User login
Official Newspaper of the American College of Surgeons
High NLR predicts poor survival in trauma patients
CHICAGO – A high neutrophil to lymphocyte ratio on days 2 and 5 of surgical ICU hospitalization independently predicts increased mortality in critically ill trauma patients, an award-winning study showed.
The risk of death was two times higher for patients with a neutrophil to lymphocyte ratio (NLR) of at least 10.45 on day 2 (adjusted hazard ratio, 2.07; 95% confidence interval, 1.38-3.13; P = .001) and 5.7 times higher for those with an NLR of at least 7.91 on day 5 (adjusted HR, 5.79; 95% CI, 2.93-11.44; P less than .001) in a multivariate analysis, after adjustment for age 65 years or older, male sex, a systolic blood pressure of 90 mm Hg or less, a Glasgow Coma Scale (GCS) score of 8 or less, an Injury Severity Score (ISS) of at least 25, and operation on admission.

“The neutrophil to lymphocyte ratio is easily accessible, the calculation is simple, it adds no additional costs, and virtually all critically ill patients will have these labs,” study author Dr. Evren Dilektasli said at the American College of Surgeons annual clinical congress.
The simple calculation has been shown to be useful in the diagnosis of appendicitis and to be associated with overall survivalin metastatic colorectal cancer, but its association with mortality in trauma patients is not known, he said.
The retrospective cohort comprised 1,356 trauma patients, at least 16 years old, admitted to the Los Angeles County–University of Southern California Medical Center surgical ICU between January 2013 and January 2014. The median NLR was calculated for each day of the surgical ICU stay. At baseline, 16% of patients had an ISS of at least 25, 16.5% had a GCS of 8 or less, 4.5% had a systolic BP of 90 mm Hg or less, 74.3% were male, 23.7% were aged 65 or older, and 86% had a blunt injury. The most common operations on admission were laparotomy (39.6%) and craniectomy/craniotomy (20.7%).
In receiver operating characteristic (ROC) analysis for the first 10 days of hospitalization, the area under the curve (AUC) values for predicting mortality were between 0.55 on day 1 and a high of 0.79 on day 5, Dr. Dilektasli reported.
Starting from day 2 to day 10, the AUCs were statistically significant for predicting mortality.
The NLRs on day 2 (AUC, 0.73; P less than .001) and day 5 (AUC, 0.79; P less than .001) were selected in order to adjust for the clinical probability of early and late complications, he said.
Subsequent ROC curve analysis revealed an NLR cutoff of 10.45 on day 2 (AUC, 0.73; sensitivity, 73.2%; specificity, 61.8%) and a cutoff of 7.91 on day 5 (AUC, 0.79; sensitivity, 82.8%; specificity, 65.2%).
A high NLR on day 2 (at least 10.45) versus a low NLR (less than 10.45) was associated with significantly more ventilator days (5 days vs. 3 days), a longer surgical ICU length of stay (5 days vs. 3 days), a longer hospital stay (11 days vs. 8 days), and greater mortality (18.3% vs. 4.8%; all P values less than .001), reported Dr. Dilektasli, who was a research fellow at USC at the time of the study and has returned to Turkey to continue his training.
On day 5, a high NLR (at least 7.91) versus a low NLR (less than 7.91) was associated with significantly more ventilator days (7 days vs. 4 days; P less than .001), a longer surgical ICU stay (9 days vs. 5 days; P less than .001), and increased mortality (20.4% vs. 2.8%; P less than .001), but not a longer hospital stay (17 days vs. 14 days; P = .119).
In Kaplan-Meier analysis, a significant difference was observed between the high and low NLR groups on day 2 (log rank P less than .001) and day 5 (log rank P less than .001), he said.
“NLR may be a promising tool for assessing the risk of in-hospital mortality,” Dr. Dilektasli concluded. “Prospective external validation is warranted in a larger heterogeneous trauma population.”
During a discussion of the study, it was noted that the ROC curves were impressive, but that other biologic markers known to be associated with poor survival such as C-reactive protein level and class II major hepatitis C expression should have been included in the analysis.
When asked whether any patients with a low NLR on day 2 went on to have a high NLR on day 5, Dr. Dilektasli said there were such patients and that they also had an increased risk of death.
The findings of the study, which earned an excellence in research award, are only an “observation” at this point and are not being used in clinical practice, he added.
The authors reported having no relevant financial conflicts of interest.
CHICAGO – A high neutrophil to lymphocyte ratio on days 2 and 5 of surgical ICU hospitalization independently predicts increased mortality in critically ill trauma patients, an award-winning study showed.
The risk of death was two times higher for patients with a neutrophil to lymphocyte ratio (NLR) of at least 10.45 on day 2 (adjusted hazard ratio, 2.07; 95% confidence interval, 1.38-3.13; P = .001) and 5.7 times higher for those with an NLR of at least 7.91 on day 5 (adjusted HR, 5.79; 95% CI, 2.93-11.44; P less than .001) in a multivariate analysis, after adjustment for age 65 years or older, male sex, a systolic blood pressure of 90 mm Hg or less, a Glasgow Coma Scale (GCS) score of 8 or less, an Injury Severity Score (ISS) of at least 25, and operation on admission.
“The neutrophil to lymphocyte ratio is easily accessible, the calculation is simple, it adds no additional costs, and virtually all critically ill patients will have these labs,” study author Dr. Evren Dilektasli said at the American College of Surgeons annual clinical congress.
The simple calculation has been shown to be useful in the diagnosis of appendicitis and to be associated with overall survivalin metastatic colorectal cancer, but its association with mortality in trauma patients is not known, he said.
The retrospective cohort comprised 1,356 trauma patients, at least 16 years old, admitted to the Los Angeles County–University of Southern California Medical Center surgical ICU between January 2013 and January 2014. The median NLR was calculated for each day of the surgical ICU stay. At baseline, 16% of patients had an ISS of at least 25, 16.5% had a GCS of 8 or less, 4.5% had a systolic BP of 90 mm Hg or less, 74.3% were male, 23.7% were aged 65 or older, and 86% had a blunt injury. The most common operations on admission were laparotomy (39.6%) and craniectomy/craniotomy (20.7%).
In receiver operating characteristic (ROC) analysis for the first 10 days of hospitalization, the area under the curve (AUC) values for predicting mortality were between 0.55 on day 1 and a high of 0.79 on day 5, Dr. Dilektasli reported.
Starting from day 2 to day 10, the AUCs were statistically significant for predicting mortality.
The NLRs on day 2 (AUC, 0.73; P less than .001) and day 5 (AUC, 0.79; P less than .001) were selected in order to adjust for the clinical probability of early and late complications, he said.
Subsequent ROC curve analysis revealed an NLR cutoff of 10.45 on day 2 (AUC, 0.73; sensitivity, 73.2%; specificity, 61.8%) and a cutoff of 7.91 on day 5 (AUC, 0.79; sensitivity, 82.8%; specificity, 65.2%).
A high NLR on day 2 (at least 10.45) versus a low NLR (less than 10.45) was associated with significantly more ventilator days (5 days vs. 3 days), a longer surgical ICU length of stay (5 days vs. 3 days), a longer hospital stay (11 days vs. 8 days), and greater mortality (18.3% vs. 4.8%; all P values less than .001), reported Dr. Dilektasli, who was a research fellow at USC at the time of the study and has returned to Turkey to continue his training.
On day 5, a high NLR (at least 7.91) versus a low NLR (less than 7.91) was associated with significantly more ventilator days (7 days vs. 4 days; P less than .001), a longer surgical ICU stay (9 days vs. 5 days; P less than .001), and increased mortality (20.4% vs. 2.8%; P less than .001), but not a longer hospital stay (17 days vs. 14 days; P = .119).
In Kaplan-Meier analysis, a significant difference was observed between the high and low NLR groups on day 2 (log rank P less than .001) and day 5 (log rank P less than .001), he said.
“NLR may be a promising tool for assessing the risk of in-hospital mortality,” Dr. Dilektasli concluded. “Prospective external validation is warranted in a larger heterogeneous trauma population.”
During a discussion of the study, it was noted that the ROC curves were impressive, but that other biologic markers known to be associated with poor survival such as C-reactive protein level and class II major hepatitis C expression should have been included in the analysis.
When asked whether any patients with a low NLR on day 2 went on to have a high NLR on day 5, Dr. Dilektasli said there were such patients and that they also had an increased risk of death.
The findings of the study, which earned an excellence in research award, are only an “observation” at this point and are not being used in clinical practice, he added.
The authors reported having no relevant financial conflicts of interest.
CHICAGO – A high neutrophil to lymphocyte ratio on days 2 and 5 of surgical ICU hospitalization independently predicts increased mortality in critically ill trauma patients, an award-winning study showed.
The risk of death was two times higher for patients with a neutrophil to lymphocyte ratio (NLR) of at least 10.45 on day 2 (adjusted hazard ratio, 2.07; 95% confidence interval, 1.38-3.13; P = .001) and 5.7 times higher for those with an NLR of at least 7.91 on day 5 (adjusted HR, 5.79; 95% CI, 2.93-11.44; P less than .001) in a multivariate analysis, after adjustment for age 65 years or older, male sex, a systolic blood pressure of 90 mm Hg or less, a Glasgow Coma Scale (GCS) score of 8 or less, an Injury Severity Score (ISS) of at least 25, and operation on admission.
“The neutrophil to lymphocyte ratio is easily accessible, the calculation is simple, it adds no additional costs, and virtually all critically ill patients will have these labs,” study author Dr. Evren Dilektasli said at the American College of Surgeons annual clinical congress.
The simple calculation has been shown to be useful in the diagnosis of appendicitis and to be associated with overall survivalin metastatic colorectal cancer, but its association with mortality in trauma patients is not known, he said.
The retrospective cohort comprised 1,356 trauma patients, at least 16 years old, admitted to the Los Angeles County–University of Southern California Medical Center surgical ICU between January 2013 and January 2014. The median NLR was calculated for each day of the surgical ICU stay. At baseline, 16% of patients had an ISS of at least 25, 16.5% had a GCS of 8 or less, 4.5% had a systolic BP of 90 mm Hg or less, 74.3% were male, 23.7% were aged 65 or older, and 86% had a blunt injury. The most common operations on admission were laparotomy (39.6%) and craniectomy/craniotomy (20.7%).
In receiver operating characteristic (ROC) analysis for the first 10 days of hospitalization, the area under the curve (AUC) values for predicting mortality were between 0.55 on day 1 and a high of 0.79 on day 5, Dr. Dilektasli reported.
Starting from day 2 to day 10, the AUCs were statistically significant for predicting mortality.
The NLRs on day 2 (AUC, 0.73; P less than .001) and day 5 (AUC, 0.79; P less than .001) were selected in order to adjust for the clinical probability of early and late complications, he said.
Subsequent ROC curve analysis revealed an NLR cutoff of 10.45 on day 2 (AUC, 0.73; sensitivity, 73.2%; specificity, 61.8%) and a cutoff of 7.91 on day 5 (AUC, 0.79; sensitivity, 82.8%; specificity, 65.2%).
A high NLR on day 2 (at least 10.45) versus a low NLR (less than 10.45) was associated with significantly more ventilator days (5 days vs. 3 days), a longer surgical ICU length of stay (5 days vs. 3 days), a longer hospital stay (11 days vs. 8 days), and greater mortality (18.3% vs. 4.8%; all P values less than .001), reported Dr. Dilektasli, who was a research fellow at USC at the time of the study and has returned to Turkey to continue his training.
On day 5, a high NLR (at least 7.91) versus a low NLR (less than 7.91) was associated with significantly more ventilator days (7 days vs. 4 days; P less than .001), a longer surgical ICU stay (9 days vs. 5 days; P less than .001), and increased mortality (20.4% vs. 2.8%; P less than .001), but not a longer hospital stay (17 days vs. 14 days; P = .119).
In Kaplan-Meier analysis, a significant difference was observed between the high and low NLR groups on day 2 (log rank P less than .001) and day 5 (log rank P less than .001), he said.
“NLR may be a promising tool for assessing the risk of in-hospital mortality,” Dr. Dilektasli concluded. “Prospective external validation is warranted in a larger heterogeneous trauma population.”
During a discussion of the study, it was noted that the ROC curves were impressive, but that other biologic markers known to be associated with poor survival such as C-reactive protein level and class II major hepatitis C expression should have been included in the analysis.
When asked whether any patients with a low NLR on day 2 went on to have a high NLR on day 5, Dr. Dilektasli said there were such patients and that they also had an increased risk of death.
The findings of the study, which earned an excellence in research award, are only an “observation” at this point and are not being used in clinical practice, he added.
The authors reported having no relevant financial conflicts of interest.
AT THE ACS CLINICAL CONGRESS
Key clinical point: A high neutrophil to lymphocyte ratio on day 2 and day 5 of surgical ICU admission may be a useful predictor of poor survival in trauma patients.
Major finding: The adjusted hazard ratios for mortality were 2.07 with a neutrophil to lymphocyte ratio of at least 10.45 on day 2 (95% CI, 1.38-3.13; P = .001) and 5.79 with an NLR of at least 7.91 on day 5 (95% CI, 2.93-11.44; P less than .001).
Data source: A retrospective study involving 1,356 trauma patients.
Disclosures: The authors reported having no relevant financial conflicts of interest.

FOTS: Minimally invasive esophagectomy viable option to reduce morbidity, mortality
BOSTON – New and innovative methodologies for conducting minimally invasive esophagectomy (MIE) offer significantly lower rates of morbidity and mortality than those normally associated with the procedure, as presented by Dr. James D. Luketich at the Focus on Thoracic Surgery: Technical Challenges and Complications meeting of the American Association for Thoracic Surgery.
While Dr. Luketich spent the bulk of his oral presentation going over the specifics of performing MIE, the accompanying literature of his presentation delved into four key studies – performed and published over the last 12 years – which show the efficacy of MIE over the more traditional approaches to esophagectomy.

“There are several different approaches to esophagectomy in general [but] the technique has evolved partly because the tumors have evolved in the United States,” explained Dr. Luketich, chairman of cardiothoracic surgery at the University of Pittsburgh. “We started off laparoscopic [and] thoracoscopic. In my opinion, that was kind of a bad idea [and] we gave that up pretty early on [...] we’re chest surgeons, we put a thoracoscope in, and we loved it.”
However, as Dr. Luketich explained, the increasing lack of experience from new general surgery residents and attendings caused esophagectomy to become the more attractive option, as it was a procedure that everyone had experience with. This began a search for an effective but minimally invasive approach, which has slowly been cultivated and refined over the years.
Luketich discussed the outcome of his 2003 study assessing 222 consecutive patients who have undergone MIE at the University of Pittsburgh. In that study, patients had lower mortality rates (1.4%) and shorter hospital stays (7 days) than those with “most open series” invasive esophagectomy procedures, with a quality of life score 19 months post operation that was similar to preoperative scores and population norms.
The success of this trial led to the development of the intergroup ECOG 222 trial to determine MIE’s viability in a multicenter setting. Out of 104 patients eligible for MIE, 95 underwent the procedure. Median length of stay in intensive care units was 2 days, and hospital stay was 9 days, with a 2.1% 30-day mortality rate. At 35.8 months (the median follow-up time), the estimated 3-year overall survival was 58.4%.
Similar work was done in 2012, also headed by Dr. Luketich. In this trial, outcomes were evaluated in 1,033 consecutive MIE patients in order to assess the differences between “the modified McKeown minimally invasive approach (videothoracoscopic surgery, laparoscopy, neck anastomosis [MIE-neck]) with our current approach [and] a modified Ivor Lewis approach (laparoscopy, videothoracoscopic surgery, chest anastomosis [MIE-chest]).” MIE-neck was performed on 481 (48%) subjects and MIE-chest on 530 (52%) subjects.
Both procedures had similar median length of stay in hospital (8 days) and in the intensive care unit (2 days), with slightly lower rates of recurrent nerve injury in the MIE-chest cohort and mortality rate of 0.9%. The median number of lymph nodes resected was 21, and total operative mortality was 1.68%, leading investigators to conclude that MIE was the “preferred approach” for resection (P less than .001).
Dr. Luketich also briefly discussed the findings of a 2012 study by Dr. S.S. Biere – an open-label, randomized controlled trial at five study centers spread across three countries from June 2009 through March 2011. Fifty-six patients were randomized into cohorts receiving open esophagectomy, and 59 received MIE; all patients were aged 18-75 years and had resectable cancer of the esophagus or gastroesophageal junction.
Results showed a statistically significant decrease in postoperative pneumonia in the MIE cohort (9% vs. 29%; relative risk 0.35, P = 0.005), compared with open esophagectomy in the first two weeks after surgery and lower postoperative pulmonary infection in the entire hospital stay. MIE patients also experienced shorter hospital stays (11 vs. 14 days), higher short-term quality of life scores at 6 weeks post surgery, lower postoperative pain scores, lower operative blood loss, and lower rates of early morbidity.
Dr. Luketich disclosed having a “shareholder relationship” with Express Scripts and Intuitive Surgical.
BOSTON – New and innovative methodologies for conducting minimally invasive esophagectomy (MIE) offer significantly lower rates of morbidity and mortality than those normally associated with the procedure, as presented by Dr. James D. Luketich at the Focus on Thoracic Surgery: Technical Challenges and Complications meeting of the American Association for Thoracic Surgery.
While Dr. Luketich spent the bulk of his oral presentation going over the specifics of performing MIE, the accompanying literature of his presentation delved into four key studies – performed and published over the last 12 years – which show the efficacy of MIE over the more traditional approaches to esophagectomy.
“There are several different approaches to esophagectomy in general [but] the technique has evolved partly because the tumors have evolved in the United States,” explained Dr. Luketich, chairman of cardiothoracic surgery at the University of Pittsburgh. “We started off laparoscopic [and] thoracoscopic. In my opinion, that was kind of a bad idea [and] we gave that up pretty early on [...] we’re chest surgeons, we put a thoracoscope in, and we loved it.”
However, as Dr. Luketich explained, the increasing lack of experience from new general surgery residents and attendings caused esophagectomy to become the more attractive option, as it was a procedure that everyone had experience with. This began a search for an effective but minimally invasive approach, which has slowly been cultivated and refined over the years.
Luketich discussed the outcome of his 2003 study assessing 222 consecutive patients who have undergone MIE at the University of Pittsburgh. In that study, patients had lower mortality rates (1.4%) and shorter hospital stays (7 days) than those with “most open series” invasive esophagectomy procedures, with a quality of life score 19 months post operation that was similar to preoperative scores and population norms.
The success of this trial led to the development of the intergroup ECOG 222 trial to determine MIE’s viability in a multicenter setting. Out of 104 patients eligible for MIE, 95 underwent the procedure. Median length of stay in intensive care units was 2 days, and hospital stay was 9 days, with a 2.1% 30-day mortality rate. At 35.8 months (the median follow-up time), the estimated 3-year overall survival was 58.4%.
Similar work was done in 2012, also headed by Dr. Luketich. In this trial, outcomes were evaluated in 1,033 consecutive MIE patients in order to assess the differences between “the modified McKeown minimally invasive approach (videothoracoscopic surgery, laparoscopy, neck anastomosis [MIE-neck]) with our current approach [and] a modified Ivor Lewis approach (laparoscopy, videothoracoscopic surgery, chest anastomosis [MIE-chest]).” MIE-neck was performed on 481 (48%) subjects and MIE-chest on 530 (52%) subjects.
Both procedures had similar median length of stay in hospital (8 days) and in the intensive care unit (2 days), with slightly lower rates of recurrent nerve injury in the MIE-chest cohort and mortality rate of 0.9%. The median number of lymph nodes resected was 21, and total operative mortality was 1.68%, leading investigators to conclude that MIE was the “preferred approach” for resection (P less than .001).
Dr. Luketich also briefly discussed the findings of a 2012 study by Dr. S.S. Biere – an open-label, randomized controlled trial at five study centers spread across three countries from June 2009 through March 2011. Fifty-six patients were randomized into cohorts receiving open esophagectomy, and 59 received MIE; all patients were aged 18-75 years and had resectable cancer of the esophagus or gastroesophageal junction.
Results showed a statistically significant decrease in postoperative pneumonia in the MIE cohort (9% vs. 29%; relative risk 0.35, P = 0.005), compared with open esophagectomy in the first two weeks after surgery and lower postoperative pulmonary infection in the entire hospital stay. MIE patients also experienced shorter hospital stays (11 vs. 14 days), higher short-term quality of life scores at 6 weeks post surgery, lower postoperative pain scores, lower operative blood loss, and lower rates of early morbidity.
Dr. Luketich disclosed having a “shareholder relationship” with Express Scripts and Intuitive Surgical.
BOSTON – New and innovative methodologies for conducting minimally invasive esophagectomy (MIE) offer significantly lower rates of morbidity and mortality than those normally associated with the procedure, as presented by Dr. James D. Luketich at the Focus on Thoracic Surgery: Technical Challenges and Complications meeting of the American Association for Thoracic Surgery.
While Dr. Luketich spent the bulk of his oral presentation going over the specifics of performing MIE, the accompanying literature of his presentation delved into four key studies – performed and published over the last 12 years – which show the efficacy of MIE over the more traditional approaches to esophagectomy.
“There are several different approaches to esophagectomy in general [but] the technique has evolved partly because the tumors have evolved in the United States,” explained Dr. Luketich, chairman of cardiothoracic surgery at the University of Pittsburgh. “We started off laparoscopic [and] thoracoscopic. In my opinion, that was kind of a bad idea [and] we gave that up pretty early on [...] we’re chest surgeons, we put a thoracoscope in, and we loved it.”
However, as Dr. Luketich explained, the increasing lack of experience from new general surgery residents and attendings caused esophagectomy to become the more attractive option, as it was a procedure that everyone had experience with. This began a search for an effective but minimally invasive approach, which has slowly been cultivated and refined over the years.
Luketich discussed the outcome of his 2003 study assessing 222 consecutive patients who have undergone MIE at the University of Pittsburgh. In that study, patients had lower mortality rates (1.4%) and shorter hospital stays (7 days) than those with “most open series” invasive esophagectomy procedures, with a quality of life score 19 months post operation that was similar to preoperative scores and population norms.
The success of this trial led to the development of the intergroup ECOG 222 trial to determine MIE’s viability in a multicenter setting. Out of 104 patients eligible for MIE, 95 underwent the procedure. Median length of stay in intensive care units was 2 days, and hospital stay was 9 days, with a 2.1% 30-day mortality rate. At 35.8 months (the median follow-up time), the estimated 3-year overall survival was 58.4%.
Similar work was done in 2012, also headed by Dr. Luketich. In this trial, outcomes were evaluated in 1,033 consecutive MIE patients in order to assess the differences between “the modified McKeown minimally invasive approach (videothoracoscopic surgery, laparoscopy, neck anastomosis [MIE-neck]) with our current approach [and] a modified Ivor Lewis approach (laparoscopy, videothoracoscopic surgery, chest anastomosis [MIE-chest]).” MIE-neck was performed on 481 (48%) subjects and MIE-chest on 530 (52%) subjects.
Both procedures had similar median length of stay in hospital (8 days) and in the intensive care unit (2 days), with slightly lower rates of recurrent nerve injury in the MIE-chest cohort and mortality rate of 0.9%. The median number of lymph nodes resected was 21, and total operative mortality was 1.68%, leading investigators to conclude that MIE was the “preferred approach” for resection (P less than .001).
Dr. Luketich also briefly discussed the findings of a 2012 study by Dr. S.S. Biere – an open-label, randomized controlled trial at five study centers spread across three countries from June 2009 through March 2011. Fifty-six patients were randomized into cohorts receiving open esophagectomy, and 59 received MIE; all patients were aged 18-75 years and had resectable cancer of the esophagus or gastroesophageal junction.
Results showed a statistically significant decrease in postoperative pneumonia in the MIE cohort (9% vs. 29%; relative risk 0.35, P = 0.005), compared with open esophagectomy in the first two weeks after surgery and lower postoperative pulmonary infection in the entire hospital stay. MIE patients also experienced shorter hospital stays (11 vs. 14 days), higher short-term quality of life scores at 6 weeks post surgery, lower postoperative pain scores, lower operative blood loss, and lower rates of early morbidity.
Dr. Luketich disclosed having a “shareholder relationship” with Express Scripts and Intuitive Surgical.
AT AATS FOCUS ON THORACIC SURGERY: TECHNICAL CHALLENGES AND COMPLICATIONS

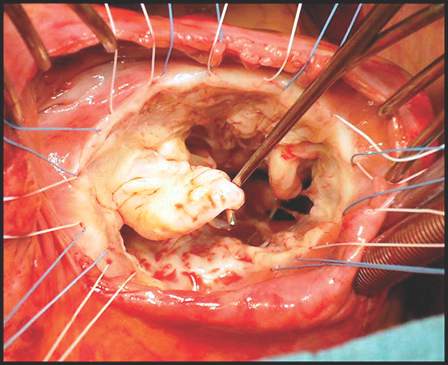
Should annular dilation be a marker for concomitant tricuspid valve repair?
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.

The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.
The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.
The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
Key clinical point: Controversy surrounds the need for concomitant tricuspid valve repair with a mitral valve procedure and what parameters the decision should be based on.
Major finding: Increasing reports have supported the use of annular dilation of 40 mm or greater as a threshold for performing concomitant tricuspid valve repair rather than grading of tricuspid regurgitation.
Data source: This Expert Opinion piece cites studies along with American and European clinical guidelines that support the 40-mm threshold.
Disclosures: Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.

Setting a new standard for aortic root repair?
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).

“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Key clinical point: Aortic root replacement surgery can be performed with minimal risk of death and complications regardless of the approach taken.
Major finding: Overall rate of death was 0.2%, with none since 2002, and the overall rate of complications was below 0.5% in the study cohort.
Data source: Review of prospective data on 890 aortic root replacement operations performed over a 17-year period at a single center.
Disclosures: The study authors had no relationships to disclose.

Functional dependence linked to risk of complications after spine surgery
SAN DIEGO – Functional dependence following elective cervical spine procedures was associated with a significantly increased risk of almost all 30-day complications analyzed, including mortality, a large retrospective analysis of national data demonstrated.
The findings suggest that physicians should “include the patient’s level of functional independence, in addition to more traditional medical comorbidities, in the risk-benefit analysis of surgical decision making,” Dr. Alpesh A. Patel said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “Those individuals with dependence need to be counseled appropriately about their increased risk of complications including mortality.”

Dr. Patel, professor and director of orthopedic spine surgery at Northwestern University Feinberg School of Medicine, Chicago, and his associates retrospectively reviewed the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data files from 2006 to 2013 and limited their analysis to patients undergoing elective anterior cervical fusions, posterior cervical fusions, cervical laminectomy, cervical laminotomy, cervical discectomy, or corpectomy. They divided patients into one of three groups based on the following preoperative functional status parameters: independent, comprising those not requiring assistance or any equipment for activities of daily living (ADLs); partially dependent, including those with equipment such as prosthetics, equipment, or devices and requiring some assistance from another person for ADLs; and totally dependent, in which patients require total assistance for all ADLs. The researchers used univariate analysis to compare patient demographics, comorbidities, and 30-day postoperative complications among the three groups, followed by multivariate logistic regression to analyze the independent association of functional dependence on 30-day complications when controlling for procedure and comorbidity variances.
Dr. Patel reported findings from 24,357 patients: 23,620 (97.0%) functionally independent, 664 (2.7%) partially dependent, and 73 (0.3%) totally dependent. Dependent patients were significantly older and had higher rates of all comorbidities (P less than .001), with the exception of obesity (P = .214). In addition, 30-day complication rates were higher for all complications (P less than .001) other than neurological (P =.060) and surgical site complications (P =.668). When the researchers controlled for type of procedure and for disparities in patient preoperative variables, multivariate analyses demonstrated that functional dependence was independently associated with sepsis (odds ratio 6.40; P less than .001), pulmonary (OR 4.13; P less than .001), venous thromboembolism (OR 4.27, P less than .001), renal (OR 3.32; P less than .001), and cardiac complications (OR 4.68; P =.001), along with mortality (OR 8.31; P less than .001).
“The very strong association between functional dependence and mortality was quite surprising,” Dr. Patel said. “It was, to the contrary, also surprising to see that, despite wide variance in medical comorbidities and functional status, surgical complications such as infection and neurological injury were similar in all groups.” He characterized the study as “the first large-scale assessment of functional status as a predictor of patient outcomes after cervical spine surgery. It fits in line with other studies utilizing large databases. Big data analysis of outcomes can be used to identify risk factors for complications including death after surgery. Identifying these factors is important if we are going to improve the care we provide. Accurately quantifying the impact of these risk factors is also critical when we risk stratify and compare hospitals and physicians.”
He acknowledged certain limitations of the study, including the fact that it is a retrospective study “with a heterogeneous population of patients, surgeons, hospitals, and procedures. This adds uncertainty to the analysis at the level of the individual patient but does provide generalizability to a broader patient population.”
Dr. Patel reported having no conflicts of interest.
SAN DIEGO – Functional dependence following elective cervical spine procedures was associated with a significantly increased risk of almost all 30-day complications analyzed, including mortality, a large retrospective analysis of national data demonstrated.
The findings suggest that physicians should “include the patient’s level of functional independence, in addition to more traditional medical comorbidities, in the risk-benefit analysis of surgical decision making,” Dr. Alpesh A. Patel said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “Those individuals with dependence need to be counseled appropriately about their increased risk of complications including mortality.”
Dr. Patel, professor and director of orthopedic spine surgery at Northwestern University Feinberg School of Medicine, Chicago, and his associates retrospectively reviewed the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data files from 2006 to 2013 and limited their analysis to patients undergoing elective anterior cervical fusions, posterior cervical fusions, cervical laminectomy, cervical laminotomy, cervical discectomy, or corpectomy. They divided patients into one of three groups based on the following preoperative functional status parameters: independent, comprising those not requiring assistance or any equipment for activities of daily living (ADLs); partially dependent, including those with equipment such as prosthetics, equipment, or devices and requiring some assistance from another person for ADLs; and totally dependent, in which patients require total assistance for all ADLs. The researchers used univariate analysis to compare patient demographics, comorbidities, and 30-day postoperative complications among the three groups, followed by multivariate logistic regression to analyze the independent association of functional dependence on 30-day complications when controlling for procedure and comorbidity variances.
Dr. Patel reported findings from 24,357 patients: 23,620 (97.0%) functionally independent, 664 (2.7%) partially dependent, and 73 (0.3%) totally dependent. Dependent patients were significantly older and had higher rates of all comorbidities (P less than .001), with the exception of obesity (P = .214). In addition, 30-day complication rates were higher for all complications (P less than .001) other than neurological (P =.060) and surgical site complications (P =.668). When the researchers controlled for type of procedure and for disparities in patient preoperative variables, multivariate analyses demonstrated that functional dependence was independently associated with sepsis (odds ratio 6.40; P less than .001), pulmonary (OR 4.13; P less than .001), venous thromboembolism (OR 4.27, P less than .001), renal (OR 3.32; P less than .001), and cardiac complications (OR 4.68; P =.001), along with mortality (OR 8.31; P less than .001).
“The very strong association between functional dependence and mortality was quite surprising,” Dr. Patel said. “It was, to the contrary, also surprising to see that, despite wide variance in medical comorbidities and functional status, surgical complications such as infection and neurological injury were similar in all groups.” He characterized the study as “the first large-scale assessment of functional status as a predictor of patient outcomes after cervical spine surgery. It fits in line with other studies utilizing large databases. Big data analysis of outcomes can be used to identify risk factors for complications including death after surgery. Identifying these factors is important if we are going to improve the care we provide. Accurately quantifying the impact of these risk factors is also critical when we risk stratify and compare hospitals and physicians.”
He acknowledged certain limitations of the study, including the fact that it is a retrospective study “with a heterogeneous population of patients, surgeons, hospitals, and procedures. This adds uncertainty to the analysis at the level of the individual patient but does provide generalizability to a broader patient population.”
Dr. Patel reported having no conflicts of interest.
SAN DIEGO – Functional dependence following elective cervical spine procedures was associated with a significantly increased risk of almost all 30-day complications analyzed, including mortality, a large retrospective analysis of national data demonstrated.
The findings suggest that physicians should “include the patient’s level of functional independence, in addition to more traditional medical comorbidities, in the risk-benefit analysis of surgical decision making,” Dr. Alpesh A. Patel said in an interview in advance of the annual meeting of the Cervical Spine Research Society. “Those individuals with dependence need to be counseled appropriately about their increased risk of complications including mortality.”
Dr. Patel, professor and director of orthopedic spine surgery at Northwestern University Feinberg School of Medicine, Chicago, and his associates retrospectively reviewed the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data files from 2006 to 2013 and limited their analysis to patients undergoing elective anterior cervical fusions, posterior cervical fusions, cervical laminectomy, cervical laminotomy, cervical discectomy, or corpectomy. They divided patients into one of three groups based on the following preoperative functional status parameters: independent, comprising those not requiring assistance or any equipment for activities of daily living (ADLs); partially dependent, including those with equipment such as prosthetics, equipment, or devices and requiring some assistance from another person for ADLs; and totally dependent, in which patients require total assistance for all ADLs. The researchers used univariate analysis to compare patient demographics, comorbidities, and 30-day postoperative complications among the three groups, followed by multivariate logistic regression to analyze the independent association of functional dependence on 30-day complications when controlling for procedure and comorbidity variances.
Dr. Patel reported findings from 24,357 patients: 23,620 (97.0%) functionally independent, 664 (2.7%) partially dependent, and 73 (0.3%) totally dependent. Dependent patients were significantly older and had higher rates of all comorbidities (P less than .001), with the exception of obesity (P = .214). In addition, 30-day complication rates were higher for all complications (P less than .001) other than neurological (P =.060) and surgical site complications (P =.668). When the researchers controlled for type of procedure and for disparities in patient preoperative variables, multivariate analyses demonstrated that functional dependence was independently associated with sepsis (odds ratio 6.40; P less than .001), pulmonary (OR 4.13; P less than .001), venous thromboembolism (OR 4.27, P less than .001), renal (OR 3.32; P less than .001), and cardiac complications (OR 4.68; P =.001), along with mortality (OR 8.31; P less than .001).
“The very strong association between functional dependence and mortality was quite surprising,” Dr. Patel said. “It was, to the contrary, also surprising to see that, despite wide variance in medical comorbidities and functional status, surgical complications such as infection and neurological injury were similar in all groups.” He characterized the study as “the first large-scale assessment of functional status as a predictor of patient outcomes after cervical spine surgery. It fits in line with other studies utilizing large databases. Big data analysis of outcomes can be used to identify risk factors for complications including death after surgery. Identifying these factors is important if we are going to improve the care we provide. Accurately quantifying the impact of these risk factors is also critical when we risk stratify and compare hospitals and physicians.”
He acknowledged certain limitations of the study, including the fact that it is a retrospective study “with a heterogeneous population of patients, surgeons, hospitals, and procedures. This adds uncertainty to the analysis at the level of the individual patient but does provide generalizability to a broader patient population.”
Dr. Patel reported having no conflicts of interest.
AT CSRS 2015
Key clinical point: Preoperative functional status is predictive of morbidity and mortality following elective cervical spine surgery.
Major finding: Patients who were dependent from a functional standpoint were significantly older and had higher rates of all comorbidities, compared with their counterparts who were partially dependent or functionally independent (P less than .001).
Data source: A retrospective analysis of 24,357 patient files from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP).
Disclosures: Dr. Patel reported having no conflicts of interest.

Study characterizes injury risk in cervical myelopathy patients
SAN DIEGO – Compared with age-matched controls, patients with cervical spondylotic myelopathy had a significantly increased incidence of falls, hip fractures, and other injuries, preliminary results from a study of Medicare data suggest.
“Cervical myelopathy is the most common cause of spinal cord dysfunction in patients over age 55,” Dr. Daniel J. Blizzard said at the annual meeting of the Cervical Spine Research Society. “In general, it’s cord compression secondary to their ossification of posterior latitudinal ligament, congenital stenosis, and/or degenerative changes to vertebral bodies, discs, and facet joints. These create an upper motor neuron lesion, which causes gait disturbances, imbalance, loss of manual dexterity and coordination, and sensory changes and weakness.”

Dr. Blizzard, an orthopedic surgery resident at Duke University, Durham, N.C., noted that myelopathy gait is the most common presenting symptom in cervical spondylotic myelopathy (CSM), affecting almost 30% of patients. “It’s present in three-quarters of CSM patients undergoing decompression,” he said. “Cord compression can lead to impaired proprioception, spasticity, and stiffness. We know that this gait dysfunction is multifactorial. Imbalance and unsteadiness lead to compensatory broad-based arrhythmic shuffling and clumsy-appearing gait to maintain balance.”
An estimated one-third of people over age 65 fall at least once per year and this may lead to significant morbidity, including institutionalization, loss of independence, and mortality, Dr. Blizzard continued. “We know that gait dysfunction is a significant risk factor for falls,” he said. “This can be CSM, lower extremity osteoarthritis, deconditioning, or poor vision. The primary cause of a gait disturbance may not be accurately identified, especially if a more obvious cause is already known.”
The researchers set out to determine the fall and injury risk of patients with CSM, “with the goal of guiding attention to what we thought might be a potentially underestimated disease with regard to morbidity, and to provide data to consider when determining the type and timing of CSM treatment,” Dr. Blizzard said. They used the PearlDiver database to search the Medicare sample during 2005-2012, and used ICD-9 codes to identify patients with CSM. They also identified a subpopulation of CSM patients that underwent decompression, “not for the purpose of comparing the effect of decompression, but to identify a population with more severe disease,” he explained. They included a control population with no CSM, vestibular disease, or Parkinson’s disease.
Dr. Blizzard reported preliminary results from a total of 601,390 patients with CSM, 77,346 patients with CSM plus decompression, and 49,550,651 controls. They looked at the incidence of falls, head injuries, skull fractures, subdural hematomas, and other orthopedic injuries including fractures of the hip, femur, leg, ankle, pelvis, and lower extremity sprains. The researchers found that when compared with controls, patients with CSM had a statistically significant increased incidence of all injuries, including hip fracture (risk ratio, 2.62), head injury (RR, 7.34), and fall (RR, 8.08). The incidence of hip fracture, head injury, and fall was also increased among the subset of CSM patients who had undergone decompression (RR of 2.25, 8.34, and 9.62, respectively).
Dr. Blizzard acknowledged certain limitations of the study, including its retrospective design. “Statistical and clinical significance are two very different things,” he emphasized. “When we get numbers this big, everything will become statistically significant, but whether things are clinically significant is up to interpretation. The presence of disease and complications is contingent upon proper coding and recognition by providers. We have no measures of severity, extent, or chronicity of disease.”
Despite such limitations, he concluded that the findings suggest that impact of CSM on morbidity “is probably underestimated by many. Symptoms of CSM can be insidious or masked. Patients can often attribute these to normal effects of aging, and often primary care physicians will not recognize these initial symptoms, especially if there is another confounding presenting complaint.”
Conservative interventions for CSM patients, he said, include gait training/physical therapy, assistive aids, hip pads, exercise programs with balance training, and an assessment of hazards in the home environment. From a surgical standpoint, the findings raise the possibility that surgeons may want to “be more aggressive” in their decision to operate on patients with CSM. “This dataset is in no way able to address this question, but I think it provides interesting information regarding the true morbidity of the disease,” Dr. Blizzard said. “There is clear risk and morbidity with cervical compression. Studies show improvement in patients regardless of age, severity, and chronicity.”
Dr. Blizzard reported having no financial disclosures.
SAN DIEGO – Compared with age-matched controls, patients with cervical spondylotic myelopathy had a significantly increased incidence of falls, hip fractures, and other injuries, preliminary results from a study of Medicare data suggest.
“Cervical myelopathy is the most common cause of spinal cord dysfunction in patients over age 55,” Dr. Daniel J. Blizzard said at the annual meeting of the Cervical Spine Research Society. “In general, it’s cord compression secondary to their ossification of posterior latitudinal ligament, congenital stenosis, and/or degenerative changes to vertebral bodies, discs, and facet joints. These create an upper motor neuron lesion, which causes gait disturbances, imbalance, loss of manual dexterity and coordination, and sensory changes and weakness.”
Dr. Blizzard, an orthopedic surgery resident at Duke University, Durham, N.C., noted that myelopathy gait is the most common presenting symptom in cervical spondylotic myelopathy (CSM), affecting almost 30% of patients. “It’s present in three-quarters of CSM patients undergoing decompression,” he said. “Cord compression can lead to impaired proprioception, spasticity, and stiffness. We know that this gait dysfunction is multifactorial. Imbalance and unsteadiness lead to compensatory broad-based arrhythmic shuffling and clumsy-appearing gait to maintain balance.”
An estimated one-third of people over age 65 fall at least once per year and this may lead to significant morbidity, including institutionalization, loss of independence, and mortality, Dr. Blizzard continued. “We know that gait dysfunction is a significant risk factor for falls,” he said. “This can be CSM, lower extremity osteoarthritis, deconditioning, or poor vision. The primary cause of a gait disturbance may not be accurately identified, especially if a more obvious cause is already known.”
The researchers set out to determine the fall and injury risk of patients with CSM, “with the goal of guiding attention to what we thought might be a potentially underestimated disease with regard to morbidity, and to provide data to consider when determining the type and timing of CSM treatment,” Dr. Blizzard said. They used the PearlDiver database to search the Medicare sample during 2005-2012, and used ICD-9 codes to identify patients with CSM. They also identified a subpopulation of CSM patients that underwent decompression, “not for the purpose of comparing the effect of decompression, but to identify a population with more severe disease,” he explained. They included a control population with no CSM, vestibular disease, or Parkinson’s disease.
Dr. Blizzard reported preliminary results from a total of 601,390 patients with CSM, 77,346 patients with CSM plus decompression, and 49,550,651 controls. They looked at the incidence of falls, head injuries, skull fractures, subdural hematomas, and other orthopedic injuries including fractures of the hip, femur, leg, ankle, pelvis, and lower extremity sprains. The researchers found that when compared with controls, patients with CSM had a statistically significant increased incidence of all injuries, including hip fracture (risk ratio, 2.62), head injury (RR, 7.34), and fall (RR, 8.08). The incidence of hip fracture, head injury, and fall was also increased among the subset of CSM patients who had undergone decompression (RR of 2.25, 8.34, and 9.62, respectively).
Dr. Blizzard acknowledged certain limitations of the study, including its retrospective design. “Statistical and clinical significance are two very different things,” he emphasized. “When we get numbers this big, everything will become statistically significant, but whether things are clinically significant is up to interpretation. The presence of disease and complications is contingent upon proper coding and recognition by providers. We have no measures of severity, extent, or chronicity of disease.”
Despite such limitations, he concluded that the findings suggest that impact of CSM on morbidity “is probably underestimated by many. Symptoms of CSM can be insidious or masked. Patients can often attribute these to normal effects of aging, and often primary care physicians will not recognize these initial symptoms, especially if there is another confounding presenting complaint.”
Conservative interventions for CSM patients, he said, include gait training/physical therapy, assistive aids, hip pads, exercise programs with balance training, and an assessment of hazards in the home environment. From a surgical standpoint, the findings raise the possibility that surgeons may want to “be more aggressive” in their decision to operate on patients with CSM. “This dataset is in no way able to address this question, but I think it provides interesting information regarding the true morbidity of the disease,” Dr. Blizzard said. “There is clear risk and morbidity with cervical compression. Studies show improvement in patients regardless of age, severity, and chronicity.”
Dr. Blizzard reported having no financial disclosures.
SAN DIEGO – Compared with age-matched controls, patients with cervical spondylotic myelopathy had a significantly increased incidence of falls, hip fractures, and other injuries, preliminary results from a study of Medicare data suggest.
“Cervical myelopathy is the most common cause of spinal cord dysfunction in patients over age 55,” Dr. Daniel J. Blizzard said at the annual meeting of the Cervical Spine Research Society. “In general, it’s cord compression secondary to their ossification of posterior latitudinal ligament, congenital stenosis, and/or degenerative changes to vertebral bodies, discs, and facet joints. These create an upper motor neuron lesion, which causes gait disturbances, imbalance, loss of manual dexterity and coordination, and sensory changes and weakness.”
Dr. Blizzard, an orthopedic surgery resident at Duke University, Durham, N.C., noted that myelopathy gait is the most common presenting symptom in cervical spondylotic myelopathy (CSM), affecting almost 30% of patients. “It’s present in three-quarters of CSM patients undergoing decompression,” he said. “Cord compression can lead to impaired proprioception, spasticity, and stiffness. We know that this gait dysfunction is multifactorial. Imbalance and unsteadiness lead to compensatory broad-based arrhythmic shuffling and clumsy-appearing gait to maintain balance.”
An estimated one-third of people over age 65 fall at least once per year and this may lead to significant morbidity, including institutionalization, loss of independence, and mortality, Dr. Blizzard continued. “We know that gait dysfunction is a significant risk factor for falls,” he said. “This can be CSM, lower extremity osteoarthritis, deconditioning, or poor vision. The primary cause of a gait disturbance may not be accurately identified, especially if a more obvious cause is already known.”
The researchers set out to determine the fall and injury risk of patients with CSM, “with the goal of guiding attention to what we thought might be a potentially underestimated disease with regard to morbidity, and to provide data to consider when determining the type and timing of CSM treatment,” Dr. Blizzard said. They used the PearlDiver database to search the Medicare sample during 2005-2012, and used ICD-9 codes to identify patients with CSM. They also identified a subpopulation of CSM patients that underwent decompression, “not for the purpose of comparing the effect of decompression, but to identify a population with more severe disease,” he explained. They included a control population with no CSM, vestibular disease, or Parkinson’s disease.
Dr. Blizzard reported preliminary results from a total of 601,390 patients with CSM, 77,346 patients with CSM plus decompression, and 49,550,651 controls. They looked at the incidence of falls, head injuries, skull fractures, subdural hematomas, and other orthopedic injuries including fractures of the hip, femur, leg, ankle, pelvis, and lower extremity sprains. The researchers found that when compared with controls, patients with CSM had a statistically significant increased incidence of all injuries, including hip fracture (risk ratio, 2.62), head injury (RR, 7.34), and fall (RR, 8.08). The incidence of hip fracture, head injury, and fall was also increased among the subset of CSM patients who had undergone decompression (RR of 2.25, 8.34, and 9.62, respectively).
Dr. Blizzard acknowledged certain limitations of the study, including its retrospective design. “Statistical and clinical significance are two very different things,” he emphasized. “When we get numbers this big, everything will become statistically significant, but whether things are clinically significant is up to interpretation. The presence of disease and complications is contingent upon proper coding and recognition by providers. We have no measures of severity, extent, or chronicity of disease.”
Despite such limitations, he concluded that the findings suggest that impact of CSM on morbidity “is probably underestimated by many. Symptoms of CSM can be insidious or masked. Patients can often attribute these to normal effects of aging, and often primary care physicians will not recognize these initial symptoms, especially if there is another confounding presenting complaint.”
Conservative interventions for CSM patients, he said, include gait training/physical therapy, assistive aids, hip pads, exercise programs with balance training, and an assessment of hazards in the home environment. From a surgical standpoint, the findings raise the possibility that surgeons may want to “be more aggressive” in their decision to operate on patients with CSM. “This dataset is in no way able to address this question, but I think it provides interesting information regarding the true morbidity of the disease,” Dr. Blizzard said. “There is clear risk and morbidity with cervical compression. Studies show improvement in patients regardless of age, severity, and chronicity.”
Dr. Blizzard reported having no financial disclosures.
AT CSRS 2015
Key clinical point: Medicare patients with cervical spondylotic myelopathy face an increased risk of falls and fractures.
Major finding: Compared with controls, patients with CSM had a statistically significant increased incidence of all injuries, including hip fracture (risk ratio, 2.62), head injury (RR, 7.34), and fall (RR, 8.08).
Data source: A retrospective analysis of Medicare patients during 2005-2012, including 601,390 patients with CSM, 77,346 patients with CSM plus decompression, and 49,550,651 controls.
Disclosures: Dr. Blizzard reported having no financial disclosures.

Perioperative statins for cardiac surgery didn’t reduce kidney injury
SAN DIEGO – High-dose perioperative atorvastatin treatment did not reduce acute kidney injury following elective cardiac surgery, and it may increase risk in patients with chronic kidney disease (CKD) who are naive to statin treatment, results from a large, randomized trial showed.
“Despite advances in patient management that have reduced mortality during cardiac surgery, acute kidney injury continues to complicate the postoperative course in 20%-30% of patients,” Dr. Frederic Tremaine Billings said during a press briefing at a meeting sponsored by the American Society of Nephrology.

“Its diagnosis is independently associated with a fivefold increase in mortality following the surgery,” Dr. Tremaine added. “Statins affect several mechanisms underlying postoperative acute kidney injury. Widely prescribed to reduce cholesterol synthesis, these drugs also reduce lipid modification of intracellular signaling molecules, which have been shown to improve perfusion and reduce oxidative stress – both mechanisms important in acute kidney injury following cardiac surgery.”
Dr. Billings of the department of anesthesiology and critical care medicine at Vanderbilt University Medical Center, Nashville, Tenn., and his associates tested the hypothesis that short-term, high-dose perioperative (preoperative, intraoperative, and postoperative) atorvastatin reduces acute kidney injury (AKI) following elective cardiac surgery.
The researchers randomly assigned preoperative statin-naive patients to 80 mg of atorvastatin on the morning before surgery, 40 mg on the morning of surgery, and 40 mg daily throughout hospitalization, or to a matching placebo regimen. In addition, they randomly assigned patients who were already using statins prior to surgery to 80 mg of atorvastatin the morning of surgery, and 40 mg on the morning after surgery, or to a matching placebo regimen.
“We felt it was important to not withhold statin treatment in patients already using statins prior to surgery, beyond what is typically done in clinical practice,” Dr. Billings explained. “For this reason, preoperative statin–using subjects continued their statin up until the day before surgery, and then resumed their statin use on postoperative day 2.”
The primary endpoint of the study was the incidence of AKI as determined by Acute Kidney Injury Network criteria (a 0.3 mg/dL increase in serum creatinine concentrations within 48 hours of surgery). Secondary endpoints included the maximum creatinine increase from baseline to 48 hours after surgery, ICU delirium diagnosed by the Confusion Assessment Method for the ICU, myocardial injury, and the incidence of atrial fibrillation, pneumonia, and stroke. Safety endpoints included liver toxicity, muscle toxicity, and adverse events.
The study was limited to adults having elective cardiac surgery and excluded those with statin intolerance, acute coronary syndrome, liver dysfunction, use of CYP3A4 inhibitors, kidney transplant recipients, those currently on dialysis, and those who were pregnant.
From November 2009 to October 2014, the researchers recruited 653 patients. But the trial was halted on recommendation of Vanderbilt’s data and safety monitoring board because of futility and an increased incidence of AKI among statin-naive patients with CKD randomized to atorvastatin.
Among all patients, AKI occurred in 20.8% of those randomized to atorvastatin, compared with 19.5% of those randomized to placebo, a difference that was neither clinically nor statistically significant (P = .75), Dr. Billings reported.
However, among the 199 patients who were statin naive, AKI occurred in 21.6% of those randomized to atorvastatin, compared with 13.4% of those randomized to placebo (P = .14). “An 8% difference in the incidence of AKI is of clinical importance, if true,” he said.
Among the 36 statin-naive patients with CKD, AKI occurred in 52.9% of those randomized to atorvastatin, compared with 15.8% of those randomized to placebo (P = .03). “While the number of patients in this subgroup is small, the magnitude of effect is striking,” Dr. Billings said.
Among the 416 patients who were using statins prior to surgery, AKI occurred in 20.4% of those randomized to atorvastatin, compared with 22.4% of those randomized to placebo (P = .63). Results were similar among the subset of those patients who had CKD (31.3% vs. 36.3%; P = .59).
Safety endpoints were similar between the two groups.
Strengths of the study, Dr. Billings said, include the fact that it’s the largest randomized, controlled trial to date to test this hypothesis, the pragmatic design of the protocol, and rigorous methodology.
Limitations include the “small number of patients in the statin-naive CKD subgroup,” he noted. “And the short duration of treatment among prestudy statin-using patients could limit the observation that short-term withdrawal is not harmful – although we felt it appropriate not to limit statins beyond what’s typical in clinical practice, based on prior reports that even short-term statin withdrawal may be harmful.”
The National Institutes of Health and the department of anesthesiology at Vanderbilt University supported the study. Dr. Billings reported having no financial disclosures.
SAN DIEGO – High-dose perioperative atorvastatin treatment did not reduce acute kidney injury following elective cardiac surgery, and it may increase risk in patients with chronic kidney disease (CKD) who are naive to statin treatment, results from a large, randomized trial showed.
“Despite advances in patient management that have reduced mortality during cardiac surgery, acute kidney injury continues to complicate the postoperative course in 20%-30% of patients,” Dr. Frederic Tremaine Billings said during a press briefing at a meeting sponsored by the American Society of Nephrology.
“Its diagnosis is independently associated with a fivefold increase in mortality following the surgery,” Dr. Tremaine added. “Statins affect several mechanisms underlying postoperative acute kidney injury. Widely prescribed to reduce cholesterol synthesis, these drugs also reduce lipid modification of intracellular signaling molecules, which have been shown to improve perfusion and reduce oxidative stress – both mechanisms important in acute kidney injury following cardiac surgery.”
Dr. Billings of the department of anesthesiology and critical care medicine at Vanderbilt University Medical Center, Nashville, Tenn., and his associates tested the hypothesis that short-term, high-dose perioperative (preoperative, intraoperative, and postoperative) atorvastatin reduces acute kidney injury (AKI) following elective cardiac surgery.
The researchers randomly assigned preoperative statin-naive patients to 80 mg of atorvastatin on the morning before surgery, 40 mg on the morning of surgery, and 40 mg daily throughout hospitalization, or to a matching placebo regimen. In addition, they randomly assigned patients who were already using statins prior to surgery to 80 mg of atorvastatin the morning of surgery, and 40 mg on the morning after surgery, or to a matching placebo regimen.
“We felt it was important to not withhold statin treatment in patients already using statins prior to surgery, beyond what is typically done in clinical practice,” Dr. Billings explained. “For this reason, preoperative statin–using subjects continued their statin up until the day before surgery, and then resumed their statin use on postoperative day 2.”
The primary endpoint of the study was the incidence of AKI as determined by Acute Kidney Injury Network criteria (a 0.3 mg/dL increase in serum creatinine concentrations within 48 hours of surgery). Secondary endpoints included the maximum creatinine increase from baseline to 48 hours after surgery, ICU delirium diagnosed by the Confusion Assessment Method for the ICU, myocardial injury, and the incidence of atrial fibrillation, pneumonia, and stroke. Safety endpoints included liver toxicity, muscle toxicity, and adverse events.
The study was limited to adults having elective cardiac surgery and excluded those with statin intolerance, acute coronary syndrome, liver dysfunction, use of CYP3A4 inhibitors, kidney transplant recipients, those currently on dialysis, and those who were pregnant.
From November 2009 to October 2014, the researchers recruited 653 patients. But the trial was halted on recommendation of Vanderbilt’s data and safety monitoring board because of futility and an increased incidence of AKI among statin-naive patients with CKD randomized to atorvastatin.
Among all patients, AKI occurred in 20.8% of those randomized to atorvastatin, compared with 19.5% of those randomized to placebo, a difference that was neither clinically nor statistically significant (P = .75), Dr. Billings reported.
However, among the 199 patients who were statin naive, AKI occurred in 21.6% of those randomized to atorvastatin, compared with 13.4% of those randomized to placebo (P = .14). “An 8% difference in the incidence of AKI is of clinical importance, if true,” he said.
Among the 36 statin-naive patients with CKD, AKI occurred in 52.9% of those randomized to atorvastatin, compared with 15.8% of those randomized to placebo (P = .03). “While the number of patients in this subgroup is small, the magnitude of effect is striking,” Dr. Billings said.
Among the 416 patients who were using statins prior to surgery, AKI occurred in 20.4% of those randomized to atorvastatin, compared with 22.4% of those randomized to placebo (P = .63). Results were similar among the subset of those patients who had CKD (31.3% vs. 36.3%; P = .59).
Safety endpoints were similar between the two groups.
Strengths of the study, Dr. Billings said, include the fact that it’s the largest randomized, controlled trial to date to test this hypothesis, the pragmatic design of the protocol, and rigorous methodology.
Limitations include the “small number of patients in the statin-naive CKD subgroup,” he noted. “And the short duration of treatment among prestudy statin-using patients could limit the observation that short-term withdrawal is not harmful – although we felt it appropriate not to limit statins beyond what’s typical in clinical practice, based on prior reports that even short-term statin withdrawal may be harmful.”
The National Institutes of Health and the department of anesthesiology at Vanderbilt University supported the study. Dr. Billings reported having no financial disclosures.
SAN DIEGO – High-dose perioperative atorvastatin treatment did not reduce acute kidney injury following elective cardiac surgery, and it may increase risk in patients with chronic kidney disease (CKD) who are naive to statin treatment, results from a large, randomized trial showed.
“Despite advances in patient management that have reduced mortality during cardiac surgery, acute kidney injury continues to complicate the postoperative course in 20%-30% of patients,” Dr. Frederic Tremaine Billings said during a press briefing at a meeting sponsored by the American Society of Nephrology.
“Its diagnosis is independently associated with a fivefold increase in mortality following the surgery,” Dr. Tremaine added. “Statins affect several mechanisms underlying postoperative acute kidney injury. Widely prescribed to reduce cholesterol synthesis, these drugs also reduce lipid modification of intracellular signaling molecules, which have been shown to improve perfusion and reduce oxidative stress – both mechanisms important in acute kidney injury following cardiac surgery.”
Dr. Billings of the department of anesthesiology and critical care medicine at Vanderbilt University Medical Center, Nashville, Tenn., and his associates tested the hypothesis that short-term, high-dose perioperative (preoperative, intraoperative, and postoperative) atorvastatin reduces acute kidney injury (AKI) following elective cardiac surgery.
The researchers randomly assigned preoperative statin-naive patients to 80 mg of atorvastatin on the morning before surgery, 40 mg on the morning of surgery, and 40 mg daily throughout hospitalization, or to a matching placebo regimen. In addition, they randomly assigned patients who were already using statins prior to surgery to 80 mg of atorvastatin the morning of surgery, and 40 mg on the morning after surgery, or to a matching placebo regimen.
“We felt it was important to not withhold statin treatment in patients already using statins prior to surgery, beyond what is typically done in clinical practice,” Dr. Billings explained. “For this reason, preoperative statin–using subjects continued their statin up until the day before surgery, and then resumed their statin use on postoperative day 2.”
The primary endpoint of the study was the incidence of AKI as determined by Acute Kidney Injury Network criteria (a 0.3 mg/dL increase in serum creatinine concentrations within 48 hours of surgery). Secondary endpoints included the maximum creatinine increase from baseline to 48 hours after surgery, ICU delirium diagnosed by the Confusion Assessment Method for the ICU, myocardial injury, and the incidence of atrial fibrillation, pneumonia, and stroke. Safety endpoints included liver toxicity, muscle toxicity, and adverse events.
The study was limited to adults having elective cardiac surgery and excluded those with statin intolerance, acute coronary syndrome, liver dysfunction, use of CYP3A4 inhibitors, kidney transplant recipients, those currently on dialysis, and those who were pregnant.
From November 2009 to October 2014, the researchers recruited 653 patients. But the trial was halted on recommendation of Vanderbilt’s data and safety monitoring board because of futility and an increased incidence of AKI among statin-naive patients with CKD randomized to atorvastatin.
Among all patients, AKI occurred in 20.8% of those randomized to atorvastatin, compared with 19.5% of those randomized to placebo, a difference that was neither clinically nor statistically significant (P = .75), Dr. Billings reported.
However, among the 199 patients who were statin naive, AKI occurred in 21.6% of those randomized to atorvastatin, compared with 13.4% of those randomized to placebo (P = .14). “An 8% difference in the incidence of AKI is of clinical importance, if true,” he said.
Among the 36 statin-naive patients with CKD, AKI occurred in 52.9% of those randomized to atorvastatin, compared with 15.8% of those randomized to placebo (P = .03). “While the number of patients in this subgroup is small, the magnitude of effect is striking,” Dr. Billings said.
Among the 416 patients who were using statins prior to surgery, AKI occurred in 20.4% of those randomized to atorvastatin, compared with 22.4% of those randomized to placebo (P = .63). Results were similar among the subset of those patients who had CKD (31.3% vs. 36.3%; P = .59).
Safety endpoints were similar between the two groups.
Strengths of the study, Dr. Billings said, include the fact that it’s the largest randomized, controlled trial to date to test this hypothesis, the pragmatic design of the protocol, and rigorous methodology.
Limitations include the “small number of patients in the statin-naive CKD subgroup,” he noted. “And the short duration of treatment among prestudy statin-using patients could limit the observation that short-term withdrawal is not harmful – although we felt it appropriate not to limit statins beyond what’s typical in clinical practice, based on prior reports that even short-term statin withdrawal may be harmful.”
The National Institutes of Health and the department of anesthesiology at Vanderbilt University supported the study. Dr. Billings reported having no financial disclosures.
AT KIDNEY WEEK 2015
Key clinical point: The use of high-dose perioperative atorvastatin did not reduce acute kidney injury in patients undergoing elective cardiac surgery.
Major finding: Among all patients, acute kidney injury occurred in 20.8% of those randomized to atorvastatin, compared with 19.5% of those randomized to placebo, a difference that is neither clinically nor statistically significant (P = .75).
Data source: A randomized, controlled trial of 653 patients to test the hypothesis that short-term, high-dose perioperative atorvastatin reduces acute kidney injury following elective cardiac surgery.
Disclosures: The National Institutes of Health and the department of anesthesiology at Vanderbilt University supported the study. Dr. Billings reported having no financial disclosures.

Core needle biopsy proves sensitive for first-line thyroid nodule diagnosis
LAKE BUENA VISTA, FLA. – The nondiagnostic result rate was significantly lower with core needle biopsy than with fine needle aspiration as a first-line biopsy method for newly detected thyroid nodules in a comparative study.
In 631 pairs of initially detected thyroid nodules that were matched based on propensity score analysis, the nondiagnostic result rate was 1.4% when core needle biopsy (CNB) was used, compared with 8.1% with ultrasound-guided fine-needle aspiration. The indeterminate result rate was 5.1% vs. 8.1% with the two approaches, respectively, and the differences between the groups were statistically significant, Dr. Hyun Kyung Lim of Soonchunhyang University Seoul Hospital, Korea, reported at the International Thyroid Congress.

The nondiagnostic rate with CNB was also significantly lower than with fine-needle aspiration for nodules with calcifications, posterior location, or diameter less than 1 cm, Dr. Lim said at the meeting at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
No difference was seen between the groups with respect to diagnostic performance based on degree of clinician experience.
The complication rate was higher with CNB than with fine -needle aspiration (3.6% vs. 1.6%), but complications were minor, Dr. Lim said.
Core needle biopsy has been suggested as a complementary tool for the diagnosis of thyroid nodules when the results of fine-needle aspiration are inconclusive, and the approach has been shown to be both safe and accurate for biopsy. However, its role as a first-line approach for thyroid nodule biopsy has been controversial and few studies have evaluated it as a first-line tool, she noted.
The current findings suggest that CNB is a safe and highly sensitive first-line biopsy method for such nodules, she concluded.
Dr. Lim reported having no disclosures.
LAKE BUENA VISTA, FLA. – The nondiagnostic result rate was significantly lower with core needle biopsy than with fine needle aspiration as a first-line biopsy method for newly detected thyroid nodules in a comparative study.
In 631 pairs of initially detected thyroid nodules that were matched based on propensity score analysis, the nondiagnostic result rate was 1.4% when core needle biopsy (CNB) was used, compared with 8.1% with ultrasound-guided fine-needle aspiration. The indeterminate result rate was 5.1% vs. 8.1% with the two approaches, respectively, and the differences between the groups were statistically significant, Dr. Hyun Kyung Lim of Soonchunhyang University Seoul Hospital, Korea, reported at the International Thyroid Congress.
The nondiagnostic rate with CNB was also significantly lower than with fine-needle aspiration for nodules with calcifications, posterior location, or diameter less than 1 cm, Dr. Lim said at the meeting at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
No difference was seen between the groups with respect to diagnostic performance based on degree of clinician experience.
The complication rate was higher with CNB than with fine -needle aspiration (3.6% vs. 1.6%), but complications were minor, Dr. Lim said.
Core needle biopsy has been suggested as a complementary tool for the diagnosis of thyroid nodules when the results of fine-needle aspiration are inconclusive, and the approach has been shown to be both safe and accurate for biopsy. However, its role as a first-line approach for thyroid nodule biopsy has been controversial and few studies have evaluated it as a first-line tool, she noted.
The current findings suggest that CNB is a safe and highly sensitive first-line biopsy method for such nodules, she concluded.
Dr. Lim reported having no disclosures.
LAKE BUENA VISTA, FLA. – The nondiagnostic result rate was significantly lower with core needle biopsy than with fine needle aspiration as a first-line biopsy method for newly detected thyroid nodules in a comparative study.
In 631 pairs of initially detected thyroid nodules that were matched based on propensity score analysis, the nondiagnostic result rate was 1.4% when core needle biopsy (CNB) was used, compared with 8.1% with ultrasound-guided fine-needle aspiration. The indeterminate result rate was 5.1% vs. 8.1% with the two approaches, respectively, and the differences between the groups were statistically significant, Dr. Hyun Kyung Lim of Soonchunhyang University Seoul Hospital, Korea, reported at the International Thyroid Congress.
The nondiagnostic rate with CNB was also significantly lower than with fine-needle aspiration for nodules with calcifications, posterior location, or diameter less than 1 cm, Dr. Lim said at the meeting at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
No difference was seen between the groups with respect to diagnostic performance based on degree of clinician experience.
The complication rate was higher with CNB than with fine -needle aspiration (3.6% vs. 1.6%), but complications were minor, Dr. Lim said.
Core needle biopsy has been suggested as a complementary tool for the diagnosis of thyroid nodules when the results of fine-needle aspiration are inconclusive, and the approach has been shown to be both safe and accurate for biopsy. However, its role as a first-line approach for thyroid nodule biopsy has been controversial and few studies have evaluated it as a first-line tool, she noted.
The current findings suggest that CNB is a safe and highly sensitive first-line biopsy method for such nodules, she concluded.
Dr. Lim reported having no disclosures.
AT THE INTERNATIONAL THYROID CONGRESS
Key clinical point: The nondiagnostic result rate was significantly lower with core needle biopsy than with fine-needle aspiration as a first-line biopsy method for newly detected thyroid nodules in a comparative study.
Major finding: The nondiagnostic result rate was 1.4% with core needle biopsy vs. 8.1% with fine-needle aspiration.
Data source: A comparative study in 631 propensity score–matched pairs of thyroid nodules.
Disclosures: Dr. Lim reported having no disclosures.

Self-reported poor functional status predicts perioperative morbidity
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”

In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”
In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”
In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point:Poor self-reported exercise tolerance by patients with pulmonary hypertension is associated with multiple comorbidities and increased hospital length of stay.
Major finding: Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035).
Data source: A study 294 PHTN patients seen in preoperative anesthesia clinic at the University of Washington for non-cardiac, nonobstetric procedures from April 2007 through September 2013.
Disclosures: The researchers reported having no financial disclosures.

FDA advisory committees support changing codeine contraindications for children
SILVER SPRING, MD. – A joint meeting of the Food and Drug Administration’s Pulmonary-Allergy Drugs Advisory Committee (PADAC) and the Drug Safety and Risk Management Advisory Committee (DSaRM) on Dec. 10 voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the joint advisory panel voted for the aforementioned contraindication, while six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. Only one member – Dr. Maureen Finnegan of the DSaRM – voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. Only one member – Dr. Lorraine J. Gudas, a temporary voting member – supported removing codeine from the monograph only for children under age 2 years. Dr. Finnegan abstained from voting on this charge, telling the committee that “this is totally out of my wheelhouse.”
The decision to vote on approving amendments to the contraindications for codeine use – which would affect not just the monogram, but labeling as well – comes on the heels of the FDA announcing this summer that they would be investigating the safety of codeine-containing drugs in children, asking health care providers and patients to report any adverse events associated with the drug.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr. Sally Seymour, the FDA’s Deputy Director for Safety.
In a presentation on codeine use for pediatric analgesia, FDA Medical Officer Dr. Timothy Jiang cited several studies detailing adverse events in children taking codeine-containing drugs. One 2007 study by Voronov et al involved a 29-month-old boy of North African heritage who took codeine/acetaminophen following adenotonsillectomy for “recurrent tonsillitis and mild-moderate sleep apnea;” the boy was found unresponsive the day after the operation, but was later resuscitated.
In another study – a 2009 study in the New England Journal of Medicine by Catherine Ciszkowski and her associates – cites a similar situation of a 2-year-old boy receiving codeine after adenotonsillectomy, only to be found unresponsive; in this case, however, the boy died 2 days after the operation. Additionally, Dr. Jiang cited a 2012 search of the Adverse Event Reporting System, looking at data from 1969 through May 1, 2012, which found that six additional cases of death, as well as seven literature cases that mentioned patients’ CYPD26 status as possibly contributing.
The FDA is not required to follow the advice of its advisory panels, but often does. No members of the panel reported any relevant financial conflicts of interest.
SILVER SPRING, MD. – A joint meeting of the Food and Drug Administration’s Pulmonary-Allergy Drugs Advisory Committee (PADAC) and the Drug Safety and Risk Management Advisory Committee (DSaRM) on Dec. 10 voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the joint advisory panel voted for the aforementioned contraindication, while six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. Only one member – Dr. Maureen Finnegan of the DSaRM – voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. Only one member – Dr. Lorraine J. Gudas, a temporary voting member – supported removing codeine from the monograph only for children under age 2 years. Dr. Finnegan abstained from voting on this charge, telling the committee that “this is totally out of my wheelhouse.”
The decision to vote on approving amendments to the contraindications for codeine use – which would affect not just the monogram, but labeling as well – comes on the heels of the FDA announcing this summer that they would be investigating the safety of codeine-containing drugs in children, asking health care providers and patients to report any adverse events associated with the drug.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr. Sally Seymour, the FDA’s Deputy Director for Safety.
In a presentation on codeine use for pediatric analgesia, FDA Medical Officer Dr. Timothy Jiang cited several studies detailing adverse events in children taking codeine-containing drugs. One 2007 study by Voronov et al involved a 29-month-old boy of North African heritage who took codeine/acetaminophen following adenotonsillectomy for “recurrent tonsillitis and mild-moderate sleep apnea;” the boy was found unresponsive the day after the operation, but was later resuscitated.
In another study – a 2009 study in the New England Journal of Medicine by Catherine Ciszkowski and her associates – cites a similar situation of a 2-year-old boy receiving codeine after adenotonsillectomy, only to be found unresponsive; in this case, however, the boy died 2 days after the operation. Additionally, Dr. Jiang cited a 2012 search of the Adverse Event Reporting System, looking at data from 1969 through May 1, 2012, which found that six additional cases of death, as well as seven literature cases that mentioned patients’ CYPD26 status as possibly contributing.
The FDA is not required to follow the advice of its advisory panels, but often does. No members of the panel reported any relevant financial conflicts of interest.
SILVER SPRING, MD. – A joint meeting of the Food and Drug Administration’s Pulmonary-Allergy Drugs Advisory Committee (PADAC) and the Drug Safety and Risk Management Advisory Committee (DSaRM) on Dec. 10 voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the joint advisory panel voted for the aforementioned contraindication, while six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. Only one member – Dr. Maureen Finnegan of the DSaRM – voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. Only one member – Dr. Lorraine J. Gudas, a temporary voting member – supported removing codeine from the monograph only for children under age 2 years. Dr. Finnegan abstained from voting on this charge, telling the committee that “this is totally out of my wheelhouse.”
The decision to vote on approving amendments to the contraindications for codeine use – which would affect not just the monogram, but labeling as well – comes on the heels of the FDA announcing this summer that they would be investigating the safety of codeine-containing drugs in children, asking health care providers and patients to report any adverse events associated with the drug.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr. Sally Seymour, the FDA’s Deputy Director for Safety.
In a presentation on codeine use for pediatric analgesia, FDA Medical Officer Dr. Timothy Jiang cited several studies detailing adverse events in children taking codeine-containing drugs. One 2007 study by Voronov et al involved a 29-month-old boy of North African heritage who took codeine/acetaminophen following adenotonsillectomy for “recurrent tonsillitis and mild-moderate sleep apnea;” the boy was found unresponsive the day after the operation, but was later resuscitated.
In another study – a 2009 study in the New England Journal of Medicine by Catherine Ciszkowski and her associates – cites a similar situation of a 2-year-old boy receiving codeine after adenotonsillectomy, only to be found unresponsive; in this case, however, the boy died 2 days after the operation. Additionally, Dr. Jiang cited a 2012 search of the Adverse Event Reporting System, looking at data from 1969 through May 1, 2012, which found that six additional cases of death, as well as seven literature cases that mentioned patients’ CYPD26 status as possibly contributing.
The FDA is not required to follow the advice of its advisory panels, but often does. No members of the panel reported any relevant financial conflicts of interest.
AT AN FDA ADVISORY COMMITTEE MEETING