User login
Official Newspaper of the American College of Surgeons
Long spine fusions can give patients improved quality of life
SAN DIEGO – When necessary, long fusions that extend from the C-spine to the pelvis can result in health-related quality of life improvements, results from a multicenter study suggest.
“Patients with spinal deformities will sometimes require long fusion constructs that extend into the cervical spine,” lead study author Dr. Han-Jo Kim said at the annual meeting of the Cervical Spine Research Society. “The prevalence of these cases is increasing, especially as revision surgery for conditions such as proximal junctional kyphosis increase. They are also indicated for other diagnoses, such a progressive cervical deformity, cervical myelopathy as well as neuromuscular disorders.”

Prior investigations that have examined outcomes for these long constructs usually focus on patients who have had fusions from the upper thoracic spine to the pelvis, added Dr. Kim, an orthopedic spine surgeon at the Hospital for Special Surgery, New York. “To my knowledge, there are no studies in the literature that report on the subset of patients who have had fusions from the cervical spine to the pelvis,” he said. “The question is, even though these revisions may be necessary, does surgical intervention result in improved outcomes for these patients despite the extent of these long fusions?”
In an effort to determine the outcomes and rates of complications in patients who had fusions from the cervical spine to the pelvis, Dr. Kim and his associates conducted a retrospective review of patients who underwent fusions from the cervical spine to the pelvis at four institutions during 2003-2014. The researchers administered outcome scores utilizing the Scoliosis Research Society 22 (SRS-22r) questionnaire; the Oswestry Disability Index (ODI); and the Neck Disability Index (NDI); and collected demographic data including age, body mass index, and follow-up time; medical history including comorbidity data, operative details, radiographic and articular outcomes data; and postoperative complications.
Of 55 patients initially included in the study, complete data were available for 46 (84%). Their average age was 42 years, nearly one-third (30%) were classified as ASA III, 4.2% were smokers, and the average follow-up time was 2.7 years. “The majority of these cases were revision operations, and osteotomies were performed in close to 60% of these patients,” Dr. Kim said. “The average operating time was over 300 minutes, and there was an average of over 2 L of blood loss for these cases.”
The researchers observed improvements in the activity, pain, and mental health domains of the SRS, as well as an improvement in the SRS total score, which improved from an average of 3.0 preoperatively to 3.5 postoperatively (P less than .01). This was greater than the minimally clinically important difference for the SRS-22r. “At least one [minimally clinically important difference] was met in all of the SRS domains, as well as in the NDI,” Dr. Kim said. “There was no change in the ODI, as we would expect for this patient subset.”
Radiographic outcomes improved significantly, he continued, with an average 31-degree correction in maximum kyphosis and a 3.3-cm improvement in sagittal vertical axis. The overall rate of complications was 71%, with major complications comprising about 39% of these cases. Medical complications were high as well (a rate of 61%), as was the rate of surgical complications (43%). More than half of the patients (54%) required reoperation during the follow-up period, and the rate of pseudarthrosis was 29%.
“These results demonstrate improved outcomes following cervical to pelvic fusions, despite the magnitude of their operations and extent of fusion,” Dr. Kim concluded. “In addition, despite the high rate of complications and reoperations, we noted a significant improvement in radiographic and clinical outcomes.”
Dr. Kim disclosed that he is a consultant for Zimmer Biomet and K2M.
SAN DIEGO – When necessary, long fusions that extend from the C-spine to the pelvis can result in health-related quality of life improvements, results from a multicenter study suggest.
“Patients with spinal deformities will sometimes require long fusion constructs that extend into the cervical spine,” lead study author Dr. Han-Jo Kim said at the annual meeting of the Cervical Spine Research Society. “The prevalence of these cases is increasing, especially as revision surgery for conditions such as proximal junctional kyphosis increase. They are also indicated for other diagnoses, such a progressive cervical deformity, cervical myelopathy as well as neuromuscular disorders.”
Prior investigations that have examined outcomes for these long constructs usually focus on patients who have had fusions from the upper thoracic spine to the pelvis, added Dr. Kim, an orthopedic spine surgeon at the Hospital for Special Surgery, New York. “To my knowledge, there are no studies in the literature that report on the subset of patients who have had fusions from the cervical spine to the pelvis,” he said. “The question is, even though these revisions may be necessary, does surgical intervention result in improved outcomes for these patients despite the extent of these long fusions?”
In an effort to determine the outcomes and rates of complications in patients who had fusions from the cervical spine to the pelvis, Dr. Kim and his associates conducted a retrospective review of patients who underwent fusions from the cervical spine to the pelvis at four institutions during 2003-2014. The researchers administered outcome scores utilizing the Scoliosis Research Society 22 (SRS-22r) questionnaire; the Oswestry Disability Index (ODI); and the Neck Disability Index (NDI); and collected demographic data including age, body mass index, and follow-up time; medical history including comorbidity data, operative details, radiographic and articular outcomes data; and postoperative complications.
Of 55 patients initially included in the study, complete data were available for 46 (84%). Their average age was 42 years, nearly one-third (30%) were classified as ASA III, 4.2% were smokers, and the average follow-up time was 2.7 years. “The majority of these cases were revision operations, and osteotomies were performed in close to 60% of these patients,” Dr. Kim said. “The average operating time was over 300 minutes, and there was an average of over 2 L of blood loss for these cases.”
The researchers observed improvements in the activity, pain, and mental health domains of the SRS, as well as an improvement in the SRS total score, which improved from an average of 3.0 preoperatively to 3.5 postoperatively (P less than .01). This was greater than the minimally clinically important difference for the SRS-22r. “At least one [minimally clinically important difference] was met in all of the SRS domains, as well as in the NDI,” Dr. Kim said. “There was no change in the ODI, as we would expect for this patient subset.”
Radiographic outcomes improved significantly, he continued, with an average 31-degree correction in maximum kyphosis and a 3.3-cm improvement in sagittal vertical axis. The overall rate of complications was 71%, with major complications comprising about 39% of these cases. Medical complications were high as well (a rate of 61%), as was the rate of surgical complications (43%). More than half of the patients (54%) required reoperation during the follow-up period, and the rate of pseudarthrosis was 29%.
“These results demonstrate improved outcomes following cervical to pelvic fusions, despite the magnitude of their operations and extent of fusion,” Dr. Kim concluded. “In addition, despite the high rate of complications and reoperations, we noted a significant improvement in radiographic and clinical outcomes.”
Dr. Kim disclosed that he is a consultant for Zimmer Biomet and K2M.
SAN DIEGO – When necessary, long fusions that extend from the C-spine to the pelvis can result in health-related quality of life improvements, results from a multicenter study suggest.
“Patients with spinal deformities will sometimes require long fusion constructs that extend into the cervical spine,” lead study author Dr. Han-Jo Kim said at the annual meeting of the Cervical Spine Research Society. “The prevalence of these cases is increasing, especially as revision surgery for conditions such as proximal junctional kyphosis increase. They are also indicated for other diagnoses, such a progressive cervical deformity, cervical myelopathy as well as neuromuscular disorders.”
Prior investigations that have examined outcomes for these long constructs usually focus on patients who have had fusions from the upper thoracic spine to the pelvis, added Dr. Kim, an orthopedic spine surgeon at the Hospital for Special Surgery, New York. “To my knowledge, there are no studies in the literature that report on the subset of patients who have had fusions from the cervical spine to the pelvis,” he said. “The question is, even though these revisions may be necessary, does surgical intervention result in improved outcomes for these patients despite the extent of these long fusions?”
In an effort to determine the outcomes and rates of complications in patients who had fusions from the cervical spine to the pelvis, Dr. Kim and his associates conducted a retrospective review of patients who underwent fusions from the cervical spine to the pelvis at four institutions during 2003-2014. The researchers administered outcome scores utilizing the Scoliosis Research Society 22 (SRS-22r) questionnaire; the Oswestry Disability Index (ODI); and the Neck Disability Index (NDI); and collected demographic data including age, body mass index, and follow-up time; medical history including comorbidity data, operative details, radiographic and articular outcomes data; and postoperative complications.
Of 55 patients initially included in the study, complete data were available for 46 (84%). Their average age was 42 years, nearly one-third (30%) were classified as ASA III, 4.2% were smokers, and the average follow-up time was 2.7 years. “The majority of these cases were revision operations, and osteotomies were performed in close to 60% of these patients,” Dr. Kim said. “The average operating time was over 300 minutes, and there was an average of over 2 L of blood loss for these cases.”
The researchers observed improvements in the activity, pain, and mental health domains of the SRS, as well as an improvement in the SRS total score, which improved from an average of 3.0 preoperatively to 3.5 postoperatively (P less than .01). This was greater than the minimally clinically important difference for the SRS-22r. “At least one [minimally clinically important difference] was met in all of the SRS domains, as well as in the NDI,” Dr. Kim said. “There was no change in the ODI, as we would expect for this patient subset.”
Radiographic outcomes improved significantly, he continued, with an average 31-degree correction in maximum kyphosis and a 3.3-cm improvement in sagittal vertical axis. The overall rate of complications was 71%, with major complications comprising about 39% of these cases. Medical complications were high as well (a rate of 61%), as was the rate of surgical complications (43%). More than half of the patients (54%) required reoperation during the follow-up period, and the rate of pseudarthrosis was 29%.
“These results demonstrate improved outcomes following cervical to pelvic fusions, despite the magnitude of their operations and extent of fusion,” Dr. Kim concluded. “In addition, despite the high rate of complications and reoperations, we noted a significant improvement in radiographic and clinical outcomes.”
Dr. Kim disclosed that he is a consultant for Zimmer Biomet and K2M.
AT CSRS 2015
Key clinical point: Following cervical to pelvic fusions, patients can achieve improved clinical and quality of life outcomes.
Major finding: The Scoliosis Research Society total score improved from an average of 3.0 preoperatively to 3.5 postoperatively (P less than .01).
Data source: A retrospective review of 55 patients who underwent fusions from the cervical spine to the pelvis at four institutions during 2003-2014.
Disclosures: Dr. Kim disclosed that he is a consultant for Zimmer Biomet and K2M.

The palliative path: Talking with elderly patients facing emergency surgery
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
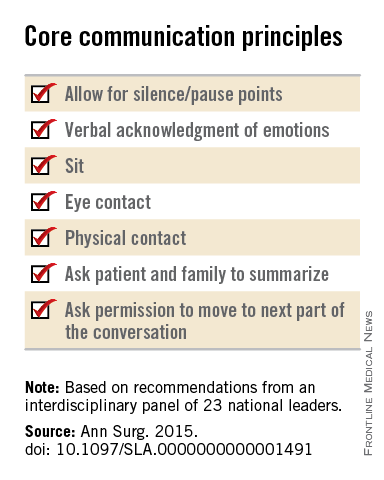
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
An expert panel has developed a communication framework to improve treatment of older, seriously ill patients who have surgical emergencies, which has been published online in Annals of Surgery.
A substantial portion of older patients who undergo emergency surgeries already have serious life-limiting illnesses such as cardiopulmonary disease, renal failure, liver failure, dementia, severe neurological impairment, or malignancy. The advisory panel based its work on the premise that surgery in these circumstances can lead to significant further morbidity, health care utilization, functional decline, prolonged hospital stay or institutionalization, and death, with attendant physical discomfort and psychological distress at the end of these patients’ lives.
Surgeons consulted in the emergency setting for these patients are hampered by patients unable to communicate well because they are in extremis, by surrogates who are unprepared for their role, and by time constraints, lack of familiarity with the patient, poor understanding of the illness by patients and families, prognostic uncertainty, and inadequate advance care planning. In addition, “many surgeons lack skills to engage in conversations about end-of-life care, or are too unfamiliar with palliative options to discuss them well,” or feel obligated to maintain postoperative life support despite the patient’s wishes, said Dr. Zara Cooper, of Ariadne Labs and the Center for Surgery and Public Health at Brigham and Women’s Hospital, both in Boston, and her associates.
To address these issues and assist surgeons in caring for such patients, an expert panel of 23 national leaders in acute care surgery, general surgery, surgical oncology, palliative medicine, critical care, emergency medicine, anesthesia, and health care innovation was convened at Harvard Medical School, Boston.
The focus of the panel’s recommendations was a structured communications framework prototype to facilitate shared decision-making in these difficult circumstances.
Among the panel’s recommendations for surgeons were the following priorities:
• Review the medical record and consult the treatment team to fully understand the patient’s current condition, comorbidities, expected illness trajectory, and preferences for end-of-life care.
• Assess functional performance as part of the routine history and physical to fully understand the patient’s fitness for surgery.
• Formulate a prognosis regarding the patient’s overall health both with and without surgery.
The panel offered a set of principles and specific elements for the meeting with the patient and family:
• The surgeon should begin by introducing himself or herself; according to reports in the literature, physicians fail to do this approximately half of the time.
• Pay attention to nonverbal communication, such as eye contact and physical contact, as this is critical to building rapport. Immediately address pain, anxiety, and other indicators of distress, to maximize the patients’ and the families’ engagement in subsequent medical discussions. “Although adequate analgesia may render a patient unable to make their own decisions, surrogates are more likely to make appropriate decisions when they feel their loved one is comfortable,” the panel noted.
• Allow pauses and silences to occur. Let the patient and the family process information and their own emotions.
• Elicit the patients’ or the surrogates’ understanding of the illness and their views of the patients’ likely trajectory, correcting any inaccuracies. This substantially influences their decisions regarding the aggressiveness of subsequent treatments.
• Inform the patient and family of the life-threatening nature of the patient’s acute condition and its potential impact on the rest of his or her life, including the possibility of prolonged life support, ICU stay, burdensome treatment, and loss of independence. Use accepted techniques for breaking bad news, and check to be sure the patient understands what was conveyed.
• At this point, the surgeon should synthesize and summarize the information from the patient, the family, and the medical record, then pause to give them time to process the information and to assess their emotional state. It is helpful to label and respond to the patient’s emotions at this juncture, and to build empathy with statements such as “I know this is difficult news, and I wish it were different.”
• Describe the benefits, burdens, and range of likely outcomes if surgery is undertaken and if it is not. The surgeon should use nonmedical language to describe symptoms, and should convey his or her expectations regarding length of hospitalization, need for and duration of life support, burdensome symptoms, discharge to an institution, and functional recovery.
• Surgeons should be able to communicate palliative options possible either in combination with surgery or instead of surgery. Palliative care can aid in managing advanced symptoms, providing psychosocial support for patients and caregivers, facilitating interdisciplinary communication, and facilitating medical decisions and care transitions.
• Avoid describing surgical procedures as “doing everything” and palliative care as “doing nothing.” This can make patients and families “feel abandoned, fearful, isolated, and angry, and fails to encompass palliative care’s practices of proactive communication, aggressive symptom management, and timely emotional support to alleviate suffering and affirm quality of life,” the panel said.
• Surgeons should explicitly support the patients’ medical decisions, whether or not they choose surgery.
The panel also cited a few factors that would assist surgeons in following these recommendations. First, surgeons must recognize the importance of communicating well with seriously ill older patients and acknowledge that this is a crucial clinical skill for them to cultivate. They must also recognize that palliative care is vital to delivering high-quality surgical care. Surgeons should consider discharging patients to hospice, which can improve pain and symptom management, improve patient and family satisfaction with care, and avoid unwanted hospitalization or cardiopulmonary resuscitation.
“There are a number of major barriers to introducing palliative care in these situations. One is an education problem - the perception on the part of patients and clinicians, and surgeons in particular, that palliative care is only limited to end-of-life care, which it is not. It is a misperception of what palliative care means in this equation - that palliative care and hospice are the same thing, which they absolutely are not,”said Dr. Cooper in an interview.
”The definition of palliative care has evolved over the past decade and the focus of palliative care is on quality of life and alleviating symptoms. End-of-life palliative care is part of that, and as patients get closer to the end of life, symptom management and quality of life become more focal than life-prolonging treatment... But for patients with chronic and serious illness, there has to be a role for palliative care because we know that when patients feel better, they tend to live longer. And when patients feel their emotional concerns and physical needs are being addressed, they tend to do better. Patients families have improved satisfaction when their loved one receives palliative care,” she noted.”
However, the number of palliative providers is completely inadequate to meet the needs of the number of seriously ill patients, she said. And a lot of hospital-based palliative care is by necessity limited to end-of-life care because of a lack of palliative resources.
Dr. Atul Gawande, a coauthor of the panel recommendations, wrote a best-selling book, Being Mortal (New York: Metropolitan Books, 2014) addressing the shortcomings and potential remaking of medical care in the context of age-related frailty, grave illness, and death. Dr. Cooper noted that there is a growing sentiment among the general public that they want to have their quality of life addressed in the type of medical care they receive. She said that Dr. Gawande’s book tapped into the perception of a lack of recognition of personhood of seriously ill patients.
“We often focus on diagnosis and we don’t have the ‘bandwidth’ to focus on the person carrying that diagnosis, and our patients and focus on the person carrying that diagnosis, but our patients and their families are demanding different types of care. So, ultimately, the patients will be the ones to push us to do better for them.”
The next steps to further developing a widely used and validated communication framework would be to create educational opportunities for clinicians to develop clinical skills in communication with seriously ill patients and palliative care, and to study the impact of these initiatives on improving outcomes most relevant to older patient. This work was supported by the Ariadne Labs, a Joint Center for Health System Innovation at Brigham and Women’s Hospital. Dr. Cooper and her associates reported having no relevant financial disclosures.
FROM ANNALS OF SURGERY

Acute care surgeons should watch for bariatric surgery complications
Acute care surgeons are likely to encounter problems related to bariatric surgery because patients have a lifelong risk of complications, said authors of a single-center retrospective study.
“Internal hernias or obstructive etiologies are the most common presentations, and often require emergent or urgent surgery,” added Dr. Joel F. Bradley of Premier Surgical Associates, Knoxville, Tenn., and his associates at Carolinas Medical Center, a quaternary care hospital in Charlotte, N.C. “We recommend that when diagnosis is unclear for former bariatric surgery patients, diagnostic laparoscopy be performed to answer definitively if a surgical complication is present.”

Bariatric surgeries in the United States have leveled off at about 100,000 per year, but postsurgical complications are rising along with the total patient population. The researchers reviewed all 33 such cases at their acute care surgical service between 2007 and 2013 (Am. J. Surg. 2015;210:456-61).
Most patients were middle-age women with a history of laparoscopic Roux-en-y gastric bypass (RYGB) surgery. Other common index procedures included open RYGB and laparoscopic gastric banding, the researchers said. The most frequent complication was internal hernia, which affected a third of patients, and in two cases involved ischemic bowel. Other complications included adhesive small bowel obstruction, laparoscopic band restriction, and biliary disease. “Of note, all three patients with biliary disease also had internal hernias at Peterson’s defect that were closed at the time of cholecystectomy,” the investigators said. Less-common complications included upper gastrointestinal bleeding or ulcer, perforated ulcer, gastric outlet obstruction, intussusception, and ventral incisional hernia.
About 91% of patients with complications needed surgery, and 43% were open rather than minimally invasive. Laparoscopic and open surgery cases had similar baseline characteristics and outcomes, but open surgery patients averaged 11 days in the hospital, compared with 5 days for laparoscopic cases (P less than .05).
Cases were often emergent (43%) or urgent (20%), the investigators emphasized. All three patients with a previous vertical banded gastroplasty were obstructed at the gastroplasty site and were converted to RYGB. Surgeons managed the single case of intussusception with laparoscopic reduction and colopexy of the proximal and distal bowel to the abdominal wall. All three patients with symptomatic cholelithiasis underwent laparoscopic cholecystectomy. Two patients underwent upper endoscopies for bleeding or ulcer, and one underwent gastric band deflation for obstruction. No patients died.
Patients who have undergone RYGB are at particular risk of obstructive internal hernias, which can be mesenteric, mesojejunal, jejunojejunal, or at the Petersen’s space, the researchers noted. Some bariatric surgeons do not routinely close mesenteric defects, and, even when closed at the index surgery, as many as 83% of patients spontaneously open their jejunojejunostomy mesenteric defect after losing weight, they added (JSLS. 2010 Apr-Jun;14[2]:213-6).
Surgeons should also watch for obstructions secondary to adhesive disease and lap band restriction, they said. “Importantly, patients presenting with bowel obstruction from adhesive disease after RYGB are indiscernible from those with internal herniation, and surgeons must have a low threshold to evaluate these patients with diagnostic laparoscopy,” they added.
Band slippage, the most common complication of gastric banding, can cause dysphagia and gastric outlet obstruction, the investigators noted. Port site infection and band erosion are thought to be rare and can be managed laparoscopically if caught early, they said. “Many general and acute care surgeons may think that these complications are rare, and do not pertain to their practice; however, as bariatric procedures have regionalized, patients’ emergent complications are often seen by the local surgeon, not at the regional center,” they added.
The researchers reported no funding sources and no disclosures.
Acute care surgeons are likely to encounter problems related to bariatric surgery because patients have a lifelong risk of complications, said authors of a single-center retrospective study.
“Internal hernias or obstructive etiologies are the most common presentations, and often require emergent or urgent surgery,” added Dr. Joel F. Bradley of Premier Surgical Associates, Knoxville, Tenn., and his associates at Carolinas Medical Center, a quaternary care hospital in Charlotte, N.C. “We recommend that when diagnosis is unclear for former bariatric surgery patients, diagnostic laparoscopy be performed to answer definitively if a surgical complication is present.”
Bariatric surgeries in the United States have leveled off at about 100,000 per year, but postsurgical complications are rising along with the total patient population. The researchers reviewed all 33 such cases at their acute care surgical service between 2007 and 2013 (Am. J. Surg. 2015;210:456-61).
Most patients were middle-age women with a history of laparoscopic Roux-en-y gastric bypass (RYGB) surgery. Other common index procedures included open RYGB and laparoscopic gastric banding, the researchers said. The most frequent complication was internal hernia, which affected a third of patients, and in two cases involved ischemic bowel. Other complications included adhesive small bowel obstruction, laparoscopic band restriction, and biliary disease. “Of note, all three patients with biliary disease also had internal hernias at Peterson’s defect that were closed at the time of cholecystectomy,” the investigators said. Less-common complications included upper gastrointestinal bleeding or ulcer, perforated ulcer, gastric outlet obstruction, intussusception, and ventral incisional hernia.
About 91% of patients with complications needed surgery, and 43% were open rather than minimally invasive. Laparoscopic and open surgery cases had similar baseline characteristics and outcomes, but open surgery patients averaged 11 days in the hospital, compared with 5 days for laparoscopic cases (P less than .05).
Cases were often emergent (43%) or urgent (20%), the investigators emphasized. All three patients with a previous vertical banded gastroplasty were obstructed at the gastroplasty site and were converted to RYGB. Surgeons managed the single case of intussusception with laparoscopic reduction and colopexy of the proximal and distal bowel to the abdominal wall. All three patients with symptomatic cholelithiasis underwent laparoscopic cholecystectomy. Two patients underwent upper endoscopies for bleeding or ulcer, and one underwent gastric band deflation for obstruction. No patients died.
Patients who have undergone RYGB are at particular risk of obstructive internal hernias, which can be mesenteric, mesojejunal, jejunojejunal, or at the Petersen’s space, the researchers noted. Some bariatric surgeons do not routinely close mesenteric defects, and, even when closed at the index surgery, as many as 83% of patients spontaneously open their jejunojejunostomy mesenteric defect after losing weight, they added (JSLS. 2010 Apr-Jun;14[2]:213-6).
Surgeons should also watch for obstructions secondary to adhesive disease and lap band restriction, they said. “Importantly, patients presenting with bowel obstruction from adhesive disease after RYGB are indiscernible from those with internal herniation, and surgeons must have a low threshold to evaluate these patients with diagnostic laparoscopy,” they added.
Band slippage, the most common complication of gastric banding, can cause dysphagia and gastric outlet obstruction, the investigators noted. Port site infection and band erosion are thought to be rare and can be managed laparoscopically if caught early, they said. “Many general and acute care surgeons may think that these complications are rare, and do not pertain to their practice; however, as bariatric procedures have regionalized, patients’ emergent complications are often seen by the local surgeon, not at the regional center,” they added.
The researchers reported no funding sources and no disclosures.
Acute care surgeons are likely to encounter problems related to bariatric surgery because patients have a lifelong risk of complications, said authors of a single-center retrospective study.
“Internal hernias or obstructive etiologies are the most common presentations, and often require emergent or urgent surgery,” added Dr. Joel F. Bradley of Premier Surgical Associates, Knoxville, Tenn., and his associates at Carolinas Medical Center, a quaternary care hospital in Charlotte, N.C. “We recommend that when diagnosis is unclear for former bariatric surgery patients, diagnostic laparoscopy be performed to answer definitively if a surgical complication is present.”
Bariatric surgeries in the United States have leveled off at about 100,000 per year, but postsurgical complications are rising along with the total patient population. The researchers reviewed all 33 such cases at their acute care surgical service between 2007 and 2013 (Am. J. Surg. 2015;210:456-61).
Most patients were middle-age women with a history of laparoscopic Roux-en-y gastric bypass (RYGB) surgery. Other common index procedures included open RYGB and laparoscopic gastric banding, the researchers said. The most frequent complication was internal hernia, which affected a third of patients, and in two cases involved ischemic bowel. Other complications included adhesive small bowel obstruction, laparoscopic band restriction, and biliary disease. “Of note, all three patients with biliary disease also had internal hernias at Peterson’s defect that were closed at the time of cholecystectomy,” the investigators said. Less-common complications included upper gastrointestinal bleeding or ulcer, perforated ulcer, gastric outlet obstruction, intussusception, and ventral incisional hernia.
About 91% of patients with complications needed surgery, and 43% were open rather than minimally invasive. Laparoscopic and open surgery cases had similar baseline characteristics and outcomes, but open surgery patients averaged 11 days in the hospital, compared with 5 days for laparoscopic cases (P less than .05).
Cases were often emergent (43%) or urgent (20%), the investigators emphasized. All three patients with a previous vertical banded gastroplasty were obstructed at the gastroplasty site and were converted to RYGB. Surgeons managed the single case of intussusception with laparoscopic reduction and colopexy of the proximal and distal bowel to the abdominal wall. All three patients with symptomatic cholelithiasis underwent laparoscopic cholecystectomy. Two patients underwent upper endoscopies for bleeding or ulcer, and one underwent gastric band deflation for obstruction. No patients died.
Patients who have undergone RYGB are at particular risk of obstructive internal hernias, which can be mesenteric, mesojejunal, jejunojejunal, or at the Petersen’s space, the researchers noted. Some bariatric surgeons do not routinely close mesenteric defects, and, even when closed at the index surgery, as many as 83% of patients spontaneously open their jejunojejunostomy mesenteric defect after losing weight, they added (JSLS. 2010 Apr-Jun;14[2]:213-6).
Surgeons should also watch for obstructions secondary to adhesive disease and lap band restriction, they said. “Importantly, patients presenting with bowel obstruction from adhesive disease after RYGB are indiscernible from those with internal herniation, and surgeons must have a low threshold to evaluate these patients with diagnostic laparoscopy,” they added.
Band slippage, the most common complication of gastric banding, can cause dysphagia and gastric outlet obstruction, the investigators noted. Port site infection and band erosion are thought to be rare and can be managed laparoscopically if caught early, they said. “Many general and acute care surgeons may think that these complications are rare, and do not pertain to their practice; however, as bariatric procedures have regionalized, patients’ emergent complications are often seen by the local surgeon, not at the regional center,” they added.
The researchers reported no funding sources and no disclosures.
FROM THE AMERICAN JOURNAL OF SURGERY
Key clinical point: Postsurgical complications from bariatric surgery are on the rise, and acute care surgeons should be familiar with them.
Major finding: The most common complication in the case series was internal hernia, followed by adhesive small bowel obstruction.
Data source: A single-center retrospective review of 33 bariatric complications treated at an acute case surgery service between 2007 and 2013.
Disclosures: The researchers reported no funding sources and had no disclosures.

‘Fear and ignorance’ drive rise in bilateral mastectomy
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.

In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.

He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.
In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.
He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
SAN ANTONIO – The worldwide upsurge in bilateral mastectomy for unilateral breast cancer in the last decade came under withering fire from prominent breast surgeons at the San Antonio Breast Cancer Symposium.
“It seems crazy, doesn’t it, that we’re spending all this time trying to conserve the breast, yet we’re facing a tsunami of requests for bilateral mastectomy,” observed Dr. Fiona MacNeill, chairman of the education and training committee of the Royal College of Surgeons of England.
“A contralateral risk–reducing prophylactic mastectomy undoubtedly will reduce the risk of contralateral breast cancer, since you’re removing the breast, but this is overtreatment for the vast majority of women who request it. At 20 years we haven’t been able to demonstrate that it offers a significant survival advantage. I think a lot of what’s driving bilateral mastectomy is fear and ignorance, a failure to understand risk by patients and often by health professionals,” said Dr. MacNeill, a breast surgeon at Royal Marsden Hospital in London.
In an invited special lecture titled, “Less is more: minimizing breast cancer surgery,” Dr. MacNeill began by observing, “Only a surgeon could give this talk, because only a surgeon can tell you why we’re doing too much surgery.”
She stressed three main points: surgery is, as she put it, “a medieval treatment in a molecular era.” Overwhelming evidence shows that breast cancer outcomes are determined by disease biology, burden, and response to systemic therapy and not by the extent of surgery. And since there is no survival benefit for more aggressive surgery, the surgeon’s goal must be to optimize breast and axillary conservation.
In a separate presentation, Dr. Ismail Jatoi, professor and chief of surgical oncology at the University of Texas, San Antonio, outlined trends in surgical treatment of early-stage breast cancer as documented in a recent major retrospective study conducted in Tennessee of 1.2 million women treated at accredited U.S. breast cancer centers during 1998-2011.
The Tennessee investigators’ analysis points to a polarization in surgical therapy: The rate of unilateral mastectomy without reconstruction has dropped steadily since the beginning of the study period in 1998 among women eligible for breast-conserving surgery (BCS), while starting around 2006 the rate of bilateral mastectomy with reconstruction has surged. This increase in bilateral mastectomies with reconstruction resulted in an adjusted 34% jump in the overall mastectomy rate during 2004-2011 as compared with 1998-2003. As a result, in 2011 nearly 40% of women with early breast cancer underwent mastectomy. Meanwhile, the rate of BCS has been waning since 2006 (JAMA Surg. 2015 Jan;150[1]:9-16).
These disturbing trends have been fueled in part by at least eight published observational studies reporting improved survival with contralateral prophylactic mastectomy (CPM) as compared with unilateral mastectomy or BCS. But these were all observational studies and hence likely compromised by unmeasured confounders, according to Dr. Jatoi.
He presented highlights of his study of National Cancer Institute Surveillance, Epidemiology, and End Results data to support his recommendation that these observational studies be taken with a grain of salt.
His study included nearly 26,000 women who underwent CPM and more than 400,000 who did not. In a multivariate regression analysis adjusted for age, race, tumor stage, hormone receptor status, and histologic grade, CPM was associated with a statistically significant and impressive-sounding 16% reduction in the 5-year risk of breast cancer–specific mortality, a 17% reduction in overall mortality, and … a highly improbable 29% reduction in noncancer mortality (Breast Cancer Res Treat. 2014 Nov;148[2]:389-96).
“Obviously bilateral mastectomy is not going to reduce your risk of dying of heart attack or stroke or other noncancer causes. So even though we adjusted for everything possible in the SEER database, it suggests there were still unmeasured confounders. What this study shows is that it’s these unmeasured confounders that pose a threat to the validity of observational studies,” the surgeon said.
“Randomized data and observational studies consistently show that breast-conserving surgery is the optimal choice for most patients. It’s the safest choice, it’s cost effective, and it should remain in 2015 the optimal treatment for breast cancer,” he declared.
The cost-effectiveness of BCS was underscored during the symposium by means of a retrospective study presented by Dr. Benjamin D. Smith.
He and his coinvestigators analyzed costs and complication rates in the first 2 years following diagnosis of early-stage breast cancer in 44,344 patients under age 65 in the MarketScan database and almost 61,000 older women in the SEER-Medicare database.
The 2-year complication rate related to local therapy in younger breast cancer patients ranged from 30% for lumpectomy plus whole breast irradiation to 56% for mastectomy plus reconstruction. In older patients, the complication rates were 38% for lumpectomy plus whole breast irradiation and 69% for mastectomy plus reconstruction.
Adding together procedural and complication costs, the most expensive therapy in younger women was mastectomy with reconstruction, at an average of $89,140, which was $23,421 more than for lumpectomy plus whole breast irradiation, according to Dr. Smith, a radiation oncologist at MD Anderson Cancer Center in Houston.
“When oncologists offer all appropriate therapy options to patients, some women may choose to avoid radiation and opt for mastectomy and reconstruction instead. This study is helpful to such patients because it provides them with information regarding the trade-offs involved in this choice,” he explained.
Dr. MacNeill noted that in addition to the increased financial cost and physical complication rate entailed by mastectomy plus reconstruction for early breast cancer, this more aggressive surgery has another important unwelcome consequence: it delays the start of adjuvant therapy, which is the intervention that truly affects outcome.
Many women who opt for CPM do so because they can’t face the prospect of going through chemotherapy again should cancer arise in the contralateral breast. What’s often overlooked, she continued, is that the greatest risks of death or need for further systemic treatment due to relapse arise from the index cancer.
“We overestimate our patients’ contralateral risk, we underestimate the risk of dying from relapse of the index cancer, and we very often fail to consider other competing health risks from smoking, obesity, age, and other factors,” according to Dr. MacNeill.
“It’s not as if additional surgery is risk-free. A bilateral mastectomy carries bilateral complications. Our patients expect a perfect outcome because that’s what they see on television, but the reality is that for some women the results can be absolutely disastrous. Whilst women may not regret their choice for bilateral mastectomy with reconstruction because they think it’s lifesaving, the psychosexual impact is phenomenal,” she said.
That being said, Dr. MacNeill continued, “the elephant in the room” regarding BCS is that re-excision rates of up to 40% are common. This high rate of repeat surgery is a huge issue because of the resultant increased costs, morbidity, poor cosmesis, increased risk of mastectomy, and delay to adjuvant therapy.
High re-excision rates aren’t due to surgical incompetence, Dr. MacNeill stressed, but rather to the difficulty in defining microscopic disease intraoperatively. But help is on the way. Several novel approaches that facilitate lower re-excision rates and more breast conservation show considerable promise.
For example, investigators at Yale University have recently demonstrated in a randomized controlled trial that routine intraoperative cavity shave margins taken circumferentially halved the re-excision rate, from 21% to 10% (N Engl J Med. 2015 Aug 6;373[6]:503-10).
A meta-analysis of studies that included nearly 9,000 breast cancer patients who underwent BCS alone or BCS with oncoplastic breast conservation techniques concluded that the re-excision rate was just 4.3% in women who underwent oncoplastic breast conservation, compared with 14.6% with BCS alone (Ann Plast Surg. 2014 Feb;72[2]:145-9).
“This is going to be a driver for many breast cancer units to look at how they can use oncoplastic breast conservation to bring down their resection rates,” Dr. MacNeill predicted.
Neoadjuvant chemotherapy or endocrine therapy, a strategy in which surgery becomes adjuvant therapy, is likely to play an important role in facilitating breast conservation in the future. In the CALGB 40603 trial, for example, neoadjuvant chemotherapy in women with triple-negative breast cancer resulted in an absolute 14% increase in eligibility for BCS. Moreover, BCS was successful with no re-excision in 93% of treated patients (Ann Surg. 2015 Sep;262[3]:434-9).
The ‘less is more’ movement in breast cancer surgery may in the future mean no surgery at all in certain cases. Now underway in the United Kingdom is LORIS (the Low Risk DCIS Trial), in which women with low-risk DCIS are being randomized to surgery or 10 years of monitoring via annual mammograms.
“I’m suggesting that surgery may not exist in the longer term,” Dr. MacNeill said.
She, Dr. Jatoi, and Dr. Smith reported having no financial conflicts regarding their presentations. Dr. Smith’s study was supported by the Cancer Prevention and Research Institute of Texas, the Conquer Cancer Foundation, and the American Society for Radiation Oncology.
EXPERT ANALYSIS FROM SABCS 2015

New definition for massive ventral hernia?
Massive ventral hernias should be defined as those with a length or width of at least 15 cm and/or an overall area of 150 cm2, according to a report published in the Journal of American Surgery.
Until now, there has been no standardized definition of these defects. Defining massive ventral hernias is the first step in collecting and analyzing data on outcomes so that the best-practice methods for managing these cases can be determined, said Dr. Samuel W. Ross and his associates in the division of gastrointestinal and minimally invasive surgery, Carolinas Medical Center, Charlotte, N.C.
Their results suggest that patients with a massive ventral hernias “can be expected to stay in hospital for approximately 8 days, have an approximately 25% wound complication rate, have an 80% rate of activity limitation, and have a 100% rate of symptomatic pain at 1 month after surgery. This not only requires a long hospital course, with incumbent morbidity, but also the subsequent follow-up and management of wound and other complications,” the investigators said.

As expected, patients with massive ventral hernias had more complications and lower postop quality of life in terms of pain, activity limitation, and “mesh sensation,” compared with patients having regular hernia.
Large hernia defects are defined in the literature as up to 10 cm in size, but Dr. Ross and his colleagues hypothesized that massive hernia needed a more accurate cutoff size. The goal of this study was to define massive ventral hernia as 15 cm or more intraoperative defect size in any dimension or area 150 cm2 or more, and validate it by comparing ventral hernia repair patients’ outcomes using an international, multicenter, prospectively collected database.
To validate that their definition correlated with patient outcomes, the investigators analyzed information in the International Hernia Mesh Registry, a prospectively collected database covering consecutive inguinal, umbilical, and ventral hernia repairs at 45 medical centers in 10 countries. They focused on 878 cases of ventral hernia treated during a 6-year period. A total of 158 cases (18%) met their criteria for massive ventral hernia.
Hernia repairs were nearly equally divided between laparoscopic (50.3%) and open (49.7%) surgeries. Approximately 18% of each group were massive ventral hernias.
Overall, there were 118 wound complications, including seromas (affecting 9.6% of patients), hematomas (2%), and superficial and deep surgical site infections (2%). Other complications included deep vein thrombosis (0.5%), pneumonia (1%), cardiac events (0.5%), and problems requiring reoperation (4.2%). At 2-year follow-up, 1.5% of the study participants had died and 5.1% had ventral hernia recurrences.
As expected, compared with patients who had regular-sized hernias, those with massive hernias were significantly more obese, had a higher percentage of previous hernia surgeries, and had larger defect sizes. In general, their outcomes were not as good as those of patients with regular-sized hernias.
In the laparoscopic group, patients with massive hernias required a longer length of hospital stay than did those with regular-sized hernias (4.8 vs. 2.6 days), but their rates of wound complications, deep vein thrombosis, cardiac events, reoperation, and recurrence were similar. They had significantly increased pain and limitation of activity for the first postoperative month, but thereafter these factors were comparable.
In the open-surgery group, patients with massive hernias required a longer length of stay and had significantly more hematomas, deep infections at the surgical site, other wound complications, and cases of pneumonia. But their rates of superficial surgical site infection, seroma, cardiac events, hernia recurrence, and death were comparable with those in patients with regular-size hernias. They had significantly increased pain and limitation of activity during the first postoperative month, but thereafter, these factors were comparable (Amer J Surg. 2015;210[5]:801-13).
Interestingly, massive hernias were associated with “increased mesh sensation” at both 1-year and 2-year follow-up only in the laparoscopic cohort. “This finding may be due to the lack of closure of the musculofascial abdominal wall during these laparoscopic repairs, which may allow the patients to directly appreciate the mesh underneath their subcutaneous tissue.” In contrast, open surgery allowed more complete closure of the abdominal wall, “which may have impacted the patients’ perception of the mesh in their abdomens,” Dr. Ross and his associates wrote.
The study had no outside funding. Dr. Ross reported having no relevant financial disclosures. His associates reported ties to W.L. Gore, Ethicon, Novadaq, Bard/Davol, and LifeCell; one associate reported holding a patent for a free mobile app predicting the rate and cost of wound complications after ventral hernia repair, for which he receives no financial gain.
Massive ventral hernias should be defined as those with a length or width of at least 15 cm and/or an overall area of 150 cm2, according to a report published in the Journal of American Surgery.
Until now, there has been no standardized definition of these defects. Defining massive ventral hernias is the first step in collecting and analyzing data on outcomes so that the best-practice methods for managing these cases can be determined, said Dr. Samuel W. Ross and his associates in the division of gastrointestinal and minimally invasive surgery, Carolinas Medical Center, Charlotte, N.C.
Their results suggest that patients with a massive ventral hernias “can be expected to stay in hospital for approximately 8 days, have an approximately 25% wound complication rate, have an 80% rate of activity limitation, and have a 100% rate of symptomatic pain at 1 month after surgery. This not only requires a long hospital course, with incumbent morbidity, but also the subsequent follow-up and management of wound and other complications,” the investigators said.
As expected, patients with massive ventral hernias had more complications and lower postop quality of life in terms of pain, activity limitation, and “mesh sensation,” compared with patients having regular hernia.
Large hernia defects are defined in the literature as up to 10 cm in size, but Dr. Ross and his colleagues hypothesized that massive hernia needed a more accurate cutoff size. The goal of this study was to define massive ventral hernia as 15 cm or more intraoperative defect size in any dimension or area 150 cm2 or more, and validate it by comparing ventral hernia repair patients’ outcomes using an international, multicenter, prospectively collected database.
To validate that their definition correlated with patient outcomes, the investigators analyzed information in the International Hernia Mesh Registry, a prospectively collected database covering consecutive inguinal, umbilical, and ventral hernia repairs at 45 medical centers in 10 countries. They focused on 878 cases of ventral hernia treated during a 6-year period. A total of 158 cases (18%) met their criteria for massive ventral hernia.
Hernia repairs were nearly equally divided between laparoscopic (50.3%) and open (49.7%) surgeries. Approximately 18% of each group were massive ventral hernias.
Overall, there were 118 wound complications, including seromas (affecting 9.6% of patients), hematomas (2%), and superficial and deep surgical site infections (2%). Other complications included deep vein thrombosis (0.5%), pneumonia (1%), cardiac events (0.5%), and problems requiring reoperation (4.2%). At 2-year follow-up, 1.5% of the study participants had died and 5.1% had ventral hernia recurrences.
As expected, compared with patients who had regular-sized hernias, those with massive hernias were significantly more obese, had a higher percentage of previous hernia surgeries, and had larger defect sizes. In general, their outcomes were not as good as those of patients with regular-sized hernias.
In the laparoscopic group, patients with massive hernias required a longer length of hospital stay than did those with regular-sized hernias (4.8 vs. 2.6 days), but their rates of wound complications, deep vein thrombosis, cardiac events, reoperation, and recurrence were similar. They had significantly increased pain and limitation of activity for the first postoperative month, but thereafter these factors were comparable.
In the open-surgery group, patients with massive hernias required a longer length of stay and had significantly more hematomas, deep infections at the surgical site, other wound complications, and cases of pneumonia. But their rates of superficial surgical site infection, seroma, cardiac events, hernia recurrence, and death were comparable with those in patients with regular-size hernias. They had significantly increased pain and limitation of activity during the first postoperative month, but thereafter, these factors were comparable (Amer J Surg. 2015;210[5]:801-13).
Interestingly, massive hernias were associated with “increased mesh sensation” at both 1-year and 2-year follow-up only in the laparoscopic cohort. “This finding may be due to the lack of closure of the musculofascial abdominal wall during these laparoscopic repairs, which may allow the patients to directly appreciate the mesh underneath their subcutaneous tissue.” In contrast, open surgery allowed more complete closure of the abdominal wall, “which may have impacted the patients’ perception of the mesh in their abdomens,” Dr. Ross and his associates wrote.
The study had no outside funding. Dr. Ross reported having no relevant financial disclosures. His associates reported ties to W.L. Gore, Ethicon, Novadaq, Bard/Davol, and LifeCell; one associate reported holding a patent for a free mobile app predicting the rate and cost of wound complications after ventral hernia repair, for which he receives no financial gain.
Massive ventral hernias should be defined as those with a length or width of at least 15 cm and/or an overall area of 150 cm2, according to a report published in the Journal of American Surgery.
Until now, there has been no standardized definition of these defects. Defining massive ventral hernias is the first step in collecting and analyzing data on outcomes so that the best-practice methods for managing these cases can be determined, said Dr. Samuel W. Ross and his associates in the division of gastrointestinal and minimally invasive surgery, Carolinas Medical Center, Charlotte, N.C.
Their results suggest that patients with a massive ventral hernias “can be expected to stay in hospital for approximately 8 days, have an approximately 25% wound complication rate, have an 80% rate of activity limitation, and have a 100% rate of symptomatic pain at 1 month after surgery. This not only requires a long hospital course, with incumbent morbidity, but also the subsequent follow-up and management of wound and other complications,” the investigators said.
As expected, patients with massive ventral hernias had more complications and lower postop quality of life in terms of pain, activity limitation, and “mesh sensation,” compared with patients having regular hernia.
Large hernia defects are defined in the literature as up to 10 cm in size, but Dr. Ross and his colleagues hypothesized that massive hernia needed a more accurate cutoff size. The goal of this study was to define massive ventral hernia as 15 cm or more intraoperative defect size in any dimension or area 150 cm2 or more, and validate it by comparing ventral hernia repair patients’ outcomes using an international, multicenter, prospectively collected database.
To validate that their definition correlated with patient outcomes, the investigators analyzed information in the International Hernia Mesh Registry, a prospectively collected database covering consecutive inguinal, umbilical, and ventral hernia repairs at 45 medical centers in 10 countries. They focused on 878 cases of ventral hernia treated during a 6-year period. A total of 158 cases (18%) met their criteria for massive ventral hernia.
Hernia repairs were nearly equally divided between laparoscopic (50.3%) and open (49.7%) surgeries. Approximately 18% of each group were massive ventral hernias.
Overall, there were 118 wound complications, including seromas (affecting 9.6% of patients), hematomas (2%), and superficial and deep surgical site infections (2%). Other complications included deep vein thrombosis (0.5%), pneumonia (1%), cardiac events (0.5%), and problems requiring reoperation (4.2%). At 2-year follow-up, 1.5% of the study participants had died and 5.1% had ventral hernia recurrences.
As expected, compared with patients who had regular-sized hernias, those with massive hernias were significantly more obese, had a higher percentage of previous hernia surgeries, and had larger defect sizes. In general, their outcomes were not as good as those of patients with regular-sized hernias.
In the laparoscopic group, patients with massive hernias required a longer length of hospital stay than did those with regular-sized hernias (4.8 vs. 2.6 days), but their rates of wound complications, deep vein thrombosis, cardiac events, reoperation, and recurrence were similar. They had significantly increased pain and limitation of activity for the first postoperative month, but thereafter these factors were comparable.
In the open-surgery group, patients with massive hernias required a longer length of stay and had significantly more hematomas, deep infections at the surgical site, other wound complications, and cases of pneumonia. But their rates of superficial surgical site infection, seroma, cardiac events, hernia recurrence, and death were comparable with those in patients with regular-size hernias. They had significantly increased pain and limitation of activity during the first postoperative month, but thereafter, these factors were comparable (Amer J Surg. 2015;210[5]:801-13).
Interestingly, massive hernias were associated with “increased mesh sensation” at both 1-year and 2-year follow-up only in the laparoscopic cohort. “This finding may be due to the lack of closure of the musculofascial abdominal wall during these laparoscopic repairs, which may allow the patients to directly appreciate the mesh underneath their subcutaneous tissue.” In contrast, open surgery allowed more complete closure of the abdominal wall, “which may have impacted the patients’ perception of the mesh in their abdomens,” Dr. Ross and his associates wrote.
The study had no outside funding. Dr. Ross reported having no relevant financial disclosures. His associates reported ties to W.L. Gore, Ethicon, Novadaq, Bard/Davol, and LifeCell; one associate reported holding a patent for a free mobile app predicting the rate and cost of wound complications after ventral hernia repair, for which he receives no financial gain.
FROM THE AMERICAN JOURNAL OF SURGERY
Key clinical point: Massive ventral hernias should be defined as having a length or width of at least 15 cm or an overall area of 150 cm2.
Major finding: Patients with a massive ventral hernias can be expected to stay in hospital for approximately 8 days, have an approximately 25% wound complication rate, have an 80% rate of activity limitation, and have a 100% rate of symptomatic pain at 1 month.
Data source: An analysis of data concerning 878 hernia cases in an international registry during a 6-year period.
Disclosures: This study has no outside funding. Dr. Ross reported having no relevant financial disclosures. His associates reported ties to W.L. Gore, Ethicon, Novadaq, Bard/Davol, and LifeCell; one associate reported holding a patent for a free mobile app predicting the rate and cost of wound complications after ventral hernia repair, for which he receives no financial gain.

CMS finalizes ruling on prior authorization for some durable goods and equipment
The Centers for Medicare & Medicaid Services today issued its final rule on prior authorization for certain durable medical equipment, prosthetics, orthotics, and supplies.
The rule moves necessary documentation earlier in the approval process, requiring all relevant coverage, coding, and clinical documentation to be completed before certain goods are provided to a beneficiary and before the claim is submitted for payment, according to a CMS statement published Dec. 30 in the Federal Register.
Prior authorization is an effective way to reduce or prevent questionable billing practices and improper payments for durable medical equipment, prosthetics, orthotics, and supplies, according to the statement.
The rule includes review and approval timeframes and a provision for expedited claims in which delayed approval could adversely impact a beneficiary’s health.
Some of the items subject to “frequent unnecessary utilization” include certain powered air mattresses, continuous airway pressure devices, power wheelchairs, oxygen concentrators, and prosthetic limbs (especially for lower extremities).
On Twitter @whitneymcknight
The Centers for Medicare & Medicaid Services today issued its final rule on prior authorization for certain durable medical equipment, prosthetics, orthotics, and supplies.
The rule moves necessary documentation earlier in the approval process, requiring all relevant coverage, coding, and clinical documentation to be completed before certain goods are provided to a beneficiary and before the claim is submitted for payment, according to a CMS statement published Dec. 30 in the Federal Register.
Prior authorization is an effective way to reduce or prevent questionable billing practices and improper payments for durable medical equipment, prosthetics, orthotics, and supplies, according to the statement.
The rule includes review and approval timeframes and a provision for expedited claims in which delayed approval could adversely impact a beneficiary’s health.
Some of the items subject to “frequent unnecessary utilization” include certain powered air mattresses, continuous airway pressure devices, power wheelchairs, oxygen concentrators, and prosthetic limbs (especially for lower extremities).
On Twitter @whitneymcknight
The Centers for Medicare & Medicaid Services today issued its final rule on prior authorization for certain durable medical equipment, prosthetics, orthotics, and supplies.
The rule moves necessary documentation earlier in the approval process, requiring all relevant coverage, coding, and clinical documentation to be completed before certain goods are provided to a beneficiary and before the claim is submitted for payment, according to a CMS statement published Dec. 30 in the Federal Register.
Prior authorization is an effective way to reduce or prevent questionable billing practices and improper payments for durable medical equipment, prosthetics, orthotics, and supplies, according to the statement.
The rule includes review and approval timeframes and a provision for expedited claims in which delayed approval could adversely impact a beneficiary’s health.
Some of the items subject to “frequent unnecessary utilization” include certain powered air mattresses, continuous airway pressure devices, power wheelchairs, oxygen concentrators, and prosthetic limbs (especially for lower extremities).
On Twitter @whitneymcknight
Treatment failure reduced in Barrett’s esophagus with endoscopic mucosal resection
The use of endoscopic mucosal resection (EMR) before radiofrequency ablation significantly reduced the risk for treatment failure among patients with Barrett’s esophagus–associated intramucosal adenocarcinoma (IMC) and dysplasia, according to new data published in the American Journal of Surgical Pathology.
Complete eradication of IMC/dysplasia on the first follow-up endoscopy after treatment was achieved in 86% of patients, while durable eradication, defined as a complete recurrence that persisted until the last follow-up, was achieved in 78% of patients. However, there was significant variation between the different study sites (P = .03) and outcomes were significantly impacted by the baseline extent of IMC and the use of EMR prior to radiofrequency ablation (RFA) therapy.
In addition, almost a quarter of all patients developed treatment-related strictures, usually in the setting of multiple EMRs, and recurrence occurred as a malignant stricture in one patient.
Radiofrequency ablation used with or without EMR, is a safe, effective, and durable treatment option for the treatment of dysplasia associated with Barrett’s esophagus. However, studies that have assessed the predictors of treatment failure in Barrett’s esophagus-associated intramucosal adenocarcinoma (IMC) are limited.
In this study, Dr. Agoston T. Agoston of the department of pathology at Brigham and Women’s Hospital, Boston, and his colleagues investigated the rate of Barrett’s esophagus–associated IMC eradication when using RFA, with or without EMR, in a multicenter setting. In addition, they attempted to identify clinical and pathologic predictors of treatment failure.
“We anticipate that these data will have significant implications for a personalized treatment approach to patients with BE [Barrett’s esophagus]–associated IMC,” wrote the authors.
They conducted a retrospective review of medical records from four tertiary care academic medical centers, and identified 78 patients who underwent RFA with or without EMR as the primary treatment for biopsy-proven IMC.
Some notable baseline differences were observed in patient characteristics at the different study sites, including baseline Barrett’s esophagus segment length (P = .06), baseline nodularity (P = .08), and percentage of tissue involved by IMC at pretreatment endoscopy and biopsy (P = .01).
Over a mean follow-up time of 26.4 months (range, 2-116 months), 86% of patients achieved complete eradication and 78% durable eradication of IMC/dysplasia.
Within the cohort, 11 patients failed to achieve complete eradication, and of the 67 patients who initially did, 6 patients (9.0%) had a subsequent recurrence of neoplasia (3.91 recurrences per 100 patient-years). This extrapolated to an overall rate of 22% for treatment failure (17/78 patients). Of the 17 patients who failed the treatment, 3 subsequently underwent esophagectomy, 1 received palliative measures in the setting of advanced neurological disease, and 1 patient is currently undergoing a repeat ablation procedure with curative intent.
Dr. Agoston and his team also identified 2 clinicopathologic factors that were significantly associated with treatment failure, and both remained significant on univariate and multivariate analysis. The first was that the use of EMR prior to RFA was associated with a significantly reduced risk for treatment failure (hazard ratio, 0.15; 95% confidence interval, 0.05-0.48; P = .001), and the second was that the extent of IMC involving at least 50% of the columnar metaplastic area was associated with a significantly increased risk for treatment failure (HR, 4.24; 95% CI, 1.53-11.7; P = .005).
They also observed similar results when the analysis of extent of IMC as a predictor was restricted to a subset of 43 cases in which the diagnosis of IMC was made on EMR specimens only (HR, 10.8; 95% CI, 2.30-50.8; P = .003).
“In conclusion, we have identified endoscopic and pathologic factors associated with treatment success in patients with BE-associated IMC treated with RFA with or without EMR,” they wrote. “Utilization of these predictors can help in identifying patients with a high probability of success and also those patients with a higher risk for treatment failure for whom a more aggressive initial approach may be justified” (Am J Surg Pathol. 2015 Dec 5. doi: 10.1097/PAS.0000000000000566).
Dr. Rothstein and Dr. Abrams have received research support previously from Barrx/ Covidien and C2 Therapeutics/Covidien, respectively. None of the other authors reported significant conflicts of interest.
The use of endoscopic mucosal resection (EMR) before radiofrequency ablation significantly reduced the risk for treatment failure among patients with Barrett’s esophagus–associated intramucosal adenocarcinoma (IMC) and dysplasia, according to new data published in the American Journal of Surgical Pathology.
Complete eradication of IMC/dysplasia on the first follow-up endoscopy after treatment was achieved in 86% of patients, while durable eradication, defined as a complete recurrence that persisted until the last follow-up, was achieved in 78% of patients. However, there was significant variation between the different study sites (P = .03) and outcomes were significantly impacted by the baseline extent of IMC and the use of EMR prior to radiofrequency ablation (RFA) therapy.
In addition, almost a quarter of all patients developed treatment-related strictures, usually in the setting of multiple EMRs, and recurrence occurred as a malignant stricture in one patient.
Radiofrequency ablation used with or without EMR, is a safe, effective, and durable treatment option for the treatment of dysplasia associated with Barrett’s esophagus. However, studies that have assessed the predictors of treatment failure in Barrett’s esophagus-associated intramucosal adenocarcinoma (IMC) are limited.
In this study, Dr. Agoston T. Agoston of the department of pathology at Brigham and Women’s Hospital, Boston, and his colleagues investigated the rate of Barrett’s esophagus–associated IMC eradication when using RFA, with or without EMR, in a multicenter setting. In addition, they attempted to identify clinical and pathologic predictors of treatment failure.
“We anticipate that these data will have significant implications for a personalized treatment approach to patients with BE [Barrett’s esophagus]–associated IMC,” wrote the authors.
They conducted a retrospective review of medical records from four tertiary care academic medical centers, and identified 78 patients who underwent RFA with or without EMR as the primary treatment for biopsy-proven IMC.
Some notable baseline differences were observed in patient characteristics at the different study sites, including baseline Barrett’s esophagus segment length (P = .06), baseline nodularity (P = .08), and percentage of tissue involved by IMC at pretreatment endoscopy and biopsy (P = .01).
Over a mean follow-up time of 26.4 months (range, 2-116 months), 86% of patients achieved complete eradication and 78% durable eradication of IMC/dysplasia.
Within the cohort, 11 patients failed to achieve complete eradication, and of the 67 patients who initially did, 6 patients (9.0%) had a subsequent recurrence of neoplasia (3.91 recurrences per 100 patient-years). This extrapolated to an overall rate of 22% for treatment failure (17/78 patients). Of the 17 patients who failed the treatment, 3 subsequently underwent esophagectomy, 1 received palliative measures in the setting of advanced neurological disease, and 1 patient is currently undergoing a repeat ablation procedure with curative intent.
Dr. Agoston and his team also identified 2 clinicopathologic factors that were significantly associated with treatment failure, and both remained significant on univariate and multivariate analysis. The first was that the use of EMR prior to RFA was associated with a significantly reduced risk for treatment failure (hazard ratio, 0.15; 95% confidence interval, 0.05-0.48; P = .001), and the second was that the extent of IMC involving at least 50% of the columnar metaplastic area was associated with a significantly increased risk for treatment failure (HR, 4.24; 95% CI, 1.53-11.7; P = .005).
They also observed similar results when the analysis of extent of IMC as a predictor was restricted to a subset of 43 cases in which the diagnosis of IMC was made on EMR specimens only (HR, 10.8; 95% CI, 2.30-50.8; P = .003).
“In conclusion, we have identified endoscopic and pathologic factors associated with treatment success in patients with BE-associated IMC treated with RFA with or without EMR,” they wrote. “Utilization of these predictors can help in identifying patients with a high probability of success and also those patients with a higher risk for treatment failure for whom a more aggressive initial approach may be justified” (Am J Surg Pathol. 2015 Dec 5. doi: 10.1097/PAS.0000000000000566).
Dr. Rothstein and Dr. Abrams have received research support previously from Barrx/ Covidien and C2 Therapeutics/Covidien, respectively. None of the other authors reported significant conflicts of interest.
The use of endoscopic mucosal resection (EMR) before radiofrequency ablation significantly reduced the risk for treatment failure among patients with Barrett’s esophagus–associated intramucosal adenocarcinoma (IMC) and dysplasia, according to new data published in the American Journal of Surgical Pathology.
Complete eradication of IMC/dysplasia on the first follow-up endoscopy after treatment was achieved in 86% of patients, while durable eradication, defined as a complete recurrence that persisted until the last follow-up, was achieved in 78% of patients. However, there was significant variation between the different study sites (P = .03) and outcomes were significantly impacted by the baseline extent of IMC and the use of EMR prior to radiofrequency ablation (RFA) therapy.
In addition, almost a quarter of all patients developed treatment-related strictures, usually in the setting of multiple EMRs, and recurrence occurred as a malignant stricture in one patient.
Radiofrequency ablation used with or without EMR, is a safe, effective, and durable treatment option for the treatment of dysplasia associated with Barrett’s esophagus. However, studies that have assessed the predictors of treatment failure in Barrett’s esophagus-associated intramucosal adenocarcinoma (IMC) are limited.
In this study, Dr. Agoston T. Agoston of the department of pathology at Brigham and Women’s Hospital, Boston, and his colleagues investigated the rate of Barrett’s esophagus–associated IMC eradication when using RFA, with or without EMR, in a multicenter setting. In addition, they attempted to identify clinical and pathologic predictors of treatment failure.
“We anticipate that these data will have significant implications for a personalized treatment approach to patients with BE [Barrett’s esophagus]–associated IMC,” wrote the authors.
They conducted a retrospective review of medical records from four tertiary care academic medical centers, and identified 78 patients who underwent RFA with or without EMR as the primary treatment for biopsy-proven IMC.
Some notable baseline differences were observed in patient characteristics at the different study sites, including baseline Barrett’s esophagus segment length (P = .06), baseline nodularity (P = .08), and percentage of tissue involved by IMC at pretreatment endoscopy and biopsy (P = .01).
Over a mean follow-up time of 26.4 months (range, 2-116 months), 86% of patients achieved complete eradication and 78% durable eradication of IMC/dysplasia.
Within the cohort, 11 patients failed to achieve complete eradication, and of the 67 patients who initially did, 6 patients (9.0%) had a subsequent recurrence of neoplasia (3.91 recurrences per 100 patient-years). This extrapolated to an overall rate of 22% for treatment failure (17/78 patients). Of the 17 patients who failed the treatment, 3 subsequently underwent esophagectomy, 1 received palliative measures in the setting of advanced neurological disease, and 1 patient is currently undergoing a repeat ablation procedure with curative intent.
Dr. Agoston and his team also identified 2 clinicopathologic factors that were significantly associated with treatment failure, and both remained significant on univariate and multivariate analysis. The first was that the use of EMR prior to RFA was associated with a significantly reduced risk for treatment failure (hazard ratio, 0.15; 95% confidence interval, 0.05-0.48; P = .001), and the second was that the extent of IMC involving at least 50% of the columnar metaplastic area was associated with a significantly increased risk for treatment failure (HR, 4.24; 95% CI, 1.53-11.7; P = .005).
They also observed similar results when the analysis of extent of IMC as a predictor was restricted to a subset of 43 cases in which the diagnosis of IMC was made on EMR specimens only (HR, 10.8; 95% CI, 2.30-50.8; P = .003).
“In conclusion, we have identified endoscopic and pathologic factors associated with treatment success in patients with BE-associated IMC treated with RFA with or without EMR,” they wrote. “Utilization of these predictors can help in identifying patients with a high probability of success and also those patients with a higher risk for treatment failure for whom a more aggressive initial approach may be justified” (Am J Surg Pathol. 2015 Dec 5. doi: 10.1097/PAS.0000000000000566).
Dr. Rothstein and Dr. Abrams have received research support previously from Barrx/ Covidien and C2 Therapeutics/Covidien, respectively. None of the other authors reported significant conflicts of interest.
FROM THE AMERICAN JOURNAL OF SURGICAL PATHOLOGY
Key clinical point: The use of EMR before radiofrequency ablation significantly reduced the risk for treatment failure for IMC associated with Barrett’s esophagus.
Major finding: The overall rate of complete and durable IMC eradication in Barrett’s esophagus was 86% and 78%, respectively, during a mean follow-up of about 2 years, but was significantly impacted by the baseline extent of IMC and the use of EMR.
Data source: A retrospective review of data from four tertiary care academic medical centers that included 78 patients and was conducted to determine the rate of IMC eradication when using RFA and EMR.
Disclosures: Dr. Rothstein and Dr. Abrams have received research support previously from Barrx/ Covidien and C2 Therapeutics/Covidien, respectively. None of the other authors reported significant conflicts of interest.
Blanket hardship exemption for 2015 meaningful use authorized by Congress
For doctors unable to meet meaningful use requirements for 2015, Congress has approved a blanket process for those applying for a hardship exemption to avoid having a penalty applied to their Medicare payments in 2017.
By voice vote in the House on Dec. 18 and a unanimous consent vote later that day in the Senate, Congress passed the Patient Access and Medicare Protection Act (S. 2425), which allows CMS to grant hardship exemptions globally, rather than on a case-by-case basis.

There are a number of reasons a hardship exemption would be issued, including infrastructure-related problems, unforeseen circumstances, lack of face-to-face interactions, and lack of available certified electronic health records.
Doctors seeking the exemption will need to apply by March 15, 2016; hospitals must do so by April 1, 2016.
“Moving forward, this process will now allow doctors to avoid erroneous penalties that would have otherwise caused harm for patients seeking quality care,” Rep. Renee Ellmers (R-N.C.) said in a statement.
For doctors unable to meet meaningful use requirements for 2015, Congress has approved a blanket process for those applying for a hardship exemption to avoid having a penalty applied to their Medicare payments in 2017.
By voice vote in the House on Dec. 18 and a unanimous consent vote later that day in the Senate, Congress passed the Patient Access and Medicare Protection Act (S. 2425), which allows CMS to grant hardship exemptions globally, rather than on a case-by-case basis.
There are a number of reasons a hardship exemption would be issued, including infrastructure-related problems, unforeseen circumstances, lack of face-to-face interactions, and lack of available certified electronic health records.
Doctors seeking the exemption will need to apply by March 15, 2016; hospitals must do so by April 1, 2016.
“Moving forward, this process will now allow doctors to avoid erroneous penalties that would have otherwise caused harm for patients seeking quality care,” Rep. Renee Ellmers (R-N.C.) said in a statement.
For doctors unable to meet meaningful use requirements for 2015, Congress has approved a blanket process for those applying for a hardship exemption to avoid having a penalty applied to their Medicare payments in 2017.
By voice vote in the House on Dec. 18 and a unanimous consent vote later that day in the Senate, Congress passed the Patient Access and Medicare Protection Act (S. 2425), which allows CMS to grant hardship exemptions globally, rather than on a case-by-case basis.
There are a number of reasons a hardship exemption would be issued, including infrastructure-related problems, unforeseen circumstances, lack of face-to-face interactions, and lack of available certified electronic health records.
Doctors seeking the exemption will need to apply by March 15, 2016; hospitals must do so by April 1, 2016.
“Moving forward, this process will now allow doctors to avoid erroneous penalties that would have otherwise caused harm for patients seeking quality care,” Rep. Renee Ellmers (R-N.C.) said in a statement.

FDA finalizes 1-year blood donor deferral for gay, bisexual men
The Food and Drug Administration announced finalized blood-donor deferral guidance that includes cutting the deferral for men who have sex with men from indefinitely to 1 year from the most recent sexual contact of this type.
The finalized guidance, which had been in development since its initial announcement in December 2014, contains 10 recommended questions that the blood industry should pose to potential donors to exclude those at greatest risk for potentially transmitting HIV in their blood.
In addition to reducing the deferral period for men who have had sex with men, the finalized guidance also cuts the deferral period for a woman who has had sex with a man who had sex with men from indefinitely to 12 months, and also reduces the deferral period for any person who has had sex with someone with a history of a positive test for HIV from indefinitely to 12 months.
The new guidance continues to recommend indefinite deferral for people who have ever tested positive for HIV, those who have exchanged sex for money or drugs, and those with a history of nonprescription injection drug use.
The FDA’s guidance document highlights that these are recommended steps for the blood products industry to take and are not required by law or legally enforceable.
The finalized guidance, which followed a public comment period on essentially unchanged draft guidance issued last May, received quick support in a statement from Dr. Andrew W. Gurman, president-elect of the American Medical Association.
“The American Medical Association commends the U.S. Food and Drug Administration for ending the lifetime ban that prohibits men who have had sex with men from donating blood,” Dr. Gurman said. “The AMA has been a strong advocate for eliminating public policies that do not align with scientific evidence and best ethical practices in public policy. The FDA’s final guidance takes important steps to improve the balance among ensuring health equity, engaging with high-risk populations, and protecting the safety of the national blood supply.”
However, a highly critical comment came from Daniel Bruner, senior director of policy for Whitman-Walker Health, a Washington-based health center focused on the LGBT community and HIV care.
“Although some may argue that a 12-month ban is better than a grossly outdated lifetime ban, the updated policy is still discriminatory and not rooted in the reality of HIV testing today,” Mr. Bruner said in a statement. “As we called for in our recommendations, the deferral period should be no longer than 30 days, given that with current testing technology an HIV infection can be detected in donated blood within several weeks of exposure.
“And even then, those that would be subject to the deferral period should be able to donate blood if they agree to return for an HIV test 30 days after donating,” Mr. Bruner said. “Sadly, and also not in line with modern science, the new guidelines continue the discriminatory lifetime bans on individuals who have ever engaged in sex work or ever used nonprescription injection drugs.”
Mr. Bruner added, “We are also disheartened that the FDA has failed to give clear guidance to prevent discrimination against transgender individuals, which occurs too often at blood donation centers. The FDA must do better than this slow chipping away at antiquated bans.”
On Twitter @mitchelzoler
The Food and Drug Administration announced finalized blood-donor deferral guidance that includes cutting the deferral for men who have sex with men from indefinitely to 1 year from the most recent sexual contact of this type.
The finalized guidance, which had been in development since its initial announcement in December 2014, contains 10 recommended questions that the blood industry should pose to potential donors to exclude those at greatest risk for potentially transmitting HIV in their blood.
In addition to reducing the deferral period for men who have had sex with men, the finalized guidance also cuts the deferral period for a woman who has had sex with a man who had sex with men from indefinitely to 12 months, and also reduces the deferral period for any person who has had sex with someone with a history of a positive test for HIV from indefinitely to 12 months.
The new guidance continues to recommend indefinite deferral for people who have ever tested positive for HIV, those who have exchanged sex for money or drugs, and those with a history of nonprescription injection drug use.
The FDA’s guidance document highlights that these are recommended steps for the blood products industry to take and are not required by law or legally enforceable.
The finalized guidance, which followed a public comment period on essentially unchanged draft guidance issued last May, received quick support in a statement from Dr. Andrew W. Gurman, president-elect of the American Medical Association.
“The American Medical Association commends the U.S. Food and Drug Administration for ending the lifetime ban that prohibits men who have had sex with men from donating blood,” Dr. Gurman said. “The AMA has been a strong advocate for eliminating public policies that do not align with scientific evidence and best ethical practices in public policy. The FDA’s final guidance takes important steps to improve the balance among ensuring health equity, engaging with high-risk populations, and protecting the safety of the national blood supply.”
However, a highly critical comment came from Daniel Bruner, senior director of policy for Whitman-Walker Health, a Washington-based health center focused on the LGBT community and HIV care.
“Although some may argue that a 12-month ban is better than a grossly outdated lifetime ban, the updated policy is still discriminatory and not rooted in the reality of HIV testing today,” Mr. Bruner said in a statement. “As we called for in our recommendations, the deferral period should be no longer than 30 days, given that with current testing technology an HIV infection can be detected in donated blood within several weeks of exposure.
“And even then, those that would be subject to the deferral period should be able to donate blood if they agree to return for an HIV test 30 days after donating,” Mr. Bruner said. “Sadly, and also not in line with modern science, the new guidelines continue the discriminatory lifetime bans on individuals who have ever engaged in sex work or ever used nonprescription injection drugs.”
Mr. Bruner added, “We are also disheartened that the FDA has failed to give clear guidance to prevent discrimination against transgender individuals, which occurs too often at blood donation centers. The FDA must do better than this slow chipping away at antiquated bans.”
On Twitter @mitchelzoler
The Food and Drug Administration announced finalized blood-donor deferral guidance that includes cutting the deferral for men who have sex with men from indefinitely to 1 year from the most recent sexual contact of this type.
The finalized guidance, which had been in development since its initial announcement in December 2014, contains 10 recommended questions that the blood industry should pose to potential donors to exclude those at greatest risk for potentially transmitting HIV in their blood.
In addition to reducing the deferral period for men who have had sex with men, the finalized guidance also cuts the deferral period for a woman who has had sex with a man who had sex with men from indefinitely to 12 months, and also reduces the deferral period for any person who has had sex with someone with a history of a positive test for HIV from indefinitely to 12 months.
The new guidance continues to recommend indefinite deferral for people who have ever tested positive for HIV, those who have exchanged sex for money or drugs, and those with a history of nonprescription injection drug use.
The FDA’s guidance document highlights that these are recommended steps for the blood products industry to take and are not required by law or legally enforceable.
The finalized guidance, which followed a public comment period on essentially unchanged draft guidance issued last May, received quick support in a statement from Dr. Andrew W. Gurman, president-elect of the American Medical Association.
“The American Medical Association commends the U.S. Food and Drug Administration for ending the lifetime ban that prohibits men who have had sex with men from donating blood,” Dr. Gurman said. “The AMA has been a strong advocate for eliminating public policies that do not align with scientific evidence and best ethical practices in public policy. The FDA’s final guidance takes important steps to improve the balance among ensuring health equity, engaging with high-risk populations, and protecting the safety of the national blood supply.”
However, a highly critical comment came from Daniel Bruner, senior director of policy for Whitman-Walker Health, a Washington-based health center focused on the LGBT community and HIV care.
“Although some may argue that a 12-month ban is better than a grossly outdated lifetime ban, the updated policy is still discriminatory and not rooted in the reality of HIV testing today,” Mr. Bruner said in a statement. “As we called for in our recommendations, the deferral period should be no longer than 30 days, given that with current testing technology an HIV infection can be detected in donated blood within several weeks of exposure.
“And even then, those that would be subject to the deferral period should be able to donate blood if they agree to return for an HIV test 30 days after donating,” Mr. Bruner said. “Sadly, and also not in line with modern science, the new guidelines continue the discriminatory lifetime bans on individuals who have ever engaged in sex work or ever used nonprescription injection drugs.”
Mr. Bruner added, “We are also disheartened that the FDA has failed to give clear guidance to prevent discrimination against transgender individuals, which occurs too often at blood donation centers. The FDA must do better than this slow chipping away at antiquated bans.”
On Twitter @mitchelzoler
SF-6D best quality of life measure in cervical spine patients
SAN DIEGO – Among patients undergoing elective surgical spine procedures, the Short Form–6D derived from the Neck Disability Index was more valid and a better responsive measure of general health and quality of life, compared with the Short Form–6D derived from the Short Form–12 or the EuroQol-5D, results from a single-center study showed.
For such quality of life measures to be useful and meaningful, they “should be reproducible, responsive, economical, easy to use, and sensitive to responder burden,” Dr. John A. Sielatycki said at the annual meeting of the Cervical Spine Research Society.

“The EQ-5D is well established and commonly used in many of these studies, as is SF-6D, which in some cases has been shown to be more sensitive in certain disease states,” explained Dr. Sielatycki, a resident in the department of orthopedics at Vanderbilt University, Nashville, Tenn. “The differences between SF-6D and EQ-5D have been studied in a wide variety of disease conditions, but to our knowledge few have looked at this specifically in the setting of cervical spine operations.”
To analyze the validity and responsiveness of the SF-6D (derived from both the SF-12 and the NDI) and the EQ-5D in determining overall health and quality of life following elective cervical spine procedures, Dr. Sielatycki and his associates compared the three tools in 420 consecutive patients who presented over the course of 2 years. Trauma and workers’ compensation cases were excluded from the study, as were patients who had a tumor or an infection.
The researchers collected outcome measures at baseline, 3 months, 6 months, 12 months, and yearly thereafter, and defined meaningful improvement as having a North American Spine Society patient satisfaction score of 1, indicating the procedure “met the patient’s expectations.” Next, they generated receiver operating characteristic curves to discriminate between meaningful and nonmeaningful improvement.
The SF-6D (NDI) was a more valid discriminator of meaningful improvement, compared with the SF-6D (SF-12) or the EQ-5D (area under the curve of .69, .65, and .62, respectively). It was also a more responsive measure, compared with the SF-6D (SF-12) and the EQ-5D (standardized response means difference of .66, .48, and .44, respectively).
“Surgeons, outcomes researchers, and payers should use health metrics that are most responsive to changes in the particular disease in question,” Dr. Sielatycki said. “Based on this analysis, SF-6D derived from NDI may be a more valid and responsive measure of improvement in patients undergoing cervical procedures. We suggest that this metric be used in cost-effectiveness analysis and in calculating quality-adjusted life years for cervical spine patients.”
Dr. Sielatycki acknowledged certain limitations of the study, including the fact that it “should have some external validation done to further corroborate our findings. Our gold standard of meaningful improvement has not been established.”
Dr. Sielatycki reported having no financial disclosures.
SAN DIEGO – Among patients undergoing elective surgical spine procedures, the Short Form–6D derived from the Neck Disability Index was more valid and a better responsive measure of general health and quality of life, compared with the Short Form–6D derived from the Short Form–12 or the EuroQol-5D, results from a single-center study showed.
For such quality of life measures to be useful and meaningful, they “should be reproducible, responsive, economical, easy to use, and sensitive to responder burden,” Dr. John A. Sielatycki said at the annual meeting of the Cervical Spine Research Society.
“The EQ-5D is well established and commonly used in many of these studies, as is SF-6D, which in some cases has been shown to be more sensitive in certain disease states,” explained Dr. Sielatycki, a resident in the department of orthopedics at Vanderbilt University, Nashville, Tenn. “The differences between SF-6D and EQ-5D have been studied in a wide variety of disease conditions, but to our knowledge few have looked at this specifically in the setting of cervical spine operations.”
To analyze the validity and responsiveness of the SF-6D (derived from both the SF-12 and the NDI) and the EQ-5D in determining overall health and quality of life following elective cervical spine procedures, Dr. Sielatycki and his associates compared the three tools in 420 consecutive patients who presented over the course of 2 years. Trauma and workers’ compensation cases were excluded from the study, as were patients who had a tumor or an infection.
The researchers collected outcome measures at baseline, 3 months, 6 months, 12 months, and yearly thereafter, and defined meaningful improvement as having a North American Spine Society patient satisfaction score of 1, indicating the procedure “met the patient’s expectations.” Next, they generated receiver operating characteristic curves to discriminate between meaningful and nonmeaningful improvement.
The SF-6D (NDI) was a more valid discriminator of meaningful improvement, compared with the SF-6D (SF-12) or the EQ-5D (area under the curve of .69, .65, and .62, respectively). It was also a more responsive measure, compared with the SF-6D (SF-12) and the EQ-5D (standardized response means difference of .66, .48, and .44, respectively).
“Surgeons, outcomes researchers, and payers should use health metrics that are most responsive to changes in the particular disease in question,” Dr. Sielatycki said. “Based on this analysis, SF-6D derived from NDI may be a more valid and responsive measure of improvement in patients undergoing cervical procedures. We suggest that this metric be used in cost-effectiveness analysis and in calculating quality-adjusted life years for cervical spine patients.”
Dr. Sielatycki acknowledged certain limitations of the study, including the fact that it “should have some external validation done to further corroborate our findings. Our gold standard of meaningful improvement has not been established.”
Dr. Sielatycki reported having no financial disclosures.
SAN DIEGO – Among patients undergoing elective surgical spine procedures, the Short Form–6D derived from the Neck Disability Index was more valid and a better responsive measure of general health and quality of life, compared with the Short Form–6D derived from the Short Form–12 or the EuroQol-5D, results from a single-center study showed.
For such quality of life measures to be useful and meaningful, they “should be reproducible, responsive, economical, easy to use, and sensitive to responder burden,” Dr. John A. Sielatycki said at the annual meeting of the Cervical Spine Research Society.
“The EQ-5D is well established and commonly used in many of these studies, as is SF-6D, which in some cases has been shown to be more sensitive in certain disease states,” explained Dr. Sielatycki, a resident in the department of orthopedics at Vanderbilt University, Nashville, Tenn. “The differences between SF-6D and EQ-5D have been studied in a wide variety of disease conditions, but to our knowledge few have looked at this specifically in the setting of cervical spine operations.”
To analyze the validity and responsiveness of the SF-6D (derived from both the SF-12 and the NDI) and the EQ-5D in determining overall health and quality of life following elective cervical spine procedures, Dr. Sielatycki and his associates compared the three tools in 420 consecutive patients who presented over the course of 2 years. Trauma and workers’ compensation cases were excluded from the study, as were patients who had a tumor or an infection.
The researchers collected outcome measures at baseline, 3 months, 6 months, 12 months, and yearly thereafter, and defined meaningful improvement as having a North American Spine Society patient satisfaction score of 1, indicating the procedure “met the patient’s expectations.” Next, they generated receiver operating characteristic curves to discriminate between meaningful and nonmeaningful improvement.
The SF-6D (NDI) was a more valid discriminator of meaningful improvement, compared with the SF-6D (SF-12) or the EQ-5D (area under the curve of .69, .65, and .62, respectively). It was also a more responsive measure, compared with the SF-6D (SF-12) and the EQ-5D (standardized response means difference of .66, .48, and .44, respectively).
“Surgeons, outcomes researchers, and payers should use health metrics that are most responsive to changes in the particular disease in question,” Dr. Sielatycki said. “Based on this analysis, SF-6D derived from NDI may be a more valid and responsive measure of improvement in patients undergoing cervical procedures. We suggest that this metric be used in cost-effectiveness analysis and in calculating quality-adjusted life years for cervical spine patients.”
Dr. Sielatycki acknowledged certain limitations of the study, including the fact that it “should have some external validation done to further corroborate our findings. Our gold standard of meaningful improvement has not been established.”
Dr. Sielatycki reported having no financial disclosures.
AT CSRS 2015
Key clinical point: The Short Form–6D derived from the Neck Disability Index is an effective measure of outcomes in cervical spine patients.
Major finding: The Short Form–6D derived from the Neck Disability Index was a more valid discriminator of meaningful improvement, compared with the Short Form–6D derived from the Short Form–12 or the EuroQol-5D (AUC of .69, .65, and .62, respectively).
Data source: A single-center study that compared three quality of life measures in 420 patients presenting for elective surgical spine procedures.
Disclosures: Dr. Sielatycki reported having no financial disclosures.
