User login
Official Newspaper of the American College of Surgeons
A Perfect Storm: The current climate in breast cancer
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
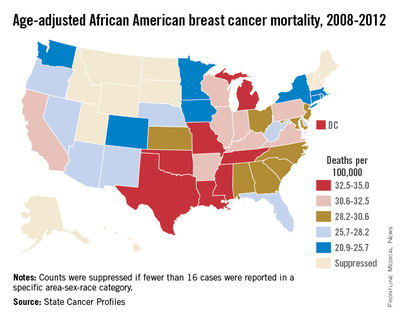
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.

There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.

Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.

Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.
There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.
This is the first installment of a five-part monthly series that will discuss the pathologic, genomic, and clinical factors that contribute to the racial survival disparity in breast cancer. The series, which is adapted from an article that originally appeared in CA: A Cancer Journal for Clinicians,1 a journal of the American Cancer Society, will also review exciting and innovative interventions to close this survival gap. This month’s column reviews the scope of this important health care issue.
The National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER) has estimated that 231,840 new cases of female breast cancer will be diagnosed in 2015, representing 14% of all new cancer cases among women. The NCI also has estimated 40,290 deaths from breast cancer, representing 6.8% of all cancer deaths among women.2 Breast cancer is the second leading cause of cancer death among women after lung cancer. It is well known that there has historically been a significant racial divide in breast cancer incidence (rate of new occurrences of breast cancer) and mortality (death) rates. Caucasian women were more likely to be diagnosed with breast cancer, but African American women were more likely to die from it.
However, in a recently released study by DeSantis et al. this incidence trend no longer holds, and in 2012 there was a convergence of breast cancer incidence rates at 135 cases per 100,000 women for both Caucasian and African American women.3 In addition, this recent analysis revealed that the mortality disparity between African American and Caucasian women has continued to increase, with a death rate 42% higher in African American than in Caucasian women in 2012. While overall improvements in therapy have led to a decrease in breast cancer death rates in the United States since 1990, the decreases in death rates began earlier and have been larger in proportionate terms for Caucasians than for African Americans.4,5 According to SEER data from 1975 to 2011, Caucasian women had a 23% increase in breast cancer incidence and a 34% decrease in mortality, whereas African American women experienced a 35% increase in incidence and a 2% increase in mortality.6
Beyond national statistics and on a more-local level, several studies have explored regional variations in breast cancer mortality by race. One such study analyzed mortality data from the National Center for Health Statistics from 1975 to 2004.5 The researchers discovered that trends in breast cancer death rates varied widely by region. While breast cancer death rates in Caucasian women decreased in all 50 states, among African American women in 37 states analyzed, breast cancer death rates increased in 2 states, were level in 24 states, and decreased in only 11 states. Many of the states in which African American breast cancer death rates were level or rising were in the South and Midwest.
There are also differences in age and stage at diagnosis between African American and Caucasian women. Although the overall incidence of breast cancer has been historically higher in Caucasians, the incidence profile changes when the data are looked at by age. Among African American women with breast cancer, 33% are diagnosed at an age younger than 50 years, compared with 21.9% among Caucasian women.7
In women younger than 35 years, the incidence of breast cancer in African Americans is 1.4-2.0 times that of Caucasians.8 In addition, African American women present with more advanced-stage disease. Again, using the SEER program and examining data from 2005-2011, 62% of Caucasians had localized disease (cancer confined to the breast and potentially curable) versus 53% of African Americans. In all, 5% of Caucasians had distant disease (cancer outside the breast and treatable but not curable), compared with 9% of African Americans.9 A recent study in JAMA of 373,563 women with breast cancer during 2004-2011 found that African American women were less likely to be diagnosed with stage I breast cancer than were non-Hispanic white women across all age groups (non-Hispanic white women, 50.8%; African American women, 37.0%).10
The researchers examined further those women with small breast cancers (breast tumors ≤ 2 cm) and the percentages of nodal metastases (cancer in the lymph nodes) and distant metastases (cancer outside the breast) by race/ethnicity. The authors found that an African American woman with a small-sized breast tumor was more likely to present with lymph node metastases and distant metastases. Significantly, African American women were also more likely to die of breast cancer with small-sized tumors than were non-Hispanic white women.
These differences in age and stage highlight important differences in tumor biology, genomics, and patterns of care that contribute to the disparity in breast cancer survival between Caucasian and African American women. The February installment of this column will explore tumor biology – the first element in the perfect storm.
Other installments of this column can be found in the Related Content box.
1. Daly B, Olopade OI: A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 65:221-38, 2015.
2. National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Stat fact sheets: Breast cancer. Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed Nov. 20, 2015.
3. DeSantis C, Fedewa S, Goding Sauer A, et al., Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer Journal for Clinicians. doi: 10.3322/caac.21320
4. DeLancey JO, Thun MJ, Jemal A, et al.: Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol Biomarkers Prev. 17:2908-12, 2008.
5. DeSantis C, Jemal A, Ward E, et al.: Temporal trends in breast cancer mortality by state and race. Cancer Causes Control. 19:537-45, 2008.
6. Howlander N NA, Krapcho M, et al. eds.: SEER Cancer Statistics Review, 1975-2011, 2014.
7. Clarke CA, West DW, Edwards BK, et al.: Existing data on breast cancer in African-American women: what we know and what we need to know. Cancer. 97:211-21, 2003.
8. Marie Swanson G, Haslam SZ, Azzouz F: Breast cancer among young African-American women: a summary of data and literature and of issues discussed during the Summit Meeting on Breast Cancer Among African American Women, Washington, DC, September 8-10, 2000. Cancer. 97:273-9, 2003.
9. National Cancer Institute. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/results_single/sect_04_table.13.pdf. Accessed, Nov. 20, 2015.
10. Iqbal J, Ginsburg O, Rochon PA, et al: Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313:165-73, 2015.
Bobby Daly, MD, MBA, is the chief fellow in the section of hematology/oncology at the University of Chicago Medicine. His clinical focus is breast and thoracic oncology, and his research focus is health services. Specifically, Dr. Daly researches disparities in oncology care delivery, oncology health care utilization, aggressive end-of-life oncology care, and oncology payment models. He received his MD and MBA from Harvard Medical School and Harvard Business School, both in Boston, and a BA in Economics and History from Stanford (Calif.) University. He was the recipient of the Dean’s Award at Harvard Medical and Business Schools.
Olufunmilayo Olopade, MD, FACP, OON, is the Walter L. Palmer Distinguished Service Professor of Medicine and Human Genetics, and director, Center for Global Health at the University of Chicago. She is adopting emerging high throughput genomic and informatics strategies to identify genetic and nongenetic risk factors for breast cancer in order to implement precision health care in diverse populations. This innovative approach has the potential to improve the quality of care and reduce costs while saving more lives.
Disclosures: Dr. Olopade serves on the Medical Advisory Board for CancerIQ. Dr. Daly serves as a director of Quadrant Holdings Corporation and receives compensation from this entity. Frontline Medical Communications is a subsidiary of Quadrant Holdings Corporation.
Published in conjunction with Susan G. Komen®.

The Right Choice? Kindness and Surgical Ethics: Reflections on a Friend and Mentor
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.

Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.
Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
As I sit down to write this column, I reflect on the news that my mentor and friend, Norman W. Thompson, M.D, FACS, passed away yesterday. I had the good fortune to spend 1 year as an endocrine surgery fellow with Dr. Thompson at the University of Michigan in 1995-96. That year was certainly the most significant of my training in terms of defining my professional life as an endocrine surgeon. However, as I think back on my time with Dr. Thompson, I am struck by how much more I learned from him than how to take out a thyroid or a parathyroid or manage multiple endocrine neoplasia.
Dr. Thompson was an excellent technical surgeon, and he would have had a tremendous career helping thousands of patients if that was all that he had done. However, he was much more than an excellent technician. He was also a great doctor. In order for a surgeon to be a great doctor, it is necessary to be technically excellent, but that alone is not sufficient. I believe that what makes a surgeon a great doctor is the combination of technical mastery with outstanding interpersonal skills and ethically sound clinical judgment. Dr. Thompson had all of that, and he was exceptionally kind.
Kindness is not a word that we commonly use in describing surgeons today. In an era of surgeons being pressured to see more patients and generate more RVUs [relative value units], it is unusual to hear kindness mentioned as an essential attribute of a great surgeon. However, Dr. Thompson’s kindness was immediately apparent to all who spent time with him. He treated each patient as a unique individual. In addition, he treated his trainees and his colleagues in Ann Arbor and around the world with respect and incredible humility. He was generous with his time and was always approachable no matter how inexperienced the surgeon asking him a question. Dr. Thompson was kind to all of us and made us feel that he valued spending time with us.
What does kindness have to do with a column that traditionally focuses on ethical issues in the practice of surgery? Although acting with kindness is not the same as acting in an ethical manner, I believe that there is more overlap of the terms than we often imagine. The kind surgeon is the one who treats people – whether they are patients or colleagues – as though they matter. The ethical surgeon respects the patient’s wishes and acts to benefit the patient as much as possible in all circumstances. I am certain that I have met ethical surgeons who were not kind, but I have met very few kind surgeons who are not ethical.
As someone who has spent significant time and energy in the last 19 years as a surgery faculty member trying to teach ethics, I am also struck by a clear truth. Actions always speak louder than words. It may be valuable to talk about the ethical principles that may come to play in a particularly difficult surgical case. Defining the competing interests and assessing the patient’s wishes are important components of the ethical practice of surgery. However, no amount of discussion of these issues can substitute for the value of behavior. Treating patients and colleagues with kindness and respect is modeling the behaviors of an ethical surgeon – perhaps learned from a wise and thoughtful mentor.
Dr. Thompson was an excellent role model for me and so many others in how he treated patients and everyone around him. As I see patients and perform surgery, I still hear myself saying many of the same things that he said many years ago. His genuine expressions of optimism before difficult operations, honesty in communicating, and sadness when things did not go well were tremendous examples to me of how a great doctor treats those around him. These lessons that I learned from Dr. Thompson have influenced my practice significantly, and I am grateful for the opportunity to try to model them on a daily basis.
Although I remain convinced that formal curricula in ethics and professionalism remain important in the education of today’s surgeons, it is valuable to remember the impact that the behaviors of those we respect have on us. Perhaps we surgeons more than other physicians are molded by the people who train us, but there is no question that the ethical behaviors of our teachers and mentors will have a greater impact than any lecture or manuscript. I want to acknowledge and commemorate the kindness and ethical behaviors that Dr. Thompson modeled daily for all who were fortunate enough to work with him.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.

Screening Mammography: Debates, Guidelines, Issues
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.

Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.
Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.
The screening mammography debate has been rekindled by the American Cancer Society’s updated guideline released in October 2015. Surgeons are now looking at yet another iteration of the optimal surveillance schedule aimed at reducing breast cancer mortality.
Nearly all breast cancer patients undergo surgery as at least one component of their care through diagnostic biopsy and/or definitive locoregional management, and many women are referred to surgeons for evaluation as well as follow-up for a variety of benign breast problems. The discussion of breast cancer screening with patients can be complicated by the many guidelines with conflicting recommendations, not to mention patient fears triggered by incompletely informed or simplistic media coverage. Surgeons are therefore obliged to remain knowledgeable regarding the status and rationale for breast cancer screening guidelines that have been developed by our colleagues in the American Cancer Society as well as other organizations.
Context of the updated guideline
The American Cancer Society and the American College of Surgeons have historically advocated in favor of annual screening mammography for average-risk women in the United States beginning at age 40 years (https://goo.gl/4W92EI). In 2009, the United States Preventive Services Task Force (USPSTF) published a recommendation that women delay initiation of screening mammography until reaching age 50, with follow-up studies performed biennially thereafter. This USPSTF guideline has remain unchanged as of 2015 (http://goo.gl/RYYWEP). Other medical societies and institutions have established their own guidelines.
The updated American Cancer Society guideline now recommends that average-risk women initiate annual mammography at age 45, but advocates in favor of availability of annual mammography beginning at age 40; the updated guideline also indicates that women can transition to biennial mammography at age 55, but should have access to continued annual mammography in accordance with personal preferences and after consideration of risks and benefits (JAMA. 2015;314[15]:1599-614).
The updated guideline can basically be interpreted as a more relaxed version of the prior guideline, which featured a straightforward mandate for average-risk women to undergo annual screening mammography beginning at age 40 years. However, the increased complexity of the more flexible guideline has generated legitimate concerns regarding the potential for confusion and misinterpretation.
Updated guideline rationale and empirical basis
The Society commissioned a systematic review to evaluate the benefits and harms of mammographic screening as well as clinical breast examination, based upon randomized clinical trials, and observational and modeling studies (JAMA. 2015;314[15]: 1615-34).
The Society then convened their Guideline Development Group (GDG) and GDG Breast Subgroup to interpret the systematic review for the purpose of drafting the breast cancer screening update. This process was further guided by a panel of External Expert Advisors. Mortality reductions were analyzed in the context of population-based breast cancer incidence rates by 5-year age increments.
Not surprisingly, the overall review confirmed the findings of several published studies that screening mammography in women aged 40-79 reduces breast cancer mortality rates by 20%-50%, with extent of benefit varying by age, as well as study design (randomized clinical trial versus observational). Since breast cancer incidence rates increase substantially among women by age (incidence rates per 100,000 population for women 35-39; 40-44; 45-49; 50-54; and 55-59 reported as 59.5; 122.5; 188.6; 224.0; and 266.4, respectively), the likelihood of a mammogram detecting a true cancer clearly increases with age. The American Cancer Society GDG Breast Subgroup balanced the mortality reductions and population-based incidence rates against the risks of mammography “harms” (defined as needing to be recalled for additional testing via imaging and/or biopsy).
The quality of evidence for estimating risk of “overdiagnosis” (detecting a breast cancer that was not destined to be biologically significant or life threatening) was deemed to be insufficient and so this controversial metric was omitted from the final analysis. However, data regarding the general tendency for breast cancers to have more favorable biologic features (and therefore presumed to be more indolent) in older-aged women were taken into account with regard to recommendations for age-based screening intervals.
Upon review of the above incidence and mortality-related issues, the Society generated their age- and interval-based mammography screening recommendations. The recommendations were stratified as either “strong” (defined as a screening practice that “most” patients should follow, and one that could be reasonably used as a “quality criterion or performance indicator”) or “qualified” (defined as a screening practice that is reasonable for the “majority” of patients, but encouraging a balanced discussion of possible alternatives and informed decision making). The recommendations for average-risk women are summarized as follows:
• Strong Recommendation: Women should initiate screening mammography at age 45 years.
• Qualified Recommendation: Screening mammography should be performed annually between ages 45 and 54 years.
• Qualified Recommendation: Women should have the opportunity to undergo annual screening mammography between ages 40 and 44 years.
• Qualified Recommendation: Women aged 55 and older should transition to biennial screening mammography but they should have the opportunity to continue annual screening.
• Qualified Recommendation: Women should continue screening mammography until they no longer have a life expectancy of at least 10 years.
The updated American Cancer Society screening mammography guideline therefore continues to support availability of annual screening mammography for average-risk women beginning at age 40 years and continuing for as long as life expectancy supports the benefit of undergoing treatment for a screen-detected breast cancer. However, in acknowledging the increasing risk of breast cancer with age and the increased prevalence of biologically favorable breast cancers among older versus younger women, the Society stresses that screening mammography is a must by the time a woman reaches age 45, and that she can safely consider transitioning from annual to biennial screening at age 55.
Other components of the updated guideline:
While the mammography component of the breast cancer screening guidelines have provoked the most substantial discussion, they have also addressed other screening practices, and these are summarized as follows:
• Qualified Recommendation: Clinical breast examination is not recommended for breast cancer screening among average-risk women at any age.
• Not addressed in the update, and therefore not changed from prior American Cancer Society recommendation: Breast self-examination is not recommended for average-risk women at any age.
Additional issues in the screening mammography debate
While the American Cancer Society and other organizations attempt to synthesize and interpret the existing data regarding the benefits and risks of various screening practices, clinicians must also consider several public health issues when deciding upon their own screening recommendation practices:
• Disparities and variation in breast cancer patterns associated with racial/ethnic identity: Although white American women have historically had higher population-based incidence rates of breast cancer, compared with African American women, incidence rates have risen among African Americans, and 2012 data indicate comparable rates for both groups. Furthermore, breast cancer outcome disparities have worsened, with breast cancer mortality rates 42% higher for African Americans (CA Cancer J Clin. 2015 Oct 29. doi: 10.3322/caac.21320 [Epub ahead of print]). African American women have a twofold higher population-based incidence rate of the biologically more aggressive triple-negative breast cancers at all ages, and the rates among African American women in their forties is higher than those among white American women in their fifties (Cancer. 2011;117[12]:2747-53; J Natl Cancer Inst. 2015;107[6]: djv048). Prevalence of breast cancer in the premenopausal age range is also higher among African American patients. Delayed initiation of breast cancer screening, and more prolonged intervals between screenings is therefore likely to have a disproportionate impact on the breast cancer burden of the African American population.
• Demographics of the American female population: While overall population-based incidence rates of breast cancer have been stable among American women younger than age 45 years, U.S. Census data reveal 10 million more women in the 20-45 years age range for 2010, compared with 1980. The absolute number of breast cancer patients belonging to this young age category has therefore increased (JAMA Oncol. 2015;1[7]:877-8).
• Scenarios that are not relevant for routine screening recommendations: Clinicians must continue to aggressively counsel patients regarding the importance of overall breast health awareness. The development of a new breast mass, inflammatory skin changes, and/or bloody nipple discharge should prompt immediate medical attention regardless of the result and timing of the most recent mammogram. Furthermore, women facing increased risk of breast cancer because of family history, chest wall irradiation in adolescence/early adulthood, and high-risk breast biopsy pathology (atypia, lobular carcinoma in situ) are candidates for more intense surveillance such as breast MRI in addition to mammography. The most appropriate management of women with increased risk based upon mammographic density remains unclear. Lastly but extremely importantly, American-based breast cancer screening recommendations do not apply to low- and middle-income countries where screening mammography is not widely available. Clinical breast examination and breast self-examination may play a different role in the breast cancer burden of these populations.
Dr. Newman is an ACS Fellow, Director of the Breast Oncology Program, Multi-Hospital Henry Ford Health System, Detroit, and founding Medical Director, Henry Ford Health System International Center for the Study of Breast Cancer Subtypes. Dr. Newman has acted as a volunteer advisor to the American Cancer Society.

Neurosurgery at the End of Life
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.
The juxtaposition between my first 2 days of neurosurgery could not have been more profound. On my first day as a third-year medical student, the attending and chief resident let me take the lead on the first case: a straightforward brain biopsy. I got to make the incision, drill the burr hole, and perform the needle biopsy. I still remember the thrill of the technical challenge, the controlled violence of drilling into the skull, and the finesse of accessing the tumor core.
The buzz was so strong that I barely registered the diagnosis that was called back from the pathologist: glioblastoma. It was not until I saw the face of the disease the next morning that I understood the reality of a GBM diagnosis. That face belonged to a 47-year-old man who hadn’t slept all night, wide eyed with apprehension at what news I might bring. He beseeched me with questions, and though his aphasia left him stammering to get the words out, I knew exactly what he was asking: Would he live or die? It was a question I was in no position to answer. Instead, I reassured him that we were waiting on the final pathology, all the while trying to forget the fact that the frozen section suggested an aggressive subtype, surely heralding a poor prognosis.
In his poignant memoir, “Do No Harm: Stories of Life, Death and Brain Surgery” (New York: Thomas Dunne Book, 2015), Dr. Henry Marsh writes beautifully about how difficult it can be to find the balance between optimism and realism. In one memorable passage, Dr. Marsh shows a house officer a scan of a highly malignant brain tumor and asks him what he would say to the patient. The trainee reflexively hides behind jargon, skirting around what he knew to be the truth: This tumor would kill her. Marsh presses him to admit that he’s lying, before lamenting at how hard it is to improve these critical communication skills: “When I have had to break bad news I never know whether I have done it well or not. The patients aren’t going to ring me up afterward and say, ‘Mr. Marsh, I really liked the way you told me that I was going to die,’ or ‘Mr. Marsh, you were crap.’ You can only hope that you haven’t made too much of a mess of it.”
I could certainly relate to Dr. Marsh’s house officer as I walked away from my own patient. I felt almost deceitful withholding diagnostic information from him, even if I did the “right” thing. It made me wonder, why did I want to become a neurosurgeon? Surely to help people through some of the most difficult moments of their lives. But is it possible to be a source of comfort when you are required so often to be a harbinger of death? The answer depends on whether one can envision a role for the neurosurgeon beyond the mandate of “life at all costs.”
While the field has become known for its life-saving procedures, neurosurgeons are called just as often to preside over the end of their patient’s lives – work that requires just as much skill as any technical procedure. Dr. Marsh recognized the tremendous human cost of neglecting that work. For cases that appear “hopeless,” he writes, “We often end up operating because it’s easier than being honest, and it means that we can avoid a painful conversation.”
We are only beginning to understand the many issues that neurosurgical patients face at the end of life, but so far it is clear that neurosurgical trainees require substantive training in prognostication, communication, and palliation (Crit Care Med. 2015 Sep;43[9]:1964-77 1,2; J Neurooncol. 2009 Jan;91[1]:39-43). Is there room in the current training paradigm for more formal education in these domains? As we move further into the 21st century, we must embrace the need for masterful clinicians outside of the operating room if we are to ever challenge the axiom set forth by the renowned French surgeon, René Leriche, some 65 years ago: “Every surgeon carries within himself a small cemetery, where from time to time he goes to pray – a place of bitterness and regret, where he must look for an explanation for his failures.” Let us look forward to the day when this is no longer the case.
Stephen Miranda is a medical student from the University of Rochester, who is now working as a research fellow at Ariadne Labs, a joint center for health systems innovation at Brigham & Women’s Hospital and Harvard T.H. Chan School of Public Health, both in Boston.

Candor laws growing, but are they effective?
Iowa is the latest state to launch a unique strategy that aims to reduce medical malpractice lawsuits and bolster doctor-patient communication after poor outcomes, while encouraging swift resolution. The Communication and Optimal Resolution (CANDOR) law, which took effect in July, permits privileged discussions between Iowa physicians and patients after medical errors and allows for compensation offers, when appropriate.
After years of failing to enact traditional tort reform, the alternative method is hoped to decrease litigation costs and keep doctors and patients out of a flawed court system, said Dr. Michael McCoy, chair of the Iowa Medical Society Ad Hoc Tort Reform Task Force and a West Burlington obstetrician-gynecologist.

“If there’s an untoward outcome, the current system creates isolation,” he said. “The patients get alienated, and the doctors get stressed. That’s the exact opposite of what should happen. You should be able to talk to patients and feel protection. That’s what this law does.”
About 36 states have so-called “apology laws” that prohibit certain statements, expressions, or other evidence from being admissible in a malpractice lawsuit, according to data from Sorry Works!, an advocacy group that tracks apology statutes. Most apology laws cover expressions of empathy or sympathy, while some statutes protect admissions of fault. At least three states – including Iowa – go a step further, laying the foundation for early disclosure of errors, communication between physicians and patients, and negotiation of potential resolutions. Oregon’s Early Discussion and Resolution (EDR) law, which passed in 2013, allows both providers and patients to initiate conversations after adverse events, discuss what happened, and resolve the issue outside of court. Massachusetts’ 2012 disclosure, apology, and offer legislation includes a 182-day waiting period before lawsuits can be filed to allow for the process. Other states, including Washington, Texas, California, and Utah have expressed interest in enacting similar laws.

Efforts in Iowa, Oregon, and Massachusetts were driven by the successes of similar programs at the University of Illinois Hospital and Health Sciences System, Chicago and at the University of Michigan Health System, Ann Arbor, among others. Since the University of Michigan began its CANDOR program in 2001, average legal expenses per case have been cut in half, according to the UM data. The health system’s presuit claims have gone from 260 annually to about 100 per year. Pilot efforts by the University of Illinois (Chicago) Hospital and Health Sciences System since 2006 have increased adverse event reports from 1,500 per year to 10,000 while decreasing malpractice premiums by $15 million dollars since 2010.
But questions remain as to whether such approaches are successful when implemented on a state level. So far, the majority of data on early discussion, apology, and offer programs have come from closed systems, such as academic medical centers.

“We’re starting to look at how this works in an open system when you try to disseminate it across a state,” said Dr. Alan C. Woodward, chair of the Massachusetts Medical Society Committee on Professional Liability and cofounder of the Massachusetts Alliance for Communication and Resolution following Medical Injury (MACRMI). “If we can show this is an effective model in a statewide distribution, the hope is that multiple other states will follow suit, because this is clearly a better alternative for patients and providers and for patient safety improvement efforts.”
Massachusetts program showing promise
In Massachusetts, the state’s CANDOR law enabled MACRMI to roll out its Communication, Apology, and Resolution (CARe) model at six hospital pilot sites. MACRMI was formed as part of a research initiative led by Beth Israel Deaconess Medical Center, Boston, and the Massachusetts Medical Society, Waltham, and funded by a 2010 grant from the Federal Agency for Health Care Research and Quality.
Under the CARe model, participating health providers communicate with patients and families after an unanticipated adverse outcome, investigate and explain what happened, and where appropriate, apologize and offer fair financial compensation. Data collection in the 3-year study trial closed in December 2015, and the alliance plans to publish its findings in spring 2016. The model has greatly expedited case resolutions, Dr. Woodward said. A case in the CARe program can be resolved in 6 months or less, compared with a lawsuit that can take up to 5 years to resolve. By April 2015, the alliance had screened 856 cases. In three-quarters of cases, the care provided was deemed appropriate, Dr. Woodward said. Of these cases, 615 were closed after full-disclosure meetings with patients. Of the total cases screened, 122 cases were referred to an insurer for resolution, and 93 cases were awaiting further evaluation.
“It’s doing extraordinarily well,” Dr. Woodward said. “We’re resolving cases very efficiently in a short period of time, rather than using litigation.”

Outside the pilot program, health providers in Massachusetts are benefiting from the state’s 182-day waiting period before malpractice lawsuits can be filed, said Elizabeth A. Cushing, vice president of claims for CRICO, a medical liability insurer for the Harvard University medical community. The law allows physicians and insurers the opportunity to review a case and decide whether the complaint requires compensation. In cases that are not considered malpractice, explaining the underlying reasoning to patients or plaintiffs’ attorneys prevents some lawsuits from being filed, she said.
However, Ms. Cushing notes that not every case fits smoothly into the alternative model. Cases in which a poor outcome is immediately known, such as a surgical mishap, lend themselves to quicker investigation, disclosure, and remedy, she said. Claims of misdiagnosed cancer for instance, where the alleged mistake occurred years before, are more challenging.
“A lot of what we are seeing are alleged failures to diagnose things sooner, so it’s 2 years later and someone says, ‘You should have picked up on the fact that I had lung cancer 2 years ago,’ Ms. Cushing said. “Those situations get tricky. What did you know, when? Those cases are not as easily amenable to this process.”
Oregon program gaining speed
Meanwhile, Oregon officials are hoping that more doctors will soon participate in the state’s Early Discussion and Resolution program. In 2014 – its first year in operation – no individual physicians initiated participation in the program. Because EDR is voluntary, both parties must agree to participate for EDR to begin and either party can choose to stop participating at any time.

In 2014, Oregon patients and health providers filed 29 EDR requests to participate in the program, according to data from the Oregon Patient Safety Commission. Patients filed 21 notices and health care professionals filed eight notices. A majority of the eight notices filed by health professionals were issued by hospital representatives. No requests were filed by individual health providers. In 9 of the 21 patient-filed notices, at least one involved health professional accepted the patient’s request to participate in EDR. In the remaining 12 patient-filed notices, the involved health provider(s) declined the request. Data is not yet available on resolution time or case outcomes.
EDR leaders are hopeful that more health professionals and patients will participate in the coming years, said Melissa Parkerton, director of the Early Discussion and Resolution program for the Oregon Patient Safety Commission.
“Widespread adoption of a new approach like EDR requires not just a new process, but a new mindset,” she said. “This kind of cultural shift takes time. In Oregon, our fervent hope is that EDR will be embraced by every health care organization and professional.”
Efforts to raise awareness about the program are ongoing, adds Dr. Robert Dannenhoffer, a Roseburg, Ore., pediatrician and past president of the Oregon Medical Association.
“It’s a little hard to get the word out,” he said in an interview. “Most [doctors] are not going to be dealing with this on a regular basis. It’s a slow uptake. We’re working on better educating physicians.”
A practical model for independent docs?
Questions remain about whether disclosure, apology, and offer models work for independent physicians in small practices.
Dr. Thad L. Anderson, an ob.gyn in private practice in Dubuque, Iowa, strongly supports his state’s law, but he does not foresee the process having much impact on his practice. Larger health systems are generally more situated to utilize the process, he said.

“A hospital system that employees physicians is probably better suited to take advantage of this law,” he said. Independent doctors “don’t have the infrastructure. You don’t have the in-house lawyer. It’s probably a little more problematic for an individual to take advantage of the process compared to a bigger system.”
With this issue in mind, MACRMI in Massachusetts recently added an 800-physician, multispecialty outpatient group to its program analysis. The goal is to evaluate how the process operates within this type of setting and identify challenges and impediments, Dr. Woodward said. In addition, the alliance is encouraging commercial insurers to assist independent physicians in participating in the CARe model.
“The independent or small practice all benefit from the statute we passed – they have the [182-day waiting period] – but if they don’t have an internal risk management structure, than we’ve been working with insurers to set up a support structure,” he said. That way, “when a patient is unhappy with their care, there is a process that can support even a small practice in going through this and working through it with a patient.”
*This story was updated 1/26/2016.
On Twitter @legal_med
Iowa is the latest state to launch a unique strategy that aims to reduce medical malpractice lawsuits and bolster doctor-patient communication after poor outcomes, while encouraging swift resolution. The Communication and Optimal Resolution (CANDOR) law, which took effect in July, permits privileged discussions between Iowa physicians and patients after medical errors and allows for compensation offers, when appropriate.
After years of failing to enact traditional tort reform, the alternative method is hoped to decrease litigation costs and keep doctors and patients out of a flawed court system, said Dr. Michael McCoy, chair of the Iowa Medical Society Ad Hoc Tort Reform Task Force and a West Burlington obstetrician-gynecologist.
“If there’s an untoward outcome, the current system creates isolation,” he said. “The patients get alienated, and the doctors get stressed. That’s the exact opposite of what should happen. You should be able to talk to patients and feel protection. That’s what this law does.”
About 36 states have so-called “apology laws” that prohibit certain statements, expressions, or other evidence from being admissible in a malpractice lawsuit, according to data from Sorry Works!, an advocacy group that tracks apology statutes. Most apology laws cover expressions of empathy or sympathy, while some statutes protect admissions of fault. At least three states – including Iowa – go a step further, laying the foundation for early disclosure of errors, communication between physicians and patients, and negotiation of potential resolutions. Oregon’s Early Discussion and Resolution (EDR) law, which passed in 2013, allows both providers and patients to initiate conversations after adverse events, discuss what happened, and resolve the issue outside of court. Massachusetts’ 2012 disclosure, apology, and offer legislation includes a 182-day waiting period before lawsuits can be filed to allow for the process. Other states, including Washington, Texas, California, and Utah have expressed interest in enacting similar laws.
Efforts in Iowa, Oregon, and Massachusetts were driven by the successes of similar programs at the University of Illinois Hospital and Health Sciences System, Chicago and at the University of Michigan Health System, Ann Arbor, among others. Since the University of Michigan began its CANDOR program in 2001, average legal expenses per case have been cut in half, according to the UM data. The health system’s presuit claims have gone from 260 annually to about 100 per year. Pilot efforts by the University of Illinois (Chicago) Hospital and Health Sciences System since 2006 have increased adverse event reports from 1,500 per year to 10,000 while decreasing malpractice premiums by $15 million dollars since 2010.
But questions remain as to whether such approaches are successful when implemented on a state level. So far, the majority of data on early discussion, apology, and offer programs have come from closed systems, such as academic medical centers.
“We’re starting to look at how this works in an open system when you try to disseminate it across a state,” said Dr. Alan C. Woodward, chair of the Massachusetts Medical Society Committee on Professional Liability and cofounder of the Massachusetts Alliance for Communication and Resolution following Medical Injury (MACRMI). “If we can show this is an effective model in a statewide distribution, the hope is that multiple other states will follow suit, because this is clearly a better alternative for patients and providers and for patient safety improvement efforts.”
Massachusetts program showing promise
In Massachusetts, the state’s CANDOR law enabled MACRMI to roll out its Communication, Apology, and Resolution (CARe) model at six hospital pilot sites. MACRMI was formed as part of a research initiative led by Beth Israel Deaconess Medical Center, Boston, and the Massachusetts Medical Society, Waltham, and funded by a 2010 grant from the Federal Agency for Health Care Research and Quality.
Under the CARe model, participating health providers communicate with patients and families after an unanticipated adverse outcome, investigate and explain what happened, and where appropriate, apologize and offer fair financial compensation. Data collection in the 3-year study trial closed in December 2015, and the alliance plans to publish its findings in spring 2016. The model has greatly expedited case resolutions, Dr. Woodward said. A case in the CARe program can be resolved in 6 months or less, compared with a lawsuit that can take up to 5 years to resolve. By April 2015, the alliance had screened 856 cases. In three-quarters of cases, the care provided was deemed appropriate, Dr. Woodward said. Of these cases, 615 were closed after full-disclosure meetings with patients. Of the total cases screened, 122 cases were referred to an insurer for resolution, and 93 cases were awaiting further evaluation.
“It’s doing extraordinarily well,” Dr. Woodward said. “We’re resolving cases very efficiently in a short period of time, rather than using litigation.”
Outside the pilot program, health providers in Massachusetts are benefiting from the state’s 182-day waiting period before malpractice lawsuits can be filed, said Elizabeth A. Cushing, vice president of claims for CRICO, a medical liability insurer for the Harvard University medical community. The law allows physicians and insurers the opportunity to review a case and decide whether the complaint requires compensation. In cases that are not considered malpractice, explaining the underlying reasoning to patients or plaintiffs’ attorneys prevents some lawsuits from being filed, she said.
However, Ms. Cushing notes that not every case fits smoothly into the alternative model. Cases in which a poor outcome is immediately known, such as a surgical mishap, lend themselves to quicker investigation, disclosure, and remedy, she said. Claims of misdiagnosed cancer for instance, where the alleged mistake occurred years before, are more challenging.
“A lot of what we are seeing are alleged failures to diagnose things sooner, so it’s 2 years later and someone says, ‘You should have picked up on the fact that I had lung cancer 2 years ago,’ Ms. Cushing said. “Those situations get tricky. What did you know, when? Those cases are not as easily amenable to this process.”
Oregon program gaining speed
Meanwhile, Oregon officials are hoping that more doctors will soon participate in the state’s Early Discussion and Resolution program. In 2014 – its first year in operation – no individual physicians initiated participation in the program. Because EDR is voluntary, both parties must agree to participate for EDR to begin and either party can choose to stop participating at any time.
In 2014, Oregon patients and health providers filed 29 EDR requests to participate in the program, according to data from the Oregon Patient Safety Commission. Patients filed 21 notices and health care professionals filed eight notices. A majority of the eight notices filed by health professionals were issued by hospital representatives. No requests were filed by individual health providers. In 9 of the 21 patient-filed notices, at least one involved health professional accepted the patient’s request to participate in EDR. In the remaining 12 patient-filed notices, the involved health provider(s) declined the request. Data is not yet available on resolution time or case outcomes.
EDR leaders are hopeful that more health professionals and patients will participate in the coming years, said Melissa Parkerton, director of the Early Discussion and Resolution program for the Oregon Patient Safety Commission.
“Widespread adoption of a new approach like EDR requires not just a new process, but a new mindset,” she said. “This kind of cultural shift takes time. In Oregon, our fervent hope is that EDR will be embraced by every health care organization and professional.”
Efforts to raise awareness about the program are ongoing, adds Dr. Robert Dannenhoffer, a Roseburg, Ore., pediatrician and past president of the Oregon Medical Association.
“It’s a little hard to get the word out,” he said in an interview. “Most [doctors] are not going to be dealing with this on a regular basis. It’s a slow uptake. We’re working on better educating physicians.”
A practical model for independent docs?
Questions remain about whether disclosure, apology, and offer models work for independent physicians in small practices.
Dr. Thad L. Anderson, an ob.gyn in private practice in Dubuque, Iowa, strongly supports his state’s law, but he does not foresee the process having much impact on his practice. Larger health systems are generally more situated to utilize the process, he said.
“A hospital system that employees physicians is probably better suited to take advantage of this law,” he said. Independent doctors “don’t have the infrastructure. You don’t have the in-house lawyer. It’s probably a little more problematic for an individual to take advantage of the process compared to a bigger system.”
With this issue in mind, MACRMI in Massachusetts recently added an 800-physician, multispecialty outpatient group to its program analysis. The goal is to evaluate how the process operates within this type of setting and identify challenges and impediments, Dr. Woodward said. In addition, the alliance is encouraging commercial insurers to assist independent physicians in participating in the CARe model.
“The independent or small practice all benefit from the statute we passed – they have the [182-day waiting period] – but if they don’t have an internal risk management structure, than we’ve been working with insurers to set up a support structure,” he said. That way, “when a patient is unhappy with their care, there is a process that can support even a small practice in going through this and working through it with a patient.”
*This story was updated 1/26/2016.
On Twitter @legal_med
Iowa is the latest state to launch a unique strategy that aims to reduce medical malpractice lawsuits and bolster doctor-patient communication after poor outcomes, while encouraging swift resolution. The Communication and Optimal Resolution (CANDOR) law, which took effect in July, permits privileged discussions between Iowa physicians and patients after medical errors and allows for compensation offers, when appropriate.
After years of failing to enact traditional tort reform, the alternative method is hoped to decrease litigation costs and keep doctors and patients out of a flawed court system, said Dr. Michael McCoy, chair of the Iowa Medical Society Ad Hoc Tort Reform Task Force and a West Burlington obstetrician-gynecologist.
“If there’s an untoward outcome, the current system creates isolation,” he said. “The patients get alienated, and the doctors get stressed. That’s the exact opposite of what should happen. You should be able to talk to patients and feel protection. That’s what this law does.”
About 36 states have so-called “apology laws” that prohibit certain statements, expressions, or other evidence from being admissible in a malpractice lawsuit, according to data from Sorry Works!, an advocacy group that tracks apology statutes. Most apology laws cover expressions of empathy or sympathy, while some statutes protect admissions of fault. At least three states – including Iowa – go a step further, laying the foundation for early disclosure of errors, communication between physicians and patients, and negotiation of potential resolutions. Oregon’s Early Discussion and Resolution (EDR) law, which passed in 2013, allows both providers and patients to initiate conversations after adverse events, discuss what happened, and resolve the issue outside of court. Massachusetts’ 2012 disclosure, apology, and offer legislation includes a 182-day waiting period before lawsuits can be filed to allow for the process. Other states, including Washington, Texas, California, and Utah have expressed interest in enacting similar laws.
Efforts in Iowa, Oregon, and Massachusetts were driven by the successes of similar programs at the University of Illinois Hospital and Health Sciences System, Chicago and at the University of Michigan Health System, Ann Arbor, among others. Since the University of Michigan began its CANDOR program in 2001, average legal expenses per case have been cut in half, according to the UM data. The health system’s presuit claims have gone from 260 annually to about 100 per year. Pilot efforts by the University of Illinois (Chicago) Hospital and Health Sciences System since 2006 have increased adverse event reports from 1,500 per year to 10,000 while decreasing malpractice premiums by $15 million dollars since 2010.
But questions remain as to whether such approaches are successful when implemented on a state level. So far, the majority of data on early discussion, apology, and offer programs have come from closed systems, such as academic medical centers.
“We’re starting to look at how this works in an open system when you try to disseminate it across a state,” said Dr. Alan C. Woodward, chair of the Massachusetts Medical Society Committee on Professional Liability and cofounder of the Massachusetts Alliance for Communication and Resolution following Medical Injury (MACRMI). “If we can show this is an effective model in a statewide distribution, the hope is that multiple other states will follow suit, because this is clearly a better alternative for patients and providers and for patient safety improvement efforts.”
Massachusetts program showing promise
In Massachusetts, the state’s CANDOR law enabled MACRMI to roll out its Communication, Apology, and Resolution (CARe) model at six hospital pilot sites. MACRMI was formed as part of a research initiative led by Beth Israel Deaconess Medical Center, Boston, and the Massachusetts Medical Society, Waltham, and funded by a 2010 grant from the Federal Agency for Health Care Research and Quality.
Under the CARe model, participating health providers communicate with patients and families after an unanticipated adverse outcome, investigate and explain what happened, and where appropriate, apologize and offer fair financial compensation. Data collection in the 3-year study trial closed in December 2015, and the alliance plans to publish its findings in spring 2016. The model has greatly expedited case resolutions, Dr. Woodward said. A case in the CARe program can be resolved in 6 months or less, compared with a lawsuit that can take up to 5 years to resolve. By April 2015, the alliance had screened 856 cases. In three-quarters of cases, the care provided was deemed appropriate, Dr. Woodward said. Of these cases, 615 were closed after full-disclosure meetings with patients. Of the total cases screened, 122 cases were referred to an insurer for resolution, and 93 cases were awaiting further evaluation.
“It’s doing extraordinarily well,” Dr. Woodward said. “We’re resolving cases very efficiently in a short period of time, rather than using litigation.”
Outside the pilot program, health providers in Massachusetts are benefiting from the state’s 182-day waiting period before malpractice lawsuits can be filed, said Elizabeth A. Cushing, vice president of claims for CRICO, a medical liability insurer for the Harvard University medical community. The law allows physicians and insurers the opportunity to review a case and decide whether the complaint requires compensation. In cases that are not considered malpractice, explaining the underlying reasoning to patients or plaintiffs’ attorneys prevents some lawsuits from being filed, she said.
However, Ms. Cushing notes that not every case fits smoothly into the alternative model. Cases in which a poor outcome is immediately known, such as a surgical mishap, lend themselves to quicker investigation, disclosure, and remedy, she said. Claims of misdiagnosed cancer for instance, where the alleged mistake occurred years before, are more challenging.
“A lot of what we are seeing are alleged failures to diagnose things sooner, so it’s 2 years later and someone says, ‘You should have picked up on the fact that I had lung cancer 2 years ago,’ Ms. Cushing said. “Those situations get tricky. What did you know, when? Those cases are not as easily amenable to this process.”
Oregon program gaining speed
Meanwhile, Oregon officials are hoping that more doctors will soon participate in the state’s Early Discussion and Resolution program. In 2014 – its first year in operation – no individual physicians initiated participation in the program. Because EDR is voluntary, both parties must agree to participate for EDR to begin and either party can choose to stop participating at any time.
In 2014, Oregon patients and health providers filed 29 EDR requests to participate in the program, according to data from the Oregon Patient Safety Commission. Patients filed 21 notices and health care professionals filed eight notices. A majority of the eight notices filed by health professionals were issued by hospital representatives. No requests were filed by individual health providers. In 9 of the 21 patient-filed notices, at least one involved health professional accepted the patient’s request to participate in EDR. In the remaining 12 patient-filed notices, the involved health provider(s) declined the request. Data is not yet available on resolution time or case outcomes.
EDR leaders are hopeful that more health professionals and patients will participate in the coming years, said Melissa Parkerton, director of the Early Discussion and Resolution program for the Oregon Patient Safety Commission.
“Widespread adoption of a new approach like EDR requires not just a new process, but a new mindset,” she said. “This kind of cultural shift takes time. In Oregon, our fervent hope is that EDR will be embraced by every health care organization and professional.”
Efforts to raise awareness about the program are ongoing, adds Dr. Robert Dannenhoffer, a Roseburg, Ore., pediatrician and past president of the Oregon Medical Association.
“It’s a little hard to get the word out,” he said in an interview. “Most [doctors] are not going to be dealing with this on a regular basis. It’s a slow uptake. We’re working on better educating physicians.”
A practical model for independent docs?
Questions remain about whether disclosure, apology, and offer models work for independent physicians in small practices.
Dr. Thad L. Anderson, an ob.gyn in private practice in Dubuque, Iowa, strongly supports his state’s law, but he does not foresee the process having much impact on his practice. Larger health systems are generally more situated to utilize the process, he said.
“A hospital system that employees physicians is probably better suited to take advantage of this law,” he said. Independent doctors “don’t have the infrastructure. You don’t have the in-house lawyer. It’s probably a little more problematic for an individual to take advantage of the process compared to a bigger system.”
With this issue in mind, MACRMI in Massachusetts recently added an 800-physician, multispecialty outpatient group to its program analysis. The goal is to evaluate how the process operates within this type of setting and identify challenges and impediments, Dr. Woodward said. In addition, the alliance is encouraging commercial insurers to assist independent physicians in participating in the CARe model.
“The independent or small practice all benefit from the statute we passed – they have the [182-day waiting period] – but if they don’t have an internal risk management structure, than we’ve been working with insurers to set up a support structure,” he said. That way, “when a patient is unhappy with their care, there is a process that can support even a small practice in going through this and working through it with a patient.”
*This story was updated 1/26/2016.
On Twitter @legal_med

3D imaging tracks causes of post-TAVR aortic regurgitation
Three-dimensional transesophageal echocardiography identified several significant predictors of aortic regurgitation after transcatheter aortic valve replacement, according to a study published online Jan. 5 in JACC Cardiovascular Imaging.
“This is the first study to demonstrate that large prosthetic expansion, elliptical prosthetic shape, and anti-anatomical position are 3D features associated with transvalvular AR,” said Dr. Kentaro Shibayama of Cedars-Sinai Heart Institute in Los Angeles, and his associates. The study also showed that paravalvular AR was inversely related to effective area oversizing, the investigators said (JACC Cardiovasc Imag. 2016 Jan. 6).
Post-TAVR AR continues to affect substantial numbers of patients, despite progress in prosthesis design. Past research has linked paravalvular AR to prosthetic undersizing, long-axis malpositioning, and aortic annular calcification, but the causes of transvalvular AR have not been adequately studied, the researchers said. Using intraprocedural 3D transesophageal echocardiography, they imaged the native annuluses and postoperative prosthetic valves of 201 patients with severe aortic stenosis who received the Edwards SAPIEN device. The investigators also used transthoracic echocardiography to separately grade post-TAVR transvalvular and paravalvular AR as none or trivial, mild, moderate, or severe according to the 2012 Valve Academic Research Consortium criteria (J Am Coll Cardiol. 2012;60:1438-54).Fully 44% of patients developed mild or moderate aortic regurgitation after TAVR, while the rest had no or trivial AR, the investigators said. About three-quarters of AR cases were mild, nearly 25% were moderate, and none were severe. Only 3% of patients had transvalvular AR only, 34% had paravalvular AR only, and 7% had both types of AR. Patients with post-TAVR transvalvular AR had significantly more prosthetic expansion (P less than .05), a more elliptical prosthetic shape at the level of the prosthetic commissure (P less than .01), and malpositioning of the prosthetic commissures in relation to the native commissures (P less than .001), compared with patients without transvalvular AR.
Patients were more likely to have paravalvular AR if they had a lower percentage of effective area oversizing, defined as the prosthetic frame area divided by the area of the native aortic annulus (odds ratio, 0.97; 95% CI: 0.93-0.99, P less than .05). “A mismatch between a larger native aortic valve annulus area and a smaller deployed prosthesis found by intra-procedural 3D TEE may increase the risk of developing mild or greater paravalvular AR,” the researchers explained. Older age also was slightly but significantly linked with mild or moderate paravalvular AR(OR, 1.05; 95% CI, 1.01-1.09, P less than .05).
“Abnormalities related to transvalvular AR after TAVR found in this study may contribute to further deterioration of the prosthesis, warranting careful prospective studies to assess the long-term prognosis of these patients,” the investigators concluded. They cautioned that the number of patients with post-TAVR transvalvular AR was too small to carry out detailed analyses.
The researchers reported no funding sources. Senior author Dr. Takahiro Shiota reported being a speaker for Philips Ultrasound, and three of the other seven coinvestigators reported financial relationships with Edwards, Medtronic, Abbott, Capricor, St. Jude Medical, Philips Ultrasound, and Venus Medtech.
This study is important because it reinforces the important role that 3D TEE can play in procedural planning for TAVR and in predicting which patients are more likely to suffer from post-TAVR AR. It is the first study that has highlighted the practical utilization of 3D TEE in this way.
Multislice computed tomography is the preferred imaging modality for TAVR planning in many centers. However, since the imaging resolution of both techniques is similar, and they both have software capable of generating multiplane reconstructions from 3D datasets, I believe that the skill and experience of the imaging expert analyzing the datasets are more important than the modality itself, and the results from this study could probably translate to MSCT.
Although the manufacturers of TAVR valves would have us believe that the issue of postimplant AR has largely been solved by newer valve design, it still remains an important issue and will continue to be so as the technique competes with surgical alternatives. Imaging will continue to play a pivotal role in procedure planning and guidance and, as has been demonstrated by Shibayama et al., 3D TEE can be extremely useful for anticipating and potentially avoiding post-TAVR AR.
Mark Monaghan, Ph.D., is the FESC director of noninvasive cardiology at King’s College Hospital Denmark Hill in London. These comments were taken from his editorial (JACC Cardiovasc Imaging 2016 Jan. 6).
This study is important because it reinforces the important role that 3D TEE can play in procedural planning for TAVR and in predicting which patients are more likely to suffer from post-TAVR AR. It is the first study that has highlighted the practical utilization of 3D TEE in this way.
Multislice computed tomography is the preferred imaging modality for TAVR planning in many centers. However, since the imaging resolution of both techniques is similar, and they both have software capable of generating multiplane reconstructions from 3D datasets, I believe that the skill and experience of the imaging expert analyzing the datasets are more important than the modality itself, and the results from this study could probably translate to MSCT.
Although the manufacturers of TAVR valves would have us believe that the issue of postimplant AR has largely been solved by newer valve design, it still remains an important issue and will continue to be so as the technique competes with surgical alternatives. Imaging will continue to play a pivotal role in procedure planning and guidance and, as has been demonstrated by Shibayama et al., 3D TEE can be extremely useful for anticipating and potentially avoiding post-TAVR AR.
Mark Monaghan, Ph.D., is the FESC director of noninvasive cardiology at King’s College Hospital Denmark Hill in London. These comments were taken from his editorial (JACC Cardiovasc Imaging 2016 Jan. 6).
This study is important because it reinforces the important role that 3D TEE can play in procedural planning for TAVR and in predicting which patients are more likely to suffer from post-TAVR AR. It is the first study that has highlighted the practical utilization of 3D TEE in this way.
Multislice computed tomography is the preferred imaging modality for TAVR planning in many centers. However, since the imaging resolution of both techniques is similar, and they both have software capable of generating multiplane reconstructions from 3D datasets, I believe that the skill and experience of the imaging expert analyzing the datasets are more important than the modality itself, and the results from this study could probably translate to MSCT.
Although the manufacturers of TAVR valves would have us believe that the issue of postimplant AR has largely been solved by newer valve design, it still remains an important issue and will continue to be so as the technique competes with surgical alternatives. Imaging will continue to play a pivotal role in procedure planning and guidance and, as has been demonstrated by Shibayama et al., 3D TEE can be extremely useful for anticipating and potentially avoiding post-TAVR AR.
Mark Monaghan, Ph.D., is the FESC director of noninvasive cardiology at King’s College Hospital Denmark Hill in London. These comments were taken from his editorial (JACC Cardiovasc Imaging 2016 Jan. 6).
Three-dimensional transesophageal echocardiography identified several significant predictors of aortic regurgitation after transcatheter aortic valve replacement, according to a study published online Jan. 5 in JACC Cardiovascular Imaging.
“This is the first study to demonstrate that large prosthetic expansion, elliptical prosthetic shape, and anti-anatomical position are 3D features associated with transvalvular AR,” said Dr. Kentaro Shibayama of Cedars-Sinai Heart Institute in Los Angeles, and his associates. The study also showed that paravalvular AR was inversely related to effective area oversizing, the investigators said (JACC Cardiovasc Imag. 2016 Jan. 6).
Post-TAVR AR continues to affect substantial numbers of patients, despite progress in prosthesis design. Past research has linked paravalvular AR to prosthetic undersizing, long-axis malpositioning, and aortic annular calcification, but the causes of transvalvular AR have not been adequately studied, the researchers said. Using intraprocedural 3D transesophageal echocardiography, they imaged the native annuluses and postoperative prosthetic valves of 201 patients with severe aortic stenosis who received the Edwards SAPIEN device. The investigators also used transthoracic echocardiography to separately grade post-TAVR transvalvular and paravalvular AR as none or trivial, mild, moderate, or severe according to the 2012 Valve Academic Research Consortium criteria (J Am Coll Cardiol. 2012;60:1438-54).Fully 44% of patients developed mild or moderate aortic regurgitation after TAVR, while the rest had no or trivial AR, the investigators said. About three-quarters of AR cases were mild, nearly 25% were moderate, and none were severe. Only 3% of patients had transvalvular AR only, 34% had paravalvular AR only, and 7% had both types of AR. Patients with post-TAVR transvalvular AR had significantly more prosthetic expansion (P less than .05), a more elliptical prosthetic shape at the level of the prosthetic commissure (P less than .01), and malpositioning of the prosthetic commissures in relation to the native commissures (P less than .001), compared with patients without transvalvular AR.
Patients were more likely to have paravalvular AR if they had a lower percentage of effective area oversizing, defined as the prosthetic frame area divided by the area of the native aortic annulus (odds ratio, 0.97; 95% CI: 0.93-0.99, P less than .05). “A mismatch between a larger native aortic valve annulus area and a smaller deployed prosthesis found by intra-procedural 3D TEE may increase the risk of developing mild or greater paravalvular AR,” the researchers explained. Older age also was slightly but significantly linked with mild or moderate paravalvular AR(OR, 1.05; 95% CI, 1.01-1.09, P less than .05).
“Abnormalities related to transvalvular AR after TAVR found in this study may contribute to further deterioration of the prosthesis, warranting careful prospective studies to assess the long-term prognosis of these patients,” the investigators concluded. They cautioned that the number of patients with post-TAVR transvalvular AR was too small to carry out detailed analyses.
The researchers reported no funding sources. Senior author Dr. Takahiro Shiota reported being a speaker for Philips Ultrasound, and three of the other seven coinvestigators reported financial relationships with Edwards, Medtronic, Abbott, Capricor, St. Jude Medical, Philips Ultrasound, and Venus Medtech.
Three-dimensional transesophageal echocardiography identified several significant predictors of aortic regurgitation after transcatheter aortic valve replacement, according to a study published online Jan. 5 in JACC Cardiovascular Imaging.
“This is the first study to demonstrate that large prosthetic expansion, elliptical prosthetic shape, and anti-anatomical position are 3D features associated with transvalvular AR,” said Dr. Kentaro Shibayama of Cedars-Sinai Heart Institute in Los Angeles, and his associates. The study also showed that paravalvular AR was inversely related to effective area oversizing, the investigators said (JACC Cardiovasc Imag. 2016 Jan. 6).
Post-TAVR AR continues to affect substantial numbers of patients, despite progress in prosthesis design. Past research has linked paravalvular AR to prosthetic undersizing, long-axis malpositioning, and aortic annular calcification, but the causes of transvalvular AR have not been adequately studied, the researchers said. Using intraprocedural 3D transesophageal echocardiography, they imaged the native annuluses and postoperative prosthetic valves of 201 patients with severe aortic stenosis who received the Edwards SAPIEN device. The investigators also used transthoracic echocardiography to separately grade post-TAVR transvalvular and paravalvular AR as none or trivial, mild, moderate, or severe according to the 2012 Valve Academic Research Consortium criteria (J Am Coll Cardiol. 2012;60:1438-54).Fully 44% of patients developed mild or moderate aortic regurgitation after TAVR, while the rest had no or trivial AR, the investigators said. About three-quarters of AR cases were mild, nearly 25% were moderate, and none were severe. Only 3% of patients had transvalvular AR only, 34% had paravalvular AR only, and 7% had both types of AR. Patients with post-TAVR transvalvular AR had significantly more prosthetic expansion (P less than .05), a more elliptical prosthetic shape at the level of the prosthetic commissure (P less than .01), and malpositioning of the prosthetic commissures in relation to the native commissures (P less than .001), compared with patients without transvalvular AR.
Patients were more likely to have paravalvular AR if they had a lower percentage of effective area oversizing, defined as the prosthetic frame area divided by the area of the native aortic annulus (odds ratio, 0.97; 95% CI: 0.93-0.99, P less than .05). “A mismatch between a larger native aortic valve annulus area and a smaller deployed prosthesis found by intra-procedural 3D TEE may increase the risk of developing mild or greater paravalvular AR,” the researchers explained. Older age also was slightly but significantly linked with mild or moderate paravalvular AR(OR, 1.05; 95% CI, 1.01-1.09, P less than .05).
“Abnormalities related to transvalvular AR after TAVR found in this study may contribute to further deterioration of the prosthesis, warranting careful prospective studies to assess the long-term prognosis of these patients,” the investigators concluded. They cautioned that the number of patients with post-TAVR transvalvular AR was too small to carry out detailed analyses.
The researchers reported no funding sources. Senior author Dr. Takahiro Shiota reported being a speaker for Philips Ultrasound, and three of the other seven coinvestigators reported financial relationships with Edwards, Medtronic, Abbott, Capricor, St. Jude Medical, Philips Ultrasound, and Venus Medtech.
FROM JACC CARDIOVASCULAR IMAGING
Key clinical point: Three-dimensional transesophageal echocardiography identified significant predictors of aortic regurgitation after transcatheter aortic valve replacement.
Major finding: Patients with post-TAVR transvalvular AR had significantly more prosthetic expansion (P less than .05), a more elliptical prosthetic shape (P less than .01), and malpositioning of the prosthetic commissures (P less than .001) compared with patients without transvalvular AR.
Data source: A 3D TEE study of 201 patients with severe aortic stenosis who underwent TAVR with the Edwards SAPIEN device.
Disclosures: The investigators reported no funding sources. Senior author Dr. Takahiro Shiota reported being a speaker for Philips Ultrasound, and three of the other seven coinvestigators reported financial relationships with Edwards, Medtronic, Abbott, Capricor, St. Jude Medical, Philips Ultrasound, and Venus Medtech.
Gun safety: HIPAA change allows providers to report on some mentally ill patients
As part of the Obama administration’s efforts to reduce gun violence, physicians and certain other health care providers will be permitted to disclose to the National Instant Criminal Background Check System (NICS) the identities of mentally ill patients who could be a danger to themselves or others.
NICS is the federal system by which firearms sellers determine whether a potential buyer has a criminal record or is otherwise ineligible to purchase firearms.

The change – a modification to the HIPAA Privacy Rule – was published in the Federal Register on Jan. 5, the same day President Obama announced new executive actions that aim to expand background checks for firearm purchases and increase federal enforcement of gun laws.
The HIPAA modification, which takes effect in February, makes clear that certain covered entities are permitted to disclose information to the NICS, including the minimum identifying information necessary about patients who have been involuntarily committed to a mental institution or who have otherwise been determined by a lawful authority to be a danger to themselves or others.
The modification is tailored to preserve the patient-provider relationship and ensure that patients are not discouraged from seeking voluntary treatment, according to officials at the U.S. Department of Health & Human Services.
The rule applies only to a small subset of HIPAA-covered entities that either make mental health determinations that disqualify patients from having firearms or are designated by states to report the information to NICS. The modification does not apply to most treating health providers and does not permit reporting of diagnostic, clinical, or other mental health treatment information.
The scope of disclosed information under the final rule is quite limited, according to Gerald “Jud” E. DeLoss, a Chicago health law attorney and cybersecurity expert. Disclosure is restricted to limited demographic data and other information. In addition, state statutes or regulations regarding mental health information disclosure that are more stringent than HIPAA would still apply regardless of the final rule, he added.
“Further, while the final rule would apply to mental health information, substance abuse treatment information held by a federally assisted program covered under the confidentiality regulations set forth under 42 CFR Part 2 would still be protected,” Mr. DeLoss said in an interview.
The HIPAA change finalizes a 2014 proposed rule that was recommended as part of President Obama’s plan to strengthen the national background check system and remove unnecessary legal barriers that prevent states from making data available to the background check system.
“Due to a history of underreporting, the NICS has lacked complete information about all individuals who are prohibited by federal law from possessing or receiving a firearm,” Jocelyn Samuels, director of the HHS Office for Civil Rights, wrote in a blog post. “The modification announced today better enables the reporting of the identities of prohibited individuals to the background check system and is an important step toward improving the public’s safety while continuing to strongly protect individuals’ privacy interests.”

Psychiatrist Dr. Daniel J. Carlat of Tufts University, Boston, said that he does not see the new rule posing a major threat to patient confidentiality.
“HIPAA already allows us to share clinical information with law enforcement under certain circumstances where a patient is thought to pose some type of danger,” Dr. Carlat said in an interview. “This new rule adds another limited instance to that list. This is certainly something that we would want to add to the HIPAA Privacy notices that we show our patients so that they are fully aware of this potential breach of confidentiality.”
Dr. Jane M. Orient, executive director of Association of American Physicians and Surgeons, said that she disagrees. She believes the modification will be harmful to both doctors and patients.
“My impression is that this supposedly narrow intrusion will get wider and wider, and will inevitably damage the patient-physician relationship,” she said in an interview. “If a person has been adjudicated by law to be ineligible to possess a firearm, then the legal authority should report. The NICS is not going to do much good anyway – if a person is an imminent danger, he needs to be restrained, not put into a database.”
In addition to the HIPAA rule change, President Obama unveiled several other initiatives to combat gun violence and asked Congress for $500 million to increase mental health care service capacity and the behavioral health workforce.
The President outlined stronger efforts by federal agencies to monitor and prevent illegal gun sales. This includes an overhaul of NICS and the hiring of 230 additional FBI examiners to process background checks. The President’s budget for fiscal 2017 will include funding for 200 new Bureau of Alcohol, Tobacco, Firearms and Explosives (ATF) agents and investigators. The ATF plans to dedicate $4 million and additional personnel to enhance the National Integrated Ballistics Information Network (NIBIN), a database that links violent crimes across jurisdictions.
Physician associations praised President Obama’s efforts to reduce gun violence and improve public safety.
“Gun violence is a public health threat to children, and like any epidemic, it can be prevented with the right interventions,” Dr. Benard Dreyer, president of the American Academy of Pediatrics, said in a statement. “Preventing gun violence is complicated, but achievable, and President Obama’s new executive actions are a welcome and needed first step in an environment where we have yet to see the enactment of commonsense federal gun violence prevention legislation.”
Dr. Renée Binder, president of the American Psychiatric Association, said the announcement highlights needed investments in mental health and necessary efforts to curb the epidemic of gun violence.
“Gun violence is a public health problem and needs to be addressed as such,” Dr. Binder said in a statement. “We support the president’s efforts to expand background checks, propose policies that respect physician-patient confidentiality, and increase funding for mental health services by $500 million. We will work with Congress to make that funding proposal a reality, as we also work with allies in Congress who are championing comprehensive mental health reform.”
On Twitter @legal_med
As part of the Obama administration’s efforts to reduce gun violence, physicians and certain other health care providers will be permitted to disclose to the National Instant Criminal Background Check System (NICS) the identities of mentally ill patients who could be a danger to themselves or others.
NICS is the federal system by which firearms sellers determine whether a potential buyer has a criminal record or is otherwise ineligible to purchase firearms.
The change – a modification to the HIPAA Privacy Rule – was published in the Federal Register on Jan. 5, the same day President Obama announced new executive actions that aim to expand background checks for firearm purchases and increase federal enforcement of gun laws.
The HIPAA modification, which takes effect in February, makes clear that certain covered entities are permitted to disclose information to the NICS, including the minimum identifying information necessary about patients who have been involuntarily committed to a mental institution or who have otherwise been determined by a lawful authority to be a danger to themselves or others.
The modification is tailored to preserve the patient-provider relationship and ensure that patients are not discouraged from seeking voluntary treatment, according to officials at the U.S. Department of Health & Human Services.
The rule applies only to a small subset of HIPAA-covered entities that either make mental health determinations that disqualify patients from having firearms or are designated by states to report the information to NICS. The modification does not apply to most treating health providers and does not permit reporting of diagnostic, clinical, or other mental health treatment information.
The scope of disclosed information under the final rule is quite limited, according to Gerald “Jud” E. DeLoss, a Chicago health law attorney and cybersecurity expert. Disclosure is restricted to limited demographic data and other information. In addition, state statutes or regulations regarding mental health information disclosure that are more stringent than HIPAA would still apply regardless of the final rule, he added.
“Further, while the final rule would apply to mental health information, substance abuse treatment information held by a federally assisted program covered under the confidentiality regulations set forth under 42 CFR Part 2 would still be protected,” Mr. DeLoss said in an interview.
The HIPAA change finalizes a 2014 proposed rule that was recommended as part of President Obama’s plan to strengthen the national background check system and remove unnecessary legal barriers that prevent states from making data available to the background check system.
“Due to a history of underreporting, the NICS has lacked complete information about all individuals who are prohibited by federal law from possessing or receiving a firearm,” Jocelyn Samuels, director of the HHS Office for Civil Rights, wrote in a blog post. “The modification announced today better enables the reporting of the identities of prohibited individuals to the background check system and is an important step toward improving the public’s safety while continuing to strongly protect individuals’ privacy interests.”
Psychiatrist Dr. Daniel J. Carlat of Tufts University, Boston, said that he does not see the new rule posing a major threat to patient confidentiality.
“HIPAA already allows us to share clinical information with law enforcement under certain circumstances where a patient is thought to pose some type of danger,” Dr. Carlat said in an interview. “This new rule adds another limited instance to that list. This is certainly something that we would want to add to the HIPAA Privacy notices that we show our patients so that they are fully aware of this potential breach of confidentiality.”
Dr. Jane M. Orient, executive director of Association of American Physicians and Surgeons, said that she disagrees. She believes the modification will be harmful to both doctors and patients.
“My impression is that this supposedly narrow intrusion will get wider and wider, and will inevitably damage the patient-physician relationship,” she said in an interview. “If a person has been adjudicated by law to be ineligible to possess a firearm, then the legal authority should report. The NICS is not going to do much good anyway – if a person is an imminent danger, he needs to be restrained, not put into a database.”
In addition to the HIPAA rule change, President Obama unveiled several other initiatives to combat gun violence and asked Congress for $500 million to increase mental health care service capacity and the behavioral health workforce.
The President outlined stronger efforts by federal agencies to monitor and prevent illegal gun sales. This includes an overhaul of NICS and the hiring of 230 additional FBI examiners to process background checks. The President’s budget for fiscal 2017 will include funding for 200 new Bureau of Alcohol, Tobacco, Firearms and Explosives (ATF) agents and investigators. The ATF plans to dedicate $4 million and additional personnel to enhance the National Integrated Ballistics Information Network (NIBIN), a database that links violent crimes across jurisdictions.
Physician associations praised President Obama’s efforts to reduce gun violence and improve public safety.
“Gun violence is a public health threat to children, and like any epidemic, it can be prevented with the right interventions,” Dr. Benard Dreyer, president of the American Academy of Pediatrics, said in a statement. “Preventing gun violence is complicated, but achievable, and President Obama’s new executive actions are a welcome and needed first step in an environment where we have yet to see the enactment of commonsense federal gun violence prevention legislation.”
Dr. Renée Binder, president of the American Psychiatric Association, said the announcement highlights needed investments in mental health and necessary efforts to curb the epidemic of gun violence.
“Gun violence is a public health problem and needs to be addressed as such,” Dr. Binder said in a statement. “We support the president’s efforts to expand background checks, propose policies that respect physician-patient confidentiality, and increase funding for mental health services by $500 million. We will work with Congress to make that funding proposal a reality, as we also work with allies in Congress who are championing comprehensive mental health reform.”
On Twitter @legal_med
As part of the Obama administration’s efforts to reduce gun violence, physicians and certain other health care providers will be permitted to disclose to the National Instant Criminal Background Check System (NICS) the identities of mentally ill patients who could be a danger to themselves or others.
NICS is the federal system by which firearms sellers determine whether a potential buyer has a criminal record or is otherwise ineligible to purchase firearms.
The change – a modification to the HIPAA Privacy Rule – was published in the Federal Register on Jan. 5, the same day President Obama announced new executive actions that aim to expand background checks for firearm purchases and increase federal enforcement of gun laws.
The HIPAA modification, which takes effect in February, makes clear that certain covered entities are permitted to disclose information to the NICS, including the minimum identifying information necessary about patients who have been involuntarily committed to a mental institution or who have otherwise been determined by a lawful authority to be a danger to themselves or others.
The modification is tailored to preserve the patient-provider relationship and ensure that patients are not discouraged from seeking voluntary treatment, according to officials at the U.S. Department of Health & Human Services.
The rule applies only to a small subset of HIPAA-covered entities that either make mental health determinations that disqualify patients from having firearms or are designated by states to report the information to NICS. The modification does not apply to most treating health providers and does not permit reporting of diagnostic, clinical, or other mental health treatment information.
The scope of disclosed information under the final rule is quite limited, according to Gerald “Jud” E. DeLoss, a Chicago health law attorney and cybersecurity expert. Disclosure is restricted to limited demographic data and other information. In addition, state statutes or regulations regarding mental health information disclosure that are more stringent than HIPAA would still apply regardless of the final rule, he added.
“Further, while the final rule would apply to mental health information, substance abuse treatment information held by a federally assisted program covered under the confidentiality regulations set forth under 42 CFR Part 2 would still be protected,” Mr. DeLoss said in an interview.
The HIPAA change finalizes a 2014 proposed rule that was recommended as part of President Obama’s plan to strengthen the national background check system and remove unnecessary legal barriers that prevent states from making data available to the background check system.
“Due to a history of underreporting, the NICS has lacked complete information about all individuals who are prohibited by federal law from possessing or receiving a firearm,” Jocelyn Samuels, director of the HHS Office for Civil Rights, wrote in a blog post. “The modification announced today better enables the reporting of the identities of prohibited individuals to the background check system and is an important step toward improving the public’s safety while continuing to strongly protect individuals’ privacy interests.”
Psychiatrist Dr. Daniel J. Carlat of Tufts University, Boston, said that he does not see the new rule posing a major threat to patient confidentiality.
“HIPAA already allows us to share clinical information with law enforcement under certain circumstances where a patient is thought to pose some type of danger,” Dr. Carlat said in an interview. “This new rule adds another limited instance to that list. This is certainly something that we would want to add to the HIPAA Privacy notices that we show our patients so that they are fully aware of this potential breach of confidentiality.”
Dr. Jane M. Orient, executive director of Association of American Physicians and Surgeons, said that she disagrees. She believes the modification will be harmful to both doctors and patients.
“My impression is that this supposedly narrow intrusion will get wider and wider, and will inevitably damage the patient-physician relationship,” she said in an interview. “If a person has been adjudicated by law to be ineligible to possess a firearm, then the legal authority should report. The NICS is not going to do much good anyway – if a person is an imminent danger, he needs to be restrained, not put into a database.”
In addition to the HIPAA rule change, President Obama unveiled several other initiatives to combat gun violence and asked Congress for $500 million to increase mental health care service capacity and the behavioral health workforce.
The President outlined stronger efforts by federal agencies to monitor and prevent illegal gun sales. This includes an overhaul of NICS and the hiring of 230 additional FBI examiners to process background checks. The President’s budget for fiscal 2017 will include funding for 200 new Bureau of Alcohol, Tobacco, Firearms and Explosives (ATF) agents and investigators. The ATF plans to dedicate $4 million and additional personnel to enhance the National Integrated Ballistics Information Network (NIBIN), a database that links violent crimes across jurisdictions.
Physician associations praised President Obama’s efforts to reduce gun violence and improve public safety.
“Gun violence is a public health threat to children, and like any epidemic, it can be prevented with the right interventions,” Dr. Benard Dreyer, president of the American Academy of Pediatrics, said in a statement. “Preventing gun violence is complicated, but achievable, and President Obama’s new executive actions are a welcome and needed first step in an environment where we have yet to see the enactment of commonsense federal gun violence prevention legislation.”
Dr. Renée Binder, president of the American Psychiatric Association, said the announcement highlights needed investments in mental health and necessary efforts to curb the epidemic of gun violence.
“Gun violence is a public health problem and needs to be addressed as such,” Dr. Binder said in a statement. “We support the president’s efforts to expand background checks, propose policies that respect physician-patient confidentiality, and increase funding for mental health services by $500 million. We will work with Congress to make that funding proposal a reality, as we also work with allies in Congress who are championing comprehensive mental health reform.”
On Twitter @legal_med

Point/Counterpoint: Self-employed community practice is still a viable proposition
YES
The recent 2-year bipartisan budget deal signed by President Obama and sent up by Congress brought the hammer down on hospitals so quickly that they did not see it coming. It is highly unusual for Congress to keep anything secreted from the American Hospital Association (AHA) lobby. The AHA spent $4.6 million in the first quarter of 2015 for an annual estimated expenditure of about $18 million. This does not include dollars spent by local and state hospital associations. The SVS is clearly dwarfed by these powerful interests. Our society spent less than $100,000 in that same quarter on advocating for over 4,000 members, the majority of whom are United States residents and most of whom depend solely on the SVS to look out for them.
As a result of the budget deal, Medicare will not pay most hospital-owned physician practices higher rates than those of independently owned practices. The reimbursement changes will apply to those hospital-owned physician practices acquired or opened since the date the law was signed and also located farther than 250 yards from a hospital’s main campus. It does grandfather in facilities prior to the signing that were being reimbursed with hospital outpatient department (HOPD) rates. The savings will prevent an increase in premiums for about 15 million Medicare beneficiaries. The AHA expressed its outrage while the AARP celebrated. So did independent physicians who have been protesting all along that costs were rising because of excessive payments to hospitals for essentially the same services.
Margot Sanger-Katz, in a column for “The Upshot” in the New York Times, wrote that it had been estimated that correcting this payment differential would save Medicare $30 billion over 10 years, more than Medicare could save if it raised the Medicare eligibility age to 67!1 She also pointed out that the Medicare Payment Advisory Committee (MedPAC), an independent group that advises Congress, thinks “that the pay differences should be narrowed, but only for a select set of medical services in which it’s really clear that there’s no difference between the care offered by a hospital and a physician office.”

The rush to buy physician practices is being done for many reasons but the disparate payment schedule favoring hospital-owned practices for many of the same services is one reason. The hospital brings in a lot more revenue through its hired physicians providing the same service in their offices that are now under the banner of the health system. The hospitals cite several justifications for the “surcharge” on care provided by employed physicians in hospital facilities, some of which may be valid. Regulatory requirements, sicker inpatients, increased cost due to training programs, and being required to support money-losing services such as burn care are some reasons. But, independent physicians say they provide the same or better quality care at a lower cost without resources such as legal, accounting, self-insurance against professional liability, and robust lobbying firms.
Hospitals have also contended that vertical integration by buying physician practices should lead to lower health care costs by squeezing efficiencies within the system. There have been conflicting reports on whether physician hospital integration leads to lower health care expenditures.2 The public debate has caught the attention of government regulators. In the recent case of Saint Lukes-Saltzer, the question before the Federal Trade Commission (the agency responsible for federal antitrust action) was: Did total medical expenditures increase or decrease for patients cared for by physician practices acquired by St. Luke’s? Indeed, the conclusions were that not only did overall costs not go down but evidence showed that the merger may have resulted in increased costs.
On appeal, the Ninth Circuit Court ruled that any future efficiency must be “substantial, verifiable and specific” to the merger. Ciliberto and Dranove looked at hospital prices after physician hospital affiliations in California and found no evidence of increase in prices.3 Baker and coauthors analyzed privately insured patients between 2001 and 2007 and the effect of physician hospital integration on hospital prices, admission volumes, and spending.4 They reported higher hospital prices and spending in hospitals with the tightest vertically integrated relationship with physicians. In one of the few studies of the issue, Capps and colleagues reviewed 7 years of administrative data from multiple insurers across the United States to estimate postintegration costs. From 2007 to 2013, they found that there was a 57% increase in the share of spending by physicians whose practices are owned by hospitals. In addition, this led to an increase in physician prices of 14% post integration.5 The larger the market share of inpatients by a hospital the larger the price increase. The authors estimate that about 25% of the price increases are precisely due to “exploitation of reimbursement rules” by charging the facility fees for their employed physicians. If these “surcharges” led to decreased utilization as one measure of increased efficiency and therefore reduced overall health care costs, it would be acceptable. But, Capps et al. found no such evidence and speculate that this scenario could lead to higher expenditures.
In a recent study, total expenditures for over 4 million patients by private physician groups or integrated groups covered by health maintenance organizations (HMOs) in California between 2009 and 2012 were analyzed.6 Mean annual expenditures were highest for large multihospital systems followed by hospital-owned physician groups and, lastly, physician-owned groups. The expenditures for multihospital systems were 19.8% higher and for local hospital-employed physician groups 10% higher compared to physician-owned organizations.
Why should prices increase after tighter physician hospital integration on a large scale? Market power. Once health systems have a large enough number of physicians in their panel, hospitals could charge insurers higher prices to access their specialists. Similarly, by employing a large number of physicians in a particular specialty, which then attracts a large pool of patients with a particular illness, they could dominate the other health systems in the region. One action specifically forbidden by anti-kickback laws is compensating physicians based on the number of referrals they make to the hospital. But, there are enough loopholes that allow hospitals to indirectly tie compensation to “productivity.” This may change with bundled payments or compensation tied to “value,” although there will always be incentives for work volume to some degree.
A further roadblock for basing merger decisions entirely on possible efficiencies is how the courts will see these activities in terms of antitrust actions. Most arguments using efficiency as the basis for merging physician groups with hospitals are vague and in general courts have not superseded antitrust actions with economic efficiency arguments.
What should be genuine reasons for hospitals employing and aligning with physicians? Addressing uneven quality of care, access and, of course, ever spiraling costs. If the object was to share responsibility for attacking these problems, health care systems and physicians would be cut a lot of slack. But, some health care systems want to not only survive the existing chaos but also dominate their local market.
I guess health care is really no different from Wall Street corporations in its focus on short-term gains versus long-term benefits. Until broader incentives change, health systems will continue to look to survive and gain market share and power. Competition, in isolation, drives tactics where the only objective may be to increase market share. However, it appears that the FTC will be busy wielding the Sherman Act of the antitrust law to keep a check on health systems to ensure consumers, payers, physicians, and the country at large are all on a fair playing field.7
Dr. Satiani is professor of clinical surgery, division of vascular diseases & surgery, department of surgery, associate director, FAME; director, Faculty Leadership Institute, and medical director, Vascular Labs, at Ohio State University College of Medicine, Columbus. He is also an associate medical editor for Vascular Specialist.
References
2. Journal of Health Economics 2006; 25: 1-28.
3. Journal of Health Economics 2006; 25: 29-38.
4. Health Affairs 2014; 33(5): 756-63.
5. www.ipr.northwestern.edu/publications/docs/workingpapers/2015/IPR-WP-15-02.pdf
6. JAMA. 2014; 312(16):1663-9.
7. Plastic & Reconstructive Surgery. 2006; 117(3): 1012-22.
NO
The days of hanging one’s shingle on a door and starting a self-employed practice are rapidly fading. While some fondly remember the practice of medicine as it was in Norman Rockwell’s classic “Before the Shot,” the realities of a current practice couldn’t be more different. Reusable syringes, analog weighing stations, an unaccompanied minor, and lack of regard for universal precautions are just a few examples from that painting that have long since disappeared. However, the humor in this painting comes from the young boy scrutinizing the doctor’s credentials, implying a sense of distrust and fear as he stands there with his buttocks partially exposed waiting for the vaccination.
This scrutiny of physician performance and results is more relevant today than ever before. Perhaps if we were to update the painting today, it would depict the boy furiously tapping away at his tablet searching through ProPublica to see what the doctor’s complication rate with the intended procedure truly is.

This is just one of the many pressures physicians are facing today. Navigating the publicly reported complication data is but one tiny portion of the regulatory red tape physicians face in taking care of their patients. If you add in the need to negotiate and contact with insurers, manage an office staff, acquire and maintain an electronic medical record (EMR) while ensuring that your EMR is properly secured against potential cyber threats and compliant with meaningful use regulations, audit your billing and coding, keep up to date with upcoming changes to bundled payments, mail out and track Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), as well as an endless list of other requirements, it is no wonder physicians are less willing to take these challenges on as solo practitioners. In fact, based on Medscape’s 2014 Employed Doctors Report, which compiled responses from over 4,600 physicians, the top three reasons for being an employed physician were not having to deal with the business of running an office (58%), not having to deal with insurers and billing (45%), and guaranteed income/even cash flow (42%).1
Multiple sources continue to confirm the trend that more physicians are moving to an employed practice.2-4 In the last decade, the rate of hospital employment has increased from 11% to 64%.1 There are many factors that have pushed physicians away from self-employment. Some of these are related to physicians’ personal choices, and many are from external pressures. As various parts of the Affordable Care Act come into play, there will continue to be increasing regulatory demands. These have the potential of increasing overhead costs, and, coupled with decreasing reimbursement, will inevitably make staying profitable more challenging in a self-employed model.
There are two other very telling trends that foretell the inevitable decline of self-employed physicians. Fewer and fewer new graduates are reporting that they are self employed. In the most recent surveys, twice as many physicians under the age of 40 are employed than self-employed.1 Furthermore, 92% of residents surveyed in their final year would prefer employment with a salary, and only 2% would consider solo practice.5 Of these graduating residents, 36% specifically were considering hospital employment, which is nearly a 10-fold increase from a decade ago. The second factor affecting new hires is their confidence that they have the necessary skills to manage a self-employed model. During the same decade, there was only a small increase in graduating residents who felt very prepared to deal with the business side of medicine (10% vs. 2%).5 This lack of knowledge will undoubtedly make it difficult for those who would consider self-employment to feel comfortable in that practice model. Some have speculated that there is soon to be a “push back” from the physicians and specifically from specialists who don’t have as much to gain in large group practices. With so few graduates considering solo and small group practice, and the overwhelming majority not feeling very prepared to manage the business of medicine, who can help lead this trend reversal?
Not only are fewer new graduates choosing self-employment, but fewer opportunities for self-employment are available as more physician groups are being bought by hospitals or other large group practices. Specifically with vascular surgery, there is a significant overhead cost requirement. Advantages to joining a large group practice include better ability to negotiate cost savings with the frequent capital requirements for new equipment, updates and maintenance of the electronic records, and professional liability. In fact, one study in California shows that as the proportion of physicians employed by the health system increased, supply chain expenses and inventory costs improved.6 Furthermore, hospitals have administrators who are hired to negotiate with insurers regarding reimbursement and respond to audits and other regulatory changes. As mentioned above, the top two reasons for avoiding self-employment are precisely these. This will no doubt draw even more physicians and specifically vascular surgeons into employed models.
Dr. Haurani is assistant professor of surgery in the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
References
1. www.medscape.com/features/slideshow/public/employed-doctors#1
3.Perspect Vasc Surg Endovasc Ther. 2013;25:46-52.
4 Tenn Med. 2012;105:38-39.
5.www.merritthawkins.com/uploadedFiles/MerrittHawkings/Surveys/2014_MerrittHawkins_FYMR_Survey.pdf.
6. Health Care Manage Rev. 2015 Jul 23. [Epub ahead of print] www.ncbi.nlm.nih.gov/pubmed/26207654
YES
The recent 2-year bipartisan budget deal signed by President Obama and sent up by Congress brought the hammer down on hospitals so quickly that they did not see it coming. It is highly unusual for Congress to keep anything secreted from the American Hospital Association (AHA) lobby. The AHA spent $4.6 million in the first quarter of 2015 for an annual estimated expenditure of about $18 million. This does not include dollars spent by local and state hospital associations. The SVS is clearly dwarfed by these powerful interests. Our society spent less than $100,000 in that same quarter on advocating for over 4,000 members, the majority of whom are United States residents and most of whom depend solely on the SVS to look out for them.
As a result of the budget deal, Medicare will not pay most hospital-owned physician practices higher rates than those of independently owned practices. The reimbursement changes will apply to those hospital-owned physician practices acquired or opened since the date the law was signed and also located farther than 250 yards from a hospital’s main campus. It does grandfather in facilities prior to the signing that were being reimbursed with hospital outpatient department (HOPD) rates. The savings will prevent an increase in premiums for about 15 million Medicare beneficiaries. The AHA expressed its outrage while the AARP celebrated. So did independent physicians who have been protesting all along that costs were rising because of excessive payments to hospitals for essentially the same services.
Margot Sanger-Katz, in a column for “The Upshot” in the New York Times, wrote that it had been estimated that correcting this payment differential would save Medicare $30 billion over 10 years, more than Medicare could save if it raised the Medicare eligibility age to 67!1 She also pointed out that the Medicare Payment Advisory Committee (MedPAC), an independent group that advises Congress, thinks “that the pay differences should be narrowed, but only for a select set of medical services in which it’s really clear that there’s no difference between the care offered by a hospital and a physician office.”
The rush to buy physician practices is being done for many reasons but the disparate payment schedule favoring hospital-owned practices for many of the same services is one reason. The hospital brings in a lot more revenue through its hired physicians providing the same service in their offices that are now under the banner of the health system. The hospitals cite several justifications for the “surcharge” on care provided by employed physicians in hospital facilities, some of which may be valid. Regulatory requirements, sicker inpatients, increased cost due to training programs, and being required to support money-losing services such as burn care are some reasons. But, independent physicians say they provide the same or better quality care at a lower cost without resources such as legal, accounting, self-insurance against professional liability, and robust lobbying firms.
Hospitals have also contended that vertical integration by buying physician practices should lead to lower health care costs by squeezing efficiencies within the system. There have been conflicting reports on whether physician hospital integration leads to lower health care expenditures.2 The public debate has caught the attention of government regulators. In the recent case of Saint Lukes-Saltzer, the question before the Federal Trade Commission (the agency responsible for federal antitrust action) was: Did total medical expenditures increase or decrease for patients cared for by physician practices acquired by St. Luke’s? Indeed, the conclusions were that not only did overall costs not go down but evidence showed that the merger may have resulted in increased costs.
On appeal, the Ninth Circuit Court ruled that any future efficiency must be “substantial, verifiable and specific” to the merger. Ciliberto and Dranove looked at hospital prices after physician hospital affiliations in California and found no evidence of increase in prices.3 Baker and coauthors analyzed privately insured patients between 2001 and 2007 and the effect of physician hospital integration on hospital prices, admission volumes, and spending.4 They reported higher hospital prices and spending in hospitals with the tightest vertically integrated relationship with physicians. In one of the few studies of the issue, Capps and colleagues reviewed 7 years of administrative data from multiple insurers across the United States to estimate postintegration costs. From 2007 to 2013, they found that there was a 57% increase in the share of spending by physicians whose practices are owned by hospitals. In addition, this led to an increase in physician prices of 14% post integration.5 The larger the market share of inpatients by a hospital the larger the price increase. The authors estimate that about 25% of the price increases are precisely due to “exploitation of reimbursement rules” by charging the facility fees for their employed physicians. If these “surcharges” led to decreased utilization as one measure of increased efficiency and therefore reduced overall health care costs, it would be acceptable. But, Capps et al. found no such evidence and speculate that this scenario could lead to higher expenditures.
In a recent study, total expenditures for over 4 million patients by private physician groups or integrated groups covered by health maintenance organizations (HMOs) in California between 2009 and 2012 were analyzed.6 Mean annual expenditures were highest for large multihospital systems followed by hospital-owned physician groups and, lastly, physician-owned groups. The expenditures for multihospital systems were 19.8% higher and for local hospital-employed physician groups 10% higher compared to physician-owned organizations.
Why should prices increase after tighter physician hospital integration on a large scale? Market power. Once health systems have a large enough number of physicians in their panel, hospitals could charge insurers higher prices to access their specialists. Similarly, by employing a large number of physicians in a particular specialty, which then attracts a large pool of patients with a particular illness, they could dominate the other health systems in the region. One action specifically forbidden by anti-kickback laws is compensating physicians based on the number of referrals they make to the hospital. But, there are enough loopholes that allow hospitals to indirectly tie compensation to “productivity.” This may change with bundled payments or compensation tied to “value,” although there will always be incentives for work volume to some degree.
A further roadblock for basing merger decisions entirely on possible efficiencies is how the courts will see these activities in terms of antitrust actions. Most arguments using efficiency as the basis for merging physician groups with hospitals are vague and in general courts have not superseded antitrust actions with economic efficiency arguments.
What should be genuine reasons for hospitals employing and aligning with physicians? Addressing uneven quality of care, access and, of course, ever spiraling costs. If the object was to share responsibility for attacking these problems, health care systems and physicians would be cut a lot of slack. But, some health care systems want to not only survive the existing chaos but also dominate their local market.
I guess health care is really no different from Wall Street corporations in its focus on short-term gains versus long-term benefits. Until broader incentives change, health systems will continue to look to survive and gain market share and power. Competition, in isolation, drives tactics where the only objective may be to increase market share. However, it appears that the FTC will be busy wielding the Sherman Act of the antitrust law to keep a check on health systems to ensure consumers, payers, physicians, and the country at large are all on a fair playing field.7
Dr. Satiani is professor of clinical surgery, division of vascular diseases & surgery, department of surgery, associate director, FAME; director, Faculty Leadership Institute, and medical director, Vascular Labs, at Ohio State University College of Medicine, Columbus. He is also an associate medical editor for Vascular Specialist.
References
2. Journal of Health Economics 2006; 25: 1-28.
3. Journal of Health Economics 2006; 25: 29-38.
4. Health Affairs 2014; 33(5): 756-63.
5. www.ipr.northwestern.edu/publications/docs/workingpapers/2015/IPR-WP-15-02.pdf
6. JAMA. 2014; 312(16):1663-9.
7. Plastic & Reconstructive Surgery. 2006; 117(3): 1012-22.
NO
The days of hanging one’s shingle on a door and starting a self-employed practice are rapidly fading. While some fondly remember the practice of medicine as it was in Norman Rockwell’s classic “Before the Shot,” the realities of a current practice couldn’t be more different. Reusable syringes, analog weighing stations, an unaccompanied minor, and lack of regard for universal precautions are just a few examples from that painting that have long since disappeared. However, the humor in this painting comes from the young boy scrutinizing the doctor’s credentials, implying a sense of distrust and fear as he stands there with his buttocks partially exposed waiting for the vaccination.
This scrutiny of physician performance and results is more relevant today than ever before. Perhaps if we were to update the painting today, it would depict the boy furiously tapping away at his tablet searching through ProPublica to see what the doctor’s complication rate with the intended procedure truly is.
This is just one of the many pressures physicians are facing today. Navigating the publicly reported complication data is but one tiny portion of the regulatory red tape physicians face in taking care of their patients. If you add in the need to negotiate and contact with insurers, manage an office staff, acquire and maintain an electronic medical record (EMR) while ensuring that your EMR is properly secured against potential cyber threats and compliant with meaningful use regulations, audit your billing and coding, keep up to date with upcoming changes to bundled payments, mail out and track Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), as well as an endless list of other requirements, it is no wonder physicians are less willing to take these challenges on as solo practitioners. In fact, based on Medscape’s 2014 Employed Doctors Report, which compiled responses from over 4,600 physicians, the top three reasons for being an employed physician were not having to deal with the business of running an office (58%), not having to deal with insurers and billing (45%), and guaranteed income/even cash flow (42%).1
Multiple sources continue to confirm the trend that more physicians are moving to an employed practice.2-4 In the last decade, the rate of hospital employment has increased from 11% to 64%.1 There are many factors that have pushed physicians away from self-employment. Some of these are related to physicians’ personal choices, and many are from external pressures. As various parts of the Affordable Care Act come into play, there will continue to be increasing regulatory demands. These have the potential of increasing overhead costs, and, coupled with decreasing reimbursement, will inevitably make staying profitable more challenging in a self-employed model.
There are two other very telling trends that foretell the inevitable decline of self-employed physicians. Fewer and fewer new graduates are reporting that they are self employed. In the most recent surveys, twice as many physicians under the age of 40 are employed than self-employed.1 Furthermore, 92% of residents surveyed in their final year would prefer employment with a salary, and only 2% would consider solo practice.5 Of these graduating residents, 36% specifically were considering hospital employment, which is nearly a 10-fold increase from a decade ago. The second factor affecting new hires is their confidence that they have the necessary skills to manage a self-employed model. During the same decade, there was only a small increase in graduating residents who felt very prepared to deal with the business side of medicine (10% vs. 2%).5 This lack of knowledge will undoubtedly make it difficult for those who would consider self-employment to feel comfortable in that practice model. Some have speculated that there is soon to be a “push back” from the physicians and specifically from specialists who don’t have as much to gain in large group practices. With so few graduates considering solo and small group practice, and the overwhelming majority not feeling very prepared to manage the business of medicine, who can help lead this trend reversal?
Not only are fewer new graduates choosing self-employment, but fewer opportunities for self-employment are available as more physician groups are being bought by hospitals or other large group practices. Specifically with vascular surgery, there is a significant overhead cost requirement. Advantages to joining a large group practice include better ability to negotiate cost savings with the frequent capital requirements for new equipment, updates and maintenance of the electronic records, and professional liability. In fact, one study in California shows that as the proportion of physicians employed by the health system increased, supply chain expenses and inventory costs improved.6 Furthermore, hospitals have administrators who are hired to negotiate with insurers regarding reimbursement and respond to audits and other regulatory changes. As mentioned above, the top two reasons for avoiding self-employment are precisely these. This will no doubt draw even more physicians and specifically vascular surgeons into employed models.
Dr. Haurani is assistant professor of surgery in the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
References
1. www.medscape.com/features/slideshow/public/employed-doctors#1
3.Perspect Vasc Surg Endovasc Ther. 2013;25:46-52.
4 Tenn Med. 2012;105:38-39.
5.www.merritthawkins.com/uploadedFiles/MerrittHawkings/Surveys/2014_MerrittHawkins_FYMR_Survey.pdf.
6. Health Care Manage Rev. 2015 Jul 23. [Epub ahead of print] www.ncbi.nlm.nih.gov/pubmed/26207654
YES
The recent 2-year bipartisan budget deal signed by President Obama and sent up by Congress brought the hammer down on hospitals so quickly that they did not see it coming. It is highly unusual for Congress to keep anything secreted from the American Hospital Association (AHA) lobby. The AHA spent $4.6 million in the first quarter of 2015 for an annual estimated expenditure of about $18 million. This does not include dollars spent by local and state hospital associations. The SVS is clearly dwarfed by these powerful interests. Our society spent less than $100,000 in that same quarter on advocating for over 4,000 members, the majority of whom are United States residents and most of whom depend solely on the SVS to look out for them.
As a result of the budget deal, Medicare will not pay most hospital-owned physician practices higher rates than those of independently owned practices. The reimbursement changes will apply to those hospital-owned physician practices acquired or opened since the date the law was signed and also located farther than 250 yards from a hospital’s main campus. It does grandfather in facilities prior to the signing that were being reimbursed with hospital outpatient department (HOPD) rates. The savings will prevent an increase in premiums for about 15 million Medicare beneficiaries. The AHA expressed its outrage while the AARP celebrated. So did independent physicians who have been protesting all along that costs were rising because of excessive payments to hospitals for essentially the same services.
Margot Sanger-Katz, in a column for “The Upshot” in the New York Times, wrote that it had been estimated that correcting this payment differential would save Medicare $30 billion over 10 years, more than Medicare could save if it raised the Medicare eligibility age to 67!1 She also pointed out that the Medicare Payment Advisory Committee (MedPAC), an independent group that advises Congress, thinks “that the pay differences should be narrowed, but only for a select set of medical services in which it’s really clear that there’s no difference between the care offered by a hospital and a physician office.”
The rush to buy physician practices is being done for many reasons but the disparate payment schedule favoring hospital-owned practices for many of the same services is one reason. The hospital brings in a lot more revenue through its hired physicians providing the same service in their offices that are now under the banner of the health system. The hospitals cite several justifications for the “surcharge” on care provided by employed physicians in hospital facilities, some of which may be valid. Regulatory requirements, sicker inpatients, increased cost due to training programs, and being required to support money-losing services such as burn care are some reasons. But, independent physicians say they provide the same or better quality care at a lower cost without resources such as legal, accounting, self-insurance against professional liability, and robust lobbying firms.
Hospitals have also contended that vertical integration by buying physician practices should lead to lower health care costs by squeezing efficiencies within the system. There have been conflicting reports on whether physician hospital integration leads to lower health care expenditures.2 The public debate has caught the attention of government regulators. In the recent case of Saint Lukes-Saltzer, the question before the Federal Trade Commission (the agency responsible for federal antitrust action) was: Did total medical expenditures increase or decrease for patients cared for by physician practices acquired by St. Luke’s? Indeed, the conclusions were that not only did overall costs not go down but evidence showed that the merger may have resulted in increased costs.
On appeal, the Ninth Circuit Court ruled that any future efficiency must be “substantial, verifiable and specific” to the merger. Ciliberto and Dranove looked at hospital prices after physician hospital affiliations in California and found no evidence of increase in prices.3 Baker and coauthors analyzed privately insured patients between 2001 and 2007 and the effect of physician hospital integration on hospital prices, admission volumes, and spending.4 They reported higher hospital prices and spending in hospitals with the tightest vertically integrated relationship with physicians. In one of the few studies of the issue, Capps and colleagues reviewed 7 years of administrative data from multiple insurers across the United States to estimate postintegration costs. From 2007 to 2013, they found that there was a 57% increase in the share of spending by physicians whose practices are owned by hospitals. In addition, this led to an increase in physician prices of 14% post integration.5 The larger the market share of inpatients by a hospital the larger the price increase. The authors estimate that about 25% of the price increases are precisely due to “exploitation of reimbursement rules” by charging the facility fees for their employed physicians. If these “surcharges” led to decreased utilization as one measure of increased efficiency and therefore reduced overall health care costs, it would be acceptable. But, Capps et al. found no such evidence and speculate that this scenario could lead to higher expenditures.
In a recent study, total expenditures for over 4 million patients by private physician groups or integrated groups covered by health maintenance organizations (HMOs) in California between 2009 and 2012 were analyzed.6 Mean annual expenditures were highest for large multihospital systems followed by hospital-owned physician groups and, lastly, physician-owned groups. The expenditures for multihospital systems were 19.8% higher and for local hospital-employed physician groups 10% higher compared to physician-owned organizations.
Why should prices increase after tighter physician hospital integration on a large scale? Market power. Once health systems have a large enough number of physicians in their panel, hospitals could charge insurers higher prices to access their specialists. Similarly, by employing a large number of physicians in a particular specialty, which then attracts a large pool of patients with a particular illness, they could dominate the other health systems in the region. One action specifically forbidden by anti-kickback laws is compensating physicians based on the number of referrals they make to the hospital. But, there are enough loopholes that allow hospitals to indirectly tie compensation to “productivity.” This may change with bundled payments or compensation tied to “value,” although there will always be incentives for work volume to some degree.
A further roadblock for basing merger decisions entirely on possible efficiencies is how the courts will see these activities in terms of antitrust actions. Most arguments using efficiency as the basis for merging physician groups with hospitals are vague and in general courts have not superseded antitrust actions with economic efficiency arguments.
What should be genuine reasons for hospitals employing and aligning with physicians? Addressing uneven quality of care, access and, of course, ever spiraling costs. If the object was to share responsibility for attacking these problems, health care systems and physicians would be cut a lot of slack. But, some health care systems want to not only survive the existing chaos but also dominate their local market.
I guess health care is really no different from Wall Street corporations in its focus on short-term gains versus long-term benefits. Until broader incentives change, health systems will continue to look to survive and gain market share and power. Competition, in isolation, drives tactics where the only objective may be to increase market share. However, it appears that the FTC will be busy wielding the Sherman Act of the antitrust law to keep a check on health systems to ensure consumers, payers, physicians, and the country at large are all on a fair playing field.7
Dr. Satiani is professor of clinical surgery, division of vascular diseases & surgery, department of surgery, associate director, FAME; director, Faculty Leadership Institute, and medical director, Vascular Labs, at Ohio State University College of Medicine, Columbus. He is also an associate medical editor for Vascular Specialist.
References
2. Journal of Health Economics 2006; 25: 1-28.
3. Journal of Health Economics 2006; 25: 29-38.
4. Health Affairs 2014; 33(5): 756-63.
5. www.ipr.northwestern.edu/publications/docs/workingpapers/2015/IPR-WP-15-02.pdf
6. JAMA. 2014; 312(16):1663-9.
7. Plastic & Reconstructive Surgery. 2006; 117(3): 1012-22.
NO
The days of hanging one’s shingle on a door and starting a self-employed practice are rapidly fading. While some fondly remember the practice of medicine as it was in Norman Rockwell’s classic “Before the Shot,” the realities of a current practice couldn’t be more different. Reusable syringes, analog weighing stations, an unaccompanied minor, and lack of regard for universal precautions are just a few examples from that painting that have long since disappeared. However, the humor in this painting comes from the young boy scrutinizing the doctor’s credentials, implying a sense of distrust and fear as he stands there with his buttocks partially exposed waiting for the vaccination.
This scrutiny of physician performance and results is more relevant today than ever before. Perhaps if we were to update the painting today, it would depict the boy furiously tapping away at his tablet searching through ProPublica to see what the doctor’s complication rate with the intended procedure truly is.
This is just one of the many pressures physicians are facing today. Navigating the publicly reported complication data is but one tiny portion of the regulatory red tape physicians face in taking care of their patients. If you add in the need to negotiate and contact with insurers, manage an office staff, acquire and maintain an electronic medical record (EMR) while ensuring that your EMR is properly secured against potential cyber threats and compliant with meaningful use regulations, audit your billing and coding, keep up to date with upcoming changes to bundled payments, mail out and track Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), as well as an endless list of other requirements, it is no wonder physicians are less willing to take these challenges on as solo practitioners. In fact, based on Medscape’s 2014 Employed Doctors Report, which compiled responses from over 4,600 physicians, the top three reasons for being an employed physician were not having to deal with the business of running an office (58%), not having to deal with insurers and billing (45%), and guaranteed income/even cash flow (42%).1
Multiple sources continue to confirm the trend that more physicians are moving to an employed practice.2-4 In the last decade, the rate of hospital employment has increased from 11% to 64%.1 There are many factors that have pushed physicians away from self-employment. Some of these are related to physicians’ personal choices, and many are from external pressures. As various parts of the Affordable Care Act come into play, there will continue to be increasing regulatory demands. These have the potential of increasing overhead costs, and, coupled with decreasing reimbursement, will inevitably make staying profitable more challenging in a self-employed model.
There are two other very telling trends that foretell the inevitable decline of self-employed physicians. Fewer and fewer new graduates are reporting that they are self employed. In the most recent surveys, twice as many physicians under the age of 40 are employed than self-employed.1 Furthermore, 92% of residents surveyed in their final year would prefer employment with a salary, and only 2% would consider solo practice.5 Of these graduating residents, 36% specifically were considering hospital employment, which is nearly a 10-fold increase from a decade ago. The second factor affecting new hires is their confidence that they have the necessary skills to manage a self-employed model. During the same decade, there was only a small increase in graduating residents who felt very prepared to deal with the business side of medicine (10% vs. 2%).5 This lack of knowledge will undoubtedly make it difficult for those who would consider self-employment to feel comfortable in that practice model. Some have speculated that there is soon to be a “push back” from the physicians and specifically from specialists who don’t have as much to gain in large group practices. With so few graduates considering solo and small group practice, and the overwhelming majority not feeling very prepared to manage the business of medicine, who can help lead this trend reversal?
Not only are fewer new graduates choosing self-employment, but fewer opportunities for self-employment are available as more physician groups are being bought by hospitals or other large group practices. Specifically with vascular surgery, there is a significant overhead cost requirement. Advantages to joining a large group practice include better ability to negotiate cost savings with the frequent capital requirements for new equipment, updates and maintenance of the electronic records, and professional liability. In fact, one study in California shows that as the proportion of physicians employed by the health system increased, supply chain expenses and inventory costs improved.6 Furthermore, hospitals have administrators who are hired to negotiate with insurers regarding reimbursement and respond to audits and other regulatory changes. As mentioned above, the top two reasons for avoiding self-employment are precisely these. This will no doubt draw even more physicians and specifically vascular surgeons into employed models.
Dr. Haurani is assistant professor of surgery in the division of vascular diseases and surgery, Ohio State University Medical Center, Columbus.
References
1. www.medscape.com/features/slideshow/public/employed-doctors#1
3.Perspect Vasc Surg Endovasc Ther. 2013;25:46-52.
4 Tenn Med. 2012;105:38-39.
5.www.merritthawkins.com/uploadedFiles/MerrittHawkings/Surveys/2014_MerrittHawkins_FYMR_Survey.pdf.
6. Health Care Manage Rev. 2015 Jul 23. [Epub ahead of print] www.ncbi.nlm.nih.gov/pubmed/26207654

FDA reclassifies transvaginal mesh for pelvic organ prolapse as ‘high risk’
The Food and Drug Administration is tightening its regulation of surgical mesh to repair pelvic organ prolapse transvaginally or through the vagina, citing continued safety risks including severe pelvic pain and organ perforation.
The agency is reclassifying surgical mesh used for transvaginal repair of pelvic organ prolapse from a class II to a class III medical device, moving the devices from the moderate-risk to high-risk category. The FDA is also requiring device manufacturers to submit a premarket approval application that supports the safety and effectiveness of surgical mesh. The premarket approval application requirement only applies to mesh used for transvaginal repair of pelvic organ prolapse, not to mesh used for other indications, such as stress urinary incontinence or abdominal repair of pelvic organ prolapse.

The first mesh device for transvaginal repair of pelvic organ prolapse was cleared for use by the FDA in 2002 and five manufacturers are currently marketing the product, according to the FDA.
For products that are already on the market, manufacturers have 30 months to comply with the premarket approval application requirements.
“These stronger clinical requirements will help to address the significant risks associated with surgical mesh for repair of pelvic organ prolapse,” Dr. William Maisel, deputy director of science and chief scientist for the FDA’s Center for Devices and Radiological Health, said in a statement. “We intend to continue monitoring how women with this device are faring months and years after surgery through continued postmarket surveillance measures.”
This is the latest move by the FDA to signal to physicians and patients that surgical mesh should be used with caution when treating pelvic organ prolapse.
In 2008 and 2011, the FDA issued warnings about increased adverse events reports for surgical mesh used in urogynecological procedures. And in 2012, the agency instructed manufacturers to conduct postmarket surveillance studies on surgical mesh used for tranvaginal repair of pelvic organ prolapse.
The agency first proposed reclassifying surgical mesh to a class III device and requiring premarket approval in May 2014.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Food and Drug Administration is tightening its regulation of surgical mesh to repair pelvic organ prolapse transvaginally or through the vagina, citing continued safety risks including severe pelvic pain and organ perforation.
The agency is reclassifying surgical mesh used for transvaginal repair of pelvic organ prolapse from a class II to a class III medical device, moving the devices from the moderate-risk to high-risk category. The FDA is also requiring device manufacturers to submit a premarket approval application that supports the safety and effectiveness of surgical mesh. The premarket approval application requirement only applies to mesh used for transvaginal repair of pelvic organ prolapse, not to mesh used for other indications, such as stress urinary incontinence or abdominal repair of pelvic organ prolapse.
The first mesh device for transvaginal repair of pelvic organ prolapse was cleared for use by the FDA in 2002 and five manufacturers are currently marketing the product, according to the FDA.
For products that are already on the market, manufacturers have 30 months to comply with the premarket approval application requirements.
“These stronger clinical requirements will help to address the significant risks associated with surgical mesh for repair of pelvic organ prolapse,” Dr. William Maisel, deputy director of science and chief scientist for the FDA’s Center for Devices and Radiological Health, said in a statement. “We intend to continue monitoring how women with this device are faring months and years after surgery through continued postmarket surveillance measures.”
This is the latest move by the FDA to signal to physicians and patients that surgical mesh should be used with caution when treating pelvic organ prolapse.
In 2008 and 2011, the FDA issued warnings about increased adverse events reports for surgical mesh used in urogynecological procedures. And in 2012, the agency instructed manufacturers to conduct postmarket surveillance studies on surgical mesh used for tranvaginal repair of pelvic organ prolapse.
The agency first proposed reclassifying surgical mesh to a class III device and requiring premarket approval in May 2014.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The Food and Drug Administration is tightening its regulation of surgical mesh to repair pelvic organ prolapse transvaginally or through the vagina, citing continued safety risks including severe pelvic pain and organ perforation.
The agency is reclassifying surgical mesh used for transvaginal repair of pelvic organ prolapse from a class II to a class III medical device, moving the devices from the moderate-risk to high-risk category. The FDA is also requiring device manufacturers to submit a premarket approval application that supports the safety and effectiveness of surgical mesh. The premarket approval application requirement only applies to mesh used for transvaginal repair of pelvic organ prolapse, not to mesh used for other indications, such as stress urinary incontinence or abdominal repair of pelvic organ prolapse.
The first mesh device for transvaginal repair of pelvic organ prolapse was cleared for use by the FDA in 2002 and five manufacturers are currently marketing the product, according to the FDA.
For products that are already on the market, manufacturers have 30 months to comply with the premarket approval application requirements.
“These stronger clinical requirements will help to address the significant risks associated with surgical mesh for repair of pelvic organ prolapse,” Dr. William Maisel, deputy director of science and chief scientist for the FDA’s Center for Devices and Radiological Health, said in a statement. “We intend to continue monitoring how women with this device are faring months and years after surgery through continued postmarket surveillance measures.”
This is the latest move by the FDA to signal to physicians and patients that surgical mesh should be used with caution when treating pelvic organ prolapse.
In 2008 and 2011, the FDA issued warnings about increased adverse events reports for surgical mesh used in urogynecological procedures. And in 2012, the agency instructed manufacturers to conduct postmarket surveillance studies on surgical mesh used for tranvaginal repair of pelvic organ prolapse.
The agency first proposed reclassifying surgical mesh to a class III device and requiring premarket approval in May 2014.
mschneider@frontlinemedcom.com
On Twitter @maryellenny

Jury still out on appendectomy vs. antibiotics-first approach
Despite a growing movement toward the antibiotics-first approach instead of surgical intervention for uncomplicated appendicitis, a new review of existing literature shows that the jury is still out on how to advise patients about their choices, according to Dr. Anne P. Ehlers and her colleagues who undertook the study.
The findings show that surgical intervention should continue to be considered a viable option and that appendectomy is not necessarily any better or worse in terms of long-term complication rates and length of hospital stay (J Am Coll Surg. 2015. doi:10.1016/j.jamcollsurg.2015.11.009).
“What we found is that treatment of acute, uncomplicated appendicitis with antibiotics first is probably a safe approach, but that there are many questions that need to be answered before we can fully inform our patients about the long-term outcomes of this treatment strategy,” Dr. Ehlers of the department of surgery at the University of Washington, Seattle, said in an interview.
Dr. Ehlers and her coinvestigators combed the PubMed and EMBASE databases for all English-language randomized controlled trials involving comparisons of antibiotic and appendectomy-based treatments for acute appendicitis. Studies were excluded if they lacked adult population investigation.
“Our study is a critical review of the literature [available] on this topic to understand the current state of evidence,” explained Dr. Ehlers, adding that the study’s main goal was to answer the most common questions she and her coauthors encountered when talking to physicians and patients about the benefits and risks of antibiotics-first over appendectomy; namely, “Is my appendicitis going to come back?” “Am I going to have a lot of extra trips to the hospital?” and “What’s my quality of life going to be?”
Ultimately, six trials, comprising 1,720 patients, were selected for inclusion. These studies were led by Dr. S. Eriksson (40 subjects), Dr. J. Styrud (252 subjects), Dr. A.N. Turhan (290 subjects), Dr. J. Hansson (369 subjects), Dr. C. Vons (239 subjects), and Dr. P. Salminen (530 subjects). The Styrud study did not enroll any women, and no study enrolled subjects older than 75 years of age, but the average age of each study’s patients ranged from 26 to 38 years.
Length-of-stay comparisons between appendectomy and antibiotics-first cohorts varied among the studies, but most showed the same or longer LOS for antibiotics-first subjects. Mean LOS was 3.3 for surgical patients vs. 3.1 for antibiotics (Eriksson), 2.6 surgical vs. 3.0 antibiotics (Styrud), 2.4 surgical vs. 3.14 antibiotics (Turhan), 3.0 for both (Hansson), 3.04 surgical vs. 3.96 antibiotics (Vons), and 3.0 for both (Salminen).
Rates of appendectomy among patients treated with an antibiotics-first approach varied as well, with a 35% rate in the Eriksson study (7 out of the 20 subjects treated with antibiotics-first) and a 24% rate in the Styrud and Turhan studies. The Hansson trial reported an unusually high crossover between cohorts of 60%, the investigators noted.
Two studies – those led by Turhan and Vons – noted higher rates of complications in antibiotics-first patients versus those who received surgical intervention: 4.7% vs. 4.4%, and 2.5% vs. less than 1%, respectively. All other studies had high rates of complications in the surgical cohorts, with the Eriksson study reporting no complications whatsoever among antibiotics-first subjects.
These findings, Dr. Ehlers stressed, are just a first step. This review’s relatively low sample size and limiting factors require that further studies be done to more firmly ascertain which option for appendicitis treatment is the most beneficial. To that end, Dr. Ehlers said that she and her coinvestigators are working on that next step.
“Our group is currently working on a study called the CODA [Comparing Outcomes of Drugs in Appendectomy] Study,” she said, with the goal of answering “questions about long-term patient-centered outcomes related to the antibiotics-first approach.” These questions include patients’ quality of life, whether patients have decisional regret about choosing one treatment strategy over another, if they develop long-term anxiety any time they experience even a small abdominal pain, how much time they miss from school or work by choosing one treatment option over another, and so on.
The goal of this study is that physicians “will be able to give [patients] a more informed view of what each treatment entails,” she said. Funded by the Patient-Centered Outcomes Research Institute, the study has no firm date of publication.
Dr. Ehlers disclosed receiving support via a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. No other conflicts of interest were reported.
Despite a growing movement toward the antibiotics-first approach instead of surgical intervention for uncomplicated appendicitis, a new review of existing literature shows that the jury is still out on how to advise patients about their choices, according to Dr. Anne P. Ehlers and her colleagues who undertook the study.
The findings show that surgical intervention should continue to be considered a viable option and that appendectomy is not necessarily any better or worse in terms of long-term complication rates and length of hospital stay (J Am Coll Surg. 2015. doi:10.1016/j.jamcollsurg.2015.11.009).
“What we found is that treatment of acute, uncomplicated appendicitis with antibiotics first is probably a safe approach, but that there are many questions that need to be answered before we can fully inform our patients about the long-term outcomes of this treatment strategy,” Dr. Ehlers of the department of surgery at the University of Washington, Seattle, said in an interview.
Dr. Ehlers and her coinvestigators combed the PubMed and EMBASE databases for all English-language randomized controlled trials involving comparisons of antibiotic and appendectomy-based treatments for acute appendicitis. Studies were excluded if they lacked adult population investigation.
“Our study is a critical review of the literature [available] on this topic to understand the current state of evidence,” explained Dr. Ehlers, adding that the study’s main goal was to answer the most common questions she and her coauthors encountered when talking to physicians and patients about the benefits and risks of antibiotics-first over appendectomy; namely, “Is my appendicitis going to come back?” “Am I going to have a lot of extra trips to the hospital?” and “What’s my quality of life going to be?”
Ultimately, six trials, comprising 1,720 patients, were selected for inclusion. These studies were led by Dr. S. Eriksson (40 subjects), Dr. J. Styrud (252 subjects), Dr. A.N. Turhan (290 subjects), Dr. J. Hansson (369 subjects), Dr. C. Vons (239 subjects), and Dr. P. Salminen (530 subjects). The Styrud study did not enroll any women, and no study enrolled subjects older than 75 years of age, but the average age of each study’s patients ranged from 26 to 38 years.
Length-of-stay comparisons between appendectomy and antibiotics-first cohorts varied among the studies, but most showed the same or longer LOS for antibiotics-first subjects. Mean LOS was 3.3 for surgical patients vs. 3.1 for antibiotics (Eriksson), 2.6 surgical vs. 3.0 antibiotics (Styrud), 2.4 surgical vs. 3.14 antibiotics (Turhan), 3.0 for both (Hansson), 3.04 surgical vs. 3.96 antibiotics (Vons), and 3.0 for both (Salminen).
Rates of appendectomy among patients treated with an antibiotics-first approach varied as well, with a 35% rate in the Eriksson study (7 out of the 20 subjects treated with antibiotics-first) and a 24% rate in the Styrud and Turhan studies. The Hansson trial reported an unusually high crossover between cohorts of 60%, the investigators noted.
Two studies – those led by Turhan and Vons – noted higher rates of complications in antibiotics-first patients versus those who received surgical intervention: 4.7% vs. 4.4%, and 2.5% vs. less than 1%, respectively. All other studies had high rates of complications in the surgical cohorts, with the Eriksson study reporting no complications whatsoever among antibiotics-first subjects.
These findings, Dr. Ehlers stressed, are just a first step. This review’s relatively low sample size and limiting factors require that further studies be done to more firmly ascertain which option for appendicitis treatment is the most beneficial. To that end, Dr. Ehlers said that she and her coinvestigators are working on that next step.
“Our group is currently working on a study called the CODA [Comparing Outcomes of Drugs in Appendectomy] Study,” she said, with the goal of answering “questions about long-term patient-centered outcomes related to the antibiotics-first approach.” These questions include patients’ quality of life, whether patients have decisional regret about choosing one treatment strategy over another, if they develop long-term anxiety any time they experience even a small abdominal pain, how much time they miss from school or work by choosing one treatment option over another, and so on.
The goal of this study is that physicians “will be able to give [patients] a more informed view of what each treatment entails,” she said. Funded by the Patient-Centered Outcomes Research Institute, the study has no firm date of publication.
Dr. Ehlers disclosed receiving support via a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. No other conflicts of interest were reported.
Despite a growing movement toward the antibiotics-first approach instead of surgical intervention for uncomplicated appendicitis, a new review of existing literature shows that the jury is still out on how to advise patients about their choices, according to Dr. Anne P. Ehlers and her colleagues who undertook the study.
The findings show that surgical intervention should continue to be considered a viable option and that appendectomy is not necessarily any better or worse in terms of long-term complication rates and length of hospital stay (J Am Coll Surg. 2015. doi:10.1016/j.jamcollsurg.2015.11.009).
“What we found is that treatment of acute, uncomplicated appendicitis with antibiotics first is probably a safe approach, but that there are many questions that need to be answered before we can fully inform our patients about the long-term outcomes of this treatment strategy,” Dr. Ehlers of the department of surgery at the University of Washington, Seattle, said in an interview.
Dr. Ehlers and her coinvestigators combed the PubMed and EMBASE databases for all English-language randomized controlled trials involving comparisons of antibiotic and appendectomy-based treatments for acute appendicitis. Studies were excluded if they lacked adult population investigation.
“Our study is a critical review of the literature [available] on this topic to understand the current state of evidence,” explained Dr. Ehlers, adding that the study’s main goal was to answer the most common questions she and her coauthors encountered when talking to physicians and patients about the benefits and risks of antibiotics-first over appendectomy; namely, “Is my appendicitis going to come back?” “Am I going to have a lot of extra trips to the hospital?” and “What’s my quality of life going to be?”
Ultimately, six trials, comprising 1,720 patients, were selected for inclusion. These studies were led by Dr. S. Eriksson (40 subjects), Dr. J. Styrud (252 subjects), Dr. A.N. Turhan (290 subjects), Dr. J. Hansson (369 subjects), Dr. C. Vons (239 subjects), and Dr. P. Salminen (530 subjects). The Styrud study did not enroll any women, and no study enrolled subjects older than 75 years of age, but the average age of each study’s patients ranged from 26 to 38 years.
Length-of-stay comparisons between appendectomy and antibiotics-first cohorts varied among the studies, but most showed the same or longer LOS for antibiotics-first subjects. Mean LOS was 3.3 for surgical patients vs. 3.1 for antibiotics (Eriksson), 2.6 surgical vs. 3.0 antibiotics (Styrud), 2.4 surgical vs. 3.14 antibiotics (Turhan), 3.0 for both (Hansson), 3.04 surgical vs. 3.96 antibiotics (Vons), and 3.0 for both (Salminen).
Rates of appendectomy among patients treated with an antibiotics-first approach varied as well, with a 35% rate in the Eriksson study (7 out of the 20 subjects treated with antibiotics-first) and a 24% rate in the Styrud and Turhan studies. The Hansson trial reported an unusually high crossover between cohorts of 60%, the investigators noted.
Two studies – those led by Turhan and Vons – noted higher rates of complications in antibiotics-first patients versus those who received surgical intervention: 4.7% vs. 4.4%, and 2.5% vs. less than 1%, respectively. All other studies had high rates of complications in the surgical cohorts, with the Eriksson study reporting no complications whatsoever among antibiotics-first subjects.
These findings, Dr. Ehlers stressed, are just a first step. This review’s relatively low sample size and limiting factors require that further studies be done to more firmly ascertain which option for appendicitis treatment is the most beneficial. To that end, Dr. Ehlers said that she and her coinvestigators are working on that next step.
“Our group is currently working on a study called the CODA [Comparing Outcomes of Drugs in Appendectomy] Study,” she said, with the goal of answering “questions about long-term patient-centered outcomes related to the antibiotics-first approach.” These questions include patients’ quality of life, whether patients have decisional regret about choosing one treatment strategy over another, if they develop long-term anxiety any time they experience even a small abdominal pain, how much time they miss from school or work by choosing one treatment option over another, and so on.
The goal of this study is that physicians “will be able to give [patients] a more informed view of what each treatment entails,” she said. Funded by the Patient-Centered Outcomes Research Institute, the study has no firm date of publication.
Dr. Ehlers disclosed receiving support via a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. No other conflicts of interest were reported.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: While the antibiotics-first approach to uncomplicated appendicitis has become increasingly popular in recent years, existing evidence shows that appendectomy is not inferior in terms of hospital stay and rates of complications.
Major finding: Length-of-stay and complication rates vary among all six included studies between antibiotics-first and surgical cohorts, indicating that neither one is definitively better or worse than the other.
Data source: Literature review of 1,720 appendicitis patients across six studies selected from PubMed and EMBASE databases.
Disclosures: The National Institute of Diabetes and Digestive and Kidney Diseases supported the study. No other conflicts of interest were reported.