User login
Official Newspaper of the American College of Surgeons
Alternative payment models: MedPAC says keep it simple
WASHINGTON – A federal advisory panel has straightforward advice for the government as it shifts towards value-based health care: Keep it simple.
At the Jan. 15 meeting of the Medicare Payment Advisory Commission (MedPAC), Commissioner Warner Thomas said, “I think one of our first principles should be to try to simplify this because it’s very complicated for a provider to try to understand what path to take and how to play in these situations. We want providers to engage in this and I think there is a lot of aversion because folks don’t understand it, and they’re not sure where to play or where not to play.”

Officials at the Centers for Medicare & Medicaid Services are drafting the regulations needed to implement the Medicare Access & CHIP Reauthorization Act (MACRA); the proposed regulations are expected in the Spring.
MedPAC staff offered a number of principles they hope to see incorporated into the final design for alternative payment models (APMs) under the law, including:
• Incentive payments to providers should be distributed only if the entities they are a part of are able to successfully control cost, improve quality, or both.
• Entities should have enough beneficiaries to detect changes in spending and quality.
• Entities should be at risk for total Part A and Part B spending; in the future, Part D also might be measured.
• Entities should be allowed to share savings with beneficiaries.
• Regulatory relief should be possible.
Several MedPAC commissioners focused on how physicians are viewing the risk they will be asked to assume in an APM.
APMs are “an attempt to sort of jump start a movement in the direction of risk taking from a group that I don’t think is very thrilled about taking financial risk and has shown it by their actual practice in the face of efforts at least to nudge them in this direction,” said Commissioner Bill Gradison Jr., a former congressman from Ohio who served on the House Committee on Ways and Means. “Having said that, I wish I had a better understanding of the motivation of physicians in terms of what might move them in this direction. The assumption here is that the money will move them, and maybe it’s that simple, but I am not too sure about that.”
Commissioner Jack Hoadley, Ph.D., of the Health Policy Institute at Georgetown University, Washington, noted that the if there is too little risk involved, there tends to be little movement in changing the behavior.
Dr. Hoadley suggested that CMS could consider “looking at some of the models by which risk can be structured so it puts plenty of money on the line but it doesn’t do it in a way that’s going to get complicated in terms of physicians owing money back.”
Commissioners also recommended a tight threshold, at least early on, to show that cost containment and/or quality improvement are well established before an entity can move into an APM and receive a financial incentive.
“Let’s keep the initial round and definition tight and actually demand a track record before we qualify something as an alternative payment mechanism,” said Commissioner Kathy Buto, a U.S. and international health policy consultant and former deputy executive secretary in the U.S. Health & Human Services Department. “Once you open this up, you can’t close it down. You cannot walk it back. We are talking about paying a lot more money, 5% more and if the definition is too loose and too many entities get into it, you can never walk it back and you will be just adding to the expenditures.”
WASHINGTON – A federal advisory panel has straightforward advice for the government as it shifts towards value-based health care: Keep it simple.
At the Jan. 15 meeting of the Medicare Payment Advisory Commission (MedPAC), Commissioner Warner Thomas said, “I think one of our first principles should be to try to simplify this because it’s very complicated for a provider to try to understand what path to take and how to play in these situations. We want providers to engage in this and I think there is a lot of aversion because folks don’t understand it, and they’re not sure where to play or where not to play.”
Officials at the Centers for Medicare & Medicaid Services are drafting the regulations needed to implement the Medicare Access & CHIP Reauthorization Act (MACRA); the proposed regulations are expected in the Spring.
MedPAC staff offered a number of principles they hope to see incorporated into the final design for alternative payment models (APMs) under the law, including:
• Incentive payments to providers should be distributed only if the entities they are a part of are able to successfully control cost, improve quality, or both.
• Entities should have enough beneficiaries to detect changes in spending and quality.
• Entities should be at risk for total Part A and Part B spending; in the future, Part D also might be measured.
• Entities should be allowed to share savings with beneficiaries.
• Regulatory relief should be possible.
Several MedPAC commissioners focused on how physicians are viewing the risk they will be asked to assume in an APM.
APMs are “an attempt to sort of jump start a movement in the direction of risk taking from a group that I don’t think is very thrilled about taking financial risk and has shown it by their actual practice in the face of efforts at least to nudge them in this direction,” said Commissioner Bill Gradison Jr., a former congressman from Ohio who served on the House Committee on Ways and Means. “Having said that, I wish I had a better understanding of the motivation of physicians in terms of what might move them in this direction. The assumption here is that the money will move them, and maybe it’s that simple, but I am not too sure about that.”
Commissioner Jack Hoadley, Ph.D., of the Health Policy Institute at Georgetown University, Washington, noted that the if there is too little risk involved, there tends to be little movement in changing the behavior.
Dr. Hoadley suggested that CMS could consider “looking at some of the models by which risk can be structured so it puts plenty of money on the line but it doesn’t do it in a way that’s going to get complicated in terms of physicians owing money back.”
Commissioners also recommended a tight threshold, at least early on, to show that cost containment and/or quality improvement are well established before an entity can move into an APM and receive a financial incentive.
“Let’s keep the initial round and definition tight and actually demand a track record before we qualify something as an alternative payment mechanism,” said Commissioner Kathy Buto, a U.S. and international health policy consultant and former deputy executive secretary in the U.S. Health & Human Services Department. “Once you open this up, you can’t close it down. You cannot walk it back. We are talking about paying a lot more money, 5% more and if the definition is too loose and too many entities get into it, you can never walk it back and you will be just adding to the expenditures.”
WASHINGTON – A federal advisory panel has straightforward advice for the government as it shifts towards value-based health care: Keep it simple.
At the Jan. 15 meeting of the Medicare Payment Advisory Commission (MedPAC), Commissioner Warner Thomas said, “I think one of our first principles should be to try to simplify this because it’s very complicated for a provider to try to understand what path to take and how to play in these situations. We want providers to engage in this and I think there is a lot of aversion because folks don’t understand it, and they’re not sure where to play or where not to play.”
Officials at the Centers for Medicare & Medicaid Services are drafting the regulations needed to implement the Medicare Access & CHIP Reauthorization Act (MACRA); the proposed regulations are expected in the Spring.
MedPAC staff offered a number of principles they hope to see incorporated into the final design for alternative payment models (APMs) under the law, including:
• Incentive payments to providers should be distributed only if the entities they are a part of are able to successfully control cost, improve quality, or both.
• Entities should have enough beneficiaries to detect changes in spending and quality.
• Entities should be at risk for total Part A and Part B spending; in the future, Part D also might be measured.
• Entities should be allowed to share savings with beneficiaries.
• Regulatory relief should be possible.
Several MedPAC commissioners focused on how physicians are viewing the risk they will be asked to assume in an APM.
APMs are “an attempt to sort of jump start a movement in the direction of risk taking from a group that I don’t think is very thrilled about taking financial risk and has shown it by their actual practice in the face of efforts at least to nudge them in this direction,” said Commissioner Bill Gradison Jr., a former congressman from Ohio who served on the House Committee on Ways and Means. “Having said that, I wish I had a better understanding of the motivation of physicians in terms of what might move them in this direction. The assumption here is that the money will move them, and maybe it’s that simple, but I am not too sure about that.”
Commissioner Jack Hoadley, Ph.D., of the Health Policy Institute at Georgetown University, Washington, noted that the if there is too little risk involved, there tends to be little movement in changing the behavior.
Dr. Hoadley suggested that CMS could consider “looking at some of the models by which risk can be structured so it puts plenty of money on the line but it doesn’t do it in a way that’s going to get complicated in terms of physicians owing money back.”
Commissioners also recommended a tight threshold, at least early on, to show that cost containment and/or quality improvement are well established before an entity can move into an APM and receive a financial incentive.
“Let’s keep the initial round and definition tight and actually demand a track record before we qualify something as an alternative payment mechanism,” said Commissioner Kathy Buto, a U.S. and international health policy consultant and former deputy executive secretary in the U.S. Health & Human Services Department. “Once you open this up, you can’t close it down. You cannot walk it back. We are talking about paying a lot more money, 5% more and if the definition is too loose and too many entities get into it, you can never walk it back and you will be just adding to the expenditures.”
AT A MEDPAC MEETING

Significant risk of relapse remains for ER-positive breast cancer patients beyond 10 years
The risk of breast cancer relapse decreases consistently for 10 years, then remains stable through 25 years, with ER-positive disease carrying higher risk than ER-negative disease from years 5 to 25, according to researchers.
At a median follow up of 24 years, the study reported outcomes of 4,105 patients who were diagnosed from 1978 to 1985 and participated in the International Breast Cancer Study Group Trials I to V. During the first 5 years of follow-up, risk of recurrence was lower for ER-positive compared with ER-negative disease: 9.9% vs. 11.5%. Beyond 5 years, risk was higher: 5-10 years, 5.4% vs. 3.3%; 10-15 years, 2.9% vs. 1.3%, 15-20 years, 2.8% vs. 1.2%. At 20-25 years, risk was 1.3% vs. 1.4% (P less than .001).

“We identified a population (ER positive) that maintains a significant risk of relapse even after more than 10 years of follow-up. New targeted treatments and different modes of breast cancer surveillance for preventing late recurrences within this population should be studied,” wrote Dr. Marco Colleoni of the European Institute of Oncology and International Breast Cancer Study Group, and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.3504).
For the entire patient group, breast cancer recurrence reached a peak at years 1-2 (15.2%), and decreased consistently through year 10 (5-10 years, 4.5%), then remained stable (10-15 years, 2.2%; 15-20, 1.5%; 20-25, 0.7%). Cumulative incidence of distant recurrence for the ER-positive group occurred less frequently than for the ER-negative group during the first 5 years and more frequently from 5 to 25 years: at 5 years, 27.1% vs. 23.4%; at 10 years, 31.9% vs. 31.8%; at 15 years, 35% vs. 33.4%; at 20 years, 37.4% vs. 34.1%; at 25 years, 38.3% vs. 35.3% (P less than .001).
All patients in the trials had undergone mastectomy and axillary clearance with at least eight nodes removed, with no locoregional radiotherapy, as was standard at the time.
Within the ER-positive group, patients who had zero to three positive nodes had had a stable risk of recurrence beyond 10 years, whereas for patients with four or more involved nodes, risk decreased gradually from 10 to 24 years.
Recent studies have shown that 10 years of adjuvant tamoxifen further improves breast cancer survival compared with 5 years of adjuvant therapy, albeit at a cost of 0.4% due to mortality resulting from endometrial carcinoma or pulmonary embolism. The studies underline the critical importance of sufficiently large patient populations and longer follow-up to provide accurate outcome data.
The report by Colleoni et al. describes clinical trial results from a median 24-year follow up. Patients with ER-positive disease require long-term follow up, which should be fundamentally different from those with ER-negative and/or human epidermal growth factor receptor 2–positive disease, who require shorter follow-up. Given these differences, adjuvant clinical studies with shorter follow-up periods will underreport events for ER-positive patients.
The study also reports a secondary malignancy rate of 4.9%, a figure likely to be underreported in studies with shorter follow-up schedules.
Limitations of the study arise from the time period in which it began. Regimens used in the study (different schedules of cyclophosphamide, methotrexate, and fluorouracil, and 1 year of tamoxifen with or without prednisone) have been shown to be inferior to newer regimens. None of the patients received postoperative radiotherapy, in accordance with data available at the time. Today, women with node-positive disease receive locoregional radiotherapy to reduce the risk of locoregional recurrence.
Studies with long-term follow up periods offer insights into both efficacy and safety; however, such studies require extensive resources. The entities that decide which types of cancer care are made available, such as insurance companies, governments, and regional health care funders, must shoulder the responsibility to ensure the required long-term evaluation of these treatments is conducted. Joint projects between pharmaceutical companies and health care providers could identify long-term benefits and adverse effects. The process may be more readily implemented in countries with population-based cancer registries.
Dr. Jonas Bergh is professor in the department of oncology-pathology at Karolinska Institutet and University Hospital, Stockholm. Dr. Kathleen Pritchard is a medical oncologist at Sunnybrook Odette Cancer Centre and professor at the University of Toronto. Dr. David Cameron is clinical director and chair of oncology at the University of Edinburgh Cancer Research Centre, Scotland. These remarks were part of an editorial accompanying the report by Colleoni et al. (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.65.2255). Dr. Bergh reported financial ties to Amgen, AstraZeneca, Bayer HealthCare Pharmaceuticals, Merck, Pfizer, Roche, and Sanofi. Dr. Pritchard reported ties to AstraZeneca, Pfizer, Roche, Amgen, Novartis, GlaxoSmithKline, and Eisai. Dr. Cameron reported ties to Novartis.
Recent studies have shown that 10 years of adjuvant tamoxifen further improves breast cancer survival compared with 5 years of adjuvant therapy, albeit at a cost of 0.4% due to mortality resulting from endometrial carcinoma or pulmonary embolism. The studies underline the critical importance of sufficiently large patient populations and longer follow-up to provide accurate outcome data.
The report by Colleoni et al. describes clinical trial results from a median 24-year follow up. Patients with ER-positive disease require long-term follow up, which should be fundamentally different from those with ER-negative and/or human epidermal growth factor receptor 2–positive disease, who require shorter follow-up. Given these differences, adjuvant clinical studies with shorter follow-up periods will underreport events for ER-positive patients.
The study also reports a secondary malignancy rate of 4.9%, a figure likely to be underreported in studies with shorter follow-up schedules.
Limitations of the study arise from the time period in which it began. Regimens used in the study (different schedules of cyclophosphamide, methotrexate, and fluorouracil, and 1 year of tamoxifen with or without prednisone) have been shown to be inferior to newer regimens. None of the patients received postoperative radiotherapy, in accordance with data available at the time. Today, women with node-positive disease receive locoregional radiotherapy to reduce the risk of locoregional recurrence.
Studies with long-term follow up periods offer insights into both efficacy and safety; however, such studies require extensive resources. The entities that decide which types of cancer care are made available, such as insurance companies, governments, and regional health care funders, must shoulder the responsibility to ensure the required long-term evaluation of these treatments is conducted. Joint projects between pharmaceutical companies and health care providers could identify long-term benefits and adverse effects. The process may be more readily implemented in countries with population-based cancer registries.
Dr. Jonas Bergh is professor in the department of oncology-pathology at Karolinska Institutet and University Hospital, Stockholm. Dr. Kathleen Pritchard is a medical oncologist at Sunnybrook Odette Cancer Centre and professor at the University of Toronto. Dr. David Cameron is clinical director and chair of oncology at the University of Edinburgh Cancer Research Centre, Scotland. These remarks were part of an editorial accompanying the report by Colleoni et al. (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.65.2255). Dr. Bergh reported financial ties to Amgen, AstraZeneca, Bayer HealthCare Pharmaceuticals, Merck, Pfizer, Roche, and Sanofi. Dr. Pritchard reported ties to AstraZeneca, Pfizer, Roche, Amgen, Novartis, GlaxoSmithKline, and Eisai. Dr. Cameron reported ties to Novartis.
Recent studies have shown that 10 years of adjuvant tamoxifen further improves breast cancer survival compared with 5 years of adjuvant therapy, albeit at a cost of 0.4% due to mortality resulting from endometrial carcinoma or pulmonary embolism. The studies underline the critical importance of sufficiently large patient populations and longer follow-up to provide accurate outcome data.
The report by Colleoni et al. describes clinical trial results from a median 24-year follow up. Patients with ER-positive disease require long-term follow up, which should be fundamentally different from those with ER-negative and/or human epidermal growth factor receptor 2–positive disease, who require shorter follow-up. Given these differences, adjuvant clinical studies with shorter follow-up periods will underreport events for ER-positive patients.
The study also reports a secondary malignancy rate of 4.9%, a figure likely to be underreported in studies with shorter follow-up schedules.
Limitations of the study arise from the time period in which it began. Regimens used in the study (different schedules of cyclophosphamide, methotrexate, and fluorouracil, and 1 year of tamoxifen with or without prednisone) have been shown to be inferior to newer regimens. None of the patients received postoperative radiotherapy, in accordance with data available at the time. Today, women with node-positive disease receive locoregional radiotherapy to reduce the risk of locoregional recurrence.
Studies with long-term follow up periods offer insights into both efficacy and safety; however, such studies require extensive resources. The entities that decide which types of cancer care are made available, such as insurance companies, governments, and regional health care funders, must shoulder the responsibility to ensure the required long-term evaluation of these treatments is conducted. Joint projects between pharmaceutical companies and health care providers could identify long-term benefits and adverse effects. The process may be more readily implemented in countries with population-based cancer registries.
Dr. Jonas Bergh is professor in the department of oncology-pathology at Karolinska Institutet and University Hospital, Stockholm. Dr. Kathleen Pritchard is a medical oncologist at Sunnybrook Odette Cancer Centre and professor at the University of Toronto. Dr. David Cameron is clinical director and chair of oncology at the University of Edinburgh Cancer Research Centre, Scotland. These remarks were part of an editorial accompanying the report by Colleoni et al. (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.65.2255). Dr. Bergh reported financial ties to Amgen, AstraZeneca, Bayer HealthCare Pharmaceuticals, Merck, Pfizer, Roche, and Sanofi. Dr. Pritchard reported ties to AstraZeneca, Pfizer, Roche, Amgen, Novartis, GlaxoSmithKline, and Eisai. Dr. Cameron reported ties to Novartis.
The risk of breast cancer relapse decreases consistently for 10 years, then remains stable through 25 years, with ER-positive disease carrying higher risk than ER-negative disease from years 5 to 25, according to researchers.
At a median follow up of 24 years, the study reported outcomes of 4,105 patients who were diagnosed from 1978 to 1985 and participated in the International Breast Cancer Study Group Trials I to V. During the first 5 years of follow-up, risk of recurrence was lower for ER-positive compared with ER-negative disease: 9.9% vs. 11.5%. Beyond 5 years, risk was higher: 5-10 years, 5.4% vs. 3.3%; 10-15 years, 2.9% vs. 1.3%, 15-20 years, 2.8% vs. 1.2%. At 20-25 years, risk was 1.3% vs. 1.4% (P less than .001).
“We identified a population (ER positive) that maintains a significant risk of relapse even after more than 10 years of follow-up. New targeted treatments and different modes of breast cancer surveillance for preventing late recurrences within this population should be studied,” wrote Dr. Marco Colleoni of the European Institute of Oncology and International Breast Cancer Study Group, and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.3504).
For the entire patient group, breast cancer recurrence reached a peak at years 1-2 (15.2%), and decreased consistently through year 10 (5-10 years, 4.5%), then remained stable (10-15 years, 2.2%; 15-20, 1.5%; 20-25, 0.7%). Cumulative incidence of distant recurrence for the ER-positive group occurred less frequently than for the ER-negative group during the first 5 years and more frequently from 5 to 25 years: at 5 years, 27.1% vs. 23.4%; at 10 years, 31.9% vs. 31.8%; at 15 years, 35% vs. 33.4%; at 20 years, 37.4% vs. 34.1%; at 25 years, 38.3% vs. 35.3% (P less than .001).
All patients in the trials had undergone mastectomy and axillary clearance with at least eight nodes removed, with no locoregional radiotherapy, as was standard at the time.
Within the ER-positive group, patients who had zero to three positive nodes had had a stable risk of recurrence beyond 10 years, whereas for patients with four or more involved nodes, risk decreased gradually from 10 to 24 years.
The risk of breast cancer relapse decreases consistently for 10 years, then remains stable through 25 years, with ER-positive disease carrying higher risk than ER-negative disease from years 5 to 25, according to researchers.
At a median follow up of 24 years, the study reported outcomes of 4,105 patients who were diagnosed from 1978 to 1985 and participated in the International Breast Cancer Study Group Trials I to V. During the first 5 years of follow-up, risk of recurrence was lower for ER-positive compared with ER-negative disease: 9.9% vs. 11.5%. Beyond 5 years, risk was higher: 5-10 years, 5.4% vs. 3.3%; 10-15 years, 2.9% vs. 1.3%, 15-20 years, 2.8% vs. 1.2%. At 20-25 years, risk was 1.3% vs. 1.4% (P less than .001).
“We identified a population (ER positive) that maintains a significant risk of relapse even after more than 10 years of follow-up. New targeted treatments and different modes of breast cancer surveillance for preventing late recurrences within this population should be studied,” wrote Dr. Marco Colleoni of the European Institute of Oncology and International Breast Cancer Study Group, and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.3504).
For the entire patient group, breast cancer recurrence reached a peak at years 1-2 (15.2%), and decreased consistently through year 10 (5-10 years, 4.5%), then remained stable (10-15 years, 2.2%; 15-20, 1.5%; 20-25, 0.7%). Cumulative incidence of distant recurrence for the ER-positive group occurred less frequently than for the ER-negative group during the first 5 years and more frequently from 5 to 25 years: at 5 years, 27.1% vs. 23.4%; at 10 years, 31.9% vs. 31.8%; at 15 years, 35% vs. 33.4%; at 20 years, 37.4% vs. 34.1%; at 25 years, 38.3% vs. 35.3% (P less than .001).
All patients in the trials had undergone mastectomy and axillary clearance with at least eight nodes removed, with no locoregional radiotherapy, as was standard at the time.
Within the ER-positive group, patients who had zero to three positive nodes had had a stable risk of recurrence beyond 10 years, whereas for patients with four or more involved nodes, risk decreased gradually from 10 to 24 years.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The risk of breast cancer recurrence continues through 24 years after primary treatments, especially for estrogen receptor–positive disease.
Major finding: During the first 5 years, risk of recurrence was lower for ER-positive disease than for ER-negative disease (9.9% vs. 11.5%). Risk was higher 5-10 years later (5.4% vs. 3.3%), at 10-15 years (2.9% vs. 1.3%), and at 15-20 years (2.8% vs. 1.2%). From 20 to 25 years on, the risk was 1.3% vs. 1.4% (P less than .001).
Data sources: The International Breast Cancer Study Group Trials I to V, comprising 4,105 patients with breast cancer diagnosed from 1978 to 1985.
Disclosures: Dr. Colleoni reported financial ties to Novartis, Boehringer Ingelheim, Taiho Pharmaceutical, AbbVie, AstraZeneca, Pierre Fabre, and Pfizer. Several of his coauthors reported ties to industry.
RCTs vs. observational studies: mortality ‘strikingly’ different following RT
Analyses of mortality after breast cancer radiotherapy using randomized clinical trial data versus observational data produced strikingly different results, according to researchers.
Analyses of randomized data indicated radiotherapy reduced mortality after breast-conserving surgery and mastectomy in node-positive disease; by contrast, SEER data analyses showed radiotherapy was associated with a significantly larger reduction in breast cancer mortality after breast-conserving surgery but higher mortality after mastectomy. Among patients with node-positive breast cancer who underwent mastectomy and axillary dissection, radiotherapy was associated with lower mortality by clinical trial data (rate ratio, 0.84; 95% CI, 0.76-0.94) but was associated with higher mortality by observational data (1.34; 1.31-1.37).
Furthermore, analyses of randomized trial data indicated increased mortality from heart disease (1.27; 1.12-1.44) and lung cancer (1.78; 1.30-2.46) following radiotherapy, but analyses of SEER data indicated reduced mortality from heart disease (0.56; 0.53-0.60) and lung cancer (0.86; 0.75-0.99) associated with radiotherapy.
“It is not plausible that these negative associations in the SEER data are causal and, clearly, they are strongly influenced by factors other than the effect or radiotherapy,” wrote Dr. Katherine Henson of the University of Oxford (England), and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
“Randomized trials are needed wherever possible to investigate the effect of treatment on mortality from the original cancer,” according to the investigators, and, “selection biases can be problematic even when analyzing treatment-related toxicities using observational data.”
Analyses of randomized data demonstrated reduced breast cancer mortality associated with radiotherapy after breast-conserving surgery (0.82; 95% CI, 0.75-0.90). Compared with randomized data, analyses of observational data showed a much greater reduction in mortality associated with radiotherapy after breast-conserving surgery (0.64; 95% CI, 0.62-0.66).
Randomized evidence came from the Early Breast Cancer Trialists’ Collaborative Group, meta analyses of 17 trials (n = 10,801) of radiotherapy after breast-conserving surgery, 14 trials (n = 3,131) of radiotherapy after mastectomy, and 78 trials (n = 42,080) of mortality from causes other than breast cancer. Observational evidence came from the SEER data base (n = 393,840).
The researchers offered plausible explanations for selection bias that may have resulted in the divergent results calculated using observational data. Because radiotherapy following mastectomy is indicated only in the presence of adverse disease characteristics, patients who did not receive radiotherapy may have survived longer because of especially favorable characteristics, despite of lack of radiotherapy.
“When evaluating rare late effects for which sufficient randomized evidence cannot reasonably be obtained, analyses of observational data comparing treated and untreated patients may often be the only source of information, but they must always be interpreted with considerable caution,” wrote the investigators.
The hierarchy of evidence establishes that meta-analyses and randomized clinical trials (RCTs) offer the highest quality of evidence, and RCTs clearly offer the best assessment of effects of therapy. Observational studies, on the other hand, have considerable limitations, yet they have helped establish key causal relationships. Large prospective cohort studies, such as Framingham Heart Study, the National Child Development Study, and the Nurse’s Health Study, among others, continue to provide important data.
The study by Henson et al. reopens the debate over the value of RCTs versus observational studies (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
It is well known the nonrandomized studies can produce misleading results due to selection bias. Selection bias favoring treatment for healthier patients produces improved survival among treated patients. On the other hand, selection bias disfavoring treatment occurs in studies of patients with more aggressive tumors who receive more treatment, and despite interventions, have worse outcomes.
The observation that postmastectomy radiotherapy is associated with worse outcomes reflects a real phenomenon, likely explained by confounding by indication. Patients treated with radiotherapy likely have worse prognoses, and despite therapy, had worse outcomes.
In the Henson et al. study, detailed data on treatment, comorbid conditions, or other health determinants were not available. In recognizing the importance of observational data for comparative effectiveness research, we must also understand and account for the limitations.
There should be no battle between RCTs and observational data, as both can provide valid and important knowledge to help clinicians make decisions and deliver evidence-based compassionate care.
Dr. Mariana Chavez-MacGregor is assistant professor in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center, Houston. Dr. Sharon Giordano is associate professor in the department of breast medical oncology at the university. These remarks were part of an editorial (J Clin Oncol. 2016 Jan. 18. doi: 10.1200/JCO.2015.64.7487). Dr. Chavez-MacGregor reported financial ties with Roche, Novarits, InVitae, Pfizer, Genomic Health, and Genentech/Roche. Dr. Giordano reported having no disclosures.
The hierarchy of evidence establishes that meta-analyses and randomized clinical trials (RCTs) offer the highest quality of evidence, and RCTs clearly offer the best assessment of effects of therapy. Observational studies, on the other hand, have considerable limitations, yet they have helped establish key causal relationships. Large prospective cohort studies, such as Framingham Heart Study, the National Child Development Study, and the Nurse’s Health Study, among others, continue to provide important data.
The study by Henson et al. reopens the debate over the value of RCTs versus observational studies (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
It is well known the nonrandomized studies can produce misleading results due to selection bias. Selection bias favoring treatment for healthier patients produces improved survival among treated patients. On the other hand, selection bias disfavoring treatment occurs in studies of patients with more aggressive tumors who receive more treatment, and despite interventions, have worse outcomes.
The observation that postmastectomy radiotherapy is associated with worse outcomes reflects a real phenomenon, likely explained by confounding by indication. Patients treated with radiotherapy likely have worse prognoses, and despite therapy, had worse outcomes.
In the Henson et al. study, detailed data on treatment, comorbid conditions, or other health determinants were not available. In recognizing the importance of observational data for comparative effectiveness research, we must also understand and account for the limitations.
There should be no battle between RCTs and observational data, as both can provide valid and important knowledge to help clinicians make decisions and deliver evidence-based compassionate care.
Dr. Mariana Chavez-MacGregor is assistant professor in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center, Houston. Dr. Sharon Giordano is associate professor in the department of breast medical oncology at the university. These remarks were part of an editorial (J Clin Oncol. 2016 Jan. 18. doi: 10.1200/JCO.2015.64.7487). Dr. Chavez-MacGregor reported financial ties with Roche, Novarits, InVitae, Pfizer, Genomic Health, and Genentech/Roche. Dr. Giordano reported having no disclosures.
The hierarchy of evidence establishes that meta-analyses and randomized clinical trials (RCTs) offer the highest quality of evidence, and RCTs clearly offer the best assessment of effects of therapy. Observational studies, on the other hand, have considerable limitations, yet they have helped establish key causal relationships. Large prospective cohort studies, such as Framingham Heart Study, the National Child Development Study, and the Nurse’s Health Study, among others, continue to provide important data.
The study by Henson et al. reopens the debate over the value of RCTs versus observational studies (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
It is well known the nonrandomized studies can produce misleading results due to selection bias. Selection bias favoring treatment for healthier patients produces improved survival among treated patients. On the other hand, selection bias disfavoring treatment occurs in studies of patients with more aggressive tumors who receive more treatment, and despite interventions, have worse outcomes.
The observation that postmastectomy radiotherapy is associated with worse outcomes reflects a real phenomenon, likely explained by confounding by indication. Patients treated with radiotherapy likely have worse prognoses, and despite therapy, had worse outcomes.
In the Henson et al. study, detailed data on treatment, comorbid conditions, or other health determinants were not available. In recognizing the importance of observational data for comparative effectiveness research, we must also understand and account for the limitations.
There should be no battle between RCTs and observational data, as both can provide valid and important knowledge to help clinicians make decisions and deliver evidence-based compassionate care.
Dr. Mariana Chavez-MacGregor is assistant professor in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center, Houston. Dr. Sharon Giordano is associate professor in the department of breast medical oncology at the university. These remarks were part of an editorial (J Clin Oncol. 2016 Jan. 18. doi: 10.1200/JCO.2015.64.7487). Dr. Chavez-MacGregor reported financial ties with Roche, Novarits, InVitae, Pfizer, Genomic Health, and Genentech/Roche. Dr. Giordano reported having no disclosures.
Analyses of mortality after breast cancer radiotherapy using randomized clinical trial data versus observational data produced strikingly different results, according to researchers.
Analyses of randomized data indicated radiotherapy reduced mortality after breast-conserving surgery and mastectomy in node-positive disease; by contrast, SEER data analyses showed radiotherapy was associated with a significantly larger reduction in breast cancer mortality after breast-conserving surgery but higher mortality after mastectomy. Among patients with node-positive breast cancer who underwent mastectomy and axillary dissection, radiotherapy was associated with lower mortality by clinical trial data (rate ratio, 0.84; 95% CI, 0.76-0.94) but was associated with higher mortality by observational data (1.34; 1.31-1.37).
Furthermore, analyses of randomized trial data indicated increased mortality from heart disease (1.27; 1.12-1.44) and lung cancer (1.78; 1.30-2.46) following radiotherapy, but analyses of SEER data indicated reduced mortality from heart disease (0.56; 0.53-0.60) and lung cancer (0.86; 0.75-0.99) associated with radiotherapy.
“It is not plausible that these negative associations in the SEER data are causal and, clearly, they are strongly influenced by factors other than the effect or radiotherapy,” wrote Dr. Katherine Henson of the University of Oxford (England), and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
“Randomized trials are needed wherever possible to investigate the effect of treatment on mortality from the original cancer,” according to the investigators, and, “selection biases can be problematic even when analyzing treatment-related toxicities using observational data.”
Analyses of randomized data demonstrated reduced breast cancer mortality associated with radiotherapy after breast-conserving surgery (0.82; 95% CI, 0.75-0.90). Compared with randomized data, analyses of observational data showed a much greater reduction in mortality associated with radiotherapy after breast-conserving surgery (0.64; 95% CI, 0.62-0.66).
Randomized evidence came from the Early Breast Cancer Trialists’ Collaborative Group, meta analyses of 17 trials (n = 10,801) of radiotherapy after breast-conserving surgery, 14 trials (n = 3,131) of radiotherapy after mastectomy, and 78 trials (n = 42,080) of mortality from causes other than breast cancer. Observational evidence came from the SEER data base (n = 393,840).
The researchers offered plausible explanations for selection bias that may have resulted in the divergent results calculated using observational data. Because radiotherapy following mastectomy is indicated only in the presence of adverse disease characteristics, patients who did not receive radiotherapy may have survived longer because of especially favorable characteristics, despite of lack of radiotherapy.
“When evaluating rare late effects for which sufficient randomized evidence cannot reasonably be obtained, analyses of observational data comparing treated and untreated patients may often be the only source of information, but they must always be interpreted with considerable caution,” wrote the investigators.
Analyses of mortality after breast cancer radiotherapy using randomized clinical trial data versus observational data produced strikingly different results, according to researchers.
Analyses of randomized data indicated radiotherapy reduced mortality after breast-conserving surgery and mastectomy in node-positive disease; by contrast, SEER data analyses showed radiotherapy was associated with a significantly larger reduction in breast cancer mortality after breast-conserving surgery but higher mortality after mastectomy. Among patients with node-positive breast cancer who underwent mastectomy and axillary dissection, radiotherapy was associated with lower mortality by clinical trial data (rate ratio, 0.84; 95% CI, 0.76-0.94) but was associated with higher mortality by observational data (1.34; 1.31-1.37).
Furthermore, analyses of randomized trial data indicated increased mortality from heart disease (1.27; 1.12-1.44) and lung cancer (1.78; 1.30-2.46) following radiotherapy, but analyses of SEER data indicated reduced mortality from heart disease (0.56; 0.53-0.60) and lung cancer (0.86; 0.75-0.99) associated with radiotherapy.
“It is not plausible that these negative associations in the SEER data are causal and, clearly, they are strongly influenced by factors other than the effect or radiotherapy,” wrote Dr. Katherine Henson of the University of Oxford (England), and colleagues (J Clin Oncol. 2016 Jan 18. doi: 10.1200/JCO.2015.62.0294).
“Randomized trials are needed wherever possible to investigate the effect of treatment on mortality from the original cancer,” according to the investigators, and, “selection biases can be problematic even when analyzing treatment-related toxicities using observational data.”
Analyses of randomized data demonstrated reduced breast cancer mortality associated with radiotherapy after breast-conserving surgery (0.82; 95% CI, 0.75-0.90). Compared with randomized data, analyses of observational data showed a much greater reduction in mortality associated with radiotherapy after breast-conserving surgery (0.64; 95% CI, 0.62-0.66).
Randomized evidence came from the Early Breast Cancer Trialists’ Collaborative Group, meta analyses of 17 trials (n = 10,801) of radiotherapy after breast-conserving surgery, 14 trials (n = 3,131) of radiotherapy after mastectomy, and 78 trials (n = 42,080) of mortality from causes other than breast cancer. Observational evidence came from the SEER data base (n = 393,840).
The researchers offered plausible explanations for selection bias that may have resulted in the divergent results calculated using observational data. Because radiotherapy following mastectomy is indicated only in the presence of adverse disease characteristics, patients who did not receive radiotherapy may have survived longer because of especially favorable characteristics, despite of lack of radiotherapy.
“When evaluating rare late effects for which sufficient randomized evidence cannot reasonably be obtained, analyses of observational data comparing treated and untreated patients may often be the only source of information, but they must always be interpreted with considerable caution,” wrote the investigators.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Analysis of randomized trial data compared with observational data on mortality after breast cancer radiotherapy shows strikingly different results.
Major finding: Radiotherapy after mastectomy and axillary dissection was associated with lower mortality by clinical trial data (rate ratio, 0.84; 95% CI, 0.76-0.94) but was associated with higher mortality by observational data (1.34; 95% CI, 1.31-1.37).
Data sources: Randomized evidence came from the Early Breast Cancer Trialists’ Collaborative Group, meta-analyses of 31 trials (n = 13,932); observational evidence came from the SEER data base (n = 393,840).
Disclosures: Dr. Henson reported having no disclosures. One of her coauthors reported ties to industry.
AHA: Bariatric surgery slashes heart failure exacerbations
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
ORLANDO – Bariatric surgery in obese patients with heart failure was associated with a marked decrease in the subsequent rate of ED visits and hospitalizations for heart failure in a large, real-world, case-control study presented at the American Heart Association scientific sessions.
“This decline in the rate of heart failure morbidity was rapid in onset and sustained for at least 2 years after bariatric surgery,” according to Dr. Yuichi J. Shimada of Massachusetts General Hospital, Boston.
In a separate study, however, he found that bariatric surgery for obesity in patients with atrial fibrillation didn’t produce a reduction in ED visits and hospitalizations for the arrhythmia.
The heart failure study was a case-control study of 1,664 consecutive obese patients with heart failure who underwent a single bariatric surgical procedure in California, Florida, or Nebraska. Their median age was 49 years. Women accounted for 70% of the participants. Drawing upon federal Healthcare Cost and Utility Project databases on ED visits and hospital admissions in those three states, Dr. Shimada and coinvestigators compared the group’s rates of ED visits and hospitalizations for heart failure for 2 years before and 2 years after bariatric surgery. Thus, the subjects served as their own controls.
During the reference period, which lasted from months 13-24 presurgery, the group’s combined rate of ED visits and hospital admission for heart failure exacerbation was 14.4%. The rate wasn’t significantly different during the 12 months immediately prior to surgery, at 13.3%.
The rate dropped to 8.7% during the first 12 months after bariatric surgery and remained rock solid at 8.7% during months 13-24 postsurgery. In a logistic regression analysis, this translated to a 44% reduction in the risk of ED visits or hospital admission for heart failure during the first 2 years following bariatric surgery.
These findings are consistent with previous work by other investigators showing a link between obesity and heart failure exacerbations. The new data advance the field by providing the best evidence to date of the effectiveness of substantial weight loss on heart failure morbidity, Dr. Shimada observed.
Nonbariatric surgeries such as hysterectomy or cholecysectomy in the study population had no effect on the rate of heart failure exacerbations.
Dr. Shimada’s atrial fibrillation study was structured in the same way. It included 1,056 patients with atrial fibrillation who underwent bariatric surgery for obesity in the same three states. The rate of ED visits or hospitalization for heart failure was 12.1% in months 13-24 prior to bariatric surgery, 12.6% in presurgical months 1-12, 14.2% in the first 12 months post-bariatric surgery, and 13.4% during postsurgical months 13-24. These rates weren’t statistically different.
Dr. Shimada reported having no financial conflicts of interest regarding the two studies.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Bariatric surgery in obese patients with heart failure results in a dramatic reduction in ED visits and hospital admission for heart failure.
Major finding: The combined rate of ED visits and hospital admissions for heart failure dropped by 44% during the 2 years after a large group of patients with heart failure underwent bariatric surgery for obesity.
Data source: This case-control study compared the rates of ED visits and hospital admissions for worsening heart failure in 1,664 patients with heart failure during the 2 years before and 2 years after they underwent bariatric surgery for obesity.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study, which utilized publicly available patient data.
West African Ebola–virus transmission ends, then resumes
A day after the World Health Organization declared on Jan. 14 that no known cases of Ebola-virus transmission or active infection had been identified in West Africa for more than 42 days, the agency revealed the existence of a new, single case of Ebola-virus infection in Sierra Leone.
The appearance of the new case highlighted the challenges that remain in fully stamping out the West African Ebola–virus outbreak. The crisis began in December 2013, raged throughout 2014, and only wound down toward a sputtering halt near the end of 2015.

When Dr. Rick Brennan, the World Health Organization (WHO) director for Emergency Risk Management and Humanitarian Response, announced during a press conference on Jan. 14, “the end of Ebola-virus transmission in West Africa” and “the first time since 2014 that all know chains of transmission have stopped in Guinea, Liberia, and Sierra Leone,” he and his colleague, Dr. Peter Graaff, also underscored the ongoing risk for sporadic, isolated cases. The main threat for new cases comes from men who survived Ebola-virus infection but harbored significant quantities of infectious virus in various body fluids and tissues, including their semen, for a period of about 1 year following their infection.
During the press conference, both Dr. Brennan and Dr. Graaff spoke of a new, strengthened infrastructure that WHO had placed in West Africa to better monitor and react quickly to these flare-up cases – the mechanism that led to quick identification of the new Sierra Leone case.
“I think you’ll see a more responsive and effective WHO,” said Dr. Graaff, WHO’s director of Ebola response. “We will use the Ebola experience to be more agile, more operational, and better able to react more quickly to whatever future problems come our way,” including infectious-disease outbreaks by pathogens other than Ebola virus.
The 42-day period without new infections that had led to the announcement of an end to Ebola-virus transmission in West Africa represents two 21-day incubation cycles for the virus. Until the Sierra Leone case reported on Jan. 15, the last confirmed West African case had been identified in Liberia in mid-November. Liberia had previously been declared Ebola free in last May, but four new, isolated infections appeared subsequent to that transmitted by Ebola-infection survivors who still harbored infectious virus. Before the Jan. 15 case, an additional three such flare-ups occurred in Sierra Leone and another three in Guinea since last March, Dr. Brennan said.

The current tally on the West African Ebola outbreak stands at roughly 28,500 confirmed cases identified, and about 11,300 deaths. Nearly three-quarters of infections occurred during 2014. The case fatality rate at the start of the outbreak ran about 80%, noted Dr. Graaff, but gradually fell as infected patients began receiving better care. Near the outbreak’s end, the case fatality rate stood at roughly 35%, when most patients were receiving optimal clinical care.
WHO staffers are maintaining close surveillance of people who recently survived Ebola-virus infection so that they can identify and isolate any new infections. WHO personnel have also counseled these survivors on the risk they pose for potential transmission, primarily by unprotected sex by men for up to 12 months following the end of active infection. The WHO also plans to launch an investigational protocol to vaccinate sexual partners and other close contacts of adult male survivors with an as-yet unapproved Ebola vaccine to further reduce risk of new infections.
“The WHO and world community reacted slowly at the start of the Ebola outbreak” in early 2014, admitted Dr. Brennan. “Without question, the disease got away from us. In retrospect, there were a number of things that we should have done better and sooner,” he said. “We have done a lot of soul-searching and we [at WHO] have identified a number of weaknesses in our structures and systems. We have already taken several important steps, and we are undergoing major reforms of our emergency operations. I think you’ll see a much more effective WHO in the future.”
Reform of WHO systems for infection prevention and control “will be much better able to detect new cases, not only of Ebola, but of other important diseases,” said Dr. Graaff.
The United States is also strengthening its health screening and monitoring system for travelers coming from affected countries and improving its hospital preparedness to manage cases, said Alice C. Hill, senior adviser for preparedness and resilience at the National Security Council and special assistant to President Obama. Hill, who spoke Jan. 6 at the Public Health Emergency Medical Countermeasures Enterprise stakeholders workshop, acknowledged that challenges still exist that must be addressed, including the development of safe and effective diagnostics, treatments, and vaccines for existing infectious diseases such as influenza and more emerging threats such as Ebola or MERS (Middle East Respiratory Syndrome), developing accurate disease forecasting capabilities to predict what will be the next threat, building rapid clinical trial networks and manufacturing capabilities, and the abilities for mass dispensing of medical countermeasures.
Gregory Twachtman also contributed to this story.
On Twitter @mitchelzoler
A day after the World Health Organization declared on Jan. 14 that no known cases of Ebola-virus transmission or active infection had been identified in West Africa for more than 42 days, the agency revealed the existence of a new, single case of Ebola-virus infection in Sierra Leone.
The appearance of the new case highlighted the challenges that remain in fully stamping out the West African Ebola–virus outbreak. The crisis began in December 2013, raged throughout 2014, and only wound down toward a sputtering halt near the end of 2015.
When Dr. Rick Brennan, the World Health Organization (WHO) director for Emergency Risk Management and Humanitarian Response, announced during a press conference on Jan. 14, “the end of Ebola-virus transmission in West Africa” and “the first time since 2014 that all know chains of transmission have stopped in Guinea, Liberia, and Sierra Leone,” he and his colleague, Dr. Peter Graaff, also underscored the ongoing risk for sporadic, isolated cases. The main threat for new cases comes from men who survived Ebola-virus infection but harbored significant quantities of infectious virus in various body fluids and tissues, including their semen, for a period of about 1 year following their infection.
During the press conference, both Dr. Brennan and Dr. Graaff spoke of a new, strengthened infrastructure that WHO had placed in West Africa to better monitor and react quickly to these flare-up cases – the mechanism that led to quick identification of the new Sierra Leone case.
“I think you’ll see a more responsive and effective WHO,” said Dr. Graaff, WHO’s director of Ebola response. “We will use the Ebola experience to be more agile, more operational, and better able to react more quickly to whatever future problems come our way,” including infectious-disease outbreaks by pathogens other than Ebola virus.
The 42-day period without new infections that had led to the announcement of an end to Ebola-virus transmission in West Africa represents two 21-day incubation cycles for the virus. Until the Sierra Leone case reported on Jan. 15, the last confirmed West African case had been identified in Liberia in mid-November. Liberia had previously been declared Ebola free in last May, but four new, isolated infections appeared subsequent to that transmitted by Ebola-infection survivors who still harbored infectious virus. Before the Jan. 15 case, an additional three such flare-ups occurred in Sierra Leone and another three in Guinea since last March, Dr. Brennan said.
The current tally on the West African Ebola outbreak stands at roughly 28,500 confirmed cases identified, and about 11,300 deaths. Nearly three-quarters of infections occurred during 2014. The case fatality rate at the start of the outbreak ran about 80%, noted Dr. Graaff, but gradually fell as infected patients began receiving better care. Near the outbreak’s end, the case fatality rate stood at roughly 35%, when most patients were receiving optimal clinical care.
WHO staffers are maintaining close surveillance of people who recently survived Ebola-virus infection so that they can identify and isolate any new infections. WHO personnel have also counseled these survivors on the risk they pose for potential transmission, primarily by unprotected sex by men for up to 12 months following the end of active infection. The WHO also plans to launch an investigational protocol to vaccinate sexual partners and other close contacts of adult male survivors with an as-yet unapproved Ebola vaccine to further reduce risk of new infections.
“The WHO and world community reacted slowly at the start of the Ebola outbreak” in early 2014, admitted Dr. Brennan. “Without question, the disease got away from us. In retrospect, there were a number of things that we should have done better and sooner,” he said. “We have done a lot of soul-searching and we [at WHO] have identified a number of weaknesses in our structures and systems. We have already taken several important steps, and we are undergoing major reforms of our emergency operations. I think you’ll see a much more effective WHO in the future.”
Reform of WHO systems for infection prevention and control “will be much better able to detect new cases, not only of Ebola, but of other important diseases,” said Dr. Graaff.
The United States is also strengthening its health screening and monitoring system for travelers coming from affected countries and improving its hospital preparedness to manage cases, said Alice C. Hill, senior adviser for preparedness and resilience at the National Security Council and special assistant to President Obama. Hill, who spoke Jan. 6 at the Public Health Emergency Medical Countermeasures Enterprise stakeholders workshop, acknowledged that challenges still exist that must be addressed, including the development of safe and effective diagnostics, treatments, and vaccines for existing infectious diseases such as influenza and more emerging threats such as Ebola or MERS (Middle East Respiratory Syndrome), developing accurate disease forecasting capabilities to predict what will be the next threat, building rapid clinical trial networks and manufacturing capabilities, and the abilities for mass dispensing of medical countermeasures.
Gregory Twachtman also contributed to this story.
On Twitter @mitchelzoler
A day after the World Health Organization declared on Jan. 14 that no known cases of Ebola-virus transmission or active infection had been identified in West Africa for more than 42 days, the agency revealed the existence of a new, single case of Ebola-virus infection in Sierra Leone.
The appearance of the new case highlighted the challenges that remain in fully stamping out the West African Ebola–virus outbreak. The crisis began in December 2013, raged throughout 2014, and only wound down toward a sputtering halt near the end of 2015.
When Dr. Rick Brennan, the World Health Organization (WHO) director for Emergency Risk Management and Humanitarian Response, announced during a press conference on Jan. 14, “the end of Ebola-virus transmission in West Africa” and “the first time since 2014 that all know chains of transmission have stopped in Guinea, Liberia, and Sierra Leone,” he and his colleague, Dr. Peter Graaff, also underscored the ongoing risk for sporadic, isolated cases. The main threat for new cases comes from men who survived Ebola-virus infection but harbored significant quantities of infectious virus in various body fluids and tissues, including their semen, for a period of about 1 year following their infection.
During the press conference, both Dr. Brennan and Dr. Graaff spoke of a new, strengthened infrastructure that WHO had placed in West Africa to better monitor and react quickly to these flare-up cases – the mechanism that led to quick identification of the new Sierra Leone case.
“I think you’ll see a more responsive and effective WHO,” said Dr. Graaff, WHO’s director of Ebola response. “We will use the Ebola experience to be more agile, more operational, and better able to react more quickly to whatever future problems come our way,” including infectious-disease outbreaks by pathogens other than Ebola virus.
The 42-day period without new infections that had led to the announcement of an end to Ebola-virus transmission in West Africa represents two 21-day incubation cycles for the virus. Until the Sierra Leone case reported on Jan. 15, the last confirmed West African case had been identified in Liberia in mid-November. Liberia had previously been declared Ebola free in last May, but four new, isolated infections appeared subsequent to that transmitted by Ebola-infection survivors who still harbored infectious virus. Before the Jan. 15 case, an additional three such flare-ups occurred in Sierra Leone and another three in Guinea since last March, Dr. Brennan said.
The current tally on the West African Ebola outbreak stands at roughly 28,500 confirmed cases identified, and about 11,300 deaths. Nearly three-quarters of infections occurred during 2014. The case fatality rate at the start of the outbreak ran about 80%, noted Dr. Graaff, but gradually fell as infected patients began receiving better care. Near the outbreak’s end, the case fatality rate stood at roughly 35%, when most patients were receiving optimal clinical care.
WHO staffers are maintaining close surveillance of people who recently survived Ebola-virus infection so that they can identify and isolate any new infections. WHO personnel have also counseled these survivors on the risk they pose for potential transmission, primarily by unprotected sex by men for up to 12 months following the end of active infection. The WHO also plans to launch an investigational protocol to vaccinate sexual partners and other close contacts of adult male survivors with an as-yet unapproved Ebola vaccine to further reduce risk of new infections.
“The WHO and world community reacted slowly at the start of the Ebola outbreak” in early 2014, admitted Dr. Brennan. “Without question, the disease got away from us. In retrospect, there were a number of things that we should have done better and sooner,” he said. “We have done a lot of soul-searching and we [at WHO] have identified a number of weaknesses in our structures and systems. We have already taken several important steps, and we are undergoing major reforms of our emergency operations. I think you’ll see a much more effective WHO in the future.”
Reform of WHO systems for infection prevention and control “will be much better able to detect new cases, not only of Ebola, but of other important diseases,” said Dr. Graaff.
The United States is also strengthening its health screening and monitoring system for travelers coming from affected countries and improving its hospital preparedness to manage cases, said Alice C. Hill, senior adviser for preparedness and resilience at the National Security Council and special assistant to President Obama. Hill, who spoke Jan. 6 at the Public Health Emergency Medical Countermeasures Enterprise stakeholders workshop, acknowledged that challenges still exist that must be addressed, including the development of safe and effective diagnostics, treatments, and vaccines for existing infectious diseases such as influenza and more emerging threats such as Ebola or MERS (Middle East Respiratory Syndrome), developing accurate disease forecasting capabilities to predict what will be the next threat, building rapid clinical trial networks and manufacturing capabilities, and the abilities for mass dispensing of medical countermeasures.
Gregory Twachtman also contributed to this story.
On Twitter @mitchelzoler

Bronchoscopic nitinol coils improve severe emphysema
Bronchoscopically placed nitinol coils to reduce lung volume markedly improved quality of life and modestly improved walk distance and lung function in a preliminary study of patients with severe emphysema, which was published online Jan. 12 in JAMA.
The magnitude and severity of serious and nonserious adverse effects were far less than has been reported for more invasive lung volume reduction surgery in this patient population. However, the short-term financial costs of coil placement were substantial, said Dr. Gaetan Deslee of University of Reims (France) Hospital and his associates.
Nitinol coils are shape-memory devices delivered into subsegmental airways to reduce regional parenchymal volume, which increases expansion of adjacent nontargeted lung. This increases the nontargeted tissue’s elastic recoil and reestablishes small-airway tethering, which improves expiratory flow and reduces air trapping.
The investigators compared this procedure against usual care in 100 patients with severe emphysema who were treated and followed for 1 year at 10 university hospitals across France. Both groups underwent pretreatment pulmonary rehabilitation and received inhaled bronchodilators with or without inhaled corticosteroids and with or without supplemental oxygen at the discretion of their treating physicians. Then patients were randomly assigned – 50 to receive the coils and 50 to receive usual care.
The coils were inserted under general anesthesia, and approximately 10 coils were placed per targeted lobe. Most patients later underwent the procedure on the opposite side, so that 47 patients received bilateral and 3 received unilateral coils during 97 bronchoscopies. The mean procedure time was 54 minutes, and the treatment significantly decreased lung hyperinflation.
The primary efficacy endpoint, improvement in 6-minute walk test scores after 6 months, was evaluable for 44 patients in each study group. A total of 18 patients (36%) who underwent coil placement and 9 (18%) who received usual care improved their scores by at least 54 m, which was a significant difference, the investigators said (JAMA. 2016 Jan 12. doi: 10.1001/jama.2015.17821).
In addition, all secondary endpoints were significantly better after coil placement than after usual care at both 6 months and 12 months. This included forced expiratory volume in 1 second, forced vital capacity, residual volume, and residual volume/total lung capacity, scores on the Medical Research Council dyspnea scale, and scores on a measure of health-related quality of life.
A cost-benefit analysis at 1 year showed that the mean increase in expenditures was $47,908 per person in the coil group, compared with the usual-care group. The 1-year incremental cost-effectiveness ratio was $782,598 per quality-adjusted life year (QALY). Assuming that the quality of life gains would be maintained over 3 years and that the costs of follow-up care would be identically low in both study groups, this ratio would decrease to $270,000 per QALY at 3 years.
However, neither of these cost-effectiveness ratios would be considered economical enough to warrant adopting this technology in most countries, Dr. Deslee and his associates noted.
At least one serious adverse event developed in 52% of the coil group and in 38% of the usual-care group, and there were four deaths (8%) in the coil group and three deaths (6%) in the usual-care group. The most frequent adverse event was pneumonia, which resolved with medical care in all cases. “The mechanism involved in pneumonia may result from local airway irritation, subsegmental airway closure, tension-induced inflammation, or local ischemia rather than from an infectious mechanism,” the researchers said.
This study was limited in that coil placement was not compared with either a sham or control procedure, patients were not blinded to treatment assignment, the sample size was relatively small, and follow-up was short. Larger studies using more rigorous statistical methods are needed “to draw a definitive conclusion regarding the long-term efficacy of coil treatment,” they added.
The improvement in health-related quality of life scores in this study represents a mean response of approximately three times the established minimal clinically important difference. By comparison, trials of pharmacologic interventions rarely achieve even the minimal clinically important difference.
Despite the high cost-effectiveness ratio of more than $700,000 per QALY – when ratios of $50,000 to $100,000 per QALY are commonly deemed to be the maximal acceptable limit – clinicians shouldn’t hesitate to use this treatment if these findings are confirmed in larger trials. Bronchoscopically placed nitinol coils are largely palliative, but the response is meaningful and offers realistic hope to patients who have few other treatment choices.
Dr. Frank C. Sciurba, Dr. Divay Chandra, and Dr. Jessica Bon are all in the division of pulmonary, allergy, and critical care medicine at the University of Pittsburgh. Dr. Sciurba reported receiving grants from PneumRX, maker of the coils used in this study, and PulmonX. Dr. Sciurba, Dr. Chandra, and Dr. Bon made these remarks in an editorial accompanying Dr. Deslee’s report (JAMA 2016;315:139-41).
The improvement in health-related quality of life scores in this study represents a mean response of approximately three times the established minimal clinically important difference. By comparison, trials of pharmacologic interventions rarely achieve even the minimal clinically important difference.
Despite the high cost-effectiveness ratio of more than $700,000 per QALY – when ratios of $50,000 to $100,000 per QALY are commonly deemed to be the maximal acceptable limit – clinicians shouldn’t hesitate to use this treatment if these findings are confirmed in larger trials. Bronchoscopically placed nitinol coils are largely palliative, but the response is meaningful and offers realistic hope to patients who have few other treatment choices.
Dr. Frank C. Sciurba, Dr. Divay Chandra, and Dr. Jessica Bon are all in the division of pulmonary, allergy, and critical care medicine at the University of Pittsburgh. Dr. Sciurba reported receiving grants from PneumRX, maker of the coils used in this study, and PulmonX. Dr. Sciurba, Dr. Chandra, and Dr. Bon made these remarks in an editorial accompanying Dr. Deslee’s report (JAMA 2016;315:139-41).
The improvement in health-related quality of life scores in this study represents a mean response of approximately three times the established minimal clinically important difference. By comparison, trials of pharmacologic interventions rarely achieve even the minimal clinically important difference.
Despite the high cost-effectiveness ratio of more than $700,000 per QALY – when ratios of $50,000 to $100,000 per QALY are commonly deemed to be the maximal acceptable limit – clinicians shouldn’t hesitate to use this treatment if these findings are confirmed in larger trials. Bronchoscopically placed nitinol coils are largely palliative, but the response is meaningful and offers realistic hope to patients who have few other treatment choices.
Dr. Frank C. Sciurba, Dr. Divay Chandra, and Dr. Jessica Bon are all in the division of pulmonary, allergy, and critical care medicine at the University of Pittsburgh. Dr. Sciurba reported receiving grants from PneumRX, maker of the coils used in this study, and PulmonX. Dr. Sciurba, Dr. Chandra, and Dr. Bon made these remarks in an editorial accompanying Dr. Deslee’s report (JAMA 2016;315:139-41).
Bronchoscopically placed nitinol coils to reduce lung volume markedly improved quality of life and modestly improved walk distance and lung function in a preliminary study of patients with severe emphysema, which was published online Jan. 12 in JAMA.
The magnitude and severity of serious and nonserious adverse effects were far less than has been reported for more invasive lung volume reduction surgery in this patient population. However, the short-term financial costs of coil placement were substantial, said Dr. Gaetan Deslee of University of Reims (France) Hospital and his associates.
Nitinol coils are shape-memory devices delivered into subsegmental airways to reduce regional parenchymal volume, which increases expansion of adjacent nontargeted lung. This increases the nontargeted tissue’s elastic recoil and reestablishes small-airway tethering, which improves expiratory flow and reduces air trapping.
The investigators compared this procedure against usual care in 100 patients with severe emphysema who were treated and followed for 1 year at 10 university hospitals across France. Both groups underwent pretreatment pulmonary rehabilitation and received inhaled bronchodilators with or without inhaled corticosteroids and with or without supplemental oxygen at the discretion of their treating physicians. Then patients were randomly assigned – 50 to receive the coils and 50 to receive usual care.
The coils were inserted under general anesthesia, and approximately 10 coils were placed per targeted lobe. Most patients later underwent the procedure on the opposite side, so that 47 patients received bilateral and 3 received unilateral coils during 97 bronchoscopies. The mean procedure time was 54 minutes, and the treatment significantly decreased lung hyperinflation.
The primary efficacy endpoint, improvement in 6-minute walk test scores after 6 months, was evaluable for 44 patients in each study group. A total of 18 patients (36%) who underwent coil placement and 9 (18%) who received usual care improved their scores by at least 54 m, which was a significant difference, the investigators said (JAMA. 2016 Jan 12. doi: 10.1001/jama.2015.17821).
In addition, all secondary endpoints were significantly better after coil placement than after usual care at both 6 months and 12 months. This included forced expiratory volume in 1 second, forced vital capacity, residual volume, and residual volume/total lung capacity, scores on the Medical Research Council dyspnea scale, and scores on a measure of health-related quality of life.
A cost-benefit analysis at 1 year showed that the mean increase in expenditures was $47,908 per person in the coil group, compared with the usual-care group. The 1-year incremental cost-effectiveness ratio was $782,598 per quality-adjusted life year (QALY). Assuming that the quality of life gains would be maintained over 3 years and that the costs of follow-up care would be identically low in both study groups, this ratio would decrease to $270,000 per QALY at 3 years.
However, neither of these cost-effectiveness ratios would be considered economical enough to warrant adopting this technology in most countries, Dr. Deslee and his associates noted.
At least one serious adverse event developed in 52% of the coil group and in 38% of the usual-care group, and there were four deaths (8%) in the coil group and three deaths (6%) in the usual-care group. The most frequent adverse event was pneumonia, which resolved with medical care in all cases. “The mechanism involved in pneumonia may result from local airway irritation, subsegmental airway closure, tension-induced inflammation, or local ischemia rather than from an infectious mechanism,” the researchers said.
This study was limited in that coil placement was not compared with either a sham or control procedure, patients were not blinded to treatment assignment, the sample size was relatively small, and follow-up was short. Larger studies using more rigorous statistical methods are needed “to draw a definitive conclusion regarding the long-term efficacy of coil treatment,” they added.
Bronchoscopically placed nitinol coils to reduce lung volume markedly improved quality of life and modestly improved walk distance and lung function in a preliminary study of patients with severe emphysema, which was published online Jan. 12 in JAMA.
The magnitude and severity of serious and nonserious adverse effects were far less than has been reported for more invasive lung volume reduction surgery in this patient population. However, the short-term financial costs of coil placement were substantial, said Dr. Gaetan Deslee of University of Reims (France) Hospital and his associates.
Nitinol coils are shape-memory devices delivered into subsegmental airways to reduce regional parenchymal volume, which increases expansion of adjacent nontargeted lung. This increases the nontargeted tissue’s elastic recoil and reestablishes small-airway tethering, which improves expiratory flow and reduces air trapping.
The investigators compared this procedure against usual care in 100 patients with severe emphysema who were treated and followed for 1 year at 10 university hospitals across France. Both groups underwent pretreatment pulmonary rehabilitation and received inhaled bronchodilators with or without inhaled corticosteroids and with or without supplemental oxygen at the discretion of their treating physicians. Then patients were randomly assigned – 50 to receive the coils and 50 to receive usual care.
The coils were inserted under general anesthesia, and approximately 10 coils were placed per targeted lobe. Most patients later underwent the procedure on the opposite side, so that 47 patients received bilateral and 3 received unilateral coils during 97 bronchoscopies. The mean procedure time was 54 minutes, and the treatment significantly decreased lung hyperinflation.
The primary efficacy endpoint, improvement in 6-minute walk test scores after 6 months, was evaluable for 44 patients in each study group. A total of 18 patients (36%) who underwent coil placement and 9 (18%) who received usual care improved their scores by at least 54 m, which was a significant difference, the investigators said (JAMA. 2016 Jan 12. doi: 10.1001/jama.2015.17821).
In addition, all secondary endpoints were significantly better after coil placement than after usual care at both 6 months and 12 months. This included forced expiratory volume in 1 second, forced vital capacity, residual volume, and residual volume/total lung capacity, scores on the Medical Research Council dyspnea scale, and scores on a measure of health-related quality of life.
A cost-benefit analysis at 1 year showed that the mean increase in expenditures was $47,908 per person in the coil group, compared with the usual-care group. The 1-year incremental cost-effectiveness ratio was $782,598 per quality-adjusted life year (QALY). Assuming that the quality of life gains would be maintained over 3 years and that the costs of follow-up care would be identically low in both study groups, this ratio would decrease to $270,000 per QALY at 3 years.
However, neither of these cost-effectiveness ratios would be considered economical enough to warrant adopting this technology in most countries, Dr. Deslee and his associates noted.
At least one serious adverse event developed in 52% of the coil group and in 38% of the usual-care group, and there were four deaths (8%) in the coil group and three deaths (6%) in the usual-care group. The most frequent adverse event was pneumonia, which resolved with medical care in all cases. “The mechanism involved in pneumonia may result from local airway irritation, subsegmental airway closure, tension-induced inflammation, or local ischemia rather than from an infectious mechanism,” the researchers said.
This study was limited in that coil placement was not compared with either a sham or control procedure, patients were not blinded to treatment assignment, the sample size was relatively small, and follow-up was short. Larger studies using more rigorous statistical methods are needed “to draw a definitive conclusion regarding the long-term efficacy of coil treatment,” they added.
FROM JAMA
Key clinical point: Bronchoscopically placed nitinol coils to reduce lung volume markedly improved quality of life and modestly improved walk distance in severe emphysema.
Major finding: 36% of patients who underwent coil placement achieved an improvement of at least 54 m in the 6-minute walk test, compared with only 18% who received usual care.
Data source: A preliminary randomized trial involving 100 patients treated at 10 university hospitals in France and followed for 1 year.
Disclosures: This study was supported by the French Ministry of Health. Dr. Deslee reported ties to PneumRx, maker of the coils tested in this study; his associates reported ties to PneumRx, Novatech, GlaxoSmithKline, Boehringer Ingelheim, Novartis, AstraZeneca, and Pulmonix.
No benefit in open massage over closed compressions in trauma cardiac arrest
SAN ANTONIO – Open-chest cardiac massage offers no benefit over closed-chest compressions in patients with traumatic cardiac arrest, according to a prospective observational study from the University of Maryland Shock Trauma Center in Baltimore.
The investigators compared 16 open-chest cardiac massage (OCCM) patients with 17 closed-chest compression (CCC) patients delivered directly to the level 1 trauma center in cardiac arrest. The open-massage group received closed compressions for a mean of 66 seconds before being converted to open massage for reasons that weren’t captured by the data.

End-tidal carbon dioxide (ETCO2) – the gold standard for determining the effectiveness of chest compressions and return of spontaneous circulation – was used as a surrogate for cardiac output and adequacy of resuscitation. Continuous high-resolution ETCO2 measurements were collected every 6 seconds in both groups.
When periods of OCCM were compared to equivalent periods of CCC, there were no differences in the initial, final, peak, or mean ETCO2 values, and there was no difference in return of spontaneous circulation (OCCM, 23.5% versus CCC, 38.9%; P = .53).
“Unless the patient has a thoracic injury that you need to get into the chest to fix, we didn’t see any benefit in opening the chest just to massage the heart. The data suggest that maybe we shouldn’t be so aggressive in doing open cardiac massage. There’s renewed interest in performing endovascular balloon occlusion techniques for the aorta to obtain hemorrhage control; if you do that and you do closed-chest compressions, it’s just as effective as opening up the chest and doing cardiac massage,” said investigator Dr. Matthew Bradley, a trauma surgeon at the Shock Trauma Center, at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Most of the patients were men, and there was a higher percentage of penetrating trauma in the OCCM group (81% versus 47%; P = .04).
The results were the same, however, in subgroup analyses limited to blunt and penetrating trauma.
All of the open massage patients died, but there were a few survivors in the CCC group. Dr. Bradley didn’t think the closed versus open approach was the reason for the survival difference.
Resuscitative endovascular balloon occlusion of the aorta patients were excluded from the trial to prevent confounding.
The investigators have no relevant disclosures.
SAN ANTONIO – Open-chest cardiac massage offers no benefit over closed-chest compressions in patients with traumatic cardiac arrest, according to a prospective observational study from the University of Maryland Shock Trauma Center in Baltimore.
The investigators compared 16 open-chest cardiac massage (OCCM) patients with 17 closed-chest compression (CCC) patients delivered directly to the level 1 trauma center in cardiac arrest. The open-massage group received closed compressions for a mean of 66 seconds before being converted to open massage for reasons that weren’t captured by the data.
End-tidal carbon dioxide (ETCO2) – the gold standard for determining the effectiveness of chest compressions and return of spontaneous circulation – was used as a surrogate for cardiac output and adequacy of resuscitation. Continuous high-resolution ETCO2 measurements were collected every 6 seconds in both groups.
When periods of OCCM were compared to equivalent periods of CCC, there were no differences in the initial, final, peak, or mean ETCO2 values, and there was no difference in return of spontaneous circulation (OCCM, 23.5% versus CCC, 38.9%; P = .53).
“Unless the patient has a thoracic injury that you need to get into the chest to fix, we didn’t see any benefit in opening the chest just to massage the heart. The data suggest that maybe we shouldn’t be so aggressive in doing open cardiac massage. There’s renewed interest in performing endovascular balloon occlusion techniques for the aorta to obtain hemorrhage control; if you do that and you do closed-chest compressions, it’s just as effective as opening up the chest and doing cardiac massage,” said investigator Dr. Matthew Bradley, a trauma surgeon at the Shock Trauma Center, at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Most of the patients were men, and there was a higher percentage of penetrating trauma in the OCCM group (81% versus 47%; P = .04).
The results were the same, however, in subgroup analyses limited to blunt and penetrating trauma.
All of the open massage patients died, but there were a few survivors in the CCC group. Dr. Bradley didn’t think the closed versus open approach was the reason for the survival difference.
Resuscitative endovascular balloon occlusion of the aorta patients were excluded from the trial to prevent confounding.
The investigators have no relevant disclosures.
SAN ANTONIO – Open-chest cardiac massage offers no benefit over closed-chest compressions in patients with traumatic cardiac arrest, according to a prospective observational study from the University of Maryland Shock Trauma Center in Baltimore.
The investigators compared 16 open-chest cardiac massage (OCCM) patients with 17 closed-chest compression (CCC) patients delivered directly to the level 1 trauma center in cardiac arrest. The open-massage group received closed compressions for a mean of 66 seconds before being converted to open massage for reasons that weren’t captured by the data.
End-tidal carbon dioxide (ETCO2) – the gold standard for determining the effectiveness of chest compressions and return of spontaneous circulation – was used as a surrogate for cardiac output and adequacy of resuscitation. Continuous high-resolution ETCO2 measurements were collected every 6 seconds in both groups.
When periods of OCCM were compared to equivalent periods of CCC, there were no differences in the initial, final, peak, or mean ETCO2 values, and there was no difference in return of spontaneous circulation (OCCM, 23.5% versus CCC, 38.9%; P = .53).
“Unless the patient has a thoracic injury that you need to get into the chest to fix, we didn’t see any benefit in opening the chest just to massage the heart. The data suggest that maybe we shouldn’t be so aggressive in doing open cardiac massage. There’s renewed interest in performing endovascular balloon occlusion techniques for the aorta to obtain hemorrhage control; if you do that and you do closed-chest compressions, it’s just as effective as opening up the chest and doing cardiac massage,” said investigator Dr. Matthew Bradley, a trauma surgeon at the Shock Trauma Center, at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Most of the patients were men, and there was a higher percentage of penetrating trauma in the OCCM group (81% versus 47%; P = .04).
The results were the same, however, in subgroup analyses limited to blunt and penetrating trauma.
All of the open massage patients died, but there were a few survivors in the CCC group. Dr. Bradley didn’t think the closed versus open approach was the reason for the survival difference.
Resuscitative endovascular balloon occlusion of the aorta patients were excluded from the trial to prevent confounding.
The investigators have no relevant disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: There’s no benefit in opening the chest just to massage the heart.
Major finding: When periods of OCCM were compared to equivalent periods of CCC, there were no differences in initial, final, peak, or mean ETCO2 values, and there was no difference in return of spontaneous circulation (OCCM, 23.5% versus CCC, 38.9%; P = .53).
Data source: Prospective observational study in 33 patients
Disclosures: The investigators have no relevant disclosures.

Hawaii healthiest U.S. state in 2015, North Carolina most improved
For the fourth year in a row, Hawaii was named the healthiest state in America by the United Health Foundation in the 2015 edition of “America’s Health Rankings.”
A low obesity prevalence, low rate of preventable hospitalizations, few poor mental health days, and an 11% increase in immunization among children aged 19-35 months in 2015 helped make Hawaii the healthiest state over second-ranked Vermont. Massachusetts ranked third, with Minnesota and New Hampshire rounding out the top five.
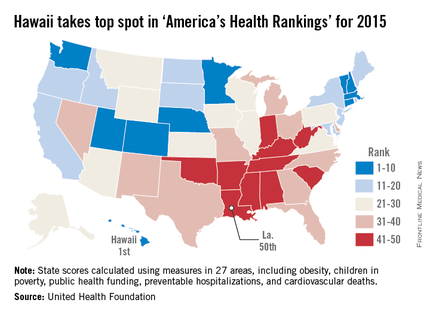
At the other end of the list, Louisiana replaced Mississippi as the least healthy state in 2015. Mississippi rose by one spot to 49th, however, followed by Arkansas at 48th, West Virginia at 47th, and Alabama at 46th.
The most improved state for 2015 was North Carolina, moving six spots up from 37th to 31st. Other states that saw significant moves upward were Maine, Washington, Delaware, and Kentucky. The largest decline was by Oregon, which dropped eight spots to 20th from 12th. New Mexico, Alabama, North Dakota, Texas, and West Virginia also made considerable downward movements.
Overall, the United States saw a significant decrease in preventable hospitalizations, physical inactivity, smoking, cardiovascular deaths, and infant mortality, and an increase in recommended vaccination coverage. Obesity rates increased, however, as did diabetes rates, drug deaths, and children living in poverty, and no progress was made in reducing premature deaths.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
For the fourth year in a row, Hawaii was named the healthiest state in America by the United Health Foundation in the 2015 edition of “America’s Health Rankings.”
A low obesity prevalence, low rate of preventable hospitalizations, few poor mental health days, and an 11% increase in immunization among children aged 19-35 months in 2015 helped make Hawaii the healthiest state over second-ranked Vermont. Massachusetts ranked third, with Minnesota and New Hampshire rounding out the top five.
At the other end of the list, Louisiana replaced Mississippi as the least healthy state in 2015. Mississippi rose by one spot to 49th, however, followed by Arkansas at 48th, West Virginia at 47th, and Alabama at 46th.
The most improved state for 2015 was North Carolina, moving six spots up from 37th to 31st. Other states that saw significant moves upward were Maine, Washington, Delaware, and Kentucky. The largest decline was by Oregon, which dropped eight spots to 20th from 12th. New Mexico, Alabama, North Dakota, Texas, and West Virginia also made considerable downward movements.
Overall, the United States saw a significant decrease in preventable hospitalizations, physical inactivity, smoking, cardiovascular deaths, and infant mortality, and an increase in recommended vaccination coverage. Obesity rates increased, however, as did diabetes rates, drug deaths, and children living in poverty, and no progress was made in reducing premature deaths.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
For the fourth year in a row, Hawaii was named the healthiest state in America by the United Health Foundation in the 2015 edition of “America’s Health Rankings.”
A low obesity prevalence, low rate of preventable hospitalizations, few poor mental health days, and an 11% increase in immunization among children aged 19-35 months in 2015 helped make Hawaii the healthiest state over second-ranked Vermont. Massachusetts ranked third, with Minnesota and New Hampshire rounding out the top five.
At the other end of the list, Louisiana replaced Mississippi as the least healthy state in 2015. Mississippi rose by one spot to 49th, however, followed by Arkansas at 48th, West Virginia at 47th, and Alabama at 46th.
The most improved state for 2015 was North Carolina, moving six spots up from 37th to 31st. Other states that saw significant moves upward were Maine, Washington, Delaware, and Kentucky. The largest decline was by Oregon, which dropped eight spots to 20th from 12th. New Mexico, Alabama, North Dakota, Texas, and West Virginia also made considerable downward movements.
Overall, the United States saw a significant decrease in preventable hospitalizations, physical inactivity, smoking, cardiovascular deaths, and infant mortality, and an increase in recommended vaccination coverage. Obesity rates increased, however, as did diabetes rates, drug deaths, and children living in poverty, and no progress was made in reducing premature deaths.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
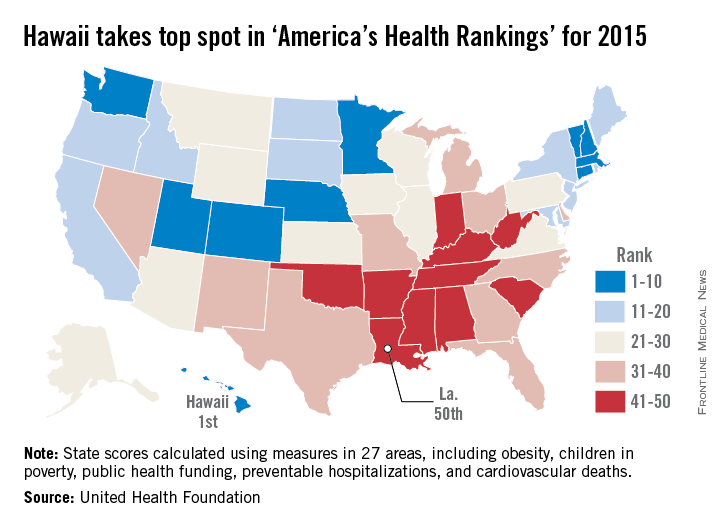
Trauma hospitalists reduce mortality, readmissions
SAN ANTONIO – Embedding a hospitalist in the trauma service reduces mortality and readmissions, according to a review from Christiana Care Health System’s Level 1 trauma center in Newark, Del.
Investigators wanted to see how their trauma hospitalist program – launched in 2013 – was working, so they matched 469 patients who were comanaged by a hospitalist in 2014 to 938 patients who were not, based on age, injury severity score, and comorbidities.
“We were pleasantly surprised to see a dramatic reduction in mortality [2.9% to 0.4%] and 30-day trauma-related readmissions [2.3% to 0.6%]” when hospitalists were involved with care, said Dr. Mark Cipolle, chief of trauma surgery at the center. The findings were statistically significant.

More hospitalist patients were upgraded to the ICU [4.3% versus 2.1%], and hospitalist patients stayed in the hospital about a day and half longer. The increased ICU upgrades is probably from the extra vigilance trauma hospitalists bring to the team. As for length of stay, hospitalists probably “kept patients an extra day to tune up their diabetes, hypertension,” and other problems, and ensure they had good follow-up. “We strongly feel that many of these patients go home with their comorbidities better managed than when they came in,” Dr. Cipolle said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Hospitalists also seemed to improve patient satisfaction on surveys.
Christiana currently employs about eight trauma hospitalists in Newark who rotate through week-long shifts. They’ve become so central to trauma care there that Dr. Cipolle suspects it would be difficult to find patients without hospitalist management for a new control group.
His hospitalists tend to work with older patients and manage comorbidities, especially insulin-dependent diabetes, heart failure, other significant heart disease, and chronic renal injury. Trauma surgeons, meanwhile, manage injury-related issues, such as additional diagnostics and pain control.
There can be some disagreements when two attendings care for the same patient, but, overall, “we get along pretty darn well,” Dr. Cipolle said.
Hospitalists in the study made no significant difference in the frequency of cardiology, nephrology, neurology, or endocrinology consultations. There was no difference in the development of venous thromboembolism, pneumonia, stroke, urinary tract infection, bacteremia, or alcohol withdrawal.
The patients were about 72 years old, on average, with a mean injury severity score of 10. Roughly 8% were recovering from a stroke, about 10% had heart failure, a quarter were diabetic, and three-quarters were hypertensive.
Dr. Cipolle said he has no relevant disclosures.
SAN ANTONIO – Embedding a hospitalist in the trauma service reduces mortality and readmissions, according to a review from Christiana Care Health System’s Level 1 trauma center in Newark, Del.
Investigators wanted to see how their trauma hospitalist program – launched in 2013 – was working, so they matched 469 patients who were comanaged by a hospitalist in 2014 to 938 patients who were not, based on age, injury severity score, and comorbidities.
“We were pleasantly surprised to see a dramatic reduction in mortality [2.9% to 0.4%] and 30-day trauma-related readmissions [2.3% to 0.6%]” when hospitalists were involved with care, said Dr. Mark Cipolle, chief of trauma surgery at the center. The findings were statistically significant.
More hospitalist patients were upgraded to the ICU [4.3% versus 2.1%], and hospitalist patients stayed in the hospital about a day and half longer. The increased ICU upgrades is probably from the extra vigilance trauma hospitalists bring to the team. As for length of stay, hospitalists probably “kept patients an extra day to tune up their diabetes, hypertension,” and other problems, and ensure they had good follow-up. “We strongly feel that many of these patients go home with their comorbidities better managed than when they came in,” Dr. Cipolle said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Hospitalists also seemed to improve patient satisfaction on surveys.
Christiana currently employs about eight trauma hospitalists in Newark who rotate through week-long shifts. They’ve become so central to trauma care there that Dr. Cipolle suspects it would be difficult to find patients without hospitalist management for a new control group.
His hospitalists tend to work with older patients and manage comorbidities, especially insulin-dependent diabetes, heart failure, other significant heart disease, and chronic renal injury. Trauma surgeons, meanwhile, manage injury-related issues, such as additional diagnostics and pain control.
There can be some disagreements when two attendings care for the same patient, but, overall, “we get along pretty darn well,” Dr. Cipolle said.
Hospitalists in the study made no significant difference in the frequency of cardiology, nephrology, neurology, or endocrinology consultations. There was no difference in the development of venous thromboembolism, pneumonia, stroke, urinary tract infection, bacteremia, or alcohol withdrawal.
The patients were about 72 years old, on average, with a mean injury severity score of 10. Roughly 8% were recovering from a stroke, about 10% had heart failure, a quarter were diabetic, and three-quarters were hypertensive.
Dr. Cipolle said he has no relevant disclosures.
SAN ANTONIO – Embedding a hospitalist in the trauma service reduces mortality and readmissions, according to a review from Christiana Care Health System’s Level 1 trauma center in Newark, Del.
Investigators wanted to see how their trauma hospitalist program – launched in 2013 – was working, so they matched 469 patients who were comanaged by a hospitalist in 2014 to 938 patients who were not, based on age, injury severity score, and comorbidities.
“We were pleasantly surprised to see a dramatic reduction in mortality [2.9% to 0.4%] and 30-day trauma-related readmissions [2.3% to 0.6%]” when hospitalists were involved with care, said Dr. Mark Cipolle, chief of trauma surgery at the center. The findings were statistically significant.
More hospitalist patients were upgraded to the ICU [4.3% versus 2.1%], and hospitalist patients stayed in the hospital about a day and half longer. The increased ICU upgrades is probably from the extra vigilance trauma hospitalists bring to the team. As for length of stay, hospitalists probably “kept patients an extra day to tune up their diabetes, hypertension,” and other problems, and ensure they had good follow-up. “We strongly feel that many of these patients go home with their comorbidities better managed than when they came in,” Dr. Cipolle said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Hospitalists also seemed to improve patient satisfaction on surveys.
Christiana currently employs about eight trauma hospitalists in Newark who rotate through week-long shifts. They’ve become so central to trauma care there that Dr. Cipolle suspects it would be difficult to find patients without hospitalist management for a new control group.
His hospitalists tend to work with older patients and manage comorbidities, especially insulin-dependent diabetes, heart failure, other significant heart disease, and chronic renal injury. Trauma surgeons, meanwhile, manage injury-related issues, such as additional diagnostics and pain control.
There can be some disagreements when two attendings care for the same patient, but, overall, “we get along pretty darn well,” Dr. Cipolle said.
Hospitalists in the study made no significant difference in the frequency of cardiology, nephrology, neurology, or endocrinology consultations. There was no difference in the development of venous thromboembolism, pneumonia, stroke, urinary tract infection, bacteremia, or alcohol withdrawal.
The patients were about 72 years old, on average, with a mean injury severity score of 10. Roughly 8% were recovering from a stroke, about 10% had heart failure, a quarter were diabetic, and three-quarters were hypertensive.
Dr. Cipolle said he has no relevant disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: The addition of a hospitalist to the trauma service resulted in statistically significant improvements in mortality and readmissions.
Major finding: When hospitalists were added to the trauma team, mortality fell from 2.9 to 0.4%, and 30-day readmissions fell from 2.3 to 0.6%.
Data source: Retrospective, single-center study of 1,407 trauma patients.
Disclosures: Dr. Cipolle said he has no relevant disclosures.

Wound-healing template approved for diabetic foot ulcers
A bilayer matrix used for dermal regeneration and first approved in 1996 as a treatment for third-degree burns is now approved as a treatment for diabetic foot ulcers.
The Integra Dermal Regeneration Template was approved for the new indication based on a study that showed that the matrix device “improved ulcer healing compared to standard diabetic foot ulcer care,” according to a Food and Drug Administration statement announcing the approval on Jan. 7. Specifically, the new indication is for treating “partial and full-thickness neuropathic diabetic foot ulcers that are greater than 6 weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care.”
The product is a dermal-replacement layer that “consists of a porous, three-dimensional matrix, comprised of bovine collagen and chondroitin-6-sulfate,” with a temporary epidermal silicone layer “to provide immediate wound coverage and control moisture loss. … [It] provides an environment for new skin and tissue to regenerate and heal the wound,” according to the agency’s approval summary.
In a multicenter, randomized controlled study, 307 patients were first treated with 0.9% sodium chloride gel, a secondary dressing, and an offloading device for 2 weeks and were then randomized to a treatment or a control group that received continued treatment with the gel. After 16 weeks, 51% of those treated with the device and 32% of those in the control group had healed completely (P = .001). Among those whose wounds healed, the median time to healing was 43 days in the treatment group and 78 days in the control group.
More patients in the control group had severe adverse events (26.8% vs. 15.6%) and moderate adverse events (42.5% vs. 31.8%).The results of the study, funded and sponsored by the manufacturer, were recently published (Wound Repair Regen. 2015;23[6]:891-900).
The product is contraindicated in patients with bovine or chondroitin allergies and in patients with infected wounds.
The manufacturer, Integra LifeSciences, is marketing the device as Integra Omnigraft Dermal Regeneration Matrix for the diabetic foot ulcer indication.
A bilayer matrix used for dermal regeneration and first approved in 1996 as a treatment for third-degree burns is now approved as a treatment for diabetic foot ulcers.
The Integra Dermal Regeneration Template was approved for the new indication based on a study that showed that the matrix device “improved ulcer healing compared to standard diabetic foot ulcer care,” according to a Food and Drug Administration statement announcing the approval on Jan. 7. Specifically, the new indication is for treating “partial and full-thickness neuropathic diabetic foot ulcers that are greater than 6 weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care.”
The product is a dermal-replacement layer that “consists of a porous, three-dimensional matrix, comprised of bovine collagen and chondroitin-6-sulfate,” with a temporary epidermal silicone layer “to provide immediate wound coverage and control moisture loss. … [It] provides an environment for new skin and tissue to regenerate and heal the wound,” according to the agency’s approval summary.
In a multicenter, randomized controlled study, 307 patients were first treated with 0.9% sodium chloride gel, a secondary dressing, and an offloading device for 2 weeks and were then randomized to a treatment or a control group that received continued treatment with the gel. After 16 weeks, 51% of those treated with the device and 32% of those in the control group had healed completely (P = .001). Among those whose wounds healed, the median time to healing was 43 days in the treatment group and 78 days in the control group.
More patients in the control group had severe adverse events (26.8% vs. 15.6%) and moderate adverse events (42.5% vs. 31.8%).The results of the study, funded and sponsored by the manufacturer, were recently published (Wound Repair Regen. 2015;23[6]:891-900).
The product is contraindicated in patients with bovine or chondroitin allergies and in patients with infected wounds.
The manufacturer, Integra LifeSciences, is marketing the device as Integra Omnigraft Dermal Regeneration Matrix for the diabetic foot ulcer indication.
A bilayer matrix used for dermal regeneration and first approved in 1996 as a treatment for third-degree burns is now approved as a treatment for diabetic foot ulcers.
The Integra Dermal Regeneration Template was approved for the new indication based on a study that showed that the matrix device “improved ulcer healing compared to standard diabetic foot ulcer care,” according to a Food and Drug Administration statement announcing the approval on Jan. 7. Specifically, the new indication is for treating “partial and full-thickness neuropathic diabetic foot ulcers that are greater than 6 weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care.”
The product is a dermal-replacement layer that “consists of a porous, three-dimensional matrix, comprised of bovine collagen and chondroitin-6-sulfate,” with a temporary epidermal silicone layer “to provide immediate wound coverage and control moisture loss. … [It] provides an environment for new skin and tissue to regenerate and heal the wound,” according to the agency’s approval summary.
In a multicenter, randomized controlled study, 307 patients were first treated with 0.9% sodium chloride gel, a secondary dressing, and an offloading device for 2 weeks and were then randomized to a treatment or a control group that received continued treatment with the gel. After 16 weeks, 51% of those treated with the device and 32% of those in the control group had healed completely (P = .001). Among those whose wounds healed, the median time to healing was 43 days in the treatment group and 78 days in the control group.
More patients in the control group had severe adverse events (26.8% vs. 15.6%) and moderate adverse events (42.5% vs. 31.8%).The results of the study, funded and sponsored by the manufacturer, were recently published (Wound Repair Regen. 2015;23[6]:891-900).
The product is contraindicated in patients with bovine or chondroitin allergies and in patients with infected wounds.
The manufacturer, Integra LifeSciences, is marketing the device as Integra Omnigraft Dermal Regeneration Matrix for the diabetic foot ulcer indication.