User login
Official Newspaper of the American College of Surgeons
President Obama calls for ‘moon shot’ to cure cancer
President Obama is calling on America’s medical research industry to cure cancer.
In his final State of the Union address, delivered Jan. 12, Mr. Obama compared this moment to that embraced by the nation in response to the Soviet Union’s foray into space: Within 12 years, Americans stepped foot on the Moon.

“Last year, Vice President [Joe] Biden said that, with a new moon shot, America can cure cancer,” President Obama said. “Tonight, I’m announcing a new national effort to get it done.”
No further details were given, except that Vice President Biden is being put “in charge of Mission Control,” after noting his role in getting increased funding in the recent budget for the National Institutes of Health.
The American Association for Cancer Research (AACR) applauded the commitment to curing cancer.
“We have indeed reached an inflection point, where the number of discoveries that are being made at such an accelerated pace are saving lives and bringing enormous hope for cancer patients, even those with advanced disease,” Dr. José Baselga, AACR president, said in a statement. “Now is the time for a major new initiative in cancer science that supports and builds upon our basic science foundation while translating these exciting scientific discoveries into improved treatments for cancer patients, such as in the areas of genomics, precision medicine, and immuno-oncology.”
The AACR said that members of its organization were among a group that met with Vice President Biden on Jan. 8 to discuss the state of cancer research.
The American Society of Clinical Oncology concurred.
“With nearly 1.7 million people in the United States diagnosed with cancer each year, and the incidence of cancer expected to rise to 2.3 million cases per year by 2030, it is imperative that we do all we can to bring more effective treatments from the laboratory bench to the patient’s bedside as quickly as possible,” Dr. Richard L. Schilsky, ASCO chief medical officer, said in a statement. “We must recommit to vastly speeding the discovery of new cancer treatments and enabling the possibility of precision medicine for every individual with cancer.”
The annual address to Congress was light on health care issues, with President Obama acknowledging U.S. leadership in helping to halt the Ebola epidemic and adding that “we are on track to end the scourge of HIV/AIDS, and we have the capacity to accomplish the same thing with malaria – something I’ll be pushing this Congress to fund this year.”
Rather, President Obama focused more on the economy and the security of the nation, as well as calling on Americans to be more active in voting and the overall political process.
President Obama is calling on America’s medical research industry to cure cancer.
In his final State of the Union address, delivered Jan. 12, Mr. Obama compared this moment to that embraced by the nation in response to the Soviet Union’s foray into space: Within 12 years, Americans stepped foot on the Moon.
“Last year, Vice President [Joe] Biden said that, with a new moon shot, America can cure cancer,” President Obama said. “Tonight, I’m announcing a new national effort to get it done.”
No further details were given, except that Vice President Biden is being put “in charge of Mission Control,” after noting his role in getting increased funding in the recent budget for the National Institutes of Health.
The American Association for Cancer Research (AACR) applauded the commitment to curing cancer.
“We have indeed reached an inflection point, where the number of discoveries that are being made at such an accelerated pace are saving lives and bringing enormous hope for cancer patients, even those with advanced disease,” Dr. José Baselga, AACR president, said in a statement. “Now is the time for a major new initiative in cancer science that supports and builds upon our basic science foundation while translating these exciting scientific discoveries into improved treatments for cancer patients, such as in the areas of genomics, precision medicine, and immuno-oncology.”
The AACR said that members of its organization were among a group that met with Vice President Biden on Jan. 8 to discuss the state of cancer research.
The American Society of Clinical Oncology concurred.
“With nearly 1.7 million people in the United States diagnosed with cancer each year, and the incidence of cancer expected to rise to 2.3 million cases per year by 2030, it is imperative that we do all we can to bring more effective treatments from the laboratory bench to the patient’s bedside as quickly as possible,” Dr. Richard L. Schilsky, ASCO chief medical officer, said in a statement. “We must recommit to vastly speeding the discovery of new cancer treatments and enabling the possibility of precision medicine for every individual with cancer.”
The annual address to Congress was light on health care issues, with President Obama acknowledging U.S. leadership in helping to halt the Ebola epidemic and adding that “we are on track to end the scourge of HIV/AIDS, and we have the capacity to accomplish the same thing with malaria – something I’ll be pushing this Congress to fund this year.”
Rather, President Obama focused more on the economy and the security of the nation, as well as calling on Americans to be more active in voting and the overall political process.
President Obama is calling on America’s medical research industry to cure cancer.
In his final State of the Union address, delivered Jan. 12, Mr. Obama compared this moment to that embraced by the nation in response to the Soviet Union’s foray into space: Within 12 years, Americans stepped foot on the Moon.
“Last year, Vice President [Joe] Biden said that, with a new moon shot, America can cure cancer,” President Obama said. “Tonight, I’m announcing a new national effort to get it done.”
No further details were given, except that Vice President Biden is being put “in charge of Mission Control,” after noting his role in getting increased funding in the recent budget for the National Institutes of Health.
The American Association for Cancer Research (AACR) applauded the commitment to curing cancer.
“We have indeed reached an inflection point, where the number of discoveries that are being made at such an accelerated pace are saving lives and bringing enormous hope for cancer patients, even those with advanced disease,” Dr. José Baselga, AACR president, said in a statement. “Now is the time for a major new initiative in cancer science that supports and builds upon our basic science foundation while translating these exciting scientific discoveries into improved treatments for cancer patients, such as in the areas of genomics, precision medicine, and immuno-oncology.”
The AACR said that members of its organization were among a group that met with Vice President Biden on Jan. 8 to discuss the state of cancer research.
The American Society of Clinical Oncology concurred.
“With nearly 1.7 million people in the United States diagnosed with cancer each year, and the incidence of cancer expected to rise to 2.3 million cases per year by 2030, it is imperative that we do all we can to bring more effective treatments from the laboratory bench to the patient’s bedside as quickly as possible,” Dr. Richard L. Schilsky, ASCO chief medical officer, said in a statement. “We must recommit to vastly speeding the discovery of new cancer treatments and enabling the possibility of precision medicine for every individual with cancer.”
The annual address to Congress was light on health care issues, with President Obama acknowledging U.S. leadership in helping to halt the Ebola epidemic and adding that “we are on track to end the scourge of HIV/AIDS, and we have the capacity to accomplish the same thing with malaria – something I’ll be pushing this Congress to fund this year.”
Rather, President Obama focused more on the economy and the security of the nation, as well as calling on Americans to be more active in voting and the overall political process.

The art of negotiation: The impact of psychosocial factors
Those of you who are either poker players or have watched those that play will understand the importance of having a poker face in some circumstances. Although poker typically results in a zero-sum game, the strategy and tactics in achieving an optimal outcome are quite similar to contract negotiations. Coming into the “game” prepared with a strategic approach and the ability to be observant, and having the aptitude to maintain a high level of emotional intelligence are fundamental to success. This is the third and final article on this special series titled “The Art of Negotiation.” In the first article, we looked at big picture concepts related to the negotiation of contracts in medicine (ACS Surgery News, October 2015, p. 13), and subsequently we delved the task of gathering information (November 2015, p. 9). We will end this series by looking at how we can put everything together in order to best position ourselves in reaching a win-win solution.
Understanding your emotional approach
One of the first things discussed early on within this series of articles is the fact that contract negotiations in medicine are far from a simple transactional deal. The relationship building in the negotiation context extends far beyond this one deal. For those new to the job market, the right job can be the culmination of dreams and ambitions years in the making. Job negotiations should not be taken lightly nor sabotaged by out-of-control emotions. You may experience a variety of emotions during a negotiation such as anxiety, anger, sadness, and excitement.
These feelings can directly affect the process, and therefore understanding how to internally deal with them can make for a smoother and potentially more beneficial end result.
Anxiety management
Anxiety is a feeling often experienced during the early stages of the negotiation process. One response to anxiety is avoidance – cut negotiations short and make a quick agreement. But avoidance can undermine some of the basic tenants of negotiation where the ability to be patient and persevere is critical. Anxious negotiators can end up making weaker offers, spending less time negotiating, and getting a less-than-optimal agreement. The ability to minimize feelings of anxiety is related to preparation and practice.
Have you ever walked into an exam feeling unprepared and wishing you had studied more or done a few more review questions? There is a clear difference in how you approach an exam you are unprepared for versus one for which you have mastered the material.
Do your homework and your anxiety will be less.
Imagine the following scenario. A colleague of mine was back for a second interview at a medical center that overall had what she was looking for, and therefore she had begun the negotiation process with the committee including the chief of the service. They began by telling her how wonderful their offer was, and even mentioned that a few other candidates were interested in taking this position if she hesitated. This technique to exert pressure on candidates is not uncommon, yet it made her anxious. As the conversation went on, her anxiety continue to build.
She was able to excuse herself for a moment and she texted me from her sanctuary, which at that time happened to be a restroom stall. “Joe, what if I don’t agree to the terms? Am I going to lose this potentially great opportunity? I should just sign the contract?” she said. I was able to remind her of a few things. First, I told her, you are at the table for a reason, which primarily has to do with the fact that you may provide value to the organization. Second, I asked her if she knew what were they looking for. It is critical to understand what the institution considers important since it will allow you to leverage your skill set. If the answer is not clear, then ask questions to help illustrate what they value to help advance their objectives.
Once you have determined what they value most, you can negotiate with greater confidence.
Finally, you should never sign a contract without taking time to really review it. If a potential employer is not willing to give you that time then it should be a red flag that something is not right!
Anger management
Anger is another emotion that, unlike anxiety, can result in an increase in intensity of the negotiation. While certain aspects of this might seem appealing and even at times beneficial, in general, anger impairs the overall process, results in a higher likelihood of an impasse, and potentially damages the long-term relationship. In fact, even if a deal is ultimately agreed upon, trust among the parties is reduced, making for a potentially difficult working relationship in the future. It is wise to make every effort to minimize aggression during the discussion and ensure the other team understands your goal of reaching a win-win solution. Remember that even in the best circumstances, these complex negotiations usually result in a combination of elements gained and lost. The most skilled negotiators will leave the table confident that they achieved a great deal, while making sure that the other party also feels good about the agreement.
The value of MESOs
The term Multiple Equivalent Simultaneous Offers (MESO) negotiation is a strategy that is used when multiple interests are involved. MESO fits perfectly with the type of compensation packages physicians aiming to negotiate where base salary is not the only aspect under discussion. The idea is to make multiple offers that, in your mind, are essentially equivalent.
The three steps required are as follows:
1. Identify and prioritize important issues, and assign them a relative weight
2. Identify different likely outcomes for each issue
3. Develop three or more equivalent offers
This strategy gives you the opportunity to gather information about the other side in order to better understand where their priorities lie, and provides you the opportunity to be assertive at the negotiating table but also flexible and cooperative. MESO does require an investment of time in putting together these plans, and will ultimately require you to reveal some of your own interests. At the end of the day, people feel good about being given multiple choices rather than a single option. This typically results in greater value, and will often enhance the probability of reaching an agreement.
Parting thoughts
The process of negotiating a contract can be unsettling. This series has aimed to provide you with some of the basic principles that might help facilitate these discussions that at some point in time you will inevitably be required to have.
The following are 10 summary points that you might find helpful:
1. Preparation is the key. (Do your research, talk to people.)
2. Maintain a high level of emotional intelligence.
3. Listen and be observant during discussions.
4. Be creative in your approach. (Remember, its not all about the base salary!)
5. Maintain discipline when responding to questions (especially when unsure).
6. The only way to guarantee an agreement is to get it in writing.
7. The goal is to reach a win-win solution.
8. Maintain honesty and integrity throughout the process.
9. Understand that you are building long-term relationships.
10. Gut instinct is not a strategy.
Napoleon Hill said, “The starting point of all achievement is desire.” Whatever that desire may be, remember to think of all the variables critical to turning that desire into achievement. My hope is that some of the techniques I have described will be useful as you prepare to take that next step into the surgical workforce.
Feel free to tweet me for questions, comments, or ideas @Josephsakran.
Dr. Sakran is an ACS Fellow, and assistant professor of surgery and Director of Global Health & Disaster Preparedness for the department of surgery at the Medical University of South Carolina. He is the immediate past chair of the ACS Resident and Associate Society and recently finished a year at the Harvard Kennedy School of Government studying public policy, economics, and leadership development. He has no relevant disclosures.
Those of you who are either poker players or have watched those that play will understand the importance of having a poker face in some circumstances. Although poker typically results in a zero-sum game, the strategy and tactics in achieving an optimal outcome are quite similar to contract negotiations. Coming into the “game” prepared with a strategic approach and the ability to be observant, and having the aptitude to maintain a high level of emotional intelligence are fundamental to success. This is the third and final article on this special series titled “The Art of Negotiation.” In the first article, we looked at big picture concepts related to the negotiation of contracts in medicine (ACS Surgery News, October 2015, p. 13), and subsequently we delved the task of gathering information (November 2015, p. 9). We will end this series by looking at how we can put everything together in order to best position ourselves in reaching a win-win solution.
Understanding your emotional approach
One of the first things discussed early on within this series of articles is the fact that contract negotiations in medicine are far from a simple transactional deal. The relationship building in the negotiation context extends far beyond this one deal. For those new to the job market, the right job can be the culmination of dreams and ambitions years in the making. Job negotiations should not be taken lightly nor sabotaged by out-of-control emotions. You may experience a variety of emotions during a negotiation such as anxiety, anger, sadness, and excitement.
These feelings can directly affect the process, and therefore understanding how to internally deal with them can make for a smoother and potentially more beneficial end result.
Anxiety management
Anxiety is a feeling often experienced during the early stages of the negotiation process. One response to anxiety is avoidance – cut negotiations short and make a quick agreement. But avoidance can undermine some of the basic tenants of negotiation where the ability to be patient and persevere is critical. Anxious negotiators can end up making weaker offers, spending less time negotiating, and getting a less-than-optimal agreement. The ability to minimize feelings of anxiety is related to preparation and practice.
Have you ever walked into an exam feeling unprepared and wishing you had studied more or done a few more review questions? There is a clear difference in how you approach an exam you are unprepared for versus one for which you have mastered the material.
Do your homework and your anxiety will be less.
Imagine the following scenario. A colleague of mine was back for a second interview at a medical center that overall had what she was looking for, and therefore she had begun the negotiation process with the committee including the chief of the service. They began by telling her how wonderful their offer was, and even mentioned that a few other candidates were interested in taking this position if she hesitated. This technique to exert pressure on candidates is not uncommon, yet it made her anxious. As the conversation went on, her anxiety continue to build.
She was able to excuse herself for a moment and she texted me from her sanctuary, which at that time happened to be a restroom stall. “Joe, what if I don’t agree to the terms? Am I going to lose this potentially great opportunity? I should just sign the contract?” she said. I was able to remind her of a few things. First, I told her, you are at the table for a reason, which primarily has to do with the fact that you may provide value to the organization. Second, I asked her if she knew what were they looking for. It is critical to understand what the institution considers important since it will allow you to leverage your skill set. If the answer is not clear, then ask questions to help illustrate what they value to help advance their objectives.
Once you have determined what they value most, you can negotiate with greater confidence.
Finally, you should never sign a contract without taking time to really review it. If a potential employer is not willing to give you that time then it should be a red flag that something is not right!
Anger management
Anger is another emotion that, unlike anxiety, can result in an increase in intensity of the negotiation. While certain aspects of this might seem appealing and even at times beneficial, in general, anger impairs the overall process, results in a higher likelihood of an impasse, and potentially damages the long-term relationship. In fact, even if a deal is ultimately agreed upon, trust among the parties is reduced, making for a potentially difficult working relationship in the future. It is wise to make every effort to minimize aggression during the discussion and ensure the other team understands your goal of reaching a win-win solution. Remember that even in the best circumstances, these complex negotiations usually result in a combination of elements gained and lost. The most skilled negotiators will leave the table confident that they achieved a great deal, while making sure that the other party also feels good about the agreement.
The value of MESOs
The term Multiple Equivalent Simultaneous Offers (MESO) negotiation is a strategy that is used when multiple interests are involved. MESO fits perfectly with the type of compensation packages physicians aiming to negotiate where base salary is not the only aspect under discussion. The idea is to make multiple offers that, in your mind, are essentially equivalent.
The three steps required are as follows:
1. Identify and prioritize important issues, and assign them a relative weight
2. Identify different likely outcomes for each issue
3. Develop three or more equivalent offers
This strategy gives you the opportunity to gather information about the other side in order to better understand where their priorities lie, and provides you the opportunity to be assertive at the negotiating table but also flexible and cooperative. MESO does require an investment of time in putting together these plans, and will ultimately require you to reveal some of your own interests. At the end of the day, people feel good about being given multiple choices rather than a single option. This typically results in greater value, and will often enhance the probability of reaching an agreement.
Parting thoughts
The process of negotiating a contract can be unsettling. This series has aimed to provide you with some of the basic principles that might help facilitate these discussions that at some point in time you will inevitably be required to have.
The following are 10 summary points that you might find helpful:
1. Preparation is the key. (Do your research, talk to people.)
2. Maintain a high level of emotional intelligence.
3. Listen and be observant during discussions.
4. Be creative in your approach. (Remember, its not all about the base salary!)
5. Maintain discipline when responding to questions (especially when unsure).
6. The only way to guarantee an agreement is to get it in writing.
7. The goal is to reach a win-win solution.
8. Maintain honesty and integrity throughout the process.
9. Understand that you are building long-term relationships.
10. Gut instinct is not a strategy.
Napoleon Hill said, “The starting point of all achievement is desire.” Whatever that desire may be, remember to think of all the variables critical to turning that desire into achievement. My hope is that some of the techniques I have described will be useful as you prepare to take that next step into the surgical workforce.
Feel free to tweet me for questions, comments, or ideas @Josephsakran.
Dr. Sakran is an ACS Fellow, and assistant professor of surgery and Director of Global Health & Disaster Preparedness for the department of surgery at the Medical University of South Carolina. He is the immediate past chair of the ACS Resident and Associate Society and recently finished a year at the Harvard Kennedy School of Government studying public policy, economics, and leadership development. He has no relevant disclosures.
Those of you who are either poker players or have watched those that play will understand the importance of having a poker face in some circumstances. Although poker typically results in a zero-sum game, the strategy and tactics in achieving an optimal outcome are quite similar to contract negotiations. Coming into the “game” prepared with a strategic approach and the ability to be observant, and having the aptitude to maintain a high level of emotional intelligence are fundamental to success. This is the third and final article on this special series titled “The Art of Negotiation.” In the first article, we looked at big picture concepts related to the negotiation of contracts in medicine (ACS Surgery News, October 2015, p. 13), and subsequently we delved the task of gathering information (November 2015, p. 9). We will end this series by looking at how we can put everything together in order to best position ourselves in reaching a win-win solution.
Understanding your emotional approach
One of the first things discussed early on within this series of articles is the fact that contract negotiations in medicine are far from a simple transactional deal. The relationship building in the negotiation context extends far beyond this one deal. For those new to the job market, the right job can be the culmination of dreams and ambitions years in the making. Job negotiations should not be taken lightly nor sabotaged by out-of-control emotions. You may experience a variety of emotions during a negotiation such as anxiety, anger, sadness, and excitement.
These feelings can directly affect the process, and therefore understanding how to internally deal with them can make for a smoother and potentially more beneficial end result.
Anxiety management
Anxiety is a feeling often experienced during the early stages of the negotiation process. One response to anxiety is avoidance – cut negotiations short and make a quick agreement. But avoidance can undermine some of the basic tenants of negotiation where the ability to be patient and persevere is critical. Anxious negotiators can end up making weaker offers, spending less time negotiating, and getting a less-than-optimal agreement. The ability to minimize feelings of anxiety is related to preparation and practice.
Have you ever walked into an exam feeling unprepared and wishing you had studied more or done a few more review questions? There is a clear difference in how you approach an exam you are unprepared for versus one for which you have mastered the material.
Do your homework and your anxiety will be less.
Imagine the following scenario. A colleague of mine was back for a second interview at a medical center that overall had what she was looking for, and therefore she had begun the negotiation process with the committee including the chief of the service. They began by telling her how wonderful their offer was, and even mentioned that a few other candidates were interested in taking this position if she hesitated. This technique to exert pressure on candidates is not uncommon, yet it made her anxious. As the conversation went on, her anxiety continue to build.
She was able to excuse herself for a moment and she texted me from her sanctuary, which at that time happened to be a restroom stall. “Joe, what if I don’t agree to the terms? Am I going to lose this potentially great opportunity? I should just sign the contract?” she said. I was able to remind her of a few things. First, I told her, you are at the table for a reason, which primarily has to do with the fact that you may provide value to the organization. Second, I asked her if she knew what were they looking for. It is critical to understand what the institution considers important since it will allow you to leverage your skill set. If the answer is not clear, then ask questions to help illustrate what they value to help advance their objectives.
Once you have determined what they value most, you can negotiate with greater confidence.
Finally, you should never sign a contract without taking time to really review it. If a potential employer is not willing to give you that time then it should be a red flag that something is not right!
Anger management
Anger is another emotion that, unlike anxiety, can result in an increase in intensity of the negotiation. While certain aspects of this might seem appealing and even at times beneficial, in general, anger impairs the overall process, results in a higher likelihood of an impasse, and potentially damages the long-term relationship. In fact, even if a deal is ultimately agreed upon, trust among the parties is reduced, making for a potentially difficult working relationship in the future. It is wise to make every effort to minimize aggression during the discussion and ensure the other team understands your goal of reaching a win-win solution. Remember that even in the best circumstances, these complex negotiations usually result in a combination of elements gained and lost. The most skilled negotiators will leave the table confident that they achieved a great deal, while making sure that the other party also feels good about the agreement.
The value of MESOs
The term Multiple Equivalent Simultaneous Offers (MESO) negotiation is a strategy that is used when multiple interests are involved. MESO fits perfectly with the type of compensation packages physicians aiming to negotiate where base salary is not the only aspect under discussion. The idea is to make multiple offers that, in your mind, are essentially equivalent.
The three steps required are as follows:
1. Identify and prioritize important issues, and assign them a relative weight
2. Identify different likely outcomes for each issue
3. Develop three or more equivalent offers
This strategy gives you the opportunity to gather information about the other side in order to better understand where their priorities lie, and provides you the opportunity to be assertive at the negotiating table but also flexible and cooperative. MESO does require an investment of time in putting together these plans, and will ultimately require you to reveal some of your own interests. At the end of the day, people feel good about being given multiple choices rather than a single option. This typically results in greater value, and will often enhance the probability of reaching an agreement.
Parting thoughts
The process of negotiating a contract can be unsettling. This series has aimed to provide you with some of the basic principles that might help facilitate these discussions that at some point in time you will inevitably be required to have.
The following are 10 summary points that you might find helpful:
1. Preparation is the key. (Do your research, talk to people.)
2. Maintain a high level of emotional intelligence.
3. Listen and be observant during discussions.
4. Be creative in your approach. (Remember, its not all about the base salary!)
5. Maintain discipline when responding to questions (especially when unsure).
6. The only way to guarantee an agreement is to get it in writing.
7. The goal is to reach a win-win solution.
8. Maintain honesty and integrity throughout the process.
9. Understand that you are building long-term relationships.
10. Gut instinct is not a strategy.
Napoleon Hill said, “The starting point of all achievement is desire.” Whatever that desire may be, remember to think of all the variables critical to turning that desire into achievement. My hope is that some of the techniques I have described will be useful as you prepare to take that next step into the surgical workforce.
Feel free to tweet me for questions, comments, or ideas @Josephsakran.
Dr. Sakran is an ACS Fellow, and assistant professor of surgery and Director of Global Health & Disaster Preparedness for the department of surgery at the Medical University of South Carolina. He is the immediate past chair of the ACS Resident and Associate Society and recently finished a year at the Harvard Kennedy School of Government studying public policy, economics, and leadership development. He has no relevant disclosures.
CMS: End of meaningful use imminent in 2016
Meaningful use is on its way out.
Andy Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, told investors attending the annual J.P. Morgan Healthcare Conference that CMS is pulling back from the health care IT incentive program in the coming months.
“The meaningful use program as it has existed will now be effectively over and replaced with something better,” Mr. Slavitt said.*

“We have to get the hearts and minds of physicians back. I think we’ve lost them,” Mr. Slavitt said. He noted that, when the meaningful use incentive program began, few physicians and practices used electronic health records and concerns were that many would not willingly embrace information technology. Now that “virtually everywhere care is delivered has a computer,” it’s time to make health care technology serve beneficiaries and the physicians who serve them, Mr. Slavitt said.
The cost, however, was too high, Mr. Slavitt said. “As any physician will tell you, physician burden and frustration levels are real. Programs that are designed to improve often distract. Done poorly, measures are divorced from how physicians practice and add to the cynicism that the people who build these programs just don’t get it.”
Soon, CMS will no longer reward health care providers for using technology, but will instead focus on patient outcomes through the merit-based incentive pay systems created by last year’s Medicare Access and CHIP Reauthorization Act (MACRA) legislation. In addition to asking physicians to work with health care IT innovators to create systems that work best according to their practice’s respective needs, CMS is calling on the private sector to create apps and analytic tools that will keep data secure while fostering true and widespread interoperability.
Anyone seeking to block data transfer will find CMS is not their friend. Mr. Slavitt said. “We’re deadly serious about interoperability. Technology companies that look for ways to practice data blocking in opposition to new regulations will find that it will not be tolerated.”

Dr. James L. Madara, CEO of the American Medical Association, echoed Mr. Slavitt’s comments on the current, negative impact of EHRs on physicians’ practices. He noted that many physicians are spending at least 2 hours each workday using their EHR and may click up to 4,000 times per 8-hour shift.
Dr. Madara outlined three AMA goals to help restore the physician-patient relationship. The first is to restructure the medical school curriculum, which he said essentially is the same as it has been for 100 years. New generations of physicians should be taught how to deliver collaborative care that includes telemedicine, more ambulatory care, and home care. Community-based partnerships, he said, would become key to treating chronic diseases like diabetes and would have to be factored into reimbursement models. The AMA also seeks to improve health outcomes and ensure thriving physician practices.
Central to the AMA’s plan for the future: Helping physicians restructure practice via technology. He announced that the AMA is a founding partner in the Silicon Valley (Calif.) based Health2047, a company focused on supporting health IT and other entrepreneurs in their efforts to provide physicians with digital tools that improve patient outcomes, among other innovations.
With MACRA set to go into full effect in 2019, Dr. Madara said that a “daunting” level of change is about to take place. Citing the successful shift to ICD-10, he said he was optimistic there would be positive changes, largely brought about through incentives to the private marketplace and by dropping meaningful use.
Although having metrics in health care delivery is important, Dr. Madara said that, up to this point, “We kinda got it wrong” with quality measures that are more processed based, rather than evidence based. “It was really great to hear about the move from meaningful use to a more aggregated program.”
*Correction, 1/12/2016: A previous version of this story included an incorrect start-up date for meaningful use changes.
On Twitter @whitneymcknight
Meaningful use is on its way out.
Andy Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, told investors attending the annual J.P. Morgan Healthcare Conference that CMS is pulling back from the health care IT incentive program in the coming months.
“The meaningful use program as it has existed will now be effectively over and replaced with something better,” Mr. Slavitt said.*
“We have to get the hearts and minds of physicians back. I think we’ve lost them,” Mr. Slavitt said. He noted that, when the meaningful use incentive program began, few physicians and practices used electronic health records and concerns were that many would not willingly embrace information technology. Now that “virtually everywhere care is delivered has a computer,” it’s time to make health care technology serve beneficiaries and the physicians who serve them, Mr. Slavitt said.
The cost, however, was too high, Mr. Slavitt said. “As any physician will tell you, physician burden and frustration levels are real. Programs that are designed to improve often distract. Done poorly, measures are divorced from how physicians practice and add to the cynicism that the people who build these programs just don’t get it.”
Soon, CMS will no longer reward health care providers for using technology, but will instead focus on patient outcomes through the merit-based incentive pay systems created by last year’s Medicare Access and CHIP Reauthorization Act (MACRA) legislation. In addition to asking physicians to work with health care IT innovators to create systems that work best according to their practice’s respective needs, CMS is calling on the private sector to create apps and analytic tools that will keep data secure while fostering true and widespread interoperability.
Anyone seeking to block data transfer will find CMS is not their friend. Mr. Slavitt said. “We’re deadly serious about interoperability. Technology companies that look for ways to practice data blocking in opposition to new regulations will find that it will not be tolerated.”
Dr. James L. Madara, CEO of the American Medical Association, echoed Mr. Slavitt’s comments on the current, negative impact of EHRs on physicians’ practices. He noted that many physicians are spending at least 2 hours each workday using their EHR and may click up to 4,000 times per 8-hour shift.
Dr. Madara outlined three AMA goals to help restore the physician-patient relationship. The first is to restructure the medical school curriculum, which he said essentially is the same as it has been for 100 years. New generations of physicians should be taught how to deliver collaborative care that includes telemedicine, more ambulatory care, and home care. Community-based partnerships, he said, would become key to treating chronic diseases like diabetes and would have to be factored into reimbursement models. The AMA also seeks to improve health outcomes and ensure thriving physician practices.
Central to the AMA’s plan for the future: Helping physicians restructure practice via technology. He announced that the AMA is a founding partner in the Silicon Valley (Calif.) based Health2047, a company focused on supporting health IT and other entrepreneurs in their efforts to provide physicians with digital tools that improve patient outcomes, among other innovations.
With MACRA set to go into full effect in 2019, Dr. Madara said that a “daunting” level of change is about to take place. Citing the successful shift to ICD-10, he said he was optimistic there would be positive changes, largely brought about through incentives to the private marketplace and by dropping meaningful use.
Although having metrics in health care delivery is important, Dr. Madara said that, up to this point, “We kinda got it wrong” with quality measures that are more processed based, rather than evidence based. “It was really great to hear about the move from meaningful use to a more aggregated program.”
*Correction, 1/12/2016: A previous version of this story included an incorrect start-up date for meaningful use changes.
On Twitter @whitneymcknight
Meaningful use is on its way out.
Andy Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, told investors attending the annual J.P. Morgan Healthcare Conference that CMS is pulling back from the health care IT incentive program in the coming months.
“The meaningful use program as it has existed will now be effectively over and replaced with something better,” Mr. Slavitt said.*
“We have to get the hearts and minds of physicians back. I think we’ve lost them,” Mr. Slavitt said. He noted that, when the meaningful use incentive program began, few physicians and practices used electronic health records and concerns were that many would not willingly embrace information technology. Now that “virtually everywhere care is delivered has a computer,” it’s time to make health care technology serve beneficiaries and the physicians who serve them, Mr. Slavitt said.
The cost, however, was too high, Mr. Slavitt said. “As any physician will tell you, physician burden and frustration levels are real. Programs that are designed to improve often distract. Done poorly, measures are divorced from how physicians practice and add to the cynicism that the people who build these programs just don’t get it.”
Soon, CMS will no longer reward health care providers for using technology, but will instead focus on patient outcomes through the merit-based incentive pay systems created by last year’s Medicare Access and CHIP Reauthorization Act (MACRA) legislation. In addition to asking physicians to work with health care IT innovators to create systems that work best according to their practice’s respective needs, CMS is calling on the private sector to create apps and analytic tools that will keep data secure while fostering true and widespread interoperability.
Anyone seeking to block data transfer will find CMS is not their friend. Mr. Slavitt said. “We’re deadly serious about interoperability. Technology companies that look for ways to practice data blocking in opposition to new regulations will find that it will not be tolerated.”
Dr. James L. Madara, CEO of the American Medical Association, echoed Mr. Slavitt’s comments on the current, negative impact of EHRs on physicians’ practices. He noted that many physicians are spending at least 2 hours each workday using their EHR and may click up to 4,000 times per 8-hour shift.
Dr. Madara outlined three AMA goals to help restore the physician-patient relationship. The first is to restructure the medical school curriculum, which he said essentially is the same as it has been for 100 years. New generations of physicians should be taught how to deliver collaborative care that includes telemedicine, more ambulatory care, and home care. Community-based partnerships, he said, would become key to treating chronic diseases like diabetes and would have to be factored into reimbursement models. The AMA also seeks to improve health outcomes and ensure thriving physician practices.
Central to the AMA’s plan for the future: Helping physicians restructure practice via technology. He announced that the AMA is a founding partner in the Silicon Valley (Calif.) based Health2047, a company focused on supporting health IT and other entrepreneurs in their efforts to provide physicians with digital tools that improve patient outcomes, among other innovations.
With MACRA set to go into full effect in 2019, Dr. Madara said that a “daunting” level of change is about to take place. Citing the successful shift to ICD-10, he said he was optimistic there would be positive changes, largely brought about through incentives to the private marketplace and by dropping meaningful use.
Although having metrics in health care delivery is important, Dr. Madara said that, up to this point, “We kinda got it wrong” with quality measures that are more processed based, rather than evidence based. “It was really great to hear about the move from meaningful use to a more aggregated program.”
*Correction, 1/12/2016: A previous version of this story included an incorrect start-up date for meaningful use changes.
On Twitter @whitneymcknight
FROM THE J.P. MORGAN HEALTHCARE CONFERENCE

Hong Kong zygomycosis deaths pinned to dirty hospital laundry
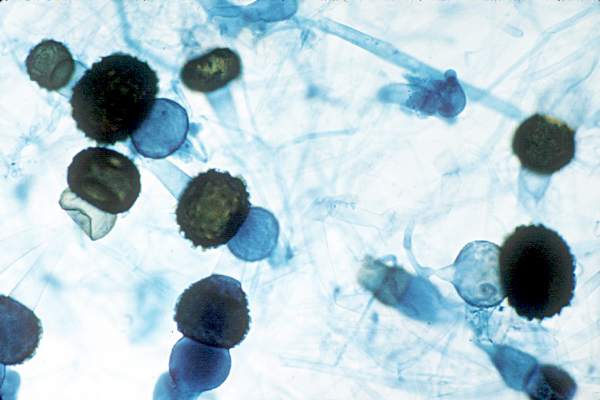
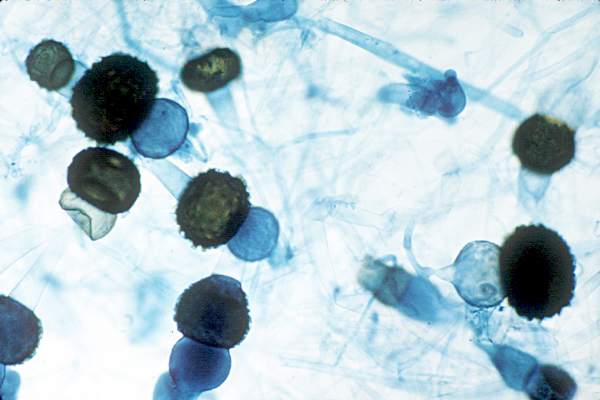
Contaminated laundry led to an outbreak of cutaneous and pulmonary zygomycosis that killed three immunocompromised patients and sickened three others at Queen Mary Hospital in Hong Kong.
The contamination was traced to a contract laundry service that was, in short, a microbe Disneyland. It was hot and humid, with sealed windows, dim lights, and a thick layer of dust on just about everything. Washers weren’t hot enough to kill spores; washed items were packed while warm and moist; and dirty linens rich with organic material were transported with clean ones (Clin Infect Dis. 2015 Dec 13. doi:10.1093/cid/civ1006).
Of 195 environmental samples, 119 (61%) were positive for Zygomycetes, as well as 100% of air samples. Freshly laundered items – including clothes and bedding – had bacteria counts of 1,028 colony forming units (CFU)/100 cm2, far exceeding the “hygienically clean” standard of 20 CFU/100 cm2 set by U.S. healthcare textile certification requirements.
Queen Mary didn’t regularly audit its linens for cleanliness and microbe counts. “Our findings [suggest] that such standards should be adopted to prevent similar outbreaks,” said the investigators, led by Dr. Vincent Cheng, an infection control officer at Queen Mary, one of Hong Kong’s largest hospitals and a teaching hospital for the University of Hong Kong.
It has since switched to a new laundry service.
The outbreak ran from June 2 to July 18, 2015, during Hong Kong’s hot and humid season, which didn’t help matters.
The six patients were 42-74 years old; one had interstitial lung disease and the rest were either cancer or transplant patients. Infection was due to the spore-forming mold Rhizopus microsporus. Two pulmonary and one cutaneous infection patient died.
Length of stay was the most significant risk factor for infection; the mean interval from admission to diagnosis was more than 2 months.
“Pulmonary zygomycosis due to contaminated hospital linens has never been reported.” Clinicians need to “maintain a high index of suspicion for early diagnosis and treatment of zygomycosis in immunosuppressed patients,” the investigators said.
The U.S. recently had a cutaneous outbreak in Louisiana; hospital linens contaminated with Rhizopus species killed five immunocompromised children there in 2015.
“Invasive zygomycosis is an emerging infection that is increasingly reported in immunosuppressed hosts;” previously reported sources include adhesive bandages, wooden tongue depressors, ostomy bags, damaged water circuitry, adjacent building construction activity, and, as Queen Mary reported previously, contaminated allopurinol tablets.
Detecting the problem isn’t easy. None of the Replicate Organism Detection and Counting contact plates at Queen Mary recovered zygomycetes from the contaminated linen items. It took sponge swapping to find it; “without the use of sponge swab and selective culture medium, the causative agents in this outbreak would have been overlooked,” the investigators said.
Hong Kong government services helped support the work. The authors did not have any financial conflicts of interest.
Contaminated laundry led to an outbreak of cutaneous and pulmonary zygomycosis that killed three immunocompromised patients and sickened three others at Queen Mary Hospital in Hong Kong.
The contamination was traced to a contract laundry service that was, in short, a microbe Disneyland. It was hot and humid, with sealed windows, dim lights, and a thick layer of dust on just about everything. Washers weren’t hot enough to kill spores; washed items were packed while warm and moist; and dirty linens rich with organic material were transported with clean ones (Clin Infect Dis. 2015 Dec 13. doi:10.1093/cid/civ1006).
Of 195 environmental samples, 119 (61%) were positive for Zygomycetes, as well as 100% of air samples. Freshly laundered items – including clothes and bedding – had bacteria counts of 1,028 colony forming units (CFU)/100 cm2, far exceeding the “hygienically clean” standard of 20 CFU/100 cm2 set by U.S. healthcare textile certification requirements.
Queen Mary didn’t regularly audit its linens for cleanliness and microbe counts. “Our findings [suggest] that such standards should be adopted to prevent similar outbreaks,” said the investigators, led by Dr. Vincent Cheng, an infection control officer at Queen Mary, one of Hong Kong’s largest hospitals and a teaching hospital for the University of Hong Kong.
It has since switched to a new laundry service.
The outbreak ran from June 2 to July 18, 2015, during Hong Kong’s hot and humid season, which didn’t help matters.
The six patients were 42-74 years old; one had interstitial lung disease and the rest were either cancer or transplant patients. Infection was due to the spore-forming mold Rhizopus microsporus. Two pulmonary and one cutaneous infection patient died.
Length of stay was the most significant risk factor for infection; the mean interval from admission to diagnosis was more than 2 months.
“Pulmonary zygomycosis due to contaminated hospital linens has never been reported.” Clinicians need to “maintain a high index of suspicion for early diagnosis and treatment of zygomycosis in immunosuppressed patients,” the investigators said.
The U.S. recently had a cutaneous outbreak in Louisiana; hospital linens contaminated with Rhizopus species killed five immunocompromised children there in 2015.
“Invasive zygomycosis is an emerging infection that is increasingly reported in immunosuppressed hosts;” previously reported sources include adhesive bandages, wooden tongue depressors, ostomy bags, damaged water circuitry, adjacent building construction activity, and, as Queen Mary reported previously, contaminated allopurinol tablets.
Detecting the problem isn’t easy. None of the Replicate Organism Detection and Counting contact plates at Queen Mary recovered zygomycetes from the contaminated linen items. It took sponge swapping to find it; “without the use of sponge swab and selective culture medium, the causative agents in this outbreak would have been overlooked,” the investigators said.
Hong Kong government services helped support the work. The authors did not have any financial conflicts of interest.
Contaminated laundry led to an outbreak of cutaneous and pulmonary zygomycosis that killed three immunocompromised patients and sickened three others at Queen Mary Hospital in Hong Kong.
The contamination was traced to a contract laundry service that was, in short, a microbe Disneyland. It was hot and humid, with sealed windows, dim lights, and a thick layer of dust on just about everything. Washers weren’t hot enough to kill spores; washed items were packed while warm and moist; and dirty linens rich with organic material were transported with clean ones (Clin Infect Dis. 2015 Dec 13. doi:10.1093/cid/civ1006).
Of 195 environmental samples, 119 (61%) were positive for Zygomycetes, as well as 100% of air samples. Freshly laundered items – including clothes and bedding – had bacteria counts of 1,028 colony forming units (CFU)/100 cm2, far exceeding the “hygienically clean” standard of 20 CFU/100 cm2 set by U.S. healthcare textile certification requirements.
Queen Mary didn’t regularly audit its linens for cleanliness and microbe counts. “Our findings [suggest] that such standards should be adopted to prevent similar outbreaks,” said the investigators, led by Dr. Vincent Cheng, an infection control officer at Queen Mary, one of Hong Kong’s largest hospitals and a teaching hospital for the University of Hong Kong.
It has since switched to a new laundry service.
The outbreak ran from June 2 to July 18, 2015, during Hong Kong’s hot and humid season, which didn’t help matters.
The six patients were 42-74 years old; one had interstitial lung disease and the rest were either cancer or transplant patients. Infection was due to the spore-forming mold Rhizopus microsporus. Two pulmonary and one cutaneous infection patient died.
Length of stay was the most significant risk factor for infection; the mean interval from admission to diagnosis was more than 2 months.
“Pulmonary zygomycosis due to contaminated hospital linens has never been reported.” Clinicians need to “maintain a high index of suspicion for early diagnosis and treatment of zygomycosis in immunosuppressed patients,” the investigators said.
The U.S. recently had a cutaneous outbreak in Louisiana; hospital linens contaminated with Rhizopus species killed five immunocompromised children there in 2015.
“Invasive zygomycosis is an emerging infection that is increasingly reported in immunosuppressed hosts;” previously reported sources include adhesive bandages, wooden tongue depressors, ostomy bags, damaged water circuitry, adjacent building construction activity, and, as Queen Mary reported previously, contaminated allopurinol tablets.
Detecting the problem isn’t easy. None of the Replicate Organism Detection and Counting contact plates at Queen Mary recovered zygomycetes from the contaminated linen items. It took sponge swapping to find it; “without the use of sponge swab and selective culture medium, the causative agents in this outbreak would have been overlooked,” the investigators said.
Hong Kong government services helped support the work. The authors did not have any financial conflicts of interest.
FROM CLINICAL INFECTIOUS DISEASES
Key clinical point: Clinicians need to maintain a high index of suspicion for early diagnosis and treatment of zygomycosis in immunosuppressed patients,
Major finding: Of 195 environmental samples at the contaminated laundry, 119 (61%) were positive for Zygomycetes, as well as 100% of air samples.
Data source: Epidemiological study in Hong Kong.
Disclosures: Hong Kong government services helped support the work. The authors do not have any financial conflicts of interest.
Noncompete clauses: Be wary, negotiate early
Noncompete clauses can severely limit a doctor’s business options and create serious financial challenges, so negotiate with employers early and watch out for tricky contract terms that could stifle future opportunities.
That is the advice from health law experts around the country. They point out that when it comes to noncompete clauses – employment contract language that limits where physicians can practice after employment ends or is terminated – doctors should pay close attention, especially to the following:
Geographical limitations
Distance requirements within noncompete provisions are a top issue that can trip up doctors, Bloomfield Hills, Mich., health law attorney Mark S. Kopson said. The clause typically specifies that a physician cannot practice within a certain radius of the former employer. However, if an employer has three offices for instance, that 10-mile radius can quickly become a 30-mile radius or more depending how the provision is worded. Mr. Kopson recalled a recent client who practiced for 5 years in one office and was transferred to an office in another town for 30 days. He was then terminated, and his employer attempted to enforce contract terms that would prevent him from practicing within a 10-mile radius of both offices. A court determined that the employer was acting in bad faith and sought an unfair competitive advantage.

“But No. 1, you don’t want to have to go to court,” Mr. Kopson said. “And No. 2, you can have the best lawyer, but once it’s in the hands of the judge or the jury, anything can happen. That’s why you really want to do the work on this up front.”
When negotiating noncompete clauses, be cognizant of where distances are being measured from and around, the legal experts stress. Also, be clear with employers about what defines a reasonable distance, based on the geographic spread of their patient base.
“What’s reasonable for a family practice physician is probably not going to be reasonable for a pediatric neurosurgeon, as they draw their patients from varying distances,” he said. “Also, negotiate to ensure that the length of time of the restriction is reasonable. Taking into account, both the distance and time period, the physician must still be able to earn a living.”
Time frame restrictions
Negotiate the shortest duration that you can, advises Greenbelt, Md., labor and employment attorney Jay P. Holland. Noncompete provisions typically limit a doctor from practicing around a certain radius for 1-5 years, but some employers may try to enforce longer time periods.

“Consider your career and lifestyle goals carefully prior to entering into a noncompete,” Mr. Holland said. “The first approach should always be an attempt to exclude the noncompete from your prospective agreement if you are joining a practice. If a noncompete is unavoidable, then strive to make it the least onerous possible. Ask yourself prior to signing an agreement, ‘If I were to leave this practice, what are the restrictions I could live with? Are the restrictions reasonable?’ ”
Knowing your state’s law is key. State regulation of noncompete provisions widely differ. States such as California broadly hold that noncompete contracts are per se invalid – even if narrowly tailored – unless necessary to protect trade secrets. States such as Maryland allow the provisions only if area and duration restrictions are reasonable and do not impose undue hardship on employees. Three states – Colorado, Delaware, and Massachusetts – have laws that strictly prohibit noncompete clauses in physician contracts.
“Most other states will generally enforce noncompete clauses so long as their terms are reasonable in light of the interests of the employer, the employee, and the general public,” Mr. Holland said. “Therefore, noncompete clauses should be no greater in scope than is necessary to protect the business or goodwill of the employer.”
Patient retention problems
Watch out for contract language referring to “trade secrets,” adds Los Angeles health law attorney Andrew H. Selesnick. Trade secret clauses are often lengthy and typically state that physicians cannot use or retain information from the employer that is considered confidential. Because patient lists are usually considered confidential, these terms could potentially prohibit patients from following their doctor.

“If you want to leave and take your patients with you, there may be some trade secret implications associated with that,” Mr. Selesnick said. “The ability to be able to move patients is significant and can have significant financial impacts. Know what you’re getting into.”
If bringing patients with them to a new practice, doctors should make sure the employment agreement excludes these patients from any nonsolicitation provision at the time the doctor leaves, notes Mr. Holland. Include language that states physicians can retain patients they originally brought to the practice when they depart without violating the agreement.
Make sure to review any proposed noncompete clauses in relation to proposed termination provisions, Mr. Kopson said. Doctors should negotiate language that ensures noncompete obligations will be null and void if physicians are terminated without cause (if such terminations are permitted by the contract), or if the employer breaches the contract.
Seeking the advice of an experienced contract attorney before signing a noncompete clause can save doctors significant time, money, and heartache in the long run, Mr. Kopson notes.
“The biggest risk is signing a contract that has such a clause with an expectation that it will not be enforced,” he said. “If [clauses are] properly drafted, they’re going to be binding. If you get the help up front, it’s going to be a lot less expensive than having your life turned upside down because you’re stuck with a noncompete that has bad terms in it.”
Unreasonable terms
Once signed, getting out of non-compete clauses can be tricky, Mr. Selesnick said. However, doctors can usually escape them if they can prove the terms are unreasonable.
“You can get out of them, especially if they’re very restrictive and say you can’t practice within an area that may prevent you from earning your livelihood,” Mr. Selesnick said. “Courts [generally] think that employees should be able to leave and be able to get a job elsewhere, even if it’s across the street.”
Courts are typically more favorable to physician-employees than independent contractors when it comes to noncompete clauses, Mr. Selesnick said. Independent contractors are generally viewed as having more power over their work than physician-employees. They may have a tougher time convincing a court that such provisions will harm their employment options.
When seeking to enforce a disputed noncompete agreement, employers frequently will request a court-ordered temporary restraining order or injunction to enforce the clause, Mr. Holland said. Judges consider general principles of fairness and equity, and balance the relative harm to the employer and the employee, when deciding whether to issue the injunction. The employee-physician can also try to beat the employer to the courthouse steps by filing a “declaratory judgment” lawsuit that seeks guidance from the court on the contract’s enforceability.
“Typically, employers attempt to do that which is in their best economic interest,” Mr. Holland said. “If a proposal can be negotiated where the employer’s economic well-being is not threatened, then the employer should have a strong interest in a compromise.”
On Twitter @legal_med
Noncompete clauses can severely limit a doctor’s business options and create serious financial challenges, so negotiate with employers early and watch out for tricky contract terms that could stifle future opportunities.
That is the advice from health law experts around the country. They point out that when it comes to noncompete clauses – employment contract language that limits where physicians can practice after employment ends or is terminated – doctors should pay close attention, especially to the following:
Geographical limitations
Distance requirements within noncompete provisions are a top issue that can trip up doctors, Bloomfield Hills, Mich., health law attorney Mark S. Kopson said. The clause typically specifies that a physician cannot practice within a certain radius of the former employer. However, if an employer has three offices for instance, that 10-mile radius can quickly become a 30-mile radius or more depending how the provision is worded. Mr. Kopson recalled a recent client who practiced for 5 years in one office and was transferred to an office in another town for 30 days. He was then terminated, and his employer attempted to enforce contract terms that would prevent him from practicing within a 10-mile radius of both offices. A court determined that the employer was acting in bad faith and sought an unfair competitive advantage.
“But No. 1, you don’t want to have to go to court,” Mr. Kopson said. “And No. 2, you can have the best lawyer, but once it’s in the hands of the judge or the jury, anything can happen. That’s why you really want to do the work on this up front.”
When negotiating noncompete clauses, be cognizant of where distances are being measured from and around, the legal experts stress. Also, be clear with employers about what defines a reasonable distance, based on the geographic spread of their patient base.
“What’s reasonable for a family practice physician is probably not going to be reasonable for a pediatric neurosurgeon, as they draw their patients from varying distances,” he said. “Also, negotiate to ensure that the length of time of the restriction is reasonable. Taking into account, both the distance and time period, the physician must still be able to earn a living.”
Time frame restrictions
Negotiate the shortest duration that you can, advises Greenbelt, Md., labor and employment attorney Jay P. Holland. Noncompete provisions typically limit a doctor from practicing around a certain radius for 1-5 years, but some employers may try to enforce longer time periods.
“Consider your career and lifestyle goals carefully prior to entering into a noncompete,” Mr. Holland said. “The first approach should always be an attempt to exclude the noncompete from your prospective agreement if you are joining a practice. If a noncompete is unavoidable, then strive to make it the least onerous possible. Ask yourself prior to signing an agreement, ‘If I were to leave this practice, what are the restrictions I could live with? Are the restrictions reasonable?’ ”
Knowing your state’s law is key. State regulation of noncompete provisions widely differ. States such as California broadly hold that noncompete contracts are per se invalid – even if narrowly tailored – unless necessary to protect trade secrets. States such as Maryland allow the provisions only if area and duration restrictions are reasonable and do not impose undue hardship on employees. Three states – Colorado, Delaware, and Massachusetts – have laws that strictly prohibit noncompete clauses in physician contracts.
“Most other states will generally enforce noncompete clauses so long as their terms are reasonable in light of the interests of the employer, the employee, and the general public,” Mr. Holland said. “Therefore, noncompete clauses should be no greater in scope than is necessary to protect the business or goodwill of the employer.”
Patient retention problems
Watch out for contract language referring to “trade secrets,” adds Los Angeles health law attorney Andrew H. Selesnick. Trade secret clauses are often lengthy and typically state that physicians cannot use or retain information from the employer that is considered confidential. Because patient lists are usually considered confidential, these terms could potentially prohibit patients from following their doctor.
“If you want to leave and take your patients with you, there may be some trade secret implications associated with that,” Mr. Selesnick said. “The ability to be able to move patients is significant and can have significant financial impacts. Know what you’re getting into.”
If bringing patients with them to a new practice, doctors should make sure the employment agreement excludes these patients from any nonsolicitation provision at the time the doctor leaves, notes Mr. Holland. Include language that states physicians can retain patients they originally brought to the practice when they depart without violating the agreement.
Make sure to review any proposed noncompete clauses in relation to proposed termination provisions, Mr. Kopson said. Doctors should negotiate language that ensures noncompete obligations will be null and void if physicians are terminated without cause (if such terminations are permitted by the contract), or if the employer breaches the contract.
Seeking the advice of an experienced contract attorney before signing a noncompete clause can save doctors significant time, money, and heartache in the long run, Mr. Kopson notes.
“The biggest risk is signing a contract that has such a clause with an expectation that it will not be enforced,” he said. “If [clauses are] properly drafted, they’re going to be binding. If you get the help up front, it’s going to be a lot less expensive than having your life turned upside down because you’re stuck with a noncompete that has bad terms in it.”
Unreasonable terms
Once signed, getting out of non-compete clauses can be tricky, Mr. Selesnick said. However, doctors can usually escape them if they can prove the terms are unreasonable.
“You can get out of them, especially if they’re very restrictive and say you can’t practice within an area that may prevent you from earning your livelihood,” Mr. Selesnick said. “Courts [generally] think that employees should be able to leave and be able to get a job elsewhere, even if it’s across the street.”
Courts are typically more favorable to physician-employees than independent contractors when it comes to noncompete clauses, Mr. Selesnick said. Independent contractors are generally viewed as having more power over their work than physician-employees. They may have a tougher time convincing a court that such provisions will harm their employment options.
When seeking to enforce a disputed noncompete agreement, employers frequently will request a court-ordered temporary restraining order or injunction to enforce the clause, Mr. Holland said. Judges consider general principles of fairness and equity, and balance the relative harm to the employer and the employee, when deciding whether to issue the injunction. The employee-physician can also try to beat the employer to the courthouse steps by filing a “declaratory judgment” lawsuit that seeks guidance from the court on the contract’s enforceability.
“Typically, employers attempt to do that which is in their best economic interest,” Mr. Holland said. “If a proposal can be negotiated where the employer’s economic well-being is not threatened, then the employer should have a strong interest in a compromise.”
On Twitter @legal_med
Noncompete clauses can severely limit a doctor’s business options and create serious financial challenges, so negotiate with employers early and watch out for tricky contract terms that could stifle future opportunities.
That is the advice from health law experts around the country. They point out that when it comes to noncompete clauses – employment contract language that limits where physicians can practice after employment ends or is terminated – doctors should pay close attention, especially to the following:
Geographical limitations
Distance requirements within noncompete provisions are a top issue that can trip up doctors, Bloomfield Hills, Mich., health law attorney Mark S. Kopson said. The clause typically specifies that a physician cannot practice within a certain radius of the former employer. However, if an employer has three offices for instance, that 10-mile radius can quickly become a 30-mile radius or more depending how the provision is worded. Mr. Kopson recalled a recent client who practiced for 5 years in one office and was transferred to an office in another town for 30 days. He was then terminated, and his employer attempted to enforce contract terms that would prevent him from practicing within a 10-mile radius of both offices. A court determined that the employer was acting in bad faith and sought an unfair competitive advantage.
“But No. 1, you don’t want to have to go to court,” Mr. Kopson said. “And No. 2, you can have the best lawyer, but once it’s in the hands of the judge or the jury, anything can happen. That’s why you really want to do the work on this up front.”
When negotiating noncompete clauses, be cognizant of where distances are being measured from and around, the legal experts stress. Also, be clear with employers about what defines a reasonable distance, based on the geographic spread of their patient base.
“What’s reasonable for a family practice physician is probably not going to be reasonable for a pediatric neurosurgeon, as they draw their patients from varying distances,” he said. “Also, negotiate to ensure that the length of time of the restriction is reasonable. Taking into account, both the distance and time period, the physician must still be able to earn a living.”
Time frame restrictions
Negotiate the shortest duration that you can, advises Greenbelt, Md., labor and employment attorney Jay P. Holland. Noncompete provisions typically limit a doctor from practicing around a certain radius for 1-5 years, but some employers may try to enforce longer time periods.
“Consider your career and lifestyle goals carefully prior to entering into a noncompete,” Mr. Holland said. “The first approach should always be an attempt to exclude the noncompete from your prospective agreement if you are joining a practice. If a noncompete is unavoidable, then strive to make it the least onerous possible. Ask yourself prior to signing an agreement, ‘If I were to leave this practice, what are the restrictions I could live with? Are the restrictions reasonable?’ ”
Knowing your state’s law is key. State regulation of noncompete provisions widely differ. States such as California broadly hold that noncompete contracts are per se invalid – even if narrowly tailored – unless necessary to protect trade secrets. States such as Maryland allow the provisions only if area and duration restrictions are reasonable and do not impose undue hardship on employees. Three states – Colorado, Delaware, and Massachusetts – have laws that strictly prohibit noncompete clauses in physician contracts.
“Most other states will generally enforce noncompete clauses so long as their terms are reasonable in light of the interests of the employer, the employee, and the general public,” Mr. Holland said. “Therefore, noncompete clauses should be no greater in scope than is necessary to protect the business or goodwill of the employer.”
Patient retention problems
Watch out for contract language referring to “trade secrets,” adds Los Angeles health law attorney Andrew H. Selesnick. Trade secret clauses are often lengthy and typically state that physicians cannot use or retain information from the employer that is considered confidential. Because patient lists are usually considered confidential, these terms could potentially prohibit patients from following their doctor.
“If you want to leave and take your patients with you, there may be some trade secret implications associated with that,” Mr. Selesnick said. “The ability to be able to move patients is significant and can have significant financial impacts. Know what you’re getting into.”
If bringing patients with them to a new practice, doctors should make sure the employment agreement excludes these patients from any nonsolicitation provision at the time the doctor leaves, notes Mr. Holland. Include language that states physicians can retain patients they originally brought to the practice when they depart without violating the agreement.
Make sure to review any proposed noncompete clauses in relation to proposed termination provisions, Mr. Kopson said. Doctors should negotiate language that ensures noncompete obligations will be null and void if physicians are terminated without cause (if such terminations are permitted by the contract), or if the employer breaches the contract.
Seeking the advice of an experienced contract attorney before signing a noncompete clause can save doctors significant time, money, and heartache in the long run, Mr. Kopson notes.
“The biggest risk is signing a contract that has such a clause with an expectation that it will not be enforced,” he said. “If [clauses are] properly drafted, they’re going to be binding. If you get the help up front, it’s going to be a lot less expensive than having your life turned upside down because you’re stuck with a noncompete that has bad terms in it.”
Unreasonable terms
Once signed, getting out of non-compete clauses can be tricky, Mr. Selesnick said. However, doctors can usually escape them if they can prove the terms are unreasonable.
“You can get out of them, especially if they’re very restrictive and say you can’t practice within an area that may prevent you from earning your livelihood,” Mr. Selesnick said. “Courts [generally] think that employees should be able to leave and be able to get a job elsewhere, even if it’s across the street.”
Courts are typically more favorable to physician-employees than independent contractors when it comes to noncompete clauses, Mr. Selesnick said. Independent contractors are generally viewed as having more power over their work than physician-employees. They may have a tougher time convincing a court that such provisions will harm their employment options.
When seeking to enforce a disputed noncompete agreement, employers frequently will request a court-ordered temporary restraining order or injunction to enforce the clause, Mr. Holland said. Judges consider general principles of fairness and equity, and balance the relative harm to the employer and the employee, when deciding whether to issue the injunction. The employee-physician can also try to beat the employer to the courthouse steps by filing a “declaratory judgment” lawsuit that seeks guidance from the court on the contract’s enforceability.
“Typically, employers attempt to do that which is in their best economic interest,” Mr. Holland said. “If a proposal can be negotiated where the employer’s economic well-being is not threatened, then the employer should have a strong interest in a compromise.”
On Twitter @legal_med

Denosumab boosts BMD in kidney transplant recipients
SAN DIEGO – Twice-yearly denosumab effectively increased bone mineral density in kidney transplant recipients, but was associated with more frequent episodes of urinary tract infections and hypocalcemia, results from a randomized trial showed.
“Kidney transplant recipients lose bone mass and are at increased risk for fractures, more so in females than in males,” Dr. Rudolf P. Wuthrich said at Kidney Week 2015, sponsored by the American Society of Nephrology. Results from previous studies suggest that one in five patients may develop a fracture within 5 years after kidney transplantation.

Considering that current therapeutic options to prevent bone loss are limited, Dr. Wuthrich, director of the Clinic for Nephrology at University Hospital Zurich, and his associates assessed the efficacy and safety of receptor activator of nuclear factor–kappaB ligand (RANKL) inhibition with denosumab to improve bone mineralization in the first year after kidney transplantation. They recruited 108 patients from June 2011 to May 2014. Of these, 90 were randomized within 4 weeks after kidney transplant surgery in a 1:1 ratio to receive subcutaneous injections of 60 mg denosumab at baseline and after 6 months, or no treatment. The study’s primary endpoint was the percentage change in bone mineral density measured by DXA at the lumbar spine at 12 months. The study, known as Denosumab for Prevention of Osteoporosis in Renal Transplant Recipients (POSTOP), was limited to adults who had undergone kidney transplantation within 28 days and who were on standard triple immunosuppression, including a calcineurin antagonist, mycophenolate, and steroids.
Dr. Wuthrich reported results from 46 patients in the denosumab group and 44 patients in the control group. At baseline, their mean age was 50 years, 63% were male, and 96% were white. After 12 months, the total lumbar spine BMD increased by 4.6% in the denosumab group and decreased by 0.5% in the control group, for a between-group difference of 5.1% (P less than .0001). Denosumab also significantly increased BMD at the total hip by 1.9% (P = .035) over that in the control group at 12 months.
High-resolution peripheral quantitative computed tomography in a subgroup of 24 patients showed that denosumab also significantly increased BMD and cortical thickness at the distal tibia and radius (P less than .05). Two biomarkers of bone resorption in beta C-terminal telopeptide and urine deoxypyridinoline markedly decreased in the denosumab group, as did two biomarkers of bone formation in procollagen type 1 N-terminal propeptide and bone-specific alkaline phosphatase (P less than .0001).
In terms of adverse events, there were significantly more urinary tract infections in the denosumab group, compared with the control group (15% vs. 9%, respectively), as well as more episodes of diarrhea (9% vs. 5%), and transient hypocalcemia (3% vs. 0.3%). The number of serious adverse events was similar between groups, at 17% and 19%, respectively.
“We had significantly increased bone mineral density at all measured skeletal sites in response to denosumab,” Dr. Wuthrich concluded. “We had a significant increase in bone biomarkers and we can say that denosumab was generally safe in a complex population of immunosuppressed kidney transplant recipients. But it was associated with a higher incidence of urinary tract infections. At this point we have no good explanation as to why this is. We also had a few episodes of transient and asymptomatic hypocalcemia.”
The researchers reported having no financial disclosures.
SAN DIEGO – Twice-yearly denosumab effectively increased bone mineral density in kidney transplant recipients, but was associated with more frequent episodes of urinary tract infections and hypocalcemia, results from a randomized trial showed.
“Kidney transplant recipients lose bone mass and are at increased risk for fractures, more so in females than in males,” Dr. Rudolf P. Wuthrich said at Kidney Week 2015, sponsored by the American Society of Nephrology. Results from previous studies suggest that one in five patients may develop a fracture within 5 years after kidney transplantation.
Considering that current therapeutic options to prevent bone loss are limited, Dr. Wuthrich, director of the Clinic for Nephrology at University Hospital Zurich, and his associates assessed the efficacy and safety of receptor activator of nuclear factor–kappaB ligand (RANKL) inhibition with denosumab to improve bone mineralization in the first year after kidney transplantation. They recruited 108 patients from June 2011 to May 2014. Of these, 90 were randomized within 4 weeks after kidney transplant surgery in a 1:1 ratio to receive subcutaneous injections of 60 mg denosumab at baseline and after 6 months, or no treatment. The study’s primary endpoint was the percentage change in bone mineral density measured by DXA at the lumbar spine at 12 months. The study, known as Denosumab for Prevention of Osteoporosis in Renal Transplant Recipients (POSTOP), was limited to adults who had undergone kidney transplantation within 28 days and who were on standard triple immunosuppression, including a calcineurin antagonist, mycophenolate, and steroids.
Dr. Wuthrich reported results from 46 patients in the denosumab group and 44 patients in the control group. At baseline, their mean age was 50 years, 63% were male, and 96% were white. After 12 months, the total lumbar spine BMD increased by 4.6% in the denosumab group and decreased by 0.5% in the control group, for a between-group difference of 5.1% (P less than .0001). Denosumab also significantly increased BMD at the total hip by 1.9% (P = .035) over that in the control group at 12 months.
High-resolution peripheral quantitative computed tomography in a subgroup of 24 patients showed that denosumab also significantly increased BMD and cortical thickness at the distal tibia and radius (P less than .05). Two biomarkers of bone resorption in beta C-terminal telopeptide and urine deoxypyridinoline markedly decreased in the denosumab group, as did two biomarkers of bone formation in procollagen type 1 N-terminal propeptide and bone-specific alkaline phosphatase (P less than .0001).
In terms of adverse events, there were significantly more urinary tract infections in the denosumab group, compared with the control group (15% vs. 9%, respectively), as well as more episodes of diarrhea (9% vs. 5%), and transient hypocalcemia (3% vs. 0.3%). The number of serious adverse events was similar between groups, at 17% and 19%, respectively.
“We had significantly increased bone mineral density at all measured skeletal sites in response to denosumab,” Dr. Wuthrich concluded. “We had a significant increase in bone biomarkers and we can say that denosumab was generally safe in a complex population of immunosuppressed kidney transplant recipients. But it was associated with a higher incidence of urinary tract infections. At this point we have no good explanation as to why this is. We also had a few episodes of transient and asymptomatic hypocalcemia.”
The researchers reported having no financial disclosures.
SAN DIEGO – Twice-yearly denosumab effectively increased bone mineral density in kidney transplant recipients, but was associated with more frequent episodes of urinary tract infections and hypocalcemia, results from a randomized trial showed.
“Kidney transplant recipients lose bone mass and are at increased risk for fractures, more so in females than in males,” Dr. Rudolf P. Wuthrich said at Kidney Week 2015, sponsored by the American Society of Nephrology. Results from previous studies suggest that one in five patients may develop a fracture within 5 years after kidney transplantation.
Considering that current therapeutic options to prevent bone loss are limited, Dr. Wuthrich, director of the Clinic for Nephrology at University Hospital Zurich, and his associates assessed the efficacy and safety of receptor activator of nuclear factor–kappaB ligand (RANKL) inhibition with denosumab to improve bone mineralization in the first year after kidney transplantation. They recruited 108 patients from June 2011 to May 2014. Of these, 90 were randomized within 4 weeks after kidney transplant surgery in a 1:1 ratio to receive subcutaneous injections of 60 mg denosumab at baseline and after 6 months, or no treatment. The study’s primary endpoint was the percentage change in bone mineral density measured by DXA at the lumbar spine at 12 months. The study, known as Denosumab for Prevention of Osteoporosis in Renal Transplant Recipients (POSTOP), was limited to adults who had undergone kidney transplantation within 28 days and who were on standard triple immunosuppression, including a calcineurin antagonist, mycophenolate, and steroids.
Dr. Wuthrich reported results from 46 patients in the denosumab group and 44 patients in the control group. At baseline, their mean age was 50 years, 63% were male, and 96% were white. After 12 months, the total lumbar spine BMD increased by 4.6% in the denosumab group and decreased by 0.5% in the control group, for a between-group difference of 5.1% (P less than .0001). Denosumab also significantly increased BMD at the total hip by 1.9% (P = .035) over that in the control group at 12 months.
High-resolution peripheral quantitative computed tomography in a subgroup of 24 patients showed that denosumab also significantly increased BMD and cortical thickness at the distal tibia and radius (P less than .05). Two biomarkers of bone resorption in beta C-terminal telopeptide and urine deoxypyridinoline markedly decreased in the denosumab group, as did two biomarkers of bone formation in procollagen type 1 N-terminal propeptide and bone-specific alkaline phosphatase (P less than .0001).
In terms of adverse events, there were significantly more urinary tract infections in the denosumab group, compared with the control group (15% vs. 9%, respectively), as well as more episodes of diarrhea (9% vs. 5%), and transient hypocalcemia (3% vs. 0.3%). The number of serious adverse events was similar between groups, at 17% and 19%, respectively.
“We had significantly increased bone mineral density at all measured skeletal sites in response to denosumab,” Dr. Wuthrich concluded. “We had a significant increase in bone biomarkers and we can say that denosumab was generally safe in a complex population of immunosuppressed kidney transplant recipients. But it was associated with a higher incidence of urinary tract infections. At this point we have no good explanation as to why this is. We also had a few episodes of transient and asymptomatic hypocalcemia.”
The researchers reported having no financial disclosures.
AT KIDNEY WEEK 2015
Key clinical point: Denosumab effectively increased bone mineral density in kidney transplant recipients in the POSTOP trial.
Major finding: After 12 months, total lumbar spine BMD increased by 4.6% in the denosumab group and decreased by 0.5% in the control group, for a between-group difference of 5.1% (P less than .0001).
Data source: POSTOP, a study of 90 patients who were randomized within 4 weeks after kidney transplant surgery in a 1:1 ratio to receive subcutaneous injections of 60 mg denosumab at baseline and after 6 months, or no treatment.
Disclosures: The researchers reported having no financial disclosures.

President vetoes bill to repeal ACA
President Obama formally vetoed, as expected, a budget reconciliation bill that would have effectively killed the Affordable Care Act.
The budget reconciliation bill, H.R. 3762, passed in the Senate in December and cleared the House nearly along party lines on Jan. 6.

In announcing the veto, President Obama said in a statement that the bill would increase the number of uninsured by 22 million after 2017 and “would cost millions of hard-working middle-class families the security of affordable health coverage they deserve. Reliable health care coverage would no longer be a right for everyone: It would return to being a privilege for a few.”
He also noted that provisions that would defund Planned Parenthood would limit access to health care and disproportionately impact low-income individuals.
“Because of the harm this bill would cause to the health and financial security of millions of Americans, it has earned my veto,” he said.
President Obama formally vetoed, as expected, a budget reconciliation bill that would have effectively killed the Affordable Care Act.
The budget reconciliation bill, H.R. 3762, passed in the Senate in December and cleared the House nearly along party lines on Jan. 6.
In announcing the veto, President Obama said in a statement that the bill would increase the number of uninsured by 22 million after 2017 and “would cost millions of hard-working middle-class families the security of affordable health coverage they deserve. Reliable health care coverage would no longer be a right for everyone: It would return to being a privilege for a few.”
He also noted that provisions that would defund Planned Parenthood would limit access to health care and disproportionately impact low-income individuals.
“Because of the harm this bill would cause to the health and financial security of millions of Americans, it has earned my veto,” he said.
President Obama formally vetoed, as expected, a budget reconciliation bill that would have effectively killed the Affordable Care Act.
The budget reconciliation bill, H.R. 3762, passed in the Senate in December and cleared the House nearly along party lines on Jan. 6.
In announcing the veto, President Obama said in a statement that the bill would increase the number of uninsured by 22 million after 2017 and “would cost millions of hard-working middle-class families the security of affordable health coverage they deserve. Reliable health care coverage would no longer be a right for everyone: It would return to being a privilege for a few.”
He also noted that provisions that would defund Planned Parenthood would limit access to health care and disproportionately impact low-income individuals.
“Because of the harm this bill would cause to the health and financial security of millions of Americans, it has earned my veto,” he said.

Consider pyoderma gangrenosum for nonhealing wounds
LAS VEGAS – Though pyoderma gangrenosum and other neutrophilic skin disorders are rare, clinicians should include them in their differential, especially for nonhealing surgical wounds or skin “infections.”
Since these painful areas of ulceration need corticosteroid treatment, not antibiotics, for resolution, accurate diagnosis is critical for healing, Dr. J. Mark Jackson said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.

In a review of pyoderma gangrenosum (PG) and its cousins at the meeting, Dr. Jackson noted that the etiology of PG is unknown, but disordered neutrophilic chemotaxis is thought to be a factor. The many different manifestations of this disease are now collectively called the “neutrophilic dermatoses,” he said.
“Pyoderma gangrenosum is a very important diagnosis to consider in the differential diagnosis for nonhealing ulcerations, as suspicion and early recognition of this debilitating condition can prevent long-term sequelae such as pain, scarring, and long-term immunosuppressive medications,” said Dr. Jackson of the department of dermatology at the University of Louisville (Ky.).
The diagnosis should be suspected in the setting of a painful cutaneous ulcer with necrolysis. The border is typically irregular, violaceous, and undermined, he said, adding that this classic undermined border is caused by the sheets of neutrophils that characterize the disease.
Noting that half of patients with PG have underlying associated conditions such as Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and hematologic malignancies, Dr. Jackson emphasized that systemic disease associated with PG should heighten suspicion. “Histopathologic findings may be consistent with but not diagnostic of PG,” and can include a sterile dermal neutrophilia, with or without mixed inflammation and a lymphocytic vasculitis.
“Where you biopsy is important,” he continued, emphasizing that the biopsy must capture the margin of ulceration, where the sheets of neutrophils characteristic of PG will be seen on pathology.

Therapy consists of corticosteroids, with or without an immunosuppressive agent, and cessation of treatments that may continue to provoke pathergy.
Other diseases should also be considered in the differential diagnosis, including dangerous infectious causes, such as atypical mycobacteria, deep fungal infections, and staphylococcal and streptococcal infections. Squamous cell carcinoma, lymphoma, and leukemia may also present with similar lesions, as may metastatic Crohn’s disease, Dr. Jackson said. Several vasculitic and vasculopathic inflammatory conditions can also have similar appearances, including Wegener’s granulomatosis and vasoocclusive disorders such as peripheral vascular disease and cryoglobulinemia.
Classically, PG presents as painful ulcerated areas, most often on the lower extremities, that have a typical undermined border, caused by the sheets of neutrophils that characterize PG, he pointed out. PG may be mistaken for venous stasis ulcers, pressure ulcers, and cellulitis, but it doesn’t improve with antibiotics and mechanical manipulation from exfoliative dressings – and debridement may worsen the condition.

For susceptible individuals, surgery may provoke a pathergic response and trigger PG at the site of the surgical wound, and dogged attempts at conventional wound care may cause continued pathergy and begin a vicious cycle, Dr. Jackson said.
Peristomal pyoderma gangrenosum is a disease subcategory that may be seen in patients whose inflammatory bowel disease has been surgically treated and who have a stoma. Patients will have ulcerating lesions around their stoma site that are often misdiagnosed and treated as infections. Some wound care therapies, such as debridement, may continue to provoke the pathergic response and worsen peristomal PG, he said.
Though associated disease is seen in up to 50% of individuals with PG, there’s no predictable timeline linking the development of PG with the course of the associated disorder. In classic PG, usually occurring on the legs, autoimmune diseases such as inflammatory bowel disease, rheumatoid arthritis or another inflammatory arthritis, and paraproteinemia may be seen. Atypical PG, occurring more commonly on the upper extremities and face, is associated with myelogenous leukemia and preleukemic states, Dr. Jackson said.
Pyoderma gangrenosum lesions improve with corticosteroid administration. Depending on disease severity and location, topical, intralesional, or systemic steroids may be used.
Adjunctive treatments for PG and other neutrophilic dermatoses can include antibiotics with anti-inflammatory properties, such as minocycline or doxycycline, dapsone, and metronidazole. Immunosuppressives such as cyclosporine, azathioprine, and mycophenolate mofetil may also help speed resolution. In some cases, skin grafts may be necessary.

PG patients with Crohn’s disease or rheumatoid arthritis who are prescribed tumor necrosis factor–alpha (TNF-alpha) inhibitors for their systemic disease may also see improvement in PG lesions, Dr. Jackson said.
Other rare categories of neutrophilic dermatoses include Sweet’s syndrome, an acute febrile neutrophilic dermatosis, and neutrophilic dermatosis of the dorsum of the hand.
Neutrophilic invasion can also occur in other organs. “These extracutaneous lesions are also ‘sterile’ neutrophilic abscesses, which are often misdiagnosed as infections,” Dr. Jackson said. The most common site of extracutaneous neutrophilic infiltration is the lungs, though any organ system may be affected.
Dr. Jackson disclosed that he has received research support, honoraria, consulting fees, and other support from Abbvie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
The Skin Disease Education Foundation and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Though pyoderma gangrenosum and other neutrophilic skin disorders are rare, clinicians should include them in their differential, especially for nonhealing surgical wounds or skin “infections.”
Since these painful areas of ulceration need corticosteroid treatment, not antibiotics, for resolution, accurate diagnosis is critical for healing, Dr. J. Mark Jackson said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
In a review of pyoderma gangrenosum (PG) and its cousins at the meeting, Dr. Jackson noted that the etiology of PG is unknown, but disordered neutrophilic chemotaxis is thought to be a factor. The many different manifestations of this disease are now collectively called the “neutrophilic dermatoses,” he said.
“Pyoderma gangrenosum is a very important diagnosis to consider in the differential diagnosis for nonhealing ulcerations, as suspicion and early recognition of this debilitating condition can prevent long-term sequelae such as pain, scarring, and long-term immunosuppressive medications,” said Dr. Jackson of the department of dermatology at the University of Louisville (Ky.).
The diagnosis should be suspected in the setting of a painful cutaneous ulcer with necrolysis. The border is typically irregular, violaceous, and undermined, he said, adding that this classic undermined border is caused by the sheets of neutrophils that characterize the disease.
Noting that half of patients with PG have underlying associated conditions such as Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and hematologic malignancies, Dr. Jackson emphasized that systemic disease associated with PG should heighten suspicion. “Histopathologic findings may be consistent with but not diagnostic of PG,” and can include a sterile dermal neutrophilia, with or without mixed inflammation and a lymphocytic vasculitis.
“Where you biopsy is important,” he continued, emphasizing that the biopsy must capture the margin of ulceration, where the sheets of neutrophils characteristic of PG will be seen on pathology.
Therapy consists of corticosteroids, with or without an immunosuppressive agent, and cessation of treatments that may continue to provoke pathergy.
Other diseases should also be considered in the differential diagnosis, including dangerous infectious causes, such as atypical mycobacteria, deep fungal infections, and staphylococcal and streptococcal infections. Squamous cell carcinoma, lymphoma, and leukemia may also present with similar lesions, as may metastatic Crohn’s disease, Dr. Jackson said. Several vasculitic and vasculopathic inflammatory conditions can also have similar appearances, including Wegener’s granulomatosis and vasoocclusive disorders such as peripheral vascular disease and cryoglobulinemia.
Classically, PG presents as painful ulcerated areas, most often on the lower extremities, that have a typical undermined border, caused by the sheets of neutrophils that characterize PG, he pointed out. PG may be mistaken for venous stasis ulcers, pressure ulcers, and cellulitis, but it doesn’t improve with antibiotics and mechanical manipulation from exfoliative dressings – and debridement may worsen the condition.
For susceptible individuals, surgery may provoke a pathergic response and trigger PG at the site of the surgical wound, and dogged attempts at conventional wound care may cause continued pathergy and begin a vicious cycle, Dr. Jackson said.
Peristomal pyoderma gangrenosum is a disease subcategory that may be seen in patients whose inflammatory bowel disease has been surgically treated and who have a stoma. Patients will have ulcerating lesions around their stoma site that are often misdiagnosed and treated as infections. Some wound care therapies, such as debridement, may continue to provoke the pathergic response and worsen peristomal PG, he said.
Though associated disease is seen in up to 50% of individuals with PG, there’s no predictable timeline linking the development of PG with the course of the associated disorder. In classic PG, usually occurring on the legs, autoimmune diseases such as inflammatory bowel disease, rheumatoid arthritis or another inflammatory arthritis, and paraproteinemia may be seen. Atypical PG, occurring more commonly on the upper extremities and face, is associated with myelogenous leukemia and preleukemic states, Dr. Jackson said.
Pyoderma gangrenosum lesions improve with corticosteroid administration. Depending on disease severity and location, topical, intralesional, or systemic steroids may be used.
Adjunctive treatments for PG and other neutrophilic dermatoses can include antibiotics with anti-inflammatory properties, such as minocycline or doxycycline, dapsone, and metronidazole. Immunosuppressives such as cyclosporine, azathioprine, and mycophenolate mofetil may also help speed resolution. In some cases, skin grafts may be necessary.
PG patients with Crohn’s disease or rheumatoid arthritis who are prescribed tumor necrosis factor–alpha (TNF-alpha) inhibitors for their systemic disease may also see improvement in PG lesions, Dr. Jackson said.
Other rare categories of neutrophilic dermatoses include Sweet’s syndrome, an acute febrile neutrophilic dermatosis, and neutrophilic dermatosis of the dorsum of the hand.
Neutrophilic invasion can also occur in other organs. “These extracutaneous lesions are also ‘sterile’ neutrophilic abscesses, which are often misdiagnosed as infections,” Dr. Jackson said. The most common site of extracutaneous neutrophilic infiltration is the lungs, though any organ system may be affected.
Dr. Jackson disclosed that he has received research support, honoraria, consulting fees, and other support from Abbvie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
The Skin Disease Education Foundation and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Though pyoderma gangrenosum and other neutrophilic skin disorders are rare, clinicians should include them in their differential, especially for nonhealing surgical wounds or skin “infections.”
Since these painful areas of ulceration need corticosteroid treatment, not antibiotics, for resolution, accurate diagnosis is critical for healing, Dr. J. Mark Jackson said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
In a review of pyoderma gangrenosum (PG) and its cousins at the meeting, Dr. Jackson noted that the etiology of PG is unknown, but disordered neutrophilic chemotaxis is thought to be a factor. The many different manifestations of this disease are now collectively called the “neutrophilic dermatoses,” he said.
“Pyoderma gangrenosum is a very important diagnosis to consider in the differential diagnosis for nonhealing ulcerations, as suspicion and early recognition of this debilitating condition can prevent long-term sequelae such as pain, scarring, and long-term immunosuppressive medications,” said Dr. Jackson of the department of dermatology at the University of Louisville (Ky.).
The diagnosis should be suspected in the setting of a painful cutaneous ulcer with necrolysis. The border is typically irregular, violaceous, and undermined, he said, adding that this classic undermined border is caused by the sheets of neutrophils that characterize the disease.
Noting that half of patients with PG have underlying associated conditions such as Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and hematologic malignancies, Dr. Jackson emphasized that systemic disease associated with PG should heighten suspicion. “Histopathologic findings may be consistent with but not diagnostic of PG,” and can include a sterile dermal neutrophilia, with or without mixed inflammation and a lymphocytic vasculitis.
“Where you biopsy is important,” he continued, emphasizing that the biopsy must capture the margin of ulceration, where the sheets of neutrophils characteristic of PG will be seen on pathology.
Therapy consists of corticosteroids, with or without an immunosuppressive agent, and cessation of treatments that may continue to provoke pathergy.
Other diseases should also be considered in the differential diagnosis, including dangerous infectious causes, such as atypical mycobacteria, deep fungal infections, and staphylococcal and streptococcal infections. Squamous cell carcinoma, lymphoma, and leukemia may also present with similar lesions, as may metastatic Crohn’s disease, Dr. Jackson said. Several vasculitic and vasculopathic inflammatory conditions can also have similar appearances, including Wegener’s granulomatosis and vasoocclusive disorders such as peripheral vascular disease and cryoglobulinemia.
Classically, PG presents as painful ulcerated areas, most often on the lower extremities, that have a typical undermined border, caused by the sheets of neutrophils that characterize PG, he pointed out. PG may be mistaken for venous stasis ulcers, pressure ulcers, and cellulitis, but it doesn’t improve with antibiotics and mechanical manipulation from exfoliative dressings – and debridement may worsen the condition.
For susceptible individuals, surgery may provoke a pathergic response and trigger PG at the site of the surgical wound, and dogged attempts at conventional wound care may cause continued pathergy and begin a vicious cycle, Dr. Jackson said.
Peristomal pyoderma gangrenosum is a disease subcategory that may be seen in patients whose inflammatory bowel disease has been surgically treated and who have a stoma. Patients will have ulcerating lesions around their stoma site that are often misdiagnosed and treated as infections. Some wound care therapies, such as debridement, may continue to provoke the pathergic response and worsen peristomal PG, he said.
Though associated disease is seen in up to 50% of individuals with PG, there’s no predictable timeline linking the development of PG with the course of the associated disorder. In classic PG, usually occurring on the legs, autoimmune diseases such as inflammatory bowel disease, rheumatoid arthritis or another inflammatory arthritis, and paraproteinemia may be seen. Atypical PG, occurring more commonly on the upper extremities and face, is associated with myelogenous leukemia and preleukemic states, Dr. Jackson said.
Pyoderma gangrenosum lesions improve with corticosteroid administration. Depending on disease severity and location, topical, intralesional, or systemic steroids may be used.
Adjunctive treatments for PG and other neutrophilic dermatoses can include antibiotics with anti-inflammatory properties, such as minocycline or doxycycline, dapsone, and metronidazole. Immunosuppressives such as cyclosporine, azathioprine, and mycophenolate mofetil may also help speed resolution. In some cases, skin grafts may be necessary.
PG patients with Crohn’s disease or rheumatoid arthritis who are prescribed tumor necrosis factor–alpha (TNF-alpha) inhibitors for their systemic disease may also see improvement in PG lesions, Dr. Jackson said.
Other rare categories of neutrophilic dermatoses include Sweet’s syndrome, an acute febrile neutrophilic dermatosis, and neutrophilic dermatosis of the dorsum of the hand.
Neutrophilic invasion can also occur in other organs. “These extracutaneous lesions are also ‘sterile’ neutrophilic abscesses, which are often misdiagnosed as infections,” Dr. Jackson said. The most common site of extracutaneous neutrophilic infiltration is the lungs, though any organ system may be affected.
Dr. Jackson disclosed that he has received research support, honoraria, consulting fees, and other support from Abbvie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
The Skin Disease Education Foundation and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Congress passes ACA repeal bill; President says he will veto
After more than 60 House-originated bills attacking the Affordable Care Act stalled before completing their congressional journey, President Obama will finally get the opportunity to veto one.
On Jan. 6, the House passed a budget reconciliation bill that would essentially gut Obamacare and defund Planned Parenthood for at least 1 year by a 240-181 vote, largely on party lines. One Democrat joined the Republicans in approving the bill, while three Republicans voted against the measure.

The Senate passed the same bill, H.R. 3762, in December. The legislation would repeal the individual and employer mandates and associated tax penalties; phase out Medicaid expansion; eliminate federal subsidies to help patients buy insurance on the federal exchange; repeal the “Cadillac tax” on high-value health insurance plans; repeal the medical device tax; and defund Planned Parenthood for 1 year and divert some of those funds to community health centers.
“This reconciliation bill would cause an estimated 22 million Americans … to lose their health care, would increase premiums by approximately 20%, would provide employers with much uncertainty, and worsen the outlook for deficits over the long term,” Rep. Steny Hoyer (D-Md.) said during floor debate prior to the vote. “Only in the first 10-year window do you have a savings. The [Congressional Budget Office] says if you go to the second 10 years, this bill is a loser and exacerbates the deficit.”
Republicans continue to argue that the Affordable Care Act is anything but affordable.
“This bill will help undermine and get rid of the foundation of Obamacare which, I know as a physician, has accelerated the negative trends in health care, of which there are many,” said Rep. Charles Boustany Jr. (R-La.). “[It] is not the affordable, patient-centered health care that the American people deserve.”
In a statement, Health and Human Services Secretary Sylvia Burwell said, “President Obama has clearly said he will veto this bill. As I travel the country, I consistently hear Americans say that they want Washington to build on the progress we have made to increase access to coverage, drive down the growth of health costs and improve the quality of care. Unfortunately, today’s partisan effort in the House of Representatives to repeal key parts of the ACA, along with its effective defunding of Planned Parenthood, does the opposite.”
After more than 60 House-originated bills attacking the Affordable Care Act stalled before completing their congressional journey, President Obama will finally get the opportunity to veto one.
On Jan. 6, the House passed a budget reconciliation bill that would essentially gut Obamacare and defund Planned Parenthood for at least 1 year by a 240-181 vote, largely on party lines. One Democrat joined the Republicans in approving the bill, while three Republicans voted against the measure.
The Senate passed the same bill, H.R. 3762, in December. The legislation would repeal the individual and employer mandates and associated tax penalties; phase out Medicaid expansion; eliminate federal subsidies to help patients buy insurance on the federal exchange; repeal the “Cadillac tax” on high-value health insurance plans; repeal the medical device tax; and defund Planned Parenthood for 1 year and divert some of those funds to community health centers.
“This reconciliation bill would cause an estimated 22 million Americans … to lose their health care, would increase premiums by approximately 20%, would provide employers with much uncertainty, and worsen the outlook for deficits over the long term,” Rep. Steny Hoyer (D-Md.) said during floor debate prior to the vote. “Only in the first 10-year window do you have a savings. The [Congressional Budget Office] says if you go to the second 10 years, this bill is a loser and exacerbates the deficit.”
Republicans continue to argue that the Affordable Care Act is anything but affordable.
“This bill will help undermine and get rid of the foundation of Obamacare which, I know as a physician, has accelerated the negative trends in health care, of which there are many,” said Rep. Charles Boustany Jr. (R-La.). “[It] is not the affordable, patient-centered health care that the American people deserve.”
In a statement, Health and Human Services Secretary Sylvia Burwell said, “President Obama has clearly said he will veto this bill. As I travel the country, I consistently hear Americans say that they want Washington to build on the progress we have made to increase access to coverage, drive down the growth of health costs and improve the quality of care. Unfortunately, today’s partisan effort in the House of Representatives to repeal key parts of the ACA, along with its effective defunding of Planned Parenthood, does the opposite.”
After more than 60 House-originated bills attacking the Affordable Care Act stalled before completing their congressional journey, President Obama will finally get the opportunity to veto one.
On Jan. 6, the House passed a budget reconciliation bill that would essentially gut Obamacare and defund Planned Parenthood for at least 1 year by a 240-181 vote, largely on party lines. One Democrat joined the Republicans in approving the bill, while three Republicans voted against the measure.
The Senate passed the same bill, H.R. 3762, in December. The legislation would repeal the individual and employer mandates and associated tax penalties; phase out Medicaid expansion; eliminate federal subsidies to help patients buy insurance on the federal exchange; repeal the “Cadillac tax” on high-value health insurance plans; repeal the medical device tax; and defund Planned Parenthood for 1 year and divert some of those funds to community health centers.
“This reconciliation bill would cause an estimated 22 million Americans … to lose their health care, would increase premiums by approximately 20%, would provide employers with much uncertainty, and worsen the outlook for deficits over the long term,” Rep. Steny Hoyer (D-Md.) said during floor debate prior to the vote. “Only in the first 10-year window do you have a savings. The [Congressional Budget Office] says if you go to the second 10 years, this bill is a loser and exacerbates the deficit.”
Republicans continue to argue that the Affordable Care Act is anything but affordable.
“This bill will help undermine and get rid of the foundation of Obamacare which, I know as a physician, has accelerated the negative trends in health care, of which there are many,” said Rep. Charles Boustany Jr. (R-La.). “[It] is not the affordable, patient-centered health care that the American people deserve.”
In a statement, Health and Human Services Secretary Sylvia Burwell said, “President Obama has clearly said he will veto this bill. As I travel the country, I consistently hear Americans say that they want Washington to build on the progress we have made to increase access to coverage, drive down the growth of health costs and improve the quality of care. Unfortunately, today’s partisan effort in the House of Representatives to repeal key parts of the ACA, along with its effective defunding of Planned Parenthood, does the opposite.”

Hospital-acquired pneumonia threatens cervical spinal cord injury patients
SAN DIEGO – The overall rate of hospital-acquired pneumonia following cervical spinal cord injury is about 20%, results from a study of national data demonstrated.
“Cervical spinal cord injury patients are at an increased risk for the development of hospital-acquired pneumonia,” lead study author Dr. Pablo J. Diaz-Collado said in an interview after the annual meeting of the Cervical Spine Research Society.

“Complete cord injuries, longer length of stay, ICU stay and ventilation time lead to significantly increased risk of HAP, which then leads to poor inpatient outcomes,” he said. “It is of crucial importance to keep these risk factors in mind when treating patients with cervical spinal cord injuries. There is a need to optimize the management protocols for these patients to help prevent the development of HAPs.”
Dr. Diaz-Collado, an orthopedic surgery resident at Yale–New Haven (Conn.) Hospital, and his associates identified 5,198 cervical spinal cord injury patients in the 2011 and 2012 National Trauma Data Bank (NTDB) to analyze risk factors for the development of HAP and inpatient outcomes in this population. They used multivariate logistic regression to identify independent associations of various risk factors with the occurrence of HAP.
The researchers found that the overall incidence of HAP among cervical spinal cord injury patients was 20.5%, which amounted to 1,065 patients. Factors independently associated with HAP were complete spinal cord injuries (compared to central cord injuries; OR 1.44; P = .009); longer inpatient length of stay (OR 3.08 for a stay that lasted 7-13 days, OR 10.21 for 21-27 days, and OR 14.89 for 35 days or more; P = .001 or less for all associations); longer ICU stay (OR 2.86 for a stay that lasted 9-11 days, OR 3.05 for 12-14 days, and OR 2.94 for 15 days or more; P less than .001 for all associations), and longer time on mechanical ventilation (OR 2.68 for ventilation that lasted 3-6 days, OR 3.76 for 7-13 days, OR 3.98 for 14-20 days, and OR 3.99 for 21 days or more; P less than .001 for all associations).
After the researchers controlled for all other risk factors, including patient comorbidities, Injury Severity Score, and other inpatient complications, HAP was associated with increased odds of death (OR 1.60; P = .005), inpatient adverse events (OR 1.65; P less than .001), discharge to an extended-care facility (OR 1.93; P = .001), and longer length of stay (a mean of an additional 10.93 days; P less than .001).
Dr. Diaz-Collado acknowledged that the study is “limited by the quality of the data entry. In addition, the database does not include classifications of fractures, and thus stratification of the analysis in terms of the different kinds of fractures in the cervical spine is not possible. Finally, procedural codes are less accurate and thus including whether or not patients underwent a surgical intervention is less reliable.”
Dr. Diaz-Collado reported having no financial disclosures.
SAN DIEGO – The overall rate of hospital-acquired pneumonia following cervical spinal cord injury is about 20%, results from a study of national data demonstrated.
“Cervical spinal cord injury patients are at an increased risk for the development of hospital-acquired pneumonia,” lead study author Dr. Pablo J. Diaz-Collado said in an interview after the annual meeting of the Cervical Spine Research Society.
“Complete cord injuries, longer length of stay, ICU stay and ventilation time lead to significantly increased risk of HAP, which then leads to poor inpatient outcomes,” he said. “It is of crucial importance to keep these risk factors in mind when treating patients with cervical spinal cord injuries. There is a need to optimize the management protocols for these patients to help prevent the development of HAPs.”
Dr. Diaz-Collado, an orthopedic surgery resident at Yale–New Haven (Conn.) Hospital, and his associates identified 5,198 cervical spinal cord injury patients in the 2011 and 2012 National Trauma Data Bank (NTDB) to analyze risk factors for the development of HAP and inpatient outcomes in this population. They used multivariate logistic regression to identify independent associations of various risk factors with the occurrence of HAP.
The researchers found that the overall incidence of HAP among cervical spinal cord injury patients was 20.5%, which amounted to 1,065 patients. Factors independently associated with HAP were complete spinal cord injuries (compared to central cord injuries; OR 1.44; P = .009); longer inpatient length of stay (OR 3.08 for a stay that lasted 7-13 days, OR 10.21 for 21-27 days, and OR 14.89 for 35 days or more; P = .001 or less for all associations); longer ICU stay (OR 2.86 for a stay that lasted 9-11 days, OR 3.05 for 12-14 days, and OR 2.94 for 15 days or more; P less than .001 for all associations), and longer time on mechanical ventilation (OR 2.68 for ventilation that lasted 3-6 days, OR 3.76 for 7-13 days, OR 3.98 for 14-20 days, and OR 3.99 for 21 days or more; P less than .001 for all associations).
After the researchers controlled for all other risk factors, including patient comorbidities, Injury Severity Score, and other inpatient complications, HAP was associated with increased odds of death (OR 1.60; P = .005), inpatient adverse events (OR 1.65; P less than .001), discharge to an extended-care facility (OR 1.93; P = .001), and longer length of stay (a mean of an additional 10.93 days; P less than .001).
Dr. Diaz-Collado acknowledged that the study is “limited by the quality of the data entry. In addition, the database does not include classifications of fractures, and thus stratification of the analysis in terms of the different kinds of fractures in the cervical spine is not possible. Finally, procedural codes are less accurate and thus including whether or not patients underwent a surgical intervention is less reliable.”
Dr. Diaz-Collado reported having no financial disclosures.
SAN DIEGO – The overall rate of hospital-acquired pneumonia following cervical spinal cord injury is about 20%, results from a study of national data demonstrated.
“Cervical spinal cord injury patients are at an increased risk for the development of hospital-acquired pneumonia,” lead study author Dr. Pablo J. Diaz-Collado said in an interview after the annual meeting of the Cervical Spine Research Society.
“Complete cord injuries, longer length of stay, ICU stay and ventilation time lead to significantly increased risk of HAP, which then leads to poor inpatient outcomes,” he said. “It is of crucial importance to keep these risk factors in mind when treating patients with cervical spinal cord injuries. There is a need to optimize the management protocols for these patients to help prevent the development of HAPs.”
Dr. Diaz-Collado, an orthopedic surgery resident at Yale–New Haven (Conn.) Hospital, and his associates identified 5,198 cervical spinal cord injury patients in the 2011 and 2012 National Trauma Data Bank (NTDB) to analyze risk factors for the development of HAP and inpatient outcomes in this population. They used multivariate logistic regression to identify independent associations of various risk factors with the occurrence of HAP.
The researchers found that the overall incidence of HAP among cervical spinal cord injury patients was 20.5%, which amounted to 1,065 patients. Factors independently associated with HAP were complete spinal cord injuries (compared to central cord injuries; OR 1.44; P = .009); longer inpatient length of stay (OR 3.08 for a stay that lasted 7-13 days, OR 10.21 for 21-27 days, and OR 14.89 for 35 days or more; P = .001 or less for all associations); longer ICU stay (OR 2.86 for a stay that lasted 9-11 days, OR 3.05 for 12-14 days, and OR 2.94 for 15 days or more; P less than .001 for all associations), and longer time on mechanical ventilation (OR 2.68 for ventilation that lasted 3-6 days, OR 3.76 for 7-13 days, OR 3.98 for 14-20 days, and OR 3.99 for 21 days or more; P less than .001 for all associations).
After the researchers controlled for all other risk factors, including patient comorbidities, Injury Severity Score, and other inpatient complications, HAP was associated with increased odds of death (OR 1.60; P = .005), inpatient adverse events (OR 1.65; P less than .001), discharge to an extended-care facility (OR 1.93; P = .001), and longer length of stay (a mean of an additional 10.93 days; P less than .001).
Dr. Diaz-Collado acknowledged that the study is “limited by the quality of the data entry. In addition, the database does not include classifications of fractures, and thus stratification of the analysis in terms of the different kinds of fractures in the cervical spine is not possible. Finally, procedural codes are less accurate and thus including whether or not patients underwent a surgical intervention is less reliable.”
Dr. Diaz-Collado reported having no financial disclosures.
AT CSRS 2015
Key clinical point: About one in five cervical spinal cord injury patients develop hospital-acquired pneumonia.
Major finding: The overall incidence of HAP among cervical spinal cord injury patients was 20.5%.
Data source: A study of 5,198 cervical spinal cord injury patients in the 2011 and 2012 National Trauma Data Bank.
Disclosures: Dr. Diaz-Collado reported having no financial disclosures.