User login
Official Newspaper of the American College of Surgeons
TH3RESA: T-DM1 prolongs survival in heavily pretreated HER2-positive breast cancer
SAN ANTONIO – The antibody–drug conjugate trastuzumab emtansine (T-DM1) is safe and efficacious for treating heavily pretreated HER2-positive metastatic breast cancer, according to data from the randomized phase III TH3RESA trial reported at the San Antonio Breast Cancer Symposium.
“T-DM1 demonstrated a clinically meaningful and statistically significant improvement in overall survival, compared to treatment of physician’s choice in patients with HER2-positive metastatic breast cancer previously treated with a taxane, trastuzumab, and lapatinib,” first author Dr. Hans Wildiers, professor of medical oncology at KU Leuven (Belgium), commented in a related press briefing. “This result was reached despite about 50% crossover and about 80% of patients in the control arm receiving trastuzumab-containing regimens,” he said.

T-DM1 is approved by the Food and Drug Administration for the treatment of less heavily pretreated advanced disease on the basis of findings from the EMILIA trial. In that trial (the results of which were updated at the symposium), T-DM1 outperformed the combination of lapatinib and capecitabine.
“The TH3RESA results together with the EMILIA overall survival benefit … further solidify the role of T-DM1 in the treatment of previously treated HER2-positive advanced breast cancer,” Dr. Wildiers said.
Press briefing moderator Dr. C. Kent Osborne, professor of medicine and molecular and cellular biology and director of the Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, asked about the durability of the T-DM1 benefit: “What is the longest patients who are still in remission have been on study?”
About a quarter of patients were still on the trial as of the data cutoff for the analysis, signifying longer-term benefit, according to Dr. Wildiers.
“Just to put this in perspective, we used to think, and still do in a way, that HER2-positive breast cancer was one of the more aggressive forms of the disease, and we hated to see a patient who would come in with a HER2-positive tumor,” Dr. Osborne commented. “Now with our treatments, based on the HER2 and the identification of targeted therapy, it’s actually turned out to be a good tumor to have. And this is just another example of the effectiveness of this drug.”

The 602 patients enrolled in TH3RESA had to have received at least two prior HER2-directed therapies for their advanced disease, although the majority had received four or more. They were randomized 2:1 to T-DM1 (brand name Kadcyla) or a treatment of the physician’s choice as a control.
The study was amended part way through when the EMILIA results became available so that patients in the control arm could cross over to T-DM1 at the time of progression, and about half did so.
The results of the second interim overall survival analysis reported at the symposium showed that T-DM1 prolonged overall survival by almost 7 months, compared with a treatment of the physician’s choice: 22.7 months vs.15.8 months (hazard ratio, 0.68; P = .0007).
“Subgroup analysis showed no clear differences in different subgroups, except for a possible trend toward greater benefit for patients outside the United States,” Dr. Wildiers commented, while cautioning that numbers of patients were small and that finding shouldn’t be overinterpreted.
The overall survival benefit was similar when patients in the control arm were censored at the time of progression and crossing over to T-DM1 (22.7 vs. 15.6 months; HR, 0.58; P = .0002).
Patients were on therapy about twice as long with T-DM1 as with the treatment of a physician’s choice (7.9 vs. 4.1 months). Even so, the agent had a favorable safety profile, he said.
The control group had higher rates of grade 3 or worse diarrhea (4.3% vs. 0.7%), neutropenia (15.8% vs. 2.5%), and febrile neutropenia (3.8% vs. 0.2%). The T-DM1 group had a higher rate of grade 3 or worse thrombocytopenia (6.0% vs. 2.7%). Reductions in ejection fraction were rare overall and no more common with T-DM1 than in the control arm, according to Dr. Wildiers.
Quality of life was not assessed in the trial. However, that outcome can be inferred from others, according to Dr. Osborne.
“You could estimate the difference in quality of life by looking at the side effects of the treatment, and this treatment [T-DM1] had far fewer side effects,” he said. “Most of the side effects come from the cancer anyway at this stage, and if you are putting patients into remission and they are staying there for long periods of time, those symptoms are markedly improved.”
SAN ANTONIO – The antibody–drug conjugate trastuzumab emtansine (T-DM1) is safe and efficacious for treating heavily pretreated HER2-positive metastatic breast cancer, according to data from the randomized phase III TH3RESA trial reported at the San Antonio Breast Cancer Symposium.
“T-DM1 demonstrated a clinically meaningful and statistically significant improvement in overall survival, compared to treatment of physician’s choice in patients with HER2-positive metastatic breast cancer previously treated with a taxane, trastuzumab, and lapatinib,” first author Dr. Hans Wildiers, professor of medical oncology at KU Leuven (Belgium), commented in a related press briefing. “This result was reached despite about 50% crossover and about 80% of patients in the control arm receiving trastuzumab-containing regimens,” he said.
T-DM1 is approved by the Food and Drug Administration for the treatment of less heavily pretreated advanced disease on the basis of findings from the EMILIA trial. In that trial (the results of which were updated at the symposium), T-DM1 outperformed the combination of lapatinib and capecitabine.
“The TH3RESA results together with the EMILIA overall survival benefit … further solidify the role of T-DM1 in the treatment of previously treated HER2-positive advanced breast cancer,” Dr. Wildiers said.
Press briefing moderator Dr. C. Kent Osborne, professor of medicine and molecular and cellular biology and director of the Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, asked about the durability of the T-DM1 benefit: “What is the longest patients who are still in remission have been on study?”
About a quarter of patients were still on the trial as of the data cutoff for the analysis, signifying longer-term benefit, according to Dr. Wildiers.
“Just to put this in perspective, we used to think, and still do in a way, that HER2-positive breast cancer was one of the more aggressive forms of the disease, and we hated to see a patient who would come in with a HER2-positive tumor,” Dr. Osborne commented. “Now with our treatments, based on the HER2 and the identification of targeted therapy, it’s actually turned out to be a good tumor to have. And this is just another example of the effectiveness of this drug.”
The 602 patients enrolled in TH3RESA had to have received at least two prior HER2-directed therapies for their advanced disease, although the majority had received four or more. They were randomized 2:1 to T-DM1 (brand name Kadcyla) or a treatment of the physician’s choice as a control.
The study was amended part way through when the EMILIA results became available so that patients in the control arm could cross over to T-DM1 at the time of progression, and about half did so.
The results of the second interim overall survival analysis reported at the symposium showed that T-DM1 prolonged overall survival by almost 7 months, compared with a treatment of the physician’s choice: 22.7 months vs.15.8 months (hazard ratio, 0.68; P = .0007).
“Subgroup analysis showed no clear differences in different subgroups, except for a possible trend toward greater benefit for patients outside the United States,” Dr. Wildiers commented, while cautioning that numbers of patients were small and that finding shouldn’t be overinterpreted.
The overall survival benefit was similar when patients in the control arm were censored at the time of progression and crossing over to T-DM1 (22.7 vs. 15.6 months; HR, 0.58; P = .0002).
Patients were on therapy about twice as long with T-DM1 as with the treatment of a physician’s choice (7.9 vs. 4.1 months). Even so, the agent had a favorable safety profile, he said.
The control group had higher rates of grade 3 or worse diarrhea (4.3% vs. 0.7%), neutropenia (15.8% vs. 2.5%), and febrile neutropenia (3.8% vs. 0.2%). The T-DM1 group had a higher rate of grade 3 or worse thrombocytopenia (6.0% vs. 2.7%). Reductions in ejection fraction were rare overall and no more common with T-DM1 than in the control arm, according to Dr. Wildiers.
Quality of life was not assessed in the trial. However, that outcome can be inferred from others, according to Dr. Osborne.
“You could estimate the difference in quality of life by looking at the side effects of the treatment, and this treatment [T-DM1] had far fewer side effects,” he said. “Most of the side effects come from the cancer anyway at this stage, and if you are putting patients into remission and they are staying there for long periods of time, those symptoms are markedly improved.”
SAN ANTONIO – The antibody–drug conjugate trastuzumab emtansine (T-DM1) is safe and efficacious for treating heavily pretreated HER2-positive metastatic breast cancer, according to data from the randomized phase III TH3RESA trial reported at the San Antonio Breast Cancer Symposium.
“T-DM1 demonstrated a clinically meaningful and statistically significant improvement in overall survival, compared to treatment of physician’s choice in patients with HER2-positive metastatic breast cancer previously treated with a taxane, trastuzumab, and lapatinib,” first author Dr. Hans Wildiers, professor of medical oncology at KU Leuven (Belgium), commented in a related press briefing. “This result was reached despite about 50% crossover and about 80% of patients in the control arm receiving trastuzumab-containing regimens,” he said.
T-DM1 is approved by the Food and Drug Administration for the treatment of less heavily pretreated advanced disease on the basis of findings from the EMILIA trial. In that trial (the results of which were updated at the symposium), T-DM1 outperformed the combination of lapatinib and capecitabine.
“The TH3RESA results together with the EMILIA overall survival benefit … further solidify the role of T-DM1 in the treatment of previously treated HER2-positive advanced breast cancer,” Dr. Wildiers said.
Press briefing moderator Dr. C. Kent Osborne, professor of medicine and molecular and cellular biology and director of the Dan L. Duncan Comprehensive Cancer Center, Baylor College of Medicine, Houston, asked about the durability of the T-DM1 benefit: “What is the longest patients who are still in remission have been on study?”
About a quarter of patients were still on the trial as of the data cutoff for the analysis, signifying longer-term benefit, according to Dr. Wildiers.
“Just to put this in perspective, we used to think, and still do in a way, that HER2-positive breast cancer was one of the more aggressive forms of the disease, and we hated to see a patient who would come in with a HER2-positive tumor,” Dr. Osborne commented. “Now with our treatments, based on the HER2 and the identification of targeted therapy, it’s actually turned out to be a good tumor to have. And this is just another example of the effectiveness of this drug.”
The 602 patients enrolled in TH3RESA had to have received at least two prior HER2-directed therapies for their advanced disease, although the majority had received four or more. They were randomized 2:1 to T-DM1 (brand name Kadcyla) or a treatment of the physician’s choice as a control.
The study was amended part way through when the EMILIA results became available so that patients in the control arm could cross over to T-DM1 at the time of progression, and about half did so.
The results of the second interim overall survival analysis reported at the symposium showed that T-DM1 prolonged overall survival by almost 7 months, compared with a treatment of the physician’s choice: 22.7 months vs.15.8 months (hazard ratio, 0.68; P = .0007).
“Subgroup analysis showed no clear differences in different subgroups, except for a possible trend toward greater benefit for patients outside the United States,” Dr. Wildiers commented, while cautioning that numbers of patients were small and that finding shouldn’t be overinterpreted.
The overall survival benefit was similar when patients in the control arm were censored at the time of progression and crossing over to T-DM1 (22.7 vs. 15.6 months; HR, 0.58; P = .0002).
Patients were on therapy about twice as long with T-DM1 as with the treatment of a physician’s choice (7.9 vs. 4.1 months). Even so, the agent had a favorable safety profile, he said.
The control group had higher rates of grade 3 or worse diarrhea (4.3% vs. 0.7%), neutropenia (15.8% vs. 2.5%), and febrile neutropenia (3.8% vs. 0.2%). The T-DM1 group had a higher rate of grade 3 or worse thrombocytopenia (6.0% vs. 2.7%). Reductions in ejection fraction were rare overall and no more common with T-DM1 than in the control arm, according to Dr. Wildiers.
Quality of life was not assessed in the trial. However, that outcome can be inferred from others, according to Dr. Osborne.
“You could estimate the difference in quality of life by looking at the side effects of the treatment, and this treatment [T-DM1] had far fewer side effects,” he said. “Most of the side effects come from the cancer anyway at this stage, and if you are putting patients into remission and they are staying there for long periods of time, those symptoms are markedly improved.”
AT SABCS 2015
Key clinical point: T-DM1 is safe and efficacious for treating heavily pretreated HER2-positive breast cancer.
Major finding: The median overall survival was 22.7 months with T-DM1 vs. 15.8 months with the treatment of a physician’s choice.
Data source: A randomized phase III trial in 602 patients with heavily pretreated HER2-positive breast cancer (TH3RESA trial).
Disclosures: Dr. Wildiers disclosed that his institution has received compensation from Roche for lectures he has presented at national meetings and for consulting work, as well as an unrestricted research grant for academic research. The trial was supported by Roche.

Docs to CMS: Delay Meaningful Use Stage 3
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).

“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.

The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.

Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).
“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.
The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.
Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).
“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.
The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.
Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med

Beta-blocker prevents trastuzumab-related LVEF drop
SAN ANTONIO – Prophylactic beta-blockade with bisoprolol during adjuvant trastuzumab therapy for HER2-positive breast cancer prevented trastuzumab-induced decline in left ventricular ejection fraction in MANTICORE, a randomized trial presented at the San Antonio Breast Cancer Symposium.
“MANTICORE provides the first intervention proven in a randomized, double-blind, placebo-controlled, multicenter way to be an effective means of preventing trastuzumab-associated left ventricular dysfunction,” said Edith Pituskin, Ph.D., of the University of Alberta, Edmonton.

MANTICORE (Multidisciplinary Approach to Novel Therapies in Cardio-Oncology Research) randomized 99 patients with HER2-positive early breast cancer and a normal-range left ventricular ejection fraction (LVEF) at baseline to bisoprolol (Zebeta), the ACE inhibitor perindopril (Aceon), or placebo shortly before starting a planned 1-year course of adjuvant trastuzumab (Herceptin). The patients had low background levels of cardiovascular risk factors. Roughly three-quarters of subjects were able to titrate up to the target dose of 10 mg once daily for bisoprolol or 8 mg once daily for perindopril.
Cardiac MRI assessments at baseline, 3, and 12 months – the point when trastuzumab and the cardioprotective medications were stopped – showed that neither bisoprolol nor perindopril prevented trastuzumab-related left ventricular remodeling, which was a disappointment, given that this was the prespecified primary endpoint.
“Our results hint that, potentially, trastuzumab exposure–related left ventricular remodeling is not reversible,” Dr. Pituskin said.
The average reduction from baseline in LVEF over the course of a year of adjuvant trastuzumab therapy was 5% with placebo, 3% with perindopril, and 1% with bisoprolol, with the differences between bisoprolol and the other two study arms being highly statistically significant.
On the plus side, both of the once-daily cardiac medications displayed an important side benefit in MANTICORE: an eightfold reduction in the number of interruptions of trastuzumab therapy mandated by a significant drop in LVEF. There were eight such interruptions in the control group versus one each in the bisoprolol and perindopril arms. That’s of practical value in terms of patient convenience, cost of care, and possibly even the efficacy of the adjuvant cancer regimen, she noted.
Audience members raised several questions: what’s the clinical significance of the asymptomatic reduction in LVEF seen in the control group in MANTICORE? Does it place affected patients at risk for overt heart failure as time passes? And since LVEF is just one aspect of cardiac function, isn’t it possible that the cardiac medications were simply propping up LVEF while the underlying cardiotoxic effects of trastuzumab remained unchecked, such that the LVEF will drop once patients are off therapy?
Dr. Pituskin replied that these are good questions, the answers to which may be forthcoming at the planned follow-up cardiac MRI to be conducted at 24 months, a full year after discontinuation of the therapies.
Asked to compare the MANTICORE findings with those of the PRADA trial presented at this year’s annual meeting of the American Heart Association, in which an LVEF drop in breast cancer patients on adjuvant anthracycline and trastuzumab was prevented by prophylactic use of the angiotensin receptor blocker candesartan (Atacand) but not the beta-blocker metoprolol, Dr. Pituskin said she can’t make a definitive comparison until PRADA is published, but that it’s her understanding PRADA was a single-center trial without serial cardiac MRIs, and it included many more participants on an anthracycline-containing regimen, long recognized as a major hazard in terms of cardiotoxicity, and one thought to have a different cardiotoxic mechanism than trastuzumab.
By way of background, she noted that roughly 20% of women with breast cancer have HER2 receptor–overexpressing tumors. In such patients it’s well established that trastuzumab reduces mortality by one-third. However, it’s also well established that one in five patients on trastuzumab experience left ventricular dysfunction, and 1%-5% of patients develop heart failure, an “extremely devastating” complication carrying a 50% 5-year mortality. Beta-blockers and ACE inhibitors or angiotensin receptor blockers are standard, guideline-recommended treatments for patients with established heart failure.
SAN ANTONIO – Prophylactic beta-blockade with bisoprolol during adjuvant trastuzumab therapy for HER2-positive breast cancer prevented trastuzumab-induced decline in left ventricular ejection fraction in MANTICORE, a randomized trial presented at the San Antonio Breast Cancer Symposium.
“MANTICORE provides the first intervention proven in a randomized, double-blind, placebo-controlled, multicenter way to be an effective means of preventing trastuzumab-associated left ventricular dysfunction,” said Edith Pituskin, Ph.D., of the University of Alberta, Edmonton.
MANTICORE (Multidisciplinary Approach to Novel Therapies in Cardio-Oncology Research) randomized 99 patients with HER2-positive early breast cancer and a normal-range left ventricular ejection fraction (LVEF) at baseline to bisoprolol (Zebeta), the ACE inhibitor perindopril (Aceon), or placebo shortly before starting a planned 1-year course of adjuvant trastuzumab (Herceptin). The patients had low background levels of cardiovascular risk factors. Roughly three-quarters of subjects were able to titrate up to the target dose of 10 mg once daily for bisoprolol or 8 mg once daily for perindopril.
Cardiac MRI assessments at baseline, 3, and 12 months – the point when trastuzumab and the cardioprotective medications were stopped – showed that neither bisoprolol nor perindopril prevented trastuzumab-related left ventricular remodeling, which was a disappointment, given that this was the prespecified primary endpoint.
“Our results hint that, potentially, trastuzumab exposure–related left ventricular remodeling is not reversible,” Dr. Pituskin said.
The average reduction from baseline in LVEF over the course of a year of adjuvant trastuzumab therapy was 5% with placebo, 3% with perindopril, and 1% with bisoprolol, with the differences between bisoprolol and the other two study arms being highly statistically significant.
On the plus side, both of the once-daily cardiac medications displayed an important side benefit in MANTICORE: an eightfold reduction in the number of interruptions of trastuzumab therapy mandated by a significant drop in LVEF. There were eight such interruptions in the control group versus one each in the bisoprolol and perindopril arms. That’s of practical value in terms of patient convenience, cost of care, and possibly even the efficacy of the adjuvant cancer regimen, she noted.
Audience members raised several questions: what’s the clinical significance of the asymptomatic reduction in LVEF seen in the control group in MANTICORE? Does it place affected patients at risk for overt heart failure as time passes? And since LVEF is just one aspect of cardiac function, isn’t it possible that the cardiac medications were simply propping up LVEF while the underlying cardiotoxic effects of trastuzumab remained unchecked, such that the LVEF will drop once patients are off therapy?
Dr. Pituskin replied that these are good questions, the answers to which may be forthcoming at the planned follow-up cardiac MRI to be conducted at 24 months, a full year after discontinuation of the therapies.
Asked to compare the MANTICORE findings with those of the PRADA trial presented at this year’s annual meeting of the American Heart Association, in which an LVEF drop in breast cancer patients on adjuvant anthracycline and trastuzumab was prevented by prophylactic use of the angiotensin receptor blocker candesartan (Atacand) but not the beta-blocker metoprolol, Dr. Pituskin said she can’t make a definitive comparison until PRADA is published, but that it’s her understanding PRADA was a single-center trial without serial cardiac MRIs, and it included many more participants on an anthracycline-containing regimen, long recognized as a major hazard in terms of cardiotoxicity, and one thought to have a different cardiotoxic mechanism than trastuzumab.
By way of background, she noted that roughly 20% of women with breast cancer have HER2 receptor–overexpressing tumors. In such patients it’s well established that trastuzumab reduces mortality by one-third. However, it’s also well established that one in five patients on trastuzumab experience left ventricular dysfunction, and 1%-5% of patients develop heart failure, an “extremely devastating” complication carrying a 50% 5-year mortality. Beta-blockers and ACE inhibitors or angiotensin receptor blockers are standard, guideline-recommended treatments for patients with established heart failure.
SAN ANTONIO – Prophylactic beta-blockade with bisoprolol during adjuvant trastuzumab therapy for HER2-positive breast cancer prevented trastuzumab-induced decline in left ventricular ejection fraction in MANTICORE, a randomized trial presented at the San Antonio Breast Cancer Symposium.
“MANTICORE provides the first intervention proven in a randomized, double-blind, placebo-controlled, multicenter way to be an effective means of preventing trastuzumab-associated left ventricular dysfunction,” said Edith Pituskin, Ph.D., of the University of Alberta, Edmonton.
MANTICORE (Multidisciplinary Approach to Novel Therapies in Cardio-Oncology Research) randomized 99 patients with HER2-positive early breast cancer and a normal-range left ventricular ejection fraction (LVEF) at baseline to bisoprolol (Zebeta), the ACE inhibitor perindopril (Aceon), or placebo shortly before starting a planned 1-year course of adjuvant trastuzumab (Herceptin). The patients had low background levels of cardiovascular risk factors. Roughly three-quarters of subjects were able to titrate up to the target dose of 10 mg once daily for bisoprolol or 8 mg once daily for perindopril.
Cardiac MRI assessments at baseline, 3, and 12 months – the point when trastuzumab and the cardioprotective medications were stopped – showed that neither bisoprolol nor perindopril prevented trastuzumab-related left ventricular remodeling, which was a disappointment, given that this was the prespecified primary endpoint.
“Our results hint that, potentially, trastuzumab exposure–related left ventricular remodeling is not reversible,” Dr. Pituskin said.
The average reduction from baseline in LVEF over the course of a year of adjuvant trastuzumab therapy was 5% with placebo, 3% with perindopril, and 1% with bisoprolol, with the differences between bisoprolol and the other two study arms being highly statistically significant.
On the plus side, both of the once-daily cardiac medications displayed an important side benefit in MANTICORE: an eightfold reduction in the number of interruptions of trastuzumab therapy mandated by a significant drop in LVEF. There were eight such interruptions in the control group versus one each in the bisoprolol and perindopril arms. That’s of practical value in terms of patient convenience, cost of care, and possibly even the efficacy of the adjuvant cancer regimen, she noted.
Audience members raised several questions: what’s the clinical significance of the asymptomatic reduction in LVEF seen in the control group in MANTICORE? Does it place affected patients at risk for overt heart failure as time passes? And since LVEF is just one aspect of cardiac function, isn’t it possible that the cardiac medications were simply propping up LVEF while the underlying cardiotoxic effects of trastuzumab remained unchecked, such that the LVEF will drop once patients are off therapy?
Dr. Pituskin replied that these are good questions, the answers to which may be forthcoming at the planned follow-up cardiac MRI to be conducted at 24 months, a full year after discontinuation of the therapies.
Asked to compare the MANTICORE findings with those of the PRADA trial presented at this year’s annual meeting of the American Heart Association, in which an LVEF drop in breast cancer patients on adjuvant anthracycline and trastuzumab was prevented by prophylactic use of the angiotensin receptor blocker candesartan (Atacand) but not the beta-blocker metoprolol, Dr. Pituskin said she can’t make a definitive comparison until PRADA is published, but that it’s her understanding PRADA was a single-center trial without serial cardiac MRIs, and it included many more participants on an anthracycline-containing regimen, long recognized as a major hazard in terms of cardiotoxicity, and one thought to have a different cardiotoxic mechanism than trastuzumab.
By way of background, she noted that roughly 20% of women with breast cancer have HER2 receptor–overexpressing tumors. In such patients it’s well established that trastuzumab reduces mortality by one-third. However, it’s also well established that one in five patients on trastuzumab experience left ventricular dysfunction, and 1%-5% of patients develop heart failure, an “extremely devastating” complication carrying a 50% 5-year mortality. Beta-blockers and ACE inhibitors or angiotensin receptor blockers are standard, guideline-recommended treatments for patients with established heart failure.
AT SABCS 2015
Key clinical point: Bisoprolol prevents the trastuzumab-related decline in left ventricular ejection fraction in breast cancer patients.
Major finding: The average reduction from baseline in LVEF over the course of a year of adjuvant trastuzumab therapy was 5% with placebo, 3% with perindopril, and 1% with bisoprolol, with the differences between bisoprolol and the other two study arms being highly statistically significant. .
Data source: MANTICORE was a randomized, double-blind, multicenter study in which 99 patients with HER2-positive breast cancer were placed on prophylactic bisoprolol, perindopril, or placebo before starting adjuvant trastuzumab.
Disclosures: MANTICORE was funded by the Canadian Institutes for Health Research and the Alberta Cancer Foundation. The study presenter reported having no financial conflicts of interest.

‘Clinical equipoise’ surrounds neoadjuvant carboplatin for TNBC
SAN ANTONIO – Should carboplatin be considered a routine part of neoadjuvant therapy in early stage triple negative breast cancer?
Not yet, Dr. Angela M. DeMichele declared at the San Antonio Breast Cancer Symposium.

“I would say it’s still an individualized decision. The hazard ratios suggest benefit, but currently there’s not enough data to be conclusive,” according to Dr. DeMichele, who served as discussant for two clinical trials with discordant results – GeparSixto and CALGB/Alliance 40603 – presented at the symposium.
She also addressed a second issue raised by the two studies: is a pathologic complete response a valid surrogate for event-free survival?
“I would say a qualified yes,” commented Dr. DeMichele, professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia.
In GeparSixto, the addition of weekly carboplatin to a neoadjuvant chemotherapy backbone comprised of an anthracycline, taxane, and bevacizumab in patients with triple negative breast cancer (TNBC) boosted the 3-year disease-free survival rate significantly, from 76.1% to 85.5%. This result prompted GeparSixto presenter Dr. Gunter von Minckwitz, president of the German Breast Group, to declare that the study supports incorporation of carboplatin as part of standard neoadjuvant therapy in TNBC.
In contrast, in CALGB/Alliance 40603, adding carboplatin to neoadjuvant chemotherapy didn’t result in a significant improvement in 3-year event-free or overall survival.
Dr. DeMichele noted that with just 3 years of followup to date in these trials, there isn’t any information yet about carboplatin’s added potential long-term bone marrow toxicity. That’s an important unanswered question. Nor is any quality of life data available from the two trials. These issues need clarification before broader use of carboplatin.
One possible explanation for the disparate results in the two studies lies in differences in the chemotherapy and carboplatin doses and treatment schedules used. Patients in GeparSixto received greater cumulative amounts of anthracycline and taxane, given over a longer time period. And if patients were randomized to receive carboplatin, they got it at area under the curve 1.5 or 2 weekly for the duration of chemotherapy, as compared to carboplatin dosed just four times at area under the curve 6 every 3 weeks in CALGB/Alliance 40603.
“Could the weekly carboplatin in GeparSixto have provided less time for DNA repair in the tumor?,” she speculated.

Dr. William M. Sikov, who presented the CALGB/Alliance 40603 findings, found this quite plausible.
“We know treatment schedule and dose are important with anthracyclines, they’re important with taxanes, and it’s certainly not far fetched to propose that they may be important for carboplatin as well. Might that have made a difference? Can’t say,” observed Dr. Sikov of Women and Infants Hospital of Rhode Island in Providence.
In any case, Dr. DeMichele said neither GeparSixto, with its 315 patients with TNBC, nor CALGB/Alliance 40603, with 443, was adequately powered to prove or disprove a therapeutic advantage for the addition of neoadjuvant carboplatin.
“This is the 50th anniversary of the discovery of carboplatin. Yet despite all of our advancements in breast cancer, we’re still trying to figure out the role of platinum-containing agents in our armamentarium for breast cancer,” she observed.
During this period of what she termed clinical equipoise regarding carboplatin, she said it’s reasonable to consider using the agent outside of a clinical trial in selected circumstances: namely, when it’s important to gain rapid control of locoregional disease in order to improve operability or reduce morbidity, or in patients at the highest risk of relapse, mainly those who are very young or have stage III disease.
The issue of the validity of pathologic complete response (pCR) as a surrogate endpoint for event-free survival was raised by the GeparSixto and CALGB/Alliance 40603 investigators. In CALGB/Alliance 40603 only 9% of patients who had a pCR developed a distant recurrence and 3-year mortality was just 6%, compared with a 27% distant recurrence rate and 25% mortality in those without a pCR. Patients with a pCR had a 70% improvement in event-free survival and an 80% improvement in overall survival compared to those without a pCR, Dr. Sikov reported.
Similarly, in GeparSixto disease relapse occurred in only 5 of 129 TNBC patients with a pCR, compared with 50 of 162 without a pCR.
Dr. DeMichele said that while these are encouraging results, neither trial was designed to evaluate pCR as a predictor of improved event-free survival in accord with the Food and Drug Administration’s formal written guidance for attaining recognition of pCR as a surrogate endpoint. The studies were underpowered for this purpose. And a pooled analysis of 12 international trials totaling nearly 12,000 patients that was led by FDA investigators concluded that the data couldn’t validate pCR as a surrogate endpoint for event-free and overall survival (Lancet. 2014 Jul 12;384[9938]:164-72).
However, four studies adequately powered to detect improvement in event-free survival in conjunction with a carboplatin-induced benefit in terms of pCR are underway, including the NRG-BR-003 trial in the U.S. and the BrighTNess study in China.
In addition, a study with an innovative post-neoadjuvant design for platinum-based therapy is underway. The ECOG-ACRIN 1131 study is a Phase III randomized postoperative trial of four rounds of carboplatin or cisplatin versus observation in patients with residual TNBC following an anthracycline-based neoadjuvant regimen. This strategy limits exposure to the toxicities of platinum-based compounds to those patients in need of additional therapy. The planned 558-patient trial is powered to detect a 33% improvement in event-free survival.
SAN ANTONIO – Should carboplatin be considered a routine part of neoadjuvant therapy in early stage triple negative breast cancer?
Not yet, Dr. Angela M. DeMichele declared at the San Antonio Breast Cancer Symposium.
“I would say it’s still an individualized decision. The hazard ratios suggest benefit, but currently there’s not enough data to be conclusive,” according to Dr. DeMichele, who served as discussant for two clinical trials with discordant results – GeparSixto and CALGB/Alliance 40603 – presented at the symposium.
She also addressed a second issue raised by the two studies: is a pathologic complete response a valid surrogate for event-free survival?
“I would say a qualified yes,” commented Dr. DeMichele, professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia.
In GeparSixto, the addition of weekly carboplatin to a neoadjuvant chemotherapy backbone comprised of an anthracycline, taxane, and bevacizumab in patients with triple negative breast cancer (TNBC) boosted the 3-year disease-free survival rate significantly, from 76.1% to 85.5%. This result prompted GeparSixto presenter Dr. Gunter von Minckwitz, president of the German Breast Group, to declare that the study supports incorporation of carboplatin as part of standard neoadjuvant therapy in TNBC.
In contrast, in CALGB/Alliance 40603, adding carboplatin to neoadjuvant chemotherapy didn’t result in a significant improvement in 3-year event-free or overall survival.
Dr. DeMichele noted that with just 3 years of followup to date in these trials, there isn’t any information yet about carboplatin’s added potential long-term bone marrow toxicity. That’s an important unanswered question. Nor is any quality of life data available from the two trials. These issues need clarification before broader use of carboplatin.
One possible explanation for the disparate results in the two studies lies in differences in the chemotherapy and carboplatin doses and treatment schedules used. Patients in GeparSixto received greater cumulative amounts of anthracycline and taxane, given over a longer time period. And if patients were randomized to receive carboplatin, they got it at area under the curve 1.5 or 2 weekly for the duration of chemotherapy, as compared to carboplatin dosed just four times at area under the curve 6 every 3 weeks in CALGB/Alliance 40603.
“Could the weekly carboplatin in GeparSixto have provided less time for DNA repair in the tumor?,” she speculated.
Dr. William M. Sikov, who presented the CALGB/Alliance 40603 findings, found this quite plausible.
“We know treatment schedule and dose are important with anthracyclines, they’re important with taxanes, and it’s certainly not far fetched to propose that they may be important for carboplatin as well. Might that have made a difference? Can’t say,” observed Dr. Sikov of Women and Infants Hospital of Rhode Island in Providence.
In any case, Dr. DeMichele said neither GeparSixto, with its 315 patients with TNBC, nor CALGB/Alliance 40603, with 443, was adequately powered to prove or disprove a therapeutic advantage for the addition of neoadjuvant carboplatin.
“This is the 50th anniversary of the discovery of carboplatin. Yet despite all of our advancements in breast cancer, we’re still trying to figure out the role of platinum-containing agents in our armamentarium for breast cancer,” she observed.
During this period of what she termed clinical equipoise regarding carboplatin, she said it’s reasonable to consider using the agent outside of a clinical trial in selected circumstances: namely, when it’s important to gain rapid control of locoregional disease in order to improve operability or reduce morbidity, or in patients at the highest risk of relapse, mainly those who are very young or have stage III disease.
The issue of the validity of pathologic complete response (pCR) as a surrogate endpoint for event-free survival was raised by the GeparSixto and CALGB/Alliance 40603 investigators. In CALGB/Alliance 40603 only 9% of patients who had a pCR developed a distant recurrence and 3-year mortality was just 6%, compared with a 27% distant recurrence rate and 25% mortality in those without a pCR. Patients with a pCR had a 70% improvement in event-free survival and an 80% improvement in overall survival compared to those without a pCR, Dr. Sikov reported.
Similarly, in GeparSixto disease relapse occurred in only 5 of 129 TNBC patients with a pCR, compared with 50 of 162 without a pCR.
Dr. DeMichele said that while these are encouraging results, neither trial was designed to evaluate pCR as a predictor of improved event-free survival in accord with the Food and Drug Administration’s formal written guidance for attaining recognition of pCR as a surrogate endpoint. The studies were underpowered for this purpose. And a pooled analysis of 12 international trials totaling nearly 12,000 patients that was led by FDA investigators concluded that the data couldn’t validate pCR as a surrogate endpoint for event-free and overall survival (Lancet. 2014 Jul 12;384[9938]:164-72).
However, four studies adequately powered to detect improvement in event-free survival in conjunction with a carboplatin-induced benefit in terms of pCR are underway, including the NRG-BR-003 trial in the U.S. and the BrighTNess study in China.
In addition, a study with an innovative post-neoadjuvant design for platinum-based therapy is underway. The ECOG-ACRIN 1131 study is a Phase III randomized postoperative trial of four rounds of carboplatin or cisplatin versus observation in patients with residual TNBC following an anthracycline-based neoadjuvant regimen. This strategy limits exposure to the toxicities of platinum-based compounds to those patients in need of additional therapy. The planned 558-patient trial is powered to detect a 33% improvement in event-free survival.
SAN ANTONIO – Should carboplatin be considered a routine part of neoadjuvant therapy in early stage triple negative breast cancer?
Not yet, Dr. Angela M. DeMichele declared at the San Antonio Breast Cancer Symposium.
“I would say it’s still an individualized decision. The hazard ratios suggest benefit, but currently there’s not enough data to be conclusive,” according to Dr. DeMichele, who served as discussant for two clinical trials with discordant results – GeparSixto and CALGB/Alliance 40603 – presented at the symposium.
She also addressed a second issue raised by the two studies: is a pathologic complete response a valid surrogate for event-free survival?
“I would say a qualified yes,” commented Dr. DeMichele, professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia.
In GeparSixto, the addition of weekly carboplatin to a neoadjuvant chemotherapy backbone comprised of an anthracycline, taxane, and bevacizumab in patients with triple negative breast cancer (TNBC) boosted the 3-year disease-free survival rate significantly, from 76.1% to 85.5%. This result prompted GeparSixto presenter Dr. Gunter von Minckwitz, president of the German Breast Group, to declare that the study supports incorporation of carboplatin as part of standard neoadjuvant therapy in TNBC.
In contrast, in CALGB/Alliance 40603, adding carboplatin to neoadjuvant chemotherapy didn’t result in a significant improvement in 3-year event-free or overall survival.
Dr. DeMichele noted that with just 3 years of followup to date in these trials, there isn’t any information yet about carboplatin’s added potential long-term bone marrow toxicity. That’s an important unanswered question. Nor is any quality of life data available from the two trials. These issues need clarification before broader use of carboplatin.
One possible explanation for the disparate results in the two studies lies in differences in the chemotherapy and carboplatin doses and treatment schedules used. Patients in GeparSixto received greater cumulative amounts of anthracycline and taxane, given over a longer time period. And if patients were randomized to receive carboplatin, they got it at area under the curve 1.5 or 2 weekly for the duration of chemotherapy, as compared to carboplatin dosed just four times at area under the curve 6 every 3 weeks in CALGB/Alliance 40603.
“Could the weekly carboplatin in GeparSixto have provided less time for DNA repair in the tumor?,” she speculated.
Dr. William M. Sikov, who presented the CALGB/Alliance 40603 findings, found this quite plausible.
“We know treatment schedule and dose are important with anthracyclines, they’re important with taxanes, and it’s certainly not far fetched to propose that they may be important for carboplatin as well. Might that have made a difference? Can’t say,” observed Dr. Sikov of Women and Infants Hospital of Rhode Island in Providence.
In any case, Dr. DeMichele said neither GeparSixto, with its 315 patients with TNBC, nor CALGB/Alliance 40603, with 443, was adequately powered to prove or disprove a therapeutic advantage for the addition of neoadjuvant carboplatin.
“This is the 50th anniversary of the discovery of carboplatin. Yet despite all of our advancements in breast cancer, we’re still trying to figure out the role of platinum-containing agents in our armamentarium for breast cancer,” she observed.
During this period of what she termed clinical equipoise regarding carboplatin, she said it’s reasonable to consider using the agent outside of a clinical trial in selected circumstances: namely, when it’s important to gain rapid control of locoregional disease in order to improve operability or reduce morbidity, or in patients at the highest risk of relapse, mainly those who are very young or have stage III disease.
The issue of the validity of pathologic complete response (pCR) as a surrogate endpoint for event-free survival was raised by the GeparSixto and CALGB/Alliance 40603 investigators. In CALGB/Alliance 40603 only 9% of patients who had a pCR developed a distant recurrence and 3-year mortality was just 6%, compared with a 27% distant recurrence rate and 25% mortality in those without a pCR. Patients with a pCR had a 70% improvement in event-free survival and an 80% improvement in overall survival compared to those without a pCR, Dr. Sikov reported.
Similarly, in GeparSixto disease relapse occurred in only 5 of 129 TNBC patients with a pCR, compared with 50 of 162 without a pCR.
Dr. DeMichele said that while these are encouraging results, neither trial was designed to evaluate pCR as a predictor of improved event-free survival in accord with the Food and Drug Administration’s formal written guidance for attaining recognition of pCR as a surrogate endpoint. The studies were underpowered for this purpose. And a pooled analysis of 12 international trials totaling nearly 12,000 patients that was led by FDA investigators concluded that the data couldn’t validate pCR as a surrogate endpoint for event-free and overall survival (Lancet. 2014 Jul 12;384[9938]:164-72).
However, four studies adequately powered to detect improvement in event-free survival in conjunction with a carboplatin-induced benefit in terms of pCR are underway, including the NRG-BR-003 trial in the U.S. and the BrighTNess study in China.
In addition, a study with an innovative post-neoadjuvant design for platinum-based therapy is underway. The ECOG-ACRIN 1131 study is a Phase III randomized postoperative trial of four rounds of carboplatin or cisplatin versus observation in patients with residual TNBC following an anthracycline-based neoadjuvant regimen. This strategy limits exposure to the toxicities of platinum-based compounds to those patients in need of additional therapy. The planned 558-patient trial is powered to detect a 33% improvement in event-free survival.
EXPERT ANALYSIS FROM SABCS 2015

Laparoscopic TAP blocks offer quick, easy, postoperative analgesia
LAS VEGAS – A laparoscopic transversus abdominis plane (TAP) block is easy to learn, quick to perform, and provides effective postoperative analgesia for women undergoing minimally invasive gynecologic surgeries.
TAP blocks are usually done by an anesthesiologist under ultrasound guidance, Dr. Shanti Mohling said at a meeting sponsored by AAGL. But they can also be performed quite efficiently during a laparoscopic procedure using anatomic landmarks.
“All you need to perform this is a knowledge of the anatomy, a beveled needle with tubing, and two syringes with 20-30 cc of analgesic,” said Dr. Mohling of the University of Tennessee, Chattanooga. “It takes about 3 minutes and it’s very time saving, compared to having an anesthesiologist do this with ultrasound guidance.”
She presented a video of her technique, which relies on identification of the lumbar triangle of Petit to deliver a large volume of anesthetic into the transversus abdominis plane – the neurovascular space between the internal oblique and transversus abdominis muscles. The area is of critical importance to pain sensation, she said. “This plane carries the afferent nociceptor nerves for T7-L1, including the ilioinguinal and iliohypogastric nerves.”
The efficacy of a laparoscopically administered TAP block during laparoscopic gynecologic surgery has been demonstrated in several studies, she noted. One – a review of 61 cases of total laparoscopic hysterectomy - found associations between the use of the TAP black and reduced length of stay and lower opioid consumption (Aust N Z J Obstet Gynaecol. 2011 Dec;51[6]:544-7.).
The video described her technique, beginning with identifying the triangle of Petit. “The triangle of Petit is the area formed between the iliac crest inferiorly, the latissimus dorsi posteriorly, and the external oblique anteriorly. Within this triangle, we find perfect access to the transversus abdominis plane.”
Once the triangle is identified, a beveled needle is advanced slowly, “as to appreciate the ‘double pop sensation’ of the needle as it passes the fascia of the external and internal oblique muscles. Laparoscopically, this can be observed,” Dr. Mohling said. “If the needle can be seen just beneath the peritoneum, then it has penetrated too far.”
Once into the space, which can easily accommodate a large volume of fluid, she delivers the anesthetic into the neurovascular plane. “Importantly, the injectate must be of sufficient volume to effectively spread throughout the neurovascular plane. Typically this requires 20-30 cc on each side,” she said.
Long-acting agents like bupivacaine or ropivacaine are preferable. Dr. Mohling uses a solution of 10 cc liposomal bupivacaine; 10 cc 0.25% bupivacaine; and 10 cc normal saline.
As the anesthetic is injected, it’s important to track it visually to assure correct placement, she noted. “The delivery can be noted laparoscopically by watching a bulge spreading beneath the transversus abdominis fascia.”
The potential for complications is low, but these include intraperitoneal injection; abdominal wall or bowel hematoma; transient femoral nerve palsy; and local anesthetic toxicity.
Dr. Mohling is in the process of conducting a randomized controlled trial of 100 women undergoing planned laparoscopic or robotic hysterectomy. They will be assigned to either TAP block with the liposomal bupivacaine solution or to traditional preincisional local anesthetic with bupivacaine alone.
“I believe we should all add this technique to our practice,” she said. “It’s easy and there is an increasing body of evidence supporting these blocks.”
Dr. Mohling reported having no financial disclosures.
LAS VEGAS – A laparoscopic transversus abdominis plane (TAP) block is easy to learn, quick to perform, and provides effective postoperative analgesia for women undergoing minimally invasive gynecologic surgeries.
TAP blocks are usually done by an anesthesiologist under ultrasound guidance, Dr. Shanti Mohling said at a meeting sponsored by AAGL. But they can also be performed quite efficiently during a laparoscopic procedure using anatomic landmarks.
“All you need to perform this is a knowledge of the anatomy, a beveled needle with tubing, and two syringes with 20-30 cc of analgesic,” said Dr. Mohling of the University of Tennessee, Chattanooga. “It takes about 3 minutes and it’s very time saving, compared to having an anesthesiologist do this with ultrasound guidance.”
She presented a video of her technique, which relies on identification of the lumbar triangle of Petit to deliver a large volume of anesthetic into the transversus abdominis plane – the neurovascular space between the internal oblique and transversus abdominis muscles. The area is of critical importance to pain sensation, she said. “This plane carries the afferent nociceptor nerves for T7-L1, including the ilioinguinal and iliohypogastric nerves.”
The efficacy of a laparoscopically administered TAP block during laparoscopic gynecologic surgery has been demonstrated in several studies, she noted. One – a review of 61 cases of total laparoscopic hysterectomy - found associations between the use of the TAP black and reduced length of stay and lower opioid consumption (Aust N Z J Obstet Gynaecol. 2011 Dec;51[6]:544-7.).
The video described her technique, beginning with identifying the triangle of Petit. “The triangle of Petit is the area formed between the iliac crest inferiorly, the latissimus dorsi posteriorly, and the external oblique anteriorly. Within this triangle, we find perfect access to the transversus abdominis plane.”
Once the triangle is identified, a beveled needle is advanced slowly, “as to appreciate the ‘double pop sensation’ of the needle as it passes the fascia of the external and internal oblique muscles. Laparoscopically, this can be observed,” Dr. Mohling said. “If the needle can be seen just beneath the peritoneum, then it has penetrated too far.”
Once into the space, which can easily accommodate a large volume of fluid, she delivers the anesthetic into the neurovascular plane. “Importantly, the injectate must be of sufficient volume to effectively spread throughout the neurovascular plane. Typically this requires 20-30 cc on each side,” she said.
Long-acting agents like bupivacaine or ropivacaine are preferable. Dr. Mohling uses a solution of 10 cc liposomal bupivacaine; 10 cc 0.25% bupivacaine; and 10 cc normal saline.
As the anesthetic is injected, it’s important to track it visually to assure correct placement, she noted. “The delivery can be noted laparoscopically by watching a bulge spreading beneath the transversus abdominis fascia.”
The potential for complications is low, but these include intraperitoneal injection; abdominal wall or bowel hematoma; transient femoral nerve palsy; and local anesthetic toxicity.
Dr. Mohling is in the process of conducting a randomized controlled trial of 100 women undergoing planned laparoscopic or robotic hysterectomy. They will be assigned to either TAP block with the liposomal bupivacaine solution or to traditional preincisional local anesthetic with bupivacaine alone.
“I believe we should all add this technique to our practice,” she said. “It’s easy and there is an increasing body of evidence supporting these blocks.”
Dr. Mohling reported having no financial disclosures.
LAS VEGAS – A laparoscopic transversus abdominis plane (TAP) block is easy to learn, quick to perform, and provides effective postoperative analgesia for women undergoing minimally invasive gynecologic surgeries.
TAP blocks are usually done by an anesthesiologist under ultrasound guidance, Dr. Shanti Mohling said at a meeting sponsored by AAGL. But they can also be performed quite efficiently during a laparoscopic procedure using anatomic landmarks.
“All you need to perform this is a knowledge of the anatomy, a beveled needle with tubing, and two syringes with 20-30 cc of analgesic,” said Dr. Mohling of the University of Tennessee, Chattanooga. “It takes about 3 minutes and it’s very time saving, compared to having an anesthesiologist do this with ultrasound guidance.”
She presented a video of her technique, which relies on identification of the lumbar triangle of Petit to deliver a large volume of anesthetic into the transversus abdominis plane – the neurovascular space between the internal oblique and transversus abdominis muscles. The area is of critical importance to pain sensation, she said. “This plane carries the afferent nociceptor nerves for T7-L1, including the ilioinguinal and iliohypogastric nerves.”
The efficacy of a laparoscopically administered TAP block during laparoscopic gynecologic surgery has been demonstrated in several studies, she noted. One – a review of 61 cases of total laparoscopic hysterectomy - found associations between the use of the TAP black and reduced length of stay and lower opioid consumption (Aust N Z J Obstet Gynaecol. 2011 Dec;51[6]:544-7.).
The video described her technique, beginning with identifying the triangle of Petit. “The triangle of Petit is the area formed between the iliac crest inferiorly, the latissimus dorsi posteriorly, and the external oblique anteriorly. Within this triangle, we find perfect access to the transversus abdominis plane.”
Once the triangle is identified, a beveled needle is advanced slowly, “as to appreciate the ‘double pop sensation’ of the needle as it passes the fascia of the external and internal oblique muscles. Laparoscopically, this can be observed,” Dr. Mohling said. “If the needle can be seen just beneath the peritoneum, then it has penetrated too far.”
Once into the space, which can easily accommodate a large volume of fluid, she delivers the anesthetic into the neurovascular plane. “Importantly, the injectate must be of sufficient volume to effectively spread throughout the neurovascular plane. Typically this requires 20-30 cc on each side,” she said.
Long-acting agents like bupivacaine or ropivacaine are preferable. Dr. Mohling uses a solution of 10 cc liposomal bupivacaine; 10 cc 0.25% bupivacaine; and 10 cc normal saline.
As the anesthetic is injected, it’s important to track it visually to assure correct placement, she noted. “The delivery can be noted laparoscopically by watching a bulge spreading beneath the transversus abdominis fascia.”
The potential for complications is low, but these include intraperitoneal injection; abdominal wall or bowel hematoma; transient femoral nerve palsy; and local anesthetic toxicity.
Dr. Mohling is in the process of conducting a randomized controlled trial of 100 women undergoing planned laparoscopic or robotic hysterectomy. They will be assigned to either TAP block with the liposomal bupivacaine solution or to traditional preincisional local anesthetic with bupivacaine alone.
“I believe we should all add this technique to our practice,” she said. “It’s easy and there is an increasing body of evidence supporting these blocks.”
Dr. Mohling reported having no financial disclosures.
EXPERT ANALYSIS FROM THE AAGL GLOBAL CONGRESS

NIH, CDC get boost in House budget bill
The National Institutes of Health would see an almost 10% increase in funding under a budget deal announced Dec. 15 by House Speaker Paul Ryan (R-Wisc.).
Other provisions in the omnibus budget agreement include an increased budget for the Centers for Disease Control and Prevention, level budgets for the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology, and a reduced budget for the Agency for Healthcare Research and Quality.

The bill also prevents any new or additional spending on the Affordable Care Act.
The National Institutes of Health will see its budget increase to $32 billion, $2 billion more than the fiscal 2015 budget and $1 billion more than the White House had requested. The increases are targeted to a number of specific research areas, including Alzheimer’s disease, the BRAIN Initiative, antibiotics research, as well as for the Precision Medicine Initiative. The NIH increase also reflects increased budget levels for all individual institutes and centers.
CDC’s budget is increased by about $308 million – almost double the White House–requested increase – to $7.2 billion. The proposal prioritizes funding on disease prevention and biodefense research to prevent against infectious diseases as well as bioterrorism attacks, and helping the agency modernize laboratory facilities and work with states to address antibiotic resistance.
It also includes $70 million to target prescription drug abuse, $160 million for the Division for Heart Disease and Stroke Prevention, $170 million to help address preventable chronic diseases, $160 million in block grants for states to address their individual health needs, and $1.4 billion in budgeting for states to use for emergency preparedness for bioterror attacks or pandemic disease emergencies.
The budget proprosal also cuts more than $30 million from the Agency for Healthcare Research and Quality (AHRQ). The White House had asked for funding of the AHRQ to remain static.
Both the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology saw their budgets remain level; however, the bill makes no changes to the Meaningful Use program.
As part of Congress’ ongoing oversight into prescription drug pricing, the budget bill is calling for the U.S. Department of Health & Human Services to prepare a report examining the prices.
According to a committee report accompanying the bill language, HHS will prepare a report on prices, net of rebate, of the top 10 most commonly prescribed drugs and the top 10 highest-cost drugs paid under Medicare Part B and Part D, Medicaid, and by the Department of Veterans Affairs since 2003. The report, due 180 days after the enactment of the bill, would also evaluate access to drugs under the four programs as well as patient satisfaction with care.
The House is expected to vote on the budget proposal as early as Dec. 18.
The National Institutes of Health would see an almost 10% increase in funding under a budget deal announced Dec. 15 by House Speaker Paul Ryan (R-Wisc.).
Other provisions in the omnibus budget agreement include an increased budget for the Centers for Disease Control and Prevention, level budgets for the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology, and a reduced budget for the Agency for Healthcare Research and Quality.
The bill also prevents any new or additional spending on the Affordable Care Act.
The National Institutes of Health will see its budget increase to $32 billion, $2 billion more than the fiscal 2015 budget and $1 billion more than the White House had requested. The increases are targeted to a number of specific research areas, including Alzheimer’s disease, the BRAIN Initiative, antibiotics research, as well as for the Precision Medicine Initiative. The NIH increase also reflects increased budget levels for all individual institutes and centers.
CDC’s budget is increased by about $308 million – almost double the White House–requested increase – to $7.2 billion. The proposal prioritizes funding on disease prevention and biodefense research to prevent against infectious diseases as well as bioterrorism attacks, and helping the agency modernize laboratory facilities and work with states to address antibiotic resistance.
It also includes $70 million to target prescription drug abuse, $160 million for the Division for Heart Disease and Stroke Prevention, $170 million to help address preventable chronic diseases, $160 million in block grants for states to address their individual health needs, and $1.4 billion in budgeting for states to use for emergency preparedness for bioterror attacks or pandemic disease emergencies.
The budget proprosal also cuts more than $30 million from the Agency for Healthcare Research and Quality (AHRQ). The White House had asked for funding of the AHRQ to remain static.
Both the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology saw their budgets remain level; however, the bill makes no changes to the Meaningful Use program.
As part of Congress’ ongoing oversight into prescription drug pricing, the budget bill is calling for the U.S. Department of Health & Human Services to prepare a report examining the prices.
According to a committee report accompanying the bill language, HHS will prepare a report on prices, net of rebate, of the top 10 most commonly prescribed drugs and the top 10 highest-cost drugs paid under Medicare Part B and Part D, Medicaid, and by the Department of Veterans Affairs since 2003. The report, due 180 days after the enactment of the bill, would also evaluate access to drugs under the four programs as well as patient satisfaction with care.
The House is expected to vote on the budget proposal as early as Dec. 18.
The National Institutes of Health would see an almost 10% increase in funding under a budget deal announced Dec. 15 by House Speaker Paul Ryan (R-Wisc.).
Other provisions in the omnibus budget agreement include an increased budget for the Centers for Disease Control and Prevention, level budgets for the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology, and a reduced budget for the Agency for Healthcare Research and Quality.
The bill also prevents any new or additional spending on the Affordable Care Act.
The National Institutes of Health will see its budget increase to $32 billion, $2 billion more than the fiscal 2015 budget and $1 billion more than the White House had requested. The increases are targeted to a number of specific research areas, including Alzheimer’s disease, the BRAIN Initiative, antibiotics research, as well as for the Precision Medicine Initiative. The NIH increase also reflects increased budget levels for all individual institutes and centers.
CDC’s budget is increased by about $308 million – almost double the White House–requested increase – to $7.2 billion. The proposal prioritizes funding on disease prevention and biodefense research to prevent against infectious diseases as well as bioterrorism attacks, and helping the agency modernize laboratory facilities and work with states to address antibiotic resistance.
It also includes $70 million to target prescription drug abuse, $160 million for the Division for Heart Disease and Stroke Prevention, $170 million to help address preventable chronic diseases, $160 million in block grants for states to address their individual health needs, and $1.4 billion in budgeting for states to use for emergency preparedness for bioterror attacks or pandemic disease emergencies.
The budget proprosal also cuts more than $30 million from the Agency for Healthcare Research and Quality (AHRQ). The White House had asked for funding of the AHRQ to remain static.
Both the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology saw their budgets remain level; however, the bill makes no changes to the Meaningful Use program.
As part of Congress’ ongoing oversight into prescription drug pricing, the budget bill is calling for the U.S. Department of Health & Human Services to prepare a report examining the prices.
According to a committee report accompanying the bill language, HHS will prepare a report on prices, net of rebate, of the top 10 most commonly prescribed drugs and the top 10 highest-cost drugs paid under Medicare Part B and Part D, Medicaid, and by the Department of Veterans Affairs since 2003. The report, due 180 days after the enactment of the bill, would also evaluate access to drugs under the four programs as well as patient satisfaction with care.
The House is expected to vote on the budget proposal as early as Dec. 18.

Aortic valve replacement: Transcatheter soars past surgical
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
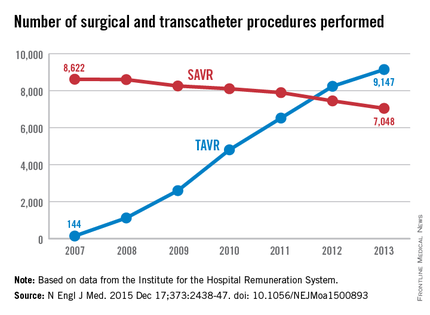
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement occurred among patients unsuited for a surgical approach.
Major finding: The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of surgical procedures declined only slightly, from 8,622 to 7,048 per year.
Data source: A retrospective analysis of all 88,573 surgical and TAVR performed in Germany in 2007-2013.
Disclosures: This study was supported by the Heart Center at Freiburg University. Dr. Reinöhl and one of his associates reported receiving personal fees from Edwards Lifesciences and Direct Flow Medical.

VIDEO: Cleveland Clinic experts provide SABCS take-home messages
SAN ANTONIO –The San Antonio Breast Cancer Symposium had a lot to offer clinicians. Cleveland Clinic breast cancer experts Dr. Jame Abraham, Dr. Holly Pederson, and Dr. Alberto Montero outline take-home messages from research presented at the San Antonio Breast Cancer Symposium. The panel agreed that some findings were practice-changing – particularly results showing adjuvant denosumab not only reduces fracture risk for women but also improves breast cancer outcomes – while findings for other treatments, including immunotherapy for breast cancer, have a long way to go before arriving in the clinic.
Dr. Pederson highlighted presentations on prevention, including findings linking aspirin with lower breast density. She also said presentations confirmed for her that gene panels are here to stay in helping identify and manage women at high risk of breast cancer.
The panelists also discussed the clinical relevance of studies on neoadjuvant carboplatin and on using capecitabine for cleanup of residual disease after neoadjuvant therapy.
The three panelists had no financial disclosures related to these studies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO –The San Antonio Breast Cancer Symposium had a lot to offer clinicians. Cleveland Clinic breast cancer experts Dr. Jame Abraham, Dr. Holly Pederson, and Dr. Alberto Montero outline take-home messages from research presented at the San Antonio Breast Cancer Symposium. The panel agreed that some findings were practice-changing – particularly results showing adjuvant denosumab not only reduces fracture risk for women but also improves breast cancer outcomes – while findings for other treatments, including immunotherapy for breast cancer, have a long way to go before arriving in the clinic.
Dr. Pederson highlighted presentations on prevention, including findings linking aspirin with lower breast density. She also said presentations confirmed for her that gene panels are here to stay in helping identify and manage women at high risk of breast cancer.
The panelists also discussed the clinical relevance of studies on neoadjuvant carboplatin and on using capecitabine for cleanup of residual disease after neoadjuvant therapy.
The three panelists had no financial disclosures related to these studies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO –The San Antonio Breast Cancer Symposium had a lot to offer clinicians. Cleveland Clinic breast cancer experts Dr. Jame Abraham, Dr. Holly Pederson, and Dr. Alberto Montero outline take-home messages from research presented at the San Antonio Breast Cancer Symposium. The panel agreed that some findings were practice-changing – particularly results showing adjuvant denosumab not only reduces fracture risk for women but also improves breast cancer outcomes – while findings for other treatments, including immunotherapy for breast cancer, have a long way to go before arriving in the clinic.
Dr. Pederson highlighted presentations on prevention, including findings linking aspirin with lower breast density. She also said presentations confirmed for her that gene panels are here to stay in helping identify and manage women at high risk of breast cancer.
The panelists also discussed the clinical relevance of studies on neoadjuvant carboplatin and on using capecitabine for cleanup of residual disease after neoadjuvant therapy.
The three panelists had no financial disclosures related to these studies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM SABCS 2015

Sugammadex OK’d to reverse neuromuscular blockade during surgery
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
Six-year Norwood-RVPA results in matched patients outperformed BT-shunt
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.

“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”

|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOTHORACIC SURGERY
Key clinical point: For newborns with critical left ventricular outflow tract obstruction (LVOTO) undergoing Norwood stage-1 procedures, Norwood with right ventricle to pulmonary artery conduit (NW-RVPA) resulted in better survival and less short-term right-ventricle dysfunction than matched patients who had the Norwood procedure with Blalock-Taussig shunt (NW-BT).
Major finding: Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group, and RV dysfunction rates three months after the procedure were 6% for NW-RVPA vs. 16% for NW-BT.
Data source: Prospective group of 454 newborns with LVOTO in the Congenital Heart Surgeons’ Society database.
Disclosures: The Congenital Heart Surgeons’ Society and Hospital for Sick Children, Toronto, provided funding for the study. The authors had no relationships to disclose.
