User login
Official Newspaper of the American College of Surgeons
Off-pump bypass may confer stroke benefit
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Off-pump coronary artery bypass is associated with a significant reduction in the odds of stroke compared with conventional coronary artery bypass grafting and should be considered in high-risk patients.
Major finding: Off-pump coronary artery bypass was associated with a 28% reduction in the odds of patients having a cerebral stroke when compared with the conventional on-pump procedure.
Data source: Meta-analysis of 100 studies with a total of 19,192 patients.
Disclosures: Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other authors had no relationships to disclose.
Post-repair MR may be worse than thought
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Residual mild mitral valve regurgitation (MR) after implantation of the MitraClip device (Abbott Vascular) was associated with worse survival, symptom relief, and risk of moderate or severe MR than residual trace MR after implantation.
Major finding: Patients with residual mild MR after MitraClip implantation had a 45% probability of recurrence of moderate or severe MR within 4 years, more than three times that of those who had residual trace MR.
Data source: Population of 223 consecutive patients with acute residual trace or mild MR after MitraClip implantation between 2008 and 2014 at a single institution.
Disclosures: Dr. Nicola Buzzatti and Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other authors had no relationships to disclose.
Sirolimus reduced posttransplant skin cancer risk
Sirolimus protects organ-transplant recipients against developing skin cancer, reducing their risk by 40%, according to a retrospective cohort study published in JAMA Dermatology on Jan. 20.
Recipients of solid organs are at three- to fourfold higher risk of developing cancer, compared with the general population, and the most common type they get is nonmelanoma skin cancer. The risk of developing cutaneous squamous cell carcinoma is 65-250 times higher in organ-transplant recipients. Drugs that reduce the growth and proliferation of tumor cells by inhibiting mTOR (mammalian target of rapamycin), including sirolimus, are believed to reduce this cancer risk, said Pritesh S. Karia of the department of dermatology, Brigham and Women’s Hospital and Harvard University, Boston, and his associates (JAMA Dermatol. 2016 Jan 20. doi: 10.1001/jamadermatol.2015.5548).
The investigators reviewed the electronic medical records of 329 patients (mean age, 56 years) who underwent organ transplantation at one of the two medical centers during a 9-year period and who then developed a cancer of any type. The study participants received renal (53.8%), heart (17.6%), lung (16.4%), liver (10.3%), or mixed-organ (1.8%) transplants. The most common index cancers they developed post transplant included cutaneous squamous cell carcinoma (31.9%), basal cell carcinoma (22.5%), and melanoma (2.7%).
Of the 329 patients, 97 (29.5%) then received sirolimus, while 232 (70.5%) did not. During a median follow-up of 38 months, 130 of these patients (39.5%) developed a second posttransplant cancer. The sirolimus-treated group showed a reduction in risk for cancer of any type, compared with the group that did not receive sirolimus (30.9% of 97 vs. 43.1% of 232).
Nearly all (88.5%) of the second posttransplant cancers that developed were skin cancers, and sirolimus reduced the risk of skin cancers by 40%. The 1-year, 3-year, and 5-year rates of skin cancer after an index posttransplant cancer were 9.3%, 20.6%, and 24.7% in the sirolimus group, compared with 17.7%, 31.0%, and 35.8%, respectively, in the untreated group, “thus demonstrating a lower risk for skin cancer with sirolimus treatment,” they said.
“Even for patients who have already had difficulty with skin cancer formation, mTOR inhibition appears to be of benefit. No difference in cancer outcomes was observable between sirolimus-treated and [untreated] groups because poor outcomes were rare,” Mr. Karia and his associates wrote.
These findings suggest that sirolimus chemoprevention should be considered for the subset of organ-transplant recipients who develop post-transplant cancer, they noted. The results also highlight the need for dermatologists and transplant physicians “to be aware of skin cancer history, coordinate regular posttransplant surveillance of skin cancers” in patients with organ transplant recipients, especially those with a history of skin cancer, and to communicate closely “as skin cancers form to consider reduction in immunosuppressive therapy or conversion to an mTOR-based regimen if skin cancer formation is of concern,” they added.
This study was supported by sirolimus manufacturer Novartis Pharmaceuticals. Mr. Karia and his associates reported having no relevant financial disclosures.
Sirolimus protects organ-transplant recipients against developing skin cancer, reducing their risk by 40%, according to a retrospective cohort study published in JAMA Dermatology on Jan. 20.
Recipients of solid organs are at three- to fourfold higher risk of developing cancer, compared with the general population, and the most common type they get is nonmelanoma skin cancer. The risk of developing cutaneous squamous cell carcinoma is 65-250 times higher in organ-transplant recipients. Drugs that reduce the growth and proliferation of tumor cells by inhibiting mTOR (mammalian target of rapamycin), including sirolimus, are believed to reduce this cancer risk, said Pritesh S. Karia of the department of dermatology, Brigham and Women’s Hospital and Harvard University, Boston, and his associates (JAMA Dermatol. 2016 Jan 20. doi: 10.1001/jamadermatol.2015.5548).
The investigators reviewed the electronic medical records of 329 patients (mean age, 56 years) who underwent organ transplantation at one of the two medical centers during a 9-year period and who then developed a cancer of any type. The study participants received renal (53.8%), heart (17.6%), lung (16.4%), liver (10.3%), or mixed-organ (1.8%) transplants. The most common index cancers they developed post transplant included cutaneous squamous cell carcinoma (31.9%), basal cell carcinoma (22.5%), and melanoma (2.7%).
Of the 329 patients, 97 (29.5%) then received sirolimus, while 232 (70.5%) did not. During a median follow-up of 38 months, 130 of these patients (39.5%) developed a second posttransplant cancer. The sirolimus-treated group showed a reduction in risk for cancer of any type, compared with the group that did not receive sirolimus (30.9% of 97 vs. 43.1% of 232).
Nearly all (88.5%) of the second posttransplant cancers that developed were skin cancers, and sirolimus reduced the risk of skin cancers by 40%. The 1-year, 3-year, and 5-year rates of skin cancer after an index posttransplant cancer were 9.3%, 20.6%, and 24.7% in the sirolimus group, compared with 17.7%, 31.0%, and 35.8%, respectively, in the untreated group, “thus demonstrating a lower risk for skin cancer with sirolimus treatment,” they said.
“Even for patients who have already had difficulty with skin cancer formation, mTOR inhibition appears to be of benefit. No difference in cancer outcomes was observable between sirolimus-treated and [untreated] groups because poor outcomes were rare,” Mr. Karia and his associates wrote.
These findings suggest that sirolimus chemoprevention should be considered for the subset of organ-transplant recipients who develop post-transplant cancer, they noted. The results also highlight the need for dermatologists and transplant physicians “to be aware of skin cancer history, coordinate regular posttransplant surveillance of skin cancers” in patients with organ transplant recipients, especially those with a history of skin cancer, and to communicate closely “as skin cancers form to consider reduction in immunosuppressive therapy or conversion to an mTOR-based regimen if skin cancer formation is of concern,” they added.
This study was supported by sirolimus manufacturer Novartis Pharmaceuticals. Mr. Karia and his associates reported having no relevant financial disclosures.
Sirolimus protects organ-transplant recipients against developing skin cancer, reducing their risk by 40%, according to a retrospective cohort study published in JAMA Dermatology on Jan. 20.
Recipients of solid organs are at three- to fourfold higher risk of developing cancer, compared with the general population, and the most common type they get is nonmelanoma skin cancer. The risk of developing cutaneous squamous cell carcinoma is 65-250 times higher in organ-transplant recipients. Drugs that reduce the growth and proliferation of tumor cells by inhibiting mTOR (mammalian target of rapamycin), including sirolimus, are believed to reduce this cancer risk, said Pritesh S. Karia of the department of dermatology, Brigham and Women’s Hospital and Harvard University, Boston, and his associates (JAMA Dermatol. 2016 Jan 20. doi: 10.1001/jamadermatol.2015.5548).
The investigators reviewed the electronic medical records of 329 patients (mean age, 56 years) who underwent organ transplantation at one of the two medical centers during a 9-year period and who then developed a cancer of any type. The study participants received renal (53.8%), heart (17.6%), lung (16.4%), liver (10.3%), or mixed-organ (1.8%) transplants. The most common index cancers they developed post transplant included cutaneous squamous cell carcinoma (31.9%), basal cell carcinoma (22.5%), and melanoma (2.7%).
Of the 329 patients, 97 (29.5%) then received sirolimus, while 232 (70.5%) did not. During a median follow-up of 38 months, 130 of these patients (39.5%) developed a second posttransplant cancer. The sirolimus-treated group showed a reduction in risk for cancer of any type, compared with the group that did not receive sirolimus (30.9% of 97 vs. 43.1% of 232).
Nearly all (88.5%) of the second posttransplant cancers that developed were skin cancers, and sirolimus reduced the risk of skin cancers by 40%. The 1-year, 3-year, and 5-year rates of skin cancer after an index posttransplant cancer were 9.3%, 20.6%, and 24.7% in the sirolimus group, compared with 17.7%, 31.0%, and 35.8%, respectively, in the untreated group, “thus demonstrating a lower risk for skin cancer with sirolimus treatment,” they said.
“Even for patients who have already had difficulty with skin cancer formation, mTOR inhibition appears to be of benefit. No difference in cancer outcomes was observable between sirolimus-treated and [untreated] groups because poor outcomes were rare,” Mr. Karia and his associates wrote.
These findings suggest that sirolimus chemoprevention should be considered for the subset of organ-transplant recipients who develop post-transplant cancer, they noted. The results also highlight the need for dermatologists and transplant physicians “to be aware of skin cancer history, coordinate regular posttransplant surveillance of skin cancers” in patients with organ transplant recipients, especially those with a history of skin cancer, and to communicate closely “as skin cancers form to consider reduction in immunosuppressive therapy or conversion to an mTOR-based regimen if skin cancer formation is of concern,” they added.
This study was supported by sirolimus manufacturer Novartis Pharmaceuticals. Mr. Karia and his associates reported having no relevant financial disclosures.
FROM JAMA DERMATOLOGY
Key clinical point: Sirolimus protects organ-transplant recipients against skin cancer.
Major finding: The 1-year, 3-year, and 5-year rates of skin cancer after an index posttransplant cancer were 9.3%, 20.6%, and 24.7% in the sirolimus group, compared with 17.7%, 31.0%, and 35.8% in the untreated group.
Data source: A retrospective cohort study of 329 organ-transplant recipients who had already developed one cancer likely related to their immunosuppressive therapy.
Disclosures: This study was supported by sirolimus manufacturer Novartis Pharmaceuticals. Mr. Karia and his associates reported having no relevant financial disclosures.
CMS: IT changes are coming, but not here yet
Don’t walk away from meaningful use quite yet. That’s the message from CMS leaders Andy Slavitt and Dr. Karen DeSalvo.
Mr. Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, announced on Jan. 11 that change would be coming to health care IT. “The meaningful use program as it has existed will now be effectively over and replaced with something better,” he said at the annual J.P. Morgan Healthcare Conference.

In a blog post intended to elaborate on those statements, Mr. Slavitt and Dr. DeSalvo, National Coordinator for Health IT, wrote that “the approach to meaningful use under the [Medicare Access & CHIP Reauthorization Act of 2015 (MACRA)] won’t happen overnight. Our goal in communicating our principles now is to give everyone time to plan for what’s next and to continue to give us input. We encourage you to look for the MACRA regulations this year; in the meantime, our existing regulations – including meaningful use stage 3 – are still in effect.”
Although CMS had been hinting since late in 2015 that it was considering dropping or modifying the meaningful use program, Mr. Slavitt made it official during the J.P. Morgan conference. The latest announcement asks providers to have patience with this process. “We will continue to listen and learn and make improvements based on what happens on the front line,” Mr. Slavitt and Dr. DeSalvo wrote. “The process will be ongoing, not an instant fix and we must all commit to learning and improving and collaborating on the best solutions.”
Since health IT changes under MACRA apply only to Medicare, the CMS leaders pointed out that electronic health record incentives for Medicaid and Medicare hospitals are unchanged; however, they noted that the agency would seek ways to help health care institutions streamline their IT needs as well.
The blog post also pointed out that late last year, CMS was given the authority to allow groups of providers – rather than individuals – to receive hardship exemptions under meaningful use. “This should make the process much simpler for physicians and their practice managers in the future. We will be releasing guidance on this new process soon,” Mr. Slavitt and Dr. DeSalvo noted.
The American Medical Association lauded the coming changes to health IT. This is “a win for patients, physicians and common sense,” Dr. Steven J. Sack said in a statement.
But as CMS forges ahead with new tech mandates, others advised the agency not to throw away the good with the bad.

“We are heartened that CMS has its ears to the ground and is trying to shape the program in a way that will be genuinely beneficial for providers and patients,” Ed Park, chief operating officer at AthenaHealth, a Boston-based health IT solutions firm, said in an interview. “With that said, just because providers found meaningful use stage 2 hard doesn’t by itself make it a bad program.”
This latest information out of CMS would seem to reinforce Mr. Slavitt’s promise to the investors at the J.P. Morgan conference that the move away from meaningful use would be to “start small and leave a lot of tool-building opportunities for the private sector.” He told attendees that CMS would level the playing field for start-ups and new entrants into the health IT space who can help providers securely transfer patient data and close the loops on referrals and other essentials of continuous care.
Some are not so optimistic about the private sector’s ability to help make MACRA a sustained reality, however. “As to whether the systems will be ready for the new payment regime, I am not holding my breath,” Johnathan Graham, a health economist and senior fellow at the National Center for Policy Analysis, Washington, D.C., said in an interview.
Even with updated technologies, physician satisfaction will not rise overall, he predicted, because of what he referred to as a too-slow rate of growth in Medicare’s Part B budget.
He also called out MACRA payment adjustments as onerous to physicians: The implementation of MACRA’s range of positive or negative payment adjustments in the MIPS program of minus 3.5% to plus 4.5% in 2019, plus or minus 5% in 2020, plus or minus 7% in 2021, and plus or minus 9% after that, meaning that the more providers who score above the threshold for the positive payment update, the narrower the update will be to each practice.
“I think MACRA will fall apart within 2 or 3 years as practicing physicians learn they are in a dog-eat-dog environment, or zero-sum game. The can will get kicked down the road just like meaningful use was,” Mr. Graham said.
But forcing doctors to face off is the point, according to Mr. Park: “Our health care system is on a transformational journey and we should all expect it to be hard. We want to encourage CMS to continue to keep the bar high on the right things and we hope that CMS doesn’t water down merit-based incentive pay so that the definition of success is that everyone succeeds.”
On Twitter @whitneymcknight
Don’t walk away from meaningful use quite yet. That’s the message from CMS leaders Andy Slavitt and Dr. Karen DeSalvo.
Mr. Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, announced on Jan. 11 that change would be coming to health care IT. “The meaningful use program as it has existed will now be effectively over and replaced with something better,” he said at the annual J.P. Morgan Healthcare Conference.
In a blog post intended to elaborate on those statements, Mr. Slavitt and Dr. DeSalvo, National Coordinator for Health IT, wrote that “the approach to meaningful use under the [Medicare Access & CHIP Reauthorization Act of 2015 (MACRA)] won’t happen overnight. Our goal in communicating our principles now is to give everyone time to plan for what’s next and to continue to give us input. We encourage you to look for the MACRA regulations this year; in the meantime, our existing regulations – including meaningful use stage 3 – are still in effect.”
Although CMS had been hinting since late in 2015 that it was considering dropping or modifying the meaningful use program, Mr. Slavitt made it official during the J.P. Morgan conference. The latest announcement asks providers to have patience with this process. “We will continue to listen and learn and make improvements based on what happens on the front line,” Mr. Slavitt and Dr. DeSalvo wrote. “The process will be ongoing, not an instant fix and we must all commit to learning and improving and collaborating on the best solutions.”
Since health IT changes under MACRA apply only to Medicare, the CMS leaders pointed out that electronic health record incentives for Medicaid and Medicare hospitals are unchanged; however, they noted that the agency would seek ways to help health care institutions streamline their IT needs as well.
The blog post also pointed out that late last year, CMS was given the authority to allow groups of providers – rather than individuals – to receive hardship exemptions under meaningful use. “This should make the process much simpler for physicians and their practice managers in the future. We will be releasing guidance on this new process soon,” Mr. Slavitt and Dr. DeSalvo noted.
The American Medical Association lauded the coming changes to health IT. This is “a win for patients, physicians and common sense,” Dr. Steven J. Sack said in a statement.
But as CMS forges ahead with new tech mandates, others advised the agency not to throw away the good with the bad.
“We are heartened that CMS has its ears to the ground and is trying to shape the program in a way that will be genuinely beneficial for providers and patients,” Ed Park, chief operating officer at AthenaHealth, a Boston-based health IT solutions firm, said in an interview. “With that said, just because providers found meaningful use stage 2 hard doesn’t by itself make it a bad program.”
This latest information out of CMS would seem to reinforce Mr. Slavitt’s promise to the investors at the J.P. Morgan conference that the move away from meaningful use would be to “start small and leave a lot of tool-building opportunities for the private sector.” He told attendees that CMS would level the playing field for start-ups and new entrants into the health IT space who can help providers securely transfer patient data and close the loops on referrals and other essentials of continuous care.
Some are not so optimistic about the private sector’s ability to help make MACRA a sustained reality, however. “As to whether the systems will be ready for the new payment regime, I am not holding my breath,” Johnathan Graham, a health economist and senior fellow at the National Center for Policy Analysis, Washington, D.C., said in an interview.
Even with updated technologies, physician satisfaction will not rise overall, he predicted, because of what he referred to as a too-slow rate of growth in Medicare’s Part B budget.
He also called out MACRA payment adjustments as onerous to physicians: The implementation of MACRA’s range of positive or negative payment adjustments in the MIPS program of minus 3.5% to plus 4.5% in 2019, plus or minus 5% in 2020, plus or minus 7% in 2021, and plus or minus 9% after that, meaning that the more providers who score above the threshold for the positive payment update, the narrower the update will be to each practice.
“I think MACRA will fall apart within 2 or 3 years as practicing physicians learn they are in a dog-eat-dog environment, or zero-sum game. The can will get kicked down the road just like meaningful use was,” Mr. Graham said.
But forcing doctors to face off is the point, according to Mr. Park: “Our health care system is on a transformational journey and we should all expect it to be hard. We want to encourage CMS to continue to keep the bar high on the right things and we hope that CMS doesn’t water down merit-based incentive pay so that the definition of success is that everyone succeeds.”
On Twitter @whitneymcknight
Don’t walk away from meaningful use quite yet. That’s the message from CMS leaders Andy Slavitt and Dr. Karen DeSalvo.
Mr. Slavitt, acting administrator of the Centers for Medicare & Medicaid Services, announced on Jan. 11 that change would be coming to health care IT. “The meaningful use program as it has existed will now be effectively over and replaced with something better,” he said at the annual J.P. Morgan Healthcare Conference.
In a blog post intended to elaborate on those statements, Mr. Slavitt and Dr. DeSalvo, National Coordinator for Health IT, wrote that “the approach to meaningful use under the [Medicare Access & CHIP Reauthorization Act of 2015 (MACRA)] won’t happen overnight. Our goal in communicating our principles now is to give everyone time to plan for what’s next and to continue to give us input. We encourage you to look for the MACRA regulations this year; in the meantime, our existing regulations – including meaningful use stage 3 – are still in effect.”
Although CMS had been hinting since late in 2015 that it was considering dropping or modifying the meaningful use program, Mr. Slavitt made it official during the J.P. Morgan conference. The latest announcement asks providers to have patience with this process. “We will continue to listen and learn and make improvements based on what happens on the front line,” Mr. Slavitt and Dr. DeSalvo wrote. “The process will be ongoing, not an instant fix and we must all commit to learning and improving and collaborating on the best solutions.”
Since health IT changes under MACRA apply only to Medicare, the CMS leaders pointed out that electronic health record incentives for Medicaid and Medicare hospitals are unchanged; however, they noted that the agency would seek ways to help health care institutions streamline their IT needs as well.
The blog post also pointed out that late last year, CMS was given the authority to allow groups of providers – rather than individuals – to receive hardship exemptions under meaningful use. “This should make the process much simpler for physicians and their practice managers in the future. We will be releasing guidance on this new process soon,” Mr. Slavitt and Dr. DeSalvo noted.
The American Medical Association lauded the coming changes to health IT. This is “a win for patients, physicians and common sense,” Dr. Steven J. Sack said in a statement.
But as CMS forges ahead with new tech mandates, others advised the agency not to throw away the good with the bad.
“We are heartened that CMS has its ears to the ground and is trying to shape the program in a way that will be genuinely beneficial for providers and patients,” Ed Park, chief operating officer at AthenaHealth, a Boston-based health IT solutions firm, said in an interview. “With that said, just because providers found meaningful use stage 2 hard doesn’t by itself make it a bad program.”
This latest information out of CMS would seem to reinforce Mr. Slavitt’s promise to the investors at the J.P. Morgan conference that the move away from meaningful use would be to “start small and leave a lot of tool-building opportunities for the private sector.” He told attendees that CMS would level the playing field for start-ups and new entrants into the health IT space who can help providers securely transfer patient data and close the loops on referrals and other essentials of continuous care.
Some are not so optimistic about the private sector’s ability to help make MACRA a sustained reality, however. “As to whether the systems will be ready for the new payment regime, I am not holding my breath,” Johnathan Graham, a health economist and senior fellow at the National Center for Policy Analysis, Washington, D.C., said in an interview.
Even with updated technologies, physician satisfaction will not rise overall, he predicted, because of what he referred to as a too-slow rate of growth in Medicare’s Part B budget.
He also called out MACRA payment adjustments as onerous to physicians: The implementation of MACRA’s range of positive or negative payment adjustments in the MIPS program of minus 3.5% to plus 4.5% in 2019, plus or minus 5% in 2020, plus or minus 7% in 2021, and plus or minus 9% after that, meaning that the more providers who score above the threshold for the positive payment update, the narrower the update will be to each practice.
“I think MACRA will fall apart within 2 or 3 years as practicing physicians learn they are in a dog-eat-dog environment, or zero-sum game. The can will get kicked down the road just like meaningful use was,” Mr. Graham said.
But forcing doctors to face off is the point, according to Mr. Park: “Our health care system is on a transformational journey and we should all expect it to be hard. We want to encourage CMS to continue to keep the bar high on the right things and we hope that CMS doesn’t water down merit-based incentive pay so that the definition of success is that everyone succeeds.”
On Twitter @whitneymcknight

Lymphedema microsurgery gaining momentum
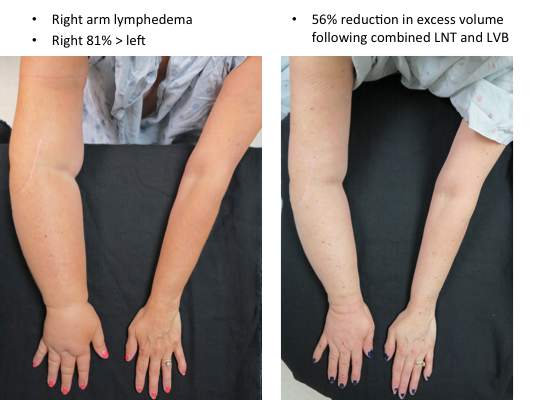
CHICAGO – Microsurgery does not cure lymphedema, in most cases. But, in most cases, it does improve the severity of lymphedema and reduce the complications of this chronic and debilitating disease. And “it certainly improves patients’ quality of life,” lymphedema treatment pioneer Dr. David W. Chang said at the 40th annual Northwestern Vascular Symposium.
Surgical treatment for limb lymphedema has come into its own since a lymphovenous shunt was first used in a dog model in 1962, with Dr. Chang and others now anastomosing subdermal lymphatics to subdermal venules less than 0.8 mm in diameter. The rationale behind “super-microsurgery” is that venous pressure is low in the subdermal venules and has minimal back flow, he said.

One of the big problems early on was knowing exactly where the lymphatic vessels were, but newer technology like indocyanine green (ICG) lymphangiography helps visualize functioning lymphatic channels for potential bypass and determine the severity of the disease. Understanding the disease stage is key to selecting the appropriate surgical procedure.
Lymphovenous bypass (LVB) is best in patients with stage 1 or 2 upper extremity lymphedema, while lymph node transfer (LNT) works for patients who are poor candidates for LVB or require combined breast reconstruction, said Dr. Chang, a plastic surgeon with the University of Chicago.
More recently, Dr. Chang has begun combining LVB and LNT, particularly for the more severe cases with stage 3 or 4 upper or lower extremity disease.
In Dr. Chang’s first 100 consecutive LVB cases while at the M.D. Anderson Cancer Center in Houston, quantitative improvement occurred in 74% of patients, symptom improvement in 96%, and the average volume differential reduction was 42% at 12 months (Plast Reconstr Surg. 2013 Nov;132:1305-14). The reduction was significantly larger in patients with earlier stage 1 or 2 vs. later stage 3 or 4 disease (61% vs. 17%).
During lymphovenous bypass, ICG is injected into the dermis of the web space and the superficial lymphatics evaluated with near-infrared fluorescence. It is easy to identify discrete functioning lymphatic channels in early-stage disease, but in late-stage disease significant dermal back flow is present, Dr. Chang said.
Dissection is performed under the microscope in the superficial subcutaneous plane to locate a good venule and lymph channel. Lymphatics are confirmed with isosulfan blue and ICG, and once the bypass site is determined, the lymphatic is anastomosed to the venule using 11-0 or 12-0 nylon, preferably in an end-to-side fashion. It’s thought this creates a more favorable flow pattern for the lymph to empty into the venule than an end-to-end anastomosis, he observed.
After the anastomosis is complete, patency is confirmed with isosulfan blue and ICG and the incision is closed under the microscope to ensure that the delicate anastomosis isn’t damaged. To avoid shear injury to the anastomosis, the limb is wrapped postoperatively for about a month without use of compression garments, he said.
Lymph node transfer (LNT) is increasingly being offered at centers to provide relief from lymphedema, although the mechanism by which it works is yet unclear; either the healthy lymph nodes act as a sponge to absorb lymphatic fluid or they induce lymphangiogenesis. Experience has shown, however, that rather than just grafting the lymph nodes, they need to be harvested with a vascular pedicle before transfer and anastomosed to the recipient artery and vein, although reconnecting the actual lymphatics may not be necessary, Dr. Chang observed.
Despite its popularity as a donor site, Dr. Chang said he is reluctant to use the groin because of the potential for iatrogenic lymphedema and prefers to harvest the supraclavicular nodes based off the transverse cervical artery. The external jugular vein can be harvested with the nodes if adequate venae comitantes are not present with the artery. Dissection of this flap can be difficult and care should be taken not to injure the lymphatic ducts, he noted.
It is also important to excise all scar tissue in the recipient site as this can impair lymphatic flow and inhibits lymphangiogenesis. If it is difficult to access or remove the scar, the vascularized lymph nodes are best placed just distal on the limb to the site of lymphatic obstruction, he added.
A recent meta-analysis (Plast Reconstr Surg. 2014 Apr;133:905-13) in five LNT studies reported that 91% of patients had a quantitative improvement, 78% discontinued compression garments, and complications were infection (8%), lymphorrhea (15%), and need for additional procedures (36%). There was great heterogeneity between studies, so the results should be interpreted with caution, Dr. Chang advised.
LNT is frequently combined with autologous breast reconstruction in patients with breast cancer, who comprise a significant percentage of Dr. Chang’s practice. The overall incidence of arm lymphedema after breast cancer can range from 8% to 56% at 2 years’ post-surgery, with the risk higher among women undergoing axillary lymph node dissection and/or axillary radiation.
Outcomes with combined LNT and breast reconstruction have been favorable, with one series reporting evidence of improved lymphatic flow on lymphoscintigraphy in five of six cases and one-third of patients no longer needing compression therapy (Ann Surg. 2012 Mar;255:468-73).
In cases where the patient requires a large skin paddle or seeks breast reconstruction after a previous mastectomy, lateral superficial groin lymph nodes can be harvested for transfer, leaving the deeper lymph nodes that drain the leg behind, Dr. Chang said. The nodes are usually clustered at the junction of the superior inferior epigastric and superficial circumflex iliac veins.
When combining LNT with breast reconstruction, this tissue is harvested together with the free abdominal flap used to reconstruct the breast. The superficial circumflex iliac vein is anastomosed in the axilla in addition to the arterial and venous anastomosis of the deep inferior epigastric vessels to the internal mammary vessels for the breast reconstruction. Reverse lymphatic mapping with technetium and ICG is used to decrease the risk of donor site lymphedema.
An algorithmic approach to simultaneous LNT with microvascular breast reconstruction proposed by Dr. Chang resulted in a 47% reduction in mean volume differential 12 months after reconstruction in 29 consecutive patients with refractory lymphedema following breast cancer treatment. These early results also showed no flap losses or donor-site lymphedema and donor-site wound complications in six patients (21%) that resolved with conservative measures (Ann Surg Oncol. 2015 Sep;22:2919-24).
The holy grail may be to strike lymphedema before it develops. To that end, Italian surgeons have proposed the Lymphatic Microsurgical Preventing Healing Approach (LYMPHA), which involves anastomosing arm lymphatics to a collateral branch of the axillary vein at the time of nodal dissection.
Over more than 4 years’ follow-up, only 3 of 74 breast cancer patients who underwent axillary nodal dissection with LYMPHA developed lymphedema, translating into a an exceptionally low 4% risk of lymphedema (Microsurgery. 2014 Sep;34:421-4). However, this approach is controversial because of unknown oncological risk and the uncertainty of its effectiveness in patients who may receive radiation after the surgery, Dr. Chang said in an interview.
Although these techniques show promise, currently no optimal solution exists and more research is needed to better understand lymphatic anatomy and physiology and the pathophysiology of lymphedema, concluded Dr. Chang, who reported no relevant conflicts of interest.
CHICAGO – Microsurgery does not cure lymphedema, in most cases. But, in most cases, it does improve the severity of lymphedema and reduce the complications of this chronic and debilitating disease. And “it certainly improves patients’ quality of life,” lymphedema treatment pioneer Dr. David W. Chang said at the 40th annual Northwestern Vascular Symposium.
Surgical treatment for limb lymphedema has come into its own since a lymphovenous shunt was first used in a dog model in 1962, with Dr. Chang and others now anastomosing subdermal lymphatics to subdermal venules less than 0.8 mm in diameter. The rationale behind “super-microsurgery” is that venous pressure is low in the subdermal venules and has minimal back flow, he said.
One of the big problems early on was knowing exactly where the lymphatic vessels were, but newer technology like indocyanine green (ICG) lymphangiography helps visualize functioning lymphatic channels for potential bypass and determine the severity of the disease. Understanding the disease stage is key to selecting the appropriate surgical procedure.
Lymphovenous bypass (LVB) is best in patients with stage 1 or 2 upper extremity lymphedema, while lymph node transfer (LNT) works for patients who are poor candidates for LVB or require combined breast reconstruction, said Dr. Chang, a plastic surgeon with the University of Chicago.
More recently, Dr. Chang has begun combining LVB and LNT, particularly for the more severe cases with stage 3 or 4 upper or lower extremity disease.
In Dr. Chang’s first 100 consecutive LVB cases while at the M.D. Anderson Cancer Center in Houston, quantitative improvement occurred in 74% of patients, symptom improvement in 96%, and the average volume differential reduction was 42% at 12 months (Plast Reconstr Surg. 2013 Nov;132:1305-14). The reduction was significantly larger in patients with earlier stage 1 or 2 vs. later stage 3 or 4 disease (61% vs. 17%).
During lymphovenous bypass, ICG is injected into the dermis of the web space and the superficial lymphatics evaluated with near-infrared fluorescence. It is easy to identify discrete functioning lymphatic channels in early-stage disease, but in late-stage disease significant dermal back flow is present, Dr. Chang said.
Dissection is performed under the microscope in the superficial subcutaneous plane to locate a good venule and lymph channel. Lymphatics are confirmed with isosulfan blue and ICG, and once the bypass site is determined, the lymphatic is anastomosed to the venule using 11-0 or 12-0 nylon, preferably in an end-to-side fashion. It’s thought this creates a more favorable flow pattern for the lymph to empty into the venule than an end-to-end anastomosis, he observed.
After the anastomosis is complete, patency is confirmed with isosulfan blue and ICG and the incision is closed under the microscope to ensure that the delicate anastomosis isn’t damaged. To avoid shear injury to the anastomosis, the limb is wrapped postoperatively for about a month without use of compression garments, he said.
Lymph node transfer (LNT) is increasingly being offered at centers to provide relief from lymphedema, although the mechanism by which it works is yet unclear; either the healthy lymph nodes act as a sponge to absorb lymphatic fluid or they induce lymphangiogenesis. Experience has shown, however, that rather than just grafting the lymph nodes, they need to be harvested with a vascular pedicle before transfer and anastomosed to the recipient artery and vein, although reconnecting the actual lymphatics may not be necessary, Dr. Chang observed.
Despite its popularity as a donor site, Dr. Chang said he is reluctant to use the groin because of the potential for iatrogenic lymphedema and prefers to harvest the supraclavicular nodes based off the transverse cervical artery. The external jugular vein can be harvested with the nodes if adequate venae comitantes are not present with the artery. Dissection of this flap can be difficult and care should be taken not to injure the lymphatic ducts, he noted.
It is also important to excise all scar tissue in the recipient site as this can impair lymphatic flow and inhibits lymphangiogenesis. If it is difficult to access or remove the scar, the vascularized lymph nodes are best placed just distal on the limb to the site of lymphatic obstruction, he added.
A recent meta-analysis (Plast Reconstr Surg. 2014 Apr;133:905-13) in five LNT studies reported that 91% of patients had a quantitative improvement, 78% discontinued compression garments, and complications were infection (8%), lymphorrhea (15%), and need for additional procedures (36%). There was great heterogeneity between studies, so the results should be interpreted with caution, Dr. Chang advised.
LNT is frequently combined with autologous breast reconstruction in patients with breast cancer, who comprise a significant percentage of Dr. Chang’s practice. The overall incidence of arm lymphedema after breast cancer can range from 8% to 56% at 2 years’ post-surgery, with the risk higher among women undergoing axillary lymph node dissection and/or axillary radiation.
Outcomes with combined LNT and breast reconstruction have been favorable, with one series reporting evidence of improved lymphatic flow on lymphoscintigraphy in five of six cases and one-third of patients no longer needing compression therapy (Ann Surg. 2012 Mar;255:468-73).
In cases where the patient requires a large skin paddle or seeks breast reconstruction after a previous mastectomy, lateral superficial groin lymph nodes can be harvested for transfer, leaving the deeper lymph nodes that drain the leg behind, Dr. Chang said. The nodes are usually clustered at the junction of the superior inferior epigastric and superficial circumflex iliac veins.
When combining LNT with breast reconstruction, this tissue is harvested together with the free abdominal flap used to reconstruct the breast. The superficial circumflex iliac vein is anastomosed in the axilla in addition to the arterial and venous anastomosis of the deep inferior epigastric vessels to the internal mammary vessels for the breast reconstruction. Reverse lymphatic mapping with technetium and ICG is used to decrease the risk of donor site lymphedema.
An algorithmic approach to simultaneous LNT with microvascular breast reconstruction proposed by Dr. Chang resulted in a 47% reduction in mean volume differential 12 months after reconstruction in 29 consecutive patients with refractory lymphedema following breast cancer treatment. These early results also showed no flap losses or donor-site lymphedema and donor-site wound complications in six patients (21%) that resolved with conservative measures (Ann Surg Oncol. 2015 Sep;22:2919-24).
The holy grail may be to strike lymphedema before it develops. To that end, Italian surgeons have proposed the Lymphatic Microsurgical Preventing Healing Approach (LYMPHA), which involves anastomosing arm lymphatics to a collateral branch of the axillary vein at the time of nodal dissection.
Over more than 4 years’ follow-up, only 3 of 74 breast cancer patients who underwent axillary nodal dissection with LYMPHA developed lymphedema, translating into a an exceptionally low 4% risk of lymphedema (Microsurgery. 2014 Sep;34:421-4). However, this approach is controversial because of unknown oncological risk and the uncertainty of its effectiveness in patients who may receive radiation after the surgery, Dr. Chang said in an interview.
Although these techniques show promise, currently no optimal solution exists and more research is needed to better understand lymphatic anatomy and physiology and the pathophysiology of lymphedema, concluded Dr. Chang, who reported no relevant conflicts of interest.
CHICAGO – Microsurgery does not cure lymphedema, in most cases. But, in most cases, it does improve the severity of lymphedema and reduce the complications of this chronic and debilitating disease. And “it certainly improves patients’ quality of life,” lymphedema treatment pioneer Dr. David W. Chang said at the 40th annual Northwestern Vascular Symposium.
Surgical treatment for limb lymphedema has come into its own since a lymphovenous shunt was first used in a dog model in 1962, with Dr. Chang and others now anastomosing subdermal lymphatics to subdermal venules less than 0.8 mm in diameter. The rationale behind “super-microsurgery” is that venous pressure is low in the subdermal venules and has minimal back flow, he said.
One of the big problems early on was knowing exactly where the lymphatic vessels were, but newer technology like indocyanine green (ICG) lymphangiography helps visualize functioning lymphatic channels for potential bypass and determine the severity of the disease. Understanding the disease stage is key to selecting the appropriate surgical procedure.
Lymphovenous bypass (LVB) is best in patients with stage 1 or 2 upper extremity lymphedema, while lymph node transfer (LNT) works for patients who are poor candidates for LVB or require combined breast reconstruction, said Dr. Chang, a plastic surgeon with the University of Chicago.
More recently, Dr. Chang has begun combining LVB and LNT, particularly for the more severe cases with stage 3 or 4 upper or lower extremity disease.
In Dr. Chang’s first 100 consecutive LVB cases while at the M.D. Anderson Cancer Center in Houston, quantitative improvement occurred in 74% of patients, symptom improvement in 96%, and the average volume differential reduction was 42% at 12 months (Plast Reconstr Surg. 2013 Nov;132:1305-14). The reduction was significantly larger in patients with earlier stage 1 or 2 vs. later stage 3 or 4 disease (61% vs. 17%).
During lymphovenous bypass, ICG is injected into the dermis of the web space and the superficial lymphatics evaluated with near-infrared fluorescence. It is easy to identify discrete functioning lymphatic channels in early-stage disease, but in late-stage disease significant dermal back flow is present, Dr. Chang said.
Dissection is performed under the microscope in the superficial subcutaneous plane to locate a good venule and lymph channel. Lymphatics are confirmed with isosulfan blue and ICG, and once the bypass site is determined, the lymphatic is anastomosed to the venule using 11-0 or 12-0 nylon, preferably in an end-to-side fashion. It’s thought this creates a more favorable flow pattern for the lymph to empty into the venule than an end-to-end anastomosis, he observed.
After the anastomosis is complete, patency is confirmed with isosulfan blue and ICG and the incision is closed under the microscope to ensure that the delicate anastomosis isn’t damaged. To avoid shear injury to the anastomosis, the limb is wrapped postoperatively for about a month without use of compression garments, he said.
Lymph node transfer (LNT) is increasingly being offered at centers to provide relief from lymphedema, although the mechanism by which it works is yet unclear; either the healthy lymph nodes act as a sponge to absorb lymphatic fluid or they induce lymphangiogenesis. Experience has shown, however, that rather than just grafting the lymph nodes, they need to be harvested with a vascular pedicle before transfer and anastomosed to the recipient artery and vein, although reconnecting the actual lymphatics may not be necessary, Dr. Chang observed.
Despite its popularity as a donor site, Dr. Chang said he is reluctant to use the groin because of the potential for iatrogenic lymphedema and prefers to harvest the supraclavicular nodes based off the transverse cervical artery. The external jugular vein can be harvested with the nodes if adequate venae comitantes are not present with the artery. Dissection of this flap can be difficult and care should be taken not to injure the lymphatic ducts, he noted.
It is also important to excise all scar tissue in the recipient site as this can impair lymphatic flow and inhibits lymphangiogenesis. If it is difficult to access or remove the scar, the vascularized lymph nodes are best placed just distal on the limb to the site of lymphatic obstruction, he added.
A recent meta-analysis (Plast Reconstr Surg. 2014 Apr;133:905-13) in five LNT studies reported that 91% of patients had a quantitative improvement, 78% discontinued compression garments, and complications were infection (8%), lymphorrhea (15%), and need for additional procedures (36%). There was great heterogeneity between studies, so the results should be interpreted with caution, Dr. Chang advised.
LNT is frequently combined with autologous breast reconstruction in patients with breast cancer, who comprise a significant percentage of Dr. Chang’s practice. The overall incidence of arm lymphedema after breast cancer can range from 8% to 56% at 2 years’ post-surgery, with the risk higher among women undergoing axillary lymph node dissection and/or axillary radiation.
Outcomes with combined LNT and breast reconstruction have been favorable, with one series reporting evidence of improved lymphatic flow on lymphoscintigraphy in five of six cases and one-third of patients no longer needing compression therapy (Ann Surg. 2012 Mar;255:468-73).
In cases where the patient requires a large skin paddle or seeks breast reconstruction after a previous mastectomy, lateral superficial groin lymph nodes can be harvested for transfer, leaving the deeper lymph nodes that drain the leg behind, Dr. Chang said. The nodes are usually clustered at the junction of the superior inferior epigastric and superficial circumflex iliac veins.
When combining LNT with breast reconstruction, this tissue is harvested together with the free abdominal flap used to reconstruct the breast. The superficial circumflex iliac vein is anastomosed in the axilla in addition to the arterial and venous anastomosis of the deep inferior epigastric vessels to the internal mammary vessels for the breast reconstruction. Reverse lymphatic mapping with technetium and ICG is used to decrease the risk of donor site lymphedema.
An algorithmic approach to simultaneous LNT with microvascular breast reconstruction proposed by Dr. Chang resulted in a 47% reduction in mean volume differential 12 months after reconstruction in 29 consecutive patients with refractory lymphedema following breast cancer treatment. These early results also showed no flap losses or donor-site lymphedema and donor-site wound complications in six patients (21%) that resolved with conservative measures (Ann Surg Oncol. 2015 Sep;22:2919-24).
The holy grail may be to strike lymphedema before it develops. To that end, Italian surgeons have proposed the Lymphatic Microsurgical Preventing Healing Approach (LYMPHA), which involves anastomosing arm lymphatics to a collateral branch of the axillary vein at the time of nodal dissection.
Over more than 4 years’ follow-up, only 3 of 74 breast cancer patients who underwent axillary nodal dissection with LYMPHA developed lymphedema, translating into a an exceptionally low 4% risk of lymphedema (Microsurgery. 2014 Sep;34:421-4). However, this approach is controversial because of unknown oncological risk and the uncertainty of its effectiveness in patients who may receive radiation after the surgery, Dr. Chang said in an interview.
Although these techniques show promise, currently no optimal solution exists and more research is needed to better understand lymphatic anatomy and physiology and the pathophysiology of lymphedema, concluded Dr. Chang, who reported no relevant conflicts of interest.
EXPERT ANALYSIS AT THE NORTHWESTERN VASCULAR SYMPOSIUM

Neurosurgeon memoir illuminates the journey through cancer treatment and acceptance of mortality
Dr. Paul Kalanithi, a neurosurgeon who had just completed his residency at the Stanford (Calif.) University, died of metastatic lung cancer last year, but he left a memoir of his experiences as a physician, a patient, and a dying man that was published on Jan. 12. His book, “When Breath Becomes Air” (New York: Random House, 2016), recounts the many years of working to exhaustion and deferring of life experiences and pleasures that are necessary to complete medical training.
In a review of the book, Janet Maslin wrote, “One of the most poignant things about Dr. Kalanithi’s story is that he had postponed learning how to live while pursuing his career in neurosurgery. By the time he was ready to enjoy a life outside the operating room, what he needed to learn was how to die.”
Dr. Kalanithi reflected on the profound grief and sense of loss that comes with a diagnosis that he knew meant imminent death. The memoir also reveals his search for meaning and joy, and finally, his acceptance of mortality. He opted for palliative care and his memoir, along with the epilogue written by his wife, Dr. Lucy Kalanithi, gives insight into the value of the palliative path to patients and their families in dire medical crises.
Dr. Paul Kalanithi, a neurosurgeon who had just completed his residency at the Stanford (Calif.) University, died of metastatic lung cancer last year, but he left a memoir of his experiences as a physician, a patient, and a dying man that was published on Jan. 12. His book, “When Breath Becomes Air” (New York: Random House, 2016), recounts the many years of working to exhaustion and deferring of life experiences and pleasures that are necessary to complete medical training.
In a review of the book, Janet Maslin wrote, “One of the most poignant things about Dr. Kalanithi’s story is that he had postponed learning how to live while pursuing his career in neurosurgery. By the time he was ready to enjoy a life outside the operating room, what he needed to learn was how to die.”
Dr. Kalanithi reflected on the profound grief and sense of loss that comes with a diagnosis that he knew meant imminent death. The memoir also reveals his search for meaning and joy, and finally, his acceptance of mortality. He opted for palliative care and his memoir, along with the epilogue written by his wife, Dr. Lucy Kalanithi, gives insight into the value of the palliative path to patients and their families in dire medical crises.
Dr. Paul Kalanithi, a neurosurgeon who had just completed his residency at the Stanford (Calif.) University, died of metastatic lung cancer last year, but he left a memoir of his experiences as a physician, a patient, and a dying man that was published on Jan. 12. His book, “When Breath Becomes Air” (New York: Random House, 2016), recounts the many years of working to exhaustion and deferring of life experiences and pleasures that are necessary to complete medical training.
In a review of the book, Janet Maslin wrote, “One of the most poignant things about Dr. Kalanithi’s story is that he had postponed learning how to live while pursuing his career in neurosurgery. By the time he was ready to enjoy a life outside the operating room, what he needed to learn was how to die.”
Dr. Kalanithi reflected on the profound grief and sense of loss that comes with a diagnosis that he knew meant imminent death. The memoir also reveals his search for meaning and joy, and finally, his acceptance of mortality. He opted for palliative care and his memoir, along with the epilogue written by his wife, Dr. Lucy Kalanithi, gives insight into the value of the palliative path to patients and their families in dire medical crises.
David Bowie’s death inspires blog on palliative care
The death of David Bowie, iconic musician and artist, on Jan. 10 inspired palliative care specialist Dr. Mark Taubert to write a blog about end-of-life scenarios and the importance of advance care planning. The blog, which begins by thanking Mr. Bowie for his many artistic contributions, continues by suggesting that his planned death at home will inspire many people in similar health crises to consider palliative care. The palliative care conversation between a doctor and a patient facing death can be challenging but can lead to what Dr. Taubert called “a good death” at home with symptoms managed and loved ones nearby. Mr. Bowie’s son, Duncan Jones, tweeted a link to the blog in the days after his father’s death.

Dr. Taubert found himself speaking with a patient who was facing probable death in the near future, and both doctor and patient found inspiration in Mr. Bowie’s final music project and his death at home with his family. Dr. Taubert and his patient were able to have the conversation about palliative care at end-of-life in part because they were both impressed with what Mr. Bowie was able to achieve in his last months. “Your story became a way for us to communicate very openly about death, something many doctors and nurses struggle to introduce as a topic of conversation,” he wrote.
Dr. Taubert of the Velindre NHS Trust in Cardiff, Wales, noted that, although palliative care is a highly developed skill with many resources to help patients at the end of life, “this essential part of training is not always available for junior healthcare professionals, including doctors and nurses, and is sometimes overlooked or under-prioritized by those who plan their education. I think if you [David Bowie] were ever to return (as Lazarus did), you would be a firm advocate for good palliative care training being available everywhere.”
The death of David Bowie, iconic musician and artist, on Jan. 10 inspired palliative care specialist Dr. Mark Taubert to write a blog about end-of-life scenarios and the importance of advance care planning. The blog, which begins by thanking Mr. Bowie for his many artistic contributions, continues by suggesting that his planned death at home will inspire many people in similar health crises to consider palliative care. The palliative care conversation between a doctor and a patient facing death can be challenging but can lead to what Dr. Taubert called “a good death” at home with symptoms managed and loved ones nearby. Mr. Bowie’s son, Duncan Jones, tweeted a link to the blog in the days after his father’s death.
Dr. Taubert found himself speaking with a patient who was facing probable death in the near future, and both doctor and patient found inspiration in Mr. Bowie’s final music project and his death at home with his family. Dr. Taubert and his patient were able to have the conversation about palliative care at end-of-life in part because they were both impressed with what Mr. Bowie was able to achieve in his last months. “Your story became a way for us to communicate very openly about death, something many doctors and nurses struggle to introduce as a topic of conversation,” he wrote.
Dr. Taubert of the Velindre NHS Trust in Cardiff, Wales, noted that, although palliative care is a highly developed skill with many resources to help patients at the end of life, “this essential part of training is not always available for junior healthcare professionals, including doctors and nurses, and is sometimes overlooked or under-prioritized by those who plan their education. I think if you [David Bowie] were ever to return (as Lazarus did), you would be a firm advocate for good palliative care training being available everywhere.”
The death of David Bowie, iconic musician and artist, on Jan. 10 inspired palliative care specialist Dr. Mark Taubert to write a blog about end-of-life scenarios and the importance of advance care planning. The blog, which begins by thanking Mr. Bowie for his many artistic contributions, continues by suggesting that his planned death at home will inspire many people in similar health crises to consider palliative care. The palliative care conversation between a doctor and a patient facing death can be challenging but can lead to what Dr. Taubert called “a good death” at home with symptoms managed and loved ones nearby. Mr. Bowie’s son, Duncan Jones, tweeted a link to the blog in the days after his father’s death.
Dr. Taubert found himself speaking with a patient who was facing probable death in the near future, and both doctor and patient found inspiration in Mr. Bowie’s final music project and his death at home with his family. Dr. Taubert and his patient were able to have the conversation about palliative care at end-of-life in part because they were both impressed with what Mr. Bowie was able to achieve in his last months. “Your story became a way for us to communicate very openly about death, something many doctors and nurses struggle to introduce as a topic of conversation,” he wrote.
Dr. Taubert of the Velindre NHS Trust in Cardiff, Wales, noted that, although palliative care is a highly developed skill with many resources to help patients at the end of life, “this essential part of training is not always available for junior healthcare professionals, including doctors and nurses, and is sometimes overlooked or under-prioritized by those who plan their education. I think if you [David Bowie] were ever to return (as Lazarus did), you would be a firm advocate for good palliative care training being available everywhere.”

Families perceive few benefits from aggressive end-of-life care
Bereaved families were substantially more satisfied with end-of-life cancer care when patients did not die in hospital, received more than 3 days of hospice care, and did not enter the ICU within 30 days of dying, according to a multicenter, prospective study published online Jan. 19 in JAMA.
The analysis is one of the first of its type to assess these end-of-life care indicators, said Dr. Alexi Wright of Harvard Medical School, Boston, and her associates. The findings could affect health policy as electronic health records expand under the Health Information Technology for Economic and Clinical Health Act, they said.
End-of-life cancer care has become increasingly aggressive, belying evidence that this approach does not improve patient outcomes, quality of life, or caregiver bereavement. To explore alternatives, the researchers analyzed 1,146 interviews of family members of Medicare patients who died of lung or colorectal cancer by 2011. Their data source was the multiregional, prospective, observational Cancer Care Outcomes Research and Surveillance (CanCORS) study (JAMA 2016;315:284-92).

Family members described end-of-life care as “excellent” 59% of the time when hospice care lasted more 3 days, but 43% of the time otherwise (95% confidence interval for adjusted difference, 11% to 22%). Notably, 73% of patients who received more than 3 days of hospice care died in their preferred location, compared with 40% of patients who received less or no hospice care. Care was rated as excellent 52% of the time when ICU admission was avoided within 30 days of death, and 57% of the time when patients died outside the hospital, compared with 45% and 42% of the time otherwise.
The results support “advance care planning consistent with the preferences of patients,” said the investigators. They recommended more extensive counseling of cancer patients and families, earlier palliative care referrals, and an audit and feedback system to monitor the use of aggressive end-of-life care.
The National Cancer Institute and the Cancer Care Outcomes Research and Surveillance Consortium funded the study. One coinvestigator reported financial relationships with the American Academy of Hospice and Palliative Medicine, National Institute of Nursing Research, National Institute on Aging, Retirement Research Retirement Foundation, California Healthcare Foundation, Commonwealth Fund, West Health Institute, University of Wisconsin, and UpToDate.com. Senior author Dr. Mary Landrum, also of Harvard Medical School, reported grant funding from Pfizer and personal fees from McKinsey and Company and Greylock McKinnon Associates. The other authors had no disclosures.
Bereaved families were substantially more satisfied with end-of-life cancer care when patients did not die in hospital, received more than 3 days of hospice care, and did not enter the ICU within 30 days of dying, according to a multicenter, prospective study published online Jan. 19 in JAMA.
The analysis is one of the first of its type to assess these end-of-life care indicators, said Dr. Alexi Wright of Harvard Medical School, Boston, and her associates. The findings could affect health policy as electronic health records expand under the Health Information Technology for Economic and Clinical Health Act, they said.
End-of-life cancer care has become increasingly aggressive, belying evidence that this approach does not improve patient outcomes, quality of life, or caregiver bereavement. To explore alternatives, the researchers analyzed 1,146 interviews of family members of Medicare patients who died of lung or colorectal cancer by 2011. Their data source was the multiregional, prospective, observational Cancer Care Outcomes Research and Surveillance (CanCORS) study (JAMA 2016;315:284-92).
Family members described end-of-life care as “excellent” 59% of the time when hospice care lasted more 3 days, but 43% of the time otherwise (95% confidence interval for adjusted difference, 11% to 22%). Notably, 73% of patients who received more than 3 days of hospice care died in their preferred location, compared with 40% of patients who received less or no hospice care. Care was rated as excellent 52% of the time when ICU admission was avoided within 30 days of death, and 57% of the time when patients died outside the hospital, compared with 45% and 42% of the time otherwise.
The results support “advance care planning consistent with the preferences of patients,” said the investigators. They recommended more extensive counseling of cancer patients and families, earlier palliative care referrals, and an audit and feedback system to monitor the use of aggressive end-of-life care.
The National Cancer Institute and the Cancer Care Outcomes Research and Surveillance Consortium funded the study. One coinvestigator reported financial relationships with the American Academy of Hospice and Palliative Medicine, National Institute of Nursing Research, National Institute on Aging, Retirement Research Retirement Foundation, California Healthcare Foundation, Commonwealth Fund, West Health Institute, University of Wisconsin, and UpToDate.com. Senior author Dr. Mary Landrum, also of Harvard Medical School, reported grant funding from Pfizer and personal fees from McKinsey and Company and Greylock McKinnon Associates. The other authors had no disclosures.
Bereaved families were substantially more satisfied with end-of-life cancer care when patients did not die in hospital, received more than 3 days of hospice care, and did not enter the ICU within 30 days of dying, according to a multicenter, prospective study published online Jan. 19 in JAMA.
The analysis is one of the first of its type to assess these end-of-life care indicators, said Dr. Alexi Wright of Harvard Medical School, Boston, and her associates. The findings could affect health policy as electronic health records expand under the Health Information Technology for Economic and Clinical Health Act, they said.
End-of-life cancer care has become increasingly aggressive, belying evidence that this approach does not improve patient outcomes, quality of life, or caregiver bereavement. To explore alternatives, the researchers analyzed 1,146 interviews of family members of Medicare patients who died of lung or colorectal cancer by 2011. Their data source was the multiregional, prospective, observational Cancer Care Outcomes Research and Surveillance (CanCORS) study (JAMA 2016;315:284-92).
Family members described end-of-life care as “excellent” 59% of the time when hospice care lasted more 3 days, but 43% of the time otherwise (95% confidence interval for adjusted difference, 11% to 22%). Notably, 73% of patients who received more than 3 days of hospice care died in their preferred location, compared with 40% of patients who received less or no hospice care. Care was rated as excellent 52% of the time when ICU admission was avoided within 30 days of death, and 57% of the time when patients died outside the hospital, compared with 45% and 42% of the time otherwise.
The results support “advance care planning consistent with the preferences of patients,” said the investigators. They recommended more extensive counseling of cancer patients and families, earlier palliative care referrals, and an audit and feedback system to monitor the use of aggressive end-of-life care.
The National Cancer Institute and the Cancer Care Outcomes Research and Surveillance Consortium funded the study. One coinvestigator reported financial relationships with the American Academy of Hospice and Palliative Medicine, National Institute of Nursing Research, National Institute on Aging, Retirement Research Retirement Foundation, California Healthcare Foundation, Commonwealth Fund, West Health Institute, University of Wisconsin, and UpToDate.com. Senior author Dr. Mary Landrum, also of Harvard Medical School, reported grant funding from Pfizer and personal fees from McKinsey and Company and Greylock McKinnon Associates. The other authors had no disclosures.
FROM JAMA
Key clinical point: Bereaved family members were more satisfied with end-of-life cancer care when patients spent more than 3 days in hospice, died outside the hospital, and were not admitted to the ICU within 30 days of dying.
Major finding: Care was described as “excellent” about 9%-17% more often when these end-of-life quality indicators were met.
Data source: A multicenter, prospective, observational study of 1,146 family members of patients who died of lung or colorectal cancer.
Disclosures: The National Cancer Institute and the Cancer Care Outcomes Research and Surveillance Consortium funded the analysis. One coinvestigator reported financial relationships with the American Academy of Hospice and Palliative Medicine, National Institute of Nursing Research, National Institute on Aging, Retirement Research Retirement Foundation, California Healthcare Foundation, Commonwealth Fund, West Health Institute, University of Wisconsin, and UpToDate.com. Senior author Dr. Mary Landrum reported grant funding from Pfizer and personal fees from McKinsey and Company and Greylock McKinnon Associates. The other authors had no disclosures.

DME: New prior authorization requirements could up the ‘hassle factor’
Starting next month, Medicare won’t pay for certain durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) without prior authorization. The regulation could mean headaches for doctors in the form of extra paperwork and frustrated patients.
“Our initial reaction is one of concern,” said Dr. Wanda Filer, president of the American Academy of Family Physicians. “This new rule could prompt DMEPOS suppliers to request additional documentation from ordering/prescribing physicians to support the suppliers’ requests for prior authorization. Such requests could lead to administrative hassles for physicians.”

Under the new requirement – effective Feb. 29 – prior CMS authorization will be required for certain DMEPOS items that are frequently subject to “unnecessary utilization,” according to a Dec. 29 announcement. The prior authorization process requires the same information currently necessary for Medicare payment, but will happen earlier in the process.
The early evaluation will assure that all relevant coverage, coding, and clinical documentation is provided before the equipment is furnished to the patient and before the claim is submitted for payment. CMS hopes the prior review will reduce improper payments for DMEPOS.
Not every piece of durable medical equipment will be subject to prior authorization; instead, CMS will prescreen items from its master list of 135 costly and overprescribed items, especially those with an average purchase price of more than $1,000 or rental fee of $100. The complete master list was published within CMS’ final rule in the Federal Register. CMS will publish a “required prior authorization list” 60 days before implementation.
The final rule primarily impacts vendors paid by Medicare to supply durable medical equipment to patients, said Dr. Yul D. Ejnes, an internist in private practice and a past chair of the American College of Physicians Board of Regents. The prescriber is responsible for meeting all Medicare coverage, coding, and payment rules. However, doctors will likely be indirectly affected because of the clinical documentation required for CMS approval, Dr. Ejnes said.

“The documentation requirement could be burdensome depending on how DME vendors interpret the regulations, and then the whole issue of increasing the amount of chart documentation that’s going out to various places raises some concern,” Dr. Ejnes said in an interview. “Even though it may all be covered under HIPAA, [there’s] the issue of content in the notes that’s irrelevant to the DME request and how we handle that. Do we need to start redacting notes to meet the documentation requirements for prior authorization?”
The new requirements also may mean that patients wait longer for needed equipment, Dr. Ejnes added. “Oftentimes, there’s the finger-pointing exercise that occurs when things don’t happen quickly enough and patients are unhappy. “It just adds to the temperature of the environment, which is already pretty high because of patients unhappy about increasing copays and deductibles and everything else.”
To prepare for the rule, physicians should identify the DMEPOS items they order or prescribe most often and engage with suppliers early to ensure they understand what kind of documentation will be needed, Dr. Filer recommended.
“If the physician understands upfront what Medicare requires and is able to provide it to the DMEPOS supplier[s] at the time the DMEPOS items are ordered/prescribed, that may save time on the back-end preventing or otherwise dealing with additional documentation requests from the DMEPOS supplier[s] in support of prior authorization requests,” she said.
Be extremely thoughtful about prescribing durable medical equipment and make sure that equipment orders are placed that meet the patient’s needs rather than their desires, Dr. Ejnes recommended. In addition, it’s helpful for practices to consider work flow and how to efficiently respond to document requests. In some cases, office staff can locate records or precomplete basic information on forms, he said.
“Figure out a way to respond to these in terms of who in the office will take the first pass if there’s a form to fill out,” he said. “Be aware that there may be some delays in getting patients what they need. Some of these items are not emergency items. Educate patients to the fact that there’s a couple steps between writing the prescription and them picking up the item.”
On Twitter @legal_med
Starting next month, Medicare won’t pay for certain durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) without prior authorization. The regulation could mean headaches for doctors in the form of extra paperwork and frustrated patients.
“Our initial reaction is one of concern,” said Dr. Wanda Filer, president of the American Academy of Family Physicians. “This new rule could prompt DMEPOS suppliers to request additional documentation from ordering/prescribing physicians to support the suppliers’ requests for prior authorization. Such requests could lead to administrative hassles for physicians.”
Under the new requirement – effective Feb. 29 – prior CMS authorization will be required for certain DMEPOS items that are frequently subject to “unnecessary utilization,” according to a Dec. 29 announcement. The prior authorization process requires the same information currently necessary for Medicare payment, but will happen earlier in the process.
The early evaluation will assure that all relevant coverage, coding, and clinical documentation is provided before the equipment is furnished to the patient and before the claim is submitted for payment. CMS hopes the prior review will reduce improper payments for DMEPOS.
Not every piece of durable medical equipment will be subject to prior authorization; instead, CMS will prescreen items from its master list of 135 costly and overprescribed items, especially those with an average purchase price of more than $1,000 or rental fee of $100. The complete master list was published within CMS’ final rule in the Federal Register. CMS will publish a “required prior authorization list” 60 days before implementation.
The final rule primarily impacts vendors paid by Medicare to supply durable medical equipment to patients, said Dr. Yul D. Ejnes, an internist in private practice and a past chair of the American College of Physicians Board of Regents. The prescriber is responsible for meeting all Medicare coverage, coding, and payment rules. However, doctors will likely be indirectly affected because of the clinical documentation required for CMS approval, Dr. Ejnes said.
“The documentation requirement could be burdensome depending on how DME vendors interpret the regulations, and then the whole issue of increasing the amount of chart documentation that’s going out to various places raises some concern,” Dr. Ejnes said in an interview. “Even though it may all be covered under HIPAA, [there’s] the issue of content in the notes that’s irrelevant to the DME request and how we handle that. Do we need to start redacting notes to meet the documentation requirements for prior authorization?”
The new requirements also may mean that patients wait longer for needed equipment, Dr. Ejnes added. “Oftentimes, there’s the finger-pointing exercise that occurs when things don’t happen quickly enough and patients are unhappy. “It just adds to the temperature of the environment, which is already pretty high because of patients unhappy about increasing copays and deductibles and everything else.”
To prepare for the rule, physicians should identify the DMEPOS items they order or prescribe most often and engage with suppliers early to ensure they understand what kind of documentation will be needed, Dr. Filer recommended.
“If the physician understands upfront what Medicare requires and is able to provide it to the DMEPOS supplier[s] at the time the DMEPOS items are ordered/prescribed, that may save time on the back-end preventing or otherwise dealing with additional documentation requests from the DMEPOS supplier[s] in support of prior authorization requests,” she said.
Be extremely thoughtful about prescribing durable medical equipment and make sure that equipment orders are placed that meet the patient’s needs rather than their desires, Dr. Ejnes recommended. In addition, it’s helpful for practices to consider work flow and how to efficiently respond to document requests. In some cases, office staff can locate records or precomplete basic information on forms, he said.
“Figure out a way to respond to these in terms of who in the office will take the first pass if there’s a form to fill out,” he said. “Be aware that there may be some delays in getting patients what they need. Some of these items are not emergency items. Educate patients to the fact that there’s a couple steps between writing the prescription and them picking up the item.”
On Twitter @legal_med
Starting next month, Medicare won’t pay for certain durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) without prior authorization. The regulation could mean headaches for doctors in the form of extra paperwork and frustrated patients.
“Our initial reaction is one of concern,” said Dr. Wanda Filer, president of the American Academy of Family Physicians. “This new rule could prompt DMEPOS suppliers to request additional documentation from ordering/prescribing physicians to support the suppliers’ requests for prior authorization. Such requests could lead to administrative hassles for physicians.”
Under the new requirement – effective Feb. 29 – prior CMS authorization will be required for certain DMEPOS items that are frequently subject to “unnecessary utilization,” according to a Dec. 29 announcement. The prior authorization process requires the same information currently necessary for Medicare payment, but will happen earlier in the process.
The early evaluation will assure that all relevant coverage, coding, and clinical documentation is provided before the equipment is furnished to the patient and before the claim is submitted for payment. CMS hopes the prior review will reduce improper payments for DMEPOS.
Not every piece of durable medical equipment will be subject to prior authorization; instead, CMS will prescreen items from its master list of 135 costly and overprescribed items, especially those with an average purchase price of more than $1,000 or rental fee of $100. The complete master list was published within CMS’ final rule in the Federal Register. CMS will publish a “required prior authorization list” 60 days before implementation.
The final rule primarily impacts vendors paid by Medicare to supply durable medical equipment to patients, said Dr. Yul D. Ejnes, an internist in private practice and a past chair of the American College of Physicians Board of Regents. The prescriber is responsible for meeting all Medicare coverage, coding, and payment rules. However, doctors will likely be indirectly affected because of the clinical documentation required for CMS approval, Dr. Ejnes said.
“The documentation requirement could be burdensome depending on how DME vendors interpret the regulations, and then the whole issue of increasing the amount of chart documentation that’s going out to various places raises some concern,” Dr. Ejnes said in an interview. “Even though it may all be covered under HIPAA, [there’s] the issue of content in the notes that’s irrelevant to the DME request and how we handle that. Do we need to start redacting notes to meet the documentation requirements for prior authorization?”
The new requirements also may mean that patients wait longer for needed equipment, Dr. Ejnes added. “Oftentimes, there’s the finger-pointing exercise that occurs when things don’t happen quickly enough and patients are unhappy. “It just adds to the temperature of the environment, which is already pretty high because of patients unhappy about increasing copays and deductibles and everything else.”
To prepare for the rule, physicians should identify the DMEPOS items they order or prescribe most often and engage with suppliers early to ensure they understand what kind of documentation will be needed, Dr. Filer recommended.
“If the physician understands upfront what Medicare requires and is able to provide it to the DMEPOS supplier[s] at the time the DMEPOS items are ordered/prescribed, that may save time on the back-end preventing or otherwise dealing with additional documentation requests from the DMEPOS supplier[s] in support of prior authorization requests,” she said.
Be extremely thoughtful about prescribing durable medical equipment and make sure that equipment orders are placed that meet the patient’s needs rather than their desires, Dr. Ejnes recommended. In addition, it’s helpful for practices to consider work flow and how to efficiently respond to document requests. In some cases, office staff can locate records or precomplete basic information on forms, he said.
“Figure out a way to respond to these in terms of who in the office will take the first pass if there’s a form to fill out,” he said. “Be aware that there may be some delays in getting patients what they need. Some of these items are not emergency items. Educate patients to the fact that there’s a couple steps between writing the prescription and them picking up the item.”
On Twitter @legal_med

Law & Medicine: Health care costs and defensive medicine
Question: Which of the following choices is best?
A. Controversy exists over whether defensive medicine is widely practiced and whether it raises health care costs.
B. Everyone agrees that defensive medicine is widely practiced.
C. Doctors who spend more for their hospitalized patients have been reported to face a lower malpractice risk.
D. A and C.
E. B and C.
Answer: D. Virtually all doctors admit they practice defensive medicine, which describes medical care specifically directed to attenuate the threat of malpractice liability rather than for a proper medical indication. Survey studies generally put the prevalence at greater than 90%, but what separates true defensive medicine from careful practice or patient expectation/demand remains controversial.

A mail survey of 824 physicians in high-risk specialties in Pennsylvania, a state where doctors pay high malpractice premiums, revealed that nearly all reported practicing defensive medicine. The respondents admitted to both assurance behavior – such as ordering more tests, especially imaging studies – as well as avoidance behavior – that is, restricting or eliminating complex procedures or perceived litigious patients.1
In another study, emergency physicians in the upper third of “malpractice fear” used more diagnostic tests and were more likely to hospitalize patients at low risk for coronary artery disease.2
On the other hand, a report using simulated clinical scenarios concluded that the extent of defensive medicine was at most 8%, and another found no correlation between individual malpractice claims experience and resource use, physician concern about malpractice, tolerance for uncertainty, or perception of risk.3
Another area of contention is whether some of our soaring health care costs may reflect defensive medicine at play.
A recent survey of 2,000 U.S. orthopedic surgeons found that 96% admitted practicing defensive medicine, with 24% of all ordered tests being for defensive reasons. The authors estimated that this amounted to about $100,000 per surgeon per year, or a total annual sum of $2 billion for the 20,400 orthopedic surgeons in the U.S.4
By correlating professional liability insurance with cost of services, the AMA estimated that in the 1980s, defensive medicine cost $12.1 billion to $13.7 billion each year.5 In an oft-cited study by Kessler and McClellan, the authors measured the effects of malpractice liability reforms using data from elderly Medicare beneficiaries treated for serious heart disease.6 They found that reforms that directly reduced provider liability pressure led to reductions of 5%-9% in medical expenditures. If such Medicare savings, which amounted to $600 million per year for cardiac disease, were extrapolated across the health care system, the annual savings would total $50 billion.
A more conservative study estimated that systemwide savings from aggressive malpractice reform would approach $41 billion over 5 years.7
Dr. Anupam B. Jena and his coauthors are the latest investigators seeking to clarify the correlation between defensive medicine and health care costs.8 Using Florida hospital admission data from 2000-2009, which covered some 24,000 physicians in seven separate specialties, the authors found that higher spending by physicians was associated with reduced malpractice claims the following year. This pattern held true for six of the seven specialties, family practitioners being the sole exception.
For example, among internists, the malpractice risk probability was reduced from 1.5% in the bottom spending fifth ($19,725 per admission) to 0.3% in the top fifth ($39,379 per admission). Among obstetricians, a separate subgroup analysis of cesarean-section rates revealed that malpractice claims were approximately halved among obstetricians with rates in the highest fifth, compared with the lowest fifth. These results comport with previous reports of higher C-section rates in obstetricians who perceived themselves at higher malpractice risk, although other studies have found no correlation or an actual lower rate.
In concluding that higher resource use by physicians was associated with fewer malpractice claims, the authors acknowledged that a principal limitation of the study was the lack of information on illness severity. Importantly, they were unable to state whether higher spending was defensively motivated. A companion editorial questioned whether increased resource expenditure was a bona fide reflection of defensive medicine or may simply have resulted in fewer errors and adverse events.9
Unfortunately, the past malpractice experience of the doctors, which could provide insight into more defensive postures, better communication, etc., was not measured in the study. In addition, claims made just 1 year after an incident may not accurately reflect the real-world situation, where the filing of a lawsuit may lag any alleged negligence by a much longer period, especially in obstetric cases.
Worryingly, the results of this timely study may be used to imply that the more doctors spend, the less likely they are to be sued – a troubling notion in our current race to stem rising health care costs.
References
1. JAMA. 2005 Jun 1;293(21):2609-17.
2. Ann Emerg Med. 2005 Dec;46(6):525-33.
3. J Health Polit Policy Law. 1996 Summer;21(2):267-88.
4. Am J Orthop (Belle Mead NJ). 2012 Feb;41(2):69-73.
5. JAMA. 1987 May 22-29;257(20):2776-81.
6. Q J Econ. 1996 May; 111(2):353-90.
7. J Am Health Policy. 1994 Jul-Aug;4(4):7-15.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: Which of the following choices is best?
A. Controversy exists over whether defensive medicine is widely practiced and whether it raises health care costs.
B. Everyone agrees that defensive medicine is widely practiced.
C. Doctors who spend more for their hospitalized patients have been reported to face a lower malpractice risk.
D. A and C.
E. B and C.
Answer: D. Virtually all doctors admit they practice defensive medicine, which describes medical care specifically directed to attenuate the threat of malpractice liability rather than for a proper medical indication. Survey studies generally put the prevalence at greater than 90%, but what separates true defensive medicine from careful practice or patient expectation/demand remains controversial.
A mail survey of 824 physicians in high-risk specialties in Pennsylvania, a state where doctors pay high malpractice premiums, revealed that nearly all reported practicing defensive medicine. The respondents admitted to both assurance behavior – such as ordering more tests, especially imaging studies – as well as avoidance behavior – that is, restricting or eliminating complex procedures or perceived litigious patients.1
In another study, emergency physicians in the upper third of “malpractice fear” used more diagnostic tests and were more likely to hospitalize patients at low risk for coronary artery disease.2
On the other hand, a report using simulated clinical scenarios concluded that the extent of defensive medicine was at most 8%, and another found no correlation between individual malpractice claims experience and resource use, physician concern about malpractice, tolerance for uncertainty, or perception of risk.3
Another area of contention is whether some of our soaring health care costs may reflect defensive medicine at play.
A recent survey of 2,000 U.S. orthopedic surgeons found that 96% admitted practicing defensive medicine, with 24% of all ordered tests being for defensive reasons. The authors estimated that this amounted to about $100,000 per surgeon per year, or a total annual sum of $2 billion for the 20,400 orthopedic surgeons in the U.S.4
By correlating professional liability insurance with cost of services, the AMA estimated that in the 1980s, defensive medicine cost $12.1 billion to $13.7 billion each year.5 In an oft-cited study by Kessler and McClellan, the authors measured the effects of malpractice liability reforms using data from elderly Medicare beneficiaries treated for serious heart disease.6 They found that reforms that directly reduced provider liability pressure led to reductions of 5%-9% in medical expenditures. If such Medicare savings, which amounted to $600 million per year for cardiac disease, were extrapolated across the health care system, the annual savings would total $50 billion.
A more conservative study estimated that systemwide savings from aggressive malpractice reform would approach $41 billion over 5 years.7
Dr. Anupam B. Jena and his coauthors are the latest investigators seeking to clarify the correlation between defensive medicine and health care costs.8 Using Florida hospital admission data from 2000-2009, which covered some 24,000 physicians in seven separate specialties, the authors found that higher spending by physicians was associated with reduced malpractice claims the following year. This pattern held true for six of the seven specialties, family practitioners being the sole exception.
For example, among internists, the malpractice risk probability was reduced from 1.5% in the bottom spending fifth ($19,725 per admission) to 0.3% in the top fifth ($39,379 per admission). Among obstetricians, a separate subgroup analysis of cesarean-section rates revealed that malpractice claims were approximately halved among obstetricians with rates in the highest fifth, compared with the lowest fifth. These results comport with previous reports of higher C-section rates in obstetricians who perceived themselves at higher malpractice risk, although other studies have found no correlation or an actual lower rate.
In concluding that higher resource use by physicians was associated with fewer malpractice claims, the authors acknowledged that a principal limitation of the study was the lack of information on illness severity. Importantly, they were unable to state whether higher spending was defensively motivated. A companion editorial questioned whether increased resource expenditure was a bona fide reflection of defensive medicine or may simply have resulted in fewer errors and adverse events.9
Unfortunately, the past malpractice experience of the doctors, which could provide insight into more defensive postures, better communication, etc., was not measured in the study. In addition, claims made just 1 year after an incident may not accurately reflect the real-world situation, where the filing of a lawsuit may lag any alleged negligence by a much longer period, especially in obstetric cases.
Worryingly, the results of this timely study may be used to imply that the more doctors spend, the less likely they are to be sued – a troubling notion in our current race to stem rising health care costs.
References
1. JAMA. 2005 Jun 1;293(21):2609-17.
2. Ann Emerg Med. 2005 Dec;46(6):525-33.
3. J Health Polit Policy Law. 1996 Summer;21(2):267-88.
4. Am J Orthop (Belle Mead NJ). 2012 Feb;41(2):69-73.
5. JAMA. 1987 May 22-29;257(20):2776-81.
6. Q J Econ. 1996 May; 111(2):353-90.
7. J Am Health Policy. 1994 Jul-Aug;4(4):7-15.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
Question: Which of the following choices is best?
A. Controversy exists over whether defensive medicine is widely practiced and whether it raises health care costs.
B. Everyone agrees that defensive medicine is widely practiced.
C. Doctors who spend more for their hospitalized patients have been reported to face a lower malpractice risk.
D. A and C.
E. B and C.
Answer: D. Virtually all doctors admit they practice defensive medicine, which describes medical care specifically directed to attenuate the threat of malpractice liability rather than for a proper medical indication. Survey studies generally put the prevalence at greater than 90%, but what separates true defensive medicine from careful practice or patient expectation/demand remains controversial.
A mail survey of 824 physicians in high-risk specialties in Pennsylvania, a state where doctors pay high malpractice premiums, revealed that nearly all reported practicing defensive medicine. The respondents admitted to both assurance behavior – such as ordering more tests, especially imaging studies – as well as avoidance behavior – that is, restricting or eliminating complex procedures or perceived litigious patients.1
In another study, emergency physicians in the upper third of “malpractice fear” used more diagnostic tests and were more likely to hospitalize patients at low risk for coronary artery disease.2
On the other hand, a report using simulated clinical scenarios concluded that the extent of defensive medicine was at most 8%, and another found no correlation between individual malpractice claims experience and resource use, physician concern about malpractice, tolerance for uncertainty, or perception of risk.3
Another area of contention is whether some of our soaring health care costs may reflect defensive medicine at play.
A recent survey of 2,000 U.S. orthopedic surgeons found that 96% admitted practicing defensive medicine, with 24% of all ordered tests being for defensive reasons. The authors estimated that this amounted to about $100,000 per surgeon per year, or a total annual sum of $2 billion for the 20,400 orthopedic surgeons in the U.S.4
By correlating professional liability insurance with cost of services, the AMA estimated that in the 1980s, defensive medicine cost $12.1 billion to $13.7 billion each year.5 In an oft-cited study by Kessler and McClellan, the authors measured the effects of malpractice liability reforms using data from elderly Medicare beneficiaries treated for serious heart disease.6 They found that reforms that directly reduced provider liability pressure led to reductions of 5%-9% in medical expenditures. If such Medicare savings, which amounted to $600 million per year for cardiac disease, were extrapolated across the health care system, the annual savings would total $50 billion.
A more conservative study estimated that systemwide savings from aggressive malpractice reform would approach $41 billion over 5 years.7
Dr. Anupam B. Jena and his coauthors are the latest investigators seeking to clarify the correlation between defensive medicine and health care costs.8 Using Florida hospital admission data from 2000-2009, which covered some 24,000 physicians in seven separate specialties, the authors found that higher spending by physicians was associated with reduced malpractice claims the following year. This pattern held true for six of the seven specialties, family practitioners being the sole exception.
For example, among internists, the malpractice risk probability was reduced from 1.5% in the bottom spending fifth ($19,725 per admission) to 0.3% in the top fifth ($39,379 per admission). Among obstetricians, a separate subgroup analysis of cesarean-section rates revealed that malpractice claims were approximately halved among obstetricians with rates in the highest fifth, compared with the lowest fifth. These results comport with previous reports of higher C-section rates in obstetricians who perceived themselves at higher malpractice risk, although other studies have found no correlation or an actual lower rate.
In concluding that higher resource use by physicians was associated with fewer malpractice claims, the authors acknowledged that a principal limitation of the study was the lack of information on illness severity. Importantly, they were unable to state whether higher spending was defensively motivated. A companion editorial questioned whether increased resource expenditure was a bona fide reflection of defensive medicine or may simply have resulted in fewer errors and adverse events.9
Unfortunately, the past malpractice experience of the doctors, which could provide insight into more defensive postures, better communication, etc., was not measured in the study. In addition, claims made just 1 year after an incident may not accurately reflect the real-world situation, where the filing of a lawsuit may lag any alleged negligence by a much longer period, especially in obstetric cases.
Worryingly, the results of this timely study may be used to imply that the more doctors spend, the less likely they are to be sued – a troubling notion in our current race to stem rising health care costs.
References
1. JAMA. 2005 Jun 1;293(21):2609-17.
2. Ann Emerg Med. 2005 Dec;46(6):525-33.
3. J Health Polit Policy Law. 1996 Summer;21(2):267-88.
4. Am J Orthop (Belle Mead NJ). 2012 Feb;41(2):69-73.
5. JAMA. 1987 May 22-29;257(20):2776-81.
6. Q J Econ. 1996 May; 111(2):353-90.
7. J Am Health Policy. 1994 Jul-Aug;4(4):7-15.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at siang@hawaii.edu.
