User login
Official Newspaper of the American College of Surgeons
ACS Surgery News December digital issue is available
The December ACS Surgery News digital issue is online - use the mobile app to download or view as a pdf.
This month features a review of the American Cancer Society revised mammogram guidelines, news on what gives your patient with an infected hernia the best chance for salvage, and an interview with ACS Operation Giving Back Medical Director, Dr. Girma Tefera.
Don't miss Dr. Peter Angelos' tribute to his late mentor, Dr. Norman W. Thompson.
The December ACS Surgery News digital issue is online - use the mobile app to download or view as a pdf.
This month features a review of the American Cancer Society revised mammogram guidelines, news on what gives your patient with an infected hernia the best chance for salvage, and an interview with ACS Operation Giving Back Medical Director, Dr. Girma Tefera.
Don't miss Dr. Peter Angelos' tribute to his late mentor, Dr. Norman W. Thompson.
The December ACS Surgery News digital issue is online - use the mobile app to download or view as a pdf.
This month features a review of the American Cancer Society revised mammogram guidelines, news on what gives your patient with an infected hernia the best chance for salvage, and an interview with ACS Operation Giving Back Medical Director, Dr. Girma Tefera.
Don't miss Dr. Peter Angelos' tribute to his late mentor, Dr. Norman W. Thompson.

Study suggests surgeons have heeded FDA warning about vaginal mesh
Surgeons seem to have heeded a beefed-up warning from the U.S. Food and Drug Administration about using transvaginal surgical mesh when repairing pelvic organ prolapse, investigators reported online Dec. 21 in JAMA Internal Medicine.
In New York state, the use of mesh fell by almost 25% just 2 years after the FDA intensified its original warning, said Dr. Art Sedrakyan of Cornell University in Ithaca, N.Y., and his associates. “Although other explanations are possible, we believe that the stronger language in the 2011 FDA warning is at least partly related to the decline in mesh use,” they said.
A prior study by the investigators found that use of mesh actually rose by almost 50% during the 3 years after the original FDA warning, issued in 2008 (BMJ. 2015 Jun 3;350:h2685 doi: 10.1136/bmj.h2685). During that time, FDA received about 1,500 reports of subsequent adverse events, such as erosion through the vagina, pain, infection, organ perforation, bleeding, dyspareunia, vaginal scarring or shrinkage, and urinary problems, the investigators noted (JAMA Intern Med. 2015 Dec 21. doi: 10.1001/jamainternmed.2015.6595).
In 2011, the FDA responded by strengthening its original warning. Instead of urging physicians to be aware of risks and training in each technique in which they used mesh, the agency noted that mesh-related complications are “not rare” and emphasized that pelvic organ prolapse (POP) can be repaired without mesh. To examine the effects of that warning, the investigators analyzed a database of all surgical procedures performed in New York state during 2011-2013. They excluded patients who had undergone previous POP repairs and broke down trends by hospital type and size.
Total annual POP repairs dropped from 6,960 in 2011 to 5,757 in 2013, they found. After the new FDA warning, the use of mesh also fell – from 30% (95% confidence interval, 29%-31%) in 2011 to 23% (95% CI, 22%-24%) in 2013. The drop was significantly less dramatic in academic and high-volume hospitals, perhaps because surgeons there were more comfortable using mesh or were treating worse disease, the researchers said. “The higher rate of decline in the use of mesh by low-volume and nonacademic providers may be related to a lower tolerance for litigation related to sizable awards and growing numbers of lawsuits in outpatient settings,” they added.
The National Institutes of Health and the FDA partially funded the study. The investigators had no disclosures.
Surgeons seem to have heeded a beefed-up warning from the U.S. Food and Drug Administration about using transvaginal surgical mesh when repairing pelvic organ prolapse, investigators reported online Dec. 21 in JAMA Internal Medicine.
In New York state, the use of mesh fell by almost 25% just 2 years after the FDA intensified its original warning, said Dr. Art Sedrakyan of Cornell University in Ithaca, N.Y., and his associates. “Although other explanations are possible, we believe that the stronger language in the 2011 FDA warning is at least partly related to the decline in mesh use,” they said.
A prior study by the investigators found that use of mesh actually rose by almost 50% during the 3 years after the original FDA warning, issued in 2008 (BMJ. 2015 Jun 3;350:h2685 doi: 10.1136/bmj.h2685). During that time, FDA received about 1,500 reports of subsequent adverse events, such as erosion through the vagina, pain, infection, organ perforation, bleeding, dyspareunia, vaginal scarring or shrinkage, and urinary problems, the investigators noted (JAMA Intern Med. 2015 Dec 21. doi: 10.1001/jamainternmed.2015.6595).
In 2011, the FDA responded by strengthening its original warning. Instead of urging physicians to be aware of risks and training in each technique in which they used mesh, the agency noted that mesh-related complications are “not rare” and emphasized that pelvic organ prolapse (POP) can be repaired without mesh. To examine the effects of that warning, the investigators analyzed a database of all surgical procedures performed in New York state during 2011-2013. They excluded patients who had undergone previous POP repairs and broke down trends by hospital type and size.
Total annual POP repairs dropped from 6,960 in 2011 to 5,757 in 2013, they found. After the new FDA warning, the use of mesh also fell – from 30% (95% confidence interval, 29%-31%) in 2011 to 23% (95% CI, 22%-24%) in 2013. The drop was significantly less dramatic in academic and high-volume hospitals, perhaps because surgeons there were more comfortable using mesh or were treating worse disease, the researchers said. “The higher rate of decline in the use of mesh by low-volume and nonacademic providers may be related to a lower tolerance for litigation related to sizable awards and growing numbers of lawsuits in outpatient settings,” they added.
The National Institutes of Health and the FDA partially funded the study. The investigators had no disclosures.
Surgeons seem to have heeded a beefed-up warning from the U.S. Food and Drug Administration about using transvaginal surgical mesh when repairing pelvic organ prolapse, investigators reported online Dec. 21 in JAMA Internal Medicine.
In New York state, the use of mesh fell by almost 25% just 2 years after the FDA intensified its original warning, said Dr. Art Sedrakyan of Cornell University in Ithaca, N.Y., and his associates. “Although other explanations are possible, we believe that the stronger language in the 2011 FDA warning is at least partly related to the decline in mesh use,” they said.
A prior study by the investigators found that use of mesh actually rose by almost 50% during the 3 years after the original FDA warning, issued in 2008 (BMJ. 2015 Jun 3;350:h2685 doi: 10.1136/bmj.h2685). During that time, FDA received about 1,500 reports of subsequent adverse events, such as erosion through the vagina, pain, infection, organ perforation, bleeding, dyspareunia, vaginal scarring or shrinkage, and urinary problems, the investigators noted (JAMA Intern Med. 2015 Dec 21. doi: 10.1001/jamainternmed.2015.6595).
In 2011, the FDA responded by strengthening its original warning. Instead of urging physicians to be aware of risks and training in each technique in which they used mesh, the agency noted that mesh-related complications are “not rare” and emphasized that pelvic organ prolapse (POP) can be repaired without mesh. To examine the effects of that warning, the investigators analyzed a database of all surgical procedures performed in New York state during 2011-2013. They excluded patients who had undergone previous POP repairs and broke down trends by hospital type and size.
Total annual POP repairs dropped from 6,960 in 2011 to 5,757 in 2013, they found. After the new FDA warning, the use of mesh also fell – from 30% (95% confidence interval, 29%-31%) in 2011 to 23% (95% CI, 22%-24%) in 2013. The drop was significantly less dramatic in academic and high-volume hospitals, perhaps because surgeons there were more comfortable using mesh or were treating worse disease, the researchers said. “The higher rate of decline in the use of mesh by low-volume and nonacademic providers may be related to a lower tolerance for litigation related to sizable awards and growing numbers of lawsuits in outpatient settings,” they added.
The National Institutes of Health and the FDA partially funded the study. The investigators had no disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Surgeons seem to have heeded stronger language from FDA about the risks of using transvaginal surgical mesh.
Major finding: The use of mesh to repair pelvic organ prolapse fell from 30% to 23% within 2 years after the FDA beefed up its original warning.
Data source: A retrospective analysis of data from the New York Statewide Planning and Research Cooperative System, which has records of all surgical procedures in the state.
Disclosures: The National Institutes of Health and the U.S. FDA partially funded the study. The investigators had no disclosures.
Six factors predicted poor surgical outcomes in toxic colitis
Older age, female sex, preoperative chronic steroid use, azotemia, respiratory insufficiency, and coagulopathy all predicted death within a month of colectomy in patients with toxic colitis in the National Surgical Quality Improvement Project database.
The study is the largest to evaluate patients undergoing colectomy for toxic colitis, according to lead investigator Dr. Anand Dayama of the University of California, Davis, and his associates.

“In a case such as multiorgan failure with toxic colitis, the decision whether ... to operate can be an immensely difficult one,” Dr. Dayama and his colleagues wrote. “This study can help in making informed decisions in order to avoid the medicolegal ramifications of either performing an unnecessary procedure or withholding a lifesaving one,” they wrote in the American Journal of Surgery.
Surgical salvage remains the preferred treatment for patients with medically refractory toxic colitis. To assess outcomes in these patients, the researchers queried the National Surgical Quality Improvement Project database for relevant International Classification of Diseases, Ninth Revision codes between 2005 and 2012 (Am J Surg. 2015 Nov;210[5]:852-8).
The results underscored the severity of toxic colitis, they said. Of 189 patients, more than 26% died within 30 days after surgery, one in five developed postsurgical sepsis, about 17% had cardiovascular complications, 15% had wound complications, and 13% had renal complications. Furthermore, patients who were 70-80 years old had 3.5 times greater odds of dying, compared with younger patients (95% confidence interval, 1.0-12.8), and the increased likelihood of death rose by 22.2 when patients were older than 80 years (95% CI, 5.7-86.4).
Other baseline predictors of 30-day mortality included female sex (odds ratio, 4.1), blood urea nitrogen levels above 40 mg/dL (OR, 4.1), an international normalized ratio exceeding 2 (OR, 7.7), preoperative respiratory insufficiency (OR, 2.73), and a history of chronic steroid use (OR, 3.9), the researchers said. In addition, patients who died within 30 days after surgery were more likely than survivors to have undergone prolonged mechanical ventilation (56% vs. 27%), to have returned to the operating room (18% vs. 14%), to have acute renal failure (28% vs. 6%), or to have suffered a cardiac arrest that required cardiopulmonary resuscitation (18% vs. 7%). Survivors averaged about 2 fewer days in the hospital, compared with patients who died after surgery.
“The high morbidity and mortality of toxic colitis requires early and intensive medical management with IV [intravenous] steroids, antibiotics, decompressive maneuvers, and other resuscitative measures to treat the underlying cause,” they emphasized. “If there is no sign of improvement within 7 days or if there are any signs of deterioration, urgent surgical intervention should be considered.”
The link between female sex and mortality might reflect hormonal changes associated with menopause, but the study did not assess hormonal status or use of hormone therapy, the investigators noted. The association between chronic steroid use and postoperative death “is highly relevant” because long-term steroids are so often used in inflammatory bowel disease, they added. Clinical guidelines (Am J Gastroenterol. 2012 Feb;107:179-94) recommend that patients with acute severe ulcerative colitis proceed to second-line therapy or surgery if they do not respond to 3 days of intravenous steroids, because unnecessary delays can increase the risk of postoperative complications, they added.
The researchers reported no funding sources and had no disclosures.
Older age, female sex, preoperative chronic steroid use, azotemia, respiratory insufficiency, and coagulopathy all predicted death within a month of colectomy in patients with toxic colitis in the National Surgical Quality Improvement Project database.
The study is the largest to evaluate patients undergoing colectomy for toxic colitis, according to lead investigator Dr. Anand Dayama of the University of California, Davis, and his associates.
“In a case such as multiorgan failure with toxic colitis, the decision whether ... to operate can be an immensely difficult one,” Dr. Dayama and his colleagues wrote. “This study can help in making informed decisions in order to avoid the medicolegal ramifications of either performing an unnecessary procedure or withholding a lifesaving one,” they wrote in the American Journal of Surgery.
Surgical salvage remains the preferred treatment for patients with medically refractory toxic colitis. To assess outcomes in these patients, the researchers queried the National Surgical Quality Improvement Project database for relevant International Classification of Diseases, Ninth Revision codes between 2005 and 2012 (Am J Surg. 2015 Nov;210[5]:852-8).
The results underscored the severity of toxic colitis, they said. Of 189 patients, more than 26% died within 30 days after surgery, one in five developed postsurgical sepsis, about 17% had cardiovascular complications, 15% had wound complications, and 13% had renal complications. Furthermore, patients who were 70-80 years old had 3.5 times greater odds of dying, compared with younger patients (95% confidence interval, 1.0-12.8), and the increased likelihood of death rose by 22.2 when patients were older than 80 years (95% CI, 5.7-86.4).
Other baseline predictors of 30-day mortality included female sex (odds ratio, 4.1), blood urea nitrogen levels above 40 mg/dL (OR, 4.1), an international normalized ratio exceeding 2 (OR, 7.7), preoperative respiratory insufficiency (OR, 2.73), and a history of chronic steroid use (OR, 3.9), the researchers said. In addition, patients who died within 30 days after surgery were more likely than survivors to have undergone prolonged mechanical ventilation (56% vs. 27%), to have returned to the operating room (18% vs. 14%), to have acute renal failure (28% vs. 6%), or to have suffered a cardiac arrest that required cardiopulmonary resuscitation (18% vs. 7%). Survivors averaged about 2 fewer days in the hospital, compared with patients who died after surgery.
“The high morbidity and mortality of toxic colitis requires early and intensive medical management with IV [intravenous] steroids, antibiotics, decompressive maneuvers, and other resuscitative measures to treat the underlying cause,” they emphasized. “If there is no sign of improvement within 7 days or if there are any signs of deterioration, urgent surgical intervention should be considered.”
The link between female sex and mortality might reflect hormonal changes associated with menopause, but the study did not assess hormonal status or use of hormone therapy, the investigators noted. The association between chronic steroid use and postoperative death “is highly relevant” because long-term steroids are so often used in inflammatory bowel disease, they added. Clinical guidelines (Am J Gastroenterol. 2012 Feb;107:179-94) recommend that patients with acute severe ulcerative colitis proceed to second-line therapy or surgery if they do not respond to 3 days of intravenous steroids, because unnecessary delays can increase the risk of postoperative complications, they added.
The researchers reported no funding sources and had no disclosures.
Older age, female sex, preoperative chronic steroid use, azotemia, respiratory insufficiency, and coagulopathy all predicted death within a month of colectomy in patients with toxic colitis in the National Surgical Quality Improvement Project database.
The study is the largest to evaluate patients undergoing colectomy for toxic colitis, according to lead investigator Dr. Anand Dayama of the University of California, Davis, and his associates.
“In a case such as multiorgan failure with toxic colitis, the decision whether ... to operate can be an immensely difficult one,” Dr. Dayama and his colleagues wrote. “This study can help in making informed decisions in order to avoid the medicolegal ramifications of either performing an unnecessary procedure or withholding a lifesaving one,” they wrote in the American Journal of Surgery.
Surgical salvage remains the preferred treatment for patients with medically refractory toxic colitis. To assess outcomes in these patients, the researchers queried the National Surgical Quality Improvement Project database for relevant International Classification of Diseases, Ninth Revision codes between 2005 and 2012 (Am J Surg. 2015 Nov;210[5]:852-8).
The results underscored the severity of toxic colitis, they said. Of 189 patients, more than 26% died within 30 days after surgery, one in five developed postsurgical sepsis, about 17% had cardiovascular complications, 15% had wound complications, and 13% had renal complications. Furthermore, patients who were 70-80 years old had 3.5 times greater odds of dying, compared with younger patients (95% confidence interval, 1.0-12.8), and the increased likelihood of death rose by 22.2 when patients were older than 80 years (95% CI, 5.7-86.4).
Other baseline predictors of 30-day mortality included female sex (odds ratio, 4.1), blood urea nitrogen levels above 40 mg/dL (OR, 4.1), an international normalized ratio exceeding 2 (OR, 7.7), preoperative respiratory insufficiency (OR, 2.73), and a history of chronic steroid use (OR, 3.9), the researchers said. In addition, patients who died within 30 days after surgery were more likely than survivors to have undergone prolonged mechanical ventilation (56% vs. 27%), to have returned to the operating room (18% vs. 14%), to have acute renal failure (28% vs. 6%), or to have suffered a cardiac arrest that required cardiopulmonary resuscitation (18% vs. 7%). Survivors averaged about 2 fewer days in the hospital, compared with patients who died after surgery.
“The high morbidity and mortality of toxic colitis requires early and intensive medical management with IV [intravenous] steroids, antibiotics, decompressive maneuvers, and other resuscitative measures to treat the underlying cause,” they emphasized. “If there is no sign of improvement within 7 days or if there are any signs of deterioration, urgent surgical intervention should be considered.”
The link between female sex and mortality might reflect hormonal changes associated with menopause, but the study did not assess hormonal status or use of hormone therapy, the investigators noted. The association between chronic steroid use and postoperative death “is highly relevant” because long-term steroids are so often used in inflammatory bowel disease, they added. Clinical guidelines (Am J Gastroenterol. 2012 Feb;107:179-94) recommend that patients with acute severe ulcerative colitis proceed to second-line therapy or surgery if they do not respond to 3 days of intravenous steroids, because unnecessary delays can increase the risk of postoperative complications, they added.
The researchers reported no funding sources and had no disclosures.
FROM THE AMERICAN JOURNAL OF SURGERY
Key clinical point: Older age, female sex, preoperative azotemia, chronic steroid use, preoperative respiratory failure, and coagulopathy predicted adverse surgical outcomes in patients with toxic colitis.
Major finding: Odds ratios for these factors in the multivariate model ranged from 2.7 (preoperative respiratory failure) to 22.2 (age older than 80 years).
Data source: A multicenter prospective analysis of data from the National Surgical Quality Improvement Project.
Disclosures: The investigators reported no funding sources and had no disclosures.

Budget deal with NIH, CDC funding boost clears Congress
A budget deal that includes increases in funding to both the National Institutes of Health and the Centers for Disease Control and Prevention quickly passed through Congress and is expected to be signed by President Obama.
The omnibus budget agreement, announced Dec. 15, cleared the House on Dec. 18 by a 316-113 vote, with five representatives not voting. The agreement was quickly passed the same day in the Senate by a 65-33 vote. If signed, the budget bill would fund the government through the end of fiscal year 2016.

The agreement would boost funding to the NIH by $2 billion, bringing the total budget to $32 billion. It would increase funding for the CDC by about $308 million, bringing the 2016 budget to $7.2 billion.
The bill would cut $30 million from the Agency for Healthcare Research and Quality budget and keep the budgets at the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology at their fiscal 2015 levels.
Absent from the bill are any changes to the Meaningful Use program, as well as any cuts to Planned Parenthood funding.
A budget deal that includes increases in funding to both the National Institutes of Health and the Centers for Disease Control and Prevention quickly passed through Congress and is expected to be signed by President Obama.
The omnibus budget agreement, announced Dec. 15, cleared the House on Dec. 18 by a 316-113 vote, with five representatives not voting. The agreement was quickly passed the same day in the Senate by a 65-33 vote. If signed, the budget bill would fund the government through the end of fiscal year 2016.
The agreement would boost funding to the NIH by $2 billion, bringing the total budget to $32 billion. It would increase funding for the CDC by about $308 million, bringing the 2016 budget to $7.2 billion.
The bill would cut $30 million from the Agency for Healthcare Research and Quality budget and keep the budgets at the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology at their fiscal 2015 levels.
Absent from the bill are any changes to the Meaningful Use program, as well as any cuts to Planned Parenthood funding.
A budget deal that includes increases in funding to both the National Institutes of Health and the Centers for Disease Control and Prevention quickly passed through Congress and is expected to be signed by President Obama.
The omnibus budget agreement, announced Dec. 15, cleared the House on Dec. 18 by a 316-113 vote, with five representatives not voting. The agreement was quickly passed the same day in the Senate by a 65-33 vote. If signed, the budget bill would fund the government through the end of fiscal year 2016.
The agreement would boost funding to the NIH by $2 billion, bringing the total budget to $32 billion. It would increase funding for the CDC by about $308 million, bringing the 2016 budget to $7.2 billion.
The bill would cut $30 million from the Agency for Healthcare Research and Quality budget and keep the budgets at the Centers for Medicare & Medicaid Services and the Office of the National Coordinator for Health Information Technology at their fiscal 2015 levels.
Absent from the bill are any changes to the Meaningful Use program, as well as any cuts to Planned Parenthood funding.

2014 sets U.S. record for drug overdose deaths
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Key clinical point: Efforts to encourage safer prescribing of opioid pain relievers should be strengthened.
Major finding: In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths.
Data source: The National Vital Statistics System multiple cause-of-death mortality files.
Disclosures: The authors had no relevant financial disclosures.
ESR1 mutations linked with poorer survival from ER-positive breast cancer
SAN ANTONIO – Women with estrogen receptor–positive advanced breast cancer who have common mutations of the estrogen receptor 1 (ESR1) gene detectable in plasma cell–free DNA have poorer overall survival, according to data presented at the San Antonio Breast Cancer Symposium.
Investigators led by Dr. Sarat Chandarlapaty, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York, analyzed archival baseline plasma samples from 541 patients enrolled in the BOLERO-2 trial, which evaluated addition of everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin). They specifically looked for the D538G and Y537S mutations of the ESR1 gene, the two most commonly seen mutations in this setting and ones that lead to activation of the receptor even in the absence of estrogen.

Overall, nearly 29% of the women had either or both mutations, he reported in a session and related press briefing. “We think that is almost certainly an underestimate of the mutation rate, because there will be some other mutations … that we didn’t assay for here,” he commented. Of note, this prevalence using plasma was sharply higher than that found when analysis was instead performed on archival tumor tissue.
Patients with these ESR1 mutations had a 40% higher risk of death than counterparts who did not have them. And those with the D538G mutation (but not those with the Y537S mutation) had better progression-free survival if they were given everolimus.
“Patients with different mutations might end up having different responses to therapies in the future, and I think that’s what we are looking for in future research,” Dr. Chandarlapaty commented.
Press briefing moderator and codirector of the San Antonio Breast Cancer Symposium, Dr. Carlos L. Arteaga, a professor of medicine at Vanderbilt University, Nashville, Tenn., and director of the Breast Cancer Program, noted the high rate of discordance in mutation prevalence between the tumor tissue and the plasma. “Can you speculate about the reasons for that discordance?” he asked.

There are three possible explanations, Dr. Chandarlapaty replied. The archival tumor was often the primary tumor, whereas plasma samples were collected in the metastatic setting. Also, the tumor tissue was often obtained before any aromatase inhibitor therapy, which precipitates a low-estrogen environment that may promote emergence of resistance mutations. Finally, mutations detected in plasma likely reflect a summation of all mutations in the body in different sites. “I think for all these reasons, plasma may have certain advantages, especially for this alteration,” he said.
In the session, attendee Dr. Daniel F. Hayes of the University of Michigan Health System in Ann Arbor wondered whether the plasma samples were treated in any special way before the mutational testing.
“This trial started before we recognized the importance of plasma tumor DNA, so I’m pretty certain these samples were not handled in a way that we all believe they should be. The reason I’m asking this question is that if you did something special, the rest of us would love to know what it is because we are all sitting on samples like this that I’ve been told are worthless, but maybe I’m wrong,” he elaborated.
The plasma samples were collected in a routine manner, without any consideration of future genomic analysis and mutational testing, according to Dr. Chandarlapaty. “These were collected as a regular spin … and frozen at –70 [degrees],” he said. And they were stored that way, in some cases for many years, at various global sites. The investigators simply performed an additional hard spin before analyzing the samples. “So I think it does tell us that some of these archival samples that we have in our freezers may be usable for this type of analysis,” he said.

Attendee Dr. Eric P. Winer of the Dana-Farber Cancer Institute in Boston said, “So on Monday morning, people can’t go home and order circulating tumor DNA in most centers. What studies need to be done and how long do you think it will be before this is something we should consider?”
Efforts are under way to try to rapidly make these assays available in the clinic, according to Dr. Chandarlapaty. “Actually, there are some that are not in the CLIA lab but sort of are available by different vendors,” he said. Additional studies still needed include validation of the observed findings in other cohorts, among others.
BOLERO-2 tested addition of the mTOR inhibitor everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin) in postmenopausal women with metastatic or locally advanced estrogen receptor–positive, HER2-negative breast cancer that had progressed despite treatment with other aromatase inhibitors.
Dr. Chandarlapaty and colleagues detected the D538G mutation in 15.3% of patients, the Y537S mutation in 7.8%, and both in 5.5% patients, for an overall prevalence of 28.8%.
In a subset of cases having both cell-free DNA and archival tumor tissue, the proportion of cases having these mutations was much higher in the former (28.4% vs. 1.3%).
Subgroup analyses showed mutations were more common for patients who had received prior aromatase therapy in the metastatic setting versus only in the adjuvant setting (P for difference less than .001).
In the study sample as a whole, median overall survival was 32.1 months with neither ESR1 mutation, 26.0 months with only the D538G mutation, 20.0 months with only the Y537S mutation, and 15.2 months with both. Compared with patients having neither mutation, patients having either or both had an increased risk of death (hazard ratio, 1.40), as did those having the D538G mutation (1.25), the Y537S mutation (2.31), and both (1.77).
Additionally, exploratory analyses showed that adding everolimus to exemestane more than doubled median progression-free survival for patients with neither mutation (8.5 vs. 3.9 months; hazard ratio, 0.40) and for those with a D538G mutation (5.8 vs. 2.7 months; hazard ratio, 0.34). In contrast and unexpectedly, adding this drug did not improve the outcome for patients with a Y537S mutation.
Numbers of patients in the Y537S group were small, and a clear explanation for lack of benefit in that group is lacking, Dr. Chandarlapaty cautioned. “But it does tell us the biology, and what we need to do going forward in the clinic is look at these mutations not just as a whole, but individually, and ask how do they impact therapies that we are developing going forward,” he said.
SAN ANTONIO – Women with estrogen receptor–positive advanced breast cancer who have common mutations of the estrogen receptor 1 (ESR1) gene detectable in plasma cell–free DNA have poorer overall survival, according to data presented at the San Antonio Breast Cancer Symposium.
Investigators led by Dr. Sarat Chandarlapaty, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York, analyzed archival baseline plasma samples from 541 patients enrolled in the BOLERO-2 trial, which evaluated addition of everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin). They specifically looked for the D538G and Y537S mutations of the ESR1 gene, the two most commonly seen mutations in this setting and ones that lead to activation of the receptor even in the absence of estrogen.
Overall, nearly 29% of the women had either or both mutations, he reported in a session and related press briefing. “We think that is almost certainly an underestimate of the mutation rate, because there will be some other mutations … that we didn’t assay for here,” he commented. Of note, this prevalence using plasma was sharply higher than that found when analysis was instead performed on archival tumor tissue.
Patients with these ESR1 mutations had a 40% higher risk of death than counterparts who did not have them. And those with the D538G mutation (but not those with the Y537S mutation) had better progression-free survival if they were given everolimus.
“Patients with different mutations might end up having different responses to therapies in the future, and I think that’s what we are looking for in future research,” Dr. Chandarlapaty commented.
Press briefing moderator and codirector of the San Antonio Breast Cancer Symposium, Dr. Carlos L. Arteaga, a professor of medicine at Vanderbilt University, Nashville, Tenn., and director of the Breast Cancer Program, noted the high rate of discordance in mutation prevalence between the tumor tissue and the plasma. “Can you speculate about the reasons for that discordance?” he asked.
There are three possible explanations, Dr. Chandarlapaty replied. The archival tumor was often the primary tumor, whereas plasma samples were collected in the metastatic setting. Also, the tumor tissue was often obtained before any aromatase inhibitor therapy, which precipitates a low-estrogen environment that may promote emergence of resistance mutations. Finally, mutations detected in plasma likely reflect a summation of all mutations in the body in different sites. “I think for all these reasons, plasma may have certain advantages, especially for this alteration,” he said.
In the session, attendee Dr. Daniel F. Hayes of the University of Michigan Health System in Ann Arbor wondered whether the plasma samples were treated in any special way before the mutational testing.
“This trial started before we recognized the importance of plasma tumor DNA, so I’m pretty certain these samples were not handled in a way that we all believe they should be. The reason I’m asking this question is that if you did something special, the rest of us would love to know what it is because we are all sitting on samples like this that I’ve been told are worthless, but maybe I’m wrong,” he elaborated.
The plasma samples were collected in a routine manner, without any consideration of future genomic analysis and mutational testing, according to Dr. Chandarlapaty. “These were collected as a regular spin … and frozen at –70 [degrees],” he said. And they were stored that way, in some cases for many years, at various global sites. The investigators simply performed an additional hard spin before analyzing the samples. “So I think it does tell us that some of these archival samples that we have in our freezers may be usable for this type of analysis,” he said.
Attendee Dr. Eric P. Winer of the Dana-Farber Cancer Institute in Boston said, “So on Monday morning, people can’t go home and order circulating tumor DNA in most centers. What studies need to be done and how long do you think it will be before this is something we should consider?”
Efforts are under way to try to rapidly make these assays available in the clinic, according to Dr. Chandarlapaty. “Actually, there are some that are not in the CLIA lab but sort of are available by different vendors,” he said. Additional studies still needed include validation of the observed findings in other cohorts, among others.
BOLERO-2 tested addition of the mTOR inhibitor everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin) in postmenopausal women with metastatic or locally advanced estrogen receptor–positive, HER2-negative breast cancer that had progressed despite treatment with other aromatase inhibitors.
Dr. Chandarlapaty and colleagues detected the D538G mutation in 15.3% of patients, the Y537S mutation in 7.8%, and both in 5.5% patients, for an overall prevalence of 28.8%.
In a subset of cases having both cell-free DNA and archival tumor tissue, the proportion of cases having these mutations was much higher in the former (28.4% vs. 1.3%).
Subgroup analyses showed mutations were more common for patients who had received prior aromatase therapy in the metastatic setting versus only in the adjuvant setting (P for difference less than .001).
In the study sample as a whole, median overall survival was 32.1 months with neither ESR1 mutation, 26.0 months with only the D538G mutation, 20.0 months with only the Y537S mutation, and 15.2 months with both. Compared with patients having neither mutation, patients having either or both had an increased risk of death (hazard ratio, 1.40), as did those having the D538G mutation (1.25), the Y537S mutation (2.31), and both (1.77).
Additionally, exploratory analyses showed that adding everolimus to exemestane more than doubled median progression-free survival for patients with neither mutation (8.5 vs. 3.9 months; hazard ratio, 0.40) and for those with a D538G mutation (5.8 vs. 2.7 months; hazard ratio, 0.34). In contrast and unexpectedly, adding this drug did not improve the outcome for patients with a Y537S mutation.
Numbers of patients in the Y537S group were small, and a clear explanation for lack of benefit in that group is lacking, Dr. Chandarlapaty cautioned. “But it does tell us the biology, and what we need to do going forward in the clinic is look at these mutations not just as a whole, but individually, and ask how do they impact therapies that we are developing going forward,” he said.
SAN ANTONIO – Women with estrogen receptor–positive advanced breast cancer who have common mutations of the estrogen receptor 1 (ESR1) gene detectable in plasma cell–free DNA have poorer overall survival, according to data presented at the San Antonio Breast Cancer Symposium.
Investigators led by Dr. Sarat Chandarlapaty, a medical oncologist at the Memorial Sloan Kettering Cancer Center in New York, analyzed archival baseline plasma samples from 541 patients enrolled in the BOLERO-2 trial, which evaluated addition of everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin). They specifically looked for the D538G and Y537S mutations of the ESR1 gene, the two most commonly seen mutations in this setting and ones that lead to activation of the receptor even in the absence of estrogen.
Overall, nearly 29% of the women had either or both mutations, he reported in a session and related press briefing. “We think that is almost certainly an underestimate of the mutation rate, because there will be some other mutations … that we didn’t assay for here,” he commented. Of note, this prevalence using plasma was sharply higher than that found when analysis was instead performed on archival tumor tissue.
Patients with these ESR1 mutations had a 40% higher risk of death than counterparts who did not have them. And those with the D538G mutation (but not those with the Y537S mutation) had better progression-free survival if they were given everolimus.
“Patients with different mutations might end up having different responses to therapies in the future, and I think that’s what we are looking for in future research,” Dr. Chandarlapaty commented.
Press briefing moderator and codirector of the San Antonio Breast Cancer Symposium, Dr. Carlos L. Arteaga, a professor of medicine at Vanderbilt University, Nashville, Tenn., and director of the Breast Cancer Program, noted the high rate of discordance in mutation prevalence between the tumor tissue and the plasma. “Can you speculate about the reasons for that discordance?” he asked.
There are three possible explanations, Dr. Chandarlapaty replied. The archival tumor was often the primary tumor, whereas plasma samples were collected in the metastatic setting. Also, the tumor tissue was often obtained before any aromatase inhibitor therapy, which precipitates a low-estrogen environment that may promote emergence of resistance mutations. Finally, mutations detected in plasma likely reflect a summation of all mutations in the body in different sites. “I think for all these reasons, plasma may have certain advantages, especially for this alteration,” he said.
In the session, attendee Dr. Daniel F. Hayes of the University of Michigan Health System in Ann Arbor wondered whether the plasma samples were treated in any special way before the mutational testing.
“This trial started before we recognized the importance of plasma tumor DNA, so I’m pretty certain these samples were not handled in a way that we all believe they should be. The reason I’m asking this question is that if you did something special, the rest of us would love to know what it is because we are all sitting on samples like this that I’ve been told are worthless, but maybe I’m wrong,” he elaborated.
The plasma samples were collected in a routine manner, without any consideration of future genomic analysis and mutational testing, according to Dr. Chandarlapaty. “These were collected as a regular spin … and frozen at –70 [degrees],” he said. And they were stored that way, in some cases for many years, at various global sites. The investigators simply performed an additional hard spin before analyzing the samples. “So I think it does tell us that some of these archival samples that we have in our freezers may be usable for this type of analysis,” he said.
Attendee Dr. Eric P. Winer of the Dana-Farber Cancer Institute in Boston said, “So on Monday morning, people can’t go home and order circulating tumor DNA in most centers. What studies need to be done and how long do you think it will be before this is something we should consider?”
Efforts are under way to try to rapidly make these assays available in the clinic, according to Dr. Chandarlapaty. “Actually, there are some that are not in the CLIA lab but sort of are available by different vendors,” he said. Additional studies still needed include validation of the observed findings in other cohorts, among others.
BOLERO-2 tested addition of the mTOR inhibitor everolimus (Afinitor) to the aromatase inhibitor exemestane (Aromasin) in postmenopausal women with metastatic or locally advanced estrogen receptor–positive, HER2-negative breast cancer that had progressed despite treatment with other aromatase inhibitors.
Dr. Chandarlapaty and colleagues detected the D538G mutation in 15.3% of patients, the Y537S mutation in 7.8%, and both in 5.5% patients, for an overall prevalence of 28.8%.
In a subset of cases having both cell-free DNA and archival tumor tissue, the proportion of cases having these mutations was much higher in the former (28.4% vs. 1.3%).
Subgroup analyses showed mutations were more common for patients who had received prior aromatase therapy in the metastatic setting versus only in the adjuvant setting (P for difference less than .001).
In the study sample as a whole, median overall survival was 32.1 months with neither ESR1 mutation, 26.0 months with only the D538G mutation, 20.0 months with only the Y537S mutation, and 15.2 months with both. Compared with patients having neither mutation, patients having either or both had an increased risk of death (hazard ratio, 1.40), as did those having the D538G mutation (1.25), the Y537S mutation (2.31), and both (1.77).
Additionally, exploratory analyses showed that adding everolimus to exemestane more than doubled median progression-free survival for patients with neither mutation (8.5 vs. 3.9 months; hazard ratio, 0.40) and for those with a D538G mutation (5.8 vs. 2.7 months; hazard ratio, 0.34). In contrast and unexpectedly, adding this drug did not improve the outcome for patients with a Y537S mutation.
Numbers of patients in the Y537S group were small, and a clear explanation for lack of benefit in that group is lacking, Dr. Chandarlapaty cautioned. “But it does tell us the biology, and what we need to do going forward in the clinic is look at these mutations not just as a whole, but individually, and ask how do they impact therapies that we are developing going forward,” he said.
AT SABCS 2015
Key clinical point: Women with estrogen receptor–positive advanced breast cancer who have an ESR1 mutation are at increased risk for death.
Major finding: Median overall survival was 32.1 months with neither ESR1 mutation, 26.0 months with only the D538G mutation, 20.0 months with only the Y537S mutation, and 15.2 months with both mutations.
Data source: An exploratory analysis of plasma cell–free DNA from 541 patients in a phase III trial evaluating everolimus plus exemestane (BOLERO-2 trial).
Disclosures: Dr. Chandarlapaty disclosed that he receives consulting fees from Chugai, Foresite Capital, and Oncothyreon, and receives grant support from Novartis. The study was supported by Novartis and the Memorial Sloan Kettering Cancer Center’s Center for Metastasis Research.

ACA marketplace sees late surge in new enrollees
Individuals new to the federal insurance marketplace made up nearly half of the last-minute enrollees, according to data released by the Centers for Medicare & Medicaid Services.
CMS officials said that of the 1.8 million people who purchased insurance coverage in the last 5 days of open enrollment, 48% were new customers. The open enrollment period was extended for 2 days past the original Dec. 15 deadline following a late surge in demand, including the single highest day of individuals enrolling for coverage – 600,000 on Dec. 15 – during the 3 years of the federal marketplace.

In total, 6 million people signed up for coverage through HealthCare.gov during this open enrollment season, which began Nov. 1, including 2.4 million newly enrolled people and 3.6 million returning to actively enroll in coverage. CMS did not have figures for how many people will be automatically reenrolled, and the figures released account for the federal marketplace only and do not include those who are enrolling through the 13 state-run marketplaces.
“It’s clear that people have been waiting for this open enrollment period to come to the marketplace and purchase coverage,” CMS Acting Administrator Andy Slavitt said during a Dec. 18 press briefing.
He cited a number of factors driving enrollment, including the increasing tax penalty for noncoverage, which can be $695 or more; a desire to have insurance; affordability, particularly when accounting for federal subsidies; and improvements to the shopping experience, including better cost estimates and decision support tools.
Individuals new to the federal insurance marketplace made up nearly half of the last-minute enrollees, according to data released by the Centers for Medicare & Medicaid Services.
CMS officials said that of the 1.8 million people who purchased insurance coverage in the last 5 days of open enrollment, 48% were new customers. The open enrollment period was extended for 2 days past the original Dec. 15 deadline following a late surge in demand, including the single highest day of individuals enrolling for coverage – 600,000 on Dec. 15 – during the 3 years of the federal marketplace.
In total, 6 million people signed up for coverage through HealthCare.gov during this open enrollment season, which began Nov. 1, including 2.4 million newly enrolled people and 3.6 million returning to actively enroll in coverage. CMS did not have figures for how many people will be automatically reenrolled, and the figures released account for the federal marketplace only and do not include those who are enrolling through the 13 state-run marketplaces.
“It’s clear that people have been waiting for this open enrollment period to come to the marketplace and purchase coverage,” CMS Acting Administrator Andy Slavitt said during a Dec. 18 press briefing.
He cited a number of factors driving enrollment, including the increasing tax penalty for noncoverage, which can be $695 or more; a desire to have insurance; affordability, particularly when accounting for federal subsidies; and improvements to the shopping experience, including better cost estimates and decision support tools.
Individuals new to the federal insurance marketplace made up nearly half of the last-minute enrollees, according to data released by the Centers for Medicare & Medicaid Services.
CMS officials said that of the 1.8 million people who purchased insurance coverage in the last 5 days of open enrollment, 48% were new customers. The open enrollment period was extended for 2 days past the original Dec. 15 deadline following a late surge in demand, including the single highest day of individuals enrolling for coverage – 600,000 on Dec. 15 – during the 3 years of the federal marketplace.
In total, 6 million people signed up for coverage through HealthCare.gov during this open enrollment season, which began Nov. 1, including 2.4 million newly enrolled people and 3.6 million returning to actively enroll in coverage. CMS did not have figures for how many people will be automatically reenrolled, and the figures released account for the federal marketplace only and do not include those who are enrolling through the 13 state-run marketplaces.
“It’s clear that people have been waiting for this open enrollment period to come to the marketplace and purchase coverage,” CMS Acting Administrator Andy Slavitt said during a Dec. 18 press briefing.
He cited a number of factors driving enrollment, including the increasing tax penalty for noncoverage, which can be $695 or more; a desire to have insurance; affordability, particularly when accounting for federal subsidies; and improvements to the shopping experience, including better cost estimates and decision support tools.

Neratinib shows consistent breast cancer benefit at 3 years
SAN ANTONIO – The investigational oral tyrosine kinase inhibitor neratinib showed continued benefit in terms of reduced invasive disease-free survival at 3 years of follow-up in women with early-stage HER2-positive breast cancer in the randomized, double-blind ExteNET trial, Dr. Arlene Chan reported at the San Antonio Breast Cancer Symposium.
The 3-year analysis was not prespecified. It was performed because she and her coinvestigators were concerned that the previously reported benefit seen at 2 years might be lost with longer follow-up, as has occurred with trastuzumab (Herceptin) in the landmark HERA (HERceptin Adjuvant) trial. Reassuringly, however, the absolute 2.3% benefit for neratinib compared to placebo seen at 2 years in ExteNET was maintained at 3 years in the updated analysis, where the absolute difference remained essentially unchanged at 2.1%, according to Dr. Chan, vice chair of the Breast Cancer Research Center of Western Australia in Perth.

Moreover, most patients have reached the 4-year mark in follow-up, where the invasive disease-free survival benefit has remained significant in favor of neratinib at 90.5% versus 88.6% with placebo, she added.
ExteNET was a large international trial of 2,840 women with stage II-IIIc HER2-positive breast cancer with node-positive disease who were randomized to oral neratinib at 240 mg/day or placebo for 1 year beginning an average of 4.4 months after completing adjuvant chemotherapy and 1 year of trastuzumab.
The impetus for ExteNET was the well-established observation that relapse occurs in up to 26% of trastuzumab-treated patients at 8-plus years of follow-up. The study hypothesis is that neratinib, a tyrosine kinase inhibitor of HER1, –2, and –4, will prevent or delay disease recurrence because it attacks the cancer through a mechanism of action different from that of trastuzumab.
At 2 years of follow-up post neratinib, the invasive disease-free survival rate was 93.9% with active therapy and 91.6% with placebo, as previously reported by Dr. Chan. At 3 years in the roughly 85% of patients who remained in the study, which changed sponsors in the interim, the rates were 92% and 89.9%.
The 3-year outcomes were most robust in patients who began neratinib less than 1 year after completing trastuzumab and who were hormone receptor positive. In this subgroup, the 3-year invasive disease-free survival rate was 93.3% with neratinib versus 88.6% with placebo. That, Dr. Chan said, is the scenario where delayed adjuvant neratinib might prove beneficial in clinical practice.
Patients with hormone receptor–negative disease didn’t benefit from neratinib.
Forty percent of patients on neratinib developed grade 3 diarrhea, the agent’s major side effect and one that is a class effect with the tyrosine kinase inhibitors. Most cases occurred within the first 30 days of treatment and lasted for a median of 5 days, with 1.4% of neratinib-treated patients being hospitalized for this complication.
Dr. Chan noted that the study protocol precluded prophylaxis with loperamide during the first month of neratinib, which has been shown by other investigators to markedly reduce the frequency and severity of diarrhea.
Another ExteNET follow-up is planned at the 5-year mark.
Audience members asked how the Food and Drug Administration’s approval of pertuzumab (Perjeta) with indications for neoadjuvant treatment of HER2-positive breast cancer as well as for metastatic disease will change the prospects for neratinib.
Dr. Chan replied that, like other medical oncologists, she’s eagerly awaiting the results of the APHINITY trial, which is testing adjuvant pertuzumab versus placebo on top of chemotherapy plus trastuzumab in women with HER2-positive disease.
“I would suspect that even if APHINITY is positive, there will be patients who will still have a risk of relapse, so we still won’t be curing all HER2-positive patients,” she said, adding that a new clinical trial would be required in order to establish that neratinib is of benefit in such individuals.
SAN ANTONIO – The investigational oral tyrosine kinase inhibitor neratinib showed continued benefit in terms of reduced invasive disease-free survival at 3 years of follow-up in women with early-stage HER2-positive breast cancer in the randomized, double-blind ExteNET trial, Dr. Arlene Chan reported at the San Antonio Breast Cancer Symposium.
The 3-year analysis was not prespecified. It was performed because she and her coinvestigators were concerned that the previously reported benefit seen at 2 years might be lost with longer follow-up, as has occurred with trastuzumab (Herceptin) in the landmark HERA (HERceptin Adjuvant) trial. Reassuringly, however, the absolute 2.3% benefit for neratinib compared to placebo seen at 2 years in ExteNET was maintained at 3 years in the updated analysis, where the absolute difference remained essentially unchanged at 2.1%, according to Dr. Chan, vice chair of the Breast Cancer Research Center of Western Australia in Perth.
Moreover, most patients have reached the 4-year mark in follow-up, where the invasive disease-free survival benefit has remained significant in favor of neratinib at 90.5% versus 88.6% with placebo, she added.
ExteNET was a large international trial of 2,840 women with stage II-IIIc HER2-positive breast cancer with node-positive disease who were randomized to oral neratinib at 240 mg/day or placebo for 1 year beginning an average of 4.4 months after completing adjuvant chemotherapy and 1 year of trastuzumab.
The impetus for ExteNET was the well-established observation that relapse occurs in up to 26% of trastuzumab-treated patients at 8-plus years of follow-up. The study hypothesis is that neratinib, a tyrosine kinase inhibitor of HER1, –2, and –4, will prevent or delay disease recurrence because it attacks the cancer through a mechanism of action different from that of trastuzumab.
At 2 years of follow-up post neratinib, the invasive disease-free survival rate was 93.9% with active therapy and 91.6% with placebo, as previously reported by Dr. Chan. At 3 years in the roughly 85% of patients who remained in the study, which changed sponsors in the interim, the rates were 92% and 89.9%.
The 3-year outcomes were most robust in patients who began neratinib less than 1 year after completing trastuzumab and who were hormone receptor positive. In this subgroup, the 3-year invasive disease-free survival rate was 93.3% with neratinib versus 88.6% with placebo. That, Dr. Chan said, is the scenario where delayed adjuvant neratinib might prove beneficial in clinical practice.
Patients with hormone receptor–negative disease didn’t benefit from neratinib.
Forty percent of patients on neratinib developed grade 3 diarrhea, the agent’s major side effect and one that is a class effect with the tyrosine kinase inhibitors. Most cases occurred within the first 30 days of treatment and lasted for a median of 5 days, with 1.4% of neratinib-treated patients being hospitalized for this complication.
Dr. Chan noted that the study protocol precluded prophylaxis with loperamide during the first month of neratinib, which has been shown by other investigators to markedly reduce the frequency and severity of diarrhea.
Another ExteNET follow-up is planned at the 5-year mark.
Audience members asked how the Food and Drug Administration’s approval of pertuzumab (Perjeta) with indications for neoadjuvant treatment of HER2-positive breast cancer as well as for metastatic disease will change the prospects for neratinib.
Dr. Chan replied that, like other medical oncologists, she’s eagerly awaiting the results of the APHINITY trial, which is testing adjuvant pertuzumab versus placebo on top of chemotherapy plus trastuzumab in women with HER2-positive disease.
“I would suspect that even if APHINITY is positive, there will be patients who will still have a risk of relapse, so we still won’t be curing all HER2-positive patients,” she said, adding that a new clinical trial would be required in order to establish that neratinib is of benefit in such individuals.
SAN ANTONIO – The investigational oral tyrosine kinase inhibitor neratinib showed continued benefit in terms of reduced invasive disease-free survival at 3 years of follow-up in women with early-stage HER2-positive breast cancer in the randomized, double-blind ExteNET trial, Dr. Arlene Chan reported at the San Antonio Breast Cancer Symposium.
The 3-year analysis was not prespecified. It was performed because she and her coinvestigators were concerned that the previously reported benefit seen at 2 years might be lost with longer follow-up, as has occurred with trastuzumab (Herceptin) in the landmark HERA (HERceptin Adjuvant) trial. Reassuringly, however, the absolute 2.3% benefit for neratinib compared to placebo seen at 2 years in ExteNET was maintained at 3 years in the updated analysis, where the absolute difference remained essentially unchanged at 2.1%, according to Dr. Chan, vice chair of the Breast Cancer Research Center of Western Australia in Perth.
Moreover, most patients have reached the 4-year mark in follow-up, where the invasive disease-free survival benefit has remained significant in favor of neratinib at 90.5% versus 88.6% with placebo, she added.
ExteNET was a large international trial of 2,840 women with stage II-IIIc HER2-positive breast cancer with node-positive disease who were randomized to oral neratinib at 240 mg/day or placebo for 1 year beginning an average of 4.4 months after completing adjuvant chemotherapy and 1 year of trastuzumab.
The impetus for ExteNET was the well-established observation that relapse occurs in up to 26% of trastuzumab-treated patients at 8-plus years of follow-up. The study hypothesis is that neratinib, a tyrosine kinase inhibitor of HER1, –2, and –4, will prevent or delay disease recurrence because it attacks the cancer through a mechanism of action different from that of trastuzumab.
At 2 years of follow-up post neratinib, the invasive disease-free survival rate was 93.9% with active therapy and 91.6% with placebo, as previously reported by Dr. Chan. At 3 years in the roughly 85% of patients who remained in the study, which changed sponsors in the interim, the rates were 92% and 89.9%.
The 3-year outcomes were most robust in patients who began neratinib less than 1 year after completing trastuzumab and who were hormone receptor positive. In this subgroup, the 3-year invasive disease-free survival rate was 93.3% with neratinib versus 88.6% with placebo. That, Dr. Chan said, is the scenario where delayed adjuvant neratinib might prove beneficial in clinical practice.
Patients with hormone receptor–negative disease didn’t benefit from neratinib.
Forty percent of patients on neratinib developed grade 3 diarrhea, the agent’s major side effect and one that is a class effect with the tyrosine kinase inhibitors. Most cases occurred within the first 30 days of treatment and lasted for a median of 5 days, with 1.4% of neratinib-treated patients being hospitalized for this complication.
Dr. Chan noted that the study protocol precluded prophylaxis with loperamide during the first month of neratinib, which has been shown by other investigators to markedly reduce the frequency and severity of diarrhea.
Another ExteNET follow-up is planned at the 5-year mark.
Audience members asked how the Food and Drug Administration’s approval of pertuzumab (Perjeta) with indications for neoadjuvant treatment of HER2-positive breast cancer as well as for metastatic disease will change the prospects for neratinib.
Dr. Chan replied that, like other medical oncologists, she’s eagerly awaiting the results of the APHINITY trial, which is testing adjuvant pertuzumab versus placebo on top of chemotherapy plus trastuzumab in women with HER2-positive disease.
“I would suspect that even if APHINITY is positive, there will be patients who will still have a risk of relapse, so we still won’t be curing all HER2-positive patients,” she said, adding that a new clinical trial would be required in order to establish that neratinib is of benefit in such individuals.
AT SABCS 2015
Key clinical point: The significant benefit of delayed adjuvant neratinib following chemotherapy and trastuzumab remains unabated at 3 years’ follow-up in women with HER2-positive breast cancer.
Major finding: At 3 years of follow-up in a large randomized trial in women with HER2-positive breast cancer, the invasive disease-free survival rate remained significantly higher with delayed adjuvant neratinib than with placebo by a margin of 92% versus 89.1%.
Data source: ExteNET, a double-blind clinical trial of 2,840 women with stage II-IIIc HER2-positive breast cancer with node-positive disease who were randomized to oral neratinib at 240 mg/day or placebo for 1 year following completion of adjuvant chemotherapy and 1 year of trastuzumab.
Disclosures: Puma Biotechnology sponsored the trial. The presenter reported serving as a consultant to Pfizer, Amgen, and Eisai.

New England the place to be for physician access
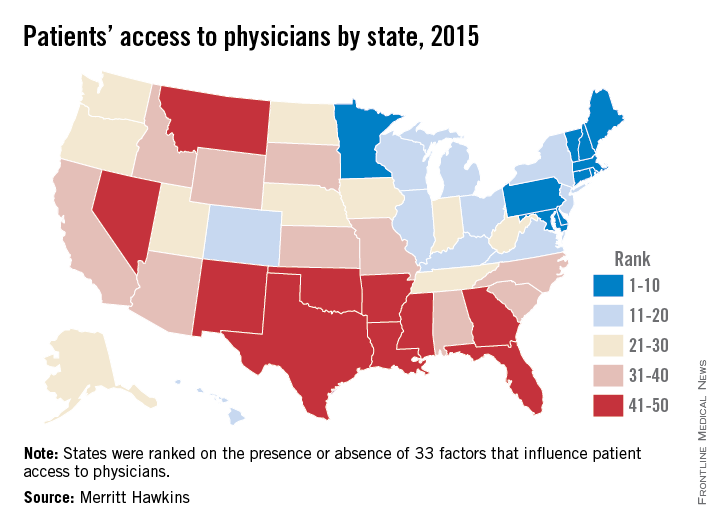
Massachusetts has the best physician access in the nation, and the rest of the New England states are not far behind, according to physician recruiting firm Merritt Hawkins.
All the New England states were ranked in the top 10 of the 2015 Physician Access Index, with New Hampshire second, Vermont third, Rhode Island eighth, Maine ninth, and Connecticut tenth. Delaware was the highest-ranked non–New England state, finishing fourth, followed by Maryland in fifth, Minnesota in sixth, and Pennsylvania in seventh.
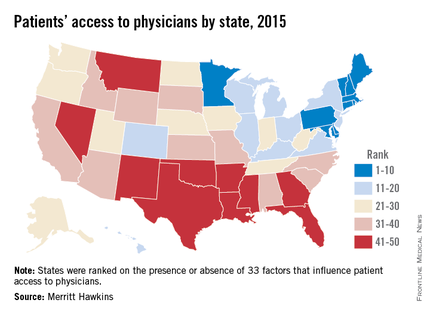
The bottom 10 states were largely clustered in the South and lower Midwest, with Oklahoma getting the not-so-coveted 50th spot, just after Nevada at 49 and New Mexico at 48.
The Physician Access Index uses 33 variables – including physicians per capita, percent of population with health insurance, urgent care centers and retail clinics per capita, and percent of physicians close to retirement. One point goes to the best-performing state and 50 to the lowest performer for each variable, so low score wins. Massachusetts had a score of 442, with Oklahoma coming in at 1,096, Merritt Hawkins said.
The report, however, also noted variability within each state. “No state is without its challenges and strong points where physician access is concerned,” Mark Smith, president of Merritt Hawkins, said in a statement. “There are pockets of patients with poor physician access in highly ranked states and pockets of patients with good physician access in states with low rankings.”
Massachusetts has the best physician access in the nation, and the rest of the New England states are not far behind, according to physician recruiting firm Merritt Hawkins.
All the New England states were ranked in the top 10 of the 2015 Physician Access Index, with New Hampshire second, Vermont third, Rhode Island eighth, Maine ninth, and Connecticut tenth. Delaware was the highest-ranked non–New England state, finishing fourth, followed by Maryland in fifth, Minnesota in sixth, and Pennsylvania in seventh.
The bottom 10 states were largely clustered in the South and lower Midwest, with Oklahoma getting the not-so-coveted 50th spot, just after Nevada at 49 and New Mexico at 48.
The Physician Access Index uses 33 variables – including physicians per capita, percent of population with health insurance, urgent care centers and retail clinics per capita, and percent of physicians close to retirement. One point goes to the best-performing state and 50 to the lowest performer for each variable, so low score wins. Massachusetts had a score of 442, with Oklahoma coming in at 1,096, Merritt Hawkins said.
The report, however, also noted variability within each state. “No state is without its challenges and strong points where physician access is concerned,” Mark Smith, president of Merritt Hawkins, said in a statement. “There are pockets of patients with poor physician access in highly ranked states and pockets of patients with good physician access in states with low rankings.”
Massachusetts has the best physician access in the nation, and the rest of the New England states are not far behind, according to physician recruiting firm Merritt Hawkins.
All the New England states were ranked in the top 10 of the 2015 Physician Access Index, with New Hampshire second, Vermont third, Rhode Island eighth, Maine ninth, and Connecticut tenth. Delaware was the highest-ranked non–New England state, finishing fourth, followed by Maryland in fifth, Minnesota in sixth, and Pennsylvania in seventh.
The bottom 10 states were largely clustered in the South and lower Midwest, with Oklahoma getting the not-so-coveted 50th spot, just after Nevada at 49 and New Mexico at 48.
The Physician Access Index uses 33 variables – including physicians per capita, percent of population with health insurance, urgent care centers and retail clinics per capita, and percent of physicians close to retirement. One point goes to the best-performing state and 50 to the lowest performer for each variable, so low score wins. Massachusetts had a score of 442, with Oklahoma coming in at 1,096, Merritt Hawkins said.
The report, however, also noted variability within each state. “No state is without its challenges and strong points where physician access is concerned,” Mark Smith, president of Merritt Hawkins, said in a statement. “There are pockets of patients with poor physician access in highly ranked states and pockets of patients with good physician access in states with low rankings.”
Physician Compare: Expanded data cause concern
Potentially inaccurate data posted on the federal Physician Compare website could misinform patients and lead to incorrect assumptions about the quality of care individual doctors provide.
With the most recent update of Physician Compare, the Centers for Medicare & Medicaid Services for the first time has posted individual physician performance scores on the 40,000 individual health care professionals who are part of the Physician Quality Reporting System (PQRS).

“Given the widespread accuracy issues with the 2014 PQRS calculations, the newly released information is premature,” American Medical Association President Steven J. Stack said in a statement. “The data inaccuracies and difficulties with CMS’s processes grew over the last couple of months and, while CMS has acknowledged these problems, it has failed to address the underlying issues. Most importantly, consumers visiting the Physician Compare website are likely to get a false impression that it provides accurate quality information for all physicians, when in fact, due to significant data problems, the newly added information covers only about 40,000 physicians.”
Although the concept of Physician Compare makes sense, the CMS needs to resolve data inconsistencies and improve how the information is being presented before posting new information to the site, said Dr. Wanda Filer, president of the American Academy of Family Physicians (AAFP). Performance scores on each measure are displayed on Physician Compare as stars followed by a percent, with each star representing 20%.
“A star rating system is too simplistic to provide for informed decisions [and] doesn’t reflect the complexity or context of care that undergirds those measures,” Dr. Filer said in an interview. “Given that complexity, it is likely that inaccurate data will be attributed to a physician’s care.”
In an effort to reduce inaccuracies, the AAFP had called for an extended period – from the current 30 days to 90 – for physicians to review their data before the data are published, Dr. Filer said.
She added that the CMS takes too long to communicate with physicians about their performance scores. Doctors do not receive reports for 6-9 months, reducing the opportunity for them to improve their performance before the next reporting period, she said.
“CMS needs to provide feedback to physicians much sooner so improvement can take place before their data are posted on the next Physician Compare,” Dr. Filer said. “Moreover, CMS must do a better job educating physicians about this website and their opportunity to review and correct any accuracies in what is reported.”

In addition to posting new PQRS measures on Physician Compare, the CMS also has posted 2014 data from group practices that report patient experience measures through the Consumer Assessment of Healthcare Providers and Systems (CAHPS) for PQRS survey. The CAHPS survey measures Medicare patients’ feedback about their care experiences. Updated performance scores for accountable care organizations, including clinical quality of care and patient experience measures for Shared Savings Program ACOs and 20 Pioneer ACOs were also added.
The reporting of the new data may be welcome for some physicians or group practices that are achieving high scores under quality-reporting programs, noted Philadelphia health law attorney Karl A. Thallner Jr.
“However, a physician who does not participate or who does not have high scores may feel that the reported data does not provide an accurate picture of the quality of care that he/she provides to patients, and therefore may be misleading to consumers,” Mr. Thallner said in an interview. “Also, physicians may not report data consistently, making differences between physicians less relevant.”
On Twitter@legal_med
Potentially inaccurate data posted on the federal Physician Compare website could misinform patients and lead to incorrect assumptions about the quality of care individual doctors provide.
With the most recent update of Physician Compare, the Centers for Medicare & Medicaid Services for the first time has posted individual physician performance scores on the 40,000 individual health care professionals who are part of the Physician Quality Reporting System (PQRS).
“Given the widespread accuracy issues with the 2014 PQRS calculations, the newly released information is premature,” American Medical Association President Steven J. Stack said in a statement. “The data inaccuracies and difficulties with CMS’s processes grew over the last couple of months and, while CMS has acknowledged these problems, it has failed to address the underlying issues. Most importantly, consumers visiting the Physician Compare website are likely to get a false impression that it provides accurate quality information for all physicians, when in fact, due to significant data problems, the newly added information covers only about 40,000 physicians.”
Although the concept of Physician Compare makes sense, the CMS needs to resolve data inconsistencies and improve how the information is being presented before posting new information to the site, said Dr. Wanda Filer, president of the American Academy of Family Physicians (AAFP). Performance scores on each measure are displayed on Physician Compare as stars followed by a percent, with each star representing 20%.
“A star rating system is too simplistic to provide for informed decisions [and] doesn’t reflect the complexity or context of care that undergirds those measures,” Dr. Filer said in an interview. “Given that complexity, it is likely that inaccurate data will be attributed to a physician’s care.”
In an effort to reduce inaccuracies, the AAFP had called for an extended period – from the current 30 days to 90 – for physicians to review their data before the data are published, Dr. Filer said.
She added that the CMS takes too long to communicate with physicians about their performance scores. Doctors do not receive reports for 6-9 months, reducing the opportunity for them to improve their performance before the next reporting period, she said.
“CMS needs to provide feedback to physicians much sooner so improvement can take place before their data are posted on the next Physician Compare,” Dr. Filer said. “Moreover, CMS must do a better job educating physicians about this website and their opportunity to review and correct any accuracies in what is reported.”
In addition to posting new PQRS measures on Physician Compare, the CMS also has posted 2014 data from group practices that report patient experience measures through the Consumer Assessment of Healthcare Providers and Systems (CAHPS) for PQRS survey. The CAHPS survey measures Medicare patients’ feedback about their care experiences. Updated performance scores for accountable care organizations, including clinical quality of care and patient experience measures for Shared Savings Program ACOs and 20 Pioneer ACOs were also added.
The reporting of the new data may be welcome for some physicians or group practices that are achieving high scores under quality-reporting programs, noted Philadelphia health law attorney Karl A. Thallner Jr.
“However, a physician who does not participate or who does not have high scores may feel that the reported data does not provide an accurate picture of the quality of care that he/she provides to patients, and therefore may be misleading to consumers,” Mr. Thallner said in an interview. “Also, physicians may not report data consistently, making differences between physicians less relevant.”
On Twitter@legal_med
Potentially inaccurate data posted on the federal Physician Compare website could misinform patients and lead to incorrect assumptions about the quality of care individual doctors provide.
With the most recent update of Physician Compare, the Centers for Medicare & Medicaid Services for the first time has posted individual physician performance scores on the 40,000 individual health care professionals who are part of the Physician Quality Reporting System (PQRS).
“Given the widespread accuracy issues with the 2014 PQRS calculations, the newly released information is premature,” American Medical Association President Steven J. Stack said in a statement. “The data inaccuracies and difficulties with CMS’s processes grew over the last couple of months and, while CMS has acknowledged these problems, it has failed to address the underlying issues. Most importantly, consumers visiting the Physician Compare website are likely to get a false impression that it provides accurate quality information for all physicians, when in fact, due to significant data problems, the newly added information covers only about 40,000 physicians.”
Although the concept of Physician Compare makes sense, the CMS needs to resolve data inconsistencies and improve how the information is being presented before posting new information to the site, said Dr. Wanda Filer, president of the American Academy of Family Physicians (AAFP). Performance scores on each measure are displayed on Physician Compare as stars followed by a percent, with each star representing 20%.
“A star rating system is too simplistic to provide for informed decisions [and] doesn’t reflect the complexity or context of care that undergirds those measures,” Dr. Filer said in an interview. “Given that complexity, it is likely that inaccurate data will be attributed to a physician’s care.”
In an effort to reduce inaccuracies, the AAFP had called for an extended period – from the current 30 days to 90 – for physicians to review their data before the data are published, Dr. Filer said.
She added that the CMS takes too long to communicate with physicians about their performance scores. Doctors do not receive reports for 6-9 months, reducing the opportunity for them to improve their performance before the next reporting period, she said.
“CMS needs to provide feedback to physicians much sooner so improvement can take place before their data are posted on the next Physician Compare,” Dr. Filer said. “Moreover, CMS must do a better job educating physicians about this website and their opportunity to review and correct any accuracies in what is reported.”
In addition to posting new PQRS measures on Physician Compare, the CMS also has posted 2014 data from group practices that report patient experience measures through the Consumer Assessment of Healthcare Providers and Systems (CAHPS) for PQRS survey. The CAHPS survey measures Medicare patients’ feedback about their care experiences. Updated performance scores for accountable care organizations, including clinical quality of care and patient experience measures for Shared Savings Program ACOs and 20 Pioneer ACOs were also added.
The reporting of the new data may be welcome for some physicians or group practices that are achieving high scores under quality-reporting programs, noted Philadelphia health law attorney Karl A. Thallner Jr.
“However, a physician who does not participate or who does not have high scores may feel that the reported data does not provide an accurate picture of the quality of care that he/she provides to patients, and therefore may be misleading to consumers,” Mr. Thallner said in an interview. “Also, physicians may not report data consistently, making differences between physicians less relevant.”
On Twitter@legal_med
