibrosis in those with moderate and severe obesity and those with overweight. Randomized trials, though, are needed to assess the management of weight loss surgery for NASH before this can be recommended, certainly in patients with a BMI of less than 35,” she concluded.
Dr. Corey reported serving on an advisory committee or review panel for Gilead, and serving in a speaking or teaching role for Synageva.
AT THE LIVER MEETING 2015
Key clinical point: Bariatric surgery is an effective treatment for nonalcoholic steatohepatitis (NASH) in obese patients, a Markov model suggests.
Major finding: The number needed to treat to prevent 1 case of cirrhosis was 6-7; to prevent 1 liver-related death, it was 8-11.
Data source: A Markov modeling study involving a hypothetical simulated cohort of patients.
Disclosures: Dr. Corey reported serving on an advisory committee or review panel for Gilead, and serving in a speaking or teaching role for Synageva.

Pediatric heart transplant results not improving
A 25-year study of heart transplants in children with congenital heart disease (CHD) at one institution has found that results haven’t improved over time despite advances in technology and techniques. To improve outcomes, transplant surgeons may need to do a better job of selecting patients and matching patients and donors, according to study in the December issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1455-62).
“Strategies to improve outcomes in CHD patients might need to address selection criteria, transplantation timing, pretransplant and posttransplant care,” noted Dr. Bahaaldin Alsoufi, of the division of cardiothoracic surgery, Children’s Healthcare of Atlanta, Emory University. “The effect of donor/recipient race mismatch warrants further investigation and might impact organ allocation algorithms or immunosuppression management,” wrote Dr. Alsoufi and his colleagues.
The researchers analyzed results of 124 children with CHD who had heart transplants from 1988 to 2013 at Emory University and Children’s Healthcare of Atlanta. Median age was 3.8 years; 61% were boys. Ten years after heart transplantation, 44% (54) of patients were alive without a second transplant, 13% (17) had a second transplant and 43% (53) died without a second transplant. After the second transplant, 9 of the 17 patients were alive, but 3 of them had gone onto a third transplant. Overall 15-year survival following the first transplant was 41% (51).
The study cited data from the Registry of the International Society for Heart and Lung Transplantation that reported more than 11,000 pediatric heart transplants worldwide in 2013, and CHD represents about 54% of all heart transplants in infants.
A multivariate analysis identified the following risk factors for early mortality after transplant: age younger than 12 months (hazard ration [HR] 7.2) and prolonged cardiopulmonary bypass (HR 5). Late-phase mortality risk factors were age younger than 12 months (HR 3) and donor/recipient race mismatch (HR 2.2).
“Survival was not affected by era, underlying anomaly, prior Fontan, sensitization or pulmonary artery augmentation,” wrote Dr. Alsoufi and his colleagues.
Among the risk factors, longer bypass times may be a surrogate for a more complicated operation, the authors said. But where prior sternotomy is a risk factor following a heart transplant in adults, the study found no such risk in children. Another risk factor previous reports identified is pulmonary artery augmentation, but, again, this study found no risk in the pediatric group.
The researchers looked at days on the waiting list, with a median wait of 39 days in the study group. In all, 175 children were listed for transplants, but 51 did not go through for various reasons. Most of the children with CHD who had a heart transplant had previous surgery; only 13% had a primary heart transplant, mostly in the earlier phase of the study.
Dr. Alsoufi and coauthors also identified African American race as a risk factor for lower survival, which is consistent with other reports. But this study agreed with a previous report that donor/recipient race mismatch was a significant risk factor in white and African American patients (Ann Thorac Surg. 2009;87:204-9). “While our finding might be anecdotal and specific to our geographic population, this warrants some investigation and might have some impact on future organ allocation algorithms and immunosuppression management,” the researchers wrote.
The authors had no relevant disclosures. Emory University School of Medicine, Children’s Healthcare of Atlanta provided study funding.
In his invited commentary, Dr. Robert D.B. Jaquiss of Duke University, Durham, N.C., took issue with the study authors’ “distress” at the lack of improvement in survival over the 25-year term of the study (J Thorac Cardiovasc Surg. 2015;150:1463-4) . Using the year 2000 as a demarcation line for early and late-phase results, Dr. Jaquiss said, “It must be pointed out that in the latter period recipients were much more ill.” He noted that 89% of post-2000 heart transplant patients had UNOS status 1 vs. 49% in the pre-2000 period.

|
Dr. Robert Jaquiss |
“Considering these between-era differences, an alternative, less ‘discouraging’ interpretation is that excellent outcomes were maintained despite the trend toward transplantation in sicker patients, undergoing more complex transplants, with longer ischemic times,” he said.
Dr. Jaquiss also cited “remarkably outstanding outcomes” in Fontan patients, reporting only one operative death in 33 patients. He found the lower survival for African-American patients in the study group “more sobering,” but also controversial because, among other reasons, “a complete mechanistic explanation remains elusive.” How these findings influence pediatric heart transplant practice “requires thoughtful and extensive investigation and discussion,” he said.
Wait-list mortality and mechanical bridge to transplant also deserve mention, he noted. “Though they are only briefly mentioned, the patients who died prior to transplant provide mute testimony to the lack of timely access to suitable donors,” Dr. Jaquiss said. Durable mechanical circulatory support can provide a bridge for these patients, but was not available through the majority of the study period.
“It is striking that no patient in this report was supported by a ventricular assist device (VAD), and only a small number (5%) had been on [extracorporeal membrane oxygenation] support,” Dr. Jaquiss said. “This is an unfortunate and unavoidable weakness of this report, given the recent introduction of VADs for pediatric heart transplant candidates.” The use of VAD in patients with CHD is “increasing rapidly,” he said.
Dr. Jaquiss had no disclosures.
In his invited commentary, Dr. Robert D.B. Jaquiss of Duke University, Durham, N.C., took issue with the study authors’ “distress” at the lack of improvement in survival over the 25-year term of the study (J Thorac Cardiovasc Surg. 2015;150:1463-4) . Using the year 2000 as a demarcation line for early and late-phase results, Dr. Jaquiss said, “It must be pointed out that in the latter period recipients were much more ill.” He noted that 89% of post-2000 heart transplant patients had UNOS status 1 vs. 49% in the pre-2000 period.
|
|
Dr. Robert Jaquiss |
“Considering these between-era differences, an alternative, less ‘discouraging’ interpretation is that excellent outcomes were maintained despite the trend toward transplantation in sicker patients, undergoing more complex transplants, with longer ischemic times,” he said.
Dr. Jaquiss also cited “remarkably outstanding outcomes” in Fontan patients, reporting only one operative death in 33 patients. He found the lower survival for African-American patients in the study group “more sobering,” but also controversial because, among other reasons, “a complete mechanistic explanation remains elusive.” How these findings influence pediatric heart transplant practice “requires thoughtful and extensive investigation and discussion,” he said.
Wait-list mortality and mechanical bridge to transplant also deserve mention, he noted. “Though they are only briefly mentioned, the patients who died prior to transplant provide mute testimony to the lack of timely access to suitable donors,” Dr. Jaquiss said. Durable mechanical circulatory support can provide a bridge for these patients, but was not available through the majority of the study period.
“It is striking that no patient in this report was supported by a ventricular assist device (VAD), and only a small number (5%) had been on [extracorporeal membrane oxygenation] support,” Dr. Jaquiss said. “This is an unfortunate and unavoidable weakness of this report, given the recent introduction of VADs for pediatric heart transplant candidates.” The use of VAD in patients with CHD is “increasing rapidly,” he said.
Dr. Jaquiss had no disclosures.
In his invited commentary, Dr. Robert D.B. Jaquiss of Duke University, Durham, N.C., took issue with the study authors’ “distress” at the lack of improvement in survival over the 25-year term of the study (J Thorac Cardiovasc Surg. 2015;150:1463-4) . Using the year 2000 as a demarcation line for early and late-phase results, Dr. Jaquiss said, “It must be pointed out that in the latter period recipients were much more ill.” He noted that 89% of post-2000 heart transplant patients had UNOS status 1 vs. 49% in the pre-2000 period.
|
|
Dr. Robert Jaquiss |
“Considering these between-era differences, an alternative, less ‘discouraging’ interpretation is that excellent outcomes were maintained despite the trend toward transplantation in sicker patients, undergoing more complex transplants, with longer ischemic times,” he said.
Dr. Jaquiss also cited “remarkably outstanding outcomes” in Fontan patients, reporting only one operative death in 33 patients. He found the lower survival for African-American patients in the study group “more sobering,” but also controversial because, among other reasons, “a complete mechanistic explanation remains elusive.” How these findings influence pediatric heart transplant practice “requires thoughtful and extensive investigation and discussion,” he said.
Wait-list mortality and mechanical bridge to transplant also deserve mention, he noted. “Though they are only briefly mentioned, the patients who died prior to transplant provide mute testimony to the lack of timely access to suitable donors,” Dr. Jaquiss said. Durable mechanical circulatory support can provide a bridge for these patients, but was not available through the majority of the study period.
“It is striking that no patient in this report was supported by a ventricular assist device (VAD), and only a small number (5%) had been on [extracorporeal membrane oxygenation] support,” Dr. Jaquiss said. “This is an unfortunate and unavoidable weakness of this report, given the recent introduction of VADs for pediatric heart transplant candidates.” The use of VAD in patients with CHD is “increasing rapidly,” he said.
Dr. Jaquiss had no disclosures.
A 25-year study of heart transplants in children with congenital heart disease (CHD) at one institution has found that results haven’t improved over time despite advances in technology and techniques. To improve outcomes, transplant surgeons may need to do a better job of selecting patients and matching patients and donors, according to study in the December issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1455-62).
“Strategies to improve outcomes in CHD patients might need to address selection criteria, transplantation timing, pretransplant and posttransplant care,” noted Dr. Bahaaldin Alsoufi, of the division of cardiothoracic surgery, Children’s Healthcare of Atlanta, Emory University. “The effect of donor/recipient race mismatch warrants further investigation and might impact organ allocation algorithms or immunosuppression management,” wrote Dr. Alsoufi and his colleagues.
The researchers analyzed results of 124 children with CHD who had heart transplants from 1988 to 2013 at Emory University and Children’s Healthcare of Atlanta. Median age was 3.8 years; 61% were boys. Ten years after heart transplantation, 44% (54) of patients were alive without a second transplant, 13% (17) had a second transplant and 43% (53) died without a second transplant. After the second transplant, 9 of the 17 patients were alive, but 3 of them had gone onto a third transplant. Overall 15-year survival following the first transplant was 41% (51).
The study cited data from the Registry of the International Society for Heart and Lung Transplantation that reported more than 11,000 pediatric heart transplants worldwide in 2013, and CHD represents about 54% of all heart transplants in infants.
A multivariate analysis identified the following risk factors for early mortality after transplant: age younger than 12 months (hazard ration [HR] 7.2) and prolonged cardiopulmonary bypass (HR 5). Late-phase mortality risk factors were age younger than 12 months (HR 3) and donor/recipient race mismatch (HR 2.2).
“Survival was not affected by era, underlying anomaly, prior Fontan, sensitization or pulmonary artery augmentation,” wrote Dr. Alsoufi and his colleagues.
Among the risk factors, longer bypass times may be a surrogate for a more complicated operation, the authors said. But where prior sternotomy is a risk factor following a heart transplant in adults, the study found no such risk in children. Another risk factor previous reports identified is pulmonary artery augmentation, but, again, this study found no risk in the pediatric group.
The researchers looked at days on the waiting list, with a median wait of 39 days in the study group. In all, 175 children were listed for transplants, but 51 did not go through for various reasons. Most of the children with CHD who had a heart transplant had previous surgery; only 13% had a primary heart transplant, mostly in the earlier phase of the study.
Dr. Alsoufi and coauthors also identified African American race as a risk factor for lower survival, which is consistent with other reports. But this study agreed with a previous report that donor/recipient race mismatch was a significant risk factor in white and African American patients (Ann Thorac Surg. 2009;87:204-9). “While our finding might be anecdotal and specific to our geographic population, this warrants some investigation and might have some impact on future organ allocation algorithms and immunosuppression management,” the researchers wrote.
The authors had no relevant disclosures. Emory University School of Medicine, Children’s Healthcare of Atlanta provided study funding.
A 25-year study of heart transplants in children with congenital heart disease (CHD) at one institution has found that results haven’t improved over time despite advances in technology and techniques. To improve outcomes, transplant surgeons may need to do a better job of selecting patients and matching patients and donors, according to study in the December issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015;150:1455-62).
“Strategies to improve outcomes in CHD patients might need to address selection criteria, transplantation timing, pretransplant and posttransplant care,” noted Dr. Bahaaldin Alsoufi, of the division of cardiothoracic surgery, Children’s Healthcare of Atlanta, Emory University. “The effect of donor/recipient race mismatch warrants further investigation and might impact organ allocation algorithms or immunosuppression management,” wrote Dr. Alsoufi and his colleagues.
The researchers analyzed results of 124 children with CHD who had heart transplants from 1988 to 2013 at Emory University and Children’s Healthcare of Atlanta. Median age was 3.8 years; 61% were boys. Ten years after heart transplantation, 44% (54) of patients were alive without a second transplant, 13% (17) had a second transplant and 43% (53) died without a second transplant. After the second transplant, 9 of the 17 patients were alive, but 3 of them had gone onto a third transplant. Overall 15-year survival following the first transplant was 41% (51).
The study cited data from the Registry of the International Society for Heart and Lung Transplantation that reported more than 11,000 pediatric heart transplants worldwide in 2013, and CHD represents about 54% of all heart transplants in infants.
A multivariate analysis identified the following risk factors for early mortality after transplant: age younger than 12 months (hazard ration [HR] 7.2) and prolonged cardiopulmonary bypass (HR 5). Late-phase mortality risk factors were age younger than 12 months (HR 3) and donor/recipient race mismatch (HR 2.2).
“Survival was not affected by era, underlying anomaly, prior Fontan, sensitization or pulmonary artery augmentation,” wrote Dr. Alsoufi and his colleagues.
Among the risk factors, longer bypass times may be a surrogate for a more complicated operation, the authors said. But where prior sternotomy is a risk factor following a heart transplant in adults, the study found no such risk in children. Another risk factor previous reports identified is pulmonary artery augmentation, but, again, this study found no risk in the pediatric group.
The researchers looked at days on the waiting list, with a median wait of 39 days in the study group. In all, 175 children were listed for transplants, but 51 did not go through for various reasons. Most of the children with CHD who had a heart transplant had previous surgery; only 13% had a primary heart transplant, mostly in the earlier phase of the study.
Dr. Alsoufi and coauthors also identified African American race as a risk factor for lower survival, which is consistent with other reports. But this study agreed with a previous report that donor/recipient race mismatch was a significant risk factor in white and African American patients (Ann Thorac Surg. 2009;87:204-9). “While our finding might be anecdotal and specific to our geographic population, this warrants some investigation and might have some impact on future organ allocation algorithms and immunosuppression management,” the researchers wrote.
The authors had no relevant disclosures. Emory University School of Medicine, Children’s Healthcare of Atlanta provided study funding.
Key clinical point: Pediatric heart transplantation outcomes for congenital heart disease haven’t improved in the current era, indicating ongoing challenges.
Major finding: Ten years following heart transplantation, 13% of patients had undergone retransplantation, 43% had died without retransplantation, and 44% were alive without retransplantation.
Data source: A review of 124 children with congenital heart disease who had heart transplantation at a single center.
Disclosures: The study authors had no relationships to disclose.
