User login
In Case You Missed It: COVID
Daily Recap: Stressed out primary care docs, ‘hospital at home’ for cancer patients
Here are the stories our MDedge editors across specialties think you need to know about today:
Racism, COVID-19 lead to sky-high stress levels
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, 12% of the survey’s 586 respondents “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement. One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being.
In a related survey of 1,111 patients conducted June 8 about 65% of patients said that racism affected emotional, psychological, and behavioral health.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers. Read more.
Medical teams take to the streets
They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go. Many are medical professionals who see parallels between the front lines of COVID-19, where they confront stark racial imbalances among those stricken by the coronavirus, and what they see as racialized police brutality.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. “I am working full time and basically being at the protest after getting straight off of work,” said Ms. Butler, who is black. That’s tiring, she added, but so is being a black woman in America. Read more.
At-home management of type 1 diabetes, COVID-19
Although hyperglycemia and diabetic ketoacidosis are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
These new findings are still preliminary and were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
The published study includes data as of May 5 on 64 individuals from a total of 64 US sites. Since the paper was submitted, there are now 220 patients from 68 sites. There were two deaths in the preliminary report, Dr. Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Overall, 34.9% of patients were able to manage COVID-19 entirely at home. At the other extreme, 22.2% of patients overall were admitted to the intensive care unit. Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to the hospital. “Even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Dr. Ebekozien said. Read more.
‘Hospital at home’ for cancer patients
Visits to the emergency department (ED) and hospitalizations are often frequent occurrences for cancer patients, but what if the “hospital” could be brought into the home instead?
A new American cohort study provides evidence that this can be a workable option for cancer patients. The authors report improved patient outcomes, with 56% lower odds of unplanned hospitalizations, 45% lower odds of ED visits, and 50% lower cumulative charges, as compared with patients who received usual care.
“The oncology hospital-at-home model of care that extends acute-level care to the patient at home offers promise in addressing a long-term gap in cancer care service delivery,” said lead author Kathi Mooney, PhD, RN, distinguished professor of nursing at the University of Utah, Salt Lake City. “In light of the current global pandemic, we are compelled to consider new ways to provide cancer care, and the oncology hospital-at-home model is on point to address critical elements of an improved cancer care delivery system.”
Dr. Mooney presented the findings during the virtual scientific program of the American Society of Clinical Oncology 2020 annual meeting (abstract 7000). Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Racism, COVID-19 lead to sky-high stress levels
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, 12% of the survey’s 586 respondents “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement. One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being.
In a related survey of 1,111 patients conducted June 8 about 65% of patients said that racism affected emotional, psychological, and behavioral health.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers. Read more.
Medical teams take to the streets
They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go. Many are medical professionals who see parallels between the front lines of COVID-19, where they confront stark racial imbalances among those stricken by the coronavirus, and what they see as racialized police brutality.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. “I am working full time and basically being at the protest after getting straight off of work,” said Ms. Butler, who is black. That’s tiring, she added, but so is being a black woman in America. Read more.
At-home management of type 1 diabetes, COVID-19
Although hyperglycemia and diabetic ketoacidosis are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
These new findings are still preliminary and were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
The published study includes data as of May 5 on 64 individuals from a total of 64 US sites. Since the paper was submitted, there are now 220 patients from 68 sites. There were two deaths in the preliminary report, Dr. Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Overall, 34.9% of patients were able to manage COVID-19 entirely at home. At the other extreme, 22.2% of patients overall were admitted to the intensive care unit. Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to the hospital. “Even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Dr. Ebekozien said. Read more.
‘Hospital at home’ for cancer patients
Visits to the emergency department (ED) and hospitalizations are often frequent occurrences for cancer patients, but what if the “hospital” could be brought into the home instead?
A new American cohort study provides evidence that this can be a workable option for cancer patients. The authors report improved patient outcomes, with 56% lower odds of unplanned hospitalizations, 45% lower odds of ED visits, and 50% lower cumulative charges, as compared with patients who received usual care.
“The oncology hospital-at-home model of care that extends acute-level care to the patient at home offers promise in addressing a long-term gap in cancer care service delivery,” said lead author Kathi Mooney, PhD, RN, distinguished professor of nursing at the University of Utah, Salt Lake City. “In light of the current global pandemic, we are compelled to consider new ways to provide cancer care, and the oncology hospital-at-home model is on point to address critical elements of an improved cancer care delivery system.”
Dr. Mooney presented the findings during the virtual scientific program of the American Society of Clinical Oncology 2020 annual meeting (abstract 7000). Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Racism, COVID-19 lead to sky-high stress levels
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, 12% of the survey’s 586 respondents “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement. One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being.
In a related survey of 1,111 patients conducted June 8 about 65% of patients said that racism affected emotional, psychological, and behavioral health.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers. Read more.
Medical teams take to the streets
They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go. Many are medical professionals who see parallels between the front lines of COVID-19, where they confront stark racial imbalances among those stricken by the coronavirus, and what they see as racialized police brutality.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. “I am working full time and basically being at the protest after getting straight off of work,” said Ms. Butler, who is black. That’s tiring, she added, but so is being a black woman in America. Read more.
At-home management of type 1 diabetes, COVID-19
Although hyperglycemia and diabetic ketoacidosis are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
These new findings are still preliminary and were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
The published study includes data as of May 5 on 64 individuals from a total of 64 US sites. Since the paper was submitted, there are now 220 patients from 68 sites. There were two deaths in the preliminary report, Dr. Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Overall, 34.9% of patients were able to manage COVID-19 entirely at home. At the other extreme, 22.2% of patients overall were admitted to the intensive care unit. Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to the hospital. “Even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Dr. Ebekozien said. Read more.
‘Hospital at home’ for cancer patients
Visits to the emergency department (ED) and hospitalizations are often frequent occurrences for cancer patients, but what if the “hospital” could be brought into the home instead?
A new American cohort study provides evidence that this can be a workable option for cancer patients. The authors report improved patient outcomes, with 56% lower odds of unplanned hospitalizations, 45% lower odds of ED visits, and 50% lower cumulative charges, as compared with patients who received usual care.
“The oncology hospital-at-home model of care that extends acute-level care to the patient at home offers promise in addressing a long-term gap in cancer care service delivery,” said lead author Kathi Mooney, PhD, RN, distinguished professor of nursing at the University of Utah, Salt Lake City. “In light of the current global pandemic, we are compelled to consider new ways to provide cancer care, and the oncology hospital-at-home model is on point to address critical elements of an improved cancer care delivery system.”
Dr. Mooney presented the findings during the virtual scientific program of the American Society of Clinical Oncology 2020 annual meeting (abstract 7000). Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Many COVID patients shed virus in feces, even without GI symptoms
Even without GI symptoms, many patients with COVID-19 shed viral RNA in feces, suggesting that stool testing and prevention of fecal-oral transmission may be needed to combat the ongoing pandemic, according to investigators.
A meta-analysis of 29 studies showed that 12% of patients with COVID-19 developed nausea, diarrhea, or vomiting, while 41% shed viral RNA in feces, reported lead author Sravanthi Parasa, MD, of Swedish Medical Center, Seattle.Writing in JAMA Network Open, Dr. Parasa and colleagues emphasized that respiratory symptoms remain the predominant form of disease; however, GI symptoms can occur.
“In fact, the first reported patient with COVID-19 in the U.S. reported GI symptoms of loose bowel movements and abdominal discomfort,” the investigators wrote, noting that the patient went on to test positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in both respiratory and stool specimens.
“This raises the question of inadvertent human-to-human transmission via the fecal route despite public health emphasis on droplet transmission and precautions for contact with respiratory secretions,” the investigators wrote.
To address this question, the investigators conducted a systematic review and meta-analysis involving 23 published and 6 preprint studies involving a total of 4,805 patients, all of whom tested positive for SARS-CoV-2 based on PCR results from nasopharyngeal swabs. Dr. Parasa and colleagues noted that most of the studies “scored between 8 and 10 on the MINORS quality assessment,” suggesting moderate quality.
Pooled data from these studies showed that 4.6% of patients reported nausea or vomiting, while 7.4% reported diarrhea. Such symptoms may serve as an early warning flag for clinicians, the investigators noted.
“[T]he presence of GI symptoms may portend a worse outcome for patients infected with SARS-CoV-2,” they wrote, citing a study by Pan and colleagues, which found that GI symptoms were associated with lower rates of recovery and hospital discharge.
Regardless of GI symptoms, 40.5% of patients in the meta-analysis tested positive for viral RNA in feces (95% confidence interval, 27.4%-55.1%). Duration of viral shedding in feces lasted up to 11 days after symptom onset, or in a single-patient case study, 18 days after hospitalization.
The investigators called these duration figures “particularly concerning,” especially in light of a study published by Xiao and colleagues, which showed that 23.3% of patients with negative respiratory tests were still shedding live virus in feces.
“[T]he fecal-oral route of transmission could be an additional potential source of infection spread,” wrote Dr. Parasa and colleagues. “Our results also suggest that testing of the virus in feces ... could be helpful in disease monitoring and surveillance.”
David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the findings confirm what has been suspected for some time: GI disease is relatively common with COVID-19.
“The evidence is clear now that a sizable percentage of patients have GI symptoms,” Dr. Johnson said in an interview.
GI issues may precede respiratory signs, he added, so clinicians should be aware that nausea, vomiting, or diarrhea could be early indicators of COVID-19, and possibly, a worse outcome.
“The other highlight of this study is that stool shedding may be extended beyond respiratory shedding,” Dr. Johnson said.
He suggested that this finding could influence current CDC criteria, which define absence of infectious risk by two consecutive, negative nasopharyngeal swabs. Instead, fecal testing may be needed, he said, along with measures to prevent fecal-oral transmission.
Dr. Johnson expressed particular concern for risk of infection via toilet plume, in which toilet flushing aerosolizes viral particles.
“As much as people try to social distance by 6 feet – you can do that when you walk into a store, or a building, but you can’t necessarily do that when you walk into a public toilet, where the plume may have been expansive for a period of time,” he said. “That toilet may never really get cleaned to a high level of disinfection, and those droplets set up potential for fecal-oral spread.”
Dr. Sharma disclosed relationships with Medtronic, Fujifilm, Boston Scientific, and others. Dr. Johnson disclosed no relevant conflicts of interest.
SOURCE: Parasa S et al. JAMA Network Open. 2020 Jun 11. doi: 10.1001/jamanetworkopen.2020.11335.
Even without GI symptoms, many patients with COVID-19 shed viral RNA in feces, suggesting that stool testing and prevention of fecal-oral transmission may be needed to combat the ongoing pandemic, according to investigators.
A meta-analysis of 29 studies showed that 12% of patients with COVID-19 developed nausea, diarrhea, or vomiting, while 41% shed viral RNA in feces, reported lead author Sravanthi Parasa, MD, of Swedish Medical Center, Seattle.Writing in JAMA Network Open, Dr. Parasa and colleagues emphasized that respiratory symptoms remain the predominant form of disease; however, GI symptoms can occur.
“In fact, the first reported patient with COVID-19 in the U.S. reported GI symptoms of loose bowel movements and abdominal discomfort,” the investigators wrote, noting that the patient went on to test positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in both respiratory and stool specimens.
“This raises the question of inadvertent human-to-human transmission via the fecal route despite public health emphasis on droplet transmission and precautions for contact with respiratory secretions,” the investigators wrote.
To address this question, the investigators conducted a systematic review and meta-analysis involving 23 published and 6 preprint studies involving a total of 4,805 patients, all of whom tested positive for SARS-CoV-2 based on PCR results from nasopharyngeal swabs. Dr. Parasa and colleagues noted that most of the studies “scored between 8 and 10 on the MINORS quality assessment,” suggesting moderate quality.
Pooled data from these studies showed that 4.6% of patients reported nausea or vomiting, while 7.4% reported diarrhea. Such symptoms may serve as an early warning flag for clinicians, the investigators noted.
“[T]he presence of GI symptoms may portend a worse outcome for patients infected with SARS-CoV-2,” they wrote, citing a study by Pan and colleagues, which found that GI symptoms were associated with lower rates of recovery and hospital discharge.
Regardless of GI symptoms, 40.5% of patients in the meta-analysis tested positive for viral RNA in feces (95% confidence interval, 27.4%-55.1%). Duration of viral shedding in feces lasted up to 11 days after symptom onset, or in a single-patient case study, 18 days after hospitalization.
The investigators called these duration figures “particularly concerning,” especially in light of a study published by Xiao and colleagues, which showed that 23.3% of patients with negative respiratory tests were still shedding live virus in feces.
“[T]he fecal-oral route of transmission could be an additional potential source of infection spread,” wrote Dr. Parasa and colleagues. “Our results also suggest that testing of the virus in feces ... could be helpful in disease monitoring and surveillance.”
David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the findings confirm what has been suspected for some time: GI disease is relatively common with COVID-19.
“The evidence is clear now that a sizable percentage of patients have GI symptoms,” Dr. Johnson said in an interview.
GI issues may precede respiratory signs, he added, so clinicians should be aware that nausea, vomiting, or diarrhea could be early indicators of COVID-19, and possibly, a worse outcome.
“The other highlight of this study is that stool shedding may be extended beyond respiratory shedding,” Dr. Johnson said.
He suggested that this finding could influence current CDC criteria, which define absence of infectious risk by two consecutive, negative nasopharyngeal swabs. Instead, fecal testing may be needed, he said, along with measures to prevent fecal-oral transmission.
Dr. Johnson expressed particular concern for risk of infection via toilet plume, in which toilet flushing aerosolizes viral particles.
“As much as people try to social distance by 6 feet – you can do that when you walk into a store, or a building, but you can’t necessarily do that when you walk into a public toilet, where the plume may have been expansive for a period of time,” he said. “That toilet may never really get cleaned to a high level of disinfection, and those droplets set up potential for fecal-oral spread.”
Dr. Sharma disclosed relationships with Medtronic, Fujifilm, Boston Scientific, and others. Dr. Johnson disclosed no relevant conflicts of interest.
SOURCE: Parasa S et al. JAMA Network Open. 2020 Jun 11. doi: 10.1001/jamanetworkopen.2020.11335.
Even without GI symptoms, many patients with COVID-19 shed viral RNA in feces, suggesting that stool testing and prevention of fecal-oral transmission may be needed to combat the ongoing pandemic, according to investigators.
A meta-analysis of 29 studies showed that 12% of patients with COVID-19 developed nausea, diarrhea, or vomiting, while 41% shed viral RNA in feces, reported lead author Sravanthi Parasa, MD, of Swedish Medical Center, Seattle.Writing in JAMA Network Open, Dr. Parasa and colleagues emphasized that respiratory symptoms remain the predominant form of disease; however, GI symptoms can occur.
“In fact, the first reported patient with COVID-19 in the U.S. reported GI symptoms of loose bowel movements and abdominal discomfort,” the investigators wrote, noting that the patient went on to test positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in both respiratory and stool specimens.
“This raises the question of inadvertent human-to-human transmission via the fecal route despite public health emphasis on droplet transmission and precautions for contact with respiratory secretions,” the investigators wrote.
To address this question, the investigators conducted a systematic review and meta-analysis involving 23 published and 6 preprint studies involving a total of 4,805 patients, all of whom tested positive for SARS-CoV-2 based on PCR results from nasopharyngeal swabs. Dr. Parasa and colleagues noted that most of the studies “scored between 8 and 10 on the MINORS quality assessment,” suggesting moderate quality.
Pooled data from these studies showed that 4.6% of patients reported nausea or vomiting, while 7.4% reported diarrhea. Such symptoms may serve as an early warning flag for clinicians, the investigators noted.
“[T]he presence of GI symptoms may portend a worse outcome for patients infected with SARS-CoV-2,” they wrote, citing a study by Pan and colleagues, which found that GI symptoms were associated with lower rates of recovery and hospital discharge.
Regardless of GI symptoms, 40.5% of patients in the meta-analysis tested positive for viral RNA in feces (95% confidence interval, 27.4%-55.1%). Duration of viral shedding in feces lasted up to 11 days after symptom onset, or in a single-patient case study, 18 days after hospitalization.
The investigators called these duration figures “particularly concerning,” especially in light of a study published by Xiao and colleagues, which showed that 23.3% of patients with negative respiratory tests were still shedding live virus in feces.
“[T]he fecal-oral route of transmission could be an additional potential source of infection spread,” wrote Dr. Parasa and colleagues. “Our results also suggest that testing of the virus in feces ... could be helpful in disease monitoring and surveillance.”
David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the findings confirm what has been suspected for some time: GI disease is relatively common with COVID-19.
“The evidence is clear now that a sizable percentage of patients have GI symptoms,” Dr. Johnson said in an interview.
GI issues may precede respiratory signs, he added, so clinicians should be aware that nausea, vomiting, or diarrhea could be early indicators of COVID-19, and possibly, a worse outcome.
“The other highlight of this study is that stool shedding may be extended beyond respiratory shedding,” Dr. Johnson said.
He suggested that this finding could influence current CDC criteria, which define absence of infectious risk by two consecutive, negative nasopharyngeal swabs. Instead, fecal testing may be needed, he said, along with measures to prevent fecal-oral transmission.
Dr. Johnson expressed particular concern for risk of infection via toilet plume, in which toilet flushing aerosolizes viral particles.
“As much as people try to social distance by 6 feet – you can do that when you walk into a store, or a building, but you can’t necessarily do that when you walk into a public toilet, where the plume may have been expansive for a period of time,” he said. “That toilet may never really get cleaned to a high level of disinfection, and those droplets set up potential for fecal-oral spread.”
Dr. Sharma disclosed relationships with Medtronic, Fujifilm, Boston Scientific, and others. Dr. Johnson disclosed no relevant conflicts of interest.
SOURCE: Parasa S et al. JAMA Network Open. 2020 Jun 11. doi: 10.1001/jamanetworkopen.2020.11335.
FROM JAMA NETWORK OPEN
Half of type 1 diabetes patients with COVID-19 manage at home
New preliminary data from the T1D Exchange suggest that, although hyperglycemia and diabetic ketoacidosis (DKA) are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
The new findings – the first US data on individuals with type 1 diabetes and COVID-19 – were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
Two UK studies are the only prior ones to previously examine the topic.
The newly published study includes data as of May 5 on 64 individuals from a total of 64 US sites, including 15 T1D Exchange member clinics and an additional 49 endocrinology clinics from around the country. Since the paper was submitted, there are now 220 patients from 68 sites. Another publication with a more detailed analysis of risk factors and adjustment for confounders is planned for later this year.
Some of the findings from the preliminary data have shifted, but many aspects remain consistent, Ebekozien told Medscape Medical News.
“One thing still very true, even with the unpublished findings, is the influence of A1c and glycemic management. ...With higher A1c levels, we’re seeing more COVID-19 hospitalizations and worse outcomes,” he said.
And as has been generally reported for COVID-19, high body mass index was a major risk factor in the preliminary dataset – and remains so.
There were two deaths in the preliminary report, both individuals with comorbidities in addition to type 1 diabetes, Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Interestingly, females predominate in both cohorts. That may be a reporting phenomenon, another factor that is being analyzed.
Hyperglycemia Remains a Major Risk Factor
The study is specifically being conducted by the T1D Exchange’s Quality Improvement Collaborative, which Ebekozien heads.
Data were obtained for 33 patients with type 1 diabetes who tested positive for COVID-19, and another 31 who were classified as “COVID-19–like” because they had symptoms consistent with COVID-19, as identified by the Centers for Disease Control and Prevention, but hadn’t been tested for the virus.
For all 64 patients, the mean age was 20.9 years and two thirds (65.6%) were aged 18 or younger. A higher proportion of the COVID-19–like patients were pediatric than the confirmed cases. The larger dataset includes more adult patients, Ebekozien told Medscape Medical News.
Overall, 60.9% of patients were female. Nearly half were white, a quarter Hispanic, and 18.8% black. More confirmed COVID-19 cases were black compared with suspected cases (30.3% vs 6.5%).
Median A1c for the overall group (including suspected COVID-19 cases) was 8.0%, but it was 8.5% among confirmed cases. Overall, six patients (9.8%) presented with new-onset type 1 diabetes after they developed COVID-19.
Hyperglycemia was present in half (32) of patients overall. DKA occurred in 19 people (30.2%): 15 of the confirmed COVID-19 cases (45.5%) versus just 4 (13.3%) of the COVID-19–like cases. Nausea was reported in 30.2% of patients overall.
Other symptoms were typical of COVID-19, including fever (41.3%), dry cough (38.1%), and shortness of breath (27.0%). Loss of taste and smell was less common, at just 9.5% overall.
Obesity was present in 39.7% of patients overall, with similar proportions in the confirmed and suspected COVID-19 groups. Hypertension and/or cardiovascular disease were present in 14.3% of patients overall, and the rate was similar between the two subgroups.
One of the two patients who died was a 79-year-old man who had hypertension and a prior stroke in addition to type 1 diabetes. The other was a 19-year-old woman with a history of asthma who developed a pulmonary embolism during the onset of COVID-19. Neither had DKA.
Even in Type 1 Diabetes, COVID-19 Can Be Managed at Home
Overall, 34.9% of patients were able to manage COVID-19 entirely at home, with 27.3% of the confirmed and 43.3% of the suspected cases able to do so.
At the other extreme, 22.2% of patients overall were admitted to the intensive care unit; 30.3% of the confirmed versus 13.3% of suspected cases.
Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to hospital.
“Interestingly, even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist. ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Ebekozien said.
“But, we’re seeing a good number of patients who are managed at home and the symptoms resolve in a week or two, and the illness runs its course, and they don’t have to even be seen,” he added.
The research team is also collecting data on barriers to remote care, including challenges with telemedicine and how frontline providers are navigating them.
“Those are all things that our future paper will be able to shed more light on,” he explained.
Endocrinologists around the country are invited to report cases of COVID-19 in patients with type 1 diabetes to the T1D Exchange by emailing QI@T1Dexchange.org.
And in fact, Ebekozien also requested that clinicians with a large type 1 diabetes population also report if they’ve had no COVID-19 cases.
“Even if they haven’t had a case, that’s very useful information for us to know. One of the things we want to calculate down the line is the incidence ratio. Not all participating sites have had a case.”
Endocrinologists from all the participating sites have formed a dedicated community that meets regularly via webinars to share information, he noted. “It’s been a very selfless effort to work collaboratively as a community to quickly answer critical questions.”
The Helmsley Charitable Trust funds the T1D Exchange Quality Improvement Collaborative. The T1D Exchange received financial support for this study from Abbott Diabetes, Dexcom, JDRF, Insulet Corporation, Lilly, Medtronic, and Tandem Diabetes Care. No other relevant financial relationships were reported.
This article first appeared on Medscape.com.
New preliminary data from the T1D Exchange suggest that, although hyperglycemia and diabetic ketoacidosis (DKA) are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
The new findings – the first US data on individuals with type 1 diabetes and COVID-19 – were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
Two UK studies are the only prior ones to previously examine the topic.
The newly published study includes data as of May 5 on 64 individuals from a total of 64 US sites, including 15 T1D Exchange member clinics and an additional 49 endocrinology clinics from around the country. Since the paper was submitted, there are now 220 patients from 68 sites. Another publication with a more detailed analysis of risk factors and adjustment for confounders is planned for later this year.
Some of the findings from the preliminary data have shifted, but many aspects remain consistent, Ebekozien told Medscape Medical News.
“One thing still very true, even with the unpublished findings, is the influence of A1c and glycemic management. ...With higher A1c levels, we’re seeing more COVID-19 hospitalizations and worse outcomes,” he said.
And as has been generally reported for COVID-19, high body mass index was a major risk factor in the preliminary dataset – and remains so.
There were two deaths in the preliminary report, both individuals with comorbidities in addition to type 1 diabetes, Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Interestingly, females predominate in both cohorts. That may be a reporting phenomenon, another factor that is being analyzed.
Hyperglycemia Remains a Major Risk Factor
The study is specifically being conducted by the T1D Exchange’s Quality Improvement Collaborative, which Ebekozien heads.
Data were obtained for 33 patients with type 1 diabetes who tested positive for COVID-19, and another 31 who were classified as “COVID-19–like” because they had symptoms consistent with COVID-19, as identified by the Centers for Disease Control and Prevention, but hadn’t been tested for the virus.
For all 64 patients, the mean age was 20.9 years and two thirds (65.6%) were aged 18 or younger. A higher proportion of the COVID-19–like patients were pediatric than the confirmed cases. The larger dataset includes more adult patients, Ebekozien told Medscape Medical News.
Overall, 60.9% of patients were female. Nearly half were white, a quarter Hispanic, and 18.8% black. More confirmed COVID-19 cases were black compared with suspected cases (30.3% vs 6.5%).
Median A1c for the overall group (including suspected COVID-19 cases) was 8.0%, but it was 8.5% among confirmed cases. Overall, six patients (9.8%) presented with new-onset type 1 diabetes after they developed COVID-19.
Hyperglycemia was present in half (32) of patients overall. DKA occurred in 19 people (30.2%): 15 of the confirmed COVID-19 cases (45.5%) versus just 4 (13.3%) of the COVID-19–like cases. Nausea was reported in 30.2% of patients overall.
Other symptoms were typical of COVID-19, including fever (41.3%), dry cough (38.1%), and shortness of breath (27.0%). Loss of taste and smell was less common, at just 9.5% overall.
Obesity was present in 39.7% of patients overall, with similar proportions in the confirmed and suspected COVID-19 groups. Hypertension and/or cardiovascular disease were present in 14.3% of patients overall, and the rate was similar between the two subgroups.
One of the two patients who died was a 79-year-old man who had hypertension and a prior stroke in addition to type 1 diabetes. The other was a 19-year-old woman with a history of asthma who developed a pulmonary embolism during the onset of COVID-19. Neither had DKA.
Even in Type 1 Diabetes, COVID-19 Can Be Managed at Home
Overall, 34.9% of patients were able to manage COVID-19 entirely at home, with 27.3% of the confirmed and 43.3% of the suspected cases able to do so.
At the other extreme, 22.2% of patients overall were admitted to the intensive care unit; 30.3% of the confirmed versus 13.3% of suspected cases.
Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to hospital.
“Interestingly, even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist. ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Ebekozien said.
“But, we’re seeing a good number of patients who are managed at home and the symptoms resolve in a week or two, and the illness runs its course, and they don’t have to even be seen,” he added.
The research team is also collecting data on barriers to remote care, including challenges with telemedicine and how frontline providers are navigating them.
“Those are all things that our future paper will be able to shed more light on,” he explained.
Endocrinologists around the country are invited to report cases of COVID-19 in patients with type 1 diabetes to the T1D Exchange by emailing QI@T1Dexchange.org.
And in fact, Ebekozien also requested that clinicians with a large type 1 diabetes population also report if they’ve had no COVID-19 cases.
“Even if they haven’t had a case, that’s very useful information for us to know. One of the things we want to calculate down the line is the incidence ratio. Not all participating sites have had a case.”
Endocrinologists from all the participating sites have formed a dedicated community that meets regularly via webinars to share information, he noted. “It’s been a very selfless effort to work collaboratively as a community to quickly answer critical questions.”
The Helmsley Charitable Trust funds the T1D Exchange Quality Improvement Collaborative. The T1D Exchange received financial support for this study from Abbott Diabetes, Dexcom, JDRF, Insulet Corporation, Lilly, Medtronic, and Tandem Diabetes Care. No other relevant financial relationships were reported.
This article first appeared on Medscape.com.
New preliminary data from the T1D Exchange suggest that, although hyperglycemia and diabetic ketoacidosis (DKA) are common in people with type 1 diabetes who develop COVID-19, many are still able to manage the illness at home and overall mortality is relatively low.
The new findings – the first US data on individuals with type 1 diabetes and COVID-19 – were published online June 5 in Diabetes Care by Osagie A. Ebekozien, MD, vice president, quality improvement and population health at the T1D Exchange, and colleagues.
Two UK studies are the only prior ones to previously examine the topic.
The newly published study includes data as of May 5 on 64 individuals from a total of 64 US sites, including 15 T1D Exchange member clinics and an additional 49 endocrinology clinics from around the country. Since the paper was submitted, there are now 220 patients from 68 sites. Another publication with a more detailed analysis of risk factors and adjustment for confounders is planned for later this year.
Some of the findings from the preliminary data have shifted, but many aspects remain consistent, Ebekozien told Medscape Medical News.
“One thing still very true, even with the unpublished findings, is the influence of A1c and glycemic management. ...With higher A1c levels, we’re seeing more COVID-19 hospitalizations and worse outcomes,” he said.
And as has been generally reported for COVID-19, high body mass index was a major risk factor in the preliminary dataset – and remains so.
There were two deaths in the preliminary report, both individuals with comorbidities in addition to type 1 diabetes, Ebekozien said. There have been a few more deaths in the larger dataset, but the mortality rate remains relatively low.
Interestingly, females predominate in both cohorts. That may be a reporting phenomenon, another factor that is being analyzed.
Hyperglycemia Remains a Major Risk Factor
The study is specifically being conducted by the T1D Exchange’s Quality Improvement Collaborative, which Ebekozien heads.
Data were obtained for 33 patients with type 1 diabetes who tested positive for COVID-19, and another 31 who were classified as “COVID-19–like” because they had symptoms consistent with COVID-19, as identified by the Centers for Disease Control and Prevention, but hadn’t been tested for the virus.
For all 64 patients, the mean age was 20.9 years and two thirds (65.6%) were aged 18 or younger. A higher proportion of the COVID-19–like patients were pediatric than the confirmed cases. The larger dataset includes more adult patients, Ebekozien told Medscape Medical News.
Overall, 60.9% of patients were female. Nearly half were white, a quarter Hispanic, and 18.8% black. More confirmed COVID-19 cases were black compared with suspected cases (30.3% vs 6.5%).
Median A1c for the overall group (including suspected COVID-19 cases) was 8.0%, but it was 8.5% among confirmed cases. Overall, six patients (9.8%) presented with new-onset type 1 diabetes after they developed COVID-19.
Hyperglycemia was present in half (32) of patients overall. DKA occurred in 19 people (30.2%): 15 of the confirmed COVID-19 cases (45.5%) versus just 4 (13.3%) of the COVID-19–like cases. Nausea was reported in 30.2% of patients overall.
Other symptoms were typical of COVID-19, including fever (41.3%), dry cough (38.1%), and shortness of breath (27.0%). Loss of taste and smell was less common, at just 9.5% overall.
Obesity was present in 39.7% of patients overall, with similar proportions in the confirmed and suspected COVID-19 groups. Hypertension and/or cardiovascular disease were present in 14.3% of patients overall, and the rate was similar between the two subgroups.
One of the two patients who died was a 79-year-old man who had hypertension and a prior stroke in addition to type 1 diabetes. The other was a 19-year-old woman with a history of asthma who developed a pulmonary embolism during the onset of COVID-19. Neither had DKA.
Even in Type 1 Diabetes, COVID-19 Can Be Managed at Home
Overall, 34.9% of patients were able to manage COVID-19 entirely at home, with 27.3% of the confirmed and 43.3% of the suspected cases able to do so.
At the other extreme, 22.2% of patients overall were admitted to the intensive care unit; 30.3% of the confirmed versus 13.3% of suspected cases.
Including the small proportion of patients sent home after being seen in emergency or urgent care, overall roughly half were not admitted to hospital.
“Interestingly, even in this preliminary study, half were managed at home via telemedicine with an endocrinologist and infectious disease specialist. ... I think it continues to be a case-by-case clinical decision between the patient and their provider,” Ebekozien said.
“But, we’re seeing a good number of patients who are managed at home and the symptoms resolve in a week or two, and the illness runs its course, and they don’t have to even be seen,” he added.
The research team is also collecting data on barriers to remote care, including challenges with telemedicine and how frontline providers are navigating them.
“Those are all things that our future paper will be able to shed more light on,” he explained.
Endocrinologists around the country are invited to report cases of COVID-19 in patients with type 1 diabetes to the T1D Exchange by emailing QI@T1Dexchange.org.
And in fact, Ebekozien also requested that clinicians with a large type 1 diabetes population also report if they’ve had no COVID-19 cases.
“Even if they haven’t had a case, that’s very useful information for us to know. One of the things we want to calculate down the line is the incidence ratio. Not all participating sites have had a case.”
Endocrinologists from all the participating sites have formed a dedicated community that meets regularly via webinars to share information, he noted. “It’s been a very selfless effort to work collaboratively as a community to quickly answer critical questions.”
The Helmsley Charitable Trust funds the T1D Exchange Quality Improvement Collaborative. The T1D Exchange received financial support for this study from Abbott Diabetes, Dexcom, JDRF, Insulet Corporation, Lilly, Medtronic, and Tandem Diabetes Care. No other relevant financial relationships were reported.
This article first appeared on Medscape.com.
Fighting COVID and police brutality, medical teams take to streets to treat protesters
Amid clouds of choking tear gas, booming flash-bang grenades and other “riot control agents,” volunteer medics plunged into street protests over the past weeks to help the injured – sometimes rushing to the front lines as soon as their hospital shifts ended.
Known as “street medics,” these unorthodox teams of nursing students, veterinarians, doctors, trauma surgeons, security guards, ski patrollers, nurses, wilderness EMTs, and off-the-clock ambulance workers poured water – not milk – into the eyes of tear-gassed protesters. They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go.
So donning cloth masks to protect against the virus – plus helmets, makeshift shields and other gear to guard against rubber bullets, projectiles and tear gas – the volunteer medics organized themselves into a web of first responders to care for people on the streets. They showed up early, set up first-aid stations, established transportation networks and covered their arms, helmets and backpacks with crosses made of red duct tape, to signify that they were medics. Some stayed late into the night past curfews until every protester had left.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. She didn’t see it as a choice.
“I am working full time and basically being at the protest after getting straight off of work,” said Butler, who is black. That’s tiring, she added, but so is being a black woman in America.
After going out as a medic on her own, she soon met other volunteers. Together they used text-message chains to organize their efforts. One night, she responded to a man who had been shot with a rubber bullet in the chest; she said his torso had turned blue and purple from the impact. She also provided aid after a shooting near the protest left someone in critical condition.
“It’s hard, but bills need to be paid and justice needs to be served,” she said.
The street medic movement traces its roots, in part, to the 1960s protests, as well as the American Indian Movement and the Black Panther Party. Denver Action Medic Network offers a 20-hour training course that prepares them to treat patients in conflicts with police and large crowds; a four-hour session is offered to medical professionals as “bridge” training.
Since the coronavirus pandemic began, the Denver Action Medic Network has added new training guidelines: Don’t go to protests if sick or in contact with those who are infected; wear a mask; give people lots of space and use hand sanitizer. Jordan Garcia, a 39-year-old medic for over 20 years who works with the network of veteran street medics, said they also warn medics about the increased risk of transmission because of protesters coughing from tear gas, and urge them to get tested for the virus after the protests.
The number of volunteer medics swelled after George Floyd’s May 25 killing in Minneapolis. In Denver alone, at least 40 people reached out to the Denver Action Medic Network for training.
On June 3, Dr. Rupa Marya, an associate professor of medicine at the University of California,San Francisco, and the co-founder of the Do No Harm Coalition, which runs street medic training in the Bay Area, hosted a national webinar attended by over 3,000 medical professionals to provide the bridge training to be a street medic. In her online bio, Marya describes the coalition as “an organization of over 450 health workers committed to structural change” in addressing health problems.
“When we see suffering, that’s where we go,” Marya said. “And right now that suffering is happening on the streets.”
In the recent Denver protests, street medics responded to major head, face and eye injuries among protesters from what are sometimes described as “kinetic impact projectiles” or “less-than-lethal” bullets shot at protesters, along with tear-gas and flash-bang stun grenade canisters that either hit them or exploded in their faces.
Garcia, who by day works for an immigrant rights nonprofit, said that these weapons are not designed to be shot directly at people.
“We’re seeing police use these less-lethal weapons in lethal ways, and that is pretty upsetting,” Garcia said about the recent protests.
Denver police Chief Paul Pazen promised to make changes, including banning chokeholds and requiring SWAT teams to turn on their body cameras. Last week, a federal judge also issued a temporary injunction to stop Denver police from using tear gas and other less-than-lethal weapons in response to a class action lawsuit, in which a medic stated he was shot multiple times by police with pepper balls while treating patients. (Last week in North Carolina police were recorded destroying medic stations.)
Denver street medic Kevin Connell, a 30-year-old emergency room nurse, said he was hit with pepper balls in the back of his medic vest – which was clearly marked by red crosses – while treating a patient. He showed up to the Denver protests every night he did not have to work, he said, wearing a Kevlar medic vest, protective goggles and a homemade gas mask fashioned from a water bottle. As a member of the Denver Action Medic Network, Connell also served at the Standing Rock protests in North Dakota in a dispute over the building of the Dakota Access Pipeline.
“I mean, as bad as it sounds, it was only tear gas, pepper balls and rubber bullets that were being fired on us,” Connell said of his recent experience in Denver. “When I was at Standing Rock, they were using high-powered water hoses even when it was, like, freezing cold. … So I think the police here had a little bit more restraint.”
Still, first-time street medic Aj Mossman, a 31-year-old Denver emergency medical technician studying for nursing school, was shocked to be tear-gassed and struck in the back of the leg with a flash grenade while treating a protester on May 30. Mossman still has a large leg bruise.
The following night, Mossman, who uses the pronoun they, brought more protective gear, but said they are still having difficulty processing what felt like a war zone.
“I thought I understood what my black friends went through. I thought I understood what the black community went through,” said Mossman, who is white. “But I had absolutely no idea how violent the police were and how little they cared about who they hurt.”
For Butler, serving as a medic with others from various walks of life was inspiring. “They’re also out there to protect black and brown bodies. And that’s amazing,” she said. “That’s just a beautiful sight.”
This article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Amid clouds of choking tear gas, booming flash-bang grenades and other “riot control agents,” volunteer medics plunged into street protests over the past weeks to help the injured – sometimes rushing to the front lines as soon as their hospital shifts ended.
Known as “street medics,” these unorthodox teams of nursing students, veterinarians, doctors, trauma surgeons, security guards, ski patrollers, nurses, wilderness EMTs, and off-the-clock ambulance workers poured water – not milk – into the eyes of tear-gassed protesters. They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go.
So donning cloth masks to protect against the virus – plus helmets, makeshift shields and other gear to guard against rubber bullets, projectiles and tear gas – the volunteer medics organized themselves into a web of first responders to care for people on the streets. They showed up early, set up first-aid stations, established transportation networks and covered their arms, helmets and backpacks with crosses made of red duct tape, to signify that they were medics. Some stayed late into the night past curfews until every protester had left.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. She didn’t see it as a choice.
“I am working full time and basically being at the protest after getting straight off of work,” said Butler, who is black. That’s tiring, she added, but so is being a black woman in America.
After going out as a medic on her own, she soon met other volunteers. Together they used text-message chains to organize their efforts. One night, she responded to a man who had been shot with a rubber bullet in the chest; she said his torso had turned blue and purple from the impact. She also provided aid after a shooting near the protest left someone in critical condition.
“It’s hard, but bills need to be paid and justice needs to be served,” she said.
The street medic movement traces its roots, in part, to the 1960s protests, as well as the American Indian Movement and the Black Panther Party. Denver Action Medic Network offers a 20-hour training course that prepares them to treat patients in conflicts with police and large crowds; a four-hour session is offered to medical professionals as “bridge” training.
Since the coronavirus pandemic began, the Denver Action Medic Network has added new training guidelines: Don’t go to protests if sick or in contact with those who are infected; wear a mask; give people lots of space and use hand sanitizer. Jordan Garcia, a 39-year-old medic for over 20 years who works with the network of veteran street medics, said they also warn medics about the increased risk of transmission because of protesters coughing from tear gas, and urge them to get tested for the virus after the protests.
The number of volunteer medics swelled after George Floyd’s May 25 killing in Minneapolis. In Denver alone, at least 40 people reached out to the Denver Action Medic Network for training.
On June 3, Dr. Rupa Marya, an associate professor of medicine at the University of California,San Francisco, and the co-founder of the Do No Harm Coalition, which runs street medic training in the Bay Area, hosted a national webinar attended by over 3,000 medical professionals to provide the bridge training to be a street medic. In her online bio, Marya describes the coalition as “an organization of over 450 health workers committed to structural change” in addressing health problems.
“When we see suffering, that’s where we go,” Marya said. “And right now that suffering is happening on the streets.”
In the recent Denver protests, street medics responded to major head, face and eye injuries among protesters from what are sometimes described as “kinetic impact projectiles” or “less-than-lethal” bullets shot at protesters, along with tear-gas and flash-bang stun grenade canisters that either hit them or exploded in their faces.
Garcia, who by day works for an immigrant rights nonprofit, said that these weapons are not designed to be shot directly at people.
“We’re seeing police use these less-lethal weapons in lethal ways, and that is pretty upsetting,” Garcia said about the recent protests.
Denver police Chief Paul Pazen promised to make changes, including banning chokeholds and requiring SWAT teams to turn on their body cameras. Last week, a federal judge also issued a temporary injunction to stop Denver police from using tear gas and other less-than-lethal weapons in response to a class action lawsuit, in which a medic stated he was shot multiple times by police with pepper balls while treating patients. (Last week in North Carolina police were recorded destroying medic stations.)
Denver street medic Kevin Connell, a 30-year-old emergency room nurse, said he was hit with pepper balls in the back of his medic vest – which was clearly marked by red crosses – while treating a patient. He showed up to the Denver protests every night he did not have to work, he said, wearing a Kevlar medic vest, protective goggles and a homemade gas mask fashioned from a water bottle. As a member of the Denver Action Medic Network, Connell also served at the Standing Rock protests in North Dakota in a dispute over the building of the Dakota Access Pipeline.
“I mean, as bad as it sounds, it was only tear gas, pepper balls and rubber bullets that were being fired on us,” Connell said of his recent experience in Denver. “When I was at Standing Rock, they were using high-powered water hoses even when it was, like, freezing cold. … So I think the police here had a little bit more restraint.”
Still, first-time street medic Aj Mossman, a 31-year-old Denver emergency medical technician studying for nursing school, was shocked to be tear-gassed and struck in the back of the leg with a flash grenade while treating a protester on May 30. Mossman still has a large leg bruise.
The following night, Mossman, who uses the pronoun they, brought more protective gear, but said they are still having difficulty processing what felt like a war zone.
“I thought I understood what my black friends went through. I thought I understood what the black community went through,” said Mossman, who is white. “But I had absolutely no idea how violent the police were and how little they cared about who they hurt.”
For Butler, serving as a medic with others from various walks of life was inspiring. “They’re also out there to protect black and brown bodies. And that’s amazing,” she said. “That’s just a beautiful sight.”
This article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Amid clouds of choking tear gas, booming flash-bang grenades and other “riot control agents,” volunteer medics plunged into street protests over the past weeks to help the injured – sometimes rushing to the front lines as soon as their hospital shifts ended.
Known as “street medics,” these unorthodox teams of nursing students, veterinarians, doctors, trauma surgeons, security guards, ski patrollers, nurses, wilderness EMTs, and off-the-clock ambulance workers poured water – not milk – into the eyes of tear-gassed protesters. They stanched bleeding wounds and plucked disoriented teenagers from clouds of gas, entering dangerous corners where on-duty emergency health responders may fear to go.
So donning cloth masks to protect against the virus – plus helmets, makeshift shields and other gear to guard against rubber bullets, projectiles and tear gas – the volunteer medics organized themselves into a web of first responders to care for people on the streets. They showed up early, set up first-aid stations, established transportation networks and covered their arms, helmets and backpacks with crosses made of red duct tape, to signify that they were medics. Some stayed late into the night past curfews until every protester had left.
Iris Butler, a 21-year-old certified nursing assistant who works in a nursing home, decided to offer her skills after seeing a man injured by a rubber bullet on her first night at the Denver protests. She showed up as a medic every night thereafter. She didn’t see it as a choice.
“I am working full time and basically being at the protest after getting straight off of work,” said Butler, who is black. That’s tiring, she added, but so is being a black woman in America.
After going out as a medic on her own, she soon met other volunteers. Together they used text-message chains to organize their efforts. One night, she responded to a man who had been shot with a rubber bullet in the chest; she said his torso had turned blue and purple from the impact. She also provided aid after a shooting near the protest left someone in critical condition.
“It’s hard, but bills need to be paid and justice needs to be served,” she said.
The street medic movement traces its roots, in part, to the 1960s protests, as well as the American Indian Movement and the Black Panther Party. Denver Action Medic Network offers a 20-hour training course that prepares them to treat patients in conflicts with police and large crowds; a four-hour session is offered to medical professionals as “bridge” training.
Since the coronavirus pandemic began, the Denver Action Medic Network has added new training guidelines: Don’t go to protests if sick or in contact with those who are infected; wear a mask; give people lots of space and use hand sanitizer. Jordan Garcia, a 39-year-old medic for over 20 years who works with the network of veteran street medics, said they also warn medics about the increased risk of transmission because of protesters coughing from tear gas, and urge them to get tested for the virus after the protests.
The number of volunteer medics swelled after George Floyd’s May 25 killing in Minneapolis. In Denver alone, at least 40 people reached out to the Denver Action Medic Network for training.
On June 3, Dr. Rupa Marya, an associate professor of medicine at the University of California,San Francisco, and the co-founder of the Do No Harm Coalition, which runs street medic training in the Bay Area, hosted a national webinar attended by over 3,000 medical professionals to provide the bridge training to be a street medic. In her online bio, Marya describes the coalition as “an organization of over 450 health workers committed to structural change” in addressing health problems.
“When we see suffering, that’s where we go,” Marya said. “And right now that suffering is happening on the streets.”
In the recent Denver protests, street medics responded to major head, face and eye injuries among protesters from what are sometimes described as “kinetic impact projectiles” or “less-than-lethal” bullets shot at protesters, along with tear-gas and flash-bang stun grenade canisters that either hit them or exploded in their faces.
Garcia, who by day works for an immigrant rights nonprofit, said that these weapons are not designed to be shot directly at people.
“We’re seeing police use these less-lethal weapons in lethal ways, and that is pretty upsetting,” Garcia said about the recent protests.
Denver police Chief Paul Pazen promised to make changes, including banning chokeholds and requiring SWAT teams to turn on their body cameras. Last week, a federal judge also issued a temporary injunction to stop Denver police from using tear gas and other less-than-lethal weapons in response to a class action lawsuit, in which a medic stated he was shot multiple times by police with pepper balls while treating patients. (Last week in North Carolina police were recorded destroying medic stations.)
Denver street medic Kevin Connell, a 30-year-old emergency room nurse, said he was hit with pepper balls in the back of his medic vest – which was clearly marked by red crosses – while treating a patient. He showed up to the Denver protests every night he did not have to work, he said, wearing a Kevlar medic vest, protective goggles and a homemade gas mask fashioned from a water bottle. As a member of the Denver Action Medic Network, Connell also served at the Standing Rock protests in North Dakota in a dispute over the building of the Dakota Access Pipeline.
“I mean, as bad as it sounds, it was only tear gas, pepper balls and rubber bullets that were being fired on us,” Connell said of his recent experience in Denver. “When I was at Standing Rock, they were using high-powered water hoses even when it was, like, freezing cold. … So I think the police here had a little bit more restraint.”
Still, first-time street medic Aj Mossman, a 31-year-old Denver emergency medical technician studying for nursing school, was shocked to be tear-gassed and struck in the back of the leg with a flash grenade while treating a protester on May 30. Mossman still has a large leg bruise.
The following night, Mossman, who uses the pronoun they, brought more protective gear, but said they are still having difficulty processing what felt like a war zone.
“I thought I understood what my black friends went through. I thought I understood what the black community went through,” said Mossman, who is white. “But I had absolutely no idea how violent the police were and how little they cared about who they hurt.”
For Butler, serving as a medic with others from various walks of life was inspiring. “They’re also out there to protect black and brown bodies. And that’s amazing,” she said. “That’s just a beautiful sight.”
This article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
If you reopen it, will they come?
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .

Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .
Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
On April 16, the White House released federal guidelines for reopening American businesses – followed 3 days later by specific recommendations from the Centers for Medicare and Medicaid Services for .
Depending on where you live, you may have already reopened (or even never closed), or you may be awaiting the relaxation of restrictions in your state. (As I write this on June 10, the stay-at-home order in my state, New Jersey, is being rescinded.)
The big question, of course, is whether patients can be convinced that it is safe to leave their homes and come to your office. The answer may depend on how well you time your reopening and adhere to the appropriate federal, state, and independent guidelines.
The federal guidelines have three sections: criteria, which outline conditions each region or state should satisfy before reopening; preparedness, which lists how states should prepare for reopening; and phase guidelines, which detail responsibilities of individuals and employers during distinct reopening phases.
You should pay the most attention to the “criteria” section. The key question to ask: “Has my state or region satisfied the basic criteria for reopening?”
Those criteria are as follows:
- Symptoms reported within a 14-day period should be on a downward trajectory.
- Cases documented (or positive tests as a percentage of total tests) within a 14-day period should also be on a downward trajectory.
- Hospitals should be treating all patients without crisis care. They should also have a robust testing program in place for at-risk health care workers.
If your area meets these criteria, you can proceed to the CMS recommendations. They cover general advice related to personal protective equipment (PPE), workforce availability, facility considerations, sanitation protocols, supplies, and testing capacity.
The key takeaway: As long as your area has the resources to quickly respond to a surge of COVID-19 cases, you can start offering care to non-COVID patients. Keep seeing patients via telehealth as often as possible, and prioritize surgical/procedural care and high-complexity chronic disease management before moving on to preventive and cosmetic services.
The American Medical Association has issued its own checklist of criteria for reopening your practice to supplement the federal guidelines. Highlights include the following:
- Sit down with a calendar and pick an expected reopening day. Ideally, this should include a “soft reopening.” Make a plan to stock necessary PPE and write down plans for cleaning and staffing if an employee or patient is diagnosed with COVID-19 after visiting your office.
- Take a stepwise approach so you can identify challenges early and address them. It’s important to figure out which visits can continue via telehealth, and begin with just a few in-person visits each day. Plan out a schedule and clearly communicate it to patients, clinicians, and staff.
- Patient safety is your top concern. Encourage patients to visit without companions whenever possible, and of course, all individuals who visit the office should wear a cloth face covering.
- Screen employees for fevers and other symptoms of COVID-19; remember that those records are subject to HIPAA rules and must be kept confidential. Minimize contact between employees as much as possible.
- Do your best to screen patients before in-person visits, to verify they don’t have symptoms of COVID-19. Consider creating a script that office staff can use to contact patients 24 hours before they come in. Use this as a chance to ask about symptoms, and explain any reopening logistics they should know about.
- Contact your malpractice insurance carrier to discuss whether you need to make any changes to your coverage.
This would also be a great time to review your confidentiality, privacy, and data security protocols. COVID-19 presents new challenges for data privacy – for example, if you must inform coworkers or patients that they have come into contact with someone who tested positive. Make a plan that follows HIPAA guidelines during COVID-19. Also, make sure you have a plan for handling issues like paid sick leave or reporting COVID-19 cases to your local health department.
Another useful resource is the Medical Group Management Association’s COVID-19 Medical Practice Reopening Checklist. You can use it to confirm that you are addressing all the important items, and that you haven’t missed anything.
As for me, I am advising patients who are reluctant to seek treatment that many medical problems pose more risk than COVID-19, faster treatment means better outcomes, and because we maintain strict disinfection protocols, they are far less likely to be infected with COVID-19 in my office than, say, at a grocery store.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Racism joins COVID-19 at the primary care table
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
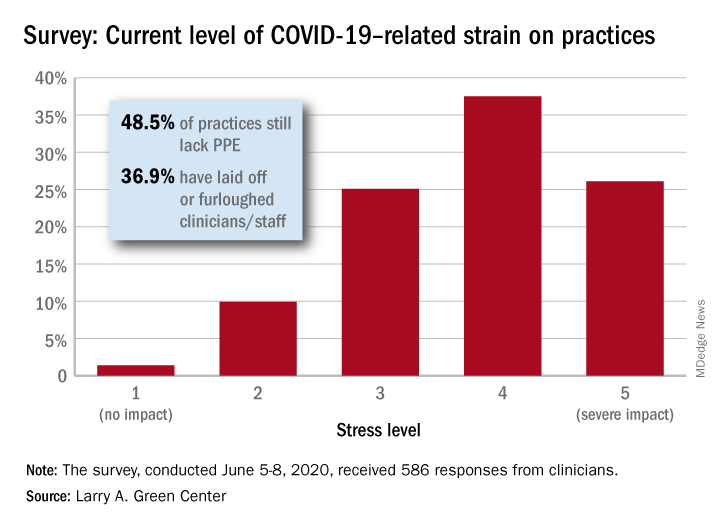
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
Primary care clinicians, already experiencing all-time high stress levels related to COVID-19, are now struggling to cope with the fallout from racism and the death of George Floyd, according to a survey conducted June 5-8.
When asked how the situation has affected their practices, two-thirds of the survey’s 586 respondents said that George Floyd’s death and related events had been the subject of practice conversations and 12% “drew clear connections between the current racial unrest and the health of their patients,” the Larry A. Green Center said in a recent statement.
One-third of the clinicians also said that recent racism-related events have had a negative effect on their own well-being, and that connection was expressed even more strongly in a related survey of 1,111 patients that was conducted June 8.
In that survey, about 65% of patients said that racism affected emotional, psychological, and behavioral health, and 40% noted that George Floyd’s death had a negative impact on the well-being of friends, the Larry A. Green Center said in partnership with the Primary Care Collaborative and 3rd Conversation.
“The fact that so many patients and clinicians agree that racism is a driver of health points to the incredible role primary care plays in creating safe spaces to process deep societal and personal issues,” said Christine Bechtel, cofounder of 3rd Conversation, a community of patients and providers.
COVID-19, in the meantime, is still doing its thing. Almost two-thirds (63%) of respondents to the clinician survey said that stress levels at their practices had reached all-time-high levels in the last 4 weeks.
Just 1.4% of the primary care clinicians said that the pandemic had put no strain on their practices (see graph), and just 10% rated that strain as a 2 on a scale of 1-5, the center said. Among the stressors:
About 49% continue to lack PPE.
About 40% still have no or limited ability for testing.
About 37% of practice settings still report layoffs and furloughs.
About 31% report that clinician salaries are still being skipped or deferred.
“Both public and private policy makers must take immediate steps to stabilize primary care,” said Ann Greiner, president and CEO of the Primary Care Collaborative. “This financial support is necessary but not sufficient. Instead, we need wholesale reform of payment in order to achieve the kind of high-performing primary care that truly meets patient needs.”
Surge in colonoscopies postponed by COVID-19 expected
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.

Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.
Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
An expected surge in the number of people seeking colonoscopy after the peak of the COVID-19 pandemic passes could cause physicians to rethink patient prioritization, could create a strain on endoscopy capacity, and might raise the specter of detecting colorectal cancer in more patients at a later stage of disease.
Furthermore, months of delay in diagnosis of colorectal cancer (CRC) could shorten survival, although more data is needed, according to expert analysis from a gastroenterologist, a medical oncologist, and a colorectal surgeon.
“It has been a big decrease in the number of colonoscopies performed at our hospital in Alicante, Spain,” Rodrigo Jover Martinez, MD, PhD, said during a COVID-19 and Digestive Health webinar presented by United European Gastroenterology (UEG). He estimated colonoscopy procedures are down 60%-90%, and the number of CRC surgeries has dropped by 60%. “As you know, the COVID-19 pandemic is hitting Europe hard.”
When patients do return, “the backlog will be huge ... in already exhausted endoscopy units,” predicted Dr. Martinez, a gastroenterologist at Hospital General Universitario in Alicante.
Multiple risks
Not knowing which patients with CRC will develop severe COVID-19 infection is another challenge, Bartomeu Massuti, MD, of the medical oncology service at the Hospital General Universitario de Alicante, said during the webinar.
Caution is warranted because “we know cancer patients have an increased risk of infection.” However, he added, most evidence supports an elevated risk for bacterial infections, not viral infections.
Therefore, physicians must continue to balance the risks associated with potential COVID-19 exposure against the risks associated with postponed treatment, Dr. Massuti said. “The goal of oncology care is to try to maintain the preplanned treatment and follow-up. We need mainly to avoid stopping or delaying treatment ... because we will lose efficacy in oncology disease outcomes.”
Imran Aslam, MD, PhD, a colorectal surgeon who moderated and presented during the webinar, agreed: “By delaying the treatment, we might do harm to our patients.”
Dr. Aslam cited data about clinical costs of delaying CRC surgery. A 2019 population-based study in PLOS ONE evaluated different times from diagnosis to treatment. The researchers found a delay of more than 150 days “significantly reduced survival, even during stage I, II, and III disease,” he said. The stage I hazard ratio was 2.66, compared with a reference HR of 1.00 for 90 days or fewer. They also reported elevated risk for people with stage II CRC (HR, 2.80), stage III CRC (HR, 2.70), and stage IV CRC (HR, 1.36).
“This could become more and more abysmal if the pandemic continues,” added Dr. Aslam, consultant colorectal surgeon at University Hospitals of Coventry and Warwickshire, England.
Prioritizing patients
Restarting endoscopy with prioritization strategies and increasing patient capacity are possible solutions. Dr. Martinez suggested a four-quadrant matrix in which physicians place patients into “now,” “next,” “delayed,” or “never” categories based on clinical indicators. The priority 1 “now” patients, for example, will be those with suspected CRC based on physical examination, imaging results, and/or an abnormal fecal immunochemical test result.
He suggested, furthermore, that more widespread CRC screening can resume once “endoscopy units have been alleviated of priority 1, symptomatic patients.”
Dr. Massuti concurred with Dr. Martinez’s call to prioritize patients carefully. He suggested a green, yellow, and red classification system based on treatment priority recommendations from the European Society for Medical Oncology. The green group, for example, should receive priority for intervention based on a condition that is immediately clinically unstable or life threatening.
“The main goal is to preserve the continuum of care,” he added.
Another concern – although data are limited – is that treatment might also increase risk of mortality among cancer patients with COVID-19, according to a cohort study of nearly 1,000 such patients reported May 2020 in The Lancet. Dr. Massuti, who was not affiliated with the research, noted that 12% of the patients had GI tumors. In addition to increased risk associated with male sex (odds ratio, 1.63), cytotoxic cancer treatment in the prior 4 weeks increased risk (OR, 1.47), as did surgery in the same time frame (OR, 1.52).
“This means patients on treatment have an increased risk of mortality,” Dr. Massuti said.
Moving forward
Implementing telehealth information and communication technologies will continue to grow in importance, Dr. Massuti said. Dr. Aslam noted that video consultation with patients before surgery is already replacing face-to-face interaction, and most follow-up care at his hospital is now done by telephone.
Postoperative care is just as essential in the COVID-19 era, if not more so. “We need to be very vigilant to manage postoperative complications – any symptoms of pyrexia or sepsis, or any sign of COVID,” Dr. Aslam said, including postoperative fever. “If there is any doubt, do a chest CT scan.”
Dr. Aslam predicted the time to perform endoscopy or surgery for each patient will be longer, “so the number of patients done in 1 day will be less than 4 months ago.” In addition, elective surgery patients at his institution undergo COVID-19 testing twice, 3 days apart, prior to intervention.
“This disease will continue in the community for a while, so we have to continue what we’ve done well, like social distancing,” Dr. Aslam said. “We’ve gone through a storm and we are awaiting a tsunami. That tsunami of patients will overwhelm us in the coming months.”
Dr. Martinez, Dr. Massuti, and Dr. Aslam had no relevant disclosures.
Daily Recap: Feds seek COVID-19 info through app, hospitalists take on new roles
Here are the stories our MDedge editors across specialties think you need to know about today:
FDA seeks COVID-19 info through CURE ID
Federal health officials are asking clinicians to use the free CURE ID mobile app and web platform as a tool to collect information on the treatment of patients with COVID-19. CURE ID is an Internet-based data repository first developed in 2013 as a collaboration between the Food and Drug Administration and the National Center for Advancing Translational Sciences, part of the National Institutes of Health. It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. “By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” said Heather A. Stone, MPH, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.” Read more.
Hospitalists take on new roles in COVID era
Whether it’s working shifts in the ICU, caring for ventilator patients, or reporting to postanesthesia care units and post-acute or step-down units, hospitalists are stepping into a variety of new roles as part of their frontline response to the COVID-19 pandemic. Valerie Vaughn, MD, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.” Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care professionals, who volunteered to manage COVID-19 patients in the ICU and other hospital units. Read more.
COVID-19 recommendations for rheumatic disease treatment
The European League Against Rheumatism (EULAR) issued provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Contrary to earlier expectations, there is no indication that patients with rheumatic and musculoskeletal diseases have a higher risk of contracting the virus or have a worse course if they do, according to the task force that worked on the recommendations. The task force also pointed out that rheumatology drugs are being used to treat COVID-19 patients who don’t have rheumatic diseases, raising the possibility of a shortage of disease-modifying antirheumatic drugs. Read more.
Mental health visits are 19% of ED costs
Mental and substance use disorders represented 19% of all emergency department visits in 2017 and cost $14.6 billion, according to figures from the Agency for Healthcare Research and Quality. The most costly mental and substance use disorder diagnosis was anxiety and fear-related disorders, accounting for $5.6 billion worth of visits, following by depressive disorders and alcohol-related disorders. Read more.
Food deserts linked to health issues in pregnancy
Living in a neighborhood lacking adequate access to affordable, high-quality food is associated with a somewhat greater risk of developing pregnancy morbidity, according to an observational study. Researchers found that women who lived in a food desert had a 1.6 times greater odds of pregnancy comorbidity than if they did not. “An additional, albeit less obvious factor that may be unique to patients suffering disproportionately from obstetric morbidity is exposure to toxic elements,” the researchers reported in Obstetrics & Gynecology. “It has been shown in a previous study that low-income, predominantly black communities of pregnant women may suffer disproportionately from lead or arsenic exposure.” Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
FDA seeks COVID-19 info through CURE ID
Federal health officials are asking clinicians to use the free CURE ID mobile app and web platform as a tool to collect information on the treatment of patients with COVID-19. CURE ID is an Internet-based data repository first developed in 2013 as a collaboration between the Food and Drug Administration and the National Center for Advancing Translational Sciences, part of the National Institutes of Health. It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. “By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” said Heather A. Stone, MPH, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.” Read more.
Hospitalists take on new roles in COVID era
Whether it’s working shifts in the ICU, caring for ventilator patients, or reporting to postanesthesia care units and post-acute or step-down units, hospitalists are stepping into a variety of new roles as part of their frontline response to the COVID-19 pandemic. Valerie Vaughn, MD, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.” Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care professionals, who volunteered to manage COVID-19 patients in the ICU and other hospital units. Read more.
COVID-19 recommendations for rheumatic disease treatment
The European League Against Rheumatism (EULAR) issued provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Contrary to earlier expectations, there is no indication that patients with rheumatic and musculoskeletal diseases have a higher risk of contracting the virus or have a worse course if they do, according to the task force that worked on the recommendations. The task force also pointed out that rheumatology drugs are being used to treat COVID-19 patients who don’t have rheumatic diseases, raising the possibility of a shortage of disease-modifying antirheumatic drugs. Read more.
Mental health visits are 19% of ED costs
Mental and substance use disorders represented 19% of all emergency department visits in 2017 and cost $14.6 billion, according to figures from the Agency for Healthcare Research and Quality. The most costly mental and substance use disorder diagnosis was anxiety and fear-related disorders, accounting for $5.6 billion worth of visits, following by depressive disorders and alcohol-related disorders. Read more.
Food deserts linked to health issues in pregnancy
Living in a neighborhood lacking adequate access to affordable, high-quality food is associated with a somewhat greater risk of developing pregnancy morbidity, according to an observational study. Researchers found that women who lived in a food desert had a 1.6 times greater odds of pregnancy comorbidity than if they did not. “An additional, albeit less obvious factor that may be unique to patients suffering disproportionately from obstetric morbidity is exposure to toxic elements,” the researchers reported in Obstetrics & Gynecology. “It has been shown in a previous study that low-income, predominantly black communities of pregnant women may suffer disproportionately from lead or arsenic exposure.” Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
FDA seeks COVID-19 info through CURE ID
Federal health officials are asking clinicians to use the free CURE ID mobile app and web platform as a tool to collect information on the treatment of patients with COVID-19. CURE ID is an Internet-based data repository first developed in 2013 as a collaboration between the Food and Drug Administration and the National Center for Advancing Translational Sciences, part of the National Institutes of Health. It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. “By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” said Heather A. Stone, MPH, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.” Read more.
Hospitalists take on new roles in COVID era
Whether it’s working shifts in the ICU, caring for ventilator patients, or reporting to postanesthesia care units and post-acute or step-down units, hospitalists are stepping into a variety of new roles as part of their frontline response to the COVID-19 pandemic. Valerie Vaughn, MD, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.” Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care professionals, who volunteered to manage COVID-19 patients in the ICU and other hospital units. Read more.
COVID-19 recommendations for rheumatic disease treatment
The European League Against Rheumatism (EULAR) issued provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Contrary to earlier expectations, there is no indication that patients with rheumatic and musculoskeletal diseases have a higher risk of contracting the virus or have a worse course if they do, according to the task force that worked on the recommendations. The task force also pointed out that rheumatology drugs are being used to treat COVID-19 patients who don’t have rheumatic diseases, raising the possibility of a shortage of disease-modifying antirheumatic drugs. Read more.
Mental health visits are 19% of ED costs
Mental and substance use disorders represented 19% of all emergency department visits in 2017 and cost $14.6 billion, according to figures from the Agency for Healthcare Research and Quality. The most costly mental and substance use disorder diagnosis was anxiety and fear-related disorders, accounting for $5.6 billion worth of visits, following by depressive disorders and alcohol-related disorders. Read more.
Food deserts linked to health issues in pregnancy
Living in a neighborhood lacking adequate access to affordable, high-quality food is associated with a somewhat greater risk of developing pregnancy morbidity, according to an observational study. Researchers found that women who lived in a food desert had a 1.6 times greater odds of pregnancy comorbidity than if they did not. “An additional, albeit less obvious factor that may be unique to patients suffering disproportionately from obstetric morbidity is exposure to toxic elements,” the researchers reported in Obstetrics & Gynecology. “It has been shown in a previous study that low-income, predominantly black communities of pregnant women may suffer disproportionately from lead or arsenic exposure.” Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Hospitalists stretch into new roles on COVID-19 front lines
‘Every single day is different’
In the midst of the COVID-19 pandemic, health systems, hospitals, and hospitalists – especially in hot spots like New York, Detroit, or Boston – have been challenged to stretch limits, redefine roles, and redeploy critical staff in response to rapidly changing needs on the ground.

Many hospitalists are working above and beyond their normal duties, sometimes beyond their training, specialty, or comfort zone and are rising to the occasion in ways they never imagined. These include doing shifts in ICUs, working with ventilator patients, and reporting to other atypical sites of care like postanesthesia care units and post-acute or step-down units.
Valerie Vaughn, MD, MSc, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.”
Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care providers, who volunteered to manage COVID-19 patients in the ICU and other hospital units. She was asked to help develop an all-COVID unit called the Regional Infectious Containment Unit or RICU, which opened March 16. Then, when the RICU became full, it was supplemented by two COVID-19 Moderate Care Units staffed by hospitalists who had “learned the ropes” in the RICU.
Both of these new models were defined in relation to the ICUs at Michigan Medicine – which were doubling in capacity, up to 200 beds at last count – and to the provision of intensive-level and long-term ventilator care for the sickest patients. The moderate care units are for patients who are not on ventilators but still very sick, for example, those receiving massive high-flow oxygen, often with a medical do-not-resuscitate/do-not-intubate order. “We established these units to do everything (medically) short of vents,” Dr. Vaughn said.
“We are having in-depth conversations about goals of care with patients soon after they arrive at the hospital. We know outcomes from ventilators are worse for COVID-positive patients who have comorbidities, and we’re using that information to inform these conversations. We’ve given scripts to clinicians to help guide them in leading these conversations. We can do other things than `use ventilators to manage their symptoms. But these are still difficult conversations,” Dr. Vaughn said.

“We also engaged palliative care early on and asked them to round with us on every [COVID] patient – until demand got too high.” The bottleneck has been the number of ICU beds available, she explained. “If you want your patient to come in and take that bed, make sure you’ve talked to the family about it.”
The COVID-19 team developed guidelines printed on pocket cards addressing critical care issues such as a refresher on how to treat acute respiratory distress syndrome and how to use vasopressors. (See the COVID-19 Continuing Medical Education Portal for web-accessible educational resources developed by Michigan Health).
It’s amazing how quickly patients can become very sick with COVID-19, Dr. Vaughn said. “One of the good things to happen from the beginning with our RICU is that a group of doctors became COVID care experts very quickly. We joined four to five hospitalists and their teams with each intensivist, so one critical care expert is there to do teaching and answer clinicians’ questions. The hospitalists coordinate the COVID care and talk to the families.”
Working on the front lines of this crisis, Dr. Vaughn said, has generated a powerful sense of purpose and camaraderie, creating bonds like in war time. “All of us on our days off feel a twinge of guilt for not being there in the hospital. The sense of gratitude we get from patients and families has been enormous, even when we were telling them bad news. That just brings us to tears.”
One of the hardest things for the doctors practicing above their typical scope of practice is that, when something bad happens, they can’t know whether it was a mistake on their part or not, she noted. “But I’ve never been so proud of our group or to be a hospitalist. No one has complained or pushed back. Everyone has responded by saying: ‘What can I do to help?’ ”
Enough work in hospital medicine
Hospitalists had not been deployed to care for ICU patients at Beth Israel Deaconess Medical Center (BIDMC) in Boston, a major hot spot for COVID-19, said Joseph Ming Wah Li, MD, SFHM, director of the hospital medicine program at BIDMC, when he spoke to The Hospitalist in mid-May. That’s because there were plenty of hospital medicine assignments to keep them busy. Dr. Li leads a service of 120 hospitalists practicing at four hospitals.
“As we speak today, we have 300 patients with COVID, with 70 or 80 of them in our ICU. I’m taking care of 17 patients today, 15 of them COVID-positive, and the other two placed in a former radiology holding suite adapted for COVID-negative patients. Our postanesthesia care unit is now an ICU filled with COVID patients,” he said.
“Half of my day is seeing patients and the other half I’m on Zoom calls. I’m also one of the resource allocation officers for BIDMC,” Dr. Li said. He helped to create a standard of care for the hospital, addressing what to do if there weren’t enough ICU beds or ventilators. “We’ve never actualized it and probably won’t, but it was important to go through this exercise, with a lot of discussion up front.”

Haki Laho, MD, an orthopedic hospitalist at New England Baptist Hospital (NEBH), also in Boston, has been redeployed to care for a different population of patients as his system tries to bunch patients. “All of a sudden – within hours and days – at the beginning of the pandemic and based on the recommendations, our whole system decided to stop all elective procedures and devote the resources to COVID,” he said.
NEBH is Beth Israel Lahey Health’s 141-bed orthopedic and surgical hospital, and the system has tried to keep the specialty facility COVID-19–free as much as possible, with the COVID-19 patients grouped together at BIDMC. Dr. Laho’s orthopedic hospitalist group, just five doctors, has been managing the influx of medical patients with multiple comorbidities – not COVID-19–infected but still a different kind of patient than they are used to.
“So far, so good. We’re dealing with it,” he said. “But if one of us got sick, the others would have to step up and do more shifts. We are physicians, internal medicine trained, but since my residency I hadn’t had to deal with these kinds of issues on a daily basis, such as setting up IV lines. I feel like I am back in residency mode.”
Convention Center medicine

Another Boston hospitalist, Amy Baughman, MD, who practices at Massachusetts General Hospital, is using her skills in a new setting, serving as a co-medical director at Boston Hope Medical Center, a 1,000-bed field hospital for patients with COVID-19. Open since April 10 and housed in the Boston Convention and Exhibition Center, it is a four-way collaboration between the Commonwealth of Massachusetts, the City of Boston, Partners HealthCare, and the Boston Health Care for the Homeless Program.
Boston Hope is divided into a post-acute care section for recovering COVID-19 patients and a respite section for undomiciled patients with COVID-19 who need a place to safely quarantine. Built for a maximum of 1,000 beds, it is currently using fewer, with 83 patients on the post-acute side and 73 on the respite side as of May 12. A total of 370 and 315, respectively, had been admitted through May 12.
The team had 5 days to put the field hospital together with the help of the Army National Guard. “During that first week I was installing hand sanitizer dispensers and making [personal protective equipment] signs. Everyone here has had to do things like that,” Dr. Baughman said. “We’ve had to be incredibly creative in our staffing, using doctors from primary care and subspecialties including dermatology, radiology, and orthopedics. We had to fast-track trainings on how to use EPIC and to provide post-acute COVID care. How do you simultaneously build a medical facility and lead teams to provide high quality care?”
Dr. Baughman still works hospitalist shifts half-time at Massachusetts General. Her prior experience providing post-acute care in the VA system was helpful in creating the post-acute level of care at Boston Hope.
“My medical director role involves supervising, staffing, and scheduling. My co-medical director, Dr. Kerri Palamara, and I also supervise the clinical care,” she said. “There are a lot of systems issues, like ordering labs or prescriptions, with couriers going back and forth. And we developed clinical pathways, such as for [deep vein thrombosis] prophylaxis or for COVID retesting to determine when it is safe to end a quarantine. We’re just now rolling out virtual specialist consultations,” she noted.

“It has gone incredibly well. So much of it has been about our ability and willingness to work hard, and take feedback and go forward. We don’t have time to harp on things. We have to be very solution oriented. At the same time, honestly, it’s been fun. Every single day is different,” Dr. Baughman said.
“It’s been an opportunity to use my skills in a totally new setting, and at a level of responsibility I haven’t had before, although that’s probably a common theme with COVID-19. I was put on this team because I am a hospitalist,” she said. “I think hospitalists have been the backbone of the response to COVID in this country. It’s been an opportunity for our specialty to shine. We need to embrace the opportunity.”
Balancing expertise and supervision
Mount Sinai Hospital (MSH) in Manhattan is in the New York epicenter of the COVID-19 crisis and has mobilized large numbers of pulmonary critical care and anesthesia physicians to staff up multiple ICUs for COVID-19 patients, said Andrew Dunn, MD, chief of the division of hospital medicine at Mount Sinai School of Medicine.

“My hospitalist group is covering many step-down units, medical wards, and atypical locations, providing advanced oxygen therapies, [bilevel positive airway pressure], high-flow nasal cannulas, and managing some patients on ventilators,” he said.
MSH has teaching services with house staff and nonteaching services. “We combined them into a unified service with house staff dispersed across all of the teams. We drafted a lot of nonhospitalists from different specialties to be attendings, and that has given us a tiered model, with a hospitalist supervising three or four nonhospitalist-led teams. Although the supervising hospitalists carry no patient caseloads of their own, this is primarily a clinical rather than an administrative role.”
At the peak, there were 40 rounding teams at MSH, each with a typical census of 15 patients or more, which meant that 10 supervisory hospitalists were responsible for 300 to 400 patients. “What we learned first was the need to balance the level of expertise. For example, a team may include a postgraduate year 3 resident and a radiology intern,” Dr. Dunn said. As COVID-19 census has started coming down, supervisory hospitalists are returning to direct care attending roles, and some hospitalists have been shared across the Mount Sinai system’s hospitals.
Dr. Dunn’s advice for hospitalists filling a supervisory role like this in a tiered model: Make sure you talk to your team the night before the first day of a scheduling block and try to address as many of their questions as possible. “If you wait until the morning of the shift to connect with them, anxiety will be high. But after going through a couple of scheduling cycles, we find that things are getting better. I think we’ve paid a lot of attention to the risks of burnout by our physicians. We’re using a model of 4 days on/4 off.”
Another variation on these themes is Joshua Shatzkes, MD, assistant professor of medicine and cardiology at Mount Sinai, who practices outpatient cardiology at MSH and in several off-site offices in Brooklyn. He saw early on that COVID-19 would have a huge effect on his practice, so he volunteered to help out with inpatient care. “I made it known to my chief that I was available, and I was deployed in the first week, after a weekend of cramming webinars and lectures on critical care and pulling out critical concepts that I already knew.”

Dr. Shatzkes said his career path led him into outpatient cardiology 11 years ago, where he was quickly too busy to see his patients when they went into the hospital, even though he missed hospital medicine. Working as a temporary hospitalist with the arrival of COVID-19, he has been invigorated and mobilized by the experience and reminded of why he went to medical school in the first place. “Each day’s shift went quickly but felt long. At the end of the day, I was tired but not exhausted. When I walked out of a patient’s room, they could tell, ‘This is a doctor who cared for me,’ ” he said.
After Dr. Shatzkes volunteered, he got the call from his division chief. “I was officially deployed for a 4-day shift at Mount Sinai and then as a backup.” On his first morning as an inpatient doctor, he was still getting oriented when calls started coming from the nurses. “I had five patients struggling to breathe. Their degree of hypoxia was remarkable. I kept them out of the ICU, at least for that day.”
Since then, he has continued to follow some of those patients in the hospital, along with some from his outpatient practice who were hospitalized, and others referred by colleagues, while remaining available to his outpatients through telemedicine. When this is all over, Dr. Shatzkes said, he would love to find a way to incorporate a hospital practice in his job – depending on the realities of New York traffic.
“Joshua is not a hospitalist, but he went on service and felt so fulfilled and rewarded, he asked me if he could stay on service,” Dr. Dunn said. “I also got an email from the nurse manager on the unit. They want him back.”
‘Every single day is different’
‘Every single day is different’
In the midst of the COVID-19 pandemic, health systems, hospitals, and hospitalists – especially in hot spots like New York, Detroit, or Boston – have been challenged to stretch limits, redefine roles, and redeploy critical staff in response to rapidly changing needs on the ground.
Many hospitalists are working above and beyond their normal duties, sometimes beyond their training, specialty, or comfort zone and are rising to the occasion in ways they never imagined. These include doing shifts in ICUs, working with ventilator patients, and reporting to other atypical sites of care like postanesthesia care units and post-acute or step-down units.
Valerie Vaughn, MD, MSc, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.”
Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care providers, who volunteered to manage COVID-19 patients in the ICU and other hospital units. She was asked to help develop an all-COVID unit called the Regional Infectious Containment Unit or RICU, which opened March 16. Then, when the RICU became full, it was supplemented by two COVID-19 Moderate Care Units staffed by hospitalists who had “learned the ropes” in the RICU.
Both of these new models were defined in relation to the ICUs at Michigan Medicine – which were doubling in capacity, up to 200 beds at last count – and to the provision of intensive-level and long-term ventilator care for the sickest patients. The moderate care units are for patients who are not on ventilators but still very sick, for example, those receiving massive high-flow oxygen, often with a medical do-not-resuscitate/do-not-intubate order. “We established these units to do everything (medically) short of vents,” Dr. Vaughn said.
“We are having in-depth conversations about goals of care with patients soon after they arrive at the hospital. We know outcomes from ventilators are worse for COVID-positive patients who have comorbidities, and we’re using that information to inform these conversations. We’ve given scripts to clinicians to help guide them in leading these conversations. We can do other things than `use ventilators to manage their symptoms. But these are still difficult conversations,” Dr. Vaughn said.
“We also engaged palliative care early on and asked them to round with us on every [COVID] patient – until demand got too high.” The bottleneck has been the number of ICU beds available, she explained. “If you want your patient to come in and take that bed, make sure you’ve talked to the family about it.”
The COVID-19 team developed guidelines printed on pocket cards addressing critical care issues such as a refresher on how to treat acute respiratory distress syndrome and how to use vasopressors. (See the COVID-19 Continuing Medical Education Portal for web-accessible educational resources developed by Michigan Health).
It’s amazing how quickly patients can become very sick with COVID-19, Dr. Vaughn said. “One of the good things to happen from the beginning with our RICU is that a group of doctors became COVID care experts very quickly. We joined four to five hospitalists and their teams with each intensivist, so one critical care expert is there to do teaching and answer clinicians’ questions. The hospitalists coordinate the COVID care and talk to the families.”
Working on the front lines of this crisis, Dr. Vaughn said, has generated a powerful sense of purpose and camaraderie, creating bonds like in war time. “All of us on our days off feel a twinge of guilt for not being there in the hospital. The sense of gratitude we get from patients and families has been enormous, even when we were telling them bad news. That just brings us to tears.”
One of the hardest things for the doctors practicing above their typical scope of practice is that, when something bad happens, they can’t know whether it was a mistake on their part or not, she noted. “But I’ve never been so proud of our group or to be a hospitalist. No one has complained or pushed back. Everyone has responded by saying: ‘What can I do to help?’ ”
Enough work in hospital medicine
Hospitalists had not been deployed to care for ICU patients at Beth Israel Deaconess Medical Center (BIDMC) in Boston, a major hot spot for COVID-19, said Joseph Ming Wah Li, MD, SFHM, director of the hospital medicine program at BIDMC, when he spoke to The Hospitalist in mid-May. That’s because there were plenty of hospital medicine assignments to keep them busy. Dr. Li leads a service of 120 hospitalists practicing at four hospitals.
“As we speak today, we have 300 patients with COVID, with 70 or 80 of them in our ICU. I’m taking care of 17 patients today, 15 of them COVID-positive, and the other two placed in a former radiology holding suite adapted for COVID-negative patients. Our postanesthesia care unit is now an ICU filled with COVID patients,” he said.
“Half of my day is seeing patients and the other half I’m on Zoom calls. I’m also one of the resource allocation officers for BIDMC,” Dr. Li said. He helped to create a standard of care for the hospital, addressing what to do if there weren’t enough ICU beds or ventilators. “We’ve never actualized it and probably won’t, but it was important to go through this exercise, with a lot of discussion up front.”
Haki Laho, MD, an orthopedic hospitalist at New England Baptist Hospital (NEBH), also in Boston, has been redeployed to care for a different population of patients as his system tries to bunch patients. “All of a sudden – within hours and days – at the beginning of the pandemic and based on the recommendations, our whole system decided to stop all elective procedures and devote the resources to COVID,” he said.
NEBH is Beth Israel Lahey Health’s 141-bed orthopedic and surgical hospital, and the system has tried to keep the specialty facility COVID-19–free as much as possible, with the COVID-19 patients grouped together at BIDMC. Dr. Laho’s orthopedic hospitalist group, just five doctors, has been managing the influx of medical patients with multiple comorbidities – not COVID-19–infected but still a different kind of patient than they are used to.
“So far, so good. We’re dealing with it,” he said. “But if one of us got sick, the others would have to step up and do more shifts. We are physicians, internal medicine trained, but since my residency I hadn’t had to deal with these kinds of issues on a daily basis, such as setting up IV lines. I feel like I am back in residency mode.”
Convention Center medicine
Another Boston hospitalist, Amy Baughman, MD, who practices at Massachusetts General Hospital, is using her skills in a new setting, serving as a co-medical director at Boston Hope Medical Center, a 1,000-bed field hospital for patients with COVID-19. Open since April 10 and housed in the Boston Convention and Exhibition Center, it is a four-way collaboration between the Commonwealth of Massachusetts, the City of Boston, Partners HealthCare, and the Boston Health Care for the Homeless Program.
Boston Hope is divided into a post-acute care section for recovering COVID-19 patients and a respite section for undomiciled patients with COVID-19 who need a place to safely quarantine. Built for a maximum of 1,000 beds, it is currently using fewer, with 83 patients on the post-acute side and 73 on the respite side as of May 12. A total of 370 and 315, respectively, had been admitted through May 12.
The team had 5 days to put the field hospital together with the help of the Army National Guard. “During that first week I was installing hand sanitizer dispensers and making [personal protective equipment] signs. Everyone here has had to do things like that,” Dr. Baughman said. “We’ve had to be incredibly creative in our staffing, using doctors from primary care and subspecialties including dermatology, radiology, and orthopedics. We had to fast-track trainings on how to use EPIC and to provide post-acute COVID care. How do you simultaneously build a medical facility and lead teams to provide high quality care?”
Dr. Baughman still works hospitalist shifts half-time at Massachusetts General. Her prior experience providing post-acute care in the VA system was helpful in creating the post-acute level of care at Boston Hope.
“My medical director role involves supervising, staffing, and scheduling. My co-medical director, Dr. Kerri Palamara, and I also supervise the clinical care,” she said. “There are a lot of systems issues, like ordering labs or prescriptions, with couriers going back and forth. And we developed clinical pathways, such as for [deep vein thrombosis] prophylaxis or for COVID retesting to determine when it is safe to end a quarantine. We’re just now rolling out virtual specialist consultations,” she noted.
“It has gone incredibly well. So much of it has been about our ability and willingness to work hard, and take feedback and go forward. We don’t have time to harp on things. We have to be very solution oriented. At the same time, honestly, it’s been fun. Every single day is different,” Dr. Baughman said.
“It’s been an opportunity to use my skills in a totally new setting, and at a level of responsibility I haven’t had before, although that’s probably a common theme with COVID-19. I was put on this team because I am a hospitalist,” she said. “I think hospitalists have been the backbone of the response to COVID in this country. It’s been an opportunity for our specialty to shine. We need to embrace the opportunity.”
Balancing expertise and supervision
Mount Sinai Hospital (MSH) in Manhattan is in the New York epicenter of the COVID-19 crisis and has mobilized large numbers of pulmonary critical care and anesthesia physicians to staff up multiple ICUs for COVID-19 patients, said Andrew Dunn, MD, chief of the division of hospital medicine at Mount Sinai School of Medicine.
“My hospitalist group is covering many step-down units, medical wards, and atypical locations, providing advanced oxygen therapies, [bilevel positive airway pressure], high-flow nasal cannulas, and managing some patients on ventilators,” he said.
MSH has teaching services with house staff and nonteaching services. “We combined them into a unified service with house staff dispersed across all of the teams. We drafted a lot of nonhospitalists from different specialties to be attendings, and that has given us a tiered model, with a hospitalist supervising three or four nonhospitalist-led teams. Although the supervising hospitalists carry no patient caseloads of their own, this is primarily a clinical rather than an administrative role.”
At the peak, there were 40 rounding teams at MSH, each with a typical census of 15 patients or more, which meant that 10 supervisory hospitalists were responsible for 300 to 400 patients. “What we learned first was the need to balance the level of expertise. For example, a team may include a postgraduate year 3 resident and a radiology intern,” Dr. Dunn said. As COVID-19 census has started coming down, supervisory hospitalists are returning to direct care attending roles, and some hospitalists have been shared across the Mount Sinai system’s hospitals.
Dr. Dunn’s advice for hospitalists filling a supervisory role like this in a tiered model: Make sure you talk to your team the night before the first day of a scheduling block and try to address as many of their questions as possible. “If you wait until the morning of the shift to connect with them, anxiety will be high. But after going through a couple of scheduling cycles, we find that things are getting better. I think we’ve paid a lot of attention to the risks of burnout by our physicians. We’re using a model of 4 days on/4 off.”
Another variation on these themes is Joshua Shatzkes, MD, assistant professor of medicine and cardiology at Mount Sinai, who practices outpatient cardiology at MSH and in several off-site offices in Brooklyn. He saw early on that COVID-19 would have a huge effect on his practice, so he volunteered to help out with inpatient care. “I made it known to my chief that I was available, and I was deployed in the first week, after a weekend of cramming webinars and lectures on critical care and pulling out critical concepts that I already knew.”
Dr. Shatzkes said his career path led him into outpatient cardiology 11 years ago, where he was quickly too busy to see his patients when they went into the hospital, even though he missed hospital medicine. Working as a temporary hospitalist with the arrival of COVID-19, he has been invigorated and mobilized by the experience and reminded of why he went to medical school in the first place. “Each day’s shift went quickly but felt long. At the end of the day, I was tired but not exhausted. When I walked out of a patient’s room, they could tell, ‘This is a doctor who cared for me,’ ” he said.
After Dr. Shatzkes volunteered, he got the call from his division chief. “I was officially deployed for a 4-day shift at Mount Sinai and then as a backup.” On his first morning as an inpatient doctor, he was still getting oriented when calls started coming from the nurses. “I had five patients struggling to breathe. Their degree of hypoxia was remarkable. I kept them out of the ICU, at least for that day.”
Since then, he has continued to follow some of those patients in the hospital, along with some from his outpatient practice who were hospitalized, and others referred by colleagues, while remaining available to his outpatients through telemedicine. When this is all over, Dr. Shatzkes said, he would love to find a way to incorporate a hospital practice in his job – depending on the realities of New York traffic.
“Joshua is not a hospitalist, but he went on service and felt so fulfilled and rewarded, he asked me if he could stay on service,” Dr. Dunn said. “I also got an email from the nurse manager on the unit. They want him back.”
In the midst of the COVID-19 pandemic, health systems, hospitals, and hospitalists – especially in hot spots like New York, Detroit, or Boston – have been challenged to stretch limits, redefine roles, and redeploy critical staff in response to rapidly changing needs on the ground.
Many hospitalists are working above and beyond their normal duties, sometimes beyond their training, specialty, or comfort zone and are rising to the occasion in ways they never imagined. These include doing shifts in ICUs, working with ventilator patients, and reporting to other atypical sites of care like postanesthesia care units and post-acute or step-down units.
Valerie Vaughn, MD, MSc, a hospitalist with Michigan Medicine and assistant professor of medicine at the University of Michigan in Ann Arbor, was doing research on how to reduce overuse of antibiotics in hospitals when the COVID-19 crisis hit and dramatically redefined her job. “We were afraid that we might have 3,000 to 5,000 hospitalized COVID patients by now, based on predictive modeling done while the pandemic was still growing exponentially,” she explained. Although Michigan continues to have high COVID-19 infection rates, centered on nearby Detroit, “things are a lot better today than they were 4 weeks ago.”
Dr. Vaughn helped to mobilize a team of 25 hospitalists, along with other health care providers, who volunteered to manage COVID-19 patients in the ICU and other hospital units. She was asked to help develop an all-COVID unit called the Regional Infectious Containment Unit or RICU, which opened March 16. Then, when the RICU became full, it was supplemented by two COVID-19 Moderate Care Units staffed by hospitalists who had “learned the ropes” in the RICU.
Both of these new models were defined in relation to the ICUs at Michigan Medicine – which were doubling in capacity, up to 200 beds at last count – and to the provision of intensive-level and long-term ventilator care for the sickest patients. The moderate care units are for patients who are not on ventilators but still very sick, for example, those receiving massive high-flow oxygen, often with a medical do-not-resuscitate/do-not-intubate order. “We established these units to do everything (medically) short of vents,” Dr. Vaughn said.
“We are having in-depth conversations about goals of care with patients soon after they arrive at the hospital. We know outcomes from ventilators are worse for COVID-positive patients who have comorbidities, and we’re using that information to inform these conversations. We’ve given scripts to clinicians to help guide them in leading these conversations. We can do other things than `use ventilators to manage their symptoms. But these are still difficult conversations,” Dr. Vaughn said.
“We also engaged palliative care early on and asked them to round with us on every [COVID] patient – until demand got too high.” The bottleneck has been the number of ICU beds available, she explained. “If you want your patient to come in and take that bed, make sure you’ve talked to the family about it.”
The COVID-19 team developed guidelines printed on pocket cards addressing critical care issues such as a refresher on how to treat acute respiratory distress syndrome and how to use vasopressors. (See the COVID-19 Continuing Medical Education Portal for web-accessible educational resources developed by Michigan Health).
It’s amazing how quickly patients can become very sick with COVID-19, Dr. Vaughn said. “One of the good things to happen from the beginning with our RICU is that a group of doctors became COVID care experts very quickly. We joined four to five hospitalists and their teams with each intensivist, so one critical care expert is there to do teaching and answer clinicians’ questions. The hospitalists coordinate the COVID care and talk to the families.”
Working on the front lines of this crisis, Dr. Vaughn said, has generated a powerful sense of purpose and camaraderie, creating bonds like in war time. “All of us on our days off feel a twinge of guilt for not being there in the hospital. The sense of gratitude we get from patients and families has been enormous, even when we were telling them bad news. That just brings us to tears.”
One of the hardest things for the doctors practicing above their typical scope of practice is that, when something bad happens, they can’t know whether it was a mistake on their part or not, she noted. “But I’ve never been so proud of our group or to be a hospitalist. No one has complained or pushed back. Everyone has responded by saying: ‘What can I do to help?’ ”
Enough work in hospital medicine
Hospitalists had not been deployed to care for ICU patients at Beth Israel Deaconess Medical Center (BIDMC) in Boston, a major hot spot for COVID-19, said Joseph Ming Wah Li, MD, SFHM, director of the hospital medicine program at BIDMC, when he spoke to The Hospitalist in mid-May. That’s because there were plenty of hospital medicine assignments to keep them busy. Dr. Li leads a service of 120 hospitalists practicing at four hospitals.
“As we speak today, we have 300 patients with COVID, with 70 or 80 of them in our ICU. I’m taking care of 17 patients today, 15 of them COVID-positive, and the other two placed in a former radiology holding suite adapted for COVID-negative patients. Our postanesthesia care unit is now an ICU filled with COVID patients,” he said.
“Half of my day is seeing patients and the other half I’m on Zoom calls. I’m also one of the resource allocation officers for BIDMC,” Dr. Li said. He helped to create a standard of care for the hospital, addressing what to do if there weren’t enough ICU beds or ventilators. “We’ve never actualized it and probably won’t, but it was important to go through this exercise, with a lot of discussion up front.”
Haki Laho, MD, an orthopedic hospitalist at New England Baptist Hospital (NEBH), also in Boston, has been redeployed to care for a different population of patients as his system tries to bunch patients. “All of a sudden – within hours and days – at the beginning of the pandemic and based on the recommendations, our whole system decided to stop all elective procedures and devote the resources to COVID,” he said.
NEBH is Beth Israel Lahey Health’s 141-bed orthopedic and surgical hospital, and the system has tried to keep the specialty facility COVID-19–free as much as possible, with the COVID-19 patients grouped together at BIDMC. Dr. Laho’s orthopedic hospitalist group, just five doctors, has been managing the influx of medical patients with multiple comorbidities – not COVID-19–infected but still a different kind of patient than they are used to.
“So far, so good. We’re dealing with it,” he said. “But if one of us got sick, the others would have to step up and do more shifts. We are physicians, internal medicine trained, but since my residency I hadn’t had to deal with these kinds of issues on a daily basis, such as setting up IV lines. I feel like I am back in residency mode.”
Convention Center medicine
Another Boston hospitalist, Amy Baughman, MD, who practices at Massachusetts General Hospital, is using her skills in a new setting, serving as a co-medical director at Boston Hope Medical Center, a 1,000-bed field hospital for patients with COVID-19. Open since April 10 and housed in the Boston Convention and Exhibition Center, it is a four-way collaboration between the Commonwealth of Massachusetts, the City of Boston, Partners HealthCare, and the Boston Health Care for the Homeless Program.
Boston Hope is divided into a post-acute care section for recovering COVID-19 patients and a respite section for undomiciled patients with COVID-19 who need a place to safely quarantine. Built for a maximum of 1,000 beds, it is currently using fewer, with 83 patients on the post-acute side and 73 on the respite side as of May 12. A total of 370 and 315, respectively, had been admitted through May 12.
The team had 5 days to put the field hospital together with the help of the Army National Guard. “During that first week I was installing hand sanitizer dispensers and making [personal protective equipment] signs. Everyone here has had to do things like that,” Dr. Baughman said. “We’ve had to be incredibly creative in our staffing, using doctors from primary care and subspecialties including dermatology, radiology, and orthopedics. We had to fast-track trainings on how to use EPIC and to provide post-acute COVID care. How do you simultaneously build a medical facility and lead teams to provide high quality care?”
Dr. Baughman still works hospitalist shifts half-time at Massachusetts General. Her prior experience providing post-acute care in the VA system was helpful in creating the post-acute level of care at Boston Hope.
“My medical director role involves supervising, staffing, and scheduling. My co-medical director, Dr. Kerri Palamara, and I also supervise the clinical care,” she said. “There are a lot of systems issues, like ordering labs or prescriptions, with couriers going back and forth. And we developed clinical pathways, such as for [deep vein thrombosis] prophylaxis or for COVID retesting to determine when it is safe to end a quarantine. We’re just now rolling out virtual specialist consultations,” she noted.
“It has gone incredibly well. So much of it has been about our ability and willingness to work hard, and take feedback and go forward. We don’t have time to harp on things. We have to be very solution oriented. At the same time, honestly, it’s been fun. Every single day is different,” Dr. Baughman said.
“It’s been an opportunity to use my skills in a totally new setting, and at a level of responsibility I haven’t had before, although that’s probably a common theme with COVID-19. I was put on this team because I am a hospitalist,” she said. “I think hospitalists have been the backbone of the response to COVID in this country. It’s been an opportunity for our specialty to shine. We need to embrace the opportunity.”
Balancing expertise and supervision
Mount Sinai Hospital (MSH) in Manhattan is in the New York epicenter of the COVID-19 crisis and has mobilized large numbers of pulmonary critical care and anesthesia physicians to staff up multiple ICUs for COVID-19 patients, said Andrew Dunn, MD, chief of the division of hospital medicine at Mount Sinai School of Medicine.
“My hospitalist group is covering many step-down units, medical wards, and atypical locations, providing advanced oxygen therapies, [bilevel positive airway pressure], high-flow nasal cannulas, and managing some patients on ventilators,” he said.
MSH has teaching services with house staff and nonteaching services. “We combined them into a unified service with house staff dispersed across all of the teams. We drafted a lot of nonhospitalists from different specialties to be attendings, and that has given us a tiered model, with a hospitalist supervising three or four nonhospitalist-led teams. Although the supervising hospitalists carry no patient caseloads of their own, this is primarily a clinical rather than an administrative role.”
At the peak, there were 40 rounding teams at MSH, each with a typical census of 15 patients or more, which meant that 10 supervisory hospitalists were responsible for 300 to 400 patients. “What we learned first was the need to balance the level of expertise. For example, a team may include a postgraduate year 3 resident and a radiology intern,” Dr. Dunn said. As COVID-19 census has started coming down, supervisory hospitalists are returning to direct care attending roles, and some hospitalists have been shared across the Mount Sinai system’s hospitals.
Dr. Dunn’s advice for hospitalists filling a supervisory role like this in a tiered model: Make sure you talk to your team the night before the first day of a scheduling block and try to address as many of their questions as possible. “If you wait until the morning of the shift to connect with them, anxiety will be high. But after going through a couple of scheduling cycles, we find that things are getting better. I think we’ve paid a lot of attention to the risks of burnout by our physicians. We’re using a model of 4 days on/4 off.”
Another variation on these themes is Joshua Shatzkes, MD, assistant professor of medicine and cardiology at Mount Sinai, who practices outpatient cardiology at MSH and in several off-site offices in Brooklyn. He saw early on that COVID-19 would have a huge effect on his practice, so he volunteered to help out with inpatient care. “I made it known to my chief that I was available, and I was deployed in the first week, after a weekend of cramming webinars and lectures on critical care and pulling out critical concepts that I already knew.”
Dr. Shatzkes said his career path led him into outpatient cardiology 11 years ago, where he was quickly too busy to see his patients when they went into the hospital, even though he missed hospital medicine. Working as a temporary hospitalist with the arrival of COVID-19, he has been invigorated and mobilized by the experience and reminded of why he went to medical school in the first place. “Each day’s shift went quickly but felt long. At the end of the day, I was tired but not exhausted. When I walked out of a patient’s room, they could tell, ‘This is a doctor who cared for me,’ ” he said.
After Dr. Shatzkes volunteered, he got the call from his division chief. “I was officially deployed for a 4-day shift at Mount Sinai and then as a backup.” On his first morning as an inpatient doctor, he was still getting oriented when calls started coming from the nurses. “I had five patients struggling to breathe. Their degree of hypoxia was remarkable. I kept them out of the ICU, at least for that day.”
Since then, he has continued to follow some of those patients in the hospital, along with some from his outpatient practice who were hospitalized, and others referred by colleagues, while remaining available to his outpatients through telemedicine. When this is all over, Dr. Shatzkes said, he would love to find a way to incorporate a hospital practice in his job – depending on the realities of New York traffic.
“Joshua is not a hospitalist, but he went on service and felt so fulfilled and rewarded, he asked me if he could stay on service,” Dr. Dunn said. “I also got an email from the nurse manager on the unit. They want him back.”

Clinicians urged to use CURE ID to report COVID-19 cases
in conjunction with ongoing clinical trial efforts.
“By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” Heather A. Stone, MPH, said during a June 9 webinar sponsored by the Food and Drug Administration. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.”
During the hour-long webinar, Ms. Stone, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research, demonstrated CURE ID, an Internet-based data repository first developed in 2013 as a collaboration between the FDA and the National Center for Advancing Translational Sciences, a part of the National Institutes of Health (NCATS/NIH). It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. The app can be downloaded for free at http://cure.ncats.io. It can also be downloaded from the Apple app store or the Google Play store by searching “CURE ID.”
According to Ms. Stone, the platform’s three main goals are to enhance the understanding of new uses of approved medical products, to facilitate clinical trials and drug development, and to serve as a resource for physicians to share information where no FDA-approved product (which has been proven to be safe and effective) exists for the new use. CURE ID enables users to report their own cases as well as read cases of neglected infectious diseases with no sufficient approved therapies from other clinicians around the world. “It also enables clinicians to engage directly with communities of disease experts around the world, breaking down geographic and specialty silos,” Ms. Stone said. “It also enables them to access information on approved therapies for each disease and as well on active clinical trials.”
To date, CURE-ID contains information on 325 infectious diseases, including 1,580 case reports and 18,907 clinical trials. Initial pilot priority diseases include COVID-19, mycetoma, atypical mycobacteria, drug-resistant gonorrhea, rare and resistant fungal infections, as well as multidrug resistant gram-negative bacteria.
As of June 9, COVID-19-related data on the platform includes 151 case reports that have been extracted from the published literature or entered by clinician users, 80 discussion posts, and links to 694 clinical trials, 303 journal articles, 212 news articles, and 34 events. A total of 65 repurposed drugs have been identified as potential treatments for the virus, including 15 drugs with 10 or more cases.
“This facilitates clinicians reporting their real-world experiences treating COVID-19 patients, when patients are unable to be enrolled in a clinical trial,” Ms. Stone said. “It includes an updated case report form tailored to COVID-19 and data fields that have been harmonized with other real-world data and clinical trial platforms.” She pointed out that voluntary submission of cases to CURE ID is not a substitute for filing information with regulatory and public health authorities, where required. The platform also enables data to be entered and adverse events to be automatically shared with the FDA’s MedWatch Adverse Reporting System.
Ms. Stone concluded the webinar by announcing the formation of a new private-public partnership between the Critical Path Institute and the FDA and NCATS/NIH known as the CURE Drug Repurposing Collaboratory. The effort will begin with a pilot project focused on furthering drug development for COVID-19 through use of the CURE ID platform. “The Collaboratory will demonstrate how data shared from clinicians in real-time can be used to inform ongoing and future clinical trials, and potentially drug labeling,” Ms. Stone said. She reported having no financial disclosures.
in conjunction with ongoing clinical trial efforts.
“By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” Heather A. Stone, MPH, said during a June 9 webinar sponsored by the Food and Drug Administration. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.”
During the hour-long webinar, Ms. Stone, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research, demonstrated CURE ID, an Internet-based data repository first developed in 2013 as a collaboration between the FDA and the National Center for Advancing Translational Sciences, a part of the National Institutes of Health (NCATS/NIH). It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. The app can be downloaded for free at http://cure.ncats.io. It can also be downloaded from the Apple app store or the Google Play store by searching “CURE ID.”
According to Ms. Stone, the platform’s three main goals are to enhance the understanding of new uses of approved medical products, to facilitate clinical trials and drug development, and to serve as a resource for physicians to share information where no FDA-approved product (which has been proven to be safe and effective) exists for the new use. CURE ID enables users to report their own cases as well as read cases of neglected infectious diseases with no sufficient approved therapies from other clinicians around the world. “It also enables clinicians to engage directly with communities of disease experts around the world, breaking down geographic and specialty silos,” Ms. Stone said. “It also enables them to access information on approved therapies for each disease and as well on active clinical trials.”
To date, CURE-ID contains information on 325 infectious diseases, including 1,580 case reports and 18,907 clinical trials. Initial pilot priority diseases include COVID-19, mycetoma, atypical mycobacteria, drug-resistant gonorrhea, rare and resistant fungal infections, as well as multidrug resistant gram-negative bacteria.
As of June 9, COVID-19-related data on the platform includes 151 case reports that have been extracted from the published literature or entered by clinician users, 80 discussion posts, and links to 694 clinical trials, 303 journal articles, 212 news articles, and 34 events. A total of 65 repurposed drugs have been identified as potential treatments for the virus, including 15 drugs with 10 or more cases.
“This facilitates clinicians reporting their real-world experiences treating COVID-19 patients, when patients are unable to be enrolled in a clinical trial,” Ms. Stone said. “It includes an updated case report form tailored to COVID-19 and data fields that have been harmonized with other real-world data and clinical trial platforms.” She pointed out that voluntary submission of cases to CURE ID is not a substitute for filing information with regulatory and public health authorities, where required. The platform also enables data to be entered and adverse events to be automatically shared with the FDA’s MedWatch Adverse Reporting System.
Ms. Stone concluded the webinar by announcing the formation of a new private-public partnership between the Critical Path Institute and the FDA and NCATS/NIH known as the CURE Drug Repurposing Collaboratory. The effort will begin with a pilot project focused on furthering drug development for COVID-19 through use of the CURE ID platform. “The Collaboratory will demonstrate how data shared from clinicians in real-time can be used to inform ongoing and future clinical trials, and potentially drug labeling,” Ms. Stone said. She reported having no financial disclosures.
in conjunction with ongoing clinical trial efforts.
“By utilizing the CURE ID platform now for COVID-19 case collection – in conjunction with data gathered from other registries, EHR systems, and clinical trials – data collected during an outbreak can be improved and coordinated,” Heather A. Stone, MPH, said during a June 9 webinar sponsored by the Food and Drug Administration. “This may allow us to find possible treatments to help ease this pandemic, and prepare us better to fight the next one.”
During the hour-long webinar, Ms. Stone, a health science policy analyst in the office of medical policy at the FDA’s Center for Drug Evaluation and Research, demonstrated CURE ID, an Internet-based data repository first developed in 2013 as a collaboration between the FDA and the National Center for Advancing Translational Sciences, a part of the National Institutes of Health (NCATS/NIH). It provides licensed clinicians worldwide with an opportunity to report novel uses of existing drugs for patients with difficult-to-treat infectious diseases, including COVID-19, through a website, a smartphone, or other mobile device. The app can be downloaded for free at http://cure.ncats.io. It can also be downloaded from the Apple app store or the Google Play store by searching “CURE ID.”
According to Ms. Stone, the platform’s three main goals are to enhance the understanding of new uses of approved medical products, to facilitate clinical trials and drug development, and to serve as a resource for physicians to share information where no FDA-approved product (which has been proven to be safe and effective) exists for the new use. CURE ID enables users to report their own cases as well as read cases of neglected infectious diseases with no sufficient approved therapies from other clinicians around the world. “It also enables clinicians to engage directly with communities of disease experts around the world, breaking down geographic and specialty silos,” Ms. Stone said. “It also enables them to access information on approved therapies for each disease and as well on active clinical trials.”
To date, CURE-ID contains information on 325 infectious diseases, including 1,580 case reports and 18,907 clinical trials. Initial pilot priority diseases include COVID-19, mycetoma, atypical mycobacteria, drug-resistant gonorrhea, rare and resistant fungal infections, as well as multidrug resistant gram-negative bacteria.
As of June 9, COVID-19-related data on the platform includes 151 case reports that have been extracted from the published literature or entered by clinician users, 80 discussion posts, and links to 694 clinical trials, 303 journal articles, 212 news articles, and 34 events. A total of 65 repurposed drugs have been identified as potential treatments for the virus, including 15 drugs with 10 or more cases.
“This facilitates clinicians reporting their real-world experiences treating COVID-19 patients, when patients are unable to be enrolled in a clinical trial,” Ms. Stone said. “It includes an updated case report form tailored to COVID-19 and data fields that have been harmonized with other real-world data and clinical trial platforms.” She pointed out that voluntary submission of cases to CURE ID is not a substitute for filing information with regulatory and public health authorities, where required. The platform also enables data to be entered and adverse events to be automatically shared with the FDA’s MedWatch Adverse Reporting System.
Ms. Stone concluded the webinar by announcing the formation of a new private-public partnership between the Critical Path Institute and the FDA and NCATS/NIH known as the CURE Drug Repurposing Collaboratory. The effort will begin with a pilot project focused on furthering drug development for COVID-19 through use of the CURE ID platform. “The Collaboratory will demonstrate how data shared from clinicians in real-time can be used to inform ongoing and future clinical trials, and potentially drug labeling,” Ms. Stone said. She reported having no financial disclosures.